Bridging the Gap: How Patient Advocacy is Shaping Access to Medications in Canada
Clinical Consequences of Delayed Medication Access
Emerging Treatments
Health Canada's recent approvals in 2025
CADTH/CDA call for patient input
Diversity, Inclusion, and Equity
Systemic Barriers to Medication Access in Canada & The Role of Patient Advocacy in Overcoming Barriers
Mental Health
Reading for Well-Being
Spring Cleaning Your Mind: Refresh Your Mental Space
Shame-Based Identity: Understanding Its Impact and Path to Healing
Senior Health
The State of Social Connection: A Life Course Matter Ageing and Social Connection
Senior Access to Medications: Why It’s
in
and What Can Be
The Importance of Access to Medications for Pediatric Patients
Advocacy Spotlight
Empowering a generation to thrive
Pancreatic Cancer: Patient Empowerment through Self-Advocacy
Introducing the Health Advisory Network
StayWell
Patient Journey
Resilience, Advocacy, and Giving Back
Stem Cell Transplant Success
Living Well
Sun Myths
Turning a diagnosis into a passion Resepies
Satisfy Your Sweet Tooth: Combat Your Cravings
the Professional
Founders Note
Welcome to our 8th Issue of E3 Advocacy. A digital magazine for Patient Advocates and Patient Centricity
This edition is deeply personal and critically important, focusing on access to medication, a cornerstone of equitable healthcare.
Across Canada, and globally, too many patients still face insurmountable barriers to getting the treatments they need— due to cost, delays in approval, supply chain issues, or lack of inclusion in formularies. For some, the wait for medication isn't just frustrating—it's life-threatening.As advocates, caregivers, professionals, and patients, we know that access is more than just about pharmaceuticals—it’s about dignity, autonomy, and the right to quality care. It's about making sure children, seniors, and marginalized communities aren’t left behind because of bureaucracy, economics, or outdated systems We hope this issue inspires you to ask bold questions, demand change, and stand firm in the belief that access to medication is not a privilege—it is a human right.
We're deeply grateful to our readers for their continued interest and support. Your engagement drives us to bring insightful and valuable content to each issue. By subscribing to Heal Canada Digital Magazine, you'll stay connected with us and gain access to future issues that explore topics that matter to you and the healthcare community. Become a subscriber and visit our websiteat https://www.healcanada.org toenjoyallthebenefits.
In each Issue, we have been adding new sections to be inclusive oftheentireHealthcareEcosystem.
We are humbled at the momentum we are gaining with the information to our readers. This digital publication is being read by patient advocates, patients and care partners across the world.
Thank you for being a part of our journey, and welcome to anotherenlighteningissue!
Bridging the Gap: How Patient Advocacy is Shaping Access to Medications in Canada
by Cheryl Petruk, MBA
Access to medications in Canada remains a pressing concern for many patients—especially those with rare, chronic, or life-threatening illnesses. While Canada’s publicly funded healthcare system is celebrated globally, the reality is more complex. Delays in drug approvals, inconsistent provincial formularies, and affordability challenges create barriers that leave patients waiting— and sometimes suffering—while the system navigates red tape. In this landscape, patient advocacy is not just helpful—it is essential.
Understanding the Canadian Drug Access Landscape
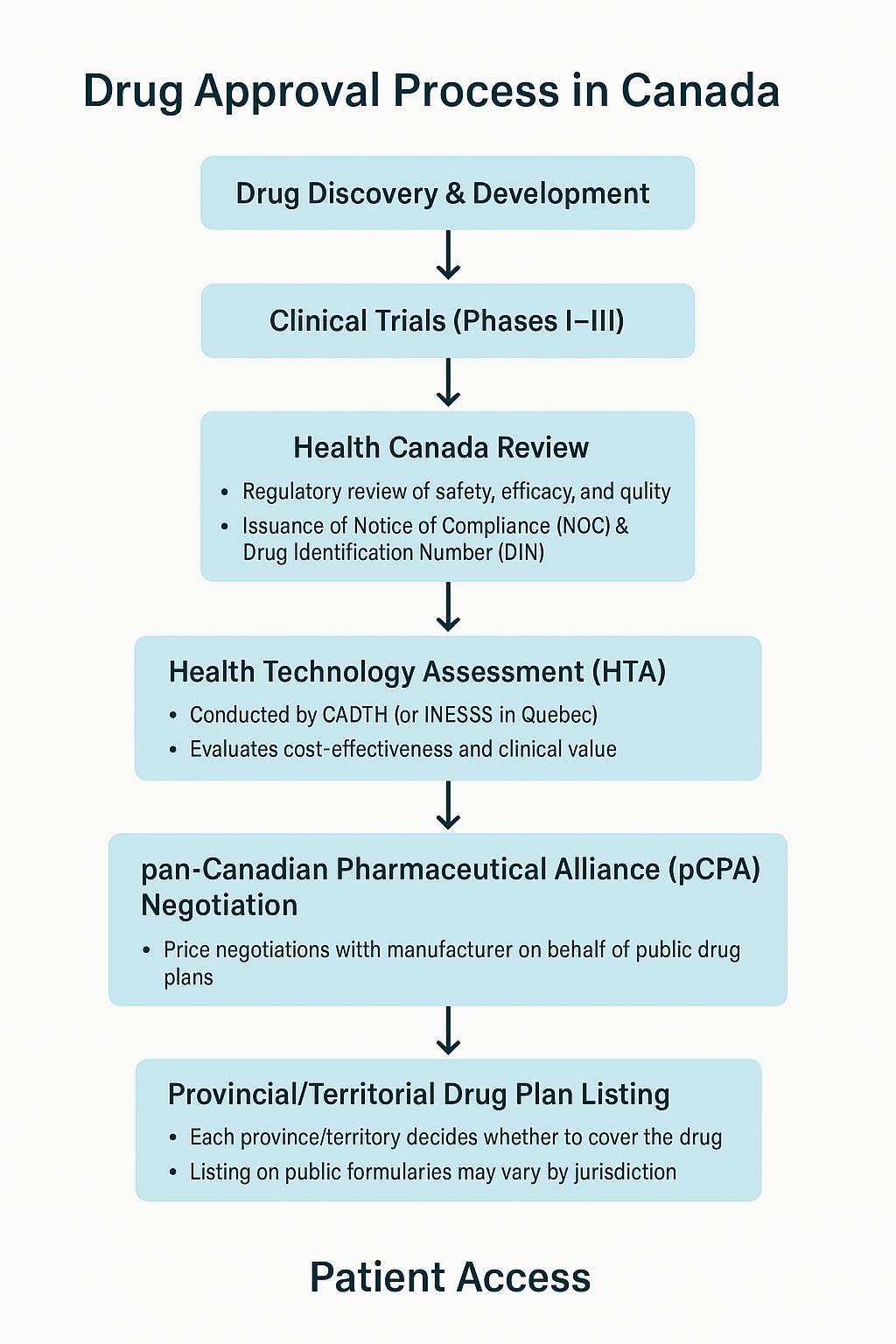
Canada has a unique, multi-layered process for bringing medications to market. Once a drug is approved by Health Canada, it undergoes a Health Technology Assessment (HTA) process—primarily conducted by the Canadian Agency for Drugs and Technologies in Health (CDA/CADTH) or INESSS in Quebec—to evaluate the cost-effectiveness and therapeutic value. This recommendation then informs negotiations with the Pan-Canadian Pharmaceutical Alliance (pCPA), which aims to secure pricing agreements with manufacturers. Only after these steps can provinces and territories choose to include the medication in theirpublicdrugplans.
This lengthy process often means patients must wait months—or even years—for publicly funded access to medications already approved in other countries. For patients with progressive or lifethreatening illnesses, these delays can mean deteriorating health, missed treatment windows, ordeath.
Furthermore, once a medication is approved, provincial coverage varies. A cancer patient in Alberta might have access to a drug that a patient in Nova Scotia does not. This "postal code lottery" canbedevastatingandinequitable.
Bridging the Gap: How Patient Advocacy is Shaping Access to Medications in Canada
WhereAdvocacyMakestheDifference
Patient advocacy has emerged as a transformative force in addressing these challenges. Advocacy groups amplify the voices of those who are too often sidelined in drug access conversations—patients themselves.
InfluencingHealthTechnologyAssessments
CDA/CADTH and INESSS increasingly invite patient submissions as part of their review process. These are not merely anecdotal stories—they are powerful qualitative evidence of how disease impacts daily life, mental health, employment, caregiving burdens, and more. By humanizing data, advocates provide a broader picture of a medication’s value beyond cost per qualityadjustedlifeyear(QALY).
Patient groups like Myeloma Canada, Cystic Fibrosis Canada, and the Canadian Organization for Rare Disorders (CORD) have become respected contributors to the HTA process, ensuring that recommendations considerreal-worldpatientperspectives.
PolicyandSystemicChange
Advocates have played a key role in shaping federal policy. The National Strategy for Drugs for Rare Diseases, announced in 2023, was a direct result of sustained lobbying, research, patient testimonies, and collaborative pressure on the government to address gaps in rare disease treatment access.
Patient groups have also influenced reforms to the Patented Medicine Prices Review Board (PMPRB) framework, which, though controversial, showed how patient engagement could both support and challenge regulatory bodies when access is at stake.
FillingtheGapswithNavigationandSupport
Advocacy organizations often act as navigators and lifelines for patients lost in the healthcare system They help individuals understand how to appeal denied drug coverage, access compassionate access programs from pharmaceutical companies, or apply for financial assistance. Without these groups, many patients especially those without private insurance would have no clearpathtotreatment.
For instance, Save Your Skin Foundation, focused on melanoma, helps patients access immunotherapydrugs.
Bridging the Gap: How Patient Advocacy is Shaping Access
Equity in Access: A Core Advocacy Goal
Advocacy isn’t just about pushing for the newest drugs it’s also about ensuring equitable access for all populations. Indigenous, rural, and racialized communities often face disproportionate barriers to care, whether due to a lack of nearby specialists, lower rates of private insurance, or historical mistrust of the healthcare system.
Patient advocates work to:
Increase awareness about systemic inequities
Push for inclusive clinical trials that reflect Canada’s diversity.
Ensure culturally competent care and materials. Advocate for decentralized delivery models (e.g., virtual care, rural infusion sites).
In this way, advocacy becomes not only a voice for the individual patient, but a mechanism for structural change.
Take the example of Trikafta, a game-changing drug for cystic fibrosis Canadian patients and their families launched coordinated campaigns under the banner of #TrikaftaNow, sharing videos, writing letters, holding media interviews, and rallying public support. Their efforts led to an accelerated Health Canada approval and a swift recommendation by CADTH. As a result, Trikafta was listed on several provincial formularies within months unheard of for a rare disease drug justyearsearlier.
Another example is the MPN (myeloproliferative neoplasm) patient community, which has pushed for early access to promising therapies through compassionate use programs, participation in clinical trials, and patient education platforms that empower people to speak directly todecision-makers
These stories show that when patients become advocates, policy can move faster, systems can bend,andlivescanbechanged.
Bridging the Gap: How Patient Advocacy is Shaping Access
Looking Ahead: Patients as Partners
Patient advocacy must evolve from a consultative role to a collaborative partnership. This means: Co-developing clinical trial protocols with patients involved from design to dissemination.
Sitting at policy tables as equal stakeholders Funding patient-led research, ensuring that research questions reflect community priorities.
Strengthening data infrastructure so that realworld patient outcomes inform access decisions continuously
To build a truly patient-centred system, we must see patients not as passive recipients of care butasexpertsinlivedexperience acritical form of expertisethatistoooftenundervalued.
AdvocacyIsAccess
Canada’s drug access system is evolving, but not fast enough Patient advocates are helping to bridge that gap not just by raising their voices but by contributing research, shaping policy, offering peersupport,andholding institutionsaccountable.
Access to medications isn’t just a logistical issue it’s a moral imperative. Every day a patient waits is a day lost to pain, uncertainty, or preventable decline. Advocacy pushes the system to act faster, to act more fairly, and to center what matters most: the person behind the prescription
Clinical Consequences of Delayed Medication Access
by Cheryl Petruk, MBA
Timely access to medications is a cornerstone of effective healthcare delivery. Delays in obtaining prescribed treatments can lead to worsened health outcomes, increased healthcare costs, and diminished quality of life for patients. This article explores the multifaceted impact of delayed medication access, examining clinical consequences, economic implications, and systemic barriers.
In acute care environments such as emergency departments and intensive care units, medication administration often plays a pivotal, time-sensitive role in patient stabilization and survival. Delays in this context are not merely inconveniences—they can be life-threatening.
Time-CriticalInterventions
Certain medications have narrow therapeutic windows, meaning they must be administered within a specific timeframe to be effective.Forinstance:
Insulin: For patients experiencing diabetic ketoacidosis (DKA), delayed insulin administration can rapidly worsen metabolic acidosis, dehydration, and eventual cardiovascular collapse. The American Diabetes Association (ADA) guidelines emphasize rapid insulin therapy within the first hour of diagnosis (Kitabchi etal.,2009).
Levodopa: In patients with Parkinson’s disease, delays in administration—even by 30 minutes—can precipitate acute dystonia, rigidity, and loss of motor function, significantly impairing recovery and extending hospital stays. A UK-based observational study by Martinez-Ramirez et al. (2015) confirmed that Parkinson’s patients who did not receive their medications on time in hospital settings had a 2.5 times greater risk of complications,includingaspirationpneumoniaandfalls.
Thrombolytics: In ischemic stroke, the delay of tissue plasminogen activator (tPA) beyond the 4.5-hour window drastically reduces efficacy. Every 15-minute delay in tPA delivery is associated with decreased odds of walking independently at discharge and increased risk of long-term disability(Saveretal.,2013).
Clinical Consequences of Delayed Medication Access
cont'd
OperationalBottlenecks
Several systemicbarrierscontributetothesedelays,including:
Nurse-to-patient ratios: A study in the BMJ Quality & Safety journal revealed that higher patient loads significantly delay medication rounds and error-checking procedures (Griffiths etal.,2018).
Shift transitions: Medication errors and omissions are most likely during nurse handoffs and shift changes. These transitions introduce information silos and lapses in continuity of care (Riesenberg,Leitzsch,&Cunningham,2010)
Pharmacy turnaround time: Centralized hospital pharmacies may take hours to deliver nonstock medications to patient floors, especially during overnight hours or weekends
Elevated 30-day readmission rates, especially in elderly populations and those with polypharmacy.
Higher mortality rates in time-sensitive conditions such as myocardial infarction, sepsis, and statusepilepticus(Kumaretal.,2006).
ChronicDiseaseManagement
For chronic conditions, delayed medication initiation or interruptions can exacerbate disease progression. In non-small cell lung cancer (NSCLC), delays in accessing oncology drugs have been associated with reduced overall survival and progression-free survival Similarly, costrelated nonadherence in chronic diseases like diabetes and hypertension has been linked to highermortalityrates.
Chronic conditions such as cancer, diabetes, cardiovascular diseases, and autoimmune disorders require long-term pharmacological management to maintain stability, slow disease progression, and prevent complications. When access to these essential medications is delayed—whether due tocost,availability,oradministrativebarriers—theclinicalramificationsareprofound.
CancerTherapyDelays
Inoncology,thetimingoftherapyinitiationpost-diagnosiscansignificantlyaffectoutcomes: In non-small cell lung cancer (NSCLC), a delay of more than 6 weeks from diagnosis to treatment isassociatedwithloweroverallsurvival(Bozcuketal.,2005). Onereasonistumorprogressiontoamoreadvanced,inoperablestage. For breast cancer, a delay of over 90 days between surgery and adjuvant chemotherapy was associatedwitha34%increasedriskofdeath(Biagietal.,2011).
Clinical Consequences of Delayed Medication Access
cont'd
Access to novel therapies like immunotherapies or tyrosine kinase inhibitors (TKIs) is often delayed due to formulary restrictions, provincial drug funding decisions (in Canada), or prolonged reimbursement approval processes, leading to inequitable access and potential survival disparities
Cost-RelatedMedicationNonadherence
Financial barriers remain a primary cause of delays in initiating or continuing treatment:
A study by Kennedy et al (2020) using NHANES data revealed that 1 in 5 adults aged 65+ in the US reported skipping or rationing medication due to cost, many of them managing chronic diseases suchashypertension,hyperlipidemia,andType2 diabetes In diabetes care, missed doses of antidiabetic medications can quickly destabilize glucose control, leading to complications like retinopathy, neuropathy, nephropathy, or hyperosmolar hyperglycemicstate(HHS).
A landmark observational study in Circulation (2006) demonstrated that nonadherence to prescribed statins or antihypertensives led to a 30%higherrisk of cardiovasculareventsover3years
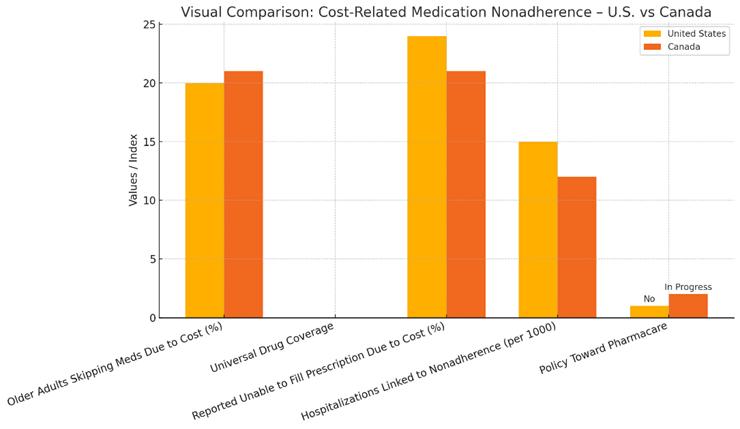
Cost-related nonadherence (CRN) is a pervasive and welldocumented challenge in both high-income and low-income countries. Despite universal health coverage in many regions, including Canada, financial barriers to accessing prescribed medications continue to delay treatment initiation and compromise disease management. The downstream effects are not only felt at the individual level, through worsened health outcomes and loss of quality of life, but also ripple across the healthcare system via preventable hospitalizations and increased healthcare expenditures.
TheCanadianPerspective
Despite Canada’s publicly funded healthcare system, prescription medications are not universally covered, creating significant disparitiesinaccessacrossprovincesandpopulations.
Gaps in Canada's Drug Coverage
Approximately 1 in 5 Canadians (21.1%) report not taking their prescribed medication due to cost (Law, Cheng, & Dhalla, 2018).
Unlike physician and hospital services, outpatient prescription medications are not comprehensively insured under the Canada Health Act. Instead, coverage is provided through a patchwork of provincial drug plans, private insurance, and out-of-pocket payments.
Clinical Consequences of Delayed Medication Access
In 2021, 3.5 million Canadians reported they could not afford to fill one or more prescriptions(StatisticsCanada,2022).
Thisdisproportionately affects:
Seniors not covered by provincial pharmacare plans, especially in provinces with limited formularies or high deductibles (e.g., British Columbia’sFairPharmacare).
Younger Canadians are less likely to have employer-sponsoreddrug plans
Patients with rare diseases, whose medications may not be listed on public formularies due to high cost or lack of provincial negotiations.
Real-WorldConsequences
The consequences of cost-related nonadherence in Canada are tangible and measurable:
A study published in CMAJ (2012) found that introducing out-of-pocket charges for essential medications, even as low as $2, resulted in higher rates of emergency department visits and hospitalizations, particularly among those with diabetes and cardiovasculardisease.
In Ontario, a delay in accessing second-line antihypertensive medications due to limited public coverage contributed to higher rates of stroke and myocardial infarction, especially among low-income individuals (Gupta et al., 2017).
Additionally, patient organizations across Canada have reported that financial stress from affording medications often leads patients to make trade-offs prioritizing rent or food over their medications, which exacerbatessocial determinantsof health.
Case Example: Diabetes in Indigenous Communities
Indigenous Canadians experience disproportionately high rates of Type 2 diabetes, and many live in remote areas with limited access to pharmacies. While the NonInsured Health Benefits (NIHB) program covers prescription costs for eligible First Nations and Inuit peoples, logistical delays, medication shortages, and bureaucratic inefficiencies lead to substantial delays in receiving treatment, resulting in increased rates of diabetic complications and earlier mortality (Reading &Wien,2009).
Canada’sMovementTowardPharmacare
In response to the growing concern over costrelated nonadherence, momentum has been building toward implementing national pharmacare The 2019 Advisory Council on the Implementation of National Pharmacare recommended establishing a universal, singlepayerpublicpharmacaresystem.
Potentialbenefitsofsuchasysteminclude:
Reduced nonadherence through lower or eliminatedout-of-pocketcosts
Streamlined access across provinces, ensuring equity regardlessof geography orincome Cost savings through bulk purchasing of medicationsandadministrativeefficiencies.
Clinical Consequences of Delayed Medication Access cont'd
The Parliamentary Budget Officer projected that national pharmacare could result in $4 to $11 billion in annual savings, largely from improved health outcomes and reduced hospitalizationsduetobettermedicationadherence(PBO,2017). However, political will and intergovernmental cooperation remain hurdles. Until pharmacare is realized, many Canadians remain underinsured and continue to face dangerous delays in accessing themedicationsthey need.
TheHiddenCostofNonadherence
While the financial burden of medication costs is clearly documented in the U.S., the Canadian healthcare system, despite its many strengths, also suffers from medication access inequities. CRN leads not only to the progression of chronic diseases but also to cascading costs for the healthcare system due to avoidable acute careandlong-term complications. Both countries reveal that without addressing cost-related access delays, even the most innovative treatments lose their value. In Canada, advancing pharmacare is not merely a policy debate it is a publichealthnecessity.
Clinical Consequences of Delayed Medication Access
Disease Progression and Complications
The long-term consequences of chronic disease mismanagement due to delayed medications include: Organ damage (e.g., renal failure in hypertension, cirrhosis in hepatitis C). Increased hospitalization rates, particularly for avoidable complications like stroke, hypoglycemia, or heart failure. Reduced quality of life and increased caregiver burden, especially in degenerative conditions like multiple sclerosis or Parkinson’s disease.
Mental Health Impact
Patients experiencing medication delays often face psychological distress Anxiety over health deterioration, feelings of helplessness, and diminished trust in the healthcare system are common.
In rheumatologic conditions such as rheumatoid arthritis, delays in initiating disease-modifying antirheumatic drugs (DMARDs) correlate with higher disease activity scores and long-term disability (Nell et al., 2004).
In major depressive disorder, delays in accessing antidepressant therapy can increase the risk of suicidal ideation, absenteeism, and social withdrawal. Treatment initiation within the first few weeks of symptom onset has been shown to improve both short- and long-term outcomes
The clinical consequences of delayed medication access span the entire spectrum of care, from acute crises in emergency departments to the slow-burning deterioration of chronic conditions.
Timely access is not just a logistical convenience—it is a clinical imperative The impact of these delays can be quantified in preventable deaths, irreversible complications, and avoidable suffering. A healthcare system that fails to prioritize and protect timely access to essential medications risks undermining its very purpose: to heal and to help.
In Canada, one of the most significant barriers to timely access to medications is the lengthy and multilayered drug approval and reimbursement process. Although Canada is internationally recognized for its rigorous regulatory standards, this same rigour can result in substantial delays, sometimes up to two years or more, between a drug’s approval in other countries, such as the United States or those in the European Union, and its availability to Canadian patients
The Canadian approval pathway involves several stages that extend beyond initial Health Canada authorization. Once Health Canada deems a drug safe and effective for use, it issues a Notice of Compliance (NOC).
Clinical Consequences of Delayed Medication Access cont'd
However, this approval alone does not guarantee patient access. To be publicly reimbursed under provincial drug plans, which is essential for many Canadians who do not have private insurance, the medication must undergo further health technology assessments (HTA).
This includes evaluation by the Canadian Agency for Drugs and Technologies in Health (CDA/CADTH) and, in Quebec, by the Institut national d’excellence en santé et en services sociaux (INESSS). These agencies assess whether a medication provides good value for money compared to existing treatments.
While this step is important for ensuring costeffectiveness and stewardship of public funds, it adds months to the timeline After the HTA, drug manufacturers must negotiate pricing with the pan-Canadian Pharmaceutical Alliance (pCPA)—a process that can last anywhere from a few months to over a year, depending on the complexity of negotiations and the therapeutic area involved.
CACHEducation is evolving to better serve the needs of patient advocates and healthcare professionals with its rebrand to CACHEducation Academy. This transformation reflects an expanded commitment to delivering high-quality, structured learning experiences tailored to the ever-changing landscape of patient advocacy and healthcare education. As part of this rebrand, CACHEducation Academy will introduce Advanced Curriculum offerings starting in April 2025, providing deeper insights, specialized training, and enhanced skill development for those looking to elevate their expertise. This next phase marks a significant step forward in strengthening the capacity and impact of patient advocates through comprehensive and innovative education.
"Enrolling in CACHEducation was a game-changer for me as a patient advocate. The program provided invaluable knowledge, practical skills, and a supportive community that empowered me to make a real impact in healthcare advocacy."
Emerging Treatments
New treatments offer hope to patients and their loved ones. Here, we present new therapies that are available to Canadians.
This section also addresses challenges around access to new medication. Our readers will find important information to help them understand Canada's drug review processes.
An informed and engaged patient is an empowered one. We aim to equip our readers with the tools and knowledge to navigate the complex healthcare landscape because, more than ever, patients need to raise their voices to get access to services. Accessing innovative medicines can save patients' lives.
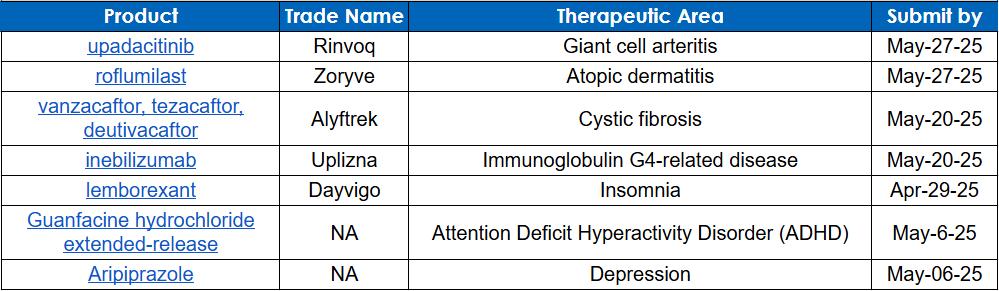
Health Canada's recent approvals in 2025
by Brigitte Leonard, Ph.D.
In 2025, Health Canada approved three highly targeted innovative treatments for rare diseases and cancers. One is for a rare disease called amyotrophic lateral sclerosis (ALS). (1) Another is for a cancer called metastatic or recurrent locally advanced Merkel cell carcinoma (MCC)(2). The third targets advanced or metastatic breast cancer (3). For more information about these disorders and innovative treatments, follow me in this publication.
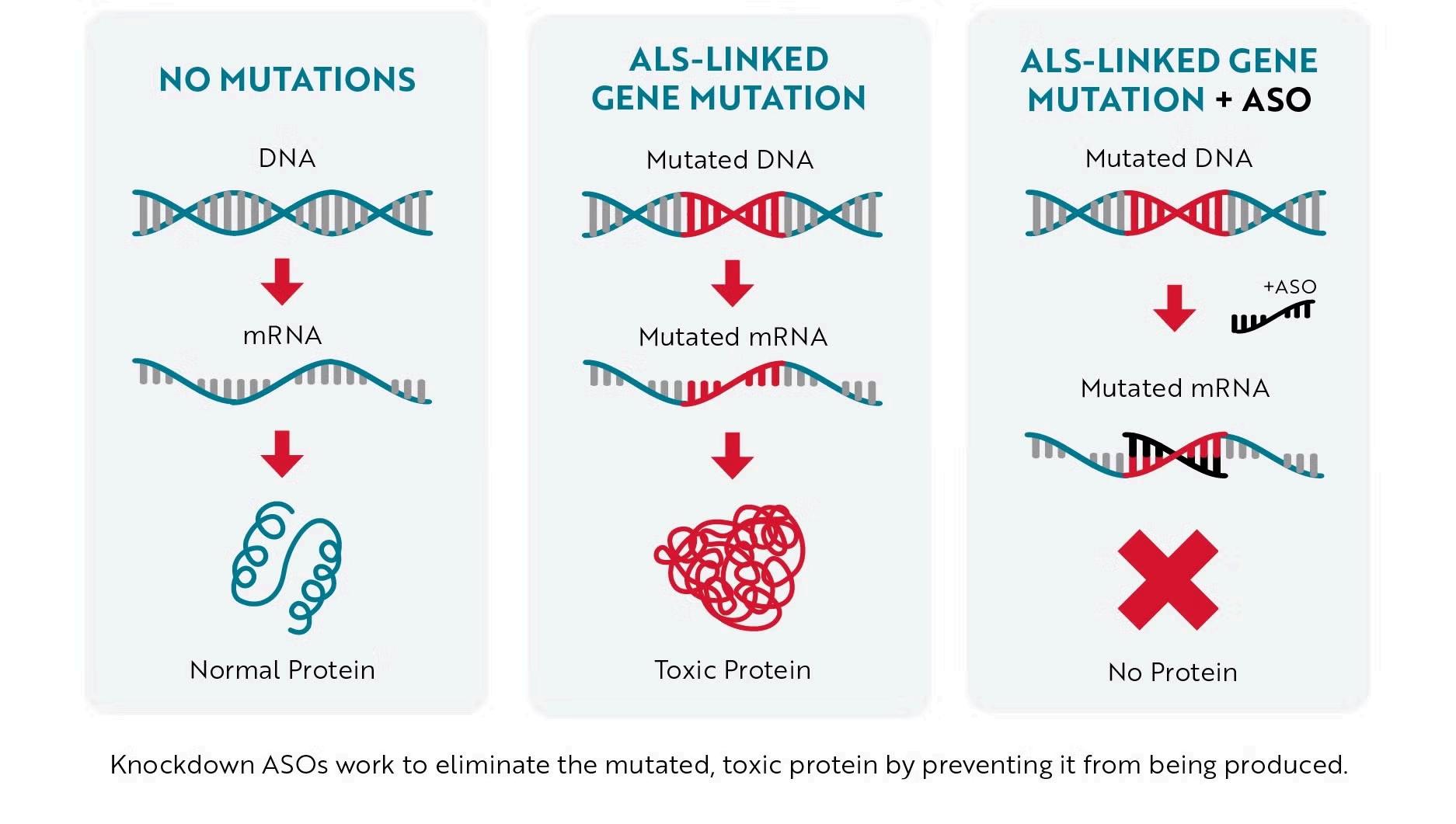
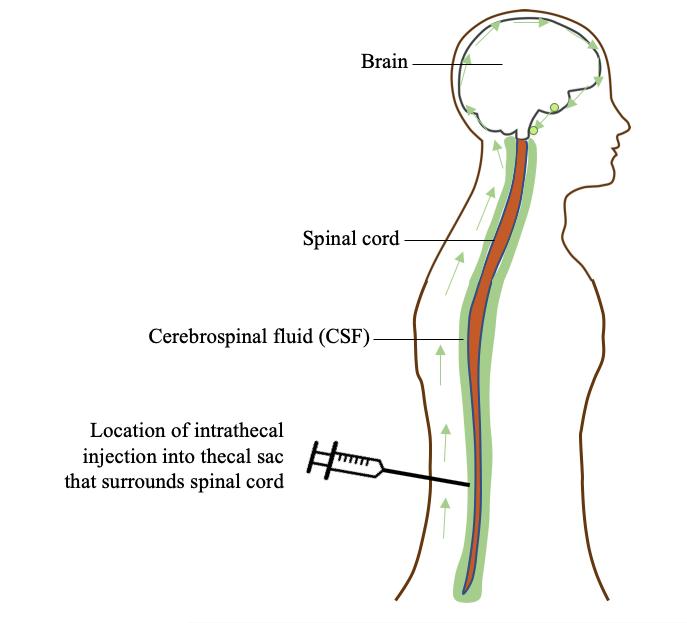
Amyotrophic lateral sclerosis (ALS) is a progressive, neurodegenerative, muscle-wasting condition affecting the body in several challenging ways. Several motor functions are impacted, such as mobility, breathing, communication, and mental health. These symptoms worsen over time. Life expectancy is 3 to 5 years after the appearance of symptoms. Approximately 2% of ALS cases are linked with mutations in a gene encoding superoxide dismutase 1 (SOD1). (4) The toxic mutant SOD1 protein causes neuron degeneration in this disorder. (4)
In February 2025, Biogen received approval for QALSODY (Tofersen) for treating adults with amyotrophic lateral sclerosis (ALS) associated with a mutation in the SOD1 gene (Figure 1). The complete indication can be found in Health Canada or on the Biogen website.
QALSODY is a molecule that can bind to the RNA messenger that produces the mutated protein. By binding to this mutated RNA, QALSODY stimulates the cellular defence mechanism, which destroys the mutated RNA. So, the toxic product cessed (Figure 2). (5)
Tofersen is an injection that needs to be delivered directly close to the spine in the back (Figure 3).
Health Canada's recent approvals in 2025 cont'd
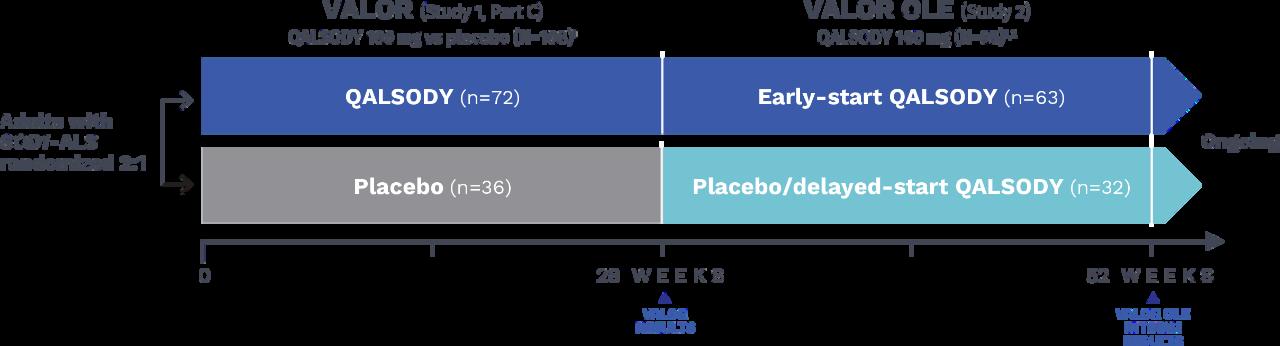
Health Canada approved QALSODY with conditions based on the VALOR phase III clinical trial results and its extension (VALOR OLE). See the design of the study in Figure 4.
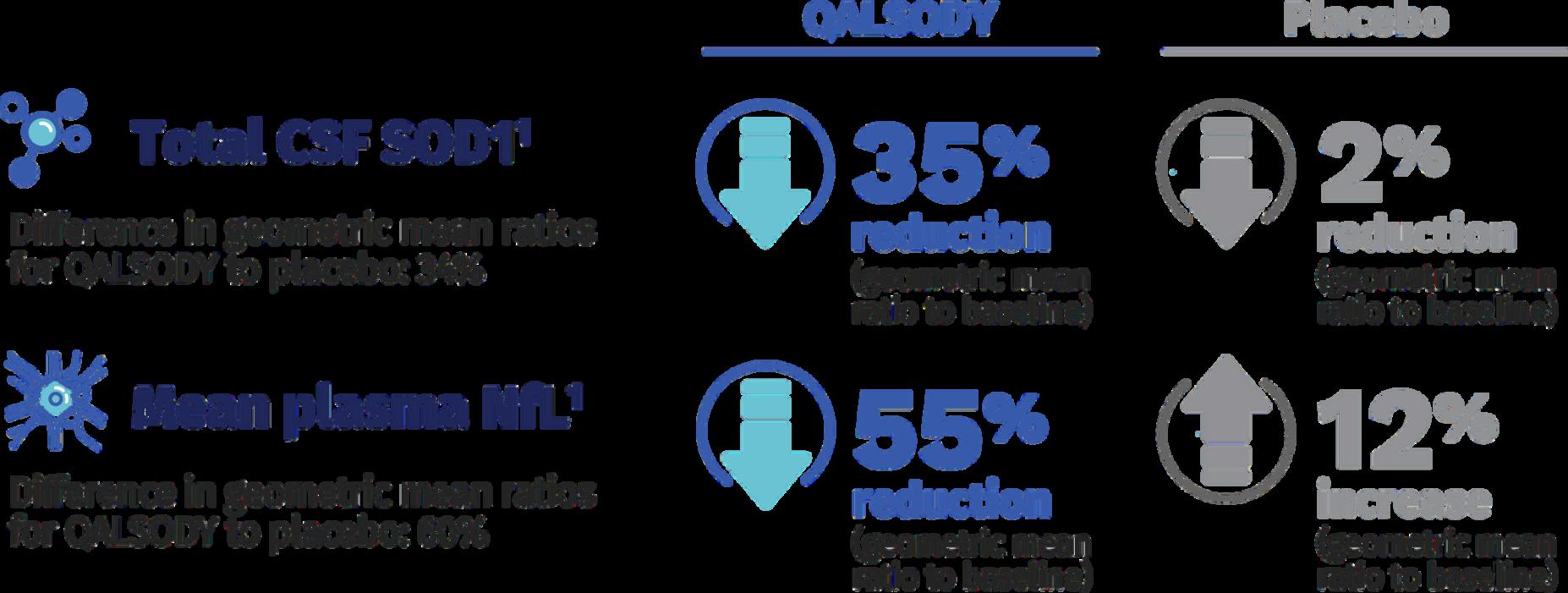
To assess the efficacy of QALSODY, two biomarkers have been used:
1) The total concentration of SOD1 protein in cerebrospinal fluid; 2) The concentration of neurofilament light (Nfl) chains in blood. Nfl is a marker of neuron degeneration.
In Figure 5, you can see that QALSODY allows a more significant reduction of the mutated protein than the placebo, 35% versus 2%.
Also, neuron degeneration seems to be reduced by QALSODY, where a 55% reduction is observed, while neuron degeneration progresses in the patient on placebo (12%).
QALSODY provides positive results with an acceptable safety profile, offering hope for these patients.
Merkel Cell Carcinoma (MCC) is a rare neuroendocrine skin cancer. MCC is associated with frequent recurrences and a high mortality rate. In recent years, the number of MCC diagnoses has increased in the USA, Australia, and Europe.(7)
Factors strongly associated with the development of MCC include aging, fair skin, history of extensive sun exposure, chronic immune suppression (e.g., kidney or heart transplantation or HIV), and the Merkel cell polyomavirus.(8)
Merkel cells are found in the lower part of the skin(epidermis). Although the exact function of Merkel cells is unknown, they are thought to be touch receptors. Also known as neuroendocrine cells, they have machinery like nerve cells and to hormone-secreting (endocrine) cells.
Health Canada's recent approvals in 2025 cont'd
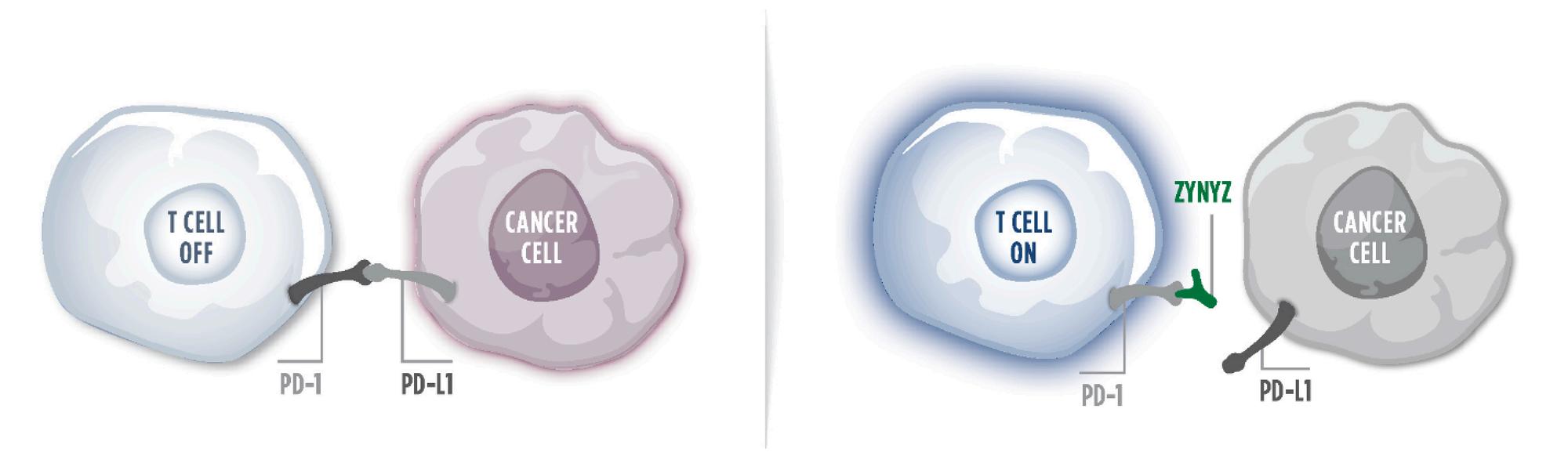
In February 2025, Incyte received approval for ZYNYZ (retifanlimab) as the first-line treatment for metastatic or advanced MCC. The complete indication can be found in Health Canada or the Incyte website (Figure 6).
Cancer cells can express a molecule called PD ligand (PD-L1) (Figure 7). When this ligand binds to the PD-1 molecule on the T cell, it inhibits the activation of the immune system. Thus, cancer cells can escape immune surveillance. ZYNYZ interferes with this process by binding PD-1 on the T cell and preventing the interaction with the cancer cells' PD ligand.(9)
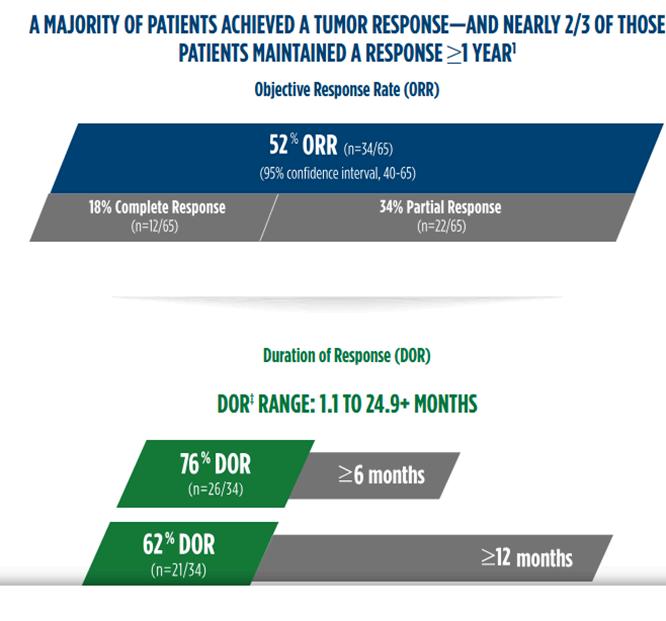
Marketing authorization was based on tumour response and the durability of response observed in the POD1UM-201 clinical trial (Figure 8). (10) This new approval offers hope for patients with MCC.
Several clinical strategies have been put in place during the last two decades to improve the survival of patients diagnosed with Breast Cancer. Preventive recommendations, early diagnosis and targeted therapies are some of these strategies. However, the war has not been won yet. Some forms of breast cancer can still be challenging.
Hormone-receptor (HR)-positive breast cancer is the most prevalent type of all breast cancers, accounting for approximately 70% of cases. A defining feature of HR-positive breast cancer is that its tumour cells have receptors that attach to one or both hormones – estrogen or progesterone – which can contribute to tumour growth. People diagnosed with HR-positive metastatic breast cancer often face the risk of disease progression and treatment side effects, creating a need for additional treatment options. The PI3K signalling pathway is commonly dysregulated in HR-positive breast cancer, due to activating mutations, which have been identified as a potential mechanism of intrinsic resistance to standard of care.
(11) (12) (13)
Health Canada's recent approvals in 2025 cont'd
In February 2025, Roche received approval for ITOVEBI® (inavolisib) to treat advanced or metastatic breast cancer (Figure 10). The complete indication can be found in Health Canada or on the Roche website. Itovebi inhibits a molecule called PI3K, which slows tumour growth and causes cancer cells to die.
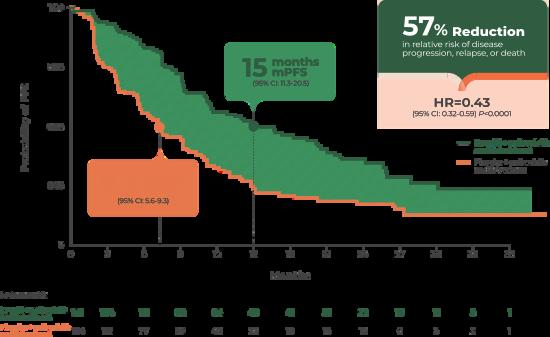
The INAVO120 study [NCT04191499] is a phase III study evaluating the efficacy and safety of Itovebi® (inavolisib) in combination with other standard treatments. Study results showed that the Itovebi-based treatment regimen more than doubled progression-free survival in the patient population (Figure 11) with an acceptable safety profile. ITOVEBI offers another chance for these women. (14)
by Brigitte Leonard, Ph.D
The Canadian Agency for Drugs and Technologies in Health (CDA/CADTH) is an independent, not-for-profit organization that provides evidence-based assessments on drugs, medical devices, and healthcare technologies to support informed decision-making in Canada's healthcare system. CDA/CADTH collaborates with federal, provincial, and territorial governments (excluding Quebec) to evaluate the clinical effectiveness, cost-effectiveness, and broader impact of new and existing healthcare interventions. By conducting Health Technology Assessments (HTAs), providing reimbursement recommendations, and developing guidance reports, CDA/CADTH plays a crucial role in shaping healthcare policies, ensuring that patients, healthcare providers, and policymakers have access to reliable, science-driven information to improve health outcomes and optimize resource allocation.
Exciting News from Heal Canada! We are thrilled to announce the launch of our new podcast series, Empowering Voices, dedicated to amplifying the stories and insights of patients, healthcare professionals, and advocates in the blood disorder and rare disease communities. Each episode will feature meaningful conversations on patient experiences, emerging research, and the evolving landscape of healthcare advocacy. Through Empowering Voices, we aim to educate, inspire, and drive change by bringing real-world perspectives to the forefront. Stay tuned for our first episode, coming soon because every voice matters!
Welcome to the Belonging, Diversity, Inclusion and Equity section of E3 Advocacy Digital Magazine. In this section, we provide information on ensuring that BDEI is part of the patient conversation in our Health ecosystem. Our focus is to illuminate the pathways through which individuals grappling with health challenges can not only find their voice but also harness it to drive their own journey.
Healthcare and the patient’s experiences should not be determined by social determinants of health.
We believe that an informed and engaged patient is an empowered one. Through enlightening articles, expert insights, and inspiring stories, we aim to equip our readers with the tools and knowledge necessary to navigate the complex healthcare landscape.
Systemic Barriers to Medication Access in Canada & The Role of Patient Advocacy in Overcoming Barriers
by Cheryl Petruk, MBA
to become available through public drug plans, a duration significantly longer than in many peer countries. These delays can detrimental, especially for patients requiring timely access innovative treatments. (Innovative Medicines Canada, Myeloma Canada)
3.StructuralandInstitutionalInequities
Systemic racism and institutional biases contribute to disparities medication access. Racialized communities often face implicit biases from healthcare providers, language barriers, and geographic challenges, such as pharmacy deserts in underserved areas. These factors collectively hinder equitable access to medications marginalizedpopulations.(PMC)
4.HealthLiteracyandSystemNavigationChallenges
Many patients struggle with understanding the healthcare system and their treatment options. This is particularly true for newcomers to Canada, who may be unfamiliar with the healthcare infrastructure, leading to difficulties in accessing and adhering to prescribed medications.(CaringforKidsNewtoCanada-Home)
Systemic Barriers to Medication Access in Canada & The Role of Patient Advocacy in Overcoming Barriers cont'd
Advocacy groups actively participate in the drug approval and pricing processes, providing patient perspectives to bodies like Health Canada and the Patented Medicines Prices Review Board (PMPRB). Their involvement ensures that patient needs and experiences are considered in policy decisions (CACHEducation)
2.PromotingEquitableAccessandAwareness
Organizations such as Arthritis Society Canada and Myeloma Canada work to highlight disparities in medication access and advocate for policies that promote equity. They engage in public education campaigns and collaborate with stakeholders to address systemic inequities Wikipedia+1MyelomaCanada+1
3.EnhancingHealthLiteracyandPatientEmpowerment
Advocacy groups provide resources and support to help patients understand their treatment options and navigate the healthcare system. For example, Asthma Canada offers educational materials and support services to empower patients in managing their condition effectively. Wikipedia
4.FacilitatingTimelyAccesstoMedications
By engaging with policymakers and healthcare providers, advocacy organizations work to streamline processes and reduce delays in medication access. Their efforts aim to ensure that patientsreceivetimely andappropriatetreatmentswithoutunnecessary bureaucratichurdles.
Systemic barriers continue to impede equitable access to medications in Canada, affecting the health and well-being of many individuals. Patient advocacy plays a vital role in identifying these challengesandworking towardssolutionsthatprioritizepatientneeds.
Through policy influence, education, and support, advocacy organizations strive to create a healthcare system where all Canadians have timely and equitable access to the medications they require
Mental Health
Welcome to the Mental Health section of E3 Advocacy Digital Magazine, a dedicated space where we embrace the journey towards mental wellness with open arms and open hearts. In this edition, we delve into the empowering world of patient advocacy, engagement, empowerment, and education. Our focus is to illuminate the pathways through which individuals grappling with mental health challenges can not only find their voice but also harness it to drive their own journey.
We believe that an informed and engaged patient is an empowered one. Through enlightening articles, expert insights, and inspiring stories, we aim to equip our readers with the tools and knowledge necessary to navigate the complex mental health care landscape.
Join us as we explore how patient advocacy, active engagement and comprehensive education can transform the experience of mental health care, turning obstacles into opportunities for growth and healing.
Reading for Well-Being
by Joanna Pozzulo, Ph.D.
For many of us who live in Canada, cold, long winters are a rite of passage. By March, we’re often ready to put away the snowshoes. What better way to usher in the brighter season than with a book to help us adopt a sunnier outlook?
Do you consider yourself a naturally happy person? This question is posed at the beginning of The Positive Shift: Mastering Mindset to Improve Happiness, Health, and Longevity (2019) by Catherine Sanderson, Ph.D.
She suggests that if you answered “yes,” you won’t need to read her book. I couldn’t disagree more! Although I consider myself on the “happier” side of the scale, I still read this book and am so glad I did. The Positive Shift is for anyone looking to implement some evidence-based strategies to help with their happiness level. Spoiler alert: We have some control over our happiness.
Sanderson states that our level of happiness, physical health, and even longevity is connected to how “we think about ourselves and the world around us”. In other words, our mindset. By making small changes, we can help improve our happiness and health (both mental and physical). And if you are wondering where to start, there are several self-assessments provided in the book to better understand your starting mindset.
The book is chock-full of pretty straightforward strategies and the science behind them to “shift your mindset.” Perhaps, not surprisingly, my favourite strategy was “read a book you love!”. Sanderson even cites a study that found reading for over 3 ½ hours a week can increase longevity! Count me in! The Positive Shift includes some great chapters on aging, memory, and health. Hint: Don’t give into the stereotypes! Mindset matters!
Reading for Well-Being
I would argue that this book is for anyone looking for strategies on how to be a little happier. By making a few changes to how we think about situations, we may be able to improve our overall well-being. If one strategy doesn’t work, not to worry; there are many included in the book to try out.
If you want to hear from Dr. Sanderson directly, check out my interview with her on the Reading for Wellbeing Podcast: https://www.youtube.com/@ReadingforWel lBeingPodcast.
Don’t forget to subscribe if you don’t want to miss any of my interviews.
For more evidence-based picks for wellbeing, sign up for the Reading for WellBeing Community Book Club https://carleton.ca/mental-health/bookclub-sign-up/
Happy reading!
Joanna Pozzulo, Ph.D.
Chancellor’s Professor Department of Psychology Director, Mental Health and Well-Being Research and Training Hub (MeWeRTH) https://carleton.ca/mental-health/ Carleton University
Spring Cleaning Your Mind: Refresh Your Mental Space
by Chris Sciberras
As the days grow longer and nature bursts into bloom, there's no better time to refresh and renew—not just your home but your mind too. Much like how we tidy up our physical spaces during spring cleaning, our mental and emotional landscapes also deserve a little attention. After all, a cluttered mind can weigh us down, leaving us feeling overwhelmed, stressed, or uninspired. So, let’s dive into some practical steps to help clear out the mental cobwebs and create a healthier, more focused state of mind.
1. Declutter Your Thoughts
Our minds are full of ideas, to-dos, worries, and emotions that can create a cluttered, chaotic feeling. Much like cleaning out a closet, it's time to sift through your mental clutter. Make a List: Write down everything on your mind. This simple exercise allows you to see your thoughts on paper, making them feel more manageable and less intimidating. Once you've written it down, you can prioritize, delegate, or even let go of what's no longer important.
Practice Mindfulness: Spend a few minutes every day simply observing your thoughts without judgment. Mindfulness techniques can help clear away the mental noise, allowing you to focus on the present moment and your emotional state.
2. Let Go of Negative Thought Patterns
Spring cleaning isn’t just about removing physical clutter; it's also about clearing out things that no longer serve us mentally. Negative self-talk, limiting beliefs, and unhealthy thought patterns can keep us stuck in a mental rut.
Challenge Negative Thoughts: Whenever a negative thought arises, ask yourself if it’s truly accurate. Are there any facts or evidence to support it, or is it just a habit of thinking? By reframing negative thoughts, you can create a more positive, balanced mindset.
Replace With Affirmations: Use positive affirmations to combat self-doubt. Repeating empowering statements, like "I am capable," "I am enough," or "I can handle this," can help shift your mindset and replace old patterns with healthier ones.
3. Clear Out Emotional Baggage
Emotions, just like physical clutter, can accumulate over time, creating unnecessary weight in our lives. Spring cleaning your mind also means letting go of emotions tied to past events that no longer serve you.
Forgiveness: Holding onto anger, resentment, or hurt can weigh heavily on your mind. Consider whether forgiving—whether it’s someone else or yourself—could help release that burden. You don't have to forget, but forgiving allows you to move forward with a lighter heart.
Spring Cleaning Your Mind: Refresh Your Mental Space cont'd
Journaling: Writing down your feelings can be a powerful way to release pent-up emotions. Whether it’s anger, grief, or confusion, journaling provides a safe space for emotional release and introspection.
4. Refresh Your Relationships
Our relationships play a crucial role in our mental health, and sometimes, they need a little spring cleaning, too.
Set Boundaries: Are there relationships that drain you? Now’s a great time to assess your social connections and consider setting healthier boundaries. Whether it's saying "no" more often or distancing yourself from toxic individuals, protecting your emotional energy is key.
Nurture Positive Connections: Spring cleaning is a chance to focus on relationships that nourish you. Reach out to friends and loved ones who lift you up, and spend quality time with those who bring positivity to your life
5. Cultivate New Habits
Just as we refresh our homes by adding new décor or plants, it’s a good idea to refresh our mental habits and routines. This could involve:
Learning Something New: Engage your brain with a new skill or hobby Whether it's learning a language, taking a class, or trying out a creative activity, stimulating your mind in new ways helps keep it sharp and focused.
Physical Exercise: A healthy body contributes to a healthy mind. Regular exercise can reduce stress, boost your mood, and improve mental clarity, helping you feel more energized and refreshed overall.
6. Practice Gratitude
Gratitude can be a powerful tool for mental spring cleaning. By focusing on the positive aspects of your life, you shift your attention away from negativity and increase your emotional well-being.
Daily Gratitude Practice: Each day, take a few moments to reflect on things you’re thankful for. Whether it’s big or small, acknowledging your blessings helps create a more positive mindset and attracts more of the good things you want in life.
Spring Cleaning Your Mind: Refresh Your Mental Space cont'd
Conclusion: Embrace the New Season with a Clear Mind
Spring cleaning isn’t just about tidying up your house—it’s an opportunity to refresh your mental state, let go of what no longer serves you, and create space for new opportunities. By decluttering your thoughts, letting go of negative patterns, and fostering positive habits, you can make room for growth, creativity, and joy. So, take a moment to clean out your mind, breathe in the fresh air, and step into the new season with a renewed sense of clarity and peace. Here’s to a fresh start, inside and out!
This article was originally published by Chris Sciberras on March 9, 2025, on his website breakthroughpsychology and is reproduced with the kind generosity and permission from Chris Sciberras.
Chris Sciberras
Registered Psychologist with a Master's of Counselling from the University of Calgary. Chris has worked extensively with youth, adults, and families for over a decade in various capacities. Through the use of Cognitive Behavioural Therapy, Dialectical Behaviour Therapy, Solution-Focused practices, and strengthbased approaches, Chris is able to develop personalized support to assist clients with the unique challenges they face. Chris excels at creating a non-judgmental and safe environment, which is key to identifying unhelpful thinking patterns and behaviours that often contribute to the spiral of poor mental health practices. Through the process of collaboration, Chris's mission is to support clients in exploring alternate options that promote resilience, confidence, and positive mental health. For more information, please get in touch with https://breakthroughpsychology.ca/ or email: info@breakthroughpsychology.ca
Shame-Based Identity: Understanding Its Impact and Path to Healing
by Dr. Amber Cohen
Shame is a powerful emotion that, when internalized, can shape how we see ourselves, interact with others, and navigate the world. A shame-based identity goes beyond feeling shame over specific actions or events - it becomes ingrained and entrenched in a person's self-concept. A shame-based identity involves chronic feelings of inadequacy, worthlessness, and self-blame that are often at the forefront of their experiences. This influences their mental health, attachment to others and overall well-being.
The Roots of a Shame-Based Identity
At its core, shame differs from guilt. While guilt focuses on behaviour ("I did something bad"), shame is about the self ("I am bad"). When someone repeatedly experiences shame, it can shift from a fleeting emotional experience to a persistent identity. This transformation often leads to harmful patterns of behaviour, including self-sabotage, difficulty accepting love or care from others, and the avoidance of vulnerability or authentic self-expression.
A shame-based identity is often formed early in life. It can be the result of various experiences, including childhood trauma, neglect, abuse, or repeated messages from caregivers, peers, or society that tell a person they are unworthy or broken. People who grow up in environments where their worth is tied to external validation or unrealistic expectations are more likely to internalize these shame messages.
For instance, children who are criticized for their emotions or behaviours or who face consistently harsh discipline may begin to associate their inherent value with these external reactions. Over time, this leads to the belief that they are fundamentally flawed, even when they haven’t done anythingwrong.
Additionally, cultural and societal factors play a significant role in shaping shame-based identities. Individuals may feel immense pressure to meet those expectations in cultures where success, perfection, and appearance are highly valued. When they inevitably fall short, feelings of shame can take root, perpetuating a sense of unworthiness that is difficulttoovercome.
The Consequences of Living with a Shame-Based Identity
The impact of living with a shame-based identity extends far beyond negative self-perception. It can manifest in several mental health challenges, including:
Shame-Based
1.
Identity: Understanding Its Impact and Path to Healing cont'd
Depression and Anxiety: They may constantly feel overwhelmed by their perceived inadequacy. This persistent sense of not being "good enough" can lead to chronic anxiety and depression.
2.
Difficulty in Relationships: Shame often leads to difficulty forming deep, authentic relationships. People may push others away or not be their authentic selves out of fear of rejection or may struggle to accept love and care, believing they don't deserve it.
4
Perfectionism and Self-Sabotage: To avoid the painful feelings of shame, individuals may overcompensate by striving for perfection, leading to burnout and disappointment. Alternatively, they may self-sabotage, unconsciously reinforcing the belief that they are unworthy of success or happiness.
3. Avoidance of Vulnerability: Vulnerability is often seen as dangerous by those with a shamebased identity. They may withdraw from emotionally open situations, fearing that exposing their true selves will only lead to further shame or rejection. This negatively impacts their ability to connect with others in a meaningful way.
Healing from a Shame-Based Identity
Healing from a shame-based identity is not a quick fix, but it is possible. It requires both selfcompassion and the willingness to challenge the deep-rooted beliefs that have defined one’s self-worth. Here are some steps on the path to healing:
1.
Awareness and Acknowledgment: The first step in healing is understanding how shame has shaped your identity. Acknowledging that shame influences your thoughts and behaviours allows you to begin untangling its hold on your life.
2.
Therapy and Counseling: Professional therapy, particularly through a trauma-informed lens, is beneficial. Approaches such as Eye Movement Desensitization and Reprocessing Therapy (EMDR), Cognitive Behavioural Therapy (CBT) and Compassion Focused Therapy (CFT) can help individuals address shame’s deep roots. Therapy provides a safe space to process emotions, challenge and shift core beliefs, and learn healthier coping strategies.
Building Self-Compassion: People with a shame-based identity often struggle with selfcompassion. Learning to treat yourself with kindness, acceptance, and understanding rather than self-criticism is key to breaking free from the cycle of shame.
4. Challenging Negative Beliefs: Cognitive restructuring can help identify and challenge the negative beliefs that perpetuate shame. By questioning the validity of these thoughts and replacing them with more balanced perspectives, individuals can begin to shift their selfconcept.
5. Seeking Support: Support from others, whether through peer groups, family, or close friends, is crucial in the healing process. Connecting with others who understand or empathize with your experience can reduce feelings of isolation and reinforce a sense of belonging.
6. Self-Expression and Vulnerability: Allowing yourself to be vulnerable and authentic in relationships is a powerful tool in healing. Practicing this with someone who feels safe can help you develop and build this skill. Over time, expressing emotions and sharing your true self can help dismantle the walls built by shame.
7. Engage in Activities that Spark Joy: By exploring and engaging in activities that bring you joy, you can connect with happiness and experience moments of confidence. This can assist in building your sense of self from a healthier perspective.
Moving Forward: Reclaiming Your Identity
While healing from a shame-based identity is a process, it’s important to remember that it’s entirely possible to shift and strengthen your sense of self. As you work through these challenges, it’s essential to recognize that your shame does not define you. You are a unique, valuable individual worthy of love, connection, and growth. Through therapy, self-compassion, and support, you can transform your relationship with yourself and, in turn, your life. Shame is not a permanent sentence. It is a painful emotion that can be released when processed and understood. By shedding the layers of shame built over time, you can reclaim your identity and live a life rooted in authenticity, self-compassion, and resilience.
Dr. Amber Cohen
Registered Clinical Psychologist and the founder and CEO of The Cohen Clinic. Dr. Cohen has special interests in trauma, anxiety, depression, and self-esteem. The Cohen Clinic is a holistic wellness therapy practice focusing on the mind-body connection. The team is composed of Psychologists, Psychotherapists, Social Workers, a Registered Dietitian and a Naturopathic Doctor. Website Link: https://thecohenclinic.com/
Seniors Health
In today's society, the health of senior citizens stands as a paramount concern, particularly within the framework of the Canadian healthcare system. This heightened focus is more than just a response to the growing number of seniors. Still, it is deeply rooted in recognizing their invaluable contribution to society and their unique challenges in their twilight years.
As people transition into their senior years, they bring unique health and social needs. This shift presents challenges and opportunities for the Canadian healthcare system and society.
In our Seniors Health section, we will provide information to help you in your journey, navigate daily life as a Senior, and provide resources to help you have the best quality of life.
The State of Social Connection: A Life Course Matter Ageing and Social Connection
by Dr. Natasha Ginnivan
Humans need connection at every age. Like many other mammals, we have evolved as a group that relies on and is sensitive to the degree to which we are in close connection.
Brené Brown’s hit TED talk was all about connection, and she asserts, “It’s why we’re here.” So, we feel it acutely when we are excluded from being in connection, whether that’s in our family, friends’ groups, work-life or community. What social impact can we make by connecting outside of our day-to-day lives, building our social resilience and networks and paying it forward with a simple, extra check-in with friends and/or relatives in midlife and beyond?
A recent New York Times article reported studies showing the significant impact a simple call or text to check in on someone can have on the people in our lives.
I study the psychology of ageing, midlife transitions, age expectations and attitudes to ageing. Having been strongly influenced by the work of Yale Psychologist Becca Levy, I am an advocate for consciously shedding negative age stereotypes and living our best life by embracing age. Though I support and advocate for embracing our ageing journey with positivity, I also recognize that various stages of the life course are not without their challenges. Many in this ageing and midlife transition space have referred to the U-curve of happiness, which speaks to the idea that the average person becomes happier with age. I would also argue for the importance of social connections, a sense of purpose and positive self-perceptions of ageing in aiding this trajectory of happiness.
Therefore, I would say as a society, we need more support in these important life stages and transitions that would include ritual, recognition, and rites of passage in our mid-life transition. Without these, we can easily psychologically stumble into that ditch of the U-curve!
The State of Social Connection: A Life Course Matter Ageing and Social Connection
Rituals that we need are ones with a positive and life-affirming frame that recognizes your past achievements while also acknowledging the challenges that you have overcome. The road ahead can be framed as one of opportunity, transformation, and change. Without intentional support mechanisms and ways of cognitively combatting ageist sentiment that promulgates the myth that we have no purpose after 50, we may struggle to move beyond that ditch.
Social isolation has been associated with poorer quality of life, lower mood and depression, and headlines are often about ‘the elderly’ suffering from loneliness and social isolation. This is no doubt a challenge for our ‘age-segregated’ society, which has three or four distinct stages of life that revolve around learning, earning, and retiring. These traditional life stages include intense activities of rituals, milestones, and progression from formative years of socializing and learning skills to transition into a state of earning a living. This also informs the psychosocial processes involving selfcategorization and self-identity. Little has been cultivated in the way of rituals and developmental transitions, as seen in earlier life chapters, to ensure our social identities, social connection, and quality of life continue to be optimized in supporting social roles and identity in midlife and beyond. Western society predominantly frames ageing as negative and of complete decline once we reach middle age
Intersectionality of our ageing journey with our individual identities, be it gender, ethnicity and life chances, can all play a role in whether we experience equal or unequal ageing However, the biggest predictor of longevity, interestingly, is how socially connected we are. Having positive social interactions is linked with a sense of purposefulness in older adults. Humans are so wired for social connection that from infancy, if babies are not receiving attention, social interaction and optimal reflection of emotion and co-regulating with their primary caregivers, this can impact the size of their brain in those formative stages. As we grow older, we continue to need connection and social stimulation, or we languish.
A memorable psychology experiment that I learned of in my undergraduate degree was looking at the impact of social exclusion on the brain by having a participant engage in a virtual game of catch while having functional magnetic resonance imaging (FMRI) taken of their brain. The participants’ role in the video game was to continue throwing and catching in this virtual game of catch between him/herself and the two virtual playmates. The ball would be thrown to you, and then you continue passing it along to the next player in the video game, and it comes back around to you.
The State of Social Connection: A Life Course Matter Ageing and Social Connection cont'd
Then, without warning, as part of the experiment, the two [virtual] playmates would exclude you and only throw the ball amongst themselves. The response of the participant shown via the FMRI scan when this happened was part of the brain that is activated and lights up is the same part of the brain that is activated when one experiences physical pain as though someone took a hammerandhityourhand!Thatreallybroughthometomejusthowwiredweareforinclusion.
A well-known Harvard study on longevity also shows the importance of social connection in having a happy, healthy longer life, while other studies on ageing affirm that men who are happily married live longer lives than those who are not married, and the quality of our social networksarealsoimportantinensuringourhappinessandlongevity.
As a society, we have come a long way with recognizing the fluidity of gender constructs, and that as we mature, there can be different identities emerging, with some people realizing that they have a preference for same-sex romantic relationships or that their internal sense of self is not aligned with the biologicalsextheycameintotheworldas.
The LGBTQI community still face many challenges in a highly gendered society where, historically, gender has been seen as binary, with social roles and constructs attached to thetwocategoriesofmaleandfemale.
Further, the cultural expectations that accompany these social constructs leave a narrow set of expectations that one feels an obligation to fulfill to belong. This intersectionality of age and gender can leave us feeling a step outside of societal membership if there aren’t social roles, rituals, and milestones to validate your identity as you progress from middle-aged into later life, and it becomes more challenging for individuals who find themselves needing high levels of care in late life without those strong social supports.
In the focus groups I ran for my research on ageing and transitioning through life stages, people between sixty and eighty-five spoke about the importance of needing an activity to go on with once they had ‘retired’ because they felt like they were giving back, contributing, but also that they belonged to something bigger than themselves. We cannot underestimate the power of belonging, and as a society, I think we are still finding our way to re-imagining what ageing and longevity look like in the state beyond midlife. We all ‘feel young’ owing to a well-known ‘youthage phenomenon’ where we don’t necessarily feel our biological age, but there remains a disconnect between societal perceptions, supporting rituals and a platform to transform our midlife and past milestones into a regenerative culminating chapter of transformation and belonging within our workplaces and wider society.
The State of Social Connection: A Life Course Matter Ageing and Social Connection cont'd
However, I can hear rumblings in the distance, and I think that perceptual change is afoot. There’s a reason why the UN have declared this the decade of Healthy Ageing (2020 – 2030): because amidst the world’s chaotic state of pandemic navigation, economic upheaval, conflict, and ‘identity wars’, we are beginning to recognize one unifying force: that we are all ageing, and this needs to be in the front of our minds with a growth mindset to seize that longer midlife transition, not be an afterthought and deny ageing as though it were only a category or stage reached only in later life.
This article was on her website Mobilising Wisdom (mobilisingwisdom.com/f/the-state-of-social-connection-a-life-coursematter?) and is reproduced with the kind generosity and permission from Dr. Ginnivan.
Dr. Natasha Ginnivan
holds a Bachelor of Science (Psych), UNSW, Grad Dip (Psych), Macquarie University and a PhD in Population Health, Psychology & Ageing, ANU.
Dr. Ginnivan is a Senior Research Associate with the School of Population Health. She is an Associate Investigator with the Ageing Futures Institute whose focus is on investigating implicit and cultural attitudes to ageing, stigma and ageing, age stereotypes and self-perceptions of ageing. Her research includes the lived experience of ageing and dementia and ageing in marginalized populations, including ageing prisoners. Her current research focuses on elder abuse in the form of financial abuse and drug mule scams and ageing prisoner health.
Senior Access to Medications: Why It’s Difficult in Canada and What Can Be Done
by Cheryl Petruk, MBA
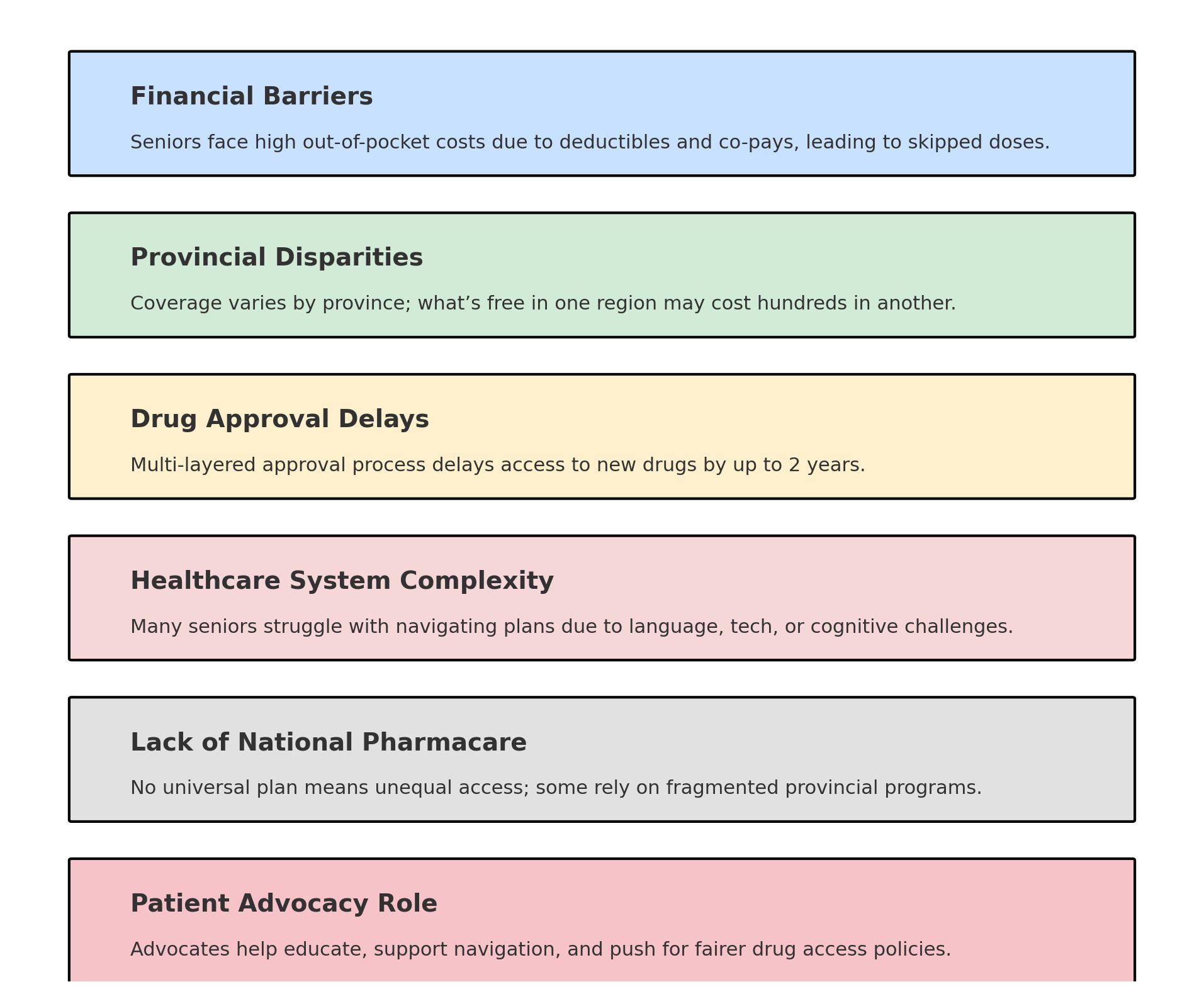
Canada prides itself on a publicly funded healthcare system designed to ensure equitable access to care for all citizens. However, for many seniors, access to necessary medications remains a persistent and complex challenge. While doctor visits and hospital stays are largely covered under the Canada Health Act, prescription medications—especially those taken outside of a hospital setting—are often not. This leaves seniors, many on fixed incomes, navigating a confusing patchwork of provincial drug plans, rising out-ofpocket expenses, and bureaucratic approval processes. This article explores the major barriers seniors face in accessing medications in Canada and discusses how systemic reform and patient advocacy can help alleviate this growing concern.
1. Financial Barriers and the Cost of Prescription Drugs
Perhaps the most prominent barrier to medication access for seniors in Canada is cost. While every province and territory offers some form of drug coverage for seniors, the specifics vary widely. Deductibles, co-pays, and eligibility requirements mean that many older adults still face significant out-of-pocket expenses.
For example, under Ontario’s Ontario Drug Benefit (ODB) Program, seniors must still pay a $100 annual deductible and $6.11 per prescription—amounts that can quickly add up for those on multiple medications. In provinces like British Columbia and Alberta, income-based plans may result in higher costs for seniors with modest retirement income, which nonetheless disqualifies them from full coverage.
The result? Many seniors report skipping doses, splitting pills, or delaying prescription refills. A 2018 study published in Health Affairs found that nearly 1 in 10 Canadians aged 55 and older said they did not take their medications as prescribed due to cost.
2. Fragmented and Inconsistent Drug Coverage Across Provinces
Canada does not have a universal pharmacare program. Instead, each province and territory administers its own public drug plan, creating inconsistencies in access and affordability A medication approved and fully covered in Quebec may not be accessible to a senior in Manitoba without significant personal cost
This fragmentation results in inequality not just by income, but by geography. Seniors living in rural and remote areas, particularly in Indigenous communities, may also struggle with additional logistical barriers such as fewer local pharmacies and delayed delivery services. Moreover, provincial drug formularies may not include all necessary medications, particularly new or highcost drugs.
Senior Access to
3. Delays in Drug Approval and Reimbursement
Another often-overlooked challenge is the time it takes for medications to become accessible to seniors through public drug plans. After Health Canada approves a drug, it must undergo further review by the Canadian Agency for Drugs and Technologies in Health (CDA/CADTH) and the pan-Canadian Pharmaceutical Alliance (pCPA) for costeffectiveness and pricing negotiations. Only then can individual provinces decide to list it on their formulary
This multi-layered process can delay access by 1 to 2 years —sometimes more—compared to countries like Germany or the United States For seniors living with chronic or progressive illnesses, such as arthritis, cancer, or heart disease, these delays can compromise quality of life and, in some cases, survival.
4. Complexity of the Healthcare System and Digital Divide
Many seniors struggle to navigate the complexities of provincial drug plans, reimbursement processes, and appeals systems. Language barriers, cognitive decline, and low digital literacy can all contribute to confusion and delay in accessing needed medications. As more provinces move to online portals for plan registration and prescription management, seniors who are not tech-savvy may be left behind.
Caregivers often step in to bridge this gap, but not all seniors have access to that support. For those living alone or with limited family engagement, the system can be overwhelming.
5. Lack of Integrated Pharmacare
The absence of a national pharmacare program continues to exacerbate disparities. While political discussions have circled around universal pharmacare for years, actual implementation has been slow. The result is a two-tiered system: those with private insurance (often employersponsored and lost upon retirement) and those who must rely on a patchwork of public programs. The 2019 Advisory Council on the Implementation of National Pharmacare recommended a single-payer public pharmacare system, but progress has been slow due to federal-provincial jurisdictional tensions and concerns about cost.
Senior Access to Medications: Why
It’s Difficult in Canada and What Can Be Done
TheRoleofPatientAdvocacy
Patient advocacy groups play a vital role in amplifying the voices of seniors and pushing for policy change Advocatescan:
Collaborate with researchers and clinicians to identify gaps in medication access and proposepatient-centeredsolutions.
Organizations like the Canadian Association for Retired Persons (CARP), Heal Canada, and the Council of Senior Citizens’ Organizations of British Columbia have actively championed these issues,calling formoreresponsivesystemsthatprioritizeseniorhealthoutcomes.
Senior Access
to Medications: Why It’s Difficult in Canada and What Can Be
While Canada’s healthcare system offers many strengths, access to medications for seniors remains an area of deep concern. The financial burden, inconsistent provincial coverage, bureaucratic delays, and system complexity create a landscape that is difficult to navigate particularly for a population that often requires the most care. Closing these gaps requires a concerted effort: policy reform, a national pharmacare plan, better patient navigation tools, and empowered advocacy. Only then can we ensure that aging in Canada does not mean aging without the medications needed to maintain health, dignity, and independence.
Patient Surveys
Your voice matters visit the Heal Canada website to take part in our patient surveys and help shape the future of care. New surveys are added regularly, so check back often and make your experience count!
Staying physically active is crucial for seniors to maintain their overall health and quality of life. Engaging in regular fitness activities helps improve strength, flexibility, balance, and cardiovascular health, reducing the risk of injury and chronic diseases. Fortunately, many free workout resources are available, particularly online. One such valuable resource to try is the
https://yes2next.com/
It is a mother-and-daughter dynamic duo showcasing a variety of exercises specifically tailored for those 50 and beyond and for individuals with limited mobility. Their YouTube channel offers you more than 200 free fitness videos.
Whether it's gentle stretches, chair exercises, or low-impact cardio routines, yes2next provides a convenient and effective way for seniors and everyone to stay active and maintain their wellbeing.
Pediatric Health
Welcome to the Pediatric Health section of E3 Advocacy Digital Magazine, a dedicated space where we embrace the journey toward pediatric wellness with open arms and open hearts.
We believe that an informed and engaged parent is an empowered one. Through enlightening articles, expert insights, and inspiring stories, we aim to equip our readers with the tools and knowledge necessary to navigate the complex pediatric health care landscape.
Join us as we explore how patient advocacy, active engagement and comprehensive education can transform the pediatric health care experience, turning obstacles into opportunities for growth and healing.
The Importance of Access to Medications for Pediatric Patients: Why Children Need Patient Advocacy the Most – A Canadian Perspective
by Cheryl Petruk, MBA
Access to timely, appropriate, and affordable medication is critical for all Canadians—but when it comes to children, the stakes are even higher. Pediatric patients are not simply “small adults”; they have unique physiological, developmental, and psychosocial needs that must be taken into account when delivering healthcare
Yet in Canada, significant barriers persist that impede access to medications for children, ranging from limited pediatric-specific drug approvals to gaps in coverage and off-label prescribing. In this context, patient advocacy becomes not only important but essential. Advocates play a key role in ensuring that children’s voices, often silent or underrepresented, are heard at all levels of the healthcare system.
This article explores the importance of medication access for pediatric patients, the unique challenges they face in Canada, and why patient advocacy must be at the forefront of change
Pediatric Pharmacotherapy: A Critical Need
Children with chronic conditions, rare diseases, cancer, or acute illnesses depend on a range of medications to manage symptoms, improve quality of life, or even survive.
Examples include insulin for Type 1 diabetes, chemotherapy for pediatric cancers, biologics for juvenile arthritis, and antiepileptics for seizure disorders. For many families, navigating access to these treatments is a complex, stressful journey.
While Canada prides itself on a universal healthcare system, prescription drug coverage is not universally insured. Instead, access to medications is determined by a patchwork of provincial drug plans, private insurance, and out-of-pocket spending. For pediatric patients, whose care often involves specialized treatments not always covered by public formularies, the result can be delayed treatment, financial burden, or in some cases, no treatment at all.
The Importance of Access to Medications for Pediatric Patients: Why Children Need Patient Advocacy the Most – A Canadian Perspective cont'd
UniqueChallengesforChildreninCanada
LimitedDrugApprovalsforPediatricUse
One of the most pressing concerns is that many medications used in children have not been formally approved for pediatric populations. According to the Canadian Pediatric Society, over 50% of medications prescribed to children are done so “off-label”—meaning they were not specifically tested or approved for that age group. This is due in part to a lack of pediatric clinical trials, regulatory hurdles, and insufficient incentives for pharmaceutical companies to pursue pediatricindicationsinCanada.
This presents risks in terms of efficacy and safety, as children metabolize medications differently than adults. Without robust pediatric data, healthcare providers must make best guessesondosage,frequency,andsideeffects,potentiallyjeopardizingoutcomes.
DisparitiesinCoverageandAccess
Access to medications varies widely across provinces and territories. While some provinces have established special programs for children (such as OHIP+ in Ontario, which covers most prescription drugs for those under 25 without private insurance), others rely heavily on meanstested public plans or require co-payments. For families with low income or those living in rural or Indigenous communities, the combination of costs, travel, and administrative hurdles can be overwhelming.
Rare Disease and Orphan Drug Access
Children represent a disproportionate share of patients with rare diseases, many of which have no Health Canada-approved treatments. Even when treatments exist, Canada’s review and reimbursement system is slow and often restrictive. For instance, while the Canadian Agency for Drugs and Technologies in Health (CADTH) conducts health technology assessments (HTAs) for public drug plans, their criteria often exclude the real-world needs and quality-of-life improvements vital to pediatric patients with rare or life-threatening diseases. This results in significant delays or outright denials in funding, despite international approvals.
The Importance of Access to Medications for Pediatric Patients: Why Children Need Patient Advocacy the Most – A Canadian Perspective cont'd
The Role of Pediatric Patient Advocacy in Canada
Advocacy organizations, caregivers, and health professionals are vital players in bridging the gap between pediatric patients and the medications they need. In a system where children often cannot advocate for themselves, adult allies must champion their voices.
1. Amplifying the Pediatric Patient Voice
Children are dependent on others to make decisions on their behalf—parents, caregivers, doctors, and policymakers. Advocacy ensures that these decisions reflect the best interests of the child, informed by lived experience, clinical evidence, and ethical considerations. Groups such as SickKids, Children’s Healthcare Canada, and various diseasespecific foundations have become powerful advocates in raising awareness of pediatric health inequities.
2. Driving Policy Reform and Coverage Expansion
Advocates push for improvements in federal and provincial policy, such as Canada’s emerging National Pharmacare strategy. A truly universal plan must account for pediatric populations, ensuring access to ageappropriate medications, eliminating co-pays for essential drugs, and prioritizing rapid review and funding of medications for children with rare diseases.
3. Fostering Pediatric Research and Trials
Advocacy organizations also play a crucial role in pushing for more pediatric-specific research. In Canada, this means advocating for funding to support pediatric clinical trials, ethical frameworks for child participation, and incentives for manufacturers to seek pediatric indications. For instance, initiatives like the Canadian Paediatric Clinical Trials Network are a step in the right direction, but they need sustained support and attention.
4. Real-World Impacts of Delayed Access
The consequences of delayed or denied access to medication can be devastating. Consider a child with a rare genetic disorder like spinal muscular atrophy (SMA), where early treatment with gene therapy or diseasemodifying drugs can significantly improve life expectancy and quality of life. Every day without treatment can mean irreversible damage. Families often turn to crowdfunding or advocacy campaigns to raise money or gain public attention—something no parent should be forced to do in a country with public healthcare.
Another example includes delays in approving medications like biologics for juvenile idiopathic arthritis Prolonged wait times can mean months of uncontrolled pain, missed school, and developmental delays Pediatric advocacy ensures that children are not treated as an afterthought in a system designed primarily for adults.
The Importance of Access to Medications for Pediatric Patients: Why Children Need Patient Advocacy the Most – A Canadian Perspective cont'd
Indigenous and Rural Pediatric Populations
Indigenous children face even greater disparities. Remote locations, jurisdictional confusion over federal versus provincial healthcare responsibilities, and historical distrust of the system all contribute to poor access. Advocacy efforts must be inclusive and collaborative with Indigenous communities to ensure culturally appropriate, equitable care.
MovingForward: WhatNeedstoChange
Inclusion of Pediatric Needs in National Pharmacare: Any future national drug strategy must be pediatric-inclusive, with equitable coverageacrossall regions.
Streamlined Access for Rare Disease Medications: Canada should adopt a pediatric fast-track process for rare disease drug approvalsandfunding,withachild-firstlens
SupportforPediatricTrials:
More funding and regulatory encouragement for pediatric research will improve the evidence base and lead to more on-label use of essential medications
Strengthening the Advocacy Infrastructure: Empowering patient advocacy organizations with resources and partnerships will ensure continued pressure on decision-makers to prioritizechildhealth.
Children in Canada deserve access to safe, timely, and affordable medications. Yet the current landscape is uneven, slow, and in many cases, ill-equipped to address their uniqueneeds.
Pediatric patients require dedicated advocacy because they can’t fight for themselves. The role of patient advocates in this space is not only to raise awareness, but to push for structural change, equity, and compassion in a healthcare system that must be reoriented to prioritize its youngest and most vulnerable members. In doing so, we create a healthier, more just future for children, families, and all Canadians.
Access to Medications for Pediatric Patients in Canada:
The Need for
Advocacy
Off-Label Presriptions in Pediatric Care
80% Of pediatric prescriptions in Canada are off label
Many medications prescribed to children haven't been specifically approved for pediatric use, leading to potential safety and efficacy concerns
Canadian Pediatric Society
Public Concern over Pediatric Healthcare Access
83%
Of Canadians are concerned about long delays in accessing time sensitive healthcare services for children and youth
+only 52% of Canadian parents feel confident in their ability to access necessary healthcare services for their child
Childrens Healthcare Canada
Challenges in Accessing Rare Disease Treatments
$100,000 to over $2 million
rare disease treatments can cost
Government of Canada
Government of Canada has committed to up to 1.5 billion over three years to improve access to drugs for rare disease
Disparities in Healthcare Access of First Nations people living off reserve land, had to travel outside their community and stay overnight to access healthcare services
18% 27% to 28%
Among children and oung without a regular healthcare provider 27% reported no one available in their area, & 28 % reported no one accepting new patients
Statistics Canada
The role of Patient Advocacy, Action to address the unique challenges forced by pediatric patients ensuring equitable access to necessay treatments
Global Partners
The My Blood My Health program is dedicated to empowering individuals affected by Hematological issues by providing trusted education, advocacy, and support. Through patientcentered resources and expert collaborations, we strive to enhance awareness and improve access to critical information for those navigating their blood health journey. Stay tuned for the next edition of the My Blood My Health digital magazine, coming in March, featuring insightful articles, patient stories, and the latest updates in hematology
Heal Canada and Pat ADV Hub in the USA have embarked on a collaborative journey, aiming to revolutionize the realm of patient advocacy across North America. This pioneering partnership brings together two influential organizations from neighbouring countries, combining their extensive expertise and resources.
The objective is to expand and enhance the access to critical information for patient advocates, ensuring that individuals across the continent receive the best possible support and guidance in their healthcare journeys.
By bridging the gap between Canadian and American healthcare advocacy, this alliance promises to foster a more informed, empowered, and connected community of patient advocates, significantly contributing to the improvement of healthcare experiences for countless individuals.
patadvhub@gmail.com www.patadvhub.org
Advocacy Spotlight
The "Advocacy Spotlight" section of E3 Advocacy Digital Magazine is a dynamic platform dedicated to shining a light on patient advocacy groups, both new and established. This unique feature aims to introduce these vital organizations to a broader audience, highlighting their missions, achievements, and the critical support they offer patients and their families.
Each edition of this segment meticulously selects a different group, delving into their specific focus areas, ranging from rare diseases to everyday health challenges. Heal Canada amplifies these groups’ voices and fosters a deeper understanding and connection within the broader healthcare community by showcasing their stories, initiatives, and community resources.
This section is more than just an informational piece; it celebrates these advocacy groups’ tireless efforts and significant impact and empowers readers by connecting them with valuable resources and support networks.
Empowering a generation to thrive
by Young Adult Cancer Canada
Cancer is a challenge at any age, but for young adults, it often feels like a particularly isolating experience. Facing cancer at a time is tough, but there are added layers of complexity when doing it while your peers are focused on school, building careers, or starting families. You’re navigating treatment, recovery, and the emotional toll of it all, while feeling like no one truly gets what you're going through. That’s where Young Adult Cancer Canada (YACC) comes in. YACC is a nonprofit organization dedicated to helping people diagnosed with cancer before the age of 40, offering support, inspiration, and connection to help people living with, through, and beyond their diagnoses.
How YACC got its start
Young Adult Cancer Canada was founded in 2000 by Geoff Eaton after he recognized a gap in the cancer care system following his own diagnosis. Young adults, typically aged 18 to 39, often fall into an awkward limbo. They're too old for pediatric cancer programs, but they're also too young for most services aimed at older adults. This leaves many feeling overlooked, unsupported, and isolated. YACC was born out of the need to create a space where people could find both practical and emotional support to overcome challenges like finishing school, starting a career, family planning, navigating relationships, planning for the future, and facing the end of your life when you are just getting started.
YACC’s
programming
After covering some ground with successful awareness campaigns, Eaton helped shape an online hub where young adults diagnosed with cancer could share their stories, ask questions, and connect with others who were going through the same things.
As the organization grew, it took this connection to the next level with its four-day Retreat Yourself program, and then a Survivor Conference, social activity-based groups in eight cities across Canada under the banner of Localife, Retreat Yourself Adventure, and more!
When the COVID-19 pandemic hit, YACC was forced to find ways to stay connected in the face of travel restrictions and a population with especially compromised immune systems. This led to the first virtual Survivor Conference, recurring informal YACC Chats where people discuss a cancer-related theme, a multi-week creative program called Writing It Out!, and closed group Support Groups.
As of 2025, YACC is dedicated to offering an evolving smorgasbord of programs that offer varying levels of connection, information, and commitment, inviting members to find the best fit for them via its web-based, virtual, and face-to-face programs.
Empowering a generation to thrive cont'd
The emotional support found through the YACC community is invaluable, providing the camaraderie and hope that are often hard to come by during a cancer diagnosis. Whether you're newly diagnosed or a survivor, being part of a community where everyone “gets it” can make all the difference.
Ways to get involved
YACC relies on support from the community to fund its vital programs and outreach efforts. Whether you’re directly affected by cancer or simply want to make a difference, there are several ways to get involved and support YACC’s mission.
Volunteer
Volunteering with YACC is an impactful way to contribute your time and energy to this important cause. Whether you're helping organize events, providing administrative support, or connecting with the YACC community, your involvement can make a real difference. Volunteering also gives you the opportunity to meet others who share your passion for supporting young adults with cancer. Fundraise
As a non-profit, YACC depends heavily on fundraising to keep its programs running. You can support the organization by participating in events like Shave for the Brave, the Climb, or online campaigns. Every dollar raised helps fund essential programs like the Retreat Yourself events and peer support services. You can also make a direct donation to YACC to ensure these programs continue to thrive.
Share your story
If you have lived experience as a young adult with cancer, YACC encourages you to share your story. Personal stories are powerful tools for raising awareness and providing emotional support to others who are facing similar challenges. Whether through YACC's website, social media channels, the Recover Study research project, or directly within the community, sharing your experience can help others feel less isolated and more empowered to seek help.
Raise awareness
One of the most important ways to get involved is by raising awareness about the unique needs of young adults with cancer. Whether through social media, school events, or community outreach, sharing information about the challenges young adults face can help drive change. YACC provides various advocacy tools to make it easier for you to spread the word and increase support for this often-overlooked group.
Why YACC matters
Young Adult Cancer Canada is more than just a support organization—it's a movement aimed at ensuring that young adults with cancer don't have to face their diagnosis alone. Through community-driven programs and initiatives, YACC helps individuals not only survive but thrive. Whether you’re personally impacted by cancer or looking for ways to give back, YACC offers a welcoming space for anyone who wants to make a difference.
Together, we can ensure that no young adult has to navigate cancer without the support, resources, and community they deserve. By getting involved, sharing your story, or simply raising awareness, you can help make sure that every young adult impacted by cancer knows they’re not alone.
Visit youngadultcancer.ca to learn more!
Young Adult Cancer Canada
The YACC team is made up of 10 passionate individuals across Canada. Most of the team works out of the headquarters in St. John’s, NL, with the goal of helping young adults live with, through, and beyond cancer.
Pancreatic Cancer: Patient Empowerment through SelfAdvocacy
by Maureen Elliott, BA, MA
Pancreatic cancer is known as the world’s toughest cancer, with only marginal advancements in survival rates over the past 50 years. Often considered to be a death sentence, a diagnosis of pancreatic cancer is incredibly distressing and can be made worse by your doctor or care team having little advice, direction or support beyond “go home and get your affairs in order.”
However, more and more patients are demanding better from their healthcare providers and the system in general; they are seeking treatment beyond Canadian borders and asking more questions of their care team to receive more personalized treatment plans. Self-advocacy can be used throughout the pancreatic cancer experience as a tool for gaining control, ensuring the best treatment, and improving both physical and emotional well-being when dealing with pancreatic cancer.
Self-Advocacy in Pancreatic Cancer: Why It Matters
1 Better Communication with Healthcare Providers: When you advocate for yourself, you establish open and clear communication with your doctors, which can help clarify your needs, preferences, and concerns. This promotes a collaborative relationship where you can ask questions, address fears, and ensure that your voice is heard in treatment planning.
3.
Personalized Care and Treatment Options: Engaging in self-advocacy allows individuals to actively participate in their treatment decisions. Pancreatic cancer treatment options can vary based on the stage and type of cancer, and advocating for oneself ensures that the patient explores the most effective and personalized treatments available.
2. Access to Clinical Trials and New Treatments: Self-advocacy can help patients stay informed about the latest clinical trials and experimental treatments. By actively seeking out opportunities, individuals may gain access to cutting-edge therapies that are not part of standard treatment protocols.
4. Emotional and Psychological Support
: Navigating a cancer diagnosis can be emotionally overwhelming. By advocating for oneself, patients can seek out necessary mental health resources, counselling, or support groups, which can provide a strong foundation for coping with the emotional challenges of the disease.
Pancreatic Cancer: Patient Empowerment through Self-Advocacy cont'd
5. Navigating the Healthcare System: The healthcare system can be complex, especially with serious illnesses like pancreatic cancer. Advocating for yourself ensures that you are aware of all available resources, insurance options, and support systems, which can be crucial for managing finances and accessing the right care.
6. Improved Outcomes: Studies have shown that patients who actively engage in their healthcare decisions and advocate for themselves tend to experience better health outcomes. This is especially true in cancer care, where timely interventions, proactive treatment, and proper monitoring are critical.
7. Empowerment and Control: Being diagnosed with pancreatic cancer can often leave patients feeling powerless. Self-advocacy restores a sense of control over the situation, enabling patients to make informed decisions and take an active role in their health journey, which can positively impact their overall well-being.
Pancreatic Cancer Canada (PCC) actively emphasizes the importance of self-advocacy for individuals diagnosed with pancreatic cancer, providing resources and support to empower patients in their healthcare journey. Our goals, programs, and supports are in place to assist the pancreatic cancer community in their selfadvocacy journey and the community that we work alongside supports this vision.
For instance, Nancy Tavares acted as an advocate and caregiver for her husband, George, during his pancreatic cancer journey. While she was initially hesitant to question the doctors and nurses, she realized that she needed to speak up on George’s behalf. To be an effective advocate and a caregiver, she learned to be persistent, inquisitive and strong.
Pancreatic Cancer Canada’s "Ask An Expert" program is designed to empower patients, caregivers, and those affected by pancreatic cancer by providing access to specialized information and support, thereby fostering self-advocacy.
Key Features of the "Ask An Expert" Program: Personalized Information: The program offers tailored responses to inquiries about pancreatic cancer, helping individuals understand their diagnosis, treatment options, and care plans.
2.
Assistance in Locating Specialists: If a second opinion or specialized care is desired, the "Ask An Expert" service can help identify and connect patients with appropriate healthcare professionals. Patients have the right to seek second opinions to ensure the best course of treatment.
Pancreatic Cancer: Patient Empowerment through
Self-Advocacy
3. Accessible Communication Channels: Individuals can submit questions through an online form or by leaving a voicemail. PCC commits to responding within two business days, ensuring timely support.
Additionally, the accessible and downloadable resources on the Pancreatic Cancer Canada (PCC) website support self-advocacy by providing individuals with the tools, information, and guidance needed to make informed decisions about their care. Here’s how these resources contribute to self-advocacy:
Easy Access to Information: PCC’s website offers a variety of downloadable resources, such as guides on treatment options, managing symptoms, and questions to ask doctors. These resources allow patients and caregivers to access vital information at any time, ensuring they are well-prepared for appointments and treatment discussions.
1. Empowerment through Knowledge: Resources like the “Questions to Ask Your Doctor” offer a comprehensive guide designed to empower patients by facilitating informed and proactive engagement with their healthcare providers. Other informational posts on available treatments enable patients to become active participants in their healthcare. By having key questions and information at their fingertips, patients can take control of their medical journey and ensure they fully understand their options.
Encouragement of Second Opinions: Access to resources supports patients in seeking second opinions to ensure the chosen treatment aligns with the patient's needs and preferences.
Support for Informed Decision-Making: The downloadable resources cover various aspects of pancreatic cancer care, from diagnosis to treatment and follow-up. By providing clear, understandable information, these resources ensure that patients can make decisions based on accurate and comprehensive knowledge, which is essential for effective self-advocacy.
4. Easier Communication with Healthcare Providers: With resources that help prepare for doctor visits and treatment decisions, patients can feel more confident and empowered when communicating with healthcare teams. They can ask the right questions, voice concerns, and advocate for their needs more effectively.
Pancreatic
Cancer: Patient Empowerment through Self-Advocacy
6. Convenient Access for Diverse Needs: PCC’s resources are designed to be easy to download and print, making them accessible to people with varying technological capabilities or those who prefer physical copies. This ensures that all patients, regardless of their background or situation, can benefit from the tools provided. Through these efforts, Pancreatic Cancer Canada underscores the vital role of self-advocacy, offering support, facilitating access to expert knowledge and resources to help patients and their supportive community become more informed, prepared, and confident in advocating for their healthcare needs, ultimately improving their ability to manage and navigate their pancreatic cancer journey.
Maureen Elliott
Maureen has over 10 years of experience in the not-for-profit and community health sectors. Passionate about patient advocacy and support, she focuses on creating accessible, sustainable programs. Currently, she serves as Senior Manager, Programs and Support at Pancreatic Cancer Canada, dedicated to innovative ways of supporting patients and their communities. melliott@pancreaticcancercanada.ca https://pancreaticcancercanada.ca/patient-and-family-support/
Introducing the Health Advisory Network: ShareYour Story, Shape the Future
by Kim Hanson
Living with diabetes has taught me the importance of sharing my story—whether it’s with researchers developing studies, companies improving medications and devices, or government agencies striving to deliver better services. But over the years, I’ve often wondered: How do my experiences compare to those of someone facing cancer or cardiovascular disease? Could we uncover valuable solutions by looking at what connects us, alongside what makes our challenges unique?
At HealthPartners, these questions inspired something big. For over 35 years, we’ve brought together workplaces, health charities, and communities they serve to improve the lives of people affected by illness. Now, we’re taking the next step.
We’re proud to introduce the Health Advisory Network (HAN)—a national platform where people like you can share your experiences, highlight challenges, and collaborate on solutions to improve healthcare across Canada.
Here’s how it works:
Share Your Voice: Participate in quick online surveys and consultations about your experiences as a patient or caregiver.
Get Paid: Your time and insights are valuable, and we make sure they’re compensated.
Drive Change: Help tackle challenges in workplaces, healthcare systems, and communities. Why now? Because the numbers speak for themselves:
45% of Canadians live with at least one major chronic condition. 2.5 million Canadians report unmet healthcare needs
1 in 2 Canadians will act as caregivers during their lifetime
The Health Advisory Network creates a unified space for people affected by health conditions to connect, share, and make a meaningful impact It’s not here to replace the incredible work of health charities or patient-oriented research groups—it’s here to amplify it. Together, we can uncover shared challenges and opportunities to build a stronger, more inclusive healthcare system.
Join the Health Advisory Network today and help shape the future of healthcare in Canada.
➡ Sign up and start making an impact
Health Advisory Network
For over 35 years, HealthPartners has brought together workplaces, health charities, and people with lived healthcare experience to improve lives across Canada. The Health Advisory Network is a national platform that invites individuals affected by illness to share their stories through paid surveys and consultations. Your lived experience can help shape research, policies, and programs that make healthcare better for everyone.
Providing Accommodation Access to Healthcare For Every Canadian: StayWell Suites Charity
Imagine being forced to choose between life-saving medical care and the financial burden of relocatingtoTorontotoaccessit.Thisistherealityformanypatients,alongsidetheircaregivers and family who must travel far from home to receive critical treatment. The added challenge of securing safe, affordable housing in an unfamiliar city often makes an already difficult journey evenharder.Thisfinancialburdenmayforcepatientstoeitherdelayorforgonecessarymedical care.
ThisiswhereStayWellSuitesCharitystepsin.
StayWell provides affordable accommodations to Canadians who must relocate for medical treatment. Through partnerships with major hotel chains and professional furnished apartment providers, we offer subsidized patient rates, alleviating the financial burden and ensuring patients can stay close to hospitals, alongside their caregivers and family, while receiving treatment
The inspiration for StayWell Suites Charity came from the personal experience of Tina Proulx, a patient from Ottawa, who faced a similar challenge in 2015. Diagnosed with a rare, lifethreateningdisease,TinaneededadoublelungtransplantatTorontoGeneralHospital,over400 kilometres from her home in Ottawa. In Toronto, the areas surrounding the hospitals are amongst the most expensive in the city. Tina and her husband Joel decided to make the move and had to take leaves of absence from work – they found themselves living in one of the most expensivecitiesinthecountrywithoutanyincome.
Matt Regush, a partner at Sky View Suites, learned of Tina's relocation challenges in the fall of 2015, when her family inquired about furnished accommodations and instantly provided them with a fully furnished unit at a reduced cost. This encounter led to the creation of StayWell Suites Charity. “If you cannot afford to live in Toronto and you’re making the choice not to accept treatment, then you are basically making the choice to die” says Tina, reflecting on her experience In December 2015, Tina received her transplant and made a full recovery, inspiring StayWell’smissiontohelpotherpatientsfacingthesamechallenges
From our start in 2018, providing three patients of the Princess Margaret Cancer Centre, including their families and caregivers, with 135 nights, we have grown significantly. By the end of 2024, we will have supported over 5,500 patients with over 90,000 room nights across all major hospitals in Toronto. Patient stays range from a few days to over a year. Earlier this year, we concluded an agreement with the SickKids Foundation to provide $250,000 in accommodationsupportoverthenextfiveyears.
Providing Accommodation Access to Healthcare For Every Canadian: StayWell Suites Charity cont'd
Looking ahead, StayWell will expand to other cities across Canada in 2025, continuing to rely on the support of dono s and partners to fill the gap between accommodation costs and what patients can afford. StayWell Suites Charity is committed to providing safe, affordable accommodations to patients, along with their caregivers and family, during their medical journey. Your support can make a life-changing difference for families like Tina’s, ensuring that no patient has to choose between their health and affordable accommodations.
Patients/caregivers can go to our website staywell.ca and select the Book Now link
Patient Journey's
The "Patient’s Journey" section of E3 Advocacy Digital Magazine is close to our hearts. This magazine is dedicated to patients and caregivers. We are proud to offer a platform to our community so that we can share, learn, and grow together. Here, patients can share their experiences and empower readers by connecting them with our Heal Canada community. By doing so, we can understand that whatever the situation we face, we are not alone! United, we stand in Advocacy!
Resilience, Advocacy, and Giving Back
by Laurie White
Life has a way of testing us. From being shot in the line of duty in 1998, losing my lower right leg, returning to operational policing, and battling PTSD to becoming a speaker on resilience, mental health, and living with a disability—my journey is one of both perseverance and purpose. Even after retiring from the RCMP in 2020 and publishing my memoir, 10-33 An Officer Down Steps Back Up, life continued to present hurdles, including a melanoma diagnosis in 2024 and a severe femur fracture requiring surgery. Yet, through every challenge, my commitment to advocacy, giving back, and being a role model for others remains steadfast.
A Defining Moment
In 1998, at 28 years old, my life changed in an instant. I heard my partner say the police radio code every officer dreads — “10-33.” It means “officer down,” and that officer was me.
Shot while executing a search warrant at the home of an alleged sex offender, I suffered an injury that led to the amputation of my lower right leg. The physical pain was immense, but the mental and emotional toll was just as significant. Soon, diagnosed with PTSD, I faced not only the trauma of that day but also the uncertainty of my future.
Determined to reclaim my life, I pushed myself through intensive rehabilitation, was fitted with a prosthetic leg, and defied expectations by returning to operational policing just ten months post-amputation. That return wasn’t about proving others wrong—it was about proving something to myself. It was about reclaiming my identity, my purpose, and my belief in what was possible.
The Power of Story-Sharing
As I rebuilt my life, I found a passion for sharing my story. At first, I wasn’t sure what people would want to hear. But I quickly realized that, while circumstances vary, emotions connect us. The challenges I faced resonated with others in ways I never expected. Story-sharing is one of the most powerful forms of human connection, and I became committed to using my experiences to inspire others to push through adversity and find strength and meaning in their struggles. Resilience isn’t just about bouncing back—it’s about adapting, learning, and finding new ways to move forward. Through my speaking engagements, I don’t just recount my experiences; I aim to empower audiences to see their own resilience, their own strength, and their own ability to persevere.
Resilience, Advocacy, and Giving Back cont'd
Advocacy in a New Chapter
Publishing my memoir allowed me to reach even more people. It was a deeply personal achievement, but more importantly, it became a tool to help others see that no matter how dire circumstances may seem, there is always a way forward. Retirement from the RCMP in 2020 didn’t mark the end of my mission—it marked a new chapter in advocacy and mentorship. Then, life threw me another test. In 2023, I was concerned with a mole on my back and had the opportunity to have it checked at the Mole Mobile. That check revealed nothing concerning, but months later, that same mole began bleeding. A check at the Skin Cancer Clinic resulted in three biopsies, including two locations which had not previously been concerning. Two biopsies, including the back mole, were negative. However, I was shocked when one on my left leg was diagnosed as invasive melanoma.
Despite being sun-conscious as an adult, my fair skin and childhood sun exposure had caught up with me. Thankfully, early detection led to successful surgery with clear margins, but the experience was a stark reminder of life’s unpredictability.
Rather than dwelling on fear and uncertainty, I chose to use my experience to help others. I became a Sun Guardian for Melanoma Canada, advocating for skin cancer awareness and the importance of regular skin checks. My diagnosis not only changed my perspective but also prompted my family members to get checked— leading to my mother’s early melanoma diagnosis. This reinforced what I already knew: awareness and early intervention save lives.
Another Setback, Another Lesson
As I began to move past the stress of melanoma, another challenge emerged—a severe femur fracture on my amputated side, requiring ORIF (open reduction and internal fixation) surgery. Suddenly, I found myself unable to walk, drive, or maintain the independence I had fought so hard to preserve.
For someone who prided herself on resilience, this forced dependence was mentally and emotionally taxing. But it also reinforced something crucial—the importance of accepting help, leaning on support systems, and recognizing that resilience isn’t just about pushing through alone. As I now await another surgery to remove hardware from my femur and a fourth biopsy for a newly identified skin spot, I remain focused on recovery and advocacy.
Turning Adversity into Purpose
My life has been defined by adversity, but more importantly, by the decision to keep pushing forward. As a young amputee and police officer, I learned to trust my instincts and advocate for what is reasonable and just in both medical and professional spaces. That commitment to advocacy has only grown—not just for first responders with PTSD or individuals with disabilities, but now also for cancer awareness. Each of us can turn our struggles into opportunities to educate, inspire, and uplift others. Together, we can drive positive change, improving policies, services, and care for those who come after us.
Resilience isn’t about never falling. It’s about rising—again and again. It’s not about a singular comeback but about continually emerging stronger, growing through each setback, and refusing to let challenges define us. It is, most certainly, a practice. Giving back is the most meaningful way to channel adversity into purpose. I want people to see that no matter how dark things may seem, there is always a way forward. Through resilience, advocacy, and a commitment to giving back, we can turn our struggles into sources of strength— not just for ourselves but for those walking a similar path.
As I navigate my own challenges, I hold onto the words of Lao Tzu: “The journey of a thousand miles begins with a single step.”
served in the Royal Canadian Mounted Police from 1996 to 2020, when she retired as a sergeant. In 1998, she survived a gunshot wound, but her injury resulted in a right lower leg amputation. She has received several awards, including the prestigious Governor General's Meritorious Service Medal, the Medal of Valour from the International Association of Women Police and the Queen’s Diamond Jubilee Medal.
Laurie is the author of 10-33 An Officer Down Steps Back Up 1033-Officer-Down-Steps-Back, and she is a sought-after speaker. She is a graduate of Brock University and the University of Ottawa, as well as the RCMP Training Academy ("Depot").
Laurie can be contacted at lawhite2023@gmail.com or on LinkedIn.
Laurie White
Stem Cell Transplant Success
by Wim Smits
In the Fall of 2018, routine blood work during my annual physical revealed that I had some abnormal blood counts. Repeating the blood tests confirmed the counts. As a result, I was referred to Dr. Nicole Laferriere, hematologist and Chief of Oncology at Thunder Bay (where I live) Regional Health Sciences Centre, for further testing. More detailed blood work was done, along with an abdominal ultrasound, CAT scan, and a bone marrow biopsy. Those tests revealed that I had a rare, terminal blood cancer called Primary Myelofibrosis (PM).
PM belongs to a group of blood cancers called myeloproliferative neoplasms. It is a chronic or slow-growing leukemia in which excessive scar tissue forms in the bone marrow (the soft, spongy tissue inside the bone), making it difficult to produce normal blood cells. This disease affects each person differently. There is no set treatment path for individuals with PM. Some medications may help with some of the symptoms, but currently, the only treatment with the potential to cure PM is a stem cell transplant. However, finding a matching donor is difficult, and the risks associated with the transplant are high.
Dr. Laferriere explained the basics of this disease to me and my wife, Harriet. One significant thing she pointed out was that there was at least a potential cure in a successful bone marrow/stem cell transplant. She also asked if I would like to be referred to Dr. Gupta, a worldrenowned expert in this disease, at Princess Margaret Cancer Centre (PMCC) in Toronto. I agreed without hesitation. We were also offered, and took advantage of, counselling at the Thunder Bay Regional HealthSciencesCentre.
When we got home, we immediately began searching for information on this disease to understand it as best we could. We needed to know what we were dealing with. Among the many sources of information available online, we found the Canadian Myeloproliferative Neoplasm ResearchFoundation(CMNPRF).Wearegladwedid.
During my first visit with Dr. Gupta, he and his team did an extensive background check. They inquired about my family history and asked me about my understanding of the disease, how I wascoping,andmy history of smoking.
They also provided more detailed information on my particular situation. They had the results of genetic testing and could tell me that I did not have the more common JAK2 mutation. I had the less common MPL mutation. At this visit, Dr. Gupta told us that this was a chronic leukemia that could progress slowly or can be aggressive. We discussed the risk factors of this disease, such as anemia, fever, high blood cell counts, leukemic cells, and the patient’s age. At this moment, only one of these was a factor for me (age over 65). He determined that my fibrosis was a grade 1 or 2 and that, at this time, I was classified as an ‘intermediate’ risk. Since I was not statistically likely to die within the next 5 years, bone marrow transplantation was not an option at this time. For now,await-and-watchapproachwaswarranted.
Stem Cell Transplant Success
The watching and waiting continued until August 18, 2021 Until then, my blood numbers were relatively stable, although there was a pattern of decline in some key indicators like red blood cells and hemoglobin At the same time, I noticed that I was eating less and losing some weight Fortunately, no ‘blasts’ had shown up. However, the overall indications were that things were deteriorating. Dr. Gupta felt that the disease was acting more aggressively and that it was time to consider‘treatmentoptions.’
Those options were limited to participating in a drug trial (MANIFEST-2) or pursuing the possibility of a stem cell transplant The drug trial was not a curative option, but the stem cell transplant held out the possibility of being curative We chose to pursue the Stem Cell Transplant Fortunately for me, a perfect 10/10 and willing, unrelated donor was found on the international stem cell registry
In October 2021, we met with Dr. Auro Viswabandya and the transplant team at Princess Margaret Cancer Centre. We discussed in detail the transplant process, the pre-transplant testing, and the adverse effects associated with the conditioning chemotherapy and radiation required. It was also decided that since my enlarged spleen would act like a sponge for the stem cells,itwouldbebesttotakesometimetoreduceitssizeby taking Jakavi
After about 3 months, the spleen was sufficiently reduced in size to proceed with the transplant. So, in March 2022, during the height of the Covid pandemic, we made the 2-day drive to Toronto to go through it. When we got there, further testing was done. Then, I checked into the hospital and received the required chemotherapy (4 days) and radiation (1 day). On March 22, 2022, five bags of stem cells were pumped into me. Then, it was a waiting game to see if the stem cells would ‘engraft’ and my blood numbers, which were extremely low at this point, would start to recover.Luckily forme,afterabout15 days,they did.
Stem Cell Transplant Success cont'd
After 5 weeks in the hospital, in isolation, when only Harriet was allowed to visit me, I was well enough to be discharged However, I had to stay within 1 hour of the hospital for the next 3 months Given that we live 1,600 km away in Thunder Bay, which meant we had to rent a condo in Toronto for that time. The good folks at Staywell were very helpful in this regard, and they arranged a lovely condo only a 15-minute walk away. Although I was readmitted to the hospital for a few days at one point, overall, the blood numbers continued to improve, and I had none of theadversesideeffectsIhadbeenwarnedabout.Attheendof June2022,wecouldgohome.
The journey had its challenges However, with the support of my wife, family, and friends, and thanks to a dedicated and wonderful team of doctors and nurses and a generous anonymous donor, it was a tremendous success To this day, I marvel at the fact that the science of it all exists I am grateful that I live in a country and province where this kind of health care is available,andonedoesn’thavetogobroketogetit.
Wim Smits
is a 71-year-old retired civil servant who lives in Thunder Bay, Ontario, Canada, with his family. He holds both a Forest Technician Diploma and a BSc. Degree in Natural Sciences.
For further information on PM, please visit https://www.cmpnrf.ca/primary-myelofibrosis
Visit our website at: https://www.healcanada.org/survey/ Check often as
gIn this vibrant corner of E3 Advocacy Digital Magazine, we're excited to introduce you to our "Living Well" section – a treasure trove of inspiration and guidance for those seeking a healthier, happier, and more balanced life. Our mission is to empower you with expert insights, the latest health trends, and personal wellness stories that resonate with real-life challenges and triumphs.
Here, we explore the many facets of well-being, from nourishing your body with wholesome nutrition to rejuvenating your mind through meditation and mindfulness. You'll find practical advice on exercise, mental health, and preventive care, all tailored to fit into your busy lifestyle.
But "Living Well" is more than just a guide; it's a community. We encourage you to engage with us, share your journeys, and learn from others who are on similar paths. Whether you're taking the first steps towards a healthier you or are further along your journey, we're here to support and inspire you at every turn.
"Living Well" will provide topics that matter the most to your health and happiness. Let's celebrate the joy of living well together!
Sun Myths
by Melanoma Canada
The facts are that there are few, if any, real risks to using sunscreen; in fact, studies show both chemical and physical sunscreens are perfectly safe and effective*. So, let’s tackle the sunscreen-related concerns we’ve seen pop up on health blogs recently.
“People need plenty of sun exposure to avoid vitamin D deficiency.” - False
do not need to expose yourself to the sun during UV times to get enough vitamin D. On days UV levels are moderate to high, most people enough vitamin D through normal activity, even sun protection. Vitamin D can be safely and obtained from a healthy diet that includes naturally rich in vitamin D, foods and beverages fortified with vitamin D, and vitamin D supplements. Because of the known side effects of exposure, vitamin D should not be obtained from unprotected exposure to ultraviolet (UV) radiation. When UV levels are 3 or above, sun protection is still needed.
It is a well-established fact that UV radiation from sun or indoor tanning can lead to skin cancer (melanoma and non-melanoma). 1,2 To live a healthy lifestyle while practicing appropriate photoprotection, the American Academy of Dermatology recommends seeking shade, wearing protective clothing and applying a broad-spectrum sunscreen with a Sun Protection Factor (SPF) of 30 or higher. Vitamin D can be safely and easily obtained from a healthy diet that includes foods naturally rich in vitamin D, foods and beverages fortified with vitamin D, and vitamin D supplements. Because of the known side effects of UV exposure, vitamin D should not be obtained from unprotected exposure to ultraviolet (UV) radiation.
“Sunscreen usage leads to vitamin D deficiency.”- False
These concerns are unfounded. A 2017 study showed that short-term sunscreen usage doesn’t affect circulating vitamin D levels and, therefore, does not increase the risk for osteoporosis. Sunscreens block cutaneous vitamin D production with only a minimal effect on circulating 25hydroxyvitamin D. Libon F, Courtois J, Le Goff C. Archives of osteoporosis, 2017, Jul.;12(1):18623514.” You don’t put yourself at risk of vitamin D deficiency if you wear sunscreen,” Ferris says. “In one large study, the amount of vitamin D in the bloodstream was no different in people who reported high versus low rates of sunscreen use. Also, vitamin D supplements are cheap and safe.” https://www.ncbi.nlm.nih.gov/pubmed/28718005
Sun Myths
"If you tan but don’t burn, you don’t need to bother with sun protection." - False
Even if you are tan, you need sun protection. If your skin turns brown, it is a sign of sun damage, even if there is no redness or peeling. Your skin turns brown as a way of trying to protect itself because the UV rays are damaging living cells. A suntan offers limited sunburn protection of around SPF3 but doesn’t protect against further DNA damage. If you tan easily, you are still at risk of skin cancer and need to use sun protection.
"You can’t get burnt in the car or through a window or under a beach umbrella." - False
You can get burnt through a window. Glass reduces but does not completely block transmission of UV radiation, so you can still get burnt if you spend a long time in the car or behind a window when the UV is high. More commonly, people are burnt in cars with the windows down, where they can be exposed to high levels of UV radiation.
Sitting in the shade or under an umbrella is smart, but it isn’t enough. A recent study in Texas compared people who applied SPF 100 with those who sat under umbrellas and found the umbrella group had triple the incidence of burns. “People get a false sense of security [under umbrellas],” Dr. Palm says. “At the beach, the sand and water are reflecting light. You’re not in a vacuum.”
You still get plenty of the sun’s rays, Dr. Marmur says, and you still need sunscreen. Apply it before you go out (a shot glass worth for your entire body); remember your hands, neck, ears, and hairline; and reapply every two hours.
"Are active ingredients in sunscreen 'toxic' or carcinogenic?" - False
Retinyl Palmitate causes cancer
This a common misinterpretation of a study examining an ingredient found in many sunscreens: retinyl palmitate. http://www.jaad.org/article/S01909622%2810%2900850-9/abstract
A lead researcher in that study actually concludes there is no evidence supporting the idea that sunscreen causes cancer. Another study (with humans, not rats) indicates that RP is photoprotective. Cosmeceuticals: focus on topical retinoids in photoaging. Serri R, Iorizzo M. Clinics in dermatology, 2009, May.; 26(6):0738-081X
Sun Myths
cont'd
Oxybenzone causes hormone disruption.
“Concerns over oxybenzone stem from animal studies where rats were fed the sunscreen ingredient and subsequently had some endocrine dysfunction, but the human studies with reallife application showed no hormone disruption,” Dosal says. “Yet you consistently find on the internet that your chemical sunscreen will cause hormone dysregulation, which simply hasn’t been shown.
"Sunscreen is damaging the world’s coral reefs." - False
Scientists do not agree with a recent study as it was done in a lab using artificial conditions and not reflective of a marine environment. http://mashable.com/2015/11/10/sunscreen-killingcoral-reefs/#cDabOvmci5qU
The bottom line: Chemical and mineral sunscreens are both safe.
"Apply sunscreen once a day, and you are good to go!" - False
One application is not going to last all day.
That’s because sunscreen (like makeup) rubs off with water, sweat, and touch. Dermatologists recommend reapplying at least every two hours or after swimming or sweating. This step is important. Not only will it wash off, but it actually breaks down in sunlight, which lessens the effectiveness.
How much sunscreen is enough sunscreen?
Studies show most people don’t apply enough sunscreen to achieve the full SPF of the product they’re using. Application patterns among participants randomized to daily sunscreen use in a skin cancer prevention trial. Neal R. Williams G. Green A. Archives of dermatology, 2002, Nov.:138(10)L0003-987X. Sunscreen should be applied liberally on all over-exposed skin.
It is recommended to use SPF30. When it comes to increasing SPF numbers, there’s a point of diminishing returns. SPF30 keeps out 97 percent, and SPF50 keeps out 98 percent. But in order for these percentages to remain accurate, you need to reapply.
Permission to reprint this important article has been graciously granted by Melanoma Canada, and we sincerely appreciate their generosity. For further details on the references cited and to learn more about Melanoma Canada’s initiatives, please visit their website https://melanomacanada.ca/sun-safety/sun-myths/ or email info@melanomacanada.ca
Turning a diagnosis into a passion
by Neeva Kedem
When I turned 40, my life took an unexpected turn. I was diagnosed with a serious thyroid disease, and my doctor informed me that I would need to rely on medication for the rest of my life. It was a moment of shock, but deep down, I couldn’t accept that this would be my only path. Instead of resigning myself to this fate, I decided to search for a natural solution. I dove into countless studies, devoured books on holistic health, and completely overhauled my lifestyle. I changed my diet to include whole, nourishing foods, and perhaps most importantly, I returned to my yoga practice with renewed purpose and dedication.
To my amazement, these changes started to make a profound difference. Through mindful movement, meditation, and strengthening my body, I began to feel better—not just physically but emotionally and mentally, too. Over time, my thyroid function improved significantly, and I was able to avoid the lifelong dependency on medication that once seemed inevitable. When I finally visited the specialist, he confirmed that my thyroid disease was completely gone! I was overjoyed and knew I had to share this incredible experience with others. Helping women achieve better health and well-being became my life’s mission. Since then, I’ve had the privilege of helping countless women transform their lives, empowering them to become healthier, stronger, and happier!
This personal journey not only restored my health but also deepened my commitment to helping other women discover the transformative power of yoga and Pilates.
As a yoga and Pilates instructor for over 15 years, I’ve witnessed firsthand how these practices can be life-changing for women, especially as they navigate the physical and emotional challenges that often arise with age. Pilates and yoga are not just about physical fitness; they are tools for holistic well-being. For women over 40, these practices can address key health concerns, such as improving bone density, enhancing flexibility, and building core strength, which supports posture and reduces the risk of injuries. They also play a vital role in hormonal balance, stress reduction, and emotional resilience.
Turning a diagnosis into a passion cont'd
One of my students, Sarah, came to me with chronic back pain that had plagued her for years. She had tried everything—physical therapy, painkillers, even surgery consultations—but nothing provided lasting relief. Together, we worked on a tailored Pilates and yoga program that focused on strengthening her core, improving her posture, and releasing tension in her back. Over the course of several months, Sarah not only found relief from her pain but also regained her confidence and energy. Today, she tells me that she feels stronger and more vibrant in her 50s than she did in her 30s.
What makes Pilates and yoga so effective for women is their adaptability. These practices can be modified to suit any fitness level or health condition, making them accessible to everyone. They also empower women to take control of their health in a way that is gentle yet powerful By focusing on mindful movement and breath, women can reconnect with their bodies, nurture their emotional well-being, and build strength from the inside out
For me, teaching yoga and Pilates is not just a career—it’s a calling. I am passionate about creating a safe and supportive space where women can prioritize their health and wellbeing. Whether it’s a woman recovering from surgery, managing stress, or simply looking to feel stronger and more balanced, I’ve seen these practices transform lives time and time again.
If there’s one message I want to share with women everywhere, it’s this: your health is your greatest investment. No matter where you are on your journey, it’s never too late to take that first step. Yoga and Pilates offer not just a path to physical strength but also a way to cultivate inner peace and resilience. And as my own journey has taught me, the body has an incredible ability to heal when we give it the tools and attention it deserves. So, roll out your mat, take a deep breath, and join me in discovering the power of movement, mindfulness, and self-care!
After years of teaching both yoga and Pilates, I developed a unique approach called Shelates. This fusion of yoga and Pilates was specifically designed with women in mind, blending the strength and flexibility of yoga with the corefocused, toning principles of Pilates.
Turning a diagnosis into a passion cont'd
Shelates offers a dynamic and holistic workout that empowers women to build strength, improve flexibility, and enhance mind-body connection in a balanced and accessible way. We focus on pelvic floor strengthening, thyroid stimulation to promote healthier metabolism, and meditation practices to release stress. Additionally, Shelates supports hormonal balance, making it not only an effective workout but also a nurturing practice for overall well-being.
Neeva Kedem
RYT, Yoga, Fitness & Pilates Teacher
Head Instructor at SHE Pilates & Yoga 3910 Bathurst St. 4th Floor, #405, North York (Toronto) https://www.shepilatesandyoga.com/
Tomato Cucumber Feta Salad
Ingredients
Dressing:
1/3 cup olive oil
3 Tbsp. white wine vinegar
2 Tbsp. fresh dill, minced
1 Tbsp. minced fresh chives
1 Tbsp. honey
1 Tbsp. dijon mustard
1/4 tsp. crushed red pepper flakes
3 garlic cloves, grated
Pinch of kosher salt
Pinch of black pepper
Salad:
3 ripe heirloom tomatoes, cut into bite-size pieces
6 Persian, Kirby, or mini cucumbers, striped with a peeler and cut into bite-size pieces
1 (8-oz.) block feta, cubed
Kosher salt, to taste
Black pepper, to taste
1/2 cup parsley leaves
3 Tbsp. fresh dill, chopped
2 Tbsp. chopped fresh chives
6 basil leaves, torn
For the dressing: Add the oil, vinegar, dill, chives, honey, mustard, red pepper flakes, garlic, salt, and pepper to a small mason jar Secure the lid and shake vigorously to combine.
Set aside
For the salad: Arrange the tomatoes, cucumbers, and feta on a platter. Give the dressing a final shake. Spoon over a few tablespoons of the dressing and season everything with a good pinch of salt and pepper. Top with the parsley, dill, chives, basil, and another few tablespoons of the dressing. 3Serve the salad with the remaining dressing on the side.
Spinach Cheese Quiche
Ingredients
1 refrigerated pie crust (from a 14-oz. box)
2 Tbsp. butter
1 small yellow onion, chopped
1 small red bell pepper, chopped
2 garlic cloves, chopped
4 large eggs
1 1/4 cups half-and-half
1/2 cup sour cream
1 1/2 tsp. salt
1/4 tsp. black pepper
Pinch of ground nutmeg
1 (10-oz.) package frozen chopped spinach, thawed and squeezed dry
1 cup shredded sharp cheddar cheese
1/4 cup finely shredded Parmesan cheese
Preheat the oven to 375°F with a baking sheet on the center rack. Fit the pie crust into a 9-inch pie plate (about 1-inch deep). Fold the edges of the crust under and crimp as desired. Chill in the refrigerator while preparing the filling.
In a medium skillet, melt the butter over medium heat. Add the onion and bell pepper, and cook, stirring occasionally, until softened, about 10 minutes
Add the garlic, and cook, stirring often, until fragrant, about 2 minutes. Remove from the heat
In a large bowl, whisk together the eggs, half-and-half, sour cream, salt, pepper, and nutmeg. Stir in the spinach, cheddar, parmesan, and bell pepper mixture. Pour into the prepared crust.
Place the quiche on the preheated baking sheet and bake until it has puffed in the center, is just set, and the crust is golden, 40 to 50 minutes.
Transfer the quiche to a wire rack to cool. Serve warm or at room temperature.
Satisfy Your Sweet Tooth: Combat Your Cravings: Are you ready for this shocking fact?
by Sue Lemoine, RHNP
The average North American, according to recent research, consumes roughly 150 pounds of sugar a year. That sounds like A LOT, and to me, that is shocking. Hopefully, it is to you as well. When you consider that as a fact, it’s not difficult to guess why we, as a nation, struggle with obesity and diabetes Mildly overweight people usually store about 5% of the sugar they eat for energy They metabolize about 60%, and they store the rest, about 35%, as fat for future energy needs. The problem is that we rarely need to tap into those fat stores, so they just keep accumulating.
Our “Sweet Tooth” is killing us. What we whimsically call a “sweet tooth” is really just a cute name for a sugar craving or a passion for sweet foods. If you’re the person most likely to hit the dessert bar twice, you probably identify as someone with a “sweet tooth.” And that might not be entirely your fault. Recent evidence suggests a genetic root to the lust for sugar PLUS research proves that “Sugar Addiction” is as real as drug addiction and probably harder to beat Hardcore metabolic roots for those sugary cravings mean that sugar junkies who really want to combat their desires need to find healthy alternatives to satisfy their sweet teeth. What are the genetic causes for a sweet tooth?
Studies in recent years show that people who crave sugar tend to have a “weak sweet taste.” That means that they need more sugar than a normal person to taste the same level of sweetness Genetics appears to account for about 30% of the differences in people's ability to taste sweetness, according to a study of identical and non-identical twins at the Monell Chemical Senses Center.
The same resear of sugar as a kid didn’t anesthetiz e just born with a sweet tooth. So wha ors?
Satisfy Your Sweet Tooth: Combat Your Cravings: Are you ready for this shocking fact?
Sweets are more appealing to you than to most people. You eat more sugar to satisfy your desire for sweetness. And that means you take in more empty calories that your body will helpfully store as fat in case you need that energy later. Thanks What is sugar addiction?
Sugar overstimulates the reward centers in your brain and, according to some experts, causes addiction. Other experts dispute whether sugar addiction exists, but what I know is that when I eat sugar, I want more and more and more. So, regardless of what the experts say, I feel like it's an uncontrollable monster within me.
Here's what we all agree on... Foods with a lot of sugar cause our brains to release massive amounts of dopamine, the same brain chemical that illicit drugs, like cocaine and meth, amp up to create euphoria. That’s what we mean by a “sugar high.”
When we eat a lot of high-sugar foods frequently, we train the brain to be less conscious of the increased dopamine levels. And once the brain is less receptive, it takes more and more sugar to create the same feeling, just like building a tolerance to an addictive drug. Because sugar manipulates our brains’ reward centers, and functions a lot like nicotine or cocaine, folks with a predisposition toward addiction are more likely to get addicted to sugar and to lose control of their ability to regulate consumption.
Well that sucks. But I have good news! You CAN satisfy your sweet tooth and put the kibosh on those crazy cravings by choosing healthier snacks and limiting the amount of sugar you swallow. You know that you need to set down the candy bars, step away from the ice cream, and lay off the sodas and desserts, but did you also know that dairy, fruit products, and white flour pack a huge sugar punch?
The top three sources for added sugar in the North American diet are: Soft drinks, energy drinks, and sports drinks; Baked desserts with a grain base, like cookies and cake; Sugar-packed fruit drinks like juices and smoothies.
Satisfy Your Sweet Tooth: Combat Your Cravings: Are you ready for this shocking fact? cont'd
But before you start to despair, let’s get back to all of the incredibly tasty options you have to satisfy that sweet tooth and curb your cravings.
Fifteen Healthier Alternatives to Sugary Foods
Baked apple.
Banana Nice Cream (aka pureed frozen bananas)
All-fruit popsicle.
Homemade trail mix.
Baked sweet potatoes with cinnamon and nutmeg.
Strawberries dipped in cashew cream sauce.
Coconut.
Grilled pineapple.
Frozen grapes.
Sliced pear, apple or banana with almond or other nut butter.
Homemade granola bar or date square (no sugar added).
Green smoothie
Berries topped with a dollop of yogurt and granola.
Fruit crisp, also known as baked fruit with a sprinkle of nuts and granola.
Homemade protein balls.
Now, if your body has become accustomed to high-fructose, super-processed snack cakes, it will take you a while to get used to eating a frozen banana instead. But I promise that if you commit to working the sugar out of your diet, you’re going to feel so much healthier and energetic. And after a while, treats you once enjoyed will seem too sweet. You’ll be able to relish a truly divine chocolate-dipped strawberry instead of eating a sleeve of Thin Mints.
Satisfy Your Sweet Tooth: Combat Your Cravings: Are you ready for this shocking fact? cont'd You will learn to satisfy your sweet tooth with less sugar. Doesn’t that sound heavenly? To be in control of what you eat? To live without cravings? I distinctly remember the first time I decided to experiment with not eating sugar. I decided I’d quit ALL sugar for one week. I wanted to see if I was addicted, and what symptoms I would experience. The symptoms showed up on day one with a headache, and I felt very tired. I couldn’t concentrate. The next day, my symptoms were worse. I actually thought I had the flu. The third and fourth day were better until finally, on the fifth day, all withdrawal symptoms were gone, and I felt FANTASTIC. I actually felt light and alive and in such a good mood. I was shocked at how profound it was.
Now I really limit my sugar intake, but when I do have too much sugar, I actually feel like I have a hangover the next day. It’s really shocking. So let’s do it. I challenge you to go without sugar for just one week (and check all food labels for sugar, which means no ingredients with “ose”)
Do not let sugar kick your butt. Jump in and try it for just one week. And let me know how you do. It’s time to kick those sugar cravings to the curb so you can live the healthy, happy life that you deserve! if you have any questions, please reach out to me anytime.
Welcome to the "Ask the Professional" section of E3 Advocacy Digital Magazine, a dedicated space where curiosity meets expertise in the realm of healthcare.
In our pursuit to empower patients and their advocates with knowledge, this section bridges the gap between medical professionals and our readers, offering clear, accurate, and practical answers to your most pressing questions. Whether you're navigating the complexities of clinical trials, seeking advice on managing chronic conditions, or exploring the latest in wellness trends, our experts are here to provide you with insights grounded in the latest research and clinical experience.
Let's embark on this journey of understanding together, fostering a community where informed decisions lead to better health outcomes.
Ask the Professional
Maureen Carpenter, BSC, RN, CD provides her insight
Access to Medication
The World Health Organization (WHO) has t (EML) The EML is compiled as a guide for nations to create their own and to ensure the demands of their healthcaresystem will bemetthroughasupply of necessary medications
Procurement, production, education and cost schemes are developed in relation to an EML. Access to medications for cancer patients around the world is dependent on many different aspects, but foremost, the wealth of their nation and what percentage of the GDP (Gross Domestic Product) is invested in health are major contributors. Countries with Universal health care often invest 10% of their GDP, whereas countries like India 2.1%, Malaysia 4.3% and Poland 6%. This type of disparity results in more out-of-pocket expenses for patients for crucial therapy medicationsontop of themany otherconcernsfacing thoseindividuals.
These poorer countries, where most individuals live below the poverty line, are also struggling with inconsistent drug pricing, limited quality monitoring, frequent drug shortages, and delays in the approval process of new drugs. In the sub-Saharan African countries, there is an estimated 41% of the population that lives below the poverty line. This means that more than 500 million peopleintheseareasof theworldcannotaffordcancerdrug therapies.
During my research into this topic, I have discovered that there are more countries in this situation than there are not. There is also a lack of transparency in oncology drug pricing between countries, as costs are confidential, leading to inequitable valuation of the drug. The tendency then falls to the patient paying elevated bills for life-saving therapies. Even those countries deemed high income with Universal Health Care are experiencing barriers to cancer therapies. Canada and the USA both list financial constraints, complex and fragmented drug coverage systems, and disparity in access for certain groups as access concerns. Canada has one of the highest global prescription drug cost issues. The inability for a patient to pay for medications leads to non-adherence or skipping doses to stretch out the quantity.
Insurance coverage can often be complex and minimal. Inconsistent coverage will contribute to hardships for the patient and increase financial pressures during stressful health journeys. Seniors, immigrants, and racialized persons typically fall into the area of disparity due to living locations, income levels, and access to care. A research project in Canada between Queen’s University, the University of Calgary, and Dalhousie University is being conducted to identify the barriers to chemotherapy drugs. The aim of this study is to identify the factors involved in delays to treatment as well as the existence of a disproportion of chemo drug/treatment availability between the Provinces and Territories of Canada. (Chafe R, et al.)
Drug shortages are a worldwide concern, as well as product discontinuations. Up until two decades ago, HIV and Hep C treatments were expensive and only accessible in high-income countries. Since 2000,thereductionincosttopatientshasdecreasedby99%.
This was a result of a multi-stakeholder approach. The focus for oncology medication access can be found in the work being carried out by the Access to Oncology Medicines Coalition (ATOM Coalition). This collaboration involves over 40 partners in both private and civil society sectors. Workshops are developed to address barriers in low and middleincome countries. Licensing, donation programs and supply chain improvements are some of the addressed areas compounding the barriers to medication access and technologies of treatment. www.uicc.org/atom/atom-coalition-home
The Canadian Cancer Society lists three areas where Canadians with cancer may face challenges in accessing chemotherapy. An oncologistrecommended drug may not be covered through their provincial or territorial benefits plan or private insurance policies. Medications taken at home may be the best option for treatment, but due to the province of residence, there may be a lack of coverage, and a patient would be forced to pay. Lastly, significant delays through the drug approval processarealsoakeycontributortoaccessissues.
Access to medications has been discussed above. Now, a superficial look at the monetary concerns with regards to oncology drugs in Canada. Half of the Canadian provinces do not have partial or full oral chemotherapy drug reimbursement programs. In December 2023, the government of Canada announced the creation of the Canadian Drug Agency, dedicated to ensuring sustainability in the Canadian drug system. This announcement included $89.5 million over 5 years on top of the current federal funding of $34.2 million annually to achieve better health outcomes.
Residents of different provinces in Canada with the same cancer will have different experiences in their cancer treatment costs. One person will have oral drugs covered, and the other will incur costs anywhere from $1800.00 per month to $132,000.00 per year. The Canada Health Act stipulates that all intravenous chemotherapy drugs administered in hospitals are fully covered in each province. Within a province, one cancer patient's optimal treatment would be oral drugs at their cost, and a second patient with the same diagnosis would be treated with intravenous chem drugs. These inequities create a need for a standardized national pharmacare.
Your resources
Patients, caregivers, Patients organizations, Healthcare professionals and other stakeholders, we want to help you.
You are looking for information on clinical trials to finish...
CADTH. (2022). Patient and community engagement. Canadian Agency for Drugs and Technologies in Health. https://www.cadth.ca/about-cadth/what-we-do/patient-andcommunity-engagement
Canadian Organization for Rare Disorders (CORD). (2023). Canada’s national strategy for drugs for rare diseases: A step in the right direction. https://www.raredisorders.ca
Health Canada. (2021). Canada’s drug and health technology approval process. Government of Canada. https://www canada ca/en/health-canada/services/drugs-health-products/drugproducts/fact-sheets/drug-review-approval-process.html
INESSS. (2023). Role of INESSS in health technology assessment. Institut national d'excellence en santé et en services sociaux. https://www.inesss.qc.ca
Office of the Auditor General of Canada. (2022). Access to new pharmaceuticals in Canada. https://www.oag-bvg.gc.ca/internet/English/parl oag_202211_02_e_44179.html
Pan-Canadian Pharmaceutical Alliance (pCPA). (2023). About us. https://www.pcpacanada.ca Save Your Skin Foundation. (2021). Patient navigation and advocacy support programs. https://saveyourskin.ca
Van Katwyk, S. R., Jones, S. L., & Hoffman, S. J. (2022). The Canadian drug approval system: Barriers to timely access. Healthcare Policy, 17(3), 27–39. https://doi.org/10.12927/hcpol.2022.26751
Wiktorowicz, M. E., Lexchin, J., Moscou, K., Eggertson, L., & Sproule, D. (2018). Keeping an eye on prescription drugs, keeping Canadians safe: Active monitoring systems for drug safety and effectiveness in Canada and internationally. Health Evidence Network Synthesis Report 62. https://apps who.int/iris/handle/10665/326377
QALSODY Canadian product monograph
ZYNYZ Canadian product monograph
ITOVEBI® Canadian product monograph
Bunton-Stasyshyn RK, Saccon RA, Fratta P, Fisher EM. SOD1 function and its implications for amyotrophic lateral sclerosis pathology: new and renascent themes. Neuroscientist 2015;21:519-29.
McCampbell A, Cole T, Wegener AJ, et al. Antisense oligonucleotides extend survival and reverse decrement in muscle response in ALS models. J Clin Invest 2018;128:3558-67. Miller TM, et al. Trial of Antisense Oligonucleotide Tofersen for SOD1 ALS, n engl j med 387;12 nejm.org September 22, 2022
MCC Survival Rates Increased More Than Two-Fold Following Immunotherapy ApprovalDermatology Advisor
References
Causes of Merkel Cell Carcinoma
Han Y, Liu D, Li L PD-1/PD-L1 pathway: current researches in cancer Am J Cancer Res 2020;10(3):727-742.
ZYNYZ® (retifanlimab-dlwr) | ZYNYZ Efficacy
Lim E, et al. The natural history of hormone receptor-positive breast cancer. Oncology (Williston Park). 2012;26(8):688-94,696.
Tomas R and Barrios CH. Optimal management of hormone receptor positive metastatic breast cancer in 2016. Ther Adv Med Oncol. 2015;7(6):304-20.
Anderson E, et al. A Systematic Review of the Prevalence and Diagnostic Workup of PIK3CA Mutations in HR+/HER2– Metastatic Breast Cancer. Int J Breast Cancer. 2020;2020:3759179
ClinicalTrials.gov. A Study Evaluating the Efficacy and Safety of Inavolisib + Palbociclib + Fulvestrant vs Placebo + Palbociclib + Fulvestrant in Patients With PIK3CA-Mutant, Hormone Receptor-Positive, Her2-Negative, Locally Advanced or Metastatic Breast Cancer (INAVO120) [Internet; cited 2025 January]. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04191499.
Biagi, J J., Raphael, M. J., Mackillop, W J., Kong, W., King, W D., & Booth, C M. (2011). Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: a systematic review and meta-analysis JAMA, 305(22), 2335-2342. https://doi.org/10.1001/jama 2011 749
Bozcuk, H., et al (2005). Does delay in starting treatment affect survival in non-small cell lung cancer? Lung Cancer, 47(1), 125-129.
Griffiths, P., et al. (2018). Nurse staffing levels, missed vital signs and mortality in hospitals: retrospective longitudinal observational study. BMJ Quality & Safety, 27(8), 633–640.
Kennedy, J., Wood, E. G., & Wang, Y. (2020). Medication cost barriers and chronic disease management among older adults in the United States. Preventing Chronic Disease, 17, 200244. https://doi.org/10.5888/pcd17.200244
Kitabchi, A. E., Umpierrez, G. E., Miles, J. M., & Fisher, J. N. (2009). Hyperglycemic crises in adult patients with diabetes. Diabetes Care, 32(7), 1335–1343.
Kumar, A., et al. (2006). Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Critical Care Medicine, 34(6), 1589–1596.
Martinez-Ramirez, D., et al. (2015). Hospitalization and Parkinson’s disease: The importance of proper medication management. Parkinsonism & Related Disorders, 21(10), 1153–1159
Nell, V P., Machold, K P., Eberl, G., Stamm, T A., Uffmann, M., & Smolen, J S (2004). Benefit of very early referral and very early therapy with disease-modifying anti-rheumatic drugs in patients with early rheumatoid arthritis. Rheumatology, 43(7), 906–914
Riesenberg, L. A., Leitzsch, J., & Cunningham, J. M. (2010). Nursing handoffs: a systematic review of the literature. American Journal of Nursing, 110(4), 24–34.
References
Saver, J. L., et al. (2013). Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA, 309(23), 2480–2488.
American Diabetes Association. (2022). Standards of Medical Care in Diabetes 2022. Diabetes Care, 45(Suppl 1), S1–S264. https://doi.org/10.2337/dc22-SINT
Gupta, N., et al. (2017). The association between public drug coverage for antihypertensive medications and health outcomes in Ontario. Canadian Journal of Cardiology, 33(10), 1305–1311.
Kennedy, J., Wood, E. G., & Wang, Y. (2020). Medication cost barriers and chronic disease management among older adults in the United States. Preventing Chronic Disease, 17, 200244. https://doi.org/10.5888/pcd17 200244
Law, M. R., Cheng, L., & Dhalla, I. A. (2018). The effect of cost on adherence to prescription medications in Canada. CMAJ, 190(1), E11–E15. https://doi.org/10.1503/cmaj.170675
Parliamentary Budget Officer (PBO). (2017). Federal cost of a national pharmacare program. https://www.pbo-dpb.gc.ca/en/blog/news/Federal-cost-of-national-pharmacare-program
Reading, C., & Wien, F. (2009). Health Inequalities and Social Determinants of Aboriginal Peoples' Health. National Collaborating Centre for Aboriginal Health. Statistics Canada. (2022). Access to healthcare and pharmaceuticals. https://www150.statcan.gc.ca/n1/pub/82-003-x/2022007/article/00001-eng.htm
Zhang, Y., Baik, S. H., & Newhouse, J. P. (2006). Geographic variation in Medicare drug spending. New England Journal of Medicine, 354(14), 1439–1449.
Arthritis Society Canada. (n.d.). Access to medications. https://arthritis.ca/about-us/what-wedo/advocacy/access-to-medications
Asthma Canada. (n.d.). About us. https://en.wikipedia.org/wiki/Asthma Canada
Canadian Institute for Health Information (CIHI). (2021). Drug spending in Canada, 2021. https://www.cihi.ca/en/drug-spending
Health Canada. (2023). Drug and health product submissions under review (SUR). https://www canada ca/en/health-canada/services/drugs-health-products/drugproducts/submissions-under-review.html
Innovative Medicines Canada. (2022). Access to innovative medicines in Canada: Comparative analysis 2022. https://innovativemedicines ca/browse-by/access-to-medicine/ Kennedy, J., Morgan, S., Wang, J., & MacKinnon, N. J. (2020). Cost-related nonadherence in Canada: Policy implications for public drug coverage. Healthcare Policy, 15(3), 27–39. https://doi.org/10.12927/hcpol.2020.26146
Kids New to Canada. (n.d.). Barriers to health care. Canadian Paediatric Society. https://kidsnewtocanada.ca/care/barriers
Myeloma Canada. (n.d.). Advocacy and drug access. https://myeloma.ca/getinvolved/advocacy-and-drug-access/ Government of Canada. (2023, March 22). Government of Canada improves access to affordable and effective drugs for rare diseases. Retrieved from https://www.canada.ca/en/health-canada/news/2023/03/government-of-canada-improvesaccess-to-affordable-and-effective-drugs-for-rare-diseases.html
References
National Pharmacare Working Group. (2022). Toward access for all: A report on gaps in public drug coverage in Canada. Canadian Health Coalition. https://www.healthcoalition.ca/nationalpharmacare-working-group-report
Public Health Agency of Canada. (2023). Equity and the determinants of health. https://www.canada.ca/en/public-health/services/health-promotion/population-health/whatdetermines-health.html
Saleh, A., & Kirchhof, M. G. (2023). Pharmacy deserts and medication access in underserved communities. Canadian Pharmacists Journal, 156(1), 45–52. https://doi.org/10.1177/17151635221110550
Statistics Canada. (2020). Access to health care services during the COVID-19 pandemic, spring 2020. https://www150.statcan.gc.ca/n1/pub/82-003-x/2020006/article/00001eng.htm
Canadian Paediatric Society. (2021). Off-label use of prescription medication in children and youth. https://cps.ca
Lexchin, J. (2018). Health Canada and the approval of new drugs: Do we need a new approach? Healthcare Policy, 14(2), 10–18
Children’s Healthcare Canada. (2020). Access Denied: The state of children’s healthcare in Canada
Gagnon, M.-A. (2020). A Roadmap to a Rational Pharmacare Policy in Canada. Globalization and Health, 16(1), 1-8
Government of Canada. (2023). Canada’s Rare Disease Drug Strategy. https://www.canada.ca/en/health-canada/services/drugs-health-products/drugproducts/funding/access-rare-disease-drugs.html
Chafe R, Culyer A, Dubrow M, Coyte P, Sawka C, O’Reilly S, Laing K, Trudeau M, Smith S, Hoch J, Morgan S, Peacock S, Abbott R, Sullivan T.
Access to Cancer Drugs in Canada: Looking Beyond Coverage Decisions. Health Policy. 2011 Fev 6(3): 27-36, doi: 10.12927/hcpol. 2011. 22177.PMID: 22294989; PMCID: PMC3082385
Barrios C, de Lima Lopes G, Yusof, M, Rubagumya F, Rutkowski R, Sengar M.
Barriers in access to oncology drugs- a global crisis. Nat Rev Clin Oncol. 2022 Nov 15: 20(1):715. Doi: 10.1038/s41571-022-00700-7. PMCID: PMC9665041 OMID: 36380066
Sorin M, Franco E, Quesnel-Vallee A.
Inter- and intraprovincial inequities in public coverage of cancer drug programs across Canada: a plea for the establishment of a pan- Canadian pharmacare program. Current Oncology A Canadian Caner Research Journal, Vol. 26, No. 4, August 2019 www uicc.org/atom/atom-coalition-home Canadian Cancer Society cmwg-advice.pdf
Alliances
Alliances
Supporters
Heal Canada Team
Cheryl Petruk, MBA B.Mgt.
Cheryl A. Petruk is a multifaceted professional whose career spans patient advocacy, business, and post-secondary education, showcasing her dedication to significantly impacting theseareas
Family circumstances drove her transition into patient advocacy During the last 15 years, she has worked tirelessly to bridge the gap between the healthcare system, patients, and pharma stakeholders Her empathetic approach and dedication to advocacy have made her a respected figure in this field. She lobbies for a healthcare system based on patientcentricity. She supports other patient organizations in becoming better advocates by leading Heal Canada and CACHEducation Cheryl has recently achieved her greenbelt in VBHC,andisinpursuitof herDBA
Wendy Reichental, B.A.
Wendy Reichental, Program Manager, Heal Canada. Wendy holds a B.A. and a Diploma in Human Relations and Family Life Education from McGill University. She is certified in foot reflexology
Throughout her career, she has showcased her insightful perspectives through her writings, which have appeared in publications such as The Montreal Gazette and Ottawa's Globe and Mail She has also contributed to specialized platforms like Booming Encore and Refresh Reflexology Magazine, demonstrating her versatility in addressing diverse audiences. Her unique observation on the initial days of the pandemic lockdown is captured in the anthology Chronicling the Days: Dispatches from the Pandemic, published by GuernicaEditionsinthespring of 2021
No part of this publication may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the publisher, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law For permission requests, please contact: admin@healcanada org
E3 Advocacy is a publication of Heal Canada, supporting education, empowerment, and engagement in patient advocacy