每年十月是国际乳癌防治月(Breast Cancer Awareness Month),也被称为“粉 红十月”(Pink October),目的是提高女性对乳癌的认识,帮助做到及早发现和 治疗。乳癌是马来西亚女性中最常见的癌症类型,因此每位女性都应多了解乳癌 相关知识,关爱自己的乳房健康。
Every year, the month of October is Breast Cancer Awareness Month. This campaign, known as “Pink October”, aims to raise awareness among women about breast cancer, and the importance of early detection and treatment. In Malaysia, breast cancer is the most common cancer among women. It is therefore vital that women are well informed about the disease and be proactive in safeguarding their breast health.
黎淞铀医生 DR. (MR.) LOI SHUNG YU
外科专科医生 Consultant General Surgeon
Risk Factors and Symptoms to Recognise
Dr. Loi Shung Yu, a general surgeon at Kek Lok Si Charitable Hospital (KLSCH), explained that there are two main types of risk factor for breast cancer:
(1) Non-modifiable factors, which cannot be altered, and (2) Modifiable factors, which can be managed through lifestyle adjustments and preventive interventions.
Non-modifiable risk factors for breast cancer include:
(1) GENDER
(2) AGE – The risk of developing breast cancer increases with age.
(3) FAMILY HISTORY – Individuals with close relatives who have had breast cancer, or those who carry the BRCA1 or BRCA2 genes, face a higher risk.
(4) EARLY MENARCHE – Starting menstruation before the age of 12.
(5) LATE MENOPAUSE – Going through menopause after the age of 50.
Modifiable risk factors include:
(1) LIFESTYLE AND HABITS – A sedentary lifestyle, lack of physical activity, and obesity are known to increase the risk.
(2) BREASTFEEDING – Research suggests that breastfeeding can lower the risk of breast cancer.
(3) HORMONE THERAPY
(4) ORAL CONTRACEPTIVES
(5) RADIATION EXPOSURE
Dr. Loi emphasised that early-stage breast cancer often presents no clear symptoms. Therefore, it’s important to seek medical advice immediately if a lump, nipple discharge, breast pain, or other abnormalities are detected.
根据马来西亚临床实践指南(Clinical Practice Guidelines,CPG)建议,年龄介于50岁至74岁、 没有症状的女性应每两年进行一次乳房X线检查筛 检,因为这是乳癌高发的年龄段。如果存在较高风 险因素,则建议每年进行一次筛检。然而,由于越 来越多30岁至49岁的女性也罹患乳癌,磁共振成像 扫描(MRI)和超声波(Ultrasound)已成为年轻女 性筛检乳房的常用方法。
“When patients with any of these abnormalities first see a general practitioner or family doctor, they are usually referred to a specialist within two weeks so that treatment can begin as soon as possible,” he said.
Dr. Loi also noted that if the cancer has spread, the patient may experience bone pain, coughing, shortness of breath, or jaundice. Regular breast screenings remain the best way to detect breast cancer early.
Screening Methods and Clinical Recommendations
The three primary methods for breast screening are:
(1) Mammography
(2) Magnetic Resonance Imaging (MRI)
(3) Ultrasound
According to Malaysia’s Clinical Practice Guidelines (CPG), women aged 50 to 74 with no symptoms should have a mammogram every two years, because this age group has the highest incidence of breast cancer. For women with higher risk factors, annual screenings are recommended. With more women aged 30 to 49 being diagnosed with breast cancer, Magnetic Resonance Imaging (MRI) and Ultrasound have become increasingly common screening methods for younger women.
Dr. Loi elaborated that for women under 40 who show no symptoms, doctors usually prefer using Ultrasound for screening. For young women with high-risk factors, such as a family history of breast cancer, doctors may consider Magnetic Resonance Imaging (MRI), depending on the patient’s circumstances. He highlighted that more and more doctors are combining mammography with Ultrasound to achieve a more accurate diagnosis.
Breast cancer is classified into stages one through four. In Malaysia, around half of patients are already in stage three or four by the time they notice symptoms and seek treatment. Stages three and four are considered advanced, with larger tumours and cancer cells spreading to the lymph nodes. In stage four, the cancer has spread to other organs such as the lungs, bones, liver, or brain, making treatment more difficult, lower survival rates and higher risk of recurrence.
治疗管理的关键
乳癌可通过“TNM”分期系统来区分其阶段,分 别代表三个主要因素:
T - 肿瘤大小(Tumour Size)
N - 淋巴结转移的态(Nodal Status)
M - 转移情况(Metastasis)
Dr. Loi explains that after surgery, cancerous tissue is tested to determine the most suitable follow-up treatments, aimed at reducing the risk of recurrence.
Thus, breast cancer screening is crucial. Dr. Loi noted that if breast cancer is identified and treated in the first or second stage, the patient’s survival rate can be greatly enhanced, the risk of recurrence reduced, and the chances for disease-free survival (DFS) improved. Ultimately, the goal of treatment is to achieve complete recovery and a cancer-free status.
Key Aspects of Treatment Management
Breast cancer stages can be classified using the “TNM” staging system, which focuses on three key factors:
T for Tumour Size
N for Nodal Status, indicating whether the cancer has spread to the lymph nodes.
M for Metastasis, referring to whether the cancer has spread to other parts of the body.
Treatment plans are tailored to a patient’s cancer stage and specific circumstances, consisting primarily of surgery and adjuvant therapy. The surgical areas include the breast and axilla (armpit).
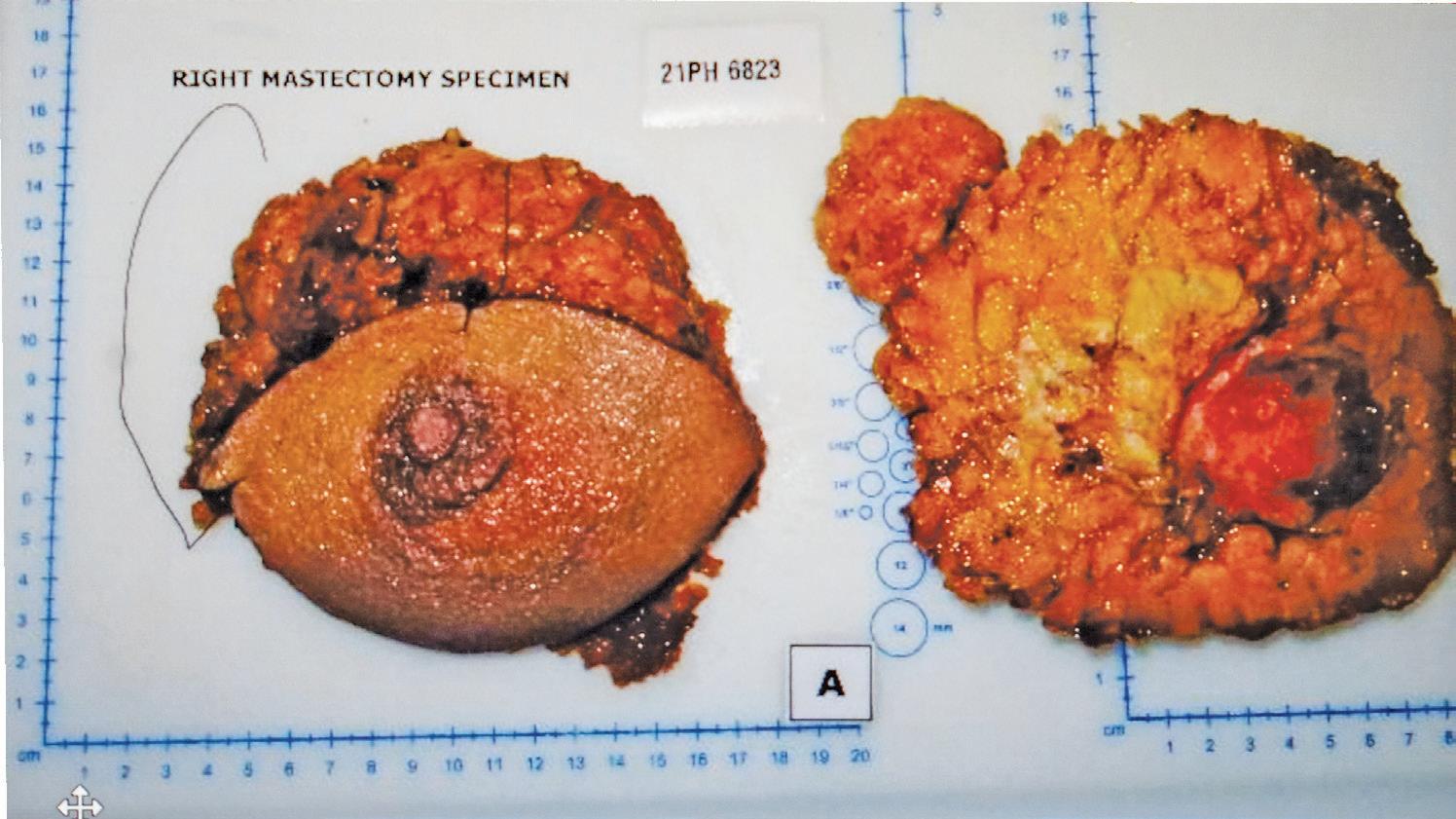
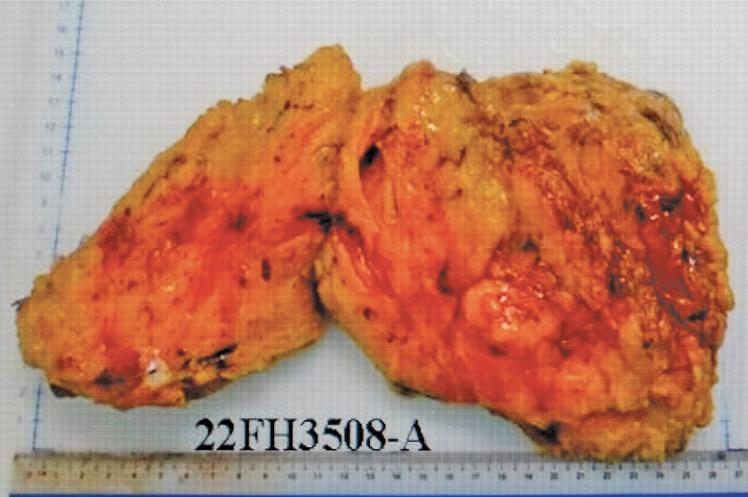
Dr. Loi mentioned that there are two main types of breast surgery: Breast Conserving Surgery (BCS) and Mastectomy. BCS is usually appropriate for patients in stages one and two, as the tumours are smaller and only the tumour itself needs to be removed. For larger tumours, a Mastectomy is necessary. This involves the complete removal of the affected breast, and is typical for patients in stages three or four.
spread to other organs through these nodes. Dr. Loi outlined two types of axillary surgery: Axillary Clearance involves removing all lymph nodes in that area to prevent cancer recurrence. However, patients may face complications like lymphedema and arm swelling as a result of this procedure. The second type of surgery is Sentinel Lymph Node Biopsy (SLNB). This involves removing a few lymph nodes that may contain cancer cells for testing. If no cancer cells are found, the cancer may not have spread. Dr. Loi noted that while SLNB may reduce the risk of lymphedema post-surgery, it is not meant for all patients. The decision to proceed with either of the two types of axillary surgery should be made by the doctor based on the patient’s unique circumstances.
Treating cancer does not conclude with surgery; appropriate adjuvant therapy – such as chemotherapy, radiation therapy, hormonal therapy, and targeted therapy – is crucial in reducing the risk of recurrence. Using hormonal therapy as an example, Dr. Loi elaborated on how a patient’s suitability for this type of adjuvant treatment is determined. After surgery, the removed tumour is sent for testing. If the results show positive Estrogen Receptors (ER) and Progesterone Receptors (PR), the patient may be eligible for hormonal therapy. However, if the results are positive for Human Epidermal Growth Factor Receptor 2 (HER2), then hormonal therapy is not appropriate, and the patient may be better suited for targeted therapy.
The primary goal of axillary surgery is to remove lymph nodes from the axilla, as cancer cells may
Dr. Loi shared a recent success story where a 66-year-old patient underwent a mammogram two years ago and noticed two small tumours. Following the diagnosis, she had a mastectomy and began hormonal therapy. Subsequent examinations showed that her cancer has not recurred, indicating a successful recovery. As part of her ongoing care,
Regular screening is the best preventive measure as early detection and treatment greatly enhance the chances of complete recovery.
she will need to undergo a mammogram every two years, and her hormonal therapy will continue until 2027, for a total of five years.
Challenges in Treatment and Future Trends
Dr. Loi acknowledged the unpredictability of cancer and the ever-present risk of recurrence, which present various challenges in caring for a cancer patient.
“A significant challenge for surgeons is margin status, which involves ensuring that the edges of the tissue removed during a mastectomy are free of cancer cells. For patients with very large tumours, chemotherapy may be required to shrink the tumour before surgery. This is to improve the surgical outcome. Sometimes, patients become too weak during chemotherapy and may choose not to proceed with surgery. There are also cases where
patients had the surgery done but did not complete the full course of chemotherapy, or when they return after some time, their condition had worsened”
He emphasised that surveillance and ongoing follow-up are crucial steps in patient care. “Patients who have completed treatment must return for regular check-ups at least once a year for a minimum of five years,” he said.
Dr. Loi reiterated, “Regular screening is the best preventive measure as early detection and treatment greatly enhance the chances of complete recovery,”
Dr Loi mentioned that the advancements in medical technology and increasing research on breast cancer is shifting the reatment paradigms where nonsurgical treatment options are preferred nowadays. If tumours are detected early and are small, patients may only require chemotherapy or other adjuvant therapies to eliminate the tumour. A surgery can therefore be avoided.
Mammography operates by positioning the breast on a flat panel, which is then compressed by the device before X-ray images are taken. Traditional 2D mammography captures images from the front and side, but overlapping breast tissue can sometimes obscure diagnostic results. With better technology, 3D mammography (Digital Breast Tomosynthesis) has overcome the limitations of 2D screenings. This new method captures multiple images from various angles and uses tomographic techniques to combine the images to create a threedimensional representation of the breast. The result is a more effective way to detect abnormal tissues. Furthermore, 3D mammography is a more comfortable process physically compared to traditional 2D mammography, with the entire process taking only 15 to 30 minutes.
黄诗幈医生 DR. WONG SEE PENG
放射学专科医生 Consultant Radiologist
The Widespread Use of 3D Mammography
Breast cancer is the most prevalent cancer among women in Malaysia, with data revealing that one in every 19 women receives a diagnosis. Dr. Wong See Peng, Consultant Radiologist at Kek Lok Si Charitable Hospital, underscores the effectiveness of 3D mammography in detecting cancer cells at earlier stages. Early detection is key to significantly improve cancer survival rates.
“Early detection makes possible the timely removal of a tumour. When tumours are identified in their early stages, they are usually smaller and easier to treat, often requiring only a lumpectomy rather than a mastectomy. Conversely, if tumours are detected at a later stage, the top concern is whether it has spread to the lymph nodes or other organs, which can significantly lower survival rates.”
Radiology staff demonstrate the operation of the newly introduced 3D mammography system.
Dr. Wong pointed out that 3D mammography is typically indicated for the following four situations:
(1) Breast Screening
Early-stage breast cancer often has no symptoms, making regular screening the most effective method for early detection. 3D mammography can better visualise calcifications that occur within breast tissue, which helps physicians identify abnormal areas more effectively. If a region appears suspicious, another 3D mammography on the same day may be ordered to obtain clearer imaging.
Additionally, breast X-rays are frequently complemented by ultrasound examinations. “Most Asian women have dense breast tissue, which can result in tightly packed structures that may appear only as shadows on mammographic images. In such cases, ultrasound is essential for confirmation. Conversely, if abnormalities are detected on the mammogram, we will also utilise ultrasound for further investigation,” said Dr. Wong.
(2)
Diagnosis
If a patient exhibits symptoms such as a palpable lump, changes in the skin, swelling in the armpit, or other concerns that raise suspicion of breast cancer, a mammogram is necessary for confirmation. Dr. Wong noted that not all lumps are indicative of cancer; they can also be associated with benign conditions such as cysts or fibroadenomas.
(3) Biopsy
When abnormalities are confirmed in breast tissue, a biopsy is typically conducted with the aid of 3D mammography or ultrasound.
This procedure involves extracting tissue from the suspicious area for further examination to ascertain the nature of the abnormalities.
(4) Surveillance
For patients diagnosed with breast cancer, whether the treatment involves unilateral disease, lumpectomy, or mastectomy, it is crucial to monitor the remaining breast or breast tissue regularly. Annual examinations are typical to ensure that there is no recurrence or the development of new cancer cells in previously healthy areas.
New Approaches to Breast Cancer Screening
Dr. Wong highlighted that, in accordance with the Malaysian Clinical Practice Guidelines (CPG), asymptomatic women aged 50 to 74 should undergo mammography screening every two years. For women aged 40 to 50 with a family history or those in highrisk groups, consulting a physician about the need for earlier screening is recommended. Those with specific circumstances, such as having a mother, aunt, or sister diagnosed with breast cancer, or being identified as a carrier of BRCA1 or BRCA2 gene mutations, may need to start screenings as early as the 30s. Physicians will recommend the appropriate screening method based on the patient’s unique situation. Some patients may also prefer a radiation-free method such as magnetic resonance imaging (MRI).
Dr. Wong emphasised that the radiation dose from 3D mammography is minimal, with its key advantage being the ability to identify issues early, and for the patient to begin treatment promptly. Consequently, the benefits of the screening significantly outweigh any associated risks. However,
she advised that pregnant women should refrain from undergoing mammography.
“Currently, the age of cancer onset is decreasing, with breast cancer cases in women aged 30 to 40 becoming increasingly frequent. There are even situations where tumours are detected during pregnancy. In these cases, we usually recommend beginning with a radiation-free ultrasound examination, after which the physician will formulate a treatment plan based on the findings.”
Dr. Wong noted that 3D mammography can occasionally result in false positives or false negatives. A false positive occurs when the results suggest a higher likelihood of cancer, but
subsequent ultrasound examinations and biopsies confirm the absence of cancer cells. In contrast, a false negative happens when early-stage cancer cells are not detected, or they appear benign, resulting in a negative finding. This underscores the importance of regular screenings every two years. Individuals who experience unusual changes in their breasts, however, should seek medical advice immediately.
Kek Lok Si Charitable Hospital has recently introduced 3D mammography to enhance its care for patients. By the end of this year, the hospital is expected to offer 3D mammography screening services to the public, enabling more women to benefit from advanced technology for the early detection and prevention of breast cancer.
依据马来西亚临床实
践指南(CPG)的建 议,50岁至74岁之间、
无症状的女性应每两年
进行一次乳房X线筛检。
In accordance with the Malaysian Clinical Practice Guidelines (CPG), asymptomatic women aged 50 to 74 should undergo mammography screening every two years.
拥抱生命最后阶段: 缓和医疗的意义
Palliative Care:A Vital Approach to Life’s Final Journey
DR. LIM LIANG YIK
40岁 ● 来自双溪大年 ● 育有两名小孩 ● 毕业于新民中学,并在 RUMC (RCSI & UCD Malaysia Campus,前Penang Medical College)修读医学系 ● 2015年考获内科专科,2019年至2021年期 间进修第二专科缓和医学 (Year 2019-2021: Ministry of Health Subspecialty Training in Palliative Medicine, Year 2021: Concord Center for Palliative Medicine, Advance Trainee in Palliative Medicine) ● 目前服务于槟城中央医院,同时也是极乐寺慈善医院的附属专科医生
Palliative care, often referred to as end-of-life or hospice care, plays a crucial role in improving the quality of life for patients facing life-threatening illnesses and their families. As defined by the World Health Organization, palliative care focuses on the early identification, thorough assessment, and management of pain and other physical, psychological, and spiritual issues to prevent and alleviate suffering. This holistic approach not only addresses physiological symptoms but also encompasses psychological, social, and spiritual dimensions. Based on a collaborative team model, palliative care supports both patients and their caregivers, meeting their practical needs and offering bereavement support. Ultimately, the goal of palliative care is to enable patients to live as fully as possible during the final stages of life.
Dr. Lim Liang Yik’s early experience with the loss of his father deeply influenced his understanding of how illnesses impact families and sparked his reflections on life and mortality. In high school, he began to seriously consider his future, and having two doctor siblings further motivated his decision to pursue medicine. He recalled being asked during his medical medical school interview why he wanted to become a doctor. While most candidates typically answered with aspirations to save lives or alleviate suffering, Dr. Lim’s responded that he wanted to focus
In his fourth year of medical school, Dr. Lim had his first encounter with Charis Hospice Penang, which ignited his passion for palliative care. He reflected, “Before this, I had intended to specialise in emergency medicine, but my exposure to palliative care led me to change my plans. Many were surprised, as this specialty is often considered niche and has yet to be fully integrated into the medical system.” He noted that support from a palliative care specialist during his internship at Penang General Hospital also played a crucial role in reinforcing his passion for this field.
After beginning work at the hospital, Dr. Lim observed that many critically ill patients were often transferred to various specialties. When these departments could no longer provide effective treatment, patients frequently found themselves stuck in the emergency room, unable to receive appropriate care. He pointed out, “These patients continue to suffer from pain and require pain management and guidance, while their families need information to plan the next steps. This highlights a significant gap in the medical system.”
Palliative Care Misconceptions
To the public, palliative care is often misconstrued as a choice to abandon treatment. Dr. Lim clarified that the main objective of palliative care is to alleviate suffering and enhance the quality of life for patients. He said, “Palliative care is not about giving up; it’s about letting go.” When curative options fail, patients still have alternatives, which means not conceding defeat but rather making the best out of a difficult situation.
In managing patients in palliative care, the
缓和医疗并不是放弃,而是放下,
以追求更重要的东西。
Palliative care is not about giving up; it’s about letting go to focus on what truly matters.
medical team must adopt a multifaceted approach to understanding and supporting them. Beyond ensuring physical comfort, patients frequently encounter psychological, social, and spiritual challenges, making communication with their families vital. Family members serve as essential support for the patient; if they feel anxious and overwhelmed, the situation can quickly become unmanageable.
Dr. Lim highlighted that when families are wellinformed and able to provide adequate support, the atmosphere of grief can become more stable. While emotional fluctuations are natural during illness, being prepared can empower both patients and families to make more thoughtful decisions as circumstances evolve.
Dr. Lim emphasise that “the common perception is that the only solution to illness is treatment. However, from conversations with patients, it is clear that they also value cherishing the present over merely striving for survival. They wish to return home, say their goodbyes to family, and enjoy quality time together. Therefore, palliative care is not about giving up; it’s about letting go to focus on what truly matters.” He further noted that seriously ill patients may lose their autonomy, and their inner voices can often be overlooked, and that palliative care is not a choice between treatment and comfort: “Even while receiving treatment, issues related to physical comfort and family time can be incorporated into the care plan.”
Many patients, in addition to dealing with physical pain, also face psychological and spiritual challenges. Doctors play a vital role in providing essential information and creating a safe, supportive environment for patients and their families to reflect on their thoughts and feelings. For example, patients who are usually active may question why they are experiencing illness despite their disciplined lifestyles, while others might grapple with religious or spiritual concerns. While physicians may not have all the answers, connecting patients with relevant support groups can be beneficial. In cases of complex psychological issues, a psychologist or medication may help.
Dr. Lim said that there is a misconception that only cancer patients require palliative care. In reality, although cancer patients do indeed benefit from more extensive palliative support, data from Malaysia indicates that the majority of patients in need are those with non-cancer conditions. Approximately 30% to 40% of these patients suffer from frailty, a condition characterised by the gradual deterioration of organ function due to aging, leading to symptoms such as weight loss, fatigue, and a reliance on others for feeding. Moreover, patients with organ failures, including renal and heart failure, also require palliative care, with cancer patients comprising only about 10% of the total demand.
Dr. Lim illustrated this with the case of a renal failure patient who, due to age or limited mobility, may decide not to pursue dialysis. In these instances, physicians continue to provide care focused on prolonging kidney function. As the patient’s condition evolves, they may face symptoms like loss of appetite, nausea, and skin discomfort. Palliative care plays a crucial role here, employing medications to alleviate these issues and enhance overall comfort.
Additionally, patients often grapple with uncertainties surrounding future care, changes in their health status, and support from caregivers. During these moments, doctors offer vital information and engage patients in discussions about their treatment preferences, while also involving family members to facilitate preparation for the road ahead.
Embracing Impermanence and Planning for the Future
Dr. Lim maintains a calm perspective on the uncertainties of life. He said, “Life and death are part of the natural order, and one shouldn’t be overly affected psychologically. The most challenging aspect is the tendency to resist; accepting reality and fostering a positive outlook are essential. I do my best to advocate for what can be changed and let go of what cannot. Understanding the value of palliative care and witnessing improvements in patients’ situations is incredibly rewarding.”
Dr. Lim welcomes the launch of palliative care services at Kek Lok Si Charitable Hospital, and recommends a comprehensive approach to enhance these services through the medical system, community support, and volunteer efforts. As the modern healthcare system has yet to fully integrate palliative care, he underscores the importance of fostering public awareness and encouraging individuals to seek tailored solutions. He believes that palliative care is not only a clinical responsibility but also a societal mindset. He advocates for the incorporation of palliative principles into everyday practices within nursing and care facilities, while promoting this understanding across government and the private sector, in medical education, and through community awareness initiatives.
病人或家属必须同意签署 拒绝心肺复苏(Do Not Resuscitate,DNR)吗?
Is signing a Do Not Resuscitate (DNR) order necessary for patients or family members?
不需要。签署DNR并不是接受缓和治疗的前 提。虽然许多接受缓和治疗的患者最终会选择拒绝 心肺复苏,但DNR主要是一种心理准备,帮助他们 在病情严重时保持冷静。No, signing a DNR is not a requirement for receiving palliative care. While many patients in palliative care may eventually choose to refuse resuscitation, the DNR primarily serves as a psychological tool to help them stay calm during critical situations.
缓和医疗是否与宗教有关? 各个种族/宗教是否都能接受
缓和医疗服务?
Is palliative care associated with religion, and can individuals from all backgrounds access these services?
缓和医疗是中立的,所有种族和宗教均可接 受。尽管一些倡导者和机构有宗教背景,但缓 和治疗不涉及宗教元素,重点是尊重患者的意 愿,倾听他们的声音。Palliative care is a neutral approach, accessible to individuals from all races and religions. While some organisations may have religious affiliations, the focus of palliative care is on respecting patients’ wishes and catering to their needs, independent of religious elements.
缓和医疗的费用昂贵吗?
How does the cost of palliative care compare to other treatments?
相较于延命治疗,缓和治疗的费用较低。马来 西亚政府医院医治公民的医疗费用相对便宜,一
些机构还通过慈善团体或公众捐款来减轻患者负 担。Generally, palliative care is more cost-effective than life-prolonging treatments. In Malaysia, medical expenses in government hospitals are relatively low, and some organisations leverage charitable donations to help ease the financial burden on patients.
是否需要医生的转介才能接 受缓和治疗服务?
Do patients need a referral from a doctor to receive palliative care services?
不需要。患者或家属可以主动请求缓和治疗服 务,只需提供足够的医疗信息。No, patients or their families can directly request palliative care services by providing adequate medical information, without needing a referral.
缓和医疗
Palliative Care
病人只能在医院里接受缓和 治疗吗?出院后是否可以在 家继续接受服务?
Is
palliative care only available in hospitals, or can it continue at home after discharge?
缓和医疗以患者的意愿为主。大约80%的患者 希望在家中接受照顾,只有20%的患者认为在医 院更好。因此,我们提倡提供社区服务,定期访 问患者家中。Palliative care is centred around the patient’s preferences. Approximately 80% of patients express a desire to receive care at home, while only 20% prefer hospital settings. Therefore, we advocate for community-based services that include regular home visits for ongoing support.
Q & A
医 者
谈 心
改变健康观念:
应对马来西亚的慢性疾病危机
Reframing Health Perspectives: Tackling the Chronic Disease Crisis in Malaysia
曾婷婷
DR. WENDY CHEN TYNG TYNG
内科 专科医生
39岁 ● 来自双溪大年,育有一名小孩 ● 毕业于双溪大年Sekolah Menengah Kebangsaan Ibrahim,尔后就读于莎亚南Universiti Teknologi MARA(UiTM) A-Level ● 之后获得公共服务 局(JPA)奖学金送往印度 Kasturba Medical College 修读医学系 ● 回国后分别在沙巴哥打京那 峇鲁Hospital Queen Elizabeth以及沙巴拿笃 (Lahad Datu)政府医院服务多年 ● 2015年12月转 至槟城中央医院服务,并于2018年考获内科专科 ● 2024年6月加入极乐寺慈善医院
Non-Communicable Diseases (NCDs), or chronic diseases, are often long-lasting and their early symptoms are subtle and may go unnoticed. Metabolic Syndrome, characterised by high cholesterol (hyperlipidaemia), high triglycerides, high blood sugar, high blood pressure (hypertension), and obesity, significantly elevates the risk of heart disease, stroke, and diabetes. Recently, the increasing prevalence of hyperlipidaemia, hypertension, and obesity among younger populations has raised concerns, highlighting the urgent need for improved public health management.
Dr. Wendy Chen Tyng Tyng harboured a childhood dream of becoming a physician, which she eventually fulfilled with a specialisation in internal medicine. A high-achieving student, she received a Jabatan Perkhidmatan Awam (JPA) scholarship to pursue her medical studies in India. The initial culture shock from the differences in language, environment, and dietary practices were a challenges, but with the support of fellow Malaysian students and the enriching experiences, she gradually adapted to her new surroundings.
Dr. Chen reflected, “My college had two branches, and the city we were assigned to had very few Malaysians; we were among the first cohort of
students there. My classmates were all locals, and while everyone spoke English, their strong accents often made comprehension challenging. During my first year in anatomy, I lived in a dormitory right above the classroom, which was quite daunting for me but typical for the locals. Our meals consisted primarily of chapati (Indian flatbread) served with curry. We once visited a Chinese restaurant and ordered stirfried vegetables, only to receive vegetable purée instead. After moving out of the dorm in my second year, I began cooking for myself and this resolved my dietary challenges.”
After completing four and a half years of medical training, Dr. Chen undertook a year-long internship at a local hospital. She remarked, “The greatest challenge in the local hospital was the language barrier, as many dialects were spoken. We also frequently travelled to rural areas, which felt like stepping into a Bollywood movie, riding local buses with loud music playing inside. The countryside we visited was picturesque, located near the coast.”
Dr. Chen also observed that in rural areas many patients sought medical attention only when their conditions had worsened, with symptoms that aligned with textbook descriptions. In contrast, patients in developed cities tended to seek care earlier, resulting in less pronounced symptoms.
After returning to Malaysia, Dr. Chen was assigned to a government hospital in Sabah and later worked at the Lahad Datu government hospital. She reflected, “My six months in the emergency department made it clear that emergency medicine was not the right fit for me. The pressure was intense, and I often found myself too busy to write patient reports until after my shift, particularly during the conflict between Malaysian security forces and armed militants from the Philippines when I dealt with
During the COVID-19 pandemic, many middle-aged patients aged 40 to 50 experienced respiratory difficulties and heart failure related to obesity and died.
numerous gunshot cases.” Dr. Chen also noted, “My boyfriend was in the internal medicine department, preparing for his specialty exams, and the doctors there provided invaluable guidance. Eventually, I was transferred to the same department, which led me to specialise in that field.”
Enhancing Awareness for Chronic Disease Prevention
Lack of public awareness and education about health often result in delayed medical attention.
During her tenure at the government hospital in Sabah, Dr. Chen noted that natives living in remote areas frequently face lengthy journeys—sometimes several hours—to reach the nearest hospital, leading them to seek care only after their conditions have worsened. Additionally, some of them believe that if they are feeling well, there is no need to seek medical consultation, thereby overlooking any potential early symptoms.
Dr. Chen pointed out that many people harbour misconceptions about Western medicine and pharmaceuticals, fearing that initiating treatment would lead to lifelong medication. With health issues such as hyperlipidemia, hypertension, and obesity becoming more prevalent among youths, including high school students, the importance of regular health check-ups cannot be ignored, so that any health risks can be identified early.
Patients with Metabolic Syndrome often have multiple conditions, including high cholesterol, fatty liver, high blood sugar, hypertension, and obesity, all of which will significantly increase their risk of heart disease, stroke, and diabetes. Dr. Wendy emphasised that the impact of chronic diseases extend well beyond the patient; they can profoundly affect families and society as a whole. For example, if
The optimal approach to tackling obesity is a dual strategy that incorporates both medication and lifestyle changes. Nutritionists also play a vital role, designing personalised dietary plans for patients and educating them on healthy eating and positive lifestyle practices.
a middle-aged patient suffers a stroke and becomes paralysed, the family loses a key financial supporter, while members face the additional burdens of caregiving and long-term medical expenses.
Currently, more than 54% of Malaysia’s population are overweight or obese. This is an urgent health concern. The primary contributors to obesity include an unhealthy lifestyle and dietary habits, such as overeating, sedentary behaviour, and lack of physical activity. While there are ongoing efforts to combat body shaming, obesity poses significant health risks, including hyperlipidemia, hypertension, and high blood sugar, as well as complications like sleep apnea and heart failure.
Furthermore, those with a pre-existing condition who are also obese face substantially increased risks. “During the COVID-19 pandemic, many middle-aged patients aged 40 to 50 experienced respiratory difficulties and heart failure related to obesity and died.”
Dr. Chen shared a success story of a diabetic patient who did the right thing. He lost weight and was able to reduce his insulin dosage. He is now able to manage his disease better and lower his risk for complications.
A combination of professional pharmacological treatment and modifications to lifestyle and diet can help patients overcome obesity. Dr. Chen said, “The optimal approach to tackling obesity is
a dual strategy that incorporates both medication and lifestyle changes. Nutritionists also play a vital role, designing personalised dietary plans for patients and educating them on healthy eating and positive lifestyle practices.” Currently, the Kek Lok Si Charitable Hospital has introduced a three-month diabetes management programme aimed at helping patients adopt a healthy lifestyle and dietary habits for the long term.
Dr. Chen noted that developing healthy habits requires time, and the programme will create sustainable plans tailored to each patient’s circumstances. “In this programme, I provide medical advice based on the patient’s blood test results and medication usage, while a professional nutritionist conducts monthly reviews of the patient’s dietary habits. Additionally, patients are required to perform daily blood glucose monitoring at home. Our goal is to achieve at least a 10% weight loss within three months, along with significant improvements in blood glucose control.”
Dr. Chen highlighted that raising public health awareness, maintaining healthy lifestyle habits, and undergoing regular health check-ups are crucial for preventing chronic diseases. For patients already diagnosed with chronic conditions, early medical intervention combined with changes in medication and lifestyle can prevent the disease from worsening.
From Public to Private: Challenges in Healthcare
After years in the medical field, Dr. Chen had her most unforgettable experiences during the COVID-19 pandemic. “During the height of the crisis, I encountered many patients who did not respond to treatment. I had to also help them make phone calls to say their final goodbyes. Simultaneously, I was concerned about bringing the virus home and potentially infecting my family, which added significant pressure. Fortunately, we all managed to get through the pandemic together.”
After years of service in government hospitals, Dr. Chen discovered Kek Lok Si Charitable Hospital and, after careful consideration, decided to make a transition to a new environment. She noted that the numerous departments and strict systems in government hospitals often limit her ability to provide effective patient care. Every day, she had to attend to a large number of patients, frequently leaving her too busy to even take a lunch break, while patients endure long wait times. In contrast, at Kek Lok Si Charitable Hospital, the processes are more streamlined. If a patient requires referral to another specialist, she can quickly facilitate that, ensuring they receive timely care.
Dr. Chen observed that patient conditions differ significantly between government and private hospitals. In private hospitals, she can focus more on educating patients about disease prevention. Furthermore, with a smaller patient load, doctors have more time to follow up on a patient’s progress and gain a deeper understanding of each patient’s condition.
The nursing and healthcare sectors are crucial in today’s society, especially as frontline workers operate under high-pressure conditions that demand quick judgments and actions to save lives. While technology and artificial intelligence continue to advance, the professionalism and compassionate care inherent in nursing remain irreplaceable. In emergency situations, the immediate responses of nursing professionals—rooted in their expertise and experience—cannot be replicated by machines.
A Journey of Compassion and Expertise in Nursing
Sister Teoh Ming Hui boasts over 20 years of experience in nursing. Her decision to pursue a career in nursing was primarily driven by the desire for job stability. She first gained insights into nursing through her involvement with the St. John Ambulance Brigade during high school and frequent visits to the hospital when she had to accompany her ailing mother for medical treatments. This exposure deepened her interest in the profession. Despite her mother’s initial concerns about the possible impact of nursing on her health and the stress of working night shifts, Sister Teoh remained steadfast. Since embarking on a professional nursing career, she has not only gained a wealth of knowledge but has also helped many, including her own family.
After graduating from Lam Wah Ee Nursing College, Sister Teoh was assigned to the Neonatology medical ward. Two years later, she had the opportunity to transition to the neonatal unit, during which she obtained a diploma in neonatal nursing (Neonatal Post Basic). In 2014, she officially became a lactation nurse and assisted Lam Wah Ee Hospital in its application to become a Baby Friendly Hospital. Throughout this journey, Sister Teoh not
only gained extensive specialised knowledge but also found joy in caring for newborns. She noted that her own experience as a mother of a preterm baby has allowed her to truly empathise with the feelings of mothers with premature infants.
Recalling her experiences in the neonatal unit, Sister Teoh described the challenges of caring for many premature infants, some of whom weighed less than one kilogram and were often unable to feed independently. Some may even forget to breathe while asleep. To prevent asphyxiation in such cases, nurses would need to gently wake them. As the discharge date for these babies nears, Sister Teoh and her team would focus on training them in essential skills such as breastfeeding and breathing. Additionally, they also teach mothers how to care for their premature babies at home and manage potential emergencies.
New Challenges and Lifelong Learning
Despite the efforts of the neonatal staff, Sister Teoh had also encountered mothers who voiced their dissatisfaction with them, who felt that as caregivers the nurses did not understand their emotions. Having gone through the experience of giving birth to a premature baby herself, she believes she is better able to understand these mothers’ feelings and be more empathetic.
Sister Teoh highlighted the challenges of working in the neonatal unit, where adults can articulate their discomfort, but infants are unable to communicate their needs. Neonatal nurses therefore must be especially perceptive to the subtle cues from newborns. It is important for neonatal nurses to provide emotional support to mothers. Some women
are particularly vulnerable to postpartum depression, and factors such as breastfeeding difficulties and a lack of understanding from family members can heighten a mother’s stress and lead to emotional turmoil.
Although Sister Teoh has become an expert in the neonatal unit, she remains committed to personal and professional growth. In 2017, she transitioned to the role of a fertility nurse, where she assisted and coordinated care for couples undergoing artificial insemination. In 2022, she decided to leave the institution where she had worked for 17 years to join Kek Lok Si Charitable Hospital (KLSCH), marking the beginning of a new chapter in her career.
A friend who had served at Kek Lok Si Charitable Hospital had encouraged Sister Teoh to explore the opportunity at KLSCH. After careful consideration, she decided to step out of her comfort zone to embrace new challenges and broaden her career horizons. She remarked:
“I believe that individuals should continually invest in themselves and not allow fear of the unknown or the comfort of familiarity impede their progress. I strive to be a role model for my children, showing them through my actions that even at a certain age, one can still forge ahead, continue to learn, and embrace the concept of lifelong learning.”
Collaborative Care in Nursing Transformation
When Sister Teoh joined KLSCH, the ward she now leads was not yet operational, with much of the preparatory work still in progress. Establishing a new department requires managing numerous tasks, and the Director of Nursing was too occupied
身为护士,这是我们的义务 和责任去照顾每一位病人。如
果连护士都害怕,不想面对, 那谁来照顾病人呢?
(1)
(1)张敏蕙护士长正协助医生 跟进病人的病情。
Sister Teoh Ming Hui assists doctors in monitoring patients’ conditions.
(2)张护士长希望她的团队可 以合作无间,一起为病人提供更 好的护理服务。
Sister Teoh envisions her team working collaboratively to deliver better care for patients.
As nurses, it is our duty and responsibility to care for every patient. If we are afraid and reluctant to confront these challenges, then who will be there to care for the patients?
to oversee everything. Other head nurses were also busy with their own responsibilities. Her arrival filled this gap and she played a crucial role in setting up the current ward. The daycare ward unit in charge of Sr. Teoh officially began operations in July last year and primarily serves patients who do not require overnight hospitalization.
When Sister Teoh transitioned into her new work environment, she had to update herself with specialised knowledge. For example, she noted that infant medication dosages differ greatly from those for adults, and management responsibilities were new to her. Despite these challenges, Sister Teoh felt fortunate to have a cohesive and supportive team. Her goal is to foster a collaborative spirit and teamwork. From the outset, she clearly communicated her expectations and encouraged open discussions and effective communication. She is open to making changes as long as the suggestions are wellreasoned. However, when it comes to patient care, she continues to maintain high standards.
In late 2023, KLSCH was called upon to support government hospitals by accepting COVID-19 patients who did not require ventilators. Sister Teoh oversaw the establishment of the hospital’s COVID-19 ward and ensured that it complied with government protocols. She worked diligently to implement the necessary protective measures despite the hospital’s limited resources, with government officials providing oversight and recommendations. She is grateful to the entire hospital team, as nurses from nearly every department remained on standby and ready to assist during that challenging period. She highlighted that teamwork was especially critical at that time:
Sister Teoh believes the communication between caregivers and patients is utmost important. When
dealing with challenging patients, it is essential for a nurse to be able to communicate effectively. As frontline caregivers, nurses often encounter patients who may be emotionally unstable. In these situations, she said nurses should put aside their personal feelings and approach patients with empathy to better understand their needs, communicate effectively and minimise any potential conflicts.
During her time at KLSCH, Sister Teoh has encountered numerous Code Blue emergencies. In these critical situations, team members must respond swiftly. She finds immense satisfaction in witnessing patients progress from illness to recovery and eventual discharge, believing that her contributions genuinely improve their well-being. She considers this to be the greatest reward for a nurse. She is also motivated by the role she can play in educating patients on managing their health post-recovery.
Due to the nature of her work, Sister Teoh is well acquainted with the realities of life and death. She candidly shares that this experience has provided her with a broader perspective on life, as death can happen at any age. This understanding drives her to cherish the present, to give her best in her work, and to live without regrets.
Vision and Dedication in Nursing Promise
During her two years at KLSCH, Sister Teoh is appreciative of the trust and support the hospital administration has shown her team, as well as their openness to feedback and suggestions. The administration also encourages ongoing education to enhance professional skills among staff. Sister Teoh is committed to upholding the core values of the hospital—compassion, commitment, and care— while leading her team to deliver high-quality nursing services and support more patients. She hopes the
administration will expand the hospital’s services and diversify its departments to better meet the needs of patients. As a head nurse, she also believes it is her duty to provide young nurses with adequate training so that the quality of care at KLSCH continues to improve.
As the population ages, the nursing profession continues to see high demand. It is a “secure career” that offers excellent opportunities for professional growth. Sister Teoh would like to encourage more youths to consider joining the nursing profession and to continually enhance their skills as they advance in their careers. She emphasised that nursing is not limited to hospital wards; nurses can leverage their abilities and interests in various areas and seek out a wide range of opportunities in areas such as management, education, clinical research, or patient education.
Madam Lim Peik Ee, now in her seventies, made a personal vow years ago to donate a portion of her savings to charity after turning 70. She spent many years working in Singapore, where she diligently accumulated a significant amount of savings in her CPF (Central Provident Fund). After retiring, she chose to return to her hometown in Penang.
In June of this year, Madam Lim learned from media reports that Kek Lok Si Charitable Hospital was undergoing an expansion project. After contacting the hospital’s welfare department to understand its needs, she generously donated RM350,000—her CPF savings from Singapore—to the Kek Lok Si Foundation. This donation will be used to acquire essential cardiology equipment for the hospital.
While Madam Lim Peik Ee’s name may not be widely recognised, her selfless act of giving has profoundly touched us. She has chosen to remain out of the public eye and has declined interviews, but her generosity speaks volumes. Her decision to donate her hard-earned savings reflects her genuine desire to give back to society with kindness and compassion.
Kek Lok Si Charitable Hospital extends its deepest gratitude to Madam Lim for her meaningful contribution. Her donation will have a lasting impact, benefiting countless patients and families. We hope her inspiring generosity will encourage others to support the well-being of our community.
跨越城市的温暖 吉隆坡前菩提精舍的善信善心
Spreading Warmth Across Cities:
The Generosity of Kuala Lumpur’s Former Bodhi Vihara Devotees
The former Bodhi Vihara in Kuala Lumpur was a Buddhist establishment managed by compassionate devotees dedicated to charity and public welfare. Although the vihara has since closed, these individuals continue to be actively engaged in philanthropic efforts.
In April of this year, a group of these devotees travelled from Kuala Lumpur to Penang, bringing with them a generous donation of RM170,000. This funding will be allocated for the purchase of medical equipment, enhancing the hospital’s service quality and benefiting more patients.
We extend our heartfelt gratitude to devotees of the former Bodhi Vihara for their generous contribution. Their support provides invaluable resources that empower us to uphold our commitment to charitable care within the community.