Terry Taylor, BSc DipMLS MNZIMLS, Southern Community Laboratories, Dunedin
Sharon Tozer, DipBis Stud, AT CAANZ, NZIMLS, Rangiora
Robyn Wells, BApllSci(MT) GradCert Haem, Milton, Australia
Formatting
Sharon Tozer, AT DipBusStud, Executive Office NZIMLS, Rangiora
About the Journal
The New Zealand Journal of Medical Laboratory Science (the Journal) is the official publication of the New Zealand Institute of Medical Laboratory Science (NZIMLS). The Journal is peer reviewed and publishes original and review articles, case studies, technical communications, and letters to the Editor on all subjects pertaining to the practice of medical laboratory science. The Journal is open access (www.nzimls. org.nz/nzimls-journal) and is published three times per year in March, July, and November. Hard copies are circulated to all NZIMLS members and universities and research units in New Zealand and overseas. Current circulation is about 2,800 copies per issue. Printing is by Blueprint Ltd, Christchurch on environmentally responsible paper using elemental chlorine free third party certified pulp sourced from well managed and legally harvested forests and manufactured under the strict ISO14001 Environmental Management System. The Journal is indexed by CINAHL, EMBASE, SCOPUS, Informit, Thomson Gale, EBSCO and Biosis Citation Index, and the Journal Editors are members of the World Association of Medical Editors (www.wame.org).
Brief instructions to authors
The Journal accepts original submissions from anyone and anywhere. Comprehensive instructions can be found on the NZIMLS website (www.nzimls.org.nz/instructions-to-authors. html). All submissions will undergo single-blind peer review and possibly plagiarism checking with iThenticate™ software. If accepted for publication, copyright is vested in the author(s) under terms of the Creative Commons Attribution License (www. creativecommons.org/licenses/by/2.5/legalcode). The authors are responsible for the scientific content and views. Opinions expressed in the Journal are not necessarily those of the Editors, Editorial Board, or Council of the NZIMLS.
What happens when commercial DNA direct-to-customer companies collapse
Michael Legge 3
Reviews
Regulatory oversight on medical laboratory tests in Aotearoa
New Zealand
Paula E Keating 4-7
Original articles
Aurora kinase A overexpression in live cancer predicts the poor prognosis of patients
Ahmed A. Mohsin and Susan Zwyea 8-12
The effects of glucose 6-phosphate dehydrogenase deficiency on some non-enzymatic antioxidants and kidney function in children in the Basra Governorate, Iraq
Zainab Shakir Abdullah Al Ali and Bushra A. M Abdul Azeez Al Salem 13-16
Integrating TREC/KREC assay and cytokines in the evaluation of the immune status of patients with DiGeorge syndrome
Assem M. Abo-Shanab, Haiam Abdel Raoul, Alaaeldin G. Fayez, Iman Helwa, Engy A. Ashaat, Naglaa Kholoussi, Nora N. Esmaiel and Rania Fawzy Mahmoud Abdelkawy 17-24
Case Studies
Implementing nanopore sequencing in a clinical laboratory: a social systems case study
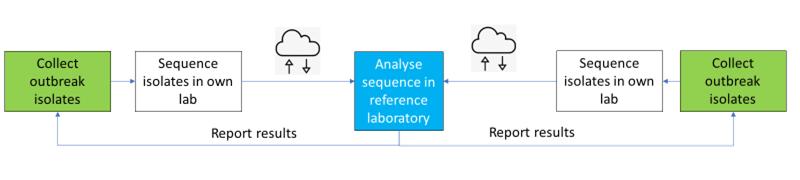
Suzanne Manning, Max Bloomfield, Samantha Hutton, Megan Burton, Charles Velasco, Claire Tarring, Rhys White and Koen van der Werff 25-29
Advertising and subscription
Advertisement bookings and enquiries should be addressed to the NZIMLS Executive Officer, Sharon Tozer: sharon@nzimls.org.nz. Phone +64 3 313 4761.
IN THIS ISSUE
Michael Legge addresses the concerns surrounding direct-tocustomer genetic testing in the Editorial, emphasising privacy, reliability and ethical concerns amidst the recent financial failure of 23andMe® and the potential risks of selling off genetic information. Many people do not realise the implications of a commercial company owning their DNA and data and that current privacy laws lack protections against misuse. Professor Legge raises important questions about informed consent and fairness in genetic information use.
Medical laboratory tests measure or detect analytes associated with pathology and wellbeing and allow clinicians to diagnose, monitor or determine treatment for disease and conditions. Many tests are developed in-house and are known as LaboratoryDeveloped-Tests (LDT). Paula Keating from Canterbury Health Laboratories, New Zealand discusses regulatory frameworks for LDTs across the world. In many jurisdictions LDTs are exempt from in vitro diagnostics (IVD) laboratory tests, however the Food and Drug Administration (FDA) in the USA, have announced their intended introduction of regulation for LDTs, affording the same protections to public safety as IVD tests. Keating invites New Zealand laboratories to consider the application of the international standards for medical laboratory testing and additional scopes of practice for medical laboratory practitioners as high-value improvements to the health service and the workforce.
Liver cancer is the second leading cause of cancer-related deaths in males and females with an estimated 1.2 million new cases yearly and 830,000 deaths worldwide, despite substantial development in liver cancer therapy, recurrence remains high and little progress has been made in early detection using hepatocellular cancer biomarkers. Zywea and colleagues at the College of Health and Medical Technology in Baghdad, Iraq investigated the role of Aurora Kinase A expression in normal, tumour and metastasis liver tissues to assess the relationship between its expression and the prognosis of liver cancer patients. Their study revealed an up-modulation in Aurora Kinases in multiple types of tumours compared to normal tissues and higher expression in metastasis liver tissues than other tumour or normal tissues. The results demonstrated that patients who suffered from high AKT and PDK1 expression had worse survival than the patients with low AKT1 and PDK1 expression. Results suggested that AURKA may drive liver cancer metastasis through PI3K/AKT signalling pathways and it might be a novel therapeutic target for liver cancer patients.
Associate Professor Al Ali and colleague Dr Salem, from the University of Basra in Iraq studied the effect of glucose 6-phosphate dehydrogenase deficiency on non-enzymatic antioxidants and kidney function in children in the Basra Governorate. The inherited mutation in the glucose-6-phosphate dehydrogenase (G6PDH) gene found on the X-chromosome causes G6PDH deficiency and can cause severe haemolytic anaemia when reactive oxygen species generation is elevated. Stress or exposure to foods high in oxidative chemicals, including fava beans or some drugs such as antimalarials may cause this. The degree of the enzyme deficiency, which in turn depends on the G6PDH variant, determines the probability and severity of
haemolysis. Results showed elevated Ievels of creatinine and urea in children suffering from severe G6PDH deficiency and lower levels of non-enzymatic antioxidants glutathione and vitamin E. Renal tests also indicated impaired renal function and are recommended as an early requirement in the early intervention to prevent future kidney disease.
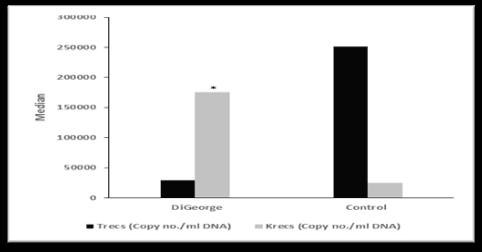
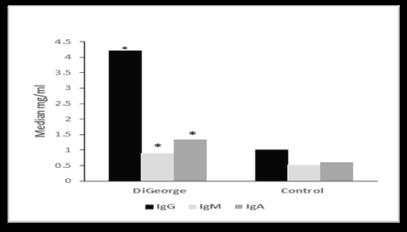
Complete and partial DiGeorge Syndrome (DGS) are conditions arising due to chromosome 22q11.2 deletion syndrome (22q11.2DS) and is the most common micro-deletion syndrome in humans, occurring in almost 1:4000 live births. Individuals who lack a thymus are classified as complete DiGeorge and partial DiGeorge syndrome is characterised by decreased thymic output. Due to this deletion there is a dysregulation of T to B cell interactions and typically low numbers of T-cell receptor excision circles (TRECs). Dr Abo-Shanab and associates from the National Research Centre in Cairo, Egypt evaluated the immune status of patients with DiGeorge syndrome by combining TREC/KREC assay and cytokines with genetic screening. Their results found KREC expression was significantly elevated in DGS patients compared to that of controls and a significant increase in immunoglobulin levels. CD8 was lower in DGS, but no significant differences were found in IL-33, Obestatin, HLA-G and procalcitonin levels in DGS compared with controls. The team concluded that combining screening of Chr22q11.2 region, immunoglobulins level patterns, and TRECS and KRECS expression could provide better genetic consultations for DiGeorge Syndrome patients.
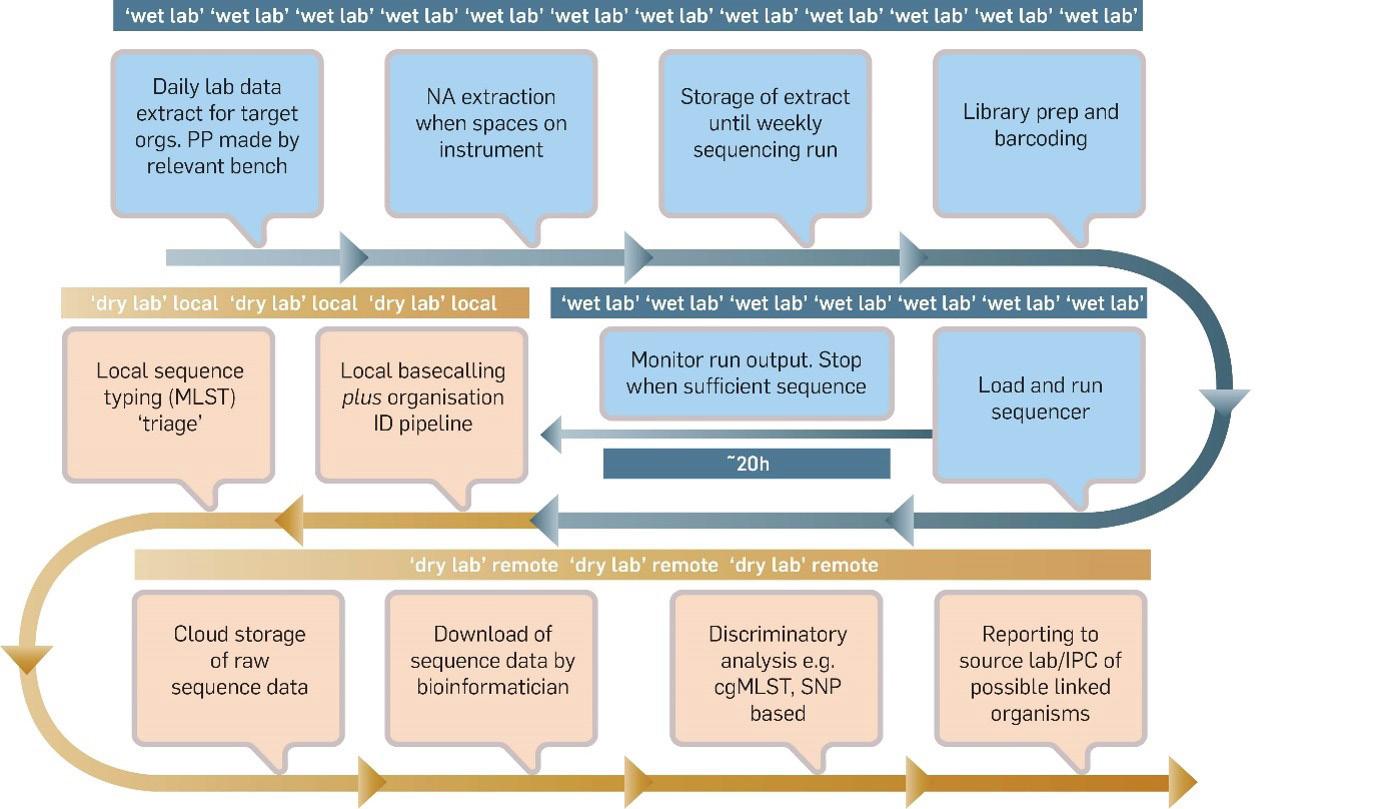
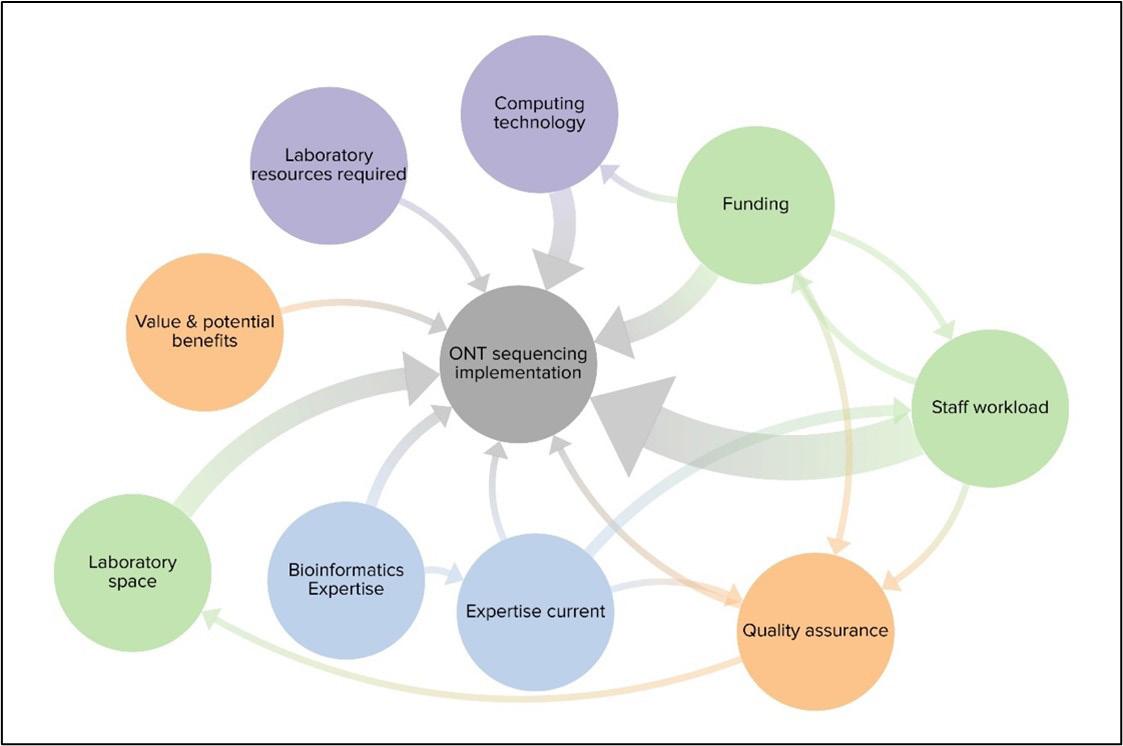
Suzanne Manning and teams at ESR in Wellington, New Zealand actively explore ways to realise the potential of technological advances in responsible ways. This qualitative case study article is written in a different format to what is normally published in the Journal but offers an enjoyable read and a unique perspective into the inner workings of a laboratory from a social perspective. The study aimed to explore the social systems around the implementation of nanopore sequencing in a clinical setting, complementing the studies that have focused on the technical aspects of implementation. They include a brief history of how nanopore long-read sequencing was implemented into the Molecular Pathology Department at Awanui Labs in Wellington and describe the social systems methodologies used and presenting their findings under the six Viable System Modelling (VSM) headings of Environment, Intelligence, Policy, Control, Coordination, and Operations to discuss their findings. They conclude that for successful implementation, attention needs to be paid to factors such as policies and practices, the mix of expertise on the team, and the access to technical and financial support. It also relies on the very human factors of team motivation and cohesion, willingness to learn, and at least one person who is willing to initiate and drive the project.
As well as our regular features; Science Digest, Recent Reviews, Questionnaire and the Pacific Way, we publish the Molecular Diagnostic SIG meeting report, interviews with two of our NZIMLS 2024 student award winners, and congratulate our new NZIMLS Life Member Geoff Herd and the retirement of Gillian Lanham.
Lisa Cambridge Editor
What happens when commercial DNA direct-to-consumer companies collapse?
Michael Legge
The recent announcement of the serious financial issues of the previously successful genetic testing company, 23andMe®, raises several issues of genetic information security. At its peak 23andMe® was valued at $US6 billion and was built on people wanting to trace ancestry links which further developed into predicting potential health risks. Customers could be tested and sell or donate their DNA results to 23andMe®, which is estimated to approximate to 15 million people with 80% giving their consent to allow their genetic information to be used for unspecified research. A similar company: Ancestry® is also in decline and has been trying to sell access to genealogical information to potential customers. Initially, 23andMe® started to offer health-based information based on an individual’s saliva DNA analysis which was subsequently limited by the FDA, to mutations linked to ten conditions. Since that limitation the company has expanded to 50 conditions. In the USA, genetic testing companies such as these are outside of the American Health Care laws and therefore are not governed by the control of genetic data.
While the numbers of people in New Zealand who have participated in direct-to-consumer testing (DTC) is not known, it is probable that most do not realise the implications of a commercial company owning their DNA and data. New Zealand privacy laws do not provide protection for insurance companies requiring the information to assess risk for life insurance. The American Government Accounting Office found important variance in genetic results obtained via different companies and that 10 out of the 15 companies investigated were engaged in some form of deceptive or questionable marketing practices relating to claims for the tests and interpretation of results.
Issues which arise from DTC not only relate to the reliability of the tests but also to skilled follow-up from genetic counsellors and clinical geneticists. Obtaining a “genetic result” does not provide information on clinical validity and utility of the information. A 2018 publication revealed that DTC results for pathological variants of genes reported by DTC companies had false positive rates of 40% when reassessed in an appropriate genetic testing laboratory. This included eight false positives for BRCA1 and 2 variants. In all variants of five genes (ATM, BRCA 1, BRCA 2, COL3A1 and COL5A1) were incorrectly identified at increased risk by the DTC data (1). This raises the issue of being misled e.g. BRCA1 and BRCA 2 mutations are highly predictive for breast cancer for women with a family history of breast cancer, but do not indicate a high risk for women with no family history (2). Without appropriate knowledge and guidance, inappropriate distress and medical intervention may occur.
So, returning to the start of this editorial, where and how does this lead to the current issues of 23andMe® and related companies?
Notwithstanding the right to own the individual’s DNA and the commercial possibilities of a genetic tests developing from the data, the issues relating to the insurance companies requiring disclosure about the results from genetic testing is significant. Similarly, expert advice about the results from genetic and clinical genetic counsellors is vital to understand both the clinical utility and the downstream issues if any result is confirmed. Confidentiality and privacy are essential to prevent discrimination in employment, insurance and in some situations within families.
These and other issues ultimately relate to the four established principles of medical bioethics: autonomy, beneficence, nonmaleficence and justice.
Autonomy provides for assurance to understand and make voluntary decisions i.e. informed consent. When undertaking DTC consumers are restricted (as a rule) to the information being provided by an overseas commercial company whereas in a suitable clinical environment the full capacity for the individual to understand and consent is assessed and obtained e.g. do they understand the requirements and implications for the tests and that adequate information has been provided? Beneficence is the act of something benefitting others. Will the individual understand that others may benefit from the outcome of the tests being undertaken (e.g. the discovery of the BRCA1 gene)? This should be considered in the context of informed consent. Nonmaleficence relates to the principle of causing no harm to others: incorrect false positives or negatives may well render a family into chaos and could in certain circumstances involve clinicians establishing incorrect or inappropriate treatment. There is also the issue of causing harm by failing to establish a genetic identity within a family for an individual. Do the extensive disclosures and complicated discussions of the technologies have the potential to limit understanding with the consequence of “harm”? Justice embodies, legal, moral and cultural principles which includes aspects of fairness and equality within a bioethical framework. Here discrimination becomes an issue, especially for employment, insurance and genetic identity. Certain DTC companies have disclaimers on their websites indicating the tests being provided are not medical tests and they are not fit for that purpose (3). Does this equate with the principle of fairness and justice and will the consumer understand the implications of the disclaimers.
As DNA technologies become easier to undertake and faster to deliver, will pathology laboratories and the necessary genetic information infrastructure be available to resolve the many issues that DTC has created? But, more importantly, when any of the DTC companies become financially unviable as with 23andMe® , what will happen to all the DNA data and personal information they have stored? An asset with considerable value that people have signed away their rights of control for companies to sell.
AUTHOR INFORMATION
Michael Legge, PhD, MRSB, FIBMS, FNZIMLS, FFSC (RCPA), University of Otago, NZIMLS.
Correspondence: mike.legge@nzimls.org.nz
REFERENCES
1. Tandy-Connor S., Guiltman MS., Krempely MS et al. Falsepositive results released by direct-to-consumer genetic tests highlight the importance of clinical confirmation testing for appropriate patient care. Genet Med 2018; 12: 1515-1521.
2. Hogarth S, Javitt G, Melzer D. The current landscape for direct-to-consumer genetic testing: legal, ethical and policy issues. Ann Rev Genomics Hum Genet 2008: 9; 161-182.
3. Phillips AM. Reading the fine print when buying your genetic self-online direct-to-consumer genetic testing terms and conditions. N Genet Soc 2017; 36: 273-295.
Regulatory oversight on medical laboratory tests in Aotearoa New Zealand
Paula E Keating
ABSTRACT
Medical laboratory tests are used to measure or detect analytes associated with pathology and wellbeing. The tests allow clinicians to diagnose, monitor, or determine treatment for diseases and conditions. This review focus is Aotearoa New Zealand legislative framework for medical laboratory tests, the medical laboratory organisation and laboratory practitioners. Regulations in other developed countries and the changes in Europe and USA on laboratory developed tests (LDT) are mentioned. Aotearoa New Zealand has a strong record in the development of laboratory developed tests and their safety and effectiveness is assured when performed under a quality management system by competent scientists. In the absence of medical device regulations, improvements in the application of the international standard for medical laboratory testing and additional scopes of practice for medical laboratory practitioners are posited to improve this vital service.
Keywords: medical device, in vitro diagnostic, regulations, scope of practice, laboratory developed test (LDT), scientist.
NZ J Med Lab Sci 2025; 79(1): 04:07
INTRODUCTION
Tests are designed to achieve at least 95% sensitivity and specificity. This means the test will return positive for 95% of people with the disease but negative (a false negative) for 5% of people who have the disease, or a negative result for 95% of people without the disease but a positive result (a false positive) for 5% of people who do not have the disease. The widely held maxim is that 70% of all diagnosis are based on a laboratory test result (1) so when results do not meet their stated level of sensitivity and specificity, they have the potential for misdiagnosis, causing public and patient harm. In 2015, a Food and Drug Administration (FDA) report highlighted twenty cases where inaccurate testing led to false positive and negative results, inappropriate testing, and delayed treatment (2). Similarly, with genetic testing for rare diseases it can be difficult to discern true genetic variants due to limitations of methods and the infrequency of rare variants in the population (3, 4). Direct to consumer genetic testing presents ethical problems when the consumer does not understand the complexity of the tests (5). False claims made by Theranos, that a pin prick of blood on its unapproved test could detect a wide array of analytes, has also brought laboratory tests into disrepute (6). More recently, the accuracy of rapid medical tests was in the spotlight during the COVID-19 pandemic, where the sensitivity of many tests was not acceptable in limiting the spread of infection (7).
In many jurisdictions, commercial in vitro diagnostic (IVD) medical laboratory tests meet legislated requirements but laboratory developed tests (LDT) also called in-house IVD (IHIVD) were often exempt. In April 2024, the regulatory authority in the USA, the FDA, announced it would introduce regulations on LDT. This aligns with the European Union introduction of regulation on IH-IVD. Prior to both USA and EU introducing regulations on LDT/ IH-IVD, Australia had regulated all IVD, both commercial and in-house developed under their therapeutic goods act implemented in 2017. Aotearoa NZ had considered working with Australia on the establishment of a joint therapeutic products regulator, however this did not proceed, and Aotearoa NZ has yet to regulate IVD tests.
To protect public safety, all IVD tests applied in our clinical laboratories should be subject to the same oversight, and the regulatory scrutiny should be proportional to the risk that a test poses to patients, or to public health, if it is inaccurate.
Aotearoa NZ IVD Regulation
The global harmonisation taskforce (GHTF), established in 1993, set about harmonising medical device regulatory practices, and their guidance documents provide the essential principles required for all manufactured medical devices. Many countries have based their legislative frameworks on GHTF guidance. The essential principles ensure medical devices do not compromise health and safety, the device design and construction are safe,
the medical device is suitable for its intended purpose, the device is not adversely affected by storage and transport and the benefits o f t he d evice o utweigh a ny u ndesirable effects. The taskforce is now superseded by the International Medical Device Regulators Forum (IMDRF). Aotearoa NZ does not have regulations on laboratory tests, nor is it a member of this organisation.
Regulatory approval on the use of devices, a mechanism for notification on device changes and a mechanism for reporting serious adverse events were introduced in Aotearoa NZ through the Therapeutic Product Act (TPA) 2023, which was to be implemented by 2026. This act was to replace the Medicines Act 1981 and introduce regulatory oversight on medical devices, however the coalition government has announced it will repeal the TPA to provide a risk-based approach (8). Until new legislation is passed, the MedicinesAct will continue to apply, with the ongoing potential for public harm through use of unregulated medical tests (9).
Laboratory Developed Tests (LDT)
The Biomedical alliance of Europe completed a questionnaire study in 2021 and found approximately 50% of tests offered in laboratories throughout Europe were developed in-house (10). Similarly, of all the tests offered at Leuven University Hospital, Belgium, 48% of tests were LDT (11). In the USA there are more than 12,000 laboratories providing LDT, while many of these laboratories offer a handful of LDT, some perform more than 100 different LDT (12).
Commercial IVD can take considerable time to gain regulatory approval. With the USA and EU being the predominant market for IVD, approval in either of these jurisdictions is generally sought. However, speed of scientific research and technological development in the diagnostics market can outpace the approval process. Furthermore, there is limited commercial incentive to develop a test for rare diseases/conditions.
Tests developed in clinical laboratories are generally the first available tests. Clinical laboratories with the requisite equipment, supplies,andexpertiseareadeptatdevelopingLDT.Thedrivefor increased efficiencies in testing has led to formation of laboratory corporations that supply a limited test repertoire, or concentrate on a speciality such as genetic testing (e.g., Blueprint Genetics, 23and Me). The expansion of this LDT market has progressed based on the ability to achieve greater performance, efficiencies and cost-effectiveness through control of the whole test process
Laboratory Developed Tests (LDT) in Aotearoa NZ
LDTs offer individualised diagnostic solutions and the need for LDTsisanticipatedtogrowaspersonalisedmedicineprogresses. Aotearoa NZ tertiary laboratories have a well-established reputation in scientific method d evelopment t hat underpins
the quality of our service. For example, embryo screening by preimplantation genetic testing for rare monogenic disorders has been performed at Canterbury Health Laboratories (CHL) since 2006. Genetics laboratories have a high usage of LDT. Comprehensive genetic testing for immunodeficiency disorders has been offered at LabPLUS laboratory in Auckland since 2005 (13). The concentration of LDT in onco-genetics speaks to the increased trend toward targeted therapy, in which individual tumours are tested for specific cancer mutations, to identify patients who are more likely to benefit from therapy. Also at CHL, the toxicology laboratory has applied in-house developed mass spectrometry testing for more than ten years. These mass spectrometry LDT provide improved accuracy at lower cost and are not yet available commercially. Similarly other disciplines within medical laboratories have kept ahead with technology and provide tests not available by global diagnostic companies. It is this application of knowledge on new technologies that enhances our service.
While half of all tests available in Europe were laboratory developed, most of the tests had no commercial equivalent (11). LDT are required for rare diseases, or to address areas with limited commercial incentive. Some tests, such as those that rely on next-generation sequencing technology, mass spectrometry, flow cytometry, are highly complex to run and require specific training to interpret. These are the specialist skills scientists and scientific officers (SO) bring to the NZ health service. It is these factors of complexity and high skill that can make a test more difficult to standardise and produce at a commercial scale. That there are no commercial alternatives for most LDT indicates the innovative capacity required of laboratories.
Organisational competence
Clinical laboratories are required to meet both technical and management system requirements to ensure consistent delivery of technically valid results. To achieve high standards the laboratory must apply best practice in quality management, the medical devices used must be effective and staff competence assured.
The International Organization for Standardization (ISO) 15189:2022 Medical laboratories — Requirements for quality and competence standard sets forth expectations on quality management. A quality management system (QMS) documents a system of processes, procedures, and responsibilities to meet regulatory requirements and customer’s needs. By embedding an expectation that quality management is the correct way of doing business, a culture of quality enhances the laboratory structure and function. The standard also provides a means of harmonising laboratory results such that clinicians and their patients can expect the same high quality regardless of where they live. International Accreditation New Zealand (IANZ) do a yearly audit of medical laboratories to confirm the competence of the laboratory management system with an audit on technical competence completed every four years. IANZ rely on laboratories to report changes to QMS in-between assessments.
The ISO 15189 standard also helps ensure the safety of laboratory workers. Laboratory workers are often exposed to hazardous materials, for example during 2023 there were two cases of laboratory acquired typhoid (14). The handling of highly infectious samples is required to be performed under physical containment in a biosafety cabinet (15), that these standards were not applied in the handling of the infectious material, in one case, is of concern. It is incumbent on all laboratory staff to know and adhere to Aotearoa NZ legislation and for laboratory management to provide the necessary equipment/facilities to enable safe practice. The knowledge and application of standards is vital in protecting medical laboratory workers from potential harm and also in provision of a high-quality service.
Competence of medical laboratory scientists
The Health Practitioners Competence Assurance Act 2003 (HPCA) ensures all health practitioners are competent and fit
to practice. The basic tenets of this act are that a consistent accountability regime is applied to all practitioners, that each practitioner has a scope of practice that sets competency requirements and that health practitioners do not work outside their scope. Ascribing a standard of competence, knowledge, and skill ensures practitioners are accountable in protecting the public from harm.
The regulatory authority, that enforces the HPCA Act for those who practice as medical laboratory scientists in Aotearoa NZ is the Medical Science Council. Medical laboratory scientists’ (MLS) scope of practice covers the collection, testing and reporting of all samples. In the laboratory the tests applied may be commercially sourced, they may be modifications to commercially sourced tests to meet specific requirements, or they may be developed in-house. The MLS scope of practice does not specifically cover aspects of test method development, nor the clinical research using the developed tests, albeit research and development are listed as discipline in the gazetted notice (16). There are legislative requirements under ISO 15189 to uphold when a laboratory introduces new tests but the competence of MLS to develop, validate, and perform ethical clinical research is not set out in the MLS competency requirements (17).
Health NZ-Te Whatu Ora employ Scientific Officers (SO) to provide research and technical leadership to the laboratory, which principally involves the development of diagnostic tests to aid clinicians. While they are employed to perform these duties under the MLS scope of practice, their competence in method validation or clinical research is not assured.
The work of SO and MLS was invaluable during the COVID-19 pandemic. SO and MLS set up and validated the first in-house COVID-19 molecular test for Aotearoa NZ, validated commercial kits and swabs for all Aotearoa NZ laboratories and developed in-house RNA extraction methods when commercial sample extraction kits were in short global supply. Scientists worked extensively to upscale testing capacity to 1000 - 2000 tests per day. COVID-19 highlighted the issues with a dependence on commercial supplies of test kits/reagents and Aotearoa NZ vulnerability in terms of its geographical location in maintaining essential supplies. The competence to independently develop and validate methods, verify commercial supplies of kits, swabs and reagents for molecular testing allowed Aotearoa NZ to test, trace, isolate and thereby limit the pandemic effects. In contrast the UK was unable to offer such testing, the move to automation with a hub and spoke laboratory service configuration has diminished scientific potential and the flexibility to innovate in a timely manner (18). The agility required during the pandemic proved a challenge in many jurisdictions but uniquely Aotearoa NZ had specialist scientists, working with academics, within our tertiary clinical laboratories with the capabilities of implementing effective LDT (19).
Regulatory improvements
Appropriate health research plays an integral role in the advancement of medical science and has health, social, and economic benefits as was demonstrated by the COVID-19 pandemic. Being cognisant of the potential for public harm, all stakeholders from scientists, laboratory management, professional organisations, government agencies, the MSC, and the laboratory accreditation body IANZ, must review practice and consider improvements to enhance the care of patients.
The latest edition of the ISO 15189:2022 standard has a focus on risk management and the need for laboratories to constantly evaluate their process and make improvements. This risk-based approach should ensure medical laboratories make improvements to enhance patient care without being prescriptive on how it is achieved. To date, the IANZ accreditation of laboratories has enforced a ‘tick box’ culture of quality; the focus on compliance had the effect of blinkering practices in the belief that they were effective, with a failure to realise further improvements. Thus the 2022 ISO revision has the potential to enhance the laboratory service.
The planned risk-based approach for medical device regulation is also encouraging. The pace of technological improvement/ research is dynamic, and we need flexibility for the early adoption of technologies. To this end it was proposed under the TPA 2023 that LDT be developed by competent scientists registered to the HPCA Act. To align with GHTF essential principles the development of medical tests must also be performed in a QMS compliant laboratory. Compliance of laboratories to QMS needs to be considered during the revision process of the TPA. Competence in QMS principles is an essential requirement for all laboratory staff with competence in the application of QMS principles required of laboratory management. Under QMS, adherence to standards/guidelines, process review and continuous improvement is required. Fewer laboratory errors indicates that the organisation of the laboratory has effective and accurate processes in place. A sustained commitment from QMS competent laboratory management to further the quality of our laboratory service will boost confidence and the value of medical laboratory testing.
In the absence of medical device regulation, the onus of public safety falls on the HPCA act. With the high usage of LDT there is no consumer protection for results issued on these tests. The provision of additional scopes of practice is required to establish both technical and quality management competence, particularly for those involved in the LDT service.
Knowledge of national and international legislation such as the following is required:
• The GHTF guidelines to ensure medical diagnostics meet essential principles and are fit for purpose.
• The international standard for clinical laboratory testing, ISO 15189 to assure compliance to QMS.
Benefits
Health service development
Public health & safety protection
Adoption of new technologies
Advance responsible innovation
Effective use of resources
Agile response to emerging pathogens
Health equity
Workforce development
Workforce engagement
• Specific knowledge of Clinical and Laboratory Standards Institute (CLSI) guidelines on laboratory QMS and validation of medical devices/technologies for clinical use. CLSI is a not-for-profit volunteer organisation that develops laboratory standards worldwide.
• The use of human tissue is regulated under the Human Tissues Act and the non-therapeutic use of human tissue standard, NZS 8135:2009.
• The ethical considerations for the use of human tissue are outlined by the National Ethical Standards for Health and Disability Research and Quality Improvement.
CONCLUSION
Consistent accountability of all practitioners within medical laboratories will facilitate our health service development. Our medical laboratory workforce has significant expertise and additional scopes of practice are required for the development of the profession. The benefit of additional scopes of practice for scientists and those in quality management are outlined in Table 1. Engaging and motivating staff through career pathways allows the health service to stay relevant and effective. Data mining and artificial intelligence are skills we will need. To garner such skills, we need to create flexible learning options such as specialised training, on-the-job training, and cross-training through placements.
New scopes of practice allow the laboratory workforce to develop additional skills which builds resilience and retains staff while improving the service. The creation of a new generation of laboratory professionals with a broader vision of health care and patient needs in a regulated QMS environment is to be encouraged.
Do nothing
Failure to maintain laboratory standards
Inconsistent accountability for public harm
Increased cost if services sourced abroad, delay in results
Loss of reputation, failure to attract investment
Waste and inefficiencies
Epidemics and disease outbreak
Poorer outcomes through misuse of information
Lack of competent scientists diminishes quality of service
Loss of motivation and staff leave the profession
CHL Canterbury Health Laboratory
CLSI Clinical and Laboratory Standards Institute
FDA Food and Drug Administration
GHTF Global Harmonisation Task Force
HPCA Health Practitioners Competence and Assurance Act
IH-IVD In-house in vitro diagnostic
IMDRF International Medical Device Regulators Forum
IANZ International Accreditation New Zealand
ISO International Organization for Standardization
IVD In-Vitro Diagnostic
LDT Laboratory Developed Test
MLS Medical Laboratory Scientist
MSC Medical Science Council
QMS Quality management system
SO Scientific Officer
TPA Therapeutic Products Act
Table 1. The benefit of an additional scope of practice
Table 2. Glossary
ACKNOWLEDGEMENTS
I thank Deborah Willis and Stewart Smith for their review of this manuscript.
DISCLOSURE OF FUNDING
No specific funding was received to support the work related to this manuscript.
CONFLICT OF INTEREST
I have no financial disclosures to declare. I am the Chair of the New Zealand Hospital Scientific Officers Association.
AUTHOR INFORMATION
Paula Keating, Immunology Section, Canterbury Health Laboratories, Christchurch, New Zealand.
Correspondence: Paula Keating.
Email: paula.keating@cdhb.health.nz
REFERENCES
1. Hallworth MJ. The ‘70% claim’: what is the evidence base? Ann Clin Biochem 2011; 48: 487-488.
2. Office of Public Health Strategy and Analysis, Office of the Commissioner of Food and Drug Administration. The public health evidence for FDA oversight of laboratory developed tests: 20 case studies. [website] 2015 Nov 16. Available at: https://www.nila-usa.org/images/nila/The%20Public%20 Health%20Case%20for%20FDA%20Oversight%20of%20 LDTs%20110915(2)_508ed%20(1).pdf.
3. Weedon MN, Jackson L, Harrison JW, Ruth KS, et al. Use of SNP chips to detect rare pathogenic variants: retrospective, population based diagnostic evaluation. BMJ 2021; 372:n214.
4. AlHilli MM and Al-Hilli Z. Perioperative management of women undergoing risk-reducing surgery for hereditary breast and ovarian cancer. J Minim Invasive Gynecol 2019; 26(2): 253-265.
5. Panacer KS. Ethical issues associated with direct-toconsumer genetic testing. Cureus 2023; 15:e39918.
6. Fiala C and Diamandis EP. The meteoric rise and dramatic fall of Theranos: lessons learned for the diagnostic industry. Clin Chem Lab Med 2018; 56:1443-1446.
7. Scheiblauer H, Filomena A, Nitsche A, Puyskens A, et al. Comparative sensitivity evaluation for 122 CE-marked rapid diagnostic tests for SARS-CoV-2 antigen, Germany, September 2020 to April 2021. Euro Surveill 2021; 26.
8. Costelloe C. Therapeutic Products Act to be repealed. [website] 2024 May 8. Available at: https://www.beehive.govt. nz/release/therapeutic-products-act-be-repealed
9. Hardcastle L. Medical device regulation and the proposed therapeutic products bill: devising a new regime. Victoria
University of Wellington Law Review 2021; 52:319-342.
10. Biomedical Alliance in Europe. Main findings IVDR Questionnaire BioMed Alliance. [website] 2021. Available at: https://www.biomedeurope.org/images/ news/2021/20211206_Findings_IVDR_Questionnaire_final. pdf.
11. Vermeersch P, Van Aelst T and Dequeker EC. The new IVD Regulation 2017/746: a case study at a large university hospital laboratory in Belgium demonstrates the need for clarification on the degrees of freedom laboratories have to use lab-developed tests to improve patient care. Clin Chem Lab Med 2020; 59:101-106.
12. Clinical and Laboratory Standards Institute. The FDA ruling on laboratory developed tests: taking control of what’s in your control. [website] 2024 July updated 2024 September 03. Available at: https://clsi.org/media/rjmpc5h1/ldt_whitepaper. pdf.
13. Woon ST and Ameratunga R. Comprehensive genetic testing for primary immunodeficiency disorders in a tertiary hospital: 10-year experience in Auckland, New Zealand. Allergy Asthma Clin Immunol 2016; 12:65.
14. George K and Macdonald N. Two lab workers in three months hospitalised with ‘rare’ typhoid infections caught at work. Stuff [web site] 2023 August 05. Available at: https:// www.stuff.co.nz/national/health/132679822/two-lab-workersin-three-months-hospitalised-with-rare-typhoid-infectionscaught-at-work.
15. Standards New Zealand. AS/NZS 2243.3:2022 Safety in laboratories - Part 3: Microbiological safety and containment published 2022 November 25.
16. New Zealand Gazette. Notice of scopes of practice and prescribed qualifications for the practice of medical laboratory science. effective 2021 June 1. Available at: https://gazette. govt.nz/notice/id/2021-gs2023
17. The Medical Sciences Council of New Zealand. Competence standards for medical laboratory science practitioners in Aotearoa New Zealand. 2018 Feb revised 2018 Nov. Available at: https://www.mscouncil.org.nz/assets_mlsb/ Uploads/2018-Nov-V2-MSC-Competence-Standards-MLS. pdf.
18. Banatvala J. COVID-19 testing delays and pathology services in the UK. Lancet 2020; 395:1831.
19. Geoghegan JL, Moreland NJ, Le Gros G and Ussher JE. New Zealand’s science-led response to the SARS-CoV-2 pandemic. Nat Immunol 2021; 22: 262-263.
Aurora kinase A overexpression in liver cancer predicts the poor prognosis of patients
Ahmed A. Mohsin and Susan Zwyea
ABSTRACT
Objectives: Aurora kinase A is a protein kinase which plays a critical role in several cancers. The role of Aurora kinase A in liver cancer metastasis is not well understood. Our study sought to investigate Aurora kinase A expression in normal, tumour and metastasis liver tissues to assess the relationship between its expression and the prognosis of liver cancer patients.
Methods: RNA-Seq data from The Cancer Genomic Atlas (TCGA), the Genotype Tissue Expression (GTEx) and the Gene Expression Omnibus (GEO) data were used for gene expression profile evaluation and prognostic analysis. Immunohistochemistry (IHC) assay of clinical specimens from the Human Protein Atlas were used for Aurora kinase A clinical value evaluation.
Results: Aurora kinase A expression was upregulated by analysed TCGA, GTEx and GEO liver cancer databases in metastasis and cancer patients when compared with normal samples. In addition, Aurora kinase A upregulation was verified by IHC assay in liver cancer tissues. Furthermore, high expression of Aurora kinase A was associated with the worst prognosis in liver cancer patients. Finally, high Aurora kinase A protein expression was positively proportionally linked to high AKT serine threonine kinase and pyruvate dehydrogenase kinase 1 protein expression in liver cancer patients.
Conclusions: Our results suggested that Aurora kinase A may act through AKT serine threonine kinase and pyruvate dehydrogenase kinase 1 to promote liver cancer, suggesting Aurora kinase A might serve as a future predictor marker and survival prognosis for patients with liver cancer.
Liver cancer is the second leading cause of cancer-related deaths in males and females with an estimated 1.2 million new cases yearly and 830,000 deaths worldwide (1-3). Hepatocellular carcinoma is the most abundant type of liver cancer. Hepatocellular carcinoma usually occurs as a consequences of chronic liver diseases, liver infections, and liver fibrosis. Despite substantial developments in liver cancer therapy, the recurrence rate remains high, and the prognosis of the disease is still poor (4). Unfortunately, only a low percentage of patients who undergo liver resection survive more than five years, due to its aggressive behaviour on the contrary little progress has been made in early detection using hepatocellular cancer biomarkers. Therefore, the identification of new effective prognosis markers for liver cancer is urgently needed.
Early detection of liver cancer is a significant key to controlling liver cancer (2). Targeting proteins such as Aurora kinase proteins precisely could enhance liver cancer detection and diagnosis. Aurora kinases are members of serine threonine family. Aurora kinases are overexpressed in several specific cancer types such as kidney, lung, and mesothelioma (5). Aurora kinases overexpression has been reported to contribute to development of a variety of cancers, particularly liver cancer. Aurora kinases overexpression causes chromosomal instability that could lead into liver cancer development. Aurora kinases play an important role in enhancing and activating specific mitotic spindle genes and oncogenes such as neurodevelopment protein 1 (NDEL1), transforming acidic coiled coil (TACC3), and aster associated protein (ASAP) (5,6). Aurora kinases have three members or subtypes. Those members are Aurora kinase A (AURKA) Aurora kinase B (AURKB), and Aurora kinase C (AURKC). The most overexpressed Aurora kinases in liver cancer tissues are AURKA and AURKB in comparison with AURKC that is not that abundant in cancer tissues (5). Both AURKA and AURKB are involved in the regulation of cell cycle, cell proliferation, cancer development, migration and metastasis (7-9). AURKA protein is well known to be interacting with certain signalling pathways like mammalian target of rapamycin (mTOR), fork head box class O (FOXO), MAP kinase (MAPK) and nuclear factor kappa B (NFkB) (10). Previous research found that AURKA protein plays important role in recruiting other signalling mitotic proteins required for tumour development (7). Importantly, several studies have identified that AURKA expression is high in certain types of
malignancies, suggesting that AURKA could be an oncogene, promoting tumorigenesis (10-13). The underlying mechanisms of AURKA promoting cancer metastasis are not fully understood. Previous studies have shown that AURKs are new promising effective prognostic biomarker in liver cancer, however no study addresses the association of the high levels of AURKA in tissues of liver cancer patients with molecular basis that promote metastasis and poor survival (14). Moreover, no study provided the prognostic value of AURKA in human liver cancer early detection.
Our study aimed to investigate Aurora kinase A expression in normal, tumour, and metastasis liver tissues, to assess the relationship between its expression and the prognosis of liver cancer patient’s prognostic marker in liver cancer.
MATERIALS AND METHODS
Public Data
The protein expression data of the liver of normal and cancer patients were obtained from the Human Protein Atlas website (https://www.proteinatlas.org) version 22.0 (15). There were 226 normal liver samples (147 male and 79 female) and 365 liver cancer samples (246 male and 119 female). The age ranged from 20-79 years. The data was used to investigate the protein expression of AURKA, AKT serine threonine kinase 1 (AKT1) and pyruvate dehydrogenase kinase 1 (PDK1) in the tissues of normal and liver cancer patients. Immunohistochemistry assay was used to investigate AURKA, AKT1 and PDK1 protein expression in samples of healthy individuals and liver cancer patients. In addition, RNA-Seq was used to check mRNA expression of AURKA in different normal and cancer tissues. The RNA levels were generated by the GEO, GTex, TCGA, and TARGET databases website (https://tnmplot.com/analysis/) (16). A ChIP assay was utilized to check the transcription level of AURKA and PDK1 genes in normal, tumour and metastasis liver tissues. The RNPDKA expression data for chip assay was obtained from GEO, GTex, and TCGA (https://tnmplot.com/ analysis/) (16).
Survival analysis
The survival dataset used in this study consists of liver cancer patients diagnosed in the United States. The dataset was obtained from Kaplan-Meier (K-M) estimator (17), and the data
used as input into K-M estimator. There were 370 liver cancer patients (249 males and 121 females). The cohort with high AURKA, AKT1, and PDK1 mRNA expression was coloured red. The cohort with low AURKA, AKT1, and PDK1 mRNA was coloured in black line. The cut off value was 620. Follow up threshold was 120 months. No restriction on cancer stage, gender, race, and cancer grade was used in the analysis.
Statistical analysis
Overall survival of liver cancer patients was measured in months after taking treatments until death. K-M estimator graphs were generated by R statistic software (version 3.6.3). Logistic rank was used to check correlation significance between the expression of AURKA, AKT1, and PDK1 genes and liver cancer patients’ survival. The results were regarded as significant when p value is less than 0.05. Kruskall-Wallis and Dunn Tests was used to investigate the multiple comparison between expression of AURKA, AKT1, and PDK1 genes in normal, tumour and metastasis samples. The Spearman Test was used to assess the correlation between liver cancer cell lines and their corresponding TCGA data sample cohorts.
RESULTS
AURKA expression in normal and cancer liver tissues
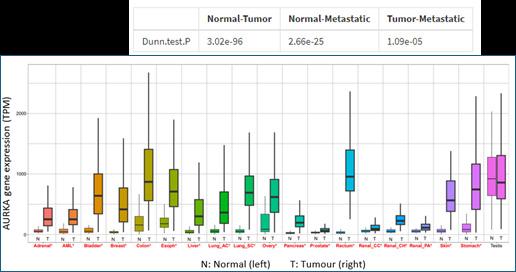
First, 56,938 samples from GEO, GTex, TCGA and TARGET databases were analysed to explore AURKA expression across 19 cancer types. This includes 15,648 normal, 40,442 tumour, and 848 metastasis samples. The data were analysed at the pan-cancer level (Figure 1a). The results showed significance difference in AURKA expression in cancer compared to normal tissue samples (p<0.05). AURKA expression was upregulated in many cancer types including liver cancer, adrenal cancer, acute myeloid leukaemia, bladder cancer, lung cancer, ovary cancer, prostate cancer, and renal clear carcinoma. However, there was no significant difference found in AURKA expression in testis cancer compared to normal (p>0.05).
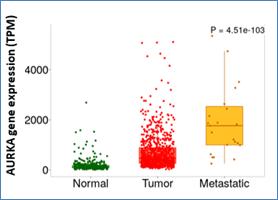
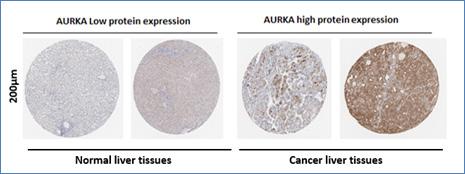
Second, AURKA expression was assessed in pairs of normal liver tissues, cancer liver tissues, and metastasis liver tissues by ChIP assay. The analysis showed that AURKA level was significantly higher in metastasis liver tissues than tumour and normal tissues (p=4.51x10e-103) as presented in Figure1b. In addition, AURKA level was significantly higher in liver tumour tissues compared to normal liver tissues (p=3.02e-93) (Figure 1b). Later, these results were confirmed by the investigation of the protein expression of AURKA in separate samples (normal and tumour liver tissues) using the human protein atlas public data set (15). The results showed that liver tumour had higher protein expression of AURKA than the normal liver tissues (Figure 1c). Consistency between cancer cell lines and their
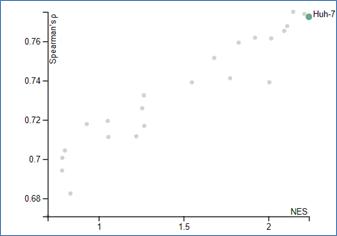
corresponding TCGA cancer cohort using spearman correlation and normalized enriched score (NES) was investigated. The results showed that high correlation between all liver cancer cell lines and their corresponding TCGA liver cancer cohort (r = 0.77) as shown in Figure 1d.
Analysis of the relationship between AURKA, AKT-1 and PDK1 in promotion liver cancer
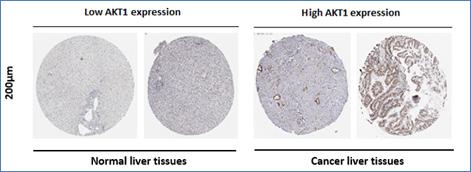
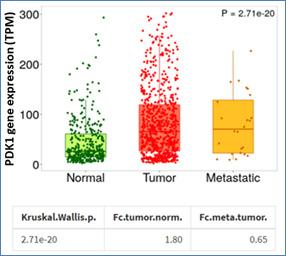
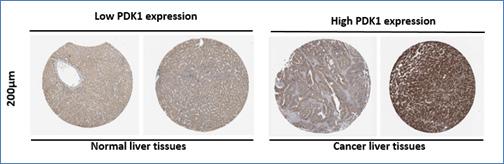
The Human Protein Atlas data for liver cancer was downloaded. AKT1 and PDK1 protein levels were analysed to determine if AURKA overexpression may be crucial to enhance AKT1 and PDK1, AURKA effectors, signal to advance liver cancer pathogenesis. First, the immunohistochemistry staining results demonstrated that AKT1 and PDK1 were upmodulated in liver cancer tissues in comparison to normal tissues (Figure 2a and 2c). Further, RNA expression of PDK1 was examined. Data from GEO, GTex, TCGA and TARGET databases were downloaded and analysed. The results showed that PDK1 was significantly higher in liver tumour tissues in comparison to normal tissues (p=2.71 e-20) (Figure 2b).
Prognostic value of AURKA in liver cancer
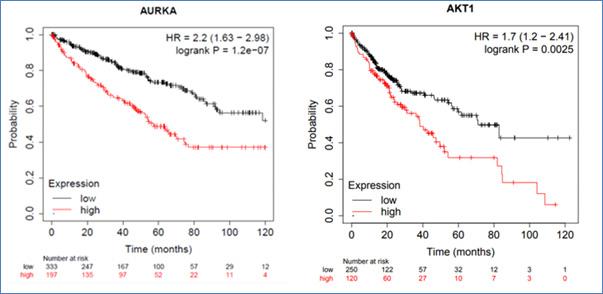
Data from Kaplan-Meier (K-M) estimator for pan cancer RNASeq were used to evaluate the prognostic value of AURKA high expression in liver tumour. Overall survival time of liver cancer patients was used as a training set (input). The results showed patients cohort was subdivided into two categories; group 1 those with low mRNA AURKA expression (n=333) and group 2 those with high mRNA expression of AURKA (n=197) as illustrated in Figure 3a. Our results showed that patients in group 2 had poorer or worse survival and two times higher risk of death than those in group 1 (HR=2.2; p=1.2e-07). Furthermore, the results revealed that survival rate of group 2 (2%; given that 4 survived out of 197) was lower than survival rate of group1 (3.6%; given that 12 survived out of 333) as shown in Figure 3a.
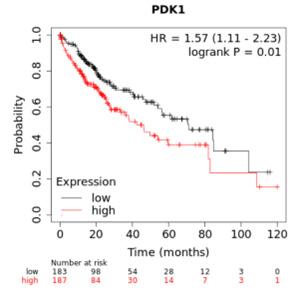
Next, the correlation between AKT1 mRNA expression and overall survival of liver cancer patient was investigated using K-M estimator. The results demonstrated that patient was subdivided into two categories; group 1 those with low mRNA AKT1 expression (n=250) and group 2 those with high mRNA expression of AKT1 (n=120) as illustrated in Figure 3b. The results showed that patients who suffer from high AKT had worse survival than the patients with low AKT1 expression (HR=1.7; p=0.0025; Figure 3b). Finally, using K-M estimator, the correlation between PDK1 mRNA expression and overall survival of liver cancer patients was examined. The results showed that patients with high PDK1 (group 2) had worse survival than patients with low PDK1 (group 1) (HR=1.57; p=0.01; Figure 3c).
Figure 1a.
Figure 1b.
1c.
1d.
Figure 1.
1a; AURKA expression in normal and liver cancer. Analysis for AURKA RNA levels in different cancer types by RNAseq assay, AML: acute myeloid leukaemia, lung AC: lung adenocarcinoma, lung S C: lung squamous cell carcinoma, renal C C: clear cell renal cell carcinoma, TPM: transcripts per million. Significant differences were tested by a Mann Whitney U and marked red. * p<0.01. 1b; Analysis for AURKA expression in normal, tumour and metastatic liver tissues using chip assay. Significant differences were tested by a Dunn test. 1c; IHC staining for AURKA in normal liver tissues were obtained from website link: (https://www.proteinatlas.org/ ENSG00000178999-AURKB/tissue/liver) and liver cancer tissues were obtained from website link: (https://www.proteinatlas.org/ ENSG00000178999AURKB/pathology/liver+cancer). 1d; Consistency correlation between cancer cell lines including Huh-7 human liver cancer cell line and their corresponding TCGA cohorts, NES: normalized enrichment score.
2a.
Figure
Figure
Figure
Figure 2b.
Figure 2c.
Figure 2.
2a; AKT1 and PDK1 expression analyses in liver cancer patients. IHC staining for AKT serine threonine kinase (AKT1) in normal (https://www.proteinatlas.org/ENSG00000142208-AKT1/tissue/liver ) and liver cancer tissues (https://www.proteinatlas.org/ ENSG00000142208-AKT1/pathology/liver+cancer) 2b; Analysis for pyruvate dehydrogenase kinase 1 (PDK1) expression in normal, tumour and metastatic liver tissues using chip assay, TPM: transcripts per million. 2c; IHC staining for PDK1 in normal (https://www. proteinatlas.org/ENSG00000152256-PDK1/tissue/liver) and liver cancer tissues (https://www.proteinatlas.org/ENSG00000152256PDK1/pathology/liver+cancer#).
3a; K-M Survival analysis of liver cancer patients AURKA expression and Survival time analyses in liver cancer patients; HR=hazard ratio 3b; AKT1 expression and Survival time analyses in liver cancer patients 3c; PDK1 expression and Survival time analyses in liver cancer patients.
Figure 3.a
Figure 3b
Figure 3.
DISCUSSION
In this study, the role of AURKA expression in liver cancer was investigated. First, AURKA expression was explored on pan cancer level across 19 cancer types using GEO, GTex, TCGA and TARGET data. Then, AURKA expression was observed in pairs of normal liver tissues, cancer liver tissues, and metastasis liver tissues to further understand its role. The study findings revealed an up modulation in AURKA in multiple types of tumours, including liver cancer tissues compared to normal tissues. These results are consistent with Goos et al research on the evaluation the role of AURKA expression in liver cancer (11). Also, the study results showed that AURKA level was higher in metastasis liver tissues than tumour and normal tissues. In addition, AURKA level was significantly higher in liver tumour tissues compared with normal liver tissues. Our results conjectured that high AURKA may have a role in driving liver cancer metastasis, consistent with what Chen found in liver cancer research (18).
Next, AURKA possible crosstalk with other signalling pathways in specific AKT1 proteins was examined using the Human Protein Atlas dataset. The immunohistochemistry results demonstrated that AKT1 was upmodulated in liver cancer tissues in comparison to normal tissues. This result was consisted with previous studies and further confirm AURKA connection and acting through other signalling pathways to drive liver cancer metastasis (9,10). Our results also suggest that AKT1 could be the downstream target of AURKA and that AURKA overexpression in liver cancer may drive AKT1 overexpression as well to promote liver cancer metastasis directly or indirectly through other signalling pathways. So, we further investigated the RNA and protein expression of one of AKT1 upstream target, namely PDK1. The results showed that PDK1 was significantly higher in liver tumour tissues in comparison to normal tissues. These results were consistent with previous studies which reported that AURKA has interactions with other signalling pathways to promote liver cancer (9,10). The results indicated that AURKA may regulate and advance liver carcinogenesis through AKT1 and PDK. These hypotheses require further research.
Finally, the prognostic value of AURKA was investigated using Kaplan-Meier (K-M) estimator. The results showed that patients with high mRNA expression of AURKA had poorer or worst survival. Therefore, AURKA may have a prognostic role in liver cancer. This result was consistent with what Du found in liver cancer research (5). In addition, the correlation between AKT1 and PDK1 mRNA expression and survival of liver cancer patients was investigated using K-M estimator. The results demonstrated that patients who suffer from high AKT and PDK1 expression had worse survival than the patients with low AKT1 and PDK1 expression. Our results suggested that AURKA may drive liver cancer metastasis through PI3K/AKT signalling pathways and it might be a novel therapeutic target for liver cancer patients. A work goal is to investigate the mechanisms behind these observations and to generate an animal model to study AURKA inhibitors effect in liver cancer.
CONCLUSIONS
Aurora kinase A expression was upmodulated in liver cancer tissues and was associated with patients’ poor survival. Aurora kinase A has the potential to be a prognostic marker for early prognosis of liver cancer. Additionally, Aurora kinase A may serve as a novel therapeutic target for the treatment of liver cancer.
AUTHOR INFORMATION
Ahmed A. Mohsin, PHD, MSc, BSc, Assistant Professor1
Susan Zwyea, PhD, MSc, BSc, Assistant Professor2
1Department of Medical Laboratory Techniques, College of Health and Medical Technology/ Baghdad, Middle Technical University, Baghdad, Iraq
2Department of Radiological Techniques, College of Health and
Medical Technology/ Baghdad, Middle Technical University, Baghdad, Iraq
Correspondence: Dr Susan Zwyea email: Dr.susanzwyea@mtu.edu.iq
REFERENCES
1. Sung H, Ferlay J, Siegel R L, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209-249.
2. Forner A, Reig M, Bruix J Hepatocellular carcinoma. Lancet 2018; 391:1301-1314.
3. Yang JD, Hainaut P, Gores GJ, et al. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol 2019; 16: 589-604.
4. Borah NA, Reddy MM. Aurora kinase B inhibition: a potential therapeutic strategy for cancer. Molecules 2021; 26:1981.
5. Du R, Huang C, Liu K, et al. Targeting AURKA in cancer: molecular mechanisms and opportunities for cancer therapy. Mol Cancer 2021; 20: 15.
6. Venoux M, Basbous J, Berthenet C, et al. ASAP is a novel substrate of the oncogenic mitotic kinase Aurora-A: phosphorylation on Ser625 is essential to spindle formation and mitosis. Hum Mol Genet. 2008; 17(2): 215–224.
7. Marumoto T, Zhang D, Saya H. Aurora-A - a guardian of poles. Nat Rev Cancer 2005; 5: 42-50.
8. Wang, Z., Qu, L., Deng, B. et al. STYK1 promotes epithelialmesenchymal transition and tumor metastasis in human hepatocellular carcinoma through MEK/ERK and PI3K/AKT signaling. Sci Rep 2016; 6: 33205.
9. Nikonova A S, Astsaturov I, Serebriiskii I G, et al. Aurora A kinase (AURKA) in normal and pathological cell division Cell Mol. Life Sci 2013; 70: 661-687.
10. Boos S L, Loevenich L P, Vosberg S, et al, Disease modeling on tumor organoids implicates AURKA as a therapeutic target in liver metastatic colorectal cancer Cell Mol. Gastroenterol Hepatol 2021; 13(2): 517-540.
11. Goos J A, Coupe V M, Diosdado B, et al, Aurora kinase A (AURKA) expression in colorectal cancer liver metastasis is associated with poor prognosis Br. J. Cancer, 2013; 109: 2445-2452.
12. Chang X, Zhang H, Lian S,Zhu W. miR-137 suppresses tumor growth of malignant melanoma by targeting aurora kinase A Biochem Biophys Res Commun 2016; 475(3): 251256.
13. Li. Y, Zhang J AURKA is a predictor of chemotherapy response and prognosis for patients with advanced oral squamous cell carcinoma Tumour Biol 2015; 36: 3557-3564.
14. Ramani P, Nash R, Rogers C A Aurora kinase A is superior to Ki67 as a prognostic indicator of survival in neuroblastoma Histopathology 2015; 66: 370-379.
15. Uhlén M et al., The human secretome. Sci Signal. 2019; 12(609): eaaz0274. doi: 10.1126/scisignal.aaz0274.
16. Bartha A, Gyorffy B, TNMplot.com: a web tool for the comparison of gene expression in normal, tumor and metastatic tissues Int J Mol Sci 2021; 22(5): 2622.
17. Győrffy B. Integrated analysis of public datasets for the discovery and validation of survival-associated genes in solid tumors. Innovation (Camb) 2024; 5(3): 100626. doi 10.1016/j.xinn.2024.100625.
18. Chen C, Song G, Xiang J, et al AURKA promotes cancer metastasis by regulating epithelial-mesenchymal transition and cancer stem cell properties in hepatocellular carcinoma. Biochem and Biophys Res Commun 2017; 486(2): 514-520.
The effects of glucose 6-phosphate dehydrogenase deficiency on nonenzymatic antioxidants and kidney function in children in the Basra Governorate, Iraq
Zainab Shakir Abdullah Al Ali and Bushra A. M Abdul Azeez Al Salem
ABSTRACT
Objective: The purpose of this study is to investigate the significance of non-enzymatic antioxidants (glutathione (GSH) and vitamin E)and kidney function tests (creatinine and urea) in children with glucose-6-phosphate dehydrogenase (G6PDH) deficiency aged 1-15 years in Basra governorate, Iraq.
Methods: A study was conducted at Ibn Ghazwan Hospital in Basra Governorate between July and October 2023 on patients with glucose-6-phosphate dehydrogenase deficiency (G6PDH) and healthy controls. Non-enzymatic antioxidants (glutathione (GSH) and vitamin E) and kidney function tests (creatinine and urea) were analysed.
Results: Severe G6PDH deficient subjects have lower mean values of vitamin E (2.93±1.00) and glutathione (0.35±0.19)*10-2 than normal subjects. Whereas the deficient subjects had elevated creatinine (1.583±0.457) and urea (21.300±3.573) levels. The correlation study shows that G6PDH was positively statistically significant (p˂0.01) correlated with glutathione and vitamin E. Conversely, G6PDH was negatively statistically significant (p˂0.01) correlated with creatinine and urea.
Conclusions: Glucose-6-phosphate dehydrogenase (G6PDH) deficiency is a common genetic disorder that can lead to a range of health complications, including increased oxidative stress and potential renal impairment.
Keywords: kidney function tests, G6PDH deficiency, non-enzymatic antioxidants, glutathione, vitamin E, creatinine; urea.
NZ J Med Lab Sci 2025; 79(1) 13:16
INTRODUCTION
Worldwide, more than 500 million people carry a mutation in the glucose-6-phosphate dehydrogenase (G6PDH) gene (1). G6PDH deficiency manifests clinically in three main ways in people with variants with decreased activity: neonatal jaundice, chronic nonspherocytic haemolytic anaemia (CNSHA), and acute haemolytic anaemia (AHA). These conditions are caused by factors such as certain foods, antibiotics, antimalarials, or infections that cause reactive oxygen species (ROS) to accumulate (1, 2). Also, there are more than 442 variants of G6PD in humans (3). Many are associated with anaemia caused by an impaired erythrocyte response to toxic stress (4, 5). A mutation in the G6PDH gene located on the X chromosome will result in full phenotypic expression for males with a mutation (hemizygote) and females with a mutation on both X chromosomes (homozygote) or one X chromosomes (heterozygote) (6-9).
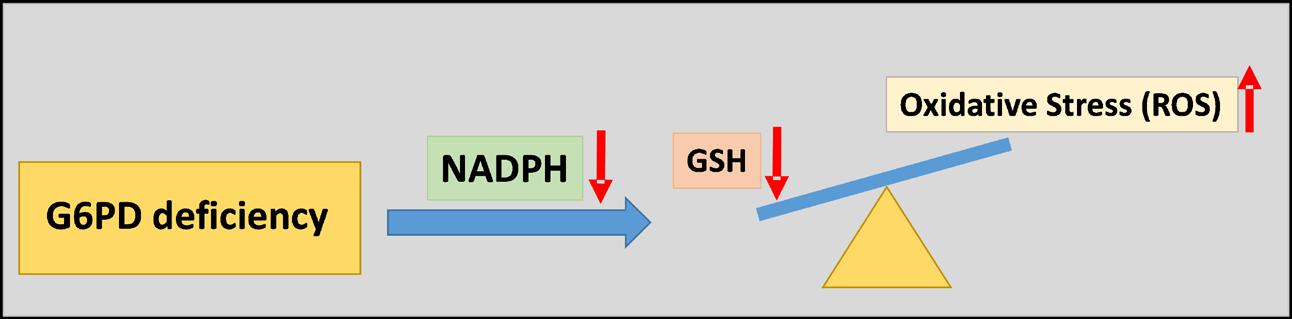
Glucose-6-phosphate dehydrogenase (G6PDH) enzyme is found in all cells in the body, in the cytoplasm. It catalyses the first step in the pentose phosphate pathway by the oxidation of glucose-6-phosphate to 6-phosphoglucono-lactone coupled to the reduction of nicotinamide adenine dinucleotide phosphate (oxidised form, NADP+) to nicotinamide adenine dinucleotide phosphate (reduced form, NADPH) (10, 11). NADPH plays a crucial role in the reduction of oxidized glutathione (GSSG) to reduced form glutathione (GSH), which is formed within red blood cells (RBCs) and prevents oxidative stress, retaining the RBC in a normally reduced state (12). G6PDH-deficient RBCs have limited reductive capacity (from decreased NADPH byproducts) and are susceptible to haemolysis caused by oxidative stress (13, 14). Thus, G6PDH prevents cellular damage from reactive oxygen species (ROS) by providing substrates that prevent oxidative damage. Because erythrocytes transport oxygen and cannot replace cellular proteins as mature cells, they are particularly vulnerable to ROS. The production of ROS during increased glucose-6-phosphate dehydrogenase deficiencies (10, 15, 16). G6PDH deficiency decreases RBC NADPH levels.
During this period, there is a decrease in GSH recycling, but a rise in ROS, which leads to oxidative stress (17). (Figure 1).
G6PDH deficiency is typically characterized by extravascular haemolysis, but intravascular haemolysis is also possible. Because haemoglobin denatures under oxidative stress and the formation of ROS in persons with G6PDH deficiency, it causes intravascular haemolysis (18-20). In intravascular haemolysis, red blood cells are destroyed by releasing their contents into the bloodstream, such as haemoglobin (21). Haemoglobinuria is one of the most prominent clinical signs of excessive intravascular haemolysis and can cause renal failure when the free plasma haemoglobin is filtered through the kidney (12, 22). Clinical manifestations of G6PDH deficiency depend on the degree of deficiency. Haemolysis does not occur in individuals with minimally reduced enzyme levels. Those with a greater degree of deficiency experience brisk haemolysis caused by infections, drugs that increase oxidative stress, eating fava beans, or experiencing ketoacidosis (23).
To combat the formation of ROS, erythrocytes and the entire body contain antioxidant defence systems containing enzymatic and non-enzymatic antioxidants (of which GSH plays a significant role) (24). Several studies have shown that individuals with G6PDH deficiencies exhibit increased oxidative stress in several tissues. Low antioxidant levels may be one factor contributing to the predisposition of deficient individuals to generate oxidative stress. For instance, it has been reported that G6PDH deficient individuals have lower vitamin E, vitamin C, carotenoids and glutathione levels (25, 26). G6PDH deficiency leads to some clinical conditions like haematuria and jaundice, which can adversely affect the kidneys and liver function in the future (12). The current research was established to investigate the oxidative stress of glucose-6-phosphate dehydrogenase and its relationship with non-enzymatic antioxidants (glutathione (GSH) and vitamin E) and kidney function tests (creatinine and urea).
Figure 1. GSH depletion and excessive oxidative stress are brought on by G6PDH deficiency
MATERIALS AND METHODS
From July to October 2023, samples were collected from Ibn Ghazwan Hospital in Basra governorate from 58 subjects (30 patients and 28 controls). Anticoagulant (EDTA) containers and non-anticoagulant containers were used to collect blood samples, which were separated into plasma and serum. All samples were stored at -20°C for further analysis within a 48-hour period. Ethics Committee approval was obtained for this study protocol by the University of Basra. No medical recommendations or prescriptions were interfered with by the research protocol.
Samples Collection and Laboratory Tests
A blood sample of 5 mL was drawn from both groups (controls and patients). To measure the activity of G6PDH, the first part of whole blood (3 mL) was collected in EDTA tubes and gently mixed. The G6PDH test kit from the G6PDHUV kinetic technique (REF97089) was obtained from Biolabo, France and used according to the manufacturer's instructions. The remainder of the whole blood was centrifuged for 20 minutes at 3000 rpm to produce plasma. The activity of plasma non-enzymatic antioxidants (glutathione and vitamin E) was measured using enzyme-linked immunosorbent assay (ELISA), using the diagnostic kit provided by the Sun Long Company (number: SL0ptHu, SL835Hu), respectively.
After coagulation at room temperature, the second part of whole blood (2 mL) was transferred to a plain tube (without anticoagulant) and centrifuged at 3000 rpm for 20 minutes to produce serum. The activity of serum kidney function tests (creatinine and urea) was measured using the diagnostic kit, namely, the creatinine kinetic method and urea colorimetric method provided by Biolabo, France and used according to the manufacturer's instructions.
Statistical Analysis
Statistical analysis of the data was undertaken using SPSS for Windows, Version 25.0. Armonk, NY: IBM Corp. The data
were expressed as mean ± standard deviation. Karl Pearson’s correlation coefficient was used to investigate the relationship between vitamin E, glutathione, creatinine, urea and G6PDH. Statistical significance between the aforesaid variables was also tested. Association between G6PDH deficiency and sex was performed with a Chi-square test statistic to study the association between the sex of the patient and G6PDH deficiency.
RESULTS
In the present study, thirty patients with glucose-6-phosphate dehydrogenase (G6PDH) deficiency were examined. The mean age of the patients was 8.0±3.58 years. As compared with the control group, 28 healthy individuals had normal G6PDH activity with an average age of 9.07±3.09 years. The mean ± SD of G6PDH activity diminished in the children group (20.64±2.15 µkat/L haemoglobin) compared to the control group (124.77±9.45 µkat/L haemoglobin) (Table 1).
The mean ± SD of vitamin E, glutathione, creatinine and urea of G6PDH normal and deficient subjects are presented in Table 2.Vitamin E and glutathione have significantly lower mean values in G6PDH deficient subjects compared to the control group. Whereas creatinine and urea levels were increased in the G6PDH deficient subjects.
The correlation and related significance (p-values) between biochemical parameters (vitamin E, glutathione, creatinine and urea) and G6PDH are shown in Table 2. Statistically significant positive correlations of G6PDH were observed with glutathione and vitamin E. Creatinine and urea demonstrated a significant negative correlation with G6PDH.
Chi-square test was used to determine the relationship between sex and G6PDH deficiency in the study participants. A cross-tabulation of sex and G6PDH deficiency is shown in Table 3. It reveals that 56.7% (n = 17) of the deficient cases were males and 43.3% (n = 13) were females. The value of Pearson Chi-square was 0.259 with a p-value <0.05, which reveals a significant relationship between sex and G6PDH deficiency.
Table 2. Pearson correlation between vitamin E, GSH, creatinine and urea of G6PDH deficient subjects
Table 1. Values of vitamin E, GSH, creatinine and urea of the severe G6PDH deficient subjects (Mean ± SD)
Table 3. Cross-tabulation of
DISCUSSION
G6PDH deficiency through X-linked inheritance can cause severe haemolytic anaemia when reactive oxygen species generation is elevated. Stress or exposure to foods high in oxidative chemicals, including fava beans, or some drugs such as antimalarials, may cause this. The haemolytic anaemia range, which varies from mild to severe haemolysis in response to oxidative stress, is a clinical manifestation of G6PDH deficiency. The degree of the enzyme deficiency, which in turn depends on the G6PDH variant, determines the probability and severity of haemolysis. Multiple abnormalities in the amounts of various vitamins, lipid profiles, blood proteins, trace elements, uric acid, and malondialdehyde are caused by a G6PDH deficit. Because of this, the concentrations of various biochemical components will vary according to age, sex, and the severity of the disease. Massive intravascular haemolysis in G6PDH deficiency can result in acute renal failure, and acute tubular necrosis may exacerbate the severe haemolytic crisis (21).
This finding aligned with an earlier finding in previous research that showed that the prevalence of deficiency G6PDH activity in males was more than in females (27-29). Females receive a copy of the X chromosome containing the G6PDH gene from both parents, whereas males only receive one copy from their mothers. Since females have two sources of the enzyme, females are less likely than males to be G6PDH deficient.
G6PDH deficiency results in the diminished effectiveness of RBC function resulting in significant health risks as well as secondary metabolic consequences (30). When the body's antioxidant defence mechanism cannot control free radical generation (reactive oxygen species, ROS), then oxidative stress results in G6PDH, which is an enzyme responsible for protecting against damage caused by ROS. Because of their function in oxygen transport and their incapacity to replenish cellular proteins as mature cells, RBCs are especially susceptible to ROS. G6PDH deficiency is associated with hidden renal injury of different degrees during acute haemolytic episodes and kidney damage may persist after the acute haemolytic crisis has passed (31, 32). This may be explained in the current work as G6PDH deficiency was demonstrated to affect levels of creatinine and urea, however, how G6PDH deficiency contributes to kidney diseases is poorly understood. (33)
Low plasma vitamin E and GSH concentrations are associated with diminished RBC survival (24) and in the current work a significant decrease in plasma vitamin E and GSH compared to controls was demonstrated, which is well documented to decrease RBC survival (26). Our findings were consistent with this outcome. The renal function tests clearly indicated some degree of impaired renal function in the G6PDH deficient children and should indicate the requirement for early intervention to prevent future kidney disease.
CONCLUSION
Children suffering from severe glucose 6-phosphate dehydrogenase deficiency in the Basra Governorate, Iraq, have elevated levels of creatinine and urea and lower levels of glutathione and vitamin E (non-enzymatic antioxidants). Therefore, G6PDH deficiency increases oxidative stress and may eventually lead to renal failure.
ACKNOWLEDGEMENTS
Thank you to patients with G6PDH deficiency for donating blood and best wishes to them.
CONFLICTS OF INTEREST
The authors have no conflict of interest to declare.
AUTHOR INFORMATION
Zainab Shakir Abdullah Al Ali, PhD MSc BSc, Associate Professor1
Bushra A. M Abdul Azeez Al Salem, PhD MSc BSc, Lecturer¹
1Department of Chemistry, College of Science, University of Basra, Basra, Iraq
Correspondence: Zainab Shakir Abdullah Al Ali, email: zainab. abdulah@uoBasra.edu.iq
REFERENCES
1. Geck RC, Powell NR, Dunham MJ. Functional interpretation, cataloging, and analysis of 1,341 glucose-6-phosphate dehydrogenase variants. Am J Hum Genet 2023; 110(2): 228-239.
2. Belfield KD, Tichy EM. Review and drug therapy implications of glucose-6-phosphate dehydrogenase deficiency. Am J Health Syst Pharm 2018; 75(3): 97-104.
3. Smith M. Chapter 11 - Analysis of variants associated with abnormal drug responses, genetics, and genomics in drug design. Progress in Genomic Medicine Smith M, Editor. Academic Press; 2022; 209-235.
4. Kwok CJ, Martin AC, Au SW, Lam VM. G6PDdb, an integrated database of glucose-6-phosphate dehydrogenase (G6PD) mutations. Hum Mutat 2002; 19(3): 217-224.
5. Roth E, Jr., Schulman S. The adaptation of plasmodium falciparum to oxidative stress in G6PD deficient human erythrocytes. Br J Haematol 1988;70(3): 363-367.
6. Bancone G, Kalnoky M, Chu CS, et al. The G6PD flowcytometric assay is a reliable tool for diagnosis of G6PD deficiency in women and anaemic subjects. Sci Rep 2017; 7(1): 9822.
7. Riskin A, Bravdo Y, Habib C, et al. The Genetics of Glucose-6-Phosphate-Dehydrogenase (G6PD) and Uridine Diphosphate Glucuronosyl Transferase 1A1 (UGT1A1) promoter gene polymorphism in relation to quantitative biochemical G6PD activity measurement and neonatal hyperbilirubinemia. Children (Basel, Switzerland) 2023; 10(7): 1172.
8. Luzzatto L, Ally M, Notaro R. Glucose-6-phosphate dehydrogenase deficiency. Blood 2020; 136(11): 12251240.
9. Ripoli C, Ricciardi MR, Angelo MR, Ripoli D. Quantifying the effect of glucose 6-phosphate dehydrogenase deficiency on glycated hemoglobin values in children and adolescents with type 1 diabetes. Sci Rep 2024; 14(1): 7311.
10. Chu CS, Freedman DO. Tafenoquine and G6PD: a primer for clinicians. J Travel Med 2019; 26(4).
11. Abdelwahab OA, Akil K, Seif A, et al. The potential role of vitamin E in patients with glucose-6-phosphate dehydrogenase deficiency: A systematic review and meta-
analysis. Medicine (Baltimore) 2023; 102(6): e32937.
12. Dorgalaleh A, Shahzad MS, Younesi MR, et al. Evaluation of liver and kidney function in favism patients. Med J Islam Repub Iran 2013; 27(1): 17-22.
13. Tiwari M. Glucose 6 phosphatase dehydrogenase (G6PD) and neurodegenerative disorders: mapping diagnostic and therapeutic opportunities. Genes Dis 2017; 4(4): 196-203.
15. Antwi-Baffour S, Adjei JK, Forson PO, et al. Comorbidity of Glucose-6-phosphate dehydrogenase deficiency and sickle cell disease exert significant effect on RBC indices. Anemia 2019; 2019: 3179173.
16. Yang WC, Tai S, Hsu CL, et al. Reference levels for glucose6-phosphate dehydrogenase enzyme activity in infants 7-90 days old in Taiwan. J Formos Med Assoc 2020; 119(1 Pt1): 69-74.
17. Dore MP, Pes GM, Mereu S, et al. Association of Rheumatoid Arthritis with Glucose-6-Phosphate Dehydrogenase Deficiency: Results from a Case-Control Study. Mediterr J Hematol Infect Dis 2024; 16(1): e2024056.
18. Glew RH, Ninomiya Y. Clinical studies in medical biochemistry: Oxford University Press, USA; 1997.
19. Chan D. Glucose-6-phosphate dehydrogenase deficiency: correlation between the genotype, biochemistry and phenotype. Ann Acad Med Singap 2008; 37(12 Suppl): 8183.
20. Arese P, Gallo V, Pantaleo A, Turrini F. Life and death of glucose-6-phosphate dehydrogenase (G6PD) deficient erythrocytes - role of redox stress and band 3 modifications. Transfus Medicine Hemother [German] 2012; 39(5): 328334.
21. Luzzatto L. Glucose 6-phosphate dehydrogenase deficiency: from genotype to phenotype. Haematologica 2006; 91(10): 1303-1306.
22. Chugh K, Singhal P, Sharma B, et al. Acute renal failure due to intravascular hemolysis in the North Indian patients. Am J Med Sci 1977; 274(2): 139-146.
23. Wang F, Boo N, Ainoon O, Wong M. Comparison of detection of glucose-6-phosphate dehydrogenase deficiency using fluorescent spot test, enzyme assay and molecular method for prediction of severe neonatal hyperbilirubinaemia. Singapore Med J 2009; 50(1): 62-67.
24. Jamurtas AZ, Fatouros IG, Koukosias N, et al. Effect of exercise on oxidative stress in individuals with glucose-6phosphate dehydrogenase deficiency. In Vivo 2006; 20(6B): 875-880.
25. Frank JE. Diagnosis and management of G6PD deficiency. Am Fam Physician 2005; 72(7): 1277-1282.
26. Georgakouli K, Fatouros IG, Draganidis D, et al. Exercise in glucose-6-phosphate dehydrogenase deficiency: harmful or harmless? a narrative review. Oxid Med Cell Longev 2019; 2019: 8080193.
27. Lauden SM, Chongwain S, Achidi A, et al. Prevalence of glucose-6-phosphate dehydrogenase deficiency in Cameroonian blood donors. BMC Res Notes 2019; 12(1): 195.
28. Sharma S, Sharma M. To determine the prevalence of glucose-6-phosphate dehydrogenase deficiency using a novel water-soluble tetrazolium-8 formazan method for neonatal screening in region of Himachal Pradesh, India. Advances in Human Biology 2019; 9(1): 37-41.
29. Basumatary N, Baruah D, Sarma PK, et al Prevalence and alteration in haematological parameters of glucose6-phosphate dehydrogenase deficient proto-australoid population of malaria endemic Himalayan belt of Assam, India. Explor Amin Med Res 2021; 11(1): 43-38.
30. Pinna A, Carru C, Solinas G, et al. Glucose-6-phosphate dehydrogenase deficiency in retinal vein occlusion. Invest Ophthalmol Vis Sci 2007; 48(6): 2747-2752.
31. Abdel Hakeem GL, Abdel Naeem EA, Swelam SH, et al. Detection of Occult Acute Kidney Injury in Glucose-6Phosphate Dehydrogenase Deficiency Anemia. Mediterr J Hematol Infect Dis 2016; 8(1): e2016038.
32. Mula-Abed W-AS, Al Rasadi K, Al-Riyami D. Estimated glomerular filtration rate (eGFR): A serum creatinine-based test for the detection of chronic kidney disease and its impact on clinical practice. Oman Med J 2012; 27(2): 108-113.
33. Jayasekara J, Dissanayake DM, Gunaratne M, et al. Prevalence of G6PD deficiency in patients with chronic kidney disease of unknown origin in North Central region of Sri Lanka: case control study. Int J Recent Sci Res 2013; 4(4): 455-458.
The NZIMLS Council has approved an Annual Journal prize to the value of NZ$1,500 for the best peer-reviewed article published by NZIMLS members in the Journal during the Calendar year. The article can be a review article, case study, research paper or technical communication. Excluded are Fellowship dissertations. Many studies are presented at Annual Scientific Meeting, SIG meeting and the North and South Island Seminars, yet are rarely submitted to the Journal for wider dissemination to the profession. Consider submitting your presentation to the Journal, if accepted, you are in consideration for the Rob Siebers Journal Prize and you will also earn valuable CPD points.
Please contact the Editor or any Editorial Board Member for advice and help. Contact details are on the NZIMLS website (www.nzimls.org.nz) as are the instruction to authors.
All articles published during the calendar year (March July and November issues) will be considered, the Editor, Deputy Editors and the President of the NZIMLS, who themselves are ineligible,
will judge all eligible articles. Their decision will be final, and no correspondence will be entered into.
The Winner of the Rob Siebers Journal prize for 2024 is Andrew Soepnel, from Pathlab, Waikato for his article ‘Evaluation of NOVA view single-well titre determination for antinuclear antibody testing under routine conditions in a New Zealand medical laboratory” published in NZ J Med Lab Sci 2024; 78(2): 77-81.
Integrating
TREC/KREC assay
and
cytokines
in the evaluation of the immune status of patients with DiGeorge syndrome
Assem M. Abo-Shanab, Haiam Abdel Raoul, Alaaeldin G. Fayez, Iman Helwa, Engy A. Ashaat, Naglaa Kholoussi, Nora N. Esmaiel and Rania Fawzy Mahmoud Abdelkawy
ABSTRACT
Aim: The study aimed to offer better genetic evaluation and consultation for DiGeorge syndrome (DGS) patients by combining screening of Chr 22q11.2 and immunologic studies. A basic immune profile including the basic CD panel and immunoglobulins estimation was performed.
Methods: All investigations were performed for DiGeorge syndrome (DGS) patients (n=33) and a matched control group ( n=45). Polymorphic 22q11.2 marker mapping was performed by PCR-STR technique. Lymphocyte subset immunophenotyping was done using flow cytometry, while measurement of serum immunoglobulins was estimated using nephelometry. Real-time PCR was the method used for T-cell receptor excision circles (TRECS) and Kappa receptor excision circles (KREC) measurement. Serum Interleukin-33 (IL-33), obestatin, histocompatibility antigen, class I, G (HLA-G), and procalcitonin levels were determined using ELISA. Data was coded, tabulated, and statistically analysed using SPSS version 19.0 software.
Results: In our case-control study, KREC expression was significantly elevated in DiGeorge syndrome compared to healthy controls (p= 0.001). There was also a significant increase in immunoglobulin levels in DGS. CD8 percentage (%) as well as CD8 absolute count in the patients with DiGeorge syndrome were significantly lower than in the healthy control (p= 0.0127 and 0.054 respectively). There were no significant differences in Interleukin-33 (IL-33), obestatin, HLA-G, and procalcitonin levels between DiGeorge syndrome patients compared to the control group. Our results concerning the distinct segment of 22q11.2 as a DiGeorge syndrome susceptibility region revealed an informative novel atypical interstitial homozygous deletion. This deletion included D22S944 and COMT absence, and D22S941 and D22S264 presence. Out of 33 DGS patients, three patients showed deletion in the D22S944 marker only in the presence of D22S941, and D22S264 markers. Therefore, we could assume that D22S944 is a common deleted marker in non-isolated DiGeorge syndrome patients.
Conclusion: Combining 22q11.2 region screening, immune profile studies, and T-cell receptor excision circles (TRECS) and Kappa receptor excision circles (KRECS) expression offers a new comprehensive approach for DiGeorge syndrome patients. This approach provides a better strategy for genetic consultation for DiGeorge syndrome patients. Moreover, this study may be the first to show a small interstitial 22q11.2 deletion stereotype in a DiGeorge syndrome patient and showed that the smallest deletion at the 22q11.2 region is enough to confer the DiGeorge syndrome phenotype.
Keywords: DiGeorge Syndrome (DGS), T-cell receptor excision circles (TREC), Kappa receptor excision circles (KREC), Interleukin-33 (IL-33), histocompatibility antigen, class I, G (HLA-G), Procalcitonin, Obestatin.
NZ J Med Lab Sci 2025; 79(1): 17:24
INTRODUCTION
Chromosome 22q11.2 deletion syndrome (22q11.2DS) is the most common micro-deletion syndrome in humans. It happens in almost 1:4000 live births and was traditionally identified as DiGeorge syndrome (DGS) which is classified as a primary immunodeficiency. It is described by T-cell lymphopenia and thymic dysplasia (1). The condition can be divided into two types: complete DGS and partial DGS. Individuals who completely lack a thymus are classified as having the complete form of the disorder (2).
In DiGeorge syndrome, there is dysregulation of T to B-cell interactions. Complete DGS patients were found to suffer from life-threatening severe T-cell lymphopenia. Whereas partial DGS is characterized by decreased thymic output demonstrate T-cell lymphopenia. This is exemplified in a low number of T-cell receptor excision circles (TRECs) (3). This resulted from recent thymic emigrant T cells and a low number of naive T cells (4). The humoral immune compartment in DGS is also affected. This is reflected in hypogammaglobulinemia, diminished response to vaccination, (12) and dysfunctional maturation of B-cells (5). This leads to increased vulnerability to infections, atopy, and autoimmune disease. There is a wide variability of phenotypic features. Hallmark features include cardiac anomalies and hypoparathyroidism, in addition to thymic aplasia or hypoplasia. Other phenotypic features include feeding and swallowing anomalies, palatal defects, renal abnormalities, and others (2). Patients do not necessarily manifest the typical features of the syndrome and severity differs considerably between patients. Even if the mutation is familiarly inherited or presented in identical twins, the deletion may be expressed with completely different phenotypes (6). Immune deficiency in such patients cannot be evaluated depending on clinical phenotype. Some
degree of T cell lymphopenia is encountered in around 70% of patients with Chr 22q11.2del (7). Therefore, immunologic assessment of affected subjects with Chr22q11.2del and any other developmental thymus deformity (DTD) is crucial to define immune status and assess infection susceptibility. T cell markers (CD3, CD4, CD8), B cell markers (CD19 or CD20), and natural killer cell markers (CD16 or CD56) should be included in the primary immunologic evaluation required for diagnosis. This is to be requested along with IgG, IgM, and IgA estimation. Moreover, T cell receptor excision circles (TREC) assay is performed if available; abnormal results increase the probability of significant T cell lymphopenia (TCL) (8).
Actual thymus-derived naive T cells, recent thymic emigrants (RTEs) can be evaluated by T cell receptor excision circles (TREC) assay. It serves as an excellent marker for this task. During V(D)J recombination of TCR in the thymus, circulating remnants of the DNA excision by-products are formed and these remnants can be measured. Neonates who may have abnormal TREC assay reflect remarkable TCL (9). Nevertheless, an assay can also detect congenital athymia as well as other severe forms of thymic hypoplasia (10). In the same context, kappa-deleting recombination excision circles (KREC) can be used to detect newly developed B cells. A conjoint TREC/KREC assay is used to distinguish patients with severe B cell disorders (11).
In another study (4), TREC was only identified in severe cases with deep lymphopenia, whereas children with incomplete DGS had normal range TREC/KREC levels both at birth and postnatally. However, a significant age-related decline in both TREC and KREC levels was observed in DGS patients compared to controls. This finding suggests that these assays are valuable complements to standard investigations and follow-up care for
patients with DGS. Based on the del22q11 background, their levels may reflect age-related immune changes along the course of the disease.
The humoral immune system is sometimes found intact in Chr22q11.2 del subjects. Yet, immunoglobulin (Ig) A deficiencies, improper response to vaccines, and transient hypogammaglobulinemia were sometimes encountered. Recently, humoral abnormalities as well as immunoglobulins have been studied in Chr22q11.2 del (12). IgG deficiency may develop even in individuals with normal immune function early in life. It may develop a picture very similar to common variable immunodeficiency (CVID) both clinically and biologically. Moreover, the US Immunodeficiency Network (USIDNET) performed a conjoint study with the European Society for Immunodeficiencies (ESID), where nearly half the subjects with confirmed Chr 22q11.2del, had IgG, IgA, and IgM abnormalities (8).
Obestatin, a ghrelin gene product, was primarily defined as an appetite suppressant; its role in metabolism remains an ongoing debate. It is believed to play a role in regulating metabolic balance and cardiovascular function. Furthermore, some prior research has suggested that obestatin can increase beta cell mass and enhance lipid metabolism; thus, inversely correlated with fasting blood glucose (13). Moreover, in obese individuals, obestatin levels were found reduced and negative with body mass index (BMI) (14, 15). In this same context, regarding adults with 22q11.2DS, there is evidence of obesity, global medical multimorbidity, and some other features, such as early onset Parkinson’s disease in these subjects (16, 17).
Procalcitonin (PCT) is one of the biomarkers released in response to bacterial infections. It has an important role in the diagnosis and management of lower respiratory tract infections and sepsis. In the same context, it is worth noting that Infections were observed in DGS and the most common infection was noted as pneumonia (18).
Interleukin-33 is a member of the IL-1 family of cytokines. It is found in multiple organs and is mainly localized to barrier epithelial cells and endothelial cells. Fibroblasts, myofibroblasts, and airway smooth muscle cells were also found to express IL33 (19, 20). It has a crucial role in innate and adaptive immune responses. It drives type 2 T-helper responses and can activate basophils, mast cells, and eosinophils (21). It is released into the extracellular space by endothelial cells following cellular insult. Necrosis can occur secondary to exposure to various factors, such as cigarette smoke, environmental pollutants, allergens, and viral or bacterial infections, hence acting as an innate immune indicator of danger (alarmin). Accordingly, IL-33 is considered to perform some immunologically important functions in the cortex and medulla of the thymus during mammalian development (22). Therefore, IL-33 in addition to acting as a nuclear transcription factor, has pro-inflammatory effects (20, 23). Infection-induced IL-33 release was found to induce thymic involution and thus T cell aging which consequently impairs host control of severe infection. Moreover, T cell immune deficiency or increased liability to infections has been related to impaired thymus function in many conditions in children such as DGS, preterm newborns, and severe combined immunodeficiency (24, 25).
Histocompatibility antigen, class I, G (HLA-G) is an HLA antigen having immunomodulatory properties. CD4 and CD8 T lymphocytes express it as well as NK cells, monocytes, and dendritic cells. T cells expressing the immunomodulatory m HLA-G molecule are identified as distinct subpopulations of regulatory T lymphocytes. These were found present in the peripheral blood of 0.1–8.3% of healthy subjects and primarily originate from the thymus. Studies confirmed their importance in health and disease (26). Moreover, quantitative, and qualitative derangements of HLA-G were detected in several immune conditions which highly suggests that HLA-G immune cells may
be involved in the pathogenesis of such disorders (27).
METHODS
Patients
This study employed a case-control design and was conducted between November 2019 and May 2022. It adhered to the ethical principles outlined in the Declaration of Helsinki. The study population included thirty-three patients diagnosed with DGS (22q11.2DS), as well as forty-five healthy individuals, matched for age and sex, who served as a control group. All participants were recruited from the Genetics Clinics at the Medical Research Centre of Excellency, National Research Centre (NRC), in Dokki, Giza, Egypt. The study protocol was approved by the Ethics Committee of the National Research Centre (NRC) in Cairo, Egypt (Ethics No. 19267-1). Written informed consent was obtained from the parents of the participating children.
Blood samples
For all patients and control subjects, 5mL of fresh peripheral blood samples were drawn. Of this, 2.5mL were divided into two sterile EDTA-containing tubes, 1mL was used for a complete blood count (CBC), The sample was divided for two analyses: flow cytometry, done within 24 hours, and DNA extraction, performed either right away or on refrigerated sample kept at 2-8°C, within one week. The remaining 2.5mL of blood was spun in a centrifuge at 3,000rpm for 10 minutes. This process separates the blood into its components, with the liquid portion (plasma) becoming isolated. The plasma was then collected and promptly divided into 0.2mL aliquots, which were frozen at -80°C until they could be analysed. The frozen samples were later tested using nephelometry to measure immunoglobulin levels and underwent ELISA testing.
Determination of IgA, IgM, and IgG Immunoglobulins
Measurement of serum immunoglobulin was performed using the method of nephelometry (28).
Flow cytometric analysis
The anticoagulated blood samples were stained using the wholeblood lysis method. Whole blood was stained with the following monoclonal antibodies targeting specific surface antigens; CD3 FITC-labelled for T lymphocytes, CD16 PE-labelled for NK cells, CD4 FITC-labelled for helper T lymphocytes, CD8 PE-labelled for cytotoxic T lymphocytes and CD19 FITC-labelled for B lymphocytes. Antibodies were purchased from BD Biosciences (USA). Lymphocyte subset immunophenotyping was then performed using flow cytometry on a BD Accuri™ C6 Cytometer (USA) (29).
Real-time PCR for TRECs and KRECs measurement
Genomic DNA was extracted from white blood cells collected from the participant's peripheral blood by using the QIAamp DNA Mini Kit (50 preps, catalogue number 51304, QIAGEN, Germany). The assay was run on a 7500 Fast Real-Time PCR system (Applied Biosystems) utilizing specific primers and probes for TRECs, KRECs, and β-actin. RT-PCR was carried out using TaqMan Universal PCR Master Mix II. A 10μL mix for PCR was prepared by combining 5μL of DNA samples with 1μL each of forward and reverse primers from Applied Biosystems, 1μL of TaqMan TAMRA probe, and 2μL of water. The reactions were set up in a sterile 48-well PCR plate and run under the following realtime cycler conditions: initial activation at 95°C for 10 minutes, followed by 45 cycles of denaturation at 95°C for 15 seconds and combined primer/probe annealing and elongation at 60°C for 1 minute. The copy numbers of TRECs, KRECs, and β-actin were obtained by extrapolating the respective sample quantities from standard curves generated by serial dilutions of human genomic DNA (Promega, USA). The initial copy numbers were calculated using the following equation: Copies of the gene of interest = mass of gDNA/mass of haploid genome. The number of TRECs and KRECs per microlitre of extracted DNA was then determined
for each sample. The β-actin copy number was used to assess the successful amplification of each sample.
Enzyme-linked immunosorbent assay (ELISA)
Serum IL-33, obestatin, HLA-G, and procalcitonin levels of all study subjects were determined using Human procalcitonin ELISA kit (EIAab, Co., Ltd, East Lake Hi-Tech Development Zone, Wuhan, China) and Human IL-33, obestatin and HLA-G ELISA kits (NOVA, Beijing, China) by following the manufacturer’s protocol.
Polymorphic Chr22q11.2 markers mapping
The PCR-STR technique was performed using specific primers for microsatellite genotyping. These primers were directly retrieved from the now-retired Electronic PCR tool (NCBI, USA). Three consecutive polymorphic loci located in the typically 3-Mb deleted region were analysed: D22S941, D22S944, and D22S264, along with the COMT marker. The PCR products were then visualized using 4% agarose gel electrophoresis.
Statistical methods
The collected data were coded, tabulated, and statistically analysed using SPSS version 19.0 software (SPSS Inc., Chicago, Illinois, USA). For comparing parametric results between groups, the t-test was used. The Mann-Whitney U Test was employed for comparing non-parametric results across groups. The data were presented as median and range. All analyses were two-tailed, and the level of significance was set at p < 0.05. Values with p ≥ 0.05 were considered non-significant.
RESULTS
This case-control study included two groups: Group I (33 children
clinically diagnosed as DGS and Group II (45 healthy controls). The demographic and clinical characteristics of DGS patients and volunteer control subjects are presented in Table 1. All the DGS patients in the study had congenital heart diseases (CHDs). KRECs expression was significantly elevated in DGS patients as compared with the healthy controls (p=0.001) (Figure 1). There was also a significant increase in immunoglobulins level between DGS patients and the healthy controls (IgA p=0.014, IgG p=0.0019 & IgM p=0.003) (Figure 2).
Table 2 summarizes laboratory findings such as Total leukocyte count (TLC) (, Lymphocytes, CD3, CD16, CD4, and CD8, in addition to CD19 in the DGS group and control group. CD8 percentage (%) as well as CD8 absolute count in the patients with DGS were significantly lower than in the healthy controls (p=0.027 and 0.054 respectively). There were no significant differences in IL-33, obestatin, HLA-G, and procalcitonin levels in DGS patients compared with the control group (Table 3).
A novel atypical interstitial homozygous Chr22q11.2 microdeletion suggested three DGS-susceptibility genes. Using three polymorphic DNA markers, an informative novel atypical interstitial homozygous deletion was found. This deletion included D22S944 and COMT absence, and D22S941 and D22S264 presence. The COMT gene, the nearest gene to the distal region of D22S264, was used to determine the minimal breakpoint loci. The distance of the identified novel deleted region was approximately 0.35 Mb leading to the deletion of 3 genes: GP1BB, TBX1, and COMT (Figure 3). Out of 33 DGS patients, three patients showed deletion in the D22S944 marker only in the presence of D22S941and D22S264 markers, as shown in Table 4. Therefore, we could assume that D22S944 is a common deleted marker in non-isolated DGS patients. None of the healthy controls had deletions.
p-value calculated using t-test
*P< 0.05 Significant versus controls (by Mann Whitney
*P< 0.05 Significant versus controls (by Mann Whitney U Test)
3. Order of STRs and genes located on the detected nested 22q11.2 microdeletion. (-) indicates the deleted loci, while (+) indicates the undeleted loci. The triangle marked white is the detected deletion breakpoint.
Table 1. Demographic and clinical characteristics
Figure 1. Expression of TRECs and KRECs in DGS patients and control subjects.
U Test)
Figure 2. Immunoglobulins median levels in subjects with DGS patients compared with control subjects.
Figure
Table 2. Comparison of the laboratory data measured between DGS cases and controls.
(2752-6958)
(159.6-1793.3)
(590-3012.8)
(5-43.1)
(212.3-1071.5)
(10.3-37.4)
(284.8-2177.9)
Results were expressed as Median (Range). * Significant versus controls (by Mann Whitney U Test) * Evaluation of the TLC count was required to calculate the absolute number of different lymphocytes.
Table 3. Biomarkers comparing apparently healthy control with DiGeorge patients
Figure 4. This image was adapted from previously published sources (62, 63) and used with permission. The image depicts the 3 Mb 22q11.2 region (based on the hg19 genome assembly) as a line spanning this chromosomal segment. The image also highlights four low copy repeats (LCR22) within this region, labelled as LCR22A, LCR22B, LCR22C, and LCR22D. Below the line representing the 22q11.2 region, most of the known coding and noncoding genes are presented. In a clear blue font, TBX1 is indicated. A clear red font indicates genes linked to recessive genetic conditions. A star indicates noncoding genes. The size and position of reported 22q11.2 deletions are indicated by a grey box, and novel, in the current study, 22q11.2 deletion is indicated by a black box. The frequencies of deletions were obtained from McDonald-McGinn and colleagues in the special AJMG issue.
DISCUSSION
Phenotypic features of DiGeorge Syndrome (Chr22q11.2DS) vary considerably; nearly 75–80% of DGS patients exhibit disorders of the immune system, which may cause them to suffer from immune instabilities such as autoimmune disease, susceptibility to infections, and atopy (1).
Our results showed that KREC expression was significantly elevated in DGS patients as compared with the healthy controls (p=0.0008). On the contrary, Dar et al., 2015 (30) and Lingman Framme et al, 2014 (31) stated that in DGS patients, KREC
levels don’t vary much from those of healthy controls, which suggests normal bone marrow output of B cells. Nevertheless, DGS patients with low TREC counts have long-term impairment of thymic output. These patients were much more susceptible to viral infections, which is analogous to the situation seen in cases of more severe T-cell lymphopenia (reduced number of T-cells) (31, 32). Moreover, the link between lower TREC levels and recurrent infections continues regardless of age (30).
Our research found a significant increase in immunoglobulin levels among DGS patients compared to healthy controls (IgA
Table 4. STS-PCR results for three genetic polymorphic STS markers in the Chr22q11.2 region
*Note: In case no. 23; novel atypical interstitial nested microdeletion about 0.35Mb p=0.014, IgG p=0.0019 & IgM p=0.0032) unlike Patel et al (2012) (12)who stated that after 3 years of age, almost 6% of DGS patients have low IgG levels. In the same context, Al-Herz et al (2004) (33) and Kung et al (2007) (34) reported selective IgM deficiency associated with DGS although less common. However, in one cohort, the most common humoral defect reported was low IgM (35). In DGS, low levels of IgG, IgA, IgM, and defective antibody responses to vaccines were described. Severe infections observed in DGS were attributed to humoral immune deficiency (12, 36, 37). In 17% of cases, humoral immunity instabilities were witnessed (38). Some autoimmune problems including juvenile rheumatoid arthritis (JRA) reported IgA deficiency in nearly 13% of patients with DGS (39). Despite the finding that hypogammaglobulinemia was found to present in the first year of life, it usually resolves. On the other hand, hypergammaglobulinemia was reported in some cases after
the age of five. Surprisingly, most affected individuals show functional antibody defects despite the normal antibody function and antibody avidity (36, 39).
Impaired T-cell production resulting from thymic hypoplasia leads to immunodeficiency. It’s quite apparent that fewer cells of thymic lineage are present in newborns with DGS. Sixtyseven percent of individuals had reduced T-cell production and more than 18% showed compromised T-cell function in previous studies (39). In another study including 1,421 DGS patients, abnormal T-cell populations were found in half the included subjects (38). Over time, the production of T-cells improves and in the first year of life, children improve despite the considerable T-cell defects they suffer from. Whereas individuals with minor T-cell decrease showed better performance against pathogens (39).
Regarding our study, CD8 percentage (%) as well as CD8
absolute count in the patients with DGS were significantly lower than healthy controls (p= 0.013 and 0.054 respectively). Another study conducted with partial DGS patients had the same opinion. It stated that 20 out of 25 patients had low CD8+T cells and recurrent bacterial and viral infections (36). On the other hand, researchers demonstrated normalization of CD4+T cell numbers in most patients up to 3 years (40). In another observational study, 81% of DGS patients reported normal levels of CD8+T at the age of 2 years when compared to healthy controls (18).
Our results showed that IL-33 levels showed no significant difference in DGS patients compared with the control group. In an experimental model of DGS, Handel et al (2022) (41) explored the changes in the non-epithelial stromal compartment of the thymus across diverse developmental stages. High levels of complexity within the thymic mesenchyme were revealed using single-cell sequencing. A Uniform Manifold Approximation and Projection (UMAP) analysis of non-thymic epithelial cell (non-TEC) stroma components identified two distinct medullary fibroblast subtypes. These were designated as medullary fibroblast subtype 1 (MedFb1) and medullary fibroblast subtype 2 (MedFb2). Both medullary fibroblast subtypes expressed transcripts for IL-33 and Cxcl16. These soluble factors are known to play important roles in dendritic cell activation and natural killer T (NKT) cell migration, respectively. The identification of these two medullary fibroblast subpopulations and their expression of key immunoregulatory molecules suggests a potential role for these stromal cells in modulating thymic microenvironmental cues that govern T cell development and function. (42, 43).
In nearly 40% of DGS patients, obesity has been reported with onset often during childhood or adolescence (16, 44, 45). In obesity, Nakahara et al (2008) (46) reported a negative correlation of plasma obestatin concentrations using measures like body mass index, insulin resistance, and plasma levels of the hormone leptin. Regarding our research, there was no statistically significant difference in obestatin levels between DGS patients and controls. Eberle et al. (2008) (47) reported that high-risk patients with DiGeorge syndrome (DGS) experienced more frequent serious infections and lymphoproliferative complications.
Procalcitonin levels are known to begin rising within 3-4 hours of a bacterial infection, typically peaking between 12 and 36 hours (48). A study by Nargis et al (2014) (49) found that procalcitonin exhibited a diagnostic accuracy of 75%, a specificity of 72%, and a sensitivity of 76% for detecting bacterial infections. These findings suggest that monitoring procalcitonin levels may be a useful diagnostic approach for identifying bacterial infections, particularly in high-risk populations such as those with DGS. They concluded as well that procalcitonin is better than CRP regarding accuracy in the identification and assessment of sepsis severity. Our results showed no significant differences in procalcitonin levels between DGS patients and healthy controls.
Persistent low numbers of CD4+, CD45RA+, and CD8+T cells in DGS patients rendered them more prone to lethal infections and lymphoproliferative disorders during the followup period (47). Feger et al (2006) (26) defined novel subsets of T cells expressing the immunomodulatory molecule HLA-G as CD4 HLA-GC distinct Regulatory T cells. Through blocking cell cycle progression, sHLA-G5 can inhibit CD4 and CD8 T cell alloproliferation (50). However, our results showed no significant differences in HLA-G levels between patients and controls.
We analysed the Chr22q11.2 region in extracted DNA from the peripheral blood of 33 DGS patients and 20 controls who were referred from our clinical genetics department at the National Research Centre (NRC). Using a set of polymorphic STR markers with known locations, we found one patient with novel atypical nested homozygous microdeletion flanked by D22S941 and D22S264 markers. None of the healthy controls had deletions. Our findings indicate a specific segment of the 22q11.2 chromosomal region, located between the genetic markers D22S941 and D22S264, as a susceptibility locus for DGS. Using the published DNA sequence data for human
chromosome 22, we estimate this identified susceptibility region contains three main genes: GP1BB, TBX1, and COMT. However, it remains unclear which of these three genes is directly responsible for the pathogenesis of DGS, and further gene dosage studies are required to elucidate the specific genetic drivers of this condition. The majority Chr22q11.2 deleted region (3 Mb) contains approximately 50 genes, and several miRNAs (Figure 4). TBX1 and COMT genes are considered the most relevant genes to DGS (51). The TBX1 gene encodes a type of transcription factor known as a T-box protein. This transcription factor is recognized as playing a crucial role in the early stages of development in vertebrate organisms. Using FISH analysis with KB1764E3 probe which encompassed TBX1, CDCrel-1, and GP1BB genes, no deletions were observed in 13 patients with DGS (52). McQuade et al (1999) (53) detected small deletions including TBX1 and COMT genes in a patient with the DGS phenotype. However, results agreed with this study but also detect novel homozygous Chr22q11.2 deletion encompassing TBX1, COMT, and in addition to GP1BB using Polymorphic STS markers mapping as illustrated in (Figure 4).
GP1BB (Glycoprotein 1b platelet subunit beta) was previously detected in DGS patients with atypical features (54, 55, 56). Using SNP-array analysis, Huang et al (2015) (57) found four 22q11.2DS patients shared the same deletion breakpoints which included TBX1, COMT, DGCR2, GP1BB, RTN4R, PRODH, SNAP29, and SERP genes. It is worth noting that DGS has phenotypic heterogeneity and severity variability. So, some patients are mildly affected, whereas others have severe features that could be due in part to the presence of genetic modifiers and dosage of the deleted gene’s haploinsufficiency. It was reported that phenotypic variability in DGS is associated with behavioural traits including autistic spectrum disorders (ASD), which are more frequent in LCRA-B deleted individuals (58, 59), schizophrenia (SCZ), and attention deficit hyperactivity disorder (ADHD) phenotypes (in LCRA-D deleted regions including COMT, PRODH, GNB1L, TBX1, SEPT5/GP1BB, ZDHHC8, PI4KA, and ARVCF genes) (60, 61, 62).
CONCLUSIONS
Our results may be given merit to adopt a new comprehensive investigation strategy for DGS patients that combines screening of Chr22q11.2 region, immunoglobulin level patterns, and TRECS and KRECS expression. This investigation strategy can provide better genetic consultations for DGS patients. The current study may be the first to show a small interstitial Chr22q11.2 deletion stereotype in a DGS patient, but it has shown that the smallest deletion at the 22q11.2 region is enough to confer the DGS phenotype. Further investigating of other DGS-relevant pathogenesis factors and their correlation with the patient’s clinical manifestations can help to provide a better explanatory model for the clinical variability of DGS disease.
FUNDING & COMPETING INTERESTS
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
AVAILABILITY OF DATA AND MATERIALS
The datasets were generated and analysed during the current study, however, a deidentified version of the dataset may be available from the corresponding author upon reasonable request.
Article Preprint: Assem Metwally Abo-Shanab, Haiam Abdel Raouf, Alaaeldin G. Fayez et al. Integrating TREC/KREC assay and some cytokines in the evaluation of the immune status of patients with DiGeorge Syndrome, 24 April 2024, PREPRINT (Version 1) Available at Research Square: [https://
AUTHOR INFORMATION
Assem M Abo-Shanab, PhD, Researcher1
Haiam Abdel Raouf, PhD, Professor of Immunogenetics, Head of Immunogenetics1
Alaaeldin G. Fayez, PhD MSc, Assistant Professor of Molecular Genetics and Enzymology2
Iman Helwa, MD, Assistant Professor of Immunogenetics1
Engy A. Ashaat, PhD, Associate Professor of Clinical Genetics3
Naglaa Kholoussi, MD, Head of Department of Immunogenetics1
Nora N. Esmaiel, PhD, Associate Professor of Molecular Genetics and Enzymology2
Rania Fawzy Mahmoud Abdelkawy, PhD, Assistant Professor of Immunogenetics1
1 Department of Immunogenetics, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt.
2 Department of Molecular Genetics and Enzymology, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt.
3 Department of Clinical Genetics, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt.
Corresponding Author: Dr Assem Metwally Abo-Shanab, Department of Immunogenetics, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt.
Email: asem_nrc@yahoo.com
REFERENCES
1. Davies EG. Immunodeficiency in DiGeorge syndrome and options for treating cases with complete athymia. Front Immunol 2013; 31(4): 322.
2. Biggs SE, Gilchrist B, May KR. Chromosome 22q11.2 deletion (DiGeorge Syndrome): immunologic features, diagnosis, and management. Curr Allergy Asthma Rep 2023; 23(4): 213-222.
3. Klocperk A, Paračková Z, Bloomfield M, et al. Follicular helper T cells in DiGeorge syndrome. Front Immunol 2018; 23(9): 1730.
4. Froňková E, Klocperk A, Svatoň M, et al. The TREC/KREC assay for the diagnosis and monitoring of patients with DiGeorge syndrome. Plos One 2014; 9(12): e114514.
5. Klocperk A, Mejstříková E, Kayserová J, et al. Low marginal zone-like B lymphocytes and natural antibodies characterize skewed B-lymphocyte subpopulations in del22q11 DiGeorge patients. Clin Immunol 2015; 161(2):144-149.
6. Digilio MC, Angioni A, De Santis M, et al. Spectrum of clinical variability in familial deletion 22q11.2: from full manifestation to extremely mild clinical anomalies. Clin Genet 2003; 63(4): 308-313.
8. Mustillo PJ, Sullivan KE, Chinn IK, et al. Clinical practice guidelines for the immunological management of chromosome 22q11. 2 deletion syndrome and other defects in thymic development. J Clin Immunol 2023; 43(2): 247270.
9. Lewis DB, Haines C, Ross D. Protein tyrosine kinase 7: a novel surface marker for human recent thymic emigrants with potential clinical utility. J Perinatol 2011; 31(1): Suppl 1: 72-81.
10. Pierdominici M, Mazzetta F, Caprini E, et al. Biased T-cell receptor repertoires in patients with chromosome 22q11.2 deletion syndrome (DiGeorge syndrome/velocardiofacial syndrome). Clin Exp Immunol 2003; 132(2): 323-331.
11. Borte S, Wang N, Óskarsdóttir S, et al. Newborn screening for primary immunodeficiencies: beyond SCID and XLA. Ann N Y Acad Sci 2011; 1246(1): 118-130.
12. Patel K, Akhter J, Kobrynski L, et al. Immunoglobulin deficiencies: the B-lymphocyte side of DiGeorge Syndrome.
J Pediatr 2012; 161(5): 950-953.
13. Cowan E, Burch KJ, Green BD, Grieve DJ. Obestatin as a key regulator of metabolism and cardiovascular function with emerging therapeutic potential for diabetes. Br J Pharmacol 2016; 173(14): 2165-2181.
14. Zou CC, Liang L, Wang CL, et al. The change in ghrelin and obestatin levels in obese children after weight reduction. Acta Paediatr 2009; 98(1):159-165.
15. Zhang N, Yuan C, Li Z, et al. Meta-analysis of the relationship between obestatin and ghrelin levels and the ghrelin/ obestatin ratio with respect to obesity. Am J Med Sci 2011; 341(1): 48-55.
16. Voll SL, Boot E, Butcher NJ, et al. Obesity in adults with 22q11.2 deletion syndrome. Genet Med 201; 19(2): 204208.
17. Malecki SL, Van Mil S, Graffi J, et al. A genetic model for multimorbidity in young adults. Genet Med 2020; 22(1): 132141.
18. Suksawat Y, Sathienkijkanchai A, Veskitkul J, et al Resolution of primary immune defect in 22q11.2 deletion syndrome. J Clin Immunol 2017; 37(4): 375-382.
19. Byers DE, Alexander-Brett J, Patel AC, et al. Long-term IL-33–producing epithelial progenitor cells in chronic obstructive lung disease. J Clin Invest 2013; 123(9):39673982.
20. Calderon AA, Dimond C, Choy DF, et al. Targeting interleukin-33 and thymic stromal lymphopoietin pathways for novel pulmonary therapeutics in asthma and COPD. Eur Respir Rev 2023; 32(167): 220144.
21. Ramesh N, Gawli K, Kiran Pasupulleti V, Unniappan S.Metabolic and cardiovascular actions of nesfatin-1: implications in health and disease. Curr Pharm Des 2017; 23(10):1453-1464.
22. Mamoor S. Interleukin 33 is differentially expressed in the thymus by developmental stage and cell type. OSF Preprints Avaliable from https://osf.io/preprints/osf/kya42_v1.
23. Liew FY, Girard JP, Turnquist HR. Interleukin-33 in health and disease. Nat Rev Immunol 2016; 16(11): 676-689.
24. Zdrojewicz Z, Pachura E, Pachura P. The thymus: a forgotten, but very important organ. Adv Clin Exp Med 2016; 25(2):369-375.
25. Xu L, Wei C, Chen Y, et al. IL-33 induces thymic involutionassociated naive T cell aging and impairs host control of severe infection. Nat Commun 2022; 13(1): 6881.
26. Feger U, Tolosa E, Huang YH, et al HLA-G expression defines a novel regulatory T-cell subset present in human peripheral blood and sites of inflammation. Blood 2007; 110(2): 568-577.
27. Contini P, Murdaca G, Puppo F, Negrini S. HLA-G expressing immune cells in immune mediated diseases. Front Immunol 2020; 11: 1613.
28. Aksu G, Genel F, Koturoglu G, et al. Serum immunoglobulin (IgG, IgM, IgA) and IgG subclass concentrations in healthy children: a study using nephelometric technique. Turk J Pediatr 2006; 48(1):19-24.
29. Rahman M. Introduction to flowcytometry. J Clin Invest 2006; 45: 345–361.
30. Dar N, Gothelf D, Korn D, et al. Thymic and bone marrow output in individuals with 22q11.2 deletion syndrome. Pediart Res 2015; 77(4): 579-585.
31. Lingman Framme J, Borte S, von Döbeln U, et al. Retrospective analysis of TREC based newborn screening results and clinical phenotypes in infants with the 22q11 deletion syndrome. J Clin Immunol 2014; 34: 514-519.
32. Framme JL, Lundqvist C, Lundell AC, et al. Long-term follow-up of newborns with 22q11 deletion syndrome and low TRECs. J Clin Immunol 2022; 42(3): 618-633.
33. Al-Herz W, McGeady SJ, Gripp KW. 22q11.2 deletion syndrome and selective IgM deficiency: an association of a common chromosomal abnormality with a rare immunodeficiency. Am J Med Genet A 2004; 127(1): 99-100.
34. Kung SJ, Gripp KW, Stephan MJ, et al. Selective IgM deficiency and 22q11.2 deletion syndrome. Ann Allergy Asthma Immunol 2007;99(1): 87-92.
35. Giardino G, Radwan N, Koletsi P, et al. Clinical and immunological features in a cohort of patients with partial DiGeorge syndrome followed at a single center. Blood 2019; 133(24): 2586-2596.
36. Gennery AR, Barge D, O’Sullivan JJ, et al. Antibody deficiency and autoimmunity in 22q11.2 deletion syndrome. Arch Dis Child 2002; 86(6): 422-425.
37. Finocchi A, Di Cesare S, Romiti ML, et al. Humoral immune responses and CD27+ B cells in children with DiGeorge syndrome (22q11. 2 deletion syndrome). Pediatric Allergy Immunol. 2006; 17(5): 382-388.
38. Campbell IM, Sheppard SE, Crowley TB, et al. What is new with 22q? an update from the 22q and You Center at the Children’s Hospital of Philadelphia. Am J Med Genet A 2018;176(10): 2058-2069.
40. Sedivá A, Bartůňková J, Zachová R, et al Early development of immunity in diGeorge syndrome. Med Sci Monit 2005; 11(4): 182-187.
41. Handel AE, Cheuk S, Dhalla F, et al. Developmental dynamics of the neural crest–mesenchymal axis in creating the thymic microenvironment. Sci Adv 2022; 8(19): eabm9844.
42. Germanov E, Veinotte L, Cullen R, et al. Critical role for the chemokine receptor CXCR6 in homeostasis and activation of CD1d-restricted NKT cells. J Immunol 2008; 181(1): 8191.
43. Kurokawa M, Matsukura S, Kawaguchi M, et al. Interleukin33-activated dendritic cells induce the production of thymus and activation-regulated chemokine and macrophagederived chemokine. Int arch Allergy Immunol 2013; 161(Suppl. 2): 52-7.
44. Bassett AS, Chow EW, Husted J, et al Clinical features of 78 adults with 22q11 deletion syndrome. Am J Med Genet A 2005; 138(4): 307-313.
45. Guzman ML, Delgado I, Lay-Son G, et al. Growth in Chilean infants with chromosome 22q11 microdeletion syndrome. Am J Med Genet A 2012; 158(11): 2682-2686.
46. Nakahara T, Harada T, Yasuhara D, et al. Plasma obestatin concentrations are negatively correlated with body mass index, insulin resistance index, and plasma leptin concentrations in obesity and anorexia nervosa. Biol Psychiatry 2008; 64(3): 252-255.
47. Eberle P, Berger C, Junge S, et al. Persistent low thymic activity and non-cardiac mortality in children with chromosome 22q11·2 microdeletion and partial DiGeorge syndrome. Clin Exp Immunol 2009; 155(2): 189-198.
48. Covington EW, Roberts MZ, Dong J. Procalcitonin monitoring as a guide for antimicrobial therapy: a review of current literature. Pharmacotherapy: Pharmacotherapy 2018; 38(5): 569-581.
49. Nargis W, Ibrahim MD, Ahamed BU. Procalcitonin versus C-reactive protein: Usefulness as biomarker of sepsis in ICU patient. Int J Crit IIIn Inj Sci 2014; 4(3): 195-199.
50. Bahri R, Hirsch F, Josse A, et al. Soluble HLA-G inhibits cell cycle progression in human alloreactive T lymphocytes. J Immunol 2006; 176(3): 1331-1339.
51. Verhoeven L, Reitsma P, Siegel LS. Cognitive and linguistic factors in reading acquisition. Read Writ 2011; 24(4): 387394.
52. Yagi H, Furutani Y, Hamada H, et al. Role of TBX1 in human del22q11.2 syndrome. Lancet 2003; 362(9393): 1366-1373.
53. McQuade L, Christodoulou J, Budarf M, et al. Patient with a 22q11.2 deletion with no overlap of the minimal DiGeorge syndrome critical region (MDGCR). Am J Med Genet 1999; 86(1): 27-33.
54. Hayashi T, Suzuki K. Molecular pathogenesis of BernardSoulier syndrome. In: Seminars in thrombosis and hemostasis 2000 [Vol. 26, No. 01, pp. 053-060] Thieme Medical Publishers, Inc, New York.
55. Kato T, Kosaka K, Kimura M, et al. Thrombocytopenia in patients with 22q11.2 deletion syndrome and its association with glycoprotein Ib-β. Genet Med 2003; 5(2): 113-119.
56. Kunishima S, Imai T, Kobayashi R, et al. Bernard–Soulier syndrome caused by a hemizygous GPIb β mutation and 22q11. 2 deletion. Pediatr Int 2013; 55(4): 434-437.
57. Huang L, Xie Y, Zhou Y, et al. Clinical and molecular cytogenetic studies of an unrecognised 22q11.2 deletion in three families. Exp ther Med 2015; 9(3): 823-828.
58. Burnside RD. 22q11. 21 deletion syndromes: a review of proximal, central, and distal deletions and their associated features. Cytogenet Genome Res. 2015; 146(2): 89-99.
59. Clements CC, Wenger TL, Zoltowski AR, et al. Critical region within 22q11.2 linked to higher rate of autism spectrum disorder. Mol Autism 2017; 8:58.
60. Jungerius BJ, Hoogendoorn ML, Bakker SC, et al. An association screen of myelin-related genes implicates the chromosome 22q11 PIK4CA gene in schizophrenia. Mol Psychiatry 2008; 13(11): 1060-1068.
61. Hiroi N, Takahashi T, Hishimoto A, et al. Copy number variation at 22q11.2: from rare variants to common mechanisms of developmental neuropsychiatric disorders. Mol Psychiatry 2018; 18(11): 1153-1165.
2025 QMLT applications are now open on our website
Applications close 15 April 2025, and no late applications will be accepted.
We process your applications as quickly as we can, however due to the number of applications we receive, there may be a slight delay. Once processed, you will receive a confirmation email from us.
Note: Membership and QMLT Examination payment must be made at the time of application.
CASE STUDY
Implementing nanopore sequencing in a clinical laboratory: a social systems case
Suzanne Manning, Max Bloomfield, Samantha Hutton, Megan Burton, Charles Velasco, Claire Tarring, Rhys White and Koen van der Werff
ABSTRACT
The Molecular Pathology Department at Awanui Labs Wellington have been trialling the implementation of nanopore long-read sequencing since 2020, initially to assist the Infection Prevention and Control team. This case study explored the social systems that enabled or constrained this implementation. The study found that implementation was enabled by systems that were set up to balance the need for continued service improvement through research and innovation with the need to maintain the current level of service to clinicians and ultimately, the patients. The process also allowed oversight and coordination by management while providing a reasonable degree of autonomy for the laboratory staff to conduct the trial, including the time and flexibility required to investigate and develop the protocols.
There were several implementation challenges. One challenge related to introducing a novel and unfamiliar technology while maintaining a busy routine workload, fitting in with the other work in the laboratory and securing funding. However, the main challenge specific to nanopore sequencing were the issues around accessing bioinformatics expertise, providing adequate computing power for data analysis, and the more systemic issue of data infrastructure in the health sector. The bioinformatics expertise and upgraded computer requirements have been addressed at a local level; however, the issue of national health data infrastructure and governance must be addressed if the potential of nanopore sequencing is to be realised
Keywords: Social Sciences, Infection Control, Genomics, Nanopore sequencing.
NZ J Med Lab Sci 2025; 79(1): 25:29
INTRODUCTION
The Genomics and Bioinformatics team at the Institute of Environmental Science and Research (ESR) utilises nextgeneration sequencing (NGS) technology in its research and service delivery, and actively explores ways to realise the potential of technological advances in responsible ways. Since 2020 the ESR team has been supporting Awanui Labs Wellington, a hospital clinical pathology laboratory, to implement NGS using the Oxford Nanopore Technologies platform (‘nanopore sequencing’). A reflection on this implementation was undertaken in conjunction with the social systems team at ESR in 2023. Many reports and reviews on implementation of new laboratory technologies focus on feasibility, technical challenges and solutions, comparison between similar technologies, and comments on cost-effectiveness (1-6). This study took a different approach, using a social systems methodology to investigate the perceptions of those involved in the implementation as well as the wider context of laboratory policies and practices, both formal and informal. The purpose was to understand the barriers and enablers from the point of view of the people involved.
This participatory research case study used a combination of Viable System Modelling (VSM) (7) and Systems Effects Mapping (8) to describe the social system in the laboratory that influenced the implementation of nanopore sequencing. VSM is a framework for organisational design and was used in this context to analyse the structural influences on the implementation of nanopore sequencing. Systems Effects Mapping further explored the factors (barriers and enablers) that affected how nanopore sequencing was implemented.
This article first outlines the characteristics of the case study laboratory, including a brief history of how nanopore sequencing was implemented, and then describes the social systems methodologies. The findings are presented under the six VSM headings of Environment, Intelligence, Policy, Control, Coordination, and Operations, with the Systems Effects Map included under Operations. A discussion of the major implications of the study is given in the discussion, with a conclusion summarising the case study.
The setting: Awanui Laboratories, Wellington Awanui Labs, formerly Southern Community Laboratories (SCL), is the largest network of diagnostic laboratories in Aotearoa New Zealand. It is a New Zealand business which contracts to the
former District Health Boards, now Te Whatu Ora/Health New Zealand¹. Awanui Labs Wellington² provides services to the Wellington, Hutt Valley and Wairarapa regions. There are 28 sample collection centres and 4 ISO 15189 accredited hospitalbased medical testing laboratories throughout the region, catering for both the community and hospitals. The Molecular Pathology Department at the Wellington Regional Hospital laboratory identify pathogens through DNA/RNA, working closely with the Microbiology Department who identify pathogens predominantly through culture-based methods. The two departments are located next to each other in the laboratory layout, and one Head of Department manages both groups.
Introducing nanopore sequencing to the laboratory
The cost of hospital-acquired infection is significant, both in terms of economic and social costs, and some of this can be reduced by effective Infection Prevention and Control (IPC) measures (9, 10). Standard hospital organism surveillance is based on species type and broad antimicrobial resistance categories, which provides limited insight into ward transmission events and infection outbreaks. The laboratory staff at Wellington Regional Hospital sought new methods for further characterising infectious organisms, which could then inform more precise IPC measures. A clinical microbiologist initiated the project to implement nanopore sequencing in the Molecular Pathology Department, starting the collaboration between Awanui Labs Wellington and the ESR Genomics group.
Oxford Nanopore Technologies (Oxford, United Kingdom) has achieved commercial success with its direct, real-time, electronics-based sequencing of native DNA/RNA through a nanopore (11-14). This achievement is largely attributed to the ultra-portable MinIONTM Mk1B device, which weighs only 87g and can be connected to a laptop or PC with a high-speed USB 3.0 cable (15). The initial cost of the Mk1B in April 2024 was USD$1,000, inclusive of the device and an initial set of reagents. Notably, no additional capital costs were required. This made nanopore long-read sequencing a cost-effective alternative to Illumina short-read sequencing, particularly for a feasibility trial.
The initial set up was funded by the Capital and Coast District Health Board (DHB) Infectious Diseases research fund. After a successful feasibility trial, the DHB funded the ongoing costs of ¹The system of District Health Boards was replaced by the centralised Te Whatu Ora | Health New Zealand in July 2022. The nanopore sequencing trial was started under the old system of District Health Boards, but this case study was carried out after the change to Te Whatu Ora. Most of the information presented here therefore relates to the previous system.
The laboratory scientists trialled protocols, working around existing workloads and workspaces. By January 2022 a routine had been established to make best use of current workflow practices (Figure 1). When target organisms in samples were identified, DNA was extracted and stored until the weekly sequencing run. The generated data were analysed on-site to produce a multi-locus sequencing type (MLST) to characterise the organism of interest. If more granular analysis was required, sequence data could be transferred via the cloud to ESR for detailed bioinformatics analysis (16).
The routine nanopore sequencing of Clostridioides difficile from patient diarrheal stool samples helped identify and manage a ward outbreak in 2022 (17). The low-discrimination genomic analysis by the nanopore sequencing, combined with routine information on ward bed occupancy, enabled IPC teams to be more precise and selective in their investigation as indicated in this feedback to the microbiologist: “Now we can be certain of possible transmissions and only review a small number of cases” (personal communication, Bloomfield). The new nanopore sequencing system also enabled the identification of an outbreak of methicillin-resistant Staphylococcus aureus (MRSA) in the hospital’s neonatal intensive care unit when there were only two known cases. Ward screening found six other infants to have been colonised with the bacteria, and appropriate infection measures were then able to control the outbreak (18).
At the time of this study, implementation was continuing. The laboratory team were publishing protocols they had developed to enable others to replicate their work (16). ESR supported the development of automated analysis pipelines to enable bespoke analyses without the laboratory team needing specialist bioinformatics expertise. Oxford Nanopore Technologies were developing nanopore sequencing technology to make it more user-friendly and include more automated analysis pipelines.
METHODS
A social system is an interconnected group of elements with at least one goal, produces relatively stable behaviour over time despite fluctuations in the environment, yet can also adapt in response to the environment (19). Awanui Labs Wellington can be seen as a system that is set up to provide diagnostic pathology services that remain relatively constant over time yet also has ways to adapt to the changing needs of patients and clinicians and changing technology. Implementing nanopore sequencing is an example of such adaptation.
This case study was conducted as participatory research, where the Molecular Pathology Department staff were involved in the data generation and making sense of the findings. Ethics review and approval was obtained from the Aotearoa Research
Ethics Committee (AREC23_21).The study explored the system of nanopore sequencing and its implementation, including describing the larger system in which it is embedded (20), that is, Awanui Labs Wellington. Two systems approaches were used: VSM and Systems Effects mapping. VSM is a model of organisational structure and design, which is used to ask questions about how the functions of intelligence gathering, policy and governance, coordination and control, and operations are structured to respond to the changing environment to meet the goals of the organisation or system (7, 20). Systems Effects mapping further explored the interconnected influences on the system of implementing nanopore sequencing in the laboratory (8).
The data were generated from interviews with two staff members, a focus group discussion with three team members, and supplied documents including expenses spreadsheets, a workflow diagram, funding applications and a seminar slide presentation. Luke Craven, founder of the Systems Effects methodology, was contracted to produce a bespoke survey tool for this project (https://systemeffects.com/#/) that was distributed to the Awanui Labs team, with five responses received. The survey asked about the factors that the team thought had influenced the implementation of nanopore sequencing, further factors that influenced the primary factors, and what connections they saw between these factors. The Systems Effects survey drew a map of the interconnections between factors, and the participant could add to or change the map. The social science researcher then used the survey tool to refine the data by grouping the factors where respondents had expressed similar ideas using slightly different language, and naming these groups as seemed appropriate. The tool produced a matrix of interconnections of the groups, and this matrix was downloaded as raw data for the Kumu Inc. system mapping online application (https://kumu. io/). The initial survey also included an open-ended question to suggest a vision for the future of nanopore sequencing, which provided additional context for the overall study.
The Kumu Inc. application was used to visualise the interconnected factors. The map generated by the downloaded matrix was adjusted for greater clarity by adding colours based on the researcher’s interpretation of related factors, placing the factors where they could be clearly seen, and ensuring the size of the arrows reflected the number of responses that contributed to that theme. The system map was then shared with the laboratory team to check that it made sense to them, as the basis for the focus group discussion.
The organisational model following the VSM framework was constructed by the social science researcher from the data inputs described above. This was written as a case study report that was circulated to the laboratory team for feedback and editing.
Figure 1. Workflow for weekly Nanopore sequencing runs – diagrammatic representation to show the locations of the work – initial ‘web lab’ work at the hospital laboratory, ‘dry lab’ computing work onsite at the hospital, and ‘dry lab’ remotely at ESR.
VIABLE SYSTEM MODEL
This model has been developed through the process outlined above. It is a model constructed by the social science researcher and checked with the rest of the laboratory team to ensure that the model fairly describes the social system surrounding their implementation of nanopore sequencing. Like all models, it is a partial view of the social system and is used to generate potentially useful insights for action.
Goal: Infection Prevention and Control
According to the VSM framework, the first step in a system analysis is to establish the goals, as by definition every social system must have at least one goal (19). Through the interview and discussions, the overall goal of the laboratory was articulated as pathological diagnostic services for the ultimate benefit of patients, through providing clinicians with high-quality information on which to base their decisions.
A more specific goal for the nanopore sequencing project was to contribute to IPC, which was a significant issue that the laboratory team was involved with. It has been estimated that up to 5-10% of hospitalised patients acquire an infection after hospital admission (9). This has negative effects on patients’ health and wellbeing, and the additional length of stay has implications for the workload of the medical staff and a flow on economic cost (21). Estimated costs of hospital-acquired infections in New Zealand were NZD$226m in 2021 (10). Some of these infections could be prevented by IPC interventions, especially if applied early in an outbreak, and it was this goal that partially motivated introducing nanopore sequencing as a monitoring method. Nanopore sequencing in the Molecular Pathology Department provided additional information to the existing procedures, enabling IPC interventions that were not possible previously. The long-term aim was articulated as the development of this technology to the point that this service was routinely available.
With these goals in mind, the following sections describe the structural influences on the implementation of nanopore sequencing in the Molecular Pathology Department, focusing on the VSM framework categories of Environment, Intelligence gathering, Policies, Control mechanisms, Coordination processes, and Operations and service delivery.
Environment
Every social system operates within a complex and changeable environment. Two environmental issues were identified that affected nanopore sequencing implementation. One was the constant development of new technology, and the other was resourcing for healthcare in general, specifically research.
New technologies for use in a clinical laboratory were continually being developed. A tension within the laboratory was balancing the core role of providing approved funded services with innovation and introduction of new services, particularly during the time of initial implementation where testing for COVID-19 placed considerable demands on the Molecular Pathology Department. Further, staff were expected to facilitate transfer of new technology from the research to the clinical laboratory setting. There were processes in place to enable the introduction of new services, however these necessarily set limits on what could be undertaken to ensure uninterrupted service delivery.
The economic resourcing of services was recognised by all the laboratory staff as the fundamentally limiting factor in all technological innovations. They saw the resourcing of public healthcare as a highly political issue, subject to changing political intentions. The challenges of limited funding were mentioned by all staff and was seen to particularly affect staffing levels and workload. Technological innovation was resourced through targeted funding streams for research, and this funding was seen as vulnerable to changes in management decisions or to decreases in overall healthcare resourcing.
Intelligence
To adapt to a changing environment, an organisation needs ways of gathering information about the environment and assessing the magnitude and longevity of changes. In this laboratory there were ‘vertical’ and ‘horizontal’ processes of gathering intelligence. The ‘vertical’ process was through the management structure of the organisation. The Head of Department was the link between the Molecular Pathology Department and the wider organisation, connecting with other Heads of Department within Awanui Wellington, and through them to the management of the Awanui Lab network throughout the country.
There were two main ‘horizontal’ intelligence networks operating. One was the close working relationship between laboratory scientists, clinical microbiologists, and clinicians and medical staff in the wider hospital. This enabled flow of information around what clinical problems needed to be addressed, the capability of new technology and potential uses for new technology. This informal network relied on frequent interactions during daily business. The second ‘horizontal’ network was between the staff at different clinical laboratories around the country. The nationwide laboratory scientist community was seen as small enough that the team felt that they knew most of the scientists in the country. This meant that a scientist in the Molecular Pathology Department at Wellington would feel confident in discussing a question or issue with scientists in a different laboratory who might be doing similar work. The Wellington scientists were aware that they were the first clinical laboratory in the country to be implementing nanopore sequencing for IPC and were conscious of developing and documenting protocols that would allow others to replicate their work.
Policy
The tension between business-as-usual services and the need to continually develop new tests and technologies was recognised through processes that made funding available for the programme. The Wellington Regional Hospital Infectious Diseases department had a small fund for testing the feasibility of an innovation, and the DHB had a larger fund that could be used to fund the ongoing delivery of new laboratory tests. For both funds, an application justifying the need for funding, detailing the method and supplying a budget was required. Despite the limited funding available, the policy provided a means to balance the tension between service delivery and development.
Control
The laboratory operations were subject to quality assurance (QA). Staff were expected to follow established QA procedures, which were externally monitored. The laboratory was accredited by International Accreditation New Zealand (IANZ) for ISO 15189:2912, as a prerequisite for health sector operations. However, the nanopore sequencing fell outside of this QA monitoring as it was not an established technology, especially in Aotearoa New Zealand. There was no relevant ISO standard to be accredited against, and no organisation available for external QA. Development of standards would be necessary for the technology to move from research to being part of the core services. However, before this could occur the protocols had to be developed and validated, work which was underway during this case study (16).
Coordination
A viable organisational system needs to balance autonomy of various units and coordination of the whole. The coordination of the lab work was achieved through related departments (Molecular Pathology and Microbiology) reporting to the same Head of Department, and the clinicians who worked across these departments in a close working relationship with the scientists. Implementing nanopore sequencing introduced a requirement for a new level of coordination. In this context, Awanui Labs Wellington was supported by ESR, especially through the
provision of bioinformatics expertise. The model that developed was of the extraction, sequencing and initial bioinformatics being done on-site at Awanui Labs Wellington, followed by transfer of data to ESR for more detailed bioinformatics analysis when required (16). It was acknowledged that there were relatively few people with required bioinformatics skills, as this was a specialised and rapidly evolving field.
Operations
The factors influencing implementation of nanopore sequencing identified through the survey were mostly operational in nature and are therefore reported in this VSM category. The interconnections of these influencing factors are shown in Figure 2. The size of the arrows corresponds to the number of people indicating that connection, hence it can be seen that ‘staff workload’ was the most identified influencing factor. The colours group the factors in terms of major issues affecting the work (green), computing equipment (purple), computing and other expertise (blue), and other (orange).
The initial set up of nanopore sequencing in the laboratory involved the purchase of new equipment and kits, costing around USD$7,500. Ongoing costs depended on the sequencing sample batch size (12, 18 or 24) and were around USD$450 per run. This was justified in comparison to the significant costs of infection events, for example around NZD$20,000 per event in one study (9). The weekly workflow of ongoing extraction and a weekly batch run was designed in part to balance the differing priorities of quick turnaround time with cost efficient batch runs, as well as balance the workloads of the scientists. The weekly
batch runs were also a way to efficiently use bench space and not disrupt routine work. A benefit of nanopore sequencing was the lack of a DNA amplification (PCR) step, which meant that there were fewer issues with contamination and therefore more flexibility as to which bench spaces could be used.
Expertise was a significant influencing factor. The laboratory scientists were largely self-taught, using online protocols published by Oxford Nanopore Technologies, designing extraction protocols using other resources, and drawing on their experience and expertise of many years. Publishing the developed protocols was seen as a way of supporting other laboratory workers. There was a general opinion in the team that nanopore sequencing required previous knowledge of working in a laboratory, although it was acknowledged that this could change over time especially if parts of the process became more automated or more familiar to the scientists. A significant limitation was the need for bioinformatics expertise. Some of the laboratory staff had acquired limited bioinformatics expertise, however the skill level required for the more granular analysis was specialised.
An unexpected expense was the need to upgrade the available computing power to be able to process and analyse the large amounts of data. Once achieved, the next issue was the transfer of large amounts of data for retrospective analysis at ESR. Because of the size of the data generated and organisational IT security policies, direct data transfers (that is, laboratory staff uploading data directly to ESR High-Performance Computers) were not possible and an indirect solution had to be implemented.
DISCUSSION
This social science study was motivated in part by research scientists wanting to better understand the social and systemic barriers to the uptake of nanopore sequencing, given that it is not yet widely used in clinical settings (1). This study showed that in this case, implementation was slow not because of unwillingness from the team involved, but rather because of a prioritisation of the needs of patients (as the ultimate beneficiaries). Implementation of new technology was balanced against the need to ensure continuity of existing services. The implementation also proceeded carefully to ensure that quality standards were maintained, again in the best interests of patients. This was shown to be the general approach to the introduction of any new technology or diagnostic tests.
A limitation of the greater use of nanopore sequencing specifically was the lack of in-depth bioinformatic expertise. This
has also been identified by other reviews of implementation of NGS (3-6). The review by Besser et al. in 2018 suggested that the future of NGS would be automated sequencing and data analysis, where a sample could be loaded into the sequencer and then without the need for further manual interaction, a standardised report would be generated and stored in the Laboratory database (6). At the time of the case study in 2023, this future was not imminent. A different solution was proposed by the research collaboration between Awanui Labs Wellington and ESR Genomics and Bioinformatics team, one that leveraged the advantages of the relatively small medical laboratory system in Aotearoa New Zealand and promoted collective working. This recommended solution was to combine decentralised sequencing carried out in routine diagnostic laboratories with a centralised bioinformatics reference laboratory service, as shown in Figure 3. The centralised collection and analysis of data would
Figure 2. Systems Effects map of factors influencing the implementation of nanopore sequencing from the perspective of staff at Wellington Regional Hospital laboratory
support further monitoring, surveillance and research for public health. This would also support making genomic research data sets publicly available, which is an increasing requirement of academic genomic research.
This scenario would require the development of appropriate data infrastructure, including data storage, transfer mechanisms, security, governance and sovereignty. While Māori data sovereignty is less of an issue when sequencing pathogens, this same system could be used for research and diagnosing of
genetic disorders which would require measures to protect Māori data sovereignty. It would be a major undertaking to develop such data infrastructure, and although work had started on digital health infrastructure for Aotearoa New Zealand, political changes created uncertainty about the future of these initiatives. The need for infrastructure highlights the difference between nanopore sequencing in a research laboratory versus a clinical laboratory, and the issues that come with scaling up a technology for widespread routine use.
Figure 3. Proposed model for efficient use of scarce bioinformatic resource – decentralised collection and initial sequencing of isolates in regional laboratories, centralised further bioinformatic analyses in a centralised reference laboratory.
CONCLUSION
This social systems case study focused on the Molecular Pathology Department at Awanui Labs, Wellington who had been trialling the implementation of nanopore sequencing for two years to assist in Infection Prevention and Control at the Wellington Regional Hospital. This trial was enabled by the systems that had been set up to balance the need for continued service improvement through research and innovation with the need to maintain the current level of service to clinicians and ultimately, the patients. The new technology implementation process allowed oversight and coordination by management while providing a reasonable degree of autonomy for the laboratory scientists to conduct the trial, including the time and flexibility required to investigate and develop the protocols as well as upskill on genomic sequencing methods. The trial was further enabled by the collaboration with ESR Genomics group, who provided advice and bioinformatics expertise to support the implementation of nanopore sequencing in the laboratory.
There were several challenges that related to implementing new technology while maintaining a busy routine workload and securing funding. The main challenges specific to nanopore sequencing were issues around accessing bioinformatics expertise, providing adequate computing power for the analysis of the data, and the wider systemic issue of data infrastructure in the health sector. The bioinformatics expertise and upgraded computing equipment had been addressed to some degree, however the issue of data infrastructure was one that was beyond the system described in this case study.
This qualitative case study aimed to explore the social systems around the implementation of nanopore sequencing in a clinical setting, complementing the studies that have focused on the technical aspects of implementation. For successful implementation, attention needs to be paid to factors such as policies and practices, the mix of expertise on the team, and the access to technical and financial support. It also relies on the very human factors of team motivation and cohesion, willingness to learn, and at least one person who is willing to initiate and drive the project.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the collaboration and support of the ESR Genomics and Bioinformatics team, in particular Donia Macartney-Coxson and David Winter [current], and Miles Benton, Matt Storey and Joep de Ligt [previous team members]. Thank you also to Mat Walton, former Technical Lead of the ESR Social Systems Team for his work on the funding proposal.
The case study was internally funded by ESR through the Strategic Science Investment Fund (SSIF), wet-lab and initial bioinformatics nanopore sequencing implementation work was internally funded by Capital Coast DHB, and the more granular
bioinformatics analyses funded by ESR through SSIF and funding from Genomics Aotearoa.
AUTHOR INFORMATION
Suzanne Manning, PhD, Technical Lead Social Systems1
Max Bloomfield, MPhil, Clinical Microbiologist2
Samantha Hutton, BMLSc, Medical Laboratory Scientist2
Megan Burton, BMLSc, Medical Laboratory Scientist2
Charles Velasco, GradDipSci, Medical Laboratory Scientist2 Claire Tarring, MSc, Scientist2
Rhys Thomas White, PhD, Scientist3
Koen van der Werff, BMLSc, Head of Department Microbiology and Molecular Pathology2
1 Social Systems Team, Institute of Environmental Science and Research (ESR), Wellington, New Zealand
2 Awanui Labs, Wellington, New Zealand
3 Genomics and Bioinformatics Team, Institute of Environmental Science and Research (ESR), Wellington, New Zealand
Correspondence: Rhys White, Genomics and Bioinformatics Team, Institute of Environmental Science and Research email rhys.white@esr.cri.nz
REFERENCES
1. Vanhee M, Floré K, Vanthourenhout S, et al. Implementation of full-length 16S nanopore sequencing for bacterial identification in a clinical diagnostic setting. Diagn Microbiol Infect Dis 2024; 108(2): 116156. doi: 10.1016/j. diagmicrobio.2023.116156.
2. Zhao W, Zeng W, Pang B, et al. Oxford nanopore long-read sequencing enables the generation of complete bacterial and plasmid genomes without short-read sequencing. Front Microbiol 2023; 14: 1179966. doi: 10.3389/ fmicb.2023.1179966.
3. Athanasopoulou K, Boti MA, Adamopoulos PG, et al. Thirdgeneration sequencing: the spearhead towards the radical transformation of modern genomics. Life 2022; 12(1): 30. doi: 10.3389/fmicb.2023.1179966.
4. Brlek P, Bulić L, Bračić M, et al. Implementing whole genome sequencing (WGS) in clinical practice: advantages, challenges, and future perspectives. Cells 2024; 13(6): 504.
5. Petersen LM, Martin IW, Moschetti WE, et al. Thirdgeneration sequencing in the clinical laboratory: exploring the advantages and challenges of nanopore sequencing. J Clin Microbiol 2019; 58(1): e01315-01319 doi: 10.1128/ jcm.01315-19.
6. Besser J, Carleton HA, Gerner-Smidt P, et al. Next-generation sequencing technologies and their application to the study and control of bacterial infections. Clinic Microbiol Infect 2018; 24(4): 335-341. doi: 10.1016/j.cmi.2017.10.013.
7. Hoverstadt P. The Viable System Model. In: Reynolds M, Holwell S, [editors]. Systems approaches to managing change: A practical guide. 2nd ed. The Open Polytechnic, London, 2020: 85-138
8. Craven LK. System Effects: A hybrid methodology for exploring the determinants of food in/security. Ann Am Assoc Geogr 2017; 107(5): 1011-1027. doi: 10.1080/24694452.2017.1309965.
9. Burns A, Bowers L, Pak N, et al. The excess cost associated with healthcare-associated bloodstream infections at Auckland City Hospital. NZ Med J 2010; 123(1324): 17-24.
10. Grae N, Singh A, Jowitt D, et al. Prevalence of healthcareassociated infections in public hospitals in New Zealand, 2021. J Hosp Infect 2023; 131: 164-172. Doi: 10.1016/j. jhin.2022.10.002.
11. Brown CG, Clarke J. Nanopore development at Oxford Nanopore. Nat Biotechnol 2016; 34(8): 810-811. doi: 10.1038/nbt.3622.
12. Heather JM, Chain B. The sequence of sequencers: the history of sequencing DNA. Genomics 2016; 107(1): 1-8. doi: 10.1016/j.ygeno.2015.11.003.
13. Jain M, Olsen HE, Paten B, Akeson M. The Oxford Nanopore MinION: delivery of nanopore sequencing to the genomics community. Genome Biol 2016; 17(1): 239. doi: 10.1186/ s13059-016-1103-0.
15. Oxford Nanopore Technologies. Available from: https:// nanoporetech.com/products/sequence
16. Bloomfield M, Hutton S, Velasco C, et al. Oxford nanopore next generation sequencing in a front-line clinical microbiology laboratory without on-site bioinformaticians. Pathology 2023 56(3): 444-447. doi: 10.1016/j.pathol.2023.07.014.
17. Bloomfield M, Hutton S, Burton M, et al. Early identification of a ward-based outbreak of Clostridioides difficile using prospective multilocus sequence type-based Oxford Nanopore genomic surveillance. Infect Control Hosp Epidemiol 2024; 45(9): 1-7. doi:10.1017/ice.2024.77.
18. White RT, Bakker S, Burton M, et al. Rapid identification and subsequent contextualization of an outbreak of methicillinresistant Staphylococcus aureus in a neonatal intensive care unit using nanopore sequencing. Microb Genom 2024; 10(7): 0011273. doi: 0.1099/mgen.0.001273.
19. Meadows DH, Wright DE. Thinking in systems: a primer. White River Junction, VT: Chelsea Green; 2008.
20. Ríos JP. Design and diagnosis for sustainable organizations: the viable system method. Berlin: Springer; 2012.
21. Sundermann AJ, Kumar P, Griffith MP, et al. Genomic surveillance for enhanced healthcare outbreak detection and control. medRxiv [preprint]. 2024: 2024.09.19.24313985. doi: 10.1101/2024.09.19.24313985
Point of Care Testing Coordinator, Pathology Services, Northland District Health Board
Acknowledging Geoff Herd’s contribution to Medical Laboratory Science with a Life Membership to NZIMLS
On Wednesday 6th November 2024 I had the privilege of awarding Geoff Herd a Life Membership of the NZIMLS. Geoff Herd is a strong advocate for best patient outcomes, and quality medical laboratory testing. This has included medical laboratory quality improvement projects in urban and rural hospitals, and workplace health screening in isolated populations in Northland.
Geoff has worked in Medical Laboratory Science since 1978 and was awarded the NZIMLS prize for Medical Microbiology in 1982. He has previously worked in Haematology and Transfusion Science, Operations Management and Medical Laboratory Accreditation. He was appointed as Point of Care Testing Coordinator for Northland in 2007.
In 2009 he set up the New Zealand Point of Care Testing Advisory Group (NZPOCTAG), which has significantly grown the reputation and quality of POCT in New Zealand, and which contributed to New Zealand’s COVID-19 response. Geoff has been fortunate to co-author 14 published articles in a variety of medical journals, advocated for clinical governance for POCT and changes to legislation for the regulation of in vitro diagnostic devices through the Ministry of Health, the Therapeutic Products Act 2023, and the proposed Medical Products Bill.
Geoff was nominated by Stephanie Williams, and the NZPOCTAG to receive this NZIMLS Life Membership, which was greatly accepted by the NZIMLS Council. The membership was awarded at the Northern Regional POCT ISO15189:2022 Quality Assurance Workshop, which came as a big surprise to
Geoff (he had no idea this was happening and was not expecting it!). It was an absolute pleasure to be a part of presenting this award, and to recognise the hard work that our Scientists and Technicians give to healthcare.
Geoff Herd, NZIMLS Life Membership, presented by Melanie Adriaansen
Interviews with the recipients of the NZIMLS top student award, 2024
Top Student Awards are offered annually by the NZIMLS for student academic achievement during the third year of the BMLSc degree or in more recent times during the fourth year. The award is made to students at the University of Otago and AUT in New Zealand who offer the BMLSc qualification and is provided in support of the recipient's final clinical training year in the BMLSc programme. The $2,000.00 prize is typically paid to the University who then present it to the winner on behalf of the NZIMLS. For the first time NZIMLS also offered awards to the top placement students who were nominated by their placement laboratories. The Placement prize was $1,000.00.
In December, Otago University recognised Tristan Cherrill and Senumi Gunawickrama as joint Top 4th Year Students and the Top Placement Students prize was shared between were Divya Patel in Semester one and Imogen Taylor for Semester two.
Firstly, congratulations to you all on winning the top BMLSc student awards! What a fantastic accolade to start your careers in medical laboratory science. Tristan and Imogen share their experiences with us.
1. Can you tell us a little about yourself?
Tristan: I am originally from Wales and moved to NZ when I was 5 years old. I grew up on the Kāpiti Coast where I played violin in orchestras, joined community groups helping organise charity events, and getting outside to experience the beautiful nature. I carried this on to university joining environmental groups and exploring the South Island.
Imogen: I’m originally from Christchurch. I’ve been into the health sciences since I was a kid but decided to study medical laboratory science during high school. I loved the degree and my time studying at Otago. My other interests include music, philosophy, running and being outdoors.
2. What interested you about the BMLSc degree?
Tristan: I really love science and have always been interested in the idea of a practical job working in a laboratory. The Health Sciences have also been a large interest of mine because of the prospect to care for the health of others. Understanding the complex system of our bodies is particularly valuable. The BMLSc degree interested me because it unifies these two ideas and also allows exploration of the different disciplines so that I could find what I enjoy doing most.
Imogen: I originally found out about the BMLSc after looking into studying forensic science. I have always been interested in science and wanted a job where I could focus on helping others. Med lab seemed like a really good fit and I was also attracted to the practical elements of the degree.
3. Was there a defining moment where you thought; ‘yes that’s what I want to do’? Can you tell us about it?
Tristan: Not really a defining moment, but since I heard about the degree when I first got to high school, I knew at that time it interested me. I worked towards the health sciences pathway and enjoyed the practical work in first year which built upon my interest to carry out the degree.
Imogen: I’m not sure there was one definite moment, but I do remember visiting a careers fair in year 12 of high school and talking to a med lab student who was really encouraging about the degree. She emphasized how personalised the course can be and how tight knit her cohort was. I was already interested in the topics and hearing positive feedback about the course definitely pushed me into med lab.
4. What did the programme entail? Was there a speciality or a particular placement that really grabbed you?
Tristan: The programme entails a wide understanding of the human body from major organ systems down to the cellular and chemical systems in both healthy and diseased states. This is built upon by teaching about the tests that help identify the healthy and disease states of the body. The course is both theoretical and practical and requires knowledge of how these tests are conducted, how they work, and what the results mean. I really loved both my Transfusion science and Haematology placements where I could feel the impact of my work on the lives of the patients. Both shared an investigative nature where transfusion science investigates the correct product or course of action to now take, while Haematology investigated the likely cause of a change seen.
Imogen: In my experience the program was a great mix of theory and lab work, with opportunities to work alongside other health professions in first and second year, and more isolated study with the med lab cohort in third year. I’m grateful to say I had two really amazing placements, one in microbiology and one in haematology. I loved my time in both placements and had the chance to greatly improve my knowledge in both specialties. Getting to experience hands on work during my placements was one of my favourite parts of the degree and gaining a better understanding of day-today life as a scientist was great for my motivation.
5. Top Student or Top Placement, what does this prize mean for you?
Tristan: I feel so proud that I could achieve such an achievement being a top 4th year student. It is gratifying that the dedication and hard work I put into my course has been so successful and appreciated. It motivates me to continue my enthusiasm for knowledge and commitment to achieving excellence in everything I do.
Imogen: It’s really great to receive a top placement award! I definitely put a lot of work into my placements this year and I’m proud of what I managed to accomplish during them. It’s great to know that I did well.
6. Was there a person/s who inspired you during this journey?
Tristan: I have been inspired by all the lecturers, researchers, scientists, and technicians I have met during my education. Their passion for the laboratory work to provide and develop the best diagnostic results and techniques for patient care, as well as their commitment to give me the best education, inspires me to be passionate about my own work. I want to
Tristan Cherrill, Senumi Gunawickrama, Lisa Cambridge (Editor) and Imogen Taylor. Absent; Divya Patel
strive hard to be capable and competent and exceed the expectations put on me.
Imogen: I was inspired by lots of people along my journey. During university I was lucky enough to have professors and teaching fellows/lab demonstrators that were excited about med lab and this helped push me through my time at Otago. During my placement year I met many scientists who inspired me to continue into the career, including my supervisors Tony Barnett and Shona Brougham. I was also greatly inspired by my fellow students and feel blessed to have studied with such a hard-working and supportive cohort.
7. What’s next for you in your career?
Tristan: I’ve enjoyed the degree and want to use it as a supporting branch to complete further education and I am now currently enrolled in a Bachelor of Dentistry. I think this degree has been invaluable to me and has allowed me to discover so much about myself, the profession and the health service, and how to best support the patients within the healthcare system
Imogen: I’ve recently started my first postgraduate role working in microbiology and am excited to continue my learning as a scientist! I’m really lucky to be working with an amazing team and I’m definitely enjoying starting my career in a supportive environment.
8. What do you enjoy about the job? And what has your experience in the laboratory taught you?
Tristan: I have really enjoyed the practical aspects of laboratory work and using my knowledge in combination with critical thinking to fulfil the laboratory work. I have enjoyed meeting so many new people, both patients and staff, at multiple labs around NZ and helping them all in one way or another. The experience has taught me how to learn different skill sets and has improved my problem solving, communication, confidence, creativity, and analytical techniques.
Imogen: I really enjoy lots of different elements about the job. I particularly love the hands-on aspects of the work. In the day-to-day lab I enjoy seeing how lab results fit together to create a full picture of different pathologies. In microbiology, I appreciate how important interpretation and background knowledge building are, and the constant need to develop new skills and further my learning.
9. The profession has featured in the media during your studies, what has been your experience or thoughts on
this so far? How do you think this has impacted both the profession, your career and you personally?
Tristan: I saw the profession featured heavily near the beginning of my degree which boosted the deserved recognition of how much work is done for patient health that isn’t seen by the public. As my degree continued, despite great efforts of the workforce, I am now left with a rather bleak outlook. The prominence in the public’s opinion has diminished and along with it so has regard for scientists and technicians. I noticed during my study this has left a mark on many people in the lab, myself included. I hope that things can change, and fair compensation can be given before the profession loses too many qualified and skilled and experienced staff.
Imogen: I think that media attention on the profession definitely has positive and negative aspects. I think that it is important to increase general public awareness of the profession as I know personally not many people are aware of the field. I think it’s also been great to see people within the profession coming together. It would be great to see increased awareness and general appreciation for med lab work in the future.
10. Do you have any advice for our up-and-coming medical laboratory scientists?
Tristan: Try to use all the resources available to you, ask questions and listen to the advice others have to offer you. Explore your options too, be curious about the different disciplines and look at the parts you really enjoy about them. This profession is so important in the healthcare system, so work hard and be proud of what you accomplish.
Imogen: Engage with all the opportunities you get, work with your classmates and lecturers as much as possible and do your best to work hard and engage in your placements, they can set you up really well for the workplace. I would definitely recommend giving every speciality a chance, even if it doesn’t interest you right away. Remember that learning in university can be very different to working in the lab!
Thank you, Tristan and Imogen, it was lovely to meet you and your experiences are inspiring and aspirational. On behalf of the NZIMLS and its members we wish you all the best in your careers and I hope we will be hearing more from you all in the future.
Lisa Cambridge Editor
REVIEWS OF INTEREST
The reviews below can be accessed for their Abstracts and “Open Access” is indicated where applicable. Unfortunately, the NZIMLS cannot provide full access to the articles due to copyright restrictions, but full access may be available through various institution arrangements. Any feedback on this can be sent to: editor@nzimls.org.nz
1. Munoz de Toro M and Ferdanez-Pol S. Systematic literature review of published cases of reactive plasmacytosis in peripheral blood and bone marrow. J Clin Pathol 2024: 77; 802-809.
2. Gong S, Zhang X, Chen X et al. The impact of bariatric surgery on gut microbiota: a bibliometric analysis of research trends and scientific contributions. Front Microbiol 2025: 16; doi: 10.3389/fmich.2025.1523809. [Open Access]
3. Coates TD. Management of iron overload: lessons from
4. Li Y, He W, Zhou Y et al. Advances in laboratory diagnosis of Sjogren’s disease in children. Clin Chim Acta 2025; 567:1200095. doi: 10.1016/j.cca.2024.120095.
6. Borkhataria CH, Sharma S, Vaja P et al. Quality management, ethical considerations, and emerging challenges in genomics and biobanking: A comprehensive review. Clin Chim Acta 2025; 569: 120161. doi: 10.1016/j.cca.2025.120161.
7. Tayeb BA, Osman AAM, Njangiru IK. Liquid biopsy biomarkers in breast cancer: an overview of systematic reviews. Clin Chim Acta 2025: 1200063. doi: 10.1016/j. cca/2024.120063.
SCIENCE DIGEST
Contributed by Michael Legge
Zombie viruses and bacteria: is there a risk?
Permafrost is any ground that remains completely frozen at 0oC or colder for long periods of time. These unique areas are usually found near polar regions in places such as in Russia and Alaska. It is estimated that about a quarter of the Northern hemisphere land area is in permafrost. In some regions the top layer may thaw in summer but below remains frozen. So, where do the zombie bacteria occur? Recent research from an international group in Sweden and Russia have monitored cycles of climate change and the changes in permafrost (1). They identified that with the warming climate there was an increased rainfall which thawed the permafrost beyond the top layer; this increased the release of carbon substrates with up to 70% of permafrost estimated to thaw by 2100. This ecological destabilisation is starting to release viruses and bacteria and potential pathogens that were frozen and at the time inactive (2). Although to date the viruses recovered have proven to be inactive for diseases such as smallpox (300 years old), H1N1 virus (Spanish flu, which was subsequently activated in the laboratory). An anthrax outbreak in 2000 was traced to thawed cattle in the thawing permafrost, and killed more than 2000 reindeer and a 12-year-old boy. Both research groups conclude that the increasing thaw now being associated in permafrost will not only change the ecology of vast Northern hemisphere regions but will also unlock viruses and bacteria that may have been captured for millennia, and this resurrection may have the potential for future pandemic associated diseases.
Anomalous results in prenatal cfDNA sequencing
The use of circulating cell-free DNA in the plasma of pregnant women has become a significant tool for the detection of fetal aneuploidy. It is superior to the use of serum biochemical screening and the nuchal transparency screening and reduces the use of amniocentesis. Typically, approximately 10% of cfDNA comes from the placenta and the remaining 90% from the person’s haematopoietic system. When analysed against controls all the data is analysed using bioinformatic algorithms. As the test develops and use increases, retrospective data analysis has indicated unusual sequencing results e.g. multiple aneuploidies, autosomal monosomies and cancer have been identified. In the case of cancer, the tumour itself can shed cfDNA into the circulation. In a recent research publication from the USA (3) the researchers looked at identifying DNAsequence patterns and other biomarkers that could identify asymptomatic people who may have cancer and establish a procedure for use with pregnant women who may get unusual results. From the initial cohort of 197 pregnant or post-partum women who had an unusual cfDNA result, 52 were identified as having cancer using clinical and laboratory criteria. Of the 52, 47 had a combination of copy number gains and losses across multiple chromosomes. Other women were identified as having sequencing abnormalities unrelated to cancer but non-malignant conditions. The authors conclude that 48.8% of participants with unusual or non-reportable cfDNA results had occult cancer and recommended that more research is needed to further understand unusual cfDNA results.
Gaps in ion-selective based analysers
Various analysers use ion-selective electrodes to measure plasma sodium which is based on two methods; an indirect method typically used on high throughput analysers and a direct method normally used on blood gas analysers. Previous research had shown that there can be clinically significant discrepancies between the two sodium results. Both methods assume a fixed non-aqueous fraction of 7% but they differ in whether a predilution step is used with an aqueous buffer. Deviations in the non-aqueous fraction caused by dilution
will affect the electrolyte concentrations and checks need to be made between results from blood gas analysers and laboratory results for validation. A recent research paper from Belgium (4) has further investigated this anomaly. The authors evaluated a new analyser from China (BioassaysTM E6 analyser) which uses direct ion-specific electrode technology and is a high throughput analyser that can measure four clinically relevant electrolytes, and pH. The authors demonstrated that there was good agreement between the other electrolyte methods and that the ability to recalculate other results obtain by alternative methods was possible using this instrument. They conclude that the instrument is an alternative to established ion-specific electrodes and provides the option of adjustment of data from blood gas analysers but needs to be evaluated in clinical conditions.
Relooking at pan-Trk in various subtypes of breast cancer
Secretory carcinoma of the breast is a rare subtype of breast cancer historically defined as juvenile breast cancer. However, it is now known that it is diagnosed in a wide range of ages and has a favourable outcome when diagnosed and treated. Typically, the diagnosis relies on a characteristic appearance from histological analysis but can vary in its architecture. It is usually negative for oestrogen receptor, progesterone receptor and no overexpression of HER2. On immunohistochemistry most demonstrate staining for CK5/6 or CK14, EGFR and expression of S100, SOX10 and MUC4. This mixed expression can make diagnosis difficult. Secretory carcinoma of the breast has been identified as having a recurrent chromosomal rearrangement t(12;15) (p13;q25) that fuses ETV6 on 12p13 to NTRK3 on 15q25 and this accounts for 95.2% of this cancer. Although the translocation can be identified by FISH and other molecular techniques these may not be readily available and are costly. A recent publication from the USA has examined the feasibility of using pan-Trk immunohistochemistry for the various sub-types of secretory carcinoma of the breast (5). The authors used material from 346 invasive breast carcinomas from differing diagnosis using a rabbit monoclonal Pan-Trk antibody and formalin fixed tissue sections and HRP. They identified that pan-Trk staining was positive for all secretory carcinoma of the breast but not in any of the non-secretory invasive breast cancers. They conclude that Trk is an ancillary test that is useful for distinguishing from triple-negative histological mimickers.
Artificial intelligence and human embryo assessment
The use of Assisted Reproductive Technologies (ART) is now considered common place in resolving fertility problems, which is primarily the use of in-vitro-fertilisation (IVF). While there are many issues associated with the use of the ART technologies one major issue is the determination of embryo quality following fertilisation and culture of the gametes and embryos. Typically, the assessment of embryo quality and subsequently a successful pregnancy is dependent on the skills and experience of the embryologist. Using a set of morphological criteria decisions are made on what constitutes a “good” embryo (essentially viability) and a “poor-quality” embryo (considered non-viable). When all is well the good/viable embryo can be transferred to the uterus and the anticipation is that a successful pregnancy is achieved. Any remaining embryos are cryopreserved. Previous research has shown that some “poor quality” embryos may develop normally whereas others die. Recently research has considered Artificial Intelligence (AI) and Machine Learning (ML) to determine whether a more accurate predication of embryo viability is possible and concluded that currently validation was a problem (6). More recently research from Australia (7) considered the ethics of using AI and ML in human embryo assessment and raised issues relating to dehumanization of an intimate process, how decision making would be determined relating to bias, who
accepts responsibility for the decision making relating to embryo quality, deskilling of a very skilled workforce and importantly transparency and explainability of how the decisions were made and should patients give ethical approval for the use of AI/ML technologies. Finally, the authors express concern whether clinics may use the use of AI/ML to “bring business”.
Should we be concerned about direct-to-consumer testing? Diagnostic testing technologies have made significant advances in recent years which has led to the proliferation of direct-toconsumer tests (DTC). Current estimates from the USA put sales in 2022 to $USD1.5 billion. Besides the genetic tests and more recently COVID-19 tests, an increasing array of tests are becoming available to the public. Companies are increasingly making tests available as wellness tests or nutritional assessment tests and increasingly as organ function tests e.g. thyroid function, prostate health, fertility and menopause tests. Progressively DTC for infectious diseases such as HIV and STDs are appearing in an unregulated market. In recent international research paper, the group explored the use of DTC tests and emerging trends (7). They identified that internationally the market is unregulated and was rife with misleading consumer information. There was no consideration of either false negatives or positives and many kits were inaccurate. Misleading information was leading to misinformed health care decisions as there was no expert interpretation or backup. In certain situations, the initial results may lead to an increased over testing or the use of unproven supplements or self-treatment. The authors expressed concern relating to tests for cancer which again had no validity or expert input. These led to increased healthcare costs as well as issues of uncertainty and possible delays in treatment. They conclude that there needs to be effective management of the DTC tests and that regulation under in-vitro devices the focus is primarily on quality and efficiency of the test and not on appropriateness
of selection and use. They recommend a regulatory framework to monitor and control the use of DTC testing including nonregulated testing facilities.
REFERENCES
1. Magnusson RI, Hamm A, Karsanaev SV et al. Extremely wet summer events enhance permafrost thaw for multiple years in Siberian tundra. Nature Comm 2022; 13(1):1556. doi: 10.1038/s41467-022-292-48-x.
2. Murray KA. Keep it in the ground: climate change could prompt the reemergence of zombie pathogens. BMJ 2025; 388: r46 doi.101136/bmjr46.
3. Malayeri AA, Annunziata CM, Malayeri AA et al. Prenatal cfDNA sequencing and incidental detection of maternal cancer. N Eng J Med 2024; 391(22): 2123-2132.
4. Oyaert M, Verougstraete N, Vandekerckhove B et al. Analytical evaluation of a diect ion-selective-based analyser: still gaps to close. Clin Biochem 2024; 133-134: 110829 doi: 10.1016/j.clinbiochem.2024.1.10829.
5. Ye Q, Chen H, Peng C et al. Nuclear staining for pan-Trk by immunohistochemistry is highly specific for secretory carcinoma of breast: pan-Trk in various sub-types of breast cancer. J Clin Pathol 2024; 77(11): 751-755.
6. Salih M, Austin C, Warty RR et al. Embryo selection through artificial intelligence versus embryologists: a systematic review. Hum Reprod Open 2023; doi: 10.1093//hropen/ hoad031. [Open Access].
7. KoplinJJ, Johnston M, Webb ANS et al. Ethics of artificial intelligence in embryo assessment: mapping the terrain. Hum Reprod 2025; 40(2): 179-185. [Open Access].
8. Gram E G, Copp T, Ransohoff DF et al. Direct-to-consumer tests: emerging trends and cause for concern. BMJ 2024; 387: e080460 doi:10113/bmj-2024-080460.
RETIREMENT ANNOUNCEMENT
Gillian Lanham
Technical Specialist
Histology Department, Waikato Hospital Laboratory, Hamilton
Gillian Lanham began her career at National Women’s Hospital (Auckland DHB) at the age of 17 on January 24, 1977. In 1990, she moved to Hamilton with her husband, Ray, a fellow scientist specialized in Haematology.
Gillian later worked at Medlab, Hamilton, for six years before taking time off to raise her twin daughters, Megan and Heather. Following this, she began part-time work on the dawn chorus (night shift) at Waikato Hospital Laboratory. In 2007, Gillian transitioned to a full-time role in the Histology Department as a Pathologist’s Assistant. At that time, there were very few Pathologist’s Assistants, and over the years, she advanced to become the Technical Specialist in the Histology Department at Waikato Hospital Laboratory. Gillian retired on 20th December 2024 after 47 years of dedicated service to our profession.
Gillian lives on a lifestyle block near Ruakura and looks forward to a fulfilling retirement with her farm animals and pets. She reflects that she will miss the patient journeys and the fascinating clinical details but is relieved to leave behind the challenges of short staffing and work-related stress.
Gillian joined the NZIMLS in February 2005 and was always a passionate member actively involved in NZIMLS activities. She particularly cherished her interactions with colleagues and enjoyed attending ASMs and SIG meetings.
Gillian’s advice for new scientists is:
“Keep learning and stay interested in what you do. Your work matters, even if it feels invisible at times. What you do is an important job that needs to be done well.”
The NZIMLS Council and your colleagues wish you all the best in your retirement. Thank you for your support of the NZIMLS and your contribution to the profession.
Read the articles carefully as most questions require more than one answer. Answers are to be submitted through the NZIMLS website. Make sure you supply your correct email address and membership number, it is recommended that you write your answers in a word document and then cut and paste your answers on the website.
You are reminded that to claim valid CPD points for successfully completing the journal questionnaire you must submit an individual entry. It must not be part of a consultative or group process. In addition, members who have successfully completed the journal questionnaire cannot then claim additional CPD points for reading the articles from which the questions were derived.
The site will remain open until Friday 13th June 2025. You must get a minimum of eight questions correct per questionnaire to obtain 5 CPD points.
The Editor sets the questions but the CPD Co-Ordinator, Jillian Broadbent, marks the answers. Direct any queries to her at cpd@ nzimls.org.nz.
MARCH 2025 QUESTIONNAIRE
1. 70% of all diagnoses are based on a laboratory test result, what can happen when results do not meet their stated levels of sensitivity and specificity? What did an FDA report of twenty cases highlight in 2015?
2. What three examples of Laboratory Developed Tests (LDT) are available in Aotearoa NZ? Where?
3. What cancers have reported overexpression of Aurora kinases? What does overexpression cause? What is are the most overexpressed members or subtypes of Aurora kinases found in liver cancer tissues?
4. What 3 findings in the Zywea study into AURKA expression in liver cancer were revealed? What was a high mRNA expression of AURKA associated with?
5. Mutations in the glucose-6-phosphate dehydrogenase (G6PDH) gene manifest as a deficiency in G6PDH enzyme activity. What are the three clinical manifestations of this deficiency? How are these conditions caused?
6. G6PDH deficiency and type of G6PDH variant present determines the probability and severity of haemolysis, what other abnormalities are caused by a G6PDH deficit? Why is the prevalence of G6PDH deficiency higher in males, than in females?
7. What is DiGeorge syndrome? What are the two forms and how are they characterised?
8. What should be defined during an immunologic evaluation of DiGeorge syndrome? What assessments are required for immunological diagnosis?
9. Implementation of novel and unfamiliar technologies into a busy laboratory is complex and challenging. What does a traditional review of implementation entail? What different methodology did ESR use to review the implementation of next-generation sequencing (NGS) using the Oxford Nanopore Technologies platform? What were the purpose of using these systems?
10. What is one limitation of the greater use of nanopore sequencing? What solution is proposed by the ESR study? And what would this scenario require?
ANSWERS NOVEMBER 2024 QUESTIONNAIRE
1. Proteinuria is defined as the presence of abnormally elevated amounts of protein in urine, what is considered normal urine protein excretion and what values indicate presence of proteinuria? What is an example of a Turbidimetric assay and what did its method validation provide?
Normal urinary protein excretion is <0.15g/day, urinary total protein values ≥ 0.15g/day indicate presence of proteinuria. An example of a turbidimetric assay is the Sulfosalicylic acid method and validated as a cost-effective method for the quantitative evaluation of proteinuria in the lower ranges (0.03—0.5g/L)
2. The 25% SSA method uses precipitation of proteins to quantitate urine protein, what 3 sample volumes were evaluated by pairwise comparison in the Siriwardhana
study, what differences were found? What conclusions were drawn about the potential for the 25% SSA method to be automated?
Pairwise comparison comparing 1mL, 0.5mL and 2mL sample volumes, showed protein concentration did not differ across the 3 samples tested. Concluded that the 25%SSA method is a reliable and cost-effective alternative for the pyrogallol red protein assay specially in the lower range of proteinuria (0.03-0.45g/L) and shows feasibility for automation with lower sample volumes
3. What do C-reactive protein (CRP), Interleukin-6 and procalcitonin levels in COVD-19 patients correlate with? What can these biomarkers determine?
C-reactive protein (CRP), Interleukin-6 and procalcitonin levels are correlated with disease severity and ICU submissions, these biomarkers are used to determine the severity of lung injury and lesions due to COVID-19 and the severity of the disease.
4. What have elevated IL-6 levels been linked to in one of COVID-19’s common symptoms? What was observed in this symptom over time and in recovery?
IL-6 levels were found to be correlated with the alterations in the ability to taste and smell. When the IL-6 levels in COVID-19 patients decreased during recovery time, it led to significant improvement in the ability to smell.
5. There are more than 4,000 chemicals in a single cigarette, including carbon monoxide. What does carbon monoxide bind to in the body and what can this cause?
Carbon monoxide binds to haemoglobin, causing diseases and impacting numerous organs, including; high blood pressure hypoxia, anaemia, pancreatic cancer, colon cancer, liver cancer, kidney cancer, lung cancer, strokes, chronic obstructive pulmonary disease, and heart disease.
6. What principal features are exhibited by the rare neurodevelopmental disorder Prader-Willi Syndrome (PWS) in infancy? Where is the chromosome deletion? What are the physical manifestations/characteristics of this disorder? Exhibit failure to thrive, feeding difficulties, hypogonadism, growth hormone deficiency. Chromosome deletion is at 15q11-q13 of the paternal chromosome. Physical manifestations/characteristics include facial features as narrow forehead, almond-shaped eyes and triangular mouth. Infants with PW have small hands and feet, short stature and intellectual impairment.
7. What is a principal feature in patients with Prader-Willi Syndrome arising in early childhood? What inflammatory processes and co-morbidities are often related to this disease?
Obesity is a principal feature in patients with PWS with related co-morbidities as diabetes mellitus, hypertension, cardiovascular disease, strokes and elevated C-reactive protein serum levels.
8. What is the estimated prevalence of the para-Bombay phenotype worldwide? Why do the two different genetic compositions seen in the para-Bombay phenotype result in poor detection of this phenotype on the ABO blood group system?
Worldwide estimated 1:1000 (mostly reported in Eastern Asia. Because the para-Bombay phenotype, only has trace H/A/B antigens present on RBCs due to these genetic compositions, the weak forms of A and B antigens
expressed are serologically undetectable using routine ABO testing methods and require additional test of adsorption and elution technique for confirmation
9. What adipocytokines are implicated in insulin resistance? What else do they influence?
Adipocytokines such as adiponectin, tumour necrosis factoralpha (TNF-α), resistin and interleukins, are implicated in the pathogenesis of insulin resistance. They have significant influence on body fat mass and distribution, modulating body weight. They also affect appetite, blood pressure and several physiological processes such as glucose
homeostasis, inflammation, and liver function
10. Non-alcoholic fatty liver disease (NAFLD) is becoming one of the most prevalent liver pathologies globally. What is the percentage of adults and children affected by NAFLD in developed countries? What is predicted to emerge from this disease?
Up to 30% Adults and 10% children. It is emerging as the primary indication for liver transplantation in the future.
MOLECULAR DIAGNOSTICS SPECIAL INTEREST GROUP MEETING
22 November 2024, Wellington
The Molecular Diagnostics SIG meeting was held at Wellington Hospital. The same venue being used to host the microbiology SIG meeting the following day in the hope of attracting a wider audience. There was a record number of registrants, several of whom attended both meetings.
Sessions within the full day programme were themed; opening with a clinical focus (germline conversion rates for tumour detected variants, mainstreaming cancer genomic testing in Aotearoa, and a malignant hypothermia diagnostic pathway update). Three elegant presentations followed using different molecular strategies (methylation, long and short read sequencing technology) in the genetic assessment of cancer.
The afternoon was infectious-disease focussed. Exciting whole genome sequencing work undertaken at ESR was presented as well as two novel ‘in house’ PCR assays developed within public hospitals leading to improved microorganism detection, reduced costs, and faster turnaround times. Awanui Laboratory Wellington, with their experience of the use of nanopore sequencing technology to support hospital infection control completed the programme.
The quality of all presentations was extremely high making awarding prizes difficult. Congratulations went to Amy Bradshaw from ESR, Porirua for the best presentation entitled Transitioning to WGS: Legionella typing and beyond. Yue Sun from Health NZ – Waikato was runner up with her presentation Validation of in-house VRE PCR assay.
As local organiser; acknowledgement and special thanks to all those who willingly presented their excellent work, which contributed to the success of this meeting as well as our local caterers who provided everyone with a generous and delicious selection of food.
Reported by: Clive Felix (Convenor) Service Leader, Genetics, Capital, Coast, Hutt Valley and Wairarapa, Te Whatu Ora
Dates may be subject to change
23-25 May NICE Weekend, Heartland Hotel, Auckland Raewyn.cameron@pathlab.co.nz
TBC South Island Seminar sharon@nzimls.org.nz
TBC North Island Seminar sharon@nzimls.org.nz
15 April QMLT Applications CLOSE admin@nzimls.org.nz
27-29 August NZIMLS Annual Scientific Meeting, Hamilton AndreaLee@adhb.govt.nz
28 August NZIMLS Annual General Meeting, Hamilton sharon@nzimls.org.nz
04 October QMLT Examinations admin@nzimls.org.nz
Best Presentation Recipient: Amy Bradshaw
Runner up: Yue Sun
2025 NZIMLS CALENDAR
JOURNAL HISTORY
Birth and early days of the Journal
Douglas Whillans (Foreword by Rob Siebers)
FOREWORD
The New Zealand Journal of Medical Laboratory Science (Journal) has been continuously published since 1946 and is now in its 79th year making it one of the oldest journals devoted to laboratory medicine in the world. The birth of the Journal originated late 1945 at the 1st Conference of the New Zealand Association of Bacteriologists (forerunner of the NZIMLS) where delegates voted to start a journal to communicate and disseminate laboratory medicine knowledge thought to be of interest to members of the Association.
Douglas Whillans from the Pathology Department at Auckland Hospital was appointed Editor and produced the 1st Journal issue in April 1946. He remained Editor until 1951 when Alan Murphy from the same department took over. The latter asked Douglas to reflect on and give his experiences in starting and producing the Journal. Douglas produces an interesting insight in the tribulations of this enterprise. He explained how he acquired a printing press and the trials and tribulations of producing the Journal. His essay was recently discovered but unfortunately, this was never published. Read below his reflections as 1st Editor on the birth and the first few years of the Journal.
Rob Siebers Emeritus Editor
BIRTH AND EARLY DAYS OF THE JOURNAL
I have been asked by the Editor of this Journal to write some notes on its birth and early days, and find that I approach the task with quiet pride and some nostalgia.
At the inaugural meeting of the Association as it became, I was appointed Editor of a non-existent publication. It was felt important for the Association to have some type of news medium to convey the feelings and views of the members to those in authority and to any others who might be interested and to keep those working in hospital laboratories in touch with one another. A further important part was the publishing of scientific papers as this was felt to be a valuable aim in itself.
A small committee was set up and this soon found that costs of even a modest venture were considerable. As the Journal would have to be self-supporting it soon became apparent that advertising space would have to be sold and this implied printing. A quick round of the printers showed that all too clearly that the price would be prohibitive even if they were not too busy to take on the work.
This left a final alternative of somehow printing it ourselves. I cast around for a printing press and was fortunate to obtain the loan of one which could handle a page at a time. Hand setting of type was an impossibility for such tyros, so I wheedled the Manager of Auckland Trade Linotypes into setting the first issue for me. This was, in itself, somewhat of an achievement as they had more work to do than they could handle with short staff and the difficult conditions which had been created by the war, but by coincidence, my wife had taken her first job in the office of this firm when she left school, and this turned the tide in our favour. I can still remember the incredulous looks which the line-setters gave me when they realised that I had never handled a press in my life before, but they were so tickled by the idea that they gave me useful hints, which, together with further information gained by pestering small printers and that obtained by reading enabled Volume 1 No. 1 to appear in April 1946.
Some 100 copies of this eight page issue were distributed to the 29 senior and 45 junior members, Pathologists and the Health Department. It contained details of a salary scale commencing at 130 pounds and finishing at 600 pounds which had come into effect from April 1st 1945, a paper on the isolation of Br. abortus in milk By J.J.G Peddie, the examination papers for the March C.O.P Examination, and a list of the members of
the New Zealand Association of Bacteriologists.
It was clear that it would be impossible to continue to print the Journal on such a small press, and while casting around for an alternative I chanced to go in a shop attached to premises of a printer to buy a typewriter ribbon. With a burst of inspiration I asked him if he knew of a machine for sale and was delighted to be told that he was storing one for a friend. He also told me in no uncertain terms that it was in the way of his expanding business and that if I had 35 pounds I could have it there and then. I closed on the deal and the machinery firm installed it in my workshop under my mother’s house in Mount Eden. The platen machine was an old “Arab” platen which I modified quite a bit over the years as it really had insufficient inking power. I also operated it by foot pedal, as in general printing was done after work and I was always fairly tired before starting. The machine had no safety devices and I felt that the attachment of a motor could cause a serious accident if anything went wrong with the hand feeding of the press.
The possession of a press was a start, but it took the whole of 100 pounds to really set the whole thing moving. I provided this myself, with the willing support of my wife, at a time when we were building a new house and I wish to place on record my thanks to her for this and other understanding help. By Volume 1 No. 3, we were running five advertisements, a publication fund had been set up to help defray the cost of the press and the Council of the Association, with great daring, asked for a top salary of 750 pounds, and had put forward a syllabus for training for C.O.P.
Publication continues, but was plagued by persistent shortages of paper, electricity, gas (which made the linotype slugs of poor quality and hard to print from) and finally, when the novelty wore off, of labour to edit, print, publish, obtain advertisements, and post. The other trouble, one common to all editors was a lack of items to print, so that getting out of a Journal finally took about six weeks of every three months. A total of 19 issues was printed under these conditions.
A subsidiary part of the work was the printing of such material as rules, headed paper, receipts, membership cards and Annual Conference circulars and voting papers. These were more interesting in that rather more time was available to do a good job on them, and quite a lot of them were hand set, but by Volume 5 No. 4 it was obvious that the time had come for the Journal to be continued as a commercial venture. Mr. Alan Murphy relieved me on the post of Editor and carried on the responsibilities of the post most ably.
The Journal had now become a publication of some 32 pages and 350 copes, with numerous advertisements and blocs and with many of the advertisements hand set. A small honorarium was paid to the Editor but the whole venture was self-supporting. It had proved a hard but interesting venture and it was not for a further five years that the press and its ancillary equipment was sold. It had been transferred to my new house in 1948 where it took up a corner of the workshop immediately beneath our bedroom and many times my wife was lulled to sleep by the rhythmic crash of the press. During this second five years a deal of the special printing was still done, but finally the work became too great with the expansion of the Laboratory Services in Auckland and the extra time required for this so that the press was sold and a very satisfactory amount of money was returned to the Association. My monetary advance had long since been repaid and I have nothing of the establishment left but my printer’s registration of 23rd May 1946.
D Whillans Sometime Editor
Warm Pacific greetings to you all from the PPTC
HAEMATOLOGY
Haematology continues to be weak in performance and this is due to a devastating lack of expertise and interpretative skill in blood film examination and interpretation throughout the Pacific. Blood cell identification and interpretation is a continual learning process and unfortunately Pacific Island laboratories do not have resident experts who are able to mentor and add to this learning experience. A comprehensive knowledge (theory and practice) of both normal Haematology and pathological Haematology is a building process and excellence in proficiency can take several years to achieve. The PPTC recognises that long term New Zealand consultancy attachments in the Pacific would be of enormous benefit but would require extensive financial resource. The PPTC continues to work towards the development of a PPTC facilitated Haematology strengthening programme for the Pacific, to be delivered in-country, utilizing New Zealand Haematology technical experts to travel regularly throughout the region. This will be subject to available funding.
The PPTC’s Haematology technical expert is currently providing on-line education focusing on Haematology cellular morphology and interpretation workshops for laboratories throughout the Pacific region, as a supplement to the PPTC Diploma, in-country teaching and training and centre-based courses.
UPDATES
Centre Based Course- Foundations of Haematology, (23rd September - 1st November 2024)
This training course was delivered over the duration of six weeks at the Pacific Pathology Training Centre, Wellington Hospital campus, to six medical laboratory personnel working in Pacific laboratories. A comprehensive theoretical component and a series of practical workshops were provided to the students in diagnostic Haematology and blood film morphology. The purpose of this training was to equip students with sufficient knowledge to be able to work confidently and competently in their home laboratories and be able to provide quality diagnostic test results to clinicians using the medical laboratory services for better patient management and better health outcomes.
Course Content and Objectives:
This course provided students with the following:
• Guidelines for the objective microscopic evaluation of white cells, red cells, and platelets in both health and disease.
• Introduction to the workings of the microscope in terms of correct operation, correct use of objectives, and essential maintenance.
• Principles of Romanowsky staining, the preparation of stains and buffers, causes of inconsistent staining quality and the correct staining techniques.
• Introduction to the blood film in terms of sample quality, the effects of anticoagulants, correct technique in blood film
making, morphological artefacts, buffy coat preparations, and the correct storage of blood films.
• Extensive teaching on the correlation of clinical details with blood film findings and results obtained from FBC for red cell, white cell and platelet parameters.
• Morphological terminology with reference to origin and correct application.
• The lineage of all blood cells systematically from the common stem cell through all stages of development.
• A comprehensive account of both normal Haematology and pathological Haematology.
• Differentiation of the white cell count into both normal and abnormal populations.
• The development of confidence and competence in morphological recognition and final commenting, with regards to abnormal film findings in an extensive range of common blood cell disorders.
• FBC analysers and principles of operation.
• Correct setting up and interpretation of the ESR test.
• Correct staining technique and interpretation of reticulocyte estimation.
• Coagulation theory and practical application.
• Coagulation instrumentation and principles of operation.
• Case studies.
Student Name Country Laboratory Funded by
Mira Vaiaso Samoa Apia Pacifica Medical Association Group
Shayena Nisha Fiji Lautoka NZ MFAT
Telehia Manuele Tokelau Nukunonu MOH
Devine Reuelu Tokelau Atafu MOH
Silivelio Sauman Tokelau Fakaofo MOH
Seleni Peleni Tokelau Fakaofo MOH
The course was delivered most successfully and students returned to their home laboratories with an enhanced knowledge base and practical skill set.
Table 1. 2024 Haematology Participants
Figure 1. Back Row; PPTC Consultants, Front Row; Haematology Students
The Pacific Way, PACIFIC PATHOLOGY TRAINING CENTRE
Both Shayena Nisha and Silivelio Sauman gained top marks in their final examinations and were both awarded a copy of Blood Cells A practical Guide by Barbara Bain as recognition of their achievement.
Silivelio Sauman (Tokolau) and Lecturer Phil Wakem
Thank you to Dr Julia Phillips for being available to present each student with their certificate of achievement on graduation day. Julia has supported the PPTC for many years now and we are so grateful to be able to consult with her should a clinical presentation be required.
Telehia Manuele (Tokelau) and Dr Julia Phillips (Haematologist)
Thank you, Sharon Cole, Senior Medical Laboratory Scientist, Kenepuru Hospital, Capital Coast Health Wellington. The PPTC would like to thank Sharon who visited the Rarotonga, Cook Islands 19-29th Feb 2024 to observe the laboratory’s processes in both Biochemistry and Haematology and assist in any corrective action that was required to be carried out to ensure the quality status of the laboratory was not under threat of being compromised. The PPTC is appreciative and most grateful to Sharon for sharing her extensive knowledge and experience with the laboratory and for the contributions made during her stay.
Thank you, Pip Sarcich, Technical Specialist Cellular Morphology, LabPlus, Haematology Laboratory, Auckland District Health Board.
The PPTC wishes to thank Pip so very much, for her ongoing support of the PPTC’s Haematology EQA programme. Her expert knowledge and practical excellence in Haematology was shared when she agreed to visit the Fiji National laboratories with our PPTC consultants (18-29 August 2024) to strengthen and offer training and teaching in blood cell morphology and
blood film interpretation. The Fiji laboratories including Labasa, Suva and Lautoka gained a great deal of valuable teaching and training from Pip during her stay and for this we are most grateful for the great contribution she made.
Gillian Rozenberg Training Workshops
Both Phil Wakem and Emmanuel Marshall will attend Gillian’s 2-day workshop in Sydney, scheduled for the 28th - 29th March 2025. This workshop will cover the following topics:
• Red cell nomenclature
• WHO Classification of myeloproliferative neoplasms
• WHO Classification of myelodysplastic syndromes
• WHO Classification of acute myeloid leukaemia and related precursor neoplasms:
• Malaria
• Lymphocytes: reactive / neoplastic
• Paediatric Haematology
• Case Studies
Gillian’s workshops are very well known and much sought after and of enormous benefit to those who attend.
Emmanuel as a PPTC consultant, is the appointed Education Manager for PPTC Centre Based Courses, Assistant manager for PPTC Diploma studies and PPTC specialist for IT and molecular platforms. He is beginning the journey of developing expertise in Haematology with the view of becoming a PPTC Haematology Consultant and Gillian’s workshop will be most valuable in assisting him on this journey.
CAN YOU HELP?
Microscopes for haematology morphology and GeneXperts for molecular diagnostics
If any New Zealand medical laboratories have items of diagnostic instrumentation as mentioned above that have been recently upgraded or continue to be stored in the laboratory but are actually surplus to requirements, the PPTC would be most grateful if such items could be donated through its Centre to Pacific Island laboratories where there is an exceptional need. Pacific laboratories have very restricted budgets and often cannot afford to replace troublesome instrumentation that continues to breakdown and which is often discontinued because it is so outdated.
Please contact:
Phil Wakem Chief Executive Officer
Pacific
Pathology Training Centre
Wellington, New Zealand
Email: pptc@pptc.org.nz or phil@pptc.org.nz
Tel: 64-4-389 6294 or 027 2305483
Shayena Nisha (Lautoka, Fiji) and Lecturer Phil Wakem
CORRECTION
Unfortunately in our November 2024 issue an original article, Jeyaraj et al was published without references 24 - 46. Below is the full list references.
Correlation
of IL-6 with D-dimer, LDH, S-ferritin biomarkers, comorbidities and clinical outcomes of COVID-19 patients admitted in a tertiary hospital in Coimbatore, India – a retrospective study based on 2,569 patients
1. WHO Coronavirus (COVID-19) Dashboard [Internet]. [cited 2023 Oct 16]. Available from: https://covid19.who.int
2. Guan WJ, Ni ZY, Hu Y, Liang WH, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020; 382(18): 1708–1720.
3. Lichter Y, Topilsky Y, Taieb P, et al. Lung ultrasound predicts clinical course and outcomes in COVID-19 patients. Intensive Care Med 2020; 46(10): 1873–1883.
4. Gershengorn HB, Hu Y, Chen JT, et al. The impact of highflow nasal cannula use on patient mortality and the availability of mechanical ventilators in COVID-19. Ann Am Thorac Soc 2021; 18(4): 623–631.
6. Cao X. COVID-19: immunopathology and its implications for therapy. Nat Rev Immunol 2020; 20(5): 269–270.
7. Ing AJ, Cocks C, Green JP. COVID-19: in the footsteps of Ernest Shackleton. Thorax 2020; 75(8): 693–694.
8. Yang R, Gui X, Xiong Y. Comparison of clinical characteristics of patients with asymptomatic vs symptomatic coronavirus disease 2019 in Wuhan, China. JAMA Netw Open 2020;3(5): e2010182.
9. Gajate-Arenas M, García-Pérez O, Chao-Pellicer J, et al. Differential expression of antiviral and immune-related genes in individuals with COVID-19 asymptomatic or with mild symptoms. Front Cell Infect Microbiol 2023; 13:1173213
10. Battaglini D, Lopes-Pacheco M, Castro-Faria-Neto HC, Pelosi P, Rocco PRM. Laboratory Biomarkers for Diagnosis and Prognosis in COVID-19. Front Immunol 2022; 27:13: 857573.
11. Leisman DE, Ronner L, Pinotti R, et al. Cytokine elevation in severe and critical COVID-19: a rapid systematic review, meta-analysis, and comparison with other inflammatory syndromes. Lancet Respir Med 2020; 8(12): 1233–1244.
12. Liu B, Li M, Zhou Z, Guan X, Xiang Y. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)induced cytokine release syndrome (CRS)? J Autoimmun 2020; 111: 102452.
13. Ye Q, Wang B, Mao J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J Infect 2020; 80(6): 607–613.
14. Smadja DM, Mentzer SJ, Fontenay M, et al. COVID-19 is a systemic vascular hemopathy: insight for mechanistic and clinical aspects. Angiogenesis 2021; 24(4): 755–788.
15. Nguyen N, Nguyen H, Ukoha C, et al. Relation of interleukin-6 levels in COVID-19 patients with major adverse cardiac events. Proc (Bayl Univ Med Cent) 2022; 35(1): 6–9.
16. Coomes EA, Haghbayan H. Interleukin-6 in COVID-19: a systematic review and meta-analysis. Rev Med Virol 2020; 30(6): 1–9.
17. Melo AKG, Milby KM, Caparroz ALMA, et al. Biomarkers of cytokine storm as red flags for severe and fatal COVID-19 cases: a living systematic review and meta-analysis. PLoS One 2021; 16(6): e0253894.
18. Herold T, Jurinovic V, Arnreich C, et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy Clin Immunol 2020; 146(1): 128-136.e4.
19. Broman N, Rantasärkkä K, Feuth T, et al. IL-6 and other biomarkers as predictors of severity in COVID-19 . Ann Med 2021; 53(1): 410–412.
20. Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med 2020; 46(5): 846–848.
21. Gohda T, Murakoshi M, Suzuki Y, et al. Circulating tumor necrosis factor receptors are associated with mortality and disease severity in COVID-19 patients. PLoS One 2022; 17(10): e0275745.
22. Zhou F, Yu T, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020; 28:395(10229): 1054–1062.
23. Yao Y, Cao J, Wang Q, et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: a case control study. J Intensive Care 2020; 8:49.
24. Zhang L, Yan X, Fan Q, Liu H, Liu X, Liu Z, et al. D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J Thromb Haemost 2020; 18(6): 1324–1329.
25. Viasus D, Del Rio-Pertuz G, Simonetti AF, et al. Biomarkers for predicting short-term mortality in community-acquired pneumonia: A systematic review and meta-analysis. J Infect 2016; 72(3): 273–282.
26. Li C, Ye J, Chen Q, et al. Elevated lactate dehydrogenase (LDH) level as an independent risk factor for the severity and mortality of COVID-19. Aging (Albany NY) 2020; 12(15): 15670–15681.
27. Viral infection in community acquired pneumonia patients with fever: a prospective observational study - PMC [Internet]. [cited 2024 Apr 2]. Available from: https://www.ncbi.nlm.nih. gov/pmc/articles/PMC6105945/.
28. Soepandi PZ, Burhan E, Mangunnegoro H, et al. Clinical course of avian influenza A(H5N1) in patients at the Persahabatan Hospital, Jakarta, Indonesia, 2005–2008. Chest 2010; 138(3): 665–673.
30. Belaid B, Lamara Mahammad L, Mihi B, et al. T cell counts and IL-6 concentration in blood of North African COVID-19 patients are two independent prognostic factors for severe disease and death. J Leukoc Biol 2022; 111(1): 269–281.
31. Copaescu A, James F, Mouhtouris E, et al. The role of immunological and clinical Biomarkers to predict clinical COVID-19 severity and response to therapy: a prospective longitudinal study. Front Immunol 2021; 12: 646095.
32. Cazzolla AP, Lovero R, Lo Muzio L, et al. Taste and smell disorders in COVID-19 patients: role of Interleukin-6. ACS Chem Neurosci 2020; 11(17): 2774–2781.
33. Campochiaro C, Della-Torre E, Cavalli G, et al. Efficacy and safety of tocilizumab in severe COVID-19 patients: a singlecentre retrospective cohort study. Eur J Intern Med 2020; 76: 43-49.
34. Tharmarajah E, Buazon A, Patel V, et al. IL-6 inhibition in the treatment of COVID-19: a meta-analysis and metaregression. J Infect 2021; 82(5): 178–185.
35. Villaescusa L, Zaragozá F, Gayo-Abeleira I, Zaragozá C. A new approach to the management of COVID-19. antagonists of IL-6: Siltuximab. Adv Ther 2022; 39(3): 1126–1148.
36. Kojima K, Yoon H, Okishio K, Tsuyuguchi K. Increased lactate dehydrogenase reflects the progression of COVID-19 pneumonia on chest computed tomography and predicts subsequent severe disease. Sci Rep 2023; 13(1): 1012.
37. Henry BM, Aggarwal G, Wong J, et al. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19 ) severity and mortality: A pooled analysis. Am J Emerg Med 2020; 38(9): 1722–1726.
38. Shi J, Li Y, Zhou X, et al. Lactate dehydrogenase and susceptibility to deterioration of mild COVID-19 patients: a multicenter nested case-control study. BMC Med. 2020; 18(1): 168.
39. Ji D, Zhang D, Xu J, et al. Prediction for progression risk in patients with COVID-19 pneumonia: the CALL score. Clin Infect Dis 2020; 71(6): 1393–1399.
40. Mehta P, McAuley DF, Brown M, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet 2020; 395(10229): 1033–1034.
41. Cecconi M, Piovani D, Brunetta E, et al. Early predictors of clinical deterioration in a cohort of 239 patients hospitalized for COVID-19 infection in Lombardy, Italy. J Clin Med 2020; 9(5): 1548.
42. Cheng L, Li H, Li L, et al. Ferritin in the coronavirus disease 2019 (COVID‐19): a systematic review and meta‐analysis. J Clin Lab Anal 2020; 34(10): e23618.
43. Wang Z, Du Z, Zhu F. Glycosylated hemoglobin is associated with systemic inflammation, hypercoagulability, and prognosis of COVID-19 patients. Diabetes Res Clin Pract 2020; 164: 108214.
44. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 3955(10223): 497–506.
45. Wang L. C-reactive protein levels in the early stage of COVID-19. Med Mal Infect 2020; 50(4): 332–334.
46. Zeng F, Huang Y, Guo Y, et al. Association of inflammatory markers with the severity of COVID-19: a meta-analysis. Int J Infect Dis 2020; 96: 467–474.
BARRIE EDWARDS & ROD KENNEDY SCHOLARSHIP
The Barrie Edwards & Rod Kennedy scholarship is one of the most significant awards offered by the NZIMLS. The scholarship provides the winner with support to attend an international or national scientific meeting up to a maximum value of $7,500 for each. Applications for this prestigious scholarship are invited from Fellows, Members and Associate Members of the NZIMLS. Applicants must be a current financial member of the NZIMLS and have been a financial member for at least two concurrent years prior to application. To be eligible applicants must make an oral presentation or present a poster as 1st author at their nominated scientific meeting.
All applications will be considered by a panel consisting of the President and Vice-President of the NZIMLS and the Editor of the New Zealand Journal of Medical Laboratory Science (who are ineligible to apply for the scholarships). The applications will be judged on your professional and academic abilities together with your participation in the profession. The panel's decision is final and no correspondence will be entered into.
Application is via https://www.nzimls.org.nz/scholarships Please email all correspondence to: NZIMLS Chief Executive Officer; sharon@nzimls.org.nz
There is one scholarship awarded in each calendar year. Closing date is December 20th in any given year.
In your application letter please provide the following details:
• Full name, position, work address, email address and contact phone number
• The length of time you have been a financial member of the NZIMLS
• The conference you wish to attend - please provide dates
• A budget comprising airfares, conference registration and accommodation costs
• The abstract of your intended oral or poster presentation and whether it has been accepted for presentation (proof required)
• Your intentions to publish your results
• State briefly your history of participation in the profession over the last 5 years
• State the reasons why you wish to attend your nominated scientific meeting
Successful applicants will be required to provide a full written report on return which will be published in the Journal. If not intended to publish elsewhere, successful applicants will be required to submit their study results for consideration by the New Zealand Journal of Medical Laboratory Science.
Barrie Edwards
Rod Kennedy
EDITORIALS
Index to Volume 78, 2024
Sustainability and green laboratory practices
Lisa Cambridge 03
Working toward translational research in pathology
Michael Legge 60
Climate change, heath and pathology
Michael Legge 107
REVIEW ARTICLES
Blood group systems and antigens described in the last 20 years: an update
Natalya J Clark and Holly E Perry 06-19
The MNS blood group system: a review
Rei Miyamoto 20-23
A review of ten years of Leptospira serology and PCR testing
Tégan A. Hall, Andrew W. Soepnel and Michael Addidle ................................................................. 25-30
Electronic crossmatch: a review
Rei Miyamoto 68-71
Factor VIII inhibitor laboratory assay: state of the art
Hamza Siyar, Hassane Mamad, Imane el Omari, Souad Benkirane and Azlarab Masrar……………………………..72-76
ORIGINAL ARTICLES
Can the use of triglyceride to glucose and triglyceride to high density lipoprotein ratios indicate metabolic syndrome in the spinal cord injured male?
Lynnette M Jones and Michael Legge 31-33
Evaluation of NOVA view single-well titre determination for antinuclear antibody testing under routine conditions in a New Zealand medical laboratory
Andrew W Soepnel 77-81
Analysis of simple markers of subclinical inflammation in Syrian patients with familial Mediterranean fever
Husam Khalil, Knida Touban and Raneem Mousa 82-86
Blocking natural antibodies with Kode technology to investigate false positives in an immunoassay
Holly E Perry and Selene S Mak 87-91
Optimisation of sample volume for the 25% sulfosalicylic acid method for quantitative evaluation of proteinuria.
Nimesha D Ranawaka, Rajika G Jinadasa, Kalani B Gunawardana, Indika D Siriwardhana 114-117
Correlation of IL-6 with D-dimer, LDH, S-ferritin biomarkers, comorbidities and clinical outcomes of COVID-19 patients admitted in a tertiary hospital in Coimbatore, India – a retrospective study based on 2,569 patients.
Immunological disturbances associated with Prader Willi syndrome in Egyptian patients.
Haiam Abdel Raouf, Rania Fawzy Mahmoud Abdelkawy, Hala T. El-Bassyouni, Shams Kholoussi, Mohammed M. Sayed-Ahmed, Azza E. Abd-Elnaby, Assem M. Abo-Shanab 131-135
The relationship between adiponectin and insulin sensitivity in obese patients with non-alcoholic fatty liver disease.
Dina Morsy A. Mohamed and Raghda M. Ghorab 136-141
CASE STUDIES
The association of MMUT mutation (NM_000255.4: c.976Q>G with wide spectrum clinical manifestations in a child affected with methylmalonic acidaemia
Para-Bombay Ah phenotype: case series from a tertiary care hospital in Malaysia.
Kaalpana Jayakumar, Rabeya Yousuf, Nur Afifah Suhemi, Nor Fadzliana Abdullah Thalith, Suria Abdul Aziz, Lailatul Hadziyah Mohd Pauzy and Qhasmira Abu Hazir 142-144
SCIENTIFIC LETTERS
Implementation of laser warning markings for equipment and instruments in the International Standard ISO15189:2022 accredited medical laboratory in New Zealand.
Dennis Mok, Naira Eloyan, Rana Nabulsi, Sharfuddin Chowdhury, María del Rocío González Guerrero, Winsome Lee and Donna Marie Gillespie 34
TH PULLAR ADDRESS
Building resilience: keeping afloat during turbulent times.
Angela Brounts 110-112
NZIMLS FELLOWSHIP TREATISE
The efficacy of general practitioner guided electronic ordering on allergy testing at Awanui laboratories
Catherine Littlechild 62-67
PROFESSIONAL AFFAIRS
Briefing for the incoming minister and associate ministers
Tony Barnett 36-38
BIOGRAPHY
Catherine Littlechild 87
BOOK REVIEWS
Most delicious poisons: the story of nature’s toxins from spices to vices by Noah Whiteman
Reviewed by Michael Legge 35
Breaking through: my life in science by Katlin Kariko
Reviewed by Michael Legge 92
Master Builder: how the new science of the cell is rewriting the story life by Alfonso Martinez Arias
Reviewed by Michael Legge 92
The Code Breaker: Jennifer Doudna, gene editing and the future of the human race by Walter Issacson
Reviewed by Ehsan Ullah 92
IN MEMORIUM
Paul McLeod, Medical Laboratory Scientist, past NZIMLS President Contributed by Tony Barnett 39
AUTHOR INDEX
Abd-Elnaby, AE 131
Abdelkawy, RFM 131
Abo-Shanab, AM 131
Addidlev, M ......................................................................... 25
Ahmadpour-kacho, M 75
Akhavan-Niaki, H 75
Al-Fawaeir, S 126
Alagesan, M 119
Arumugam, J 119
Aziz, SA 142
Barnett, T ...................................................................... 36, 39
Benkirane, S 72
Brounts, A 110
Cambridge, L 03
Chowdhury, S 34
Clark, NJ 06
El Omari, I 72
El-Bassyouni, HT 131
Eloyan, N 34
Etraj, D 119
Fattahi, S 75
Ghorab, RH 136 Gillespie, DM 34
Guerrero, M 34
Gunawardana, KB 114
Hall, TA 25
H
S
Hazir, QA 142 Jayakumar, K
NATIONAL CYTOLOGY TEAMS GROUP:
NAME: CYTOLOGY NZ
Organiser: Megon Schubel
(About Megon: Cytology scientist, practising since 2008 with experience in Gynae and NonGynae, ROSE, conventional, sure path and Thin prep).
Coordinator: Tamaki Inoue
(About Tamaki: Cytology scientist, practicing since 1992 with experience in Gynae and NonGynae, ROSE, ThinPrep application specialist in Cytyc. Currently practicing Electron Microscopy as well.
Contact me on Email: megon.schubel@ waikatodhb.health.nz or tinoue@adhb.govt.nz and we will add you to our group.
Rajasekaran, R 119 Ramalingam, S 119 Ramaraju, K 119
Ranawaka, ND 114 Raouf, HA 131
Sayed-Ahmed, MM 131 Siriwardhana, ID 114 Siyar, H 72
Soepnel, AW 25, 77 Sriramajayam, L 119
K
E
N
Join us and enjoy:
√ Space to meet cytology practitioners in NZ
√ Present any interesting Gynae or Non-Gynae cytology cases and EARN EASY CPD points with fellow cytologists. (Our own “Online SIG”)
√ Ask any cytology question from lab processes.
√ Share ideas, future events or resources.
The 34th NZIMLS Annual NICE Weekend (National Immunohaematology Continuing Education)
23rd May 2025 – 25th May 2025
Heartland Hotel Auckland Airport, Auckland
REGISTRATION COSTS
$730 NZIMLSMember
$835 Non-MemberNZIMLS
$780 NZIMLSMemberLatefee
$885 Non-memberNZIMLSLatefee
$420 Aucklandbasedregistration
What’s included?
Two night’s accommodation – twin share basis (Extra cost for single room)
Breakfast, morning and afternoon teas, and lunches on Saturday and Sunday
Great presentations on topics relating to Transfusion Science
CPD Points!
Themed dress-up Dinner on Saturday night!
This year’s dress theme is The Roaring Twenties
THE CATCH: Present a poster or 2-5 minute oral presentation on any topic on Immunohaematology or Transfusion Science (can also be a question or problem etc…)
Trades delegates attending do not present. There are no Trades stands as this an education weekend. Send all abstracts to Raewyn Cameron* in word format on or BEFORE closing date.