• Defends against microleakage via mineral apatite formation 2
• Biofilm modulation6
Shaping the future of pediatric dentistry
Pediatric dentistry stands at the forefront of a major transformation. Fueled by technological innovation, a surge of new leadership, and a renewed commitment to prevention, our field is evolving to meet the complex demands of today’s families and communities.
Artificial Intelligence: concept to clinical ally
AI is no longer theoretical — it’s transforming pediatric dentistry today. More than 60% of dental practices now use some form of AI, from diagnostic imaging to administrative automation. AI-driven caries risk assessments, digital treatment planning, insurance verification systems, and smart scheduling tools are freeing providers to focus on what truly matters: educating families and building trust with our young patients and their parents. These tools not only enhance accuracy but also enable earlier intervention, which is vital given that we all know that over 40% of children aged 2–11 still experience tooth decay.
A workforce transformed
The demographic makeup of pediatric dentistry is also shifting. Today, women account for over 85% of pediatric dental residency program applicants, and we now represent nearly 60% of active pediatric dentists. When I started dental school (more than 20 years ago), roughly only 10% of my graduation class were women. This significant change brings fresh leadership styles that emphasize collaboration, equity, empathy, and mentorship. As the profession becomes more inclusive, it is critical that our institutions, employers, and partners adapt to support work-life balance, flexible practice models, and leadership development.
Prevention and medical management of dental caries take center stage
Preventive care is the cornerstone of our specialty — and it is now being reimagined. Innovations like Cavisense and other
Lisa Bienstock, DMD, is a Board-certified Pediatric Dentist, a Fellow of the American Academy of Pediatric Dentistry, and currently serves as Vice President of the Arizona State Board of Dental Examiners. She is the Associate Director of NYU Langone’s Advanced Education in Pediatric Dentistry program in Phoenix and the proud owner of two thriving private practices dedicated to creating positive, prevention-focused dental experiences for children.
A graduate of Columbia University/NewYork-Presbyterian Medical Center’s prestigious Pediatric Dentistry residency program, Dr. Bienstock has held hospital privileges at Phoenix Children’s Hospital since 2013. Beyond the clinic, she is a passionate educator, national speaker, and philanthropist, with a growing presence on social media where she shares oral health tips (and plenty of real-life parenting humor). Most recently, she did a commercial for Sensodyne Pronamel Toothpaste. Follow her on IG @lisabienstock and on TikTok @doctorb.thatsme.
caries lesion assessment tools, the Willo® automated toothbrush for children, Curodont™ and other remineralization solutions, salivary diagnostics, digital health education platforms, and riskbased caries management systems are allowing dentists to detect caries lesions before they become radiographically visible, recognize the disease process, treat caries lesions before cavitation without removing tooth structure, and tailor prevention with precision like never before.
These changes shift our antiquated thought processes of “waiting and watching” to identifying the disease process early before it evolves into a cavitated lesion that needs treatment. Rather than being reactive, our profession will increasingly become proactive. The focus will become on treating the disease process before it progresses, instead of fixing the damage the disease has irreversibly done. These innovative tools are also critical in addressing disparities: children from low-income families are twice as likely to have untreated cavities compared to those from higher-income households. By focusing on prevention, we can narrow this gap and elevate oral health outcomes across populations.
Integrated practices: a model for the future
Another trend gaining momentum is the rise of integrated pediatric and orthodontic group practices, which are “co-located.” These models promote continuity of care, streamlined communication, and operational efficiency. For families, they offer the convenience of one-stop dental care, and even more of an opportunity for Airway/Phase I treatment. For providers, they foster interdisciplinary alignment and support long-term practice sustainability with a competitive edge. With 75% of dental graduates now preferring group or DSO-affiliated settings, these collaborative practices are poised to become the new norm. If you are a practice owner who is not part of a DSO, you may wish to consider adding an orthodontist to your practice as a potential strategic partner.
Looking ahead
This issue of Pediatric Dental Practice explores the forces redefining our field — from technology trends to leadership transitions and practice management to patient management with prevention-first strategies. Whether you are launching your career, scaling your practice, or simply looking to stay ahead of the curve, these insights offer both inspiration and practical direction.
As pediatric dentists we are fortunate — Howard Farran’s “AI Susceptibility Ranking of the ADA Dental Specialties (over the next 10 years)” ranked pediatric dentistry last. We are here to stay. Our future is bright, data-driven, and deeply human. And it is all being shaped by all of us — today. PD
Cooper courtesy of NuSmile.
✓ EndoSequence BC Pediatric Putty works exceptionally well for pulpotomies
PEDIATRIC SOLUTIONS
Enhance practice efficiency and patient comfort with a comprehensive range of products tailored specifically for pediatric dental care.
✓ EndoSequence BC Liner works during pulpal treatments to add a protective layer over the putty
✓ MINI Diamonds deliver unprecedented access in pediatric cases and patients with limited openings
✓ Brasseler MINI Electric Attachment offers a super miniature head size that provides maximum access
✓ GEM Digital Sensor in size 10 for pediatric patients provides outstanding image quality
SCAN THE QR CODE TO EXPLORE OUR PEDIATRIC FAVORITES PLUS RECEIVE AN EXCLUSIVE OFFER ON THE PEDIATRICS PRODUCT LINE.
TECHNOLOGY
Seeing the invisible
Dr. Chung-Min Kang discusses the transformative role of quantitative light-induced fluorescence technology in pediatric caries diagnosis ......... 20
PRODUCT PROFILE
Breaking through clinical barriers in everyday dentistry
Dr. Jennifer Hechko shares how she reduced anesthesia, improved healing, and uncovered practice growth ............................. 22
GOING VIRAL
Integrating AI in dental practices
Gary Salman explains how to reap the benefits of AI more safely
PRODUCT PROFILE
Magnification and behavior management in dentistry
Dr. Jarod Johnson discusses how to manage pediatric patients for the best use of magnification tools ................................................... 25
PRODUCT SPOTLIGHT
Anaphylaxis preparedness in dental practices: what to know to be prepared
J. Wesley Sublett, MD, MPH, Board-Certified Allergist in Louisville, Kentucky, and Donald Cohen, DMD, from New York State, inform dentists on how to approach this dangerous allergic reaction ............................................ 26
SERVICE PROFILE
Positive separation in pediatric dental sedation
Dr. Denise Chan, Pediatric Anesthesiologist, explains a helpful approach to anesthesia used by Pediatric Dental Anesthesia Associates ................ 30
PRODUCT SPOTLIGHT
Your “third hand” in pediatric dentistry — less stress, more smiles
Dr. Lawrence Kotlow discusses products that make dentistry easier and more comfortable
Published by
Editor in Chief, Publisher, and Senior Strategic Advisor
Scott S. De Rossi, DMD, MBA scott.derossi@nexusdentalsystems.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
Director of Business Development Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Director of Publishing Amanda Culver amanda@medmarkmedia.com
Director of Operations Melissa Minnick melissa@medmarkmedia.com
Director of Marketing Amzi Koury amzi@medmarkmedia.com
Don’t just be their first dentist — be their favorite dentist.
What if you could eliminate dental anxiety for many of your patients? And what if you could perform more multi-quadrant, same-day dentistry?
That is what anesthesia-free, blood-free, and pain-free procedures can do.1 Less blood, sweat and tears - more smiles, efficiency, and revenue for your practice.
A fresh beginning and a grateful heart
American Poet T.S. Eliot wrote, “Every moment is a fresh beginning.” These words have become my North Star — my entire journey with MedMark has been a tapestry of transformative new beginnings, each one more meaningful than the last.
Looking back on these incredible 21 years, my heart is full thinking about how we’ve scaled our impact within the dental community. When I founded Doctor of Dentistry back in 2004, it felt like launching a passion project into the unknown. But watching it evolve, and then witnessing the game-changing expansion with Implant Practice US and Endodontic Practice US in 2007, followed by Orthodontic Practice US in 2009, and Dental Sleep Practice in 2014 — each launch was like watching my children take their first steps. Through this incredible journey, we’ve successfully published 297 publications to date since MedMark’s inception — that’s countless late nights, early mornings, weekend marathons, and probably tens of thousands of road-warrior travel hours poured into every single issue. Each publication represents not just content, but sleepless nights, endless revisions to ensure excellence, and the unwavering commitment to advancing our profession. The authentic connections I’ve built with some of the most visionary minds in dentistry have been nothing short of life-changing.
souls willing to challenge outdated paradigms and pioneer bold new methodologies. Every single author who graced our pages didn’t just bring their expertise — they brought their authentic selves, their infectious passion, and often, their friendship. What started as professional relationships blossomed into an ecosystem where readers don’t just become industry leaders — they become mentors, collaborators, and genuinely cherished friends.
Lisa Moler Founder, MedMark Media
When MedMark became part of the Nexus Dental Systems family in 2020, it marked a pivotal moment in our growth story. Now, as I step into my next-level adventure as Chief Marketing Officer for Nexus Dental Systems, I’m overwhelmed with gratitude. I’ll still be championing the dental community, driving purpose-driven innovation at the intersection of dental and medical breakthroughs. And MedMark? Our publications will continue disrupting the status quo, empowering excellence across all specialties while scaling our content reach and finding new ways to innovate.
These 2 decades have been the most beautiful discovery — our dental community isn’t just an industry, it’s a family of mission-driven change-makers, visionary innovators, and most importantly, treasured friends who have enriched my life beyond measure. The relationships I’ve built with these healthcare heroes, these brilliant minds determined to revolutionize patient care, have become some of the most meaningful friendships of my lifetime. Every revolutionary thought leader, inventor, and disruptor I’ve had the privilege to know personally hasn’t just shared their next-generation technologies with me — they’ve shared their hopes, their dreams, their breakthrough moments, and even their setbacks over countless conversations that turned strangers into lifelong friends.
Our publications became so much more than a showcase for disruptive innovations in imaging, instrumentation, equipment, patient communication, and practice management — they became the bridge that connected hearts and minds. We’ve amplified the voices of clinicians who became dear friends, brave
I’m tearing up just thinking about the incredible people I’ve encountered on this journey. Some of my closest confidants, the people I turn to for advice, the friends who celebrate my victories and support me through challenges — many of them came from this extraordinary profession. I have always said that I didn’t find my dental profession; it found me. It has been a career built on divine alchemy and serendipitous moments. Twenty years of shared experiences, industry events that felt more like family reunions, deep conversations about life, work passions that turned into lifelong friendships, and a network of support that extends far beyond business cards and LinkedIn connections. This community has given me a chosen family I never expected to find. And for that, I am eternally grateful. Our content strategy has always been laser-focused on realtime relevance and community impact. We survived even during the darkest chapter of the pandemic shutdown; our team’s resilience was extraordinary. We pivoted to address the moment’s most pressing challenges — how to continue serving patients with unwavering safety protocols for patients, staff, and doctors. Watching the rise of tele-dentistry and other innovative platforms during that time, seeing our community’s incredible adaptability of hope — it was a masterclass in transformation that redefined the entire profession, and one that I was proud to be a part of.
But never fear, MedMark publications will continue their exponential growth trajectory, serving our loyal community with cutting-edge topics, breakthrough innovations, and an unwavering commitment to helping you scale the successful businesses of your dreams. I’m thrilled to welcome our new Publisher/Editor in Chief Scott S. De Rossi, DMD, MBA, and I’m genuinely excited about the fresh perspective and seasoned expertise he’ll bring to our brand. Scott is a true professional and one of the best author/ writers that I’ve had the pleasure to be associated with lately. Look for his contributions to be informative, smart, and engaging!
As I embark on this new adventure, my heart is filled with excitement while simultaneously overflowing with pride for what we’ve built together from the ground up. I’ll always be part of this incredible MedMark family, and my commitment remains rocksolid — I still remain in our industry to empower your journey to unprecedented success!
With endless gratitude, anticipation for the new journey, and always…to your best success!
Lisa Moler
The Problem: Mouth breathing can lead to underdevelopment of the upper jaw and restricted forward growth of the lower jaw. This can cause crowding and restriction of the airway. Left untreated, the child may develop Sleep Disordered Breathing (SDB).
The Solution: Whole team education and training from Nexus.
Helping you grow healthy kids. Join us: nexusdentalsystems.com/pediatrics/
Setting a new standard of pediatric care in the Texas panhandle
Amarillo Pediatric Dentistry & Orthodontics prides itself on delivering familyfriendly convenience and exceptional clinical outcomes
One of the country’s largest and most cutting-edge pediatric dental practices is situated in a surprising location: the Texas Panhandle. Amarillo Pediatric Dentistry & Orthodontics (APDO) has six offices: four in Amarillo, one in Lubbock, and one in a boarding school 36 miles northwest of Amarillo that provides residential programs and therapeutic services for at-risk boys and girls ages 11 to 17. The six offices are served by eight board-certified specialists — five pediatric dentists, two orthodontists, one oral surgeon, and 120 support staff members.
Amarillo’s welcoming community and strategic location make it a regional hub for advanced pediatric dental care. APDO draws patients from a population of nearly 2 million within a 3 to 4 hour drive, including families from across the Texas Panhandle as well as New Mexico, Oklahoma, Kansas, and Colorado. Founded in 1999, the practice has built a strong reputation for delivering exceptional pediatric outcomes in a compassionate, family-friendly environment. Caring for patients who travel up to 5 hours has inspired APDO to develop efficient systems that allow for comprehensive, same-day treatment and access to specialists without compromising quality of care.
Two of APDO’s current owners, Dr. David Harney and Dr. Devon Cooper, first connected during their pediatric residency interviews, bonding over their shared values and shared vision for providing truly exceptional care. Years later, Dr. Harney reached out to Dr. Cooper to join the growing APDO team, and in Cooper’s words, “That was all she wrote.”
Practicing in a smaller metropolitan area like Amarillo presents unique challenges, from staffing to access to advanced technology. But rather than limiting the practice, those challenges have shaped APDO’s forward-thinking systems designed to balance efficiency and excellence while supporting a patient population spanning parts of five states. The practice’s unique approach to delivering a new standard of pediatric care rests on two pillars: a special passion for family-friendly service, and a commitment to exceptional clinical outcomes.
A special passion for family-friendly service
There are three key elements supporting APDO’s passion for family-friendly service: a special focus on parents, unprecedented convenience, and a “pawsitive” workplace culture.
A special focus on parents
From day one, the doctors at APDO were determined to perfect a unique approach to running a pediatric practice that would foster strong, long-lasting relationships with patients and
In the moments before the procedure, Dr. Harney connects with the patient and parent to go over the plan and ensure they feel comfortable every step of the way
Dr. David Harney and Dr. Devon Cooper in front of Amarillo Pediatric Dentistry & Orthodontics
parents alike. One of their first moves to set their practice apart was to create a trusting, family-friendly environment by welcoming parents chairside during treatments. “We want parents to leave our office feeling confident that their child received top-tier care in a compassionate environment,” says Dr. Harney. “Equally important, we want children to look forward to their next visit. And they almost always do.”
Unprecedented convenience
To improve access and reduce the burden on families, APDO integrates pediatric dentistry, orthodontics, and oral surgery within each of its six well-staffed locations. This comprehensive model allows patients to receive multiple treatments and specialist consultations in a single visit, reducing the need for repeat appointments — an approach especially beneficial for families who travel long distances for care. Each site is staffed with cross-trained team members to ensure efficient, high-quality service for both rural and urban communities. Further enhancing its offerings, APDO is also home to the only AAHC-certified ambulatory surgical center in the region, Domain Surgical. This advanced facility provides dental surgical care under general anesthesia for patients with complex needs, serving families not only in Amarillo but throughout the surrounding states. Together, these efforts reflect APDO’s commitment to making expert care accessible, safe, and convenient for every family it serves.
A
“pawsitive”
workplace culture
“We believe that our ability to create positive relationships with patients and their parents is greatly enhanced by creating a positive work environment,” says Dr. Cooper, and that culture is evident in everything APDO does. Weekly leadership meetings bring together the owners, office leads, team leads, HR, and clinical leadership, with feedback encouraged at all levels. This open, collaborative structure empowers the team and creates an environment where staff can truly thrive.
The doctors emphasize mentorship, work-life balance, and celebrating wins. “You spend more waking hours with your coworkers than with your family most days,” Dr. Cooper points out, “so having the right work environment is essential.” That mindset has helped APDO cultivate a culture of kindness,
APDO also has a unique team member who brings extra comfort to patients. Myko, a miniature goldendoodle therapy dog is lovingly known as the office’s most “pawsitive” presence. His “dad” is none other than Dr. Cooper.
What truly sets APDO apart, though, is its team members’ shared mission: to treat every child like their own, and every parent like a partner. That spirit defines their every interaction.
A commitment to exceptional clinical outcomes
Long-lasting clinical success is always every practice’s goal, but APDO’s ability to deliver on that goal — while also reducing chair time — is particularly appreciated by patients who drive to APDO from as far as 300 miles away. To that end, APDO’s doctors take pride not only in using the latest proven technologies and products, but in achieving a mastery of the techniques necessary to ensure that all technologies and products are utilized to their fullest potential for optimal patient care.
To achieve this mastery, all five APDO pediatric dentists received practical, real-world training by attending a hands-on NuSmile® RESTORE workshop in Las Vegas in the fall of 2024. This workshop introduced the doctors to Soan, a cordless electronic local anesthetic delivery system designed to provide a painless experience that enhances patient comfort and reduces dental anxiety. Incorporating this device into the practice epitomizes APDO’s mission of providing a better experience for
Frontal view of a young patient’s smile showing anterior NuSmile ZR crowns and posterior restoration completed with NuSmile SSC crowns.
A warm welcome from Myko helps make each dental visit feel safe and friendly for patients of all ages
Members of the APDO team gather for a morning meeting, sharing updates, plans, and laughs before the day begins
patients and parents alike. Soon after introducing the Soan to its patients, APDO switched from its prior brand of zirconia crowns to NuSmile ZR crowns. “Our patients now experience not only a much more natural-looking result, but shorter appointment times due to easier placement,” says Dr. Harney. The switch to ZR was rooted in the practice’s mission to provide the highest quality clinical care. “Parents often compliment us on the reduced chair time and the natural-looking appearance of the ZR crowns. They’re just thrilled with the esthetic outcome.”
APDO also chose to adopt two state-of-the-art bioceramic products introduced to them at the workshop: NuSmile’s NeoPUTTY® and NeoLINER® LC. “Our staff appreciates how both of these bioceramics make complex cases feel more manageable,” says Dr. Cooper.
“Since participating in the NuSmile workshop, we’ve been able to enhance the quality and efficiency of our entire system,” says Dr. Harney. “We’ve seen real improvements in how we run things.” As a result, APDO’s owners have decided that all future new associates will gain the same hands-on real-world training through this workshop.
Redefining pediatric dental care
APDO has truly redefined what pediatric dental care can be in a rural area, as all six of its locations enjoy a Google rating of 4.9/5.0. What truly sets them apart, however, is the volume of positive feedback — with over 5,000 Google reviews across all locations, the practice has earned not just high marks but widespread trust and appreciation from the community. Dr. Harney, Dr. Cooper, and their associates hope families leave their visits to APDO feeling genuinely cared for and heard. They aim for every experience to be fun, stress-free, and professional, and for every child and parent to leave smiling. “I have never met a more genuine, caring provider” is the kind of comment they love to hear.
Whether through minimizing wait times, delivering same-day care, or creating a comforting environment for anxious patients and parents, APDO focuses on eliminating friction points and building trust. “We want to be the reason someone says, ‘Today was a good day,’” says Dr. Cooper. “That’s the heart of what we do.”
“It’s hard to put into words the thrill of watching a child walk out of our practice with a bright, beautiful, confident smile after having had to deal with a fractured, decayed tooth or a conspicuous stainless-steel crown,” says Dr. Harney. “And their parents are wearing smiles that are just as big. When they thank us, it’s an emotional moment for them as they say goodbye. And for us.”
And that’s why APDO is committed to investing in education for the next generation, maintaining their reputation for clinical excellence, and protecting the culture that’s gotten them this far. “We have one of the largest private pediatric dental offices in the country,” says Dr. Harney, “but at the end of the day, it’s still about doing right by each family that walks through our doors.”
The team at APDO takes great pride in their ability to make such exceptional care, comfort, and convenience available in a place like Amarillo. They are also very proud that Amarillo is a caring, affordable, close-knit community, that they consider George Strait’s “Amarillo by Morning” to be one of the greatest songs of all time, and that, according to Dr. Cooper, “We have the best steaks in the country, too!”
Demonstrating that location is no barrier to excellence, this Texas Panhandle practice has proven that with the right culture, tools, training, and passion for family-friendliness, the highest standard of pediatric dental care is achievable anywhere. PD
Dr. Harney and Dr. Cooper outside the iconic Big Texan Steak Ranch, showcasing their love for Amarillo and its vibrant local culture
Building trust beyond the chair — Dr. Harney connects with his patient after a successful procedure
Dr. Cooper uses the NuSmile Soan device to deliver gentle, painless anesthesia — keeping the young patient calm and comfortable throughout
Bridging the gap: aligning daily oral care with parents’ primary health concerns
Kristin Evans, BS, RDH, discusses the importance of educating patients on children’s overall health
As a dental hygienist with over 30 years of experience and now a grandmother, I’ve always prioritized oral health in my family. I assumed that the lessons I passed down about cavity prevention and oral health would naturally continue with my grandchildren. But as I’ve observed my adult children raising families of their own, it’s clear that today’s parenting landscape is very different. Busy schedules, shifting priorities, and new stressors have changed how oral care fits into their daily lives.
Yet, some things haven’t changed. Dental caries remains one of the most prevalent, preventable health conditions affecting around 50% of preschool children.¹ Many of these cases go undiagnosed and untreated, increasing the risk of spreading decay to other teeth and even other people. In children under 6 years old, dental decay continues to be a leading cause of preventable hospitalizations.2
From birth through age 5, children depend almost entirely on their caregivers to help build healthy oral hygiene habits.3 These habits are formed through consistent daily routines, yet many parents struggle to maintain them. Brushing can often feel like a daily battle or be forgotten all together after a long, exhausting day. These situations may help explain why just over half of children brush the recommended two times a day, both morning and night, with many missing a few brushing sessions each week.4
Pain, appearance, and self-esteem
As both a dental hygienist and a grandmother, I wonder if we are going about this the wrong way. Sources show that today’s parents may be more concerned about their children’s mental health, nutritional health, and the cost and access to healthcare than having cavities in baby teeth that will “fall out” eventually.5,6 What if we shifted our approach and met caregivers where they are, connecting daily oral care to the concerns that matter most to them?
1. Mental health: the hidden role of oral health in emotional well-being
Mental health is front and center in today’s conversations about children’s health and for good reason. According to the World Health Organization, more than 280 million people worldwide are living with depression, and 23 million of them are our younger population.7 While parents might not immediately connect mental health with oral care, the two are interrelated. Research shows that poor oral hygiene could actually worsen mental health challenges, affecting a child’s confidence, social interactions, and overall quality of life.8 It’s a connection worth exploring and sharing with families.
Untreated dental caries, malocclusion, halitosis, and gum disease can significantly impact a child’s well-being. Beyond physical pain and discomfort, these conditions often lead to sleep disturbances, clenching and grinding, poor nutrition, impact speech, and social embarrassment, all of which can contribute to psychological distress.8 This distress may manifest as low mood, reduced self-esteem, and impaired school performance. Children who feel self-conscious about their teeth may withdraw socially, smile less, or experience more anxiety and depression.8
Kristin Evans, BS, RDH, brings over 30 years of clinical experience and a passion for education to dental professionals nationwide. A graduate of Idaho State University, she is widely recognized as “The pH RDH” for her expertise in pH balance, bone health, and the oral-systemic connection. Since 2019, Evans has delivered engaging, research-based product trainings that connect science with real-world application. Her dynamic style and deep knowledge make her a trusted educator, speaker, and industry contributor. Through personalized education and prevention-focused care, Evans empowers dental teams to elevate outcomes and embrace their vital role in improving whole-body health.
Routine and empowerment to support emotional wellness
Brushing and flossing twice daily helps to build consistent routines and predictable habits. Core daily activities, such as sleep, personal hygiene, and regular meals, form the foundation of what are known as primary routines.9 These routines can reduce the impact of stress and contribute to better mental health outcomes.9 Prioritizing them gives children a sense of control over their bodies and their well-being, helping to build resilience and support emotional wellness. As Harvey Mackay wisely said, “Good habits are as addictive as bad habits, and a lot more rewarding.”
What if we shifted our approach and met caregivers where they are, connecting daily oral care to the concerns that matter most to them?”
Periodontal health and systemic inflammation
Other improvements for both mental health and oral health
• Regular dental visits starting with the eruption of the first primary tooth help build a positive relationship with dental professionals.
• Stress can be reduced with things like: optimal sleep, exercise, meditation, and breathing techniques.
• Do oral hygiene routine together as a family using the Tell-Show-Do model.
• Say to the caregiver: “Cavities can affect how your child eats, sleeps, and feels about themselves. We can help prevent that with good routine home care.”
2. Nutrition, obesity, and chronic inflammatory diseases: oral health’s overlapping role
Nutrition starts in the mouth. Poor nutrition along with the rise in childhood obesity and Type 2 diabetes are critical concerns for today’s families. A survey in 2019 showed that 1 in 3 children are living with a chronic health condition that will have a significant effect on their long-term health outcomes.10 This figure is likely even higher in 2025, prompting many parents to actively seek guidance on improving their children’s diet and metabolic health. Dental professionals can and should play a key role in this conversation.
The systemic risk of sugar and ultra-processed foods
Poor diet choices, stress, and inadequate oral hygiene can disrupt the oral microbiome, a critical system that helps regulate inflammation, protect teeth and gums, and support a child’s immune function.11,12 When pathogenic bacteria outnumber beneficial microbes, a condition known as dysbiosis occurs.11,12 This imbalance can contribute to not only oral diseases but also diabetes, cardiovascular problems, and digestive issues.11
Sugar and ultra-processed foods are shared risk factors for both dental disease and metabolic conditions. Pediatric dental teams are able to educate families on how frequent consumption of these foods impacts not only oral health, but also weight regulation and insulin resistance. Insulin resistance is a precursor to diabetes and other chronic inflammatory diseases.
By promoting a balanced microbiome with optimal oral hygiene alongside the reduction of non-beneficial foods, dental professionals can help reinforce healthy dietary behaviors through a more integrated, whole-child health approach.
Emerging evidence highlights a bi-directional relationship between gum disease and diabetes.13 Even in younger children, gingival inflammation (shaped by factors such as diet, socioeconomic status, and poor oral hygiene) may contribute to elevated systemic inflammatory markers.14 For children diagnosed with diabetes, prediabetes (including fatty liver disease), or other chronic inflammatory diseases, maintaining optimal oral hygiene is essential for preventing the progression of periodontal disease and improving future health outcomes.
Other ways to help children improve oral health and nutrition
• Neutralize pH by staying hydrated with water.
• Eat fiber rich foods, healthy fats, and clean proteins that support beneficial bacteria.
• Avoid alcohol-based mouth rinses that kill the beneficial bacteria.
• Say to the caregiver: “Brushing twice a day is one of the easiest and most powerful ways to support your child’s immune system, help prevent cavities and gum disease, and set them up for better overall health.”
3. Improved home care to help offset barriers to dental services
Access to dental care remains a significant challenge for many families. Barriers such as provider shortages, financial limitations, geographic isolation, and restricted insurance coverage often prevent children from receiving timely preventive or restorative dental services. While these barriers may not be immediately fixable, empowering parents with strategies they can control can help protect children’s oral health despite limited access to professional care.
Prioritizing home-based prevention
In the face of these barriers, home-based oral care becomes a vital first line of defense. Daily oral hygiene practices are among the most accessible and cost-effective strategies for preventing dental disease. It is essential that parents and caregivers are empowered with the knowledge and tools to protect their children’s oral health at home.
Pediatric dental teams can play a central role by educating families on how to:
• Establish consistent brushing and flossing routines appropriate for the child’s age and developmental stage.
• Choose effective, evidence-based products such as hydroxyapatite, nano-hydroxyapatite, fluoride, and nano-silver formulations.
• Use soft-bristled toothbrushes and age-appropriate flossing tools.
• Monitor and reinforce healthy oral hygiene behaviors at home.
When implemented consistently, these home care strategies can significantly reduce the incidence of caries and gingival inflammation. They also help mitigate the broader economic and health burdens associated with untreated oral disease especially in settings where access to regular dental care is limited. By improving oral health through consistent home care, families can reduce the need for costly dental interventions and ultimately save money in the long run.
Conclusion
For pediatric dental professionals, there is an opportunity to reposition oral hygiene not as an isolated dental habit, but as a foundational contributor to children’s well-being. Daily oral hygiene, when practiced effectively, supports mental well-being, improves systemic health, and helps with healthcare barriers. By aligning oral health messaging and routines with today’s top parental concerns, we shift oral care from a task to a tool that benefits both children and parents.
REFERENCES
1. Zhai L, Kong J, Zhao C, Xu Y, Sang X, Zhu W, Yao N. Global trends and challenges in childhood caries: a 20-year bibliometric review. Transl Pediatr. 2025 Jan 24;14(1):139152. doi: 10.21037/tp-24-415. Epub 2025 Jan 21.
2. Walsh O, Chauhan A, Trinh MV, Lin C, Marshall S, Gray-Burrows KA, Silva M. Parents’ perceived barriers and enablers to providing optimal infant oral care. BMC Public Health. 2025 Apr 5;25(1):1292. doi: 10.1186/s12889-025-22487-9.
3. Kaushik M, Sood S. A Systematic Review of Parents’ Knowledge of Children’s Oral Health. Cureus. 2023 Jul 6;15(7):e41485. doi: 10.7759/cureus.41485.
4. Clark SJ, Schultz SL, Gebremariam A, Beel L, Woolford. Oral hygiene is key to
healthy smiles. C.S. Mott Children’s Hospital National Poll on Children’s Health. January 27, 2025:46(5). https://mottpoll.org/reports/oral-hygiene-key-healthy-smiles. Accessed June 26, 2025.
5. Scripps Health. Top 6 concerns parents have about their children’s health. Scripps.org. January 8, 2020. https://www.scripps.org/news_items/5938-top-6-concerns-parentshave-about-their-children-s-health. Accessed June 26, 2025.
6. ParentBee. The Top 10 Concerns Regarding Children’s Health in USA. 2024. ParentBee. org. October 26, 2024. https://www.parentbee.org/blog/the-top-10-concerns-regarding-childrens-health-in-usa-2024/ (parentbee.org). Accessed June 26, 2025.
7. Global Mental Health Statistics 2025: WHO Uncovers Crisis. LealMind. Published 2025. https://lealmind.com/global-mental-health-statistics-2025/. Accessed June 26, 2025.
8. Garzon J. Oral Health and Mental Health: Reduce Stress, Improve Teeth. World of Dentistry. https://worldofdentistry.org/oral-health-and-mental-health-improve-teeth/. Accessed June 27, 2025.
9. Hou WK, Lai FT, Ben-Ezra M, Goodwin R. Regularizing daily routines for mental health during and after the COVID-19 pandemic. J Glob Health. 2020;10(2):020315. doi:10.7189/jogh.10.020315
10. UCLA Health (Internal Medicine). Pediatric chronic disease prevalence has risen to nearly 30% in the last 20 years. UCLA Health. March 10, 2025. https://www.uclahealth.org/news/release/pediatric-chronic-disease-prevalence-has-risen-nearly-30 uclahealth.org. Accessed June 26, 2025.
11. Dental Health Society. What is the Oral Microbiome and How Does it Affect Overall Health? DentalHealthSociety.com. April 21, 2025. https://dentalhealthsociety.com/ oral-health/what-is-the-oral-microbiome-and-how-does-it-affect-overall-health/. Accessed June 26, 2025.
12. Sedghi L, DiMassa V, Harrington A, Lynch SV, Kapila YL. The oral microbiome: Role of key organisms and complex networks in oral health and disease. Periodontol 2000. 2021 Oct;87(1):107-131. doi: 10.1111/prd.12393. Accessed June 27, 2025.
13. Nygaard N, Eriksen AK, Ängquist L, Belstrøm D, Stankevic E, Hansen T, Olsen A, Markvart M. A nationwide registry-based cohort study of the association between childhood dental caries and gingivitis with type 2 diabetes in adulthood. Acta Diabetol. 2025 Jan 13. doi: 10.1007/s00592-024-02437-4. Epub ahead of print.
14. Rajasekaran JJ, Krishnamurthy HK, Bosco J, Jayaraman V, Krishna K, Wang T, Bei K. Oral Microbiome: A Review of Its Impact on Oral and Systemic Health. Microorganisms. 2024 Aug 29;12(9):1797. doi: 10.3390/microorganisms12091797
Disclosure: AI was used by the author of this article for editing content and grammar.
Pediatic Dental Practice US Webinar
LEARN about the lastest techniques and technology from industry leaders with our free live and archived educational webinars. Our online seminars are a convenient way to access great information and upskill. Check out our most recent webinar:
• The Use of Bioceramics in Pediatric Dentistry along with Successful Behavior Management Techniquesg with host Dr. Sara Ruby WATCH NOW at https://pediatricdentalpractice.com/webinars/ Connect. Be Seen. Grow. Succeed. | www.medmarkmedia.com
Reflections from a case study
Drs. Dara L. Rinchuse and Donald J. Rinchuse reflect on delaying orthodontic
treatment for very young patients
The primary author’s 3-year-old daughter, JoJo (and co-author’s granddaughter), had used a pacifier (“binky”) since birth. The pacifier (Philips Avent Soothie) adversely altered JoJo’s oral facial complex creating severe maxillary anterior protrusion. Family photographs document the progress of JoJo’s case from pacifier use (Figures 1A-1C) to months afterwards when the pacifier was discontinued (Figures 2A-2B). Figures 1A-1C show the profound untoward effects the pacifier had on her dentition causing severe maxillary protrusion (Class II division 1 malocclusion with a large overjet). After stopping the pacifier at age 3 years, 4 months, her malocclusion returned to a rather normal state 4 months later (Figures 2A and 2B). Of note, JoJo had a tongue thrust while using the pacifier, and the tongue thrust disappeared after discontinuing the pacifier. Notably, JoJo’s malocclusion corrected without any kind of treatment. If JoJo had had treatment, the outcome of her bite correction could have reasonably been assumed to be due to an orthodontic intervention rather than a natural occurrence, i.e., the return to homeostatic balanced oral soft-tissue forces.
Discussion
Observations in clinical practice can be misleading if a practitioner does not consider and account for clinical results being due to factors other than
Figures 1A-1C: Severe dental protrusion for a 3-year-old-child caused by the long-term use of a pacifier
Dara L. Rinchuse, DMD, graduated from the University of Pittsburgh School of Dental Medicine (DMD) in 2008 and Jacksonville University School of Orthodontics (Certificate) in 2010. She is in private orthodontic practice in Rostraver, Pennsylvania. She has authored several papers, including several in the American Journal of Orthodontics and Dentofacial Orthopedics. She can be reached at dararinchuse13@gmail.com.
Donald J. Rinchuse, DMD, MS, MDS, PhD, graduated from the University of Pittsburgh School of Dental Medicine in 1974 with degrees in Dentistry (DMD) and Pharmacology/Physiology (MS). He received his certificate and MDS degree in orthodontics in 1976 and a PhD in Higher Education in 1985 from the University of Pittsburgh. He is a Diplomate of the American Board of Orthodontics. In addition, Dr. Rinchuse is on the editorial review board of many professional journals including the American Journal of Orthodontics and Dentofacial Orthopedics. He has published over 150 articles, two books, several book chapters, and has made many presentations. He can be reached at rinchuse21@gmail.com.
clinical treatments. JoJo’s case illustrates why controls are necessary in clinical experimental research. Importantly, research controls serve as baselines that allow researchers to compare the effects of experimental treatments against subjects who did not receive treatment. Further, control groups help by eliminating or reducing the effects of confounding factors, account for placebo effects, measure natural changes, reduce bias, establish causality, and enhance validity.1
JoJo’s case brings to mind several additional considerations. For one, are many of the orthodontic phase I treatments necessary? Are many orthodontic problems self-correcting, particularly for very young children? And, what about the evidence-based literature which suggests that many of the early phase I treatments may be unnecessary, at least for certain malocclusions and certain appliances; i.e., better treated at a later time.2-6
Of note, several recent studies have indicated that a number of occlusal discrepancies can improve and/or correct in the transition from the mixed dentition to the early permanent dentition.7,8 The occlusal variants that showed favorable changes were: crowding, maxillary midline diastema, overjet, posterior crossbite, anterior openbite, and class II occlusion.7,8
On further reflection of JoJo’s case, a contemplated question comes to mind. That is, “Why don’t all cases similar to JoJo’s return to the pre-existing state after the pacifier or habit is discontinued?” Could it be that the children with rather normal dental-facial features (normal soft and hard tissue) prior to habit use are in the best position for the malocclusion to be self-correcting? Conversely, would children who have facial and dental imbalances before the habit started, be less likely to have their malocclusions self-correct (at least fully correct)?
In addition, JoJo’s case stimulates the discussion of the never-ending debate of the question as to what comes first, the proverbial “chicken or egg.” This is regard to dental open bites and tongue thrusts. Parenthetically, this debate often ignores the possibility that both the open bite and tongue thrust developed and then ceased concomitantly.
Lastly, although case studies are not the best type of research, they can provide useful information. For instance, they can stimulate the formation of hypotheses that then provoke experimental research. The disadvantages of case studies are many. For one, with a sample size of “one,” there is not much that can be gleaned from an evidence-based perspective.
Conclusions
The results of clinical treatments, at times, may have little or nothing to do with the interventions that were rendered. Some outcomes in clinical practice and in research are best explained as natural or chance occurrences. It is advantageous for clinicians to contemplate the importance of bringing the knowledge of science, evidence-based medicine, and research to the patient care arena.
REFERENCES
1. Leotti LA, Iyengar SS, Ochsner KN. Born to choose: the origins and value of the need for control. Trends Cogn Sci. 2010 Oct;14(10):457-463. doi: 10.1016/j.tics.2010.08.001.
2. Proffit WR. The timing of early treatment: an overview. Am J Orthod Dentofacial Orthop. 2006 Apr;129(4 Suppl):S47-49. doi: 10.1016/j.ajodo.2005.09.014. PMID: 16644417.
3. O’Brien K, Wright J, Conboy F, Appelbe P, Davies L, Connolly I, Mitchell L, Littlewood S, Mandall N, Lewis D, Sandler J, Hammond M, Chadwick S, O’Neill J, McDade C, Oskouei M, Thiruvenkatachari B, Read M, Robinson S, Birnie D, Murray A, Shaw I, Harradine N, Worthington H. Early treatment for Class II Division 1 malocclusion with the Twin-block appliance: a multi-center, randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2009 May;135(5):573-579. doi: 10.1016/j.ajodo.2007.10.042.
4. Rinchuse DJ, Miles P. Chapter 2. Early intervention: The evidence for and against. pgs. 7-16. In: PS Miles, DJ Rinchuse, DJ Rinchuse. eds. Evidence-Based Clinical Orthodontics. Quintessence Publishing: Chicago;2012:7-16.
5. Schneider-Moser UEM, Moser L. Very early orthodontic treatment: when, why and how? Dental Press J Orthod. 2022 Jun 10;27(2):e22spe2. doi: 10.1590/2177-6709. 27.2.e22spe2.
6. Perillo L. Editorial: Early treatment: Where are we today? Sem Orthod. 2023;29(2): 117-118.
7. Carneiro DPA, Moraes CN, de Menezes CC, de Castro Meneghim M, Vedovello SAS. A longitudinal study of intermaxillary and intraarch relationships from mixed to permanent dentition: A 4-year follow-up. Am J Orthod Dentofacial Orthop. 2025 Jul;168(1):56-62. doi: 10.1016/j.ajodo.2025.02.006. Epub 2025 Mar 11.
8. Khda M, Kiliaridis S, Antonarakis GS. Spontaneous correction and new development of posterior crossbite from the deciduous to the mixed dentition. Eur J Orthod. 2023 May 31;45(3):266-270. doi: 10.1093/ejo/cjac061.
Figures 2A-2B: Normalization of the dentition 4 months after cessation of pacifier use
Jazz Imaging partners with Overjet for an endto-end, AI-powered imaging suite for dentists
Jazz Imaging, an independent provider of dental imaging sensors and integrated software suite, and Overjet, a leader in dental AI, has announced their new partnership to bring Overjet’s FDA-cleared technology to Jazz users. Overjet technology is FDA-cleared to detect, outline, and quantify major oral health conditions so that dentists can detect pathologies with precision and educate patients with confidence. Through Jazz’s interoperability, clinicians will be able to capture images and get near realtime AI analysis to detect caries, calculus, bone-levels, PARLs, anatomical structures, and more, all in one platform. The partnership makes it easier for doctors to educate patients and for patients to understand their oral health. The shared guiding principle for both companies in this new collaboration is enhancing patient outcomes. Customers using Overjet’s AI annotations for patient education and treatment presentation see an average of 27% higher care acceptance. In Overjet’s recent Patient Survey, 85% of patients were more likely to accept care when they could clearly see oral pathologies.
For more information, please visit Jazzimaging.com and Overjet.com.
The Association for Dental Safety announces new nonprofit: The ADS Institute For Dental Safety And Science
The Association for Dental Safety (ADS), a 501(c)(3) nonprofit formerly known as OSAP, has launched a new organization called the ADS Institute for Dental Safety and Science. This organization takes on the primary national responsibility for developing, updating, and disseminating dental infection control guidelines and best practices — a role previously filled by the CDC’s Division of Oral Health until its elimination on April 1. The Institute will be chaired and led by longtime ADS Foundation Board Member Eve Cuny, who brings decades of experience working across the public and private sectors on issues of infection control and patient safety. Through private and public partnerships, the ADS Institute for Dental Safety and Science will continue and strengthen the crucial work of ensuring safety in oral healthcare across the United States.
For more information, visit https://www.myads.org/.
FDA issues 510K clearance for BlueCheck™ Caries Detection and Monitoring
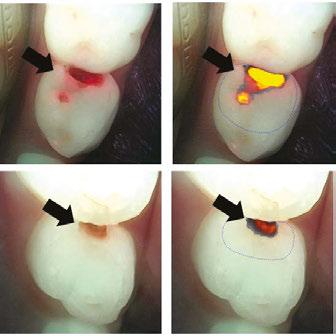
Incisive Technologies has announced that the US Food and Drug Administration (FDA) has issued 510K clearance for BlueCheck™ Caries Detection and Monitoring, a novel caries detection device used by clinicians in dental examinations to aid the detection of early caries. BlueCheck specifically binds to active caries lesions and provides a visible blue color, aiding dental professionals by providing a direct and objective measure of disease. The product’s novel mode of action uses the natural hydroxyapatite-binding chemistry of proteins the BlueCheck molecule has an affinity for and targets porous surface and sub-surface lesions. The specifically designed biomolecule, consisting of a protein, linker and dye, selectively and reversibly binds to sites of dental demineralization. BlueCheck is painted on, and then a simple rinse washes away unbound BlueCheck, to reveal the active caries via the remaining bound blue color. Due to the electrostatic interaction, removal of any bound BlueCheck is via brushing with toothpaste and interaction with saliva.
Headquartered in Melbourne, Australia, Incisive Technologies is a private company that develops, manufactures, and markets dental products supporting prevention. To learn more, visit incisive-technologies.com.
OraCare unveils OraPro — a game-changing toothpaste
OraCare has introduced OraPro, engineered with next-level technology and exclusively available through dental professionals. This unique toothpaste is powered by Micro Netting Technology (MNT) — an innovation that acts like a microscopic net, sweeping away plaque from places other toothpastes can’t reach. OraCare’s other product is OraCare Health Rinse, a professional chlorhexidine alternative.
Clinical statistics show OraPro’s results:
• Reduces plaque 359% more effectively than over-thecounter toothpaste.
• Delivers 209% increased fluoride absorption when compared to regular OTC toothpaste, helping to enhance enamel strength.
• Whitens just as effectively as leading whitening toothpastes with far less abrasion (RDA 88) leading to a brighter smile.
For more information, visit www.OraProPaste.com.
Seeing the invisible
Dr. Chung-Min Kang discusses the transformative role of quantitative lightinduced fluorescence technology in pediatric caries diagnosis
In pediatric dentistry, early detection is everything. Yet, for clinicians working with very young or behaviorally uncooperative children, conventional tools often fall short. Enter quantitative light-induced fluorescence (QLF) technology, an innovative technique in non-invasive caries detection that is gaining traction across Korean clinics — and increasingly, across the global dental landscape.
What is QLF?
Quantitative light-induced fluorescence allows clinicians to visualize dental lesions by detecting fluorescence loss in demineralized enamel. Its key strength lies in capturing early caries that may not yet appear on radiographs, and doing so without radiation exposure. For pediatric practitioners, this means faster, more comfortable exams — and fewer tears in the chair.
A device that provides this type of fluorescence, called Qray, provides quantitative data such as the ΔF value (fluorescence loss percentage) and lesion area, which can be used to track progression or arrest over time. A greater ΔF value has been associated with active lesions requiring clinical attention, while smaller fluorescence losses may indicate arrested or remineralized lesions.
Why use this technology for children?
Children present unique diagnostic challenges. Cooperation may be limited, lesion progression is often rapid, and parental involvement is critical. This technology offers a real-time, visual, and objective caries detection method, especially valuable in:
• Early caries detection in anterior and posterior teeth
• Behavioral management, allowing for quick, non-invasive assessments
Disclosure: Dr. Kang reports no financial conflicts of interest.
• Parental communication, with fluorescence images making caries visibly evident, enhancing understanding and treatment acceptance
• Monitoring lesion progression or arrest over time
• Reducing radiation exposure, aligning with ALARA principles
In Korea, this technology has received new medical technology accreditation and is currently covered under the country’s national health insurance, reflecting strong clinical support and public health value.
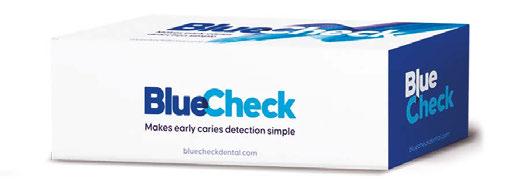
Although the visual size of the lesions appears similar, analysis with this device shows significantly higher quantitative values in tooth #L (ΔF: −38.6%, ΔQ: −41.7, ΔR: 122%) compared to tooth #B. This indicates that the lesion in #L is more active
Chung-Min Kang, DDS, PhD, is an Associate Professor, at the Department of Pediatric Dentistry, Yonsei University College of Dentistry, Seoul, South Korea.
Figure 1: Interproximal caries lesions on primary molars #L and #B.
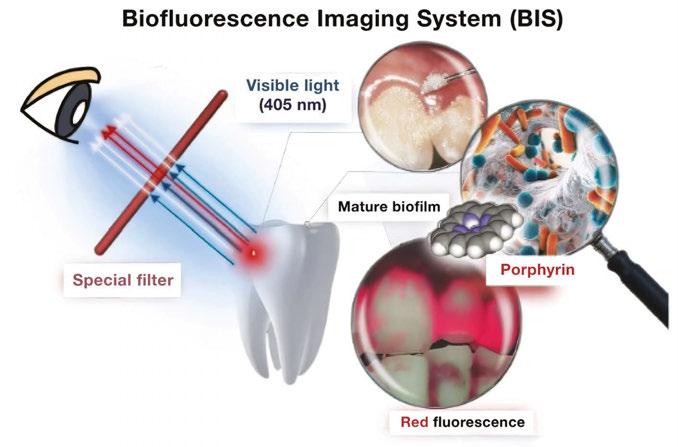
Figure 2: Schematic view illustrating the working of a biofluorescence imaging system
and likely to progress, demonstrating the value of this device in objectively assessing lesion severity beyond visual inspection.
What the research says
Multiple studies have validated Qray’s diagnostic efficacy in primary teeth. In a study by Cho, et al. (2021), Qray demonstrated 88% sensitivity and 90% specificity for detecting dentin caries in primary molars compared with histologic validation.1 A 2022 in vitro study confirmed its robustness in controlled conditions, showing clear separation between sound and carious tissues based on ΔF thresholds.2
Qray also enables clinicians to evaluate caries activity. Kim, et al. (2022), found that active lesions exhibited significantly larger ΔF values and lesion areas, and were associated with distinct microbial profiles, including higher levels of Streptococcus mutans and Lactobacillus spp.3 This opens the door for a more biologically informed approach to caries management, reducing overtreatment of inactive lesions.
In a 2023 randomized controlled clinical trial, Qray was used to assess lesion depth and healing in pulpotomized primary molars, showing potential as a non-invasive follow-up tool for restorative outcome evaluation.4
The Future is bright
As dentistry continues to embrace minimally invasive diagnostics and technology-assisted care, quantitative light-induced fluorescence (QLF) technology is well-positioned as a bridge between clinical accuracy and child-friendly care. For providers in pediatric and preventive settings, this tool doesn’t just illuminate teeth — it illuminates trust, understanding, and better outcomes.
REFERENCES
1. Cho KH, Kang CM, Jung HI, Lee HS, Lee K, Lee TY, Song JS. The diagnostic efficacy of quantitative light-induced fluorescence in detection of dental caries of primary teeth. J Dent. 2021 Dec;115:103845. doi: 10.1016/j.jdent.2021.103845. Epub 2021 Oct 9.
2. Cho KH, Kang CM, Jung HI, Lee TY, Song JS. Assessment of the caries detection ability of quantitative light-induced fluorescence (QLF) in primary teeth in vitro. Journal Korean Acad Pediatr Dent. 2022;49(1):65-75. doi: http://doi.org/10.5933/ JKAPD.2022.49.1.65.
3. Kim CH, Bae K, Lee TY, Song JS, Kim SO, Kang CM. Assessment of dental caries lesion activity status using quantitative parameters obtained from the quantitative light-induced fluorescence method and difference of microbial distribution in primary molars. Photodiagnosis Photodyn Ther. 2022 Sep;39:102942. doi: 10.1016/j. pdpdt.2022.102942. Epub 2022 May 28.
4. Joo Y, Lee T, Jeong SJ, Lee JH, Song JS, Kang CM. A randomized controlled clinical trial of premixed calcium silicate-based cements for pulpotomy in primary molars. J Dent. 2023 Oct;137:104684. doi: 10.1016/j.jdent.2023.104684. Epub 2023 Sep 1.
Leadership Starts Here...
Serendequity Education: Your Success, Our Mission
Whether you’re an owner looking to sharpen your business acumen, a practice manager striving for operational excellence, or an aspiring leader eager to make an impact, this Mini MBA for Dental Professionals lays out a step-by-step roadmap. In the 12 modules, you’ll gain hands-on templates, real-world case studies, and actionable frameworks that translate immediately into your day-to-day—and long-term—success.
Breaking through clinical barriers in everyday dentistry
Dr. Jennifer Hechko shares how she reduced anesthesia, improved healing, and uncovered practice growth
As a pediatric dentist, my mission has always been to create a gentle, efficient, and positive dental experience for children and their parents. Over the years, I have integrated therapy dogs, created a calming environment, and constantly sought out tools that elevate clinical care. One of the most transformative decisions I made was getting into laser dentistry, followed closely by upgrading from an erbium laser to a 9.3micron CO2 all-tissue laser.
I initially trained on an erbium laser hoping to reduce anesthesia, vibration, and aerosols while expanding my soft tissue offerings. While it had some benefits, I quickly learned its limitations. The wavelength’s absorption depth in soft tissue was shallow, leading to more bleeding and less effective coagulation than I wanted. I also found that my hard tissue preparations lacked depth and consistency, more often than not requiring me to switch back to a highspeed handpiece. The fiberoptic cables were costly and delicate — I burned out four of them at significant expense — and the unit frequently needed service with weekslong wait times for repairs. While I was committed to leveraging laser dentistry, I knew I needed something more reliable, efficient, and capable of delivering true hard-and-soft tissue versatility.
When I began researching alternatives, the Solea All Tissue Laser (9.3micron CO2) immediately stood out. Unlike the erbium, Solea’s wavelength is highly absorbed by hydroxyapatite and water, making it uniquely effective for both enamel and soft tissue. The result? Smoother, faster cutting, excellent coagulation, and little to no need for local anesthesia. For pediatric patients, that difference is life-changing. Instead of the stress of injections, I can treat multiple quadrants in a single visit. Parents appreciate the reduced chair time and fewer school absences, and I see dramatically less procedural anxiety.
Clinically, the transition was profound. My Class II production more than doubled after adopting Solea, and my work-
Jennifer Bryk Hechko, DDS, MS, FAAPD, graduated from The Ohio State University College of Dentistry in 2002, completed a 2-year pediatric dental residency at Nationwide Children’s Hospital, and began working in a private practice. Now, she is the proud owner of Brecksville Kids Dentistry. Dr. Jen is Board-certified in Pediatric Dentistry and a member of the American Dental Association, Ohio Dental Association, a fellow of the American Board of Pediatric Dentistry, American Academy of Pediatric Dentistry, and Ohio Academy of Pediatric Dentistry. She has received her Laser Certification from the World Clinical Laser Institute. In addition, she is honored to be recognized by Cleveland Magazine as one of the Top Dentists in Northeast Ohio.
flow became dramatically more efficient. I can sit down and go straight to work — no waiting for anesthesia, no switching between tools. I feel like a better practitioner providing my patients and their caregivers with the best clinical outcomes and the best patient experience.
Soft tissue surgery has also improved. For maxillary frenectomies, uncovering permanent teeth, and even gingival recontouring, I now achieve blood-free, suture-free results that heal beautifully. Parents are amazed when their child needs nothing more than a single dose of ibuprofen, if that, and a week later, the tissue is nearly fully healed.
I’ve expanded into treatments I never thought I would do in private practice: managing aphthous ulcers that now resolve in days instead of a week, removing fibromas and mucoceles (always sending to a lab to confirm the diagnosis), gently decontaminating lesions after extractions, and shaping gingiva to improve eruption or esthetics. Orthodontists in my area now refer their frenectomies and uncoveries to me because the laser allows quick recovery without delaying treatment.
All of this means fewer visits, less anesthesia, and less stress for everyone. Parents comment that their children aren’t anxious about appointments anymore, and many kids don’t want to “graduate” to a general dentist because they don’t want to leave this experience behind. For me, the change has been energizing. I’m accomplishing more in fewer visits, my schedule runs more smoothly, and I genuinely enjoy my days again.
Solea has elevated my practice in every way. It’s reliable, efficient, and delivers on everything it promises — something I could never say about my erbium. For any pediatric or general dentist looking to take their practice to the next level, this technology can be truly game-changing. This information was provided by Convergent. PD
Integrating AI in dental practices
Gary Salman explains how to reap the benefits of AI more safely
As artificial intelligence (AI) continues to permeate various healthcare sectors, dental specialty practices such as orthodontics, endodontics, implants, and pediatric dentistry stand to benefit significantly from its integration. AI offers vast potential to enhance diagnostics, streamline patient management, and boost operational efficiency. However, with these advancements come critical considerations around patient data protection and regulatory compliance as well as the need to maintain compliance with the Health Insurance Portability and Accountability Act (HIPAA) security and privacy rules.
The benefits of artificial intelligence
1. Enhanced diagnostics and patient care
AI has revolutionized diagnostic processes by leveraging machine-learning algorithms to analyze complex datasets, such as radiographic images. This technology can assist in predicting tooth movement and treatment outcomes, enhancing the diagnostic accuracy of decay and anomalies in x-rays, and monitoring patient treatment progress.
2. Streamlined patient management
The automation of routine administrative tasks that AI can handle, from appointment scheduling to patient follow-ups, frees up valuable time for dental professionals to focus on patient care. It also facilitates better patient communication through personalized reminders and post-treatment care instructions, enhancing patient satisfaction and engagement.
3. Operational efficiency
AI tools can optimize inventory management and predict patient flow, leading to better resource allocation and reduced operational costs. Predictive analytics can also take multiple data inputs from systems such as practice management, financial reporting, and insurance claims to identify areas where your practice could improve for growth.
Gary Salman is CEO and co-founder of Black Talon Security (www.blacktalonsecurity.com). A leader in the cybersecurity field, Salman has a 25+ year background in law enforcement and healthcare technology. His firm monitors and secures approximately 50K computers and networks worldwide and has trained tens of thousands of dental and other healthcare professionals.
Protecting patient records and ensuring HIPAA compliance
With the integration of AI, safeguarding patient information becomes paramount. Dental practices must adhere to HIPAA regulations, which mandate the protection of individual health information. Here are key considerations:
• Data storage and flow: Encrypt all stored and transmitted patient data to prevent unauthorized access. This ensures that even if data is intercepted, it remains unreadable to unauthorized individuals. AI often requires your data to be analyzed and stored in many places at a given time. This creates additional risk for your practice, because the bigger your digital footprint, the bigger the risk. Some AI applications can store your data on 3-4 different server networks at a given time.
• Data access controls: Implement strict access controls, ensuring that only authorized personnel have access to sensitive information. Use multi-factor authentication to add an extra layer of security. Many AI companies either purposely or inadvertently share your patient data, with or without your permission. Ask the AI company for their policies for data sharing and retention.
• Regular internal and external audits: Conduct regular security audits to identify vulnerabilities and ensure compliance with HIPAA standards. Internal audits help maintain the integrity of the data protection mechanisms put in place within your practice — but don’t neglect third-party risk. Unfortunately, many AI companies are still in “start-up” mode. Often hiding behind a “HIPAA Compliant” badge, they may fail to have anything more than basic security precautions in place to protect your patient data, putting you at a tremendous risk in the event of a breach.
Best practices for cybersecurity
To protect against cyber threats, dental practices should adopt comprehensive cybersecurity measures so they can identify and mitigate cyber risk. The “Cybersecurity Standard of Care for Dental Practices” includes the following:
• Vulnerability identification and remediation: Hackers use sophisticated tools to identify vulnerabilities on your firewall and computers and leverage these weaknesses to break in and exploit your network. Cybersecurity companies offer sophisticated tools that scan your computers and firewalls daily looking for these exploitable vulnerabilities. The more sophisticated scanners not only identify the vulnerabilities on the computers but can autonomously remediate them.
• Staff cyber training: Educate staff on cybersecurity best practices, including recognizing phishing attempts and safe internet usage. Regular training sessions will help maintain a security-conscious culture within the practice. To be HIPAA compliant, this must be an ongoing, documented process, not a quick “over lunch” conversation. Seek out cybersecurity companies that offer comprehensive training and understand the unique vulnerabilities in workflows of dental practices.
• Penetration testing: An ethical hacker should be attempting to break into your network at least twice per year to test the defensive measures of your network. This test should not be performed by your IT company, but an independent cybersecurity company.
• Incident response plan: Develop a written response plan for potential cyberattacks or any emergency that could disrupt your practice. This plan should outline the steps for containment, investigation, and communication to minimize the impact of the emergency. Rehearse the plan annually to ensure all team members know their role when responding, and to evaluate for any needed improvements to the plan.
• AI-based anti-virus: Utilize more advanced anti-virus software that leverages AI to detect and fight back against more sophisticated attacks. This software must be managed and watched 24/7 by security engineers to be most effective.
Practical steps for successful AI integration
1. Choosing the right AI tools
Select AI solutions that meet the specific needs of your practice. Evaluate various tools based on their functionality, ease of integration, and compliance features. Consider solutions that offer seamless integration with existing systems and have a proven track record in the dental industry. Ask to review their third-party cybersecurity evaluation and HIPAA risk assessment. You don’t want their breach to become your breach.
2. Staff adoption
Ensure that your team is well-prepared to work with AI technologies. Comprehensive training and documented processes will facilitate a smoother transition in their workflows and help staff understand the benefits, risks, and limitations of AI tools. Staff should always use caution when uploading any data that contains confidential information such as employee or patient data into these systems. You may be violating State and Federal laws without realizing it.
3. Ask for a proof of concept
The best way to assess if adding AI to your practice will provide value is to ask for a 90-day proof of concept period to fully understand how it will function. However, you’ll want to be sure you have reviewed their data handling and security protocols prior to giving the tool access to your data.
Balancing advanced technologies with data security
Integrating AI offers transformative benefits, from improved diagnostics to enhanced operational efficiency. However, this technological advancement requires a balanced approach that prioritizes patient data protection and regulatory compliance. By implementing robust cybersecurity measures and choosing the right AI tools, dental specialty practices can harness the power of AI successfully. As AI continues to evolve, embracing these technologies while maintaining vigilance over data security will ensure that your practice remains both innovative and compliant in its operations. PD
Integrating AI offers transformative benefits, from improved diagnostics to enhanced operational efficiency. However, this technological advancement requires a balanced approach that prioritizes patient data protection and regulatory compliance.”
Magnification and behavior management in dentistry
Dr. Jarod Johnson discusses how to manage pediatric patients for the best use of magnification tools
Dentistry continues to progress with advancements that not only enhance precision but also improve practitioner longevity. Among these advancements are dental magnification tools such as Ergo™ loupes and dental microscopes. These advancements are widely accepted in the field of endodontics and general dentistry. One untapped area exists in the field of pediatric dentistry.
One of the most common types of feedback I get when talking to other dental practitioners about using a microscope with kids is, “They move too much.” That simply is a myth that needs to be debunked. 90% of the kids at my office are treated under magnification using a dental microscope. With good behavior management techniques, kids sit still and can benefit from care delivered under a higher level of vision.
Behavior management in pediatric dentistry
Managing patient behavior, particularly in children, is one of the most complex and rewarding parts of modern dentistry. Combining behavioral science with empathetic care is crucial to ensuring procedures run smoothly for patients with varying cooperation levels.
The role of dental magnification in precision
For today’s dental professionals, maintaining precision in diagnostic and procedural tasks is important. This is where dental magnification tools, such as dental loupes and surgical microscopes, come into play.
Benefits of dental magnification
• Enhanced visualization and accuracy: Magnification sharpens focus on minute details, making it easier to detect the early stages of decay, cracks, or other minor issues that may be missed with the naked eye. It can also improve procedural outcomes.
• Improved ergonomics: Magnification devices promote better posture, reducing neck, back, and shoulder strain often associated with long clinical hours. This can provide for career longevity and support practitioner wellbeing.
• Boosted confidence with patients: Visualizing clinical details enhances both patient trust and confidence.
Jarod Johnson, DDS, owns and practices at Arctic Dental in Muscatine, Iowa. He graduated from the University of Iowa and has a Certificate of Pediatric Dentistry from University of Nevada. He is also a Diplomate of the American Board of Pediatric Dentistry. Over the last decade, Dr. Johnson has presented at numerous conferences and presents a hands-on course twice a year at the Enova Training Center in Minneapolis. More information can be found at www.goenova.com/trainingcenter.
Basic strategies for managing pediatric behavior
1. Tell-Show-Do: This widely used method introduces children to each step of a procedure in a non-threatening way. For example, demonstrating on a finger how polishing tools feel before starting can alleviate anxiety. I often let children hold the dental handpiece without a bur and let it run prior to using it for treatment.
2. Positive reinforcement: Offering praise or rewards after cooperative behavior encourages trust and makes future visits smoother. I can always find one thing that a patient is doing well to compliment them on even in the most difficult situations.
3. Non-verbal communication: Maintaining a welcoming demeanor, smiling, and being approachable helps ease tension. When greeting a young patient, I will often sit on the foot of the dental chair (where an adult patient’s legs usually rest) with them to start engagement.
4. Distraction techniques: Tools like ceiling-mounted TVs or virtual reality experiences can distract young patients from their surroundings, minimizing stress. A huge plus is being able to be a great storyteller and develop a story on the spot based on the child’s interests.
Integrating behavior management with magnification
For dentists, combining behavior management with dental magnification creates a powerful synergy. Magnification helps dental practitioners refine their work, and with the right behavior management protocol, it ensures the child remains as comfortable as possible.
I once thought that “kids move too much.” But after implementing a dental microscope at my office last year, I learned that simply wasn’t true. With the right behavior management techniques, magnification and pediatric dentistry can work synergistically, improve outcomes for the patient, and provide career longevity through ergonomics. This information was provided by Enova. PD
Anaphylaxis preparedness in dental practices: what to know to be prepared
J. Wesley Sublett, MD, MPH, Board-Certified Allergist in Louisville, Kentucky, and Donald Cohen, DMD, from New York State, inform dentists on how to approach this dangerous allergic reaction
One of the most dangerous emergencies you may encounter in a dental office is anaphylaxis, a severe allergic reaction that can happen within minutes and can be fatal if not treated immediately with epinephrine. The American Dental Association (ADA) recommends that dental practices have plans in place for responding to allergic emergencies, including using epinephrine auto-injectors to treat anaphylaxis. We asked J. Wesley Sublett, MD, and Donald Cohen, DMD, about the key facts every dental practice should know about anaphylaxis and how to prepare for it.
Q: What are common triggers for anaphylaxis in a dental office?
Dr. Cohen: The most common triggers of anaphylaxis in dental practice are antibiotics, antiseptics, and latex-containing products, such as gloves, bite-wing tabs, adhesive tape, and rubber dams. But these are not the only possible triggers.1 Medications, such as NSAIDs, local anesthetics, sedatives, and the materials used in endodontics and impressions can also cause anaphylaxis.1
Q: What are the symptoms of anaphylaxis?
Dr. Sublett: Because anaphylaxis is life-threatening and can occur quickly, it’s critical for dentists and their staff to recognize symptoms and respond immediately. Symptoms can occur in a number of different systems in the body.2 For example, there may be skin changes, including rash, hives, redness, itching, or swelling below the skin surface. The patient’s mouth, throat, or tongue can become swollen, causing swallowing or breathing difficulties such as wheezing or rapid breathing. The patient may experience nausea, vomiting, or other gastrointestinal symptoms. Cardiac symptoms, such as rapid heartbeat and a drop in blood pressure, can also occur.
Q: How can dentists and their staff treat anaphylaxis when it happens in the office?
Dr. Sublett: Epinephrine is the first-line treatment for anaphylaxis,4 and administering epinephrine early has been shown to reduce the risk of hospitalization and life-threatening consequences.5,6 A dose of epinephrine appropriate to the patient’s weight class should be given immediately.7 I recommend Intramuscular Injection (IM), as it is a proven route of administration that reliably delivers the full dose of epinephrine and whose effects have a rapid onset.8 The ADA recommends that practices
have a plan in place, which includes using epinephrine to deliver a premeasured dose to treat anaphylaxis.7
In addition, the World Allergy Organization Anaphylaxis Guidance recommends implementing the following protocol immediately if anaphylaxis is suspected:5
1. If the trigger can be identified, remove it immediately (if feasible).
2. Activate emergency medical services.
3. Assess the patient’s vitals and weight.
4. And, simultaneously, give the weight-appropriate dose of epinephrine.
5. If necessary, give the patient high-flow supplemental oxygen via a face mask.
Q: What are considerations during surgery for administering epinephrine to respond to anaphylaxis?
Dr. Cohen: Since use of a nasal cannula is common during dental surgery,10 I recommend IM epinephrine since it can easily be given during use of a nasal cannula and IV.
Q: When choosing an epinephrine device, what features should dental practices consider?
Dr. Sublett: Epinephrine auto-injectors, like AUVI-Q, simplify administration during an emergency because they can be administered through clothing and are pre-measured with a weight-appropriate dose to keep anaphylaxis symptoms from
J. Wesley Sublett, MD, (left) and Donald Cohen, DMD (right)
Is Your Dental
Practice Prepared?
It’s critical to recognize the symptoms of anaphylaxis and to respond quickly.
Choose a Dental Kit that includes AUVI-Q
• Can administer epinephrine through clothing
• Features voice instructions to help users confidently administer epinephrine
• Is the only epinephrine device available in three weight-appropriate doses
• Common adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties.
Indication
Scan code to equip your practice
AUVI-Q (epinephrine injection, USP) is indicated in the emergency treatment of allergic reactions (Type I) including anaphylaxis to allergens, idiopathic and exercise-induced anaphylaxis. AUVI-Q is intended for patients with a history of anaphylactic reactions or who are at increased risk for anaphylaxis.
Important Safety Information
AUVI-Q is intended for immediate self-administration as emergency supportive therapy only and is not a substitute for immediate medical care. In conjunction with the administration of epinephrine, the patient should seek immediate medical or hospital care. Each AUVI-Q contains a single dose of epinephrine for single-use injection. More than two sequential doses of epinephrine should only be administered under direct medical supervision. Since the doses of epinephrine delivered from AUVI-Q are fixed, consider using other forms of injectable epinephrine if doses lower than 0.1 mg are deemed necessary.
Please see additional Important Safety Information on next page, and full Prescribing Information and Patient Information available at www.auvi-q.com.
The only epinephrine device with voice instructions.
Designed to provide confidence from start to finish—no experience required.1-3
A calm voice in a moment of anxiety
Voice instructions guide users through administration during anaphylaxis.
Simply press and hold
For 2-second administration that patients may not even feel.
Important Safety Information (continued)
Hear the voice instructions for yourself
Reassuring dose delivery confirmation LED lights flash red and voice instructions confirm administration.
Scan code to equip your practice
AUVI-Q should ONLY be injected into the anterolateral aspect of the thigh. Do not inject intravenously, or into buttock, digits, hands, or feet. Instruct caregivers to hold the leg of young children and infants firmly in place and limit movement prior to and during injection to minimize the risk of injection-related injury.
Rare cases of serious skin and soft tissue infections have been reported following epinephrine injection. Advise patients to seek medical care if they develop any of the following symptoms at an injection site: redness that does not go away, swelling, tenderness, or the area feels warm to the touch.
Epinephrine should be administered with caution to patients with certain heart diseases, and in patients who are on medications that may sensitize the heart to arrhythmias, because it may precipitate or aggravate angina pectoris and produce ventricular arrhythmias. Arrhythmias, including fatal ventricular fibrillation, have been reported in patients with underlying cardiac disease or taking cardiac glycosides or diuretics. Patients with certain medical conditions or who take certain medications for allergies, depression, thyroid disorders, diabetes, and hypertension, may be at greater risk for adverse reactions. Common adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties.
Please see the full Prescribing Information and the Patient Information available at www.auvi-q.com.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088
References: 1. Kessler C, et al. Usability and preference of epinephrine auto-injectors: Auvi-Q and EpiPen Jr. Ann Allergy Asthma Immunol. 2019;123(3):256-262. 2. Turner P, et al. Pharmacokinetics of adrenaline autoinjectors. Clin Exp Allergy. 2022;52(1):18-28. 3. Camargo CA Jr, et al. Auvi-Q versus EpiPen: preferences of adults, caregivers, and children. J Allergy Clin Immunol Pract. 2013;1(3):266-272. e1-e3.
and
progressing. AUVI-Q is the only epinephrine device available in three weight-appropriate doses: 0.1 mg for young children weighing 16.5-33 pounds, 0.15 mg for children weighing 33 to 66 pounds, and 0.3 mg for adults and children weighing 66 pounds and above.
In addition, AUVI-Q has voice instructions that guide untrained users through administration during a moment of anxiety. In a recent usability study, users of AUVI-Q were significantly more likely to correctly demonstrate its use compared to other epinephrine auto-injectors.14
Q: What other steps can dental practices take to ensure their anaphylaxis preparedness?
Dr. Cohen: It’s critical to ensure the dental team is always prepared and confident in their ability to respond to allergic emergencies. To this end, regular team training in recognizing anaphylaxis and how to properly use emergency devices, like AUVI-Q, is essential.15
Dental practices should also keep emergency medical kits on hand.15 The ADA Member Advantage program has endorsed HealthFirst as its exclusive provider of dental emergency medical kits for ADA members. Dental professionals can learn more about emergency kits from HealthFirst that include AUVI-Q by visiting healthfirst.com/EMK.
Disclosure: Dr. Sublett is a paid advisor of Kaléo This information was provided by Kaléo.
Indication
AUVI-Q® (epinephrine injection, USP) is indicated in the emergency treatment of allergic reactions (Type I) including anaphylaxis to allergens, idiopathic and exercise-induced anaphylaxis. AUVI-Q is intended for patients with a history of anaphylactic reactions or who are at increased risk for anaphylaxis.
Important Safety Information
AUVI-Q is intended for immediate self-administration as emergency supportive therapy only and is not a substitute for immediate medical care. In conjunction with the administration of epinephrine, the patient should seek immediate medical or hospital care. Each AUVI-Q contains a single dose of epinephrine for single-use injection. More than two sequential doses of epinephrine should only be administered under direct medical supervision. Since the doses of epinephrine delivered from AUVI-Q are fixed, consider using other forms of injectable epinephrine if doses lower than 0.1 mg are deemed necessary.
AUVI-Q should ONLY be injected into the anterolateral aspect of the thigh. Do not inject intravenously, or into buttock, digits, hands, or feet. Instruct caregivers to hold the leg of young children and infants firmly in place and limit movement prior to and during injection to minimize the risk of injection-related injury.
Rare cases of serious skin and soft tissue infections have been reported following epinephrine injection. Advise patients to seek medical care if they develop any of the following symptoms at an injection site: redness that does not go away, swelling, tenderness, or the area feels warm to the touch.
Epinephrine should be administered with caution to patients with certain heart diseases, and in patients who are on medications that may sensitize the heart to arrhythmias, because it may precipitate or aggravate angina pectoris and produce ventricular arrhythmias. Arrhythmias, including fatal ventricular fibrillation, have been reported in patients with underlying cardiac disease or taking cardiac glycosides or diuretics. Patients with certain medical conditions or who take certain medications for allergies, depression, thyroid disorders, diabetes, and hypertension, may be at greater risk for adverse reactions. Common adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties.
Please see the full Prescribing Information (https://bit.ly/4j9fPAQ) and the Patient Information (https://bit.ly/4iZ2o6o).
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088.
Emergency dental kits from HealthFirst
REFERENCES
1. Goto T. Management of Anaphylaxis in Dental Practice. Anesth Prog. 2023;70(2):93-105. doi: 10.2344/anpr-70-02-16. Epub 2023 Jun 28.
2. Jevon P, Shamsi S. Management of anaphylaxis in the dental practice: an update. Br Dent J. 2020 Dec;229(11):721-728. doi: 10.1038/s41415-020-2454-1. Epub 2020 Dec 11.
3. Asthma and Allergy Foundation of America (AAFA). Food Allergy Anaphylaxis in Infants and Toddlers. https://aafa.org/asthma-allergy-research/our-research/food-allergy-anaphylaxis-in-infants/. Accessed March 24, 2025.
4. Brown JC, Simons E, Rudders SA. Epinephrine in the Management of Anaphylaxis. J Allergy Clin Immunol Pract. 2020 Apr;8(4):1186-1195. doi: 10.1016/j.jaip.2019.12.015. Erratum in: J Allergy Clin Immunol Pract. 2021 Jan;9(1):604. doi: 10.1016/j.jaip.2020.11.035.
5. Bock SA, Muñoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. 2007 Apr;119(4):1016-1018. doi: 10.1016/j.jaci.2006.12.622. Epub 2007 Feb 15.
6. Fleming JT, Clark S, Camargo CA Jr, Rudders SA. Early treatment of food-induced anaphylaxis with epinephrine is associated with a lower risk of hospitalization. J Allergy Clin Immunol Pract. 2015 Jan-Feb;3(1):57-62. doi: 10.1016/j.jaip.2014.07.004. Epub 2014 Sep 8.
7. Cardona V, Ansotegui IJ, Ebisawa M, El-Gamal Y, Fernandez Rivas M, Fineman S, Geller M, Gonzalez-Estrada A, Greenberger PA, Sanchez Borges M, Senna G, Sheikh A, Tanno LK, Thong BY, Turner PJ, Worm M. World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020 Oct 30;13(10):100472. doi: 10.1016/j.waojou.2020.100472.
8. HealthFirst. Dr. Malamed: The Importance of Epinephrine Auto-Injectors. https://www. healthfirst.com/videos/dr-stanley-malamed-the-importance-of-epinephrine-auto-injectors/. Accessed March 24, 2025.
9. American Academy of Pediatric Dentistry. Managing Professional Risks, ADA Guidelines for Practice Success™ (GPS™), ADA Tip Sheet on Managing Patients’ Medical Emergencies. https://www.aapd.org/globalassets/media/safety-toolkit-2.0/tip-sheet-on-managing-patients-medical-emergencies.pdf. Accessed March 24, 2025.
10. Becker DE, Rosenberg MB, Phero JC. Essentials of airway management, oxygenation, and ventilation: part 1: basic equipment and devices. Anesth Prog. 2014 Summer;61(2):78-83. doi: 10.2344/0003-3006-61.2.78.
11. Krishnamurthy M, Venugopal NK, Leburu A, Kasiswamy Elangovan S, Nehrudhas P. Knowledge and attitude toward anaphylaxis during local anesthesia among dental practitioners in Chennai - a cross-sectional study. Clin Cosmet Investig Dent. 2018 Jun 28;10:117-121. doi: 10.2147/CCIDE.S159341.
12. Çetinkaya F, Sezgin G, Aslan OM. Dentists’ knowledge about anaphylaxis caused by local anaesthetics. Allergol Immunopathol (Madr). 2011 Jul-Aug;39(4):228-231. doi: 10.1016/j. aller.2010.07.009. Epub 2011 Jan 13.
13. Smereka J, Aluchna M, Aluchna A, Szarpak Ł. Preparedness and attitudes towards medical emergencies in the dental office among Polish dentists. Int Dent J. 2019 Aug;69(4):321328. doi: 10.1111/idj.12473. Epub 2019 Mar 7.
14. Zhang E, Sicherer S, Agyemang A. Proper use of epinephrine autoinjectors is related to device type, prior physical demonstration, and sociodemographic factors. J Allergy Clin Immunol Pract. 2025 Feb;13(2):418-420.e1. doi: 10.1016/j.jaip.2024.11.006. Epub 2024 Nov 19.
15. Rosenberg M. Preparing for medical emergencies: the essential drugs and equipment for the dental office. J Am Dent Assoc. 2010 May;141 Suppl 1:14S-19S. doi: 10.14219/jada. archive.2010.0351.
Dr. Denise Chan, Pediatric Anesthesiologist, explains a helpful approach to anesthesia used by Pediatric Dental Anesthesia Associates
For many families, dental visits can be an emotional experience — especially when sedation or anesthesia is involved.
A thoughtful, developmentally appropriate approach to separating children from their parents or caregivers before procedures can significantly reduce distress and promote a smoother clinical experience. This is known as “positive separation.”
Positive separation is rooted in pediatric psychology and anesthesia practices. While some parents wish to be present during induction, research and experience have shown that many children — particularly toddlers and young school-aged kids — cope better when separation is handled calmly and confidently by the care team.
Children take emotional cues from the adults around them. If a parent appears anxious or tearful, the child is more likely to become upset. By contrast, when the dental and anesthesia team confidently explains what to expect and offers reassurance, the child is more likely to transition calmly. Using age-appropriate language, offering choices (e.g., mask flavor), and engaging the child with distraction techniques like bubbles or toys can all help ease the process.
Timing and tone are also essential. Positive separation works best when it is brief, direct, and supported by a consistent message from both parents and providers. Phrases like, “Mom will be waiting for you as soon as you wake up,” delivered with a smile and gentle redirection, help normalize the process.
It’s equally important to prepare parents in advance. Many parents are understandably apprehensive about being separated from their child. Preoperative discussions should explain why separation is recommended and how it benefits the child. Most parents are receptive when they understand that their presence during induction could inadvertently increase anxiety or interfere with clinical procedures.
Additionally, allowing parents to reunite with their child as soon as it is safe in the recovery phase reinforces trust. Seeing their child wake up peacefully and be cared for by trained pro-
Denise Chan, MD, is a board-certified pediatric anesthesiologist. She graduated summa cum laude from Rice University and earned her medical degree from Baylor College of Medicine, where she was inducted into the Alpha Omega Alpha Honor Medical Society. Dr. Chan completed her residency at Brigham and Women’s Hospital, Boston, Massachusetts, in Anesthesiology, and fellowships at Boston Children’s Hospital in Pediatric Anesthesiology and Boston Children’s Hospital in Global Pediatric Anesthesia.
fessionals helps parents feel included, reassured, and grateful for the care their child received.
Ultimately, positive separation is not about excluding parents — it’s about promoting a safe, calm, and efficient environment for the child. With a skilled and compassionate team such as Pediatric Dental Anesthesia Associates (PDAA), most children handle separation well and even bounce back with smiles. When implemented thoughtfully, this practice supports a child-centered approach that prioritizes emotional well-being alongside clinical excellence.
Pediatric Dental Anesthesia Associates (PDAA) is a team of board-certified physician (MD) anesthesiologists with vast experience in the care of pediatric dental patients providing sedation services directly and exclusively to pediatric dental offices across the country. After more than 18 years of helping over 400,000 patients with zero incidents, PDAA is now serving more than 700 different pediatric dental offices in 25 states. Please visit pediatricsedation.com to learn more, and see PDAA’s Google Business page for more than 3,500 5-star reviews from previous satisfied parents.
This information was provided by Pediatric Dental Anesthesia Associates.
Your “third hand” in pediatric dentistry — less stress, more smiles
Dr. Lawrence Kotlow discusses products that make dentistry easier and more comfortable
The practice of dentistry has made significant strides in the past 50 years. Innovative products that seem so simple have made dental treatment so much easier. Zyris Isolite® has created two such devices. Their initial product is known as the Isolite system — the introduction of the Isolite system made doing restorative dentistry much easier than using the rubber dam, especially as lasers become more available allowing painless anesthetic-free restorative dentistry. When using lasers, we need to prevent any type of reflection, and the material used is nonreflective and gentle to the tissues.
The latest innovation from Zyris is called the Hoopla™ Retractor. Both devices are perfect for the practice of pediatric dentistry, general dentistry, oral surgery, dental hygiene, and orthodontics. The Hoopla Retractor is especially beneficial for patient management, when treating a young child or patients suffering from dementia. In crown and bridge, the Hoopla also makes the scanning of teeth easier. I call both devices the “third hand,” since it frees up a hand usually relegated to retraction in many procedures, allowing the assistant to be more effective and valuable. A wide range of procedures can be completed in less time and with less stress for the patient using the Hoopla Retractor.
Oral hygiene
The dental hygienist can use the Hoopla Retractor to keep the lips and cheeks away from the treatment area when placing fluoride and scaling teeth, by hand or with the ultrasonic scaler. It works exceptionally well with semi-cooperative patients.
Lawrence Kotlow, DDS, is board-certified in Pediatric Dentistry. He has a solo practice in Albany, New York since 1974. Dr. Kotlow attended the Albany College of Pharmacy, graduated SUNY Buffalo School of Dentistry, and completed his pediatric dental residency at Cincinnati Children’s Hospital. He is a life member of the American Dental Association (ADA), life fellow of the American Board of Pediatric Dentistry (FABPD), life member of the NYSDA and 3rd District Dental Society of New York, member of American Academy of Physiologic Medicine and Dentistry (AAPMD), Member of Academy of Laser Dentistry, and has Mastership Academy of Laser Dentistry (MALD). He was recognized by NY Top Docs as a Top Dentist from 2021-2025 and received Dentistry Today’s recognition in 2021 and 2022-2025 as a Leader in Education.
Oral surgery
During soft tissue procedures such as gingivectomy, reshaping hypoplastic gingival tissue, or depigmentation, the Hoopla Retractor is beneficial. It is also helpful when releasing the lingual frenum.
Restorative dentistry
The Isolite is the perfect addition to hard tissue laser restorative dentistry. When using a hard tissue laser to remove tooth tissue, it is imperative to make sure the tooth remain well hydrated to prevent discomfort and burning the tooth. Often when using the high-speed suction, there is the potential to pull the water away from the tooth. I call it the “J effect.” When using the Isolite, water is pulled over the tooth; this keeps the tooth hydrated and prevents pooling of water in the area, which can interfere with hard tissue ablation. The Isolite protects the cheeks and also acts as a mouth prop eliminating the scissor-type mouth prop extending outside the mouth.
Orthodontics
Orthodontic treatment using Invisalign is quicker and easier for the orthodontist and patient with Isolite when placement and removal of buttons are required to be placed on the buccal areas of the upper and lower teeth to retain the Invisalign retainers. Both the Isolite and Hoopla come in sizes for adults, children, and toddlers. I have found in every case for which I choose to use the Isolite or the Hoopla Retractor, the procedures are completed in less time. Patients seem very comfortable and accept both devices with ease. This information was provided by Zyris Isolite®.
PD
The new biodegradable Hoopla™ Retractor from Zyris maximizes oral cavity access and visibility by comfortably retracting a patient’s lips and cheeks during hygiene, soft tissue, restorative, and orthodontic procedures
Discover why over 2,600 pediatric dentists use Isolite dental isolation in their practice.
Isolite offers pediatric dentists the ability to improve care and productivity during a single-visit. Our advanced technology allows you to address complex and unpredictable patient needs while avoiding those costly call-backs.
Create a positive and anxiety-free environment that helps young patients feel safe and relaxed during their visits, while giving parents confidence and peace of mind.
I could not do what I do as a pediatric dentist without Isolite.