24 minute read
Cultural and Western influences on the nutrition transition in Thailand

from P&E

References
Bartholemew, L. K., Parcel, G. S., Kok, G. & Gottlieb, N. H. (2001). Intervention mapping: designing theory- and evidencebased health promotion programs. Mountain View: Mayfield. Durlak, J. A. & Welsh, A. M. (1997). Primary prevention mental health programs for children and adolescents: A meta-analytic review. Am J Commun Psychology, 25, 115-152. Glanz, K., Lewis, F. M. & Rimer, B. K. (Eds.) (2002) Health behavior and health education: theory, research and practice. San Francisco: Jossey-Bass. IUHPE (1999). The evidence of health promotion effectiveness: shaping public health in New Europe. Paris: Jouve Composition & Impression. Jong, M. D. T. d. & Schellens, P. J. (2000) Formatieve evaluatie. In Schellens, P. J., Klaassen, R. and Vries, S. d. (eds), Communicatief ontwerpen. Methoden, perspectieven en toepassingen. Assen: Van Gorcum.
Advertisement
Koelen, M. A., Vaandrager, L. & Colomèr, C. (2001) Health promotion research: dilemmas and challenges Journal of Epidemiology and Community Health, 55, 257-262. Kok, G. J., Borne, B. v. d. & Mullen, P. D. (1997) Effectiveness of health education and health promotion: meta-analyses of effect studies and determinants of effectiveness. Patient Education and Counseling, 30, 1927.
McQueen, D. V. & Anderson, L. M. (2002) What counts as evidence: issues and debates on evidence relevant to the evaluation of community health programs. In Rootman, I., Goodstadt, M., McQueen, D., Potvin, L., Springett, J. and Ziglio, E. (eds), Evaluation in Health Promotion: principles and perspectives. Copenhagen: WHO/EURO.
Meurs, L. H. v. (2002) Concept Preffi2.0; reliability and usefulness, research-paper (in Dutch). Woerden: NIGZ. Molleman, G. R. M. (1999) Implementing the Preffi: the use of guidelines for practitioners in the Netherlands in Best Practices, a selection of papers on Quality and Effectiveness in Health Promotion. Helsinki/Talinn: Finnish Centre for Health Promotion.
Molleman, G. R. M., Peters, L. H. M., Hommels, L. H. & Ploeg, M. A. (2003) Assessment Package; Health Promotion Effect Management Instrument Preffi2.0. Woerden: NIGZ. Available: http://www.nigz.nl/english/index.cfm?code= 904
Molleman, G. R. M., Peters, L. W. H., Hosman, C. M. H. and Kok, G. J. (2004) Implementation of a quality assurance instrument (Preffi1.0) to improve the effectiveness of health promotion in The Netherlands Health Educ. Res., 20(4): 410-422. Molleman, G. R. M. (2005) Preffi2.0: Health Promotion Effect Management Instrument; Development, validity, reliability and usability. NIGZ, Woerden, Netherlands.
Peters, L. H. M., Molleman, G. R. M., Hommels, L. H., Ploeg, M. A., Hosman, C. M. H. & Llopis, E. (2003) Expanatory Guide Preffi2.0. Woerden: NIGZ. Available: http://www.nigz.nl
Katherine L. Craven and Steven R. Hawks
Abstract: The impact of economic development and urbanisation on nutrition and dietary changes in transitional countries has been well researched. It generally has been found that there is a positive correlation between economic development, urbanization, and negative nutrition transitions with the result of growing levels of obesity and diet related noncommunicable diseases. However, the impact of Western influences and culture on specific eating styles associated with the nutrition transition has been less studied. There is limited information about cultural and Western influences on eating styles in Thailand. Recent findings suggest that Thailand may have progressed further along the nutrition transition model, in terms of unhealthy eating styles, than would be expected based on economic development. This study was designed to determine the prevalence of current eating styles and eating motivations among Thai university students. University students were chosen for evaluation as they are thought to represent the forefront of dietary trends and nutrition changes in a population. Convenience samples from four different universities in south-central and northern Thailand were selected. The following scales were used to assess eating and dieting styles and attitudes among 662 Thai undergraduate and graduate students: Motivation For Eating Scale (MFES), Eating Attitudes Test-26 (EAT-26), and Cognitive Dieting Behavior Scale (CBDS). All scales have been shown to be reliable and valid in previous research. For this study, scales were translated into Thai, reverse translated, and pilot tested to ensure cultural relevancy and the conveyance of intended meanings. Basic demographic information was also obtained, including age, gender, year in school, marital status, height and weight, and income. Results indicated that Thai students exhibit significant levels of dieting behaviour and extrinsic eating based on CBDS and MFES scores (with the exception of environmental eating). For most negative eating styles, females scored higher than males. It was also found that high levels of dieting and extrinsic eating were positively correlated with body mass index, suggesting the possible risk of future weight gain and obesity. While the occurrence of eating disordered attitudes based on EAT-26 scores was low (13%), analysis of EAT26 scores indicated that the occurrence of eating disordered attitudes was strongly correlated with dieting behaviour among this population. The results support the need for a programme to educate Thai students, especially females, regarding healthy patterns of dieting and eating attitudes in order to prevent future weight gains and eating disorders predicted by the nutrition transition model.
This manuscript was submitted on November 8, 2004. It received blind peer review and was accepted for publication on September 23, 2005.
The nutrition transition in Thailand Over the past 30 years, economic development and demographic changes in Thailand have led to significant changes in nutrition and eating styles (Kosulwat, 2002). As the economy has moved from agriculture to the industrial sector, demographics have also changed resulting in a greater urban population. Increased urbanisation and an increase in income per capita have led to the availability of more expensive, Westerntype foods. Greater availability of inexpensive fats and oils has contributed to a change in dietary intake from traditional meals of fruits, vegetables, and grains to foods containing fats and animal products for middle and lower income families (Kosulwat, 2002). A more hectic urban lifestyle has led to a decreased consumption of home-prepared meals and an increased consumption of readymade foods, which tend to be high in fat and carbohydrates. The transition from labor-intensive agricultural lifestyles to more sedentary manufacturing occupations has resulted in lower energy expenditure (Kosulwat, 2002).
As a result of this nutrition transition, adulthood obesity has increased markedly in recent years, particularly in urban areas where one-third of middle class women are overweight or obese (Aekplakorn et al., 2004). The impact of the nutrition transition may be compounded for Thai adults by the fetal origin hypothesis. This theory suggests that a history of childhood
Katherine L. Craven, BS Department of Physical Education Brigham Young University Provo, UT 84602
Steven R. Hawks, EdD, MBA, CHES Professor of Health Science College of Health and Human Performance Brigham Young University 229L-Richards Building Provo, UT 84602, USA Tel: (801)422-1706 Fax: (801)422-0273fax Email: steve_hawks@byu.edu Figure 1
malnutrition and underdevelopment, a legacy shared by many Thai adults, may alter metabolism in a way that promotes obesity among those who later become over nourished (Binns, Lee, & Scott, 2001).
In Thailand, obesity among children and adolescents has also greatly increased from 5% during 1986-1995 to 17.9% during 1996-1999 (Likitmaskul et al., 2003). While childhood obesity may be linked to genetic factors, the rapid increase seen in Thailand is primarily the result of the socioeconomic and demographic changes associated with the nutrition transition (Mo-suwan & Geater, 1996; Sakamoto, Wansorn, Tontisirin, & Marui, 2001).
Increased obesity has led to a growing prevalence of diet-related noncommunicable diseases (DR-NCDs) in Thailand such as diabetes, cardiovascular disease, stroke, cancer and hypertension among adults and children who become over nourished (Chaisiri et al., 1998; InterASIA, 2003; Likitmaskul et al., 2003). An increase in DR-NCDs has become a burden on the health care system and thus on the economy, and has decreased the quality of life for persons affected (Ke-You & DaWei, 2001; Popkin, 1994, 2001).
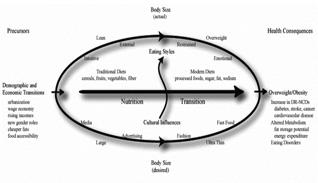
Eating styles and the nutrition transition In a previous study conducted by Hawks and colleagues, samples from the US and four Asian countries (China, Japan, the Philippines, and Thailand) were analysed to determine to what extent each of the countries had progressed within the nutrition transition model based on economic development and Western influences (see Figure 1). The general hypothesis of Hawks’ research was that the progression of certain types of eating styles associated with the nutrition transition relate directly to economic development. He found that an increase of urbanisation and income correlated with a trend towards adopting a diet of readymade foods, a more sedentary lifestyle and the adoption of negative eating styles and dieting habits. However, the results from the Thailand portion of the study showed that Thailand had moved further along in the nutrition transition, in terms of eating styles, than would be predicted by economic development (Hawks et al., 2004). This suggests that understanding the nutrition transition in Thailand may require the additional consideration of Western influences.
Traditionally, the preferred body type in Thailand was a large and robust figure as it signified wealth and prosperity. However, most of the population had slim and lean figures because of the lack of excess food and the physically-demanding nature of a traditional, agricultural lifestyle. As Thailand has undergone economic transition and been increasingly exposed to Western influences, the
Keywords
•Thailand •dieting behaviour •eating disorders •nutrition transition •eating attitudes
preferred body type has changed according to Western ideals now favoring thinness (Sharps, Price-Sharps, & Hanson, 2001). At the same time, the actual body type also changed, becoming larger, because of the changing diet and lifestyle (Aekplakorn et al., 2004). The contrast between the actual body type (heavier) and the preferred body type (thin) has prompted high levels of dieting behaviour, social and emotional eating styles, and even eating disorders (Hawks et al., 2004).
While the occurrence of eating disorders in Asia is generally lower than in the west, Thai women have been shown to prefer an even smaller body type than their western counterparts (Lucero, Hicks, Bramlette, Brassington, & Welter, 1992; Sharps et al., 2001; Tsai, 2000). This trend may contribute to a growing prevalence of dysfunctional eating styles and eating disordered attitudes in Thailand which further complicate our understanding of the nutrition transition.
Purpose and objectives In order to understand Thailand’s unpredicted advancement in negative eating styles within the nutrition transition model, it is necessary to further explore eating styles and eating motivations among the Thai people. The purpose of this study was to determine current prevailing motivations for eating and to identify eating styles. It was hypothesized that despite the lower level of economic development when compared to the US, Thailand would demonstrate high levels of extrinsic eating and dieting behaviour. Extrinsic eating is characterised by food consumption motivated by factors other than the physical satisfaction of hunger. These factors include eating for emotional satisfaction, environmental influences, and social influences (Hawks, Madanat, Merrill, Goudy, & Miyagawa, 2003; Hawks et al., 2004). Dieting behaviour is defined as restricting food intake to control weight gain. Confirmation of the hypothesis would support the need for educational programmes in Thailand that might help prevent the unhealthy progression of a nutrition transition based on negative eating styles associated with Western influences that promote a culture of thinness and excessive dieting.
Methods
A cross-sectional research design was used to analyse the prevalence of different eating styles among college students in two regions of Thailand.
Population and sample The target population for this study was students attending four universities in two regions of Thailand. College students were chosen as they are most susceptible to the nutrition transition because they reside in urban centers and are exposed to Western media influences and current eating fads and fashions. They are also more likely to embrace change and experiment with food and image fashions in order to enhance their personal image or experience crosscultural vogues. Although Thai students may not be representative of the Thai population as a whole, or of young Thai people in particular, they are nevertheless harbingers of future trends in middle-class fashion and lifestyle, including those that impact eating styles and obesity.
Non-random, convenience samples were taken from general education courses at four different universities in Thailand. Ramkamhaeng University is an openadmission, low-cost university in Bangkok. Julalongkorn University, also in Bangkok, is a closed-admission university and the most competitive in the country. The University of Chiang Mai and Payap University are both closed-admission universities in Chiang Mai, a northern province of Thailand. The four universities enroll students that represent college students throughout the country, both geographically and economically.
Instrumentation Data was collected using the 26-item version of the Eating Attitudes Test (EAT26), the Cognitive Behavioral Dieting Scale (CBDS), and the Motivation for Eating Scale (MFES). The EAT-26 was designed to evaluate the presence of eating disorders through three subscales that measure: bulimic tendencies and preoccupation with food, excessive preoccupation with dieting and dietary restraint, and preoccupation with anorexic tendencies and oral control (Garner, Olmsted, Bohr, & Garfinkel, 1982). The CDBS is designed to evaluate current dieting behaviour and how it relates to eating disorders, dietary restraint, and obesity (Martz, Sturgis, & Gustafson, 1996). The MFES has four subscales: emotional eating (eating motivated by the emotional state of the eater—loneliness, boredom, anxiety, etc.), environmental eating (food consumption motivated by environmental surroundings—advertisements, presence of palatable food, eating during meal preparation, etc.), social eating (food consumption influenced by social situations or pressure—family celebration, eating out with friends, etc.), and physical eating (eating motivated by hunger or physical need—growling stomach, fatigue, etc.). Based on relative scores on the four subscales, the MFES evaluates the dominant motivation for eating (Hawks et al., 2003; Hawks, Merrill, Gast, & Hawks, 2004).
Based on previous studies performed in the US, the EAT-26 yielded three factor groupings that correspond to the following three subscales: bulimia, with a possible score from 0 to 18; dieting, with a possible score from 0 to 39; and oral control, with a possible score from 0 to 21. A cut-off score of 20 or higher for the Total EAT-26 signifies the potential presence of an eating disorder and indicates a need for further diagnostic follow-up (Garner et al., 1982; Koslowsky et al., 1992). Similar analysis of the CBDS yielded a single factor grouping related to current dieting behavior with possible scores ranging from 14 to 70 (Martz et al., 1996). Analysis of the MFES yielded four factor groupings that correspond to four subscale constructions, including: emotional eating (scored between 19 and 95), environmental eating (scored between 11 and 55), physical eating (scored between 7 and 35), and social eating (scored between 5 and 25) (Hawks et al., 2004).
For this study, the EAT-26, CBDS, and MFES were translated into Thai. Reverse translation was used to further refine the translations. Surveys were administered to a small group of Thai students prior to data collection to ensure that understanding in Thai matched the original meaning and that each item was culturally meaningful. In addition to each of these scales, demographic and personal data was also collected including gender, age, year in school, residence, height, weight, health and weight of parents, and parent’s income.
Height and weight values collected from the demographic questionnaire were used to calculate body mass index (BMI). BMI (weight in kilograms divided by height in meters squared) is generally thought to correlate with percent body
Table 1 Descriptive statics for study variables
Age BMI
n Minimum Maximum Mean Median Std. Deviation 659 17 44 21.83 21 3.645 655 13.17 33.20 20.23 19.7 2.994
EAT-26
Diet 655 0 32 4.95 2 6.320 Bulimia 654 0 17 1.88 1 2.413 Oral 655 0 15 3.31 2 3.214 Total EAT-26 655 0 55 10.23 8 9.088 CBDS 656 14 67 38.90 39 10.500
MFES
Emotional 613 19 87 38.29 36 12.874 Environmental 625 11 48 29.00 29 6.967 Social 628 5 25 14.45 14 2.474 Physical 628 7 35 21.58 19 5.777 Income (in Baht) 557 1500 10000000 290048 120000 653334
fat and the risk of obesity related illness. It is acknowledged that BMI categories for Asians should probably differ from Caucasians as Asian populations tend to experience higher levels of body fat at lower BMI values (Kanazawa et al., 2002). For this study, BMI was not used to categorise overweight or obesity, but rather as a correlate of eating styles and as a basis of comparison among demographic variables.
Data collection EAT-26, CBDS, MFES, and demographic data were collected using paper and pencil questionnaires. Questionnaires were given to undergraduate and graduate students on college campuses by general education course instructors and research assistants who were trained in data collection methodologies. It was explained to the students that participation was voluntary and that there was no penalty for not participating. Ten to fifteen minutes were required to complete the questionnaires. Institutional Review Board (IRB) approval for human subjects was obtained prior to data collection.
Data analysis Pearson’s correlations were obtained for a 2-tailed, bivariate analysis of each subscale in relation to other eating scales, to BMI, and to other continuous demographic variables. The correlations were used to indicate the strength of linear correlation between each variable. Independent T-tests were performed to compare mean BMI values and eating style scores with various demographic variables (gender, year in school, and marital status). Frequencies were also obtained for each of the above demographic factors. Statistical analysis was completed using the SPSS Graduate Pack 12.0 for Windows.
Results
The sampling strategy resulted in a total of 662 participants: 191 from Ramkamhaeng University, 199 from Julalongkorn University, 173 from Payap University, and 99 from Chiang Mai University. Response rates on each campus exceeded 90%. Frequencies showed that the population included 395 (59.7%) females and 267 (40.3%) males. Participants had a mean age of 22 years (3.64 standard deviation) and included both graduate students (6.5%) and undergraduate students (93.5%). Ninetyfive percent of the participants were single (See Table 1).
Approximately 45% of respondents scored higher than 40 on the CBDS indicating high levels of purposeful dieting behaviour among this sample. Similarly, the dieting subscale of the EAT-26 accounted for nearly half of the total EAT score, further suggesting the presence of problematic dieting attitudes and behaviors. An unexpected 13% of respondents scored 20 or higher on the EAT-26 indicating the possibility of an eating disorder. Females scored significantly higher than males (p < .001) on the dieting and bulimia subscales of the EAT-26, as well as the total EAT-26 and the CBDS. On the MFES, females also scored higher than males on emotional eating (p < .001), environmental eating (p = .005), and social eating (p = .001). There were no differences between male and female scores on the physical subscale of the MFES, or the oral subscale of the EAT-26.
Results of Pearson’s correlations showed that BMI was positively correlated with age, the dieting subscale of the EAT-26 and the CBDS. (Age, however, did not significantly correlate with any of the other subscales of the EAT-26, the CBDS, or the MFES, indicating that age has no significant relationship with various eating styles.) BMI correlated negatively with the oral subscale of the EAT-26, the environmental subscale of the MFES, and the physical eating subscale of the MFES (see Table 2).
Both the dieting subscale of the EAT-26 and the CBDS had significant positive correlations with the bulimia subscale of
Table 2 Significant correlations with body mass index (BMI)
BMI Age Diet Oral CBDS Environmental Physical Pearson Correlation .222 .141 -.309 .254 -.109 -.105 Sig.(2-tailed) .000 .000 .000 .000 .006 .009 n 652 649 649 649 619 623
Table 3 Significant correlations with cognitive behavioural dieting scores (CBDS)
CBDS BMI Diet Bulimia Oral Total EAT-26 Emotional Social Pearson Correlation .254 .628 .304 -.195 .453 .199 .158 Sig.(2-tailed) .000 .000 .000 .000 .000 .000 .000 n 649 650 649 650 650 608 623
the EAT-26, the total EAT-26 score, the emotional eating subscale and the social eating subscale of the MFES. Interestingly, the CBDS also demonstrated a significant negative correlation with the oral subscale of the EAT-26 (see Table 3). The oral subscale of the EAT-26 also had an unexpected significant positive correlation with the physical eating subscale of the MFES and a significant positive correlation at the 0.05 level with the environmental eating subscale of the MFES.
The results of an independent samples ttest showed that BMI did not differ significantly with grade level, although there were significant differences in BMI between males and females and between married and single participants (see Table 4).
Discussion
Thailand has a lower risk of occurrence of eating disorders based on EAT-26 scores (>20) when compared to results of a similar study conducted among US college students (Anstine & Grinenko, 2000). However, Thailand had an unexpectedly high frequency of dieting among undergraduate and graduate students, indicated by the mean CBDS score which is higher than the mean CBDS score of a similar US population of university students (Psujek, Martz, Curtin, Michael, & Aeschleman, 2004). In addition, those who scored higher in both the dieting subscale of the EAT-26 and the CBDS tend to have a larger BMI, indicating a positive association between larger body mass index and excessive dieting behavior. It is also clear from the correlation between the dieting subscale and the CBDS that while the occurrence of eating disorders was not excessive, a significant occurrence of dieting behavior occurred in cases where the presence of an eating disorder would be predicted by the EAT-26, suggesting that dieting behavior in Thai students is associated with an increase in eating disordered attitudes (see Table 5).
The results also showed that in Thai culture dieting behaviour is strongly correlated with emotionally and sociallymotivated eating. Because emotionally and socially-motivated eating define extrinsic eating, these results confirm previous findings that Thai students who tend to diet are extrinsic eaters—a significant risk factor for future weight gain and obesity (Hawks et al., 2004). The participants who tended to engage in dieting behaviour also engaged in emotional and social eating. Emotional and social eating are also unhealthy eating styles that frequently lead to weight gain and eating disorders.
Although it was expected that those physically-motivated eaters would have a lower BMI as found in this study, the negative correlation between BMI and environmental eating was unexpected. Environmental eating, a characteristic of extrinsic eating, should correlate positively with an increasing BMI. The expected negative correlation between BMI and oral control (high dietary restraint, anorexic tendencies) was also supported in this study.
The primary purpose of this research was to identify the current status of Thai college students in the nutrition transition as measured by eating styles. Based on past research, it was hypothesized that Thailand had progressed further than economic development would predict, especially in terms of dieting and extrinsic eating styles. The hypothesis was supported by this data as BMI was most positively correlated to dieting behaviour and did not have significant positive correlations with any other particular eating style or motivation. The hypothesis was also supported by the high CBDS scores, indicating that dieting behaviour may be more prevalent among Thai students than among their American peers.
Excessive extrinsic eating would be indicated by a strong positive correlation between dieting and each of the subscales of the MFES excluding physical eating. This hypothesis was generally supported with a notable exception of the environmental subscale, which had no correlation with dieting.
The unexpected negative correlation of the environmental eating subscale of the MFES with BMI did not support the research hypothesis. Environmental eating, a characteristic of extrinsic eating, was predicted to correlate positively with CBDS and EAT-26 dieting scores. This
Table 4 Comparisons of mean BMI by demographic variables
n Mean BMI Std. Deviation t Sig.(2-tailed) Freshmen 114 19.39 2.85 -1.409 .163 Graduate 43 20.13 2.95 Male 265 21.50 2.97 9.536 .000 Female 388 19.36 2.69 Single 623 20.15 2.95 -4.452 .000 Married 20 23.34 3.16
Table 5 Cross-cultural comparison of EAT-26 and CBDS scores
EAT-26 CBDS n %>20 n Mean US 402 17% 461 32.10 Thailand 655 13% 656 38.90
anomaly may be the result of unique Thai cultural influences. Environmental eating in the United States is generally characterised by eating while watching television or other such things associated with weight gain. In Thailand, however, environmental eating may be associated with less negative habits and attitudes that do not lead to weight gain. This unexpected result opens an avenue for exploring the Thai culture and motivation for eating.
Limitations The findings of this study are limited by the use of convenience samples which may not be representative of all university students in Thailand. A further limitation is that no test/retest correlations are available to verify the reliability of the instruments in the study population (although all instruments have been shown to be valid and reliable in similar populations). The design used in this study is capable of identifying associations between variables of interest, but is not able to establish cause and effect relationships.
Conclusion
To understand the irregularity of Thailand in the relationship between economic development and the nutrition transition (specifically extrinsic eating habits and dieting behavior) it is necessary to explore in depth Thai students eating styles and motivations for eating (Hawks et al., 2004). Without a more complete understanding of the current eating styles and attitudes of Thai students, it is impossible to establish an accurate educational program to correct unhealthy eating styles and attitudes to prevent further deterioration of healthy eating styles among the Thai people.
The general hypothesis of this study was supported by the data. While Thailand does not exhibit a more frequent occurrence of eating disorders than other Asian countries or the United States, there is a significantly larger occurrence of dieting behavior among Thai university students which in turn is positively correlated with eating disordered attitudes and higher BMI. This could be the result of western influence on body image as well as a growing Thai tendency to control food intake and body size (Sharps et al., 2001).
The hypothesis that Thai students tend to be extrinsic eaters (eating motivated by emotion, environment, or social influences) is supported by the strong correlation between dieting behaviour and extrinsic eating characteristics (with the exception of environmental motivation). This tentatively indicates that extrinsic eating is accompanied by high levels of dieting behavior among Thai students. This is of concern as dieting behaviour tends to be associated with higher BMI as well as the risk for eating disorders. While environmental eating did not support the hypothesis, it does present the opportunity for further exploration into Thai culture in relation to eating styles and attitudes.
The results of this study indicate that Thai students, especially females, should be discouraged from participating in dieting behaviour as it is associated with eating disordered attitudes and an increase in BMI. The progression toward dieting behaviour and disordered eating is not unique to Thailand. There is a global preference for a thin, lean figure which motivates the adoption of dieting behaviour and propels progression within the nutrition transition model toward disordered eating. As in Thailand, this negative progression may be prevented by the implementation of educational programmes to introduce healthy eating styles among the affected population.
Acknowledgements
This research was generously supported by the David M. Kennedy Center for International and Area Studies, the Office of Research and Creative Activities, the Honors Program, and the College of Health and Human Performance—all at Brigham Young University.
References
Aekplakorn, W., Chaiyapong, Y., Neal, B., Chariyalertsak, S., Kunanusont, C., Phoolcharoen, W., et al. (2004). Prevalence and determinants of overweight and obesity in Thai adults: results of the Second National Health Examination Survey. Journal of the Medical Association of Thailand, 87(6), 685-693.
Anstine, D., & Grinenko, D. (2000). Rapid screening for disordered eating in collegeaged females in the primary care setting. Journal of Adolescent Health, 26(5), 338342.
Binns, C. W., Lee, M., & Scott, J. A. (2001). The fetal origins of disease hypothesis: public health implications for the Asia-Pacific region. Asia Pacific Journal of Public Health, 13(2), 68-73. Chaisiri, K., Pongpaew, P., Tungtrongchitr, R., Phonrat, B., Kulleap, S., Sutthiwong, P., et al. (1998). Nutritional status and serum lipids of a rural population in Northeast Thailand—an example of health transition. International Journal for Vitamin and Nutrition Research, 68(3), 196-202. Garner, D. M., Olmsted, M. P., Bohr, Y., & Garfinkel, P. E. (1982). The eating attitudes test: psychometric features and clinical correlates. Psychological Medicine, 12(4), 871-878.
Hawks, S. R., Madanat, H. N., Merrill, R. M., Goudy, M. B., & Miyagawa, T. (2003). A cross-cultural analysis of ‘motivation for eating’as a potential factor in the emergence of global obesity: Japan and the United States. Health Promotion International, 18(2), 153-162. Hawks, S. R., Merrill, C. G., Gast, J. A., & Hawks, J. F. (2004). Validation of the Motivation for Eating Scale. Ecology of Food and Nutrition, 43(4), 307-326. Hawks, S. R., Merrill, R. M., Madanat, H. N., Miyagawa, T., Suwanteerangkul, J., Guarin, C. M., et al. (2004). Intuitive eating and the nutrition transition in Asia. Asia Pacific Journal of Clinical Nutrition, 13(2), 194-203. InterASIA. (2003). Cardiovascular risk factor levels in urban and rural Thailand—The International Collaborative Study of Cardiovascular Disease in Asia (InterASIA). European Journal of Cardiovascular Prevention and Rehabilitation, 10(4), 249257.
Kanazawa, M., Yoshiike, N., Osaka, T., Numba, Y., Zimmet, P., & Inoue, S. (2002). Criteria and classification of obesity in Japan and Asia-Oceania. Asia Pacific Journal of Clinical Nutrition, 11 Suppl 8, S732-S737. Ke-You, G., & Da-Wei, F. (2001). The magnitude and trends of under- and overnutrition in Asian countries. Biomededical and Environmental Sciences, 14(1-2), 5360.
Koslowsky, M., Scheinberg, Z., Bleich, A., Mark, M., Apter, A., Danon, Y., et al. (1992). The factor structure and criterion validity of the short form of the Eating Attitudes Test. Journal of Personality Assessment, 58(1), 27-35.



