HUMAN PAPILLOMA VIRUS (HPV)-RELATED ORAL CANCER AND HPV-RELATED ORAL EPITHELIAL DYSPLASIA
MADHU SHRESTHA, PHD, MS, MDS, BDS ASHIM SHRESTHA
84
PRE-RADIATION HEAD AND NECK EXAMINATION FOR DENTAL CLEARANCE PRIOR TO TREATMENT
AMERIAN D. SONES, DMD, MS 90
TOOTH-LEVEL PREDICTORS OF TOOTH LOSS AND EXPOSED BONE AFTER RADIATION THERAPY FOR HEAD AND NECK CANCER
RAJESH V. LALLA, DDS, PHD; JAMES S. HODGES, PHD; NATHANIEL S. TREISTER, DMD, DMSC;
THOMAS P. SOLLECITO, DMD; BRIAN L. SCHMIDT, DDS, MD, PHD; LAUREN L. PATTON, DDS; ALEXANDER LIN, MD; MICHAEL T. BRENNAN, DDS, MHS
Reprinted with permission from The Journal of the American Dental Association
104
WHEN TEETH TELL TALES: THE VITAL ROLE OF DENTAL RECORDS IN LAW AND ETHICS
KATHLEEN NICHOLS, DDS
DIANE RHODES
DEBRAH ROGERS
THANK YOU, 2025 TDA PERKS PROGRAM SIGNATURE SPONSORS, FOR HELPING MAKE THIS AWESOME PARTY POSSIBLE!
TDA Perks Aisle
Jacqueline
Madhu Shrestha, PhD, MS, MDS, BDS
Ashim Shrestha
Rajesh V. Lalla, DDS, PhD; James S. Hodges, PhD; Nathaniel S. Treister, DMD, DMSc; Thomas P. Sollecito, DMD; Brian L. Schmidt, DDS, MD, PhD; Lauren L. Patton, DDS; Alexander Lin, MD; Michael T. Brennan, DDS, MHS
The article was reprinted with permission
TEETH TELL TALES: THE VITAL ROLE
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Don’t Get Locked Out— Ensuring Ethical Record Access
Kathleen Nichols, DDS
Diane Rhodes
Debrah Rogers
108 MEMBER SPOTLIGHT: FAMILY TIES—THE DOCTORS VAN WART 112 FBI: FOUND BUT NOT IDENTIFIED (YET)
Kathleen A. Kasper, DDS, D-ABFO
66 In Memoriam
118 Value for Your Profession: Equipped for the Unexpected: Essential Tools for Successful Sedation Outcomes
122 Classifieds
127 Index to Advertisers
About the Cover April is Oral Cancer Awareness Month. This special issue of the Texas Dental Journal provides insight into what some patients experience before and after receiving a diagnosis of oral cancer in a dental office and the value they place in that care.
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 142 | No. 2
Texas Dental Journal (ISSN 0040-4284) is published monthly, except January-February, March-April, July-August, and November-December, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2025 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement at tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Georganne P. McCandless, DDS TDA President, 2024-2025
One Big Thing: Membership Matters
It has been my great honor to be your TDA president and to work on behalf of our beloved profession. As I have traveled the state proudly representing you as your president, one thing has been apparent: membership in organized dentistry and our shared experiences as essential health care providers does matter. Dentistry can be hard in the best of ways. And when we come together in our various roundtables we can share our experiences and help one another.
Why it Matters: As mental health and well being in our profession has moved to the forefront, membership in our association is even more important today. One is but the loneliest number. When dental professionals come together in an organized way with one big voice, the dividends are innumerable. The benefits of membership in a professional association have long been reported on. It can not only improve personal and professional growth but can lead to opportunities unseen. Such benefits include:
• Opening yourself up to new professional possibilities—like becoming TDA president
• Being a part of a larger community that not only understands you, but can support you in every way
• Mentorship
• Fellowship
• The ability to influence and direct the future of our profession
• Tangible benefits like affordable health care, CE opportunities, partnerships with endorsed vendors, political advocacy
The Big Picture: There is plenty of hidden value in organized dentistry. There are plenty of tangible benefits in organized dentistry. But what there is not is plenty of active participation by our members. So as I end my year as your president, I would challenge you, what are you giving to your profession?
• Are you participating in your local components?
• Are you inviting your friends to these meetings?
• Are you saying yes to a leadership position?
• Are you offering to be an ear to listen to our younger colleagues?
Giving to your profession and receiving are different things and I promise you that what you give to your profession will give back to you 10 times over. Our members are the ties that bind our association together and I have been the beneficiary of our shared experiences.
Thank you for that!
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com
Board of Directors Texas Dental Association
PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PRESIDENT-ELECT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
VICE PRESIDENT, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and 4
Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
P R E V I E W
SPEAKER
Karen Reisman, MS
will be presenting the following session at the TDA Meeting:
Communicate like Duct Tape: Gain Traction with Your Patients, Team, and Colleagues
Friday, May 9
1:00 PM – 3:30 PM
Event #: F32
How Do You Get Your Message Heard in a Case Presentation?
You use duct tape from time to time. It’s sticky, reliable, and does the trick.
Using duct tape as our analogy, I want you to communicate more like duct tape. Namely, get stickier with your case presentations. And while we’re at it, get stickier at your team huddles, your dental study clubs, and your board reports if you’re active in your local dental society and/or with the Texas Dental Association.
I guarantee you’ll have more fun delivering your messages with a higher chance that your listeners will retain more of what you’ve said. And that patients, team, peers and maybe even your teenage kids!
Context
You are a “sieve head”. Yes, you read correctly. You and everyone you talk to is wearing a metaphorical sieve on their heads. This kitchen utensil, very helpful when making pasta and draining the hot water from your cooked noodles, has holes. Lots of water goes through those holes.
This same “sieve” process happens when you communicate. Think of the 24/7 buffet of information that hits you these days. You probably hear most of the info, but 75% lands in the sink, just like cooked pasta water. This is unacceptable!
Umm…. How often do your patients ask your chair side assistant once you’ve left to check hygiene, “What did the doctor say?” (just sayin’…).
We are in the midst of an attention crisis! Let’s talk about how to keep 75% IN the sieve and only lose 25% of your content.
three predicable ways to have stickier content
1. Use the Magic Power of 3 Rule
My favorite number is 3. If you want your patients and team to retain what you’re saying—divide your thoughts into 3 categories, reasons, or points. You can use the Magic Power of 3 on email too.
Give each section a SHORT label and number your categories/ reasons. Then discuss each of your 3 main points.
Example: “ There are 3 aspects to your case plan—#1 time involved, #2 our outcome, and #3 the process. Let’s start with talking about time—how long will this take to accomplish…”
Another example about addressing obstacles: “Patient, you’re probably concerned about time, pain, and money. Let’s discuss these 3 concerns now. First, time…”
2. Think “Less is More”
A study was done at a jam tasting. OK—you’ve never been to a jam tasting so just imagine this study as a wine tasting, it’s sexier anyway. In this study 1 table had 6 bottles of wine. The other table had 24. Rounding the numbers, 60 percent of the people went to the table with 24 bottles. Forty percent went to the table with only 6 bottles. More people gravitated to where there were more choices. BUT WHEN IT CAME TO PURCHASING THE WINE —only 3% bought from the table of 24 bottles. A whopping 30% bought
from the table with ONLY 6 bottles. Less options—more sales.
Too many options become a paradox of choice. A confused listener tunes out. A confused buyer says, “NO.”
You talk too much! So do I. The more we talk the less “sticky” we get. Embrace your inner editor by asking yourself, “So what? Who cares? Is anyone interested besides me?”
How cluttered is your space where you’re doing your case presentation? Are you showing too many models? Too many before/ after photos? Too many diplomas?! Too many options?
3. Use “Velcro” Velcro consists of 2 pieces of cloth, 1 with loops and the other with hooks, that attach to each other. I use Velcro as an analogy for a way to communicate with even more listener retention.
Let’s use the Super Bowl for our Velcro example. There are always 2 main sports commentators per game. Several times recently the Super Bowl announcers have been Jim Nance and Tony Romo (that cute guy with the dimples who was once the Dallas Cowboys quarterback… but I digress here!). Jim Nance describes the “play-byplay” aka the data. Tony Romo provides “color commentary” aka the “Velcro”—background stats, interesting factoids, stories about the athletes, the stadium, the history of the teams, on and on. TOGETHER these 2 announcers form 1 memorable voice.
The great news for you: use this method to communicate like duct tape. You, too, will be more memorable.
The challenging news for you: You have to be both Jim (convey your data) and Tony (add your “Velcro” examples, visuals, understandable stats, stories, analogies and humor.)
In this article (and congrats if you’ve gotten this far!) I’ve used Velcro throughout from “duct tape” to the jam study to the sports announcers.
In your practices, you get involved—and rightfully so— with your facts and figures. But if you only do that half of the puzzle you will not be sticky. Please add in the creative support material.
Next steps for you
1. Have clarity by using the Magic Power of 3.
2. Be concise by adopting a less is more philosophy.
3. Communicate with creativity by adding Velcro.
A compelling case presentation, team huddle, conversation or even a dinner table exchange is never just about the data.
Karen Cortell Reisman, communication speaker, author, and coffee ice cream eater, works with dentists on their case presentations and dental lectures, speaks to dental associations from Yankee to Pankey, and coaches leaders on how to “Speak For Yourself” to make even more money. Learn more at www.KarenCortellReisman.com. She’s looking forward to speaking for the fourth time at the TDA Meeting in May!
Malpractice insurance that’s all about you .
As a dentist, you face unique challenges every day. That’s why at MedPro Group, we created an industry-leading malpractice policy that keeps you safe. Here’s what else you can expect with MedPro on your side.
Get unmatched coverage. Practice more safely.
You’ll get great coverage at a great price. We also offer policy options that others don’t — including Occurrence and a pure consent clause, which gives you more control during a claim.
With 24/7 access to our free risk resources and on-staff experts, you and your practice will be better prepared for every day challenges. We don’t just defend claims, we help you avoid them.
Protect your good name.
The average dentist is sued at least once in their career, which is why we’re in your corner when it matters most. We lead the industry with a 95% dental trial win rate (plus 8 out of 10 claims close without payment).
Notice
Texas Dental Association Delegates
Per the TDA Bylaws, “The proposed annual budget shall be submitted by the Board of Directors to the members of the House of Delegates at least thirty (30) days prior to the opening of the annual session of the House of Delegates.”
Thus, the 2026 Proposed Budget, including a financial report from TDA Secretary-Treasurer
Dr Carmen Smith, will be available on tda.org no later than April 8, 2025.
LAW OFFICES OF MARK J. HANNA
• Representation Before the Texas State Board of Dental Examiners
Mark J. Hanna JD Former General Counsel, Texas Dental Association
Oral Cancer: Managing Awareness and Diagnosis
Jacqueline M. Plemons, dds, ms
Clinical Professor, Department of Periodontics, Texas A&M University College of Dentistry, Dallas, Texas; Director, Stomatology Division, Texas A&M University College of Dentistry, Dallas Texas; Periodontist, Private Practice, Dallas, Texas; Editor, Texas Dental Association
Dr jacqueline M. Plemons
Introduction
Have you found your passion in dentistry? I often tell my friends and colleagues that I make my living practicing periodontics, but I probably contribute my share of the “good in the world” by helping patients with oral medicine problems. These patients are often in pain and struggle with the challenge of navigating the bridge between medicine and dentistry. Nowhere is this feeling more palpable than when managing patients with oral cancer.
Dentists are often the first health professionals to notice the signs of oral cancer. Because we routinely examine patients at least twice a year on a regular basis, we have the unique opportunity to recognize the nuances of tissue changes. I often tell dental students that you don’t always have to know what the lesions or conditions are, you just need to know that something is not right and follow up by appropriate referral.
April is Oral Cancer Awareness Month, and this special issue on oral cancer of the Texas Dental Journal provides insight into what some patients experience before and after receiving a diagnosis of oral cancer in a dental office and the value they place in that care. In addition, we review procedures that are commonly included when dentists are asked to provide “clearance” for patients to begin radiation therapy. Finally, we examine the relationship between human papilloma virus-associated oral cancers and the potential for early cancer detection as well as prediction for future progression.
As we begin, I’ve included a short description of 3 patients I examined in a rather unusual week and a half in my practice. This special issue on oral cancer is dedicated to them.
95-year-old female with SCC on the anterior gingiva.
57-year-old female with SCC on the right ventral tongue.
51-year-old female with SCC on the mandibular right facial gingiva.
A Walk in Their Shoes: Interviews with Oral Cancer Patients
Deborah M. Foyle, DDS, MS, MSc
Diplomate of the American Board of Periodontology, Clinical Associate Professor, Interim Department Head of Periodontics, Director of Predoctoral Periodontics, Interim Department Head of Endodontics, Texas A&M University College of Dentistry, Dallas, Texas
Having the opportunity to speak with several patients who were diagnosed with oral squamous cell carcinoma was a humbling and uplifting experience. Without exception and despite their diagnoses, this small sample of patients expressed gratitude to have been diagnosed appropriately and treated. Their collective resilience and positive attitudes were remarkable considering what they had experienced up to this point. I felt very fortunate to spend time with each of them.
Patient #1
Patient #1 had a lesion on her tongue that she first noticed 6 or 7 years ago, and at that time, her dentist referred her to an oral surgeon for a biopsy, which was negative. Her dentist continued to monitor the lesion for several years until a significant change was noted. She was referred to her original surgeon for another biopsy. This proved to be a challenging experience for the patient as she felt discussions were very abrupt and her dentist felt that her visit was a waste of his time. No biopsy was performed, and she was very upset by his attitude and apparent lack of empathy. After about 9 months with no improvement, her dentist referred her to the Stomatology Clinic at Texas A&M College of Dentistry.
The faculty member and resident advised an immediate biopsy which confirmed squamous cell carcinoma and she was subsequently referred to a local ENT for treatment. As she had a previous history of aggressive renal cancer, she joked that she did not have a meltdown when she was diagnosed with squamous cell carcinoma (SCC), and that if she was going to get bad news, her periodontist at the Stomatology Clinic was a wonderful person to have to deliver it. She was grateful to finally know what she was dealing with but expressed regret for the 9-month delay in getting her diagnosis, although thankfully there appeared to be no spread to her lymph nodes.
Her treatment involved surgery on the right ventro-lateral surface of her tongue, which went well, but she was totally unprepared for the pain and discomfort following the surgery. It significantly
Dr deborah m. Foyle
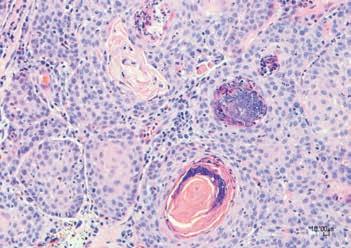
Histologic features of a cancer. Courtesy of Celeste Abraham, DDS, MS
affected her ability to eat, sleep, and talk. Recovery was difficult and it took several weeks before she could function normally again. She admitted that she hadn’t really looked beyond the actual surgery to imagine how recovery would be! As it was caught early, she felt very fortunate that the only treatment she needed was surgery and she did not require radiation or chemotherapy.
She feels very confident in her healthcare providers and very fortunate regarding her treatment. However, she did mention that should her cancer recur, she would probably not elect to have any more surgery as it significantly affected the quality of her life at that time.
She commented that her providers should have been involved much sooner than they were. She regrets the 9-month delay in getting her second biopsy; although, she is so very grateful that she got treatment before it spread further.
Patient #2
Patient #2 noted a small sore in his mouth in the lower left retromolar pad area adjacent to one of his dental implants. He mentioned it to his restorative dentist who initially prescribed Chlorhexidine (CHX) mouthrinse, followed by another rinse as the CHX was ineffective. When no resolution of the lesion was seen, the patient was referred to the Stomatology Clinic at Texas A&M College of Dentistry. An excisional biopsy was performed which confirmed squamous cell carcinoma (SCC), and the patient was referred to a surgeon for further treatment. As he was waiting for his biopsy results, he had it in the back of his mind that it was probably cancer as he had a previous history of treated Stage 4 Non-Hodgkins lymphoma 16 years ago. He stated that having some knowledge of cancer and its treatment made him better able to cope with his new diagnosis. His previous
cancer treatment involved a kidney transplant which limited some of his treatment options for the new SCC. For example, immunotherapy was not recommended as this could interfere with his anti-rejection medication.
His treatment involved aggressive surgery to remove almost half his jaw, with the mandible replaced with bone from his leg and a titanium rod placed in his leg. Two of his lymph nodes were removed. Following the surgery, he was treated with 30 rounds of radiation and 8 rounds of chemo. He felt that recovery from the treatment, especially the radiation, was very difficult. The pain from the radiation burns continues to require serious pain medication and the side effect of losing his sense of taste and the facial hair on his left side was an adjustment—although he joked that shaving doesn’t take nearly as long now!
His chief concern now is being able to have teeth on his lower arch again. Treatment is on hold until he is cleared by his surgeon and then there is the added concern of the cost for his treatment going forward. Medical insurance does not pay for his dental rehabilitation.
Patient #3
Patient #3 was diagnosed with papillary thyroid cancer in 1994 and was treated with surgery and radioactive iodine at that time and again in 2020 and 2022 when the cancer recurred. She also had breast cancer in 1996 and was treated with surgery, chemo, and radiation.
In January 2025 the patient was referred by her dentist to a periodontist for a white lesion on the left side of her mouth, which was diagnosed following biopsy as mild dysplasia. At that time, a lesion was also noted on her right posterior facial gingiva which was also biopsied. That lesion was indicative of
Patient 2: Squamous cell carcinoma involving the retromolar pad posterior to dental implant.
Patient 3: Oral cancer (SCC) affecting the facial gingival (example).
SCC. The patient said she wasn’t as surprised or shocked as would be expected when she got her diagnosis, based on her previous cancer history. She stated that she was very positive about her outcome as she’d beaten it before. She felt like she was in good hands and her recommendation was to find the right doctors—she feels very fortunate that was her current experience.
Her treatment included surgery to remove the tumor, 3 teeth, and their associated bone. She is still recovering and is not in as much pain as she was expecting. Opening her jaw is a little difficult and painful. She reports that grinding her teeth is not helping much, especially as her bite guard no longer fits.
She is scheduled to start 30 rounds of Proton radiation therapy in a few weeks (2 months after her surgery). She is aware that she may have a lot of pain after the radiation but is determined to beat this cancer. She was also concerned that her medical insurance won’t cover her dental rehabilitation.
Patient #4
Patient #4 was diagnosed with SCC on the right lateral border of his tongue in May 2024. His dentist noted a spot on the left side of his tongue several years ago and referred him to an oral surgeon. A biopsy was performed which confirmed that it was negative for cancer. Two years later, the patient noticed a spot on the right side of his tongue and went to his dentist
who referred him to a local periodontist. Tissue specimens were obtained via biopsy and confirmed as SCC. He praised his dental care provider’s delivery of the bad news and was grateful for her kindness and empathy. She referred him to an ENT for further treatment which included surgery resulting in loss of a significant portion of his tongue along with 27 lymph nodes, one of which was positive for SCC. He subsequently endured 30 rounds of radiation which was painful and left his mouth extremely dry which nothing sems to help. He needed dental clearance prior to radiation, and it was recommended that he had a tray made for fluoride delivery, however he could not tolerate the tray following treatment and instead has frequent check-ups with his dentist where he receives fluoride treatment to prevent caries.
Post surgery he has noticed considerable drooping of the right side of his mouth which exacerbates his difficulty in speaking. He is undergoing speech therapy. He still has sores from the radiation both intraorally and on his face and neck. The lotion he was prescribed for his skin seems to help but he reported that nothing works intraorally. Recently he noticed pain in his ear and an enlarged and hard lump in one of his lymph nodes. He is currently awaiting the results of a biopsy for that.
After talking to these inspiring people, it was interesting to note that they seemed to be coping with their medical challenges in a positive way. Their fear following diagnosis had been replaced by hope for the future with the help of their family and friends. They were so grateful for the care they received and the empathy and kindness with which they were treated.
A resounding theme I noticed was that none of the patients felt prepared for how difficult the healing phase would be after either the surgery or the radiation. Perhaps this is an important opportunity we can all take to help provide the best care available for our patients.
Patient 4: Lesion on right ventral surface of the tongue.
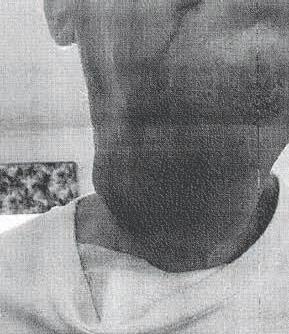
Patient 4: Significant lymphadenopathy in the neck prior to treatment.
Human Papilloma Virus (HPV)related oral cancer (HPV-OSCC)
and HPV-related Oral epithelial dysplasia (HPV-OED)
understanding the spectrum of the HPV-related cancers and pre-cursor lesions in the oral cavity
Madhu Shrestha, PhD, MS, MDS, BDS
Clinical Assistant Professor, Texas A&M University College of Dentistry, Dallas, Texas
Ashim Shrestha
Year 1 Grad Student, Oral and Maxillofacial Pathology, Texas A&M University College of Dentistry, Dallas, Texas
Abstract
Human papillomavirus (HPV)-related cancers have gained significant attention due to their increasing incidence and evolving demographic trends. While oropharyngeal HPV-related carcinomas are well studied, the role of HPV in non-oropharyngeal sites remains underexplored. HPV-related oral epithelial dysplasia (OED) represents a potential precursor lesion for malignancy in the oral cavity. Unlike HPV-driven oropharyngeal squamous cell carcinoma (OPSCC), which has well-defined diagnostic and prognostic markers, HPV-related OED remains poorly understood. This review aims to provide a comprehensive overview of HPV-driven dysplasia in non-oropharyngeal regions, including its epidemiology, histopathology, diagnostic criteria, and potential for malignant transformation. This review also highlights the emerging role of tests such as p16 and HPV DNA in identifying high-risk lesions and highlights the need for long-term studies to better understand the natural history of HPV-related OED.
Dr Madhu Shrestha
Ashim Shrestha
Human Papilloma Virus and Oral cancer
Human papillomavirus (HPV), a doublestranded DNA virus, is linked to about 5% of cancers, including those of the cervix, penis, vulva, vagina, anus, and oropharynx.1 High-risk types like HPV-16 and HPV-18 can persist in the body and may lead to precancerous lesions that could progress to cancer if untreated, while low-risk types such as HPV-6 and HPV-11 are generally non-cancerous but can cause benign conditions like genital warts.2 HPV is also the leading cause of HPV-related oral cancers. HPV-related oral cancers are the cancers that belong to the category of “oropharyngeal cancers”, a type of head and neck cancer, that mostly develops in the oropharyngeal regions, which includes the tonsils, the base of the tongue, the soft palate, the posterior and lateral pharyngeal walls and uvula (the side and back walls of the throat).
Changing trends in Oral cancer
While the incidence of conventional oral carcinoma (oral squamous cell carcinoma, non-HPV) that are mostly attributed to smoking are decreasing in the United States, oropharyngeal cancer (HPV-related) is the eighth leading cancer in males in 2024 with an estimated 58,450 new cases (2.9% of all new) and 12,230 cancer related deaths (2% of all cancer deaths). HPVrelated oral cancer (HPV-OSCC) has surpassed cervical cancer as the fourth most common cancer with the fastest increasing mortality rate.3-5 In the past 20 years, the rate of HPV-positive oral
squamous cell carcinoma (OSCC) has risen from under 20% to over 70% in the United States and some European countries.6
This epidemiological shift is attributed to changes in sexual behaviors, including increased oral-genital contact, earlier onset of sexual activity, and a reduction in tobacco-associated head and neck cancers. Unlike traditional tobacco and alcohol-related head and neck malignancies, HPV-positive OPSCC is more common in younger, nonsmoking individuals and is associated with a favorable prognosis due to its increased sensitivity to radiation and chemotherapy.7 In the UK and USA, oropharyngeal cancer in men has become more common than cervical cancer in women.8 Recently, an increase in the incidence of oropharyngeal HNSCC, specifically the tonsil and tongue base has been documented in the United States, most notably among individuals ranging in age between 40 and 55 years.8
Challenges in HPV-related oral cancer
As mentioned earlier, HPV-related oral cancers are the cancers that belong to the category of “oropharyngeal cancers”, a type of head and neck cancer, that mostly develops in the oropharyngeal regions, which includes the tonsils, the base of the tongue, the soft palate, the posterior and lateral pharyngeal walls and uvula.
Despite increasing numbers currently in the United States, lack of awareness of HPV-OSCC remains a challenge in
diagnosis and management. Routine screening in high-risk populations could improve early detection and outcomes. However, unlike oral cavity proper lesions (lesions that are in the anterior aspect of the oral cavity), which can be detected visually, oropharyngeal precancerous lesions are often hidden in deep anatomical structures of the oro-pharynx which is located deep down in the throat and often poses significant difficulty in early visual changes or palpation methods. This makes early detection challenging, leading to delayed diagnosis and treatment. Moreover, due to the asymptomatic nature of early HPV-driven dysplastic lesions in the oropharynx, most patients present with advanced-stage disease. There is also a limitation to studying the precursor cancer model in oropharyngeal cancer. Current animal models fail to replicate the full spectrum of HPV-driven carcinogenesis in the oropharyngeal region.9 Developing more accurately invivo models is crucial for understanding disease progression and testing therapeutic interventions. There are subtle histopathological differences between HPV-OED and conventional dysplasia.10-13
An experienced oral pathologist may be able to differentiate between such. HPVrelated OED presents histopathological features such as koilocytosis, nuclear pleomorphism, and increased mitotic figures. Understanding these distinctions is essential for accurate diagnosis and risk stratification.12
Diagnostic
Approaches for HPV-Related OED and use of p16 IHC (immunohistochemistry) as a Surrogate Marker
P16INK4a immunohisto-chemistry (IHC) is commonly used to help diagnose HPV-related precancerous cervical lesions, with most results being clearly positive or negative. However, there are instances where the p16 expression is unclear, meeting some but not all the characteristics of a “block-positive” pattern. This uncertainty leads to questions about whether the p16 immunoreactivity genuinely points to an oncogenic HPV infection or suggests a possible risk of progression.14 Recent research, especially in oropharyngeal carcinoma, has found a clear link between HPV detection and increased p16 protein levels in tumor cells. This has led to suggestions that p16 expression could replace traditional HPV testing in clinical practice. The reason for this shift is that p16 IHC is simpler, more affordable, and easier to perform, making it a useful alternative for identifying HPV infection, particularly in places where more complex HPV testing isn’t easily accessible.15 Confirmatory Molecular Testing PCR and ISH are gold-standard methods for confirming HPV presence. PCR detects viral DNA, while ISH visualizes HPV RNA or DNA within tissue samples, providing spatial context and confirming the association with dysplastic cells. A positive DNA ISH result means that the test detected the presence of HR-HPV DNA in the sample, indicating that the cells contain the viral DNA. An additional marker such as Ki-67 can supplement HPV diagnosis by indicating increased
Clinical presentation of an oropharyngeal carcinoma in the tonsillar area: Extensive ulceroproliferative, erythematous lesion. Note the challenging and limited accessibility of monitoring the early pre-neoplastic changes.
2. HPV-related oral carcinoma in non-oropharyngeal site (NOP-HPVOSCC): Notice the ulceroproliferative, nodular lesion with a granular surface architecture in a non-oropharyngeal site such as the mandibular gingiva.
(Image courtesy of Dr Nicolas Bebeau, Oral & Maxillofacial Surgeon).
3. Precursor lesions of HPV-related oral cancers: High-grade HPV-related oral epithelial dysplasia (HPV-OED) may present as simple whitish appearing papillary surfaced leukoplakic plaques or as thick velvety white corrugated leukoplakia and may occur in the non-oropharyngeal sites such as lateral and ventral tongue/floor of mouth.
(Image courtesy: Dr Stephen S. Walker, Periodontist).
Figure 1.
(Image courtesy: Professor John M Wright, DDS, Professor Texas A&M University)
Figure
Figure
cellular proliferation and dysregulation. These markers help differentiate HPVdriven dysplasia from other epithelial abnormalities.
Precursor lesions in HPV-related oral cancer
Causation remains unclear regarding the role of HPV infection in HPVrelated OSCC (non-HPV-OSCC) and its pre-malignant precursor, oral epithelial dysplasia (HPV-OED). There is no specific clinical presentation or reliable histologic criteria to differentiate HPV-related oral epithelial dysplasia (HPV-OED) from conventional non-HPV-related oral epithelial dysplasia (non-HPV-OED).10,12,13 While immunohistochemical (IHC) testing for p16 is used as a surrogate marker, it is not sensitive enough and specific to determine high-risk HPV status compared to DNA/RNA in-situ hybridization. Most HPV-OED are high grade (2-tier grading) or moderate or severe (3-tier system) at diagnosis. Currently, there are no guidelines to routinely screen for p16 and/or highrisk HPV status in cases of oral epithelial dysplasia. Although studies indicate the role of HPV infection in oral epithelial dysplasia (HPV-OED) as well as its progression to either HPV-related oral squamous cell carcinoma (HPV-OSCC) or non-HPV related (non-HPV-OSCC) or conventional OSCC, there are few long-term follow-up or large-scale longitudinal studies. In addition, there is a lack of large molecular studies to understand the pathogenetic mechanisms and risk progression of HPV-OED to HPV-OSCC.9
Figure 4: Methods of detection of early pre-cursor lesions of HPV-related oral epithelial dysplasia (HPV-OED).
A
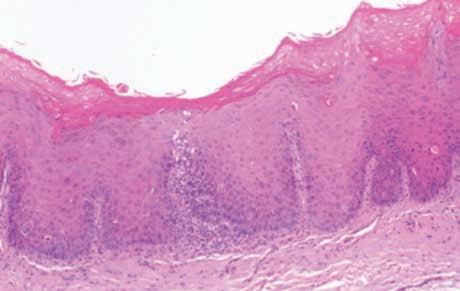
4A. H&E section of an HPV-OED exhibiting a brightly eosinophilic layer of parakeratin, with a monotonous basaloid cell with a high N:C ratio. Two types of cytopathic effect of HPV: a) karyorrhectic cells with a pericellular halo (black arrow) and b) apoptotic keratinocytes (bold arrow); both act as a surrogate for HPV-OED histologically.
B
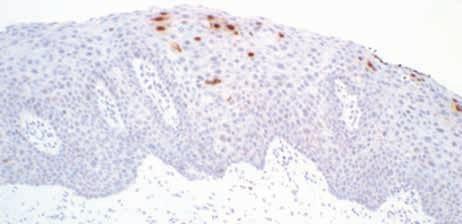
4B. Strong and diffuse nuclear and cytoplasmic positivity for p16 by immunohistochemistry, in a continuous band (block positivity, >50%) that is often sharply demarcated from the adjacent non-dysplastic epithelium.
C
4C. High-risk HPV DNA-ISH (In situ hybridization) showing punctate dot-like nuclear and cytoplasmic positivity, which indicates a high-risk HPV infection.
Emerging
Problems with persistence of HPV infection in aging and Immunocompromised population
Oral HPV infections are generally transient and are typically cleared within 1–2 years without the need for clinical intervention.9 However, in some cases, the virus evades elimination, leading to persistent infection that can last anywhere from 10 to 30 years.7 The distribution of oral HPV infection follows a bimodal pattern, peaking at ages 30–34 and again at 60–64 years—a trend that aligns with the peak incidence of HPV-positive oropharyngeal
squamous cell carcinoma (OPSCC) at 60–64 years.7 This persistence becomes particularly significant in individuals with immunosuppression, which can trigger viral reactivation, potentially explaining the higher incidence of HPVrelated cancers in older populations.17 It remains a subject of ongoing research whether this pattern arises primarily due to age-related immune changes or shifting lifestyle habits. Moreover, while not all HPV genotypes lead to malignancy, HPV16 is the predominant type associated with over 80% of HPV-positive OPSCC cases, followed by HPV35 and HPV33. This contrasts with cervical cancer, where HPV16 and HPV18 are the most common genotypes. Understanding these patterns of persistence and reactivation is crucial for early detection and prevention strategies.
Global prevention programs and challenges in control of HPVrelated oral cancer
The spread and impact of HPV infection differ widely around the world, with the related illness and death rates influenced by a mix of factors. These include geographic location, socioeconomic conditions, cultural practices, and genetic differences in the virus itself. Additionally, individual characteristics like age, gender, the specific area of the body affected, and overall health also play an important role.16 HPV vaccines are recognized as a major pharmaceutical breakthrough meant to benefit women worldwide.
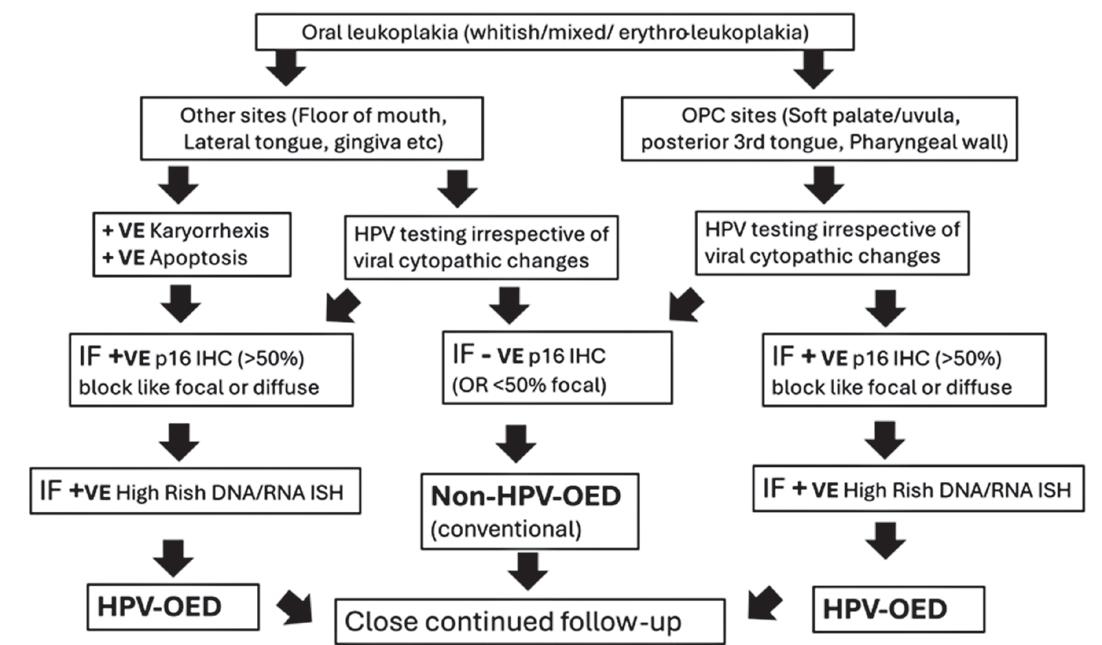
1: Proposed Schematic flowchart to manage leukoplakias of the oral cavity
Chart
However, their rollout has been neither universal nor equitable. Women from socioeconomically disadvantaged backgrounds, whether in developing, emerging, or even some advanced economies, continue to bear a disproportionately high burden of cervical cancer. Despite being promoted as a key solution to this disease, the licensing of HPV vaccines has not ensured fair and widespread access. Implementation efforts for vulnerable girls and women face numerous challenges, such as high vaccine costs, poor healthcare delivery infrastructure, and a lack of community engagement needed to raise awareness about cervical cancer and early screening methods. HPV vaccine programs must prioritize affordable, qualityassured vaccines alongside enhanced community-based health education and screening initiatives to truly function as a public health solution.18
Current Centers of Screening and Testing of the
HPV related oral cancer
Many institutions offer a comprehensive checkup for any changes that occur in the oral cavity for the detection of HPV active infection. Although oropharyngeal cancer might be challenging due to the complex location and inaccessibility to early detection in the oropharyngeal area, sites such as the posterior tongue, pharyngeal arches, soft palate, and other parts of the oral cavity can always be screened for such. It is important to ask your dental provider to provide a detailed examination of the soft tissues to screen for any such changes. If such changes are noted, it is important
to take a biopsy of that area and submit the tissue for histopathological examination. The pathologist can use the IHC staining of p16 and high-risk DNA/RNA HPV-ISH to determine the HPV infection.
Conclusion and
Future Direction
HPV-related OED represents a growing field of study with significant implications for early cancer detection and prevention. Regular vaccination in both male and female adolescents, education regarding the global burden of HPV-OSCC, and enabling HPV-OED screening, detection, and prevention as one of the accessible measures within the community could be the best preventive efforts to reduce the burden of HPV-OSCC in Texas. Current literature is unclear about the difference in treatment modalities for HPV-related oral cancers in the non-oropharyngeal sites to that of conventional oral cancer. Currently, there is no mandate for routine testing of p16 IHC and high-risk HPV testing in the epithelial dysplasia in non-oropharyngeal sites. However, the author strongly recommends establishing a diagnosis of HPV-related oral epithelial dysplasia in the oral cavity is important for 2 reasons. First, we must not forget that HPV-ISH positivity means that there is transcriptionally active virus in the oral cavity that may be able to transmit the infection to another person or to other sites such as the oro-pharynx. HPV virus is oncogenic, meaning it has a capacity to cause cancerous lesion in the oral cavity as it does to cervix and other ano-genital sites. With changing sexual practices, it might even lead to the transmission of this virus to high-risk sites such as oropharynx and cervix,
etc. Second, HPV viruses may be cleared or remain inactive for most of the time it is present, however, we must not forget that it also has a tendency to be persistent. When there is any form of immunosuppression such as aging, HIV infection, transplant, and medications that leads to a lowered immunity, this opportunistic virus may become active and progress to cancer even in non-oropharyngeal sites. Thus, if there is a leukoplakia in the oral cavity, which histologically presents as epithelial dysplasia, it is important to know the HPV status of that lesion to be cautious. Testing all oral epithelial dysplasia (OED) cases for the presence of active HPV-infection by making it a standard protocol to mandatorily test for p16 IHC and high-risk HPV-ISH will be able to detect the presence of transcriptionally active viruses, and this can be an important measure to ensure prevention of transmission to others as well as close continued follow-up for progression (Chart 1). Addressing current gaps in research through longitudinal studies and improved diagnostic methods will improve patient outcomes and public health strategies.
REFERENCES
1. Williamson, A.-L. (2023). Recent Developments in Human Papillomavirus (HPV) Vaccinology. Viruses, 15(7). https://doi. org/10.3390/v15071440
2. Wolf, J., Kist, L. F., Pereira, S. B., Quessada, M. A., Petek, H., Pille, A., Maccari, J. G., Mutlaq, M. P., & Nasi, L. A. (2024). Human papillomavirus infection: Epidemiology, biology, host interactions, cancer development, prevention, and therapeutics. Reviews in Medical Virology, 34(3), e2537. https://doi. org/10.1002/rmv.2537
3. G. A. J. A. Siegel RL, “Cancer statistics, 2024,” CA Cancer J Clin, pp. 12-49, Jan-Feb 2024.
4. SEER Cancer Stat Facts: Oral Cavity and Pharynx Cancer. National Cancer Institute. Bethesda.
5. Chan, C. K., Aimagambetova, G., Ukybassova, T., Kongrtay, K., & Azizan, A. (2019). Human Papillomavirus Infection and Cervical Cancer: Epidemiology, Screening, and Vaccination-Review of Current Perspectives. Journal of Oncology, 2019, 3257939. https:// doi.org/10.1155/2019/3257939
6. Kokkinis, E., Bastas, N. S., Mega, I., Tsironis, C., & Lianou, A. D. (2024). Association of HPV with Oral and Oropharyngeal Cancer: Current Evidence. Maedica, 19(4), 801–806. https://doi.org/10.26574/ maedica.2024.19.4.8012024;
7. Mahal, B. A., Catalano, P. J., Haddad, R. I., Hanna, G. J., Kass, J. I., Schoenfeld, J. D., Tishler, R. B., & Margalit, D. N. (2019). Incidence and Demographic Burden of HPVAssociated Oropharyngeal Head and Neck Cancers in the United States. Cancer Epidemiology, Biomarkers & Prevention : A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology, 28(10), 1660–1667. https://doi. org/10.1158/1055-9965.EPI-190038
8. Lechner, M., Liu, J., Masterson, L., & Fenton, T. R. (2022). HPVassociated oropharyngeal cancer: epidemiology, molecular biology and clinical management. Nature Reviews. Clinical Oncology, 19(5), 306–327. https://doi.org/10.1038/ s41571-022-00603-7
9. Lim, Y. X., & D’Silva, N. J. (2024). HPV-associated oropharyngeal cancer: in search of surrogate biomarkers for early lesions. Oncogene, 43(8), 543–554. https:// doi.org/10.1038/s41388-02302927-9
10. Khanal S, Trainor PJ, Zahin M, Ghim SJ, Joh J, Rai SN, et al. Histologic variation in high grade oral epithelial dysplasia when associated with high-risk human papillomavirus. Oral Surg Oral Med Oral Pathol Oral Radiol. (2017) 123:566–85. doi: 10.1016/j. oooo.2017.01.008
11. V.-G. M. Anaya-Saavedra G, “Oral HPV-associated dysplasia: is koilocytic dysplasia a separate entity?,” Front Oral Health, vol. 16, no. 5, p. 1363556, 2024.
12. Woo SB, Cashman EC, Lerman MA. Human papillomavirus-associated oral intraepithelial neoplasia. Mod Pathol. (2013) 26:1288–97. doi: 10.1038/modpathol.2013.70
13. Zhang L, Jr LJ, El-Mofty SK, Gandhi M, Chernock RD. Nonkeratinizing squamous cell carcinoma in situ of the upper aerodigestive tract: an HPV-related entity. Head Neck Pathol. (2017) 11:152–61. doi: 10.1007/s12105-016-0749-y
14. Liu, Y., Alqatari, M., Sultan, K., Ye, F., Gao, D., Sigel, K., Zhang, D., & Kalir, T. (2017). Using p16 immunohistochemistry to classify morphologic cervical intraepithelial neoplasia 2: correlation of ambiguous staining patterns with HPV subtypes and clinical outcome. Human Pathology, 66, 144–151. https://doi.org/10.1016/j. humpath.2017.06.014
15. El-Naggar, A. K., & Westra, W. H. (2012). p16 expression as a surrogate marker for HPV-related oropharyngeal carcinoma: A guide for interpretative relevance and consistency. Head & Neck, 34(4), 459–461. https://doi.org/10.1002/ hed.21974
16. Kombe Kombe, A. J., Li, B., Zahid, A., Mengist, H. M., Bounda, G.-A., Zhou, Y., & Jin, T. (2020). Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Frontiers in Public Health, 8, 552028. https://doi.org/10.3389/ fpubh.2020.552028
17. Della Fera, A. N., Warburton, A., Coursey, T. L., Khurana, S., & McBride, A. A. (2021). Persistent Human Papillomavirus Infection. Viruses, 13(2), 321. https://doi. org/10.3390/v13020321
18. Graham, J. E., & Mishra, A. (2011). Global challenges of implementing human papillomavirus vaccines. International Journal for Equity in Health, 10, 27. https://doi. org/10.1186/1475-9276-10-27.
Pre-Radiation Head and Neck Examination for Dental Clearance Prior to Treatment— What
You Need to Know
Amerian D. Sones, DMD, MS
Clinical Associate Professor, Diplomate American Board of Prosthodontists, Maxillofacial Prosthodontist and Dental Oncologist, Baylor University Medical Center and Texas A&M University College of Dentistry, Dallas, Texas
Dr AMERIAN D. SONES
As skilled dental professionals, dentists, dental hygienists, and assistants are often the first individuals to detect an early oral lesion during regular dental and oral cancer examinations. The increased frequency of dental office visits compared to medical visits provides this unique opportunity. A biopsy is the gold standard to confirm a diagnosis, and treatment often involves surgery, head and neck radiation, and chemo or immunotherapy.
An early complete oral examination prior to oral cancer treatment is ideal, however is not always possible.1 Often surgical resection has been performed prior to referral to dental colleagues in preparation for head and neck radiation (HRT) and/or chemotherapy/immunotherapy. Head and neck radiation treatment (HRT) requires dental clearance and dental professionals will be given the charge to provide important dental recommendations.2 Your diagnosis and treatment plan today will impact patients’ oral health and often survival in the future.
At
the clearance appointment, careful attention should be given to the following:
1. Full medical history including a list of current medications—especially those that may cause xerostomia and dry mouth.
2. Screening for current or past bisphosphonate therapy.
3. Evaluation for the presence and risk of dental caries.
4. Determination of patient’s periodontal status (Periodontal Classification).
5. Identification of occlusal and airway problems.
6. Evaluate the condition of the remaining teeth—supra-eruption, migration and impactions.
7. Assessment of the fit and stability of existing dentures or removable partial dentures.
8. Assessment of the quality and quantity of saliva.
9. Evaluation of oral hygiene ability and patient compliance.
10. Patient demeanor and both the ability and desire to care for teeth in the future.
11. Communication with the radiation oncologist to determine the diagnosis, ports or fields of radiation, and the dose of radiation to be delivered at individual sites.
12. Assessment of jaw opening and the potential need for exercises or stents.
13. Assessment of the potential need for radiation sparing appliances.
14. Evaluation of swallowing ability.
15. Determination of future need for placement a feeding tube (Patients who have been prescribed a feeding tube will need antibiotic prophylaxis for dental care.)
Indications for tooth extractions are the following: Remember that “when in doubt, pull it out.” A more aggressive extraction protocol is important for these patients to avoid complications (osteoradionecrosis, dental caries and medical/dental expenses) in the future.
Remember that “when in doubt, pull it out.” A more aggressive extraction protocol is important for these patients to avoid complications (osteoradionecrosis, dental caries and medical/dental expenses) in the future.
Indications for tooth removal
1. High caries index score with multiple nonrestorable teeth.
2. Periodontal pocket depths greater than 6 mm with accompanying attachment loss.
3. Clinical and radiographic furcation involvement especially in mandibular molars.
4. Lack of periodontal attached mucosa.
5. Malposed or super-erupted teeth which may cause occlusal problems.
6. Partially impacted third molars.
If teeth are recommended for extraction, consider referral to an oral surgeon requesting generous alveoloplasty and primary closure. Post-operative evaluation to assess adequate wound healing should also be performed by the oral surgeon. A healing period of 14-21 days post-extraction is advised prior to commencement of head and neck radiation.
If teeth are to be removed at the time of cancer surgery, discuss the need for generous alveoloplasty and tori/ exostosis removal with the surgeon prior to treatment. In addition, request primary closure of extraction sites to encourage healing.
Patient Education and Instructions
1. Sequelae of head and neck radiation will affect the production of saliva from the major and minor salivary glands for life. Diminished saliva will likely result in dry mouth and severe xerostomia which predispose patients to accelerated caries.3
2. Decrease salivary function also results in an increased incidence of candida oral infections including angular cheilosis. This is especially prevalent in the hemimandibulectomy patients.
3. After head and neck radiation, avoid any tooth extractions. Radiation affects the fine capillaries of the bone and the blood supply which normally encourage bone remodeling. With decreased vascularity to the mandible and alveolar bone, the occurrence of osteoradionecrosis is high. The precursor to osteoradionecrosis and debilitating alveolar bone disease is often a tooth which was not removed prior to treatment or an area of sharp bone remaining post extraction. Ill-fitting
dentures and partial dentures may exacerbate the problem by traumatizing tissues and exposing the underlying bone. Recovery and treatment of osteoradionecrosis is lengthy as well as costly, involving multiple dental appointments and may include hyperbaric oxygen treatment. It is important to note that almost all osteoradionecrosis occurs in the mandible.
4. Perform exercises to increase flexibility of the muscles of mastication to prevent trismus. Also swallow often during and after treatment to prevent difficulties eating following radiation therapy.
5. Consider shortening dental recall intervals to every 3 months and maintain dental restorations as needed.
Patient presents with previous cancer that perforated the sinus cavity.
6. Use prescription fluoride toothpaste or gels with or without delivery trays to prevent caries.
7. Consider silver diamine fluoride as a non-invasive, cost-effective approach to arresting or preventing caries.
8. Foster excellent communication with all medical and dental providers in the treatment team including radiation oncologists, medical oncologists, and the otolaryngologist/head and neck surgical colleagues.
The dental professional plays a key role in the treatment and journey of wellness for the head and neck cancer patient.4 This area of dental practice is not only rewarding but offers true interprofessional collaboration of all medical and dental specialists to obtain
the highest level of patient care.5 The general dentist and all dental specialists may significantly impact the ultimate prognosis of this special patient population.
REFERENCES
1. White, JM, Panchal, NH., Wehler, C, Bestgen, S, Colon, Jose, Desai, H., Department of Veterans Affairs Consensus: Pre-radiation dental treatment guidelines for patients with head and neck cancer, Head and Neck, Journal of the Sciences of Head and Neck, Vol 41, Issue 5, May 2019, pages 1153-1160
2. Beumer, J, III, Curtis, T., Harrison, RE, Radiation therapy of the oral cavity: sequelae and management, part 1, Head Neck Surg, 1979 MarApr;1(4):301-12.
3. Schiødt, M., Hermund, NU, Management of oral disease prior to radiation therapy, Support Care Cancer 2002 Jan;10(1):40-3
4. Ward, M, Carpenter, M., Noll, J, Carrizosa, D, Moeller, B, Helgeson, E. Lalla, R, Brennan, M., Oncologists’ Perspective on Dental Care Around the Treatment of Head and Neck Cancer: A Pattern of Practice Survey, JCO Oncology Practice, Volume 18 Issue, pg 67e-28-e-35.
5. Bertl, K., Savvidis, P., Kukla, E., Schneider, S., Zauza, K., Bruckmann, C. Stavropoulos, A, Including dental professionals in the multidisciplinary treatment team of head and neck cancer patients improves long term oral health status, Clinical Oral Investigations (2022) 26:2937–2948
Ready to take the next step? Scan the QR code to learn more or call (833) 275-3372 Ext 2 www.texasdentalsleepservices.com
Friday, May 16, 2025 8:30 aM to 4:30 PM (CSt) Texas A&M College of Dentistry - Room 605 - Dallas, TX
Linda C Niessen, DMD, MPH, MPP Professor and Dean Kansas City University College of Dental Medicine Vice Provost for Oral Health Affairs
Helena Tapias Perdigon, DDS, MS Clinical Associate Professor Texas A&M College of Dentistry Comprehensive Dentistry Department
Jennifer Hartshorn DDS, DABSCD
Clinical Associate Professor Preventive and Community Dentistry
University of Iowa College of Dentistry
Jhanvi Desai BDS, MDS
Clinical Assistant Professor Preventive and Community Dentistry
University of Iowa College of Dentistry
Iowa City, Iowa 7 Hours CE credits provided through Texas A&M University College of Dentistry Office of Lifelong Learning
Iowa City, Iowa
REGISTER ONLINE: for additional information and to register, please scan this QR code: Questions? Contact Dr. Helena Tapias: 214.828.8940 or htapias@tamu.edu
Event Organizer
Tooth-level predictors of tooth loss and exposed bone after radiation therapy for head and neck cancer
Rajesh V. Lalla, DDS, PhD; James S. Hodges, PhD; athaniel S. Treister, DMD, DMSc; Thomas P. Sollecito, DMD; Brian L. Schmidt, DDS, MD, PhD; Lauren L. Patton, DDS; Alexander Lin, MD; Michael T. Brennan, DDS, MHS
This article has an accompanying online continuing education activity available at: http://jada.ada.org/ce/home.
ABSTRACT
BACKGROUND. The objective of this study was to identify tooth-level risk factors for use during preradiation dental care management to predict risk of tooth failure (tooth lost or declared hopeless) and exposed bone after radiation therapy (RT) for head and neck cancer (HNC).
METHODS. The authors conducted a prospective observational multicenter cohort study of 572 patients receiving RT for HNC. Participants were examined by calibrated examiners before RT and then every 6 months until 2 years after RT. Analyses considered time to tooth failure and chance of exposed bone at a tooth location.
RESULTS. The following pre-RT characteristics predicted tooth failure within 2 years after RT: hopeless teeth not extracted pre-RT (hazard ratio [HR], 17.1; P < .0001), untreated caries (HR, 5.0; P < .0001), periodontal pocket 6 mm or greater (HR, 3.4; P = .001) or equaling 5 mm (HR, 2.2; P = .006), recession over 2 mm (HR, 2.8; P = .002), furcation score of 2 (HR, 3.3; P = .003), and any mobility (HR, 2.2; P = .008). The following pre-RT characteristics predicted occurrence of exposed bone at a tooth location: hopeless teeth not extracted before RT (risk ratio [RR], 18.7; P = .0002) and pocket depth 6 mm or greater (RR, 5.4; P = .003) or equaling 5 mm (RR, 4.7; P = .016). Participants with exposed bone at the site of a pre-RT dental extraction averaged 19.6 days between extraction and start of RT compared with 26.2 days for participants without exposed bone (P = .21).
CONCLUSIONS. Individual teeth with the risk factors identified in this study should be considered for extraction before RT for HNC, with adequate healing time before start of RT.
ABBREVIATION KEY
BL: Baseline.
CEJ: Cementoenamel junction.
CEJ-GM: Cementoenamel junction to gingival margin.
DMFS: Decayed, missing, and filled surfaces.
GM: Gingival margin.
HNC: Head and neck cancer.
IMRT: Intensity-modulated radiation therapy.
PD: Probing depth.
RT: Radiation therapy.
PRACTICAL IMPLICATIONS. The findings of this trial will facilitate evidence-based dental management of the care of patients receiving RT for HNC. This clinical trial was registered at Clinicaltrials.gov. The registration number is NCT02057510.
Key words
Head and neck cancer; radiation therapy; tooth loss; exposed bone; evidence-based dentistry.
authors
DR LALLA is a professor and the associate dean for research, School of Dental Medicine, University of Connecticut, Farmington, CT. Address correspondence to Dr Lalla, School of Dental Medicine, University of Connecticut, 263 Farmington Ave, Farmington, CT 06030, email lalla@uchc. edu.
DR HODGES is a professor, Division of Biostatistics, School of Public Health, University of Minnesota, Minneapolis, MN.
DR TREISTER is the chief, Division of Oral Medicine and Dentistry, Brigham and Women’s Hospital, Boston, MA, and an associate professor, Department of Oral Medicine, Infection and Immunity, Harvard School of Dental Medicine, Boston, MA.
DR SOLLECITO is a professor and the chair, Department of Oral Medicine, and the associate dean of Hospital and Extramural Affairs, University of Pennsylvania School of Dental Medicine, and the chief of Oral Medicine, University of Pennsylvania Health System, Philadelphia, PA.
DR SCHMIDT is a professor, Department of Oral and Maxillofacial Surgery, and director, Translational Research Center, New York University College of Dentistry, New York, NY.
DR PATTON is a professor, Division of Craniofacial and Surgical Care, Adams School of Dentistry, University of North Carolina, Chapel Hill, NC. Dr. Lin is a professor, Department of Radiation Oncology, University of Pennsylvania, Philadelphia, PA.
DR LIN is a professor, Department of Radiation Oncology, University of Pennsylvania, Philadelphia, PA.
DR BRENNAN is the chair, Department of Oral Medicine/Oral and Maxillofacial Surgery, Atrium Health Carolinas Medical Center, Charlotte, NC, and a clinical professor, Department of Otolaryngology/Head and Neck Surgery, Wake Forest University School of Medicine, Winston-Salem, NC.
Disclosures. None of the authors reported any disclosures.
The Observational Study of Dental Outcomes in Head and Neck Cancer Patients (also know as OraRad) is funded by grant U01 DE022939 from the National Institute for Dental and Craniofacial Research awarded to the study principal investigators Drs Brennan and Lalla.
The authors gratefully acknowledge the contributions of all the study participants and of study personnel at each clinical site and the Data Coordinating Center.
ORCID Numbers
Rajesh V. Lalla: https://orcid.org/0000-0002-7662-6937; James S. Hodges: https://orcid.org/0000-0001-7467-6941; Nathaniel S. Treister: https://orcid.org/0000-0002-5596-7222; Thomas P. Sollecito: https://orcid.org/0000-0003-0569-7743; Lauren L. Patton: https://orcid.org/0000-0002-8253-4588; Alexander Lin: https://orcid.org/0000-0003-1254-8324. For information regarding ORCID numbers, go to http://orcid.org.
Head and neck cancers (HNCs) are among the 10 most common cancers worldwide.1 Most patients with HNC receive radiation therapy (RT), often with concomitant chemotherapy. RT usually is delivered in fractions of approximately 2 Gy per day, 5 days per week, for 5 through 7 weeks, for a total dose of 50 through 70 Gy (5,0007,000 cGy). Short-term adverse effects may include oral mucositis, oral candidiasis, hyposalivation, and taste changes.2 Longer-term adverse effects can include hyposalivation, gingival recession, caries, tooth loss, and osteoradionecrosis.3-8 Osteoradionecrosis manifests as persistent exposure of intraoral bone and can result in significant morbidity, including pain, infection, fistula, paresthesia, and jaw fracture. It commonly occurs after dental extraction but also can occur owing to odontogenic or periodontal infection and denture trauma or without an identified cause.9
Because of increased risk of experiencing osteoradionecrosis and other oral complications, patients with HNC should be referred for dental evaluation and care management before RT. The primary goal is to restore or extract diseased teeth before RT, so as to avoid the need for dental extraction and potential resulting osteoradionecrosis after RT.10 Therefore, teeth with poor long-term prognosis often are extracted pre-RT. However, there is limited evidence to guide decision making on which teeth should be extracted or retained. As a result, pre-RT dental care management varies widely across dental practices, driven by expert opinion, access, and practitioner experience.11
The objective of our study was to identify tooth-level risk factors before RT that predict tooth loss and exposed bone at that specific site after RT. Such information would guide evidence-based dental care management for this patient population.
METHODS
Study Design
We conducted a prospective observational cohort study called Observational Study of Dental Outcomes in Head and Neck Cancer Patients (also known as OraRad). Study participants were assessed before beginning RT and then every 6 months until 2 years after RT. We enrolled 572 participants across 6 clinical sites. Institutional review board approval was obtained at each site. All participants provided written informed consent.
Inclusion and Exclusion Criteria
Inclusion criteria were 18 years or older; diagnosis of head and neck squamous cell carcinoma or salivary gland cancer and intending to receive external beam RT with curative intent, or a diagnosis of a nonsquamous cell carcinoma, nonsalivary gland cancer head and neck malignancy and expected to receive at least 4,500 cGy RT to the head and neck region; and having at least 1 natural tooth remaining after pre-RT dental extractions. Patients receiving palliative RT or with a history of curative RT for HNC were excluded.12
Study Procedures
Study visits were conducted before RT and 6, 12, 18, and 24 months after RT initiation. The baseline (pre-RT) assessment was conducted after completing clinical pre-RT dental care management, including extractions.
Study assessments included missing teeth, hopeless teeth, exposed bone, caries, periodontal measures, mobility, and other assessments.12
A tooth was recorded as missing if no part of the tooth was clinically visible. A tooth was recorded as hopeless if it was present and met any of these criteria: nonrestorable due to fracture or extensive caries, amputated crown with root remaining, and persistent or uncontrolled odontogenic or periodontal infection. Tooth failure was defined as a tooth that was either newly missing or declared hopeless since the last study visit.5
Exposed bone was defined as visible exposed bone in the mouth, with loss of the overlying soft tissue. Location of exposed bone was recorded using tooth numbers of teeth present or normally present in that location.8
Caries assessment was done by recording decayed, missing, and filled surfaces (DMFS) at the baseline and 6-, 12-, 18-, and 24-month visits. A no. 23 or no. 2A explorer was used to detect caries. Four tooth surfaces on the anterior teeth and 5 tooth surfaces on the posterior teeth (except third molars) were scored for DMFS.4
Periodontal measures were collected on all teeth except third molars at the baseline and 12- and 24-month visits. Pocket depth and the distance from the cementoenamel junction (CEJ) to the gingival margin (CEJ-GM) was measured using a UNC 15 probe at 6 sites per tooth. Bleeding on probing was recorded at each tooth’s 6 periodontal probing sites. Furcation involvement was scored on multirooted teeth as Class 0, 1, 2, 3, or 4, using Glickman classification and a Naber probe.6,13
Because of increased risk of experiencing osteoradionecrosis and other oral complications, patients with HNC should be referred for dental evaluation and care management before RT. The primary goal is to restore or extract diseased teeth before RT, so as to avoid the need for dental extraction and potential resulting osteoradionecrosis after RT.
Mobility was measured on all teeth present except third molars, using the nonworking ends of the dental mirror and probe, pressed on the buccal and lingual surfaces of the tooth. Mobility was rated as Class 0, 1, 2, or 3, using the classification by Grace and Smales.14
All study personnel received detailed training on conducting clinical assessments, completing study forms, entering data, and other procedures. All clinical examiners underwent annual inperson calibration on healthy volunteers for DMFS and periodontal measurements.
Statistical Methods
The statistical methods are described briefly here; the Appendix, available online and at the end of this article, gives a detailed description.
Time to Tooth Failure
These were time-to-event (survival) analyses, in which the event was tooth failure and possible event times were 6, 12, 18, and 24 months. Third molars were excluded. The analyses had the form of Cox regression, so that relative hazards are reported for comparisons. The Appendix, available online and at the end of this article, gives detailed definitions of at-risk teeth and events, analysis methods, and software. Adjusted analyses added person-level characteristics, listed in the Appendix.
Exposed Bone
The location of an exposed-bone lesion was defined using the tooth numbers to which it was closest. The outcome, an exposed-bone report, occurred for a tooth if that tooth was included in an exposed bone lesion’s location at a follow-up visit. Analyses used generalized estimating equations to estimate the probability of an exposed bone at a tooth location, so that relative
risks are reported for comparisons. Adjusted analyses added person-level characteristics, listed in the Appendix, available online and at the end of this article.
RESULTS
We enrolled 572 participants across 6 clinical sites from 2014 through 2018. Of these, 52 participants had no follow-up visits. Tooth failure data were thus available for 520 participants. Exposed bone data were available for 1 additional participant based on chart review. Table 1 provides pre-RT characteristics of the 521 participants with follow-up for exposed bone.
Tooth Failure After RT
The 520 participants with follow-up for tooth failure after RT had a total of 11,993 teeth present when RT began (excluding third molars) that were not considered to be hopeless, as defined in the Methods section above. Of these 11,993 teeth, 214 (1.8%) failed (were exfoliated, extracted, declared hopeless) within 2 years of follow-up after RT. Eighty-two of the 520 participants had at least 1 tooth failure within 2 years.5
Several pre-RT characteristics of individual teeth were associated significantly with risk of failure of that particular tooth within 2 years after RT. Table 2 and eTable 1, available online and at the end of this article, list unadjusted and adjusted hazard ratios (HRs), 95% CIs, and P values.
A tooth that was declared hopeless at the pre-RT examination but retained going into RT had the largest risk of extraction within 2 years, with adjusted HR of 17.1 compared with teeth not declared hopeless (P < .0001). The next strongest predictor of tooth failure was untreated caries pre-RT, with adjusted
HR of 5.0 compared with teeth without untreated caries (P < .0001).
Compared with teeth with a maximum probing depth (PD) less than 4 mm, a maximum PD of 6 mm or more predicted tooth failure, with an adjusted HR of 3.4 (P = .001), whereas a maximum PD of 5 mm and 4 mm predicted tooth failure with adjusted HRs of 2.2 (P = .006) and 1.7 (P = .018), respectively.
A furcation score of 2 was predictive of tooth failure with an adjusted HR of 3.3 compared with a furcation score of 0 (P = .003). Gingival recession with the gingival margin 2 mm or more below the CEJ predicted tooth failure with an adjusted HR of 2.8 compared with teeth with gingival margin at or above the CEJ (P = .002). Finally, the presence of any degree of tooth mobility before RT predicted tooth failure with an adjusted HR of 2.2 compared with teeth with no mobility (P = .008).
Exposed Intraoral Bone After RT
Thirty-five participants received diagnoses of a total of 37 exposed bone lesions during 2 years after RT.8 Average (SD) maximum RT dose to the exposed bone area was 5,456 (1,768) cGy. Of these 37 lesions, 13 occurred at the site of dental extraction performed for pre-RT management. Participants with exposed bone at the site of preRT dental extraction had a mean (SE) of 19.6 (5.0) days between extraction and start of RT compared with 26.2 (1.4) days for participants who did not experience exposed bone (P = .21).
Several pre-RT characteristics of individual teeth predicted risk for exposed bone at that particular site within 2 years after RT. Table 3 and eTable 2, available online and at the end of this
article, list unadjusted and adjusted relative risks (RRs), 95% CIs, and P values.
A tooth declared hopeless at the pre-RT examination but retained going into RT had the largest risk of developing exposed bone at that site, with an adjusted RR of 18.7 compared with teeth already missing (P = .0002). Leaving a hopeless tooth in place was associated with a 6.4-fold higher adjusted risk of developing exposed
bone compared with extracting a tooth shortly before RT (P = .034). Extraction of a tooth as part of pre-RT dental care management was associated with a 2.9fold greater risk of developing exposed bone at that site compared with a missing tooth; however, this was not statistically significant (P = .096).
a maximum PD of 5 mm predicted exposed bone with an adjusted RR of 4.7 (P = .003).
Patients who are to undergo RT for HNC should be referred for dental evaluation and care management before starting RT.15 This includes identifying teeth with poor long-term prognoses, considering the expected hyposalivation and
* These analyses include the same participants and teeth included in the adjusted analyses. Unadjusted analyses including all participants and teeth (that is, that have the data needed for the unadjusted analysis) are in eTable 1. † Adjusted analyses omitted teeth with missing data for adjusters. With exceptions as noted, analyses were adjusted for these person-level characteristics: baseline number of teeth (5 categories: < 14, 15-24, 25-26, 27, 28); age (continuous); whether the person had untreated caries at baseline; alcohol use (< 12 drinks per year vs > 12 drinks per year); radiation type (any intensity-modulated radiation therapy [RT] vs proton); smoking (never, former, or current); clinic; compliance change baseline to follow-up (4 categories, defined in the Methods section); radiation dose; nadir of saliva after RT as a percentage of baseline. Exceptions were as follows. For the tooth-level predictor untreated caries, the person-level adjuster "whether the person had untreated caries at baseline" was not included. For furcation score, only teeth with furcations were included, and a further adjuster was added, premolar vs molar. ‡ For this comparison only, teeth were at risk at baseline if they were present in the mouth, and only newly missing teeth were counted as events.
increased risk of developing caries and gingival recession after RT. Such teeth often are extracted pre-RT if they will be in the field of high-dose RT (> 5,000 cGy). The rationale is to avoid extractions after RT owing to increased risk of developing osteoradionecrosis. In some cases (for example, fractured teeth), the determination of poor longterm prognosis is clear. However, in many situations with varying degrees of severity (for example, periodontal disease), this determination is not as clear. This decision making is complicated by the fact that a tooth with a good long-term prognosis in an otherwise healthy patient may have a poor long-term prognosis in a patient with significant hyposalivation after RT for HNC. Owing to limited evidence
to guide such decision making, preRT dental care management, when available, often varies widely between centers, which can lead to suboptimal outcomes.11
Our study provides evidence at the tooth level to help guide this complex decision-making process. We examined pre-RT tooth-level risk factors that increased risk of experiencing tooth failure, defined as a tooth being extracted or declared hopeless after RT. We used this definition because extractions are often avoided in areas that have received high-dose RT owing to risk of developing osteoradionecrosis. We found that the greatest risk of experiencing tooth failure after RT was for teeth that were already identified as
hopeless but not extracted before RT. Such teeth had a 17-fold higher risk of experiencing tooth failure after RT than other teeth present in the mouth. The next highest risk of experiencing tooth failure was for teeth with untreated caries going into RT, which had a 5-fold higher risk of experiencing tooth failure than teeth without active caries at the pre-RT assessment. Because there is urgency to start RT to treat cancer, limited time is available for pre-RT dental care management. Priority is given to completing needed extractions, and caries management is sometimes deferred until after RT. However, our data show that if carious teeth are not restored before or soon after RT, there is a high risk of experiencing tooth failure.
* These analyses include the same participants and teeth included in the adjusted analyses. The adjusters had little missing data; unadjusted analyses including all participants and teeth (that is, that had the data needed for the unadjusted analysis) give nearly identical results. † Adjusted analyses omitted teeth with missing data for adjusters. With exceptions as noted, analyses were adjusted for these person-level characteristics: baseline [BL] status (had BL extractions vs had no BL extractions but at least 1 tooth declared hopeless at BL vs had no BL extractions or teeth declared hopeless), number of teeth extracted at BL, smoking status (current, former, never), enrollment site, primary radiation therapy (RT) site (5 categories listed in Table 1), and total dose to the primary site. Exceptions were for the tooth-level predictor BL tooth status (missing before pre-RT care, extracted during pre-RT care, hopeless, present and not hopeless), these adjusters were omitted: person-level BL status and number of teeth extracted at baseline. For furcation involvement, only molar teeth were included and only these adjusters were used: BL status (had BL extractions vs had no BL extractions but at least 1 tooth declared hopeless at BL vs had no BL extractions or teeth declared hopeless), number of teeth extracted at BL, and smoking status (current, former, never).
Periodontal disease presents a particular challenge during the preRT dental assessment because of its varying degrees of severity. A finding reported in 2022 was that RT for HNC led to a significant increase in gingival recession.6 Our analyses showed that teeth with the gingival margin already at 2 mm or more apical to the CEJ before RT had a 2.8-fold increased risk of experiencing tooth failure after RT. We also found that teeth with at least 1 periodontal pocket 5 mm or greater had significantly increased risk of experiencing tooth failure than teeth with maximum pocket depth less than 4 mm. A furcation score of 2 or above
and any degree of mobility pre-RT also predict increased risk of tooth failure after RT.
We also examined characteristics of teeth at the pre-RT assessment that predicted exposed bone at those sites after RT. Like tooth failure, the highest risk of developing exposed bone was for teeth already identified as hopeless but not extracted before RT. Leaving a hopeless tooth in place was associated with a 6.4-fold higher risk of developing exposed bone at that site than extracting such teeth before RT. We also found that a tooth with at least 1 periodontal pocket of 5 mm or greater
was at increased risk of developing exposed bone at that site. Pocket depth of 6 mm or greater was associated with still greater risk. This finding is relevant as not all cases of exposed bone follow an extraction. Thus, our data confirm previous reports that periodontal disease is also a risk factor for exposed bone after RT.16 Although not the focus of our report, person-level factors such as tobacco and alcohol use can also increase risk of developing exposed bone.8
actually can cause osteoradionecrosis if the extraction site is not allowed to heal adequately before RT begins.17 Of the 37 exposed bone lesions recorded in our study, 13 lesions (35%) occurred at the site of a dental extraction completed for pre-RT management. A factor governing this risk is the duration of the healing period between the extraction and first day of RT. This period was an average of 19.6 days for participants who experienced exposed bone at the extraction site vs 26.2 days for those who did not. Although this difference was not statistically significant (both groups had few exposed bone events, so statistical power was low for this comparison), these findings are clinically significant. This difference of 6.6 days suggests that from a purely dental perspective, a healing period of at least 3 weeks is preferable compared with the recommendation of 2 weeks being used now.15 Our results are supported by a 2022 systematic review, which reported a significantly greater risk of experiencing osteoradionecrosis in patients with less than 2 weeks between extractions and start of RT compared with a period of 2 weeks through 1 month.18 In some cases, however, an optimal healing period may not be achievable owing to an urgent need to start RT for tumor control. The desirable healing period is also likely to be influenced by the degree of trauma to bone due to extraction. As most cases of osteoradionecrosis occur in the posterior mandible, preRT extractions of mandibular molars likely require a longer healing period than extractions in other areas. Risk of developing osteoradionecrosis posed by pre-RT dental extractions also raises the question of whether such extractions should be performed at all shortly before RT, especially given the urgency to start RT. It is worth repeating, however, that leaving a hopeless tooth
in place is associated with a 6.4-fold higher risk of developing exposed bone at that site than extracting a tooth shortly before RT. Thus, our findings support the rationale for the practice of pre-RT dental extractions of teeth with poor prognosis but also indicate that if the healing period is not adequate, this practice can lead to osteoradionecrosis, the problem it is intended to prevent. On the basis of our findings, the Box lists characteristics of teeth that should be considered for extraction before RT, if they are in an area expected to receive more than 5,000 cGy of RT. It should be noted that the final decision about which teeth to extract should take into account all relevant factors, including oral hygiene status and practices as well as the presence of single vs multiple risk factors for tooth loss and osteoradionecrosis.
Two important systematic reviews on this topic were published in 2022. Urquhart and colleagues reported that patients with HNC who needed pre-RT dental intervention may have had an increased risk of experiencing osteoradionecrosis compared with those who did not.19 As the studies reviewed included both pre- and postRT extractions, the authors could not exclude the possibility that post-RT extractions contributed to the increased risk of developing osteoradionecrosis. These findings are consistent with published evidence that patients with poor dental status at the start of RT,
who are more likely to need pre-RT dental extractions, are also more likely to lose additional teeth after RT.5 Another systematic review and metaanalysis by Normando and colleagues reported a significant association between osteoradionecrosis and postRT dental extractions but not pre-RT dental extractions.20 They concluded that performing dental extractions before RT reduces the risk of developing osteoradionecrosis compared with post-RT extractions. This is consistent with our study, which reports a 6.4fold higher risk of developing exposed bone for hopeless teeth that were not extracted before RT compared with teeth extracted before RT.
The strengths of our study include the prospective multicenter design with a large sample size, rigorous annual calibration and training of study personnel, and external monitoring by multiple groups. A limitation of this analysis is that there were relatively few tooth failures and exposed bone events during the 2-year study period. However, this is not surprising because the study participants all received comprehensive pre-RT dental care management. Furthermore, the number of events was adequate to identify multiple risk factors for each of the outcomes. We were not able to separately assess risk only for teeth receiving high doses of RT, as such tooth-level dose data were not available for most teeth. Another limitation is that
we assessed and recorded the presence of exposed intraoral bone, whereas a diagnosis of osteoradionecrosis was only made by the treating clinician. As the commonly used definitions of osteoradionecrosis require persistence of exposed bone for at least several weeks, we were unable to determine definitively such a diagnosis for each case of exposed bone.21 Additional studies with longer follow-up times would be helpful in identifying risk factors for long-term risk of developing osteoradionecrosis.
CONCLUSIONS
This study provides quantitative estimates of risk of experiencing tooth failure and exposed bone after RT, based on pre-RT characteristics of individual teeth. These risk ratios will help guide the evidence-based dental care management of patients undergoing RT for HNC.
Supplementa Data
Supplemental data related to this article can be found at: https://doi. org/10.1016/j.adaj.2023.03.009.
References
1. Chow LQM. Head and neck cancer. N Engl J Med. 2020;382(1):60-72.
2. Sroussi HY, Epstein JB, Bensadoun R-J, et al. Common oral complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med. 2017;6(12):29182931.
3. Lalla RV, Treister N, Sollecito T, et al.; OraRad Study Group. Oral complications at 6 months after radiation therapy for head and neck cancer. Oral Dis. 2017;23(8):1134-1143.
4. Brennan MT, Treister NS, Sollecito TP, et al. Dental caries postradiotherapy in head and neck cancer. JDR Clin Transl Res. Published online April 11, 2022. doi:10.1177/23800844221086563
5. Brennan MT, Treister NS, Sollecito TP, et al. Tooth failure post-radiotherapy in head and neck cancer: primary report of the Clinical Registry of Dental Outcomes in Head and Neck Cancer Patients (OraRad) study. Int J Radiat Oncol Biol Phys. 2022;113(2):320-330.
6. Lalla RV, Treister NS, Sollecito TP, et al. Radiation therapy for head and neck cancer leads to gingival recession associated with dental caries. Oral Surg
Oral Med Oral Pathol Oral Radiol. 2022;133(5):539546.
7. Lin A, Helgeson ES, Treister NS, et al. The impact of head and neck radiotherapy on salivary flow and quality of life: results of the ORARAD study. Oral Oncol. 2022; 127:105783.
8. Treister NS, Brennan MT, Sollecito TP, et al. Exposed bone in patients with head and neck cancer treated with radiation therapy: an analysis of the Observational Study of Dental Outcomes in Head and Neck Cancer Patients (OraRad). Cancer. 2022;128(3):487-496.
9. Singh A, Huryn JM, Kronstadt KL, Yom SK, Randazzo JR, Estilo CL. Osteoradionecrosis of the jaw: a mini review. Front Oral Heal. 2022;3:980786.
10. Levi LE, Lalla RV. Dental treatment planning for the patient with oral cancer. Dent Clin North Am. 2018; 62(1):121-130.
11. Barker GJ, Epstein JB, Williams KB, Gorsky M, Raber-Durlacher JE. Current practice and knowledge of oral care for cancer patients: a survey of supportive health care providers. Support Care Cancer. 2005;13(1): 32-41.
12. Lalla RV, Long-Simpson L, Hodges JS, et al.; OraRad Study Group. Clinical Registry of Dental Outcomes in Head and Neck Cancer patients (OraRad): rationale, methods, and recruitment considerations. BMC Oral Health. 2017;17(1):59.
13. Pilloni A, Rojas MA. Furcation involvement classification: a comprehensive review and a new system proposal. Dent J. 2018;6(3):34.
14. Mani S, Mani A, Sachdeva S, Maniyar S, Anuraga S, Kale P. Indices to assess tooth mobility: a review. Int J Dent Sci Innov Res. 2019;2(2):630-635.
15. Clinical Practice Guidelines for Head and Neck Cancers. Version 2-22. 2022. National Comprehensive Cancer Network. Accessed December 6, 2022. https://www.nccn.org/ professionals/physician_gls/pdf/head-and-neck. pdf
16. Schuurhuis JM, Stokman MA, Witjes MJH, et al. Patients with advanced periodontal disease before intensity-modulated radiation therapy are prone to develop bone healing problems: a 2-year prospective follow-up study. Support Care Cancer. 2018;26(4):1133-1142.
17. Lajolo C, Gioco G, Rupe C, et al. Tooth extraction before radiotherapy is a risk factor for developing osteoradionecrosis of the jaws: a systematic review. Oral Dis. 2021;27(7):1595-1605.
18. Mazzetti T, Sergio da Silva Santos P, Spindola Antunes H, Fernandes Montagner A, Hélène van de Sande F, Timm Maske T. Required time for preoncological dental management: a rapid review of the literature. Oral Oncol. 2022:134.
19. Urquhart O, DeLong HR, Ziegler KM, et al. Effect of preradiation dental intervention on incidence of osteoradionecrosis in patients with head and neck cancer: a systematic review and meta-analysis. JADA. 2022;153(10): 931-942.e32.
20. Normando AGC, Pérez-de-Oliveira ME, Guerra ENS, et al.; Oral Care Study Group, Multinational Association of Supportive Care in Cancer (MASCC)/ International Society of Oral Oncology (ISOO). To extract or not extract teeth prior to head and neck radiotherapy? A systematic review and metaanalysis. Support Care Cancer. Published online November 1, 2022. doi: 10.1007/s00520-02207215-y
21. Chronopoulos A, Zarra T, Ehrenfeld M, Otto S. Osteoradionecrosis of the jaws: definition, epidemiology, staging and clinical and radiological findings: a concise review. Int Dent J. 2018;68(1):22-30.
APPENDIX: DETAILED STATISTICAL METHODS
Number of Participants with Follow-up Data
Of the 572 participants who enrolled in the Observational Study of Dental Outcomes in Head and Neck Cancer Patients (OraRad) study and were eligible for follow-up, 520 had 1 or more followup visits and provided data about tooth failure. One more person provided data about exposed bone based on chart review, giving a total of 521 participants. Table 1 describes the 521 with some follow-up for exposed bone.
Time to tooth failure
This study was a time-to-event analysis. Possible event times were 6, 12, 18, and 24 months, as discussed in the article by Brennan and colleagues.e1 Third molars were excluded from all analyses because the study did not record whether third molars were present at baseline. Otherwise, the definitions of teeth at risk and of the event are as follows:
A. For comparisons other than those in items B and C below: Teeth were at risk if they were present at baseline and had not been deemed hopeless. An at-risk tooth had an event during follow-up if it was deemed hopeless or exited the mouth via extraction or exfoliation.
B. For the comparison of retained hopeless teeth at baseline vs teeth extracted pre-radiation therapy (RT) vs teeth missing pre-RT vs teeth present and not hopeless: The group of teeth at risk was increased to include the 77 teeth that were declared hopeless at baseline but retained in the mouth. An at-risk tooth had an event if the tooth exited the mouth via extraction or exfoliation.
C. For the comparison of furcation
scores: The group of teeth at risk was as under item A except that it included only teeth with furcations, that is, molars and premolars 5 and 12. The event was defined as under item A.
Analyses were clustered Cox regressions computed in the R system (R Project) using the survival package (https:// CRAN.R-project.org/package=survival), specifically using the cluster option and the estimating equation method with robust SEs (Huber sandwich estimator) and Wald P values, with ties handled using the Efron approximation. Sample code is
Adjusted analyses were computed by adding adjusters to the analyses described above. Adjusters included person-level characteristics that had P value below .05 in figure 2 of the article from Brennan and colleagues.e1 With exceptions noted below, analyses were adjusted for the following person-level characteristics: baseline number of teeth (5 categories: <14, 15-24, 25-26, 27, 28; Brennan and colleaguese give the rationale for these categories), age (continuous), whether the person had untreated caries at baseline, alcohol use (<12 drinks per year vs >12 drinks per year), radiation type (any intensity-modulated RT vs proton), smoking (never, former, current), clinic, compliance with hygiene (4 categories: compliant at baseline and follow-up, compliant at baseline but not follow-up, compliant at follow-up but not baseline, compliant at neither baseline nor follow-up), radiation dose to the parotid glands (the first principal component of 4 measures, the maximum and mean dose to the right and left parotid glands), and nadir of salivary flow after
RT as a percentage of baseline.e1 Exceptions were for the tooth-level predictor of untreated caries, the person-level adjuster of whether the person had untreated caries at baseline was not included. For furcation score, a further adjuster was added: premolar vs molar.
These analyses omitted teeth that had missing data for the comparison variable (for example, baseline maximum pocket depth) or for the adjusters. Because some adjusters had substantial amounts of missing data (especially periodontal measures and compliance with hygiene), the teeth included in the unadjusted analyses were a rather larger superset of the teeth included in the adjusted analyses. The Results section shows unadjusted analyses of the same subset of teeth that were included in the adjusted analyses. eTable 1 shows unadjusted analyses using all teeth that had data for a given comparison; the results are similar to those shown in Table 2.
Exposed bone
In OraRad, the location of an exposedbone lesion was defined using the tooth numbers to which it was closest, so a lesion’s location could extend across more than 1 tooth number; for example, 1 lesion extended across 4 teeth. For this analysis, the outcome, an exposed bone report at a tooth, was defined as occurring if that tooth was included in an exposed bone lesion’s location at a followup visit and not occurring otherwise. With this definition, 35 participants and 63 teeth had events.
Analyses used generalized estimating equations computed in the R system using the geepack package (https:// cran.r-project.org/web/packages/ geepack/index.html), specifically the geeglm function, with the log (not logit)
link with offset natural log of years to the last follow-up visit (that is, 0.5, 1, 1.5, or 2 years), working correlation AR1 within person for teeth included in the analysis, fixed scale parameter, and robust standard errors.e2 Pairwise comparisons between categories used the R system emmeans package (https://cran.r-project.org/ web/packages/emmeans/index.html), specifically the emmeans function with Satterthwaite degrees of freedom, no adjustment for multiple comparisons, and default settings otherwise. Sample code is
eb12un <- geeglm (`Exposed bone` ~ offset (`ln(MAXVISIT/12) for EB`)
For comparisons involving pocket depth, bleeding on probing, tooth mobility, furcation involvement, and recession, many teeth (locations) had missing data; for example, if a tooth was missing, none of these measurements was defined for that tooth. The analysis thus included a category for teeth that otherwise would have been included but for which the predictor was missing; for example, for bleeding on probing, a tooth was in 1 of these categories: yes (that is, a site on the tooth bled on probing), no (no site on the tooth bled on probing), or missing (the tooth was missing but would have been included had it not been missing). The missing category did not include third molars, for which periodontal measurements were not made, nor did it include participants who did not have periodontal measurements because they would need antibiotic prophylaxis.
Except as described in the previous paragraph, these analyses omitted teeth that had missing data for the comparison variable or for the
adjusters. The adjusters (described in the following paragraph) had little missing data, so the Results section presents unadjusted analyses including all participants and teeth that have the data needed for the unadjusted analysis.
With exceptions noted below, analyses were adjusted for personlevel characteristics that had P values below .05 in Table 3 of the article by Treister and colleaugese baseline status (had baseline extractions vs had no baseline extractions but at least 1 tooth declared hopeless at baseline vs had no baseline extractions or teeth declared hopeless), number of teeth extracted at baseline, smoking (current, former, never), enrollment site, primary RT site (5 categories: oropharynx, oral cavity, larynx or hypopharynx, salivary gland, other), and total dose to the primary site.e3 Exceptions were as follows: for the tooth-level predictor baseline tooth status (missing before pre-RT care, extracted during pre-RT care, hopeless, present and not hopeless), these adjusters were omitted: person-level baseline status and number of teeth extracted at baseline. For furcation involvement, only molars were included and only these person-level adjusters were used: baseline status (as above), number of teeth extracted at baseline, and smoking (current, former, never).
e-References
e1. Brennan MT, Treister NS, Sollecito TP, et al. Tooth failure post-radiotherapy in head and neck cancer: primary report of the Clinical Registry of Dental Outcomes in Head and Neck Cancer Patients (OraRad) study. Int J Radiat Oncol Biol Phys. 2022;113(2):320-330.
e2. Højsgaard S, Halekoh U, Yan J. The R package geepack for generalized estimating equation. J Statistic Software. 2006;15(2):1-11.
e3. Treister NS, Brennan MB, Sollecito TP, et al. Exposed bone in patients with head and neck cancer treated with radiation therapy: an analysis of the Observational Study of Dental Outcomes in Head and Neck Cancer Patients (OraRad). Cancer. 2022;128(3):487-496.
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Excellent opportunity for growth by adding a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02332
FANTASTIC RETAIL LOCATION: Plano GP that is highly visible in a retail center. This practice operates with the owner and 1 PT associate, is open 7 days a week and provides regular dental care as well as emergency services. The practice has over 1,750 active patients who are 20% FFS, 70% PPO, and less than 10% Medicaid. The office has 4 ops and is in excellent condition. This is a great opportunity for growth by capitalizing on the existing patient base and expanding services. Opportunity ID: TX-02219
MILLION DOLLAR PRACTICE OPPORTUNITY: Frisco GP in a professional building with great access for patients and staff. The practice operates on 3.5 doctor and hygiene days per week. The office has 5 fully equipped ops, is digital, paperless, and is in excellent condition. There are over 2,800 active patients who are a blend of FFS and PPO. The seller currently refers out Perio, O.S., dentures, Pedo and Endo, giving a purchaser more potential for growth by adding those procedures. Opportunity ID: TX-02180
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano and has paperless charts. The practice is 90% FFS with a small amount of PPO. The office collected over $876K in a four-day workweek. Opportunity ID: TX-02041
Hieu Huynh, DDS, JD
DENTAL SCHOOL ADMISSIONS PANEL
Calling all Pre-dental students! Don’t miss this unique Q&A session with admissions officers from top dental schools. Get insider tips on the application process and have your questions answered directly by the experts. Room host volunteers during the TDA Meeting receive free admission to the panel. Scan the QR code below to learn more!
Event Code: F42
Time: Friday, May 9, 2:00 pm – 4:00 pm
Fee: $25 (FREE for room host volunteers!)
PARTICIPATING SCHOOLS
VOLUNTEER AT THE TDA MEETING!
Join us and make this year’s TDA Meeting a memorable experience for everyone!
We offer two different roles: Room Host or Speaker Host. By volunteering at the meeting, you can enjoy:
• Free course registration and CE credit for hosted course(s).
• Complimentary breakfast and lunch (for full-day volunteers).
• Networking opportunities and the chance to meet new friends!
When Teeth Tell Tales:
The
Ethics
Don’t Get Locked Out:
Ensuring Ethical Record Access
Kathleen Nichols, DDS, TDA Council on Ethics & Judicial Affairs, ADA Council on Ethics, Bylaws and Judicial Affairs Consultant; Diane Rhodes, TDA Senior Policy Manager; Debrah Rogers, TDA Program Manager
Scenario 1
Dr Lee, a new dentist, is considering a position at a practice but notices a clause in the contract stating she won’t be able to access patient records if she leaves the practice. She is concerned about her ability to follow up with patients if she changes practice locations.
Solution
Dr Lee negotiates with the practice owner to remove or adjust the clause, ensuring she has a clear, reasonable way to access patient records if she ever needs to leave. This allows her to provide continuity of care without legal or ethical challenges down the line. Further, the contract should include verbiage that the clinic agrees to maintain the records in accordance with the parameters set out by the Texas State Board of Dental Examiners, and the TDA Principles of Ethics & Code of Professional Conduct (the Code).
The Texas Dental Practice Act (DPA) and Texas State Board of Dental Examiners (TSBDE) rules clearly state that a patient’s dental records are “the property of the dentist performing
the dental service.”1 Records may only be transferred to the patient or, in specific circumstances, as a voluntary submission to an insurance company or another dentist in compliance with TSBDE rules.1,2
In this scenario, Dr Lee identified a clause in her employment contract stating that she would not be able to access patient records if she left the practice. This clause is problematic because it interferes with Dr Lee’s ability to exercise her independent professional judgment and adherence to the Code. It also prevents her from fulfilling her legal obligation to provide patients with the required notice upon her departure.3
The dental board rule governing improper influence on professional judgment presumes that entering into an agreement allowing anyone other than a dentist to control or restrict access to patient records violates the (DPA).4
Moreover, TSBDE regulations require that a dentist leaving a practice, for any reason, must provide patients with at least 30 days’ written notice, in accordance with the specific requirements of the notice rule.5 Our concern extends beyond a complaint regarding notice. In the future, if a complaint is filed against Dr Lee related to treatments provided or not provided, it will be essential for her to have access to those records for her defense.
If the TSBDE receives a complaint against Dr Lee for failure to provide patient notice, the dental board will take action against Dr Lee—not her non-dentist employer. Potential consequences include administrative penalties, licensure warnings, reprimands, suspension, or other disciplinary measures.
References
1. Texas Occupations Code §258.051, Dentist Records
2. 22 Texas Administrative Code §108.8, Records of the Dentist
3. Texas Occupations Code §251.003, Practice of Dentistry
4. 22 Texas Administrative Code §108.70(b)(1), Improper Influence on Professional Judgment
Application of the TDA Principles of Ethics and Code of Professional Conduct
The dentist providing the care to the patient MUST ENSURE:
1. The patient’s right to choose their dentist a. The dentist should inform the patient of the proposed treatment, and any reasonable alternatives, in a manner that allows the patient to become involved in treatment decisions.
2. The patient has a right under the code to participate in a meaningful way in the decision making process of their care.
3. Patient records are maintained appropriately, and confidentiality is assured.
a. Dentists are obliged to safeguard the confidentiality of patient records.
b. Dentists shall maintain patient records in a manner consistent with the protection of the welfare of the patient.
c. Upon request of a patient or another dental practitioner, dentists shall provide any information in accordance with applicable law that will be beneficial for the future treatment of that patient.
4. Patients have the ability to get a copy of their records with confidentiality is safeguarded.
5. Treatment cannot be discontinued without the patient being given adequate notice and the ability to find another dentist.
Section 1
PRINCIPLE: PATIENT AUTONOMY (“self-governance”). The dentist has a duty to respect the patient’s rights to self-determination and confidentiality.*
This principle expresses the concept that professionals have a duty to treat the patient according to the patient’s desires, within the bounds of what a reasonable and prudent dentist would do under the same or similar circumstances and in accordance with applicable Texas laws as found in the Dental Practice Act and to protect the patient’s confidentiality. Under this principle, the dentist’s primary obligations include involving patients in treatment decisions in a meaningful way, with due consideration being given to the patient’s needs, desires and abilities, and safeguarding the patient’s privacy.
ADVISORY OPINIONS
1.B.1. FURNISHING COPIES OF RECORDS.
A dentist has the ethical obligation on request of either the patient or the patient’s new dentist to furnish, in accordance with applicable law, either gratuitously or for nominal cost, not to exceed the schedule set forth by the Texas Administrative Code §108.8 (g), such dental records or copies or summaries of them, including dental x-rays or diagnostic copies of them, as will be beneficial for the future treatment of that patient. This obligation exists whether or not the patient’s account is paid in full.
A dentist has the ethical obligation on request of either the patient or the patient’s new dentist to furnish…such dental records or copies or summaries of them, including dental x-rays or diagnostic copies of them, as will be beneficial for the future treatment of that patient. This obligation exists whether or not the patient’s account is paid in full.
Section 2
PRINCIPLE: NON-MALEFICENCE (“do no harm”). The dentist has a duty to refrain from harming the patient.
This principle expresses the concept that professionals have a duty to protect the patient from harm. Under this principle, the dentist’s primary obligations include keeping knowledge and skills current, knowing one’s own limitations and when to refer to a specialist or other professional, and knowing when and under what circumstances delegation of patient care to auxiliaries is appropriate.
ADVISORY OPINION
2.F. PATIENT ABANDONMENT.
Once a dentist has undertaken a course of treatment, the dentist should not discontinue that treatment without giving the patient adequate notice and the opportunity to obtain the services of another dentist. Care should be taken so that the patient’s oral health is not jeopardized in the process.
Section 3
PRINCIPLE: BENEFICENCE (“do good”). The dentist has a duty to promote the patient’s welfare.
This principle expresses the concept that professionals have a duty to act for the benefit of others. Under this principle, the dentist’s primary obligation is service to the patient and the public-at-large. The most important aspect of this obligation is the competent and timely delivery of dental care within the bounds of clinical circumstances presented by the patient, with due consideration being given to the needs, desires and values of the patient. The same ethical considerations apply whether the dentist engages in fee-for-service, managed care or some other practice arrangement. Dentists may choose to enter into contracts governing the provision of care to a group of patients; however, contract obligations do not excuse dentists from their ethical duty to put the patient’s welfare first.
Section 5
PRINCIPLE: VERACITY (“truthfulness”). The dentist has a duty to communicate truthfully.
This principle expresses the concept that professionals have a duty to be honest and trustworthy in their dealings with people. Under this principle, the dentist’s primary obligations include respecting the position of trust inherent in the dentist-patient relationship, communicating truthfully and without deception, and maintaining intellectual integrity.
Once a dentist has undertaken a course of treatment, the dentist should not discontinue that treatment without giving the patient adequate notice and the opportunity to obtain the services of another dentist. Care should be taken so that the patient’s oral health is not jeopardized in the process.
Prior to the COVID-19 pandemic, TDA members who had reached their 10year, 25-year (Good Fellow), 30-year (Life), 50-year, and 60-year memberships were recognized at a special luncheon and the House of Delegates at the TDA Meeting each May. In 2020, at the height of the pandemic, the TDA discontinued the in-person luncheon due to limitations with social distancing and increased costs.
In 2021, TDA began including current-year recipients who reach those membership milestones in the TDA House of Delegates minutes and in the July special membership issue of the Texas Dental Journal each year, featuring their quotes and personal and professional experiences. Please keep an eye out for the special membership issue to be published in a few months and read stories and experiences that are like Dr Van Wart’s (right).
Note: If you received your membership award prior to 2021, your name was also published in the official House of Delegates minutes, and you were mailed a certificate of recognition. If you have lost or misplaced your certificate and need a replacement, please email Debbie Rogers at drogers@ tda.org.
Member SPOTLIGHT
Each Member Has a Story
Family Ties:
The 3 Generations of the Drs Van Wart
After years of working together, many of us view our coworkers as family, but what if they really are your family? Such is the case for the 3 generations of Drs Van Wart at Van Wart Dental in Houston.
In 1966, Dr William H. Van Wart purchased a cozy cottage bungalow in the Southampton neighborhood near Rice University. He renovated it for a dental office and hung his shingle in 1967. Now, almost 60 years later, his 2 daughters, Drs Sherry Van Wart-Noblett
and Tammy Van Wart-Hemann, and a granddaughter, Dr Christina NoblettThomas, continue the family dental practice in the same building and location.
“My most proud accomplishment is having 2 daughters come into the practice, and best of all, my granddaughter joined the practice in 2018!” says Dr Van Wart, a Life member of TDA, retiring in 1997.
Dr Van Wart’s granddaughter Dr Christina (right) began practicing with him and his daughter (left), her mother Dr Sherry, in 2018.
William (Bill) Haley Van Wart was born in 1932 in Dallas, and he said it cost $50 for the doctor and hospital bill combined. “My parents didn’t have the $50, so they paid it off weekly. The doctor who delivered me was named Dr Haley; my parents gave me his name as my middle name in hope of a discount. It didn’t work,” says Dr Van Wart.
The Van Warts moved to West University, a suburb of Houston, when he was 2 years old so his father could find work during the Depression. He attended West University Elementary, Persing Junior High, Lamar Senior High, and Rice Institute/University, which offered free tuition if you were admitted. He received his dental degree at the University of Texas Dental Branch—Houston (UTDB).
“My family couldn’t afford the tuition of dental school, so I signed up for the US Army,” says Dr Van Wart. “The requirement was I would pay back with 4 years active duty, and 4 more years reserve. I’m really glad I did, because it allowed me to gain experience in dentistry, and of course to pay for dental school.”
He and his wife Kathryn were stationed in a small town in Germany, where his first 2 children were born. They returned to the US in the early 1960s when Dr Van Wart opened his practice on Sunset Boulevard in Houston. He continued in the US Army Reserves for 32 more years.
“It became my hobby as well. I enjoyed the continuing education opportunities, the travel for 2 weeks in the summer, and the structure of the military always appealed to me. I became great friends with many military doctors and dentists.”
He says dentistry has been an excellent career choice. “It allowed me to feed my family, raise 3 daughters (2 dentists and a nurse), put them through school, and pay for 3 weddings. Dentistry allowed me to be my own boss, to have comradery with other dentists, and to give back to my community.”
He credits an interest in dentistry to his childhood dentists. “When I was a kid growing up just outside of Houston, in West University, my mom would take my brother and me on the bus into Houston to see Dr Farrell, our dentist. He and his office looked and smelled so clean, attention to detail, nice, neat, and that really appealed to me. In later years, I had a wonderful mentor, Dr Frank Hawk, who was our dentist after I was a young boy. These 2 men really influenced me in my dental career.”
Above and below: Dr Van Wart is pictured treating patients in the 1970s.
Dr Van Wart assesses a patient in the 1960s.
Through retirement, Dr Van Wart continued helping with paperwork and visiting patients of his daughters’ and granddaughter’s twice a week until he turned 90. They followed in his dental school footsteps—Drs Tammy and Sherry graduated from UTDB in Houston in 1985 and 1988, respectively, and Dr Christina from UT Health School of Dentistry in Houston (UTSD) in 2018. Dr Christina is married to an oral surgeon, UTSD alum Dr Andrew Thomas, and the family is hoping to continue the dental profession bloodline to 4th and 5th generations.
“I grew up working at our family dental practice summers and Christmas breaks from school,” says Dr Sherry. “I developed X-rays, seated the patients, worked chairside, made appointments, cleaned the office, and even did outside yard work regularly. It was a profession that I had learned every aspect of, so I think it felt comfortable.”
She says she is in the unique position of being a mentee of her father and mentor to her daughter, and many of their patients have become close, one time she treated 5 generations of the same family.
“My dad said it was a good career for women because our hands are smaller, we are very compassionate, and it allows the flexibility for a family; he was correct. One of the things I like the most about our practice is that we still have patients who started with us in 1960, saw me grow up, saw my daughters grow up, and are still special patients 65 years later.”
Dr Sherry says she loves to work with her daughter and son in law, also members of TDA. “Warranties of our work can be upheld by the next generation of dentists. We share experiences, advice, treatment planning
ideas, new technology, and experience of 36 years. Dr Christina is such an upbeat person; she is a joy to be around! It is also nice to get oral surgery advice from my son-in-law.”
Dr Van Wart passed along the importance of involvement in organized dentistry, says Dr Sherry. “He definitely led by example! We must help carry our profession on through continuing education, comradery, and affecting our state laws influencing our profession.”
Like her mother, Dr Christina grew up working at Van Wart Dental, so she knew it was a rewarding profession. “I knew I wanted to follow in their footsteps early on. My grandfather and mother have provided outstanding dentistry to many patients and families over the last 65 years. Their hard work and compassion created a perfect opportunity for me to come in and continue their legacy. I have big shoes to fill!”
The family ties are the ones that bind, and Dr Christina says she is blessed to work with her mother every day, and her grandfather enjoys hearing about her endeavors as a young dentist.
“My first patient after my licensing exam was a gentleman who started seeing my grandfather in 1976 when he was 10 years old,” says Dr Christina. “He saw my mother throughout his 20s, 30s, and 40s and me in his 50s. We were both excited to take the Van Wart family practice into its 3rd generation together. I look forward to carrying on the Van Wart Dental Legacy for the next 30+ years.”
Van Wart Family Dental: Dr Van Wart purchased this cottage on Sunset Boulevard in Houston in 1966 and converted it into a dental office that his daughters and granddaughter continue to use to treat patients.
FBI: Found But not Identified (yet)
A series of articles intended to assist Texas Medical Examiners in giving a name to “unidentified” individuals using postmortem dental evidence.
Do you recognize the dental work/conditions presented?
Kathleen A Kasper, DDS, D-ABFO
The Extent of the Problem
Over 600,000 individuals go missing in the United States every year. Fortunately, many missing children and adults are quickly found, alive and well. However, tens of thousands of individuals remain missing for more than 1 year—what many agencies consider “cold cases”.1
It is estimated that 4,400 unidentified bodies are recovered each year, with approximately 1,000 of those bodies remaining unidentified after 1 year.2
Medical examiner and coroner offices reported 11,380 unidentified remains on record as of 2018.3
The challenge in giving a name to these unidentified decedents is that the research and time invested can be extensive and expensive, and after normal protocols have been exhausted, many individuals still remain unidentified. The hope in writing this series of articles on long-term unidentified in Texas is that one of the many Texas dentists who read the Texas Dental Journal will recognize the dental work presented as theirs or possibly remember a dental condition or feature that can give a name to the unidentified and help bring closure to the family.
The Medical Examiner’s Protocol to Legally Identify Individuals
Medical examiners follow a specific protocol to identify individuals who are found without any presumptive identity. This protocol is described below and, in this order, depending on the condition of the body.
By far Latent Prints (finger, palm, sole) are the fastest and least expensive way to make a positive identification. This method of identification is not always possible if remains are severely decomposed, incinerated, or skeletonized.
Medically Implanted Devices (hip/joint replacements, pacemakers) require knowing what hospital/physician placed the device to get the matching serial number, which can be difficult.
Dental Records are also an easy, fast, and inexpensive way to identify a decedent; however, success depends on a presumptive identity and availability/existence/ quality of those antemortem (before death) dental records. If all leads for a presumptive identity are exhausted, then a postmortem (after death) dental charting/ profile is created and entered in the NamUs (National Missing and Unidentified Persons System) and NCIC (National Crime Information Center) databases.
Anthropologic Methods will use skeletal features to make a positive identification.
DNA samples are collected. This takes the longest period of time and is most expensive. Depending upon the individual, it may involve obtaining DNA samples not only from the decedent but also from family members or multiple family members if known. If no matches are obtained, then:
DNA Samples are submitted to CODIS (Combine DNA Index System), which is a computer program that operates local, state, and national databases of DNA profiles
Author
Kathleen A. Kasper, DDS, D-ABFO
Dr Kasper has been practicing general dentistry in Carrollton, Texas, for 29 years. She is a graduate of the University of Iowa College of Dentistry.
She provides 3 counties in the Dallas-Ft. Worth Area with forensic dental services. These include Collin, Dallas, and Tarrant Counties. She is currently the only active board certified forensic dentist in north Texas.
She received her formal forensic odontology training at the University of Texas Health Science Center San Antonio, Texas, Center for Education and Research in Forensics (CERF) in 2003-2004.
Dr Kasper obtained Board Certification from the American Board of Forensic Odontology in 2010.
She is a fellow of the American Academy of Forensic Sciences, a member of the American Board of Forensic Odontology, and a member of the American Society of Forensic Odontology.
She is the current American Board of Forensic Odontology Dental Age Assessment Committee Chair.
Dr Kasper is also a published author in the Journal of Forensic Sciences and coauthor of a chapter in each of 3 forensic textbooks.
Perhaps one of her greatest undertakings was chairing a working group for the American Dental Association that has published the “Technical Report” for Forensic Dental Age Estimation which went on to become a “standard” for the Organization of Scientific Area Committees (OSAC) for Forensic Science.
from convicted offenders, unsolved crime scene evidence, unidentified remains and missing persons. This is maintained by the Federal Bureau of Investigation. If this search fails then, the State of Texas requires medical examiners to submit a DNA sample from long-term unidentified decedents to the University of North Texas Center for Human Identification for additional genetic testing and comparison. This comparison may take up to a year to process, and a decedent may still remain unidentified once completed. This is the proverbial end of the road; therefore, all Texas dentists, dental auxiliaries, and staff: Can you help the Tarrant County Medical Examiner’s Office give a name to the unidentified male decedent described below?
The Unidentified Individual:
Tarrant County Medical Examiner (TCME) Case #2419568
Date of Death (Decedent found): November 23, 2024
Cause of Death: Pending Medical Examiner Testing
Manner of Death: Pending Medical Examiner Testing
Body Condition: Near complete skeletal/complete skeletal
Sex: Male
Ancestry: White
Age Interval: 36-61 years
Height: 5 feet, 8 inches
DNA analysis produced no matches
Scene Description: The decedent was an unidentified individual that was found decomposing and partially skeletonized in a creek bed. The Fort Worth Police Department investigated the scene and has not ruled out foul play. The decedent was lying supine dressed in white socks, light colored, possibly, cargo shorts, red/green plaid boxers, and a brown belt with black buckle. The decedent’s head was tilted toward the left shoulder. The decedent’s left arm was above the head and right arm stretched out to the side. Both hands appeared to be missing. The tissue was absent from the decedent’s back. A small bone was found disarticulated below the right knee. The decedent was bent nearly in half at the waist with the legs stretched out along the side. Evidence of decomposition was noted to include skeletonization, sun bleaching, adipocere, and scavenger activity.
The medical history of the decedent is unknown.
Details of the incident: The investigating officer with the Fort Worth Police Department reported that a homeless individual was passing by looking for items of value in the creek bed off of 1300 Green Oaks Rd, Fort Worth, Texas 76116 and noted the decedent. Emergency services were contacted at 2:06 PM on 11-23-2024 and the individual was pronounced dead by a medic with MedStar Emergency Services at 2:12 PM that same day. The TCME investigator assigned to this case documented the scene with photographs. The location was a drainage ditch that extended out from under the parking lot north of 1300 Green Oaks Rd. The area where the decedent was found was rocky with a large amount of debris. Tall grasses and small trees were growing throughout, and the tall grasses were bent toward the east. West of the decedent’s location was a shallow pool area. The detective with the Fort Worth Homicide Unit reported there was a homeless camp located upstream from the location.
If you believe you have any dental records, dental radiographs, intraoral/extraoral dental photographs, dental scans, or other dental information regarding the unidentified white male decedent described above as TCME Case #2419568, please contact the Tarrant County Medical Examiner’s Office, 817-920-5700, ext 8387, and ask for Christian Crowder, PhD, D-ABFA, Chief of Human Identification Services.
Let’s give this individual a name!
References
1. Between 2007 and 2020, an average of 664,776 missing persons records annually were entered into the National Crime Information Center. See https://www.fbi.gov/ services/cjis/ncic.
2. Medical Examiners And Coroners’ Offices, 2004. Matthew J. Hickman, Ph.D., Kristen A. Hughes, M.P.A., Bureau of Justice Statistics, Kevin J. Strom, Ph.D., Jeri D. Ropero-Miller, Ph.D., DABFT, RTI International.
3. Medical Examiner and Coroner Offices, 2018. Connor Brooks, Bureau of Justice Statistics, November 2021.
value for your profession
Provided by: PERKS
P R O G R A M
Equipped for the Unexpected: Essential Tools for Successful Sedation Outcomes
By Rose Dodson, MSc, CEO Sedation Resource, Inc.
Sedation can make dental procedures easier for everyone—patients feel more comfortable, and the procedure runs more smoothly. But what if things do not go as planned? For instance, imagine a patient falling into a deeper level of sedation than intended and the patient’s breathing slowing as a result. The dental team must respond with skill and careful judgment to manage the situation.
Sedation-related events such as this have the potential to lead to more serious complications. That is why it is so important for the whole dental team to be engaged. The good news? With the right tools and preparation, you can handle these moments calmly, efficiently, and with confidence.
This article provides a simple guide to the key tools and devices for keeping sedation safe, with tips on staying prepared and using simulation to improve readiness.
Three Common Sedation Issues
When something goes wrong during sedation, it usually falls into one of these three categories:
1. Breathing Problems: If breathing slows or the airway becomes blocked, oxygen levels can decrease quickly, requiring a rapid response to prevent further deterioration.
2. Blood Pressure Changes: Patients might experience a drop in blood pressure or fainting. Keeping blood pressure stable is key to making sure the brain and other vital organs receive proper blood perfusion.
3. Nausea and Vomiting: Patients might feel nauseated or vomit during or after sedation. The big concern here is aspiration—when stomach contents enter the lungs, which can cause serious complications.
Spotting these issues early is crucial. Monitoring tools not only help detect problems but also provide critical time for the team to intervene and manage the situation effectively.
Tools That Help Detect Problems Early
Paying close attention to the patient and using your clinical skills are your first line of defense. Monitoring tools are your next line of defense. They help you identify problems early so you can act fast. Here are some essential devices:
1. Pulse Oximeters
A pulse oximeter detects the oxygen level in the patient’s blood. If oxygen levels drop, it sounds an alarm so you can take action.
• Tip: Always have a backup pulse oximeter in case the main one stops working.
2. Capnography Monitors
These devices measure how much carbon dioxide the patient is exhaling. They are great for identifying early signs of breathing difficulties.
• Why it matters: If a patient’s breathing slows or stops, a capnography monitor can alert you before oxygen levels get too low.
3. Pretracheal Stethoscopes
Pretracheal stethoscopes, including wireless amplified models, allow you to listen to the patient’s airway sounds. They give you real-time information about breathing and are a key part of your monitoring system. For example, you can hear changes in the airway’s patency and the patient’s breathing pattern, even before drops in the oxygen level are noted on pulse oximeters. This allows early identification of a problem and an early response.
• Tip: The wireless design lets you move around during the procedure while keeping track of the patient’s airway.
4. Automated Blood Pressure Monitors
Automated blood pressure monitors continuously track the patient’s blood pressure throughout the procedure. Sudden changes in blood pressure can signal a developing problem, so getting an early alert from the monitor allows the team to act quickly to stabilize the patient.
• Tip: Ensure the monitor’s alarms are set correctly so you do not miss important changes.
Backup Devices: Be Ready for the Unexpected
Even with great monitoring, you still need to be ready to act when the unexpected occurs. That is where backup devices come in. Here are a few vital backup devices:
1. Portable Oxygen Tanks
If the main oxygen supply fails, a portable oxygen tank can save the day. Make sure it is always full and ready.
• Tip: Check your oxygen tank in conjunction with a repeated event such as checking it every payday.
2. Battery-Powered Suction Systems
A patient’s airway can get blocked by fluids. A battery-powered suction system clears the airway fast, even if there is a power outage.
• Tip: Check the battery regularly to make sure it is fully charged.
3. Bag-Valve Masks (BVMs)
A bag-valve mask is a positive pressure oxygen device that helps manually deliver oxygen to a patient who is not breathing well or who has stopped breathing entirely. Regular practice using a BVM with the proper head tilt-chin lift maneuver is essential so you are prepared when needed.
4. Backup Monitors
Having an extra pulse oximeter or capnography unit ensures you can keep an eye on the patient if your main monitor fails.
5. Headlamps
Good lighting is critical during any procedure. A fully charged, battery-powered, basic LED headlamp is sufficient to ensure visibility if your primary light source stops working.
How to Stay Ready: Practice and Maintenance
Having the right tools is only part of the solution. Regular simulation drills and having a simulation toolkit readily available can simplify emergency preparation and ensure your team stays confident and ready. Here’s how:
1. Practice Emergency Drills
Hold monthly simulation drills to help everyone stay calm and confident in real emergencies. For example, you can simulate a scenario where a patient’s airway becomes obstructed, allowing the team to practice using suction devices and bag-valve masks efficiently. Use these sessions to practice different scenarios and utilize all your monitoring tools and backup devices. A simulation toolkit, stocked with items like airway adjuncts, bag-valve masks, and mock medication vials, can make running these drills more efficient.
One of the best ways to prepare for emergencies is through simulationbased training. Various dental organizations offer high-fidelity workshops designed to help teams handle real-life sedation emergencies. These workshops provide an excellent opportunity to practice managing adverse events in a controlled environment.
2. Follow Clear Protocols
Make sure everyone knows their role and what to do in an emergency. Clear, step-by-step instructions can save valuable time when it matters most.
3. Keep Equipment in Good Shape
Check your equipment regularly to make sure everything works properly. This includes:
• Keeping oxygen tanks full
• Checking that suction devices and monitors are in good working order
• Replacing batteries as needed
Real-Life Training: Get Hands-On
Practice
One of the best ways to prepare for emergencies is through simulation-based training. Various dental organizations offer high-fidelity workshops designed to help teams handle real-life sedation emergencies. These workshops provide an excellent opportunity to practice managing adverse events in a controlled environment. For those looking for in-office training, Dental Simulation Specialists brings handson simulation training directly to your practice. This tailored approach allows your team to work together in the actual environment where emergencies may occur.
Programs like Ten Minutes Saves a Life®, created by the American Dental Society of Anesthesiology (ADSA), also offer video-based learning modules to guide dental teams through common emergency scenarios. For example, one module covers recognizing early signs of airway obstruction and practicing quick interventions, helping teams build confidence in managing such situations. While not a standalone course, these modules provide valuable foundational knowledge and can supplement more immersive training experiences.
If you get a chance to attend a training or use these resources, take it! The experience can be invaluable.
Conclusion
When it comes to sedation, being prepared makes all the difference. By using the right monitoring tools, keeping essential backup devices ready, and practicing emergency drills regularly, you can turn a challenging situation into a success story. Emergencies might be rare, but being ready equips you and your team to handle them confidently and to keep your patients safe.
Sedation Resource, Inc. is endorsed by TDA Perks Program. It is dedicated to supporting dental professionals in providing safe and effective care with the help of advanced monitoring technologies. For more information regarding Sedation Resource, visit tdaperks.com (Compliance and Supplies) or call (903) 634-5333.
Emergencies might be rare, but being ready equips you and your team to handle them confidently and to keep your patients safe.
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/MemberResources/TDA-Classified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN
(ID #691): Unique opportunity to purchase a GD practice with 2 locations in the Austin area. The offices have a total of 10 operatories with computers in each room and digital radiography. The offices serve a large FFS/PPO patient base with a healthy new patient flow and strong hygiene recall with over 20-25% of total annual production coming from the hygiene department.
AUSTIN (ID #723): Large, general dentistry practice (with a recent focus on implants) located in a free-standing building with great visibility in north Austin. Large facility with 8 fully equipped operatories, digital radiography, an iTero digital scanner, and a 3D CBCT unit. FFS/PPO patient base, over 2,000 active patients, and has a stellar reputation. The owner invested heavily in growing the implant side of the business.
AUSTIN (ID #729): Legacy GD office located in the heart of Austin in a high visibility location. Majority PPO patient base, 1300+ active patients, 15 new patients visit the office per month, and an impeccable reputation online and in the community. The 2,050 sq ft office space contains 6 total operatories (4 equipped), computers throughout, digital x-ray sensors,
and intra-oral cameras. They generated revenue of mid-6 figures during each of the past 3 years with abundant upside potential.
DALLAS (ID #728): Well-established GD office in a growing suburb southeast of Dallas. This practice has an impeccable reputation, treats a majority FFS patient base with 1,700+ active patients. The 1,800 sq ft facility features 4 fully equipped operatories (with a 5th plumbed and ready to be equipped), computers throughout, digital x-ray sensors, digital panoramic x-ray, digital scanner, CAD/CAM milling unit, dental laser, and intra-oral cameras. This turn-key office has strong net cash flow and significant upside potential.
DALLAS/FORT WORTH-
ORAL SURGERY (ID #711): Legacy, oral surgery practice in a bustling suburb between Dallas and Fort Worth. A heavily tenured team, large patient base, and a fantastic reputation in the local community. 3,300 sq ft office in an easily accessible medical office park, 4 fully equipped operatories, 2 plumbed operatories for future expansion, computers throughout, digital x-ray sensors, and a 3D cone beam CT. With over seven figures in 2023 revenue and profit margins trending at 50%, the foundation for a successful future has already been laid with abundant upside potential available.
HOUSTON-SOUTH (ID #682): Established,
multi-specialty dental office in a suburb ~20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
DSO C S PRACTICE SALES
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com PRACTICE APPRAISALS
www.dentaltransitions.com
classifieds
restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose. HOUSTON-NORTH (ID #712): Established, GD office located north of Houston. 6 fully equipped operatories, digital x-rays, a CBCT, a digital scanner, and a CAD/ CAM milling unit. PPO/FFS patient base, over 1500+ active patients, and boasts a near-perfect Google rating across 100+ reviews. Strong net cash flow in 2024 and a robust hygiene recall program with over 20% of production coming from the hygiene department annually.
HOUSTON-SOUTHWEST (ID #724): Legacy GD office located southwest of Houston. Majority PPO patient base, 2000+ active patients, great online reputation with 100+ reviews. 5 total operatories (4 equipped), with computers in each, digital x-rays, digital Pano, a CAD/CAM milling unit, and a digital scanner. The practice realized revenue of over 7 figures in 2024 with robust net cash flow margins (>40%) and a robust hygiene recall program. SAN ANTONIOTX HILL COUNTRY (ID #685): Well-established dental practice and real estate nestled in the Hill Country north of San Antonio. The office relies mostly on word-of-mouth- referrals
with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023 and the trend continued into 2024. SAN ANTONIOEAST (ID #716): Legacy GD practice and real estate in a rural community east of San Antonio. The large office space offers ample room for expansion and features 5 fully equipped operatories with computers in each op, digital x-ray sensors, a digital pano, a digital scanner, intraoral cameras and paperless charts. This practice has strong profit margins and serves a large, multi-generation 100% FFS patient base.
SOUTH TEXAS (ID #651): General dentistry practice located in south Texas. This state-ofthe-art office occupies 3,500 sq ft with room for 10 total operatories, is fully digital with CBCT, a digital scanner, handheld x-ray units, and a 3-D printer. The practice serves a large PPO/ Medicaid patient base with over 3,000 active patients seen over the last 24 months with a strong monthly new patient flow. TO REQUEST MORE INFORMATION ON MCLERRAN &
ASSOCIATESí LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@dentaltransitions. com.
CENTRAL TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural four operatory dental practice for sale in the heart of the beautiful Texas Hill Country. This all-digital practice with a new pano produces mid six figure income with just two days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@gmail.com for more information and showings.
HOUSTON: General practice (reference: (“Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid-6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475
sq ft with 3 total operatories: 2 for dentistry and one for hygiene. Please let me know if you need anything else from me. A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 35 years. Practice sees patients about 16 to 19 days per month. Collection ratio of 99%. Practice is a fee for service and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
HOUSTON: Houston Metro periodontal practice for sale: 5 operatories, 7-figure collections, $245K EBITDA, 1,555 active patients, and strong growth potential. Contact Bailey Jones at bailey@professionaltransition.com or 719-6948320. #TX101624.
NEW BRAUNFELS: Dental practice for sale in high traffic area and very visible building. Beautifully renovated recently, with 3 operatories, move-in ready, with 1,250 sq ft. No HMO or DMO. If interested, please email to salemydentalpractice@yahoo.com or leave message on landline, 830-606-4544.
classifieds
NEW BRAUNFELS: Dental practice for sale in high traffic area and very visible building. Beautifully renovated recently, with 3 operatories, move-in ready, with 1,250 sq ft. No HMO or DMO. If interested, please email to salemydentalpractice@yahoo.com or leave message on landline, 830-606-4544.
SAN ANTONIO: General practice, 42 years established generational, exceptional patients in growing southwest San Antonio, with 2000+ active patients, 25/30 N.P monthly. Exceptionally trained team. High 6-figures revenue, based on a 4-day work week, with high collections rate and low overhead. Range of services include: restorative, endo, restore implants, CB, removables, oral surgery, nonsurgical perio. Patients primarily FFS, PPO, cash pay, 6% Medicaid. Great potential for expansion of services would include, molar endo, ortho, implant placement, perio surgery, and hygiene expansion, open up Fridays and Saturdays. Physical plant consists of a 5,300 sq ft free standing corner lot building on a busy street. Six operatories are in use, the facility is plumbed for 11 operatories. Tech includes: CBCT,
scanner, digital x-ray units, computers / TVís in ops, phone system. Doctor is willing to work part time for transition as associate. Practice is for sale, real estate is available as well or longterm lease. Interested buyers please contact Kaylor Karlin at 210-500-3431, kaylorkarlin@ kw.com.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.