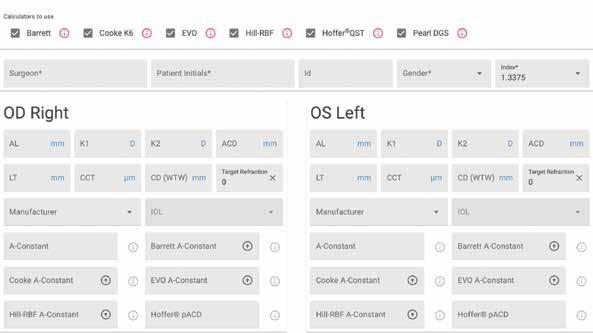
New cataract IOL for Enhanced Intermediate Vision: Precizon Go
Created by Ophtec
Gain extra intermediate vision without compromising the quality of far distance
Precizon Go is the newest addition to Ophtec’s premium line of cataract intraocular lenses (IOLs). This innovative lens represents a significant advancement in enhanced intermediate vision, and closes the gap between traditional monofocal and presbyopic cataract lenses.
Cutting-Edge Design and Technology
The new Precizon Go is a purely refractive lens, precisely engineered with an ingenious technology to provide patients with enhanced intermediate vision while maintaining superior distance vision and visual quality. Its unique optics is characterized by a diopter profile with combined spherical aberrations, which extend the depth of focus without compromising vision quality.
Proven Performance
The new Precizon Go IOL has demonstrated excellent performance both in bench and clinical studies.*
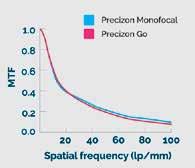
• Modulation Transfer Function (MTF): bench study results show similar MTF curves for both Precizon Go and Precizon Monofocal, confirming the high manufacturing standards of the new design (Figure 1)
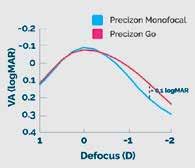
• Simulated Defocus Curve: the simulated defocus curve obtained during bench studies demonstrate a clear advantage of Precizon Go within the defocus range of -0.50 D to -2 D (Figure 2)
“The aspherical profile of the Precizon Go IOL is a stroke of genius. It provides excellent far and intermediate vision without causing dysphotopsia and corrects the corneal positive spherical aberration according to the pupil size.”
Professor Youngsub Eom, MD, PhD
Professor Youngsub Eom, MD, PhD, from the Korean University College of Medicine and Ansan Hospital, performed one of the first surgeries in the clinical marketing study. He remarked, “The aspherical profile of the Precizon Go IOL is a stroke of genius. It provides excellent far and intermediate vision without causing dysphotopsia and corrects the corneal positive spherical aberration according to the pupil size”.
• Visual and satisfaction outcomes: clinical outcomes highlight excellent performance at both far and intermediate distances (CDVA 0,00 ± 0,06 LogMAR, DCIVA80 0,14 ± 0,09 LogMAR & DCIVA66 0,2 ± 0,07 LogMAR), as well as high rates of patient satisfaction with 100% and 94% of patients reporting to be very satisfied or satisfied with far and intermediate vision respectively.
Figure 1. MTF levels of the studied IOLs at the best focus for a 4.5-mm aperture.
Figure 2. Defocus and LogMAR VA simulations as a function of spectacle defocus.
* The scientific data is the result of research studies conducted to evaluate the performance of the Precizon Go IOL, and/or the outcomes in patients receiving surgical implantation of the IOL. The results are summarized in a compendium and can be downloaded at www.ophtec.com/product-overview/precizon-go
With the participation of the Hellenic Society of Intraocular Implant and Refractive Surgery
08 Cover
Which Farsighted Fix?
Evolving technologies opening new doors to best treatments.
16 Expanding the Limits of KLEx
Sri Ganesh MBBS, MS, DNB, DSC(Hon), FRCS(Glasg), FWCRS
22 Second Global Consensus on Keratoconus
Farhad Hafezi MD, PhD, FARVO
24 Corneal Cross-Linking (CXL): From Origins to Modern Innovations
Farhad Hafezi MD, PhD, FARVO; Mark Hillen PhD; and Emilio Torres-Netto MD, PhD, FWCRS
32 New Gene Therapy for LCA Tested Alvin Luk PhD, MBA, CCRA
33 Reducing Injections for nAMD
Sobha Sivaprasad FRCS, FRCOphth, DM
34 Frugal Wet AMD Treatment
Haras Mhmud MD, MPH
Publisher Filomena
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin Roibeárd O’hÉineacháin
Contributors
Laura Gaspari Soosan Jacob
Timothy Norris
Colour and Print CitiPost
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
In Memoriam: Dr I Howard Fine
It is with a heavy heart that we extend our deepest condolences for the loss of Dr I Howard Fine. His passing on 29 August 2024, marks the end of an era for the world of ophthalmology, and we are all profoundly saddened by his departure.
Dr Fine was not just an extraordinary physician; he was a pioneer, a mentor, and a true visionary. His groundbreaking contributions, from new phacoemulsification techniques to refractive lens exchange and clear corneal surgery, have transformed the field, and his work continues to improve the lives of countless individuals around the world. His dedication to advancing eye care through research and innovation, particularly in the clinical evaluation of the Crystalens AT-45, has left an indelible mark that will endure for generations.
Beyond his remarkable achievements, Dr Fine’s engagement with the ESCRS was truly exceptional. His educational contributions to our Society were invaluable, as he generously shared his expertise and passion for teaching. Dr Fine’s lectures and presentations were always eagerly anticipated, and his ability to break down complex surgical techniques and innovations into understandable lessons has educated and inspired generations of ophthalmologists. His commitment to shaping future leaders in ophthalmology through his teaching will forever be remembered and appreciated by the ESCRS community.
But, more than his professional brilliance, what truly set Dr Fine apart was his kindness, compassion, and genuine care for every patient and colleague he encountered. He always took the time to listen, to understand, and to offer his wisdom with a gentle heart. Those of us who had the privilege of learning from him, both professionally and personally, will forever be grateful for the generosity he showed in sharing his knowledge and his time.
His legacy of excellence and empathy will continue to inspire us, but the loss of his presence will be deeply felt by all who knew him.
With heartfelt sympathy,
H Burkhard Dick MD, PhD, ESCRS Secretary
EDITORIAL BOARD
Noel Alpins (Australia)
Bekir Aslan (Turkey)
Roberto Bellucci (Italy)
Hiroko Bissen-Miyajima (Japan)
John Chang (China)
Béatrice Cochener-Lamard (France)
Thomas Kohnen Chief Medical Editor
Oliver Findl (Austria)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Vikentia Katsanevaki (Greece)
Daniel Kook (Germany)
Boris Malyugin (Russia)
José Güell Medical Editor
Paul Rosen Medical Editor
Marguerite McDonald (US)
Cyres Mehta (India)
Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands)
Filomena Ribeiro (Portugal)
Leigh Spielberg (The Netherlands)
Sathish Srinivasan (UK)
Robert Stegmann (South Africa)
Ulf Stenevi (Sweden)
Marie-José Tassignon (Belgium)
Manfred Tetz (Germany)
Carlo Enrico Traverso (Italy)
Research. Education. Innovation.
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
Research Committee is Engine Driving the Future of ESCRS
Commitment to evidence-based medicine anchors studies and other projects.
BY LAURA GASPARI
Medicine advances more and more thanks to the research efforts behind innovations great and small. This is the core assumption behind the work of the ESCRS Research Committee, which is “the brain and heart behind advancing ophthalmic research within the ESCRS community,” according to the committee’s chair, Joaquín Fernández MD, PhD.
The Research Committee does not just decide how much funding to give to a study or a clinical trial, Dr Fernández notes; it aims to nurture research from the very beginning, to support and encourage individuals and groups involved in clinical research, ensuring their work improves science and translates into better patient care. Such commitment to research enhances the prestige of ESCRS and, thus, its influence in the ophthalmic field.
“By supporting groundbreaking research, we help the ESCRS stay at the forefront of clinical innovation and education,” Dr Fernández said.
The main concept driving the Research Committee’s work is evidence-based medicine (EBM). Supporting studies grounded in EBM makes it more likely that physicians will implement the findings in their daily clinical practice and make well-informed decisions for their patients. The studies also help drive innovations in surgical techniques, new standards of care, improved patient outcomes in cataract and refractive surgery and corneal diseases, and systematic reviews and consensus guidelines strongly relying on scientific evidence.
Several Research Committee projects are currently underway, the most important one being the EPICAT study, a multi-arm investigation comparing different interventions during cataract surgery. The preliminary results of EPICAT were presented at the recent
By supporting groundbreaking research, we help the ESCRS stay at the forefront of clinical innovation and education.
ESCRS Annual Congress in Barcelona. “This study is expected to yield critical insights that could change surgical practices globally,” Dr Fernández stated.
Also in Barcelona, the Clinical Research Symposia were fundamental in showcasing the latest research advances and encouraging discussions that could lead to new research initiatives. The Spotlight Symposia on industry-sponsored clinical trials, which are also an important part of the Research Committee’s portfolio of projects, were intended partly to help foster collaboration between academia and industry, which could accelerate the translation of research into clinical practice. To have impact, however, research results need to be communicated properly and effectively. For this reason, the Research Committee also helped produce a medical writing workshop to assist researchers in honing their publication skills and sharing their findings more successfully.
Future projects include establishing specialised working groups focusing on various clinical areas. “These groups are tasked with generating consensus and developing proposals for the scientific community,” Dr Fernández said. The groups will conduct multicentric studies and systematic reviews in collaboration with basic scientific societies, aiming to advance translational research and support the adoption of new technologies and techniques. Specifically, one project will create a unified data collection approach that uses AI and other advanced methodologies to provide ophthalmologists with a reliable data source.
The Research Committee also plays a leading role in the new Functional Vision Working Group and in efforts to create a worldwide consensus on the classification of IOLs. Future projects include implementing patient-reported outcome measures (PROMs) tools and setting up collaborative platforms with other scientific organisations, regulators, and industries.
According to Dr Fernández, the strength of the Research Committee is its commitment to EBM and its respect for the vision of previous leaderships. “I am immensely proud of the outstanding work initiated under the leadership of Burkhard Dick,” Dr Fernández said. “His exceptional vision and dedication have laid a solid foundation for our committee’s success.”
The capillary efforts of working groups are also fundamental to the committee’s success. “The collaborative spirit and innovative approach of these groups are what make me especially proud and optimistic about the future impact of our committee’s work,” Dr Fernández said.
Dr Fernández summed up the Research Committee’s impact by saying it is like having a powerful engine driving the ESCRS mission and ophthalmology forward. “We are not just supporting research,” he said. “We are shaping the future of eye care.”
Joaquín Fernández Pérez MD, PhD is the CEO and Medical Director in the Ophthalmology Department at Qvisión in Vithas Virgen del Mar Hospital (Almería). He can be reached at joaquinfernandezoft@qvision.es
ESCRS forms Functional Vision Working Group
Should enhanced monofocal intraocular lenses (IOLs) be the standard of care? Can IOLs be classified in such a way as to avoid mixing categories and prevent confusion for the user? A group of ESCRS members are working to answer these and similar questions and produce a functional classification that more directly correlates with the effect on patients’ quality of vision.
The ESCRS Functional Vision Working Group, formed by ESCRS President Filomena Ribeiro and led by Research Committee Chair Joaquín Fernández, announced its intentions in a report in the August issue of the Journal of Cataract & Refractive Surgery, which is jointly published by ESCRS and its US counterpart, ASCRS.
“Classifying intraocular lens (IOL) technologies is not an easy task, primarily because of the various categories that can be integrated into a classification,” the working group stated. “Some of these categories represent different characteristics that may be inappropriately combined in an attempt to create a simplified taxonomy, which is not always feasible. Therefore, when defining an IOL, it is crucial to differentiate between various categories and avoid mixing them, to prevent confusion for the user.1
The working group’s report listed categories, subcategories, and options used to classify IOLs, reviewed the optical technologies historically used to classify IOLs, discussed the four main categories of IOLs recognized by the International Organization for Standardization, and presented an evidence-based functional classification that incorporates the scientific method. The report concluded that shifting to a functional vision classification is important because it more directly correlates with the effect on patients’ quality of vision—but conceded additional functional outcomes (such as patient-reported outcomes) should be included in future analyses.
The working group also authored a guest editorial in the same issue of the JCRS titled “Should enhanced monofocal intraocular lenses be the standard of care? An evidence-based appraisal by the ESCRS Functional Vision Working Group.”2 The editorial presented the results of a literature review to analyse the level of scientific evidence on enhanced monofocal IOLs. The working group concluded the literature review justified the use of enhanced monofocal IOLs as the standard of care in cataract surgery, but noted studies are still needed to demonstrate their cost effectiveness vis-à-vis conventional monofocal IOLs.
In addition, the working group met at the ESCRS Annual Congress in Barcelona. The meeting was designed to serve as a foundational session toward building a global consensus for adopting an evidence-based functional classification that integrates patient-reported outcomes. Building this consensus will require including scientific societies, standards organisations, and industry in discussions.
“With an evidence-based approach, the ESCRS Functional Vision Working Group aims to ensure that decisions in cataract surgery not only reflect the true visual needs of the patient, but also advance the field of ophthalmology and strengthen ESCRS’s role in shaping global standards of care,” Dr Fernández said.
For citation notes, see page 38.
Rock concert raises funds for charity vision projects Flamenco music gave way to rock and roll in Barcelona on 8 September when OftalmoRock, a group of musician ophthalmologists, performed a charity concert to benefit ESCRSsupported projects in low- to middle-income countries, principally in Sub-Saharan Africa.
The projects include a “Training the Trainers” programme with the Community Eye Healthcare Unit at the University of Cape Town, which trains ophthalmic surgeons from more than 20 African countries. Another project provides direct expert support with wet labs at the College of Ophthalmology of Eastern, Central, and Southern Africa (COECSA) Annual Congress.
It was an inspiring celebration of community, diversity, and compassion.
ESCRS has also partnered on a major project with the Barcelona-based charity Eyes of the World to provide cataract surgery in northern Mozambique as well as another cataract-oriented project with the Blantyre Institute for Community Outreach (BICO) in Malawi.
“The OftalmoRock concert was nothing short of spectacular!” said one attendee. “It was not just a musical event. It was an inspiring celebration of community, diversity, and compassion. With an incredible turnout, the energy in the room was electric, fuelled by the passion of ophthalmologists from all over the world coming together to support a meaningful cause.”
“The most likely reason for the effective larger zone is that there is less peripheral expansion of fibres after SMILE compared to LASIK and, therefore, less shortening of the OZ. This also probably explains why the refraction is more stable after SMILE—less regression, suggesting SMILE might also provide better optical quality.”
Optimising outcomes after LASIK
Discussing hyperopic LASIK, Dr Carp noted research conducted at the London Vision Clinic, UK, provides guidance on treating high hyperopia/hyperopic astigmatism.3 He focused on the proper technique for ablation centration and deciding on the correction limit for a given eye.
“LASIK for higher levels of hyperopia can be done with reliable safety by centring the ablation on the visual axis and respecting epithelial thickness,” he advised.
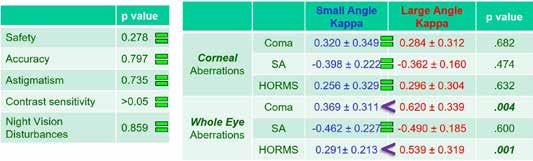
Evidence supporting centring the ablation on the visual axis (i.e., the coaxially sighted corneal light reflex, CSCLR) rather than the Benham of the entrance pupil comes from findings of a retrospective study comparing outcomes of hyperopic LASIK in eyes with a small (≤0.25 mm) versus large angle kappa (≥0.55 mm).4,2 All treatments centred on the CSCLR, and the postoperative results showed no differences between groups in safety, accuracy, induced astigmatism, contrast sensitivity, night vision disturbances, or corneal aberrations.
1
Figure
“Patients with a small angle kappa were effectively treated with pupil-based centration, and if it is correct that the treatment should be pupil-centred, the eyes with a large angle kappa would have had a decentred ablation. [These eyes] should have had poorer vision with higher levels of corneal aberrations. The fact that the outcomes were similar supports the visual axis centration hypothesis,” said Dr Carp, adding other published literature shows consensus on the topic. (see Figure 2)
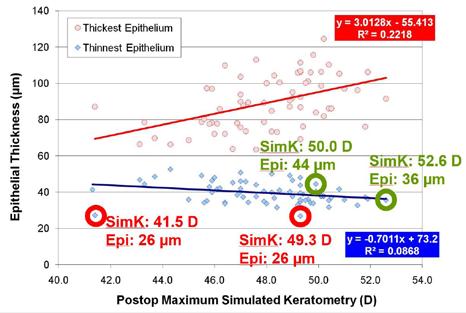
Addressing limits for LASIK treatment of hyperopia/ hyperopic astigmatism, Dr Carp said the amount of correction that can be safely done is determined by considering post-treatment epithelial thickness rather than keratometry.
“Most surgeons will tell you that when performing hyperopic LASIK, you should not steepen the cornea above 49.00 D because excessive steepening can lead to epithelial breakdown (apical syndrome),” he said. “What is more important for understanding epithelial breakdown is to look at the rate of change of curvature of the stromal surface.”
Dr Carp’s research at the London Vision Clinic shows that overall, the central epithelium progressively thins and the peripheral cornea progressively thickens the higher the attempted correction and postoperative keratometry value.3 However, he noted outliers to this pattern, presenting cases of hyperopic LASIK-treated eyes with a thin central epithelium and flat cornea and others with a thick central epithelium despite a steep cornea (>49.00 D).
“Some flat corneas will already have excessive central epithelial thinning, but some steep corneas can be steepened further if the epithelial thickness is sufficient,” Dr Carp said. (see Figure 1)
SMILE
LASIK ICL
Figure 2
A New High for Hyperopia
Hyperopia patients can expect a rise in the array of treatments.
SEAN HENAHAN REPORTS
Spectacle correction of hyperopia has been the standard of care for many centuries. Yet many patients who received them were probably asking, “Thank you for helping me see better, doctor, but isn’t there something you can do that doesn’t involve glasses?” The ophthalmology world has listened to these pleas and currently offers an array of effective interventions.
With an estimated prevalence of hyperopia in Europe of 32% among patients 35 to 74 years of age, the demand for treatment is likely to grow. The current options for hyperopia treatment include spectacles and contact lenses, LASIK, PRK, transPRK, kerato-lenticule extraction (KLEx), small incision lenticule extraction (SMILE), phakic IOL implantation, and refractive lens exchange (RLE). Each has its advantages and limitations.
While spectacle correction can be effective in most cases, patients are obliged to wear glasses, maintain and keep track of them, and replace them regularly. Glasses for hyperopia tend to be heavy and come with problems associated with all glasses, such as limited peripheral vision, fogging, and discomfort. Contact lenses, for their part, also offer effective treatment but carry well-known risks of sight-threatening bacterial and fungal infection and significant maintenance and long-term cost issues.
The desire to be spectacle free drives patients to seek other options. LASIK, which has been used to treat hyperopia since the 1990s, involves both hardware and software. A primary advantage is it allows younger patients to maintain accommodation while reducing the need for glasses. Predictability and regression are a concern, along with regular LASIK issues such as glare and halos.
“It seems there is currently a consensus on the limits of LASIK for hyperopia treatment,” Professor Burkhard Dick MD, PhD said. “It is generally agreed the upper limit for hyperopia correction via LASIK is between +4.00 D and +6.00 D, with the exact range depending on factors such as corneal and epithelial thickness, shape, optical zone, model of excimer laser, and the surgeon’s experience. It is advisable to avoid corrections beyond this range, as the risk of undercorrection, regression, and induced aberrations increases, making outcomes less predictable.”
Lenticule extraction procedures, now known under the umbrella term KLEx, have served in myopia treatment for many years, but have only recently been tried as an alternative to LASIK for hyperopia treatment. The recent ESCRS Congress in Barcelona featured the announcement of the first EU approval of a lenticular extraction hyperopia treatment using SMILE pro technology (Zeiss).
There is still debate and discussion about the relative merits of KLEx versus femtosecond-LASIK (FS-LASIK) for
hyperopia. The general thought is KLEx may be comparable to FS-LASIK in mild to moderate hyperopia cases, particularly when a flapless procedure is a priority. However, Prof Dick said it is worth noting that FS-LASIK has a more established track record for hyperopia and has been refined over decades.
“Compared to myopic KLEx, KLEx for hyperopia is more challenging for the surgeon because of the different shape and larger diameter of the lenticule requiring the use of a larger patient interface,” he noted. “Still, hyperopic KLEx is a minimally invasive procedure with a lower risk of severe complications compared to intraocular options, which could make it a suitable choice for some patients. As of today, it remains to be seen whether KLEx will have less regression over time due to its greater optical and transition zones.”
Phakic IOL
One possible option for hyperopia is a phakic IOL. In cases where the patient is experiencing moderate to high hyperopia (typically beyond +4.00 D) or when the corneal thickness or shape does not allow for safe laser correction, phakic IOLs may be preferable.
“Phakic IOLs may be an especially attractive option for younger patients with good lens clarity, as phakic IOLs preserve accommodation,” Prof Dick said. “Unfortunately, the anterior chamber depth and configuration in these hyperopic eyes often do not allow implantation of a phakic IOL, especially considering the increasing lens thickness in younger patients over time.”
Refractive lens exchange
Prof Dick suggested refractive lens exchange (RLE) may be the best option for select patients who may not be suitable candidates for other surgical approaches. It carries the same small risks as standard cataract surgery, including infection, capsular rupture, and posterior capsule opacification.
It may also be suitable for hyperopic patients older than 40 to 45 years old, particularly when presbyopia begins to manifest or when the degree of hyperopia exceeds the safety limits for laser or phakic IOL treatments. Those with early cataracts may find it beneficial, Prof Dick explained, as RLE offers a long-term solution by removing the dysfunctional lens and correcting vision in a single procedure.
Please see related articles in this issue for the latest studies on hyperopia treatment.
H Burkhard Dick MD, PhD is Professor of Ophthalmology and Chairman, Ruhr University Eye Hospital Bochum, Bochum, Germany. He is also Secretary of the ESCRS. dickburkhard@aol.com
New ESCRS Guidelines for Cataract Surgery
After an exhaustive study and review process, the ESCRS has announced new cataract surgery guidelines that provide practical, evidence-based recommendations to improve care quality and decision making.
ESCRS formed a multidisciplinary guideline panel balanced to minimise potential bias from conflicts of interest. The panel prioritised clinical questions and outcomes according to their importance for clinicians and patients. The guideline-development process used a Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach and a GRADE Evidence to Decision framework—supported by a team of methodologists.
The panel agreed on recommendations concerning 31 questions for patient pathways for cataract management. Key recommendations of these guidelines include (according to level of evidence):
1. An intracameral injection should be used (e.g., cefuroxime 1 mg in 0.1 mL) at the end of the cataract surgery to lower the risk of postoperative endophthalmitis. (GRADE +++)
2. Topical anaesthesia appears to be the most used anaesthesia technique during cataract surgery, if suitable for the patient. (GRADE ++/+++) For further reducing pain during the cataract surgery, an additional intracameral lidocaine injection can be considered. (GRADE ++/+++)
3. Toric IOLs should be considered in eyes with a degree of corneal astigmatism of 1.0 D or more, with strong evidence for corneal astigmatism above 2.0 D, moderate evidence for corneal astigmatism above 1.5 D, and may be beneficial above 1.0 D. (GRADE ++)
4. The selection of a specific target refraction highly depends on the selected IOL, expectations, and preferences of the patient. The patient and ophthalmologist should take the shared decision for IOL target selection. (GRADE ++)
5. The primary treatment options for CME after cataract surgery are topical NSAIDs or steroids. However, there is a lack of sufficient evidence to establish the optimal treatment approach for this condition. (GRADE ++)
6. Both conventional cataract surgery (CCS) and femtosecond laser-assisted cataract surgery (FLACS) can be used, as they are both safe and effective procedures. (GRADE +/++). They give comparable visual acuity and refractive outcomes and overall intraoperative and postoperative complication rates. (GRADE +/++)
7. A combination of NSAIDs and corticosteroid eye drops is more effective to use after routine cataract surgery to prevent inflammation and CME compared to monotherapy. (GRADE +/++)
8. In diabetic patients without diabetic retinopathy, it is recommended to use a combination of corticosteroid and NSAID eye drops to prevent cystoid macular oedema. (GRADE +/++) In patients with diabetic retinopathy, a supplementary depot of triamcinolone should be considered to reduce this risk. Intraocular pressure must be monitored postoperatively when using a triamcinolone depot. (GRADE +)
9. Immediate Sequential Bilateral Cataract Surgery (ISBCS) is effective and safe, has a high degree of patient satisfaction, and can be considered in patients without complicationinducing ocular comorbidities. (GRADE +)
10. EDF IOLs or pseudophakic monovision can be recommended for patients who desire a good intermediate visual acuity, with significantly less dysphotopsia compared to patients who received multifocal IOLs. (GRADE +)
11. In general, posterior segment OCT in cataract surgery should be used when there is a clinical indication, such as age-related macular degeneration, diabetic retinopathy, glaucoma, or when the visual acuity is worse than expected. (GRADE +)
12. Patient selection for pseudophakic presbyopia-correcting IOLs should be based on the presence of ocular comorbidities, the desire for spectacle independence, and realistic patient expectations. (GRADE +)
13. In the case of a toric IOL implantation, the preoperative assessment should encompass not only general mandatory evaluations but also corneal topography and/or tomography. (GRADE +) Methods that include measurements of factors such as additional posterior corneal astigmatism and effective lens position are preferred for toric IOL calculation. (GRADE +)
14. Specific IOL formulas are recommended for eyes with certain conditions to ensure accurate outcomes. In extreme long and short eyes, new-generation formulas are recommended. (GRADE +)
15. Postoperative remote care after cataract surgery might replace short-term clinical examination to better allocate hospital resources and increase time and cost efficiency. Accuracy and validity of remote care and telemonitoring are still to be evaluated. (GRADE +)
ESCRS EPICAT Study Updates
Early results suggest subconjunctival 10 mg triamcinolone an effective strategy for dropless cataract surgery.
NORRIS REPORTS
Preliminary results of the long-awaited ESCRS EPICAT study suggest subconjunctival 10 mg triamcinolone injection could be the most effective dropless strategy for cataract surgery, with lower impact on IOP, less incidence of postoperative cystoid macular oedema (CME), and clinically significant macular oedema (CSME).
According to lead investigator Nienke Visser MD, the EPICAT study aims to find a valid alternative to periocular anti-inflammatory drug use for pseudophakic cystoid macular oedema prevention. A dropless cataract surgery can effectively cut costs and reduce treatment burden for both patients and caregivers, she said.
The European multicentred randomised clinical trial was conducted on 808 patients who underwent cataract surgery in 10 sites across 4 European countries. Patients in the control group received topical dexamethasone and bromfenac eye drops 2 days preoperatively and in a 4-week tapering scheme postoperatively. Patients in the Intervention 1 group received subconjunctival injections of 10 mg triamcinolone, while the Intervention 2 group received intracameral ketorolac added to the irrigation fluid—both during cataract surgery. Finally, the Intervention 3 group received a combination of triamcinolone and ketorolac intraoperatively.
The main study outcome is the mean change in central subfield macular thickness (CSMT) at 6 weeks compared to preoperative measures, Dr Visser said. Secondary outcomes of the study included the incidence of CME, CSME, mean corrected distance, visual acuity, and IOP. An extensive ophthalmic examination was conducted on patients at baseline, 6 weeks postoperatively, and 12 weeks postoperatively.
The results showed significantly higher mean and mean change in CSMT in the ketorolac group compared to the other groups at 6 weeks. No significant differences between groups were observed at the 12-week follow-up.
Within 12 weeks, the incidence of CME was 12.7% in the ketorolac group—significantly higher than the other three groups, Dr Visser noted. Incidence in the control group was 2.6%, 0.6% in the triamcinolone group, and 0.7% in the combined triamcinolone-ketorolac group. The incidence of CSME was also significantly higher in the ketorolac group, with 5.1% compared to 0.6% in the control and triamcinolone groups and 0% in the combined group. Escape medications due to CSME or severe anterior chamber inflammation were also 12 times more likely in the ketorolac group. Mean IOP was higher in the triamcinolone group compared to the other three groups, but, she added, the mean difference was very small. IOP spikes were irrelevant, with only 3.1% of cases in the triamcinolone group compared to 1.3% in the control group and 0% in the other groups.
The preliminary results of the ESCRS EPICAT study showed that triamcinolone 10 mg is an effective dropless strategy for the prevention of CME or CSME, with the potential to save millions in healthcare costs. Final results are expected next year, she concluded.
Dr Visser presented the findings at the 2024 ESCRS Congress in Barcelona.
Nienke Visser MD is a medical specialist at Maastricht UMC+, Netherlands. nienke.visser@mumc.nl
TIMOTHY
Expanding the Limits of KLEx
Hyperopia treatment receives CE approval; mixed astigmatism may follow.
HOWARD LARKIN REPORTS
The potential applications of keratorefractive lenticule extraction (KLEx) are expanding for refractive corrections of all types, including hyperopia, according to Sri Ganesh.
“Commercial software has been limited to myopia and myopic astigmatism, and hyperopic software has just been introduced,” Dr Ganesh said. Mixed astigmatism correction is in the works and may soon follow, as may wavefront and topography guided KLEx, he added.
Current commercial CE limits on KLEx for myopia are -1.00 D to -10.00 D with up to -5.00 D astigmatism and -12.00 D spherical equivalent. For hyperopia, commercial corrections are available for up to +6.00 D with up to +5.00 D astigmatism and up to +7.00 spherical equivalent in hyperopic meridian.
Myopia
Dr Ganesh has had success with KLEx across the myopic range, including for low myopia. “For low myopia, there is some consensus that KLEx might not work as well, and PRK might be better.”
However, a study Dr Ganesh and colleagues conducted found better quality of vision, including better contrast sensitivity, and greater patient satisfaction due to better postoperative comfort among low myopia KLEx patients three months after surgery.
Pushing the commercial limit for high myopia, Dr Ganesh reported a case of -10.00 D with -1.75 D astigmatism correcting to 0.00 D sphere and -0.50 D astigmatism, and uncorrected distance vision of 6/5.
He has even had success with very high myopia using research software. For example, a patient with -15.00 D sphere and -3.50 D cylinder was corrected to -0.50 D sphere and -1.25 D cylinder with UDVA of 6/9. “It’s possible to treat very high myopia, but commercially, it’s not available.”
Yet Dr Ganesh said very high myopia may be corrected by combining a phakic intraocular lens with KLEx. A study of 12 eyes in 7 patients undergoing combined phakic implant and KLEx with a mean preoperative -23.30 D ultimately resulted in gains of two to four lines of corrected distance visual acuity in all eyes.
Astigmatism
High myopic astigmatism is also treatable with KLEx, Dr Ganesh added. He emphasised the need to adjust for cyclotorsion in correcting myopic astigmatism, especially those with a higher cylinder.
Mixed astigmatism is another question because it is not currently available with commercial software. Even so, Dr Ganesh has done it with research software with good results. The procedure involves correcting the astigmatism first, followed by the hyperopia. He published a series of 13 mixed
92%
He published a series of 13 mixed astigmatism eyes, in which 92% reached UDVA of 6/9.5 and 54% reached 6/6 or better after KLEx correction.
astigmatism eyes, in which 92% reached UDVA of 6/9.5 and 54% reached 6/6 or better after KLEx correction.
“Hopefully, we will have the commercial software in the near future.”
Hyperopia
Hyperopia corrections are possible with newly CE-marked software, Dr Ganesh said. “The results are quite similar to LASIK, but the long-term stability is better,” he said of the global registration study for hyperopic KLEx.
“I have treated hyperopia from the age group of 18 to 60 years. The ideal amount of hyperopia where we get good results is up to 4.50 D, but you can treat up to 6.00 D and a spherical equivalent of 7.00 D,” he told EuroTimes. “In higher corrections for hyperopia, you can expect some regression and induction of higher-order aberrations which can potentially reduce the BCVA (similar to hyperopic LASIK).”
Dr Ganesh spoke at the 2024 ESCRS Congress in Barcelona.
Sri Ganesh MBBS, MS, DNB, DSC(Hon), FRCS(Glasg), FWCRS is chairman and managing director of Nethradhama Hospitals in Bangalore, India.
Post-LASIK Tonometer Takes ESCRS Innovators Den Prize
Good ideas lead to solutions to unmet needs.
Ophthalmologists are full of ideas to meet unmet eye care needs. But taking an innovation from concept to clinic is a long journey. ESCRS set up the Innovators Den: Eye Care Pioneers programme to help doctors along the way, providing the mentors and business advisors needed as guidance and contacts.
“This is the future of how we meet those unmet needs through innovation,” said Dr Vance Thompson, who chaired this year’s session. “The goal is to speed up the process.”
LASIK tonometer
Each year, dozens of doctors submit ideas through the ESCRS website, from which three finalists are selected. Leading off this year’s finalists was María Iglesias MD, PhD. She presented a new tonometer designed to more accurately measure intraocular pressure (IOP) in patients who have undergone corneal refractive surgery.
Because removing tissue reduces the cornea’s profile and stiffness at the centre, the widely used Goldmann applanation tonometer tends to underestimate IOP in post-LASIK patients—potentially delaying glaucoma diagnosis and treatment. However, if a convex lens is applied to the cornea, depressing it centrally while applying pressure peripherally, its biomechanical responses are similar to pre-LASIK values, Dr Iglesias explained.
Quantifying vision quality
Next up, Harilaos Ginis PhD presented a diagnostic device designed to quantify retinal vision quality in patients with multifocal or other advanced technology intraocular lenses (IOLs). It will help ophthalmologists understand the visual complaints of patients with good visual acuity but poor vision by near-instantaneous measurement of, among other things, contrast, diffractive phenomena, astigmatism, refraction, chromatic and other aberrations, and stray light at the retina, which degrade image quality.
The device should help find solutions by identifying the sources of near, intermediate, and far vision problems, such as astigmatism and dry eye, Dr Ginis said. “This can boost your confidence to use premium lenses because you know what is going on.” Understanding how lenses work may also help improve outcomes, he added.
Watch the finalist presentations and meet the mentors from the 2024 Innovators Den.
Improving on eye drops
Last, Jean Garrec described a biopolymer pill that resides under the lower eyelid, steadily releasing topical medications for seven days. The device would address eye drop limitations, including inconsistent concentration, wasted drugs, and poor compliance, without the need for invasive inserts.
Placed similarly to a contact lens, the weekly pill has shown efficacy in phase 1 glaucoma clinical trials, he said. It is also under development for macular oedema and could be used for other conditions, including dry eye, and as a gene therapy.
Considering factors including the size of the opportunity, feasibility, and the people behind the products, the judges— Professor Filomena Ribeiro, ESCRS president, Diana Saraceni, founder of Panakès Partners venture capital, and Dr Shahzad Malik, general partner at Advent Life Sciences venture capital—found Dr Iglesias’ presentation most compelling.
“It’s difficult to make this decision,” Prof Ribeiro said. “The ideas are all brilliant.”
This prize was presented at iNovation Day at the 2024 ESCRS Congress in Barcelona.
María Iglesias MD, PhD, FEBO is an ophthalmologist and inventor with the Barraquer Ophthalmology Centre, Barcelona, Spain. mariaiglesiasalvarez@gmail.com
Harilaos Ginis PhD is senior scientist and co-founder of Diestia Systems, Athens, Greece. dimetirios@diestia.com
Jean Garrec PharmD is founder and CEO of Biophta, Paris, France. contact@biophta.com
HOWARD LARKIN REPORTS
Several companies developed platforms, which may vary slightly in terms of laser frequency, energy distribution, and treatment range and need more data in the long term. This second generation of devices contains new features which gain advantages and a smaller footprint of the laser to better fit in the surgical rooms and ease the surgeon learning curve.
The ESCRS Annual Congress in Barcelona saw the first option for hyperopia presented by Zeiss, supported by a multicentre, prospective, European study with excellent results at 12 months—showing 81% of treated eyes were within ±0.50 D and 93% within ±1.00 D with a good safety index and no loss of control sensitivity.4 Finally, Prof Nubile showed the possibility of using the extracted KLEx lenticules for therapeutic and refractive purposes instead of throwing them away.
Many studies are considering different applications of these lenticule—such as the treatment of irregular or diseased corneas avoiding keratoplasty or the correction of ametropias through allogeneic lenticule implantation—supported by several groups, especially for hyperopia, and the results are improving year after year.5 Lenticule implantation can also be used for correcting post-LASIK ectasia or keratoconus and to correct mixed astigmatism; one group suggest-
ed rotating the lenticule internally in the cornea without any extraction.
Nonetheless, the new frontier is to bioengineer human stromal lenticules, decellularising them to avoid any DNA trace and use them for therapeutic purposes, such as longterm sustained drug release intrastromally using implanted nanoparticles or microparticles of the extracted lenticules. Other possibilities are on the horizon, and Prof Nubile said the best has yet to come.
“The lenticule era just started, and we have much more to see in the future.”
Prof Nubile presented at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 38.
Mario Nubile MD, PhD is Associate Professor of Ophthalmology and Director of the Cornea Service at the “G. D’Annunzio” University of Chieti-Pescara, Italy, and National High-Tech Eye Centre, University of Chieti-Pescara, Italy, respectively. m.nubile@unich.it
Double Down On Your Decision
Screening for ectasia with double safety
The Tomographic Biomechanical Index, or TBI, provides a unique combined expression of Corvis® ST und Pentacam® measurement data. It allows the risk of corneal ectasia to be assessed with greater reliability than ever before. The TBI assists you in selecting the optimal treatment based on sound reasoning.
More safety for you and your patients!
Automating Cataract Surgery Assessment
AI system measures eye stability and centration in procedures.
In cataract surgery, the eye is something of a moving target. Keeping it relatively still is essential to safely and efficiently perform the procedure. Doing so requires experience and may be one way to measure surgical skill.
A newly developed artificial intelligence (AI)-powered program automatically measures surgeons’ ability to keep the eye stable, centred, and in focus during cataract surgery from video images. Using these measurements, the system also distinguishes between resident and attending surgeons with about 87% accuracy.
Resident surgeons perform as many as 150 cataract procedures during training, and many studies have shown trainees have a higher rate of intraoperative complications than experienced surgeons, noted Dena Ballouz MD. With further development, an automated system such as the one she helped develop might eventually be used to objectively assess surgical skill for training and certification.
Measuring eye movement
The AI-powered system works by analysing video images taken throughout the cataract procedure to identify three metrics for assessing eye motion: the distance between the limbus centroid and Purkinje image 1 (LCP1), a stability metric; the distance between the limbus centroid and the centre of the video frame (LCFC), a centration metric; and the focus level of the recorded video frame (FS), a focus metric. For each metric, a lower score indicates less movement and a higher level of surgical skill.
cases. The three surgical steps during which residents struggled with eye stability and centration most were cortical removal, with mean LCP1 nearly 20% greater and LCP1 standard deviation more than 50% greater than for attending surgeons; viscoelastic removal, with mean LCP1 more than 50% greater; and wound closure, with LCP1 standard deviation 22% greater. Residents also struggled to maintain adequate focus throughout surgery, with mean FS scores higher than for attending surgeons across all surgical steps. In addition, the system correctly classified surgeons as resident or attending with about 87% accuracy.
“This is just the beginning of how AI can be used for cataract surgery assessment,” Dr Ballouz said. Future applications might include objective feedback—possibly in real time—for cataract surgery training and surgical skills competency tests.
Dr Ballouz presented at ARVO 2024 in Seattle, US.
Dena Ballouz MD is an ophthalmology resident at the University of Michigan, Ann Arbor, Michigan, US. dballouz@umich.edu
Several models were tested for each assessment com ponent. They pre-processed images to correctly identify and measure the desired anatomical features; assessed the relationships among those features according to the proposed metrics; and assessed the skill level required to achieve a given measure.
The preprocessing component was developed with a deep-learning model trained and validated on 5,700 annotat ed images from 190 cataract surgeries. Then, images from 411 cataract surgeries—211 from attending surgeons and 195 from residents—were evaluated on the three proposed metrics. Finally, a skills assessment module was developed using a machine learning model to evaluate the differences in metrics between attending and resident surgeons.
Meaningful results
Using the best-performing models of each component, the case-level mean and standard deviation for all three metrics were significantly lower for attending cases than for resident
HOWARD LARKIN REPORTS
Second Global Consensus on Keratoconus
Forthcoming position paper to provide an updated and expanded view on evaluation and management.
CHERYL GUTTMAN KRADER REPORTS
In 2013, the recognition of revolutionary advances in keratoconus diagnosis and management led experts to organise a Delphi panel and create a Global Consensus on Keratoconus and Ectatic Diseases. This work, which addressed controversies and open questions and introduced a new definition of the disease, was published as a position paper in the journal Cornea in April 2015.1
“The fact that, to date, this paper has been cited by authors of more than 1,000 published articles speaks to its importance,” said Farhad Hafezi MD, PhD.
In the decade after work on the Global Consensus began, new knowledge accumulated at a rapid rate, and with the acknowledgement that the first consensus received criticism because it involved representatives from cornea societies but not refractive groups, work on a Second Global Consensus on Keratoconus began in 2023.
“Led by Dr José Alvaro Gomes, myself, and Dr Renato Ambrósio, more than two-thirds of the work on this new project is complete, as of September 2024,” he said. “Hopefully, a manuscript will be ready to be submitted for publication in a high-impact journal in the spring of 2025 and will be available to all in the summer.”
Providing an update on the process and progress of the Second Global Consensus group, Dr Hafezi began with its predecessor. He explained that it was a direct collaboration of four supranational cornea societies (PanCornea, Asia Cornea Society, EuCornea, and Cornea Society), whose participants divided among three subcommittees to address three major topics: definition/diagnosis, medical/clinical treatment, and surgical management. Each subcommittee was comprised
of 3 coordinators and 12 experts, all selected because of their knowledge and experience and an aim of global representation. The project was led by Brazilian ophthalmologist José AP Gomes MD, who also served as a coordinator in the clinical treatment subcommittee.
Content was derived using the Delphi method to reach a consensus where more than two-thirds of the experts arrived at the same opinion.
“Our mission was not to create a guideline, but rather a momentary view of the prevailing opinion of leading experts in the field,” Dr Hafezi explained. “We realised it would never be possible to achieve 100% consensus of opinions among leading experts.”
A more inclusive worldview
An aim in organising the Second Global Consensus on Keratoconus group was to be more inclusive. To that end, participants were not only drawn from the same four supranational cornea societies but other international refractive surgery/ophthalmology/keratoconus societies (Middle East Council of Ophthalmology, Australia and New Zealand Cornea Society, Brazilian Association of Cataract and Refractive Surgery, International Society of Refractive Surgery, and the Keratoconus and Crosslinking Experts). The effort receives financial support from the Light for Sight and Violet June foundations and industry stakeholders.
“We asked every major player in industry to support us with the same amount of funding,” Dr Hafezi noted. “The industry sponsors have no influence on the outcome, but they all recognise how important it is for medical professionals to have a common view.”
Corneal Cross-Linking (CXL): From Origins to Modern Innovations
The first of a three-part series by Professor Farhad Hafezi MD, PhD; Mark Hillen PhD; and Emilio Torres-Netto MD, PhD.
It has been 25 years since the introduction of corneal cross-linking (CXL) to clinical practice.1 Since then, CXL has revolutionised the treatment of keratoconus and other corneal ectatic diseases, and its list of indications has expanded far beyond its original scope.2 Invented in Dresden, Germany, and pioneered in Zurich, Switzerland, the story of how CXL was invented by Professors Theo Seiler and Eberhard Spoerl is one of lateral thinking, inspiration from outside sources, and a little bit of luck.
Prior to CXL, few treatment options were available for corneal ectasias. The visual symptoms could be (somewhat) corrected by special contact lenses, but this did nothing to halt the progression of the underlying disease. Once the ectasia had progressed to a point where hydrops kept occurring, risking perforation, the final treatment option was keratoplasty.
CXL represented the first (and remains the only) treatment method proven to halt ectasia progression. It is worth noting that, in the first three years since its introduction, CXL had dramatically reduced the need for keratoplasties: it was calculated to have reduced the number of corneal transplantation procedures performed in the Netherlands by 25%.
Seiler and Spoerl’s early work
The concept emerged in the 1990s when Seiler and Spoerl sought methods to halt the progression of corneal ectasias,
particularly keratoconus. At that time, it was already known that keratoconic corneas were approximately 60–70% weaker than normal corneas and contained significantly fewer cross-linked collagen fibrils in the cornea’s principal structural layer, the stroma. Seiler and Spoerl knew corneal stiffness increases with age and, thanks to the formation of advanced glycation end-products, occurred at a far faster rate in people with diabetes compared with people without the condition.
Could chemical agents cross-link and, therefore, perhaps stiffen the cornea? To find out, they investigated a range of chemical agents capable of inducing covalent cross-links in stromal collagen and extracellular matrix proteins. Among these, glutaraldehyde and aldehyde sugars showed the most promise, but they presented challenges in localising the effect to just the cornea (i.e., avoiding leaks) and required impractically long times to achieve any significant stiffening.
Seiler’s “eureka!” moment came during a dental appointment. He noticed his dentist used ultraviolet (UV) light to solidify the dental resins used as fillings. This ultimately gave him the idea of using UV light with a chromophore to catalyse the chemical cross-linking process. The advantages were clear: catalysis speeds the chemical process, and light limits the reaction to the region being irradiated.
Riboflavin (vitamin B2) was soon identified as the chromophore of choice for CXL. Unless photoactivated, riboflavin is
relatively inert and has a broad absorption spectrum, particularly in the UV-A range (300–370 nm). The only drawback is that riboflavin is a large molecule with a high molecular weight of 376.36 g/mol.
Terminology
The terminology used today (corneal cross-linking/CXL) was defined by consensus at the 2008 annual CXL Experts’ Meeting in Zurich. The adoption of ‘CXL’ has since been widely accepted in both academic literature and clinical practice, providing a consistent and accurate reference for discussing and comparing cross-linking protocols and outcomes. But it wasn’t always like this.
In the early days, ‘CCL’ (corneal collagen cross-linking) and ‘X-linking’ were used, and ‘C3-R’ (a commercial trademark) was adopted by some surgeons as a general term for the procedure, particularly in India and some centres in the US. Seiler and his colleagues originally called the procedure ‘corneal collagen cross-linking’ to emphasise the interaction between photoactivated riboflavin and the collagen fibres in the cornea. This was reconsidered after it was understood that cross-links form not only within collagen fibres but also between collagen and proteoglycans; the name did not fully capture the complexity of the biochemical interactions. A single, standardised name was necessary, and CXL was how the ‘CXL experts’ defined it.
The Dresden protocol: the original blueprint for CXL
The first method of performing CXL, known as the ‘Dresden protocol,’ was effective at halting ectasia progression.1 Remarkably, it has stood the test of time, remaining the ‘gold standard’ method for performing CXL for most of the procedure’s existence. Studies have shown its ability to halt the progression of progressive keratoconus persists for more than 15 years.4
It has its drawbacks. Dresden protocol CXL requires the removal of an approximately 8 mm region of the central corneal epithelium, as riboflavin is too large to penetrate between the tight junctions of the corneal epithelial cells and reach the stromal layer below where the cross-linking effect is required. Although the epithelial cells regrow and repopulate the endothelial cell layer (typically over the next 3–7 days), this requires careful pain management and antimicrobial drug prophylaxis until the epithelial defect is closed.
After epithelium removal, the stroma is saturated by the application of a 0.1% riboflavin solution, dropped from above, for approximately 30–60 minutes. This is followed by UV irradiation of the stroma to photoactivate the riboflavin and generate reactive oxygen species (ROS),5 which then go to oxidatively and covalently cross-link together stromal collagen and proteoglycan molecules together, thereby strengthening the cornea and counteracting the ectasia weakening.6 This has advantages and disadvantages. The disadvantage is that the UV irradiation takes 30 minutes to deliver the total dose (fluence) of UV energy required to cross-link the cornea (5.4 J/ cm²). The Dresden protocol irradiation intensity is a relatively weak 3 mW/cm²—a function of the fact that 25 years ago, this was the maximum output that affordable, commercially available mercury vapour UV lamps could achieve.
Some important concepts are associated with CXL. At about 2 weeks after the procedure, a visible ‘demarcation line’ in the stroma can be observed either at the slit lamp or through anterior segment optical coherence tomography (AS-OCT) imaging. Although the stroma is mostly acellular, the ROS generated by CXL kills stromal keratocytes, and the demarcation line appears to be the boundary where viable keratocytes persist. Many view the demarcation line as correlating with the depth of cross-linking effect procedure, but others have found the depth of the demarcation line bears no relation to in-vivo markers of biomechanical strengthening.7, 8
Generally, Dresden protocol CXL cross-links approximately the top 330 µm of the stroma, which was by design. Seiler and his team calculated that a 70 µm uncross-linked region at the base of the stroma was required to protect the corneal endothelium from UV-related damage. This brought the final drawback of the Dresden protocol: it required a minimum stromal thickness of 400 µm for the procedure to be performed.9 The problem with corneal ectasias that progressively weaken and thin the cornea is many of these ‘thin corneas’ have advanced disease and would likely benefit from CXL, yet cannot receive it.
For citation notes, see page 38.
A video discussing this topic can be seen at bit.ly/cxl25years.
Farhad Hafezi MD, PhD, FARVO is the Medical Director of the ELZA Institute in Zurich, Switzerland and is an ESCRS board member.
Mark Hillen PhD is the Communications Director of the ELZA Institute.
Emilio Torres-Netto MD, PhD, FWCRS is a cornea, cataract, and refractive surgeon at the ELZA Institute.
Knowing Iris Repair: Pinhole Pupilloplasty Instead of Keratoplasty
Which scenarios require PPP and which PK?
BY DR SOOSAN JACOB MS, FRCS, DNB
There are many conditions where the presence of a corneal scar necessitates a penetrating keratoplasty (PK). When the scar traverses through the centre of the visual axis, the indication for a PK is generally considered absolute for visual rehabilitation. Other conditions where a PK is not a must but still often opted for include a scar close to the visual axis and a central scar almost but not fully covering the pupil. In all these cases, the higher-order aberrations are quite significant; and even if the visual axis is spared, a PK is often still performed to attain a more uniform surface and, thereby, better visual quality. However, PK has its own disadvantages, including the risk of permanent vision-threatening complications such as expulsive haemorrhage, endophthalmitis, and traumatic wound dehiscence. In addition, other intraoperative complications such as difficult surgery, risk of vitreous loss and lens, or IOL expulsion, as well as postoperative complications (such as irregular astigmatism, rejection, glaucoma, surface- and suture-related complications, and Urrets-Zavalia syndrome), can result in limitation of vision or progressive loss of vision, pain, and cosmetic disfigurement.
Primary or secondary comorbidities such as corneal neovascularisation and peripheral anterior synechiae are often seen in such patients, and performing corneal transplantation in such conditions can greatly increase the chances of rejection of the graft. Thus, PK in patients with corneal scars on or near the visual axis is not always an uncomplicated way forward. The pinhole pupilloplasty (PPP) technique is an option to overcome the disadvantages of PK in such situations, and it can give visual results as good or even better than a PK would have despite the persistence of the corneal scar.
Preoperative marking and assessment
Patients with corneal scar very close to the visual axis causing irregular astigmatism may undergo PPP instead. The desired location of the pinhole pupil is marked preoperatively by slit lamp examination over the coaxially sighted corneal light reflex (CSCLR). While marking, the patient fixates with the eye on the slit lamp light kept perpendicularly and with the other eye occluded. If the CSCLR overlies a large scar covering the pupil, the pinhole pupil is shifted slightly.
The size of the pinhole pupil is determined preoperatively by using the Holladay pinhole device, which essentially consists of an opaque disc with a series of different-sized apertures created on a metal template. The patient will view the visual acuity chart through the template and try different apertures. The desired pinhole pupil size is the one the patient sees most clearly through. The Holladay device is autoclavable and can also be used intraoperatively to assess the created pupil size. However, as the corneal magnification factor comes into play intraoperatively, the apparent size of the pupil created is larger than the real size by about 8 to 10%. Therefore, the real pupil size may be created very slightly smaller than that estimated by the Holladay device.
Surgical technique
It is important to preoperatively mark the CSCLR while still avoiding the scar. During surgery, this mark acts as a guide to position the eye under the reflection of the operating microscope lights.
Since the pupil will be fixed into a pinhole size and multiple needle passes go through the iris close to the pupil, the patient undergoes phacoemulsification with IOL implantation in the same sitting just before iris surgery. The anterior chamber (AC) is then filled with viscoelastic in an eye with an intact posterior capsule. In a vitrectomised eye, a trocar anterior chamber maintainer is used. The patient’s head and eye position are first adjusted to avoid parallax error by bringing the first and fourth Purkinje images to overlap. This is easily possible if the scar does not cut across the first Purkinje image. Pupilloplasty is then performed using any preferred technique, such as the single-pass, four-throw pupilloplasty (SFT) or the modified Siepser knot technique. For SFT, essentially a 10-0 or 9-0 polypropylene suture on a straight needle is drawn through the proximal and distal iris segments, following which a loop of the suture from ahead of the proximal pass moves through the distal paracentesis. The distal end of the suture is then cut and passed through this loop four times, and the two suture ends on either side of the limbus are drawn apart to pull the loop into the AC and tighten the knot. A few knots are taken consecutively next to each other on either side of the pupil to decrease the pupil size to the desired diameter. The pupil location is also shifted to the desired spot. It is important to ensure a careful needle pass to avoid tearing the iris stroma. Knots are cut close without long ends.
Pinhole pupilloplasty for corneal scar: A) Linear scar running across the cornea and traversing the visual axis; B, C) PPP performed for corneal scar instead of penetrating keratoplasty. (Image courtesy Prof Amar Agarwal)
With the Zeiss Lumera™ microscope, if the pupil touches the Purkinje image (P1) all around, the size is around 1.0 mm, and if the pupil is just slightly larger than the P1, the size of the pupil is approximately 1.5 mm. In case the pupil becomes too small, it can be enlarged to the desired side using either a retinal endodiathermy probe (iridodiathermy) applied to the iris stroma on the side needing pupil enlargement or a vitrector for trimming iris tissue gently and carefully using a low cut rate and vacuum. A not-so-round pupil can similarly be made more circular using either the vitrector or endodiathermy probe.
Pinhole optics
A pinhole narrows the beam of light entering the eye, thereby decreasing image blurring on the retina. It decreases peripheral aberrations and increases visual acuity and depth of focus. The decreased pupillary size also lowers the chord mu value. Pinhole optics may be used non-surgically via pinhole glasses or contact lenses. They may also be implanted into the eye either within the cornea—e.g., the Kamra™ inlay (Acufocus)—or as an intraocular lens, such as the IC-8 Apthera (Bausch + Lomb) and the XtraFocus (Morcher). For these implants, the aperture comes in fixed sizes. Additionally, the location of the aperture in pinhole IOLs is generally controlled by IOL centration within the bag. Intracorneal synthetic devices such as the Kamra may be associated with haze and other complications.
The advantage PPP holds is the individual customisation of the location and size of the pupil. It can be performed by anyone without large additional costs, such as those associated with flap creation or IOLs, and the pinhole size is easily reversible postoperatively if required, as a YAG laser can be used to enlarge the pupil. A disadvantage is the greater learning curve needed for surgery.
A disadvantage of all pinhole optics also includes possible decreased retinal illumination, diffraction rings, and mild visual field narrowing. Therefore, excessively small pupil size to less than 1.0 mm should be avoided to retain a balance between vision, illumination, and field.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
Real-World Outcomes for Vortigene Neparvovec
Majority show improved visual function out to 3 years; atrophy seen in some.
HOWARD LARKIN
REPORTS
Amajority of patients receiving voretigene neparvovec (VN; Luxturna) gene therapy for RPE65-associated retinal dystrophies showed improved visual function with no reduction in visual acuity for up to 3 years after treatment, M Dominik Fischer MD reported at a recent conference. However, more than half experienced ocular adverse events, including chorioretinal atrophy in about one-quarter and cataract in about 13%.
These interim findings from the 5-year real-world PERCEIVE study are in line with VN’s known safety profile and suggest that it is safe and effective in the long term for treating inherited retinal diseases caused by RPE65 gene mutations, Dr Fischer added. The study’s primary objective is to collect information on adverse events, and secondarily on pregnancy outcomes, and visual function and structure outcomes.
VN is injected only once subretinally to insert a functional copy of the RPE65 gene into photoreceptor cells using a viral vector. This allows photoreceptors to produce proteins needed to complete the visual cycle, potentially improving visual function while slowing or preventing further retinal degeneration. It is the first ocular gene therapy for a genetic disease approved by the European Commission and the US FDA.
At the 3-year cut-off, PERCEIVE enrolled 198 patients from countries around the world.
Interim findings
At the 3-year cut-off, PERCEIVE enrolled 198 patients from countries around the world. Mean age was 22.9±14.2 years, about half were adults, and 53% were male. Mean follow-up length was 1.4±0.8 years with a maximum of 3.4 years.
At least one ocular adverse event was reported in 123 patients (62%). Ocular adverse events of special interest occurred in 109 patients (55%). These included chorioretinal atrophy in 49 patients, increased intraocular pressure in 32 patients, intraocular inflammation and/or infection related to the procedure in 28 patients, and foveal thinning in 12 patients. The most frequent chorioretinal atrophy adverse events were retinal degeneration in 39 patients and injection site atrophy in 15 patients.
Serious ocular adverse events occurred in 10 patients, including retinal fovea disorder in 2 and reduced visual acuity in 2. Non-ocular adverse events were seen in 22 patients and were generally mild, with headaches and reactions to systemic steroids among the most common, Dr Fischer said.
Overall, visual function saw sustained improvement. Mean full-field visual stimulus threshold (FST) improved by -18.41±14.66 decibels from baseline for 96 patients at 1-year follow-up, -13.37±19.56 for 39 patients at 2 years, and -14.73±19.04 for 10 patients at 3 years. “FST improved dramatically within 1 month, and was sustained 3 years down the line,” Dr Fischer said.
Even patients with chorioretinal atrophy saw visual function improve, Dr Fischer said. In fact, these patients saw greater improvement in retinal sensitivity than those who did not develop atrophy. The causes of chorioretinal atrophy are unclear, likely multifactorial, and may be related to the disease’s natural history, he added.
No reduction in mean best-corrected visual acuity was observed up to year 3. However, Dr Fischer noted no real improvement was seen either. As the PERCEIVE study continues, he concluded it will provide more information on the real-world durability and safety of VN treatment.
Dr Fischer presented at ARVO 2024 in Seattle, US.
dominik.fischer@eye.ox.ac.uk
M Dominik Fischer MD, DPhil, FEBO, MRCOphth is an ophthalmic surgeon at the Oxford Eye Hospital and professor at the University of Oxford, UK, and professor at the Centre for Ophthalmology of the University of Tübingen, Germany.
AI-Assisted nAMD Treatment
Automated system quantifies retinal fluid and correlates with vision loss.
HOWARD LARKIN REPORTS
With most neovascular age-related macular degeneration (nAMD) patients progressing despite treatment, assessing retinal fluid build-up is essential to guide injection intervals of anti-vascular endothelial growth factor (VEGF) medications. Yet the growing prevalence makes it impossible to do such assessments manually for every patient, even with ocular coherence tomography (OCT) imaging.
An artificial intelligence-derived program that automatically quantifies retinal fluid using OCT data could help. The algorithm automatically segments the retina into layers and counts every pixel in each, yielding precise measurements of both the volume and location of fluid in the intraretinal, subretinal, and pigment epithelial detachment spaces. The Fluid Monitor by RetInSight, Austria, is EU Medical Device Regulation (MDR) approved.
This fluid segmentation is important because both the volume and the location of retinal fluid correlate with vision loss and photoreceptor deterioration, Sophie Frank MD added. The same AI-based program quantifies the photoreceptor condition, allowing tracking over time.
Counting pixels
Dr Frank reported findings of a prospective clinical trial involving 290 nAMD patients. All received an anti-VEGF injection, OCT imaging, best-corrected visual acuity (BCVA) testing, and retinal sensitivity using microperimetry at baseline. After four weeks, patients again received OCT and BCVA testing.
At both visits, the AI program automatically quantified intraretinal (IRF), subretinal (SRF), and pigment epithelial detachment (PED) fluid using OCT data. It also automatically classified photoreceptors at the ellipsoid zone (EZ) level, measuring EZ thickness and loss. Three experienced graders determined macular neovascularisation (MNV) type, finding about two-thirds were type 1 and about one-fourth type 3. Fluid volumes were correlated with MNV type, visual acuity, retinal sensitivity, and photoreceptor thickness and integrity.
Vision and photoreceptor loss
Greater total fluid volume at baseline was associated with greater loss of photoreceptor integrity at one month. However, fluid in different areas affected vision loss differently, Dr Frank noted.
All fluid types significantly reduced visual acuity in the central 6 mm area, though the loss was less for pigment epithelial detachment. However, while IRF was responsible for most loss in visual function, SRF slightly improved BCVA and retinal sensitivity in the 1 mm zone, though the gain was not significant.
Similarly, total fluid volume at baseline was significantly associated with photoreceptor thinning and integrity loss in the 6 mm zone. However, SRF was not significantly associated with photoreceptor thinning in the 1 mm zone, while IRF was associated with EZ thinning and loss. High fluid volumes in all segments reduced retinal sensitivity in both the 1 mm and 6 mm zones.
Comparing MNV types, type 1 patients had low amounts of IRF, while type 3 patients had low amounts of SRF in both zones.
Overall higher fluid volumes have an impact on the structural integrity of photoreceptors, as well as visual function which makes it the most important biomarker for disease activity, Dr Frank said.
“Since it cannot be measured manually for every patient,” she concluded, “AI is needed to measure it for us.”
Dr Frank spoke at ARVO 2024 in Seattle, US.
Sophie Frank MD is a doctoral research scientist at the Medical University of Vienna, Austria. sophie.frank@meduniwien.ac.at
New Gene Therapy for LCA Tested
Switching vector virus could lower doses, improve vision.
HOWARD LARKIN REPORTS
Anew experimental gene therapy using a different viral vector may improve the efficiency and efficacy of Leber congenital amaurosis (LCA) treatment. In an early test, the new therapy improved visual acuity by about three lines in some patients at a much lower dose than an approved gene treatment.
Both treatments are for LCA caused by a mutation in the RPE65 gene, known as LCA2. The mutation prevents the eye from metabolizing vitamin A, disrupting the visual cycle and leading to photoreceptor degeneration and eventual blindness. Gene therapies replace the defective gene with a functional copy, enabling vitamin A metabolization and restoring some vision.
Our study provides a promising alternative gene therapy approach for the treatment of inherited blindness.
The currently approved LCA2 gene therapy uses adeno-associated virus serotype 2 (AAV2) to insert the functional gene into photoreceptor cells. In animal models, this has partially restored vision. However, an alternate therapy using AAV serotype 9 (AAV9) as a delivery vector is much more efficient in inserting the gene in animal photoreceptors, improving vision more at a much lower dose. This AAV9-based gene treatment, HG004, is now being tested in humans in the LIGHT trial.
Improved visual function
Preliminary six-month data from six patients injected with low and middle doses of HG004 show quick, significant, and continuous improvement in visual and retinal functions, reported Alvin Luk PhD. At the 6x109 and 1x1010 vector genomes, the vector doses are 15 and 25 times smaller; and at 0.2 mL, the injection volume is one-third smaller than the AAV2 therapy,
he added. The lower vector dose may reduce the risk of off-target effects, and the lower injection volume may reduce the risk of complications such as inflammation and retinal detachment. HG004 is administered by subretinal injection in several locations to reach more of the retina.
On average, the three patients in the low dose group, which included two children and one adult, saw best-corrected visual acuity (BCVA) improve by +11 ETDRS letters. The three in the middle dose group (which included one child and two adults) improved an average of +7.5 letters. Several patients reached +14 to +18 letters BCVA improvement at either the three- or six-month follow-up, Dr Luk noted.
For both groups, mean white light full-field visual stimulus threshold (FST) fell by -2.268 log cd.s/m2 and -1.408 log cd.s/m2 respectively for the low and medium doses, while kinetic visual field (KVF) increased by +554.25 deg2 (III4e) and +691.77 deg2 (III4e).
As for safety, no serious adverse events—such as macular hole, retinal detachment, or chorioretinal atrophy—were observed. Neither was any dose-limiting toxicity. Most adverse events were mild and transient and resolved without intervention, Dr Luk said.
Dr Luk concluded the results suggest HG004 may potentially be a safer and more efficacious therapy to treat LCA2.
“Our study provides a promising alternative gene therapy approach for the treatment of inherited blindness,” he said.
The US FDA has granted HG004 both orphan drug and rare paediatric disease designations. HG004 also received investigational new drug approval from the FDA and China Center for Drug Evaluation to conduct clinical trials in the US and China.
Dr Luk presented at ARVO 2024 in Seattle, US.
Alvin
Luk PhD, MBA, CCRA is co-founder and chief executive officer of Hudgens Therapeutics, Clinton, New Jersey, US, and Shanghai, China. PR@huidagene.com
Frugal Wet AMD Treatment
Netherlands vision outcomes better than others at 5 years.
HOWARD LARKIN REPORTS
Atreatment protocol that calls for starting neovascular age-related macular degeneration (nAMD) patients on an inexpensive anti-VEGF drug preserved vision for at least 5 years as well as for patients started on far more expensive drugs in other countries. The study findings could have important implications for improving both patient outcomes and health system finances.
The study compared visual acuity outcomes of 1,617 eyes of 1,331 nAMD patients treated in the Netherlands with 8,667 eyes of 7,086 patients in 13 other high-income countries with ethnic white majorities. Data came from participants in the Fight Retinal Blindness! registry, which collects information from clinics in 23 countries.
In keeping with Dutch Ophthalmological Society treatment guidelines first adopted in 2014, 91.1% of the Netherlands patients began treatment with intravitreal injections of compounded bevacizumab, at a drug cost of roughly €36 per treatment. In the 13 reference countries, 82.7% of patients started on aflibercept or ranibizumab, at a drug cost of roughly €700–800 per treatment.
Vision at 5 years
At the 5-year follow-up, the Netherlands patients saw mean visual acuity improve by 1.0 ETDRS letters over baseline. Over the same period, patients in the reference countries saw mean visual acuity fall by 1.6 letters, returning to baseline at about 36 months.
These results suggest the frugal Netherlands protocol— which Haras Mhmud MD noted was adopted to save money after studies showed no statistical difference in nAMD outcomes between patients treated with bevacizumab and ranibizumab—is as effective as treatment approaches favouring far more expensive drugs. However, he stressed other factors are also at play in the good results in the Netherlands.
For one, mean baseline visual acuity was better in the Netherlands, suggesting patients may be discovered and treated earlier than elsewhere. Other factors influencing when treatment begins may include waiting times to see ophthalmic specialists for urgent referrals, which may be shorter in the Netherlands than in many countries, and the average distance to reach specialists, which varies dramatically between countries like Australia and the Netherlands.
More injections
Another potentially important factor may be that nAMD patients in the Netherlands received significantly more injections,
averaging 42.4 over the 5 years compared with 28.9 in the reference countries. Again, this may be partly due to the efficiency of the Netherlands healthcare system in handling urgent referrals, where patients bear no cost of additional treatments, Dr Mhmud said. Patients in the Netherlands also were more likely to switch treatments, with about two-thirds changing over 5 years compared with about half in the reference group.
Even with a high conversion rate to more expensive drugs, the Netherlands protocol probably saves money without sacrificing outcomes, Dr Mhmud said.
“We expect to be saving money,” he said. “The other drugs cost almost 20 times more. Even though we have more injections, the cost difference is so big we still think we are getting savings.”
His research group is undertaking a cost-effectiveness analysis to assess cost savings.
Dr Mhmud reported at ARVO 2024 in Seattle, US.
Haras Mhmud MD, MPH is a clinical research fellow and PhD candidate at Radboud University Medical Center, Nijmegen, Netherlands. Haras.Mhmud@radboudumc.nl
Zeiss receives CE mark for hyperopic SMILE
Zeiss Medical Technology announced they received a CE mark for treating hyperopia with lenticule extraction with the SMILE Pro platform. Additionally, the company is celebrating more than 10 million eyes treated with its SMILE and SMILE Pro with the VISUMAX 800 femtosecond laser. The Zeiss AI IOL Calculator also recently received its CE mark. The calculator does not require IOL constants: in short eyes, it has outperformed most state-of-the-art formulas. The company also introduced Zeiss CIRRUS PathFinder, a fully integrated AI decision support tool to automatically identify macular abnormalities in OCT B-scans and its new digital ophthalmic microscopes, the Zeiss ARTEVO® 850 3D heads-up ophthalmic microscope and the ARTEVO 750.
zeiss.com
Rayner celebrates trifocal and RayOne IOL
Rayner launched the RayOne Galaxy and Galaxy Toric IOLs. The non-diffractive trifocal IOLs come fully preloaded in their injection cartridge and have a diffractive spiral optic created using a proprietary AI engine trained on patient outcomes. The IOL is designed to progressively elongate focus and deliver a full range of vision with smooth transitions and minimal dysphotopsias. The company also recently celebrated the four millionth RayOne IOL implantation in a year that also marks the 75th anniversary of Harold Ridley’s first implantation of an IOL, which Rayner manufactured.
rayner.com
New Scheimpflug OCT combo from Oculus
OCULUS announced the premiere of the Pentacam® Cornea OCT, which combines Scheimpflug technology with the world’s first pericentric ultra-high-resolution OCT scanning system. Simultaneous bimodal imaging enables detailed observations and precise measurement of the layers of the corneal tissue, essential for ectasia diagnosis and treatment.
pentacam.com
Haag-Streit introduces METIS system
Haag-Streit presented its new METIS Ophthalmic Microscope System that integrates advanced Haag-Streit optics with a coaxial red reflex to ensure clear visualisation during procedures, even under low light conditions. In addition, surgeons can control tilt, filter, focus, and zoom using hand or foot switches. The modular design allows for potential upgrades like 3D heads-up displays.
haag-streit.com
New Sinusoidal trifocal
VSY Biotechnology introduced two new IOLs, the Maestro® Sinusoidal trifocal IOL and the preloaded Enova Advanced™ EDOF IOL. The Maestro lens has sinusoidal ridges on the surface of its optic to create a smooth transition across a continuous range of focus from distance to near. The Advanced EDOF proprietary Light Tailoring Technology Biotechnology provides distance and intermediate vision with a similar aberration profile to a monofocal IOL.
vsybiotechnology.com
NO TIME FOR SUSTAINABILITY FATIGUE
William J Dupps MD, PhD cautioned against complacency in the looming climate crisis, adding cataract surgeons can make a significant contribution to promoting environmental sustainability. He noted healthcare accounts for 4.4% of global net emissions, 70% of which are generated by the production, transportation, and disposal of goods and equipment such as drugs, food, medical devices, equipment, and instruments. Regulations in many Western countries prohibit the reuse of surgical equipment because of the fears of cross-contamination, despite the lack of clinical data to support the efficacy of many mandated infection control measures. The Aravind Eye Care System (AECS) postoperative endophthalmitis (POE) registry, which follows standardised equipment sterilisation protocols, reported a POE rate of only 0.04% in 2 million consecutive cataract surgeries. Those results were identical to those of the American Academy of Ophthalmology Intelligent Research in Sight registry, which reported a 0.04% POE rate in 8.5 million consecutive cataract surgeries. Furthermore, by adopting their standardised protocols across all 14 regional eye hospitals, AECS reduces the carbon footprint of phacoemulsification procedures by 95% compared to procedures performed in the UK. Government regulations and the cost of relabelling products as multiuse remain obstacles to adopting approaches like the AECS. Some of the most crucial work will involve aligning surgeons, hospitals, industry, and regulatory agencies around common sense, data-driven strategies for reducing climate impact and cost.
STERILISED REUSABLE INSTRUMENTS GET CLEAN BILL OF HEALTH
A sterile protocol can eliminate cross-contamination risk of reusable cataract surgery instruments, according to the findings of a prospective cohort study at the Aravind Eye Hospital. In the study, no bacterial or fungal growth was found in 3,333 discrete samples collected from extensive microbiological cultures of immediate use steam-sterilised ophthalmic surgical instruments and cataract surgical products reused in consecutive cataract surgeries in multiple patients. Of the 3,241 cataract surgeries involved in the study, there were no cases of postoperative endophthalmitis over a six-week follow-up period.
AG Shukla, et al. “Reusing surgical materials for cataract surgery: an assessment of potential contamination,” 50(10): 993–999.
LOW-ENERGY FLACS EASIER ON EYES
Low-energy femtosecond laser-assisted cataract surgery (FLACS) appears to have some advantages over conventional phacoemulsification (CPS), according to a new meta-analysis and systematic review. The meta-analysis included 11 studies involving 1,680 eyes, of which 637 underwent FLACS and 1,043 underwent CPS. The study showed that, compared to CPS, FLACS procedures used significantly less balanced salt solution, had a shorter effective phacoemulsification time, and resulted in lower corneal endothelial cell counts. However, there were no differences between the two groups in cumulative dissipated energy, corrected distance visual acuity, change in central corneal thickness, or aqueous cytokine levels.
CY Yeh, et al. “Comparison of low-energy FLACS and conventional cataract surgery: meta-analysis and systematic review,” 50(10): 1074–1082.
ESCRS Patient Portal
Patients are understandably curious to learn as much as they can about their upcoming cataract or refractive surgery. ESCRS has developed a Patient Portal on its website to help inform patients about these surgeries.
The Portal is split into two sections: Cataract and Refractive. Each section provides an easy-to-understand summary of the different types of conditions, including the benefits, risks, procedures, and aftercare of common conditions. Each section is easily navigable, with clear diagrams and a glossary to convey all the information patients might need to help prepare for surgery or during aftercare.
Cited in this Issue
ESCRS Update
ESCRS forms Functional Vision Working Group
Page 7
1. Ribeiro F, Dick HB, Kohnen TM, Findl O, Nuijts R, Cochener B, and Fernandez J. “Evidence-based functional classification of simultaneous vision intraocular lenses: seeking a global consensus by the ESCRS Functional Vision Working Group,” Journal of Cataract & Refractive Surgery, 2024 Aug; 50(8): 794–798. doi: 10.1097/j.jcrs.0000000000001502
2. Ribeiro F, Pinero D, Dick HB, Findl O, Cochener B, and Kohnen TM. “Should enhanced monofocal intraocular lenses be the standard of care? An evidence-based appraisal by the ESCRS Functional Vision Working Group,” Journal of Cataract & Refractive Surgery, 2024 Aug; 50(8): 789–793. doi: 10.1097/j. jcrs.0000000000001479
Which Farsighted Fix?
Page 8
1. Reinstein DZ, Sekundo W, Archer TJ, et al. “SMILE for Hyperopia with and Without Astigmatism: Results of a Prospective Multicenter 12-Month Study,” J Refract Surg, 2022; 38(12): 760–769.
2. Reinstein DZ, Pradhan KR, Carp GI, Archer TJ, Gobbe M, Sekundo W, Khan R, Dhungana P. “Small Incision Lenticule Extraction (SMILE) for Hyperopia: Optical Zone Diameter and Spherical Aberration Induction,” J Refract Surg, 2017 Jun 1; 33(6): 370–376.
3. Reinstein DZ, Carp GI, Archer TJ, et al. “LASIK for the Correction of High Hyperopic Astigmatism with Epithelial Thickness Monitoring,” J Refract Surg, 2017; 33(5): 314–321.
4. Reinstein DZ, Gobbe M, Archer TJ. “Coaxially sighted corneal light reflex versus entrance pupil center centration of moderate to high hyperopic corneal ablations in eyes with small and large angle kappa,” J Refract Surg, 2013; 29(8): 518–525.
Refractive Surgery with the Modern Posterior Chamber Phakic IOL
Page 15
1. Cake 21 supplement. “Building Proficiency with Phakic IOLs,” February 2024. https://issuu.com/mediamice/docs/ cake_21_supplement_building_proficiency_with_phaki.
Unveiling Secrets of the Lenticule
Page 18
1. Yao L, et al. “Small Incision Lenticule Extraction (SMILE) and Laser in Situ Keratomileusis (LASIK) Used to Treat Myopia and Myopic Astigmatism: A Systematic Review and Meta-analysis of Randomized Clinical Trials,” Semin Ophthalmol, 2023 Apr; 38(3) 283–293.
2. Liu J, Lu Y, Liu J, Wei C. “Meta-analysis of efficacy, safety, stability and predictability of Small Incision Lenticule Extraction (SMILE) for myopia,” Lasers Med Sci, 2024 Feb; 39(1): 57.
3. Song J, et al. “Small Incision Lenticule Extraction (SMILE) Versus Laser-Assisted Stromal in Situ Keratomileusis (LASIK) for Astigmatism Corrections: A Systematic Review and
Meta-analysis,” Am J Ophthalmol, 2023 Mar; 247: 181–199.
4. Reinstein DZ, Sekundo W, Archer TJ, Stodulka P, Ganesh S, Cochener B, Blum M, Wang Y, Zhou X. “SMILE for Hyperopia with and Without Astigmatism: Results of a Prospective Multicenter 12-Month Study,” J Refract Surg, 2022 Dec; 38(12): 760–769.
5. Mastropasqua L, Nubile M, Acerra G, Detta N, Pelusi L, Lanzini M, Mattioli S, Santalucia M, Pietrangelo L, Allegretti M, Dua HS, Mehta JS, Pandolfi A, Mandatori D. “Bioengineered Human Stromal Lenticule for Recombinant Human Nerve Growth Factor Release: A Potential Biocompatible Ocular Drug Delivery System,” Front Bioeng Biotechnol, 2022 Jun; 10: 887414.
Second Global Consensus on Keratoconus
Page 22
1. Gomes JA, Tan D, Rapuano CJ, et al; Group of Panelists for the Global Delphi Panel of Keratoconus and Ectatic Diseases. “Global consensus on keratoconus and ectatic diseases,” Cornea, 2015; 34(4): 359–369.
Corneal Cross-Linking (CXL): From Origins to Modern Innovations
Page 24
1. Wollensak G, Spoerl E, Seiler T. “Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus,” Am J Ophthalmol, 2003 May; 135(5): 620–627. doi: 10.1016/s0002-9394(02)02220-1
3. Spoerl E, Seiler T. “Techniques for stiffening the cornea,” J Refract Surg, 1999 Nov–Dec; 15(6): 711–713. doi: 10.3928/1081597X-19991101-21
4. Raiskup F, Herber R, Lenk J, et al. “Corneal Crosslinking with Riboflavin and UVA Light in Progressive Keratoconus: Fifteen-Year Results,” Am J Ophthalmol, 2023 Jun; 250: 95–102. doi: 10.1016/j.ajo.2023.01.022
5. Sel S, Nass N, Potzsch S, et al. “UVA irradiation of riboflavin generates oxygen-dependent hydroxyl radicals,” Redox Rep, 2014 Mar; 19(2): 72–79. doi: 10.1179/1351000213Y.0000000076
6. Raiskup F, Spoerl E. “Corneal crosslinking with riboflavin and ultraviolet A. I. Principles,” Ocul Surf, 2013 Apr; 11(2): 65–74. doi: 10.1016/j.jtos.2013.01.002
8. Vinciguerra R, Tzamalis A, Romano V, Arbabi EM, Batterbury M, Kaye SB. “Assessment of the Association Between In Vivo Corneal Biomechanical Changes After Corneal Cross-linking and Depth of Demarcation Line,” J Refract Surg, 2019 Mar 1; 35(3): 202–206. doi: 10.3928/1081597X-20190124-0
9. Hafezi F. “Limitation of collagen cross-linking with hypoosmolar riboflavin solution: failure in an extremely thin cornea,” Cornea, 2011 Aug; 30(8): 917–919.
Upcoming Events
November 20–24
The 58th TOA National Congress Antalya, Turkey
November 28–29
UKISCRS
75th Anniversary of the IOL London, United Kingdom
January 17–19
LBI Weekend Workshop: London 2025 London, United Kingdom
February 28–March 2
29th ESCRS Winter Meeting Athens, Greece
April 25–28
ASCRS
Los Angeles, US
September 12–16
20 Nov
43rd Congress of the ESCRS Copenhagen, Denmark 28 Feb 28 Nov 12 Sept
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in depth overview on current clinical outlooks.
escrs.org/education/forum/
By Hanita Lenses
THE FIRST AND ONLY IOL OF ITS KIND:
De veloped using a patented algorithm
Cr eated for maximum light utilization
Designed to redefine clarity and precision
Benefit from proven technology that minimizes disturbances while maximizing performance, ensuring unparalleled visual outcomes for every patient.