August 2022 TEXAS DENTAL 487 ENCOUNTERSWILD IN DENTISTRY 495 WHAT TO KNOW MONKEYPOXABOUT



478 Texas Dental Journal | Vol 139 | No. 8 More at (Compliancetdaperks.com&Supplies) Dailey Solutions sells directly to businesses at wholesale prices. Toner Cartridges • 20%–50% off retail pricing • TDA members save additionally with preferred pricing. • Brand-new, 100% guaranteed cartridges only • All cartridges meet and/or exceed all manufacturer warranties, specs • Next Business Day UPS delivery customary on most orders • Shipping cost included in pricing Office Supplies • 2%–30% off retail pricing • TDA members save additionally with preferred pricing. • Over 70,000 items —paper and pens to toilet paper, cleaning supplies, PPE, and coffee • Furniture options such as desks, chairs and couches, bookcases, file cabinets, more • Next-Business-Day UPS delivery on most orders • Shipping included on orders $49.99 and higher 800-601-4505 Mention “TDA Perks” to access preferred pricing. Pay less for the same supplies sold at major box retailers.


Join 200,000+ medical professionals who get free CE with Texas Health Steps Online Provider Education. Choose from a wide range of courses developed by experts, for dental experts like you. Courses such as caries risk assessment and dental quality measures are available 24/7.




www.tda.org | August 2022 479 Learn more at TXHealthSteps.com
Content on the Texas Health Steps Online Provider Education website has been accredited by the UTHSCSA Dental School Office of Continuing Dental Education, Texas Medical Association, American Nurses Credentialing Center, National Commission for Health Education Credentialing, Texas State Board of Social Worker Examiners, Accreditation Council for Pharmacy Education, Texas Academy of Nutrition and Dietetics, Texas Academy of Audiology, and the International Board of Lactation Consultant Examiners. Continuing Education for multiple disciplines will be provided for some online content. Texas Health Steps is health care for children birth through age 20 who have Medicaid.
Brush

up on healthdental CE.
480 Texas Dental Journal | Vol 139 | No. 8 contents Ronald C. Auvenshine, DDS, PhD Barry K. Bartee, DDS, MD Patricia L. Blanton, DDS, PhD William C. Bone, DDS Phillip M. Campbell, DDS, MSD Michaell A. Huber, DDS Arthur H. Jeske, DMD, PhD Larry D. Jones, DDS Paul A. Kennedy Jr, DDS, MS Scott R. Makins, DDS, MS Daniel Perez, DDS William F. Wathen, DMD Robert C. White, DDS Leighton A. Wier, DDS Douglas B. Willingham, DDS Texas Dental Journal (ISSN 0040-4284) is published monthly (one issue will be a directory issue), by the Texas Dental Association, 1946 S IH-35, Austin, TX, 78704-3698, 512-443-3675. Periodicals Postage Paid at Austin, Texas and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 1946 S IH 35, Austin, TX 78704. Copyright 2022 Texas Dental Association. All rights Annualreserved.subscriptions: Texas Dental Association members $17. Instate ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated, September issue $17 ADA Affiliated, $65 Non-ADA Affili ated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement printed in the September Annual Membership Directory or on the TDA website: tda. org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made of it by its manufacturer.
487FEATURESWILD ENCOUNTERS IN DENTISTRY Kyle King, DDS 495 WHAT TO KNOW ABOUT MONKEYPOX Allison M. Lee, DDS John M. Wright, DDS 502 ASSESSMENT CONVENTIONALLYOF AND DIGITALLY REVIEWACOMPLETEFABRICATEDDENTURES:COMPREHENSIVE Manal Q. ShankargoudaArtakJoãoShilpaFuadAmitSaeedMansoorAbdulrahmanMohammedMubarakiM.AlMoaleemH.AlzahraniShariffM.AlqahtaniPorwalA.Al-SanabaniBhandiPauloMendesTribstHeboyanPatil 481editorialsEditor’s Letter 483 President’s Message 485 ADA Now! 492HIGHLIGHTS Oral and MonthPathologyMaxillofacialCaseofthe 497 Calendar of Events 498 Value for Your Profession: Anatomy of a $25,000 OSHA Citation 516 Pathology Case Diagnosis and Management 520 Advertising Briefs 526 Index to Advertisers Board of Directors TexasAssociationDental PRESIDENT Duc “Duke” M.
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 139 | No. 8 Texas Dental Association 1946 S IH-35 Ste 400, Austin, TX 78704-3698 Phone: 512-443-3675 • FAX: 512-443-3031 Email: tda@tda.org • Website: www.tda.org Ho, DDS 281-395-2112, 512-879-6225,214-585-0268,936-598-2626,325-648-2251,CodyPRESIDENT-ELECTducmho@sbcglobal.netC.Graves,DDSdrc@centex.netPASTPRESIDENTDebrahJ.Worsham,DDSworshamdds@sbcglobal.netVICEPRESIDENT,SOUTHEASTGlendaG.Owen,DDS713-622-2248,Dr.owen@owendds.comVICEPRESIDENT,SOUTHWESTCarlosCruz,DDS956-627-3556,ccruzdds@hotmail.comVICEPRESIDENT,NORTHWESTTeriB.Lovelace,DDS325-695-1131,lovelace27@icloud.comVICEPRESIDENT,NORTHEASTElizabethS.Goldman,DDStexasredbuddental@gmail.comSENIORDIRECTOR,SOUTHEASTShaileeJ.Gupta,DDSsgupta@stdavidsfoundation.orgSENIORDIRECTOR,SOUTHWESTRichardM.Potter,DDS210-673-9051,rnpotter@att.netSENIORDIRECTOR,NORTHWESTSummerKetronRoark,DDS806-793-3556,summerketron@gmail.comSENIORDIRECTOR,NORTHEASTJodiD.Danna,DDS972-377-7800,jodidds1@gmail.comDIRECTOR,SOUTHEASTLajiJ.James,DDS281-870-9270,lajijames@yahoo.comDIRECTOR,SOUTHWESTKrystelleAnaya,DDS915-855-1000,krystelle.barrera@gmail.comDIRECTOR,NORTHWESTStephenA.Sperry,DDS806-794-8124,stephenasperry@gmail.comDIRECTOR,NORTHEASTMarkA.Camp,DDS903-757-8890,macamp1970@yahoo.comSECRETARY-TREASURER*CarmenP.Smith,DDS214-503-6776,drprincele@gmail.comSPEAKEROFTHEHOUSE*JohnW.BaucumIII,DDS361-855-3900,jbaucum3@gmail.comPARLIAMENTARIAN**GlenD.Hall,DDS325-698-7560,abdent78@gmail.comEDITOR**JacquelineM.Plemons,DDS,MS214-369-8585,drplemons@yahoo.comLEGALCOUNSELCarlR.Galant*Non-votingmember**Non-voting
Editorial Staff Editorial Advisory Board Jacqueline M. Plemons, DDS, MS, Editor Paras B. Patel, DDS, Associate Editor Nicole Scott, Managing Editor Barbara Donovan, Art Director Lee Ann Johnson, CAE, Director of Member Services
Editor’s Letter
Jacqueline Plemons, DDS, MS

Change is coming to the Texas Dental Journal—can you spot it? Over the past 4 months, a task force has been working to reimagine the TDJ. The group explored the perceived value of the Journal, decided on categories of content, considered publication manner, timing and frequency, and restructured editorial support. As their work nears completion, the fun part is really just beginning! The TDJ will take on a fresh new look over the next few months. I’m incredibly grateful to work with an amazing and talented publications team at the TDA—Lee Ann Johnson (Director of Member Services), Nicole Scott (Managing Editor) and Barbara Donovan (Art Director). Together, we will experiment…with everything from colors and font size/ style to layout and presentation—all while continuing to provide you with content you can use in your professional, and sometimes personal, life. Here’s a hint of a piece in this issue that explores some ideas for change —this article comes with a “growl of Canappreciation”.youseethe changes? Let us know what you think. We are listening!
www.tda.org | August 2022 481
482 Texas Dental Journal | Vol 139 | No. 8 Our Smile Pass gives you access to 120+ courses, the Opening Session with Dr. Brené Brown, SmileCon Street Fest, Dental Central (the exhibit hall), the Closing Session, and more. Register today for this mighty meeting at SmileCon.org. SMILECON is a trademark of the American Dental Association. isRegistrationSmileConOpen Scan to see the full session list on the Agenda Builder!Houston, TX Oct. 13–15, 2022

• The Council on the Annual Meeting, Continuing Education, and Programs—is working on a high-end, member-only networking and CE conference to be held at the Omni Barton Creek Resort and Spa in 2023, as well as shaping the educational and entertainment programs for the May 2023 TDA Meeting in San Antonio.
• The Council on Membership, New Dentists, and Students—gathered via Zoom to discuss projects to promote the activities of your local components (such as the Southwest Dental Conference put on by the Dallas County Dental Society and the “A Taste & Tour of Diversity & Technology in Dentistry” presented by the San Antonio District Dental Society). They are also working to develop more individual membership growth (such as creating our own Texas Institute for Diversity in Leadership).
RELATIONSHIP. MENTORSHIP. COMMUNICATION. by your Board of Directors) which will focus on issues that solve problems for all member dentists, such as seeking insurance reform, decreasing administrative burdens and increasing Medicaid reimbursements; while DENPAC (your state political action committee) met to discuss upcoming fund-raising efforts in anticipation of the upcoming legislative year.
• The Council on Legislative, Regulatory, and Governmental Affairs—met with several other dental organizations, to develop a legislative agenda (to be approved

“Pay no attention to that man behind the curtain.”
—The Wizard, The Wizard of Oz Duc “Duke” M. Ho, DDS, FAGD TDA President
• TDA perks program continues to push more member dentists to seek the services of ERC Specialists to help with the Employee Retention Credit (ERC) application. At the time of this writing, our members are scheduled to receive almost $7 million of this fully forgiven tax credit. Please check eligibilitythecompany-erc-tax-credittdaperks.com/specialty-payroll-https://tostartprocessofcheckingyourifyouhaven’tyet.
www.tda.org | August 2022 483
I have always believed that contrary to the quote above, the success of the Association depends upon each of us knowing “that man” behind the curtain and all that’s happening around them. Given such, my goal through these monthly addresses is to be authentic, transparent, and clearly communicate how we are working to serve you. So, although the summer months are slowly beginning to wind down, your Texas Dental Association, alongside your local components, is starting to ramp up our work—behind the curtain. Here’s how: Money back to you:
Continuing Membership,Education,andOurPatients:
Advocacy, Compliance and Regulatory issues prior to the upcoming legislative session:
• TDA Smiles Foundation—is finalizing details prior to the upcoming Texas Mission of Mercy (TMOM) in Luling on September 9 and 10 with volunteer registration open for those who want to provide care.
Associates looking to own a practice or owners looking to grow or sell their practices:
Of course, we will continue to work hard to do more and share more so that you can better know the Association “behind the curtain.”
Dentist to Dentist
• TDA Perks Program hosted a complimentary networking and happy hour event connecting TDA members while they learned from TDA Perks Program vendors about topics such as real estate, practice financing, insurance negotiation with credentialing, and practice marketing. If you’re interested in an event in your area, reach out to to Josh Epstein at jepstein@tda.org.
484 Texas Dental Journal | Vol 139 | No. 8 346-221-0316 Rule 110.16 High-Risk Sedation Management 20 CE HRS Abuse & Misuse of Controlled Substances and Dental Pain Management 4 CE HRS Adult RecertificationSedation Level 1-3 Initial Pediatric & Adult Certification CONTACT US 888-761-2442 SPEAKER DR. SHAWN SEIFIKAR Dentist Anesthesiologist, President of Southwest Sedation Education, Adjunct Professor, Texas A&M College of Dentistry 6-8 CE HRS 16 CE HRS Pediatric RecertificationSedationLevel 1-2 6-8 CE HRS ONLINE OR IN-PERSONONLINE ONLY ONLINE OR IN-PERSON REGISTER ONLINE AT SWSEDATIONEDUCATION.COM ON-DEMAND AND IN-PERSON COURSES! COMMITTED TO QUALITY & SAFETY! RATED! EXPERIENCE US! Dallas, Houston, San Marcos Rule 110.17 Pediatric Sedation Management 20 CE HRS HY RID (ONLINE & IN-PERSON) HY RID (ONLINE & IN-PERSON) HY RID (ONLINE & IN-PERSON)
















Things are changing at the ADA!
www.tda.org | August 2022 485
Craig S. Armstrong, DDS ADA 15th District Trustee ADA Now!

Amidst this time of change, we continue to push forward with the important job of advocating for you, our grassroots member. Issues we continue to pursue include; fighting for dental insurance reform using over $600,000 in dedicated State Public Affair dollars, lobbying successfully for student debt reform giving much needed relief for our young dentists, and attempting to address the needs of our vulnerable senior population via an expansion of an adult benefit in Medicaid instead of going the way of our colleagues in medicine and entering the Medicare arena. Change at the ADA is taking us in a new direction. Everything is targeting you, the customer. Three big areas of change that are coming to the ADA: 1. The development of a long overdue mobile app; 2. The development of a strategic forecasting model that will be presented to the House of Delegates in October for approval. This will allow us be more agile and make changes to our budget all year round instead of one time a year at the House of Delegates; 3. The implementation of a new management software platform that has augmented intelligence capabilities along with a more robust security component. These changes will allow us to deliver laser focused messaging to you, the customer, via your preferred method of communication and puts the entire menu of products and services that the ADA offers at your fingertips. Finally, I want to be your messenger and improve the level of communication between the ADA and TDA. Please do not hesitate to reach out to me via the following email address with your questions or concerns: armstrongc@ada.org.
Our new executive director Dr Ray Cohlmia has been on the job for approximately 6 months and his arrival brings a sense of excitement and optimism to the ADA. The definition of insanity is doing the same thing over and over and expecting a different result. I am afraid that at times the ADA has fallen into this trap. What do Sears, Kodak, Blockbuster, Xerox, and Nokia all have in common? Their refusal to change or adapt led to their demise. Change is needed at the ADA, and it’s needed now!
It is my honor to represent all of the dentists of the state of Texas.
486 Texas Dental Journal | Vol 139 | No. 8

Kyle King, DDS, Jordan Family Dentistry, Lufkin, Texas
www.tda.org | August 2022 487
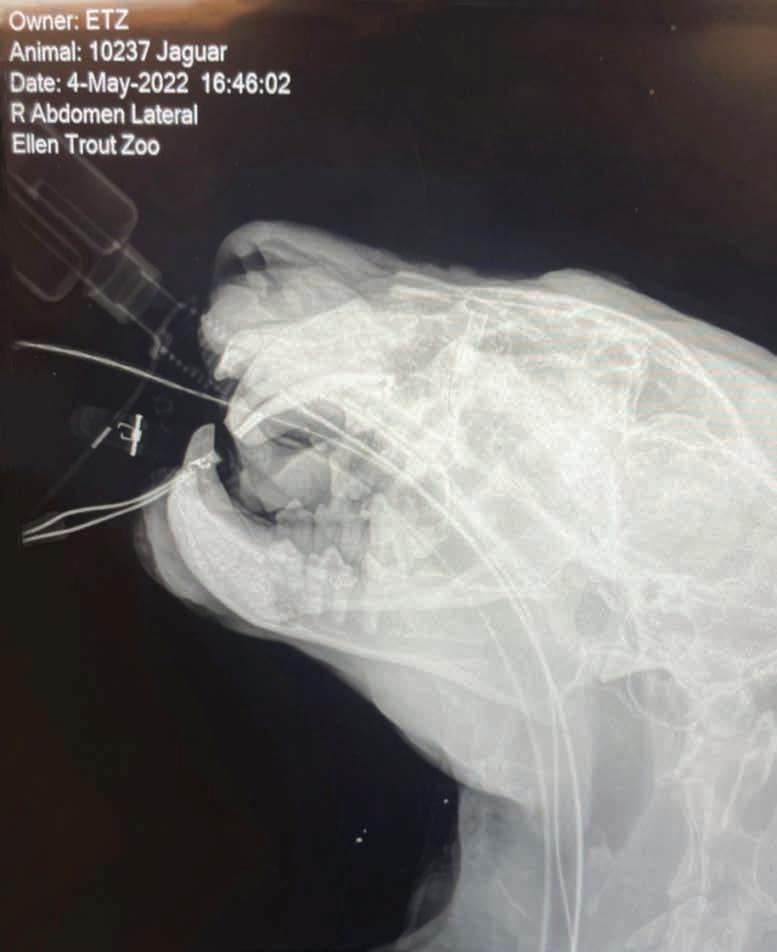
Due to the procedure being done at the zoo, Dr Dunavant had to hand-instrument the entire canal space of necrotic and infected tissue, which ultimately ended up at 54 mm. After numerous rounds of cleaning and shaping with our newly obtained 60 mm endodontic files, the canal was obturated with gutta percha and the access opening was closed with amalgam.
On follow-up, Sarah has done extremely well and regained the weight she had lost from her inability to eat.
Dr jaguartreatsDunavantRustyaat the Ellen Trout Zoo in Lufkin.
On May 4, 2022, Sarah the jaguar successfully underwent her endodontic treatment with a full team at her side. Entering the room once she was sedated, my first question was, “How long is she out for?” Hearing the reply, “It depends on...” I think the shock on my face was Oscar worthy!
treatment on humans can be challenging, the veterinarian estimated that the cuspid was around 50 mm in length, far longer than anything I have ever treated in my office. Thankfully, Dr Rusty Dunavant with East Texas Endodontics in Longview answered my call for help.
Wild
Encounters in Dentistry
In April 2022, I was on vacation when I received a message from my front desk, “The zoo veterinarian needs to speak with you about an animal.” They had noticed the local zoo jaguar
From time to time, various crazy and interesting dental stories catch my eye on social media, especially those that combine animals and oral health. Seeing police or service canines in need, I have always had a soft spot for our furry friends. In private practice, I’ve gotten to know many of the local veterinarians in the area and have offered my services if ever needed.
“Sarah” had been losing weight and not eating her normal diet. Upon labs and examination, it was discovered that she had fractured her maxillary left cuspid, which had in turn become necrotic and Whileabscessed.endodontic
It took a few weeks and several phone calls to locate an armamentarium for a case of this nature. We received instruments and materials through donations from Henry Schein (veterinary branch) and Ultradent.
488 Texas Dental Journal | Vol 139 | No. 8
Pictured is the team that worked on Sarah the jaguar: veterinarian Dr Lindsay Syler, Amber Maddox, Hadlee Hollis, Joanne Burch, Dr Kyle King, and Dr Rusty Dunavant (back).
www.tda.org | August 2022 489

490 Texas Dental Journal | Vol 139 | No. 8 • Representation Before the Texas State Board of Dental Examiners • Medicaid Audits and Administrative Hearings • Employment Issues—Texas Workforce Commission Hearings • Administrative (SOAH) Hearings and Counsel • Professional Recovery Network (PRN) Compliance • Employment/Associateship Contract Reviews • Practice Acquisition and Sales • Business Organizations, PAs, PCs, and PLLCs • Civil Litigation 2414 Exposition Blvd., Suite A1 • Austin, Texas 78703 • Phone: 512-477-6200 • Fax: 512-477-1188 • Email: mhanna@markjhanna.com Not Board Certified by the Texas Board of Legal Specialization Mark J. Hanna JD Former General Counsel, Texas Dental Association LAW OFFICES OF MARK J. HANNA EXPERIENCED LEGAL REPRESENTATION FOR TEXAS DENTISTS

4. With the webcast, you can enjoy real time interaction with the course instructor, utilizing a question and answer format
2. There may be a post test after the online course concludes, so you will receive immediate CE credit for attendance
www.tda.org | August 2022 491
ways to register: Call us
8/1/2018implyFAGD/MAGDProviderCredit.ApprovaldoesnotacceptancebyastateofprovincialboardofdentistryorAGDendorsement.to7/31/2022ProviderID#217924
Two at 214 384 0796 mail at sedationce@aol.com on the web: www.sedationce.com
is no need to travel to the program location. You can stay at home or in your office to view and listen to the cou rse. 3. There
Visit us
Anesthesia Education & Safety Foundation
PACE Program

NOW Available: In -Office ACLS & PALS renewals; In -Office Emergency Program Live Programs Available Throughout Texas
You can receive continuing education credit for simultaneous live lecture CE hours.

OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels. Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedat ion permits.
Approved
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796 OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs. Dr. Canfield New TSBDE requirement of Pain Management Two programs available (satisfies rules 104.1 and 111.1) Live Webcast (counts as in-class CE) or Online (at your convenience) All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs: Principles of Pain Management Fulfills rule 104.1 for all practitioners Use and Abuse of Prescription Medications and Provider Prescription Program Fulfills rules 104.1 and 111.1 SEDATION & EMERGENCY PROGRAMS: Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists: Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part) Level 1 Initial Minimal Sedation Permit Courses: *Hybrid program consisting of Live Lecture and online combination Credit: 20 hours lecture with 20 clinical experiences SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2 (ONLINE, LIVE WEBCAST AND IN CLASS) ONLINE LEVEL 3 AND 4 SEDATION RE PERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and 4 Program WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home Here are the distinct advantages of the webcast (contact us at 214 -384-0796 to see which courses are available for webcast):
or e
us
1.
AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation

This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs.
Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
ORAL
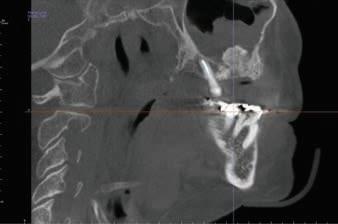
A 58-year-old Caucasian female presented with a 6-month history of right facial pain with occasional sinus drainage. Over the last 2 months, she also developed a right facial swelling. The patient had undergone a sinus lift surgery (sinus augmentation) involving the right maxilla about five years ago with placement of an implant. However, the implant failed and was removed last year. Her dental history also includes osteomyelitis of the left jaw that was treated by surgical debridement and IV antibiotics. Furthermore, the patient’s medical history is significant for two autoimmune disease conditions, Hashimoto’s thyroiditis and ankylosing spondylitis, and she also has severe osteoporosis. She was treated with IV Prolia for her severe osteoporosis, but she discontinued taking the medication 3 years ago. CBCT scan revealed an expansile lesion of the right maxilla with small focal radiopacities, and a space occupying lesion of the right maxillary sinus (Figure 1A, B). Biopsies of the right alveolus and the right sinus were subsequently performed.
Figure 1A. Cone Beam CT scan (coronal section), showing opacification of the right maxillary sinus, and an expansile mixed radiopaque-radiolucent lesion of the right maxilla.

Figure 1B. Cone Beam CT scan (sagittal section).
492 Texas Dental Journal | Vol 139 | No. 8

Ngozi Nwizu BDS, MMSc, PhD, TTS Associate Professor Board Certified Oral and Maxillofacial Pathologist, Department of Diagnostic and Biomedical Sciences, UTHealth at Houston School of Houston,Dentistry,Texas Steve DDSKoo Board Certified Oral & Maxillofacial Surgeon, Piney Point Oral and Maxillofacial Surgery, Chief of Oral and Maxillofacial Surgery, Memorial Hermann at Memorial City, Houston, Texas
and maxillofacial pathology case of the month AUTHORSCase History

www.tda.org 2022 493
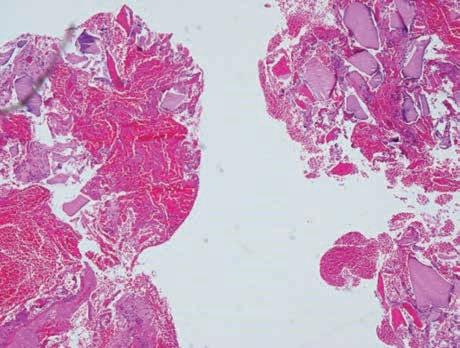
Figure 2. (Original magnification x 20) Biopsy revealing allograft material, interspersed with areas of hemorrhage, fragments of viable and partially viable bone trabeculae, as well as fibrous tissue and tissue debris.
| August
Microscopic examination of the contents from the right alveolus revealed non-specific findings comprising of fragments of allograft material, interspersed with areas of hemorrhage, fragments of viable and partially viable bone, and fibrous tissue with tissue debris (Figure 2).
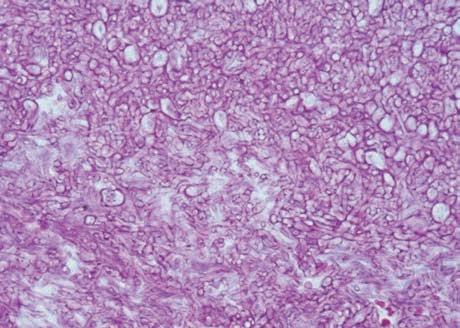
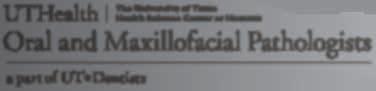
Microscopic examination of the sinus contents showed multiple soft tissue fragments, comprising of chronically inflamed fibrous tissue displaying numerous hyperemic capillaries, areas of surgical hemorrhage, and patchy infiltrates of acute and chronic inflammatory cells, consisting of mostly neutrophils, lymphocytes, plasma cells, and histiocytes. Some of the soft tissue fragments were covered by respiratory type epithelium exhibiting inflammatory cell exocytosis. A prominent feature of the tissue specimen was the presence of multiple densely packed aggregates of microorganisms, composed of septate hyphae that branch at 45 degrees (Figure 3). These microorganisms were observed in all of the biopsy specimens obtained from the sinus. What is the differential diagnosis? What is the final diagnosis? See page 516 for the answer and discussion.
Figure 3. (Original magnification x 200) presence of a tangled mass of densely packed aggregates of fungal organisms, composed of septate hyphae that branch at 45 degrees.
494 Texas Dental Journal | Vol 139 | No. 8

Allison M. Lee, DDS, resident, and John M. Wright, DDS, regents professor, Department of Diagnostic Sciences, Texas A&M College of Dentistry
www.tda.org | August 2022 495
What to Know MONKEYPOXAbout
Clinical symptoms of monkeypox: Febrile prodrome accompanied by generalized headache and fatigue. Fever lasts 8 days on average (range, 2-13 days).
Rash that usually begins about 2 days after symptom onset. The rash will appear in a centrifugal distribution on the body, with most of the lesions concentrated on the head and extremities. The rash presents as macules and papules that later develop into vesicles and pustules. They can
Monkeypox is a zoonotic orthopoxvirus. Other orthopoxviruses include cowpox, camelpox, and variola (smallpox) viruses. While similar in name, monkeypox is not related to chickenpox (Varicella-Zoster virus), but it does have a clinically similar presentation. Monkeypox is also not a sexually transmitted infection but can be spread through close or intimate contact.
Monkeypox was first reported in 1958 in 2 colonies of monkeys kept for research. The first human case of monkeypox was recorded in an infant in 1970 in the Democratic Republic of the Congo. While the virus was first reported in monkeys, the name “monkeypox” is a misnomer as the original source of the disease remains unknown. Rodents as well as humans and non-human primates can harbor the virus and spread infection. Monkeypox can spread to anyone through direct contact with monkeypox rash, scabs, or bodily fluids from a person with an active monkeypox infection. It can also spread through contact with objects or fabrics that have been used by someone infected with monkeypox. Monkeypox can also be spread through respiratory droplets. Research is still ongoing regarding how easily monkeypox is spread via respiratory secretions and at what point of infection a person is most likely to transmit the virus through respiratory droplets. However, it does not appear to be as easily communicable through respiratory droplets as COVID-19. It is also possible to get monkeypox from infected animals, either by being bitten or scratched by an infected animal or by preparing or consuming the meat of an infected animal. A person or animal infected with monkeypox can spread it to others from the time of symptom onset until the rash has completely healed. People with a monkeypox infection or suspected monkeypox infection should self-isolate to prevent the spread of infection.
Cervical or inguinal lymphadenopathy with enlarged (1-4 cm in diameter), firm, and often tender lymph nodes.
5. World Health Organization. (2022, June 27). Multi-country monkeypox outbreak: situation update. Retrieved July 29, 2022, DON396disease-outbreak-news/item/2022-https://www.who.int/emergencies/from
1.References:Bunge, Eveline M., et al. “The changing epidemiology of human monkeypox—A potential threat? A systematic review.” PLoS neglected tropical diseases 16.2 (2022): e0010141.
496 Texas Dental Journal | Vol 139 | No. 8 range from a few in number to hundreds. Lesions are often noted in the oral cavity and cause difficulty with eating and drinking. The rash will usually last about 12 days on average with a range of 7-24 days. The lesions can easily become infected and tend to heal with pitted scarring.
3. Huhn, G.D., Bauer, A.M., Yorita, K., Graham, M.B., Sejvar, J., Likos, A., Damon, I.K., Reynolds, M.G. and Kuehnert, M.J., 2005. Clinical characteristics of human monkeypox, and risk factors for severe disease. Clinical infectious diseases, 41(12), pp.1742-1751.
• While the fatality rate is relatively low for the variant of monkeypox associated with the current outbreak, those that are immunocompromised are at a much higher risk for serious complications and death. Anyone infected with monkeypox or a suspected monkeypox infection should contact their healthcare provider immediately.

2. Centers for Disease Control and Prevention. (2022, July 29). Monkeypox. Retrieved July 29, 2022, from monkeypox/index.html.https://www.cdc.gov/poxvirus/
• While there are currently no treatments available for the monkeypox virus specifically, antiviral drugs and vaccines developed to protect against smallpox may be used as these viruses are genetically similar. Currently, there are 2 vaccines available that may be used for the prevention of monkeypox or shortly following an exposure, however, there is currently not enough data available on the effectiveness of these vaccines regarding the current outbreak.
4. McCollum, A.M. and Damon, I.K., 2014. Human monkeypox. Clinical infectious diseases, 58(2), pp.260267.

www.tda.org | August 2022 497 JKJ Pathology Oral Pathology Laboratory John E Kacher, DDS • Available for consultation by phone or email • Color histology images on all reports • Expedited specimen shipping with tracking numbers • Reports available online through secure web interfaceProfessional, reliable service with hightechnology solutions so that you can better serve your patients. Call or email for free kits or johnkacher@jkjpathology.com281-292-7372281-292-7954jkjpathology.comconsultation.(T)(F) Protecting your patients, limiting your liability Calendar of events Due to COVID-19, please check each meeting’s website for up-to-date information related to cancellations or rescheduling. THE TEXAS DENTAL JOURNAL’S CALENDAR will include only meetings, symposia, etc., of statewide, national, and international interest to Texas dentists. Because of space limitations, individual continuing education courses will not be listed. Readers are directed to the monthly advertisements of courses that appear elsewhere in the Journal. TMOM 2022 SCHEDULE Luling—September 9-10, 2022 Dallas—November 4-5, 2022 TMOM Bonham: April 14-15, 2023 TMOM Abilene: July 14-15, 2023 TMOM McAllen: September 15-16, 2023 or September 22-23, 2023 (TBD by venue) SMILECON Houston—October 13-15, 2022 House of Delegates, October 15-18

OSHA cited the practice for in the
OSHA CITATION DEATH OF DENTAL ASSISTANT PROMPTS INVESTIGATION
By Lee Slaton, Vice President of Healthcare, Smart Training
Although 22 states opted to manage their own OSH programs, all 50 states’ investigations are included in the federal government’s database of OSHA investigations. Over 60% of OSHA investigations are generated by anonymous complaints, according to the latest calculations of inspections reported through the database. Those anonymous complaints can come from a variety of sources—ex or disgruntled employees with an axe to grind, employees with genuine safety concerns, or ex-spouses and ex-partners, to name a few. No matter the seriousness or source of the complaint, OSHA is compelled to open an investigation. This is the story of how an anonymous complaint regarding a serious concern played out.
This article isn’t about the validity of the complaint, nor is it about a tragedy that befell a dental healthcare professional while practicing their profession. In over ten years working with dental practices around the country and representing dental practices in hundreds of OSHA investigations, the worst accident, far and away, that I’ve encountered was a clinician who fell and fractured their arm and had to be hospitalized. The point of the article is to show exactly how much havoc can be wrought on a dental practice by the ensuing investigation an anonymous complaint to OSHA can lead to. When delivering more than I can keep track of continuing education seminars, I always point out that a complaint, valid or not, results in what I refer to as letting the OSHA camel’s nose under the tent flap. In other words, once an OSHA investigation commences, all bets are off. Anything an OSHA investigator sees is fair game. As you continue reading, most of you will hopefully realize the violations
COVID
498 Texas Dental Journal | Vol 139 | No. 8 VALUE forprofessionyour Provided by: ANATOMY OF A $25,000

In mid-2021, a state-run OSH plan received an anonymous complaint regarding a dental practice. The complaint (which has been edited only for clarity) read, in part: “The doctor had Covid. Had girls work next week without patients. The doctor, however, came in 3 times that week with Covid. Three of the staff got Covid. The first one went to the hospital, then stayed home 2 weeks. The second one stayed home for two weeks, then went back to work. The third went to the hospital, was put on a ventilator, developed pneumonia, and died.”
The OSH Fatality/Catastrophe Report stated that the “Employee developed symptoms of Covid-19 after a potential work-related exposure to another Covid-19 positive employee. The employee passed away on xxxxxxxx.”
This article is based on information obtained from multiple Freedom of Information Act requests detailing an OSHA investigation that ensued from an anonymous complaint received by that agency. The references to the investigator’s actual case notes and the practice owner’s replies are denoted in italics and quotes. The actual complaint received by the agency, which is outlined below, has been edited only for clarity and is also denoted in italics and quotes. Any underlining of items for emphasis is mine.
Let’s jump in and review the major violations—starting with the Bloodborne Pathogens standard cited, as this is the standard that most affects dental practices. You’ll see the specific standard in bold and the description of the practice’s violation of that standard immediately below it. To repeat, everything you see in quotes and italics comes directly from the investigator’s notes and the practice owner’s replies.
1910.1030(c)(1)(iv) — The Exposure Control Plan shall be reviewed and updated at least annually and whenever necessary to reflect new or modified tasks and procedures which affect occupational exposure and to reflect new or revised employee positions with occupational exposure.“When practice owner provided the Bloodborne Pathogen Program, the inspector asked if the 09/2017 date located on the program was accurate for the date of most recent review of the document. Practice owner stated that it was put in place by a previous employee and that was the most recent review. A citation is recommended for this violation.”
1910.1030(f)(2)(i) Hepatitis B vaccination shall be made available after the employee has received the training required in paragraph (g)(2) (vii)(I) and within 10 working days of initial assignment to all employees who have occupational exposure unless the employee has previously received the complete hepatitis B vaccination series, antibody testing has revealed that the employee is immune, or the vaccine is contraindicated for medical reasons.
1910.1030(f)(2)(iv) — The employer shall assure that employees who decline to accept hepatitis B vaccination offered by the employer sign the statement in appendix A.
“The inspector inquired to the policy surrounding the facility’s Hepatitis B vaccination. Practice owner stated that practice owner did not believe in asking employees about their medical
MAJOR VIOLATIONS OF THE BLOODBORNE PATHOGENS STANDARD 29 CFR 1910.30 — Bloodborne Pathogen Standard: Multiple Violations 1910.1030(c)(1)(iii) — Each employer shall ensure that a copy of the Exposure Control Plan is accessible to employees in accordance with 29 CFR 1910.20(e) “The inspector requested the facility’s Bloodborne Pathogen Program, practice owner stated that it was locked away and no one had access to this document since practice owner was in XXXXX at the time. Practice owner stated that the employees do not have access to the safety programs while practice owner is not in the office as these documents are locked away in practice owner’s personal office. A citation is recommended for this violation.”
www.tda.org | August 2022 499 following incident weren’t obscure ones cited by an investigator playing gotcha; they were what a football coach would refer to as basic blocking and tackling, to use a sport analogy. Let’s look at the inspector’s narrative and proceed through the bulk of the major (serious) violations. Due to space constraints, I won’t address every violation, but I will attempt to give you a 10,000-ft view. Any way you slice it, the practice ended up with $25,000 worth of violations and a heightened regulatory awareness regarding their practice that will probably follow them for years to come. The purpose and scope of the investigation was set thusly: “This unprogrammed inspection was the result of a non-employer reported SARCoV-2 related employee hospitalization was forwarded to the XXXXXXXXXXXXX of OSH Compliance on XXXXXX by the XXXXXXXX Board of Dentistry. This report included an anonymous complaint on the XXXXXXX complaint form stating the XXXXXX associated hospitalization of XXXXXXXXXXXX was work-related. This was processed as a complaint and assigned to XXXXXX on XXXXXX. This inspection was limited in scope to an investigation of the conditions and circumstances related to the xxxxxxxxx SARS-CoV-2 related hospitalization and consequent XXXXXXXX death of XXXXXXXX, Any additional serious safety and health violation in view of the inspector during the investigation will also be addressed during the course of the inspection.” The inspector was on site at the dental practice on 2 occasions. During the initial walkthrough, “upon the discovery of a violation involving 29 CFR 1910.1030 (the Bloodborne Pathogens standard) the inspection was expanded to cover the entirety of that standard.” And there goes that proverbial camel’s nose under the tent flap.
VIOLATED 29 CFR 1910.30 — Hazard Communication Standard 1910.1200(g)(8) — The employer shall maintain in the workplace copies of the required safety data sheets for each hazardous chemical, and shall ensure that they are readily accessible during each work shift to employees when they are in their work area(s).
“During employee interviews, inspector learned that the employees were not familiar with the hazards associated with the chemicals they use every day. Employees also stated that they did not receive any formal training on the chemicals used when they first were hired by practice owner. It is important to note that practice owner also never evaluated the employees’ knowledge of these chemicals.”
1910.1030(d)(2)(i) — Engineering and work practice controls shall be used to eliminate or minimize employee exposure. Where occupational exposure remains after institution of these controls, personal protective equipment shall also be used.“The employer did not use work practice controls such as employees touching surfaces with contaminated gloves and then touching that same surface with the ungloved hands without cleaning. Inspector observed both practice owner and another employee touching a computer keyboard with contaminated gloved hands and then touching the same keyboard with ungloved bare hands. The computer keyboards are used for every patient both prior to their procedures as well as following the procedures. Inspector observed practice owner exhibiting the same work practice controls as the employees. This was performed over multiple visits the same way.” 1910.1030(d)(2)(v) — Employers shall ensure that employees wash their hands immediately or as soon as feasible after removal of gloves or other personal protective“Inspectorequipment.observed employees removing gloves and not washing their hands prior to completing other tasks. Employees would work on a patient with gloves and touch the keyboard and other surfaces in and around the procedure area and touch these same surfaces with ungloved unwashed hands. Neither practice owner or the employees washed their hands after removing gloves prior to touching the computer keyboard, the work surfaces in the lab, bench counters, procedure tray, tools, doorknobs, and paper documents.” 1910.1030(d)(2)(ix) Eating, drinking, smoking, applying cosmetics or lip balm, and handling contact lenses are prohibited in work areas where there is a reasonable likelihood of occupational exposure.“Employees were observed drinking beverages in the work area where aerosol generating procedures are performed. During both onsite visits, inspector observed different employees drinking in the procedure area. Inspector observed employee drinking a beverage in the operatory while in the presence of practice owner during a visit. Inspector learned through interviews that employees often keep beverages on the counter while they’re working. Both of these conditions were in plain sight and appeared to be a common work practice at this facility.”
Practiced owner elaborated in a later conversation with inspector that practice owner did not inquire about any type of vaccination status including the Hepatitis B vaccination because “it wasn’t any of practice owner’s business.”
500 Texas Dental Journal | Vol 139 | No. 8 histories. The inspector explained that the standard requires the employer to provide the vaccination and if an employee declines the series, then a declination form must be signed for documentation purposes.
ADDITIONAL STANDARDS
“On or about xxxxxx the employer had locked the SDSs in employer’s office while employer was out of the office and the employees could not access them online.
1910.1200 (h)(1) — “Employers shall provide employees with effective information and training on hazardous chemicals in their work area at the time of their initial assignment, and whenever a new chemical hazard the employees have not previously been trained about is introduced into their work area…
CLOSING THOUGHTS
“On or about xxxxx the employer did not have an emergency eyewash for five (5) employees exposed to phosphoric acid while working in the operatory/ procedure area. During a xxxxx conversation with the Practice Owner, xxxx stated that their facility did not have an eyewash station or alternate means of flushing the eyes as prescribed by ANSI, which is incorporated by reference. As the employer does not have an emergency eyewash station, a violation has occurred.”
713.486.4411 go.uth.edu/Pathology • Complimentary biopsy kits • Delivery via FedEx, local courier or USPS • Diagnosis within two business days of receiving most biopsy specimens. • UT M.D. Anderson Cancer Center and UTHealth Medical School available for consultations as needed. • Affiliated with UT School of Dentistry at Houston. Our Pathologists: Specializing in: • Conventional biopsy testing • Cytopathology • Histochemistry • Immunohistochemistry • Direct immunofluorescence testing Jerry E. Bouquot, DDS, MSD Ngozi N. Nwizu, BDS, MMSc, PhD Kalu U.E. Ogbureke, BDS, DMSc, JD, MSc Nadarajah Vigneswaran, DMD, DrMedDent
This investigation and the ensuing violations should serve as a cautionary tale for some and a wake-up call for others. The time to address deficiencies in your safety programs—like the ones detailed above—is not after an accident occurred; or a complaint, no matter how frivolous it seems, is lodged.
www.tda.org | August 2022 501 29 CFR 1910.151 — Medical Services and First Aid 1910.151(c) — Where the eyes or body of any person may be exposed to injurious corrosive materials, suitable facilities for quick drenching or flushing of the eyes and body shall be provided within the work area for immediate emergency use.
Sadly, in many, many practices Smart Training inspects the first time, we see the same violations listed above.
Yet, anyone of reasonable intelligence can pull together a good compliance program for their office, given the time. Some choose to focus on ensuring great outcomes for their patients and leave the heavy lifting of regulatory compliance to professionals. Either way, don’t put off what the law requires and good business sense dictates. Let’s stay safe out there! With a little help from an expert, it’s not a heavy lift to make your practice a compliant and safer place for your employees and patients. Compliance advisors at TDA Perks Program-endorsed Smart Training have conducted over 1,500 inspections of dental practices all over the country. For more information on Smart Training, visit tdaperks.com (Compliance & Supplies) or call Smart Training at 469342-8300.
ShankargoudaArtakJoãoShilpaFuadAmitSaeedMansoorAbdulrahmanMohammedMubarakiM.AlMoaleemH.AlzahraniShariffM.AlqahtaniPorwalA.Al-SanabaniBhandiPauloMendesTribstHeboyanPatil
Reprinted from Materials 2022, 15(11), 3868; https:// doi.org/10.3390/ma15113868. Published: 28 May 2022. Copyright: © 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/4.0/). Modification includes photo on pages 502 and 503.

Manal Q.
Assessment
502 Texas Dental Journal | Vol 139 | No. 8
Dentures:CompleteFabricatedandConventionallyofDigitally
A ReviewComprehensive
Keywords computer-engineered complete denture; digital complete denture; polymers; CAD/CAM complete denture; denture base material
www.tda.org | August 2022 503
Abstract CAD/CAM technology is gaining popularity and replacing archaic conventional procedures for fabricating dentures. CAD/CAM supports using a digital workflow to reduce the number of visits, chair time, and laboratory time, making it attractive to patients. This study aimed to provide a comparative review of complete dentures manufactured using CAD/CAM and conventional methods. The PubMed/Medline, Science Direct, Cochrane, and Google Scholar databases were searched for studies published in English within the last 11 years (from 2011 to 2021). The keywords used were “computer-engineered complete dentures”, “CAD/CAM complete dentures”, “computer-aided engineering complete dentures”, and “digital complete dentures”. The search yielded 102 articles. Eighteen relevant articles were included in this review. Overall, computer-engineered complete dentures have several advantages over conventional dentures. Patients reported greater satisfaction with computer-engineered complete dentures (CECDs) due to better fit, reduced chair time, shorter appointments, and fewer post-insertion visits. CAD/CAM allows for precision and reproducibility with fewer procedures compared to conventional dentures. Polymethyl methacrylate is used as the denture base material for conventional dentures. For CECDs, the resin can be modified and cross-linked to improve its mechanical properties. The advantages of CECDs include a reduced number of appointments, saving chairside time, a digital workflow allowing easy reproducibility and greater patient satisfaction with a better fit.

504 Texas Dental Journal | Vol 139 | No. 8
Complete dentures are removable dental prostheses that rehabilitate the whole dentition as well as the related structures of the maxilla and/or mandible.1 According to the Glossary of Digital Dental Terms, a digital denture is a complete prosthesis that is formed by or through automation using CAD/CAM (computer-aided design and computer-aided manufacturing) and computer-aided engineering (CAE).2 CAE refers to the field of engineering where data are gathered and investigated before being applied to design procedures, including in the manufacturing methods for biomedical prostheses.3,4 Conventional complete dentures (CDs) are the most commonly used prosthetic modality to rehabilitate edentulous patients. They have drawbacks such as requiring multiple visits and high laboratory expenses. The denture base of CDs may not have an intimate fit with the underlying tissues due to polymerization shrinkage of the acrylic resin. Creating a duplicate complete denture is a cumbersome process.5-7
The Authors Manal Q. Mubaraki, Saudi Board Prosthodontic PGY3, College of Dentistry, King Khalid University, Abha 62529, Saudi MohammedArabia M. Al Moaleem*, Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan 45142, Saudi Arabia; Faculty of Dentistry, University of Ibn al-Nafis for Medical Sciences, Sana’a 4337, AbdulrahmanYemen H. Alzahrani, Faculty of Dentistry, Taif University, Taif 21944, Saudi Arabia Mansoor Shariff, Prosthetic Department, College of Dentistry, King Khalid University, Abha 62529, Saudi SaeedArabia M. Alqahtani, Prosthetic Department, College of Dentistry, King Khalid University, Abha 62529, Saudi AmitArabiaPorwal, Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan 45142, Saudi Arabia Fuad A. Al-Sanabani, Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan 45142, Saudi Arabia Shilpa Bhandi, Department of Restorative Dental Sciences, Division of Operative Dentistry, College of Dentistry, Jazan University, Jazan 45142, Saudi Arabia João Paulo Mendes Tribst, Department of Dental Materials, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije Universiteit Amsterdam, 1081 LA Amsterdam, The Netherlands Artak Heboyan, Department of Prosthodontics, Faculty of Stomatology, Yerevan State Medical University after Mkhitar Heratsi, Str. Koryun 2, Yerevan 0025, Armenia Shankargouda Patil,* Department of Maxillofacial Surgery & Diagnostic Sciences, Division of Oral Pathology, College of Dentistry, Jazan University, Jazan 45142, Saudi Arabia
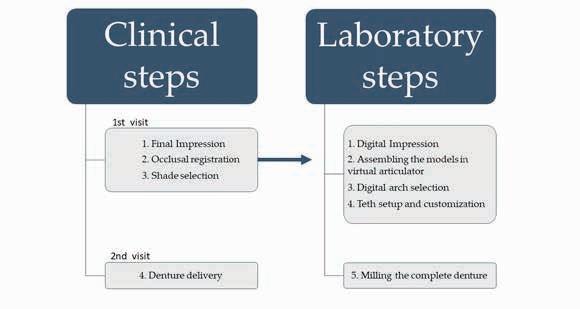
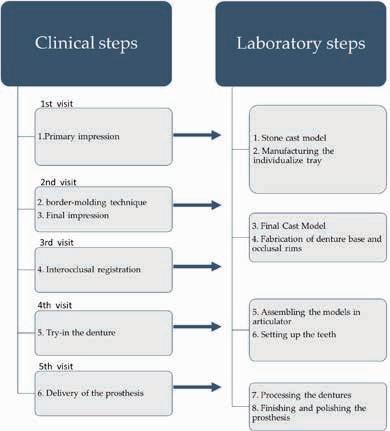
Dentists and prosthodontists are believed to be familiar with the workflow of the clinical and laboratory steps required for conventional denture fabrication. For the purposes of this article, Table 1 presents the details of case reports on the use of CECDs (computer-engineered complete dentures) technology that have been published in different countries.10,12,14-25 The table includes the names of the authors, the year of the case report’s publication, the country in which the case study was carried out, the number of visits, the patients’ gender, the age of the patient, the type of edentulous arches, the technique used, conclusions, and positive points. Figure 1 shows the workflow of manufacturing CECDs.
1. Introduction
* Correspondence: malmoaleem@jazanu.edu.sa or drlmoaleem2014@gmail.com or drmoaleem2014@ gmail.com (M.M.A.M.); dr.ravipatil@gmail.com (S.P.)
Traditional conventional complete dentures remain a valuable solution. However, newer treatments such as “all on four” rehabilitation are gaining popularity.8
The implementation of CAD/CAM systems in dentistry four decades ago ushered in a new age for the successful fabrication of full-coverage crowns, fixed dental prostheses, and superstructures for natural teeth as well as dental implants.5,9,10 Complete dentures manufactured using CAD/CAM represents a new era in removable prosthodontics. Numerous commercial CAD/CAM systems are available for the design and manufacture of CDs.5,6,11 They allow customization of tooth setup, verification of preceding steps before the trial appointment, and the ability to design a product that is clinically predictable.7,12,13 CAD/CAM systems allow for improvements in both the mechanical and surface properties.14
Kattadiyil et al. produced CAD software that processed an automatic tooth setup, ferentcountries[10,12,14 25].Thetableincludesthenamesoftheauthors,theyearof thecasereport’spublication,thecountryinwhichthecasestudywascarriedout,the numberofvisits,thepatients’gender,theageofthepatient,thetypeofedentulousarches, thetechniqueused,conclusions,andpositivepoints.Figure 1 showstheworkflowof manufacturingCECDs. different countries [10,12,14–25]. The table includes the names of the authors, the year of the case report’s publication, the country in which the case study was carried out, the number of visits, the patients’ gender, the age of the patient, the type of edentulous arches, the technique used, conclusions, and positive points. Figure 1 shows the workflow of manufacturing CECDs.
Figure 1. Workflow of CECDs. This study aimed to provide a comparative analysis of complete dentures fabricated by both digital and conventional methods. We outline the techniques and materials used Figure1. WorkflowofCECDs.
2.3. Manufacturing of ComputerEngineered Complete Dentures
This study aimed to provide a comparative analysis of complete dentures fabricated by both digital and conventional methods. We outline the techniques and materials used for the fabrication of digital and conventional complete dentures and highlight their advantages and disadvantages.
The PubMed/Medline, Science Direct, Cochrane, and Google Scholar databases were searched for literature published in English within the last 11 years (from 2011 to 2021). The keywords used were “computer engineered complete denture”, “CAD/CAM complete dentures” “computer-aided engineering complete dentures”, and “digital complete dentures”. The inclusion criteria were studies carried out in clinics, case reports or series, and reviews. The search strategy included revising the titles and abstracts to select articles that met the inclusion criteria and exclude those that did not. Only papers published in the English language were reviewed (A. P. and M. Al M) by reading the title and abstract. The contents of each paper were then summarized. A researcher evaluated the validity of the studies and identified duplications. Two investigators (Al M.M and M.Y) read all of the titles and abstracts individually and carefully evaluated them. The researchers had to agree as to whether each study was relevant. Finally, 18 full-text articles were selected and analyzed. Interventional studies involving animals or humans and other studies requiring ethical approval had to contain the approval information and the corresponding ethical approval code. Didactically, the present review was divided into subtopics presented below.
Thisstudyaimedtoprovideacomparativeanalysisofcompletedenturesfabricated bybothdigitalandconventionalmethods.Weoutlinethetechniquesandmaterialsused forthefabricationofdigitalandconventionalcompletedenturesandhighlighttheiradvantagesanddisadvantages.
2.1. Data Collection
Computer-engineered complete dentures (CECDs) can be manufactured in two ways: The first method is additive manufacturing; 3D objects are manufactured through the successive deposition of material in layers to achieve a model.15,30 The second method is subtractive manufacturing; 3D objects are manufactured using the successive milling of extra material from a solid volume of material according to the digital model.31,32 In prosthodontics, subtractive manufacturing is commonly associated with CAD/CAM technology and has been extensively used to fabricate partial or complete veneers or/and crowns, both of which are types of removable dentures; implant abutments; and prostheses replacing maxillofacial structures.30-35 Figure 1 shows the workflow of manufacturing CAD/CAMCECDs. manufacturing of computerengineered complete dentures is associated with several advantages, such as fewer clinical visits with reduced chair time. The denture itself has superior strength and uniform
Figure 1. Workflow of CECDs. semiautomatic aesthetic scheming, individualized gingival contouring, and base plate establishment.29 Kanazawa et al. used cone-beam CT scanning combined with either a rapid prototyping method or a milling method to fabricate computer-engineered complete dentures (CECDs).24 In 2012, Goodacre et al. recommended the use of recorded intaglio and the cameo surfaces of CD denture bases with the areas where teeth were located.9 The first denture base was milled from polymethyl methacrylate (PMMA) to which denture teeth were bonded by hand and placed in the patient’s mouth.
www.tda.org | 2022 505
2.2. History of CAD/CAM
2. Literature Review
August
The first digitally made removable complete denture was generated using 3D printing technology by Maeda et al.26 In 1997, Kawahata et al. used a wax block with computerized arithmetic regulator milling technology.27 Later on, Busch et al. described a digital tooth arrangement based on anatomic dimensions and averages.28
TheBalticDentureSystem,andVITAVIONICmaterialtypes,ontheotherhand,have anopenframeworkthatallowsuserstoselectfromavarietyofhandlingprocedures.Itcanbe usedwithavarietyofopen-endeddigitalscanners,CADapplications,andmillingequipment.
506 Texas Dental Journal | Vol 139 | No. 8 thickness and proper fitting. The digital nature of the system means that they are easily reproducible with less time-consuming tooth setups, easy data backup, and the ease of construction of duplicate prostheses.33
Thedentist sprosthodonticskill,thenumberofdenturesrequired,anddentureindividualizationrequirementsmayallinfluencetheprocedurethatischosen.Techniques andtechnologiesareconstantlyevolvingtoovercomeorminimizepatientdispleasure withaesthetics,bulkiness,andretention.Inallprocedures,post-insertionmodifications aremade.OlddenturescanbeusedformanufacturingnewCECDs.Mostsystemsaccept externaldenturestaining.Esthetic,retention,toothsize,verticaldimensions,horizontal relationship,andthepatientprofileareallimprovedwithvirtualdenturetry-inandare highlyrecommended.Mosttechniquesusewhiteacrylicresin.Theinterpretationofthe digitalpreviewischallenging.Allprocedureskeepadigitalrecord.Thisisbeneficial forseniorswithreducedaccesstooralcare.Castfabricationandpolymerizationproceduresareeliminated,asistheuseofmonomersaswellastheconsequencesofusingthis material[36].
Figure 2. Workflow of conventional CDs.
Figure 2. Workflow of conventional CDs.
2.4.FabricationofConventionalCompleteDentures Fabricationconsistsofclinicalsessionsalongwiththerequiredlaboratorysessions andlaterpost-operativeadjustmentvisits.Figure 2 showsthesequenceoftheclinicaland laboratorysteps. Materials 2022, 15, x FOR PEER REVIEW 5
3. Results
The dentist′s prosthodontic skill, the number of dentures required, and denture individualization requirements may all influence the procedure that is chosen. Techniques and technologies are constantly evolving to overcome or minimize patient displeasure with aesthetics, bulkiness, and retention. In all procedures, post-insertion modifications are made. Old dentures can be used for manufacturing new CECDs. Most systems accept external denture staining. Esthetic, retention, tooth size, vertical dimensions, horizontal relationship, and the patient profile are all improved with virtual denture try-in and are highly recommended. Most techniques use white acrylic resin. The interpretation of the digital preview is challenging. All procedures keep a digital record. This is beneficial for seniors with reduced access to oral care. Cast fabrication and polymerization procedures are eliminated, as is the use of monomers as well as the consequences of using this material.36 2.4. Fabrication of Conventional Complete Dentures Fabrication consists of clinical sessions along with the required laboratory sessions and later post-operative adjustment visits. Figure 2 shows the sequence of the clinical and laboratory steps. canalsobeselected[34].
3.1. Study Selection and Collections A total of 102 articles were obtained from the databases using the literature search strategy. A total of eighteen articles were included in this review. Table 1 summarizes salient details of the studies [10,12,14–25].
However, CECDs have some drawbacks. It is difficult to assess proper occlusal vertical dimensions (OVDs), the incisal edge position of the maxillary anterior teeth, and appropriate lip support. CAD/CAM dentures are more expensive and require dimensionally stable and temperature-resistant scanning.11,31,33 Regardless of the prosthesis design and manufacturing method, patient selection is a critical point to be considered when creating a treatment plan. The candidate or subject should be well informed. An adequate bulk of alveolar bone and an even maxilla–mandibular occlusal relationship (avoiding Angle class 2) allow for better prognostic cases. Edentulous patients with non-aesthetic demands and who do not have TM joint problems can also be Currently,selected.34six systems are available for the fabrication of CAE-CDs: the 3Shape Dental System, AvaDent Digital Dentures, Dentca Digital Denture, Wieland Digital Denture, and the Ceramill Full Denture System, the Baltic Denture System, and the VITA VIONIC Digital System.5-7, 31-36 The majority of the systems use subtractive manufacturing to make their dentures and only use closed systems. The Baltic Denture System, and VITA VIONIC material types, on the other hand, have an open framework that allows users to select from a variety of handling procedures. It can be used with a variety of open-ended digital scanners, CAD applications, and milling equipment.
Currently,sixsystemsareavailableforthefabricationofCAE-CDs:the3ShapeDental System,AvaDentDigitalDentures,DentcaDigitalDenture,WielandDigitalDenture,and theCeramillFullDentureSystem,theBalticDentureSystem,andtheVITAVIONICDigital System[5 7,31 36].Themajorityofthesystemsusesubtractivemanufacturingtomake theirdenturesandonlyuseclosedsystems.
Figure2. WorkflowofconventionalCDs.
AlHelaletal.,2017/ Casereport[39] SaudiArabia/ 2Visits Male/20-MaxillaryCD* VDFP*/CAD-CAM* MonolithicDenture CECDsminimizedthenumberof appointments,enhancedfitting,and retention,andallowedautomated archiving.
Atotalof102articleswereobtainedfromthedatabasesusingtheliteraturesearch strategy.Atotalofeighteenarticleswereincludedinthisreview.Table 1 summarizesthe salientdetailsofthestudies[10,12,14 25].
Table1. SummaryofarticleswhereCAD/CAMtechnologieswereusedinthefabricationofCECDs indifferentcountries. Author(s)/Year/ StudyType Country/Numberof Visits Subjects Technique Findings
BajunaidSO/2016/Case report[10] SaudiArabia/ 2Visits Female/67years/Maxillary CD*andMandibular CompleteOverdenture VDFP*/CAD-CAM* Excellentdenturebasecontact,which reducedthenumberofrequireddental appointments. Unsatisfactoryaestheticoutcomescan becorrectedwithmoreexperience. Authorsrecommendedtheuseofthis techniqueindentalschoolforalllevels ofstudy.
Janevaetal.,2017/Case report[17] Macedonia/ 3Visits Male/63years/Maxillaryand MandibularCD* VDFP*/AnatomicMeasuring Device(AMD*) AvaDent/CAD-CAM* CombinedadvantagesofCAD/CAM* andtraditionalclinicalrecording methods.CAD/CAM*technology eliminatedmanylaboratorystepsand simplifiedtheprocess.
Yilmazetal.,2017/ CastModelstudy[12] Turkey/ 2Visits EdentulousJawModelsof MaxillaandMandible VDFP*/CAD-CAM* CECDsdonotoptimallyassess maxillomandibularrelationships, maxillaryincisaledgeplacement,and lipsupport. Creatingamandibularocclusalplane wasnotpossibleandresultedin highercosts.
3.1. Study Selection and Collections
Table 1. Summary of articles where CAD/CAM technologies were used in the fabrication of CECDs in different countries.
3.1.StudySelectionandCollections
www.tda.org | August 2022 507
3.Results
Maietal.,2020/CastModel study[13] RepublicofKorea/ 2Visits EdentulousJawModelsof MaxillaandMandible VDFP*/CAD-CAM* Baseanddentalpartsofnewdentures weredesignedefficientlyand predictably. Digitalprotocolfacilitatesthedesign process,borderseal,andtooth arrangement.
Contrepoisetal.,2018/Case report[16] France/ 2Visits Female/78years/Maxillary andMandibularCD* VDFP*/CAD-CAM* Designingtheshapeoftheteethfor eachpatientresultsinbetterdenture customizationaswellasthe appropriateleveloftoothstainingand anappropriatedenturebase.Full CECDfabricationensuredagood aestheticresult.
A total of 102 articles were obtained from the databases using the literature search strategy. A total of eighteen articles were included in this review. Table 1 summarizes the salient details of the studies.10,12,14-25 Materials 2022, 15,3868 5of13
Goodacreetal.,2018/Case report[38] USA/ 2Visits Male/78years/MaxillaryCD *andMandibular OverdenturebyDental Implants VDFP*/AnatomicMeasuring Device(AMD*) AvaDent/CAD-CAM* Intraoralscanningcapturedtrue mucostaticimpression,achievinggood retentionandstabilityoftheCECD prostheses.Digitallyrecordingtooth locationandbasemorphologyofthe presentdenturesreducedthenumber ofclinicalstepsandeliminatedthe needtotransportconventional impressionstothelaboratory.
3. Results
Ohkuboetal.,2017/Case report[18] Japan/ 2Visits Female/82years/Maxillary andMandibularCD* VDFP*/DENTCA PiezographyTechnique CAD-CAM* Conceptofneutralzoneanddenture spacewereverified,anddentureteeth andflangeformswereappropriately designed.
Srinivasan,2019/Casereport [37] Switzerland/ 3Visits Male/65years/Maxillaryand MandibularCD* VDFP*/AnatomicMeasuring Device(AMD*) AvaDent/CAD-CAM* Productionofclinicallyacceptable CECDsreducedthenumberofclinical visitswithouttheuseofcomplex equipment. Male/71years/Maxillaryand MandibularResinRPD Leeetal.,2019/ Casereport[15] Korea/ 2Visits Male/53years/Maxillaryand MandibularCD* VDFP*/CAD-CAM*
Additionofconventionalimpression andmaxillomandibularrelationship withlaboratorystepsusingCAD-CAM *technology.Minimizedthe clinicaltime.
Jodaetal.,2016/Casereport [25] Switzerland/ 4Visits Male/75years/Maxillaryand MandibularCD* Patientwithdentalimplants VDFP*/DigitalDenture Provisional(DDP) CAD-CAM* Virtuallydesignedandmonolithic milledstructure. Patientbenefitsfromtimeandcost savings. Digitalizationtechniqueisidealfor planningandprovisionalsteps.
Kattadiyiletal., 2013/Case report[40] USA/ 2Visits Female/56years/Maxillary andMandibularCD* VDFP*/AnatomicMeasuring Device(AMD*) AvaDent/CAD-CAM*
Dental3DCBCT*usedtoprocessthe 3DSTLmorphologicalfileforthe artificialteeth. CD*manufacturingusingCAD/CAM *causedlargedeviationsbetween manufacturedteethandsocketsonthe prosthesesbase.
Kimetal.,2016/Casereport [20] RepublicKorea/ 3Visits Male/75years/Maxillaryand MandibularCD* VDFP*/Dentca;CAD/CAM* Denturesweredeliveredduring2nd visitwithareductioninthenumberof clinicalandlaboratorysteps. ClinicallyacceptableCECDswith smoothsurfaces. Female/61years/Maxillary andMandibularCD*
Infanteetal.,2014/Case report[23] USA/ 2Visits Male/62years/Maxillaryand MandibularCD* VDFP*/AnatomicMeasuring Device(AMD*) AvaDent/CAD-CAM* UsedAMD*clinicalrecordsduringa one-stepappointment. AMD*deviceallowedthecollectionof allofthenecessaryclinicalinformation Virtualdenturewasmilledwithoutthe useofstonemodelsandprocessing.
CECDseliminateacrylicbase shrinkageanddecreasedporosity comparedtoconventionally processeddentures. CECDsdecreasedtheretentionof Candidaalbicans. Posteriorly,teethmodifiedandmerged intomilledsocketswithamilledbase.
AmajorityofthestudieswerepublishedinFirstWorldcountriesofEuropeandNorth America.AsiaisrepresentedbyKoreaandJapan.SaudiArabia,Turkey,andMacedonia representthepublishingonCECDsfromtheMiddleEastandNorthAfricaregion.
Mostofthestudieswerepublishedafter2015(15studies:83%).Twelvewerecase reportsthatwerepublishedaftera1-yearfollow-up,onestudywasacaseseries[20], andonewasaclinicalstudy[22]involving20maxillaryandmandibulararcheswith implant-retainedprosthesesanda12-monthfollow-up,andfourstudieswerecastor modelevaluations.Thefollowingwereincludedinthepresentedstudies:17maxillary CDs;13mandibularCDs,4oncastmodel;10maxillarieswithanimplant;11mandibular overdentureswithimplants;and3mandibularoverdentures.Outofthetotalnumber,
Finalimpressionsforbotharches, bordermolding,jawrelationship,and tootharrangementsweremadeinthe firstappointment. Lessclinicaltimewasrequired. Polymerizationshrinkagewas eliminated. USA/ 2Visits Male/54year/Maxillaryand MandibularCD* VDFP*/DentcaCAD/CAM*
3.2.StudyCharacteristicsandQualityoftheReports
Most of the studies were published after 2015 (15 studies: 83%). Twelve were case reports that were published after a 1-year follow-up, one study was a case series, and one was a clinical study involving 20 maxillary and mandibular arches with implantretained prostheses and a 12-month follow-up, and four studies were cast or model evaluations.20,22 The following were included in the presented studies: 17 maxillary CDs; 13 mandibular CDs, 4 on cast model; 10 maxillaries with an implant; 11 mandibular overdentures with implants; and 3 mandibular overdentures. Out of the total number, 17 (almost 95%) were VDFP-fabricated using CAD/CAM and the One set aligned Artificial tooth System CAD/CAM and Rapid Prototyping (RP). The maximum
3.2. Study Characteristics and Quality of the Reports
*Abbreviations:virtualdesignandfabricationprocess—VDFP;computer-aideddesign/computer-aided manufacturing—CAD/CAM;computer-aidedengineering—CAE;anatomicmeasuringdevice—AMD;complete denture—CD;removablepartialdenture—RPDcentricrelation—CR;conebeam-computedtomography—CBCT.
Table 1. continued
Bilginetal.,2015/CastModel study[21] Turkey/ 3Visits EdentulousJawModelsof MaxillaandMandible One-setalignedArtificial toothSystemCAD-CAM* andRapidPrototyping(RP) CAD/CAM*andRPreducechairtime. Achievedself-designedaesthetics, occlusion,andincreaseddurability. GoodforsingleCD*opposednatural dentitionfabricatedusingRPor CAD/CAM*.
* Abbreviations: virtual design and fabrication process—VDFP; computer-aided design/computer-aided manufacturing—CAD/CAM; computer-aided engineering—CAE; anatomic measuring device—AMD; complete denture—CD; removable partial denture—RPD centric relation—CR; cone beam-computed tomography—CBCT.
508 Texas Dental Journal | Vol 139 | No. 8
Bidraetal.,2016/Clinical Study[22] Canada/ 2Visits 10MaxillaryCD*or Implant-Retained Overdentures VDFP*/CAD-CAM* MonolithicDenture
Alldenturesinagoodstateaftera 12-monthsfollow-up. Retentionlossandexcessivetooth wearwereobservedinfivecases. Higherpatientsatisfaction(79%) regardingtheirCECDs. Canada/ 2Visits 10MandibularCompleteor Implant-Retained Overdentures
Kanazawaetal.,2011/Cast Modelstudy[24] Japan/ 2Visits EdentulousJawModelsof MaxillaandMandible VDFP*/CAD-CAM* MonolithicDenture
A majority of the studies were published in First World countries of Europe and North America. Asia is represented by Korea and Japan. Saudi Arabia, Turkey, and Macedonia represent the publishing on CECDs from the Middle East and North Africa region. Materials 2022, 15,3868 6of13 Table1. Cont. Author(s)/Year/ StudyType Country/Numberof Visits Subjects Technique Findings deMendonçaetal., 2016/Casereport[19] Brazil/ 3Visits Female/63years/Maxillary CD*andMandibular CompleteOverdenture VDFP*/Prototypethen3D CAD-CAM*
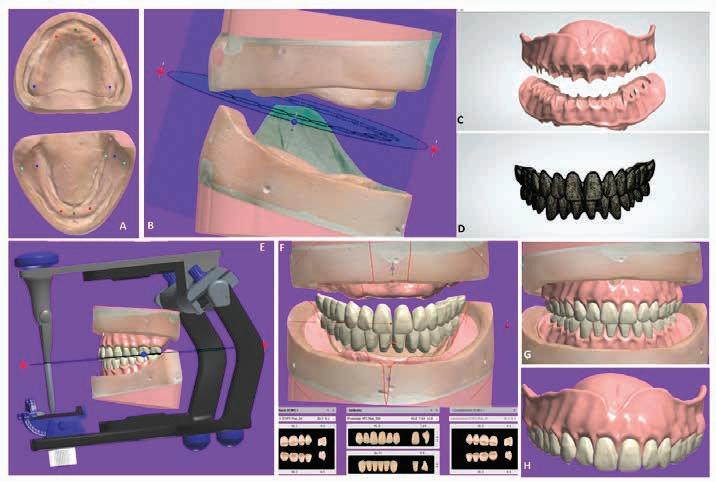
Figure3. CECDsduringdigitalprocessing(A H).(A)Virtualmodels.(B)Interocclusalrelationship. (C)Denturebaseplanning.(D)Toothsetupdesign.(E)Victualarticulator.(F)Aestheticparameters andminorcorrections.(G)Finalmodel.(H)Milledprosthesisafterfabrication.
3.3. Synthesis of Results
retained prostheses and a 12-month follow-up, and four studies were cast or model evaluations. The following were included in the presented studies: 17 maxillary CDs; 13 mandibular CDs, 4 on cast model; 10 maxillaries with an implant; 11 mandibular overdentures with implants; and 3 mandibular overdentures. Out of the total number, 17 (almost 95%) were VDFP-fabricated using CAD/CAM and the One set aligned Artificial tooth System CAD/CAM and Rapid Prototyping (RP). The maximum number of VDFP CAD/CAM obtained by VDFP with AMD AvaDent/CAD-CAM was eight (44%); two were obtained in the form of a Monolithic Denture and using the DENTCA Piezography Technique and the Digital Denture Provisional technique. The majority of the patients were above 50 years old.
Figure 3 summarizes CECD planning and manufacturing according to the workflow presented in the literature. The mounting of the final maxillary and mandibular cast with the occlusal rims can be performed digitally by software that has been connected to CAM. Then, the tooth arrangements are completed with denture teeth (SR Vivodent DCL, Ivoclar Vivadent GmbH) bonded in the milled recesses followed by a clinical try-in for the maxillary and mandibular arch. Finally, computer-engineered complete denture insertion is performed (Figure 3A–H).
During the trial periods for both sets of dentures, the phonetics, aesthetics, and vertical dimensions should be checked. At the time of insertion, the following factors need to be evaluated: retention, stability, occlusion, teeth arrangement, aesthetics, and patient satisfaction.
Duringthetrialperiodsforbothsetsofdentures,thephonetics,aesthetics,andvertical dimensionsshouldbechecked.Atthetimeofinsertion,thefollowingfactorsneedto beevaluated:retention,stability,occlusion,teetharrangement,aesthetics,andpatient satisfaction. 3.3.SynthesisofResults
Materials 2022, 15,3868 7of13 17(almost95%)wereVDFP-fabricatedusingCAD/CAMandtheOnesetalignedArtificial toothSystemCAD/CAMandRapidPrototyping(RP).ThemaximumnumberofVDFP CAD/CAMobtainedbyVDFPwithAMDAvaDent/CAD-CAMwaseight(44%);two wereobtainedintheformofaMonolithicDentureandusingtheDENTCAPiezography TechniqueandtheDigitalDentureProvisionaltechnique.Themajorityofthepatientswere above50yearsold. Figure 3 summarizesCECDplanningandmanufacturingaccordingtotheworkflow presentedintheliterature.Themountingofthefinalmaxillaryandmandibularcast withtheocclusalrimscanbeperformeddigitallybysoftwarethathasbeenconnectedto CAM.Then,thetootharrangementsarecompletedwithdentureteeth(SRVivodentDCL, IvoclarVivadentGmbH)bondedinthemilledrecessesfollowedbyaclinicaltry-inforthe maxillaryandmandibulararch.Finally,computer-engineeredcompletedentureinsertion isperformed(Figure 3A–H).
Fewstudiessufferedfromalackofdetailintheirreportingi.e.,theydidnotmention genderorreportanycomplications.Detailsregardingthetry-inwerenotreported.Authors reportedproblemsrelatedtoaesthetics,thesizesofthearrangedteeth,thepositionofthe Figure 3 summarizes CECD planning and manufacturing according to the workflow presented in the literature. The mounting of the final maxillary and mandibular cast with the occlusal rims can be performed digitally by software that has been connected to CAM. Then, the tooth arrangements are completed with denture teeth (SR Vivodent DCL, Ivoclar Vivadent GmbH) bonded in the milled recesses followed by a clinical try-in for the maxillary and mandibular arch. Finally, computerengineered complete denture insertion is performed (Figure 3A–H).
www.tda.org | August 2022 509 number of VDFP CAD/CAM obtained by VDFP with AMD AvaDent/CAD-CAM was eight (44%); two were obtained in the form of a Monolithic Denture and using the DENTCA Piezography Technique and the Digital Denture Provisional technique. The majority of the patients were above 50 years old. Figure 3. CECDs during digital processing (A–H). (A) Virtual models. (B) Interocclusal relationship. (C) Denture base planning. (D) Tooth setup design. (E) Victual articulator. (F) Aesthetic parameters and minor corrections. (G) Final model. (H) Milled prosthesis after fabrication.
Few studies suffered from a lack of detail in their reporting i.e., they did not mention gender or report any complications. Details regarding the tryin were not reported. Authors reported problems related to aesthetics, the sizes of the arranged teeth, the position of the teeth with the arches, and the profile of the patient in the summarized studies. In addition to the information in Figure 4, most of the patients were more than 53 years old, and studies from around the world were included.
The objective of this review was to examine and contrast the fabrication techniques of a computer-engineered complete denture and conventional CD dental prostheses. We examined various relevant parameters such as materials, retention, the accuracy of fitting, aesthetics, fabrication time, patient satisfaction, and the number of post-placement adjustment appointments. 4.1. Retention and Fitting The retention offered by milled pre-polymerized computer-engineered complete denture (CECD) bases with polymethyl methacrylate can be higher than that offered by Figure4. Summaryofthestudycharacteristicsusedinthereview.
The objective of this review was to examine and contrast the fabrication techniques of a computer-engineered complete denture and conventional CD dental prostheses. We examined various relevant parameters such as materials, retention, the accuracy of fitting, aesthetics, fabrication time, patient satisfaction, and the number of post-placement adjustment appointments.
Theretentionofferedbymilledpre-polymerizedcomputer-engineeredcompletedenture(CECD)baseswithpolymethylmethacrylatecanbehigherthanthatofferedbyconventionalheat-polymerizeddenturebases[39].TheCECDsshowedamoreprecisebase fit,betterclinicalretention,andaminimizedoccurrenceofdenture-relatedtraumaticlesions[4,31,41,42].Steinmassletal.reportedthatthemilleddigitalremovablecomplete denturedemonstratedasignificantincreaseandimprovementinretention,fitting[30], andhigherdimensionalaccuracy,contour,fitting,extension,andstabilitycomparedtothe polymerized computer-engineered complete denture (CECD) bases with polymethyl methacrylate can be higher than that offered by conventional heat-polymerized denture bases.39
Figure 4. Summary of the study characteristics used in the review.
4.1.RetentionandFitting
Steinmassl et al. reported that the milled digital removable complete denture demonstrated a significant increase and improvement in retention, fitting, and higher dimensional accuracy, contour, fitting, extension, and stability compared to the conventionally fabricated CDs.30,40,43,44 However, in a pilot cohort screening, Bidra et al. stated that about 50% of participants did not record retention, adaptation, and stability as having a good or excellent outcome.22 In CECDs, the greatest amount of misfit is usually on the intaglio surface in the posterior palatal and the border seal areas.30 These dentures need to be rebased after long periods of use to improve retention and to compensate for physiological bone resorption.
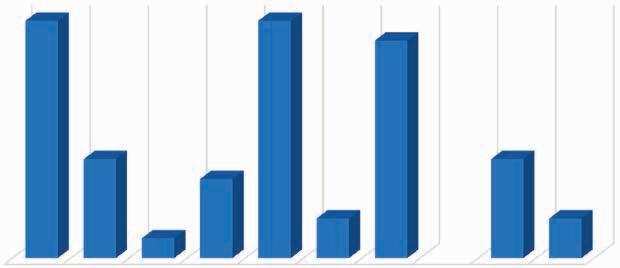
gender or report any complications. Details regarding the try-in were not reported.
2 3 4 OFMODELSJAWEDENTULOUS MANDIBLEANDMAXILLA REPORTCASE CLINICAL VDFP/CAD-CAM DENTUREMONOLITHIC AVADENT/CAD-CAM CAMCAD/DENTCA; NUMBER OF VISITSSUBJECTS SYSTEM USED 12 5 1 4 12 2 11 5 2
4.Discussion
Theobjectiveofthisreviewwastoexamineandcontrastthefabricationtechniques ofacomputer-engineeredcompletedentureandconventionalCDdentalprostheses.We examinedvariousrelevantparameterssuchasmaterials,retention,theaccuracyoffitting,aesthetics,fabricationtime,patientsatisfaction,andthenumberofpost-placement adjustmentappointments.
4.1. Retention and Fitting The retention offered by milled preFigure 4. Summary of the study characteristics used in the review. teethwiththearches,andtheprofileofthepatientinthesummarizedstudies.Inaddition totheinformationinFigure 4,mostofthepatientsweremorethan53yearsold,andstudies fromaroundtheworldwereincluded.
The CECDs showed a more precise base fit, better clinical retention, and a minimized occurrence of denturerelated traumatic lesions.4,31,41,42
510 Texas Dental Journal | Vol 139 | No. 8
Authors reported problems related to aesthetics, the sizes of the arranged teeth, the position of the teeth with the arches, and the profile of the patient in the summarized studies. In addition to the information in Figure 4, most of the patients were more than 53 years old, and studies from around the world were included.
4. Discussion
4. Discussion
CECDs are slightly lacking in terms of aesthetics, since no try-in steps are involved in their manufacture.42 Alhallak and Nankali stated that the biocompatibility of CECDs still requires better follow-up and documentation.63
www.tda.org
The CAD-CAM monolithic removable prostheses produced the best combination of precision and duplicability.38 A smooth surface is important in every restorative treatment to reduce biofilm formation. It lends better esthetics, patient acceptance, and clinical success.45 Al Moaleem et al. concluded that the presence of smooth restoration, as well as oral prostheses, clinically minimizes adherence and biofilm Alteringformation.46thedenture-fitting surfaces characteristics, such as porosity and surface irregularity, is essential for reducing Candida adhesion on the polymer surface. Denture stomatitis (DS) is an inflammatory condition affecting the palatal mucosa beneath dentures. Candida plays a role in palatal inflammation due to accumulation and colony formation, establishing a biofilm.47 The smooth surface characteristics of CECDs offered less purchase for Candida adherence.48,49 CECDs had lower porosity and polymerization shrinkage. Even after proper finishing and polishing, conventional CDs were associated with increased Candida adhesion compared to the CAD/CAM polymers.50 4.3. Clinical Time Computer-engineered complete dentures required fewer post-insertion adjustments. Saponaro et al. reported that 6 out of 48 contributors did not require any post-insertion adjustment appointment; 16 of the patients only required one post-insertion visit; less than 16 participants required two visits, and 25% (12) of applicants required three or more visits.51 Bidra et al. found that 3.3% of dentures required modifications after 12 months for all patients.22 CECDs can be an effective and time-efficient option for completely edentulous patients in terms of reduced time and overall results.40 Finally, 77% of the patients with edentulism agreed that their new CECDs were “better” than their previous set of CDs.52 CECDs are a viable alternative to conventional CDs based on the treatment duration and the reduced number of clinical and follow-up appointments, adjustments, and maintenance required.11 In conventional complete dentures, the follow-up starts immediately after the first 24 h, and as many as three adjustment visits are required.53 4.4. Patient Satisfaction Participants who received computerengineered complete dentures showed high levels of satisfaction.20,40,52 Patient outcomes were clinically acceptable. The retention with milled pre-polymerized denture bases was comparable to that of conventional denture bases.39 Inokoshi et al. observed that patients were equally satisfied with digital and conventional Asdentures.54theclinical try-in step is not performed in CECDs, it is not possible to perform an aesthetic or phonetic evaluation, which can lead to better patient satisfaction later on. In conventional CDs, there is a try-in stage (in wax) that makes it possible to change the tooth set-up, meaning that adjustments can be made to customize the denture based on the facial characteristics of each patient. 4.5. Manufacturing Time The digital method was associated with reduced fabrication time and higher technique accuracy.40,41,54 However, Schwindling and Stober and Wulfman et al. dissented from this characterization and reported a longer working time using the digital procedure.55,56 CAD/CAM technology simplifies the laboratory effort, allowing the dental technician to conveniently construct precise and well-organized prostheses.11,57 4.6. Materials Selection Polymethyl methacrylate (PMMA) is the most widely used material for complete denture fabrication due to its aesthetics, low water absorption and solubility, adequate strength, ease of maintenance, and simple manufacturing process.58 However, the material has a few disadvantages namely porosity, residual monomer, possible allergens, increased finishing time, brittleness, and uneven thickness.59 PMMA is also used in computer-engineered complete dentures, which can be pre-polymerized, cross-linked, or highimpact resistant. When used with CAD/ CAM, this material shows reduced residual monomer, superior fit, and strength.60 4.7. Complementary Aspects Computer-engineered complete dentures (CECDs) are superior to the rapidly prototyped conventional dentures in terms of the trueness of the intaglio surfaces.37,56,61 Bacali et al. stated that it was possible to achieve improved speed, precision, data reproducibility, comfort, chewing efficiency, and reduced costs due to the standardization of the treatment steps in CECDs.62 Any limitations and disadvantages could be overcome once the digital workflow became familiar.16
| August 2022 511
Denture Surface Quality
4.2.
Author Contributions: Conceptualization, M.Q.M., M.M.A.M. and A.H.A.; methodology, M.S. and S.M.A.; validation, A.H.A. and M.M.A.M.; formal analysis, A.P., S.M.A., S.B. and A.H.; investigation, A.P.; resources, M.Q.M.; data curation, F.A.A.-S.; writing—original draft preparation, M.M.A.M., S.B. and A.H.; writing—review and editing, A.P., A.H.A., S.P., A.H.A. and J.P.M.T. supervision, M.M.A.M.; project administration, M.S.; funding acquisition, M.Q.M., A.H.A., M.S. and S.M.A. All authors have read and agreed to the published version of the manuscript. Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable. Informed Consent Statement: Not applicable. Data Availability Statement: Data are available upon request. Acknowledgments: Mahmoud Rashd Alshadad, a dental technician, is thanked for the assistance in manufacturing the digital prosthesis in Figure 3.
References: 1. Ferro, K.J.; Morgano, S.M.; Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L.; McGarry, T.J.; Twain, M. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [CrossRef]
Dental Journal |
A remarkable feature of CECDs is the ease of fabrication and reduced chair time required. This is of particular relevance in light of the ongoing COVID-19 pandemic. CECDs would reduce the risk of virus transmission as well as minimize contacts and droplet-generating procedures. This is advantageous for patients, clinicians, and auxiliary staff. The digital storage of patient data would allow for the fabrication of a denture even without the patient visiting a prosthodontist, reducing the risk to older, vulnerable patients.69 Using the chlorhexidine mouthwash as an antiseptic therapy can have clinical and microbiological benefits.70 Chlorhexidine gels cause limited changes to the color and mechanical properties of PMMA denture bases. Newer formulations contain anti-discoloring agents that can be safely used with CECDs for maintaining oral hygiene. 5. Conclusions Based on the available literature, it is clear that computer-engineered complete dentures made using CAD/ CAM with a digital workflow have several advantages over conventional dentures. The digital workflow can reduce clinical and laboratory time. The patient data stored are invaluable during future appointments. Meticulous care must be taken at each stage from the initial impression to milling to minimize processing errors. Further randomized clinical trials are essential to extensively cover all of the parameters used in computerengineered complete dentures manufacturing. This paper will aid in the decision-making process during treatment planning for oral healthcare providers.
2. Grant, G.T.; Campbell, S.D.; Masri, R.M.; Andersen, M.R. American College of Prosthodontists Digital Dentistry Glossary Development Task, F. Glossary of Digital Dental Terms: American College of Prosthodontists. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2016, 25 (Suppl. 2), S2–S9. [CrossRef] [PubMed] 3. Bahman, A.; Ianuzzo, F. Computer-aided engineering simulations. In Wide Bandgap Power Semiconductor
512 Texas Vol 139 | No. 8 Data storage allows for a quick replacement of dentures when they are missing or damaged.43,44,56 Additionally, the time needed for the manufacturing and processing of CECDs was only two visits, resulting in one less hour of chair time for the dentist and five hours less time for the dental laboratory. Ultimately, Peroz et al. concluded that positive changes in the oral healthrelated quality of life were observed in the participants.64 The production of CECDs using 3D printing technology is becoming more popular in dental centers. Nevertheless, evidence regarding biocompatibility, the clinical or long-term follow-up of the patients, the chewing load capability, and data on the clinical performance of 3D printed dentures are still lacking.65,66 Further studies are essential to elucidate these parameters.
Conflicts of Interest: The authors declare no conflict of interest.
Variables related to occlusal forces were examined between CECDs and conventional methods employing various occlusal schemes. CECDs showed better retention of occlusal schemes. Bilateral balanced and lingualized occlusal schemes provided better centralization of forces, improved distribution, and high maximum occlusal forces.67 This is important, as a significant relationship exists between the distribution of occlusal contacts and temporomandibular joint disorders (TMD).68 Any asymmetry in the occlusal contact pattern may precipitate TMD over time.
21. Bilgin, M.S.; Erdem, A.; Aglarci, O.S.; Dilber, E. Fabricating Complete Dentures with CAD/CAM and RP Technologies. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2015, 24, 576–579. [CrossRef] 22. Bidra, A.S.; Farrell, K.; Burnham, D.; Dhingra, A.; Taylor, T.D.; Kuo, C.L. Prospective cohort pilot study of 2-visit CAD/CAM monolithic complete dentures and implantretained overdentures: Clinical and patient-centered outcomes. J. Prosthet. Dent. 2016, 115, 578–586. e571. [CrossRef] [PubMed]
7. Masri, G.; Mortada, R.; Ounsi, H.; Alharbi, N.; Boulos, P.; Salameh, Z. Adaptation of Complete Denture Base Fabricated by Conventional, Milling, and 3-D Printing Techniques: An In Vitro Study. J. Contemp. Dent. Pract. 2020, 21, 367–371. 8. Gherlone, E.F.; Ferrini, F.; Crespi, R.; Gastaldi, G.; Capparé, P. Digital Impressions for Fabrication of Definitive “All-on-Four” Restorations. Implant. Dent. 2015, 24, 125–129. [CrossRef]
11. Baba, N.Z.; Goodacre, B.J.; Goodacre, C.J.; Muller, F.; Wagner, S. CAD/CAM Complete Denture Systems and Physical Properties: A Review of the Literature. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2021, 30, 113–124. [CrossRef]
12. Yilmaz, B.; Azak, A.N.; Alp, G.; Ek¸si, H. Use of CAD-CAM technology for the fabrication of complete dentures: An alternative technique. J. Prosthet. Dent. 2017, 118, 140–143. [CrossRef] [PubMed]
9. Goodacre, C.J.; Garbacea, A.; Naylor, W.P.; Daher, T.; Marchack, C.B.; Lowry, J. CAD/CAM fabricated complete dentures: Concepts and clinical methods of obtaining required morphological data. J. Prosthet. Dent. 2012, 107, 34–46. [CrossRef]
5. Heikal, M.M.A.; Nabi, N.A.; Elkerdawy, M.W. A Study Comparing Patient Satisfaction and Retention of CAD/CAM Milled Complete Dentures and 3D Printed CAD/CAM Complete Dentures versus Conventional Complete Dentures: A Randomized Clinical Trial. Braz. Dent. Sci. 2022, 25, e2785. [CrossRef]
10. Bajunaid, S.O. A first experience with digital complete overdentures. Saudi Dent. J. 2016, 28, 148–153. [CrossRef]
16. Contrepois, M.; Sireix, C.; Soenen, A.; Pia, J.P.; Lasserre, J.F. Complete denture fabrication with CAD/CAM technology: A case report. Int. J. Esthet. Dent. 2018, 13, 66–85.
17. Janeva, N.; Kovacevska, G.; Janev, E. Complete Dentures Fabricated with CAD/CAM Technology and a Traditional Clinical Recording Method. Open Access Maced. J. Med. Sci. 2017, 5, 785–789. [CrossRef]
18. Ohkubo, C.; Shimpo, H.; Tokue, A.; Park, E.J.; Kim, T.H. Complete denture fabrication using piezography and CAD-CAM: A clinical report. J. Prosthet. Dent. 2018, 119, 334–338. [CrossRef]
23. Infante, L.; Yilmaz, B.; McGlumphy, E.; Finger, I. Fabricating complete dentures with CAD/CAM technology. J. Prosthet. Dent. 2014, 111, 351–355. [CrossRef] [PubMed] 24. Kanazawa, M.; Inokoshi, M.; Minakuchi, S.; Ohbayashi, N. Trial of a CAD/CAM system for fabricating complete dentures. Dent. Mater. J. 2011, 30, 93–96. [CrossRef] [PubMed]
25. Joda, T.; Müller, P.; Zimmerling, F.; Schimmel, M. CAD/CAM produced complete dentures with the “Digital Denture Professional System”. Swiss
www.tda.org | August 2022 513
4. Kattadiyil, M.T.; AlHelal, A. An update on computer-engineered complete dentures: A systematic review on clinical outcomes. J. Prosthet. Dent. 2017, 117, 478–485. [CrossRef] [PubMed]
6. Han,W.; Li, Y.; Zhang, Y.; Lv, Y.; Zhang, Y.; Hu, P.; Liu, H.; Ma, Z.; Shen, Y. Design and fabrication of complete dentures using CAD/CAM technology. Medicine 2017, 96, e5435. [CrossRef]
13. Mai, H.N.; Lee, D.H. A Digital Technique to Replicate Edentulous Arches with Functional Borders and Accurate Maxillomandibular Relationship for Digital Complete Denture. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2020, 29, 356–359. [CrossRef] [PubMed] 14. Çakmak, G.; Donmez, M.B.; Atalay, S.; Yilmaz, H.; Kokat, A.M.; Yilmaz, B. Accuracy of single implant scans with a combined healing abutmentscan body system and different intraoral scanners: An in vitro study. J. Dent. 2021, 113, 103773. [CrossRef] [PubMed] 15. Lee, Y.; Kwon, K.-R.; Pae, A.; Noh, K.; Paek, J.; Hong, S.-J. Rehabilitation of fully edentulous patient using Ceramill full denture system (FDS). J. Korean Acad. Prosthodont. 2019, 57, 232–237. [CrossRef]
19. de Mendonca, A.F.; Furtado de Mendonca, M.; White, G.S.; Sara, G.; Littlefair, D. Total CAD/ CAM Supported Method for Manufacturing Removable Complete Dentures. Case Rep. Dent. 2016, 2016, 1259581. [CrossRef] Materials 2022, 15, 3868 12 of 13
Packaging;Woodhead Publishing: Sawston, UK, 2018; pp. 199–223.
20. Kim, M.-J.; Kim, K.-H.; Yeo, D.H. Fabrication of computeraided Sci.Caseandmanufacturingdesign/computer-aidedcompletedentureconventionalcompletedenture:report.J.Dent.Rehabil.Appl.2016,32,141–148.[CrossRef]
26 Maeda, Y.; Minoura, M.; Tsutsumi, S.; Okada, M.; Nokubi, T. A CAD/CAM system for removable denture. Part I: Fabrication of complete dentures. Int. J. Prosthodont. 1994, 7, 17–21.
42. Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [CrossRef]
43. Thalji, G.; Jia-mahasap,W. CAD/ CAM removable dental prostheses: A review of digital impression techniques for edentulous arches and advancements on design and manufacturing systems. Curr. Oral Health Rep. 2017, 4, 151–157. [CrossRef] 44. Andreescu, C.F.; Ghergic, D.L.; Botoaca, O.; Hancu, V.; Banateanu, A.M.; Patroi, D.N. Evaluation of different materials used for fabrication of complete digital denture. Mater. Plast. 2018, 55, 124. [CrossRef] 45. Paolone, G.; Moratti, E.; Goracci, C.; Gherlone, E.; Vichi, A. Effect of Finishing Systems on Surface Roughness and Gloss of FullBody Bulk-Fill Resin Composites. Materials 2020, 13, 5657. [CrossRef] [PubMed] 46. Al Moaleem, M.M.; Porwal, A.; Alahmari, N.; Shariff, M. Oral Biofilm on Dental Materials Among Khat Chewers. Curr. Pharm. Biotechnol. 2020, 21, 964–972. [CrossRef] 47. Ramage, G.; Coco, B.; Sherry, L.; Bagg, J.; Lappin, D.F. In vitro Candida albicans biofilm induced proteinase activity and SAP8 expression correlates with in vivo denture stomatitis severity. Mycopathologia 2012, 174, 11–19. [CrossRef] 48. Al-Fouzan, A.F.; Al-Mejrad, L.A.; Albarrag, A.M. Adherence of Candida to complete denture surfaces in vitro: A comparison of conventional and CAD/ CAM complete dentures. J. Adv. Prosthodont. 2017, 9, 402–408. [CrossRef] Materials 2022, 15, 3868 13 of 13
514 Texas Dental Journal | Vol 139 | No. 8 Dent. J. Sso 2016, 126, 899–909.
28. Busch, M.; Kordass, B. Concept and development of a computerized positioning of prosthetic teeth for complete dentures. Int. J. Comput. Dent. 2006, 9, 113–120. 29. Kattadiyil, M.T.; Goodacre, C.J.; Baba, N.Z. CAD/CAM complete dentures: A review of two commercial fabrication systems. J. Calif. Dent. Assoc. 2013, 41, 407–416.
27. Kawahata, N.; Ono, H.; Nishi, Y.; Hamano, T.; Nagaoka, E. Trial of duplication procedure for complete dentures by CAD/CAM. J. Oral Rehabil. 1997, 24, 540–548. [CrossRef]
30. McLaughlin, J.B.; Ramos, V., Jr.; Dickinson, D.P. Comparison of Fit of Dentures Fabricated by Traditional Techniques Versus CAD/CAM Technology. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, 428–435. [CrossRef] 31. Baba, N.Z.; AlRumaih, H.S.; Goodacre, B.J.; Goodacre, C.J. Current techniques in CAD/CAM denture fabrication. Gen. Dent. 2016, 64, 23–28. 32. Steinmassl, O.; Dumfahrt, H.; Grunert, I.; Steinmassl, P.A. CAD/ CAM produces dentures with improved fit. Clin. Oral Investig. 2018, 22, 2829–2835. [CrossRef] [PubMed] 33. Hirayama, H. Digital removable complete denture (DRCD). In Digital Restorative Dentistry; Springer: Berlin/Heidelberg, Germany, 2019; pp. 115–136. 34. Edition, P.T. Parameters of Care for the Specialty of Prosthodontics. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2005, 14, 1–103. 35. Bonnet, G.; Batisse, C.; Bessadet, M.; Nicolas, E.; Veyrune, J.L. A new digital denture procedure: A first practitioners appraisal. BMC Oral Health 2017, 17, 155. [CrossRef] 36. Al Moaleem, M.M.; Al-layl, O.; Alhomood, M.; Ageeli, W.; Qsadi, A.; Mohammed, T.; Baraqt, E.; Zubayni, B.; Alalmaie, N.; Huraysi, A. Computer Engineering Complete DenturesWorkflow: Systematic Techniques Review. J. Pharm. Res. Int. 2021, 33, 207–220. [CrossRef] 37. Srinivasan, M.; Schimmel, M.; Naharro, M.; O’Neill, C.; McKenna, G.; Muller, F. CAD/CAM milled removable complete dentures: Time and cost estimation study. J. Dent. 2019, 80, 75–79. [CrossRef] 38. Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of denture tooth movement between CAD-CAM and conventional fabrication techniques. J. Prosthet. Dent. 2018, 119, 108–115. [CrossRef] [PubMed] 39. AlHelal, A.; AlRumaih, H.S.; Kattadiyil, M.T.; Baba, N.Z.; Goodacre, C.J. Comparison of retention between maxillary milled and conventional denture bases: A clinical study. J. Prosthet. Dent. 2017, 117, 233–238. [CrossRef] 40. Kattadiyil, M.T.; Jekki, R.; Goodacre, C.J.; Baba, N.Z. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J. Prosthet. Dent. 2015, 114, 818–825. [CrossRef] 41. Janeva, N.M.; Kovacevska, G.; Elencevski, S.; Panchevska, S.; Mijoska, A.; Lazarevska, B. Advantages of CAD/CAM versus Conventional Complete Dentures—A Review. Open Access Maced. J. Med. Sci. 2018, 6, 1498–1502. [CrossRef]
50. Murat, S.; Alp, G.; Alatali, C.; Uzun, M. In Vitro Evaluation of Adhesion of Candida albicans on CAD/ CAM PMMA-Based Polymers. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, e873–e879. [CrossRef]
64. Peroz, S.; Peroz, I.; Beuer, F.; Sterzenbach, G.; von Stein-Lausnitz, M. Digital versus conventional complete dentures: A randomized, controlled, blinded study. J. Prosthet. Dent. 2021. [CrossRef] [PubMed]
www.tda.org | August 2022 515
61. Kalberer, N.; Mehl, A.; Schimmel, M.; Muller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637–643. [CrossRef]
49. Taebunpakul, P.; Jirawechwongsakul, P. Palatal Inflammation and the Presence of Candida in DentureWearing Patients. J. Int. Soc. Prev. Community Dent. 2021, 11, 272–280. [CrossRef]
65. Paes Junior, T.J.D.A.; Tribst, J.P.M.; Dal Piva, A.M.D.O.; de Figueiredo, V.M.G.; Borges, A.L.S.; Inagati, C.M. Influence of Fibromucosa Height and Loading on the Stress Distribution of a Total Prosthesis: A Finite Element Analysis. Braz. Dent. Sci. 2021, 24, 2. [CrossRef] 66. Todescan, F.F.; Hayashi, M.M.; Giugni, L.R.; Bottino, M.A.; Tribst, J.P.M. From Denture to the Final Implant-Supported Prosthesis Using a Full-Digital Protocol: A Dental Technique. Oral 2021, 1, 332–339. [CrossRef] 67. Chaturvedi, S.; Addes, M.K.; Al Qahtani, N.M.; Al Ahmari, N.M.; Alfarsi, M.A. Clinical analysis of CADCAM milled and printed complete dentures using computerized occlusal force analyser. Technol. Health Care 2022, 29, 1–15. [CrossRef] 68. Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [CrossRef] 69. Gherlone, E.; Polizzi, E.; Tetè, G.; Capparè, P. Dentistry and COVID-19 pandemic: Operative indications post-lockdown. New Microbiol. 2021, 44, 1–11. [PubMed] 70. Calderini, A.; Pantaleo, G.; Rossi, A.; Gazzolo, D.; Polizzi, E. Adjunctive effect of chlorhexidine antiseptics in mechanical periodontal treatment: First results of a preliminary case series. Int. J. Dent. Hyg. 2013, 11, 180–185.
62. Bacali, C.; Mesaros, A.S, Nastase, V.; Constantiniuc, M. Particularities of CAD-CAM commercial systems with applicability in the orofacial sphere; digital complete denture. Health Sports Rehabil. Med. 2019, 20, 22–25. [CrossRef] 63. Alhallak, K.R.; Nankali, A. 3D Printing Technologies for Removable Dentures Manufacturing: A Review of Potentials and Challenges. Eur. J. Prosthodont. Restor. Dent. 2021, 30, 14–19. [CrossRef]
51. Saponaro, P.C.; Yilmaz, B.; Johnston,W.; Heshmati, R.H.; McGlumphy, E.A. Evaluation of patient experience and satisfaction with CAD-CAM-fabricated complete dentures: A retrospective survey study. J. Prosthet. Dent. 2016, 116, 524–528. [CrossRef] 52. Saponaro, P.C.; Yilmaz, B.; Heshmati, R.H.; McGlumphy, E.A. Clinical performance of CAD-CAMfabricated complete dentures: A cross-sectional study. J. Prosthet. Dent. 2016, 116, 431–435. [CrossRef]
53. Kivovics, P.; Jahn, M.; Borbely, J.; Marton, K. Frequency and location of traumatic ulcerations following placement of complete dentures. Int. J. Prosthodont. 2007, 20, 397–401. [PubMed] 54. Inokoshi, M.; Kanazawa, M.; Minakuchi, S. Evaluation of a complete denture trial method applying rapid prototyping. Dent. Mater. J. 2012, 31, 40–46. [CrossRef] [PubMed] 55. Schwindling, F.S.; Stober, T. A comparison of two digital techniques for the fabrication of complete removable dental prostheses: A pilot clinical study. J. Prosthet. Dent. 2016, 116, 756–763. [CrossRef] [PubMed] 56. Wulfman, C.; Bonnet, G.; Carayon, D.; Lance, C.; Fages, M.; Vivard, F.; Daas, M.; Rignon-Bret, C.; Naveau, A.; Millet, C. Digital removable complete denture: A narrative review. Fr. J. Dent. Med. 2020, 10, 1–9. [CrossRef] 57. Baba, N.Z. Materials and processes for CAD/CAM complete denture fabrication. Curr. Oral Health Rep. 2016, 3, 203–208. [CrossRef] 58. Urechescu, H.; Pricop, M.; Pricop, C.; Mateas, M.; Natanael, S.; Galatanu, S.V.J.M.P. Thermoplastic materials used for fabrication of maxillary obturator prostheses. Mat. Plast. 2017, 54, 477. [CrossRef] 59. Bechir, A.; Pacurar, M.; Bechir, E.S.; Comaneanu, M.R.; Cires, M.C.; Maris, M.; Barbu, H.J.M.P. Aesthetic importance of resin based dental materials used for orthodontic appliances. Mater Plast. 2014, 51, 57–61. 60. Baba, N.Z.; Charles, J.G.; Kattadiyil, M.T. CAD/CAM Inc.:Masri,Applicationsprosthodontics.removableInClinicalofDigitalTechnology;R.D.C.,Ed.;JohnWiley&Sons,Hoboken,NJ,USA,2015.
The maxillary sinus becomes infected, causing localized pain with nasal discharge, while the oral tissues may develop a diffuse swelling with a gray or violaceous discoloration, that may be followed by widespread necrosis.1
page 493
Aspergillosis disease, which is the most severe form and can be life threatening, especially among those who have weakened immune systems.2 Risk factors for developing invasive aspergillosis, include patients on immunosuppressive therapy to prevent hematopoietic stem cell transplant or solid organ transplant rejection, those receiving chemotherapy for cancer, or on corticosteroid or other immunosuppressive agents.5,6 Other factors include patients with inherited or acquired immunodeficiencies, and lung diseases such as chronic obstructive pulmonary disease, tuberculosis, sarcoidosis, or severe influenza.6-8Patientswith allergic aspergillus sinusitis are allergic to components of the fungus and present with symptoms mimicking a sinus infection, including headaches, nasal congestion and rhinorrhea.9 When allergic aspergillosis involves the lungs, it causes inflammation of the airways and air sacs, causing wheezing, worsening of symptoms of asthma, and a productive cough.10 Sometimes, aspergillus may form tangled masses within the sinuses or the lungs, and is termed fungus ball(s) or aspergilloma(s).11 Although aspergillomas may sometimes progress and become chronic in duration, the disease is usually limited to the respiratory system.11 Patients with aspergillomas may be asymptomatic, especially in the initial stages. If left untreated however, patients may become symptomatic, and demonstrate wheezing, difficulty breathing, hemoptysis, fatigue and unintentional weight loss. Invasive aspergillosis is characterized by the invasion of blood vessels, causing thrombosis and tissue necrosis. Invasive aspergillosis is not limited to the lungs and can disseminate rapidly to involve other organs such as the brain, gastrointestinal tract, liver, skin, and other organs. In rhinocerebral aspergillosis, patients often present with fever, unilateral facial swelling, headaches, nasal/sinus congestion that may be accompanied by pain, and blood-tinged nasal discharge. With disease progression, ptosis, proptosis and vision changes may occur and black necrotic lesions may develop within the nasal and/or oral cavities.12 Invasive aspergillosis may also develop following tooth extraction or root canal therapy involving posterior maxillary teeth.
The microscopic features revealed the presence of a non-invasive fungal infection, consistent with Aspergillosis.
516 Texas Dental Journal | Vol 139 | No. 8
Discussion Aspergillus is a fungal microorganism that is commonly seen all over the world, present in soil, dust, water, and other organic matter, and is the second most common fungi after candidiasis.1 As such, many of the spores are regularly inhaled and do not produce any significant disease in the vast majority of humans.2 There are about 180 different Aspergillus species, but the 2 most common species that cause most infections in humans are the A. fumigatus and A. flavus.1,2 Previously, A. fumigatus was responsible for 90% of aspergillus infections. Recently, the number of cases caused by nonfumigatus species have seen steady Theincreases.4development of aspergillosis is dependent on the host’s immune response. Its clinical presentation can vary widely, from an allergic, hypersensitivity response, typified by asthma-like symptoms and allergic sinusitis, through developing fungus balls which cause cavitating lung disease, to having disseminated invasive and maxillofacial pathology diagnosis and management—from
Periodic acid-Schiff (PAS) and Grocott (or Gomori) Methenamine silver (GMS) stains with appropriate controls, confirmed the presence of fungal hyphae, consistent with Aspergillus species (Figure 4A, B).
ORAL
The patient in our case report presented with right sided facial pain of 6 months duration with intermittent drainage. Four months later, the patient developed facial swelling on the ipsilateral side. The differential diagnosis for this clinical and radiographic presentation could include an untreated odontogenic infection that likely spread to contiguous tissues, involving the right maxilla with draining fistulas, and the right buccal fascial space as well
| August
www.tda.org 2022
Figure 4A. (Original magnification x 200), PAS (Periodic Acid-Schiff) stain highlighting the fungal organisms.
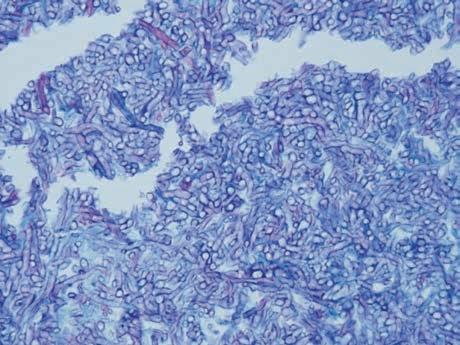
Figure 4B. (Original magnification x 200), GMS (Grocott Methenamine Silver) stain highlighting the mass of densely packed aggregates of Aspergillus species. as the right maxillary sinus. Other considerations would include maxillary sinusitis of non-odontogenic origin, medication-related osteonecrosis of the jaws, osteoradionecrosis, and sinus malignancy. Chronic sinusitisoriginosteomyelitismaxillaryofodontogenicwithmaxillary
Osteomyelitis is caused primarily by an infection that leads to inflammation of the bone/bone marrow. The majority of (suppurative) osteomyelitis of the jaws are due to an odontogenic origin, often involving a polymicrobial bacterial infection, especially those of staphylococcus species.13 Patients who present with symptoms of less than 1 month duration are usually classified as acute osteomyelitis, while those with symptoms of more than a month, (similar to our patient), are categorized as chronic osteomyelitis. Chronic osteomyelitis typically presents as chronic, low-grade pain and swelling,
517
518 Texas Dental Journal | Vol 139 | No. 8 with or without fistulous tracts, abscess formation and sequestra. Ill-defined osteolytic changes, with or without the presence of radiopaque sequestra are observed on radiographic examination. Chronic osteomyelitis is uncommon, especially in the United States, and is dependent on the quantity and virulence of pathogens, the host’s immune response, and degree of tissue perfusion in the area.14 Patients with compromised immune response or poor blood supply to the affected area are at increased risk of developing osteomyelitis14. The mandible is more susceptible than the maxilla to osteomyelitis because it is less vascularized and has thicker cortical plates.15Duetothe proximity of dentoalveolar structures to the maxillary sinus, odontogenic infection can spread to involve the maxillary sinus, which accounts for about 10% - 40% of all maxillary sinusitis cases.16,17
Dentoalveolar surgery, complicated by the formation of an oroantral fistula, is the main cause of odontogenic maxillary sinusitis.18 Periapical or periodontal infection, impacted third molar and odontogenic cysts are other common sources of odontogenic infection that promote odontogenic maxillary sinusitis. Management of odontogenic maxillary sinusitis usually involves a combination of dental and endoscopic sinus surgeries. Computed tomography (CT) is the most reliable imaging of choice for sinus pathology, especially in cases of chronic sinus disease. The CT scan generates several images of the sinus that can be reformatted in multiple planes, which allows for critical evaluation of the sinus and the surrounding anatomic bony tissues.19
osteonecrosisMedication-relatedofthe jaws and osteoradionecrosis
Maxillary sinusitis from nonodontogenic causes More than 30 million individuals in the U.S. suffer from acute or chronic sinusitis. When inflammation of the paranasal sinuses persists for more than 3 months, it is termed chronic maxillary sinusitis. Chronic sinusitis may develop from a pre-existing acute sinusitis, where there is poor drainage within the antrum or in the presence of a foreign body.20 Poor drainage may be associated with mechanical obstruction of the ostium, reduced mucin clearance from damaged cilia or abnormally thick mucus.20 Sinusitis presents as congestion, stuffy nose, post nasal drip with mucopurulent discharge, fever, headaches, throbbing pain and tenderness, especially around the maxillary teeth, eyes, infraorbital region and the canine fossa. This type of pain resembles a toothache, but it does not respond to hot, cold, or sweet stimuli and worsens when the individual bends over.20Sinusitis can also occur as a result of non-odontogenic factors. Non odontogenic factors include environmental allergens, bacteria, fungi and foreign bodies.21 Published scientific reports cite the prevalence of fungal sinusitis at around 10% of patients with chronic sinusitis.22 However, this depends on whether it references invasive or non-invasive forms of fungal sinusitis, and also whether the population consists predominantly of immunocompromised or immunocompetent individuals. The consensus is that fungal sinusitis infections tend to occur in patients who are immunocompromised and where there has been exposure to large amounts of fungus. Sinusitis can spread to involve bones contiguous to the maxillary sinus. The frontal bone is more often affected compared to the maxilla, because of the rich blood supply and thin bone structures of the maxilla.
ORALand maxillofacial pathology, continued
Maxillary sinus malignancy A malignant tumor of the maxillary sinus, though uncommon, may present as facial pain and swelling, as observed in this patient. Approximately 2,000
Patients with osteonecrosismedication-relatedofthejaw(MRONJ) or osteonecrosis of the jaws, frequently show bony involvement with draining fistulas. In order to diagnose a patient with medication-related osteonecrosis of the jaw (MRONJ), there must be the presence of nonhealing exposed bone and a positive history of use of antiresorptive or antiangiogenic agents.23 The possibility of radiation exposure to the head and neck region must also be ruled out in such patients. Osteoradionecrosis (ORN) of the jaws is also characterized by the presence of necrotic and exposed bone, but it occurs as a complication of radiation therapy in patients treated for head and neck cancers.
6. Ledoux MP, Guffroy B, Nivoix Y, Simand C, Herbrecht R. Invasive Pulmonary Aspergillosis. Semin Respir Crit Care Med. 2020 Feb;41(1):80-98. doi: 10.1055/s0039-3401990. Epub 2020 Jan 30. PMID: 32000286.
14. Morrison A. Acute PathologyOutlines.comsuppurative.website. Accessedmandiblemaxillaacuteosteomyelitis.html.www.pathologyoutlines.com/topic/https://July11th,2022.
16. Melen I, Lindahl L, Andreasson L, Rundcrantz H. Chronic maxillary sinusitis: Definition, diagnosis and relation to dental infections and nasal polyposis. Acta otolaryngol (Stockh) 1986;101:320–327. [PubMed] [Google Scholar]
12. Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Foodborne, Waterborne, and Environmental Diseases (DFWED). Atlanta. February 2014. Clinical features of aspergillosis. https://www.cdc.gov/fungal/ features.diseases/aspergillosis/symptoms/clinical-
17. Puglisi S, Privitera S, Maiolino L, et al. Bacteriological findings and antimicrobial resistance in odontogenic and nonodontogenic chronic maxillary sinusitis. J Medical Microbiology 2011;60:1353–1359. [PubMed] [Google Scholar] 18. M. Troeltzsch, C. Pache, M. Troeltzsch, G. Kaeppler, M. Ehrenfeld, S. Otto, et al. Etiology and clinical characteristics of symptomatic unilateral maxillary sinusitis: a review of 174 cases. J Craniomaxillofac Surg, 43 (2015), pp. 1522-1529.
4. Steinbach WJ, Benjamin DK Jr, Kontoyiannis DP, et al. Infections due to Aspergillus terreus: a multicenter retrospective analysis of 83 cases. Clin Infect Dis 2004;39(2):192–8.
13. Koorbush GF, Fotos P, Goll TK. Retrospective study of osteomyelitis. Aetiology, demographics, risk factors and management in 35 cases. Oral Surg Oral Med Oral Pathol1992; 74: 149–54.
5. Baddley JW. Clinical risk factors for invasive aspergillosis. Med Mycology. 2011 Apr;49 Suppl 1:S7-S12.
www.tda.org | August 2022 519 cases of nasal/paranasal sinus cancers occur each year in the United States24. Patients with cancer of the maxillary sinus are usually asymptomatic, or display features that sometimes mimic sinusitis. This may cause diagnostic confusion and may delay appropriate management. Imaging studies reveal the presence of a space occupying lesion with bone destruction. Our patient presented with right facial swelling and draining fistulas. Radiographic imaging revealed a space occupying lesion of the right maxillary sinus and an expansile lesion of the maxilla, but the margins appeared intact. The CT scans of our patient are not consistent with features observed in cases of sinus malignancy. Additionally, the patient stopped taking IV Prolia 3 years ago and has no biopsy proven cancer of the jaws or history of radiation therapy to the jaws. All of which rule out sinus malignancy, MRONJ and osteoradionecrosis, respectively.
Microscopically, large balls of fungi were observed in biopsy specimens obtained from the right sinus. The specimen from the right alveolus revealed the presence of failed bone graft material and partially viable bone, but fungal hyphae were not present. The lack of fungal hyphae in the alveolus might be because of a sampling issue or that the type of fungal infection this patient had was noninvasive. The presence of fungal balls within the sinuses, in the absence of involvement of the surrounding connective tissues and bone, suggests that this patient likely has non-invasive aspergillosis. However, a referral to an infectious disease expert is needed to properly classify the type of Aspergillosis. The patient’s past medical history was significant for Hashimoto’s thyroiditis and ankylosing spondylitis. The possibility of the patient taking corticosteroids for her ankylosing spondylitis, although not documented in our clinic notes, does exist and if present could increase her susceptibility for developing a fungal infection.
11. Denning DW, Riniotis K, Dobrashian R, Sambatakou H. Chronic cavitary and fibrosing pulmonary and pleural aspergillosis: case series, proposed nomenclature change, and review. Clin Infect Dis. 2003 Oct 1;37 Suppl 3:S265-80.
8. Crum-Cianflone NF. Invasive aspergillosis associated with severe influenza infections. Open Forum Infec Dis. 2016 Aug;3(3). 9. Glass D, Amedee RG. Allergic fungal rhinosinusitis. Ochsner J. 2011 Fall;11(3):271-5.
7. Schweer KE, Bangard C, Hekmat K, Cornely OA. Chronic pulmonary aspergillosis. Mycoses. 2014 May;57(5):257-70.
10. Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification. Clin Exp Allergy. 2013 Aug;43(8):850-73.
2. Barnes PD, Marr KA. Aspergillosis: spectrum of disease, diagnosis, and treatment. Infect Dis Clin North Am. 2006 Sep;20(3):545-61, vi. doi: 10.1016/j. idc.2006.06.001. PMID: 16984868.
1.ReferencesNeville, B.W., Damm, D.D., Allen, C.M. and Chi, A.C. (2016) In: Fungal and Protozoal Diseases, Chapter 6. Oral & Maxillofacial Pathology. 4th Edition, WB Saunders, Elsevier, Missouri, 191-217.
15. Brady B.A., Leid J.G., Costerton J.W., Shirtliff M.E. Osteomyelitis: clinical overview and mechanisms of infection persistence. Clin. Microbiol. Newsletter. 2006;28:65–72. [Google Scholar]
19. Leo G, Triulzi F, Incorvaia C. Diagnosis of chronic rhinosinusitis. Pediatr Allergy Immunol. 2012 Aug;23 Suppl 22:20-6. doi: 10.1111/j.1399-3038.2012.01320.x. PMID: 22762850.
20. Taylor KH, The Maxillary Antrum, in Oral and Maxillofacial Surgery (second edition), 2007, pp 215 - 227.
21. Little RE, Long CM, Loehrl TA, Poetker DM. Odontogenic sinusitis: A review of the current literature. Laryngoscope Investig Otolaryngol. 2018 Mar 25;3(2):110-114. doi: 10.1002/lio2.147. PMID: 29721543; PMCID: PMC5915825. 22. Karthikeyan P, Nirmal Coumare V. Incidence and presentation of fungal sinusitis in patient diagnosed with chronic rhinosinusitis. Indian J Otolaryngol Head Neck Surg. 2010 Oct;62(4):381-5. doi: 10.1007/s12070-010-0062-0. Epub 2011 Jan 5. PMID: 22319697; PMCID: PMC3266098. 23. AlDhalaan NA, BaQais A, Al-Omar A. Medication-related Osteonecrosis of the Jaw: A Review. Cureus. 2020 Feb 10;12(2):e6944. doi: 10.7759/cureus.6944. PMID: 32190495; PMCID: PMC7067354.
24. American Cancer Society. © 2020 American Cancer Society, Inc. diagnosis-staging/survival-rates.htmland-paranasal-sinus-cancer/detection-www.cancer.org/cancer/nasal-cavity-https://
3. Morgan J, Wannemuehler KA, Marr KA, et al. Incidence of invasive aspergillosis following hematopoietic stem cell and solid organ transplantation: interim results of a prospective multicenter surveillance program. Med Mycol 2005;43(Suppl 1):S49–58.
DALLAS/FORT WORTH (ID #551): Premier cosmetic dentistry practice located in the heart of the Dallas-Fort Worth metro area. The practice realized annual revenue of $2M+ and strong net cash flow of under 7 figures in 2021 and is on pace to grow significantly in 2022. The office is located in an attractive, free-standing building featuring 5 operatories and the real estate is available for purchase. EAST TEXAS (ID #486): Located in a growing east Texas community, this general practice caters to a dedicated multigenerational active patient base. The wellappointed 2,500 sq ft space contains 5 fully equipped operatories, digital pano, plumbed
AUSTIN (ID #538): State-of-the-art GD practice located in one of the most popular areas of Austin with great visibility in a busy retail center that draws over 30 new patients per month. The approximately 2,700 sq ft office features 6 total operatories (3 fully equipped) with modern finish out, digital radiography, paperless charts, a digital pano, and iTero Scanner. AUSTIN-WEST (ID #539): 100% fee-for-service practice in the Texas hill country with strong hygiene recall (approximately 30% of total production) and an increasing revenue trend over the past 3 years. The practice is located in a freestanding building that features 3 fully equipped operatories, newly installed computers in each room, digital sensors, hand-held X-ray units, practice management software (Dentrix Ascend), and paperless charts. The real estate is also for sale.
520 Texas Dental Journal | Vol 139 | No. 8 ADVERTISING BRIEFS PRACTICE OPPORTUNITIES Opportunities Online at TDA.org and Printed in the Texas Dental Journal ADVERTISING BRIEF INFORMATION CopyDEADLINEtextisdue the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.) MONTHLY RATES PRINT: First 30 words—$60 for ADA/TDA members & $100 for non-members. $0.10 each additional word. ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60. AdsSUBMISSIONmustbesubmitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy. ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. TO REQUEST MORE INFORMATION ON OUR LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@ dentaltransitions.com.
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
HOUSTON, PERIODONTAL (ID #494): Located in a growing suburb south of downtown Houston. There are 5 fully equipped www.dentaltransitions.com
EAST TEXAS (ID #542): Large practice and real estate in east Texas with over 7 figures in revenue. The recently updated 2,400 sq ft facility features 5 fully equipped operatories with digital radiography, paperless charts, CBCT, digital pano, and an iTero digital scanner. The practice serves a large FFS/PPO, multi-generational patient base with over 3,000 active patients and a stellar online reputation. The seller is open to providing a long-term transition period to the buyer.
NORTHEAST TEXAS (ID #554): 100% FFS general fentistry practice in a desirable town in northeast Texas with 7 figures in revenue and strong net income. The turn-key practice features 4 fully equipped operatories with digital radiography, intra oral cameras, paperless charts, CBCT, and a digital scanner. HOUSTON, ORTHODONTICS (ID #480): This productive, FFS orthodontic practice occupies an attractive free-standing building situated on a high traffic street in a desirable community in the heart of east Texas. The practice has realized annual revenue of seven figures with exceptional profitability. The office features a 4-chair ortho bay, 2 exam rooms, and digital pan/ceph unit. The real estate is also available for purchase.
HOUSTON-NORTHEAST (ID #488): FFS/PPO practice and real estate, growing suburb 45 minutes NE of Houston. 1,800 total patients, steady flow of new patients, solid hygiene recall, and consistent revenue of high-6 figures per year. The office contains 6 fully equipped operatories, plumbed nitrous, digital X- rays, CBCT, and computers throughout.
DSO C S PRACTICE SALES Email: texas@dentaltransitions.comPRACTICE
www.tda.org | August 2022 521 nitrous, and computers throughout.
EAST TEXAS (ID #489): This highly profitable, general dentistry practice and real estate is located in an east Texas town. The practice serves a large FFS/PPO patient base and is on pace to exceed 7 figures in revenue in 2021 while maintaining a 45%+ profit margin. The office has 3 fully equipped operatories with possible room for expansion, digital radiography, and computers throughout.
APPRAISALS Austin 512-900-7989 DFW 214-960-4451 Houston 281-362-1707 San Antonio 210-737-0100 South Texas 361-221-1990
SAN ANTONIO, ORTHODONTIC (ID #547): Rare opportunity to purchase a primarily FFS orthodontic practice in north central San Antonio. The facility has a modern feel and is equipped with a 3-chair open bay, 2 additional private treatment rooms, and digital radiography. In 2021, revenue was high-6 figures with strong net cash flow. The practice has been a staple in the community with over 40 years at its present location and is located near several highly desirable neighborhoods.
ADVERTISING BRIEFS
522 Texas Dental Journal | Vol 139 | No. 8 operatories, digital radiography, computers throughout, and a 3D Cone Beam CT in the well-appointed 2,400 sq ft modern space. Annual revenues are around 7 figures, and the owner is open to a phased transition in which they provide support to the incoming buyer to ensure they are set up for long term success.
SAN ANTONIO (ID #550): Established general dentistry practice and real estate in northeast San Antonio. The approximately 3,600 sq ft office is located in a free-standing building and is equipped with 7 operatories, digital radiography, intra oral cameras, and computers in operatories. The practice has a strong hygiene recall program, over 2,700 active patients, and provides tremendous upside potential. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions. com or contact us at 512-900-7989 or info@ dentaltransitions.com.
HOUSTON-CENTRAL (ID #552): Established, boutique practice located in the highly desirable Museum/River Oaks district of central Houston. The practice provides general, implant, and cosmetic dentistry services to a 100% FFS patient base and has an excellent reputation in the local community. The beautiful facility features high-end finishes/ decor, 3 fully equipped operatories, digital radiography, and a CBCT.
BEAUMONT—GENERAL (REFERENCE “BEAUMONT”): Small town practice near a main thoroughfare. 80 miles east of Houston. Collections in 7 figures. Country living, close enough to Houston for small commute. Practice in a stand-alone building built in 1970. The office is 1,675 sq ft with 4 total operatories, 2 operatories for hygiene and 2 operatories for dentistry. Contains, reception
HOUSTON-NORTH (ID #553): Large, extremely profitable practice and real estate in north Houston (Spring/ Woodlands). The 5,600 sq ft standalone building contains 10 fully equipped operatories, computers throughout, digital technology, and room for future expansion. The massive active patient base is comprised of Capitation (40%), PPO (35%), Medicaid (15%), and FFS (10%) with 175+ new patients visiting the office per month. The owner is open to exploring a sale to a DSO, multi-location owner, or a well-qualified private practitioner. The 10,000+ sq ft property is also available for sale which offers additional rental income and the possibility for future development.
CORPUS CHRISTI: Want to enjoy coastal living? Allen Dental Group is a dentist-owned and operated private practice with 3 locations and 5 dentists in the Corpus Christi area, just minutes away from the beach! We are proud to say that we have been serving our community for 75 years under the leadership of a third generation dentist, Dr Chad Allen. We have consistently grown over the last decade and are looking for a dentist with excellence and integrity to join our group. We are proud to provide patient focused treatment using the latest technology. We believe in having high standards of patient care and how we treat our team. The ideal addition to our team has the ability to be a team player, excel at the specific skills required and have a willingness to grow. Services provided include operative, cosmetic, implant, endodontic, and clear aligner dentistry. We are selective about insurances we are in contract with, no Medicaid. Ownership options are available to dentists within our practice along with invaluable mentorship. Come be a part of a group that strives for excellence in patient care and friendship amongst dentists! Please submit your CV to Lindsey at allendentalgrouplinds@gmail.com.
ADVERTISING BRIEFS area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 38 years. Practice sees patients about 16 days a month. Collection ratio of 100%. The Practice is a fee-for-service practice. Building is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com. HOUSTON (SHARPSTOWN AREA) —GENERAL (REFERENCE “SHARPSTOWN GENERAL”) MOTIVATED SELLER. Well established general dentist with high6 figure gross production. Comprehensive general dentistry in the southwest Houston area focused on children (Medicaid). Very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. Over 1,200 active patients. 20% Medicaid, 45% PPO, and 35% fee-for-service. 30% of patients younger than 30. Office open 6 days a week and accepts Medicaid. Contact Christopher Dunn at 800-930-8017 or Christopher@ DDRDental.com. HOUSTON (BAYTOWN AREA)— GENERAL (REFERENCE “BAYTOWN GENERAL”). MOTIVATED SELLER. Well established general practice with mid-6 figure gross production. Comprehensive general dentistry in Baytown on the east side of Houston. Great opportunity for growth! 1,400 sq ft, 4 operatories in single story building. 100% collection ratio. 100% fee-for-service. Practice focuses on restorative, cosmetic and implant dental procedures. Office open 3 - 1/2 days a week. Practice area is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
www.tda.org | August 2022 523
HOUSTON—GENERAL (SHARPSTOWN): Well established general dentist with high-6 figure gross production. Comprehensive general dentistry in the southwest Houston area focused on children (Medicaid). Very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. Over 1,200 active patients. 20% Medicaid, 45% PPO, and 35% fee-for-service. 30% of patients younger than 30. Office open 6 days a week and accepts Medicaid. Contact Chrissy Dunn at 800-930-8017 or chrissy@ddrdental.com and reference “Sharpstown General or TX#548”.
HOUSTON, COLLEGE STATION, AND LUFKIN (DDR DENTAL Listings). (See also AUSTIN for other DDR Dental listings and visit www. DDRDental.com for full details. LUFKIN— General practice on a high visibility outer loop highway near mall, hospital and mature neighborhoods. Located within a beautiful single-story, free-standing building, built in 1996 and is ALSO available for purchase. Natural light from large windows within 2,300 sq ft with 4 operatories (2 hygiene and 2 dental). Includes a reception area, dentist office, a sterilization area, lab area, and break room. All operatories fully equipped. Does not have a pano but does have digital X-ray. Production is 50% FFS and 50% PPO (no Medicaid), with collection ratio above 95%. Providing general dental and cosmetic procedures, producing mid-6 figure gross collections. Contact Christopher Dunn at 800930-8017 or Christopher@DDRDental.com and reference “Lufkin General or TX#540”.
HOUSTON—PEDIATRIC (NORTH HOUSTON): This practice is located in a highly soughtafter upscale neighborhood. It is on a major thoroughfare with high visibility in a strip shopping center. The practice has 3 operatories for hygiene and 2 for dentistry. Nitrous is plumbed for all operatories. The practice has digital x-rays and is fully computerized. The practice was completely renovated in 2018. The practice is only open 3 - 1/2 days per week. Contact Christopher Dunn at 800-9308017 or christopher@ddrdental.com and reference “North Houston or TX#562”. WEST
ADVERTISING BRIEFS
524 Texas Dental Journal | Vol 139 | No.8 HOUSTON AREA: Several acquisition opportunities in the greater Houston area. General, ortho, pedo practices available for sale. Visit lonestarpracticesales.com or email houstondentist2019@gmail.com.
HOUSTON—GENERAL (PEARLAND AREA): General located in southeast Houston near Beltway 8. It is in a freestanding building. Dentist has ownership in the building and would like to sell the ownership in the building with the practice. One office currently in use by seller. 60% of patients age 31 to 80 and 20% 80 and above. Four operatories in use, plumbed for 5 operatories. Digital pano and digital X-ray. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com and reference “Pearland General or TX#538”.
www.tda.org
HOUSTON—MOTIVATED SELLER: Medicaid practice with production over 6 figues. Three operatories in 1,200 sq ft in a strip shopping center. Equipment is within 10 years of age. Has a pano and digital X-ray. Great location. If interested contact chrissy@ddrdental.com. Reference “West Houston General or TX#559”.
INTERIM SERVICES HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512517-2826 or drzoch@yahoo.com.
SAN ANGELO: To those desiring the perfect balance between work and play: Are you interested in taking over a successful readymade practice with a great salary low-to-mid 6 figures. Located in west central Texas, San Angelo is a city of 100,000+ but offers a small town feel and excellent quality of life. The city was named the Visual Arts Capital of Texas in 2021 and is alive with a vibrant mixture of arts and culture for children and adults. It is consistently ranked as one of the best small cities for business and employment. San Angelo is home to award winning Angelo State University, 3 lakes, the beautiful Concho Riverwalk, an incredible nationally ranked Art Museum, and one of the best preserved forts in the nation, Fort Concho—all with numerous kid-involved programs. As a Texas friendly city, live music is offered almost daily at one of many venues and one-of-a-kind restaurants in town. The community is diverse, with an active young professional group, outstanding medical facilities, ranked sports teams, great hunting and fishing, and a low cost of living. Easy traffic takes you anywhere in the city within 10 minutes. It’s a great place to raise a family and a great place to live, work, and play. The 2,400 sq ft newly remodeled dental office, built to accommodate 2 dentists, is a free-standing building with natural light in each operatory. An extremely healthy hygiene program is in place with 2 hygienist. There are 6 operatory rooms—4 equipped. The majority of practice is FFS cash, with over 3,000 active patients. The practice has an excellent reputation in the local community. A bonus package is included for preferred equipment needs. Contact Geremy Haseloff @ 806-777-4732 or geremy.haseloff@ henryschein.com.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
| August 2022 525
ADVERTISING BRIEFS
526 Texas Dental Journal | Vol 139 | No. 8 PRN Helpline (800) 727-5152 Visit us online www.txprn.com YOURTRUSTPATIENTSYOU. WHO CAN YOU TRUST? If you or a dental colleague are experiencing impairment due to substance use or mental illness, The Professional Recovery Network is here to provide support and an opportunity for confidential recovery. Anesthesia Education & Safety Foundation ......... 491 Choice Transitions .......................... Inside Back Cover JKJ Pathology ............................................................. 497 Law Offices of Hanna & Anderton ...................490 McLerran & Associates......................................521 Penumbra Diagnostics ......................................484 Professional Recovery Network ............................. 526 SmileCon 2022 ......................................................... 482 Southwest Sedation Education .............................. 484 TDA Perks ........................................ Inside Front Cover Texas Health Steps .................................................. 479 UTHealth Houston Pathology................................. 501 ADVERTISERS