Reprinted with permission from the San Antonio District Dental Society.
148
SURGICAL REPOSITIONING OF INTRUSIVE LUXATION INJURY WITH 15-YEAR FOLLOW-UP: A CASE REPORT
PRIYANSHI RITWIK, BDS, MS ELSA ALFONSO-ECHEVERRI, DDS ANTONIO DARIO CARDENAS, DDS, MS
156
SHINGLES: A CASE REPORT
MICHELE WHITE, DDS
RYAN VAHDANI, DDS, MHA
JOSEPH D. YADIN, BS, (MS1)
GARY N. FREY, DDS CLEVERICK (C.D.) JOHNSON, MS, DDS
BEN F. WARNER, MS, DDS, MD
164
ASK THE POWERS CENTER
MALIK ABUMANSOUR, BDS
MARIA GONZALEZ, DDS, MS
RUBEN SAUCEDA, DDS, MS
GUEST EDITOR RADE D. PARAVINA, DDS, MS, PHD
Dental practice financing1
Our practice specialists can help you achieve your goals practice solutions
We’ll work with you to determine the financing solutions that best fit your plans, and help guide you through the process.
New office startups
Get started with up to 100% project financing.¹
Practice sales and acquisitions
Benefit from our many years of experience helping clients purchase practices.
Business debt consolidation¹
Let us help you restructure your debt and improve your cash flow.
Office improvement and expansion
Enjoy competitive terms when you remodel or expand.
Commercial real estate ²
Buy, refinance¹ or relocate with conventional or Small Business Administration (SBA)³ loan options.
Equipment financing
Choose from a variety of options and flexible terms tailored to meet your needs.
To learn more, call 800.428.2847 to talk to a practice specialist, or visit bankofamerica.com/practicesolutions.
Bank of America can also help you with cash management, employer solutions and your personal banking and financial needs.
Proudly endorsed by:
1 All programs subject to credit approval, and loan amounts are subject to creditworthiness. The term, amount, interest rate, and repayment schedule for your loan, and any product features, may vary depending on your creditworthiness and on the type, amount, and collateral for your loan. Bank of America may prohibit use of an account to pay off or pay down another Bank of America account. Repayment structure, prepayment options and early payoff are all subject to product availability and credit approval. Other underwriting standards and restrictions may apply. Products and restrictions are subject to change.
2 Owner occupied commercial real estate will be determined in underwriting and requires occupancy by the borrower/guarantor. Please note SBA guidelines require at least 51% occupancy to be considered Owner Occupied.
3 Small Business Administration (SBA) financing is subject to approval through the SBA 504 and SBA 7(a) programs. Loan terms, collateral and documentation requirements apply. Actual amortization, rate and extension of credit are subject to necessary credit approval. Bank of America credit standards and documentation requirements apply. Other restrictions may apply.
All promotional and marketing materials are Bank of America Practice Solutions property and, as such, cannot be changed, altered or modified, orally or in writing. All questions regarding these materials should be directed or referred to a Bank of America Practice Solutions Sales Associate.
Sponsorship of endorser’s products and services is not an expressed opinion or approval by the Bank.
136 “GOOD-BYE MY YELLOW-BRICK ROAD…” ARTIFICIAL INTELLIGENCE: FACT OR FICTION?
Eric Shapira, DDS, MAGD, MA, MHA
Reprinted with permission from the San Antonio District Dental Society. The article was originally published in the November/December 2023 San Antonio District Dental Society Journal and received the Division II Golden Pen award from the International College of Dentists.
148 SURGICAL REPOSITIONING OF INTRUSIVE LUXATION INJURY WITH 15-YEAR FOLLOW-UP: A CASE REPORT
Priyanshi Ritwik, BDS, MS
Elsa Alfonso-Echeverri, DDS
Antonio Dario Cardenas, DDS, MS
156 SHINGLES: A CASE REPORT
Michele White, DDS
Ryan Vahdani, DDS, MHA
Joseph D. Yadin, BS, (MS1)
Gary N. Frey, DDS
Cleverick (C.D.) Johnson, MS, DDS
Ben F. Warner, MS, DDS, MD
164 ASK THE POWERS CENTER
Malik Abumansour, BDS
Maria Gonzalez, DDS, MS
Ruben Sauceda, DDS, MS
Guest Editor Rade D. Paravina, DDS, MS, PhD
HIGHLIGHTS
134 In Memoriam
168 Value for Your Profession: Treating OSHA and HIPAA Guidelines as Mere Formalities is Risky in Dentistry 170 Classifieds
175 Index to Advertisers
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 142 | No. 3
Texas Dental Journal (ISSN 0040-4284) is published monthly, except January-February, March-April, July-August, and November-December, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2025 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement at tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE!
(Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available):
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
JKJ Pathology
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com
Board of Directors Texas Dental Association
PRESIDENT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PRESIDENT-ELECT Elizabeth Goldman, DDS 214-585-0268, texasredbuddental@gmail.com
PAST PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
VICE PRESIDENT, SOUTHEAST Matthew J. Heck, DDS 512-280-8800, matthewjheckdds@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN** Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR** Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL** Carl R. Galant
INTERIM EXECUTIVE DIRECTOR** Duc M. Ho, DDS 281-395-2112, ducmho@sbcglobal.net
*Non-voting member **Non-voting
Those in the dental community who have recently passed
William Lawson Jr
Garland
7/4/52–4/8/25
Good Fellow: 2012 Life: 2017
Joe Merrill Ellis
Houston 2/16/42–1/18/25
Good Fellow: 1991 Life: 2007
Fifty Year: 2016
David Edward Snyder
Boerne 8/15/30–3/14/25
Life: 1995
Fifty Year: 2025
Roy Berkley Jones Jr
Benbrook 11/12/35–3/10/25
Good Fellow: 1986
Life: 2000
Fifty Year: 2011
Malpractice insurance that’s all about you .
As a dentist, you face unique challenges every day. That’s why at MedPro Group, we created an industry-leading malpractice policy that keeps you safe. Here’s what else you can expect with MedPro on your side.
Get unmatched coverage. Practice more safely. Protect your good name.
You’ll get great coverage at a great price. We also offer policy options that others don’t — including Occurrence and a pure consent clause, which gives you more control during a claim.
With 24/7 access to our free risk resources and on-staff experts, you and your practice will be better prepared for every day challenges. We don’t just defend claims, we help you avoid them.
The average dentist is sued at least once in their career, which is why we’re in your corner when it matters most. We lead the industry with a 95% dental trial win rate (plus 8 out of 10 claims close without payment).
“Good-bye My Yellow-Brick Road…” Artificial Intelligence: Fact or Fiction?
Eric Shapira, DDS, MAGD, MA, MHA
Reprinted with permission from the San Antonio District Dental Society. The article was originally published in the November/December 2023 San Antonio District Dental Society Journal and received the Division II Golden Pen award from the International College of Dentists.
The Road Not Taken
—Robert Frost 1874-1963
Two roads diverged in a yellow wood, And sorry I could not travel both And be one traveler, long I stood And looked down one as far as I could To where it bent in the undergrowth.
Then took the other, as just as fair, And having perhaps the better claim, Because it was grassy and wanted wear; Though as for that the passing there Had worn them really about the same,
And both that morning equally lay In leaves no step had trodden black. Oh, I kept the first for another day!
Yet knowing how way leads on to way, I doubted if I should ever come back.
I shall be telling this with a sigh Somewhere ages and ages hence: Two roads diverged in a wood, and I— I took the one less traveled by, And that has made all the difference.
Dr Hinton believes AI could spread misinformation and, eventually, threaten humanity. This is a very frightening thought, to say the least; especially from the man that has created it mechanically and electronically. The frightening thing is all of this was a prophecy by Professor Hinton who has stated that this is “the first time in history that a system has been created that is more intelligent than us (humans)!” He has stated that machines like this can have the ability to be “self-aware” or what is known as being sentient, an accident born from a failure to create a neural network to mimic the human brain. He failed with the human mind but did generate artificial intelligence after 50 years of experimenting.
AI can learn to do bad things through manipulation or negligent oversight, such as getting people to make decisions without fully understanding the complexity of the ramifications. We might have never thought of an algorithm as harmful, because it has not happened yet in our lifetime.
AI has the ability to create meaning of which Dr Hinton has strongly advocated that “we don’t really understand AI and its risks!” In the industrial age we delegated action, now in the AI age we are delegating thought with decision making, and it may not have our best interests at hand. It seems that there is a great deal of apprehension on his part that AI will be smarter than mankind and with that knowledge, it carries with it a relatively imminent “existential threat,” through its growing influence on all levels.
There is much general concern at the present time about the fact that there are those among us humans, who may want to build robotic armies that kill people. ChatGPT is a powerful form of GAI that can perform many of these functions. AI can learn to do bad things through manipulation or negligent oversight, such as getting people to make decisions without fully understanding the complexity of the ramifications. We might have never thought of an algorithm as harmful because it has not happened yet in our lifetime. Labor market experts predict the impact may come to close to 1/3 of workers on the planet by 2030 if wide AI adoption takes place. The United States currently has 11 million unfilled jobs that AI could affect since the “pandemic has turbocharged its adoption.”
Present Examples of AI
There have been medical uses of AI for some time, for example, with the use of the great computer “IBM Watson,” which was developed from 2004 to 2011. It was originally created to beat the best humans at the television game show, “Jeopardy!” Watson Health failed due to high costs, and expense in maintenance. The company spent millions of dollars on research and development, and it also had to pay for the data that Watson needed to train. Apparently, a machine learning tool is only as good as the data that goes into it. One of Watson Health’s biggest setbacks was the revelation that its cancer diagnostics tool was not trained with real patient data! Instead, with hypothetical cases provided by a small group of doctors in a single hospital. Watson did not seem to account for the fact that this data reflected the doctor’s own biases and blind spots and specifically it was not generalizable to all patient cases. The computer was scrutinized and as a result blamed for making inaccurate and unsafe recommendations, leading high-profile hospital partners to cancel their collaborations with Watson. This is one of the largest risks of AI in general: “garbage-in, garbage out!” Facts should not be based on assumptions or generalization of limited populations. It is important for AI systems of all kinds to offer users clear and concise information about how reliable their predictions are… and to fail gracefully when they are uncertain (which often means abstaining from making predictions).
and outcomes. It can summarize multiple studies on the same issues from different sources, assisting researchers not only how to understand the dynamics of the information, but also provide the outputs to educate others in the process of caring for wounds of all kinds. Telemedicine and teledentistry are considered an avenue that will allow clinicians the ability to treat wounds, to some extent, remotely with diagnoses, through measurements of wounds, the depth, and color, as well as other characteristics that will aid in treating the wound, or wounds in question. AI algorithms are not an intervention to provider care, but can be integrated into supplementing healthcare treatment plans.
Dental AI:
Dental AI is revolutionizing how dentists diagnose and present treatment as well. Overjet, an AI utilization company, has created an AI process whereby it can assist dentists in predictive analytics. AI algorithms will be able to analyze patient data, including medical history, lifestyle, and genetics, to predict the risk of developing dental problems such as tooth decay, gum disease, and oral cancer. Dentists will be able to use this information to create personalized prevention plans for their patients, including recommendations for diet, oral hygiene, and other lifestyle factors that can help reduce the risk of developing dental problems. This type of analytics is already in action in the medical fields and has demonstrated the potential for AL in assisting dentists with diagnosis and eventual treatment in the long run.
• Predicting the risk of tooth decay
AI algorithms can analyze patient data. For example, AI can identify patients who consume a lot of sugar, have poor oral hygiene habits, or have a history of tooth decay, in turn giving recommendations for reducing the risk of developing dental caries, with the use of providing fluoride, decreasing sugar intake in the diet and improving oral hygiene habits using goals and outcome assessments.
• Predicting the risk of gingival disease
AI algorithms can analyze patient data such as smoking history, medical history, and genetics to predict the risk of developing periodontal disease. For example, AI could identify patients who smoke, have a history of periodontitis, or have a genetic predisposition to gingival disease and generate recommendations to reduce the risk of developing this type of disease.
• Predicting the risk of oral cancer
Dental AI software can analyze patient data such as age, gender, medical history, family history of cancer, lifestyle factors to predict the risk of developing oral cancer, and the like. For example, AI could identify patients who are over a certain age, have a history of smoking, using drugs, or alcohol, partaking of specific oral sexual activities, or have a family history of oral cancer and provide personalized recommendations for reducing the risks.
• Predicting the need for orthodontic extractions
A study published in March 2022 found that machine learning models accurately predicted the orthodontic need for tooth extractions up to 93.9% of the time, according to the National Library of Medicine, National Center for Biotechnology Information.
These are just some of the ways that AI will assist dentists in determining which patients may be at risk for oral health issues and create appropriate treatment plans to reduce the risk and promote optimal health in general.
This author has seen Overjet technology at work, whereby caries from the patients’ radiographs are marked in different electronic hues and can be substantiated clinically after-thefact by exploration. Periodontal probing can be calibrated and verified through radiographic and algorithmic layers of information within the system to determine the need for advanced cleaning techniques and/or surgical treatment. In these cases, the patients’ own radiographs are interpreted by the AI algorithms, which changes the spectrum of shade within the film denoting caries that were not picked up by the traditional radiographs. The issue is that the results are based on a multitude of factors utilizing thousands of bits of information used to make the algorithm that essentially makes a diagnosis. One just needs to know how to interpret what the program does to utilize the information for a particular patient. This is risky in some respects because the information going into the algorithm is not just the patient being diagnosed but is totally based on thousands of pieces of non-personalized data for each specific patient it is used with to coordinate a diagnosis. A similar issue exists regarding the periodontal pockets, which are marked by algorithms when a defect in or on the boney ridge is noted on the radiograph and predictions based on other information can be used in diagnosing the state of periodontal disease and need for subsequent treatment in each patient’s radiographs it analyzes. Again, probing depths should be done regardless of the electronic programs one has available.
• AI and Robotic Technology
Several dental technology companies are now making and selling robotic AI integrated machines to place implants. The first robotic dental surgery system was cleared by the Food and Drug Administration for dental implant procedures in 2017. Yomi is a dental implant robot with a cost of $150,000! This dental robot highlights its tools, monitors the operation, and sends alerts should the operator assisting the robot go off course in placing the implant. The robotic arm can guide the surgical procedure to ensure a more streamlined process and one that may be a bit safer in the long run. However, on the downside, unsolved issues to be aware of include accountability, trust issues and data bias. This poses a variety of ethical, legal, and regulatory issues. In addition, the rapid development of AI continues to be ahead of the process to develop the appropriate regulatory frameworks to deploy it. Despite these concerns, the robotic implant system is operative and being used at the present time and is probably here to stay.
An editorial from the National Institutes of Health, National Center for Biotechnology Information, published in August of 2023, indicates that “the use of AI in implant dentistry holds immense promise for enhancing the precision, efficiency, and overall success of dental implant procedures.” Robots equipped with advanced algorithms and sensors can perform intricate tasks with unparalleled accuracy, ensuring optimal placement of implants and minimizing the margin for error. But this author asks, where is the human factor in all of this besides the leery patient at the other end of the robotic arm? Dentists must come to a meeting of the minds to find balance between the advantages of these advancements while maintaining their professional autonomy ultimately stewarding the empathetic outcomes for their patient, should something go awry.
It might be an important note to know that AI processes vast datasets of information, which in turn can provide evidencebased, individualized treatment plans and invaluable feedback before, during and after surgical procedures. Ethically can an AI robot replace the human practitioner in making ethical decisions? Are the algorithms that are fed into the computer valid or are they based on trial and error? In light of integrating this kind of dental technology in one’s dental office, it will take a lot of forethought and the need to consider buying this type of AI unit and justifying it with the speed, accuracy, and precision of
Robots equipped with advanced algorithms and sensors can perform intricate tasks with unparalleled accuracy, ensuring optimal placement of implants and minimizing the margin for error. But this author asks, where is the human factor in all of this besides the leery patient at the other end of the robotic arm?
the “tool” versus the peace-of-mind of the practitioner and the patient in knowing that it, the robotic unit, knows exactly what it is doing and will not harm the patient in any way, let alone the practitioner morally and ethically. It is expected that the robot that is doing the surgical procedure is in control, when in reality it is the practitioner, or is it? So, who’s on first? There is much to be illuminated here, but in the meantime, there are more AI-assisted implants being placed now and much more data placed in the memory banks of the AI computer. Hopefully, this will add some security to the system. Tailoring the robot to the myriad of different implant systems out there needs to be a consideration. More research needs to be done to determine the survival rate of an AI assisted robotic placement of an implant versus one placed by the practitioner to determine the future risks and benefits of each process.
Conclusion
Take everything new to heart. Try to remember what it was like in dental school learning techniques, instruments, and restorative materials. And then, the unthinkable, a new one of everything came out and you had to learn all over again. Frustrating, to say the least, and time consuming as well. Then getting out of dental school (which one never does while practicing), you start out in the real world relearning what you need in your own practice or what you need to learn about the equipment and materials and procedures in the office you have chosen to work in, at least for a while. It is a never-ending cycle. And now, we are faced with advanced technology, and away we go again. This author went into private practice feeling secure and ready to go. It took a few weeks to realize that I had to learn about business and running a practice, let alone promoting my practice to get patients to “try me.” It was not easy, to say the least. Now after many years of practicing dentistry, one can see the evolution of dental practice by looking back and recognizing the most interesting of events that happened in the practice with respect to procedures, materials and new equipment that were supposed to make one’s “practice life” easier, more efficient, and lucrative. I invested in every new modality that came out while in private practice. Most of these allowed me to teach my patients about themselves and how the modality itself made my dentistry easier for me and more precise. Now, with AI-connected equipment, one must ask other questions about what it will do for your practice and your patients above all, and who will be in control.
• Anticipate the issues that will arise when your algorithm meets the real world of your office. Issues one might be concerned about when looking at new AI products: Don’t assume that if a “tool” succeeds in one setting, it will work in others. Get ahead of potential problems by debugging your models, performing rigorous error analysis, and evaluating and investing in the stability and robustness of your models. After receiving an AI product, continue to measure performance at regular intervals using effective testing and monitoring practices. If you don’t have the knowledge to do this, seek out someone who can assist you.
• Manage expectations and learn from errors…yours and the AI program. It is very important and necessary for companies to provide accurate evidence based real life performance statistics and, where possible, to share details of the test dataset on how these metrics were calculated. Where fees are charged monthly for analyzing data sets for radiographic analysis of caries, one must understand that the information is not just from your patient.
It is also important for AI systems to offer users clear and concise information about how reliable their predictions are—and to fail gracefully when they are not. For example, as in the Tesla model presented, automated vehicles with AI controls are designed to hand off control to drivers in unexpected situations where their models have less confidence. Certain AI-installed radiographic equipment with chest X-ray classifiers can signal to a radiologist when it has a low confidence about a diagnosis and greater scrutiny from a human is warranted. Don’t let marketing hype outpace accountability.
With the fervor around AI, it is easy for companies that are in competition with other similar companies and products to adopt a publicity-first approach that inevitably falls short when they are forced to deliver. It is essential to clear away the hype in a crowded field of competitors and focus on building great and life-changing products with their new technology. Always study the situation first before moving forward.
• Looking at one’s ability to learn new technology and realistically utilize it in one’s practice. In the long run, do you have the resources to afford a new AI product, and can you trust your instincts to
And remember that most AI systems are “trained” on databases of things that happened in the past. Good dental entrepreneurs are the ones that are thinking about what might happen in the future.
purchase one? Do you have the time and energy to learn how to use it efficiently and effectively? Will it benefit your patients? Will it decrease time spent at the dental chair and will it allow you to take up the slack and be productive in other ways? Are you able to spend the time necessary to work the AI product enough to be secure in your own mind that the responsibility for what it does for you and ultimately your patient, is basically all your responsibility? Is the AI rendered treatment accurate, ethical, and essential? Will the algorithms need to be upgraded on a regular basis and how will that change its use and fees for servicing?
These are just a few things that came to mind after researching this topic and writing this article. Find them useful in your decision-making process within the possibility of having a piece of this technology in your practice, but make sure you are taking the right road. You may make the wrong choice and must own it or turn around and look for the other road less travelled. What AI will do is sense what people say they want, which is often different from what they truly desire, especially in business prospects. And remember that most AI systems are “trained” on databases of things that happened in the past. Good dental entrepreneurs are the ones that are thinking about what might happen in the future.
This author wrote an article some 30 years ago about the “Future of Robotic Dental Assistants in Dental Practice.” Make sure that you interview your “new” unit when it arrives and that you can make commands for it to function in the way that you want it to function, and not sit there and be shocked when the automaton tells you what to do, or where to go in the process!
“Caveat Emptor” —Let the buyer beware.
Practices For Sale
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Excellent opportunity for growth by adding a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02332
FANTASTIC RETAIL LOCATION: Plano GP that is highly visible in a retail center. This practice operates with the owner and 1 PT associate, is open 7 days a week and provides regular dental care as well as emergency services. The practice has over 1,750 active patients who are 20% FFS, 70% PPO, and less than 10% Medicaid. The office has 4 ops and is in excellent condition. This is a great opportunity for growth by capitalizing on the existing patient base and expanding services. Opportunity ID: TX-02219
MILLION DOLLAR PRACTICE OPPORTUNITY: Frisco GP in a professional building with great access for patients and staff. The practice operates on 3.5 doctor and hygiene days per week. The office has 5 fully equipped ops, is digital, paperless, and is in excellent condition. There are over 2,800 active patients who are a blend of FFS and PPO. The seller currently refers out Perio, O.S., dentures, Pedo and Endo, giving a purchaser more potential for growth by adding those procedures. Opportunity ID: TX-02180
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano and has paperless charts. The practice is 90% FFS with a small amount of PPO. The office collected over $876K in a four-day workweek. Opportunity ID: TX-02041
Surgical Repositioning of Intrusive Luxation Injury with 15-Year Follow-up: A Case Report
Priyanshi Ritwik, BDS, MS
Professor, University of Texas Health Science Center at Houston School of Dentistry, Department of Pediatric Dentistry, Houston, Texas. priyanshi.ritwik@uth.tmc.edu. The role of Dr Ritwik was to prepare the manuscript.
Elsa Alfonso-Echeverri, DDS
Clinical Associate Professor, University of Texas Health Science Center at Houston, School of Dentistry, Department of Pediatric Dentistry, Houston, Texas. The role of Dr Alfonso-Echeverri was to provide the treatment to the patient.
Antonio Dario Cardenas, DDS, MS
Professor, University of Texas Health Science Center at Houston School of Dentistry, Department of Pediatric Dentistry, Houston, Texas. The role of Dr Cardenas was to help prepare the manuscript.
Introduction
Intrusive luxation is the axial displacement of a tooth in an apical direction into the alveolar bone subsequent to a traumatic impact.
A tooth which has suffered intrusive injury is usually immobile, exhibits a high metallic (ankylotic) sound on percussion and is unlikely to respond to pulp vitality testing.1
Radiographically, the periodontal ligament (PDL) space may be absent from all or part of the root and the cemento-enamel junction appears (CEJ) located more apically in the intruded tooth than in adjacent non-injured teeth. Depending on the severity of intrusion, the CEJ is often apical to the marginal bone level.1
Abstract
This case report documents a 15-year follow-up of severe intrusive luxation in a 7-year old boy. The patient sustained 6-7mm intrusive injury to his maxillary left permanent central incisor at school. The patient was brought to his pediatric dentist within 30 minutes of the injury. The treating pediatric dentist elected to perform surgical repositioning due to the severity of intrusion and the advanced stage of root development. A physiologic splint was bonded to all the maxillary permanent incisors to secure the repositioned tooth. The patient was prescribed systemic amoxicillin suspension and advised to maintain a soft diet. The splint was removed in 13 days. The patient was followed up for 15 years, during which he also received orthodontic treatment. The maxillary left permanent incisor exhibited root maturogenesis and did not develop any pulpal or periodontal complications during the 15 years. This case report exemplifies that prompt treatment can lead to long-term favorable outcomes in intrusive dental injuries.
Key words
Intrusive luxation, surgical repositioning
The current guidelines by the International Association of Dental Traumatology recommend that an immature permanent tooth with intrusion be monitored for spontaneous eruption for 4 weeks.1 If no occlusal movement of the tooth is noted over a 4-week period, then orthodontic extrusion should be initiated.1 The management of a permanent tooth with a mature root and closed apex is slightly different due to the reduced potential for spontaneous eruption. The management of an intruded permanent tooth depends on the degree of intrusion. Teeth with less than 3 mm intrusion should be monitored for spontaneous eruption for 8 weeks.1 Should re-eruption not occur within 8 weeks, surgical repositioning and placement of a passive flexible splint is recommended for 4 weeks.1 Mature teeth with 3-7 mm of intrusion can be repositioned either surgically or orthodontically.1 Mature teeth with greater than 7 mm intrusion ought to be surgically repositioned.1 In all intrusive luxation injuries, pulp vitality should be monitored. Endodontic treatment should be initiated for mature teeth within 2 weeks after the injury, or as soon as endodontic access is feasible.1
Intrusive injuries result in severe damage to the neurovscular bundle as well as the PDL. The alveolar socket sustains comminuted fracture(s). Timely management of intrusive luxation injuries is important to prevent untoward sequelae such as inflammatory root resorption or replacement resorption. Other possible complications of intrusive luxations include pulp canal obliteration, pulp non-vitality, arrested root development and periodontal defects arising from discrepancy in bone and gingival levels.
The authors present the management and 15-year follow-up of a young patient who sustained intrusive luxation of his maxillary permanent central incisor.
Case Report
A 7-year-old boy fell on his school playground and sustained dental trauma. His parents brought him to his pediatric dentist within 30 minutes of the injury. The patient was healthy and did not have underlying health problems. He had received all scheduled immunizations, including tetanus vaccination. The pediatric dentist performed a rapid neurological assessment. The patient did not exhibit any neurological deficits, loss of consciousness or memory lapse, and he was oriented to time and place. Extraoral assessment of the head, neck, jaws and the temporomandibular joint were within normal limits.
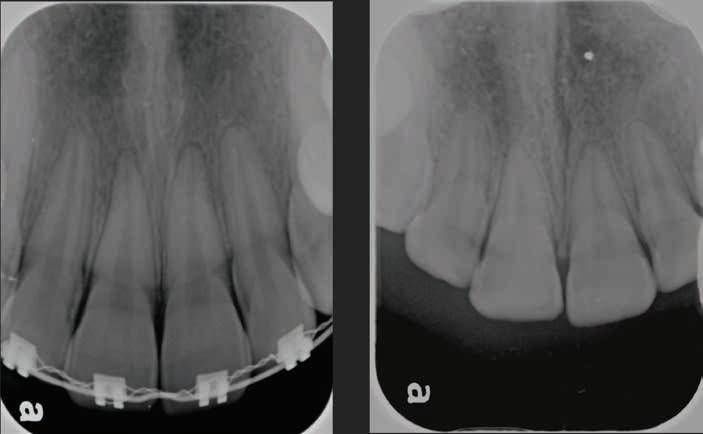
Intraoral assessment revealed that the maxillary left permanent central incisor was intruded 6-7 mm along with buccal displacement. No other extraoral, intraoral or dental injuries were noted. Intraoral radiographs taken confirmed the intrusive luxation injury. The permanent lateral incisors had erupted and the primary canines were not mobile. The initial clinical presentation of the child and associated radiograph are shown in Figure 1. Informed consent was obtained from the patient’s parents to initiate treatment.
Figure 1. Initial clinical presentation and radiograph of the child at approximately 30 minutes of the dental injury.
Treatment Rendered
Due to the severity of intrusion, the treating dentist decided to perform surgical repositioning and stabilize with a physiologic splint. Local anesthesia was achieved with the use of 20% topical benzocaine gel and infiltration with 25 mg of 2% lidocaine with 1:100,000 epinephrine. Surgical repositioning of the maxillary left permanent central incisor was achieved with the use of gentle force with straight maxillary forceps (#99C). Figure 2 shows the position of the tooth after surgical repositioning.
A 0.016” Nitinol wire with bonded composite resin was used to secure the repositioned tooth. The physiologic splint engaged all the 4 maxillary permanent incisors. The radiograph in Figure 3 shows the repositioned tooth with splint in place. The patient was very anxious about feeling pain and about how much it would hurt. However, the pediatric dentist was able to use basic behavior guidance techniques such as tell-show-do, verbal reassurance and positive reinforcement to complete the treatment.
The patient was prescribed 250 mg/5 cc amoxicillin suspension to be taken 3 times a day for 10 days. The parents were advised to administer 100 mg/5 cc of ibuprofen as needed for pain management and to maintain a soft diet.
The long-term prognosis of the intruded tooth was discussed with parents. The scope of potential future complications was identified as pulp necrosis, need for endodontic treatment and ankylosis. However, due to the short time elapsed since the injury and level of root maturity, the anticipated prognosis was favorable.
The patient returned for follow-up care in 13 days. The patient was comfortable, and in good spirits at the follow-up appointment. There were no dental or soft tissue pathologies noted at this appointment. A radiograph taken confirmed that the traumatized tooth and supporting bone did not exhibit
Figure 2. Position of the intruded tooth after surgical repositioning.
Figure 3. Radiograph of repositioned tooth with physiologic splint in place.
any pathology. Figure 4 shows the radiograph taken at this appointment. The splint was removed after confirming that the maxillary left permanent central incisor did not exhibit pathologic mobility.
The patient returned for his routine preventive visit after two months. At this visit, the traumatized tooth was free of pain or discomfort, maintained a favorable position and did not exhibit any discoloration. Thermal testing was performed and all the maxillary permanent incisors responded comparably without any lingering sensitivity. The clinical picture and radiograph at this 2-month mark is shown in Figure 5.
The patient continued to return to his pediatric dentist for routine dental check-ups and preventive visits. Figure 6 shows the clinical and radiographic appearance at 5 years after the traumatic intrusion. Root maturogenesis and apical closure of the maxillary left permanent central incisor is notable. The patient received orthodontic treatment when he was 14 years old, which was 7 years after sustaining dental trauma. Orthodontic treatment spanned one-and-a-half years, during the course of which the pediatric dentist monitored the
Figure 4. Radiograph taken at 13 days after the intrusive injury.
Figure 5. Clinical picture and radiograph at two months after intrusion injury.
maxillary left permanent central incisor for any root and/or pulpal pathosis. Figure 7 shows the radiographic presentation of the tooth during and after orthodontic treatment.
The patient continued to return to his pediatric dentist for routine preventive care till he turned 22 years old. His maxillary left permanent central incisor remained free of
years after intrusion injury).
Figure 6. Clinical and radiographic appearance at 5 years after intrusion injury.
Figure 7. Radiographic presentation of the tooth during and after orthodontic treatment (7-8
pulpal and periodontal pathoses for 15 years since the initial trauma. Figure 8 shows the radiograph at 15 years after the traumatic injury.
Discussion
Intrusion is a complex dental injury due to the concomitant disruption of marginal gingival seal, PDL, alveolar bone and neurovascular supply to the tooth.2 Long term sequelae due to intrusion include pulp necrosis, pulp calcification, inflammatory root resorption, replacement resorption (ankylosis), and loss of marginal bone support.3 Pulp necrosis is the most common complication after intrusion in mature intruded teeth.3 External root resorption can occur in 54.8% of dental intrusion injuries.2 The objective of prompt management of intrusive dental injuries is twofold: 1) to bring the intruded tooth to the appropriate clinical position, and 2) prevent or minimize pulpal and periodontal complications.
The dental age of our patient was advanced, compared to his chronologic age. The stage of root maturity of the intruded central incisor was estimated to be at Cvek stage 4, with nearly complete root length but with an open apex.4 The degree of intrusion was assessed to be severe, with 6-7 mm of displacement. The treatment options were: 1) allow spontaneous repositioning, 2) orthodontic repositioning, and 3) surgical repositioning. The treating pediatric dentist elected to utilize surgical repositioning out of concerns for pulp vitality (based on the severity of intrusion and stage of root development). This child was treated in the year 2002, and it should be kept in mind that regenerative endodontic treatment was not a mainstream modality of management at the time.5 This was also a time when the guidelines for management of traumatic dental injuries set forth by the American Academy of Pediatric Dentistry recommended surgical or orthodontic repositioning of intruded permanent teeth if the root exhibited greater than twothirds development.6
The most effective treatment modality for intrusive dental injuries remains debatable and the quality of evidence for any of the treatment recommendations is poor.7,8 Spontaneous re-eruption is recommended for immature permanent teeth with intrusion injuries.1 However, the term “spontaneous eruption”
The objective of prompt management of intrusive dental injuries is 2-fold: 1) to bring the intruded tooth to the appropriate clinical position, and 2) prevent or minimize pulpal and periodontal complications.
Figure 8. Radiograph at 15 years after intrusion injury.
is falsely optimistic as tooth movement after intrusion is unpredictable.9 A meta-analysis comparing surgical repositioning versus spontaneous re-eruption found no significant differences in outcomes.10 Further, pulp non-vitality in these immature teeth poses endodontic complications, which may necessitate regenerative procedures in the future.9 In cases of mature teeth with severe intrusion, endodontic management may need to be deferred till adequate pulpal access can be achieved.
Surgical repositioning for the current case with a 15-year follow-up resulted in long-term retention of a vital permanent central incisor without any periodontal complications. The patient also underwent orthodontic treatment without complications. The authors attribute this success to prompt treatment which alleviated sustained trauma to the neurovascular supply and PDL. It has been shown that teeth which are repositioned within 90 minutes of the displacement injury exhibit lower frequency of root resorption.11 Clinicians who treat intrusive traumatic dental injuries should assess pulp and PDL prognosis, and not just the clinical positioning and esthetics when making treatment decisions.
Conclusion
This case report with the 15-year follow-up shows that prompt treatment of intrusive luxation can lead to long-term favorable outcomes with retention of the tooth without pulpal and periodontal complications.
acknowledgment
The author is thankful to Grand Parkway Pediatric Dental for the ability to provide care for these patients. The author is grateful to Anoushka Debnath for assistance with editing and graphics.
References
1. Bourguignon C, Cohenca N, Lauridsen E, et al. International association of dental traumatology guidelines for the management of traumatic dental injuries: 1. fractures and luxations. Dent Traumatol. 2020;36(4):314-330.
2. Ghafoor R. Conservative management of progressive external inflammatory root resorption after traumatic tooth intrusion. J Conserv Dent. 2013;16(3):265-268.
3. de Alencar AH, Lustosa-Pereira A, de Sousa HA, Figueiredo JH. Intrusive luxation: A case report. Dent Traumatol. 2007;23(5):307-312.
4. Cvek M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with guttapercha. A retrospective clinical study. Endod Dent Traumatol. 1992;8(2):45-55.
5. Tzanetakis GN. Management of intruded immature maxillary central incisor with pulp necrosis and severe external resorption by regenerative approach. J Endod. 2018;44(2):245-249.
6. American Academy of Pediatric Dentistry Reference Manual. Guideline on management of acute dental trauma. American Academy of Pediatric Dentistry Reference Manual of Pediatric Dentistry Chicago, Ill. 2001;32(6):202-12.
7. Costa LA, Ribeiro CC, Cantanhede LM, Santiago Junior JF, de Mendonca MR, Pereira AL. Treatments for intrusive luxation in permanent teeth: A systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2017;46(2):214229.
8. Kirzioglu Z, Karayilmaz H. Repositioning of a completely intruded permanent incisor with surgical extrusion: A 4-year follow-up case. Pediatr Dent. 2009;31(3):253-256.
9. Gungor HC, Cengiz SB, Altay N. Immediate surgical repositioning following intrusive luxation: A case report and review of the literature. Dent Traumatol. 2006;22(6):340-344.
10. Elkhadem A, Kotb A. Spontaneous re-eruption, surgical or orthodontic extrusion: What is the choice for intrusive luxation in permanent teeth? Evid Based Dent. 2017;18(3):74.
11. Andreasen JO. Luxation of permanent teeth due to trauma. A clinical and radiographic follow-up study of 189 injured teeth. Scand J Dent Res. 1970;78(3):273-286.
Shingles: A Case Report
Michele White, DDS
Ryan Vahdani, DDS, MHA
Joseph D. Yadin, BS, (MS1)
Gary N. Frey, DDS
Cleverick (C.D.) Johnson, MS, DDS
Ben F. Warner, MS, DDS, MD
Abstract
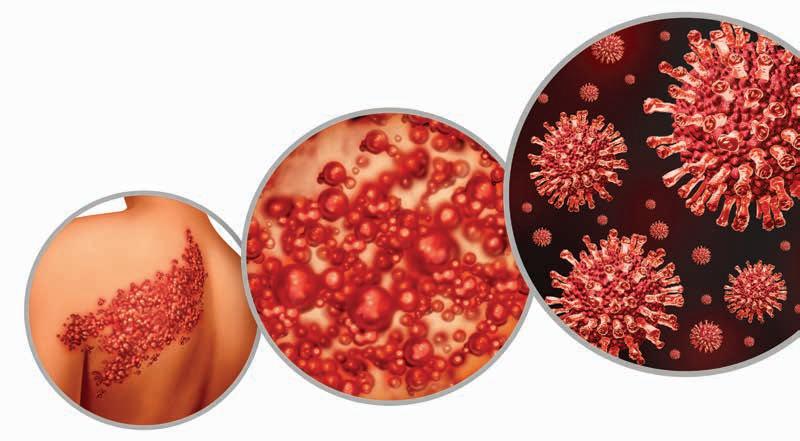
Shingles or herpes zoster is a condition that affects approximately 1 million people in the United States, with half of these being persons aged 60 or older. Herpes zoster arises from previous infection with the varicellazoster virus, known as chickenpox. After the initial infection, the varicella-zoster virus becomes dormant and remains suppressed in nerves or dorsal root ganglia. Reactivation of the varicella-zoster virus causes shingles. Stress, medication, illness, and other causes trigger shingles in which a painful blistering rash presents along dermatomes. Shingles is contagious and preventable through vaccination. The original infection of chickenpox is also preventable with vaccination. The location of symptoms is dermatome dependent. Shingles that affect the face, ears, and oral cavity are due to reactivation of the virus along cranial nerve VII. However, symptoms might also include one-sided facial paralysis, known as Ramsay Hunt Syndrome. It can also present with paralysis and no rash and is known as Zoster sine herpete. This can be confused with a condition called Bell’s palsy which is not shingles, but rather damage to cranial nerve VII, and is of an unknown origin. Patients often seek consultation with dental providers with a rash in or near the oral cavity. This is a case report of a patient that sought care with a dental urgent care clinic with a chief complaint of facial rash and oral pain. Patient symptoms, clinical examination, and differential diagnosis rational are presented. Treatment, complications such as Post-herpetic Neuralgia, and other information on shingles are also discussed, followed by the Conclusion, which advocates for the usefulness of this case report for primary care medical and dental clinicians.
Michele White, DDS, Associate Professor, Corresponding Author: Michele.r.white@uth.tmc.edu, Department of General Practice and Dental Public Health, UTHealth Houston School of Dentistry, 7500 Cambridge Street, Houston, Texas
Ryan Vahdani, DDS, MHA, Department of General Practice and Dental Public Health, UTHealth Houston School of Dentistry, 7500 Cambridge Street, Houston, Texas
Joseph D. Yadin, BS, Medical student first year, American University of the Caribbean School of Medicine, Cupecoy, Sint Maarten, Dutch Lowlands
Gary N. Frey, DDS, Professor, Department of General Practice and Dental Public Health, UTHealth Houston School of Dentistry, 7500 Cambridge Street, Houston, Texas
Cleverick (C.D.) Johnson, DDS, M2, Professor, Department of General Practice and Dental Public Health, UTHealth Houston School of Dentistry, 7500 Cambridge Street, Houston, Texas
Ben F. Warner, MS, DDS, MD, Professor, Department of General Practice and Dental Public Health, UTHealth Houston School of Dentistry, 7500 Cambridge Street, Houston, Texas
Introduction
The varicella-zoster virus, a member of the human herpes virus family, is the cause of chickenpox and remains suppressed in cranial nerves or dorsal root ganglia after the primary infection clears. Reactivation of the virus can occur due to physical stress or impaired immunity and can present almost anywhere on the body as herpes zoster, known as “shingles”. Ramsay Hunt syndrome can be described as a reactivation of the varicella-zoster virus that affects the face, including the oral cavity and ears.2 Shingles symptoms start with malaise, fatigue, fever, and the beginnings of a rash that develop fluid-filled blisters resembling chickenpox.3 This vesicular rash is painful and presents along corresponding nerve pathways called dermatomes.3 Dermatomes are areas of skin supplied with the nerve fibers of a single, posterior, spinal root. Ramsay Hunt Syndrome effects the geniculate ganglion of the facial nerve (cranial nerve VII) and presents a trio of symptoms including one-sided facial paralysis, otalgia, and a vesicular rash.2 There is variability in the clinical presentation of Ramsay Hunt Syndrome, where some patients demonstrate facial paralysis before the rash, or with no rash. This variant, known as Zoster sine herpete, can be difficult to clinically distinguish from Bell’s palsy.2 Bell’s palsy also presents due to damage of cranial nerve VII though from an unknown cause. Loss of taste of the anterior 2/3rds of tongue (cranial nerve VII) and sometimes vertigo and hearing loss (cranial nerve VIII—vestibulocochlear nerve) are experienced. Differences in skin color can also hinder diagnoses.3
Secondary bacterial infection, and post-herpetic neuralgia, are the most common complications of herpes zoster.8 For most people, the duration of shingles is from 2 to 4 weeks with complete healing of the rash with no visible scarring.3 However, postherpetic neuralgia (PHN), can present as a complication in approximately 10-18% of resolved shingles rashes. PHN symptoms include a lengthy continuance of pain in the area of the previous rash.6
The following is a case report of a patient who was seen at a dental urgent care clinic with a chief complaint of oral pain and the signs and symptoms of a shingles infection. Symptoms of shingles include: fever, headache, muscle aches, stomach pain, vomiting, and blistering rash on the skin.
The following is a case report of a patient who was seen at a dental urgent care clinic with a chief complaint of oral pain and the signs and symptoms of a shingles infection.
Symptoms of shingles include: fever, headache, muscle aches, stomach pain, vomiting, and blistering rash on the skin.
Case Report
An otherwise healthy African American male, age 58 years old, presented to the UTHealth Houston School of Dentistry with a chief complaint of a facial rash. (right and below).
The patient’s vital signs were: Blood Pressure: 142/92; Pulse: 72/minute; Respiration: 14/minute; Patient’s height: 5’10”; and Weight: 175 pounds. The patient stated that he was not taking medications for systemic diseases, had no allergies, and had not received a current shingles, pneumonia, or influenza vaccine. The patient also stated that he visits his dentist, “once every year or so,” which indicates a slightly less than recommended twice a year clinical exam, but also suggests the patient seeks semi-routine dental examination.
Upon clinical examination the patient exhibited good oral hygiene and had no visible caries. The patient’s existing dental findings included several crowns and amalgam restorations.
Intraoral examination showed multiple ulcerative type lesions located on the non-keratinized tissue of the inner mandibular lip. The lesions
simultaneously presented with a leukoplakic covering over an ulcerated base. Given the patient’s outer facial appearance of the rash with many of the lesions crusted over, it can be postulated that the intraoral lesions were previously blistering and at clinical examination were beginning to heal. The patient did not complain of dental pain. No radiographs were obtained due to the nature of the chief complaint of a facial vesicular rash.
Further, the patient did not exhibit the trio of symptoms of Ramsay Hunt Syndrome; one-sided facial paralysis, otalgia, and a vesicular rash and was removed as a possible diagnosis. Because there was no facial paralysis, a Bell’s palsy diagnosis was also eliminated. Additionally, herpes simplex virus was not considered in the differential diagnosis due to the presentation of lesions on the nonkeratinized mucous membranes of the inner lip. Herpes simplex virus most often is seen on the keratinized gingival mucosa and are commonly referred to as oral cold sores that are often reported as recurrent in the patient medical history. Given the patient had not been vaccinated against shingles and the clinical presentation of the rash, differential diagnosis was determined to be herpes zoster.
The patient was referred to his primary care physician for evaluation and treatment of a possible facial shingles outbreak. The patient was also advised to consider consultations with an ophthalmologist, otolaryngologist, and or ear, nose, and throat specialist if symptoms included the eyes, ears, nose or throat.
The dental urgent care clinic at our institution attends to persons with urgent dental needs. However, patients
also seek care through the urgent care clinic for concerns other than that of a dental origin. Especially in the head and neck region. These patients are able to be seen without the requirement of being a patient of record and can make an immediate appointment. Since the patients are not patients of record, many of them are lost to follow up as this patient was. No diagnosis was confirmed. Also unknown, were any treatments, medications, or complications such as PHN, with this patient.
The strength of this case report is in the education of primary care medical and dental clinician who may see patients with oral related symptoms of herpes zoster. As exampled in the case report, the patient’s symptoms were not complex but rather diffuse as in the “oral pain, and facial rash” complaint given by the patient. The case report shows how the dental providers were able to differentiate a possible shingles diagnosis. The limitations of this case report are the lack of extensive diagnostic testing as well as the loss to follow up.
Discussion
Reactivation of herpes zoster can occur due to many factors. Examples include, stress, immunosuppressant medications, illness, exposure to the varicella-zoster virus, or malignancies.9
Once activated, the varicella-zoster virus spreads along nerve fibers in specific dermatomes and proliferate herpes zoster, or Ramsay Hunt syndrome, or Zoster sine herpete. Herpes zoster of the facial nerve does not always become Ramsay Hunt syndrome but produces symptoms similar to the case report patient. Early prodrome of
herpes zoster encompasses otalgia, non-specific headache, fever, and fatigue for 1-3 days, followed by rash. During this acute phase, a myriad of additional symptoms may occur such as dysgeusia, epiphora, xerophthalmia, drooling, smile asymmetry, vertigo, tinnitus, hearing loss, hoarseness, hyperacusis, and facial numbness. This can be a confusing array of symptoms for the patient and the medical and dental team. The case report patient complained only of the rash and oral discomfort.
Further symptoms such as severe pain in the absence of facial palsy and vesicular rash, are diagnosed with what is known as Zoster sine herpete, which accounts for approximately 30% of Ramsey Hunt syndrome presentations and can be challenging to differentiate from Bell’s palsy.2 Bell’s palsy presents as an acute peripheral paralysis of the face associated with the facial nerve (cranial nerve VII).
Shingles can affect all races, ethnicities, age and gender. However, African Americans are 50% less likely than White Americans to develop shingles in the United States. Whereas, 16% of Latinx and 17% of Asian or Pacific Islander peoples are more likely to get it. In addition, females have a 33% higher risk of developing shingles than males.5
In the United States, approximately 1 million persons, or 1 in 3 people develop shingles. Half of these persons are age 60 or older. Further, 1 in 15 get shingles a second time. Cases of shingles in young adults have increased, whereas rates of shingles for older adults have leveled off since 2008.5 This is likely due to improved vaccination rates in younger generations.
The prognosis of facial paralysis recovery from Ramsay Hunt syndrome is worse at 70% when compared to that of Bell’s palsy at 90%. Further sequela can involve synkinesis, in which atypical reinnervation connects axons with neuromuscular junctions differently from the ones they were associated prior to the inflammation. This has the effect of dyscoordination amongst the affected muscles, and glands, and significantly effects patients’ quality of life.1
Since herpes zoster is usually selflimiting, the goal of treatment is to reduce complications such as facial paralysis and postherpetic neuralgia.9 Diagnosis is mostly clinical and early intervention is very important. Further, vaccination is very effective with an efficacy of approximately 90% at preventing disease in most populations other than in immunocompromised adults. Lastly, chickenpox is also preventable by vaccine and recommended for children starting at age 12.5
Treatment
Recommendations for treatment are to initiate therapy as soon as possible and most successful if begun within 72 hours of first signs or symptoms. In addition, patients that receive early antiviral medication intervention experience less PHN, according to the American Academy of Dermatology Association. (Table 1, 2).7
Further, the Food and Drug Administration (FDA) and Advisory Committee on Immunization Practices (ACIP) has recommended two doses of RSV for persons considered at or will be at risk for herpes zoster because of immunodeficiency or immunosuppression due to disease or therapy. Available vaccination for this group includes persons age 18 or greater for the FDA recommendation and age 19 or greater for the ACIP recommendation.7
Additional treatment includes pain reducing medications such as Acetaminophen and Ibuprofen and rash hygiene care for comfort and reduction of complications such as secondary infection.7
Prevention
Regardless of the successful efficacy rates with shingles prevention and vaccination, 96.6% in persons aged 50-59 years, 97.4% in persons aged 60-69 years, and 91.3% in persons aged 70 years or older, coverage in the United States remains low. Vaccination with two doses of recombinant zoster vaccine (RZV) (Shingrix) given 2-6 months apart is recommended for adults ages 50 years or older, whether or not the patient has had a previous outbreak of herpes zoster or received the zoster vaccine live (ZVL) (Zostavas).7
Herpes zoster is contagious during the rash phase of the outbreak. However, this only affects persons if they have not had chickenpox or the chickenpox vaccine. It is recommended to avoid contact with pregnant women, infants younger than 12 months, persons will illness, especially cancer or AIDS.7
Conclusion
The significance of this report is in its value as an educational tool for the medical and dental communities as it reviews this common disease and
Table 1. Zoster confined to dermatome (immunocompetent or immunocompromised patients)
Table 2. Visceral, central nervous system, or disseminated VZV infections, and zoster in severely immunocompromised patients
Acyclovir 800 mg PO 5 times daily
Famciclovir 500mg PO TID for 7d
Valacyclovir 1000 mg PO TID for 7-10d for 7d
Acyclovir 10 mg/kg (500 mg/m2 in children < 12 y) IV q8h for 7-10d
shows its presentation, possible complications, differential diagnoses, treatment, and prevention strategies.
Recognition of the signs and symptoms of shingles will expedite collaborative care, patient referral, and treatment options that support best practices in patient care.
Acknowledgement statement: Not Applicable.
Funding statement: This research received no specific grant from any funding agency in the public, commercial, or not-forprofit sectors.
Conflict of interest: The authors declare no conflict of interest in preparing this article.
3. Shilpa Amin, M.D., CAQ, FAAFP. Shingles. Medically reviewed by the Healthline Editorial Team, 2022 Mar. 7.
4. American Academy of Dermatology Association. Shingles: Signs and Symptoms 2023.
LAW
OFFICES
5. Dorwart, Laura, Wetchler, Brian H. Shingles Facts and Statistics: What you Need to Know. Verywell health. Oct.17, 2022.
6. Gulick, Roy M. Shingles: more common in women, but few have gotten the vaccine: get your shingles shot to reduce your risk of shingles and its painful complications and after-effects. The Free Library.
7. Wharton M. The epidemiology of varicella-zoster virus infections. Infect Dis Clin North Am. 1996 Sep;10(3):57181. doi: 10.1016/s0891-5520(05)70313-5. PMID: 8856352.
Precision-Guided Flapless Placement of a Maxillary Single Implant: A Minimally Invasive Approach
The aim of this case report is to describe a flapless implant placement technique designed to enhance both esthetic, and biological outcomes for single implant restoration in the anterior area.
Case Report
This case involves a 43-year-old female patient presenting with a defective fixed partial denture (FPD) spanning teeth #7, X, 9, and 10 (figure A). Following clinical and radiographic examination, it was determined that teeth #7, #9, and #10 were restorable upon removal of the old prosthetic restoration. Cone beam computed tomography (CBCT) and virtual wax up were created. Dental implant treatment planning software was used to evaluate the edentulous location in 3 dimensions (figure B). A flapless, fully guided implant placement approach was chosen to maximize procedural efficiency and patient outcomes while minimizing surgical invasiveness (figure E).
Malik Abumansour, BDS; Maria Gonzalez, DDS, MS; Ruben Sauceda, DDS, MS
Guest Editor Rade D. Paravina, DDS, MS, PhD
Figure A. Pre-op
Figure B. Virtual Implant Plan
Figure C. Radiograph after placement
Figure D. Implant Provisional
Given the patient’s adequate soft and hard tissue volume. Three months after the flapless placement of implant #8 using a surgical guide, a provisional crown was delivered to facilitate soft tissue maturation (figures C and D). By the end of this 3-month period, the interproximal papilla and midfacial gingiva were well-formed, achieving a natural, esthetic contour.
Outcome
To enhance the final aesthetic outcome, a zirconia abutment was selected to mask the gray hue of the titanium custom abutment beneath. The definitive implant crown was cemented onto the hybrid abutment, with the zirconia abutment’s finish line positioned 1 mm apical to the free gingival margin for optimal gingival esthetics. Additionally, adjacent teeth #6, #7, #9, #10, #11, and #12 were restored with zirconia crowns and lithium disilicate veneers to achieve cohesive shade matching, translucency, and seamless integration with the implant crown. This approach provided an aesthetically pleasing and functionally stable result across the entire maxillary anterior segment (figure F).
The patient demonstrated excellent healing, and routine follow-up appointments were scheduled to ensure successful implant integration and functional restoration. The technique showed a positive outcome, with
a 12-month follow-up confirming stable integration and well adapted soft tissue around the implant crown (figure G).
Conclusions
In conclusion, when there is sufficient bone volume, adequate keratinized tissue, and an absence of hard tissue undercut, a flapless approach can be considered as an effective alternative to conventional flap technique.
Figure G. Final smile
Figure E. Intraoral implant placement
Figure F. Final restorations
APP-SOLUTELY RE-IMAGINED!
Designed for dentists, with dentists, the new ADA Member App is here and ready to put the resources you need in the palm of your hand.
• Chat 1:1 or with your network
• Newsfeed customized to your interests
• Digital wallet to store your important documents
• Stream the new “Dental Sound Bites” podcast
Tap into possibility at ADA.org/App
value for your profession
Provided by: PERKS
P R
O G R A M
Treating OSHA and HIPAA Guidelines as Mere Formalities is Risky in Dentistry
By Smart Training
In the dental industry, maintaining safety and privacy is not just a legal obligation—it’s essential to the well-being of patients and staff.
Two key regulations—OSHA (Occupational Safety and Health Administration) and HIPAA (Health Insurance Portability and Accountability Act)—help ensure safe working environments and protect sensitive health information.
But many practices give in to the temptation to meet these superficially, often because of time constraints, a lack of resources, or a misunderstanding of the regulations’ importance. Fulfilling basic requirements without truly embracing them can have serious consequences.
“Checking the box” for OSHA compliance is not enough
OSHA regulations are designed to protect dental professionals from workplace hazards and govern everything from infection control procedures to the proper handling of sharp instruments and hazardous materials.
Some practices take a minimalistic approach to OSHA compliance. An office might provide basic personal protective equipment (PPE) like gloves and masks without fully training staff on how to handle potentially infectious materials or failing to regularly update safety protocols, for example. While this approach may seem to meet the bare minimum, it puts the practice at risk in several ways.
It increases the risk of occupational injury or illness.
Dental professionals face unique hazards, such as exposure to blood and bodily fluids, sharp instruments, and hazardous chemicals.
This opens them to exposure to bloodborne pathogens and injuries, and an improperly trained team may not handle an exposure incident correctly or it may fail to notice an unsafe setup that could lead to an accident.
It could result in serious financial and legal consequences. Failing to meet OSHA standards can result in substantial fines, legal fees, and even litigation. In the event of an injury or infection, the costs associated with non-compliance can far exceed the investment needed to create a safer, fully compliant environment.
It can damage patient trust.
Trust is key in the dental field and patients expect their providers to take every necessary step to ensure their health and safety. If patients perceive safety measures are being implemented superficially, it can undermine their confidence in the practice.
Ignoring HIPAA is dangerous
HIPAA regulations are essential for protecting patient privacy and ensuring the confidentiality of sensitive health information. In a dental practice, this includes safeguarding personal patient data such as medical histories, treatment plans, and billing information.
While most dental offices implement some form of HIPAA compliance, many may fall short in creating a robust privacy culture.
For instance, staff may undergo HIPAA training once a year without a thorough understanding of what constitutes a breach or how to properly handle electronic health records (EHR). Some offices might neglect updating security measures or conducting regular audits to ensure compliance.
This leaves the office vulnerable to:
Data Breaches and Privacy Violations
A practice that does not take proactive steps to safeguard patient data is in violation of HIPAA and at risk of
a security breach. This could result in unauthorized access to sensitive information leading to identity theft or other forms of fraud.
Loss of Patient Trust and a Damaged Reputation
Patients trust dental professionals with some of their most private information. If they believe their data is not being adequately protected, it could lead them to seek care elsewhere. A breach in patient confidentiality can have longlasting effects on the practice’s patient retention and reputation.
Legal and Financial Penalties
HIPAA violations can result in catastrophic financial and legal repercussions. The penalties for a data breach can range from fines to lawsuits; and a practice could even face criminal charges if the violation is deemed willful.
Genuine OSHA and HIPAA compliance provides 3 elements critical to creating a strong practice
Patient Safety and Trust
Ensuring compliance means providing a safe and secure environment for patients. When patients feel their safety and privacy are top priorities, they’re more likely to return and recommend the practice to others.
Employee Well-Being
OSHA compliance helps protect the team from occupational hazards, improves job satisfaction, and reduces turnover. A workplace that prioritizes safety creates a positive and productive environment.
Legal Protection
True compliance reduces the likelihood of legal issues arising from violations. Time and resources spent ensuring full compliance will help protect your
practice from costly lawsuits and penalties down the road.
How to Ensure Real Compliance
To take a genuine approach to compliance, practices must do the following.
Provide regular, comprehensive training to staff.
Make sure all staff—front desk to hygienists and assistants—are thoroughly trained in OSHA safety protocols and HIPAA privacy rules. Training should be ongoing; not an annual event.
Conduct regular compliance audits and reviews.
Conduct regular audits of your practice’s OSHA and HIPAA compliance. Include reviews of safety equipment, infection control procedures, and privacy protocols. Ensure the practice is up-todate with the latest regulations and best practices.
Foster a culture of safety and privacy.
Compliance should be a part of the practice’s culture. Staff should be encouraged to speak up about potential risks or security vulnerabilities, and management should lead by example in reinforcing the importance of safety and confidentiality.
Prioritize genuine compliance to safeguard your patients and employees; make it a core part of the practice’s values. In turn, you will safeguard your practice’s future.
As a member of TDA, you have access to exclusive resources and discounts at Smart Training to help ensure compliance with OSHA and HIPAA regulations, which will in turn reduce risk and enhance safety and confidentiality at your practice. For more information, visit TDAPerks.com (Compliance & Supplies) or call Smart Training at 469-342-8300.
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/MemberResources/TDA-Classified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN (ID #691): Unique
opportunity to purchase a GD practice with 2 locations in the Austin area. The offices have a total of 10 operatories with computers in each room and digital radiography. The offices serve a large FFS/PPO patient base with a healthy new patient flow and strong hygiene recall with over 20-25% of total annual production coming from the hygiene department. AUSTIN (ID #729): Legacy GD office located in the heart of Austin in a high visibility location. Majority PPO patient base, 1300+ active patients, 15 new patients visit the office per month, and an impeccable reputation online and in the community. The 2,050 sq ft office space contains 6 total operatories (4 equipped), computers throughout, digital x-ray sensors, and intra-oral cameras. They generated revenue of mid-6 figures during each of the past three years with abundant upside potential. DALLAS (ID #728): Well-established GD office in a growing suburb southeast of Dallas. This practice has an impeccable reputation, treats a majority FFS patient base with 1,700+ active
patients. The 1,800 sq ft facility features 4 fully equipped operatories (with a 5th plumbed and ready to be equipped), computers throughout, digital x-ray sensors, digital panoramic x-ray, digital scanner, CAD/CAM milling unit, dental laser, and intra-oral cameras. This turn-key office has strong net cash flow and significant upside potential.
ORAL
SURGERY
DALLAS/FORT
WORTH-
(ID #711): Legacy oral surgery practice in a bustling suburb between Dallas and Fort Worth. A heavily tenured team, large patient base, and a fantastic reputation in the local community. 3,300 sq ft office in an easily accessible medical office park, 4 fully equipped operatories, 2 plumbed operatories for future expansion, computers throughout, digital x-ray sensors, and a 3D cone beam CT. With over 7 figures in 2023 revenue and profit margins trending at 50%, the foundation for a successful future has already been laid with abundant upside potential available.
HOUSTON-SOUTH
(ID #682): Established, multi-specialty dental office in a suburb approximately 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base
(3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose.
HOUSTON-SOUTHWEST
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
PRACTICE SALES
DSO C S
PRACTICE APPRAISALS
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com
www.dentaltransitions.com
classifieds
(ID #724): Legacy GD office located southwest of Houston. Majority PPO patient base, 2000+ active patients, great online reputation with 100+ reviews. 5 total operatories (4 equipped), with computers in each, digital x-rays, digital pano, a CAD/CAM milling unit, and a digital scanner. The practice realized revenue of over 7 figures in 2024 with robust net cash flow margins (>40%) and a robust hygiene recall program.
HOUSTON-CENTRAL (ID #734): Well-established GD practice in a modern, high visibility location in Houston. Beautiful modern office, 2,600 sq ft, 7 fully equipped operatories, computers throughout, digital x-ray sensors, 3D cone beam CT, digital scanner, dental laser, intra oral cameras and paperless charts. The practice treats a FFS/PPO patient base with nearly 2,000 active patients, adds 30 new patients per month, and boasts a near-perfect Google rating across 400+ reviews.
HOUSTON-NORTH (ID
HILL COUNTRY (ID #685):
Well-established dental practice and real estate nestled in the hill country north of San Antonio. The office relies mostly on word-of-mouth referrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023 and the trend continued into 2024.
SAN
ANTONIO-EAST (ID
#737): Well-established, GD office located 30 miles north of Houston. The practice occupies 4,300 sq ft in a standalone building, with only one additional tenant. Four fully equipped operatories with four additional prepped for future expansion. Well equipped with computers throughout, digital x-ray sensors, a 3D cone beam CT, digital scanner, intra oral cameras, and paperless charts. The practice has a robust hygiene recall program and incredible growth potential. SAN ANTONIO-TX
#716): Legacy GD practice and real estate in a rural community east of San Antonio. The large office space offers ample room for expansion and features 5 fully equipped operatories with computers in each op, digital x-ray sensors, a digital pano, a digital scanner, intraoral cameras and paperless charts. This practice has
strong profit margins and serves a large, multigeneration 100% FFS patient base. TO REQUEST
MORE INFORMATION ON MCLERRAN & ASSOCIATESí LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@dentaltransitions. com.
CENTRAL TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural 4 operatory dental practice for sale in the heart of the beautiful Texas hill country. This all-digital practice with a new pano produces mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@gmail. com for more information and showings.
HOUSTON: General practice (reference: “Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid-6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475 square feet with 3 total operatories: 2 for dentistry and 1 for hygiene. Please let me know if you need anything else from me. A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 35 years. Practice sees patients about 16 to 19 days per month. Collection ratio of 99%. Practice is a fee-for-service and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
NEW BRAUNFELS: Dental practice for sale in high traffic area and very visible building.
Beautifully renovated recently, with 3 operatories, move-in ready, with 1,250 sq ft. No HMO or DMO. If interested, please email to salemydentalpractice@yahoo.com or leave message on landline, 830-606-4544.
classifieds
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states. For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
OFFICE SPACE
TYLER: Perfect location for dental office at one of the top intersections in Tyler, TX; Troup & Loop 323. 70,000 cars per day providing unmatched visibility to both highways. Benefits from the tallest (35’) freestanding pole sign and electronic reader board at the intersection and would be impossible to get approved today. Ready for immediate occupancy. Please call Rick, 937-367-6656.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.