31 PROMs in the Cataract Pathway Yarrow Scantling-Birch MD
32 Never Go In Blind Elizabeth Wen Ling Lim MD
RETINA
34 Is Cataract Surgery a Risk Factor for Wet AMD? Anniken Burés-Jelstrup MD
CORNEA
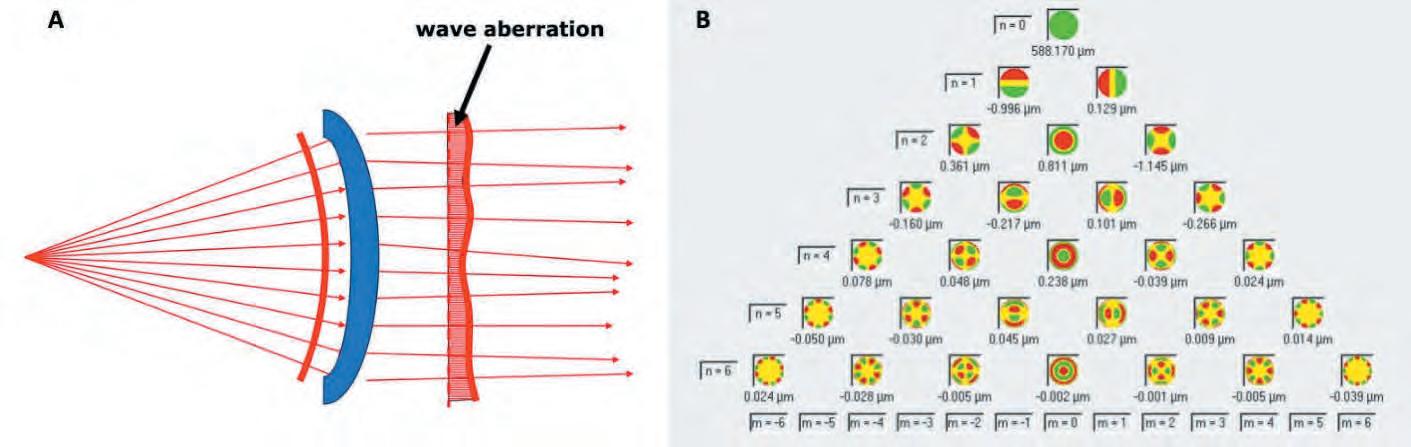
36 Need to Know: Higher-Order Aberrations and Polynomials Soosan Jacob MS, FRCS, DNB
38 Portuguese Research Shows Promising Results Mariana Domingues Vaz MD
FIRST PERSON
40 José Güell: Trends in Cornea Treatment
DIGITAL OPHTHALMOLOGY
42 Advancing AI in Medicine Dimitri T Azar MD, MBA
US UPDATE
43 “This would be a disaster” Dan Ignaszewski and Paul Sternberg Jr MD
Publisher Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin Roibeárd O’hÉineacháin
Contributors
Laura Gaspari
Soosan Jacob
Timothy Norris
Andrew Sweeney
Colour and Print CitiPost
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Let’s Get Busy!
The freshly graduated fledgling ophthalmologist exiting the cosy nest of academia enters an intimidating world of stressful workloads, never-ending institutional bureaucracy, labyrinthine insurance rules, government regulations, industry inducements, and macroeconomic forces. All of these must be navigated while maintaining the highest ethical standards and providing the best care to patients.
Most are poorly prepared to meet these challenges. Medical school does not cover the business side of the profession, yet graduates must make key decisions early on that will determine the course of their careers and personal lives.
This issue delves into the business of ophthalmology. Our cover article by Howard Larkin looks at the choice an ophthalmologist might make to go into a public or private practice setting through the eyes of those who have gone through the process of building successful, rewarding careers.
The medical world, especially ophthalmology, is driven by innovation: A doctor has an idea for solving a common problem, gets support from mentors, finds a company willing to consider providing support, and with luck (after surviving the clinical trial process), makes a lasting contribution to eye care. Harold Ridley’s bold idea to create an intraocular lens made of PMMA, developed in partnership with the Rayner company, is the best example. There are many others in cataract and refractive surgery.
A related article considers how partnerships with academia and industry continue to drive innovation in ophthalmology. As Professor Burkhard Dick notes in the article, “With a strategic approach based on clinical insight and multidisciplinary collaboration, ophthalmologists can continue to play a central
role in the development of transformative new technologies. The future of sight-saving care depends on it.”
The ESCRS recognises its members want to know more about career development, practice management, and innovation. ESCRS provides extensive resources online and at conferences in all of these areas. We invite our members to visit our online LBI library, attend seminars in person and online, and take advantage of the many offerings at ESCRS conferences.
One such offering was the Leadership, Business, and Innovation (LBI) session at our Winter Meeting in Athens. Another article in this issue examines how acquiring precise soft skills is extremely important for ophthalmologists when dealing with their team, clinical and public practice, and maintaining relationships with the industry.
We have a special LBI practice management weekend planned for 27–29 June in Zurich, where members can dig into the financial fine points of running a practice, including learning how to use AI to digitally transform the clinic.
We will once again have iNovation Day coincide with the ESCRS Annual Congress in Copenhagen. iNovation Day offers a unique opportunity to network with colleagues, industry executives, emerging companies, and financial community leaders from across Europe and other parts of the world to review, discuss, and shape the future of our profession.
Hope to see you there!
Sean Henahan Editor-in-Chief, EuroTimes
EDITORIAL BOARD
Adi Abulafia (Israel)
Bruce Allan (UK)
Noel Alpins (Australia)
Juan Alvarez de Toledo (Spain)
Gerd Auffarth (Germany)
Başak Bostancı (Turkey)
John Chang (Hong Kong SAR, China)
Béatrice Cochener-Lamard (France)
Burkhard Dick (Germany)
Mor Dickman (The Netherlands)
Joaquín Fernández (Spain)
Oliver Findl (Austria)
Nicole Fram (US)
Sri Ganesh (India)
Fahrad Hafezi (Switzerland)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Jack Kane (Australia)
Yao Ke (China)
Mika Kotimäki (Finland)
David Lockington (UK)
Artemis Matsou (Greece)
Cyrus Mehta (India)
Jod Mehta (Singapore)
Sorcha Ní Dhubhghaill (Belgium)
Rudy Nuijts (The Netherlands)
Catarina Pedrosa (Portugal)
Konrad Pesudovs (Australia)
Nic Reus (The Netherlands)
Filomena Ribeiro (Portugal)
Andreia Rosa (Portugal)
Giacomo Savini (Italy)
Julie Schallhorn (US)
Sathish Srinivasan (UK)
Paola Vinciguerra (Italy)
Shin Yamane (Japan)
Ron Yeoh (Singapore)
Mihail Zemba (Romania)
Thomas Kohnen
José Güell
Paul Rosen
ESCRS
Leadership, Business & Innovation
ESCRS Practice Management Weekend
27–29 June
Zurich, Switzerland
Business and Practice Management Education Geared Specifically to ESCRS Members
Want a better handle on the financial operations of your department or clinical practice? Wondering how to evaluate AI tools and incorporate them into your daily work?
Join Hilary Hough, Vanessa Foser, and the ESCRS Leadership, Business & Innovation (LBI) team for a Practice Management Weekend Workshop in Zurich on 27–29 June!
In this workshop, ESCRS will be partnering with the Trinity College (Dublin) Business School Executive Education programme. Trinity College offers one of the top-ranked MBA programmes in Europe and will be delivering business and practice management courses and workshops that are geared specifically for ESCRS members. In addition, it means Weekend Workshop attendees will earn continuing education credits for their participation.
Weekend Workshop Programme
Finance for Ophthalmologists
Led by Trinity Adjunct Professor Hilary Hough, this session is based on Trinity’s workshop on Finance for Healthcare Professionals. Prof Hough is a certified accountant and chartered director with a wide range of corporate finance, accounting, and general management experience. He lectures in the full-time and executive Trinity MBA courses and a range of other executive education programmes.
Gain an understanding of fundamental financial principles.
Develop the skills to analyse and interpret key financial statements, including balance sheets, income statements, and cash flow statements.
Learn to create, manage, and optimise budgets to ensure the efficient use of resources within your department/ clinical practice.
Apply financial knowledge to improve operational efficiency, streamline processes, and achieve better patient outcomes.
Engage in peer-to-peer learning to share insights, best practices, and innovative financial solutions.
What You Really Need to Know About AI Right Now
Join AI Business School Co-Founder/Chief Commercial Officer Vanessa Foser as she cuts through all the noise and hype about AI and focuses on what ophthalmologists need to know about using AI in clinical practice. Based in Zurich, the AI Business School supports organisations in their digital transformation. Ms Foser and her team are leaders in making workforces literate in (Generative) AI and its everyday use/application. In addition, members of the LBI Committee will share the AI tools they currently use in daily practice/daily life to improve efficiency and effectiveness.
Gain a better understanding of what exactly AI means.
Learn how to evaluate if an AI tool is valuable to incorporate into use.
Understand how to begin implementing AI into your clinical practice.
Attendance is limited to 30
Register for the workshop and save 50% on ESCRS Congress registration! Plus: ESCRS members enjoy an extra 15% off the LBI Workshop!
ESCRS Update
ESCRS Announces 2025 Masterclass Programmes
ESCRS is following up its successful 2023 and 2024 masterclass programmes with 2025 classes in the clinical areas of minimally invasive glaucoma surgery (MIGS) and complex cataract.
The goal of ESCRS masterclasses is to improve practice patterns, enhance clinical outcomes, and significantly grow the number of patients treated in each field. Each masterclass will have 50 student positions available, and each student will be assigned to a personal mentor who will guide them through the programme. Masterclass students will participate in mentor-guided didactic workshops, interactive live webinars, and in-person case review grand rounds, wet labs, and sessions in Copenhagen at the ESCRS Annual Congress.
The MIGS masterclass will offer four online modules: (1) Introduction to glaucoma and MIGS, (2) Angle surgery using implants, (3) Angle surgery without implants, and (4) Subconjunctival and suprachoroidal implants.
The complex cataract masterclass will offer the following online modules:
• Cornea: opacities of various causes, endothelial issues, optimising visibility cataract during surgery, when to use adjunctive corneal surgery
• Iris and pupil: Uveitic cataract, small pupil, intraoperative floppy iris syndrome (IFIS), and congenital and acquired iris defects
• The cataractous lens: soft cataracts, intumescent cataracts, hard cataracts, posterior polar cataracts
• Cataract surgery in long and short eyes
• Cataract surgery in post vitrectomy eyes
The deadline to register for the masterclasses is 1 June. Scan the QR code for information on each masterclass, including eligibility criteria, curriculum details, and instructions on how to apply.
Childcare Service to Be Provided at Congress
ESCRS will be providing a childcare crèche service during the 2025 Annual Congress in Copenhagen. The service will be available at a cost of €10 per day for registered Congress attendees and will be available 12–16 September.
The hours for the service are as follows:
• Friday, 12 September, 08:00 to 19:00
• Saturday, 13 September, 08:00 to 19:00
• Sunday, 14 September, 08:00 to 20:30
• Monday, 15 September, 08:00 to 18:00
• Tuesday, 16 September, 08:00 to 15:00
Online reservations for this service will be available through the Annual Congress website. The deadline to place a reservation is 13 August.
The childcare service is available for children aged 0–12 years only. Children may stay for up to a maximum of 4 hours at any one time. Parents must take their children out of the setting for food and fresh air and are welcome to return to the crèche after 1 hour.
New Video Interviews Added to Education Forum
Three new video interviews have been posted to the Education Forum on the ESCRS website as part of the Society’s independent medical education (IME) programme.
The three videos, which are also available as podcasts, feature Drs Ramza Diamanti and Nic Reus discussing the following topics:
• EDF in Focus: Patient Education and Effective Communication
• Achieving Accurate IOL Power
• Key Preoperative Considerations to Prevent Refractive Surprises
The ESCRS Educational Forum is supported by several industry partners and provides independent didactic education in selected therapeutic areas. The platform combines presentations from ESCRS Winter Meetings and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth look at current clinical topics.
19.5 CME CREDITS
7 SPECIAL ACTIVATIONS
2.5 DAYS
2 INSTRUCTIONAL COURSES
12 WET LABS
4 MAIN
1,924 PARTICIPANTS
6 WORLD CAFÉ SESSIONS
76 FREE PAPERS
9
20 SPEED MENTORING SESSIONS
20 PRESENTED POSTERS
1 SPOTLIGHT THEATRE
Combined Cataract and iStent inject® W Surgery
as a Preparatory Strategy for Filtering Surgery in Moderate Open-Angle Glaucoma
INTRODUCTION
The management of open-angle glaucoma associated with cataract presents therapeutic challenges, particularly in patients with moderate to advanced functional damage who fail to achieve optimal intraocular pressure (IOP) control despite maximal treatment. In such cases, a sequential surgical approach is generally preferred over combined surgery to avoid compromising the prognosis of filtering procedures.
However, standalone cataract surgery may lead to hypertensive spikes that could worsen the patient’s clinical situation.
Therefore, the addition of MIGS procedures in these patients may be beneficial to control such spikes and reduce the medication burden, thereby preparing the eye for future filtering surgery.
We present the case of a young patient with a visually significant cataract and moderate glaucoma with a high medication burden, in whom a combined cataract and iStent inject® W procedure was performed with the aim of reducing hyperemia and medication load before subsequent trabeculectomy under more favorable conditions.
CASE REPORT
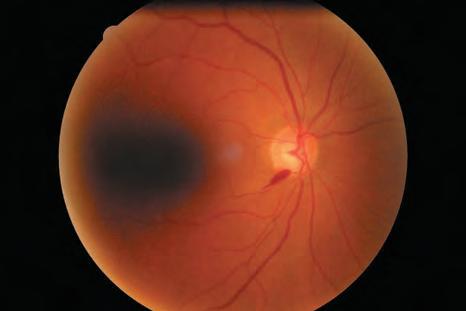
A 52-year-old male with no significant systemic history was diagnosed with bilateral primary open-angle glaucoma. In the right eye (RE), the IOP was 22 mmHg under maximum medical therapy consisting of three topical hypotensive agents (a prostaglandin and a fixed combination of betablocker and dorzolamide). Optic nerve examination revealed an optic nerve with rim thinning and an inferior temporal splinter haemorrhage. (figure 1) The visual field showed glaucomatous defects consistent with moderate functional damage.
Clinically, the patient had a grade III nuclear cataract, with symptoms of glare and reduced visual acuity (corrected VA of 0.4). Conjunctival examination showed chronic hyperemia with signs of medicationinduced toxicity. Gonioscopy revealed an open iridocorneal angle over 360°, without synechiae.
THERAPEUTIC JUSTIFICATION
Considering the patient’s age, documented functional progression, and poor tolerance to topical
A clinical case
BY JOSÉ MARÍA MARTÍNEZ DE LA CASA, MD
medications, surgical treatment was deemed necessary. As an initial approach, combined cataract surgery with iStent inject® W implantation was chosen. This decision was based on several objectives:
This decision was based on several objectives:
1. Additional IOP control via enhanced trabecular outflow without compromising the conjunctiva.
2. Reduction of the pharmacological burden, potentially improving quality of life and reducing ocular toxicity.
3. Preservation of the bulbar conjunctiva, minimising chronic hyperemia and inflammation, thereby facilitating future filtering surgery under better conditions.
SURGICAL
TECHNIQUE
The procedure was performed under topical anaesthesia. Standard phacoemulsification was carried out with intraocular lens implantation in the capsular bag. After filling the anterior chamber with viscoelastic, two iStent inject® W microstents (Glaukos Corp., USA) were implanted in the nasal trabecular meshwork (figure 2). Both stents were correctly
positioned. No intraoperative complications occurred.
POSTOPERATIVE COURSE
During follow-up, the patient showed satisfactory visual recovery (corrected VA of 0.9 at one month), without significant inflammation or adverse events. At 6 weeks, IOP was 16 mmHg with only one medication and remained stable at 3 months. A 32% reduction in IOP from baseline and a 66% reduction in topical medication use were achieved.
At 3 months, trabeculectomy was performed uneventfully, with good IOP control maintained to date without the need for further hypotensive treatment (figure 3).
DISCUSSION
DMIGS surgery, particularly the iStent inject® W, is a valid therapeutic option for patients with
open-angle glaucoma and cataract, especially when filtering surgery is to be avoided or delayed. Several studies have shown that iStent inject® W improves IOP control with a high safety profile and minimal surgical trauma.
In this case, the main objective was not to achieve extremely low IOP values or to eliminate future surgery altogether, but to create a more favorable ocular environment for subsequent filtering procedures by reducing chronic conjunctival inflammation induced by topical medications and minimizing the risk of postoperative fibrosis.
From a functional perspective, the achieved IOP reduction was clinically significant, sufficient to stabilize progression and reduce the need for topical medications.
The stability of the visual field defect and the subjective improvement in visual quality reinforce the benefit of this approach.
3
References
CONCLUSION
Combined iStent inject® W implantation with cataract surgery may be considered a useful strategy in patients with moderate open-angle glaucoma who require additional IOP control, present with medicationinduced toxicity, and may benefit from conjunctival preservation for future filtering surgery. In selected cases, this approach may enhance quality of life, reduce the risk of complications, and optimise long-term surgical outcomes.
JOSÉ MARÍA MARTÍNEZ DE LA CASA, MD
Professor of Ophthalmology, Universidad Complutense de Madrid, Madrid, Spain
Head of the Glaucoma Department, Hospital Clinico Universitario San Carlos, Madrid, Spain
1. Samuelson TW, et al. A Schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract. Ophthalmology. 2019;126(6):811–821. 2. Fea AM, et al. Prospective unmasked evaluation of the iStent inject system for open-angle glaucoma: synergy trial. J Cataract Refract Surg. 2014;40(5):843–849 . 3. Lindstrom R, et al. Six-month outcomes of the iStent inject trabecular micro-bypass in cataract surgery patients with open-angle glaucoma. Clin Ophthalmol. 2019;13:2337–2345.
Improving access through financially and environmentally sustainable innovation.
LAURA GASPARI
To meet future economic, resource, and personnel challenges, the global ophthalmological community needs frugal innovations and strategies to sustainably improve global eye care access, especially to underserved communities, explained David F Chang MD, who delivered the International Kelman Award lecture at the 2025 ESCRS Winter Meeting in Athens.
Cataract surgery has seen tremendous advances in the past 5 decades, primarily through new, expensive technologies. However, many of these advances are too costly for patients in low- and middle-income countries (LMIC) to benefit. In fact, the backlog of global blindness continues in many LMICs due to resource constraints and a shortage of cataract surgeons.
Doing more with less
Dr Chang introduced the Hindi concept of Jugaad, which means to find unconventional ways to achieve similar benefits with fewer resources or at a lower cost. In healthcare, frugal innovation would lower rather than raise the costs and resource consumption of delivering quality care. He cited 5 examples of how the Aravind Eye Care System (AECS) in Southern India has brought frugal innovation to cataract surgery.
The 14 hospitals within the AECS perform approximately 450,000 cataract operations each year, of which approximately 60% are at little to no cost to indigent patients who have extremely advanced cataracts. AECS uses a lower-tech method for them—sutureless, manual small-incision cataract surgery (MSICS)—that is well suited for mature cataracts and costs
REPORTS
much less than phaco.1 These patients receive non-foldable, PMMA IOLs with excellent functional outcomes.
Having the surgeons operate in an assembly line fashion allows them to achieve extremely high surgical volumes. For example, the team minimizes turnover time by including two adjacent operating tables per surgeon so the next patient can be prepared while the ophthalmologist operates on the other OR table. With phaco, surgeons position the machine between the two OR tables and don’t change the handpiece, tubing, cassette, or irrigation bottle between cases. Instead, that same phaco cassette is discarded at the end of the OR day.
Dr Chang collaborated with AECS on two other frugal innovations. Posterior capsular opacification (PCO) is an inconvenience in high-income countries (HIC) but a major cause of visual disability in LMICs where access to follow-up examinations and YAG lasers is often limited. Fortunately, adding a square edge to the PMMA IOL dramatically lowers the PCO rate to levels comparable to the best foldable IOLs and costs only US$1 per IOL.2 AECS’s manufacturing company, Aurolab, produces the other collaboration he helped introduce: intracameral (IC) moxifloxacin. Approved in India, a 1.0 mL vial of intraocular moxifloxacin costs only US$1 and is enough to inject 0.1 mL into 7 eyes. By adopting the treatment, AECS lowered its endophthalmitis rate from 0.07% to 0.02%.3
450,000
The 14 hospitals within the AECS perform approximately 450,000 cataract operations each year, of which approximately 60% are at little to no cost to indigent patients who have extremely advanced cataracts.
Dr Chang believes ophthalmologists in HICs can learn lessons in frugal innovation from LMIC settings, such as the AECS. A prime example is the fifth AECS innovation—reuse of most cataract surgical supplies and drugs that must be discarded after a single use in most HICs. AECS has found reusing surgical gowns, phaco cassettes and tubing, irrigation bottles, cannulas, blades, and intraocular drugs does not result in higher infection rates. Indeed, looking at 2 million consecutive cataract operations in which these supplies were routinely reused, the endophthalmitis rate was only 0.04% (half of the cases didn’t receive IC moxifloxacin)3—identical to the endophthalmitis rate reported in 10.5 million consecutive American cataract operations reported in the AAO IRIS registry. These findings are compelling because reuse of these same supplies is not allowed in the US because of the theoretical risk of infection.
Additionally, this data supports the opinions of most North American and European cataract surgeons who, in surveys, felt OR waste is excessive and single-use mandates for virtually all eye surgical supplies and drugs are unnecessary.4 Dr Chang collaborated in another AECS study that found no evidence of bacterial contamination when irrigation bags and phaco handpieces and tubing were cultured after multiple uses.5
Spurred by these studies and other data, Dr Chang and others co-founded EyeSustain.org, a global coalition of 53 international eye societies dedicated to advancing sustainability in eye care through education, research, innovation, and advocacy. He currently chairs the advisory board. One of EyeSustain’s goals is to collaborate with industry to develop more multi-use products and environmentally friendly packaging and materials. For example, AECS data suggest an all-day phaco cassette is safe and need not be changed and discarded after one case. Manufacturers could charge a click fee to maintain per-case revenues while passing along some of the savings to surgical facilities. This would dramatically improve OR turnover times and reduce packaging, shipping emissions, shelf storage requirements, and plastic landfill waste.
He concluded by calling on the profession—ophthalmologists, researchers, engineers, industry, and eye societies—to aspire to frugal innovation that can democratize access to quality eye care while reducing unnecessary costs and waste.
For more information on sustainability in ophthalmology, please visit eyesustain.org.
For citation notes, see page 46.
David F Chang MD is Clinical Professor, University of California, San Francisco, US. He chairs the advisory board for EyeSustain. He has no relevant financial disclosures.
Organising for Success
Professional and personal goals drive practice ownership and operational choices.
BY HOWARD LARKIN
For Başak Bostancı MD, the goal of ophthalmic practice was always clear.
“From the very beginning of my residency, I knew I wanted to focus on surgical fields that offered rapid, tangible outcomes and high patient satisfaction,” she said. “I became fascinated by the potential of refractive technologies—not only in corneal surgery but also through premium intraocular lenses (IOLs).”
This led Dr Bostancı to focus more and more on refractive and cataract refractive services. After residency, she worked in public care for 4 years before switching to private practice, then university. She implants premium IOLs in about 90% of her cataract cases.
“This role gives me both the clinical freedom and the strategic responsibility to implement state-of-the-art technologies and patient-centred approaches,” Dr Bostancı added. “I provide refractive services primarily in Istanbul, but I also consult internationally and participate in collaborative research and training projects across Europe.”
In addition, Dr Bostancı serves on the faculty of a university hospital. “Sharing innovative diagnostic and treatment algorithms with the next generation keeps me constantly engaged with the latest technologies and evidence. Teaching, for me, is a two-way street—it helps me stay up to date while contributing to the field.”
Emerging trends?
Dr Bostancı may not be alone. Annual clinical trends surveys from ESCRS and The Fundingsland Group show a recent decline in respondents practising primarily at public hospitals from 37% in 2021 to 32% in 2023. Over that same period, those reporting private hospitals as their primary practice site increased from 19% to 21% and those in surgeon-owned clinics from 14% to 16%. Those reporting academic medical centres remained steady at 10%, although pre-pandemic surveys show no trends in these categories.
Similarly, the proportion of eligible patients implanted with ‘premium’ IOLs rose slowly but steadily to 18% for toric and 13% for presbyopia-correcting lenses in 2023, up from 7% for both in 2016.
While not conclusive, these numbers may reflect greater confidence in and acceptance of the efficacy and benefits of refractive surgery—as well as increasing reliance on patient out-of-pocket income.
Indeed, growing worries about declining payment for standard cataract surgery may be another factor. Concerns about reimbursement came in second in a survey of doctors participating in ESCRS’s 2024 iNovation Day. Refractive IOLs were their top innovation investment interest.
“The climate for ophthalmology (particularly for refractive solutions) is dynamic and full of potential in Turkey and Europe,” Dr Bostancı said. “We are seeing a growing awareness of and demand for refractive procedures—not only from younger patients but also those seeking spectacle independence after the age of 40. The population is relatively young and well-informed, which contributes to a receptive and evolving market.”
However, economics, local regulations, and practice culture are big factors, said management consultant Kristine Morrill. “Many places in Europe still don’t allow partial payment for implanting premium lenses in cataract cases. It varies from country to country and within countries that have multiple insurance plans with different reimbursement rules,” including Germany and Italy.
Still, demand for ophthalmic services is growing as the number of ophthalmologists shrinks, Ms Morrill added. As pay for standard cataract surgery declines, some surgeons are turning to growth areas such as intravitreal injections and glaucoma procedures.
But revenue is only half the story, Ms Morrill emphasised. “Every ophthalmologist is going to do well because of the shortage, bringing in a lot of money. But are you charging enough to cover expenses? Are you paying staff enough for them to stick with you and help you grow? You can take home a lot of money, but after expenses, is there anything left? Learning financial management helps you figure it all out.”
Finding a balance between professional and personal goals is critical to overall practice success.
Patient and personal benefits
Reaching private practice professional and personal goals requires constant innovation in technology and workflows. Innovative practice structures can support that, according to Erik L Mertens MD. In 2009, he opened one of the first private ophthalmic clinics in Belgium—and the first private chain in 2018.
He now heads a network of 8 clinics employing more than 55 doctors across the country, with an equity stake in each. Most of the doctors also own shares. A few non-physician investors own a minority of shares and hold 3 of 12 board positions in the mother company, which employs a full-time CEO.
Though his early efforts faced pushback among conservative colleagues, his approach has gained acceptance. For example, the national medical council began allowing nonMD shareholders to invest in medical practices in 2018. “An evolution is underway in Europe that we have already seen in the [US],” Dr Mertens said.
In part, building the network was a risk diversification strategy to fund his eventual retirement—an important personal financial goal given the difficulty in transferring a solo or small group practice to younger partners, Dr Mertens said. “I’d rather have 9% of 8 clinics than 50% of 1 clinic. The financial risk we are carrying is much lower, and it is easier to attract young doctors. They can buy in 1–2% easily and
I’d rather have 9% of 8 clinics than 50% of 1 clinic. The financial risk we are carrying is much lower, and it is easier to attract young doctors.
create some value.” Lowering the buy-in cost also makes it possible for younger doctors to work 3–4 days a week, maintaining work-life balance, he added.
But patient service, not financial security, has always been Dr Mertens’ primary goal. He and a partner went out on their own in large part because the public hospital clinic he worked in was inefficient and impersonal. There were plenty of meetings and struggles with the board for control, but they handled only about 2 cataract cases per hour.
“We wanted to deliver a high-quality service—where patients see the same team. My team knows your name; you are not a number like in the hospital,” Dr Mertens said. This reduces patient stress, creating a welcoming, personalised experience that helps improve outcomes while building the practice’s reputation—and economic success.
Focusing on improving patients’ quality of life, Dr Mertens’ Antwerp clinic offers refractive and cataract refractive services in addition to general ophthalmology and glaucoma and retinal treatments. He does a lot of research in IOLs, working closely with industry. The clinic also offers dental and aesthetic care.
Facing rising tech costs
Though the explosion of new ophthalmic technologies enables ever-better refractive outcomes, the cost can be prohibitive. Rather than considering only theoretical financial return, how a new technology improves patient care should guide investment decisions, said Arthur B Cummings.
With new diagnostics, for example, “a more-informed decision gives you confidence. If you provide better results based on better data, ensure a great patient experience, the money will follow,” Dr Cummings said. Essentially, ophthalmologists don’t have to chase it.
Other technology, such as AI-powered records, can dramatically improve practice efficiency, Dr Cummings added. Pulling together all the diagnostic data needed to plan a case now takes seconds rather than minutes or hours, thanks to the implementation of systems that create efficiencies.
Technology is only one part of improving practice efficiency, Dr Cummings said. Staffing and training are also critical. He makes extensive use of optometrists in working up patients. That leaves him more time for surgery. All staff meet regularly to review and improve practice procedures. And once that trained, efficient staff is in place, it makes sense to pay them enough to stick around.
Dr Cummings performs privately paid surgery in his clinic and publicly insured standard cataract procedures in an adjacent hospital. His son Brendan, who shares his goals, has joined the practice.
In marketing his practice, Dr Cummings emphasises selling the result, which is better vision and the subsequent life benefits, rather than the technology. “Sell the destination, not how you will get there.”
Patients may not be eligible for a specific solution, so Dr Cummings markets his assessment services as a ‘lifestyle vision design’ consultation. Factors including age, lifestyle, eye health, anatomy, and physiology are considered before recommending a specific procedure. His entire practice, including training staff, is organised around this approach.
Still, Dr Cummings advised understanding the market before making major investments in new technology. For example, laser vision correction has generally been slow since the pandemic. “You are making a big investment in a flat market.” He noted implantable collamer lenses as a growth area, as are glaucoma and myopia prevention.
Due diligence
Indeed, in these days of stricter underwriting, banks will also look at the market and the practice’s structure and track record before lending, Ms Morrill noted. This makes it difficult for young surgeons to go out on their own. For equipment, leasing can be an attractive option. But she advised to read and run the numbers on any contract, particularly if it is a package deal—including using other products, such as the manufacturer’s IOLs. “You don’t want to end up paying twice as much for your laser.”
Similarly, Ms Morrill recommended caution when dealing with private equity investors. She’s seen several surgeons who sold their practices leave before their service agreements expired. Loss of control to the new owner was usually the cause. “Be sure you know what you are getting into before you sign.”
Başak Bostancı MD, FEBO is an assistant professor of ophthalmology in Bahçeşehir University School of Medicine and cataract and refractive surgeon in Dünyagöz Hospital, Istanbul, Turkey. drbbostanci@gmail.com
Erik L Mertens MD, FEBO, PCEO, FWCRS is founder of, and medical director and ophthalmic surgeon at Medipolis, Antwerp, Belgium. e.mertens@medipolis.be
Arthur B Cummings MMed (Ophth), FCS(SA), FRCS(Edin), FWCRS is an ophthalmologist at the Wellington Eye Clinic and Beacon Hospital, Dublin, Ireland, and Associate Clinical Professor at UCD, Dublin. abc@wellingtoneyeclinic.com
Kristine Morrill is co-founder and president of Medevise Consulting, Strasbourg, France. kris@medevise-consulting.com
EMERGING OPPORTUNITIES IN OPHTHALMOLOGY
Ophthalmology has long stood at the crossroads of precision technology and patient-centred care, according to H Burkhard Dick MD, PhD. From microinvasive surgical instruments to AI-based diagnostic tools, it is a field where innovation can rapidly translate into improved outcomes.
Yet, with the implementation of the European Medical Device Regulation (MDR), shifting investment patterns, and the pressures of global supply chains, today’s innovation climate is fraught with complexity. Nonetheless, emerging technology continues to create practice opportunities, Professor Dick said. He identified several areas:
1. Advanced cataract and refractive surgery
Cataract surgery remains the most frequently performed surgical procedure worldwide. The next frontier includes smart, customisable intraocular lenses (IOLs), such as light-adjustable lenses and simultaneous vision designs, Prof Dick said. Laser-assisted cataract surgery (LCS) continues to evolve—with more spaces integrating digital surgical guidance and imaging technologies. Refractive surgery is experiencing a resurgence, bolstered by better patient screening and novel lenticule extraction techniques.
2. AI-driven diagnostics and imaging
Artificial intelligence is transforming screening and early detection in ophthalmology. Deep learning tools are already FDA-cleared for diabetic retinopathy screening, and similar models are in development for keratoconus, glaucoma, and AMD. Future systems will likely combine multimodal data—including OCT, fundus photography, and visual field tests—for comprehensive, automated diagnostic support, Prof Dick noted.
3. Minimally invasive therapies and robotics
Minimally invasive glaucoma surgery (MIGS) and robotic assistance in vitreoretinal surgery are on the rise, Prof Dick said. These innovations reduce surgical trauma, increase precision, and improve recovery times. Enhanced visualisation systems and 3D heads-up displays are also making surgery more ergonomic and accessible.
4. Sustained-release drug delivery (SRDD)
The burden of chronic intravitreal injections for conditions like wet AMD and diabetic macular oedema has led to a wave of innovation in drug delivery. Biodegradable implants, refillable reservoirs, and microneedle technologies aim to improve compliance and outcomes, Prof Dick said. He noted a lot of progress in SRDD for treating glaucoma and inflammation, which is promising as ophthalmologists face an increasing number of patients with longer life expectancies.
5. Teleophthalmology and home monitoring
The pandemic has accelerated the adoption of telemedicine, and ophthalmology is no exception. Home-based OCT and IOP monitoring devices are under development, potentially enabling remote management of retina and glaucoma patients. Prof Dick expects the role of teleophthalmology after uneventful cataract surgery to increase as well.
H Burkhard Dick MD, PhD, FEBOS-CR is professor and chairman of the Ruhr University Eye Hospital in Bochum, Germany, and ESCRS president elect. dickburkhard@aol.com
From Concept to Clinic
Partnerships with academia and industry promote innovation.
Have an idea for a new intraocular lens (IOL), surgical instrument, or drug? The first step might be coffee with an engineer, according to Sorcha Ní Dhubhghaill MBBCh, PhD.
Many universities have research groups, including optical and biomaterial engineers, hungry for clinical perspectives, Professor Ní Dhubhghaill said. Informal meetings can break the ice. “You don’t always have an unfiltered approach on Zoom.” But it’s just the beginning of a complex journey to market that can take years and cost millions.
Early on, the key is bringing together ideas about what needs to be done—the unmet clinical need—with what can be done technically. “Engineers want a problem they can tackle, but you don’t always have the cross talk you need [among disciplines],” said Prof Ní Dhubhghaill, who works extensively with clinical trials and spinoff companies as head of a university ophthalmology department.
H Burkhard Dick MD, PhD agreed. “Innovations should originate from real-world clinical frustrations. Whether improving visualisation in deep-set eyes or reducing variability in IOL positioning, starting with a focused problem leads to more relevant solutions.”
Clinical input also helps ensure new products will be viable in the real world, said Luis Diaz-Santana PhD, who advises eye care product start-ups. Developing a new technology “is not a technology question per se; it needs to be profitable; it needs to live in a system of [clinical] workflows, guidelines, and regulations; and it needs to solve a problem and live in a consumer space.” Early ophthalmologist involvement also can build acceptance by often-conservative physicians, he added.
Experts in intellectual property, regulatory requirements, and business strategy should be consulted early, said Prof Dick, who also has extensive experience bringing new technologies to market. “No single person can bring a medical device from concept to clinic.”
Approval, payment, and partners
While regulatory approval may seem like a late step, it should be an early goal. Working with regulators early helps guide everything from design to preclinical testing to clinical trials. “There is a very formal structure. It’s not worth doing a clinical trial that doesn’t count [towards approval], and regulators may give you advice on animal studies,” Prof Ní Dhubhghaill noted.
Health plan reimbursement also should be considered early, Prof Dick said. “Design clinical trials that not only demonstrate safety and efficacy but also cost-effectiveness,” he advised.
Adding business partners helps, Prof Ní Dhubhghaill added. “It takes time and money. That’s why you need industry support. The FDA and EMEA make early clinical development very expensive. If you rely on grants, you’ll never make it.”
In addition, “established companies offer access to distribution networks, regulatory experience, and R&D resources that can accelerate time to market,” Prof Dick said.
“Strong intellectual property protection and publication in peer-reviewed journals build credibility with investors, partners, and regulatory bodies,” he added. Most universities provide services that help entrepreneurs balance the complex relationship between these two needs, Prof Ní Dhubhghaill said.
HOWARD LARKIN REPORTS
Business partners are not the only audience to consider: “How will customers see value in your proposition? You need to articulate this in a way your audience can understand,” Dr Diaz-Santana said. He also stressed that a new technology needs to actually solve a problem rather than push it off to someone else.
And investors want to see a continuing revenue stream, Dr Diaz-Santana noted. A product that requires ongoing supplies or a service contract is more attractive than a one-off sale. Scaling manufacturing and maintaining complex supply chains are also important partner concerns.
“Use familiar clinical environments for initial testing, but ensure your innovation has global applicability in design and scalability,” Prof Dick advised.
Building teams—and trust
Attracting investors and business partners requires answering key questions about every step in the development and commercialisation process, Prof Ní Dhubhghaill said. Achievable business and development plans are crucial. “Be realistic to the point of conservative. Most experienced investment teams will not be fooled.”
Dr Diaz-Santana recommended seeking early collaborators who will challenge assumptions. “You need to talk to people who don’t agree. […] Don’t be married to a technology—focus on the problem.”
Team members with the necessary development skills also enhance investor trust, Prof Ní Dhubhghaill said. “They don’t fund the idea; they fund the team.”
Though the regulatory and economic hurdles are daunting, the innovation climate in ophthalmology remains vibrant, Prof Dick said. “With a strategic approach based on clinical insight and multidisciplinary collaboration, ophthalmologists can continue to play a central role in the development of transformative new technologies. The future of sight-saving care depends on it.”
Sorcha Ní Dhubhghaill MBBCh, PhD, MRCSI(Ophth), FEBO, FEBOS-CR, BaO, Dip(stats) is chair and head of the Department of Ophthalmology at University Hospital Brussels, Belgium, and a member of the ESCRS Council of Management. sorcha.ni.dhubhghaill@uzbrussel.be; nidhubhs@gmail.com
H Burkhard Dick MD, PhD, FEBOS-CR is professor and chairman of the Ruhr University Eye Hospital in Bochum, Germany, and ESCRS president elect. dickburkhard@aol.com
Luis Diaz-Santana PhD is founder of LDSH Strategy, a consultancy specialising in assisting eye care product start-ups in Cambridge, UK. luis@ldshstrategy.com
Double Down On Your Decision
Screening for ectasia with double safety
The Tomographic Biomechanical Index, or TBI, provides a unique combined expression of Corvis® ST und Pentacam® measurement data. It allows the risk of corneal ectasia to be assessed with greater reliability than ever before. The TBI assists you in selecting the optimal treatment based on sound reasoning. More safety for you and your patients!
In 2017, young ophthalmologists competing in the John Henahan Writing Prize were asked to discuss the challenges of industry influence while maintaining the highest professional ideals. The top prize went to Clare Quigley, then a second-year resident at the Mater Misericordiae University Hospital, Dublin, now a Consultant Eye Surgeon in Dublin. Her essay remains relevant today.
Declare Disclosures
BY CLARE QUIGLEY MD
Ihave some things to disclose. On a cold, wet November morning, when my rain gear was not sufficient to prevent me from getting saturated on my cycle to work, I arrived at the ophthalmology department shortly before morning teaching was to start. After peeling off my dripping outerwear, I trudged to the orthoptist’s room, where the consultant-delivered lecture would soon begin. Entering the room, the smell of freshly roasted coffee beans banished my disgruntlement at the wintry morning. Coffee, tea, orange juice, and a tray of fresh pastries, granola, fruit, and yoghurt were arranged on display. Less immediately drawing my gaze, next to the lavish breakfast, were product information booklets for glaucoma drops and a bouquet of pharmaceutical company pens on offer. I was greeted by a smiling industry representative, who invited me to help myself to whatever took my fancy. Filling a cardboard plate, I settled down for teaching with coffee in hand; colleagues arriving each helped themselves to the generous spread. Following this hearty breakfast, we were happily awake and alert for teaching, and afterwards, in clinic, we were likely friendlier and more attentive to our patients than our unfed selves would have been.
My second disclosure: I recently arrived at the theatre for my usual afternoon session. I had picked out the cataract patient from the list of those most suitable for me, the most junior team member. As I expectantly waited for them to be portered in, a friendly surgical devices company representative approached me. She asked me my name, where I had worked previously, and spoke about a recently developed innovative intraocular lens they were newly offering, explaining some advantages of the lens. Would I like to try a sample? I was flattered by the attention; I duly chose one of her lenses. I found it injected nicely, just as she had set it would.
Disclosures aside, it is an intriguing question: How does commercial interest affect my career? ‘Career’ is a particular term that does not bring to mind patient care specifically, but rather calls up ideas of personal goals of success, financial and otherwise. One’s career is an individual journey— planned for with particular trajectories. For our career dreams, we pour endless hours of toil into research, writing papers, preparing presentations; we travel to conferences; we pay for surgical courses; we limit our annual leave; we sacrifice time that could be spent with loved ones, family, and friends. Commercial interests, I imagine, have a positive impact on any given career in ophthalmology. A commercial interest may lead to sponsorship to travel for an important meeting or to attend an otherwise prohibitively expensive
training course. An industry may sponsor a study, allowing for a greater sample size, a superior standard of research, and a higher impact factor target journal than what would be possible under a teaching hospital’s standard budget.
But what if the question was slightly altered? What if a more vocational term was used? How does commercial interest affect my patient care? Shifting emphasis away from career and towards patient beneficence has a significant effect. As medical professionals, we have ready access to best practice guidelines, derived from systematic reviews of high-grade evidence. We can map out our patients’ care—the best drop, the most appropriate implant to choose—based on this knowledge at our fingertips and also on the individual’s characteristics and preferences. But if we have been generously looked after by a particular company, be that wined and dined, given a research grant or sponsorship for an education course to run in our hospital, or perhaps funding to attend an interesting meeting, then bias surely creeps in, accompanying our gratitude and good feeling towards this company.
Pharmaceutical companies and surgical device manufacturers contribute positively to patient outcomes, as they support research that ultimately improves eye care. We must, however, recall that the primary objective for these businesses is not in the best interest of patients but rather to generate profits for their shareholders. Consider then, as ophthalmologists, our bottom line: We have a duty to do what is in our patients’ best interest. This duty should not be affected by relationships with industry and any commercial interests we develop. We must be cautious, too, of zealous rejection of any association with industry. Separation of clinicians from cutting-edge industry developments, where advances in the field of ophthalmology push forward, would be to the detriment of patient care overall.
Commercial interest will affect my career; I will be exposed to different industry forces, products marketed for prescription or implantation. As an ophthalmologist, I have a solid grounding point to return to for guidance: my duties as a professional. Epstein and Hundert define professional behaviour as “the habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values, and reflection in daily practice for the benefit of the individual and community being served.” I will therefore undertake to declare all my disclosures, and I will recall that a tasty breakfast or friendly face may influence my disposition towards treatment choices, but my first priority must be to the best interests of my patients.
iNovation Innovators Den Boosts Eye Care Pioneers
New ideas and industry, colleague, and funding contacts among the benefits.
HOWARD LARKIN REPORTS
At last year’s Innovators Den during the annual ESCRS iNovation Day in Barcelona, Maria Iglesias MD, PhD, picked up a valuable idea for a tonometer she is developing that more accurately measures intraocular pressure (IOP) in post-LASIK patients. The device uses a convex prism to applanate the cornea, which helps compensate for central corneal weakening, producing readings that more closely replicate pre-LASIK IOP values than the flat prism in the standard Goldmann applanation tonometer.
“Winning the Innovators Den brought interest in [lenticle extraction refractive surgery] patients as a possible research group,” Dr Iglesias explained. “We will be able to get new information that has never been evaluated before about the potential applicability of this device, which may lead us to new market possibilities.”
She also added more clinical trial partners on advice from the competition judges.
Strength through competition
Innovators Den is an iNovation competition in which ophthalmic entrepreneurs pitch their developing technologies. Dozens of contestants receive mentors, advice on business models and pitches, and exposure to key opinion leaders, investors, and other expert resources. Three finalists present during a designated session on iNovation Day. One is chosen the winner by an expert panel in front of an audience of ophthalmologists, investors, and industry representatives.
“Participating in this contest has been incredible in terms of visibility and international recognition,” she said. “It has allowed us to connect with people that would be quite difficult to access otherwise.”
The contacts helped secure needed resources in business planning, marketing, financing, design, and manufacturing, Dr Iglesias added. “The LASIK tonometer project has reached the point where we needed to start a company to access the market. We are currently in the process of getting its CE marking and approval by the Spanish Agency for Medicines and Health Products.” She anticipates it will be commercially available in 2026.
Towards a phase 1 trial
Jean Garrec, another Innovators Den finalist, also gained valuable exposure for his company’s topical bioadhesive tablet that resides under the lower eyelid, steadily releasing eye medications for 7 days. On track to begin a Phase 1 clinical trial as a new glaucoma drug, this self-applied insert addresses limitations of eye drops—including inconsistent concentration, wasted drugs, and poor compliance—without the need for invasive injectable implants. The start-up, BIOPHTA, is also developing a treatment for macular oedema, clearing the way for gene therapy to one day be possible.
In addition to informing influential ophthalmologists about BIOPHTA’s innovations, iNovation Day helped inform representatives of several large pharmaceutical companies. Big Pharma’s involvement as co-development partners or licensees is crucial to bringing new pharmaceutical products to market, which takes 10 to 15 years and large investments, Dr Garrec said.
“We are a young start-up at a very early stage of development (compared to other pharmaceutical companies),” he said. “Any opportunity to gain visibility, any opportunity to stand up on the stage and tell people what we are doing is beneficial.”
Finishing design touches
The third finalist, Harilaos Ginis PhD, is now finalising software for a device designed to quantify retinal vision quality in patients with multifocal or other advanced technology intraocular lenses. It will help ophthalmolo gists understand the visual complaints of patients with good visual acuity but poor vision by near-instantaneous measurement of factors that can degrade image quality, such as contrast, diffractive phenomena, and chromatic and other aberrations.
we’re now refining the interface to ensure it integrates seamlessly into clinical workflows,” he said.
While the core functionality of the device is complete, we’re now refining the interface to ensure it integrates seamlessly into clinical workflows.
On the commercialisation side, Dr Ginis’ company, Diestia Systems, recently secured two European research and innovation grants and seeks additional funding from investors. “We’re preparing for the regulatory pathway ahead—which, as with any medical device, can be lengthy and complex.”
Dr Ginis, too, found the Innovators Den experience rewarding. “The mentorship we received was incredibly valuable in helping us sharpen our pitch, identify key strategic priorities, and better align our messaging with market expectations. Just as importantly, the positive feedback from the committee, audience, and fellow innovators was both encouraging and validating. […] Being selected as one of the three finalists in such a competitive field was a great honour and helped raise awareness of our technology.”
The 4th ESCRS iNovation Day is on Friday, 12 September 2025, from 8:30–16:00 at the Bella Center in Copenhagen, Denmark, immediately before the opening of the main ESCRS Congress. For information or to apply for the Innovators Den, go to https://iNovation.escrs.org/.
Maria Iglesias MD, PhD, FEBO is an ophthalmologist and inventor with Barraquer Ophthalmology Centre, Barcelona, Spain. mariaiglesiasalvarez@gmail.com
Jean Garrec PharmD, MBA is founder and CEO of BIOPHTA, Paris, France. jean.garrec@biophta.com
Harilaos Ginis PhD is senior scientist and co-founder of Diestia Systems, Athens, Greece. harilaos@diestia.com
LEADERSHIP AND BUSINESS RESOURCES at Your Fingertips
What is the one leadership skill you would like to improve? What is the one business management challenge you would like to overcome?
The ESCRS Leadership, Business, and Innovation (LBI) programme provides ophthalmologists, clinic managers, and administrators and their teams with a variety of content to enable both online and in-person learning. Podcasts, webinars, video interviews, and more are available in the LBI library to help answer questions about topics such as selling a practice, finding a good work-life balance, facilitating patient decision making, and more.
Lead, Negotiate, Innovate
Leadership, public relations, and management skills are essential in all aspects of ophthalmic clinical practice.
TIMOTHY NORRIS REPORTS
Acquiring precise soft skills is extremely important for ophthalmologists when dealing with their team, clinical and public practice, and relationships with the industry. This message emerged during a TOGA Session at the 2025 ESCRS Winter Meeting in Athens during a debate organised by the ESCRS Leadership, Business, and Innovation (LBI) Committee.
“If you are running a department, an academic institution, a professional department, or a small business, you are managing people, finances, and budget,” said LBI Committee Chair Paul Rosen. “Wherever you work, developing business skills is extremely important.”
The very nature of leadership was the first point of discussion expressed by David Lockington MBBCh, PhD. “Leadership is doing the next right thing, bringing people with you,” he said. “How can the ESCRS help members show the right traits? How can we help you in your situation?”
He addressed the audience, encouraging them to get involved in the many compelling initiatives held by the LBI Committee, such as podcasts, meetings, and webinars.
Sometimes ophthalmologists are technicians, and sometimes they are not entirely aware of the soft skills essential to succeed, either in private or public practice, Vincent Qin MD pointed out. “You know how to successfully operate a cataract or lift a LASIK flap, but sometimes you also need to understand all the complex interplays of your practice, with the team, and the environment.”
The main goal of the LBI Committee, according to Dr Qin, is to give insight and effective indications about leading, managing a team, and bringing people together. This can help ophthalmologists learn how to market their services and leverage social media ethically and efficiently, he added.
All about innovation
Christina Grupcheva MD, PhD brought up the second topic regarding innovation and how to facilitate its access. As she pointed out, there is a need to clearly define innovation, how this can be integrated, and how it interacts with leadership.
“In the academic environment, you have more challenges but fewer risks,” she explained. “In the private environment, you are the decision maker, with fewer challenges but more risks that need to be taken.”
Through information and discussion, she added, the LBI Committee aims to find the proper way to make ophthalmology increasingly on the verge of innovation and render said innovation more accessible worldwide.
Information is key to making this possible. According to Dr Qin, articles, reviews, easy-access podcasts, and especially books need to be constantly at the disposal of the ophthalmologist to keep them up to date with all the most
Wherever you work, developing business skills is extremely important.
recent developments and provide them with the necessary soft skills—especially for business.
For this reason, the group is inaugurating the LBI book club, which aims for ophthalmology to develop key takeaways in management, leadership, and business. Professor Rosen suggested two books to consider for starters: Leading: Learning from Life and My Years at Manchester United by former football manager Alex Ferguson and Management in 10 Words by Tesco’s former CEO Terry Leahy.
Communication and negotiation with management
Good and well-practised communication and negotiation skills are of the utmost importance for implementing new technologies in the ophthalmologist’s daily practice, Artemis Matsou MD stressed. There is a real language barrier between the physician and the upper management that needs to be addressed because doctors are not used to speaking the language of management.
Dr Matsou said regardless of its private or public sector status, the practice needs to be constantly innovating, and the physician needs to overcome this barrier to push things in the right direction.
“You can present all the randomised control trials, all the evidence, but they do not get that,” she pointed out. “The
important thing is how you can generate income. We have a different mindset.”
Every innovation or discovery will be analysed under an economic lens. According to Dr Lockington, the discovery of a cure for cancer would also get an immediate response in the form of the question, “Is it cheaper than what we currently do?” Failing to understand that, he observed, will put barriers to every chance of development.
Developing negotiating skills, therefore, needs to be at the very core of everything for which LBI stands. “I went on a negotiation skill course and sat down. They said, ‘you are a doctor, why are you on a negotiation skill course?’ So, I said that I need to negotiate with my wife,” Prof Rosen joked. “But the truth is I need to negotiate for my job. Negotiation covers all aspects of what we need to do.”
Paul Rosen FRCS, FRCOphth is a Consultant Ophthalmic Surgeon at Oxford Eye Hospital, UK, Chairman of the Trustees of ESCRS, former President of ESCRS, and Chairman of the ESCRS Practice Management and Development Committee.
David Lockington MBBCh, BaO(Hons), FRCOphth, PhD is Consultant Ophthalmologist at the Tennent Institute of Ophthalmology, NHS Greater Glasgow and Clyde, UK.
Vincent Qin MD, MBA, MPH, FEBO, SSL is an ophthalmologist and surgeon based in Belgium. vincent.qin@live.be
Christina Grupcheva MD, PhD, DSc, FEBO, FICO(Hon), FBCLA, FIACLE is Vice Rector at the Medical University of Varna, Bulgaria.
Artemis Matsou MD, FEBO, MRCP(UK) is a consultant ophthalmic surgeon at Queen Victoria Hospital, East Grinstead, UK. art.matsou@gmail.com
Apply Now for the
ESCRS Systematic Research Award
ESCRS is now accepting applications for the 2025 Systematic Research Award (SRA) programme. The SRA is open to all ophthalmologists and researchers (MD and/or PhD or experienced ophthalmic nurses) who currently hold a full- or part-time clinical/research position at a clinical or academic institution.
Established in 2022, the SRA aims to encourage high-quality research that documents and codifies existing knowledge in cataract, refractive, and cornea medicine or surgery. The goal of the SRA is to provide new scholarly output in the field of cataract, refractive, and cornea medicine or surgery, focused on the methodology created by the Cochrane Library.
Up to six (6) awards are available, with a total maximum of €10,000 per award.
Preliminary applications will be accepted until 31 May 2025. Applicants are encouraged to refer to online resources at the Cochrane Library and/ or at PROSPERO and/or with PRISMA. The lead applicant should be an ESCRS member.
Retinal Re-Detachment Following Cataract Surgery
Are all patients without vitreous at risk of it?
LAURA GASPARI REPORTS
There is an urgent need to identify the risk factors and mechanisms associated with the increased risk of retinal re-detachment following cataract surgery in patients who underwent pars plana vitrectomy (PPV), according to Syed Ahmed MD, PhD.
Victrectomised eyes suffer a major risk of re-detachment after cataract extraction. The risk appears highest with a disturbance and destabilisation in the vitreous, causing a major traction on the retina.
“However, there is a significant research gap in eyes that have had previous PPV and then following cataract surgery to see whether they have had increased rates of RD or not,” Dr Ahmed explained.
He and colleagues at Moorfield Eye Hospital, London, conducted a study to assess the incidence of re-detachment and its impact on visual outcomes. The study was a retrospective review of seven years (2011–2022) of data and included all patients who underwent previous PPV for retinal detachment (RD) before cataract surgery. The exclusion criteria involved patients who had multiple RD repairs prior to their cataract surgery, those who had combined cataract procedures such as vitrectomy or glaucoma surgery, those whose procedures were complicated, and non-phacoemulsification surgeries. The statistical analysis on the results was performed using chi-square tests and logistic regression with minimum one-year follow-up.
The primary outcome measure was to see the incidence of recurrent RD after cataract extraction in people with previous PPV and compare it to the incidence of RD postoperatively. The secondary outcomes included identifying the risk factors, evaluating visual and anatomic outcomes after the re-detachment repair, and assessing the postoperative timing of re-detachment.
1,808
Of the 110,670 analysed patients, 1,808 had RD repair before cataract surgery.
Of the 110,670 analysed patients, 1,808 had RD repair before cataract surgery. Researchers found a 2.4% rate of redetachment in this cohort, whereas the rest had only a 0.34% rate of RD following cataract extraction. Concerning visual outcomes, patients with no RD had a mean visual acuity of 0.1 logMAR, and those who experienced a detachment before cataract surgery surprisingly had a visual outcome of 0.15 logMAR. However, patients who suffer RD following cataract surgery had poor visual outcomes, with 0.5 logMAR for those with a primary RD and 0.6 logMAR for those with re-detachment.
In terms of timing, the study found patients who experienced a repeated RD tended to have cataract surgery earlier than those who did not, Dr Ahmed reported. Most of them had the re-detachment after one year of follow-up.
What is important is understanding the mechanism causing the re-detachment, he said.
“There are a limited number of studies looking into this,” he observed. “Previous literature has focused on thoughts that maybe there is an increased inflammatory state that causes the remaining vitreous to contract and cause the peripheral tears, or whether there is missed vitreous that remains in the anterior vitreous face, contracting and causing the RD.”
Most of the patients in the study were highly myopic white males. Visual outcomes showed reduced BCVA due to proliferative vitreoretinopathy, multiple breaks, and associated complications. Understanding the mechanism of re-detachment and the risk factors is crucial for clinical decision making and patient management. Moreover, Dr Ahmed concluded this study indicated that not all patients without the vitreous necessarily go on to have an increased risk of RD.
Dr Ahmed spoke at the 2025 ESCRS Winter Meeting in Athens.
Syed Ahmed MD, MBBS, FRCOphth, PhD is an ophthalmologist at Moorfields Eye Hospital NHS Foundation Trust, London.
The Art of PIOL Implantation
Expert advice to overcome the challenges of phakic IOL procedures.
TIMOTHY NORRIS REPORTS
History teaches us when we listen.” With this remark, Başak Bostancı MD reviewed the state of the art in surgical procedures for the implantation of phakic IOLs (PIOLs).
There is still a learning curve—despite the new models and procedures developed to reduce the many complications, such as endothelial decompensation and glaucoma, caused by the first PIOL models developed in the 20th century.
“The most recent models of phakic IOLs did move towards new designs and materials for higher levels of safety and efficacy,” she said. “With the addition of more precise sizing and imaging techniques, it is possible to make this procedure even more safe and effective.”
Today, implanting a phakic IOL has many advantages, starting with correcting high refractive errors with predictable postoperative outcomes. Unlike RLE techniques, the natural crystalline lens is preserved along the natural accommodation, making PIOL more reversible and adjustable. As Dr Bostancı underlined, PIOLs can be explanted and exchanged if necessary, offering a satisfactory level of flexibility. Moreover, PIOLs offer reduced higher-order aberration and improved contrast sensitivity compared to refractive laser-based procedures, making them suitable for thin corneas and patients with irregular corneal topographies.
Dr Bostancı stressed sizing is crucial, since the majority of complications come from under- or oversized phakic IOLs. Many surgeons still use white-to-white measurements, but she emphasised these are not good enough.
Despite being a little more expensive, adopting advanced sizing techniques such as high-frequency digital ultrasound or anterior segment OCT is essential for optimal surgical qualities. Alternatively, using artificial intelligence or machine learning on an intraoperative OCT can be useful to track and monitor the implantation during surgery, she said.
In the preoperative phase, Dr Bostancı recommends four steps for preparation: a laser iridotomy one week in advance for ICL models without a central hole, a full mydriasis in the patient, 100 cc of mannitol one hour before surgery, and marking for toric models if there is no chance of using a digital marking tool. Marking is important, as the axis might be slightly different from the patient’s axis due to manufacturing limits, she observed.
Dr Bostancı had insights on the pitfalls to avoid during a PIOL implantation. She showed a surgical video where, during the operation, the ICL flipped suddenly because the opening was not carefully observed. By misreading the side where to inject more viscoelastic, inadvertent OVD was put on the top, completely opening the lens on the wrong side. In this scenario, she said the best course of action would have been to remove the ICL and reload it in the cartridge for a reimplantation. However, flipping the ICL inside the eye (a desperate manoeuvre) could have the potential to damage the endothelium and the lens at the same time.
“Phakic IOL surgery may seem easy, but both preparation and procedure still have their learning curves. Do not make common mistakes many surgeons may do in the beginning: take your time, learn and practise every step, and learn all the ‘dos and don’ts’ before performing this procedure,” she advised.
Dr Bostancı spoke during the ‘Innovations and Best Practices in Phakic Intraocular Lenses' session at the 2025 ESCRS Winter Meeting in Athens.
Başak Bostancı MD, FEBO is an assistant professor at Bahçeşehir University of Istanbul and a cataract and refractive surgeon at World Eye Hospital, Istanbul. drbbostanci@gmail.com
Making IOLs a More Personal Choice
Surgeons may prefer some IOLs for their patients, but what about for themselves?
TIMOTHY NORRIS REPORTS
During her presentation at the ESCRS Winter Meeting in Athens, Athina Lazaridou MD asked the audience a fundamental question: “What if it is up to cataract and refractive surgeons to choose a lens for themselves?”
The increased personalisation and standardisation of the most performed surgical procedure in Europe have allowed further patient involvement in the decision-making, particularly in selecting the desired intraocular lens, she observed, especially given the plethora of lenses and options available.
Informative devices such as virtual reality and smart devices can now grant the patient the opportunity to be an even greater participant in the process. “Still, what can be said about the patients who possess the highest level of knowledge?” she asked.
To answer this question, Dr Lazaridou and her team conducted a prospective study asking 72 male and 28 female Greek ophthalmologists to complete a 20-item, multiple-choice questionnaire. Of the 100 eye doctors, 47 were myopes, 17 were hyperopes, and 36 were emmetropes. By age, 61% of the doctors involved were 45 to 55, 24% were 55 to 65, and 15% were older than 65.
The majority of participants had more than 20 years of experience, with 44% performing 40 phacoemulsifications per month, while 28% of doctors performed more. Two-thirds of the doctors declared they did implant premium IOLs in their everyday practice but mostly preferred monofocal plus and toric lenses for their patients, followed by EDOF and multifocal IOLs.
However, Dr Lazaridou observed a discrepancy. Of the 38 surgeons that do implant multifocal lenses, only 15 would choose them for themselves. Almost 50% prefer EDOFs and the vast majority reject the idea of refractive lens exchange.
A mix-and-match approach was divisive, with 50% in favour and 50% either against or hesitant.
According to Dr Lazaridou, these results may differ between countries. Citing a similar study conducted in Spain and South America, 60% of Spanish and Latin ophthalmologists would more likely opt for a multifocal lens, with only 15% more prone to choose an EDOF. On the other hand, recent research conducted in the United Kingdom showed a preference for EDOF lenses, with 60% of doctors rejecting mix and match for their patients.1 Moreover, a study conducted by Hercules Logothetis and Robert S Feder in the United States showed a preference for monofocal plus, also concluding the higher the number of premium lenses implanted by a surgeon, the higher the possibility of choosing them for themselves.2
The study confirmed a general lack of consensus about surgeon preference regarding intraocular lenses.
“There is a tendency to minimise refractive errors and presbyopia after cataract surgery,” she said. “And despite the lack of consensus, there seems to be a correlation between years of experience with a specific technique and the type of IOLs used.”
Dr Lazaridou presented at the 2025 ESCRS Winter Meeting in Athens.
For citation notes, see page 46.
Athina Lazaridou MD is an ophthalmology resident at the Aristotle University of Thessaloniki, Greece. alazaridou11@gmail.com
Predicting Pseudoaccommodation
MERoV study data and logistic regression for a precise probability calculation.
TIMOTHY NORRIS REPORTS
While the many factors responsible for pseudoaccommodation in pseudophakic patients have been known for the past 20 years, a precise formula to predict this outcome still needs to be determined in cataract surgery.
“Technologies have advanced, and [over] the years, surgeons have modified these factors accordingly,” noted Mayank Nanavaty MBBS, PhD. “However, we are still struggling to predict pseudoaccommodation in most of the eyes implanted with a monofocal IOL.”
Citing data from the Monofocal Extended Range of Vision (MERoV) study supported by ESCRS, Dr Nanavaty observed that 9.6% of patients who received a monofocal IOL do not wear glasses for distance and reading. Four factors are responsible for this phenomenon. Understanding how these factors interact to find a mathematical prediction formula based on this ratio was one of the study’s aims.
MERoV was a prospective, non-blinded, non-randomised, single-eye cohort study conducted in Brighton, UK.1 The study enrolled 412 patients, with follow-ups conducted at one month and three to nine months after surgery. Despite the COVID pandemic hampering follow-up data collection, the study gathered information on 301 patients.
According to Dr Nanavaty, four main factors identified as responsible for pseudoaccommodation were used in a mathematical function suggested by Dr Catey Bunce and her team, linking all the predictor variables.
Using logistic regression, the formula considered preoperative axial length, mesopic pupil size, spherical equivalent, and total eye spherical aberration (SA). The formula is Logit(P)=12.54 - (0.484 x preoperative axial length) - (0.884 x mesopic pupil size) - (13.1 x total eye SA) - (0.714 x spherical equivalent), where Logit(P), natural log(P/1-P), and P being the probability of pseudoaccommodation.
While it looks complex, the formula is relatively simple, Dr Nanavaty explained. Using random values, he showed the interaction between the four variables and their weight on the final probability value.
Keeping everything the same in the formula but changing the spherical equivalent in the range of almost one point does not change the probability of pseudoaccommodation. Dr Nanavaty noted changing preoperative axial length as well does not show very convincing predictability, while on the other hand, pupil size is inversely proportional to the percentage of pseudoaccommodation.
The total spherical aberration is much more incisive than the other parameters—especially when negative—changing pseudoaccommodation predictability in the formula from 0 to 98% when transitioning from 0.5 to -0.3 µm as the other parameters remain unchanged, he showed the audience.
“Just changing the total spherical aberration of the eye to -0.3 to -0.5 microns gave a predictability of pseudoaccommodation to greater than 98%, which basically means that you just aim for this parameter in the eye, and you can almost convince the patient that he will have reasonable reading vision following a monofocal lens implantation,” he concluded.
Dr Nanavaty spoke at the 2025 ESCRS Winter Meeting in Athens.
For citation notes, see page 46.
Mayank A Nanavaty MBBS, DO, FRCOphth, PhD is Consultant Ophthalmologist and surgeon at the University Hospitals Sussex NHS Foundation Trust, Brighton, UK. mayank.nanavaty@nhs.net
When Does Posterior Capsular Rupture Occur?
Understanding the timing could lead to better management of this complication.
LAURA GASPARI REPORTS
Posterior capsular rupture (PCR) is one of the most fearsome complications of cataract surgery, and assessing and characterising when it occurs could help surgeons better understand the complication, reported Akshay Narayan MD.
PCR occurs in 0.9% of NHS cataract surgeries and may increase the risk of postoperative complications, especially macular oedema, endocytosis, and retinal detachment.
“Although we have got quite a good handle of the preoperative and intraoperative risk factors for PCR, understanding when it occurs has quite a limited literature,” he pointed out.
Dr Narayan presented a five-year retrospective and observational cohort study conducted at Moorfields Eye Hospital in London that considered all the cataract surgeries complicated with a PCR performed in the centre. The primary outcome measure was the timing of PCR during cataract surgery— while the secondary outcome was the incidence of anterior capsular (AC) tears and other intraoperative complications and the location of the IOL implantation. The study included 1,042 eyes, and the average age of patients was 70 years, with an identical proportion of females and males. The phacoemulsification machine was an Alcon system, and the predominantly implanted lens was an Alcon MA60AC.
Researchers observed a similar number of PCRs across the five years. Other intraoperative complications were vitreous loss, AC tears, dropped nucleus, and zonular dialysis. The lens was most frequently implanted in the sulcus. Cataract surgery was broadly classified into six stages: hydrodis-
section, phacoemulsification, irrigation, aspiration, IOL implantation, removal of OVD, and wound hydration. The majority of PCRs (60%) occurred during the phacoemulsification stage and included sculpting, cracking, chopping, and segment removal.
Moreover, the study compared eyes based on whether they had AC tears, finding higher proportions of PCR occurred in the earlier stages of cataract surgeries for those eyes with an AC tear while it occurred at later stages for unaffected eyes. Also, there was a significant difference in the location of the lens implantation: in eyes suffering an AC tear, the lens was implanted at an alternative location (like at the anterior chamber) or left aphakic; eyes without an AC tear had predominantly sulcus haptic capture and some lenses implanted in the bag.
The study suggested PCR is most likely to occur during the sculpting and segment removal stage of cataract surgery, and its timing is affected by the presence or absence of anterior capsular tears. Finally, Dr Narayan said surgeons should be aware that the latter, alongside PCR, will likely influence the choice of the IOL implantation location.
Dr Narayan spoke at the 2025 ESCRS Winter Meeting in Athens.
Akshay Narayan MD is an ophthalmology resident at Stoke Mandeville Hospital, Aylesbury, UK.
ESCRS Power Calculator: Fast and Effective
Study compares older and modern formulas for IOL power calculation using the ESCRS power calculator.
LAURA GASPARI REPORTS
Modern IOL power calculation formulas perform better, and the ESCRS online IOL calculator proved a valuable tool for IOL power choice, according to a study presented by Sophia A Reifeltshammer MD.
According to the 2002 EUREQUO report, the mean absolute refractive error after cataract surgery is approximately 0.40 D, with 75% of patients within 0.50 D. For short eyes, as suggested by the literature, the situation is even more challenging, with only 50% of eyes within a refractive error of 0.50 D.1
“With the ESCRS IOL power calculator, we now have a useful tool to compare all of these different formulas and further refine our IOL choice,” Dr Reifeltshammer said.
The study aimed to compare the outcomes of the ESCRS IOL power calculator to the classical formulas provided by the biometry devices regarding mean absolute error, median absolute error, and standard deviation, with a focus on feasibility and effectivity during routine clinical practice.
The multicentred prospective study included 337 patients receiving the same monofocal IOL (Tecnis™ ZBC00 by Johnson & Johnson Vision): two-thirds were women and one-third were men. The axial length (AL) of 288 eyes was regular (AL 22.00–25.50 mm), while 29 eyes were short (AL < 22.00 mm) and the other 29 were long (AL > 25.50 mm). The data set included the preoperative biometry data, the implanted IOL power, the postoperative biometry data, and subjective refraction and autorefraction. The axial line length ranged from 19.86 to 28.89 mm.
The investigators put the preoperative biometry data in the ESCRS calculator, cross-checking it by a different examiner to avoid typos. The outcomes underlined how the BUII performed better than the other formulas, with a mean absolute error of 0.38 D. HofferQ provided the lowest result with 0.43 D. Regarding the ESCRS calculator formulas, the best performance in mean absolute error was with Kane and EVO. Kane also performed well in the median absolute error and standard deviation. HofferQST provided the lowest mean absolute error. Comparing the older and modern formulas, there was no significant difference. However, when excluding HofferQST, there was a significant difference between the older and modern formulas.
Evaluating the clinical side, the examiners tried to look at the similarity of IOL power chosen by each formula, selecting the IOL power closest to target refraction, which was either emmetropia or myopia at -2.50 D. Kane and EVO resulted in the highest similarity and correlation with approximately 80% of cases choosing the same IOL power.
We now have a useful tool to compare all of these different formulas and further refine our IOL choice.
When reviewing all the formulas, Dr Reifeltshammer stated they only found seven matches (6.5% of cases). However, 68.8% of cases showed an overlap of at least five formulas. Moreover, the ESCRS calculator proved faster than other tools, saving 5 minutes and 38 seconds per patient.
“As already known, modern formulas perform better. However, they are not often included in the biometry devices,” she said. “Even modern formulas are discordant, and the number of refractive surprises could be reduced with the use of the ESCRS calculator, which also provides a reduction in time.”
The free ESCRS online calculator is available at https://iolcalculator.escrs.org/.
Dr Reifeltshammer spoke at the 2025 ESCRS Winter Meeting in Athens.
For citation notes, see page 46.
Which Technique Provides Faster Visual Acuity Recovery?
A Chilean study revealed that Yamane allows early rehabilitation compared to scleral-suture lens Micropure ® for traumatic aphakia patients.
LAURA GASPARI REPORTS
The Yamane technique allows for faster recovery of visual acuity in the early postoperative period compared to sutured Micropure® IOLs (BVI Medical) in traumatic aphakia management in severe ocular trauma, according to a retrospective study presented by Marilia Santibáñez MD.
The secondary lens implant is performed in various conditions involving support issues; Traumatic aphakia is among these conditions. “Over the years, several techniques were described, including different IOLs and fixation methods,” Dr Santibáñez explained. “Two of them involving the scleral-sutured lens are the Yamane technique and the Micropure.”
The retrospective study was conducted at the Ocular Trauma Unit (UTO), based at the Hospital del Salvador in Santiago, Chile—a specialised centre for managing severe ocular trauma. Its main objective was to compare the visual outcome of the two techniques in managing traumatic aphakia. The study involved 142 patients with traumatic aphakia with an IOL sutured to the sclera with a follow-up completed up to three months postoperatively between 2021–2023. They were divided into two surgical groups: 87 patients for the Yamane technique and 55 with scleral-sutured Micropure IOL.
The study showed no differences between the two groups related to age, sex, or mechanism of trauma. The mean initial visual acuity recorded was 0.84 logMAR for the Yamane group and 1.95 logMAR for the Micropure group. The postoperative average recorded was 1.38 logMAR in the Yamane group and 1.2 logMAR in the Micropure group. The threemonth mark revealed no statistically significant difference between the two groups.
This study will help our research group lay the groundwork for conducting a prospective study that considers refractive errors and the loss of records and information.
Regarding the complications, Dr Santibáñez reported there was not a statistically significant difference between the two groups, considering both postoperative complications and reinterventions. In fact, 26.4% of Yamane patients suffered different adverse events such as exposed haptics, decentration, ocular hypertension, macula oedema, pupil capture, and tilt, while 12.6% needed reinterventions (repositioning, change to Micropure, haptic suture, pupilloplasty, or haptic trimming and repositioning).
For the Micropure group, 28.8% of patients had postsurgical complications, such as ocular hypertension, macular oedema, and suture exposure, while 13.4% needed reinterventions (glaucoma surgery, pupilloplasty, and suture repositioning).
Even if the Yamane technique allows a faster visual acuity recovery in the immediate postoperative period than Micropure, the results in the long-term BCVA are comparable between the two. They are both effective for traumatic aphakia management, with an advantage to Yamane in early rehabilitation. In terms of complications, there was no significant difference in numbers although tilt was more frequent in Yamane and ocular hypertension in scleralsutured lens Micropure.
“This study will help our research group lay the groundwork for conducting a prospective study that considers refractive errors and the loss of records and information,” she concluded.
Dr Santibáñez spoke at the 2025 ESCRS Winter Meeting in Athens.
Marilia Santibáñez MD is a resident ophthalmologist at the Department of Ophthalmology, Hospital del Salvador, University of Chile. marilia.santibanez@gmail.com
PROMs
in the Cataract Pathway
Cataract surgery should be assessed not just in the final outcomes, but in the whole journey.
LAURA GASPARI REPORTS
When evaluating the results of cataract surgery, patients’ functional and visual outcomes often receive more weight than the entire surgical experience, according to Yarrow Scantling-Birch MD.
Prioritising patients’ needs is now an essential value in healthcare, and ophthalmologists try to deliver good vision to them. This approach is facilitated through patient-reported outcome measures (PROMs), which quantify patients’ subjective experiences—their postoperative visual functions and what quality of life parameters matter to them.
“However, all these forms and prompts typically do not measure the experience within the actual cataract pathway of our patients, from the referral process to the comfort of the operation and the postoperative care we deliver,” Dr Scantling-Birch reported.
Dr Scantling-Birch and colleagues conducted a prospective study whose primary objective was to create a PROM to capture the whole cataract pathway experience. The team designed a binary response questionnaire with a few Likert scales to assess patients’ satisfaction following surgery. The questionnaire was very simple and quick to overcome the huge language barriers present in many parts of North London, where the study took place. However, the questionnaire was internally validated in the ophthalmology unit, not externally validated.
The 140 questionnaires were collected between 1 January and 31 March 2024.
70
A mean participant age of 70 years old matched the typical demographic of the cataract cohort.
The 140 questionnaires were collected between 1 January and 31 March 2024, with a mean participant age of 70 years old, matching the typical demographic of the cataract cohort. The mean waiting time for a public system like the NHS was about 50 days. The study showed an overall positive response, with 53.6% of patients very satisfied and 31.4% satisfied with the cataract pathway experience. Most of them underwent cataract surgery for the first time (68.3%) and were referred by community practitioners (81.8%). While 50 days might seem long, 97.1% of patients were satisfied with the waiting time. Also, they were happy with receiving information about the surgery via a cataract leaflet prior to surgery (96.9%), reported receiving clear postoperative instructions (97.1%), and felt comfortable during surgery, noticing a significant visual improvement during and after surgery (81.8%).
The study underscores the idea that tools like PROMs should capture the whole patient experience and provide feedback at all points of the cataract pathway. Dr Carlos Rocha de Lossada pointed out these tools are extremely useful but should be externally evaluated before extensive use, especially in different countries or contexts.
“Future research should hopefully focus more on patient-centred prompts and on the whole cataract pathway, not just visual function alone, to promote more patient-centred care,” Dr Scantling-Birch concluded.
Dr Scantling-Birch presented at the 2025 ESCRS Winter Meeting in Athens.
Yarrow Scantling-Birch MD was an ophthalmology resident at the Department of Ophthalmology, North Middlesex University Hospital, London, and presented on behalf of his wider team who contributed equally to this research. This included Ms Sally Utting, Dr Salini Pillai, and Mr George Palexas. yarrow.scantling-birch@nhs.net
Never Go In Blind
Novel ophthalmic block simulator promises higher rates of confidence and competence in trainees.
TIMOTHY NORRIS REPORTS
Anovel and realistic ophthalmic block simulator has been shown effective in helping trainees gain confidence and competence performing blocks in a safe environment, reported Elizabeth Wen Ling Lim MD. Although commonly performed, poorly conducted ophthalmic regional blocks could increase the risk of intraoperative complications, longer operative time, and therefore poor outcomes.
According to Dr Lim, trainees in Singapore undergo minimal training before attempting their first ophthalmic block on a patient in the operating theatre—a procedure that grants little to no visualisation of the target tissues—essentially going in blind.
“There are some potentially blinding complications while performing a peribulbar block, including the most feared— perforation of the globe and retrobulbar haemorrhage,” she said. “And the risk factors increase when an inexperienced student makes multiple attempts.”
With her colleagues at the Singapore National Eye Centre and Singapore Eye Research Institute, Dr Lim developed a model to target this issue and respond to a large unmet need in ophthalmic surgery. She described the model as a multipurpose and realistic ophthalmic block simulator. This device can incorporate sham eyes of different axial lengths to better simulate even cases of high myopia, which is notably a highrisk factor for globe perforation.
Moreover, the simulation features a 3D-printed bony orbit modelled after actual CT orbit dimensions made of long-lasting and non-biodegradable materials. Its transparent properties allow direct real-time visualisation of needle positioning, making it the first model in literature able to simulate the
conjunctiva. The model is portable, and every part can be replaced individually instead of changing the whole device.
Dr Lim noted this model also allows for the practice of multiple types of blocks on the same model, such as infra-orbital, sub-tenons, and supraorbital blocks. To better study model efficacy, a pilot study was performed at the Singapore National Eye Centre to engage residents and consultants in providing feedback before and after using the simulation for training purposes.
Both confidence and competence were higher postworkshop compared to pre-workshop. Residents felt there was improved akinesia after performing blocks in the operating theatre, and while it was not statistically relevant, residents’ competence also improved, Dr Lim reported. No penetrating injuries on patients were reported in the training group after the workshop.
“With no simulators commercially available at present, our ophthalmic block simulator meets a large unmet need. This simulator is realistic, life-like, modifiable, versatile, long-lasting, and especially effective in helping ophthalmic trainees gain confidence and competence in performing blocks in a safe environment,” she concluded.
Dr Lim presented at the 2025 ESCRS Winter Meeting in Athens.
Elizabeth Wen Ling Lim MD is a resident of the Singapore National Eye Centre and Singapore Eye Research Institute of Singapore. limelizabeth@gmail.com
Need a quick introduction or refresher about a surgical procedure? Have a tip to share about a technique or approach you use that makes surgery easier?
The ESCRS 100 is the place to go. It’s a library of short (roughly 100 seconds), high-quality instructional videos about all fields of cataract and refractive surgery.
More than three dozen videos have already been created, and additional videos are being uploaded each month. Current videos include the following topics:
• IOL explantation
• Incisions in cataract surgery
• CTR insertion
• Inserting the DMEK graft
MAKE EVERY SECOND COUNT
—PUT THE ESCRS 100 VIDEO SERIES ON YOUR LIST OF MUST-WATCH EDUCATIONAL RESOURCES !
Is Cataract Surgery a Risk Factor for Wet AMD?
With no clear answer, surgeons have many factors to consider.
LAURA GASPARI REPORTS
Does cataract surgery increase the risk of progression to wet AMD? Is prophylactic anti-VEGF treatment a useful solution to avoid such a scenario? The jury is still out on both questions, according to Anniken BurésJelstrup MD.
An analysis of the Age-Related Eye Disease Study (AREDS) found no increased AMD progression associated with cataract surgery.1 However, a recent meta-analysis suggested there may indeed be an increase in the risk of progression to neovascular age-related macular degeneration (AMD),2 which Dr Burés-Jelstrup emphasises as a reason to avoid opting for any change in the patient’s treatment protocol.
“We have to take into consideration that cataract and AMD are both strongly age-related disorders, with cataract status acting as a confounding factor when we are talking about AMD patients,” she said, underlining how the multifactorial nature of the disease makes it difficult to pinpoint its exact pathogenesis.
Besides age, patients’ genetic background and many different variables are associated with progressive oxidative stress, decreased choroidal flow, drusen formation, and especially inflammation. All of these are part of a mechanism that leads to a progressive damage of the RPE receptors that may or may not trigger neovascularisation—which Dr Burés-Jelstrup noted is a variable disease with many different phenotypes. Wet AMD is based on a genetic predisposition, and for this reason, there is no obvious mechanism by which cataract surgery should trigger its development, she added.
There is a real difference between the risk for AMD patients and the risk of postoperative macular oedema in diabetic patients. Cataract surgery can indeed lead to an inflammatory response that, in patients with an already compromised vascular permeability, results in macular oedema, she observed. There is no doubt some diabetic patients could potentially benefit from a prophylactic anti-VEGF treatment before undergoing cataract surgery. However, macular oedema and neovascularisation are vastly different phenomena.
As a result, there is no evidence supporting the prophylactic use of anti-VEGF during cataract surgery in patients
We have to take into consideration that cataract and AMD are both strongly age-related disorders.
with no evidence of choroidal neovascularisation. Instead, these patients need to be closely monitored for their high risk of developing wet AMD—not because they underwent surgery, but rather due to the natural history of their disease, she emphasised.
Even more, patients with an active wet AMD diagnosed before surgery may really benefit from cataract surgery. There is no reason to delay the surgery because of a diagnosis, meaning the anti-VEGF treatment should continue per protocol. Moreover, cataract surgery should not affect the frequency of injections or the treatment regimen.
“Cataract surgery is not an important risk factor for the development of wet AMD. So, prophylactic anti-VEGF treatment is usually not recommended as a measure to avoid progression from dry to wet AMD,” she said.
“Patients with a diagnosed wet AMD will even benefit from cataract surgery, and as long as the treatment remains the same, there is no need to worry about any potential worsening of the condition as a result of the procedure.”
Dr Burés-Jelstrup spoke at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 46.
Anniken Burés-Jelstrup MD is a vitreoretinal specialist from the Instituto de Microcirugía Ocular, Barcelona, Spain. anniken.bures@imo.es
Need to Know: Higher-Order Aberrations and Polynomials
This first instalment in a tutorial series will discuss more on the measurement and clinical implications of HOAs.
BY SOOSAN JACOB MS, FRCS, DNB
Aberrations of the eye can be chromatic or monochromatic. Chromatic aberrations are caused by light dispersing into its component wavelengths, with different wavelengths focused at slightly different points. Thick lenses and materials with low Abbe value have higher dispersion and can decrease image quality—which is important for optical design and material selection in applications such as intraocular lenses, operating microscopes, and cameras.
Monochromatic aberration, on the other hand, is what we ophthalmologists often must deal with in the clinic while seeing patients with different corneal and lenticular pathologies. Defocus and astigmatism contribute to 85% of monochromatic aberrations; these are referred to as lower-order aberrations (LOA). These are typically fully corrected with spherocylindrical lenses and do not result in degradation of vision.
The other 15% constitute higher-order aberrations (HOA), which lead to decreased vision that is not fully correctable by spherocylindrical lenses. They result in an irregular wavefront rather than plane (parallel rays) or spherical (converging or diverging rays coming to a point of focus) wavefronts. HOAs are primarily due to corneal pathology, though other conditions such as a crystalline lens or the IOL may also be responsible.
Wave aberration
Total ocular aberrations are composed of corneal aberrations and internal aberrations. This quantifies the overall magnitude of wavefront deviations from an ideal wavefront, plotted in microns on the exit pupil and dependent on pupil size.
Root mean square (RMS) wavefront error (WE) refers to the square root of the mean of these squared deviations. This is preferred over a simple mean to avoid aberrations of opposite signage cancelling each other out. The RMS thus helps estimate the average magnitude, independent of sign.
Mean absolute deviation (MAD) takes the absolute value of each deviation before averaging. However, it gives equal weight to all deviations irrespective of size. On the other hand, the RMS squaring process gives more weight to larger deviations to make it a better measure of the optical performance and error in a system. RMS is thus generally higher than MAD.
Standard deviation (SD) of WE is generally used for statistical analysis to reveal the variation of values around the mean. In contrast, RMS measures deviation from the reference plane and estimates the total wavefront quality. Therefore, it is the RMS and not MAD or SD of WE used to evaluate human eyes.
Wavefront representation
The American National Standards Institute (ANSI) representation of WE uses the two-dimensional polar coordinate system: (a) r, the radial coordinate (normalised pupil radius: zero at the centre, one at the edge), and (b) θ/ theta, the azimuthal angle (angle in radians around the pupil centre). The mean of the wavefront is assigned zero level (green) and separated into two halves, the advanced from the delayed phases. The WE refers to the optical path difference from the reference surface (green level).
The wavefront can be represented by the Zernike polynomial system, the Fourier, or the Gatinel–Malet systems.
Zernike polynomials
The shape of the wavefront appears as a sum of Zernike polynomials, each describing a certain deformation. The weight of each Zernike mode is determined by the RMS coefficient of a Zernike wavefront decomposition. The magnitude of the coefficient of each mode indicates its relative contribution to total WE. However, the largest Zernike coefficient need not affect vision the most. Different Zernike modes affect vision to different extents. Zernike modes may also interact with each other, increasing or decreasing the effect on image quality.
The RMS value of the Zernike modes is dependent on pupil size, with larger pupil size exposing higher RMS values. The amplitude of variation with pupil diameter is exponential—with larger variation seen with higher radial degrees when the pupil diameter increases.
Zernike polynomials are represented on the Zernike pyramid, which has infinite modes. The first 6 orders contain 28 modes, each mode having a mean of 0. In the polynomial domain, there are multiple modes—each in a different dimension, represented by its unit vector, and orthogonal to all others. The WE in this multidimensional space is represented by a vector, which is the sum of the weighted unit vectors or the Zernike modes.
Additionally, the polynomials may be represented by a single index system (Noll’s index), which assigns a single number (j) to each Zernike polynomial in a standardised sequence and is useful for plots, charts, and software analysis. They may also be represented by the double index Optical Society of America (OSA) and Vision Science and Its Applications (VSIA) system which uses two indices: radial order (n) and azimuthal order (m). Each Zernike mode has a numerator (m), a continuous function that repeats every 2π radians and gives the number of affected meridia. The ‘m’ indicates the type of function (cosine or sine component) and a denominator (n, a
radial function proportional and corresponding to the order of polynomials). This is often used in scientific publications and clinical ophthalmology.
The mathematical expression for each Zernike mode (Znm) consists of: (a) a normalising constant that converts the RMS of each function to a value of 1 on a pupil radius of 1; (b) a polynomial function in r composed of n (radial degree/order, which is always positive), m (azimuthal/angular frequency, which may be positive or negative), and k [0≤k≤(n-m)/2 or 0≤k≤(n+m)/2]; and (c) a trigonometric function in t for rotationally asymmetric azimuthals. Rotationally symmetrical azimuthals have no angular dependency as m=0. The central column of the Zernike pyramid contains these rotationally symmetrical modes. Defocus and spherical aberration are examples of m=0.
Fourier transform
Fourier transform uses trigonometry-based decomposition, unlike the polynomial-based expansion in Zernike. The measured WE is subjected to a Fourier transform, which decomposes the wavefront into sinusoidal components (sine and cosine waves)— i.e., into its constituent spatial frequencies (frequency domain representation). Low spatial frequencies show the overall shape and are constituted by large refractive errors such as myopia and hyperopia. High spatial frequencies represent finer details and are constituted by HOAs. Fourier works well for rotationally symmetrical WE and describing corneal shape abnormalities. Unlike Zernike, which is defined over a unit circle, Fourier is defined over all the space or periodic domains. It is not limited to a circular domain and can be adapted to irregular pupil shapes. It works in both spatial (Fourier optics) and temporal (signal analysis) domains. It is thus effective for keratoconus detection and contact lens fitting, image processing, diffraction analysis, and filtering while Zernike polynomials are useful for customised refractive surgery and adaptive optics.
Gatinel–Malet polynomials
Some higher-order Zernike modes are impure and contaminated by lower-order modes. The RMS of these higher-order modes also reflects lower radial degrees of identical azimuthal frequency. For example, spherical aberration and secondary astigmatism also contain
lower-order defocus and astigmatism, whereas coma contains tilt. These contaminations bring unnecessary central distortions into the HOAs, which then require an offset by introducing unwanted LOAs such as defocus or tilt.
Thus, Zernike polynomials have the disadvantage of failing to completely separate LOA from HOA and even decreasing the values of certain HOAs. This property makes it difficult to predict the sphero-cylindrical correction, astigmatism orientation, point spread function, and retinal image quality from the wavefront. It can also interfere with contrast evaluation and accurate customisation of refractive surgery.
LOAs mostly affect the centre of the wavefront while most HOAs are flat in the centre, meaning HOAs degrade acuity with larger pupil diameters. In the Zernike expansion, LOAs are calculated with quadratic polynomial functions (highest exponent value of two) while HOAs are calculated with polynomial functions that are cubic or higher. However, many HOA polynomials are contaminated by the presence of significant LOAs. This creates artefactual central distortions in the HOAs, which are more significant towards the centre of the Zernike pyramid (e.g., coma, spherical aberration, secondary astigmatism). These central distortions are then cancelled in the Zernike expansion by artefactually creating LOAs.
Positive spherical aberration contains hidden hyperopia, negative spherical aberration contains hidden myopia, coma contains tilt, and secondary astigmatism contains some lower astigmatism. Dr Damien Gatinel and colleagues therefore defined a new polynomial function to separate the two aberration types. Some Zernike modes are retained on the pyramid sides since these are pure. However, to the centre, the conventional Zernike modes are replaced with modes that have a flat centre, thus interfering less with paraxial refraction. Gatinel–Malet’s LD/HD decomposition gives the added advantage of being able to study the actual influence of the uncontaminated HOAs on vision.
This is the first in a multipart tutorial on higher-order aberrations.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
FIGURE: A) The wave aberration; B) Zernike pyramid.
Portuguese Research Shows Promising Results
Toleration of off-label losartan treatment opens the door to further trials.
LAURA GASPARI REPORTS
Topical losartan shows promise in reducing postoperative corneal haze, improving the best corrected visual acuity (BCVA) and cornea transparency with a good safety profile, reports Mariana Domingues Vaz MD.
Postoperative corneal haze is a common complication that may lead to visual impairment due to corneal scarring and fibrosis, and until now, there has been no effective treatment. As Dr Vaz noted, some studies from Brazil suggested the potential of using topical losartan off-label in reducing corneal scarring.
“Losartan is an angiotensin II receptor blocker usually used in systemic hypertension, but it also inhibits the TGF-β signalling, which we know is linked to the fibrotic changes of the cornea,” Dr Vaz explained.
Based on these assumptions, the main goal of the study Dr Vaz presented was to evaluate the efficacy and safety of a 0.8 mg/mL concentration of topical losartan six times a day as an adjuvant treatment for postoperative corneal haze. The case series included six patients with central corneal scarring and fibrosis following refractive or corneal surgical procedures, adding the topical losartan to the protocol treatment. Patients with active or recent ocular infections (within three months), inflammatory or systemic conditions such as uveitis, or conditions that may impair corneal healing (such as diabetes or autoimmune diseases) were excluded.
In the baseline and follow-up at four months post-baseline, the study evaluated the BCVA, slit lamp biomicroscopy, Goldmann applanation tonometry and corneal Scheimpflug tomography in all six patients. The primary outcomes included BCVA, subjective visual function, and corneal optical densitometry on Pentacam (Oculus).
All six patients had a significant reduction of the corneal haze. The mean BCVA changed from 0.6 to 0.4 logMAR, and the mean corneal optical densitometry reduced from 32 grayscale units (GSU) to 19 GSU. Moreover, all the patients tolerated the treatment.
However, as underlined during the discussion by session chair Dr Pavel Stodůlka, losartan drops are not easy to obtain due to European Union overregulation.
Dr Vaz agreed, stating there is only one pharmacy in Portugal compounding losartan using the raw active pharmaceutical ingredient, and the patients involved in the study had some problems obtaining it. Considering the protocol required applying the eye drops six times a day for six months, there was no guarantee they could continue the treatment without issues.
Both Dr Stodůlka and Dr Vaz voiced a hope some regulations would loosen to put some challenges in scientific research for the sake of the patients, especially when there are promising treatments like losartan.
“This study opens the door to future clinical trials to explore the optimal dosage and duration of the treatment with losartan for postoperative corneal haze,” she concluded.
Dr Vaz spoke at the 2025 ESCRS Winter Meeting in Athens.
Mariana Domingues Vaz MD is an ophthalmologist from the Hospital Garcia de Orta EPE, Almada, Portugal. marianadomvaz@gmail.com
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
Endothelial damage, cellular treatments, human tissue, and infections are key concerns on the horizon.
The World Cornea Congress convened on 21 March in Washington, DC, US, bringing together experts from around the world for a three-day examination of trends and developments affecting cornea care. EuroTimes talked to José Güell, head of the Cornea, Cataract, and Refractive Surgery Department at IMO Grupo Miranza in Spain, about the Congress programme and the key issues he sees in the field of cornea treatment.
How long have you been attending the World Cornea Congress, and why are you attending this year?
The World Cornea Congress takes place for two or three days and is performed every four or five years. The last time it met was in Chicago in 2019, just before COVID. I’ve been attending from the beginning—since it started.
I’m participating in a panel presentation titled “Two Decades of DMEK: What Have We Learned.” It was a special
and difficult speaking invitation for me because, as a surgeon, it’s much better to talk about a particular surgical technique or the number of patients treated with this or that procedure. Anyway, it has allowed me to evaluate all we have accomplished along these years, and I must say it has been an extraordinary journey.
What do you see as the two or three biggest issues or trends today in the field of cornea treatment?
I would say one of the hottest issues is endothelial damage, both congenital and acquired, and its management. Today, DMEK—Descemet membrane endothelial keratoplasty— represents the standard of care for irreversible endothelial problems. This has been, as my lecture today points out, what we have been doing and improving for the last two decades. But I think, as we start another decade, we will now be much more focused—and a lot of talks are being presented
about it during this meeting—on cellular treatments. Cell culture techniques and cell injection techniques will definitely be the way to treat patients in the next few years.
Improving the positioning of the cells once injected inside the eye, and promoting and stimulating cell growth, will be what we will see in the next 5 to 10 years. Some of these treatments are already being investigated and implemented. So I would say that this is the hottest topic right now.
The second hottest topic, from my point of view—and also the subject of many presentations here—is the use of human tissue to be introduced into the corneal stroma in different ways, such as in the form of CAIRS, which means segments of the stroma instead of PMMA segments, which we have been using up to now. Another technique is SLAK, stromal lenticule addition keratoplasty. The use of human stroma, obtained from a human donor or through bioengineering techniques, is something that is getting relevant in the world of corneal surgery.
Third is the relevance of infections. This is nothing new because, as you will agree, it will be an issue not only in ophthalmology but [generally] for the next 30 years. So, at some point in the not-too-far future, cancer or tissue culturing will be controlled, but I think we will start suffering from new infections. And the eye is not an exception.
Infectious keratitis is an issue—it is becoming more frequent. Also, the distribution of pathogens is changing. Fungal infections, for example, were for many years a problem mostly in India and South America, but today, the number of fungal infections in the so-called Occidental World is significantly increasing. So there is a growing interest in new drugs for fungal infections, new antibiotics, and new drugs for parasites such as the Acanthamoeba
Finally, I would say that artificial corneas, keratoprostheses, and its long term management, are also a hot issue. There are many other things I could mention, but this covers the main items.
How would you describe the response to these challenges? Is it fragmented, such as between Europe and the United States? Or is there a unified effort to address them?
I think we’re much more unified on cornea issues than on things like intraocular lenses. Many of the companies that are working hard on some of the things I just mentioned, like stimulators for cell growth and tissue cultures, are American. So this is an integration, a cooperation, between different corneal surgeons from around the world.
Does ESCRS have strong representation at the World Cornea Congress?
There are not too many ESCRS people here, as the main ESCRS focus is on cataract and refractive surgery. Béatrice Cochener-Lamard is here. She is a former president of the ESCRS and also the president of EuCornea. Mario Nubile is here; he is on the Programme Committee of the ESCRS. Sorcha Ní Dhubhghaill is here as well—she is the chair of the Cornea Committee and also a board member. And probably some other members are around.
Because anterior segment surgeons do at least some cornea work, we know there are a lot of ESCRS members with an interest in cornea. So we cover cornea topics on Cornea Day at our Annual Congress and in some courses and talks, but cornea is covered most thoroughly at EuCornea meetings.
Thank you for your insights, and good luck with your presentation.
I will do my best!
José Luis Güell MD, PhD is head of the Cornea, Cataract, and Refractive Surgery Department at IMO Grupo Miranza in Barcelona, Spain. He served as president of ESCRS in 2010–2011 and president of EuCornea from 2012–2014. guell@imo.es
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.
Advancing AI in Medicine
Taking advantage of new technologies while looking out for inequity, bias, and errors.
LAURA GASPARI REPORTS
The use of artificial intelligence in corneal, cataract, and refractive surgery has grown exponentially, proving valuable for clinical practice. However, Dimitri T Azar MD noted some remaining obstacles to consider, which can involve potential biases and inaccuracies.
Since the 1910 Flexner Report, which transformed medical education and practice worldwide, there have been three major revolutions in medical science: the molecular biology revolution, the genomics revolution, and the convergence/ AI revolution.
“Many people are working on AI, and it is prevalent because of the trend of big data, cloud connectivity, and devices that are getting smaller,” he said.
Generative AI attracts many investments and publications. It is used in clinical practice by physicians to facilitate their work and, in research, to help write the first draft or gather data. The significant use of this tool is in diagnosis and screening, as anterior segment applications have made great steps recently, even if retina applications still lead the field.
AI is an extremely interesting tool with difficult patients, such as those with keratoconus or Fuchs’ dystrophy, and it is also starting to be used in refractive surgery, IOL calculation, and dry eye diagnostics, he reported.
Even so, Prof Azar emphasised some important aspects of how these tools work need disclosure.
“The idea is that the program will learn to interpret the images as the training starts. These networks will start without any fine-tuning and give random results,” Prof Azar said. “We correct them over time and, as opposed to [humans], as they learn more, they will ignore all the unimportant features—and that comes with a problem.”
One of the technology’s major pitfalls is the risk of institutionalising inequity and bias. Prof Azar said bias in AI may result from representing and collecting the data and developing the model or during processing, evaluation, deployment, and performance monitoring. If the source of learning is biased, that bias will inevitably be perpetrated when developing AI systems. For instance, AI can correctly answer a Basic and Clinical Science (BCSC) exam. However, fewer than 1% of images in the BCSC textbook depict people of colour, meaning the information is biased.
Prof Azar said the situation remains the same for clinical trials, where databases do not fully represent the general population.
“When Google did the AI program for diabetic retinopathy screening, it was successful. But when it was moved to India, it failed because the choroid pigmentation is different,” he explained. “You cannot just use a program and generalise it; [generalising] is a big problem.”
The way to fix this, he said, is not by recalibrating or updating the model—which can generate new inaccuracies—but
by considering all the potential biases, thinking about how the data is collected, and understanding what kind of data make up larger data sets and how this data can be used and interpreted.
“It is important to assess the performance across marginalised cohorts and acknowledge these models may not fully capture the true extent of algorithmic fairness. Metrics that rely only on accuracy or other characteristics may run the risk of perpetuating health inequities that are already present in data,” he concluded.
Prof Azar presented at the 2025 ESCRS Winter Meeting in Athens.
Dimitri T Azar MD, MBA is Distinguished Professor of Ophthalmology, BA Field Chair in Ophthalmic Research, and Dean Emeritus of the University of Illinois College of Medicine, US, and former Senior Director for Alphabet’s Verily Life Sciences. dazar@uic.edu
“This would be a
disaster”
US budget cuts risk global medical research; ophthalmology is not immune.
HOWARD LARKIN REPORTS
Consider the US National Institutes of Health (NIH). With a budget of $47 billion in 2024, it is the largest single funder of medical research in the world.
And with a budget of nearly $900 million, the National Eye Institute (NEI) holds a similar position in eye care research— sponsoring everything from large, long-term population studies, such as the Age-Related Eye Disease Study (AREDS), to countless projects from basic research through assessing existing treatments.
Now consider cutting those budgets by nearly half—and possibly folding the NEI in with brain and neurological research. As of April, that’s just what proposals pending before the US Congress and tied up in the courts intend to do. And while it’s too early to tell exactly how it will shake out, the impact is already being felt in the US and beyond.
For starters, nearly 800 existing NIH and other health grants worth more than $2.3 billion already have been terminated. The bulk of the grants were related to HIV/AIDS (29%), trans health (24%), COVID-19 (17%), and climate (3.5%), and according to an April analysis by Nature, many disrupt ongoing clinical studies and public health initiatives.1
However, a cursory review of a government list by EuroTimes also revealed at least a few related to nearly every stage of eye care research.2 Cancelled grants include studies of the Drosophila visual system, human retinal degeneration, artificial vision, and vision sciences training and core facilities at Columbia University. Also cut were studies examining the impact of vaccines and post-exposure antibiotics on preventing Chlamydia trachomatis infections at the University of Washington, and the impact of the herpes vaccine on herpes zoster ophthalmicus at the University of California–San Francisco.
“What we’re seeing is a targeted review process that identifies programmes like DEI initiatives that the administration doesn’t prioritize and removes their funding,” said Dan Ignaszewski, who heads a US eye research advocacy group. “It’s a ‘Ctrl+F’ approach: search, find, cut. But these programmes are embedded across NIH and play a foundational role in sustaining the broader research enterprise.”
Rotting the roots
But perhaps the most significant threat to ophthalmic research—and research generally—may be a proposed restriction to 15% of grant awards to pay for overhead, Mr Ignaszewski said. That’s about half the historic level of 27–28% seen in recent years—a figure that can range up to 60% for some institutions.3 And though the measure is on hold pending judicial review, it is part of the proposed 2025 budget.
Overhead sounds like a lot of red tape. But in addition to required administrative tasks such as grant monitoring and compliance, overhead funds a range of facilities and services necessary for research to exist, including laboratories, IT, and
even maintenance support. It’s part of a long-standing unwritten agreement to split the cost of research between private entities and the US government that is now threatened.
“The federal funding freeze that impacted several research grants around the country—and the proposed cuts to the NIH budget through the 15% indirect cap—threaten not only the future of vision research but also the stability of an entire scientific ecosystem that fuels medical innovation, job creation, and public health,” Mr Ignaszewski said.
Local and global impact
Even though the market has yet to feel the full brunt of the cuts, the direction is clear—and the shockwaves evident.
For example, the ophthalmology department at Vanderbilt University stands to lose an estimated $6 million due to the overhead pay cuts alone, said Paul Sternberg Jr MD.
“What is of concern is that our capacity to grow research programmes will be limited. … [Offering] development packages to promising young scientists by promising a level of support will be more difficult. It will be more challenging to support highrisk research that is [no longer] amenable to funding from NIH, requiring more dependence on philanthropy,” Dr Sternberg said.
These and other threatened cuts, along with fear of interference in research, might be pushing some US researchers overseas. Indeed, in a recent Nature poll, 75% of US researchers in all science fields said they are considering leaving the country, with Europe and Canada the top potential destinations.4
Ophthalmology is not immune. Several European academic eye surgeons contacted by EuroTimes said they knew of or had heard of one or more recent American applicants for European academic and research positions—though it’s not entirely certain some of them wouldn’t have applied anyway, one noted.
While this ‘brain drain’ may seem like Europe’s gain at America’s expense there’s plenty of pain to go around, one surgeon said.
“If [the NEI funding] suddenly stopped, this would be a disaster for everybody, not just the US,” the surgeon said.
“Many US researchers are at the top of their fields. If they lose their positions, we all lose.”
For citation notes, see page 46.
Dan Ignaszewski is executive director of the National Alliance for Eye and Vision Research (NAEVR) and the Alliance for Eye and Vision Research (AEVR), eye research advocacy groups based in Rockville, Maryland, US. dan@eyeresearch.org
Paul Sternberg Jr MD is professor, former director and chief medical officer, and current medical director for development of the Vanderbilt Eye Institute of Vanderbilt University, Nashville, Tennessee, US. He is also CEO of the Association of University Professors of Ophthalmology. paul.sternberg@vumc.org
Rayner doubles IOL manufacturing capacity
Rayner has expanded its Worthing, UK, production facility, doubling its annual intraocular lens production to four million. Since 2017, Rayner has produced all its IOLs in Worthing, including more than six million RayOne systems. The RayOne family includes the EMV lens platform and the rapidly growing Galaxy and Galaxy Toric lenses. rayner.com
CE Mark for Alcon’s new vitreoretinal cataract system
Alcon announced its UNITY® Vitreoretinal Cataract System (VCS) has received CE Mark approval. UNITY VCS, the first product in Alcon’s UNITY portfolio, enhances workflow efficiency compared to the CONSTELLATION® Vision System and CENTURION® Vision System with ACTIVE SENTRY®. It integrates advanced vitreoretinal and cataract surgical innovations, maximising operating room space. UNITY VCS features a new phacoemulsification modality that can remove the nucleus up to twice as fast using 40% less energy, with cutting speeds up to 30,000 cuts per minute and improved stability and efficiency via a proprietary fluidics system. alcon.com
Bausch + Lomb update enVista recall
The US FDA updated details on 7 April regarding Bausch + Lomb’s voluntary recall of certain IOLs on its enVista platform because of increased reports of toxic anterior segment syndrome (TASS) associated with the devices. The affected lenses are the enVista monofocal models starting with EE and toric models starting with ETE, enVista Aspire intermediate-optimised models starting with EA and toric models starting with ETA, enVista Envy trifocal models starting with EN and toric models starting with ETN. All reported cases responded quickly to treatment without requiring lens removal. Doctors are advised to check their inventories for affected lenses and return them to the manufacturer. bausch.com
Presbyopia eye drops launched in US
Orasis Pharmaceuticals announced that Qlosi (pilocarpine hydrochloride ophthalmic solution) 0.4%, a novel prescription eye drop for treating presbyopia in adults, is now available in the US. The FDA approved Qlosi in October 2023, following the Phase 3 NEAR-1 and NEAR-2 clinical trials. Qlosi enhances depth of focus through the pinhole effect by inducing pupil dilation, lasting up to eight hours. It contains a preservative-free solution in single-use vials, with a near-neutral pH for optimal bioavailability and lubricants (HA & HPMC) for ocular comfort. orasis-pharma.com
NDA for new presbyopia eye drop
Tenpoint Therapeutics announced the submission of a new drug application (NDA) to the US FDA for BRIMOCHOL PF, a treatment for presbyopia that combines brimonidine and carbachol in a miotic eye drop designed to increase depth of focus through the pinhole effect. The NDA submission includes efficacy and safety data from the Phase 3 BRIO-II study—the largest and longest study conducted in the presbyopia eye drop category. tenpointtherapeutics.com
Nordic’s dry eye therapy receives CE mark
Nordic Group’s dry eye therapy, Lacrifill, has received CE mark approval, enabling its launch across European markets in the coming months. Lacrifill is a hyaluronic acid gel that temporarily blocks tear drainage, preserving natural tears to manage dry eyes for up to six months. Following its earlier US launch in May 2024, Nordic Pharma is preparing for the commercial rollout in Europe, with more details to be shared soon. nordicgroup.eu
UPDATE ON ASTIGMATISM ANALYSIS
The June issue of JCRS includes two articles by a working group initiated by the journal’s editors to update and establish astigmatic reporting guidelines. The first paper provides an overview of astigmatism, covering definitions, measurement technologies, and sources of error. The second paper offers recommendations for the statistical analysis of astigmatic outcomes.
The authors note astigmatism as the difference between the orthogonal principal planes of minimal and maximal powers of a toric surface or lens. Corneal astigmatism is a common condition, and studies indicate 60–78% of individuals have more than 0.5 D of astigmatism, and 20% have more than 1.5 D.
As the magnitude of astigmatism increases, the incidence of against-the-rule (ATR) astigmatism is nearly constant, varying from 26% to 31%. By contrast, the incidence of with-the-rule (WTR) astigmatism increases as magnitude increases, from 26% to 64%, corresponding to a decreased incidence of oblique astigmatism. Corneal astigmatism also changes with age. Most population studies show an age-related shift in anterior corneal astigmatism from a vertical steepness (WTR) to a horizontal steepness (ATR).
Total corneal astigmatism is calculated through raytracing, using anterior and posterior curvature measurements and corneal thickness. Various imaging technologies and algorithms help perform these measurements, including reflection (rings or single-point mires), Scheimpflug imaging, and optical coherence tomography. However, measurements from different devices are generally not interchangeable because distance differences from the centre can result in both magnitude and axis variations. Zonal keratometry (topography/tomography) over the patient’s mesopic entrance pupil samples a larger region of the central cornea, with the zone size customisable to each specific patient.
Astigmatism can be represented as a vector since it has both magnitude and direction. The magnitude is the absolute power difference between principal meridians, and the direction is defined by the meridian of greatest positive (or least negative) power. Since meridians extend in two directions from the centre, the angle must be doubled for Euclidean vector calculations. Using double-angle plots allows for vector algebra and statistical analyses, after which the angle is halved for single-angle results. JCRS will use double-angle plots to report astigmatic outcomes.
The vector prediction error (PE) is the key expression for evaluating surgically induced astigmatic change—defined as the vector difference between the postoperatively observed and refractive astigmatism predicted from preoperative measurements. Vector calculations can be performed independent of or relative to a reference meridian or axis. Double-angle plots with convex polygons and statistical analysis for astigmatism data can be easily obtained with the wrap-up functions from the Wilcox-Holladay-Wang-Koch Statistical Software using the free R Project for Statistical Computing software or with Eyetemis software, also available online.
T Kohnen, et al. “Review/Update: Standards for Analyzing Astigmatic Outcomes: Part I,” 51(6): ahead of print.
D Koch, et al. “Review/Update: Standards for Analyzing Astigmatic Outcomes: Part II,” 51(6): ahead of print.
ESCRS Patient Portal
Patients are understandably curious to learn as much as they can about their upcoming cataract or refractive surgery. ESCRS has developed a Patient Portal on its website to help inform patients about these surgeries.
The Portal is split into two sections: Cataract and Refractive. Each section provides an easy-to-understand summary of the different types of conditions, including the benefits, risks, procedures, and aftercare of common conditions. Each section is easily navigable, with clear diagrams and a glossary to convey all the information patients might need to help prepare for surgery or during aftercare.
Cited in this Issue
Is Frugal Innovation Possible in Ophthalmology?
Page 10
1. Haripriya A, Chang DF, Reena M, Shekhar M. “Complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital,” J Cataract Refract Surg, 2012; 38(8): 1360–1369.
2. Haripriya A, Chang DF, Vijayakumar B, Niraj A, Shekhar M, Tanpreet S, Aravind S. “Long-term posterior capsule opacification reduction with square-edge polymethylmethacrylate intraocular lens,” Ophthalmology, 2017; 124(3): 295–302.
3. Haripriya A, Chang DF, Ravindran RD. “Endophthalmitis reduction with intracameral moxifloxacin in eyes with and without surgical complications: Results from two million consecutive cataract surgeries,” J Cataract Refract Surg, 2019; 45(9): 1226–1233.
5. Shukla AG, Chang DF, Dhanaseelan T, Vivekanandan VR, Gubert J, Robin AL, Venkatesh R. “Reusing Surgical Materials for Cataract Surgery: An Assessment of Potential Contamination,” J Cataract Refract Surg, 2024; 50(10): 993–999.
Making IOLs a More Personal Choice
Page 26
1. Kabbani J, Price L, Patel R, Din N, Bizrah M. “A survey of intraocular lens preferences of UK refractive surgeons for cataract surgery and refractive lens exchange,” BMC Ophthalmology, 2024; 24(1): 397. doi:10.1186/s12886-024-03639-8
2. Logothetis HD and Feder RS. “Which intraocular lens would ophthalmologists choose for themselves?” Eye, 2019; 33(10): 1635–1641. doi:10.1038/s41433-019-0460-9
Predicting Pseudoaccommodation
Page 27
1. Nanavaty, et al. “Incidence and factors for pseudoaccommodation after monofocal lens implantation: the Monofocal Extended Range of Vision study,” J Cataract Refract Surg, Dec 2023; 49(12): 1229–1235.
ESCRS Power Calculator: Fast and Effective
Page 29
1. Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. “Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry,” J Cataract Refract Surg, 2011; 37(1): 63–71. doi:10.1016/j.jcrs.2010.07.032
Is Cataract Surgery a Risk Factor for Wet AMD?
Page 34
1. Bhandari S, et al. “Cataract surgery and the risk of progression of macular degeneration,” Curr Opin Ophthalmol, 2022 Nov 21; 34(1): 27–31.
2. Yang L, et al. “Association between Cataract Surgery and Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis,” J Ophthalmology, 2022 May 5; 2022: 6780901.
“This would be a disaster”
Page 43
1. Kozlov M, Ryan C. “How Trump 2.0 is slashing NIH-backed research—in charts,” Nature, 10 April 2025. doi:https://doi. org/10.1038/d41586-025-01099-8
2. Awarding Office FAIN Award Number. https://taggs.hhs. gov/Content/Data/HHS_Grants_Terminated.pdf
3. NIH Supplementary Tables, p 13, https://officeofbudget. od.nih.gov/pdfs/FY21/br/5-SupplementaryTables.pdf.
4. Witze A. “75% of US scientists who answered Nature poll consider leaving,” Nature, 27 March 2025. doi:https://doi. org/10.1038/d41586-025-00938-y
https://escrs.org/special-interest-groups/yos/
Apply for the
John Henahan Writing Prize
Applicants to the 2025 contest must answer this prompt:
Diversity, equity, and inclusion (DEI) programmes, however well-intentioned, stir a variety of responses in the corporate and political worlds and in the scientific and medical spheres.
What DEI and unconscious bias issues are present in the current culture of ophthalmology training, practice, and clinical research? What are the potential benefits of addressing these issues for patients and ophthalmologists? What kind of meaningful changes need to happen to move beyond ‘talking the talk’ to ‘walking the walk’?
The competition is open to ESCRS members (including the free membership available to trainees) age 40 or younger on 1 January 2025. Submit your essay no later than 20 June 2025 to seanh@eurotimes.org
Cover page: All essays must include a cover page with the following information:
• Author’s name
• Contact information (email and phone)
• Institution/affiliation
• Stage of ophthalmology training
• Date of birth
• ESCRS member number
Writing tips: Submit your essay in Microsoft Word or a similar text format (no PDFs, please). The punctuation, syntax, and grammar should reflect the high standard of content published in EuroTimes. Please remember to limit your essay to 800 words. We encourage you to have a colleague read your essay before you send it to check for style and grammar mistakes. Please include citations for any studies mentioned and state whether AI tools were used in the production of the essay.
Deadline: The closing date for entries is 20 June 2025. Send your essay with cover page to seanh@eurotimes.org.
Winning essays: Past winners have all shown some original insight and personal style in their essays. You can read the recent winning essays on our website .
Upcoming Events
May 23–25
EuCornea Prague, Czech Republic
June 7–9
European Society of Ophthalmology (SOE) Lisbon, Portugal
June 12–14
2nd World Keratoconus Congress (WKC 2025) Athens, Greece
September 4–7
EURETINA
Paris, France
September 12–16
2025 ESCRS Congress
Copenhagen, Denmark
September 12
ESCRS iNovation Day Copenhagen, Denmark
September 25–28
German Ophthalmology Society Berlin, Germany
October 18–20
American Academy of Ophthalmology Orlando, Florida, US