Expert Opinion on IV Infusion Therapy Safety in Dermatology & Aesthetics
Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser
Effective Management of Irritant Contact Dermatitis with Desonide and Ceramide-Based Moisturizer
Alopecia Unraveled:
Diagnostic Pearls and Multimodal Management for Hair Restoration
Precision and Aesthetics in Dermatology: Radiofrequency Ablation for Skin Tags
EXECUTIVE
EDITOR & PUBLISHER
Dom Daniel CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
Printed, Published, Edited and Owned by Dom Daniel
Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078.
Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of September -2025
Skin Health in a Changing World: Science, Art, and Innovation in Aesthetic Dermatology
Skin, the body’s largest organ, reflects overall well-being. In India, rising pollution, stress, and lifestyle factors have intensified skin health concerns, with diseases impacting not just physical health but also emotional and psychological well-being. Encouragingly, rapid advances in scientific research and technological innovations are transforming the fields of dermatology and cosmetology, offering new hope and possibilities.
Welcome to the September issue of The Aestheticians Journal, where science meets artistry in aesthetic dermatology. This edition brings you “Alopecia Unraveled: Diagnostic Pearls and Multimodal Management for Hair Restoration”, offering a comprehensive perspective on one of the most challenging and emotionally impactful conditions. “Irritant Contact Dermatitis Successfully Managed with Desonide and Ceramide-Based Moisturizing Cream” showcases the value of targeted precision therapy in restoring skin health.
We also feature Radiofrequency Ablation for Skin Tags, highlighting a minimally invasive approach, and Hair Transplantation Redefined, an exploration of evolving surgical innovations. An Expert Opinion on IV Infusion Therapy Safety emphasizes the critical role of medical supervision, while a case report on Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser underscores the transformative potential of advanced pigment management technologies.
This issue embodies our mission to empower practitioners with trusted knowledge, encourage innovation, and celebrate the dynamic synergy of science and art in modern dermatology. We hope the insights shared here enrich your practice and inspire you to continue delivering excellence in patient care.
Hope you have a great read!
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher
Editorial Board
Dr. Satish Bhatia
MD (Skin) IFAAD (USA)
Dermatologist and Cutaneous Surgeon Dermetics, Indian Cancer Society Mumbai
Dr. Ratnakar Shukla
MD (Dermatology)
Consultant Dermatologist
Cosmetologist & Hair Transplant
Surgeon Dermagenix, Gorakhpur
Dr. Diwakar Sharma
MBBS, DNB
Consultant Dermatologist
BVP Hospital, Kota, Rajasthan
Dr. Ashutosh A. Garudkar
MBBS, FCPS (DVL)
Consultant Dermatologist
DerMédica Clinic
Ahilyanagar, Maharashtra
Dr. Neha Chaitanya Shukla
MBBS, MD
Consultant Dermatologist
Cosmetologist and Laser Surgeon EYE and SKIN Plus Advance Hospital Gandhinagar, Gujarat
Dr. Dhiral Shah
MBBS, MD (DVL), Fellowship in Aesthetic Medicine
Consultant Dermatologist
Kaytra Skin & Aesthetic Clinic
Vadodara, Gujarat
Hair Transplantation Redefined: Techniques, Outcomes and Innovations
Alopecia, or hair loss, is a multifactorial dermatological condition that affects individuals across all age groups and often results in significant psychological distress. It is broadly classified into non-scarring and scarring types, based on the preservation or destruction of hair follicles.1 Non-scarring alopecia involves the retention of viable follicles, allowing for potential regrowth once the underlying cause is addressed. Common subtypes include androgenetic alopecia (AGA), a genetically determined condition characterized by progressive, patterned hair loss—typically affecting the vertex, bitemporal, and midfrontal scalp in men, and presenting as diffuse central thinning with frontal hairline preservation in women. AGA is primarily driven by dihydrotestosterone (DHT)-induced follicular miniaturization. Alopecia areata (AA), an autoimmune
disorder, presents with abrupt, patchy hair loss and may progress to alopecia totalis or universalis. Telogen effluvium (TE) is marked by acute or chronic diffuse shedding, triggered by premature transition of follicles from the anagen to telogen phase, often in response to systemic illness, hormonal fluctuations, psychological stress, or certain medications. Pattern hair loss is categorized using several well-established systems. In female pattern hair loss (FPHL), the Ludwig classification outlines three grades of severity, from mild crown thinning to advanced baldness. The Sinclair scale provides a broader stratification, while Olsen’s classification emphasizes frontal accentuation with diffuse thinning. The BASP system classifies patterns based on basic types (L, M, C, U) and specific types (F, V), and the Kaneko scale evaluates disease progression through parameters such as
midline density, hair diameter variability, shedding, and follicular unit morphology.2 In male pattern hair loss (MPHL), the Hamilton-Norwood scale remains the standard, ranging from Stage I (minimal recession) to Stage VII (extensive vertex and frontal loss), with variant stages (IIa–Va) indicating anterior recession without vertex involvement. Psychological stress plays a pivotal role in exacerbating alopecia via neuroendocrine and immune mechanisms. Elevated cortisol levels degrade extracellular matrix components, promote follicular miniaturization, and induce premature telogen transition. Stress mediators such as substance P, ACTH, and prolactin further impair follicular function and trigger perifollicular inflammation. A comprehensive understanding of these classifications and pathophysiological pathways is essential for accurate diagnosis and effective, individualized management.3
Diagnosis
Diagnosing hair loss requires a comprehensive clinical evaluation, beginning with a detailed history that includes family background, onset and progression, potential triggers (e.g., stress, medications), and systemic symptoms. Physical examination focuses on the pattern, distribution, and type of hair loss (diffuse, patchy, or patterned). The hair pull test, performed on all scalp regions, is positive when >5–6 hairs are
extracted from a group of 50–60, indicating active shedding. The card test distinguishes new hair growth (tapered ends) from breakage (blunt ends), while the tug test assesses hair fragility. Hair mount microscopy can reveal abnormalities in the hair shaft and cycle. Trichoscopy, a noninvasive diagnostic tool, provides real-time visualization of scalp and hair shaft changes and helps guide biopsy site selection. Scalp biopsy— typically a 4-mm punch—is reserved for ambiguous cases and includes both vertical and horizontal sectioning to evaluate follicular architecture. Relevant laboratory investigations include CBC, thyroid profile, serum ferritin, vitamin D, zinc, ANA, CRP/ESR, and androgen levels (e.g., DHT), aiding in the identification of nutritional, hormonal, autoimmune, or inflammatory etiologies. Hair shaft analysis under microscopy can further detect structural anomalies such as trichorrhexis nodosa or monilethrix, useful in diagnosing brittle hair disorders.4,5,6
An accurate and systematic diagnostic approach is essential to determine the underlying etiology and guide effective treatment planning.
Treatment
Hair transplantation demonstrated successful outcomes in treated patients, with significant hair growth
and graft retention. This surgical intervention is typically indicated for individuals with non-scarring, stable alopecia who have adequate donor hair and have not responded to medical therapies such as minoxidil or finasteride. It offers a permanent and durable solution for hair restoration when conservative treatments prove insufficient. Ideal candidates possess a healthy scalp, sufficient donor density, good general health, and realistic expectations. Common indications include androgenetic alopecia (both male and female), traction alopecia, and select cases of frontal fibrosing alopecia and lichen planopilaris, when inactive. Contraindications include diffuse unpatterned alopecia, unstable cicatricial alopecias (e.g., lichen planopilaris, discoid lupus erythematosus), active alopecia areata, progressive hair loss, young age, unrealistic expectations, and psychiatric conditions such as body dysmorphic disorder. Ensuring medical stabilization of hair loss prior to surgery is essential to optimize long-term outcomes.7
A comprehensive preoperative assessment is essential to ensure optimal surgical outcomes. This includes a detailed medical history, review of current medications, and allergy screening. Certain agents require temporary discontinuation—minoxidil....... should be stopped one week prior, NSAIDs
withheld 12–24 hours before surgery, and vitamin/herbal supplements discontinued at least three weeks in advance. Alcohol should be avoided for seven days, and smoking minimized. Antihypertensives (except beta-blockers) may be continued, and anxiolytics can be considered if needed. Routine preoperative investigations include CBC, platelet count, coagulation profile, ECG, fasting glucose, and screening for hepatitis B, C, and HIV. Local anesthetic sensitivity testing is advised. Standardized preoperative photographs from multiple angles should be obtained for documentation and comparison.7
The donor area, typically the occipital scalp, is prepared by trimming the hair and administering local anesthesia prior to follicle harvesting. Two primary techniques are employed: Follicular Unit Transplantation (FUT) and Follicular Unit Extraction (FUE). FUT involves excising a scalp strip, which is then dissected into individual follicular units for implantation, leaving a linear scar concealed by surrounding hair. FUE uses a micro-punch tool to extract individual units, resulting in small, scattered scars that are less visible. Harvested grafts are carefully dissected under magnification to preserve follicular integrity and stored in chilled saline to maintain viability before implantation.7, 8
Recipient site creation
is crucial for achieving a natural aesthetic result. Sites are typically made in the frontal scalp using cutto-size blade or by needle of size 19 &18 no. with the number of sites precisely matching the planned graft count.9 Grafts are implanted using fine-angled forceps to minimize follicular trauma. Reconstructing a natural hairline generally requires 250–300 single-hair grafts, while 2,000–3,000 follicular units may be transplanted per session. In multiple sessions, a cumulative total of 4,000–6,500 grafts can be achieved, with a sessional limit of 2,500–3,000 grafts to preserve donor area integrity.10
Postoperative care is vital for graft survival and minimizing complications. Antibiotics and analgesics are prescribed to manage pain and reduce infection risk. Forehead swelling, typically seen around day three due to anesthetic fluid migration, is managed with ice compresses, intradermal triamcinolone, and a short course of oral corticosteroids. Strict adherence to postoperative protocols helps prevent complications such as infection and keloid formation. Patients demonstrated favourable outcomes, with visible hair growth noted during followup.7
Minimally invasive therapies such as platelet-rich plasma
(PRP), growth factor concentrates (GFC), and exosome therapy promote hair regeneration by delivering bioactive growth factors directly to the scalp, stimulating follicular activity. Microneedling, often combined with PRP, enhances treatment efficacy by improving transdermal absorption and inducing collagen production. Noninvasive options like lowlevel laser therapy (LLLT) support hair growth in non-scarring alopecias by increasing ATP synthesis, modulating oxidative stress, and improving follicular oxygenation—showing enhanced outcomes when used with finasteride. LED therapies, including red, orange, and blue light, further aid by boosting circulation and reducing inflammation.¹¹, ¹² The goal of treatment is to arrest progression, stimulate regrowth, and restore hair density, individualized to the alopecia type and stage for optimal results.
Result
Significant hair regrowth was observed after hair transplantation, with notable improvement in hair density and graft retention.
Discussion
Hair loss is a multifactorial condition influenced by genetic predisposition, hormonal imbalances, nutritional deficiencies, medications, environmental factors, and cosmetic practices. A thorough understanding of the hair growth cycle—anagen, catagen, telogen, and exogen—is crucial for identifying the underlying etiology. While androgenetic alopecia and stressinduced shedding are common, systemic conditions such as telogen effluvium, endocrine disorders, and autoimmune diseases also play a significant role. Topical and systemic therapies remain first-line treatments; however, in refractory cases, hair transplantation serves as an effective surgical option, offering both aesthetic restoration and psychological improvement.13
Modern hair transplantation has advanced significantly, evolving into a precise surgical technique with improved aesthetic outcomes. Follicular Unit Extraction (FUE) is now the preferred method due to its minimally invasive approach, reduced scarring, and faster recovery compared to Follicular Unit Transplantation (FUT). Innovations such as the Follicular Isolation Technique (FIT)— using depth-controlled punches—and robotic-assisted FUE systems have enhanced accuracy, efficiency, and graft survival.
While generally safe, potential complications include druginduced gastritis, persistent crusting, donor site discomfort, sterile pustules, and delayed regrowth. Educating patients about transient telogen effluvium and the gradual nature of regrowth is essential for managing expectations. Optimal outcomes depend on careful patient selection, individualized planning, and meticulous postoperative care.10, 14
Hair transplantation is a pivotal advancement in hair loss management, especially for patients unresponsive to medical therapy. Ongoing innovations in FUE, FIT, and robotic-assisted techniques have significantly improved outcomes. However, optimal results rely on careful patient selection, personalized surgical planning, and diligent postoperative care to achieve natural, durable restoration.
Conclusion
Hair transplantation has evolved into a highly effective and precise surgical technique, with FUE and FUT as foundational methods. The incorporation of robotic assistance has enhanced accuracy, graft survival, and procedural safety. Future advancements will focus on minimally invasive techniques, next-generation robotics, and personalized treatment planning to further improve outcomes. Continued innovation and research promise greater patient satisfaction and consistent clinical success.
References
1. Al Aboud AM, Syed HA, Zito PM. Alopecia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 26, 2024.
2. Fabbrocini G, Cantelli M, Masarà A, Annunziata MC, Marasca C, Cacciapuoti S. Female pattern hair loss: A clinical, pathophysiologic, and therapeutic review. Int J Womens Dermatol. 2018; 4(4):203-211. Published 2018 Jun 19. doi:10.1016/j.ijwd.2018.05.001
3. Wirya CT, Wu W, Wu K. Classification of Male-pattern Hair Loss. Int J Trichology. 2017; 9(3):95-100. doi:10.4103/ijt. ijt_46_17.
4. Singh S, Muthuvel K. Practical Approach to Hair Loss Diagnosis. Indian J Plast Surg. 2021; 54(4):399-403. Published 2021 Dec 27. Doi: 10.1055/s0041-1739240.
5. Jackson AJ, Price VH. How to diagnose hair loss. Dermatol Clin. 2013; 31(1):2128. doi:10.1016/j.det.2012.08.007.
6. Dhurat R, Saraogi P. Hair evaluation methods: merits and demerits. Int J Trichology. 2009; 1(2):108-119. doi:10.4103/0974-7753.58553.
7. Zito PM, Raggio BS. Hair Transplantation. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 12, 2024.
8. Khanna M. Hair transplantation surgery. Indian J Plast Surg. 2008; 41(Suppl):S56-S63.
9. Sethi P, Bansal A. Direct hair transplantation: a modified follicular unit extraction technique. J Cutan Aesthet Surg. 2013; 6(2):100-105. doi:10.4103/09742077.112672.
10. Mysore V, Kumaresan M, Garg A, et al. Hair Transplant Practice Guidelines. J Cutan Aesthet Surg. 2021; 14(3):265-284. doi:10.4103/JCAS.JCAS_104_20.
11. Nestor MS, Ablon G, Gade A, Han H, Fischer DL. Treatment options for androgenetic alopecia: Efficacy,
side effects, compliance, financial considerations, and ethics. J Cosmet Dermatol. 2021; 20(12):3759-3781. doi:10.1111/jocd.14537.
12. Bhargava A, Singh VK, Tiwari R, Arya A, Chokshi K. Revitalizing Hair Growth: A New Regimen Utilizing Growth Factor Concentrate for Hair Loss Treatment. Cureus. 2024; 16(6):e63354. Published 2024 Jun 28. doi:10.7759/cureus.63354.
13. Gokce N, Basgoz N, Kenanoglu S, et al. An overview of the genetic aspects of hair loss and its connection with nutrition. J Prev Med Hyg. 2022; 63(2 Suppl 3):E228-E238. Published 2022 Oct 17. doi:10.15167/2421-4248/ jpmh2022.63.2S3.2765.
14. Patwardhan N, Mysore V; IADVL Dermatosurgery Task Force. Hair transplantation: standard guidelines of care. Indian J Dermatol Venereol Leprol. 2008; 74 Suppl: S46-S53.
Biologic Therapy Shows Promise for Severe Acne Conglobata
Bimekizumab, a dual inhibitor of interleukin 17A and interleukin 17F, is showing early promise as an off-label treatment option for acne conglobata (AC), a rare and severe form of nodulocystic acne characterized by deep, interconnected inflammatory lesions. AC frequently proves resistant to conventional therapies such as high-dose isotretinoin and systemic corticosteroids. Recent reports have demonstrated rapid and substantial lesion reduction with bimekizumab in treatmentrefractory AC, highlighting its potential as a targeted immunomodulatory therapy. The mechanistic rationale stems from increasing evidence implicating the IL-17/Th17 axis in the pathogenesis of AC, where Cutibacterium acnes drives cytokine-mediated inflammation. Bimekizumab’s dual inhibition of IL-17A and IL-17F may provide a more comprehensive anti-inflammatory effect compared to agents targeting IL-17A alone. Given its recent FDA approval for hidradenitis suppurativa, a chronic inflammatory skin disease with immunologic and clinical overlap, bimekizumab offers a biologically plausible therapeutic alternative for AC. While current data are limited to early off-label use, the rapid onset of clinical improvement and potential psychosocial benefit underscore the need for controlled clinical trials to establish its safety, efficacy, and long-term role in managing severe, treatment-resistant acne conglobata.
Current Aesthetic Preferences among Gen Z and Millennial Patients
A survey of 40 experienced aesthetic clinicians revealed key generational differences between Millennials and Generation Z/Centennials in aesthetic dermatology. Millennials comprised a larger portion of patient bases compared to Centennials. Millennials primarily sought botulinum toxin, dermal fillers, and skincare for wrinkle reduction and rejuvenation, while Centennials focused on fillers, skincare, and neuromodulators to address structural or genetic concerns and modify features. Lip augmentation was the most common filler request in both groups, followed by cheek, nasal, and tear trough treatments. Millennials typically used more syringes per treatment cycle than Centennials. Centennials primarily discovered providers through social media, while Millennials depended on peer referrals. Despite technical ease in treating both, clinicians found Centennials harder to satisfy due to higher expectations, budget constraints, and lower retention. Authors recommend tailored, efficient treatment plans with clear communication and realistic outcome guidance for younger patients. Study limitations include small sample size and potential bias, highlighting the need for further research to optimize aesthetic care across generations.
Dr. Satish Bhatia MD (Skin) IFAAD (USA) Dermatologist and Cutaneous Surgeon Dermetics, Indian Cancer Society Mumbai
The recent IV therapy-related incident highlights serious concerns about patient safety, clinical protocols, and the commercialization of aesthetic procedures. As an experienced dermatologist, I believe this is a crucial time to provide evidence-based insights to educate patients, ensure ethical practice and reinforce strict medical standards in IV and aesthetic treatments.
1. What is your opinion of IV infusion therapies in dermatology?
IV infusion therapies have gained popularity in dermatology, primarily for aesthetic purposes like skin brightening, hydration, and energy enhancement.
2. What is your experience with IV infusion therapies, including safety and patient outcomes?
My experience with IV infusion therapies is mainly in medically indicated cases, with good outcomes when done under strict supervision. They are generally safe in proper settings, but misuse for non-medical purposes can lead to serious complications.
3. In your practice, do you recommend IV infusion therapy for any dermatological indications or just aesthetics? I recommend IV infusion therapy
Expert Opinion on IV Infusion Therapy Safety in Dermatology & Aesthetics
only for genuine medical needs like severe nutritional deficiencies, not for routine aesthetic purposes due to limited evidence. Patient safety is paramount, and I prefer evidence-based topical, oral, or procedural treatments over unregulated IV drips.
4. Based on your experience, which indications do you treat, and which IV formulations are most commonly requested?
The most commonly treated indications for IV infusion therapy include dull or tired-looking skin, general fatigue, and pre-event rejuvenation— particularly in the form of “bridal packages.” The most frequently requested formulations typically include Glutathione (up to 1,880,000 mg per month), Vitamin C or ascorbic acid (up to 500,000 mg), Hyaluronic acid, Alpha lipoic acid, and various trace additives such as Kojic acid, multivitamins, copper peptides, and placental extract. These combinations are often aimed at skin brightening, hydration, and boosting overall energy levels.
5. What baseline evaluations, including necessary laboratory tests, must be performed before initiating aesthetic IV therapy?
First, baseline evaluations must include a complete blood count (CBC) and erythrocyte sedimentation rate (ESR). It is essential to test for IgE levels and screen for G6PD deficiency, as the latter poses a potentially fatal risk. Additionally, bleeding and clotting times should be assessed, along with any use of blood thinners, including aspirin. If any of these criteria indicate risk, administering the IV therapy should be avoided. Next, it is important to consider the potential complications that may arise if a patient requests an IV drip, particularly when administered outside a clinical setting, such as at home.
6. Do you utilize a standard informed consent document before administering IV drip therapy in your practice?
Yes, absolutely. We have a strict protocol that includes a standard informed consent form. Patients are briefed about the treatment, expected benefits, possible side effects, ingredients, and potential risks. For minors, written parental consent is mandatory.
7. Are there specific contraindications or patient conditions for which you avoid doing IV infusion therapies even if the patient asks for it?
Contraindications for IV infusion therapy are strictly observed to ensure patient safety. These include G6PD deficiency, allergies to infusion components, use of blood thinners like aspirin, cardiac or renal disease and abnormal bleeding or clotting parameters. These conditions pose significant risks such as oxidative stress, anaphylaxis, fluid overload, or embolism. If any are identified during pre-infusion screening, the therapy is not administered. Patient safety remains the top priority.
8. What are the risks associated with IV drips given by unauthorized non-medico providers without proper medical supervision?
IV drips administered by unauthorized or untrained non-medical personnel pose extremely serious and potentially fatal risks. These include sepsis or infections due to non-sterile techniques, air embolism, liver or kidney damage, allergic reactions or anaphylaxis, contamination from unsafe or unverified products, and incorrect dosages. Additionally, there is a high risk of cross-contamination, especially in poorly regulated settings. These dangers are significantly amplified when IV drips are given in salons, spas, or other nonclinical environments without proper medical oversight.
9. Have you encountered patients who have had a negative IV treatment experience from unauthorized providers and later came to you?
Yes, I have seen patients with complications from IV treatments by unqualified providers, often presenting with infections, allergic reactions, or systemic side effects. Most come from non-medical setups and many require extensive management. Due to poor quality of the products, usually sold from cheap vendors who were non-licensed in the black market and or IV infusions. This highlights the need for strict medical supervision, regulation, and patient awareness.
10. How do you counsel patients who express interest in self-injecting aesthetic or vitamin therapies?
We strongly discourage self-injection due to the significant risks involved, including infections, incorrect dosages, and the potential use of counterfeit or unsafe products. Patients are educated about these dangers and reminded that IV therapy is a medical procedure that requires professional supervision— not a do-it-yourself treatment. We emphasize that even if the products are purchased over-the-counter, administering them without proper clinical oversight can be life-threatening.
11. What patient education or counselling do you provide before administering any aesthetic IV drips?
Before administering any aesthetic IV drips, patients are thoroughly counselled about the contents of the infusion, the expected benefits and their limitations, as well as the known risks and potential side effects. They are informed about the necessity of pre-infusion blood tests, including CBC, G6PD screening, and allergy markers. Patients are also made aware that the results are temporary and the importance of medical supervision and maintaining strict sterility throughout the procedure is emphasized.
12. What is your opinion on "feel good" party/ after-party IV drips?
“Feel good” or “party drips” have become a popular fad, but in most cases, they lack medical justification and can be extremely dangerous, especially when administered by non-medical personnel. These treatments typically contain a mix of vitamins and fluids intended to ‘detoxify’ or ‘energize,’ but they often have no clear scientific evidence to support their use, and their formulations are frequently unknown or unregulated, posing significant health risks.
13. In your opinion, what should be the safety protocols for using IV drips in aesthetic practice—or should it be stopped due to potential risks?
IV therapy in aesthetics should not be stopped but must follow strict safety protocols. It should only be administered by licensed medical professionals after proper screening and blood tests. Approved, sterile formulations must be used with informed consent and continuous monitoring. IV drips should be strictly banned in salons or by non-medical personnel to prevent serious health risks.
14. To what extent is social media marketing influencing the use of IV drips for aesthetic purposes?
Social media has heavily influenced the rising demand for IV drips in aesthetics, with many people selfprescribing after seeing trends online. Some even buy drips from chemists and get them administered without medical supervision, reflecting the market’s lack of regulation. Unapproved agents like NAD, peptides, and amino acids are often used, and glutathione is frequently combined with vitamin C and steroids without evidence-based protocols. These “glow drips” are favored for their quick results, especially in practices like “bridal packages” done at home, despite being potentially fatal. Glutathione is not approved for cosmetic use, yet some dermatologists prescribe it with caution, following proper screening and dosing. Social media influence is so strong that even teenagers request these treatments; in such cases, we require parental presence and written consent.
15. In your opinion, who should take responsibility in the case of an adverse event—the injector or the product company?
Primary responsibility lies with the injector, especially if the procedure is performed without proper protocol, screening, or training. However, if the product is substandard or falsely marketed, the product company also shares accountability. Both parties must ensure ethical practice and safety compliance.
Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser: A Case Report
Dr. Diwakar Sharma
MBBS, DNB Consultant Dermatologist
BVP Hospital, Kota, Rajasthan
Introduction
Nevus of Ota, also known as ocular
dermal melanosis, is a benign condition characterized by gray-blue hyperpigmentation primarily affecting the distribution of the ophthalmic (V1) and maxillary (V2) divisions of the trigeminal nerve. This dermatological condition presents with bluish pigmentation involving the periocular region, including the conjunctiva, sclera, eyelids, and extending to the ipsilateral facial skin. The hyperpigmentation results from melanocytes entrapped in the dermis, distinguishing it from conditions like the Mongolian spot where melanocytes reside deeper in the dermal layer. Clinically, nevus of Ota manifests as macular, patchy brown, slate-blue, or grey-black pigmented lesions with poorly defined margins, occasionally appearing nodular or papular. Although typically asymptomatic, rare cases may present with sensory loss. The condition is usually unilateral but can rarely be bilateral, with
deeper lesions appearing blue due to melanocyte localization.1
The etiopathogenesis of nevus of Ota is linked to aberrations in the dorso-lateral migratory pathway of melanoblasts originating from the neural crest during embryogenesis, occurring between the second and eighth gestation weeks. Various classifications exist based on the extent and characteristics of cutaneous manifestations. One classification categorizes the condition into four types: minimal involvement, which includes orbital, zygomatic, frontal, and nasal wing subtypes; moderate involvement encompassing upper and lower eyelids, periocular region, cheekbone, temple, wing, and root of the nose; severe involvement extending to parietal and temporal regions of the scalp, forehead, eyebrow, and nose in addition to type 2 areas; and bilateral involvement, observed in approximately 10% of cases. Another classification is based on histopathological
features superficial dominant, diffuse, deep dominant, and deep types. A differentiation based on response to laser treatment, categorizing nevus of Ota into subtypes based on presence or absence of periorbital involvement, other birthmarks, and extracutaneous manifestations. A classification based on the innervation areas of trigeminal nerve branches: type I, II, and III involve pigmentation macules of the first, second, and third trigeminal nerve branches, respectively; type IV denotes bilateral lesions and pigmentation macules of the cheeks; and type V is associated with additional complications classification focusing on ocular involvement (conjunctiva, sclera, iris, and choroid) and the extent of ocular pigmentation by number of quadrants affected.2, 3
Nevus of Ota is a distinctive dermatological condition characterized by its unique distribution along the trigeminal nerve divisions and its association with ocular and extracutaneous pigmentation. Effective management involves early diagnosis, comprehensive ophthalmic assessment, and tailored treatment strategies to address cosmetic concerns and mitigate potential ocular complications, ensuring optimal patient outcomes and quality of life.
Case Report
A 24-year-old female patient presented bluish hyperpigmentation on her face. On examination, the hyperpigmentation was observed along the maxillary
A Case Report
area of the face. The confirmation of the diagnosis of nevus Ota was made based on the clinical appearance and examination. Treatment was initiated using Nd:YAG (neodymium-doped yttrium aluminum garnet) laser therapy. Over the course of several treatment sessions, there was a significant resolution of the pigmentation, resulting in a noticeable improvement in the patient's facial appearance. The Nd:YAG laser works by targeting the melanin in the affected areas, effectively breaking down the pigment and allowing the body to naturally eliminate it. Regular monitoring will be essential to assess long-term outcomes, ensure sustained improvement, and promptly address any potential recurrence or complications.
Before treatment After treatment
Diagnosis
Reflectance confocal microscopy (RCM) is a non-invasive imaging technique providing real-time, high-resolution images of the skin at a cellular level. In nevus of Ota, RCM reveals increased melanin pigment deposition in the dermis and the presence of melanocytes in both superficial and deep layers. This helps differentiate nevus of Ota from other pigmented lesions and assess lesion depth and distribution. RCM visualizes melanocyte patterns in affected areas, following the distribution of the ophthalmic and maxillary divisions of the trigeminal nerve, including regions like the periocular area, forehead, and zygomatic area. For diagnosis, a biopsy is performed, usually with a punch or excisional technique under local anesthesia, to examine the pigmented lesion and surrounding skin. Histopathological
Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser:
Figure 1: Bluish hyperpigmentation along the maxillary area on face
examination confirms melanocytes with melanin accumulation, using special stains like Fontana-Masson, and assesses for malignancy. Slit lamp examination is crucial in diagnosing Nevus of Ota by visualizing the anterior eye segment, including the conjunctiva, sclera, cornea, and iris, revealing characteristic blue-gray or brownish pigmentation. Gonioscopy complements this by assessing trabecular meshwork pigmentation and glaucoma risk, while tonometry measures intraocular pressure to monitor potential glaucoma development from pigment dispersion.
Ultrasound biomicroscopy (UBM) further aids diagnosis by providing high-resolution images of the anterior chamber angle, iris morphology, ciliary body, and cornea, as well as episcleral and scleral pigmentation. This detailed assessment helps monitor the risk of secondary glaucoma in Nevus of Ota patients.2
Fundus Autofluorescence (FAF) visualizes melanin distribution in the posterior eye, revealing hypoautofluorescent areas in Nevus of Ota corresponding to choroidal pigmentation. Fluorescein Angiography (FA) assesses retinal and choroidal vasculature, showing hyperfluorescence and hypoautofluorescent areas.
Indocyanine Green Angiography (ICGA) enhances visualization of deeper choroidal vessels, revealing hypercyanescent areas indicating choroidal hyperpigmentation. Spectral
Domain Optical Coherence Tomography (SD-OCT) provides cross-sectional images, identifying hyperreflective areas of melanin and associated changes. OCT Angiography (OCTA) detects vascular alterations without dye injection. Ultrasonography uses sound waves to assess nevus size, shape, and internal reflectivity, useful when media opacity limits other imaging methods.2
These advanced diagnostic techniques play a crucial role in the comprehensive evaluation of Nevus of Ota, offering detailed anatomical and functional information essential for accurate diagnosis, monitoring disease progression, and guiding treatment decisions.
Treatment
Hydroquinone is a depigmenting agent used to treat hyperpigmentation disorders like Nevus of Ota by inhibiting the enzyme tyrosinase, crucial in melanin synthesis. Applied topically as cream, gel, or lotion directly to affected areas, hydroquinone reduces melanin production locally by targeting melanocytes.4
Tranexamic acid (TXA), known for its antifibrinolytic properties, is employed in dermatology orally and topically to manage hyperpigmentation disorders, including nevus of Ota. TXA may inhibit melanocyte activation and melanin synthesis, potentially improving skin appearance through its antiinflammatory effects.5
Liquid nitrogen cryotherapy is a treatment method that utilizes
extreme cold (approximately -196°C) to target and destroy abnormal tissues, including pigmented lesions like nevus of Ota. During the procedure, liquid nitrogen is applied directly to the affected area using a cryospray or a cotton-tipped applicator. The rapid freezing induces ice crystal formation within the cells, causing damage to the melanocytes responsible for the pigmentation. As the treated area thaws, the damaged cells are gradually eliminated by the body's natural immune response. This process can effectively lighten or reduce the pigmentation associated with nevus of Ota.6
The combination treatment of nevus of Ota using autologouscultured epithelium grafting and dermabrasion aims to improve skin pigmentation and texture. Healthy keratinocytes are harvested from an unaffected area, cultured in a lab, and transplanted onto the affected area to replace pigmented cells with non-pigmented epithelial cells. Dermabrasion follows to remove the outer layers of pigmented skin. Microsurgical treatment involves a specialized surgeon using advanced techniques and a surgical microscope to precisely excise the pigmented lesion, ensuring minimal trauma to adjacent healthy tissue.7,8
Nd:YAG (neodymium-doped yttrium aluminum garnet) laser treatment has emerged as a preferred modality for the treatment of nevus Ota, a benign congenital pigmented lesion typically found on the
Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser:
face. This laser operates at a wavelength of 1064 nanometers, which allows it to penetrate deep into the skin while minimizing damage to surrounding tissues.
Nd:YAG laser treatment for nevus ota utilizes a principle known as selective photothermolysis. The laser emits light energy that is absorbed by the melanin pigment within the pigmented lesions. This absorption leads to the generation of heat, which selectively destroys the melanocytes (pigmentproducing cells) responsible for the discoloration. By targeting melanin specifically, the Nd:YAG laser effectively lightens or removes the pigmented areas without causing significant harm to the normal surrounding skin. Before initiating Nd:YAG laser treatment, a thorough evaluation is conducted to assess the characteristics of the nevus Ota, including its size, depth, and location. Skin type and medical history are also considered to determine the appropriate treatment parameters. The laser settings such as wavelength, pulse duration, and energy level are carefully adjusted based on the individual's skin type and the extent of pigmentation. This customization ensures optimal treatment efficacy while minimizing the risk of adverse effects. The Nd:YAG laser is applied to the affected area in short pulses. Patients may feel a mild sensation of warmth or tingling during treatment, but discomfort is usually minimal. After Nd:YAG laser treatment, patients are advised on postprocedure care, which typically
includes applying soothing creams or ointments to the treated area and avoiding sun exposure. Sunscreen with high SPF is recommended to prevent hyperpigmentation recurrence. Benefits of Nd:YAG laser treatment is it targets melanin specifically, minimizing damage to surrounding tissues. Significant lightening or complete removal of nevus ota lesions can be achieved over multiple treatment sessions. When performed by trained professionals, Nd:YAG laser treatment is generally safe with minimal risk of scarring or other adverse effects. Depending on the size and depth of the lesion, several treatment sessions spaced weeks apart may be necessary to achieve desired results. Nd:YAG laser treatment may not be suitable for all skin types or conditions. A thorough consultation with a dermatologist or laser specialist is crucial to assess candidacy and potential outcomes. Nd:YAG laser therapy has revolutionized the management of nevus Ota by offering a safe, effective, and minimally invasive treatment option. Continued advancements in laser technology and treatment protocols hold promise for further improving outcomes and expanding the applications of Nd:YAG laser in dermatology.9
The combination of Q-switched Nd:YAG laser and fractional CO2 laser represents an advanced treatment approach for nevus of Ota, a pigmented birthmark. The Q-switched Nd:YAG laser emits light at
1064 nanometers, specifically targeting melanin pigment in the skin to selectively destroy melanocytes through photothermolysis. This process gradually lightens or removes the pigmented areas. In parallel, the fractional CO2 laser operates at approximately 10,600 nanometers, delivering laser energy in a fractionated pattern to create microscopic columns of thermal injury. This stimulates collagen production and remodeling, thereby improving skin texture and overall tone.10
Discussions
Ocular dermal melanosis, also known as nevus of Ota is an increased risk of developing uveal melanoma and glaucoma in affected individuals. The etiology of nevus of Ota involves abnormal migration of melanocytes from neural crest cells to the basal layer of the epidermis during embryonic development resulting in the typical bluish-gray pigmentation observed in affected areas. Monosomy of chromosome 3 and gain of the long arm of chromosome 8q are significant genetic alterations associated with increased risk of uveal melanoma and poorer clinical outcomes. Genetic mutations in genes like BRAF, NRAS of the MAP kinase pathway, and GNAQ are known contributors. These mutations lead to constitutive activation of G-coupled proteins, contributing to the characteristic pigmentation seen in the skin and uveal tissues. Factors such as previous radiotherapy, radiation exposure,
Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser: A Case Report
and hormonal influences are also implicated. Ocular dermal melanosis predominantly affects individuals of Asian and African descent, with a prevalence ranging from 0.014% to 0.034% in the population. The condition typically presents at birth but can also manifest during puberty or pregnancy due to hormonal changes. Females are more commonly affected than males, with a ratio of 5:1. The incidence is lower in individuals of White ethnicity, although the risk of malignant melanoma is higher in this population compared to other racial groups.1
Ocular involvement in Nevus of Ota spans several critical areas within the eye. Melanocyte accumulation on the episclera and sclera is a notable feature, commonly observed in the superior temporal and lower medial regions. Iris heterochromia is frequently present, characterized by a darker brown coloration in the affected eye, often accompanied by iris mammillations that can contribute to irregularities in the iris surface and potentially elevate intraocular pressure. In some cases, the ciliary body may be affected, increasing the risk of developing ciliary body melanoma.2
Ocular complications associated with Oculodermal Melanocytosis (ODM) encompass significant risks, necessitating vigilant monitoring and intervention. Glaucoma can develop due to abnormalities in the irido-corneal angle or pigment accumulation in the trabecular meshwork
and Schlemm's canal, resulting in obstructed aqueous humor outflow. It typically manifests ipsilateral to the pigmentation and affects approximately 10% of individuals with ODM. Approximately one in 400 white individuals with pre-existing ODM may develop uveal melanoma during their lifetime, underscoring the heightened risk association. ODM is also linked to atypical presentations of uveal melanoma, such as bilateral and multifocal forms. Genetic mutations, such as somatic activating mutations in the GNAQ gene and biallelic mutations in the BAP1 gene, are prevalent in both uveal melanoma and ODM, potentially influencing the progression to metastatic disease.2
In neonates presenting with pigmented skin lesions, the differential diagnosis includes several conditions. Facial café-au-lait macules (CALM) are benign patches ranging from light to dark brown, often sporadic or seen in genetic syndromes like neurofibromatosis type 1 (NF1), distinct from nevus of Ota by lacking deep blue or slate-gray coloration and involvement beyond the skin. Speckled lentiginous nevus presents as multiple small brown to black macules on normal skin, unlike nevus of Ota's bluish-gray pigmentation, often requiring biopsy to rule out neurocutaneous melanosis. Congenital blue nevus, characterized by blue to blue-gray lesions due to deep melanin deposition, differs from nevus of Ota by sparing the ophthalmic and maxillary divisions of the trigeminal nerve and ocular structures. Ochronosis, a metabolic disorder accumulating homogentisic acid, causes bluish-black discoloration in connective tissues, distinct from nevus of Ota by lacking dermatomal distribution and presenting systemic features like arthritis and dark urine. Diagnosis involves biochemical and genetic testing to differentiate it from primarily pigmentary dermatoses. Clinical examination and sometimes dermatoscopic evaluation or imaging helps to confirm the extent of pigmentation. Treatment options include observation with periodic follow-up, laser therapy for cosmetic improvement, or surgical excision for localized lesions. Patients should be informed that transformation into malignancy is exceedingly rare. They should seek medical evaluation promptly if there are any changes in lesion size or appearance.1, 2
Conclusion
Nevus Ota presents a significant challenge in clinical practice due to its varied presentations and potential confusion with other pigmented lesions, demanding a heightened level of clinical suspicion, especially in regions with less familiarity with such conditions. Beyond diagnostic intricacies, the condition's visibility profoundly impacts patients' psychosocial well-being, influencing self-esteem and quality of life. Addressing these complexities with advancing medical knowledge is crucial for accurate diagnosis and tailored management strategies that improve patient outcomes. Nd:YAG laser therapy has shown promising results in mitigating pigmentation associated with nevus Ota, contributing positively to
Oculodermal Melanocytosis (Nevus of Ota) Treated with Nd:YAG Laser: A Case Report
cosmetic outcomes and patient satisfaction. However, physicians continue to encounter challenges in refining treatment protocols and managing patient expectations amidst evolving technological advancements. These efforts underscore the ongoing commitment to optimizing care and enhancing the therapeutic efficacy of Nd:YAG laser in dermatological practice.
References
1. Agarwal P, Patel BC. Nevus of Ota and Ito. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 10, 2023.
2. Abdolrahimzadeh S, Pugi DM, Manni P, et al. An update on ophthalmological perspectives in oculodermal melanocytosis (Nevus of Ota). Graefes Arch Clin Exp Ophthalmol. 2023; 261(2):291-301. Doi: 10.1007/s00417022-05743-1.
3. Chan HH, Kono T. Nevus of Ota: clinical aspects and management. Skinmed. 2003; 2(2):89-98. doi:10.1111/j.15409740.2003.01706.x.
4. Nam JH, Kim HS, Choi YJ, Jung HJ, Kim WS. Treatment and Classification of Nevus of Ota: A Seven-Year Review of a Single Institution's Experience [published correction appears in Ann Dermatol.
5. Yang X, Bi C, E T, Lin L, Cao Y. A retrospective study of 1064-nm Q-switched Nd:YAG laser therapy for acquired bilateral nevus of Ota-like macules. Skin Res Technol. 2023; 29(3):e13298. doi:10.1111/ srt.13298.
6. Hosaka Y, Onizuka T, Ichinose M, et al. Treatment of nevus Ota by liquid nitrogen cryotherapy. Plast Reconstr Surg. 1995; 95(4):703-711. Doi: 10.1097/00006534199504000-00012.
7. Kumagai N, Fukushi S, Matsuzaki K, Ishida H. Treatment of nevus of Ota with autologous-cultured epithelium grafting combined with dermabrasion. Ann
8. Kobayashi T. Microsurgical treatment of nevus of Ota. J Dermatol Surg Oncol. 1991; 17(12):936-941. doi:10.1111/j.1524-4725.1991. tb01693.x.
9. Aurangabadkar S. QYAG5 Q-switched Nd:YAG Laser Treatment of Nevus of Ota: An Indian Study of 50 Patients. J Cutan Aesthet Surg. 2008; 1(2):80-84. doi:10.4103/0974-2077.44164.
10. Mann KK, Khunger N, Yadav AK. Nevus of Ota: Combination Treatment with Q-Switched Neodymium-Doped Yttrium Aluminum Garnet Laser and Fractional CO2 Laser. J Cutan Aesthet Surg. 2023; 16(3):214-220. doi:10.4103/JCAS. JCAS_116_21. Oculodermal
Effective Management of Irritant Contact Dermatitis with Desonide and Ceramide-Based Moisturizer
Dr. Neha Chaitanya Shukla MBBS, MD
Consultant Dermatologist, Cosmetologist and Laser Surgeon
EYE and SKIN Plus Advance Hospital
Gandhinagar, Gujarat
Introduction
Irritant contact dermatitis (ICD) is a common and prevalent cutaneous disorder characterized by inflammation and damage to the skin barrier, typically caused by exposure to irritant substances. The condition results from the disruption of the skin's natural barrier function, leading to symptoms that can range from mild to severe.1 It is a common condition that can present in two distinct clinical forms: acute and chronic. Acute ICD is characterized by the rapid onset of sharply bordered, erythematous, blistering, and erosive lesions, often accompanied by pruritus or pain, which are typically localized to the area of contact and exhibit an asymmetric distribution. This acute phase is usually self-limiting and resolves with removal of the causative agent. In contrast, chronic ICD is marked by a more insidious onset, with diffuse or localized, poorly defined erythematous scaly patches and plaques, skin dryness, lichenification, and
desquamation. This chronic form often affects the hands and forearms, which have a natural barrier function that is more susceptible to disruption. Allergic contact dermatitis, on the other hand, exhibits a more rapid onset and a tendency to spread, presenting with erythematous, edematous, erosive, crusty, and squamous lesions that can disseminate and cause pruritus. In some cases, ACD can also lead to chronic inflammation, characterized by a symmetric distribution, less sharply defined borders, and distant spread, accompanied by lichenification, fissures, and pruritus. Understanding the distinct clinical features of ICD and ACD is essential for accurate diagnosis and effective management of these conditions.2 Contributing factors to irritant contact dermatitis include exposure to harsh chemicals, environmental factors like extreme temperatures and dry air, and biological agents like bacteria and viruses. Additionally, atopic diathesis,
skin dryness, and genetic predisposition can also play a role. Other factors, such as allergens, acidic or alkaline substances, and systemic diseases like diabetes or kidney disease, can also contribute to the development of ICD.3
The pathogenesis of irritant contact dermatitis includes an immunological response. Irritation can occur through direct damage to epidermal cells, disruption of the epidermal barrier, or a combination of both. Disruption of the epithelial barrier allows for increased permeability of irritants, leading to activation of keratinocytes as "signal transducers." Keratinocytes convert exogenous stimuli into the secretion of cytokines, adhesion molecules, and chemotactic factors, initiating cutaneous inflammation. Upon keratinocyte damage, primary cytokines such as IL-1α, IL-1β, and TNF-α are upregulated, triggering keratinocyte proliferation and lipid formation to restore the epidermal barrier. Subsequently, additional cytokines including IL-6, IL-8, and GM-CSF are secreted, activating langerhans cells, dermal dendritic cells, and endothelial cells to recruit inflammatory cells to the site of chemical trauma. The adhesion molecule ICAM1 is upregulated on endothelial cells and fibroblasts in the skin, resulting in the secretion of chemokines including CXCL8, CCL20, and IFN-gamma. CCL21, a chemokine that enables naive T lymphocyte migration, is also upregulated in ICD. Recruited T lymphocytes often express the CLA antigen, which plays a crucial role in transendothelial T
lymphocyte migration. Irritants can also trigger pattern recognition receptors such as toll-like receptors (TLRs) and NOD-like receptors, activating the innate immune response via inflammasome and NFκB pathways.4, 5 Effective management of irritant contact dermatitis necessitates a comprehensive approach involving identification of triggers, use of topical anti-inflammatory agents, promotion of skin barrier integrity, and implementation of lifestyle modifications. These interventions not only mitigate symptoms but also reduce recurrence rates, thereby enhancing long-term dermatological health and quality of life.
Case report
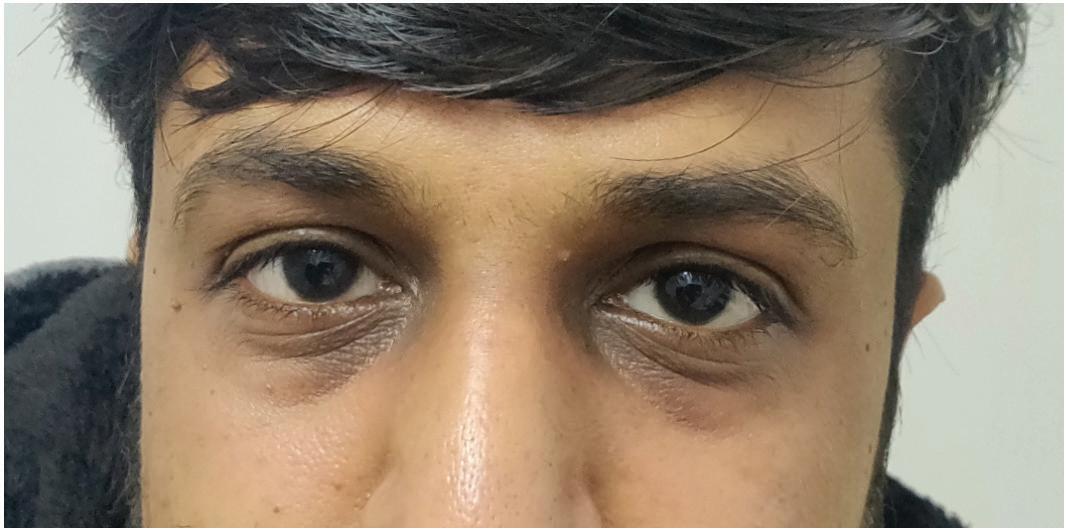
A 32-year-old male patient presented with symptoms consistent with retinoid dermatitis, which was attributed to the use of an overthe-counter undereye cream containing retinoids, used without a doctor's prescription. On examination, the patient exhibited erythema, scaling, and mild itching localized around the eyes. Based on these clinical signs, a diagnosis of retinoid dermatitis was made. Treatment was promptly initiated with desonide cream, a low-potency topical corticosteroid, applied twice daily to reduce inflammation. Additionally, a ceramide-based moisturizing cream was prescribed to be applied alongside the desonide, aiming to restore the integrity of the skin barrier. This treatment regimen was followed for 7 days. The patient showed significant improvement, with a notable reduction in erythema and scaling, and complete resolution of itching. The combined anti-inflammatory and barrierrepair approach proved effective in managing the dermatitis and alleviating the patient's symptoms.
Before treatment
After treatment
Figure 1: Erythema, scaling, and mild itching around the eyes
Diagnosis
The diagnosis of irritant contact dermatitis involves a comprehensive clinical evaluation, including detailed history-taking and physical examination to rule out other conditions like allergic contact dermatitis. Key aspects include assessing occupational and domestic exposure to skin irritants, focusing on the frequency, intensity, and duration of exposure, and examining the pattern and distribution of dermatitis, which typically begins at the site of irritant contact and does not spread. Patch testing is recommended to differentiate ICD from ACD by identifying potential allergens or irritants causing the reaction. Additionally, bioengineering techniques such as Trans-epidermal water loss (TEWL) measurement provide quantitative data on skin barrier integrity, crucial for diagnosing and assessing ICD severity. Reflectance-mode confocal microscopy (RCM) offers highresolution imaging to visualize skin structures and inflammatory changes, aiding in understanding acute tissue responses to irritants.6
Treatment
In the management of irritant contact dermatitis, the primary approach involves avoidance of irritants and protective measures to safeguard the skin from exposure, both at work and home. Additionally, topical therapy, particularly the regular application of moisturizing creams, is essential. Strontium salts have emerged as a promising therapy for managing irritant contact dermatitis by selectively blocking cutaneous
nociceptors, thereby alleviating symptoms of itching, burning, and pain associated with acute irritant dermatitis.
Topical calcineurin inhibitors (TCIs) like tacrolimus and pimecrolimus are effective alternatives in ICD treatment, particularly when corticosteroids are impractical. They inhibit calcineurin, reducing inflammation and alleviating symptoms such as redness, swelling, and itching, especially suitable for sensitive areas like the face and neck. Oral immunomodulators, such as cyclosporine and methotrexate, play a crucial role in managing severe and treatment-resistant forms of ICD by suppressing immune responses, particularly T-cell activation and folate metabolism inhibition, respectively. Monoclonal antibodies (mAbs) like dupilumab offer a targeted approach in refractory cases of hyperkeratotic ICD by modulating IL-4 receptor signaling, which reduces inflammatory cytokine production and enhances skin barrier repair. Antihistamines such as cetirizine and diphenhydramine are adjunctive therapies in ICD management, mitigating symptoms associated with histamine release, including itching and discomfort. Their use complements primary treatments focused on removing irritants, protecting the skin barrier, and promoting healing.7
Topical corticosteroids, such as desonide cream, are crucial in managing irritant contact dermatitis by modulating skin inflammation. These medications penetrate the skin and bind to glucocorticoid
receptors in dermal cells, altering gene transcription to suppress immune cell activity and reduce production of inflammatory mediators. This anti-inflammatory action effectively alleviates symptoms like erythema, edema, and pruritus associated with ICD, providing rapid relief from discomfort, itching, and pain. Moreover, corticosteroids aid in restoring compromised skin barrier function by mitigating inflammation, facilitating skin repair, and preventing further damage. Desonide cream is particularly suitable for sensitive areas such as the face and skin folds, offering a balanced approach to managing ICD with effective symptom relief while minimizing risks associated with stronger corticosteroids over prolonged use, such as dermal atrophy. These attributes make desonide cream a preferred choice for therapeutic management, ensuring both symptom relief and skin barrier protection.8
Ceramide-based are integral in managing irritant contact dermatitis by restoring and strengthening the skin's natural barrier. Ceramides, essential lipids found in the stratum corneum, replenish the lipid barrier compromised by irritants. This restoration enhances skin hydration, soothes dryness, and reduces the risk of ongoing irritation. Regular use of ceramide-based moisturizers not only provides immediate relief but also supports longterm skin health by maintaining barrier integrity. These creams are suitable for maintenance therapy, helping to prevent flareups and sustain skin health by
protecting against recurrent episodes of ICD. Therefore, ceramide-based moisturizers are crucial in the comprehensive management of ICD, facilitating skin healing and maintaining skin integrity over time.7
Phototherapy, specifically UV light therapy, is an established treatment for irritant contact dermatitis, effectively reducing inflammation and symptoms such as erythema, pruritus, and edema. UVB therapy penetrates the epidermis to restore skin barrier function, improving overall dermatological health in challenging cases of ICD. Grenz-ray therapy, employing low-energy X-rays, targets superficial skin layers to mitigate inflammation and promote healing by modulating immune responses.7 Together, these therapies underscore their pivotal role in managing refractory ICD and enhancing patient outcomes.
Discussion
Irritant contact dermatitis results from skin damage, direct toxic effects, or inflammation triggered by exposure to irritant substances. Symptoms can appear immediately upon contact and persist without removal of the irritant. The onset and severity of ICD vary based on factors such as the type and frequency of exposure, affected body areas, and individual susceptibility. Clinical types of ICD encompass various presentations, acute ICD occurs rapidly due to potent irritants like acids and solvents, causing immediate burns. Delayed acute ICD develops hours after exposure, seen with substances such as benzalkonium chloride. Non-erythematous ICD involves
early irritation detectable through assays. Cumulative ICD results from repeated exposure to weak irritants, leading to chronic conditions like lichenification. Frictional dermatitis arises from repeated trauma, causing thickened skin. Traumatic ICD follows acute skin injury, such as burns or cuts, leading to chronic eczematous lesions. Pustular and acneiform dermatitis arises from exposure to specific chemicals in predisposed individuals. Asteatotic irritant dermatitis occurs in dry, lowhumidity environments, causing dryness and scaling. Airborne ICD results from exposure to airborne irritants like fibers and solvents, causing skin irritation upon contact.7
The strategies to prevent irritant contact dermatitis focus on eliminating or substituting irritants, isolating processes, engineering controls, administrative measures, and using appropriate personal protective equipment (PPE). Pre-employment screening tools are advocated for early detection of hand dermatitis. PPE selection hinges on the type of irritants and skin exposure areas. Gloves, crucial for hand protection, should be chosen based on specific tasks and potential chemical exposures; neoprene gloves are effective against acrylate monomers. Risks of sensitization and allergic reactions are associated with glove materials like latex and nitrile. Training on glove use reduces errors and allergen exposure. Education on irritant recognition, correct PPE usage, and early ICD signs is essential. Soap-free cleansers with neutral pH and high-free fatty acids are
preferred for hand hygiene, while alcohol-based sanitizers with moisturizers are recommended. Barrier creams offer limited protection against mild irritants and require proper application. Emerging therapies targeting inflammatory pathways, such as topical disulfiram, show promise in ICD prevention.7
Maintaining cleanliness is critical in preventing occupational dermatitis, emphasizing the use of approved industrial skin cleansers and ensuring adequate washing facilities for workers. An effective skin cleanser for occupational settings should be versatile, soluble in various water types (hard, soft, cold, hot), capable of efficiently removing fats, oils, and contaminants without damaging the skin or causing defatting. It should not contain harsh abrasives, remain stable during storage to prevent degradation or contamination, and dispense easily without clogging plumbing systems. These criteria ensure that skin cleansers effectively support skin hygiene without compromising skin barrier integrity, essential for preventing occupational skin diseases.7
Understanding the complexities of contact dermatitis and individualized treatment approaches are crucial for optimizing patient outcomes and ensuring long-term skin health.
Conclusion
Irritant contact dermatitis poses ongoing challenges in dermatology. Diagnosis is straightforward in acute cases but requires repeated historytaking and tests for subacute or chronic ICD. Preventive measures are crucial once
irritants are identified (primary, secondary, tertiary) to minimize exposure in both work and home environments, aiming to prevent flare-ups and maintain skin integrity. Unlike allergic contact
References
1. Nosbaum A, Vocanson M, Rozieres A, Hennino A, Nicolas JF. Allergic and irritant contact dermatitis. Eur J Dermatol. 2009;19(4):325-332. doi:10.1684/ ejd.2009.0686.
2. Novak-bilić g, vučić m, japundžić i, meštrović-štefekov j, stanić-duktaj s, lugović-mihić l. Irritant and allergic contact dermatitis - skin lesion characteristics. Acta clin croat. 2018; 57(4):713-720. Doi:10.20471/acc.2018.57.04.13
3. Hu CH. Sweat-related dermatoses: old concept and new scenario. Dermatologica. 1991;182(2):73-76. doi:10.1159/000247748.
4. Ale IS, Maibach HI. Irritant contact dermatitis. Rev Environ Health.
dermatitis, ICD can persist despite irritant removal, compromising the skin barrier and increasing susceptibility to other irritants. Comprehensive preventive strategies are essential to reduce ICD incidence, emphasizing proactive dermatological care and patient education to manage this prevalent condition effectively.
2014;29(3):195-206. doi:10.1515/ reveh-2014-0060.
5. Spiekstra SW, Toebak MJ, SampatSardjoepersad S, et al. Induction of cytokine (interleukin-1alpha and tumor necrosis factor-alpha) and chemokine (CCL20, CCL27, and CXCL8) alarm signals after allergen and irritant exposure. Exp Dermatol. 2005;14(2):109-116. doi:10.1111/j.09066705.2005.00226.x.
6. Maarouf M, Costello CM, Gonzalez S, Angulo I, Curiel-Lewandrowski CN, Shi VY. In Vivo Reflectance Confocal Microscopy: Emerging Role in Noninvasive Diagnosis and Monitoring of Eczematous Dermatoses. Microscopia confocal de reflectancia in vivo: papel emergente en el diagnóstico no invasivo, así como en el seguimiento
de las dermatosis eccematosas. Actas Dermosifiliogr (Engl Ed). 2019;110(8):626-636. doi:10.1016/j. ad.2018.08.008
7. Patel K, Nixon R. Irritant Contact Dermatitis - a Review. Curr Dermatol Rep. 2022;11(2):41-51. doi:10.1007/s13671021-00351-4.
8. Cohen DE, Heidary N. Treatment of irritant and allergic contact dermatitis. Dermatol Ther. 2004;17(4):334-340. doi:10.1111/j.1396-0296.2004.04031.x
Vitamin C Enhances Epidermal Thickness and Skin Regeneration through Epigenetic Activation
Recent research has demonstrated that vitamin C significantly enhances epidermal thickness by stimulating keratinocyte proliferation through epigenetic regulation, specifically DNA demethylation. Using advanced laboratory skin models that closely replicate human epidermis, investigators found that VC maintains the activity of ten eleven translocation (TET) enzymes, which drive active DNA demethylation, a process that removes methyl groups from DNA, thereby reactivating genes critical for cell growth and differentiation. This epigenetic modulation results in upregulation of multiple proliferation related genes, leading to a notable increase in the thickness of the living epidermal cell layers without compromising the protective stratum corneum. By promoting keratinocyte renewal and epidermal regeneration, Vitamin C helps restore the skin’s structural integrity and barrier function, making it a promising therapeutic option for addressing age related epidermal thinning and skin fragility, particularly in older adults or patients with damaged or compromised skin. These findings underscore the potential role of Vitamin C in dermatologic treatments aimed at enhancing skin resilience and repair through targeted molecular pathways.
Botulinum Toxin A Shows Therapeutic Potential in Melasma Management beyond Cosmetic Use
Botulinum toxin A (BoNT A) is emerging as a promising adjunctive therapy for melasma, a persistent and recurrent pigmentary disorder often unresponsive to traditional topicals. A split-face clinical study showed that using intradermal BoNT A alongside a standard triple combination cream accelerated pigment clearance and maintained results for a longer duration, with improvements continuing even after stopping the topical therapy ceased, contrasting with recurrence on the control side. BoNT A appears to inhibit melanogenesis via acetylcholine mediated pathways and modulate inflammation and vascular components, addressing multiple melasma mechanisms. Additional studies report visible benefits including pore reduction and sebum control, while in vitro data confirm reduced melanin and tyrosinase activity without cytotoxicity. Well tolerated with minimal local reactions and no neuromuscular effects, BoNT A is gaining recognition in pigmentary dermatology as a neurotoxin with both cosmetic and therapeutic value.
Alopecia Unraveled: Diagnostic Pearls and Multimodal Management for Hair Restoration
Dr. Ashutosh A. Garudkar
MBBS, FCPS (DVL)
Consultant Dermatologist
DerMédica Clinic
Ahilyanagar, Maharashtra Introduction
Alopecia describes the partial or total absence of hair in areas where it typically grows and represents a common dermatologic issue with multiple underlying causes. It may manifest as localized or widespread hair loss, which can be either temporary or long-lasting, and can affect individuals across all age groups and genders. Its presentation and progression depend on the specific type and contributing factors. The hair growth cycle has four stages: anagen (growth), catagen (regression), telogen (rest), and exogen (shedding). The anagen phase, lasting between 2 to 7 years, includes around 85–90% of scalp hair follicles and plays a key role in determining hair length. Disruptions in this cycle—due to hormonal, autoimmune, pharmacologic, or environmental factors—can cause excessive shedding or permanent loss.1,2
Alopecia is generally categorized into scarring and nonscarring types, depending on whether the hair follicles remain intact. Nonscarring alopecias, often
reversible, include androgenetic alopecia (AGA), the most common variant, affecting about 50% of men by age 50 and 40% of women by age 70. Men typically exhibit bitemporal recession and vertex thinning, while women show diffuse central scalp thinning with a preserved frontal hairline. AGA involves progressive miniaturization of terminal hair follicles into velluslike hairs, primarily driven by dihydrotestosterone (DHT), a potent androgen derived from testosterone via 5α-reductase. DHT binds to androgen receptors in dermal papilla cells, promoting early transition from anagen to telogen, reducing hair shaft diameter and density. Occipital follicles are relatively resistant to DHT, explaining their preservation. In female-pattern hair loss (FPHL), the androgenic role is less defined but may involve increased receptor sensitivity or altered enzyme activity, leading to miniaturization without follicular destruction.1,2
Other nonscarring alopecias involve distinct mechanisms.
Telogen effluvium results from a synchronous shift of anagen follicles into telogen, triggered by systemic stressors like febrile illness, endocrine dysfunction, malnutrition, or surgery. Alopecia areata, an autoimmune disorder targeting anagen follicles, presents with well-demarcated patches of hair loss and may progress to totalis or universalis. Anagen effluvium, often chemotherapy-induced, stems from toxic damage to rapidly dividing matrix cells in the hair bulb, causing sudden loss. Scarring (cicatricial) alopecias involve irreversible follicular destruction and replacement with fibrous tissue, leading to permanent hair loss. Classified as primary or secondary, primary types result from follicle-targeted inflammation. Lymphocytic forms (e.g., lichen planopilaris, frontal fibrosing alopecia, discoid lupus) cause perifollicular inflammation and patchy hair loss, mainly in women. Neutrophilic types (folliculitis decalvans, dissecting cellulitis) show pustules and progressive scarring. Mixed forms like acne keloidalis display overlapping features. Secondary cicatricial alopecias result from external insults—trauma, radiation, infections, neoplasms, autoimmune diseases, or deposition disorders—that destroy follicles and cause permanent alopecia.1,2
Alopecia can have a profound psychosocial impact, particularly among women and adolescents, since hair is closely tied to self-image and confidence. Noticeable hair loss often leads to emotional distress, including anxiety, low mood, and social withdrawal. Effective management should
address both biological and psychological factors, including patient education and mental health support.
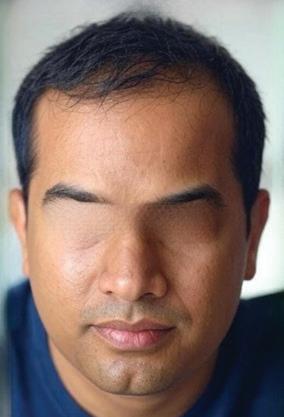
Case 1
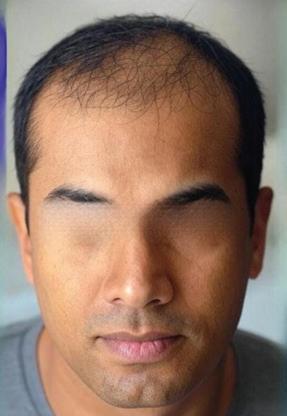
A 32-year-old male presented with progressive hair thinning over the frontal scalp and vertex region for the past two years. Clinical evaluation confirmed a diagnosis of androgenetic alopecia, classified as Hamilton-Norwood Scale III Vertex. Examination revealed diffuse thinning and follicular miniaturization in the vertex and frontal zones, with preserved occipital density. There was no significant family history of early-onset baldness. The patient was initiated on a combination treatment regimen comprising oral Dutasteride 0.5 mg once daily, low-dose oral Minoxidil (LDOM) 2.5 mg once daily, and a topical hair serum containing peptides, growth factors, and caffeine complex, applied nightly. At the 2-month follow-up, marked improvement was observed in hair density and texture, particularly in the vertex and frontal areas. Photographic comparison demonstrated visible thickening of previously sparse regions. The patient reported increased confidence and satisfaction with the results. No adverse effects were noted during the treatment course, and regular monitoring of blood pressure and laboratory parameters was unremarkable. This case highlights the early effectiveness and tolerability of combining oral Dutasteride, LDOM, and topical peptides in managing early to moderate androgenetic alopecia, offering a promising non-surgical therapeutic approach.
Case 2
A 29-year-old male presented with progressive hair thinning and recession over the vertex and fronto-temporal scalp, ongoing for the past three years. He was clinically diagnosed with androgenetic alopecia, classified as Hamilton-Norwood Grade IV. Examination revealed diffuse miniaturization of hair follicles across the frontal and vertex scalp, with preservation of the occipital region. For this case we had given 2 sessions of GFC-PRP also along with oral and topical medications includes oral Dutasteride 0.5 mg once daily,
Before treatment
After 2 months of treatment
Alopecia Unraveled: Diagnostic Pearls and Multimodal Management
low-dose oral Minoxidil (LDOM) 2.5 mg once daily, and a topical hair serum applied nightly containing peptides, growth factors, and caffeine-based complexes aimed at enhancing follicular health and prolonging the anagen phase. At the 5-month follow-up, the patient demonstrated a marked improvement in hair density and scalp coverage, particularly in the crown and mid-scalp regions. Baseline and follow-up photographs revealed significant increases in hair volume and density. The patient reported improved confidence and satisfaction with the treatment, and no adverse effects such as hypotension, excessive shedding, or sexual dysfunction were noted. Clinical parameters and laboratory values remained within normal limits. This case underscores the synergistic efficacy and tolerability of combining oral Dutasteride, LDOM and a topical growth serum as a non-surgical therapeutic approach for moderate-to-advanced androgenetic alopecia, with visible clinical benefits observed within five months.
Diagnosis
The card test distinguishes new hairs from broken or miniaturized ones by placing a contrasting black-and-white card (8 × 12 cm) next to the scalp, making it easier to identify tapered tips of new hairs, blunt ends of broken hairs, and reduced shaft diameter of miniaturized hairs. The hair pull test evaluates active shedding by gently pulling 50–60 hairs from various scalp areas; loss of more than 5–6 hairs suggests active hair fall. Patients should avoid shampooing for 24 hours prior. The tug test checks shaft strength by pulling the hair from its midpoint to end; breakage indicates structural weakness. Though microscopic hair mount analysis can reveal shaft and cycle abnormalities, it has largely been replaced by trichoscopy for routine evaluation.3 Trichoscopy is a rapid, non-invasive tool to assess scalp and hair follicles, aiding diagnosis and biopsy site selection. Contrast felt examination helps differentiate active shedding from patterned hair loss. Scalp biopsy, often with two 4-mm punches, is reserved for challenging cicatricial alopecia cases. The standardized wash
test distinguishes CTE from female pattern hair loss based on shed hair length. Global photography and dermoscopy help track density and detect miniaturization or inflammation. Trichogram and UAT assess hair cycle phases and follicular density. An integrated approach combining technology and patient-centered care is key to managing alopecia effectively.4
Treatment
Low-dose oral minoxidil (LDOM), initiated at 1–5 mg/ day in males with androgenetic alopecia (AGA) and 0.5–1 mg/day in females with female pattern hair loss (FPHL), is emerging as a safe and effective therapeutic option. It acts as a potassium channel opener, inducing vasodilation by activating ATP-sensitive K⁺ channels, leading to enhanced perifollicular blood flow and nutrient delivery. Minoxidil promotes hair growth by upregulating VEGF, HGF, and PGE2, downregulating EGF, and stimulating the Wnt/βcatenin signaling pathway in dermal papilla cells. It also suppresses IL-1α, reduces perifollicular inflammation, and may downregulate 5α-reductase type II, contributing to potential antiandrogenic effects. These mechanisms result in anagen induction, shortened telogen phase, increased hair shaft diameter, and follicular proliferation.5 Dutasteride, a dual inhibitor of type I and II 5α-reductase, reduces dihydrotestosterone (DHT) levels more effectively than finasteride, thereby preventing follicular miniaturization and promoting hair regrowth in AGA.6 The combination of LDOM and
Before treatment
After 5 months of treatment
Alopecia
dutasteride offers a synergistic approach by addressing both the vascular and androgenic components of AGA. Dutasteride halts miniaturization via DHT suppression, while minoxidil enhances follicular viability and hair cycle modulation. This dual therapy has demonstrated superior efficacy over monotherapy in improving hair density, regrowth, and patient satisfaction, with an acceptable safety profile.5,6 Hair serums optimize the scalp microenvironment by reducing inflammation, oxidative stress and enhancing follicular signalling. They support scalp integrity, microcirculation, and hair shaft strength, creating a conducive baseline for therapy. When combined with minoxidil and dutasteride, serums potentiate therapeutic efficacy and improve treatment adherence by promoting overall scalp and hair health.7
Other medications include spironolactone, an antiandrogenic diuretic mainly used in women to block androgen receptors and reduce ovarian androgen production, preventing follicular miniaturization and promoting regrowth.8 Finasteride, a selective 5α-reductase II inhibitor, lowers DHT levels to slow hair loss and improve density, particularly in the vertex and mid-scalp.² Topical corticosteroids like clobetasol propionate help control localized immune inflammation in mild to moderate alopecia areata, while intralesional or systemic corticosteroids are reserved for extensive disease.² JAK inhibitors (tofacitinib, baricitinib, ruxolitinib) restore
immune privilege and promote regrowth by blocking proinflammatory cytokine signaling.² Diphenylcyclopropenone (DPCP) induces a localized allergic response to modulate autoimmunity.² Adjunct therapies such as PRP injections, lowlevel laser therapy (LLLT), and microneedling stimulate follicular regeneration, enhance absorption of topical agents, and prolong the anagen phase.9,10,11 In advanced or resistant cases, hair transplantation using FUT or FUE techniques relocates resistant follicles for natural restoration.¹² Tailored treatment combined with scalp health optimization improves outcomes, safety, and patient adherence.
Discussion
Alopecia commonly presents as patterned hair loss in both sexes after puberty, typically involving two simultaneous processes: macroscopic and microscopic. The macroscopic pattern reflects genetically predetermined, region-specific progression, often beginning at the vertex and expanding centrifugally in a uniform manner. Microscopically, the hallmark is progressive miniaturization of follicles within compound follicular units, reducing the number of terminal hairs and overall density, ultimately leading to visible scalp and baldness. To standardize assessment, several classification systems exist. The Hamilton classification stratifies hair loss by the extent of frontoparietal and vertex recession. Early stages include no recession (Type I) or a high anterior hairline (Type IA), while advanced stages
show triangular frontoparietal recession (Type II) progressing to extensive loss (Types IV–VIII), often forming a horseshoe pattern. The Norwood-Hamilton classification further refines this system, offering a standardized staging framework for accurate diagnosis and consistent clinical evaluation.13
Hormonal influences, particularly androgens, play a key role in the pathogenesis of patterned hair loss in both sexes. The absence of hair loss in individuals with androgen deficiency highlights the necessity of androgenic stimulation— especially testosterone and dihydrotestosterone (DHT)—in the condition’s development. Interestingly, systemic androgen levels are typically normal in affected individuals, pointing to the importance of local androgen metabolism and follicular sensitivity. Elevated DHT in balding scalp areas correlates with increased local androgen receptor expression, enhanced 5-alpha reductase activity, and reduced DHT degradation. Of the two scalp 5-alpha reductase isoenzymes (types 1 and 2), type 2 predominates in regulating follicular activity and is the main target of pharmacologic inhibitors.1,2 This reflects a genetically determined hypersensitivity of follicles to androgens, forming the basis for targeted treatments. Preventive strategies focus on early risk identification, lifestyle optimization, and preserving follicular health. Nutritional status plays a crucial role—vitamin D regulates the hair cycle, while biotin (B7) supports keratin production. Antioxidants like
Alopecia Unraveled: Diagnostic Pearls and Multimodal
vitamins C and E protect against oxidative stress, and vitamin A aids cell turnover (though excess can cause shedding). Comprehensive prevention should also address hormonal imbalances, metabolic disorders, and external stressors like traction, chemicals, or inflammation. Supporting overall wellness through proper nutrition, stress management, and scalp care helps maintain follicular function and slow alopecia progression.
References
1. Qi J, Garza LA. An overview of alopecias. Cold Spring Harb Perspect Med. 2014; 4(3):a013615. Published 2014 Mar 1. doi:10.1101/cshperspect.a013615.
2. Al Aboud AM, Syed HA, Zito PM. Alopecia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 26, 2024.
3. Singh S, Muthuvel K. Practical Approach to Hair Loss Diagnosis. Indian J Plast Surg. 2021;54(4):399-403. Published 2021 Dec 27. doi:10.1055/s-0041-1739240
4. Dhurat R, Saraogi P. Hair evaluation methods: merits and demerits. Int J Trichology. 2009;1(2):108-119. doi:10.4103/0974-7753.58553
5. Gupta AK, Talukder M, Shemer A, Piraccini BM, Tosti A. Low-Dose Oral Minoxidil for Alopecia: A Comprehensive Review. Skin Appendage Disord. 2023; 9(6):423-437. Doi: 10.1159/000531890
6. Choi GS, Sim WY, Kang H, et al.
Conclusion
Hair loss refers to a multifactorial clinical entity arising from a combination of genetic susceptibility, hormonal imbalances and immune dysregulation. Accurate diagnosis through clinical evaluation and specialized investigations is crucial for distinguishing between different types of alopecia and guiding appropriate treatment strategies. Advances in understanding the underlying pathophysiology, particularly the role of androgens and follicular sensitivity, have facilitated the development of targeted pharmacologic and procedural therapies. Early recognition and a comprehensive, multidisciplinary approach are essential to optimize therapeutic outcomes and enhance quality of life for affected individuals.
Long-Term Effectiveness and Safety of Dutasteride versus Finasteride in Patients with Male Androgenic Alopecia in South Korea: A Multicentre Chart Review Study. Ann Dermatol. 2022; 34(5):349-359. doi:10.5021/ad.22.027
7. Dhurat R, Kulkarni GR, Ganjoo A, et al. Real-World Efficacy and Safety of Cuticapil Stem Hair Serum as an Add-On to Minoxidil in Androgenetic Alopecia: A Prospective Observational Study. J Cosmet Dermatol. 2025;24(5):e70247. doi:10.1111/ jocd.70247
8. Wang C, Du Y, Bi L, Lin X, Zhao M, Fan W. The Efficacy and Safety of Oral and Topical Spironolactone in Androgenetic Alopecia Treatment: A Systematic Review. Clin Cosmet Investig Dermatol. 2023; 16:603612. Published 2023 Mar 9. doi:10.2147/ CCID.S398950 (spiro)
9. Paichitrojjana A, Paichitrojjana A. Platelet Rich Plasma and Its Use in Hair Regrowth: A Review. Drug Des Devel Ther.
2022; 16:635-645. Published 2022 Mar 10. doi:10.2147/DDDT.S356858.
10. Avci P, Gupta GK, Clark J, Wikonkal N, Hamblin MR. Low-level laser (light) therapy (LLLT) for treatment of hair loss. Lasers Surg Med. 2014; 46(2):144-151. doi:10.1002/lsm.22170.
11. Fertig RM, Gamret AC, Cervantes J, Tosti A. Microneedling for the treatment of hair loss? J Eur Acad Dermatol Venereol. 2018; 32(4):564-569. doi:10.1111/ jdv.14722
12. Farjo B, Farjo N, Williams G. Hair transplantation in burn scar alopecia. Scars Burn Heal. 2015; 1:2059513115607764. Published 2015 Oct 1. doi: 10.1177/2059513115607764
13. Asfour L, Cranwell W, Sinclair R. Male Androgenetic Alopecia. In: Feingold KR, Ahmed SF, Anawalt B, et al., eds. Endotext. South Dartmouth (MA): MDText. com, Inc.; January 25, 2023.
Link between Alopecia Areata
Severity and Increased Risk of Atopic Dermatitis: Implications for Targeted Therapy
Alopecia areata (AA) is an autoimmune disorder that typically begins in childhood and can vary from small, patchy hair loss to complete loss of scalp and body hair in severe cases such as alopecia totalis and universalis. The disease is driven by immune dysregulation involving cytotoxic CD8+ NKG2D+ T cells and a Th1type inflammatory response mediated through the JAK STAT signaling pathway. AA is commonly linked with other immune-mediated conditions, especially atopic dermatitis (AD), indicating shared underlying immune mechanisms. Recent analysis reveals that both the prevalence and incidence of AD rise with increasing AA severity, particularly among adolescents, and that more severe AA correlates with greater AD severity. The findings highlight the potential benefit of JAK inhibitors, which target key immune pathways involved in both diseases, offering a promising and streamlined treatment approach. Early identification and screening for AD in patients with severe AA could improve clinical outcomes, though further research is necessary to confirm the results and optimize integrated management strategies.
Advancements in Alopecia Epidemiology through Artificial Intelligence-Based Data Analysis
A groundbreaking analysis leveraging anonymized AI-sourced data mapped contemporary patterns in alopecia epidemiology. The cross-sectional study confirmed that androgenetic alopecia remains the most prevalent form of hair loss, affecting tens of millions, and revealed that its severity escalates with age. The dataset, predominated by females, demonstrated that while women reported a higher incidence of early, mild hair thinning indicative of earlier clinical presentation, men exhibited a greater burden of severe hair loss and a stronger genetic predisposition. Hormonal influences were affirmed by significantly higher odds of advanced hair thinning in postmenopausal women and increased sudden shedding among the postpartum cohort. Additional predictors included polycystic ovary syndrome, thyroid dysfunction, and high stress, while a history of COVID-19 infection was notably linked to episodes of acute telogen effluvium. Dietary habits and shampoo frequency showed minimal association with hair loss severity, underscoring the primacy of intrinsic biological factors. Despite limitations such as self-report bias and the inability to establish causality, the findings validate established risk factors and illuminate novel associations, affirming the utility of AI-mediated, large-scale data in refining clinical screening, identifying at-risk populations, and personalizing alopecia management strategies.
Precision and Aesthetics in Dermatology: Radiofrequency Ablation for Skin Tags
Dr. Dhiral Shah
MBBS, MD (DVL), Fellowship in Aesthetic Medicine
Consultant Dermatologist
Kaytra Skin & Aesthetic Clinic
Vadodara, Gujarat
Introduction
Acrochordons, or skin tags, are common benign fibroepithelial proliferations frequently encountered in dermatological practice. Clinically, they present as soft, pedunculated lesions composed of redundant skin, with coloration ranging from flesh-toned to hyperpigmented. They typically arise in intertriginous areas subject to repetitive friction, such as the axillae, neck, eyelids, inframammary regions, and groin folds. Although usually asymptomatic, they may cause pruritus, irritation, or bleeding due to mechanical trauma.1 Lesion size generally ranges from 1 to 5 mm, but some may enlarge up to 1–2 cm or more, occasionally becoming symptomatic.
Histopathologically, ................ acrochordons display an epidermis with mild acanthosis or hyperkeratosis overlying a fibrovascular dermal core containing loosely arranged collagen, dilated vascular channels, and lymphatics, typically lacking adnexal
elements. Despite their benign nature, lesions exhibiting atypical features such as rapid growth, ulceration, or irregular pigmentation warrant further evaluation to exclude differential diagnoses, including melanocytic nevi, neurofibromas, seborrheic keratoses, or early cutaneous neoplasms.2
Acrochordons are highly prevalent benign skin lesions, affecting approximately 46–60% of adults, with frequency increasing with advancing age. Incidence peaks in the fifth and sixth decades, while occurrence beyond 70 years is uncommon. Though occasionally seen in adolescents, particularly those with elevated body mass index (BMI), their development is multifactorial. Mechanical friction in individuals with obesity and redundant skin folds is a wellrecognized trigger. Beyond local mechanical factors, acrochordons demonstrate strong systemic associations. Multiple studies have linked them with insulin resistance, type 2 diabetes mellitus, obesity,
dyslipidemia, and cardiovascular disease, establishing their role as cutaneous markers of metabolic syndrome. The presence of multiple or rapidly developing lesions should prompt clinicians to investigate underlying metabolic dysfunction through targeted evaluation, including fasting glucose, glycated hemoglobin (HbA1c), lipid profile, and BMI. Endocrine influences further contribute to pathogenesis. Elevated estrogen, progesterone, and growth hormone levels— such as during pregnancy or in acromegaly—stimulate fibrovascular proliferation and epidermal hyperplasia. Molecular pathways involving epidermal growth factor (EGF) and alpha tissue growth factor have also been implicated, reinforcing the concept that acrochordons arise from complex interactions between metabolic, hormonal, and mechanical factors.1,2
In addition to their clinical and metabolic relevance, acrochordons may exert a substantial psychosocial impact. Lesions situated in cosmetically conspicuous regions such as the face and neck can lead to diminished self-esteem, body image dissatisfaction, and psychological distress. Moreover, physical discomfort may arise from friction, pruritus, or repetitive trauma, all of which may interfere with daily activities and reduce quality of life. As such, a comprehensive management approach that addresses both the dermatologic and psychological dimensions is essential to optimize patient care and improve overall well-being.1, 2
Case Report
A 54-year-old male patient presented with a solitary skin tag located in the left pre-orbital region. Owing to the anatomical sensitivity of the site, the lesion was treated with radiofrequency ablation (RFA). The procedure allowed for precise excision with minimal bleeding and no intraoperative complications. Postoperatively, healing was rapid and uneventful, resulting in an excellent cosmetic outcome without scarring or pigmentary alterations. The patient expressed high satisfaction with the results, highlighting the efficacy and safety of RFA for the removal of cutaneous lesions in cosmetically sensitive areas.
Diagnosis
The diagnosis of acrochordons primarily relies on careful clinical examination, including visual inspection and palpation. Clinically, these lesions are asymptomatic, presenting as soft, non-tender, pedunculated papules or nodules with demonstrable mobility and a slow, progressive course. In most cases, this typical presentation suffices for diagnosis. However, additional evaluation becomes necessary when lesions display atypical features such as rapid growth, irregular surface architecture, pigmentary alterations, ulceration, or bleeding. In such instances, differential diagnoses— including melanocytic nevi, seborrheic keratoses, or verrucae— must be excluded. Dermoscopy serves as a valuable, non-invasive diagnostic adjunct. Characteristic findings include homogeneous coloration with smooth or digitiform projections, absence of pigment networks, and lack of atypical vascular structures. These features reinforce the benign nature of acrochordons and often obviate
Before treatment
Figure 1: Solitary skin tag located in the left pre-orbital region
After treatment
the need for invasive testing.3 Histopathological confirmation is reserved for clinically suspicious or diagnostically uncertain cases. Shave biopsy is the preferred technique, typically demonstrating a polypoid lesion with a fibrovascular core composed of loosely arranged collagen bundles and dilated blood vessels, covered by mildly acanthotic but nonatypical stratified squamous epithelium.4 Hematoxylin and eosin (H&E) staining highlights these features, confirming the benign nature of the lesion and aiding in differentiation from other cutaneous pathologies.5 Accurate recognition and characterization of acrochordons are crucial to distinguish them from clinically mimicking entities and to avoid unnecessary interventions. In routine practice, the integration of clinical assessment, dermoscopy, and selective histopathology provides a reliable framework for establishing the diagnosis and guiding appropriate management.
Treatment
Radiofrequency ablation (RFA) is a sophisticated, minimally invasive procedural modality employed in dermatology for the excision of benign cutaneous lesions, notably acrochordons (skin tags). It uses highfrequency alternating electrical current to generate localized heat through tissue resistance, resulting in controlled tissue destruction, coagulation, or excision.6 Radiofrequency ablation (RFA) is a wellestablished, minimally invasive technique frequently utilized
in dermatological practice for the removal of benign cutaneous lesions, including acrochordons. The procedure involves the delivery of highfrequency alternating current (typically 0.5–4.0 MHz) through a fine, insulated electrode, generating localized thermal energy due to inherent tissue resistance. This heat induces intracellular and extracellular protein denaturation, leading to coagulative necrosis and desiccation of the targeted lesion. As thermal accumulation progresses, disruption of cellular membranes facilitates precise tissue cleavage. Moreover, the regulated lateral dispersion of heat induces thermal coagulation of surrounding microvasculature, consequently reducing bleeding and facilitating efficient hemostasis. This controlled tissue destruction, combined with reduced collateral damage, makes RFA a safe, efficient, and cosmetically favorable method for skin tag removal.7, 8, 9
Procedure
The procedure begins with proper patient positioning and the attainment of informed consent. The treatment site is disinfected with an antiseptic solution to minimize infection risk, followed by infiltration of local anesthesia at the base of the acrochordon to provide analgesia and hemostasis. Electrode selection—loop, fine needle, or ball tip—depends on the lesion’s size, site, and morphology. The radiofrequency (RF) generator is adjusted to “cut” mode for precise excision and to “coagulation” mode for hemostasis, with power levels tailored to tissue response and
device specifications. The lesion is stabilized with sterile forceps to expose its fibrovascular stalk, and RF energy is applied at the base, producing smooth transection with minimal resistance while simultaneously coagulating adjacent microvasculature, thereby limiting intraoperative bleeding. Following excision, coagulation mode may be reapplied to secure hemostasis and reduce microbial burden. The site is cleansed with sterile saline, and a topical antibiotic is applied. A light dressing may be placed for larger lesions or those in frictionprone areas. Postoperative instructions include keeping the site dry for 24 hours, avoiding trauma, and monitoring for infection or delayed healing. RF ablation offers several advantages, including precise tissue removal with minimal collateral damage, effective intraoperative hemostasis, and favorable cosmetic outcomes with low risk of scarring, dyspigmentation or textural change. Healing is typically rapid, with re-epithelialization within one to two weeks. The technique is efficient—often completed in under 10 minutes per lesion—well tolerated and safe for cosmetically sensitive areas such as the face, eyelids, neck, and genitalia. Radiofrequency ablation (RFA) is contraindicated in malignant or suspicious lesions without prior histopathological confirmation and requires caution in patients with pacemakers or implanted electronic devices. It is also contraindicated in active cutaneous infections, inflamed skin, and during pregnancy when treating the abdominal or pelvic regions. Meticulous
technique is essential to avoid prolonged contact time, thereby preventing deep thermal injury and delayed wound healing. Post-procedural erythema or crusting typically resolves within days, with minimal risk of scarring. Recurrence rates remain low, even among patients with metabolic syndrome, obesity, or insulin resistance. Alternative therapeutic options for benign cutaneous lesions include surgical excision, laser modalities (CO₂, Er:YAG, pulsed dye, KTP, Nd:YAG), intense pulsed light (IPL), topical chemical agents such as trichloroacetic acid, and cryotherapy. Although laser and light-based therapies provide effective treatment—especially for vascular lesions—their use is often limited by high costs and maintenance demands. Snip excision facilitates immediate removal through mechanical transection of the fibrovascular stalk, while electrosurgical cautery achieves concurrent tissue ablation and hemostasis via high-frequency current. Cryotherapy induces intracellular ice formation and vascular stasis, resulting in ischemic necrosis and subsequent auto-amputation of the lesion. Collectively, these modalities offer safe, efficacious, and cosmetically favorable treatment tailored to lesion morphology and patient factors.10, 11, 12
Discussion
Acrochordons, or skin tags, are among the most frequently encountered benign cutaneous appendages in routine dermatological practice. Though histologically benign, these lesions often draw clinical attention because of their visible
nature and their tendency to undergo irritation from repetitive mechanical trauma. Such irritation may lead to localized discomfort as well as cosmetic or psychosocial concern, prompting patients to seek removal. Effective therapeutic approaches therefore need to ensure precise lesion clearance, adequate hemostatic control, and excellent cosmetic outcomes. The clinical differential diagnosis of acrochordons is broad and includes several mimicking conditions. Melanocytic nevi may appear as pigmented or pedunculated papules that resemble skin tags in morphology. Neurofibromas, often associated with neurofibromatosis type 1, may present similarly but tend to be softer and may coexist with systemic findings. Seborrheic keratoses, with their raised, verrucous texture and variable pigmentation, can also mimic skin tags. In addition, certain morphologic variants of basal cell carcinoma— particularly superficial and nodular subtypes—may initially resemble benign acrochordons, especially in cosmetically sensitive regions. Careful clinical evaluation, and in select cases dermoscopy or histopathology, is essential to establish the correct diagnosis. A variety of treatment modalities exist for acrochordon removal; however, radiofrequency ablation (RFA) has emerged as a modality of choice due to its precision, inherent hemostatic properties, minimal postoperative infection risk, and consistently favorable cosmetic outcomes. Its ability to precisely excise lesions while sparing adjacent uninvolved tissue makes it
particularly advantageous in sensitive or high-friction sites such as the face, eyelids, and neck. The procedure is quick, often completed in a single, well-tolerated session with minimal discomfort, thereby improving patient adherence, streamlining workflow, and reducing morbidity. Beyond acrochordons, RFA has demonstrated significant utility in treating other benign cutaneous lesions, including dermatosis papulosa nigra (DPN), verrucae vulgaris, xanthelasma palpebrarum, and benign melanocytic nevi. Safety and tolerability of RFA are generally excellent, though minor complications may occur. Transient erythema, edema, and mild discomfort are the most common, typically resolving spontaneously within days. Rare adverse effects include pigmentary alterations (hypopigmentation or hyperpigmentation), particularly in darker skin phototypes, due to thermal injury to melanocytes. Superficial scarring and delayed healing may occur in areas subject to mechanical stress or with inadequate postprocedural care. Infection is uncommon but underscores the importance of aseptic technique. Very rarely, neuropathic pain or paresthesia may arise when treating lesions near sensory nerve branches. Overall, RFA provides an efficient, safe, and cosmetically favorable technique for the removal of acrochordons and other benign lesions. Thorough patient counselling regarding potential risks and adherence to post-procedural care further enhance outcomes, reinforcing RFA as a valuable tool in dermatologic and aesthetic
Precision and Aesthetics in Dermatology: Radiofrequency Ablation for Skin Tags
practice.1,2,10,11,12
Conclusion
Radiofrequency ablation is an effective, low-risk, and cosmetically favorable treatment modality for a wide variety of benign skin lesions, including skin tags (acrochordons). The procedure is straightforward to perform, requires minimal post-procedural care, and
References
1. Pandey A, Sonthalia S. Skin Tags. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 31, 2023.
2. Belgam Syed SY, Lipoff JB, Chatterjee K. Acrochordon. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 8, 2023.
3. Fredman G, Qiu Y, Ardigò M, Mogensen M. Skin tags imaged by reflectance confocal microscopy, optical coherence tomography and multispectral optoacoustic tomography at the bedside. Skin Res Technol. 2021; 27(3):324-331. doi:10.1111/srt.12943.
4. Ramsey ML, Rostami S. Skin Biopsy. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 4, 2023.
5. Ahkami S, Hahn D, Fowler-Kim H, Domingo RJ. An Expanding Large Acrochordon on the Labia Majora
is well-suited for outpatient settings as well as resource-limited environments. Its precision and ability to minimize bleeding and tissue damage contribute to excellent aesthetic outcomes, making it a preferred option for the removal of skin tags and other superficial lesions. Furthermore, its versatility and favourable safety profile position radiofrequency ablation as a valuable alternative to more invasive surgical excision or costly laser therapies. Ongoing clinical research and expanded application will further delineate its efficacy, optimize treatment protocols, and confirm its role as a mainstay treatment for benign cutaneous growths such as skin tags.
Requiring Surgical Intervention. Cureus. 2025; 17(2):e79017. Published 2025 Feb 14. doi:10.7759/cureus.79017.
6. Sachdeva, Silonie; Dogra, Alka. RADIOFREQUENCY ABLATION IN DERMATOLOGY. Indian Journal of Dermatology 52(3): p 134-137, Jul–Sep 2007. | DOI: 10.4103/0019-5154.35091.
7. Kim DH, Hyun DJ, Piquette R, Beaumont C, Germain L, Larouche D. 27.12 MHz Radiofrequency Ablation for Benign Cutaneous Lesions. Biomed Res Int. 2016; 2016:6016943. doi:10.1155/2016/6016943.
8. Mutalik S. Standard guidelines for electrosurgery with radiofrequency current. Indian J Dermatol Venereol Leprol 2009; 75:83-89.
9. Wray JK, Dixon B, Przkora R. Radiofrequency Ablation. In: StatPearls. Treasure Island (FL): StatPearls Publishing;
June 12, 2023.
10. Coakley A, Wu MJ, Kumar J, et al. A Comparison of Ferric Subsulfate Solution, Silver Nitrate, and Aluminum Chloride for Pain Assessment, Time to Hemostasis, and Cosmesis in Acrochordon Snip Excision. J Clin Aesthet Dermatol. 2020; 13(12):32-37.
11. Hainer BL. Electrosurgery for the skin [published correction appears in Am FAM Physician 2002 Dec 15; 66(12):2208]. Am FAM Physician. 2002; 66(7):1259-1266.
Impact of Psychological Stress on Wound Healing and Scar Treatment: Integrating Holistic Care into Dermatology
A recent comprehensive review highlights the critical impact of psychological stress on wound healing and the efficacy of scar treatments, emphasizing how chronic stress disrupts essential biological processes such as collagen synthesis, immune response, and tissue regeneration. Stress induced activation of the sympathetic nervous system and hormonal imbalances, particularly elevated cortisol levels, interfere with keratinocyte migration and neocollagenesis, resulting in delayed wound closure and suboptimal remodeling of scar tissue. Consequently, commonly used collagen dependent therapies like chemical peels, laser resurfacing, subcision, and surgical scar revision may demonstrate reduced effectiveness, with patients experiencing slower recovery and less noticeable improvements. The review also draws attention to a detrimental feedback loop in which the presence of scars exacerbates psychological distress, further impairing healing outcomes. To address this complex interplay, the authors advocate for integrating stress management techniques including mindfulness, breathing exercises, and routine psychological assessments into dermatologic practice to better identify at risk patients and support holistic care. They call for future randomized controlled trials and longitudinal studies to validate these interventions and refine personalized treatment protocols that simultaneously target physical healing and mental wellbeing, ultimately aiming to enhance patient outcomes and quality of life in scar management.
Vitiligo’s Significant Impact on Quality of Life
Vitiligo impact extends far beyond the visible skin changes, profoundly affecting patient’s quality of life and influencing major life decisions across various domains. A recent study revealed that vitiligo significantly affects personal choices such as clothing, social interactions, lifestyle habits, and professional opportunities. This impact is especially pronounced when the condition involves the face, often resulting in appearance based discrimination that can hinder career advancement. The research also identified specific groups including women, single individuals, those without children, and patients with longer disease duration as experiencing greater disruptions in life decisions, highlighting the role of social and demographic factors in the disease burden. Importantly, the study found a strong association between perceived stigmatization and reduced emotional well-being, independent of the clinical severity of vitiligo, underscoring that patient’s subjective experiences and social perceptions are critical determinants of psychological distress. Experts stress the importance of a holistic, patient centered approach to care that goes beyond treating skin symptoms to include comprehensive psychosocial assessment and support. Early screening for psychosocial challenges and tailored interventions such as counselling and access to support networks are essential to improve overall patient outcomes.