Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Lou Shuman, DMD, CAGS
Julius Wolff has a bone to pick
In the realm of full-arch implant dentistry, our primary goal should be to provide long-lasting, functional, and esthetically pleasing outcomes for our patients while prioritizing their overall oral health. A cornerstone of achieving this lies in the principle of bone preservation. Recognizing the critical role of the alveolar ridge, not only in supporting dental implants but also in maintaining facial structure and gingival architecture, is paramount.
Traditional approaches to full-arch rehabilitation, such as some All-on-X protocols, necessitate the removal of healthy bone to accommodate a prosthetic designed with an artificial acrylic, zirconia, or ceramic gumline. While these methods offer a solution for edentulous patients, the removal of viable bone can have several physiological disadvantages. This can lead to compromised proprioceptive feedback, potentially affecting the patient’s ability to perceive the function and position of their restoration.
Furthermore, the reduced bone volume can limit future implant placement options should the need arise. The prosthetics can also create difficult-to-clean areas that are prone to plaque accumulation, potentially increasing the risk of periimplant disease.
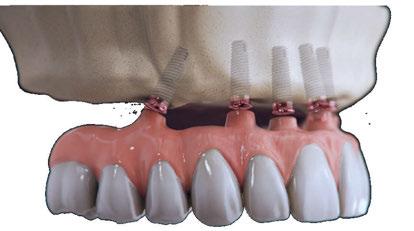
In contrast, the FP1 classification of implant-supported prostheses prioritizes the preservation of the patient’s existing alveolar bone and natural gingiva. Procedures like the 3 on 6™, which utilize multiple TRI implants to support individual bridges, exemplify this philosophy. By focusing on replacing only the missing teeth, FP1 restorations avoid the need for extensive bone removal. This approach allows for the emergence of prosthetic teeth directly from the patient’s natural gingival tissues, contributing to a more natural appearance and improved patient comfort.
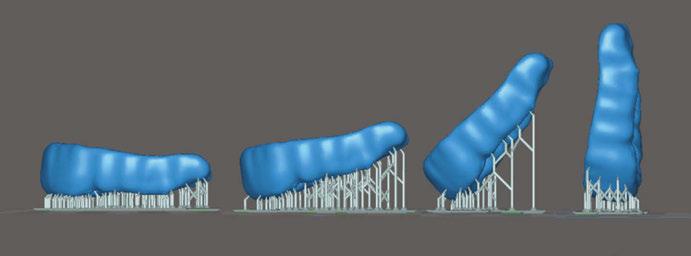
A significant physiological benefit of FP1 restorations, particularly those utilizing segmented bridges, is the potential for continued bone stimulation. Julius Wolff, a German anatomist and surgeon, coined what would be known as Wolff’s Law, which stated that bone in a healthy animal will adapt to the loads under which it is placed. In other words: our bones degrade without significant loads placed on them. We need only to look at a limb that has been splinted in a cast to see this theory in action.
Unlike a monolithic full-arch prosthesis, segmented bridges allow for a degree of independent movement of each segment during mastication. This functional loading on the individual implant fixtures and the surrounding bone can stimulate bone modeling and help prevent resorption over time. The distribution of occlusal forces across multiple, independently supported units may contribute to greater physiologic stresses within the alveolar bone and bone modeling. This contrasts with single-unit, full-arch restorations where occlusal forces are distributed across all implants as a single unit, potentially leading to bone remodeling.
By embracing sound principles and techniques that prioritize bone preservation and physiological stimulation, we can strive for more predictable long-term success and enhanced quality of life for our patients undergoing full-arch rehabilitation.
Randy Roberts, DDS, graduated Doctor of Dental Surgery from New York University College of Dentistry and later received an ALM from Harvard University. He founded Utah Smile Clinic and subsequently Smile Systems. Dr. Roberts pioneered the industrychanging 3 on 6™ full-mouth restoration procedure. Dr. Roberts is highly sought after for lecturing and training other dentists in the area of dental implants and full-mouth smile restoration. His unique conservative approach to smile restoration, including an emphasis on bone preservation, has garnered attention from dental professionals and patients worldwide.
Cover image of Dr. Randy Roberts courtesy of Smile Systems and TRI Dental Implants
TECHNOLOGY
Detection and removal of biofilm on implant surfaces using a biofluorescence imaging system: case reports
Drs. Young-Jun Ko, Jeong-Ho Yun, Hong-Cheol Yoon, Baek-Il Kim, and Dong-Won Lee illustrate the use of a new device to measure biofilm on implants.... 18
CONTINUING EDUCATION
Dentistry management essentials: leading specialty practices to success
Ali Oromchian, JD, LLM, offers guidance on creating a less stressful and more productive environment in the dental
Dr. Aaron Glick, Zain Moin, and Dr. Elham Abbassi offer a comprehensive overview of 3D printing and its applications
Beating burnout
The ADA cites that “more than 82% of dentists report feeling major stress about their careers.” In this very competitive and quickly changing world, the responsibilities can often feel like the walls of the office are closing in. Recognizing burnout symptoms and taking steps to calm your emotions can make a huge difference.
First, what does burnout feel like? Just a few signs are:
• Feeling tired, emotionally drained, or unenthusiastic
• Often feeling frustration toward work
• Negative outlook
• Problems concentrating
• Getting sick often
Lisa Moler Founder/Publisher, MedMark Media
It is important to recognize and treat burnout to avoid issues such as heart disease and diabetes, sleep-related disorders, and in some cases, substance misuse.
Some ways to overcome burnout
Get enough sleep: We’ve all had our nights of staring at the ceiling in bed while mulling over Plan A, Plan B, Plan C, and more, to solve the next day’s problems. Try to break your non-sleeping cycle. For example, ask your doctor about a possible supplement to lull your brain into the sleep cycle, or discover new relaxation techniques.
Detox from technology: Set specific technology-free windows where patient management systems and email notifications are completely turned off.
Eat and drink for health: Remembering to eat and keeping hydrated helps your brain function (improves memory, attention, and problem solving), raises your mood, and boosts your mental abilities.
Exercise: Exercising has been proven to help fight depression. It doesn’t have to take up much time – about 15-20 minutes per day should do it. A walk along a favorite path, around your neighborhood, on the beach, or even doing yoga or stretching can give your mind some time to reset.
Talk to trusted friends and mentors: There is nothing better than finding out that others can empathize with you and confirm that you are not “crazy.” Colleagues can tell you how they have navigated through similar times of burnout, or give some helpful tips, like reduced hours on Fridays or more intentional spacing of appointments. Look for summer dental retreats or workshops that combine professional development with wellness activities. Aside from work, friends or family can just listen, provide some good advice, or go along on that walk or for a quick cup of coffee and a shoulder to lean on. Finding a therapist can also be very helpful in working out your feelings and providing anti-anxiety techniques.
Give yourself a break: When you feel that burnout starting to eat away at your stomach lining, decide how you will take care of yourself at that moment. Take a few seconds. Grab your journal, and write a few lines. Go outside of the office and breathe some fresh air or look at the scenery. Research shows even 20 minutes of nature exposure significantly reduces cortisol levels. For more extreme situations, taking one day or a few days off, or a more extended vacation can bring you back with renewed spirits.
The ADA has some interesting resources just for dentists on its Wellness Resources page (https://www.ada.org/resources/practice/wellness) to help you start dealing with burnout. You can’t always control what happens in your office, but you can control the way you cope, put out those every day inner fires, and move forward to a fulfilling future with a positive outlook.
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor
Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Subscription Rate 1 year (4 issues) $149 https://implantpracticeus.com/subscribe/
Necessity may be the mother of invention, but compassion drives innovation
The path to innovation rarely begins in ideal circumstances.
After graduating from NYU’s College of Dentistry in 2011, Dr. Randy Roberts moved to Utah to start a practice with his brother, John. The two youngest of eight children, they prioritized staying close to family, even if it meant starting a dental business in one of the country’s most competitive regions for dentistry.
They purchased a bank-owned dental office in Taylorsville and launched what would eventually become Utah Smile Clinic. Like most general dentists, Dr. Roberts offered the usual array of services: fillings, crowns, veneers, and orthodontic aligners. But it wasn’t long before his curiosity pushed him to explore the world of implants. After a series of advanced implant courses and hundreds of successful surgeries, he discovered a passion — and a particular aptitude — for dental implant restoration. In short order, he became one of Utah’s top dental implant providers.
In 2013, Dr. Roberts faced a crossroads that would redefine his career and influence the future of full-mouth rehabilitation. His cousin, worn down by years of dental neglect and substance abuse, turned to him with a mouth full of failing teeth and a treatment plan he couldn’t afford. The only widely accepted solution was an All-on-4, but Dr. Roberts knew the procedure came with compromises: aggressive bone reduction, removable dentures that trapped food, and an unnatural-feeling prosthetic. Furthermore, the splinted design minimized physiological bone stimulation, potentially accelerating resorption over time.
All-on-4 changed the game when it was introduced, offering edentulous patients a fixed solution supported by just four implants. But like most things, it came with trade-offs. When faced with restoring the teeth of a close family member, Dr. Roberts didn’t like the idea of removing his healthy bone. He wondered, “If I can replace three or four teeth with a natural-looking bridge without bone removal or artificial gums, why can’t I restore an entire arch of teeth using the same methods?”
His cousin’s case was the catalyst, and he began developing a protocol that would solve some of the common pain points of All-on-4 while staying in a similar price range. Drawing on his extensive implant experience and a deep understanding of restorative biomechanics, Dr. Roberts envisioned a new kind of permanent smile solution. Instead of relying on a monolithic prosthesis, he imagined three individual zirconia bridges, each supported by two implants, preserving native bone, improving hygiene and phonetics, and creating a more natural-feeling result.
Dr. Randy Roberts
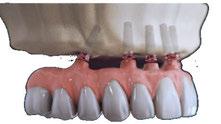
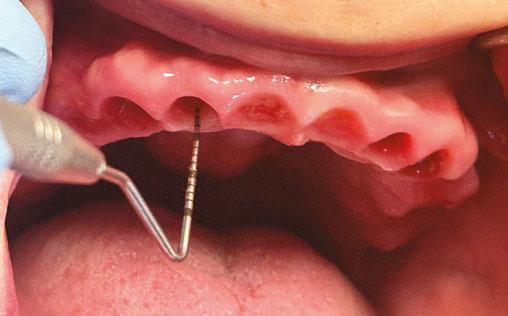
Probing tissue 3-months after 3 on 6 surgery with about 5 mm of tissue above the TRI implants
3 on 6 final result with three zirconia bridges seated. Thinner teeth and no artificial gums make it look and feel more natural
Over the course of several months, he began engineering what would become a defining advancement in FP1 restoration — the 3 on 6™. On January 28, 2014 — his birthday — he performed the first 3 on 6™ procedure. The outcome was transformative, and not just for his cousin. What started as an act of family service quickly evolved into a paradigm shift in implant dentistry.
The concept behind the 3 on 6™ is elegantly simple and biomechanically sound: six dental implants are placed to support one solid arch of teeth, providing cross-arch stabilization. After allowing time for osseointegration, the single arch is replaced with three segmented zirconia bridges — one on the anterior and one on each posterior quadrant. No bone removal necessary. No artificial gum material. No bulky prosthetics. Just permanent, implant-supported teeth that feel and function more like the real thing.
This segmentation turned out to be a game-changer. Unlike a monolithic denture-like restoration, segmented bridges allowed for healthier force distribution, improved hygiene, and superior phonetics. Patients retained their natural bone architecture, which allowed for better esthetics and long-term oral health. Because the bridges sat directly over the ridge rather than floating over pink acrylic, food impaction was minimized — and when it did occur, cleaning was far more manageable. There were also nearly no cases of prosthetic fractures with the final segmented zirconia bridges, and in cases where there were needs for replacement, it was much cheaper and easier to replace a 4-unit bridge than an entire full-arch fixed prosthetic.
Most importantly, patients loved the feel. The 3 on 6™ doesn’t rely on the palate for stability, doesn’t need to be removed for cleaning, and doesn’t simulate tissue — it replaces only the teeth. For patients who had struggled with dentures or the “false” feeling of All-on-4, this was a restoration that felt like they had their real teeth back.
Unlike All-on-4 hybrids, which often require complex removal and maintenance protocols, the 3 on 6 system shouldn’t need to be removed. In fact, the ultra-polished tissue surface of the bridges can actually adhere to the gums making it significantly more difficult for food and bacteria to get under the bridges or around the implants. This reduces long-term prosthetic complications that may otherwise result in surgical re-intervention.
As the number of successful 3 on 6™ cases grew, so did demand for this revolutionary approach to full-arch restoration. Dr. Roberts began seeing patients from across the country and even internationally. The demand from patients and popularity of the treatment approach led to inquiries from colleagues who wanted to learn how they could offer 3 on 6™ in their own practices. In response, Smile Systems was founded in 2019 to serve as the official training, support, and innovation platform for the 3 on 6™ procedure.
The success of the 3 on 6™ procedure is due in large part to its adaptability to modern digital workflows. Technologies such as CBCT imaging, intraoral scanning, 3D facial scanning, 3D printing, and photogrammetry allow for extreme precision in surgical planning and prosthetic fabrication. The use of zirconia — a durable and esthetically superior material — ensures longterm stability without sacrificing appearance.
Smile Systems continues to push boundaries by integrating emerging tools and techniques into the 3 on 6™ process. Same-day design and delivery of screw-retained temporaries is now common practice, allowing patients to leave surgery with a beautiful, fixed smile. The result is a process that feels like the future of restorative dentistry — minimally invasive, highly esthetic, and customized to each patient’s anatomy.
For decades, FP1 restorations — those replacing only the crowns of the teeth, without artificial gums — have been considered ideal but often impractical for full-arch cases. They required precise implant placement, excellent patient anatomy, and meticulous restorative planning. Many den-
3D renderings showing the 3 on 6 bridges and TRI implants
A group of new 3 on 6 providers receiving their certificate after completing training (left). Dr. Randy Roberts instructing new 3 on 6 providers (right)
tists would use the term “unicorns” when describing how rare they felt it was for a patient to qualify for FP1 treatment. Over 10 years of 3 on 6™ treatment has proven that is not the case. Today, Dr Roberts believes the vast majority of patients in need of full arch teeth restoration qualify for FP1 or FP2 treatment. Many patients have even converted from All-on-4 prosthetics that they hated to more natural feeling 3 on 6™ bridges that they love.
If there is one thing the 3 on 6 has accomplished, it has shown that there isn’t a one-size- fits-all solution to full arch restoration. The 3 on 6™ makes FP1 predictable and accessible for a wide range of patients. It provides dentists with a repeatable, trainable process that can be integrated into their practice with the right training and tools. It doesn’t just offer an alternative to All-on-4 — it redefines what full-mouth implant dentistry can look like when guided by sound prosthodontic principles and modern digital dentistry.
While the 3 on 6 was providing incredible results, Dr. Roberts faced an uphill battle to find an implant system designed for FP1 treatment. Most implant manufacturers cater to the needs of dentists providing single implants or the All-on-4 treatment, neglecting the unique treatment protocols and needs of dentists performing FP1 restorations. Dr. Roberts felt that he had two unresolved pain points with his 3 on 6™ treatment protocol: weak abutments and prosthetic screws coming loose.
A full-arch splinted prosthetic reduces the forces on implants and abutments. But with segmented bridges, they receive significantly higher forces. While the increase in forces was an important part of 3 on 6™ treatment in increasing bone stimulation modeling, it also meant increased stresses on weaker abutments and screws. After trying dozens of implant designs from a multitude of manufacturers, he thought his only option might be to create his own implants. That was when he discovered the implant he had been looking for, TRI®
The TRI implant was revolutionary in that it doesn’t require an abutment. The direct-to-connection design meant one less weak point to worry about. In addition, the prosthetic screws of TRI are nearly 10x larger than traditional screws, designed to withstand the full forces of oral function and reducing the likelihood of the screw loosening over time. Most prosthetic screws recommended torque value is 15-20ncm. TRI’s, however, is about double at 35ncm.
Dr. Roberts began testing the implants with 3 on 6 treatment and fell in love with the results. Unlike traditional implant systems that rely on intermediary abutments, TRI implants allow for direct-to-implant screw-retained restorations — eliminating the need for an abutment altogether. For FP1 treatments, where prosthetics sit directly on the ridge, and precision is key, this simplification reduces potential points of failure while improving esthetics and stability. By removing the abutment layer, there’s less micromovement, fewer opportunities for bacterial infiltration, and a more passive fit between the implant and the final zirconia bridge. These benefits are extremely valuable in fullarch cases, where long-term peri-implantitis can compromise the entire restoration.
Another standout feature Dr. Roberts gravitated to was TRI’s proprietary connection system, which utilizes a robust screw and deep conical interface. The design is significantly more resistant to mechanical fatigue, making it ideal for full-arch load scenarios.
In high-function cases like the 3 on 6™, where patients expect their teeth to perform like natural ones, the strength of this connection helps avoid loosening or screw fracture over time. The result is a restorative system that’s not only strong and hygienic, but also beautifully compatible with modern FP1 philosophy — prioritizing tissue preservation, esthetics, and patient comfort.
Today, the 3 on 6 is being performed in clinics across the U.S. and Canada by trained and licensed providers. Thousands of patients each year are receiving permanent smile restorations that are more affordable, more hygienic, and more natural-feeling than traditional options. Patients love that their teeth never have to be removed. They love that there is no transition line beneath their gums, and they love how it feels inside their mouth. In a street survey where patients were shown side-by-side retracted photos of All-on-4 and 3 on 6 smiles, 98% of respondents said they felt the 3 on 6 looked better and more natural.
Dr. Roberts and his team at Smile Systems continue to accelerate the adoption of FP1 treatment protocols by implant dentists across the country. Through their rigorous training program, they are expanding access to treatment while preserving the values that inspired the original innovation: compassion, practicality, and a commitment to long-term oral health.
For dentists, the 3 on 6 represents more than just a new treatment option — it’s a chance to offer something better. Imagine being one of the first dentists to offer All-on-4 to the market 25 years ago. 3 on 6 clinicians are at the tip of the spear when it comes to smile rehabilitation. The future of dentistry is more hygienic, more esthetic, and more natural feeling.
If you are interested in becoming a 3 on 6 Provider, you can visit SmileSystems.com for more information or to register for an upcoming course. IP
Dr. Roberts filming content at a recent 3 on 6 Providers Summit in Mexico
The critical need for business and leadership excellence in the dental industry: empowering the future through Serendequity Education
Scott S. De Rossi, DMD, MBA, discusses two new programs that develop business and leadership excellence
The modern healthcare landscape is undergoing a profound transformation. Technological advancements, shifting patient expectations, regulatory complexities, and the rise of corporate delivery models have converged to redefine what it takes to succeed — not only as a clinician but as a leader. Nowhere is this evolution more evident than in the dental industry, where the traditional solo-practitioner model is rapidly giving way to Dental Support Organizations (DSOs), group practices, and dental education models that demand far more than clinical competency. In this changing environment, the value of business and leadership excellence is not ancillary — it is foundational.
To thrive in the future of healthcare, every member of the dental team must be equipped with knowledge, skills, abilities, and judgment that transcend the operatory. Business acumen, strategic thinking, and people leadership are no longer optional soft skills; they are essential survival traits. Serendequity Education’s Mini MBA for Dentistry and Leadership Excellence to Advance Practice (LEAP) certificates respond to this need with urgency, clarity, and action. These programs are not just academic exercises; they are transformational platforms that bridge the long-standing gap between clinical mastery and business and leadership excellence.
The business of dentistry is now central to the practice of dentistry
For decades, dental education has produced competent clinicians who were expected to “figure out” business on their
Scott S. De Rossi, DMD, MBA, Vice President of Strategic Growth and Innovation of Nexus Dental Systems, is passionate about driving strategic growth and innovation in healthcare. He has led initiatives to improve access, quality, outcomes, efficiency, patient satisfaction, and affordability by integrating medicine and dentistry. He has integrated cutting-edge technology and resources to optimize clinical and academic sectors, solving long-term issues and driving exponential growth. He has prioritized and communicated the importance of oral-systemic connections in patient-centered care, increasing endowment funds and ensuring compliance with accreditation and regulations. Dr. De Rossi has fostered innovative cultures by mobilizing cross-functional teams, balancing optimism with transparency and trust, and inspiring continuous improvement.
own. As a result, thousands of private practitioners found themselves unprepared for the financial, operational, and strategic realities of running a dental practice. Today, with declining insurance reimbursements, rising operating costs, and patient expectations shaped by consumer-centric industries, the challenge is even greater.
Meanwhile, DSOs have surged in influence, offering dentists opportunities for support, stability, and scale. Yet the success of these organizations hinges on local leaders who can manage P&Ls, build high-performing teams, and deliver exceptional patient experiences. Even the best DSO infrastructure fails without empowered clinicians who understand how to run their practices as businesses and lead their teams effectively.
At the same time, dental education must also evolve. Schools are increasingly recognizing the need to graduate dentists who are not only clinically competent but also strategically agile and prepared for multifaceted roles — as clinicians, managers, educators, entrepreneurs, and change agents. However, few institutions offer meaningful and practical structured business or leadership development integrated into their core curriculum.
Why leadership matters at every level of the dental team
Leadership in dentistry is not confined to owners or executives. It manifests in every interaction that shapes a patient’s
experience and every decision that influences a team’s culture. From the front office administrator who manages scheduling efficiency, to the hygienist who educates patients and supports treatment acceptance, to the associate dentist managing chairside dynamics — every team member impacts the overall success of a practice.
Yet these professionals are rarely given formal training in conflict resolution, change management, communication strategy, or operational improvement. This lack of leadership development is a missed opportunity not just for individual growth, but for organizational excellence.
By embedding leadership training across all team levels, practices and DSOs can build a culture of shared accountability, continuous improvement, and adaptive problem-solving. Empowered teams are resilient teams — and resilient teams are those that can navigate staffing shortages, integrate new technologies, respond to shifting payer models, and deliver better outcomes under pressure.
The Serendequity Solution: Mini MBA and LEAP Certificates
Serendequity Education’s Mini MBA and LEAP programs were created to address this urgent gap with precision and practicality.
The Mini MBA for Dentistry
This intensive, modular online program is designed for dentists and staff, specialists, practice owners, and DSO executives seeking a comprehensive foundation in business disciplines essential to healthcare leadership. With 12 interactive modules — including financial management, marketing strategy, team dynamics, operations, legal compliance, and strategic planning — the Mini MBA provides real-world tools rooted in dental practice realities. Through capstone projects and case-based learning, participants do not merely absorb knowledge, they apply it — building business plans, operational improvements, and leadership strategies that can be deployed immediately in their settings.
The Serendequity Education Mini MBA for Dentistry is an innovative, industry-tailored certificate program designed to equip dentists, hygienists, and dental leaders with core business competencies to thrive in today’s rapidly evolving dental landscape. This online, self-paced curriculum offers a practical, high-impact educational experience and essential tools to lead, grow, and future-proof dental practices and organizations.
At its core, this Mini MBA bridges the long-standing gap between clinical training and business knowledge in dental education. With deep roots in real-world practice scenarios and trends, this program empowers dental professionals to make data-informed decisions, navigate competitive pressures, and create scalable, patient-centered businesses. It is a critical step forward in redefining how dentistry prepares its current and future leaders.
Leadership Excellence to Advance Practice (LEAP) Certificates
Targeted toward all dental professionals — dentists, hygienists, assistants, and administrative leaders — LEAP focuses on ele-
To thrive in the future of healthcare, every member of the dental team must be equipped with knowledge, skills, abilities, and judgment that transcend the operatory.”
vating leadership capacity within teams. These shorter, focused certificates develop core skills in emotional intelligence, decision-making, team building, coaching, and adaptability. LEAP cultivates confident, collaborative professionals who understand how to inspire others, align around vision, and foster cultures of trust, innovation, and excellence.
Both programs are designed with flexibility in mind: online, asynchronous, and accessible to working professionals. They combine world-class faculty with evidence-based frameworks ensuring that content is both cutting-edge and grounded in dental practice.
Value proposition for the dental industry and profession
Bridging the business education gap in dentistry
Most dental curricula prioritize clinical expertise but neglect business acumen. As a result, many dentists enter practice ownership or leadership roles ill-equipped to manage operations, finances, or strategy. The Serendequity Mini MBA directly addresses this gap by offering business and management education specifically contextualized for the dental industry. Unlike traditional MBA programs, this certificate is lean, focused, and immediately applicable — helping participants lead with confidence from day one.
Strategic preparedness for a changing industry
The dental profession is undergoing significant transformation:
• Consolidation and the rise of DSOs: The Mini MBA offers insights into how to collaborate with, compete against, or even build a DSO, including practical tools for assessing affiliation and acquisition opportunities.
• Technology-driven disruption: From teledentistry to AI, participants learn how to evaluate, adopt, and leverage technologies that enhance productivity, reduce overhead, and elevate the patient experience.
• Consumer expectations and patient-centered care: The curriculum trains participants to develop marketing strategies, service excellence frameworks, and patient feedback systems that drive retention and satisfaction.
Practice performance optimization
The modules on financial management, team dynamics, operations, and marketing help practitioners:
• Analyze P&L statements and manage cash flow
• Build and retain high-performing teams
• Streamline workflows using lean principles
• Attract and retain patients using data-driven marketing
• Advanced Education with Mini MBA Program and Other Advanced Certificates in Business Management and Leadership
• Retention Strategies
• Operational Support
• Technology Implementation
• Patient Trends & Analytics
• Efficiency Audit
• Competitive Fee Survey
• Production Analysis
• Increase profitability while delivering high-quality care
These are not theoretical skills; they are mission-critical for any practice owner, associate, or DSO leader aiming for sustainable growth and resilience.
Empowering clinicians as leaders
The Mini MBA cultivates leadership capacity by introducing proven frameworks in change management, organizational behavior, and strategic planning. Participants learn how to adapt their leadership styles to different situations, manage conflict, align teams around a shared vision, and drive performance in a clinical setting.
Curriculum overview
The Mini MBA spans 12 core modules delivered in a dynamic, flexible online format. Each module features video lectures by dental and business experts, interactive tools, real-world case studies, assessments, and peer discussion forums.
Highlights include:
Modules 1–3: Foundation in Business, Finance, and Leadership
• Business Foundations for Dental Practices
• Financial Management Essentials
• Leadership in Dental Practice
Modules 4–6: Team, Communication, and Marketing
• Team Management and Communication
• Marketing Strategies for Dental Practices and DSOs
• Patient Experience and Relationship Management Modules 7–9: Operations, Legal, and Strategy
• Operational Excellence in Dental Practices and DSOs
• Legal and Ethical Considerations
• Strategic Planning in Dental Practices and DSOs
Modules 10–12: Financial Planning and Capstone Project
• Financial Planning and Investment
• Capstone Business Plan Project
• Professional Reflection and Integration
The Capstone Project is a distinctive feature, allowing learners to develop and present a real-world business plan addressing a current challenge or opportunity within their own practice or the broader industry.
Differentiators and Innovation
• Dental-specific, practitioner-focused: Unlike generic business programs, every topic is translated for dental application — using dental-specific examples, case studies, and metrics.
• Expert-led and evidence-based: Instruction draws from Harvard Business Review, McKinsey, ADA policy, and successful DSO operators. This ensures that learners receive best-in-class thinking tailored to their world.
• Flexible, asynchronous learning: Designed for busy professionals, this online model supports learning on-demand while still enabling community interaction through discussion forums and coaching sessions.
• Scalable across roles and organizations: The program is valuable not only for private practitioners and owners but also for emerging leaders in DSOs, group practices, and
even dental schools seeking to embed leadership into predoctoral curricula.
Professional impact and career relevance
Graduates of the Serendequity Mini MBA will be equipped to:
• Launch or expand successful private practices or DSOs
• Increase efficiency, profitability, and patient satisfaction
• Lead multidisciplinary teams with clarity and purpose
• Make strategic financial and operational decisions
• Explore new career paths in executive leadership, consulting, or education
In a field where business illiteracy can hinder career progression, this program becomes a strategic enabler of growth, security, and fulfillment.
Equipping the profession for the future
As we enter an era of precision health, artificial intelligence, value-based care, and growing integration between oral and systemic health, the expectations placed on dental professionals will only increase. To lead in this new age, our profession must rethink how we define excellence.
• Excellence is no longer just about clinical outcomes; it is about organizational agility.
• Success is no longer just about solo achievement; it is about team empowerment.
• Impact is no longer limited to the dental chair; it is measured by systems thinking, strategic foresight, and the ability to lead change.
The Serendequity Mini MBA and LEAP programs offer a clear path forward. They democratize access to elite business and leadership education and bring it into the hands of those who need it most — practicing dental professionals and staff navigating real-world complexity.
Conclusion
The dental industry stands at an inflection point. Clinical skill will always be the foundation of dental medicine, but it is no longer sufficient to ensure success. Business literacy and leadership excellence must now be core competencies for every member of the dental team. Whether navigating the complexities of private practice, driving performance in a DSO, or preparing students in dental education, the need for strategic, empowered, and adaptive leaders has never been greater.
Serendequity Education’s Mini MBA and LEAP certificates are more than programs — they are movements. They represent a shift in how we prepare dental professionals for impact, resilience, and sustainable success. By embracing business and leadership education, the dental profession will not only meet the demands of today; it will shape the healthcare systems of tomorrow. As the profession evolves, so too must the way we prepare our clinicians — not just to drill, fill, and bill — but to lead, build, and grow.
This is not optional education — it is essential. Serendequity Education prepares people not only to survive the future of dentistry but to shape it. IP
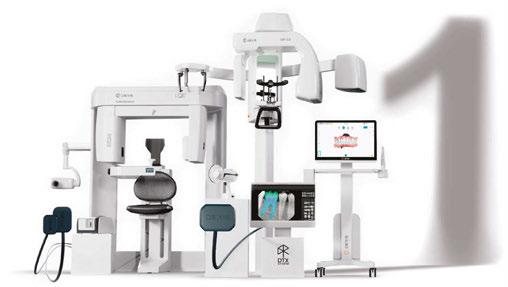
The DEXIS digital ecosystem
Your all-in-one, AI-powered solution — combining 2D and 3D imaging, intraoral scanning, diagnostics, and treatment planning into one integrated workflow
“Having all my technology integrated in one place is a game-changer,” says Dr. Lupe Poussin. “It saves time, reduces errors, and improves the overall quality of care we provide.”
Intraoral X-ray
Best known for high-clarity images, durable hardware, and user-friendly software, DEXIS™ 2D X-ray solutions connect and simplify workflows for the modern dental practice. The award-winning 2D X-ray line includes digital sensors as well as handheld and wall-mounted units to maximize flexibility.
DEXIS has the world’s most recognized intraoral sensor brand, and DEXIS sensors capture over 167 million images annually. To put it into perspective, 6 images are captured using a DEXIS intraoral sensor every second.
“We’ve been using DEXIS sensors for 20 years now,” says Dr. Paresh Shah. “We’ve never even bothered looking at others because of the quality and convenience — we’ve just always wanted to stay in the family.”
To maximize the power of DEXIS sensors, users can automatically export their 2D images to DTX Studio™ Clinic — the AI-driven diagnostics and treatment planning software that unifies the ecosystem.
Extraoral imaging
From the beloved i-CAT™ to the innovative ORTHOPANTOMOGRAPH™ OP 3D™ series, clinicians can expand their diagnostic capabilities with the DEXIS 3D imaging lineup.
Best known for precise 3D images, flexible FOV sizes, and intuitive workflows, DEXIS 3D imaging sets the industry standard for reliable performance and cutting-edge innovation.
Over 17,000 OP 3D units have been successfully installed in clinics around the world, and a 2023 survey found DEXIS to have the highest 3D market share in the United States at 31%.
“I needed a CBCT unit with a large sensor, predictable acquisition, good image quality, and intuitive software that wouldn’t slow me down,” says Dr. Tyler Tolbert. “Once the OP 3D EX got here, and we started taking some scans, I thought to myself, ‘Ok, wait … we made a REALLY good choice here.’”
Once again, the true power of DEXIS 3D imaging is seen through the software’s direct integration with DTX Studio Clinic. 3D scans can be automatically exported
into a patient workspace where clinicians can use advanced AI tools to help them with case setup, diagnostics, and treatment planning.
Intraoral scanning
World renowned for accurate digital impressions, powerful patient engagement tools, and smooth scanning workflows, DEXIS intraoral scanners and DEXIS IS ScanFlow software are setting the global precedent for precision and usability.
The DEXIS line of intraoral scanners and IS ScanFlow software are constantly evolving to help clinics communicate visually with their patients and deliver exceptional results.
“It’s like we’re standing on the tooth,” says Dr. John Zalesky. “I can show the patient where they have wear or other issues, so they can understand what’s going on. This leads to increased treatment acceptance which also increases my productivity.”
Once again, to maximize the capabilities of DEXIS intraoral scanners, users can use their direct integration with DTX Studio Clinic.
Diagnostics and treatment planning
At the very heart of the DEXIS digital ecosystem is DTX Studio Clinic, a diagnostics and treatment-planning software that automatically consolidates all data (2D, 3D, intraoral scans, and photography) into an AI-powered patient workspace.
Through the software, users can make diagnoses, educate patients, plan treatments, and generate surgical guides — all with the help of AI.
DTX Studio Clinic processes over 500,000 images per month globally and is praised by users for its ease of use and advanced AI tools.
“The major reason we were able to implement the OP 3D EX and start taking scans so quickly was largely due to DTX Studio Clinic,” says Dr. Nicholas Varney. “Once we got going, we found that so much of the work involved in prepping a 3D scan was done by the software automatically. It has improved how we work in all aspects — communicating with patients, implant planning, and even treatment team collaboration.” IP
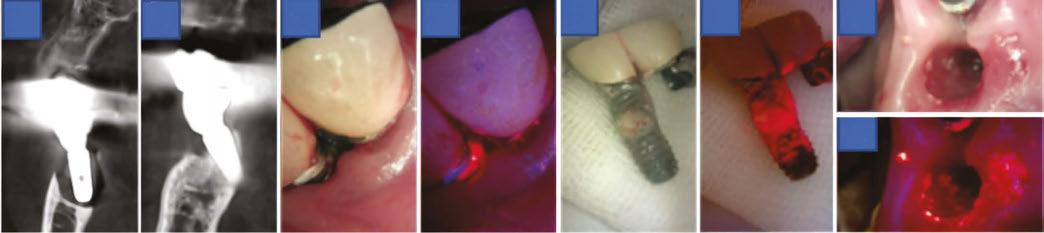
Detection and removal of biofilm on implant surfaces using a biofluorescence imaging system: case reports
Drs. Young-Jun Ko, Jeong-Ho Yun, Hong-Cheol Yoon, Baek-Il Kim, and Dong-Won Lee illustrate the use of a new device to measure biofilm on implants
Introduction
As the prevalence of dental implant treatments continues to rise, the incidence of peri-implantitis has also increased, posing a significant threat to the long-term success of implants.1 Peri-implantitis is characterized by inflammation and bone loss caused by the accumulation of biofilm on the implant surface, where metabolic byproducts produced by pathogenic bacteria trigger inflammatory responses and accelerate disease progression.2 However, conventional biofilm removal methods have shown limited efficacy, and clinical examinations combined with radiographic imaging are often insufficient for accurately assessing early-stage lesions.3 In particular, small lesions or subtle biofilm accumulations are difficult to detect visually, highlighting the need for more precise diagnostic and therapeutic technologies.4
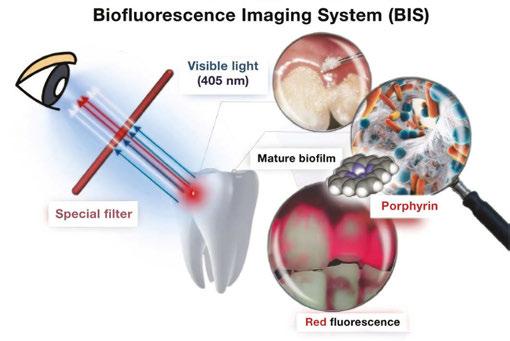
To overcome these limitations, biofluorescence imaging systems (BIS), such as quantitative light-induced fluorescence (QLF), have recently gained attention as innovative alternatives.5 QLF utilizes blue visible light at a specific wavelength (405 nm) to detect red fluorescence emitted by porphyrins produced by mature bacterial colonies, allowing for the quantitative assessment of biofilm location and maturity (Figure 1).6 This real-time visualization enables immediate evaluation of biofilm removal
Dr. Young-Jun Ko is from the Department of Periodontology, Gangnam Severance Hospital, Seoul, South Korea.
Dr. Jeong-Ho Yun is from the Department of Periodontology, College of Dentistry and Institute of Oral Bioscience, Jeonbuk National University, Jeonju, South Korea, and the Research Institute of Clinical Medicine of Jeonbuk National University-Biomedical Research Institute of Jeonbuk National University Hospital, Jeonju, South Korea.
Dr. Hong-Cheol Yoon is from the BESTDEN Dental Clinic, Seoul, South Korea.
Dr. Baek-Il Kim is from the Department of Preventive Dentistry & Public Oral Health, BK21 FOUR Project, Yonsei University College of Dentistry, Seoul, South Korea.
Dr. Dong-Won Lee is from the Department of Periodontology, Gangnam Severance Hospital, Seoul, South Korea and the Department of Periodontology, Research Institute for Periodontal Regeneration, Yonsei University College of Dentistry, Seoul, South Korea.
Disclosure: HC Yoon is employed by AIOBIO Co., Ltd. Other authors declare that they have no conflicts of interest.
from the implant surface, ultimately enhancing treatment precision.6,7
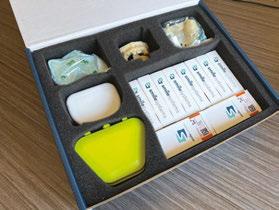
In these case reports, we present a clinical cases in which QLF (Qraypen C, AIOBIO, Seoul, South Korea; Figure 2) was used to assess biofilm accumulation on the implant surface of a patient with peri-implantitis and to confirm biofilm removal during surgical/non-surgical therapy. Additionally, clinical parameters such as probing depth, bleeding on probing, and radiographic bone loss were evaluated to assess treatment outcomes. Furthermore, we discuss the limitations of this technology and its potential for future advancements. This case highlights the utility of biofluo-
Figure 1: Schematic view illustrating the working of a biofluorescence imaging system
Figure 2: QLF device (Qraypen C, AIOBIO, Seoul, South Korea)
rescence technology as an effective and precise tool for biofilm detection and removal in the treatment of peri-implantitis.
Case presentations
Patients diagnosed with peri-implantitis reported experiencing persistent discomfort and irritation around the implant site over an extended period. Clinical examination revealed moderate gingival inflammation, bleeding on probing, and pus discharge. Radiographic assessment confirmed the diagnosis by demonstrating significant bone loss around the affected implant.
A biofluorescence imaging system (BIS) was used to identify sites of biofilm accumulation on the implant surfaces prior to the initial mechanical debridement. The effectiveness of biofilm removal was evaluated by re-examining the implant surfaces using BIS, and the disappearance of fluorescence was confirmed.
Clinical parameters including probing depth, bleeding on probing, and radiographic bone loss were recorded at baseline and post-treatment to evaluate the overall treatment outcome.
Results
Case 1
An 80-year-old female patient visited the Department of Periodontology at Gangnam Severance Dental Hospital, complaining of an odor emanating from the upper right implant site. Due to the long distance from her residence, she had been unable to attend regular check-ups consistently. The patient had a medical history of osteoporosis and had been receiving Denosumab (Prolia®) injections every 6 months for the past 6 years.
Clinical examination revealed probing depths of 5–6 mm around implant Nos. 4 and 5, with thread exposure at implant No. 5 above the gingival margin. Radiographic examination revealed bone loss around implant Nos. 4 and 5, leading to a diagnosis of peri-implantitis (Figure 3A). Although no significant biofilm accumulation was visible to the naked eye (Figure 3B), evaluation using QLF clearly detected biofilm that was not observable under conventional visual inspection (Figure 3C). Considering the patient’s osteoporosis and the fact that only 4 months had passed since her last denosumab (Prolia®) injection, flap surgery was not performed. Instead, curettage was selected as the treatment approach.
For biofilm removal, cleansing was performed using an ultrasonic scaler (Megagen, Seoul, South Korea), a curette, and a microbrush. After mechanical debridement, QLF imaging was conducted again to compare pre- and post-treatment findings. While no biofilm was visible to the naked eye (Figure 3D), QLF revealed residual biofilm on the implant threads (Figure 3E). Additional debridement was carried out, followed by another round of clinical and QLF imaging for confirmation (Figures 3F-3G). This process enabled a more thorough evaluation of biofilm removal and served as a visual aid for patient education on oral hygiene. Targeted brushing instruction (TBI) was also provided.
The area was then rinsed with 0.2% chlorhexidine, and 2% minocycline ointment (Periocline®, Sunstar, Osaka, Japan) was topically applied to the peri-implant lesion for inflammation control.
At the 2-week follow-up, peri-implant inflammation had significantly decreased, and the patient reported relief from discomfort. At the 6-month follow-up, only mild inflammation was observed in the surrounding area, but the patient remained symptom-free, and the peri-implant tissues were well maintained.
Case 2
A 70-year-old female patient visited the Department of Periodontology at Gangnam Severance Dental Hospital, reporting bleeding from the lower left implant site during brushing. The patient had been regularly attending follow-up appointments at our department but had only received non-surgical treatments due to her dental phobia. Medical history revealed no significant underlying medical conditions.
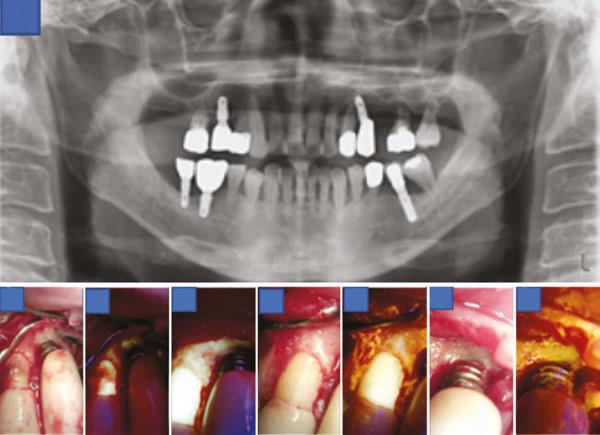
Clinical examination revealed a probing depth of 5–6 mm around implant No. 20, with the implant threads exposed above the gingiva. Although no significant biofilm attachment was observed with the naked eye (Figure 4B), QLF revealed the presence of biofilms (Figure 4C). In addition, periapical radiography revealed bone loss around implant No. 20, leading to a diagnosis of peri-implantitis (Figure 4A). Despite her dental phobia, the patient consented to undergo flap surgery after a thorough explanation of the necessity of actively removing factors contributing to infection from the implant surface.
A sulcular incision was made from the mesial line angle of No. 21 to the distal line angle of implant No. 19 using #15T and
Figures 3A-3G: Pre- and post-treatment images for Case No. 1
A.
D. F. E.
G.
B.
C.
#12 blades. Upon flap elevation, visible biofilm was observed (Figure 4D), and its presence was confirmed with QLF imaging (Figure 4E). Biofilm removal was performed using an ultrasonic scaler (Megagen, Seoul, South Korea), a curette, and a microbrush. Tetracycline was additionally applied for implant surface decontamination. Subsequent clinical and QLF imaging confirmed the successful removal of residual biofilm and infectious material (Figure 4F-4G). The surgical site was then closed using 4-0 absorbable synthetic sutures (Coated Vicryl™, Ethicon, Johnson & Johnson, Somerville, New Jersey) with an interrupted suture technique.
One week after the flap surgery, the patient returned for suture removal. The healing process was satisfactory, with no abnormal findings. At 6-month and 1-year follow-ups, the patient reported no discomfort, implant surface hygiene had improved compared to the pre-treatment condition, and the overall oral health remained stable.
Case 3
An 86-year-old female patient initially visited a local dental clinic, where she was advised to seek evaluation and treatment at a university hospital due to severe bone loss around the lower left implant. She subsequently presented for her first visit to the Department of Periodontology at Gangnam Severance Dental Hospital. The patient had no significant underlying medical conditions aside from hyperlipidemia.
Clinical examination revealed a probing depth of 12 mm around implant No. 19, accompanied by active pus discharge above the gingival margin (Figure 5C). Furthermore, QLF imaging detected red fluorescence from porphyrins, indicating a mature biofilm (Figure 5D). Cone-beam computed tomography revealed bone loss around implant Nos. 18 and 19, leading to a diagnosis of peri-implantitis (Figures 5A-5B). Notably, implant
No. 19 exhibited bone loss extending to the apex, and during prosthesis removal, it was spontaneously exfoliated (Figure 5E). Although no significant biofilm was observed macroscopically on the tissue and fixture surfaces (Figure 5G), QLF evaluation detected porphyrin fluorescence, confirming the presence of a biofilm (Figures 5F-5H).
Subsequently, a sulcular incision was made using #15T and #12 blades, followed by socket curettage with tetracycline. The wound was then closed using a figure-eight suture technique with 4-0 absorbable synthetic sutures (Coated Vicryl™, Ethicon, Johnson & Johnson, Somerville, New Jersey).
One week after the implant removal procedure, the patient returned for suture removal. Healing was satisfactory, with no notable complications. At the 6-month follow-up, the patient reported no significant discomfort, and overall oral health was stable compared to the preoperative condition.
Case 4
A 56-year-old male patient presented for his first visit to the Department of Periodontics at Gangnam Severance Dental Hospital, complaining of frequent food impaction around the upper left implant area and mobility posterior teeth. Medical history revealed no significant underlying medical conditions.
Clinical examination revealed a subgingival calculus at site tooth No. 11 and a probing depth of 6 mm at site implant No. 12. Furthermore, based on the panoramic radiography findings, the prognosis of tooth No. 14 was hopeless (Figure 6A); therefore, extraction of tooth No. 14 and flap surgery for implant No. 12 were planned. An intrasulcular incision was made from the mesial line angle of tooth No. 10 to the distal aspect of implant No. 12 using #15T and #12 blades. After flap elevation, subgingival calculus and bone loss were confirmed around tooth No. 11 and implant No. 12, respectively (Figure 6B).
Figures 5A-5H: Clinical and radiographic findings in Case 3
A. B.
G. H.
A.
B. C. D. E. F. G.
Figures 4A-4G: Preoperative and intraoperative findings in Case 2
Although no biofilm was visible to the naked eye on the implant No. 12 threads, QLF imaging revealed its presence (Figure 6C). Biofilm removal was performed using an ultrasonic scaler (Megagen, Seoul, South Korea), curette, and microbrush. Follow-up QLF imaging was conducted to evaluate the pre- and post-treatment difference, confirming successful biofilm removal (Figure 6D). The area was irrigated with tetracycline, and additional clinical photographs and QLF images were taken to verify the elimination of biofilm and infection at tooth No. 11 and implant No. 12 (Figures 6E-6H). Interrupted sutures were placed using 4-0 absorbable synthetic sutures (Coated Vicryl™, Ethicon, Johnson & Johnson, Somerville, USA). The importance of oral hygiene management was emphasized using visual aids, and tooth brushing instruction (TBI) was provided.
One week after the flap surgery and implant surface decontamination, the patient returned for suture removal and reported significant relief from discomfort. Healing was uneventful, with no notable complications.
At the 6-month follow-up visit, the patient’s clinical symptoms had resolved. Through regular TBI, implant surface hygiene had improved compared to the pre-treatment condition, and the overall oral health remained stable.
Follow-up summary (Cases 1–4)
At the 1-week and 6-month follow-up after treatment in Cases 1 through 4, clinical reassessments demonstrated significant improvements in gingival inflammation, bleeding on probing, and pus discharge. Radiographic examinations showed that peri-implant conditions remained stable.
This case series highlights the potential of BIS technology in the clinical management of peri-implantitis. Its non-invasive nature and absence of adverse effects further support its value as a precise and patient-friendly diagnostic and therapeutic adjunct in implant dentistry.
Discussion
In this case series, QLF was used as a supplementary diagnostic tool for real-time visualization of the lesion status before and after treatment. This enabled clinicians to identify residual biofilms following the initial debridement, allowing for more thorough implant-surface cleaning.
The use of the BIS contributed to the development of more systematic and individualized treatment plans, ultimately enhancing the precision and success rate of peri-implantitis management. However, biofluorescence imaging has some limitations. First, the biofilm we aim to detect is primarily located in the apical region rather than in the coronal region. However, currently available QLF devices have large heads, making access to the apical area difficult. Second, in addition to the surgeon retracting the cheek and gingiva, an assistant is required to aid in capturing images. Furthermore, effective control of bleeding is necessary during imaging. Third, areas actively exuding pus should be detected as red on QLF imaging; however, this
was not observed in few cases. Further studies are required to investigate this phenomenon. Additionally, studies establishing the long-term clinical efficacy of peri-implantitis treatment with adjunctive biofluorescence imaging and verifying the effectiveness of biofluorescence imaging through comparative studies with existing diagnostic methods are required.
Conclusion
This case series highlights the usefulness of biofluorescence imaging in the clinical management of peri-implantitis. Biofluorescence imaging is a noninvasive, safe, precise, and patient-friendly diagnostic and therapeutic adjunct in implant dentistry.
Editor’s Note: The Lead Author was responsible for the data collection, performing the data analysis, and the composition of the abstract.
REFERENCES
1. Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015 Apr;42 Suppl 16:S158-171. doi: 10.1111/ jcpe.12334.
2. Berglundh T, Armitage G, Araujo MG, Avila-Ortiz G, Blanco J, Camargo PM, Chen S, Cochran D, Derks J, Figuero E, Hämmerle CHF, Heitz-Mayfield LJA, Huynh-Ba G, Iacono V, Koo KT, Lambert F, McCauley L, Quirynen M, Renvert S, Salvi GE, Schwarz F, Tarnow D, Tomasi C, Wang HL, Zitzmann N. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018 Jun;45 Suppl 20:S286-S291. doi: 10.1111/jcpe.12957.
3. Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Clin Periodontol. 2018 Jun;45 Suppl 20:S246-S266. doi: 10.1111/jcpe.12954.
4. Lee JW, Lee ES, Kim BI. Can red fluorescence be useful in diagnostic decision making of residual dentin caries? Photodiagnosis Photodyn Ther. 2019 Jun;26:43-44. doi: 10.1016/j.pdpdt.2019.02.016. Epub 2019 Feb 20.
5. Han SY, Kim BR, Ko HY, Kwon HK, Kim BI. Assessing the use of Quantitative Light-induced Fluorescence-Digital as a clinical plaque assessment. Photodiagnosis Photodyn Ther. 2016 Mar;13:34-39. doi: 10.1016/j.pdpdt.2015.12.002. Epub 2015 Dec 9.
6. Kim YS, Lee ES, Kwon HK, Kim BI. Monitoring the maturation process of a dental microcosm biofilm using the Quantitative Light-induced Fluorescence-Digital (QLFD). J Dent. 2014 Jun;42(6):691-696. doi: 10.1016/j.jdent.2014.03.006. Epub 2014 Mar 19. Erratum in: J Dent. 2014 Dec;42(12):1626.
7. Khudanov B, Jung HI, Kahharova D, Lee JW, Hamidov I, Lee ES, Kim BI. Effect of an oral health education program based on the use of quantitative light-induced fluorescence technology in Uzbekistan adolescents. Photodiagnosis Photodyn Ther. 2018 Mar;21:379-384. doi: 10.1016/j.pdpdt.2018.01.012. Epub 2018 Jan 31.
IP
Figures 6A-6H: Clinical and radiographic findings in Case 4
A.
B.C.D. E.F. G. H.
Clinical applications and innovations of 3D printing in dentistry and dental implants
Dr. Aaron Glick, Zain Moin, and Dr. Elham Abbassi offer a comprehensive overview of 3D printing and its applications
Introduction to 3D Printing
3D printing is a relatively new field starting in the 1980s with the understanding of sequentially polymerizing materials with a beam of UV light or laser.1 Since its inception, there has been significant interest and adoption of 3D printing in multiple fields. For example, a 400-square-foot 3D-printed house in Russia was made in 24 hours and at a cost of $10,000.2 Other fields use 3D printing for making automotive parts, fabricating tools in space, concocting custom edible foods, creating educational displays, and executing rapid prototyping for engineering projects. In the health field, bioprinting is being used to build bioactive scaffolds, create human cells, and synthesize implantable tissues.3
Subtractive versus additive manufacturing
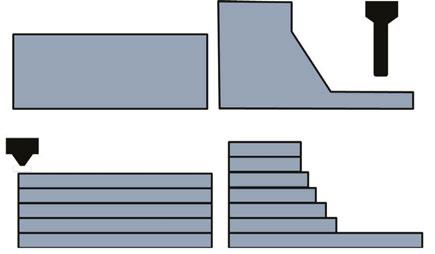
Generally, manufacturing techniques are either subtractive or additive. In subtractive manufacturing (i.e., CNC milling), the material is removed through carving or grinding away at the substructure. In additive manufacturing (i.e., 3D printing), the finished product is built through successive layers of material. Subtractive manufacturing involves a number of axes around which the block of material is rotated so the drill can remove the material, compared with additive manufacturing that will build layers of material in one plane as shown in Figure 1.
The additive nature of 3D printing holds a deep advantage in ease, cost, and flexibility. Due to the rotational axes required, there are some complex parts and internal geometries that are more difficult to manufacture through subtractive manufacturing (Figure 2). For instance, GE changed their manufacturing of some jet fuel nozzles since they could print one piece instead of assembling 20 separate parts.4 The decision to change their manufacturing method resulted in reducing manufacturing costs by 75%. Additive manufacturing allows for flexibility since the setup is minimal compared with retooling that is required for most high scale production facilities. In dentistry, the flexibility
Aaron Glick, DDS, is an Adjunct Clinical Associate Professor, General Practice and Dental Public Health, at the University of Texas Health Science Center at Houston School of Dentistry.
Zain Moin is an MD/MEng Candidate at the Texas A&M School of Engineering Medicine (EnMed).
Elham Abbassi, DDS, is Assistant Professor and Group Practice Director, General Practice and Dental Public Health, University of Texas Health Science Center at Houston School of Dentistry.
Educational aims and objectives
This self-instructional course for dentists aims to discuss 3D printing, how it works, and its benefits and drawbacks and applications for the implant dentist.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the differences between subtractive and additive manufacturing techniques.
• Recognize multiple applications for additive manufacturing in dentistry.
• Realize some oral surgery applications for 3D printing. Identify the clinical workflow for chairside 3D printing.
• Define bioprinting and realize its potential for dental applications.
is underscored by multiple types of materials that can be used to build specific appliances.
Additive manufacturing technologies
The major categories of 3D printers are fused deposition modeling (FDM), stereolithography (SLA)/digital light projection (DLP), selective laser sintering (SLS), powder binder jetting (BJ), and photopolymer jetting (PJ) (Table 1). FDM printing is the most widely used type of printing that melts a thermoplastic filament. SLA/DLP use UV to cure a liquid photopolymer resting in a vat.
This modality is most commonly used for dental applications due to its ability to accurately create small complex parts with resin materials. SLS printers are utilized more commonly in industrial settings and can be found in dental labs as opposed to offices. These printers can output nylon and metal components that have high mechanical properties. BJ printing uses a bed of binder where the printhead deposits a binding agent. PJ jets and cures droplets of liquid photopolymer materials and can build structures that are composed of multiple types of material.5
3D printing in dentistry
3D printing is most cited in manufacturing (automotive and avionics) and consumer good fields followed by the health field.6 In the dental field, the current usage of 3D printers is low according to an American Dental Association (ADA) survey conducted in late 2023 with 17% of dentists owning a 3D printer.7 Yet, the adoption rate is high with those who noted they own a printer, 67% of the dentists have owned the printer for 2 years or less. Additionally, there is interest in this field since 56% of those surveyed noted that they are considering buying a 3D printer or completing training in 3D printing. Manufacturers have been recently rapidly developing new techniques for faster post processing, material sciences, and development of low-cost printers due to the expiration of multiple key patents of additive processes.8
Multiple applications for
additive manufacturing
in dentistry
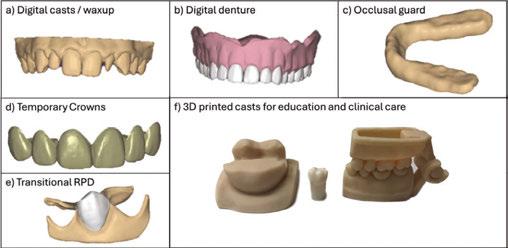
There are many applications of 3D printing in the field of dentistry. For instance, 3D printing can be used to create patient models, dentures, occlusal guards, temporary crowns, transitional RPDs, indirect orthodontic bonding trays, direct print aligners, retainers, surgical guides, implants, mandibular advancement devices, and educational devices (Figure 3). The patient models can be static or articulated and flexibly designed or altered digitally depending on the intended use. 3D printed dentures can offer reduced number of clinical appointments and higher intaglio accuracy, however have reduced esthetics compared with conventional dentures.9 The material properties of occlusal guards are similar to conventional and milled methods. Furthermore, wear resistance is not appreciably different between methods.10 Surgical guides can be used in implant
2: Internal structures of additive manufacturing. The internal structure of this 3D printed model allows for bending that is easier with additive manufacturing compared to subtractive manufacturing
Figures 3A-3F: Applications of 3D printing and computer-aided design in general dentistry. Various applications of computer-aided design and subsequent 3D printing for 3A. Patient models and treatment planning mock-up. 3B. Complete dentures. 3C. Occlusal guards. 3D. Temporary crowns. 3E. Transitional RPDs, and 3F. Articulated patient models and scaled models for education (please note that the typodont tooth in the middle is used for scale purposes and is not 3D printed)
placement, complicated root canal morphology, and complex craniofacial surgeries. Static dental implant surgical guides are accurate when 3D printed, however additional factors such as image acquisition with cone beam computed tomography (CBCT), computer aided design (CAD), and slicer software can add errors that affect overall clinical accuracies.11,12
Oral surgery applications
Alongside restorative dentistry applications, 3D printing has revolutionized surgical aspects of the field by enhancing preoperative planning, patient-specific implant fabrication, and surgical simulation. Specifically, patient-specific anatomical models
SLS Powder (nylon, metal)Heat application
$500,000Functional prototypes with high mechanical properties
$30,000Consumer electronics, multi-material medical models or dentures
Washing, curing, support removal
Depowdering, media blasting
Curing or sintering (depending on material)
Dissolvable support removal
Figure
Table 1: Common types of 3D printing techniques
derived from CT or MRI scans enable surgeons to visualize complex structures, which facilitates precise surgical planning and reduces intraoperative errors.13 These advancements allow for improved accuracy in complex reconstructions and better overall surgical outcomes.
The most notable developments in oral surgery involve the creation of custom implants and prosthetics. Advances in material science have allowed for implantable materials that are compatible with 3D printing. For instance, when using the inert material polyetheretherketone (PEEK), osseointegration can be increased using FDM with tunable porosity for diffusion of cells within the microstructure.14 Additionally, 3D-printed surgical guides allow for precise bone cutting and implant placement, further improving surgical efficiency and accuracy.15
Nevertheless, 3D-printed implants have raised concerns among clinicians regarding stress shielding for ceramic materials, long-term remodeling of the bone, and causing a potential immune response.16 Addressing these issues, novel bioprinting techniques are emerging with potential applications in tissue engineering for cartilage and bone regeneration in reconstructive head and neck surgeries.17 These bioprinted constructs aim to better replicate the mechanical properties of native bone while promoting host-derived healing and reducing the risk of immune rejection.18
As 3D printing technology continues to evolve, its applications in surgery are expanding, offering significant promise for future surgical innovations. With the ongoing development of bioprinting and improvements in material science, the integration of 3D printing in dental surgery is expected to further enhance surgical precision, reduce complications, and improve patient outcomes.
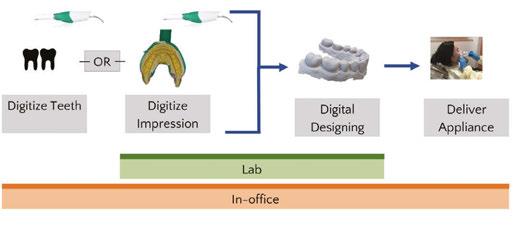
Clinical workflow for chairside 3D printing
The integration of these applications in a dental office might vary based on the device that is printed. Generally, the teeth are digitized and altered within a digital design software program and subsequently sent to a 3D printer. Given the cost of SLA/ DLP printers, it is more practical to complete all steps chairside instead of sending impressions to a traditional lab. The decision of how to complete these steps also depends on the materials required. Chairside 3D printing has been shown to be less time consuming, more cost efficient, and display similar trueness compared with lab-fabricated single unit crowns using subtractive methods.19
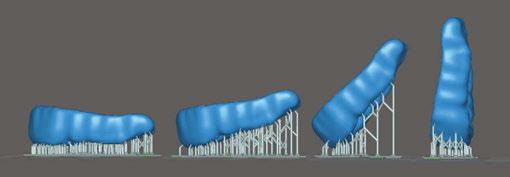
For SLA/DLP printing there are four main steps that deviate from milling: 1) slicing software and G-code creation, 2) 3D printing via vat polymerization, 3) isopropyl wash, and 4) final cure. The initial step after digitally designing the appliance is importing the digital file — usually in standard tessellation language file type (stl). This triangulated mesh surface geometry is encoded by slicing software that identifies the movements and curing protocols of the 3D printer based on user inputs (G-code). Figure 5 shows an example of an occlusal guard in multiple print orientations within the slicer software. The print orientation will affect material properties such as accuracy, strength, surface roughness, and microbial adhesion.21 For example, a dental model has been shown to have better material properties in a horizontal orientation (0°), however, mass-producing dental models in the vertical orientation in dental labs allows for sub-
stantially higher throughput yet sacrifices trueness and surface quality. There are also additional factors such as layer thickness and material property that affect the final outcome.22
After slicing the stl, the automatically generated G-code can be used to operate the 3D printer. Within the context of a SLA/ DLP printer, there is a range of resins that can be used. The manufacturers are required to seek Food and Drug Administration (FDA) clearance for each indication of use.23 Therefore, there will be a set of materials that have been tested for the specific indication and are specifically formulated to have the appropriate mechanical properties.
Once printed, the device will have uncured resin surrounding the printed structure. The process of removing the uncured resin and attaining the structure’s final mechanical properties for a finished, functional product is called post-processing. This is completed in two steps: 1) Submerging the structure in isopropyl wash, 2) Curing the structure. The specifics of post-processing depends on the resin material manufacturer and the resin specifications. It is recommended to closely follow these instructions for use because deviations can result in underperforming mechanical properties and biocompatibility.24-26
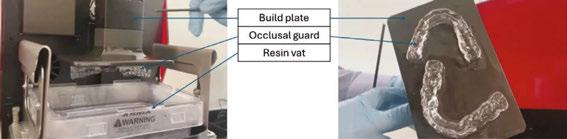
After removing the printed solid from the build plate (Figure 6), the supports (if any) can be removed and excess resin washed off. The most widely used solvent washes are isopropyl alcohol and ethanol. Distributing the solvent evenly over the device is an important step to remove uncured liquid resin that has cytotoxic effects on the body. The exposure and permeation time of these solvents reduces the physical properties of the final product. Therefore, there is a fine balance of washing the structure long enough to reduce cytotoxicity but not too long to decrease its flexural strength.27-28
After the solvent has been completely evaporated, the final cure (post-polymerization) is initiated to complete the polymer-
Figure 4: Chairside and lab workflows for additive manufacturing. There are multiple pathways for lab or chairside fabricated dental appliances using additive manufacturing (Adapted figure20)
Figure 5. Print orientations in slicer software. Occlusal guard in different print orientations from horizontal (0°) [on left of the picture] to vertical (90°) [on right of the picture]
ization reaction. The product is placed in a UV chamber where the temperature, method, and duration will influence the mechanical properties of the end-product. The oxygen-inhibited layer will prevent full polymerization in subsequent steps. For instance, glycerin immersion, nitrogen chamber, and low-pressure vacuum have been methods to reduce the oxygen-inhibited layer. Reducing the oxygen-inhibited layer and reducing viscosity of the resin with higher temperatures has been shown to improve the mechanical properties of the resin.29-30 Generally, an increase of duration and intensity of the UV post-polymerization improves end-product strength.31
The rapid evolution of 3D printing technology is expanding the indications of use, reshaping clinical workflows, and reducing patient case limitations. Ongoing advancements, such as enhanced material properties and increased print speeds, allow for chairside integration. As of 2022, there were approximately 100 rigid and 30 flexible biocompatible resin materials on the market.32 Multiple advanced formulations continue to become FDA cleared, therefore increasing the selections and indications for printing. Additionally, the many types of 3D printing technology allow dental labs to reduce cost and increase throughput.
Future of 3D printing
Bioprinting
Bioprinting, a specialized subset of 3D printing, has gained significant traction in regenerative medicine by enabling the fabrication of functional tissues through layer-by-layer deposition of bioinks containing living cells and biomaterials. This technology has been explored for applications in tissue engineering, drug development, and personalized medicine. Bioprinting has been used to vascularize tissues, skin grafts, and organ models for transplantation and disease modeling.33 The field is rapidly expanding, with research focusing on enhancing cell viability, structural integrity, and biomimetic properties of printed tissues to bridge the gap between laboratory models and clinical applications.34
In dentistry, bioprinting has shown potential for regeneration of soft and hard tissues including bone, cartilage, and mucosa. The development of bioengineered scaffolds infused with stem cells and growth factors has facilitated tooth, periodontal ligament, and alveolar bone regeneration.35-36 In vivo assessments in animal models have been investigated in bone, periodontal ligament, and dentin regeneration with generally positive results.37 As bioprinting technology matures, its integration into clinical practice could revolutionize regenerative treatments in dental surgery by offering patient-specific, bioengineered tissues that improve functional and esthetic outcomes. These tools show promise in maintaining the structural integrity of patient anatomy and in reducing the immune response seen with conventional bone grafts.
Regulation in point-of-care printing
The ability to print custom devices for patients chairside disrupts the traditional workflow of dental offices. Traditionally, dental labs have fabricated all indirect prostheses. However, to maintain patient safety and effectiveness of the devices, the Food and Drug Administration (FDA) has identified software, material, and post-processing controls.38 Because the FDA regulates finished products, it also regulates dental devices at the point of
care. Manufacturers will test their material with specific software along the workflow, and any modifications that a dentist makes to the lawfully marketed device could potentially have safety consequences.39 Due to increased controls by the FDA, free market competition is reduced, thus incentivizing manufacturers to build proprietary systems with higher upfront costs to the dentist. Despite commonly used controls, like quality management systems (i.e., ISO 13485), that are common in the industrial manufacturing sector, the specific guidelines for regulatory requirements for chairside 3D printing are sparce.32
Prototypes and innovation
The benefits of 3D printing for small scale, custom products are a notable reason that this technology fits well in dentistry because the majority of extraorally fabricated devices are patient-specific. As more dentists adopt this technology, the path toward fabricating dental-specific prototypes will increase early stages of innovation. Sites similar to thingiverse (thingiverse. com) or makerworld (makerworld.com) have accelerated userbased innovation and pose a possibility for democratizing supply chains — particularly for spare parts manufacturing.40 A recent example showing the importance of supply chain diversification was demonstrated during the COVID-19 pandemic when many dental offices began printing face shields, masks, and other medical devices as demand exceeded supply inventories.41
Re-thinking the application of current innovations in dental material science allows for boundless iterations of traditional designs. For instance, custom implants that do not require surgery (placement at time of extraction), hollow implants that allow for time-based release of anti-inflammatory mediators, and reductions of thickness or chairside implant printing through SLA compatible zirconium dioxide.42
3D printing technology can also be used in tandem with AI (artificial intelligence) in novel ways.43 For instance, AI frameworks have been used to reduce human error and automate critical steps in 3D-printing processing.44 Additionally, both tools can be used in the full digital workflow to create a dental prosthesis: a generative AI computer-aided design can be automatically created, then 3D printed and fitted to the patient.45-46
Summary
Additive manufacturing has multiple applications that are currently used in dental offices. There are still barriers for wide adoption, however the application of a personalized manufacturing approach combined with 3D technologies fits well into a digital clinical workflow. In order to adopt 3D printing in dentistry, an understanding of the different additive technologies and available materials is important. Each type of 3D printing
Figure 6. Anatomy of SLA/DLP vat resin type printer. Images of an SLA/DLP vat resin = printer with associated labels for a) build plate that adheres to the printed device, b) occlusal guards as an example of a printed device, c) resin vat of splint-specific uncured liquid resin
technology has different upfront costs that can preclude its use in a dental clinic. Additionally, the post-processing criteria will vary on the type of print technology selected. Based on current research, 3D printing technology has the potential to reduce time spent and incurred costs for a semi-automated solution of custom dental prostheses.
REFERENCES
1. Pei E, Kabir IR, Leutenecker-Twelsiek B. History of AM. In: Springer Handbook of Additive Manufacturing. 2023 Oct 18 (pp. 3-29). Cham: Springer International Publishing.
2. Sakin M, Kiroglu YC. 3D Printing of Buildings: Construction of the Sustainable Houses of the Future by BIM. Energy Procedia. 2017 Oct 1;134:702-711.
3. Gu Q, Hao J, Lu Y, Wang L, Wallace GG, Zhou Q. Three-dimensional bio-printing. Sci China Life Sci. 2015 May;58(5):411-9. doi: 10.1007/s11427-015-4850-3. Epub 2015 Apr 29.
4. D’Aveni R. The 3-D printing revolution. Harvard Business Review. 2015 May;93(5):40-48.
5. Jakus AE. An introduction to 3D printing—past, present, and future promise. In: 3D printing in Orthopaedic Surgery. Elsevier;Jan 2019:1-15. doi:10.1016/B978-0-323-58118-9.00001-4.
6. Ukobitz DV. Organizational adoption of 3D printing technology: a semisystematic literature review. Journal of Manufacturing Technology Management. 2021 Dec 17;32(9):48-74.
7. Revilla-León M, Frazier K, da Costa J, Haraszthy V, Ioannidou E, MacDonnell W, Park J, Tenuta LM, Eldridge L, Vinh R, Kumar P. Prevalence and applications of 3-dimensional printers in dental practice. J Am Dent Assoc. 2023 Apr 1;154(4):355-356. doi: 10.1016/j.adaj.2023.02.004.
8. Kessler A, Hickel R, Reymus M. 3D Printing in Dentistry-State of the Art. Oper Dent. 2020 Jan/ Feb;45(1):30-40. doi: 10.2341/18-229-L. Epub 2019 Jun 7.
9. Alhallak K, Hagi-Pavli E, Nankali A. A review on clinical use of CAD/CAM and 3D printed dentures. Br Dent J. 2023 Jan 9. doi: 10.1038/s41415-022-5401-5. Epub ahead of print.
10. Valenti C, Federici MI, Coniglio M, Betti P, Pancrazi GP, Tulli O, Masciotti F, Nanussi A, Pagano S. Mechanical and biological properties of polymer materials for oral appliances produced with additive 3D printing and subtractive CAD-CAM techniques compared to conventional methods: a systematic review and meta-analysis. Clin Oral Investig. 2024 Jun 25;28(7):396. doi: 10.1007/s00784-024-05772-6.
11. Ashtiani RE, Ghasemi Z, Nami M, Mighani F, Namdari M. Accuracy of static digital surgical guides for dental implants based on the guide system: A systematic review. J Stomatol Oral Maxillofac Surg. 2021 Dec 1;122(6):600-6077. doi: 10.1016/j.jormas.2020.10.010.
12. Juneja M, Thakur N, Kumar D, Gupta A, Bajwa B, Jindal P. Accuracy in dental surgical guide fabrication using different 3-D printing techniques. Additive Manufacturing. 2018 Aug 1;22:243-255. doi: 10.1016/j.addma.2018.05.012.
13. Javaid M, Haleem A, Singh RP, Suman R. 3D printing applications for healthcare research and development. Glob Health J [Internet]. 2022;6(4):217–226. http://dx.doi.org/10.1016/j. glohj.2022.11.001.
14. Rendas P, Figueiredo L, Machado C, Mourão A, Vidal C, Soares B. Mechanical performance and bioactivation of 3D-printed PEEK for high-performance implant manufacture: a review. Prog Biomater [Internet]. 2022;12(2):89–111. Available from: http://dx.doi.org/10.1007/ s40204-022-00214-6.
15. Wu P, Hu L, Li H, Feng L, Liu Y, Zhang S, Li XC, Zhang ML, Yang SY, Lu RJ. Clinical application and accuracy analysis of 3D printing guide plate based on polylactic acid in mandible reconstruction with fibula flap. Ann Transl Med [Internet]. 2021;9(6):460. Available from: http:// dx.doi.org/10.21037/atm-20-6781.
16. Zhao M, Xiong G, Fang Q, Dong X, Wang F, Han Y, Shen Z, Wang FY. Enlarge the Error Prediction Dataset in 3-D Printing: An Unsupervised Dental Crown Mesh Generator. IEEE Transactions on Computational Social Systems. Dec 2024;PP99:1-12. doi:10.1109/ TCSS.2024.3417388.
17. Chia HN, Wu BM. Recent advances in 3D printing of biomaterials. J Biol Eng [Internet]. 2015;9(1):4. Available from: http://dx.doi.org/10.1186/s13036-015-0001-4.
18. Hollister SJ. Porous scaffold design for tissue engineering. Nat Mater [Internet]. 2005;4:518–524. Available from: https://www.nature.com/articles/nmat1421.
19. Mangano FG, Cianci D, Pranno N, Lerner H, Zarone F, Admakin O. Trueness, precision, time-efficiency and cost analysis of chairside additive and subtractive versus lab-based workflows for manufacturing single crowns: An in vitro study. J Dent. 2024 Feb;141:104792. doi: 10.1016/j.jdent.2023.104792. Epub 2023 Nov 25.
20. Glick A and Flamenco D. Clinical application and implementation of 3D Printing. J Greater Houston Dent Soc. 2023; 94(4):16-19.
21. Shim JS, Kim JE, Jeong SH, Choi YJ, Ryu JJ. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J Prosthet Dent. 2020 Oct;124(4):468-475. doi: 10.1016/j.prosdent.2019.05.034. Epub 2019 Dec 4.
22. Alghauli MA, Almuzaini SA, Aljohani R, Alqutaibi AY. Impact of 3D printing orientation on accuracy, properties, cost, and time efficiency of additively manufactured dental models: a systematic review. BMC Oral Health. 2024 Dec 26;24(1):1550. doi: 10.1186/ s12903-024-05365-5.
23. Da Silva TM, Immich F, De Araujo TS, Lund RG, Da Silva AF, Piva E, Da Rosa WLO. Photosensitive resins used in additive manufacturing for oral application in dentistry: A scoping review from lab to clinic. J Mech Behav Biomed Mater. 2023 May;141:105732. doi:10.1016/j.
jmbbm.2023.105732. Epub 2023 Mar 1.
24. Cao J, Liu X, Cameron A, Aarts J, Choi JJE. Influence of different post-processing methods on the dimensional accuracy of 3D-printed photopolymers for dental crown applicationsA systematic review. J Mech Behav Biomed Mater. 2024 Feb;150:106314. doi: 10.1016/j. jmbbm.2023.106314. Epub 2023 Dec 12.
25. Vasques MT, Mulder JN, Machado DS, Lagana DC. The influence of the post-processing method on knoop hardness of photosensitive resins for 3D SLA printer used in Dentistry. Clinical and Laboratorial Research in Dentistry. 2019 Dec 31. Available at: https://www.revistas. usp.br/clrd/article/view/161294.
26. Cabrol A, Chuy V, Fron-Chabouis H, Naveau A. Effectiveness of postprocessing on 3D printed resin biocompatibility in prosthodontics: A systematic review. J Prosthet Dent. 2024 Sep 19:S0022-3913(24)00588-2. doi: 10.1016/j.prosdent.2024.08.014. Epub ahead of print.
27. Xu Y, Xepapadeas AB, Koos B, Geis-Gerstorfer J, Li P, Spintzyk S. Effect of post-rinsing time on the mechanical strength and cytotoxicity of a 3D printed orthodontic splint material. Dent Mater. 2021 May;37(5):e314-e327. doi: 10.1016/j.dental.2021.01.016. Epub 2021 Feb 18.
28. Hwangbo NK, Nam NE, Choi JH, Kim JE. Effects of the Washing Time and Washing Solution on the Biocompatibility and Mechanical Properties of 3D Printed Dental Resin Materials. Polymers (Basel). 2021 Dec 16;13(24):4410. doi: 10.3390/polym13244410.
29. Kim YJ, Kim HN, Kim DY. A study on effects of curing and machining conditions in post-processing of SLA additive manufactured polymer. Journal of Manufacturing Processes. 2024 Jun 15;119:511-519. doi:10.1016/j.jmapro.2024.03.112.
30. Lim JH, Lee SY, Gu H, Jin G, Kim JE. Evaluating oxygen shielding effect using glycerin or vacuum with varying temperature on 3D printed photopolymer in post-polymerization. J Mech Behav Biomed Mater. 2022 Jun;130:105170. doi: 10.1016/j.jmbbm.2022.105170. Epub 2022 Mar 13.
31. Lin YC, Tarrazzi D, Schoenbaum T, Knoernschild K. Effect of postprocessing parameters on the flexural strength of vat-polymerized additively manufactured interim fixed dental prostheses: A systematic review with postprocessing guidelines. J Prosthet Dent. 2024 Aug 13:S00223913(24)00497-9. doi: 10.1016/j.prosdent.2024.07.016. Epub ahead of print.
32. Guttridge C, Shannon A, O’Sullivan A, O’Sullivan KJ, O’Sullivan LW. Biocompatible 3D printing resins for medical applications: A review of marketed intended use, biocompatibility certification, and post-processing guidance. Annals of 3D Printed Medicine. 2022 Mar 1;5:100044. https://doi.org/10.1016/j.stlm.2021.100044.
33. Murphy SV, Atala A. 3D bioprinting of tissues and organs. Nat Biotechnol [Internet]. 2014;32:773–785. Available from: https://www.nature.com/articles/nbt.2958.
34. Groll J, Burdick JA, Cho D-W, Derby B, Gelinsky M, Heilshorn SC, Jüngst T, Malda J, Mironov VA, Nakayama K, Ovsianikov A, Sun W, Takeuchi S, Yoo JJ, Woodfield TBF. A definition of bioinks and their distinction from biomaterial inks. Biofabrication [Internet]. 2018;11(1):013001. doi: 10.1088/1758-5090/aaec52Available from: http://dx.doi.org/10.1088/1758-5090/aaec52.
35. Morrison DG, Tomlinson RE. Leveraging Advancements in Tissue Engineering for Bioprinting Dental Tissues. Bioprinting. 2021 Aug;23:e00153. doi: 10.1016/j.bprint.2021.e00153. Epub 2021 Jun 13.
36. Ostrovidov S, Ramalingam M, Bae H, Orive G, Fujie T, Shi X, Kaji H. Bioprinting and biomaterials for dental alveolar tissue regeneration. Front Bioeng Biotechnol. 2023 Apr 14;11:991821. doi: 10.3389/fbioe.2023.991821.
37. Mohd N, Razali M, Fauzi MB, Abu Kasim NH. In Vitro and In Vivo Biological Assessments of 3D-Bioprinted Scaffolds for Dental Applications. Int J Mol Sci. 2023 Aug 17;24(16):12881. doi: 10.3390/ijms241612881.
38. Food and Drug Administration. Technical considerations for additive manufactured medical devices: guidance for industry and food and drug administration staff. 2017. Accessed 3/19/2025 at: https://www.fda.gov/media/97633/download
39. Kuo RF, Lin YS, Yang TH, Nguyen AT. 3D printing: limitations, safety, and regulatory considerations for oral health science. In: 3D Printing in Oral Health Science: Applications and Future Directions 2022 Sep 27: 269-291. Cham: Springer International Publishing. 10.1007/978-3-031-07369-4_13.
41. Longhitano GA, Nunes GB, Candido G, da Silva JVL. The role of 3D printing during COVID-19 pandemic: a review. Prog Addit Manuf. 2021;6(1):19-37. doi: 10.1007/s40964-020-00159-x. Epub 2020 Nov 24.
42. Joda T, Yeung AWK, Hung K, Zitzmann NU, Bornstein MM. Disruptive Innovation in Dentistry: What It Is and What Could Be Next. J Dent Res. 2021 May;100(5):448-453. doi: 10.1177/0022034520978774. Epub 2020 Dec 16.
43. Glick A, Tipton N, Manila N, Chang J. AI in implant dentistry: clinical implementation and considerations for use. Implant Practice US. 2024;17(1):20-24, Quiz 25.
44. Martinez G, Huang K, Lou Y, Bai Y. Innovative Applications of AI and 3D Printing in Digital Dentistry: Enhancing Accuracy and Efficiency in Dental Care. In: 2024 International Conference on Identification, Information and Knowledge in the Internet of Things (IIKI). 2024 Dec 6:237-242. 10.1109/IIKI65561.2024.00048.
45. Chau RCW, Chong M, Thu KM, Chu NSP, Koohi-Moghadam M, Hsung RT, McGrath C, Lam WYH. Artificial intelligence-designed single molar dental prostheses: A protocol of prospective experimental study. PLoS One. 2022 Jun 2;17(6):e0268535. doi: 10.1371/journal. pone.0268535.
46. Zhao X, Li N, Zhang Z, Hong J, Zhang X, Hao Y, Wang J, Xie O, Zhang Y, Li H, Liu M, Zhang P, Ren X, Wang X. Beyond hype: unveiling the Real challenges in clinical translation of 3D printed bone scaffolds and the fresh prospects of bioprinted organoids. J Nanobiotechnology [Internet]. 2024;22(1):500. Available from: http://dx.doi.org/10.1186/s12951-024-02759-z.
Continuing Education Quiz
Clinical applications and innovations of 3D printing in dentistry and dental implants
GLICK/MOIN/ABBASSI
1. ________ printing is the most widely used type of printing that melts a thermoplastic filament.
a. Fused deposition modeling (FDM)
b. Selective laser sintering (SLS)
c. Powder binder jetting (BJ)
d. Digital light projection (DLP)
2. Manufacturers have been recently rapidly developing new techniques for _________ due to the expiration of multiple key patents of additive processes.
a. faster post processing
b. material sciences
c. development of low-cost printers
d. all of the above
3. 3D printing can be used to create patient models, _______, transitional RPDs, indirect orthodontic bonding trays, direct print aligners, retainers, surgical guides, implants, mandibular advancement devices, and educational devices.
a. dentures
b. occlusal guards
c. temporary crowns
d. all of the above
4. Specifically, patient-specific anatomical models derived from ________ enable surgeons to visualize complex structures, which facilitates precise surgical planning and reduces intraoperative errors.
a. 2D digital imaging
b. panoramic imaging
c. CT or MRI scans
d. impressions
5. 3D-printed surgical guides allow for precise bone cutting and implant placement, further improving surgical efficiency and accuracy.
a. True
b. False
6. For _________ there are four main steps that deviate from milling: 1) slicing software and G-code creation, 2) 3D printing via vat polymerization, 3) isopropyl wash, and 4) final cure.
a. PEEK printing
b. SLA/DLP printing
c. powder-binder jetting
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: June 30, 2025
Expiration Date: June 30, 2028 2 CE CREDITS
d. photopolymer jetting
7. The specifics of post-processing depends on ________.
a. the resin material manufacturer
b. the resin specifications
c. microbial adhesion
d. both a and b
8. _________, a specialized subset of 3D printing, has gained significant traction in regenerative medicine by enabling the fabrication of functional tissues through layer-by-layer deposition of bioinks containing living cells and biomaterials.
a. Bioprinting
b. Microbial adhesion
c. Static surgical guides
d. Slicer software
9. To maintain patient safety and effectiveness of the devices, the _______ has identified software, material, and post-processing controls.
a. American Dental Association
b. Food and Drug Administration (FDA)
c. Environmental Protection Agency
d. National Institutes of Health
10. AI frameworks have been used to reduce human error and automate critical steps in 3D-printing processing.
a. True
b. False
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Dentistry management essentials: leading specialty practices to success
Ali Oromchian, JD, LLM, offers guidance on creating a less stressful and more productive environment in the dental practice
Whether a clinician is placing implants, straightening teeth, or performing root canals, the way the office runs behind the scenes can be as important as the clinical care. Patients expect top-tier clinical expertise, but they also want a smooth, stress-free experience — from the moment they walk in to the time they leave. When applied consistently, good leadership and smart practice management can turn a busy office into a thriving one.
The strategies discussed in this article focus on the everyday realities of managing a specialty dental office. From hiring the right people to coaching your team and staying on top of compliance, these core principles help create a well-run, positive environment for patients and employees.
Laying the foundation: understanding practice management in specialized dentistry
The unique challenges of specialty practices
According to the American Dental Association, more than 1 in 5 dentists are specialists.1 Unlike many general dental clinics, specialty practices often see a narrower range of patients who have specific conditions or needs requiring advanced procedures. For example, an endodontic practice may handle fewer but more complex root canal treatments, whereas an orthodontic clinic must manage lengthy patient relationships throughout multi-year treatment plans.
In addition, since specialists depend on regular referrals to grow their practices, effective communication with referring doctors, clear treatment protocols, and well-coordinated follow-up are crucial for fostering trust and ensuring ongoing patient inflow. This reliance on professional networks shows the
Ali Oromchian, JD, LLM, is the founding attorney of the Dental & Medical Counsel, PC law firm and is renowned for his expertise in legal matters pertaining to dentists. Oromchian has served as a key opinion leader and legal authority in the dental industry with dental CPAs, consultants, banks, insurance brokers, and dental supplies and equipment companies. He serves as a legal consultant for numerous dental practice management firms that rely on his expertise for their clients’ businesses. He is also recognized as an exceptional speaker and educator who simplifies complex legal topics and has lectured extensively throughout the United States. To contact Ali Oromchian and the HR for Health team, please email hello@hrforhealth.com.
Disclosure: Ali Oromchian, JD, LLM, is CEO and Co-Founder of HR for Health. The author reports no other financial relationships related to products or services mentioned in this article.
Educational aims and objectives
This self-instructional course for dentists aims to discuss fundamental management principles for specialty dental practices, highlighting leadership, hiring, coaching, and compliance strategies that foster a cohesive and productive environment.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can: Identify the unique operational challenges of specialty dental practices and how to address them.
• Recognize core leadership principles that enhance accountability, engagement, and patient satisfaction.
• Realize the importance of structured hiring and onboarding for long-term team success.
• View methods for establishing and monitoring key performance indicators (KPIs) to drive practice growth.
• Appreciate approaches to maintaining a positive workplace culture, reducing stress, and mitigating legal risks.
2 CE CREDITS
importance of establishing and maintaining a reputation for clinical excellence and organizational efficiency.
Defining clear goals and vision for the specialty practice
Every practice benefits from clarity of purpose. A straightforward mission statement keeps everyone on the same page, whether that mission emphasizes best-in-class orthodontic care for adolescents or cutting-edge implant procedures for adult patients. Translating this overarching mission into concrete, measurable targets helps team members align daily tasks with broader practice goals.
For instance, a pediatric dental practice might set a goal to reduce patient anxiety by a specified percentage over a 6-month period. To achieve this, leadership might implement new behavioral management training or invest in child-friendly operatory designs. The same is true for other specialty practices that may see patients who may have increased anxiety because of their upcoming treatment. By defining specific goals and mapping out the steps required to achieve them, specialty practices ensure
that their vision is a central guiding force in clinical and administrative decision-making.
Leadership 101: key principles for specialty dentists
Establishing a leadership style
In any dental setting, leadership style directly influences the workplace atmosphere. Common leadership approaches include:
• Authoritative: Centralized decision-making, well-suited for high-stakes or urgent scenarios (e.g., a complex implant surgery needing immediate clarity on procedural steps).
• Coaching: Leaders guide employees through questions and feedback, encouraging professional growth (beneficial for new team members in a practices learning advanced technology).
• Democratic: Encourages collective input and consensus-building, useful when team buy-in is essential (e.g., reorganizing patient flow in a busy office).
A one-size-fits-all leadership approach rarely works. Instead, effective leaders adapt their style to the practice’s current stage of growth and the specific makeup of their team. Periodic self-evaluation and employee feedback can pinpoint which leadership tactics are working and where adjustments are needed.
Creating a culture of accountability
Accountability begins at the top. When leaders model punctuality, thorough recordkeeping, and patient-centered care, team members are more likely to follow suit. Clinicians should regularly review assigned tasks to confirm they are being completed on time and properly and encourage employees to take ownership of their responsibilities by clearly delineating roles and establishing transparent expectations in an employee handbook.
To embed accountability into daily routines, consider implementing:
• Task checklists: For example, implement a sterilization protocol checklist that must be completed before each shift ends.
• Progress updates: Brief daily or weekly huddles that help the group track ongoing initiatives and resolve potential bottlenecks.
• Open-door policies: Employees can discuss concerns, mistakes, or feedback without fear of repercussion, promoting a supportive learning environment.
Hiring
and onboarding strategies for a highperforming team
Despite offering wage increases to both hygienists and dental assistants over the past year, specialty practices — like their general dentistry counterparts — continue to face major hiring challenges.
According to a June 2023 poll from the ADA Health Policy Institute of about 1,100 dentists, 94.5% of those recruiting dental hygienists found it “very” or “extremely” difficult to fill vacancies, while 83.7% reported the same for dental assistants. Notably, 4 in 5 responding practice owners increased wages for
these roles, with most wage hikes ranging from 4% to 6%, yet the staffing gap persists.2
A May 2021 poll likewise showed that 35.8% of surveyed dentists were seeking assistants, 28.8% were seeking hygienists, and more than 80% found recruitment for both positions to be very or extremely challenging. These shortages, which predated COVID-19, have been further intensified by early retirements, safety concerns, and higher salary expectations, leaving many specialty practices struggling to attract and retain the skilled team members necessary for efficient operations.3
Effective recruitment for specialized skill
sets
Specialty dental practices often require team members with a deeper or more nuanced skill set than general dental offices. When writing job descriptions, highlight the core clinical and administrative abilities needed for that specialty. This clarity helps candidates self-select based on their experience and also ensures you attract the right talent. During the interview process, ask scenario-based questions that reveal how a candidate might handle specialty-specific tasks, such as managing sedation protocols in a pediatric practice or tracking inventory for implant, endodontic, or orthodontic components.
Comprehensive orientation and training
A strong onboarding process does more than educate new hires on practice policies; it helps them feel confident and part of the team from day one. Try to pair each newcomer with a seasoned employee who can act as a mentor during the initial weeks. This allows new employees to quickly learn the nuances of daily operations, from patient check-in procedures to specialized clinical workflows.
Orientation should cover:
• Clinical guidelines: Specialty-specific protocols, infection control measures, and charting processes.
• Communication standards: Preferred channels for interoffice messaging, meeting cadences, and conflict-resolution procedures.
When well executed, comprehensive orientation and training set a tone of professionalism and structure that bolsters both employee retention and patient satisfaction. Employee retention is incredibly important, as the cost of hiring a new dental employee can be three to four times that position’s overall salary.4
Coaching, mentorship, and ongoing development
Building a coaching culture
Continuous improvement is at the heart of high-performing dental teams. Coaching is better than traditional top-down instruction by fostering a two-way dialogue that benefits both the instructor and the learner. In a coaching culture, senior team members regularly share best practices with junior employees, and open communication channels allow everyone to contribute ideas for refining processes or enhancing patient care.
Encourage short, focused feedback sessions to address issues as they arise. Rather than waiting for an annual review, a quick “check-in” after a challenging case or a complex surgery can solidify learning and reinforce positive behavior. This supportive, real-time feedback model keeps employees engaged, motivated, and aligned with the practice’s mission.
Performance reviews and professional growth plans
While informal feedback is valuable, structured performance reviews remain a cornerstone of comprehensive team development. These reviews typically occur semi-annually or annually and offer an opportunity for leaders and employees to jointly assess progress, celebrate successes, and set new benchmarks.
When preparing for a performance evaluation, gather data on key metrics like:
• Treatment acceptance rates for front-office employees or patient coordinators.
• Quality of clinical notes and adherence to safety protocols.
• Patient satisfaction scores or feedback directly tied to an employee’s responsibilities.
Following the review, collaborate with each team member to create an individualized professional growth plan. This plan might include attending relevant continuing education courses, cross-training in other specialty services, or participating in leadership workshops.
Team dynamics and communication
Establishing clear roles and responsibilities
A specialty practice often employs team members with overlapping skill sets. For instance, an orthodontic practice may have multiple treatment coordinators, each handling digital impressions, bracket changes, and patient education. To avoid confusion and duplicate effort, explicitly define each individual’s duties, authority level, and accountability.
Job descriptions should be updated regularly as the practice grows or introduces new technologies. Clear boundaries and well-communicated responsibilities minimize task redundancy, reduce mistakes, and improve efficiency. For instance, if a treatment coordinator’s primary role is to educate patients (or their parents) on sedation options and post-op care, that information must be spelled out so other team members understand to whom they should direct relevant questions.
Conflict
resolution and collaboration tools
Even well-managed practices encounter interpersonal tension. Whether it’s a disagreement about employee scheduling or a miscommunication on clinical protocols, conflicts can esca-
Continuous improvement is at the heart of high-performing dental teams.”
late if not addressed promptly. Adopting a step-by-step approach to conflict resolution can keep issues from harming team morale or patient care:
1. Acknowledge the conflict: Encourage team members to speak openly and respectfully about the issue.
2. Clarify the underlying problem: Determine if the tension arises from miscommunication, differing priorities, or misunderstandings of role boundaries.
3. Develop a solution: Work collaboratively to find common ground, focusing on how resolving the conflict benefits the patient and the practice.
4. Monitor outcomes: Check back in after a set period to ensure the resolution remains effective.
Modern collaboration tools, such as compliant messaging apps or shared project management boards, also streamline communication and help avert potential misunderstandings. Daily or weekly team huddles can reinforce clarity and ensure everyone has up-to-date information about protocols, appointments, and treatment plans.
Measuring
success: key performance indicators (KPIs) for specialty practices
Clinical versus business metrics
Balancing patient care with business finances is a constant juggling act for specialty dentists. Tracking both clinical and financial metrics can reveal hidden inefficiencies or highlight effective strategies. Examples of KPIs relevant to specialty practices include:
• Treatment acceptance rate: This is especially crucial for practices where high-value procedures often require detailed patient education and financing.
• Patient retention and recall: For offices that typically rely on recurring visits, tracking retention rates helps gauge satisfaction and loyalty.
• Average production per patient: Offers insights into how effectively the team communicates and provides bundled or adjunctive treatments.
• Net Promoter Score (NPS): Reflects how likely patients are to recommend the practice to peers in their community, often correlating with overall patient experience.
Tracking
progress and refining strategies
Data interpretation is just as important as data collection. Holding monthly or quarterly KPI reviews provides a structured opportunity to celebrate achievements and identify areas needing course correction. For instance, if a specialty practice notices a decline in patient referrals from general dentists, leadership can investigate whether the issue stems from longer patient wait times, communication breakdown, or external market factors.
After analyzing data, scheduling protocols can be adjusted, employee training refined, or new marketing efforts deployed. This continuous improvement cycle — assess, adjust, and advance — keeps a practice agile in a competitive and evolving healthcare environment. According to the Bureau of Labor and Statistics, the dental industry is projected to grow at 5 percent per year between 2023 and 2033, highlighting the need for versatile, responsive dental practices.6
Maintaining a positive practice culture
Stress management and burnout
prevention
Long appointments, anxious patients, and complex treatments can heighten stress levels in a specialty dental setting. Whether it’s a busy clinic with intricate surgical schedules or a practice balancing dozens of active treatment plans, employee burnout remains an ongoing concern. A stressed-out team not only affects office morale but can also compromise patient safety and satisfaction.
In one study investigating psychological health among dentists, 63% of respondents reported feeling burned out.5 These findings underscore how chronic workplace stress not only diminishes office morale but can also compromise patient safety and satisfaction.
Practical strategies include:
• Streamlined workflow: Use technology to automate routine tasks like appointment reminders or supply ordering, reducing clerical burdens.
• Wellness initiatives: Provide access to stress-management resources (e.g., seminars on mindfulness, short meditation breaks, or Employee Assistance Programs).
• Time off and flexibility: Offer flexible scheduling or adequate time off to recuperate between busy patient sessions.
Risk management and legal considerations
Employment law basics for specialty practices
Specialty practices often face the same employment laws as general dental offices but with unique twists, such as employing specialized assistants with additional licensure requirements. To stay compliant:
1. Stay informed: Follow state and federal guidelines for wage-and-hour regulations, breaks, overtime, and licensure requirements.
2. Create clear policies: Document attendance expectations, disciplinary procedures, and confidentiality standards in your employee handbook.
3. Seek professional guidance: Complex matters, such as handling workplace harassment complaints or ensuring Americans with Disabilities Act (ADA) compliance, often require legal counsel or specialized HR services.
Failure to comply can lead to legal penalties, reputational damage, and diminished employee morale, so proactive risk management is a must.
Documentation and compliance essentials
Thorough documentation is a non-negotiable aspect of practice management, from medical record-keeping to employee
Additional resources
• Take your handbooks from helpful to heroic: https://bit.ly/4joNI05
• How to Write Job Descriptions for Your Healthcare Employees: https://bit.ly/4i8fUmZ
• Onboarding Best Practices in Healthcare: https://bit.ly/42aUjFO
files. Detailed charting is critical for patient care and insurance claims while also protecting against possible legal issues. Specialty offices, which frequently involve multi-visit treatment plans, should maintain clear records of patient progress, informed consent, and any modifications to the planned procedure.
Investing in HR software, like that of HR for Health, can streamline these processes, ensuring that HR files are easy to access, properly backed up, and compliant with privacy regulations like HIPAA. With all employee records stored in one secure, digital location, practice owners and managers can quickly retrieve essential documents when needed — whether for audits, legal compliance, or internal reviews.
In the staffing domain, consistent paperwork around credentials, performance reviews, and continuing education fosters transparency and accountability. A well-organized HR system also reduces the risk of misplaced or incomplete files, helping avoid compliance issues that could lead to costly penalties or operational disruptions. HR compliance is key, and investing in advanced software to streamline processes and limit opportunities for human error can help make these goals a reality.
Key takeaways
Leading a specialty dental practice requires seamlessly merging clinical expertise with adept management. From defining clear goals and leadership styles to establishing robust hiring and onboarding protocols, every aspect of operations influences patient experiences and internal team well-being. By embracing a coaching culture, measuring progress through KPIs, and diligently managing legal and compliance risks, specialists set the stage for sustainable growth and a positive work environment.
• Don’t just manage your team. Make it better: https://bit.ly/3EiCmfk IP
REFERENCES
1. American Dental Association. “Dentist Workforce: Percentage of Dentists by Specialty.” American Dental Association, 2023, https://www.ada.org/resources/research/ health-policy-institute/dentist-workforce#:~:text=What%20percentage%20of%20 dentists%20are,is%20an%20ADA%2Drecognized%20specialty.
2. American Dental Association. “Recruiting Hygienists, Assistants Still Challenging for Practice Owners.” July 2023, https://adanews.ada.org/ada-news/2023/july/recruitinghygienists-assistants-still-challenging-for-practice-owners/.
3. American Dental Association. “Dentists Face Applicant Shortages as They Emerge from COVID-19 Pandemic.” June 2021, https://adanews.ada.org/ada-news/2021/june/ dentists-face-applicant-shortages-as-they-emerge-from-covid-19-pandemic/.
4. Society for Human Resource Management. “The Real Costs of Recruitment.” SHRM, 2023, https://www.shrm.org/topics-tools/news/talent-acquisition/real-costs-recruitment.
5. Two-thirds of dental professionals ‘burnt out and exhausted’. Br Dent J 238, 295–296 (2025). https://doi.org/10.1038/s41415-025-8523-8.
6. U.S. Bureau of Labor Statistics. “Dentists.” Occupational Outlook Handbook, 2022, https://www.bls.gov/ooh/healthcare/dentists.htm.
Continuing Education Quiz
Dentistry management essentials: leading specialty practices to success OROMCHIAN
1. A _________ mission statement keeps everyone on the same page, whether that mission emphasizes best-in-class orthodontic care for adolescents or cutting-edge implant procedures for adult patients.
a. straightforward
b. broadly-written
c. generalized
d. one-size-fits-all
2. A/An ___________ leadership approach includes centralized decision-making, well-suited for high-stakes or urgent scenarios (e.g., a complex implant surgery needing immediate clarity on procedural steps).
a. democrative
b. authoritative
c. coaching
d. one-size-fits-all
3. __________ can pinpoint which leadership tactics are working and where adjustments are needed.
a. Periodic self-evaluation
b. Employee feedback
c. Strict managers
d. both a and b
4. Clinicians should regularly review assigned tasks to confirm they are being completed on time and properly and encourage employees to take ownership of their responsibilities by clearly delineating roles and establishing transparent expectations in an employee handbook.
a. True
b. False
5. When writing job descriptions, ________.
a. keep the descriptions as open-ended as possible to encourage creativity
b. don’t include any tasks that may cause the candidate to feel stressed
c. highlight the core clinical and administrative abilities needed for that specialty
d. avoid creating boring daily routines
6. For the onboarding process, try to ________.
a. pair each newcomer with a seasoned employee who can act as a mentor during the initial weeks
b. give each newcomer space to develop in the workplace on their own terms
c. keep newcomers isolated from the staff so they will not be
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 550
Date Published: June 30, 2025
Expiration Date: June 30, 2028
influenced by office politics
d. pair the newcomer with the last employee hired
7. Employee retention is incredibly important, as the cost of hiring a new dental employee can be _______ that position’s overall salary.
a. two to three times
b. four to five times
c. six to seven times
d. 10 times
8. When updating job descriptions, clear boundaries and well-communicated responsibilities _______.
a. minimize task redundancy
b. reduce mistakes
c. improve efficiency
d. all of the above
9. In one study investigating psychological health among dentists, _______ of respondents reported feeling burned out.
a. 15%
b. 36%
c. 63%
d. 85%
10. ________ is critical for patient care and insurance claims while also protecting against possible legal issues.
a. Detailed charting
b. Weekly huddles
c. Storing employee files in several locations
d. Eliminating automation of routine tasks
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
WSP/AMED 2025
ANNUAL SESSION
“Integrating the Surgical and Restorative Teams for Superior Esthetic Outcomes”
Frank Spear, DDS, MSD
KEYNOTE SPEAKER
“Interdisciplinary Management of Compromised Teeth”
Robert A. Levine, DDS
The “Eight Keys for the Reconstructive Therapy of Peri-Implantitis-Related Intrabony Defects”
Richard Miron, DDS, PhD, dr. med. dent.
“Platelet Rich Fibrin in Combination with Exosomes in Periodontology and Implant Dentistry Abstract”
Homa H. Zadeh, DDS, PhD
“Preventing and Managing Technical & Biologic Complications in Implant Dentistry: Evidence-Based Strategies for Success”
Ali Sajadi, DDS, MSD, FACD, FICD
“Practical Plastics for a Regenerative Tomorrow: Make Alloplasts Great Again”
Fereidoun Daftary, DDS, MSD
“Craniofacial Changes & Aging: Implications for Oral Rehabilitation with Implant Treatment”
Thaer Alqadoumi, DDS, MS
“Biologic Innovations in Sinus Surgery: Amnion Chorion for Schneiderian Membrane Perforation Repair”
Eduardo R. Lorenzana, DDS, MS
“Minimally Invasive Periodontal Therapy: Patient-Centered Practice Satisfaction with the Periodontal Endoscope”
Edward A. Mclaren, DDS, MDC
“CONTEMPORARY MONOLITHIC CERAMICS AND THE DIGITAL DENTAL TEAM: The Evolution of Ceramic Technologies with the Human Touch”
Cherilyn D. Sheets, DDS, W. Peter Nordland DMD, MS, FISPPS, Jean C. Wu, DDS & David Clark, DDS
“The Restoration of the Lost Interdental Papillae Using Collaborative Efforts”
Jim Janakievski, DDS, MSD
Laurence R. Rifkin, DDS
Lora Hooper, RDH
“The Value of a Tooth for Alveolar Ridge Management”
Dr. Yasuko Nemoto, DDS
“Strategies to Enhance the Predictability of Alveolar Ridge Augmentation”
Makoto Ono, DDS
“Exploring the Potential of the Laterally Closed Tunnel Technique in the Treatment of Gingival Recession”
Susan Wingrove, RDH, BS & George Kotsakis DDS, MS
“Peri-implantitis: Prevention, Maintenance, and Evidence-Based Dental Treatment”
Paul P. Chang, DDS, MS
“A Modern Perspective on Managing Peri-Implant Complications and Peri-Implant Diseases”
Dr. Lauralee Nygaard, DDS, MS
“Metabolic Dysfunction and Periodontal Disease”
Irene Marron-Tarrazzi
“Decoding the Anterior Enigma: A Magnified Hacker’s Playbook”
Mario Zuolo, DDS, MSc, PhD
“Microscope and Endodontic Retreatment: The Perfect Match”
Masoud Hasaanzadeh, DDS
“Reaching Deep Defects: The Role of Microscopy in Margin Elevation”
Sadaki Sakamoto, DDS
“Seeing The Trees And Forest-Looking Through A Microscope To See The Overall Picture”
Eason Chen, DDS
“Minimally Invasive Periodontics”
Christopher A. Laing, DDS, FAMED
“The Value of Visual Acuity - The Benefit of Magnification” in Decision Making”
“Aesthetic Dentistry and Cosmetic Surgery…. a Team Algorithm!”
Rashad Riman, DDS
“Mastering the Microscope: Practical Lessons and Transformative Techniques to Elevate Your Practice”
Judy McIntyre, DMD
“Clarity in Endodontics: Treating What You Can See - The Value of 3D! “
Kiyotaka Shibahara, DDS
“The Use of Microscope in Oral Surgery & Implant Therapy”
Andras Forster, DMD, PhD
“Diagnosis and Biomimetic Restoration of Cracked Teeth”
Satish Kumar, DMD, MDSc, MS
“How Periodontal Disease Impacts Systemic Health – A Call to Action”
Dr. Kami Hoss, DDS
“The 2025 Oral Health Revolution: Rethinking Oral Care Products, Ingredients & Protocols”
Kathy Bassett, BSDH, RDH, MEd, QOM, FADHA
“Unconventional Wisdom for Local Anesthesia Success”
Lynn Atkinson, RDH
“Periodontal Protocols Prevail -A Dental Hygienist’s Guide to Excellence in Care”
Jodi Deming, RDH
“Demystifying Biofilms and the Microbiome: The Ultimate Social Network”
Anne Rice, RDH
“Brain Health Matters: Integrating Alzheimer’s Risk Reduction Strategies”
Sherri Lukes, RDH, MS, FAADH
“Medical History Front and Center – Oral Pathologies as Manifestations of Systemic Conditions”
“Cracking the Code: Saliva Diagnostics for Personalized Periodontal and Peri-Implant Care”
Nancy Miller, RDH, BA
“Maximizing Your Power Instrumentation Abilities”
Tricia Osuna, BSDH, RDH, FAADH
“Update Your Products and Protocols for Improved Patient Care”
HANDS-ON WORKSHOPS
SATURDAY, SEPT 13TH • 8AM-5PM
Richard Miron, DDS, PhD, dr. med. dent. Exosomes, PRF, and the Future of Regenerative Medicine/ Dentistry - Member $895...Non-Member $995
SATURDAY, SEPT 13TH • 1PM-5PM
Juan Carlos Ortiz Hugues, DDS, FAMED, CEAS Dental Microscope User Guidelines Course Member $415....Non-Member $495
SUNDAY, SEPT 14TH • 8AM-12PM
Kiaresh Karimi, DDS & Masoud Hasaanzadeh, DDS “Deep Margin Elevation (DME) in Complex Cases with the Copper Band Technique and Luting Indirect Restorations with Pre-heated Composite (Thermo Modified Luting)” Member $425....Non-Member $495
SUNDAY, SEPT 14TH • 9AM-12PM
Juan Carlos Ortiz Hugues, DDS, FAMED, CEAS “Advanced Dental Ergonomics with Ergonomic Loupes” One Price....Only $199
SCAN HERE TO REGISTER! SCAN FOR HOTEL RESERVATIONS!
Dr. Jean Wu
Dr. David Clark
Dr. Jim Janakievski
Dr. Yasuko Nemoto
Lorenzana
Mclaren
Daftary Dr. Cherilyn Sheets Dr.
Nordland
Dr. Makoto Ono Susan Wingrove, RDH
Kotsakis
Chang
Nygaard
Dr. Laurence R. Rifkin
Dr. Christopher Laing
Dr. Irene Marron-Tarrazzi
Dr. Mario Zuolo
Dr. Masoud Hasaanzadeh
Dr. Sadaki Sakamoto
Dr. Eason Chen
Dr. Rashad Riman
Dr. Kiyotaka Shibahara
Dr. Andras Forster
Dr. Juan Carlos Ortiz Hughes
Kathy Bassett, RDH
Lynn Atkinson, RDH
Jodi Deming, RDH
Anne Rice, RDH Sherri Lukes, RDH
Lora Hooper, RDH
Nancy Miller, RDH, BA
Tricia Osuna, RDH Dr. Kami Hoss
Satish Kumar
Dr. Judy McIntyre
Kiaresh Karimi
• In-Network options with major payors and plans
• Out-of-Network when appropriate
• Reliable, timely, predictable results with best rates
• Access to the Nexus Specialty Physician Network
• Nexus billing portal ensures error-free claim submission and tracking
• Personal billing representative
• Complete solution for:
º Implants
º Surgical Guides
º Bone Grafts
º Extractions
º CBCT
Bill Nexus Bill Makes Reimbursement for Medically Necessary Oral Care Simple, Easy and Reliable
Getting reimbursement from medical insurance can be a nightmare for dentists. With the Nexus Bill system, you can avoid the common pitfalls of inconsistent payments, endless delays, constantly fighting with insurance companies, and patients refusing care because you are not “In-Network” for medical.