Additive manufacturing in clinical endodontics: current applications and future directions
Drs. Aaron Glick & Elham Abbassi
Perforating internal root resorption: a closer look
Dr. Joseph Stern
My endodontic journey
Dr. Rico D. Short
A model of integrated care
Drs. Scott Price, Steven Frost, Christopher Kayafas, and Jonathan Peterson
Designed to enable shaping without an initial glide path in most cases.*
X-Smart® Pro+ provides the genuine reciprocating motion, enabling Reciproc™ Blue – an instrument designed for one file endo.
* Zuolo, M.L., M.C. Carvalho, and G. De-Deus, Negotiability of Second Mesiobuccal Canals in Maxillary Molars Using a Reciprocating System. J Endod, 2015. 41(11): p. 1913-7. Based on treatment of MB2 canals of more than 300 patients. The aim was to assess the frequency in which Reciproc R25 was able to directly scout and reach working lengths in comparison with hand fi les. In the hand fi le group working length was successfully reached in 57.48%. In the Reciproc R25 group the working length was successfully reached in 85.63% of cases.
PERFECT MATCH Longing for one file endo?
Summer 2025 n Volume 18 Number 2
Editorial Advisors
Dennis G. Brave, DDS
David C. Brown, BDS, MDS, MSD
L. Stephen Buchanan, DDS, FICD, FACD
Gary B. Carr, DDS
Arnaldo Castellucci, MD, DDS
Gordon J. Christensen, DDS, MSD, PhD
Stephen Cohen, MS, DDS, FACD, FICD
Samuel O. Dorn, DDS
Josef Dovgan, DDS, MS
Luiz R. Fava, DDS
Robert Fleisher, DMD
Marcela Fridland, DDS
Gerald N. Glickman, DDS, MS
Jeffrey W Hutter, DMD, MEd
Syngcuk Kim, DDS, PhD
Kenneth A. Koch, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, DICOI
Joshua Moshonov, DMD
Richard Mounce, DDS
Yosef Nahmias, DDS, MS
David L. Pitts, DDS, MDSD
Louis E. Rossman, DMD
Stephen F. Schwartz, DDS, MS
Ken Serota, DDS, MMSc
E Steve Senia, DDS, MS, BS
Michael Tagger, DMD, MS
Martin Trope, BDS, DMD
Peter Velvart, DMD
Rick Walton, DMD, MS
John West, DDS, MSD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions.
ISSN number 2372-6245
My endodontic journey
This past spring, I attended the annual AAE meeting in Boston, Massachusetts. It was packed with new innovation, technology, and doctors. Key lecturers spoke on using various technologies for optimum results. Some advocated if you don’t use this particular solution, device, or technique, then you are doing it wrong. This made me do some serious self-reflection.
I thought about my second year at The Medical College of Georgia School of Dentistry in 1996. We learned the basics on extracted teeth before working on a real live patient. We had only hand files, bleach (household), and gutta percha after accessing the tooth.
Balanced force and step-back procedures were all done by hand instrumentation. It took a long time to perform the cleaning and shaping procedure, and most cases were done in 2 or 3 visits. Once the case was cleaned and shaped, irrigated with bleach, and canals dried, it was time for filling the canal. The sealer was mixed and was placed inside the canal. The gutta-percha cone was seated. An alcohol torch or bunson burner was used for the warm vertical condensation technique. A sharp metal instrument was heated to a cherry-red color, and then carefully placed inside the canal to heat up the gutta percha (all the while, we prayed not to burn the patient’s lip). Most procedures took over 2 hours. Despite this “ancient” technology, root canals still were very successful. In fact, success rates have not changed dramatically in the past 50 years despite the new technologies.
What’s the point? Technology changes but teeth don’t.
When you think of the best root canals, do you envision sleek dental offices and the most modern technology? Most of us do, but the practice of treating infected teeth has roots (literally) that stretch back over 2,000 years. The core idea — to relieve pain and save the natural tooth — remains the same.
Root canal therapy has advanced significantly, thanks to innovations like:
• X-rays (discovered in 1895), for accurate imaging of internal tooth structure.
• Local anesthetics, which made procedures more comfortable and accessible.
• Digital radiography and 3D cone-beam imaging for detailed diagnosis.
• Rotary endodontic systems and ultrasonics for faster, cleaner procedures.
• Heat-treated endodontic files, which allow files to be pre-curved to reach smaller areas and around severely curved canals.
• Dental operating microscopes that offer unparalleled visibility.
• Bioceramic sealers that improve sealing and biocompatibility.
These advancements have helped endodontics to become more precise and efficient. However, the success rates have not changed significantly over the past 50 years. If endodontics is performed according to the basic biological principles, a successful outcome of 90% or more is still the standard.
Root canal therapy has a fascinating history, evolving from early attempts with bronze tools to today’s precise, comfortable procedures. Despite the fears and myths, endodontics remains one of the most important ways to save natural teeth — and its long history proves it still works
Dr. Rico D. Short is a world-renowned, board-certified endodontist, author, professor, and speaker with over 25 years of dental experience. At the Medical College of Georgia School of Dentistry, he attained a Doctor of Dental Medicine degree, and then, he earned his post doctorate degree in Endodontics from Nova Southeastern University. He is a Diplomate of the American Board of Endodontics and is in private practice, Apex Endodontics P.C, located in Smyrna, Georgia. He is a national board examiner for The ADEX Testing Agency, which administers the licensure exam for oral healthcare professionals in the United States, Puerto Rico, and Jamaica. He is a member of the Fellow International College of Dentists, a graduate of the ADA Institute of Diversity In Leadership Program, an ADA Success Speaker, consultant in endodontics to the Georgia Board of Dentistry, and an assistant clinical professor at The Dental College of Georgia in Augusta.
A model for integrated care
How Red Mountain Endodontics, Superstition Springs Endodontics, East Valley Periodontics, and Mesa Implants & Periodontics are redefining collaborative specialty care in Mesa, Arizona
Cover image courtesy of Specialized Dental Partners.
ENDOSPECTIVE
CONTINUING EDUCATION
Perforating internal root resorption (IRR): a closer look
Dr. Joseph Stern explores IRR from causes to treatment
Dr. L. Stephen Buchanan shows how cavitation enhancement of irrigants can be accomplished with PulpSucker™ Irrigation
PRODUCT PROFILE
Improving endodontic success by utilizing EndoCeramic® Sealer
Dr. George Just discusses research on a bioceramic sealer from Endo Direct ........................ 27
SMALL TALK
Leadership is a choice
Drs. Joel C. Small and Edwin McDonald discuss dynamic leadership ........................................ 28
Additive manufacturing in clinical endodontics: current applications and future directions
Drs. Aaron Glick and Elham Abbassi offer a comprehensive overview of 3D printing and its applications
PRODUCT DEBUT
Improving endodontic success with advances in NiTi rotary files and bioceramic sealers
Dr. Gregori M. Kurtzman describes the characteristics of new hand files and bioceramic sealer ......................................... 30
*Paid subscribers can earn 4 continuing education credits per issue by passing the 2 CE article quizzes online at https://endopracticeus.com/category/continuing-education/
Did you miss us at AAE 2025?
WATCH the Endodontic Practice US AAE highlight reel by scanning the QR code or view more in-depth interviews and demos from the American Association of Endodontists 2025 Annual Meeting. We didn’t miss anything!
While we hope to see you at the AAE26 in Salt Lake City next year...
CONNECT with us on social media for more exclusive content.
ZenFlex
NiTi Rotary Shaping Files
High Cutting Efficiency
Preserves Tooth Integrity
Lower Risk of Breakage & Transportation
Control Memory
Corresponding ZenFlex Gutta Percha Points
Reciprocating Files
High
ZenFlex CM
Rotary NiTi Files
Excellent Flexibility
Increased Performance
Reach More
High Cutting Efficiency ZenFlex ONE
images courtesy of Dr. Judy McIntyre
Case images courtesy of Dr. Rodrigo Vargas. ZenFlex CM taper .04, Gutta Percha ZenFlex. Canals Mesials until 20/.04, Canal Distal until 30/.04
Case images courtesy of Dr. Ferras Mashtoub, DDS
Beating burnout
The ADA cites that “more than 82% of dentists report feeling major stress about their careers.” In this very competitive and quickly changing world, the responsibilities can often feel like the walls of the office are closing in. Recognizing burnout symptoms and taking steps to calm your emotions can make a huge difference.
First, what does burnout feel like? Just a few signs are:
• Feeling tired, emotionally drained, or unenthusiastic
• Often feeling frustration toward work
• Negative outlook
• Problems concentrating
• Getting sick often
It is important to recognize and treat burnout to avoid issues such as heart disease and diabetes, sleep-related disorders, and in some cases, substance misuse.
Some ways to overcome burnout
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor
Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Sales Assistant & Client Services
Get enough sleep: We’ve all had our nights of staring at the ceiling in bed while mulling over Plan A, Plan B, Plan C, and more, to solve the next day’s problems. Try to break your non-sleeping cycle. For example, ask your doctor about a possible supplement to lull your brain into the sleep cycle, or discover new relaxation techniques.
Detox from technology: Set specific technology-free windows where patient management systems and email notifications are completely turned off.
Eat and drink for health: Remembering to eat and keeping hydrated helps your brain function (improves memory, attention, and problem solving), raises your mood, and boosts your mental abilities.
Exercise: Exercising has been proven to help fight depression. It doesn’t have to take up much time – about 15-20 minutes per day should do it. A walk along a favorite path, around your neighborhood, on the beach, or even doing yoga or stretching can give your mind some time to reset.
Talk to trusted friends and mentors: There is nothing better than finding out that others can empathize with you and confirm that you are not “crazy.” Colleagues can tell you how they have navigated through similar times of burnout, or give some helpful tips, like reduced hours on Fridays or more intentional spacing of appointments. Look for summer dental retreats or workshops that combine professional development with wellness activities. Aside from work, friends or family can just listen, provide some good advice, or go along on that walk or for a quick cup of coffee and a shoulder to lean on. Finding a therapist can also be very helpful in working out your feelings and providing anti-anxiety techniques.
Give yourself a break: When you feel that burnout starting to eat away at your stomach lining, decide how you will take care of yourself at that moment. Take a few seconds. Grab your journal, and write a few lines. Go outside of the office and breathe some fresh air or look at the scenery. Research shows even 20 minutes of nature exposure significantly reduces cortisol levels. For more extreme situations, taking one day or a few days off, or a more extended vacation can bring you back with renewed spirits.
The ADA has some interesting resources just for dentists on its Wellness Resources page (https://www.ada.org/resources/practice/wellness) to help you start dealing with burnout. You can’t always control what happens in your office, but you can control the way you cope, put out those every day inner fires, and move forward to a fulfilling future with a positive outlook.
✓ Efficient Organization: Keepallyourtools in oneplace.
✓ Wall Charts and Labels Included: Personalizedwithproductcodes and images for easy re-ordering.
✓ Various Size Options: Choosefrom 18, 26, or44compartment options.
A model for integrated care
How Red Mountain Endodontics, Superstition Springs Endodontics, East Valley Periodontics, and Mesa Implants & Periodontics are redefining collaborative specialty care in Mesa, Arizona
When the term “Integrated Care” was introduced at the 2023 Specialized Dental Partners Vision Summit, it struck a chord with those in attendance. But for Drs. Steven Frost of Red Mountain Endodontics, Christopher Kayafas of Superstition Springs Endodontics, Scott Price of East Valley Periodontics, and Jonathan Peterson of Mesa Implants & Periodontics, it wasn’t a novel concept — it was validation.
“That’s what we’ve been doing all along,” Dr. Price recalled.
In Mesa, Arizona, Integrated Care isn’t a buzzword, it’s a daily reality. Four leading specialty practices — Red Mountain Endodontics, Superstition Springs Endodontics, East Valley Periodontics, and Mesa Implants & Periodontics — have organically developed a care model rooted in collaboration, trust, and a shared commitment to clinical excellence. Now aligned under the Specialized Dental Partners umbrella, their partnership offers a glimpse of what’s possible when specialists remove barriers and prioritize the patient journey together.
Defining integrated care
For Dr. Chris Kayafas of Superstition Springs Endodontics, integrated care is simple in concept but profound in impact:
Steven Frost, DDS, is an endodontist and founder of Red Mountain Endodontics. Dr. Frost is an experienced endodontist and Arizona native with a deep family legacy in dentistry. He earned his undergraduate degree from Brigham Young University, his DDS from the University of the Pacific in San Francisco, and completed his specialty training in endodontics at Tufts University School of Dental Medicine in Boston. In 1994, Dr. Frost founded Red Mountain Endodontics to provide compassionate, high-quality root canal therapy to the East Valley community. He is a member of the American Dental Association, American Association of Endodontists, and Arizona State Dental Association. Dr. Frost is known for his calming presence, clinical excellence, and dedication to preserving natural teeth using the latest in endodontic care.
Christopher Kayafas, DDS, MS, is an endodontist at Superstition Springs Endodontics. He is a board-certified endodontist with over 2 decades of clinical experience and a reputation for precision, compassion, and patient comfort. He earned his BS from Duquesne University and completed his DDS, endodontic certificate, and MS at the West Virginia University School of Dentistry. He was honored with the Pierre Fauchard Award and inducted into the Omicron Kappa Upsilon honorary dental society for academic excellence. A dedicated professional, Dr. Kayafas has remained involved in local, state, and national dental societies throughout his career. He is a member of the American Dental Association, American Association of Endodontists, the College of Diplomates of the American Board of Endodontics, and Arizona State Dental Association. He utilizes the latest root canal technologies to deliver efficient, effective care, making the endodontic experience surprisingly pleasant for his patients.
Scott Price, DMD, MS, is a periodontist at East Valley Periodontics. Dr. Price combines a strong work ethic with a compassionate approach to care, values shaped by growing up in a family of nine children and honed as a collegiate football player at the University of Utah. He earned his undergraduate degree in psychology from the University of Utah and went on to complete his Doctorate of Medical Dentistry and a master’s degree in periodontics at the University of Kentucky. Dr. Price is a Diplomate of the American Board of Periodontology and an active member of the American Academy of Periodontology, Academy of Osseointegration, and Spear Masters Program, among others. He prioritizes education, research-based treatment, and close collaboration with general dentists to ensure predictable, high-quality outcomes. Known for his personalized and respectful approach, Dr. Price takes pride in making every patient feel heard, informed, and comfortable throughout their treatment journey. His greatest reward comes from restoring health and confidence — one smile at a time.
Jonathan Peterson, DMD, MS, DICOI, is a periodontist at Mesa Implants and Periodontics. He is an Arizona native and highly credentialed periodontist dedicated to creating healthy, confident smiles. He studied biology at Arizona State University before earning both his DMD and a master’s in oral biology from Temple University School of Dentistry. He later completed a full fellowship at the Misch International Implant Institute and achieved Diplomate status with the International Congress of Oral Implantologists. He is a proud member of the American Academy of Periodontology, Arizona Dental Association, and ICOI. Dr. Peterson’s approach combines advanced clinical skills with a warm, individualized focus that helps patients achieve optimal oral health with confidence and comfort.
Back row: Christopher Kayafas, DDS, MS, and Steven Frost, DDS. Front row: Scott Price, DMD, MS, and Jonathan Peterson, DMD, MS, DICOI
“Integrated care is a model that enables trusted specialists to work together in a more efficient way to provide effective, patient-centered care.”
That efficiency is built on proximity, communication, and culture. In Mesa, those pieces have come together over years of collaboration. What makes this model exceptional is not the business structure; it’s the everyday commitment by clinicians to make specialty care more accessible, intuitive, and unified.
A legacy of collaboration
The roots of this care model stretch back more than 2 decades. For years, East Valley Periodontics and Superstition Springs Endodontics co-hosted “Spring into Dentistry,” a CE and golf event designed to connect general dentists and specialists in a relaxed, relationship-building environment.
“It wasn’t just about CE or fun,” said Dr. Price. “It was about trust — about strengthening the connections that make collaboration possible.”
That trust flowed naturally into clinical workflows. Overthe-shoulder consultations became routine. Referrals moved faster. When East Valley Periodontics opened a second location within Red Mountain Endodontics’ building, those same values transferred effortlessly into a new space, setting the stage for the collaborative care model Mesa is now known for.
Proximity with purpose
Having specialists under one roof has transformed patient care.
“We were literally passing patients down the hallway,” said Dr. Price. “If someone needed a consult, it could happen instantly.”
This “hand-off in real time” model means patients can be seen by multiple specialists, sometimes on the same day. It removes common delays, like waiting for an outside referral or scheduling an entirely new visit. The result is faster diagnoses, quicker pain relief, and significantly higher patient satisfaction.
“From the patient’s perspective,” said Dr. Kayafas, “It feels like one unified team is taking care of them. That’s a powerful experience.”
Teamwork at work: Immediate specialist collaboration leads to fast relief and comprehensive treatment — all in one visit
A patient-centered model in action: Specialists collaborate in real time to deliver seamless, efficient care under one roof
Case in point: a seamless hand-off
Dr. Kayafas recalled a recent case involving a patient with a cracked root and severe pain. The patient’s general dentist typically worked with a periodontist who only visited their office once a week.
“This patient couldn’t wait,” said Dr. Kayafas. “We called EVP, and they saw her that same day. The tooth was extracted, the site was prepared for an implant, and the patient left our building completely relieved.”
Such outcomes are common in Mesa. They aren’t the result of luck; they’re the result of coordination, proximity, and a culture that prioritizes immediate, compassionate care.
More than just logistics
In a world where specialty referrals often mean navigating insurance, scheduling delays, and duplicated paperwork, the Mesa model offers a welcome alternative. There is a focus on patient experience. Patients are seen faster, experience fewer handoffs, and receive care from a cohesive, aligned team.
Collaboration in action: Specialists combine expertise to deliver seamless, patientcentered care
agement systems, making it difficult to share notes, images, and intake information smoothly.
For Dr. Peterson, creating a positive patient experience goes beyond clinical outcomes. It’s about building trust through listening, creating consistent “WOW” moments, and guiding patients through their care journey in a way that feels personalized and respectful.
He recommends pre-appointment welcome calls, phasing large treatment plans across multiple visits, and celebrating small wins in hygiene. These intentional touchpoints improve comfort, case acceptance, and retention — while reinforcing the specialist’s role as a partner in the patient’s long-term health.
“Never let the patient leave your office without a pre-appointment for the next visit,” Peterson advises. “You are a guide — a Sherpa — on their journey to better oral health.”
Backed by Specialized Dental Partners
The Mesa group’s integration has been further strengthened through its affiliation with Specialized Dental Partners. With Specialized Dental Partners, practices gain access to operational and administrative support — HR, marketing, finance, and more — while maintaining complete clinical autonomy.
“They don’t tell us how to practice,” said Dr. Kayafas. “They help us do more of what we’re best at — treating patients.”
That support has freed up time and energy for the doctors to deepen collaboration, innovate in their workflows, and build experiences that feel seamless to patients.
“We were already working together,” added Dr. Price. “Now, with SDP’s help, we’re doing it better and smarter.”
Overcoming the challenges
Despite the cultural and operational alignment, the team acknowledges that technology integration remains a challenge. Many periodontists and endodontists use different practice man-
“The easy part has been working with these amazing specialists,” said Dr. Kayafas. “The harder part is making integrated care fully operational behind the scenes.”
Efforts are ongoing to align intake forms, image sharing, and documentation. The goal? A single streamlined experience that’s as frictionless on the back end as it is in the operatory.
“Patients shouldn’t have to fill out their medical history three different times,” he added. “That’s not what great care looks like.”
Educating together, growing together
One standout benefit of the partnership is the ability to educate as a team. The practices regularly co-host CE events, dinner lectures, and appreciation nights for local referring providers. These events not only elevate community awareness but showcase how integrated care creates stronger outcomes.
“Our CE nights are a reflection of how we practice,” said Dr. Price. “Collaborative, accessible, and grounded in what’s best for the patient.”
A blueprint for the future
What’s happening in Mesa isn’t just a success, it’s a scalable model. Other practices across the Specialized Dental Partners network are beginning to replicate its principles: co-location, unified communications, shared case management, and patient experience grounded in empathy and intention.
“This is the future of specialty care,” said Dr. Price. “Not because it’s more efficient — but because it’s better for patients.”
Dr. Peterson agrees. From small gestures to large systems, each component contributes to a care experience that is more human, more accessible, and more complete.
“By focusing on how we make patients feel,” he writes, “we elevate not just outcomes — but trust, connection, and lifelong health.” EP
Imagine More for Your Patients
Partner with Specialized Dental Partners to enjoy unmatched business support and collaboration across specialties, clinical autonomy, and equity ownership.
Clinical application of a closed-system negative pressure system
Dr. L. Stephen Buchanan shows how cavitation enhancement of irrigants can be accomplished with PulpSucker™ Irrigation
Cavitation to the rescue
Enhanced endodontic irrigation methods have garnered a great deal of interest over the last decade, beginning with Fotona’s Photon-Induced Photo-acoustic Streaming (PIPS) laser enhancement, then afterwards Sonendo’s GentleWave® multisonic enhancement, and also BioLase’s intra-canalar laser enhancement. What do they have in common? All three of them induce cavitation in endodontic irrigants — the lasers by super-heated pulses of light energy that blow up micro-bubbles of steam in aqueous solutions and GentleWave technology by applying vacuum pressure to a closed system which causes gas bubbles to form, expand, and collapse, releasing intense energy into irrigants. After 8 years of researching alternatives, I have accomplished the cavitation enhancement of irrigants with the PulpSucker™ Irrigation system.
Why is cavitation important to endodontic irrigation? Consider our clinical challenge when treating root canal systems to their full apical and lateral extents. Because minimally invasive canal preparations may be no more than 0.2 mm in terminal diameter, they are not large enough to allow entry of our smallest irrigating cannulas, not to mention that the majority of lateral canals — which can only be cleaned with irrigation — are found branching off of primary canals in this most inaccessible region.
This implosion of collapsing gas bubbles within a fluid creates sonic shock waves that travel to the ends of canals, and this sound energy is amplified when pushed into these smaller canal diameters, just like the ear trumpets that people with hearing loss used before we had electronic hearing aids (Figure
L. Stephen Buchanan, DDS, FICD, FACD, has taught endodontic procedures, with live patient demonstrations, to dentists for over 35 years. He has over 25 US and international patents for endodontic tools ranging from his EndoBender plier, to Obtura Spartan’s Buc Ultrasonic Tips, Dentsply’s variably-tapered GT rotary files, his PulpSucker negative pressure irrigation device, and Kerr’s Continuous Wave of Obturation electric heat pluggers and filling technique.
He has logged nearly 2 million air miles as he has traveled to present lectures and hands-on courses domestically and worldwide. Despite providing root canal therapy to patients for over 45 years, he still enjoys doing dangerous things safely in human beings and lives for that sense of anticipation whenever he invades yet another pulp chamber. Dr. Buchanan lives in Santa Barbara, California, where he maintains a practice limited to endodontics and trains dentists to do newly developed procedures at his Dental Education Laboratories facility. You can find his website at delendo.com.
Disclosure: Dr. Buchanan is the inventor of the PulpSucker negative pressure irrigation device.
1). Cavitated fluids transmit this energy very effectively because water is incompressible, therefore energy applied some distance away can easily affect the solutions in the apical third. Hence the all-important “forward effect” of cavitation.
The advantages of cavitating NaOCl in root canals was first described by Dr. Adrian Lussi and colleagues in his paper, “The balanced force and the GT-rotary technique in comparison with the non-instrumental technique (NIT).”1 He showed pulp chambers and the coronal two-thirds of canals in extracted teeth completely cleaned, without a single file being brought to bear, by the cavitation induced by the alternating positive and negative pressures applied to sodium hypochlorite by his prototype “tooth sucker” console. Sadly, the prototype created a net positive pressure inside the RCS, causing NaOCl to be forced beyond the ends of canals, killing the dogs in the first animal study.
The new kid on the block
I have questioned for some time whether it is necessary to spend $60K-$80K for technologies to deliver efficient irrigation enhancement? My irrigation Christmas list includes cavitation, simultaneous multi-canalar function for efficiency in molars, and automatic operation after staging because irrigation is a deadly boring procedure.
After 8 years of development, I’ve proven that cavitation enhancement of irrigants can be accomplished without any capital investment at all. If you create a closed system by luting an airtight stage to a tooth in treatment and then apply the chairside vacuum to the inside of the stage and RCS, it will not only pull irrigating solutions from a supply bag into and through the internal passageways of teeth, but also the negative pressure induces cavitation with remarkable cleaning results and a forward effect of 5 mm. Because of the closed system, multiple cannulas, and the chairside vac, this can be accomplished without a power
Figure 1: Diagram illustrating how gas bubbles initiate, expand, and violently explode when fluid pressure is reduced
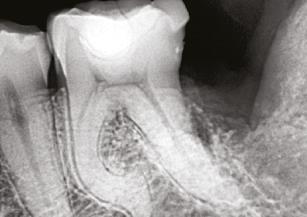
Figure 2 (left): PulpSucker Irrigation device with its stage, manifold, and supply lines feeding catheters placed to midroot in each canal, and its vacuum port exiting the top plate of the stage. Staging is a 3-minute procedure after which PulpSucker Irrigation runs by itself. Figure 3 (center): Preoperative radiography of this irreversibly inflammed mandibular molar shows incipient lucencies at both root apices and in the furcation between the roots. Figure 4 (right): PS cannulas in place 3 mm-5 mm short of the canal terminus
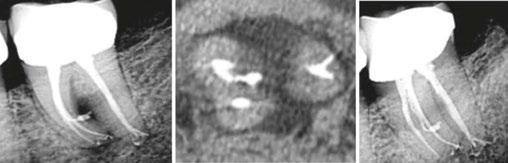
Figure 5 (left): The immediate post-op radiograph revealing a mid-root mesial canal exiting into the furcal lesion and a multiplicity of apical lateral canals in both roots. Figure 6 (center): Axial CBCT slice showing the mid-mesial canal filled into the center of the mid-root pathosis. Figure 7 (right): 3-month recall showing complete regeneration of periradicular bone adjacent to the lateral ports of exit
cord. Once the tooth is staged and catheterized, PulpSucker™ runs by itself (Figure 2).
Case report
Figures 3-7 show a lower molar treated with PulpSucker Irrigation after instrumenting the mesial canals to a 20-.03 shape and the distal canal to a 25-.05 shape. Obturation was accomplished with bioceramic sealer and the Continuous Wave filling technique.
Conclusion
Why are we so thrilled when we see lateral anatomy filled in our post-op radiography? It’s because 3D obturation of lateral recesses is a proxy for our irrigating efficacy. If you have not cleaned a lateral canal during irrigation procedures, you are not going to see it filled afterwards. Conversely, when several lateral canal projections are seen after treatment is finished, we can give ourselves a pat on the back for doing a thorough job of irrigation. This is no small accomplishment, especially in light of the recent trend toward minimally invasive endodontic procedures. In fact, MIE concepts and procedures up the ante of our mission to clean these uninstrumentable parts of root canals, and in fact, enhanced irrigation methods that produce cavitation have played a serious part in driving this trend (Figure 9). This case shows how really complex endodontic anatomy can
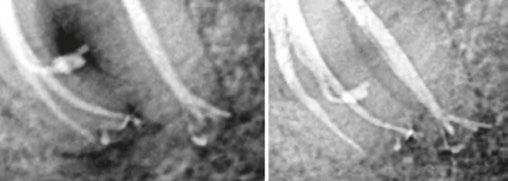
Figure 8: Close-up views of the apical two-thirds of the roots. The mid-mesial canal is 6 mm long; preoperatively, it contained vital pulp tissue, and it was never touched with a file, yet it has been definitively treated by PulpSucker Irrigation. Note the four lateral canals in the apical 2 mm of the roots, again, never touched by a file. Cavitation rocks
Figure 9: Mandibular molar treated with PulpSucker Irrigation through three independent MIE access openings. Note the apical delta system of lateral and accesssory canals in the apical third of the distal root. No dentin was cut in this canal by instruments, yet PulpSucker Irrigation was able to clear out the 5-7 portals of exit. This took 5 minutes to stage and catheterize, then ran by itself for the 15 minutes it took to run 100 mls of sodium hypochlorite through this super-complex root canal system
be effectively and automatically irrigated with a low cost, completely disposable PulpSucker device.
REFERENCE
1. Lussi A, Hotz M, Stich H. Die Balanced Force und die GT-Rotary-Technik im Vergleich zur nicht instrumentellen Technik (NIT) [The balanced force and the GT-rotary technique in comparison with the non-instrumental technique (NIT)]. Schweiz Monatsschr Zahnmed. 2004;114(1):12-8. German.
Perforating internal root resorption (IRR): a closer look
Dr. Joseph Stern explores IRR from causes to treatment
Introduction
Confusion surrounding root resorption is common within the general dental community. This is likely due to the numerous subtypes — such as internal, external, cervical, and apical resorption — and the wide variety of potential causes, including trauma, pressure, infection, inflammation, and systemic factors. Much of this confusion appears to stem from the terminology used to describe the location and etiology of root resorption. This article focuses on perforating internal root resorption (IRR), exploring its causes, diagnosis, and successful nonsurgical treatment, utilizing cone beam computed tomography to assess the extent of the lesion and bioceramics to fill the defect effectively.
Root resorption: defined
Root resorption is defined as the loss of dental hard tissues as a result of clastic activities, which can occur as a pathologic or physiologic process depending on the location and timing of the resorptive process.1 While most internal and external resorption is pathologic in nature, the resorption associated with the primary dentition is most often a normal physiologic process.2 The primary theory for what initiates internal root resorption (IRR) is multinucleated giant cells located in the granulation tissue that form in response to infected coronal pulp tissue. These odontoclasts are believed to be responsible for the resorption of the lining of the pulp space.
A second theory suggests that the granulation tissue arises from the vascular system, outside of the pulp space. Damage and/or loss of the predentin and odontoblastic layer must occur prior to the resorptive process.3 Trauma is suspected as an initiating cause, possibly supported by continuous stimulation from infection. Iatrogenic causes of continued inflammatory excitation of the coronal pulp include overheating the tooth.4-8 IRR is insidious and often progresses without symptoms. Pain and/or swelling may not occur until the process perforates
Joseph C. Stern, DDS, is a Diplomate of the American Board of Endodontics and serves as the Director of Endodontics at Touro College of Dental Medicine. He frequently lectures on clinical endodontics, having spoken at various local county dental societies, the New Jersey Dental Association Annual Session, and the Greater New York Dental Meeting. In addition to lecturing, Dr. Stern has published multiple articles on various topics within endodontics in the New York State Dental Journal, Dentistry Today, and Endodontic Practice US.
Disclosure: The author reports no conflicts of interest.
Educational aims and objectives
This self-instructional course for dentists aims to examine perforating internal root resorption (IRR), its causes, diagnosis, and successful nonsurgical treatment.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Define internal root resorption and its causes.
• Outline a standard non-surgical treatment protocol for IRR.
• Realize how IRR is different than external root resorption.
• Observe diagnosis and treatment of two IRR patients.
• Recognize bioceramic sealers as a more standardized and effective endodontic approach for managing perforating internal resorption.
• Realize the crucial need for the use of CBCT during the diagnostic planning phase of IRR for accurately visualizing the full extent of the lesion. 2
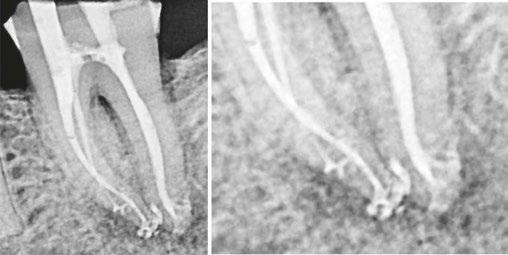
Figures 1A-1B: Two periapical radiographs of tooth No. 24 taken at different angles. Resorptive defect changes position relative to root canal, which according to buccal object rule, means defect is separate from canal and, hence, external to canal
the root, at which time the prognosis for a successful outcome becomes more questionable. As long as the apical portion of the pulp retains vital tissue, the resorptive process continues. Another requirement for continued resorption is bacterial infection, as a microbial stimulus is required for the continuation
of IRR.7 When and/if the pulp tissue becomes necrotic, before perforation, the process can be self-limiting. Usually, internal root resorption is first observed at a routine radiographic exam. Because it begins in the pulp space, the lesion is contiguous with the space. It can be confirmed if two acute-angled radiographs, taken from extreme mesial and distal positions, show no separation between the lesion and the pulp space. Cone beam computed tomography (CBCT) can help make this differential diagnosis between external and internal resorption.
Treatment protocol
Our treatment of IRR follows the standard protocol for nonsurgical endodontics. The root canal space is debrided and decontaminated to the apical constriction and, subsequently, filled. Interrupting the vital tissue pathway at the apex arrests the resorptive process. Extra care, mechanically and chemically, may be in order to remove tissue from the undercut areas that are created by the resorptive process. Creating a straight-line access to the resorptive defect is often not feasible, as this would require removal of more dentin, further weakening the root structure. It is interesting to note that internal resorption can be perceived as a misplaced periapical lesion found inside the root canal rather than at the apex. Both are caused by the presence of bacteria and the triggering of resorptive cells. Both form in a symmetrical manner. However, the periapical lesion has surrounding vital tissue, which allows these lesions to grow in size, unlike IRR, which is self-limiting. Because active IRR requires a pulp space that is partially vital and partially necrotic, vitality testing is unreliable. One cannot be sure whether the pulp tissue at the time of diagnosis is necrotic and, therefore, the resorptive process is arrested, or vital tissue remains, and the IRR is ongoing. Regardless, if perforation has occurred, the external lesion has a life of its own, and treatment is essential.
Differential diagnosis
While external root resorption comes in many forms, such as transient surface resorption, pressure resorption, external inflammatory root resorption, invasive cervical root resorption, and replacement resorption (ankylosis), internal root resorption is uniquely different. The differential diagnosis is made by taking multiple radiographs at different angles.9,10 Utilizing the buccal object rule, a lesion of internal origin will remain close to the canal regardless of the angle, while a lesion of external origin will move away from the canal depending on the angle of the radiograph (Figures 1A and 1B).
Additionally, with IRR, the outline of the root canal is usually distorted and appears contiguous with the resorptive defect, while with external resorption, the root canal outline appears normal and can usually be seen running through the radiolucent resorptive defect, as there remains a thin layer of dentin separating the canal from the resorptive area9-10 (Figures 2A-2D).
The radiographic appearance of IRR is a fairly uniform radiolucent enlargement of the root canal. There would only be alveolar bone loss adjacent to the resorption if the resorption perforates into the PDL. The best and most accurate tool we have for diagnosing IRR and determining the path of the perforating
lesion is cone beam computed tomography (CBCT). It is best to use a limited field of view (FOV), as opposed to the larger FOV used with other disciplines in dentistry. A smaller FOV increases image resolution, while at the same time providing a lower effective radiation dose to the patient. It is worth noting that in Case 2, one cannot visualize the resorptive defect from just looking at the periapical radiograph. It has been shown in countless studies that CBCT gives a more accurate diagnosis and better visualization of periapical pathology.11-13
Case report 1
A 41-year-old male presented with a chief complaint of pain and swelling adjacent to tooth No. 10. The patient reported a history of trauma as a teenager, though he had not experienced issues until the recent onset of pain and swelling. Clinical examination revealed tenderness on the buccal gingiva around tooth No. 10, with sensitivity to percussion and biting. A small, fluctuant intraoral swelling was noted near the apex of tooth No. 10, and the tooth did not respond to vitality testing. Radiographic examination showed a large perforating internal resorptive defect near the apical third of the root (Figure 3A). CBCT (Veraviewepocs 3D R100; J. Morita) revealed significant alveolar bone loss adjacent to the defect, extending along the entire mesial side of
Figures 2A-2D: 2A: Periapical radiograph of tooth No. 21. Large resorptive defect is noted in external cervical region. Blue arrows point to a thin layer of predentin that appears to be running through defect. Outline is what remains of root canal wall. Tooth tested vital, and diagnosis of invasive cervical root resorption was made. Due to minimal remaining tooth structure, extraction was advised. 2B-2D: Sagittal, coronal, axial slices show resorptive defect external to root canal
A. B.
C.
D.
the apical half of the root of tooth No.10 and reaching the root of tooth No. 9 (Figures 3B and 3C).
A diagnosis of pulpal necrosis with acute apical abscess was made. All treatment options, including extraction with replacement by an implant or bridge, were discussed. The patient, motivated to retain the tooth, opted for root canal therapy and repair of the resorptive defect. Informed consent was obtained.
First visit
The patient was anesthetized with 1.7 mL of 4% articaine with 1:100,000 epinephrine (Septocaine®; Septodont®, Lancaster, Pennsylvania) via labial infiltration. Rubber dam isolation was achieved, and the tooth was accessed using a No. 2 surgical length carbide round bur. Necrotic pulp was encountered. Working length was established with a Root ZX® apex locator (Morita, Tokyo, Japan), and the canal was instrumented to a size 35 .04 Vortex Blue® rotary file (Dentsply Tulsa Dental, Johnson City, Tennessee). Care was taken to ensure that the files passed through the resorptive defect and entered the apical portion of the canal. The canal was irrigated with 5.25% sodium hypochlorite, and the EndoActivator® (Dentsply, Tulsa, Oklahoma) was used to sonically agitate the irrigant to promote thorough disinfection of the resorptive defect. The canal was dried with paper points, and calcium hydroxide (Ultracal™ XS, Ultradent Products Inc, South Jordan, Utah) was syringed into the canal and the defect. The tooth was then temporarily restored with Cavit® (3M ESPE, Neuss, Germany).
Second visit
Two weeks later, the patient returned for completion of the endodontic treatment, reporting that all symptoms had subsided. Clinical examination confirmed that the swelling had resolved. Calcium hydroxide was removed from the canal through instrumentation, irrigation, and activation with the EndoActivator. The canal was dried with paper points, and excess irrigant was removed using surgical suction with a micro-tip. A master gutta-percha cone was placed to the working length and confirmed with radiographic examination (Figure 3D). The canal was coated with EndoSequence® BC (bioceramic) sealer (Brasseler USA, Savannah, Georgia) to ensure sufficient sealer filled the resorptive defect. It was then obturated with gutta percha and BC sealer using the technique of warm vertical condensation (Figure 3E). The lingual access opening was restored with TPH Spectra® ST composite (Dentsply Sirona, Charlotte, North Carolina), and the patient was scheduled for recall to monitor healing.
At 1-year, 2-year, and 5-year recall visits, the patient was asymptomatic, and radiographs showed complete healing with full restoration of bone and lamina dura adjacent to the resorptive defect (Figures 3F and 3H). The patient expressed satisfaction with the outcome, having retained a tooth originally planned for extraction.
Case report 2
A 56-year-old male presented with a chief complaint of vague discomfort in the left mandible. The patient reported that the discomfort had been intermittent for more than 6 months but
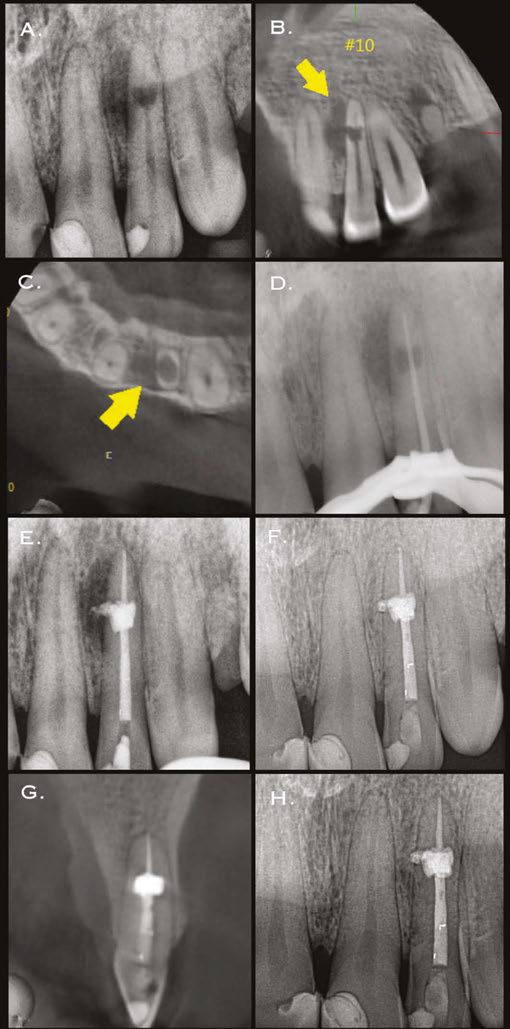
Figures 3A-3H: 3A. Preoperative periapical radiograph of tooth No.10 showing internal root resorption in apical third of root. There is significant alveolar bone loss adjacent to defect. 3B. Sagittal CBCT image of tooth No. 10 showing internal resorptive defect perforating on mesial aspect of root. Note adjacent alveolar bone loss extending proximally to tooth No. 9. 3C. Axial CBCT image of internal resorptive defect perforating on mesial aspect of root. There is thin layer of circumferential dentin remaining and extensive alveolar bone loss adjacent to the defect. 3D. Periapical radiograph showing gutta-percha cone fit. Gutta-percha cone passes through resorptive defect to contact apical portion of root canal. 2E. Immediate postoperative periapical radiograph of tooth No.10 once root canal was completed and resorptive defect was restored. 2F. Two-year follow-up showing complete healing of radiolucency adjacent to defect and reestablishment of PDL. 2G. Two-year follow-up CBCT. Coronal slice showing complete healing of radiolucency adjacent to defect and reestablishment of PDL. 2H. Five-year follow-up radiograph. Patient is completely asymptomatic
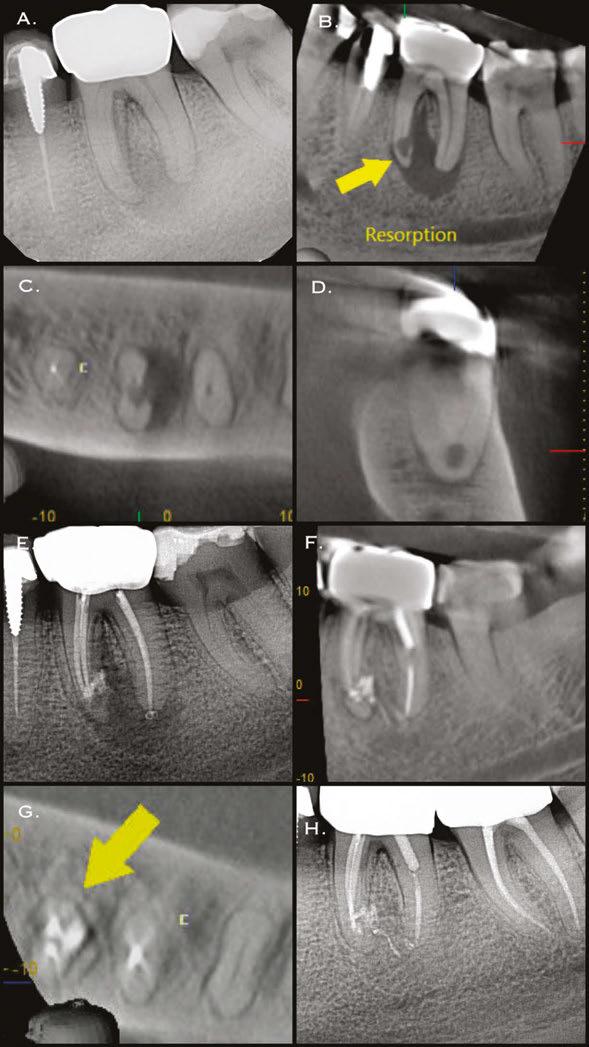
Figures 4A-4H: 4A. Preoperative periapical radiograph of tooth No. 19. Visualization of periapical radiolucency associated with mesial root is possible. Root also appears to be calcified in middle and apical thirds. 4B. Sagittal CBCT slice showing internal resorption in apical portion of mesial root. Visualization of resorptive defect perforating on distal aspect of mesial root, and significant periapical pathology extending close to furcation is possible. Defect and extent of pathology was not visualized on periapical radiograph. 4C. Axial CBCT slice showing resorptive defect encapsulating both MB and ML canals and perforating on distal aspect of mesial root. There is significant bone loss adjacent to perforating defect. 4D. Coronal CBCT slice showing internal resorptive defect encapsulating both mesiobuccal and mesiolingual canals. 4E. Immediate postop radiograph after completion of endodontic treatment. 4F,4G. Coronal and axial CBCT slice at 16-month follow-up. Note resorptive defect filled with bioceramic sealer and complete healing of adjacent bone and reestablishment of PDL. Patient returned at 16-month point for endodontic treatment of tooth No.18. 4H. Three-year follow-up radiograph. Patient remained completely asymptomatic on tooth No 19
had recently worsened. Clinical examination revealed pain to percussion on tooth No. 19. No swelling was observed, and the tooth was not sensitive to palpation or biting. Radiographic and CBCT (Veraviewepocs 3D R100; J. Morita) examination revealed a crowned tooth No.19 with perforating internal root resorption near the apical end of the mesial root, accompanied by periapical pathology extending distally to involve the distal root and coronally toward the furcation (Figures 4A-4D). A diagnosis of pulpal necrosis with symptomatic apical periodontitis was made.
The prognosis for treating the tooth with root canal therapy was discussed, along with alternative options such as extraction and replacement with an implant or bridge. Due to financial constraints, the patient opted for endodontic treatment rather than extraction. It was also explained that follow-up treatment, including an apicoectomy of the mesial root, might be necessary if the lesion persists. Informed consent was obtained.
First visit
The patient was anesthetized with 1.7 mL of 3% mepivacaine (Carbocaine, Dentsply Pharmaceutical, York, Pennsylvania) via left inferior alveolar nerve block and 1.7 mL of 4% articaine with 1:100,000 epinephrine (Septocaine; Septodont, Lancaster, Pennsylvania) via buccal infiltration. After achieving rubber dam isolation, access was made through the porcelain-fused-to-metal (PFM) crown using a combination of a round diamond bur and a No. 2 surgical length carbide round bur. Necrotic pulp was encountered. Working length was established with a Root ZX apex locator (Morita, Tokyo, Japan). The canals were instrumented to a size 35 .04 Vortex Blue rotary file (Dentsply Tulsa Dental, Johnson City, Tennessee) and irrigated with 5.25% sodium hypochlorite. The EndoActivator (Dentsply, Tulsa, Oklahoma) was used to sonically agitate the irrigant to ensure thorough disinfection of the resorptive defect. The canals were dried with paper points, and calcium hydroxide (Ultracal XS, Ultradent Products Inc, South Jordan, Utah) was syringed into the canals and defect. The tooth was then temporarily restored with Cavit (3M ESPE, Neuss, Germany).
Second visit
The patient returned after 3 weeks for completion of endodontic treatment. He reported that all symptoms had subsided. Calcium hydroxide was removed from the canals with instrumentation, irrigation, and activation with the EndoActivator. The canals were dried with paper points, and excess irrigant was removed using a surgical suction with a micro-tip. The canals were coated with BC sealer to allow for sufficient amounts of sealer to fill the resorptive defect and were then obturated with gutta percha and BC (bioceramic) sealer using the technique of warm vertical conden-
sation (Figure 4E). The occlusal access opening was restored with TPH Spectra ST composite (Dentsply Sirona, Charlotte, North Carolina), and the patient was put on a recall schedule to monitor healing. The patient returned at the 16-month point for endodontic treatment of tooth No. 18. At a 16-month recall visit, the patient was completely asymptomatic on tooth No.19. And radiographic/CBCT examination revealed complete healing of the lesion adjacent to the resorptive defect on tooth No. 19 (Figures 4F and 4G). At the 3-year recall, the patient was asymptomatic on both teeth Nos.18 and 19.
Conclusion
Two cases of extensive perforating internal root resorption (IRR) successfully treated nonsurgically are presented. A discussion of the biologic process of IRR, combined with the importance of accurate diagnosis, underscores that a nonsurgical approach should be the primary treatment plan in such cases. The advent of bioceramic sealers has enabled a more standardized and effective endodontic approach for managing perforating internal resorption. Additionally, the use of CBCT during the diagnostic planning phase is crucial for accurately visualizing the full extent of the lesion.
REFERENCES
1. Patel S, Ford TP. Is the resorption external or internal? Dent Update. 2007 May;34(4):218220, 222, 224-226, 229. doi: 10.12968/denu.2007.34.4.218.
2. Harokopakis-Hajishengallis E. Physiologic root resorption in primary teeth: molecular and histological events. J Oral Sci. 2007 Mar;49(1):1-12. doi: 10.2334/josnusd.49.1.
3. Wedenberg C, Zetterqvist L. Internal resorption in human teeth--a histological, scanning electron microscopic, and enzyme histochemical study. J Endod. 1987 Jun;13(6):255-259. doi: 10.1016/S0099-2399(87)80041-9.
4. Tronstad L. Root resorption--etiology, terminology and clinical manifestations. Endod Dent Traumatol. 1988 Dec;4(6):241-252. doi: 10.1111/j.1600-9657.1988.tb00642.x.
5. Calişkan MK, Türkün M. Prognosis of permanent teeth with internal resorption: a clinical review. Endod Dent Traumatol. 1997 Apr;13(2):75-81. doi: 10.1111/j.1600-9657.1997. tb00014.x.
6. Fuss Z, Tsesis I, Lin S. Root resorption--diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol. 2003 Aug;19(4):175-182. doi: 10.1034/ j.1600-9657.2003.00192.x.
7. Haapasalo M, Endal U. Internal inflammatory root resorption: the unknown resorption of the tooth. Endodontic Topics. 2006;14(1), 60–79. https://doi.org/10.1111/j.1601 1546. 2008.00226.x.
8. Patel S, Ricucci D, Durak C, Tay F. Internal root resorption: a review. J Endod. 2010 Jul;36(7):1107-1121. doi: 10.1016/j.joen.2010.03.014. Epub 2010 May 20.
10. Gulabivala K, Searson LJ. Clinical diagnosis of internal resorption: an exception to the rule. Int Endod J. 1995 Sep;28(5):255-260. doi: 10.1111/j.1365-2591.1995.tb00310.x.
11. Lofthag-Hansen S, Huumonen S, Gröndahl K, Gröndahl HG. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 Jan;103(1):114-119. doi: 10.1016/j.tripleo.2006.01.001. Epub 2006 Apr 24.
12. Ee J, Fayad MI, Johnson BR. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J Endod. 2014 Jul;40(7):910-916. doi: 10.1016/j.joen.2014.03.002. Epub 2014 Apr 16.
13. Rodríguez G, Abella F, Durán-Sindreu F, Patel S, Roig M. Influence of Cone-beam Computed Tomography in Clinical Decision Making among Specialists. J Endod. 2017 Feb;43(2):194-199. doi: 10.1016/j.joen.2016.10.012.
A version of this article appeared in New York State Dental Journal.
“INTEGRATING THE SURGICAL AND RESTORATIVE TEAMS FOR SUPERIOR ESTHETIC OUTCOMES”
WSP/AMED 2025 ANNUAL SESSION
Hilton La Jolla Torrey Pines
Frank Spear
Miron Dr. David Clark
Dr. Jim Janakievski
Dr. Yasuko Nemoto
Continuing Education Quiz
Perforating internal root resorption (IRR): a closer look STERN
1. ______ is defined as the loss of dental hard tissues as a result of clastic activities, which can occur as a pathologic or physiologic process depending on the location and timing of the resorptive process.
a. Root resorption
b. Granulization
c. Internal erosion
d. Inflammatory excitation
2. The primary theory for what initiates internal root resorption (IRR) is located in the granulation tissue that forms in response to infected coronal pulp tissue.
a. vascularization
b. multinucleated giant cells
c. a fistula
d. perforation
3. Damage and/or loss of the predentin and odontoblastic layer
___________.
a. must occur during the resportive process
b. must occur after the resorptive process
c. must occur prior to the resorptive process
d. will seldom occur
4. Iatrogenic causes of continued inflammatory excitation of the coronal pulp include _______.
a. overheating the tooth
b. over-irrigating the tooth
c. over-irradiation from X-rays
d. none of the above
5. IRR is insidious and often progresses without symptoms.
a. True
b. False
6. Because active IRR requires a pulp space that is partially vital and partially necrotic, vitality testing ________.
a. must be performed
b. is very reliable
c. is unreliable
d. is recommended
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 070
Date Published: July 5, 2025
Expiration Date: July 5, 2028
7. If perforation has occurred, the external lesion has a life of its own, and __________.
a. treatment is unnecessary
b. treatment is essential
c. the patient should be carefully monitored
d. will no longer grow in size
8. While external root resorption comes in many forms, such as transient surface resorption, _______, and replacement resorption (ankylosis), internal root resorption is uniquely different.
a. pressure resorption
b. external inflammatory root resorption
c. invasive cervical root resorption
d. all of the above
9. The best and most accurate tool we have for diagnosing IRR and determining the path of the perforating lesion is _______.
a. 2D radiographs
b. cone beam computed tomography (CBCT)
c. visual examination
d. transillumination
10. The advent of bioceramic sealers has enabled a endodontic approach for managing perforating internal resorption.
a. more standardized
b. more effective
c. less effective
d. both a and b
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Additive manufacturing in clinical endodontics: current applications and future directions
Drs. Aaron Glick and Elham Abbassi offer a comprehensive overview of 3D printing and its applications
Introduction to 3D Printing
3D printing is a relatively new field starting in the 1980s with the understanding of sequentially polymerizing materials with a beam of UV light or laser.1 Since its inception, there has been significant interest and adoption of 3D printing in multiple fields. For example, a 400-square-foot 3D-printed house in Russia was made in 24 hours and at a cost of $10,000.2 Other fields use 3D printing for making automotive parts, fabricating tools in space, concocting custom edible foods, creating educational displays, and executing rapid prototyping for engineering projects. In the health field, bioprinting is being used to build bioactive scaffolds, create human cells, and synthesize implantable tissues.3
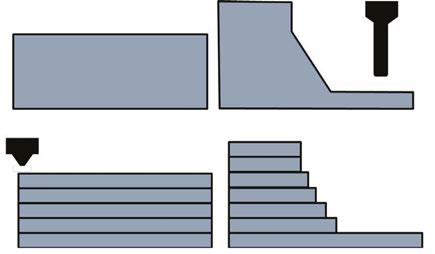
Subtractive versus additive manufacturing
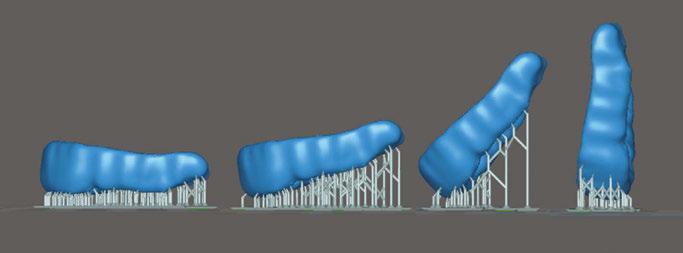
Generally, manufacturing techniques are either subtractive or additive. In subtractive manufacturing (i.e., CNC milling), the material is removed through carving or grinding away at the substructure. In additive manufacturing (i.e., 3D printing), the finished product is built through successive layers of material. Subtractive manufacturing involves a number of axes around which the block of material is rotated so the drill can remove the material, compared with additive manufacturing that will build layers of material in one plane as shown in Figure 1.
The additive nature of 3D printing holds a deep advantage in ease, cost, and flexibility. Due to the rotational axes required, there are some complex parts and internal geometries that are more difficult to manufacture through subtractive manufacturing (Figure 2). For instance, GE changed their manufacturing of some jet fuel nozzles since they could print one piece instead of assembling 20 separate parts.4 The decision to change their manufacturing method resulted in reducing manufacturing costs by 75%. Additive manufacturing allows for flexibility since the setup is minimal compared with retooling that is required for most high scale production facilities. In dentistry, the flexibility is underscored by multiple types of materials that can be used to build specific appliances.
Aaron Glick, DDS, is an Adjunct Clinical Associate Professor, General Practice and Dental Public Health, at the University of Texas Health Science Center at Houston School of Dentistry.
Elham Abbassi, DDS, is Assistant Professor and Group Practice Director, General Practice and Dental Public Health, University of Texas Health Science Center at Houston School of Dentistry.
Educational aims and objectives
This self-instructional course for dentists aims to discuss 3D printing, how it works, and its benefits and drawbacks and applications for the endodontist.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the differences between subtractive and additive manufacturing techniques.
• Recognize multiple applications for additive manufacturing in dentistry.
• Recognize some endodontic applications for 3D printing.
• Identify the clinical workflow for chairside 3D printing.
• Define bioprinting and realize its potential for dental applications. 2 CE CREDITS
Additive manufacturing technologies
The major categories of 3D printers are fused deposition modeling (FDM), stereolithography (SLA)/digital light projection (DLP), selective laser sintering (SLS), powder binder jetting (BJ), and photopolymer jetting (PJ) (Table 1). FDM printing is the most widely used type of printing that melts a thermoplastic filament. SLA/DLP use UV to cure a liquid photopolymer resting in a vat. This modality is most commonly used for dental applications
Figures 1A-1B: Subtractive and additive manufacturing. Differences of subtractive (1A) and additive (1B) manufacturing techniques A.
due to its ability to accurately create small complex parts with resin materials. SLS printers are utilized more commonly in industrial settings and can be found in dental labs as opposed to offices. These printers can output nylon and metal components that have high mechanical properties. BJ printing uses a bed of binder where the printhead deposits a binding agent. PJ jets and cures droplets of liquid photopolymer materials and can build structures that are composed of multiple types of material.5
3D printing in dentistry
3D printing is most cited in manufacturing (automotive and avionics) and consumer good fields followed by the health field.6 In the dental field, the current usage of 3D printers is low according to an American Dental Association (ADA) survey conducted in late 2023 with 17% of dentists owning a 3D printer.7 Yet, the adoption rate is high with those who noted they own a printer, 67% of the dentists have owned the printer for 2 years or less. Additionally, there is interest in this field since 56% of those surveyed noted that they are considering buying a 3D printer or completing training in 3D printing. Manufacturers have been recently rapidly developing new techniques for faster post processing, material sciences, and development of low-cost printers due to the expiration of multiple key patents of additive processes.8
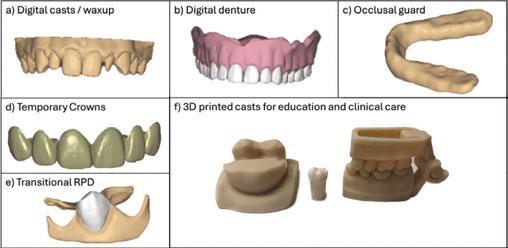
Multiple applications for additive manufacturing in dentistry
There are many applications of 3D printing in the field of dentistry. For instance, 3D printing can be used to create patient models, dentures, occlusal guards, temporary crowns, transitional RPDs, indirect orthodontic bonding trays, direct print aligners, retainers, surgical guides, implants, mandibular advancement devices, and educational devices (Figure 3). The patient models can be static or articulated and flexibly designed or altered digitally depending on the intended use. 3D printed dentures can offer reduced number of clinical appointments and higher intaglio accuracy, however have reduced esthetics compared with conventional dentures.9 The material properties of occlusal guards are similar to conventional and milled methods. Furthermore, wear resistance is not appreciably different between methods.10 Surgical guides can be used in implant placement, complicated root canal morphology, and complex
Figures 3A-3F: Applications of 3D printing and computer-aided design in general dentistry. Various applications of computer-aided design and subsequent 3D printing for 3A. Patient models and treatment planning mock-up. 3B. Complete dentures. 3C. Occlusal guards. 3D. Temporary crowns. 3E. Transitional RPDs, and 3F. Articulated patient models and scaled models for education (please note that the typodont tooth in the middle is used for scale purposes and is not 3D printed)
craniofacial surgeries. Static dental implant surgical guides are accurate when 3D printed, however additional factors such as image acquisition with cone beam computed tomography (CBCT), computer aided design (CAD), and slicer software can add errors that affect overall clinical accuracies.11,12
Endodontic applications
3D printing is a tool with multiple applications in the field of endodontics. Some applications include: 1) static guides for access preparation, 2) regenerative transplantation, 3) transplantation of obturation material, 4) pre-surgical planning/educational modeling. Static guides can facilitate guided access with pulp
SLS Powder (nylon, metal)Heat application
BJ Powder (metals, ceramics, sand, polymers)
and adhesive
PJ Photopolymer liquidLight application
and
models, occlusal guards, dentures Washing, curing, support removal
$500,000Functional prototypes with high mechanical properties
$30,000Consumer electronics, multi-material medical models or dentures
Depowdering, media blasting
Curing or sintering (depending on material)
Dissolvable support removal
Figure 2: Internal structures of additive manufacturing. The internal structure of this 3D printed model allows for bending that is easier with additive manufacturing compared to subtractive manufacturing
Table 1: Common types of 3D printing techniques
canal obliteration or provide minimally invasive access. The benefits of guided access include improving predictability of locating the root canal, greater preservation of sound tooth structure, and reducing risk of iatrogenic damage.13 Additionally, static guides can be used in microsurgeries and have been shown to increase accuracy of localizing root apices for apical resections.14
Innovative techniques, such as 3D bioprinting, are being investigated to replace teeth, where printing the microstructures of the scaffolding allows for the proliferation and maturation of undifferentiated cells. 3D printing has been used in the regeneration of dentin and pulpal tissues in addition to the full tooth complex.15 Revascularization of pulpal tissues can be aided through the creation of complex scaffolding that mimics natural vascular systems otherwise difficult to achieve with traditional hydrogels.16
The continued expansion of 3D printing applications in dentistry heavily relies on advancements in material sciences, as current common printing processes often involve high temperatures or photopolymerizing chemicals. Notably, a recent study demonstrated the custom printing of a modified gutta percha with a ZnO biocomposite replicating the radiographic root anatomy and which was shown to inhibit the growth of E. coli and S. aureus.17
Educational models generated through 3D printing can offer advantages for both before and during complex procedures by reproducing the patients’ specific spatial anatomies for full viewing with tactile input. In dental education, traditionally, extracted teeth are used to learn access, cleaning/shaping, and obturation. These teeth can be difficult to procure, not disinfected properly, or brittle, leading to a non-standardized learning experience. 3D printed models can provide a more acceptable and consistent educational experience. Printed models have been shown to allow for tailored learning experiences based on levels of difficulty.18 Ultimately, 3D printing is a tool that can be used in various settings and applications within the field of endodontics.
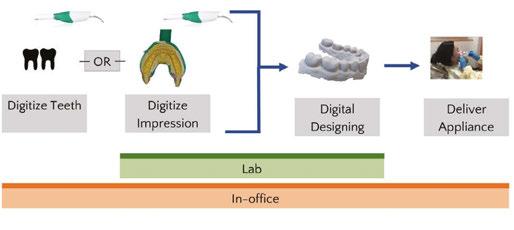
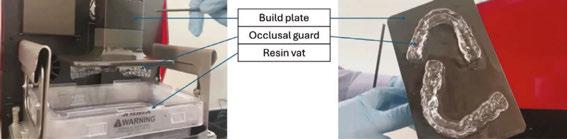
Clinical workflow for chairside 3D printing
The integration of these applications in a dental office might vary based on the device that is printed. Generally, the teeth are digitized and altered within a digital design software program and subsequently sent to a 3D printer. Given the cost of SLA/ DLP printers, it is more practical to complete all steps chairside instead of sending impressions to a traditional lab. The decision of how to complete these steps also depends on the materials required. Chairside 3D printing has been shown to be less time consuming, more cost efficient, and display similar trueness compared with lab-fabricated single unit crowns using subtractive methods.19
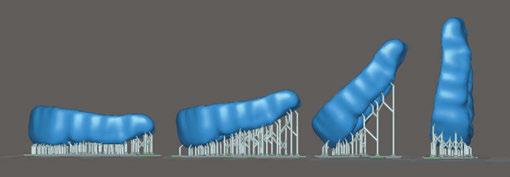
For SLA/DLP printing there are four main steps that deviate from milling: 1) slicing software and G-code creation, 2) 3D printing via vat polymerization, 3) isopropyl wash, and 4) final cure. The initial step after digitally designing the appliance is importing the digital file — usually in standard tessellation language file type (stl). This triangulated mesh surface geometry is encoded by slicing software that identifies the movements and curing protocols of the 3D printer based on user inputs (G-code). Figure 5 shows an example of an occlusal guard in multiple print orientations within the slicer software. The print orientation will affect material properties such as accuracy, strength, surface roughness, and microbial adhesion.21 For example, a dental model has been shown to have better material properties
in a horizontal orientation (0°), however, mass-producing dental models in the vertical orientation in dental labs allows for substantially higher throughput yet sacrifices trueness and surface quality. There are also additional factors such as layer thickness and material property that affect the final outcome.22
After slicing the stl, the automatically generated G-code can be used to operate the 3D printer. Within the context of a SLA/ DLP printer, there is a range of resins that can be used. The manufacturers are required to seek Food and Drug Administration (FDA) clearance for each indication of use.23 Therefore, there will be a set of materials that have been tested for the specific indication and are specifically formulated to have the appropriate mechanical properties.
Once printed, the device will have uncured resin surrounding the printed structure. The process of removing the uncured resin and attaining the structure’s final mechanical properties for a finished, functional product is called post-processing. This is completed in two steps: 1) Submerging the structure in isopropyl wash, 2) Curing the structure. The specifics of post-processing depend on the resin material manufacturer and the resin specifications. It is recommended to closely follow these instructions for use because deviations can result in underperforming mechanical properties and biocompatibility.24-26
After removing the printed solid from the build plate (Figure 6), the supports (if any) can be removed and excess resin washed off. The most widely used solvent washes are isopropyl alcohol and ethanol. Distributing the solvent evenly over the device is an important step to remove uncured liquid resin that has cytotoxic effects on the body. The exposure and permeation time of these solvents reduces the physical properties of the final product. Therefore, there is a fine balance of washing the structure long enough to reduce cytotoxicity but not too long to decrease its flexural strength.27-28
Figure 4: Chairside and lab workflows for additive manufacturing. There are multiple pathways for lab or chairside fabricated dental appliances using additive manufacturing (Adapted figure20)
Figure 5: Print orientations in slicer software. Occlusal guard in different print orientations from horizontal (0°) [on left of the picture] to vertical (90°) [on right of the picture]
After the solvent has been completely evaporated, the final cure (post-polymerization) is initiated to complete the polymerization reaction. The product is placed in a UV chamber where the temperature, method, and duration will influence the mechanical properties of the end-product. The oxygen-inhibited layer will prevent full polymerization in subsequent steps. For instance, glycerin immersion, nitrogen chamber, and low-pressure vacuum have been methods to reduce the oxygen-inhibited layer. Reducing the oxygen-inhibited layer and reducing viscosity of the resin with higher temperatures has been shown to improve the mechanical properties of the resin.29-30 Generally, an increase of duration and intensity of the UV post-polymerization improves end-product strength.31
The rapid evolution of 3D printing technology is expanding the indications of use, reshaping clinical workflows, and reducing patient case limitations. Ongoing advancements, such as enhanced material properties and increased print speeds, allow for chairside integration. As of 2022, there were approximately 100 rigid and 30 flexible biocompatible resin materials on the market.32 Multiple advanced formulations continue to become FDA cleared, therefore increasing the selections and indications for printing. Additionally, the many types of 3D printing technology allow dental labs to reduce cost and increase throughput.
Future of 3D printing
Bioprinting
Bioprinting, a specialized subset of 3D printing, has gained significant traction in regenerative medicine by enabling the fabrication of functional tissues through layer-by-layer deposition of bioinks containing living cells and biomaterials. This technology has been explored for applications in tissue engineering, drug development, and personalized medicine. Bioprinting has been used to vascularize tissues, skin grafts, and organ models for transplantation and disease modeling.33 The field is rapidly expanding, with research focusing on enhancing cell viability, structural integrity, and biomimetic properties of printed tissues to bridge the gap between laboratory models and clinical applications.34
In dentistry, bioprinting has shown potential for regeneration of soft and hard tissues including bone, cartilage, and mucosa. The development of bioengineered scaffolds infused with stem cells and growth factors has facilitated tooth, periodontal ligament, and alveolar bone regeneration.35-36 In vivo assessments in animal models have been investigated in bone, periodontal ligament, and dentin regeneration with generally positive results.37 As bioprinting technology matures, its integration into clinical practice could revolutionize regenerative treatments in dental surgery by offering patient-specific, bioengineered tissues that improve functional and esthetic outcomes. These tools show promise in maintaining the structural integrity of patient anatomy and in reducing the immune response seen with conventional bone grafts.
Regulation in point-of-care printing
The ability to print custom devices for patients chairside disrupts the traditional workflow of dental offices. Traditionally, dental labs have fabricated all indirect prostheses. However, to maintain patient safety and effectiveness of the devices, the Food and Drug Administration (FDA) has identified software, material,
and post-processing controls.38 Because the FDA regulates finished products, it also regulates dental devices at the point of care. Manufacturers will test their material with specific software along the workflow, and any modifications that a dentist makes to the lawfully marketed device could potentially have safety consequences.39 Due to increased controls by the FDA, free market competition is reduced, thus incentivizing manufacturers to build proprietary systems with higher upfront costs to the dentist. Despite commonly used controls, like quality management systems (i.e., ISO 13485), that are common in the industrial manufacturing sector, the specific guidelines for regulatory requirements for chairside 3D printing are sparce.32
Prototypes and innovation
The benefits of 3D printing for small scale, custom products are a notable reason that this technology fits well in dentistry because the majority of extraorally fabricated devices are patient-specific. As more dentists adopt this technology, the path toward fabricating dental-specific prototypes will increase early stages of innovation. Sites similar to thingiverse (thingiverse. com) or makerworld (makerworld.com) have accelerated userbased innovation and pose a possibility for democratizing supply chains — particularly for spare parts manufacturing.40 A recent example showing the importance of supply chain diversification was demonstrated during the COVID-19 pandemic when many dental offices began printing face shields, masks, and other medical devices as demand exceeded supply inventories.41
Re-thinking the application of current innovations in dental material science allows for boundless iterations of traditional designs. For instance, custom implants that do not require surgery (placement at time of extraction), hollow implants that allow for time-based release of anti-inflammatory mediators, and reductions of thickness or chairside implant printing through SLA compatible zirconium dioxide.42
3D printing technology can also be used in tandem with AI (artificial intelligence) in novel ways.43 For instance, AI frameworks have been used to reduce human error and automate critical steps in 3D-printing processing.44 Additionally, both tools can be used in the full digital workflow to create a dental prosthesis: a generative AI computer-aided design can be automatically created, then 3D printed and fitted to the patient.45-46
Summary
Additive manufacturing has multiple applications that are currently used in dental offices. There are still barriers for wide adoption, however the application of a personalized manufacturing approach combined with 3D technologies fits well into a digital clinical workflow. In order to adopt 3D printing in
Figure 6: Anatomy of SLA/DLP vat resin type printer. Images of an SLA/DLP vat resin = printer with associated labels for a) build plate that adheres to the printed device, b) occlusal guards as an example of a printed device, c) resin vat of splint-specific uncured liquid resin
dentistry, an understanding of the different additive technologies and available materials is important. Each type of 3D printing technology has different upfront costs that can preclude its use in a dental clinic. Additionally, the post-processing criteria will vary on the type of print technology selected. Based on current research, 3D printing technology has the potential to reduce time spent and incurred costs for a semi-automated solution of custom dental prostheses.
REFERENCES
1. Pei E, Kabir IR, Leutenecker-Twelsiek B. History of AM. In: Springer Handbook of Additive Manufacturing. 2023 Oct 18 (pp. 3-29). Cham: Springer International Publishing.
2. Sakin M, Kiroglu YC. 3D Printing of Buildings: Construction of the Sustainable Houses of the Future by BIM. Energy Procedia. 2017 Oct 1;134:702-711.
3. Gu Q, Hao J, Lu Y, Wang L, Wallace GG, Zhou Q. Three-dimensional bio-printing. Sci China Life Sci. 2015 May;58(5):411-9. doi: 10.1007/s11427-015-4850-3. Epub 2015 Apr 29.
4. D’Aveni R. The 3-D printing revolution. Harvard Business Review. 2015 May;93(5):40-48.
5. Jakus AE. An introduction to 3D printing—past, present, and future promise. In: 3D printing in Orthopaedic Surgery. Elsevier;Jan 2019:1-15. doi:10.1016/B978-0-323-58118-9.00001-4.
6. Ukobitz DV. Organizational adoption of 3D printing technology: a semisystematic literature review. Journal of Manufacturing Technology Management. 2021 Dec 17;32(9):48-74.
7. Revilla-León M, Frazier K, da Costa J, Haraszthy V, Ioannidou E, MacDonnell W, Park J, Tenuta LM, Eldridge L, Vinh R, Kumar P. Prevalence and applications of 3-dimensional printers in dental practice. J Am Dent Assoc. 2023 Apr 1;154(4):355-356. doi: 10.1016/j.adaj.2023.02.004.
8. Kessler A, Hickel R, Reymus M. 3D Printing in Dentistry-State of the Art. Oper Dent. 2020 Jan/ Feb;45(1):30-40. doi: 10.2341/18-229-L. Epub 2019 Jun 7.
9. Alhallak K, Hagi-Pavli E, Nankali A. A review on clinical use of CAD/CAM and 3D printed dentures. Br Dent J. 2023 Jan 9. doi: 10.1038/s41415-022-5401-5. Epub ahead of print.
10. Valenti C, Federici MI, Coniglio M, Betti P, Pancrazi GP, Tulli O, Masciotti F, Nanussi A, Pagano S. Mechanical and biological properties of polymer materials for oral appliances produced with additive 3D printing and subtractive CAD-CAM techniques compared to conventional methods: a systematic review and meta-analysis. Clin Oral Investig. 2024 Jun 25;28(7):396. doi: 10.1007/s00784-024-05772-6.
11. Ashtiani RE, Ghasemi Z, Nami M, Mighani F, Namdari M. Accuracy of static digital surgical guides for dental implants based on the guide system: A systematic review. J Stomatol Oral Maxillofac Surg. 2021 Dec 1;122(6):600-6077. doi: 10.1016/j.jormas.2020.10.010.
12. Juneja M, Thakur N, Kumar D, Gupta A, Bajwa B, Jindal P. Accuracy in dental surgical guide fabrication using different 3-D printing techniques. Additive Manufacturing. 2018 Aug 1;22:243-255. doi: 10.1016/j.addma.2018.05.012.
13. Ribeiro D, Reis E, Marques JA, Falacho RI, Palma PJ. Guided Endodontics: Static vs. Dynamic Computer-Aided Techniques-A Literature Review. J Pers Med. 2022 Sep 15;12(9):1516. doi: 10.3390/jpm12091516.
14. Zhao D, Xie W, Li T, Wang A, Wu L, Kang W, Wang L, Guo S, Tang X, Xie S. New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: a study of 14 upper anterior teeth. Sci Rep. 2023 Sep 19;13(1):15512. doi: 10.1038/s41598-023-42767-x.
15. Ma Y, Xie L, Yang B, Tian W. Three-dimensional printing biotechnology for the regeneration of the tooth and tooth-supporting tissues. Biotechnol Bioeng. 2019 Feb;116(2):452-468. doi: 10.1002/bit.26882. Epub 2018 Dec 14.
16. Bertassoni LE. Progress and Challenges in Microengineering the Dental Pulp Vascular Microenvironment. J Endod. 2020 Sep;46(9S):S90-S100. doi: 10.1016/j.joen.2020.06.033.
17. Yan S, Wan M, Liao W, Dai Z, Chen G, Li H, Cai H, Zhang H, Zheng W, Ding K, Zhou W. Alternative Polyurethane/Gutta-Percha/ZnO Biocomposite for Root Canal Therapy Based on an Efficient Melt Extrusion Additive Manufacturing Strategy. ACS Applied Polymer Materials. 2023 May 23;5(6):4106-4117.Hollister SJ. Porous scaffold design for tissue engineering. Nat Mater [Internet]. 2005;4:518–524. Available from: https://www.nature.com/articles/ nmat1421.
18. Tawasinchanadech N, Thammasitboon S, Buranadham S, Thammasitboon K. Mastery Learning in Preclinical Endodontics Using Customized 3D-Printed Tooth Models for Deliberate Practice: An Application of Educational Design Research. J Endod. 2024 Sep;50(9):1273-1280. doi: 10.1016/j.joen.2024.06.002. Epub 2024 Jun 19.
19. Mangano FG, Cianci D, Pranno N, Lerner H, Zarone F, Admakin O. Trueness, precision, time-efficiency and cost analysis of chairside additive and subtractive versus lab-based workflows for manufacturing single crowns: An in vitro study. J Dent. 2024 Feb;141:104792. doi: 10.1016/j.jdent.2023.104792. Epub 2023 Nov 25.
20. Glick A and Flamenco D. Clinical application and implementation of 3D Printing. J Greater Houston Dent Soc. 2023; 94(4):16-19.
21. Shim JS, Kim JE, Jeong SH, Choi YJ, Ryu JJ. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J Prosthet Dent. 2020 Oct;124(4):468-475. doi: 10.1016/j.prosdent.2019.05.034. Epub 2019 Dec 4.
22. Alghauli MA, Almuzaini SA, Aljohani R, Alqutaibi AY. Impact of 3D printing orientation on accuracy, properties, cost, and time efficiency of additively manufactured dental models: a systematic review. BMC Oral Health. 2024 Dec 26;24(1):1550. doi: 10.1186/ s12903-024-05365-5.
23. Da Silva TM, Immich F, De Araujo TS, Lund RG, Da Silva AF, Piva E, Da Rosa WLO. Photo-
sensitive resins used in additive manufacturing for oral application in dentistry: A scoping review from lab to clinic. J Mech Behav Biomed Mater. 2023 May;141:105732. doi:10.1016/j. jmbbm.2023.105732. Epub 2023 Mar 1.
24. Cao J, Liu X, Cameron A, Aarts J, Choi JJE. Influence of different post-processing methods on the dimensional accuracy of 3D-printed photopolymers for dental crown applicationsA systematic review. J Mech Behav Biomed Mater. 2024 Feb;150:106314. doi: 10.1016/j. jmbbm.2023.106314. Epub 2023 Dec 12.
25. Vasques MT, Mulder JN, Machado DS, Lagana DC. The influence of the post-processing method on knoop hardness of photosensitive resins for 3D SLA printer used in Dentistry. Clinical and Laboratorial Research in Dentistry. 2019 Dec 31. Available at: https://www.revistas. usp.br/clrd/article/view/161294.
26. Cabrol A, Chuy V, Fron-Chabouis H, Naveau A. Effectiveness of postprocessing on 3D printed resin biocompatibility in prosthodontics: A systematic review. J Prosthet Dent. 2024 Sep 19:S0022-3913(24)00588-2. doi: 10.1016/j.prosdent.2024.08.014. Epub ahead of print.
27. Xu Y, Xepapadeas AB, Koos B, Geis-Gerstorfer J, Li P, Spintzyk S. Effect of post-rinsing time on the mechanical strength and cytotoxicity of a 3D printed orthodontic splint material. Dent Mater. 2021 May;37(5):e314-e327. doi: 10.1016/j.dental.2021.01.016. Epub 2021 Feb 18.
28. Hwangbo NK, Nam NE, Choi JH, Kim JE. Effects of the Washing Time and Washing Solution on the Biocompatibility and Mechanical Properties of 3D Printed Dental Resin Materials. Polymers (Basel). 2021 Dec 16;13(24):4410. doi: 10.3390/polym13244410.
29. Kim YJ, Kim HN, Kim DY. A study on effects of curing and machining conditions in post-processing of SLA additive manufactured polymer. Journal of Manufacturing Processes. 2024 Jun 15;119:511-519. doi:10.1016/j.jmapro.2024.03.112.
30. Lim JH, Lee SY, Gu H, Jin G, Kim JE. Evaluating oxygen shielding effect using glycerin or vacuum with varying temperature on 3D printed photopolymer in post-polymerization. J Mech Behav Biomed Mater. 2022 Jun;130:105170. doi: 10.1016/j.jmbbm.2022.105170. Epub 2022 Mar 13.
31. Lin YC, Tarrazzi D, Schoenbaum T, Knoernschild K. Effect of postprocessing parameters on the flexural strength of vat-polymerized additively manufactured interim fixed dental prostheses: A systematic review with postprocessing guidelines. J Prosthet Dent. 2024 Aug 13:S00223913(24)00497-9. doi: 10.1016/j.prosdent.2024.07.016. Epub ahead of print.
32. Guttridge C, Shannon A, O’Sullivan A, O’Sullivan KJ, O’Sullivan LW. Biocompatible 3D printing resins for medical applications: A review of marketed intended use, biocompatibility certification, and post-processing guidance. Annals of 3D Printed Medicine. 2022 Mar 1;5:100044. https://doi.org/10.1016/j.stlm.2021.100044.
33. Murphy SV, Atala A. 3D bioprinting of tissues and organs. Nat Biotechnol [Internet]. 2014;32:773–785. Available from: https://www.nature.com/articles/nbt.2958.
34. Groll J, Burdick JA, Cho D-W, Derby B, Gelinsky M, Heilshorn SC, Jüngst T, Malda J, Mironov VA, Nakayama K, Ovsianikov A, Sun W, Takeuchi S, Yoo JJ, Woodfield TBF. A definition of bioinks and their distinction from biomaterial inks. Biofabrication [Internet]. 2018;11(1):013001. doi: 10.1088/1758-5090/aaec52Available from: http://dx.doi.org/10.1088/1758-5090/aaec52.
35. Morrison DG, Tomlinson RE. Leveraging Advancements in Tissue Engineering for Bioprinting Dental Tissues. Bioprinting. 2021 Aug;23:e00153. doi: 10.1016/j.bprint.2021.e00153. Epub 2021 Jun 13.
36. Ostrovidov S, Ramalingam M, Bae H, Orive G, Fujie T, Shi X, Kaji H. Bioprinting and biomaterials for dental alveolar tissue regeneration. Front Bioeng Biotechnol. 2023 Apr 14;11:991821. doi: 10.3389/fbioe.2023.991821.
37. Mohd N, Razali M, Fauzi MB, Abu Kasim NH. In Vitro and In Vivo Biological Assessments of 3D-Bioprinted Scaffolds for Dental Applications. Int J Mol Sci. 2023 Aug 17;24(16):12881. doi: 10.3390/ijms241612881.
38. Food and Drug Administration. Technical considerations for additive manufactured medical devices: guidance for industry and food and drug administration staff. 2017. Accessed 3/19/2025 at: https://www.fda.gov/media/97633/download
39. Kuo RF, Lin YS, Yang TH, Nguyen AT. 3D printing: limitations, safety, and regulatory considerations for oral health science. In: 3D Printing in Oral Health Science: Applications and Future Directions 2022 Sep 27: 269-291. Cham: Springer International Publishing. 10.1007/978-3-031-07369-4_13.
41. Longhitano GA, Nunes GB, Candido G, da Silva JVL. The role of 3D printing during COVID-19 pandemic: a review. Prog Addit Manuf. 2021;6(1):19-37. doi: 10.1007/s40964-020-00159-x. Epub 2020 Nov 24.
42. Joda T, Yeung AWK, Hung K, Zitzmann NU, Bornstein MM. Disruptive Innovation in Dentistry: What It Is and What Could Be Next. J Dent Res. 2021 May;100(5):448-453. doi: 10.1177/0022034520978774. Epub 2020 Dec 16.
43. Glick A, Tipton N, Manila N, Chang J. AI in implant dentistry: clinical implementation and considerations for use. Implant Practice US. 2024;17(1):20-24, Quiz 25.
44. Martinez G, Huang K, Lou Y, Bai Y. Innovative Applications of AI and 3D Printing in Digital Dentistry: Enhancing Accuracy and Efficiency in Dental Care. In: 2024 International Conference on Identification, Information and Knowledge in the Internet of Things (IIKI). 2024 Dec 6:237-242. 10.1109/IIKI65561.2024.00048.
45. Chau RCW, Chong M, Thu KM, Chu NSP, Koohi-Moghadam M, Hsung RT, McGrath C, Lam WYH. Artificial intelligence-designed single molar dental prostheses: A protocol of prospective experimental study. PLoS One. 2022 Jun 2;17(6):e0268535. doi: 10.1371/journal. pone.0268535.
46. Zhao X, Li N, Zhang Z, Hong J, Zhang X, Hao Y, Wang J, Xie O, Zhang Y, Li H, Liu M, Zhang P, Ren X, Wang X. Beyond hype: unveiling the Real challenges in clinical translation of 3D printed bone scaffolds and the fresh prospects of bioprinted organoids. J Nanobiotechnology [Internet]. 2024;22(1):500. Available from: http://dx.doi.org/10.1186/s12951-024-02759-z.
Continuing Education Quiz
Additive manufacturing in clinical endodontics: current applications and future directions
GLICK/ABBASSI
1. ___________ printing is the most widely used type of printing that melts a thermoplastic filament.
a. Fused deposition modeling (FDM)
b. Selective laser sintering (SLS)
c. Powder binder jetting (BJ)
d. Digital light projection (DLP)
2. Manufacturers have been recently rapidly developing new techniques for ___________ due to the expiration of multiple key patents of additive processes.
a. faster post processing
b. material sciences
c. development of low-cost printers
d. all of the above
3. 3D printing can be used to create patient models, ___________, transitional RPDs, indirect orthodontic bonding trays, direct print aligners, retainers, surgical guides, implants, mandibular advancement devices, and educational devices.
a. dentures
b. occlusal guards
c. temporary crowns
d. all of the above
4. Applications for 3D printing in endodontics include: _______ and pre-surgical planning/educational modeling.
a. static guides for access preparation
b. regenerative transplantation
c. transplantation of obturation material
d. all of the above
5. Static guides can facilitate guided access with pulp canal obliteration or provide minimally invasive access.
a. True
b. False
6. For _________ there are four main steps that deviate from milling: 1) slicing software and G-code creation, 2) 3D printing via vat polymerization, 3) isopropyl wash, and 4) final cure.
a. PEEK printing
b. SLA/DLP printing
c. powder-binder jetting
d. photopolymer jetting
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 070
Date Published: July 5, 2025
Expiration Date: July 5, 2028
2 CE CREDITS
7. The specifics of post-processing depend on ___________.
a. the resin material manufacturer
b. the resin specifications
c. microbial adhesion
d. both a and b
8. ________, a specialized subset of 3D printing, has gained significant traction in regenerative medicine by enabling the fabrication of functional tissues through layer-by-layer deposition of bioinks containing living cells and biomaterials.
a. Bioprinting
b. Microbial adhesion
c. Static surgical guides
d. Slicer software
9. To maintain patient safety and effectiveness of the devices, the __________ has identified software, material, and post-processing controls.
a. American Dental Association
b. Food and Drug Administration (FDA)
c. Environmental Protection Agency
d. National Institutes of Health
10. AI frameworks have been used to reduce human error and automate critical steps in 3D-printing processing.
a. True
b. False
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Improving endodontic success by utilizing EndoCeramic ® Sealer
Dr. George Just discusses research on a bioceramic sealer from Endo Direct
The American Association of Endodontists’ Guide to Clinical Endodontics outlines the acceptable standards for the nonsurgical treatment of permanent teeth.1
Sealer is a highly important component of successful endodontic treatment. It ensures a hermetic seal thus filling voids in the gutta-percha core material, as well as preventing bacteria from reentering the canal system via the apex and/or lateral canals.
The properties of an ideal sealer are the following:
1. Preventing leakage and reinfection of the peri apical tissues, and or inflammation of the periapical tissues
2. Functioning as an antimicrobial agent, thus destroying microbes that were not eliminated in the cleaning, shaping, and disinfection of the canal system, as well as those that might attempt to leak in over time
3. Solubility — an ideal sealer must exhibit low solubility in tissue fluids, thus preventing microleakage and reinfection
4. Good dimensional stability
Recent research by Abdoul R. Koroni, DDS, at the University of Maryland School of Dentistry tested these properties in several different sealers. His research compared EndoCeramic® by Endo Direct, EndoSequence® BC Sealer by Brasseler USA, NeoSealer® Flo by AvalonBiomed, and ProRoot® MTA by Dentsply Sirona. His evaluation methods used ISO 6876. All tests were performed in triplicate.
Dr. Koroni’s research evaluated the following properties of endodontic sealers:
1. Dimensional stability
2. Solubility — ability of the sealer not to dissolve
3. Film thickness
4. Flowability — the ability of the sealer to spread and fill the canal, thus preventing leakage
5. Working time — time it takes the sealer to set, thus allowing time to place the gutta-percha cone and seal the root canal system
George Just, DDS, is an endodontist practicing in Monroeville, Pennsylvania. He has lectured globally for the past 30 years.
Results
EndoCeramic® Sealer from Endo Direct
1. Dimensional Stability: EndoCeramic® by Endo Direct had the least amount of dimensional changes after 30 days (0.48%).
2. Solubility: EndoCeramic® by Endo Direct had the lowest rate of solubility at (2.08%)(p>.05).
3. Setting time: EndoSequence® had the longest at 1,428.67 minutes, ProRoot MTA the shortest at 251.33 minutes.
4. Flowability: All tested sealers were comparable.
5. Film thickness: All sealers tested were comparable. The exception was ProRoot MTA (repair material) which was very thick.
Discussion
This research paper demonstrates that EndoCeramic® sealer by Endo Direct exhibits outstanding results when compared to NeoSealer® Flo, EndoSequence® BC Sealer, and ProRoot® MTA. It far surpassed the other sealers in the two most important properties of a sealer for long-term success, solubility, and dimensional stability. Both are of paramount importance in preventing microleakage and failure of the root canal. In all other attributes tested, EndoCeramic® sealer was comparable to the others tested. Dr. Koroni noted: “EndoCeramic® offers superb dimensional stability and low solubility making it ideal for long term treatment applications.”
REFERENCE
1. American Association of Endodontists. Guide to Clinical Endodontics. 5th ed. 2015. https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/. This information was provided by Endo Direct.
Leadership is a choice
Drs. Joel C. Small and Edwin McDonald discuss dynamic leadership
Effective leadership begins with intentionality. To be an effective leader, we must have a clear understanding of our purpose and the mission for our practice. This clarity allows us to align our actions with our values, creating a cohesive narrative that our team can commit to and rally around. When we lead with purpose, we establish a vision that inspires our team, fostering a shared sense of direction.
From a practice perspective, the benefits of purposeful effective leadership are significant. When leaders intentionally engage with their teams, the result is often improved performance. Employees who feel supported and valued are more likely to be productive, engaged, and committed to their work. This commitment translates into higher quality outputs and better patient care in healthcare settings. Organizations led by engaged leaders tend to experience lower turnover rates. When employees feel connected to their leaders and the organization’s mission, they are more likely to remain loyal, reducing recruitment and training costs associated with high turnover. Moreover, organizations with effective leaders are better equipped to navigate challenges and adapt to change. When leaders model emotional intelligence and demonstrate commitment to their teams, they build a resilient workforce that can respond effectively to unexpected situations. This resilience is crucial in the healthcare sector, where changes can happen rapidly and require immediate adaptation.
Furthermore, it has been our experience that teams that are empowered through effective leadership become capable of handling many of the tasks whose time and effort diminish the leader’s work/life balance. Research has shown that leaders who make time for family and personal development are much less likely to suffer from burnout.
Being the boss versus being the leader
It is important that we distinguish between being a boss and being a leader. Being a boss does not mean that we are being a leader unless we choose to do so. A boss is simply someone one who exercises control over workers. A leader is someone who influences others so that they willingly and eagerly commit to his or her purpose and vision for an organization.
Drs. Joel C. Small and Edwin (Mac) McDonald have a total of over 75 years of dental practice experience. Both doctors are trained and certified Executive Leadership Coaches. They have joined forces to create Line of Sight Coaching, a business dedicated to helping their fellow dentists discover a better and more enjoyable way to create and lead a highly productive clinical dental practice. Through their work, clients experience a better work/life balance, find more joy in their work, and develop a strong practice culture and brand that positively impact their bottom line. To receive their free ebook, 7 Surprising Steps to Grow Your Practice Through Leadership, go to www.lineofsightcoaching.com.
Bosses who abrogate their leadership responsibilities maintain a quid pro quo relationship and culture with their team; basically, you work so you can receive pay — nothing more. Influential leaders, on the other hand, create team synergy and a culture of commitment that, by their very nature, improve the lives of everyone on the team. Values become the guidelines defining the way the team works together and how they fulfill the practice’s mission. There is clarity regarding the practice’s prevailing purpose and vision that translates into action and enthusiasm within the team.
Authoritarian versus influencer approach
Transactional leaders often exhibit authoritarian tendencies, relying on top-down control and strict adherence to rules and protocols. This approach can create an atmosphere of compliance rather than creativity, potentially leading to resentment or disengagement among team members. Feedback is sought by authoritative leaders as a means of assessment or evaluation, often using it to enforce accountability and highlighting the shortcomings of team members. Knowing this, individual team members become reluctant to offer valuable and creative feedback that can prove essential for team development.
Outwardly, authoritarian leadership may create cultures that appear productive and profitable. While authoritative leadership can lead to immediate results, particularly in environments that require strict adherence to processes, it often lacks the flexibility to adapt to changing conditions. Teams may excel at meeting shortterm goals but struggle with long-term innovation and growth, as the emphasis remains on compliance rather than creativity. Such practice cultures often lack resilience and are unable to thrive when placed under stress.
Transformational leaders are influencers who produce peak performing teams by bringing out the best that their team has to offer. They can tap into their team’s discretionary energy that is never offered to authoritarians. They do this by creating an open environment where team members feel comfortable sharing their insights and suggestions. This openness not only fosters trust but also empowers staff to contribute to the decision-making process, enhancing their commitment and engagement.
Research shows that organizations characterized by transformational leadership tend to have higher levels of open communication and feedback, leading to a more agile and responsive culture. This culture encourages continual learning and adaptation, which is essential in today’s fast-paced healthcare environment.
Ultimately, the choice between transactional and transformational leadership reflects the values and priorities of the organization itself. As healthcare practices continue to evolve in an increasingly complex landscape, the need for leaders who inspire and elevate their teams has never been more important. By prioritizing these essential aspects of leadership, we empower our teams to reach their full potential, paving the way for ongoing success and innovation in our field.
EP
Improving endodontic success with advances in NiTi rotary files and bioceramic sealers
Dr. Gregori M. Kurtzman describes the characteristics of new hand files and bioceramic sealer
Endodontic treatment has advanced over the past 4 decades. Instrumentation, traditionally performed utilizing hand files that were 02 in taper, led to potentially being unable to instrument canals easily and efficiently, as certain canals had greater tapers than the files available at the time. Filing was performed with a reciprocal motion which added to procedure inefficiency. The introduction of rotary files improved treatment efficiency. Tapers that more closely matched the shape of the canal and rotary motion with the file were able to clean and shape the canal better than reciprocal motion utilized with hand files. Additionally, hand files were fabricated with stainless steel which does not have the flexibility of NiTi rotary files. More flexible files can follow the canals’ curvature without overinstrumenting the canal when a curved canal is more pronounced.
Rotary NiTi files aid in maintaining as much native tooth structure as possible, especially in the coronal and cervical portion of the root by cleaning the canal walls without removing excess tooth structure following the canals’ natural anatomy and taper.
Obturating the canal system also has undergone advances in recent years. Traditional sealers, zinc oxide and eugenol (ZOE) or calcium hydroxide-based have been in use for many decades.
ZOE sealers are extremely sensitive to moisture in the canal system, which can inhibit their setting reaction. This can result in incomplete or inadequate sealing of the canal system. Studies have demonstrated a higher leakage than the other sealers.1
ZOE sealers, as they contain eugenol, have been shown to have potential toxic effects on surrounding tissues, especially if sealer is extruded apically during obturation. This can irritate the extra apical periodontal tissue causing an inflammatory response.2 ZOE sealers are also soluble in the presence of oral fluids or moisture,
Gregori Kurtzman, DDS, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 900 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@maryland-implants.com.
Disclosure: Dr. Kurtzman is a key opinion leader for SS White.
which can lead to the gradual loss of the sealer creating pathways for bacterial leakage and reducing the longevity of the seal.3
Calcium hydroxide-based sealers have been used due to their bactericidal nature and tissue healing properties. However, these sealers also have limitations related to their poor sealing ability and potential for gaps or shrinkage. This may lead to leakage and subsequent failure of the endodontic treatment.4 These sealers exhibit significant solubility in oral fluids that can lead to the gradual breakdown of the material, resulting in loss of the sealing function. Additionally, these types of sealers do not strongly adhere to dentin, which may lead to gaps or poor adaptation between the sealer and the canal walls. This lack of adhesion increases the likelihood of microbial leakage, potentially compromising the success of treatment.5
With those issues of traditional endodontic sealers, the shift was to a sealer type that is not affected by moisture during setting, is insoluble to eliminate potential leakage, and is bio-compatible if extruded apically. Bioceramic sealers met those expectations and originated in orthopedics in the 1970s for treatment of bone defects.6 Use in dentistry began a few decades ago, and use as an endodontic sealer was a natural transition related to its biocompatibility, bond to dentin, and insolubility once set.
The EXIMIA7™ file system
EXIMIA7™ endodontic files are designed with precision, flexibility, and durability to improve and simplify instrumentation of the canal system. These NiTi files are heat treated to increase resistance to cyclic fatigue and enhance the files’ strength and flexibility, minimizing shape memory for optimal precision. This also allows for extreme flexibility of the file in curved canals, reducing file shape memory, preserving canal anatomy, and limiting or eliminating over-instrumentation of the inner curve that may happen with stiffer files. Additionally, the files allow for instrumentation in challenging canal anatomy. The “controlled memory” of EXIMIA7™ files allows the file to return to its original shape after being bent during instrumentation in curved canals, thus maintaining the desired path in the canal. The files have a parabolic cross section, maximizing the files’ cutting efficiency for smoother procedures. They have a 1mm maximum flute diameter that allows for minimally invasive preparation, preserving tooth structure in the critical cervical area of the root. A non-cutting tip on the files provides precise guidance and centering the files within the canal, aiding in elim-
inating file transportation away from canals’ true path or perforation of the lateral aspect of the root.
EXIMIA7™ files’ sharp cutting edges allow for efficient and smooth removal of debris and tissue from the canal, minimizing the risk of ledging or zipping. The constant taper with a variable pitch design improves cutting efficiency while reducing file binding, or potential file separation.
They are available in .04 and .06 constant tapers with an ISO tip size of 17-45 in available lengths of 21 mm, 25 mm, and 29 mm (Figure 1). The system additionally provides gutta-percha cones and paper points that match the files’ taper and size to allow single cone obturation, allowing the fitted cone to press
comes in a pre-mixed syringe with disposable intraoral tips to aid in placement of the sealer into the canal system if that method is desired
sealer into the adjacent canal anatomy (Figures 2 and 3). The gutta-percha cones and paper points have length markings on them to aid in assuring working length (WL) is achieved when drying the canals and during obturation.
PURE-Ca-SEAL™ bioceramic sealer
PURE-Ca-SEAL™, an FDA-approved premixed bioceramic endodontic sealer, releases calcium ions to form mineralized tissue within the canal system and apically. The alkaline pH and low solubility of the sealer creates a hermetic seal within the canal system, making the environment within the canal system and at the apical orifice inhospitable for bacterial growth. In cases of non-communicating internal resorption, the high pH of PURE-Ca-SEAL™ neutralizes the acidic environment, assisting in halting the progression of the resorption.
This ready-to-use formulation simplifies the obturation procedure (Figure 4), resulting in less chair time and increased patient comfort. PURE-Ca-SEAL™ can be utilized with any obturation technique, including those that involve heat. The resin-free formula features a small particle size, providing a thin film thickness and excellent flow characteristics.7 Unlike ZOE and calcium hydroxide-based sealers, its hydrophilic properties are ideal for setting in a moist environment. Additionally, it is well accepted by the tissue should any sealer be extruded apically.8 The components of the sealer provide high radiopacity, mechanical resistance to calcium ion release, and other factors enhancing clinical results (Figure 5). The sealer has a setting time of ~240 minutes, good flowability, and high compressive strength once set (Figure 6). The sealers’ mechanisms of action are closely associated with contact with tissue moisture and fluids. After the calcium oxide present in the sealer comes into contact with the water present in the dentin tubules, calcium hydroxide is formed which interacts with the fluids, dissociating in calcium ion and hydroxyl. The hydroxyl ions are responsible for the increase in pH promoting its bactericidal action.9 The released Ca2+ ions react with CO2 from the bloodstream, forming calcium carbonate (calcite), and extra-cellular matrix rich in fibronectin is secreted attracted by calcite, triggering formation of hard tissue.
Component Function
Tricalcium Silicate (C3S) Mechanical resistance over time Calcium ions release
Dicalcium Silicate (C2S) Mechanical resistance over time Calcium ions release
Tricalcium Aluminate Initial setting
Calcium Oxide Calcium ions release
Zirconium Oxide Radiopacity
Silicon Dioxide Rheology agent
Polyethylene Glycol Dispersing agent
Iron Oxide Pigmentation
Figure 5: Composition and function of the components of PURE-Ca-SEALTM endodontic sealer
Figure 1: The EXIMIA7™ files available in sizes shown and 04 or 06 taper with lengths 21 mm, 25 mm, and 29 mm
Figure 2 (left): EXIMIA7™ gutta-percha cones are available in size 15, 20, 25,
Figure 4: PURE-Ca-SEAL™ sealer
% Calcium Silicates 25 - 40%
Setting Time ≤ 240 minutes
Radiopacity ≥ 7.0 mm AI
pH ~ = 12
Flowability
Particle
Solubility
mm
Compressive Strength 9.724 ± 2.484 MPa
Figure 6: Properties of the PURE-Ca-SEAL™ endodontic sealer
Case report
A 32-year-old male patient presented with a complaint of a loose filling on the maxillary right central incisor (Tooth No. 8). Examination noted a large composite filling that was loose on the tooth. A periapical radiograph showed a large periapical lesion on the right central incisor (Figure 7). The pulp of the tooth appeared larger than the adjacent central incisor, and when questioned, the patient indicated previous trauma to the tooth. He further indicated no hot, cold, or biting sensitivity on the tooth. The tooth tested negative for percussion as well as when tested with Endo-Ice® (Coltene Dental, Cuyahoga Falls, Ohio) or heat. The patient was advised that endodontic treatment was indicated as the pulp was non-vital and had an apical lesion. He indicated he would speak to his spouse about the purpose of treatment.
The patient returned several weeks later related to the old filling falling out of the tooth and fracturing a portion of the coronal. The patient indicated he was still not having any pain or sensitivity in the tooth. Local anesthetic was administered via infiltration into the vestibule adjacent to the tooth to be treated with 1 carpule 4% Septocaine with 1:200,000 epi (Septodont, New Castle, Delaware). A rubber dam was placed with rubber dam clamps on teeth Nos. 6 and 11. Access was created on tooth No. 8 with a 330-carbide bur in a high-speed handpiece. A size 25 hand file was introduced into the canal to the estimated working length (18 mm) as measured on the initial radiograph and verified with an apex locator. No bleeding was noted in the canal, confirming that the pulp was non-vital.
The canal was instrumented to a size 35 with a 04 taper EXIMIA7™ rotary file. The canal was irrigated with a 2.5% NaOCl solution followed by a 17% EDTA solution while using the last rotary file to aid in distributing the irrigation into the canal system. The canal was dried with paper points matching the final file size of 35 with a 04 taper. PURE-Ca-SEAL™ bioceramic sealer was dispensed on a pad, and a gutta-percha cone matching the final file (35 with 04 taper) was coated with the sealer and introduced into the canal to WL. The excess cone coronally was cut off with a heated instrument at the canal orifice. A periapical radiograph was taken (Figure 8). The radiographs demonstrated complete obturation of the canal with slight extrusion of sealer at
Figure 7 (left): Periapical radiograph with a fractured composite filling on the right maxillary central incisor and a large periapical lesion apically. Figure 8 (right): Periapical radiograph of the right maxillary incisor following instrumentation and obturation, noting some apical resorption of the root
the apical. Also noted was slight external resorption at the apical related to the lesion. The patient was scheduled for placement of a fiber post with composite core and a full crown.
Conclusion
Endodontics is a 2-part process, encompassing instrumentation and obturation. Success requires both parts to be performed well. The EXIMIA7™ file system provides improved canal instrumentation with flexibility of the files to follow canal anatomy while aiding in preserving root structure to improve tooth longevity. When combined with a bioceramic sealer like PURECa-SEAL™ a predictable obturation can be achieved that is insoluble to oral fluids, antibacterial, and well tolerated apically should any sealer be extruded during obturation.
REFERENCES
1. Hakke Patil A, Patil AG, Shaikh S, Bhandarkar S, Moharir A, Sharma A. Comparative Evaluation of the Sealing Ability of Mineral Trioxide Aggregate (MTA)-Based, Resin-Based, and Zinc Oxide Eugenol Root Canal Sealers: An In Vitro Study. Cureus. 2024 Jan 13;16(1):e52201. doi: 10.7759/cureus.52201.
2. Huumonen S, Lenander-Lumikari M, Sigurdsson A, Ørstavik D. Healing of apical periodontitis after endodontic treatment: a comparison between a silicone-based and a zinc oxide-eugenol-based sealer. Int Endod J. 2003 Apr;36(4):296-301. doi: 10.1046/j.13652591. 2003.00651.x.
3. Poggio C, Arciola CR, Dagna A, Colombo M, Bianchi S, Visai L. Solubility of root canal sealers: a comparative study. Int J Artif Organs. 2010 Sep;33(9):676-81. doi: 10.1177/ 039139881003300914.
4. Desai S, Chandler N. Calcium hydroxide-based root canal sealers: a review. J Endod. 2009 Apr;35(4):475-80. doi: 10.1016/j.joen.2008.11.026. Epub 2009 Feb 26.
5. Lee KW, Williams MC, Camps JJ, Pashley DH. Adhesion of endodontic sealers to dentin and gutta-percha. J Endod. 2002 Oct;28(10):684-8. doi: 10.1097/00004770-200210000-00002.
6. Daculsi G. History of Development and Use of Bioceramics and Biocomposites. In: Antoniac I, ed. Handbook of Bioceramics and Biocomposites. Springer, Cham;2016. https:// doi.org/10.1007/978-3-319-09230-0_2-2.
7. Tanomaru-Filho M, Esteves Torres FF, Pinto JC, Guerreiro Tanomaru JM, Pereira MC, de Souza PFF. Flow, Filling Ability and Apical Extrusion of New Calcium Silicate-Based Sealers: A Micro-Computed Tomographic Study. Dental Oral Biology and Craniofacial Research. June 2020;1-6. 10.31487/j.DOBCR.2020.03.04.
8. Alves Silva EC, Tanomaru-Filho M, da Silva GF, Delfino MM, Cerri PS, Guerreiro-Tanomaru JM. Biocompatibility and Bioactive Potential of New Calcium Silicate-based Endodontic Sealers: Bio-C Sealer and Sealer Plus BC. J Endod. 2020 Oct;46(10):1470-1477. doi: 10.1016/j.joen.2020.07.011. Epub 2020 Jul 17.
9. Viana FLPP. Antimicrobial activity of biocerose endodontic cements in front of enterococcus faecalis in biofilm – in vitro study. 2019. 46 f. Dissertation (Master in Dentistry) - Faculty of Pharmacy, Dentistry and Nursing, Federal University of Ceará, Fortaleza, 2019. EP
Advanced Endodontic File System
Precision, Power, and Adaptability in Every Procedure
Strong to significantly increase resistance to cyclic fatigue. Heat treated NiTi enables the EXIMIA7™ file extreme flexibility reducing shape memory, preserving canal anatomy e ortlessly following the canal as you shape.
Heat Treated NiTi
Parabolic Cross Section
Available in 3 lengths: 21, 25 & 29 mm
Maximum flute diameter 1 mm
• Heat treatment process improves strength and flexibility
• Available in .04 and .06 Constant Taper - Variable Pitch
• Maximum flute diameter 1mm allows for minimally invasive preparation
• Parabolic Cross Section non cutting tip maximizes file cutting efficiency
• ISO tip size 17-45
• Available lengths: 21, 25 & 29 mm
PURE-Ca-SEAL™ comes premixed in (1)2g Syringe and Includes 20 applicator tips
The non-resorbable hydrophilic nature, dimensional stability, biocompatibility, antibacterial property, bioactivity, and ease of delivery makes PURE-Ca-SEAL™ BioCeramic Endodontic Sealer a promising NEW option.