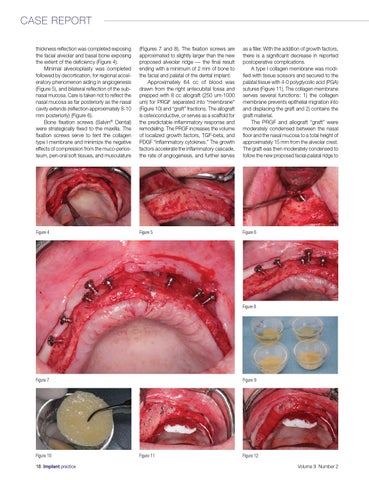
CASE REPORT thickness reflection was completed exposing the facial alveolar and basal bone exposing the extent of the deficiency (Figure 4). Minimal alveoloplasty was completed followed by decortication, for regional acceleratory phenomenon aiding in angiogenesis (Figure 5), and bilateral reflection of the subnasal mucosa. Care is taken not to reflect the nasal mucosa as far posteriorly as the nasal cavity extends (reflection approximately 8-10 mm posteriorly) (Figure 6). Bone fixation screws (Salvin® Dental) were strategically fixed to the maxilla. The fixation screws serve to tent the collagen type I membrane and minimize the negative effects of compression from the muco-periosteum, peri-oral soft tissues, and musculature
(Figures 7 and 8). The fixation screws are approximated to slightly larger than the new proposed alveolar ridge — the final result ending with a minimum of 2 mm of bone to the facial and palatal of the dental implant. Approximately 64 cc of blood was drawn from the right antecubital fossa and prepped with 8 cc allograft (250 um-1000 um) for PRGF separated into “membrane” (Figure 10) and “graft” fractions. The allograft is osteoconductive, or serves as a scaffold for the predictable inflammatory response and remodeling. The PRGF increases the volume of localized growth factors, TGF-beta, and PDGF “inflammatory cytokines.” The growth factors accelerate the inflammatory cascade, the rate of angiogenesis, and further serves
as a filler. With the addition of growth factors, there is a significant decrease in reported postoperative complications. A type I collagen membrane was modified with tissue scissors and secured to the palatal tissue with 4-0 polyglycolic acid (PGA) sutures (Figure 11). The collagen membrane serves several functions: 1) the collagen membrane prevents epithelial migration into and displacing the graft and 2) contains the graft material. The PRGF and allograft “graft” were moderately condensed between the nasal floor and the nasal mucosa to a total height of approximately 15 mm from the alveolar crest. The graft was then moderately condensed to follow the new proposed facial-palatal ridge to
Figure 4
Figure 5
Figure 6
Figure 8
Figure 7
Figure 10 18 Implant practice
Figure 9
Figure 11
Figure 12 Volume 9 Number 2