On July 18, 2025, Kek Lok Si Charitable Hospital (KLSCH) enters its fourth year of operation. Since its establishment in 2021, this non-profit medical institution has gradually transitioned from a community-based primary care provider to a mid-sized specialist centre. With the completion of its Phase II building in mid2025, the hospital is currently undergoing final review by the Ministry of Health—marking a pivotal milestone that will shape its strategic direction moving forward.
Unlike capital-intensive large-scale hospitals, KLSCH has not pursued expansion as a primary goal. Instead, it has advanced methodically through spatial growth, the introduction of specialty services, medical equipment upgrades, and the development of institutional mechanisms - steadily shaping a replicable model for non-profit medical development. Beginning with a five-storey facility, the hospital continues to confront a pressing question: amid limited resources and escalating healthcare demands, how can a non-profit hospital define the rhythm and direction of its own growth?
极乐寺慈善医院首席执行长
Chief Executive Officer of Kek Lok Si Charitable Hospital
The hospital’s development pathway stands in marked contrast to conventional private healthcare institutions. The Phase II expansion project, launched in December 2023, culminated in teh addition of three floors over eighteen months — an uncommon achievement within the local healthcare landscape. As Dr. Thor Teong Gee, Chief Executive Officer of Kek Lok Si Charitable Hospital, notes: “Our progress is not driven by large-scale budgets or a singular master plan. Rather, we follow the rhythm of phased resource availability, ensuring the synchronized growth of physical space, manpower, and service delivery — thereby avoiding fragmentation across growth stages.”
The number of consultation rooms has expanded from eight to thirteen, and the number of specialist medical staff is projected to reach fourteen by year-end—twice the number at the hospital’s inception. This spatial expansion has resolved previous bottlenecks in personnel allocation and laid the physical groundwork for an expanded portfolio of specialist services. Under these conditions, the growth of the medical team is no longer constrained by consultation space but has evolved into a practical and strategic undertaking.
Patient data further affirm the effectiveness of this development strategy. In the second year, total patient load increased by over 40% compared to the inaugural year, followed by a further 15% increase in the third year. By the close of the current
We do not see this as an act of charity, but as an institutional distribution of social responsibility.
fourth year, projected growth is expected to reach 60%. This sustained upward trend – driven not by marketing campaigns but by the quality of care and patient trust — reflects the community’s enduring confidence in the hospital’s services.
Expanding Service Capacity and Upgrading Technological Infrastructure
The hospital’s development extends beyond the expansion of clinical personnel; more importantly, it involves a systematic enhancement of medical equipment and technological capabilities. Among the most significant milestones is the establishment of a Cardiac Catheterization Laboratory (Cath Lab), which has empowered the hospital to offer a suite of minimally invasive cardiac procedures, including coronary angiography (angiogram), percutaneous coronary intervention (PCI), and pacemaker implantation.
“Catheter-based procedures are non-surgical and do not require general anesthesia, significantly reducing intraoperative risks and postoperative recovery time, particularly for elderly patients,” emphasized Dr. Thor. The launch of the Cath Lab
has not only strengthened the hospital’s capability in cardiovascular care but also marks a substantive leap forward in its specialist service provision.
Alongside other developments, the installation of magnetic resonance imaging (MRI) and dualenergy X-ray absorptiometry (DEXA) systems has further strengthened the hospital’s diagnostic capabilities in neurology, musculoskeletal health, and bone density assessment. DEXA is utilized not only for osteoporosis evaluation but also for detecting sarcopenia—an important risk factor for falls and functional decline. Complemented by the Fracture Liaison Service (FLS), launched two years ago, the hospital is progressively building a robust framework for preventative care.
The completion of its imaging infrastructure has also unlocked new potential for regional collaboration. With MRI, CT, and DEXA systems now fully operational, the hospital has reached a key diagnostic threshold—enabling it to serve both internal patients and function as a diagnostic support hub for neighbouring healthcare providers.
“Many patients from central hospitals visit us first for imaging before returning to public specialists with completed reports. It saves time and avoids
delays in follow-up care,” explained Dr. Thor. This informal mechanism of resource sharing is gradually positioning the charitable hospital as an intermediary within the regional healthcare network.
Institutional Frameworks and Resource Allocation Mechanisms
The effective distribution of healthcare resources requires robust institutional support. At KLSCH, the non-profit model is sustained not through ad hoc donations or isolated sponsorships, but through a structured Welfare Subsidy system that ensures consistent and equitable financial assistance. Targeting individuals in the B40 and M40 income groups, the fund operates through a streamlined application process – approvals are typically completed within 72 hours, requiring only basic income documentation such as Employees Provident Fund (EPF) statements or EA Forms.
For general patients, the fund offers standardized subsidies. In cases involving complexity or high treatment costs, a special review mechanism may be initiated to ensure that individuals with urgent needs receive sufficient financial support. For instance, if a surgery initially budgeted at RM15,000 incurs unforeseen expenses due to complications or extended hospitalization, the fund can be flexibly adjusted to provide additional assistance as needed.
affordable rate of RM2,900—without transferring capital costs to patients. For those who continue to face financial hardship, the Welfare Subsidy fund provides additional support, ensuring that resources are allocated to those with the greatest need.
“We do not see this as an act of charity, but as an institutional distribution of social responsibility,” emphasized Dr. Thor. The core of the system lies in ensuring predictability and equity in resource allocation—structuring philanthropic intent into a sustainable operational model, while mitigating the irregularities and imbalances that often accompany ad hoc charitable acts.
Preventive Governance and Regional Synergy
Cataract surgery offers a clear illustration of this mechanism in practice. As the surgical equipment was acquired through charitable donations, the hospital is able to offer the procedure at an
KLSCH’s development strategy has progressively expanded from curative services to encompass preventive care and regional integration. As the paradigm of long-term care continues to take shape, the hospital is deepening its early intervention efforts for geriatric patients – offering anticipatory services such as DEXA screening, nutritional assessments, and rehabilitation planning.
极乐寺慈善医院致力于为社区打造一 个病患可以依靠的健康支持系统。
KLSCH is committed to building a healthcare support system that patients can truly rely on.
“Many elderly patients are hospitalized due to falls or minor infections. After just a few days of bed rest, they begin to lose muscle mass—recovering from the illness but suffering a loss of functional independence,” explained Dr. Thor. “Preventive intervention is not only more cost-effective than post-incident treatment; it is also more aligned with patients’ long-term well-being.”
In addition, the hospital has increasingly taken on the role of a regional resource support platform, helping to ease scheduling pressures for imaging services at both public and private hospitals. It is also proactively exploring institutional models for postoperative rehabilitation, chronic disease management, and long-term care. This progression not only addresses the specific healthcare needs of targeted communities but also positions the charitable hospital as a critical node within the broader healthcare ecosystem—facilitating resource integration and optimizing service pathways across institutions.
Building Institutional Depth in Charitable Healthcare
The viability of this development model hinges on the synchronized advancement of multiple components: calibrated pacing of spatial and infrastructural growth, steady expansion of a qualified professional workforce, systematic enhancement of diagnostic capacity, phased realization of regional collaboration frameworks, and the formalization of an equitable subsidy system. Key indicators – including rising patient volumes, increasing physician numbers, and the diversification of service offerings – demonstrate the model’s practicality and success in real-world implementation.
As Dr. Thor observed, “Our goal is not merely to build a hospital, but to establish a healthcare support system that instills trust and stability within the community.” At its core, this system is not defined by charitable giving, but by the institutionalization of social resources and the standardization of care delivery. Within the existing healthcare landscape, it forges an intermediary space that harmonizes human-centred values with professional efficiency.
Over the past four years, the development of KLSCH has not simply been a story of physical expansion or facility upgrades. Rather, it charts an institutionalized, strategic, and traceable path of healthcare advancement. This evolution is neither propelled by capital-driven growth nor based on a benevolence-driven model of charity. Instead, it embodies the construction of a sustainable, professional service framework – carefully built within the constraints of limited resources.
医者谈心
耳鼻喉医疗的初心与实践
From the Details Up: Foundational Values and Real-World Practices in Otorhinolaryngology
黄 种 贤
DR. (MR.)
SHAUN NG CHONG SIAN
耳鼻喉及头颈内外 专科医生
Consultant Ear, Nose, and Throat (Otorhinolaryngologist), Head & Neck Surgeon
37岁
从小在雪兰莪长大,后来在吉 打 AIMST University 就读医学系
毕业后被派往沙巴哥打基纳巴 鲁中央医院 (Queen Elizabeth Hospital) ,期间曾在古达 (Kudat Hospital) 服务两年,总 共在沙巴待长达8年的时间
从马来西亚国立大学 (Universiti Kebangsaan Malaysia, UKM) 硕 士毕业后被派往巴生 (Hospital Tengku Ampuan Rahimah Klang, HTAR) 服务3年
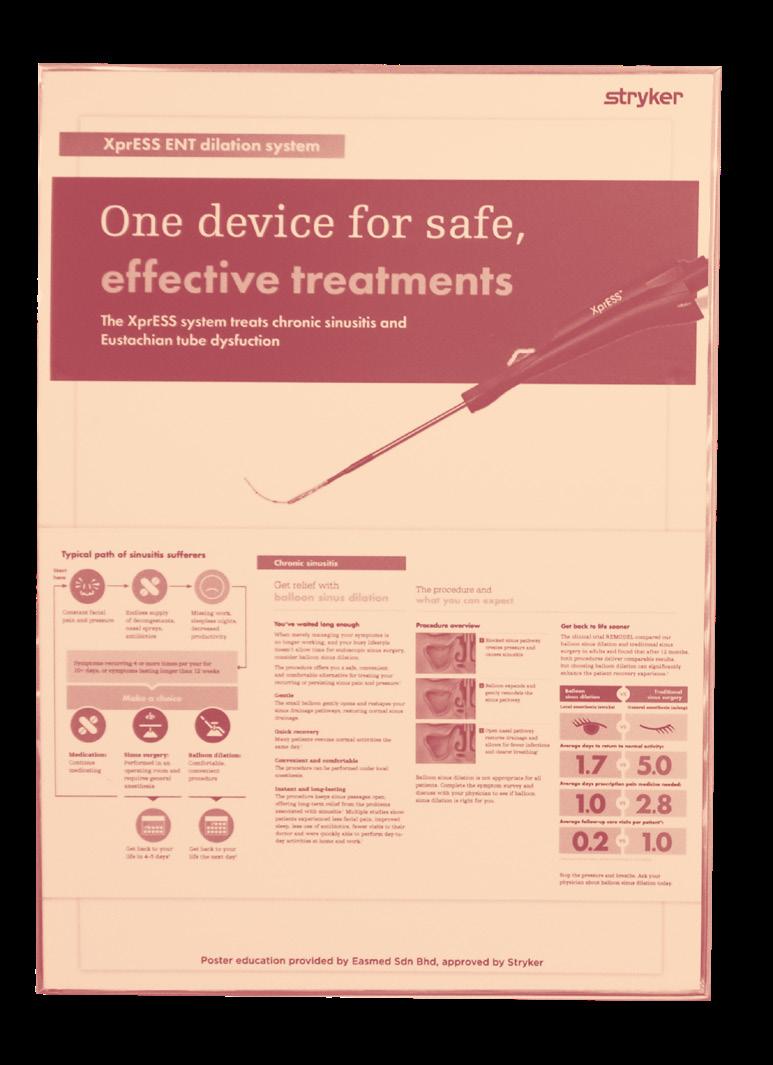
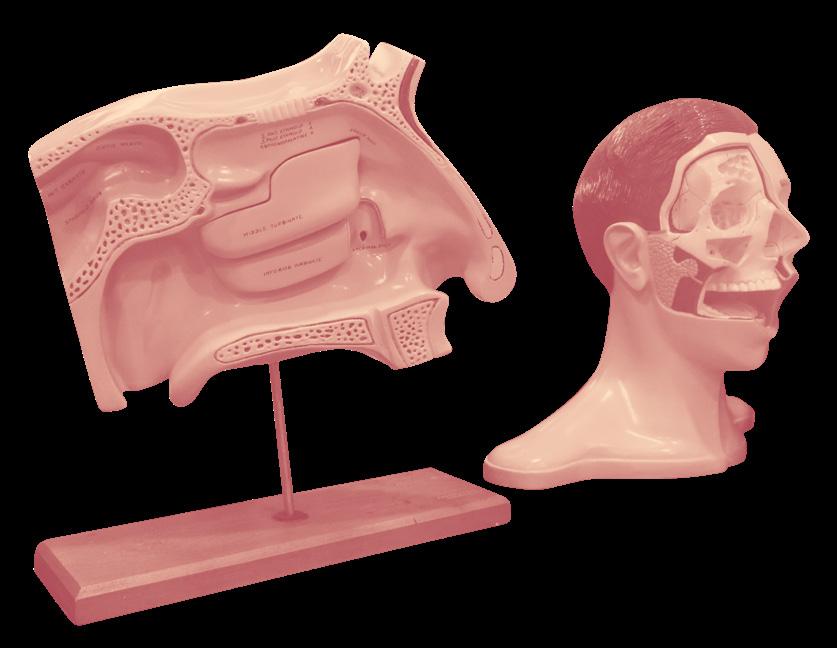
The ear, nose, and throat system governs our senses of hearing, smell, and taste – functions essential not only to basic physiology but also to the richness of everyday life. A soothing melody can ease emotional tension, while a fragrant, flavourful meal can offer moments of comfort and joy. Since many ear, nose, and throat conditions are not immediately life-threatening, they are often deprioritized in personal health management. However, nasopharyngeal cancer ranks among the most common cancers in Malaysia, with many patients diagnosed only at advanced stages – well past the optimal window for treatment. Raising public awareness about ear, nose, and throat health can promote earlier symptom recognition and timely medical intervention, ultimately improving recovery prospects and enhancing quality of life.
Dr. Shaun Ng Chong Sian’s earliest encounters with the medical field were shaped by his mother, a nurse, whose influence left a lasting impression. From an early age, he grew to understand the responsibilities and mission that physicians bear, and developed a deep respect for their ability to alleviate suffering. As a teenager, he resolved to one day join the medical frontline – to be a doctor who brings hope.
Despite his clear ambition, the path to medicine was far from easy, especially specialist training, which demands long-term dedication and perseverance. Reflecting on his academic journey,
Did you know that the smallest bones in the human body are actually located in the ear?
Dr. Ng shares, “The pressure was intense, but my passion for medicine helped me find a sense of achievement and fulfillment throughout the process.”
After completing his medical degree, Dr. Ng began his internship at Central Hospital in Kota Kinabalu, the Sabah’s state capital, before being posted to Kudat – a remote town in northern Sabah nearly a three-hour drive from the city. At first, he was not particularly enthusiastic about this deployment. However, a surgical specialist who had previously served at Kudat encouraged him to embrace the opportunity, sharing that “It would be an unforgettable experience.” That assurance gave Dr. Ng the conviction to accept the posting – a decision that would profoundly shape his clinical growth.
transfer to Kota Kinabalu Central Hospital often missed the critical lifesaving treatment window due to distance.
“During that time, whether it was internal medicine, surgery, pediatrics, or obstetrics, we all had to take turns managing every case,” Dr. Ng recalls. He faced various urgent situations—from assisting police with postmortem examinations, to performing immediate surgeries for acute appendicitis, to handling complicated deliveries such as emergency cesarean sections and ruptured ectopic pregnancies causing severe hemorrhage. Without specialist support, he and his team had to rapidly assess and act fast to save lives. Fortunately, most patients pulled through.
That chapter proved a defining moment in Dr. Ng’s professional development. He reflects, “During those two years in Kudat, I frequently faced life-and-death decisions. Some cases demanded immediate surgery – any delay could mean the patient wouldn’t make it. That period transformed me from a nervous young doctor into one with growing experience and confidence, honing my ability to make independent judgments and swift interventions.” He also notes that the local nurses’ rich experience and the strong spirit of teamwork among doctors were vital in overcoming these challenges. “Seeing patients who arrived on the brink of death and later walked out of the hospital – that was an indescribable sense of fulfillment.”
As in many small-town hospitals in Malaysia, resources at Kudat were limited. With only seven to eight doctors on rotating duty and no resident specialists, emergency or critical cases that require
By the end of his two-year service, Dr. Ng had grown fond of life in Kudat. He smiled, “Kudat is a small town,” he smiled. “People are warm and friendly. People on the street know who you are, and I gradually adapted to the local slower pace of life and hospital’s rhythms.”
This experience also sparked his keen interest in surgery. He observed that surgical treatment often brought rapid improvement to patients’ conditions—“For example, acute appendicitis, once operated on promptly, allows patients to recover and be discharged within a few days.” He developed a particular fondness for delicate minimally invasive procedures, and ear, nose, and throat (ENT) and head and neck surgery stood out as specialties requiring exceptional focus and fine technical skills. Ultimately, he chose to pursue further specialization in ENT and head and neck surgery.
Signals Too Often Ignored: Understanding Ear, Nose, and Throat Health
“Did you know that the smallest bones in the human body are actually located in the ear?”
While people typically seek prompt medical attention for vision problems, they often delay or dismiss issues like nasal congestion or hearing loss in one ear. According to Dr. Shaun Ng Chong Sian, this stems from a widespread perception that ear, nose, and throat (ENT) conditions are rarely serious or life-threatening – yet such assumptions can prove costly. Left untreated, early symptoms may evolve unnoticed until the optimal treatment window has passed.
“Nasopharyngeal cancer is one of Malaysia’s most common cancers,” he explains. Tumors often emerge behind the nasal cavity near the Eustachian tube, causing middle ear fluid accumulation and resulting in hearing loss on one side. Besides hearing changes, recurrent nosebleeds, persistent nasal blockage, double vision, and neck lumps may
also signal the presence of nasopharyngeal cancer. “Regrettably, nearly 70% of patients are diagnosed at an advanced stage,” he cautions, urging the public to remain vigilant and seek timely examinations.
In clinical practice, common ENT conditions Dr. Ng frequently encounters include sinusitis, allergic rhinitis, ear blockage, and tonsillitis. Many of his patients at Kek Lok Si Charitable Hospital are elderly, some experiencing chronic dizziness due to inner ear balance disorders. Although these symptoms may not be severe, dizziness-related falls among seniors can lead to fractures and subsequent complications such as pneumonia, which must not be overlooked.
Another condition that often flies under the radar is obstructive sleep apnea (OSA). Patients with OSA experience repeated breathing pauses or shallow breaths during sleep, resulting in poor sleep quality. They often feel fatigued, suffer headaches, and experience daytime sleepiness. Over time,
this may increase the risk of chronic conditions like hypertension. Dr. Ng advises anyone with suspected sleep disturbances to seek early medical assessment and care.
“Some patients grow so used to their discomfort that only after treatment do they realize what they were missing,” he shares. One young patient, who had long suffered from nasal congestion due to a nasal septum deviation, described experiencing effortless breathing for the first time after surgery. Dr. Ng emphasizes that any deviation from normal health should never be ignored. Prompt medical consultation is crucial to prevent seemingly minor ailments from escalating into more serious health problems.
The Healing Power of Doctor-Patient Dialogue
Although Dr. Shaun Ng Chong Sian grew up in the Klang Valley, he has developed a special affection for Penang. With many family members and friends residing there, he is familiar with the city and has grown fond of its pace of life through frequent visits. After careful consideration, he decided to settle in Penang to pursue his ideal of achieving a work-life balance—allowing him to devote himself fully to medical practice while also being present for his family.
His decision to join Kek Lok Si Charitable Hospital was shaped by more than geography or lifestyle – It was also rooted in alignment of values. The hospital’s mission resonated strongly with his belief that the role of a physician is not limited to treating physical symptoms, but encompasses care for the patient as a whole: physiologically, psychologically, and even spiritually. “When patients
fall ill, the issue often goes beyond the physical. It may involve psychological stress, family dynamics, and more. Therefore, doctors should provide holistic care—that is, comprehensive attention to body, mind, and spirit.”
Reflecting on his experience in government hospitals, he admits that the high patient volume often forces doctors to complete consultations rapidly, leaving little room for meaningful interaction. “We are treating people—individuals with emotions and feelings,” he says with some regret. Under such systems, it becomes difficult for doctors to build genuine connections, and clinical encounters tend to become mechanical. At KLSCH, by contrast, he found a different rhythm—one that allows time for conversation, understanding, and the gradual cultivation of trust.
“I recently saw a patient who had been anxious and suffering from insomnia due to ear problems. He had previously been treated at a government hospital where tests were arranged, but the wait time was four months,” Dr. Ng recalls. “Here, I could take the time to explain his condition and reassure him. When he left, he told me he’d finally be able to sleep well that night. In that moment, I truly felt I’d done the right thing.”
attributed to medication or surgery; rather, communication and interaction between doctor and patient account for up to 80%. “It’s through listening, empathizing, and building understanding that we can help patients move past the fear and uncertainty illness often brings.”
Medical Practice Rooted in Compassionate Commitment
Since joining Kek Lok Si Charitable Hospital a few months ago, Dr. Shaun Ng Chong Sian has been struck by the warmth and collegiality of the team. Both clinical and administrative staff demonstrate a strong spirit of cooperation. He smiles as he says, “Waking up each day knowing I am going to work is a joy. I truly enjoy communicating with patients and feel fortunate to effectively help them resolve their issues. Seeing them leave with a sense of relief and a smile brings me the greatest satisfaction.”
He also values the hospital’s provision of relatively affordable medical services, which allow patients with limited financial means to receive appropriate care. For those facing genuine hardship, patients can seek assistance through the Kek Lok Si Foundation. “Here, doctors do not have to carry excessive financial burdens and can fully focus on patient care. That means a great deal to me.”
He further emphasizes that treatment effectiveness does not rely solely on the 20%
Looking ahead, Dr. Ng is committed to further honing his clinical skills and hopes that, when resources allow, the hospital will be able to invest in more advanced equipment. Doing so, he believes, will enhance diagnostic accuracy and efficiency— helping even more patients reclaim their health and renew their hope.
眼科医学的温度与深度
Vision and Horizons: The Sensibility and Depth of Ophthalmology
杜 施 瑾
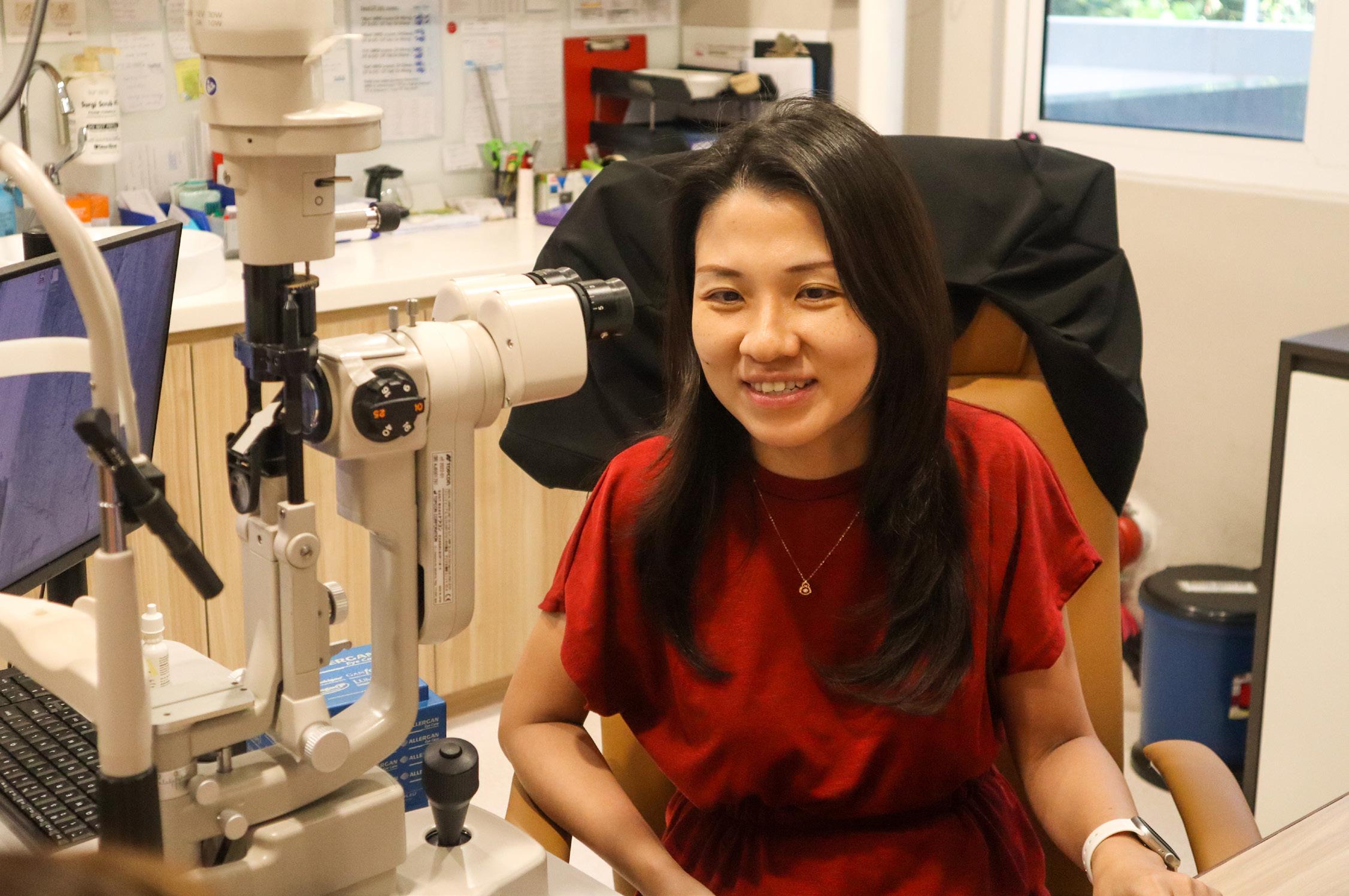
DR. DIANA TOH SHI JIN
眼科 专科医生
Consultant Ophthalmologist
39岁,槟城人
毕业于槟城槟华女子中学,获 得公共服务局(JPA)奖学金远 赴俄罗斯莫斯科 RSMU (Russian State Medical University) 修读 医学系
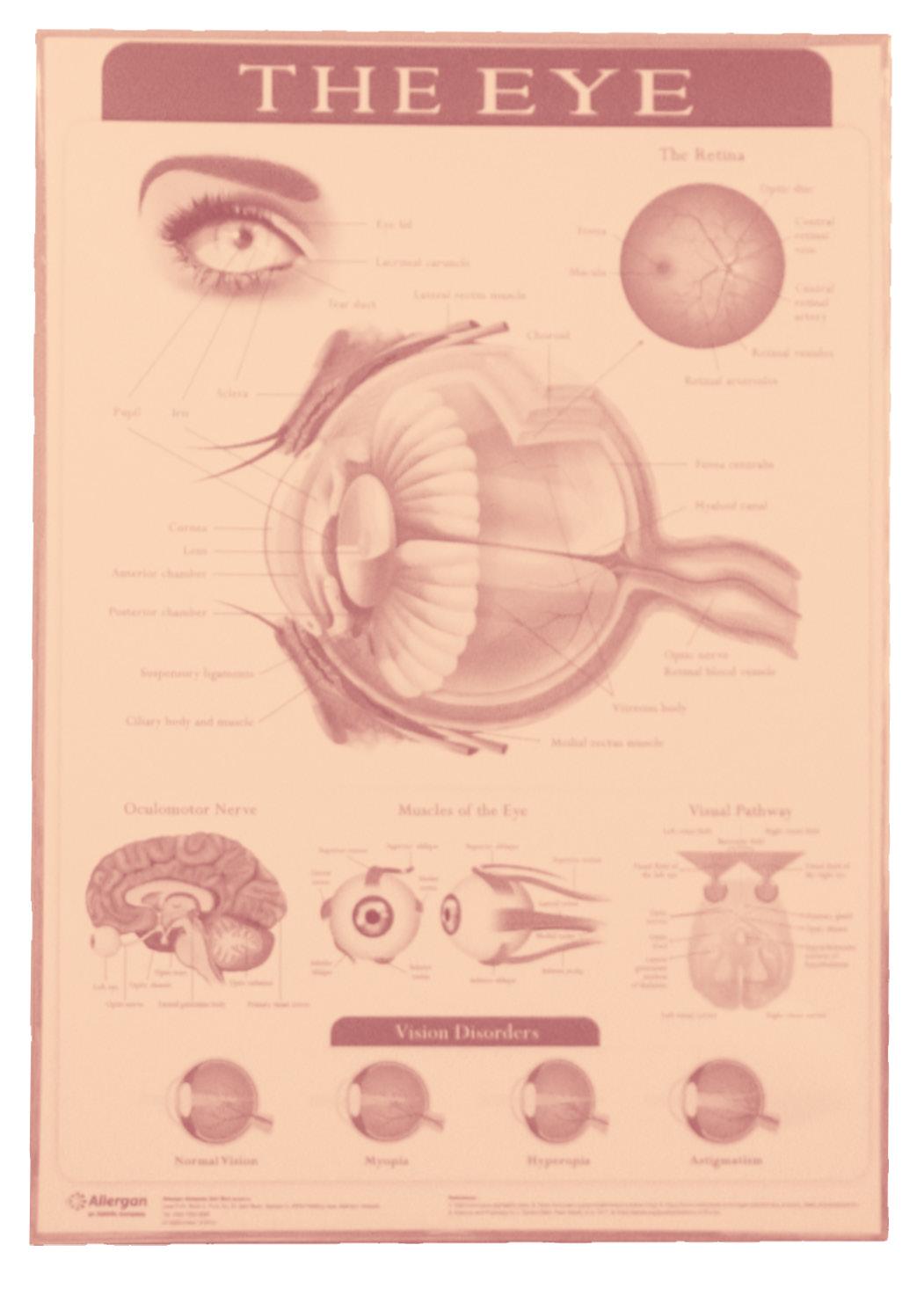
Common ophthalmic conditions, such as cataracts, diabetic retinopathy, glaucoma, and age-related macular degeneration, often present with subtle early symptoms that can easily lead to delayed diagnosis and treatment. Therefore, regular eye examinations are crucial for middle-aged and elderly individuals, as well as for patients with diabetes. These check-ups are essential for the early detection of abnormalities and facilitate timely intervention and treatment.
Dr. Diana Toh Shi Jin’s journey into medicine began during her secondary school years, when she joined the St. John Ambulance Brigade. That early exposure sparked a lasting aspiration to become a doctor. After graduating from high school, she was awarded a Public Service Department (JPA) scholarship to pursue her medical degree in Russia. Faced with the challenges of language barriers and cultural differences, she admits she once hesitated between “chasing her dream” abroad and staying in Malaysia for local preparatory studies. Ultimately, she chose to step beyond her comfort zone. “My family was understandably worried—I had grown
up sheltered and had never lived on my own. But that experience taught me independence and helped me discover who I really was.”
During her six years in Russia, she adapted to the harsh winters, homesickness, and the rigors of medical training. The first three years of her program were conducted in English, but the latter half required fluency in medical Russian for clinical rotations and coursework. At times, she also encountered subtle discrimination from some older locals, which added emotional strain. Still, she views the experience as a formative chapter in her life.
Upon returning to Malaysia, Dr. Toh began her internship at a government hospital. As someone with severe myopia—over 1,000 degrees—she underwent LASIK surgery toward the end of her training. “Without glasses, I could barely see,” she recalls. “Once, when my glasses broke in Russia, I was completely immobilized.” The transformation after surgery was profound: “It felt like the world had become bright again.” That personal experience of restored vision deepened her interest in ophthalmology.
After completing her internship, she was accepted into the ophthalmology master’s program at Universiti Sains Malaysia (USM) in Kelantan—a four-year commitment. The decision was not without sacrifice. “My family and children were in Penang, but the training required me to be based full-time in Kelantan,” she shares. With her parents’ unwavering support in caring for her children, she took on the challenge of commuting nearly every weekend. Despite the academic demands and the added strain of pandemic-related travel restrictions, she persevered. “My career matters
deeply to me, but so does my role as a mother. The journey was tough, but it solidified my commitment to this path.”
Hidden and Overt Signs in Ophthalmology
Progressive blurring of vision or a decline in sight in one eye are symptoms that are often overlooked—yet they may be early warning signs of serious conditions such as glaucoma or retinal disease. Delayed diagnosis can lead to irreversible vision loss. “In many cases,” explains Dr. Diana Toh Shi Jin, “when one eye begins to blur, patients may not notice the problem because the other eye compensates. Daily life continues as usual, and the severity goes undetected.”
She especially urges diabetic patients to remain vigilant. Diabetic retinopathy is one of the leading causes of adult blindness. In its early stages, it may involve only minor retinal microvascular leakage—often without any symptoms. But as vascular blockage and oxygen deprivation worsen, the retina begins to form abnormal new blood vessels. These fragile vessels are prone to rupture and bleeding, which can result in permanent vision loss. Because central vision is typically unaffected in the early phase, many patients only seek help when their sight has already deteriorated—by which time the optimal treatment window may have passed. Dr. Toh strongly recommends that all diabetic patients undergo annual eye examinations to enable early detection and timely intervention.
Glaucoma is another highly insidious condition. “It first affects peripheral vision,” she explains. “The visual field gradually narrows, like a slow inward
collapse, until only a small central area remains.”
Many patients are unaware of the change—until it affects daily activities. “Some may not notice a car in their blind spot while changing lanes, assuming the road is clear. That’s when it becomes dangerous.”
Those with a family history of glaucoma are at higher risk, and Dr. Toh advises individuals over 40 to have yearly eye exams—especially those previously flagged as “glaucoma suspects.”
With the widespread use of digital devices, prolonged screen time has become a major contributor to eye strain. Dr. Toh recommends practicing the “20-20-20” rule: every 20 minutes, look at something 20 feet (about 6 meters) away for at least 20 seconds. This simple habit helps reduce fatigue and gives the eyes a chance to rest. She also emphasizes maintaining proper lighting and reading distance, and suggests using artificial tears to relieve dryness when needed. If symptoms such as dry eyes, visual fatigue, or headaches persist, she advises seeking medical attention early to avoid complications.
Reflecting on her clinical journey, Dr. Toh shares two patient stories that left a lasting impression.
The first was an elderly woman whose cataracts had rendered her nearly blind. Financial hardship had delayed her treatment for years. With the hospital’s support, she finally underwent surgery. At her follow-up visit, she beamed with joy: “For the first time, I can clearly see my granddaughter’s face.”
That moment deeply moved Dr. Toh. “Restoring sight isn’t just about vision—it’s about restoring warmth, connection, and hope.”
The second patient was an elderly gentleman from Balik Pulau who had long relied on family members to accompany him due to cataractrelated vision loss. After successful surgery, he smiled and said, “Now I can go to the market by myself.” A simple statement—but one that struck a chord. “The true meaning of charitable healthcare often lies in these quiet, everyday moments,” Dr. Toh reflects. “It’s not just about restoring sight—it’s about helping people reclaim their independence and dignity.”
From Institutional Service to Patient-Centered Care
“Joining Kek Lok Si Charitable Hospital was one of the most meaningful decisions of my life,” reflects Dr. Diana Toh Shi Jin, describing her transition from the public healthcare system. After years of service in government hospitals, she had long hoped to continue her medical practice in a setting rooted in community engagement and charitable values. The hospital’s guiding philosophy—“people-centered, serving the public”—deeply resonated with her, revealing the possibility of integrating clinical professionalism with genuine compassion. “It’s rare
to find a hospital that balances medical excellence with empathy. The mission here convinced me that this is truly fertile ground for meaningful medical practice.”
Through this platform, Dr. Toh aspires to apply her expertise where it is most needed—offering high-quality, compassionate care at reasonable costs to underserved communities. “Of course, we can help people in the public system too,” she acknowledges, “but large institutions come with many limitations and layers beyond our control.” She recalls how scheduling surgeries in the past often involved complex, time-consuming processes. In contrast, her current work rhythm allows for greater efficiency: “I can perform surgeries in the morning and continue with outpatient consultations in the afternoon. Every minute counts.”
For Dr. Toh, the most significant difference at KLSCH isn’t just procedural—it’s cultural. “In government hospitals, the pace is relentless, the patient load is heavy, and administrative pressure is high. Here, both the clinical and administrative teams are united by a shared goal: prioritizing the well-being of every patient.” She describes a work environment built on mutual respect and empathy, where patients are not just case numbers, but individuals deserving of understanding and care.
“There’s a warmth to the medical culture here,” she says. “It allows me to adapt treatments to each patient’s unique needs and brings me closer to the kind of doctor I’ve always aspired to be.” For Dr. Toh, ophthalmology is not just about restoring sight—it’s about helping patients reclaim confidence, independence, and dignity. “This philosophy of holistic care is something I hold very close to my heart.”
Building a More Comprehensive Ophthalmology Service Network
Kek Lok Si Charitable Hospital (KLSCH) has long partnered with corporations and nongovernmental organizations to implement medical subsidy programs that ease the financial burden on underserved patients. Dr. Diana Toh Shi Jin believes such cross-sector collaboration is not only meaningful but essential. “Healthcare has never been the sole responsibility of a single institution— it is a shared mission across society. When hospitals, businesses, charitable foundations, and non-profits work together, resources can be more effectively integrated, expanding both the reach and depth of care for those in need.”
She cites the hospital’s cataract subsidy program as a clear example: “It’s a very practical form of support. Once patients regain their vision, they often recover their independence—and in some cases, even return to work. Their quality of life improves dramatically.” Dr. Toh advocates for the continued expansion of such collaborative models, alongside stronger public education to raise awareness of eye health. The hospital also offers targeted financial assistance for patients whose vision loss affects their daily functioning or employment, helping to reduce the cost of surgery.
Looking ahead, Dr. Toh hopes to further strengthen community-based outreach, with a focus on early screening and preventive education. “Many eye conditions can be detected and treated early, preventing long-term damage. I hope we can
理想的医疗
环境不仅止于 “治病”,更应 在日常中提升 公众的视力健 康意识。
An ideal healthcare environment is not limited to treating illness—it also nurtures public awareness and long-term wellness.
expand mobile eye clinics, host public talks on eye health, and build closer partnerships with schools and eldercare homes.”
She also emphasizes that even within a charitable healthcare model, investment in advanced medical equipment and clinical expertise must remain a priority. “I hope we can continue to introduce cutting-edge diagnostic and surgical technologies, so that our ophthalmology services approach international standards.” For Dr. Toh, an ideal healthcare environment is not limited to treating illness—it also nurtures public awareness and long-term wellness. “What I strive for is a healthcare culture that values prevention, promotes well-being, and is grounded in human compassion.”
当 专 业 遇 见 人 性 ——
重 症 护 理 的 日 常
When Professionalism
Meets Compassion: Daily Life in Intensive Care
黄春燕 护士长 / 重症护理 Intensive Care Unit SISTER OOI CHOON YEN
在重症护理(Intensive Care Unit)的第一 线,护士往往是最贴近病人的人。他们不仅与仪 器和数据为伍,更要读懂无法言语的身体讯号— 一个眼神的变化、一口呼吸的异常,都是不容忽 视的讯息。身处重症病房(ICU)多年的黄春燕深 知这种工作节奏与心理强度,她说:“虽然工作很 疲惫,但每当看到病人康复出院,便觉得一切付 出都是值得的。”
On the frontlines of the Intensive Care Unit (ICU), nurses are often the closest observers of a patient’s condition. Their role goes far beyond reading monitors and interpreting data—they must also attune themselves to the body’s unspoken signals: a flicker in the eyes, a change in breathing rhythm, a subtle shift that could mean everything. With years of experience in critical care, Sister Ooi Choon Yen of Kek Lok Si Charitable Hospital (KLSCH) understands the relentless pace and emotional demands of the ICU. “The work can be exhausting,” she admits, “but every time I see a patient recover and walk out of the ward, it feels like every effort was worth it.”
A
Nursing Vocation Grounded in Reality
Sister Ooi Choon Yen is the Head Nurse of the Intensive Care Unit (ICU) at Kek Lok Si Charitable Hospital (KLSCH), bringing with her years of clinical experience and specialized training as a Coronary Care Nurse. After completing high school, she began her career as a ward assistant at Pantai Hospital Penang. When the opportunity arose, she enrolled in a three-year nursing program and became a fully registered nurse.
She shares candidly that her decision to pursue nursing was shaped by practical realities. “At the time, my family faced financial difficulties. Nursing offered a stable career path—it was both a livelihood and a pragmatic choice.” Even while working, she continued to advance her training, completing a coronary care specialty and eventually serving as Head Nurse in the Coronary Care Unit (CCU).
In the ICU, most patients are either unconscious or in unstable condition, requiring round-theclock monitoring of vital signs. “Although we now have advanced monitoring systems that trigger automatic alerts when readings are abnormal, we still conduct hourly rounds,” she explains. “Before every shift handover, we meticulously review and verify each patient’s medical records to ensure nothing is overlooked.”
A Nine-Month Journey to Recovery
Among the many patients she has cared for, one case remains indelibly etched in Sister Ooi Choon Yen’s memory. A 21-year-old man was admitted to the ICU with a rare and life-threatening form of meningitis. His condition was critical. Even with high doses of sedatives, his seizures remained uncontrollable. During one episode, he bit through his tongue, resulting in severe bleeding that required emergency suturing.
“We arranged one-on-one, round-the-clock care,” Sister Ooi recalls. “Each time he seized, the nursing staff had to act immediately—restraining his limbs to prevent self-injury. The entire team was under immense pressure, but no one backed down.”
After three months, the patient miraculously regained consciousness—but with complete memory loss. Slowly, he was weaned off the ventilator and other life-support equipment. By the sixth month, he began to feed himself and recognize written words. And nine months after his admission, he walked out of the ward on his own.
“In that moment,” Sister Ooi reflects, “all our exhaustion and stress found release. That’s why we keep going. That’s why we hold on.”
Witnessing Life’s Fulfillment and Its Imperfections
Since joining Kek Lok Si Charitable Hospital in March 2021, Sister Ooi Choon Yen has stood beside countless patients at critical turning points in their lives. The hospital’s ICU, though limited in bed capacity, primarily serves elderly patients suffering from conditions such as pneumonia and respiratory failure—many of whom require intubation and lifesustaining interventions.
She recalls one particularly poignant case: an octogenarian who had fallen while traveling in Thailand. The accident resulted in a traumatic brain injury and coma. By the time he was admitted, he had suffered extensive intracranial bleeding. Because he had been on long-term anticoagulant therapy, the bleeding proved difficult to control and continued to worsen, making surgical intervention impossible. The medical team focused on stabilizing his condition, but ultimately, the family made the decision to bring him home for end-of-life care.
“We accompanied him home,” Sister Ooi recounts. “We helped remove the medical equipment and stayed by his side in silence, supporting him through his final journey.” She pauses, then adds, “This too is part of intensive care. We witness recovery and rebirth—but we must also learn to face the sorrow that comes with life’s impermanence.”
Mutual Support Among Colleagues
In a healthcare system continually stretched by staffing shortages, the ICU often faces the challenge of operating with limited personnel. Sister Ooi Choon Yen shares that during times of unexpected absences or sudden surges in emergency admissions, her team members consistently step up to support one another. “We all understand the pressures we face, and we share the same purpose. It’s not about obligation—it’s a quiet understanding, a mutual commitment,” she says.
She smiles as she reflects on what keeps her going: “The greatest motivation comes from seeing patients improve and recover. That’s the most direct and meaningful reward.”
To address the ongoing manpower gap, the hospital actively recruits young nurses. Sister Ooi frequently speaks with the younger generation about the value and meaning of the nursing profession. “This job has taught me so much and continues to help me grow,” she says. “And when you’re able to care for your own loved ones with the skills you’ve gained, that sense of reassurance is something few other professions can offer.”
A Human-Centered Vision of Medical Care
Reflecting on her experience at Kek Lok Si Charitable Hospital, Sister Ooi Choon Yen affirms that “people-centered care” is the hospital’s most defining quality. “There are no rigid departmental boundaries here. Wherever help is needed, someone
steps forward,” she says. She recalls a moment when the Emergency Department received two critical cases back-to-back, straining available staff. Without hesitation, nurses from other departments rushed in to assist. “No one was concerned about recognition or reward. In this kind of environment, every day feels meaningful.”
She also appreciates the flexibility and trust extended by hospital leadership, which empowers department heads to adapt to on-the-ground realities and lead with autonomy. Currently, the ICU houses only two beds, but expansion plans are underway to increase capacity—including the ability to care for post-operative cardiac and neurosurgical patients.
Looking ahead, Sister Ooi hopes to pass on the professional knowledge and clinical wisdom she has accumulated to the next generation of passionate nurses. “I want the strength of nursing to continue growing—to reach further, and to last longer.”
聚焦社区健康,
佳能落实社会责任
Canon’s Commitment to Community Health and Social Responsibility
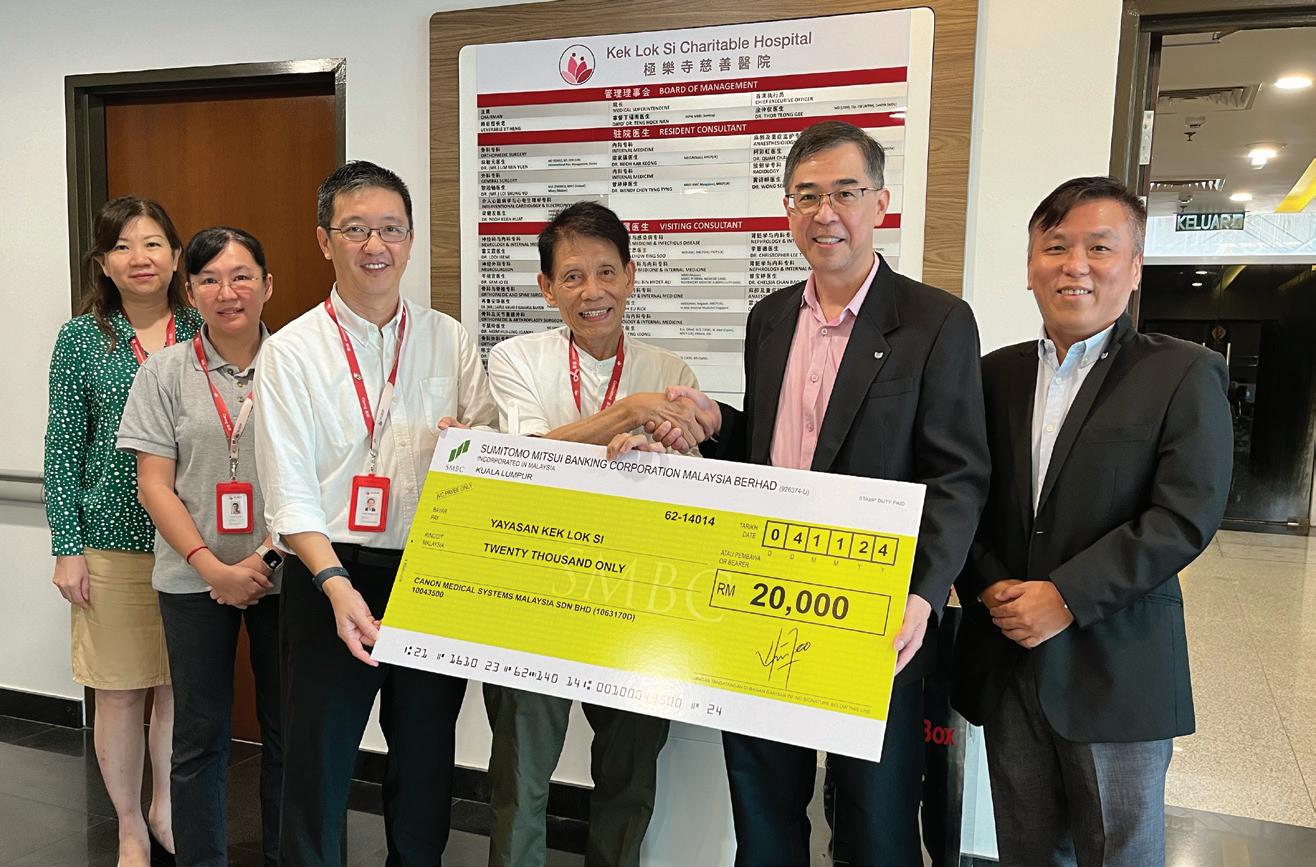
跨国日企 Canon Medical Systems Malaysia Sdn Bhd 于2024年捐 出一笔2万令吉的款项予极乐寺慈善医院。总部位于吉隆坡的 Canon Medical Systems Malaysia Sdn Bhd,此次是首次向极乐寺慈善医院 捐款。该公司总经理 Mr Tan Khoon Eng 接受访问时表示,这也是他 们首次将资金用于慈善用途。
Mr Tan 表示:“我们公司每年都会举办相关活动,以配合 ESG(环 境、社会与公司治理)指标,过去主要着重在环境保护方面,例如种 树等项目。不过,自从新冠疫情爆发后,许多人失去了工作或经济来 源,我们开始意识到有必要支持并协助慈善机构。”该公司于2024年正 式启动慈善捐助计划,而极乐寺慈善医院正是名单中的其中一家。
谈到如何筛选捐助对象时,Mr Tan 表示,最重要的条件是这些 慈善机构确实将善款用于帮助贫困群体。他也补充,这是一项非常 有意义的计划,并期望未来有机会继续推动慈善捐助项目。
In 2024, Canon Medical Systems Malaysia Sdn Bhd—a subsidiary of the multinational Japanese corporation—made its first-ever charitable donation, contributing RM20,000 to Kek Lok Si Charitable Hospital (KLSCH). Headquartered in Kuala Lumpur, this marked not only the company’s inaugural support for KLSCH, but also its first philanthropic initiative.
“This is the first time we are channeling funds toward a charitable cause,” said Mr. Tan Khoon Eng, General Manager of Canon Medical Systems Malaysia. “Each year, our company organizes activities aligned with ESG (Environmental, Social, and Governance) goals. In the past, we focused primarily on environmental efforts, such as tree-planting. But after the COVID-19 pandemic, when so many people lost their jobs or sources of income, we realized the importance of supporting charitable organizations.”
In response to these shifting social needs, Canon Medical Systems Malaysia officially launched its charitable giving program in 2024, with KLSCH selected as one of its first beneficiaries.
When asked about the criteria for selecting recipients, Mr. Tan emphasized that the most important factor is ensuring that donations are genuinely used to support underprivileged communities. “This is a deeply meaningful initiative,” he said, expressing hope that the company will continue to expand its philanthropic efforts in the years ahead.
“There are many in the B40 income group who need assistance,” he added. “The establishment of Kek Lok Si Charitable Hospital is a commendable step forward—it brings tangible benefits to the community. Its affordable medical services help ensure that more low-income patients can access the care they need.”
Mr. Tan also extended his best wishes for the hospital’s ongoing expansion, expressing hope that it will continue to grow and provide essential healthcare services to those who need them most.
“健康长寿,应该是‘健康’而‘长寿’,而不只是活得久。” 涂医生强调,慢性病并非无法逆转,只要及早调整饮食与生 活习惯,仍有机会改善。他以极乐寺慈善医院的减重项目为 例,说明通过生活调养,有患者成功减药,甚至逆转病情。 他以一句话作结:“Today if you don’t take food as medicine, tomorrow you will have to take medicine as your food。(今天 如果我们不把食物当药吃,明天我们就要把药当食物吃。)”
On June 19, Kek Lok Si Charitable Hospital and Dalin Tzu Chi Hospital in Taiwan signed a Memorandum of Understanding (MoU), formalizing a bilateral partnership. The two institutions will engage in ongoing collaboration across several key areas, including clinical medicine, hospital administration, medical education, and humanistic care, with a shared vision of promoting sustainable, compassion-driven healthcare.
The signing ceremony took place at Kek Lok Si Charitable Hospital and was witnessed by Dato’ Dr. Teng Hock Nan, Medical Superintendent of Kek Lok Si Charitable Hospital; Dr. Thor Teong Gee, Chief Executive Officer; Ms. Harriet Shen, Director of Strategy and Planning at The International Medical Centre of Dalin Tzu Chi Hospital; and Dr. Yang Chang-Chen, Orthopaedic Surgeon and Director of Spine Surgery. Also in attendance were Ms. Chen Tzu-Ying, Manager of the International Medical Centre, Dalin Tzu Chi Hospital; Dato’ Simon Wong, Deputy CEO of Buddhist Tzu Chi Merits Society Malaysia and Dato’ Khoo Boo Leong, Commissioner of Tzu Chi Malaysia.
In his remarks, Dato’ Dr. Teng Hock Nan emphasized that although the two hospitals are geographically distant, they are grounded in similar values, both drawing on Buddhist compassion as the foundation of their medical practice. Since opening in 2021, Kek Lok Si Charitable Hospital has advanced steadily despite limited resources—expanding infrastructure, developing specialty services, upgrading medical equipment, and investing in staff training—while remaining focused on providing charitable care for underserved patients.
“Compassion is the core value of our medical mission,” Dr. Teng stated. “This agreement is more than administrative—it is a meeting of shared beliefs.” He noted that Dalin Tzu Chi Hospital’s extensive experience in hospital operations, volunteer systems, and holistic care offers valuable guidance for Kek Lok Si Charitable Hospital as it continues to grow.
“There are times when our progress has felt slow, and we’ve questioned our path—but seeing Tzu Chi’s example reaffirms our direction,” he added. Dr. Teng also stressed that while medical technology is essential, what truly resonates with patients is sincere, compassionate care. For this reason, the hospital places strong emphasis on nurturing the humanistic qualities of its staff, encouraging medical professionals to combine technical excellence with empathy and kindness.
Speaking on behalf of Dalin Tzu Chi Hospital, Ms. Harriet Shen praised Kek Lok Si Charitable Hospital’s quiet yet consistent commitment to delivering quality healthcare across Penang and the surrounding region. She highlighted the alignment between the hospital’s approach and Tzu Chi’s guiding mission: “safeguarding life, safeguarding health, and safeguarding love.”
“Though we are 3,185 kilometers apart, the connection between these two Buddhist hospitals is profound,” she said. “This partnership is not driven by profit, but by a deep resonance of shared ideals.” In each other’s visions and practices, the two institutions have recognized striking similarities—as well as opportunities for mutual growth.
This agreement, witnessed by all present, marks both an institutional milestone and a meaningful extension of the spirit of compassion. Moving forward, the two hospitals will continue their dialogue and practical collaboration, jointly exploring models of care that combine professional rigor with humanistic sensitivity—contributing enduring strength and warmth to the regional healthcare landscape.
极乐寺基金会主席、极乐寺慈善医院管理理
事会主席 CHAIRMAN OF YAYASAN KEK LOK SI AND KLSCH BOARD OF MANAGEMENT
释日恒长老 VENERABLE JIT HENG
极乐寺基金会董事、极乐寺慈善医院院长
DIRECTOR OF YAYASAN KEK LOK SI, MEDICAL SUPERINTENDENT OF KLSCH
拿督丁福南医生 DATO’ DR. TENG HOCK NAN
极乐寺慈善医院首席执行长
CHIEF EXECUTIVE OFFICER OF KLSCH
涂仲仪医生 DR. THOR TEONG GEE
极乐寺慈善医院首席营运长
CHIEF OPERATING OFFICER OF KLSCH
叶爱琴 CONSTANCE YEAP AI KHIM
极乐寺慈善医院首席财务长
CHIEF FINANCIAL OFFICIAL OF KLSCH
周君慧 JANICE CHOW KUAN WAI
极乐寺慈善医院护理总监
DIRECTOR OF NURSING OF KLSCH
柯诗晴 QUAH HSI CHING
极乐寺慈善医院医院负责人
PERSON-IN-CHARGE OF KLSCH
林敏元医生 DR. LIM MIN YUEN
驻院专科医生 RESIDENT CONSULTANTS
骨科专科
ORTHOPAEDIC SURGERY
林敏元医生 DR. (MR.) LIM MIN YUEN
MD (RSMU), MS Orth (UM), Fellowship in Interventional Pain Medicine (Korea)