Pediatric Dental Practice US Spring/Summer 2025 Vol 3 No 1
Pediatric Dental Anesthesia Associates
Hector Vila, MD, with Brandon Larkin, DDS
The importance of calcium hydroxide in dental trauma cases
Dr. Sonia Chopra
Are we meeting our patient’s individual needs?
Dr. Kelly Tanner
The role of dentists in ensuring proper growth of the craniofacial-respiratory complex from infancy
Drs. Lynda and Krystle Dean-Duru
Running a “kool” practice for “kidz”
Iam Dr. Morghan Teeters. I was born and raised in Phoenix, Arizona, graduated from Northwest Christian High School, and attended ASU and UNLV where I earned my Bachelor of Science in Biology. I attended dental school at the University of Nevada, Las Vegas School of Dental Medicine, where I graduated with honorable mention. My husband and I were in the same dental class and got married during our third year of school. After dental school, I practiced as a general dentist in Minnesota, allowing my husband to complete an orthodontic specialty residency program. My family returned to Arizona where I completed an intensive 2-year pediatric specialty program at NYU Lutheran Medical Center in Tucson, Arizona in 2015. I knew from a young age that I had a passion for dentistry because of my dad. I began working in my dad’s office at the age of 12 in the lab.
Building trust and consistency is crucial, and my dental team works closely with families or caregivers to understand each patient’s specific needs.”
My passion is providing comprehensive pediatric dentistry with an emphasis on preventative care. I gained valuable experience during my residency with many different populations of children, including children with special needs. I have specialized training in higher-level behavior management methods such as sedation and hospital dentistry. I am especially drawn to children and adolescents affected by Autism Spectrum Disorders and medically compromising conditions.
Morghan Teeters, DMD
Working in dentistry with patients who have special needs, including those with Autism Spectrum Disorders, requires a unique combination of compassion, adaptability, and specialized training. These patients often face sensory sensitivities, communication challenges, or heightened anxiety, which can make dental visits particularly difficult. I approach care with patience and empathy, using individualized strategies such as visual aids, desensitization techniques, or modified appointment structures to create a comfortable and supportive environment. Building trust and consistency is crucial, and my dental team works closely with families or caregivers to understand each patient’s specific needs.
I am board certified by the American Association of Pediatric Dentistry, the highest official level of pediatric dentistry training. I am also a member of several professional organizations including the American Academy of Pediatric Dentistry, the American Dental Association, and the Arizona Dental Association. I regularly attend national meetings, conferences, and seminars for continuing education in my specialty.
I run my practice, Kidz-R-Kool Pediatric Dentistry, with my husband Chris. We live in Peoria with our three sons, one
daughter, and 2 goldendoodles. In my spare time, I enjoy traveling, going to the lake, and spending time with family and friends. As a mother of four children, I feel that my commitment to my family helps me to relate and empathize with parents and patients alike. I am committed to my patients and treat each patient with the same gentle care and respect that I would for my own child. I have a large extended family in the Phoenix area, and am fully committed to helping the dental needs of the community.
The entire Kidz-R-Kool Pediatric Dentistry staff loves working with children. We realize that the initial experiences a child has with their dentist will be reflected throughout their lifetime. Our goal is to provide a warm and fun atmosphere for the family while providing the utmost quality of care.
I have always believed in the power of teamwork when it comes to creating healthy, confident smiles. One of the most impactful collaborations I focus on is the partnership between pediatric dentistry and orthodontics. By working next door to my husband, both of us are better able to monitor growth, development, and tooth alignment from the very beginning — often catching potential issues before they become complex problems. This proactive approach not only supports healthier outcomes but can also reduce the need for extensive treatments later on.
Through this interdisciplinary connection, we ensure our patients receive seamless, well-coordinated care. Regular communication with orthodontic professionals means that decisions about space maintenance, eruption guidance, and timing of braces are personalized and precise. This team-based strategy empowers families, supports long-term oral health, and transforms smiles with both function and esthetics in mind — making every visit to the dental chair part of a thoughtfully designed journey.
Morghan Teeters, DMD Pediatric Dentist
COVER STORY
Pediatric Dental Anesthesia Associates (PDAA)
Dr. Brandon Larkin describes how in-office sedation improves patient’s safety and the quality of dental care
Cover image of Hector Vila, MD, and Brandon Larkin, DDS, courtesy of PDAA.
Drs. Lynda Dean-Duru and Krystle Dean-Duru explain the importance of early diagnosis and intervention
Dr. Jenny C. Jackson explains how the Solea® All-Tissue Laser enhanced her practice .............. 14
✓ EndoSequence BC Pediatric Putty works exceptionally well for pulpotomies
PEDIATRIC SOLUTIONS
Enhance practice efficiency and patient comfort with a comprehensive range of products tailored specifically for pediatric dental care.
✓ EndoSequence BC Liner works during pulpal treatments to add a protective layer over the putty
✓ MINI Diamonds deliver unprecedented access in pediatric cases and patients with limited openings
✓ Brasseler MINI Electric Attachment offers a super miniature head size that provides maximum access
✓ GEM Digital Sensor in size 10 for pediatric patients provides outstanding image quality
SCAN THE QR CODE TO EXPLORE OUR PEDIATRIC FAVORITES PLUS RECEIVE AN EXCLUSIVE OFFER ON THE PEDIATRICS PRODUCT LINE.
Discover why over 2,600 pediatric dentists use Isolite dental isolation in their practice.
Isolite offers pediatric dentists the ability to improve care and productivity during a single-visit. Our advanced technology allows you to address complex and unpredictable patient needs while avoiding those costly call-backs.
Create a positive and anxiety-free environment that helps young patients feel safe and relaxed during their visits, while giving parents confidence and peace of mind.
I could not do what I do as a pediatric dentist without Isolite.
DR. ANNA FENCL
See for yourself!
Beating burnout
The ADA cites that “more than 82% of dentists report feeling major stress about their careers.” In this very competitive and quickly changing world, the responsibilities can often feel like the walls of the office are closing in. Recognizing burnout symptoms and taking steps to calm your emotions can make a huge difference.
First, what does burnout feel like? Just a few signs are:
• Feeling tired, emotionally drained, or unenthusiastic
• Often feeling frustration toward work
• Negative outlook
• Problems concentrating
• Getting sick often
It is important to recognize and treat burnout to avoid issues such as heart disease and diabetes, sleep-related disorders, and in some cases, substance misuse.
Some Ways to Overcome Burnout
Get enough sleep: We’ve all had our nights of staring at the ceiling in bed while mulling over Plan A, Plan B, Plan C, and more, to solve the next day’s problems. Try to break your non-sleeping cycle. For example, ask your doctor about a possible supplement to lull your brain into the sleep cycle, or discover new relaxation techniques.
neighborhood, on the beach, or even doing yoga or stretching can give your mind some time to reset.
Lisa Moler Founder/Publisher, MedMark Media
Detox from technology: Set specific technology-free windows where patient management systems and email notifications are completely turned off.
Eat and drink for health: Remembering to eat and keeping hydrated helps your brain function (improves memory, attention, and problem solving), raises your mood, and boosts your mental abilities.
Exercise: Exercising has been proven to help fight depression. It doesn’t have to take up much time – about 15-20 minutes per day should do it. A walk along a favorite path, around your
Talk to trusted friends and mentors: There is nothing better than finding out that others can empathize with you and confirm that you are not “crazy.” Colleagues can tell you how they have navigated through similar times of burnout, or give some helpful tips, like reduced hours on Fridays or more intentional spacing of appointments. Look for summer dental retreats or workshops that combine professional development with wellness activities. Aside from work, friends or family can just listen, provide some good advice, or go along on that walk or for a quick cup of coffee and a shoulder to lean on. Finding a therapist can also be very helpful in working out your feelings and providing anti-anxiety techniques. Give yourself a break: When you feel that burnout starting to eat away at your stomach lining, decide how you will take care of yourself at that moment. Take a few seconds. Grab your journal, and write a few lines. Go outside of the office and breathe some fresh air or look at the scenery. Research shows even 20 minutes of nature exposure significantly reduces cortisol levels. For more extreme situations, taking one day or a few days off, or a more extended vacation can bring you back with renewed spirits.
The ADA has some interesting resources just for dentists on its Wellness Resources page (https://www.ada.org/resources/ practice/wellness) to help you start dealing with burnout. You can’t always control what happens in your office, but you can control the way you cope, put out those every day inner fires, and move forward to a fulfilling future with a positive outlook.
To your best success,
Lisa Moler Founder/Publisher, MedMark Media
Pediatric Dental Anesthesia Associates (PDAA)
Dr. Brandon Larkin describes how in-office sedation improves patient’s safety and the quality of dental care
Pediatric Dental Anesthesia Associates (PDAA) is a team of board certified physician (MD) anesthesiologists providing sedation services directly and exclusively to pediatric dentists. Having safely served more than 350,000 patients for nearly 2 decades, PDAA serves 700 different pediatric dental offices across 25 states. Recently, during a Sedation Day with longtime partner, pediatric dentist Dr. Brandon Larkin, PDAA’s founding physician anesthesiologist Dr. Hector Vila, and Chief Executive Officer Justin Horne sat down with Dr. Larkin to ask him how in-office sedation has impacted his practice.
Dr. Larkin, can you give us some background on yourself?
I am originally from Flint, Michigan, and completed my undergraduate degree at The University of Michigan-Ann Arbor. Afterward, I pursued my dental degree at The University of Michigan and then further specialized in pediatric dentistry at Miami Children’s Hospital. My education and training have been instrumental in shaping my approach to pediatric dentistry, focusing on providing the best care for children in a comfortable and friendly environment.
Where is your practice located, and how long have you all been serving your community?
My practice is located in New Port Richey, Florida and I have been serving the community for over 10 years. Over that time, we’ve developed strong relationships with families in the area and established a reputation for being a trusted and compassionate dental provider for children.
What attracted you to a specialty in pediatric dentistry?
From the start of my dental training, I was drawn to the idea of working with children to provide a positive experience with the dentist. Pediatric dentistry allows me to combine my love for working with kids with my passion for dentistry. The opportunity to help children establish healthy oral habits and create a positive experience is incredibly rewarding.
What different behavioral management options do you use regularly in your practice?
We use a variety of behavioral management techniques, depending on the child’s age, temperament, and the procedures
being performed. These include positive reinforcement, tellshow-do, distraction techniques, and a sedation option. Our goal is to make sure each child feels safe, comfortable, and at ease during their visit to create a lifetime of good oral health and a positive relationship at the dental office.
How long have you been utilizing an officebased anesthesia option in your practice?
We’ve been offering office-based anesthesia for 10 years. It has not only allowed us to perform more complex procedures
Pediatric anesthesiologist Dr. Hector Vila (PDAA) and pediatric dentist Dr. Brandon Larkin discuss another successful Sedation Day in the office
in a setting where the child is comfortable but also made the parents’ experience better as well.
What prompted your decision to use an independent anesthesia team as opposed to taking sedation patients to a hospital or ASC?
The decision was based on convenience and patient safety. Using an independent anesthesia team allows us to provide sedation in our office, which is less stressful for the child to be in a familiar environment and more convenient for the families. In this fashion, we can provide the care children need without requiring hospital visits.
Why did you decide to partner with Pediatric Dental Anesthesia Associates (PDAA) for your in-office sedation solutions?
We chose to partner with PDAA because they have an outstanding reputation for safety and professionalism. Their team is highly trained — all of their providers are board-certified physician (MD) anesthesiologists with several years of pediatric training. Their experience and credentials ensure positive outcomes for all our patients.
How has PDAA changed your practice since you started partnering with them? How have patients and parents responded?
PDAA has greatly improved the safety and efficiency of our practice. Their team ensures that sedation is administered safely and effectively, reducing the stress on both the patient and the parents. Parents have expressed tremendous relief knowing that their child is in the hands of a board-certified pediatric anesthesiologist and in a familiar environment. Their knowledge and skills have allowed us to treat more patients in a shorter period of time than we otherwise would in a hospital setting. This has helped our patients tremendously since they are not waiting weeks on end in pain or with infections for a hospital operating room to become available.
Having PDAA in my office has also allowed me to pivot away from doing traditional oral sedation. Their techniques are much more effective for me to treat the patients, and I’m able to execute shorter cases with very efficient turnover, so I can help more patients. Shorter cases also benefit the parents because their financial responsibility is much lower, which only adds to the tremendous value that PDAA provides. We regularly schedule 10 to 12 patients with PDAA that normally would have been oral sedation cases, and now we have a much safer day that is finished by 1pm.
How do you determine when a patient is an ideal candidate for in-office sedation with PDAA?
An ideal candidate for in-office sedation is typically a younger child who may have anxiety or difficulty remaining still during procedures, or those who need more extensive dental work that cannot be performed under local anesthesia alone. For their safety and best treatment outcomes, those situations are best done under anesthesia. We also consider the child’s medical history and behavioral needs. Many parents who have special needs children have also expressed appreciation for the option to safely care for their child in the comfort of the office.
How does a typical sedation day flow with PDAA?
A typical sedation day with PDAA starts with a pre-sedation consultation to review medical histories and confirm the sedation plan with the parent. The PDAA team administers the anesthesia, ensuring that the child is comfortable and relaxed before any dental work begins. Throughout the procedure, the PDAA
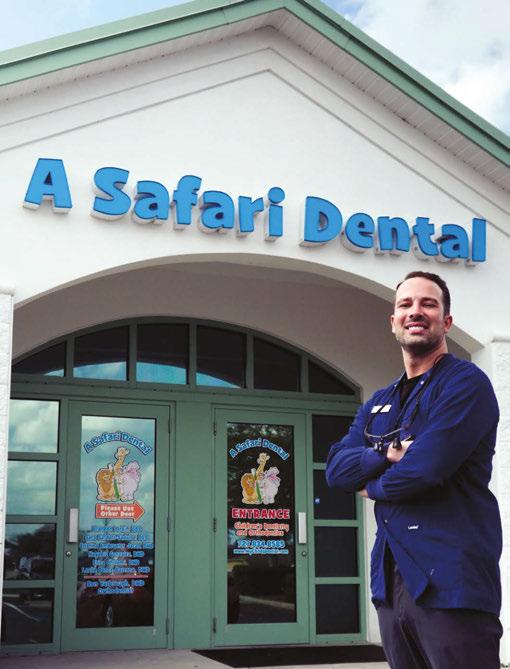
Pediatric dentist Dr. Brandon Larkin of A Safari Dental in New Port Richey, Florida
team monitors the child’s safety closely, allowing me to focus on the dental procedures. Afterward, the child is monitored until they’re awake and ready to go home with their parents.
How safe and efficient does your dental work feel during the cases with PDAA?
The cases feel incredibly safe and efficient. PDAA provides a level of expertise that allows us to focus on the dental procedures while they handle the sedation process. This partnership ensures that both the patient’s safety and the quality of the dental care are always our top priorities. I’m proud to say we have done thousands of cases over the last decade all with positive outcomes.
“PDAA has revolutionized the way we care for our patients. Previously, our options were cumbersome, inefficient, or financially burdensome for our patients. With PDAA, they now receive care from a highly skilled team of professionals within a system that is safe, reliable, efficient, and reflective of our practice’s patient-centered values.” — Dr. Richard Facko, pediatric dentist, Palos Pediatric Dentistry, Palos Heights, Illinois
Would you recommend Pediatric Dental Anesthesia Associates to your colleagues?
Absolutely! I highly recommend PDAA to my colleagues. Their professionalism, expertise, and commitment to patient safety are exceptional, and they have truly enhanced the quality of care we’re able to offer our young patients. It’s been a gamechanger for our practice as we are able to complete twice as many cases in a day than in a traditional hospital setting. This shortens the wait time for our patients so they are not waiting on OR time while in pain or with dental infections.
About PDAA
Pediatric Dental Anesthesia Associates (PDAA) is the nation’s largest pediatric anesthesia practice solely focused on pediatric dental patients. PDAA outfits each Sedation Day with a physician anesthesiologist, all of the essential equipment (monitoring, medications, emergency), 1-2 pediatric nurses for pre-op and recovery, and the necessary liability insurance. Thirty percent of their patient base includes special needs children. There are no narcotic/opioids used, and cases are typically turned over in 10 minutes or less. PDAA’s administrative team facilitates all patient
payments, financing options, insurance assistance when applicable, and supports the clinical professionals in medical screening/ clearance so pediatrician visits are not necessary. Pediatric dental offices across the country regularly schedule sedation days with PDAA weekly, monthly, quarterly, or as needed depending on their practice needs.
For more information, please visit pediatricsedation.com or contact CEO Justin Horne at 813-480-1857. Be sure to check out their Google Business listing for nearly 3,000 5-star reviews from previous satisfied parents. PD
Beyond First Latch: the role of dentists in ensuring proper growth of the craniofacial-respiratory complex from infancy
Drs. Lynda Dean-Duru and Krystle Dean-Duru explain the importance of early diagnosis and intervention
The connection between breastfeeding and craniofacial development begins remarkably early, setting the foundation for proper sleep and breathing patterns throughout life.
Many babies have restrictions that make it difficult, sometimes impossible, to breastfeed. Typically, these situations involve anatomic, functional, and sometimes neurological issues with the baby. The tongue acts as a natural pump while breastfeeding and drives the development of the face, jaws, and airway, and when tongue function is compromised, breastfeeding, breathing, sleep, and the growth of the face and jaws are adversely affected.
Where does it all start?
At 4 weeks gestation, the neural tube is specializing, mesoderm growing the vascular system and seeding the skeletal, and endoderm invaginating into the gut tube. The endoderm is also forming the pharyngeal pouches, which contain the neuro/meso/ skeletal blueprints for the face, mouth, and throat. Neural crest cells are migrating through all tissues, illuminating cranial nerve
Lynda Dean-Duru, DDS, pursued a degree in dental surgery from the University of Benin in Nigeria and continued her training in the United States, completing her general practice residency at Howard University Hospital and pediatric dentistry specialty training at Children’s National Medical Center. She holds board certification from the American Board of Pediatric Dentistry, Mastership from the World Clinical Laser Institute, and Fellowship Laser Certification from the Academy of Laser Dentistry. In 2000, Dr. Lynda established Ashburn Children’s Dentistry in Virginia and now, Womb2Grow Wellness LLC with a mission to provide comprehensive, holistic dental care for children and promote overall well-being. From the very beginning, she focused on early intervention, starting by helping moms with breastfeeding and nursing difficulties through tongue and lip-tie releases using laser technology. Dr. Lynda was a pioneer, bringing laser dentistry to Ashburn and mentoring countless dentists and dental professionals along the way. She is certified in Advanced Light Functionals (ALF) therapy, a treatment that uses brain-friendly custom-made appliances to promote proper neurology, craniofacial development, and optimal airway function, and is a member of the prestigious Gnathos Orthodontic Education Group and a Fellow at the United States Dental Institute.
Krystle Dean-Duru, DDS, followed in her mother’s footsteps. With a bachelor’s degree in psychology from Columbia University and a dental degree from Virginia Commonwealth University, Dr. Krystle further honed her skills during her specialty pediatric residency at the Interfaith Department of Dental Medicine in Brooklyn, New York, where she served as Chief Resident. Her specialized training includes pediatric dental sleep medicine, airway orthodontics, and functional frenuloplasty. She is a Diplomate of the American Board of Pediatric Dentistry.
The brainstem is a stalk-like projection of the brain extending caudally from the base of the cerebrum, bridging communication between the cerebrum with the cerebellum and spinal cord.1,2 It has three sections: midbrain, pons, and medulla oblongata, combining to maintain functions necessary for life, such as breathing, consciousness, maintaining blood pressure, heart rate, and sleep regulation.
The brainstem contains both collections of white and grey matter: The grey matter consists of nerve cell bodies and includes important brainstem nuclei; for example, 10 of the 12 cranial nerves’ nuclei originate there. The white matter tracts involve neuron axons traveling between the cerebrum, cerebellum, and spinal cord to the peripheral nervous system. These tracts carry information to the brain (afferent pathways, such as the somato-
sensory pathways) and from the brain (efferent pathways such as the corticospinal tract).3
State of ideal development
People are born obligate nose breathers. For survival, the baby needs to be able to suck-swallow and breathe. The important steps include: first breath, breast crawl, and breastfeeding, which all help decompress the cranium, setting the stage for graceful transition of the autonomic nervous system as well as loosening the fascia connections. The healthy swallow is most critical in re-igniting and maintaining rhythmic motion and, with breathing, coordinates fascia, visceral motion, and the brainstem.
Birth trauma and developmental challenges
It follows then, that intrauterine factors, birth trauma, and intervention could affect these important areas and compromise function and structure. These include the normal process of descent through the birth canal, abnormal position of the baby, and interventions such as epidural and pitocin, which increase compressive forces via stronger contractions. Others are caesarean births, vacuum, and/or forceps-assisted deliveries. These can lead to somatic dysfunction, notably, occipital condylar compression/dysfunction.5
With extra compressive forces, the skull bones and the surrounding fascia can affect the function of the nerves and muscles. The occipital bone, which at this stage is in four parts, is in close proximity to the vagus and hypoglossal nerves, which partially control tongue function, breathing, rest, and digestion. Cranial nerves IX (glossopharyngeal and XI (accessory nerve) are in close proximity as well.
Symptoms of occipital condylar compression
Occipital condylar compression manifests through various interconnected symptoms affecting multiple bodily functions. Common manifestations include difficulties with nursing, sucking, and swallowing, often accompanied by digestive issues such as reflux, vomiting, and colic. Respiratory challenges frequently arise, and patients may experience constipation and bloating. Physical manifestations can include torticollis, and many infants display notable irritability as a result of these combined challenges.
Where it goes wrong
Somatic function, early cranial nerve mapping, and integration are most critical for successful breastfeeding, and problems are best detected and treated within 24-48 hours after birth. Breastfeeding is a baby’s innate function and should be effortless. Suck, swallow, and nasal breathing set the foundation of good function and flow throughout the body.
Infant symptoms for compromised tongue function and breastfeeding
Infants experiencing compromised tongue function display a complex array of feeding-related symptoms. During breastfeeding, they often exhibit clicking sounds, chomping or gumming behaviors, and struggle to maintain proper flange formation. The latch is typically shallow and frequently slides off the nipple, leading to extended feeding times and frequent sleep episodes at the breast. These babies commonly show signs of acid reflux, notably clicking sounds and air swallowing during nursing,
accompanied by frequent feeding sessions and excessive spit-up. Digestive issues manifest through gassiness and hiccups, while nursing blisters may develop. The inadequate milk transfer often results in slow weight gain and, in severe cases, failure to thrive. Physical manifestations include a preference for feeding on one side and development of a high vaulted palate. Breathing difficulties become apparent through open mouth posture, heavy breathing patterns, and inability to retain a pacifier. Sleep disturbances often present as congestion upon waking, along with snoring. Skin manifestations such as baby acne or rash may also occur.
Maternal symptoms during breastfeeding
Mothers experiencing breastfeeding challenges due to infant tongue dysfunction face a range of physical and emotional difficulties. Physical symptoms predominantly affect the breast and nipple area, including soreness and discomfort, creased or lipstick-shaped nipples, and flattened nipples. More severe complications can develop, such as plugged ducts, open wounds, and mastitis. Many mothers struggle with low milk supply and may need to resort to using nipple shields. The presence of inverted nipples can further complicate the feeding process. The persistent physical challenges, including ongoing nipple pain and repeated episodes of mastitis, often contribute to low milk supply and can lead to depression.
Differential diagnosis for difficulty breastfeeding
The challenges in breastfeeding can stem from various underlying conditions and factors that require careful consideration for proper diagnosis. Primary physical factors include fascial restrictions resulting from in-utero positioning or traumatic birth experiences, along with occipital condylar compression. Oral structure issues such as restrictive tethered oral tissues, which can be either functional or structural in nature, play a significant role. Additionally, conditions like hypotonia, laryngomalacia, and Pierre Robin sequence can impact feeding ability. Structural abnormalities such as cleft palate and/or cleft lip must be considered, as well as complications related to prematurity. Maternal metabolic issues can also contribute to breastfeeding difficulties, highlighting the importance of examining both infant and maternal factors in the diagnostic process.
The importance of early intervention and proper diagnosis is foundational in a child’s lifelong, overall health. It’s critical that healthcare providers, particularly dentists, understand these developmental processes as they directly impact craniofacial development for the children we treat, so we can set them up for a healthy and happy life.
REFERENCES
1. Haines DE. Fundamental neuroscience for basic and clinical applications. 4th ed. Elsevier Saunders; 2012.
2. Netter FH. Atlas of human anatomy. 6th ed. Elsevier Saunders; 2014.
4. Nolte J. The Human Brain: An Introduction to its Functional Anatomy. 3rd ed. Mosby; 1993.
5. Tobey AH, Kozar AJ. Frequency of Somatic Dysfunction in Infants With Tongue-Tie: A Retrospective Chart Review, AAO Journal. 2018;28(4):10–14. https://doi.org/10.53702/ 2375-5717-28.4.10
6. Bonuck K, Freeman K, Chervin RD, Xu L. Sleep-disordered breathing in a population-based cohort: behavioral outcomes at 4 and 7 years. Pediatrics. 2012 Apr;129(4):e857-865. doi: 10.1542/peds.2011-1402.
A game-changer in clinical excellence
The Solea Laser has also elevated Dr. Jackson’s clinical capabilities. Procedures that once required invasive techniques or referrals can now be completed in-office with greater precision and better patient outcomes.
“Previously, I would have placed stainless steel or zirconia crowns on certain first molars,” she explains. “With Solea, I can conservatively restore them with resins with incredible predictability and beautiful outcomes.”
The laser has also enabled her to expand into new treatment areas, including frenuloplasties, hemangioma removals, bloodless tooth exposures, and other soft tissue surgeries. Patients have increasingly sought her expertise, even traveling internationally for treatment, further validating the value this technology has brought to her practice.
A strong return on investment
Though Dr. Jackson invested in the laser for its clinical and patient-care benefits, the financial benefits became evident quickly. Despite acquiring it just before the COVID-19 shutdown, her practice rebounded strongly, going from a 36% revenue decline in Q2 of 2020 to closing the year just 1% below 2019 levels, even with having to close half her open-bay chairs for distancing during that period.
Some of the key financial impacts included:
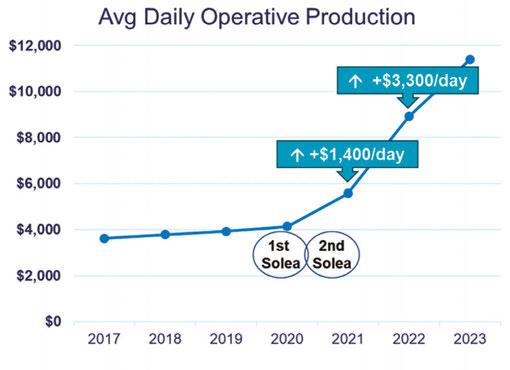
• Increased operative production: Her average daily operative production grew by $1,400 per day in the first full year with Solea, and total production was up over $800k.
• Expanded treatment options: In addition to increasing restorative and operative efficiencies, the laser allowed Dr. Jackson to perform a wider range of soft-tissue procedures, further increasing practice revenue.
• Efficiency gains and new patient flow: The laser streamlined workflows, allowing more patients to be treated daily and more procedures per patient. She saw a 53% growth in new patient starts in her first full year with Solea.
• Work-life balance: By optimizing productivity, Dr. Jackson was able to reduce her workdays while still increasing production.
“At the end of my first year with Solea, I asked my accountant if I should pay off the first laser. She said, ‘No, you should get another one.’ So, we did — and we saw even more growth.”
The second laser allowed her and her associate to seamlessly integrate the technology into each of their workflows, ensuring that every patient benefits from the best available treatment.
Her message to fellow dentists is clear: If you do what is right for every patient, as an individual, every time, everything else falls into place. The financial aspect works itself out by doing the right thing for the patient.
“While you have to conserve resources and have a budget, you must always do what’s in the best interest of your patients. If you do, and that’s truly where your heart is, it’s felt. It’s palpable in the energy of your practice and in all you do. Solea allows you to take this mentally to the next level, providing compassionate care that feels good and is better for the patient and their families, resulting in superior outcomes as well. It’s beautiful how we can stay truly present and love the care we are providing, knowing it’s unlike anything previously available.
“Parents ask me all the time, why isn’t everyone doing this (offering Solea)? I tell them, that I believe they will be, once they realize the true impact of this laser and how it changes their level of care for their patients.” This information was provided by
Dr. Jackson (center) and her team at Asheville Pediatric Dentistry
Ormco™ announces the launch of Spark™ Retainers and Spark BiteSync™ Class II Corrector System
Ormco Corporation, announced the official launch of Spark™ Retainers and BiteSync Class II Corrector in the United States. Developed for doctors and patients, Spark Retainers bring a new level of comfort, durability, and clinical flexibility to orthodontic retainers whether treating with Spark™ Clear Aligners, Ormco Digital Bonding, or fixed brackets. With the debut of BiteSync, Spark now offers an innovative solution for mandibular advancement for Class II patients in growing stage and for adults, consisting of the Occlusion Guide for mandibular advancement and the SideBar for maxillary distalization, which can be used combined or separate. The BiteSync system allows a flexible workflow customized for each patient’s needs and added simplicity within the Spark software.
For more information on Spark Retainers, visit https://ormco. com/en-us/spark-retainers. For information on BiteSync, visit https://ormco.com/en-us/spark-clear-aligner-solution#BiteSync.
Orion Innovations announces that its NoGag® Gag Reflex elimination solution achieves 2,000th dental office milestone
Orion Innovations, a healthcare technology platform company, highlighted that the 2,000th dental practice has adopted its breakthrough product, NoGag. The five-time patented consumable powder — a unique mixture of salt and citric acid — begins working in only 10 seconds and eliminates the gag reflex from patients for a minimum of an hour. With no contraindications for age and no allergens, NoGag stands poised to change the global dental and medical fields forever for adults and children alike. NoGag is a smart, simple, and stress-free solution that has proven to eliminate the gag reflex, which improves patient experience, and it enables dentists to capture lost patients, procedures, and revenue. As many as 8 percent of patients gag every time they are in the dentist’s chair, with 50% gagging at least once. As a result, these individuals have procedures fail or delayed, all while dealing with rising oral safety issues, costs, and pain.
NoGag was developed by Robert Olson, DDS, a dental professional of over 3 decades, who saw the gag reflex’s impact on his patients along with the cost of lost patients and revenue. Made in the US, and available in over 20 major markets across the US and EU; NoGag is expanding quickly into the Middle East and Southeast Asia.
To learn more, visit https://www.orioninnovationsgroup.com.
Convergent Dental reaches 2,000 Solea Dental Lasers across North America
Convergent Dental, a privately owned dental equipment and technology company whose flagship product is the Solea® All-Tissue Dental Laser, announced the installation of the 2,000th Solea laser. This significant milestone underscores the rapidly growing adoption of Solea among dental professionals across North America. Solea, the only 9.3-micron CO2 laser, has elevated the way dentists deliver care by enabling anesthesia-free, blood-free, and pain-free procedures in hard and soft tissue. Its versatility allows dentists to expand their treatment offerings, enhance clinical outcomes, and increase efficiency, including more same-day and multi-quadrant dentistry. Patients benefit from less discomfort and anxiety, fewer appointments, and an overall improved dental experience. Solea®, is the only CO2 laser to be cleared by the FDA for all-tissue indications.
For more information about Solea, visit www.convergentdental.com/solea.
Dentsply Sirona takes Primescan 2 to the next level
Dentsply Sirona has announced major enhancements to its Primescan 2. Only 6 months after the initial introduction of Primescan 2, the first cloud-native intraoral scanning solution has an additional emphasis on seamless connectivity, faster workflows, and smarter integrations. Primescan has implemented these next-level enhancements:
• Integrated caries detection: Featuring advanced near-infrared and fluorescence technologies, complementing conventional methods to help clinicians effectively identify and successfully treat caries, and help patients better understand their treatment needs via DS Core.
• Optimized Smart Compression: Cutting bandwidth requirements by up to 50% and making Primescan 2 more accessible without additional infrastructure and therefore simplifying installation procedures.
• Faster SureSmile® simulations: The automatic initiation of tooth segmentation and smile simulation right after taking a Primescan 2 treatment scan reduces calculation times by up to 90%, allowing for a more efficient patient consultation.
For more details about Primescan 2, visit www.dentsplysirona.com/primescan2.
Simplifying Space Maintainers: a faster, smarter approach
Dr. Ben Curtis breaks down how Universal Chairside Space Maintainers reduce time, hassle, and complexity in pediatric dentistry
Space maintainers have been an important part of preserving the developing arch length in our pediatric patients for generations. The simplification of the unilateral spacer has been revolutionized by the release of the Universal Chairside Space Maintainer. The long-standing lab-created unilateral (Band and Loop) space maintainer can have an excellent fit and makes a strong, sturdy appliance. The downside of the lab-created Band and Loop is that it requires a model to be created of the area and an additional appointment to deliver the appliance. This additional appointment can create a barrier for the patient due to time missed from school, hours missed from work for the parent, and additional chair time for the clinician.
This barrier of time was overcome by the introduction of a chairside space maintainer system where the band has an attached pre-soldered or welded tube and a custom trim and fit wire loop to slide into the tube that is then crimped tight. Several of these systems have been utilized over the years, but there are so many pieces that have to be ordered and stored that it can be confusing and frustrating. Some of these systems have bands for upper molars and then bands for lower molars that come in both wide tube sizes and narrow tube sizes. There are plain wires and curved wires that have to be ordered in narrow and wide. There are so many parts that it can make using a chairside spacemaintainer system inefficient and cumbersome.
With the introduction of the NuSmile Universal Chairside Space Maintainer, many of these frustrations are resolved, and the process is simplified. The NuSmile system utilizes the same universal band for both the upper and lower arches. This eliminates the need for the storage, ordering, and hassle of having maxillary and mandibular bands like other systems, all while still creating a good fit and adaptation to the tooth. There are no wide and narrow wire/loop sizes, so that helps to once again streamline and simplify the process of making
Ben Curtis, DDS, graduated as valedictorian from Wills Point High School in Texas before earning a summa cum laude degree in Biomedical Sciences from Texas A&M University. He continued his education at Baylor College of Dentistry, where he was honored with induction into the Omicron Kappa Upsilon Honor Society. Dr. Curtis then completed his pediatric residency at Children’s Medical Center in Dallas, Texas, Scottish Rite Hospital for Children, and Baylor College of Dentistry, where he was recognized with the Provider of the Month award and awarded the prestigious AAPD Harris Fellowship. He is passionate about children’s healthcare advocacy and is a Board-certified Pediatric Dentist and a Diplomate of the American Board of Pediatric Dentistry.
Figure 1 (above): Preoperative periapical radiograph of tooth number B with a large distal radiolucency that is approximating the pulp. Patient is reporting significant pain. Figure 2 (below): Placement of NuSmile Universal Chairside Space Maintainer to preserve the arch length for extracted tooth number B
them chairside and also having to order additional pieces to keep stocked. The metal tube on the band of the NuSmile Universal Chairside Space Maintainer is also shorter in length than other space maintainers. This reduces the time and hassle of having to trim the tube to make it shorter so it will fit in a smaller space.
By being able to simplify the process of fabricating a unilateral space maintainer chairside, the provider is able to more efficiently manage the chair time for the patient. It is possible for these to even be quickly placed on sedated patients or in the operating room. By reducing the parts and pieces needed to create a unilateral spacer maintainer, the provider’s team will have less to order, less to store, and less to keep up with. All in all, the NuSmile Universal Space Maintainer is more efficient for the provider, less fussy for the team, and a great service for the patient. For my practice, that’s a win-win-win!
This information was provided by NuSmile. PD
The importance of calcium hydroxide in dental trauma cases
Dr. Sonia Chopra illustrates her treatment of tooth avulsion in a teenager
Dental trauma is unfortunate and can be scary for patients because it can happen to anyone and at the most inopportune times. As a dental provider, I am so happy that I know the exact steps to handle this situation so I can help a patient (or loved one) through the chaos of a traumatic incident. I invite you to share this knowledge with all of your patients too — you never know when they may need it.
In my opinion, the most traumatic of all dental injuries is the avulsion, when the tooth is completely dislodged from its socket, aka, “the knocked out tooth.” This type of injury typically happens to young children in the anterior region of the mouth, so it is not just traumatic for the child, but for the parent as well. As a mother myself, I can empathize. With the knowledge that I have, I can feel confident that everything will be okay. Being able to tell a parent, “We can fix this,” is pure gold in a moment like this. However, we must adhere to a particular protocol to be able to guarantee such a tall order. In conversation, the clinician can try to calm and support the parent, with comments such as, “I don’t know who the trauma is worse for, the child or the parent.” “These teeth didn’t actually come out completely, and they were still able to soak in his own blood.” “Don’t give up hope; we see a lot of these types of traumas, and we’re able to restore their smiles.”
The following is a truly successful tooth story that outlines a scenario of a very scary moment for both mother and child, and how my team and I were able to put things back together as if no trauma happened at all.
A teenager’s avulsion tooth story
This 14-year-old boy was play-fighting with his brother in the kitchen with a broom. That broom hit him in the face and knocked out his front teeth.
Sonia Chopra, DDS, was the first female board-certified endodontist in Charlotte, North Carolina, where she founded Ballantyne Endodontics in 2008. As a mentor and impact entrepreneur, Dr. Chopra improves endodontic education for general dentists, dental residents, and patients. She is a TEDx speaker, Dentistry Today and Forbes contributor, and the author of Tooth Wisdom, a book designed to inform and empower patients in their own oral health. She teaches endodontists how to grow their practices and improve efficiencies in their workflows, so they can be more effective and profitable through her Heal Your Practice program. Dr. Chopra is also co-founder of A Night for Smiles, a gala bringing Charlotte-area dentists together to support dental health initiatives. She is an active member of the American Association of Endodontics and is a Key Opinion Leader for Sonendo, Dentsply Sirona, J Morita, and Kerr. When she’s not treating patients or teaching dentists about endodontics, she loves to travel, garden, and spend time with her family. Follow her on Instagram at @drsoniachopra.
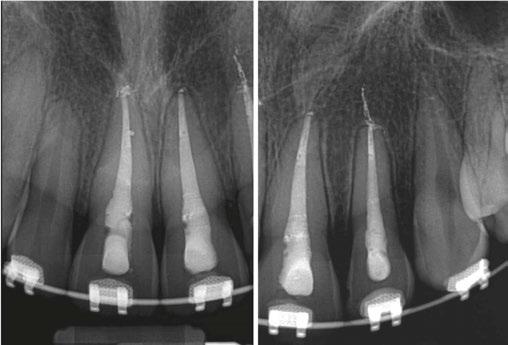
Luckily, the young boy was undergoing orthodontic treatment so the avulsed teeth remained in the oral cavity. As you can see from the clinical photograph in Figure 1, teeth Nos. 8, 9, and 10 would not have remained in the mouth if the orthodontic wire was not in place.
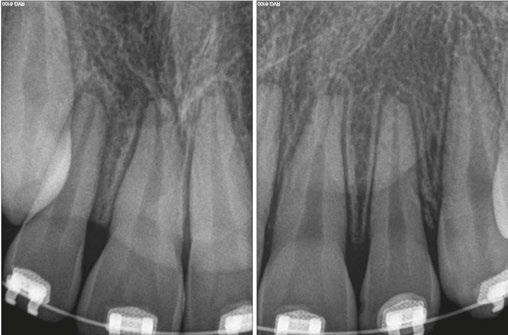
Two days after treatment, the patient was seen in my practice after the teeth were splinted back in place by the orthodontist. Figures 2A-2B are the preoperative radiographs after the teeth were reimplanted.
One can already appreciate the inflammatory resorption that is occurring at the apices of teeth Nos. 9 and 10. These images were taken just two days after the trauma.
My goal at the first visit was to understand the trauma with respect to the extraoral dry time of the teeth (how long were
Figure 1
Figures 2A-2B
There was some sealer extrusion at the apex of these teeth (Figure 7), especially 10, but this was due to the inflammatory resorption occurring at the apex as a result of the trauma, which started to eat away the apical stop. I am confident that, over time, this sealer will resorb away, and this extrusion should not impede the healing at all. Figure 8 is the final outcome of the case.
And now that the patient is stable, he can go back into his brackets and orthodontic wire. Figure 9 is him 6 months later, and we will continue to follow him up for the next 5 years.
Top tips to keep in mind
Dental trauma is distressing for patients and their loved ones, but when you can confidently reassure them that they’re in good hands, you’ll help them feel safe. And posttreatment, you’ll be their hero.
Some key points to remember following avulsion is:
1. Stabilize the teeth and get a baseline for your diagnostic tests.
2. Start root canal therapy 7–10 days after the trauma to preserve the PDL and avoid inflammatory resorption.
3. Place calcium hydroxide in the teeth as the first step.
4. Keep the teeth medicated (the medication may need to be replenished over time).
6. Follow up with the patient after 1 month, 3 months, 6 months, 1 year, 2 years, 3 years, 4 years, and 5 years.
REFERENCE
1. Zare Jahromi M, Kalantar Motamedi MR. Effect of calcium hydroxide on inflammatory root resorption and ankylosis in replanted teeth compared with other intracanal materials: a review. Restor Dent Endod. 2019 Aug 1;44(3):e32.
5. Once the teeth are no longer tender to percussion and the PDL looks normal radiographically, the teeth may be obturated.
Figures 9A-9B
experience and every decision that influences a team’s culture. From the front office administrator who manages scheduling efficiency, to the hygienist who educates patients and supports treatment acceptance, to the associate dentist managing chairside dynamics — every team member impacts the overall success of a practice.
Yet these professionals are rarely given formal training in conflict resolution, change management, communication strategy, or operational improvement. This lack of leadership development is a missed opportunity not just for individual growth, but for organizational excellence.
By embedding leadership training across all team levels, practices and DSOs can build a culture of shared accountability, continuous improvement, and adaptive problem-solving. Empowered teams are resilient teams — and resilient teams are those that can navigate staffing shortages, integrate new technologies, respond to shifting payer models, and deliver better outcomes under pressure.
The Serendequity Solution: Mini MBA and LEAP Certificates
Serendequity Education’s Mini MBA and LEAP programs were created to address this urgent gap with precision and practicality.
The Mini MBA for Dentistry
This intensive, modular online program is designed for dentists and staff, specialists, practice owners, and DSO executives seeking a comprehensive foundation in business disciplines essential to healthcare leadership. With 12 interactive modules — including financial management, marketing strategy, team dynamics, operations, legal compliance, and strategic planning — the Mini MBA provides real-world tools rooted in dental practice realities. Through capstone projects and case-based learning, participants do not merely absorb knowledge, they apply it — building business plans, operational improvements, and leadership strategies that can be deployed immediately in their settings.
The Serendequity Education Mini MBA for Dentistry is an innovative, industry-tailored certificate program designed to equip dentists, hygienists, and dental leaders with core business competencies to thrive in today’s rapidly evolving dental landscape. This online, self-paced curriculum offers a practical, high-impact educational experience and essential tools to lead, grow, and future-proof dental practices and organizations.
At its core, this Mini MBA bridges the long-standing gap between clinical training and business knowledge in dental education. With deep roots in real-world practice scenarios and trends, this program empowers dental professionals to make data-informed decisions, navigate competitive pressures, and create scalable, patient-centered businesses. It is a critical step forward in redefining how dentistry prepares its current and future leaders.
Leadership Excellence to Advance Practice (LEAP) Certificates
Targeted toward all dental professionals — dentists, hygienists, assistants, and administrative leaders — LEAP focuses on ele-
To thrive in the future of healthcare, every member of the dental team must be equipped with knowledge, skills, abilities, and judgment that transcend the operatory.”
vating leadership capacity within teams. These shorter, focused certificates develop core skills in emotional intelligence, decision-making, team building, coaching, and adaptability. LEAP cultivates confident, collaborative professionals who understand how to inspire others, align around vision, and foster cultures of trust, innovation, and excellence.
Both programs are designed with flexibility in mind: online, asynchronous, and accessible to working professionals. They combine world-class faculty with evidence-based frameworks ensuring that content is both cutting-edge and grounded in dental practice.
Value proposition for the dental industry and profession
Bridging the business education gap in dentistry
Most dental curricula prioritize clinical expertise but neglect business acumen. As a result, many dentists enter practice ownership or leadership roles ill-equipped to manage operations, finances, or strategy. The Serendequity Mini MBA directly addresses this gap by offering business and management education specifically contextualized for the dental industry. Unlike traditional MBA programs, this certificate is lean, focused, and immediately applicable — helping participants lead with confidence from day one.
Strategic preparedness for a changing industry
The dental profession is undergoing significant transformation:
• Consolidation and the rise of DSOs: The Mini MBA offers insights into how to collaborate with, compete against, or even build a DSO, including practical tools for assessing affiliation and acquisition opportunities.
• Technology-driven disruption: From teledentistry to AI, participants learn how to evaluate, adopt, and leverage technologies that enhance productivity, reduce overhead, and elevate the patient experience.
• Consumer expectations and patient-centered care: The curriculum trains participants to develop marketing strategies, service excellence frameworks, and patient feedback systems that drive retention and satisfaction.
Practice performance optimization
The modules on financial management, team dynamics, operations, and marketing help practitioners:
• Analyze P&L statements and manage cash flow
• Build and retain high-performing teams
• Streamline workflows using lean principles
• Attract and retain patients using data-driven marketing
• Increase profitability while delivering high-quality care
These are not theoretical skills; they are mission-critical for any practice owner, associate, or DSO leader aiming for sustainable growth and resilience.
Empowering clinicians as leaders
The Mini MBA cultivates leadership capacity by introducing proven frameworks in change management, organizational behavior, and strategic planning. Participants learn how to adapt their leadership styles to different situations, manage conflict, align teams around a shared vision, and drive performance in a clinical setting.
Curriculum overview
The Mini MBA spans 12 core modules delivered in a dynamic, flexible online format. Each module features video lectures by dental and business experts, interactive tools, real-world case studies, assessments, and peer discussion forums.
Highlights include:
Modules 1–3: Foundation in Business, Finance, and Leadership
• Business Foundations for Dental Practices
• Financial Management Essentials
• Leadership in Dental Practice
Modules 4–6: Team, Communication, and Marketing
• Team Management and Communication
• Marketing Strategies for Dental Practices and DSOs
• Patient Experience and Relationship Management
Modules 7–9: Operations, Legal, and Strategy
• Operational Excellence in Dental Practices and DSOs
• Legal and Ethical Considerations
• Strategic Planning in Dental Practices and DSOs
Modules 10–12: Financial Planning and Capstone Project
• Financial Planning and Investment
• Capstone Business Plan Project
• Professional Reflection and Integration
The Capstone Project is a distinctive feature, allowing learners to develop and present a real-world business plan addressing a current challenge or opportunity within their own practice or the broader industry.
Differentiators and Innovation
• Dental-specific, practitioner-focused: Unlike generic business programs, every topic is translated for dental application — using dental-specific examples, case studies, and metrics.
• Expert-led and evidence-based: Instruction draws from Harvard Business Review, McKinsey, ADA policy, and successful DSO operators. This ensures that learners receive best-in-class thinking tailored to their world.
• Flexible, asynchronous learning: Designed for busy professionals, this online model supports learning on-demand while still enabling community interaction through discussion forums and coaching sessions.
• Scalable across roles and organizations: The program is valuable not only for private practitioners and owners but also for emerging leaders in DSOs, group practices, and
even dental schools seeking to embed leadership into predoctoral curricula.
Professional impact and career relevance
Graduates of the Serendequity Mini MBA will be equipped to:
• Launch or expand successful private practices or DSOs
• Increase efficiency, profitability, and patient satisfaction
• Lead multidisciplinary teams with clarity and purpose
• Make strategic financial and operational decisions
• Explore new career paths in executive leadership, consulting, or education
In a field where business illiteracy can hinder career progression, this program becomes a strategic enabler of growth, security, and fulfillment.
Equipping the profession for the future
As we enter an era of precision health, artificial intelligence, value-based care, and growing integration between oral and systemic health, the expectations placed on dental professionals will only increase. To lead in this new age, our profession must rethink how we define excellence.
• Excellence is no longer just about clinical outcomes; it is about organizational agility.
• Success is no longer just about solo achievement; it is about team empowerment.
• Impact is no longer limited to the dental chair; it is measured by systems thinking, strategic foresight, and the ability to lead change.
The Serendequity Mini MBA and LEAP programs offer a clear path forward. They democratize access to elite business and leadership education and bring it into the hands of those who need it most — practicing dental professionals and staff navigating real-world complexity.
Conclusion
The dental industry stands at an inflection point. Clinical skill will always be the foundation of dental medicine, but it is no longer sufficient to ensure success. Business literacy and leadership excellence must now be core competencies for every member of the dental team. Whether navigating the complexities of private practice, driving performance in a DSO, or preparing students in dental education, the need for strategic, empowered, and adaptive leaders has never been greater.
Serendequity Education’s Mini MBA and LEAP certificates are more than programs — they are movements. They represent a shift in how we prepare dental professionals for impact, resilience, and sustainable success. By embracing business and leadership education, the dental profession will not only meet the demands of today; it will shape the healthcare systems of tomorrow. As the profession evolves, so too must the way we prepare our clinicians — not just to drill, fill, and bill — but to lead, build, and grow.
This is not optional education — it is essential. Serendequity Education prepares people not only to survive the future of dentistry but to shape it. PD
Are we meeting our patients’ individual needs?
Dr. Kelly Tanner discusses how to help patients make informed decisions
As dental professionals, we often fall into the routine of giving standardized advice: “Remember to floss daily,” “Try to limit those sweets,” and “We’ll keep watching this area.” While these recommendations aren’t wrong, they over look a crucial fact — every patient sitting in our chair brings unique challenges and risk factors.
Our patients trust us to be their oral health advocates. They rely on us to not only identify problems but also to help them understand the connection between their habits and their oral health outcomes. Without comprehensive information tailored to their specific situation, how can they make informed decisions about their care? We typically see our patients for just 2 hours each year. The real question becomes: How are we supporting their oral health journey during the other 8,758 hours?
Let’s explore three key areas where we can provide more individualized care:
Understanding the nutrition connection
When we take time to provide targeted nutritional counseling, we help patients grasp how their food choices impact both their gingival health and oral pH levels. This goes beyond simply saying, “Watch your sugar intake.” We can educate them about the surprising acidity of alternative sweeteners and help them make informed dietary choices that benefit both their oral and overall health.
Staying current with medical changes
Six months between visits is plenty of time for significant changes in a patient’s health. As dental professionals, we’re often the first to identify systemic health changes through oral manifestations. Over 80% of our patients take medications that cause xerostomia, fundamentally affecting their mouth’s ability
Kelly Tanner, RDH, PhD, is a renowned leader and pioneering force in transforming dental care and fostering professional growth within the industry. She holds a Ph.D. in Business and Leadership and leverages her expertise to empower dental teams. As a sought-after consultant and trainer, Dr. Tanner specializes in developing sustainable systems for enhanced productivity and accountability, cultivating a culture of ownership in case acceptance, and strengthening patient-team relationships through trust-building strategies. Recognized for her ability to inspire and motivate, Dr. Tanner has catalyzed positive change in dental practices nationwide. Her work consistently results in more engaged teams, satisfied patients, and thriving practices. Dr. Tanner can be reached at www.drkellytanner.com.
to buffer, remineralize, and maintain healthy tissues. By staying alert to these changes, we can make timely referrals and help patients understand how their medications might impact their oral health.
Providing effective take-home solutions
Our care shouldn’t stop when patients leave the office. Recommending personalized protective products can help bridge the gap between visits. While electric toothbrushes and remineralizing agents are valuable, products like Profisil® by Kettenbach offer unique benefits. This innovative fluoride treatment uses a non-allergenic dimethicone formula that patients actually look forward to receiving — a welcome change from traditional varnishes that leave them counting the hours until they can brush it off! The smooth, non-sticky application makes it especially popular among our patients who previously declined fluoride treatments due to texture concerns.
What sets Profisil apart is its sophisticated delivery system. Not only does it occlude dentinal tubules, but it also deposits calcium fluoride crystals, achieving deeper remineralization than traditional varnishes. The dimethicone formula continuously releases fluoride ions for up to 24 hours, providing extended protection without the uncomfortable sticky residue that patients typically associate with fluoride treatments. The fact that it can be applied to wet surfaces and doesn’t require prior prophylaxis for effectiveness makes it a practical choice for both clinicians and patients alike.
The key to providing exceptional care lies in recognizing and responding to each patient’s individual risk factors. By tailoring our approach to their specific needs, we can better support them in achieving optimal oral health. After all, isn’t that why we chose this profession in the first place? PD
Profisil comes in mild flavors, Mint, Berry and Unflavored
New possibilities in aligner therapy
Drs. Steven R. Olmos, Kristina Wolf, and Emily B. Levy discuss craniofacial and respiratory dysfunction therapy for all ages
The importance of proper respiration, temporomandibular joint disorder (TMD), facial pain, malocclusion, and posture have been covered in the orthodontic literature. Aligner therapy has an increasing presence as a delivery choice of patients and clinicians. This article compares various systems for arch development and aligner mechanisms and how they can improve whole body function — specifically, in combination with removable functional maxillary arch development devices for adults and children.
Non-surgical craniofacial changes and resolution of chronic TMD and respiratory pathology (mouth breathing and obstructive sleep apnea [OSA]) of a late-20s adult case study was published in a previous article for this journal.1 A case study of pediatric severe apnea/obesity/TMD/headache was resolved through functional development of the maxilla and was also published in this journal.2 These cases required fixed and removable functional development orthopedic devices to achieve these results. We investigate the possibility of replacing these traditional techniques with 3D-printed removable functional development devices in combination with aligner therapy and photobiomodulation (laser).
The relationships between improper respiration (sleep disordered breathing, mouth breathing, nasal obstruction) and malocclusion are well known.3,4 These conditions are comorbid with maxillary deficiency and position to cranial base. This is demonstrated by the incidence of children with Down syndrome who have pediatric obstructive sleep apnea (POSA) after tonsil and adenoid (T and A) surgery at 65%-73%.5,6,7,8
Maxillary insufficiency results in nasal pathology which can result in mouth breathing, snoring, aggravation of obstructive sleep apnea, and forward head posture. This is supported by studies demonstrating that maxillary development can improve OSA and nasal function by increasing volume.9,10 It has been shown
Steven R. Olmos, DDS, DABCP, DABCDSM, DABDSM, DAAPM, FAAOP, FAACP, FICCMO, FADI, FIAO, is Founder and Director of Education at TMJ and Sleep Therapy Centres International. www.tmjtherapycentre.com
Kristina Wolf, MS, DMD, DABDSM, is from the TMJ and Sleep Therapy Centre of Cleveland, and is a Lecturer, Mini-Residency, TMJ and Sleep Therapy Centres International.
Emily B. Levy, DDS, FAACP, FOM, is from the TMJ and Sleep Therapy Centre of New Orleans, and is a Lecturer, Pediatric OSA Mini-Residency, TMJ and Sleep Therapy Centres International.
Disclosure: BioResearch and Nuvola are sponsors of T & S Therapy Centre International, LLC courses.
that maxillary expansion can shrink T and A and increase the width of the internal nasal valve (which is the first point of entry of air into the nose).11,12 Nasal valve compromise (narrowing of the internal nasal valve) has been found to result in a 7-times greater chance of TM joint capsulitis and facial and cervical myositis, via mouth breathing, when compared to other nasal obstructions.13 Maxillary expansion has been demonstrated to reduce mouth breathing and upright head posture.14,15 Forward head posture is a compensatory mechanism in order to improve respiratory muscle function in children with mouth breathing, which results in submaximal exercise performance.16
Comparisons to other orthodontic aligner and functional orthodontic systems
In recent years, there has been an increase in the use of clear or “invisible” aligner systems in adult populations in lieu of traditional orthodontic treatments. The use of clear aligners provides a more esthetic and comfortable treatment option and allows for better oral hygiene. Clear aligners have commonly been used in simpler orthodontic cases; however, over the years, clear aligners have been utilized in more complex cases of malocclusion.
In 1997, Align Technologies brought to market the original aligner product that set the standard for clear aligner therapy. With this application of light and constant forces by use of the aligners, teeth can move biomechanically. However, when assessing and addressing any root cause dysfunctions, such as muscle function, tongue position, or more completely treating the entire craniofacial complex, Invisalign™ and other clear aligners have significant limitations to their functionality. Furthermore, because of the simplistic nature of the biomechanics and dento-alveolar tooth movement, the complexity of cases able to be treated with Invisalign™ is diminished, allowing treat-
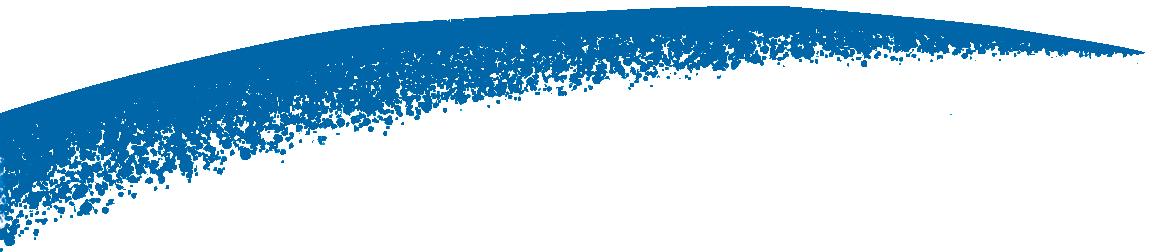
Figure 1: The blue line shows what traditional orthodontics focuses on (achieved with the Nuvola Pro™ clear aligners); the green wave shows the cyclic forces (achieved with the Freedom™ appliance)
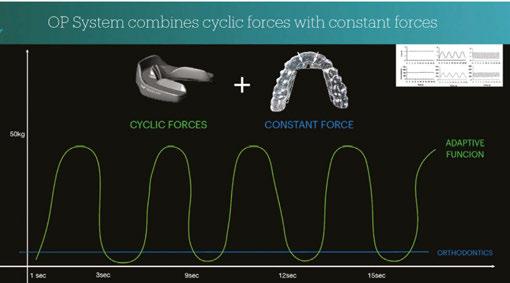
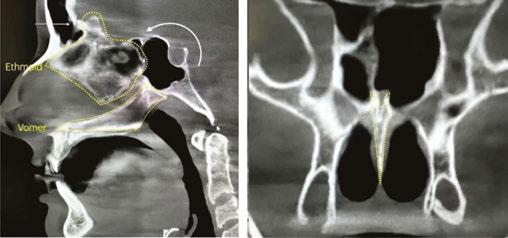
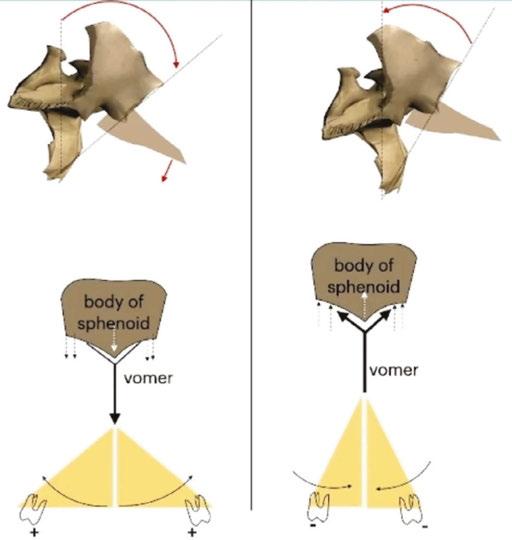
cyclic deformation of the aligners. This allows the cyclic force system to be activated, which is the driving force needed at the sutural level (Figure 1). The maxillary spine (anterior nasal spine) is engaged by the action of the lingual ramp of the Freedom™ appliance and the lingual pins of the aligners. This results in a piston action on the vomer which engages the sphenoid (cranial base) and is the mechanism of cranial remodeling (Figures 6 and 7). The frontal shield of the Freedom™ device, acting as a PMA, activates the orbicularis oris muscle promoting lip competency and proper nasal breathing. This system, therefore, combines the constant and light forces of traditional orthodontics (via the Nuvola Pro™ aligners) with stronger cyclical forces by contraction of the muscles of mastication and adaptation of cranial sutures (via the Freedom™ appliance) (Figure 8).19
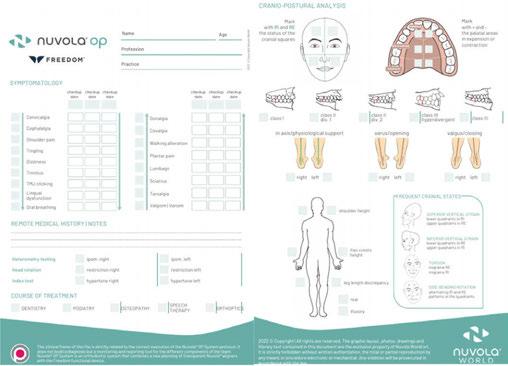
A comprehensive examination is recommended for all patients with malocclusion and functional deficits. Nuvola® has a custom medical information form to be used during an exam, including a posture evaluation (Figure 9).
Pediatrics
When treating the pediatric patient population, early intervention is especially critical to redirect abnormal craniofacial growth, especially because the mandible and maxilla have both reached approximately 85% of their adult size by 5 years of age.20,21 Maxillary insufficiency contributes to mouth breathing, snoring, obstructive sleep apnea (OSA), and forward head posture. Breathing disorders can be functional (with regards to mouth breathing) or sleep-related, but all dysfunctional breathing cases are underdeveloped when compared to cases of nasal respiration.
A comprehensive exam for children is required prior to treatment, including intraoral photographs, postural photos, cephalometric radiography and tracing of the skull, CBCT scan, and intraoral scan impressions. Lingual frenulum function should also be evaluated, as literature shows a relationship between a short lingual frenulum and maxillary hypoplasia, as well as increased risk for the onset of OSA.22,23 A referral for a sleep evaluation may be necessary to diagnose an underlying breathing disorder.
Figure 7: Distribution of cyclic forces resulting in piston action of vomer and engagement of sphenoid (cranial base) for cranial remodeling
Figure 8: Benefits of the Nuvola® OP System
Figures 9A-9B: Nuvola® Medical Examination Form
TECHNIQUE
pain associated with orthopedics and orthodontics.28,29 The MLS and M Hi-D (BioResearch) and NdYag (DEKA) lasers facilitate osteoblast and osteoclast activity on the maxillary sutures and decrease inflammation (Figure 15).
Future studies will determine efficacy of the Nuvola® OP/ Nuvola Junior™ system to treat pediatric OSA. If proved to be efficacious for treatment of sleep breathing disorders, the Nuvola Junior™ system can begin treatment on even younger patients to facilitate craniofacial development and habitual nasal breathing, the only valid endpoint of treating pediatric OSA.30
REFERENCES
1. Olmos SR. Improving quality of life and faces nonsurgically Orthodontic Practice US. 2017;8(3):36-43.
2. Olmos SR. Pediatric severe apnea/obesity/TMD/headache — Class III. Orthodontic Practice US. 2016;7(3): 20-24.
3. Aroucha Lyra MC, Aguiar D, Paiva M, Arnaud M, Filho AA, Rosenblatt A, Thérèse Innes NP, Heimer MV. Prevalence of sleep-disordered breathing and associations with malocclusion in children. J Clin Sleep Med. 2020 Jul 15;16(7):1007-1012. doi: 10.5664/ jcsm.8370.
4. Huynh NT, Morton PD, Rompré PH, Papadakis A, Remise C. Associations between sleep-disordered breathing symptoms and facial and dental morphometry, assessed with screening examinations. Am J Orthod Dentofacial Orthop. 2011 Dec;140(6):762770. doi: 10.1016/j.ajodo.2011.03.023.
5. Shott SR, Amin R, Chini B, Heubi C, Hotze S, Akers R. Obstructive sleep apnea: Should all children with Down syndrome be tested? Arch Otolaryngol Head Neck Surg. 2006 Apr;132(4):432-436. doi: 10.1001/archotol.132.4.432.
6. Maris M, Verhulst S, Wojciechowski M, Van de Heyning P, Boudewyns A. Prevalence of obstructive sleep apnea in children with down syndrome. Sleep. March 2016;39:699–704.
7. Hill CM, Evans HJ, Elphick H, Farquhar M, Pickering RM, Kingshott R, Martin J, Reynolds J, Joyce A, Rush C, Gavlak JC, Gringras P. Prevalence and predictors of obstructive sleep apnoea in young children with Down syndrome. Sleep Med. 2016 Nov-Dec;27-28:99-106. doi: 10.1016/j.sleep.2016.10.001. Epub 2016 Oct 22. Erratum in: Sleep Med. 2017 Jun;34:249. doi: 10.1016/j.sleep.2017.02.003.
8. Dyken ME, Lin-Dyken DC, Poulton S, Zimmerman MB, Sedars E. Prospective polysomnographic analysis of obstructive sleep apnea in down syndrome. Arch Pediatr Adolesc Med. 2003 Jul;157(7):655-660. doi: 10.1001/archpedi.157.7.655.
9. Cistulli PA, Palmisano RG, Poole MD. Treatment of obstructive sleep apnea syndrome by rapid maxillary expansion. Sleep. 1998 Dec 15;21(8):831-835. doi: 10.1093/ sleep/21.8.831.
10. Motro M, Schauseil M, Ludwig B, Zorkun B, Mainusch S, Ateş M, Küçükkeleş N, Korbmacher-Steiner H. Rapid-maxillary-expansion induced rhinological effects: a retrospective multicenter study. Eur Arch Otorhinolaryngol. 2016 Mar;273(3):679-687. doi: 10.1007/s00405-015-3584-y. Epub 2015 Apr 3.
11. Yoon A, Abdelwahab M, Bockow R, Vakili A, Lovell K, Chang I, Ganguly R, Liu SY, Kushida C, Hong C. Impact of rapid palatal expansion on the size of adenoids and tonsils in children. Sleep Med. 2022 Apr;92:96-102. doi: 10.1016/j.sleep.2022.02.011. Epub 2022 Feb 19.
12. Yoon A, Abdelwahab M, Liu S, Oh J, Suh H, Trieu M, Kang K, Silva D. Impact of rapid palatal expansion on the internal nasal valve and obstructive nasal symptoms in children. Sleep Breath. 2021 Jun;25(2):1019-1027. doi: 10.1007/s11325-020-02140-y. Epub 2020 Jul 9.
13. Olmos SR. Nasal airway obstruction and orofacial pain: a multicenter retrospective analysis. Gen Dent. 2022 Nov-Dec;70(6):28-33.
14. Tecco S, Festa F, Tete S, Longhi V, D’Attilio M. Changes in head posture after rapid maxillary expansion in mouth-breathing girls: a controlled study. Angle Orthod. 2005 Mar;75(2):171-176. doi: 10.1043/0003-3219(2005)075<0167:CIHPAR>2.0.CO;2.
15. McGuinness NJ, McDonald JP. Changes in natural head position observed immediately and one year after rapid maxillary expansion. Eur J Orthod. 2006 Apr;28(2):126-34. doi: 10.1093/ejo/cji064. Epub 2005 Sep 12.
16. Okuro RT, Morcillo AM, Ribeiro MÂ, Sakano E, Conti PB, Ribeiro JD. Mouth breathing and forward head posture: effects on respiratory biomechanics and exercise capacity in children. J Bras Pneumol. 2011 Jul-Aug;37(4):471-479. English, Portuguese. doi: 10.1590/s1806-37132011000400009.
17. Perrotti G, Carrafiello A, Rossi O, Karanxha L, Baccaglione G, Del Fabbro M. Clinical Use of Aligners Associated with Nuvola® OP System for Transverse Maxillary Deficiency: A Retrospective Study on 100 Patients. Int J Environ Res Public Health. 2022
Figures 16A-16C: A. 4 yo/5 months tx. B. 16 yo/6 months tx. C. 40yo/2 months tx. Photo Credit: Emily Levy, DDS, TMJ and Sleep Therapy Centre of New Orleans
May 9;19(9):5751. doi: 10.3390/ijerph19095751. PMID: 35565146;
18. Camacho M, Certal V, Abdullatif J, Zaghi S, Ruoff CM, Capasso R, Kushida CA. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep. 2015 May 1;38(5):669-675. doi: 10.5665/sleep.4652.
19. Carrafiello A. Recovery of craniofacial proportions using the Nuvola Op System protocol. Journal of Oral Health and Craniofacial Science. December 2022;7(2):022–026. doi:10.29328/journal.johcs.1001041.
20. Midori Albert A, Payne AL, Brady SM, Wright C. Craniofacial Changes in Children-Birth to Late Adolescence. ARC Journal of Forensic Science. 2019;4(1):1–19.
21. Capote R, Preston K, Kapadia H. Craniofacial Growth and Development: A Primer for the Facial Trauma Surgeon. Oral Maxillofac Surg Clin North Am. 2023 Nov;35(4):501513. doi: 10.1016/j.coms.2023.04.007.
22. Bussu S. Nuvola aligners combined with a myofunctional device in paediatric treatment: A case report. Aligners. 2023;2:38–44.
23. Huang YS, Quo S, Berkowski JA, Guilleminault C. Short Lingual Frenulum and Obstructive Sleep Apnea in Pre-Pubertal Children. International Journal of Pediatric Research. 2015;1:003. doi: 10.23937/2469-5769/1510003.
24. Align Technology. Align Technology Receives US FDA 510(k) Clearance for the Invisalign® Palatal Expander System to Address Skeletal and Dental Expansion in Growing Patients, Including Teenage Patients Which Represent the Majority of Orthodontic Case Starts Globally [Press Release]. Align. Published: December 2023. https://investor.aligntech.com/news-releases/news-release-details/align-technology -receives-us-fda-510k-clearance-invisalignr.
25. Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, Liu SY. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional - morphological study. Orthod Craniofac Res. 2017 Nov;20(4):237-244. doi: 10.1111/ocr.12206.
26. Sadowsky C, Sakols EI. Long-term assessment of orthodontic relapse. Am J Orthod. 1982 Dec;82(6):456-463. doi: 10.1016/0002-9416(82)90312-8.
27. Steinnes J, Johnsen G, Kerosuo H. Stability of orthodontic treatment outcome in relation to retention status: An 8-year follow-up. Am J Orthod Dentofacial Orthop. 2017 Jun;151(6):1027-1033. doi: 10.1016/j.ajodo.2016.10.032.
28. Ojima K, Dan C, Schupp W, Kumagai Y. Invisalign Treatment Accelerated by Photobiomodulation. J Clin Orthod. 2016 May;50(5):309-317.
29. Doshi-Mehta G, Bhad-Patil WA. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: a clinical investigation. Am J Orthod Dentofacial Orthop. 2012 Mar;141(3):289-297. doi: 10.1016/j.ajodo.2011.09.009.
30. Guilleminault C, S Sullivan S. Towards Restoration of Continuous Nasal Breathing as the Ultimate Treatment Goal in Pediatric Obstructive Sleep Apnea. Enliven: Pediatrics and Neonatal Biology. 2014;1(1):01.
The Problem: Mouth breathing can lead to underdevelopment of the upper jaw and restricted forward growth of the lower jaw. This can cause crowding and restriction of the airway. Left untreated, the child may develop Sleep Disordered Breathing (SDB).
The Solution: Whole team education and training from Nexus.
Helping you grow healthy kids. Join us: nexusdentalsystems.com/pediatrics/