Quarter 2
June 2020
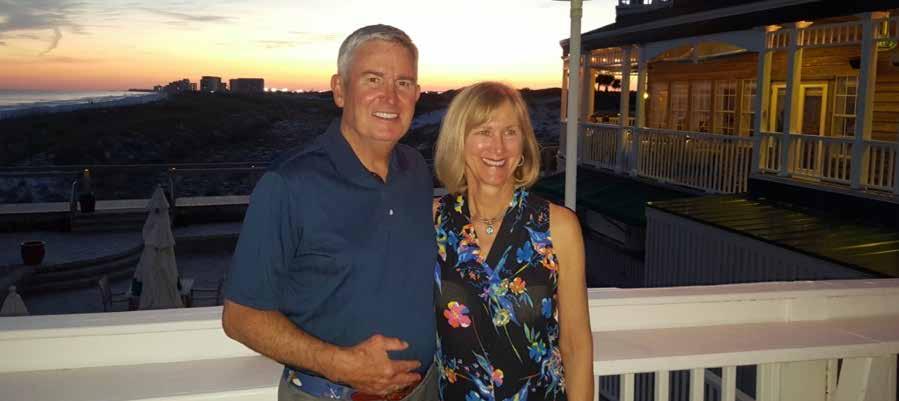
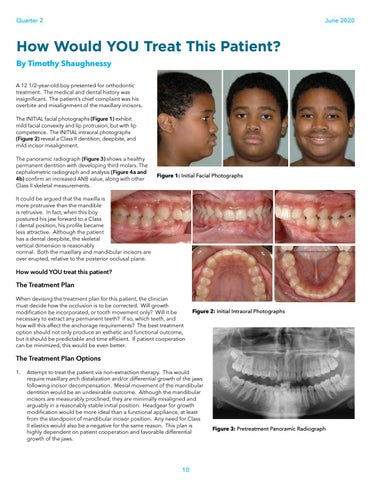
How Would YOU Treat This Patient? By Timothy Shaughnessy A 12 1/2-year-old boy presented for orthodontic treatment. The medical and dental history was insignificant. The patient’s chief complaint was his overbite and misalignment of the maxillary incisors. The INITIAL facial photographs (Figure 1) exhibit mild facial convexity and lip protrusion, but with lip competence. The INITIAL intraoral photographs (Figure 2) reveal a Class II dentition, deepbite, and mild incisor misalignment. The panoramic radiograph (Figure 3) shows a healthy permanent dentition with developing third molars. The cephalometric radiograph and analysis (Figure 4a and 4b) confirm an increased ANB value, along with other Class II skeletal measurements.
Figure 1: Initial Facial Photographs
It could be argued that the maxilla is more protrusive than the mandible is retrusive. In fact, when this boy postured his jaw forward to a Class I dental position, his profile became less attractive. Although the patient has a dental deepbite, the skeletal vertical dimension is reasonably normal. Both the maxillary and mandibular incisors are over erupted, relative to the posterior occlusal plane.
How would YOU treat this patient?
The Treatment Plan When devising the treatment plan for this patient, the clinician must decide how the occlusion is to be corrected. Will growth modification be incorporated, or tooth movement only? Will it be necessary to extract any permanent teeth? If so, which teeth, and how will this affect the anchorage requirements? The best treatment option should not only produce an esthetic and functional outcome, but it should be predictable and time efficient. If patient cooperation can be minimized, this would be even better.
Figure 2: Initial Intraoral Photographs
The Treatment Plan Options 1. Attempt to treat the patient via non-extraction therapy. This would require maxillary arch distalization and/or differential growth of the jaws following incisor decompensation. Mesial movement of the mandibular dentition would be an undesirable outcome. Although the mandibular incisors are measurably proclined, they are minimally misaligned and arguably in a reasonably stable initial position. Headgear for growth modification would be more ideal than a functional appliance, at least from the standpoint of mandibular incisor position. Any need for Class II elastics would also be a negative for the same reason. This plan is highly dependent on patient cooperation and favorable differential growth of the jaws.
10
Figure 3: Pretreatment Panoramic Radiograph