Understanding NSAIDs: essential knowledge for dentists
Dr. Lisa Chan and Barbara Madej, RPh
The
Dr. Sonia Chopra
Canal Cleanliness Score in 5 Seconds?
The Endocator® is the first and only chairside device that detects residual contamination invisible to microscopes and radiographs, optimizing your disinfection protocol.*
Spring 2025 n Volume 18 Number 1
Editorial Advisors
Dennis G. Brave, DDS
David C. Brown, BDS, MDS, MSD
L. Stephen Buchanan, DDS, FICD, FACD
Gary B. Carr, DDS
Arnaldo Castellucci, MD, DDS
Gordon J. Christensen, DDS, MSD, PhD
Stephen Cohen, MS, DDS, FACD, FICD
Samuel O. Dorn, DDS
Josef Dovgan, DDS, MS
Luiz R. Fava, DDS
Robert Fleisher, DMD
Marcela Fridland, DDS
Gerald N. Glickman, DDS, MS
Jeffrey W Hutter, DMD, MEd
Syngcuk Kim, DDS, PhD
Kenneth A. Koch, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, DICOI
Joshua Moshonov, DMD
Richard Mounce, DDS
Yosef Nahmias, DDS, MS
David L. Pitts, DDS, MDSD
Louis E. Rossman, DMD
Stephen F. Schwartz, DDS, MS
Ken Serota, DDS, MMSc
E Steve Senia, DDS, MS, BS
Michael Tagger, DMD, MS
Martin Trope, BDS, DMD
Peter Velvart, DMD
Rick Walton, DMD, MS
John West, DDS, MSD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Circulation Disclosure: Total Circulation May Vary. Publisher retains the right to adjust circulation based on a number of factors including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions.
ISSN number 2372-6245
Seeking validation
The need for validation is a complex interplay of social, psychological, and emotional factors. Validation serves as a mirror reflecting our worth and competence, helping to build self-esteem and confidence by affirming that we are valued and respected. This is especially relevant to endodontists who often seek validation for our treatment philosophies, technology, and protocols.
Negotiating complex root canal anatomy and achieving high levels of disinfection are among the most challenging aspects of performing endodontics. To address these challenges, we have incorporated various technologies designed to activate chemical solutions. These technologies include sonic, ultrasonic, multisonic, and laser activation using different wavelengths and protocols.
Validation of these technologies and protocols is often empirical, relying primarily on research conducted with extracted teeth featuring artificially created biofilm, which lack complications associated with treating patients. Caution must be exercised when applying this data to patient scenarios. Moreover, many endodontists frequently modify or adjust manufacturers’ protocols, rendering the original data less valid.
We no longer perform bacterial testing to validate protocols. The culturing technique is no longer performed due to its arduous nature and the time-consuming process involved in identifying microorganisms. DNA-based identification methods such as polymerase chain reaction (PCR) are expensive and prone to high false-positive readings due to the detection of DNA from dead bacterial cells. However, there is much interest and excitement surrounding the recently introduced rapid, inexpensive, chairside adenosine triphosphate (ATP) assay test (Endocator™) for identifying viable bacteria in the root canal.
ATP, the primary energy source for cellular functions, serves as an indicator of metabolic activity in viable cells and degrades rapidly; thus, any detectable ATP indicates recent viability. The test is highly sensitive and capable of detecting small variations in root canal contamination, identifying bacterial levels below 10 culturable bacteria. Additionally, ATP high/low findings correlate with culture positive/ negative results. The Endocator™ reader measures bioluminescence emitted when ATP is reduced to AMP in the presence of oxygen and the enzyme luciferase. The device converts the detected light intensity into a score ranging from 0 to 100.
In essence, the test scores can validate (or invalidate) the endodontic protocol used. Elevated scores can be mitigated by modifying or reapplying the activation protocol and chemical irrigant used. Using the Endocator™ to assess the laser-assisted Radial Apical Cleansing protocol (Biolase and EdgePro®) showed its high effectiveness in root canal disinfection, with scores usually between 0-5. Higher scores were often lowered by repeating the disinfection phase. After testing over 200 cases in patients, it was determined that NaOCl concentration, laser energy per pulse, laser tip diameter, and duration of activation are important factors in achieving low ATP scores, indicating high levels of disinfection.
The addition of this highly sensitive ATP assay test will play a pivotal role validating endodontic protocols, providing accurate data on their efficacy as well as readiness of canal systems for obturation.
Justin Kolnick, DDS, received his dental degree, cum laude, from the University of the Witwatersrand in South Africa, where he was the first dental school graduate to be awarded the University Scholarship for Overseas Postgraduate Study. He completed his postdoctoral endodontic training at Columbia University in New York City. Dr. Kolnick has held positions as an Associate Clinical Professor in Endodontics at Columbia University, an Attending at Westchester Medical Center, and an Associate Clinical Professor in Endodontics at New York Medical College. He continues to lecture around the world and has published several articles on endodontics. Dr. Kolnick works to advance endodontics through education and the integration of modern technology. For the past 20 years, his experience with lasers has contributed to the development of laser-assisted treatment concepts in endodontics. Dr. Kolnick practices full time in Westchester County, New York. He is also a consultant for Biolase and EdgeEndo.
Dr. Beth Ann Damas
A shared vision and Dentsply products create a satisfying endodontic experience
Cover image of Dr. Beth Ann Damas courtesy of Dentsply Sirona.
The importance of calcium hydroxide in dental trauma cases
Dr. Sonia Chopra illustrates her treatment of tooth avulsion in a teenager
CONTINUING EDUCATION
Dr. Lisa Chan and Barbara Madej, RPh,
Imagine More with the Power of Partnership
Dr. Juan Carlos Ortiz Hugues explains how dental microscopes can improve
An Interconnected System elements™ Connect and Apex Connect
Dual Light Indicators With intuitive light indicators in both motor handpiece and the Apex file clip, you’ll have greater visibility for more confident shaping.
Patient Safety
The intuitive, easy-to-see smart light and audible indicators, as well as a large, bright viewing display alert you when you’re reaching the apex.
Portable Convenience
Easily move between operatories with this interconnected system; lightweight, ergonomic and cordless design.
Continuous Use-Comes with 2 removable and rechargeable batteries.
Apex Connect
Built-in Self Calibration that activates everytime the device is turned on.
Light and Audible Indicators for real-time working length information.
Making the world a better place
Every day, in newspapers, on TV, and social media we see humanitarian efforts across the world. Whether it’s for saving endangered animals, survivors of natural disasters, cures for diseases, or other causes closer to home, we all try as much as possible to open our hearts and wallets for those who could use a boost in life. Dental practices’ own little corners of the world can have their own distinctive ways to create a better place.
Lisa Moler Founder/Publisher, MedMark Media
It’s easy being green: One of the most popular ways dental offices can show environmental responsibility is by employing “green” programs. The ADA has a page on its website titled “80 ways to make your practice green” (https://bit.ly/4gbMrra) — with suggestions like investing in energy efficient technologies, purchasing furniture made from recycled products, or something as small as using biodegradable cups. Replacing high-energy consuming office lights with energy-efficient lighting will conserve energy and also probably help lower some of the electric bill as well.
One patient at a time: MedMark publications always feature new equipment, technology, and materials. Researchers and inventors of these new dental solutions spend hours of their time, effort, and money improving the dental experience and creating new options for better and more individualized patient care. Whether it’s taking the pain out of root canal treatment, bringing new treatments to those with sleep-breathing issues, inventing implant solutions for those who need special care, creating new aligner and bracket-and-wire systems to help patients smile again after years of low self-esteem, or taking the fear out of the office for even the youngest dental patients, our articles can help improve patients’ quality of life, while also improving your business.
Pay it forward: Some of the most famous key opinion leaders in the dental industry were mentored and encouraged by their peers. Implementing any new protocol or procedure from the simple to the complex is less stressful when there is someone to call on for advice. We’ve all been there — in any occupation, moving to a higher level means being educated not only from text books or lectures, but hands-on, chairside guidance from someone who has “been there and done that.” Articles in our publications also feature authors who want to share their expertise, and who are often happy to follow up with constructive pointers on how to add their protocols to your practice options.
Love thy neighbor: Dental offices can be a productive part of any community. From contributing to local schools, to visiting classes to talk about better oral care, to participating in veteran’s events, clinicians and their teams can expand their reputation, referrals, and hearts by showing the surrounding areas that their community is important to you too. It isn’t hard to find these activities. Check with your local Chamber of Commerce, community newspaper, school volunteer event staff, or even ask your patients what organizations they may be involved in. Your practice name will stay in potential patients’ minds long after the event is over.
The spring issue is ready to share concepts that will help to build your world. We hope you enjoy this issue’s well thought out/interesting articles, and make some ideas into realities.
It is a small world — and by making it better, your potential patients will be happy you are a part of it.
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Subscription Rate 1 year (4 issues) $149 https://endopracticeus.com/subscribe/
How to submit an article to Endodontic Practice US
Endodontic Practice US is a peer-reviewed, quarterly publication containing articles by leading authors from around the world. Endodontic Practice US is designed to be read by specialists in Endodontics, Periodontics, Oral Surgery, and Prosthodontics.
Submitting articles
Endodontic Practice US requires original, unpublished article submissions on endodontic topics, multidisciplinary dentistry, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,400 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Endodontic Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Articles are classified as either clinical, continuing education, technology, or research reports. Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to endodontics. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio and author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple) Doe JF Doe JF, Roe JP
Permissions
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased after the issue is published.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to: Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
Dr. Beth Ann Damas
A shared vision and Dentsply products create a satisfying endodontic experience
Tell us about yourself and your practice.
I currently own and manage an all-female endodontic practice with two locations in the south and west suburbs of Chicago, Illinois. Drs. Sara Iampaglia, Morgan McCall, and I share the same vision and collaborate in a boutique setting to provide excellence to patients of all ages.
Why did you choose to enter the field of endodontics?
My father was an orthodontist and many, including myself, thought that I would simply follow in his footsteps. My very first Cabbage Patch® doll had brackets on her front teeth. I attended the same dental school as my father and even shadowed him for a year after I graduated. I realized that my true passion was in endodontics. I appreciate the complexity of the job and providing a service that gets people out of pain. Endodontics is often completed in one step which provides immediate satisfaction to both the patient and the practitioner. I value the depth of the work and that it covers surgical aspects as well as the occasional cosmetic procedure. I feel fulfilled and am proud to be a specialist partner with my referring doctors.
Have you seen the “face” of endodontics change in recent years?
All of dentistry has seen a shift as equal numbers of men and women are currently choosing a career in dentistry. We provide an incredible service to patients in an environment that allows us to achieve great balance between our home and work life. My practice works as a team. Our schedules are flexible, but communication is key to making this work. Women make excellent communicators and that, combined with an astute attention to detail, helps us excel in our field.
What inspired you to open your own practice?
My father inspired me to be a business owner. Growing up watching him build something that benefited the community that he was proud of as well was something I strived for myself. Not a week goes by where there isn’t a person sitting in my chair telling me that my dad put on their braces. I am proud to be an extension of that journey.
What is your biggest challenge as an endodontist, especially as a woman?
The biggest challenge I face is managing unrealistic patient
Dr. Beth Ann Damas
expectations. If an additional procedure is necessary, patients question whether the provider guarantees their work. Is the next procedure going to be free, or if they need to be referred out to a specialist, is the original provider going to refund their money? I don’t think too many people question their medical doctors like this. It can be frustrating and emotionally draining. Instead, I encourage clinicians to spend more time educating the patient before treatment on the risks and benefits, so they can make the best informed decision for themselves.
Another challenge is building a cohesive brand, and ensuring that our quality of work is universal for both locations so that every patient has a great experience, from setting their appointment to posttreatment.
What is your future goal clinically?
I want to continue providing excellent patient care for my community and grow my practice with like-minded clinicians. I hope to continue my father’s legacy, so that if patients hear my name, they say, “She is excellent at what she does, just like her dad was.”
What else has led to your practice’s success?
We always want to provide consistent, seamless, safe, and predictable appointments. We keep up to date with the latest advancements and innovations in imaging and instrumentation
techniques. We educate our staff to help guide the patients through their appointments. When patients leave that chair out of pain and with a smile on their faces asking if they can give us a hug, we know we are doing something right.
What guidance would you give other endodontists?
I would advise to find a mentor. Work in an office where you would be a patient yourself. Don’t be afraid to ask questions. Trust that you will be able to do it all in the timeline that makes you most comfortable. I had my first child 3 months into my endodontic residency. My director, Dr. Michael M. Hoen, was a wonderful family man and gave me the confidence that I could be a great mom as well as a great endodontist, spouse, friend, colleague, and mentor. When my kids were young, I worked less. Now that they are more self-sufficient, I feel comfortable working more, whether seeing patients or lecturing others on the specialty I love.
Do you think your efforts with them help endodontics?
Women in dentistry need to spend more time supporting one another. This is not a competition. We can all learn from each other to find what works best for us as individuals. We just need a forum and outlet to talk about these things more.
As a Dentsply Sirona KOL, why do you choose to spend your time helping GPs complete successful RCTs?
The majority of root canals performed in the United States are done by GPs. Why not help them be the absolute best while at the same time gaining the knowledge to know their limitations? If a GP wants to do better dentistry, then I am proud and honored to be a part of their journey.
Do you think your efforts help the specialty?
The more GPs learn about the complexity of endodontics, they ultimately become better referring partners for the specialist. When practicing endodontists teach GPs the most up-todate instrumentation, irrigation, and obturation protocols, they become better clinicians. The more GPs know what they can master or what they need to refer to their specialist team helps everyone win.
What Dentsply Sirona products do you depend on to get you through your day?
At the beginning of my procedure, I rely on imaging to aid in diagnosis and treatment planning. Our office utilizes Schick 33 X-Ray sensors. The most cost-effective aspect of these sensors is the ability to replace or repair the cords without having to replace the entire sensor.
Dr. Beth Ann Damas examining a patient’s x-rays
Left: XSmart ProPlus. Right: Reciproc Blue file
I utilize the X-Tip needle system routinely to provide profound anesthesia to all of my patients. Often, I will use the needle in this system for my PDL injections when I encounter a hot tooth.
I recently switched to the X-Smart® Pro+ in some ops with the combined apex locator. Other ops still have the ProMark motor, and it really just comes down to provider preference.
I use a variety of Dentsply files, and it all depends on the individual tooth. On any given day, I will likely have used ProTaper Ultimate™, ProTaper Gold®, Pro Taper® Universal, WaveOne® Gold, and now Reciproc™ Blue. I often customize my protocol and sequence based on the anatomy from the cone beam scan.
The EndoActivator® is one of my favorite adjuncts to my irrigation protocol. It is simple to use, lightweight, and leaves me with a clean canal space to obturate. It has become something that I cannot live without. I use custom-matched paper points to dry out the canal space. Utilizing the precision matched conform-fit gutta percha has helped streamline my obturation. I really like how well the gutta percha heats and sears with warm vertical obturation.
On the rare occasion that I place a core buildup, I use Dentsply Fluorocore 2 and cure it with the curing light attachment for the EndoActivator.
How has the new X-Smart Pro+ streamlined your workflow and impacted your day?
The combination of the apex locator and motor into one single piece of equipment really streamlines the work setup and leaves less clutter on the work surface. The X-Smart Pro+ allows us to work efficiently and effectively to ensure the canals are instrumented to length. I appreciate not having to stop and switch back to the apex locator to confirm working lengths. For appointments where every second counts, this combination method is a game changer. The added light source is especially helpful when accessing through small spaces, crowns, and heavily restored teeth. The file library is also advantageous to my daily workflow. Like most endodontists, I tend to hybridize the file systems to match the anatomy of the case in front of me. I can custom set specific file sequences among the systems to create the instrumentation pattern that best matches my needs.
When and how did you learn about Reciproc Blue?
I was introduced to Reciproc Blue in the summer of 2023 at the Dentsply Global Endodontic KOL event. It has been used in European countries for a decade. Bringing their expertise into the mix really streamlined the introduction of the file to the U.S. and Canada.
How did Reciproc Blue help overcome some of the challenges you see as an endodontist?
The biggest change is integrating this file into my retreatment protocol. This file can be used to retreat cases without the addition of a solvent. You just need to give the file a few seconds to gently peck at the center core of the gutta percha, and then once it engages, it quickly and effectively removes everything in the canal system. This file is also really efficient at engaging Thermafil carriers and removing those in one piece without the fear of
breakage. Not having to use a ton of different files for retreatment is both time and cost efficient.
How has integrating Reciproc Blue into your practice streamlined your workflow?
I am no longer flipping back and forth between multiple file systems in the same tooth during retreatments. This has eliminated my guesswork. My assistant and I are less frustrated, and my patient often leaves my office telling us that this retreatment procedure took less time than the original root canal.
In your opinion, why do some clinicians remain hesitant to adopt innovations like Reciproc Blue?
Dentists as a whole do not really like change. Conceptually, Reciproc Blue is different from how endodontics is routinely taught in dental schools in the U.S. It takes a bit of time to grasp and accept the concept of a one-file system that matches the safety and efficiency of a multi-file system. It is also tough to replicate or simulate a procedure benchtop. This is not just limited to files. All of our demos in dentistry are hard to recreate outside the mouth. Reciproc Blue functions much differently inside an actual tooth than a plastic one. That is where the trust and expertise from our European colleagues came into play. With a decade of experience, they were able to walk us through how to truly use Reciproc Blue to its full potential and what ultimately made me decide to incorporate it into my practice on a regular basis for my retreatment protocols. EP
Dr. Beth Ann Damas speaking with a patient
game changer you’ve been waiting for.
X-Smart® Pro+
Endo Motor with Apex Locator
Reciproc™ Blue Treatment Solution
Sign up now
During retreatments, Reciproc™ Blue has eliminated my guesswork. My assistant and I are less frustrated, and my patient often leaves my office telling us that this retreatment procedure took less time than the original root canal.” Dr. Beth Damas
Listen to Dr. Beth Damas at AAE April 2-5 2025
Treating Complex Cases: Management of Calcified Canals and Severe Curvatures Dentsply Sirona Booth #1401 Exhibit Hall D www. dentsplysirona.com/reciprocblue
The importance of calcium hydroxide in dental trauma cases
Dr. Sonia Chopra illustrates her treatment of tooth avulsion in a teenager
Dental trauma is unfortunate and can be scary for patients because it can happen to anyone and at the most inopportune times. As a dental provider, I am so happy that I know the exact steps to handle this situation so I can help a patient (or loved one) through the chaos of a traumatic incident. I invite you to share this knowledge with all of your patients too — you never know when they may need it.
In my opinion, the most traumatic of all dental injuries is the avulsion, when the tooth is completely dislodged from its socket, aka, “the knocked out tooth.” This type of injury typically happens to young children in the anterior region of the mouth, so it is not just traumatic for the child, but for the parent as well. As a mother myself, I can empathize. With the knowledge that I have, I can feel confident that everything will be okay. Being able to tell a parent, “We can fix this,” is pure gold in a moment like this. However, we must adhere to a particular protocol to be able to guarantee such a tall order. In conversation, the clinician can try to calm and support the parent, with comments such as, “I don’t know who the trauma is worse for, the child or the parent.” “These teeth didn’t actually come out completely, and they were still able to soak in his own blood.” “Don’t give up hope; we see a lot of these types of traumas, and we’re able to restore their smiles.”
The following is a truly successful tooth story that outlines a scenario of a very scary moment for both mother and child, and how my team and I were able to put things back together as if no trauma happened at all.
A teenager’s avulsion tooth story
This 14-year-old boy was play-fighting with his brother in the kitchen with a broom. That broom hit him in the face and knocked out his front teeth.
Sonia Chopra, DDS, was the first female board-certified endodontist in Charlotte, North Carolina, where she founded Ballantyne Endodontics in 2008. As a mentor and impact entrepreneur, Dr. Chopra improves endodontic education for general dentists, dental residents, and patients. She is a TEDx speaker, Dentistry Today and Forbes contributor, and the author of Tooth Wisdom, a book designed to inform and empower patients in their own oral health. She teaches endodontists how to grow their practices and improve efficiencies in their workflows, so they can be more effective and profitable through her Heal Your Practice program. Dr. Chopra is also co-founder of A Night for Smiles, a gala bringing Charlotte-area dentists together to support dental health initiatives. She is an active member of the American Association of Endodontics and is a Key Opinion Leader for Sonendo, Dentsply Sirona, J Morita, and Kerr. When she’s not treating patients or teaching dentists about endodontics, she loves to travel, garden, and spend time with her family. Follow her on Instagram at @drsoniachopra.
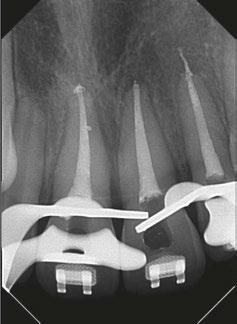
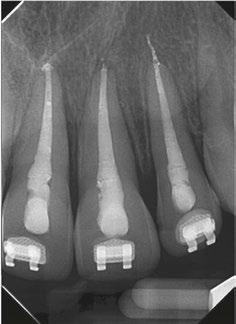
Luckily, the young boy was undergoing orthodontic treatment so the avulsed teeth remained in the oral cavity. As you can see from the clinical photograph in Figure 1, teeth Nos. 8, 9, and 10 would not have remained in the mouth if the orthodontic wire was not in place.
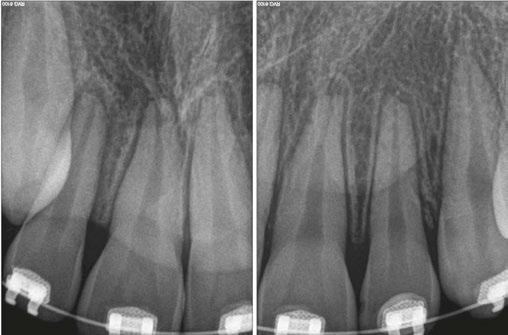
Two days after treatment, the patient was seen in my practice after the teeth were splinted back in place by the orthodontist. Figures 2A-2B are the preoperative radiographs after the teeth were reimplanted.
One can already appreciate the inflammatory resorption that is occurring at the apices of teeth Nos. 9 and 10. These images were taken just two days after the trauma.
My goal at the first visit was to understand the trauma with respect to the extraoral dry time of the teeth (how long were
Figure 1
Figures 2A-2B
the teeth outside of the mouth), get a full picture of the type of trauma that occurred, and to make sure that the teeth were stabilized.
Endodontic treatment began a few days after my initial examination. We did not want to start treatment right away, but we also didn’t want to wait too long to start treatment — we needed to give the periodontal ligament a moment to restabilize prior to treatment so we didn’t get further unwanted consequences down the road. But if we waited too long, inflammatory resorption would start to set in, and we would start to lose tooth structure. Endodontic treatment should be started within 7–10 days after the trauma to avoid these two potential consequences.
Figures 6-8
Using calcium hydroxide in a dental trauma case
One of the most critical steps in treating dental trauma is making sure you don’t rush things. That means that obturation is often postponed until the patient is asymptomatic (i.e., no pain to percussion) and the periodontal ligament has radiographically re-established itself. Clinicians must also make sure the tooth is completely disinfected of bacteria. Both of these steps are achieved by placing calcium hydroxide as an intracanal medicament during the treatment as seen in Figure 4.
Calcium hydroxide has been shown to be extremely beneficial in the long-term retention of teeth after they have experienced trauma. It can arrest and even repair inflammatory resorption and eliminate harmful bacteria from the root canal system after trauma. Its antimicrobial properties come from its alkaline pH and its ability to dissolve necrotic tissue, bacteria, and their byproducts.1
My personal favorite calcium hydroxide product to use in these delicate clinical situations is UltraCal™ XS paste by Ultradent. It is syringeable, making it very simple to use, since there is no mixing involved. The syringe tip is thin and comes with a rubber stopper that allows placement of the material to be safe and contained within the canal.
Next steps in the post-trauma treatment process
As I mentioned earlier, in any dental trauma situation, you never want to rush the treatment. The key to success is to watch the periodontal ligament and how it heals. Once you see the ligament re-establish itself into its normal resting place, then you know that the teeth are ready to be obturated.
You will also notice that during the endodontic treatment phase of this case, the orthodontic wire was removed until the periodontal ligament could heal. You don’t want to over-stabilize the teeth during the healing process after trauma because this can induce replacement resorption (aka, ankylosis). Therefore, the orthodontic wire was removed during this time when the calcium hydroxide was placed.
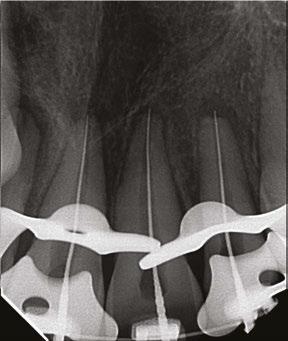
From here (Figure 6), I could see that my gutta percha was slightly overextended so I trimmed my master cones a bit prior to permanently obturating the teeth here.
Figure 3
Figure 4
Figure 5
There was some sealer extrusion at the apex of these teeth (Figure 7), especially 10, but this was due to the inflammatory resorption occurring at the apex as a result of the trauma, which started to eat away the apical stop. I am confident that, over time, this sealer will resorb away, and this extrusion should not impede the healing at all. Figure 8 is the final outcome of the case.
And now that the patient is stable, he can go back into his brackets and orthodontic wire. Figure 9 is him 6 months later, and we will continue to follow him up for the next 5 years.
Top tips to keep in mind
Dental trauma is distressing for patients and their loved ones, but when you can confidently reassure them that they’re in good hands, you’ll help them feel safe. And posttreatment, you’ll be their hero.
Some key points to remember following avulsion is:
1. Stabilize the teeth and get a baseline for your diagnostic tests.
2. Start root canal therapy 7–10 days after the trauma to preserve the PDL and avoid inflammatory resorption.
3. Place calcium hydroxide in the teeth as the first step.
4. Keep the teeth medicated (the medication may need to be replenished over time).
6. Follow up with the patient after 1 month, 3 months, 6 months, 1 year, 2 years, 3 years, 4 years, and 5 years.
REFERENCE
1. Zare Jahromi M, Kalantar Motamedi MR. Effect of calcium hydroxide on inflammatory root resorption and ankylosis in replanted teeth compared with other intracanal materials: a review. Restor Dent Endod. 2019 Aug 1;44(3):e32.
5. Once the teeth are no longer tender to percussion and the PDL looks normal radiographically, the teeth may be obturated.
Custom
equipment, as precise as you are.
At Boyd, we understand that precision is everything in endodontics. That's why we design every piece of equipment with the same meticulous care you bring to your procedures. From our customizable chairs to our ergonomic features, each element is crafted to support your exact standards.
You can trust Boyd’s custom equipment to provide the comfort, reliability, and precision you need—every time. Ready to get started? Scan the QR code or visit boydindustries.com.
Figures 9A-9B
PURE-Ca-SEAL™ BioCeramic formulation, releases Ca 2+ ions to form mineralized tissue. The alkaline pH and low solubility of PURE-Ca-SEAL™ hermetically seals the root canal system, making the environment inhospitable for bacterial growth enhancing safety and endodontic treatment success. The premixed, ready-to-use formulation simplifies the obturation procedure, resulting in less chair time and increased patient comfort.
Understanding NSAIDs: essential knowledge for dentists
Dr. Lisa Chan and Barbara Madej, RPh,
review the benefits and drawbacks of NSAID use in the dental practice
Introduction
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) are a widely used class of medications that effectively manage pain, inflammation, and fever by inhibiting cyclooxygenase (COX) enzymes responsible for prostaglandin production. In dental practice, NSAIDs play a crucial role in controlling pain and inflammation associated with common procedures such as extractions, root canals, and periodontal treatments. Their proven efficacy, accessibility, and non-opioid mechanism make them a preferred choice for both acute and chronic dental pain management.
The purpose of this article is to provide dental practitioners with comprehensive knowledge about NSAID use, including their mechanisms, benefits, risks, prescribing guidelines, and considerations for special populations, to ensure safe and effective pain management for patients.
How do NSAIDs work?
NSAIDs work by targeting enzymes in the body called cyclooxygenases (COX-1 and COX-2), which are essential for producing prostaglandins — hormone-like chemicals that promote inflammation, pain, and fever.
There are two main types of COX enzymes in the body: COX-1 and COX-2.1 Both enzymes are responsible for making prostaglandins, but the effects of these prostaglandins differ based on their origin:
Lisa Chan, DDS, co-founder and Chief Executive Officer, MedAssent DDS, has over 35 years of dentistry experience, including roles as a hospital dentist at Kaiser Permanente, a private practitioner, and a California State Dental Board consultant. With a DDS from USC, she focuses on promoting equity and integrated care, addressing challenges in patient safety. Dr. Chan also serves on educational and community boards, including Santa Monica College, UC San Diego, Los Angeles FBI, and the Salvation Army.
Barbara Madej, RPh, Chief Science Officer, MedAssent DDS, is a licensed pharmacist with a passion for improving lives through education on proper medication use. After earning her pharmacy degree from the University of Saskatchewan, she has served both Canada and Los Angeles, California. Through MedAssent DDS, Barbara aims to reduce medication errors at the intersection of dentistry and pharmacy, enhancing workplace efficiency and patient safety. Her lifelong goal is to make a meaningful impact in healthcare for all involved.
Disclosures: The authors of this article are affiliated with MedAssent DDS (www.medassentdds.com), a platform designed to support dental professionals in medication management and patient care.
Educational aims and objectives
This self-instructional course for dentists aims to provide dental practitioners with a comprehensive understanding of the mechanisms, benefits, and risks of nonsteroidal anti-inflammatory drug (NSAID) use in dental practice.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the mechanisms of action of NSAIDs, including their impact on COX enzymes and prostaglandin production and their relevance to dental pain management.
• Recognize the benefits of NSAIDs as a non-opioid alternative for managing pain and inflammation in dental practice.
• View the risks and potential adverse effects of NSAIDs in patient populations with comorbid conditions, including gastrointestinal, cardiovascular, and renal complications.
• Realize the importance of tailoring NSAID prescribing practices based on individual patient factors, including age, medical history, and concurrent medications.
• Pinpoint strategies to educate patients on the safe use of NSAIDs, emphasizing proper dosing, duration, and awareness of drug interactions and side effects.
• COX-1 enzymes: These produce prostaglandins that help protect the stomach lining and intestinal tract from digestive acids, as well as thromboxane which regulates blood clotting. While COX-1 inhibitors block inflammation, they also interfere with these protective functions, potentially leading to side effects like stomach ulcers and bleeding.2 A common COX-1 enzyme used in dental practices is indomethacin.
• COX-2 enzymes: These primarily produce prostaglandins involved in inflammation and pain. By selectively blocking COX-2, these NSAIDs can reduce inflammation effectively without significantly affecting the protective prostaglandins made by COX-1.2,3 Celecoxib, etodolac, and meloxicam are common examples of COX-2 NSAIDs.
• Traditional NSAIDs (COX-1 & COX-2): These block both COX-1 and COX-2 enzymes. This dual action reduces
inflammation and alleviates pain by decreasing the production of prostaglandins involved in these processes, while also affecting prostaglandins that regulate other bodily functions like stomach lining protection and blood clotting. Many NSAIDs block both COX-1 and COX-2, although one can be better than the other depending on the medication. Some traditional NSAIDs include aspirin, ibuprofen, naproxen, diclofenac, ketorolac, ketoprofen, and nabumetone.
NSAID use in dentistry
NSAIDs are essential in dental pain management due to their effective dual action in alleviating pain and reducing inflammation.4,5 Acetaminophen is often used in combination with NSAIDs because of its complementary action. While most NSAIDs exert their effects peripherally by reducing inflammation and pain at the site of tissue injury, acetaminophen works centrally, inhibiting prostaglandin synthesis in the central nervous system.6 This complementary action blocks pain signal transmission centrally while NSAIDs address inflammation locally, making their combined use highly effective in managing mild to moderate pain.6
Key applications
1. Postoperative pain and inflammation management: NSAIDs are widely used after dental procedures, such as extractions, root canals, and periodontal surgeries, to reduce pain and swelling, promoting faster recovery and enhancing patient outcomes.
2. Adjunctive use in inflammatory conditions: NSAIDs have shown potential as adjuncts to controlling inflammation in dental conditions like periodontitis.7 By targeting localized swelling and pain, they may complement conventional periodontal treatments and aid in managing discomfort. However, their use should be carefully weighed against potential risks, highlighting the need for a tailored approach in incorporating NSAIDs into dental care plans.8
3. Non-opioid pain management alternative: In light of the opioid crisis, NSAIDs offer a safer, non-addictive alternative for pain management. This makes them particularly beneficial for patients at risk of dependency or those with a history of substance abuse.
4. Patient accessibility and compliance: NSAIDs are widely available both over-the-counter and by prescription, with various formulations (e.g., tablets, capsules, topical gels) that accommodate individual patient preferences. Their familiarity and convenience encourage adherence to pain management regimens, improving treatment outcomes.
Pharmacokinetics and pharmacodynamics
NSAIDs are well-absorbed after oral administration, typically reaching peak plasma concentrations within hours.9 Once in the bloodstream, they bind extensively to plasma proteins, primarily albumin, and are metabolized in the liver by enzymes like cytochrome P450 (e.g. CYP2C9, CYP3A4).9 These processes yield inactive metabolites that undergo further processing, often through glucuronidation, to enhance water solubility, facilitating excretion primarily via urine and, to a lesser extent, bile in the feces.10
The plasma half-life of NSAIDs closely determines their onset and duration of action.11 Short-acting NSAIDs, including aspirin, diclofenac, and ibuprofen, are effective for rapid relief of acute pain or inflammation due to their half-lives of less than 6 hours. Long-acting options like naproxen and celecoxib, with half-lives exceeding 10 hours, are better suited for managing chronic conditions such as arthritis, maintaining therapeutic levels over extended periods. Choosing between short- and long-acting NSAIDs depends on the clinical need for immediate relief versus sustained control of chronic symptoms.
Patient response to NSAIDs is influenced by pharmacokinetic profiles, genetic variations (e.g., CYP2C9 activity), and individual factors like age, organ function, and comorbidities.11 Personalized treatment strategies and clear communication are essential for optimizing outcomes, ensuring proper adherence to dosing schedules, and tailoring therapy to meet patient-specific needs.
Risks and side effects of NSAIDs
NSAIDs are effective medications but can cause a range of side effects, from mild to severe.12,13 Common mild side effects include:4
• Nausea, vomiting, bloating, and heartburn
• Dizziness, headache, and drowsiness
• Tinnitus (ringing in the ears)
• Diarrhea, constipation, and stomach discomfort
More serious complications may include:4
• Gastrointestinal (GI) toxicity: ulcers, bleeding, or perforation
• Cardiovascular issues: hypertension, heart attack, and stroke
• Kidney damage (nephrotoxicity) and liver damage (hepatotoxicity)
• Thrombocytopenia, hyperkalemia, and anemia
• Rare hypersensitivity reactions like Stevens-Johnson Syndrome
These risks underscore the importance of careful patient selection and ongoing monitoring during NSAID use.
Contraindications and special considerations
NSAIDs are contraindicated in specific situations, including:
• Patients undergoing coronary artery bypass graft (CABG) surgery for perioperative pain
• Individuals with known hypersensitivity to NSAIDs or aspirin
• Patients with a history of asthma, urticaria, or allergic reactions triggered by NSAIDs
Special caution is required for:
• Older adults
• Patients with a history of peptic ulcer disease (PUD) or GI bleeding
Prescription NSAIDs carry black box warnings for cardiovascular thrombotic events and GI risks. Similarly, prescription acetaminophen warns against hepatotoxicity, particularly at doses exceeding 4,000 mg/day, which can cause acute liver failure. In cases where NSAIDs are contraindicated, consider alternatives like acetaminophen or acetaminophen-based opiate combinations (e.g., Tylenol #3).
Risks with prolonged use
Chronic NSAID use increases the risk of severe complications, especially in older populations. These include:
• Peptic ulcer disease14 and acute kidney injury (AKI)15
• Worsening pre-existing conditions such as hypertension and heart failure
The inhibition of prostaglandin production — vital for protecting the GI mucosa and maintaining kidney function — can lead to gastrointestinal damage, reduced renal perfusion, and impaired drug clearance. Patients with moderate to severe renal issues or those on dialysis should be closely monitored, as NSAIDs can exacerbate renal dysfunction and increase the risk of AKI.15
Patient education
Educating patients on the safe use of NSAIDs is crucial. Key points to emphasize include:
• Use the lowest effective dose for the shortest duration.
• Avoid combining prescription and OTC NSAIDs to reduce adverse effects.
• Carefully review OTC medication labels to prevent duplicate or excessive dosing.
Patients should be informed about potential side effects and encouraged to report symptoms promptly. Clear communication helps minimize risks and maximize treatment effectiveness.
NSAID interactions with other medications
NSAIDs commonly interact with other medications, leading to adverse effects.3,17
Common drug interactions
• Other NSAIDs or aspirin: Co-administration increases the risk of gastrointestinal ulcers, bleeding, hypertension, and hyperkalemia.
• Corticosteroids (e.g. prednisone, methylprednisolone): Combination heightens the likelihood of GI bleeding, fluid retention, and hypertension.
• Anticoagulants (e.g. warfarin, rivaroxaban, dabigatran, apixaban, edoxaban): Combination significantly elevates the risk of serious bleeding.
• Methotrexate, lithium, phenytoin, and calcium channel blockers: Some NSAIDs, such as celecoxib, can increase blood levels of these drugs, raising the risk of nephrotoxicity.18
• Oral antidiabetic drugs: NSAIDs may increase the risk of hypoglycemia.
• Antifungals (e.g. fluconazole): Can elevate celecoxib levels, amplifying side effects.
• Quinolone antibiotics (e.g. ciprofloxacin, levofloxacin): May enhance the risk of central nervous system stimulation and seizures when combined with NSAIDs.
Patient risk factors
Special caution is necessary for patients with the following conditions, as NSAID use must be carefully monitored to prevent exacerbation:19
• Cardiovascular conditions (e.g., heart failure, uncontrolled high blood pressure, history of stroke or heart attack).
• Diabetes, bleeding disorders, or poorly managed chronic illnesses.
Best practices for safe NSAID use
1. Patient evaluation: Thoroughly review the patient’s medical history to identify potential risks or contraindications.
2. Appropriate NSAID selection: Choose the safest option based on the patient’s health status, and prescribe the lowest effective dose for the shortest duration.
3. Monitoring: Regularly assess kidney and liver function, particularly in long-term NSAID users.
4. Patient education: Inform patients about:
a. Risks of overuse or combining NSAIDs with other medications.
b. The importance of adhering to dosing instructions.
c. Recognizing early signs of adverse effects (e.g., gatrointestinal bleeding, swelling, unusual fatigue).
5. Reevaluation: Periodically reassess the need for NSAIDs and consider alternative therapies where appropriate. By understanding and mitigating potential interactions, healthcare providers can enhance patient safety and reduce the risks associated with NSAID therapy in dental practice.
Special considerations for pediatric, geriatric, and perinatal patients
Pediatrics
Prescribing NSAIDs for children requires careful attention to their unique needs.20
• Dosing and formulation: Always calculate doses based on weight to avoid toxicity, and choose age-appropriate formulations for ease of use.
• Precautions: Use NSAIDs cautiously in children with asthma or kidney problems, as these conditions can worsen with their use.
• Aspirin contraindication: Avoid aspirin in children under 18 due to the risk of Reye’s Syndrome, a rare but serious condition.
• Safer options: Ibuprofen is a well-studied and reliable choice for children when used at the right dose.
Geriatrics
For older adults, NSAIDs can be effective, but they come with increased risks due to age-related changes in the body.21,22
• Risks: For geriatric patients, increased sensitivity to NSAIDs, slower metabolism, and a higher likelihood of adverse effects, such as gastrointestinal bleeding, renal impairment, and cardiovascular complications, necessitate a more cautious approach.
• Strategies: Start with the lowest effective dose, limit how long the medication is used, and monitor regularly for any side effects.
Pregnant and breastfeeding patients
NSAIDs require extra caution during pregnancy and breastfeeding to protect both mother and child.23
• Pregnancy:
o In 2020, the FDA updated the prescribing information for prescription NSAIDs to highlight the risk of kidney problems in unborn babies, which can lead to low amniotic fluid levels (oligohydramnios). The updated guidance advises avoiding NSAIDs in pregnant women starting at 20 weeks of pregnancy, a change from the previous recommendation of 30 weeks.
o Avoid NSAIDs in the third trimester, as they can lead to serious complications for the baby, including renal injury, oligohydramnios, ductus arteriosus constriction, persistent pulmonary hypertension, necrotizing enterocolitis, and intracranial hemorrhage.
• Breastfeeding:
o NSAIDs generally result in low infant exposure through breastmilk and are considered safe, with ibuprofen and naproxen preferred over aspirin due to their more favorable risk profiles.
Best practices for NSAID prescribing
Effective dental pain management involves tailoring analgesics to the expected level of pain. These evidence-based guidelines offer a structured approach to prescribing based on pain severity:4
NSAIDS are a cornerstone of care that, when used thoughtfully, can profoundly impact a patient’s comfort and recovery.
Anticipated pain level: mild
For patients experiencing mild pain, a non-prescription NSAID is often sufficient:
• Oral analgesic option: Ibuprofen 200–400 mg as needed for pain, every 4 to 6 hours.
Anticipated pain level: mild to moderate
For mild-to-moderate pain, a fixed dosing schedule initially ensures better pain control, followed by as-needed administration:
• Oral analgesic option: Ibuprofen 400–600 mg on a fixed interval, every 6 hours for the first 24 hours. Then, ibuprofen 400 mg as needed for pain, every 4 to 6 hours.
For patients requiring longer-term pain management, meloxicam can be considered as an option due to its once-daily dosing and favorable safety profile when used appropriately.
• Meloxicam dosage:24 Start with 7.5 mg orally once daily, and adjust based on individual response. The maximum recommended daily dose is 15 mg. In patients undergoing hemodialysis, the dose should not exceed 7.5 mg/ day. To minimize gastrointestinal upset, it can be administered with food. Use the lowest effective dose for the shortest duration to align with treatment goals.
Anticipated pain level: moderate to severe
For moderate-to-severe pain, combining an NSAID with acetaminophen offers enhanced analgesic efficacy:
• Oral analgesic option: Ibuprofen 400–600 mg plus acetaminophen 500 mg on a fixed interval, every 6 hours for the first 24 hours. Then, ibuprofen 400 mg plus acetaminophen 500 mg as needed for pain, every 6 hours.
Anticipated pain level: severe
For severe pain, a combination of an NSAID, acetaminophen, and an opioid is recommended initially, with a step-down approach as pain diminishes:
• Oral analgesic option: Ibuprofen 400–600 mg plus acetaminophen 650 mg with hydrocodone 10 mg on a fixed interval, every 6 hours for 24 to 48 hours. Then, ibuprofen 400–600 mg plus acetaminophen 500 mg as needed for pain, every 6 hours.
After prescribing NSAIDs, careful monitoring is essential to ensure patient safety and prevent adverse effects.25 Key considerations include assessing kidney function through renal studies and liver health with liver function tests. Coagulation studies, such as prothrombin time and international normalized ratio (INR), are particularly important in patients on anticoagulants. A complete blood count (CBC) can help detect signs of anemia
or other blood-related issues, as well as symptoms of gastrointestinal bleeding. Patients should also be advised to monitor for warning signs of bleeding, such as nosebleeds, unusual bruising, blood in the stool or urine, or feelings of dizziness.26
Additionally, regular monitoring of blood pressure is necessary, as NSAIDs can contribute to hypertension, especially in patients with pre-existing cardiovascular conditions. These measures help identify potential complications early and ensure the safe, effective use of NSAIDs.
Case studies and clinical scenarios
The importance of thorough medication review and patient history cannot be overstated, as highlighted by the experiences of this paper’s co-authors.
Dr. Lisa Chan shared a harrowing case from her husband who is a hospitalist. A patient was prescribed ibuprofen by their dentist to manage dental pain. Soon after, they were rushed to the emergency room with severe gastrointestinal bleeding, requiring two pints of blood. The cause? The patient had already been taking celecoxib, another NSAID, prescribed by their physician. Similarly, over many years in pharmacy practice, Barbara Madej, RPh, encountered situations where combining NSAIDs with selective serotonin reuptake inhibitors (SSRIs)—such as citalopram, sertraline, fluoxetine, or paroxetine — significantly increased the risk of upper gastrointestinal bleeding. In these scenarios, careful consideration of the risks and benefits is crucial. When such combinations are unavoidable, co-prescribing a proton pump inhibitor (PPI) can help mitigate the risk of serious complications.
These examples highlight the critical importance of reviewing patient histories and checking for drug interactions before prescribing NSAIDs. A simple review of current medications using new, dentistry-specific technology such as the MedAssent DDS Digital Drug Handbook could have prevented the severe, avoidable outcomes in these cases.
Conclusion
NSAIDs are more than just a tool for managing dental pain — they are a cornerstone of care that, when used thoughtfully, can profoundly impact a patient’s comfort and recovery. Yet, their power comes with responsibility. As dental professionals, the choices we make in prescribing NSAIDs can mean the difference between relief and harm, between trust and fear.
Each patient brings a unique story, a medical history that demands our attention and respect. By taking the time to review drug interactions, anticipate risks, and educate our patients, we reinforce the trust they place in us that forms the foundation of excellent care.
REFERENCES
1. Cryer B, Feldman M. Cyclooxygenase-1 and cyclooxygenase-2 selectivity of widely used nonsteroidal anti-inflammatory drugs. Am J Med. 1998;104(5):413-421. doi: 10.1016/s0002-9343(98)00091-6.
2. Qureshi O, Dua A. COX Inhibitors. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www. ncbi.nlm.nih.gov/books/NBK549795/
3. Cleveland Clinic. COX-2 inhibitors: Uses, side effects, and more. Cleveland Clinic website. Last reviewed: May 24, 2022. https://my.clevelandclinic.org/health/drugs/
23119-cox-2-. https://my.clevelandclinic.org/health/drugs/23119-cox-2-inhibitors. Accessed January 14, 2025.
4. American Dental Association. Oral analgesics for acute dental pain. American Dental Association. https://www.ada.org/resources/ada-library/oral-health-topics/oral-analgesics-for-acute-dental-pain. Updated February 2, 2024. Accessed December 18, 2024.
5. Pergolizzi JV, Magnusson P, LeQuang JA, Gharibo C, Varrassi G. The pharmacological management of dental pain. Expert Opin Pharmacother. 2020;21(5):591-601. doi:10. 1080/14656566.2020.1718651
6. Altman RD. A rationale for combining acetaminophen and NSAIDs for mild-to-moderate pain. Clin Exp Rheumatol. 2004;22(1):110-117.
7. Salvi GE, Lang NP. The effects of non-steroidal anti-inflammatory drugs (selective and non-selective) on the treatment of periodontal diseases. Curr Pharm Des. 2005;11(14):1757-1769. doi:10.2174/1381612053764878.
8. Ren J, Fok MR, Zhang Y, Han B, Lin Y. The role of non-steroidal anti-inflammatory drugs as adjuncts to periodontal treatment and in periodontal regeneration. J Transl Med. 2023;21(1):149. Published 2023 Feb 25. doi:10.1186/s12967-023-03990-2.
9. Verbeeck RK, Blackburn JL, Loewen GR. Clinical pharmacokinetics of non-steroidal anti-inflammatory drugs. Clin Pharmacokinet. 1983;8(4):297-331. doi: 10.2165/00003088-198308040-00003.
10. Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem Pharmacol. 2020; 180:114147. doi:10.1016/j.bcp.2020.114147.
11. Davies NM, Skjodt NM. Choosing the right nonsteroidal anti-inflammatory drug for the right patient: a pharmacokinetic approach. Clin Pharmacokinet. 2000;38(5):377-392. doi:10.2165/00003088-200038050-00001.
12. NAPROSYN (naproxen). DailyMed website. National Library of Medicine. https:// dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=8bff5df5-d856-4237-b6a8ae445b454844. Updated January 2 2025. Accessed January 14, 2025.
13. Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16(5):821-847. doi:10.18433/j3vw2f.
14. Drini M. Peptic ulcer disease and non-steroidal anti-inflammatory drugs. Aust Prescr. 2017;40(3):91-93. doi:10.18773/austprescr.2017.037.
15. Lucas GNC, Leitão ACC, Alencar RL, Xavier RMF, Daher EF, Silva Junior GBD. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J Bras Nefrol. 2019;41(1):124-130. doi:10.1590/2175-8239-JBN-2018-0107.
16. Varga Z, Sabzwari SRA, Vargova V. Cardiovascular Risk of Nonsteroidal Anti-Inflammatory Drugs: An Under-Recognized Public Health Issue. Cureus. 2017;9(4):e1144. doi:10.7759/cureus.1144.
17. Moore N, Pollack C, Butkerait P. Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Ther Clin Risk Manag. 2015;11:1061-1075. doi:10.2147/TCRM.S79135.
18. Kim SJ, Seo JT. Selection of analgesics for the management of acute and postoperative dental pain: a mini-review. J Periodontal Implant Sci. 2020;50(2):68-73. doi:10.5051/ jpis.2020.50.2.68.
19. Cleveland Clinic. Non-steroidal anti-inflammatory medicines (NSAIDs). Cleveland Clinic website. https://my.clevelandclinic.org/health/treatments/11086-non-steroidalanti-inflammatory-medicines-nsaids. Updated July 24, 2023. Accessed January 14, 2025.
20. American Academy of Pediatric Dentistry. Useful Medications for Oral Conditions. The Reference Manual of Pediatric Dentistry. 2024-2025/ P. 644-651. https://www.aapd. org/research/oral-health-policies--recommendations/useful-medications-for-oral-conditions/. Accessed December 19, 2024.
21. Wongrakpanich S, Wongrakpanich A, Melhado K, Rangaswami J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The Elderly. Aging Dis. 2018;9(1):143-150. doi:10.14336/AD.2017.0306.
22. Buckinghamshire Healthcare NHS Trust/Buckinghamshire, Oxfordshire and Berkshire West Integrated Care Board. 299FM.5 Guideline For Prescribing Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) In Adults. https://www.bucksformulary.nhs.uk/docs/ Guideline_299FM.pdf. Published July 26, 2023. Accessed January 14, 2025.
23. Bloor M, Paech M. Nonsteroidal anti-inflammatory drugs during pregnancy and the initiation of lactation. Anesth Analg. 2013;116(5):1063-1075. doi:10.1213/ANE. 0b013e31828a4b54.
24. Boehringer Ingelheim Pharmaceuticals, Inc. Mobic (Celebrex) [package insert]. U.S. Food and Drug Administration. Revised March 2012. Accessed December 19, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020938s022lbl.pdf
25. Specialist Pharmacy Service. NSAIDs: Monitoring Requirements. Published June 22, 2021. Accessed December 19, 2024. https://www.sps.nhs.uk/monitorings/ nsaids-monitoring/.
26. de Jong JC, van den Berg PB, Tobi H, de Jong-van den Berg LT. Combined use of SSRIs and NSAIDs increases the risk of gastrointestinal adverse effects. Br J Clin Pharmacol. 2003;55(6):591-595. doi:10.1046/j.0306-5251.2002.01770.x.
Continuing Education Quiz
Understanding NSAIDs: essential knowledge for dentists CHAN/MADEJ
1. NSAIDs work by targeting enzymes in the body called cyclooxygenases (COX-1 and COX-2), which are essential for producing prostaglandins — hormone-like chemicals that promote ________.
a. inflammation
b. pain
c. fever
d. all of the above
2. _________ produce prostaglandins that help protect the stomach lining and intestinal tract from digestive acids, as well as thromboxane which regulates blood clotting.
a. COX-1 enzymes
b. COX-2 enzymes
c. CYP2C7 activity
d. genetic deficiencies
3. primarily produce prostaglandins involved in inflammation and pain.
a. COX-1 enzymes
b. COX-2 enzymes
c. Anticoagulants
d. Antidiabetic drugs
4. While most NSAIDs exert their effects peripherally by reducing inflammation and pain at the site of tissue injury, work(s) centrally, inhibiting prostaglandin synthesis in the central nervous system.
a. plasma proteins
b. cytochrome P450
c. acetaminophen
d. anticoagulants
5. NSAIDs have shown potential as adjuncts to controlling inflammation in dental conditions like periodontitis.
a. True
b. False
6. Patient response to NSAIDs is influenced by _______.
a. pharmacokinetic profiles
b. genetic variations
c. individual factors like age, organ function, and comorbidities
d. all of the above
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 010
Date Published: March 1, 2025
Expiration Date: March 1, 2028
7. Educating patients on the safe use of NSAIDs is crucial. One key point to emphasize is to use _______.
a. the lowest effective dose for the shortest duration
b. the highest effective dose for the longest duration
c. the highest effective dose for the shortest duration
d. the lowest effective dose for the longest duration
8. Quinolone antibiotics (e.g. ciprofloxacin, levofloxacin) may enhance the risk of central nervous system stimulation and seizures when combined with NSAIDs.
a. True
b. False
9. When prescribing NSAIDs for children, always calculate doses based on ________, and choose age-appropriate formulations for ease of use.
a. the parents’ previous experience with it
b. weight to avoid toxicity
c. the likelihood of compliance
d. height
10. For geriatric patients, ___, necessitate(s) a more cautious approach.
a. increased sensitivity to NSAIDs
b. slower metabolism
c. a higher likelihood of adverse effects, such as gastrointestinal bleeding, renal impairment, and cardiovascular complications
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Endodontic access cavities: science versus trends
Dr. Chafic Safi discusses how the design of access cavities can affect root canal treatment
Introduction
The prevention and treatment of apical periodontitis has always been paramount for any clinician performing a root canal treatment. By prevention, the clinician aims at stopping an ingress of microbes into the root canal system before affecting the periapical tissues. Once these microbes colonize the root canal system and reach a certain critical concentration, periapical tissues develop a radiolucency, a sign of endodontic disease. The removal of these microbes and lowering their count restores the health of the diseased tissues. In other words, the aim of a root canal treatment is microbial control.1
This control is achieved through a series of steps involving the chemo-mechanical debridement and disinfection of the root canal system. Mechanically, root canal systems are instrumented with files up to a certain diameter.2,3,4 The resulting space is chemically disinfected by the action of irrigation solutions and then filled and sealed using various available techniques.4,5,6 Finally, a proper coronal restoration is placed to ensure a fluid tight seal as well as to consolidate the tooth.7,8 The prognosis of such a goal has been reported to be in the range of 90%-96%. 9,10
In the recent decade, technological advancements have simplified root canal treatments. The advent and accessibility of magnification and illumination, as well as cone beam computed tomography (CBCT), and other techniques made it possible to localize and visualize the pulpal space and canal orifices with more ease. This resulted in a shift in the design of access cavities, going from traditional cavities to less invasive ones such as conservative, ultra conservative (ninja), truss, caries-oriented, and restorative-oriented access cavities.
Endodontic access cavities: the science
The access cavity is the first clinical step in a root canal treatment. Its design and execution can dictate the healing or the per-
Chafic Safi, DMD, completed his postgraduate residency in Endodontics at the University of Pennsylvania in 2015 where he also completed a Master of Science in Oral Biology researching the outcome of endodontic microsurgery and factors affecting prognosis. Dr. Safi is a published researcher and lectures on various endodontic topics nationally and internationally. He is certified by the American Board of Endodontics. Dr. Safi remains on the faculty at the University of Pennsylvania’s department of Endodontics as well as University of Montreal, as an adjunct professor. He is also a faculty lecturer for Next Level Endodontics. He founded Centre Endodontique Saint-Laurent in Montreal, Canada where he lives and practices since 2016.
Educational aims and objectives
This self-instructional course for dentists aims to give a general understanding of the various endodontic access cavities, their impact on tooth structure, and the current scientific recommendations.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify the role of endodontic access cavities. Identify various access cavity designs.
• Recognize advantages and shortcoming for those various designs.
• Realize the most current scientific recommendations.
2 CE CREDITS
sistence of apical periodontitis. The purpose of an access cavity is to offer the clinician a proper entry into the pulpal chamber, the canal orifices, and into the canals all the way to the working length. It should allow the easy way-in and way-out of all the mechanical and chemical armamentarium during a root canal treatment.11
Traditionally, the endodontic access cavity was designed in a way that aimed to remove any obstruction in the way of reaching the canal orifices. This included the complete unroofing of the chamber, exposing all pulp horns, and obtaining a straight-line access to the apex — avoiding the need to alter visual angulation. This design also aimed at reducing the likelihood of iatrogenic errors.
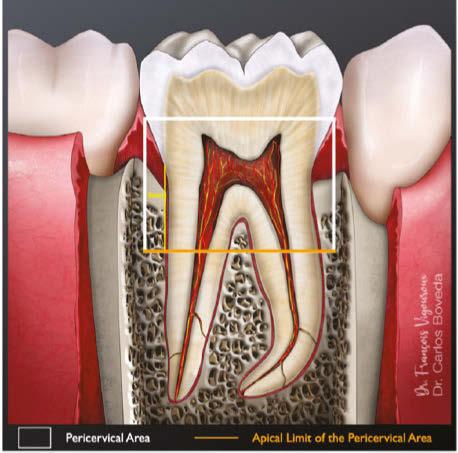
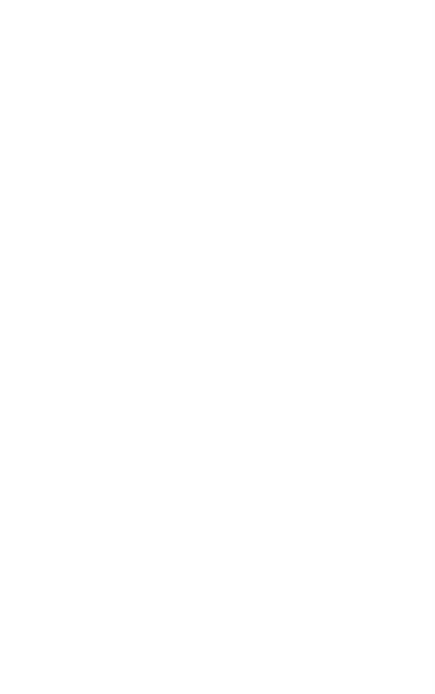
There are various factors that influence the size of such cavities, notably the anatomical location of the orifices and visualizing these orifices without tilting the mirror.12 This results in an access cavity that is widest occlusally and smallest at the level of the orifices.12,13 Hence the drawback of such access cavity design is that it requires the removal of healthy tooth structure, specifically the pericervical dentin — the dentin present 4 mm above and 6 mm below the crestal bone which helps to distribute any forces placed on the tooth (Figure 1).14 This access design, known as Traditional Endodontic Cavity (TEC) is presently being questioned, giving rise to various access designs emphasizing the preservation of this pericervical dentin.14,15
Endodontic access cavities: The trends
The increasing popularity of magnification, illumination, and CBCT technology, along with the goal to preserve pericervical dentin, gave rise to a series of new endodontic access cavities. These include conservative, ultra conservative (ninja), truss, guided, caries-oriented, and restorative access cavities.
Conservative Endodontic Cavity (Figure
2A)
The Conservative Endodontic Cavity (CEC) is a first step towards a less invasive access cavity while executing a root canal treatment. It is based on the partial deroofing of the pulpal chamber while preserving pulpal horns, resulting in a slight occlusal convergence. This elimination of straight-line access makes orifices visible one at a time using different visual angulation.16
It has been shown that CEC might increase the strength of endodontically treated teeth especially in mandibular premolars and molars.17 However, there are concerns about the ability of effective chemo-mechanical debridement and disinfection of the root canal system as well as procedural errors due to reduced direct vision.18
The Ultraconservative Endodontic Cavity (UEC), also known as Ninja access, is a more minimalistic version of the CEC. It is performed by creating a cavity in the occlusal surface starting from the central fossa or incisal edge and reaching the pulpal floor with an extremely conservative deroofing of the chamber and preservation of the pulp horns. No further extension is made.15 This results in a super convergent cavity and the preservation of not only percervical dentin but also occlusal enamel. This ultraconservative shape makes it more challenging to locate, clean, disinfect, and obturate the root canal system. It also increases the risks of missed canals which can then lead to failure of the treatment. The increased mechanical stability and increased long-term survival claimed to be attributes to such cavity design are limited and debatable.17 There is also increased treatment time to be considered.
Truss Access Cavity (Figure
2C)
In the discussion of smaller access cavities with the aim of preserving pericervical dentin, we include the Truss Access Cavity. This design yields separate access cavities on the occlusal surface, aligned with the corresponding canals, to expose the orifices and leaving the truss of dentin intact in between.19
On mandibular molars, this yields two separate cavities, one mesial and one distal. On maxillary molars, the mesiobuccal and distobuccal orifices are accessed through one opening and the palatal through a separate opening. One of the major challenges of such design is inaccuracy which may lead to perforations and other errors.15
In a study comparing CEC to truss cavities, there was no difference in fracture resistance between the two. Considering the higher risk and difficulty of the truss access, it is advisable to opt for the conservative access.20
There is a major lack of evidence to support the use of truss access cavities and whether they can result in effective tissue cleaning.
Guided
Access Cavity (Figure 3)
The advancements in CBCT and in imaging software make it possible for a clinician to have an access cavity guide. Similar to a surgical guide in implant dentistry, this access guide/stent
Figures 1A and 1B: Pericervical dentin. Schematic representation (A) and location on a periodontal film (B). Adapted from Boveda C, Kishen A, Millan B, Camejo MV, Gomez-Sosa JF. Pericervial Dentin Metrics in Mandibular First Molars Determined with Digital Periapical Radiography and Cone-beam Computed Tomography. J Endod. 2024 May;50(5);637-643
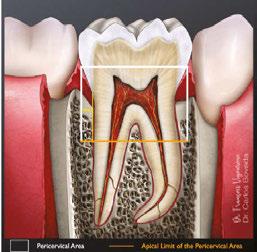
Figures 2A-2E: Comparison of the traditional access cavity (TradAC) with other types of cavities. A. ConsAC = conservative access. B. UltraAC = ultraconservative access (ninja). C. TrussAC = truss access. D. CariesAC = caries-oriented access. E. RestoAC = restorative-oriented access. Adapted from Silva EJNL, Pinto KP, Ferreira CM, Belladonna FG, De-Deus G, Dummer PMH, Versiani MA. Current status on minimal access cavity preparations: a critical analysis and a proposal for a universal nomenclature. Int Endod J. 2020 Dec;53(12):1618-1635
A.
C.
B.
D. E.
A.
B.
is placed in the patient’s mouth and allows for guided dentin removal. This allows the clinician to plan their access cavity in a way that conserves the dentin and saves time. This access cavity design is mainly used in obliterated root canal systems to reduce the risks of canal deviation and perforation. However, the lack of accuracy of the stent as well as its cumbersomeness in posterior regions tend to make this kind of access cavity less popular.15, 21
Caries
The increasing popularity of magnification, illumination, and CBCT technology, along with the goal to preserve pericervical dentin, gave rise to a series of new endodontic access cavities.”
Oriented and Restorative-Oriented Access Cavity (Figures 2D and 2E)
Remaining in the quest of maximizing tooth structure to reduce post-endodontic fractures, comes the caries and restorative-oriented access cavities. The cavities are done through the caries or through an existing restoration, allowing this to dictate the overall design and preserve sound tooth structure.19 One main disadvantage of these designs is the increased stress and strain on instruments, and hence an increased risk of instrument separation. Due to the restricted access, there is a debate that appropriate chemo-mechanical debridement is compromised, therefore increasing the risk of post treatment disease.15
Science versus trends
The transformational shift into more restricted endodontic access cavities with the claim of stronger teeth was investigated by many, especially TEC versus CEC and UEC.
In a study comparing TEC versus CEC and UEC, extracted premolars and molars with TEC showed lower fracture strength than the ones prepared with CEC or UEC. The ultraconservative “ninja” endodontic cavity access did not increase the fracture strength of teeth compared with the ones prepared with CEC.15 It seems consistent in many other studies that UEC does not offer an increased resistance to fracture compared to TEC or CEC. Moreover, there is evidence that UEC makes cleaning procedures more difficult, increasing the total time required for a root canal treatment.20
The effect of CEC is, however, not consistent in the literature, with systematic reviews showing no evidence that supports the use of CEC over TEC for the increase of fracture resistance in human teeth.20,22 It should be mentioned, however, that TEC does sacrifice more percervical dentin, but it is not clear if that can impact the fracture resistance of endodontically treated teeth.
However, not only did many studies’ results show no benefits associated with CECs, but some also present evidence that this access modality resulted in less root canal detection, less preservation of the original canal anatomy particularly at the apical level, and more complications regarding the restoration.16,23,24
As for guided access cavities and caries and restoration-oriented cavities, there are only case reports and case series pertaining to them, hence questioning the validity of their clinical implementation.
Lastly, what seems important in terms of fracture resistance is not the access cavity design but rather the number of walls remaining at time of access. It has been shown that molars with two remaining walls are significantly less resistant to fracture compared to four- and three-walled cavities, regardless of the cavity design.20 This of course, raises the importance of post-endodontic cuspal coverage.
Conclusion
The wave of technological advancements that the field of endodontics has experienced in the last decade has transformed the way a root canal treatment is executed. However, the main purpose remains the same — microbial control. This control relies heavily on the action of chemo-mechanically debriding the root canal system and sealing it afterwards. This in turn relies on having an adequate access cavity opening. The traditional access opening has been redesigned into more restricted preparations with the claim of better preservation of tooth structure. However, at the present time, there is not enough supporting evidence for the incorporation of such cavities into clinical practice, and clinicians must remain cautious and base themselves on current scientific evidence.
REFERENCES
1. Bergenholtz G, Hörsted-Bindslev P, Reit C (eds). Textbook of endodontology. Chichester : John Wiley & Sons; 2013.
2. Sundqvist G, Figdor, D. Endodontic treatment of apical periodontitis, in Ørstavik, D, Pitt Ford T (eds). Essential Endodontology Oxford, UK:Blackwell Science Ltd; 1998:242–277.
3. Byström A, Sundqvist G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981 Aug;89(4):321328. doi: 10.1111/j.1600-0722.1981.tb01689.x.
4. Shuping GB, Orstavik D, Sigurdsson A, Trope M. Reduction of intracanal bacteria
Figure 3: Navigation stent used for guided endodontic access cavity design. Adapted from Serota K. Dynamic navigation — The future of minimally invasive endodontics. Dental Tribune. March 2020
using nickel-titanium rotary instrumentation and various medications. J Endod. 2000 Dec;26(12):751-755. doi: 10.1097/00004770-200012000-00022.
5. Byström A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J. 1985 Jan;18(1):35-40. doi: 10.1111/ j.1365-2591.1985.tb00416.x.
6. Byström A, Sundqvist G. Bacteriologic evaluation of the effect of 0.5 percent sodium hypochlorite in endodontic therapy. Oral Surg Oral Med Oral Pathol. 1983 Mar;55(3):307-312. doi: 10.1016/0030-4220(83)90333-x.
7. Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995 Jan;28(1):12-18. doi: 10.1111/j.1365-2591.1995.tb00150.x.
8. Hommez GM, Coppens CR, De Moor RJ. Periapical health related to the quality of coronal restorations and root fillings. Int Endod J. 2002 Aug;35(8):680-689. doi: 10.1046/j.1365-2591.2002.00546.x.
9. Sjögren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990 Oct;16(10):498-504. doi: 10.1016/ S0099-2399(07)80180-4.
10. López-Valverde I, Vignoletti F, Vignoletti G, Martin C, Sanz M. Long-term tooth survival and success following primary root canal treatment: a 5- to 37-year retrospective observation. Clin Oral Investig. 2023 Jun;27(6):3233-3244. doi: 10.1007/s00784-02304938-y. Epub 2023 Mar 18.
11. American Association of Endodontics. Colleagues for Excellence: Access opening and canal location. Spring 2010. https://www.aae.org/specialty/newsletter/access-opening-canal-location/. Accessed January 26, 2025.
12. Rankow HJ, Krasner PR. The access box: an ah-ha phenomenon. J Endod. 1995 Apr;21(4):212-214. doi: 10.1016/S0099-2399(06)80569-8.
13. Krasner P, Rankow HJ. Anatomy of the pulp-chamber floor. J Endod. 2004 Jan;30(1):516. doi: 10.1097/00004770-200401000-00002.
14. Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010 Apr;54(2):249-273. doi: 10.1016/j.cden.2010.01.001.
15. Al-Helou N, Zaki AA, Al Agha M, Moawad E, Jarad F. Which endodontic access cavity is best? A literature review. Br Dent J. 2023 Mar;234(5):335-339. doi: 10.1038/s41415023-5581-7. Epub 2023 Mar 10.
16. Shabbir J, Zehra T, Najmi N, Hasan A, Naz M, Piasecki L, Azim AA. Access Cavity Preparations: Classification and Literature Review of Traditional and Minimally Invasive Endodontic Access Cavity Designs. J Endod. 2021 Aug;47(8):1229-1244. doi: 10.1016/j.joen.2021.05.007. Epub 2021 May 28.
17. Plotino G, Grande NM, Isufi A, Ioppolo P, Pedullà E, Bedini R, Gambarini G, Testarelli L. Fracture Strength of Endodontically Treated Teeth with Different Access Cavity Designs. J Endod. 2017 Jun;43(6):995-1000. doi: 10.1016/j.joen.2017.01.022. Epub 2017 Apr 14.
18. Krishan R, Paqué F, Ossareh A, Kishen A, Dao T, Friedman S. Impacts of conservative endodontic cavity on root canal instrumentation efficacy and resistance to fracture assessed in incisors, premolars, and molars. J Endod. 2014 Aug;40(8):1160-1166. doi: 10.1016/j.joen.2013.12.012. Epub 2014 Jan 28.
19. Silva EJNL, Pinto KP, Ferreira CM, Belladonna FG, De-Deus G, Dummer PMH, Versiani MA. Current status on minimal access cavity preparations: a critical analysis and a proposal for a universal nomenclature. Int Endod J. 2020 Dec;53(12):1618-1635. doi: 10.1111/iej.13391. Epub 2020 Sep 18.
20. Corsentino G, Pedullà E, Castelli L, Liguori M, Spicciarelli V, Martignoni M, Ferrari M, Grandini S. Influence of Access Cavity Preparation and Remaining Tooth Substance on Fracture Strength of Endodontically Treated Teeth. J Endod. 2018 Sep;44(9):1416-1421. doi: 10.1016/j.joen.2018.05.012. Epub 2018 Jul 23.
21. Connert T, Weiger R, Krastl G. Present status and future directions - Guided endodontics. Int Endod J. 2022 Oct;55 Suppl 4(Suppl 4):995-1002. doi: 10.1111/iej.13687. Epub 2022 Feb 4.
22. Ballester B, Giraud T, Ahmed HMA, Nabhan MS, Bukiet F, Guivarc’h M. Current strategies for conservative endodontic access cavity preparation techniques-systematic review, meta-analysis, and decision-making protocol. Clin Oral Investig. 2021 Nov;25(11):6027-6044. doi: 10.1007/s00784-021-04080-7. Epub 2021 Oct 8.
24. Alovisi M, Pasqualini D, Musso E, Bobbio E, Giuliano C, Mancino D, Scotti N, Berutti E. Influence of Contracted Endodontic Access on Root Canal Geometry: An In Vitro Study. J Endod. 2018 Apr;44(4):614-620. doi: 10.1016/j.joen.2017.11.010. Epub 2018 Jan 12.
Continuing Education Quiz
Endodontic access cavities: science versus trends
SAFI
1. The aim of a root canal treatment is _________.
a. To remove tooth structure
b. To detect radiopacity
c. Microbial control
d. To obtain a wide occlusal access cavity
2. The design and execution of the access cavity can dictate the healing or the persistence of apical periodontitis.
a. True
b. False
3. Traditionally, the endodontic access cavity was designed in a way that aimed to remove any obstruction in the way of reaching the canal orifices. This included _______ — avoiding the need to alter visual angulation.
a. the complete unroofing of the chamber
b. exposing all pulp horns
c. obtaining a straight-line access to the apex
d. all of the above
4. The drawback of ________ design is that it requires the removal of healthy tooth structure, specifically the pericervical dentin — the dentin present 4 mm above and 6 mm below the crestal bone which helps to distribute any forces placed on the tooth.
a. Traditional Endodontic Cavity (TEC)
b. Truss Access Cavity
c. Guided Access Cavity
d. Ultraconservative Endodontic Cavity (UEC)
5 The increasing popularity of _______, along with the goal to preserve pericervical dentin, gave rise to a series of new endodontic access cavities.
a. magnification
b. illumination
c. CBCT technology
d. all of the above
6. ________ is based on the partial deroofing of the pulpal chamber while preserving pulpal horns, resulting in a slight occlusal convergence.
a. The Conservative Endodontic Cavity (CEC)
b. The Magnified Access Cavity
c. The Truss Access Cavity
d. Caries-Oriented Access Cavity
7. The ultraconservative shape (of the Ultraconservative Endodontic
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://endopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://endopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 070
Date Published: March 1, 2025
Expiration Date: March 1, 2028
Cavity) __________ to locate, clean, disinfect, and obturate the root canal system.
a. makes it considerably easier
b. makes it totally impossible
c. makes it more challenging
d. is the best way
8. The ________ design is mainly used in obliterated root canal systems to reduce the risks of canal deviation and perforation.
a. Conservative Endodontic Cavity
b. Guided Access Cavity
c. Restorative Access Cavity
d. Truss Access Cavity
9. In a study comparing Traditional Endodontic Cavity (TEC) versus Conservative Endodontic Cavity (CEC) and Ultraconservative Endodontic Cavity (UEC), extracted premolars and molars with TEC showed ______ than the ones prepared with CEC or UEC.
a. higher fracture strength
b. lower fracture strength
c. equal fracture strength
d. none of the above
10. There is evidence that ______ access makes cleaning procedures more difficult, increasing the total time required for a root canal treatment.
a. Ultraconservative Endodontic Cavity (UEC)
b. Truss Access Cavity
c. Guided Access Cavity
d. Caries Oriented Access Cavity
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Exploring the dental microscope’s benefits
Dr. Juan Carlos Ortiz Hugues explains how dental microscopes can improve precision and clinical accuracy
The introduction of the dental microscope into clinical dentistry in the 1990s marked a significant milestone in the field, with its adoption in endodontic programs accredited by the Commission on Dental Accreditation (CODA) in 1998.1 This technology has fundamentally transformed dental practice by offering superior magnification and lighting, which have enhanced the precision of procedures and improved clinical outcomes.
One of the key advantages of the dental microscope is its ability to provide high levels of magnification, allowing clinicians to detect minute details that are often invisible to the naked eye. This is especially important in complex procedures like root canal therapy, where precision is crucial for successful outcomes. The microscope’s superior illumination also ensures that the working area is brightly lit, reducing the risk of errors caused by poor visibility and facilitating better diagnosis and treatment.
magnifying glasses, enhancing diagnostic and procedural accuracy significantly.
Addressing precision and ergonomics in dentistry
Magnification: transforming visual precision
Dental microscopes offer various magnification levels, typically in increments of 5 to 6, ranging from low to high magnification. At the highest setting (20x), these microscopes provide up to 400 times more visual information than the naked eye and 100 times more than 2x magnifying glasses.2 As magnification increases, the resolution and clarity of the visual field improve, enabling dental professionals to achieve exceptional precision in clinical procedures.
Illumination: eliminating shadows for optimal visualization
A key feature of dental microscopes is their coaxial illumination system, which is integrated into the optical structure. This system ensures 100% shadow-free lighting along the operator’s visual axis, providing a uniformly illuminated field of vision. This advanced lighting surpasses the limitations of traditional
Juan Carlos Ortiz Hugues, DDS, CEAS II, AEP, is a master of the Academy of Microscope Enhanced Dentistry (AMED), and current president of the AMED. He is an endodontist in private practice in Panama. Dr. Ortiz Hugues lectures and provides hands-on training throughout the world on endodontics, microscope dentistry, and advanced ergonomics. He wrote the book, Ergonomics Applied to Dental Practice.
Incorporating ergonomic principles into the use of the dental microscope has further amplified its benefits. With the addition of adjustable positions, optimal posture can be maintained during lengthy procedures, thereby reducing operator fatigue and musculoskeletal strain. This focus on ergonomics not only promotes the longevity and health of the practitioner but also enhances comfort and efficiency during treatment.3
Real-time documentation: building trust and transparency
The ability to document procedures through the microscope’s built-in camera enables practitioners to capture high-quality images and videos for educational purposes, patient records, and legal documentation. This fosters a more comprehensive understanding of the treatment process and allows for better communication with patients.
The integration of the dental microscope, coupled with ergonomic principles, has significantly elevated both the quality of care provided and the well-being of dental professionals. The continued adoption of this technology, along with the emphasis on ergonomic best practices, promises to further refine clinical outcomes and optimize the working environment for dental practitioners.
REFERENCES
1. American Association of Endodontists (AAE). Position Statement – Use of Microscopes and Other Magnification Devices. 2020. www.aae.org. Accessed January 6, 2025.
2. van As GA. Magnification alternatives: seeing is believing, Part I. Dent Today. 2013 Jun;32(6):82-87. PMID: 23802377.
3. Juan Carlos Ortiz Hugues. Applied Ergonomics and Microscope Dentistry, A Need for Quality Dentistry, and Prolonged Performance. Systematic Approach Concept: Applied Ergonomics and Microscope Dentistry. Inter Ped Dent Open Acc J. 2023;8(4):706-708. Published August 10, 2023. doi: 10.32474/IPDOAJ.2023.08.000295. Accessed January 6, 2025.
Dr. Travis Parker
Dr Samantha Jeffery
EP
Kerr Dental
Cutting-edge solutions in dentistry
Kerr Dental, a distinguished leader in dental care, offers an extensive range of Endodontic, Restorative, Rotary, and TotalCare products. Known for its commitment to innovation, Kerr has introduced several groundbreaking advancements in endodontics. Among these are the minimally invasive ZenFlex™ NiTi Rotary Shaping File, the elements™ IC obturation unit, and the new cordless motor elements™ Connect. Kerr has also revolutionized the field with the introduction of the K-File, a product that has become a staple in most dental practices.
Kerr’s success is built on its close collaboration with key opinion leaders in the dental industry. This partnership ensures that Kerr remains responsive to the needs of doctors, practices, and their patients. Dr. Matthew Miller, a member of Kerr’s Endodontic and Restorative Advisory Board, emphasizes this point: “Kerr truly listens to the feedback from dentists and incorporates our input into their design. This results in products that are intuitive to use, drive workflow efficiencies, adapt to the doctor’s preferred techniques, and support improved patient outcomes with exceptional results.”
Recently, Kerr Dental was recognized by Dental Advisor as the “Innovative Company of the Year” for its cutting-edge solutions in dentistry. This accolade highlights Kerr’s dedication to excellence and its continuous efforts to advance dental care. Several standout products were also awarded, further cementing Kerr’s reputation as a leader in the industry.
In conclusion, Kerr Endodontics provides a comprehensive solution for endodontic procedures, addressing the diverse needs of dental practices. We invite you to visit the Kerr Dental Booth No. 1311 to discover how our products can help you save on your everyday dental supplies. For more information, you can refer to the detailed awards issue by Dental Advisor. https:// dentaladvisor.com/wp-content/uploads/2005/05/Vol_42-2025Awards-Issue.pdf
Letting go of our reactivity is the hardest leadership lesson
Drs.
Joel C. Small
and Edwin McDonald discuss ways to control reactive tendencies
Finding and bringing forth the leader that resides within each of us is an amazing and uniquely personal experience.
Those of us who have experienced this amazing transformation understand that mitigating our reactive tendencies is the right of passage and must precede our personal and professional leadership transformation. Without this essential first step, our leadership development becomes difficult; often impossible.
Bob Anderson, the founder of the Leadership Circle, researcher, and author of numerous leadership books, describes two competing aspects of effective leadership. Creative competencies are the eighteen leadership characteristics that have a high correlation with effective leadership. Reactive tendencies are the eleven characteristics that correlate negatively with effective leadership. The reactive tendencies and creative competencies have an inverse relationship. For example, the greater the reactive tendencies, the less the creative competencies, and consequently the more our leadership effectiveness is diminished.
Anderson’s findings indicated that most human beings are hard wired to be reactive. Given this finding, our leadership development must begin by overcoming our inherent reactive tendencies so that our creative competencies can flourish. This can be a daunting task, especially when we realize that our reactive tendencies are subconscious, habitual, and the manifestations of previous life experiences that are deeply engrained within our psyche and create the lens through which we view the world. They are the stories that continuously play in our subconscious background and dictate our thoughts and actions.
Drs. Joel C. Small and Edwin (Mac) McDonald have a total of over 75 years of dental practice experience. Both doctors are trained and certified Executive Leadership Coaches. They have joined forces to create Line of Sight Coaching, a business dedicated to helping their fellow dentists discover a better and more enjoyable way to create and lead a highly productive clinical dental practice. Through their work, clients experience a better work/life balance, find more joy in their work, and develop a strong practice culture and brand that positively impact their bottom line. To receive their free ebook, 7 Surprising Steps to Grow Your Practice Through Leadership, go to www.lineofsightcoaching.com.
Unless we mitigate and/or reframe these tendencies, our attempts at becoming a transformational leader are rendered ineffective. There is a prevailing theory that we can never reach our full leadership potential if our attempts at generating creative competencies, or any positive change, are in competition with an underlying narrative that does not support our efforts. Our subconscious reactive narratives are powerful negative forces that can easily foil any attempt at positive change.
Furthermore, and even more concerning, is the fact that these subconscious reactive tendencies and narratives have served as a psychological protective mechanism that shields us from vulnerability. Thus, in order to bring forth our innate leadership capabilities, we must consciously let go of them and expose ourselves to a degree of vulnerability that we have been avoiding our entire life.
Once our unconscious and habitual reactive tendencies are identified and brought to a conscious level, we can begin a process of mitigating these tendencies and their negative impact on how we show up for those we lead. Carl Jung stated this most eloquently in this famous quote:
“Until we make the unconscious conscious, it will rule our life, and we will call it fate.”
According to Viktor Frankl, the Austrian psychologist and Nazi concentration camp survivor, there is a space between stimulus and response, and within that space is our choice to respond. Having brought our unconscious reactive tendencies to a conscious level allows us to substitute a different and more appropriate response than the habitual knee jerk responses that are driven by our underlying reactive tendencies and negative narratives. It is in this very brief moment between stimulus and response that our leadership is defined and either flourishes or flounders.
Currently there are several useful assessments designed to increase our awareness of our reactive tendencies as well as our creative competencies. Line of Sight Coaching’s Leadership Circle Profile 360 assessment is simple, yet it delivers a clear and powerful picture of how someone is showing up for those they lead and pinpoints those areas of needed improvement.
Letting go of our life-long reactive tendencies and engrained narratives is difficult and may require the help of a coach who collaborates with developing new leaders.
Specialty1 Partners
Better care. Better business. Better oral health.
“Our primary focus has always been patient and partner satisfaction, and we have found that this approach truly resonates with the specialists we bring on board.” – Dr. Daryl Dudum, Founding Partner and Co-CEO
Specialist founded — Specialist led — Specialist supported
We are proud to be the only Specialty Partnership Organization founded, led, and supported by dental specialists. Specialty1 Partners (S1P) is your best choice for taking your specialty dental practice to the next level of success and patient care.
With over 225 partner practices spanning 28 states, S1P is the leader in enabling its partners to focus on patient care while benefiting from the support of a network of seasoned professionals dedicated to the success of their practices. S1P provides operational, financial, and administrative support services to fuel clinical excellence, growth, and financial security. Ensuring your ability to focus on your patients and your future is what we do best.
225+ practices — 350+ specialists — 28 states
Practice owners — your focus, our support
Joining Specialty1 Partners is the starting point for a more fulfilling career and a path to a more secure future. You’ll have
a professional team behind you to manage the administrative tasks currently consuming time and energy better spent caring for your patients.
Realize your vision
We enable our Partner practices to maintain clinical autonomy in caring for their patients without also having to manage the back-office aspects of their business.
Focus on patient care — Your specialty practice will no longer need to manage back-office complexities, enabling you to spend more time and energy keeping patients healthy.
Secure your future — As a member of our growing family of practices, you’ll have the potential to realize financial upside from our continued successful growth.
Do more of what you love — By no longer having to manage all the complexities of running a practice, you’ll have the time and energy to pursue other personal and professional interests.
Level up your practice — Elevate your ability to focus on patient care while a team of professionals manages the complexities associated with running a specialty practice.
If you would like more information about Specialty1 Partners and to see how we can work together, please visit https://www. specialty1partners.com/.
This information was provided by Specialty1 Partners.
Endodontic Artistry
Cutting Edge File System with Flexibility and Strength
Strong to significantly increase resistance to cyclic fatigue. Heat treated NiTi enables the EXIMIA7™ file extreme flexibility reducing shape memory, preserving canal anatomy e ortlessly following the canal as you shape.
Matching Gutta Percha and Paper Points Available
• Heat treatment process improves strength and flexibility
• Available in .04 and .06 Constant Taper - Variable Pitch
• Maximum flute diameter 1mm allows for minimally invasive preparation
• Parabolic Cross Section non cutting tip maximizes file cutting efficiency