



Dr. Sunita Tandulwadkar President, FOGSI (2025)
Dear Readers,
It gives me immense pride and joy to introduce the inaugural edition of YTP FUTURE CHRONICLES, the official digital newsletter of FOGSI’s Young Talent Promotion (YTP) Committee. This initiative is a milestone in our ongoing journey of nurturing the future torchbearers of obstetrics and Gynecology in India.
FOGSI, since its inception in 1950, has stood as the largest professional organization of obstetricians and Gynecologists in the country, committed to advancing women’s health, fostering academic excellence, and supporting professional growth. Over the decades, FOGSI has not only upheld clinical standards but has also provided a vibrant platform for continuous education, research, and innovation. Our strength lies in our vast network of 45,000+ members who share a common goal—empowering women through quality healthcare.
The Young Talent Promotion Committee (YTP) of FOGSI is committed to inspiring and empowering the next generation of Gynecologists. It bridges youthful curiosity with expert mentorship, turning ideas into impactful innovations. YTP Future Chronicles reflects this vision, delivering insights, trends, and voices shaping modern Gynecology.
A space to learn, exchange, and evolve with the rapidly advancing field of women’s health. Together, we aim to build a strong, future-ready community of leaders.
As President of FOGSI 2025, I am deeply committed to strengthening this bridge between today’s leaders and tomorrow’s pioneers. With credibility, authenticity, and a collaborative spirit, this newsletter will serve as both a resource and an inspiration for our younger colleagues.
I warmly invite all our members to engage, contribute, and grow with us through this platform. Together, let us continue FOGSI’s legacy of excellence while shaping the next generation of Gynecologists who will carry forward our mission with passion and integrity.
Preeti

EXECUTIVE EDITOR & PUBLISHER
Dom Daniel

CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: paradigminfocomobgyn@gmail.com
Website: ytpfuturechronicles.com
Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“YTP FUTURE CHRONICLES” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of September -2025







Dr. Surakshith Battina
MBBS, MD (Obstetrics and Gynaecology) Specialist in Reproductive Medicine Endoscopic Surgery, and Cosmetic Gynaecology Indigo Women’s Center, Chennai
Dr. Khushbu Dubey
MS OBGYN, FMAS(AIIMS, BHOPAL) Senior Resident in AIIMS BHOPAL
Dr. Preeti Jindal
MD, DNB, MRCOG (London), FICOG Director – The Touch Clinic (Advanced Gynae & IVF Centre, Mohali)
High Risk Pregnancy, Recurrent Miscarriage Expert IVF Treatment Specialist, Robotic Surgeon & Cosmetic Gynecologist.
Dr. Ragini Agrawal
MS, FICOG , FICMCH
Sr. Consultant, Cosmetic Gyn & Laser Surgeon, AA Derma science “ Complete Women Rejuvenation Center” Gurgaon
Dr. Bhaskar Pal
MBBS, DGO, MD, DNBE (Obs & Gynae) MRCOG, FICOG, and FRCOG
Senior Consultant Obstetrician & Gynaecologist, Apollo Hospital, kolkata President Elect- FOGSI
Dr. Parul Saoji
MS, DNB, MNAMS, FMAS, Dip. (CosGyn) Cosmetic Gynaecologist, Laparoscopic Surgeon and Infertility Specialist Oracle Clinic, Nagpur
Dr. Gurkiran Kaur
MBBS, MS (Obstetrics and Gynaecology), Fellowship in Reproductive Medicine
Consultant Gynecologist and Infertlity specialist Kuldip Hospital and IVF Centre, Jalandhar

Dr. Rohan Palshetkar President, YTP (2025)
Dear Readers,
I am pleased to present the inaugural edition of YTP FUTURE CHRONICLES, a platform dedicated to empowering Gynecologists with the latest insights, innovations, and perspectives shaping the future of women’s healthcare.
This publication bridges knowledge and practice, delivering evidence-based updates, thought-provoking insights, and practical solutions for your clinical journey. Each issue explores emerging trends, transformative technologies, and expert perspectives shaping modern Gynecology. Since 1950, FOGSI has championed women’s health and professional growth, with the YTP Committee dedicated to nurturing young talent through mentorship and opportunities. YTP drives FOGSI’s mission to empower young Gynecologists with leadership, innovation, and academic excellence. YTP FUTURE CHRONICLES reflects this mission by showcasing clinical advancements, emerging trends, resident voices, and achievements, ensuring the future of women’s health remains strong in the hands of the next generation.
We are deeply thankful to FOGSI office bearers, advisors, and contributors for their faith, encouragement, and coordination and on behalf of my editorial team at YTP I present the first issue of YTP FUTURE CHRONICLES for your reading.
This first edition features thought-provoking contributions from eminent Gynecologists on a diverse range of topics which includes an insightful discussion on Vaginismus in India: A Cultural Conundrum, the challenges and management strategies of Premature Ovarian Failure: Dealing with Early Menopause, and the evolving role of Vaginal Rejuvenation in Perimenopausal Women. We also explore the Changing Scenario: Cosmetic to Functional and Regenerative Gynecology, alongside a reflective piece titled In Today’s World, What A Woman Need to Be? A Rani, a Laxmi, or a Bai?
We hope this first edition inspires curiosity, encourages dialogue, and supports your commitment to advancing care for women everywhere.
We wish all our readers a blissful and enriching reading journey.

Dr.Prerna Keshan
Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1
Masters in Cosmetic Gynecology

Dr. Gurkiran Kaur
MBBS, MS (Obstetrics and Gynaecology), Fellowship in Reproductive Medicine
Consultant Gynecologist and Infertlity specialist Kuldip Hospital and IVF Centre, Jalandhar
Dear Readers,
With immense delight, I am proud to present the inaugural edition of YTP FUTURE CHRONICLES, something we had been working on to bring a fresh perspective to obstetrics and gynaecology practice in India.
FOGSI has always been on a mission to educate and enhance the clinical skills and practice of all the members. With this publication, it’s a step ahead in it’s mission, as we have tried to cover a lot of recent advancements, latest clinical research and emerging trends in women’s healthcare in India. Women’s health is a vast topic, especially with the changing needs and mindsets of the present community, it is very important to understand each aspect to give the best possible care. From a working woman in a 9-5 job supporting a family, or home makers working day in and night to raise their families, each woman needs to be heard and given treatments tailored specifically to them. This edition of YTP FUTURE CHRONICLES is dedicated to provide insights into the latest problems of women of all age groups, and solutions that we can offer and work with them to give them a better quality of life.
As we dive into some very interesting and wide range of topics that are currently shaping the future of modern gynaecology, like tackling vaginismus and premature menopause, changing scenarios: cosmetic to functional and regenerative gyanecology, it makes us ponder that at the end, what does the world really want a woman to be? Can we ever really understand what it takes to be HER?
I thank Dr Rohan Palshetkar for giving me this wonderful opportunity in bringing this newsletter together and always encouraging me to learn and work hard as a member of YTP.
We hope this edition will bring you up to date with everything a modern woman needs, and help you make your practice more advanced and oriented. Wishing you a delightful and enriching reading experience.


Dr. Surakshith Battina
MBBS, MD (Obstetrics & Gynaecology)
Specialist in Reproductive Medicine, Endoscopic Surgery, and Cosmetic Gynaecology
Indigo Women’s Center Chennai
Vaginismus, a condition where involuntary muscle spasms prevent vaginal penetration, presents a unique challenge in India. The socio-cultural context of the country deeply influences the understanding, diagnosis, and treatment of this condition. Unlike many parts of the world, India’s cultural intricacies, the emphasis on virginity, a patriarchal society, and the portrayal of women in Bollywood significantly impact the lives of those affected by vaginismus.
................ INFLUENCES AND VIRGINITY
In India, the concept of
virginity is often held sacred. A woman's virginity is seen as a symbol of purity and family honor. This societal pressure can create immense anxiety around sexual intercourse, contributing to the development of vaginismus. The fear of pain, coupled with the fear of losing virginity, can make the very thought of intercourse terrifying for many women. In a culture where open discussions about sex are taboo, women often lack the necessary information and support, leading to an increase in sexual anxieties and dysfunctions.
India's patriarchal structure
exacerbates the issue. Women are often seen as possessions transferred from one family to another through marriage. This objectification can lead to a lack of agency and autonomy over their bodies. The societal expectation that women should be sexually passive and submissive further discourages them from seeking help for sexual issues, including vaginismus.
Bollywood, India's prolific film industry, has not been particularly helpful. Movies often depict unrealistic and idealized notions of romance and sexuality, contributing to societal misconceptions. Women are frequently portrayed as objects of desire, whose primary role is to please men. Such portrayals reinforce harmful stereotypes and discourage women from addressing their sexual health issues openly.
The healthcare system in India, particularly in the realm of gynecology, faces significant challenges. Doctors are often overwhelmed by the sheer number of patients, leaving them little time to engage in meaningful conversations about sensitive issues like vaginismus. Moreover, there is a notable lack of training in cosmetic gynecology and the treatment of sexual dysfunctions. Many medical professionals are not equipped to handle these conditions effectively, leading to misdiagnosis or inadequate treatment.
Historically, India was not always such a closed society. The temples of Khajuraho, with their intricate erotic sculptures, and the ancient text of the Mahabharata, which included references to sex, suggest a more open attitude towards sexuality. However, modern interpretations and editions of these texts have often excluded sexual content, reflecting the current conservative mindset. This shift away from a historically rich and open sexual discourse has further marginalized discussions about sexual health.
To improve the diagnosis and treatment of vaginismus in India, it is essential to treat it as a genuine medical condition. This involves adopting a multidisciplinary approach that includes gynecologists, pelvic floor therapists, physiotherapists, and psychologists. Creating awareness is crucial; educational programs and campaigns can help destigmatize sexual health issues and encourage women to seek help.
Statistics highlight the urgency of this issue. According to a study published in the Journal of Sexual Medicine, around 1-6% of women globally are affected by vaginismus, and the prevalence is likely higher in conservative societies like India due to underreporting. Another study found that 80% of Indian women experience pain during their first intercourse, a factor that can contribute to vaginismus if not addressed properly.
Vaginismus in India is a multifaceted issue influenced by cultural, societal, and healthcare system challenges. Addressing this condition requires a comprehensive understanding of these factors and a concerted effort to bring about change. By recognizing vaginismus as a legitimate medical condition and employing a multidisciplinary approach to its treatment, India can take significant strides in improving the sexual health and overall well-being of its women. Awareness and education are key to breaking the cycle of silence and stigma, allowing women to reclaim autonomy over their bodies and their health.
Premature ovarian failure (POF), also known as premature ovarian

Dr. Khushbu Dubey
MS OBGYN, FMAS(AIIMS, BHOPAL) Senior Resident in AIIMS BHOPAL
Addisons disease, diabetes type 1, coeliac disease, albinism, Rheumatoid arthritis, SLE & Myasthenia gravis, & iatrogenic, or idiopathic. Understanding and managing this condition is crucial for maintaining the quality of life and long-term health of affected women.
A physician might come across this condition when evaluating a young female patient who is having trouble conceiving or dealing with secondary amenorrhea. To help with diagnosis, checking for signs of menopause can be important. In many cases of premature ovarian failure (POF), the patient’s medical history shows a normal age for menarche and regular menstrual cycles, which later shift to infrequent insufficiency (POl), was defined by de Moraes-Ruehsen and Jones in 1967. It is a condition characterized by the loss of ovarian function before the age of 40. In 1939, the hormone profile in women with POF was described as hypergonadotropic hypoestrogenism. In 1950, the clinical features of POF were discussed in detail by Atria. This leads to early menopause and presents unique challenges for affected women. Diagnosis is based on criteria including amenorrhea or oligomenorrhea, elevated FSH levels, low estradiol levels, and age under 40 years. The causes can be genetic (Turner’s syndrome, fragile X syndrome), autoimmune disease such as Hashimoto’s disease,
periods or sudden absence of menstruation. Sometimes, the loss of periods is noticed after stopping birth control pills. Common symptoms include hot flashes, excessive sweating, hair loss, and dryness of the skin and mucous membranes.
Diagnostic criteria:
• Amenorrhea for atleast 4 months
• Elevated FSH levels (>40 IU/L) on two occasions, at least 4 weeks apart
• Low estradiol level (<50 pmol/L)
• AMH <0.5 ng/ml
• Low inhibin levels
Hormonal Therapy
• Hormone replacement therapy (HRT) is the mainstay of treatment
• Aim: Restore sex hormones to premenopausal levels
• Duration: Continue until the average age of natural menopause (51 years) HRT Options
• Estrogen + progestogen for women with an intact uterus
• Estrogen-only for women who have undergone hysterectomy
• Combined hormonal contraception as an alternative
Bone Health
• Increased risk of osteoporosis. Maternal aging and oestrogen deficiency as a result of declining ovarian activity have been implicated in the aetiology of osteoporosis. Oestrogen is cardio protective in prevention of cardiovascular disease. Oestrogen also increases HDL and decreases LDL, cholesterol and triglycerides. Oestrogen
receptors have been found throughout the cardiovascular system. A typical oestrogen effect is a relaxation in arterial tone and a decrease in resistance.
Management:
• Calcium and vitamin D supplementation
• Weight-bearing exercises
• Bone density monitoring
Cardiovascular Health
• Elevated risk of cardiovascular disease. Oestrogen is cardio protective in prevention of cardiovascular disease. Oestrogen also increases HDL and decreases LDL, cholesterol and triglycerides. Oestrogen receptors have been found throughout the cardiovascular system. A typical oestrogen effect is a relaxation in arterial tone and a decrease in resistance.
• Interventions: Regular exercise, Healthy diet, Blood pressure and lipid profile monitoring
Cognitive Function
• Potential increased risk of cognitive decline
• Strategies:
- Mental stimulation activities
- Social engagement
- Consider cognitive screening
Psychological Support
• Address potential psychological distress
• Offer counseling or support groups
• Consider cognitive behavioral therapy if needed
Fertility Concerns
• Discuss fertility preservation options early
• Consider oocyte or embryo cryopreservation
• Donor oocyte in vitro fertilization may be an option
The possible theoretical reasons for high pregnancy rates in ovum donation programmes are:
1. Absence of the state of hypoestrogenism,
2. Absence of other causes of infertility,
3. Lack of endometrial hyperstimulation,
4. Absence of episodes of premature lutenization,
5. Better control of the window of receptivity.
Long-term Management
• Regular Monitoring
• Annual health check-ups
• Hormone level assessments
• Bone density scans
• Cardiovascular risk assessment
Lifestyle Modifications
• Smoking cessation
• Maintain healthy body weight
• Regular physical activity
• Balanced diet
Ongoing Support
• Provide education about POF POI
• Encourage participation in support networks
• Regular review of treatment efficacy and side eftects
Managing premature ovarian failure requires a comprehensive approach addressing hormonal, physical, and psychological aspects. Early diagnosis, prompt initiation of hormone therapy, and ongoing monitoring are crucial for optimizing quality of life and long-term health outcomes in women with POF/ POl.


MD, DNB, MRCOG (London), FICOG Director – The Touch Clinic (Advanced Gynae & IVF Centre, Mohali)
High Risk Pregnancy, Recurrent Miscarriage Expert
IVF Treatment Specialist, Robotic surgeon & Cosmetic Gynecologist.
General Secretary – InSARG (Indian Aesthetic & Regenerative Gynecologists Society)
Past President – Mohali Obstetrics & Gynaecology Society.
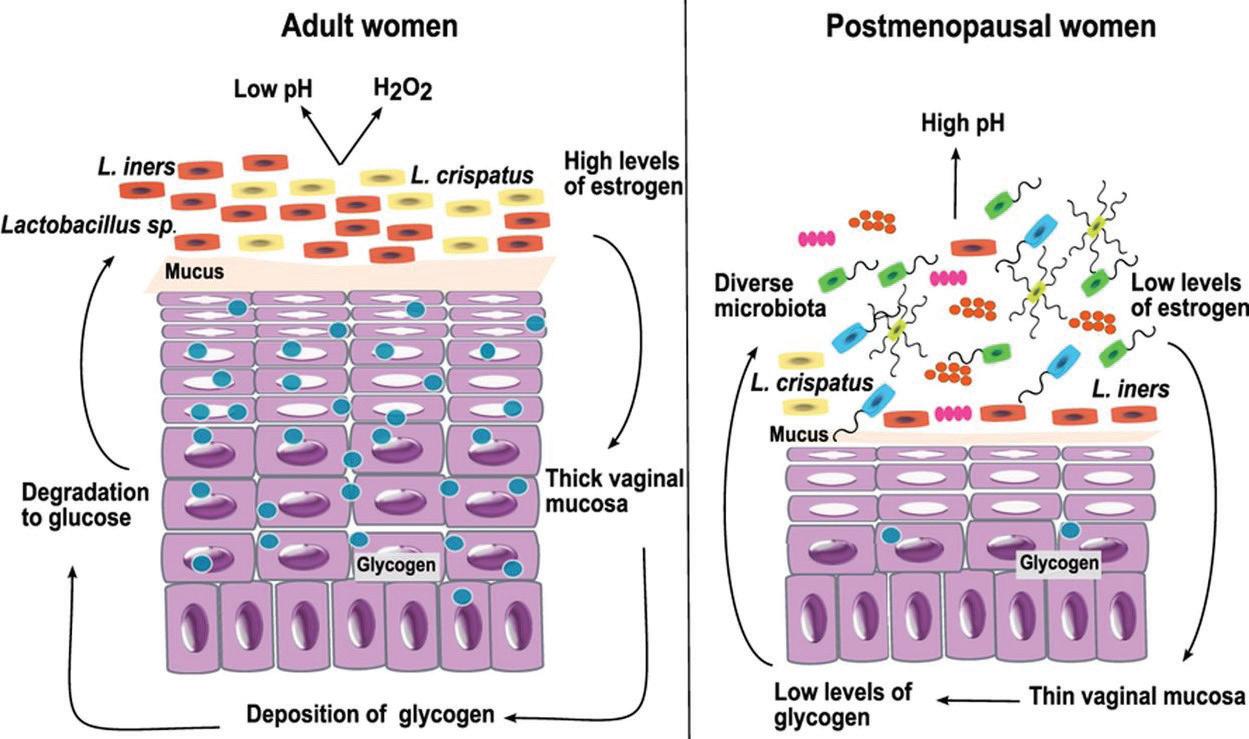
often brings about significant physiological changes in a woman’s body. Among these changes, many women experience a decline in vaginal health, characterized by symptoms such as vaginal dryness, laxity, discomfort during intercourse, and a decrease in overall sexual satisfaction. These changes can have profound impacts on a woman’s quality of life, self esteem, and intimate relationships.
erimenopause, the transitional period leadingup to menopause, decline in estrogen levels leads to a reduction in vaginal moisture and elasticity. The vaginal walls may become thinner, less lubricated, and more prone to irritation and discomfort. These changes are often accompanied by symptoms such as vaginal dryness, itching, burning and dyspareunia (painful intercourse). Additionally, pelvic floor muscles may weaken due to pregnancy, child birth and aging leading to stress urinary incontinence and vaginal laxity.
Vaginal rejuvenation, a term encompassing various surgical and non–surgical treatments, has gained increasing attention as an effective solution for addressing these perimenopausal issues.
During perimenopause, the
Non-Surgical Vaginal Rejuvenation treatments have gained popularity due to their minimally invasive nature. They are painless, patient friendly, coffee break procedures with relatively short recovery times.
Laser, Radiofrequency and High intensity focussed usg (HIFU) are energy based devices which focus energy to raise the temperature of tissues to 40-45 degree Celsius, leading to thermo neo collagenogenesis and neo elastogenesis.

1) Laser Therapy: Fractional CO2 and Erbium: YAG lasers are commonly used to stimulate collagen production and improve vaginal tissue elasticity and hydration. Laser therapy can also enhance blood flow and reduce symptoms of vaginal atrophy. It is also used to treat genitor urinary syndrome of menopause.
2) Radiofrequency (RF) Therapy: RF devices uses thermal energy to tighten vaginal tissues and promote collagen remodelling. This treatment can improve vaginal laxity and alleviate symptoms of dryness and discomfort.
3) Platelet – Rich Plasma (PRP) Therapy: PRP involves injecting a concentration of
the patient’s own platelets into the vaginal tissues to stimulate tissue regeneration and enhance lubrication. PRP is very rich in different growth factors and is used widely for rejuvenation. It is safe, non allergic , easy to prepare and has beautiful results. Author does ovarian PRP also in low AMH infertility patients.
4) Topical Estrogen Therapy: While not strictly classified as rejuvenation, topical estrogen creams or tablets can be effective in addressing vaginal dryness and atrophy. They work by replenishing local estrogen levels and improving tissue health. They are not as effective as newer energy based devices.
In women with old episiotomy scarring, abnormal size of labia minora and deficient perineum these surgical options can be given-
1) Labiaplasty: This procedure involves reshaping and reducing the size of the labia minora for aesthetic and functional purposes. It can alleviate discomfort caused by elongated labia and enhance the overall appearance of the genital area.
2) Vaginoplasty: Vaginoplasty aims to tighten the vaginal canal by removing excess vaginal mucosa and tightening the surrounding muscles. But this usually tightens only introitus and not the whole canal.
3) Perineoplasty: Often performed in conjunction with vaginoplasty, perineoplasty repairs and tightens the perineal area, which may have been stretched or damaged during childbirth.
When considering vaginal rejuvenation for perimenopausal
women, it is crucial to conduct a thorough evaluation of each patient’s medical history, symptoms, and expectations. Factors such as the severity of symptoms, overall health, and individual goals should guide the selection of the most appropriate treatment modality. Pap smear, breast examination and pelvic USG should not be forgotten. Holistic health should be remembered.
Informed consent and realistic expectations are essential components of the patient consultation process. Practitioners should provide comprehensive information about the benefit, risks, and potential outcomes of each treatment option, ensuring that patients are well–informed and comfortable with their decisions.
Newer field of cosmetic gynecology offers perimenopausal women a range of effective solutions to address the physical and emotional challenges associated with this transitional phase. By restoring vaginal health and function, these treatments can significantly enhance a woman’s quality of life, sexual satisfaction, and overall wellbeing. As the field of esthetic gynecology continues to evolve, ongoing research and advancements will further refine and expand the options available for perimenopausal women seeking rejuvenation.
“Aesthetic and Regenerative gynecology”, book published by Springer.
Editors- Dr. Preeti Jindal etal.


Childbearing trauma, aging, and inherited irregularities affect not only the aesthetic look of the external female organs, but also create feelings of being different or inadequate. It can have an effect on intimate relationships and women's emotions.
- Dr. Adam Ostrzenswski
Cosmetic Gynecology is emerging new subspecialty of gynecology which started as something like media driven and frivolous subspecialty but within a decade it has established itself as a fourth dimension of aesthetic medicine. It addresses a need of women which was not addressed adequately for ages and forced to live women a poor quality of life. There has never been a shortage of opinion on cosmetic surgery, but in every culture
that has ever existed people have willingly availed themselves of the methods and technologies available at that time. People have long been driven to painful, surgical measures to “correct” their facial features and body parts, even prior to the use of anesthesia and discovery of antiseptic principles. From the milk and honey baths used by the ancient Egyptians to the light zaps of today’s cosmetic lasers, people are constantly searching for the latest and greatest procedures to help achieve a younger, healthier, more rejuvenated look.
Incorporation of medical aesthetics in women’s intimate organs rejuvenation has swept the medical field and opened many new discussion points. Most important discussion is “is it really needed. Is it really demand of women or just a hype created by industry,” Answer of both questions is, “Yes it is needed by women itself.” It is a subject totally neglected and swept under closet. Aesthetic gynecology may represent unmet functional needs partly/ completely. It has given answer to unmet needs of women. An insight to many women sexual disorders, her poor quality of life, her low self-esteem and even social isolation.
What is changed today is economic independence of women, and it is boosted by advent of nonsurgical rejuvenation methods along with safe use of adjuvants and developments in anti-aging medicine. It has completely changed the field of cosmetic gynecology to functional to regenerative gynecology.
A) Physiological
➢ Genitourinary syndrome of menopause
➢ Postmenopausal vaginal
dryness and dyspareunia
➢ Recurrent vaginal infections
➢ Recurrent UTI
➢ OAB and nocturia
B) Anatomical
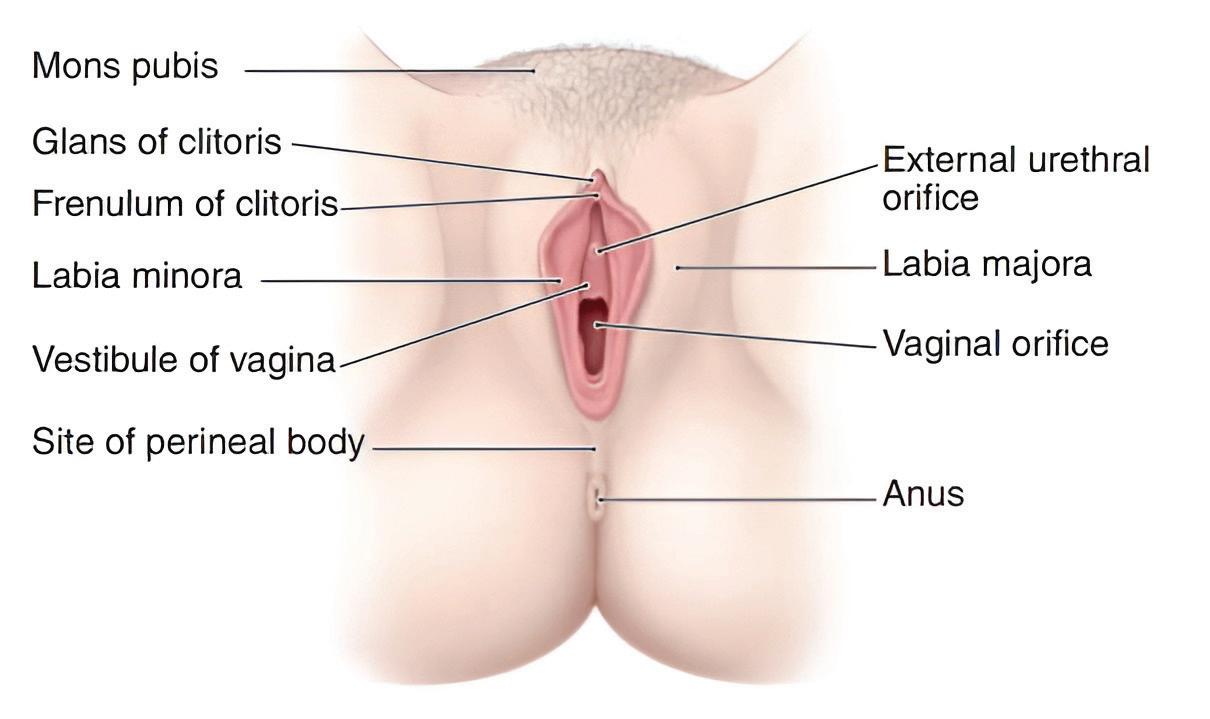
1. Need for reduction/ augmentation/ smooth appearance: - Labia MinoraLabia Majora - Clitoral hoodMons pubis
2. Vaginal walls - length, laxity
3. Vaginal caliber narrowing, widening
4. Gaping vaginal introitus versus intact hymen
Case Discussion - Mrs SONUM Age: 53 P2+0 both NVD
▶ Chief Complaint: “I don’t feel like being intimate anymore. I haven’t had sex for three years. I don’t enjoy it as it’s not comfortable and I feel dry. It’s affecting our relationship. I feel
embarrassed talking about it.”
Examination:
▶ Vaginal dryness
▶ Good vaginal wall support
▶ No lesions on the vagina/ vulva
▶ Normal pap smear
Petrova et al, 2013
This patient needs vaginal rejuvenation “Ability to make a tissue functionally younger”
FDA cleared the first cosmetic lasers to reduce unwanted hair and wrinkles.
Evolution of Energy Based Devices -1st laser in 1990. Today Medical aesthetics has grown to include more than just lasers. Infrared light, RF energy and Ultrasound technology and hybrid technology is being used to reduce the appearance of cellulite, improve skin texture & tighten sagging skin and addressing many functional disorders like SUI, GSM. Not only this aesthetic treatments are done with injectable also along with EBDs. Botox, Dermal fillers, Fat, PRP, & Stem Cells are being used to address vulvo vaginal rejuvenation.
We have come long way from surgical treatment to nonsurgical
and regenerative treatments. It is now affordable to masses. It includes both functional vaginal repairs cosmetic procedures to enhance the aesthetic appearance of the vulvo/vaginal region & to enhance or help to restore sexual function and pelvic floor disorders like stress incontinence, urge incontinence of menopause, following the changes that may occur following childbirth and/or aging. Studies have also recently shown that
this is a trend driven by women themselves not their sexual partners because today’s women need to address her intimate health problems. New technology like lasers as well as “An aesthetic uplift can lead to a psychological uplift”. radiofrequency, HIFU, Hybrid lasers treatments and adjuvant regenerative therapies with PRP, and fat grafting has been introduced in the field offering non-surgical/office based procedures to treat female
Physiologic changes in a woman’s life are
Childbirth, Weight fluctuations
Hormonal changes due to again and menopause
Alter the laxity of the vaginal canal
Damage the pelvic floor

Devitalize the mucosal tone of the vaginal wall
Development of genitourinary
Conditions such as
Stress urinary incontinence
Vaginal atrophy
Dryness

Physiologic distress affecting a woman’s quality of life, selfconfidence, and sexuality.
sexual dysfunction (VLS), vaginal health and vulvo/vaginal cosmetic issues for women and functional disorders like mild SUI, GSM and Mild Prolapse & Medical Conditins Like Vulvodynia And Lichen Sclerosis And Vaginismus
• Surgical procedures and systemic and topical treatments have been supplemented with new, noninvasive, energy based systems, which is a welcome development for the many women wary of surgery due to the risk, expense, and downtime involved. These devices have opened up a new market for nonsurgical vulvovaginal correction procedures for women. Although numerous studies have demonstrated the therapeutic efficacy of energy-
based devices in rejuvenation of the face, neck, and decollete, their application in the vaginal canal is a fairly new concept with a paucity of clinical studies currently available to validate their efficacy.
Medico Legal Considerations -
▶ Fully informed consent is fundamental when offering FGCS, as is the case for all medical treatment.
▶ Clinicians who perform FGCS must be aware that they are operating without a clear evidence base.
▶ Women should be advised accordingly.
▶ Owing to anatomical development during puberty, FGCS should not normally be offered to individuals below 18 years of age.
My role as a designer is to make a woman feel her very best - Oscar de la renta

Q.1 Can you describe your journey in FOGSI as a member and prominent leader? How did you start out? How has your experience been through all these years in this organization?
Ans- I have been associated with FOGSI since 1991 when I was a lecturer. Late Prof MY Rawal introduced me to participation in FOGSI as a member of medical disorders committee in 1995 and since then there has been no looking back. From organizing conferences to chairing them, it has been such a pleasant journey. I have seen this organization grow through all these years, and it gives me immense pleasure and pride to have been a significant part of this growth and progress.
Q.2 How do you manage to maintain a work life balance with your busy schedule?
Ans- Honestly speaking, there is no work life balance. There has never been a work life balance. I travel every weekend, meet my friends in FOGSI to recharge myself almost every week. So there has never actually been a need of a balance since my wife has always taken the responsibility of the kids and household very well. And that has worked out pretty well for both of us. With my academics, meetings and practice, I have really enjoyed each and every aspect of my life.
Q.3 What is the most rewarding thing that FOGSI has given you in all these years?
Ans- Friendship. I am just so proud to say that FOGSI has given me so much love and friendship almost all over India. I am so grateful for my FOGSI family, because be it any city, anyone is in any problem, everyone reaches out. I remember one of my colleagues suffered an RTA once somewhere and help reached through FOGSI within an hour. That is the level of love and respect I have found in FOGSI in all these years.
Q.4 Who has been your mentor or guide who has inspired you all these years? Someone whom you look up to and learn from everyday?
Ans- There was my professor and unit head Prof Geeta Niyogi who encouraged me to participate in
FOGSI activities. I have always looked up to Dr. Narendra Malhotra, Dr. Hema Diwakar for their passion to work and shine, I have always admired Dr. Jaydeep Tank, Dr. Parikshit Tank, for their grit and integrity, and Dr. PL Mohapatra and Dr. Hrishikesh Pai for their inclusiveness. I have always followed the principle of learning good things from a leader, to make a good leader.
Q.5 What would be your message to the young generation of FOGSI who wants to follow in your footsteps?
Ans- I have always believed in giving the youngsters a suitable platform. I remember I gave a chance to Dr. Neharika to speak on a topic in AICOG and she was fantastic. So the youngsters in FOGSI are full of talent and potential, and they deserve to be given a suitable platform. Having chaired this committee before, YTP is something that is very close to my heart.
Q.6 What is Your Agenda for Your Upcoming Presidential Candidature?
My belief and agenda is continuity and progress. I want to work to make this organization more inclusive and representative, so that it can become an even more close knit community, there can be even more opportunities for everyone to learn and participate. I want to give each and every FOGSI member a platform to work hard and progress.

Dr. Bhaskar Pal
MBBS, DGO, MD, DNBE (Obs & Gynae), MRCOG, FICOG, and FRCOG Senior Consultant Obstetrician & Gynaecologist, Apollo Hospital, kolkata
President Elect- FOGSI
Polycystic ovary syndrome (PCOS), affecting 1113% of women of reproductive age, is linked
to fertility challenges, higher miscarriage rates, and increased endometrial cancer risk. A recent study published in Nature Medicine analysed nearly 250,000 endometrial cell nuclei from healthy women and those with PCOS, revealing that PCOS is associated with insulin resistance, obesity, and elevated male hormones, causing endometrial dysfunction. Women with PCOS showed a higher proportion of epithelial cells and fewer stromal cells, which may contribute to implantation issues, miscarriage risk, and heightened endometrial cancer risk.
The study identified significant molecular changes in the endometrium of women with PCOS, particularly in epithelial cells, with upregulation of genes involved in cell adhesion, ECM, and integrin signaling (ITGA2, ITGA3, ITGAV) in SOX9+LGR5+ and androgen receptor-positive cells. These alterations contribute to increased epithelial cell proliferation, impaired differentiation, and a higher risk of endometrial cancer. Immune cells, including uNK2 and uM1, showed gene expression linked to implantation failure and cancer. Disruption in epithelial, stromal, and immune cell communication, particularly in collagen, laminin, and IGF signaling, was also observed. Women with PCOS underwent metformin treatment, with or without lifestyle management, over a 16-week period. This treatment reversed the molecular changes, reducing testosterone and androgen levels, and improving endometrial health by addressing hyperandrogenism and insulin resistance. The study underscores the role of metformin in modulating endometrial dysfunction, improving reproductive outcomes, and identifies potential therapeutic targets such as integrin inhibitors, offering valuable insights into PCOSrelated endometrial diseases, including cancer.

AA recent retrospective study published in CHEST assessed the impact of cystic fibrosis
transmembrane conductance regulator (CFTR) modulators on pregnancy outcomes in individuals with cystic fibrosis (CF). Analyzing data from 307 pregnancies between 2010 and 2021 across 11 U.S. adult CF centers, the study aimed to evaluate how CFTR modulator use affects maternal health during and after pregnancy. CFTR modulators, which improve CFTR protein function, significantly enhance lung health, weight, and quality of life in CF patients. Historically, fewer than 200 pregnancies per year occurred in women with CF in the
U.S., as many did not survive to childbearing age or were unable to carry a pregnancy to term due to the disease. Pregnancy outcomes have improved for women using modulators, and babies exposed to modulators during pregnancy were generally healthy. The researchers reviewed medical records comparing women who used CFTR modulators to those who did not. Pregnant individuals on CFTR modulators experienced significant improvements in lung function, as measured by percent predicted FEV1 (ppFEV1), while those not using modulators showed a decline.
These findings suggest that CFTR modulator use during pregnancy may positively impact maternal lung health and is likely safe for the exposed infants. However, given the limited number of centers and the short study duration, further research is needed to understand the long-term effects of CFTR modulator use during pregnancy. The ongoing Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS) study is prospectively tracking these outcomes during pregnancy and postpartum.
As I reflect on this statement, one name echoes powerfully in my mind — Rani Laxmi Bai. And that’s exactly what inspired me to write this.
I am privileged to be a daughter, a wife, a mother — A WOMAN. From the moment we are born, we daughters are surrounded by love. Our parents would do anything to see a smile on our faces. It feels safe to have that permanent armour of protection around us.
We are born princesses a RANI— yes, we are! Even if dressed in rags, carrying a few extra inches around our waists, or living in attics, we are still beautiful. We are princesses — if not to the world, then certainly to our parents, for whom we are the world. Our throne walk begins the day we are born. So girls, our once upon a time is now.
To our fathers, we will always be the little princesses they once carried in their arms — the ones who playfully decked them up in role-play games with all kinds of colourful, girly stuff.
The moment we think of getting married, we are given an intaglio engraved with the words “The LAXMI of the house.” From being honored as the Finance Minister of the family to becoming CEOs and financial advisors in MNC’s, many more women are stepping out not just because it is fashionable, but because it makes a lot more
business sense. We women tend to be more nurturing, and our approach is often more customer service–oriented. Even Lord Ganesha is always worshipped alongside Goddess Laxmi.
I believe one should never underestimate what a woman can bring to the table, —the skills she is blessed with and has imbibed. Their behaviour is naturally nurturing with risk aversion always on their plate as priority. It should be a dogma for all the men to entrust their wives not just with household finances, but also with other investments made by them, as women, by ethos, are protective and foreseeing.
Women, Empower the Laxmi in you.
Coming to the 3rd locution — BAI. I believe it would not be wrong to spell Bai as BAE — Before Anyone Else — because they truly form the epicentre of any family. Even house helpers’ work incredibly hard, and their role is not at all demeaning or downtrodden echelon. They are simply an extension of us, filling in the gaps where we cannot.
This reminds me of a beautiful line from Sex and the City:
"I can scrub and rub the house till it shines like a dime, I can feed the baby and put some powder on my face at the same time, because I am a woman."
There is no single answer to what a woman’s role in society
is or who she should be. She is powerful soul with or without any of these titles.
She is Rani. She is Laxmi. She is Bai.
“It’s the fire in my eyes, and the flash in my teeth, The swing in my waist, and the joy in my feet —
I am a woman. Phenomenally.”
A woman is Magnanimous — she should be who she wants to be.
Embrace yourself as RANI, support your family as LAXMI, spend time with your kids , parents and husbands as BAE
But when we hear of horrific incidents like Nirbhaya , Calcutta rape-murder, it sends chills down our spines. It is in these moments that we realise — we must become no one else but Rani Laxmi Bai, and rise to fight for our basic human rights.

MS, DNB (ObGy), MNAMS, FMAS, Dip (CosGyn) Director Oracle Clinics, Nagpur
There is an air of sweetness and poise around her, A quiet strength that everyone admires and loves. They call her pretty, they call her beautiful — But it does not really matter to her, she says.
Deep down, she keeps her heartbreaks safe, From the people who gave them to her in the first place. Yet, she keeps the warrior in her alive — Feeds it, tames it, trains it, For she knows it alone will save her From this cruel world, And help her stay strong and thrive.
She wants to learn new things every day, And walks the streets with her head held high. She is a mother, a daughter, a sister, a wife — And a very doting one, I will not lie.
She enjoys her one cup of evening tea everyday With no sugar and less milk, “It is my reward to myself,” she says — Her moment to relax, to pause, to think. Her office is full of the degrees she earned, From working hard work, both day and night. But it has always been her beautiful mind, That won everyones heart . There is probably a part of her In each of us.
Because after all, do not we all know What it takes — to be her?

Dr. Gurkiran Kaur
MBBS, MS (Obstetrics and Gynaecology), Fellowship in Reproductive Medicine
Consultant Gynecologist and Infertlity specialist
Kuldip Hospital and IVF Centre, Jalandhar

The recent Fungal Master Class on “Overview of Effective Management Strategies for Vulvar and Perianal Infections,” held in Pune, was organized under the auspices of the Young Talent Promotion (YTP) committee of FOGSI (The Federation of Obstetric and Gynaecological Societies of India) in association with POGS (Pune Obstetric and Gynaecological Society) and drscourseslive.com. The event assembled leading specialists in Gynaecology and Urology to address the evolving challenges in diagnosing and managing vulvar and perianal fungal infections. Conducted as a hybrid event with over 2000 Gynaecologists in attendance Online on drscourseslive.com, it marked the fourth edition of a wellestablished educational series committed to evidence-based, multidisciplinary, and patient-centered approaches to women’s health. The keynote speaker, Dr. Kiran Kurtkoti, President of AMOGS (2024–2026), presented key insights. The session, moderated by Dr. Manish Machave, President of POGS 20252026, featured Panelists Dr. Vaishali Chavan, Vice President Elect of POGS (2025–26), Dr. Vaishali Korde-Nayak, Executive Vice President of POGS (2025–26) and Dr. Shirish Yande, Urologist, who has served as the Hon. Secretary and President of the West Zone Chapter of the Urological Society of India, discussed urinary conditions, diagnostic challenges, and treatment-resistant infections.
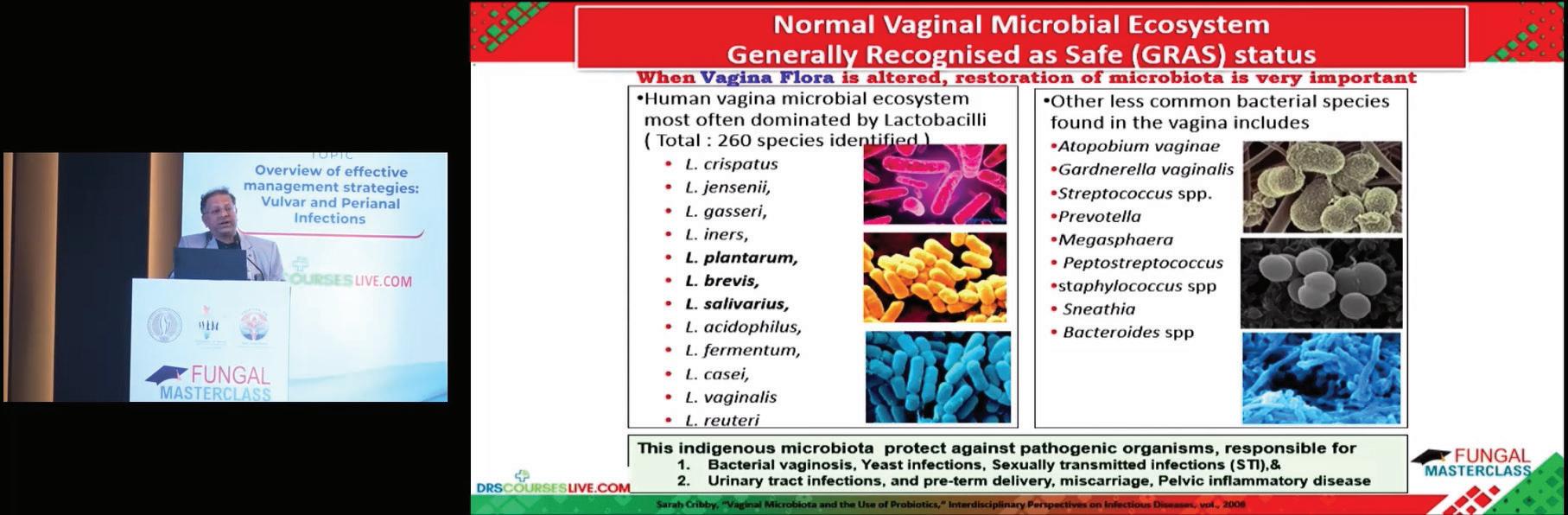
Speaker Dr. Kiran Kurtkoti shared his insightful presentation
The masterclass featured a detailed presentation by Dr. Kiran Kurtkoti, who provided valuable insights into diagnosing and managing vulvar and perianal fungal infections, emphasizing pH testing, microscopy, and targeted treatments. Recurrent cases were addressed with species identification, extended therapy, probiotics, and partner treatment. Highlighting that UTIs can mimic these infections, the importance of appropriate antibiotic use and further evaluation was emphasized. His session concluded by stressing patient education and ongoing care to reduce recurrence and improve outcomes.

Dr. Vaishali Korde-Nayak
The interactive panel session, moderated by Dr. Manish Machave, offered expert insights from Dr. Shirish Yande, Dr. Vaishali Chavan and Dr. Vaishali Korde-Nayak. Key topics included adolescent vulvovaginitis with psychosocial care, differentiating vulvovaginal infections from UTIs, and managing asymptomatic infections in IVF patients. The panel emphasized culture media for diagnosing non-albicans candidiasis, long-term estrogen therapy for postmenopausal urethritis, and the importance of hygiene, antibiotic stewardship, and IUCD safety, especially in underserved populations to reduce recurrence. The discussion was rounded off with audiencedriven questions, enriching the discussion on realworld clinical challenges and best practices.


Closing Ceremony Glenmark Team along with L to R: Dr. Kiran Kurtkoti, Dr. Shirish Yande, Dr. Manish Machave, Dr. Vaishali Korde-Nayak, Dr. Vaishali Chavan and Dr. Kalyani Ingale
This Fungal Master Class was supported by Glenmark and the event ended with a warm note of appreciation from the Glenmark team to the esteemed Facultys’s Dr. Kiran Kurtkoti, Dr. Shirish Yande, Dr. Manish Machave, Dr. Vaishali Korde-Nayak, Dr. Vaishali Chavan, Dr. Kalyani Ingale and all other contributors for their valuable support in making the event meaningful, informative and a grand success.
Dr. Aarti Nimkar:
The topic was comprehensively explained, covering infections across all stages of women’s health. The presentation was well-delivered, and the panelists engaged in thorough and insightful discussions.
Dr. Ashwini Devdikar:
An excellent and highly informative event, offering valuable insights applicable to current clinical practice. The panelists demonstrated strong expertise, making the session very beneficial.
Dr. Pradnya Badge:
The presentation was outstanding and filled with relevant information. The panel discussion was engaging, with all speakers providing valuable perspectives.

This Event was conceptualized and executed by Paradigm Infocom Pvt. Ltd, Publisher of this Newsletter.
For more information, Contact: +919820507771 Email id: - paradigminfocomobgyn@gmail.com
regnancy complications like gestational hypertension,
gestational diabetes mellitus (GDM), preeclampsia (PE), preterm birth (PTB), maternal inflammation, and fetal growth restriction can impact pregnancy outcomes and offspring health. Researchers at the University of Queensland developed a rapid, portable sensor to detect placental-derived extracellular vesicles (EVs) in maternal plasma for early GDM detection. Published in Science Advances, the study used targeted proteomics to identify peptides quantifying circulating

placental EVs, aiding in assessing risks for GDM, PE, and PTB. EVs expressing CD9, CD63, CD81, TSG101, and PLAP are elevated in pregnancy, reflecting placental function and monitoring maternal and fetal health.
The sensor developed in this study uses superparamagnetic nanoflower particles (SMNFs) to isolate target EVs and enable sensitive detection through nanozyme activity. The system combines SMNFs with a nanozyme-based readout on a 4-flex glass strip, isolating target EVs in 30 minutes and allowing for rapid assay formation and detection. The sensor demonstrated excellent enzyme-like activity, detecting as few as 1,000 EVs per million cells within 24 hours, outperforming previous nanostructure-based methods. By integrating isolation and detection in one step, the system simplifies the process, reduces costs by eliminating complex exosome isolation, and provides high specificity, verified through three control samples. Additionally, it remains stable for repeated use, making it adaptable for clinical settings. While the sensor showed strong performance in training cohorts, further validation in larger, multicenter studies is needed. With over 90% accuracy in identifying women at risk for GDM, this cost-effective, portable sensor has the potential for widespread use in point-of-care settings for early detection of pregnancy complications.

Alandmark study has confirmed that bacterial vaginosis (BV), affecting one-third of women
globally and linked to infertility, premature births, and neonatal death, is a sexually transmitted infection (STI). Researchers from Monash University and Alfred Health published their findings in the New England Journal of Medicine, challenging the current practice of treating BV as a microbiome imbalance. The study demonstrated that treating both sexual partners simultaneously with oral and topical antibiotics significantly reduced BV recurrence, halving the rate compared to the standard treatment of women alone.
In a trial of 164 monogamous couples, women treated with antibiotics alongside their male partners showed a marked improvement in BV cure rates. This cost-effective and brief intervention has the potential to improve BV outcomes and prevent complications. The study also reinforces that BV increases susceptibility to other STIs, due to shared risk factors like multiple partners.
Previous studies showed that men might harbor BV-related bacteria, but did not demonstrate improved cure rates in female partners. This trial, however, used combined oral and topical antibiotics to clear BV from male partners, revealing that reinfection from partners contributes to BV recurrence. These results suggest BV is indeed an STI and could lead to changes in clinical practice and treatment guidelines.

