Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions. ISSN number 2372-8396
Shaping the future
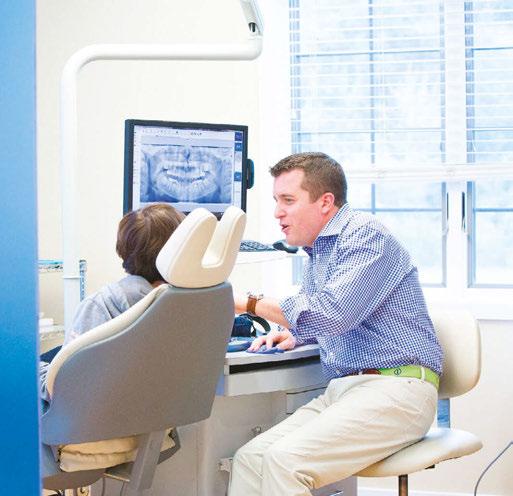
Iam Dr. Chris Teeters, a board-certified orthodontist dedicated to advancing the field of orthodontics through innovation, education, and collaboration. As the co-founder of the Mother of Pearls Orthodontic Conference (MOPC), I have helped create one of the most influential continuing education events in the industry. This annual conference brings together top experts from around the world to share cutting-edge techniques, research, and advancements in orthodontics. We are preparing to host our 7th Annual MOPC this coming October 10-11 at the Kennedy Space Center featuring over 500 attendees, 20 of our industry’s best speakers, 50 exhibits, incredible food and beverages, and a phenomenal Pearls Party under the Apollo Saturn V rocket with space exhibits and live music from the world’s only all-orthodontist band, RELAPSE. Through this educational platform, I have been able to help foster an environment where orthodontists can learn, grow, and elevate their practices to new levels of success. Learn more about our upcoming conference at orthodonticpearls.org.
Beyond the conference, I spend time as admin and co-founder of Orthodontic Pearls, the world’s largest orthodontic study group on Facebook, with over 9,400 vetted and verified orthodontists worldwide. This online community has become an invaluable resource for orthodontists looking to exchange knowledge, discuss complex cases, and refine their treatment approaches. It was through the shared experiences of this group that I ultimately decided to use Angel Aligner™ in my practice, as the overwhelming feedback on their effectiveness has been incredible.
In my practice at Teeters Orthodontics in Peoria, Arizona, I have fully integrated Angel Aligner into my treatment protocols. One of the key innovations I utilize is the angelButton™, a unique feature designed to enhance sagittal bite correction and correct crossbites more efficiently and effectively. By incorporating these built-in buttons with elastics, I am able to achieve more predictable and efficient outcomes for my patients, improving their overall bite alignment with greater precision.
Additionally, I have embraced the A6 Mandibular Advancement solution to help patients with mandibular retrusion. This system allows me to simultaneously correct occlusion issues while advancing the mandible, leading to improved facial profiles and functional benefits. Having utilized the twin block in practice for over 12 years with remarkable results, I have embraced this new technology to combine orthopedic and orthodontic treatment in a single phase, reducing overall treatment time while delivering superior results.
My passion for orthodontics extends beyond my practice. I am deeply committed to sharing knowledge and advancing the profession through education and collaboration. I frequently lecture at orthodontic conferences across the United States and internationally and have contributed to the field by developing appliances and treatment techniques that are now used by orthodontists worldwide. As a Key Opinion Leader for Angel Aligner, I look forward to sharing my cases and clinical techniques with my colleagues for years to come.
Outside of orthodontics, I enjoy spending time with my family, playing guitar for my church, and staying active with hobbies like piano, running, and weightlifting. My goal is to continue pushing the boundaries of what’s possible in orthodontics while helping both my patients and colleagues achieve the best outcomes possible. By staying at the forefront of innovation and fostering a strong professional community, I am committed to shaping the future of orthodontics.
Chris Teeters, DMD, MS
Maximize efficiency with Clarity™ Digital Bonding
Save time, boost performance
Streamline procedures that reduce repositioning appointments by up to 1.2 per case
Statistically, doctors can expect to save treatment time with Clarity™ Digital Bondingmonths 6 up to
Ready to elevate your practice with the unmatched flexibility of Clarity™ Digital Bonding? < Scan to get started
CONTINUING EDUCATION The DOME approach to breathing, bite, and beauty
Drs. Claudia Pinter and Stanley Liu illustrate a protocol to improve nasal breathing in orthodontic care 31
Dr. Lisa Chan and Barbara Madej, RPh,
PRACTICE MANAGEMENT Selling with integrity — the CliffsNotes ®1
Dr. Jamie Reynolds explains how marketing skills and Ormco products can lead to long-term success .......................................... 38
Dr. Anthony Serrano discusses how the LightForce personalized IDB system, LightTray, changed his practice
Making the world a better place
Every day, in newspapers, on TV, and social media we see humanitarian efforts across the world. Whether it’s for saving endangered animals, survivors of natural disasters, cures for diseases, or other causes closer to home, we all try as much as possible to open our hearts and wallets for those who could use a boost in life. Dental practices’ own little corners of the world can have their own distinctive ways to create a better place.
Lisa Moler Founder/Publisher, MedMark Media
It’s easy being green: One of the most popular ways dental offices can show environmental responsibility is by employing “green” programs. The ADA has a page on its website titled “80 ways to make your practice green” (https://bit.ly/4gbMrra) — with suggestions like investing in energy-efficient technologies, purchasing furniture made from recycled products, or something as small as using biodegradable cups. Replacing high-energy consuming office lights with energy-efficient lighting will conserve energy and also probably help lower some of the electric bill as well.
One patient at a time: MedMark publications always feature new equipment, technology, and materials. Researchers and inventors of these new dental solutions spend hours of their time, effort, and money improving the dental experience and creating new options for better and more individualized patient care. Whether it’s taking the pain out of root canal treatment, bringing new treatments to those with sleep-breathing issues, inventing implant solutions for those who need special care, creating new aligner and bracket-and-wire systems to help patients smile again after years of low self-esteem, or taking the fear out of the office for even the youngest dental patients, our articles can help improve patients’ quality of life, while also improving your business.
Pay it forward: Some of the most famous key opinion leaders in the dental industry were mentored and encouraged by their peers. Implementing any new protocol or procedure from the simple to the complex is less stressful when there is someone to call on for advice. We’ve all been there — in any occupation, moving to a higher level means being educated not only from text books or lectures, but hands-on, chairside guidance from someone who has “been there and done that.” Articles in our publications also feature authors who want to share their expertise, and who are often happy to follow up with constructive pointers on how to add their protocols to your practice options.
Love thy neighbor: Dental offices can be a productive part of any community. From contributing to local schools, to visiting classes to talk about better oral care, to participating in veteran’s events, clinicians and their teams can expand their reputation, referrals, and hearts by showing the surrounding areas that their community is important to you too. It isn’t hard to find these activities. Check with your local Chamber of Commerce, community newspaper, school volunteer event staff, or even ask your patients what organizations they may be involved in. Your practice name will stay in potential patients’ minds long after the event is over.
The spring issue is ready to share concepts that will help to build your world. We hope you enjoy this issue’s well thought out/interesting articles, and make some ideas into realities.
It is a small world — and by making it better, your potential patients will be happy you are a part of it.
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Subscription Rate 1 year (4 issues) $149 https://orthopracticeus.com/subscribe/
Innovative Orthodontics growing with DentalMonitoring
In 2008, Dr. Dan Bills started Innovative Orthodontics with one location in New Jersey. Over the next decade, he used technology to deliver efficient care and grow his practice, adding two more locations and two associate orthodontists. Dr. Bills’s wife, Dr. Emily Eilerman, expanded the practice to include pediatric dentistry with a focus on clinical excellence and technology. While Dr. Bills is an orthodontist with an interest in new technology, he doesn’t consider himself an early adopter. Instead, he’s happy to learn from his colleagues’ experiences before making a purchase and bringing it to his team. He had been watching DentalMonitoring for years before utilizing it to improve his patients’ treatment experience. In 2018, he began using asynchronous, virtual visit apps, but at that stage, remote monitoring was more useful as a marketing tool for the practice than as a clinical tool for improving treatment outcomes. Dr. Bills initially considered remote monitoring as a tool to compete
with direct-to-consumer orthodontics. As that segment of the orthodontic market collapsed, the pandemic created a whole new need for remote monitoring as everyone struggled to see patients. Patients appreciated the convenience of the asynchronous appointments and the new patient process. Additionally, Innovative Orthodontics has nearly 3,000 patients in observation because of the pediatric component of the practice, so remote care became useful for managing those appointments.
Before implementing DentalMonitoring, Dr. Bills explains, remote monitoring took too much doctor and staff time to manage. They started working on virtual and remote care options to make the treatment experience more convenient for patients, but that didn’t mean the practice staff was sharing in the convenience. ”We created a remote treatment platform using barebones technology to stay open during COVID. We realized then that patients loved it, and they wanted it to stay. We started
Dr. Dan Bills
searching for a better solution and onboarded DentalMonitoring 2 years ago.”
Dr. Bills knew his team was ready to onboard DentalMonitoring because he’d been discussing the platform with them and showing them parts of it for years. He’d built trust with his team about new technology; they know he’s vetted each new tool he brings to the practice and that they aren’t getting “a shiny toy” he brought back from a trade show. “After 2 years of using DentalMonitoring,” he says, “I want to go back and kick myself for not bringing it on sooner. The AI component of DentalMonitoring has made our lives so much simpler.”
The key to success, Dr. Bills explains, was going all in with DentalMonitoring from day one. “Aligner patients, braces patients, retention patients, and observation patients all get DentalMonitoring. We use DM Engage as a lead management tool, which is helping us with new patient growth.”
Dr. Bills had already recognized that allocating chair time for pretreatment observation patients was wasteful for everyone involved. With DentalMonitoring fully integrated into the practice workflow, “The team immediately saw how AI-powered monitoring was the robust platform we needed. Our headcount has decreased through attrition by one or two team members while the practice has grown. Production has increased, but our number of doctor days needed has decreased.”
“My remote care coordinator utilizes the DentalMonitoring AI to troubleshoot just about anything. When there is a question that needs a doctor’s attention, they’re able to get that directly. DentalMonitoring decreased my digital homework, and I can accomplish more during business hours.”
Treatment philosophy
Dr. Bills’ treatment philosophy is focused on delivering what patients want and deserve. As he tells it, it boils down to three key elements: great patient experience, clinical excellence, and optimal efficiency.
Great patient experience
From the first phone call to the last visit, we make sure that patients feel like they’re part of the family.
Clinical excellence
Clinical excellence is the bare minimum. Every patient expects a great smile, and we make sure to deliver upon that.
Shortest treatment times
People are busy and want the quickest treatment without sacrificing great outcomes.
Efficiency
According to Gaidge, the national average of months in treatment is 27, with an average of 19 visits. For Dr. Bills, that number is too high. “We’ve always embraced the patient side of this journey. We believe that excellent work and efficient treatment is a win-win. If you care about efficiency at all, DentalMonitoring is a solution to a real problem that we all have.”
Emergencies
For Dr. Bills, there are no emergencies in orthodontics. “We call them comfort checks.” His practice now uses DentalMonitoring to triage when someone calls or messages over the app and says they have a broken bracket and need to come in. This is where the patient experience and clinical efficiency meet. The team makes sure that patients know they’re receiving immediate care via the DentalMonitoring app, and they will make sure the patients are out of discomfort as soon as possible. “We let the patients know that they’re taken care of, then send them a scan request and get eyes on the situation immediately,” Dr. Bills explains. With DentalMonitoring scans, the team knows how to schedule the patient’s next appointment. “We’re finding that nearly half of those appointments don’t require an office visit. We no longer have any surprises on those visits,” Dr. Bills says.
Referrals
One way to get referrals, Dr. Bills knows from experience, is to partner with a pediatric dentist. Another good way is to use technology. For Dr. Bills, both have worked out great. He met his wife, Dr. Emily Eilerman, through the dental community. They have a daughter, “who just became a better skier than me,” Dr. Bills proudly shares.
It’s common for orthodontic practices to spend time and money buying snacks and drinks for referring dentists; however, Dr. Bills explains, “Our community appreciates the fact that we use technology that makes the patient experience better.” General practitioners continually hear how much patients love DentalMonitoring and the convenience that it brings them so the practice has become known in their region as an efficient and convenient practice. Dr. Bills has been teaching about the need for efficiency and the way that DentalMonitoring allows him to boost the value-per-visit of every treatment. He says, “Our referral base knows that their patients are not going to have their time wasted.”
Dr. Bills loves the DM Insights component of DentalMonitoring, explaining, that “DM Insights data means you can’t hide.” The Innovative Orthodontics team is focused on clinical efficiency. “We use DM Insights to validate our efficiency, but I see how it would also help other orthodontists become more efficient as they pull reports on breakages and treatment planning.”
Prioritizing growth might seem more logical because some inefficiency won’t hurt practices that aren’t feeling the pressure in their schedule. Dr. Bills is very clear that this is an unacceptable choice. He says, “There’s no such thing as being 100% efficient, but efficiency needs to be central to your treatment philosophy. You’re stealing the time you need to grow if you let your team and procedures take longer than necessary.”
Data
One part of DentalMonitoring is the powerful DM Insights data hub, which Dr. Bills uses as a quality management system. With close to no additional work for his team, he’s able to explore practice data and validate their efficiency. While there’s no such thing as 100% efficiency, there’s honesty in data that lets Dr. Bills know that he’s delivering the level of care that patients deserve. “We can use DM Insights and see that we are well below the national average for breakage rates and other issues; it makes sure that we’re not fooling ourselves. We aim for excellence and clinical efficiency at every step of treatment, every appointment. DM Insights data shows the success of that intentionality.”
But efficiency is more than a set of numbers; it’s a way of practicing. Dr. Bills says, “I can sit down with my team and DM Insights and look at bond failure rates using real numbers. We can get granular, and look at outliers, people with the most breakage or attachment loss, and use it in our training to help individual assistants improve.”
Partnering with DentalMonitoring
Dr. Bills can’t help but express his enthusiasm for the new releases that DentalMonitoring has been working on. “It’s really fun to work with a company as visionary as DentalMonitoring. I don’t see any other companies attempting to innovate at this speed. It’s amazing to just have a group of people who are all rowing the boat in the same direction. There are some companies out there that haven’t made a new product in 20 years. I can’t think of another company in orthodontics that is trying to continue to develop tools to make our lives easier and our patients’ lives better.”
He explains that DentalMonitoring CEO Philippe Salah has been teasing the upcoming product release of DentalMonitoring+,
One of the benefits of a highly efficient practice is that Dr. Bills has more
which features updated 3D models based on remote scans. Dr. Bills can’t wait to get his hands on the new tool to monitor and customize treatment. “I’ve never been this excited about where the profession is going and where technology is going as I am today. DentalMonitoring+ will be the new standard of care.”
Orthodontic education
Dr. Bills is on the faculty at Harvard University and the University of Pennsylvania, where he teaches a year-long mini-residency on technology-based solutions. He also teaches an annual inoffice course for working practitioners looking to increase practice efficiency. “We talk through all the different technological options in the orthodontic office from patient acquisition, marketing, clinical treatment efficiencies, digital workflows, retention, patient experience, and experiential branding.” His takeaway from his time teaching is that the next generation is not only embracing this, they’re demanding technological innovation.
“I started my residency the year after Invisalign® started and was able to use it during my residency, but other programs at that time did not allow clear aligners in their program.” The correlation for Dr. Bills is that DentalMonitoring and remote care are just as transformative for the orthodontic industry as the clear aligners. “The spirit of technological revolution of 2000 to 2001 is happening again in 2024 and 2025. It’s exciting that educational programs are putting this into the hands of residents.” OP
time to connect with patients
MY BEST ORTHODONTIC EXPERIENCE.
> HAPPY USER FROM APP STORE <
“I love not having to be in the orthodontics office every time you breath (like I did with my older son)! And although the treatment was excellent with my eldest, I think this treatment is even better
“I love not having to be in the orthodontics office every time you breath (like I did with my older son)! And although the treatment was excellent with my eldest, I think this treatment is even better with the scans and feedback from the app”.
Discover how DentalMonitoring will transform your practice.
Discover how DentalMonitoring will transform your practice.
Use it to keep treatment on track. Unlock your potential to start more patients. ·WEEKLY
Use it to keep treatment on track. Unlock your potential to start more patients.
·WEEKLY REMOTE MONITORING ·AI PROCESSING
·AUTOMATED NOTIFICATIONS
·AUTOMATED NOTIFICATIONS
·SCHEDULING EFFICIENCIES
·SCHEDULING EFFICIENCIES
·PRACTICE OPTIMIZATION
Treatment length comparison between DIBS AI digital bonding and traditional direct bonding: a preliminary assessment
Milan Detweiler, senior vice president of OrthoSelect, LLC, discusses the results of a study comparing two bonding methods
Introduction
Direct bonding to enamel has been the traditional method of placing brackets in orthodontic treatment since the 1960s.1 As indirect bonding methodologies have appeared on the market, controversy has arisen over the preferability of either direct or indirect bonding techniques.2
Various approaches to indirect bonding have been developed, with varying levels of effectiveness and accuracy.3 While many practitioners who have used indirect bonding to treat their patients report that it shortens the clinical time required for the initial bonding appointment, the question remains as to whether this approach can measurably shorten the overall length of treatment. The purpose of this study is to specifically assess the DIBS AI digital bonding technique provided by OrthoSelect and compare treatment times among similar patients treated using direct bonding to determine if there are differences in treatment times and number of office visits required, and, if so, the extent of those differences.
OrthoSelect uses the term digital bonding as opposed to indirect bonding. While the concepts are somewhat similar, DIBS AI does all the modeling digitally, so there is no longer a need for physical study models, and most of the work is automated through artificial intelligence. Additionally, transfer trays are 3D printed rather than using older vacuum-formed appliances. For purposes of this article, digital bonding is used when referring to the DIBS AI technique.
Methodology
For this study, patients treated at four unrelated orthodontic practices (located in Ft. Collins, Colorado; Orlando, Florida; Las Vegas, Nevada, and Port Orange, Florida) that provide both types of treatment were selected post hoc, anonymized, and then segmented into two groups: those who received bracket placement via direct bonding and those who had brackets placed via DIBS AI digital bonding. Data from a total of 286 completed cases were
collected for this study (168 direct bonding cases and 118 digital bonding cases). Selected patients constituted a mix of genders and ages ranging from 9 to 45 years old, with the majority of the patients being in their teenage years. The orthodontists followed the prescribed protocols for DIBS AI software treatment planning and clinical procedures as provided by OrthoSelect. No guidelines were given for their use of direct bonding techniques. Therefore, some variance in approach for direct bonding cases may have occurred.
Using data stored in each practice’s Patient Management System (PMS), information on treatment lengths and number of appointments was collected and aggregated for both direct and digital bonding cases.
The sample data were analyzed using standard statistical testing methods to determine if meaningful differences exist. In the case of comparing the mean results of both samples, an independent two-sample t-test was used with a p-value threshold < 0.05. An F-test was used for comparing standard deviations between samples, p-value threshold also < 0.05.
Results
Based on analysis of the data, the combined results across practices show that mean treatment time for direct bonding was 23.4 months compared to 15.8 months for digital bonding, an average reduction of treatment time of 7.6 months (32.5%) for digital bonding. An independent group’s t-test was performed to compare and validate the mean treatment time differences between the two treatment modalities. The t-statistic was significant at the 0.05 critical alpha level, t(284)=10.191, p<0.001. Therefore, we conclude that there is a significant difference between the mean treatment times between direct and digital bonding protocols. Likewise, the mean number of treatment appointments for direct bonding cases was 15.6 compared to 11.6 for digital bonding cases — an average reduction of four appointments (25.6%) for digital bonding (again, statistically significant at the 0.05 critical alpha level: t(284)=7.023, p<0.001).
Table 1:
Table 2: Summary Results Number of Appointments
Along with shorter average treatment times for digital bonding cases, it also appears that the treatment-time variability is less for digital bonding cases, as borne out by the significantly smaller standard deviation of the indirect bonding sample (see Table 3).
Conclusions
Based on this analysis, the DIBS AI digital bonding approach appears to significantly reduce the amount of treatment time required and the number of office visits necessary to complete orthodontic treatment by an average of 7.6 months (32.5%) and 4.0 visits (25.6%) respectively compared to traditional direct bracket bonding. While one would expect that treatment time and the number of office visits would be positively correlated, the fact that both are significantly lower for DIBS AI treatment demonstrates that no unusual cadence of treatment or timing was required to achieve the indicated outcomes.
Further, the fact that the standard deviation of treatment time for the DIBS AI treatment sample is statistically lower than for the direct bonding sample indicates that the DIBS AI treatment protocol, in addition to being shorter, is also more predictable. In other words, the smaller standard deviation indicates that there is less variability in average treatment times for the DIBS AI approach. This narrowed range could make treatment planning and setting expectations for the patient easier for the practitioner.
It is important to note that the orthodontists in this study closely followed established clinical procedures for DIBS AI treatments. Deviation from these techniques would likely yield sub-optimal results and may change the outcomes as presented in this study.
As indicated in the title of this article, this is a preliminary study, though the results do appear promising for DIBS AI as an effective means to shorten overall orthodontic treatment times. Further examination is warranted across a broader number of practices and cases.
Doctor insights
To get a fuller understanding of the clinical experience with digital bonding, we also spoke with Dr. TC Hardy of Ft. Collins, Colorado, who participated in the study, to gain some additional insights into his experience and results with DIBS AI.
What has been your experience using DIBS AI?
Dr. Hardy: I have been using DIBS AI for approximately 5 years. When I first began, I was excited to explore a new digital solution within the orthodontic community. Something I particularly liked with DIBS AI is that it could be seamlessly integrated into my existing practice. Transitioning to a digital setup with DIBS AI immediately improved both my bracket placement and treatment outcomes. Once I saw these improvements, there was no turning back.
The data from the study indicate that using DIBS AI versus direct bonding shortens overall treatment time. Any further thoughts on this from either a clinical or practice perspective?
Dr. Hardy: With DIBS AI, I noticed an immediate improvement in the precision of bracket positioning. The details in the software measurements allow for greater confidence in bracket
Table 3: Standard Deviation of Sample Datasets
Standard deviation direct bonding treatment time
Standard deviation DIBS AI bonding treatment time F-Test Results (P
all cases
placement. The predictive treatment simulator continues to improve, allowing to make further adjustments based on these outcomes. This is, I am finding, of tremendous value. From my experience, transitioning from chairside bonding to digital bonding with DIBS AI has significantly reduced the need for additional visits for wire bending or bracket repositioning in most cases. This directly correlates to the overall treatment time for the patient.
The initial bonding procedure has become highly efficient for my clinical team, with the process now taking approximately the same amount of time as an aligner start. By utilizing DIBS AI, I no longer need to be directly involved in bracket checks for initial bonding. Instead, I can complete the digital setup between patient appointments at a time more convenient for me and the office flow. This has alleviated the pressure on the treatment coordinator and other assistants, as they no longer need to wait for me to conduct the full bracket start procedure.
What recommendations do you have for doctors considering switching to DIBS AI?
Dr. Hardy: I strongly recommend investing time in training yourself on the software. DIBS AI offers on-site clinical training and excellent resources on dibsai.com, including instructional videos that provide a solid foundation. Don’t hesitate to reach out to other doctors who are already using the system if you have any questions. I’m always available to share my thoughts as well!
It is especially important to dedicate significant time to training your team on the digital bonding chairside process, especially if they have not previously worked with digital indirect bonding trays.
While DIBS AI does allow for in-office printing, I highly recommend utilizing their lab for printing. The quality, detail, and turnaround time offered by DIBS AI’s lab provide distinct advantages, particularly when you’re new to the system. Even if you are already using 3D printing for models and other appliances in your practice, I strongly advise using their lab services to get the best results.
About DIBS AI
For more information on DIBS AI, visit DIBSAI.com or scan the QR code.
REFERENCES
1. Gange P. The evolution of bonding in orthodontics. Am J Orthod Dentofacial Orthop. 2015 Apr;147(4 Suppl):S56-563. doi: 10.1016/j.ajodo.2015.01.011.
2. Menini A, Cozzani M, Sfondrini MF, Scribante A, Cozzani P, Gandini P. A 15-month evaluation of bond failures of orthodontic brackets bonded with direct versus indirect bonding technique: a clinical trial. Prog Orthod. 2014 Dec 30;15(1):70. doi: 10.1186/ s40510-014-0070-9.
3. Xue C, Xu H, Guo Y, Xu L, Dhami Y, Wang H, Liu Z, Ma J, Bai D. Accurate bracket placement using a computer-aided design and computer-aided manufacturing-guided bonding device: An in vivo study. Am J Orthod Dentofacial Orthop. 2020 Feb;157(2):269-277. doi: 10.1016/j.ajodo.2019.03.022.
How to submit an article to Orthodontic Practice US
Orthodontic Practice US is a peer-reviewed, quarterly publication containing articles by leading authors from around the world. Orthodontic Practice US is designed to be read by specialists in Orthodontics, Periodontics, Oral Surgery, and Prosthodontics.
Submitting articles
Orthodontic Practice US requires original, unpublished article submissions on orthodontic topics, multidisciplinary dentistry, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,400 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Orthodontic Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Articles are classified as either clinical, continuing education, technology, or research reports. Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to orthodontics. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio
• Author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple)
Doe JF Doe JF, Roe JP
Permissions
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased after the issue is published.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to: Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
Dr. Dan Bills
Insights from Orthopreneurs Summit
In the midst of the 2008 economic freefall, a young orthodontist in Southern New Jersey took a bold leap of faith by opening Innovative Orthodontics. Over a decade later, Dr. Dan Bills stands at the forefront of orthodontic innovation — with three thriving locations, faculty roles at Harvard and the University of Pennsylvania, and a reputation as one of the industry’s sharpest minds. Ahead of his session, “The Algebra of Orthodontic Efficiency: How to Work Smarter and Live Better,” at the Orthopreneurs Summit in Las Vegas, Dr. Bills to discussed his revolutionary approach to orthodontic practice.
Q: What inspired you to launch Innovative Orthodontics in 2008, despite the challenging economic climate?
Dr. Bills: I saw an opportunity where others saw risk. While many were tightening their belts, I believed that by rethinking our workflows and embracing efficiency, we could not only weather the storm but set new industry standards. It was a calculated gamble that has paid off, both in patient satisfaction and profitability.
Q: How do you define “efficiency” in orthodontics?
Dr. Bills: Efficiency for me isn’t about cutting corners — it’s about making every appointment count. Many orthodontists assume their patients want more frequent visits, but when you look at the numbers, reducing unnecessary check-ups not only streamlines the process but also enhances patient experience and boosts your bottom line.
Q: Technology seems to play a major role in your practice. Can you share how it factors into your approach?
Dr. Bills: Absolutely. We leverage remote monitoring to eliminate needless visits, use data-driven strategies in appliance selection, and optimize treatment planning with clear aligners. Every decision — from bracket placement to biomechanics — is backed by data. We take the emotion out of the process; if the numbers don’t support a system, we simply don’t use it.
Q: You’ve mentioned “value per visit” as a key metric. Why is this so important?
Dr. Bills: Knowing your numbers is crucial. Tracking value per visit helps us identify inefficiencies and opportunities to enhance both care and profitability. In our practice, these numbers are nearly double the national average. If we can eliminate even one unnecessary visit, it can drastically improve profitability and patient satisfaction. If you don’t know how many visits it takes you to finish a case, you’re flying blind.
Q: What can attendees expect from your upcoming lecture at the Orthopreneurs Summit?
Dr. Bills: I’ll be breaking down real clinical cases that illustrate the transformative power of a data-driven approach in everyday orthodontic practice. We’re talking about optimizing everything from bracket placement to clear aligner treatment planning for maximum efficiency. The session isn’t just theoretical — it’s filled with actionable strategies you can start implementing as soon as Monday morning.
Q: How has your experience as both a speaker and an attendee shaped your view of the Summit?
Dr. Bills: The Orthopreneurs Summit is unique — it’s clinical, high-level, and extremely practical. What sets it apart is the real, actionable takeaways. Plus, with someone like Glenn [Krieger] putting on a hell of a show, the entire experience is both informative and inspiring.
Q: Finally, what’s your message to orthodontists looking to revolutionize their practices?
Dr. Bills: I want them to understand that efficiency isn’t a luxury — it’s a necessity. By embracing data and rethinking traditional workflows, you can work smarter and ultimately provide better care. The only question is: are you ready to work smarter?
The Orthopreneurs Summit is your gateway to transforming your orthodontic practice with cutting-edge strategies and actionable insights from leaders like Dr. Dan Bills. Join us in Las Vegas Sept 18-20, 2025 to learn how to work smarter, optimize every appointment, and dramatically boost your profitability. Don’t miss this unique opportunity to revolutionize your practice — sign up today and take the first step towards a more efficient, data-driven future in orthodontics!
This information was provided by Orthopreneurs. OP
3M Health Care becomes Solventum
A new chapter in innovation and commitment
On April 1, 2024, 3M Health Care became Solventum — an independent healthcare company with a rich legacy of creating innovative solutions. This marks a new era as we continue to be an independent, innovation-driven healthcare company dedicated to addressing your toughest challenges.
What’s
behind the name “Solventum”?
The name Solventum originates from two words: “solving” and “momentum.” “Solving” captures our dedication to finding breakthrough solutions, while “momentum” symbolizes swifter and nimbler innovation.
Our name and logo are expressions of our renewed commitment to tackling your biggest challenges in a responsive, imaginative way — and to never stop solving for you.
A legacy of innovation, a future of possibility
For over 70 years, we’ve partnered with providers to improve patient outcomes and transform practices. But we won’t stop
there. Our experts in dentistry and orthodontics share your deep passion for oral health. We’re pioneering game-changing innovations, connecting leading-edge materials with data science to advance dental care. Most of all, we’re focused on beautiful, healthy smiles.
What does this mean for customers?
Though our name may be new, our experienced team, trusted technologies, and exceptional service remain unchanged. Solventum continues to provide the same products, teams and services you’ve relied on. The same experienced professionals and innovative technologies will continue to support clinicians and improve patient care worldwide.
Looking ahead
Solventum represents more than just a name change; it’s a renewed promise to tackle the evolving challenges of global healthcare. With our roots firmly planted in trusted solutions and a forward-looking mindset, Solventum is positioned to drive the next generation of breakthroughs in healthcare.
For more information, visit Solventum.com/en-us/home/ oral-care/.
NEW! Clarity™ Precision Grip Attachments The first 3D-printed, custom aligner attachments. Available exclusively with Clarity™ Aligners.
Leave inconsistency behind. Scan to learn more.
created attachments
Information related to orthodontics changes constantly, stay on top of the latest news and resources with Orthodontic Practice US. Your subscription gets you...
• Opportunities to earn 16+ CE Credits Per Year
• Live & On-demand Webinars
• Bi-monthly enewsletters
• Digital editions
• Exclusive online content
• Special event invitations
• Podcasts, and more Visit our booth #2152 to take advantage
Dental Alignment Jaw/Bone Development
April 25th – April 27th ––– AAO 2025, Philadelphia – Booth #2027 Live Speaker Sessions | Cutting-Edge Insights | Exclusive Demos
Join us at the DentalMonitoring Booth #2027 in Philadelphia and hear from 10 industry-leading speakers as they unveil the latest innovations in remote monitoring and AI-driven patient care.
Discover how DentalMonitoring, the only FDA-approved Software as a Medical Device (SaMD) in remote monitoring, is transforming orthodontic workflows—enhancing efficiency, elevating patient care, and maximizing practice growth.
Zac Varble: Evolve Your Practice with DentalMonitoring
Josh Adcox: The Digital Practice Difference
Barry Benton: Transformative Care with DentalMonitoring+
Terry Sellke: Ortho Meets AI: The Future is Now
Mike Ragan: Advancing Braces Treatment Through DentalMonitoring+
Jacquee Scheick: Dynamic Scheduling: Optimize Time & Elevate Care
Bill Layman: Smarter Workflows with SmartSTL
Ed Davis: The Power of Observation Monitoring
Shannon Patterson: Consumer Trends and Expectations are Changing the Delivery of Orthodontic Care
Tara Gostovich: Shifting the Standard: Discover DentalMonitoring+
Elegance and Engineering in Equal Measure The GC Orthodontics Collection
Beauty by Design… Performance by GC Orthodontics. From Self-Ligation to Aesthetics to Twins, the GC Orthodontics Collection provides your patients Stylish and Sensible ways to outfit their Orthodontic treatment. Our innovation in digital treatments deliver on efficiency with the New GC IDB giving a boost to your chairshare savings.
Through GC Ortho's exclusive partnership with the renowned "TOMY Brackets and Wires," we can consistently achieve reliable and repeatable clinical results. All powered by the GC Ortho 3-Wire sequence… One wire for each stage… Leveling, Working and Finishing. Stage One is Initialloy, Stage Two is Stainless Steel, and Stage Three is Bioactive. These wires have intelligence and technology for treatment inside the mouth, moving the fundamentals of mechanics from the 1980’s to 2025!
gcorthonline.com
Understanding NSAIDs: essential knowledge for dentists
Dr. Lisa Chan and Barbara Madej, RPh, review the benefits and drawbacks of NSAID use in the dental practice
Introduction
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) are a widely used class of medications that effectively manage pain, inflammation, and fever by inhibiting cyclooxygenase (COX) enzymes responsible for prostaglandin production. In dental practice, NSAIDs play a crucial role in controlling pain and inflammation associated with common procedures such as extractions, root canals, and periodontal treatments. Their proven efficacy, accessibility, and non-opioid mechanism make them a preferred choice for both acute and chronic dental pain management.
The purpose of this article is to provide dental practitioners with comprehensive knowledge about NSAID use, including their mechanisms, benefits, risks, prescribing guidelines, and considerations for special populations, to ensure safe and effective pain management for patients.
How do NSAIDs work?
NSAIDs work by targeting enzymes in the body called cyclooxygenases (COX-1 and COX-2), which are essential for producing prostaglandins — hormone-like chemicals that promote inflammation, pain, and fever.
There are two main types of COX enzymes in the body: COX-1 and COX-2.1 Both enzymes are responsible for making prostaglandins, but the effects of these prostaglandins differ based on their origin:
Lisa Chan, DDS, co-founder and Chief Executive Officer, MedAssent DDS, has over 35 years of dentistry experience, including roles as a hospital dentist at Kaiser Permanente, a private practitioner, and a California State Dental Board consultant. With a DDS from USC, she focuses on promoting equity and integrated care, addressing challenges in patient safety. Dr. Chan also serves on educational and community boards, including Santa Monica College, UC San Diego, Los Angeles FBI, and the Salvation Army.
Barbara Madej, RPh, Chief Science Officer, MedAssent DDS, is a licensed pharmacist with a passion for improving lives through education on proper medication use. After earning her pharmacy degree from the University of Saskatchewan, she has served both Canada and Los Angeles, California. Through MedAssent DDS, Barbara aims to reduce medication errors at the intersection of dentistry and pharmacy, enhancing workplace efficiency and patient safety. Her lifelong goal is to make a meaningful impact in healthcare for all involved.
Disclosures: The authors of this article are affiliated with MedAssent DDS (www.medassentdds.com), a platform designed to support dental professionals in medication management and patient care.
Educational aims and objectives
This self-instructional course for dentists aims to provide dental practitioners with a comprehensive understanding of the mechanisms, benefits, and risks of nonsteroidal anti-inflammatory drug (NSAID) use in dental practice.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the mechanisms of action of NSAIDs, including their impact on COX enzymes and prostaglandin production and their relevance to dental pain management.
• Recognize the benefits of NSAIDs as a non-opioid alternative for managing pain and inflammation in dental practice.
• View the risks and potential adverse effects of NSAIDs in patient populations with comorbid conditions, including gastrointestinal, cardiovascular, and renal complications.
• Realize the importance of tailoring NSAID prescribing practices based on individual patient factors, including age, medical history, and concurrent medications.
• Pinpoint strategies to educate patients on the safe use of NSAIDs, emphasizing proper dosing, duration, and awareness of drug interactions and side effects.
• COX-1 enzymes: These produce prostaglandins that help protect the stomach lining and intestinal tract from digestive acids, as well as thromboxane which regulates blood clotting. While COX-1 inhibitors block inflammation, they also interfere with these protective functions, potentially leading to side effects like stomach ulcers and bleeding.2 A common COX-1 enzyme used in dental practices is indomethacin.
• COX-2 enzymes: These primarily produce prostaglandins involved in inflammation and pain. By selectively blocking COX-2, these NSAIDs can reduce inflammation effectively without significantly affecting the protective prostaglandins made by COX-1.2,3 Celecoxib, etodolac, and meloxicam are common examples of COX-2 NSAIDs.
• Traditional NSAIDs (COX-1 & COX-2): These block both COX-1 and COX-2 enzymes. This dual action reduces
inflammation and alleviates pain by decreasing the production of prostaglandins involved in these processes, while also affecting prostaglandins that regulate other bodily functions like stomach lining protection and blood clotting. Many NSAIDs block both COX-1 and COX-2, although one can be better than the other depending on the medication. Some traditional NSAIDs include aspirin, ibuprofen, naproxen, diclofenac, ketorolac, ketoprofen, and nabumetone.
NSAID use in dentistry
NSAIDs are essential in dental pain management due to their effective dual action in alleviating pain and reducing inflammation.4,5 Acetaminophen is often used in combination with NSAIDs because of its complementary action. While most NSAIDs exert their effects peripherally by reducing inflammation and pain at the site of tissue injury, acetaminophen works centrally, inhibiting prostaglandin synthesis in the central nervous system.6 This complementary action blocks pain signal transmission centrally while NSAIDs address inflammation locally, making their combined use highly effective in managing mild to moderate pain.6
Key applications
1. Postoperative pain and inflammation management: NSAIDs are widely used after dental procedures, such as extractions, root canals, and periodontal surgeries, to reduce pain and swelling, promoting faster recovery and enhancing patient outcomes.
2. Adjunctive use in inflammatory conditions: NSAIDs have shown potential as adjuncts to controlling inflammation in dental conditions like periodontitis.7 By targeting localized swelling and pain, they may complement conventional periodontal treatments and aid in managing discomfort. However, their use should be carefully weighed against potential risks, highlighting the need for a tailored approach in incorporating NSAIDs into dental care plans.8
3. Non-opioid pain management alternative: In light of the opioid crisis, NSAIDs offer a safer, non-addictive alternative for pain management. This makes them particularly beneficial for patients at risk of dependency or those with a history of substance abuse.
4. Patient accessibility and compliance: NSAIDs are widely available both over-the-counter and by prescription, with various formulations (e.g., tablets, capsules, topical gels) that accommodate individual patient preferences. Their familiarity and convenience encourage adherence to pain management regimens, improving treatment outcomes.
Pharmacokinetics and pharmacodynamics
NSAIDs are well-absorbed after oral administration, typically reaching peak plasma concentrations within hours.9 Once in the bloodstream, they bind extensively to plasma proteins, primarily albumin, and are metabolized in the liver by enzymes like cytochrome P450 (e.g. CYP2C9, CYP3A4).9 These processes yield inactive metabolites that undergo further processing, often through glucuronidation, to enhance water solubility, facilitating excretion primarily via urine and, to a lesser extent, bile in the feces.10
The plasma half-life of NSAIDs closely determines their onset and duration of action.11 Short-acting NSAIDs, including aspirin, diclofenac, and ibuprofen, are effective for rapid relief of acute pain or inflammation due to their half-lives of less than 6 hours. Long-acting options like naproxen and celecoxib, with half-lives exceeding 10 hours, are better suited for managing chronic conditions such as arthritis, maintaining therapeutic levels over extended periods. Choosing between short- and long-acting NSAIDs depends on the clinical need for immediate relief versus sustained control of chronic symptoms.
Patient response to NSAIDs is influenced by pharmacokinetic profiles, genetic variations (e.g., CYP2C9 activity), and individual factors like age, organ function, and comorbidities.11 Personalized treatment strategies and clear communication are essential for optimizing outcomes, ensuring proper adherence to dosing schedules, and tailoring therapy to meet patient-specific needs.
Risks and side effects of NSAIDs
NSAIDs are effective medications but can cause a range of side effects, from mild to severe.12,13 Common mild side effects include:4
• Nausea, vomiting, bloating, and heartburn
• Dizziness, headache, and drowsiness
• Tinnitus (ringing in the ears)
• Diarrhea, constipation, and stomach discomfort
More serious complications may include:4
• Gastrointestinal (GI) toxicity: ulcers, bleeding, or perforation
• Cardiovascular issues: hypertension, heart attack, and stroke
• Kidney damage (nephrotoxicity) and liver damage (hepatotoxicity)
• Thrombocytopenia, hyperkalemia, and anemia
• Rare hypersensitivity reactions like Stevens-Johnson Syndrome
These risks underscore the importance of careful patient selection and ongoing monitoring during NSAID use.
Contraindications and special considerations
NSAIDs are contraindicated in specific situations, including:
• Patients undergoing coronary artery bypass graft (CABG) surgery for perioperative pain
• Individuals with known hypersensitivity to NSAIDs or aspirin
• Patients with a history of asthma, urticaria, or allergic reactions triggered by NSAIDs
Special caution is required for:
• Older adults
• Patients with a history of peptic ulcer disease (PUD) or GI bleeding
Prescription NSAIDs carry black box warnings for cardiovascular thrombotic events and GI risks. Similarly, prescription acetaminophen warns against hepatotoxicity, particularly at doses exceeding 4,000 mg/day, which can cause acute liver failure. In cases where NSAIDs are contraindicated, consider alternatives like acetaminophen or acetaminophen-based opiate combinations (e.g., Tylenol #3).
Risks with prolonged use
Chronic NSAID use increases the risk of severe complications, especially in older populations. These include:
• Peptic ulcer disease14 and acute kidney injury (AKI)15
• Worsening pre-existing conditions such as hypertension and heart failure
The inhibition of prostaglandin production — vital for protecting the GI mucosa and maintaining kidney function — can lead to gastrointestinal damage, reduced renal perfusion, and impaired drug clearance. Patients with moderate to severe renal issues or those on dialysis should be closely monitored, as NSAIDs can exacerbate renal dysfunction and increase the risk of AKI.15
Patient education
Educating patients on the safe use of NSAIDs is crucial. Key points to emphasize include:
• Use the lowest effective dose for the shortest duration.
• Avoid combining prescription and OTC NSAIDs to reduce adverse effects.
• Carefully review OTC medication labels to prevent duplicate or excessive dosing.
Patients should be informed about potential side effects and encouraged to report symptoms promptly. Clear communication helps minimize risks and maximize treatment effectiveness.
NSAID interactions with other medications
NSAIDs commonly interact with other medications, leading to adverse effects.3,17
Common drug interactions
• Other NSAIDs or aspirin: Co-administration increases the risk of gastrointestinal ulcers, bleeding, hypertension, and hyperkalemia.
• Corticosteroids (e.g. prednisone, methylprednisolone): Combination heightens the likelihood of GI bleeding, fluid retention, and hypertension.
• Anticoagulants (e.g. warfarin, rivaroxaban, dabigatran, apixaban, edoxaban): Combination significantly elevates the risk of serious bleeding.
• Methotrexate, lithium, phenytoin, and calcium channel blockers: Some NSAIDs, such as celecoxib, can increase blood levels of these drugs, raising the risk of nephrotoxicity.18
• Oral antidiabetic drugs: NSAIDs may increase the risk of hypoglycemia.
• Antifungals (e.g. fluconazole): Can elevate celecoxib levels, amplifying side effects.
• Quinolone antibiotics (e.g. ciprofloxacin, levofloxacin): May enhance the risk of central nervous system stimulation and seizures when combined with NSAIDs.
Patient risk factors
Special caution is necessary for patients with the following conditions, as NSAID use must be carefully monitored to prevent exacerbation:19
• Cardiovascular conditions (e.g., heart failure, uncontrolled high blood pressure, history of stroke or heart attack).
• Diabetes, bleeding disorders, or poorly managed chronic illnesses.
Best practices for safe NSAID use
1. Patient evaluation: Thoroughly review the patient’s medical history to identify potential risks or contraindications.
2. Appropriate NSAID selection: Choose the safest option based on the patient’s health status, and prescribe the lowest effective dose for the shortest duration.
3. Monitoring: Regularly assess kidney and liver function, particularly in long-term NSAID users.
4. Patient education: Inform patients about:
a. Risks of overuse or combining NSAIDs with other medications.
b. The importance of adhering to dosing instructions.
c. Recognizing early signs of adverse effects (e.g., gastrointestinal bleeding, swelling, unusual fatigue).
5. Reevaluation: Periodically reassess the need for NSAIDs and consider alternative therapies where appropriate. By understanding and mitigating potential interactions, healthcare providers can enhance patient safety and reduce the risks associated with NSAID therapy in dental practice.
Special considerations for pediatric, geriatric, and perinatal patients
Pediatrics
Prescribing NSAIDs for children requires careful attention to their unique needs.20
• Dosing and formulation: Always calculate doses based on weight to avoid toxicity, and choose age-appropriate formulations for ease of use.
• Precautions: Use NSAIDs cautiously in children with asthma or kidney problems, as these conditions can worsen with their use.
• Aspirin contraindication: Avoid aspirin in children under 18 due to the risk of Reye’s Syndrome, a rare but serious condition.
• Safer options: Ibuprofen is a well-studied and reliable choice for children when used at the right dose.
Geriatrics
For older adults, NSAIDs can be effective, but they come with increased risks due to age-related changes in the body.21,22
• Risks: For geriatric patients, increased sensitivity to NSAIDs, slower metabolism, and a higher likelihood of adverse effects, such as gastrointestinal bleeding, renal impairment, and cardiovascular complications, necessitate a more cautious approach.
• Strategies: Start with the lowest effective dose, limit how long the medication is used, and monitor regularly for any side effects.
Pregnant and breastfeeding patients
NSAIDs require extra caution during pregnancy and breastfeeding to protect both mother and child.23
• Pregnancy:
o In 2020, the FDA updated the prescribing information for prescription NSAIDs to highlight the risk of kidney problems in unborn babies, which can lead to low amniotic fluid levels (oligohydramnios). The updated guidance advises avoiding NSAIDs in pregnant women starting at 20 weeks of pregnancy, a change from the previous recommendation of 30 weeks.
o Avoid NSAIDs in the third trimester, as they can lead to serious complications for the baby, including renal injury, oligohydramnios, ductus arteriosus constriction, persistent pulmonary hypertension, necrotizing enterocolitis, and intracranial hemorrhage.
• Breastfeeding:
o NSAIDs generally result in low infant exposure through breastmilk and are considered safe, with ibuprofen and naproxen preferred over aspirin due to their more favorable risk profiles.
NSAIDS are a cornerstone of care that, when used thoughtfully, can profoundly impact a patient’s comfort and recovery.
Anticipated pain level: mild
For patients experiencing mild pain, a non-prescription NSAID is often sufficient:
• Oral analgesic option: Ibuprofen 200–400 mg as needed for pain, every 4 to 6 hours.
Anticipated pain level: mild to moderate
For mild-to-moderate pain, a fixed dosing schedule initially ensures better pain control, followed by as-needed administration:
• Oral analgesic option: Ibuprofen 400–600 mg on a fixed interval, every 6 hours for the first 24 hours. Then, ibuprofen 400 mg as needed for pain, every 4 to 6 hours.
For patients requiring longer-term pain management, meloxicam can be considered as an option due to its once-daily dosing and favorable safety profile when used appropriately.
• Meloxicam dosage:24 Start with 7.5 mg orally once daily, and adjust based on individual response. The maximum recommended daily dose is 15 mg. In patients undergoing hemodialysis, the dose should not exceed 7.5 mg/ day. To minimize gastrointestinal upset, it can be administered with food. Use the lowest effective dose for the shortest duration to align with treatment goals.
Anticipated pain level: moderate to severe
For moderate-to-severe pain, combining an NSAID with acetaminophen offers enhanced analgesic efficacy:
• Oral analgesic option: Ibuprofen 400–600 mg plus acetaminophen 500 mg on a fixed interval, every 6 hours for the first 24 hours. Then, ibuprofen 400 mg plus acetaminophen 500 mg as needed for pain, every 6 hours.
Anticipated pain level: severe
For severe pain, a combination of an NSAID, acetaminophen, and an opioid is recommended initially, with a step-down approach as pain diminishes:
• Oral analgesic option: Ibuprofen 400–600 mg plus acetaminophen 650 mg with hydrocodone 10 mg on a fixed interval, every 6 hours for 24 to 48 hours. Then, ibuprofen 400–600 mg plus acetaminophen 500 mg as needed for pain, every 6 hours.
Best
practices for NSAID prescribing
Effective dental pain management involves tailoring analgesics to the expected level of pain. These evidence-based guidelines offer a structured approach to prescribing based on pain severity:4
After prescribing NSAIDs, careful monitoring is essential to ensure patient safety and prevent adverse effects.25 Key considerations include assessing kidney function through renal studies and liver health with liver function tests. Coagulation studies, such as prothrombin time and international normalized ratio (INR), are particularly important in patients on anticoagulants. A complete blood count (CBC) can help detect signs of anemia
or other blood-related issues, as well as symptoms of gastrointestinal bleeding. Patients should also be advised to monitor for warning signs of bleeding, such as nosebleeds, unusual bruising, blood in the stool or urine, or feelings of dizziness.26
Additionally, regular monitoring of blood pressure is necessary, as NSAIDs can contribute to hypertension, especially in patients with pre-existing cardiovascular conditions. These measures help identify potential complications early and ensure the safe, effective use of NSAIDs.
Case studies and clinical scenarios
The importance of thorough medication review and patient history cannot be overstated, as highlighted by the experiences of this paper’s co-authors.
Dr. Lisa Chan shared a harrowing case from her husband who is a hospitalist. A patient was prescribed ibuprofen by their dentist to manage dental pain. Soon after, they were rushed to the emergency room with severe gastrointestinal bleeding, requiring two pints of blood. The cause? The patient had already been taking celecoxib, another NSAID, prescribed by their physician.
Similarly, over many years in pharmacy practice, Barbara Madej, RPh, encountered situations where combining NSAIDs with selective serotonin reuptake inhibitors (SSRIs)—such as citalopram, sertraline, fluoxetine, or paroxetine — significantly increased the risk of upper gastrointestinal bleeding. In these scenarios, careful consideration of the risks and benefits is crucial. When such combinations are unavoidable, co-prescribing a proton pump inhibitor (PPI) can help mitigate the risk of serious complications.
These examples highlight the critical importance of reviewing patient histories and checking for drug interactions before prescribing NSAIDs. A simple review of current medications using new, dentistry-specific technology such as the MedAssent DDS Digital Drug Handbook could have prevented the severe, avoidable outcomes in these cases.
Conclusion
NSAIDs are more than just a tool for managing dental pain — they are a cornerstone of care that, when used thoughtfully, can profoundly impact a patient’s comfort and recovery. Yet, their power comes with responsibility. As dental professionals, the choices we make in prescribing NSAIDs can mean the difference between relief and harm, between trust and fear.
Each patient brings a unique story, a medical history that demands our attention and respect. By taking the time to review drug interactions, anticipate risks, and educate our patients, we reinforce the trust they place in us that forms the foundation of excellent care.
REFERENCES
1. Cryer B, Feldman M. Cyclooxygenase-1 and cyclooxygenase-2 selectivity of widely used nonsteroidal anti-inflammatory drugs. Am J Med. 1998;104(5):413-421. doi: 10.1016/s0002-9343(98)00091-6.
2. Qureshi O, Dua A. COX Inhibitors. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www. ncbi.nlm.nih.gov/books/NBK549795/
4. American Dental Association. Oral analgesics for acute dental pain. American Dental Association. https://www.ada.org/resources/ada-library/oral-health-topics/oral-analgesics-for-acute-dental-pain. Updated February 2, 2024. Accessed December 18, 2024.
5. Pergolizzi JV, Magnusson P, LeQuang JA, Gharibo C, Varrassi G. The pharmacological management of dental pain. Expert Opin Pharmacother. 2020;21(5):591-601. doi:10. 1080/14656566.2020.1718651
6. Altman RD. A rationale for combining acetaminophen and NSAIDs for mild-to-moderate pain. Clin Exp Rheumatol. 2004;22(1):110-117.
7. Salvi GE, Lang NP. The effects of non-steroidal anti-inflammatory drugs (selective and non-selective) on the treatment of periodontal diseases. Curr Pharm Des. 2005;11(14):1757-1769. doi:10.2174/1381612053764878.
8. Ren J, Fok MR, Zhang Y, Han B, Lin Y. The role of non-steroidal anti-inflammatory drugs as adjuncts to periodontal treatment and in periodontal regeneration. J Transl Med. 2023;21(1):149. Published 2023 Feb 25. doi:10.1186/s12967-023-03990-2.
9. Verbeeck RK, Blackburn JL, Loewen GR. Clinical pharmacokinetics of non-steroidal anti-inflammatory drugs. Clin Pharmacokinet. 1983;8(4):297-331. doi: 10.2165/00003088-198308040-00003.
10. Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem Pharmacol. 2020; 180:114147. doi:10.1016/j.bcp.2020.114147.
11. Davies NM, Skjodt NM. Choosing the right nonsteroidal anti-inflammatory drug for the right patient: a pharmacokinetic approach. Clin Pharmacokinet. 2000;38(5):377-392. doi:10.2165/00003088-200038050-00001.
12. NAPROSYN (naproxen). DailyMed website. National Library of Medicine. https:// dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=8bff5df5-d856-4237-b6a8ae445b454844. Updated January 2 2025. Accessed January 14, 2025.
13. Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16(5):821-847. doi:10.18433/j3vw2f.
14. Drini M. Peptic ulcer disease and non-steroidal anti-inflammatory drugs. Aust Prescr. 2017;40(3):91-93. doi:10.18773/austprescr.2017.037.
15. Lucas GNC, Leitão ACC, Alencar RL, Xavier RMF, Daher EF, Silva Junior GBD. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J Bras Nefrol. 2019;41(1):124-130. doi:10.1590/2175-8239-JBN-2018-0107.
16. Varga Z, Sabzwari SRA, Vargova V. Cardiovascular Risk of Nonsteroidal Anti-Inflammatory Drugs: An Under-Recognized Public Health Issue. Cureus. 2017;9(4):e1144. doi:10.7759/cureus.1144.
17. Moore N, Pollack C, Butkerait P. Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Ther Clin Risk Manag. 2015;11:1061-1075. doi:10.2147/TCRM.S79135.
18. Kim SJ, Seo JT. Selection of analgesics for the management of acute and postoperative dental pain: a mini-review. J Periodontal Implant Sci. 2020;50(2):68-73. doi:10.5051/ jpis.2020.50.2.68.
19. Cleveland Clinic. Non-steroidal anti-inflammatory medicines (NSAIDs). Cleveland Clinic website. https://my.clevelandclinic.org/health/treatments/11086-non-steroidalanti-inflammatory-medicines-nsaids. Updated July 24, 2023. Accessed January 14, 2025.
20. American Academy of Pediatric Dentistry. Useful Medications for Oral Conditions. The Reference Manual of Pediatric Dentistry. 2024-2025/ P. 644-651. https://www.aapd. org/research/oral-health-policies--recommendations/useful-medications-for-oral-conditions/. Accessed December 19, 2024.
21. Wongrakpanich S, Wongrakpanich A, Melhado K, Rangaswami J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The Elderly. Aging Dis. 2018;9(1):143-150. doi:10.14336/AD.2017.0306.
22. Buckinghamshire Healthcare NHS Trust/Buckinghamshire, Oxfordshire and Berkshire West Integrated Care Board. 299FM.5 Guideline For Prescribing Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) In Adults. https://www.bucksformulary.nhs.uk/docs/ Guideline_299FM.pdf. Published July 26, 2023. Accessed January 14, 2025.
23. Bloor M, Paech M. Nonsteroidal anti-inflammatory drugs during pregnancy and the initiation of lactation. Anesth Analg. 2013;116(5):1063-1075. doi:10.1213/ANE. 0b013e31828a4b54.
24. Boehringer Ingelheim Pharmaceuticals, Inc. Mobic (Celebrex) [package insert]. U.S. Food and Drug Administration. Revised March 2012. Accessed December 19, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020938s022lbl.pdf
25. Specialist Pharmacy Service. NSAIDs: Monitoring Requirements. Published June 22, 2021. Accessed December 19, 2024. https://www.sps.nhs.uk/monitorings/ nsaids-monitoring/.
26. de Jong JC, van den Berg PB, Tobi H, de Jong-van den Berg LT. Combined use of SSRIs and NSAIDs increases the risk of gastrointestinal adverse effects. Br J Clin Pharmacol. 2003;55(6):591-595. doi:10.1046/j.0306-5251.2002.01770.x.
3. Cleveland Clinic. COX-2 inhibitors: Uses, side effects, and more. Cleveland Clinic website. Last reviewed: May 24, 2022. https://my.clevelandclinic.org/health/drugs/ 23119-cox-2-. https://my.clevelandclinic.org/health/drugs/23119-cox-2-inhibitors. Accessed January 14, 2025.
Continuing Education Quiz
Understanding NSAIDs: essential knowledge for dentists CHAN/MADEJ
1. NSAIDs work by targeting enzymes in the body called cyclooxygenases (COX-1 and COX-2), which are essential for producing prostaglandins — hormone-like chemicals that promote ________.
a. inflammation
b. pain
c. fever
d. all of the above
2. _________ produce prostaglandins that help protect the stomach lining and intestinal tract from digestive acids, as well as thromboxane which regulates blood clotting.
a. COX-1 enzymes
b. COX-2 enzymes
c. CYP2C7 activity
d. genetic deficiencies
3. primarily produce prostaglandins involved in inflammation and pain.
a. COX-1 enzymes
b. COX-2 enzymes
c. Anticoagulants
d. Antidiabetic drugs
4. While most NSAIDs exert their effects peripherally by reducing inflammation and pain at the site of tissue injury, work(s) centrally, inhibiting prostaglandin synthesis in the central nervous system.
a. plasma proteins
b. cytochrome P450
c. acetaminophen
d. anticoagulants
5. NSAIDs have shown potential as adjuncts to controlling inflammation in dental conditions like periodontitis.
a. True
b. False
6. Patient response to NSAIDs is influenced by _______.
a. pharmacokinetic profiles
b. genetic variations
c. individual factors like age, organ function, and comorbidities
d. all of the above
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 010
Date Published: March 15, 2025
Expiration Date: March 15, 2028
7. Educating patients on the safe use of NSAIDs is crucial. One key point to emphasize is to use _______.
a. the lowest effective dose for the shortest duration
b. the highest effective dose for the longest duration
c. the highest effective dose for the shortest duration
d. the lowest effective dose for the longest duration
8. Quinolone antibiotics (e.g. ciprofloxacin, levofloxacin) may enhance the risk of central nervous system stimulation and seizures when combined with NSAIDs.
a. True
b. False
9. When prescribing NSAIDs for children, always calculate doses based on ________, and choose age-appropriate formulations for ease of use.
a. the parents’ previous experience with it
b. weight to avoid toxicity
c. the likelihood of compliance
d. height
10. For geriatric patients, ___, necessitate(s) a more cautious approach.
a. increased sensitivity to NSAIDs
b. slower metabolism
c. a higher likelihood of adverse effects, such as gastrointestinal bleeding, renal impairment, and cardiovascular complications
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
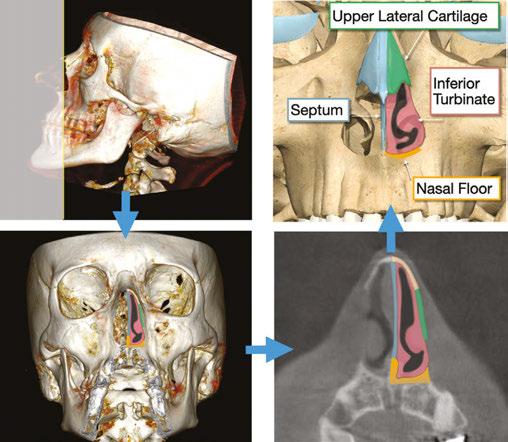
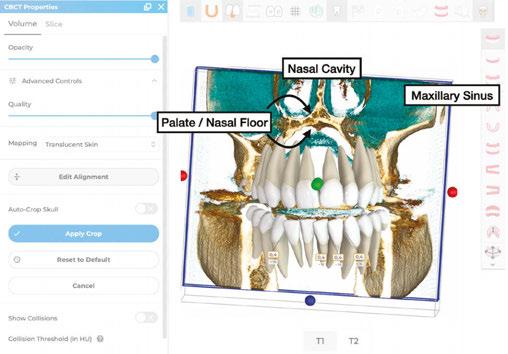
The DOME approach to breathing, bite, and beauty
Drs. Claudia Pinter and Stanley Liu illustrate a protocol to improve nasal breathing in orthodontic care
Bestselling author James Nestor highlights in his book, Breath:
The New Science of a Lost Art that nasal breathing has profound effects on overall health, including respiratory function, cardiovascular health, mental clarity, sleep quality, and athletic performance. Of all the contributors to overall wellness, a healthy way to breathe has eluded attention from modern medicine and dentistry. This is especially true with breathing during sleep.
Breathing interruptions during sleep make up a constellation of conditions called “sleep-disordered breathing,” (SDB) with common diagnoses including snoring, upper airway resistance syndrome, and obstructive sleep apnea. A contemporary population-based study on adults estimates SDB to be present in 23.4% of women, and 49.7% of men. SDB is independently associated with hypertension, diabetes, metabolic syndrome, and depression.1
Regarding nasal breathing, the internal nasal valve (INV) is the narrowest part of the nasal cavity and is the location of greatest airflow resistance.2,3 Located about 1.3 cm posterior to the nostril opening, it is surrounded by the dorsal septum medially, the head of inferior turbinate laterally, upper lateral cartilages superiorly, and the maxillary roof (nasal floor) inferiorly. Anatomic causes of nasal obstruction frequently involve structures of the INV. Beyond anatomy, there are physiologic and pathophysiologic causes of nasal obstruction (Figure 1).
When it comes to anatomic treatment, surgical approaches to the septum, inferior turbinate, and upper lateral cartilage of
Claudia Pinter, DMD, is an orthodontist in private practice in Vienna and Wels, Austria, specializing in esthetic orthodontic treatments with aligners. She is also an Affiliate Professor at Nova Southeastern University in Florida. Her passion for education led her to become the Course Director for the Fellowship in Aligner Orthodontics at Ripeglobal. In 2024, she received the Award for Best Aligner Case at the European Aligner Society Congress. A published author in peer-reviewed journals, Dr. Pinter regularly lectures at international dental, orthodontic, and sleep conferences.
Dr. Stanley Liu, MD, DDS, FDSRC(ed), FACS, is the Chair of Oral & Maxillofacial Surgery at Nova Southeastern University and Director of the NSU Breathe and Sleep Wellness Center. Previously, he was an Associate Professor of Otolaryngology at Stanford University School of Medicine, where he directed the sleep surgery fellowship. He has published over 120 original articles, with an emphasis on sleep-disordered breathing. His updated surgical and medical treatment of OSA is published in textbooks across a broad range of specialties. He has been honored as a keynote speaker at both the American and World Sleep Medicine Congresses. You can also find him at www.drstanleyliu.com
Disclosure: Dr. Claudia Pinter is a key opinion leader and paid speaker for Ormco Spark Aligners.™
Educational aims and objectives
This self-instructional course for dentists aims to educate readers on the implications of poor nasal breathing with maxillary hypoplasia on wellness and the importance of addressing sleep-disordered breathing through the DOME approach.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Define different types of sleep-disordered breathing.
• Identify anatomy that affects nasal breathing. Identify the DOME approach to treating nasal obstruction.
• Observe patient outcomes after being treated with the DOME approach.
2 CE CREDITS
the INV are well described. What has been less discussed until recently is maxillary expansion at the nasal floor.4 This is likely a byproduct of otolaryngologists (ear, nose, throat surgeons) focusing on structures treated within their scope. Historically though, otolaryngologists have collaborated with orthodontists to treat nasal obstruction via maxillary expansion.5
Figure 1: Structures of the Internal Nasal Valve (INV)
In 2017, Dr. Ryan Williams and Dr. Stanley Liu at Stanford Otolaryngology performed a retrospective case-control study to identify phenotypes of patients who complain of persistent nasal obstruction after surgery.6 Eighty-nine subjects with perioperative validated questionnaires and computed tomography imaging were included. The study showed that patients with persistent nasal obstruction after intranasal surgery (septoplasty, inferior turbinate reduction) presented with a narrower maxilla (and nasal floor), near the region of the internal nasal valve.
In parallel, Dr. Christian Guilleminault mentored Dr. Audrey Yoon and Dr. Stanley Liu at Stanford Sleep Medicine to apply maxillary expansion techniques for SDB patients. From around 2015, Dr. Stanley Liu described the change as converting a high-arched palate to a “dome”-shaped palate. As the surgical-orthodontic techniques progressed, “dome” became an acronym of “maxillary expansion” with “distraction osteogenesis.” This shifted maxillary expansion from a dentoalveolar-first to a nasal-floor first process, and as an approach rather than specific surgical or dental techniques.
Subsequent studies were undertaken to understand the mechanism of action of DOME using treatment-specific rhinomanometry and patient-specific computational fluid dynamics analysis. With expansion at the INV region, nasal airflow slows significantly, and the downstream negative pressure that collapses the pharyngeal airway decreases.7 DOME for both the adult and pediatric populations had similar outcomes, most notably a patient-reported decrease in nasal obstruction.8-10 The decrease in apnea-hypopnea index (AHI) was associated with increase of INV surface area and angle.8,11
For patients requiring surgical osteotomies, endoscopic approaches to DOME were introduced.12 Finally, to complete the full circle dating back to Williams and Liu’s original study, patients who underwent DOME after nasal surgery were examined. The study found that a transverse increase of at least 6 mm at the INV was associated with resolution of nasal obstruction and improvement of sleep-related symptoms.13 Since then, many colleagues in the field of SDB across different disciplines have continued to expand (puns intended) upon DOME.14,15
Today, the need of invasive maxillary osteotomy to expand the adult maxilla has become markedly reduced. The advent of custom, temporary anchorage device supported expanders have increased the phenotype of eligible patients for non-surgical expansion. Moreover, restoration of cosmesis and occlusion evolved rapidly. European leaders including Dr. Christian Leonardt and Dr. Claudia Pinter have further streamlined the DOME approach to a dentist-friendly ecosystem. In this article, the contemporary DOME approach for dentists is highlighted.
Case report No. 1
A 51-year-old male was referred by the treating dentist to address malocclusion before doing extensive restorative work. The patient presented equal facial thirds and pronounced buccal corridors. Intraorally, the teeth presented in Class I, with an anterior open bite, a narrow upper jaw, and a high-arched palate.
In cases with maxillary deficiency, the narrowing of the nasal cavity increases airflow resistance, potentially leading to nasal obstruction snoring and resulting in sleep breathing disturbances.
Upon investigation, the NOSE Score indicated nasal obstruction, and the patient reported frequent and loud snoring. Insufficient lateral overjet could have been addressed with dental expansion of the upper arch, which would not have effects on the nasal cavity.
Figure 2 (left): Patient presenting pronounced buccal corridors and narrow upper arch in need of pre-restorative orthodontic treatment. Figure 3 (right): Intraorally, the teeth present with negative overbite and lacking lateral overjet
Figure 4: The CBCT integration into the aligner treatment plan demonstrates how the palate is not only the roof of the mouth, but also the floor of the nose
Figure 5: The configuration of the palate is high-arched with a transpalatal width of 30 mm measured at the closest points of the first molars
The patient opted for a DOME (Distraction Osteogenesis Maxillary Expansion) approach to address malocclusion, create more space for the tongue, and to facilitate nasal breathing both during wakefulness and sleep.
To ensure predictable suture separation of the maxillary halves, minimally invasive osteotomies were performed (Periodontist: Dr. Christian Leonhardt). During the same appointment, four mini-screws were placed: two in the anterior palate (Benefit PSM Medical, 2 mm x 11 mm) and two between the roots of the second premolar and first molar (Benefit PSM Medical, 2 mm x 13 mm). Surgical guides were used to place the mini-screw in areas with sufficient bone and navigate from the roots. An intraoral scan was then taken to produce a custom-made expander that could be mounted onto the bone screws.
Following the successful orthopedic expansion, aligners were employed to close the diastema and restore the occlusion.
The initial setup in the aligners software (Spark™ Approver™) yielded an esthetically pleasing result, with ideal incisor inclination. While aligners generally perform well in expressing root movements, clinicians should anticipate that not all lingual root torque will be fully expressed in the upper incisors. To prevent
retroclination and a steep interincisal angle, an additional 10° of palatal root torque should be incorporated into the ideal inclination.
The result shows an adequate overjet and overbite in both the incisors and the posterior teeth. The palate is now dome-shaped, allowing for proper tongue positioning. Additionally, after the palatal expansion, the patient ceased to snore.
Case report No. 2
A 12-year-old female presented with her mother to evaluate a need for orthodontic treatment.
Clinical examination revealed maxillary transverse deficiency, high-arched palate, mild crowding, and enlarged tonsils. The mother reported that the patient exhibited mouth breathing and “loud breathing” sounds during sleep. To further assess nasal breathing, the patient completed the Nasal Obstruction Symptom Evaluation (NOSE) questionnaire, which indicated nasal obstruction. A home sleep study showed an apnea-hypopnea index (AHI) of 6.4, confirming the presence of moderate obstructive sleep apnea. Patient also was referred to an ENT specialist.
Although the patient’s malocclusion could be corrected with dental expansion, skeletal expansion was chosen to achieve greater effect on the nasal cavity. Her DOME approach aimed to enhance nasal breathing both during wakefulness and sleep.
A bone-borne expander was selected to maximize skeletal expansion while minimizing dentoalveolar bending. Aligners were then used to restore the occlusion while the expander remained on the palate as a skeletal retainer for another 6 months.
After maxillary expansion, the mother reported that the patient’s breathing during sleep had become silent and that she now slept with her mouth closed. Additionally, the patient’s NOSE score improved from 6/20 to 0/20 — indicating a significant improvement in nasal breathing. The patient also noted that she previously woke up during the night, but this ceased after orthopedic expansion of the maxilla.
After completion of orthodontic treatment, a repeat sleep study may help determine need of further treatment including tonsillectomy.
Figure 6: NOSE Score: (Nasal Obstruction Symptom Evaluation) is a validated questionnaire for nasal obstruction
Figure 9 (left): Diastema closure with aligners: Two vertical mesially beveled vertical 5 mm attachments were employed to ensure bodily movement of the incisors and prevent excessive crown tipping. Figure 10 (right): Initial: Diastema between incisors. Space Closure: superimposition for initial position in blue.
Overcorrection: additional lingual root torque has been added to incisors
Figure 7: Four weeks after the osteotomies have been done, the expander was inserted, and the patient was instructed to activate the expander at a rate of 1 turn per day (each turn equating to 0.17 mm of expansion of the screw). After 5 weeks, a substantial diastema had developed between the upper incisors, and sutural separation was confirmed with a CBCT
Resolving nasal obstruction is central to the care of sleep-disordered breathing (SDB). Nasal breathing confers significant advantages over mouth breathing during sleep, particularly with the physiologic stimulation of upper airway dilator muscles.16 Effective treatment of SDB is based on changing the negative pressure that can collapse the downstream pharyngeal airway. This is the critical negative pressure, referred to as P-crit, and is the basis of anatomic treatment of SDB.17 Slower and smoother airflow through the internal nasal valve results in less negative pressure to collapse pharyngeal muscles during sleep. Procedures such as septoplasty, inferior turbinate reduction, and upper lateral cartilage grafts including spreaders reduce and realign structures of the INV. To expand the actual INV surface area with volumetric increase of the nasal passage, maxillary expansion is our most efficient means today. Beyond changes to the INV to improve nasal breathing, expansion of the maxilla also allows the tongue to be positioned favorably during sleep. This process is further augmented by breathing and myofunctional exercises.18,19
that allows proper tongue positioning, contributing to the prevention of relapse of the anterior open bite
A great day begins with consistent, high-quality sleep. One of the most prevalent, but under-diagnosed and under-treated detractors, is sleep-disordered breathing. Ranging from snoring, upper airway resistance syndrome (UARS) to obstructive sleep apnea (OSA), airflow interruptions during sleep take a detrimental toll on cognitive, mental, and physical health. In 2001, Dr. Christian Guilleminault called upon the dental profession to help, stating that “dentists and orthodontists have the greatest opportu-
nity to [identify these patients] … and may obviate the need for aggressive surgical treatment later in life.”16 In the past, the collaboration of an orthodontist and surgeon to treat SDB began with maxillomandibular advancement (MMA). MMA is still needed for severe, persistent OSA, or patients with concomitant dentofacial deformity. Today, for mild OSA and UARS patients, the creation of a dome-shaped palate by the orthodontist, alongside any necessary intranasal treatments for SDB fills in the gap (puns intended again). As restoring sleep airway health is a gateway to wellness, the contemporary orthodontist is the chief architect of the “dome” to breathe.
REFERENCES
1.
Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobback N, Mooser V, Preisig M, Malhotra A, Waeber G, Vollenweider P, Tafti M, Haba-Rubio J. Prevalence of sleep-dis-
Figure 11 (left): Result after orthopedic expansion with a bone-borne expander and tooth alignment using Spark Aligners. Figure 12 (right): The occlusal view of the upper jaw shows a palate
Figure 13 (left): 12-year-old female patient with sleep study confirmed obstructive sleep apnea and malocclusion. Figure 14 (center): Mild transverse deficiency in the upper jaw . Figure 15 (right): Red arrow pointing towards enlarged tonsils visible in the lateral ceph. The adenoids were also enlarged
Figure 16 (left): The upper jaw presents with a high-arched palate and crowded teeth. Figure 17 (center left): A purely bone-borne expander on 2 mini screws in the anterior palate (PSM Benefit Screw 2 mm x 9 mm) was used to maximize skeletal effects. Power arms on the palatal side of central incisors were employed to support bodily movement into the area of newly formed bone. Figure 18 (center right): in the CBCT, new bone formation is visible in the midpalatal suture. Figure 19 (right): After the DOME approach, the patient is very satisfied with her smile, and transition from observed mouth breathing to nasal breathing during sleep
ordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015 Apr;3(4):310-318. doi: 10.1016/S2213-2600(15)00043-0. Epub 2015 Feb 12.
2. Chandra RK, Patadia MO, Raviv J. Diagnosis of nasal airway obstruction. Otolaryngol Clin North Am. 2009 Apr;42(2):207-225, vii. doi: 10.1016/j.otc.2009.01.004.
3. Rhee JS, Weaver EM, Park SS, Baker SR, Hilger PA, Kriet JD, Murakami C, Senior BA, Rosenfeld RM, DiVittorio D. Clinical consensus statement: Diagnosis and management of nasal valve compromise. Otolaryngol Head Neck Surg. 2010 Jul;143(1):48-59. doi: 10.1016/j.otohns.2010.04.019.
4. Kiki A, Özdoğan A, Kiki MA, Genç YS. Bibliometric Analysis of Maxillary Expansion Publications Trends. Turk J Orthod. 2024 Sep 30;37(3):193-200. doi: 10.4274/ TurkJOrthod.2023.2023.113.
5. Gray LP. Results of 310 cases of rapid maxillary expansion selected for medical reasons. J Laryngol Otol. 1975 Jun;89(6):601-614. doi: 10.1017/s0022215100080804.
6. Williams R, Patel V, Chen YF, Tangbumrungtham N, Thamboo A, Most SP, Nayak JV, Liu SYC. The Upper Airway Nasal Complex: Structural Contribution to Persistent Nasal Obstruction. Otolaryngol Head Neck Surg. 2019 Jul;161(1):171-177. doi: 10.1177/ 0194599819838262.
7. Iwasaki T, Yoon A, Guilleminault C, Yamasaki Y, Liu SY. How does distraction osteogenesis maxillary expansion (DOME) reduce severity of obstructive sleep apnea? Sleep Breath. 2020 Mar;24(1):287-296. doi: 10.1007/s11325-019-01948-7. Epub 2019 Dec 10.
8. Abdelwahab M, Yoon A, Okland T, Poomkonsarn S, Gouveia C, Liu SY. Impact of Distraction Osteogenesis Maxillary Expansion on the Internal Nasal Valve in Obstructive Sleep Apnea. Otolaryngol Head Neck Surg. 2019 Aug;161(2):362-367. doi: 10.1177/0194599819842808. Epub 2019 May 14.
9. Liu SY, Guilleminault C, Huon LK, Yoon A. Distraction Osteogenesis Maxillary Expansion (DOME) for Adult Obstructive Sleep Apnea Patients with High Arched Palate. Otolaryngol Head Neck Surg. 2017 Aug;157(2):345-348. doi: 10.1177/0194599817707168. Epub 2017 Jul 4.
10. Yoon A, Guilleminault C, Zaghi S, Liu SY. Distraction Osteogenesis Maxillary Expansion (DOME) for adult obstructive sleep apnea patients with narrow maxilla and nasal floor. Sleep Med. 2020 Jan;65:172-176. doi: 10.1016/j.sleep.2019.06.002. Epub 2019 Jun 13.
11. Yoon A, Kim TK, Abdelwahab M, Nguyen M, Suh HY, Park J, Oh H, Pirelli P, Liu SY. What changes in maxillary morphology from distraction osteogenesis maxillary expansion (DOME) correlate with subjective and objective OSA measures? Sleep Breath. 2023 Oct;27(5):1967-1975. doi: 10.1007/s11325-022-02761-5. Epub 2023 Feb 20.
12. Liu SY, Ibrahim B, Abdelwahab M, Chou C, Capasso R, Yoon A. A Minimally Invasive Nasal Endoscopic Approach to Distraction Osteogenesis Maxillary Expansion to Restore Nasal Breathing for Adults with Narrow Maxilla. Facial Plast Surg Aesthet Med. 2022 NovDec;24(6):417-421. doi: 10.1089/fpsam.2021.0154. Epub 2022 Feb 17.
13. Liu SY, Yoon A, Abdelwahab M, Yu MS. Feasibility of distraction osteogenesis maxillary expansion in patients with persistent nasal obstruction after septoplasty. Int Forum Allergy Rhinol. 2022 Jun;12(6):868-871. doi: 10.1002/alr.22931. Epub 2022 Jan 5.
14. Jara SM, Thuler ER, Hutz MJ, Yu JL, Cheong CS, Boucher N, Evans M, Dedhia RC. Posterior Palatal Expansion via Subnasal Endoscopy (2PENN) for Maxillary Deficiency: A Pilot Study. Laryngoscope. 2024 Apr;134(4):1970-1977. doi: 10.1002/lary.31060. Epub 2023 Sep 29.
15. Thuler E, Rabelo FAW, Yui M, Tominaga Q, Dos Santos V Jr, Arap SS. Correlation between the transverse dimension of the maxilla, upper airway obstructive site, and OSA severity. J Clin Sleep Med. 2021 Jul 1;17(7):1465-1473. doi: 10.5664/jcsm.9226.
16. Fitzpatrick MF, McLean H, Urton AM, Tan A, O’Donnell D, Driver HS. Effect of nasal or oral breathing route on upper airway resistance during sleep. Eur Respir J. 2003 Nov;22(5):827-832. doi: 10.1183/09031936.03.00047903.
17. Carberry JC, Amatoury J, Eckert DJ. Personalized Management Approach for OSA. Chest. 2018 Mar;153(3):744-755. doi: 10.1016/j.chest.2017.06.011. Epub 2017 Jun 16..
18. Camacho M, Certal V, Abdullatif J, Zaghi S, Ruoff CM, Capasso R, Kushida CA. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep. 2015 May 1;38(5):669-675. doi: 10.5665/sleep.4652.
19. Cavalcante-Leão BL, de Araujo CM, Ravazzi GC, Basso IB, Guariza-Filho O, Taveira KVM, Santos RS, Stechman-Neto J, Zeigelboim BS. Effects of respiratory training on obstructive sleep apnea: systematic review and meta-analysis. Sleep Breath. 2022 Dec;26(4):15271537.. doi: 10.1007/s11325-021-02536-4. Epub 2021 Dec 1.
20. Guilleminault C, Quo SD. Sleep-disordered breathing. A view at the beginning of the new Millennium. Dent Clin North Am. 2001 Oct;45(4):643-656.
We’ve got your back— literally.
At Boyd Industries, we’ve always been committed to one thing: supporting you.
The trust you place in Boyd products drives us to continually raise the bar—delivering equipment built for unmatched durability, precision, and design excellence. So go ahead, sit back, and experience the comfort of our ergonomic seating. We’ll handle the rest. Ready to get started? boydindustries.com | (727) 561-9292 Built to last. Built for you. Built by Boyd!
Continuing Education Quiz
The DOME approach to breathing, bite, and beauty
PINTER/LIU
1. Bestselling author James Nestor highlights in his book, Breath: The New Science of a Lost Art that nasal breathing has profound effects on overall health, including respiratory function, _________, and athletic performance.
a. cardiovascular health
b. mental clarity
c. sleep quality
d. all of the above
2. A contemporary population-based study on adults estimates sleep-disordered breathing (SDB) to be present in _________.
a. 23.4% of women, and 49.7% of men
b. 49.7% of women, and 23.4% of men
c. 16.4% of women and 65.4% of men
d. 25.6% of women and 87.4% of men
3. SDB is independently associated with _________ and depression.
a. hypertension
b. diabetes
c. metabolic syndrome
d. all of the above
4. Regarding nasal breathing, the internal nasal valve (INV) is the _______ part of the nasal cavity and is the location of greatest airflow resistance.
a. widest
b. narrowest
c. most important
d. hardest to identify
5. From around 2015, Dr. Stanley Liu described the change as converting a _________ to patients.
a. a “dome”-shaped palate to a v-shaped palate
b. “dome”-shaped palate to a high-arched palate
c. high-arched palate to a “dome”-shaped palate
d. a high-arched palate to a v-shaped palate
6. With expansion at the INV, nasal airflow _________, and the downstream negative pressure that collapses the pharyngeal airway decreases.
a. increases
b. slows significantly
c. stays the same
d. expands
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 730
Date Published: March 15, 2025
Expiration Date: March 15, 2028
7. (In an examination of patients outcomes of those who underwent DOME with a history of nasal surgery) A study found that a transverse increase of at least _______ at the INV was associated with resolution of nasal obstruction and improvement of sleep-related symptoms.
a. 6 mm
b. 8 mm
c. 10 mm
d. 12 mm
8. The advent of ______ have increased the phenotype of eligible patients for non-surgical expansion.
a. clear aligners
b. lingual braces
c. custom, temporary anchorage device supported expanders
d. various types of attachments
9. (When the clinician screens for symptoms of impaired nasal breathing) ________ is a validated questionnaire for nasal obstruction.
a. DOME Symptom Questionnaire
b. Nasal Obstruction Symptom Evaluation (NOSE)
c. Polysomnography Evaluation
d. none of the above
10. Slower and smoother airflow through the internal nasal valve results in less negative pressure to collapse pharyngeal muscles during sleep.
a. True
b. False
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Selling with integrity — the CliffsNotes ® 1
Dr. Jamie Reynolds explains how marketing skills and Ormco products can lead to long-term success
Ithink it’s fair to say that the competition to acquire new orthodontic patients is plentiful. There are many professionals in the dental space, and most are attempting to incorporate orthodontic treatment into their revenue stream. Straightening teeth is no longer the exclusive domain of the orthodontist, who graduates from dental school with increasingly suffocating debt obligations and faces increased competition for patients/customers. And, because most orthodontic consumers don’t even know how many teeth they should have in their mouth, we as specialists, need to understand how to communicate the value of our services to our potential patients — as it is in their best interest to be treated by an orthodontist who specializes in teeth and jaw alignment versus a provider with less training.
Communicating the value of your services to a potential customer such that they become an actual customer is formally known as a sales process. Sales can be a dirty word in healthcare as some think it implies selling things people don’t need, and unfortunately, the reputation has been well-earned on occasion. But sales don’t need to be unscrupulous. In a local, referral-based family business such as orthodontics, the sales process must be based on integrity. Otherwise, the community will smell foul play, and the business will suffer. Although a great sales process has many steps, here are three key factors that may not be obvious but will contribute to successful sales efforts:
1. Set expectations: The number one factor correlated to Treatment Recommended Conversion (TRC) is the frequency with which you do same-day starts, which should not surprise you. I have found the key ingredient to sameday starts is to set expectations for the consumer leading up to the exam, which can be easily achieved via a confirmation call. If your patient or their parents are surprised
Jamie Reynolds, DDS, MS, is a private-practice orthodontist at Reynolds Orthodontics in Novi, Rochester Hills, Troy, and West Bloomfield, Michigan. He received his undergraduate and dental degrees from the University of Michigan and his master’s in orthodontics from the University of Detroit-Mercy. Dr. Reynolds is a Diplomate of the American Board of Orthodontics and a member of the American Dental Association and the American Association of Orthodontists. He co-founded OrthoFi, is a “Certified Damon Educator,” has been a featured speaker at most Ormco Forums, and is co-founder of Orthodontic Partners OSO. He’s an author and co-author of two books and has received Hour Detroit Magazine’s “Top Orthodontist” awards from 2009 to the present.
Disclaimer: Dr. Reynolds is a paid consultant of Ormco. Ormco is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients.
when you offer same-day treatment during the exam, it is tough for you, the doctor, or your treatment coordinator not to seem “pushy” — which is the archenemy of a great sales process.
2. Marketing matches reality: We have always used the PSL Damon™ System and a premium aligner brand (Invisalign®2 for many years before switching to Spark™ Clear Aligners a few years ago). We have marketed our practice brand around being a premium provider as such. Should we switch to a lower-cost bracket or aligner to help the bottom line? Our team, especially our TCs, would likely view the cost-cutting measure as a departure from our quality-driven marketing. Believe it or not, your team is involved in selling the practice just as much as you are. If you are marketing premium products and services, you had better provide premium products and services like Ormco’s comprehensive range of products and solutions for your practice; otherwise, your team will not be on board, and your sales will suffer.
3. Play the long game: OrthoFi™3 data shows the average Treatment Recommended Percentage (the percentage of treatment recommended for new patient exams) around 71%.4 I am part of the Orthodontic Partners™5 OSO, which is comprised predominantly of large practices ($4M to $15M annual production), and our Treatment Recommended Percentage collectively is 51%. I share this information because I have heard countless times, “The only reason practices grow large is they recommend treatment for people who do not need it.” The data shows that recommending treatment less frequently may actually be a prerequisite for growing larger, likely because it builds trust over time. And, in a local, community-driven business, developing trust takes time, but it is the currency that allows for both production growth and maintenance of that growth — the long game. Recommending treatment initially to a higher percentage of patients may lead to a temporary boost in sales. However, it contradicts the practice’s sustained growth and long-term success.
REFERENCES
1. CliffsNotes® is a registered trademark of Learneo, Inc.
2. Invisalign® is a registered trademark of Align Technology, Inc.
3. OrthoFi™ is a trademark of OrthoFi, Inc.
4. Data on file at Reynolds Orthodontics.
5. Orthodontic Partners™ is a trademark of Orthodontic Partners, LLC.
*All other referenced trademarks are the property of Ormco Corporation.
16
Clinical articles enhanced by high-quality photography
Analysis of the latest groundbreaking developments in orthodontics
Technology reviews of the latest products
Real-life profiles of successful orthodontic practices
Practice management advice on how to make orthodontics more profitable
LightForce Orthodontics — breaking the mold
Dr. Anthony Serrano discusses how the LightForce personalized IDB system, LightTray, changed his practice
Remember the first time you tried indirect bonding (IDB) with stock brackets? Me too. The concept sounded like a game-changer — greater efficiency, better bracket placement — but the reality was anything but. I spent hours manually placing brackets on models in the lab, only to face inevitable “round-tripping” when adjustments were needed. This process was cumbersome, error-prone, and time-consuming.
That’s why LightForce’s fully customized bracket and indirect bonding system, along with its broader advancements in digital orthodontics, have completely transformed how I practice. It finally solves the issues that traditional IDB systems never could. By combining computer-aided design, 3D printing, and intraoral scanning, LightForce has transformed indirect bonding into a precise, predictable process. In practice, what used to take hours in the lab now takes my team only 5 to 10 minutes in the chair. And because the accuracy is so dialed in — down to hundredths of a millimeter — bracket placement is right the first time, drastically reducing the need for adjustments later on.
But LightForce isn’t just about efficiency — it’s about continuous improvement. Their latest innovation, LightTray, takes the bonding process to the next level by making it even more predictable and user-friendly for my team. Built from both data and direct feedback from orthodontists and staff, LightForce redesigned its IDB trays with personalized segments that adapt to each patient’s anatomy. This means each segment is designed to incorporate patient-specific factors like spacing, crowding, and erupting teeth, leveraging historical data to optimize bond success. For my assistants, that translates to a smoother workflow — no more rocking trays over partially erupted teeth or tearing trays during removal. Simply put, LightTray makes indirect bonding easier, faster, and more reliable than ever.*
Beyond the bonding process, the real game-changer is the ability to fully customize bracket placement. Unlike stock brackets, which force every patient into the same generic setup,
Dr. Andrew Serrano attended Brown University, where he completed his degree in technology management with a focus on biotechnology. Dr. Serrano then went on to complete his Doctorate of Medicine in Dentistry, Master in Public Health, and Orthodontic Residency at Arizona School of Dentistry and Oral Health. Dr. Serrano is a Diplomate of the American Board of Orthodontics and the American Sleep and Breathing Academy. As a secondgeneration orthodontist, Dr. Serrano has observed firsthand the evolution of the modern orthodontic practice and changing patient population. Today’s patients demand efficiency in all aspects of treatment, and Dr. Serrano is passionate in leveraging technology to meet patient expectations.
LightForce customizes each bracket to the patient’s exact dental anatomy. No more FA point bracket placement required. No more wire slop. I can adjust torque, rotation, and prescription from the start without compromise. And the impact on treatment is undeniable — I’ve cut treatment times from 23 months to about 15 or 16 months, with five fewer office visits per case.** For adult patients, that’s a huge motivator to start treatment.
On the practice side, the impact has been just as profound. With shorter treatment times and fewer visits, I’ve reclaimed nearly 30 extra days each year — time I can spend growing my practice, training my team, or just enjoying life outside the office. And the best part? Patients notice. They want efficiency, customization, and fewer office visits.
Looking back, I’ve come to realize that digital orthodontics is more than just stock brackets on a computer screen. It’s about eliminating inefficiencies, simplifying workflows, and delivering better results with less guesswork. LightForce has redefined indirect bonding, and it’s been one of the most impactful changes I’ve ever made in my practice.
This information was provided by LightForce. OP
* The LightForce system was honored as the 2024 Townie Choice Award Winner for Best Digital Indirect Bonding System. ** Individual results may vary.
April 25th – 9:15-3:15
Available in Mini & Standard Size
or individual patient packs - Offset bicuspids & vertical slot also available
BUY 100 CASES GET 80 CASES FREE (only 67¢ ea.)
+200 FREE MOLAR TUBES +1 FREE CURING LIGHT!
"I've been using the Allure Ortho Mini twin in my office for the better part of the last decade and I love it. I'm able to keep a low overhead without sacrificing quality. This is all wrapped up in Allure Ortho's exceptional customer service. You get great quality, great prices and service that is the best around. I highly recommend using this bracket."
twin bracket system Used by some of the largest practices in the
--- Dr. David Harmon, Jr. | Former President of MASO | Mitchellville, MD
*Allure Ortho does not imply endorsement by Dr. Roth or by Doctors McLaughlin, Bennett and Trevisi.