Editor
Lisa Cambridge, NZCS DipQA B.ApplManagement, MNZIMLS, NZIMLS, Rangiora
Deputy Editors
Michael Legge, PhD MRSB FIBMS FNZIMLS FFSc(RCPA), University of Otago, Dunedin
Holly Perry, DipMLS MAppSc(Hons) PhD MNZIMLS, University of Otago
Emeritus Editor
Rob Siebers, PGCertPH FNZIC FNZIMLS FRSB HonFNZAP, Wellington
Editorial Board
Paul Austin, MSc(Hons) DipMLT MNZIMLS, LabPlus, Auckland
Jillian Broadbent, FNZIMLS, NZIMLS, Rangiora
Julie Creighton, DipMLS, FNZIMLS, Canterbury Health Laboratories, Christchurch
Sujata Hemmady, PGDipMLSc, MMLSc, MNZIMLS, LabPlus, Auckland
Chris Kendrick, GradDipSci MSc MNZIMLS, Massey University, Palmerston North
Craig Mabbett, BMLSc PGDipHSM, LabCare Pathology, New Plymouth
Holly Perry, DipMLS MAppSc(Hons) PhD MNZIMLS, University of Otago
Mohd. Shahid, MBBS MD PhD FNZIMLS, PGDipHSM, Arabian Gulf University, Bahrain
Terry Taylor, BSc DipMLS MNZIMLS, Southern Community Laboratories, Dunedin
Sharon Tozer, DipBis Stud, AT CAANZ, NZIMLS, Rangiora
Robyn Wells, BApllSci(MT) GradCert Haem, Milton, Australia
Formatting
Rangiora
About the Journal
The New Zealand Journal of Medical Laboratory Science (the of Medical Laboratory Science (NZIMLS). The Journal is peer reviewed and publishes original and review articles, case studies, technical communications, and letters to the Editor on all subjects pertaining to the practice of medical laboratory science. The Journal is open access (www.nzimls. org.nz/nzimls-journal) and is published three times per year in April, August, and November. Hard copies are circulated to all NZIMLS members and universities and research units in New Zealand and overseas. Current circulation is about 2,800 copies per issue. Printing is by Blueprint Ltd, Christchurch on environmentally responsible paper using elemental chlorine free harvested forests and manufactured under the strict ISO14001 Environmental Management System. The Journal is indexed by CINAHL, EMBASE, SCOPUS, Informit, Thomson Gale, EBSCO and Biosis Citation Index, and the Journal Editors are members of the World Association of Medical Editors (www.wame.org).
Brief instructions to authors
The Journal accepts original submissions from anyone and anywhere. Comprehensive instructions can be found on the NZIMLS website (www.nzimls.org.nz/instructions-to-authors. html). All submissions will undergo single-blind peer review and possibly plagiarism checking with iThenticate™ software. If accepted for publication, copyright is vested in the author(s) under terms of the Creative Commons Attribution License (www. creativecommons.org/licenses/by/2.5/legalcode). The authors
expressed in the Journal are not necessarily those of the Editors, Editorial Board, or Council of the NZIMLS.
Advertising and subscription
Advertisement bookings and enquiries should be addressed to org.nz. Phone +64 3 313 4761.
Journal cover © Joseph Manieda, Te Whatu Ora Hawke’s Bay
Editorial
Professional input into a national pathology service provision strategy.
Terry Taylor 104
TH Pullar address
Thos Pullar and the philosphers stone.
Michael Legge................................................................105-106
Original articles
on haematological parameters among patients in Central Hospital, Benin City, Nigeria
Christopher O Elemuwa, Joe O Isibor, Nyoho J Inyang, Uchenna Geraldine Elemuwa, Richard Omoregie and Mary Ayanlere................................................................. 109-112
fever in Egyptian patients.
Hala T El-Bassyouni, Hisham Megahed, Eman R Youness, Hisham A Aziz Orban, Maha M Kobesiy, Rania A Ellethy, Mina Wassef Girgiss, Adel Mohamed Ashour, Ahmed Helal El Sayed and Moushira E Zaki....................................................... 114-118
cross-sectional study.
Moushira Zaki, Wafaa Kandeel and Eman Refaat Youness....................................................120-123
Comparison of the BD Max™ vaginal panel, against standard methods, for the detection of common vaginitis conditions.
Julie A Creighton and Bethany J Mills............................124-127
Sue Calvert.....................................................................128-129
Book reviews
This is going to hurt by Adam Kay.........................................130
A nurse on the edge of the desert by Andrew Cameron
Reviewed by Elaine Booker............................................130-131
Regular features
Advertisers ............................................................................103
Call for nominations for Life Membership of the NZIMLS......136
Governor General Welcome Speech SPC2023....................108
this issue
questionnaire ...........................................................138
Otago 4th year BMLSc student research project abstracts, semester 1, 2023............................................................139-146
...........................................................................103
Laboratory
NZIMLS
..................................................................129
In
Journal
Christmas quiz..............................................147-149
calendar
.....................................................................132-134
Recent
Science
New Zealand Journal of Medical Laboratory Science 2023 102
QMLT curriculum review .......................................................137
reviews......................................................................112
digest................................................................135-136
In this issue
last 30 years of working in pathology in this issue’s Editorial. He writes that one of his most apparent and disappointing aspects has been the complete lack of voice from professional expertise
dominance and poor professional knowledge were some of the key reasons as to why the pathology section is in unprecedented crisis in New Zealand. The major role of the NZIMLS professional body is the continued advocation and promotion of the profession, with genuine input from professional leads who represent the workforce and those directly involved in the service delivery for a national pathology strategy. Taylor encourages all in the profession, to be a strong and consistent voice for the sector.
Each year the NZIMLS invites a prominent New Zealand medical laboratory scientist or pathologist to deliver the TH Pullar Address. Retired Associate Professor, Michael Legge from the University of Otago is this years’ recipient, addressing the 2023 philosophers stone” and reprinted in this issue.
Escherichia coli food-borne pathogen of considerable public health concern. Elemuwa and colleagues at the Central Hospital, Benin City, Nigeria conducted a study of patients presenting with various gastrointestinal complaints. Their results show that gender did E. coli
and those with diarrhoea. The prevalence of E. coli in the study was 1.19% of total faecal specimens, lower than studies reported in Lagos and Zaria and prevalence was shown to be varied depending on geographic locations, regions within the same country and even over time. Authors advocate further studies and measures to prevent the spread of this food-borne pathogen.
Mediterranean fever (FMF) is characterised by persistent and cause endothelial dysfunction and atherosclerosis. Professor ElBassyouni and colleagues from the National Research Centre in
aim of the study was to assess if Chemerin could be used as a diagnostic index in FMF patients. Results showed that FMF serum amyloid A and serum lipids (cholesterol, total triglycerides correlated with high-density lipoprotein (HDL). There was no correlation between Chemerin and gene mutations studied. The the atherogenic factors amongst FMF patients compared to that adipokine and could be considered as a biomarker of chronic for Vitamin D supplementation for FMF patients.
Zaki and researchers at the National Research Centre in Cairo, of the triglyceride to HDL-C ratio for insulin resistance amongst
Egyptian obese premenopausal women. Insulin Resistance progression of cardiovascular disease and diabetes mellitus. The current gold standard test for IR is complex and of high cost, preventing its use in daily clinical practice and epidemiological assessment for insulin resistance (HOMA-IR) index to gauge insulin resistance in adults. This diagnostic procedure utilised a routine test for triglycerides and high-density lipoprotein cholesterol (HLD-C) ratio and measurements of plasma fasting insulin and glucose in 220 obese women. Results showed an indication of IR in these patients and provide a tool to recognise high-risk individuals.
Bacterial vaginosis (BV), vulvovaginal candidiasis, and Trichomonas vaginalis infections are common cause of vaginitis
Researchers Julie Creighton and Bethany Mills from the Microbiology Laboratory at Canterbury Health, New Zealand compared the performance of BD Max™ Vaginal Panel, against standard methods, for the detection of common vaginitis conditions. Gram Stain interpretation can be subjective even with an experience operator and correct distinction of bacterial Panel (BD MAX) is a qualitative diagnostic test using real-time
and correlated well with Gram stain interpretation for the diagnosis of BV. Creighton and Mills concluded that laboratories stain is inconclusive or indeterminate.
Congress, Sue Calvert the CEO of the Medical Science Council of New Zealand clears up some of the confusion around the and their roles.
Elaine Booker, from Southland, New Zealand pens two
and A nurse on the edge of the desert by Andrew Cameron.
Congress by The Right Honourable, Dame Cindy Kiro, Governor General of New Zealand, a QMLT curriculum review update and the Otago University 4th year BMLSc student abstracts for some fun break-time debate.
2023 has been another challenging year for the profession and the voices of frustration and uncertainty echo throughout this issue, in the Editorial, the TH Pullar Address and in the book reviews. I hope that from shared knowledge and connection, we
Lisa Cambridge Editor
Advertisers in this issue Abacus Dx ................................................................................................Inside front cover Bio-Strategy ....................................................................................................................107 Stago ..............................................................................................................................113 Temprecord..................................................................................................................... 119 New Zealand Journal of Medical Laboratory Science 2023 103
Professional input into a national pathology service provision strategy
Terry Taylor
One of the most apparent and disappointing aspects of my 30 years working in pathology in Aotearoa New Zealand has been the complete lack of voice from professional expertise in operational service decisions. The irony of political interference, vested has left our country with a pathology structure that is fragmented, poorly controlled, and embedded in competitive and anti-trust issues. The only saving grace has been the professionalism of a workforce that has continued to operate at a consistently high level despite the governance mess that hangs above them. But the cracks that widened during the pandemic are now breaking apart and the reality for our Pathology sector is that we are in an unprecedented crisis.
One of the questions I get asked most by health and political leadership, is ‘how did things get this bad?’ We all know there are several reasons that have led to where we are, but I am going to stress that one of the big ones has been the lack of an authoritative professional voice at the political and health leadership level.
Medical laboratory professionals are by their nature typically introverts with a strong systems approach to what is in front of them. No fuss, no need to speak outside of their expert scope, and most certainly not ones to chase publicity and attention. Unfortunately for our sector this has been taken advantage of by many in health and business management, particularly during the well documented ‘contracting wars’ that began in 2007. It is fair to say at that time the New Zealand Institute of Medical Laboratory Science (Inc.) (NZIMLS), unions and our other professional colleagues were just not equipped to deal with the the pathology sector under our noses. I well remember at that time thinking this is all too big and we just need to adapt and get has clearly shown that we all should have done more to provide a professional perspective of what history has clearly shown, and pathology sector in Aotearoa New Zealand.
correspondence with the Prime Minister and Governor General in August 2023, it is fair to say the pathology sector is now seen in the light it should always have been. We have respect and knowledge across all of Parliament, and this needs to continue to governance clout than the current Director General of Health, policy to go to Parliament, so they remain important for our sector to be engaged with. And now we have Te Whatu Ora and Te Akai Whai Ora who provide the operational governance for all health sectors, who currently lack operational pathology expertise apart from the input from professional organisations like the NZIMLS and the Royal College of Pathologists Australasia (RCPA). Your professional body, the NZIMLS, has spent literally thousands of volunteer hours and numerous in-person and virtual meetings to get us in the door at the leadership level of these important national entities. My frustrations continue to be around national strategy and governance, and the lack of progress on this has been incredibly disheartening. This has led to the ‘posturing’ within providers and stakeholders in our sector to gain favour
for future service provision. Entirely predictable but this could have been addressed with strong direction from government and then Te Whatu Ora, through an integrated national strategy
-directed post pandemic testing review (1). Put simply this led to the profession’s inherent problems being swept and hidden from public, political and health leadership scrutiny until mid-2023 when workforce and service issues hit the mainstream media with full impact.
My expectation is that as part of any national pathology strategy there needs to be genuine input from the professional leads who represent the workforce and are directly involved in service delivery. This process should never again be solely driven by
(2)and Te Pae Tata (NZ Health Plan) (3). These may well be foreign words to many in corporate and health bureaucracy but when we look at the result of the many past poor service decisions without professional input there is one massive chance to put things right for the pathology sector in Aotearoa New Zealand.
I encourage all practitioners to utilise the new situation we have in our sector. We need to keep having our say and taking solace that as a prominent professional group we deserve to sit at the same table as all other stakeholders when strategies and decisions are worked through. There is simply no excuse for the ‘one way’ approach to be tolerated in 2023. A major role of the NZIMLS is to continue to advocate and promote our professional voice while providing the context of the historical damage that
the seasoned professional experience in our ranks that will drive our involvement forward.
One thing you can do as a medical professional is to provide a strong consistent expert voice for the direction that the pathology sector needs to aspire towards. It is no longer a time to sit back and put up with processes and strategies that are not in the best interest of our expert workforce and the patients we provide
scientist from Dunedin can discuss issues on equal terms with health and political royalty, then what is stopping any of you from doing the same thing?
AUTHOR INFORMATION
Terry Taylor, BSc, DipMLS, MNZIMLS, Immediate Past President, New Zealand Institute of Medical Laboratory Science
REFERENCES
1.Allen + Clark. Covid-19 PCR Testing Backlog - Rapid www.health.govt.nz/system/files/documents/publications/
2.
3.
o-rongo-nz-health-charter/
–Health New Zealand. Te Pae Tata Interim New Zealand tewhatuora.govt.nz/publications/te-pae-tata-interim-newzealand-health-plan-2022/
EDITORIAL
New Zealand Journal of Medical Laboratory Science 2023 104
TH PULLAR ADDRESS
Thos Pullar and the philosophers stone
Michael Legge
First I would like to acknowledge the honour of being asked by the NZIMLS to give this very important address which is part of the ongoing tradition of the profession and one I believe should not be lost.
TH Pullar
Pullar to both Pathology and Medical Laboratory Scientists education and career structure. I doubt now if anyone has had personal contact with Thos Pullar as he was known. I certainly have not but I have heard a lot of TH Pullar addresses. So a
and initially worked as a Biochemist before moving to London where he became an authority on tumour pathology, before moving to a new position in New Plymouth where he would work with a strong clinical biochemistry background at that time. During this time he was largely responsible for the introduction of the BCG vaccination in New Zealand and the establishment of a blood group reference laboratory in Auckland. In his day he was one of New Zealand’s leading clinical pathologists with a passion for training and establishing education structures for the then, Technologists and travelled New Zealand as an
New Zealand Medical Technologists Training Board to produce in 1965 after a long illness. In 1966 in Thos Pullar’s Obituary it is
Meeting in 1967 by one of his colleagues and acknowledged Thos Pullar’s contribution to pathology, science and education. The topic was cytogenetics and the cell cycle, which at the time
lasted well over a good hour, which brings me to the main body of this presentation. What I found interesting in the TH Pullar address was the speculation that genes are presumed to consist of the structure of DNA by James Watson, Francis Crick and Maurice Williamson in 1953. Maurice Williamson was a New Zealand scientist working in the UK, often forgotten that he was a New Zealand Nobel Prize winner, and all three received the Nobel Prize for their work. Until this discovery, inheritance was presumed to be by proteins. So 14 years after the discovery of DNA structure, there was still speculation on the roles of genes Watson and Crick on the structure of DNA they announced that Harry Potter.
So what did Watson and Crick mean by the “Philosophers Stone of Life”?
A second century Egyptian Alchemist, Maria Hebrea described time was translated and corrupted into making gold from base metals. This quest consumed alchemists up to and including the 17th century. However, it is believed that Maria’s original meaning of the Philosophers Stone related to transforming knowledge. However in their quest for the impossible alchemists, including Isaac Newton, started laying the basis for modern science by systematic observations and documenting experimental techniques. By commenting on the discovery of the
they had unlocked the essential key to the knowledge of life. By making this statement they were starting to merge centuries of magic and alchemy into a foundation for modern science and
ultimately genomics.
Fast forward now to 1967, where we had the knowledge of chromosomes but there was incomplete knowledge of DNA, from Mendel’s work and his subsequent contemporaries and William Bateson in 1905 provide the term genetics from the Greek but what they were was unknown. At that time science and knowledge progressed by the decade and was frequently not accepted by all. Take for example a German physician who cut inherited as a physical characteristic.
Thos Pullar have would been fascinated by our science, knowledge and training today and just as he had published in the New Zealand Medical Journal in 1965 in an article on training laboratory technologists being at a crossroads, we as a profession profession had to evolve and that education and training were paramount to establishing a skill base for pathology. He was using university graduates. Of course the universities in those days considered anything of a ‘technical nature’ well below their image of an academic institution, how things have changed.
Today we take for granted diagnostic pathology and the massive amount of data being produced every day. But, genetic technologies progressed slowly. In 1977, Fredrick Sanger introduced a method for sequencing the genome which is still used today, and in 1983 Kary Mullis invented PCR by transforming knowledge into application. The billion dollar Human Genome it is possible to get a genome sequence in a few days and costs less than $US1000. Genetic technologies now form an important diagnostic component for understanding inheritance, cancer and genetic diseases – and the list goes on.
We accumulate knowledge and skills faster now than any other time in the history of pathology and life sciences. This has led to the evolution of a highly skilled and competent workforce. We
comments by Watson and Crick, a question I would pose here of Life” with our unprecedented transformational knowledge and technologies that did not even exist in the realms of science molecular biology, genetics and metabolomics has revolutionised the understanding of these insidious diseases. We can classify cancer, track its inheritance patterns and we are beginning to understand the metabolism of tumours and the potential of targeting cancer metabolism therapy with novel drugs inhibiting cancer metabolism as an alternative to chemotherapy.
of previously incurable cancers, longer survival times and the development of new medications. The concept of tailoring cancer medication is beginning to be based on pharmacogenomics, where by clinical treatment can be tailored for both the cancer
is leading to successful treatment or alleviating the worst complications. For example, the life expectancy of a cystic
USA aged 86 years. When the disease was explained to her as a
New Zealand Journal of Medical Laboratory Science 2023 105
to orange juice.
So not only is the technology and diagnosis important, so are
We tend to think that genetic diseases are rare but a recent publication from Europe indicates that 1 in 20 of the population carry a mutation for a rare disease. As carriers it should not manifest itself but may account for an unusual diagnostic pathology result. I think it is safe to say that irrespective of a disease, diagnostic pathology services are the key to modern medicine.
So, how can we as a profession move forward, both in the quest for knowledge and the practical applications?
We are fortunate in New Zealand to have two excellent BMLSc degrees, which are in tune with the increasingly sophisticated requirements of the profession. These are linked to a range a highly skilled workforce. The NZIMLS has for over 40 years with new knowledge and developments for technician training. and cannot be replaced by a science related BSc or a simple examination to transit technicians to ‘registered scientists’. Whilst the HPCA Act protects the public with the regulation process, registration alone does not provide either the knowledge or workforce.
In the 1970s we entered the age of automation, especially in chemical pathology, which was being signalled as the end of a skilled workforce. All that was needed were people to load the analysers and send the printed results to the wards. Of course, this proved to be incorrect as new skill sets emerged including knowledge of computerisation. What was starting to happen was the evolution of new knowledge, an understanding of multiple data outputs and the speed that results could be produced. New methods and technologies emerged as well as
the pathology information revolution in diagnostic laboratories. Changes such as these started the long road to the creation of the BMLSc degree. This recognised the necessity for a skilled graduate workforce to meet the changes starting to occur.
Today, I think we are at another major crossroads for our profession. For me, it is evident that just as Thos Pullar had a vision of a graduate profession we now have to consider how diagnostic pathology services may evolve and the nature of the workforce needed to progress these changes. I consider that there are three emerging issues, stabilisation of the workforce, on a single pathology provider who is not linked to returning common data bases and the freedom to exchange information.
continuing education for scientists and technicians is recognised as being essential for both good practice as well as career progression. Unless someone wishes to be a ‘manager’ the career progression in diagnostic pathology basically does not exist. Again, this is hampered in part, by private providers with
Practice” document in December 2022 indicated that they lacked both the knowledge of the disciplines in diagnostic pathology and the profession itself.
So where to from here?
It is hopeful that Te Whata Ora will heal the fractured pathology services and bring together a national pathology service under a single authority. This is essential to try and resolve the ongoing issues in New Zealand Pathology. Pathways for continuing education exist but the workforce is restricted on access. There
needs to be clear pathways that can be followed to allow new these can be best achieved. I think it is safe to say that career progression is virtually non-existent and we need to work on how this can be implemented for the profession as a whole. As an adjunct to this is perhaps the Medical Sciences Council could employ medical laboratory scientists to advise on the profession.
In this ideal world, what could the future of pathology look like? The key is an equitable system across the country and the profession that it is not considered as an ‘add-on’. Like Thos Pullar I have tried to renew his vision. For me the key is the security of the BMLSc programmes at the two universities with an appropriate funding model to sustain a four year programme. Graduates need to be employed as scientists and not technicians and both groups need to see a way ahead. Career progression is key to the security of New Zealand’s diagnostic pathology services. We need to recognise special skill sets working within pathology and based on experience and post-graduate
has been available in the United Kingdom for over 40 years and in Australia for over 12 years. We need a clear route for the training programme similar to that of pathology registrars and the recognition of the knowledge, skills and seniority these scientists bring to pathology.
Finally, where do we place research?
of Health, Te Whata Ora and other health agencies are to be
Translational research links with Precision Medicine, providing the new knowledge by linking research to routine pathology. We will see new emerging disciplines, which will deliver unprecedented of disease signatures. We have already entered the ‘genomics era’ as well as the progressive development of metabolomics and proteomics. These technologies will evolve into stem cell therapies, therapeutic gene editing, pharmacogenomics,
(AI) in data management and decision making as well as new, as yet unthought of laboratory technologies emerge. When such powerful technologies are linked with image analysis, computational biology, informatics systems etc, we will have more powerful diagnostic tools than ever before in the laboratory.
from pathology laboratories in New Zealand have changed or transformed people’s lives, often for the better and longer, a of medicine and diagnostic pathology is central to many of the new innovations. Just as Thos Pullar many years ago had faith in the profession, now is the time for the profession to have faith in itself.
Thank you.
AUTHOR INFORMATION
Michael Legge, PhD, MRSB, FIBMS, FNZIMLS, FFSc(RCPA), University of Otago
Correspondence
distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
New Zealand Journal of Medical Laboratory Science 2023 106
New Zealand Journal of Medical Laboratory Science 2023 107
Her Excellency, Dame Cindy Kiro, Govenor General of New Zealand
-zealand-institute-
the New Zealand Institute of Laboratory Science, and Mary-Ann Just, CEO of the Australian Institute of Medical and Clinical
immense and ongoing public scrutiny.
I’d like to read out a passage from one of the New Zealand Institute of Medical Laboratory Science’s press releases, from
‘In the early hours of this morning, in a diagnostic medical laboratory somewhere in New Zealand, the three-millionth PCR test will be performed with no fuss or celebration. That medical past the other more visible health professionals on their way home. They will watch and listen as news outlets question why it should take so long for an individual test result to come back –
I’m delighted to be here to open the New Zealand Institute of and to welcome medical and clinical scientists from across New special event.
The Covid-19 pandemic emphasised just how important medical laboratory scientists and technicians are to our healthcare system. The work of such highly skilled and dedicated professionals, in our laboratories and testing stations, played a vital role in how we were able to respond to the outbreak of the virus.
I know that throughout each new and unknown phase of the pandemic – and, in particular, throughout the Omicron outbreak –the strain on laboratories processing PCR tests was immense and unrelenting.
However, without those test results, we would have lost a vital tool in protecting ourselves and each other from the spread of the virus – and even more lives would certainly have been lost.
I also know, during those periods, the huge strain that was important, but so often unacknowledged – while also under such


I want to take this opportunity to thank you – on behalf of all New Zealanders – for your immense work over the past three years to help keep us all safe, on top of the hugely important work you
I also want to take this opportunity to acknowledge Terry Taylor –our CEO here in New Zealand – for being such a staunch advocate for medical laboratory scientists across the country. I
–and I know how hard you work to advocate on behalf of those in this room and throughout New Zealand.
In my role as Governor-General, I often have the great privilege of meeting New Zealanders, in communities across the country, who do extraordinary things in the services of others.
One of the most common things I’ve noticed about such people is that they are motivated, not by the promise of any kind of reward or recognition, but by the belief in what they’re doing, and the knowledge of the good that comes in helping others. And that seems to me the case with those in this room. My sincere thanks once again for your outstanding dedication and sense of duty.
The theme for this congress is Sailing into the Future. I wish all here in attendance, a rich and rewarding time over these next few days – and all the very best for your future. It brings me great pleasure to declare this Congress open.

 Dame Cindy Kiro and NZIMLS (Immediate Past) President, Terry Taylor
Ailsa Bunker, Middlemore Hospital receives her Life Membership from Dame Cindy Kiro
Dame Cindy Kiro and NZIMLS (Immediate Past) President, Terry Taylor
Ailsa Bunker, Middlemore Hospital receives her Life Membership from Dame Cindy Kiro
New Zealand Journal of Medical Laboratory Science 2023 108
The Rt Hon. Govenor General, Dame Cindy Kiro delivering her speech to the SPC23 delegates
Occurrence of Escherichia coli
haematological parameters among patients in Central Hospital, Benin City, Nigeria
Christopher O Elemuwa, Joe O Isibor, Nyoho J Inyang, Uchenna Geraldine Elemuwa, Richard Omoregie and Mary Ayanlere
ABSTRACT
Objectives Escherichia coli
This study was conducted against the background of the paucity of data on its prevalence in secondary healthcare facilities in Benin City, Nigeria.
Methods
at Central Hospital, Benin City, Nigeria. The stool specimens were cultured on MacConkey agar to recover Escherichia coli. The recovered Escherichia coli isolates were further subjected to sorbitol fermentation and the sorbitol non-fermenting isolates were further subjected to Escherichia coli count of the patients.
Results
Escherichia coli were recovered from the 420 stool specimens. The gender of the patients did not Escherichia coli isolates (p=0.9114). Patients within the age group of 11 – 20 years had Escherichia coli recovery and recovery of Escherichia coli
Escherichia coli isolates
Escherichia coli
Escherichia coli
Conclusion Escherichia coli haematological parameters. Measures to prevent the spread of this food-borne pathogen are advocated.
Keywords Escherichia coli
NZ J Med Lab Sci 2023; 77(3): 109-112
INTRODUCTION
Escherichia coli (E. coli) is a Gram-negative bacteria and strains that cause diarrhoea in humans are enterotoxigenic E. coli (ETEC), enteroaggregative E. coli (EAEC), enteropathogenic E.coli (EPEC), enteroinvasive E. coli
E.coli (DAEC) or verocytotoxigenic E. coli (VTEC) (1). One of the VTEC stains associated with diarrhoea, bloody diarrhoea, haemorrhagic colitis and haemolytic uremic syndrome (HUS) is the Shiga toxin-producing Escherichia coli (2, 3). Shiga toxin-producing E. coli (STEC) are important causes of diarrhoea, haemorrhagic colitis, bloody diarrhoea,
transmitted via the faecal-oral route by ingestion of contaminated food and water as well as from person to person (5). Escherichia coli of considerable public health concern, because of the severity of infection which it causes (6). This is due to characteristics such long survival time in the environment, unusual acid tolerance, association with ruminants that are used for food (7-13). Studies in Nigeria have demonstrated the presence of E. coli in humans, animals and the environment (14-16). No studies among patients accessing care at a secondary health facility in E. coli
the literature. This is important as E. coli be associated with haemorrhagic colitis, bloody diarrhoea, and HUS (4).
Against this background, this study aimed to determine the prevalence of E. coli complaints seeking care at a public secondary healthcare facility E. coli haematological parameters was also determined.
MATERIALS AND METHODS
Study area
The study was carried out in Central Hospital, Benin City (Oredo Local Government Area of Edo State, Nigeria), located on latitude 6.3298oN and longitude 5.6225oE. Oredo LGA has a population
is a government-owned secondary-level hospital that serves the health needs of people in Benin City as well as other LGAs in Edo State as it attends to referral cases from primary health care centres. The study was conducted between June 2017 and May 2018.
Study population
A total of 420 patients with gastrointestinal complaints (diarrhoea, stomach discomfort and abdominal pain) attending Central Hospital, Benin City, Nigeria, were recruited for this study. Information on patients’ age, gender and whether or not they had diarrhoea was obtained. Informed consent was obtained from all subjects or their parents/guardians in case of children prior to specimen collection. Approval for the study was given by the Ethical Committee of the Edo State Ministry of Health, Benin City.
Specimen collection and processing
Blood and stool specimens from each patient were collected into ethylene diamine tetra-acetic acid (EDTA) containers and sterile universal containers respectively and analysed in the laboratory within one hour of collection. The full blood count of all patients was determined using a haematology autoanalyzer –Sysmex K21N (Sysmex Corporation, Kobe, Japan) following the manufacturer’s instructions.
The stool specimens were inoculated onto MacConkey agar plates. The plates were incubated at 37oC overnight. Lactose fermenting colonies were processed to get pure cultures, and
E. coli if it was a Gram-negative bacillus, oxidase negative, lactose fermenting, motile, indole positive, citrate negative and urease negative.
Screening for Escherichia coli O157: H7
Escherichia coli were screened using MacConkey sorbitol agar to determine if they were presumptive E. coli E. coli isolates were cultured on MacConkey sorbitol agar and the plates were incubated at 37oC overnight. Isolates that did not ferment sorbitol (appear colourless) were taken as presumptive E. coli
ORIGINAL ARTICLE
New Zealand Journal of Medical Laboratory Science 2023 109
Escherichia coli O157:H7
Escherichia coli
agglutination kit (Rim E. coli
Santa Fe, CA, USA) following the manufacturer’s instructions. For each isolate to be tested, one drop of Test Latex reagent was dispensed into a well of the test slide, labelled test. One drop of E.coli Control Latex was dispensed into a separate well of the test slide labelled control. Using a plastic stick (provided with the kit), a small portion of a non-sorbitol fermenting E. coli colony
E.
coli O157 Test Latex on the slide. Using a fresh plastic stick, the remaining portion of the non-sorbitol fermenting E. coli colony was
E. coli Control Latex. The mixtures in the slide were rotated for 1 minute and agglutination watched out for. If there is agglutination in the test E. coli O157 area labelled test and no agglutination in the area labelled control, the isolate is positive for E. coli O157. The positive isolate was subcultured on blood agar, incubated overnight and the emergent colonies used to repeat the above process but using the E. coli H7 Latex reagent. However, the control latex is not used in this E. coli was E. coli
Statistical analysis
The parametric data were analysed using unpaired student t–test. The non-parametric data were analysed using Chi square 2) test and odd ratio (OR) analysis. The statistical software INSTAT® (Graph Pad Software Inc., San Diego, CA, USA) was used for the analysis.
RESULTS
A total of 107 (25.48%) Escherichia coli were recovered from the associated with E. coli E. coli was group of 11 – 20 years compared to the other age groups (Table 1). The recovery of E. coli associated with diarrhoea (OR= 2.376, 95%CI = 1.079, 5.232, p = 0.0489) (Table 1). Of the 107 E. coli isolates, 7 (6.54%) were E.coli Escherichia coli
(Table 2).
Male16142 (26.09)
Female25965 (25.10) Age (Years)
308 (26.67)
11 – 204625 (54.35)
21 – 308312 (14.46)
31 – 409324 (25.81)
41 – 507316 (21.92)
9522 (23.16)
Diarrhoea2911 (37.93)
Non-diarrhoea39180 (20.46)
5.2320.0489
CharacteristicsSubjects Tested Subjects with E.coli (%) OR95%CIP value Gender1.0530.672, 1.6530.9114
Type of stool2.3761.079,
Table 1: Distribution of Escherichia coli isolates among the studied subjects
Parameters Patients infected with E. coli O157 H7 (n=5) Patients infected with non-E. coli O157: H7 (n=102) P value Haemoglobin (g/L)116.7 ± 7.3131.1 ± 25.00.5816 Haematocrit (%)35.43 ± 2.5138.72 ± 6.110.6198 White blood cell count (x103/μL) 3.27 ± 0.90 5.36 ± 2.57 0.4447 Neutrophil count (%)40.71 ± 8.94 50.78 ± 12.090.5085 Lymphocyte count (%)40.86 ± 6.23 37.90 ± 10.510.8097
Table 2: Haematological parameters of patients infected with and without E. coli
New Zealand Journal of Medical Laboratory Science 2023 110
Figures are in mean ± standard error of the mean (SEM)
DISCUSSION
The prevalence of E. coli prevalence. E. coli participants within 11 – 20 years of age and those with diarrhoea. The presence of E. coli haematological parameters.
Among the bacterial agents responsible for diarrhoea and other gastrointestinal complaints, E. coli has been reported to be the most prevalent (1,19). In this study, a total of 107 (25.48%) of the 420 stool specimens yielded E. coli. This is comparable to the 27.3% reported by Ifeanyi et al. (20).
E. coli in this study (p= 0.9114). This is in agreement with a previous report (20), albeit the study subjects in Ifeanyi et al (20) study were prevalence of E. coli generally in females and among EPEC (enteropathogenic E. coli), EIEC (enteroinvasive E. coli), EAEC (enteroaggregative E. coli) and EHEC (enterohaemorrhagic E. coli), statistical analysis was not performed on the data. E. coli
prevalence. The reason for this is unclear. However, diarrhoea is a leading cause of morbidity and mortality among children less pathogen most associated with endemic forms of childhood diarrhoea is Escherichia coli (21, 22). The use of antibiotics in Nigeria is unregulated and over-the-counter sales of antibiotics without prescriptions are rife (23). It is possible that children less health centre before they arrived at the secondary health centre, and one may surmise that this may be responsible for the lower
A higher prevalence of E. coli was recovered from diarrheagenic stool specimens compared to non-diarrhoea stool specimens. E.coli is the most prevalent bacterial agent associated with
The E. coli O157 serogroup does not usually ferment sorbitol unlike typical E. coli and this characteristic is usually used to screen for E. coli O157 (24). Of the 107 E. coli isolates, 7 (6.54%)
6% reported in Lagos, Nigeria (14). The prevalence reported in this study is higher than the 3.6% reported in Tanzania (25) but lower than the 11.4% reported in Zaria, Nigeria (15). The higher value reported by Chigor et al (15) may be because the isolates were recovered from water and faecal specimens. The lower prevalence reported by Raji et al (25) compared with the and geographical location. Raji et al. (25) study sampled only patients with diarrhoea compared to this study where patients with gastrointestinal complaints (not only diarrhoea patients) were used.
Serological analysis revealed that 5 (71.4%) out of the 7 nonsorbitol fermenting E. coli was E. coli have reported that not all non-sorbitol fermenting E. coli are E. coli study. The prevalence of E. coli
in this study was 1.19% (5/420). This is lower than 6% reported due to geographical location and the type of patients used. Both studies (14, 15) used patients with diarrhoea. This study used patients with and without diarrhoea. This study was conducted
study was carried out in Zaria – Northwest geopolitical zone while Olorunshola et al. (14) study was in Lagos – southwest geopolitical zone. Also, the prevalence of the infection varies among children who had diarrhoea depending on geographic locations, regions within the same country, and even over time in the same location and population (28).
The presence of E. coli
alter the studied haematological parameters. Patients infected with E. coli
experience watery non-bloody diarrhoea or it may lead to haemorrhagic colitis, the haemolytic uremic syndrome (HUS), thrombocytopenia purpura and death (29). Patients with haemorrhagic colitis, HUS, and thrombocytopenia purpura usually have altered haematological picture. None of the patients used in this study presented with bloody diarrhoea. There was no physician to help ascertain if the patients had haemorrhagic colitis, HUS and/or thrombocytopenia purpura at the point of specimen collection. It is safe to assume that the patients recruited for this study came with signs and symptoms that did help to explain the results of this study.
CONCLUSION
In conclusion, the prevalence of E.coli
gastrointestinal complaints it sustained. Further studies in this regard are highly recommended and measures to prevent the spread of this food-borne pathogen are advocated.
AUTHOR INFORMATION
Christopher O Elemuwa, PhD, FMLSCN, FWAPCMLS (IMMUNIOL), Research/Director1
Joe O Isibor, PhD, Professor/Lecturer2
Nyoho J Inyang, PhD, ResearcherAssociate Professor/Lecturer3 Uchenna Geraldine Elemuwa, BPharm, MPharm, MILR, FWAPC, PhD Researcher/Director4
Richard Omoregie, PhD, FMLSCN, Researcher and Senior Lecturer5, 6
Mary Ayanlere, PhD, FMLSCN, Researcher and Senior Lecturer7
1National Primary Healthcare Development Agency, Garki, Abuja, Nigeria.
2Department of Microbiology, Faculty of Life Sciences, Ambrose Alli University, Ekpoma, Nigeria.
3Department of Medical Microbiology, Faculty of Medical Laboratory Sciences, Ambrose Alli University, Ekpoma, Nigeria.
4Pharmacovigilance Directorate, National Agency for Foods and Drugs Administration (NAFDAC), Abuja, Nigeria.
5Medical Microbiology Division, Medical Laboratory Services, University of Benin Teaching Hospital, Benin City, Nigeria 6School of Medical Laboratory Sciences, University of Benin Teaching Hospital, Benin City, Nigeria.
7Laboratory Department, Central Hospital, Benin City, Edo State, Nigeria.
Corresponding author Email
REFERENCES
1.Nataro JP, Kaper JB. Diarrheagenic escherichia coli. Clin Microbiol Rev
2.Wells JG, Davis BR, Wachsmuth IK, et al. Laboratory investigation of hemorrhagic colitis outbreaks associated with a rare escherichia coli serotype. J Clin Microbiol
3.Lupindu AM. Epidemiology of Shiga toxin-producing S Afri J Infect Dis
4.Ardissino G, Salardi S, Colombo E, et al. Epidemiology of haemolytic uremic syndrome in children. Data from the North Italian HUS network. Eur J Pediatr
5.Lupindu AM, Olsen JE, Ngowi HA, et al. Occurrence and characterization of Shiga Toxin-producing escherichia coli
and humans in urban areas of Morogoro, Tanzania. Vector Borne Zoonotic Dis
6.Coia JE. Clinical, microbiological and epidemiological aspects of escherichia coli O157 infection. FEMS Immunol Med Microbiol
New Zealand Journal of Medical Laboratory Science 2023 111
7.Hancock DD, Besser TE, Kinsel ML, et al. The prevalence of escherichia coli O157.H7 in dairy and beef cattle in Washington State. Epidemiol Infect.
8.
escherichia coli. Food Technol
9.Germani Y, Soro B, Vohito M, et al. Enterohaemorrhagic escherichia coli in Central African Republic. Lancet
10.Strachan NJC, Fenlon DR, Ogden ID. Modelling the vector pathway and infection of humans in an environmental outbreak of Escherichia coli O157. FEMS Microbiol Lett
11.Howie H, Mukerjee A, Cowden J, et al. Investigation of an outbreak of escherichia coli O157 infection caused by environmental exposure at a scout camp. Epidemiol Infect
12. in organic wastes destined for land application. J Appl Microbiol
13.Caprioli A, Morabito S, Brugère H, Oswald E. virulence and modes of transmission. Vet Res 289-311.
14.Olorunshola ID, Smith SI, Coker AO. Prevalence of EHEC APMIS
15.Chigor VN, Umoh VJ, Smith SI, et al. Multidrug resistance and plasmid patterns of escherichia coli O157 and other E. coli isolated from diarrhoeal stools and surface waters from some selected sources in Zaria, Nigeria. Int J Environ Res Pub Health
16.Ojo OE, Ajuwape ATP, Otesile EB, et al. Potentially zoonotic shiga toxin-producing escherichia coli serogroups in the faeces and meat of food-producing animals in Ibadan, Nigeria. Int J Food Microbiol
17.National Population Commission. Population and housing census of the Federal Republic of Nigeria, 2006. Available of-publications.
18.Barrow GI. Feltham RKA. Cowan and Steel’s manual for the University Press, Cambridge, UK. 2003.
19.Nweze EI. Aetiology of diarrhoea and virulence properties of diarrhoeagenic escherichia coli among patients and health subject in Southeast, Nigeria. J Health Popul Nutr
20.Ifeanyi CIC, Ikeneche NK, Bassey EB, et al. Diarrheagenic escherichia coli pathotypes isolated from children with diarrhea in the Federal Capital Territory Abuja, Nigeria. J Infect Dev Ctries.
21.Huilan S, Zhen LG, Mathan MM, et al. Etiology of acute
Bull World Health Organ
22.Okeke IN, Lamikanra A, Steinruck H, Kaper JB. Characterization of escherichia coli strains from cases of childhood diarrhea in provincial southwestern Nigeria. J Clin Microbiol
23.Okeke IN, Lamikaran A, Edelman R. (1999). Socioeconomic and behavioural factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerg Infect Dis
24.Abbott SL, Hanson DF, Felland TD, et al. Escherichia
panels. J Clin Microbiol
25.Raji MA, Minga UM, Machang’u RS. Prevalence and characterization of verotocytoxin producing escherichia coli O157 from diarrhoea patients in Morogoro, Tanzania. Tanzan J Health Res
26.Ojeda A, Prado V, Martinez J, et al. Sorbitol-negative phenotype among enterohemorrhagic escherichia coli J
Clin Microbiol
27.Dahiru M, Uraih N, Enabulele SA, Shamsudeen U.
beef in Kano City, Nigeria. Bayero J Pure Appl Sci
28.Petri WA Jr, Miller M, Brinder HJ, Levine MM, Dillingham R, Guerrant RL. Enteric infections, diarrhea, and their impact on function and development. J Clin Invest. 1277–1290.
29.
Sci
J Vet
distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
RECENT REVIEWS
The reviews below can be accessed for their Abstracts and the NZIMLS cannot provide full access to the articles due to copyright restrictions, but full access may be available through various institution arrangements.
1.Finlay WS. What is cancer metabolism? Cell 1670-1688.
2.Mosnaim G. Asthma in adults. N Eng J Med 1023-1031.
3.Xu J, Yang P, Xue S. et al. Translating cancer genomics into challenges, and future prospects. Hum Genet 109-124.
4.Shakerdi L, Ryan A. Drug-induced hyperammonia. J Clin Path
5.Kolter R, Balaban N, Julou T. Bacteria grow swiftly and live thriftily. Curr Biol cub.2022.05.005.
6. metabolism. Signal Transduct Target Ther 10.1038/s41392-023-01380-0.
7.Yekani M, Memar MY. Immunologic biomarkers for bacterial meningitis. Clin Chim Acta cca.2023.117470.
8. infection and vaccination. Clin Chim Acta
New Zealand Journal of Medical Laboratory Science 2023 112

Chemerin: an exploitable biomarker for familial Mediterranean fever in Egyptian patients
Hala T El-Bassyouni, Hisham Megahed, Eman R Youness, Hisham A Aziz Orban, Maha M Kobesiy, Rania A Ellethy, Mina Wassef Girgiss, Adel Mohamed Ashour, Ahmed Helal El Sayed and Moushira E Zaki
ABSTRACT
Aim
in Familial Mediterranean Fever patients.
Methods
Chemerin, vitamin D3
Results
lower in Familial Mediterranean Fever patients.
Conclusion status in the Familial Mediterranean Fever patients and may facilitate the development of Chemerin as a new therapeutic modality in the treatment of Familial Mediterranean Fever. Furthermore, vitamin D supplementation is recommended in the Familial Mediterranean Fever patients.
Keywords 3
NZ J Med Lab Sci 2023; 77(3): 114-118
INTRODUCTION
Familial Mediterranean Fever (FMF) is a chronic systemic
(1). It is an inherited autosomal recessive trait associated with missense mutation in the MEFV gene located on the short arm of chromosome 16 (2). The MEFV gene encodes the protein pyrin-
MEFV gene mutation leads to loss of Pyrin function resulting in
Activated platelets in FMF patients react with neutrophils (4). The MEFV mutations are responsible for dysregulation of
and interleukin-1-beta. Accordingly, FMF has self-limited febrile attacks of polyserositis, followed by free periods. However, during the symptom-free intervals, FMF patients have subclinical atherosclerosis are facilitated by this mechanism.
sex and age served as a control group. All patients were recruited from the Clinical Genetics Department, National Research Centre (NRC). This study received ethical approval from the Al-
the Declaration of Helsinki of the World Medical Association. After receiving a thorough explanation of the study, each participant and legal guardian in the study also signed a written informed consent agreement. All the datasets used and/or analysed during the current study are available from the corresponding author (Hala T El-Bassyouni) upon reasonable request.
Anthropometry
The International Biological Programme (IBP) was followed for the anthropometric measures. Tanita’s SC-330 body composition analyser evaluated fat mass (9).
Biochemical examinations
Total cholesterol (TC) and triglycerides (TG) in serum were assessed. Also, high-density lipoprotein cholesterol (HDL cholesterol) was assessed using an automatic biochemistry analyzer (Olympus America Inc., Centre Valley, Pennsylvania, USA), and the Friedewald algorithm was used to calculate lowdensity lipoprotein cholesterol (LDL cholesterol) (Olympus and Beckman Coulter).
5(OH) vitamin D3
linked immunosorbent assay (ELISA) (DiaSorin 25-OHD assay, still water, Minnesota, USA) (10).
than those of healthy controls and the expression of Chemerin in serum is positively correlated with the erythrocyte sedimentation rate (ESR) and C-reactive protein levels (7). Moreover, Chemerin is mainly related to regulating adipogenesis and the progression of atherosclerosis (8). Therefore, Chemerin can be used as a
The aim of the study is to highlight the role of Chemerin in FMF
SUBJECTS AND METHODS
Subjects
Our research comprised 66 patients diagnosed with FMF, according to the FMF criteria and 60 healthy children matching
immunosorbent assay (ELISA) assay produced by Sinogeneclon Biotech, Co., Ltd. China, catalogue No.SG-10381 (7).
Serum Oxidized LDL was determined in by enzyme-linked immunosorbent assay (ELISA) assay produced by Sinogeneclon Biotech, Co., Ltd. China, catalogue No.SG-11266 (11).
Amyloid A was determined by enzyme-linked immunosorbent assay (ELISA) assay produced by Sunlong Biotech Co., Ltd. China, catalog No.SL 1571Hu (12).
ORIGINAL ARTICLE
New Zealand Journal of Medical Laboratory Science 2023 114
Molecular analysis
Peripheral blood sample of 3mL volume was collected from all participants in EDTA tubes and DNA was extracted from white blood cells using PREP-MP Genetics kit (MP Biomedicals,
equal to 1.0ng per reaction.
Familial Mediterranean Fever Real-Time PCR Genotyping Kit (DNA Technology, Mosco, Russia) was used for mutation
480 Instrument (Software Version 1.2.9.11, Roche) according to the manufacturer’s instructions. Exons 2, 3, 5 and 10 were
elongation for 30 seconds. The 13 gene variants analysed with E148Q in exon 2, P369S and R408Q in exon 3, F479L in exon 5, and M694V, M694I, M680IG/C, M680IG/A, I692del, V726A, A744S, K695R and R761H in exon 10.
Statistical analysis
Statistics used to characterize the data included mean (+/SD), range, and median, or frequencies (number of cases). The Kolmogorov-Smirnov test was used to determine whether numerical data supported the normal premise. The Mann Whitney U test for independent samples was used to compare non-normal data and the student test for independent samples was used to compare numerical variables between the research groups. We
the anticipated frequency is less than 5, the CExact test was used in its place. The Spearman rank correlation equation for non-normal variables and non-linear monotonic relation was
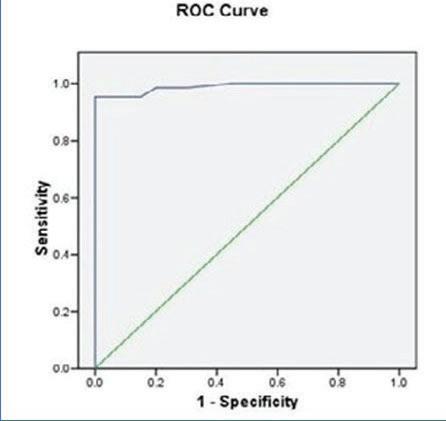
Corp., Armonk, NY, USA) release 22 for Microsoft Windows was used to perform all statistical computations. Receiver operator characteristic (ROC) curve was performed to detect the importance of Chemerin in the diagnosis of FMF.
RESULTS
The age of FMF patients ranged from 5 years to eighteen years was detected in 41.3%, while positive family history was present in 39.7%. The anthropometric measurements showed that all absolute and z-scores are within normal ranges (Table 1). Our serum Chemerin, serum amyloid A and serum lipids (cholesterol, triglycerides, and low-density lipoprotein) compared to controls (Table 2). The current study indicated that Chemerin positively inversely correlated with the high-density lipoprotein (Table 3).
correlated with vitamin D. But there was no correlation between Chemerin and Colchicine intake (Table 4).
Genetic analysis of MEFV gene in our FMF patients revealed that 39 cases showed M6941 mutations, 26 cases had M6801 mutations, and one case only showed V726A mutation. There was no correlation between Chemerin, and gene mutations except that Chemerin had a high level in the case with V726A mutation, but it was only one case (Table 5). Receiver Operator Characteristic (ROC) analysis was done to determine the best cut
Chemerin in the diagnosis of FMF (Figure 1).
Table1
ParametersFMF Weight (kg)25.5±10.1 Weight-Z score-0.38±0.03 Height (cm)122.4±21.2 Height -Z score-0.144±0.01 Head circumference (cm)51.4±2.5 Head circumference Z score-0.21±0.49 BMI (kg/m2)17.53±8.62 BMI-Z score-0.26±0.01
FMF (n=66) Controls (n=60) p-value Chemerin (nmol/L)76.3±16.956.2±5.40.05 35.2±22.210.3±17.40.01 Vitamin D (nmol/L)21.2±2.124.8±1.70.01 Cholesterol (mmol/L)114.8±14.7103.4±8.40.1 Triglycerides (mmol/L)113.6±34.578.8±9.50.01 High density lipoprotein (HDL) (mmol/L)40.9±6.755.4±5.70.01 Low density lipoprotein (LDL) (mmol/L)50.4±13.918.9±6.90.01 New Zealand Journal of Medical Laboratory Science 2023 115
Table 2
3 CorrelationsCholTGsHDLLDL Spearman’s rhoChemerin -0.32-0.16-0.270.14 p value0.010.210.030.25 N66666666
Table
Vit. D -0.24 p value0.05 Colchicine -0.21 p value0.11 Chemerin ESR 0.3 p value0.02 Serum Amyloid A 0.37 p value0.002
Table 4
Table 5
Number of Mutations MutationVariantPatient Number MeanStd DevMedianMinMax M680I2040 G>C & 2040 G>A 2686.6514.018867110 M694I2082 G>A 3982.2616.727859120 V726A2177 T>C 1112-112112112 New Zealand Journal of Medical Laboratory Science 2023 116
MEFV gene mutations in FMF cohort patients
hyperactivation and increased atherosclerotic burden (13).
between the atherogenic factors in the form of total cholesterol, total triglycerides and low-density lipoprotein in FMF patients, while there was an inverse correlation of the high-density lipoprotein amongst the FMF patients compared to normal 14). While Tasliyurt et al. did not detect an increase in the lipid both physiologic and pathophysiologic processes, according to recent investigations (16, 6). Chemerin and its receptor CMKLR1 form a complex which is implicated in the regulation of immune of pre-adipocytes (17). Additionally, Chemerin contributes to the
report, the Chemerin level showed positive correlation with the ESR and serum amyloid A level amongst the FMF patients, which is similar to former reports (21, 22). The increased concentration of Chemerin in adipose tissue causes recruitment of immune amyloid A (23). Moreover, Chemerin highly positively correlated to total cholesterol and negatively correlated with HDL in the cholesterol, triglyceride and LDL and negative correlation with HDL. The HDL function reverses the cholesterol transmission and prevents the LDL oxidation accordingly diminishing its atherogenic activity (25). Chemerin is suggested to play a role in the regulation of the enzyme responsible for lipid metabolism by diminishing the gathering of adenosine cyclic monophosphate (CAMP) and stimulates the calcium release in the adipocytes (6). The current research revealed no correlation between Chemerin and colchicine intake. Moreover, no association was detected between the Chemerin level and M6941 and M6801 mutations while a high level of Chemerin was reported in the patient with V726A mutation. Similarly, earlier research found that high V726A allele (26). While a previous study reported that patients with V726A mutations were related to the mild form of the disease, this is in contrary to our results, but this may be due to the presence of only one patient with V726A mutation (27). Furthermore, low vitamin D levels were determined among the FMF patients.
Therefore, we recommend vitamin D supplementation to these patients.
In addition, the ROC analysis was done to determine the best limitation is the small sample size and only one case showed V726A mutation.
CONCLUSION
status in the FMF patients and may facilitate the development of Chemerin as a new therapeutic modality in the treatment of FMF. It is recommended that a follow-up study be conducted to
Chemerin levels in FMF patients low. In addition, vitamin D supplementation is recommended for FMF patients.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
AUTHOR INFORMATION
Hala T El-Bassyouni, MD, Professor of Clinical Genetics1
Hisham Megahed, MD, Professor of Clinical Genetics1
Eman R. Youness, MD, Professor of Medical Biochemistry2
Hisham A. Aziz Orban, MD, Assistant Professor of Medical Biochemistry2
Maha M Kobesiy, PhD, Researcher at Molecular and Enzymology Department3
Rania A. Ellethy, PhD, Lecturer at Chemistry Department4
Mina Wassef Girgiss, PhD, Assistant Professor at Medical Department5
Adel Mohamed Ashour, MD, Professor of Clinical Genetics1
Ahmed Helal El Sayed, PhD, Professor at Pediatric Department6
Moushira E Zaki, PhD, Professor of Human Genetics7
1Clinical Genetics Department, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt.
2Medical Biochemistry Department, Medical Research and Clinical Studies Institute, National Research Centre, Cairo, Egypt
3Molecular and Enzymology Department, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt
4Chemistry Department, Faculty of Science, Helwan University, Cairo, Egypt.
5Medical Department, Medical Research and Clinical Studies Institute, National Research Centre, Cairo, Egypt.
6Pediatric Department, Faculty of Medicine for Boys, Al-Azhar University, Cairo, Egypt.
7Biological Anthropology Department, Medical Research Division, National Research Centre, Cairo, Egypt
Correspondence
Email
REFERENCES
1.Mahmoud SSE, Ismail NA, Farag YM, et al. Intima media thickness as an early predictor of atherosclerosis in Egyptian children with familial Mediterranean fever. Arch Med Sci Atheroscler Dis
2.
3.
lessons from the study of familial mediterranean fever. J Autoimmun
Mediterranean fever and in heterozygous carriers of MEFV mutations. Rheumatology (Oxford)
4.Bakogiannis C, Sachse M, Stamatelopoulos K, et al. PlateletCytokine
5.Zekry ME, Sallam AM, AbdelHamid SG, et al. Genetic and Epigenetic Regulation of MEFV gene and their impact on fever patients. Curr Issues Mol Biol
6. diseases. Clin Chim Acta
7.Lehrke M, Becker A, Greif M, et al. Chemerin is associated metabolic syndrome but does not predict coronary atherosclerosis. Eur J Endocrinol
8.Sun JX, Zhang C, Cheng ZB, et al. Chemerin in atherosclerosis. Clin Chim Acta
9.Leite Portella D, Arruda M, Gómez-Campos R, et al. Physical growth and biological maturation of children and Ann Nutr Metab
10.Lotfy HM, Marzouk H, Farag Y, et al. Serum vitamin D level in Egyptian children with familial mediterranean fever. Immunol Lett
11.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin
DISCUSSION
New Zealand Journal of Medical Laboratory Science 2023 117
Chem
12.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol
13.Ozalper V, Kara M, Tanoglu A, et al. Evaluation of endothelial dysfunction in patients with familial mediterranean
dimethylarginine and endocan with carotid intima-media thickness and endothelium-dependent vasodilation. Clin Rheumatol
14.Mohamed R, El-Bassyouni HT, Elwan HS, et al. Carotid vitamin D status in children with familial mediterranean fever. Egyptian Rheumatologist
15.Tasliyurt, T, Gokce, E, Sahin, S, et al. Prevalence of nonalcoholic fatty liver disease in familial mediterranean fever. Endocr Metab Immune Disord Drug Targets 952-958.
16.
pulmonary disease and pulmonary rehabilitation. Biomed Res Int
17.Fischer TF, Czerniak AS, Weiß T, et al. Ligand-binding and -scavenging of the Chemerin receptor GPR1. Cell Mol Life Sci
18.Acewicz M, Kasacka I. Chemerin activity in selected pathological states of human body - a systematic review. Adv Med Sci
19.Gonzalez-Ponce F, Gamez-Nava JI, Perez-Guerrero EE, et PLoS ONE
20.Macvanin MT, Rizzo M, Radovanovic J, et al. Role of Chemerin in cardiovascular diseases. Biomedicines
21.Vazquez-Villegas ML, Gamez-Nava JI, Saldaña-Cruz AM, et al. Functional disability is related to serum Chemerin levels in rheumatoid arthritis. Sci Rep
22.Kolahdouzi S, Baghadam M, Kani-Golzar FA, et al. biomarkers and insulin resistance in obese men. Physiol Behav
23.Szpakowicz A, Szpakowicz M, Lapinska M, et al. Serum status in chronic coronary syndrome. Biomolecules
24.
Genes Dis
25.Duan H, Song P, Li R, et al. Attenuating lipid metabolism in low-density lipoprotein of herbal medicines. Front Pharmacol
26.Lofty HM, Marzouk H, Farag Y, et al. Serum amyloid a level in Egyptian children with familial mediterranean fever. Int J Rheumatol
27.
28.
Ital J Pediatr
amelioration of the clinical status and cognitive functions of familial mediterranean fever patients. Kobe J Med Sci
29.Abdallah HR, Thomas MM, Abuelhamd WA, et al. The presentation, body mass index, and osteoprotegerin (OPG) level in a sample of Egyptian children with familial Mediterranean fever. Egypt Pediatric Association Gazette
distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
• Have been a member of the New Zealand Institute of Medical Laboratory Science (Inc) for a minimum period of two years
• Are currently employed in an IANZ accredited Laboratory
• report, to be in the hands of the NZIMLS Journal Editor within 12 months of completion of the project for consideration of publication
• The decision of the NZIMLS Council on the awarding entered into
• The Application Form is available from www.nzimls. org.nz and must be fully completed
New Zealand Journal of Medical Laboratory Science 2023 118

New Zealand Journal of Medical Laboratory Science 2023 119
among Egyptian obese premenopausal women: a cross-sectional study
Moushira Zaki, Wafaa Kandeel and Eman Refaat Youness
ABSTRACT
Background
ethnic groups.
Objective
Methods
were divided into an insulin resistance (IR) group and a non-insulin resistance group, using homeostasis model assessment (HOMA). A receiver operating characteristic (ROC) analysis was conducted to evaluate the ability of the developed clinical prediction rule to correctly discriminate between subjects of insulin resistance (IR) positive and insulin resistance negative groups.
Results
Conclusion
resistance among premenopausal obese women.
Keywords
NZ J Med Lab Sci 2023; 77(3): 120-123
INTRODUCTION
The most prevalent aspect of obesity, insulin resistance (IR), progression of cardiovascular disease and diabetes mellitus (DM) (1–3). Despite insulin’s normal or elevated blood levels, insulin resistance is a condition of glucose homeostasis characterized by a diminished sensitivity of the liver, adipose tissue, muscles and other body tissues to the hormone(4). The hyperinsulinemic euglycemic clamp is the gold standard technique for measuring IR. However, the complexity and high cost of the test has prevented its use in daily clinical practice and in epidemiological studies(5). As a substitute, the homeostasis model assessment for insulin resistance (HOMA-IR) index is frequently utilized to gauge insulin resistance in adults. The measurements of plasma fasting insulin and glucose are necessary for the HOMA calculations. A simple diagnostic procedure that can identify insulin resistance is required, which provides good precision, is inexpensive and a routine test for triglycerides (TG) and HDL-C is less expensive than an insulin test. Currently, portable analysers
utility of the triglyceride to HDL-C ratio (TG/HDL-C ratio) as a predictor or marker of IR and its ethnic dependence have been
levels increased whereas HDL-C levels decreased in people with insulin resistance. An alternate method for determining insulin resistance is presented in the current work, using a lipoprotein cholesterol (TG/HDL-C) (9). The TG/HDL-C ratio of resistance in previous studies (10). TG/HDL-C ratio has been recognized as a simple clinical indicator of IR and a predictor of diabetes (11) and coronary heart disease (9). In a previous study, the TG/HDL-C ratio and HOMA-IR in obese children were
The goal of the current study was to evaluate whether the use of the TG/HDL-C can identify IR among the middle-aged Egyptian women and assess its clinical utility.
METHODS
Two hundred and twenty obese women between ages of 30 and 35 years were recruited from the obesity clinic, National Research Centre. Written informed consent was gained from each woman after a complete description of the study. The research has been authorized by the Ethical Committee of National Research Centre, Egypt (number = 16361), in accordance with the World Medical Association’s Declaration of Helsinki.
These subjects underwent a detailed clinical, biochemical and hormonal evaluation and were found to be free of any systemic illness. HOMA-IR was calculated by fasting glucose (mmol/L) × fasting insulin (mU/mL)/22.5. HOMA-IR was used to identifying those with insulin resistance (13, 14).
Anthropometric examinations
All patients and controls underwent thorough clinical examinations and medical histories. Weight in kilograms divided by height in square metres (kg/m2) is used to calculate Body Mass Index (BMI). A plastic, non-stretchable tailor’s tape, the circumferences of the hips and the waist have been measured in centimetres (cm). The Waist-to-Hip-Ratio (WHR) was then determined by dividing the waist circumference (WC) by the hip circumference (HC). The measurements’ complete description has been provided elsewhere (15).
Exclusion criteria
Women with other chronic illnesses, with type 2 diabetes mellitus, gestational diabetes mellitus, thyroid disease history, heart, hepatic, and muscular problems and those with irregular cycles also were not included.
Statistical analysis
The statistical analyses were conducted using SPSS version 20.0 (SPSS Inc. Chicago, USA). The information is displayed as mean standard deviation. The independent student t-test was used to assess all parametric data in categorical groups. The use of TG/HDL-C and the presence or absence of IR allowed for the plotting of receiver operator characteristic (ROC) curves. Using calculate Youden’s index. The highest Youden’s index value was
RESULTS
Table 1 demonstrates the basic participant characteristics as
increase of WC, HC, WHR and diastolic blood pressure (referred to as DBP and SBP) levels was observed in IR positive group compared to IR negative group. As shown in Table 2, the ideal
ORIGINAL ARTICLE
New Zealand Journal of Medical Laboratory Science 2023 120
The ROC curve for TG/HDL-C as a predictor for HOMA-IR index is shown in Figure 1. The HOMA-IR index was predicted
value to use for predicting the HOMA-IR index using the TG/ HDL-C ratio. In addition, it had the highest diagnostic accuracy and positive predictive value. The point with the shortest distance
value from the point (0,1) has a Youden index of [sensitivitydetermined (16). The positive probability ratio (PLR), which compares the likelihood of individuals with the disease to have a certain test result to those of patients without the disease, determine PLR.
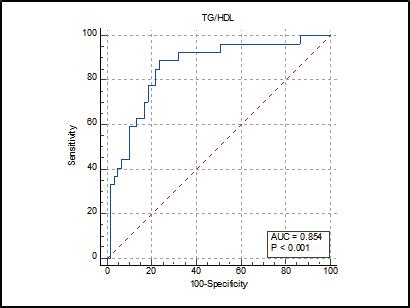 Table 1. Clinical characteristics of IR positive and IR negative participants
Table 1. Clinical characteristics of IR positive and IR negative participants
TG/HDL Sensitivity % (95% CI) (95% CI) +LR +PV (95% CI) AUC (95% CI) Youden index 3.39 88.89 (57.7-91.4) 76.27 (69.1- 90.3)4.17 65.6 (51.9 - 77.1) 0.854 (0.762- 0.921) 0.87 (0.76- 0.92
Table 2.
IR NegativeIR PositiveP-value Age (years)33.44±2.4531.41±2.350.65 BMI (kg/m2)29.67±9.8832.83±10.120.06 MUAC (cm)28.35±7.6535.91±8.230.07 WC (cm)79.88±10.8189.54±12.990.01 HC (cm)94.59±9.78105.77±10.110.01 WHR0.76±0.660.84±0.990.03 SBP (mmHg)139.8±11.8159.8±12.80.02 DBP (mmHg)84.5±5.9595.5±9.910.02 New Zealand Journal of Medical Laboratory Science 2023 121
Figure 1. ROC curve for TG/HDL-C marker for IR among obese women
DISCUSSION
The adipose tissue captures and maintains less fatty acid in IR condition, which is the mechanism of high TG and low HDL-C (17). As a result, more free fatty acids are delivered to the liver, where they are used to produce more TG and TG-containing very low-density lipoproteins (VLDL). In addition, as the plasma TG concentration rises, the TG content of TG-containing VLDL and the cholesteryl ester of HDL-C exchange. The TG-rich HDL-C that results from this process is easily metabolized (18). As a result, IR patients have a high TG, high TG/HDL-C, and low HDL-C levels (18). According to several research, the TG, rather than factors such the TG/HDL-C index, visceral adiposity index, leptin, Apo-B/Apo-AI, and lipid parameters, more accurately predicts HOMA-IR values (18,19). TG levels are elevated whereas HDL-C levels diminished in people with insulin resistance (2,10,19). A higher ratio would indicate a worsening state of health since there are more fats circulating in the blood and/or less good cholesterol. Insulin resistance has been proven to be closely demonstrated that among Iranian men, the TG/HDL-C ratio represents a distinct risk factor for coronary heart disease(20). A prior research among healthy Spanish children indicated that both girls and boys HOMA-IR gradually increased with age (21). While the association between WHR and HOMA-IR was weak, HOMA-IR had strong relationships with BMI, WC, and WHR. seen in other research, including one from India (22–24). In other work, WHR has also been demonstrated that strongly correlated
by HOMA-IR) in middle-aged Egyptian women is strongly correlated with the TG/HDL-C ratio (26). Adipose tissue traps and retains less fatty acid in IR condition, which is the cause of high TG and low HDL-C (27,28). The present optimal threshold
and 76.27% in middle-aged obese women, we concluded that TG/HDL-C is a suitable marker that can be utilized alone for IR assessment. Another study suggested that middle-aged and elderly Taiwanese might detect IR just using the TG/HDL-C ratio (29, 31). A study of 812 Taiwanese adults (31) demonstrated that models incorporating the TG/HDL-C ratio, sex, larger waist values of the TG/HDL-C ratio had been reported in other studies
28). Previously, TG/HDL-C ratio was used as a predictor of IR in cross-sectional research of 258 participants. Previously, the TG/HDL-C ratio was studied that predict metabolic syndrome in overweight individuals (19). However, other cross-sectional cohort of 90 overweight African Americans (32) reported that the TG/HDL-C ratio was not reliable marker for IR.
A limitation of this study is that the blood samples of all women were not collected at the same point of the menstrual cycle.
CONCLUSION
In conclusion, our results demonstrate that the elevated TG/ as an indicator of IR amongst the middle-aged Egyptian obese women and might be a useful tool to recognize high risk individuals for early intervention and thereby delay or prevent the onset of IR-related illnesses such as hypertension and type 2 diabetes.
AUTHOR INFORMATION
Moushira Zaki, PhD, Professor of Human Genetics1
Wafaa Kandeel, PhD, Professor of Biological Anthropology1
Eman Refaat Youness, PhD, Professor of Medical Biochemistry2
1Biological Anthropology Department, Medical Research and Clinical Studies Institute, National Research Centre, Cairo, Egypt.
2Medical Biochemistry Department, Medical Research and Clinical Studies Institute, National Research Centre, Cairo, Egypt.
Correspondence
REFERENCES
1.Xin Z, Yuan J, Hua L, et al. A simple tool detected diabetes and prediabetes in rural Chinese. J Clin Epidemiol
2.Wang H, Wang C, Xuan X, et al. Association between triglyceride to high-density lipoprotein cholesterol ratio and type 2 diabetes risk in Japanese. Sci Rep
3.Fu Q, Zhang Z, Hu W, Yang Y. The correlation of triglyceride/ high-density lipoprotein cholesterol ratio with muscle mass in type 2 diabetes patients. BMC Endocr Disord 1-5.
4.Gierach M, Gierach J, Junik R. Insulin resistance and thyroid disorders. Endokrynol Pol
5.Kim-Dorner S-J, Deuster PA, Zeno SA, et al. Should triglycerides and the triglycerides to high-density lipoprotein cholesterol ratio be used as surrogates for insulin resistance? Metabolism
6.Gianotti G, Cenni A, Bianchi G, et al. Diastolic dysfunction with NAFLD? Arch Gerontol Geriatr
7.Kang H-T, Yoon J-H, Kim J-Y, et al. The association between the ratio of triglyceride to HDL-C and insulin resistance according to waist circumference in a rural Korean population. Nutr Metab Cardiovasc Dis 1060.
8.Olusi SO. Obesity is an independent risk factor for plasma lipid peroxidation and depletion of erythrocyte cytoprotectic enzymes in humans. Int J Obes Relat Metab Disord
9.Kannel WB, Vasan RS, Keyes MJ, et al. Usefulness of the triglyceride–high-density lipoprotein versus the cholesterol–high-density lipoprotein ratio for predicting insulin resistance cohort). Am J Cardiol
10.McLaughlin T, Abbasi F, Cheal K, et al. Use of metabolic markers to identify overweight individuals who are insulin resistant. Ann Intern Med
11.Hadaegh F, Hatami M, Tohidi M, et al. Lipid ratios and of Iranian men and women. Lipids Health Dis 1–9.
12.Behiry EG, El Nady NM, AbdEl Haie OM, et al. Evaluation of TG/HDL-C ratio Instead of HOMA ratio as insulin resistance marker in overweight and children with obesity. Endocr Metab Immune Disord Drug Targets
13. resistance using HOMA-IR for Americans of Mexican descent using machine learning. PLoS One e21041.
14.Madeira FB, Silva AA, Veloso HF, et al. Normal weight obesity is associated with metabolic syndrome and insulin resistance. PLoS One
15.Zaki M, Kholoussi S, Ismail S, et al. Metabolic abnormalities in young Egyptian women with polycystic ovary syndrome and their relation to ADIPOQ gene variants and body fat phenotype. Egypt J Med Hum Genet
16.Martin BC, Warram JH, Krolewski AS, et al. Role of glucose and insulin resistance in development of type 2 diabetes Lancet
17.Fazakerley DJ, Krycer JR, Kearney AL, et al. Muscle mechanism? J Lipid Res
18.Kolovou GD, Anagnostopoulou KK, Cokkinos DV.
New Zealand Journal of Medical Laboratory Science 2023 122
Pathophysiology of dyslipidaemia in the metabolic syndrome. Postgrad Med J
19.Kosmas CE, Rodriguez Polanco S, Bousvarou MD, et al. The triglyceride/high-density lipoprotein cholesterol (TG/ HDL-C) ratio as a risk marker for metabolic syndrome and cardiovascular disease. Diagnostics (Basel) 929.
20.Hadaegh F, Khalili D, Ghasemi A, et al. Triglyceride/HDLcholesterol ratio is an independent predictor for coronary heart disease in a population of Iranian men. Nutr Metab Cardiovasc Dis
21.García Cuartero B, García Lacalle C, Jiménez Lobo C, et al. The HOMA and QUICKI indexes, and insulin and C-peptide
An Pediatr (Barc)
22.Hirschler V, Aranda C, de Luján Calcagno M, et al. Can waist circumference identify children with the metabolic syndrome? Arch Pediatr Adolesc Med 744.
23.Bitsori M, Linardakis M, Tabakaki M, Kafatos A. Waist adolescents with the metabolic syndrome phenotype. Int J Pediatr Obes
24.Ren X, Chen ZA, Zheng S, et al. Association between triglyceride to HDL-C ratio (TG/HDL-C) and insulin resistance in Chinese patients with newly diagnosed type 2 diabetes mellitus. PLoS One
25.Kondaki K, Grammatikaki E, Pavón DJ, et al. Comparison of several anthropometric indices with insulin resistance Study. Eur J Pediatr
26.Hegab WS, Omar GA, Hussein MA. Assessment of the eligibility of triglyceride–glucose index and triglyceride–highdensity lipoprotein cholesterol ratio as applicable insulin resistance indices among overweight/obese Egyptians. J Med Sci Res
27.
ratio as insulin resistance marker for metabolic syndrome in children with obesity. Front Endocrinol (Lausanne)
28.Yeh W-C, Tsao Y-C, Li W-C, et al. Elevated triglyceride-toHDL cholesterol ratio is an indicator for insulin resistance sectional study. Lipids Health Dis
29.Yen SSC. The polycystic ovary syndrome. Clin Endocrinol (Oxf)
30.Sheikh A. Polycystic ovary syndrome and metabolic Edition, Elsevier
31.Chiang J-K, Lai N-S, Chang J-K, Koo M. Predicting insulin resistance using the triglyceride-to-high-density lipoprotein cholesterol ratio in Taiwanese adults. Cardiovasc Diabetol
32.Sumner AE, Finley KB, Genovese DJ, et al. Fasting triglyceride and the triglyceride–HDL cholesterol ratio are not markers of insulin resistance in African Americans. Arch Intern Med
distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Advertise your company in the NZIMLS Journal of Medical Laboratory Science
The Journal is distributed free to all members of the NZIMLS, which at present numbers approximately 3,000. This means that the Journal is read by most medical laboratory scientists and technicians and enters all hospital and community medical laboratories in New Zealand. It is also sent to members employed in commercial and veterinary laboratories as well as some government establishments, and a few are sent to members overseas.
New Zealand Journal of Medical Laboratory Science 2023 123
Comparison of the BD Max™ vaginal panel, against standard methods, for the detection of common vaginitis conditions
Julie A Creighton and Bethany J Mills
ABSTRACT
Objectives Trichomonas vaginalis infections are common causes of vaginitis to compare the performance of the BD MAX™ Vaginal Panel (MAX VP), a qualitative molecular test against routine laboratory procedures for the detection of these conditions. The primary focus was for the detection of bacterial vaginosis as Gram stain assessment is a particularly challenging area for microbiology laboratories, due to subjective interpretation.
Methods
included in the study. Routine methods including Gram stain and culture were performed before the swabs were transferred into
Results
diagnosis of T. vaginalis
Conclusion
diagnosis BV, candidiasis and T. vaginalis and correlated well with Gram stain interpretation. The overall results of our study are in line with other evaluations of BD MAX™ Vaginal Panel. We suggest that BD MAX™ Vaginal Panel would be a useful adjunct to Gram stain testing when the Gram is inconclusive or indeterminate.
Keywords Trichomonas vaginalis, molecular test, BD MAX™ Vaginal Panel.
NZ J Med Lab Sci 2023; 77(3): 124-127
INTRODUCTION
Vaginal swab analysis, commonly including culture and Gram stain, represents one of the high-volume sample processes in a clinical microbiology laboratory. The laboratory receives samples from both symptomatic and asymptomatic women. Vaginitis and vaginal discharge conditions are frequent complaints among women, especially during the reproductive years, and are most commonly caused by bacterial vaginosis (BV), vulvovaginal candidiasis, and Trichomonas vaginalis infections (1,2). Sexually transmitted infectious agents such as Neisseria gonorrhoeae and Chlamydia trachomatis can also be responsible for abnormal vaginal discharge, as can non-infectious syndromes such as cytolytic vaginosis, atrophic vaginosis and desquamative vaginitis. In addition to vaginal discharge investigations, the laboratory receives vaginal swabs for antenatal screening, rupture of membranes, post-partum infections, and sexualarray of clinical settings.
characterised by a predominance of aerobic lactobacilli, including Lactobacillus crispatus, L. jensenii and L. gasseri, which helps to confer a protective environment against the development of BV partly due to the production of lactic acid and hydrogen peroxide. In contrast, symptomatic BV is associated with a reduction or absence of lactobacilli with a corresponding increase of a diverse group of facultative and anaerobic bacteria, most frequently including Gardnerella vaginalis, Atopobium vaginae, BV-associated bacterium-2 (BVAB-2), Prevotella species and Megasphaera-1 (2,3). G. vaginalis is the precursor vaginal epithelial cells, and may contribute to therapy resilience and BV recurrence (2).
Diagnosis of vaginitis consists of a physical examination by a clinician, followed by laboratory analysis of a vaginal swab. Bacterial vaginosis has the highest prevalence in vaginitis, ranging from 6% - 60%, depending on the population studied (3,4). BV can be asymptomatic in many women, perhaps
hormonal cycle, rather than a true dysbiosis (3). Gram stain testing of vaginal smears, is low cost and only requires a microscope, has become the standard for diagnosing BV (2). However, Gram stain interpretation can be subjective, even with an experienced operator, and the correct distinction of bacterial morphotypes
collected after a physical examination may contain gel lubricant residue which can result in very poor-staining smears, often
especially if they require review by one or more senior scientist.
The diagnosis of a Candida infection consists of Gram stain and culture for yeasts on selective media such as chromogenic Candida agar or Sabouraud-Dextrose Agar. Gram stain analysis for yeast cells and pseudohyphae can be insensitive and yeast presence of yeast, either found in a Gram stain or from culture, asymptomatic vaginal colonisation by Candida species can be found in 20% of women (1).
T.vaginalis is a sexually transmitted protozoan parasite,
Laboratory diagnosis of T. vaginalis can range from an insensitive, but low-cost, wet-mount microscopy analysis, to more sensitive but progressively more expensive assays such as immunochromatographic rapid antigen strips or nucleic acid
As an alternative to Gram stain or wet-mount, molecular analysis of the vaginal microbiome is non-subjective and rapid, potentially enabling an improved service for the clinicians. The BD MAX™ Vaginal Panel (MAX VP) is an automated qualitative multiplex molecular test for the direct detection of BV, Candida species (including C. albicans, C. tropicalis, C. parapsilosis, C. dubliniensis), Pichia kudriavzevii (formally known as C. krusei), C.glabrata and T. vaginalis, from vaginal swabs, performed using the BD MAX System.
The aim of this study was to compare the performance of the BD MAX™ Vaginal Panel against routine laboratory procedures for the detection of BV, Candida spp., and T. vaginalis. The primary focus was for the direct detection of BV-associated bacteria, as Gram stain assessment is a particularly challenging area for microbiology laboratories.
METHODS
Study design and setting
This comparative study was conducted at Canterbury Health Laboratories (CHL) to compare the performance of the BD MAX™ Vaginal Panel for the direct detection of BV, and to
ORIGINAL ARTICLE
New Zealand Journal of Medical Laboratory Science 2023 124
compare the Candida spp., yeast culture, and AlinityM molecular detection of Trichomonas vaginalis
Sample population and specimen selection
The study included vaginal swabs collected in Amies Transport medium and AlinityM multi-collect tubes from patients attending hospitals, sexual health clinics, and after-hours clinics in the Canterbury area. From a pool of specimens received between November to December 2022, 96 vaginal swabs in Amies Transport medium were selected for inclusion in the study. The majority of specimens were randomly selected, while approximately 20% were retrospectively included based on a Gram stain result inconclusive for BV during routine testing.
BD MAXTM Vaginal Panel and comparator methods
The BD MAX™ Vaginal Panel (MAX VP) is a qualitative
(Gardnerella vaginalis, Atopobium vaginae, BV-associated bacterium-2 (BVAB-2) and Megasphaera-1), Candida spp., and T.vaginalis. Testing of the vaginal swabs in Amies Transport medium with the BD MAX Vaginal Panel was performed following completion of routine laboratory procedures, including a Gram stain and culture on Sabouraud-Dextrose Agar. At is used for Gram stain diagnosis of BV (5). A selective protocol is enforced for testing of T. vaginalis, with diagnosis made by swabs, therefore only 27/96 samples were available for the comparison of T. vaginalis detection, which limited our ability to fully evaluate the performance of MAX VP. As vaginal swabs at the time of collection, the vaginal swabs were transferred from
refrigerated overnight and vortexed again. Testing of samples was then performed on the BD MAX System, in line with the instructions provided in the MAX VP package insert.
Interpretation of results and statistical methods
The performance of the MAX VP was determined based on concordance with results obtained by Gram staining analysis, yeast culture, and AlinityM T. vaginalis NAAT. For the purpose by the presence of classic or indeterminate/intermediate BV
classed as BV negative. In some instances, re-evaluation of a Gram stain was triggered by discordance between the reported was determined using the above criteria under the guidance of an experienced Senior Scientist. Where the initial recorded decision, a false positive or negative Gram stain result was recorded for statistical analysis. A true Candida positive result positive T. vaginalis by a positive AlinityM NAAT result. It is of note that routine testing for T. vaginalis is only performed on highrisk patients or on request and so there was limited data on the true T. vaginalis rates of the 96 samples collected. Using these
positive predictive value, and negative predictive values for both the BD MAX™ Vaginal Panel and Gram stain analysis.
RESULTS
A total of 96 vaginal swabs were included in this study for the detection of BV and yeast, with a subset of 27/96 samples
available for the comparison of T. vaginalis detection. Results are shown in Table 1. MAX VP was negative for BV, Candida spp. and T. vaginalis
in 73 samples.
Overall the MAX VP performed with high sensitivity and positive predictive value (PPV) and negative predictive value (NPV) are shown in Table 2.
There were 34 (35.4%) patients determined to be a true positive VP was positive in 35 samples, which included 3 false positive results and 2 false negative results, achieving a sensitivity of determined to be a false positive and there were 4 false negative was 88.2% and 98.4%.
Regarding Candida infection, there were 25/96 (26%) patients determined to be true positives, based on a combination of culture and molecular results. Of note were two samples which were positive by MAX VP, but negative by both Gram stain and culture, but the patients had recurrent Candida infections samples were regarded as true positives. MAX VP was positive for 26 samples, which included 2 false positive results and 1 false 97.2%. Conversely, the sensitivity of Gram stain for the detection
With respect to the detection of T. vaginalis, all 96 samples performance of MAX VP, compared to AlinityM PCR, was limited to 27 samples from a subgroup of high-risk patients. Five samples returned a positive MAX VP result for the detection of T. vaginalis, compared with only 2 positive samples on the AlinityM. One case where MAX VP was positive, but AlinityM negative, immediately preceded a true positive sample and was presumed to be contaminated during processing. The AlinityM results on the two remaining samples were not able to be accessed due to selective testing for T. vaginalis. Hence, the sensitivity of MAX
Incidence of co-infection for both BV and yeast was 8.3% (8/96). Two patients who tested positive for TV also tested positive
T. vaginalis. No patients had a dual infection with yeast and T. vaginalis
DISCUSSION
Analysis of female genital samples is commonly performed in a clinical laboratory, with Gram stain interpretation considered the laboratory standard for the diagnosis of BV. However, the subjective and widely accepted challenging nature of Gram stain assessment prompted us to investigate a molecular alternative.
While there is some controversy over what constitutes a true BV disease state, the laboratory needs to alert the clinician to the possibility of BV due to the association with serious outcomes such as preterm birth, spontaneous abortion, or acquisition of sexually transmitted diseases. BV involves complex vaginal (3,6). Importantly, many of the microorganisms involved may not be culturable, easily distinguished or even seen in a Gram stain, strengthening the potential for improved diagnosis using molecular analysis.
The results of our study demonstrated that the MAX VP provided stain interpretation for the diagnosis of BV. The prevalence of BV in this study was 35.4%, which is likely higher than our routine sample baseline due to some retrospective selective sample
New Zealand Journal of Medical Laboratory Science 2023 125
Patients with Bacterial vaginosis
BV = bacterial vaginosis, TP = True Positive, FN = False Negative, TN = True Negative, FP = False Positive, PPV = Positive Predictive Value, NPV = Negative Predictive Value, ND = Not Determined.
The prevalence of Candida species group in our study was 26%, with the MAX VP achieving superior sensitivity and higher NPV compared to Gram stain. The MAX VP can separately detect and identify C. glabrata and Pichia kudriavzevii (C. krusei) from other Candida spp. While none of our samples tested positive or C. glabrata and Pichia kudriavzevii is clinically important due to their inherent
The overall results of our study are in line with other evaluations of MAX VP (1,7,8). A trial by Hillier et al, of 290 vaginal samples from symptomatic women, determined that the detection of BV by Gram stain was similar to MAX VP with frequencies of 36% and 37% respectively (1). For the detection of yeast, they found culture to be more sensitive than MAX VP, resulting in a concordance of 90% for Candida spp. Group and 98% for C. glabrata. In Hillier’s study, the incidence of T. vaginalis was 7%, returning 100% concordance between MAX VP and GeneXpert PCR. The authors concluded that the utilisation of standardised testing, as provided by MAX VP, would improve patient care compared to in-clinic diagnosis of vaginitis.
Schwebke et al, compared the performance of MAX VP against a clinician’s assessment and various in-clinic tests for the diagnosis of vaginitis attributed to BV, Candida spp. And T. vaginalis prevalence rates of BV 58%, Candida spp. 32% and T. vaginalis 8%, the MAX VP out-performed clinical assessment, especially with multiple-cause vaginitis, achieving high rates of sensitivity
The Ison-Hay’s Gram stain method for BV diagnosis was also used in a United Kingdom study of 196 symptomatic women
attending a sexual health service (8). MAX VP was compared to standard tests, revealing a high sensitivity of 94.4% for the authors attributed to possible vaginal dysbiosis due to a high rate of sexually transmitted diseases in the study group. The Candida species was 86.4% and 86.0% respectively. The lower performance level for Candida spp. Was considered to be due to asymptomatic colonisation.
particularly for the diagnosis of BV, may be best utilised when the patient is symptomatic. Molecular detection of multiple etiologicdecrease inappropriate treatment and improve patient care (1,2,7).
Limitations of this study include a lack of correlation of laboratory results against clinical diagnosis, as no clinical records were able to be accessed. The Nugent criteria is the recognised gold-standard method for the determination of BV by Gram stain. Our laboratory uses a qualitative Ison-Hay’s method, which has been found to have excellent agreement with Nugent
limitations involve those which are recognised as being intrinsic to molecular detection including non-viable organisms may test positive, the diagnosis of BV may not always be linked to a disease state, and the presence of yeast in small numbers may swabs which had already been used for routine testing, which
Result Max VP Gram (BV, Yeast) Culture (Yeast) Alinitym (T. vaginalis) BV 41 53 73 25 BV (Indeterminate)24 21 -BV + Yeast - 8 -BV + T. vaginalis 922T.vaginalis 2--Yeast 3 - - 2 BV + Yeast 17 12 21BV = bacterial vaginosis
Table 1. Results for 96 vaginal samples, showing the number of positives tests for each method.
POS =34NEG = 62 Sensitivity PPVNPV TPFNTNFP BD MAX 322593 94.1%95.2%91.4%96.7% GRAM 304611 88.2%98.4%96.8%93.8%
with Yeast POS =25NEG = 71 Sensitivity PPVNPV TPFNTNFP BD MAX 241692 96.0%97.2%92.3%98.6% GRAM 1411710 56.0%100%100%86.6%
with T. vaginalis POS =2NEG = 94 Sensitivity PPVNPV TPFNTNFP BD MAX 20913 100%NDND100%
Table 2. Performance results for BD MAX™ Vaginal Panel compared with routine testing.
Patients
Patients
New Zealand Journal of Medical Laboratory Science 2023 126
performance of MAX VP.
CONCLUSION
molecular test for the determination of BV, yeast and T. vaginalis from vaginal swabs. The test is easy to perform, can be used with vaginal swabs collected in Aimes transport medium, and is complete in approximately three hours. Clinicians should be aware that there is a potential for overdiagnosis of either BV, when a patient is transiently colonised with bacteria other than Lactobacillus species, or candidiasis, when yeast are present as commensal organisms. A Gram stain smear would still have to be examined for uncommon syndromes such as atrophic vaginitis, cytolytic vaginosis and desquamative vaginitis. Clinical when the Gram stain is inconclusive or indeterminate.
ACKNOWLEDGMENTS
used in this trial were supplied by BD.
AUTHOR INFORMATION
JulieACreighton, DipMLT, FNZIMLS, Senior Medical Laboratory Scientist1 and Clinical Lecturer2
Bethany J Mills, BMLSc, Medical Laboratory Scientist1
1Department of Microbiology, Canterbury Health Laboratories, Christchurch, New Zealand
2University of Otago, Christchurch, New Zealand.
Correspondence
Canterbury Health Laboratories email
REFERENCES
1.Hillier SL, Austin M, Macio I, et al. Diagnosis and treatment of vaginal discharge syndromes in community practice settings. Clin Infect Dis
2.Coleman JS, Gaydos CA. Molecular diagnosis of bacterial J Clin Microbiol
3.Diop K, Dufour JC, Levasseur A, Fenollar F. Exhaustive repertoire of human vaginal microbiota. Hum Microb J
4.Kenyon C, Colebunders R, Crucitti T. The global Am J Obstet Gynecol
5. stained vaginal smears for use in genitourinary medicine clinics. Sex Transm Infect
6.Srinivasan S, Morgan MT, Liu C et al. More than meets morphotypes using molecular phylogenetic analysis. PloS One
7.Schwebke JR, Gaydos CA, Nyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol
8.Sherrard J. Evaluation of the BD MAXTM Vaginal Panel for the detection of vaginal infections in a sexual health service in the UK. Int J STD AIDS
distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
BARRIE EDWARDS & ROD KENNEDY SCHOLARSHIP
Applications for this prestigious scholarship are invited from Fellows, Members and application. To be eligible applicants must make an oral presentation or present a poster

All applications will be considered by a panel consisting of senior medical laboratory scientists (who are ineligible to apply for the scholarships). The applications will be judged on the quality of the presentation and your professional and academic abilities together the decision making process. In the event of the presentation being declined by the conference organisers the successful Scholarship NZIMLS.
Evidence of travel insurance is required following all travel bookings and conference arrangements.
Application is by using the Scholarship Application form and Curriculum Vitae form. All correspondence and applications should be
Rangiora 7440
There is one scholarship awarded in each calendar year. Closing date is December 20th in any given year.
Successful applicants will be required to provide a full written report within three months on return from the conference, which will be published in the New Zealand Journal of Medical Laboratory Science. If not intending to publish elsewhere, successful applicants will be required to submit their study results for consideration by the New Zealand Journal of Medical Laboratory Science within 12 months following the conference.
Acknowledgement of the Barrie Edwards and Rod Kennedy Scholarship in both the presentation and any subsequent publication is a required condition of this award. The NZIMLS Council reserves the right to request the full conference presentation.
New Zealand Journal of Medical Laboratory Science 2023 127
Barrie Edwards Rod Kennedy
PROFESSIONAL AFFAIRS
Sue Calvert
and professional associations. This article hopes to clear up some of the confusion to support practitioners’ understanding. are established under legislation, which in the case of those the Medical Sciences Council, is the Health Practitioners Competence Assurance Act (HPCA) (2003) (1). The role of regulators is to protect the public by making sure that people their profession. The focus therefore of the regulator is the safety of the person receiving health care.
Members of the Council are appointed by the Minister of Health and are accountable to the Minister. Council members are appointed to govern the organisation, that is they are responsible for setting the organisation’s strategic direction. This is an important role as it means they are setting the direction for the
regulation for members of the profession. Each year the Council provides an annual report to the Minister that describes the work it has undertaken in relation to its obligations under the Act. Professional Associations are not established because of members. The focus of the professional association is the practitioner. The executive of the professional association is accountable to its membership.
in order to be able to practise within the medical laboratory membership of a professional association is not mandatory. Further, while the Council accredits programmes of education, its role is not to provide education to its registrants. The provision of education and programmes of ongoing competence is one of the primary purposes of the professional association. (Figure 1.)
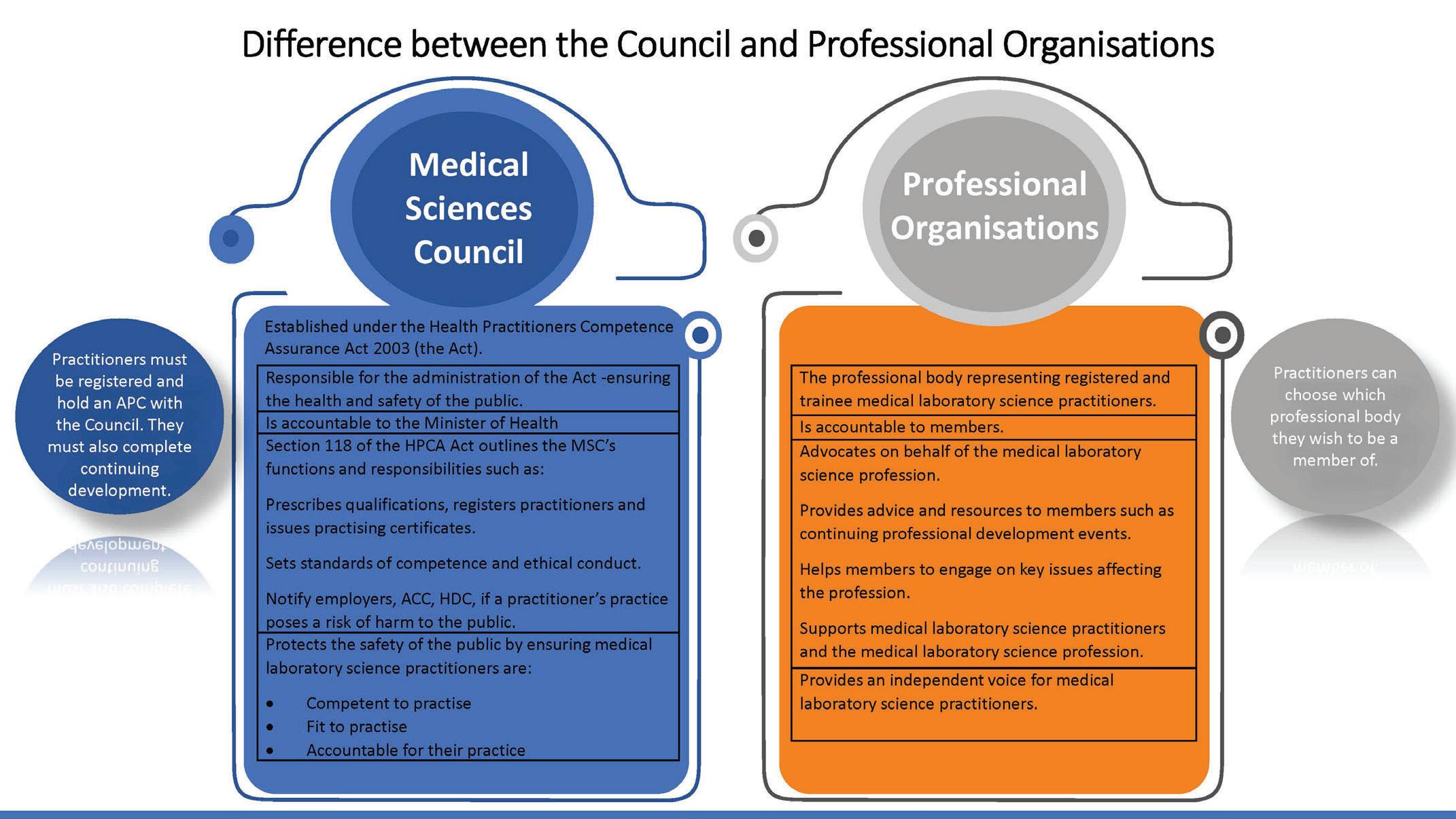
So what do regulators do?
The purpose of the Medical Sciences Council is described within the HPCA Act. The functions are clearly articulated in section
• and to accredit and monitor programmes of education. The Council does this through its approval and accreditation also monitors these programmes against the accreditation standards. As part of this work, the programmes of education that lead to entry to the register for Medical Laboratory Technicians have been approved by the Council.
• Once
education programmes. Each year practitioners must apply to work.
•To set standards of competence, cultural competence
be observed by health practitioners. This is one of the key functions of the Council and the codes and competencies are the standards against which practice is assessed.
• To set programmes of ongoing competence to be observed by members of the profession. One of the key aspects of the HPCA Act is the requirement for practitioners to be able to demonstrate their ongoing competence. The Council uses compliance with these requirements to reassure itself of the ongoing competence of practitioners. While the Council set the standards, i.e. the hours and requirements for
Figure 1.
New Zealand Journal of Medical Laboratory Science 2023 128
practitioners, it is the professional association that takes the lead in the provision of programmes of ongoing competence. As with the pre-registration programmes, the Council has also approved the association’s ongoing professional development programme as a way that its members can comply with the Council’s continuing professional development requirements.
• and to notify certain agencies if a person’s practice poses a risk of harm. While the number of complaints and large. For example, if there is a belief that a practitioner may pose a risk of serious harm because of a lack of knowledge, to practise, or because their professional behaviour may bring the profession into disrepute, then the Council has the ability to restrict or stop someone from practising while it takes the necessary actions. While people may complain to the professional association it has no mandate to act on any complaints about a practitioner, nor to take any action in that regard. Some professional associations do provide advocacy, support or legal advice for practitioners who are conduct.
• To promote education, inter-collaborative practice and public awareness of the authority.
The functions outlined above are the day-to-day business of the to ensure that we carry out these functions and that we have the right systems and processes in place to ensure a responsive but proportionate regulatory approach to matters. Our work is predominantly focused around registration, practising group that focusses on education accreditation matters and
requirements of section 118 of the Act. The report following our audit can be found on our website (2). Since this time, we have an update on those matters can be found in our most recent annual report.
The interface with the professional association
The professional association is one of the Council’s key stakeholders. The Council liaises with professional associations
on matters of common interest, for example as part of the review of the scopes of practice, members of the professional association provided advice to the Council. The Council also seeks its advice on matters related to practise. Media enquiries regarding pay or employment issues are always referred to the professional association or union, as setting pay and conditions of employment are not the role of the regulator.
The professional association is the key agency with regards to promotion of the profession. Its role is to advocate for the needs of practitioners. While both the regulator and the professional
Whatu Ora and Te Aka Whai Ora, for example, our focus and
For example, the professional association would have an interest to advocate for terms and conditions for its members, while the regulator would note that there were issues or questions about the workforce but would consider the implications for the public. While the professional association would actively promote careers in science, the Council needs to ensure that its policies and procedures for entry to the profession ensure that those seeking registration have the required knowledge and skills for contemporary professional practice.
In summary, both the regulator and the professional association are essential for the development of a profession and for the safety and wellbeing of the communities they serve. Regulators are focused on using the regulatory mechanisms that they are enabled with to ensure the health and safety of members of the public. While professional associations advocate for their members and provide education to support their ongoing competence to practise.
AUTHOR INFORMATION
Medical Sciences Council of New Zealand, Wellington.
Correspondence email
1.Health Practitioners Competence Assurance Act (HPCA)
legislation.govt.nz/act/public/2003/0048/latest/DLM203312. html
2.Ministry of Health, Medical Sciences Council of New Zealand.
REFERENCES
2023/24 NZIMLS CALENDAR Dates may be subject to change Visit https://www.nzimls.org.nz/calendar for updates November04Microbiology, Palmerston North November11Preanalytical, Auckland November11Mortuary, Whangarei December/January 22/12/2308/01/24 Closed for Christmas Break All NZIMLS events will be held in conjunction with current NZ Government COVID-19 regulations. New Zealand Journal of Medical Laboratory Science 2023 129
BOOK REVIEWS
This is going to hurt
Author: Adam Kay, Picador, 2018
ISBN: 1509858636
This book is hilarious. It is pungent. It is heart-breaking. It is the story of Adam Kay as we follow him bright eyed and bushy tailed just out of medical school through the ranks of junior doctor (and as he points out, many so called junior doctors are not that he left the profession.
The best thing about this book is that it is broken down into bite size pieces. Really bite size pieces so it is easy to read while on shift, just before bed or anytime you want to just read a few funny stories as an amusing interlude. And it’s so easy to read. Unlike many medical memoirs, it is free of medical jargon, or at least there is a full lay-persons explanation provided for the uninitiated.
The other great thing about this book is how relatable it is. Scarily so. Even though as a medical scientist, we may not be working on labour ward ourselves, but we are still involved whether we like it or not. Lab work is a bit like watching from the wings as we process the platelet count for an epidural, the haemoglobin for a patient with post-partum haemorrhage or take stage front and centre for a massive transfusion, we are still involved.
One can understand Adam’s occasional annoyance with patients’ ignorance of their own normal bodily functions, his understandable disgust at some retrieved objects that
wonder at some of humanities more bizarre accidents and in some cases, especially brain-dead behaviour (penis degloving anyone?).
Especially easy to understand is his frustration at the hospital
The painfully slow computer systems, the never-ending confetti of paperwork, the gruelling shifts and lack of support. Sound familiar anyone?
for Adam. The last story is not so funny. Not so funny at all. It is heart wrenching. It is raw. It is real. And so very, very relatable. As I too am leaving the health sector for a bit, it may be
that not only has Adam written this book, but that he has settled happily into Life Without Medicine. I only hope that I can do the same.
Reviewed by: Elaine Booker, BMLSc, Invercargill
A nurse on the edge of the desert
Author: Andrew Cameron, Massey University Press, 2017
ISBN: 9780994140791
Nurse on the edge of the desert is a really good read, especially if you have ever wondered what nursing is about. Andrew Cameron is a real down home Otago boy, and from his writing style, you immediately feel like you know him. He’s very relatable school” New Zealand, land of innovation, hard work and number eight wire. One day his Mum decided they needed a holiday. So, she packed the three younger kids into the car and dropped For a week.
By the time he was in his late teens, he had had twelve jobs, could weld, drive any class of vehicle, fence, milk cows and assemble cars. So what attracted him to nursing? The promise not what he told the formidable matron of Lower Hutt Hospital,
where he starts work. Learning at the bedside, as you did in those days, he is something of a novelty, being the only male nurse in his uptake. He pioneers the way for other male nurses and describes many of his trials and tribulations along the way, especially the rule that male nurses could not train in obstetrics and gynaecology. Despite many of the obstetrics doctors being pro feminis, a feminis” or by for women by women. Knowing full well that this is not a subject that can be glossed over or learnt from a textbook, it
and I nearly choked on my porridge when I read his account of some of the bullying old battle axes he encounters on labour
experienced the sexual pleasure in their lives that they ought to have, so they take their frustrations out on other people.” Yes, she said some quite odd things to me on occasion, my mother.”
Able to turn his hand to anything and any aspect of nursing, we follow Andrew on his adventures around both New Zealand and Australia and then around the world to various war-torn countries on missions for the Red Cross. The take home message for me is how fortunate we are that people like Andrew, are willing to dedicate their lives, at the expense of their own, to better the outcomes of humanity.
It takes a very special person to mentally
It takes a river of compassion to hold the hand of the school bully so he does not die alone, and a very strong stomach to watch someone’s leg dissolve into a bucket. Indeed, we need more people like Andrew in this world.
Reviewed by: Elaine Booker,
 BMLSc, Invercargill
BMLSc, Invercargill
So what does Nurse on the edge of the desert and This is going to hurt have in common? One is the story of a Kiwaussie nurse, and one is the tale of a UK doctor. The underlying themes in both books are the brutally long hours and anti-social shifts
hospital. In the case of Adam, we watch his relationship with H gradually break down, as he is never home. He virtually lives at the hospital, or on the commute. There is a high personal price to pay in medicine, with broken relationships and children growing up in a solo parent household. The hours are at odds with the rest of humanity.
The other underlying theme is the lack of support within the
than one occasion, and these episodes always left me shaking such times, but our administrators never seemed to realise how Andrew Cameron really dealing with it, I was just getting on with it. I went six months without laughing, every smile was just an impression of one – I felt bereaved. I should have had counselling – in fact, my hospital should have arranged it. But there’s a mutual code of silence that keeps help from those who need it most.” Adam Kay
New Zealand Journal of Medical Laboratory Science 2023 130
constantly pitted against actually helping the patients and possible for patients. Everything from pitifully slow computers to distinct lack of resources hinder these caring and hardworking professionals at every step.
While I cannot change anything with a mere book review, I can





The nurse of today is the patient of tomorrow. There clearly needs to be a global shift in the way healthcare is managed. Because we need people likeAndrew andAdam, and everyone, human relationships, which are clearly unable to be maintained in the current model.
Elaine Booker, MScMLS, Invercargill
Introducing the NZIMLS Council 2023-2025
President
SueMelvin
Tony Barnett Region 5 Representative
Awanui Labs, Nelson Awanui Labs, Clyde

Sujata Hemmady
Emma Potton Vice-President Technician Representative
Te Whatu Ora, Auckland Communio NZ Ltd, Dunedin

Ajesh Joseph
Mike Legge
Secretary/Treasurer ProfessionalAdvisor
Te Whatu Ora - Waikato Otago University

Melanie Adriaansen
Sharon Tozer

Holly Beall
Jillian Broadbent
Region 2 Representative CPD & Membership Coordinator
Te Whatu Ora, Waikato NZIMLS
Gavin Atkinson
Region 4 Representative
NZ Blood Service

New Zealand Journal of Medical Laboratory Science 2023 131

Greetings to you all
PPTC in Wellington and funded by the New Zealand government
Laboratory Quality Management: 19th June - 13th July, 2023
Pathology Training Centre, to medical laboratory personnel in potential leadership or senior quality positions, who can then
Laboratory environments.
Aim: The purpose of the training was to provide knowledge and practical insight into quality management principles in medical laboratories. This also included workplace Health and Safety laboratory issues and risk factors heightened by the recent
15189 requirements, best practice standards and government level expectations so as to enable their laboratory to function
The course expanded on all components of the medical laboratory service in its teaching and implementation of practical examples and development pathways that will eventually lead to laboratories achieving International Accreditation status. Enhanced service delivery of quality diagnostic test results to clinicians and healthcare communities was considered the greatest outcome for students attending this course.
Course Content and Objectives: This course provided students
Overview of Quality Management Systems and associated laboratory guidelines. (ISO15189 standards, WHO Minimum Standards, International Accreditation requirements) Laboratory Director, Laboratory Manager, Quality Manager and organisational role discussions.
laboratory services.
Developing a quality statement, devising a quality plan, performance indicators and organisational goals or responsibilities.
Practical and interactive workshops on organisation charts, template documents, title page, document formats, formulating policies, creating designated SOP manuals, etc. were included in the course.
Quality manual structure and contents, contents of personnel, Health & Safety manuals, department Standard Operating Procedure (SOP) essentials were discussed.
copies, draft SOPs, obsolete documents, worksheets, record keeping, result reporting and presentation.
Equipment management and associated maintenance requirements and monitoring major incident response, emergency planning.
Monitoring and evaluation of new work, validation of new methods and diagnostic tests.
The establishment of Human Resource and Personnel
competency records.
Job descriptions, orientation, skill listing exercises, rosters
Quality improvement projects, customer service feedback and dealing with complaints.
Implementation of a laboratory health and safety programme. and design aspects, biohazard waste and disposal of contaminated material, disinfection and sterilisation. Personal protection, code of conduct, equipment risk factors. issues.
Chemical and dangerous goods storage including Material Data Safety Sheets. concepts.
Reema Kumar- Centre for Disease Control (CDC) Laboratory, Suva, Fiji
Tiina Faaalo- Princess Margaret Hospital Laboratory, Tuvalu
Feao Muli- Vaiola Hospital Laboratory, Tonga
Dhanbhagium Gounder- Centre for Disease Control (CDC) Laboratory, Nadi, Fiji

 Figure 1. Laboratory Quality Management Course
Figure 1. Laboratory Quality Management Course
New Zealand Journal of Medical Laboratory Science 2023 132
Figure 2. Laboratory Quality Management Consultants (back row) students (front row), 2023
Microbiology Course 28th Aug - 22nd Sept 2023
Pathology Training Centre, to medical laboratory personnel region.
Aim
practical workshops were provided to students in the diagnostic
able to provide quality diagnostic test results to clinicians using their medical laboratory services for patient management and better health outcomes.
Course Content and Objectives: This course provided students
Processing of all sample types, performing cell counts and
The theoretical and practical aspects of current methods isolated from various microbiology specimens.
Antimicrobial susceptibility testing of micro-organism pathogens using the CLSI and EUCAST guidelines.
The monitoring of resistance patterns for multi drug resistant bacterial pathogens.
Discussions on emerging and re-emerging bacterial organisms likely to cause infectious diseases.
Emergence of automation in microbiology, in-house media production for bacterial isolation and choosing the right resources to carry out microbiological testing.
Health and Safety in a microbiology laboratory including disposing of infectious rubbish.
The reporting and presenting of Microbiology results to clinicians.
The role of the microbiology laboratory in the surveillance
public health importance.
bacterial and viral diseases including Hepatitis A, B, and C, HIV and other STIs.
Standard Operating Procedures and written documents in microbiology.
Laboratory Quality Management issues, including performing / managing quality controls and documentation. UN/IATA shipping requirements for infectious substances category B.
Four students from the Reeves Brown- Tupua Tamasese Meole Hospital Laboratory, Samoa
April Sendito- Rarotonga Hospital Laboratory, Cook Islands Shanon Prasad- Centre for Disease Control (CDC) Laboratory, Suva, Fiji Patilupe Pikona- Princess Margaret Hospital Laboratory, Tuvalu

Blood Transfusion
PACIFIC CONFERENCES
PPHSN (EPINET Regional Meeting, 25-28th July, Hawaii (PIHOA-SPC)
Phil Wakem (PPTC’s CEO) accompanied by Filipo Faiga (PPTC’s Biochemistry Consultant and REQA programme Manager) attended the 4 day conference in Honolulu organized
1.To discuss and outline the roles, compositions and resources available to EpiNet teams
2.Provide training opportunities to build capacity for
3.Identify current and future needs for EpiNet
4.Discuss laboratory support for surveillance activities and sub-regional harmonisation.
Background with reference to PPHSN (from SPC Research, Evidence and Information Programme, Public Health Division,
Body
is a voluntary network of countries and organisations dedicated to the promotion of public health surveillance and appropriate and territories. PPHSN includes six services to prevent and
PacNet
For alert and communication. PacNet connects 900 health
rapid overall communication, especially early warnings for epidemic threats and consequently makes it possible to raise awareness and preparedness levels in the region. It also gives access to resources, including technical expertise.
EpiNet
For preparedness and response. Initiated in 2001 to function as the response arm of the network, EpiNet is made up of multi-disciplinary national / territorial outbreak response teams. The EpiNet (or equivalent) teams were formed territory. On top of coordinating surveillance and response and maintaining relevant PPHSN target disease surveillance and response protocols, including technical and resourcerelated aspects of public health operations.
Syndromic Surveillance System (PSSS) serves as an early warning tool for common outbreak-prone diseases. The PSSS is both indicator- and event-based surveillance. Data are collected weekly on four syndromes – acute fever and –from over 200 health care facilities in 23 countries across information that could indicate the start of an outbreak.
LabNet
PPHSN, LabNet is a three-tier network of public health
Polynesia, Guam and New Caledonia) that have agreed to provide select diagnostic services to neighbouring countries or territories according to their individual capacity. Level 3
Rim (Australia, New Zealand and United States). These include WHO Collaborating Centres.
Figure
3. Microbiology Course students, 2023
Science: 6th Nov – 30th Nov 2023
New Zealand Journal of Medical Laboratory Science 2023 133
PICNet
For Infection control. Launched in 2006, PICNet is the infection control network of PPHSN. It is to be used as a tool for communication and sharing of experiences, particularly how to be innovative with limited resources to ensure patient and health care worker safety from infectious diseases. Major activities of PICNet include the development of regional infection prevention and control guidelines, incountry technical assistance and training in infection control.
ShipNet (DDM)
Capacity building in core epidemiological skills for health from health ministers in the region. In response, PPHSN
Epidemiology (PGCFE) at Fiji National University – as the
undergoing a development process following endorsement at the Heads of Health meeting in 2014 to establish a regional entity that integrates training with capacity development. SHIP builds on the principle ‘from work, at work, for work’, and incorporates already existing initiatives for capacity building in essential public health functions.
Informal Consultation on Strengthening Surveillance Systems of Antimicrobial Resistance and Antimicrobial
18-20 September
2023, Manila, Philippines
This informal consultation aims to stimulate stakeholder engagement in WHO initiatives and drive progress in establishing and strengthening national surveillance systems for AMR pathogens and AMC in countries and areas across the Western
1.Stimulate engagement of stakeholders in WHO initiatives on surveillance of AMR pathogens and AMC, including recently published global and regional guidance and tools.
2.Facilitate the exchange of country experiences and good
systems and how to best utilize the data to inform the development of evidence-based policies and clinical practice
3.Discuss and recommend feasible approaches to establishing and strengthening sustainable systems for AMR and AMC at national, subnational and facility levels to address the threat of AMR.
Angela Lewis, the PPTC’s Molecular and Microbiology Specialist has been nominated to attend this meeting.
Can you help?
If any New Zealand medical laboratories have items of diagnostic instrumentation that have been recently upgraded or continue to be stored in the laboratory but are actually surplus to requirements, the PPTC would be most grateful if such items
troublesome instrumentation that continues to breakdown and which is often discontinued because it is so outdated.
The PPTC would also welcome teaching resources in terms of projector slides, textbooks and journals (within 10 years of longer have a use for them. Any contribution is so valuable to us. Please contact
Phil Wakem
Wellington, New Zealand


New Zealand Journal of Medical Laboratory Science 2023 134
Science Digest
Michael Legge
A new approach to childhood febrile illness
most common causes for seeking medical intervention. Often there are challenges in the diagnosis and treatment of childhood infections with the conventional approach is often slow due to the time for culture. Additionally, infections may be in inaccessible sites and conventional samples may fail to identify the infection. A recent publication from a European collaboration may provide a new direction for the diagnosis of childhood febrile illnesses (1). The multi-author publication used whole blood transcriptomic microarray, linked to medical learning incorporating 12 publicly available data sets. This included 1,212 children with 18
investigated using a new RNA dataset panel. Overall, the 161
broad classes of diseases such as malaria and tuberculosis. The authors concluded that a single panel of RNA transcripts can be used to identify causative organisms resulting in fever in a nonreducing diagnostic delays and improving antibiotic use.
Serum potassium and seasonal change
Serum potassium is an important electrolyte with a reference range of 3.5 to 5.3mmol/L depending on the method used.
above 5.5mmol/L and below 3.0mmol/L respectively are used as triggers for clinical intervention. Many of the spurious changes in serum potassium concentrations are due to pre-analytical
addition, transport temperature of whole blood can increase serum potassium concentrations and blood collection in winter
the serum potassium concentration and ACE inhibitors are known to increase potassium excretion. ACE inhibitors are a widely prescribed group of medication. In a recent publication (2)the authors investigated the relationship of serum potassium levels in patients prescribed ACE inhibitors and the association
national anonymised database for general practice. Overall, 10,680,825 serum potassium results were obtained from 5,600,741 prescriptions. Their analysis clearly demonstrated seasonal changes in serum potassium concentrations which was linked to changes in prescribing ACE inhibitors. They conclude that clinicians need to be more aware of seasonal variability and their prescribing activity.
Transgender women and prostate cancer
to reduce health disparities in this group. An area of healthcare frequently overlooked is the susceptibility of cancer in birth organs. Transgender women (assigned male sex at birth) retain
doing so remain at risk for prostate cancer. Until recently, the medical and few case studies or short reports. A recently published study (3) using medical records over the last 11 years has provided some additional data on this issue. A total of 449 transgender patients oestrogen, 17 had used previously used oestrogen and 22 were active oestrogen users at the time of diagnosis. The PSA values not used oestrogens and the lower grade prostate biopsies and non-oestrogen group. The authors emphasise the necessity for prostate cancer screening for transgender women especially for
(GAHTs). However, they further indicate that those using GAHTs of GAHTs need further research.
Leftover samples in diagnostic laboratories
Tens of thousands of patient samples pass through pathology laboratories every day that are clinically characterised and provide valuable diagnostic information. For research, new test development, validation studies, quality control etc., many of the leftover samples may provide useful options for secondary require ethical consideration as a range of data exists such as personal records, age, disease status and family history which may be readily available. Access to and use of such samples could reduce the necessity to recruit new people into a research project. A recent publication from Argentina (4) considers the ethical issues for using leftover samples. The authors consider justice. It was considered appropriate to respect the autonomy of the individual as the consent for use was only originally given to obtain further informed consent. Would the secondary use of the sample cause harm to the individual such as breach of privacy, access to medical information, the risk of harm to
several historical unethical practices. Collecting samples from vulnerable populations only, especially when their autonomy is compromised is against the principles of justice. The authors conclude that clear informed consent underpins good ethical practice and the individual’s right to know. They provide seven recommendations for the use of leftover samples to guide investigators and management of medical laboratories.
Endometriosis: a new insight for its origins
Endometriosis results from endometrial like tissue growing outside of the uterus which may attach to abdominal organs. and a widely accepted cause is retrograde menstruation. However, although most women of reproductive age experience retrograde menstruation, around 85% do not develop endometriosis. Although the endometrial growths are considered benign, the disease results in chronic pain and infertility. The current information indicating that most women do not develop endometriosis suggest that there may be alternative mechanisms underlying this disease process. In a recently published study
from the vagina could contribute to the pathology (5). Amongst the vaginal bacteria previously described there were members of the Fusobacterium species, which although a normal commensal in the gastrointestinal tract, are considered to be an opportunistic pathogen. Using a range of molecular techniques, the authors analysed endometrial tissues for the presence for the presence of Fusobacterium species and in particular Fusobacterium nucleatum, which has a role in carcinogenesis with endometriosis had tissue analysed for Fusobacterium matched with 79 women who had normal endometrium. When
in endometriosis compared to controls. The upregulated genes endometriosis patients was analysed, 64% demonstrated a Fusobacterium
New Zealand Journal of Medical Laboratory Science 2023 135
tissue into mice who subsequently developed endometriosis. Direct infection with Fusobacterium but not with other bacterial species resulted in the development of endometriosis. The vaginal swabs from women with endometriosis showed a higher Fusobacterium population than the controls. Antibiotic treatment of the Fusobacterium development of endometriosis. The authors conclude that progress to clinical trials is required to reduce the pathogenesis of endometriosis by Fusobacterium infection to develop a treatment for endometriosis.
Human scent and mosquito guidance
unsuspecting targets and their presence is known only after their blood meal. This uncanny ability to select their human targets is known to be associated with a series of factors such as visual cues, body heat, humidity, breath carbon dioxide and chemicals are annoying, a more serious issue is malaria caused by the Anopheles mosquito with an estimated 247 million cases and 619,00 deaths worldwide from 2021 data provided by WHO. If there was a better understanding of attractants, it could help reduce the incidence of this disease. In a recent publication (6)an international collaboration investigated what cues guide mosquitos to their blood source. Anopheles gambiae has a strong preference for humans and the authors designed an experiment to test and validate mosquito attraction. They constructed a of hungry Anopheles gambiae mosquitos who prefer to feed at midnight. Eight one-person tents were erected around the structure containing a single person with each having their own scent which was ducted to the cage to individual heated (37oC) aluminium plates. Over six nights the mosquitos were observed using infra-red cameras. Each tent had the scent analysed to compounds were detected of which 15 controlled mosquito
attraction. The most frequently sought odour was a participant with high levels of carboxylic acids which are produced by the
attractive, was a person with low levels of carboxylic acids and a high level of eucalyptol which is present in high concentration of eucalyptus. It is also found in foods such as rosemary and sage as well as beauty products and mouth wash. This person was a
cues and both visual and odour cues from 5 to 15 metres. Heat and humidity cues were detected from 0.3 to 0.5 metres. The authors conclude that human scent is the primary attractant and speculate whether these data may provide a mechanism for mosquito control.
REFERENCES
Habgood-Coote D, Wilson C, Shmizu C, et al. Diagnosis of childhood febrile illness using a multi-class blood RNA signature. Med medj.2023.06.007.
Thayakaran R, Hothan R, Gokhale KM, et al. Seasonal variation of serum potassium and related prescription J Clin Path
Nik-Ahd F, deHoedt A, Butler C, et al. Prostate cancer in 2000-2002. JAMA
Lenicov FR, Fink NE. Ethical issues in the use of leftover samples and associated personal data obtained from diagnostic laboratories. Clin Chim Acta
Muraoka A, Suzuki M, Hamaguchi T, et al. Fuscobacterium infection facilitates the development of endometriosis
Sci Transl Med scitranslmed.add1531
Giraldo D, Rankin-Turner S, Corver A, et al. Human scent guides mosquito thermotaxis and host selection under naturalistic conditions. Curr Biol
Call for nominations for Life Membership of the NZIMLS
The Council of the New Zealand Institute of Medical Laboratory Science (Inc.) (NZIMLS) is calling for nominations for suitable candidates for Life Membership. A Life Member is any member of the NZIMLS who the Council considers has given outstanding service to the Institute of Medical Laboratory Science (typically but not exclusively) who notwithstanding anything to the contrary in these rules shall retain the privileges of his/her previous category of membership.
Guidelines for Life Membership:
Publications
Oral Presentations
Voluntary contributions to Institute activities, e.g. Council, SIGs, Conferences etc.
Special projects
Other areas considered relevant by nominators. will be considered.
or download from our website.
New Zealand Journal of Medical Laboratory Science 2023 136
NZIMLS QMLT Curriculum Review
30 September 2023
Present
Barnett (President, NZIMLS, Microbiology), Ajesh Joseph (Secretary/Treasurer, NZIMLS, Specimen Services), Kate Stewart (Histology), Shugo Kowamoto (Biochemistry), Diane Woolcott (Transfusion), Annette Bissett (Phlebotomy), Shane French (Mortuary), Andrew Soepnel (Immunology), Pippa Grainger (Diagnostic Genetics), Sandy Beckman (Transfusion), Tane Segismar (Transfusion), Rod Smith (Mortuary), Lyndia Rios (Phlebotomy), John Fainsan (Phlebotomy), Lynne Morgan, (Specimen Services).
Apologies
(Donor), Ash Nishimura (Donor), Matthew Pynegar (Anatomical Pathology), Sue Melvin (General), Catherine Littlechild (Immunology), Sarah Burge (Immunology), Coral Olsen (Transfusion Science), Nathan Peacock (Transfusion Science).
Laboratory Technician (QMLT) Board of Examiners (BoE) organised a one-day face-to-face workshop on September 30th 2023 in Auckland, to review both the discipline and common curricula as well as the discipline Practical Assessments. The overall aim was to identify any commonality between disciplines, update in relation to laboratory practices and review the common curriculum
This was a very successful workshop. All participants were highly engaged and the resultant discussions provided useful guidance for the NZIMLS Board of Examiners to progress the review of the QMLT curricula and practical assessments.
review was required. Many of the suggested changes focussed
on the common curriculum and whether this is retained as part of the examination or incorporated into the practical assessment logbooks. Additionally, standardisation and improvements to the
for this review. Several updates for the discipline curricula were noted and further work needs to be done regarding these.
The next step for this review will be for the BoE to review the common curriculum with a view to identifying those components which would be better considered as examples relating to each discipline. These could then be moved to each discipline curriculum or to the practical assessments. This is not considered a loss of common curriculum topics but rather a more meaningful
the written examination.
The suggestions for common curriculum will be forwarded to the participants in this group for incorporation as the discipline curricula are updated. Review of the practical assessments will be undertaken as a second phase of the project. All potential changes for the QMLT Curricula are expected to be in place by 2025.
Thank you to all the participants who gave up their Saturday to assist with this review, your involvement was invaluable and highly appreciated.
Michael Legge, NZIMLS Board of Examiners
Mary-Ann Janssen, NZIMLS Board of Examiners

Royal College of Pathologists of Australasia, Faculty of Science honour for Otago Scientist
Honorary Associate Professor Michael (Mike) Legge, Department of Biochemistry and former Director of the Bachelor of Medical Laboratory Science (BMLSc) Programme in the Department of Pathology, University of Otago has recently been appointed as Royal College of Pathologists Australasia (RCPA), commencing in November 2023. Associate Professor Legge has recently been working on the Faculty of Science Strategic Plan and Chaired the 10 Year Review of the Faculty of Science for the RCPA. He has been involved with developing an on-line Pathological Sciences self-assessment programme and considers that the work as the Director of the BMLSc programme provided strong
direction for his work with the RCPA. Currently, he is assisting in developing pathways in the Faculty of Science for the creation of Clinical Scientists who will be
in the wide range of Pathology disciplines. He considered that the BMLSc degree Fellowship of the Faculty of Science. Associate Professor Legge has continued his research and publications with University of Otago colleagues following his retirement.

New Zealand Journal of Medical Laboratory Science 2023 137
Journal Questionnaire
Read the articles carefully as most questions require more than one answer. Answers are to be submitted through the NZIMLS website. Make sure you supply your correct email address and membership number. It is recommended that you write your answers in a word document and then cut and paste your answers on the web site.
You are reminded that to claim valid CPD points for successfully completing the journal questionnaire you must submit an individual entry. It must not be part of a consultative or group process. In addition, members who have successfully completed the journal questionnaire cannot then claim additional CPD points for reading the articles from which the questions were derived.
The site will remain open until Friday 17 February 2024. You must get a minimum of eight questions right per questionnaire to obtain
NOVEMBER 2023 QUESTIONNAIRE
1.How is Shiga toxin-producing Escherichia coli (STEC)
2.Why is E.coli what are the characteristics of infection?
3.What was the percent prevalence of E.coli study? And in what age group?
4.What is Familial Mediterranean Fever (FMF)? How is it characterised? And what genetic trait causes the disorder?
5.What role does Chemerin play in the early stages of
6.Chemerin levels in FMF patients in this study were support therapeutic treatment for FMF patients?
7.What is insulin resistance (IR)? And in what diseases does
8.What is the gold standard technique for measuring Insulin Resistance? What prevents the use of this technique? What substitute is frequently used?
9.In the diagnosis of vaginitis, what laboratory analysis of the vaginal swab is performed? And what are the problems with this standard method?
10.The laboratory needs to alert the clinician to the possibility of Bacterial Vaginosis (BV) due to the association of what serious outcomes? What is only revealed by molecular diagnosis? And how can this strengthen the potential for improved diagnosis?
ANSWERS JULY 2023 QUESTIONNAIRE
1.What is glycated haemoglobin (HbA1c) testing used for and how often is it measured in children? Used to diagnose children with type 2 diabetes mellitus and guide management of children with T2DM and T1DM. measured every 3 months in children with diabetes and complements home monitoring of blood glucose.
2.What is the utility of Point of Care Testing (POCT) using the smaller handheld devices for HbA1c testing? They can be used by patients at home, also hard to reach and underserved populations, marginalised groups and remote peoples, where quick decision making is needed.
3.What group is common in the misreporting of selfmonitored glucose levels? What else has attributed to misreporting of blood glucose in recent times? The adolescent population. Recent lockdown restrictions in response to the global COVID 19 pandemic have highlighted
4.What viral infections have been reported to increase the incidence of Coeliac Disease (CD)? What is associated Viral infections such as adenovirus, enterovirus, hepatitis C virus,
5.Natural cytotoxic receptors (NCRs) such as NKp46, Nkp44 and NKp30 are important cell-activating receptors that after engagement with their ligands deliver potent signals to Natural Killer cells. What do these signals lead to and what do defects in expression of these activating receptors cause? Lysis of harmful tumour-transformed or infected cells and regulation of the homoeostasis of immune responses. Defects to epithelial cell death and villous atrophy in extreme cases.
6. and cytokines secreted by adipose tissue. What subjects has decreased NKp30 expression been found in? What is this linked to? And what is believed to happen to NK cell activity following weight loss? Decreased expression of NKp30 is seen in normal obese subjects and linked to the people’s susceptibility to infections and increased cancer risk. NK cell activity is disturbed in obesity and could be reactivated following weight loss.
7.What is Klinefelter’s Syndrome? How do patients present and what state may be involved in the syndrome’s pathogenesis?
Klinefelter’s syndrome is a sex chromosome aneuploidy, phenotypically males but carry an extra X chromosome (47, XXY). It is the most common form of aneuploidy witha prevalence estimated to about 1 in 650 new-born boys. Patients present with tall stature, cryptorchidism, gynecomastia, cognitive impairment, infertility and hypergonadotropic hypogonadism. A state of chronic
8. in this study?
Low levels of testosterone in Klinefelter’s syndrome patients.
9.What is Methylmalonic Acidemia (MMA)? and what tests are performed for initial diagnosis? MMA is an autosomal recessive inherited metabolic disorder and appears in early infancy due to methylmalonyl CoA mutase lethargy, hypotonia, seizure, acid-base disturbances, tachypnea and death Initial diagnosis tests include assessing metabolites including urine organic acids (UOA), plasma acylcarnitines, plasma methylmalonic acid, plasma amino acids (PAA), total homocysteine, and vitamin B12 levels
10. to breakdown what substances in their diet? Patients are unable to breakdown certain amino acids and lipids.
New Zealand Journal of Medical Laboratory Science 2023 138
OTAGO BMLSC student research project abstracts: Semester 1, 2023
Evaluation of the CerTest VIASURE Bordetella real time BDMAX PCR assay
Grace Adams1 and Trevor Anderson2
1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives
house multiplex PCR assay to the CerTest VIASURE RT-PCR BDMAX assay for the detection of Bordetella in the clinical microbiology laboratory.
Methods
nasopharyngeal samples with varying bacterial loads for Bordetella pertussis (n=8) or Bordetella parapertussis (n=8), Bordetella negatives were sampled. The twenty-four samples that were previously run on the inhouse multiplex PCR assay were run on BDMAX using the CerTest VIASURE RT-PCR assay kit as recommended by the manufacture.
Results
sixteen positive samples that were previously detected on the in-house multiplex PCR assay. The Viasure assay missed two B.pertussis and three B. parapertussis weakly detected on the in-house assay. One B. pertussis positive on the in-house PCR assay was B. holmesii positive by Viasure PCR.
Conclusion
multiplex PCR assay and the CerTest VIASURE RT-PCR assay for BD MAX are suitable for diagnosis of a Bordetella infection. However, the in-house falsely called the B. holmesii positive as B. pertussis due to cross-reaction in the PCR target. The CerTest VIASURE assay kit, although less sensitive than the in-
The BDMAX assay would be appropriate for use in smaller rapid diagnostics service.
Validation of sexually transmitted infections PCR Assay on the BD MAXTM System
Swaleha Ali1 and Paul Ogbuigwe2
1University of Otago, Dunedin and 2Molecular Biology Laboratory, Te Whatu Ora – Waikato, Hamilton
Objectives Chlamydia trachomatis, Trichomonas vaginalis and Neisseria gonorrhoeae are the top three non-viral organisms responsible for a large portion of sexually transmitted infections of these infections can reduce the public health burden. The detection of these infections. Waikato Hospital currently tests STI specimens using the Abbott STI PCR Assay on the AIinity volumes, establishing another method for conducting STI PCR was important in case this analyser became non-operational. This study aimed to validate testing of STI samples collected in Alinity M collection tubes on the BD MAX Analyzer.
Methods
MAX collection tubes were provided but to reduce time costs and resources, multiple methods were trialled to determine the
this method, as alternative methods either failed to accurately detect the presence of all pathogens (10.8%) or yielded inhibitory results (32.4%).
Conclusion
using various specimen swabs, revealed that swabbing
MAX can serve as a backup testing system for STI PCR at Waikato Hospital.
Eva Bell1 and Regie Inigo2
1University of Otago, Dunedin and 2LabPLUS, Auckland
Objectives
(PRAME) has been involved in various studies demonstrating its use as a biomarker in diagnosis of melanoma. Pathologists at LabPLUS believed incorporating a PRAME antibody test into the was to optimize PRAME antibody to be used in supporting the diagnosis of melanoma at LabPLUS.
Methods
optimization, with all protocols being run on the Leica Bond III machine. Known positive controls were included and the antibody-antigen complexes via a red precipitate. Adaptations were made to the protocol recommended by Cell Marque to identify the optimal PRAME antibody protocol for LabPLUS. Variables trialled in this experiment included primary antibody incubation time, epitope retrieval method and pH.
Results
experiment with heat induced epitope retrieval quickly being discovered as the only epitope retrieval method to produce positive PRAME staining. The testis control demonstrated consistent positive PRAME staining with appropriate protocols, whilst the SOX10 and known cases of melanoma presented with antibody protocol demonstrated great nuclear intensity and compatibility with current protocols at LabPLUS.
Conclusion
the optimal protocol for PRAME antibody included a 15-minute primary antibody incubation, heat induced epitope retrieval for 60 minutes and a high pH.
Usefulness of the Sysmex XN 2000 Body-Fluid HF-BF Panel
Laura Bungard1, YiiSen Wee2 and Paul Spek2
1University of Otago, Dunedin and 2Southern Community Laboratories, Dunedin
Objectives
diseases. BF cell counts have previously been performed manually, but automation allows for faster and more accurate analysis. The BF mode on the haematology analyser, Sysmex
(HFC). The aim of this study was to evaluate the performance of HFC in the detection of malignant cells in pleural and ascites of malignancy.
Methods
Results
Valid results were only obtained from specimens tested using
to investigate. Samples received during the permitted time frame were analysed on the Sysmex XN-2000, and if greater than the
New Zealand Journal of Medical Laboratory Science 2023 139
manual microscopy.
Results
detected by cytological microscopic examination in all samples that were received over the data collection period.
Conclusion
could be an alternative method for BF cell counts, with the HFBF parameter acting as a screening tool to determine whether samples require further investigation by microscopy but has its limitations. Therefore, in cases where the concentration of HFmalignancy, additional microscopic review will be required.
Evaluation of Fortress and Bio-Rad TPHA kits as
Abbey Burgess1 and Bronwyn Findon2
1University of Otago, Dunedin and 2Waikato Hospital Laboratory, Hamilton
Objectives
Treponema pallidum antibodies are an essential requirement for the diagnosis of syphilis infection. The objective of this study was to assess the performance of two Treponema pallidum haemagglutination assays in order to validate a new assay to replace the discontinued Serodia kit,
Methods
Waikato Hospital were selected for repeat testing to evaluate the performance of the Bio-Rad and Fortress haemagglutination kits. Previously positive sera (n=30) were selected, including samples from Waikato Hospital, Hamilton Sexual Health, surrounding rural laboratories and the Royal College of Pathologists of Australasia. Negative samples (n=10) were selected based on a negative Treponema pallidum immunoassay result. Serodia, BioRad and Fortress procedures were performed on each sample and results were compared.
Results
were achieved with the Fortress kit, detecting 30 true positives, but only 9 of the 10 true negatives. Of the 30 positive results
the 30 showed repeat equivocal results. Both the Bio-Rad and Fortress haemagglutination methods describe a repeatable equivocal as a positive result.
Conclusion
assays provided results concordant with the current Serodia kit.
Rad is the best replacement for the current Serodia kit.
Investigating CD61 as a novel marker for identifying vascular invasion in follicular thyroid cancer
Megan Casey1 and Michael Lau2
1University of Otago, Dunedin and 2Southern Community Laboratories, Dunedin
Background
cancer with vascular invasion being the predominant route of metastasis, hence vascular invasion is seen as a key marker for diagnosing malignancy. Currently the only way to diagnose vascular invasion in follicular thyroid cancer is through a haematoxylin and eosin (H&E) stain. The study aimed to determine if CD61 could be a relevant marker in helping to
Methods
thyroid cancer and one adrenal cancer case were chosen based on the uncertainty of vascular invasion. Tissue samples were stained with H&E stain using a Leica autostainer XL, and a CD61 monoclonal mouse antibody using the Ventana Benchmark Ultra machine. The resulting stains were viewed and interpreted by
a pathologist to determine if the CD61 marker provided a clear view of vascular invasion.
Results
invasion in the known positive cases of follicular thyroid cancer, while not showing any vascular invasion in cases that were diagnosed as non-invasive from a H&E stain. In the non-invasive cancers, there was still staining of the platelets within the vessels in the capsule, but no breach of the capsule wall into the vasculature was evident.
Conclusion
investigation using more known positive vascular invasion cases and a larger sample size is needed before it can be fully implemented into the thyroid cancer immunohistochemistry panel.
Acknowledgement supervision. assay
Katelyn Carter1, Jenna Paterson2, Gayleen Parslow2, James Ussher1,2 and Juliet Elvy2
1University of Otago, Dunedin and 2Southern Community Laboratories, Dunedin
Objectives for women to visit the doctor. The majority of cases are Bacterial to anaerobic pathogens including Gardnerella vaginalis and Atopobium vaginae. Abnormal discharge can also be caused by vulvovaginal candidiasis and Trichomonas vaginalis. The aim of this study was to compare two molecular real-time transcription-
Aptima CV/TV, to gold standard methods in women with relevant symptoms.
Methods
Nugent scoring for bacterial vaginosis, SAB culture for candidiasis and Aptima T. vaginalis assay for T. vaginalis. Nugent scoring was performed on Gram stains from Amies swabs with a score were streaked onto sabouraud dextrose agar (SAB) to observe Candida growth. Aptima swabs were run on Aptima BV, CV/TV, and T. vaginalis assays.
Results
sensitivity of 97.4%, with 97.4% concordance against Nugent scoring. 45 specimens with indeterminant Nugent scores were excluded from these calculations and require further investigation. The Aptima CV/TV assay for candidiasis performed sensitivity, and concordance for T. vaginalis.
Conclusion
to current methods. Although cost per assay is more expensive than current reference methods, time saved performing manual gram stain readings is valuable and promotes a shift to molecular testing.
Stability of vitamin B12
Sathu Chandrasiri1, Heather Hughes2 and Teresa Wong2
1University of Otago, Dunedin and 2Canterbury Southern Community Laboratories, Christchurch
Objectives (CSCL), the current levy to add tests for vitamin B12 is 24 hours. This is based on a published study by the World Health Organization in 2002. However, the laboratory receives many test-adds for vitamin B12 beyond 24 hours. This study aimed to
New Zealand Journal of Medical Laboratory Science 2023 140
evaluate the stability of vitamin B12, to see whether the results
tubes, then centrifuged to separate the serum. Each sample was aliquoted into four sample cups labelled day 0, 1, 2, and 3. These samples were then frozen periodically over three days. They were all thawed and tested on the same day to eliminate kit variations on the Cobas.
Results
Royal College of Pathologists of Australasia Quality Assurance
the upper limit. Based on the data collected from days 1, 2 and 3, and comparing each sample to its respective result from day 0, it was evident that all results were within 15% of the allowable limit.
Conclusion
B12 is within the allowable limit of performance according to the Royal College of Pathologists of Australasia Quality Assurance Program, for the upper limit. However, further testing with samples is required to make any changes to the allowable testadd time at CSCL.
Application of the GeneXpert in a 3-step algorithm for indeterminate diagnostic
results
Ysaure Chemaslé1, Tina Lusher2 and Rebecca Lucas-Roxburgh2 1University of Otago, Dunedin and 2Med Lab Central, Palmerston North
Objectives
step testing algorithm for patient samples with indeterminate (GDH positive/Toxin negative) results using the GeneXpert Dx System, ensuring higher diagnostic sensitivity and accurate results for clinicians, thereby providing better patient outcomes.
Methods
April 6th 2023. A total of 17 samples had previously been tested using the current GDH/Toxin testing algorithm, these samples comprised four GDH positive/Toxin positive, three GHD negative, and 10 indeterminates. An additional three samples previously tested using an alternative molecular method (Aus Diagnostics faecal PCR) were also included to allow comparison across molecular platforms.
Results
yielded the same respective results on the GeneXpert, verifying its function. Two of 10 indeterminate (GDH positive/Toxin negative) samples were PCR positive on the GeneXpert with Ct also had a Binary Toxin Ct value of 24.3. One sample negative for both GDH and Toxins was positive by PCR on the GeneXpert with a Ct value of 34.4.
Conclusion
positive/Toxin negative results increases the sensitivity and ensures positive infections are detected giving clinicians more accurate results. In turn, this reduces transmission and upholds infection and prevention controls, thereby improving patient outcomes.
clotting time
Jessie Chen1, Aileen Wemyss2, Nalita Bali2 and Laura Chen2
1University of Otago, Dunedin and 2Middlemore Hospital Laboratory, Auckland
Objectives
dilute thrombin clotting time (DTCT) by performing DTCT and Dabigatran assays on patients on Dabigatran, where performing a Dabigatran assay would be unnecessary as the Dabigatran
levels would be below detectable levels.
Methods
receiving Dabigatran therapy over a 5-week period. The plasma was aliquoted, and frozen at -35 degrees Celsius after routine testing was completed. Testing was carried out in two batches. Both DTCT and Dabigatran assays were performed on the Diagnostica Stago STA R® Max 2 analyser. A retrospective study was performed using the same reagents and methods due to the relatively few samples collected in this study.
Results
had a Dabigatran assay result which ranged from 42 ng/mL to 413 ng/mL. For DTCT results within the range of 40 to 68 seconds, 10 patients had a Dabigatran level between 11 ng/mL to 82 ng/mL. There were 12 patients in the range of 30 to 38 seconds for DTCT with a Dabigatran level between 3 ng/mL to 25 ng/mL. One patient had a Dabigatran level of 9 ng/mL below DTCT of 30 seconds.
Conclusion
Dabigatran assay on patients who had a DTCT of 30 seconds or less would be unnecessary as Dabigatran levels would be below detectable levels. The retrospective study, which was performed for DTCT to be 30 seconds. Due to the relatively few samples collected, further testing is required before implementing a
Case Study: Immune acquired anti-D antibody in pregnancy
Yi Xuan Chong1 and
Talalelei Teu2
1University of Otago, Dunedin and 2Middlemore Hospital Blood Bank, Auckland
RhD negative individuals who are exposed to the D antigen may be sensitised and start producing anti-D antibodies. This can be through blood transfusions or fetomaternal bleeds during pregnancy where the fetus has RhD positive blood. Production of anti-D in pregnancy is dangerous for the fetus as it can cause haemolytic disease of the fetus and new-born (HDFN). A pregnant woman who was previously admitted to the hospital pregnancy. She was 37 weeks pregnant and was admitted in preparation for the birth of the second baby. The patient had a history of immune anti-D and the routine antibody screen rather than the usual probable passive anti-D that is the result of routine antenatal anti-D prophylaxis (RAADP). The baby was slightly jaundiced but healthy, and further testing and an elution determined that maternally acquired anti-D was bound on the surface of the baby’s red cells. True immune acquired anti-D is uncommon because any situation where there is a risk of fetal cells in the maternal circulation indicates that a dose of anti-D anti-D is that the patient had a miscarriage or bleed between pregnancies that she did not know about. Due to a gap in the cause of sensitisation that produced the anti-D.
Validation of the BioFire FilmArray Torch Gastrointestinal (GI) panel
1 and Tony Barnett2
1University of Otago, Dunedin and 2MedLab South, Nelson
Objectives
gastrointestinal pathogens in inpatient faecal samples received during the weekend. Methods sample to establish a base solution in which to spike with positive
New Zealand Journal of Medical Laboratory Science 2023 141
synthetic genetic material, and to ensure no contamination was present within the instrument or reagents. Then, two synthetic positive control samples were run, as well as a positive faecal sample, and a 1 in 4 dilution of the positive faecal sample. Each to test for potential user to user variation.
Results
positive control samples outputting results as expected. Only one result was unexpected, which was the initial attempt at a negative control sample. However, this unexpected result has
E. coli strain O157 from other pathogenic strains of E. coli, which was
negative control also additionally uncovered an unexplained false positive to or low-level detection of Norovirus, which was
Conclusion
samples, has the ability to identify all pathogens listed in the panel, can identify pathogens at 25% of the ideal concentration, and has no risk of user-to-user variation.
Kleihauer testing requests in Canterbury Health Laboratories; audit of testing and alignment with ANZSBT guidelines
Margaret Lilley1,2 and Catherine Neal2
1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives
haemorrhage in RhD-negative mothers to determine the dosage of RhD immunoglobulin (anti-D). It is important to give anti-D to RhD-negative mothers to prevent alloimmunisation that could cause haemolytic disease of the fetus and newborn in current/ future pregnancies. This study aimed to evaluate Canterbury Health Laboratories standard operating procedures against the Australian and New Zealand Society of Blood Transfusion guidelines.
Methods
2021 to January 2023 and November 2022 to January 2023) was used to assess if Canterbury Health Laboratories standard operating procedures are in line with the Australian and New Zealand Society of Blood Transfusion guidelines. Data was
Results
at Canterbury Health Laboratories across the two quarters were not recommended based on the Australian and New Zealand Society of Blood Transfusion guidelines. The majority of the not recommended Kleihauer tests performed at Canterbury Health Laboratories were for antepartum haemorrhage and abdominal pain in RhD-positive mothers.
Conclusion
at Canterbury Health Laboratories each quarter are not recommended by the Australian and New Zealand Society of Blood Transfusion guidelines. This should prompt Canterbury Health Laboratories to review and update their Kleihauer test standard operating procedure. A clinician will need to oversee and give input to ensure the proposed standard operating procedure is appropriate before being put into practise.
prostate adenocarcinomas
The aim of this study was to optimise NKX3.1 antibody within prostate cancer (adenocarcinomas).
Methods
selected and PSA staining was rerun as well as NKX 3.1 staining. This IHC staining was run on a Ventana Benchmark Ultra using an Optiview detection kit. PSA staining was carried out using a protocol optimised within our laboratory. For NKX 3.1 staining, the NordiQC recommend protocol was used.
Results
for PSA and NKX 3.1. For these cases similar staining patterns were seen, although it did appear that NKX 3.1 was staining slightly more cells than PSA. The other two cases had weak or patchy PSA staining but a majority of cells still stained positively for NKX 3.1.
Conclusion is useful for identifying cells of prostate origin even when PSA expression has been decreased or lost. Due to this added
Acknowledgement
Palmerston North for their supervision and support of this project.
Celeste Linley
University of Otago, Dunedin
Objectives
chromosome 8p. NKX 3.1 has been shown to be positive in most primary prostatic adenocarcinomas as well as being highly
Kyle McLean, Harrison Dolan, Francesc March de Ribot, and Tania Slatter
University of Otago, Dunedin
Objectives
over 196 million people worldwide. AMD pathogenesis involves several complex retina changes not fully understood, involving
VEGF production. The basis of this study was to optimise an was increased in a model of AMD.
Methods
preparations of RPE cells (serum-starved and non-serum starved) were made. Slides were stained using the RNAscope 2.5 HD Detection Reagent – RED method. The probes used were UBC (positive control), DapB (negative control) and Tp53
alterations in the standard procedure, which included additional time for protease and AMP5 hybridisation steps. Slides were visualised using digital pathology, positive cells counted, and the percentage of positive cells compared between serum starved and non-serum starved cells.
Results
by strong positive staining in the UBC control and negative in the AMD model of serum-starved cells and not in the control.
Conclusion was increased in the model of AMD and if it contributes to
Comparison of a one-point calibration system with a sixpoint calibration system for the Opiate assay performed on the Roche Cobas c502 analyser
Abi McCullagh1, Sian Horan2 and Christian Christian2 1University of Otago, Dunedin and 2Southern Community Laboratories, Dunedin
Objectives
Cobas c502 analyser. The opiate assay is currently programmed
New Zealand Journal of Medical Laboratory Science 2023 142
to perform a six-point calibration and the c502 analyser reports results as a numerical value (semi-quantitative). The purpose of this project was to assess the implications of a one-point calibration system (rendering the assay qualitative) and
Methods
c502 analyser using the six-point calibration system and the new one-point system. All samples were sent to the liquid chromatography-tandem mass spectrometry laboratory for performance of the one-point calibration system in comparison liquid chromatography-tandem mass spectrometry laboratory. Results to 100% (six-point method had a sensitivity of 86.6%). The
changed by only 1% for both positive and negative quality control material tested daily over a period of ten days.
Conclusion point method is implemented. All positive samples are sent to the liquid chromatography-tandem mass spectrometry laboratory for detected and corrected. A one-point calibration will also save time in terms of preparation and money.
concentrations for the detection of extended-spectrum
Rei Miyamoto1, Catherine Gordon2 and Bronwyn Davison2
1University of Otago, Dunedin and 2Canterbury SCL, Christchurch
Objectives
combination disc tests using cefotaxime 5μg and ceftazidime 10μg discs with and without clavulanic acid 10μg, with the cefotaxime 30μg and ceftazidime 30μg discs with and without detection at Canterbury SCL.
Methods
negative Enterobacterales (n=31) were used to carry out the combination disc tests. For each isolate, a bacterial suspension was inoculated across two Mueller Hinton Agar plates and incubated according to the MAST combination disc kit manual. Each set consisted of a plate with MAST® cefotaxime 5μg and ceftazidime 10μgdiscs with and without clavulanic acid 10μg, and a plate with MAST® cefotaxime 30μg and ceftazidime 30μg discs with and without clavulanic acid 10μg. The inhibition zone sizes were measured and recorded in Microsoft Excel, then analysed using RStudio version 4.3.0.
Results
and 93%, respectively. They both displayed good repeatability
Laboratories, Dunedin
Objectives
homeostasis, and thus measurements for the iCa are increasingly requested in patient care. Smaller laboratories are often unable to do an immediate analysis of the iCa due to the method’s unavailability, analytical performance, and stringent sample collection and handling. The study aimed to compare the measurement of iCa in heparinised whole blood syringes to vacutainer tubes, and to compare the iCa concentration of whole blood to plasma. The study can help to determine whether samples can be sent from remote laboratories to Dunedin for analysis of iCa.
Methods
Southern Community Laboratories, Dunedin, on both blood gas syringes and lithium heparinised tubes to compare the stability of iCa. The measurement was done on heparinised whole blood syringes, whole blood, and plasma (immediate, 24 hours and 48 hours), and the plasma samples were further divided into two Hitachi cups and stored at 40C and –200C. Measurements were done using a direct Ion Selective Electrode (ISE) blood gas
ionised calcium (4%) criteria established by the Royal College of Pathology of Australasia.
Results
blood gas syringe for iCa.
Conclusion
blood syringe for analysis of iCa. It is not recommended to send samples from remote areas for analysis of iCa.
Secretor status and susceptibility to IgG ABO antibodyassociated haemolysis
Annabel Parker1 and Krishna Badami2
1University of Otago, Dunedin and 2New Zealand Blood Service, Christchurch
Objectives
a variety of disorders. Haemolysis is a complication of IVIg, especially in non-O (A, B, AB) group individuals. This is due to the presence of IgG anti-A, anti-B, and anti-AB in IVIg. Haemolysinpositive plasma poses a similar risk. This in-vitro study aimed to investigate secretor substance as a possible mitigation of haemolysis due to IgG ABO antibodies.
Methods
IgG anti-A), fresh group AB serum as a complement source, and serum with or without secretor substance was tested for haemolysis against group AB red cells. Appropriate controls were used. As Lewis phenotype is correlated to secretor status, samples were phenotyped to determine the presence of secretor substances. Haemolysis was detected using an adapted button width. Direct antiglobulin testing (DAT) was performed to investigate extravascular haemolysis.
Results
detected with these combination discs alone in isolates with
Conclusion and ceftazidime 10μg discs with and without clavulanic acid 10μg were similar to the discs with 3μg of cefotaxime and 30μg of ceftazidime. This allows standardised detection and other susceptibility testing using the same antimicrobial concentrations.
Stability of ionised calcium measured in vacutainer tubes compared to blood gas syringes, and the potential
Nasrin Neyyan1, Sian Horan2, and Christian Christian2 1University of Otago, Dunedin and 2Southern Community
samples containing non-secretor serum and 12/16 secretor serum samples. The relative risk of haemolysis in samples containing non-secretor serum was 1.33 times higher than in samples containing secretor serum. However, IVIg did not induce haemolysis, regardless of the secretor status of additional serum. The DAT results with IVIg were positive using both group AB and O RBC.
Conclusion
substance potentially conveys a lower risk for IVIg-, or haemolysin plasma-related haemolysis. Results using IVIg were inconclusive. Explanations for the IVIg results may be relatively low titres of IgG ABO antibodies and, for the DAT result, the presence of anti-D.
New Zealand Journal of Medical Laboratory Science 2023 143
Investigation of INNOVANCE® D-dimer QC reagent stability past expiration date
Anjali Raju1
1University of Otago, Dunedin
Objectives
the stability of the INNOVANCE® D-dimer quality control reagents can be extended to an extra seven days past the expiry date as originally stated by the manufacturer.
Methods
according to manufacturer’s directions and used to perform a quality control assay on the Sysmex CS 2500 automated coagulation analyser. The QC assay was performed twice daily
The same QC vial was then assayed for an extended 7 days, with the same procedure of performing two QC assays per day from day 8-14. This method was used to analyse seven vials each of D-dimer QC1 and QC2. The results for each vial from days 1-7 were compared to days 8-14 to evaluate whether there
the QC set expired.
Results
INNOVANCE® D-dimer QC1 and QC2 measured on the days after expiration met the limit of allowable performance set by the Royal College of Pathologists of Australasia. However, further statistical analysis showed increased variability of the data, suggesting there were procedural errors in the experimental phase of this study.
Conclusion
from assays using expired QC reagents for D-dimers were within acceptable limits. However, due to the variability and experimental errors, the results were not reliable. Further testing is required to validate the results.
Acknowledgement
Southern Community Laboratories for their and supervision and support of this project.
Shortened erythrocyte sedimentation rate evaluation in community patients
Jacinta Richardson1 and Nicole Keegan2
1University of Otago, Dunedin and 2Taranaki Pathology Services, New Plymouth
Objectives The erythrocyte sedimentation rate (ESR) test is most erythrocyte sedimentation rate (ESR) result can be estimated based on values from earlier set times.
Methods from patients who had ESR requests sent to Taranaki Pathology services between the 5th of April and the 24th of May 2023. Once the ESRs for these patients were set up, the results were recorded at 15, 30, 45, and 60 minutes. These results were then result, and the values collected at earlier times.
Results patients was 64.3 +/- 17.4. Thirty-six percent of the patients were male and 64% were female. The mean ESR value at 15 minutes was 1.2 (SD+/-1.8), the 30-minute mean was 5.2 (SD+/- 5.7), the 45-minute mean was 11.4 (SD+/- 11.3), and a 60-minute was found between 15 and 60 minutes (r=0.731), and 30 and correlation was between 45 and 60 minutes (r=0.979). In order to estimate the 60-minute (y) value based on the 45-minute (x) 45-minute estimation was the most reliable regardless of age, gender, and if the end result was normal or not.
Conclusion
helpful in cases where an ESR result is time critical.
Stemcell EasySep positive cell selection kits for isolation of T cells and granulocytes for chimerism analysis
Sneha Sathish1, Michelle Burns2 and Geraldine Duncan2
1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives
myeloid and lymphoid cells to determine the success of a stem method to isolate cells from smaller volumes of blood than the CD3 and CD66b+ kits for isolating T cells (lymphoid) and granulocytes (myeloid) respectively.
Methods
using antibody complexes and magnetic particles. Purity was Qiagen kit. The DNA was used as a template for PCR using the kit, and cell numbers/purity were checked, DNA extracted and chimerism PCR performed. Chimerism results (% donor) for T cells and granulocytes from two patients were compared using cells prepared by the current method or the EasySep kits.
Results
DNA obtained for the chimerism PCR. Over several experiments cells or granulocytes. The kits also successfully isolated pure cell populations from blood two days after collection which is important for non-Christchurch patients. Percent donor results for T cells and granulocytes from two patients were similar for cells isolated by the current method or EasySep kits.
Conclusion populations. The EasySep CD3 and CD66b+ kits are easy to use, rapid (30 minutes hands-on), require small blood volumes, and are relatively inexpensive. Further parallel testing will now be conducted for patients with chimerism analysis requests.
Validation of the N435 and XN25 VITEK 2 AST cards
Johnny Slade1
2, Rachel Roth2
1University of Otago, Dunedin and 2Wellington Southern Community Laboratories, Wellington
Objectives
of two new Vitek 2 cards (N435 and XN25) for antimicrobial susceptibility testing (AST). This project aimed to determine whether the new cards are viable options for routine AST based on the reproducibility of expected results.
Methods
with a range of known resistance phenotypes were used. The N435 card validation compared the resistance determination to the current standard N311 AST card, as both cards contain
and measuring zones of inhibition to compare to the resistance determinations from the card.
Results
identical results to their reference standard. The results from the tazobactam of the XN25 card showed an increased number of resistances detected relative to their reference method. We hypothesise that this is a result of increased accuracy due to the clinical outcomes and treatment availability in some cases if these are false positives.
Conclusion
microbroth dilution and E-test strips and utilising more bacterial
New Zealand Journal of Medical Laboratory Science 2023 144
validation of any discrepant results before these cards become used routinely in the WSCL microbiology laboratory.
mediated platelet clump dissociation
Judea Smith1 and Linda Williams2
1University of Otago, Dunedin and 2Canterbury Southern Community Laboratories, Christchurch
Objectives
platelets in platelet clumped samples. This study investigated the the stability of open gentamicin over its 24-hour limit.
Methods
(if available) of 14 patients with known platelet clumping were tested. Mixed patient sample (400uL) was pipetted into a tube and mixed with 200uL of gentamicin. After 15 minutes at room temperature, the sample was remixed and manually sampled through an XN20 unit. The diluted platelet count was obtained by multiplying by 1.5 to correct for dilution. The diluted WBC, RBC and HGB values were also multiplied by 1.5 and compared to the undiluted values. If the diluted values were within 5% of the undiluted values, the platelet count was accepted. A dissociation. This method was repeated hourly for 6 hours using one gentamicin vial and daily for 5 days (120 hours) using one gentamicin vial and repeated using a new gentamicin vial as a control.
Results
counts when gentamicin was added to EDTA tubes over 6 hours and added to EDTA and citrate tubes over 5 days, with similar patterns in results between both open gentamicin and gentamicin from the same vial, revealed platelet clumps were present at hour 0 and hour 24 then began to appear again by hour 120.
Conclusion
gentamicin can be extended beyond the current 24 hour limit.
Cobas 6800
Brandon Su1 and Megan Burton2
1University of Otago, Dunedin and 2Southern Community Laboratories, Wellington
Objectives
virus quantitative DNA assay was evaluated and compared to that of the Cobas 4800. This was to verify the use of the Cobas Community Laboratories (SCL), Wellington.
Methods
assessed by comparing the results of hepatitis B viral loads from historic samples evaluated by the Cobas 4800 to the results obtained when tested by the Cobas 6800. Precision was assessed through a serial dilution of a sample with a high viral load tested in triplicate to assess the variability in the results at three titres.
Results
across the tested range of 1.0 log IU/ml to 8.4 log IU/ml when compared to results from the Cobas 4800. There was excellent agreement between results from the two systems, with a mean
were false negatives at the limit of detection for the assay. At the investigated titres, there was great precision within and run variation all below 5% for their respective titres.
Conclusion
level of agreement and precision when compared with the Cobas 4800. Thus, the Cobas 6800 is suitable for testing hepatitis B viral loads at SCL, Wellington.
syphilis
Mosie S’ua1 and Helen Vanderloo2
1University of Otago, Dunedin and 2Southern Community Laboratories, Dunedin
Objectives
syphilis (detection of the bacterium, Treponema pallidum) between
Methods
currently used analyser at SCL Dunedin and reference point for this research. Patient samples (n=116) that were previously screened on the Alinity were re-run on the Liaison XL, supplied by DiaSorin, to see if the two analysers gave concordant results. Results
results displayed a low positive signal on the Alinity analyser, indicated by values equal to or exceeding 1.0 S/CO. However, when compared to the Liaison XL analyser, the majority of these discrepant results (15 out of 17) exhibited negative signals, falling below the threshold of 1.0 S/CO. Notably, the remaining 2 discrepant results obtained from the Liaison XL analyser yielded equivocal signals, ranging between 0.9 and 1.0 S/CO.
Conclusion
than the Liaison XL, picking up a few false positives from time to time. However, it is preferred that the method of screening has a high sensitivity. The Liaison XL analyser was, for the most part, concordant with the Alinity for the vast majority of patient samples and was actually more accurate when it came to the 17 discrepant results obtained. It seems the Liaison would be a good alternative to the Alinity if a backup screening test for syphilis is ever needed, albeit a larger sample size would need to be tested to see the true measure of agreement between these two analysers.
Determining the optimal input DNA concentration range for TM assay
Harry Ward-Hayes1 and Amanda Dixon-McIver2
1University of Otago, Dunedin and 2Igenz, Auckland
Objectives
retrospectively analysed to determine an optimal DNA Methods assessed on the Nanodrop to determine an optimal range which would reduce the number of re-runs and fails. Other factors such as sex, age and collection location were also examined to
Results
had a 62.5% pass rate, along with 20% Rerun rate and 17.5% Fail rate. DNA concentration ranged from 0.263 ng/uL to 6.54 ng/uL with no clear correlation between DNA concentration assessed using absorbance ratios 260/280 and 260/230, and values between 1.08 and 1.88 and 0.25 to 1.07 were obtained, respectively. Again, with no correlation to pass rates. There was also no correlation to pass rate between age, sex or collection location found.
Conclusion
New Zealand Journal of Medical Laboratory Science 2023 145
concentration range which could be implemented to reduce the number of failed samples and in turn to reduce cost and time
Collection location, age and sex did not appear to have an impact on pass/failure rate.
The impact of various pre-analytical centrifugation settings on ABO/D typing
Chloe Williams1 and Amy Christie2
1University of Otago and 2New Zealand Blood Services, Dunedin
Objectives
Dunedin Blood Bank is 1000 RCF for a duration of 5 min. This have on the analytical quality of samples for card ABO/D typing. By conducting this research, the aim is to further reduce the centrifuge duration. Reducing the duration could potentially decrease the laboratory turnaround time.
Methods
other centrifuge settings were chosen based on guidance from the manufacturer’s literature of the tubes used. The four other
individuals. The analytical quality of both manual and automated card ABO/D typing was assessed.
Results
the analytical quality of manual or automated card ABO/D typing among the three individuals. Each manual ABO/D result was compared to results obtained from the control centrifuge conditions. Furthermore, the automated system successfully tested and accepted samples spun at each centrifuge setting.
Conclusion results in manual and automated card ABO/D typing for each healthy individual. This suggests the possibility of reducing the duration to 3 min for a broader population of healthy individuals.
further investigation involving a larger and more diverse sample population, including both patients and healthy individuals. Additionally, future research should encompass a comprehensive range of blood bank tests beyond just ABO/D typing.
distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.


New Zealand Journal of Medical Laboratory Science 2023 146



Laboratory Christmas Quiz: light relief from CPD questions
The Christmas quiz was very successful again last year and The NZIMLS Council has agreed to sponsor another quiz this year. As with last year it is a General Knowledge Quiz and the NZIMLS Council has agreed to award a single prize of $300 towards a laboratory Christmas function for the most correct answers. While individuals can also complete the quiz, the prize is only to a laboratory team entry to encourage teamwork. There are no CPD points for this quiz and it is not discipline related. The NZIMLS Council have not participated in the question setting or have knowledge of the answers. An answer sheet is available on the NZIMLS website, and the quiz answers can be submitted electronically as for the CPD questions. The answers will be published on the NZIMLS website after the quiz closes and the winner is announced. Closing date for all answers is December 8th and please indicate if the entry is a team or individual entry.
and subject Christmas Quiz.
1. The word ‘diagnosis’ is derived from the Greek to mean?
a.To indicate disease
b.To tell apart
c.To treat disease
d.To indicate normality
2.From the celebrities’ listed below, who has a fear of balloons?
a.Celine Dion
b.Tom Hanks
c.Oprah Winfrey
d.Johnny Depp
from which of the following countries?
a.Japan
b.Philippines
c.China
d.Indonesia
4.Which famous ‘rock’ guitarist made his own guitar?
a. Beck
b.Eric Clapton
c.Brian May
d.Andy Taylor
5.In which country is the Stock Exchange believed to have started?
a.Netherlands
b.England
c.Germany
d.France
6.The Brooklyn-style hat is considered the main precursor of what head gear?
a.Base-ball cap
b.Fedora
c.Beanie
d.Trilby
7.What gas gives Neptune its blue colour?
a.Ammonia
b.Carbon dioxide
c.Ionised oxygen
d.Methane
8.Which French criminologist was considered to be the
a.Maigret
b.Lacassagne
c.Locard
d.Peroit
9.What country was known to the Romans as Hibernia?
a.England
b.Ireland
c.Wales
d.Scotland
a.8
b.4 c.6
d.10
11.Who of the following had koumpounophobia?
a.Steve Jobs
b.Elon Musk
c.Mark Zuckerberg
d.Julian Assange
Manhattan?
a.Port
b.Vermouth
c.Marsala
d.Lillet Dry
13.Which of the following plants was used as eye-drops by Renaissance women to enhance their beauty?
a.Belladonna
b.White henbane
c.Black nightshade
d.Oleander
14.What is the highest selling computer model of all time?
a.Commodore 64
b.Apple 111
c.ZX Spectrum
d.iMac
15.Which of the following was a historic baselard?
a.Short dagger
b.Long sword
c.Long dagger
d.Short sword
16.Modern ballet evolved from which 15th century European Court?
a. France
b. Italy
c. Spain
d. Portugal
New Zealand Journal of Medical Laboratory Science 2023 147
following cultures?
a.Indian
b.Greek
c.Latin
d.Arabic
century by?
a.An Edinburgh ‘gentleman’ surgeon
b.An English anaesthetist
c.A French clinician
d.Two Irish general practitioners
19.In which sport would a ‘nutmeg’ be performed?
a.Cricket
b.Soccer
c.Tennis
d.Curling
20.On an Indian menu, what does ‘aloo’ mean?
a.Potato
b.Lamb
c.Spinach
d.Goat
parrot?
a.Mr Swordes
b.Captain Blood
c.Little John
d.Captain Flint
a.Water polo
b.Hockey
c.Basketball
d.Volleyball
23.What is historically the best-selling movie soundtrack?
a.Saturday Night Fever
b.Dirty Dancing
c.The Bodyguard
d.Grease
th
24.Which of the following words can be used to describe a wasteful project?
a.Boondoggle
b.Loblolly
c.Blepharospasm
d.Rigmarole
25.Which is thought to have originated in New Zealand?
a.Lolly cake
b.Fairy bread
c.Caramel slice
d.Neenish tart
a.Phoenician
b.Babylonian
c.Egyptian
d.Persian
27.What was the original purpose for the small side pocket in Levi jeans?
a.Guitar pick
b.Pocket watch
c.Keys d.Money
28. Play-Doh was originally developed for which of the following?
a.Plumbing sealant
b.
c.Potential toy
d.Wallpaper cleaner
29.Which cricket team was beaten only once in 43 games in 1741?
a.Arindel team
b.Duke of Richmond’s team
c.Slidon team
d.Duke of Sussex team
30.In the TV series MASH, what was the number of the unit?
a.4017
b.4077
c.4777
d.4707
31.What is the traditional Welsh dish Laverbread made from?
a.Leeks
b.Barley
c.Seaweed
d.Oats
32.Bastet was the Egyptian revered god of which of the following animal?
a.Ibis
b.Crocodiles
c.Cats
d.Scarab beetles
33. When using traditional ale barrel sizes, which of the following was the smallest?
a.Kilderkin
b.Firkin
c.Hogshead
d.Pin
34.Who of the following had a fear of eggs?
a.Alfred Hitchcock
b.Steven Spielberg
c.Woody Allen
d.Keanu Reeves
35.What is a group of bears called?
a.A sleuth
b.A skulk
c.A mob
d.A gang
a.Homer
b.Erasmus
c.Pepys
d.Aristotle
37.The concept of ‘herd immunity’ is believed to be derived from?
a.The Greeks
b.The Druids
c.The Romans
d.The Egyptians
the following?
a.Alice through the rabbit hole
b.There’s a wockert in my pocket
c.The owl and the pussy cat
d.Jamberry
New Zealand Journal of Medical Laboratory Science 2023 148
39.Which of the Rolling Stones songs was written by Paul McCartney and John Lennon?
a.Lady Jane
b.I want to be your man
c.Ruby Tuesday
d.Let’s spend the night together
40.In which country was the concept of zero created?
a.China
b.Greece
c.India
d.Phoenicia
41.From which country did the Periodic Table of the elements
a.Russia
b.Germany
c.Netherlands
d.England
42. Which of the following authors grandparents-built lighthouses?
a.Arthur Conan Doyle
b.Robert Louis Stevenson
c.Herman Melville
d.Charles Dickens
a.Intelligence
b.Good looks
c.Generosity
d.Good taste
44.How many Astronomical Units is the planet Saturn from the Sun?
a.6.2
b.9.5
c.11.5
d.8.4
45.The pigment sepia is obtained from which animal?
a.A tropical sea snail (Murex)
b.Cochineal insect
c.Cows force fed mango
d.
46.The most common sheep breed in New Zealand is which of the following?
a.Romney
b.Drysdale
c.Merino
d.Copworth
47.The cricket ground in Australia known as the Richmond Police Paddock in 1877 is which of the following?
a.SGC – Sydney
b.The Gabba – Brisbane
c.Bellerine Oval - Hobart
d.MCG – Melbourne
48.Which toxin is found naturally in castor beans?
a.Cyanide
b.Solanines
c.Ricin
d.Oxalic acid
49. Which golf course established the 18-hole round as standard?
a.Augusta
b.Carnoustie
c.
d.St Andrews
a.A platinum rod held in a vacuum in France
b.Light from krypton spectrum in a vacuum
c.Speed of light in a vacuum in 1/299,792,458 of a second
d.A platinum-iridium rod held in a vacuum in France
New Zealand Journal of Medical Laboratory Science 2023 149



NZIMLS
Pre-Analytical Services Special Interest Group (PASSIG) Seminar on November 11, 2023 at
Waipuna Conference Centre, Auckland
For registration visit: www.nzimls.org.nz
Call for presentations
Contact: Ajesh Joseph (SIG Convenor)
email: ajesh.joseph@waikatodhb.health.nz