Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions. ISSN number 2372-8396
Your clinic vibe: the patient experience beyond customer service
Your office vibe is talking. The real question is — what’s it saying about you? You can have the most advanced tools, the most efficient systems, and a rockstar team — but if your clinic “feels” off, your patients feel it too. Before I became an orthodontist, I studied fine arts and interior architecture. So, I see space differently. I notice light, flow, texture, and proportion. But even more than that, I notice how a space feels. And here’s what I’ve come to believe: so do our patients. Even if they don’t have the words to describe it, they’re picking up on everything from the lighting to the temperature to the sound of the front desk phone ringing. They’re asking themselves, “Do I feel welcome here? Is this place clean, calm, cool, warm, or chaotic?” These visceral impressions shape their perception of care before we’ve even started treatment.
Orthodontics today is about more than straight teeth. It’s about the experience, the journey a patient takes from consultation to final scan. And that experience is deeply influenced by the physical environment. The smell of a custom-curated scent versus disinfectant. The warmth of a welcome versus the beep of an iPad. The softness of a chair, the artwork on the walls, the way your team interacts when they don’t think anyone’s watching. It all matters.
And yet, most of us were trained to focus on mechanics and outcomes. We learned how to diagnose and plan, not how to set a mood. But I believe now, more than ever, the mood is part of the plan.
The beauty is, you don’t need a full renovation to elevate your space. It starts with intention. Ask yourself: What do you want your office to feel like? Calm and spalike? Energetic and youthful? High-end? Cozy? Community-driven? Then take a walk through your office with fresh eyes. What do you see? What do you hear? Is the lighting welcoming? Is your seating inviting? Are your spaces cluttered or clear? All these things work together to tell a story, and that story becomes part of the care you deliver.
Patients today want more than great results. They want to feel seen, safe, and comfortable along the way. And when you create a space that truly reflects your values, your personality, and your patient promise, everything aligns. So here’s my challenge to you: Walk through your space tomorrow like a brand-new patient. What do you feel? What do you notice? What story are you telling?
Because you can have the most beautifully executed treatment in the world, but if your space feels cold, chaotic, or impersonal, that’s what your patients will remember. And in today’s world, how your care feels matters just as much as how it turns out. Now go check your vibe!
Dr. Farah Kar (aka The Ortho Queen)
Farah Kar, DDS, MS, MSc, has a background in fine arts and architecture and worked in the design field before changing careers and becoming an orthodontist. She attended the University of Minnesota School of Dentistry for her DDS, Master of Science degree, and Certificate of Orthodontics. She is double-Board certified and a Diplomate of the American Board of Orthodontics and Royal College of Dentists of Canada. Dr. Kar has been an Invisalign®-certified orthodontist since 2014 and an Invisalign Diamond Plus Provider who has treated over 4,000 cases. She enjoys merging her background in fine arts, architecture, and project management with practicing orthodontics efficiently and with flare! Check out Dr. Kar’s Instagram for a snapshot of her life as an orthodontist: @the.ortho.queen
Dr. Farah Kar
Drs. Dara L. Rinchuse and Donald J. Rinchuse reflect
Drs. Aaron Glick, Joseph Ryan, and Elham Abbassi
Cover image of Dr. Jennifer Messenger courtesy of Ormco
Anaphylaxis preparedness in dental practices: what to know to be prepared
J. Wesley Sublett, MD, MPH, Board-Certified Allergist in Louisville, Kentucky, and Donald Cohen, DMD, from New York State, inform dentists on how to approach this dangerous allergic reaction
to
Smiles that Heal. Confidence that Lasts
Embracing Our Warriors began with one powerful question from Dr. Glenn Krieger: That question, and one veteran named Darrel, inspired a movement. After years of service as a Navy special operator, Darrel came to Dr. Krieger not just for orthodontic care, but for a second chance. He was ready to rebuild his life, regain confidence, and return to the workforce.
“How can someone who risked everything for our freedom be left without the support they need to smile again?”
At the same time, nonprofit leader Robin Coen was reshaping another mission. In 2019, she became executive director of Smile for a Lifetime, a national charity providing free braces to children in foster care and low-income homes. She saw how untreated orthodontic issues left kids isolated, bullied, and struggling with selfesteem.
Together, Dr. Krieger and Ms. Coen combined their expertise and passion to launch Embracing Our Warriors. Their mission: to restore confidence and dignity through free orthodontic care for veterans with service-related disabilities and their children. Since launching in 2024, more than 120 volunteer providers have joined the cause, changing lives one smile at a time.
Now, we’re asking the orthodontic community to stand with us. Here’s how you can help:
Orthodontists: Volunteer to treat just one patient a year. Your skill can restore confidence and hope.
Companies & Partners: Make a lasting impact through financial support. Your donation helps cover the cost of essential care and coordination.
The OP Summit Silent Auction: Hosted by Dr. Krieger and the OP Summit, this industry-wide auction benefits both children and veterans. Make in-kind donations of products, trips, and unique experiences.
Bid now or buy today: www.BiddingForGood.com/smile
The ADA cites that “more than 82% of dentists report feeling major stress about their careers.” In this very competitive and quickly changing world, the responsibilities can often feel like the walls of the office are closing in. Recognizing burnout symptoms and taking steps to calm your emotions can make a huge difference.
First, what does burnout feel like? Just a few signs are:
• Feeling tired, emotionally drained, or unenthusiastic
• Often feeling frustration toward work
• Negative outlook
• Problems concentrating
• Getting sick often
It is important to recognize and treat burnout to avoid issues such as heart disease and diabetes, sleep-related disorders, and in some cases, substance misuse.
Some ways to overcome burnout
Lisa Moler Founder/Publisher, MedMark Media
Get enough sleep: We’ve all had our nights of staring at the ceiling in bed while mulling over Plan A, Plan B, Plan C, and more, to solve the next day’s problems. Try to break your non-sleeping cycle. For example, ask your doctor about a possible supplement to lull your brain into the sleep cycle, or discover new relaxation techniques.
Detox from technology: Set specific technology-free windows where patient management systems and email notifications are completely turned off.
Eat and drink for health: Remembering to eat and keeping hydrated helps your brain function (improves memory, attention, and problem solving), raises your mood, and boosts your mental abilities.
Exercise: Exercising has been proven to help fight depression. It doesn’t have to take up much time – about 15-20 minutes per day should do it. A walk along a favorite path, around your neighborhood, on the beach, or even doing yoga or stretching can give your mind some time to reset.
Talk to trusted friends and mentors: There is nothing better than finding out that others can empathize with you and confirm that you are not “crazy.” Colleagues can tell you how they have navigated through similar times of burnout, or give some helpful tips, like reduced hours on Fridays or more intentional spacing of appointments. Look for summer dental retreats or workshops that combine professional development with wellness activities. Aside from work, friends or family can just listen, provide some good advice, or go along on that walk or for a quick cup of coffee and a shoulder to lean on. Finding a therapist can also be very helpful in working out your feelings and providing anti-anxiety techniques.
Give yourself a break: When you feel that burnout starting to eat away at your stomach lining, decide how you will take care of yourself at that moment. Take a few seconds. Grab your journal, and write a few lines. Go outside of the office and breathe some fresh air or look at the scenery. Research shows even 20 minutes of nature exposure significantly reduces cortisol levels. For more extreme situations, taking one day or a few days off, or a more extended vacation can bring you back with renewed spirits.
The ADA has some interesting resources just for dentists on its Wellness Resources page (https://www.ada.org/resources/practice/wellness) to help you start dealing with burnout. You can’t always control what happens in your office, but you can control the way you cope, put out those every day inner fires, and move forward to a fulfilling future with a positive outlook.
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
1 year (4 issues) $149 https://orthopracticeus.com/subscribe/
Breaking the bonding barrier: a new era with Ormco™ EtchFree Bonding
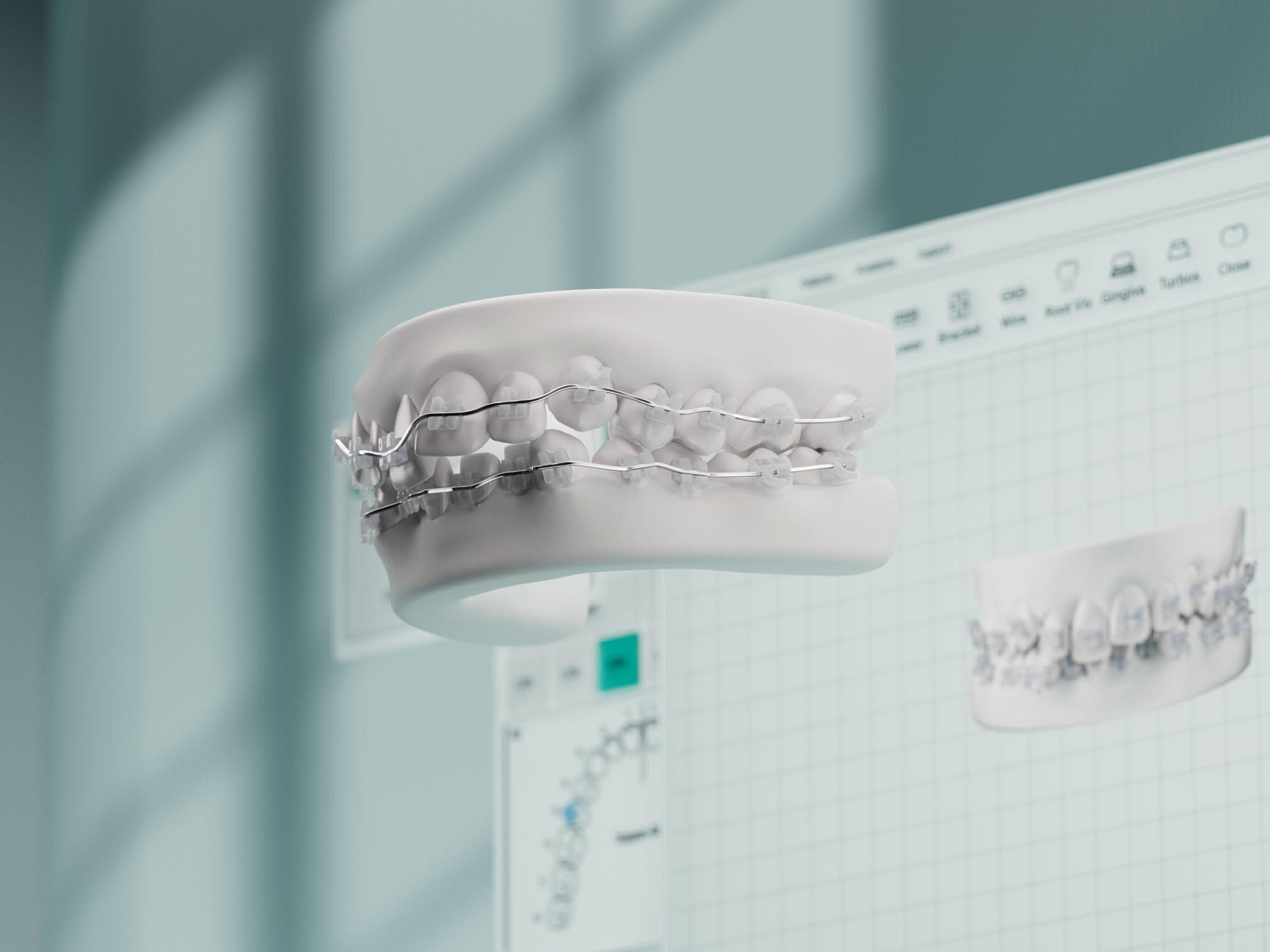
Dr. Jennifer Messenger explores a new bonding system that improves the patient and doctor experience
My orthodontic journey began in 2011. After moving back to my hometown and practicing general dentistry for a few years, I decided to pursue my true dream of becoming an orthodontist. That decision meant packing up my family — my husband and our two young daughters, then just 1 and 3 years old — and moving from California to Oregon to attend Oregon Health & Science University (OHSU). It turned out to be one of the best decisions we ever made. OHSU was an outstanding program, and our time in the Pacific Northwest as a young family was truly magical.
For my master’s thesis at OHSU, I conducted a bonding study comparing two traditional bracket-pad designs with a novel design fabricated by a local orthodontic company. The goal was to evaluate whether the retentive features of the new design significantly affected bond strength, adhesive thickness, and adhesive cure. Ironically, more than a decade after defending my master’s thesis in front of fellow residents, dental students, and a panel of experts, I was invited by Ormco™ to evaluate a
Jennifer Messenger, DDS, MS, is a board-certified orthodontic specialist based in Huntington Beach, California. She completed her undergraduate education at UC Santa Barbara. Dr. Messenger earned her Doctor of Dental Surgery (DDS) degree from the UCLA School of Dentistry, followed by a certificate in Advanced Education in General Dentistry (AEGD) at the University of Southern California, where she focused on cosmetic and restorative dentistry. After practicing general dentistry in Orange County, California for 3 years, she completed her orthodontic residency at Oregon Health & Science University.
In 2018, Dr. Messenger founded Messenger Orthodontics, a boutiquestyle practice known for its personalized approach to patient care. She is committed to delivering individualized treatment and exceptional results.
Disclosure: Dr. Messenger is a paid consultant for Ormco, a medical device manufacturer, which does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients.
product that has the potential to revolutionize bonding: Ormco’s EtchFree Bonding material.
This time, however, I wasn’t spending hours in a lab surrounded by extracted teeth, brackets, universal testing machines, microscopes, and a Fourier Transform Infrared Spectrometer. Instead, I had the opportunity to apply the product in a realworld clinical setting — on patients in my own practice. What made the experience especially rewarding was that many of the study participants were parents of my young and teen patients who had never had orthodontic treatment. While parents often prioritize their children’s needs, this opportunity gave them a gentle nudge to begin treatment for themselves, even if just for 6 months. Most were thrilled with their results by the end of the study, and a few chose to continue treatment to achieve an ideal finish.
At Messenger Orthodontics, I’m always looking for ways to improve both the patient and doctor experience, so I was excited to evaluate this new bonding system. Ormco EtchFree Bonding streamlines clinical workflows, reduces common risks, and promotes better enamel preservation.1 In a field that’s constantly evolving, innovations like this allow us to align our techniques with our core values: clinical precision, patient safety, and longterm oral health. For those looking to update their bonding protocols, Ormco EtchFree Bonding offers a compelling alternative worth exploring.
Dr. Jennifer Messenger
Rethinking an outdated standard
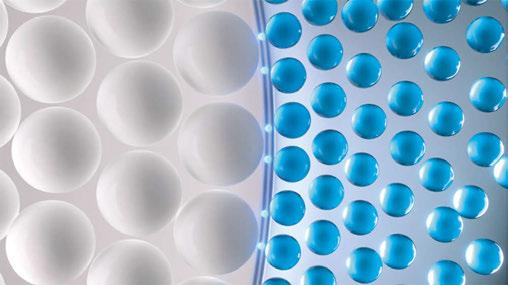
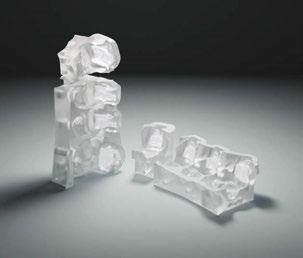
With minimal bonding modification developments in over 100 years, orthodontic bonding has revolved around a single process: acid etching. Despite significant advancements in nearly every other aspect of our profession, this one critical step has remained stuck in time, bringing with it a host of clinical challenges. As a practicing orthodontist, I’ve experienced firsthand the complications that acid etching can introduce: risk of patient discomfort or injury, post-debonding sensitivity, an enamel surface that is more susceptible to demineralization in the presence of poor oral hygiene, and the ever-frustrating bracket failures caused by moisture contamination. But that era is over. Ormco’s new EtchFree Bonding system marks a true turning point in orthodontics. For the first time, we have a clinically viable alternative that completely eliminates the need for acid etching (Figure 1).
No etching, no rinsing, no waiting — just brush and go
One of the most remarkable advantages of Ormco EtchFree Bonding is its simplicity. Traditional etch, prime, and bond procedures can take up to 11 technique-sensitive steps. In contrast, Ormco EtchFree Bonding reduces the process to just nine streamlined steps, eliminating the need for etching, rinsing, or drying. One of the most helpful features of Ormco EtchFree is that it’s hydrophilic, allowing it to perform reliably even in the presence of moisture — from initial drying through adhesive application (Figure 2).
Consistency you can count on — wet or dry
In day-to-day practice, using Ormco EtchFree Bonding has reduced concerns about salivary contamination and helped minimize debond failures, ultimately increasing confidence in each bond placed. According to data from Gaidge Analytics, emergency repair visits accounted for 8% of all orthodontist appointments in 2022. Bonding problems contribute to 22% of these emergency visits, with moisture contamination as a contributing factor. Each emergency visit can cost the orthodontist up to $300.2*
Ormco EtchFree Bonding becomes especially important when working with younger patients. In children and adolescents, maintaining a completely dry field during bonding can be a real challenge. Whether it’s due to smaller oral anatomy, limited cooperation, or simply the difficulty of isolation in certain areas, moisture control is often less predictable. Having a bonding system that is moisture-tolerant at every stage has been a welcome shift in my practice. It helps reduce the stress of trying to achieve perfect dryness and allows for more consistent results, even in less-than-ideal conditions. Moisture contamination is no longer a cause for concern. Whether the field is perfectly dry or slightly moist, the bond strength remains consistent — something that simply isn’t possible with traditional systems.
A healthier bond for healthier enamel
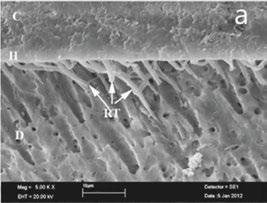
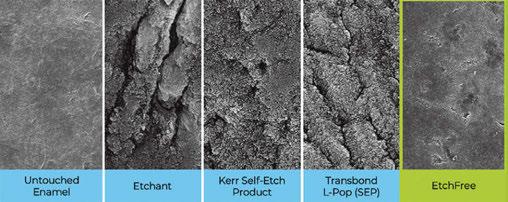
Where traditional etching roughens and demineralizes enamel to create a mechanical bond (Figure 3), Ormco EtchFree Bonding forms ionic bonds directly with calcium in the enamel, achieving strong adhesion without damaging the tooth surface (Figure 4). The difference is visible to the naked eye: Enamel remains smooth and intact. And because there’s no acid involved, there’s also no risk of etch burns or sensitivity.
Figure 1: 3D illustration of the ionic bonding utilized by EtchFree Bonding
Figure 2: Bonds in wet or dry environments
Figures 3A (left) and 3B (center): EtchFree Bonding images and description from Ormco. How it Works: Etch-based bonding — Resin infiltrates the etched surface, and is cured to create a mechanical bond.1 Figure 4 (right): Unmatched enamel protection3,4
Figures 5A and 5B: Damon Ultima bond/debond example. 5A. Bond: Damon Ultima patient, day of bond. Split-mouth design: Ormco EtchFree Bonding on the right side. 37% phosphoric acid etch applied during bracket bonding on the left side. 5B. Debond: Debonded at 6 months per clinical trial protocols and requirements. Archwire Progression: 014 NT 8 weeks, 018 NT 8 weeks, 14x0275 NT 8 weeks. No debonded brackets during treatment. Good initial alignment and leveling are noted; no signs of decalcification or white spot lesions
Synergy with the Damon Ultima™ System, Symetri™ Clear Brackets, and Spark™ Clear Aligners
In our practice, we’ve paired Ormco’s EtchFree Bonding with the Damon Ultima System using Ormco Digital Bonding, Symetri Clear Brackets, and Spark Clear Aligners. Working with a company that offers high-quality solutions across every treatment modality allows for a more integrated and consistent approach to care. One of the added benefits is the convenience of ordering supplies from a single source, which streamlines logistics. Additionally, being able to work up cases on the same platform — whether for aligners or fixed appliances like the Ormco Digital Bonding featuring the Damon Ultima System — makes treatment planning both efficient and precise.
REFERENCES
1. Data on file with Ormco Corporation.
2. Yakoby Epstein S. The 411 on 911s in Orthodontic Treatments. Oral Health. Published September 2023. https://www.oralhealthgroup.com/features/the-411-on-911s-in-orthodontic-treatments/. Accessed May 7, 2025.
Kerr Self-Etch is a trademark of Kerr Corporation.
3M™ Transbond™ Plus Self-Etching Primer is a trademark of Solventum.
*Costs may vary from $100-$300.
Figures 6A and 6B: Spark Aligners. 6A. Bond: Spark Aligner patient, day of attachment delivery. Split-mouth design: 37% phosphoric acid etch applied during attachment bonding on the right side; Ormco EtchFree Bonding on the left side. 6B. Debond: Debonded at 6 months per clinical trial protocols and requirements. 19 Active Spark Aligners. No debonded attachments during treatment. Good initial alignment, leveling, and arch expansion, no signs of decalcification or white spots noted. Patient continued the study to finish the alignment of UL2
Figures 7A and 7B: Symetri Clear. 7A. Bond: Symetri Clear patient, day of bond. Split-mouth design: Ormco EtchFree Bonding on the right side. 37% phosphoric acid etch applied during bracket bonding on the left side. 7B. Debond: Debonded at 6 months per clinical trial protocols and requirements. Archwire Progression: 014 NT 16 weeks, 20x20 NT 8 weeks. No debonded brackets during treatment. Good initial alignment and leveling; no decalcification or white spots noted. Patient switched to Spark Aligners to continue treatment
WAVE IN ADHESIVES
EASIER AND FASTER BONDING PROCEDURES
No etching, rinsing, drying or waiting FEWER DEBONDS2
-Dr. Jennifer Messenger, Huntington Beach, CA
Tolerates moisture in every bonding step IMPROVED PATIENT EXPERIENCE
It’s always been a problem in orthodontics to maintain our moisture control. We’re working on children and small spaces. So having any product that helps us with that is a game changer. Ormco EtchFree Bonding takes out the moisture sensitivity in every step.1
May help prevent white spot lesions by removing acid etching2
The importance of controls in research and implications for clinical practice
Drs. Dara L. Rinchuse and Donald J. Rinchuse reflect on delaying orthodontic treatment for very young patients
The primary author’s 3-year-old daughter, JoJo (and coauthor’s granddaughter), had used a pacifier (“binky”) since birth. The pacifier (Philips Avent Soothie) adversely altered JoJo’s oral facial complex creating severe maxillary anterior protrusion. Family photographs document the progress of JoJo’s case from pacifier use (Figures 1A-1C) to months afterwards when the pacifier was discontinued (Figures 2A-2B). Figures 1A-1C show the profound untoward effects the pacifier had on her dentition causing severe maxillary protrusion (Class II division 1 malocclusion with a large overjet). After stopping the pacifier at age 3 years, 4 months, her malocclusion returned to a rather normal state 4 months later (Figures 2A and 2B). Of note, JoJo had a tongue thrust while using the pacifier, and the tongue thrust disappeared after discontinuing the pacifier. Notably, JoJo’s malocclusion corrected without any kind of treatment. If JoJo had had treatment, the outcome of her bite correction could have reasonably been assumed to be due to an orthodontic intervention rather than a natural occurrence, i.e., the return to homeostatic balanced oral soft-tissue forces.
Discussion
Observations in clinical practice can be misleading if a practitioner does not consider and account for clinical results being due to factors other than clinical treatments. JoJo’s case illustrates why controls are necessary in clinical experimental research. Importantly, research controls serve as baselines that allow researchers to compare the effects of experimental treatments against subjects who did not receive treatment. Further, control groups help by eliminating or reducing the effects of confound-
Dara L. Rinchuse, DMD, graduated from the University of Pittsburgh School of Dental Medicine (DMD) in 2008 and Jacksonville University School of Orthodontics (Certificate) in 2010. She is in private orthodontic practice in Rostraver, Pennsylvania. She has authored several papers, including several in the American Journal of Orthodontics and Dentofacial Orthopedics. She can be reached at dararinchuse13@gmail.com.
Donald J. Rinchuse, DMD, MS, MDS, PhD, graduated from the University of Pittsburgh School of Dental Medicine in 1974 with degrees in Dentistry (DMD) and Pharmacology/Physiology (MS). He received his certificate and MDS degree in orthodontics in 1976 and a PhD in Higher Education in 1985 from the University of Pittsburgh. He is a Diplomate of the American Board of Orthodontics. In addition, Dr. Rinchuse is on the editorial review board of many professional journals including the American Journal of Orthodontics and Dentofacial Orthopedics. He has published over 150 articles, two books, several book chapters, and has made many presentations. He can be reached at rinchuse21@gmail.com.
ing factors, account for placebo effects, measure natural changes, reduce bias, establish causality, and enhance validity.1
JoJo’s case brings to mind several additional considerations. For one, are many of the orthodontic phase I treatments necessary? Are many orthodontic problems self-correcting, particularly for very young children? And, what about the evidence-based literature which suggests that many of the early phase I treatments may be unnecessary, at least for certain malocclusions and certain appliances; i.e., better treated at a later time.2-6
On further reflection of JoJo’s case, a contemplated question comes to mind. That is, “Why don’t all cases similar to JoJo’s return to the pre-existing state after the pacifier or habit is discontinued?” Could it be that the children with rather normal dental-facial features (normal soft and hard tissue) prior to habit use are in the best position for the malocclusion to be self-correcting? Conversely, would children who have facial and dental imbalances before the habit started, be less likely to have their malocclusions self-correct (at least fully correct)?
In addition, JoJo’s case stimulates the discussion of the never-ending debate of the question as to what comes first, the proverbial “chicken or egg.” This is regard to dental open bites and tongue thrusts. Parenthetically, this debate often ignores the
Figures 1A-1C: Severe dental protrusion for a 3-year-old-child caused by the long-term use of a pacifier
possibility that both the open bite and tongue thrust developed and then ceased concomitantly.
Lastly, although case studies are not the best type of research, they can provide useful information. For instance, they can stimulate the formation of hypotheses that then provoke experimental research. The disadvantages of case studies are many. For one, with a sample size of “one,” there is not much that can be gleaned from an evidence-based perspective.
Conclusions
The results of clinical treatments, at times, may have little or nothing to do with the interventions that were rendered. Some outcomes in clinical practice and in research are best explained as natural or chance occurrences. It is advantageous for clinicians to contemplate the importance of bringing the knowledge of science, evidence-based medicine, and research to the patient care arena.
REFERENCES
1. Leotti LA, Iyengar SS, Ochsner KN. Born to choose: the origins and value of the need for control. Trends Cogn Sci. 2010 Oct;14(10):457-463. doi: 10.1016/j.tics.2010.08.001.
2. Proffit WR. The timing of early treatment: an overview. Am J Orthod Dentofacial Orthop. 2006 Apr;129(4 Suppl):S47-49. doi: 10.1016/j.ajodo.2005.09.014. PMID: 16644417.
3. O’Brien K, Wright J, Conboy F, Appelbe P, Davies L, Connolly I, Mitchell L, Littlewood S, Mandall N, Lewis D, Sandler J, Hammond M, Chadwick S, O’Neill J, McDade C, Oskouei M, Thiruvenkatachari B, Read M, Robinson S, Birnie D, Murray A, Shaw I, Harradine N, Worthington H. Early treatment for Class II Division 1 malocclusion with the Twin-block appliance: a multi-center, randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2009 May;135(5):573-579. doi: 10.1016/j.ajodo.2007.10.042.
4. Rinchuse DJ, Miles P. Chapter 2. Early intervention: The evidence for and against. pgs. 7-16. In: PS Miles, DJ Rinchuse, DJ Rinchuse. eds. Evidence-Based Clinical Orthodontics. Quintessence Publishing: Chicago;2012:7-16.
5. Schneider-Moser UEM, Moser L. Very early orthodontic treatment: when, why and how? Dental Press J Orthod. 2022 Jun 10;27(2):e22spe2. doi: 10.1590/2177-6709. 27.2.e22spe2.
6. Perillo L. Editorial: Early treatment: Where are we today? Sem Orthod. 2023;29(2): 117-118.
Figures 2A-2B: Normalization of the dentition 4 months after cessation of pacifier use
Clinical applications of 3D printing in orthodontics and future technologies
Drs. Aaron Glick, Joseph Ryan, and Elham Abbassi offer a comprehensive overview of 3D printing and its applications
Introduction to 3D Printing
3D printing is a relatively new field starting in the 1980s with the understanding of sequentially polymerizing materials with a beam of UV light or laser.1 Since its inception, there has been significant interest and adoption of 3D printing in multiple fields. For example, a 400-square-foot 3D-printed house in Russia was made in 24 hours and at a cost of $10,000.2 Other fields use 3D printing for making automotive parts, fabricating tools in space, concocting custom edible foods, creating educational displays, and executing rapid prototyping for engineering projects. In the health field, bioprinting is being used to build bioactive scaffolds, create human cells, and synthesize implantable tissues.3
Subtractive versus additive manufacturing
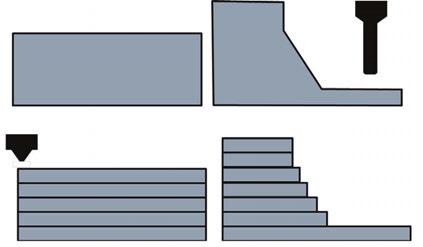
Generally, manufacturing techniques are either subtractive or additive. In subtractive manufacturing (i.e., CNC milling), the material is removed through carving or grinding away at the substructure. In additive manufacturing (i.e., 3D printing), the finished product is built through successive layers of material. Subtractive manufacturing involves a number of axes around which the block of material is rotated so the drill can remove the material, compared with additive manufacturing that will build layers of material in one plane as shown in Figure 1.
The additive nature of 3D printing holds a deep advantage in ease, cost, and flexibility. Due to the rotational axes required, there are some complex parts and internal geometries that are more difficult to manufacture through subtractive manufacturing (Figure 2). For instance, GE changed their manufacturing of some jet fuel nozzles since they could print one piece instead of assembling 20 separate parts.4 The decision to change their manufacturing method resulted in reducing manufacturing costs by 75%. Additive manufacturing allows for flexibility since the setup is minimal compared with retooling that is required for most high scale production facilities. In dentistry, the flexibility is underscored by multiple types of materials that can be used to build specific appliances.
Aaron Glick, DDS, is an Adjunct Clinical Associate Professor, General Practice and Dental Public Health, at the University of Texas Health Science Center at Houston School of Dentistry.
Elham Abbassi, DDS, is Assistant Professor and Group Practice Director, General Practice and Dental Public Health, University of Texas Health Science Center at Houston School of Dentistry.
Joseph Ryan, DDS, MSD, is in private practice in McAllen, Texas.
Educational aims and objectives
This self-instructional course for dentists aims to discuss 3D printing, how it works, and its benefits and drawbacks and applications for the orthodontic practice.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the differences between subtractive and additive manufacturing techniques.
• Recognize multiple applications for additive manufacturing in dentistry.
• Realize some orthodontic applications for 3D printing. Identify the clinical workflow for chairside 3D printing.
• Define bioprinting and realize its potential for dental applications. 2
Additive manufacturing technologies
The major categories of 3D printers are fused deposition modeling (FDM), stereolithography (SLA)/digital light projection (DLP), selective laser sintering (SLS), powder binder jetting (BJ), and photopolymer jetting (PJ) (Table 1). FDM printing is the most widely used type of printing that melts a thermoplastic filament. SLA/DLP use UV to cure a liquid photopolymer resting in a vat. This modality is most commonly used for dental applications due to its ability to accurately create small complex parts with resin materials. SLS printers are utilized more commonly in industrial settings and can be found in dental labs as opposed to offices.
These printers can output nylon and metal components that have high mechanical properties. BJ printing uses a bed of binder where the printhead deposits a binding agent. PJ jets and cures droplets of liquid photopolymer materials and can build structures that are composed of multiple types of material.5
3D printing in dentistry
3D printing is most cited in manufacturing (automotive and avionics) and consumer good fields followed by the health field.6 In the dental field, the current usage of 3D printers is low according to an American Dental Association (ADA) survey conducted in late 2023 with 17% of dentists owning a 3D printer.7 Yet, the adoption rate is high with those who noted they own a printer, 67% of the dentists have owned the printer for 2 years or less. Additionally, there is interest in this field since 56% of those surveyed noted that they are considering buying a 3D printer or completing training in 3D printing. Manufacturers have been recently rapidly developing new techniques for faster post processing, material sciences, and development of low-cost printers due to the expiration of multiple key patents of additive processes.8
Multiple applications for additive manufacturing in dentistry
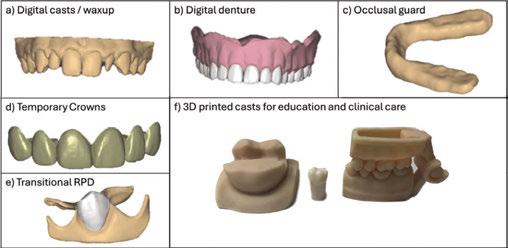
There are many applications of 3D printing in the field of dentistry. For instance, 3D printing can be used to create patient models, dentures, occlusal guards, temporary crowns, transitional RPDs, indirect orthodontic bonding trays, direct print aligners, retainers, surgical guides, implants, mandibular advancement devices, and educational devices (Figure 3). The patient models can be static or articulated and flexibly designed or altered digitally depending on the intended use. 3D printed dentures can offer reduced number of clinical appointments and higher intaglio accuracy, however have reduced esthetics compared with conventional dentures.9 The material properties of occlusal guards are similar to conventional and milled methods. Furthermore, wear resistance is not appreciably different between methods.10 Surgical guides can be used in implant placement, complicated root canal morphology, and complex craniofacial surgeries. Static dental implant surgical guides are accurate when 3D printed, however additional factors such as image acquisition with cone beam computed tomography (CBCT), computer aided design (CAD), and slicer software can add errors that affect overall clinical accuracies.11,12
Figures 3A-3F: Applications of 3D printing and computer-aided design in general dentistry. Various applications of computer-aided design and subsequent 3D printing for 3A. Patient models and treatment planning mock-up. 3B. Complete dentures. 3C. Occlusal guards. 3D. Temporary crowns. 3E. Transitional RPDs, and 3F. Articulated patient models and scaled models for education (please note that the typodont tooth in the middle is used for scale purposes and is not 3D printed)
Orthodontic
applications
There are also many applications of 3D printing with regards to orthodontic applications. For instance, 3D printing of models can aid in the treatment planning process to evaluate tooth position, occlusion, arch coordination for jaw surgery, act as records, or even act as templates for orthodontic appliances. Orthodontic appliances made from 3D printers include laser-sintered metal appliances which can include expanders or space maintainers. 3D printing can also be used to sequentially move teeth with clear aligner therapy. There are two main pathways for the fabrication of clear aligners: 1) serial changes replicated in 3D-printed models which are then used to vacuum-form thermoplastic sheets
$30,000Consumer electronics, multi-material medical models or dentures
Depowdering, media blasting
Curing or sintering (depending on material)
Dissolvable support removal
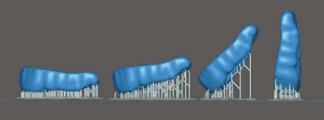
Figure 2: Internal structures of additive manufacturing. The internal structure of this 3D printed model allows for bending that is easier with additive manufacturing compared to subtractive manufacturing
Table 1: Common types of 3D printing techniques
into aligners and 2) directly 3D printing clear aligners. Multiple workflows exist, and the 3D-printed fabrication of aligners and/or models can be done in-office or through a third-party company. In both pathways, digital planning can allow clinicians or technicians to stage movements of individual teeth with software. Typical non-rotational tooth movement will be 0.25 mm per aligner, but in maximal anchorage cases has been shown up to 0.33 mm per aligner.13 Directly printing aligners will reduce manufacturing steps that have the potential to reduce overall fabrication time, labor costs, and errors in accuracy. In fact, accuracy, trueness, and precision is generally improved in directly 3D-printed aligners.14 Additionally, the mechanical properties of thermoformed aligners have a tendency to reduce force transmission overtime compared to directly 3D-printed aligners with TC-85 resin.14 Clinically, these biomechanical properties of thermoformed aligners are such that they have a potentially lower performance overtime, yet with improved patient comfort.
There are third-party companies that 3D print custom braces. After the clinician decides on an end position for teeth/occlusion, the underlying digital technology builds bracket-specific prescriptions based on the initial tooth positions. This allows for a simple archwire progression to arrive at aligned teeth without traditional repositioning of brackets. In severely rotated teeth, a bracket is bonded in the best available position to allow initial derotation. As the tooth straightens, and ideal bracket position is achieved, the bracket must be repositioned to said ideal position to achieve proper positioning. Generally, the 3D-printed custom braces are more comfortable, reduce treatment time, and allow for higher torque although debond more frequently with lower debonding forces.15 Ultimately, 3D printing of brackets can allow customization where some cases would additionally benefit due to discrepancies in craniofacial anatomy and tooth morphology. The material for 3D printing varies and can be made from resins or a slurry of zirconia through a lab service or chairside.16
3D printing as a clinical tool can allow for additional opportunities for reimagining the orthodontic workflow. For instance, indirect bonding trays can be more easily and quickly fabricated digitally based on AI and digital enhancements.17 Other 3D technologies can reduce lab wait times though chairside 3D printing of mandibular advancement devices, which are custom removable devices to treat obstructive sleep apnea.18 As technology continues to progress, the potential applications of 3D printing in orthodontics will likely expand, leading to more innovative, effective, and patient-friendly treatment options.
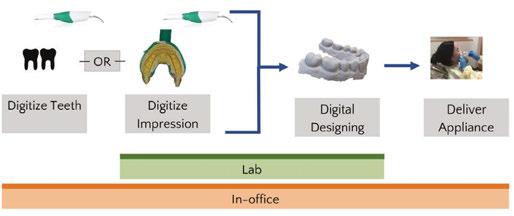
Clinical workflow for chairside 3D printing
The integration of these applications in a dental office might vary based on the device that is printed. Generally, the teeth are digitized and altered within a digital design software program and subsequently sent to a 3D printer. Given the cost of SLA/DLP printers, it is more practical to complete all steps chairside instead of sending impressions to a traditional lab. The decision of how to complete these steps also depends on the materials required. Chairside 3D printing has been shown to be less time consuming, more cost efficient, and display similar trueness compared with lab-fabricated single unit crowns using subtractive methods.19
For SLA/DLP printing there are four main steps that deviate from milling: 1) slicing software and G-code creation, 2) 3D printing via vat polymerization, 3) isopropyl wash, and 4) final cure.
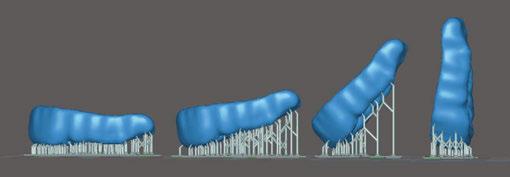
The initial step after digitally designing the appliance is importing the digital file — usually in standard tessellation language file type (stl). This triangulated mesh surface geometry is encoded by slicing software that identifies the movements and curing protocols of the 3D printer based on user inputs (G-code). Figure 5 shows an example of an occlusal guard in multiple print orientations within the slicer software. The print orientation will affect material properties such as accuracy, strength, surface roughness, and microbial adhesion.21 For example, a dental model has been shown to have better material properties in a horizontal orientation (0°), however, mass-producing dental models in the vertical orientation in dental labs allows for substantially higher throughput yet sacrifices trueness and surface quality. There are also additional factors such as layer thickness and material property that affect the final outcome.22
After slicing the stl, the automatically generated G-code can be used to operate the 3D printer. Within the context of a SLA/ DLP printer, there is a range of resins that can be used. The manufacturers are required to seek Food and Drug Administration (FDA) clearance for each indication of use.23 Therefore, there will be a set of materials that have been tested for the specific indication and are specifically formulated to have the appropriate mechanical properties.
Once printed, the device will have uncured resin surrounding the printed structure. The process of removing the uncured resin and attaining the structure’s final mechanical properties for a finished, functional product is called post-processing. This is completed in two steps: 1) Submerging the structure in isopropyl wash, 2) Curing the structure. The specifics of post-processing depends on the resin material manufacturer and the resin specifications. It is recommended to closely follow these instructions for use because deviations can result in underperforming mechanical properties and biocompatibility.24-26
After removing the printed solid from the build plate (Figure 6), the supports (if any) can be removed and excess resin washed
Figure 4: Chairside and lab workflows for additive manufacturing. There are multiple pathways for lab or chairside fabricated dental appliances using additive manufacturing (Adapted figure20)
Figure 5. Print orientations in slicer software. Occlusal guard in different print orientations from horizontal (0°) [on left of the picture] to vertical (90°) [on right of the picture]
off. The most widely used solvent washes are isopropyl alcohol and ethanol. Distributing the solvent evenly over the device is an important step to remove uncured liquid resin that has cytotoxic effects on the body. The exposure and permeation time of these solvents reduces the physical properties of the final product. Therefore, there is a fine balance of washing the structure long enough to reduce cytotoxicity but not too long to decrease its flexural strength.27-28
After the solvent has been completely evaporated, the final cure (post-polymerization) is initiated to complete the polymerization reaction. The product is placed in a UV chamber where the temperature, method, and duration will influence the mechanical properties of the end-product. The oxygen-inhibited layer will prevent full polymerization in subsequent steps. For instance, glycerin immersion, nitrogen chamber, and low-pressure vacuum have been methods to reduce the oxygen-inhibited layer. Reducing the oxygen-inhibited layer and reducing viscosity of the resin with higher temperatures has been shown to improve the mechanical properties of the resin.29-30 Generally, an increase of duration and intensity of the UV post-polymerization improves end-product strength.31
The rapid evolution of 3D printing technology is expanding the indications of use, reshaping clinical workflows, and reducing patient case limitations. Ongoing advancements, such as enhanced material properties and increased print speeds, allow for chairside integration. As of 2022, there were approximately 100 rigid and 30 flexible biocompatible resin materials on the market.32 Multiple advanced formulations continue to become FDA cleared, therefore increasing the selections and indications for printing. Additionally, the many types of 3D printing technology allow dental labs to reduce cost and increase throughput.
Future of 3D printing
Bioprinting
Bioprinting, a specialized subset of 3D printing, has gained significant traction in regenerative medicine by enabling the fabrication of functional tissues through layer-by-layer deposition of bioinks containing living cells and biomaterials. This technology has been explored for applications in tissue engineering, drug development, and personalized medicine. Bioprinting has been used to vascularize tissues, skin grafts, and organ models for transplantation and disease modeling.33 The field is rapidly expanding, with research focusing on enhancing cell viability, structural integrity, and biomimetic properties of printed tissues to bridge the gap between laboratory models and clinical applications.34 In dentistry, bioprinting has shown potential for regeneration of soft and hard tissues including bone, cartilage, and mucosa. The development of bioengineered scaffolds infused with stem cells and growth factors has facilitated tooth, periodontal ligament, and alveolar bone regeneration.35-36 In vivo assessments in animal models have been investigated in bone, periodontal ligament, and dentin regeneration with generally positive results.37 As bioprinting technology matures, its integration into clinical practice could revolutionize regenerative treatments in dental surgery by offering patient-specific, bioengineered tissues that improve functional and esthetic outcomes. These tools show promise in maintaining the structural integrity of patient anatomy and in reducing the immune response seen with conventional bone grafts.
Regulation in point-of-care printing
The ability to print custom devices for patients chairside disrupts the traditional workflow of dental offices. Traditionally, dental labs have fabricated all indirect prostheses. However, to maintain patient safety and effectiveness of the devices, the Food and Drug Administration (FDA) has identified software, material, and post-processing controls.38 Because the FDA regulates finished products, it also regulates dental devices at the point of care. Manufacturers will test their material with specific software along the workflow, and any modifications that a dentist makes to the lawfully marketed device could potentially have safety consequences.39 Due to increased controls by the FDA, free market competition is reduced, thus incentivizing manufacturers to build proprietary systems with higher upfront costs to the dentist. Despite commonly used controls, like quality management systems (i.e., ISO 13485), that are common in the industrial manufacturing sector, the specific guidelines for regulatory requirements for chairside 3D printing are sparce.32
Prototypes and innovation
The benefits of 3D printing for small scale, custom products are a notable reason that this technology fits well in dentistry because the majority of extraorally fabricated devices are patient-specific. As more dentists adopt this technology, the path toward fabricating dental-specific prototypes will increase early stages of innovation. Sites similar to thingiverse (thingiverse.com) or makerworld (makerworld.com) have accelerated user-based innovation and pose a possibility for democratizing supply chains — particularly for spare parts manufacturing.40 A recent example showing the importance of supply chain diversification was demonstrated during the COVID-19 pandemic when many dental offices began printing face shields, masks, and other medical devices as demand exceeded supply inventories.41
Re-thinking the application of current innovations in dental material science allows for boundless iterations of traditional designs. For instance, custom implants that do not require surgery (placement at time of extraction), hollow implants that allow for time-based release of anti-inflammatory mediators, and reductions of thickness or chairside implant printing through SLA compatible zirconium dioxide.42
3D printing technology can also be used in tandem with AI (artificial intelligence) in novel ways.43 For instance, AI frameworks have been used to reduce human error and automate critical steps in 3D-printing processing.44 Additionally, both tools can be used in the full digital workflow to create a dental prosthesis: a generative AI computer-aided design can be automatically created, then 3D printed and fitted to the patient.45-46
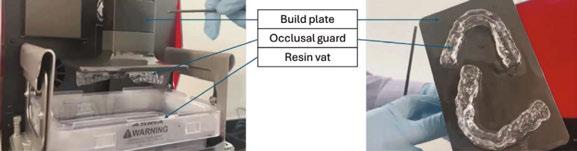
Figure 6. Anatomy of SLA/DLP vat resin type printer. Images of an SLA/DLP vat resin = printer with associated labels for a) build plate that adheres to the printed device, b) occlusal guards as an example of a printed device, c) resin vat of splint-specific uncured liquid resin
Summary
Additive manufacturing has multiple applications that are currently used in dental offices. There are still barriers for wide adoption, however the application of a personalized manufacturing approach combined with 3D technologies fits well into a digital clinical workflow. In order to adopt 3D printing in dentistry, an understanding of the different additive technologies and available materials is important. Each type of 3D printing technology has different upfront costs that can preclude its use in a dental clinic. Additionally, the post-processing criteria will vary on the type of print technology selected. Based on current research, 3D printing technology has the potential to reduce time spent and incurred costs for a semi-automated solution of custom dental prostheses.
REFERENCES
1. Pei E, Kabir IR, Leutenecker-Twelsiek B. History of AM. In: Springer Handbook of Additive Manufacturing. 2023 Oct 18 (pp. 3-29). Cham: Springer International Publishing.
2. Sakin M, Kiroglu YC. 3D Printing of Buildings: Construction of the Sustainable Houses of the Future by BIM. Energy Procedia. 2017 Oct 1;134:702-711.
3. Gu Q, Hao J, Lu Y, Wang L, Wallace GG, Zhou Q. Three-dimensional bio-printing. Sci China Life Sci. 2015 May;58(5):411-9. doi: 10.1007/s11427-015-4850-3. Epub 2015 Apr 29.
4. D’Aveni R. The 3-D printing revolution. Harvard Business Review. 2015 May;93(5):40-48.
5. Jakus AE. An introduction to 3D printing—past, present, and future promise. In: 3D printing in Orthopaedic Surgery. Elsevier;Jan 2019:1-15. doi:10.1016/B978-0-323-58118-9.00001-4.
6. Ukobitz DV. Organizational adoption of 3D printing technology: a semisystematic literature review. Journal of Manufacturing Technology Management. 2021 Dec 17;32(9):48-74.
7. Revilla-León M, Frazier K, da Costa J, Haraszthy V, Ioannidou E, MacDonnell W, Park J, Tenuta LM, Eldridge L, Vinh R, Kumar P. Prevalence and applications of 3-dimensional printers in dental practice. J Am Dent Assoc. 2023 Apr 1;154(4):355-356. doi: 10.1016/j.adaj.2023.02.004.
8. Kessler A, Hickel R, Reymus M. 3D Printing in Dentistry-State of the Art. Oper Dent. 2020 Jan/ Feb;45(1):30-40. doi: 10.2341/18-229-L. Epub 2019 Jun 7.
9. Alhallak K, Hagi-Pavli E, Nankali A. A review on clinical use of CAD/CAM and 3D printed dentures. Br Dent J. 2023 Jan 9. doi: 10.1038/s41415-022-5401-5. Epub ahead of print.
10. Valenti C, Federici MI, Coniglio M, Betti P, Pancrazi GP, Tulli O, Masciotti F, Nanussi A, Pagano S. Mechanical and biological properties of polymer materials for oral appliances produced with additive 3D printing and subtractive CAD-CAM techniques compared to conventional methods: a systematic review and meta-analysis. Clin Oral Investig. 2024 Jun 25;28(7):396. doi: 10.1007/s00784-024-05772-6.
11. Ashtiani RE, Ghasemi Z, Nami M, Mighani F, Namdari M. Accuracy of static digital surgical guides for dental implants based on the guide system: A systematic review. J Stomatol Oral Maxillofac Surg. 2021 Dec 1;122(6):600-6077. doi: 10.1016/j.jormas.2020.10.010.
12. Juneja M, Thakur N, Kumar D, Gupta A, Bajwa B, Jindal P. Accuracy in dental surgical guide fabrication using different 3-D printing techniques. Additive Manufacturing. 2018 Aug 1;22:243-255. doi: 10.1016/j.addma.2018.05.012.
13. Martínez-Lozano D, Castellanos-Andrés D, López-Jiménez A-J. Staging of Orthodontic Tooth Movement in Clear Aligner Treatment: Macro-Staging and Micro-Staging—A Narrative Review. Applied Sciences. 2024; 14(15):6690. https://doi.org/10.3390/app14156690.
14. Torkomian T, de la Iglesia F, Puigdollers A. 3D-printed clear aligners: An emerging alternative to the conventional thermoformed aligners? - A systematic review. J Dent. 2025 Apr;155:105616. doi: 10.1016/j.jdent.2025.105616. Epub 2025 Feb 5.
15. Elabed I, Zheng Z, Zhang Y, Chung CH, Li C. The Mechanical and Clinical Properties of Customized Orthodontic Bracket Systems-A Comprehensive Review. J Funct Biomater. 2024 Oct 7;15(10):299. doi: 10.3390/jfb15100299.
16. Panayi NC. In-house three-dimensional designing and printing customized brackets. J World Fed Orthod. 2022 Dec;11(6):190-196. doi: 10.1016/j.ejwf.2022.10.004. Epub 2022 Nov 5.
17. Gardner S, Khosravi R, Detweiler M, Owen B. 3D printing digitally planned in-direct bonding tray. Seminars in Orthodontics. 2022;28(2):61-72. doi: 10.1053/j.sodo.2022.10.009.
18. Glick A, Abbassi E, Farach-Carson M. Novel 3D-printed custom oral appliance therapy: a pilot study. Sleep. May 2022;45(Suppl1):A165. doi:10.1093/sleep/zsac079.364.
19. Mangano FG, Cianci D, Pranno N, Lerner H, Zarone F, Admakin O. Trueness, precision, time-efficiency and cost analysis of chairside additive and subtractive versus lab-based workflows for manufacturing single crowns: An in vitro study. J Dent. 2024 Feb;141:104792. doi: 10.1016/j.jdent.2023.104792. Epub 2023 Nov 25.
20. Glick A and Flamenco D. Clinical application and implementation of 3D Printing. J Greater Houston Dent Soc. 2023; 94(4):16-19.
21. Shim JS, Kim JE, Jeong SH, Choi YJ, Ryu JJ. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J Prosthet Dent. 2020 Oct;124(4):468-475. doi: 10.1016/j.prosdent.2019.05.034. Epub 2019 Dec 4.
22. Alghauli MA, Almuzaini SA, Aljohani R, Alqutaibi AY. Impact of 3D printing orientation on accuracy, properties, cost, and time efficiency of additively manufactured dental models: a systematic review. BMC Oral Health. 2024 Dec 26;24(1):1550. doi: 10.1186/ s12903-024-05365-5.
23. Da Silva TM, Immich F, De Araujo TS, Lund RG, Da Silva AF, Piva E, Da Rosa WLO. Photosensitive resins used in additive manufacturing for oral application in dentistry: A scoping review from lab to clinic. J Mech Behav Biomed Mater. 2023 May;141:105732. doi:10.1016/j. jmbbm.2023.105732. Epub 2023 Mar 1.
24. Cao J, Liu X, Cameron A, Aarts J, Choi JJE. Influence of different post-processing methods on the dimensional accuracy of 3D-printed photopolymers for dental crown applicationsA systematic review. J Mech Behav Biomed Mater. 2024 Feb;150:106314. doi: 10.1016/j. jmbbm.2023.106314. Epub 2023 Dec 12.
25. Vasques MT, Mulder JN, Machado DS, Lagana DC. The influence of the post-processing method on knoop hardness of photosensitive resins for 3D SLA printer used in Dentistry. Clinical and Laboratorial Research in Dentistry. 2019 Dec 31. Available at: https://www.revistas. usp.br/clrd/article/view/161294.
26. Cabrol A, Chuy V, Fron-Chabouis H, Naveau A. Effectiveness of postprocessing on 3D printed resin biocompatibility in prosthodontics: A systematic review. J Prosthet Dent. 2024 Sep 19:S0022-3913(24)00588-2. doi: 10.1016/j.prosdent.2024.08.014. Epub ahead of print.
27. Xu Y, Xepapadeas AB, Koos B, Geis-Gerstorfer J, Li P, Spintzyk S. Effect of post-rinsing time on the mechanical strength and cytotoxicity of a 3D printed orthodontic splint material. Dent Mater. 2021 May;37(5):e314-e327. doi: 10.1016/j.dental.2021.01.016. Epub 2021 Feb 18.
28. Hwangbo NK, Nam NE, Choi JH, Kim JE. Effects of the Washing Time and Washing Solution on the Biocompatibility and Mechanical Properties of 3D Printed Dental Resin Materials. Polymers (Basel). 2021 Dec 16;13(24):4410. doi: 10.3390/polym13244410.
29. Kim YJ, Kim HN, Kim DY. A study on effects of curing and machining conditions in post-processing of SLA additive manufactured polymer. Journal of Manufacturing Processes. 2024 Jun 15;119:511-519. doi:10.1016/j.jmapro.2024.03.112.
30. Lim JH, Lee SY, Gu H, Jin G, Kim JE. Evaluating oxygen shielding effect using glycerin or vacuum with varying temperature on 3D printed photopolymer in post-polymerization. J Mech Behav Biomed Mater. 2022 Jun;130:105170. doi: 10.1016/j.jmbbm.2022.105170. Epub 2022 Mar 13.
31. Lin YC, Tarrazzi D, Schoenbaum T, Knoernschild K. Effect of postprocessing parameters on the flexural strength of vat-polymerized additively manufactured interim fixed dental prostheses: A systematic review with postprocessing guidelines. J Prosthet Dent. 2024 Aug 13:S00223913(24)00497-9. doi: 10.1016/j.prosdent.2024.07.016. Epub ahead of print.
32. Guttridge C, Shannon A, O’Sullivan A, O’Sullivan KJ, O’Sullivan LW. Biocompatible 3D printing resins for medical applications: A review of marketed intended use, biocompatibility certification, and post-processing guidance. Annals of 3D Printed Medicine. 2022 Mar 1;5:100044. https://doi.org/10.1016/j.stlm.2021.100044.
33. Murphy SV, Atala A. 3D bioprinting of tissues and organs. Nat Biotechnol [Internet]. 2014;32:773–785. Available from: https://www.nature.com/articles/nbt.2958.
34. Groll J, Burdick JA, Cho D-W, Derby B, Gelinsky M, Heilshorn SC, Jüngst T, Malda J, Mironov VA, Nakayama K, Ovsianikov A, Sun W, Takeuchi S, Yoo JJ, Woodfield TBF. A definition of bioinks and their distinction from biomaterial inks. Biofabrication [Internet]. 2018;11(1):013001. doi: 10.1088/1758-5090/aaec52Available from: http://dx.doi.org/10.1088/1758-5090/aaec52.
35. Morrison DG, Tomlinson RE. Leveraging Advancements in Tissue Engineering for Bioprinting Dental Tissues. Bioprinting. 2021 Aug;23:e00153. doi: 10.1016/j.bprint.2021.e00153. Epub 2021 Jun 13.
36. Ostrovidov S, Ramalingam M, Bae H, Orive G, Fujie T, Shi X, Kaji H. Bioprinting and biomaterials for dental alveolar tissue regeneration. Front Bioeng Biotechnol. 2023 Apr 14;11:991821. doi: 10.3389/fbioe.2023.991821.
37. Mohd N, Razali M, Fauzi MB, Abu Kasim NH. In Vitro and In Vivo Biological Assessments of 3D-Bioprinted Scaffolds for Dental Applications. Int J Mol Sci. 2023 Aug 17;24(16):12881. doi: 10.3390/ijms241612881.
38. Food and Drug Administration. Technical considerations for additive manufactured medical devices: guidance for industry and food and drug administration staff. 2017. Accessed 3/19/2025 at: https://www.fda.gov/media/97633/download
39. Kuo RF, Lin YS, Yang TH, Nguyen AT. 3D printing: limitations, safety, and regulatory considerations for oral health science. In: 3D Printing in Oral Health Science: Applications and Future Directions 2022 Sep 27: 269-291. Cham: Springer International Publishing. 10.1007/978-3-031-07369-4_13.
41. Longhitano GA, Nunes GB, Candido G, da Silva JVL. The role of 3D printing during COVID-19 pandemic: a review. Prog Addit Manuf. 2021;6(1):19-37. doi: 10.1007/s40964-020-00159-x. Epub 2020 Nov 24.
42. Joda T, Yeung AWK, Hung K, Zitzmann NU, Bornstein MM. Disruptive Innovation in Dentistry: What It Is and What Could Be Next. J Dent Res. 2021 May;100(5):448-453. doi: 10.1177/0022034520978774. Epub 2020 Dec 16.
43. Glick A, Tipton N, Manila N, Chang J. AI in implant dentistry: clinical implementation and considerations for use. Implant Practice US. 2024;17(1):20-24, Quiz 25.
44. Martinez G, Huang K, Lou Y, Bai Y. Innovative Applications of AI and 3D Printing in Digital Dentistry: Enhancing Accuracy and Efficiency in Dental Care. In: 2024 International Conference on Identification, Information and Knowledge in the Internet of Things (IIKI). 2024 Dec 6:237-242. 10.1109/IIKI65561.2024.00048.
45. Chau RCW, Chong M, Thu KM, Chu NSP, Koohi-Moghadam M, Hsung RT, McGrath C, Lam WYH. Artificial intelligence-designed single molar dental prostheses: A protocol of prospective experimental study. PLoS One. 2022 Jun 2;17(6):e0268535. doi: 10.1371/journal. pone.0268535.
46. Zhao X, Li N, Zhang Z, Hong J, Zhang X, Hao Y, Wang J, Xie O, Zhang Y, Li H, Liu M, Zhang P, Ren X, Wang X. Beyond hype: unveiling the Real challenges in clinical translation of 3D printed bone scaffolds and the fresh prospects of bioprinted organoids. J Nanobiotechnology [Internet]. 2024;22(1):500. Available from: http://dx.doi.org/10.1186/s12951-024-02759-z.
Continuing Education Quiz
Clinical applications of 3D printing in orthodontics and future technologies
GLICK/RYAN/ABBASSI
1. ____________ printing is the most widely used type of printing that melts a thermoplastic filament.
a. Fused deposition modeling (FDM)
b. Selective laser sintering (SLS)
c. Powder binder jetting (BJ)
d. Digital light projection (DLP)
2. Manufacturers have been recently rapidly developing new techniques for ___________ due to the expiration of multiple key patents of additive processes.
a. faster post processing
b. material sciences
c. development of low-cost printers
d. all of the above
3. 3D printing can be used to create patient models, ___________, transitional RPDs, indirect orthodontic bonding trays, direct print aligners, retainers, surgical guides, implants, mandibular advancement devices, and educational devices.
a. dentures
b. occlusal guards
c. temporary crowns
d. all of the above
4. 3D printing of models can aid in the treatment planning process to evaluate tooth position, _____ or even act as templates for orthodontic appliances.
a. occlusion
b. arch coordination for jaw surgery
c. act as records
d. all of the above
5. The mechanical properties of thermoformed aligners have a tendency to _____ force transmission overtime compared to directly 3D-printed aligners with TC-85 resin.
a. reduce
b. increase
c. equalize
d. expand
6. For _________ there are four main steps that deviate from milling: 1) slicing software and G-code creation, 2) 3D printing via vat polymerization, 3) isopropyl wash, and 4) final cure.
a. PEEK printing
b. SLA/DLP printing
c. powder-binder jetting
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 070
Date Published: July 18, 2025
Expiration Date: July 18, 2028
d. photopolymer jetting
7. The specifics of post-processing depend on ___________.
a. the resin material manufacturer
b. the resin specifications
c. microbial adhesion
d. both a and b
8. ________, a specialized subset of 3D printing, has gained significant traction in regenerative medicine by enabling the fabrication of functional tissues through layer-by-layer deposition of bioinks containing living cells and biomaterials.
a. Bioprinting
b. Microbial adhesion
c. Static surgical guides
d. Slicer software
9. To maintain patient safety and effectiveness of the devices, the _____________ has identified software, material, and post-processing controls.
a. American Dental Association
b. Food and Drug Administration (FDA)
c. Environmental Protection Agency
d. National Institutes of Health
10. AI frameworks have been used to reduce human error and automate critical steps in 3D-printing processing.
a. True
b. False
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Early orthodontic intervention: enhancing oral hygiene compliance in the transitional dentition
Dr. Christina Carter points out the importance of oral hygiene education for early orthodontic patients
Introduction: framing the hygiene challenge in mixed dentition
The mixed dentition stage represents a critical window of opportunity in a child’s oral development. Between the ages of 6 and 12, the eruption of permanent teeth alongside retained primary teeth creates a complex oral environment prone to plaque retention, gingival inflammation, and early signs of periodontal stress.1 At the same time, children in this stage often lack the dexterity, motivation, and maturity to maintain adequate oral hygiene independently. These compounding factors set the stage for increased risk of caries, demineralization, and compromised outcomes from both restorative and orthodontic care.
Traditionally, orthodontic treatment has been reserved for adolescence, but clinical evidence increasingly supports the benefits of early interceptive treatment — not only for skeletal and dental correction but also for behavioral shaping and hygiene compliance.2 Early orthodontic intervention provides a platform for education, habit formation, and caregiver engagement that can dramatically influence long-term oral health outcomes.
Christina R. Carter, DMD, is a graduate of Haverford College in Haverford, Pennsylvania. She earned her dental degree at UMDNJ-NJDS, now Rutgers School of Dental Medicine and her Certificate in both Pediatric Dentistry and Orthodontics at New York University College of Dentistry. She completed a fellowship in Cleft, Craniofacial and Surgical Orthodontics at the Institute of Reconstructive Plastic Surgery-New York University Langone Medical Center and earned her Certificate as a Holistic Health Coach from the Institute of Integrative Nutrition in New York. She is a Diplomate of the American Board of Pediatric Dentistry and American Board of Orthodontics. Dr. Carter is in private practice in Madison, New Jersey. She is an Assistant Professor at New York University College of Dentistry in the Departments of Pediatric Dentistry and Orthodontics, a Board member for the NYU Oral Health Center for People with Disabilities, and a member of the Academy of General Dentistry’s Advisory Board. She served on the AAO Council of Orthodontic Health Care and multiple AAO committees. She is a PastPresident of the Northeastern Society of Orthodontists (NESO) and served as Delegate Chair to the House of Delegates. She often appears on Sirius Radio “Doctor Radio”, AAPD Podcasts, and has appeared on Inside Edition, WPIX News, and Today.com. She lectures nationally and internationally on pediatric dentistry, orthodontics, and treating special-needs patients.
Disclosure: Dr. Carter is a KOL for WildSmiles, but does not have any financial interest in the company.
Educational aims and objectives
This self-instructional course for dentists aims to discuss the role of early orthodontic treatment in improving long-term oral hygiene outcomes and enhancing patient compliance during the mixed dentition stage.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify key risk factors that compromise oral hygiene in early mixed dentition.
• Recognize behavioral and developmental barriers to hygiene compliance in children.
• View early orthodontic interventions as part of a preventive care strategy.
• Realize the clinical impact of customized appliance strategies on hygiene outcomes.
• Identify age-specific communication and compliance strategies for pediatric patients.
Clinical evidence: hygiene risk in the transitional dentition
Oral hygiene in children undergoing orthodontic treatment presents a unique clinical challenge. The presence of orthodontic appliances, combined with the eruptive pattern of the mixed dentition stage, often results in increased areas for plaque retention and difficulty with access during brushing. Crowded arches, exfoliating primary teeth, and partially erupted molars can hinder effective hygiene even before brackets are placed. In many cases, this age group tends to show inconsistent brushing habits, and their oral hygiene tends to require more caregiver involvement than that of older adolescents. When orthodontic appliances are introduced in this already vulnerable stage, plaque accumulation becomes more likely without active prevention and support strategies. These patterns emphasize the need for early, targeted hygiene instruction tailored to this developmental window. Clinical teams should not assume that the absence of obvious gingival inflammation or caries in early appointments equates to effective hygiene.
Preventive protocols — especially in the context of interceptive treatment — must begin with behavioral engagement and education at the first signs of eruptive transition.
Developmental barriers: why hygiene habits fail in younger patients
It is critical to recognize the unique developmental stage of early mixed dentition patients. At this age, many children are still developing the cognitive and motor skills necessary for consistent hygiene.3 They may struggle with toothbrush angulation, flossing technique, and time perception.
Furthermore, emotional and behavioral factors often play a role. Younger patients are more prone to oppositional behavior, have less intrinsic motivation for hygiene, and often rely heavily on caregivers to enforce routines. Without consistent reinforcement, oral hygiene becomes inconsistent at best, and neglectful at worst.
Clinical success in early treatment depends not just on tooth movement, but on fostering compliance through age-appropriate tools, visual feedback, and parental guidance. Without this foundation, long-term orthodontic results are at risk.
A picture is worth a thousand words and shows real repercussions that cannot be repaired. When trying to convey to patients the risk of white-spot lesions, I show a clinical photograph of a patient’s teeth after debond with unattractive white-spot lesions and decalcification. We also keep this picture in all the operatories so it stays fresh in the patient’s mind, and also we include a picture in our take-home care material. Parents have found that placing this picture on the bathroom mirror as a reminder is helpful. As we explain this picture, our patients are empowered with the knowledge that they have complete control over what their teeth will look like after we remove braces if they follow our protocol. We recommend brushing above, below, and between the braces using a prescription toothpaste such as Elevate Fluorimax® 5000, Just Right 5000® (Elevate Oral Care®), or PreviDent® 5000 Plus (Colgate).
We advocate checking to “shine your smile and see your shape” as a visual target to guide their efforts. We recommend flossers that fit under the wire for easy use such as Plackers Orthopick® Flossers and Gum® Proxabrushes® for in between difficult spots.
The role of early orthodontic intervention in hygiene shaping
Early orthodontic treatment presents a unique opportunity: the ability to use appliance therapy as a catalyst for hygiene improvement. Designer braces in this stage can be leveraged to minimize plaque traps, facilitate easier brushing markers, and engage patients with visual cues that reinforce hygiene behavior. The AAO website notes, “Children can make their orthodontic journey fun with designer braces that feature brackets in various shapes like stars, hearts, and even sports-themed designs. These braces are equally effective and safe as their conventional counterparts.”4
An example of designer braces is WildSmiles whose shaped brackets come in various shapes, college logos, and Disney designs.5 These fun shapes of WildSmiles brackets have a broader base that sits on the tooth and extends beyond the tie wing, which protects more of the tooth from risk of decalcification. This fun shape is part of a child’s “signature smile,” and brushing to see the shape helps provide a visual target and achievable goal that
is more tangible than “go brush your teeth.” Guiding a child to their brushing goal eliminates the struggle between parents and children. With the proper and fun direction, they will not need to re-brush because they were not effective the first time.
Early treatment protocols also encourage more frequent visits or remote monitoring scans, which create additional opportunities for clinicians to reinforce brushing technique, monitor oral health, and educate caregivers. In these regular intervals, oral hygiene is repositioned from an abstract instruction into a visible, trackable goal. For patients who are not yet ready for independent hygiene, these visits or scans can serve as anchor points for accountability and encouragement.
This proactive strategy reframes interceptive orthodontics not as an isolated biomechanical phase, but as a developmental milestone where habits and healthcare literacy are actively shaped.
Compliance
tools and strategies: from chairside
to homecare
1. Behavioral reinforcement: Positive reinforcement strategies — such as sticker charts, progress photos, and digital rewards — have shown effectiveness in improving pediatric compliance.
2. Visual tracking tools: Tools that allow children to see plaque accumulation, such as disclosing tablets or color-coded brackets, enhance awareness and ownership.
3. Parental coaching: Chairside modeling, instructional videos, and take-home materials empower parents to serve as hygiene coaches.
4. Technological aids: Smartphone apps with reminders, timers, and gamified elements encourage consistency and make brushing feel like a routine rather than a chore.
5. In-office protocols: Every visit can include a hygiene check-in, verbal praise or correction, and visual tracking of progress.
6. Brushing cues for younger patients: Simple strategies such as encouraging patients to “brush to see the shape” of their appliance or teeth have proven effective. By prompting children to reveal the clean contours of designer brackets, clinicians can guide attention to thorough brushing without complex instructions. This method promotes ownership and an easily understood visual goal for the young patient and caregiver.
Integrating these strategies into interceptive treatment fosters a stronger clinician-patient-parent partnership and reinforces the value of early compliance.
Appliance considerations: supporting hygiene through design
Fixed and removable appliances used in early treatment should prioritize hygienic access and minimize plaque-retentive areas. For example:
• Bands versus bonds: Where clinically appropriate, bonded molar tubes may provide easier access for brushing compared to full bands.
• Archwire simplicity: Reducing the number of auxiliaries or unnecessary archwire accessories can limit areas prone to plaque accumulation.6
• Customized designs: Incorporating appliance features that are visually engaging for children — such as personalized color choices and themed shapes — can make oral hygiene more goal-oriented and fun. Customized options allow patients to take ownership of their appliance design and help clinicians tailor appliance selection to each patient’s motivational profile.
Clinicians should assess appliance options not only by mechanical function but also by their potential to increase brush-
Case
example: a compliance-centered
inter-
ceptive
case
A 9-year-old female presented with moderate crowding, anterior crossbite, and poor hygiene scores despite parental supervision. Treatment was initiated using a limited fixed-appliance approach with bonded tubes and esthetic bracket designs chosen by the patient. Brushing instruction and a hygiene chart were provided at each visit.
What made the brushing instruction effective was the integration of visual, child-led feedback tools. The patient was taught to use disclosing tablets before brushing at home and to “brush to see the shape” of her appliance — a cue that helped her recognize missed plaque in a nonjudgmental way. In-office praise for visible improvements and monthly plaque tracking built intrinsic motivation. The chart used a simple weekly reward system that both patient and caregiver could monitor. (Figures 1-3)
By the third month, plaque scores had improved by 32%, and the patient reported brushing twice daily with caregiver oversight. At 6 months, the anterior crossbite was resolved, and hygiene scores remained in the optimal range. The patient was retained with a removable appliance and transitioned to monitoring until phase II.
This case illustrates the compounding success that occurs when early treatment goals include both biomechanical correction and behavioral hygiene shaping.
Conclusion: hygiene as a clinical priority in early orthodontics
For orthodontists and pediatric dentists, the mixed dentition stage represents more than a biomechanical phase — it is a formative window for habit shaping, behavior reinforcement, and preventive care. Oral hygiene compliance is not a secondary outcome but a foundational one.
By embracing early treatment as an opportunity to influence behavior, reinforce family education, and integrate hygiene into appliance design, clinicians can improve both immediate outcomes and lifelong oral health trajectories. The intentional alignment of treatment goals, communication strategies, and compliance tools transforms interceptive treatment into a comprehensive care experience.
REFERENCES
1. American Academy of Pediatric Dentistry. Periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. The Reference Manual of Pediatric Dentistry. Chicago, Ill.: American Academy of Pediatric Dentistry; 2024:293-305.
3. Piaget J. The Psychology of the Child. New York: Basic Books; 1969.
4. American Association of Orthodontics. How Do Braces Work? Designer Braces. https://aaoinfo.org/treatments/braces. Accessed June 13, 2025.
5. Wild Smiles. https://www.wildsmilesbraces.com/. Accessed June 13, 2025.
6. Artun J, Brobakken BO. Prevalence of carious white spots after orthodontic treatment. Eur J Orthod. 1986;8(4):229-234.
Author’s note: This article was developed with the assistance of AI-based writing tools under the direction of the author. The author takes full responsibility for the accuracy, clinical integrity, and originality of the final manuscript.
Figure 1: Showing the plaque that had accumulated gingivally over the bracket pad
Figure 2: Showing the instruction to brush to see the shape
Figure 3: Showing the result of the brush-to-see-the-shape instruction in the office
Continuing Education Quiz
Early orthodontic intervention: enhancing oral hygiene compliance in the transitional dentition CARTER
1. The ___________ stage represents a critical window of opportunity in a child’s oral development.
a. mixed dentition
b. permanent dentition
c. deciduous dentition
d. transitional adult dentition
2. Between the ages of 6 and 12, the eruption of permanent teeth alongside retained primary teeth creates a complex oral environment prone to _____.
a. plaque retention
b. gingival inflammation
c. early signs of periodontal stress
d. all of the above
3. Children in this stage (between 6 and 12 years old) often lack the _______, motivation, and maturity to maintain adequate oral hygiene independently.
a. intelligence
b. proper tools
c. dexterity
d. tooth morphology
4. The presence of orthodontic appliances, combined with the eruptive pattern of the mixed dentition stage, often results in ______.
a. increased areas for plaque retention
b. difficulty with access during brushing
c. the need for extractions
d. both a and b
5. Crowded arches, exfoliating primary teeth, and partially erupted molars can hinder effective hygiene even before brackets are placed.
a. True
b. False
6. Clinical teams should not assume that the absence of obvious gingival inflammation or caries in early appointments equates to effective hygiene.
a. True
b. False
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 250
Date Published: July 18, 2025
Expiration Date: July 18, 2028
7. Younger patients are more prone to ________.
a. oppositional behavior
b. have less intrinsic motivation for hygiene
c. often rely heavily on caregivers to enforce routines
d. all of the above
8. Disclosing tablets or color-coded brackets are examples of _____.
a. visual tracking tools
b. archwire simplicity
c. in-office technology aid
d. plaque traps
9. Smartphone apps with reminders, timers, and gamified elements
_______.
a. are expensive and unnecessary
b. make children dependent on outside cues and are not recommended
c. encourage consistency and make brushing feel like a routine rather than a chore
d. eliminate the need for parental involvement
10. The _________ of treatment goals, communication strategies, and compliance tools transforms interceptive treatment into a comprehensive care experience.
a. spontaneous creation
b. intentional alignment
c. unintentional outcome
d. random selection
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
DentalMonitoring — the future is now
Orthodontics is at a pivotal moment. Technological advancement is no longer just an option — it’s a necessity. As patient expectations evolve, and staffing shortages persist, orthodontists are faced with a crucial question: How can I deliver exceptional care more efficiently, with fewer resources, and still maintain a competitive edge?
The answer is DentalMonitoring.
What began as a pioneering remote monitoring solution has now become the only FDA- and MDR-approved Software as a Medical Device (SaMD) in its category. DentalMonitoring isn’t just helping doctors monitor patients remotely — it’s clinically transforming how we practice.
By leveraging AI to detect and track up to 18 intraoral indications, including archwire passivity, aligner fit, occlusion, and even midline deviations, DentalMonitoring provides orthodontists with near real-time data between appointments. It’s like having eyes on every patient, every week — without requiring them to step into the office.
This shift to AI-driven, data-supported care is not only smarter — it’s faster. What used to take 6 to 8 weeks for a patient issue to be flagged and resolved can now happen in under 7 days. That kind of responsiveness isn’t just nice to have — it’s becoming the new expectation.
And we’re just getting started.
This summer, DentalMonitoring+ is launching a gamechanger that automatically generates interactive 3D models from every patient scan. From within the dashboard, doctors can now assess detailed tooth movements, manipulate teeth virtually, and
track occlusal changes with surgical precision. No special hardware. No waiting. Just instant, dynamic insight.
But perhaps the most powerful evolution isn’t a feature — it’s a philosophy: Dynamic Scheduling.
Instead of the rigid, pre-set appointment intervals that define traditional orthodontics, DentalMonitoring enables a patientdriven cadence. You bring patients in only when their biology — and your clinical insight — says it’s time. That means fewer unnecessary appointments, faster treatment times, and more efficient practices.
Think of it as orthodontic care finally catching up with modern expectations: personalized, responsive, and intelligently optimized.
And it doesn’t stop at treatment.
With innovations like SmartSTL, doctors can now generate up-to-date STL files remotely using a patient’s latest scan — no in-office visit required. Whether you’re prepping for a refinement or fabricating a new retainer, DentalMonitoring has turned what used to be a logistical hurdle into a seamless, on-demand experience.
We’ve also partnered with leading orthodontic platforms — Ormco™, Spark™, Angel Aligners™, Dolphin, Ortho2, GreyFinch®, BrightReferral, 3Shape, Medit, and others — to ensure that DentalMonitoring integrates smoothly into your existing workflow, keeping your team efficient and your focus on what matters most: patient care.
So what does this all mean?
It means the standard of care is shifting. It means practices that embrace AI-driven tools like DentalMonitoring will be the ones patients talk about, staff want to work for, and competitors try to keep up with.
It means the future of orthodontics isn’t 5 years away. It’s already here.
And it’s time to step into it. This information was provided by DentalMonitoring.
THE FIRST DATA-DRIVEN RECOGNITION PROGRAM
DentalMonitoring’s AI-powered monitoring identifies the world’s top orthodontic practices based on objective clinical data. At the TOP Summit, these elite leaders reveal the proven strategies behind their outstanding patient outcomes. September 18, 2025 from 2:00 - 5:30 PM
Anaphylaxis preparedness in dental practices: what to know to be prepared
J. Wesley Sublett, MD, MPH, Board-Certified Allergist in Louisville, Kentucky, and Donald Cohen, DMD, from New York State, inform dentists on how to approach this dangerous allergic reaction
One of the most dangerous emergencies you may encounter in a dental office is anaphylaxis, a severe allergic reaction that can happen within minutes and can be fatal if not treated immediately with epinephrine. The American Dental Association (ADA) recommends that dental practices have plans in place for responding to allergic emergencies, including using epinephrine auto-injectors to treat anaphylaxis. We asked J. Wesley Sublett, MD, and Donald Cohen, DMD, about the key facts every dental practice should know about anaphylaxis and how to prepare for it.
Q: What are common triggers for anaphylaxis in a dental office?
Dr. Cohen: The most common triggers of anaphylaxis in dental practice are antibiotics, antiseptics, and latex-containing products, such as gloves, bite-wing tabs, adhesive tape, and rubber dams. But these are not the only possible triggers.1 Medications, such as NSAIDs, local anesthetics, sedatives, and the materials used in endodontics and impressions can also cause anaphylaxis.1
Q: What are the symptoms of anaphylaxis?
Dr. Sublett: Because anaphylaxis is life-threatening and can occur quickly, it’s critical for dentists and their staff to recognize symptoms and respond immediately. Symptoms can occur in a number of different systems in the body.2 For example, there may be skin changes, including rash, hives, redness, itching, or swelling below the skin surface. The patient’s mouth, throat, or tongue can become swollen, causing swallowing or breathing difficulties such as wheezing or rapid breathing. The patient may experience nausea, vomiting, or other gastrointestinal symptoms. Cardiac symptoms, such as rapid heartbeat and a drop in blood pressure, can also occur.
Q: How can dentists and their staff treat anaphylaxis when it happens in the office?
Dr. Sublett: Epinephrine is the first-line treatment for anaphylaxis,4 and administering epinephrine early has been shown to reduce the risk of hospitalization and life-threatening consequences.5,6 A dose of epinephrine appropriate to the patient’s weight class should be given immediately.7 I recommend Intramuscular Injection (IM), as it is a proven route of administration that reliably delivers the full dose of epinephrine and whose effects have a rapid onset.8 The ADA recommends that practices
have a plan in place, which includes using epinephrine to deliver a premeasured dose to treat anaphylaxis.7
In addition, the World Allergy Organization Anaphylaxis Guidance recommends implementing the following protocol immediately if anaphylaxis is suspected:5
1. If the trigger can be identified, remove it immediately (if feasible).
2. Activate emergency medical services.
3. Assess the patient’s vitals and weight.
4. And, simultaneously, give the weight-appropriate dose of epinephrine.
5. If necessary, give the patient high-flow supplemental oxygen via a face mask.
Q: What are considerations during surgery for administering epinephrine to respond to anaphylaxis?
Dr. Cohen: Since use of a nasal cannula is common during dental surgery,10 I recommend IM epinephrine since it can easily be given during use of a nasal cannula and IV.
Q: When choosing an epinephrine device, what features should dental practices consider?
Dr. Sublett: Epinephrine auto-injectors, like AUVI-Q, simplify administration during an emergency because they can be administered through clothing and are pre-measured with a weight-appropriate dose to keep anaphylaxis symptoms from
J. Wesley Sublett, MD, (left) and Donald Cohen, DMD (right)
Is Your Dental
Practice Prepared?
It’s critical to recognize the symptoms of anaphylaxis and to respond quickly.
Choose a Dental Kit that includes AUVI-Q
• Can administer epinephrine through clothing
• Features voice instructions to help users confidently administer epinephrine
• Is the only epinephrine device available in three weight-appropriate doses
• Common adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties.
Indication
Scan code to equip your practice
AUVI-Q (epinephrine injection, USP) is indicated in the emergency treatment of allergic reactions (Type I) including anaphylaxis to allergens, idiopathic and exercise-induced anaphylaxis. AUVI-Q is intended for patients with a history of anaphylactic reactions or who are at increased risk for anaphylaxis.
Important Safety Information
AUVI-Q is intended for immediate self-administration as emergency supportive therapy only and is not a substitute for immediate medical care. In conjunction with the administration of epinephrine, the patient should seek immediate medical or hospital care. Each AUVI-Q contains a single dose of epinephrine for single-use injection. More than two sequential doses of epinephrine should only be administered under direct medical supervision. Since the doses of epinephrine delivered from AUVI-Q are fixed, consider using other forms of injectable epinephrine if doses lower than 0.1 mg are deemed necessary.
Please see additional Important Safety Information on next page, and full Prescribing Information and Patient Information available at www.auvi-q.com.
The only epinephrine device with voice instructions.
Designed to provide confidence from start to finish—no experience required.1-3
A calm voice in a moment of anxiety
Voice instructions guide users through administration during anaphylaxis.
Simply press and hold
For 2-second administration that patients may not even feel.
Important Safety Information (continued)
Hear the voice instructions for yourself
Reassuring dose delivery confirmation LED lights flash red and voice instructions confirm administration.
Scan code to equip your practice
AUVI-Q should ONLY be injected into the anterolateral aspect of the thigh. Do not inject intravenously, or into buttock, digits, hands, or feet. Instruct caregivers to hold the leg of young children and infants firmly in place and limit movement prior to and during injection to minimize the risk of injection-related injury.
Rare cases of serious skin and soft tissue infections have been reported following epinephrine injection. Advise patients to seek medical care if they develop any of the following symptoms at an injection site: redness that does not go away, swelling, tenderness, or the area feels warm to the touch.
Epinephrine should be administered with caution to patients with certain heart diseases, and in patients who are on medications that may sensitize the heart to arrhythmias, because it may precipitate or aggravate angina pectoris and produce ventricular arrhythmias. Arrhythmias, including fatal ventricular fibrillation, have been reported in patients with underlying cardiac disease or taking cardiac glycosides or diuretics. Patients with certain medical conditions or who take certain medications for allergies, depression, thyroid disorders, diabetes, and hypertension, may be at greater risk for adverse reactions. Common adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties.
Please see the full Prescribing Information and the Patient Information available at www.auvi-q.com.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088
References: 1. Kessler C, et al. Usability and preference of epinephrine auto-injectors: Auvi-Q and EpiPen Jr. Ann Allergy Asthma Immunol. 2019;123(3):256-262. 2. Turner P, et al. Pharmacokinetics of adrenaline autoinjectors. Clin Exp Allergy. 2022;52(1):18-28. 3. Camargo CA Jr, et al. Auvi-Q versus EpiPen: preferences of adults, caregivers, and children. J Allergy Clin Immunol Pract. 2013;1(3):266-272. e1-e3.
and
progressing. AUVI-Q is the only epinephrine device available in three weight-appropriate doses: 0.1 mg for young children weighing 16.5-33 pounds, 0.15 mg for children weighing 33 to 66 pounds, and 0.3 mg for adults and children weighing 66 pounds and above.
In addition, AUVI-Q has voice instructions that guide untrained users through administration during a moment of anxiety. In a recent usability study, users of AUVI-Q were significantly more likely to correctly demonstrate its use compared to other epinephrine auto-injectors.14
Q: What other steps can dental practices take to ensure their anaphylaxis preparedness?
Dr. Cohen: It’s critical to ensure the dental team is always prepared and confident in their ability to respond to allergic emergencies. To this end, regular team training in recognizing anaphylaxis and how to properly use emergency devices, like AUVI-Q, is essential.15
Dental practices should also keep emergency medical kits on hand.15 The ADA Member Advantage program has endorsed HealthFirst as its exclusive provider of dental emergency medical kits for ADA members. Dental professionals can learn more about emergency kits from HealthFirst that include AUVI-Q by visiting healthfirst.com/EMK.
Disclosure: Dr. Sublett is a paid advisor of Kaléo This information was provided by Kaléo.
Indication
AUVI-Q® (epinephrine injection, USP) is indicated in the emergency treatment of allergic reactions (Type I) including anaphylaxis to allergens, idiopathic and exercise-induced anaphylaxis. AUVI-Q is intended for patients with a history of anaphylactic reactions or who are at increased risk for anaphylaxis.
Important Safety Information
AUVI-Q is intended for immediate self-administration as emergency supportive therapy only and is not a substitute for immediate medical care. In conjunction with the administration of epinephrine, the patient should seek immediate medical or hospital care. Each AUVI-Q contains a single dose of epinephrine for single-use injection. More than two sequential doses of epinephrine should only be administered under direct medical supervision. Since the doses of epinephrine delivered from AUVI-Q are fixed, consider using other forms of injectable epinephrine if doses lower than 0.1 mg are deemed necessary.
AUVI-Q should ONLY be injected into the anterolateral aspect of the thigh. Do not inject intravenously, or into buttock, digits, hands, or feet. Instruct caregivers to hold the leg of young children and infants firmly in place and limit movement prior to and during injection to minimize the risk of injection-related injury.
Rare cases of serious skin and soft tissue infections have been reported following epinephrine injection. Advise patients to seek medical care if they develop any of the following symptoms at an injection site: redness that does not go away, swelling, tenderness, or the area feels warm to the touch.
Epinephrine should be administered with caution to patients with certain heart diseases, and in patients who are on medications that may sensitize the heart to arrhythmias, because it may precipitate or aggravate angina pectoris and produce ventricular arrhythmias. Arrhythmias, including fatal ventricular fibrillation, have been reported in patients with underlying cardiac disease or taking cardiac glycosides or diuretics. Patients with certain medical conditions or who take certain medications for allergies, depression, thyroid disorders, diabetes, and hypertension, may be at greater risk for adverse reactions. Common adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties.
Please see the full Prescribing Information (https://bit.ly/4j9fPAQ) and the Patient Information (https://bit.ly/4iZ2o6o).
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.
Emergency dental kits from HealthFirst
REFERENCES
1. Goto T. Management of Anaphylaxis in Dental Practice. Anesth Prog. 2023;70(2):93-105. doi: 10.2344/anpr-70-02-16. Epub 2023 Jun 28.
2. Jevon P, Shamsi S. Management of anaphylaxis in the dental practice: an update. Br Dent J. 2020 Dec;229(11):721-728. doi: 10.1038/s41415-020-2454-1. Epub 2020 Dec 11.
3. Asthma and Allergy Foundation of America (AAFA). Food Allergy Anaphylaxis in Infants and Toddlers. https://aafa.org/asthma-allergy-research/our-research/food-allergy-anaphylaxis-in-infants/. Accessed March 24, 2025.
4. Brown JC, Simons E, Rudders SA. Epinephrine in the Management of Anaphylaxis. J Allergy Clin Immunol Pract. 2020 Apr;8(4):1186-1195. doi: 10.1016/j.jaip.2019.12.015. Erratum in: J Allergy Clin Immunol Pract. 2021 Jan;9(1):604. doi: 10.1016/j.jaip.2020.11.035.
5. Bock SA, Muñoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. 2007 Apr;119(4):1016-1018. doi: 10.1016/j.jaci.2006.12.622. Epub 2007 Feb 15.
6. Fleming JT, Clark S, Camargo CA Jr, Rudders SA. Early treatment of food-induced anaphylaxis with epinephrine is associated with a lower risk of hospitalization. J Allergy Clin Immunol Pract. 2015 Jan-Feb;3(1):57-62. doi: 10.1016/j.jaip.2014.07.004. Epub 2014 Sep 8.
7. Cardona V, Ansotegui IJ, Ebisawa M, El-Gamal Y, Fernandez Rivas M, Fineman S, Geller M, Gonzalez-Estrada A, Greenberger PA, Sanchez Borges M, Senna G, Sheikh A, Tanno LK, Thong BY, Turner PJ, Worm M. World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020 Oct 30;13(10):100472. doi: 10.1016/j.waojou.2020.100472.
8. HealthFirst. Dr. Malamed: The Importance of Epinephrine Auto-Injectors. https://www. healthfirst.com/videos/dr-stanley-malamed-the-importance-of-epinephrine-auto-injectors/. Accessed March 24, 2025.
9. American Academy of Pediatric Dentistry. Managing Professional Risks, ADA Guidelines for Practice Success™ (GPS™), ADA Tip Sheet on Managing Patients’ Medical Emergencies. https://www.aapd.org/globalassets/media/safety-toolkit-2.0/tip-sheet-on-managingpatients- medical-emergencies.pdf. Accessed March 24, 2025.
10. Becker DE, Rosenberg MB, Phero JC. Essentials of airway management, oxygenation, and ventilation: part 1: basic equipment and devices. Anesth Prog. 2014 Summer;61(2):78-83. doi: 10.2344/0003-3006-61.2.78.
11. Krishnamurthy M, Venugopal NK, Leburu A, Kasiswamy Elangovan S, Nehrudhas P. Knowledge and attitude toward anaphylaxis during local anesthesia among dental practitioners in Chennai - a cross-sectional study. Clin Cosmet Investig Dent. 2018 Jun 28;10:117-121. doi: 10.2147/CCIDE.S159341.
12. Çetinkaya F, Sezgin G, Aslan OM. Dentists’ knowledge about anaphylaxis caused by local anaesthetics. Allergol Immunopathol (Madr). 2011 Jul-Aug;39(4):228-231. doi: 10.1016/j. aller.2010.07.009. Epub 2011 Jan 13.
13. Smereka J, Aluchna M, Aluchna A, Szarpak Ł. Preparedness and attitudes towards medical emergencies in the dental office among Polish dentists. Int Dent J. 2019 Aug;69(4):321328. doi: 10.1111/idj.12473. Epub 2019 Mar 7.
14. Zhang E, Sicherer S, Agyemang A. Proper use of epinephrine autoinjectors is related to device type, prior physical demonstration, and sociodemographic factors. J Allergy Clin Immunol Pract. 2025 Feb;13(2):418-420.e1. doi: 10.1016/j.jaip.2024.11.006. Epub 2024 Nov 19.
15. Rosenberg M. Preparing for medical emergencies: the essential drugs and equipment for the dental office. J Am Dent Assoc. 2010 May;141 Suppl 1:14S-19S. doi: 10.14219/jada. archive.2010.0351.
A new generation of aligners designed for effortless compliance and predictability
OrthoFX™, a leading innovator in clear aligners, is redefining clear aligner therapy with a portfolio of products designed to deliver effortless compliance and predictability. This includes FXClear™, which features stain-resistant material and smooth, scalloped edges for enhanced comfort and fit. FXBright™ is a translucent aligner that gives teeth a naturally whiter and straighter appearance, without the use of whitening gels, from day one of the treatment. At the forefront of OrthoFX’s aligners is AirFlex™, previously branded as NiTime™, a patented aligner engineered for comfort, compliance, and groundbreaking predictability.
AirFlex is the first and only FDA-cleared aligner system designed explicitly for 9-12 hours of continuous daily wear time. It has been proven to straighten teeth with 50% less wear time without extending treatment duration.* The secret behind AirFlex’s performance is its patented HyperElastic™ technology. It is the only aligner made from a proprietary multi-copolymer, unlike leading aligner brands that rely on off-the-shelf aligner materials. This advancement in material engineering enhances aligner performance and delivers efficient orthodontic movements.
“My number one priority is to provide the most efficient, predictable, and comfortable orthodontic treatment for my patients, regardless of the complexity of their cases. From my experience, patients are not wearing their aligners as required for 20 to 22 hours a day,” said Dr. Neil Warshawsky, orthodontist, professor, and OrthoFX provider. “This is why AirFlex, with 50% less wear time, is a gamechanger to get patient compliance and treatment outcomes as planned. AirFlex allows me to get the efficiency and outcome I want, while giving my patients a better treatment experience.”
The multi-copolymer features a highly adaptable inner surface designed to conform precisely to the tooth’s outer surface, ensuring an exact fit and preventing the aligner from unseating. HyperElastic technology expands the elastic range, accommodating up to 4 weeks of tooth movement, reducing relapse from non-wear and minimizing refinements.
The science behind AirFlex
Biologically optimal forces
AirFlex aligners are designed with a favorable cellular environment to stimulate timely generation of osteoclasts and osteoblasts. Bone-tissue remodeling happens naturally, allowing teeth to move predictably to their destination.
Consistent force delivery
With industry aligners, very little strain (5%) results in excessive stress that is greater by 20x the optimal force. With AirFlex™ aligners, stress and strain have been decoupled, resulting in strain control within the working range without increasing stress. AirFlex exerts 8.4x less force than other aligner brands.*
4x greater fit range
AirFlex boasts a 4x greater fit range than industry-standard aligners, promoting effortless compliance and reducing the need for refinements.* Its innovative multi-copolymer structure ensures an exact fit and prevents the aligner from unseating.
AirFlex completed 89.4% of treatments with one or fewer refinements,* compared to only 28.6% for the leading aligner brand.** This high predictability rate offers a smoother treatment experience for both the provider and the patient.
Discover AirFlex at www.orthofx.com/discover-airflex/.
Supercharging orthodontics with DentoAI
In today’s orthodontic landscape, balancing efficiency with personalized care has become increasingly challenging. As administrative burdens grow, and patients expect clearer communication, many practices are turning to AI to support their workflows. One software leading the way is DentoAI, the world’s first AI-powered case acceptance platform and ambient scribe built for orthodontists.
Developed by Orthodontist Dr. Amanda Cheng, DentoAI was designed to solve the very challenges she encountered during her decade in clinical practice. At its core, DentoAI gives time back to orthodontists and treatment coordinators (TCs) by automating documentation and streamlining workflows.
A key feature is its ambient scribe, which passively records and structures clinical notes during the consult. This feature alone saves an average of 11 minutes and 57 seconds per visit, adding up to nearly 2 extra hours a day in a busy clinic. That time can be used for additional consultations, increased production, or a less rushed pace for orthodontists and TCs.
The benefits extend beyond documentation. By handling note taking automatically, DentoAI enables TCs to focus entirely on the patient. This shift has been shown to improve same-day start rates. With less typing, TCs can listen more closely, build rapport, and guide patients through important financial or treatment decisions with greater confidence and empathy.
DentoAI also includes an instant treatment plan explanation tool that converts clinical terminology into easy-to-understand layman’s terms. This helps ensure that patients and families
understand the proposed treatment while still in the consult room, allowing for quicker decision-making. For practices serving multilingual communities, the platform can translate the plan into multiple languages instantly, reducing the need for a translator and keeping the decision-making process moving forward during the visit.
Administrative tasks are also simplified. DentoAI can generate referral letters to general dentists instantly, helping orthodontists maintain consistent communication with their referring network. This not only improves the continuity of care but also supports long-term professional relationships, which are essential for practice growth.
What makes DentoAI stand out is its origin. Unlike generic software retrofitted for healthcare, DentoAI was created by a practicing orthodontist who understands the day-to-day complexities of clinical care. Dr. Cheng designed the platform to support existing workflows rather than overhaul them, making the technology easy to adopt and impactful from day one.
As orthodontic practices continue to evolve alongside rapid advances in AI, those that embrace tools designed for efficiency and connection will be best positioned for sustainable success. DentoAI allows teams to operate more smoothly, reduce stress, and focus more fully on their patients.
For orthodontists looking to modernize operations, boost case acceptance, and empower their treatment coordinators, DentoAI is the only AI platform designed specifically for orthodontists.
This information was provided by DentoAI.
Insight to impact: how LightForce is redefining digital orthodontics
In today’s rapidly evolving orthodontic landscape, delivering truly personalized care can feel more complex than ever. That’s where LightForce stands apart. Designed by orthodontists for orthodontists, the LightForce Ecosystem brings together fully customized 3D-printed appliances, intuitive treatment planning software, expert clinical support, and continuous feedback from peers and practices across the country. Every element of the system is built around the real-world needs of clinicians making it easier to deliver exceptional outcomes for every patient.
But LightForce is more than just a set of tools, it’s a complete care platform that supports you from the moment records are submitted to the final debond. Treatment planning, bonding, education, and feedback are all connected to help you streamline your workflow, improve efficiency, and reduce variability in outcomes. With built-in clinical education and peer-to-peer guidance, you and your team can confidently delegate tasks and stay focused on what matters most: delivering personalized, high-quality care to every patient.
introduced a new bracket design featuring thicker tie wings and an optimized base. Early clinical evaluations showed promising improvements in bond reliability.*
Historically, hardware updates in orthodontics take years to implement. But the LightForce ecosystem has enabled something no other system can claim: hardware innovation at the speed of software. Thanks to the real-time feedback loop between practices, our internal product teams, and clinical educators, we can take insight from chairside experiences and turn it into product improvements in a matter of weeks. There are no molds or stock prescriptions holding us back. Every appliance is made-to-order and digitally designed from the start.
Take, for example, one recent update. After hearing customer feedback around tie wing durability and bonding performance in specific regions, our team analyzed bracket reorder data. This is a unique advantage enabled by the LightForce ecosystem. We identified the lower premolars, particularly the gingival tie wings, as a common challenge. In just 12 weeks, we
But we didn’t stop there. In some clinical scenarios, we saw that manual adjustments to our indirect bonding jigs were creating bonding challenges. In response, we partnered with top-performing practices to develop a smarter software algorithm. Built from real-world feedback and clinical expertise, this algorithm can now identify challenging bond cases in advance and pre-segment the LightTrays to simplify the process. The result? A new generation of fully personalized trays that reduce the need for in-office modifications and enhance bond efficiency.
Since launching the updated LightBracket and LightTray designs, we’ve seen a 40% reduction in bracket reorders within 60 days of bonding* — a clear testament to the power of our data-driven innovation cycle.
This is what the LightForce Advantage is all about: empowering orthodontists with a system that listens, adapts, and evolves with them and their needs. If you would like to read more about the LightForce Ecosystem and explore the data behind the improvements highlighted above, please check out our latest LightForce white paper.
Scan the QR code to download the LightForce Bond Success white paper.
Aligners By Allure brings German Innovation from the largest European Aligner Company and engineering to the world of orthodontic treatment as a renowned specialist within the clear aligner industry. Boasting a dedicated customer support team throughout the entire process, we ensure a smooth transition from start to finish for your practice. Combining orthodontic designed treatment plans with our elite manufacturing experience from aesthetic to complex cases, Aligners By Allure delivers exceptional results, every time. Additionally, we pride ourselves on offering the most competitive prices you will find in the market, ensuring that our high-quality aligners are accessible to a wide range of practices. Plus, we understand the importance of timely treatment initiation, which is why the average time for aligners to ship is just 2 weeks, guaranteeing a swift start to your patient's orthodontic journey.
Align Yourself with the Best
Allure Ortho has partnered with ARCAD*, a leader in technology for dental aligners and digital orthodontics.
We are now able to provide a full service Aligner System by pairing the popular Zendura Flex Aligner Material with ARCAD’s revolutionary software system.
Orthodontic designed treatment plans
Market leading, Zendura FLX multi-layered material for ultimate patient comfort
Available in either straight or scallop cut finish
Zendura Flex Material—the benchmark material for Aligners and Retainers
Innovative, user friendly software with AI technology for automatic scanning/segmentation preparation
Direct access to our team of specialists on the connected platform
Doctor created treatment plans
The Workflow
The Workflow
No Extra Fees! WHAT DRS. ARE SAYING This All-Inclusive Aligner System Features a Full Sequence of Aligners, PLUS: FREE Expert Treatment Planning, FREE Aligner Case, FREE Aligner Chewies, FREE Aligner Remover, FREE Align-EEZ Perfect Aligner Seater, & FREE Ultrasonic + UV Light Cleaning Pod FREE Ultrasonic Pod Included with Every Aligner Case of 10 or More Aligners! Powered by
BEFORE AFTER Benefits
Rapid turnaround time Take intraoral scans 1 2 3 4
Take intraoral scans
Upload case on platform
Upload case on platform
Review and confirm treatment plan
Review, modify & confirm treatment plan
Receive Allure Aligners
Receive Allure Aligners
SCAN THIS QR CODE & CREATE AN ACCOUNT Or, visit: allure.arcadlab.com "The software, great pricing, incredible customer service, and of course, the Aligners, have made using Aligners by Allure a great choice for my office." --- Dr. Jerald Hawk | Rockville, MD
$19 per Aligner
Allure Ortho 1 Main Street #10, Whitinsville, MA 01588 sales@allureortho.com made in Germany