
She discusses how she started making jewellery and her own experience with loss, as well as how that experience has evolved throughout her life.
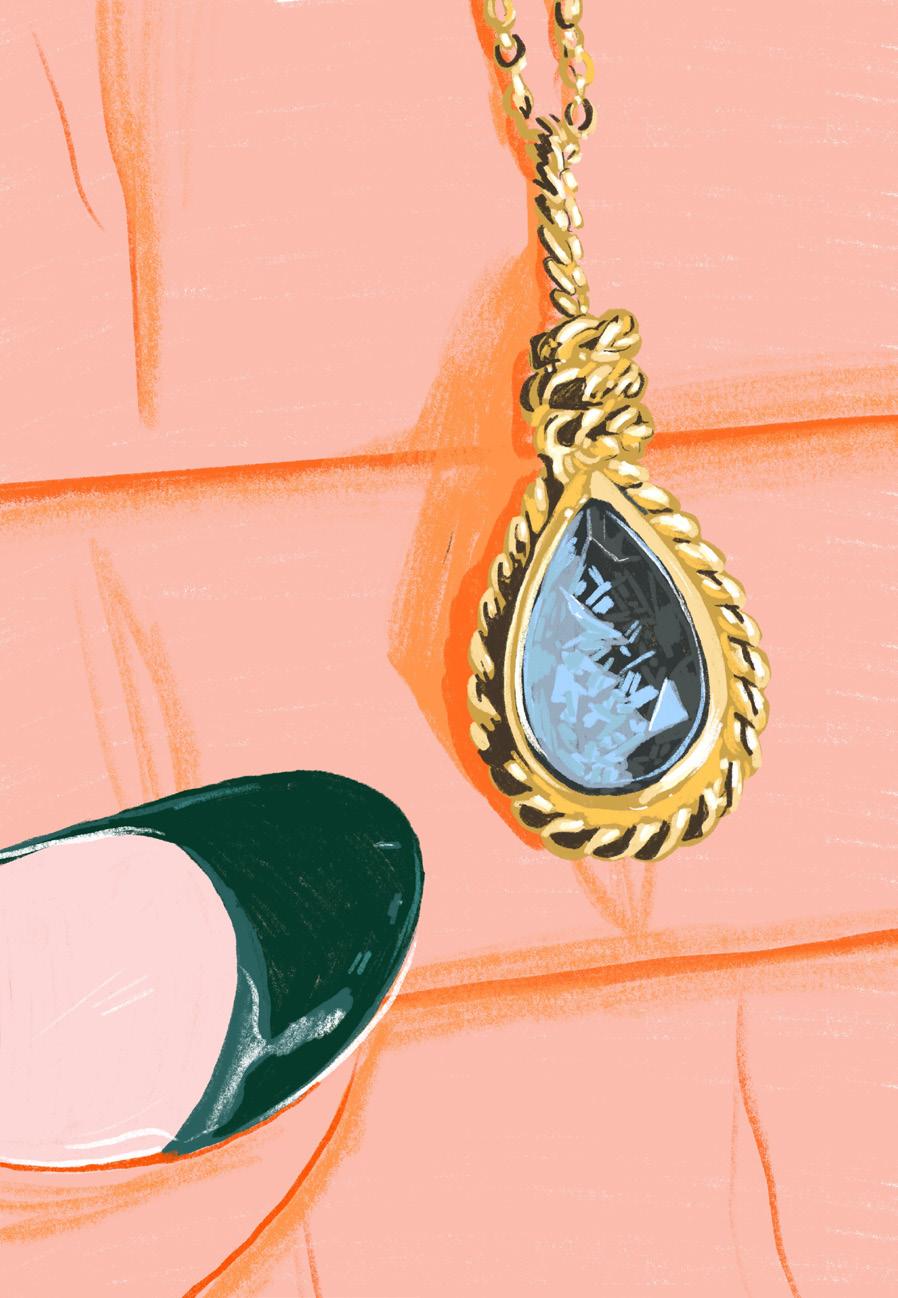
Margaret Cross is an artist who makes love and loss jeweller y Her mourning pieces are created using vintage techniques to preserve mementos of loved ones, often posted on her Instagram accompanied by a story about the memor y.
Margaret uses everything from hair and ashes to love letters and petals to make her designs. In a world of digital photographs and text messages, she creates a beautiful physical way to remember people, places and pets.
MourningwithMargaret
61G rowing Pains

“That night I dragged myself to work a very public event at the Brooklyn Museum. I brushed my hair for the first time in weeks. I spoke to people who didn’t know him or us, or what I was going through. And I had fun. I was distracted and it felt momentous. I kept myself very busy that winter in the jewellery studio. It wasn’t a conscious decision. It also felt like a way of letting friends and fam ily know, ‘I’m ok, I’m working through this’.”
“There is a C.S. Lewis quote , ‘the death of a beloved is an amputation’. That stuck with me, it is not a wound that heals , it’s a new way of learning how to live. I think that’s why I was drawn to jewellery. It’s a physical extension of ourselves.”
62
The first few years without Jamie, Margaret would throw a slice of cake into the r iver on his birthday. Over time it became a ritual which changed shape. She began t aking a bite out of the slice, lowering it into the water and watching it float away. A decade has passed and last year she took her children to the beach, where they swam in the ocean and ate cupcak es instead. “I think the way that tradition has evolved is a nice reminder of my own per sonal gr owth and that time really does heal.”
“I think my earliest memories of mourning jewellery are the hairwork pieces, but more specifically the response to the sight of hair when detached from one’s head. As a particularly hir sute person I’ve always found that r epulsion so interesting! It struck me that hair is so personal and intimate, it’s expressive and it contains our DNA. It’s a beautiful token of love to share with someone.”
After finishing her BFA and wor king full time as an artist’s assistant, she dec ided to post the jeweller y she was making in her spare time on her Ins tagram page. Requests started to pour in and Margaret quit her beloved job of seven years in order to create jewellery full “time.The first mourning pieces I made were for myself. I went through a very per sonal tragedy of losing my best friend Jamie suddenly in 2009. It was an avoidable death, just before the holiday s. I knew that I wanted to gift his family something special, so I went into the studio and made them all memorial necklaces. I was having a hard time interacting with friends and colleagues. I felt responsible and apologetic for their discomfort with my grief. Their woes seemed trivial. I wanted to isolate.”
Whilst studying for a BFA in printmaking, Margaret took a jewellery class as an elective in 2003 and fell in love with lost-wax casting. This is where a wax model is used to make a mould, whic h is then filled with molten metal.
63G rowing Pains

Do you have a favourite piece you’ve worked on? “I love the custom work. It’s not all mourning, I am frequently commiss ioned to create an engagement r ing or wedding band that incorporates the love and loss they’ve experienced in life. There is a particular mourning piec e that comes to mind. A young woman c ontacted me asking to create an ashes reliquary piece for her father who took his own life. She reques ted his ashes be set in a noose. Grieving a stigmatised death such as suicide or an overdose can be especially hard. I tend to lean on the denial side of things s o I deeply admire her bravery and acceptance and willingnes s to face the reality of her father’s death by his own hands head on.”
64
Do you ever f ace any sort of criticism for your work? “Not to my face! People are actually quite kind on the internet/in the comments , offering condolenc es and tender remarks to each other. Occasionally when I post a hairwork piec e that gets a lot of engagem ent from people who don’t follow my account there’s alway s one comment that says ‘gross ’ or ‘creepy’. The disgust at the sight of hair when seen in an unexpected place really fascinated me. There is so much emotion tied to hair, it has so much power, it can really freak people out.”

Is there any advice you would offer to anybody who is thinking of commissioning a piece of mourning jewellery? “I would suggest waiting 6 months to a year before parting with any sacred remains of your loved one, be it their ashes, hair, or if neither of those is available, a dried flower from their funeral service or garden. A scrap of their clothing or a piece of a love letter. We can create a reliquary with any tactile object that makes you feel connected to them. I know in the early days of my own grief, in that first year I made regretful decisions, while simultaneously being indecisive. It’s hard to know what you want when your world has been flipped upside down. With time comes clarity.”
What hang-ups do you think people have about mourning jewellery, if any?
Is there any advice you would offer to anybody who is thinking of commissioning a piece of mourning jewellery? “I would suggest waiting 6 months to a year before parting with any sacred remains of your loved one, be it their ashes, hair, or if neither of those is available, a dried flower from their funeral service or garden. A scrap of their clothing or a piece of a love letter. We can create a reliquary with any tactile object that makes you feel connected to them. I know in the early days of my own grief, in that first year I made regretful decisions, while simultaneously being indecisive. It’s hard to know what you want when your world has been flipped upside down. With time comes clarity.”
65G rowing Pains
“I don’t know that anyone would have any hang ups with my memorial/mourning pieces such as my hand engraved Love Tokens with a deceased loved ones name on it. I think the only hang ups would with the pieces containing ashes or hair, or any other sacred bodily remains. Some people think ashes are ‘gross’. To each their own. When I first started working with ashes I did a tour of a crematorium to better understand the process. Visually the ashes vary greatly from person to person (or pet to pet). Recently I worked with ashes that ranged in pastel pinks to blues.”
To see more of Margaret’s work or to order a custom piece, visit mourningjewelry.com or @Margaretcross on Instagram
What hang-ups do you think people have about mourning jewellery, if any?
“I don’t know that anyone would have any hang ups with my memorial/mourning pieces such as my hand engraved Love Tokens with a deceased loved ones name on it. I think the only hang ups would with the pieces containing ashes or hair, or any other sacred bodily remains. Some people think ashes are ‘gross’. To each their own. When I first started working with ashes I did a tour of a crematorium to better understand the process. Visually the ashes vary greatly from person to person (or pet to pet). Recently I worked with ashes that ranged in pastel pinks to blues.”

be strong LOCKMANHEEDAYAHBYILLUSTRATION 66
•Intense •Financial•Drug-seeking•Physical•Withdrawal•Tolerancecravingssymptomsdependencebehaviourstroublerelatedtodruguse •Neglecting responsibilities •Isolating •Engagingbehavioursinincreasingly risky •Developingbehavioursrelationshipsunhealthywithpeople who support addiction A d d i c t i o n i s d e f i n e d a s a c h r o n i c , r e l a p s i n g d i s o r d e r c h a r a c t e r i s e d b y a c o m p u l s i v e b e h a v i o u r. T h i s c o u l d b e s u b s t a n c e a b u s e , g a m b l i n g o r a n y o t h e r h a r m f u l b e h a v i o u r w h i c h w i l l r e s u l t i n l o n g la s t i n g c h a n g e s t o t h e b r a i n a f t e r c o n t i n u e d u s e . I t i s c o n s i d e r e d b o t h a c o m p l e x b r a i n d i s o r d e r a n d a m e n t a l h e a l t h i l l n e s s . Symptoms those abusing will be aware AddictionofAddictionAddiction 67G rowing Pains
Signs other people will be aware of Diagnosis The first place to seek a diagnosis is with your general practitioner. They will talk through the options available, depending on how severe the addiction is and will discuss what appropriate services are available. They will do a baseline assessment and create a referral to the addiction team. The team then allocate a support worker to develop a care plan, taking into account the risks and relapse potential. They maintain medication with a focus on reduction and support. Treatment Treatment can vary from person to person but will usually involve•Detoxification (detox) • Talking therapies such as Cognitive Behaviour Therapy (CBT) • Charity or private therapy clinics •Reduction •Self-helpmaintenanceandclinicsgroupslikeNarcoticsAnonymous (NA) or AnonymousAlcohol(AA) •Change in personality and •Irritabilitybehaviouror agitation •Bloodshot eyes •Frequent bloody noses •Shakes or tremors •Lack of motivation •Slurred speech •Change in their daily routines •Lack of concern for personal •Unusualhygiene need for money •Ongoing financial problems 68
BeatingAddictions.co.uk
GamblersAnonymous.org.uk
How to help Resources for support
TalkToFrank.com – Con dential help and advice about drugs.
– Information about a range of addictive behaviours and treatments.
NACOA.org.uk – National Association for Children of Alcoholics provides information, support and advice for everyone a ected by a parent ’s drinking, including adults.
•Exercisingwoodworkcanmakesleepingeasier–offer to go swimming, walking or hiking 69G rowing
– Health and social care services for drug, alcohol and mental health issues.
Turning-point.co.uk
– Support groups for anyone wanting to stop gambling.
Pains
M-alliance.org – Organisation led by recovering users which provides information and advocacy for people accessing treatment for drug and alcohol problems.
Addaction.org.uk – Support for people with drug, alcohol or mental health issues, and their loved ones.
•Offer to go along with a loved one to meetings
•Offer alternative ways to occupy their time •Join a recreational activity class like gardening, pottery, joinery or
•Be there to listen and make them feel safe
When did you first notice that your alcohol use was becoming an issue?
Des Sober advocate
70
“I’ve kind of suffered with agoraphobia and panic attacks even before alcohol entered my life, since I was a young boy, and I still do at times. I was first referred for treatment when I was nine but back then anxiety was very much seen as more common in young girls than boys. I’d be nervous about going somewhere so I’d have a couple of drinks and that would usually get me through. It sort of dulled the senses and numbed the anxiety, which probably made me more comfortable going out. Initially it was little things like a couple of pints before I went on the train to go out but in the end it was really bad. I couldn’t leave the house without having a drink. It was real ridiculous, I was so scared to leave the house at one point and alcohol made me feel a bit braver. It just fools you into thinking you can do stuff and it fools you into thinking you need it. It would be much worse when the drink wore off, it would be worse than being back at square one, it was minus square one.” Was there a relationship for you between anxiety and alcohol? “The alcohol got rid of the anxiety basically, it totally eliminated it for a short time. It can seem like a quick fix, I mean I think any doctor will tell you that - a doctor said to me once that’s why they used to keep brandy in every doctor’s kit, because it would calm you down instantly It made me a bit bolder and a bit more comfortable in situations but again it’s a vicious circle. It comes back tenfold when the alcohol wears off, so in the interim you need to drink more alcohol. The relationship with alcohol and anxiety was really the fact that the alcohol made me think I could beat the anxiety but in turn it was actually making it worse in the long term.”
“I would notice the next day after drinking that I didn’t want to do anything, and that I wouldn’t particularly want to go anywhere. That was quite early on in late teenage years and I probably missed work because of that, just feeling really quite down and very, very anxious. Where most people have hangovers, I would get really bad anxiety.” What was your experience with agoraphobia whilst you were drinking?
I started coming down by drinking say sixteen cans then down to twelve, but the guess mark wasn’t accurate and I went down too quickly, which caused me to have seizures and I ended up in hospital for ten days. That meant a lot of my detox was done whilst I was a bit out of the game but to anybody who wants to start detoxing, the first port of call is your GP. Ask for the help. Go through the proper channels, it’s not advisable to do it on your own unsupervised, definitely not.
Do you think there is a stigma around addiction that people face? If so, how has that affected your journey to sobriety? “I think there absolutely is a stigma around addiction. I think I’m a lot more empathetic now too. People see others struggling in the street and they’re very dismissive - ‘there’s a junkie, there’s an alkie, they’re just a waste of space’. Everybody has a story, something that has affected them and a reason as to why they’ve ended up where they are. You’ve got to try and look at the human aspect of everything really, in any situation.
Do you think there is a stigma around addiction that people face? If so, how has that affected your journey to sobriety? “I think there absolutely is a stigma around addiction. I think I’m a lot more empathetic now too. People see others struggling in the street and they’re very dismissive - ‘there’s a junkie, there’s an alkie, they’re just a waste of space’. Everybody has a story, something that has affected them and a reason as to why they’ve ended up where they are. You’ve got to try and look at the human aspect of everything really, in any situation.
What was the detox process like for you and do you have any advice for anyone who wants to start detoxing?
It doesn’t matter whether it’s addiction or money troubles, we need to get away from this judgemental thing in society. People judge you but they’ve never walked in your shoes. Or at least until it affects them or their family, but that’s just a fact of life that happens with anything and not just addiction.
71G rowing Pains
“The detox process was long but obviously it had to be done. When I started to detox, I went through official channels because with the amount of drinking I’d been doing, it was too dangerous to just stop. The issue was that we couldn’t figure out how much I was drinking so we put a guess mark number on it - I thought I was drinking about twenty cans a day and maybe a bottle of gin or a half bottle of gin on top of that.
What was the detox process like for you and do you have any advice for anyone who wants to start detoxing?
There are great people out there who will help you, who will come out and see you and make sure you’re okay. Go into it with open eyes and an open mind and get in touch with your doctor and ask for help. That’s the biggest thing you need to do, just ask for help. I didn’t go down the Alcoholics Anonymous route but I know plenty of people who have and still do. They swear by it. It wasn’t for me but we are all different and there is more than one way of doing things so I would just say to anyone to keep an open mind when they are trying to get help or fix something in their life.”
It doesn’t matter whether it’s addiction or money troubles, we need to get away from this judgemental thing in society. People judge you but they’ve never walked in your shoes. Or at least until it affects them or their family, but that’s just a fact of life that happens with anything not just addiction. As for me I did not feel any adverse effect from being stigmatised against. I knew I was focused; I knew what I had to do and why I had to do it but I think there definitely is a stigma out there and that is something which needs to be looked at.”
“The detox process was long but obviously it had to be done. When I started to detox, I went through official channels because with the amount of drinking I’d been doing, it was too dangerous to just stop. The issue was that we couldn’t figure out how much I was drinking so we put a guess mark number on it - I thought I was drinking about twenty cans a day and maybe a bottle of gin or a half bottle of gin on top of that. I started coming down by drinking say sixteen cans then down to twelve, but the guess mark wasn’t accurate and I went down too quickly, which caused me to have seizures and I ended up in a hospital ward for ten days. That meant a lot of my detox was done whilst I was a bit out of the game, but to anybody who wants to start detoxing, the first port of call is your GP Ask for the help. Go through the proper channels, it’s not advisable to do it on your own unsupervised, definitely not. There are great people out there who will help you, who will come out and see you and make sure you’re okay. Go into it with open eyes and an open mind and get in touch with your doctor and ask for help. That’s the biggest thing you need to do, just ask for help. I didn’t go down the Alcoholics Anonymous route but I know plenty of people who have and still do. They swear by it. It wasn’t for me but we are all different and there is more than one way of doing things, so I would just say to anyone to keep an open mind when they are trying to get help or fix something in their life.”
As for me I did not feel any adverse effect from being stigmatised against. I knew I was focused; I knew what I had to do and why I had to do it but I think there definitely is a stigma out there and that is something which needs to be looked at.”
When did you first notice signs of addiction in someone in your life and what were they?
72
Joan nurse
- Addiction
“People need to understand why other people begin to abuse substances Sometimes it’s recreational and other times it’s because of an underlying issue like depression, feeling like they don’t fit in to the world, a lack of family structure and support, loneliness or trying to avoid dealing with life.
“There are things you notice when you are talking to someone, for example their pupils are usually notably large and their behaviour is very elated or very flat. Sometimes the way they talk will be different, they slur their words and they don’t realise they’re doing it but it’s obvious to you. It depends how it affects them too –some people might smoke cannabis and not change very much and other people might smoke cannabis and change drastically. Often when someone is taking drugs they can seem ‘tuned to the moon’ and not realise they are talking at you instead of to you. If it’s someone close to you, you might notice that the things they talk about when you see them have changed drastically Sometimes people who smoke cannabis believe that they see the world a different way to other people and gravitate towards talking about things like conspiracy theories. People who are taking things like cocaine or amphetamines often lose their social inhibitions and may uncharacteristically overshare personal details. It depends on what they have been taking. There are people who take cocaine to party or to stay awake longer but before they know it, they need it in their day-to-day activities. If it's something like heroin, you can tell from the changes a person’s body will go through. Even if they try to hide it initially, they will lose weight rapidly. Another giveaway is that when they come down from the drug, they need to eat a lot of sugary things. If you ever watch a regular heroin user in a shop, they will go and pick up things like chocolate bars or fizzy drinks, they won’t go and get themselves something like a sandwich. In a broader sense, their behaviour changes –they lie and steal then deny it was them. They withdraw from you and everyone they normally spend time with because they don’t want anybody to know they are using drugs. They miss work and lose their jobs. They lose their friends and/or their friends are always changing. They get in debt, become unwell and ashamed, they have suicidal thoughts. The most problematic thing is that they won’t talk about what’s happening, they won’t take help and they don’t think they have a problem.” What’s something you wish more people understood about addiction?
empathy and compassion , but you also need to be firm that you won’t buy drugs for them, and that you won’t give them money to buy drugs either. Tell them that emotionally you will be there for them any time they are ready to change - that way they know you care about them as a person and don’t just see them as an addict.”
What can you do for someone who doesn’t want to seek help themselves? “People who don’t want help need to get to the point where they do, but if it is someone you care for then let them know you are there to support them in any way that would benefit them in going into recover y. Let them know you value them as a person and let them know you value their Showfriendship.
What people don’t realise when they start taking drugs, is that when they get a hold of you, the things you run from only become worse.” What more could the healthcare system and government be doing to help people who are suffering from addictions?
“People who don’t want help need to get to the point that they do, but if it is someone you care for then let them know you are there to support them in any way that would benefit them in going into recovery. Let them know you value them as a person and let them know you value their friendship. Show empathy and compassion but you also need to be firm that you won’t buy drugs for them, and that you won’t give them money to buy drugs either. Tell them that emotionally you will be there for them any time they are ready to change - that way they know you care about them as a person and don’t just see them as an addict.” with life. What people don’t realise when they start taking drugs, is that when they get a hold of you, the things you run from only become worse.”
TARRANTLAOISEBYILLUSTRATION 73G rowing Pains
“The government needs to open more rehabilitation long term rehabilitation centres so that people can get clean and then have the time to look beyond the drugs and determine why people have taken them. That can take a lot of counselling and therapies to understand the triggers and develop coping tools to stay clean instead of introducing them to a methadone problem.”
What can you do for someone who doesn’t want to seek help themselves?
with life. What people don’t realise when they start taking drugs, is that when they get a hold of you, the things you run from only become worse.” What more could the healthcare system and government be doing to help people who are suffering from addictions?
What more could the healthcare system and government be doing to help people who are suffering from addictions?
“The government needs to open more rehabilitation long term rehabilitation centres so that people can get clean and then have the time to look beyond the drugs and determine why people have taken them. That can take a lot of counselling and therapies to understand the triggers and develop coping tools to stay clean instead of introducing them to a methadone problem.”
What can you do for someone who doesn’t want to seek help themselves?
“People who don’t want help need to get to the point that they do, but if it is someone you care for then let them know you are there to support them in any way that would benefit them in going into recovery. Let them know you value them as a person and let them know you value their friendship. Show empathy and compassion but you also need to be firm that you won’t buy drugs for them, and that you won’t give them money to buy drugs either. Tell them that emotionally you will be there for them any time they are ready to change - that way they know you care about them as a person and don’t just see them as an addict.”
“The government needs to open more long term rehabilitation centres so that people can get clean and then have the time to look beyond the drugs and determine why they first began to take them. That can take a lot of counselling and therapies for someone to understand their triggers and develop coping tools to stay sober, instead of introducing someone to a methadone problem in an attempt to give them a short-term solution.”

SMITHKATIEBYILLUSTRATION 74

75G rowing Pains
76
the gender roles or stereotypes were still quite traditional in that many of the men were the 'workers', and by that I mean people who went to work to earn money. The women were mostly part time 'workers' but full time looking Nothing creative was nurtured. You weren’t really allowed to think or feel emotion, you had to keep it all in. For example, say you were at school and had an argument with someone and they punch you in the face, you couldn’t cry. You might have wanted to. It might have felt like somebody has broken your nose and you wanted to burst into tears but you couldn’t. You had to hit them back. You had to fight. I think it’s better now for my kids because people talk about their feelings and it’s more acceptable to do different kinds of things. In the same breath I don’t envy anyone growing up in this generation where everything is all about social media and the pressure that comes with that.”
When he mov ed out of the house, on a Friday night my mum and my auntie would have dinner and a couple of drink s and put their records on. I’d alway s be dancing about the house and jumping about to the music and singing. I loved that, I loved Michael Jackson films and videos and I wanted to dance about lik e him. I always remember going to places like parties –birthday s, christenings and weddings , and they’d have a karaoke and they’d say ‘right go on, you sing, watch my boy sing on the karaoke’ or they’d tell you to go up and dance. Even though I loved all that stuff I’d think ‘I can’t’, cause I knew I would get laughed at. You would get made fun of because people said dancing was for ‘poofs’. If you wer e dancing about people would say ‘you’re a wee fair y’ and all that stuff. Hugh “I was brought up in a town k nown for its shipbuilding in the eighties. My m um and d ad were really good, k ind, har dworking and loving people. I went to bed every night knowing I was cared for, fed, clothed, loved etc. I was alway s encouraged to do the best I could at whatever I was interested. I'll always be eternally grateful to them for that. My upbr inging wasn't well off or lav ished with loads of excess. I wasn't spoiled but I felt I wanted for nothing. It was a hard place to grow up in at times and it was no countryside idyll, plus the eighties wer e a period of huge c hange for the town, as the shipyards were in their death throes by then and many people were losing their jobs. I was brought up between tenement flats and high r ise flats but trust me, those were (or could be) some great places to grow up, and to grow up with some really good, interesting Ipeople.suppose
77G rowing Pains
78
The way that I deal with my anxiety is through physical exercis e and mak ing sure I do enough self-care. Getting up in the morning, running and sorting out my serotonin levels. In points throughout m y recovery, I’ve had to go on medication for anxiety and that’s something I’m okay with bec ause it can get a bit overwhelming at times.”
Over the years I learned a lot about anxiety and I learned that anxiety always has a peak. All the stuff happening with your s ystem; the adrenaline, the blood rushing, the fight or flight response – it can only last so long. It always has a peak , and say this peak is at ten. Most people with s ocial anxiety will leave a s ituation when their anxiety reaches eight, not realising if they had just waited another five, ten, fifteen minutes, the trajectory would start to go back down.
my head but eventually, I visited my doctor and asked to speak to a psychologist. I described what was happening and she told me that it sounded like an obs essive compulsive dis order anxiety, where I was ruminating on these obsessive thoughts.
79G rowing Pains
Those were all enc ouraged and nur tured really. If I was interested in something spec ific I would get gifts related to it at Christmas or birthdays to suppor t me. I suppose it c ould have been different if I wanted to do something unusual for the times or maybe even aimed more for girls or a different gender stereotype - I'll never know. If I'm honest, I think anything I wanted to do would have been enc ouraged and nothing would be off limits Paul “I grew up in a ver y tough hous ing scheme. The impact of that kind of environment, especially at home… Sometimes you could be s urrounded by psychopaths – guys who were craz y, guys who actually enjoyed going out and stabbing people, who wanted to fight with people. You would find yourself running about with these sorts of guys and inside you would know everything was wrong and you didn’t want to be there. You’re really, very scared but you would find yourself getting carried along in this wave. We grew up in this place where you didn’t use the polic e. If you stepped out of line, you got attacked or y ou got slashed. You would see stuff like that happening on a daily Ibasisnever thought that I had anxiety problems but when I cam e out of rehab, I started to find out what anx iety was. After I had been clean for a year, I started to get hundreds of horrible intrusive thoughts . They were all sexual and violent. I was kind of convincing myself that I was mentally ill, that I had damaged my self. I couldn’t speak to anybody about it because I was so embarr assed about what was g oing o n in Being rais ed in a standard industrial town then, I'd doubt I would have had a ballet school or anything like that for me to attend (just using that as an example) but I'd say if I had expressed an interest in that, it would have been encouraged by my parents if not my friends. Possibly nowadays thes e things would not be an issue at all. I think things are much more open now and there's a lot less 'boys play soldiers or football' and 'girls play with dolls or skipping' type of attitudes that were prevalent then.”
80
81G rowing Pains
Music is still a massive thing that really, really keeps me going. It's something I can throw myself into. Like I said, I need structure in my life. I need focus in my day to day life and when I’v e not got that I fall apart. I’ve put on a lot of weight since I broke my leg so I want to start looking after my body again because you only get one. I’m tr ying to Hugh “As I mentioned, I've played guitar s ince I was twelve and I'd s ay that was my release. In some ways (albeit different now) it still is. First was learning it - still learning today and that will never stop but I mean learning from being a beginner, then on to my first times playing with others, to being in bands and writing songs. All those phases were probably wrapped around the ages of thirteen to seventeen and it was a great outlet to dis appear into. I didn't really have much else until getting a bit older and getting into pubs, nightclubs, gigs etc. All that was on the go by the early to midnineties , plus the whole music, drinking and drugs scenes going on. I've Graham “I think people s tart drinking and tak ing drugs because it blocks out s omething. They want to get obliterated to a point where they’re stupefied. For a lot of people, it’s a social thing too. We’re always doing what our dad’s used to do; finish look at exercising more and what’s going to be good for my diet, what food, supplem ents etc. will mak e me function a bit better . Having that in my head about better ing my self and look ing after myself in my mind and body is working for me right now too. As much as we all think we’re invincible, we need to look after ourselves .”
82
So, I think that’s kind of the start of that lifestyle and booze culture and then if people have any problems, that’s what they revert to. Or like me, they want some Dutch courage. People need that one or two to get going and then they’re looking for that next thing. Whether it’s alcohol or smoking green or snorting cocaine, before you know it, it’s got a grip of you. It’s controlling you and your lifestyle because you need that to function.
83G rowing Pains
I’m not against anybody who wants to use recreational drugs. If people want to go get drunk all night that’s fine but I know for a fact that when I’m in a bad mood and I start drinking it’s only going one way, it’s a slippery slope because alcohol is a depressant. If you’re already not feeling good about yourself and you add alcohol into the mix, it only makes it ten times worse. Anything stupid that I’ve ever done and any of my problems in life, I could probably start the story off by saying I was drunk.”
84
After a week or so I was hallucinating - I was seeing ants in my bed and things like that. When the paink illers wor e off, I would start to feel really agitated, frustrated and angr y. After a while that turned into a feeling of really bad anxiety If somebody dropped a pen or the kids changed the TV channel , I would jump out of my skin. I was strung out because I wasn’t sleeping even with the painkiller s and I wasn’t going anywhere. I just sat in one plac e all day l ong. When the painkiller s wore off the withdrawal was horrible too. I was constantly on edge apart from when I’d feel the tablets kick in. I was worried and thinking to myself ‘I’m getting addicted’. I could feel myself becoming reliant on the tablets s o I stopped tak ing them. I took only paracetamol and ibuprofen, and don’t get me wrong I was in a lot more pain physically but the cravings started disappear ing. After that though, I started jumping out of m y skin whenever I went into the front garden on my crutches and heard noises like cars going by. I still had this feeling of being ultra-alert that wouldn’t go away. All the sitting about had an effect on me too but I didn’t know I was depressed. I felt like I had no control over anything and that everything in my life was upside down. I had no structure or routine. I was used to being bus y with the kids, going from nursery to school, to work and now I had nothing. I didn’t know what I was dealing with and I didn’t know what was wrong with m e. I was snappy and irritable. People would come to see me and I would pretend I was going to my bed so that I could get rid of them. I didn’t want anybody near me but I didn’t know why I didn’t know it the time but I’d s tarted falling into a really deep depression. Prior to this accident I’d had a couple of deaths in my family so I had a lot of time to be thinking about that kind of stuff, which was all dragged up by the stretch of free time in front of me. After I stopped taking the painkiller s, I started drinking at night when I couldn’t sleep. I’d try to get really drunk so I could just fall asleep where I was on the couch with my leg in a brace. Eventually when I did start getting a bit better and going out, I was petrified. 85G rowing
Pains
86
MARTINCOOPERBYILLUSTRATION 87G rowing Pains
88
Psychosis
SHRINIVASROSALINDBYILLUSTRATION
Psychosis is classically associated with schizophrenic disorders. Although there are other symptoms for schizophrenia, one of the defining symptoms is experiencing psychosis.
During a psychotic episode, a person might have sensory experiences that do not exist and/or persistant beliefs with no basis in reality, known as delusions. They may see or hear things that do not exist, which can be frightening for the person and their loved ones.


During paranoid delusions, the person may become very suspicious, believing other people or organisations are plotting to cause them harm. They might begin to per ce ive non-exis t e nt threats in every day life, s uc h as thinking one of their coworkers is planning to hurt them or that their hous e is under surveillance.
Hallucinations – Hearing, seeing or feeling things which do not exist.
Delusions – False beliefs, especially based on fear or suspicions about situations that aren’t real.
• S leep problem s – insomnia or fatigue
The most comm on exam ples of delus ions are par anoid delusions or delus ions of grandeur.
During delusions of grandeur, a pers on may have clearly false but very strong beliefs in having special abilities or powers - they might believe that they are a world leader or religious Dependingicon.
Hallucinations can affect any of the senses (sight, sound, smell, taste and touch). The most common exam ples of auditory hallucinations are a voice giving commentary on what the person is doing, a voice repeating what the person is thinking, or several voices talking about the person affected with ps ychosis, often negatively.
.
Delusions c an be m or e extrem e too, a per s on may be c onvinced extra-terrestrials are going to come into their home or that other people want to steal their identity This can be hard for other s to empathise with or take seriously at fir s t, and the per s on them s elves m ay initially be s om ewhat aware that thes e delusions are strange and s tr uggle to share how they are feeling.
on the c ause, psychosis can c ome on quickly or s lowly. In slow cases there may be milder initial s ymptoms of psychosis such as•Feelings of suspicion •General anxiety •Distorted per •Obses•Depresceptionssionsivethinking
Disordered thinking – Jumping between unrelated topics and m aking abnormal connections with loose correlations. This is when a person sees a connection between two topics where there are clearly no connections
89G rowing Pains
Disorganisation – In thought, speech or behav iour.
Catatonia – Entering an unresponsive state.
Symptoms


Lifestyle – e xtreme stress, drug use and hormonal changes can induce psychosis in people with a genetic disposition to develop the disor der. Methylphenidate (a common ADHD medication als o known as Ritalin, Adder al or Concerta) can also create a stimulant-induced ps ychosis
Causes
Lifestyle – Extreme stress, drug use and hormonal changes can induce psychosis in people with a genetic disposition to develop the disorder. Methylphenidate (a common ADHD medication also known as Ritalin, Adderal or Concerta) can also create a stimulant-induced psychosis. Early detection signs Getting a diagnosis of psychosis for someone as early as possible will improve their long-term outcome. Recognising the signs quickly can be difficult, as sometimes symptoms can initially appear relative to a current situation the person is going through. Some early signs in young people can be poor performance in school or work for a long period of time, becoming more socially withdrawn or becoming more distressed and agitated but unable to explain why.
There are no biological tests to determine psychosis due to it being a mental health condition, however drug interactions, side effects, toxins or delirium (the sudden onset of a confused mental state) can cause similar symptoms, so laboratory tests are common to check for another potential diagnosis. These laboratory tests might be a urine sample, brain scan or a electroencephalography (E.E.G.) which tests electrical activity and may help to rule out delirium, epilepsy or a head injury.
Pregnanc y – p ostpartum psy chosis occurs v ery soon after giving birth , normally within two weeks. The exact cause is unknown but some researchers believe the onset is due to dis rupted sleep and c hanges in hormonal levels.
Diagnosis
Receiving a diagnosis of psychosis for someone as early as possible will improve their longterm outcome. Rec ognising the s igns quickly can be difficult because sometimes symptoms ( inc luding delus ions ) ar en't initially taken s er ious ly and acted upon by friends and family. S y m ptom s m ay appear r elative to a current situation the person is going through , or they c an be passed off as mis understandings or jokes Although m os t symptoms appear between the ages of 18- 24, they can begin as late as 30 or as early as 13.
Diagnosis
Brain changes – a lterations in brain structure and the changes of certain chemicals are found in people diagnos ed with psychosis. Some people with a history of psychosis have reduced grey matter in their brain which may explain the effect psychosis has on thought process ing.
Early detection signs
Some early signs in young people might be poor performance in school or work for a long period of time, becoming mor e socially withdr awn or bec oming more dis tressed and agitated but unable to ex plain why.
The condition is first diagnosed during an examination where history, symptoms, experiences, thoughts and daily activities will be discussed. There are no biological tests to determine psychosis due to it being a mental health condition, however dr ug interactions, side effects, toxins or delirium (the sudden onset of a confused mental s tate) can cause similar symptoms , s o l abor atory tests are common to c heck for another potential diagnosis. Thes e labor atory tests might be a urine sample, brain scan or a n electroencephalogr aphy which tests electrical activity and may help to rule out delir ium, epileps y or a head in jur y 90 Causes Brain changes – Alterations in brain structure and the changes of certain chemicals are found in people diagnosed with psychosis. Some people with a history of psychosis have reduced grey matter in their brain which may explain the effect psychosis has on thought processing.
Pregnancy – Postpartum psychosis occurs very soon after giving birth (normally within two weeks). The exact cause is unknown but some researchers believe the onset is due to disrupted sleep and changes in hormonal levels.
The condition is first diagnosed during an examination where history, symptoms, experiences, thoughts and daily activities will be discussed.

There are a number of these treatments available and they can r educ e the anx iety c aused by ps y c hos is .
Cognitive Behavioural Ther apy (CBT) for psychosis is based on an understanding of how a person makes sense of their experiences and how to avoid accompanying distress. A CBT therapis t may encourage the person to try different ways of understanding what is happening to them. The aim is to help them identify and achieve meaningful goals like reducing stress, regaining a sense of control, and retur ning to work, education or training. Family intervention
include discussing the condition and how it might progress, available treatment options, ex ploring ways of supporting one another, and deciding how to solve practical iss ues such as managing any future psychotic epis odes.
A person experiencing episodes of psychosis might benefit from being around other people who have had sim ilar experienc es. C ommunity support groups and mental health charities have a range of services to connect with other people going through the same thing.
Treatments
P sychological treatment
Ant i-psychot ic drugs
S elf - help groups
These side effects c an be severe but they can also lessen over time as the body becom es used to the drug . I f a person is struggling with any side effects, they can contact their GP or their community psychiatric nurses to dis cuss changing their medication. Finding the right medic ation and dos age can take a few tr ies.
This is a way of helping both the person and their family process the condition and move forward. After having an episode of psychosis, someone may rely on their family members for care and suppor t. Whilst most family members are happy to help, the stress of caring for someone and uncertainty of the future can place a strain on any family, so it can be beneficial to receive psychiatric suppor t. Family therapy involv es a series of meetings which take place over thr ee months or Mmore.eetings
91G rowing Pains 91rowing
Treatment with this class of drugs is t he most common therapy for psychosis. They work by blocking m essage transmissions in the brain, which can reduce symptoms. Although this can be the most effective form of treatment, side effects are common and c an vary from drowsines s, shaking and trembling, weight gain, restlessness, blurred vision, dizziness, loss of libido, dr y mouth and musc les spasms.
• Avoid using metaphors or sarcas m as this could lead to misunderstandings.
If someone is experiencing a particularly sever e psychotic episode and their loved ones are worried about danger occurring to them or others, they can be detained at a hospital under The Mental Health A ct of 1983. If someone is detained under the Act, they can receiv e treatment without their c onsent if it is deemed absolutely necessary, however ev ery effort will be made first for consent to be given for any treatment.
•T ry not to deny a person’ s r eality or argue with them about the logistics of their delusions. Keep your voice calm and quiet, and respect their per s onal space.
•Do your best to take concerns and fears seriously but try not to encourage them either . If you are struggling with the right wor ds, try to be s upportive without necessarily agreeing, statem ents like ‘that sounds scary’ can be a good way to keep an open line of communication with someone.
The Mental Health Act is there to guide mental health workers to ensure that no harm comes to a person or their loves ones during a severe episode of psychosis, and that they are supported whilst their condition improv es.
•Paranoia can make people can feel suspic ious about any relationship they have with any person. Try not to take any suspicion or los s of trust personall y
Hospitalisation
•Make them feel like they can tell you everything but don’t react negatively if they won’t. It’s better to hear about events even if they ar en’t real, than to make someone feel like they c an’t talk to you anymore.
•Pointing out to a person that they are having a psychotic episode will not suddenly c hange the way their mind is working and revert their senses back to realit y
•Keep their treatment team informed to make s ur e everyone involved in their care is on the same page and up to date with all infor mation. A treatment team (including doctors) can’t s peak to you directly about their patient due to confidentiality laws, but if y ou believe there is something they should know, there are ways to get in touch. You c an get a message thr ough to them by calling them and leaving a voicemail, writing them a letter, c alling the patient’s GP directl y, or even asking the police to relay y our message to their G P
How you can be there for a loved one who is going through a period of psychosis
9292
BYILLUSTRATION IGWELAEZOHHALI 93G rowing Pains

94
• Abnormal body sensations (hardening, stretching, hollowness) which have no medical cause Hebephrenic or disorganised schizophrenia
95G rowing Pains
• Unusual thoughts or beliefs
I \ I I \ I ' I '---�
• A lack of interest in personal hygiene and self-care
• Suspicion and fear of other people and their motives
Symptoms
• Using made up words
• Unpredictable or inappropriate emotional responses - they may sometimes laugh at sad things, or exhibit the 'flat effect' where they show little to no emotion with their facial expressions, tone and mannerisms
• Lack of impulse control
There are mainly five different types of schizophrenia which have different sets of symptoms. Paranoid schizophrenia
• Isolating behaviour
• Strange or purposeless behaviours
• Repetition of phrases and words
• Experiencing things which others don't through senses like sight, sound and taste
• Difficulty concentrating
This is characterised by disorganised behaviour and speech with a disturbance to emotional expressions. Hallucinations and delusions are less common with this type although the disorder can be so severe that it can render the affected person unable to communicate in an understandable way. The onset of symptoms is usually between the ages of 15 to 29 and they include
• Neglect of personal hygiene
• Shifting between topics with no obvious connection
• Using words which rhyme without any meaning
This is characterised by delusions and hallucinations which make the person struggle to identify what is real and what is not. This type is considered the most common and initially symptoms can seem ordinary or realistic, especially in relation to other stressors like relationships, friendships, family, work and education. The onset of symptoms is usually between the ages of 18 to 30 and these symptoms include



•
• Mutism (no verbal communication) Repeating words Repeating movements
•
This is where a person experiences schizophrenic symptoms and symptoms of a mood disorder. If a person has schizophrenic symptoms and major depressive episodes, this is known as the 'depressive type'. Those who experience schizophrenic symptoms and depressive episodes alongside episodes of mania are known to have the 'bipolar type'. Symptoms can be different for each person but generally there may be Delusional beliefs • Auditory or visual hallucinations
• Stupor (a near unconscious state)
Residual schizophrenia
• Manic episodes where they don't feel the need to sleep and seem to have a lot of energy Depression • Difficulty excelling in school or work as well as maintaining relationships
•
•
This used to be a type of schizophrenia but now it's widely understood that catatonia can happen alongside any medical condition. A person can move between the three forms of catatonia - akinetic (slow movements, mute speech), excited (moving quickly and appearing manic) and malignant which is very dangerous (fever, delirium, organ failure, increased heart and breathing rates). Symptoms can include
• Copying the body movements of others
• Difficulty concentrating Schizoaffective Disorder
• Unusual facial expressions
• Lack of hygiene
96
• Behaviour which seems out of the ordinary or significantly impulsive Schizophrenia with catatonia
• Waxy flexibility (a person will allow their limbs to be moved and may hold them in that position)
This is characterised by a history of psychosis where there are continuing non-psychotic symptoms including • Memory problems Slow movements
•



The specific cause of schizophrenic spectrum disorders are unknown but it's thought that a combination of factors can lead to their development
•
• Stressful events - moving home, losing a job, losing a loved one Environment Brain chemistry
Diagnosis
After the first episode of psychosis or symptoms of schizophrenia, a person will normally be referred by their doctor to an early intervention team. This team consists of a psychologist, a psychiatrist, a mental health nurse, a social worker and a support worker.
The team specialises in providing treatment and support for people experiencing symptoms for the first time. A psychiatrist will make a diagnosis after a full psychological assessment of the symptoms. Some areas don't have early intervention teams but no matter where you are, you should have access to a crisis or home treatment team.
• Birth
- research shows that cannabis users are six times more likely to develop schizophrenia, especially if they start using it before the age of eighteen
I \ I I I\ ' I , ___ ,,, Cause
Strongcomplicationscannabisuse
There is no test for schizophrenia and it can be difficult to diagnose due to the fact many people who have it don't believe they are unwell. Some recreational drugs can cause schizophrenia-like symptoms too.
Symptoms are separated into three main categories.
Positive symptoms are symptoms which "add" to a person's behaviour - these are hallucinations, delusions, repetitive movements.
-
•
• Genetics - people with schizophrenia often have a genetic predisposition for developing the disorder. Research shows that schizophrenia and bipolar disorder may share a common genetic disease.
Negative symptoms "detract" from a person's behaviour - these are difficulties communicating, apathy, poor hygiene, low sex drive, withdrawing from social activities. Cognitive symptoms are anything which relate to functions of the mind. These are disorganised thinking, memory issues, and difficulties with paying attention or focusing.
97G rowing Pains




Treatment
There are resources like hearing-voices.org which have information and support including local support groups, and there are forums like voicesforum.org where people can discuss living with schizophrenia.PhysicalhealthDiet,exercise and healthy sleep patterns are beneficial for overall wellbeing. Without these, symptoms can be worse. It's important to stick to treatment plans in order to avoid symptoms which are detrimental to a person's day to day life. Although there is no cure for schizophrenia, many people recover and lead a meaningful and sociable life. Recovery can be different for each individual person. Half of all people diagnosed with schizophrenia have entirely manageable symptoms with treatment, and 25% improve with treatment but still require support from mental health and social services. These outcomes are known as clinical recovery. Others will go on to have what is known as a personal recovery, where they live a meaningful life but it will be slightly different to that of other people. With a personal recovery, someone can set goals which are achievable for them. Any type of recovery for schizophrenia is going to be ongoing and there may be difficulties or setbacks along the way but don't lose hope.
Psychosocial treatments
98
Talking treatments like CBT, psychoeducation, art therapies and family therapies.
Coping strategies
AMedicationntipsychotics can have a range of side effects, which means it may take a while for someone to find the right medication for them. Even when the right medication is found, it should be reviewed at least once a year. If a person has tried two types of antipsychotics which didn't work for them, they are able to try clozapine. This can work for some people who are treatment resistant but it can be a very dangerous medication due to its side effects. It's often used as a last resort and frequent blood tests are necessary to monitor any damage clozapine may cause. Although it can b e dangerous, the side effects are known to lessen once a person's body becomes adjusted.

99G rowing Pains
SHRINIVASROSALINDBYILLUSTRATED 100
101G rowing Pains
How did you first know your family members were experiencing symptoms of schiz ophrenic disorders? “My brother was the first person I noticed to be experiencing symptoms. In hindsight, there were small s igns before the tell-tale signs emerged. He was diagnosed with A ttention D eficit D isorder (ADD) when he was about twelve years old, then he was prescribed Adderall and it helped him with his schoolwork. He did better in school and was doing well on a low dose for years. I think he may have been misdiagnosed and his attention difficulty was actually a very early onset cognitive symptom of Whenschizophrenia.Iwasthir
teen my mother divorc ed my father. She was awarded pr imary custody by default and my dad was forced to leave the house. She got a restraining order against him, and my brother and I were allowed to see m y dad br iefly for one weekend each month. After the divorce she tried to begin a relationship with my music teacher. I didn’t know it at the time but my mother was suffering from delusions and mania when this was occurring. My mother had a formal diagnosis of post traumatic s tress disorder, anxiety, depress ion, attention deficit disorder and her therapis t has noted ‘bipolar lik e symptoms’. I know my mother’s treatment is inadequate and suspect she suffers from schizoaffective disorder. She has a pers istent delusion that our music teacher is making her and our family do things through mind control. She believes he is a Wiccan, a Satanist or involved with the Illuminati. Later she wanted to undo the divorce with my dad because she said it wasn’t her who did it. She left my brother and I for almost a month to go model s ome dress es for an independent designer in California, I think. A family friend checked in on us weekly. My dad got in trouble for trying to meet with us whilst she was away During this time, my brother would drive me back and forth to school and sec retly I wanted to move in with him when he turned eighteen, to escape the problems of our parent’s divorce. I think he sensed this pressure from me on some level. The stress of what was happening pushed him over the edge. I didn’t hav e many friends at the time and my brother was my rock. The next time my mother left us, we stayed with a family friend and this is when my brother’s firs t psychotic break began. He was acting strangely, making weird notes and drawings the whole tim e we were there. He didn’t talk to me much. He didn’t r eally eat and stayed downstairs the entire time. I thought it was odd but I was playing with my friends upstairs during a lot of this. When it was time to leave and our mother came to pick us up, I ask ed him to get his suitcase. He had no idea what that meant. I knew something was wrong then and I was afraid, I insisted five times that he get his stuff so we could leave and he did. My brother’s first psychotic episode lasted about 3 months. I was only thirteen at the time but I remember he wrecked a game system because he thought it was watching him and he lined up shoes in the hallway in the shape of a pyramid. He made all sorts of strange doodles and notes, said that he needed to go to the equator to play a rock concert to save the world and he kept wanting to walk out into the woods Various things would trigger different behaviors He made tons of loosely correlated m edia referenc es and insisted he wasn’t to be addressed by his own name. He rarely showered, dressed bizarr ely and laid out objects in odd patterns in the carpet. My mother was fully in denial the entire time. We had to go to the grocery store and my mother let my brother drive me. We were on the freeway and he let go of the steering wheel say ing I should take the wheel. I realized I was in real danger then. I’m happy he was very cooperative at this time because he lis tened when I told him he needed to drive. We got to the store and I directed him through. People were look ing at us strangely, I think they knew something was wrong but I guided him. I never let him drive me again until after he got treatment.
What sort of treatment did they receive and how did they react? “I went to the therapist with my mother and brother. I explained what was happening to my brother and she prescribed him an antipsychotic (Abilify/Aripiprazole) and took him off his ADD medication. He took it for a while and got better. He got off that medicine and eventually ended up on Adderall again half a year later after his first therapist retired. That is when his second psychotic break occ urred.
I was scared he wouldn’t be released from the hospital even though he seemed to be doing well again. He was very sleepy at first, had bradycardia ( a slower than normal heart rate), tremors and he put on a lot of weight. As his dose was lowered, he got better and is now almost totally back to how I remember him, on a management dose of Clozapine. He will have to get blood tests to make sure his meds aren’t hurting him for the rest of his life, but the meds made him so much better. He’s doing well in school now (even without the ADD meds) My mother got on an antipsychotic which helps with bipolar disorder and schizophrenia about 6 months ago. She still avoids going outside unaccompanied and is suspicious of everything.
I thought my mother was faking her symptoms for a long time to avoid blame for what she did to our family. Looking back, I now recognise that throughout my whole childhood she was suffering from a mental illness. She had hypomanic episodes where she would get erratic waves of motivation to stay up all night cleaning, cooking, decorating or exercising. She had lots of depressive episodes where the house got really dirty too.”
102102
I fully prepared myself to lose my brothe r, m y best friend, my emotional rock but he came back and by all standard measures he’s doing amazing for what he’s been dealt with.
To be diagnos ed with bipolar disorder you must have at least one manic or hypomanic episode ( h ypomanic means low mania ) . A manic episode involves psychotic symptoms and is more extreme than a hypomanic episode.”
E v eryone around me was insane I remember grieving my brother as if he were dead during his first psychotic break. I cried and I laughed at the same time, which is nothing like anything I’ve felt since. He was a completely different pers on and the fact he gave himself a different name just punctuated the separation.
He was freshly eighteen at the time and had started wearing three outfits worth of clothing at once, with a shirt on the bottom part of his body He jumped out of a second story window and was found standing on a bridge in the town by a police officer, who took him to a psychiatric hospital. He spent six months there and went through a series of antipsyc hotic medication s and counselling until the last resort drug Clozapine worked. After that he stabilized enough to where we could take him on day trips.
I didn’t connect in m y mind how neglectful what my mother did was until much later. This was one of the scariest times in my life.
How would you describe a manic episode? “A manic episode is an extended period of time where someone has an unreasonably high amount of energy and motivation. They will pursue goals relentlessly, feel awesome, have extremely high self-esteem. They may also sleep very little or not at all for many days at a time. They will spend money recklessly and make extreme decisions they often regret later.
“I wish I had known everything but I wouldn’t change anything. I don’t know if my brother would have gotten the treatment he did if things went differently. I would have liked to have known that things turn out mostly okay. All of this is a big part of who I am, I don’t know who I would be without that stuff.”
I wish people would have more compassion too. My brother can’t talk to a lot of his old friends and he’s pretty socially isolated despite being treated for his psychosis. People still feel uncomfortable about having a schizophrenic roommate despite them being totally fine when treated. People feel unsure about hiring a schizophrenic worker because they don’t understand what that means.
I wish things didn’t always have to get really bad before people could get help. I wish there were medical day programmes where people could be safely looked after for a period of time without being fully committed to a psychiatric ward. No one person can take care of someone with psychosis alone.”
Is there anything you’ve learned that you wish you had known at the start of their diagnosis?
103G rowing Pains
Finding a job that is low stress (stress can induce psychosis), part time (so you can sleep off the medicine), with minimal education requirements (school can be hard because of cognitive symptoms and many don’t finish due to disruptions), with minimal overtime and a normal schedule that pays well can be very difficult.
Her treatment doesn’t work yet, I think she needs a different dose or a different antipsychotic. She’s still in denial about my brother and has no awareness her delusions might not be real. I really hope her therapist will spend more time trying to get to the bottom of what’s happening so I can meet my real mother who is free of psychosis or bipolar symptoms.” How did you support them and how has the whole experience affected you? “I try to be there for them and offer rational grounded advice. I suggest what they should do to try and keep them out of trouble. It’s hard but I’m stronger and more empathetic than how I would be without them. I’d be very lonely without my brother. I always felt safe around him. I was more afraid of what he’d accidentally do to himself or do to my stuff than what he’d do to me. I was scared of him once when my mother and I had backed him into a corner, trying to persuade him to take a sleeping tablet and he didn’t trust it. I don’t know what he thought was happening. He said he didn’t want to hurt us but would do what he would have to. I don’t blame him for that, but the situation could have gone badly if we kept pushing him. People in psychosis need twenty-four-hour supervision and it’s exhausting. They don’t sleep at normal hours. Mostly I wish people would talk more openly about severe psychiatric disorders. I feel like I can’t talk about my family a lot of the time or my childhood because of what happened. I’m afraid that it will come back to hurt them or me if I talk about it. I wish our infrastructure were built to support psyche cases in the way they need to be supported. I wish there were definitive testing (not interviews or surveys) for psychiatric disorders and more effective treatment. There are lingering impacts and side effects associated with antipsychotic medication. Some people gain tons of weight, some people faint, some people end up with lowered immune systems and many have to sleep much more.