Feeding tubes –placement and maintenance
Blood gas –it doesn’t need to be scary

Feeding tubes –placement and maintenance
Blood gas –it doesn’t need to be scary
It’s time to start planning your attendance at the 29th VNCA Conference in Perth …

The VNCA aspires to strengthen the position of Veterinary Nurses as part of the veterinary healthcare profession.
MISSION
The VNCA: Serves and represents all Veterinary Nurses Protects the professionalism of Veterinary Nurses
Promotes the value of Veterinary Nurses as vital in delivery of quality veterinary care Advocates for the increased recognition of Veterinary Nurses across Australia
Supports Veterinary Nurses through the provision of continuing education and networking opportunities
Strengthens the position of Veterinary Nurses across the veterinary industry

Engages all Veterinary Nurses across the veterinary industry.

It’s beginning to look a lot like Christmas ... the silly season is upon us and what would normally be our nice hot summer is instead presenting unprecedented weather. I want to start by sending my thoughts to all those affected by floods over the past few months; it has not been an easy time for the communities affected. Please know our thoughts are with you all.
As we come into our happy holiday period, I have been reflecting on all that we have achieved as an organisation, not only the challenges we have faced, but also the community we have built coming out of lockdown and living with COVID. Just as we have steered the VNCA ship through some tough times, we are finally emerging in smoother waters.
As president, I have been extremely lucky to have so many opportunities to connect with industry at forums, conferences and meetings where I have been promoting the interests of veterinary nurses and technicians nationally. We know as an industry we face staff shortages, and we at the
VNCA believe the utilisation of nurses and technicians will go a long way to supporting industry to meet our animal health and welfare outcomes. We will continue to promote utilisation and registration as a way forward.
We at the VNCA have an amazing team of volunteers in each state and on every committee who dedicate many hours to supporting you, our members. We know it hasn’t been an easy year, so I would like to thank everyone for all their efforts and recognise the work they have achieved.
We had a very successful year of CPD with conferences, state events and webinars, and we have some very exciting plans for next year, including our Perth conference – and the program of speakers is amazing! Launching our values and aligning them to our vet nurse and technician week, we celebrate and recognise two amazing individuals in our industry awards for the Vet Nurse/Technician of the Year, Anita Parkin, and our Student Vet Nurse of the Year, Kristie Wallace – two amazing humans who
The VNCA announced on Friday 25 November 2022 that the Australasian Veterinary Boards Council (AVBC) has agreed to work with the VNCA and AVNAT Regulatory Council towards mandatory registration of veterinary nurses and technicians across Australia.

Dr Peter Gibbs, AVBC Chair, said 'Following last week’s Council decisions, work will continue to take this initiative forward. Next steps include refining the definitions of “veterinary nurse” and “veterinary technician”, defining the acts they can perform, and identifying processes required for registration.'
The VNCA President, Rebecca Coventry stated ‘Today is a tremendous step
forward for our professions. The VNCA has been working towards regulation of veterinary nurses and technicians for 25 years and is looking forward to collaborating with AVBC to strengthen the veterinary team by improving role clarity and career progression for veterinary nurses and technicians. While there is much work to be done, agreement across all parties to progress this long-awaited development is warmly welcomed.’
Ms Jo Hatcher, Australian Veterinary Nurse and Technician Registration Scheme Chair said, 'When the VNCA developed the AVNAT registration scheme our main goal was for registration to move from voluntary to national regulation of all veterinary nurses and technicians in Australia.
 Rebecca Coventry VNCA President
Rebecca Coventry VNCA President
are excellent role models and leaders in our industry. Congratulations, once again!
We are working with divisions and finalising our planning for 2023–24. There are so many exciting things in the pipeline and we look forward to continuing to support nurses and technicians nationally.
On behalf of the Board, I want to thank you for your continued membership, and we hope that you get to spend some time over the holiday period with family and friends, that you celebrate your successes with your team, and have a work celebration to recognise your efforts this year.
Stay safe, be merry and we will reconnect with you all in 2023, which I know will be an amazing year!
Rebecca Coventry VNCA PresidentThe AVNAT Regulatory Council welcomes this significant move by the AVBC and looks forward to working together to achieve this goal.'
There is much work to be done to progress this initiative and VNCA members can be assured that we will continue to work to ensure optimal outcomes for veterinary nurses and technicians across Australia. Keep an eye out for further developments which will be published as they become available.
The AVNAT Regulatory Committee welcomes our new and renewed AVNAT registrants. Thank you all for your commitment, dedication and enthusiasm as we continue to build the profile of our role within the workplace and the communities in which we live and work. We also thank our education partners who are a part of the AVNAT scheme in providing high quality education events for all. These partners provide a number of events and courses throughout the year, and I encourage you to check out their events as there will be a CPD event for everyone on a variety of topics. For a list of education partners and their events, go to the VNCA website and the AVNAT page for details.
The AVNAT Regulatory Committee completed the audit process over the last few months. It was pleasing for the committee to see most of those audited ensuring that they had all their documentation in place and CPD activities clearly listed. This was certainly aided by the online CPD activity tracker that makes everything clear and easy to follow. If you have not used the tracker, I encourage you to do so, and every time you undertake a CPD activity, log it straightaway.
The committee did note during the audit process that there are several registered veterinary nurses and technicians who are logging CPD events that have no formal points system approved, and these CPD events are therefore ineligible for CPD points to use for AVNAT. While listing all CPD you undertake on the CPD tracker is a good idea, you must ensure that a minimum of 20 points is either AVNAT, RACE or NZVNA approved to be eligible to use for AVNAT CPD requirements.
• AVNAT CPD Points are awarded by the AVNAT Regulatory Council on application by the training provider. The certificate of completion/ attendance will often feature the following logo and/or wording with the number of eligible points clearly specified.

Another area to check when you receive your certificate for a CPD event is to understand the difference between CPD hours and CPD points applied to the event. Some certificates will state a number for hours that the event or course was undertaken in, but this is not necessarily the same as the actual CPD points applied. For example, a course may list on the certificate that the length was 20 hours, but the CPD points applied may only be 5 points. It is the CPD points that you can use towards your overall CPD yearly total, not the hours.
• RACE CPD Points are awarded by the American Association of Veterinary State Boards (AAVSB) on application by the training provider for a wide range of international programs and veterinary medical professionals. As such, some activities may only be approved as CPD for veterinarians, while others will have wider approval.
While some training providers may include a RACE logo on their certificates, the following wording must always appear:
‘This program has been approved for _____ hours of continuing education credit in jurisdictions that recognize RACE approval.’
• NZVNA CPD Points are awarded on a training provider basis and will include a logo and wording similar to that shown for AVNAT CPD Points.
If you are undertaking CPD and the course or event does not have any formal points system applied, ask the provider why not and if they would apply for points with AVNAT. While the AVNAT Committee does contact providers to encourage them to apply for points for their events, your voice can also assist us with this process and ensure even more approved events for all.

Work continues on the path towards the formal regulation of veterinary nurses and technicians in Australia with the VNCA and AVNAT Regulatory Council continuing to liaise with associations and government bodies at both state and national level. The Sustainable Practice Committee (SPC) of the Australasian Veterinary Boards Council (AVBC) continues to meet and is reviewing the feedback from the survey on the potential for a national registration scheme with the consultation of the VNCA, AVNAT and relevant industry representatives.
In South Australia, the Minister for Primary Industries and Regional Development, the Honourable Clare Scriven MLC, has advised that a drafting of a New Veterinary Services Bill for South Australia is underway and is considering feedback from the discussion paper in 2021 that the VNCA and AVNAT provided on the registration of veterinary nurses and technicians. We will keep you updated on further developments as they occur.
As we enter the second half of our registration and CPD cycle, plan your CPD events to ensure you gain your minimum of 20 points for your renewal in July. For all AVNAT enquiries, please email avnat@vnca.asn.au
Gone are the days where we can assume to live in a world of neurotypical students and colleagues. Where everyone is expected to learn, act, think and behave the same. International Attention Deficit/ Hyperactivity Disorder (ADHD) Awareness Month runs through October; a time to celebrate individual differences and educate others while tackling the misconceptions of ADHD.
ADHD is a common neurobiological condition that affects 5–8% of children. These children have symptoms that can persist into adulthood. Young girls can be difficult to diagnose by health professionals due to masking, whereas boys can be diagnosed as early as 7 years of age.
A recent increase in media awareness of the neurodiverse condition indicates that more adults are now being diagnosed. One in twenty Australian adults are affected by ADHD. The majority are males, whereas females are often diagnosed when they recognise symptoms in adulthood.
People with ADHD have different neurophysiology, where the brain has different anatomy, electrical activity and metabolism. The precise causes are not known, but there are multiple factors that make a person more likely to develop ADHD. Currently, researchers are still trying to isolate which genes are linked to ADHD.
Neurodiversity is best described as a variance in brain function in some people. This enables them to think differently from the way others expect. Many who are diagnosed with ADHD will often have another neurodevelopmental condition such as autism spectrum disorder (ASD), specific learning disorders, Tourette syndrome or other neuro syndromes and anxiety.

Medical literature within the last 200 years has described the human behaviour and characteristics of modern traits of ADHD. These can include differences in focus/ attention, regulating emotions, movement, and impulse control. German physicians Franz Kramer and Hans Pollnow importantly started to identify these differences in the early 1930s, where it was concluded that these behaviours were from other underlying causes. These included the nervous system and differences in the brain structure, which were not intellectual deficits. As medical studies advanced, Dr Charles Bradley in America discovered that stimulant medication could help improve symptoms of ADHD. However, it wasn’t until 1994 that there were three sub-types of ADHD officially recognised.
The 3 types of ADHD:

• Inattentive means a person is easily distractible or inattentive but isn’t hyperactive or impulsive.
• Hyperactive-impulsive means a person has symptoms of impulsivity and hyperactivity.
• Combined means a person has a mixture of symptoms including hyperactivity, inattention and impulsivity.
Diagnosis can be expensive, prolonged and involves a team of health professionals, usually starting with a patient’s general practitioner, who refers them on to a psychologist, psychiatrist or neurologist. There is no pathology testing currently available, only cognitive and behavioural awareness testing. Adults must exhibit at least five of the symptoms in multiple settings to be diagnosed with ADHD.
Once diagnosed, treatment can begin based on the individual, who may benefit from stimulant/non-stimulant medications, biomedical treatment, neurofeedback, psychology and ADHD coaching.
Self-awareness is the first step to creating tactics that help overcome any specific challenges. Communicate your diagnosis with your workplace mentor/supervisors and employer and how this can affect your workday. This will be difficult; however, having an employer and team who understand can help enhance and shape your career.
SO
There are many benefits that these behaviours can bring to the workplace. Nurses with neurodivergent minds can be creative and can hyperfocus on complex cases, turning the way their brain processes tasks and activities into a ‘superpower’.
Other advantages include:
• the ability to find unique solutions to difficult problems
• being adventurous, courageous and thinking ‘outside the box’
• constantly evolving, continually learning
• endlessly desiring to try new ideas, tasks and projects
• being empathetic and intuitive to feelings/emotions
• being conversationalists, humourists
• being resourceful.
Some struggles that the neurodiverse nurse may encounter within the workplace may include problems prioritising, starting or completing tasks and maintaining focus.

Employers and other team members can help create a supportive environment for the neurodiverse to help optimise their abilities to see them thrive within the workplace.
How ADHD affects the neurodiverse person:
• poor attention; excessive distractibility
• physical restlessness or hyperactivity
• excessive impulsivity such as saying or doing things without thinking
• excessive and chronic procrastination
• difficulty getting started on tasks
and completing tasks, poor organisation, planning, and time management skills
• excessive forgetfulness
• insomnia
• sensory processing disorders.
Besides medication and therapies … you need to look after yourself.
• If full-time hours don’t work for you, consider fewer hours – speak to your employer.
• Take your full lunch break at work. Go outside and walk, get into the sunshine. Do not feel guilty. If you don’t look after you, how will you have the energy to look after your patients or work cohesively to help your team?
• Ear buds, earmuffs – muffs may look funny, but if you’re on the kennel shift, these can be a lifesaver.
• Take your annual leave!
• Have a personal schedule to exercise, rest and try to sleep.
• Find a hobby you love outside of work.
• Grounding techniques – seek occupational therapy (OT) advice or breathing techniques i.e. what are 5 things you can physically touch, smell or see?
• Wear and use antiglare glasses.
• Have visual lists of tasks on the wall.
• Set timers/alarms such as visual clocks, smart watches, etc.
• Surround yourself with a good support system, including family and friends, who understand your neurodiversity.
Self-awareness is the first step to creating tactics that help overcome any specific challenges. Communicate your diagnosis with your workplace mentor/supervisors and employer and how this can affect your workday. This will be difficult; however, having an employer and team who understand can help enhance and shape your career.
Speak to your registered training organisation (RTO) or university educators; ensure to disclose this diagnosis at time of enrolment to get the support you may need. This can help with your learning and help your educators create effective techniques to assist your learning.
Use time management and organisational strategies to streamline your day. To help get more organised, you can:
• set goals, write to-do lists, and use these to plan and prioritise tasks for the day
• use a diary and set reminders for jobs that need doing
• group similar tasks that can be done together
• be mindful of sensory overload – loud noises, bright lights within your environment. Modify your
environment to ensure it is comfortable and quiet
• listen to podcasts, webinars or PDF readers to mix up your learning (don’t just read text)
• break down tasks into smaller chunks – smaller tasks are easier to complete, easier to organise and are less overwhelming
• Pomodoro technique – this involves a time management system that encourages you to work with the time you have – rather than against it. Break your tasks up into 25-minute chunks and separate with fiveminute breaks. These intervals are referred to as Pomodoro
• try different brainstorming with others to solve common problems. Remember, there is often more than one solution to a problem.
The workplace can help by:
• promoting health and wellbeing within the workplace
• encouraging employer diversity, equality and fair treatment
• being mindful of each staff member’s workload and flexibility
• encouraging personal and career development
• focusing on the individual’s specific love/area of nursing (Are they great with medical, reception, surgical, client focus, etc.?) and get this individual to specialise in this area of the clinic
• encouraging employers to educate themselves regarding neurodiverse conditions.
If the neurodivergent nurse is happy, this may promote and improve the retention of skilled and motivated staff, both in their workplace and in the industry overall. A healthy workplace will also be more likely to cope well with unexpected challenges.
When neurodivergent nurses understand their differences, and can harness their superpower, we can achieve brilliant things. After all, if we all saw the world from the same perspective, we wouldn’t see depth, shade or an alternative viewpoint. In daring to think differently, we not only support staff better, but also unlock potential in the workplace by unleashing much needed skills to create a positive change.
Sources Australian Psychological Society Access EAP
Australian Evidence-based Clinical Practice Guideline for ADHD, published July 2022, Australian ADHD Guideline Development Group ADHDFoundation.org.au adhdsupportaustralia.com.au adhdaustralia.org.au – National Resource Centre on ADHD

 by Anita Parkin RVN, AVN, Dip (Surg & ECC), VTS (Anes & Analgesia), CVPP, TAE
by Anita Parkin RVN, AVN, Dip (Surg & ECC), VTS (Anes & Analgesia), CVPP, TAE
Nutrition is a very important component of patient management, especially in the critical care setting. There is significant information indicating that animals may be hypermetabolic during many disease states. For this reason, understanding and meeting nutritional requirements cannot be overlooked when managing a critically ill or severely traumatised animal. Other factors, such as immune system function and maintaining a healthy gastrointestinal mucosal barrier, may also play a role in managing diseased dogs and cats.
Enteral feeding is indicated in patients who cannot ingest adequate calories but have sufficient gastrointestinal function to allow digestion and
absorption of feeding solutions delivered into the gastrointestinal tract via an enteral feeding device. The most important stimulus for mucosal cell proliferation is the direct presence of nutrients in the intestinal lumen.
For the most part, the old adage ‘If the gut works, use it’ applies in most situations. Practical measures to improve food intake include the use of highly odorous foods, warming the foods prior to feeding and stimulating eating by positive reinforcement with petting and stroking behaviour. Assisted feeding, appetite stimulation and tube feeding (orogastric) methods can all be used.
Assisted feeding by gently syringing a liquid food into the corner of the patient’s mouth
or ‘pilling’ balls of food used to be suggested; however, this method can be exceptionally stressful to the patient and will foster the development of food aversion. Enteral nutrition is the most appropriate choice of providing protein and calories. It is simple, well tolerated and the most cost-effective.
Significant anorexia (> 3 days, > 1-day neonates). Significant weight loss (> 10%, > 5% neonates). Increased nutritional losses (diarrhoea, vomiting, renal disease, wounds and burns). Increased nutritional requirements (fever/infection, trauma/surgery, cancer, burns). Anticipated loss of appetite (animal not expected to eat for 3 days). Bypass of specific parts of alimentary canal (head injury, surgical site, pancreatitis).
It has been well established that nutritional support in critically ill
patients will decrease morbidity and mortality, improve tolerance to invasive procedures, shorten hospitalisation periods, decrease incidence of infections, enable earlier ambulation, hasten wound healing, and reduce complications.
The type of formula to feed the patient will depend on the selected route of feeding, the functional status of the gastrointestinal tract and the patient’s nutrient requirements. Other factors such as cost, availability and ease of use may also be important. Patients that are fed via naso-oesophageal or jejunostomy feeding tubes are limited to receiving liquid enteral formulas. Most commercially available liquid diets have a caloric density of approximately 1 kcal per ml.
Commercial blended pet food diets should be used for feeding into the stomach via esophagostomy or gastrostomy tubes. In select cases, the feeding of a liquid enteral formulation may be indicated (naso-oesophageal or jejunostomy tube feeding). There are a

number of complete and balanced veterinary enteral formulations that contain adequate amounts of protein, taurine, and micronutrients, precluding the need for supplementation in most situations. Feeding should be delayed for 24 hours after placing a gastrostomy tube to allow gastric motility to return and to allow formation of a fibrin seal.
An estimate of an animal’s nutrient requirements is needed to determine the minimum amount of food necessary to sustain critical physiologic processes. The resting energy requirement (RER) is the animal’s energy requirement at rest in a thermoneutral environment and in a postabsorptive state. A linear formula can be applied to determine the RER of dogs and cats weighing at least 2 kg but less than 45 kg. Alternatively, one can utilise an allometric formula that can be applied to dogs and cats of all body weights.
Linear formula: RER (kcal/day) = (30 x BWkg) + 70
Allometric formula: RER (kcal/day) = 70 (BWkg)0.75
Hospitalised patients should be fed a third of their calculated RER initially, increasing to their full RER over 3 days, realising that their actual energy requirement is likely to change over the course of the disease process through recovery. Close observation of changes in body weight, physical examination findings (decreased subcutaneous fat stores, muscle wasting, and presence of oedema or ascites), and ongoing losses (diarrhoea, vomiting, exudative wounds), will help determine whether to increase or decrease the patient’s caloric intake towards the illness energy requirement (IER) or RER, respectively.
IER (kcal/day) in dogs = 1.25-1.5 x RER: in cats 1.10-1.25 x RER
Feeding can be instituted immediately following oesophagostomy tube placement once the animal has fully recovered from anaesthesia. Diet can be administered as bolus feedings or continuous infusion when feeding via oesophagostomy and gastrostomy tube.
Capacities for cats and dogs are 5 to 10 ml/kg body weight during initial food reintroduction. Maximum capacities as high as 45 to 90 ml/kg body weight have been measured in cats and dogs when fully realimented. Most often, meeting the patient’s RER can be done in volumes far less than these maximums. Salivating, gulping, retching and even vomiting may occur when too much food has been infused or when the infusion rate is too fast.
With bolus feeding, the required daily volume of food should be divided into four to six feeds. Patients are usually fed approximately 33% of their caloric requirement on the first day of feeding, with a gradual increase of 33% of the caloric requirement per day. Most patients can reach their energy requirement by the third or fourth day of feeding. The food should be warmed to room temperature and
fed slowly through the tube to prevent vomiting. Flushing of the tube with 10 to 15 ml of lukewarm to warm water helps prevent clogging. Before each feeding, aspirate the tube with an empty syringe to check for residual food left in the stomach from the previous feeding. If more than half the last feeding is removed from the stomach, skip the feeding and recheck the residual volume at the next feeding.
Naso-oesophageal/nasogastric intubation is an easy, effective, and efficient means of providing enteral nutritional support. The availability of small bore, soft polyvinyl and silastic feeding tubes, low viscosity, nutritionally complete liquid diet formulations and patient tolerance of tube placement has made naso-oesophageal/ nasogastric tube placement a popular avenue for feeding malnourished patients. Naso-oesophageal/ nasogastric tube placement is indicated in any patient with proteincalorie malnutrition that will not undergo oral, pharyngeal, oesophageal, gastric or biliary tract surgery.
Tube management: Place a column of water in the tube and cap it when not in use; this prevents intake of air, reflux of oesophageal contents, and occlusion of the tube by diet. Tube occlusion by diet can frequently be unblocked by flushing the tube with a little carbonated soft drink, leaving it in situ for 10–15 minutes then flushing with a little pressure. Naso-oesophageal/ nasogastric tubes can be left in place for several weeks, are well tolerated, easily removed, the patient can drink and swallow around the tube, and repeated orogastric intubation is prevented.
Complications: Tracheal intubation, inadvertent dislodgement (use Elizabethan collars), dislodgement through sneezing, vomiting or regurgitation, rhinitis, unilateral dacryocystitis tube occlusion are uncommonly encountered. Reflux
oesophagitis can result from improper tube placement (i.e. through the lower oesophageal sphincter) or oesophageal irritation from the tube itself.
Indications: Oesophagostomy tube feeding is indicated in anorexic patients with disorders of the oral cavity or pharynx or anorexic patients with a functional gastrointestinal tract distal to the oesophagus.
Contraindications: Oesophagostomy tube placement is contraindicated in patients with a primary or secondary oesophageal disorder (for example, oesophageal stricture after oesophageal foreign body removal or oesophageal surgery, oesophagitis, megaoesophagus).
Advantages: Advantages of oesophagostomy tube feeding include ease of tube placement, tubes are well tolerated by the patient, large bore feeding tubes (8 Fr or greater) can be used allowing the use of blended diets, tube care and feeding is easily performed by the client, patients can eat and drink around the tube, and tube removal can be performed any time after placement. Oesophageal tube placement eliminates coughing, laryngospasm, or aspiration occasionally associated with pharyngostomy tubes.
Disadvantage: The major disadvantage of the oesophagostomy tube is the need for general anaesthesia during placement.
Complications: Complications associated with oesophagostomy tube placement include early removal by the patient or vomiting. No significant long-term complications have been reported (for example, oesophagitis, oesophageal stricture, oesophageal diverticulum or subcutaneous cervical cellulitis). As with naso-oesophageal tubes reflux oesophagitis can result from improper tube placement (i.e. through the lower oesophageal sphincter) or oesophageal irritation from the tube itself.
Obstruction of the feeding tube is one of the most common complications of enteral feeding. Most obstructions are secondary to coagulation of formula, although obstruction by tablet fragments, tube kinking, and precipitation of incompatible medications can also result in tube obstruction. Naso-oesophageal tubes are prone to obstruction because of their small diameters and obstruction also occurs up to three times more frequently in patients fed by continuous vs bolus feedings. Sucralfate and antacids have been reported to precipitate with enteral formulas and cause tube obstruction. Several ‘remedies’ have been advocated to relieve tube obstruction. Warm water injected with gentle pressure and suction will relieve most obstructions. For more unyielding obstructions, carbonated water is instilled into the tube and allowed to sit for up to one hour before applying gentle pressure and suction. Tube obstructions can be minimised by flushing the feeding tube with warm water before and after administering medications or enteral feedings. Tablets should be crushed and dissolved in water prior to administration through the feeding tube if no alternative form of medication is available.
• ‘If the gut works, use it’.
• Warm food before feeding –even if using the tubes.
• Keep a column of water in the tube between feeds.
• Use carbonated drink to unblock the tube if required.
• Introduce food slowly (even via the tubes).








Dip VN (ECC), Cert IV VN, Cert IV TAA, VTS (ECC), RVN, AVN
Kate presented on this topic at the 2022 VNCA Conference
The information a venous blood gas tells us can vary slightly depending on the brand of machine. The most common results will include a patient’s pH, electrolytes, lactate, bicarbonate, base deficit and partial pressure of dissolved carbon dioxide. In addition, an arterial blood gas will provide all the above as well as the partial pressure of dissolved oxygen. Why is this information important? Many patients who present to the veterinary practice for injury or illness are likely to have changes in values associated with parameters measured on the blood gas. Significant changes on some of these parameters have the potential to be life-threatening without intervention.

To maintain normal cellular function, the body tries to keep a patient’s pH within a narrow window of normal. For cats and dogs, this is 7.35–7.45, with some slight variation expected depending on the machine used or text read. Blood pH is a measure of a patient’s hydrogen ion concentration and the ratio of bicarbonate and carbon dioxide. A pH that is too low indicates an acidemia and a pH that is too high indicates an alkalemia.
There are three major processes that maintain a normal acid-base:
• regulation of dissolved carbon dioxide
• buffering of acids with bicarbonate and non-bicarbonate buffering systems
• changes to the renal excretion of acid or base.
Carbon dioxide (CO2) is the main respiratory indicator; CO2 acts as an acid in the body due to its ability to react with water and produce carbonic acid. Changes in a patient’s alveolar ventilation, and therefore CO2 levels, can change very quickly to maintain a normal pH.
Bicarbonate (HCO3) is the body’s main extracellular buffer and is regulated by the kidneys. Bicarbonate can
either donate or absorb an H+ ion to minimise pH disturbances and gives us a representation of the metabolic component. Changes in bicarb values take much longer than changes to CO2 and can represent a process that can be days/weeks. As there are additional buffers in the body, the patient’s base excess may be a more accurate way to assess the metabolic component.
So how does all this help us? By identifying which of the 4 primary disturbances the patient is suffering from helps to guide both their treatment plan and understand their nursing care.
Metabolic acidosis is the most common disturbance. On a blood gas with a simple metabolic acidosis you
would expect to see a low pH, low HCO3 negative base excess and a decrease in CO2.
Common examples of metabolic acidosis:
• lactic and pyruvic acidosis
• ketoacidosis
• renal disease
• ethylene glycol intoxication
• GI loss.
Consequences of a metabolic acidosis include:
• decreased myocardial contractility
• decreased cardiac output
• decreased response to catecholamines
• arterial vasodilation
• impaired coagulation
• decreased renal and hepatic perfusion
• insulin resistance
• altered central nervous system
• secondary hyperkalaemia.
Metabolic alkalosis is the less common metabolic disturbance. On a blood gas sample with a simple metabolic alkalosis you would expect to see a high pH, high HCO3, positive base excess and an increase in CO2.
The most common examples of a metabolic alkalosis:
• upper gastrointestinal obstruction
• administration of loop diuretics or sodium bicarbonate
• refeeding syndrome
• severe hypokalaemia.
Consequences of a metabolic alkalosis include:
• changes to myocardial contractility
• arrhythmias
• decreased cerebral perfusion
• increased neuromuscular excitability
• impaired peripheral oxygen unloading.
Many patients who present to the veterinary practice for injury or illness are likely to have changes in values associated with parameters measured on the blood gas. Significant changes on some of these parameters have the potential to be life-threatening without intervention.
Respiratory acidosis is seen more commonly than respiratory alkalosis. Remember that metabolic compensation takes time, and so an acute respiratory disturbance may have little to no HCO3 compensation, but a more chronic respiratory disturbance will have more HCO3 compensation.
On a blood gas for a respiratory acidosis, you would expect to see a low pH, high CO2, and depending on the duration of the condition, a normal to high HCO3.
Causes of a respiratory acidosis include:
• airway obstruction (such as laryngeal paralysis, tracheal collapse, foreign body)
• neuromuscular disease (lower motor neuron disease, cervical spinal cord disease)
• pleural space disease
• decreased respiratory centre (anaesthetics and opioids)
• asthma
• severe hypokalaemia.
Consequences of a respiratory acidosis include:
• marked dilation of cerebral arteries and increased cerebral blood flow
• increased intracranial pressure
• arrythmias
• variable effect on heart rate
• decreased myocardial contractility
• decreased systemic vascular resistance
• catecholamine release
• increased systemic blood pressure
• sodium and water retention
• hyperkalaemia.
On a blood gas for a respiratory alkalosis, you would expect to see a high pH, low CO2 and depending on the duration of the condition, a normal to low HCO3.
Causes of a respiratory alkalosis:
• hypoxemia (chemoreceptor stimulation to increase respiratory rate)
• diseases that stimulate the respiratory centre (sepsis, drugs, hyperthermia)
• pulmonary disease
• exercise
• pain
• stress.
Consequences of a respiratory alkalosis include:
• marked constriction of cerebral arteries and decreased cerebral blood flow
• decreased intracranial pressure
• seizures
• reduced cardiac output
• decreased systemic blood pressure.
To help identity a disturbance, you must first be familiar with normal ranges:
Venous normal ranges
pH normal 7.35–7.45 PCO2 35–45 mmHg HCO3 18–24 mEq/L
Then you can use the tic-tac-toe method to draw the following grid.
Acid Normal Alkaline
1. Look at the patient’s pH. Is it normal, low or high? Place this in the table under the appropriate column.
2. Look at the patient’s HCO3/base excess. Is it low, normal or high? Place this in the table under the appropriate column.
3. Look at the CO2. Is it low, normal or high? Remember that CO2 is an acid, so a high CO2 needs to be placed under the acid column and a low CO2 needs to be placed under the alkaline column.
4. For simple disorders, the column that has 2 in a row vertically is the primary disorder. It is important to remember that the body never overcompensates. If you get more than 2 in a row, you may be dealing with a mixed disorder. Here is an example of a metabolic acidosis
pH 7.14 HC03 12.1 B/E –10.1 CO2 28
1st – Look at the patient’s pH. Is it normal, low or high? Place this in the table.
2nd – Look at both the bicarb/base excess and place them in the column that reflects if they are low, normal or high.
3rd – Look at the CO2. Is it low, normal or high? (Remember, CO2 acts like acid, so if CO2 is low, it is more alkaline on the pH scale, and if CO2 is high, it will be more acid on the pH scale.)
Acid Normal Alkaline pH Bicarb CO2
Example of respiratory acidosis
Acid Normal Alkaline pH HCO3
CO2
pH 7.23
HCO3 27.2 CO2 65
Example of metabolic alkalosis
Acid Normal Alkaline CO2 pH HCO3
pH 7.55 HCO3 36.0 CO2 46
In addition to all the information that a venous blood gas provides, an arterial blood gas provides the
partial pressure of oxygen in arterial blood (PaO2). Arterial samples must be collected anaerobically and run immediately to get accurate results. The PaO2 gives a measurement to evaluate the lungs’ ability to oxygenate blood. Normal PaO2 is approximately 80–100 mmHg on room air.
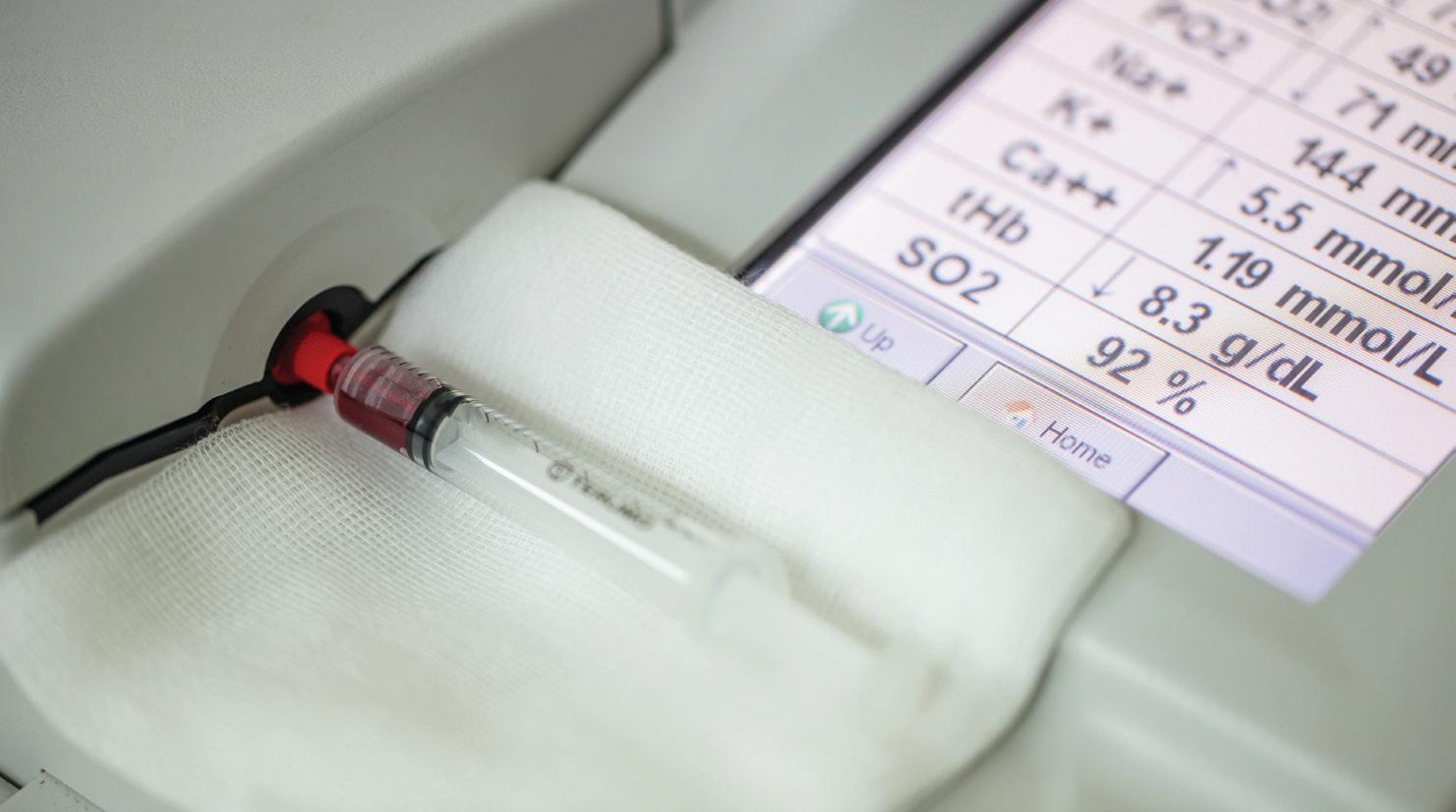
The 5 causes of hypoxemia are: 1. hypoventilation 2. decreased inspirated oxygen content (low fiO2) 3. ventilation/perfusion (V/Q) mismatch 4. intrapulmonary shunt 5. diffusion impairment.
When a patient is receiving supplemental oxygen, the PaO2 should be close to 5 times the fiO2.
Some patients will be suffering from a mixed disorder. This mixed disorder leads to often significant changes in a patient’s pH. To determine a mixed disorder, first you must calculate the expected compensation. When treating a mixed disorder, it is important to treat the most life-threatening process first. Often, this is the respiratory component.

Hypersomatotropism is where the pituitary gland is excessively producing growth hormone (GH). GH is the hormone responsible for tissue growth and cell reproduction and regeneration. It consists of a long, single chain of amino acids called a polypeptide, and is produced in the cells of the anterior pituitary gland. Excessive GH production then leads to an increase in production of insulin growth factor 1 (IGF-1). IGF-1 is mainly produced in the liver. They both follow the same trend in the blood; if one is increased, the other follows suit.1
The pituitary gland is an integral part of the body. Located at the base of the brain, it regulates multiple hormones in the body. There are two main parts to the pituitary gland: the adenohypophysis (anterior pituitary) and the neurohypophysis (posterior pituitary). Each side controls its own certain hormones; however, together they control the production of seven major hormones in the body. The first five are controlled by the adenohypophysis2 and the last two are controlled by the neurohypophysis.
1. adrenocorticotropic hormone (ACTH), which stimulates the adrenal glands to produce cortisol
2. thyroid stimulating hormone (TSH), which stimulates the thyroid gland to produce thyroxin
3. growth hormone (GH), which regulates muscle and bone growth
4. follicle stimulating hormone (FSH)/ luteinising hormone (LH), which together aid in follicular growth and ovulation
5. prolactin (PRL), which enables milk production in mammals
6. oxytocin (OXY), which plays key parts in reproduction and social behaviour
7. antidiuretic hormone (ADH), which regulates the water balance in the body. It tells the kidneys when to release water (via urine) and when to retain it. This helps maintain blood pressure, fluid volume of the blood vessels and sodium concentrations.
Cats can present to the veterinary hospital with a vast range of clinical signs. Cats in early stages of disease still have excessive GH being produced. Even before diabetes has been diagnosed, the patient may present

with weight gain and signs of excess GH production, such as polyphagia (increased appetite), polydipsia (increased thirst) and polyuria (increased urination).3 There may be a period after diabetes is diagnosed where insulin requirements are considered relatively normal (1–3 international units (IU) per cat).1 There will eventually be a notable pattern of poor response to insulin requiring over 3 IU per kilogram and still resulting in persistent hyperglycaemia (normal range 4.5–7 mmol/L).
A cat with hypersomatotropism will usually be overproducing growth hormone for a period of months before they develop the symptoms of acromegaly, which is the condition seen when this occurs. A cat with acromegaly will usually have a diabetes mellitus (DM) diagnosis beforehand, though DM can sometimes present after the acromegaly diagnosis.4 It occurs predominantly in male cats over 8 years of age (can range from 4–17 years).1 The symptoms may also not be very noticeable at first as they can develop slowly. Clinical signs of chronic, increased
Pituitary picture (https://en.wikipedia.org/ wiki/Posterior_pituitary)


levels of IGF-1 are prognathia inferior (enlarged mandible), enlarged or clubbed paws, degenerative arthropathy, a stertor or snore due to thickening of the oropharyngeal tissue, cardiac changes such as myocardial hypertrophy (enlargement and thickening of the heart muscle) and often organomegaly (enlarged liver, spleen, kidneys or even thyroid).1
A physical exam is always the best place to start. Start by getting a baseline heart rate, respiratory rate and effort, temperature, and weight. In a patient that is having historical weight gain (extra muscle and bone growth due to increased IGF-1 levels) despite poorly controlled diabetes, acromegaly should be considered. A systolic heart murmur can also be a clinical sign of acromegaly (due to the heart wall thickening). Collecting and submitting a complete blood panel is also helpful to identify any additional, concurrent issues. A patient with acromegaly and concurrent unregulated diabetes will usually have serum abnormalities such as hyperglycaemia (high glucose), hyponatraemia (low sodium) and hypochloraemia (low chloride),
hyperkalaemia (high potassium), and some elevated liver enzymes such as total bilirubin (Tbil), alanine amino transferase (ALT) and alkaline phosphatase (ALKP). In the absence of underlying haematological disease, only the occasional mild increase in haematocrit was seen on a complete blood count.5
There are a few places that run validated immunoassays for IGF-1 testing. Royal Veterinary College in the UK and the Diagnostic Centre at Michigan State University are two. Conveniently, Idexx Laboratory here in Australia now has IGF-1 testing available. They will send samples to the RVC in the UK for testing. Otherwise, samples can be submitted straight from the consulting vet clinic to the RVC. Results greater than 1000 ng/mL (normal is < 795 ng/mL6) is abnormal and considered a marker for hypersomatotropism.7
Computed tomography, or CT, is recommended to assess the brain to identify a mass or growth of the pituitary gland. This helps in diagnosis of hypersomatotropism and is helpful when planning a radiation or surgical approach for treatment.
There are a few different treatment options available for a cat with a pituitary mass causing an increased GH production. The two main recognised ways to treat this condition are by radiation therapy and surgery.7

Radiation therapy involves the use of a linear accelerator (commonly referred to as a LINAC), which delivers high doses of energy or electrons as a beam targeting a patient’s tumour with the intent to shrink it. The more conventional and safer approach is definitive radiotherapy (DR). Definitive radiotherapy delivers radiation in the safest way, as it splits up a large dose into multiple small ones. The patient needs to undergo 20 radiation treatments, Monday to Friday over 4 weeks, each one requiring a short general anaesthetic.
A newer protocol starting to be used is stereotactic radiotherapy (SRT). This approach delivers 3 large doses over 1 week, each also requiring a general anaesthetic. With the availability of newer planning capabilities and delivery techniques, SRT has good
safety margins, though because of the large doses there is still a risk of harmful radiation effects on the surrounding normal brain tissue. Overall, the mean survival rate of a patient undergoing SRT is longer than the survival rate of one undergoing DR, whether it is due to less anaesthesia time or that SRT delivers doses more effective to pituitary tumours.8
Radiotherapy generally has few side effects but is not usually successful in decreasing the level of GH and therefore IGF-1 being produced. While increased insulin sensitivity and possibly even diabetic remission can be seen with radiotherapy, the clinical manifestations (arthropathies, myocardial changes, etc.) associated with increased IGF-1 levels can take years if at all to rectify.1
The surgical approach, called a hypophysectomy, removes the pituitary tumour and gland in one go due to the small size. The patient is anaesthetised during the procedure and placed into sternal recumbency with the head held up by a surgical head frame. The rigid head frame is needed to keep the patient as still as possible. The pituitary gland with tumour may only measure a few
millimetres in diameter and can be extremely close to important nerves and arteries. The site is then accessed through the soft palate in the mouth. Surgery is the best option for curing acromegaly. It is considered the optimal approach with a much higher incidence of diabetic remission and decrease of IGF-1 and GH levels, as most cats (60–80%) have much better diabetic control or go into diabetic remission within one month.7 Surgical success is dependent on the size of the tumour as well as the experience of the surgery and postoperative care teams. Success rates with an established team (neurosurgeons, surgical nurses, internal medics, and nurses, criticalists and ICU nurses) are 90–96% (4–10% mortality rate)7; they help see the patient through to discharge and beyond.
It is good practice to place a multiple lumen central venous catheter into the cat before proceeding to surgery. It will allow for easy access for serial blood glucose monitoring in theatre and will help with all the blood collections needed for the first few days postoperatively without compromising peripheral veins with multiple blood draws.

There are several fluids and medications a hypophysectomy patient needs to receive while in theatre and postoperatively. Cats undergoing hypophysectomies usually have some degree of heart disease due to the thickening of the heart from the increased GH production. For this reason, fluid rates need to be conservative during surgery, preferably not going above 4 millilitres per kilogram per hour (mL/kg/hr).
Pain management: A fentanyl constant rate infusion (CRI) is recommended intraoperatively for pain relief. This should be delivered at an undiluted concentration of 50 micrograms per millilitre (ug/mL) to allow for smaller volumes to be delivered.

Fluids: The patient should be on a fluid drip of compound sodium lactate (Hartmann’s) during surgery and an appropriate isotonic (0.9% NaCl/ Hartmann’s) or hypotonic (0.45% NaCl or glucose 5%) fluid postoperatively. The electrolyte levels of sodium and potassium postoperatively will dictate which IV fluid is chosen. It is expected, once the pituitary gland is removed, that the cat will become hypernatremic (increased sodium levels) due to the lack of ADH being produced by the neurohypophysis (posterior pituitary).9
Insulin: An actrapid (regular insulin) CRI will need to be started to help keep control of the cat’s hyperglycaemia. A special, highly concentrated dose of 11 international units per kilogram (normal is 1.1 iu/kg) is added to a 240 mL bag of regular 0.9% sodium chloride. The infusion is then adjusted as needed in response to the blood glucose, only needing to run at low rates to keep our fluid volumes low.
Cortisone: Since the adrenals will no longer be receiving any ACTH stimulus from the pituitary signalling them to release cortisol, a hydrocortisone sodium succinate (HSS) CRI will need to be started as soon as the
pituitary is reached. This CRI is diluted to a 1 milligram per millilitre (mg/mL) concentration. Without any cortisol in the body, the patient can develop hypotension, weakness, inappropriate mentation and even seizures and death. All these infusions need to be running no higher than a combined 4 ml/kg/hr.
The fentanyl CRI can be discontinued once awake and buprenorphine started. The Actrapid CRI will continue for a few days postoperatively until the cat can be transitioned back onto their subcutaneous insulin (most commonly for cats it would be the long-acting insulin glargine, though some may be on another type). Sublingual (under the tongue) or subconjunctival (under the conjunctiva of the eye) synthetic diuretic hormone (called Vasopressin or DDAVP) will need to be administered for the rest of the cat’s life (in most cases three times daily). The hydrocortisone CRI should be continued until the cat is eating well and can be transitioned to oral cortisone. Oral cortisone and oral thyroxine (since no more TSH will be produced) will be lifelong medications for the cat as well.
There are multiple areas in the process of diagnosis, treatment and postoperative care where nurses can put their skills to good use. Diagnosis of this condition requires blood collection and sample submission to both local and international laboratories. Accurate recording of patient health statuses is required (weight monitoring, auscultation of any new heart murmurs) and is something that the nurse can keep on top of. For preoperative planning, working with the veterinarian to calculate appropriate fluid and medication rates as well as working with an anaesthesiologist to create an appropriate anaesthetic plan for the patient. Postoperatively, a hypophysectomy patient will need intensive care. Recovery in the ICU for multiple days is required. If
There are multiple areas in the process of diagnosis, treatment and postoperative care where nurses can put their skills to good use. Diagnosis of this condition requires blood collection and sample submission to both local and international laboratories.
available, placing a Freestyle Libre glucose sensor can be helpful for less invasive monitoring of the cat’s glucose levels as well. Blood glucose readings will fluctuate postoperatively, and electrolyte levels (sodium, potassium and chloride) will be greatly affected due to the loss of antidiuretic hormone production from the neurohypophysis..9 These will be monitored quite closely for the first 5–7 days by the intensive care nursing and veterinary teams and fluid plans can be altered accordingly.
Postoperatively, cats should be offered food as soon as they are up and walking around. Nurses can offer a variety of soft, warmed cat foods to tempt the patient into eating. Anti-nausea drugs such as maropitant and ondansetron can be used to combat any nausea and mirtazapine can be administered as an appetite stimulant. Nurses should take care when tableting a postoperative hypophysectomy patient as the surgical site is on the roof of the mouth and fingers or pill poppers can damage the site. Urine outputs should be monitored closely, without using a urinary catheter. This can be done by weighing the clean litter and box before offering it to the cat, then reweighing it after urination. Unfortunately, this is only accurate if the cat doesn’t kick litter out of the box or doesn’t do a bowel movement in it. Monitoring urine output is important as when there is a lack of ADH (or Vasopressin) being produced by the neurohypophysis, the urine becomes excessively dilute, and the animal becomes polyuric. If the patient isn’t getting appropriate replacement of water or IV fluids, they become
hypernatremic.10 Care for a central line, or jugular catheter, includes close monitoring for slipping or swelling, and at least every 8 to 12-hour inspections of the site. Any unused ports need to be flushed with small amounts of saline every 4 hours to keep patent. Proper flushing techniques and sampling techniques need to be adhered to so that it is kept as aseptic as possible and no air is introduced into the lines. Mentation status should be monitored closely for dullness, ataxia, head pressing, or other signs of intracranial pressure post-surgery. The blood glucose levels should be monitored quite closely for the first several days in case the cat quickly develops a sudden sensitivity to insulin and becomes hypoglycaemic, especially if they are not eating well.
The hope is the cat will start to go into diabetic remission over the first week to month post-surgery. The nursing team can counsel the owners of the cat on what to watch for in the event of hypoglycaemia, such as dullness, weakness, or even partial or full seizures. These are some of the things owners probably are not used to looking out for, since they have had an insulin resistant cat for so long. After discharge, weekly to fortnightly rechecks may be required while medication doses are being stabilised or altered. Once on a stable dose of medications, every three months should be adequate for rechecks, to continue monitoring the cat’s electrolyte levels and general wellbeing post hypophysectomy.





Using a combination of clinical signs, advanced imaging and validated growth hormone testing, a diabetic cat that shows an increased resistance to insulin can be considered as having hypersomatotropism. Radiation therapy is considered the most common treatment form but is not as successful in resolving overproduction of IGF-1 as is surgical treatment. With surgery and postoperative care from a well-established team, recovery with a decrease in serum GH and IGF-1 levels and diabetic remission rates have been recorded above 80%, with an average survival rate of approximately 850 days.7
1-Feldman E, Nelson R et al. Ch 2. – Disorders of growth hormone. Canine and feline endocrinology. 4th ed. Elsevier Saunders, Missouri. 2015:37–72.
2-Sanders K, Galac S. Pituitary tumour types in dogs and cats. Veterinary Journal. 2021;270:105623.
3- Rijnberk A, Kooistra H. Clinical hypothalmus –Pituitary system. Clinical Endocrinology of Dogs and Cats, Schluterche, Germany. 2010:13–45.
4- Nelson R, Couto G. Ch 49 – Disorders of the hypothalamus and pituitary gland. Small Animal Internal Medicine. 5th ed. Elsevier, Missouri. 2014:713–726.
5-Niessen SMJ, Petrie F. Feline acromegaly: An underdiagnosed endocrinopathy. Journal of Veterinary Internal Medicine. 2007;21(5):899–905.
6- Raiman Y. Reference range of the IGF-1. Utrecht University. 2014.






































































7-Kenny P et al. Efficacy of hypophysectomy for the treatment of hypersomatotropism. JVM. 2021:16080.
8-Wormhoudt T, Boss M et al. Stereotactic radiation therapy for the treatment of functional pituitary adenomas associated with feline acromegaly. Journal of Veterinary Internal Medicine. 2018:15212.
9-Magno S, Van Rijn S. Plasma sodium and potassium concentrations after hypophysectomies in dogs with corticotroph adenomas. Journal of Veterinary Internal Medicine. 2021:16337.













































10-DiBartola S. Fluid, electrolyte and acid base disorders in small animal practice. Ch 3. –Disorders of sodium and water: Hypernatremia and hyponatremia. 4th ed. Elsevier, Missouri, 2012;4:45–75.













We are thrilled at how our community came together and promoted the VNCA values of Inclusiveness, Integrity, Inspiration, and Innovation for our inaugural Veterinary Nurse & Technician Awareness Week held in October 2022. The week was a wonderful way to show our vet nurses and technicians how important they are to our industry and how much we
The week culminated with our notable Appreciation Day on Friday 14 October with workplaces across the country honouring and celebrating their staff with lunch and gifts. Additionally, the VNCA was pleased to announce the two winners of this year’s awards:
Anita Parkin – Veterinary Nurse/ Technician of the Year, and Kristie Wallis – Student Veterinary Nurse/Technician of the Year.
Both have shown a great commitment to our industry and continue to inspire our community to evolve, grow and live by our values. Congratulations once again to Anita and Kristie – we look forward to formally presenting you both with your awards at next year’s conference.

The VNCA also gratefully acknowledges the support of our sponsor of the 2022 Veterinary Nurse/ Technician of the Year Awards












8:00 AM - 10:00 AM
Leadership Symposium 2023
Masterclass One: 10-minute TED talksJanet Murray
Masterclass Three: wound management and suturingGeorgia Marsden
10:00 AM - 10:30 AM MORNING TEA
10:30 AM - 12:30 PM Leadership Symposium 2023 (continued)
Masterclass Two: Debriefing - it’s the missing piece of the jigsaw puzzle - Erica Honey
Masterclass Three: Wound management and suturing - Georgia Marsden (continued)
12:30 PM - 1:00 PM LUNCH
1:00 PM - 3:00 PM Leadership Symposium 2023 (continued)
Masterclass Four: Tube feedingVictoria Koks
Masterclass Five: Creating a community with education and supportbehaviour consults with a veterinary nurseDr Liam Clay
3:00 PM - 3:30 PM AFTERNOON TEA
3:30 PM - 5:30 PM Leadership Symposium 2023 (continued)
Masterclass Four: Tube feedingVictoria Koks (continued)
Masterclass Five: Creating a community with education and supportbehaviour consults with a veterinary nurseDr Liam Clay (continued)
5:30 PM - 7:00 PM PRESIDENT’ S WELCOME DRINKS
1
8:00 AM - 8:45 AM Conference Opening Ceremony & Welcome to Country
RECOVER CPR: Rescuer Certification Workshop - basic and advanced life support - presented by Andrea Steele, Harold Davis and Marcia Fletcher
RECOVER CPR: Rescuer Certification Workshopbasic and advanced life support (continued)
RECOVER CPR: Rescuer Certification Workshopbasic and advanced life support (continued)
RECOVER CPR: Rescuer Certification Workshopbasic and advanced life support (continued)
8:45 AM - 9:45 AM Being a fully-fledged professional: what does this mean for veterinary nurses and veterinary technicians in Australia? - Patricia Clarke
9:45 AM - 10:30 AM MORNING TEA
10:30 AM - 11:30 AM Gasping for breath I: Respiratory emergencies - Andrea Steele
11:30 AM - 12:30 PM Gasping for breath II: Respiratory diseases - Andrea Steele
Your pet ate what? Understanding toxicological casesAsha Yeoman
Electrocardiography - understanding the basics - Asha Yeoman
Common presentations of avian and exotic patients - Rebecca De Gier
Endotracheal intubation of avian and exotic patients - Iffy Glendinning
12:30 PM - 1:30 PM LUNCH
1:30 PM - 2:30 PM Intravenous access: Considerations and alternativesHarold Davis
2:30 PM - 3:30 PM Oh oh, respiratory failure! Get that patient on a ventilatorAndrea Steele
3:30 PM - 4:00 PM
4:00 PM - 5:00 PM CPR: an overviewHarold Davis
Class is now in session! Going back to the basics of small animal nutrition - Kim Healy
Feeding hospitalised and post-operative patients - Victoria Koks
Monitoring reptile anaesthesia – because surgeons need heroes too! (Part 1) - Emma Jane Newton-Dinning
Monitoring small mammal anaesthesia – because surgeons need heroes too! (Part 2) - Emma Jane Newton-Dinning
AFTERNOON TEA
Fluid therapythe essentialsJo Hatcher
5:00 PM - 5:30 PM VNCA Annual General Meeting
5:30 PM - 6:30 PM Happy Hour with the Exhibitors
Workshop One: Radiographic positioning - Jasmine Pengelly
Workshop One: Radiographic positioning - Jasmine Pengelly (continued)
Workshop Two: The perfect puppy programLaura Ryder
Workshop Two: The perfect puppy programLaura Ryder (continued)
Wildlife triage, hospitalisation and rehabilitationRebecca De Gier
9:00 AM - 10:00 AM Understanding palliative care - Jackie Campbell
Creating a community with education and support: behaviour consults with veterinary nurses - Liam Clay
Biosecurity disasters - emergency animal disease (EAD)Erica Honey
10:00 AM - 10:30 AM MORNING TEA
10:30 AM - 11:30 AM Pain management, the role of veterinary technicians - Andrea Steele
11:30 AM - 12:30 PM Pain management, the role of veterinary technicians - Andrea Steele (continued)
Creating a gold standard preschool for your pup-ils - Narelle Braunack
Identifying fear, stress and anxiety in your patients and when to actNarelle Braunack
Nursing the equine endocrine patient - Isobel Entwisle
Workflow efficiency in clinical practice and the role of veterinary nursesGraham Swinney
Now you’re a nurse managerErica Honey
The stinky end of the tail - nursing the equine colitis patient - Gemma Murphy
12:30 PM - 1:30 PM LUNCH
1:30 PM - 2:30 PM Taking the ‘nurse dental check’ to the next level - the transformation to the consulting dental nurse - Maggie Burley
Recumbent patient careJenni Andrews
Case Study Session One Presentations by Penny Lim, Sophie Peignon and Kimberley Kitster
Working smarter not harder: an inclusive team approach to veterinary care - Abby McGougan
Workshop Three: Theatre escape room - Anita Parkin and Trish Farry
Workshop Three: Theatre escape room - Anita Parkin and Trish Farry (continued)
Building an inclusive community through remote indigenous community animal management - programs, challenges, and opportunities – Roper Gulf Regional Council and AMRRICMichelle Hayes
Workshop Four: What kind of manager are you? Discover your full potential!Navin Prakash
2:30 PM - 3:30 PM Cats are not small dogs - a spotlight on feline dentistry - Maggie Burley
Supporting grieving clients before and after euthanasia - Rosie Overfield
Case Study Session Two Presentations by Kristie Balding and Rebecca Cameron
Principles of community centred veterinary care – what can veterinary nurses/ technology students and graduates learn from these principles to create inclusive veterinary practices? - Courtnay Baskerville
Workshop Four: What kind of manager are you? Discover your full potential!Navin Prakash (continued)
3:30 PM - 4:00 PM
4:00 PM - 5:00 PM Introduction to LGBTIQA+ inclusivity in practiceAndrew Thompson
7:00 PM - late
Empowering your team to tackle climate changeVfCA Climate Care ProgramJeannet Kessels
AFTERNOON TEA
Case Study Session Three Presentations by Tenneal Prebble, Mallory Johnstone and Katherine Moore
Levelling up your consultation game! Taking the leap to consulting vet nurse - Kim Healy
CONFERENCE DINNER - 'ALL THAT GLITTERS '

8:00 AM - 9:00 AM The heart of the matter: cardiac nursingAndrea Steele
9:00 AM - 10:00 AM Anaesthesia for the broken heartMarcia Fletcher

10:00 AM - 10:30 AM


10:30 AM - 11:30 AM Shock, an overview - Harold Davis
11:30 AM - 12:30 PM Rough inductions and difficult recoveries - Marcia Fletcher





Understanding blood gas pathologyGeorgia Marsden

Capnographya key anaesthetic monitoring deviceJo Hatcher


IPP... what?!Samantha Dhatt
How to perfect general anaesthesia monitoring charting - Eileen O’Doherty
MORNING TEA
Complications of IV and medicationsAndrea Steele

A twist on the mid-life crisis - emergency nursing of the neonate and paediatrics - Kate Tinney

Nursing GIT patients - Jasmine Pengelly

Using radiographs to improve your nursing care - Keegan Diwell

12:30 PM - 1:30 PM LUNCH
1:30 PM - 2:30 PM
2:30 PM - 3:00 PM
TECH-niques in critical careAndrea Steele
Mums and bubs: anaesthesia in pregnancy and caesareansMarcia Fletcher

CONFERENCE CLOSING SESSION
Workshop Five: The end-of-life journeybecoming a palliative care advocate in your practice - Jackie Campbell and Rosie Overfield
Workshop Five: The end-of-life journeybecoming a palliative care advocate in your practice - Jackie Campbell and Rosie Overfield (continued)
Workshop Six: Anaesthesia escape room - Anita Parkin and Trish Farry
Workshop Six: Anaesthesia escape room - Anita Parkin and Trish Farry (continued)

*Program subject to change without notification.

Signalment: ‘Clarabelle’ – 4 year & 6-month-old female, Isa Brown chicken

Presenting complaint: Dyspnoea with a distended coelom
History: The patient was purchased from a local produce centre at the age of 3 months and had been kept in a large chicken coop with two other hens and a single rooster. All the chickens were fed a staple diet consisting of a complete chicken pellet, vegetable food scraps and occasionally a grain mix. The patient had not laid an egg since January 2018 and at the time of presentation had been dyspnoeic for the previous 24 hours with a distended coelom.
On physical examination, the patient was bright, alert and responsive. Had a heart rate (HR) of 248 beats per minute (bpm) and respiratory rate (RR) of 60 breaths per minute with normal lung/ air sac and heart sounds. The eyes and nares were clear without discharge. The patient’s body weight was 2.76 kg with a body condition score assessed as good with a score of 3/5. The feathers and skin were normal with no evidence of external parasites. On palpation, the crop was empty and the coelom was moderately distended, and fluid filled. The patient’s respiratory effort was increased with a tail bob at each breath and intermittent open mouth breathing.
Problem list/Differential diagnosis: The patient’s problem list included. 1: Coelomic effusion and distension; differentials include: yolk coelomitis,
coelomic neoplasia. 2: Dyspnoea of lower respiratory cause; differentials include: egg yolk coelomitis, fungal infections e.g. Aspergillus spp., bacterial pneumonia (Reavill, 2007).
The patient was admitted to hospital for a coelomic ultrasound and coelomocentesis. The ultrasound identified a large amount of free fluid and multiple ovoid/irregular-shaped structures with a combination of anechoic fluid and hypoechoic nodular structures. The patient was pre-oxygenated prior to the coelomocentesis with 100% O2 for 5 minutes prior and throughout the procedure via an anaesthetic mask. The skin of the ventral midline was aseptically prepared and a 20 g, 1-inch catheter was inserted into the coelomic cavity and stylet removed. A 50 cm extension set and threeway tap were attached, and using a 60 ml syringe, fluid was aspirated. A total of 440 ml of amber-coloured, slightly cloudy fluid was aspirated. The fluid was examined microscopically but was of low cellularity and was unremarkable. The patient’s respiratory effort returned to normal after the coelomocentesis with no further open mouth breathing.
Treatment plan: The patient was dispensed meloxicam 2.8 mg (1 mg/
kg) PO 12H × 5d and scheduled for an exploratory celiotomy to differentiate yolk coelomitis vs neoplasia.
Final diagnosis: The coelomic ultrasound identified a significant volume of free fluid within the coelomic cavity and multiple ovoid/irregularshaped structures with a combination of anechoic fluid and hypoechoic nodular structures indicating a yolk coelomitis or potential neoplasia, carcinomatosis, or lymphoma. As the respiratory symptoms returned to normal, post-coelomocentesis, it was presumed that these symptoms were associated with the coelomic effusion, compression and reduced tidal volume of the caudal and abdominal air sacs. Plans were made for a surgical exploratory celiotomy to differentiate yolk coelomitis vs neoplasia and to potentially perform a salpingohysterectomy if indicated.
Outcome: The patient presented for surgery and was bright, alert and responsive. Blood was collected via basilic vein venipuncture and submitted to an internal laboratory for PCV, total protein (TP) and blood glucose analysis. The results of the PCV/TP (40%/48g/L) were within normal limits, but the blood glucose was mildly elevated at 24.1 mmol/L (12–17 mmol/L) indicating a stress-induced hyperglycaemia. A 22 g, 1-inch intravenous catheter was aseptically placed into the left medial metatarsal vein. Warmed Hartmann’s solution was started at 27.6 ml/hr (10 ml/ kg/hr). The patient was premedicated with methadone 1.38 mg (0.5 mg/kg) IV and midazolam 0.55 mg (0.2 mg/ kg) IV. The patient’s American Society of Anaesthesiologists (ASA) status was determined to be ASA III. Preoxygenation was administered with 100% oxygen via an anaesthetic mask for 10 minutes prior to induction. Anaesthesia was induced with sevoflurane in O2 (5%/2.0L/ min). The patient was intubated with a 4.0 mm uncuffed Murphy Eye endotracheal (ET) tube connected to a non-rebreathing circuit with a small animal ventilator and maintained on sevoflurane in O2 (1–3%/2.0L/min) for the anaesthetic duration. The patient was positioned in right lateral recumbency with the wings extended dorsally. A 24 g, 1-inch arterial catheter was aseptically placed in the left superficial ulna artery and connected to a transducer to monitor invasive blood pressure. Prior to the surgery, cephazolin 276 mg (100 mg/kg) IV was administered over 15 minutes. A fentanyl CRI (2–10 µg/kg/hr) IV was administered intraoperatively and titrated to effect. Throughout the anaesthetic and surgical procedure, the patient was monitored using capnography, pulse oximetry, ECG, invasive blood pressure, oesophageal temperature and physical parameters including HR and RR and corneal reflex. Immediately into the procedure the patient experienced an extreme hypotensive event, with mean arterial
Adenocarcinomas of the ovary or oviduct are a very common diagnosis of reproductive neoplasia in older chickens. A study addressing the cause of mortality in backyard chickens identified neoplasia as the most common cause of mortality, of which the most common non-virally induced neoplasms were ovarian adenocarcinoma and carcinomatosis
pressures (MAP) ranging between 35–45 mm Hg. The fentanyl CRI was increased to 13.8 µg/hr (5 µg/kg/hr) and the inhalant, isoflurane, was titrated down from 1. 75–1%. An anticholinergic was administered consisting of atropine 0.11 mg (0.04 mg/kg) IV with a crystalloid fluid bolus and Hartmann’s 27.6 ml (10 ml/kg) IV. This raised the MAP to above 40 mm Hg, but the patient was still hypotensive. At this point, a dopamine 27.6 µg/min (10 µg/kg/min) IV CRI was initiated, including a fresh frozen plasma (FFP) infusion 5.5 ml (2 ml/kg) IV in conjunction with a crystalloid over 30 minutes. This combined treatment resolved the hypotension and the patient’s MAP rose to above 70 mm Hg for the remainder of the procedure. As the surgery included incising through the left caudal and abdominal air sacs, the patient was manually ventilated, which removed the ability to monitor end tidal CO2 (ETCO2) during this period of the surgery.
The feathers of the left lateral coelom were plucked, and the skin aseptically prepared for surgery. A linear incision was made in the left lateral flank extending from the caudal rib to the pubic bone through the superficial layers of muscles and air sacs. A Lone Star retractor was used to facilitate visualisation of the coelomic cavity. A yellow/brown gelatinous fluid was identified within the coelom and removed with suction. Digital exploration was performed through the peritoneum
and mesentery identifying the presence of nodules throughout the coelomic cavity. Multiple ovarian cysts were present within the ovary ranging from 1 cm to 5 cm in diameter.
Due to the presentation, the patient was diagnosed with diffuse metastatic adenocarcinoma. Due to the presence of diffuse carcinomatosis the owner elected for euthanasia, which was performed while under anaesthesia, and pentobarbitone sodium 977 mg (254 mg/kg) IV was administered.
Conclusion/Case summary:
Adenocarcinomas of the ovary or oviduct are a very common diagnosis of reproductive neoplasia in older chickens. A study addressing the cause of mortality in backyard chickens identified neoplasia as the most common cause of mortality, of which the most common non-virally induced neoplasms were ovarian adenocarcinoma and carcinomatosis (Cadmus et al., 2019). Ovarian neoplasia is often associated with secondary egg retention, ascites, cystic ovaries or oviductal impaction (Echols, 2015).
Chickens with ovarian neoplasm often present for nonspecific symptoms such as coelomic distension, dyspnoea and ascites, lethargy and altered reproductive performance. Diagnostic imaging in the form of radiography, ultrasonography, computed tomography and magnetic resonance imaging can assist with a
Diffuse metastatic adenocarcinoma originating from the ovary in an Isa Brown chicken (Gallus gallus domesticus)
non-invasive definitive diagnosis. More invasive techniques, such as exploratory coeliotomy, biopsy and endoscopy, are also used as diagnostic tools (Echols, 2015).
Treatment should be aimed at the eradication of the tumour; this will often require multiple therapies concurrently. Surgical excision or debulking of the tumour, followed by chemotherapy or radiotherapy, can be used. Unfortunately, due to the ovary being associated with the aorta, total removal is virtually impossible (Filippich, 2004). Often, before an attempt can be made to surgically excise or debulk the tumour, treatment of secondary disease such as egg yolk coelomitis is required. This involves managing pain and inflammation with pure mu opioids and nonsteroidal anti-inflammatory drugs. Coelomic distension can be immediately treated with coelomocentesis to provide rapid relief. In the majority of cases, it is appropriate to remove as much of the coelomic effusion as possible to relieve respiratory compromise. Unfortunately, all cases have a poor prognosis unless complete surgical excision of the tumour is achieved (Echols, 2015).
Mutations on the TP53 gene are thought to contribute to the development of ovarian carcinomas in chickens. Recent studies have been able to reduce the incidence of ovarian or oviductal cancer in chickens with the use of a trial chemoprevention therapy (Mocka et al., 2017). However, due to these tumours generally occurring towards the end of a chicken’s commercial lifetime, euthanasia is the general outcome (Cadmus et al., 2019; Tobias et al., 2011).
Discussion: As the patient was dyspnoeic and had coelomic distension on physical exam, ultrasound was utilised as it could be performed on a conscious patient and would also assist a guided coelomocentesis to remove as much of the coelomic effusion as possible. Unfortunately, the ultrasound
was unable to definitively diagnose ovarian carcinoma so an exploratory coeliotomy was performed.
A significant challenge of this case was the hypotension experienced immediately after induction. Initial attempts to lower the inhalant requirement by increasing the constant rate infusion of fentanyl, a pure mu opioid, were unsuccessful. Initial fluid boluses to counteract the vasodilatory shock and administration of an anticholinergic were only mildly successful at increasing the patient’s blood pressure. Due to the extent of the hypotension, mean arterial blood pressure (MAP) of 40 mm Hg, the use of intravenous dopamine was instigated at a dose of 10 µg/kg/min concurrently with a natural colloid, fresh frozen plasma infusion. This aggressive treatment and the capability to monitor real-time invasive blood pressure via arterial catheterisation succeeded in raising the MAP to 70 mm Hg.
Dopamine is commonly used in dogs and cats to treat severe hypotension but use in avian patients is poorly understood. Dopamine has direct activity at the β- and α-dopamine receptors dependent on dose. The dopaminergic effects predominating in low doses 1–3 µg/kg/min, the β- effects at moderate doses, 5– 10 µg/kg/min and the α- effects at higher doses > 15 µg/kg/min (Silverstein et al., 2015). Schnellbacher et al. (2012) examined the effects of dopamine on isofluraneinduced hypotension and found the dose rates of 7–10 µg/kg/min caused the greatest increase in arterial blood pressure in Hispaniolan Amazon parrots. Therefore, dopamine appears to be an appropriate treatment for severe hypertension in birds and potentially aided the restoration of normotension in this case.
Another potential preventive may have been to induce general anaesthesia with an injectable agent. The high dose of inhalant anaesthesia required for
mask induction is known to have a dose dependent vasodilation. This effect may have been mitigated by use of a shortacting injectable induction agent such as alfaxalone. Alfaxalone has minimal cardiovascular side effects when titrated to effect and is metabolised quickly.
Due to the advanced nature of the diffuse carcinomatosis, it was unlikely that adequate debulking and surgical removal of the tumours could be performed and therefore a poor prognosis was determined even if followed up with chemo or radiotherapy. This resulted in the pragmatic decision to euthanise.
Cadmus KJ, Mete A, Harris M, Anderson D, Davison S, Sato Y, Helm J, Boger L, Odani J, Ficken
MD & Pabilonia KL. Causes of mortality in backyard poultry in eight states in the United States. Journal of Veterinary Diagnostic Investigation. 2019;31(3):318–326. doi:10.1177/1040638719848718
Echols MS. Soft tissue surgery. In CB Greenacre & TY Morishita (eds.). Backyard Poultry Medicine and Surgery. 2015:220–259. Hoboken, NJ, USA: John Wiley & Sons, Inc.
Filippich LJ. Tumor control in birds. Seminars in Avian and Exotic Pet Medicine. 2004;13(1):25–43. doi:10.1053/ S1055-937X(03)00055-0
Mocka EH, Stern RA, Fletcher OJ, Anderson KE, Petitte JN & Mozdziak PE (2017). Chemoprevention of spontaneous ovarian cancer in the domestic hen. Poultry Science. 2017;96(6):1901–1909. doi:10.3382/ps/ pew422
Reavill D. The Differential Diagnosis. Paper presented at the Association of Avian Veterinarians, Rhode Island. 2007.
Schnellbacher RW, da Cunha AF, Beaufrère H, Queiroz P, Nevarez JG & Tully TN. Effects of dopamine and dobutamine on isofluraneinduced hypotension in Hispaniolan Amazon parrots (Amazona ventralis). American Journal of Veterinary Research. 2012;73(7):952–958. doi:10.2460/ ajvr.73.7.952
Silverstein DC, Hopper K & Silverstein DC. Small animal critical care medicine. 2nd ed. Saint Louis, Missouri: Elsevier. 2015.
Tobias JR, Barnes HJ & Law JM. Pathology in Practice. Journal of the American Veterinary Medical Association, 2011;239(8):1065–1067. doi:10.2460/ javma.239.8.1065
 By Andrea Suesskow Cert IV VN, CIV TAE, AVN, RVN
By Andrea Suesskow Cert IV VN, CIV TAE, AVN, RVN
Doesn’t the idea of being ‘cat friendly’ sound lovely? Especially if you are an avid cat lover like me. But what does ‘cat friendly’ mean? The term ‘cat friendly’ has its strongest links with the ‘Cat Friendly Clinic’ program, an international program developed and run by the International Society of Feline Medicine (ISFM). ISFM is a not-forprofit veterinary organisation and a veterinary division of International Cat Care, which is a charity dedicated to improving the health and wellbeing of cats internationally through education.
The ISFM Cat Friendly Clinic Standard is an international standard that can be adopted by clinics everywhere, making changes to the clinic ethos, procedures, equipment and infrastructure to demonstrate a clinic’s cat friendly practices to current and new clients. It’s important to note that the ISFM provides a program in which clinics register for accreditation as a Cat Friendly Clinic at 3 various levels; however, you do not need to complete accreditation to implement changes and work towards becoming a more cat friendly clinic. The
recommendations provided in this article are formulated following the ISFM recommended guidelines. When it comes to a cat friendly approach, a holistic view is needed to understand cat basics and how this affects our approach to cats as patients. Understanding the behaviour and inherent traits of cats is vital, as this shapes our approach in most areas to ensure we are providing care in a way that meets the needs of the cat and prevents the difficult reactions that can occur when inappropriate care is provided.
In simple terms, when we understand more about feline behaviour, we are able to tailor our care to meet their needs, resulting in a happier, stressfree interaction where the cat’s needs are met.
The topic of being cat friendly is enormous, and there are many specific areas we can look at, such as client education and preparation for veterinary visits, reception and waiting areas, consultation techniques, restraint and handling, hospitalisation and enrichment. These are just a few. This article will focus on hospitalisation of the feline patient, looking first at 5 key facts about cats that help us understand and shape our hospitalisation techniques around their needs.
Cats are hunters and obligate carnivores who prefer to catch and eat small regular meals.
Because cats are predators, they can often defend themselves (fight) when they feel threatened, especially when they do not have the option of flight. Cats do also have two other defence strategies: freeze and appeasement. However, flight and/or fight are the more common responses. This increases the risk of bites, scratches and resulting infection as a handler, so it is ideal to follow protocols that minimise fear and the resulting defensive aggression in the first place.
Cats being hunters, this also tells us that cats need an outlet to express their natural hunting behaviours. This can be facilitated through enrichment strategies such as toys.
In a natural environment, cats could consume between 10–20 small meals a day, so feeding 1 or 2 big meals a day may not always be ideal. If cats had a choice, the hunting and feeding process would happen in complete solitude with no social interaction (excluding queens and kittens), as food is a survival resource for cats and they prefer to eat alone. Drinking behaviour is important too, as cats may avoid water placed close to their food source due to the instinct to avoid contamination. In the hospital
environment, this information can guide us to implement a suitable and individualised feeding and enrichment plan, as well as appropriate cage setup.
Cats are territorial.
While cats are fed by their owners so do not need to hunt to survive, cats do still have a strong drive to hunt, and this fuels the need for cats to establish territories. The sex of the cat is also a factor to consider, as the male’s territory can extend 3–10 times that of a queen. Territory marking is an important aspect of feline communication and they use a range of methods including spraying urine, rubbing and scratching.
With this information, we can consider the most appropriate ways to house cats within the hospital, recognising that being out of their normal territory is extremely stressful for a cat. (Cats bond more to a territory than they do to owners!) This will enable us to implement strategies of hospitalisation to limit stress and cater to their needs.
Cat’s are sensitive to scent.
It’s important to understand that scent is one of the main methods of communication between felines. Have you ever handled a stressed and cranky cat one morning and for the rest of the day your remaining feline patients seemed stressed and cranky too? It’s likely your first stressed patient released an alarm pheromone, and this scent signal was picked up by your next feline patients, resulting in higher stress and fear levels. Cats have scent glands in various locations on the body (as well as release from urine and faeces), where they release pheromones and leave their unique scent as a form of communication. These scent signals can indicate
alarm, fear, stress, territorial marking, bonding facilitation, happiness, sexual viability, plus many more. During hospitalisation, there are many key strategies to implement when it comes to scent and managing scents that we must consider for our feline patient’s emotional wellbeing.
Cats are clean.
Grooming forms an important aspect of a cat’s instinct and serves many purposes. Being a predator, cats must be in great condition ready to hunt. Grooming ensures they are removing parasites or any contaminants that may cause smells or degradation to the coat. Grooming is important for social bonding and self-comfort too. When cats are unable to maintain cleanliness due to environmental or illness factors, this can negatively impact our patients, and we may even see excessive grooming occur as a displacement behaviour.
Cats are independent, emotional and highly aware.
Let’s start this section with a key phrase here: It is vital that cats feel in control of their situations. Cats are independent and do not rely on other felines to form social groups. They can (in certain circumstances) live in social groups; however, any assumptions of cats requiring company is a human perception of sociability. When a cat can act on their own terms (i.e. approaching a human), they will be at their most content. While it’s not possible in a hospital environment to let cats run the show, it’s important to remember that when we remove a cat’s control completely, this can result in a cascade of effects that could make handling much more difficult and cause emotional distress to our patients.
Continued from previous page
Before admitting a cat to the hospital, it can be very helpful to ensure we have some additional information about the individual patient that may not have been covered in the consultation with the veterinarian. Consider asking questions such as:
What type of cat litter do you use at home? If your clinic does not stock this type, perhaps consider asking the client to drop some off, as changing litter suddenly could cause a litter tray aversion.
What food do you normally feed at home, how often, and from what type of food receptacle? While diet is often required to be changed during hospitalisation, if the situation permits, continuing the patient’s regular diet may help avoid food aversions. In consultation with the veterinarian, they may direct that a new diet is commenced at home once the patient has been discharged, allowing a transition period from their existing diet to the new one. If no special diet is required, it may be helpful to ask the client to provide some of the cat’s normal food to increase patient emotional comfort.
Don’t forget these patients are in a brand-new environment where nothing at all is familiar. This is extremely stressful, and if we provide any elements of familiarity, that is a great thing.
Utilising the same or a similar style of food receptacle as the cat is used to may assist as well.
What activities does your cat normally enjoy? Do they like being groomed or do they enjoy a particular type of toy? Are there any other important behavioural notes for your pet that we should know? This information can be very helpful in assisting with the development and implementation of enrichment strategies that cater to the specific patient.
Do you have a blanket, soft bed or toys that have your home scent that you would consider leaving with your pet during their stay? As we remember, scent is extremely important for our felines, and providing a familiar scent in an unfamiliar environment can assist with emotional resilience. It’s best to explain to owners that it’s not always possible to return the items so they can select something suitable.
So, now we have a bit more information regarding our patient, we are ready to transfer them into their housing.
When transporting the patient from consultation room to the hospitalisation facilities, if possible, ensure this is a direct transfer with no interaction with other patients. It’s best to keep their cages covered with a blanket to reduce visual, auditory and olfactory stimuli.
If a direct transfer is not possible, ensure the patient’s cage is always placed in a raised and safe location, away from other patients, and with a covering over the enclosure. Placement on the floor is not acceptable.
All clinics will have a different layout and individual challenges when it comes to the clinic infrastructure, as there is no one-size-fits-all approach. There are some key considerations we should aim to implement when housing any feline patients.
Ideally, cats and dogs should be housed completely separately with a separation of solid walls and doors. If this is simply not possible in your clinic, you may like to consider appropriate scheduling to limit crossover of species and specific cage housing to limit visualisation between species.
The use of synthetic dog appeasing pheromones (e.g. Adaptil diffuser) may prevent emotional disturbances such as agitation and barking from
the canine patients. Feline facial pheromones i.e. Feliway, can be run concurrently in the same location and each product respectively will not affect the other species.
If you do have a cat only ward, there are some additional considerations to have in place where possible and appropriate.
Ward location – In addition to separation from the dog ward, where possible, an ideal cat ward should be easily accessible without obstacles through noisy and busy areas of the clinic.
Cages should be positioned in a manner so that visibility is reduced or eliminated to other areas of the clinic. It is also ideal that the cat ward position limits exposure to noisy treatment areas where other cats may be vocalising or protesting medical treatment.
Ideally, it will also be in an area that is not too isolated from the rest of the clinic, so that cats can be observed frequently without being forgotten and it does not require long distances for the cats to be transported from the ward to the treatment area.
Ward specifications – There are a few considerations to make in terms of the ward environment, such as size, ventilation and temperature. Temperature should be controlled and ambient, between 18 to 23 degrees Celsius, and adequate ventilation should be in place. The size of the ward should be taken into consideration, if possible, as staff should have enough space to observe cats from a suitable distance, perform all required tasks and move with ease, as well as transferring patients with the ability to limit exposure to other patients in the room.
Enclosure positioning and layout –There are a few considerations when it comes to the positioning and layout of
When transporting the patient from consultation room to the hospitalisation facilities, if possible, ensure this is a direct transfer with no interaction with other patients. It’s best to keep their cages covered with a blanket to reduce visual, auditory and olfactory stimuli
the housing within the cat ward. If possible, visual contact between patients should be avoided as this is an additional stressor and may increase the risk of spread of infectious particles between patients. If it is not possible to avoid visual contact with cages facing one another, ensure at least 2 metres remains between cages.
A safe height should be considered for staff, so that patients are easily visualised and removed from cages, avoiding strain and injury to the staff.

If there are multiple rows of cages together, consider raising the lowest level to at least 20 cm above floor level, if possible, to ensure the patient is not at floor level. An ideal height for the lowest cage is 90–100 cm.
Enclosure material – Any cage used should be constructed of a solid material and solid flooring must be used. There are a few options out there, with the two most common enclosure options being:
1. Stainless steel – The advantages of stainless steel are that it is easily cleaned and disinfected, easily accessible and may be a more affordable option for clinic housing. The disadvantages are that they conduct heat away from the patient, are highly reflective (which may scare the patient) and can be noisy.
If stainless steel is used, it is necessary to insulate using appropriate flooring and bedding, and it would be ideal to modify the cage door latches with rubber or plastic stoppers to reduce noise.
2. Fibreglass – This is also an excellent option for comfortable feline housing as it can also be cleaned and disinfected easily, it is durable, and compared to stainless steel, it is quieter, warmer and not as reflective. Latches are often still made of metal, so stoppers are also recommended here.
Enclosure doors – The front of the cage should also be considered. While toughened glass poses an excellent option for visibility, durability and infection control, this option is not always an accessible or affordable option.
If using metal bar doors, it is important to consider the size of any spaces. They should be far enough apart to support visibility into the cage, but close enough together to ensure no injury or escape could occur with smaller patients.
Internal enclosure design – When it comes to design of the enclosure, there are small considerations we can make to ensure maximum comfort for the patient.
Shelves and ledges – As we know, cats often feel more comfortable and safer in higher positions, which is a natural desire we can often accommodate.
Cages with built-in shelves or ledges should be considered, particularly for patients hospitalised for longer than 24 hours.
However, if this is not available, makeshift shelves can be easily implemented using disposable cardboard boxes turned upsidedown or using the cat’s carrier if it is constructed with a solid and flat roofing.
Cage specifications – Often a cat ward will contain cages of varying sizes, with smaller sizes ideal for daystay patients, and larger cages more suitable for hospitalised patients housed for longer than 24 hours.
It is important to consider that at a minimum for day-stay surgical patients, the cages must be large enough to facilitate full stretching of the patient with their neck extended to ensure a safe recovery from anaesthesia.
ISFM does provide specifications for both cage options, which are the suggested minimum internal measurements.
Day patients < 24 hours: 60 x 60 cm (3600 cm2) floor area
Longer hospitalisation periods > 24 hours: 90 x 70 cm (6300 cm2) floor area
With the above in mind, it’s now time to set up and furnish the cage. At this point, we are going to continue reflecting on our 5 feline facts to ensure we are furnishing the cage in a way that meets our cats’ physiological, safety and emotional needs.
Before we furnish the cage, we must first ensure our cage is ready for set-up.
Scent management – Don’t forget our felines are sensitive to scent and use scent marking due to their territorial nature. Besides the obvious
reasons of adequate infection control, previous hospital patients may have also released fear pheromones, which future patients could potentially detect if the cage has not been cleaned appropriately.
Before furnishing an enclosure for a new patient, always ensure all surfaces including doors and surrounding catchments have been thoroughly cleaned, using a veterinary grade disinfectant to the correct dilutions and contact time.
Ensure any objects entering the cage, such as bedding, litter trays or feeding receptacles, have also been cleaned and disinfected appropriately for infection control. Any toys and enrichment items used should also follow the same protocol.
Just as it is important to remove any undesirable scents, it is equally important to implement positive and familiar scents. Familiar scents could include items from home, such as bedding, cat carriers, clothing items of the owners, favourite toys, etc.
Another easy step we can take to introduce positive scent is through the use of feline facial pheromones (FFPs) in the form of Feliway diffusers

and spray. The FFP is a stress reducing pheromone released from facial glands, which marks an area as safe, and Feliway is the synthetic analogue of this pheromone. When we have constant diffusion of this pheromone in the hospital environment, this can contribute to a sense of safety for the patient. This product can also be sprayed onto bedding 30 minutes before use.
Cage flooring and bedding – Here we want to ensure we are applying a base that is not only hygienic, but also comfortable and warm, particularly if our cage is stainless steel material.
If underfloor heating is utilised, it is also important to ensure there is bedding to insulate and protect against overheating.
There are many options here, some disposable and some reusable. Newspapers only are not enough when it comes to flooring and bedding!
Towels are great as a cost and environmentally friendly option as they can be cleaned thoroughly for reuse and are comfortable and warm. It’s important to check towels and
I’m feline good: how to support your patient’s wellbeing through cat friendly hospitalisation
Implementing a cat friendly approach can seem daunting but does not need to be an expensive or complicated process. The core sentiment of these guidelines reflects a positive shift in attitude and culture surrounding the specialised needs of cats and an effort to understand their inherent needs.
If we reflect on our feline facts, we remember that cats need to feel clean, and bedding and flooring is an important consideration when considering the most suitable option for each individual patient.
Litter trays – Litter trays are a necessary addition for all hospitalised cats and it is ideal to have multiple sizes and styles of litter trays available to cater to the individual cat’s needs. For example, if we are housing a geriatric patient with suspected or diagnosed osteoarthritis, it would not be suitable to select a litter tray with elevated sides as this may be difficult and uncomfortable to enter and exit. Some cats may prefer more privacy and in this case using a covered litter tray, or simply placing a large cardboard box over the top, can meet this need.
shallow sides to avoid whisker irritation. The ceramic material is also much less permeable than plastic, meaning they do not become tainted with odours like plastic can. The food and water bowls should be placed far apart.
Privacy – Privacy is extremely important to cats and we must cater to this physiological need by providing access to a private area where they can hide. As discussed earlier, we know cats are not only solitary predatory hunters, but they are also independent, emotional and highly aware.
blankets for any loose threads or holes. These should be disposed of to avoid injury or interference with medical paraphernalia such as fluid lines. It is also important to note that towels and blankets absorb moisture, so they must be changed if they become soiled. Disposable absorbent pads are another great option, particularly if a patient is suspected of carrying an infectious disease or is in isolation. The downside to absorbent pads is they are not as cost and environmentally friendly, and often a towel or blanket is still required underneath to have an ideal level of comfort and insulation.
There are other purpose-made reusable bedding options available through veterinary suppliers that can be cut to size, are soft and padded, and enable moisture to be drawn away from the surface. While these types of bedding need to be purchased, they are reusable in the long term, which makes them more cost-effective and environmentally friendly than the disposable options. These types of bedding are excellent for recumbent patients or FLUTD patients due to their quick absorbing nature and soft padding.
Litter substrate – As discussed earlier, we should aim to ask clients about their cat’s litter preferences at admission. A variety of suitable options should be available, and if necessary, we can request a client brings in some litter if it is a particularly niche type or we feel it is necessary for the patient.
Food and water receptacles – As we remember from our feline facts, cats are hunters and obligate carnivores, and because of this they have an instinct to avoid contamination to their water source by consuming food away from their water. It’s important to place food and water apart, which means a big no to the double bowl if we can avoid it. Double bowls are often used in clinic due to them being easily sourced, cost-effective and easily cleaned and disinfected. When double bowls are used this may also increase the likelihood of food aversions. These types of bowls are often deep set with raised sides, which means it is also difficult for a cat to eat and drink without their whiskers touching the side, which can be irritating and uncomfortable.
Ideal receptables would be ceramic material, single bowls or dishes with
Hospitalisation for a cat is a huge loss of control and safety, as they cannot retreat from perceived danger. We know that cats will attack if they feel threatened and cannot retreat, which means an increased risk of injury to staff. Ensuring cats have a space where they can hide will help them to regain some feeling of control over their situation and provide some safety and retreat from environmental stimuli.
We can make some small changes to introduce a private area to the cage, including a blanket covering half the enclosure door in one corner, an upturned disposable cardboard box that’s an appropriate size for the cage, the patient’s cat carrier with the door removed (remember those familiar scents are important), and enclosed soft bedding igloos can also work very well.
Implementing a cat friendly approach can seem daunting but does not need to be an expensive or complicated process. The core sentiment of these guidelines reflects a positive shift in attitude and culture surrounding the specialised needs of cats and an effort to understand their inherent needs. It’s important to understand that even small steps towards improving feline nursing care is beneficial not only to our misunderstood feline patients and their health outcomes, but also reflects rewarding, skilled and compassionate veterinary care.
Species: Equine
Breed: Thoroughbred Age: 12 years old Sex: Gelding Colour: Brown Weight: 520 kg
A gelding was assessed on farm by one of our ambulatory veterinarians for the acute onset of severe colic symptoms. The gelding was uncomfortable, showing marked abdominal distention but permitted a basic examination. His heartrate was slightly increased at 52, which is above the ideal reference range of 28–48 beats per minute. His respiration rate of 16 and a rectal temperature of 37.6 degrees Celsius were within normal limits for his breed and age group. To permit further examination, intravenous analgesia was provided with 10 ml of flunixin meglumine (1 mg/kg) and 2 ml of xylazine (0.4 mg/kg). His mucous membranes were pink and moist with a capillary refill time of less than 2 seconds, indicating adequate perfusion. Gastrointestinal auscultation was reduced in all four quadrants, but with tympanic sounds throughout. The gelding indicated increasing pain despite analgesia and was reluctant to stand. This uncontrollable pain indicated the need for further diagnostics with the possibility of surgical intervention. The gelding was to be referred to the
hospital for further evaluation by our surgeons and internists. For the aid of transportation, 0.5 ml of butorphanol (0.1 mg/kg) was administered intravenously.
On arrival at the hospital the gelding’s condition had deteriorated and he was recumbent in the trailer. Cardinal signs were consistent with the onfarm assessment, but physically he was showing severe pain. A rectal examination performed by the afterhours surgeon found moderate gas distention and displacement of the large colon.
These findings, in combination with the uncontrollable pain exhibited by the gelding, indicated the need for surgical correction. With consent for surgical intervention, the team prepared the patient and the theatre for an emergency exploratory laparotomy.
A blood sample was collected from the left jugular vein to run a pre-anaesthetic panel. The results showed a mild hyperlactatemia, as blood lactate levels were at 2.6 mmol/L, with a normal range below 2 mmol/L in adults. The packed cell volume or PCV of 32% was on the low end of normal, with the reference range at 32–48%. The total protein result of 42 g/L, a mild hypoproteinemia was apparent, as the suggested range is 57–80 g/L (Zoetis LLC, 2022). These values can be suggestive of compromised blood circulation and can be representative of an early intestinal strangulation.
The right jugular vein was clipped and prepped using a chlorhexidine and methylated spirit preparation. The nurse aseptically placed a 14-gauge Extended Use MILACATH®, attached a heparinised extension set and sutured into position. Antimicrobials were given prophylactically, 38 ml of procaine penicillin (22 IU/kg) was given into the muscle, and 34 ml of gentamicin (6.6 mg/kg) was given intravenously.
As premedication, 3.1 ml of xylazine (0.6 mg/kg) and 5.2 ml of methadone (0.1 mg/kg) were calculated. With 2 ml of xylazine and the full dose of methadone administered intravenously, his mouth was rinsed to clear any food material and a nasogastric tube passed to ensure no accumulation of fluid in the stomach. The remaining 1.1 ml of xylazine was given in the induction box and he was allowed to settle. The patient was induced with 11.4 ml of ketamine and 4.2 ml of midazolam at the listed rates. The patient was intubated with a 26 mm ET tube and connected to a rebreathing circuit with mechanical ventilation. Isoflurane was used as the anaesthetic agent with 8L of oxygen as the carrier.
The surgery site preparation begins in the induction box as the clip starts from the base of the sternum and caudally to include the entire area around the sheath. The area was scrubbed with a chlorhexidine-based detergent. To transfer the patient from induction to the surgery room, hobbles were attached around the
These findings, in combination with the uncontrollable pain exhibited by the gelding, indicated the need for surgical correction. With consent for surgical intervention, the team prepared the patient and the theatre for an emergency exploratory laparotomy.

pasterns and connected to an electric hoist from the ceiling. Together the team transported the gelding onto the surgical bed and positioned in dorsal recumbency. While anaesthetised, the patient received Hartmann’s at 5 L/hr for the first hour, reducing to 3 L/hr afterwards. To ensure adequate fluid therapy was provided, urine output was monitored by the placement of an indwelling 28 French Foley catheter. The sheath was sutured closed to ensure a sterile preparation of the surgical site could be achieved
The surgical site was prepared with a 4% chlorhexidine solution, methylated spirits, and sterile gauze swabs were used to prepare the surgical site. The chlorhexidine was used in a circular motion starting over the incision site and working towards the periphery. The chlorhexidine was removed with the spirit-soaked swabs using the same principle. The surgical scrub was repeated three times to ensure an aseptic technique.
Prior to the gelding moving into the surgery room, the instrument table was prepared. The surgical table provided basic instrumentation for the surgeon to gown and glove, drape the patient, and open the abdomen via a ventral midline incision.
The laparotomy revealed a right dorsal displacement of the large colon, although with further exploration there also seemed to be a strangulating lesion. A portion of the small intestine was herniated within the epiploic foramen, which caused the blood supply and motility to become compromised. A small intestinal resection was performed, removing 3 feet of damaged bowel.
To complete the resection, further instrumentation was needed by the
surgeon. The following instrumentation was provided to the surgical assistant:
• an extensive instrument kit
• two doyen intestinal clamps
• two medium Penrose drains
• a Caiman® seal and cut device
• additional abdominal sponges
• warmed saline
• Poole suction tube
• new gloves.
The surgeon exteriorised the strangulation to understand the extent of the comprised small intestine and how much would need to be removed to allow for healthy margins. With the damaged bowel identified, the surgeon marked the two outer edges of the resection with the Penrose drains. The surgeon utilised the Caiman to seal and cut the vessels
to ensure a clean removal of the damaged bowel.
The abdomen was lavaged using 10 L of warmed sterile saline to remove any contamination and withdrew under suction using the Poole suction tube. The surgeon continued to investigate the abdomen, ensuring the placement of bowel was correct, and prepared for closure. A 5 Safil on a cutting needle was used to close the linea, with a 2/0 Monosyn for subcutaneous and skin closure. A stent was sutured over the top of the incision with a non-absorbable suture and a Hypafix dressing placed over the top.
The surgery team transferred the patient into recovery where he was provided with flow-by oxygen at 15 L/ min and monitored closely on camera. The gelding sat into sternal and stood on his first attempt.
An abdominal bandage was placed in recovery to ensure the incision remained clean and dry prior to moving to the ICU. The nursing team removed the Hypafix dressing in a sterile manner, ensuring the stent was intact. An additional sterile bandage was placed along the incision and

covered with a layer of cohesive bandage and a layer of Elastoplast over the top.
As he was transferred to ICU, he was placed on intravenous fluid therapy (IVFT), with Hartmann’s at a rate of 1.5 L/hr through a gravity fed administration set allowing 4–5 drops per second. Analgesia was provided with lignocaine as a continuous rate of infusion (CRI), administered through a fluid pump at 78 ml/hour. Lignocaine CRIs require an initial loading dose at 1.3 mg/kg, to be given intravenously over a 15-minute period. The lignocaine CRI required careful patient monitoring to ensure no signs of toxicity or neurological side effects presented. Flunixin meglumine was continued postoperatively at 1.1 mg/kg for the first 12 hours and reduced to 0.5 mg/kg twice daily. Antimicrobials were continued postoperatively at the same rates given at the time of surgery.
At 48 hours post-surgery, the gelding had passed cowpat-like faeces and was urinating well. His appetite and demeanour strengthened with an increasing interest in gradual feeding and surrounding activity. IVFT was reduced to 1 L/hr, with the lignocaine CRI discontinued, but continuation of
flunixin intravenously twice daily. To monitor fluid therapy, PCV and TP were monitored showing a PCV of 40% and total protein of 60 g/L, which indicated we were providing adequate fluid therapy.
At 72 hours post-surgery, mild intermittent colic symptoms presented, with him becoming agitated and flank watching. A nasogastric tube was passed, and 3 L of gastric reflux was obtained. Additional flunixin was administered and fluid therapy increased to compensate the loss.
Six hours after the additional flunixin, the gelding demonstrated mild colic signs and a further 2 L of gastric reflux. He was then refluxed every 2 hours, consistently producing upwards of 1 L each time. The owner was contacted to discuss the likelihood of a small intestinal obstruction. His poor prognosis was noted, and the owner unfortunately decided to subject the gelding to euthanasia. Despite best efforts with medical management, it was evident that a small intestinal obstruction was present. This was most likely at the anastomosis site leading to the accumulation of fluid proximal to this (Rubio Martinez and Hendrickson, 2021).
Afterhours emergency admissions of such a large animal take a team of highly trained and skilled members, and this case highlights the utilisation of multiple departments in the equine industry.

With the slow introduction of feed, IVFT and analgesia as medical support, postoperative ileus still became evident. Cases that present financial limitations are challenging, as the patient may have recovered with continued medical management or further surgical investigation, but this was not an option for our client.
Afterhours emergency admissions of such a large animal take a team of highly trained and skilled members, and this case highlights the utilisation of multiple departments in the equine industry. The cases aren’t always successful, but they can offer learning experiences for what we can do better or what we can change next time.


Coumbe KM. Equine Veterinary Nursing 2nd ed. Wiley-Blackwell. 2012. Rubio Martinez L & Hendrickson D. Complications in equine surgery. 1st ed. Wiley & Sons inc., 2021:332–337.
Services LLC, z. Vetscan VS2 Reference Ranges. Retrieved 5 June 2022, from https://www2.zoetisus.com/content/_assets/docs/Diagnostics/technicalpapers/VETSCAN-VS2-Reference-Ranges-VTS-00038.pdf
Zoetis LLC. HM5 Reference Ranges. Retrieved 5 June 2022, from https://www2. zoetisus.com/content/_assets/docs/Diagnostics/technical-papers/HM5Reference-Ranges-iPad-VTS-00426.pdf
Casual or part-time – what’s the difference? This is a question we often get asked on the HR Helpdesk. Casual and part-time employees both have different sets of entitlements, each with their own pros and cons for you as an employee, and it’s important to know about the different employment conditions you should receive accordingly so you’re not caught short.
This article will outline the key differences between casual and part-time employment, as well as a pathway from casual to part-time for longstanding regular casuals.
The first thing to note is that there is no such thing as a ‘permanent casual’. This is a common misconception, but as an employee you will be one or the other, not both. A part-time employee is a ‘permanent employee’, while a casual employee is, of course, casual.
Modern awards clarify how both casual and part-time employees must be engaged under that award. For most employees in a veterinary practice, the relevant award is the Animal Care and Veterinary Services Award 2020 (ACVS), which states that a casual employee:
• works on an hourly basis
• can work up to and including 38 hours per week
• is paid a 25% loading instead of receiving certain paid leave entitlements
• must be engaged for a minimum of three hours each time they work (or 2.5 hours under certain circumstances).
Meanwhile, a part-time employee:
• works less than 38 hours per week on a regular and systematic basis
• receives the pay and conditions a full-time employee receives on a pro-rata basis (e.g. accrues annual leave at a proportionate rate).
Further differences between casual and part-time employees include:
The first thing to note is that there is no such thing as a ‘permanent casual’. This is a common misconception, but as an employee you will be one or the other, not both. A part-time employee is a ‘permanent employee’, while a casual employee is, of course, casual.
A casual employee should have no expectation of ongoing work. Rather, their work is more intermittent, and they should only be engaged on an ‘as-needs’ basis. A genuine casual employee should not be expecting to receive regular hours each week.
In comparison, a part-time employee should have agreed minimum hours of work each week and there should be a clear expectation of an ongoing employment relationship.
A part-time employee is entitled to paid annual leave, as well as paid personal/carer’s (sick) leave. A casual employee is not entitled to either. While
a part-time employee is entitled to paid compassionate leave, a casual employee is only entitled to unpaid compassionate leave.
While part-time employees are entitled to the notice provisions stipulated in the ACVS (1 month), the ‘as-needs’ nature of casual employment means a casual employee is not entitled to notice of termination. This also applies to longterm casuals, even if they have access to unfair dismissal.
If a casual position is made redundant, the casual employee who held that position is not entitled to redundancy pay. Keep in mind, redundancy pay only applies if a practice has more than 15 employees.
If a casual has worked for 12 months on a regular and systematic basis, and has a reasonable expectation of ongoing work, they will also be entitled to unpaid parental leave.
This means they will also have a return-to-work guarantee at the same or similar position after finishing their parental leave period.
Similarly, a casual employee who has worked regularly and systematically for 12 months can request flexible working arrangements.
While traditionally a genuine casual employee should have no expectation of ongoing employment, if a casual employee has worked on a regular and systematic basis for 6 months, they are also entitled to make a claim for unfair dismissal if they feel
they were unfairly dismissed. For small businesses, this must be for a period of 12 months.
While each state and territory has its own long service leave legislation and entitlements, casual employees are generally afforded the same long service leave entitlement as permanent employees.
There were recent changes to the NES that allowed casual employees to convert to part-time employment if they meet certain criteria:
• For the past 6 months they have worked regular and systematic hours
• They have a reasonable expectation of ongoing employment
• Their hours would not change significantly should they transition to permanent employment.
Within 21 days of their 12-month anniversary, an employer must inform a casual employee in writing whether they are offering the employee casual conversion or declining to make an offer. An employer may only decline to
offer casual conversion if the employee does not meet the requirements, or on reasonable business grounds – such as that the position will not exist in the next 12 months.
For small businesses there is no positive obligation to offer casual conversion, but as an employee you may still request conversion to permanent employment if you believe you meet the criteria.
There are key differences between casual and part-time employees, but it’s not uncommon for employers to lump some of them together interchangeably, or miss them altogether, so it’s important to be aware of how you should be engaged.
When making up your mind about what sort of employment you would prefer, it’s important to consider:
• Do you want more flexibility to accept shifts when available and take time away from work? If so, casual employment might be better.
• Do you want more job security where you are guaranteed hours each
week? If so, part-time might be a better fit.
If you are unsure about your entitlements as an employee and whether you are receiving the correct entitlements, or whether you might be eligible for casual conversion, please contact the VNCA HR Service on 02 8448 3266 or email helpline@ myadvantage.com.au for assistance. Alternatively, templates and other resources can be found online at the HR Portal available to members.

The material contained in this publication is general comment and is not intended as advice on any particular matter. No reader should act or fail to act on the basis of any material contained herein. The material contained in this publication should not be relied on as a substitute for legal or professional advice on any particular matter. Wentworth Advantage Pty Ltd, expressly disclaim all and any liability to any persons whatsoever in respect of anything done or omitted to be done by any such person in reliance whether in whole or in part upon any of the contents of this publication. Without limiting the generality of this disclaimer, no author or editor shall have any responsibility for any other author or editor. For further information please contact Wentworth Advantage Pty Ltd.
©Wentworth Advantage Pty Ltd 2022
When faced with a diagnosis of a tumour, it can instantly instil fear. The veterinary approach to any tumour diagnosis is a methodical one that allows for a thorough diagnosis and optimal treatment pathway.
Identifying the tumour type is essential in determining the prognosis and treatment required. There are a number of methods to identify the type e.g. cytology and biopsy.
The examination of the lymph nodes and the use of ultrasound, CT scan or MRI helps determine if the tumour is malignant and has spread to other parts of the body. For a benign tumour i.e. a tumour that only occurs locally, staging is not required.
T describes the size and invasiveness of the tumour N describes the status of the local lymph nodes
M describes the presence or absence of metastases
The grade refers to the aggressiveness of the tumour.
There are 3 grades
1 least aggressive
2 moderately aggressive
3 highly aggressive
The grading helps to predict tumour behaviour.
Once the tumour has been identified, staged, and graded, the treatment plan is determined, and the prognosis can be estimated.
The VNCA and VetCheck have supplied this information to assist vet nurses to educate, brief and assist their clients to care for and manage their pets.
These are the main therapies used to treat cancer in animals:
Chemotherapy The administration of chemotherapeutic medications every 1–3 weeks for an appropriate course length. Alternatively, oral medications can be prescribed.
Surgery Surgery can be performed to remove the entire tumour, to remove the partial tumour as a debulking procedure, or as palliative care to decrease pain.
Immunotherapy
The use of ionising radiation to kill cancer cells with responses seen within 2–8 weeks of therapy.
Using the pet’s immune system to fight the cancer.
They can be used together or separately. Depending on the location of the disease, local tumours typically call for local therapy and systemic disease requires systemic therapy.
The ultimate goal for cancer treatment is complete remission or cure.
There are 5 responses to cancer therapy.
Complete remission The disappearance of all clinical evidence of an active tumour
Partial remission 50% or greater decrease in tumour size
Stable disease No appearance of new lesions or worsening clinical signs
Progressive disease Increase of at least 50% in tumour size
Relapse The appearance of new lesions following complete remission
Source: VetCheck is a powerful client education platform that helps veterinary teams save time, increase client engagement, retention and grow the practice through digital pet health summaries, handouts, best practice tools (digital dental charts, GA monitoring charts, hospital workflow) and forms with e-sign. To add your practice logo and start sharing directly to the pet owner’s mobile phone, visit www.vetcheck.it
© VetCheck Technologies Pty Ltd.® VetCheck is a registered trademark. All rights reserved.
For digital case reports, handouts and request forms for veterinary teams visit www.vetcheck.it


We asked Brittney a few questions on her achievement
Congratulations on becoming the first Australian to gain your Vet Tech Specialist in Diagnostic Imaging. You are the only non-North American and one of less than 20 worldwide to gain this speciality. How does it feel?

It feels great to be part of what I hope is a growing movement! Diagnostic imaging is an area of vet med growing at a rapid speed, and it only makes sense that we should have specialised nurses and techs to run these machines to acquire these high quality images. As our equipment is on par with human medicine, many hospitals are choosing to hire human radiographers, but apart from the licensing hurdles, there is no reason why we can’t be training our own people. I am passionate about diagnostic imaging, both as subject matter and as an area of veterinary medicine that desperately needs more nurses and techs.
Tell us about what you had to do to gain this VTS?
To sit for the VTS DI, I required 10,000 hours (or 5 years) in practice with at least 75% of that being imaging-specific work, to have 2 VTS or veterinary radiologist mentors and 40 hours of imaging CE in the years immediately prior. The application required the submission of 50 case logs and 6 detailed case reports covering an extensive skills list that required mastering. The skills included radiography, CT, MRI, ultrasound and scintigraphy across small and large animals. Once this application was accepted, the final step was an examination. To complete my skills list, case logs and study, I worked at 2 specialist clinics across multiple species and departments.
What made you decide to undertake this further study?
When I started my role as a vet tech in imaging, I struggled to find other people in similar roles. I was the first in my clinic and most clinics with advanced modalities seemed to be hiring human diagnostic radiographers for image acquisition. Nurses in clinics who were taking most of the X-rays were juggling so much else they had little time to dedicate to specifically imaging. I also found it hard to
The industry is expanding and developing so quickly that the options for specialisation feel almost endless, and people who love and are good at what they do will always be in demand.
find imaging-specific CE and wanted to be part of the change. I was fortunate to work alongside a diagnostic radiographer who taught me so much and I fell in love with imaging early on, pursuing additional licensing and teaching opportunities at every chance. As a person who loves a challenge, learning new things, and still trying to find my niche in vet med, this constantly evolving specialty was a great fit for me. When the diagnostic imaging academy was finally officially recognised by NAVTA and considering the limited Australian qualifications for techs for clinical specialisation, it seemed like the logical next step.
What advice do you have for those interested in furthering their career?
It sounds very cheesy but find what you love and pursue it even when you’re not sure where it will lead, or the pathway is unclear. The industry is expanding and developing so quickly that the options for specialisation feel almost endless, and people who love and are good at what they do will always be in demand. When I started on my DI pathway, there were no vet nurses or techs licensed for CT in Queensland. We didn’t have an MRI in my clinic and all I was doing was radiographing stifles, chests and abdomens, day in and day out. I put in the hours, jumped at every opportunity to expand my skills, relentlessly hounded QLD Health for further radiation licensing and everything else fell into place.
BAppSc (Veterinary Technology), Cert IV VN, VTS (Exotic Companion Animal) RVN, RVT
Veterinary nurses and technicians are a very talented bunch! Gary Fitzgerald, a current director on the Veterinary Nursing Council of Australia’s (VNCA) Board of Directors and the 2020 VNCA Nurse/Technician of the Year, is a shining example!

Gary, Practice Manager at The University of Queensland’s UQ Vets Veterinary Teaching Hospital, attained Veterinary Technician Specialist certification on 27 June this year after meeting the rigorous requirements set by the Academy of Veterinary Technicians in Clinical Practice (AVTCP) in the United States of America. AVTCP is modelled after the American Veterinary Medical Association accredited college, the American Board of Veterinary Practitioners (ABVP). Gary’s subspeciality in this academy is Clinical Practice (Exotic Companion Animal). Completing the specialisation required a minimum of five years’ prior clinical experience, a minimum of 50 hours advanced continuing professional development that is RACE certified (or equivalent) and delivered by other specialists, 50–75 case studies, four case reports and mastery of skills linked to the case log, plus a written examination. Gary is the only technician to hold this qualification in the southern hemisphere and there are only 11 technicians worldwide with this qualification. Congratulations to Gary on such an outstanding achievement!
Gary is at the forefront of advancing the professional status of veterinary nursing in Australia, not only with this specialisation, but he has also co-authored a book on nursing the reptile patient, and published articles on exotics in the Australian Veterinary Nurse Journal, and in The Veterinary Nurse, a peer-reviewed international journal. Gary regularly presents at VNCA conferences,
If you could give other nurses one piece of advice or a tip you have learnt, what would it be?
Your most valuable asset will always be your support team. At UQ, I am blessed to be surrounded by an incredible group of techs and nurses passionate about both personal development and patient outcomes. This means gold standard care with gold standard people, always pushing you to do your best. I never would have pursued this specialty without the support of my team.
and in 2019 he was invited to present at the VMX Veterinary Meeting & Expo in Orlando, Florida, which is the largest veterinary conference in the world with over 17,000 delegates. In between these professional activities, Gary finds time to help train and mentor veterinary technology students and handles the occasional venomous brown snake in a clinical capacity at the UQ Vets Veterinary Teaching Hospital. As a qualified veterinary nurse and veterinary technician, Gary has dual AVNAT registration: leading by example in the pursuit of mandatory registration of veterinary nurses and technicians in Australia!
Outside of work, I have a great network of family friends who keep me busy, along with whatever hobby of the moment I’m fixated on. Right now, that means crochet gifts for everyone, including my ever-so-patient dog and cat that keep me sane and focused on what’s important. I am also fortunate to have a supportive partner who is also in the industry. She knows when to let me ramble on about MRI physics for 45 minutes and when to help me switch my work brain off. It’s so easy to burn yourself out in this industry and I feel very strongly about maintaining a healthy work/ life balance.





If you could give other nurses one piece of advice or a tip you have learnt, what would it be? Something I heard a speaker say at this year’s VNCA Gold Coast Conference, about how vital it is to have courage … the courage to keep trying and learning, because it’s the process of repetition that will build competency and then confidence will follow.
How do you keep a work/life balance?
Qualification: Certificate IV Veterinary Nursing
Currently studying anything?
Yes, slowly! A Diploma in Leadership and Management.
Experience in the profession:
I completed my Certificate IV in Veterinary Nursing in 2012, while working in clinic. Since then, I have worked full time as a veterinary nurse and head veterinary nurse. More recently, I’ve been part of the management team at our practice, which has been an exciting new challenge!
Why did you choose veterinary nursing as your career?
I’ve always had a love of animals and all things science. Veterinary nursing presented as a good way to combine my interests. I love the practical aspect of nursing; there is always something interesting happening – a new patient to meet and a new skill to learn. I also found a great practice to work in from the start, which got me hooked.
What has been your most memorable moment as a veterinary nurse and why?
I love being involved in complex procedures and learning new technical skills, such as the process for CT scans. I have also given a home to two animals through veterinary nursing, so they are very fond memories.
I try not to take work home with me, but it can definitely be difficult to switch off at times. I like to take my dog out and spend time outside to help reset from the day, talk with family, or watch something easy on TV. If there is something I’m feeling stressed about, I will set a limit on how much time I spend thinking about it (which sometimes works).
What animals do you own?
I have a greyhound/staffy mix (at least that’s what I say she is) named Rosie and a cat called Coco. I adopted Rosie when she was around 16 weeks, after she presented at the clinic with HOD (hypertrophic osteodystrophy). She was being cared for by a local rescue group, but her disease made it difficult for her to be adopted out. I pretty much fell in love with her straightaway and being her nurse every day for a week cemented that. Rosie is a comedian at home and will play up to make people laugh. She has also been called a kangaroo and a tiger by people we’ve met (it’s the ears and the stripes). As for Coco, I found her at a local vet who had taken in some kittens and she is now about 15 years old. She is occasionally grumbly, but also loves nothing more than to sit in my lap and have cuddles.
How long have you been a VNCA Member?
Five years, on and off. I enjoy attending conferences when I can.
Name:
Qualification: ISFM Diploma of Feline Nursing, Cert IV Veterinary Nursing, RECOVER certified, RVN, AVN
Currently studying anything?
Safe Use of Chemotherapy in Practice run by VETcpd.
Experience in the profession
I recently celebrated ten years as a vet nurse. My first eight years were in GP: working with amazing people, fostering countless kittens, knowing all my regulars and their families, and learning so much every year. Two years ago, I moved into a specialist setting which has pushed me to learn more and develop new skills.

I now work as an oncology and departmental nurse at SASH Tuggerah, which has been an amazing experience that I didn’t even know was possible when I started nursing.
Why did you choose veterinary nursing as your career?
I started as a vet nurse because I love animals and thought I wasn’t a people person. Why I stayed a vet nurse was because of the people: the hardworking, intelligent and caring colleagues, as well as the dedicated and vulnerable families of the pets.
 Michelle Reeves
Michelle Reeves
What has been your most memorable moment as a veterinary nurse and why?


No single moment but an accumulation of memories of moments of kindness seen throughout my career – a senior nurse or vet taking time to teach me something, an extra break after a rough euthanasia, the comradery of a late-night surgery, someone scheduling a Burmese patient for a day I’m working ... all the moments that turned me into a people person.
If you could give other nurses one piece of advice or a tip you have learnt, what would it be?
Be kind to yourself. Always make sure you’re giving enough of your energy to your own needs before caring for others.
I work part time and make sure I fill my cup back up on my days off.
I am the lucky companion of 4 senior rescue Burmese cats, a senior Bordoodle (I know, I know), a rescue Indian Ringneck Parrot and a senior chicken.
How long have you been a VNCA Member?
Six years in January 2023. I joined the NSW Division Committee last year and it’s been very interesting seeing all the work that goes into making the VNCA great.
If you are considering publishing in AVNJ as your next career goal but are not sure how to get started, we are here to help!
There are lots of options available – from clinical and research articles through to case studies, opinion pieces and the everpopular ‘Member Vitals’.
As a starting point, check out the Author Guidelines on our website at www.vnca.asn.au/resources/avnj/authorguidelines/
When you are ready to submit, or if you have further questions, please email us on media@vnca.asn.au – whether it is the first time or you are a frequent contributor, we’ll make sure your journey to publishing in AVNJ is rewarding.
THE AUSTRALIAN VETERINARY NURSES JOURNALAVNAT Registered Veterinary Nurses and Registered Veterinary Technicians demonstrate their commitment to their profession by:
• meeting entry level education
• completing ongoing continuing professional development
• abiding by a Code of Professional Conduct and Ethical Practice and related standards.
Find an AVNAT registered professional today via the AVNAT Online Register

The AVNAT Registration Scheme has been established by the VNCA to set the standards of professionalism across the veterinary industry. Congratulations to our newest AVNAT registered veterinary nurses and technicians for their commitment to quality practice.
Zarena Andrew
Alyssia Balbi
Rachelle Balfe
Amy Bishop
Peta Black
Theneal Brits
Georgia Brown
Carly Calavetta
Mimi Calvin
Evangeline Charles
Taylor Chesters
Emma Corbett
Christina Dalagiorgos
Jasmine Davey
Stacy Devenish
Tegan Dziurek
Karen Hasthorpe
Helle Heesen
Simone Heywood
Emma Holder
Gabrielle Houston
Benjamin Hunter
Jessica Hyde
Sarah Jafer Shauna James
Tegan Jennings
Pei En Keong
Shannon Knoth
Nikeah Locke
Fiona Matarrese
Rebecca McKelvey
Samantha Melamdowitz
Olivia Morrissy
Erin Murnane
Brittany Nash
Annabel Newell
Amy Padman
Talia Pasche
Mia Peters
Tamryn Plummer
Eva Potocnik
Elizabeth Puglisi
Anita Renzullo
Abigail Russell-Brereton
Megan Rutter
Stephanie Scaife
Jaimie Screaigh
Emma Sullivan
Jessica Van Arend
Raine van Rensburg
Kathryn Veale
Ellie Vilardi
Emma Ward
Jordan Weeks
Rebecca Welsh
Melanie Werner
Kaytlyn Williams
Bethany Wilson