Peptides for Hair Loss: A Dermatologist’s Perspective on Their Use and Benefits
Comprehensive Facial Rejuvenation with Hyaluronic Acid Fillers
Fractional CO2 Laser Ablation for Hypertrophic Nasal Scar Treatment
Idiopathic Chronic Urticaria
Atopic Dermatitis
Chronic Idiopathic Urticaria
Histamine-Mediated Pruritus
Desloratadine 5 mg
Montelukast 10 mg
Loratadine 10mg
EXECUTIVE EDITOR & PUBLISHER
Dom Daniel
CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
Printed, Published, Edited and Owned by Dom Daniel Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of February -2025
Cover Model: Rozalyn Khan
Photography: Dhananjay Pratap Singh
Hair & make up: by Sima Samir
Advancing Excellence in Skin and Hair Care Treatments
As both medical and aesthetic dermatology rapidly evolve, new treatments and technologies are providing more effective, targeted, and minimally invasive options for a range of skin conditions, from acne and hair loss to aging signs and pigmentation disorders.
Key innovations, including nanotechnology for peptide delivery, advanced injectable therapies, and the personalization of treatment regimens, are reshaping patient care. These advancements not only improve clinical outcomes but also place a strong emphasis on patient comfort, safety, and satisfaction.
As the field continues to evolve, dermatologists must stay at the cutting edge of these innovations, adapting new solutions to meet the growing demands of patients seeking sustainable, effective treatments. This editorial underscores the importance of embracing these advancements while ensuring dermatologists continue to offer individualized care, addressing the unique needs and concerns of each patient.
This issue highlights significant innovations in dermatology, focusing on advancements in both medical and aesthetic practices. It features four key articles: one exploring the role of peptides in hair loss; another examining the use of hyaluronic acid fillers in facial rejuvenation, with an emphasis on personalized techniques for natural results; and a third offering a comprehensive approach to acne vulgaris, addressing its complex pathogenesis and emerging therapies. Additionally, it features the use of Fractional CO2 Laser Ablation for treating hypertrophic nasal scars. These articles showcase the dynamic progress in dermatology, emphasizing the integration of science, technology, and individualized care to enhance patient outcomes.
HOPE YOU HAVE A GREAT READ
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher
Editorial Board Advisory Board
Dr. Geetanjali Shetty
MD, FCPS, DDV, FRSPH, FAAD
Consultant Dermatologist and Cosmetologist
Revitalis, Hair Laser Aesthetics
Mumbai
Dr. Sonali Kohli
MD
Consultant Dermatologist
Sir H.N. Reliance Foundation Hospital
Mumbai
Dr. Mamta Dhayal
MBBS, DDV
Dermatologist, Dr. Dhayal's Skin, Hair & Nails Clinic, Mumbai
Consultant Dermatologist, DFY NGO
Dermatologist, K J Somaiya Hospital & Research Centre, Mumbai
Peptides for Hair Loss: A Dermatologist’s Perspective on Their Use and Benefits
Dr. Geetanjali Shetty
MD, FCPS, DDV, FRSPH, FAAD
Consultant Dermatologist and Cosmetologist
Revitalis, Hair Laser Aesthetics, Mumbai
Introduction
Peptides have emerged as a revolutionary ingredient in dermatology
and trichology, offering a new approach to managing hair loss and promoting hair health. These small protein fragments, composed of amino acids, act as signaling molecules in the skin and scalp, encouraging cellular repair, growth, and rejuvenation. For individuals dealing with hair thinning, alopecia, or weakened hair follicles, peptide-based treatments can be an effective addition to their regimen.
Key Benefits of Peptides in Hair Care
1. Stimulates Hair Follicles
Peptides work at the follicular level to activate dormant hair follicles, encouraging the growth phase (anagen) of the hair cycle. Research has demonstrated their ability to boost the production of proteins essential for hair growth, such as keratin.
2. Improves Scalp Health
A healthy scalp is crucial for hair growth. Peptides help reduce
inflammation, improve hydration, and enhance the scalp’s barrier function, creating a conducive environment for heal thier hair.
3. Increases Blood Circulation
Peptides like copper peptides play a role in improving blood flow to the scalp, ensuring that hair follicles receive essential nutrients and oxygen, which are vital for healthy hair growth.
4. Blocks DHT (Dihydrotestosterone)
Certain peptides inhibit the activity of DHT, a hormone associated with androgenetic alopecia (pattern baldness). By reducing DHT’s effects, peptides help prevent further hair loss and thinning.
5. Reduces Scalp Inflammation
Chronic inflammation can damage hair follicles and contribute to hair loss. Peptides possess anti-inflammatory properties, soothing irritated scalps and promoting recovery.
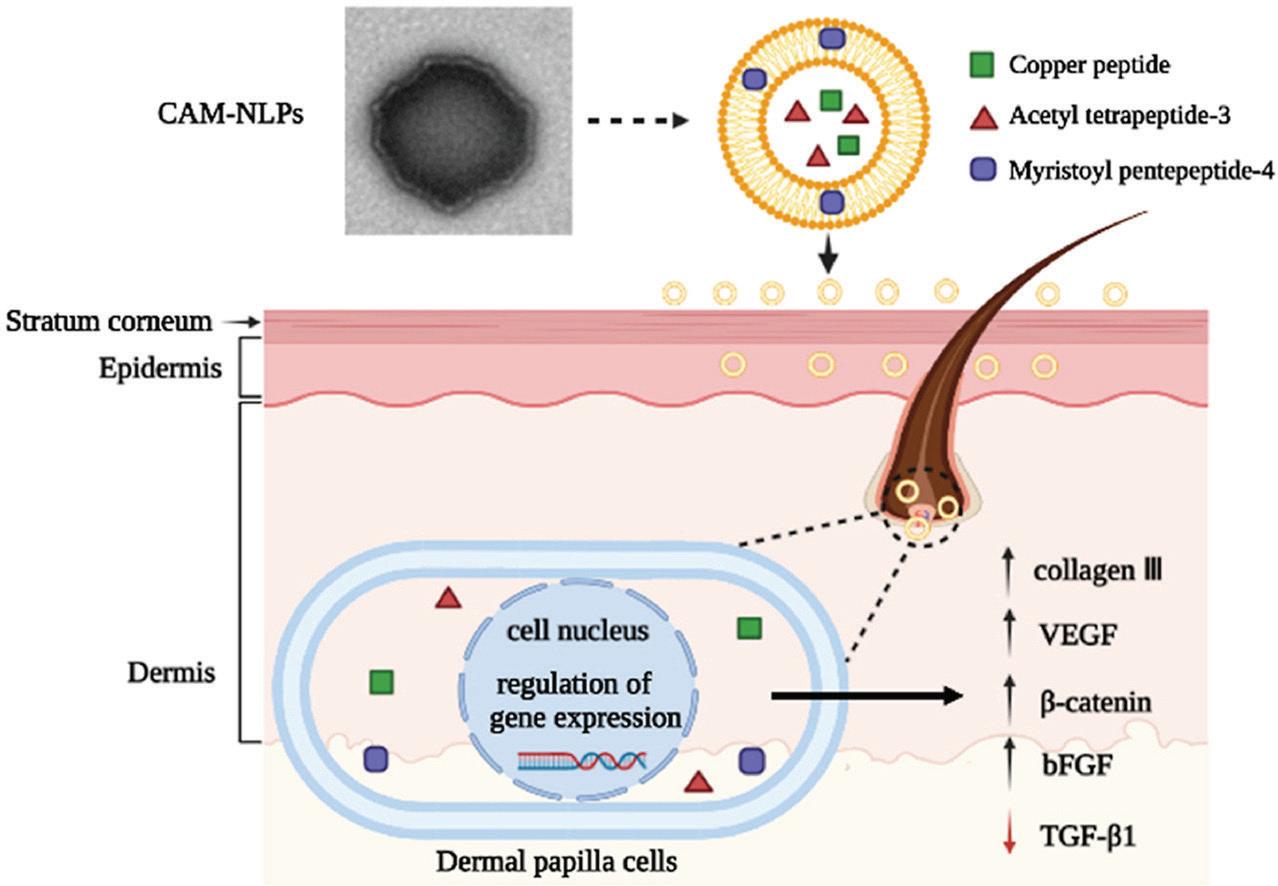
Co-delivery of bioactive peptides by nanoliposomes for promotion of hair growth
Types of Peptides Used in Hair Care
1. Copper Peptides
• Enhances hair growth by stimulating blood flow to the scalp.
• Promotes collagen and elastin production, supporting hair follicle structure.
2. Keratin Peptides
• Strengthens the hair shaft and prevents breakage.
• Repairs damaged hair, improving texture and elasticity.
3. Biotinyl-GHK (Biotin Peptides)
• Combines biotin’s benefits with peptides to improve follicular strength.
• Boosts keratin production and addresses hair thinning.
4. Collagen-Derived Peptides
• Improves scalp hydration and elasticity.
• Supports overall scalp health to create a robust base for hair growth.
Peptides for Hair Loss: A Dermatologist’s Perspective on Their Use and Benefits
Incorporating Peptides into Hair Care
Peptide-Infused Products
Peptides are commonly included in hair care formulations such as serums, shampoos, conditioners, and masks. Each product type has its unique application:
• Serums: Apply a few drops directly onto the scalp and massage gently. These leave-in treatments work best when used consistently.
• Shampoos and Conditioners : Follow the product’s instructions, usually 2-3 times a week.
• Masks: Ideal for a weekly intensive treatment to repair damage and nourish the scalp.
Best Practices for Use
1. Daily Use: Lightweight leave-in serums with peptides can be applied daily for sustained benefits.
2. Avoid Overuse: Concentrated peptide treatments like masks should be used sparingly to avoid scalp buildup.
3. Consistency Matters: Results take time, often visible after 8-12 weeks of regular use.
Clinical Perspective: Evidence Supporting Peptides for Hair Growth
In Vitro Studies
Laboratory studies have highlighted peptides’ ability to enhance keratinocyte and fibroblast activity, crucial for hair follicle regeneration.
In Vivo Studies
Human trials have shown that consistent application of peptidebased products improves hair density, reduces hair shedding, and enhances scalp health within three to six months.
Dermatologist-Recommended Application Tips
• Always conduct a patch test before incorporating new products into your routine.
• Combine peptides with other effective treatments like minoxidil or platelet-rich plasma (PRP) therapy for enhanced results.
• Ensure proper scalp hygiene to maximize peptide absorption.
Conclusion
Peptides offer a scientificallybacked, non-invasive approach to combating hair loss and improving overall hair health. As a dermatologist, I recommend incorporating peptide-based products into your hair care regimen to complement existing treatments. When used consistently, they not only improve hair thickness and density but also restore confidence in individuals struggling with hair loss.
Remember: Consult a dermatologist to customize your treatment plan and determine the best products for your specific hair and scalp needs.
Innovative RF and HIFES Device Proven Effective for Improving Facial Laxity in Asian Patients.
A novel device combining synchronized radiofrequency (RF) and high-intensity facial electrical stimulation (HIFES) was evaluated for its safety and efficacy in treating facial laxity, particularly in Asian patients. A prospective, evaluatorblinded study showed significant improvements in facial lifting, skin firmness, texture, and pigmentation. The RF component heated the dermis to promote collagen stimulation, while HIFES targeted deeper tissues to enhance muscle tone and skin elasticity. Significant reductions in skin wrinkles, pore
volume, and melanin levels were noted, with sustained improvements in eyebrow and forehead lifting. The therapy was well-tolerated with decreasing pain scores over the treatment sessions and no serious adverse events. The results suggest the therapy is effective for noninvasive facial rejuvenation, though the small sample size and predominantly female cohort call for further investigation in larger, more diverse populations. Future studies should explore comparing this dual-modality approach to other noninvasive treatments, particularly considering ethnic variations in treatment response.
New Cysteamine and Isobionicamide Combination Enhances Skin Rejuvenation and Reduces Signs of Aging.
A novel case study evaluated the combination of cysteamine and isobionicamide in a topical formulation for skin rejuvenation and anti-aging. The study involved patients with varying Fitzpatrick skin types who applied the product daily. The treatment resulted in improved skin radiance, evenness, reduced fine lines, and diminished hyperpigmentation. Wrinkle depth and skin texture were also significantly improved, with enhanced hydration and overall skin health.
Both clinical assessments and patient self-reports showed noticeable improvements. The product demonstrated excellent safety, with no signs of erythema, irritation, or dryness. The combination of cysteamine, a potent antioxidant, and isobionicamide, a melanosomal transfer inhibitor, showed a synergistic effect on tyrosinase inhibition and may reduce oxidative stress. Further studies with larger sample sizes and objective measurements are needed to better understand the formulation's mechanisms of action and potential for use alongside in-office procedures like laser therapies and chemical peels.
Comprehensive Facial Rejuvenation with Hyaluronic Acid Fillers
Dr. Sonali Kohli MD
Consultant Dermatologist
Sir H.N. Reliance Foundation Hospital
Mumbai
Introduction
The field of aesthetic medicine has experienced substantial
advancements, culminating in the development of innovative therapies designed to enhance skin quality and address specific concerns associated with aging and dermal laxity. One notable advancement is the introduction of bio-remodelling injectables, a novel class of products that harness the properties of hyaluronic acid (HA) to facilitate rejuvenation at the cellular level. Unlike conventional dermal fillers, which primarily function to increase volume, these injectables emphasize the stimulation of collagen and elastin production, thereby promoting the integrity and resilience of the skin. By targeting the fundamental structural components of the dermis, bio-remodelling injectables offer a multifaceted approach to aesthetic enhancement, improving overall skin texture and appearance while addressing the underlying mechanisms of skin aging.1
The periorbital region, commonly known as the under-eye area, is often among the first to
exhibit signs of aging due to its notably thinner skin compared to other facial regions, making it particularly susceptible to aesthetic concerns such as periorbital hyperpigmentation (dark circles), edema (puffiness), and volume loss (hollowness). Several factors contribute to the deterioration of this area with advancing age, including genetic predisposition, hormonal fluctuations, lifestyle choices, and environmental influences such as ultraviolet (UV) exposure and pollution. As the skin loses elasticity and volume, pronounced fine lines and wrinkles may appear, leading to a fatigued and aged look. Dark circles, or periorbital hyperpigmentation, can be exacerbated by psychological stress, sleep deprivation, and hereditary factors, imparting a tired appearance that diminishes perceived vitality. Additionally, periorbital edema can result from fluid retention, allergic reactions, or inflammatory processes, with lifestyle factors such as poor dietary habits and excessive sodium intake further exacerbating this issue. Age-related changes in
subcutaneous fat and bone density can lead to noticeable volume loss in the periorbital region, resulting in hollowness or trough formation that accentuates dark circles and contributes to a gaunt facial contour, significantly affecting the overall aesthetic balance of the face.2
The aesthetic concerns associated with the under-eye area can significantly impact an individual's daily life and self-esteem. For many, the appearance of dark circles, puffiness, or hollowness can lead to feelings of self-consciousness and insecurity. This discomfort may affect social interactions, professional opportunities, and even personal relationships, as individuals might go to great lengths to conceal these imperfections with makeup or other temporary solutions. Moreover, the psychological effects of under-eye concerns can extend beyond physical appearance. Individuals may experience a lack of confidence or feel judged based on their appearance, which can influence their mental well-being. The pursuit of youthful and vibrant skin often becomes a focus for those experiencing these issues, leading to increased interest in aesthetic treatments. Bio-remodelling injectables present a promising solution for those seeking to rejuvenate the under-eye area. By stimulating collagen and elastin production, these injectables not only improve the skin’s texture and hydration but also address issues such as dark circles and hollowness, providing a more youthful and refreshed appearance. As aesthetic
medicine continues to advance, bio-remodelling injectables stand out as a versatile and effective option for enhancing facial aesthetics, particularly in the delicate under-eye region.1, 2
Case 1
A 30-year-old female patient presented for facial rejuvenation utilizing biomedical injectable fillers, hyaluronic acid, targeting the facial region, cervical area, and bilateral periorbital zones. The objective of the intervention was to restore volume, enhance skin texture, and reduce the appearance of fine lines and wrinkles. After a comprehensive consultation and assessment of her aesthetic goals, a synergistic combination of hyaluronic acid-based fillers was administered to achieve optimal outcomes. Post-procedure evaluations demonstrated immediate enhancements in facial contours, skin hydration, and overall dermal quality. The patient expressed a high level of satisfaction with the aesthetic results, noting improved facial symmetry and a more youthful appearance. Scheduled follow-up assessments will be conducted to monitor the longevity of the results and ensure the maintenance of the desired effects.
Comprehensive Facial Rejuvenation with Hyaluronic Acid Fillers
Before treatment
After treatment
Figure 1: Filler for face
Case 2
A 36-year-old female, presented with dark circles and under-eye hollowness contributing to a tired appearance. Clinical evaluation revealed bilateral tear trough deformity with mild periorbital volume loss (Fitzpatrick Type IV). Tear trough correction was performed using hyaluronic acid fillers. Post-procedure, mild erythema and swelling resolved within 48 hours. At a 2-week follow-up, significant improvement in under-eye hollowness and brightness was noted, with no adverse effects. The patient expressed high satisfaction with the refreshed and natural aesthetic outcome.
Figure 2: Filler for neck
Figure 3: Filler for under eye (left side) After
Figure 4: Filler for under eye
Diagnosis
The primary goal of diagnosing under-eye concerns is to differentiate between vascular, pigmentary, and structural causes, enabling targeted treatment. A thorough assessment of the patient's medical history and lifestyle is essential, considering hereditary factors, previous treatments, and underlying health issues like thyroid dysfunction, along with aspects such as sleep quality and diet. This comprehensive approach allows for personalized treatment strategies that optimize aesthetic outcomes.3 Visual inspection of the periorbital region is crucial for identifying conditions like dark circles and edema, helping to distinguish between vascular hyperpigmentation and melanin deposition.4 Dermoscopy provides high-resolution imaging to enhance diagnostic precision for conditions such as vascular lesions.5 Additionally, allergy testing, including skin prick tests and specific IgE blood assays, is important for diagnosing periorbital edema and hyperpigmentation, enabling appropriate avoidance strategies and treatments like antihistamines.6 Imaging techniques, such as ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI), are also vital for evaluating undereye conditions, collectively enhancing diagnostic accuracy and optimizing patient outcomes.7
Treatment
This advanced injectable bioremodeling agent consists of stabilized hybrid hyaluronic acid (HA) complexes, specifically formulated to address skin laxity, dehydration, and fine lines in the under-eye region. Utilizing patented thermal treatment technology, it combines high and low molecular weight HA for optimal skin rejuvenation. The formulation contains 32 mg of high molecular weight hyaluronic acid (HA) with a molecular weight ranging from 1100 to 1400 kDa and 32 mg of low molecular weight HA with a molecular weight ranging from 80 to 100 kDa, presented in a 2 mL syringe. This balanced formulation facilitates comprehensive facial bioremodeling through targeted delivery to the dermal layers.6
The low molecular weight HA activates CD44 receptors on fibroblasts and keratinocytes, stimulating the endogenous production of hyaluronic acid, collagen, and elastin, enhancing hydration and promoting a youthful appearance in the undereye area. The high molecular weight HA provides structural support within the extracellular matrix (ECM), increasing skin turgor and overall density, thereby improving the appearance of fine lines and wrinkles around the eyes. The hybrid HA complexes exhibit enhanced resistance to bovine testicular hyaluronidase (BTH), being up to eight times more stable than conventional high molecular weight HA. This stability translates
to prolonged action within the tissue, ensuring sustained hydration and remodeling effects. The formulation is characterized by low TGF-B expression, leading to minimal inflammatory response postinjection, which is beneficial for the delicate under-eye area, where inflammation can exacerbate concerns such as swelling or bruising. The agent is injected using 29G thin wall needles, allowing for precise administration despite its high concentration (32 mg/ ml). Its low viscosity facilitates easy and rapid distribution within the dermis, promoting even bioremodeling effects.7
A range of aesthetic treatments for under-eye concerns exists beyond bio-remodelling injectables. Topical agents like retinoids and vitamin C serums enhance skin texture and brightness. Chemical peels promote exfoliation and address pigmentation issues. Laser therapies, including fractional laser resurfacing and pulsed dye laser, stimulate collagen and reduce dark circles. Intense pulsed light (IPL) improves skin tone by treating pigmentation and vascular irregularities. Microdermabrasion and radiofrequency therapy enhance texture and tighten skin, respectively. Microneedling promotes collagen synthesis, while cryotherapy reduces puffiness. Additionally, tear trough fillers restore volume, and lifestyle changes such as adequate sleep and a
balanced diet can support skin health. These treatments collectively provide effective alternatives for rejuvenating the periorbital region, warranting consultation with a qualified practitioner for individualized care.6
Minimally invasive procedures have transformed the treatment landscape for facial and body rejuvenation, significantly impacting the recent evolution of cosmetic surgery. Initially designed solely for addressing fine lines and wrinkles, the application of dermal fillers has broadened to encompass the correction of volume loss associated with aging, enhancement of damaged and scarred tissues, and the overall success of cosmetic interventions. The ideal soft tissue filler should possess several characteristics: it must be effective, nonimmunogenic, nontoxic, noncarcinogenic, nonmigratory, easily applicable, nonpalpable, painless, and long-lasting.8
As a linear polysaccharide comprised of repeated disaccharide units of glucuronic acid and N-acetylglucosamine, hyaluronic acid is a crucial component of the natural extracellular matrix and is abundantly present in various connective tissues, including the skin, vitreous humor of the eye, and synovial fluid. Due to its hygroscopic properties, biocompatibility, and reversibility, hyaluronic acid (HA) has become the most
commonly used dermal filler for the correction of volume loss associated with aging.8
Injection Technique
The technique employed in this procedure is referred to as Bio Aesthetic Points (BAP) and is specifically designed for this product. The BAP technique has been developed by a team of experts. The location of the five BAP technique points stems from a selection criteria that aims to minimize risks and maximize hyaluronic acid (HA) distribution while reducing the number of intradermal injection points and treatment sessions required.8
• Zygomatic Protrusion: Located at the apex of the zygomatic arch, positioned at least 2 cm from the orbital area.8
• Nasal Base: Identified at the intersection of two reference lines: one horizontal extending from the tip of the nose to the inferior aspect of the tragus, and the other vertical, originating from the center of the pupil.8
• Tragus: Situated 1 cm anterior to the most inferior point of the tragus.8
• Chin: Defined as 2.5 cm from the midpoint of a horizontal line bisecting the distance between the lower lip and the chin, where the inferior segment is twice the length of the superior segment.8
• Mandibular Angle: Should be positioned 1 cm superior
to the mandibular angle.8
Following any similar aesthetic treatments, it is recommended that no aggressive procedures be conducted in the treated area for a period of 24 hours. Additionally, patients should adhere to an appropriate facial hygiene regimen during this initial recovery phase. Beyond this, no specific aftercare is required.
Discussion
Facial aging is a complex physiological process characterized by reduced skin hydration and alterations in the elastin and collagen fibers of the dermis, leading to diminished turgor and skin tone. While studies indicate that the loss of facial volume typically begins after the age of thirty, many patients visiting clinics express greater concern regarding declining skin hydration, tone, and elasticity.8 Research supports the efficacy and safety of hyaluronic acid (HA) in volume restoration; however, the primary focus remains on enhancing skin quality, hydration, and texture. Recent advancements in understanding the cutaneous aging process have facilitated more targeted therapeutic interventions. Various treatments for skin regeneration, including calcium hydroxyapatite, polylactic acid, polycaprolactone, and platelet-rich plasma, as well as devices such as lasers, pulsed light, and radiofrequency,
have been explored. HA is notable for its ability to restore hydration, elasticity, and skin tone through the application of varying molecular weights, achieving a synergistic effect that combines deep hydration with mechanical lifting. Furthermore, HA plays a crucial role in the extracellular matrix, creating optimal conditions for cellular proliferation, migration, and organization. Hybrid complexes demonstrate resistance to hyaluronidase, as shown in vitro by D’Agostino et al., thereby prolonging their effects despite utilizing natural HA. Existing literature on similar biostimulation treatments has primarily focused on reticulated HA; however, formulations of high and low molecular weight HA are particularly effective for delivering hydrating and bio-stimulatory effects while providing structural support. The natural composition of HA results in minimal inflammatory reactions, and its thermal treatment enhances resistance to hyaluronidase, extending its duration compared to conventional long-chain HA. The administration of this treatment involves a straightforward technique that minimizes complications and ensures consistent replicability. Despite some limitations regarding sample size and study duration, the low incidence of complications— most of which were minor— affirms the safety of the BAP
technique. The treatment's efficacy is evidenced by patient evaluations, with over 70% reporting improvements exceeding 75% at 60 days post-treatment. Notably, the subjective satisfaction levels reported by patients significantly surpassed objective assessments made by professionals at this time point, likely due to enhanced understanding of expected outcomes. While acknowledging the limitations of this preliminary study, including its brief duration and limited patient population, the clarity of the results encourages further long-term investigations and the potential for multi-center studies to evaluate efficacy and safety comprehensively.8
Hyaluronic acid (HA) is a naturally occurring glycosaminoglycan polysaccharide that serves as the foundation for dermal fillers, restoring volume, improving skin hydration, and enhancing tissue structure. Upon injection, HA attracts and retains moisture, increasing skin elasticity and providing immediate volumization through a gel-like matrix. It also stimulates fibroblasts to produce collagen and elastin, leading to long-term improvements in skin quality.3 Aging reduces HA and collagen levels, resulting in wrinkles, which HA fillers can counteract by replenishing lost volume. They can be either animal-derived or non-animal-derived, with variations in manufacturing affecting their durability. HA is also used intra-articularly, where it mimics synovial fluid, aiding in osteoarthritis treatment through its antiinflammatory effects. Adverse effects from HA treatments are minimal, with rare cases of ecchymosis and pain, making it a safe and popular option for facial rejuvenation, offering immediate results and long-term benefits while maintaining a low risk of allergic reactions and the ability to be reversed using hyaluronidase.5
Conclusion
The application of hyaluronic acid for periorbital rejuvenation has significantly transformed both aesthetic and medical practices by offering a safe and effective intervention for conditions such as periorbital dark circles, volume loss, and hollowness. The immediate volumetric and hydrating properties of hyaluronic acid facilitate observable enhancements in skin texture and elasticity. Its biocompatibility markedly reduces the risk of allergic reactions, rendering it suitable for a diverse patient population. Furthermore, the minimally invasive nature of the procedure involves minimal to no recovery period, allowing for personalized treatment regimens. For healthcare practitioners, the use of hyaluronic acid fillers not only improves aesthetic outcomes but also enhances patient satisfaction and self-confidence, effectively addressing both symptomatic manifestations and underlying pathophysiological factors to optimize overall patient well-being.
References
1. Razi S, Truong TM, Khan S, Sanabria B, Rao B. Hydradermabrasion through the lens of Line-Field Confocal Optical Coherence Tomography. Skin Res Technol. 2024;30(4):e13684. doi: 10.1111/ srt.13684.
2. Humzah D, Molina B, Salti G, Cigni C, Bellia G, Grimolizzi F. Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine?. Int J Mol Sci. 2024;25(6): 3216. Published 2024 Mar 12. doi:10.3390/ ijms25063216
3. Liew S, Doreian S, Kunathathorn W, Lam S, Jorge A, Lan LB, Selkon E, Arendse S, Silleri J, Telfer T. Lower Eyelid Dark Circles (Tear Trough and Lid-Cheek Junction): A Stepwise Assessment Framework.
Aesthet Surg J. 2024 Jun 14; 44(7): NP476NP485. doi: 10.1093/asj/ sjae058. PMID: 38489829; PMCID: PMC11177555.
4. Schneider KJ, Flaharty KG, Ellis CN, Bitar OM, Barinova H, Tejasvi T, Nelson CC. Dermoscopy can be safely and reliably used in ophthalmology. Heliyon. 2024 Apr 28; 10(9):e30293. doi: 10.1016/ j.heliyon.2024.e30293. PMID: 38737239; PMCID: PMC11088248.
5. Leonardi A, Doan S, Fauquert JL, Bozkurt B, Allegri P, Marmouz F, Rondon C, Jedrzejczak M, Hellings P, Delgado L, Calder V. Diagnostic tools in ocular allergy. Allergy. 2017 Oct; 72(10):1485-1498. doi: 10.1111/ all.13178. Epub 2017 May 10. PMID: 28387947.
6. Nguyen VP, Zhe J, Hu J, Ahmed U, Paulus YM. Molecular and cellular imaging
of the eye. Biomed Opt Express. 2023 Dec 21; 15(1):360-386. doi: 10.1364/ BOE.502350. PMID: 38223186; PMCID: PMC10783915.
7. Cassuto D, Delledonne M, Zaccaria G, Illiano I, Giori AM, Bellia G. Safety Assessment of High- and Low-MolecularWeight Hyaluronans (Profhilo®) as Derived from Worldwide Postmarketing Data. Biomed Res Int. 2020 Jun 20; 2020:8159047. doi: 10.1155/ 2020/ 8159047. PMID: 32685528; PMCID: PMC7327616.
8. Rodriguez Abascal M. et al. Facial bioremodeling by intradermal injection of a stabilized hybrid complex of high and low molecular weight hyaluronic acid: prospective study on 30 patients. Eur Aesth Plast Surg J 2015; 5(2): 124-131.
MUMBAI 2025
Acid 6%
Reduces acne and blemishes
Reduces pigmentation and dark spots
Repairs skin from photo-aging damages
Unplugs clogged pores and improves skin texture
Reduces small bumps caused by acne
Acid 12%
Treatment and prevention of hyperpigmentation
Glycolic acid 12% exfoliates the skin by dissolving dead skin cells
Treat certain skin conditions like melasma, acne, wrinkles, etc.,
Prevents the skin from photoaging
Glycolic
Glycolic
Tablets 40mg
Urticaria Chronic Spontaneous Urticaria (CSU)
A potent and highly selective HI -antihistamine approved for the treatment of urticaria
Has a rapid onset of action and long duration of action
Does not undergo significant metabolism and does not interact with the CYP450 system, which limits its potential for drug-drug interactions
Bilastine
Eczema
Rozlyn Khan is an Actress and PETA model, known for her Breast Cancer Awareness, while sharing her skincare and haircare routine under the guidance of her Dermatologist.
In this exclusive interview, Rozlyn Khan discusses her personalized skincare and haircare routines, emphasizing the importance of maintaining a healthy lifestyle and proper care. She highlights the connection between emotional well-being and overall health, underscoring how self-care plays a crucial role in supporting both. Despite her demanding schedule, Rozlyn remains dedicated to consistently following her skincare and haircare regimen, including the daily application of sunscreen, with expert guidance from her Dermatologist.
1. What is your daily skincare and hair care routine to keep them healthy and glowing?
My daily skincare routine starts with a gentle face wash, followed by a toner to maintain my skin pH balance. After applying Vitamin C and a moisturizer, I make sure to use sunscreen to protect my skin from UV rays. For my hair, I use argan oil shampoo and conditioner to keep it nourished. Before bed, I remove my makeup, cleanse my skin, and exfoliate for 2–3 minutes, I apply a toner or retinol for anti-aging and an under-eye cream for added care.
2. What are the most common skin and hair concerns you encounter as a model, and how do you manage them with your Dermatologist's advice?
As a model, I often experience frizz and dryness in my hair. To address this, I undergo
regular spa treatments and apply nourishing oils to maintain hydration and reduce frizz. Additionally, under the guidance of my Dermatologist, I adhere to a comprehensive skincare regimen designed to hydrate and treat my skin effectively.
3. How do you maintain healthy, glowing skin and strong, shiny hair during long photoshoots or events?
During long shoots, I make sure to stay hydrated by drinking a lot of water. I also do eye exercises to reduce fatigue. For my hair, I apply argan oil serum to protect it and keep it shiny while styling. These steps help maintain my skin and hair health, even after hours of exposure.
4. What care did you take to maintain your skin and hair during the chemotherapy treatment? and what food restrictions were particularly observed
during that period.? During chemotherapy, I prioritized skin and hair care to manage treatment effects, much like a model preparing for a flawless shoot. I used mild, fragrance-free cleansers, thick emollients, and sunscreen for hydration and protection. For my hair, I relied on sulfate-free shampoos, avoided heat styling, and used a soft brush or scalp cooling therapy to minimize hair loss. Nail care involved keeping them short and moisturized. My diet focused on well-cooked, protein-rich foods while avoiding raw, processed, or sugary items. Staying hydrated and avoiding spicy, acidic foods and grapefruit helped maintain both my health and a radiant glow.
5. How do you protect your skin and hair from the sun during extended outdoor exposure, with recommendations from your Dermatologist? I follow my Dermatologist advice
by applying sunscreen regularly, including on my hands and body. This helps protect my skin from harmful UV rays during outdoor shoots. For my hair, I use argan oil to keep it nourished and shielded from the sun damaging effects.
6. While on medication, how do you take care of your skin and hair under your Dermatologist's supervision to manage any side effects?
Medications can sometimes cause dryness or other side effects. To counteract these effects, I incorporate a diet rich in vegetables, fruits, green tea, and buttermilk. I follow my Dermatologist advice and stick to my skincare routine, using hydrating products like retinol and Vitamin C to keep my skin healthy and moisturized.
7. What habits, including exercise, sleep, and diet, contribute to improving your skin and hair health?
I start my day with yoga, meditation, and breathing exercises, which help me stay balanced and calm. In the evening, I take a walk to stay active and enjoy fresh air. I prioritize 8 hours of sleep each night to ensure proper rest and rejuvenation for my body. My diet includes an abundance of fresh vegetables, fruits, and green tea, all of which support the health and vitality of my skin and hair.
8. How do you protect your skin from irritation caused by makeup removers and your hair from damage due to styling tools or chemicals?
I use gentle makeup removers to avoid irritating my skin, and I make sure to cleanse thoroughly at the end of the day. For my hair, I protect it from heat damage by using argan oil serum before styling. I also keep my hair hydrated with regular spa treatments and avoid overuse of styling tools or harsh chemicals.
9. How do you maintain your mental health, and what impact does it have on the overall health of your skin and hair?
I maintain my mental health by practicing yoga and meditation, which help me stay calm and positive. I also enjoy reading inspirational books and spending time with my pets, who bring a sense of joy and unconditional love into my life. This emotional well-being has a positive impact on the health of my skin and hair, as stress can often manifest in both.
10. What advice would you give for maintaining optimal skin and hair health, based on your experience and insights from your Dermatologist?
My advice is to stay consistent with your skincare and hair care routine. Always wear sunscreen, stay hydrated, and get enough sleep. A balanced diet, full of vitamins and nutrients, is essential for healthy skin and hair. It is also important to manage stress, as it can directly affect your skin and hair health. Lastly, regularly consult with your Dermatologist to ensure you are using the right products and techniques for your skin and hair type.
Comprehensive Treatment Strategies for Acne Vulgaris
Dr. Mamta Dhayal
MBBS, DDV
Dermatologist, Dr. Dhayal's Skin, Hair & Nails Clinic, Mumbai,
Consultant Dermatologist, DFY NGO
Dermatologist, K J Somaiya Hospital & Research Centre, Mumbai
Introduction
Acne vulgaris is a common chronic inflammatory condition
affecting the pilosebaceous unit. It typically presents with papules, pustules, or nodules, predominantly on the face, though it can also involve the upper arms, trunk, and back. The pathophysiology of acne vulgaris is multifactorial, involving several key factors such as increased sebum production, follicular hyperkeratinization, dysbiosis of the pilosebaceous microbiome, and the inflammatory response, which together contribute to the formation of the primary lesion, the comedo. The condition is most prevalent during adolescence but can affect individuals across all age groups. Sebaceous glands in the skin, particularly those of the face, chest, and back, show hypersensitivity to circulating androgens, resulting in excessive sebum production (Seborrhea) his sebum, along with keratin, accumulates within the follicular infundibulum, forming the microcomedo, a hyperkeratotic plug that serves as the precursor to various acne lesions.1 As the microcomedo evolves, it can
form either closed comedones (whiteheads) or open comedones (blackheads), the latter characterized by the dark color resulting from the oxidation of sebum lipids and melanin. The accumulation of sebum, keratin, and the proliferation of Cutibacterium acnes (formerly Propionibacterium acnes) leads to follicular inflammation, resulting in papules, pustules, and nodules. Follicular rupture further exacerbates inflammation by releasing keratin, sebum, proinflammatory lipids, and bacteria into the dermis, promoting deeper inflammatory responses and nodule formation. The severity of acne can range from mild, characterized primarily by comedones, to severe, involving extensive inflammatory lesions that may lead to complications such as post-inflammatory hyperpigmentation, scarring, and significant psychological distress. Factors such as genetic predisposition, hormonal influences, and dietary components also contribute to the pathogenesis of acne vulgaris.2
The etiological factors, including
pharmacological agents like lithium, corticosteroids, and anticonvulsants, which can exacerbate the condition. UV radiation and excessive sun exposure increase inflammation and sebaceous gland activity, while mechanical occlusion from materials like headbands, backpacks, and underwire brassieres can promote follicular obstruction. Endocrine disorders, such as polycystic ovary syndrome (PCOS) and pregnancy, trigger or worsen acne, with premenstrual flares occurring in 70% of women. Genetic factors, particularly those affecting sebum composition, play a significant role, with heritability estimates ranging from 50% to 90%. Other contributing factors include mechanical trauma, highglycaemic diets, and increased milk consumption, which may elevate insulin-like growth factor (IGF) levels. Psychological stress also exacerbates acne through cortisol release.3 Acne vulgaris significantly affects quality of life (QoL) due to its psychological and social impact, often causing embarrassment,
low self-esteem, anxiety, and depression, particularly in adolescents and young adults. Visible lesions and potential scarring or hyperpigmentation contribute to emotional distress and reduced confidence. Physical discomfort from inflammatory lesions and the need for ongoing treatment further burden individuals, collectively diminishing well-being and life satisfaction.1,2
Case report
A 17-year-old male presents with moderate to severe acne vulgaris primarily affecting the face, with some involvement on the back and shoulders. The patient has been struggling with persistent acne for the past two years, characterized by comedones, papules, and pustules, despite trying over-the-counter topical treatments with minimal improvement. The acne has caused significant emotional distress and affected the patient's self-esteem. The medical history is unremarkable, with no known allergies or previous treatments with oral isotretinoin or other systemic medications. The patient is a high school student, active in sports, and maintains a balanced diet, though occasional consumption of high-sugar foods is reported. A family history of acne is noted, with the patient's mother having experienced similar issues during adolescence. On physical examination, numerous comedones, papules, and pustules are noted on the forehead, cheeks, and chin, with some scarring observed on the back, but no signs of active infection or other skin conditions. The patient was started on a treatment regimen consisting of oral isotretinoin 20 mg at night, a pulse dose of azithromycin 500 mg to reduce inflammatory lesions, and topical treatments including a ceramide-based gentle cleanser, ceramide-based moisturizer, mineral sunscreen, and azelaic acid serum applied twice daily for its anti-inflammatory and comedolytic properties. Follow-up is scheduled in four weeks to evaluate treatment response and side effects, with education provided on the importance of adherence to the treatment regimen and skin care routine. The goal of this treatment plan is to reduce the severity of acne, improve the patient's quality of life, and monitor for potential side effects of isotretinoin.
After treatment
Diagnosis
Diagnosing acne vulgaris involves identifying its presence, severity, and contributing factors through detailed patient history and physical examination. Tools like the Global Acne Grading System (GAGS) assess lesion type and distribution, classifying acne as mild, moderate, or severe to guide treatment. Lesion count quantifies comedones, papules, pustules, and nodules for severity assessment. Hormonal evaluation, including tests for testosterone, DHEAS, and FAI, is essential in persistent or severe cases to identify underlying endocrine issues like PCOS or adrenal hyperplasia, aiding in tailored management.4,5,6 Microbial culture for Cutibacterium acnes is not routine in acne diagnosis but may be considered in refractory cases or suspected secondary infections. While C. acnes is part of normal skin flora, its overgrowth can contribute to inflammation, warranting evaluation in complicated cases.7 A skin biopsy is rarely needed for diagnosing acne vulgaris but may be used in atypical or severe cases to rule out conditions like rosacea, folliculitis, or hidradenitis suppurativa. Histopathology helps differentiate acne from other disorders, especially in uncertain or resistant cases.8 Imaging studies may be considered in severe or atypical cases of acne vulgaris. Pelvic ultrasound is used when polycystic ovary syndrome (PCOS) is suspected, aiding in the assessment of ovarian cysts. In rare instances, computed tomography (CT) or magnetic resonance imaging (MRI) may be utilized to exclude other underlying conditions, such as adrenal tumours, when the presentation is atypical or suggests an alternative pathology. These imaging modalities provide additional diagnostic insight when necessary.9 Laboratory tests are important in evaluating associated conditions in acne vulgaris. Fasting glucose and insulin levels can be measured in patients suspected of insulin resistance, which may contribute to acne. A lipid profile is also useful for assessing metabolic syndrome, particularly in obese patients, as these factors can influence acne severity and progression.10
Treatment
The management of acne vulgaris is tailored to its severity and
type. For mild to moderate acne, topical retinoids like tretinoin, adapalene, and tazarotene normalize keratinization, reduce comedones, and have anti-inflammatory effects. Topical antimicrobials such as clindamycin and benzoyl peroxide target Cutibacterium acnes and reduce inflammation, with benzoyl peroxide offering additional comedolytic properties. Hormonal therapies, including oral contraceptives and anti-androgens like spironolactone, are effective in androgen-driven acne, particularly in female patients. Isotretinoin is reserved for severe or refractory cases, significantly reducing sebaceous activity and keratinization, with strict monitoring for teratogenic risks. Other treatments include salicylic acid, a keratolytic effective for comedonal acne, and macrolides like erythromycin, used selectively due to resistance concerns. Mineral sunscreen, containing zinc oxide or titanium dioxide, serves as a physical barrier to UV radiation, preventing skin damage and inflammation. It is
Figure 1: Numerous comedones, papules and pustules are noted on the forehead, cheeks, and chin
particularly beneficial for acne patients, as it is less likely to irritate or worsen acne compared to chemical sunscreens. Zinc oxide possesses antiinflammatory properties, which aid in alleviating erythema and irritation.11
Azithromycin, a macrolide antibiotic, is used for moderate to severe inflammatory acne vulgaris. It inhibits Cutibacterium acnes and has anti-inflammatory effects, reducing erythema, edema, and pain. Typically prescribed in a pulse dosing regimen, it targets bacterial load and inflammation while minimizing the risk of resistance. Azithromycin is considered a second-line therapy when other treatments are insufficient. Azelaic acid is a dicarboxylic compound with antimicrobial and keratolytic effects. It inhibits the growth of Cutibacterium acnes, a key microorganism in acne vulgaris, and normalizes keratinization in the follicular epithelium to prevent comedone formation. Its depigmenting effect also helps reduce post-inflammatory hyperpigmentation, making it effective for mild to moderate acne, especially in individuals with darker skin tones. Isotretinoin, a potent oral retinoid, is the most effective treatment for severe acne. It reduces sebaceous gland size, decreases sebum production, and normalizes epithelial turnover, which helps prevent comedones and reduces inflammation. Due to its potential side effects, it is typically used for recalcitrant cases of acne. Ceramide-based creams are used to restore skin hydration and maintain the skin barrier, particularly in patients
using isotretinoin, which can cause dryness and irritation. These creams help prevent trans-epidermal water loss, improve skin elasticity, and reduce discomfort from other acne treatments.11
Discussion
Acne vulgaris is a common condition, especially among adolescents, with prevalence ranging from 35% to 90%. It typically starts between ages 7-12 and may resolve by the third decade, though it can persist into adulthood. Adolescent acne is more common in males, while postadolescent acne mainly affects females. Urban populations are more affected, with 20% developing severe forms leading to scarring. Severity varies by race, with Asians experiencing more severe cases and Caucasians having milder forms. Darker skin types are prone to post-inflammatory hyperpigmentation. Neonatal acne resolves on its own, but acne in infants or children may need further evaluation. Acne vulgaris accounts for 99% of acne cases, presenting as noninflammatory comedones and inflammatory lesions (papules, pustules, nodules, cysts). Its global prevalence is 9.38%, with 35%-100% of adolescents affected and 0.74% of adults, with higher rates linked to diet and reporting.1 Acne vulgaris is classified from Grade 1 to Grade 4: Grade 1 (comedones), Grade 2 (inflammatory papules), Grade 3 (pustules), and Grade 4 (nodulocystic acne). Severity is determined by lesion type, scarring, psychological impact, and treatment response. Common in adolescents,
especially in the T-zone, acne in adult women often flares with the menstrual cycle. Acne can cause scarring (boxcar, ice-pick, rolling scars) and is linked to seborrhea. Hyperandrogenism may present with hirsutism, irregular periods, and weight gain. Post-inflammatory hyperpigmentation is common in darker skin tones. Other forms include acne conglobata, fulminans, and conditions like SAPHO and PAPA syndromes. A thorough history and physical exam, including assessment for hyperandrogenism, are key for diagnosis.2,3
The differential diagnosis of acne vulgaris includes conditions with distinct features: rosacea (lacking comedones, with telangiectasia), perioral dermatitis (erythematous papules around the mouth), Demodex folliculitis (nonresponsive to acne treatments), and facial angiofibromas (red papules in children). Other conditions include pseudofolliculitis barbae, adnexal tumors, nevus comedonicus, sebaceous hyperplasia, and Favre-Racouchot syndrome. Acne complications can include psychological effects, acne fulminans, solid facial edema, and Gram-negative folliculitis. Prevention involves non-comedogenic cleansers, avoiding triggers like smoking and high-glycemic diets, and using oil-free sunscreen. Topical treatments (retinoids, benzoyl peroxide) and systemic treatments are used for moderate to severe acne. Hormonal therapy is effective in females with acne linked to menstrual cycles or hyperandrogenism. Isotretinoin
Comprehensive Facial Rejuvenation with Hyaluronic Acid Fillers
remains the key treatment for severe acne, with careful dosing and combination therapies to improve efficacy and reduce adverse effects.4,5,9
Conclusion
Acne vulgaris is a prevalent, multifactorial disorder impacting patients' psychosocial well-
References
1. Santer M, Burden-Teh E, Ravenscroft J. Managing acne vulgaris: an update. Drug Ther Bull. 2023; 62(1):6-10. Published 2023 Dec 27. doi:10.1136/dtb. 2023.000051.
2. Oge' LK, Broussard A, Marshall MD. Acne Vulgaris: Diagnosis and Treatment. Am FAM Physician. 2019 Oct 15; 100(8):475-484. PMID: 31613567.
3. Reynolds RV, Yeung H, Cheng CE, CookBolden F, Desai SR, Druby KM, Freeman EE, Keri JE, Stein Gold LF, Tan JKL, Tollefson MM, Weiss JS, Wu PA, Zaenglein AL, Han JM, Barbieri JS. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024 May; 90(5): 1006.e1-1006.e30. doi: 10.1016/ j.jaad. 2023.12.017. Epub 2024 Jan 30. PMID: 38300170.
4. Hacivelioglu S, Gungor AN, Gencer M, Uysal A, Hizli D, Koc E, Cosar E. Acne severity and the Global Acne Grading System in polycystic ovary syndrome. Int J Gynaecol Obstet. 2013 Oct; 123(1):33-
being. Despite various treatment options, management is challenging due to the condition’s variability, patient responses, and potential adverse effects, particularly with isotretinoin. A personalized approach, considering acne severity, triggers, and comorbidities, is crucial for optimizing outcomes. Recent advancements in understanding acne's pathophysiology—focusing on inflammation, microbiome, genetics, and hormones—have led to novel treatments targeting specific pathways, like nitric oxidereleasing agents. Ongoing research aims to improve acne treatment, scarring management, and psychological well-being through more targeted interventions.
6. doi: 10.1016/ j.ijgo.2013.05.005. Epub 2013 Aug 12. PMID: 23948280.
5. Adityan B, Kumari R, Thappa DM. Scoring systems in acne vulgaris. Indian J Dermatol Venereol Leprol. 2009 May-Jun; 75(3):3236. doi: 10.4103/ 0378-6323. 51258. PMID: 19439902.
6. Borzyszkowska D, Niedzielska M, Kozłowski M, et al. Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with ContraceptiveBased Therapies in Young Adult Women. Cells. 2022; 11(24): 4078. Published 2022 Dec 16. Doi: 10.3390/ cells11244078.
7. Hassanzadeh P, Bahmani M, Mehrabani D. Bacterial resistance to antibiotics in acne vulgaris: an in vitro study. Indian J Dermatol. 2008; 53(3):122-124. doi:10.4103/ 00195154.43213.
8. Eichenfield DZ, Sprague J, Eichenfield LF. Management of Acne Vulgaris: A Review. JAMA. 2021 Nov 23; 326(20):20552067. doi: 10.1001/ jama.2021.17633.
PMID: 34812859.
9. Fuchs CSK, Ortner VK, Hansen FS, Philipsen PA, Haedersdal M. Subclinical effects of adapalene-benzoyl peroxide: a prospective in vivo imaging study on acne micromorphology and transfollicular delivery. J Eur Acad Dermatol Venereol. 2021 Jun; 35(6): 1377-1385. doi: 10.1111/ jdv.17140. Epub 2021 Mar 5. PMID: 33508886.
10. Hasrat NH, Al-Yassen AQ. The Relationship between Acne Vulgaris and Insulin Resistance. Cureus. 2023; 15(1 ):e34241. Published 2023 Jan 26. doi:10.7759/ cureus.34241.
11. Vasam M, Korutla S, Bohara RA. Acne vulgaris: A review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023; 36:101578. Published 2023 Nov 23. doi:10.1016/ j.bbrep.2023.101578.
Fractional CO2 Laser Ablation for Hypertrophic Nasal Scar Treatment
Hypertrophic nasal scars are abnormal scars that form on
the nose due to excessive collagen deposition during the wound healing process. Unlike normal scars, which mature and fade over time, hypertrophic nasal scars are characterized by their elevated, thickened, and often discoloured appearance. These scars remain confined to the area of the original wound and are associated with significant cosmetic and functional concerns. They present with several distinct symptoms, including elevation and thickening, where the scar forms a noticeable bump due to overproduction of collagen and extracellular matrix components; redness or pinkness, especially in the early stages due to increased blood vessel formation; itching or discomfort; and irregular texture, with a rough or nodular surface compared to surrounding skin.1
The pathogenesis of hypertrophic scars involves a complex interplay of cellular and molecular processes that disrupt the normal wound healing continuum, which is traditionally divided into three phases: inflammation, proliferation, and remodelling. Inflammation is the initial phase triggered by the disruption of capillary blood vessels, leading to the activation of the haemostatic cascade. This results in the extravasation of intravascular components and the formation of fibrin clots, which are composed of a fibrin mesh and platelets. This provisional extracellular matrix (ECM) acts as a scaffold for the migration and recruitment of various cellular elements essential for subsequent healing stages. Proliferation typically begins around days 4 to 5 postinjury. During this phase, fibroblasts migrate into the wound matrix and become highly activated, replacing the
initial fibrin matrix with a more robust collagenous matrix by approximately 2 to 4 weeks. In mature wounds, the initial elastic fibre network is often no longer detectable, which contributes to the firmness and reduced elasticity typical of scars. Additionally, this phase involves the inward epithelialization of keratinocytes from the wound margins, and wound contraction usually begins around days 10 to 12, although this timing can be influenced by wound severity and the patient's overall condition. Remodelling starts approximately 3 weeks after tissue injury. During this phase, fibroblast density decreases, blood vessels occlude, and collagen fibres harden. Continuous collagen synthesis and degradation contribute to the remodelling of the wound matrix over about 6 months. At this stage, the rates of collagen production and degradation reach equilibrium, leading to minimal further changes in collagen content. This phase is crucial in determining the final appearance of the scar, with both intra- and interpersonal variations in scar characteristics being prominent. Consequently, a healing incisional wound may develop into a conspicuous scar during this period.1
Hypertrophic nasal scars arise from an aberrant wound healing process characterized by excessive collagen deposition and dysregulated
remodeling. Clinically, these scars manifest as elevated, discolored, and occasionally pruritic lesions on the nose, posing both cosmetic and functional challenges. A thorough understanding of their pathogenesis and symptoms is essential for devising effective prevention and treatment strategies to mitigate their impact.1
Hypertrophic nasal scars present with a range of distinctive clinical features that affect both aesthetics and function, stemming from an aberrant wound healing process characterized by excessive collagen deposition and deregulated remodelling. These scars are notably elevated above the surrounding skin due to the overproduction of collagen, resulting in a prominent, often unsightly lump or bump on the nose. The scar tissue may exhibit an irregular contour, including nodular or ridged formations, deviating from the smooth texture of normal skin. Initially, hypertrophic scars often appear reddish or pinkish due to increased vascularity (angiogenesis) and the abundance of newly formed blood vessels. Over time, they may develop hyperpigmentation or hypopigmentation, particularly in darker skin types, with colour changes potentially persisting long after the initial injury. The texture of these scars is typically coarse and uneven, feeling firm and fibrous to the touch,
and may sometimes show keloid-like characteristics such as significant hardness and protrusion. Patients may experience localized itching, discomfort, or tenderness, and in some cases, pain, especially if the scar is subjected to trauma or mechanical irritation. Functional concerns include potential nasal deformity that can affect cosmetic appearance and, in severe cases, impact nasal function or airflow due to significant distortion. Additionally, scarring on the nose can interfere with facial expressions, leading to psychological distress. Hypertrophic nasal scars evolve over time, initially being more inflamed and red but gradually becoming less vascularized and more fibrotic. While some may improve, others may persist or worsen, particularly if exacerbated by ongoing tension or recurrent trauma. Understanding these clinical features is crucial for effective management and treatment planning.2
Case report
A 33-year-old female patient presented with hypertrophic scars on her nose, accompanied by noticeable dyspigmentation. To address these issues, Fractional CO2 laser ablation therapy was initiated. This treatment effectively targeted the hypertrophic scar tissue, promoting collagen remodeling and improving the overall texture of the scars. Following the therapy, the
patient exhibited significant improvement in the appearance of the scars, with a notable reduction in their height and prominence. Additionally, the laser treatment managed the dyspigmentation effectively, resulting in a more even skin tone. The patient demonstrated marked improvement in both the texture and color of the affected area, highlighting the efficacy of Fractional CO2 laser therapy for managing hypertrophic scars and associated pigmentation issues.
Diagnosis
The diagnosis of hypertrophic nasal scars principally involves a thorough clinical evaluation and detailed patient history, supported by a range of diagnostic modalities. These methods are crucial for assessing scar severity, determining its functional and aesthetic impact, and devising appropriate therapeutic strategies.
Hypertrophic scars are characterized by excessive, disorganized Type I collagen, leading to a raised and firm texture. Biopsies reveal increased fibroblast activity, abnormal cells, heightened vascularity, and reduced elastic fibers, resulting in disrupted dermal architecture and chronic inflammation. Ultrasound is crucial in diagnosing these scars by measuring increased thickness, visualizing dense collagen,
and assessing blood flow with Doppler, aiding in treatment planning and monitoring scar progression over time.2,3 Optical Coherence Tomography (OCT) is vital for diagnosing hypertrophic scars, providing highresolution images that measure scar thickness, visualize disorganized collagen fibers, and capture surface and subsurface features, including vascularity. Scar rating scales complement this by quantifying scar height, thickness, color, texture, elasticity, and symptoms like itching or pain. These tools assess the scar's impact on function and quality of life, guiding treatment decisions and monitoring effectiveness.4,5 A skin tensiometer evaluates hypertrophic nasal scars by measuring increased tension, reduced elasticity, and greater firmness, highlighting the scar's rigidity and abnormal mechanical properties due to disorganized collagen. Complementing this, 3D imaging and computerassisted analysis offer precise insights by capturing detailed scar geometry, surface texture, and volume. Together, these tools provide a comprehensive assessment, track scar progression, and support effective treatment planning and monitoring.6,7
Treatment
Silicone cream is commonly used to treat hypertrophic scars by hydrating the tissue, regulating collagen
Fractional
Figure 1: Dyspigmented hypertrophic scars on nose
production, and improving texture. Flavonoids reduce inflammation and promote healing, while Botulinum toxin-A decreases fibroblast activity to minimize scar formation. Scar excision is a surgical option for severe cases. Microneedling stimulates collagen remodelling by creating microinjuries, and corticosteroids reduce inflammation and scar thickness. Paper tape, silicone sheets, and wound compression further enhance scar management by promoting hydration, reducing friction, and accelerating collagen maturation. Together, these treatments provide a comprehensive approach to improving the appearance and texture of hypertrophic scars.8
Laser therapy for hypertrophic scars uses focused light to destroy tiny blood vessels within the scar, reducing blood flow and oxygen supply. This process stimulates healing, breaks down excess collagen, and improves scar texture and color, resulting in a smoother and less noticeable scar. The CO2 laser is a powerful tool in managing hypertrophic scars due to its ablative properties. It emits a wavelength of light that is highly absorbed by water in the skin, allowing precise vaporization of the outer layers of scar tissue. This targeted removal of damaged skin reduces scar thickness and improves texture by eliminating disorganized collagen and stimulating the
production of new, healthier skin. During treatment, the laser's energy vaporizes the thickened, raised layers of the scar, creating a more even surface while the thermal effect promotes natural collagen production, leading to improved texture and reduced scar elevation. The CO2 laser is particularly effective for addressing surface texture and thickness, significantly flattening and smoothing scars, and encouraging the formation of organized collagen for a more refined appearance.8 1064 nm ND Laser operates at a wavelength of 1064 nm, allowing it to penetrate deeply into the dermal layers of the skin. It is particularly effective for treating deeper scar tissue by targeting and reducing excess blood vessels and improving scar texture. The laser promotes collagen remodelling within the dermis, which helps in flattening and smoothing the scar over time. By stimulating the deeper layers of the skin, it encourages the formation of new, more organized collagen, leading to an improved texture and reduced scar elevation. Pulsed-dye lasers (PDL) are designed to address the vascular component of hypertrophic scars. They emit light at a wavelength that is absorbed by haemoglobin, the protein in blood vessels. This targeted approach helps to reduce the redness and vascularity of the scar by constricting the blood vessels
within it. By decreasing the blood flow and the number of visible blood vessels, PDLs can effectively minimize the discoloration and improve the overall appearance of the scar.8
Tensile reduction suture closure flattens hypertrophic scars by placing sutures under tension, often combined with silicone gel, laser therapy, or steroids for enhanced results. Surgical excision is effective for severe scars, with careful technique and adjuvant treatments like pressure garments or silicone gel. Recent advancements include 5-Fluorouracil (5FU), Losartan, Oxandrolone, and Dipeptidyl Peptidase-4 inhibitors, which target fibroblast activity and collagen synthesis. Other innovative approaches, such as 1,4-Diaminobutane, autologous fat grafting, stem cell therapy, PRP, CD206, IL-6, and IFN-y, offer diverse strategies for scar management, improving texture and appearance by addressing underlying scar formation mechanisms.8 The treatment of hypertrophic scars involves a variety of strategies designed to address the underlying mechanisms of scar formation and improve overall appearance. By targeting different aspects of the scar's development— such as collagen production, vascularity, and inflammation— these treatments offer a
Fractional
comprehensive approach to managing and optimizing scar outcomes.
Discussion
Hypertrophic scars affecting an estimated 100 million individuals annually in developed nations due to 55 million elective and 25 million trauma-related procedures, these scars can substantially impair quality of life through symptoms such as pruritus, pain, and contractures. The incidence of hypertrophic scarring is reported to be between 40% and 70% following surgical procedures and may reach up to 91% in the context of burn injuries, with a notable prevalence peak occurring in individuals during their second to third decades of life.9 Although, several predictors for severe scarring, particularly following burn injuries, have been identified and categorized into intrinsic (patient-related) and extrinsic (injury-related) factors. Intrinsic factors associated with a higher risk of hypertrophic scarring include female sex, younger age (≤30 years), darker skin types (Fitzpatrick skin types IV–VI), and burn injuries located on anatomical sites such as the neck, chest, and upper limbs. Racial differences also play a significant role, with hypertrophic scarring being more prevalent among Black/ African American and Asian populations. Genetic factors, especially those related to skin pigmentation, have been investigated in relation
to hypertrophic scarring. The melanocortin 1 receptor (MC1R) gene, which encodes a G-protein-coupled receptor involved in pigment regulation, is of particular interest. MC1R interacts with a-melanocytestimulating hormone (a-MSH), which promotes eumelanin production in melanocytes. Additionally, MC1R is expressed in leukocytes, fibroblasts, and keratinocytes, where it modulates inflammatory responses and collagen synthesis. a-MSH has been demonstrated to downregulate proinflammatory cytokines while up-regulating anti-inflammatory cytokines such as interleukin-10 (IL-10). Furthermore, melanocortin signaling is implicated in reducing collagen synthesis in fibroblasts in response to transforming growth factor-B1 (TGF-B1). Research has identified over 80 variant alleles of the MC1R gene, including the loss-of-function R163Q single-nucleotide polymorphism (SNP), which is common among East/ Southeast Asians and Native Americans and is associated with an increased risk of hypertrophic scarring in these populations. However, this SNP is absent in Black/ African American individuals, who are at an elevated risk for hypertrophic scarring. This indicates that while genetic variations such as the R163Q SNP may contribute to susceptibility in specific populations, other
genetic and environmental factors likely also influence the predisposition to hypertrophic scar formation.9 Several conditions can mimic hypertrophic scars, requiring careful differential diagnosis. Keloids extend beyond the original wound and may continue to grow, affecting individuals with darker skin tones and having a tendency to recur. Contractures involve tightening of scar tissue, leading to restricted movement and significant functional impairment, particularly in large burns or improperly managed injuries. Normal scars may initially resemble hypertrophic scars but typically flatten and fade over time. Granulomas, which are raised inflammatory lesions, can be distinguished by histopathological examination revealing inflammatory cell patterns and foreign material. Dermatofibromas are benign nodules with a firm texture and dimpled appearance, sometimes mistaken for hypertrophic scars. Basal cell carcinoma (BCC) may present as raised lesions but typically has a pearly appearance with visible blood vessels and may ulcerate. Other dermatologic conditions like lichen planus or psoriasis can present with scarring-like lesions but usually have distinct features such as scaling or pruritus.2
Patients with hypertrophic scars should be advised to adopt lifestyle modifications that may mitigate scar exacerbation. Such
Fractional
modifications include avoiding physical activities or exercises that involve repetitive motions or excessive tension on the scar tissue. In addition to managing existing scars, preventative measures are crucial for reducing the risk of hypertrophic scars and keloids. Initially, when addressing a wound, it is imperative to thoroughly clean and disinfect the area, apply topical antibiotics as indicated, and use fixation materials to protect the wound from local tension. This precautionary approach is essential even for minor wounds, as hypertrophic scars and keloids can arise from wounds that initially
References
1. Son D, Harijan A. Overview of surgical scar prevention and management. J Korean Med Sci. 2014; 29(6):751-757. doi:10.3346/ jkms.2014.29.6.751.
2. Schmieder SJ, Ferrer-Bruker SJ. Hypertrophic Scarring. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 4, 2023.
3. Ogawa R, Akita S, Akaishi S, et al. Diagnosis and Treatment of Keloids and Hypertrophic Scars-Japan Scar Workshop Consensus Document 2018. Burns Trauma. 2019; 7:39. Published 2019 Dec 27. Doi: 10.1186/ s41038-019-0175-y.
4. Abrouk M, Gianatasio C, Li Y, et al. An Atlas of Optical Coherence Tomography (OCT): Elucidating In Vivo Differences of Scar Types Using OCT in Order to Guide Laser Treatment Parameters. J Clin Aesthet Dermatol. 2022; 15(9):30-39.
appear insignificant. Moreover, for all patients, treatment should commence with the least invasive options. This strategy helps to minimize potential complications and promotes more effective management of hypertrophic scars.10
Conclusion
Hypertrophic scars present a significant clinical challenge due to their intricate pathophysiology and variable response to treatment. Effective management is complicated by the scars' tendency to recur, their potential for causing functional impairment, and their psychological impact on patients. Accelerating the wound-healing process is critical in reducing the incidence of hypertrophic scars, emphasizing the need for proper management and timely interventions in the early stages of wound healing. Strategies informed by molecular evidence can be instrumental in preventing hypertrophic scar formation. Despite recent advancements offering new hope, continued research into the underlying mechanisms of wound healing and hypertrophic scar development is essential. This ongoing exploration of novel technologies and treatment modalities is crucial for improving patient outcomes and addressing the complex challenges associated with hypertrophic scars.
5. Choo AMH, Ong YS, Issa F. Scar Assessment Tools: How Do They Compare? Front Surg. 2021; 8:643098. Published 2021 Jun 23. doi:10.3389/fsurg.2021.643098.
6. Scheepens KMJ, Marsidi N, Genders RE, Horeman- Franse T. The Compressiometer: Toward a New Skin Tensiometer for Research and Surgical Planning. IEEE J Transl Eng Health Med. 2021; 10:2500109. Published 2021 Dec 6. doi:10.1109/ JTEHM.2021.3133485.
7. Verhiel SH, Piatkowski de Grzymala AA, Van den Kerckhove E, Colla C, van der Hulst RR. Three-dimensional imaging for volume measurement of hypertrophic and keloid scars, reliability of a previously validated simplified technique in clinical setting. Skin Res Technol. 2016; 22(4):513-518. doi:10.1111/ srt.12296.
8. Mony MP, Harmon KA, Hess R, Dorafshar AH, Shafikhani SH. An Updated Review of Hypertrophic Scarring. Cells. 2023; 12(5):678. Published 2023 Feb 21. Doi: 10.3390/ cells12050678.
9. Nabai L, Pourghadiri A, Ghahary A. Hypertrophic Scarring: Current Knowledge of Predisposing Factors, Cellular and Molecular Mechanisms. J Burn Care Res. 2020; 41(1): 48-56. doi:10.1093/ jbcr/ irz158.
10. Ogawa R, Akita S, Akaishi S, et al. Diagnosis and Treatment of Keloids and Hypertrophic Scars-Japan Scar Workshop Consensus Document 2018. Burns Trauma. 2019; 7:39. Published 2019 Dec 27. Doi: 10.1186/ s41038-0190175-y.
Cacao Nutraceutical Supplement Proven Effective and Safe for Male Hair Loss.
A randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a nutraceutical supplement in male patients with androgenetic alopecia. Participants received either the active supplement or placebo. The supplement, containing saw palmetto, ashwagandha, vitamin E, curcumin, and other botanicals, significantly improved hair growth and quality, with a higher percentage of the active group reporting improvement compared to the placebo group. No significant changes in sexual function were observed, and both groups
remained moderately stressed. Gastrointestinal adverse events were reported in a small number of patients, but no serious adverse events occurred. The nutraceutical was well-tolerated, suggesting potential for hair restoration without adverse effects. Further studies with phototrichogram assessments are recommended.
Study Investigates Patient and Clinician Priorities in Psoriatic Arthritis Management
Psoriatic arthritis (PsA) presents significant management challenges due to its multifaceted nature, encompassing both inflammatory joint and skin involvement. A recent study highlighted discrepancies in priorities between patients and clinicians, with patients emphasizing issues such as fatigue, sleep disturbances, and access to care, while clinicians prioritized clinical manifestations and structural damage. Key patient concerns included healthcare access and uncertainty regarding long-term outcomes. Integrating patient perspectives into clinical decisionmaking is essential for optimizing care. Future research should focus on refining individualized treatment strategies to enhance disease management and improve health-related quality of life.
Synergistic Effect of IPL and BoNT/A in the Treatment of Rosacea
A recent study assessed the efficacy of combining Intense Pulsed Light (IPL) and Botulinum Neurotoxin Type A (BoNT/A) for treating erythematotelangiectatic rosacea in Fitzpatrick skin type III patients. IPL targets erythematous telangiectasia and inflammatory lesions via effects on mast cells and inflammatory mediators, although monotherapy often lacks sustained efficacy. BoNT/A reduces vasodilation and inflammation, particularly facial erythema, by inhibiting acetylcholine release and modulating neuropeptides. Patients underwent IPL followed by BoNT/A
injections. Outcomes were evaluated through photographic analysis and the Global Physician Assessment (GPA). Results demonstrated significant improvements in rosacea severity, with the majority of patients achieving mild or normal status post-treatment. High patient satisfaction was noted, with significant reductions in erythema and telangiectasia. The study's limitations warrant larger, controlled trials. IPL and BoNT/A may synergistically address vascular and inflammatory rosacea components.
Fractional Radiofrequency Microneedling is an Effective and Safe Treatment for Acne Scarring.
A systematic review evaluated the use of fractional radiofrequency microneedling (FRM) as a monotherapy for facial acne scarring, demonstrating significant improvements in skin rejuvenation. FRM was found to be equally effective as other treatment modalities, such as fractional ablative CO2 lasers, and superior to bipolar radiofrequency for certain scar types. The treatment was welltolerated with minimal downtime and adverse events, primarily transient erythema. Pain was mild to moderate and resolved promptly. Patient satisfaction was high, with improvements in psychosocial well-being and quality of life. The study's limitations included variability in scoring systems, precluding meta-analysis. Further randomized controlled trials with extended follow-up are needed to confirm long-term efficacy and safety, as well as to establish standardized treatment protocols.