10 minute read
SAO 2019 Leadership Project – Orange Team


Awareness Program (CAP) and Career Services. The main reasons these members maintain their memberships are the AAOendorsed Insurance Programs (AAOIC), the Annual Session continuing education, and the Legal Advocacy/Political Action Committee (PAC).
When asked about the CAP directly, 70% of respondents report that the CAP is valuable; however, the perception of value for the CAP decreases with years in practice. When asked directly about the AAO-endorsed insurance programs, most respondents (73%+) reported that they value the AAOIC. This benefit is valued most by mid-career members (11-20 years), and members later in their career value this benefit the least (20+ years). When asked directly about the value of membership in organized orthodontics, most (70%+) respondents value membership as GoodExcellent. Furthermore, the perception of Good to Excellent value from membership increases with years in practice. Chris Baker • Eddy Sedeño • Robin Mayo • Arghavan Welch • Wallie McCarlie • Ahmad Abdelkarim • Debbie Sema (EC Liaison) • As specialists in orthodontics, we are in a strong position to impact some of our fundamental responsibilities: to educate patients and to improve patient care. We can do these things individually. We can also do them collectively by being an active participant in organized dentistry. The mission of organized dentistry and of organized orthodontics is to advocate for patient-centered orthodontic care. Therefore, orthodontists and dentists have the legal, ethical, and moral duty to seek and advocate for treatment modalities that are in the best interest of patients.
RECOMMENDATIONS
Find a way to efficiently and effectively ensure sure that every AAO member has access to the breakdown of how dues are spent. Increase efforts to educate members about the benefits and results of CAP. This is a great benefit of AAO membership and should be promoted as such.
Members earlier in their careers may need additional assistance with dues and a way of enhancing their perception of the value of membership in the AAO. Market/promote the VALUE OF MEMBERSHIP to the orthodontic residents and early (young) orthodontists.
In general, do not reduce fees for the purpose of increasing membership. In general, continue to find ways to “stay relevant” in an ever-changing
REFERENCES
(1) Mission and history, American Association of Orthodontists: https://www1.aaoinfo.org/ about-us/mission-history/.
(2) “10 reasons to renew your AAO membership,” AAO: The Practice Management Bulletin, 2019; 37(3): 3-8.
(3) Dunn, Dr Courtney. Does membership matter? The Progressive Orthodontist, Q2 2016; 78-79. www.orthopundit.com/doesmembership-matter/.
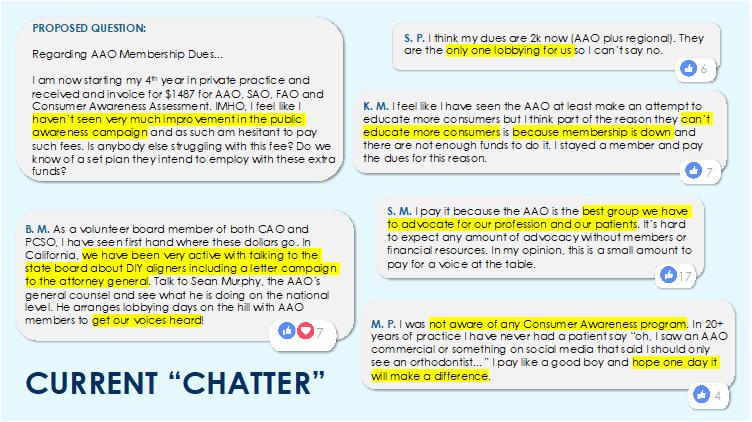
(4) OrthoPreneurs (Facebook Private Group) August 26, 2019; Dr Nick Mann post
SAO Orange Team Leadership Project 2019
Patient Advocacy and Organized Dentistry: Identify the Issue and its Impact on Orthodontists
culture There are currently a number of dental service organizations that seek to provide patients options to self-managed orthodontic care or do-it-yourself (DIY) orthodontics. These dental service organizations are located throughout the United States and successfully reach millions of consumers through marketing and promises to cut the “middle man”. These organizations follow several telemodels already adopted in retail, travel, dining, entertainment, and banking. Through these telemodels, patients can generate data from their own devices that can be immediately analyzed, graphed and shared. Challenges inherent to teledentistry that apply to DIY orthodontics are patient confidentiality, different standards of care across different states and deceptive marketing. 1
DEFINITION OF ISSUES
Teledentistry is a combination of telecommunications and dentistry delivered in order to provide care across
long geographic distances. 2 Teledentistry involves exchange of clinical information that is transferred in digital format between doctors and patients. It can be used for multiple purposes, including diagnosis and treatment planning, oral health consultation, treatment monitoring, appliance fabrication, or even on-site job training. Although modern teledentistry appears to be largely internet-based, teledentistry is vastly different from Web browsing and distance learning. Essentially, it is the sharing of digital information through communication technology, not direct personal contact, to provide dental care when distance separates the patient and the doctor. Technological advances in computers, smartphones, and digital diagnostic imaging have made partial or complete management of orthodontic patients by teledentistry more “vulnerable” than ever before. What follows is a review of the history, applications, legal concerns, and potential abuses of teledentistry in orthodontics, as well as its role in the emergence of do-it-yourself (DIY) braces and remote treatment-monitoring software. 3
TELEDENTISTRY
In 1984, computer aided design/computer aided manufacturing (CAD/CAM) entered the dental world with the advent of Chairside Economical Restoration of Esthetic Ceramics (CEREC) restorations. 4 Three dimensional digital impressions in dentistry were first introduced in 1987 by CEREC (Siemens, Munich, Germany) using an infrared camera and optical power on the teeth to create a virtual model. In 2001, Cadent introduced the OrthoCAD® system for the production of 3D digital models, virtual occlusal setups, and indirectbonding trays. This was the first use of this technology in orthodontics and it had significant teledentistry implications. Either cast models or polyvinyl siloxane (PVS) impressions were sent to the OrthoCAD scanning center where the model or impression was scanned. The data was processed into a digital file that was downloaded into the practitioner’s office network. In 2006, Cadent developed the in-office iTero® digital impression system. The first in-office digital impression system capable of full-arch intraoral scanning came online in 2008. In late 2009, Cadent launched the iOC® system for iTero users. Align Technology purchased Cadent in 2011 and encouraged clinicians who had iOC to begin submitting 3D digital scans in place of physical impressions for the fabrication of Invisalign appliances. 5
Intra-oral scanner devices offer numerous applications in orthodontics – study casts, indirect bonding, customized arch wires, customized fixed appliances (both labial and lingual), aligners, removable orthodontic appliances, and diagnostic procedures in both orthodontic and orthodontic/orthognathic surgical combined treatment. Advances in hardware and software technologies over time have drastically perfected this technology to effectively replace traditional alginate and polyvinyl siloxane (PVS) impressions in dentistry. This technology has led to increased possibilities for teledentistry in orthodontics.
The “teledentistry” idea first started in “telemedicine”. Patients could contact medical specialists who were not in their specific location because specialists were not available in the patient’s location. Teledentistry was first implemented in 1994 by the US Army. Teledentistry has evolved in order to “increase access to dental care,” especially in rural areas. 6 It has been used in advanced dental education to connect students at one location via telecommunications to doctors at another location who have specialized training. 7
DIY ORTHODONTICS
An example of DIY orthodontics is the practice of using rubber bands to close midline diastema gaps based on YouTube videos. In some of these cases, there are reports of severe damage to teeth and to the periodontal structures which have, on some occasions, resulted in loss of teeth.
Currently, a trend is “at-home” clear aligners. The American Dental Association House of Delegates has considered and debated do-it-yourself (DIY) orthodontics in the past few years. This “at home” trend seems to include patients who are looking for less expensive treatment, putatively shorter treatment time, anonymity or something else. Today, there are many DIY dental service organizations. One DIY dental service organization, for example, is backed by a venture capital group that has also funded other large, successful companies. 7 This DIY organization currently employs over 4000 people, has 200 “smile shop” locations and is valued at over 3 billion dollars – three times its valuation the previous year. 8 It employs 225 licensed dentists/orthodontists who are the prescribing doctors for every patient. This organization collaborated in May 2019 with an American multinational information technology company to make the largest multi-jet Fusion 3D production facility in the US. In spite of all the market excitement, the company has not been free of patient complaints.
In the last few years, several state dental boards have fulfilled their duty-bound responsibilities to enforce their respective dental practice acts which were passed and codified to insure that the public received a high standard of care. Recently, two state dental boards have been sued by DIY entities that claim that the DIY is not practicing dentistry. In both cases, the claims have been dismissed. In at
least one of these cases, the AAO’s legal team served as the sole advocate for patient care, because not one practicing orthodondist was available to provide
supporting testimony. Although the Association’s legal team is organized at the national level, there seems to be little or no locally organized infrastructure at the component or constituent level that can help with these issues. The minimal infrastructure found at the local level is an area that we have identified that has great potential for growth, especially with regard to advocating for patients.
ANALYSIS OF ROOT CAUSE(S)
One of the reasons for the lack of minimal organized political infrastructure at the component or constituent level for patient advocacy is perhaps historical. State issues that impacted the practice of dentistry did not necessarily require a certain infrastructure or a nimble response system because the local issues originated externally rather than internally. With teledentistry, factors outside the locale may have a more significant influence upon local issues.
POSSIBLE SOLUTIONS OF THE ISSUE
Though there are differing opinions, even within the orthodontic community, about how to advocate for patients, organized orthodontics offers balance to disparate factions and provides a basis for rational agreement as to how to best advocate for patients.
Improving patient advocacy through constituent and component levels of the Association can happen at the state level in the following ways:
Encourage state dental board members to carry out duty-bound responsibilities to advocate for patients.
Develop relationships with legislators and educate them regarding patient advocacy through a localized, formal structure.
Reframe state dental boards in a way that strengthens the board’s ability to advocate for patients.
Because the practice of dentistry is regulated by each state, local infrastructure is best suited to advocate for patients. A state dental board can enforce state laws that regulate the authorized practice of dentistry. We propose that the Southern Association of Orthodontists Board of Directors consider formally re-structuring component leadership to include a “legislative liaison” who would become a point-person and organizer of events and activities such as hosting a political “get to know you” for elected officials or for those running for office. This person would organize patient advocacy with state legislators. In conjunction with this suggestion, we propose the creation of a model or template in each state so that in each district of the state there is a team of orthodontists who form a political infrastructure that is charged to connect with every single representative and senator at the state level, similar to the Georgia Dental Association’s model for general dentistry.
HOW WILL PROGRESS BE MONITORED?
Progress will be monitored by assessing whether or not these positions and teams have been created by the time of our next annual session. Events that are designed to engage more orthodontic specialists in the political process must be scheduled.
WHO WILL MONITOR PROGRESS AND BE ACCOUNTABLE?
Common sense dictates that local leadership, and SAO component organizations should be accountable. Those components within the SAO include: West Virginia, Kentucky, Virginia, Tennessee, North Carolina, Mississippi, Alabama, Georgia, South Carolina, Louisiana, and Florida.
References:
1. Sfikas, PM. Teledentistry: Legal and regulatory issues explored, J. Am. Dent. Assoc. 128:1716- 1718, 1997.
2. Khan, SA, Omar, H. Teledentistry in practice: Literature review, Telemed. J.E. Health 19:565- 567, 2013.
3. Kravitz ND, Burris B, Butler D, Dabney CW. Teledentistry, Do-It-Yourself Orthodontics, and Remote Treatment Monitoring. J Clin Orthod. 2016;50(12):718-726.
4. Mörmann W, Brandestini M, Ferru A, Lutz F, Krejci I. Marginal adaptation of adhesive porcelain inlays in vitro. Schweiz Monatsschr Zahnmed. 1985;95:1118–1129.
5. Kravitz ND, Groth C, Jones PE, Graham JW, Redmond WR. Intraoral digital scanners. Journal of Clinical Orthodontics 2014;48: 337-47
6. Chen, Jung-Wei, et al. “Teledentistry and its use in dental education.” The Journal of the American Dental Association 134.3 (2003): 342-346.
7. Kravitz, N, et al. “Teledentistry, Do-ItYourself Orthodontics, and Remote Treatment Monitoring.” Journal of Clinical Orthodontics L.12 (2016): 718-726
8. Dickey, Megan Rose. “Teeth-Straightening Startup SmileDirectClub Is Now Worth $3.2 Billion.” TechCrunch, TechCrunch, 10 Oct. 2018, https://techcrunch.com/2018/10/10/teethstraightening-startup-smiledirectclub-is-nowworth-3-2-billion/.