Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Lou Shuman, DMD, CAGS
A promising option
Remote anchorage of dental implants is an innovative concept in implant dentistry designed to improve the stability, retention, and overall effectiveness of implant-supported restorations. Traditionally, dental implants are anchored directly into the alveolus to replace missing teeth, with the goal of providing strong, functional, and esthetic replacements. However, in cases where the bone density is insufficient or the anatomical structures are compromised, remote anchorage can offer an alternative solution.
The term remote anchorage refers to the use of alternative support structures outside of the typical alveolar bone housing to stabilize dental implants. Examples include the pterygoid region of the maxilla, the zygoma, and the lateral nasal wall/inferior turbinate, nasopalatine duct, and anterior nasal spine. These anchorage points are typically located outside the immediate area of traditional implant sites, providing greater flexibility in cases where the direct implant site cannot provide enough support. These techniques circumvent challenges related to bone volume and quality, making it an effective solution for patients with insufficient bone, such as those with severe periodontal disease, extensive bone loss, sinus pneumatization, or after tooth extraction.
Benefits of remote anchorage
1. Reduced need for bone grafting: One of the most significant advantages of remote anchorage is that it reduces the need for invasive bone-grafting procedures. By using existing bone at remote sites, clinicians can avoid the additional pain, surgeries, and cost of bone augmentation, which carries with it lower success rates.
2. Improved implant stability: In cases where the local bone is compromised or soft, remote anchorage can offer enhanced stability by shifting the load and stress to more stable structures and allowing immediate loading.
3. Expanding treatment options: Remote anchorage broadens the possibilities for patients who would otherwise be considered unsuitable candidates for dental implants due to insufficient bone or complex anatomical challenges.
4. Reduced treatment time: With appropriate remote anchorage, patients may avoid the lengthy healing times associated with bone grafting or sinus lift procedures, reducing the overall duration of treatment.
5. Higher success rates: As we are typically engaging native cortical bone sites, higher success rates are achievable.
6. Elimination of cantilevers: The use of pterygoids and posteriorly placed zygomas can eliminate cantilevers and allow restoration back to second molar.
Remote anchorage of dental implants provides a promising solution for patients with insufficient bone or challenging anatomical conditions and allows immediate function. By utilizing adjacent structures or extraoral support systems, this technique can enhance implant stability, reduce the need for bone grafting, and offer greater flexibility in complex cases. However, careful planning and precise execution are crucial to ensuring the long-term success and stability of the restoration. As research and technology advance, remote anchorage is likely to become an increasingly important tool in the field of implant dentistry.
Sami Nizam II, MD, DMD, is a dual degree and double board-certified oral and maxillofacial surgeon and facial cosmetic surgeon. He owns and operates Alabama Surgical Arts, an outpatient surgical center located in Montgomery, Alabama that is accredited by the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF). Follow Dr. Nizam on Instagram, Facebook, and Tiktok @Alabamasurgicalarts.
A new angle in full-arch implantology
Dr. Sundeep Rawal; Eric Kukucka, DD; and Dr. Nassif Youssef discuss experience with angled implants for full-arch cases and how LOCATOR Angled fits into their clinical practices
Cover image courtesy of Zest Dental Solutions.
Dr. Dan Holtzclaw describes one of the newest methods of implant treatment
Dr. Leke Olowokere
PRACTICE MANAGEMENT How to help your team thrive when there’s a change in ownership
Dr. Samson Liu discusses how to make practice transitions more productive 28
PRACTICE DEVELOPMENT
The art of the referral
JoAn Majors offers four simple steps for delivering referrals for less than a dollar ........................... 30
• Advanced Education with Mini MBA Program and Other Advanced Certificates in Business Management and Leadership
• Retention Strategies
• Operational Support
• Technology Implementation
• Patient Trends & Analytics
• Efficiency Audit
• Competitive Fee Survey
• Production Analysis
Making the world a better place
Every day, in newspapers, on TV, and social media we see humanitarian efforts across the world. Whether it’s for saving endangered animals, survivors of natural disasters, cures for diseases, or other causes closer to home, we all try as much as possible to open our hearts and wallets for those who could use a boost in life. Dental practices’ own little corners of the world can have their own distinctive ways to create a better place.
Lisa Moler Founder/Publisher, MedMark Media
It’s easy being green: One of the most popular ways dental offices can show environmental responsibility is by employing “green” programs. The ADA has a page on its website titled “80 ways to make your practice green” (https://bit.ly/4gbMrra) — with suggestions like investing in energy efficient technologies, purchasing furniture made from recycled products, or something as small as using biodegradable cups. Replacing high-energy consuming office lights with energy-efficient lighting will conserve energy and also probably help lower some of the electric bill as well.
One patient at a time: MedMark publications always feature new equipment, technology, and materials. Researchers and inventors of these new dental solutions spend hours of their time, effort, and money improving the dental experience and creating new options for better and more individualized patient care. Whether it’s taking the pain out of root canal treatment, bringing new treatments to those with sleep-breathing issues, inventing implant solutions for those who need special care, creating new aligner and bracket-and-wire systems to help patients smile again after years of low self-esteem, or taking the fear out of the office for even the youngest dental patients, our articles can help improve patients’ quality of life, while also improving your business.
Pay it forward: Some of the most famous key opinion leaders in the dental industry were mentored and encouraged by their peers. Implementing any new protocol or procedure from the simple to the complex is less stressful when there is someone to call on for advice. We’ve all been there — in any occupation, moving to a higher level means being educated not only from text books or lectures, but hands-on, chairside guidance from someone who has “been there and done that.” Articles in our publications also feature authors who want to share their expertise, and who are often happy to follow up with constructive pointers on how to add their protocols to your practice options.
Love thy neighbor: Dental offices can be a productive part of any community. From contributing to local schools, to visiting classes to talk about better oral care, to participating in veteran’s events, clinicians and their teams can expand their reputation, referrals, and hearts by showing the surrounding areas that their community is important to you too. It isn’t hard to find these activities. Check with your local Chamber of Commerce, community newspaper, school volunteer event staff, or even ask your patients what organizations they may be involved in. Your practice name will stay in potential patients’ minds long after the event is over.
The spring issue is ready to share concepts that will help to build your world. We hope you enjoy this issue’s well thought out/interesting articles, and make some ideas into realities.
It is a small world — and by making it better, your potential patients will be happy you are a part of it.
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor
Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Subscription Rate 1 year (4 issues) $149 https://implantpracticeus.com/subscribe/
How to submit an article to Implant Practice US
Implant Practice US is a peer-reviewed, quarterly publication containing articles by leading authors from around the world. Implant Practice US is designed to be read by specialists in Periodontics, Oral Surgery, and Prosthodontics.
Submitting articles
Implant Practice US requires original, unpublished article submissions on implant topics, multidisciplinary dentistry, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,400 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Implant Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Articles are classified as either clinical, continuing education, technology, or research reports. Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to implant dentistry. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio
• Author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple) Doe JF Doe JF, Roe JP
Permissions
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased after the issue is published.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to:
Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
A new angle in full-arch implantology
Dr. Sundeep Rawal; Eric Kukucka, DD; and Dr. Nassif Youssef discuss experience with angled implants for full-arch cases and how LOCATOR Angled fits into their clinical practices
The evolution of implant dentistry continuously seeks to address the complexities clinicians face in achieving optimal prosthetic outcomes. One persistent challenge has been the management of non-ideal implant angulations, which can compromise the functional and esthetic results of both removable and fixed prosthetic designs.
In removable prosthetic cases, the success of overdentures heavily depends on the alignment and distribution of the supporting implants. Suboptimal implant positioning, whether due to anatomical limitations or surgical inconsistencies, can create functional and esthetic issues for the patient. Traditional Locator® abutments, while effective, are sometimes insufficient to overcome angulation challenges, particularly in cases exceeding 10 - 15 degrees of divergence. With Locator abutments, the housing compensates for the malposition of implants, allowing a maximum divergence of 20 degrees total with standard hous-
Sundeep Rawal, DMD, is a proud alumnus of University of Florida College of Dentistry. He completed his prosthodontics training at the University of California San Francisco in 2009. Since then, he has worked extensively to utilize CAD/CAM technologies within the scope of clinical dentistry and enhance patients’ restorative treatments. He is a renowned lecturer globally and has held numerous positions with national organizations. After 10 successful years of private practice, he joined Aspen Dental in 2019 as the Senior Vice President of Implant Support, where he’s continued to drive the industry forward through integrating the latest technologies that shape the future of dentistry.
Eric Kukucka, DD, currently serves as Vice President, Clinical Removable Prosthetics and Design Technologies at Aspen Dental. He is an active researcher, educator, author, and key opinion leader who helps develop protocols, processes, and materials used by practicing clinicians around the world. After many years of private practice, working in research and development and most importantly, treating patients with removal therapy, Kukucka joined Aspen Dental to work alongside Dr. Sundeep Rawal and guide the company through its digital transformation. Today, he is a critical member of the team who is responsible for innovation of digital technology and prosthetics and provides doctors, dental technicians, and team members with the training they need to deliver the best possible removable prosthetic experience.
Nassif Youssef, BDS, CAGS, is the Director of Implant Prosthodontics and Educational Support, recognized for his leadership in advancing implant dentistry and education. With years of expertise as a prosthodontist, Dr. Youssef has transformed clinical operations and educational programs at the oral care center for excellence, which serves U.S. Army veterans and low-income communities in Illinois. A passionate educator, he has taught hundreds of courses to doctors, focusing on implantology, advanced surgical techniques, and restorative procedures. Dr. Youssef is also a respected researcher and author, contributing to advancements in implant and prosthetic dentistry through his published work. His career exemplifies a dedication to patient care, innovation, and mentorship in dentistry.
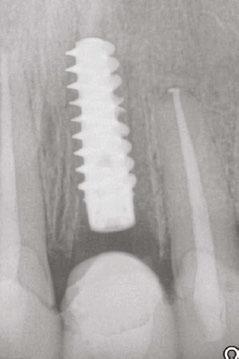
1: Due to anatomical features and bone position, some implants require placement at increased angulation (right) compared to scenarios where less angulation is required (left)
ings and up to 40 degrees total with extended range inserts. In a typical 4-implant overdenture case, this equates to either only 5 or 10 degrees of correction per implant, often falling short in managing significant angulation issues.
Locator Angled abutments present a transformative solution to this challenge when utilizing individual stud-type connections of prosthetics to implants, offering clinicians enhanced flexibility and predictability in their cases. The pre-angled Locator Angled abutment corrects 15 degrees of angulation and allows for the clinician to restore implants up to 35 degrees of angulation.
Clinically, this innovation eliminates the need for invasive corrective surgeries or additional components to accommodate for angulation discrepancies, which can lead to a reduction in
Eric Kukucka, Drs. Sundeep Rawal and Nassif Youssef
Figure
the prosthetic restorative space due to the height of additional components needed to compensate. For instance, in a recent case involving a mandibular overdenture, the use of Locator Angled abutments allowed seamless adaptation to significant divergence between anterior and posterior implants. The result was a prosthesis with superior retention, stability, and patient satisfaction without compromising the gingival esthetics or the longevity of the attachment system. Moreover, the Locator Angled system simplifies chairside adjustments, reducing the need for extensive prosthetic modifications or complex restorative solutions that could increase treatment time and cost. By
providing a predictable seating path and robust retention, these abutments ensure a streamlined workflow and fewer prosthetic and post-delivery complications. For the patient, this translates to improved comfort and confidence in their removable prosthetic solution.
While traditionally associated with removable prosthetics, Locator Angled abutments have demonstrated equal impact in the realm of fixed implant-supported prostheses. Fixed full-arch restorations often face angulation challenges due to implant placement dictated by anatomical constraints or previous restorative work. In these scenarios, Locator Angled abutments
Figure 2: Locator Angled abutment placed using a hex driver
Figure 3: Angled Locator abutment in place
Figure 4: Standard Locator abutments (upper left) presented with increased angulation (top right). Locator Angled abutments placed (bottom left) resulting in more parallelism (bottom right)
provide a solution that combines the precision of fixed restorations with the adaptability of angled correction.
Consider a clinical case of a maxillary full-arch restoration where implants (Straumann® BLX) were placed with significant buccal angulation due to the constraints of the patient’s anatomy. Traditional abutments would have necessitated excessive prosthetic bulk or compromised the anterior posterior spread (A-P Spread) of the restoration. Utilizing Locator Angled abutments, the divergence was corrected efficiently, ensuring proper prosthetic alignment, and reducing stress on the framework while ensuring maximum A-P spread. The ability to adjust angulation without complex laboratory workflows also supports cost-effective treatment solutions.
By mitigating the need for custom abutments or extensive laboratory work, Locator Angled abutments enable clinicians to deliver high-quality fixed solutions with enhanced efficiency. Additionally, their compatibility with modern digital workflows ensures seamless integration into both analog and digital treatment paradigms.
These clinical cases demonstrate that the Locator Angled abutment addresses one of the most critical problems in implant dentistry: the reconciliation of “less-than-ideal” implant positions with the need for predictable and durable prosthetic outcomes. Whether used in removable or fixed applications, these abutments simplify complex cases, reduce the need for surgical or prosthetic compromises, and enhance patient satisfaction. However, another benefit of this innovation is the ability to enable a comprehensive treatment plan that spans the entire “life cycle of care” for patients.
Historically, the formulation of a patient’s treatment plan and subsequent planned implant positioning was dictated by the proposed definitive restoration being either fixed or removable. If the patient was planned for a removable prosthesis with individual stud-type attachments without the use of a CAD/CAM milled framework, then parallelism of implant placement was paramount, even at the expense of the Anterior-Posterior distribution of implants. This planned positioning was much different than when planning for a fixed solution where tilting of implants to diverge them and increase the A-P spread has become the prevailing technique over the past two decades for achieving optimal implant positioning.
Unfortunately, these two approaches to implant placement are not synergistic, and in most cases, planning one modality of placement precluded the ability to deliver the other type of restoration at a future date. If parallel implants were placed for removable therapies, the distribution was less than ideal for a fixed, fully implant-supported restoration in the future. If that transition was desired, further surgical intervention was needed to place more implants with or without adjunctive procedures such as bone augmentation. This was a similar situation if implants were tilted for maximum spread in preparation of a fully implant-supported restoration. In those cases, the use of stud-type attachments like the Locator abutment system were precluded due to divergence unless a CAD/CAM milled framework was utilized as well to splint the implants together and create the ability for the attachment system to have parallelism for a path of insertion. Unfortunately, these methods of treatment are costly, laborious, and hinder optimal prosthetic outcomes.
The Locator Angled abutment system allows clinicians to overcome this dichotomy in treatment planning. Today, a patient can be treatment planned to maximize the distribution of implants with a fully implant-supported restoration in mind, tilting implants to accomplish this while simultaneously avoiding critical anatomical structures and circumventing the need for complex grafting procedures. With the use of Locator Angled abutments, the initial definitive restoration can be a removable prosthesis with individual stud-type locator abutments and attachments, which can transition to a fixed, fully implant-supported restoration later. Along with the advent of the Locator Fixed concept in conjunction with the innovation of the Locator Angled abutment, a uniform methodology can be applied to the treatment planning of full-arch implant solutions with four or more implants allowing versatility in how a patient can progress through a life cycle of therapy without necessitating further surgical intervention.
In summary, Locator Angled abutments empower clinicians to overcome angulation challenges with precision and ease. Their versatile application and synergistic convergence in implant placement planning for both removable and fixed prosthetics highlight their crucial role in modern implant dentistry by enabling a standardized, cohesive methodology. This unified approach offers exceptional versatility in how patients progress through the treatment progress, eliminating the need for additional surgeries or interventions at later stages.
REFERENCES
1. Amato F, Polara G. Clinical Application of the New LOCATOR F-Tx Fixed Attachment System for Immediate Rehabilitation of Complete Edentulous Cases: 1-Year Prospective Clinical Study. Compend Contin Educ Dent. 2018;39(1). https://www. compendiumlive.com/2018/zest-supplement/clinical-application-of-the-new-locator-f-tx-fixed-attachment-system-for-immediate-rehabilitation-of-complete-edentulous-cases-1-year-prospective-clinical-study/. Accessed January 30, 2025.
2. Al-Shehri AN. Overdenture Treatment of Angled Implant with Extended Range Locator Attachment: Clinical Report. J Am Sci. 2020;16(2):9-15.
3. Alqutaibi AY, Kaddah AF. Effect of Mastication Load on Retention Force of Custom-Made LOCATOR Attachments for Implant Overdentures. J Prosthet Dent. 2023;129(4):680. e1-680.e7.
4. Alikhasi M, Siadat H, Hashemloo A, Bassir SH. CAD-CAM Fabrication of Semiprecision LOCATOR-Style Abutments to Correct Implant Angulation. J Prosthet Dent. 2024;131(2):181-184. IP
Figure 5: Completed Locator FIXED case with Locator Angled abutments
Transnasal dental implant placement using PLACATE guidelines
Dr. Dan Holtzclaw describes one of the newest methods of implant treatment
Background
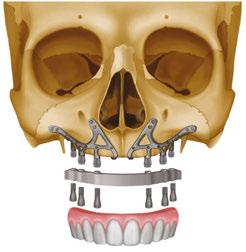
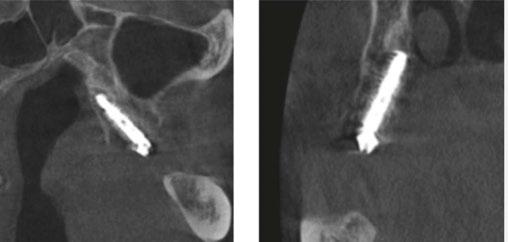
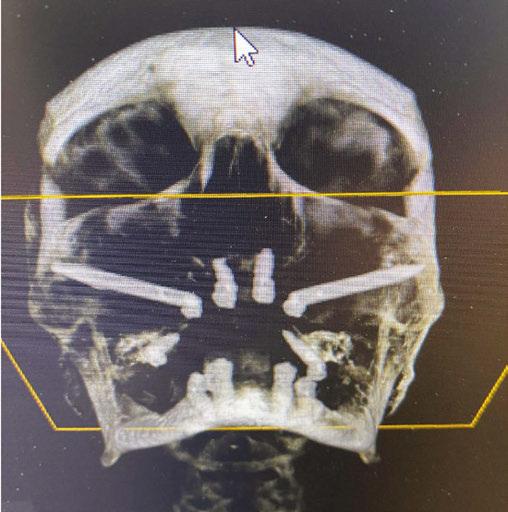
Treatment of severely atrophic maxillae often requires highly advanced procedures such as quad-zygomatic implants1-3 (Figure 1) or customized subperiosteal implants (Figure 2).4,5 Quad-zygomatic implant treatment has a long history of success, but requires significant surgical expertise due to limited malar bone availability and propinquity to anatomic structures such as the orbit and infraorbital nerve.6 Customized subperiosteal implants, on the other hand, are a promising new treatment option but have limited long-term follow-up data and significant expense.7 Transnasal dental implants have recently been introduced as another option for treatment of severely atrophic maxillae, specifically as an alternative to quad-zygomatic implant placement (Figure 3).8 Transnasal implants may serve as a replacement for anterosuperior zygomatic implants as they tangentially traverse the interior lateral nasal wall and achieve high insertion torque via 3 mm-5 mm of apical engagement in the confluence of the inferior concha, lateral nasal wall, and frontal process of the maxilla (Figure 4).8-16
In 2019, the first report on transnasal implants, called the Vanderlim technique, was published in Brazil as an alternative to the quad-zygomatic implant configuration.8 In this publication, the authors described using 16 mm–25 mm long implants placed tangentially along the interior of the lateral nasal wall to achieve insertion torque of 40-50 Ncm for immediate loading. In 2021, Almeida published a case report documenting use of an “extralong transnasal implant” as an alternative to the quad-zygoma,10 and Vanderlim supported his 2019 publication with a series of 12 cases using “transnasal implants placed using the Vanderlim technique” with follow-up of 2-26 months.9 In 2023, Holtzclaw published a textbook with a case series of seven transnasal implant cases performed by himself and other dental implant surgeons.6
Dan Holtzclaw, DDS, MS, is President of Holzklau Full Arch Implant Consulting and maintains practices limited to remote anchorage implantology in multiple states. He is a Diplomate of the American Board of Periodontology and Diplomate of the International Congress of Oral Implantologists. Dr. Holtzclaw has published over 60 articles in peer reviewed journals in addition to multiple textbooks. He served as the Editor-In-Chief of the Journal of Implant and Advanced Clinical Dentistry for 13 years in addition to serving as an editorial board member and/or editorial reviewer for several other dental journals.
3 (left): 3-dimensional CBCT rendering of patient treated with transnasal dental implants as an alternative to quad-zygomatic implant treatment. Figure 4 (right): Intrasurgical photo of transnasal dental implant traversing the nasal cavity and engaging the base of the inferior concha
While there were no transnasal dental implant articles published in 2022, case reports on a handful of patients were published by Oh, et al.,12 and Sahin14 in 2023. In this same year, Holtzclaw published an article discussing protocols addressing atrophic maxillae which featured one case of unilateral transnasal implant treatment.17 In 2024, Sales echoed Holtzclaw’s 2023 publication with a case report on a unilateral transnasal implant in the treatment of an atrophic maxilla15 while Nunes, et al., published a case series of three patients treated with both unilateral and bilateral transnasal fixtures.13 Up to this point, all transnasal publications had been case reports or case series. This changed in late 2024 when Gelpi, et al., published a retrospective multi-center study of 45 transnasal implants placed in patients who underwent surgery between July 2021 and November 2023. In this largest study to date on transnasal implants, the survival rate was 100%, although mean follow-up was relatively short.
Disclosure: The author reports no conflicts of interest with any products mentioned in this article. He is the developer of the HESIAn, PFAST, PLACATE, and PHARS protocols and co-developer of the PATZi protocol.
Initial guidelines for transnasal dental implant placement as noted in the initial publications by Vanderlim8,9 and Almeida10:
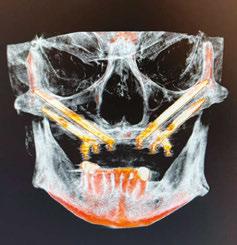
Figure 1 (left): 3-dimensional CBCT rendering of patient treated with quad-zygomatic implants. Figure 2 (right): Example of customized subperiosteal dental implant for treatment of an atrophic maxilla
Figure
1. Minimum bone volume of 3 mm for apical anchorage in the inferior concha and frontal process of the maxilla
2. Minimum bone height of 4 mm between the ridge of the maxilla and the nasal cavity
3. Insufficient premaxillary bone volume for the placement of two conventional implants
4. Insufficient bone volume for the placement of two zygomatic implants in a single malar process
5. Infraorbital nerve position which would be violated by placement of a zygomatic implant
6. Large concavity of the anterior maxillary wall which may facilitate soft tissue recession with placement of a zygomatic implant
7. Avoid placing transnasal implants in wide nasal cavities
8. Avoid tearing the nasal mucosa during elevation
PLACATE guidelines
In 2023, Holtzclaw expanded the guidelines for transnasal dental implant placement with (P)re(LAC)rimal (A)ssesment of (T) ransnasal Implant (E)ngagement — PLACATE.6 Under PLACATE guidelines, appropriate transnasal dental implant candidates must meet the following parameters:
1. Simmen 2 or 3 classification of the nasolacrimal canal
2. Prelacrimal bone width ≥3 mm
3. Subnasal bone height ≥2 mm
4. Vertical measurement from residual subnasal bone, or anticipated anterior alveolar ridge reduction level, to
prelacrimal bone engagement point that does not exceed 25 mm
Failure to meet all four PLACATE criteria prevented a patient from being an appropriate transnasal implant candidate.
A recent 2025 retrospective review by Holtzclaw, et al.,11 evaluated anonymized cone beam computer tomography (CBCT) scans from 300 sequential referrals using PLACATE guidelines to determine transnasal dental implant feasibility. In this study, inferior conchae were initially located in the coronal plane, and imaging crosshairs were positioned just superior to this structure in the axial plane. To evaluate the ipsilateral and contralateral transnasal engagement points, imaging crosshairs were next positioned over each concha in the sagittal plane. This prelacrimal engagement point, sometimes referred to as the “Z-Point”,6,12 was then evaluated according to PLACATE guidelines as follows:
1. Simmen classification19 determined by measurement from the external aspect of the frontal maxilla to the most anterior aspect of the nasolacrimal canal (Figure 5)
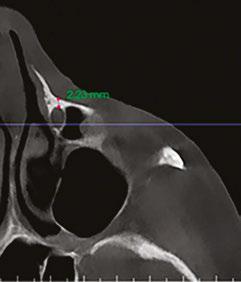
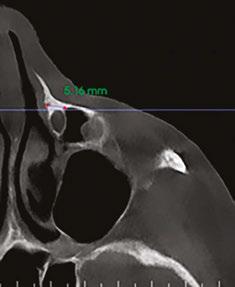
2. Mediolateral measurement of prelacrimal bone width (Figure 6)
3. Vertical measurement of subnasal bone height
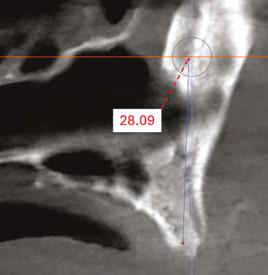
4. Vertical measurement from subnasal bone to prelacrimal bone engagement point (Figure 7)
The results of this study found that only 30.54% of patients qualified for transnasal dental implants anatomically. The most common disqualification was inadequate prelacrimal bone width which affected 49.71% of patients. Excessive subnasal bone height, which could foster placement of conventional dental implants, eliminated 28.74% of patients. The third most common reason for patient disqualification from transnasal dental implant placement, 22.16% of patients, was Simmen 1 classification which would result in potential violation of the nasolacrimal canal.
Case report
An 80-year-old male with a relatively clean medical history was referred for full-arch immediately loaded maxillary implant treatment. The patient had been previously treated with maxillary dental implants in a traditional All-on-X approach. The referring clinician noted that the patient’s bone was extremely “soft” and that insertion torque for most of the implants was very low. Although these implants were not immediately loaded, they ultimately failed and created large oroantral communications. While the communications were ultimately closed, extremely large
Figure 6 (right): CBCT slice (axial view) for mediolateral measurement of prelacrimal bone width
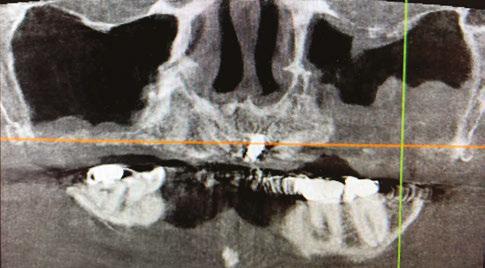
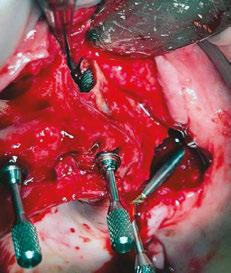
Figure 7 (left): CBCT slice (sagittal view) for vertical measurement from subnasal bone to prelacrimal bone engagement point. Figure 8 (middle): Panoramic radiograph of patient with history of failed All-on-X treatment, oroantral fistulae, and thickened Schneiderian membranes. Figure 9 (right): Intrasurgical photo of transnasal dental implant traversing the nasal cavity and engaging the base of the inferior concha
defects resulted in the floor and walls of the maxillary sinuses (Figure 8). CBCT analysis revealed a significantly thickened left Schneiderian membrane and occluded osteomeatal complex. The patient was referred to ENT for a Functional Endoscopic Sinus Surgery (FESS) procedure. Upon healing, a new CBCT was taken and evaluated for potential treatment.
Due to the atrophic nature of the maxilla, treatment following the PATZi protocol was planned.6,17,20 CBCT evaluation revealed pterygomaxillary bone appropriate for pterygoid implants allowing for posterior arch support and cantilever elimination. The zygomas were of adequate height and width to accommodate multiple zygomatic implant fixtures bilaterally. PLACATE guidelines were used to evaluate the patient for potential treatment with transnasal implants. With Simmen 3 nasolacrimal canal classification, ≥ 3 mm of prelacrimal bone, ≥2 mm subnasal bone, and ≤ 25 mm to the Z-point, the patient satisfied all PLACATE parameters. Accordingly, a treatment plan of bilateral pterygoid, single zygomatic, and transnasal implants was agreed upon.
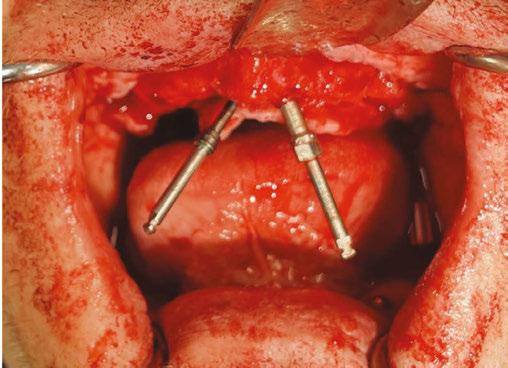
Following the induction of general anesthesia, extraoral and intraoral local anesthesia was applied. To avoid exposing the large subantral bony defects, mini-flaps were elevated at the pterygoid landing areas to expose the hamular notch. The pterygoid fossa was identified via probing, and pterygoid implant placement ensued. Following the PATZi protocol, bilateral pterygoid implants were placed first and both achieved insertion torque between 45+ Ncm.
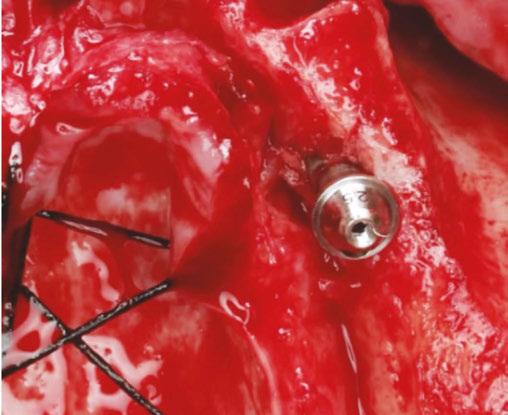
Following PATZi, anterior support was sought next. As such, the nasal mucosa was elevated to expose the floor of the nasal cavity and the bone of the inferior conchae. A pair of 25 mm transnasal implants were placed, and each achieved high insertion torque of 45+ Ncm (Figures 9-11). Continuing with the PATZi protocol and treatment plan, 42.5 mm long zygomatic implants were placed in both zygomas. The zygomatic implants were placed using an extrasinus approach and both achieved insertion torque of 45+Ncm. Buccal fat pedicles were advanced bilaterally to cover extrasinus portions of the zygomatic implants, and flap closure was achieved with 4-0 chromic gut suture. The patient was immediately temporized with a screw-retained transitional bridge (Figure 12), and a final zirconia restoration was delivered after 8 months of healing (Figure 13).
Discussion
With fewer than 200 published cases and less than 7 years of follow-up, transnasal dental implants are one of the newest styles of treatment in implant dentistry. The limited number of studies which have evaluated this treatment have generally found transnasal implants to be of diameters ranging from 3.5 mm to 4.2 mm and lengths of 20 mm-25 mm.6,8-16 Having multicortical anchorage points in subnasal and prelacrimal bones, transnasal implants have been found to have high insertion torques appropriate for immediate loading.6,8-16 A unique feature of transnasal dental implants is that the midbody of the fixture remains exposed in the nasal cavity. Regarding exposed transnasal implant threads in the nasal cavity, there is currently no consensus on the need for grafting.
Although transnasal implants can be placed under direct visualization, their proximity to certain antatomic structures requires intimate anatomic knowledge and surgical skill. Iatrogenic damage to Kesselbach’s complex may result in excessive hemorrhaging while tearing of the nasal mucosa may lead to oronasal fistulae.6 Careless mucoperiosteal flap elevation can result in damage to the infraorbital nerve, and poor placement of transnasal implant fixtures may lead to dacryostenosis, epiphora, and dacryocystitis.6 Fortunately, to date, published studies have shown few complications with transnasal dental implants and few failures.
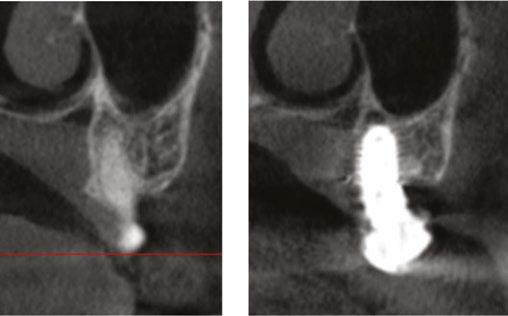
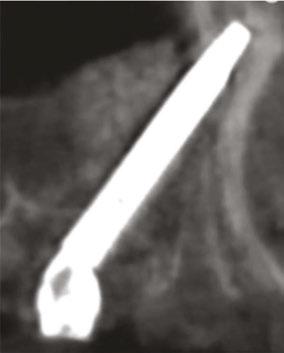
Figure 10 (left): CBCT slice (coronal view) of transnasal dental implants engaging the Z-point. Figure 11 (middle): CBCT slice (sagittal view) of transnasal dental implant engaging prelacrimal bone ventral to the nasolacrimal duct. Figure 12 (right): 3-dimensional CBCT rendering of patient treated with transnasal, zygomatic, and pterygoid dental implants via the PATZi protocol
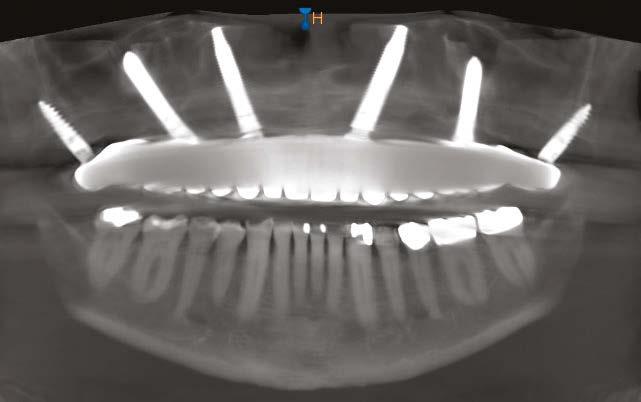
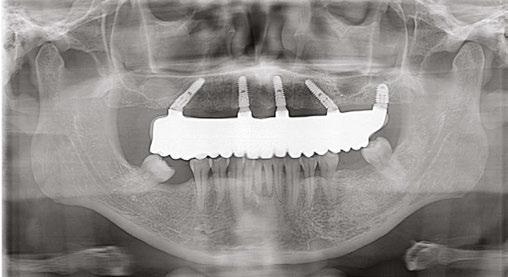
Figure 13: Panoramic radiograph of patient with final zirconia restoration
Conclusion
When anatomic conditions are appropriate, transnasal dental implants are a promising alternative to anterosuperior zygomatic implant fixtures in quad-zygo treatment. While continually emerging updates such as PLACATE guidelines are improving the safety and predictability of transnasal dental implants, more studies with longer follow-up times are needed to confirm the reliability of this relatively new treatment.
REFERENCES
1. Bothur S, Jonsson G, Sandahl L. Modified technique using multiple zygomatic implants in reconstruction of the atrophic maxilla: a technical note. Int J Oral Maxillofac Implants. 2003 Nov-Dec;18(6):902-904. PMID: 14696667.
2. Varghese KG, Gandhi N, Kurian N, Daniel AY, Dhawan K, Joseph M, Varghese MG. Rehabilitation of the severely resorbed maxilla by using quad zygomatic implant-supported prostheses: a systematic review and meta-analysis. J Prosthet Dent. 2023 Oct;130(4):543-552. doi: 10.1016/j.prosdent.2021.11.007. Epub 2021 Dec 14.
3. Lan K, Wang F, Huang W, Davó R, Wu Y. Quad Zygomatic Implants: A Systematic Review and Meta-analysis on Survival and Complications. Int J Oral Maxillofac Implants. 2021 JanFeb;36(1):21-29. doi: 10.11607/jomi.8417.
4. Anitua E, Eguia A, Staudigl C, Alkhraisat MH. Clinical performance of additively manufactured subperiosteal implants: a systematic review. Int J Implant Dent. 2024 Feb 5;10(1):4. doi: 10.1186/s40729-024-00521-6.
5. Onică N, Budală DG, Baciu ER, Onică CA, Geleău GL, Murariu A, Balan M, Pertea M, Stelea C. Long-Term Clinical Outcomes of 3D-Printed Subperiosteal Titanium Implants: A 6-Year Follow-Up. J Pers Med. 2024 May 18;14(5):541. doi: 10.3390/jpm14050541.
6. Holtzclaw D Remote Anchorage Solutions for Severe Maxillary Atrophy: Zygomatic, Pterygoid, Transnasal, Nasal Rim, Piriform Rim, Nasopalatine, and Trans-Sinus Dental Implants. Austin, Texas: Zygoma Partners; 2023.
7. Herce-López J, Pingarrón MDC, Tofé-Povedano Á, García-Arana L, Espino-Segura-Illa M, Sieira-Gil R, Rodado-Alonso C, Sánchez-Torres A, Figueiredo R. Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics (Basel). 2024 Jan 22;9(1):61. doi: 10.3390/biomimetics9010061.
Custom equipment, as precise as you are.
At Boyd, we understand that precision is everything in implant dentistry. That's why we design every piece of equipment with the same meticulous care you bring to your procedures. From our customizable chairs to our ergonomic features, each element is crafted to support your exact standards.
You can trust Boyd’s custom equipment to provide the comfort, reliability, and precision you need—every time.
8. Vanderlim BC, Baptista D, Manfro R. Transnasal Implant (Vanderlim Technique) as an option to the second zygomatic implant. Solucoes Clinicas para Reabilitacoes Totais Sobre Implantes Sem Enxertos Osseos. 2019;12:199-215.
9. Vanderlim BC, Baptista D, Almeida JR. Transnasal implants: Vanderlim technique as an alternative to the Zygoma Quad technique in atrophic total jaws - series of 12 cases in immediate load and follow-up of two to 26 months. Implant News. 2021;6(5):1-14.
10. Almeida PHT, Cacciacane SH, Arcazas Junior A. Extra-long transnasal implants as alternative for Quad Zygoma: Case report. Ann Med Surg (Lond). 2021 Jul 27;68:102635. doi: 10.1016/j. amsu.2021.102635.
11. Holtzclaw D, Zelig D, Bulot D, Nelson S, Nguyen A. Feasibility of Transnasal Dental Implant Placement Determined by PLACATE Guidelines. Dent Res Oral Health. 2025;8(1):21-26.
12. Oh S, Zelig D, Aalam AA, Kurtzman GM. Case report: utilization of Z-Point fixture “Trans-nasal” implants. Ann Med Surg (Lond). 2023 Apr 11;85(5):1959-1965. doi: 10.1097/ MS9.0000000000000520.
13. Nunes M, de Araújo Nobre M, Camargo V. All-on-4 Hybrid with Extra-Long Transnasal Implants: Descriptions of the Technique and Short-Term Outcomes in Three Cases. J Clin Med. 2024 Jun 6;13(11):3348. doi: 10.3390/jcm13113348.
14. ăahin O. Treatment of Severely Atrophic Maxilla by Using Zygomatic, Pterygoid, and Transnasal Implants. J Craniofac Surg. 2024 Mar-Apr 01;35(2):e145-e146. doi: 10.1097/ SCS.0000000000009896. Epub 2023 Nov 20.
15. Sales P, Amaral G. The use of the Transnasal implant associated with the zygomatic implants in the treatment of atrophic maxilla: A Case Report. Eur J Stomatol Oral Fac Surg. 2024;1(1):1-6.
16. Montanari Dalmolin CA, Baptista D, Meurer E, Andretti F, Almeida Grossi JR, Vanderlim BC. A Transnasal Implant Technique. Inside Dent. 2023;19(6):22-26.
17. Holtzclaw D. Treatment of Severely Atrophic Maxillae using the PATZI Remote Anchorage Protocol: A Case Series. Impl Prac US. 2023;16(4):26-32.
18. Gelpi F, Alberti C, De Santis D, Bevilacqua M, Mellone F, Tealdo T. A Retrospective Multicentric Study of 52 Nasal and Transnasal Implants in 31 Severely Atrophic Patients to Reduce Anterior Cantilever Bending in Full-Arch Implant-Supported Fixed Rehabilitations. Int J Oral Maxillofac Implants. 2025 Feb 7;40(1):69-75. doi: 10.11607/jomi.10921.
19. Simmen D, Veerasigamani N, Briner HR, Jones N, Schuknecht B. Anterior maxillary wall and lacrimal duct relationship - CT analysis for prelacrimal access to the maxillary sinus. Rhinology. 2017 Jun 1;55(2):170-174.
20. Ponnusamy S, Gonzalez J, Holtzclaw D. A Systematic Approach to Restoring Full Arch
Ready to get started? Scan the QR code or visit boydindustries.com.
Primary stability — an overview of options for the full-arch implantologist
Dr. Leke Olowokere offers guidelines for repeatable and predictable full-arch implant protocols
The concept of a full-arch, implant-supported, immediately loaded prosthetic has been well studied and has become a predictable treatment modality to provide the edentulous population, as well as individuals with terminal dentition, with an implant-supported restoration at the same time as implant placement.1 Of the many factors that need to be considered when planning an immediately loaded prosthetic, achieving primary stability is imperative. Here lies the challenge that the full-arch implantologist must be able to predictably and habitually overcome — obtaining sufficient primary stability utilizing implants that are mechanically fixated, biologically stable, and prosthetically driven. Primary stability can be quantified in multiple ways, but a common measurement is via torque values (in general, minimum values considered sufficient for immediate load include 30ncm per implant or 120ncm cumulative torque).2,3 The aim of this article is to provide the full-arch implantologist with a basic guideline of anatomical considerations, armamentarium, and finally surgical techniques to consider in order to obtain sufficient primary stability for full-arch immediately loaded implants.
Anatomical considerations
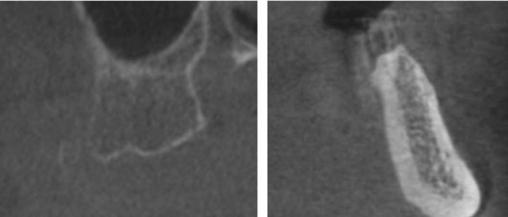
Evaluation of hard tissue quantity and quality (Figures 1 and 2) is a key diagnostic factor when determining potential sites for sufficient primary stability. The implant surgeon needs to be able to evaluate a patient’s CBCT to locate areas of hard tissue for dental implants to be placed in a prosthetically driven, mechanically fixed, and biologically stable position. This is done by identifying and evaluating the patient-specific variations of common anatomical structures such as the maxillary sinus, nasal aperture, neurovascular canals, and the bone density (classified as D1, D2, D3, or D4 bone by Misch). Common areas of bone used for full-arch immediately loaded implants in the maxilla include: the alveolar ridge and basal bone apical to extraction sockets, palatal
Leke Olowokere, DDS, FICOI, obtained his Doctor of Dental Surgery degree from Texas A&M College of Dentistry in Dallas, Texas. Following graduation, he completed a general practice residency at the Dallas VA Medical Center and has since devoted his practice to dental implantology, dentoalveolar surgery, and removable dentures. He has committed hundreds of hours toward continuing education and worldwide training with a focus in fullarch implant-supported rehabilitation all in order to best “restore health, wellness, and hope one smile at a time.” Dr. Olowokere currently practices in Springdale, Arkansas and serves as a mentor with Shared Practices Group, a nationwide DSO focused on full arch implantology.
Educational aims and objectives
This self-instructional course for dentists aims to discuss an overview of guidelines and protocols for obtaining adequate primary stability for full-arch immediately loaded implant-supported rehabilitation.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify anatomic structures that are associated with the full-arch immediate-load protocol.
• Recognize characteristics about implant macro design that make them more favorable for increased primary stability. Recognize surgical techniques used to obtain primary stability.
• Realize protocols that serve as guidelines for repeatable and predictable immediate load.
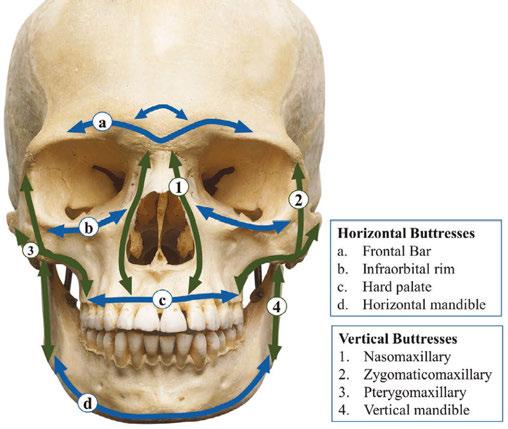
walls, the piriform rim of the nasal aperture, and the nasal crest of the maxilla. Facial buttresses can also be suitable areas of implant anchorage. These include the nasomaxillary, zygomaticomaxillary, and pterygomaxillary buttresses as seen in Figure 3.
In the mandible, common anatomical sites suitable for anchorage include: the alveolar ridge and basal bone apical to extraction sockets, and in severely atrophic mandibles or mandibles with exceptionally soft trabecular bone, the inferior border of the jaw.
These anatomical landmarks will be further discussed later in this article as it relates to the surgical technique for obtaining satisfactory primary stability.
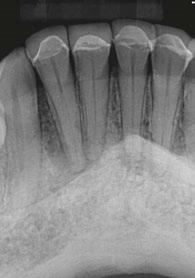
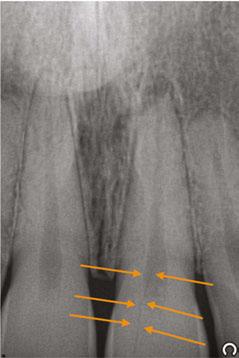
Figure 1 (left): Radiographic example of soft D4 bone. Figure 2 (right): Radiographic example of more dense D1/D2 bone
Armamentarium
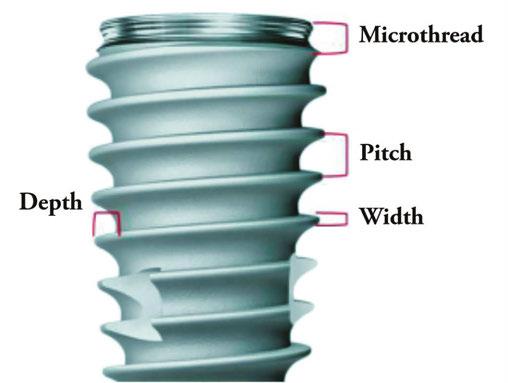
Implant design can play a significant role in the immediate-load process. Considerations include choosing an implant with appropriate width and length for the desired anatomical site (generally falls between 10 mm -15 mm in length and 3.5 mm -5.0 mm in width) and the use of a tapered implant design. Implants with deeper thread depths and shorter thread pitches can increase the bone-to-implant contact and increase primary stability5 (Figure 4 shows a visual of these terms). V-shaped threads are more aggressive and allow for greater stability of implants, while more square-shaped threads allow for greater distribution of stress and greater bone-to-implant contact.6 An implant design that is self-tapping is also advantageous for increasing primary stability.7 Although drilling protocols for osteotomies are guided by manufacturer’s recommendation, in general, primary stability can be increased when the osteotomies are under-prepared in width.8
Surgical techniques
After proper anatomic evaluation and prosthetic planning, it can be determined which techniques and implants can be utilized.
The traditional All-on-4 configuration is performed by placing two axial implants in the anterior jaw and two distally tilted implants in the posterior jaw in both the maxilla and the mandible. The posterior implants are placed tilted in order to 1) obtain sufficient anterior-posterior (AP) spread, 2) avoid disrupting anatomical structures, and 3) (which most pertains to this article) to increase the bone-to-implant contact for increased primary stability.10
Maxilla
In the maxilla, the areas of most common apical fixation include the apical bone of the anterior and premolar zones. Following the traditional All-on-4 protocol, the posterior-angled implants should aim to have their apices anchored in the point of maximum bone mass just lateral to the piriform rim and mesial to the anterior sinus wall. This area is termed the M-point by Ole Jensen.3
The anterior implants have slightly more options as they can either be placed axially, directed distally to the M-point, or directed anteriorly toward the point of maximum bone mass at the superior midline near the junction of the nasal crest and the
Figure 3: Arrangement of vertical and horizontal facial buttresses supporting the bony structure of the face4
Figure 4: Implant macro-design parameters
Figure 5: Anterior implant osteotomies angled more towards the mesial to engage the V point. Photo contributed by Dr. Paige Moorhead
Figure 6: All-on-4 configuration with anterior two implants slightly engaging the piriform rim in order to increase primary stability
vomer. This point is called the V-point, also termed by Jensen3 (Figure 5).
If more stability is needed, both the posterior as well as the anterior implants can slightly perforate and engage the cortical bone of the piriform rim for bicortical stabilization11 as seen in Figure 6.
Mandible
Similar to the maxilla, mandibular implants are commonly fixated to the apical bone of the anterior and premolar zones utilizing tilted distal implants and axially placed anterior implants. In certain circumstances, the length of these implants can extend as far as to the inferior border of the mandible to engage its dense cortical bone.3 An additional point of anchorage are implants placed behind the mental foramen. Typically there is limited bone height availability in these areas due to the proximity to the inferior alveolar nerve following alveoloplasty or due to atrophy. When enough vertical bone is available, shorter and wider implants can be axially placed in these retroforaminal positions.
Alternative alveolar sites for implant anchorage
When the degree of atrophy increases, other techniques can be utilized to obtain primary stability in biologically stable positions. The remainder of this article will focus on the techniques and protocols available for the maxillary jaw.
Palatal approach and palatal root
Two techniques that take advantage of the dense palatal bone of the maxilla are implant insertion via the palatal approach and implant insertion into the palatal roots of maxillary molars. “Palatal approach” focuses on placing the implant on the palatal side of the alveolar ridge in the presence of advanced buccolingual atrophy. These implants apically engage the dense bone of the hard palate.12 This will many times lead to thread exposure on the lingual side of the implant as seen in Figure 7. This exposed area should be in a position where the thick keratinized gingiva of the palate can passively cover the lingual threads while suturing. The palatal approach allows for implants to be anchored with sufficient primary stability in sites with narrow buccolingual dimensions.
Figure 7: Implant placed via palatal approach due to buccolingual atrophy of the maxillary jaw. Photo contributed by Dr. Thomas Kaczynski
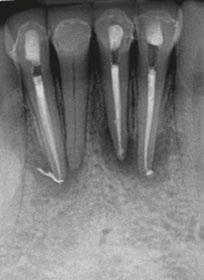
Figure 8: Implants placed using the palatal root approach can obtain high torque values of 60ncm as seen here. Photo contributed by Dr. Parker Gill
Figure 11: Pano of final zirconia of the same case. Photos of Figures 9-11 contributed by Dr. Kyle Hargis
The second anchorage site to consider is the palatal root of the maxillary molars. If there is a maxillary molar present pre-operatively, and there is sufficient vertical bone height at this area post-alveoplasty, the palatal root can be utilized as an anchorage point (Figures 8-11). This implant will generally be shorter and wider (ex. 5 mm x 8 mm). If an implant is being placed into the palatal root, then generally the drilling protocol should be more focused on expanding and shaping the socket and starting with wider drills in preparation for the desired implant to be placed. This is different from situations where the interradicular bone of the maxillary molars are utilized, and the drilling protocol follows a more standard sequence.
Remote anchorage
In cases of severe maxillary atrophy, there are remote sites of implant anchorage that deviate from the traditional sites of the alveolar bone. These remotely anchored implants include pterygoid, trans-sinus, zygomatic, trans-nasal, and subperiosteal implants. These techniques require advanced training due to their increased degree of difficulty and should only be performed when clinically appropriate. Pterygoid, zygomatic, and trans-sinus implants will be generally discussed in this article. These descriptions serve as a basic understanding of these implants. Resources such as Dan Holtzclaw’s Remote Anchorage Solutions for Severe Maxillary Atrophy (Zygoma Partners, LLLP), Carlos Aparicio’s Advanced Zygomatic Implants: The ZAGA Concept (Quintessence Publishing), and many others can be studied if the reader would like a deeper didactic understanding and insight into remotely anchored implants.
Pterygoid implants
The pterygoid implant utilizes the dense bone of the pyramidal process of the palatine bone and the pterygomaxillary junction (pterygoid pillar) to gain primary stability in the posterior maxillary regions.13 These implants not only increase the amount of cumulative torque values, but also eliminate the posterior cantilever allowing there to be reduced stress on the distal mid-maxillary implants.14 The pterygoid implant is placed in a
medial-superior-distal direction to allow for greater engagement of the pyramidal process and pterygoid pillar (Figures 12-14). Great care needs to be taken to avoid critical anatomical structures that are adjacent to this anchorage spot. These include the infratemporal fossa and the pterygopalatine fossa, both which contain vasculature that could be life threatening if severed. Precision is of importance when seeking to engage the desired target area of hard tissue and avoid hitting any vital anatomical structures that could lead to significant hemorrhage and complications. The pterygoid implant is a useful multifunctional tool to obtain primary stability in distal sites, increase the A-P spread, and eliminate the cantilever.
Zygomatic implants
Zygomatic implants are significantly longer implants which engage the dense bone of the zygoma and were originally placed to provide posterior support in the severely atrophic maxilla15 (Figure 15). These implants are indicated when there
Figure 12: 3D CBCT rendering
Figure 13 (left): Sagittal slice of pterygoid implant angled in a superior-distal angle. Figure 14 (right): Coronal slice of pterygoid implant angled in a superior-medial direction
Figure 15: 3D CBCT rendering of zygomatic implants. Photo contributed by Dr. Frank Nelson
is little to no remaining bone height of the alveolar ridge as well as severe anterior pneumatization of the maxillary sinuses.15 Carlos Aparicio created the Zygoma Anatomy Guided Approach (ZAGA) in 2011 which serves as a guide for zygomatic implant planning with respect to patient specific anatomy of the zygoma and favorable prosthetic planning.15 As previously mentioned, the zygomaticomaxillary buttress is one of the several buttresses of the skull that provide a mass of cortical bone that can be used for predictable immediate loading. Although predictable, these implants should be reserved for severely atrophic cases and revisions as indicated.
Trans-sinus implants
Lastly, the trans-sinus implant can also be used to obtain primary stability in the midst of severe anterior pneumatization of the maxillary sinuses. With traditional All-on-4 configurations, the posterior implants are angled to the distal and are positioned just anterior to the anterior border of the maxillary sinuses to remain enclosed in bone. When the sinuses are significantly pneumatized anteriorly, the trans-sinus implant can be a suitable technique to establish posterior support. This implant is similar to
the traditional All-on-4 distal implant; however, it intentionally penetrates the anterior portion of the maxillary sinus on its way to engage the cortical bone lateral to the nasal aperture (M-point) as seen in Figures 16 and 17. These implants have shown high success rates since first documented in 2012.16
Protocols
There are a vast amount of techniques to utilize different anatomical structures in order to obtain the primary stability needed for immediate load. With the multitude of approaches, it is up to the implant surgeon to select what approach to use for each case. In addition to Malo’s traditional All-on-4 protocol, several guidelines have been proposed as roadmaps for full-arch implant placement with a focus on engaging bone best fit for load bearing in prosthetically favorable positions.
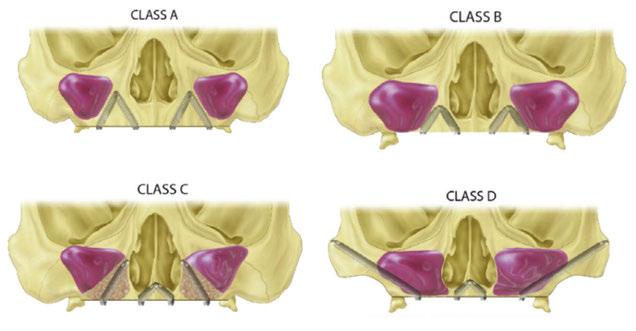
Ole Jensen developed an immediate loading site classification for the maxilla utilizing four implants.3 His protocol classifies the maxilla into four groups based on the degree of atrophy. He describes the maxillary and mandibular jaws as Class A, Class B, Class C, or Class D in order from less-to-more jaw resorption (Figure 18). Jensen describes utilizing longer tilted implants to engage the dense bone of the maxilla, and as atrophy increases, the length and configuration of implants change accordingly.
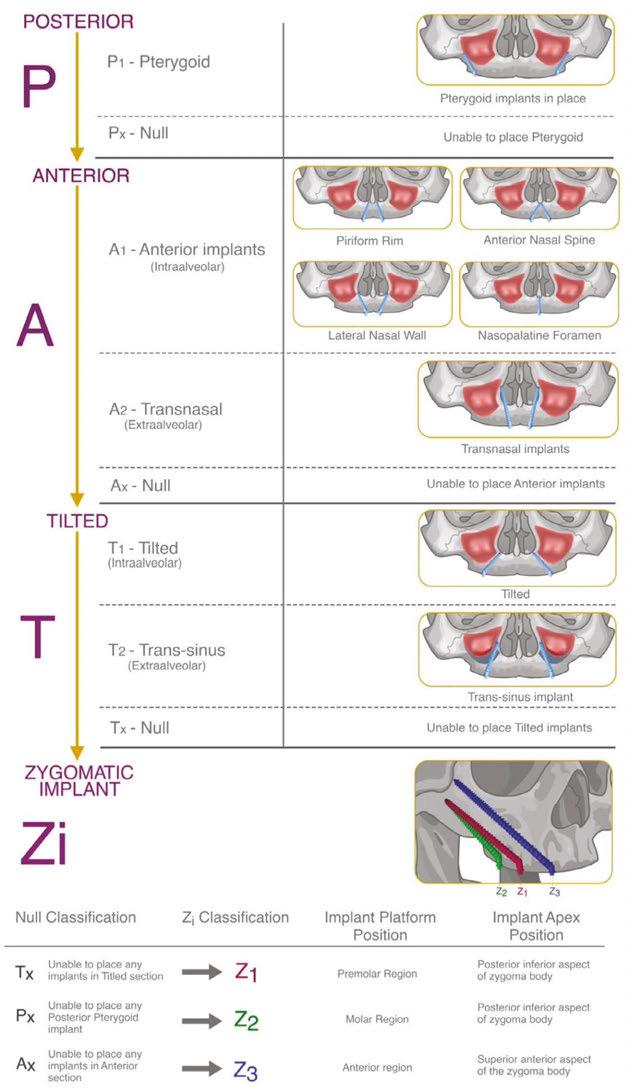
The PATZI protocol is another approach described by Shouvik Ponnusamy, Juan Gonzalez, and Dan Holtzclaw which aims to improve cumulative torque values, AP spread, and prosthetic planning using a systematic algorithm17 (Figure 19). “PATZI” is an acronym for Pterygoid Anterior Tilted Zygomatic Implants. This protocol begins with placement of the pterygoid implant. The next step is implant placement in the anterior. These implants include axial, nasopalatine, piriform rim, or transnasal implants. Next is the placement of the tilted implant. These implants provide support for the mid-maxillary region and consist of either traditional All-on-4 tilted implants or trans-sinus implants. Lastly, if the tilted implants are not able to be placed, zygomatic implants are utilized in this region. As it relates to the implant’s apical position within the zygoma, a posterior-inferiorly placed zygomatic implant can be used for posterior prosthetic support, and an anterior-superiorly placed zygomatic implant can be used for more anterior prosthetic support. The PATZI protocol is a novel approach to mechanically anchoring implants into favorable positions and decreasing/eliminating cantilever stresses with fixed full arch maxillary rehabilitation.
In addition to the general treatment planning considerations for dental implants (medical history, occlusion, patient habits, soft tissue, etc.), the full-arch immediate-load treatment modality depends heavily on the ability to achieve adequate primary stability. The implant surgeon should be aware of predictable points of anchor-
Figure 16 (left): Intraoral photo of trans-sinus implant traversing the anterior portion of the maxillary sinus. Figure 17 (right): Radiograph of trans-sinus implant. Photos in Figures 16 and 17 contributed by Dr. Thomas Kaczynski
Figure 18: Illustrations of implant placement in Jensen’s four classifications of the maxilla
age and should be able to identify and use these areas as indicated for each patient’s unique anatomy. Failure to have this knowledge could lead to a delayed loading of the prosthetic at best, or an aborted procedure with added time, procedures, and finances at worst. With proper training, experience, and knowledge, obtaining predictable and consistent primary stability is a goal that every fullarch surgeon should be able to achieve.
REFERENCES
1. Gallardo YNR, da Silva-Olivio IR, Gonzaga L, Sesma N, Martin W. A Systematic Review of Clinical Outcomes on Patients Rehabilitated with Complete-Arch Fixed Implant-Supported Prostheses According to the Time of Loading. J Prosthodont. 2019 Dec;28(9):958-968. doi: 10.1111/jopr.13104. Epub 2019 Oct 18.
2. Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2014;29 Suppl:256-270. doi: 10.11607/jomi.2014suppl.g4.3.
3. Jensen OT. Complete arch site classification for all-on-4 immediate function. J Prosthet Dent. 2014 Oct;112(4):741-751.e2. doi: 10.1016/j.prosdent.2013.12.023. Epub 2014 May 13.
4. Ghosh SG, Patra SK. Fractures involving bony orbit: A comprehensive review of relevant clinical anatomy. Translational Research in Anatomy, 2021;24(Suppl 1):100125. https://doi.org/10.1016/j. tria.2021.100125.
5. Abuhussein H, Pagni G, Rebaudi A, Wang HL. The effect of thread pattern upon implant osseointegration. Clin Oral Implants Res. 2010 Feb;21(2):129-136. doi: 10.1111/j.1600-0501.2009.01800.x. Epub 2009 Aug 25.
6. Menini M, Bagnasco F, Calimodio I, Di Tullio N, Delucchi F, Baldi D, Pera F. Influence of Implant Thread Morphology on Primary Stability: A Prospective Clinical Study. Biomed Res Int. 2020 Aug 5;2020:6974050. doi: 10.1155/2020/6974050.
7. Toyoshima T, Wagner W, Klein MO, Stender E, Wieland M, Al-Nawas B. Primary stability of a hybrid self-tapping implant compared to a cylindrical non-self-tapping implant with respect to drilling protocols in an ex vivo model. Clin Implant Dent Relat Res. 2011 Mar;13(1):71-78. doi: 10.1111/j.1708-8208.2009.00185.x.
8. Degidi M, Daprile G, Piattelli A. Influence of underpreparation on primary stability of implants inserted in poor quality bone sites: an in vitro study. J Oral Maxillofac Surg. 2015 Jun;73(6):1084-1088. doi: 10.1016/j.joms.2015.01.029. Epub 2015 Feb 7.
9. Ryu HS, Namgung C, Lee JH, Lim YJ. The influence of thread geometry on implant osseointegration under immediate loading: a literature review. J Adv Prosthodont. 2014 Dec;6(6):547-554. doi: 10.4047/jap.2014.6.6.547. Epub 2014 Dec 17.
10. Taruna M, Chittaranjan B, Sudheer N, Tella S, Abusaad M. Prosthodontic perspective to all-on-4® concept for dental implants. J Clin Diagn Res. 2014 Oct;8(10):ZE16-19. doi: 10.7860/JCDR/ 2014/9648.5020. Epub 2014 Oct 20.
11. Wu HC, Huang HL, Fuh LJ, Tsai MT, Hsu JT. Influence of implant length and insertion depth on primary stability of short dental implants: An in vitro study of a novel mandibular artificial bone model. J Dent Sci. 2024 Jan;19(1):139-147. doi: 10.1016/j.jds. 2023.05.019. Epub 2023 May 31.
Figure 19: Visualization of the PATZi workflow algorithm17
12. Andreasi Bassi M, Lopez MA, Andrisani C, Ormanier Z, Gargari M. Full arch rehabilitation in severe maxillary atrophy with palatal approach implant placement: a case report. Oral Implantol (Rome). 2016 Nov 13;9(3):115-122. doi: 10.11138/orl/2016.9.3.115.
13. D’Amario M, Orsijena A, Franco R, Chiacchia M, Jahjah A, Capogreco M. Clinical achievements of implantology in the pterygoid region: A systematic review and meta-analysis of the literature. J Stomatol Oral Maxillofac Surg. 2024 Sep;125(5S1): 101951. doi: 10.1016/j.jormas.2024.101951. Epub 2024 Jun 19.
14. Wilkirson E, Chandran R, Duan Y. Rehabilitation of Atrophic Posterior Maxilla with Pterygoid Implants: A 3D Finite Element Analysis. Int J Oral Maxillofac Implants. 2021 May-Jun;36(3):e51-e62. doi: 10.11607/jomi.8185.
15. Aparicio C, Manresa C, Francisco K, Claros P, Alández J, González-Martín O, Albrektsson T. Zygomatic implants: indications, techniques and outcomes, and the zygomatic success code. Periodontol 2000. 2014 Oct;66(1):41-58. doi: 10.1111/prd.12038.
16. Jensen OT, Cottam J, Ringeman J, Adams M. Trans-sinus dental implants, bone morphogenetic protein 2, and immediate function for all-on-4 treatment of severe maxillary atrophy. J Oral Maxillofac Surg. 2012 Jan;70(1):141-148. doi: 10.1016/j. joms.2011.03.045. Epub 2011 Jul 28.
17. Ponnusamy S, Gonzalez J, Holtzclaw D. A Systematic Approach to Restoring Full Arch Length with Maxillary Fixed Implant Reconstruction: The PATZi Protocol. Int J Oral Maxillofac Implants. 2023 Oct 17;38(5):996-1004. doi: 10.11607/jomi.10153.
Continuing Education Quiz
Primary stability — an overview of options for the full-arch implantologist OLOWOKERE
1. Here lies the challenge that the full-arch implantologist must be able to predictably and habitually overcome — obtaining sufficient primary stability utilizing implants that are ________.
a. mechanically fixated
b. biologically stable
c. prosthetically driven
d. all of the above
2. Primary stability can be quantified in multiple ways, but a common measurement is via torque values (in general, minimum values considered sufficient for immediate load include ________ per implant or 120ncm cumulative torque)
a. 30ncm
b. 35ncm
c. 40ncm
d. 45ncm
3. (When evaluating a patient’s CBCT to locate areas of hard tissue for dental implants to be placed) This is done by identifying and evaluating the patient-specific variations of common anatomical structures such as the ________ and the bone density (classified as D1, D2, D3, or D4 bone by Misch).
a. maxillary sinus
b. nasal aperture
c. neurovascular canals
d. all of the above
4. Facial buttresses can also be suitable areas of implant anchorage.
a. True
b. False
5. Implants with deeper thread depths and shorter thread pitches can _______.
a. decrease the bone-to-implant contact and increase primary stability
b. increase the bone-to-implant contact and increase primary stability
c. increase the bone-to-implant contact and decrease primary stability
d. decrease the bone-to-implant contact and decrease primary stability
6. _______ focuses on placing the implant on the palatal side of the alveolar ridge in the presence of advanced buccolingual atrophy.
a. “Palatal root approach”
b. “Bicortical approach
c. “Palatal approach”
d. “M-point approach”
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: March 5, 2025
Expiration Date: March 5, 2028
2 CE CREDITS
7. When anchoring to the palatal root of the maxillary molars, and the palatal root is being utilized as an anchorage point, the implant will generally be _______.
a. longer and thinner
b. shorter and wider
c. longer and tapered
d. zygomatic
8. (For pterygoid implants) Precision is of importance when seeking to engage the desired target area of hard tissue and avoid hitting any vital anatomical structures that could lead to significant hemorrhage and complications.
a. True
b. False
9. __________ is/are indicated when there is little to no remaining bone height of the alveolar ridge as well as severe anterior pneumatization of the maxillary sinuses.
a. Short and wide implants
b. Palatal approach to implants
c. Zygomatic implants
d. Intra-sinus implants
10. _________ developed an immediate loading site classification for the maxilla utilizing four implants.
a. Ole Jensen
b. Shouvik Ponnusamy
c. Juan Gonzalez
d. Dan Holtzclaw
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Anesthesia in endodontic and implant practices — reducing the fear of “the shot”
Drs. Gary Glassman and Mazen Dagher discuss various forms of anesthesia and how to improve the patient experience
What are the biggest fears of life? There’s the fear of dying, the fear of public speaking, fear of animals and crawling insects, but one of the most prevalent, is fear of pain from the dentist’s needle. (Trypanophobia is the medical term for fear of receiving an injection.) Dentists have spent much time and money on local anesthetic products, distraction techniques, and buffered anesthetic agents.1 And, over the years, much time and research has been spent on developing anesthetic delivery systems that are more comfortable and easier on the patient and the doctor.
Historical background
In the annals of anesthetic delivery history, Dr. Harvey S. Cook is a pioneer and visionary. In 1917 during World War I, he was a physician for the U.S. Army in France. He found that on the battlefield, it was not efficient to draw up the solution into
Gary Glassman, DDS, FRCD(C), graduated from the University of Toronto, Faculty of Dentistry in 1984 and graduated from the Endodontology Program at Temple University in 1987. Dr. Glassman lectures globally on endodontics and is on staff at the University of Toronto, Faculty of Dentistry in the graduate department of endodontics. Dr. Glassman helped develop the dental school curriculum for the Oral Health Science program for the University of Technology, Kingston, Jamaica. He is a fellow of the Royal College of Dentists of Canada, Fellow of the American College of Dentists, endodontic editor for Oral Health dental journal, Editorial Advisory Board for Inside Dentistry, Faculty Chair for DC Institute, and Chief Dental Officer for dentalcorp Canada. He maintains a private practice, Endodontic Specialists, in Toronto, Ontario, Canada. His personal/professional website is www.drgaryglassman. com, and his office website is www.rootcanals.ca. He can be reached at gary@rootcanals.ca.
Mazen Dagher, DMD, is the founder and chief education officer of Dagher Institute, a learning center for professionals who wish to advance their skills in implant dentistry, prosthodontics, endodontics, and periodontal surgery. Dr Dagher also founded the Hawkesbury Dental Centre in 1999, a top tier group practice. Dr. Dagher has acquired a high level of expertise in implantology from some of the most prestigious schools which includes the Kois Center for Advanced Dentistry (Washington), the Canadian Implant Institute, the Misch Implant Institute (Michigan), and the Sapo-Implant Institute of the University Paul IV in Paris. His practice is focused on implant dentistry and complete functional rehabilitation. He is also the founder of Chapter2Dental, a new generation of fully interactive education platform for patients and dental staff.
Disclosure: As of the time of this writing, Drs. Glassman and Dagher were not KOLs for Andau Medical or Milestone Scientific, nor do they have any financial interest in the STA/Wand device.
Educational aims and objectives
This self-instructional course for dentists aims to discuss anesthetic delivery options and how technology has improved the process and patient perception.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Realize some history of early anesthesia.
• Identify various anesthesia delivery methods over the years.
• Define the C-CLAD — computer controlled local anesthetic delivery category of anesthesia. Recognize some contraindications to single tooth anesthesia.
• Realize some ergonomics specific to the STA system in the C-CLAD category.
• Identify some possible reasons for positive reactions from patients when using less painful and stressful anesthesia methods.
the metal syringe every time anesthesia was needed. He created a faster and more efficient design after observing soldiers load their rifles and watching the empty shells being dispensed after firing. He cut glass tubing and filled them with anesthetic solution, creating the first prepackaged cartridges of anesthetic. For the stopper, he used the erasers from the heads of pencils. This was the forerunner to all future types of carpules and syringes. After patenting the system in 1925 after the war, he founded Cook Laboratories in Chicago, which eventually partnered with RB Waite, a dentist who also had created an improved syringe system. The result was the Cook-Waite Company, whose dental products are still available today.2
Over my 40 years of endodontic practice and treating teeth with “live” nerves, I have tried many options for anesthesia. Like many of my peers, when in dental school, I started with a foot pedal and pulley system to drive my slow handpiece, and using that traditional syringe and anesthetic reinforced the fearsome reputation of dental anesthesia. Even when improvements to the syringe were made, they were still large, cumbersome, and anxiety-producing. In my own childhood memories, I remember my dentist sneaking up with the dreaded shot. It’s one of the
reasons I became a dentist — I knew there had to be a better way to induce patients to get dental care, by reducing their fear of “the shot.”
Implant patients often suffer from fear of pain during the procedure, and this can cause several negative effects. Implant placements can last 1 to 2 hours or more depending on the complexity of the procedure. During this time, the patient could have increased anxiety and stress that can cause increased blood pressure, heart rate, cardiac output, and behavioral activation (alertness, vigilance).3
In an implant practice, this can lead to reduced treatment acceptance. Anxiety related to surgery may get patients to refuse implant solutions which can interfere with their esthetic and functional rehabilitation. They may also choose a treatment option, such as dentures, that would not give them as much functionality, but that are perceived as less painful a process. All of this may lead to them perceiving an unsatisfied experience in the practice.4
Anesthetic delivery options
I have tried many different anesthetic delivery systems over the years. I’ve tried the Ligmaject syringe with its pistol-grip handle and a ratchet system that injects a small amount of anesthetic per “click” and the Calaject Computer-Assisted Local Anesthesia unit (Aseptico). I have also used the QuickSleeper Intraosseous Anaesthesia Delivery System. It has a blue tooth-connected foot pedal to a rotating syringe mechanism providing an effective intraosseous injection, but I could not hide the large obtrusive handpiece from the patient, which, in my opinion, is very important to my objective of positive patient experience. In a 2020 study, some children reported that seeing the needle would increase their anxiety.5 The fear and pain of dental treatment also often results in not only avoiding dental care but also uncooperative behavior and unwanted movements while in the chair.6
Many years ago, I implemented the STA Single Tooth Anesthesia® System instrument from Milestone Scientific, which at the time was called “The Wand,” because of its pen-like shape. Patel, et al., notes that Single Tooth Anesthesia has the advantages of “not causing anticipatory worry, not hurting, and having no lingering numbing effects on the lips, tongue, or cheeks.”1
Often patients require an inferior alveolar nerve block, but in my opinion, that in itself is not enough to provide profound anesthesia for conditions like irreversible pulpitis; most often the lower second molar (the proverbial “hot tooth”). Single tooth anesthesia (STA) is effective because even though it is injected into the gingival tissue, it really is an intraosseous injection. The anesthetic reaches the bone itself, as it surrounds the tooth in a very painless manner. In this way, the “hot tooth” can be anesthetized without the patient experiencing pain. Studies have shown that the Wand® system resulted “in a significant reduction in the perception of pain compared with traditional injections (p=0.04), during induction of local anaesthesia.”6
This type of effective, profound anesthesia is very helpful in reducing fear, for both adults and pediatric patients. It helps to alleviate many of the causes of pain from syringe methods including soft tissue damage during penetration of the oral mucosa and pressure from the spread of the anesthetic solution.
C-CLAD category
The STA is in the category of C-CLAD — computer controlled local anesthetic delivery. According to Kwak, et al., the most widely known devices of this type include the Wand® (Milestone Scientific, Livingstone, New Jersey), Comfort Control Syringe (CCS; Dentsply), QuickSleeper (Dental HiTec, France), and iCT (Dentium, Seoul, Korea).7 Weight is a valid consideration for units such as this. The article notes that the STA is light weight, with a circumference that is about half that of traditional anesthetic syringes. In contrast, the Quicksleeper® and CCS® devices are about three times the size and weight of traditional anesthetic syringes, which can present difficulties in handling for operators with small hands. The increased weight of the Quicksleeper® and CCS® are due to the syringes and motors being combined in the handpiece. The Kwak, et al., article continues, “C-CLAD devices must be held stationary for long periods of time in order to ensure safe administration of anesthesia. If the device is too heavy, operation is difficult, and may lead to chance movement while the needle is inside the tissue, which may cause the needle to break” and cause undo patient discomfort. Therefore, it is important for clinicians to select the right product with appropriate weight for their needs.
While Milestone Scientific actually created the C-CLAD category with their debut of the Wand in 1997, the technology of this system is unique because it allows for certain injections that cannot be accomplished with other C-CLAD devices, such as areas of the oral cavity with difficult access. Kwak, et al., notes that the STA cartridge is installed in the main unit, which allows for the cartridge to be changed during anesthesia without having to change the needle position. During an inferior alveolar nerve block for instance, clinicians using traditional syringe methods must remove the needle from the tissue, reload with a new anesthetic carpule, and once again search the landmarks to provide a predictable nerve block. With the STA, the needle is already in position, and practitioner can change the anesthetic carpule on the unit to continue an almost uninterrupted delivery of additional anesthetic. This is especially helpful if the patient needs two or three carpules for the nerve block.
The STA device offers the needles in the 30G ½”, 30G 1” and 27G 1-1/4” to do all the different types of injections. For the mandibular block, the needle of choice would be the 27G 1-1/4”.
STA Single Tooth Anesthesia® System instrument from Milestone Scientific
The STA is a plastic wand with a little needle at the end of a small tube. The practitioner can actually break down the plastic cover that holds the delivery tubing along specific scored indentations in order to make the handpiece shorter. This is particularly useful with young patients or patients with “needlephobia” as the needle is barely visible and can be covered by the doctor’s hand.
Speed of anesthetic delivery is a concern as an injection that is performed too fast may distend the soft tissues too quickly and lead to increased discomfort for the patient compared to a slow measured delivery. Because of its computerization, the STA system provides a slow, controlled flow of anesthetic, greatly reducing pain or discomfort during its delivery due to the slow distension of the soft tissue. The injection is delivered in a controlled flow rate of one drop every other second, which allows the bone to absorb the anesthetic, prevents “oozing” of the anesthetic, and ultimately delivers the injection under the patient’s pain threshold. Continuous positive pressure yields a constant anesthetic drip that precedes the needle during its insertion.4 With some patients, the total quantity of required anesthetic is markedly reduced, due to a very precise injection and consequent rapid onset of anesthesia.8
mal apical tissues. Anesthesia was delivered with the STA at the buccal and lingual papillas of the involved teeth, and endodontic treatment was completed painlessly without lip, chin, and tongue anesthesia. The 6-month recall revealed excellent periapical healing, and tooth No. 25 remained asymptomatic with a normal pulp and normal apical tissues.
Case report from Dr. Dagher (Figures 4-8)
While some say that local anesthesia is not necessary for sedation patients, in my practice, sedation patients are anesthetized while they are sedated so they will not have pain after awakening.
The Dynamic Pressure Sensing (DPS) technology replaces the traditional hand syringe, which is much harder to control. The technology allows the anesthetic to be precisely administered to just the treatment site — allowing for complete numbness of the tooth being treated, while eliminating the numbing and morbidity effect on the cheek, lip and tongue.
That avoids the patient chewing on their lip, which is especially helpful with children, since they are more likely to cause tissue damage from biting themselves after the procedure while they are still numb. And because the anesthesia is so exact, patients don’t have to worry about 4 to 6 hours of numbness after treatment.
With lower anterior teeth, due to cross innervation, it is not uncommon where clinicians must give bilateral mandibular blocks or technically savvy bilateral mental nerve blocks to provide adequately profound anesthesia. The following case shows how I was able to complete endodontic treatment comfortably on multiple mandibular anterior teeth without the need for nerve blocks or infiltrations which would have caused the patient to have a “numb” lip, chin, and tongue for several hours. Rather STA about each tooth allowed for profound anesthesia without the soft tissue morbidity issues.
Case report from Dr. Glassman (Figures 1-3)
A 58-year-old female with a non-contributory medical history presented with a dental history of porcelain veneers on her lower anterior teeth. Teeth Nos. 23, 24, and 26 were diagnosed with pulpal necrosis with symptomatic apical periodontitis. Tooth No. 25 was asymptomatic with a normal pulp with nor-
A 37-year-old male with a non-contributory medical history presented at the office following an all-terrain vehicle accident involving teeth Nos. 7, 8, 9, and 10. The accident resulted in lip lacerations and a minor chin injury, but with no involvement of the temporomandibular joint (TMJ). Blunt force trauma to the upper anterior teeth led to pulp necrosis in teeth Nos. 7, 8, and 10, all of which exhibited normal apices. Tooth No. 9 sustained a non-restorable vertical root fracture.
For anesthesia, an anterior and middle superior alveolar (AMSA) nerve block was administered using the Single Tooth Anesthesia (STA) system, ensuring effective pulpal and hard tissue anesthesia for the affected teeth. Buccal papilla infiltrations were performed on tooth No. 9 for additional localized anesthesia. The STA system’s ability to minimize discomfort and
Figure 1 (left): Pre-op radiograph of teeth Nos. 23, 24, and 26. Figure 2 (center): Post-op radiograph of teeth Nos. 23, 24, and 26. Figure 3 (right): 6-month radiograph of teeth Nos. 23, 24, and 26 revealing healing of the apical lesions and the permanent restoration of all teeth completed.
Figure 4 (left):Vertical fracture extending to the root beyond 7 mm subgingival. Figure 5 (right): Extraction and implant placement, Straumann BLX 4.0 mm x 12 mm with temporization
6 (left): Temporization stage. Figure 7 (center): Final restoration. Note: Visible titanium tacs used during bone grafting procedure. Figure 8 (right): Final restorations, IPS.emax crowns
reduce anxiety was particularly advantageous in this case, given the patient’s recent traumatic experience.
After administering anesthesia, painless endodontic treatment was completed for teeth Nos. 7, 8, and 10. Immediate implant placement and temporization were successfully performed for tooth No. 9, addressing both functional and esthetic concerns.
At the 12-month recall, teeth Nos. 7, 8, and 10 exhibited excellent periapical healing, with no signs of complications. The implant in position of tooth No. 9 demonstrated excellent osseointegration, ensuring long-term stability and function.
The treatment effectively addressed the trauma’s clinical and psychological impacts, leveraging advanced anesthesia techniques to ensure patient comfort and a successful outcome.
Contraindications9
As with any dental technology, there are some contraindications. For severe periodontal cases with deep pockets, the area would not become sufficiently anesthetized.
According to Milestone Scientific, the single tooth injection can be an adjunct to a traditional injection in the case of areas of primary apical periodontitis and infection in general. The single tooth injection may not be indicated as a primary injection for surgical procedure, like an apicoectomy. I often use the Wand for traditional injections, (i.e., infiltration, IANB) for these procedures as the delivery is slower, more comfortable for the patient, and may provide longer duration of anesthesia.
Ergonomics
Another advantage of the STA is its ergonomics for the dentist. With repeated use of a traditional syringe, some dentists report overuse injuries to their wrists and hands because of the pushing and pulling of the wrist while injecting.10 The STA is a very tactile handpiece. The computer does the pushing and pulling for the clinician. For doctors suffering from carpal tunnel syndrome and/ or repeated strain syndrome this may provide relief.
Patient loyalty and improved practice reputation
Positive patient experience may influence the reputation and growth of a dental practice. A negative patient experience may lose a whole family’s support.
When going to the dentist, especially an endodontist, patients imagine the worst. This generates real anxiety around any procedure and the injection process in particular, since they often are already in pain. If the process is indeed painful, often they will not return to the practice, or will seek out a practice
with better pain management. According to Ost, 56% of patients who had injection phobia could trace their fear back to negative conditioning from a health-care experience.11 Moreover, 24% of patients could trace their fear to having seen another child, often a sibling, experiencing a negative event (i.e., painful or traumatic) associated to needles.12 If their expectation of pain is eliminated, patients will tell their family, friends, and post favorable comments on their social media platforms.
A number of studies investigating the origin of dental fear have been published. Most of them indicate needle phobia as the primary etiological factor, potentially leading to avoidance of dental treatment.13-15 Having an anesthesia option that is digital, quick, efficacious, and flexible enough to meet the diverse needs of various ages is a valuable asset to any dental practice.
REFERENCES
1. Patel BJ, Surana P, Patel KJ. Recent Advances in Local Anesthesia: A Review of Literature. Cureus. 2023 Mar 17;15(3):e36291.
2. Nathan J, Asadourian L, Erlich MA. A Brief History of Local Anesthesia. Int J of Head and Neck Surg. January-March 2016;7(1):29-32.
3. Turer OU, Ozcan M, Alkaya B, Demirbilik, Alpay N, Daglioglu G, Seydaoglu G, Haytac MC. The effect of mindfulness meditation on dental anxiety during implant surgery: a randomized controlled clinical trial. Sci Rep. 2023;13;21686. https://doi.org/10.1038/ s41598-023-49092-3.
4. Xie X, Zhang Z, Zhou J, Deng F. Changes of dental anxiety, aesthetic perception and oral health-related quality of life related to influencing factors of patients’ demographics after anterior implant treatment: a prospective study. Int J Implant Dent. 2023; 9(22). https://doi. org/10.1186/s40729-023-00486-y.
5. Noble F, Kettle J, Hulin J, Morgan A, Rodd H, Marshman Z. ‘I Would Rather Be Having My Leg Cut off Than a Little Needle’: A Supplementary Qualitative Analysis of Dentally Anxious Children’s Experiences of Needle Fear. Dent J (Basel). 2020 May 13;8(2):50.
6. Patini R, Staderini E, Cantiani M, Camodeca A, Guglielmi F, Gallenzi P. Dental anaesthesia for children - effects of a computer-controlled delivery system on pain and heart rate: a randomised clinical trial. Br J Oral Maxillofac Surg. 2018 Oct;56(8):744-749.
7. Kwak EJ, Pang NS, Cho JH, Jung BY, Kim KD, Park W. Computer-controlled local anesthetic delivery for painless anesthesia: a literature review. J Dent Anesth Pain Med. 2016 Jun;16(2):81-88.
8. Grassi FR, Rapone B, Scarano Catanzaro F, Corsalini M, Kalemaj Z. Effectiveness of computer-assisted anesthetic delivery system (sta™) in dental implant surgery: a prospective study. Oral Implantol (Rome). 2017 Jan 21;10(4):381-389.
10. Abichandani S, Shaikh S, Nadiger R. Carpal tunnel syndrome - an occupational hazard facing dentistry. Int Dent J. 2013 Oct;63(5):230-236.
11. Ost LG. Acquisition of blood and injection phobia and anxiety response patterns in clinical patients. Behav Res Ther. 1991;29:323-332.
12. Re D, Del Fabbro M, Karanxha L, Augusti G, Augusti D, Fessi S, Taschieri S. Minimally-invasive dental anesthesia: Patients’ preferences and analysis of the willingness-to-pay index. J Invest Clin Dent. 2017;00:e12275.
13. Kleinknecht RA, Klepac RK, Alexander LD. Origins and characteristics of fear of dentistry. J Am Dent Assoc. 1973;86:842-848.
14. Sokolowski CJ, Giovannitti JA Jr, Boynes SG. Needle phobia: Etiology, adverse consequences, and patient management. Dent Clin North Am. 2010;54:731-744.
15. Willershausen B, Azrak A, Wilms S. Fear of dental treatment and its possible effects on oral health. Eur J Med Res. 1999;4:72-77.
Figure
Continuing Education Quiz
Anesthesia in endodontic and implant practices — reducing the fear of “the shot” GLASSMAN/DAGHER
1. ________ is the medical term for fear of receiving an injection.
a. Trypanophobia
b. Thalassophobia
c. Tonitrophobia
d. Trypophobia
2. The STA is in the category of _______.
a. M-CLAD — manually controlled local anesthetic delivery
b. C-CLAD — computer controlled local anesthetic delivery
c. PGRS — pistol grip and rachet system
d. RSDS — rotating syringe delivery system
3. _______ is a valid consideration for units such as this (in the C-CLAD category).
a. Price
b. Complexity
c. Weight
d. Amount of anesthesia
4. Speed of anesthetic delivery is a concern as an injection that is performed too fast may distend the soft tissues too quickly and lead to ________ compared to a slow measured delivery.
a. increased discomfort for the patient
b. infection
c. delivery of too little anesthetic
d. widespread numbness
5. (For the STA) The technology allows the anesthetic to be precisely administered to just the treatment site — allowing for complete numbness of the tooth being treated, while eliminating the numbing and morbidity effect on the _______.
a. cheek
b. lip
c. tongue
d. all of the above
6. As with any dental technology, there are some contraindications. ________, the area would not become sufficiently anesthetized.
a. For single teeth
b. For mandibular anterior teeth
c. For severe periodontal cases with deep pockets
d. For patients who are sedated
7. _____________, some dentists report overuse injuries to their wrists
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 340
Date Published: March 5, 2025
Expiration Date: March 5, 2028 2 CE CREDITS
and hands because of the pushing and pulling of the wrist while injecting.
a. With the use of a M-CLAD device
b. With repeated use of a traditional syringe
c. With Dynamic Pressure Sensing (DPS) technology
d. With inferior alveolar nerve blocks
8. According to Ost, _________ of patients who had injection phobia could trace their fear back to negative conditioning from a healthcare experience.
a. 25%
b. 38%
c. 56%
d. 84%
9. Moreover, _______ of patients could trace their fear to having seen another child, often a sibling, experiencing a negative event (i.e., painful or traumatic) associated to needles.
a. 6%
b. 24%
c. 45%
d. 67%
10. A number of studies investigating the origin of dental fear have been published. Most of them indicate needle phobia as the primary etiological factor, potentially leading to avoidance of dental treatment.
a. True
b. False
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
How to help your team thrive when there’s a change in ownership
Dr. Samson Liu discusses how to make practice transitions more productive
Achange in ownership can be a fretful time at any dental practice as team members wonder what the future holds for them under the new management. But it doesn’t have to be that way. The right moves can help make the transition smoother and alleviate the unsettled feelings people naturally experience when the world they have grown accustomed to shifts beneath them.
Alleviating those concerns is necessary because a happy, engaged office leads to higher morale, better decision-making, and greater creativity. If the team’s concerns are allowed to fester, and rumors and gossip fill the void left by a lack of communication, then the opposite can happen. This impacts how everyone in the office interacts with the doctor, patients, and others.
Fortunately, there are steps leaders can take to avoid such undesirable results, and this is true whether the dentist who previously owned the practice is retiring and will no longer be actively involved, or whether that dentist plans to continue to practice under the new ownership.
It begins with what could be viewed as a new ownership version of the medical adage, “First, do no harm.”
Less is more
As much as possible, and contrary to common beliefs, it is preferred to keep changes to a minimum, when legally feasible. Check with your legal counsel for your individual situation. Unless there is an overriding necessity to do so, don’t rename the practice or create a new sign that greets patients when they arrive. Keep the same website and the same phone number, so that these simple things patients are accustomed to will remain comfortingly familiar. Ideally, the patients won’t even know or care that new ownership has taken over.
Certainly, some things may need to change, but the team will feel less stress if those changes are minimal –– especially early on –– and patients will not feel so disoriented when they arrive for an appointment.
Another reason to avoid rushing in with too many changes is that we need to spend time with the team to learn and understand
Samson Liu, DDS, MAGD, MBA, is the author of the Amazon bestseller Grit Your Teeth: Building a People-First Organization Through Tenacity and Purpose. He is the founder of SOHDental (mysohdental.com), a national dental support organization that is purpose-driven, people-first focused, and legacyminded. Before starting SOHDental, Dr. Liu was a veteran senior executive at Heartland Dental for more than 18 years. A frequent speaker, he has a dual Master’s degree in business administration and corporate finance and a Master’s in the Academy of General Dentistry.
what makes the practice successful in the first place. (Or, conversely, where any problems lie.) Every practice has its unique path to success, and there will always be a few nuggets, ideas, or takeaways that we can gather so that we don’t unwittingly change a process that has proved successful for the practice. Once we have handled this fact-finding mission, we will have a much better idea of what works and what doesn’t with the practice, why certain procedures are followed, and what was found to not work in the past. This will put us in a better place to understand where improvements are needed so we can make them in a strategic way. The team will be more open to this type of change, rather than if we had thoughtlessly proclaimed, “This is the way we are going to do it now.”
These learning conversations also allow us to begin building a relationship and trust with those who work in the practice. Who are they? How long have they been there? What are they passionate about? What are their concerns? If we show that we care about them, their well-being, and their successes, they will be more open to our recommendations later.
At the same time, if we rush in and begin implementing significant changes without building relationships first, we will be perceived as a threat and create within the practice a mentality of us versus them. Even good, well thought-out improvements may be met with resistance if the new ownership becomes viewed as the enemy rather than an ally.
The need for transparency
If we do deem that some changes are necessary early in the transition, though, it’s imperative to be transparent with the team about what those changes are and how the decisions we make will affect each of them. This is not a one-way conversation.
Allow them to express their thoughts without judgment, and tell them we are available to hear their questions or concerns and listen to any ideas or suggestions.
Having such open and honest conversations with team members helps establish trust, which promotes respect and a willingness to do what needs to be done. People feel valued when we take the time to communicate with them. This also helps pave the way for good working relationships going forward. The team is more likely to respond well if we explain why a change is needed, set clear expectations, and expect positive results. The biggest mistake I have made in the past is taking advantage of the communication and trust we had built with the team and implemented too many changes which ultimately backfired.
Of course, there are many communication styles and approaches, but for me, communicating with team members is similar to communicating with patients. As a clinician, I use the Problem-Consequence-Solutions-Benefits (PCSB) concept to communicate to patients about the current state of their oral health. First, I identify the problem/issue. Then I explain the consequences of doing nothing with whatever that issue might be. Next, we discuss a solution and finally, I confirm the benefits of the solution.
When used to communicate with team members, PCSB can be a great tool that allows us and the team to be transparent with each other about any issues we are facing. This will help with understanding the consequences of doing nothing and the benefits of a proposed solution. All of this can help improve the quality of the work, reduce turnover, and provide excellent patient care.
Even as we encourage the team to be open about what works, and where there may be a problem, we also want to welcome their input to improve operations. Keep communication open, productive, and positive. They will be more effective in carrying out their duties when they know we have their back and support them as a team.
Celebrate the past, look to the future
One final important lesson I have learned as an entrepreneur and leader is that micromanaging great employees is not necessary or productive. They will chafe at this, especially if they suspect a new owner doesn’t trust them to do their jobs correctly. They will worry that the new owner’s excessive control of even the most minute details isn’t just for the transition but will be what they can expect for their long-term future. They may decide they want to spend that future somewhere else –– and the best employees usually have the option to do so.
By empowering and trusting team members, we will let them do what they do best and will often find that they do the job better than we (and our micromanaging) could. Every time I have put a skilled team member in a position that I feel they will do well in, it works out better than I could ever imagine.
There is no getting around the fact that a change in ownership can be challenging as the new owner and the existing team learn about each other and begin to demystify the unknowns that lie between them. But this also can be a time to celebrate the past by acknowledging the successes of the practice under the previous owner, while embracing the future and generating optimism about the days and years ahead. IP
Implant Practice US Webinars
LEARN about the lastest techniques and technology from industry leaders with our free live and archived educational webinars. Our online seminars are a convenient way to access great information and upskill. Check out our most recent webinar:
• Full Arch and Remote Anchorage Implant Complications with hosts Drs. Justin Moody and Dan Holtzclaw
• Remote Anchorage Solutions – Making the Impossible, Possible! with hosts Drs. Justin Moody and Dan Holtzclaw
The art of the referral
JoAn Majors offers four simple steps for delivering referrals for less than a dollar
No, it’s not a typo! Some of you think art doesn’t apply to the referral process. However, I’d like you to consider a different attitude about this bedrock part of any healthy practice. Art, is defined as, “a visual object or experience consciously created through an expression of skill or imagination.” Think about this granularly, and focus on an experience created through an expression of skill. Best practices for the referral process are precisely that. The problem is often that there is no actual process in place.
I often ask offices about their referral process and get many answers. If it is a specialty office, they immediately launch into how they maintain the referrals from their professional circle. If it is a GP, it is often about a single question randomly asked at or during check-out. I want to share the simple process that will produce patients like those you especially like. The old “like likes like” proverb applies here, as does “Birds of a Feather.” The English term means people of the same sort or the same tastes and interests will be found together. If we ask patients who we like, who like and trust us, their referrals become a more predictable fit for our practice culture and care.
JoAn Majors works with organizations in the dental industry who want to improve predictability, profitability, and passion. She knows the dental industry because she comes from it and has spent 3 decades focused on the soft skills that create substantial outcomes. Fondly referred to as the “verbal word surgeon,” she creates ways to turn tough or technical conversations into scalable systems that produce value and stronger connections. She’s passionately dedicated to an exceptional patient experience. She’s a Registered Dental Assistant, Certified Speaking Professional, and Certified Virtual Presenter. She co-founded The Soft Skills Institute, a nationally recognized AGD PACE provider, with her husband, Dr. Chuck Majors.
Published in 25 magazines, newsletters, and blogs, she’s also written five books. Her latest, Permission to Be Honest, is available on Amazon. Her happy place is at the front of the room, inspiring the entire team to action with her signature “open arms” communication and savvy lingo. JoAn’s speaking and writing voice are the same as her storytelling style. She is candid but not crude, funny but serious about results. Her seminars and workshops can be followed with high-value online training content for greater implementation and scalability.
JoAn earned the distinguished CSP Award from the National Speakers Association, the highest award among professional speakers. Less than 12% of professional speakers worldwide have earned the designation. She is a 2022 DENOBI award winner and serves on the board for Dental Entrepreneurial Women (DeW) as Co-Director of Education. Serving as Team Training Faculty member for the Misch Implant Institute for 20 years, she was the first non-dentist appointed by the late Dr. Misch. Lastly, JoAn is the VP of Training and Development for ICON Dental Partners, a truly doctor-owned, doctor-led, completely doctor-centric group. For more information, or to see her in action, visit www.joanmajors.com.
The process is the 4 P’s: plan, pick, postcard, and process. It sounds pretty simple and can be if you complete the process. Think of it as baking a cake or, more to your mindset, a procedure you follow. You wouldn’t bake a cake and leave out the flour, or you’d have a terrible cake. You, the doctor, wouldn’t start a process and not complete each step. This is no different. Systems and processes followed correctly more often produce the results we expect.
Plan
The planning portion of the process is pretty simple. I’m going to start by assuming that you have a morning huddle. If you do not have a morning huddle, planning likely isn’t your thing.
During the morning huddle each day, I’d like you and your team to review the schedule to choose just one patient daily. There will be days when you may have more and days when you have none who fit the standard you are looking to grow in your practice. Consider that your goal is to find four per week.
Pick
You’re looking for happy paying patients who like you and your team, and when you see their name on the schedule, you actually smile. As a team, we agree that this person is someone you’d like to duplicate in your patient base. Although not always, often it is a fee-for-service patient. It’s your patient to duplicate. Sometimes, discussing as a team to outline this person is helpful. It could be a patient with a particular procedure you’d love to have talking about their outcome or someone you’ve found to
Implant Practice US
be courteous to your team and complimentary of your office. This referral is by your design.
Decide among the team who has the best relationship with the person or will have more time to have the “referral convo” while they are in that day. Once the team members are assigned to them in the huddle, they will be the ones to have the conversation, send the notes, and document the process.
Sample Convo
Scenario 1
You’re looking for happy paying patients who like you and your team, and when you see their name on the schedule, you actually smile.”
“Hi, Happy Holly; this morning, when we were planning our day and saw your name on our schedule, I have to share that we all smiled. I want you to know how much we appreciate patients like you who fill in this blank. What we do isn’t easy, and it really makes our day. Could you help me with something?
Wait for the answer. People appreciate the ask.
“You may not know this, but we are expanding our practice and would love more patients like you. I’d love it if you’d consider sharing your experience with us with a work colleague or family member like yourself. Would you keep us in mind when chatting with people like yourself?”
Scenario 2
“Hi Happy Holly; this morning, when we were planning our day and saw your name on our schedule, I have to share that we all smiled. I wanted to ask you about your (experience/treatment) with us. How do you feel we’ve done?”
Wait for the answer. If you plan well, the patient will respond favorably.
“I was hoping you would feel that way. Could you help me with something?
Wait for the answer.
“You may not know this, but we are expanding our practice and would love more patients like you. I’d love it if you’d consider sharing your experience with us with a work colleague or family member like yourself. Would you keep us in mind when chatting with people like yourself?”
Postcard
This is the part of the process most leave out. Imagine, doctor, that you’ve given a finely crafted delivery of a beneficial and easily deliverable treatment to a patient. Yet, when they are transferred to the front desk, no one offers the appointment or completes the process. The art of the referral process is no different. It shouldn’t be started if we aren’t willing to complete it.
Now, to the postcard. No matter how small, a handwritten note is still considered an act of endearment. It’s not a text follow-up; it has a purpose. I can’t tell you how many female patients (most naturally appreciate being recognized for their influence and being asked for help) have dropped this little card into a purse and handed it off to a friend, colleague, or family member within a few days. A recent article in Forbes, “Who
Runs The World? Women Control 85% of Purchases,” showed proof of female referrals’ power.
The U.S. Post Office sells a pre-stamped postcard. A postcard is great because it is lightweight; others can’t help from being nosey and reading it when it is being transferred or lying around. The cost ranges from .53 cents to .73 cents, depending on size. You keep these stocked up and in the area where you have your huddle. My mantra is to make it easy for people to do what you want them to and hard for them to do what you don’t want them to. This will apply here. Make it easy for the team member you are asking to write a quick address in the huddle.
Sample Note:
“Happy Holly. It was great visiting with you today in the office. I loved hearing about fill in the blank personal to the individual. I want to thank you in advance for referring others to our office. We really enjoy patients like you and look forward to our next visit.
Personal close, name.”
Hint: Choose a great return address label in color! Write your card with colored ink that matches the label. As I have written about in the past, this now becomes a handout from your “walking-talking marketing tool.” This will be the most affordable marketing you’ll do; I promise!
Process
Remember to complete the process. In our office, the card was handed off to the admin team for mailing and for putting a patient note in the record. Use a code you create or in the note section. Ours simply said, “Referral Convo.” It was noted in the record the day the card went out. Mail it quickly so that it is still fresh in their minds.
In my 20 years of teaching this system to our team members, I’ve never had someone say no when we asked for help. They may not all produce a referral, but most are so surprised that you asked them for help that they are moved to a yes simply because you complimented them and asked. The word “help” is most important.
If you have issues with this process, it will be because you chose the wrong person. Remember, “like likes like.” Picking the right person to ask is significant to the outcome.
I’ve taught the system for years to many offices, and it amazes me how many team members and doctors I hear from. They are often amazed that something so simple and so affordable can make such a difference in the patient’s mind. If you have an interest, I’d love to share more about our other Soft Skill Systems. Choosing the right communication is really affordable; it’s the intention behind it that makes it significant and profitable.
See you on the road.
• In-Network options with major payors and plans
• Out-of-Network when appropriate
• Reliable, timely, predictable results with best rates
• Access to the Nexus Specialty Physician Network
• Nexus billing portal ensures error-free claim submission and tracking
• Personal billing representative
• Complete solution for:
º Implants
º Surgical Guides
º Bone Grafts
º Extractions
º CBCT
Bill Nexus Bill Makes Reimbursement for Medically Necessary Oral Care Simple, Easy and Reliable
Getting reimbursement from medical insurance can be a nightmare for dentists. With the Nexus Bill system, you can avoid the common pitfalls of inconsistent payments, endless delays, constantly fighting with insurance companies, and patients refusing care because you are not “In-Network” for medical.