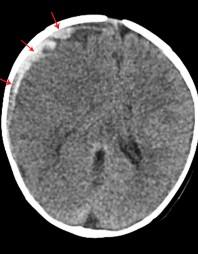
Unwitnessed fall from couch, no impact injury, scalp contusion
CT Great for Vascular Assessment (CTA/CTV) and metallic foreign bodies (precludes MRI)
Fall while playing, “foreign body”
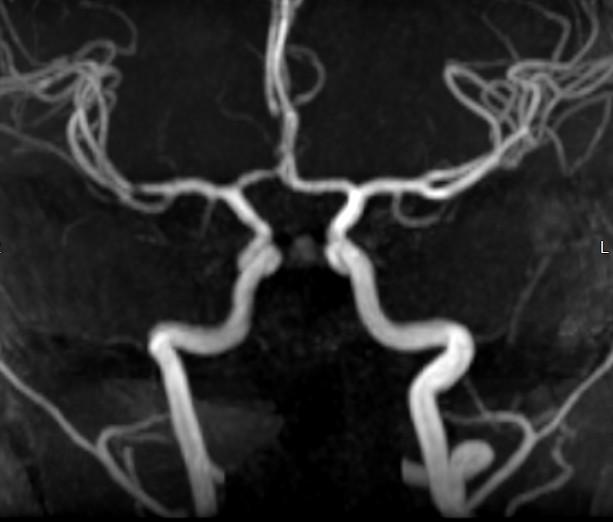
CTA/CTV: No vascular injury.
CT: Signs of Ischemic/Anoxic Injury
Loss of grey white juncture
White cerebellar sign
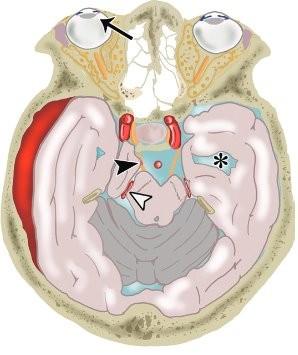
Pseudo Subarachnoid Hemorrhage Reversal of Basal Ganglia
Normal 2-year-old
CT: Signs of Ischemic/Anoxic Injury
Loss of grey white juncture
White cerebellar sign
Normal 2-year-old
Pseudo Subarachnoid Hemorrhage Reversal of Basal Ganglia
CT: Signs of Ischemic/Anoxic Injury
Loss of grey white juncture
White cerebellar sign
Normal 2-year-old
Pseudo Subarachnoid Hemorrhage Reversal of Basal Ganglia
CT: Signs of Ischemic/Anoxic Injury
Loss of grey white juncture
White cerebellar sign
Normal 2-year-old
Pseudo Subarachnoid Hemorrhage Reversal of Basal Ganglia
8-yearold, encephalopa thy:
Reversal of Basal Ganglia density
Day 1 Admittance
Day 3, Progressive encephalopathy with seizures
How Fast Can I Go? MRI
How do I capture Motion?
Use of strobes in “high speed flash photography”
1957
“Edgerton’s Coronet”
Harold Doc Edgerton
“Father of High-Speed Flash Photography” MIT professor E. Engineering Created the “stroboscope”
TOOLBox: QUICK BRAIN
ssfse - “single shot fast spin echo”
Heavily T2 weighted image acquired in seconds 6-20 sec per sequence
• HASTE Siemans
• ssfse GE
Good for large masses, mass effects, hydrocephalus
QUICK BRAIN with DL Deep Learning
Trauma Post Decompression , Neurosurgery
Quick Brain with (GE) EpiMix
Quick
Brain with (GE) EpiMix = Quick Mix
QuickMix: Surveillance Cavernoma with DVA Developmental Venous Anomaly
Ssfse T2 Pseudoswan
Ssfse T2 Pseudoswan
DWI
QuickMix: Surveillance Cavernoma with DVA Developmental Venous Anomaly
First attempt: Remember, chasing moving targets!
Ssfse T2 Pseudoswan
Ssfse T2 Pseudoswan
DWI
PEDS MRI Tool Box
ACC Techniques:
ARC...undersampling K space
ASSET...undersampling Image space
DL...Deep Learning, AI
HyperSense...Compressed Sensing
Quick : No Sedation
FAST: No Sedation
Accelerated Comprehensive
FAST Brain:
Stroke in Adults, neg CTA/perfusion, 5 minutes w/o contrast
Brain 1 or 3 views
FAST Stroke in both Adults & Pediatrics
• FAST:
• "face, arm, speech, time"
• Hesitancy to sedate children in the acute setting
• Stroke often presents with HA or Seizure
Addition of Perfusion after contrast Core versus Penumbra
PEDS FAST Stroke MRI/MRA Brain 10 mins
Addition of Contrast, COW MRA, Black Blood T1 VASC
FAST "Black Blood" Imaging ACC T1 COR VASC 2 minutes
Focal Cerebral Arteriopathy of Childhood FCA-i
Mechanism unknown
Inflammation/Infection leading to Endothelial disruption, vasculopathy/vasculitis
In children, Moya Moya?
Black Blood Imaging (T1 VASC) vs Vessel Wall Imaging (VWI)
BB T1 COR VASC .8 mm resolution
Pick up collateral enhancement
• High Res VWI
• 3T (double the signal)
• .5 mm slice thickness
• Isotrophic
• When to image: 5-10 window after contrast administration
• 7-9 minutes sequence acquisition time
Hemorrhagic
Stroke:
Hemorrhagic Venous Infarction
Thanks to H. Rowley
PEDS MRI ToolBox
ACC Lesional Brain: Surveillance Exams for Tumor, NF I, or in children where No sedation +/AV Distraction or Limited Sedation is being considered. The total exam time (30 min) is not necessarily shorter (COMP Brain 35 mins) but each sequence is "faster" and tolerates more motion.
Quick : No Sedation
FAST: No Sedation
Accelerated Comprehensive
Acc Lesional Protocol: Surveillance Scans
OP/IP
Subpackages: Post Fossa, Chiasm, Seizure
Gilardi et al, Radiographics, 2019
Subfalcine
oMidline Shift Transtentorial Descending
oUnilateral or bilateral Uncal Transtentorial Ascending Tonsillar Extracranial