Cell-Free DNA BCT is a blood collection tube with a preservative stabilising nucleated blood cells and preventing the release of gDNA, allowing isolation of high-quality cell-free DNA.
• High-quality cell-free DNA recovery for reduced variability associated with cell-free DNA sample preparation.
• Reduced need for immediate plasma preparation and CTC processing.
• Multiple applications – suitable for use in clinical research studies, drug discovery and diagnostic assay development.
• Confidence in stability and a trusted solution – with over 17 million tubes shipped worldwide.
• No need to centrifuge immediately after collection.
Editor
Lisa Cambridge, NZCS DipQA B.ApplManagement, MNZIMLS, NZIMLS, Rangiora
Deputy Editors
Michael Legge, PhD MRSB FIBMS FNZIMLS FFSc(RCPA), University of Otago, Dunedin
Holly Perry, DipMLS MAppSc(Hons) PhD MNZIMLS, University of Otago
Emeritus Editor
Rob Siebers, PGCertPH FNZIC FNZIMLS FRSB HonFNZAP, Wellington
Editorial Board
Paul Austin, MSc(Hons) DipMLT MNZIMLS, LabPlus, Auckland
Jillian Broadbent, FNZIMLS, NZIMLS, Rangiora
Heather Brooks, PhD, PGDip MLS, BSc(Hons), University of Otago, Dunedin
Julie Creighton, DipMLS, FNZIMLS, Canterbury Health Laboratories, Christchurch
Terry Taylor, BSc DipMLS MNZIMLS, Southern Community Laboratories, Dunedin
Sharon Tozer, DipBis Stud, AT CAANZ, NZIMLS, Rangiora
Robyn Wells, BApllSci(MT) GradCert Haem, Milton, Australia
Formatting
Sharon Tozer, AT DipBusStud, Executive Office NZIMLS, Rangiora
About the Journal
The New Zealand Journal of Medical Laboratory Science (the Journal) is the official publication of the New Zealand Institute of Medical Laboratory Science (NZIMLS). The Journal is peer reviewed and publishes original and review articles, case studies, technical communications, and letters to the Editor on all subjects pertaining to the practice of medical laboratory science. The Journal is open access (www.nzimls. org.nz/nzimls-journal) and is published three times per year in March, July, and November. Hard copies are circulated to all NZIMLS members and universities and research units in New Zealand and overseas. Current circulation is about 2,800 copies per issue. Printing is by Blueprint Ltd, Christchurch on environmentally responsible paper using elemental chlorine free third party certified pulp sourced from well managed and legally harvested forests and manufactured under the strict ISO14001 Environmental Management System. The Journal is indexed by CINAHL, EMBASE, SCOPUS, Informit, Thomson Gale, EBSCO and Biosis Citation Index, and the Journal Editors are members of the World Association of Medical Editors (www.wame.org).
Brief instructions to authors
The Journal accepts original submissions from anyone and anywhere. Comprehensive instructions can be found on the NZIMLS website (www.nzimls.org.nz/instructions-to-authors. html). All submissions will undergo single-blind peer review and possibly plagiarism checking with iThenticate™ software. If accepted for publication, copyright is vested in the author(s) under terms of the Creative Commons Attribution License (www. creativecommons.org/licenses/by/2.5/legalcode). The authors are responsible for the scientific content and views. Opinions expressed in the Journal are not necessarily those of the Editors, Editorial Board, or Council of the NZIMLS.
The rewards of publishing and guidance for authors Lisa Cambridge 93
TH Pullar Address
The call of the Pacific Philip Wakem 95-97
Original articles
COVID-19 severity and mortality in Pakistani male patients: the predictive role of pituitary-gonadal axis dysfunction
Kaleem Maqsood, Shaaf Ahmad, Azeem Saeed, Zulfiqar Ali Beg, Muhammad Ahsan Raza and Nabila Roohi 99-103
Platelet hyperactivation and haemostatic derangements of persons living with human immunodeficiency virus infection on highly active antiretroviral therapy
Josephine E Okon, Patience A Akpan and Anthony O Emeribe 105-110
Comparative analysis of white blood cell differential counts in acute exacerbation and stable chronic obstructive pulmonary diseases
A rare presentation of apolipoprotein B - related familial hypobetalipoproteinaemia: a case report
Reza Nemati and Christopher James McEntyre 117-119
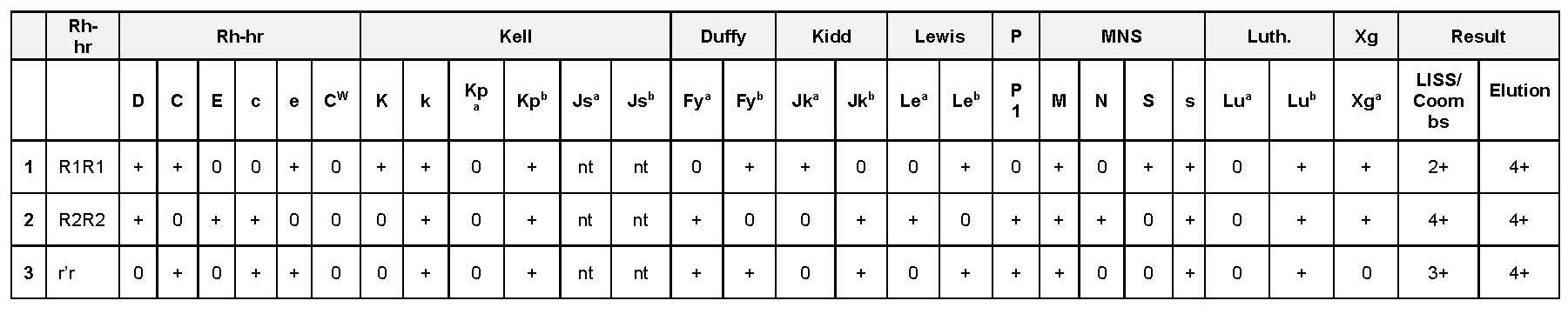
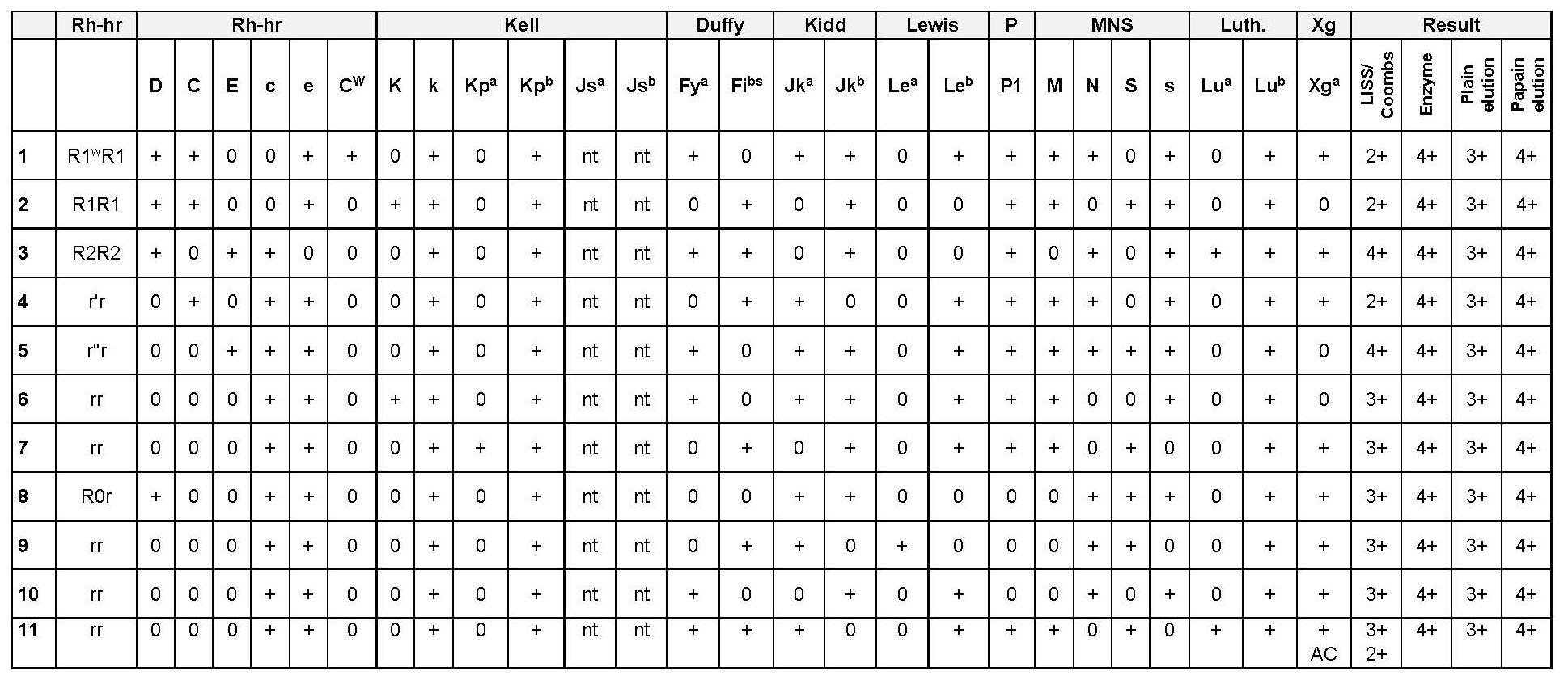
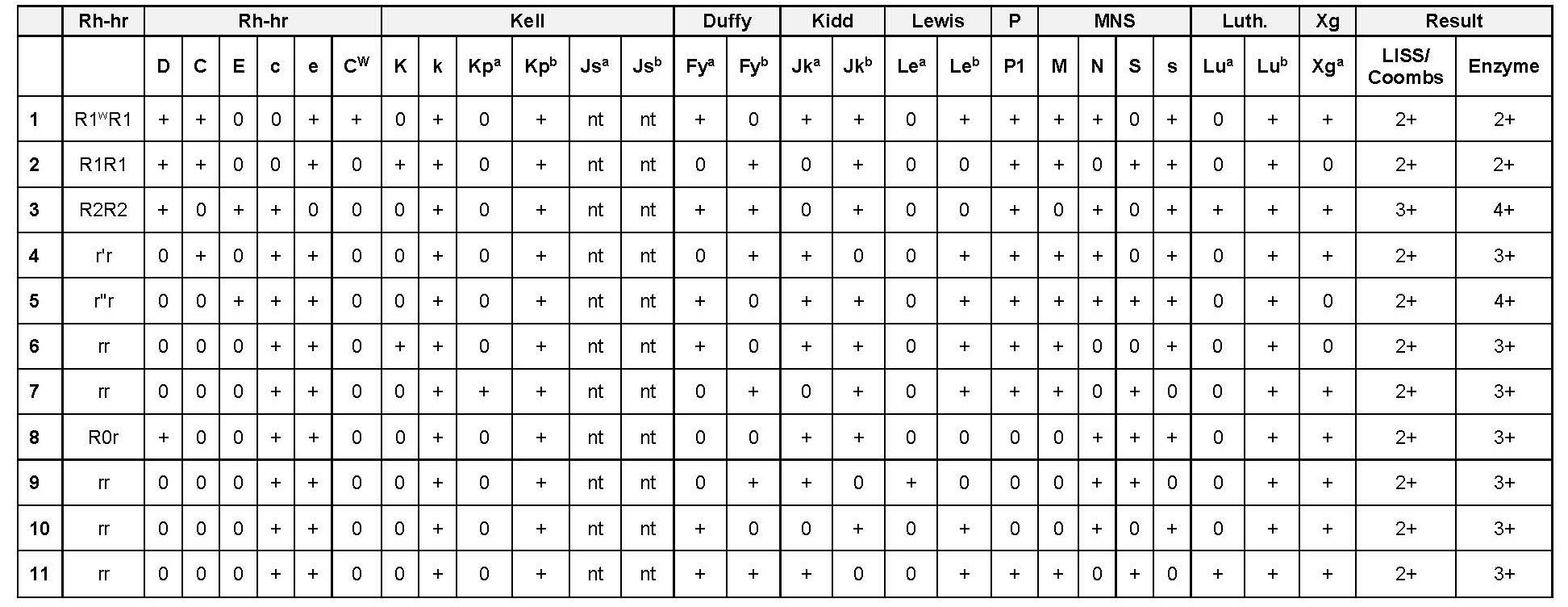
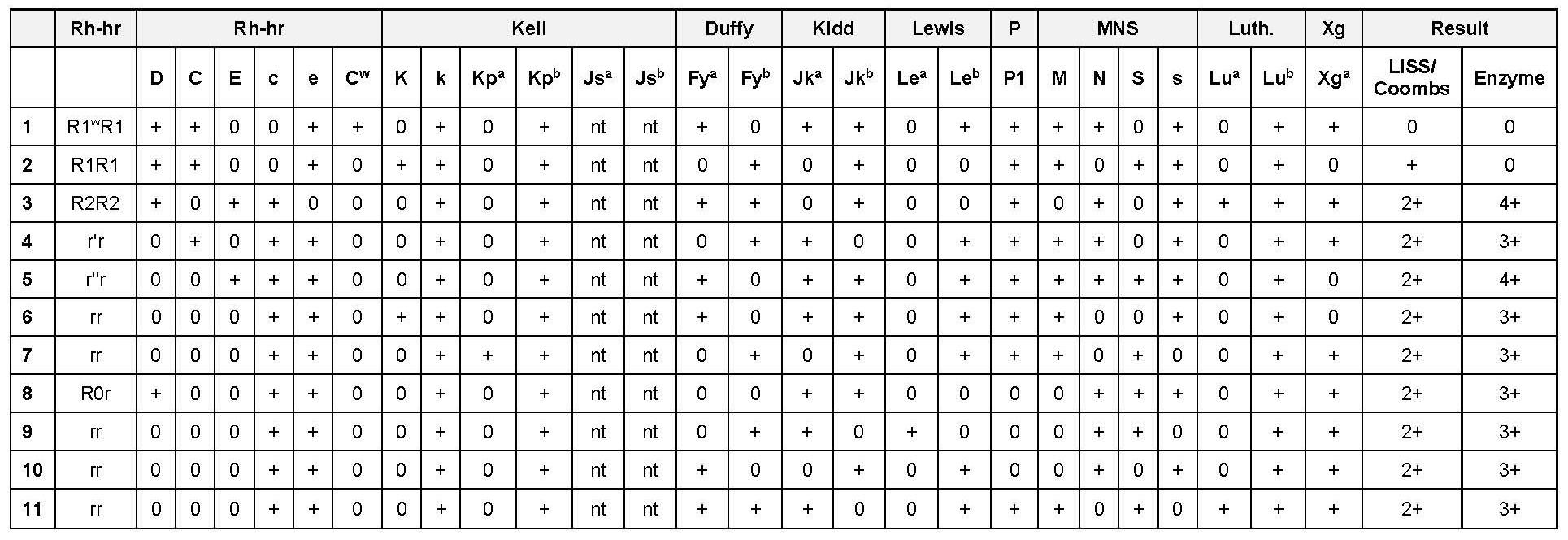
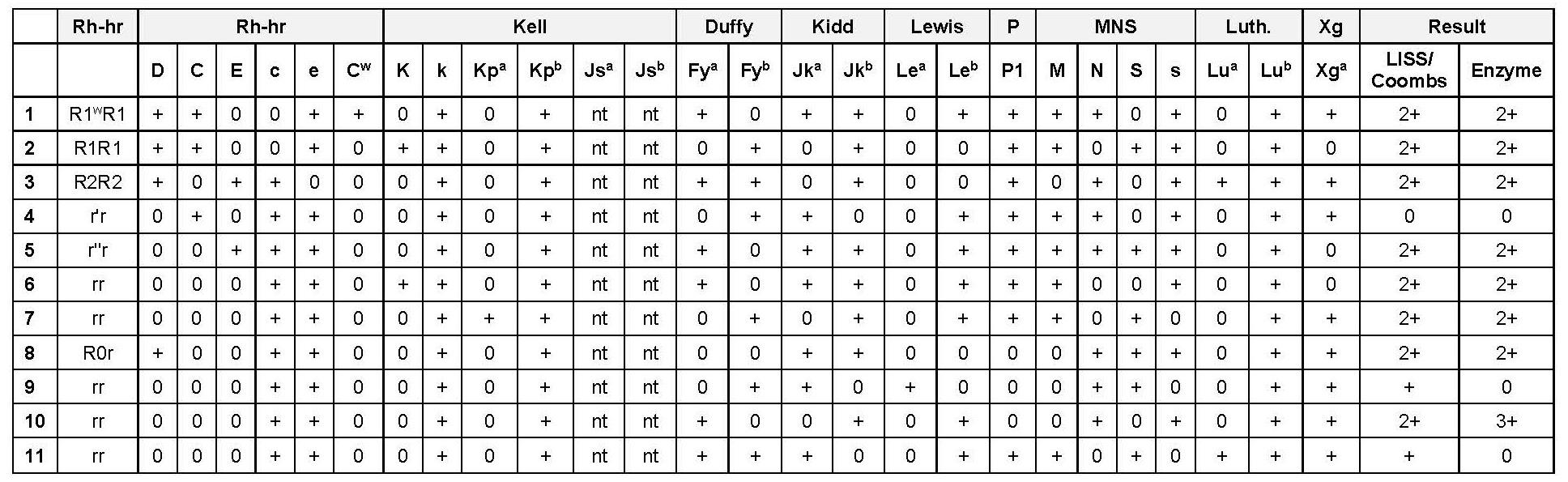
Unravelling the presence of multiple alloantibodies and autoantibodies in a patient - a case report from a tertiary care centre in Malaysia
Rabeya Yousuf, Kaalpana Jayakumar, Siti Nurrazan Zulkifli, Nur Afifah Suhemi, Nor Fadzliana Abdullah Thalith, Yee Loong Tang, Hari Priya Raghvan and Qhasmira Abu Hazir 120-124 Book reviews
The age of diagnosis by Suzanne O’Sullivan
final diagnosis by Cynric Temple-Camp
by Michael Legge
The intention of this issue’s editorial is to encourage authorship across the profession, provide some guidance and not to underestimate the value of laboratory experiences to provide a wealth of material that can be shared with the wider community.
Each year the NZIMLS invites a prominent New Zealand medical laboratory scientist, technician or pathologist to deliver the TH Pullar Address at its Annual Scientific Meeting. This year, Philip Wakem, from the Pacific Pathology Training Centre shared his eternal enthusiasm and joy of his experiences in the Pacific with attendees at the NZIMLS ASM 2025 in Hamilton and it is reprinted in this issue.
Maqsood and colleagues at the University of Punjab, the King Edward and Allama Iqbal Hospitals and the National University of Science and Technology in Pakistan report on a study of the predictive role of pituitary-gonadal axis dysfunction in COVID-19 severity and mortality. Males are more likely to experience infection and associated symptoms than females in both SARS and COVID-19 cases, however the potential for the SARS-CoV-1 virus to cause viral orchitis, its effects on male reproductive organs have not been thoroughly studied. Angiotensin-converting enzyme 2 (ACE2) and TMPRSS2 genes play essential roles in virus transmission and ACE2 expression patterns in adult human testes revealed a predominant distribution in Leydig, Sertoli cells and spermatogonia, implying the susceptibility of the human testis to SARS-CoV-2. This study revealed that serum level of Testosterone and Sex-hormone-binding globulin (SHBG) were negatively linked with the severity of the disease. For mortality prediction, the study showed that these declined levels of testosterone and SHBG were also significantly linked with severe outcomes in men with COVID-19.
Highly active antiretroviral therapy (HAART) has achieved significant improvements with respect to the quality and length of life for persons infected with Human immunodeficiency virus (HIV). Infection with HIV is becoming a common chronic disease however, patients may experience an increased risk of nonHIV/AIDS causes of end-stage organ disease and haemostatic complications, including risk of cardiovascular disease, venous thromboembolic disease, and microvascular disease. The toxicity of antiretroviral therapy also contributes significantly to chronic inflammation as certain protease inhibitors in the HAART regimens have been linked to dyslipidaemia, a risk factor for thrombosis. Okon, Akpan and Emeribe from the University of Calabar in Nigeria investigated platelet hyperactivation and haemostatic derangements in patients living with HIV who were being treated with HAART. Results showed an increased platelet count, mean platelet volume (MPV), platelet distribution width (PDW), platelet large cell ratio as well as prothrombin F1+2, α2-antiplasmin and P-selectin levels indicating platelet hyperactivation, thrombin generation and inhibition of clot digestion, posing a risk for the development of thrombosis.
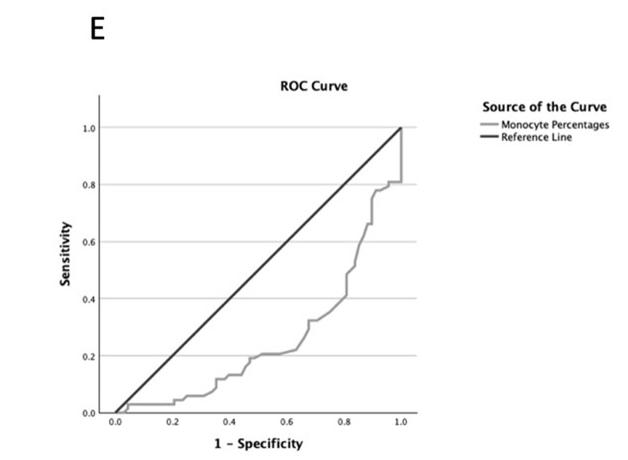
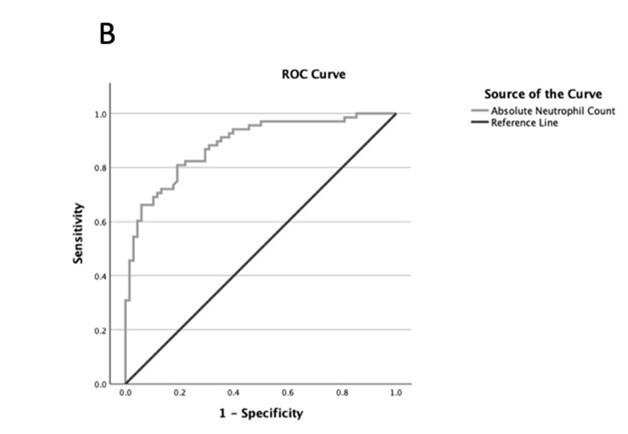
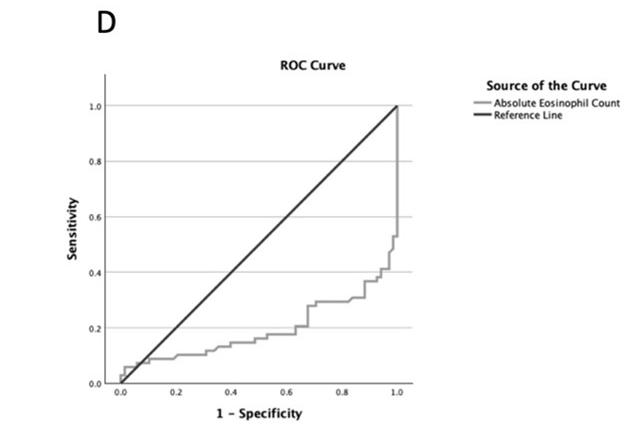
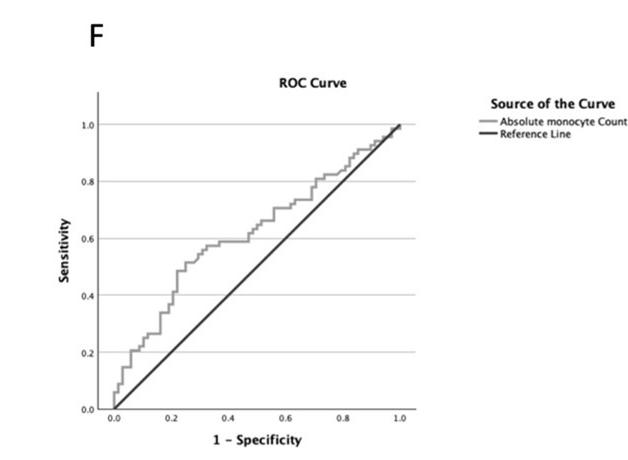
Chronic obstructive pulmonary disease (COPD) is a progressive pulmonary disorder characterised by airflow restriction, manifested by classic respiratory symptoms such as dyspnoea, and persistent coughing, resulting from structural changes in the airways and/or alveoli. Data from the World Health Organisation indicates that COPD is the fourth major contributor to global mortality and in 2021 COPD, accounted for 3.5million deaths worldwide. Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are frequently characterised with heightened inflammatory responses, often induced by bacterial or viral infections. Baharuddin and investigators at the Hasanuddin University in Indonesia conducted a cross-sectional observational study to compare white blood cell differential counts of neutrophils, eosinophils, and monocytes between patients experiencing acute exacerbations of chronic obstructive pulmonary disease (AECOPD) and those with stable COPD to assess their utility as predictive biomarkers. Their results identified significant differences in the percentages and counts of
neutrophils, eosinophils, and monocytes between patients who had acute exacerbations of COPD and those with stable disease. Neutrophils were significantly higher in AECOPD, with higher absolute monocyte counts and lower eosinophil and monocyte counts and percentages. Reducing the risk of exacerbation is central to COPD management, as acute exacerbations are related with increased inflammation, hospitalizations, worse lung function, and higher mortality. Their findings support routine blood testing as a simple and effective indicator of the systemic inflammatory response in COPD.
Nemati and McEntyre from Canterbury Health Laboratories in Christchurch, New Zealand report a rare presentation of Apolipoprotein B-related familial hypobetalipoproteinaemia (APOB-FHBL), an autosomal co-dominant inherited disorder of lipid metabolism caused by a mutation in the APOB gene. Homozygous APOB-FHBL patients typically have symptoms of fat malabsorption, steatorrhea, diarrhoea, failure to thrive, deficiencies in fat-soluble vitamins, and neurologic dysfunction along with hepatomegaly and steatosis, however heterozygous APOB-FHBL is often diagnosed incidentally due its asymptomatic nature or mild liver dysfunction and treatment of heterozygous FHBL focuses on dietary management, managing symptoms and preventing complications, especially those related to fat malabsorption and vitamin deficiencies and conducting regular monitoring. Their case study highlights the importance of persistence low lipid profile monitoring and the role of specific age-related reference interval for lipid profile and liver function tests in affected individuals.
The presence of multiple alloantibodies discovered during pretransfusion testing complicates subsequent selection of red cells for transfusion. Hazir and researchers at the National University of Malaysia report a case of multiple alloantibodies with autoantibodies in a 42-year-old patient with multiple comorbidities. This thorough investigation highlights the importance of complex antibody and clinically significant alloantibodies identification during immunohaematological work ups and demonstrates the need for attention to detail and immunohaematology expertise to ensure appropriate management of transfusion and minimise risk to patient safety.
Dr Michael Legge reviewed three books; Crypt, by Alice Roberts, The age of diagnosis, by Suzanne O’Sullivan and The final diagnosis, by Cynric Temple-Camp, between writing his regular Science Digest snippets and Recent Reviews.
Chris Kendrick looks back on his life as a medical laboratory scientist, lecturer and past NZIMLS President and we announce the retirement of Bronwen Johnson, from Labplus, Auckland. The NZIMLS, Journal and the profession thank them both for their services to the profession and wish them both all the best.
Regular features include the University of Otago BMLSc student research project abstracts from Semester 1, 2025, updates from the Pacific Pathology Training Centre (PPTC) in the Pacific Way, CPD Questionnaire and Reports from special interest group meetings. The Christmas Quiz is back with the coveted laboratory team prize and kudos up for grabs so, we invite you to take a break, have a laugh and have some fun!
Lisa Cambridge, Editor
The rewards of publishing and guidance for authors
Lisa Cambridge
Seeing my name as a published author in a scientific journal for the first time was exciting, it was a short one-page communication reporting a new polymorphism and printed in Animal Genetics, but it sparked my career-long passion for writing and learning the craft.
Do not underestimate the value of laboratory experiences to provide a wealth of material that can be published and shared with the wider community. Medical Laboratory Scientists (MLS) and Technicians (MLT) are essential to the diagnostic process in healthcare, generating the objective data and evidence that informs up to 80% of clinical decisions (1). Medical Laboratory Scientists and Technicians are skilled observers, critical thinkers, problem-solvers and innovators throughout technology, pathology, biology and patient care, however, the full value and impact of this work often remain invisible to the wider public and even to other healthcare professionals.
The long-term rewards and significant benefits of publishing in a peer-reviewed journal for individuals and the profession lie beyond just sharing information. Publication can contribute to professional development, recognition, career capability, subjectmatter expertise and own understanding. Publishing builds on the body of knowledge, increases field visibility, presents new methodologies, advances the profession, encourages investigation, establishes best practices, informs policymakers and provides a direct pathway to improving patient care by presenting verified and evidence-based practices.
Academia and research institutions rely heavily on publication to support their work and have at their disposal, preferred Journals, support systems and guidance to help their authors throughout the publishing process. Prolific, prominent, highly cited and ranked authors are rewarded with professional recognition, titles and grants. However, in the laboratory environment, these opportunities, support mechanisms and accolades are rare. Some organisations do not allow or are constrained by the inclusion of support and research laboratory staff as contributing authors, co-authors nor formally named in article acknowledgements. With these barriers and the demands of daily laboratory work, research and writing may seem a bridge too far and given no encouragement, guidance, reward or mentoring, impossibly hard.
What can we do as a profession to foster, encourage, support, advocate and mentor those wishing to write, publish and share knowledge?
Opportunities for publishing may come from small beginnings, for example a poster or a presentation given at a meeting can be fleshed out into a Case Report. The importance of case report publication is underestimated for the novice author in medical research, but they can succinctly communicate rare conditions , act as guides for cause analysis and problem-solving in-patient care and ultimately clinical decisions (2). New or improved methodology or even a perceived laboratory ‘failure’ can be written as a Scientific Letter or a Technical Report. Literature searches and investigation into relevant research material for a project could be the beginning of a Review article. Reading a new textbook or non-fiction book by the profession and pathologyrelated topics could become a Book Review.
The New Zealand Institute of Medical Laboratory Science (NZIMLS) website (3) provides information about the New Zealand Journal of Medical Laboratory Science, including the Journal’s background (Editors, Editorial Board and independence), Instructions for Authors (article type, word limits, referencing, peer-review process and style requirements), Author Forms, guidance on how to write a laboratory based case study, plagiarism policy and article review CPD proforma. There are also links to online medical science sites and MLS education. Next year (2026) we are going to be updating the website information and adding links offering more guidance material, useful tools
and reviewer guidelines. The NZIMLS offers monetary and recognition incentives for its member authors including The Hugh Bloore Poster Award presented at NZIMLS Annual Scientific Meetings. The Barrie Edwards & Rod Kennedy Scholarship to attend an international or national scientific meeting and present an oral or poster presentation as first author. A Research Grant to fund projects with final report submission for consideration of publication. The Rob Sieber’s Journal Prize for the best peerreviewed article published by an NZIMLS member in the Journal during a calendar year. Continuing Professional Development (CPD) programme also supports author activities with up to 20 substantive points for a scientific paper publication as an author and other written presentations where 5 to 10 points can be awarded.
Laboratory management and organisations could play an active role in supporting authorship and would go a long way to improving staff motivation, engagement, career recognition, satisfaction and the reputation of the organisation itself. For example, shared resource laboratories (SRL) participate in clinical research studies and are heavily involved in key aspects of experimental design, protocol development, data analysis and interpretation and troubleshooting of data. These activities are considered significant contributions for co-authorship. Guidelines are recommended for organisations, laboratory management and principal investigators to ensure advocacy and appropriate recognition for laboratory contribution in publications early during the planning stages of the study design including Intellectual Property (IP) policies and requirements (4). Discussion of authorship incentives and resources (for example, staff time and funding) during performance reviews, setting Key Performance Indicator (KPI) goals, recognition or promotion opportunities. Other ideas include a mentoring programme, expected participation in Journal clubs to present recent relevant published articles to colleagues. Although not directly linked to authorship, these activities encourage peer discussion and critical thinking to build an understanding of the writing and publishing process and if nothing else, then it is an opportunity to write a CPD reflective document. On an individual level, reading this Journal’s articles and completing CPD questionnaires also develops an awareness of content and structure required for writing scientific material. For the keen individual, there are many writing and publishing courses available online as well as guidance by education institutes and large publishing houses including Wiley, Sage and Elsevier to support your writing journey.
There are possibilities and rewards out there for aspiring authors and based on what I saw and heard at the recent ASM there is no lack of great material or enthusiastic presenters, so I urge you to reach out to the Editorial Team - ask questions, seek direction and feedback on ideas and send us those submissions, we are happy to guide you through the process and review.
AUTHOR INFORMATION
Lisa Cambridge, BApplManagement, MNZIMLS, Editor NZ J Med Lab Sci
Email: editor@nzimls.org.nz
REFERENCES
1. Sikaris KA. Enhancing the Clinical Value of Medical Laboratory Testing. Clin Biochem Rev 2017; 38(3): 107-114
2. Fawcett MA, Sinclair MK. Navigating the path to publication: A guide for the novice researcher. Kans J Med. 2023; 16(3): 247-250.
3. https://www.nzimls.org.nz/about-the-journal
4. Ferrer-Font L, Schimdt A, Ronchese F, Price KM. A guideline for the appropriate recognition of shared resource laboratories in publication. Cytometry 2023; 103(3): 193197.
TH PULLAR ADDRESS
The call of the Pacific
Philip Wakem
E nga mana, e nga reo o te motu. Tena koutou katoa
Avery good morning to you all and thank you for the opportunity of presenting the TH Pullar Address, the responsibility of which I am honoured to be given, especially when one considers the list of esteemed and highly achieved presenters who have gone before me and I am now to follow.
You all absolutely deserve to be on this stage receiving the same acknowledgement and accolades that you have worked so hard for, and so I salute you all for the enormous contribution you have made and continue to make to the medical and clinical sciences, each one of you playing a pivotal role in diagnosing disease, guiding treatment plans and improving patient outcomes.
My name is Philip Wakem, and I am a Medical Laboratory Scientist who commenced a 6-year training programme at Wellington Hospital back in 1978, a time when automation especially in Haematology was just beginning its introduction into the diagnostic services. It was a time when the beginnings of my working life were absorbed into a strict scientific environment of absolute structure, absolute discipline, absolute focus, absolute learning, and absolutely no fun. It was a time to leave behind the remnants of secondary education and move into the world of professionalism where science took on a whole new level.
I remember when guinea pigs were still being used in the laboratory to culture urine TB. I remember when as a trainee in Haematology, a human brain was requested several times in the yearfromthehospitalmortuarytobecutupbylaboratorystaffand emulsified by way of a food blender in the preparation of tissue thromboplastin for use in coagulation testing. I can remember the revolutionary changes that Haematology underwent with the introduction of automated blood cell counting specifically the Coulter S Full Blood Count analyser where the operator would sit in front of a mass of exposed precision glassware watching blood taking its leave from the aspirator, being then divided by a sample valve and then finally distributed by way of numerous glass coils and mixing baths to final FBC measurement. The infamous Hemalog D, a revolutionary wonder was also a new addition, the first instrument to perform automated white cell differentials in Wellington’s Hospital’s Haematology Department. It was a floor-based monstrosity, approximately 7 feet in length, and 5 feet in height and when it was functional it performed adequately well. Being continuous flow with numerous mixing coils and pumps however, it became an operational nightmare most of the time and finally outstayed its welcome only to be replaced by more advanced automation at a much-reduced size, greater capability, greater sensitivity and far greater reliability. I can also still remember in Biochemistry as a rotational first year trainee being absolutely mesmerised by the science of flame photometry as I watched the magical changing colours of emitted light as samples were aspirated into the flame, for the quantification of electrolytes.
How times have progressed and how scientific advancement has now reached unparalleled heights. The mid 1970’s was also a time when a good number of you hadn’t even been born so if that doesn’t make me feel slightly ancient, I just have to take a look in the mirror every morning and who should pop up, Father Christmas! After 30 yrs of hospital service, I joined the Pacific Pathology Training Centre in 2008 as Educational Programme Coordinator, later graduating to CEO in 2012, a position that I still currently hold.
Pacific Pathology Training Centre (PPTC)
For those of you who are unfamiliar with the Pacific Pathology Training Centre, I will at least explain in a nutshell what this organisation is all about.
The PPTC is a New Zealand based initiative that was established way back in 1980 as a response to a need for teaching and training in the medical
laboratory diagnostic sciences throughout the Pacific region. In 1990 the PPTC gained WHO status as a “Collaborating Centre for External Quality Assessment in Health Laboratory Services.”
The PPTC has a 40 plus year history of excellence in providing developmental assistance to medical diagnostic laboratories operating in the Pacific and Southeast Asia.
Strongly supported primarily by the New Zealand Ministry of Foreign Affairs and Trade, and to a lesser extent by numerous other organisations both in New Zealand and overseas, the PPTC has advanced and strengthened clinical laboratory services in Pacific neighbouring countries through its delivery of scientific teaching programmes, Regional External Quality Assurance Programmes and professional workforce development pathways. Staffed by six specialist scientists, the PPTC has impacted Pacific laboratories in providing management consultation, service development plans and advice on technology and equipment installations. These specialist scientists or PPTC consultants as they are referred to, are also experts in their respective fields with all having years of experience in the diagnostic sciences, laboratory management and healthcare delivery. They each play a crucial role in delivering specialized training programmes and ensuring that the Centre’s curriculum is both scientifically rigorous and contextually appropriate. Moreover, they serve as mentors, guiding trainees not only in technical skills but also in disease diagnosis, leadership and management, auditing and assessment, health and safety and ethical practices.
From the onset through to the conclusion of the 2020-2022 pandemic, every nation around the globe struggled and were shaken by the infective threatening force of COVID-19. The Pacific Island nations were no exception. In the South Pacific, many Pacific Island countries and territories braced themselves to be potentially overwhelmed by mass infection rates estimated by the increasing number of patients visiting sample collection centres and laboratory testing sites.
Suddenly the calibre and status of national diagnostic laboratory services for all the Pacific nations was in the spotlight, looking exposed and highly vulnerable. It was at this time that inadequate laboratory testing facilities in Pacific countries were recognised as a reality. Requests began to pour in from the Pacific for much needed support, and development partners such as WHO, the New Zealand Ministry of Foreign Affairs and Trade, Australian Department of Foreign Affairs and Trade and the Pacific Community, responded by requesting the PPTC to be involved in the development of portable laboratory systems that could be transported to the Pacific and made operational within an accepted time frame.
The PPTC accepted this challenge which involved the outfitting of new shipping containers with appropriate infrastructure and laboratory instrumentation, thereby increasing testing capabilities of Pacific laboratories in the critical testing sectors of microbiology, clinical biochemistry, haematology, serology, blood transfusion science as well incorporating rapidly developing molecular PCR platforms. Once completed, these portable laboratories were shipped across the Pacific to their final destinations where they, on arrival were immediately positioned, wired and plumbed ready for operation.
The PPTC is considered not only as the “go to” organization for the delivery of teaching and training programmes in the Pacific, but also portable laboratory construction which continues to be just as popular and necessary now as it was during the pandemic.
Many have commented in the past how lucky PPTC consultants are being able to work in such a Pacific paradise especially having yearlong opportunities travelling around the Pacific Islands. What is it really like they ask to be absorbed into the beauty of the tropical south seas warmly fanned by swaying coconut palms, swimming in turquoise, crystal clear waters and resting on golden sands with a martini in one hand and an olive in the other? My answer to that is I don’t know what’s it like because I never venture away from air conditioning units in laboratories or in hotels. I don’t do well in extreme humidity or in fact 35-degree temperatures, so if you need me for any good reason, follow
the layout as to where air conditioning units will be, and it’s a certainty that I will be under one of them.
Let’s now turn ourselves to the theme of this conference
The “Interweaving of Science and People” takes us on a specific exploratory journey which firstly sets out to explain how science and people are interwoven in Pacific Island laboratories, secondly, which identifies the significance of technological advances, and thirdly, promotes emphatically the importance of ISO15189 the International Accreditation Standard in strengthening healthcare systems across the region. The Pacific Islands described as an eclectic tapestry of over 25,000 islands distributed across the Pacific region is home to diverse cultures, traditions, customs and histories.
Within the Pacific Islands, medical diagnostic laboratories are vital components of the healthcare system serving as bridges between scientific knowledge and the communities they serve. Pacific medical laboratories serve as a hub where scientific innovation and human expertise converge to enhance healthcare delivery. The “Interweaving of Science and People” is evident in various aspects including capacity building, inviting and appreciating advances in the diagnostic sciences, community engagement, and the application of scientific knowledge to address local health challenges.
In Pacific cultures, healthcare has historically been intertwined with indigenous knowledge, community-based practices and spiritual beliefs. Such practices, even though they have in previous years been effective in their own right, still do exist often standing in contrast to western medical approaches which characteristically emphasize diagnostics through technology and empirical science. Adopting modern scientific approaches is not without its challenges, but as time moves on, these two systems of knowledge have been seen as complementary rather than conflicting.
Medical professionals and diagnostic laboratories currently operational in the Pacific region are beginning to incorporate traditional understanding with modern medical diagnostics to establish a model that accommodates both cultural and clinical needs of Pacific communities. These laboratories are at the crossroads of science and people, bridging the gap between traditional medicine in terms of healing practices and modern medical advancements while at the same time addressing unique challenges specific to the Islands themselves.
Scientific progress has long played a pivotal role in shaping societies, improving healthcare and fast-forwarding sustainable development. Pacific Island nations are continually faced with on-going challenges, in the form of geographical isolation, resource limitations, financial instability, compromised healthcare, uncontrolled climate change, and inefficient disease control, and for this reason, Pacific health systems necessitate robust scientific infrastructure to ensure improved public health outcomes, enhanced disease management and strengthened disaster response.
A large number of Pacific Island nations constantly struggle with high incidences of communicable and non-communicable diseases. Infectious disease such as malaria, HIV, Dengue fever, Leptospirosis, STI’s, Tuberculosis, Zika and Chikungunya remain prevalent while NCD’s such as diabetes and cardiovascular disease are considered major causes of mortality.
Working with the Pacific laboratories for over 17 years, I have come to terms with the negative impact that these challenges have caused and to be honest I believe that financial instability would have to be one of the most significant facing laboratories in the Pacific as this affects all areas of diagnostic operation. It’s important to remember that many laboratories in the Pacific region have small economies and are heavily reliant on tourism, agriculture and foreign aid. Tourists often when visiting Pacific Islands will invariably stay in luxury hotels offered by selected Pacific countries, but one needs to ask the question is this truly a representation as to how Pacific communities actually live. It is not. Poverty is reality to so many communities and is graded at different levels throughout the Pacific, the highest being in countries having no export markets where absolute economy is totally dependent on aid given by such counties as NZ, Australia, and the US. Because of this, national budgets must prioritize placing at the top of the list immediate social needs such as healthcare, infrastructure, and education, leaving scientific
institutions such as diagnostic medical laboratories underfunded.
As medical laboratory scientists you can appreciate that laboratories require substantial investment to function effectively at the highest levels of quality. Analytical systems over a broad spectrum of the diagnostic disciplines including molecular platforms such as PCR are expensive in terms of purchase and maintenance. In reality, Pacific laboratories continuously struggle with outdated or broken equipment due to financial constraints compromising repairs or essential replacements. Furthermore, reagents and consumables critical for laboratory operation are costly often at levels far more than one would expect to pay in New Zealand.
Laboratory personnel are also impacted by the lack of funding in terms of competitive salaries. This unfortunately often leads to staff shortages, as trained professionals migrate to countries with better career prospects. The scientific capacity of Pacific nations is significantly weakened by this “brain drain” effect, perpetuating a movement towards non progression of scientific development. It must be said that without financial support, Pacific laboratories will suffer from operational insufficiency with limitations in their ability to contribute to public health environmental protection and scientific innovation.
The Education Gap as it exists continues to hinder progress of Pacific laboratories and this is due to limited accessibility to scientific education and training. Students whose families can afford financial support will be considered fortunate to be able to enrol into a four-year Bachelor of Medical Laboratory Science programme at a registered university e.g. FNU in Fiji. On completion of this degree however, laboratory positions can be long awaited for. Students who do not have financial support from their families, can apply as an alternative, to the NZ Ministry of Foreign Affairs, Australia Aid, US Aid or the World Health Organisation for long term scholarship funding provided if, and when it may be available. It is important to note that universities or research institutions throughout the Pacific offering specialised laboratory science programmes, are limited in number and because of this, young aspiring scientists who live in Pacific countries where universities or university programmes are unavailable, are often required to travel internationally for higher education which can be extremely costly, and logistically challenging. In reality very few scholarships are offered yearly to a very small number of successful applicants and for those who remain unsuccessful in receiving such a scholarship which is the majority of cases, laboratory education can be given only at an extremely basic level to students once employed which is often inadequate to meet the ISO15189 Standards of quality.
PPTC now makes its grand entry into this conversation
For decades, Pacific medical laboratories were often underdeveloped, relying on external testing services or delayed diagnoses that hindered timely treatment. However, the interweaving of science with the lives of Pacific peoples has transformed this landscape. Laboratories in the region are no longer silent spaces of technology but are dynamic intersections where scientific innovation and community values converge. This partnership has revolutionized disease diagnosis and the management of treatment, significantly improving health outcomes. Weaving modern science into Pacific medical laboratory diagnostics has meaningfully improved speed and accuracy of diagnosis, surveillance and treatment decisionswhich in turn reduces transmission, shortens time-to-treatment, and strengthens outbreak response and health-system planning.
Installing PCR and molecular platforms (e.g., GeneXpert) has enabled many Pacific islands to have the capability of performing TB, COVID-19 and other tests locally rather than sending samples overseas. This in turn shortens turnaround from days into weeks to hours into days and enables faster treatment or isolation.
In terms of TB detection and drug resistance for instance, the introduction of the GeneXpert into the Pacific region has increased case detection and allows rapid identification of Rifampicin resistance, so communities can receive the correct therapy much sooner. A key step toward TB control in settings where access and geography are barriers. Improved HIV care through point-of-care and near-patient viral-load testing reduces the time between testing and clinical action improving treatment outcomes.
Investments in sequencing and pathogen-genomics give countries real-time information on variants and transmission chains so public-health measures can be targeted locally rather than reactively, an example of which is Fiji and its launching of an in-country pathogen genomics lab this year.
Genetic sequencing technologies identify mutations associated with diseases that are inherited, provide guidance to targeted therapies, and track pathogen evolution. This holds a great deal of significance in the Pacific region especially taking into consideration genetic predispositions to conditions like diabetes and obesity which we know to be high. Additionally genomic surveillance of viruses and bacteria enables proactive “Public Health” responses to emerging threats. It is vitally important that investment in molecular diagnostic capabilities is ensured so that Pacific islands remain at the forefront of global health security
Faster, accurate diagnostics reduce unnecessary antibiotic use, improve case surveillance data for policy, enable decentralised care (less travel for patients), and make epidemic/pandemic response faster and more efficient. Studies of COVID-19 responses in the Pacific highlight how lab investments improved preparedness and routine surveillance.
When I look back over the 17 years of absolute involvement with the PPTC and even on a part time basis throughout the years before this time, I can honestly say that even though Pacific laboratories can be overwhelmed with ongoing challenges, scientific progress has been made and continues to be so, certainly not at the same speed as you would experience in your own laboratories here in New Zealand, but one which is far slower, often hampered by the lack of affordability, resource availability, and sustainability. An example of this is the alignment and accreditation to the International Standard ISO15189. Where it would take NZ laboratories probably no more than 8-12 months to reach accreditation, the same process would stretch into years with regards to Pacific laboratories possibly even up to 15 years to reach alignment or possible accreditation to the standard, not to mention the challenge of sustainability which would naturally follow. Continual commitment from Pacific Ministries of Health in conjunction with support given by the PPTC is absolutely vital to progress and maintain quality achievement.
What contribution is the PPTC making?
The Pacific Pathology Training Centre was established with a clear mission: to provide quality Pathology training and education to Pacific Island healthcare professionals particularly pathologists, laboratory managers, quality officers, medical laboratory scientists, and laboratory technicians. The PPTC’s primary goal is to improve the quality of healthcare in the Pacific region through capacity building in pathology services as well as through the promotion of effective laboratory management. An increase in the globalization of diseases, exemplified by the COVID pandemic, clearly indicates the importance of wellequipped and technologically advanced laboratories.
A laboratory’s ability to quickly identify pathogens, sequence genomes and conduct surveillance is critical towards prevention of widespread outbreaks and protecting vulnerable populations especially those of the Pacific. One of the most significant contributions to Pacific healthcare systems of the Pacific islands that the PPTC makes, is its role in advancing the quality of pathology education and practise in the Pacific. This is executed through structured scientific teaching and training programmes examples of which include:
1. Short-term New Zealand-based courses at the PPTC Centre in Wellington covering the disciplines of Haematology, Biochemistry, Microbiology, Molecular Diagnostics, Laboratory Quality Management, and Blood Transfusion Science.
2. PPTC Distance Learning Diploma Programme, covering the same spectrum of diagnostic disciplines.
3. Short-term teaching and training programmes delivered in-country - covering the same diagnostic disciplines.
4. New Zealand attachments for Pacific students to New Zealand accredited laboratories.
5. PPTC Regional External Quality Assessment Programme which encompasses over 90 diagnostic
laboratories throughout the Pacific to Southeast Asia.
6. PPTC Laboratory Quality Management Programme and PPTC’s mentorship towards ISO15189 Accreditation.
The PPTC continues to be instrumental in guiding Pacific laboratories by providing on site mentorship and ongoing remote support towards ISO15189 alignment as the first stage towards international accreditation. Throughout this process, the PPTC assists laboratories in the execution of the 12 Essentials of Quality Management, prepares audits and assists in the implementation of generated corrective action. The PPTC funded by the New Zealand Ministry of Foreign Affairs and Trade is currently working with 7 countries in terms of ISO15189 alignment over a 5-year programme and these include Fiji, Samoa, Tonga, Cook Islands, Kiribati, Vanuatu and the Solomon Islands. PPTC consultants work closely with national health ministries and laboratory managers to align national quality objectives with international best practices. Through the PPTC’s commitment to quality, education and sustainable development, it has been a catalyst for elevating laboratory standards, throughout the Pacific.
It is important to remember, that science should not be a privilege of well-funded institutions alone. It should be a tool accessible to all, empowering Pacific communities to build and continue to build a healthier and more sustainable future. With continued investment in education technology and international collaboration, the future of medical diagnostics in the Pacific islands looks promising as each country strives toward global accreditation, greater professional development and enhanced healthcare outcomes for all.
PPTC consultants who tirelessly carry the flame of hope every day of their working lives, set out to make a difference to Pacific communities that are in desperate need of help and guidance. Our journey is a rewarding one but it can be tough at times having to deal with the barrage of limiting challenges that threaten to compromise progress made, not to mention annoying mosquitos, lizards who insist on spending the night with you either above your bed or in it, bed bugs, biting centipedes, cellulitis, rodents, food poisoning and explosive diarrhoea, I have experienced the lot!
Oh, I had forgotten about the time in the north Pacific when I had just arrived in the Federated States of Micronesia, checked into the hotel, couldn’t wait to have a shower, finally got in, trickled a little water over myself, then soaped up completely from head to toe turned on the water to full capacity, to rinse, only to find the hotels water supply had dried up. And there I was, the abominable snowman of the Pacific, a vision that you probably would desperately want to forget. I say this with affection only because it doesn’t really matter at all. Everyone has their fair share of experiences no matter what country in the world they are in and I’m sure they have all had their share of unwanted flying, stinging, crawling or biting guests so it’s no big deal. Not at all. What’s far more important is the appreciation that I have for being given so many opportunities while travelling around the Pacific to meet and be part of the most warm, the most gentle, the most giving, the most caring and the most loving people you will ever be privileged during your lifetime to meet, who will welcome you with open arms and unsurpassable generosity and who will make you feel that you have always been treasured as part of their immediate family.
It is important to once again extend my sincerest acknowledgements to everyone here today. To conclude, I wish for everyone to consider this Māori proverb:
Hei whakakapi i tenei wa, ka tika me mihi ano kia koutou katoa. He aha te mea nui o tenei ao? He tangata, he tangata, he tangata!
What is the most important thing in the world? It is the people, it is the people, it is the people!
AUTHOR INFORMATION
Philip Wakem, NZCS, DipMLSc, MMLSc, MNZIMLS, RNZIMLS, Chief Executive Officer, Pacific Pathology Training Centre, Wellington, New Zealand. Email: phil@pptc.org.nz
Atellica LumIQ Analyser
Illuminating the intelligence of urinalysis
The CLINITEK Status® Family of analysers has evolved.
Accelerate decision-making without compromising on accuracy or compliance
80+ years of reliable chemistry, same precision and assay versatility, modern technology and design. Accelerate decisionmaking without compromising on accuracy or compliance.
Broad menu. Trusted results.
Routine urinalysis, microalbumin, hCG, and quality control with streamlined workflows and built-in safe guards to help reduce user error.
Designed for simplicity and scalability
Compact, intuitive, and portable. Scalable to meet the demands of different clinical settings and test volumes.
Built-in secure connectivity
Bluetooth-enabled for encrypted data transfer. Seamlessly connects to LIS/HIS/EMR systems for clinical decision support and quality assurance.
COVID-19 severity and mortality in Pakistani male patients: the predictive role of
pituitary-gonadal axis dysfunction
Kaleem Maqsood, Shaaf Ahmad, Azeem Saeed, Zulfiqar Ali Beg, Muhammad Ahsan Raza and Nabila Roohi
ABSTRACT
Introduction: The global threat of the COVID-19 pandemic persists, prompting extensive efforts to identify risk factors for severity and mortality Increasing infections among males have raised concerns about the potential impact on male health. The objective of this study was to analyse the predictive power of sex hormones for severity and mortality in male patients.
Method: Blood samples of 94 male patients with moderate (n=68) and severe (n=26) PCR-positive patients hospitalized with COVID-19 and 40 healthy males as the controls were collected. The serum level of testosterone, sex hormone-binding globulin (SHBG), Follicle stimulating hormone (FSH) and luteinizing hormone (LH) was done through ELISA, and obtained data were analysed statistically by One-Way ANOVA and Regression analysis through IBM-SPSS software.
Results: In patients, the serum level of testosterone and SHBG was significantly low, while the level of LH and FSH was high. Multinomial regression analysis between moderate, severe and control categories indicated that serum testosterone and SHBG were negatively associated while LH and FSH were positively associated with COVID‐19 severity Among these predictors, testosterone was a significant predictor for severity (OR: 0.20; P<0.001) even after adjusting for SHBG, FSH and LH in Multivariate analysis. Binary logistic regression showed that low levels of testosterone (OR: 0.443; P=0.003) and SHBG (OR: 0.876; P=0.017) were associated with mortality even after adjusting for FSH and LH.
Conclusions: Our study demonstrated that reduced testosterone and SHBG levels play a substantial role in increasing the risk of COVID-19 severity and mortality amongst adult male patients.
Keywords: Andrology, COVID-19, mortality, sex hormone-binding globulin (SHBG), Testosterone.
NZ J Med Lab Sci 2025; 79(3): 99-103
INTRODUCTION
COVID-19 pandemic has had a devastating influence on the world (1), resulting in millions of deaths, overwhelming public health systems, and causing immense social and economic disruption (2).
The European Union has been the most affected area of the world in terms of the daily increase of confirmed COVID-19 cases, which is estimated to be between 26% and 30% (3). As of the 1st of February 2023, World Health Organization has reported 753,651,712 confirmed cases of COVID-19 worldwide with 6,813,845 deaths. In Pakistan, between the 3rd of January 2020 and the 6th of February 2023, the WHO recorded 1,576,343 confirmed cases of the virus and 30,640 deaths (4).
Males are more likely to experience infection and associated symptoms than females in both SARS and COVID-19 cases (5-7). Despite the potential for the SARS-CoV-1 virus to cause viral orchitis, its effects on male reproductive organs have not been thoroughly studied (8). The exact reasons for the genderbased variations in severe COVID-19 development remain not entirely clear. However, due to the transcriptional regulation of angiotensin-converting enzyme 2 (ACE2)- the primary cellular receptor for SARS-CoV-2 and Transmembrane protease, serine 2 (TMPRSS2) - a crucial viral fusogenic protease by androgens, it was anticipated that men would be more susceptible to SARSCoV-2 infection and likely to experience more severe disease compared to women (9). There is growing evidence that severe COVID-19 in male patients is accompanied by diminished levels of circulating testosterone (10). Role of testosterone in coagulation should be considered a factor in pathogenesis of COVID-19 (11).
Crucial for virus transmission, angiotensin-converting enzyme 2 (ACE2) and TMPRSS2 play essential roles. SARS-CoV-2 primarily spreads through respiratory aerosols and infiltrates human cells using ACE-2 receptors (12). Furthermore, an analysis of ACE2 expression patterns in the adult human testes revealed a predominant distribution in Leydig, Sertoli cells and spermatogonia, implying the susceptibility of the human testis to SARS-CoV-2 (13). Spermatids and spermatogonia predominantly express TMPRSS2 (14).
Given the impact of male sex on COVID-19 mortality risk, there is a plausible connection between sex hormones and the incidence or severity of SARS-CoV-2 infection. To comprehend the relationship between testosterone status and disease severity, an analysis focused on total testosterone, SHBG (sex hormone-binding globulin), FSH (Follicle stimulating hormone) and LH (luteinizing hormone) associations with COVID-19 severity and death. The study tested the hypotheses linking total
testosterone concentrations in men to SARS-CoV-2 infection severity and the risk of death.Additionally, the research explored associations of SHBG, FSH, and LH with these outcomes.
METHOD
For this observational prospective study ninety-four PCRpositive male COVID-19 patients, including 68 with moderate infection and 26 with severe infection from Mayo Hospital, Lahore, were recruited for this investigation. 40 healthy males of the same age group were also recruited as study controls from University of the Punjab, Lahore. Exclusion criteria included COVID-19 patients who had a self-reported history of cardiovascular disease, diabetes or cancer, and who died from other causes.
The Ethical Review Board of University of the Punjab, Lahore approved the research plan and written informed consent from all participants was taken before blood sampling, after explaining the complete study design and objective. The research was conducted following the principles of the Declaration of Helsinki. Complete information about the subjects was gathered using a predesigned proforma, and the questionnaire was planned according to the standards of Demographic and Health Surveys (DHS) (https://dhsprogram). Demographic variables such as the subject’s height, weight, age, education, work and disease history were also noticed.
For phlebotomy, a registered technician was recruited. Collected blood samples were poured into clot activator tubes to separate the serum. The blood samples were immediately carried to the Physiology Laboratory of the Institute of Zoology, University of the Punjab, and left for 30-40 minutes to allow coagulation. Centrifugation was performed for 15 minutes at 3000rpm. Serum was transferred to labelled Eppendorf vials and stored at -80°C until hormone analysis.
Analysis of serum levels of hormones (Testosterone, LH, FSH and SHBG) using commercially available ELISA kits of PerkinElmer (USA) was conducted at the Physiology/Endocrinology Laboratory, Institute of Zoology, University of the Punjab, Lahore.
Statistical analysis of obtained data from the biochemical analysis was statistically analysed through OneWay ANOVA, univariate and multivariate multinomial logistic regression, and binary logistic regression to find the variations between the study groups and the best predictor of severity and mortality in patients. IBM-SPSS (version 20) was used for this purpose.
RESULTS
A total of 134 eligible subjects were included in this study, among them 94 were COVID-19 patients categorized into moderate and severe groups (68 and 26, respectively), while 40 were controls of the same age group (Table 1). Clinical symptoms fever and cough were most prevalent (69.15% and 62.77%, respectively) among all patients. While diarrhoea, ICU admission and olfactory dysfunction were more prevalent (23.08%, 30.77% and 50.00%, respectively) in severe patients (Table 2).
Intergroup comparisons of serum levels of hormones were conducted through One-Way ANOVA. The results showed that serum testosterone and SHBG levels were considerably lower (p<0.001) in mild and severe patient groups than control group. But FSH and LH levels in both the mild and severe patient groups were significantly higher (p=0.029 and 0.002, respectively) compared to the control group (Table 3). We used univariate multinomial regression analysis to calculate the predictive power of each parameter separately and observed highly significant ORs
for the severity of the disease. After that, we go for the predictive power of the whole panel and only testosterone was a significant predictor in both the severe vs. control (OR; 0.20, CI; 0.12-0.34, P<0.001) and moderate vs. control (OR: 0.366; CI: 0.23-0.57; p<0.001) (Table. 4). We next used univariate and multivariate binary logistic regression analysis to calculate the mortality OR by comparing the survivors and non-survivors’ groups. In univariate analysis, all the predictors produced significant results. Among the predictors testosterone and SHBG were negatively associated with mortality (OR: 0.375; CI: 0.23-0.61; p<0.001 and OR: 0.871; CI: 0.79-0.95; p=0.002, respectively). However, the FSH and LH were positively associated with the mortality of patients (OR: 1.22; CI: 1.06-1.42; p=0.006 and OR: 1.17; CI: 1.05-1.31; p=0.005, respectively). In multivariate analysis, only testosterone and SHBG were significant predictors of mortality (OR: 0.443; CI: 0.26-0.75; p=0.003 and OR: 0.876; CI: 0.780.97; p=0.017, respectively) (Table 5).
Table 2. Prevalence (%) of clinical symptoms among the moderate and severe patients
Table 1. Socio-demographic characteristics of study subjects
Table 3. Intergroup comparison of serum level of hormones in control and patients
Tukey post-hoc; a significance for
Table 4. Multinomial logistic regression for the severity of COVID-19
Table 5. Binary logistic regression analysis for mortality (survivors vs. non-survivors) predictors
DISCUSSION
Male COVID-19 patients having fatal disease experience more detrimental inflammatory processes than female patients (15), as in other viral infections of respiratory system (7, 16). In male patients critically declined levels of serum testosterone, along with other predictive factors, are demonstrated to be a riskfactor for severe COVID-19 disease (17-19). Notably, indicators of inflammation (such as IL-6 and CRP) and tissue damage (LDH), which demonstrated effective prognostic capabilities for outcomes in initial sample assessments upon admission, exhibited a decline in their prognostic efficacy in longitudinalanalyses conducted on male patients throughout the period leading up to discharge or death (20).
In our study, the serum level of testosterone and SHBG were negatively linked with the severity of the disease, however, FSH and LH showed direct association in univariate analysis. When all these predictors were combined in multivariate analysis only testosterone was a significant predictor of severity. For mortality prediction, our study showed that declined levels of testosterone and SHBG were significantly linked with severe outcomes in men with COVID-19.
In COVID-19 lower levels of SHBG predicted worse outcome, as in a study of Zou, (21) 95.1% patients had normal or lower
SHBG levels. Non-survivor patients had lower than normal levels of sex hormone-binding globulin as compared to survivor patients. This decline in SHBG levels may be directly related to testosterone. The link between SHBG and mortality can be elucidated through various mechanisms. Factors like insulin levels, age, nutrition, and BMI can influence levels of SHBG. COVID-19 patients often exhibit obesity and elevated levels of insulin due to insulin resistance, which can partially explain lower SHBG levels observed in them (22). Moreover, severely ill patients show an increase in vascular-permeability and leakage of capillaries which causes hypoalbuminaemia (23), same mechanism can cause SHBG levels to drop. There is a documented association between SHBG levels and thyroid hormone levels (24). Individuals in intensive care units (ICUs) frequently exhibit reduced thyroid hormones concentrations, including thyroxine and tri-iodothyronine, a condition recognized as non-thyroidal illness syndrome, linked to an unfavourable prognosis (25). The observed lower SHBG levels in our findings could be explained by this association, especially considering that lower levels of tri-iodothyronine have been testified in COVID-19 patients and are correlated with disease severity (26).
The most significant findings of our study were the negative association of testosterone with the severity and fatality of
COVID-19 patients, these results were in agreement with the study of Salonia, (27). Lower levels of testosterone are associated with an increase in respiratory disorders susceptibility andpredictworseoutcomesanddeathfromCOVID-19.Inastudy by Kelada, (28), it was demonstrated that COVID-19 can likely reduce circulating testosterone levels. Lower testosterone levels can increase the risk of severe symptoms necessitating ventilator support. This is attributed to the upregulation of ACE2 receptors in respiratory system cells, heightening the likelihood of lungs damage and death. Additionally, connection between testosterone and immune surveillance in respiratory organs suggests that decreased level of testosterone may elevate the susceptibility to respiratory system infections (13). Coronavirus’s spike protein activates and downregulates ACE2 receptors so this disease can infiltrate epithelial cells of respiratory system (29).Therefore, the expression ofACE2 receptors may decrease upon viral attachment, which then degrades protective pathway of lungs and may disturb production of testosterone in male patients, increasing levels of pro-inflammatory cytokines in them (30).
SARS-CoV-2 might act directly on ACE2-positive Sertoli and Leydig cells, and spermatogonia and disrupt gonadal function and spermatogenesis in males (31). In context of viral infection, inflammation triggered by the virus results in the production of cytokines either systemically or locally. These cytokines have detrimental effects on testicular cells e.g. IL-6 prevents Leydig cells from differentiating. Additionally, IFN-γ suppresses rate-limiting enzyme - steroidogenic acute regulatory-protein (StAR) expression, thereby inhibiting the production of testosterone (32). Additionally, COVID-19 can also affect the hypothalamohypophyseal axis in central nervous system (33).
Aromatase enzyme converts androstenedione and testosterone into oestrone and estradiol (E2) respectively (34). In men, critical illness can upregulate the production of aromatase in adipose tissues (possibly because of excessive proinflammatory cytokines production) which converts testosterone into estradiol (35) and results in a reduction of testosterone level and enhanced disease severity ultimately result in an adverse outcome.
It is important to recognize some limitations of this study. The sample size is comparatively modest, and there is a restricted number of adverse outcomes. Additionally, hormonal assessments were conducted only once and not through the gold standard method, e.g. mass spectrometry, which was unavailable in this clinical setting. Instead, the measurements were carried out using a commercially available immunoassay. Our study indicates the need for future research to assess whether hormone-replacement therapies can play a part in COVID-19. This evaluation could explore the potential impact, whether protective and anti-inflammatory, or through the anticatabolic effect on respiratory muscles.
CONCLUSION
Our study revealed that variations in the concentrations of male sex hormones, such as decreased Testosterone and SHBG levels, can strongly prognosticate COVID-19 severity and mortality in male patients. We propose that clinicians remain attentive of the alterations in sex hormone parameters of male COVID-19 patients and seek advice for precise treatment.
ACKNOWLEDGEMENT
We gratefully acknowledge the Institute of Zoology, University of the Punjab, Lahore for providing financial support for this study.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR INFORMATION
Kaleem Maqsood, PhD, Researcher1
Shaaf Ahmad, MBBS, Researcher2
Azeem Saeed, MBBS, Researcher3
Zulfiqar Ali Beg, PhD, Director of Field Administration4 Muhammad Ahsan Raza, PhD, Researcher1
Nabila Roohi, PhD, Professor, Department of Zoology1
1 Institute of Zoology, University of the Punjab, Lahore, Punjab,
Pakistan
2 King Edward Medical University/Mayo Hospital, Hospital Road, Lahore, Punjab, Pakistan
3 Allama Iqbal Medical College/Jinnah Hospital, Lahore, Punjab, Pakistan
4 National University of Science and Technology, Islamabad, Pakistan
Corresponding Author; Dr. Kaleem Maqsood, Institute of Zoology, University of the Punjab, Lahore, Punjab, Pakistan
Email: kaleemmaqsood4@gmail.com
REFERENCES
1. Blaylock RL. Covid update: What is the truth? Surg Neurol Int 2022; 13:167.
2. Saravanan K, Panigrahi M, Kumar H, et al. Role of genomics in combating COVID-19 pandemic. Gene 2022; 823: 146387
3. Riou J, Althaus CL. Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Euro Surveill 2020; 25(4): 2000058.
4. WHO. WHO Coronavirus (COVID-19) Dashboard 2023 [Available from: https://covid19.who.int/?mapFilter=death].
5. Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020; 579(7798): 270-273.
6. Guan W-j, Ni Z-y, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020; 382(18): 1708-1720.
7. Karlberg J, Chong D, Lai W. Do men have a higher case fatality rate of severe acute respiratory syndrome than women do? Am J Epidemiol 2004; 159(3): 229-231.
8. Xu J, Qi L, Chi X, et al. Orchitis: a complication of severe acute respiratory syndrome (SARS). Biol Reprod 2006; 74(2): 410-416.
9. Baratchian M, McManus JM, Berk MP, et al. Androgen regulation of pulmonary AR, TMPRSS2 and ACE2 with implications for sex-discordant COVID-19 outcomes. Sci Rep 2021; 11(1): 11130.
10. Dhindsa S, Zhang N, McPhaul MJ, et al. Association of circulating sex hormones with inflammation and disease severity in patients with COVID-19. JAMA Netw Open 2021; 4(5): e2111398.
11. Agledahl I, Brodin E, Svartberg J, Hansen J-B. Impact of long-term testosterone treatment on plasma levels of free TFPI and TF-induced thrombin generation ex vivo in elderly men with low testosterone levels. Thromb Haemost 2009; 102(11): 945-950.
12. South AM, Diz DI, Chappell MC. COVID-19, ACE2, and the cardiovascular consequences. Am J Physiol Heart Circ Physiol 2020; 318(5): H1084-1090.
13. Wang Z, Xu X. scRNA-seq profiling of human testes reveals the presence of the ACE2 receptor, a target for SARS-CoV-2 infection in spermatogonia, Leydig and Sertoli cells. Cells 2020; 9(4): 920.
14. Cai Z, Zhong J, Jiang Y, Zhang J. Associations between COVID-19 infection and sex steroid hormones. Front Endocrinol (Lausanne) 2022; 13: 940675.
15. Peckham H, de Gruijter NM, Raine C, et al. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat Commun 2020; 11(1): 6317.
16. Noymer A, Garenne M. The 1918 influenza epidemic’s effects on sex differentials in mortality in the United States. Popul Dev Rev 2000; 26(3): 565-581.
17. Zhang J, Yu M, Tong S, et al. Predictive factors for disease progression in hospitalized patients with coronavirus disease 2019 in Wuhan, China. J Clin Virol 2020; 127: 104392.
18. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395(10223): 497-506.
19. Laguna-Goya R, Utrero-Rico A, Talayero P, et al. IL-6–based mortality risk model for hospitalized patients with COVID-19. J Allergy Clin Immunol 2020; 146(4): 799-807. e9.
20. Rastrelli G, Di Stasi V, Inglese F, et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology 2021; 9(1): 88-98.
21. Zou X, Chen K, Zou J, et al. Single-cell RNA-seq data analysis
on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med 2020; 14: 185-192.
22. Pugeat M, Crave JC, Elmidani M, et al. Pathophysiology of sex hormone binding globulin (SHBG): relation to insulin. J Steroid Biochem Mol Biol 1991; 40(4-6): 841-849.
23. Caironi P, Gattinoni L. The clinical use of albumin: the point of view of a specialist in intensive care. Blood Transfus 2009; 7(4): 259.
24. Krassas G, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev 2010; 31(5): 702-755.
25. Fliers E, Bianco AC, Langouche L, Boelen A. Thyroid function in critically ill patients. Lancet Diabetes Endocrinol 2015; 3(10): 816-825.
26. Chen M, Zhou W, Xu W. Thyroid function analysis in 50 patients with COVID-19: a retrospective study. Thyroid 2021; 31(1): 8-11.
27. Salonia A, Pontillo M, Capogrosso P, et al. Severely low testosterone in males with COVID‐19: a case‐control study. Andrology 2021; 9(4): 1043-1052.
28. Kelada M, Anto A, Dave K, Saleh SN. The role of sex in the risk of mortality from COVID-19 amongst adult patients: a systematic review. Cureus 2020; 12(8): e10114.
29. La Vignera S, Cannarella R, Condorelli RA, et al. Sexspecific SARS-CoV-2 mortality: among hormone-modulated ACE2 expression, risk of venous thromboembolism and hypovitaminosis D. Int J Mol Sci 2020; 21(8): 2948.
30. Abass RA, Rasheed MK, Saeed GT. The Relation between
the Plasma Level of Testosterone Hormone and the Severity of COVID-19 in Iraqi Patients. Indian J Forensic Med Toxicol 2022; 16(2): 326-333.
31. Carlsen E, Andersson AM, Petersen JH, Skakkebæk NE. History of febrile illness and variation in semen quality. Hum Reprod 2003; 18(10): 2089-2092.
32. Hu B, Huang S, Yin L. The cytokine storm and COVID‐19. J Med Virol 2021; 93(1): 250-256.
33. Stocco C. Tissue physiology and pathology of aromatase. Steroids 2012; 77(1-2): 27-35.
34. Carreau S, Lambard S, Delalande C, et al. Aromatase expression and role of estrogens in male gonad: a review. Reprod Biol Endocrinol 2003; 1(1): 35.
35. Spratt DI, Morton JR, Kramer RS, et al. Increases in serum estrogen levels during major illness are caused by increased peripheral aromatization. Am J Physiol Endocrinol Metab 2006; 291(3): E631-638.
National conference a ‘fantastic’ opportunity for Māori tauira
Three Māori tauira from Otago’s Department of Medical Laboratory Science have attended a national conference –marking another first for Ōtākou Whakaihu Waka.
The New Zealand Institute of Medical Laboratory Science (NZIMLS) Annual Scientific Meeting is an event for medical laboratory professionals in New Zealand, bringing together specialists for educational presentations, networking opportunities, and an industry exhibition.
Fourth-year tauira Ashleigh Brett (Ngāpuhi), Caitlin Huria (Ngāi Tahu/Kāi Tahu, Ngāti Raukawa, Ngāti Apa ki Te Rā Tō, Muaūpoko), and Tanya Taimana (Ngāpuhi, Ngāti Maniapoto) attended the conference last month – the first group of students from Otago to do so.
Olivia Moreton (Kāti Māmoe & Ngāi Tahu / Kāi Tahu), from the Department of Medical Laboratory Science who helped organise thestudents'attendance, saysattending sucheventsisvaluable.
“It gives students the opportunity to network with others in the profession,” Olivia says.
“There are not many Medical Laboratory Scientists who are Māori, so events such as this give a chance for them to interact not just with other MLS but multiple different professions outside of a university setting.
“It also gives them a taster of what they can expect if they attend conferences once they have graduated and joined the profession, especially for those who might not have been able to experience something like this previously. MedLabSci students receive very limited opportunities, so this was a fantastic chance for us to be able to provide something new.”
While at the conference, Ashleigh, Caitlin and Tanya were able to listen to and support a fellow Otago student, who was presenting at the same conference.
Tanya says she took a lot away from the conference - new knowledge,anewperspective,andaplanastohowshewantsto help shape the next generation of medical laboratory scientists.
“The NZIMLS conference was definitely an enjoyable experience, and I am very fortunate that I was able to attend; from networking with others in the laboratory sector to meeting representatives from companies across the world. The three-day event allowed me to look into the question that has always been on my mind since starting this degree: what does the future of the laboratory sector look like?” Tanya says.
“The theme of this conference was Tinana Rongoaa: Interweaving Science and People, a theme I believe was well chosenbecausethereisnothingmoreimportantinthehealthcare sector than the connection you have to yourself, your culture, and in turn, the patients that you help.”
Ashleigh, Caitlin, and Tanya are all currently on clinical lab placements around Aotearoa. Ashleigh is completing a placement in Molecular Diagnostics at Canterbury Health Labs in Christchurch. Caitlin is completing a placement in Rural Health for Medical Laboratory Science at Awanui Labs Hutt Hospital in the Lower Hutt while Tanya is completing a placement in Molecular Diagnostics at IGENZ - Auckland.
The Department of Medical Laboratory Science would like to thank Dr Griffin Leonard in the Kōhatu Centre for Hauora Māori and Dr Holly Perry from the Department of Medical Laboratory Science for their assistance.
Korero by Māori Communications Adviser Brigham RiwaiCouch Reprinted with permission from the University of Otago, first published in Newsroom, media releases, University of Otago, 22 September 2025
At the New Zealand Institute of Medical Laboratory Science Annual Scientific Meeting, from left to right, is Tanya Taimana, Ashleigh Brett, and Caitlin Huria.
Mediray is a proud New Zealand-owned and operated distributor with comprehensive portfolio of high-quality laboratory equipment, diagnostic systems, and consumables. We aim to contribute to better patient outcomes by ensuring labs and clinics have access to the tools they need for accurate and timely diagnostics.
NEW BIOFIRE® SPOTFIRE® SOLUTION
COMPREHENSIVE PCR RESULTS IN ~15 MINUTES.
ENSURE YOUR LAB’S ACCURACY WITH EPPENDORF AND CHECK OUT OUR CURRENT PROMOTIONS FOR SPECIAL OFFERS ON THESE ESSENTIAL TOOLS! and more...
Multipette® M4/E3 with Combitips
Platelet hyperactivation and haemostatic derangements of persons living with human immunodeficiency virus infection on highly active antiretroviral therapy
Josephine E Okon, Patience A Akpan and Anthony O Emeribe
ABSTRACT
Objectives: Human immunodeficiency virus (HIV) infection remains a significant public health challenge globally and in Nigeria with dysfunctional haemostasis as a concern in HIV pathogenesis. This study assessed platelet indices and markers of haemostatic activation of HIV patients on highly active antiretroviral therapy (HAART).
Methods: With ethical approval and informed consent, 45 HIV patients aged 18-60 years on HAARTwere enrolled at University of Uyo Teaching Hospital along with 45 HIV sero-negative control. Data on demographics and antiretroviral therapy were compiled. Platelet indices, CD4+ count, viral load, prothrombin fragment 1+2, α2-antiplasmin and P-Selectin were determined by standard techniques. Data analysis was on statistical package for social sciences with P set at ≤ 0.05.
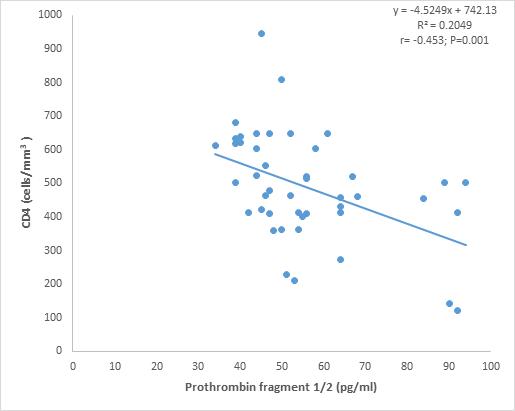
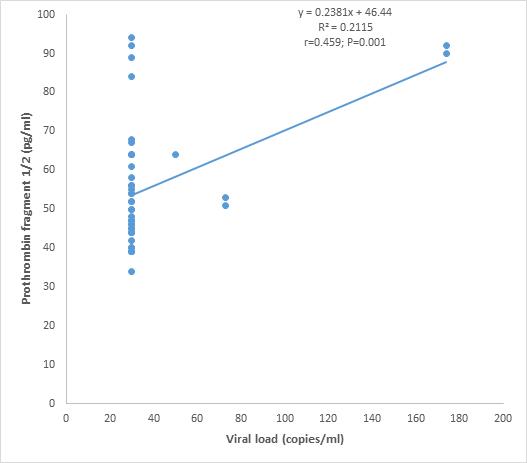
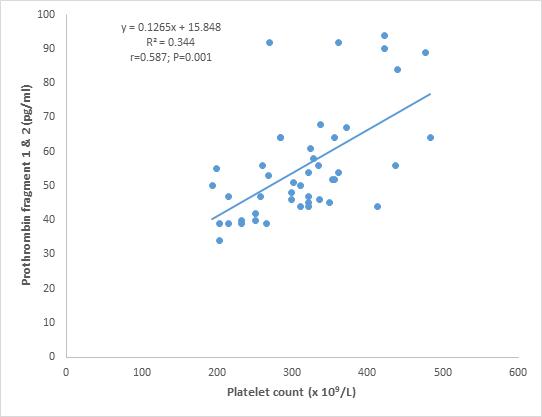
Results: The HIV patients on HAART were aged 47.0±7.5 years, mostly females (57.8%) with 55.6% being married; 80% had tertiary education (80%) and were government workers (64.4%). While CD4 count was significantly lower (p = 0.001), viral load (p = 0.001), platelet count, mean platelet volume and platelet distribution width were significantly higher (p = 0.001) for HIV patients compared to control. Prothrombin F1+2, α2-antiplasmin and P-selectin levels were significantly higher (p = 0.001, p = 0.012 and p = 0.001 respectively) for HIV patients compared to control. Prothrombin F1+2 correlated negatively with CD4 count (r = -0.453, p= 0.001) but positively with viral load (r = 0.459, p= 0.001) and platelet count (r = 0.587, p= 0.001). P-selectin increased significantly (p = 0.001) for those on HAART for more than 36 months.
Conclusions: Patients with HIV on HAART have increased platelet count, mean platelet volume (MPV), platelet distribution width (PDW), platelet large cell ratio as well as prothrombin F1+2, α2-antiplasmin and P-selectin levels indicating platelet hyperactivation, thrombin generation and inhibition of clot digestion, which pose a risk for development of thrombosis.
Keywords: Platelets, Coagulation, Human immunodeficiency virus (HIV), highly active antiretroviral therapy (HAART)
NZ J Med Lab Sci 2025; 79(3): 105:110
INTRODUCTION
Human immunodeficiency virus (HIV) infection remains one of the world’s most significant public health challenges. Unfortunately, Africa remains the most severely affected with 3.2% HIV prevalence in the adult population compared to 0.7% rate for the same group worldwide (1). From the era of monotherapy to combination antiretroviral therapy (c-ART) also known as highly active antiretroviral therapy (HAART), significant improvements have been achieved with respect to the quality and length of life for persons infected with HIV. Infection with HIV is becoming a common chronic disease however patients may experience an increased risk of non-HIV/AIDS causes of end-stage organ disease, which includes haemostatic complications. Risks of cardiovascular disease, venous thromboembolic disease, and microvascular disease together with their attendant mortality are thought to be relatively higher in people living with HIV (2). While antiretroviral therapy has been shown to address HIV viremia, the ability of the therapy to resolve associated derangements remains unclear. Moreover, the drugs are also suspected to cause adverse effects that compound these derangements (3).
Higher risk of thrombosis and occurrence of deep vein thrombosis and venous thromboembolism has been reported in HIV infection (4, 5). The HIV virus attacks the immune system, resulting in immunosuppression. This provokes the inflammatory response, triggering the release of tissue necrotic factor (TNFα) thereby increasing the production of plasminogen activator inhibitor 1 (PAI-1). The PAI-1 inhibits clot dissolution, increasing the risk of thrombosis. The toxicity of antiretroviral therapy also contributes significantly to chronic inflammation as certain protease inhibitors in the HAART regimens have been linked to dyslipidaemia, a risk factor for thrombosis (6). In HIV-induced chronic inflammation, endothelial injury persists with subsequent activation of platelets and coagulation and increased likelihood of thrombotic complications (7).
Persons living with HIV might also experience a relatively higher risk of dysfunctional haemostasis in the case of a lower plasma CD4+ T-cell count or/and higher viral load as well as current opportunistic infections. In fact, thrombosis associates significantly with poorer survival in HIV (8, 9). Dysfunctional haemostasis in association with HIV infection is an area of concern despite phenomenal achievements in lowering HIV viremia to undetectable levels. In the face of newer and better HAART regimens, there is need to investigate platelet indices and markers of haemostatic activation in persons on HAART particularly in our locality where such data is lacking. This study aims to contribute to the understanding of haemostatic aspects
of HIV morbidity and is expected to enhance the management of patients with HIV infection and provide information on platelet indices and markers of haemostatic activation of HIV patients on HAART in Uyo, Akwa Ibom State, Nigeria.
MATERIALS AND METHODS
Study scope and participants
The study site was the University of Uyo Teaching Hospital (UUTH), a tertiary health facility and referral centre in Uyo, Nigeria. A case-control descriptive study design was adopted. With ethical approval (NHREC/24/06/22.UUTH) and informed consent, 45 HIV patients aged 18-60 years on HAART and 45 apparently healthy HIV sero-negative individuals (control) were enrolled. Participants who were pregnant, those on hormonal contraceptives and those not on HAART as well as those who did not consent were excluded.
Data and sample collection
A structured questionnaire was administered to capture bio and demographic data; information on antiretroviral therapy was retrieved from patients’ case notes. A volume of 6.5mL of blood was collected aseptically through venipuncture with minimal stasis (within one minute of applying the tourniquet), 2mL was transferred into potassium ethylene diamine tetra acetic acid (K2EDTA) container at a concentration of 2mg/mL of blood. The remaining 4.5mLof blood was dispensed into 3.13% trisodium citrate container (9 parts to 1 part) and centrifuged within 20 minutes of collection to obtain plasma. The EDTA blood was used for platelet indices, CD4 count and viral load assay, while the citrated plasma samples were stored at -20oC for subsequent analysis of prothrombin fragment 1+2 (F1+2), α2-antiplasmin and P-selectin levels within four weeks of storage.
Sample analysis
Platelet indices were determined using HEMIA 5D Auto Hematology Analyzer based on the principle of electrical impedance. The CD4+ cell count was analysed using Partec Cyflow Counter (Germany, 2006) based on the principle of light scattering and emission wavelength spectrum. Viral load was measured using Abbott Laboratories Real Time polymerase chain reaction (PCR) primer mediated enzymatic amplification of DNA. Prothrombin F1+2, α2-Antiplasmin and P-Selectin levels were determined using enzyme-linked immunosorbent assay (ELISA) technique with kits obtained from Bioassay Technology Laboratory, China. The ELISA testing was done alongside
controls and standards according to the instruction of the manufacturer.
Statistical analysis
Data analysis was on statistical package for social sciences (SPSS) version 22.0; Chi-squared test analysed frequencies while student t-test compared means. Pearson’s correlation coefficient was used to establish relationship between variables. A two-tailed p-value of ≤ 0.05 denotes a statistically significant difference.
RESULTS
Table 1 shows the demographic data of HIV patients and control.
The HIV patients on HAART had a mean age of 47.0±7.5 years. 57.8% were females with the majority being (55.6%) married. The HIV patients had tertiary education (80%) and were mainly government workers (64.4%).
The CD4 count was significantly lower (p = 0.001), while the viral load was significantly higher (p = 0.001) for HIV patients
compared to controls as shown in Table 2. Platelet count, mean platelet volume (MPV) platelet distribution width (PDW) (coefficient of variation and standard deviation) (p = 0.001) and platelet large cell ratio (p = 0.037) were significantly higher for HIV patients compared to control.
As presented in Table 3, prothrombin F1+2, α2-antiplasmin and P-selectin levels of HIV patients were significantly higher (p = 0.001, p = 0.012 and p = 0.001 respectively) compared to the control group. Prothrombin F1+2 correlated negatively with CD4 cell count (r = -0.453, p= 0.001) but positively with viral load (r = 0.459, p= 0.001) as seen in Figures 1 and 2. In addition, prothrombin F1+2 correlated positively with platelet count (r = 0.587, p= 0.001) as shown in Figure 3.
Table 4 shows that the CD4, viral load and platelet parameters as well as prothrombin F1+2 and α2-antiplasmin of HIV patients did not differ significantly (p > 0.05) based on duration of antiretroviral therapy. Conversely, P-selectin level increased significantly (p = 0.001) for those on HAART for more than 36 months when compared to those treated for 36 months and less.
Table 1. Demographic data of HIV patients and controls.
Table 2. CD4, viral load and platelet indices of HIV patients and control.
Table 3. Prothrombin fragments 1+2, α2-antiplasmin and P-selectin levels of HIV patients and control.
Table 4. CD4, viral load, platelet and haemostatic activation markers of HIV patients based on duration of antiretroviral therapy
Figure 1. Correlation between prothrombin fragment 1+2 and CD4 count of HIV patients
Figure 2. Correlation between prothrombin fragment 1+2 and viral load of HIV patients
Figure 3. Correlation between prothrombin fragment 1+2 and platelet count of HIV patients
DISCUSSION
This study assessed platelet indices and markers of haemostatic activation of HIV patients on HAART. The HIV patients and control were aged-matched, and more females were affected. This is in line with reports that women are more at risk due to biological, social and cultural factors. Biologically, the vagina has a large surface area hence there is more exposure. Social barriers to care, economic constraints as well as hormonal contraceptive use are also risk factors for women (10, 11). The HIV patients receiving treatment at UUTH were more of married females of reproductive age. This is attributable to the mandatory antenatal screening that facilitates detection and therapy commencement for infected pregnant women which continues post-delivery (12, 1).
The lower CD4 count, and higher viral load observed for HIV patients in this study is in line with the behaviour of the HIV virus as it has been known to attack and destroy the T-helper cells (CD4 cells) and replicate itself thus reducing CD4 numbers while increasing the viral load (13). A direct consequence of viral replication is that T-cell colony formation is adversely affected; there is profound depletion in the CD4 T-cell population resulting in diminished CD4 T-cell proliferative response to many stimuli. Decline in CD4 cells mediates several disease manifestations relating to poor immunologic response (14). The CD4 cell count has been identified as an indicator for severity of HIV infection. It remains useful in the assessment of disease progression, while the viral load is an indication of invasiveness or otherwise of the virus. Addressing these challenges has long been the focus of antiretroviral therapy resulting in the emergence of improved drugs. The study participants were HIV-infected persons receiving HAART with varying treatment durations. These parameters were comparable between those who had received therapy for up to 36 months and those beyond 36 months of treatment (Table 4).
Changes in platelet parameters were observed in HIV infection (Table 2). Reduction in all blood cell lines was previously a major concern in HIV infection; owing to improved therapy, the pattern of derangement appears to be changing. Higher platelet count was observed in the HIV subjects on HAART in this study in contrast to several reports of thrombocytopenia in HIV infection (15, 16). Thrombocytopenia in HIV has been attributed to increased peripheral destruction of platelets and ineffective production of platelets from infected megakaryocytes and is linked to CD4 counts of <200 cells/µL, high viral load as well as the presence of opportunistic infections. However, thrombocytopenia has been observed to improve with antiretroviral therapy (17). Platelets play crucial roles in primary haemostasis and thrombosis. In addition, their complex reactions to viral (and bacterial) signals result in immune responses, and may be protective, or may contribute to significant systemic inflammation. The immune and inflammatory responses of platelets to HIV are therefore thought to be of great significance in mediating thrombosis (18, 17). A possible reason for higher platelet numbers in HIV infection as observed in this study is that the body signals the bone marrow to produce more platelets as a measure to repair damaged tissues. This is a characteristic response of the immune system in the face of inflammation (19). Consequently, larger platelets are released into the circulation hence the higher MPV observed for the HIV patients. A higher MPV could be a risk factor for cardiovascular complications (20). Similarly, the PDW which reflects variation in size of platelets, was observed to be significantly higher for the HIV patients. The PDW is considered to be a marker of platelet activation and can be used to assess inflammatory reactions. The presence of larger platelets in the circulation is also confirmed by the higher value of platelet large cell ratio of HIV patients when compared to the control. The observed value for mean platelet volume, platelet distribution with and platelet large cell ratio for HIV patients, all points to the fact that there is platelet activation along with increase in platelet numbers as part of the immune response against the HIV infection (21).
Higher levels of prothrombin fragments 1 + 2 and α2-antiplasmin were seen in HIV infection (Table 3). Haemostatic abnormalities occur frequently and is linked with increased mortality in patients with HIV. This could arise from increased concentrations of coagulation and fibrinolytic markers. Chronic immune activation and inflammatory state in both untreated and treated HIV infections can result in abnormal haemostatic changes (22).
Prothrombin fragment 1+2 is considered the best marker of thrombin generation and hence of coagulation activation (23, 24). The plasmin-antiplasmin system plays a key role in blood coagulation and fibrinolysis. Plasmin and α (2)-antiplasmin are primarily responsible for a controlled and regulated dissolution of the fibrin polymers into soluble fragments hence elevated levels as observed is consistent with increase in thrombin generation (25-27). Prothrombin fragment 1+2 correlated negatively with CD4 counts and positively with viral load (figures 1 and 2) indicating that its increase as observed is directly related to the presence of the HIV virus and its consequent effect on CD4 lymphocytes. However, the moderate positive correlation (r=0.459) observed between prothrombin fragment 1+2 and viral load is a consequence of few data points arising from a narrow range of viral load values obtained for a small sample size and a high margin of error (calculated as 23.32%). The small sample size of 45 is a limitation of the study. Prothrombin fragment 1+2 also correlated positively with platelet count (Figure 3) as a reflection of the ongoing activation of platelets as well as the coagulation system occasioned by the chronic state of inflammation in HIV infection.
P-selectin is synthesized by megakaryocytes and endothelial cells, where it is sorted into the membranes of secretory granules. When megakaryocytes and endothelial cells are activated by agonists such as thrombin and antihistamine during inflammation, P-selectin is rapidly translocated to the plasma membrane from granules. P-selectin plays an essential role in the initial recruitment of leukocytes (white blood cells) to the site of injury during inflammation (28-30). P-selectin level increased for HIV patients in this study and remained elevated for those who had received treatment for more than 36 months (Tables 3 and 4) reflecting sustained activated coagulation even with longer duration of therapy.
CONCLUSIONS
Persons living with HIV on highly active antiretroviral therapy have increased platelet count, MPV, PDW, platelet large cell ratio as well as prothrombin F1+2 , α2-antiplasmin and P-selectin levels, indicating platelet hyper-activation, thrombin generation and inhibition of clot digestion, which pose a risk for development of thrombosis. Platelet hyperactivation persists even with longer duration of HAART.
Improvement of HAART by the pharmaceutical industry should focus on addressing platelet hyperactivation and derangement of coagulation. Future studies will focus on flow cytometric analysis of platelet immune markers as well as platelet ribonucleic acid profiling and sequencing in HIV infection.
ACKNOWLEDGEMENTS
The authors acknowledge the staff at the HIV Clinic, University of Uyo Teaching Hospital for their assistance in enrolling HIV infected persons. We also appreciate the study participants for consenting to be part of the study.
AUTHOR INFORMATION
Josephine E Okon, PhD, Director Medical Laboratory Services1 Patience A Akpan, PhD, Associate Professor2 Anthony O Emeribe, PhD, Professor2
1 Department of Haematology, University of Calabar Teaching Hospital, Nigeria.
2 Department of Haematology and Blood Transfusion Science, Faculty of Medical Laboratory Science, University of Calabar, Nigeria
Corresponding author: Patience A Akpan, Department of Haematology and Blood Transfusion Science, Faculty of Medical Laboratory Science, University of Calabar, Nigeria. Email: apu0520@unical.edu.ng
REFERENCES
1. World Health Organization. [cited 2025 January 7] Available from https://www.who.int/publication/i/item/WHO-UCNHHS-SIA-2023-01
2. Post WS, Cardiovascular disease in HIV. Trans Am Clin Climatol Assoc 2022; 132: 126-134
3. Matoga MM, Hosseinipour MC, Aga E, et al. Hyperlipidaemia in HIV-infected patients on lopinavir/ritonavir monotherapy in resource-limited settings. Antivir Ther 2017; 22(3): 205-213
4. Vululi ST, Bugeza S, Zeridah M, et al. Prevalence of lower limb deep vein thrombosis among adult HIV positive patients attending an outpatient clinic at Mulago Hospital AIDS Res Ther 2018; 15(1): 3.
5. Agrati C, Mazzotta V, Pinnetti C, et al. Venous thromboembolism in people living with HIV infection (PWH) Transl Res 2021; 227: 89-99.
6. Rasmussen LD, Dybdal M, Gerstoft J, et al. HIV and risk of venous thromboembolism: a Danish nationwide populationbased cohort study. HIV Med 2010; 12(4): 202-210.
7. Perkins MV, Joseph SB, Dittmer JD, et al. Cardiovascular disease and thrombosis in HIV infection Arterioscler Thromb Vasc Biol 2022; 43(2): 175-191.
8. Nou E, Lo J, Grinspoon SK. Inflammation, immune activation, and cardiovascular disease in HIV. AIDS 2016; 30(10): 1495–1509.
9. Taylor KA, Smyth E, Rauzi F. Pharmacological impact of antiretroviral therapy on platelet function to investigate human immunodeficiency virus‐associated cardiovascular risk. Br J Pharmacol 2019; 176(7): 879 – 889.
10. US Department of Health and Human Services. Women and HIV- Office on Women’s Health [Internet], 2023 [cited 2025 January 15] Available from https://womenshealth.gov/hivand-aids/women-and-hiv
11. National Institute of Health. HIV and women (based on assigned sex at birth)-Office of AIDS Research [Internet], 2024 [cited 2025 January 18] Available from https://www. oar.nih.gov/women
12. United Nations Programme on AIDS. UNAIDS DATA 2020 [Internet] 2020 [cited 2025 January 24] Available from https:// www.unaids.org/en/resources/documents/2020/unaids-data
13. Jain V, Peterson M, Havlir DV. Population HIV viral load metrics for community health Lancet HIV 2021; 8(9): e523-e524.
14. World Health Organization. HIV and AIDS Fact sheets [Internet] 2021 [cited February 8] Available from https:// www.who.int/news-room/fact-sheets/detail/hiv-aids
15. Getawa S, Aynalem M, Bayleyegn B, et al. The global prevalence of thrombocytopenia among HIV-infected adults: a systematic review and meta-analysis Intl J Infect Dis 2021; 105: 495-504.
16. Ayanaw MA, Yabeyu AB, Lenjiso G, et al. Prevalence and predictors of thrombocytopenia among HAART naïve HIV positive patients at Ambo University Referral Hospital. Clin Epidemiol Glob Health 2022; 15: 101049.
17. Marchionatti A, Parisi MM. Anemia and thrombocytopenia in people living with HIV/AIDS: a narrative literature review Int Health 2021; 13(2): 98–109.
18. Vishnu P, Aboulafia DM. Haematological manifestations of human immune deficiency virus infection. Br J Haematol 2015; 171(5): 695-709.
19. Rokkam VR, Killen RB. Kotagiri R. Secondary thrombocytosis Statpearls Treasure Island [Internet] 2024 [cited 2025 February 10] Available from https://pubmed.ncbi.nlm.nih. gov/32809645
20. Handtke S, Thiele T. Large and small platelets – (when) do they differ? J Thromb Haemost 2020; 18(6): 1256-1267.
21. Pogorzelska K, Kretowska A, Krawczuk-Rybak M, SawickaZukowska M. Characteristics of platelet indices and their prognostic significance in selected medical condition- a systematic review. Adv Med Sci 2020; 65(2): 310-315.
22. Zhang Q, Peng F, Li M, et al. Elevated risk of venous thromboembolism in people living with HIV. Viruses 2022, 14(3): 590.
23. Acquasaliente L, Pelc LA, Di Cera E. Probing prothrombin structure by limited proteolysis. Sci Rep 2019; 9(1): 6125.
24. Friedmann AP, Koutychenko A, Wu C. et al. Identification and characterization of a factor Va-binding site on human prothrombin fragment 2. Sci Rep 2019; 9(1): 2436.
25. Abdul S, Leebeek FW, Rijken DC, et al. Natural heterogeneity of á2-antiplasmin: functional and clinical consequences. Blood 2016; 127(5): 538–545.
26. Reed GL, Houng AK. Singh S, Wang D. á2-Antiplasmin: new insights and opportunities for ischemic stroke. Semin. Thromb Hemost 2017; 43(2): 191–199.
27. Abdul S, Dekkers DH, Ariëns RA, et al. On the localization of the cleavage site in human alpha-2-antiplasmin, involved in the generation of the non-plasminogen binding form. J Thromb Haemost 2020; 18(5): 1162–1170.
28. Setiadi H, Yago T, Liu Z, McEver RP. Endothelial signaling by neutrophil-released oncostatin M enhances P-selectindependent inflammation and thrombosis. Blood Adv 2019; 3(2): 168–183.
29. Hellen N, Mashanov GI, Conte IL, et al. P-selectin mobility undergoes a sol-gel transition as it diffuses from exocytosis sites into the cell membrane. Nat Commun 2022; 13(1): 3031.
30. Liu CH, Jheng PR, Rethi L, et al. P-Selectin mediates targeting of a self-assembling phototherapeutic nanovehicle enclosing dipyridamole for managing thromboses. J Nanobiotechnology 2023; 21(1): 260.
Objectives: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are frequently characterised with heightened inflammatory responses, often induced by bacterial or viral infections. Identifying accessible biomarkers is essential for early detection of exacerbations and prevention of complications. This study aimed to compare white blood cell (WBC) differential counts, specifically neutrophils, eosinophils, and monocytes, between patients experiencing AECOPD and those with stable chronic obstructive pulmonary disease (COPD).
Methods: This cross-sectional observational study analysed data from 136 patients with chronic obstructive pulmonary disease treated at Wahidin Sudirohusodo Hospital from January 2024 to May 2025. Patients were categorized into two groups: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD; n = 68) and stable chronic obstructive pulmonary disease (COPD) (n = 68). Peripheral blood counts of neutrophils, eosinophils, and monocytes were measured. Statistical analyses included the chi-square test, Student’s t-test, Mann–Whitney U test, and receiver operating characteristic (ROC) curve analysis. A p-value of < 0.05 was considered statistically significant.
Results: Of the 136 patients with chronic obstructive pulmonary disease enrolled in this study, 68 (50%) were experiencing an acute exacerbation (AECOPD), while the remaining 68 (50%) were in a stable condition. Compared to patients with stable chronic obstructive pulmonary disease, those in the AECOPD group exhibited significantly higher neutrophil percentages and absolute neutrophil counts (p < 0.001). Conversely, both eosinophil percentage and absolute count were significantly lower in the AECOPD group (p < 0.001). Monocyte percentage was also significantly lower in AECOPD patients (p < 0.001), whereas absolute monocyte count was significantly higher (p = 0.018) compared to those of stable chronic obstructive pulmonary disease. Receiver operating characteristic (ROC) curve analysis identified optimal diagnostic cut-off values for neutrophil parameters. A neutrophil percentage cut-off of 69.8% demonstrated both a sensitivity and specificity of 82.4%, while an absolute neutrophil count cut-off of 6.76 x109/L demonstrated a sensitivity and specificity of 80.9%.
Conclusions: Differential counts of neutrophils, eosinophils, and monocytes may serve as simple and costefficient biomarkers for predicting acute exacerbations in patients with chronic obstructive pulmonary disease.
Chronic obstructive pulmonary disease (COPD) is a progressive pulmonary disorder characterised by airflow restriction, manifested by classic respiratory symptoms such as dyspnoea, and persistent coughing, with or without sputum production, resulting from structural changes in the airways and/or alveoli (1). Data from World Health Organization indicates that COPD is now the fourth major contributor to global mortality worldwide and a significant major to chronic morbidity (1,2). In 2021, COPD accounted for 3.5 million fatalities, with 90% of them happening in individuals under 70 years of age (3). The global incidence of COPD is forecast to reach an estimated 600 million cases by 2050 (4). Inflammatory cascades in the airway and lung are associated with various risk factors which have been identified as contributors to COPD, including cigarette smoking, biomass fuel exposure, occupational and environmental pollutants, genetic predisposition, impaired lung function trajectory, and childhood or adult respiratory infections (1,4).
Reducing the risk of exacerbation is central to COPD management, as acute exacerbations are related with increased inflammation, hospitalizations, worse lung function, and higher mortality (5-8). Approximately 46% of people with COPD encounter at least one exacerbation each year, and nearly 20% require hospitalization (9). Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are typically triggered by respiratory infections, inhalational irritants, comorbidities, or seasonal factors, resulting in intensified airway and systemic inflammation (8,10-11). Respiratory infections remain the primary triggers of AECOPD, with viral infections accounting for approximately 60% and bacterial infection for 40-50% of cases (12,13).
Since the predominant cause of AECOPD was infection, identifying reliable and accessible biomarkers are essential for early detection and appropriate management, especially in settings with limited access to immediate diagnostic resources (11-13). Components of the white blood cell (WBC) population, such as neutrophils, eosinophils, and monocytes, offer potential as cost-effective inflammatory markers. Previous studies have shown individuals with AECOPD exhibit higher levels of leukocytes and neutrophil counts, suggesting their utility in
distinguishing exacerbations from stable disease (14-16). Therefore, this study aimed to evaluate and compare WBC differential counts of neutrophils, eosinophils, and monocytes between AECOPD and stable COPD to assess their utility as predictive biomarkers.
MATERIALS AND METHODS
Study Population and Data Collection
This cross-sectional observational study was conducted at Wahidin Sudirohusodo Hospital in Makassar, Indonesia, from January 2024 to May 2025. A total of 136 patients with COPD were included based on electronic medical records and divided into two groups: 68 (50%) with AECOPD and 68 (50%) with stable COPD. The diagnosis was determined utilizing the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, confirmed by spirometry test showing a post-bronchodilator FEV₁/FVC ratio < 70% (1). AECOPD is characterized by recorded emergency room visits or hospital admissions due to an acute worsening of respiratory symptoms necessitating further intervention (1). Stable COPD is defined as the absence of symptom exacerbation in the past month (17). Inclusion criteria included patients aged 25 years or older who presented to outpatient clinic or emergency departments. Exclusion criteria were patients with incomplete CBC data. Demographic and clinical data were obtained from medical records. Demographic data included age, sex, smoking status, and brinkman index. The study was conducted with the highest ethical standards, with approval secured from the Hasanuddin University Research Ethics Committee (348/UN4.6.4.5.31/PP36/2025). All data were handled in compliance with ethical and data protection standards.
White Blood Cell Differential Counts
Laboratory data included both the percentage and absolute counts of neutrophils, eosinophils, and monocytes. Blood samples were collected upon admission to the emergency department for patients with AECOPD and during routine outpatient visits for those with stable COPD. The percentages of neutrophils, eosinophils, and monocytes were calculated as the proportion of each cell type relative to the total white blood cell count (x109/L)
and expressed as percentages. Absolute counts represented the actual number of each cell type per microlitre (µL) of blood and were expressed in SI units (x 109/L). Venous blood samples were collected in ethylenediaminetetraacetic acid (EDTA) tubes to prevent coagulation. To minimize pre-analytical variability, all samples were processed within 2 hours of collection. White blood cell differential counts were performed using the Mindray BC6800 automated haematology analyser, which employs a flow cytometric method based on dual-angle laser light scattering and fluorescence signals to perform complete blood counts (CBC) and five-part white blood cell differentials (18).
Statistical Analysis
Data were analysed using IBM SPSS Statistics, version 29. Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as means ± standard deviations or medians (interquartile ranges). The normality distribution was assessed with the Kolmogorov–Smirnov test. Comparison between group were conducted utilising the chi-square test for categorical data, and either the independent samples t-test or Mann–Whitney U test for continuous data. Receiver operating characteristic (ROC) curve analysis was used to calculate the sensitivity and specificity of neutrophils, eosinophils and monocyte in detecting COPD patients with acute exacerbation. Statistical significance was defined as a p-value < 0.05.
RESULTS
Baseline Characteristics of patients with AECOPD and Stable COPD
The mean age in the AECOPD group was 63.7 ± 12.8 years, while in the stable COPD group was 67.9 ± 10.5 years. Both groups showed a predominance of male patients. Smoking was prevalent in both groups, with 82.4% of AECOPD patients and 89.7% of stable COPD patients identified as current or former smokers. According to the Brinkman Index, most participants in
both groups were categorized as moderate smokers: 44.1% in the stable COPD group and 46.8% in the AECOPD group. Table 1 shows the basic characteristics of subjects in this study.
Comparative Analysis of WBC Differential Counts Between AECOPD and Stable COPD
The comparative analysis of WBC Differentials Counts between the two groups is presented in Table 2. Both the percentage (79.51% vs. 61.97%) and count of neutrophils (9.62 x 109/L vs. 4.54 x 109/L) were significantly higher in the AECOPD compared to the stable COPD (p < 0.001). The eosinophil percentages (0.75% vs. 5.15%) and eosinophil counts (0.072 x 109/L vs. 0.361 x 109/L) were significantly lower in AECOPD (p < 0.001) compared to stable COPD. The monocyte percentage was significantly lower in AECOPD (6.8% vs. 8.86%, p < 0.001), whereas the absolute monocyte count was significantly higher (0.78 x 109/L vs. 0.63 x 109/L, p = 0.018) compared to stable COPD.
Receiver operating characteristic (ROC) curve analysis was conducted to evaluate the diagnostic performance of neutrophils, eosinophils, and monocytes in detecting AECOPD. Optimal cut-off values were determined for both the percentage and absolute count of neutrophils, as well as for the absolute count of monocytes. A neutrophil percentage cut-off of 69.8% yielded a sensitivity and specificity of 82.4% (Table 3, Figure 1A). For neutrophil count, the optimal cut-off was 6.76 x 109/L, with a sensitivity and specificity of 80.9% (Table 3, Figure 1B). The best cut-off value for monocyte count was 0.677 x 109/L, which provided a sensitivity of 58.8% and a specificity of 60.3% (Table 3, Figure 1F). In contrast, eosinophil parameters and monocyte percentage demonstrated the lowest diagnostic accuracy. A cutoff value of 2.65% for eosinophil percentage provided a sensitivity of 20.6% and specificity of 17.6% (Table 3, Figure 1C), while an absolute eosinophil count cut-off of 0.229 x 109/L yielded a sensitivity and specificity of 29.4% (Table 3, Figure 1D). The cutoff for monocyte percentage was 7.65%, with both sensitivity and specificity at 32.4% (Table 3, Figure 1E).
Table 1. Basic Characteristics of patients with AECOPD and stable COPD
Variables
•
•
Brinkman Index
• Non-smoker
• Mild
• Moderate
• Severe
(17.6)
Note: *Independent samples t-test; **Chi-square test; Data presented as mean ± SD or numbers (%)
Abbreviation: AECOPD, acute exacerbation of chronic obstruction pulmonary disease; SD, Standard deviation.
Table 2. Comparative Analysis of WBC differential Counts Between AECOPD and Stable COPD
Variables
Note: *Independent samples t-test; ***Mann-Whitney U test; Data presented as mean ± SD or median (IQR) Abbreviations: AECOPD, acute exacerbation of chronic obstruction pulmonary disease; IQR, Interquartile range; SD, Standard deviation.
Table 3. The cut-off value, sensitivity dan specificity of neutrophils, eosinophils and monocytes in detecting AECOPD
Figure 1. Receiver operating characteristic (ROC) curves and corresponding area under the curve (AUC) values for differentiating acute exacerbation of COPD (AECOPD) from stable COPD: (A) ROC curve based on neutrophil percentage; (B) ROC curve based on absolute neutrophil count; (C) ROC curve based on eosinophil percentage; (D) ROC curve based on absolute eosinophil count; (E)ROC curve based on monocyte percentage; (F) ROC curve based on absolute monocyte count.
DISCUSSION
This study identified significant differences in the percentages and counts of neutrophils, eosinophils, and monocytes between patients had acute exacerbations of COPD and those with stable disease. COPD is a multifactorial, chronic inflammatory disorder primarily affecting the lung parenchyma and surrounding airways, involving diverse molecular pathogenic mechanisms (11,19,20). Several mechanisms have been proposed in the pathogenesis of COPD, including the inactivation of lung antiproteases, elevated oxidative stress, and persistent inflammation (21). The inflammatory response in COPD is typified by increased infiltration of immune cells such as macrophages, lymphocytes, neutrophils, and, in some patients, eosinophils—primarily within the pulmonary vasculature, peripheral airways, and lung tissue (20,21). During COPD exacerbations, both pulmonary and systemic inflammation are significantly intensified, most New Zealand Journal of
commonly triggered by an underlying infectious aetiology. This is reflected by elevated levels of inflammatory markers, contributing to an exaggerated systemic inflammatory response (11,15,22).
In the present study, both the percentage and absolute count of neutrophils were significantly higher in patients with AECOPD compared to those with stable COPD, consistent with findings from previous studies (14-16,22,23). Diagnostic ROC curve analysis identified optimal cut-off values for neutrophil parameters to distinguish between AECOPD and stable of COPD. A neutrophil percentage threshold of 69.8% demonstrated a sensitivity and specificity of 82.4%, while an absolute neutrophil count cut-off of 6.76 x 109/L achieved a sensitivity and specificity of 80.9%. These cut-offs are intended to support the identification of AECOPD in clinical settings. Neutrophilic inflammation during AECOPD is commonly triggered by infection, leading to an amplified systemic inflammatory response. As primary innate immune cells, neutrophils play a critical role during the acutephase response (21,24,25). Neutrophils are rapidly recruited from the vascular compartment to infected tissues in response to pathogen exposure, where they mediate various antimicrobial mechanism, predominantly through phagocytosis (24,25). During this process, neutrophil elastase (NE) is activated and released, contributing to microbial clearance but also contributing local tissue injury (24–26). Notably, neutrophils in the induced sputum of COPD patients also exhibit elevated levels of matrix metalloproteinases MMP-8 and MMP-9, which have been associated with disease exacerbations. Additionally, increased NE levels in sputum correlate with more frequent exacerbations of COPD (26). A study by Lonergan et al. reported elevated blood neutrophil counts in COPD patients were associated with a significantly elevated rates and severity of exacerbation episodes (27). Similarly, Yoon et al. demonstrated that elevated blood neutrophil counts were associated with a heightened risk of acute exacerbations over a three-year follow-up period (14). While neutrophil parameters show promise as adjunctive diagnostic tools, especially in resource-limited settings, they should be interpreted in conjunction with clinical assessment and other diagnostic indicators to improve diagnostic accuracy for AECOPD.
In this study, both the percentage and absolute count of eosinophils were significantly lower in patients with AECOPD compared to those with stable COPD. Similarly, Lv Mei-Yu et al. reported that COPD patients with blood eosinophil levels <2% exhibited significantly greater systemic inflammation, poorer lung function, longer hospitalization, and elevated fatalities compared to those with higher eosinophil levels (28). Ruiyang et al. also reported that patients with higher eosinophil levels experienced lower incidence of complications, less severe obstructive impairment, a predominance of non-infectious inflammation, and lower three-year mortality (29). A meta-analysis further reported that individuals with COPD and elevated eosinophil counts had lower mortality rates and shortened inpatient hospitalization than those with low eosinophil levels; however, they were slightly more predisposed be readmitted following discharge (30). In contrast, studies suggest that increased eosinophil counts were correlated with a heightened risk of exacerbations and responsiveness to inhaled corticosteroids (31–33). A study from Copenhagen involving a cohort of over 7,225 individuals with COPD found that higher eosinophil counts (>0.34 × 10⁹ cells/L) were correlated with a 1.76-fold enhanced susceptibility to severe exacerbations (33). In this study, eosinophil-related parameters exhibited the poorest diagnostic performance. The potential of blood eosinophils as a biomarker for COPD exacerbation risk continues to draw attention, though findings remain inconsistent (34).
Eosinophils, typically present in low numbers in peripheral blood and tissues, are most commonly associated with parasitic infections, as well as allergic and autoimmune disorders (21,32). Among individuals with COPD, sputum eosinophil counts are significantly higher in those with a history of asthma or allergy (21). Although eosinophil levels may also be elevated in the blood of COPD patients, blood and sputum measurements are poorly correlated and provide distinct prognostic insights (18). Furthermore, lower blood eosinophil counts have been linked to an increased risk of bacterial infections (35). Pavord et al. reported that patients with blood eosinophil levels < 2% experienced slightly greater incidence of pneumonia compared to those with levels ≥2%, regardless of inhaled corticosteroid use
(36).
In the present study, monocyte percentages were lower in patients with acute exacerbation of COPD (AECOPD), while absolute monocyte counts were higher compared to those with stable COPD. In contrast, a previous study reported significantly higher monocyte percentages and absolute counts at admission in AECOPD patients compared to healthy controls, with no substantial reduction observed during remission (37). The optimal cut-off value for absolute monocyte counts in detecting AECOPD was 0.677 x 109/L, yielding a sensitivity of 58.8% and a specificity of 60.3%. Monocyte percentage, however, demonstrated the poorest discriminative performance among the tested parameters. Given relatively low sensitivity and specificity observed, monocyte parameters demonstrated limited diagnostic performance and do not appear to be potential independent biomarkers for identifying acute exacerbations of COPD. A study conducted in Taiwan found that patients with a monocyte percentage >10% or <7.4%, combined with an absolute monocyte count <0.62 × 10⁹/L, had a significantly increased risk of AECOPD (38). The AECOPD risk matrix developed in Lin et al study indicated that both low monocyte percentages with absolute counts and isolated increases in monocyte percentage were associated with an elevated exacerbation risk in COPD (38).
Monocytes are primarily derived from the bone marrow and differentiate into macrophages in response to inflammatory stimuli (38,39). In individuals with COPD, these macrophages display impaired phagocytic and bactericidal functions, resulting in recurrent bacterial persistence, deposition of cellular debris, and chronic airway inflammation (39). The intensity and duration of smoking, major risk factors for COPD, are strongly associated with elevated circulating monocyte levels. Notably, elevated monocyte counts, particularly among individuals with substantial smoking histories, have been linked to greater risk of lung injury and increased mortality (40).
CONCLUSIONS
Routine blood tests, which are simple, accessible, and costeffective, can serve as useful indicators of the systemic inflammatory response in COPD. This study reveals that, relative to patients with stable COPD, those undergoing acute exacerbations had higher neutrophil counts and percentages, lower eosinophil counts and percentages, lower monocyte percentages, and higher absolute monocyte counts. Optimal diagnostic thresholds were established for neutrophil percentage, absolute neutrophil count, and absolute monocyte count.
Although this study established optimal diagnostic cut-off for neutrophil percentage, absolute neutrophil count, and absolute monocyte count in differentiating stable COPD from acute exacerbations, offering supportive value in clinical assessment, especially in resource-limited settings, several limitations should be considered before these findings are adopted in clinical practice. The relatively small sample size and single-centre design may limit the generalizability of the results, highlighting the need for external validation in larger and multi-centre populations.
ACKNOWLEDGMENTS
The authors acknowledge the Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, South Sulawesi, Indonesia for data analysis on this study. The authors also gratefully acknowledge the Indonesia Endowment Fund for Education (Lembaga Pengelola Dana Pendidikan - LPDP), Ministry of Finance of the Republic of Indonesia.
CONFLICT OF INTEREST AND FUNDING
The authors declare no conflicts of interest. No external funding was received for this study.
AUTHOR INFORMATION
Ria Mustika Baharuddin, MD, Resident in Internal Medicine1
Erwin Arief, MD, Pulmonologist and Lecturer in Internal Medicine1
Faridin HP, MD, Internist and Lecturer in Internal Medicine1
Syakib Bakri, MD, Professor of Internal Medicine1
Rahmawati Minhajat, MD, PhD, Professor of Internal Medicine1
Andi Alfian Zainuddin, MD, Lecturer in Public Health & Community Medicine2
1Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
2Department of Public Health and Community Medicine, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Corresponding author: Ria Mustika Baharuddin Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Email: ria.mustika.b@gmail.com
REFERENCES
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2024 GOLD Report: Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (Internet). 2024. (cited 01 July 2025). Available from https://goldcopd.org/2024-goldreport/
2. World Health Organization. The top 10 causes death (Internet). 7 August 2024. (cited 01 July 2025). Available from https://www.who.int/news-room/fact-sheets/detail/thetop-10-causes-of-death.
3. World Health Organization. Chronic obstructive pulmonary disease (COPD) (Internet). 6 November 2024. (cited 01 July 2025). Available from https://www.who.int/news-room/ fact-sheets/detail/chronic-obstructive-pulmonary-disease(copd).
4. Boers E, Barrett M, Su JG, Benjafield AV, Sinha S, Kaye L, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw Open 2023; 6(12): e2346598. doi: 10.1001/jamanetworkopen.2023.46598.
5. Zhang J, Chen F, Wang Y, Chen Y. Early detection and prediction of acute exacerbation of chronic obstructive pulmonary disease. Chin Med J Pulm Crit Care Med 2023; 1(2):102-107. doi: 10.1016/j.pccm.2023.04.004.
6. Vogelmeier CF, Román-Rodríguez M, Singh D, et al. Goals of COPD treatment: focus on symptoms and exacerbations. Respir Med 2020; 166:105938. doi: 10.1016/j.rmed.2020.105938.
7. Ritchie AI, Wedzicha JA. Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med 2020; 41(3):421438.doi: 10.1016/j.ccm.2020.06.00.
8. Crisafulli E, Barbeta E, Ielpo A, Torres A. Management of severe acute exacerbations of COPD: an updated narrative review. Multidiscip Respir Med 2018; 13: 36. doi: 10.1186/ s40248-018-0149-0.
9. Lim S, Lam DC, Muttalif AR, et al. Impact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: the EPIC Asia population-based survey. Asia Pac Fam Med 2015; 14: 4. doi: 10.1186/s12930-015-0020-9.
10. Qian Y, Cai C, Sun M, et al. Analyses of factors associated with acute exacerbations of chronic obstructive pulmonary disease: a review. Int J Chron Obstruct Pulmon Dis 2023; 18: 2707-2723. doi: 10.2147/COPD.S433183.
11. Ko FW, Chan KP, Hui DS, et al. Acute exacerbation of COPD. Respirology 2016; 21(7): 1152-1165. doi: 10.1111/ resp.12780.
12. Kuwal, A., & Joshi, V. (n.d.). Bacterial infection in hospitalized patients of acute exacerbation of COPD and their relation to lung function: A prospective study. European Respiratory Journal 2016; 48(suppl 60); OA1789. doi: 10.1183/13993003.congress-2016.OA1789.
13. Messous S. Elargoubi A, Pillet S, et al. Bacterial and viral infection in patients hospitalized for acute exacerbation of chronic obstructive pulmonary disease: implication for antimicrobial management and clinical outcome. COPD; 2021; 18(1): 53-61. doi: 10.1080/15412555.2020.1854210.
14. Yoon EC, Koo SM, Park HY, et al. Predictive role of white blood cell differential count for the development of acute exacerbation in Korean chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 2024; 19: 17-31. doi: 10.2147/COPD.S435921.
15. Şahin F, KoŞar AF, Aslan AF, et al. serum biomarkers in
patients with stable and acute exacerbation of chronic obstructive pulmonary disease: a comparative study. J Med Biochem 2019; 38(4): 503-511. doi: 10.2478/jomb-20180050.
16. Aida M. Yousef, Wael Alkhiary. Role of neutrophil to lymphocyte ratio in prediction of acute exacerbation of chronic obstructive pulmonary disease. Egypt J Chest Dis Tuberc 2017;16(1):43-48.doi:10.1016/j.ejcdt.2016.09.006.
17. Mao R, Liu Z, Zhao Y, et al. Stable chronic obstructive pulmonary disease (COPD) management under a tiered medical system in China. Int J Chron Obstruct Pulmon Dis 2022; 17: 181-194. doi: 10.2147/COPD.S333274.
18. Lee HT, Park PW, Seo YH, et al. Performance evaluation of Mindray CAL 8000(BC-6800 and SC-120) hematology analyzer and slidemaker/stainer. J Clin Lab Anal 2017; 31(4): e22065. doi: 10.1002/jcla.22065.https://doi. org/10.1016/j.pccm.2023.04.004.
19. Hikichi M, Mizumura K, Maruoka S, Gon Y Pathogenesis of chronic obstructive pulmonary disease (COPD) induced by cigarette smoke J Thorac Dis 2019; 11(Suppl 17): S2129-S2140. doi: 10.21037/jtd.2019.10.43
20. Xu J, Zeng Q, Li S, et al. Inflammation mechanism and research progress of COPD. Front Immunol 2024; 15: 1-11. doi: 10.3389/fimmu.2024.1404615.
21. Wechsler ME, Wells JM. What every clinician should know about inflammation in COPD. ERJ Open Res 2024; 10(5): 00177-2024. doi: 10.1183/23120541.00177-2024.
22. Perng DW, Chen PK. The relationship between airway inflammation and exacerbation in chronic obstructive pulmonarydisease. Tuberc Respir Dis (Seoul) 2017; 80(4): 325-335. doi: 10.4046/trd.2017.0085.
23. Taylan M, Demir M, Kaya H, et al. Alterations of the neutrophil-lymphocyte ratio during the period of stable and acute exacerbation of chronic obstructive pulmonary disease patients. Clin Respir J 2017; 11(3): 311-31.
24. Cowburn AS, Condliffe AM, Farahi N, et al. Advances in neutrophil biology: clinical implications. Chest 2008; 134(3): 606-612. doi: 10.1378/chest.08-0422.
25. JasperAE,McIverWJ,SapeyE,WaltonGM.Understanding the role of neutrophils in chronic inflammatory airway disease. F1000Res 2019; 8: F1000 Faculty Rev-557. doi: 10.12688/f1000research.18411.1.
26. Ham J, Kim J, Ko YG, Kim HY The dynamic contribution of neutrophils in the chronic respiratory diseases. Allergy Asthma Immunol Res 2022; 14(4): 361-378. doi: 10.4168/ aair.2022.14.4.361
27. Lonergan M, DickerAJ, Crichton ML, et al. Blood neutrophil counts are associated with exacerbation frequency and mortality in COPD. Respir Res 2020; 21(1): 166. doi: 10.1186/s12931-020-01436-7.
28. Lv MY, Qiang LX, Li ZH, Jin SD. The lower the eosinophils, the stronger the inflammatory response? The relationship of different levels of eosinophils with the degree of inflammation in acute exacerbation chronic obstructive pulmonary disease (AECOPD). J Thorac Dis 2021; 13(1): 232-243. doi: 10.21037/jtd-20-2178.
29. Ruiying W, Zhaoyun, Jianying X. Clinical features and three-year prognosis of AECOPD patients with different levels of blood eosinophils. Heart Lung 2022; 56: 29-39. doi: 10.1016/j.hrtlng.2022.05.012.
30. Liu H, Xie Y, Huang Y, et al. The association between blood eosinophils and clinical outcome of acute exacerbations of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Respir Med 2024; 222: 107501. doi: 10.1016/j.rmed.2023.107501.
31. Juthong S, Kaenmuang P Association between blood eosinophils with exacerbation and patient-reported outcomesinchronicobstructivepulmonarydiseasepatients in an endemic area for parasitic infections: a prospective study. J Thorac Dis 2020; 12(9): 4868-4876. doi: 10.21037/ jtd-19-4101.
32. Brusselle G, Pavord ID, Landis S, et al. Blood eosinophil levels as a biomarker in COPD Respir Med 2018; 138: 2131. doi: 10.1016/j.rmed.2018.03.016.
33. Vedel-KroghS,NielsenSF,LangeP,etal.Bloodeosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am
J Respir Crit Care Med 2016; 193(9): 965-74. doi: 10.1164/rccm.201509-1869OC.
34. Chen F, Yang M, Wang H, et al. High blood eosinophils predict the risk of COPD exacerbation: a systematic review and meta-analysis. PLoS One 2024; 19(10): e0302318. doi: 10.1371/journal.pone.0302318.
35. Mésinèle L, Pujol T, Brunetti N, et al. Association between low eosinophil count and acute bacterial infection, a prospective study in hospitalized older adults. BMC Geriatr 2023; 23(1): 852. doi: 10.1186/s12877-023-04581-y.
36.
37. Pavord ID, Lettis S, Anzueto A, Barnes N. Blood eosinophil countandpneumoniariskinpatientswithchronicobstructive pulmonary disease: a patient-level meta-analysis. Lancet Respir Med 2016; 4(9): 731-741. doi: 10.1016/ S2213-2600(16)30148-5. Yang J, Qiao M, Li Y, et al. Expansion of a population of large monocytes (atypical monocytes) in peripheral blood of patients with acute exacerbations of chronic obstructive pulmonary diseases. Mediators Inflamm 2018; 2018:9031452. doi: 10.1155/2018/9031452.
38. Lin CH, Li YR, Lin PR, et al. Blood monocyte levels predict the risk of acute exacerbations of chronic obstructive pulmonary disease: a retrospective case-control study. Sci Rep 2022; 12(1): 21057.
39. Shiba Prasad Dash, Saloni Gupta, Pranita P Sarangi. Monocytesandmacrophages:origin,homing,differentiation, and functionality during inflammation. Heliyon 2024;1 0(8): 1-14. doi: 10.1016/j.heliyon. 2024.e29686.
40. Sangani RG, Deepak V, Anwar J, et al. Cigarette smoking, and blood monocyte count correlate with chronic lung injuries and mortality. Int J Chron Obstruct Pulmon Dis 2023; 18: 431-446. doi: 10.2147/COPD.S397667.
rare presentation of apolipoprotein B - related familial hypobetalipoproteinaemia: a case report
Reza Nemati and Christopher J McEntyre
Familial Hypobetalipoproteinaemia or FHBL is an autosomal co-dominant inherited disorder of lipid metabolism. Individuals with biallelic apolipoprotein B (APOB) - related familial hypobetalipoproteinaemia (APOB-FHBL) may show clinical presentation from infancy through to adulthood. A 12-year-old boy with obesity (BMI 41kg/m2) presented with hip and lower limb pain. On examination, significant abdominal adiposity and acanthosis nigricans on the neck were seen. Abdominal ultrasound indicated fatty liver. Laboratory testing showed a low lipid profile, a low level of the fat-soluble vitamin E, and acanthocytosis was observed in the complete blood count (CBC). We present a case of FHBL and highlight the importance of persistence low lipid profile monitoring and the role of specific age-related reference interval for lipid profile and liver function tests.
Familial Hypobetalipoproteinaemia or FHBL is an autosomal codominant inherited disorder of lipid metabolism indicated by <5th percentile plasma level of low-density lipoprotein-cholesterol (LDL-C) or total apolipoprotein B that is caused by a mutation in the APOB gene. The symptoms include deficiency in fat soluble vitamins and gastrointestinal and neurological dysfunction. People with APOB-FHBL often have lower levels of plasma total cholesterol, and APOB levels compared to non-affected people for age and sex. Generally, acanthocytosis, increased plasma level of liver enzymes, and hyperbilirubinemia are observed. Clinically, these patients often present with hepatomegaly, steatorrhea, liver failure, and growth deficiency, but they may also be asymptomatic. In the absence of appropriate management, the patient can develop atypical pigmentation in the retina, progressive loss in tendon reflexes, vibratory sense, kinaesthesia, muscle pain and weakness, ataxia, steatohepatitis, or even life-threatening cirrhosis of the liver.
Individuals with heterozygous variant of APOB typically have a truncated gene that is associated with abnormal phenotype or increased risk of disease (i.e., pathogenic variant). The pathogenic variant can cause a mild or asymptomatic liver dysfunction and hepatic steatosis. Nevertheless, a small portion of people with the heterozygous variant can still develop severe non-alcoholic steatohepatitis. Severe non-alcoholic steatohepatitis needs medical care to avoid a very rare but possible chance of cirrhosis. Diagnosis is usually confirmed by molecular genetic testing. Lipid studies may reveal an unexpected low level of low-density lipoprotein-cholesterol (LDL-C). Unlike hypercholesteremia which is characterised by an increased blood plasma level of LDL-C, in hypocholesterolaemia a reduced LDL-C level is observed that can be caused either by genetic mutations or is acquired (1). Hypocholesterolaemia is defined when LDL-C is < 5th percentile or 1.29 mmol/L in the absence of lipid-lowering therapy (2). Usually, the genetic cause of the disorder can manifest in infancy or adulthood. Genetic causes of low LDL-C in early childhood include abetalipoproteinemia, a rare autosomal recessive disorder, by mutations in the gene encoding microsomal transfer protein (MTP) (3). MTP is responsible for the intracellular assembly of apolipoprotein B (APOB) and lipids in the liver and intestine (4). Due to the lack of APOB, very low-density lipoprotein (VLDL) and LDL-C is very near to zero. Therefore, high-density lipoprotein-cholesterol (HDL-C) is the only way to transport cholesterol and as a result APOE is increased because increased APOE expression on HDL particles enables them to bind to the LDL receptor (2). The other genetic cause of low LDL-C is chylomicron retention disease (Anderson's disease) (5). Anderson's disease is an autosomal recessive cause of low LDL-C by a mutation in SAR1B
(6). It has been shown that the most frequent genetic cause of low LDL-C is heterozygous familial hypobetalipoproteinaemia (FHBL) with the incidence of 1 in 10,000 or 0.01% (4). This genetic disorder is caused by a mutation in the APOB gene APOB makes APOB-100 and APOB-48. APOB-100 is the main lipoprotein to make VLDL, intermediate-density lipoprotein (IDL), LDL and lipoprotein (a). APOB-48 is derived from APOB-100, representing 48% of the APOB-100 sequence. It is involved in the formation of chylomicrons and chylomicron remnants. APOB exists in two isoforms in plasma: APOB-100, synthesized in the liver, and APOB-48, synthesized in the intestine. APOB-100 is the major structural component of VLDL, IDL, LDL, and Lp (a). APOB-100 is the ligand for the LDL receptor (LDLR) with the important role of clearing lipoprotein particles (8).
The aim of this case report is to summarise a confirmed case of APOB-FHBL in a 12-year boy with low apolipoprotein B (APOB) and LDL-C.
Case presentation and examination
The proband, a Caucasian 12-year-old male presented with hip and lower limb pain on a background of morbid obesity with BMI 41kg/m2 (weight 121 kg, height 172 cm) and obstructive sleep apnoea (by polysomnography). On examination, considerable abdominal adiposity, with significant striae on his back and acanthosis nigricans around his neck was observed. In the early clinical stages, diffuse hepatic steatosis indicative of fatty liver was detected via ultrasound. Additionally, early investigations revealed that his father had retinitis pigmentosa (RP), which was diagnosed when his father was five years old.
Diagnostic assessment
Lipid studies consequently showed low HDL-C and LDL-C. As HDL-C was low, different investigations were requested to investigate any underlying reason for obesity and/or dyslipidaemia. Fasting blood for complete blood count (CBC) to detect acanthocytosis, biochemical tests including thyroid function, lipase, and fat-soluble vitamin measurement (A, E, and D), HbA1C, apolipoprotein B (APOB) and apolipoprotein A1 (APOA1) with its ratio, and lipid profile was requested. There was no abnormality seen in thyroid function tests, and other routine biochemical tests. However, there were some low results in the lipid and lipoprotein profiles, and low plasma vitamin E was also observed. Table 1 shows more related information regarding laboratory tests done for the case.
In addition to biochemical and haematological testing, a genetic next generation sequencing test of DNA was performed on peripheral whole blood to find any possible linkage between elevated BMI with low LDL and APO (A1 and B). The sequencing
was performed on the panel of LDLR, APOB, PCSK9, APOE, and LDLRAP1, and a mutation in APOB was identified. The finding indicated a diagnosis of heterozygous APOB-FHBL in this patient, which is associated with primarily asymptomatic hepatic steatosis with rare clinical symptoms. The mutation that was identified, APOB c.3322_3323del p. (Gly1108Profs*5), is a rare deletion. This deletion introduces a frameshift in exon 21 which is predicted to result in nonsense-mediated decay (NMD) and a loss of function of this allele. This variant is classified as pathogenic (ACMG Class 5: PVS1, PM2). This variant along with the presence of low APOAB and extremely low LDL confirmed the diagnosis of heterozygous APOB-FHBL.
Treatment and management
Patients with homozygous APOB-FHBL typically have symptoms of fat malabsorption, steatorrhea, diarrhoea, failure to thrive, deficiencies in fat-soluble vitamins, and neurologic dysfunction along with hepatomegaly and steatosis. Such patients may need to be put on a low fat diet and supplemented with fat-soluble vitamins (5). However, the current case is a heterozygous form of APOB-FHBL, asymptomatic with mild liver dysfunction and steatosis and incidentally diagnosed. There is no need for special treatment or restriction in fat intake. It is only important to reduce risk factors, such as alcohol consumption and excessive calorie intake, and to have regular follow-ups to monitor for cirrhosis and/or hepatocellular carcinoma, which occur rarely (5,7,9). Follow up should also include liver function tests and, lipid profiles (every 2 years), as well as radiographic examinations such as hepatic ultrasonography (every three years) (7) . It is important to note that the low vitamin E result for the patient can be caused by hypolipidemia and/or malnourishment (obesity). Vitamin E supplement may be indicated in this case.
Table 1. Biochemical laboratory results
Tests Result Reference Interval*
Cholesterol (mmol/L) 1.5 2.88-5.23M
Triglycerides (mmol/L) 0.8 0.51-2.38
HDL cholesterol (mmol/L) 0.78 0.9-1.79M
LDL cholesterol (mmol/L) 0.3 1.18-3.4A, M
CHOL/HDL ratio 1.9 -
Apolipoprotein A1 (g/L) 0.8 1.18-3.4A
Apolipoprotein B (g/L) 0.18 0.31-0.84A, M
Apo B/Apo A1 ratio (mass ratio) 0.23 -
Total Bilirubin (µmol/l) 6 3-12A
Alk. Phosphatase (U/L) 224 141-460A, M
GGT (U/L) 27 7-21A
ALT (U/L) 37 9-25A, M AST (U/L) 24 14-35A, M
Total Protein (g/L) 73 65-81A
Albumin (g/L) 39 37-47A, M, B
Vitamin A(ug/L) 634 610-1330M, IH
Vitamin E (µmol/L) 8 17-32IH
Vitamin D (nmol/L) 60 50-150Diasorin
*All Reference intervals adopted from CALIPER (https://caliper. research.sickkids.ca/#/), except vitamin A and E. A, Abbott Architect; B Bromocresol purple; IH in-house method, M, reference interval in males.
DISCUSSION
Heterozygous APOB-FHBL is often diagnosed incidentally due to its asymptomatic nature or mild liver dysfunction (7). To diagnose and evaluate this condition effectively, it is important to start by obtaining a comprehensive patient history, including a detailed
family history of low LDL-C in first-degree relatives, and assessing for any concurrent or recent severe underlying diseases. Following this, conduct a thorough physical examination to identify any relevant signs such as hepatomegaly, jaundice or any indicators of liver disease. Hypocholesterolaemia can be attributed to both secondary and primary causes; secondary factors should be considered first, while primary hypocholesterolaemia often results from genetic mutations affecting cholesterol absorption, biosynthesis, or metabolism. Table 2 shows the most common primary and secondary causes of hypocholesterolaemia plus assay interferences.
In infants or early childhood with malabsorption, diarrhoea, and failure to thrive, the differential diagnosis needs to include abetalipoproteinemia, homozygous familial hypobetalipoproteinaemia, and chylomicron retention disease. An undetectable LDL-C indicates either abetalipoproteinemia or homozygous hypobetalipoproteinaemia and if LDL-C is detectable but low (0.39 mmol/L), this suggests the presence of Anderson’s disease (11).
FHBL is a dominantly inherited condition, meaning that if one parent is affected, there is a 50% chance that the offspring will inherit the condition (13). Parental testing is helpful in identifying this condition (5). An easy way to start is by measuring Apolipoprotein B (APOB). Once a low level of APOB is detected, genetic testing can be performed to confirm the diagnosis. It is crucial to mention that all first-degree relatives should be screened through cascade screening. This includes siblings, as they may also carry the same genetic mutation and be at risk for the condition. Genetic counselling is vital for parents who have a child diagnosed with FHBL, especially if they wish to have more children. During genetic counselling, parents are informed about the inheritance patterns and risks associated with FHBL, as well as the availability and role of pre-implantation genetic testing (PGT). This information helps parents make informed reproductive choices and understand the genetic implications for future offspring. PGT allows embryos to be screened for the specific genetic mutation before implantation during in vitro fertilisation (IVF). This can help parents have children who do not carry the genetic mutation. It is also recommended for other siblings and other first-degree relatives to undergo genetic testing to determine their risk and take appropriate preventive measures if needed. In this group of patients, it is recommended that they be monitored and managed at a lipid clinic (13).
There is no specific treatment for APOB-FHBL. Treatment for heterozygous FHBL typically focuses on managing symptoms and preventing complications, especially those related to fat malabsorption and vitamin deficiencies (5). There are several general approaches for managing FHBL, including dietary management and regular monitoring. Dietary management involves supplementation with fat-soluble vitamins (A, D, E, and K)and adjustments to ensure a balanced diet rich in essential fatty acids and nutrients, along with increased fat consumption. Regular liver function tests and blood tests for nutrient status are also recommended to monitor and maintain optimal health. Additionally, healthy lifestyle and avoidance of alcohol consumption are recommended (14).
At the early stage of the investigations, no abnormality was seen on the patient’s liver function tests (LFTs) because they did not flag according to the testing lab’s reference intervals. However, ultrasound detected fatty liver. Therefore, having a specific reference interval for adolescents may be useful to better manage patients. The role of the laboratory is crucial in defining a reasonable reference interval. Establishing accurate reference ranges is essential for the correct interpretation of test results, because it helps to differentiate between normal and abnormal values. This ensures that healthcare providers can make informed decisions based on reliable data, improving diagnostic accuracy and patient care. In addition, there are several disorders that can mimic hypocholesterolaemia such as liver dysfunction (cirrhosis or hepatitis), hyperthyroidism, chronic anaemia, malnutrition and acute illness; thus the laboratory plays
a crucial role to assist in making a more accurate diagnosis.
Table 2. Most common causes of low LDL-C.
Hypocholesterolaemia Causes (9)
Primary Secondary
Abetalipoproteinemia
Hypobetalipoproteinaemia
Chylomicron retention disease
Familial combined hypolipidemia
PCSK9 deficiency
Primary bile acid malabsorption
Smith-Lemli-Opitz syndrome
Anaemia
Hyperthyroidism
Malignancy
Severe liver disease
End-stage renal disease
Critical illness
Severe physiological stress
Cachexia and malabsorption
Strict vegan diet
High-dose lipid lowering therapy
*N-acetylcysteine and N-acetyl-p-benzoquinoneimine
CONCLUSION
Any persistent hypolipidemia should be considered for FHBL, especially when along with even a mild liver dysfunction. This case study also shows how important is to have a paediatric specific reference interval for lipid profile and liver function tests.
ACKNOWLEDGMENTS
We would like to sincerely thank Dr. Simon Thompson for his invaluable guidance, insightful feedback, and significant contribution to the preparation and writing of this case report. His expertise and support were essential throughout the process.
AUTHOR INFORMATION
Reza Nemati, PhD, Medical Laboratory Scientist1 Christopher James McEntyre, PhD, Scientific Officer1
1 Specialist Chemistry, Canterbury Health Laboratories, Christchurch, New Zealand
Corresponding Author: Reza Nemati, Specialist Chemistry, Canterbury Health Laboratories, Christchurch, New Zealand Email: reza.nemati@cdhb.health.nz
REFERENCES
1. Vyroubal P, Chiarla C, Giovannini I, et al., Hypocholesterolemia in clinically serious conditions-review. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2008; 152(2): 181-189.
2. Rosenson RS, Durrington P. Low LDL-cholesterol: etiologies and approach to evaluation. UpToDate. Waltham (MA): UpToDate. [accessed 14 August 2022]. https://www. uptodate.com/contents/search.
3. Sirtori CR, Pavanello C, Bertolini S. Microsomal transfer protein (MTP) inhibition-a novel approach to the treatment of homozygous hypercholesterolemia. Ann Med 2014; 46(7): 464-474.
4. Linton M, Farese R, Young S. Familial hypobetalipoproteinemia. J Lipid Res 1993; 34(4): 521-541.
5. Burnett JR, Hooper AJ, Hegele RA. APOB-related familial hypobetalipoproteinemia. 2021 In: Adam MP, Feldman J, Mirzaa GM, et al. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025.
Common assay interferences caused by supplements (11, 12)
NAC & NAPQI*
Vitamin C
6. Peretti N, Sassolas A, Roy CC et al. Guidelines for the diagnosis and management of chylomicron retention disease based on a review of the literature and the experience of two centers. Orphanet J Rare Dis 2010; 5(1): 1-13.
7. Park SY, Kim HS, Chu MA et al., Case report of familial hypobetalipoproteinemia: a novel APOB mutation and literature review. Ann Pediatr Endocrinol Metab 2023; 28(Suppl1): S9-11
8. Bednarska-Makaruk M, Ługowska A. Rare monogenic disorders of cholesterol metabolism, [In Cholesterol 2022, Elsevier. 553-607].
9. McRae MP. Vitamin C supplementation lowers serum low-density lipoprotein cholesterol and triglycerides: a meta-analysis of 13 randomized controlled trials. J Chiropr Med 2008; 7(2): 48-58.
10. Genzen JR, Hunsaker JJ, Nelson LS et al. N-acetylcysteine interference of trinder-based assays. Clin Biochem 2016; 49(1-2): 100-104.
11. Levy E, Poinsot P, Spahis S. Chylomicron retention disease: genetics, biochemistry, and clinical spectrum. Curr Opin Lipidol 2019; 30(2): 134-139.
12. Schonfeld G. Familial hypobetalipoproteinemia: a review. J Lipid Res 2003; 44(5): 878-883.
13. Burnett JR, Bell DA, Hooper AJ, et al., Clinical utility gene card for: Familial hypobetalipoproteinaemia (APOB)–Update 2014. Eur J Hum Genet 2015; 23(6): 889-889.
14. Bredefeld C, Hussain MM, Averna M, et al. Guidance for the diagnosis and treatment of hypolipidemia disorders. J Clin Lipidol 2022; 16(6): 797-812.
Unravelling the presence of multiple alloantibodies and autoantibodies in a patient - a case report from a tertiary care centre in Malaysia
Rabeya
Yousuf, Kaalpana Jayakumar, Siti Nurrazan Zulkifli, Nur Afifah Suhemi, Nor Fadzliana Abdullah Thalith, Yee Loong Tang, Hari Priya Raghvan and Qhasmira Abu Hazir
ABSTRACT
Detection of multiple antibodies during pre-transfusion testing is a complicated and time-consuming process that might delay bloodsupply However,itiscrucialtosupplyantigen-negativecrossmatchcompatiblebloodtopreventtransfusion-relatedadverse events. Here we report a case of multiple alloantibodies with autoantibodies in a 42-year-old patient with multiple comorbidities. She was admitted for left forearm cellulitis and had multiple history of blood transfusions, including recent transfusion (less than three months). During the current admission, two units of red cells were requested due to symptomatic anaemia. The patient was grouped as O RhD positive with positive antibody screening on pre-transfusion investigation.Antibody identification showed pan reactivity with variable reaction strengths with positive auto control in which multiple alloantibodies were suspected. Direct antiglobulin test (DAT) was positive with anti-IgG monospecificity The elution study revealed pan-agglutination of similar reaction strength which indicate presences of non-specific auto-IgG. Further extended test of alloadsorption with selected enzyme-treated donor cells of i) R1R1, Jk(a+b-), K- ii) R1R1, Jk(a-b+), K- and iii) R2R2, Jk(a+b-), K-, confirmed the presence of anti-E, anti-c, anti-Jkb and anti-S. The patient’s probable red cell phenotypes were R1R1, ss, kk, with inconclusive Kidd and MN phenotyping due to recent transfusion. Patient had subsequently received antigen-negative blood accordingly and the transfusion was uneventful. The presence of multiple alloantibodies indeed complicates the investigation process. However, with advanced immunohaematology methods, we have successfully identified all the clinically significant antibodies. Keywords: Multiple alloantibodies, Autoantibody, Alloadsorption
NZ J Med Lab Sci 2025; 79(3): 120:124
INTRODUCTION
The presence of multiple alloantibodies discovered during the pre-transfusion testing complicates subsequent selection of red cells for transfusion (1). The hurdle includes delay in transfusion due to difficulty in obtaining compatible blood without the antigen. As opposed, if antigen-negative red cells cannot be provided, presence of alloantibody together with the corresponding antigen will decrease the survival of transfused red cells (2). Therefore, it is crucial to supply the corresponding antigen-negative and crossmatch compatible blood to prevent transfusion-related adverse events, which might lead to haemolysis (1).
Red cell alloimmunization occurs when the patient is exposed to a non-self-antigen through previous transfusion or pregnancy (3). There are numerous RBC antigens present which differ structurally and functionally (4). Only a minority of transfusion recipients will ever develop detectable RBC alloantibodies from hundreds of non-self RBC antigens in every transfused RBC unit. For an alloantibody to develop, an individual must, at least be exposed to a non-self RBC antigen and have an HLA-binding motif capable of presenting a portion of the non-self-antigen (5).
The reagent red cells or donor red cells with known phenotypes can be used for antibody identification or alloadsorption (6).
The process of identification of multiple alloantibodies is a complicated and time-consuming process that includes different immunohaematological tests, such as using extended cell panel or selective cells or using enzyme, elution, adsorption, neutralization, titration and other specialized tests (7). A skilled workforce is also very important to perform the different tests (6).
In this case report, we highlighted a patient with multiple alloantibodies and autoantibodies and the methodical workup done during pre-transfusion testing to identify the antibody specificities.
CASE REPORT
This patient is a 42-year-old female with diabetes mellitus, hypertension, ischemic heart disease and end-stage-renalfailure (ESRF), admitted for left forearm cellulitis. She had previous history of hospitalisation at our centre two months prior for sepsis secondary to left forearm cellulitis and her underlying ESRF complications. She also had a recent history of two units of red cell transfusion during her previous admission. At that time, antibody screening was negative, and she was
transfused with group O RhD positive crossmatched compatible blood at 37°C and anti-human globulin (AHG) phase by using column agglutination technique. For current admission, she had symptomatic anaemia with haemoglobin of 72 g/L and required two units of red cells transfusion during haemodialysis.
A blood sample was sent for group, screen and crossmatch (GXM). Test was run by using Bio-Rad automated analyser IH500 which revealed the patient’s blood group of O RhD positive and antibody screening was positive in all three screening cells with different reaction strength. The antibody screening was repeated manually with the Bio-Rad three cell screening panel (ID-DiaCell I-II-III Asia) using gel card which revealed a similar reaction (Figure 1 and Table 1). Antibody identification using BioRad 11-cell panel with plain and papain treated cells showed pan-agglutination of variable strength with positive auto control (2+) (Figure 2 and Table 2). Direct antiglobulin test (DAT) was positive with polyspecific AHG (3+) and monospecific Anti-IgG (2+). Acid elution study revealed pan-agglutination of similar reaction strength. These findings were suggestive of non-specific auto-IgG with concomitant presence of clinically significant alloantibodies. In view of the recent transfusion, autoadsorption was not done. To identify the alloantibodies, we proceeded with alloadsorption using three different RBC phenotypic donor cells and tested at plain and papain phase. First alloadsorption was done with R1R1, Jk(a+b-) and K negative cells and the postadsorbed plasma was tested with the 11-cell panel. The result showed likely presence of anti-E, anti-c and anti-Jkb (Figure 3 and Table 3) in correlation with the individual strength of reaction for each corresponding antibodies with the selective positive panel cells of phenotype specific. This was further supported by the patient’s probable Rhesus phenotyping of R1R1 with red cell phenotyping for Jkb antigen negative. Second alloadsorption was done with R1R1, Jk(a-b+) and K negative cells and testing the post-adsorbed plasma further confirmed the presence of anti-E, anti-c with highly suspicious of anti-S (Figure 4 and Table 4). Anti-E and anti-c were confirmed due to stronger reaction at the E positive cells 3 and 5 and stronger reaction at c positive cells 4 respectively. This was also based on the individual strength of reaction of the corresponding antibodies with the selective positive panel cells of phenotype specific. Thus, anti-S cannot be excluded in view of positive reaction seen at the S positive cells 2. Patient’s probable red cell phenotyping for S
antigen was also negative. The final alloadsorption with R2R2, Jk(a+b-) and K negative cells and subsequent testing of the adsorbed plasma confirmed the presence of anti-Jkb and anti-S (Figure 5 and Table 5). These two antibodies corresponded with variable strengths of reactions on the panel cells respectively for anti-Jkb and anti-S, further correlating with the patient’s probable red cells phenotype.
As mentioned before, patient had previous history of blood transfusion which was less than three months prior to this admission. There was no baseline Rhesus or red cells phenotyping in our centre. Based on current testing, the probable red cell phenotyping was R1R1, kk, ss with inconclusive Duffy, Kidd and MN phenotyping. The inconclusive phenotyping was
due to mixed field reaction strength from recent transfusion. It was recommended to repeat red cell phenotyping three months from the last transfusion or to send for red cells genotyping which need to be outsourced to the reference centre for confirmation. At this point, based on the all the immunohaematological testing results, we concluded the presence of multiple alloantibodies of anti-E, anti-c, anti-Jkb, anti-S and non-specific auto-IgG. For transfusion, red cells of group O, R1R1, Jkb antigen and S antigen negative, crossmatched least incompatible with the plain plasma were supplied. The transfusion was closely monitored and it was uneventful. Table 6 summarises the results of immunohaemotological tests done for this patient.
Positive antibody screening (indirect antiglobulin test) and positive elution test.
Table 2. Antibody identification showed pan-agglutination of variable strength with positive auto control of 2+ suggestive of presence of auto-IgG with multiple alloantibodies.
Table 3. Antibody identification of post-adsorbed plasma (alloadsorption using R1R1, Jk(a+b-), and K- donor cells) showed likely presence of anti-E, anti-c and anti-Jkb.
Table 4. Antibody identification of post-adsorbed plasma (alloadsorption using R1R1, Jk(a-b+), and K- donor cells) showed the presence of anti-E, anti-c and unable to exclude anti-S.
Table 1.
Table 5. Antibody identification of post-adsorbed plasma (alloadsorption using R2R2, Jk(a+b-) and K- donor cells) confirmed the presence of anti-Jkb and anti-S.
Alloadsorption with R2R2
with R2R2
Table 6. Results of immunohaematological testing
ABO and RhD Blood Group
Probable Rh genotype
Other probable red cell phenotype
DAT polyspecific
DAT monospecific
Acid elution
Antibody screening (3-cell panel)
Antibody identification (11-cell panel)
First alloadsorption with R1R1, Jk(a+b-) and K- cell
Second alloadsorption with R1R1, Jk(a-b+) and K-cell
Final alloadsorption with R2R2, Jk(a+b-) and K- cell
Antibodies detected
O RhD positive
CDe/CDe (R1R1)
kk, ss and inconclusive for Duffy, Kidd and MN
Positive (2+)
Positive anti-IgG (2+), negative anti-C3d
Pan-agglutination of similar strength
Pan-agglutination (different strength)
Pan-agglutination (different strength)
Likely presence of anti-E, anti-c and anti-Jkb
Confirmed anti-E, anti-c and unable to exclude anti-S
Confirmed anti-Jkb and anti-S.
Anti-E, anti-c, anti-Jkb, anti-S and non-specific auto IgG autoantibody
Figure 1. Positive antibody screening (indirect antiglobulin test) and positive elution test, Bio-Rad I-II-III Asia Screening panel.
Figure 2 Antibody identification showed pan-agglutination of variable strength with positive auto control of 2+ suggestive of presence of auto-IgG with multiple alloantibodies (Bio-Rad 11 cell panel).
Figure 3. Antibody identification of post-adsorbed plasma (alloadsorption using R1R1, Jk(a+b-), and K- donor cells) showed likely presence of anti-E, anti-c and anti-Jkb.
Figure 4. Antibody identification of post-adsorbed plasma (alloadsorption using R1R1, Jk(a-b+), and K- donor cells) showed the presence of anti-E, anti-c and unable to exclude anti-S.
Figure 5. Antibody identification of post-adsorbed plasma (alloadsorption using R2R2, Jk(a+b-) and K- donor cells) confirmed the presence of anti-Jkb and anti-S.
DISCUSSION
Red cell alloimmunisation is a common adverse effect in patients having multiple transfusions as seen in our patient. The frequency of alloimmunisation varies from 2.6% to 9% in multitransfused hospitalised patients while a higher frequency of 3.7 to 50% is noted in thalassaemia patients (8). The underlying factors that influence the alloimmunisation are the antigenic difference between recipient and donor, the recipient’s immune status, recipient’s age of first transfusion, dose of transfusion and the immunogenicity of the red cell antigen (7,9). It is challenging work to identify multiple alloantibodies, where extended cell panels are required and special techniques need to be applied.
In this patient, we suspect multiple alloantibodies as the reaction pattern did not match a single antibody specificity or did not show any distinct antibody pattern, and the reaction strengths were variable. The red cell elution test results were of similar strength, suggestive of nonspecific auto IgG as DAT was positive with IgG monospecificity and positive auto control.
In our patient, due to history of recent transfusion, it was not recommended to proceed with auto-adsorption to determine the presence of alloantibodies. The solution was to proceed with an extended supplementary test which involves alloadsorption with selected donor cells. This was indeed a complex process in which
the selection of certain donor cells was taken into consideration for possibilities only. Adsorption removes or adsorbs antibodies from plasma by incubating the sample with red cells possessing the corresponding antigen whereby the antibody binds to the red cell antigen and thus is removed from the plasma. The antigen-antibody complex or the adsorbed cell is separated from the adsorbed plasma by centrifugation and subsequently the adsorbed antibody to the cell can be separated using elution methods and tested against RBC panel for specificity identification. The adsorbed plasma can also be tested using RBC panel to detect the unabsorbed remaining alloantibody and to proceed for crossmatching (10).
Alloadsorption is recommended if the patient’s phenotype is unknown and DAT is positive or if the patient is recently transfused. Group O, R1R1, R2R2 and rr donor cells are used where one cell should be negative for K, another negative for Jka and another negative for Jkb antigen. (10).
In our patient, we used two R1R1 and one R2R2 cells including cells negative for K, Jka and Jkb antigen. The alloadsorption with selected donor cells has proved the presence of anti-E, anti-c, anti-Jkb and anti-S. This patient’s DAT is also positive with monospecific Anti-IgG (2+) and auto-control strength of 2+. Further test with acid elution reveals presence of non-specific auto-IgG.
The significance of differentiating presence of autoantibodies with alloantibodies is crucial in transfusion field as autoantibodies may coat the cells, forming a "mask" over the alloantibodies that would otherwise react with antigens on the donor's cells. Essentially, the autoantibodies obscure or hide the presence of the alloantibodies that would normally participate in the crossmatch reaction. Despite the autoantibodies masking the alloantibodies, the crossmatch may still appear incompatible because the autoantibodies are interfering with the ability of the test to detect the true interaction between the recipient's alloantibodies and the donor's antigens. This can lead to a false impression of incompatibility been the donor and recipient, even though the crossmatch might have been compatible had the autoantibodies not been present. Therefore, it is highly recommended to supply crossmatch compatible with autoabsorped plasma and antigen negative red cells in such cases to minimize antibody-mediated destruction of transfused red cells. However, in our case the patient has recent history of blood transfusion therefore restrict the decision to supply crossmatch least incompatible (weaker than auto-control) red cells with patient’s original plasma and antigen negative red cells.
She was supplied with two units of group O, R1R1, Jkb antigen-negative, S antigen-negative least incompatible red cells and the transfusion was uneventful. This whole process of identifying, resolving and supplying red cells for this patient took us whole three working days. Time is very crucial; at the same point it is also important to supply correct blood to ensure patient safety. Clinician were very understanding with the complicated work process and decided to wait for confirmation rather than to rush for transfusion. In this case, patient was haemodynamically stable and had no evidence of bleeding, the transfusion was still necessary to correct the anaemia and proceed for operation. Besides that, red cells phenotyping using serological method in recently transfused patient may not be feasible like in our patient as some of the results were inconclusive. In such instances, red cell genotyping can be utilised (10).
CONCLUSION
This case highlights the importance of thorough immunohaematological workup in identifying complex antibody, including clinically significant alloantibodies. The identification of such antibodies through methods like alloadsorption underscores the need for advanced expertise in immunohaematology to ensure appropriate management of transfusion. Mastery of these techniques is crucial in resolving challenging cases and minimizing risks to patient safety.
ACKNOWLEDGEMENTS
We would like to express our gratitude to the hospital management and staff for making the publication of this case possible.
AUTHOR INFORMATION
Rabeya Yousuf, MBBS, MSC1
Kaalpana Jayakumar, MBBS 1
Siti Nurrazan Zulkifli, MBBS 2
Nur Afifah Suhemi, MBBS 1
Nor Fadzliana Abdullah Thalith, Dip MLT1
Yee Loong Tang, MD, DrPath, (Haematology)3
Hari Priya Raghvan MD, (Haematology) 2
Qhasmira Abu Hazir, MBBS, DrPath (Haematology)1
1 Blood Bank Unit, Department of Laboratory Diagnostic Services, Hospital Canselor Tuanku Muhriz, National University of Malaysia, Kuala Lumpur, Malaysia.
2 Department of Pathology, Faculty of Medicine, National University of Malaysia, Kuala Lumpur, Malaysia.
3 Laboratory Department, Sunway Medical Centre Velocity, Kuala Lumpur, Malaysia.
Corresponding author: Dr. Qhasmira Binti Abu Hazir, Blood Bank Unit, Department of Diagnostic Laboratory Services, Hospital Canselor Tuanku Muhriz, National University of Malaysia, Kuala Lumpur, Malaysia.
Email: qhasmira@hctm.ukm.edu.my
REFERENCES
1. Bhuva DK, Vachhani JH. Red cell alloimmunization in repeatedly transfused patients. Asian J Transfus Sci 2017;11(2): 115-120.
2. El-Beshlawy A, Salama AA, El-Masry MR, et al. A study of red blood cell alloimmunization and autoimmunization among 200 multitransfused Egyptian β thalassemia patients. Sci Rep 2020; 10(1): 21079.
3. Hendrickson JE, Tormey CA. Understanding red blood cell alloimmunization triggers. Hematology Am Soc Hematol Educ Program 2016; 2;2016(1): 446-451.
4. Reid ME, Mohandas N. Red blood cell blood group antigens: structure and function. Semin Hematol 2004; 41(2): 93-117.
5. Hendrickson JE. Red blood cell alloimmunization and sickle cell disease: a narrative review on antibody induction. Ann Blood 2020; 5: 33.
6. Ray GK, Mukherjee S, Sahoo D, et al. Resolution of the complexity of transfusion support by alloadsorption in a patient of thalassaemia intermedia with multiple alloantibodies. J Appl Hematol 2020; 11: 195-198.
7. Walker PS, Hamiltaon JR. Identification of antibodies to red cell antigens. In: Fung MK, Grossman BJ, Hillyer CD, Westhoff CM, eds. Technical Manual 18th ed. Bethesda, Maryland: AABB. 2014; 391-424.
8. Thapa S, Jagannathan L, Mathur A, et al. Systematic approach in identification and management of multiple alloantibody: A case of triple alloantibody. Glob J Transfus Med 2019; 4: 93-95.
9. Pahuja S, Chauhan R, Sharma G, et al. Dual Red Cell Alloimmunization with Anti-c and anti-E Antibodies. A Systematic Approach to Workup and Transfusion Management in Different Clinical Scenarios in ResourceLimited Settings. Glob J Transfus Med 2023; 8(1): 71-78.
10. Yadav BK, Chaudhary RK, Elhence P, et al. Red cell alloimmunization and associated risk factors in multiply transfused thalassemia patients: A prospective cohort study conducted at a tertiary care center in Northern India. Asian J Transfus Sci 2023; 17(2): 145-150.
Otago BMLSc student research project abstracts: Semester 1, 2025
Change in probable passive anti-D prevalence in Canterbury, New Zealand
Laurraine Aperocho1 and Krishna Badami2
1University of Otago, Dunedin and 2New Zealand Blood Service, Christchurch
Objectives: The detection of probable passive anti-D (PPAD) during red cell antibody screening (RCAS) has become increasingly common, presenting challenges in clinical interpretation and management. PPAD results from the presence in RCAS samples, of prophylactic RhD immunoglobulin (RhIG), which is widely administered to Rh-D negative individuals, especially during pregnancy, and in other females with childbearing potential, at risk of alloimmunization. In Canterbury New Zealand, the growing uptake of routine antenatal anti-D prophylaxis (RAADP) has coincided with a notable rise in PPAD determinations. We aimed to assess prevalence of PPAD in Canterbury from 2015 to 2024, identify contributing factors, including RhIG administration, and adherence to testing guidelines.
Methods: A retrospective review of RCAS and antibody identification data from Christchurch Hospital between January 2015 and December 2024 was conducted. PPAD prevalence was calculated annually and compared with RhIG administration rates. Repeat RhIG dosing patterns were also analysed.
Results: Among 179,529 individuals tested, 1,807 (1.0%) had PPAD determined of whom 96.8% were females. PPAD prevalence increased over the study period, mirroring the 49.3% rise in RhIG administration. The majority of the RhIG doses were the 625 IU formulation used in RAADP. Poor adherence to guidelines recommending pre-RhIG RCAS blood sampling appears to be the primary driver of rising PPAD prevalence, compounded by increased RAADP uptake and improved antibody detection methods.
Conclusion: The rising prevalence of PPAD in Canterbury reflects both improved RhIG prophylaxis coverage and suboptimal adherence to testing protocols. However, the decline in immune anti-D occurring at the same time supports the effectiveness of RAADP and improved transfusion practices. Strengthening compliance with RCAS testing is essential to optimise the RhIG use and improve maternal-fetal outcomes.
A comparative evaluation of Gill’s II and Harris’ haematoxylin for use in haematoxylin and eosin staining at the Oral Pathology Centre
Abigail Bennett, Remeny Weber and Benedict Seo University of Otago, Dunedin
Objectives: Haematoxylin and Eosin (H&E) staining is a fundamental technique in histology, essential for accurate assessment and diagnosis of patient samples. This research compares the current H&E staining method in the Oral Pathology Laboratory (progressive staining using Gill’s II haematoxylin) with alternative methods utilising Harris’ haematoxylin, with the aim of determining whether the new approach provides improved staining quality.
Methods: Eight different rat tissue types were selected to ensure a representative range of histological samples. Both progressive and regressive H&E staining methods using Harris haematoxylin were optimised through multiple rounds of testing prior to evaluation. For assessment, pathologists were presented with forty H&E slides (five per tissue type). These included one slide stained with the current Gill’s II protocol, and four slides stained with Harris haematoxylin – two using progressive methods and two using regressive methods, each with slight procedural variations. The slides were graded on a five-point scale in a blinded manner, without knowledge of the staining methods used.
Results: Initial results indicate a significant improvement in staining quality with the use of Harris haematoxylin in both progressive and regressive methods. When compared to Gill’s II haematoxylin, Harris haematoxylin produced sharp and more defined nuclear staining. It also enhanced contrast with eosin, resulting in a clearer distinction between nuclear and cytoplasmic material.
Conclusion: These findings support the implementation of Harris haematoxylin as a superior alternative to Gill’s II for improved H&E staining quality at the Oral Pathology Centre.
Investigating carry-over contamination in Levetiracetam assays on the AU5822 Beckman Coulter analyser
Ash R Brett1 and Hank Ploeg2 1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives: Levetiracetam, manufactured by ARK, is a widely used antiepileptic requiring accurate therapeutic-drug monitoring. Because it is not a manufacturer-validated assay on the AU5822, carry-over contamination could compromise patient management. This study aimed to determine whether levetiracetam transfers to and from other routine chemistry assays on the AU5822 and identified any need for corrective measures such as additional wash cycles.
Methods: Carry-over was assessed using a donor-recipient sequence on the AU5822. For the forward sequence (levetiracetam to other assays), five initial saline “blank” assays were run to equilibrate the system, followed by five baseline measurements of each recipient analyte. Next, five high-concentration levetiracetam (donor) samples were analysed consecutively, immediately followed by five postdonor measurements of each recipient analyte. The first postdonor result was compared to the average of the five baseline measurements and to the subsequent four post-donor results; a significant deviation in the first post-donor result would indicate carry-over. The reverse sequence (other assays to levetiracetam) was conducted identically, using the other assays as donors and levetiracetam as the recipient.
Results: Across the eight recipient analytes assessed in both forward and reverse sequences, the initial post-donor results did not differ significantly from their corresponding baseline or other post donor results being within the acceptability threshold. This indicated no clinically meaningful contamination between levetiracetam and the other assays studied in either direction.
Conclusion: Under routine operating conditions, the AU5822 exhibits negligible carry-over for the levetiracetam assay. Implementation of additional wash cycles, extended probe soaks, or instrument reconfiguration is not required. These findings support the continued use of levetiracetam therapeuticdrug monitoring on the AU5822 without modification.
Amiloride to the rescue? A Histological study of NGAL and NRF2 expression in kidney damage and repair in a rat model
Bente Captijn, Kahla Tyson, Tania Slatter and Robert Walker University of Otago, Dunedin
Objectives: Within New Zealand, chronic kidney disease poses a large burden on the healthcare system and is associated with significant treatment costs. Reducing the incidence or severity of kidney disease will substantially reduce kidneyrelated mortality. Previous research found that the drug amiloride down-regulated fibrosis in three models of kidney fibrosis (lithium-, folic acid-, and adenine- induced). However, amiloride’s effects on kidney damage and oxidative stress pathways remain unclear. This study aimed to extend the analysis and understanding of amiloride’s potential benefits.
Methods: Immunohistochemistry for NGAL as a marker of kidney damage, and NRF2 as a marker of protection against oxidative damage was performed on 56 rat kidney sections from the adenine and folic acid studies. NGAL expression was quantified using ImageScope analysis software, while NRF2 analysis is ongoing.
Results: Statistical analysis of NGAL expression revealed a significant increase in the cortex and medulla of adenine-treated rats compared to controls, with no statistical difference between the adenine and adenine plus amiloride treatment groups. No statistically significant differences were observed between folic acid treated groups in the cortex and medulla. Neutrophil counts were also significantly increased in the adenine group compared to controls, with no significant differences between adenine and adenine plus amiloride groups or between the folic acid groups. Conclusion: These findings suggest that amiloride does not significantly reduce NGAL tissue expression. This may reflect the increased recruitment of neutrophils that were evident as opposed to lack of modification of kidney injury. Further studies into amiloride’s method of action in reducing kidney inflammation and fibrosis are underway. This could reveal novel therapeutic targets for kidney disease, addressing a critical unmet need in kidney disease treatment.
Comparative analysis of body fluid cell count: automated XN-1000 vs. manual microscopy
Russell Cheng1 and Charisse Guino-o2
1University of Otago, Dunedin and 2Awanui Labs, Blenheim
Objectives: White blood cell (WBC) counting and differentiation in body fluids are essential for accurate clinical diagnoses. This study compared the performance of the Sysmex XN1000 automated analyser with manual microscopy for total and differential WBC counts in body fluids.
Methods: A total of 26 body fluid samples were analysed using the Sysmex XN-1000. Manual counts were performed using a counting chamber and Wright-Giemsa-stained slides. Correlation analysis, Bland-Altman plots, and the Wilcoxon Signed-Rank Test were used to compare the two methods.
Results: Total WBC counts showed strong correlation between methods (r = 0.81). However, Bland-Altman analysis indicated substantial bias and wide limits of agreement, particularly at higher WBC concentrations. The Wilcoxon Signed-Rank Test (p < 0.0001) confirmed statistically significant differences between the methods. Differential counts for mononuclear (MN) and polymorphonuclear (PMN) cells showed very strong correlations (r = 0.96 for both). Bland-Altman plots for MN and PMN differentials revealed narrow limits of agreement (±0.3), suggesting better consistency. Although statistically significant differences were also found for differential counts (p < 0.0001), the variation was minor and likely not clinically significant.
Conclusion: The Sysmex XN-1000 demonstrated strong correlation with traditional methods for both total WBC and differential cell analysis in body fluids. However, the wide limits of agreement for total WBC counts indicate that two methods may have different clinical values, especially at higher concentrations. In contrast, the limits of agreement for the differential counts were narrow, supporting the potential reliability of the XN-1000 for routine classification of mononuclear cells and polymorphonuclear cells. While automation provides efficiency and consistency, manual review remains important in cases where accurate cell quantification is critical.
Comparing the performance of HpSA PLUS enzyme immunoassay with CerTest and RIDA QUICK chromatographic immunoassays for the detection of Helicobacter pylori
Stella Cory-Wright1, Chiara Galang2 and Tina Neilson2
1University of Otago, Dunedin and 2Te Whatu Ora Waikato
Microbiology,
Hamilton
Objectives: The HpSA PLUS enzyme immunoassay is currently
in use for the detection of Helicobacter pylori at Waikato Hospital Laboratory. This investigation aimed to compare the performance of the current assay, with the lateral flow immunochromatographic assays by CerTest and R-Biopharm. This study determined if either rapid antigen test would be an acceptable alternative for a less laborious and faster diagnosis of an important gastric pathogen.
Methods: Stool samples (50) were tested including 43 provided by Pathlab Hamilton. The selected samples included positive, negative and equivocal results for H. pylori. Each sample was tested for H. pylori by HpSA immunoassay, CerTest and RIDA QUICK immunoassays as per manufacturer instructions. Results for each sample were compared between the three test protocols and validated by the Pathlab provided results.
Results: HpSA had 100% sensitivity, specificity, negative and positive predictive values. CerTest showed 100% sensitivity, 85% specificity, negative predictive value of 100%, positive predictive value of 79% and an error rate of 11%. RIDA QUICK had 95% sensitivity, 100% specificity, 97% negative predictive value, 100% positive predictive value and 2% error rate.
Conclusion: RIDA QUICK was more specific than CerTest and performed nearly as perfectly as the current protocol immunoassay. RIDA QUICK could be validated for permanent use at Waikato Hospital Laboratory reducing turnaround time and labour for detection of H. pylori
Detection of NPM1 variants in acute myeloid leukaemia (AML) patients at diagnosis using stored RNA in Cepheid’s Xpert NPM1 Mutation assay
Robert Yoshiki Dalziel1 and Geraldine Duncan2 1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives: 4bp insertion variants in the NPM1 gene occur in 30% of AML patients at diagnosis and are classified as Type A/B/D (90% cases) or other rare types depending on sequence. Detection of NPM1 variants allows for prognosis, accurate treatment decisions, and disease monitoring. Cepheid’s Xpert NPM1 assay detects NPM1 variants using bone marrow or blood within 72 hours of collection. This study assessed a method using stored RNA to test NPM1 variant presence in retrospect. Methods: The Cepheid protocol processes blood/marrow cells to liberate RNA before applying to a cartridge for real-time PCR. The NPM1 variant is reported as a percentage in respect to an ABL1 control. The alternative method in this study added patient RNA directly to the cartridge and was used to test 22 patient samples tested previously as positive/negative for NPM1 variants. Additional replicate testing of the blood/RNA of a newly diagnosed patient, and a simple dilution series of 1 positive RNA sample was performed to investigate reliability of quantitation. Results: All samples had results concordant with previous diagnostic testing. The range of results for Types A/B/D were 188% to >500%. Rare types had lower percentages of <0.5%. Replicate testing showed similar percentages between blood/ RNA methods. The simple dilution series demonstrated assay linearity.
Conclusion: RNA can be used in the Xpert NPM1 assay to detect NPM1 variants in AML patients at diagnosis. Statistical inferences can be made from this study on the reliability of percentage quantitation. However, these are to be investigated further due to low sample size in this study resulting from limitations including cartridge cost and availability.
Human Herpesvirus type 6 assay evaluation
Ava Elsmore1 and Andrew Strathdee2
1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives: This report outlines a comparative analysis of the detection of human betaherpesvirus type 6 (HHV-6) between the new BD Max (Becton Dickinson) and the current NucliSENS
easyMAG (Biomerieux) /ABI7500 (Applied Biosystems) methods. This experiment aimed to demonstrate the consistency between these methods in support of validating the new process.
Methods: Probe and primer titration experiments were carried out to determine the most efficient concentrations for the new assay. HHV-6 primers and probes remained unchanged from the current method. The current internal control was switched to SPC (sample processing control), already incorporated into the BD DNA-1 test kits, and primers and probes were changed accordingly. The new method pre-prepares a master mix that can be frozen rather than preparing it with each run. A 10-fold dilution series of an HHV-6 DNA-positive CSF sample was tested to determine the analytical sensitivity for both methods. Limited positive clinical samples were available; 23 external quality control (QCMD) plasma samples were used to compare results from the original method to the new one. These samples consisted of HHV-6 types A, B, and Cytomegalovirus samples. 15 known HHV-6 DNA-negative plasma samples were tested to evaluate specificity.
Results: The limit of detection from the HHV-6 dilution for both the current method and the new method was 10-2. One QCMD sample not detected by the current method was detected by the new method. All other QCMD and the negative plasma results from the new method were consistent with the current method, resulting in 100% sensitivity and specificity in the new method compared with 97% in the current method.
Conclusion: This evaluation demonstrated consistency in analytical sensitivity between both methods. The new flexible method increases workflow efficiency, reducing chances for error.
Evaluating histological stains for bacteria and application of the Brown and Hopps stain for detecting intratumoral bacteria
Erin Formo, Heather Brooks and Tania Slatter University of Otago, Dunedin
Objectives: Histological stains are routinely used for identifying cellular architecture and microorganisms. Research suggests that bacteria can colonise tumours and have a role in carcinogenesis and tumorigenesis of primary cancers. It is not known whether bacteria are able to metastasise with cancerous cells to the brain. We aimed to evaluate histological stains for detecting bacteria in formalin-fixed paraffin embedded (FFPE) positive controls known to contain bacteria and apply the most effective technique to identify intratumoral bacteria in primary tumours and brain metastases.
Methods: The Gram Twort, DAB, BacLightTM red, and Brown and Hopps stain were assessed using FFPE positive controls, consisting of rat lungs incubated with Staphylococcus aureus (Gram positive coccus) and Escherichia coli (Gram negative rod) prior to fixation. Stains were evaluated and examined for bacteria by light and fluorescent microscopy.
Results: In the FFPE positive control, the Gram Twort, DAB, and BacLightTM red stains failed to clearly distinguish bacterial morphology. In contrast, the Brown and Hopps stain successfully demonstrated rods and cocci, but rods appeared purple rather than the expected pink. This method was applied to FFPE samples from prostate, melanoma, and metastatic brain tumours. Cocci and rod-shaped bacteria were observed in the prostate and melanoma samples, but identification in brain metastases was challenging due to necrosis and debris.
Conclusion: The Brown and Hopps stain offers a possible histological approach for detecting intratumoral bacteria. Despite limitations in sensitivity and specificity, it provides a foundation for future studies involving complementary molecular techniques to further explore the tumour associated microbiota in brain metastasis.
Assessing homologous recombination deficiency: A pathway to personalized PARPi therapy in ovarian cancer patients in Aotearoa
Shivannee Ganeshan, Magda Ratajska and Tania Slatter
University of Otago, Dunedin
Objectives: High-grade serous ovarian cancer (HGSOC) is the most aggressive subtype of ovarian cancer (OC) and is frequently diagnosed at stage IIIc. Approximately 50% of OC cases exhibit homologous recombination deficiency (HRD), commonly due to pathogenic variants in BRCA1/2 or other homologous recombination repair (HRR) genes. The remaining cases are homologous recombination proficient (HRP). HRD status is a key biomarker for determining eligibility for poly (ADP-ribose) polymerase inhibitors (PARPi), which target defective DNA repair pathways. Access to HRD testing in Aotearoa is limited, involving expensive overseas processing. In 2024, PHARMAC approved the use of Niraparib, a PARPi, regardless of HRD status, raising safety concerns for HRP patients.
Methods: Formalin-fixed paraffin-embedded (FFPE) ovarian cancer tissue from 45 Polish patients was processed for DNA extraction, quality assessment, and targeted library preparation using Qiagen HRD assay. Sequencing was analysed via the CLC Genomics Workbench. HRD scoring was based on the detection of loss of heterozygosity (LOH), large-scale state transitions (LST), and telomeric allelic imbalance (TAI) from 13,809 SNPs. Pathogenic variants were curated following ClinGen/CGC/VICC guidelines.
Results: Among the 45 samples, 23 harboured germline BRCA1/2 mutations, 13 somatic mutations, and 9 had no BRCA1/2 alterations. HRD (score ≥50) was observed in 30 cases. 12 patients exhibited both germline BRCA1 and somatic BRCA2 mutations, suggesting dual HRR pathway disruption. Samples with low tumour tissue content or sequencing depth were flagged for cautious interpretation. The assay performed well across varying DNA quality, with unique molecular indices (UMIs) enhancing variant reliability.
Conclusion: HRD scoring needs to be considered for various factors, including tumour tissue content, depth coverage and specific mutations. Comparison with the Agilent HRR17 panel and using New Zealand Aotearoa samples are recommended for further studies.
Comparative evaluation of two commercially available enrichment broths for Staphylococcus aureus detection
Ambryme Guergoua1, Hui Wang2 and Michael Kwong2 1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives: Enrichment broths selectively enhance growth of Staphylococcus aureus from nasal samples of suspected carriers. Due to supply depletion, the current in-house CAS (Colistin Aztreonam Sodium Chloride) broth is no longer producible. This project aimed to validate two commercially available enrichment broths.
Methods: Reference strains of S. aureus and Staphylococcus epidermidis were serially diluted from 10⁸ to 10² CFU/mL, and 100 microlitres inoculated into 20 Tryptone Mannitol Salt Broths (TMSB) and 20 7% Salt Broths. Following overnight incubation at 35°C, broths were subcultured onto blood agar. To simulate in vivo conditions characterized by low levels of S. aureus amidst competing flora, a mixed culture of coagulase-negative Staphylococcus spp. was diluted from 10⁸ to 10⁴ CFU/mL. The S.aureus reference strain was added at low concentration (10¹ CFU/mL). In the final study phase, nasal swabs from a known S. aureus carrier were inoculated into the laboratory’s current CAS enrichment broth, as well as the two commercial alternatives. Following incubation, cultures were plated onto Staph CHROMagar.
Results: Growth outcomes were analysed, assessing the relative performance of each medium in recovering S. aureus from clinical samples. TMSB and 7% Salt Broth demonstrated comparable growth patterns. No significant advantage was observed in terms of presumptive identification due to a mannitol fermentation. TMSB demonstrated reduced accuracy, evidenced by a lack of growth at low S. aureus dilution on one plate
and mixed growth from the patient nasal swab, in contrast to consistent performance of CAS and 7% Salt Broth.
Conclusion: The commercially available broths showed good comparative results, making them viable for integration without risking patient outcomes. Based on cost-effectiveness and performance, the 7% Salt Broth was deemed the more practical option for routine use.
Optimising Legionella detection: Evaluating the use of Dithiothreitol for sputum treatment
Georgina Harris1 and Paul Ogbuigwe2 1University of Otago, Dunedin and 2Waikato Hospital Laboratory, Hamilton
Objectives: Legionella testing requires liquefying sputum samples for pipetting during extraction. This study aimed to assess Dithiothreitol (DTT) as a chemical alternative for sputum breakdown compared to a manual washing method.
Methods: 17 sputum samples were tested for Legionella with both washing and DTT methods over a range of DTT concentrations (0.1%, 5%, 10%). In addition, a set of 10 external quality assessment (EQA) samples were measured, and a dilution series of extracts from a spiked Legionella positive sputum sample was run to compare the limit of detection. Standard qualitative Legionella PCR testing protocol was followed on all samples with extraction of DNA via an EZ1 system and PCR on a LightCycler 480 using melting curve analysis. Legionella sample results and inhibition control Ct values of both methods were compared.
Results: Initial testing found DTT 10% more effective at sputum breakdown, producing more consistent results, and therefore was used for subsequent testing. A Bland-Altman plot for inhibition control Ct values (95% limits of agreement = -1.92 to 1.89, mean difference = 0.311) and the Legionella sample results displayed agreement between methods. One discordant result occurred where a negative Legionella result in a washed sample was subsequently positive with DTT 10% treatment. This was confirmed positive for Legionella longbeachae by ESR. EQA results were congruent with those expected, and the dilution series showed an improvement in the limit of detection for DTT 10%.
Conclusion: Sputum treatment with DTT 10% provided increased sensitivity, proving clinically significant in detecting previously missed Legionella cases while providing a workflow advantage. However, further investigations with a larger sample pool and examining specific DTT procedures should be explored.
Optimising Bp53-11 in immunohistochemistry: Expediting endometrial carcinoma diagnosis at Taranaki Histology Laboratory
Alena Hojdelewicz1 and Gareth Ashton2
1University of Otago, Dunedin and 2Awanui Labs, Taranaki
Objectives: Endometrial carcinoma is a common gynaecological malignancy, and accurate diagnosis is essential for guiding treatment decisions. p53 immunohistochemistry (IHC) is a widely requested reflex test for detecting TP53 mutation. This study aimed to optimise the Bp53-11 IHC protocol for Taranaki, expediting endometrial carcinoma diagnosis by transitioning to in-house testing.
Methods: Five tests were conducted to optimise the Bp53-11 protocol, refining antigen retrieval, antibody application, and detection. Each slide included three tissue sections—a vulval biopsy, a p-multi control, and an endometrial biopsy sample— ensuring thorough assessment and validation of staining consistency for precise diagnostic results. After optimising the protocol, adenocarcinoma, endometrial tissue, rectosigmoid carcinoma, and an MSI control were assessed to determine the
most effective routine control, ensuring clear and reproducible staining.
Results: Observational analysis showed that Test 5 achieved superior staining performance, producing a clear background. The addition of a signal amplification step further enhanced signal intensity. The MSI control emerged as the most reliable choice for routine quality assurance, providing consistent and reproducible staining under optimised conditions.
Conclusion: The optimisation of the Bp53-11 IHC protocol has significantly improved staining consistency, expedited turnaround times, and enhanced diagnostic accuracy for endometrial carcinoma in Taranaki. The introduction of in-house p53 testing enhances accessibility for the Taranaki Histology Lab, ensuring reliable and reproducible staining, particularly with the MSI control for quality assurance, while also improving diagnostic efficiency, patient care, and clinical outcomes.
Validation of the Roche Cobas c 513 for clinical HbA1c testing: Method comparison with the Bio-Rad D-100
Caitlin Huria1, Philippa Holdaway2, Joanne Webb2, Cassandra Muir2 and Lee Barrass2
1University of Otago, Dunedin and 2Awanui Labs, Wellington
Objectives: HbA1c is a key biomarker for diagnosing and monitoring diabetes. As part of a methodological transition, this study aimed to assess the analytical agreement between the BioRad D-100 (cation-exchange HPLC) and the Roche Cobas c 513 (turbidimetric immunoassay) analysers for HbA1c measurement. Additionally, the suitability of the Roche Cobas c 513 for routine clinical use was evaluated by assessing the validity of its results.
Methods: Evaluation of the Roche Cobas c 513 analyser included assessment of intra-run precision using in-house Roche quality control (QC) materials, and inter-run precision using external Bio-Rad QC materials, both at normal and pathological HbA1c levels. Patient samples (n = 102) covering a clinically relevant range of HbA1c values were tested on both platforms. Method agreement was evaluated using correlation analysis, Passing-Bablok regression, and Bland-Altman analysis. Analytical performance was compared against the Royal College of Pathologists of Australasia (RCPA) Allowable Performance Specifications (APS).
Results: For both normal and pathological quality control levels, the Roche Cobas c 513 demonstrated acceptable coefficients of variation for intra-run and inter-run precision. Comparison of patient samples revealed a strong correlation between the two analysers, with a Pearson’s correlation coefficient = 0.9987. Passing-Bablok regression indicated a constant positive bias and minimal proportional bias, while Bland-Altman analysis revealed a mean bias of +4.2 mmol/mol.
Conclusion: This method validation demonstrated strong analytical agreement with the Roche Cobas c 513 and BioRad D-100 analysers. The Roche Cobas c 513 met established performance criteria and is therefore suitable for routine clinical implementation for HbA1c testing at Awanui Labs, Wellington.
Optimisation of Haematoxylin and Eosin staining in a diagnostic hospital laboratory
Erin Jacobsen1, Matt Pynegar2 and Kelly Jones2
1University of Otago, Dunedin and 2Christchurch Hospital Laboratory, Christchurch
Objectives: Haematoxylin and Eosin staining is the gold standard in the histopathological diagnosis of tissue samples. Dye interactions between basophilic and eosinophilic features in tissue allow for visualisation of different pathological microanatomy. The aim of this investigation was to optimise the Haematoxylin and Eosin protocol established at Canterbury Health Laboratories while maintaining standard lab practices.
Methods: A panel of three pathologists scored skin slides 1 to 5 based on quality of stained features. Three formalin fixed quality control slides were assessed to provide a baseline. Fifteen formalin fixed skin experimental protocols were produced by manipulating reagent timings to increase haematoxylin intensity and contrast. Seven protocol slides were then chosen to be assessed by pathologists based on thickness, reproducibility, and preferences. These were then given alphabetical identifiers.
Results: Three quality control slides collected over a 3-month period scored an overall average mean score of 4.22 out of 5. Slide A was not optimised with a recorded mean score of 3.67 out of 5. Slides B and G did not improve with mean scores of 4 out of 5. Slide C scored similar to QC slides with a mean score of 4.33 out of 5. Slides D, E, and F produced optimised protocols with a mean score of 4.67 out of 5.
Conclusion: Optimisation of a diagnostic laboratory Haematoxylin and Eosin protocol was achieved by manipulating reagent timings for Slides D, E, and F. In this instance, qualitative and quantitative analysis indicated optimisation while the ability to maintain standard lab practices allows for practical use. Validation of various tissue types and large-scale throughput should be considered before incorporating new protocols. By optimising a histological process, the ultimate result is the improvement of patient care.
Evaluation of the methotrexate assay on the Cobas Pro 503 unit at Middlemore Hospital Laboratory
Jeniffer Jude1 and Wendy Shaddick2
1University of Otago, Dunedin and 2Middlemore Hospital Laboratory, Auckland
Objectives: This study aimed to evaluate the analytical performance of the methotrexate assay on the newly implemented Roche Cobas pro 503 analyser, which has replaced the Cobas 502 at Middlemore Hospital Laboratory. It also compared methotrexate reagents from ARK Diagnostics (Cobas 502) and Roche (Cobas Pro 503) to validate manufacturer claims and assess their suitability for routine laboratory use.
Methods: Precision and interference studies were performed using 32 patient samples. Pooled low and high concentration samples were analysed over 5 days to assess intra- and interrun precision. Linearity was evaluated using serial dilutions of a high concentration methotrexate sample with the ARK dilution buffer. Stability was evaluated by storing a random sample at 4 °C and analysing it daily over 7 days. Interference from haemolysis and lipaemia was assessed using spiked samples. For the correlation study, 24 patient samples ranging from 0.04 to 12.10 µmol/L were analysed on both Cobas analysers.
Results: High-level precision met acceptable criteria, however, low-level precision did not. Linearity demonstrated excellent correlation coefficient of 0.999. Methotrexate remained stable for up to 3 days at 4 °C. Minimal interference from haemolysis (less than 1710) and lipaemia (less than 2043), within percent difference of 10%. The correlation study displayed excellent agreement between the two analysers.
Conclusion: The methotrexate assay on the Cobas Pro 503 unit displayed strong linearity, acceptable interference and stability, and comparable performance to the Cobas 502, supporting manufacturer claims. It is suitable for routine clinical use. Further investigation into low-level precision is recommended.
Verification of the Idylla BRAF mutation assay for melanoma: a comparison with MassARRAY
Rae Kwan1 and Amanda Dixon-McIver2
1University of Otago, Dunedin and 2IGENZ, Auckland
Objectives: Accurate detection of BRAF mutations is essential
for timely treatment decisions in melanoma cases, particularly to guide the use of targeted therapies such as BRAF and MEK inhibitors. The Idylla BRAF assay was evaluated for its potential use in urgent diagnostic settings or when MassARRAY testing is unavailable. This study aimed to verify the assay's performance in detecting BRAF V600 mutations in melanoma by assessing its concordance with established MassARRAY results.
Methods: Five archived melanoma samples with known BRAF mutation status were analysed using both the Idylla and MassARRAY platforms. Samples included formalin-fixed paraffin- embedded (FFPE) sections and extracted DNA. Idylla results were interpreted through amplification curves and Cq values in Idylla Explore, while MassARRAY data were analysed via MALDI-TOF mass spectra to identify mutations at codon 600.
Results: The Idylla assay demonstrated complete concordance with MassARRAY in four of five samples, accurately detecting BRAF V600E mutations in FFPE tissues. Amplification curves aligned well with MassARRAY profiles. One low-input DNA sample failed to amplify on Idylla, highlighting sensitivity limitations. No non-V600E variants were identified, limiting evaluation of broader mutation coverage.
Conclusion: The Idylla platform demonstrates potential as a rapid and user-friendly tool for urgent melanoma cases and as a backup when MassARRAY is unavailable or impractical. While further validation is needed – particularly for detecting rarer variants and low-input samples – it could serve as a valuable adjunct in time-sensitive clinical scenarios.
Optimisation of Restriction Fragment Length Polymorphism (RFLP) in Secretor genotyping, for the investigation of discrepancy rate between Lewis phenotype and Secretor genotype in Aotearoa New Zealand
Selene Mak and Holly Perry University of Otago, Dunedin
Objectives: Secretor status of an individual is determined by the FUT2 genotype. The FUT2 genotype can be established by multiplex Polymerase Chain Reaction (PCR) - Restriction Fragment Length Polymorphism (RFLP) method using four restriction enzymes. The aim of this project was to optimise the RFLP step for clear visibility of DNA band patterns upon imaging. The subsequent aim was to establish the discrepancy rate between Lewis phenotyping and genotyping of the Secretor blood group.
Methods: Four conditions were investigated to optimise the RFLP step in FUT2 genotyping – enzyme incubation temperatures, enzyme concentrations, reaction buffers and gel electrophoresis conditions. Quantification of band intensity was performed in the Image Lab Software (BioRad) to determine whether modifications were effective. The optimised RFLP protocol was then used to genotype the secretor status of study participants recruited as part of a wider study.
Results: The optimal RFLP protocol was found to be a singletemperature incubation of 37oC for 180 minutes and using a buffer recommended for one of the four restriction enzymes. Increasing the concentration of one of the four enzymes decreased the quantity of RFLP product. Gel electrophoresis ran at 100V for 90 minutes proved most effective for band separation. Of 181 participants in the wider study, 6.1% (n = 11) showed discrepancy between Lewis phenotyping and secretor status genotyping. All were of non-Caucasian ancestry.
Conclusion: The PCR-RFLP method is a valid method for secretor genotyping but requires optimisation in individual laboratories to give high performance. Discrepancy between Lewis phenotyping and secretor genotyping highlighted the unreliability of serological methods. Molecular methods are preferred for an accurate determination of secretor status.
A comparative study of two commercial Kleihauer-Betke staining kits for quantifying fetomaternal haemorrhage
Samantha McGregor1, Sonette Kruger2 and Rajesh Lakhani2 University of Otago, Dunedin1 and Medlab Central, Palmerston North2
Objectives: The Kleihauer-Betke test is essential for detecting fetal red blood cells in maternal circulation, particularly in suspected cases of fetomaternal haemorrhage. Accurate quantification of fetal cells is critical for timely administration of Anti-D immunoglobulin in Rhesus D-negative mothers. This study compared fetal cell counts in two commercial Kleihauer-Betke staining kits; the Guest Medical Fetal Red Cell Detection Kit, currently used at MedLab Central and the Sigma-Aldrich Fetal Haemoglobin Kit, to assess their effectiveness and reliability.
Methods: Fifty fetal red cell counts were conducted for each method using artificially spiked adult male blood with known concentrations of cord blood. Standardised inclusion criteria were followed, and controls were prepared for each staining batch. Staining protocols were followed per manufacturer instructions, with minor time optimisations made for the SigmaAldrich method. Each slide was analysed by a single examiner using light microscopy, counting 2000 adult cells and the number of fetal cells present. Statistical analysis, including tables, graphs and paired t-tests were performed to evaluate differences between the methods.
Results: The Guest Medical method consistently demonstrated higher fetal cell counts than the Sigma-Aldrich method. In samples with known elevated fetal haemoglobin, both methods detected fetal cells, however, differences in staining intensity and background clarity were identified. Statistical analysis showed a significant difference between methods (p < 0.05), with a mean difference in fetal cell counts of approximately 7 fetal cells. However, this variation was not considered clinically meaningful. Conclusion: Although statistically different, both methods revealed broadly similar fetal cell counts suitable for clinical use. Each has advantages and limitations, making either a viable option for use in the laboratory.
Validation of the Redox InnovationTM Protein Carbonyl Assay: A new biotin hydrazide ELISA-based method
Aevia Monoy1 , Nicholas Magon2 , Mark Hampton2 and Christine Winterbourn2
1University of Otago, Dunedin and 2Mātai Hāora - Centre for Redox Biology and Medicine, University of Otago, Christchurch
Objectives: Oxidative stress is associated with various diseases and ageing. Physiological oxidants can directly oxidise proteins, forming stable carbonyl groups. Protein carbonyls are a general biomarker of oxidative stress and are traditionally quantified by derivatisation with 2,4-dinitrophenylhydrazine (DNP), followed by detection with an antibody Our laboratory recently redeveloped an ELISA assay that replaced DNP and a biotinylated anti-DNP antibody with biotin hydrazide (BH), removing the requirement for an antibody This study aimed to test and validate various aspects of the new assay.
Methods: In this ELISA-based assay, protein samples are derivatised with BH and bound to a plate. Streptavidinhorseradish peroxidase binds strongly to the biotin group, and tetramethylbenzidine oxidation is used to detect and measure protein carbonyls. Critical steps in the protocol were slightly modified and tested to determine the impact on protein carbonyl quantification.
Results: Comparable performance was observed between freshly reconstituted standards and those subsequently stored at 4°C for one week. The optimum BH concentration for derivatisation was found to be 2 mM (tested range: 1-4 mM). No statistically significant differences were observed between
derivatisation time variations (30-90 minutes). No significant difference was observed when the amount of protein added to wells was varied (0.5-2.0 µg). Varying chromogen development time did not affect protein carbonyl levels. The assay was determined to have a limit of detection of 0.08 nmol carbonyls/ mg protein.
Conclusion: Critical evaluation of various parameters in the new assay confirmed its robustness to slight deviations from the protocol and identified optimal conditions.
Clinical correlation and method comparison of NT-proBNP with BNP
Ryan Muirhead1, Bobby Tagore2 and Jacob Kay2
1University of Otago, Dunedin and 2Pathlab Bay of Plenty, Tauranga
Objectives: B-type natriuretic peptide (BNP) and N-terminal proB-type natriuretic peptide (NT-proBNP) are critical biomarkers used for diagnosing and managing heart failure. This study aimed to evaluate whether the NT-proBNP assay performed on the DxI-9000 analyser can replace the BNP assay performed on a DxI-800 as the primary method of analysis by assessing the analytical and clinical agreement between the two analysers and an external Roche Cobas NT-proBNP assay.
Methods: Fifty-two SST and EDTA samples were simultaneously collected across various locations during BNP requests. Frozen aliquots were sent to Pathlab Bay of Plenty for analysis on the DxI analysers, while the primary SST sample was sent for analysis on the Cobas. BNP analysis was performed with the EDTA samples, while NT-proBNP was measured using the SST samples. Results were compared between the analysers using SPSS and Analyse-it for the statistical analysis.
Results: The DxI-9000 demonstrated excellent agreement and correlation with the Cobas (y = 0.3304 + 1.05x, r = 0.997), while the Bland-Altman analysis showed a mean difference of 7.8 pmol/L with acceptable limits of agreement. Comparison between the DxI analysers showed an expected proportional bias, with a Passing-Bablok regression of y = -6.765 + 1.948x and Pearson’s r = 0.964. Bland Altman showed a mean difference of 68.1 pmol/L. Clinical concordance showed 96.2% agreement with the Cobas and 90.2% with the DxI-800.
Conclusion: The strong statistical and clinical agreement displayed by the DXI-9000 NT-proBNP assay with both the Roche Cobas NT-proBNP and DxI-800 BNP assays, combined with the benefits of NT-proBNP such as improved sample stability, validates that the DxI-9000 NT-proBNP is a viable and clinically reliable replacement for the DxI-800 BNP assay.
Validation of the specimen stability at room temperature and 4°C, permitting a reliable reticulocyte count
Chloe Present1 and Tao Meng2
1University of Otago, Dunedin and 2LabPLUS, Auckland
Objectives: Blood collected in Ethylenediamine tetraacetic acid (EDTA) is stable for up to 24 hours at room temperature and up to 48 hours when refrigerated, allowing reticulocytes to be reported, respectively, within those storage conditions. Reticulocyte counts are requested to assess bone marrow activity and investigate anaemia, often as an additional add-on test. This study aimed to assess if the current guidelines set for specimen stability at room temperature and 4°C result in a reliable reticulocyte count. Methods: Samples (20) collected in EDTA tubes were selected to analyse the reticulocyte count using the Sysmex XN 9000 XN-20 analyser. To anonymise the data, the blood was aliquoted into separate EDTA tubes, each given a numbered barcode label from 1-20 with a ‘RT’ or ‘4°C’ suffix. The room temperature and 4°C samples were run manually every 6 hours after baseline measurement. A Bland-
Altman graph was utilised to comment on the reticulocyte stability, and a paired t-test was used to strengthen the results further.
Results: The mean bias between baseline measurement and measurement at 24 hours stored at room temperature and 48 hours stored at 4 °C was minimal. The Bland-Altman for 4°C demonstrated that 95% of the samples lie within the limits of agreement, showing stability. In comparison, the room temperature demonstrated that 90% lie within the limits of agreement, which also suggests stability. The p-values demonstrated no statistically significant differences between baseline measurements and measurements taken at 24 and 48 hours.
Conclusion: Whole blood EDTA samples are stable when stored at room temperature for 24 hours and 48 hours when refrigerated, so the reticulocytes can be reported confidently and should remain implemented.
Culturing periprosthetic joint specimens: A comparison of automated and manual incubation methods
Xander Pritchard1 and Melanie Williams2
1University of Otago, Dunedin and 2Health New Zealand (HNZ) Taranaki Laboratory, New Plymouth
Objectives: Periprosthetic joint infections are commonly investigated in the microbiology laboratory. At HNZ Taranaki Laboratory, the current diagnostic method involves manual incubation and monitoring of culture media for 14 days. A proposed automated incubation method involves the use of automated blood culture systems to incubate the specimens, theoretically resulting in quicker, more energy efficient and more sensitive detection. The objective of this project was to compare the two methods and discover which method would be superior, with the intentions of routinely implementing the automated method.
Methods: This project entailed processing specimens using both methods simultaneously. Received specimens were first streaked onto agar plates of enriched media to enable growth of any present bacteria or fungi, as well as incubated in an enrichment broth, as per the current method. Following this, a small amount of specimen was homogenised and transferred into a blood culture bottle for automatic incubation, as per the proposed method. Any detected growth, either on agar or by the blood culture system, was recorded with reference to the timeto-positivity.
Results: The results indicated that the automated method was just as sensitive as the manual method. The automated method was quicker at detecting growth 100% of the time. Of the 11 significant positive specimens wherein both methods detected growth, the microorganism isolated was the same, indicating true positive results.
Conclusion: This study demonstrated that the proposed automated method is consistently superior to the current method, having the desired qualities of being quicker, more energy efficient, and more sensitive. Due to the small sample size of specimens studied, the proposed method should be studied further but is reliable enough to be implemented.
Optimised solid-phase extraction methods for simultaneous extraction of four antibiotics from urine
Karina Soh and Natalie Hughes
University of Otago, Dunedin
Objectives: An initial investigation using Solid-phase extraction (SPE) coupled with Liquid Chromatography Triple Quadrupole Tandem Mass Spectrometry (LC-QqQ-MS/MS) aimed to detect a panel of antibiotics potentially sourced outside the formal
healthcare system in developing countries. While two detection methods were successfully developed, antibiotic recovery using SPE proved challenging, highlighting the need for further optimisation. This study focused on refining SPE methods for simultaneous extraction of four antibiotics—amoxicillin, benzylpenicillin, phenoxymethylpenicillin, and flucloxacillin— from urine.
Methods: Two SPE approaches were evaluated: a reversephase method by Chiesa et al. and a weak cation-exchange method by Phenomenex. Extraction was optimised for four antibiotics spiked into mimic and human urine. Key parameters— concentration effects, matrix interactions, sample pre-treatment pH, sorbent equilibration, wash conditions and evaporation stability—were systematically investigated to enhance analyte retention and minimise matrix interferences. Eluates were analysed using gradient and isocratic LC-QqQ-MS/MS methods, detecting all four antibiotics within 10 and 5 minutes, respectively. Chromatographic separation was performed with Phenomenex Kinetex C18 column with 0.1% v/v formic acid in water and acetonitrile as mobile phases.
Results: Sample pH affected analyte-sorbent interaction, lowering retention and overall recovery. Antibiotic concentration affected recovery, with lower recovery results as concentration increases. Amoxicillin showed poor recovery in urine, while other antibiotics showed minor matrix impact. The antibiotics were prone to degradation from excessive time in the concentrating centrifuge and use of methanol as a wash solvent led to low recovery.
Conclusion: Two SPE protocols were optimised, achieving consistent recovery rates of 50–70% for three of the four target antibiotics in urine. Amoxicillin consistently exhibited poor recovery from urine (~10%), suggesting that urine matrix effects may inhibit extraction or promote degradation.
Validation of the iLAB alpha thalassaemia screening kit
Dhilka Sookdev1, Julia Bennet2 and Ramesh Tiwari2
1University of Otago, Dunedin and 2Canterbury Health Laboratories, Christchurch
Objectives: Alpha thalassaemia is a recessively inherited haemoglobin disorder of red blood cells causing abnormal production of globin chains. The screening test used by Canterbury Health Laboratories to detect this disorder utilises a commercial lateral flow and immunochromatographic test strip to mark the presence of gamma chain tetramers (Hb Bart’s). Due to thenatureofantibody-antigencomplexbeingformedonsamples potentially containing interfering proteins, cross reactivity and non-specific binding can cause false positives. This study aimed to investigate whether incorporating a red cell wash step reduces the potential risk of non-specific binding and concomitant false positive results.
Method: Packed red cells were aliquoted into 20 separate microcentrifuge tubes, spiked with an equal volume of autoantibody or paraprotein positive serum, and incubated at room temperature for 15 minutes. Thereafter, lysis buffer was added to 10 of these tubes, and results were read from the immunochromatographic strip after a 5-minute incubation. The remaining10samplesunderwentthreewashingstepswith800uL of 0.9% saline and were centrifuged after each addition, with the saline layer above the packed red cells removed. Following the third wash, lysis buffer was added to the samples and results were read after a 5-minute incubation.
Results: From a total of 30 samples tested, 19 immunochromatographic strips returned false positive results when incubated in unwashed red cell samples, and 3 of the 30 samples returned false positives when incubated in washed red cell samples. Statistic validation using the Chi-Square Test returned a p-value < 0.05, suggesting statistical significance. Conclusion: The results are suggestive that the addition of a
washing step likely reduces incidence of false positives occurring in the alpha thalassaemia screening procedure, due to removal of non-specific antibody binding.
Investigating the pathogenicity of TAB2 missense variants
Emily Swasbrook, Emma Wade and Stephen Robertson
University of Otago, Dunedin
Objectives: TGF-beta-activated kinase 1 binding protein 2 (TAB2) is a key regulatory protein in inflammatory and developmental pathways. While the pathogenic role of gainof-function variants in TAB2 is recognized, particularly in the context of frontometaphyseal dysplasia (FMD), the molecular mechanisms driving this phenotype remain poorly understood. To further characterize the impact of gain-of-function missense mutations, we combined a cell-based luciferase reporter assay with AI-driven protein structural predictions –AlphaFold– to assess their effects on transcriptional regulation.
Methods: Ten TAB2 missense variants were analysed for their effect on activator protein-1 (AP-1) transcriptional activity using a luciferase assay. Of these, seven were identified in individuals with FMD, including one previously characterised gain-offunction variant. One additional variant included in the cohort has been a reported loss-of-function. Variants were transfected into HEK293T cells alongside an AP-1 luciferase reporter, and luciferase activity was measured to evaluate functional impact.
Results: Our results did not demonstrate that specific gain-offunction variants enhance AP-1 signalling, suggesting a potential mechanism for TAB2-mediated pathology. While these did not show significant results, the findings contribute to understanding the potential mechanisms underlying TAB2-mediated pathology.
Conclusions: Furthermore, this study demonstrates the value of integrating functional assays with protein structural prediction tool such as AlphaFold, which may support future variant interpretation and diagnosis, and highlights the utility of integrative functional and structural approaches in variant characterisation.
Establishing new means and acceptable limits for haematological parameters using XB/XM analysis
Kayla Syben 1, Vandhana Lal2 and Alan Neal2
1University of Otago, Dunedin, and 2Pathlab, Bay of Plenty
Objectives: The aim of this study was to calculate new means and acceptable ranges using XB/XM analysis and to adjust the current complete blood count (CBC) values being used on the DxH900 analysers to better represent the Tauranga patient population.
Methods: Means (500) from batches of 20 patient results were put into an Excel spreadsheet. The overall mean and standard deviation for each parameter was calculated. Coefficient of variation percentage (%CV) was calculated for the parameters considered stable to assess variation. Upper and lower acceptable values for the parameters were calculated using XB/ XM analysis. The newly calculated values were compared to current. All data was reviewed before parameters were adjusted on the analysers.
Results: The current means for each parameter showed slight changes compared to the newly calculated means. Therefore, none of the current mean values were adjusted. The newly calculated acceptable ranges were also very similar to the current ones. The new ranges for the white blood cell count (WBC), neutrophils (NE), and lymphocytes (LY) were slightly wider than the current ones.
Conclusion: New values for CBC parameters were successfully calculated using XB/XM analysis. It was decided that the current ranges for the WBC, NE and LY were to be adjusted to the new values. Overall, patient moving averages allow the continuous monitoring of analyser performance, while saving money on commercial quality control material.
OBITUARY
Jenny Bennett
Born in the United Kingdom, Jenny immigrated to Wellington, New Zealand with her family at the age of seven. She began her career at a young age as a laboratory assistant, training and working across several hospital laboratories before completing her qualifications to become a Medical Laboratory Scientist. Determined and hardworking, she went on to complete a Master’s degree in Medical Laboratory Science at Massey University while working at ESR in Kenepuru, Wellington. Her research in microbiology, particularly in gram-negative bacilli led to the publication of several scientific papers. In recognition of her contributions to the profession, Jenny was awarded a Fellowship of The New Zealand Institute of Medical Laboratory Science (NZIMLS) July 2003. Title of the dissertation was: “Vibrio Species: A Review of the current literature with reference to the importance of Vibrio Species as a cause of both enteric and non-enteric disease in humans”
At ESR, Jenny gained experience in both Microbiology and Molecular Biology, where she developed a passion for molecular science and research. Her colleagues remember her as deeply committed, often working long hours beyond what was required, driven by her dedication to laboratory science and patient care.
In 2007, Jenny and her husband Mark moved to Hamilton, where she joined Waikato Hospital as a Medical Laboratory Scientist. She later became the Technical Specialist in Molecular Biology. In this role, Jenny’s expertise and vision helped shape the department, where she introduced a range of inhouse molecular assays. Her leadership and foresight were critical during the COVID-19 pandemic. Jenny developed and validated assays for COVID-19 testing inhouse and played an important role in supporting the country’s COVID response. During this period she displayed resilience, efficiency, and generosity, always ready to support her colleagues in unprecedented challenges.
Beyond her professional achievements, Jenny’s greatest pride was her family. She and Mark were blessed with three daughters and four grandchildren, all of whom brought immense joy to her life. She cherished weekends spent cooking and sharing meals with her extended family. She enjoyed travelling, camping, sewing, gardening, and her daily morning walks with the dog.
In later years, due to a medical condition, Jenny made the difficult decision to step back from her career during the COVID-19 to spend more time with her family. True to her nature, she faced this period with courage and grace.
Jenny will be remembered as a brilliant scientist, a supportive colleague, and a deeply caring wife, mother, and grandmother. Her contributions to medical laboratory science and to the people around her will leave a lasting legacy
Jenny Bennett, a devoted scientist, colleague, wife, mother, and grandmother, passed away peacefully in August 2024, surrounded by her loving family.
Contributed by Ajesh Joseph, NZIMLS Secretary/Treasurer
Chris Kendrick: my life as an MLS
A baby boomer from Whanganui, I grew up in a family at a time when life was less complicated and the technology of the day were the bikes we rode, the household telephone (used by our parents) and the family entertainment centre was the television. Growing up was fun with fishing, tree climbing, rugby and a lot of our time was spent racing our bikes around the parks that surrounded the Whanganui River. We were the original BMX racers with plenty of puddles and jumps that tested our riding skills. There were always plenty of things to do and we were never idle. As time moved on my school days came to an end and finally it was time to look for a job. Throughout my time at secondary school, I came to enjoy science thanks to inspirational teachers in both the 5th and 6th form years at St Augustine’s College. There was something exciting about becoming a laboratory technician and soon I was employed as a Laboratory Technician at the Wanganui Milk Treatment plant. This job lasted about a year before both my sister Alison and I commenced careers as Trainee Medical Laboratory Technologists at Wanganui Hospital in 1971.
Back in the day, the career pathway to becoming a registered Medical Laboratory Technologist was five years of in-house apprentice-style learning. There was little formal teaching provided by the laboratory staff and most training was practically focused. With four trainees we all managed to complete the first hurdle which was the basic training examination at the end of the third year. From here we moved on to the final two years with O level examinations to complete the Technologist Registration requirements. We all became registered Technologists with the Medical Laboratory Technologists Board in 1975. For the next few years I worked in the Wanganui Hospital Laboratory, initially in Microbiology and then in Immunohaematology. I was appointed Charge Technologist of the Blood Bank at Wanganui in 1981 and in 1985 moved to the Manawatu Regional Blood Service in Palmerston North. I practised as a Senior Medical Laboratory Scientist initially in the Blood Bank before moving to the Tissue-Typing section of the Blood Centre. This section provided tissue typing for the National Transplant Service and disease association testing for local clinicians. It was during my time here that an exciting career opportunity came along. In 1992 I was appointed to a Lectureship in the Department of Microbiology & Genetics at Massey University. The appointment was to help with setting up the recently approved Bachelor of Medical Laboratory Science (BMLSc) programme and my task was to create new courses from scratch for Haematology & Transfusion Science for both 300 and 400 levels of the BMLSc. In 1992 Massey enrolled its first intake of 30 students enrolled into the second year of the BMLSc. Most students moved over from first-year biological science courses offered at Massey. The BMLSc was an internal programme developed for delivery only to internal students and was delivered as lectures and laboratory practicals. The courses were later modified to accommodate students in the Massey GradDipSci, an extramural bridging course setup as a venture between Massey and Diagnostic Laboratories throughout New Zealand. Over time the number of students enrolling in the BMLSc faded until it was closed in 2017. By this time the GradDipSci was a popular pathway for Laboratory
Technicians to become registered scientists in New Zealand. At around the time of the closure of the BMLSc, the GradDipSci was restructured to become the Post Graduate Diploma in Health Science and continued until the last students completed their courses in 2025. Throughout my time at Massey, my teaching in the clinical sciences of Haematology & Transfusion Science grew into contributions to the 202.371 Human Genetics and Molecular and Clinical Diagnosis offering. In this I provided the introductory cytogenetics teaching and its use in the clinical diagnosis of leukaemia and other cancers. Nearing the end of my time at Massey I was one of a group offering Immunology and Microbiology and some of the Physiology courses mainly to students in the Health Sciences.
While employed at Massey I completed a Post Graduate Diploma of Science in Microbiology and Immunology and in 2000 graduated with an MSc following the publication of my research thesis into cases of New Zealand transfusion reactions caused by infected donor blood. The title of my research was “Novel screening methods for the detection of Yersinia enterocolitica in infected blood used for transfusion in New Zealand”.
In 2001 Massey University offered a Masters MSc (MLSc) programme for Laboratory Scientists wanting to extend their studies and to undertake some laboratory related research. The MSc (MLSc) was a workplace course of study that allowed students to maintain employment and study at University Post Graduate level. The programme was comprised of part coursework and part research. Numbers enrolled in the MSc (MLSc) gradually increased with the MSc (MLSc) becoming a popular option for some registered scientists. I delivered the Haematology/Transfusion Science components into 202.781 Current Topics in Medical Laboratory Science updating students on recent developments in Thrombosis, Iron Overload Disease and Transfusion Transmitted Infections. Other updates were offered in Microbiology, Histology & Clinical Biochemistry. For these students the research element of the MSc (MLS) was jointly supervised by university staff as principal supervisors, with external supervisors appointed for onsite student supervision. I supervised many MSc projects during this time covering a diversity of subjects with some of the research topics presented below.
1. Method development of an Elisa assay for the quantitative evaluation of Factor VIII binding activity of von Willebrand Factor.
2. The application of linkage analysis in Haemophilia A diagnosis.
3. Measurement of ultra-large molecular weight von Willebrand factor multimers in patients with Thrombotic Thrombocytopenia Purpura.
4. Haematological and related reference ranges for people of sixty years of age and over.
5. Development of a flow cytometric method for the measurement of Zap-70 in Chronic Lymphocytic Leukaemia.
6. Investigation into the seroprevalence of antibodies to West Nile virus infection in NZ blood donors.
7. Assessment and validation of methods for the quantitation of feto-maternal haemorrhage using flow cytometry.
8. Comparison of screening methods for feto-maternal haemorrhage in Rh(D) negative women.
9. Development of a Flow cytometric method to determine rates of red cell contamination in platelet components prepared for transfusion at NZBS Waikato.
10. Helicobacter pylori infection and its effect on the platelet count in patients presenting at Middlemore Hospital and Manukau Surgical Centre Gastroenterology clinics
11. Single dimension gel electrophoresis with immunofixation, with & without Heparin – a new laboratory method for the detection of heparin-binding site defects in antithrombin deficiency.
12. Biomarkers as predictors of six-month survival outcomes of patients presenting with solid tumours.
13. DNA sequencing to determine HLA-DQA1 tissue types.
14. Assessment and validation of two flow cytometry methods for the determination and quantitation of fetal Rh(D) positive red cells in Rh(D)negative mothers post-delivery.
15. Comparison of methods available for the determination of feto-maternal haemorrhage in Rh(D) negative mothers.
16. Antenatal cell free fetal DNA genotyping to predict the presence of the Rh(D) blood group.
17. Zinc protoporphyrin analysis to predict early onset iron deficiency in blood donors.
In 1993 I was elected by the NZIMLS Membership to join the NZIMLS Council, the professional body of Medical Laboratory Science in NZ. During my time on the Council, I was fortunate to be involved in the profession’s activities at many levels. At about the time I joined Council, university degree programmes were just commencing, and it was timely for me with my new job at Massey to update/inform the Council with details of Massey’s BMLSc programme. Other involvement on Council was my lead in the creation and development of the initial NZIMLS website, redevelopment of the Competence & Professional Development programme and its adoption by the Medical Laboratory Science Board (MLSB) as a tool for competence assessment in conjunction with the Annual Practicing Certificate, setup of the NZIMLS Journal archive and its publication on the NZIMLS website. During my time in the profession, I was co-opted to the Editorial Board of the NZIMLS Journal, a role that allowed me to review potential publications submitted to the Editor. Over my 13 years with the NZIMLS I had the privilege to work with many of the profession whom I came to count as friends. My final four years on the NZIMLS Council I spent as President and at the Hamilton ASM in 2012 I was awarded Life Membership. These and many other events/activities that are too numerous to recall (or I have forgotten) I look back on with pride.
In 2006 as part of an external consultancy, I developed a Transfusion Science course for technicians working in laboratories in the Pacific Islands. The course was used for the education of laboratory personnel spread across the Pacific Island nations. The programme was offered as a series of lectures and laboratory practicals delivered to students through the Pacific Paramedical Training Centre in Wellington.
Having stood down as NZIMLS President, I was asked by the Minister of Health to accept a nomination to become a Member of the MLSB - soon to become the Medical Sciences Council (MSC). The appointment was for an initial three years and was a time of change for the profession’s regulatory body following the introduction of the Health Professions Competence Assurance Act. In addition to my university roles, I was appointed by the Health & Disability Commissioner to review complaints from the public about MLS practitioners or MLS practice in general. These activities were interspersed with my time on the Health Practitioners Tribunal in which my role was to review the complaints about MLS practitioners that contravened the regulations of the MSC.
My career in the Medical Laboratory Science profession over the years has had enormous variety. Starting off as a Trainee ML Technologist with my sister at Wanganui Hospital, to becoming a senior Scientist in charge of the Blood Bank. With my move to the Regional Blood Centre in Palmerston North, my experience in the laboratory led me to a Lectureship at Massey University and many happy years working as part of the team teaching graduates about their future roles in Diagnostic Pathology. I was fortunate enough to get in to research and was able to study and to graduate with my MSc. My election to the NZIMLS and subsequent involvement in that organisation through to becoming President and a Life Member has left me with a feeling of deep belonging, and I am proud to call myself a Medical Laboratory Scientist.
At the end of 2024 and after 32 years I finished at Massey University as a University Academic and informed the MSC that I was now inactive in the profession after 54 years. I can look back with pride on the things I accomplished and the fun in a career that spanned over half a century. There are many other activities I recall from time to time that because of space restraints I cannot include in this summary of my life as an MLS.
In closing, I encourage any “wannabe” scientists among the youth of New Zealand thinking about a career in health, to consider the clinical sciences. The profession can be very rewarding, and the work of our MLS and the information provided from their work, plays an essential role in the diagnoses of patients in the New Zealand’s public health system. It is sometimes disappointing to realise that the work of Technicians and Scientists in our country continues to receive minimal credit from employers, regulating bodies and other health workers. From retirement I look forward to positive developments in this respect in the future.
AUTHOR INFORMATION
Chris Kendrick, PGDipSci, MSc, LMNZILMS, MNZIMLS. Retired Senior Lecturer, PGDipHealth Sciences, Massey University, New Zealand.
Email: bmkendri@inspire.net.nz
On behalf of the NZIMLS Council, the Journal and your colleagues, thank you for your contribution and for your enduring support to the profession. We wish all the best in your retirement. Lisa Cambridge, Editor
Crypt: life, death and disease in the middle ages
Author: Alice Roberts, Simon & Schuster Ltd, 2025
ISBN: 1398519251
This is the third book in a series written by the author relating to the intersection between archaeology, anatomy and genetics.
Professor Alice Roberts is an osteoarchaeologist and an acknowledged expert on the communication of science to the public. In “Crypt” she examines “Life, death and disease patterns in the Middle Ages”. Here she investigates six historic case studies using skeletal discoveries in historic graves. The author describes how combining multiple scientific disciplines can describe
the lives and diseases of those long ago forgotten. The cases are systematically placed in their respective historic period, in the context of what life would have been in that time. Particularly interesting are the chapters on leprosy, black death and syphilis. These are not only placed in the historical context but also illustrate how archaeogenetics and archeopathology can trace disease patterns and predict the social consequences at each historical period. For those interested in historic diseases, the use of osteoarchaeology and how new technologies are revealing previous secrets locked up in bones, this is a must read. It is also interesting what can be found by browsing bookshops rather than staring at a computer screen.
Reviewed by: Michael Legge, PhD
The age of diagnosis: how the overdiagnosis epidemic is making us sick
Author: Suzanne O’Sullivan, Hodder Press, 2025
ISBN: 1399727656
The author poses the question:” Sickness and health and why medicine has gone too far”. The author is a consultant neurologist specializing in complex epilepsy and psychogenic disorders. She is an award-winning author on public communications in medicine. In this her third book she examines two important concepts relating to medicine: “the right to know” and does “modern medicine lead down the path of overdiagnosis”. To do this the author discusses real clinical cases and her experience with patient interactions. The medical conditions described in the book are complex in their presentation and how or should people be informed and when. The examples used are Huntington’s Disease, Lyme Disease and Long Covid, Autism, Cancer, ADHD Depression and Neurodiversity, and finally an interesting case of a “Syndrome without a name”. Each chapter considers the implications of the disease for both the patient and their family,
the increasing diagnostic power of technology and the “right to know”, especially with late onset inherited diseases.
The author questions whether technologies could lead to an overdiagnosis and whether some disorders e.g. ADHD would be in the spectrum of “normality”. The book is well written, and the author links the chapters very effectively, and raises the question whether a diagnosis could do more harm than good.
Reviewed by: Michael Legge, PhD
The final diagnosis: obscure cases of death, disease & murder
The author is a New Zealand Pathologist who has written two previous books based on his experiences as a Pathologist.
The current book continues his stories of a Pathologist’s experiences. Additionally, the author re-examines some of the more notable murder cases using publicly available information. The personal experiences of the strange and unusual during his time as a Pathologist are interesting and varied. They highlight the diverse ways people die or the tricky linking of medical information
with pathology outcomes and offer insights into the Pathologist and autopsies in reaching a final diagnosis which may differ from the clinical diagnosis. The author provides an excellent mix of medical puzzles and includes his own personal experiences outside of the laboratory to help explain how he understands the problems of the deceased. The re-examining of evidence from some of the well-publicised murders is interesting. The sub-title “Obscure causes of death, disease and murder” fully describes an interesting reflection of a Pathologist’s career!
The book is not complex to read and is well written. However, the reader who has followed the previous two books is left to wonder whether, this is the authors, “Final Diagnosis” in print!
Reviewed by: Michael Legge, PhD
The Pacific Way Warm Pacific greetings to you all from the PPTC
Congratulations to the PPTC Consultancy Team
It is with great pleasure to inform you all that the Pacific Pathology Training Centre has been successful in gaining registration status as a NZ Private Training Establishment, a prestigious achievement that has been granted by the New Zealand Qualifications Authority under Subpart 5 of Part 4 of the Education and Training Act 2020. The PPTC has also been awarded Signatory to the Education Code of Practice 2021. For the PPTC, this means that the Centre Based Courses offered by the PPTC at its home base in Wellington are being certified by NZQA as New Zealand approved teaching programmes. Over the last 2 years, the PPTC has contributed an enormous amount of time and effort in order to reach this milestone, and I sincerely thank our PPTC consultancy team for bringing our application to the successful outcome which will now benefit the entire Pacific region. What does this mean for Pacific students? It means that Pacific medical laboratory personnel can now apply to the New Zealand High Commissions in their own countries for NZ Short Term Training Scholarships to attend courses provided by the PPTC in Wellington NZ, throughout each academic year. Each scholarship provides appropriate funding (supplied by the NZ Government) for Pacific students to attend courses in Wellington, and this funding accommodates airfares, hotel accommodation expenses and living allowances for students wishing to attend either 2 weeks, 4 weeks or 6 weeks courses. Before applying to attend courses in Wellington, students are advised to contact the PPTC Education Manager (Emmanuel Marshall) for the purpose of establishing eligibility to attend the course of choice. Each applicant will be assessed by two authorities ie, the Education Manager who is responsible for the arrangement and coordination of the course and the PPTC Consultant responsible for teaching the course. Once eligibility is granted by the PPTC, the applicant will receive a signed letter of acceptance from the PPTC which can then be submitted to the NZ High Commission along with a completed application for the scholarship process to begin. If the scholarship application is successful, it will be awarded to the student and from this point, the SKILLS Organisation of NZ on behalf of the NZ Ministry of Foreign Affairs will take responsibility for the student throughout the duration of the course. If a student is granted a PPTC based Scholarship, then the PPTC itself will take full responsibility for the student throughout the duration of the course.
UPDATES
Courses delivered and completed in 2025
Clinical Biochemistry, 23rd June- 18th July 2025 (4 weeks)
The Biochemistry Course involved four participants:
The Biochemistry centre based course provided a comprehensive theoretical component to students in the diagnostic medical field of Clinical Biochemistry. The purpose of the training is to equip the students with sufficient knowledge to be able to work confidently in providing quality diagnostic testing to clinicians using the medical laboratory services available in their home countries for patient management and better health outcomes.
Course Content and Objectives
This course provided students with the following:
• Overview of basic equipment used in Biochemistry including pipettes, pH meters, water baths, centrifuges and balances.
• Overview of analytical principles utilised by most analytical systems for the analysis of Biochemistry tests, such as spectrophotometry, immunoassay, blood gas analyser and other Biochemistry analysers.
• Overview of Diabetes in terms of pathology diagnosis and laboratory testing.
• Overview of cardiac tests in health and disease focusing on Myocardial Infarction, diagnosis and laboratory analysis.
• Overview of protein analysis, liver function tests and specialist biochemical analysis.
• Overview of endocrine tests such as tumour markers, thyroid function tests, fertility hormones, other hormones (eg PTH), and associated abnormalities.
• Molecular approach to biochemical pathology.
• Organisation and effective management of the Biochemistry laboratory.
• Emphasis on quality indicators such as TAT.
• Reporting of urgent and critical results.
• Presentations from various Biochemistry suppliers will be incorporated.
• Quality Control; IQC, and External Quality Assessment in the Biochemistry laboratory.
• Overview of reference intervals and Uncertainty of Measurement (UoM).
• Discussion of quality systems, Standard Operating Procedures, stock control and its management, result processing, audit trails, reducing error and process improvement.
• Overview of the validation process for introducing new methods and analysers.
The Blood Transfusion centre based course provides a comprehensive theoretical component and a series of practical workshops to students in the medical laboratory field of Blood Transfusion Science. The purpose of the training like all PPTC courses is to equip the students with sufficient knowledge to be able to work confidently in their home laboratories and be able to provide quality diagnostic test results to clinicians using the medical laboratory services for patient management and better health outcomes.
Course Content and Objectives
This course provides students with the following:
• Transfusion transmitted diseases (including HIV, Syphilis, Hepatitis B and C).
• Donor selection criteria and collection.
• Blood processing, blood transfusion practise, ABO, Rh and other blood group systems
• Blood group genetics and basic immunology.
• Preparation of Coombs control cells, technical methods.
• Antibody screening and identification.
• Compatibility testing.
• Haemolytic Disease of the Newborn.
• Transfusion reaction investigations and Haemovigilance.
• Blood Bank quality management processes.
• Equipment maintenance.
• Organisation of a Blood Bank including emergency planning, major trauma cases, backup planning.
• Appropriate use of blood components in Transfusion Medicine.
• Referral laboratory network.
• Provision of practical sessions focusing on correct technique and fundamental basic procedure.
• Tours of NZBS crossmatch laboratory and the blood donor centre
Content of this course ensures that the practical needs of all students attending are met and the practical sessions will focus on repeated basic methodology, so as techniques are mastered to levels of excellence.
Courses scheduled for the remainder of 2025
Foundations of Haematology, October 27th – 5th December (6 weeks)
The final course for 2025 is 6 weeks of “Foundational Haematology” It is unfortunate that Haematology continues to be weak in performance and this is due to a devastating lack of expertise and interpretative skill in blood film examination and interpretation throughout the Pacific region. Blood cell identification and interpretation is a continual learning process and unfortunately Pacific Island laboratories do not have resident experts who are able to mentor and add to this learning experience.
Phil Wakem, the PPTC´s CEO and Haematology specialist will be offering a six week Haematology course at the PPTC in Wellington which is designed to deliver a comprehensive theoretical component and a series of practical workshops in foundational Haematology and blood film morphological examination. The purpose of this training once again is to equip students with sufficient knowledge to be able to work confidently and competently in their home laboratories and be able to provide quality test results to clinicians using the medical laboratory services in the diagnosis and treatment management of patients.
Figure 4. Blood Transfusion students, Lecturer and PPTC Consultants
International / National Conferences/ Professional Development
NZIMLS Annual Scientific Meeting, Hamilton, 27th – 29th August 2025
We are pleased to announce that the PPTC’s Chief Executive Officer, Philip Wakem was recently awarded Life Membership with the New Zealand Institute of Medical Laboratory Science at the 2025 Annual Scientific Meeting held in Hamilton.
Phil was also nominated to deliver the “TH Pullar Memorial Address”, the title of which for 2025 was “The call of the Pacific”. Each year the NZIMLS Council invites a person who has made a significant contribution towards Medical Laboratory Science as a profession to deliver the TH Pullar Memorial Address at the Annual Scientific Meeting. This prestigious Address is in honour of Dr TH Pullar who passed away on the 29th of August 1966. The TH Pullar Memorial Address is given at the opening ceremony of the NZIMLS ASM and is published in this issue of the Journal.
The entire team of PPTC Consultants attended the ASM to show support and acknowledge Phil for his leadership and welldeserved award. The following Māori proverb quoted at the end of Phil’s address and sums up in a small number of words why PPTC Consultants carry the flame of hope every day of their working lives to make a difference to Pacific communities who are in desperate need of help.
Hei whakakapi i tenei wa, ka tika me mihi ano kia koutou katoa. He aha te mea nui o tenei ao? He tangata, he tangata, he tangata!
What is the most important thing in the world? It is the people, it is the people, it is the people
Ngā Mihi
Meeting on strengthening the use of data from AMR and antimicrobial consumption and use surveillance in the human health sector in the Western Pacific Region, Manila, Philippines. 9th – 11th September 2025
Angela Lewis, (PPTC’s laboratory contracts manager for portable laboratories and resident Microbiology specialist) attended this meeting in Manila representing the PPTC.
Surveillance data must be used to strengthen understanding of AMR, factors that influence it and the impact of mitigating actions. This 2025 meeting aimed to stimulate stakeholder engagement in WHO initiatives and drive progress in how AMR and antimicrobial consumption and use (AMC/U) surveillance data can be synthesised, analysed and used to accelerate the fight against AMR. The objectives of the meeting were to:
1. Stimulate engagement of stakeholders on the use of data from surveillance of AMR pathogens and AMC/U, including recently published WHO guidance and tools.
2. Share country experiences and good practices on using AMR and AMC/U surveillance data to improve clinical management, infection prevention and control, antimicrobial stewardship and outbreak response, and to
inform the development and implementation of national and local, evidence-based policies.
3. Decide on feasible approaches towards strengthening the use of AMR and AMC/U surveillance data at national, subnational and facility levels, taking advantage of regional AMR surveillance guidance, the WPRACSS platform and capacity-building.
Fifth Regional Forum of WHO Collaborating Centres in the Western Pacific. Manila, Philippines, 4th - 5th November 2025. Two participants have been invited by WHO to attend, John Elliot as Chairman (PPTC) and Filipo Faiga (EQA Programme Manager and Biochemistry specialist) have been nominated by the CEO of the PPTC to attend this Forum which occurs once every 2 years. The objectives of the Forum are to:
1. Reflect on the progress made and lessons learnt from WHO and WHO CC collaborations since the Fourth Forum.
2. Reassess the role of WHO CCs in advancing health goals within the context of a new financial setting.
3. Expand effective mechanisms for collaboration and acceleration to achieve strategic, impactful and sustainable outcomes.
CAN YOU HELP?
MICROSCOPES for Haematology morphology and GENEXPERTS for Molecular diagnostics
If any New Zealand medical laboratories have items of diagnostic instrumentation as mentioned above that have been recently upgraded or continue to be stored in the laboratory but are actually surplus to requirements, the PPTC would be most grateful if such items could be donated through its Centre to Pacific Island laboratories where there is an exceptional need. Pacific laboratories have very restricted budgets and often cannot afford to replace troublesome instrumentation that continues to breakdown and which is often discontinued because it is so outdated.
Please contact:
Phil Wakem Chief Executive Officer
Pacific Pathology Training Centre
Wellington New Zealand
E-mail : pptc @ pptc.org.nz or phil @ pptc.org.nz
Tel: 64-4-389 6294 or 027 2305483
Figure 6. PPTC consultants and Phil Waken, ASM
RECENT REVIEWS
The reviews below can be accessed for their Abstracts, and “Open Access” is indicated where applicable. Unfortunately, the NZIMLS cannot provide full access to the articles due to copyright restrictions, but full access may be available through various institution arrangements. Any feedback on this can be sent to: editor.nzimls.org.nz.
1. Bernier ED, Bartnick E, Khanna KM. Macrophages: sentinels, warriors, and healers. Hum Mol Genet 2025; 34(R1): R110-R120. doi:1093/hmg/ddaf87.
5. Do LAH, Mulholand K. Measles 2025. N Eng J Med 2025; doi:10.1056/NEJMra2504516.
6. Orth M, Sanberg S, Shih P. Direct-to-consumer testing: benefits and concerns of commercially accessed laboratory tests. Clin Chem 2025; 71(6): 652-663.
7. Maqsood Q, Khan MU, Fatima T, et al. Recent insights into breast cancer: Molecular pathways, epigenetic regulation, and emerging targeted therapies. Breast Cancer (Auckl) 2025; 19: doi:10.1177/1782234251355663. [Open Access]
8. Vella G, Rescigno M. Cancer microbiota: a focus on tumorresident bacteria. EMBO Rep 2025; 26(12): 2977-2993.
9. Chen JT, Dadheech N, Pin Tan E et al. Stem cell therapies for diabetes. Nature Med 2025; 31(7): 2147-2160. doi: 10.1038/s41591-025-03767-8.
10. Basar M, Duzuc T. The burnout: a silent saboteur in in vitro fertilization laboratories. J Ass Reprod Genet 2025; 42(8): 2497-2513. doi: 10.1007/s10815-025-03537-y.
11. Gong S, Zhang X, Chen X, et al. The impact of bariatric surgery on gut microbiota: a bibliometric analysis of research trends and scientific contributions. Front Microbiol 2025; 16: 1523809. doi:10.3389/fmcb.2025.1523809. [Open Access]
12. Glokerth RD, Sampson BA, Graham JK. Forensic Pathology. jNEJMra2406208.
13. Treger RS, Menza TW, Truong TT et al.Advances in syphilis diagnostics to address the 21st-century epidemic. Clin Chem 2025; 71(9): 935-948. doi: 10.1093/clinchem/ hvaf072. [Open Access]
14. Dartois VA, Mizrahi V, Savic RM et al. Savic RM et al. Strategies for shortening tuberculosis therapy. Nature Med 2025; 31(6): 1765-1775. doi: 10.1038/s41591-025-037423.
15. Hagerman RJ, Hagerman PJ. The spectrum of fragile X disorders. N Eng J Med 2025; 393(3): 281-288. doi.1056/ NEJMra2300487.
16. Aba N, Ducos C, More E et al. Influence of genetic biomarkers on cardiac diseases in childhood cancer survivor: systematic review. Pharmacogenomics J 2025; 25(3): 15. doi: 10.1038/s41397-297-025-00369-y [Open Access]
17. Fang W, Wu J, Cheng M et al. Diagnosis of invasive fungal infections: challenges and recent developments. J Biomed Sci 2023; 30 (42): doi: 10.1186/s12929-023-00926-2. [Open Access].
18. Spies NC, Farnsworth CW, Wheeler S et al. Validating, implementing, and monitoring machine learning solutions in the clinical laboratory safety and effectively. Clin Chem 2024; 70(11): 1334-1343. doi: 10.1093/clinchem/hvae126. [Open Access]
19. Walch PDK, Broz P. Molecular mechanisms of co-infections. 2025; EMBO Rep2025; 26(15): 3714-3729. doi: 10.1038/ s44319-025-00517-2. [Open access]
20. Wallmuth EM, Angert ER. Microbial circadian clocks: hostmicrobe interplay in diel cycles. BMC Micobiol 2023; 23(1): 124.24.doi:186/s12866-023-02839-4. [Open Access]
21. Naghdi M, Cao P, Essers R et al. Artificial intelligencesimplified information to advance reproductive genetic literacy and health equality. Hum Reprod (2025); 40(9): 1681-1688. doi: 10.1093/humreprod/deaf135. [Open Access]
22. Metcalf RA, Nahimtak S, Guyatt G. et al. Platelet transfusion: 2025 AABB and ICTMG clinical practice guidelines. JAMA 2025; 334(7): 606-617. doi: 10.1001/jama.2025.7529. [Open Access]
Prepared by: Michael Legge
Making memories at the 2025 Annual Scientific Meeting, Hamilton
JOURNAL QUESTIONNAIRE
Read the articles carefully as most questions require more than one answer. Answers are to be submitted through the NZIMLS website. Make sure you supply your correct email address and membership number, it is recommended that you write your answers in a word document and then cut and paste your answers on the website.
You are reminded that to claim valid CPD points for successfully completing the journal questionnaire you must submit an individual entry. It must not be part of a consultative or group process. In addition, members who have successfully completed the journal questionnaire cannot then claim additional CPD points for reading the articles from which the questions were derived.
The site will remain open until Friday 13 February 2026. You must get a minimum of eight questions correct per questionnaire to obtain 5 CPD points.
The Editor sets the questions but the CPD Co-Ordinator, Jillian Broadbent, marks the answers. Direct any queries to her at cpd@nzimls.org.nz.
NOVEMBER 2025 QUESTIONNAIRE
1. Angiotensin-converting enzyme 2 (ACE2) receptors are crucial for SARS-CoV-2 virus transmission. In what organ was ACE2 expression pattern analysed and what were the predominant cell types where it was distributed?
2. Which hormone levels declined in the Masqood et al study and was found to be a predictor of COVID-19 severity? What were these lower levels associated with?
3. HIV infection is increasingly viewed as a manageable chronic condition, but what non-HIV/AID causes are persons living with HIV at higher risk of experiencing? How does the toxicity of highly active antiretroviral therapy (HAART) contribute significantly to chronic inflammation and subsequent activation of what?
4. What role does P-selectin play in inflammation? What observations were made with P-selectin levels in HIV patients on HAART?
5. What are the primary triggers of Acute Exacerbations of Chronic Obstructive Pulmonary Disease (AECOPD)? What are their approximate percentages of cases? What offer potential as cost-effective inflammatory markers of this disease?
6. The Baharuddin et al study identified what differences in routine blood tests between patients with AECOPD and those with stable COPD?
7. What is apolipoprotein B - related Familial Hypobetalipoproteinaemia (APOB-FHBL)? What is indicated by this condition? What is the heterozygous (pathogenic) variant of the APOB gene and what may this cause?
8. APOB-FHBL has no specific treatment, how are symptoms managed for patients of the heterozygous APOB FHBL phenotype? Provide two examples of dietary management of the condition.
9. When does red cell alloimmunisation occur? What two conditions must be present for an individual to develop an alloantibody? What types of immunohaematological tests are needed to identify multiple alloantibodies in pretransfusion testing?
10. Why is it crucial to differentiate the presence on autoantibodies and alloantibodies in pre-transfusion? Why would the crossmatch appear incompatible?
ANSWERS JULY 2025 QUESTIONNAIRE
1. What is familial hypercholesterolemia (FML)? What is considered as the disease risk of this disorder? What three genes have mutations shown to give rise to FML?
Familial hypercholesterolaemia (FH) is a genetic disorder distinguished by elevated levels of low-density lipoprotein cholesterol (LDL-C). Risk of early cardiovascular disease. LDL receptor gene, (LDLR) apolipoprotein B gene (or the proprotein convertase subtilisin/kexin 9 gene (PCSK 9).
2. FH patients are classified into two clinical types: homozygous (HoFH) and heterozygous (HeFH). What is the prevalence of each type in a population? How is each type characterised?
HoFH is approx. 1 in 1 million, while HeFH occurs in fewer than 1 in 500 individuals, but depends on the population. HeFH patients are characterised by tendon xanthomas, corneal arcus, and CVD complications and have a Total cholesterol of >5.18 and LDL-C >3.37 mmol/L. HoFH patients are typically diagnosed earlier, within the first two decades of life, exhibiting severe manifestations such as extremely premature atherosclerosis and elevated Total cholesterol levels >12.95mmol/L, with untreated individuals at risk of dying by age 20.
3. Where is Low-density lipoprotein receptor (LDLR) located? What does it encode for? And why is it crucial?
Found on chromosome 19(p13.1 - 13.3) and encodes a glycoprotein of 860 amino acids, crucial for cholesterol homeostasis.
4. Why is antithetical M antigen typically considered as clinically insignificant and rarely responsible for Haemolytic disease of the fetus and newborn (HDFN) or haemolytic transfusion reactions (HTR)?
Anti-M is a naturally occurring IgM antibody reacting at temperatures below 37°C, anti-M is predominantly an IgM antibody which is unable to cross the placenta due to its size and pentameric structure.
5. How is the identification of anti-M antigen aided in the laboratory?
Its demonstration of dosage and susceptibility to enzymes ficin, bromelain, and papain in antibody identification panels.
6. What is the severe clinical syndrome Haemophagocytic Lymphohistiocytosis (HLH) caused by? What differences in presentation of the syndrome are seen between paediatric and adult populations?
Serious hyperinflammatory syndrome caused byabnormal activity in cytotoxic T-lymphocytes and macrophages, leading to a cytokine storm and potential organ damage and risk of increased mortality. Primary HLH is seen mostly in paediatric population and occurs mostly due to chromosomal/genetic alteration. Secondary HLH occurs mostly in adults and common triggers would be infection, malignancies, and autoimmune conditions, including lymphoma.
7. In reported neoplasm-associated HLH cases in adults, lymphoma accounts for 67%, what are the majority of cases linked to? What is the survival rate? What are the
challenges in defining treatment? (LA-HLH) are linked to T-cells/NK cells lymphoma. Survival is less than 1-2 months. HLH can mask underlying lymphoma, challenging diagnosis due to its low incidence rate, diagnostic complexities, rapid progression and the often-compromised physical condition of affected individuals.
8. Why can the initial diagnosis of HLH be delayed? And how?
Due to the resemblance between HLH and other inflammatory disorders. Histological diagnosis might be obstructed by tissue infiltration with activated lymphocytes and macrophages, which enables tumour cells to conceal themselves within the inflammatory infiltrates.
9. What medications are implicated in Pyroglutamic acidosis (PGA)?
10. How does PGA develop? Other than the medications above, what other factors contribute to the risk of PGA?
Due to inference with glutathione metabolism, relative deficiency in cysteine/glycine and/or reduced clearance of pyroglutamate. Malnutrition, acute kidney injury (AKI), being female, advancing age, epilepsy, multi-morbidity, including renal and hepatic failure.
SEMINAR REPORTS
South Island Seminar
3 May 2025, Christchurch
The South Island seminar was held at Manawa, Christchurch with a great turnout of 145 people attending from Canterbury, West Coast, Nelson/Marlborough and even the North Island. In the week prior to the event the South Island experienced a severe weather event with a state of emergency being declared in Canterbury due to heavy rain and flooding. Fortunately, the worst had passed by the weekend, and all attendees were able to travel safely to Christchurch.
The winner of Best Presentation was Jaya Montecillo, MLT, Core Biochemistry, Canterbury Health Laboratories (CHL). Jaya’s topic was Deglycosylation Improves Performance of suPAR for Acute Heart Failure Diagnosis. Her research was carried out as part of her PhD study with the Christchurch Heart Institute, University of Otago. The runner up was Ricci Bergin, MLS, Genetics, Canterbury Health Laboratories. Ricci’s topic was Spinal Muscular Atrophy – Screening in New Zealand.
Casey Davies, from Chemical Guidance & Design gave an informative presentation on Laboratory Safety, and Mike Legge (University of Otago) tackled the topic of Cultural Competency in laboratories. Esther Lau (CHL) gave an update on emerging fungal pathogens, Kirsty Sewell (CHL) spoke on the importance of building better working relationships with our referrers with a focus on histology. Henry Hole (West Coast) presented a Malaria case study. Chris Sies (CHL) gave a thought-provoking presentation on the Science of Compassion in Healthcare. Erin Boshier (CHL) presented an interesting case study of a multiple myeloma patient undergoing CAR-T cell therapy. Allize Mangar (Awanui Labs) told his story of coming to New Zealand as a refugee and gaining his qualification as a phlebotomist.
Thank you to all the speakers for their efforts and high-quality presentations, to the chairs and the NZIMLS for their support, and to the attendees for their enthusiastic participation.
Report by: Ginna Alston, SIS 2025 Convenor, Microbiology Service Manager, Canterbury Health Laboratories, Christchurch.
Biochemistry Seminar
28 June 2025, Wellington
The 2025 Biochemistry Seminar was held in The Cable Room, Harbourside, Wellington in June and brought together medical laboratory scientists and technicians from across New Zealand for a day of professional learning, discussion, and networking. THERE WERE 45 delegates representing both hospital and community laboratories nationwide.
The programme covered a broad range of topics relevant to modern clinical biochemistry practice. Presentations included updates on artificial intelligence in laboratory medicine, patientbased real-time QC, ferritin harmonisation, ECMO and free haemoglobin, changes in the medical laboratory science profession in New Zealand, recent developments in pathology and research, and point-of-care testing. Speakers provided both clinical and scientific depth alongside practical take-home messages, sparking lively Q&A sessions throughout the day.
Emerging technologies were also a highlight, with wellreceived talks on artificial intelligence in clinical diagnostics. These sessions generated significant interest, reflecting the profession’s growing focus on digital transformation and the need to future-proof laboratory services. Ferritin harmonisation also stimulated strong engagement. Variations in assay methods between manufacturers were highlighted as a major challenge; fortunately, Max Reed represented New Zealand in international discussions with experts across Australasia and provided the latest update on harmonisation progress.
The seminar also celebrated excellence within the discipline. Prizes were awarded for outstanding presentations: Max Reed received the prize for Best Presentation, and Shugo Kawamoto was awarded Runner-Up.
Beyond the formal sessions, the seminar created valuable opportunities for collegial interaction. Participants shared experiences, discussed challenges around accreditation and quality, and exchanged ideas for improving collaboration across regions.
Overall, the 2025 Biochemistry Seminar proved to be a valuable professional day, balancing scientific rigour with practical relevance. The event not only strengthened the biochemistry community but also reinforced the importance of continued dialogue and shared learning as laboratories navigate an evolving healthcare landscape.
Report
by: Leo Luk, Biochemistry SIG Convenor
Failure of POCT testing for HbA1c
SCIENCE DIGEST
Contributed by Michael Legge
With the worldwide incidence of type 2 diabetes increasing, there is a worldwide attempt to reduce the incidence of this disorder. Currently it is estimated that there are approximately 6.7 million deaths each year from diabetes and the associated complications. The major areas affected by the complications of diabetes are the low- and middle-income countries where access to testing for diabetes is severely limited. Since 2011 the WHO has advocated the use of HbA1c for testing for the diagnosis of type 2 diabetes. The use of point of care testing (POCT) is considered to help overcome the limited resources in low-income countries without laboratory infrastructure and POCT devices have increased in availability. In this paper (1) jointly coauthored from the UK and the Netherlands the authors evaluated the analytical performance of 19 POCT devices against the IFCC laboratory medicine criteria and the National Glycohaemoglobin Standardisation Programme (NGSP). A total of 19 POCT HbA1c devices were tested from different suppliers and a range of different methods. Overall testing included, precision, trueness, variant interference, high HbA1c and manufacturers certification procedures. Only five passed the IFCC and NGSP criteria. In addition, many devices that had previously been certified could not replicate their performance in this study. The authors conclude that while the performance of all devices was undertaken under optimal laboratory condition the outcomes were very concerning when the devices may be used in limited clinical settings with little or no oversight.
Fine tuning the flavour of chocolate
The history of chocolate dates back more than 5000 years with the original cacao trees being domesticated in Mexico and cacao drinks were a significant part of both Maya and Aztec cultures. The introduction of cacao by the Spanish to Europe created a drink for the elite and many properties were ascribed to cacao including aphrodisiac, medical and religious. The Swiss and British chocolate makers became dominant in the manufacture of chocolate, but the cacao source is fundamental to the flavour of chocolate. In an international collaboration between scientists in the UK, West Indies, and Columbia, the initial processing of the cacao beans was investigated (2). The initial stage after cacao been harvest is to allow them to ferment in their mucilaginous coating before being dried and ready for processing. The investigators monitored the microbial communities from beans collected from three different farms and established that pH, temperature, and the microbiota communities were the critical actors in flavour development. Using metagenomics, they established the metabolic networks involved in flavour development which differed depending on the location of the initial bean fermentation by the abiotic and biotic bacteria and yeasts, which influenced the quality of the chocolate. By identifying the critical involvement of abiotic and biotic factors in the initial fermentation process the authors conclude that it should be possible in the future to manipulate the initial labour intensive first steps in chocolate manufacture in the same way that beer and wine are produced and to be able to manipulate flavour profiles.
Cancer diagnosis from blood samples
Being able to diagnose and monitor cancer using a specific blood test has long been the goal of many cancer researchers. While cancer biomarkers and imaging technologies are available these often rely on the presence of a protein or enzyme being produced by the tumour or the resolution of the imaging technique and have their respective limitations. The discovery in 2011 that cancer could be diagnosed from circulating cancer cells and cell tumour DNA (ctDNA) led to the development of liquid biopsies, and particularly the use of a blood sample. This is based on the
concept that tumour cells shed cells and DNAinto the blood and other fluids e.g. CSF. Using molecular techniques liquid biopsies have progressively been used for both diagnosis and monitoring of treatment. The technology is limited however by the amount of circulating ctDNAagainst the background of normal circulating DNA. A recent publication from the USA studied 162 plasma samples from 18 subjects undergoing treatment for colorectal cancer (3). The authors developed a modification of a technique called BEAMing (beads, emulsion, amplification and magnetics) to quantify ctDNA. They found that using the modified ctDNA techniques, ctDNA was detectable in all the patients and that serial ctDNA had oscillations that coincided with surgery and increased with when new lesions were identified by radiology. The authors concluded that the modified technique provides a more sensitive method for diagnosing and monitoring tumour dynamics and provides improved sensitivity for ctDNA use.
Effects of EDTA contamination on magnesium and iron
EDTA contamination during blood collections is identified as a noticeable pre-analytical error for certain clinical biochemistry analytes. While there are clear contamination issues for potassium and calcium, there are variable reports in the literature regarding the effect of EDTA on magnesium and iron as well as calcium and ALP These variable reports appear to relate to the analytical platform being used e.g. enzymatic analysis or dye binding techniques. In addition, other reports indicate that iron may be influenced by EDTAbut again depending on the platform being used. In the present publication from Canada, the authors evaluated the effects of EDTA on magnesium, iron, calcium and ALP using two analytical platforms: the Abbot Alinity c and the Roche cobas c303 (4). Four sample pools were created from residual serum or plasma and were free from haemolysis and lipaemia. Potential icterus interference for theAbbotAlinity c was below that stated by the manufacturer Eight aliquots of sample 1 to 4 were spiked with increasing concentrations of NaEDTAfrom 0.10 to 8.05mmol/L plus 0. Two hours post spiking the samples were analysed on both analysers and the results analysed. The outcome was that EDTA has differing effects on magnesium which was method dependent with the enzymatic method (Abbot) being least affected and the dye method (Roche) having a significant decrease. Iron, similarly the chelator used in the Roche methods was more affected that that used in the Abbot method. Both calcium and ALP showed similar decreases using analytical platform. The authors conclude that both magnesium and calcium dye binding methods are affected by small amounts of EDTA. Iron andALP will be influenced by the method used on the analyser and indicated for an understanding of the chemistry taking place during analysis.
Greening the laboratory
Healthcare in general is a greenhouse gas contributor, and international studies indicate that there is variability between countries e.g. UK 4% and Australia 7%. For pathology data is available for the greenhouse gas contribution for certain routine tests and that 60 to 90% of the individual test is contributed by the phlebotomy process i.e. plastics collection and transport systems. Previous research has calculated the annual carbon dioxide contribution for individual pathology tests in a 1000 be hospital and the carbon footprint for a full blood count over the year was 26,100Kg. A research collaboration between Australia, Turkey, Finland and Nigeria has investigates a possible pathway to create a sustainable laboratory (5). The authors direct readers to resource that are available and provide key steps for developing an “Action Plan” for the laboratory. In addition, they provide direction on obtaining certification for a “Green Laboratory” and emphasize the importance of involvement and education for providing environmentally sustainable laboratories.
Promoting laboratory medicine
Who appreciates the value of laboratory medicine (read pathology)? Despite laboratory medicine being involved with virtually all modern medicine and is essential for concept of “patient centred care” it is a “faceless profession”. It is a fundamental part of the concept of wellness, preventative care and identification and treatment for disease as well as being innovators of new diagnostic biomarkers. Despite the innovative nature of laboratory medicine more recently it has fallen victim to reducing costs per tests, economies of scale, turnaround times etc. This has effectively moved to a “commodity based” function rather that the link in the clinical based context. In a collaboration between scientists from Italy and Turkey they have investigated a route for an innovative clinical laboratory (6). They propose a “value based” process where the laboratory results are not a mere transactional event but have direct relevance to both response time and communication. Misinterpretation of laboratory results is the second most medical error from diagnostic tests. The authors propose that more attention should be given to longitudinal data for clinical decision making which would accommodate biological variation. They encourage the use of “well care” biomarkers which may be used in modelling wellness or disease patterns. This development would lead to integrated diagnostics and remove the current fragmentation of multiple subspecialities that can create a silo effect. The authors conclude that a new way of considering the interactions of laboratory professionals and clinicians would result in improved outcomes for both the health care professionals and the patients.
REFERENCES
1. Lenters-Westra E, Singh P, Vetter B, English E. Challenges in HbA1c point of care testing: Only 5 of 19 HbA1c point of care devices meet IFCC and NGSP certification criteria on independent valuation. Clin Chem 2025; 71: 775-788. doi: 10.1093/clinchem/hvaf059. [Open Access]
2. Gopaulchan D, Moore C, Ali N, Sukha D et al. A defined microbial community reproduces attributes of fine flavour chocolate fermentation. Nature Microbiol 2025; 10(9): 21302152. doi: 10.38/s41564-025-02077-6. [Open Access]
3. Diehl F, Schmidt K, Choti MA, Romans K et al. Circulating mutant DNA to assess tumor dynamics. Nat Med 2008; 14(9): 985-990. doi: 10.1038/nm.1789.
4. Brinc D, Lu C-Y, Rodrigues O, Rokforooz F et al. Assay dependant effects of EDTA contamination on magnesium and iron, Clin Chim Acta 2025:1:577:120453. doi: 10.1016j. cca.2025.120442.
6. Plebani M, Coskun A. Promoting value-based laboratory medicine. Moving towards an innovative model of clinical laboratory. Clin Chim Acta 2025; 15:572:120269. doi: /1016/j.cca.2025.120269. [Open Access]
RETIREMENT ANNOUNCEMENT
Bronwen Johnson, Laboratory Medical Scientist
Automation & Laboratory Support Services, Labplus, Auckland
After more than five decades in the laboratory, Bronwen Johnson is hanging up her lab gown and heading into a well-earned retirement.
She started her journey on 20 January 1974 as one of nine fresh-faced trainees at Auckland Hospital - back when computers filled a room, and automation meant having two hands. Her training involved rotating through every department imaginable, studying at AUT by day (and night!), and surviving the dreaded midnight-to-8am blood bank shift.
Bronwen officially qualified with O-levels in Microbiology and Biochemistry, with Biochemistry stealing her heart, especially the automation side. She worked at Princess Mary, took a short break to raise her family, then returned to what became her long-standing evening shift at Labplus - 33 years and countless samples later!
She’s seen it all, from manual pipettes to high-speed analysers, floppy disks to LIS upgrades (too many to count). Through it all, she’s remained calm, capable, and wonderfully down-to-earth.
As she steps into retirement, we thank Bronwen for her incredible contribution and wish her endless cups of tea, sleepins, and no more on-calls. Happy retirement, Bronwen, you have more than earned it!
Laboratory Christmas Quiz: Light relief from CPD questions
The Christmas quiz was very successful again last year and the NZIMLS Council has agreed to sponsor another quiz this year. As with last year it is a General Knowledge Quiz and the NZIMLS Council has agreed to award a single prize of $300.00 towards a laboratory Christmas function for the most correct answers. While individuals can also complete the quiz, the prize is only to a laboratory team entry to encourage teamwork. There are no CPD points for this quiz, and it is not discipline related. The NZIMLS Council have not participated in the question setting or have knowledge of the answers. An answer sheet is available on the NZIMLS website. The answers will be published on the NZIMLS website after the quiz closes, and the winner(s) is announced. Closing date for all answers is 8 December 2025. All completed quiz answers with a Laboratory contact person should be sent to: mike.legge@nzimls.org.nz and subject Christmas Quiz. Please indicate if the entry is a team or individual entry as indicated below. No correspondence will be entered into relating to the quiz.
Team entry: Yes No
Name of Team and Laboratory:
(Delete One)
1. The word ‘derrick’ used for a construction on commercial oil rigs is named after?
a. An 18th century crinoline support frame
b. Old English for a scaffold
c. A 17th century hangman
d. A 16th century engineer
2. In which European city was Karl Marx buried?
a. London
b. Paris
c. Moscow
d. Berlin
3. Which of the following European countries is the biggest banana producer in Europe?
a. Spain
b. Denmark
c. Iceland
d. Italy
4. Denim was first produced in which French city?
a. Nice
b. Lyon
c. Marseille
d. Nimes
5. Lewis Caroll was a pen name for which author?
a. C.S. Lewis
b. Henry Auber Fletcher
c. Charles Lutwidge Dodgson
d. Harry Hart Frank
6. Vernal relates to which season?
a. Autumn
b. Winter
c. Spring
d. Summer
7. In which field would the word Oulipo be found?
a. Geology
b. Writing
c. Painting
d. Medicine
8. In the Greek mythology Erebus is the persons function of what?
a. Sky
b. Day
c. Sea
d. Darkness
9. In which opera does Don Jose play a leading role?
a. La Boheme
b. Carmen
c. Lakme
d. Pagliacci
10. Which European city was known as ‘Olisipo during the Roman Empire?
a. Lisbon
b. Paris
c. Tangier
d. Madrid
11. Which country is generally accredited with the invention of the ‘ute’?
a. New Zealand
b. Germany
c. Australia
d. America
12. How many ‘face off’ circles are marked in the rink for an ice hockey game?
a. Eight
b. Five
c. Nine
d. Four
13. The Phoenician people lived mainly in the equivalent of which modern country?
a. Greece
b. Turkey
c. Lebanon
d. Egypt
14. At sea level, approximately how far can the horizon be seen?
a. 15Km
b. 5Km
c. 10Km
d. 20Km
15. Which country outside of Europe has more than three million German speakers?
a. Argentina
b. Columbia
c. Uruguay
d. Brazil
16. The meaning of the car manufacturers trademark “Volvo” means which of the following?
a. To role
b. To move
c. To service
d. To use
17. Which blues guitarist was born Ellas Bates?
a. Chuck Berry
b. Muddy Waters
c. Bo Diddly
d. Eric Clapton
18. The modern Italian language originated from which Italian City State?
a. Venice
b. Rome
c. Naples
d. Florence
19. Where is the Sargasso Sea?
a. Pacific Ocean
b. Indian Ocean
c. Artic Ocean
d. Atlantic Ocean
20. The fashion house “Prada” has been involved in designing which of the following?
a. Sun protection clothing
b. Space suits
c. Antarctic protection clothing
d. Personal protection clothing
21. In the 17th century which country did lens makers learn to combine lenses?
a. England
b. Germany
c. Italy
d. Holland
22. In which Western movie did the “Man with no name” use body armour?
a. For a few dollars more
b. The good the bad and the ugly
c. Pale Rider
d. A fistful of dollars
23. The Normans from France originated from which culture?
a. Celtic
b. Germanic
c. Gaelic
d. Norse
24. Besides the Vatican, which of the following is the only country to have a square flag?
a. Switzerland
b. Austria
c. Nepal
d. Finland
25. Norway’s Svalbard Island is home to a refuge for which of the following?
a. Seeds
b. Threatened species embryos
c. DNA bank
d. Data bank
26. How many emirates are in the United Arab Emirates?
a. Five
b. Nine
c. Three
d. Seven
27. Which metallic element takes its name from the ancient Greek word for stone?
a. Lithium
b. Zinc
c. Tin
d. Lead
28. The pattern of alternating rectangles of colour on emergency vehicles, is known as?
a. Quadrant colour
b. Crossover tartan
c. Bauhaus block
d. Battenberg markings
29. What colour are the tennis courts at Melbourne Park for the Australian Open?
a. Green
b. Brown
c. Blue
d. Red
30. Where did tomatoes originate from?
a. South America
b. India
c. China
d. Italy
31. Which modern city is on the site of the ancient Greek city of Byzantium?
a. Tunis
b. Istanbul
c. Beirut
d. Athens
32. Who wrote the music “Adagio for Strings”?
a. Leonard Bernstien
b. Claude DeBussey
c. Benjamin Britten
d. Samuel Barber
33. How many official national languages are there in Switzerland?
a. Three
b. Four
c. Two
d. Five
34. In which year was the first in-flight movie screened?
a. 1948
b. 1925
c. 1950
d. 1955
35. Which country produces most of the world’s emeralds?
a. India
b. Columbia
c. South Africa
d. Australia
36. On which island did halloumi cheese originate?
a. Corsica
b. Sardinia
c. Cyprus
d. Crete
37. What is the main ingredient in a “Singapore Sling”?
a. Whisky
b. Cognac
c. Vodka
d. Gin
38. From which country did the word “spa” as in “spa pool” originate?
a. France
b. Italy
c. Belgium
d. Portugal
39. What does a cordwainer make?
a. Shields
b. Ships
c. Shoes
d. Shirts
40. Which of the following is the world’s driest non-polar desert?
a. Gobi
b. Atacama
c. Saraha
d. Kalahari
41. In which country is the province of Zeeland?
a. Belgium
b. Sweden
c. Denmark
d. Netherlands
42. What was the group Queen’s first name for the group?
a. Grin
b. The Smirk
c. Smile
d. The Beams
43. In which year was the first web page served on the open internet?
a. 1990
b. 1992
c. 1988
d. 1985
44. Where would you find a serac?
a. On a glacier
b. In the ocean
c. In a desert
d. On the moon
45. Bumbershoot is the old-fashioned word for which of the following?
a. Umbrella
b. Shotgun
c. Automobile
d. Fly swat
46. What kind of pastry is used to make eclairs and profiteroles?
a. Flaky
b. Choux
c. Puff
d. Filo
47. Which of the following countries has no capital city?
a. Belgium
b. Netherlands
c. Switzerland
d. Austria
48. Putiputi is the te rao Mâori word for which of the following?
a. Flower
b. Tree
c. Bird
d. Animal
49. A thermopolium in the ancient Greece-Roman world was what?
a. A blacksmith
b. A public spa
c. A smelting foundry
d. A takeaway
50. Which technique was essential for creating flavoured crisps?
a. Gas chromatography
b. Thin-layer chromatography
c. Mass spectrometry
d. Liquid chromatography
51. Who is the only person below to win the Nobel prize in two different sciences?
a. Louis Pasteur
b. Marie Curie
c. Albert Einstein
d. Nikola Tesla
52. Where would you find a millum?
a. Plants
b. Skin
c. Astronomy
d. Mathematics
53. Robert Galbraith is a ‘pen name’ of which of the following authors?
a. JK Rowling
b. John le Carrier
c. Val Mcdermid
d. Ian Rankin
54. The island of Upola is in which country?
a. Samoa
b. Tonga
c. Rarotonga
d. Fiji
55. Which of the following English rulers banned Christmas? Charles II George IV Oliver Cromwell Charles
a.
b.
c.
d.
56. What was the nationality of the person who invented the internal combustion engine?
a. Swiss
b. German
c. American
d. English
57. Which country is the ‘home’ of the fondue
a. France
b. Switzerland
c. Holland
d. Sweden
58. The nationality of Agatha Christie’s fictional detective Hercule Poirot was?
a. Dutch
b. French
c. Italian
d. Belgian
59. The ancient Greek goddess Selene represented which heavenly body?
a. Venus
b. Moon
c. Sun
d. Jupiter
60. What was the occupation of the person who wrote “Alice in Wonderland”?
a. Scientist
b. Philosopher
c. Priest
d. Mathematician
Enter your answers online at: https://irp.cdn-website.com/102112c1/files/uploaded/Laboratory+Christmas+Quiz+2025+online+answer+sheet.pdf
2026 NZIMLS CALENDAR
Dates may be subject to change
January 01
09
Membership and CPD enrolment due for renewal Admin@nzimls.org.nz
Material for the March issue of the Journal must be with the Editor sharon@nzimls.org.nz
09 QMLT applications open www.nzimls.org.nz
31 Last day for 2025 CPD points to be entered cpd@nzimls.org.nz
February 21 Haematology SIG, Waipuna Events Centre, Auckland Mala.govender@awanuilabs.co.nz
26/27 Council Meeting, Christchurch sharon@nzimls.org.nz
April 15
May 08
South Island Seminar (TBC)
Closing date for QMLT applications admin@nzimls.org.nz
Material for the July Journal must be with the Editor sharon@nzimls.org.nz
NICE Weekend (TBC) raewyn.cameron@pathlab.co.nz
28/29 Council meeting (venue to be confimed) sharon@nzimls.org.nz
August 06
Annual Reports and Balance Sheet to be with the Membership (14 days prior to AGM) sharon@nzimls.org.nz
17/18 Council Meeting, Wellington sharon@nzimls.org.nz
19-21
NZIMLS 80th Annual Scientific Meeting, Tākina Events Centre, Wellington sharon@nzimls.org.nz
20 NZIMLS Annual General Meeting sharon@nzimls.org.nz
September 11
October 03
Material for the November Journal must be with the Editor sharon@nzimls.org.ng
QMLT Examinations admin@nzimls.org.nz
November Pre-Analytical SIG, Auckland (TBC)
26/27 Council Meeting, Christchurch
Ajesh.joseph@waikatodhb.health. nz
More events (and dates) will be added as they are confirmed.