A look at the evidence for tasty ways of lowering risks and improving ocular health.
Extending Depth of Satisfaction
Avoiding patient dissatisfaction with EDOFs before it happens. ALSO IN THIS ISSUE
Tips for Toric IOL Alignment
Accurate preoperative measurement and digital marking can help.
Enhancing Glaucoma Care with AI
New tools can aid clinical decision making and improve patient engagement.
Artiplus A big plus
Finally, a presbyopia correcting IOL, with clear vision at any distance. To help presbyopia patients regain natural eye sight, with full spectacle independence.
Unique Patented CTF Technology
Artiplus is a new premium solution for young presbyopes (40-60 years) to become spectacle independent. The unique, refractive optic of Artiplus with patented CTF technology employs smooth transitions between far and near zones, minimizing glares and halos and offers natural vision at all distances.
With a low add power of +2.5 D, it delivers excellent intermediate and near vision. The iris-fixated design enhances decentration tolerance and reduces cataract risk, making it also ideal for myopic patients.
“The results from the clinical study for uncorrected distance, intermediate and near visual acuity were extraordinarily good. In my experience with Artiplus, the results have been extremely consistent.”
Prof. Dr. José Güell
N=48
Outstanding Clinical Performance
The one-year follow-up from the international multicenter clinical trial demonstrates extraordinary visual acuity at all distances. Defocus curve results highlight the benefits of residual accommodation, enhancing patients’ overall vision experience.
Binocular defocus curve showed a VA ≤ 0.10 logMAR between defocus levels of +1.00 to -3.00 D (Figure 1).
Alessandro Mularoni
11 The Doctor Recommends… Alessandro Mularoni MD
Sharing a Vision for the Future
Filomena Ribeiro MD, PhD, FEBO; Oliver Findl MD, MBA, FEBO; Joaquín Fernández MD, PhD; and Roberto Bellucci MD
14 Long-Term Outcomes of EK for Failed Grafts
Erika M Ellis MD, PhD
15 Accurately Aligning Toric IOLs
Douglas D Koch MD
16 Extending Depth of Satisfaction
Artemis Matsou MD, MRCP(UK), FEBOS-CR, FEBO, PgDip CRS; Alfredo Borgia MD, FEBO; Victoria Till MD; Rudy MMA Nuijts MD, PhD; and Andreia Rosa MD, PhD
18 Conventional Versus Laser-Assisted Cataract Surgery
Joaquín Fernández MD, PhD
CORNEA
20 Need to Know: Spherical Aberration
Soosan Jacob MS, FRCS, DNB
23 The True Cost of Shingles Shots
Bita Manzouri BSc, MBBS, MRCP, FRCOphth, PhD
24 Endothelial Keratoplasty in Vitrectomised Eyes
Ibrahim Qozat MD
25 DMEK Following AC-IOL Explantation
Ayça Bulut Ustael MD
26 Pharmacological Treatment for Corneal Oedema
Itay Lavy MD
27 Amphotericin B-Supplemented Corneal Storage Media
Nicole R Fram MD
28 AI Analysis and the Cornea
Marcus Ang MBBS, MMed(Ophth), MCI, FRCS(Ed), FAMS, PhD
RETINA
30 AI and Gene Therapy as the Next Frontier
Andrew Dick BSc, MBBS, MD, MRCP, FRCS, FRCP, FRCOphth, FMedSci
GLAUCOMA
32 Opportunities for Enhancing Glaucoma Care with AI
Robert T Chang MD and Benjamin Y Xu MD, PhD
34 Novel Strategy for Lowering Nocturnal IOP
Leon W Herndon Jr MD
DIGITAL OPTHALMOLOGY
35 AI Scribing and Telephone Management
Robert T Chang MD
36 Generating AI’s Potential
Bruce Allan MD, FRCS; Nino Hirnschall MD, PhD, MBA, FEBO; Sorcha Ní Dhubhghaill MBBCh, PhD, MRCSI(Ophth), FEBO, FEBOS-CR, BaO, Dip(stats); Mor Dickman MD, PhD; Ernest Lim MBBS, BSc(Hons), PhD; and Nic J Reus MD, PhD
Publisher
Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin Roibeárd O’hÉineacháin
Contributors
Laura Gaspari
Soosan Jacob
Priscilla Lynch
Timothy Norris
Andrew Sweeney
Colour and Print
CitiPost
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Correction: An earlier version of “A Look at Innovative Treatments in Late-Stage Development” (March/April 2025) mistakenly reported the Ciliatech Intercil device received the CE mark. The device has not been approved yet and does not have the CE mark. The article has since been corrected, and updated versions are available on the ESCRS website.
Learn more about EuroTimes or connect with ESCRS at ESCRS.org
Just the Facts
Take a look towards the bottom of this page and you’ll notice the pictures of our three medical editors: Thomas Kohnen, José Güell, and Paul Rosen. We meet regularly to discuss content, themes, upcoming conferences, and issues involving ESCRS. These are well-known, highly respected ophthalmic surgeons and educators with many years of experience in ESCRS governance. Below the three stars, you will see some new names, constituting our freshly updated list of editorial advisors.
We recently organised a video call to get to know the new advisors, during which I gave a brief overview of EuroTimes’ mission. This got me thinking of the long road EuroTimes has taken. EuroTimes was the brainchild of the great Emanuel Rosen, the first president of the ESCRS, who wanted the Society to have its own magazine along the lines of the ASCRS and EyeWorld. The idea was to provide members with reliable clinical news from conferences and share information on ESCRS endeavours. The first issue appeared in print in 1996, under the editorship of John F Henahan (for whom the John Henahan Writing Prize is named). Russian and Turkish versions followed, and the online version launched in the early 2000s.
Emanuel Rosen insisted the magazine maintain the highest standards of editorial integrity. News and features were to be factual, evidence-based reports free of industry influence. Much has changed over the years. We now produce six print
and four online-only issues per year. What has not changed is our total commitment to editorial independence.
In recent years, EuroTimes coverage has reflected the ESCRS response to some of the great social issues affecting ophthalmology and the wider world—COVID, sustainability, gender and inclusivity issues, and artificial intelligence. The current issue explores the role ophthalmologists can play in influencing patients to prioritise nutrition and lifestyle to help maintain eye health.
Our articles are prepared and edited by professional medical journalists. The value of this cannot be overstated. In these times of media misinformation when it can be near impossible to sort fact from fiction, we hold the line. We respect the growing influence of AI, but it has no role in choosing content, fact-checking, and approvals here. If we should make an error, we report it and fix it.
Our meeting with our new editorial board went very well. There were useful suggestions on integrating more didactic content, improving our social media outreach, and developing resources for young ophthalmologists. We welcome the new advisors, and we also welcome any ideas from the wider ESCRS membership on how we can continue to improve EuroTimes.
Sean Henahan Editor-in-Chief
EDITORIAL BOARD
Adi Abulafia (Israel)
Bruce Allan (UK)
Noel Alpins (Australia)
Juan Alvarez de Toledo (Spain)
Gerd Auffarth (Germany)
Başak Bostanci (Turkey)
John Chang (Hong Kong SAR, China)
Béatrice Cochener-Lamard (France)
Burkhard Dick (Germany)
Mor Dickman (The Netherlands)
Joaquín Fernández (Spain)
Oliver Findl (Austria)
Nicole Fram (US)
Sri Ganesh (India)
Farhad Hafezi (Switzerland)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Jack Kane (Australia)
Yao Ke (China)
Mika Kotimäki (Finland)
David Lockington (UK)
Artemis Matsou (Greece)
Cyrus Mehta (India)
Jod Mehta (Singapore)
Sorcha Ní Dhubhghaill (Belgium)
Rudy Nuijts (The Netherlands)
Catarina Pedrosa (Portugal)
Konrad Pesudovs (Australia)
Nic Reus (The Netherlands)
Filomena Ribeiro (Portugal)
Andreia Rosa (Portugal)
Giacomo Savini (Italy)
Julie Schallhorn (US)
Sathish Srinivasan (UK)
Paola Vinciguerra (Italy)
Shin Yamane (Japan)
Ron Yeoh (Singapore)
Mihail Zemba (Romania)
Thomas Kohnen
José Güell
Paul Rosen
Get Ahead of Bias and Burnout and Build Your Career!
Are you concerned about burning out early? Wondering what you can do to help promote equitable eye care for all patients? Looking for advice on building your career?
The ESCRS BoSS (Building Our Sustainable Society) initiative is addressing these questions by sponsoring a symposium and courses as well as a speed mentoring programme at the ESCRS Annual Congress in Copenhagen.
Check out the details below and make plans to attend.
BoSS Symposium:
Are you satisfied?
From burned out to burning bright
Date: 14 September
Time: 11:00–12:30
Location: Hall B2-M1 (300 seats)
Speed Mentoring Sessions
(Held at the ESCRS membership booth)
BoSS Course:
Implicit bias
Date: 14 September
Time: 16:45–18:15
Location: Hall D2 (450 seats)
Speaker: Amy Johnson
Speed mentoring is a dynamic and interactive session where mentees have the opportunity to engage with experienced mentors in short, focused conversations. This format allows for the exchange of knowledge, guidance, and networking in a time-efficient manner. It also offers an excellent opportunity to build your professional network by meeting mentors and fellow mentees, fostering connections that could benefit your career for years to come.
BoSS Course:
Combatting unconscious gender bias in ophthalmology, industry, and research
Promoting Family Integration at Ophthalmic Conferences
BY LAURA MAUBON
Prioritising attendance at ophthalmic conferences (such as the ESCRS Annual Congress) while balancing parenthood, work, and family life can often feel like a juggling act.
Through the efforts of the BoSS (Building Our Sustainable Society) initiative, ESCRS is committed to making conference attendance more accessible for working parents. Over the past two years, ESCRS has supported Congress and Winter Meeting delegates through affordable childcare services provided by accredited professionals. We have also enhanced on-site facilities by creating safe breastfeeding and baby-changing stations to foster a more inclusive and supportive environment. Our mission is to break down barriers to education and promote inclusivity for all.
As a working mama of young children and a member of the BoSS Working Group, I know first-hand what it’s like to choose between career opportunities and caring for my family. I have often had to decide whether to miss out on an opportunity or bite the bullet and bring my babies along. Thankfully, I’ve had the support of my non-ophthalmic ‘conference husband’ (yes, it’s a growing trend), which was particularly helpful when I was still breastfeeding, as he could hold the baby whilst I popped on and off the stage.
I asked some fellow ESCRS members who have conferenced with kids to share their experiences and top tips as well as their vision of a future ‘kid-friendly’ conference. Aida Hajjar Sesé (Ophthalmic Surgeon at King’s College Hospital, London) and David Shahnazaryan (Ophthalmic Surgeon at Centre for Sight, London), the parents
The carers were warm and professional, and the set-up included a library, art area, sports zone, play kitchen, slides, and plenty of soft play.
of two young girls, said they used the childcare service at ESCRS 2024 in Barcelona and came away impressed.
“The carers were warm and professional, and the set-up included a library, art area, sports zone, play kitchen, slides, and plenty of soft play,” Aida said. “It was perfect for the little ones. I only needed a few hours to attend specific sessions. I wouldn’t use it for the whole day, but it was fantastic for focused sessions.”
Amanda Cardwell Carones (founder of OPHTHALPRENEURS) and Francesco Carones (founder and medical director of ADVALIA Vision, Milan) live in Italy with their two boys, ages nine and ten. The oldest attended ESCRS 2014 in London when he was just six weeks old and then attended ESCRS 2015 in Barcelona the following year.
“Don’t bring your children unless you will have some time to spend with them as well,” counselled Amanda. “Our kids love to travel and experience new places, food, and cultures. When they travel with us, we clearly define in advance which meetings and events we will attend and which we won’t, and we stick to it. Work will have a way of creeping in on family time, so we find it best to stick with a hard ‘no’.”
Amanda’s vision is for industry meetings to include events that families
Interested in registering for childcare at ESCRS 2025 in Copenhagen? Scan the QR code for details.
can attend together—for example, dinners where children are invited or at least allowed to attend.
“This is already happening at smaller conferences,” she said. “Having childcare is useful as a service provision that enables parents to attend ESCRS meetings; otherwise, they may not be able to attend due to a lack of childcare, nursing, etc. But it would be great to have events that extend to the children themselves, especially since so many eventually follow in the footsteps of their parents.”
Aida agreed and suggested additional accommodations. “On-site
childcare, family rooms, and live-streamed sessions aren’t luxuries, they’re enablers,” she said. “I know brilliant female ophthalmologists who have missed meetings due to childcare barriers. There’s also the added pressure on women to hit both personal and professional milestones before 40—a reality we don’t talk about enough.”
Both couples are pleased to see ESCRS leading the way. We saw progress in Milan at ESCRS 2022, and subsequently BoSS was launched. The introduction of on-site childcare felt overdue; in other subspecialities—general practitioners, obstetrics, surgery—it already existed for years. I am glad we are finally achieving this.
My own observation is that if ophthalmic professionals bring their children, we should be prepared to welcome them. It’s a juggle, but sometimes it’s hard to justify leaving them behind, especially after a busy working week or when conferences clash with family events. I’d love to see our community accept whatever professionals choose.
As more ophthalmologists balance parenthood with professional development, the need for inclusive, family-friendly environments will only grow. At ESCRS, we’re proud to help lead that change. When we support parents, we strengthen our entire community.
ESCRS Update
New Award to Encourage Research into Sustainable Practices
ESCRS is deepening its commitment to sustainable ophthalmology by launching a new award to drive high-quality translational research that can reduce the carbon footprint and enhance the circularity of global cataract, refractive, and corneal practices.
The Sustainability Research (SURE) Award will fund projects examining meaningful, practical ways to promote environmental responsibility in ophthalmic care. From reducing surgical waste to analysing life-cycle efficiencies in clinical workflows, the award aims to support research that aligns with ESCRS’s commitment to longterm sustainability in ophthalmology. Award details. Two awards of up to €10,000 each will be presented per research project. Applications can be submitted 28 July through 01 November. The project duration is 12 months.
Award recipients must submit an article to a peer-reviewed journal within 6 months after the research period concludes. The article should be made open access if accepted and submitted to the Journal of Cataract & Refractive Surgery in the first instance. Evidence of this submission should be shown on request to the ESCRS Research Committee in order to release the final instalment of funding. Evaluation criteria. Applications will be assessed on the following criteria:
• A well-defined research question that addresses a gap in sustainability literature and is appropriate for the proposed methodology
• A strong methodology design (e.g., RCTs, systematic reviews, and life-cycle analyses)
• A realistic scope for a 12-month project
• Clear, justified and feasible use of award funds
• A dissemination plan that includes publication, conference presentation, and novel dissemination (e.g., podcasts/webinars)
clinical or academic institution. Early-career researchers and young ophthalmologists are especially encouraged to apply.
Note that applications from current ESCRS Research Committee members as well as the Society’s executive leaders, trustees, council members, and co-opted council members will not be accepted. This abstention extends to submissions from their respective departments and/or clinics. Please check with the ESCRS Head Office (escrs@ escrs.org) if you are unsure of your eligibility.
Survey to Establish Benchmarks for Quality of Life Factors
The ESCRS BoSS (Building Our Sustainable Society) initiative is conducting an anonymous survey to determine how income, workload, and employment benefits influence the well-being of ophthalmologists and create an evidence base for policies and practices that contribute to sustainable career paths.
The European Eye Surgeons’ Compensation and Life Satisfaction Survey (EyE-CLaSS) is intended for ophthalmic surgeons, ophthalmic surgeons in training, and retired ophthalmic surgeons and takes approximately 5–8 minutes to complete. It asks questions about income, workload, and employment benefits from three internationally validated survey instruments: the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form, the Satisfaction with Life Scale, and the Cantril SelfAnchoring Ladder.
The survey data will be used to—
• Establish a global benchmark for ophthalmologists’ compensation;
• Clarify the extent to which earnings, protected time, and practice setting influence day-to-day well-being; and
• Provide an evidence base for professional organisations and policymakers seeking to promote equitable and sustainable career structures.
All responses are strictly confidential, and an executive summary of the findings will be circulated. The deadline for completion is Monday, 18 August.
Laura Maubon FRCOphth, BMBS, BMedSci, PGCert (Surg Ed) is a consultant ophthalmologist specialising in anterior segment surgery, ocular surface disease, and surgical education.
Eligibility. The award is open to ophthalmologists and researchers (MD and/or PhD) and experienced ophthalmic nurses who are active ESCRS members. Applicants must hold a current full- or part-time clinical or research position at a
The deadline to complete the survey is Monday, 18 August.
Nutrition and the Eye: A Recipe for Success
A look at the evidence for tasty ways of lowering risks and improving ocular health.
BY SEAN HENAHAN
Reportedly, the first medical text was a cookbook. As long ago as 1500 BCE, Egyptian physicians observed a connection between nutrition and eye disease, including prescribing liver, high in vitamin A, to treat night blindness. Chinese doctors in the early 14th century also made the connection between vitamin A and ocular health, prescribing leafy greens, carrots, liver, and egg yolks for patients with eye problems.1
The association between good vision and eating carrots and fish seems baked into our DNA. While modern medicine has innovated so many useful pharmaceutical treatments, devices, and surgical practices, nutrition remains a central factor in overall health, particularly ocular health.
“As ophthalmologists, even within the constraints of a busy clinic, we have a valuable opportunity to advocate for long-term visual health by promoting simple, science-based lifestyle advice,” Filomena Ribeiro MD, PhD told EuroTimes. “I still remember being told as a child that eating carrots would give me ‘beautiful eyes’—a charming myth, but one rooted in a deeper truth: nutrition does matter.”
Key nutrients—including polyunsaturated omega-3 fatty acids (PUFA) such as docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA); lutein; zeaxanthin; and vitamins A, B3, B9, and E—are all known to play a role in visual development and cognitive function. DHA is abundant in the retina and plays a role in phototransduction and neuroprotection.2
This knowledge supports advising patients to include sources of omega-3 PUFA in their diets. Some of the bestknown examples include salmon and other fatty fish, nuts, seeds, olive oil, and eggs, which contribute to the increasing popularity of the Mediterranean diet.
Even a brief word from us can carry weight—especially when patients understand that what they eat today may influence how well they see tomorrow.
“As ophthalmologists, we have an important role in helping patients understand how their daily habits—especially nutrition and lifestyle—can affect their eye health,” noted Başak Bostanc� MD. “This applies not only to preventing future problems but also to managing conditions already present.”
The potential benefit of omega-3 in the diet has not been lost on supplement marketers. The size of the eye health supplement market is eye-opening, to say the least. A recent global study valued the eye health supplement market at USD 2.5 billion in 2023, predicting it would grow to USD 4.48 billion by 2032.3
In general, there is little evidence to support the use of nutritional supplements in maintaining general health. However, ophthalmology research has produced some of the few examples where supplements do provide benefits.
The Age-Related Eye Disease Studies (AREDS and AREDS2), conducted by the US National Eye Institute (NEI), followed 4,700 participants aged 55–80 with different degrees of AMD.4 Patients received a combination of antioxidants and zinc or placebo over 6 years. While the supplement did not prevent the onset of AMD, it did significantly reduce the risk of progression to advanced disease in patients with intermediate or advanced AMD and the risk of moderate vision loss. No study of dietary supplements in any area of medicine produced such dramatic effects on health.
The follow-up AREDS2 study addressed some of the concerns raised in the first study, including concerns about beta-carotene and cancer risk, the side effects of zinc, and the lack of lutein. The AREDS2 protocol added lutein, zeaxanthin, and/or omega-3 fatty acids but removed zinc and beta-carotene from the formula. In that study, lutein and zeaxanthin were found to be safe and effective, while omega-3 fatty acids did not appear to provide additional benefit in reducing AMD progression.
“While our primary focus is often diagnosis and treatment, patients trust us as experts in vision, and this trust gives us an opportunity to deliver concise, evidence-based guidance,” Dr Bostanc� said. “We know from the AREDS and AREDS2 studies that targeted nutritional supplementation can slow the progression of age-related macular degeneration. But our responsibility doesn’t stop with vitamins. Encouraging a healthy diet, regular exercise, smoking cessation, screen-time management, and adequate sleep are all evidence-backed measures that support ocular and systemic health alike.”
Dry eye disease is another area where omega-3 fatty acids play a role. The need is great, with some 5% of the public experiencing symptoms of dry eye. A recent global survey conducted by Bausch + Lomb indicated 58% of adult dry eye sufferers experience frequent or occasional symptoms, but only 1 in 5 have been diagnosed. Population studies suggest a benefit among those practising an eye-healthy diet, with some studies indicating additional potential for omega-3 supplements.5–7
“Beyond supplements, encouraging patients to adopt a diet rich in leafy greens, oily fish, and colourful vegetables, along with good sleep hygiene and regular physical activity, contributes not just to ocular health, but to overall well-being. Even a brief word from us can carry weight—especially when patients understand that what they eat today may influence how well they see tomorrow,” Professor Ribeiro said.
“And beyond the science, the simple pleasure of selecting fresh ingredients and preparing meals thoughtfully can itself be a powerful act of self-care—a source of balance and well-being in daily life.”
For citation notes, see page 40.
Filomena Ribeiro MD, PhD, FEBO is Head of the Department of Ophthalmology at the Hospital da Luz, Lisbon, Portugal, and president of the ESCRS. filomenajribeiro@gmail.com
Başak Bostancı MD, FEBO is Assistant Professor of the Bahçeşehir University of Istanbul and a cataract and refractive surgeon at World Eye Hospital, Istanbul, Turkey. drbbostanci@gmail.com
Cooking a Feast for the Eyes
A cookbook to promote ocular health through thoughtful and traditional cuisine.
LAURA GASPARI
REPORTS
Nutrition can be the best ally for eye health without giving up flavour, culinary traditions, or the joy of cooking, according to Alessandro Mularoni MD.
The correlation between healthy food habits and eye health is no news in the ophthalmological world. For example, a balanced diet can play a key role in the prevention of systemic diseases such as diabetes mellitus, which is known to have significant ocular complications. Nutrition plays an increasingly significant role in overall health and, more specifically, ocular health—especially now life expectancy has increased.
“We live in an age where a considerable number of diseases can be, at least in part, prevented. While the market offers hundreds of dietary supplements, the most effective and beneficial are often those naturally integrated into our daily nutrition,” Dr Mularoni emphasised.
Under this rationale, Dr Mularoni co-authored a 300-page Italian cookbook in 2017 titled Eye on Food (original title, Occhio al Cibo). The book, structured in two parts, seeks to offer a comprehensive and accessible perspective—presented in clear and straightforward language, suitable even for patients—on the vital role of nutrition in ocular health. The first part, which is more scientific, provides a full description of the micronutrients (such as vitamins, proteins, minerals, polyunsaturated fatty acids, and fibres) and their impact on ocular health, as well as a complete explanation of ocular diseases of both anterior and posterior segments that bad nutritional habits can exacerbate. The second part is entirely devoted to recipes, and this is where Dr Mularoni’s book becomes special and innovative.
Contrary to widespread belief, Italian cuisine is far from being a single, monolithic tradition. Italy is administratively
divided into twenty regions and from north to south, each of them with culinary traditions and peculiarities. The cookbook differentiates them accordingly. Moreover, each recipe presents the nutritional values for the quantity described to help the readers know the exact micronutrients they are intaking.
“Our goal was to show readers that maintaining good health through nutrition does not require sacrificing flavour,” he explained. “By slightly adapting traditional recipes, we can promote a model in which prevention and tradition coexist harmoniously.”
In addition, two special menus created by Michelin-starred chefs complete the book, featuring a selection of seafood and land-based recipes, each accompanied by their respective nutritional values.
The book also provides insight into the several types of cooking and their benefits, the chemistry applied to cooking, the right choice for kitchen tools, and some tips on balancing a good diet with sport and a healthy lifestyle.
As Dr Mularoni pointed out, all proceeds from the book were donated to the Italian charity Associazione Medici Oculisti per l’Africa (Association of Ophthalmologist Doctors for Africa). The book is only available in Italian, but Dr Mularoni hopes to see it translated into other languages to promote a deeper understanding of Italian cuisine and its application in supporting eye health.
Alessandro Mularoni MD is an anterior segment surgeon and director of the ophthalmological unit of the Hospital of the Republic of San Marino. alessandro.mularoni@iss.sm
The Doctor Recommends…
Dr Alessandro Mularoni shares two delicious recipes that promote ocular health.
Ingredients for 8 servings
• 1 cod or desalinated salted cod fillet, about 600 g
• 100 g mascarpone
• 100 g fish broth
• 500 g fresh pasta for ravioli
• 500 g Pachino cherry tomatoes
• sage
• 50 g butter
Preheat the oven to 180°C (350°F). Place the cod in an ovenproof dish, pour the fish broth over it, add a few sage leaves, and cover with aluminium foil. Turn off the oven, place the dish with the cod inside, and let it cool down slowly. This slow cooking keeps the cod tender.
Retrieve the cooking liquid and emulsify it with the butter, warm it up, and let the sage infuse in the sauce.
Prepare the filling by blending the cod and mascarpone in a food processor. Make ravioli using pasta discs about 6 cm (2.4 in) in diameter.
Blend the raw cherry tomatoes with just a little sugar and salt to make the tomato cream.
Cook the ravioli, toss them with the tomato sauce, and dress with the sage butter sauce.
Nutritional Profile per Serving
Energy: 273 Kcal
Protein: 21 g
Fat: 12 g
Cholesterol: 53 mg
Carbohydrates: 21 g
Vitamin A (preformed): 112 mcg
Vitamin C: 16 mg
Calcium: 42 mg
Iron: 3 mg
Phosphorus: 217 mg
Potassium: 214 mg
Magnesium: 21 mg
Sodium: 16 mg
Beta-carotene (pro-Vitamin A): 183 mcg
Lycopene: 1,900 mcg
Lutein/Zeaxanthin: 59 mcg
Omega-3: 420 mg
Ingredients for 4 servings
• 400 g boneless rabbit loin with belly attached
• 200 g curly lettuce
• 50 g ginger
• 100 g rabbit juices
• 30 g white wine
• salt, pepper, and extra virgin olive oil
Grate the ginger and soak it in white wine. Separate the loin from the belly. Heat a pan and sauté the salted and peppered loin in extra virgin olive oil until cooked. Remove from heat and let the loin rest. Cut the belly into julienne strips and cook them in the pan until crispy.
In a saucepan, place the grated ginger to heat it up, adding the rabbit juices. Season with salt and pepper, then strain the sauce. Finally, emulsify it with extra virgin olive oil.
Season the curly lettuce with salt and oil, then spread it on the plates. Slice the loin into even pieces, arrange them over the lettuce, and dress with the sauce and the crispy belly strips. Serve immediately.
Nutritional Profile per Serving Energy: 258 Kcal
Protein: 21 g
Fat: 19 g
Cholesterol: 60 mg
Vitamin A (preformed): 5 mcg
Vitamin C: 18 mg
Vitamin E: 3 mg
Calcium: 47 mg
Phosphorus: 16 mg
Potassium: 190 mg
Sodium: 105 mg
Beta-carotene (pro-Vitamin A): 2,613 mcg
Lutein/Zeaxanthin: 1,156 mcg
Cod Ravioli, Raw Tomato Cream, Butter, and Sage
Ginger Rabbit Salad
Sharing a Vision for the Future
ESCRS leaders update Trieste conference on ESCRS initiatives.
TIMOTHY NORRIS REPORTS
Affiliation in the name of collaboration: The tight partnership between the ESCRS and their national counterparts has always been a key value for the development of a greater scientific network on a continental scale, with the common goal of improving ophthalmology by sharing information, encouraging and financing new research, and creating a common language towards standardisation and consensus for the benefit of the patient.
The Italian Society of Cataract and Refractive Surgery (AICCER) remains one of the most important points of reference for ophthalmologists specialised in the anterior segment.
“We have a lot in common with AICCER,” explained Filomena Ribeiro MD, PhD, president of the ESCRS, during the 26th AICCER congress held in Trieste in late March 2025. “This is a society that is clearly committed to providing a high level of scientific information, not only in refractive surgery, not only in intraocular surgery, but also corneal surgery and many different aspects of ophthalmology. We are very proud to be able to benefit from all this knowledge.”
Many the most important topics ESCRS promotes were presented to a crowded and interested audience in Trieste. For example, a session dedicated to the EPICAT study shared the compelling option of a dropless cataract surgery.
Oliver Findl MD pointed out that sharing the recent findings of this study on a national level could be game changing, given the impact that dropless cataract surgery could have on the Italian healthcare system, as well as its surgeons, patients, and caretakers.
The new ESCRS functional classification system of presbyopia-correcting IOLs was another hot topic at the congress. This evidence-based classification defines IOLs based on different ranges of field, aiming to streamline the description of existing and future IOLs for researchers, clinicians, patients, and industry.
Joaquín Fernández MD, PhD noted the development of this classification is still ongoing, with plans to include contrast sensitivity and photic phenomena, among others. This process will start with national societies before returning to the collaboration between ESCRS and ASCRS as part of a broader strategy.
IOL classification is a topic that has become more pressing every year due to the sheer number of premium lenses, added Robert Bellucci MD. He stressed it is essential for the ESCRS to provide eye doctors with all the instruments to better communicate with the patient, helping them better understand what they will achieve and not achieve.
Another hot topic in Trieste was artificial intelligence in healthcare, particularly its application in the field of ophthalmology. AI is destined to be increasingly important, eventually becoming a central part of the ophthalmologist’s everyday professional life, Dr Bellucci noted.
The AICCER congress was also conducted with an eye towards sustainability and equity—principles that resonate with and guide ESCRS, as evidenced by initiatives such as the BoSS (Building Our Sustainable Society) project, Professor Ribeiro observed. She added the idea of national societies following the same goals and the same path is rewarding.
Yet the AICCER congress has some characteristics that differentiate it from the ESCRS. According to Dr Findl, the most interesting part of the congress was the live surgery events, something that would be difficult to replicate on a broader scale. Despite the language barrier, he said, it was interesting to sit down and watch a live surgery, something in which the Italians have always been at the forefront.
This is a further reason to commit ESCRS to share its projects with this society, and by doing that, we are sharing their projects with all cataract and refractive surgeons in Europe.
Some of the topics discussed on a national level may provoke conversations on a continental scale. “There are some new approaches regarding the preoperative treatment of patients (related to the severity of dry eye) that need to be broadened,” Dr Bellucci said. “Some of these preoperative protocols discussed in Trieste really inspired me to change my approach to the patient.”
“There are a lot of talks regarding communication with the patient,” Prof Ribeiro echoed. “This is something that really makes a change in our practice. As physicians, we are not always prepared to deal with the patient, and I think this is an extremely good topic to develop and integrate in our clinical practice.”
Prof Ribeiro said the success of the 26th AICCER congress represents an additional step for tighter collaboration between national and international societies. “This is a further reason to commit ESCRS to share its projects with this society, and by doing that, we are sharing their projects with all cataract and refractive surgeons in Europe.”
Filomena Ribeiro MD, PhD, FEBO is president of ESCRS and Head of Department at Hospital da Luz, Lisbon, Portugal. filomenajribeiro@gmail.com
Oliver Findl MD, MBA, FEBO is Chief of the Department of Ophthalmology at Vienna Hanusch Hospital, Austria, and past president of the ESCRS. oliver@findl.at
Joaquín Fernández Pérez MD, PhD is Managing Director at Qvision, Almería, Spain, and secretary of the ESCRS. joaquinfernandezoft@qvision.es
Roberto Bellucci MD is Chief of the Ophthalmic Unit at the Hospital and University of Verona, Italy, and past president of the ESCRS. roberto.bellucci52@gmail.com
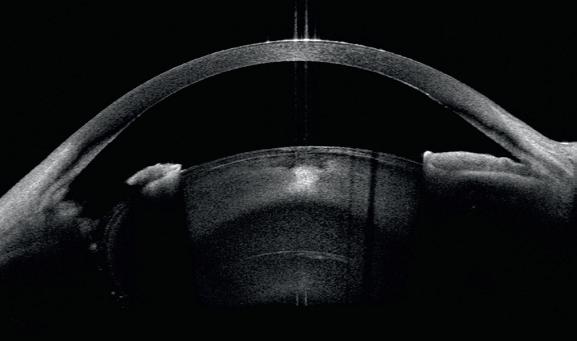
CASIA2 User Experience
Post-DSAEK Complications and Cataract Surgery in Fuchs’ Dystrophy*
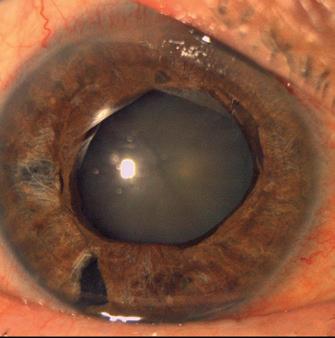
This concerns a patient with bilateral Fuchs’ dystrophy whose history includes DSAEK surgery in the right eye with subsequent ocular hypertension due to misdirection syndrome, requiring pars plana Vitrectomy and Goniosynechialysis in the same procedure. The patient presented significant photophobia and cataract, with intraocular pressure of 18 mmHg (figure 1).
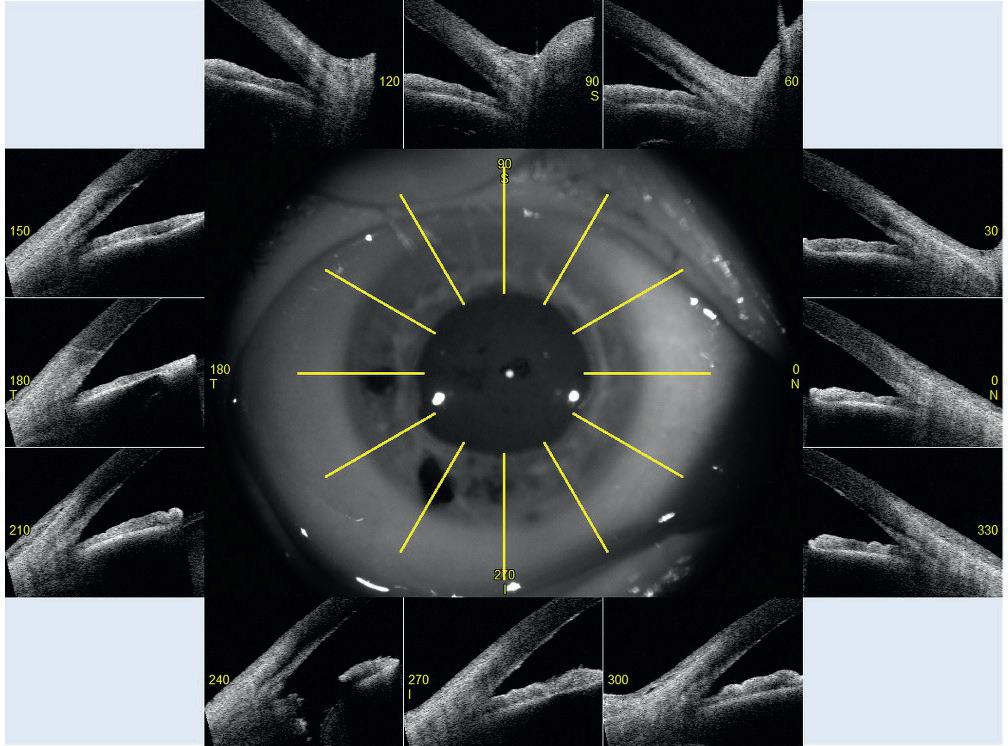
CASIA2 images inform us about corneal transparency and good adaptation of the endothelial graft, but also allows us to visualise the integrity of the lens after inferior iridectomy and gives us a 360° visualisation of the iridocorneal angle (figure 2).
In this case, a narrow angle with no presence of previous synechiae in all four quadrants is observed (figure 3). Given this situation, cataract surgery will be proposed with pupillary sphincter reconstruction using iris cerclage, with no associated glaucoma surgery as part of the procedure at this time.
* This use case was provided with kind permission of Dr. Pau Romera, Hospital Universitari Germans Trias i Pujol, Barcelona (Spain)
CASIA2 at tomey.de
Visit TOMEY at the ESCRS 2025: Booth C4.045
Figure 1
Figure 2
Figure 3
Long-Term Outcomes of EK for Failed Grafts
Research seeks evidence for guiding future management.
CHERYL GUTTMAN KRADER REPORTS
Aretrospective study investigating the long-term outcomes of endothelial keratoplasty (EK) in eyes with a history of failed corneal transplantation confirmed graft survival time decreases after every subsequent graft and showed that eyes having failed multiple grafts retained good visual potential.
“We wanted to better understand long-term outcomes of EK in eyes with prior failed corneal transplants to help guide clinical decision making for their further management,” said Erika Ellis MD, PhD. “Our findings showing they retained good visual potential despite experiencing decreased graft survival time support efforts to continue pursuing alternative treatments that can provide sustained functional improvement for these patients. Perhaps emerging keratoprostheses and cell-based treatment options may improve outcomes in patients with multiple graft failures.”
Data for the study were extracted from records of patients who had undergone Descemet stripping endothelial keratoplasty (DSEK) or Descemet membrane endothelial keratoplasty (DMEK) after prior keratoplasty. The EK procedures were performed over a 10-year period (2014–2024) by 2 UCLA Jules Stein Eye Institute surgeons. The analysis included 295 EK procedures (60% DSEK, 40% DMEK) performed for prior graft failure in 221 eyes of 208 patients. Mean follow-up was about 33 months.
The team explored the effect of the number of prior grafts on graft survival by comparing results for 252 eyes with 1 to 2 prior grafts and 43 eyes with 3 or more prior grafts.
“When we looked at survival for all our grafts after prior graft failure, we found the 50% survival rate was approximately 3 years, and the 5-year survival rate was about 30%,” said Dr Ellis, explaining the rationale for this analysis. “However, within the subgroup of eyes that had 3 or more prior grafts, the 50% survival rate was just about 2 years, and the 5-year survival rate was less than 5%.”
These patients are put in a difficult situation, and many choose to defer another surgery.
The results for the eyes included in the retrospective chart review showed that while the graft failure rate at 1 year was higher among eyes with 3 or more prior failed grafts than among those with 1 to 2 (12% versus 8%), there was no difference between the 2 groups in the rate of repeat EK within the first year.
“This is probably because we know if the current graft fails in less than 1 year, the subsequent graft is likely to fail in even less time. Therefore, these patients are put in a difficult situation, and many choose to defer another surgery for some time,” Dr Ellis said.
Data on change in vision after repeat graft showed that 88.4% of eyes with 3 or more prior grafts and 84.7% of eyes with 1 to 2 prior grafts achieved a significant improvement in corrected distance visual acuity (CDVA) after undergoing EK (defined as an improvement from preoperative VA of 20/200 or worse to better than 20/200 or an improvement of at least 2 lines for patients with preoperative VA of 20/200 or better).
The study also analysed complication rates after EK as a secondary outcome and found that eyes with 3 or more prior grafts had a higher rate of graft rejection, although the difference compared to the group with fewer failed grafts did not achieve statistical significance.
Dr Ellis spoke at the 2025 ASCRS annual meeting in Los Angeles.
Erika M Ellis MD, PhD is an ophthalmology resident at Jules Stein Eye Institute, University of California, Los Angeles, US. emellis@mednet.ucla.edu
Accurately Aligning Toric IOLs
Careful measurement and alignment are key, but issues persist.
HOWARD LARKIN REPORTS
When aligning toric intraocular lenses (IOL), just how accurate do surgeons need to be? It depends in part on the type of lens, said Douglas D Koch MD.
For monofocal IOLs, it’s generally acceptable to get within 0.75 D of residual cylinder, depending on individual patient needs. But for trifocals, the ideal goal is 0.5 D or less, which Professor Koch noted is more difficult, as the magnitude of astigmatic correction increases.
For 1.0 D of correction, alignment can be off by up to 14 degrees and still leave 0.5 D or less residual astigmatism. That drops to 7 degrees for 2.0 D correction and 3 degrees for 4.0 D correction.
“If we all set targets for ourselves to be well under 10 degrees, hopefully within 5 degrees of target, we [will] meet the needs of almost all our patients,” Prof Koch said.
Still, challenges persist that cannot be entirely overcome. Therefore, surgeons should be ready to deal with residual astigmatism after surgery.
Measurement and prediction formulas
An essential first step, Prof Koch said, should be to address corneal surface issues to obtain accurate corneal measurements.
Device variability is another source of potential measurement error, Prof Koch said. In a snapshot of 129 right eyes measured with the IOLMaster (Zeiss) and Lenstar (Haag-Streit), agreement between the two devices on the location of the steep meridian was within 5 degrees in only 60.5% of eyes and 82.9% within 10 degrees. He recommends taking multiple measurements to reduce the chance of error.
Axis prediction formula performance is another source of variability, Prof Koch said. “You can run three different toric formulas and get three different recommendations.” Still, running multiple formulas may help target an accurate recommendation.
Alignment issues
Manual versus digital alignment is debated, with some studies suggesting digital solutions are more accurate, and others finding no significant difference. In a study Prof Koch and colleagues conducted, there were no significant differences between manual and automated markings, with all deviations less than 10 degrees.1
“You don’t need to feel compelled to use a digital system, but it offers the advantages of speed and efficiency in the operating room,” he said.
The flaws of manually “eyeballing it” at the slit lamp include marks that are too wide and run before use or are simply misplaced, Prof Koch said. He recommends observing and accounting for shifts in markings measured upright at the slit lamp to lying down on the operating table.
80%
About 80% within 0.5 D might be the best you can expect.
Several digital solutions are available, and Prof Koch’s team uses a digital marking system with manual marks as a backup. If the patient’s head is not in the same position for each, errors can be introduced by recording the axis on one device and the landmarks for finding it on another.
“Ideally, you should measure and mark using the same device.”
So how accurate are surgeons? An American Academy of Ophthalmology technology assessment reviewing 21 toric IOL studies rated level I or II found that less than half showed 80% of cases with 0.5 D or less residual astigmatism.2
“In the end, about 80% within 0.5 D might be the best you can expect,” Prof Koch concluded. “Therefore, be ready to deal with residual astigmatism at the outset.”
Prof Koch spoke at the 2025 ASCRS Refractive Day in Los Angeles.
For citation notes, see page 40.
Douglas D Koch MD is professor and Allen, Mosbacher, and Law Chair in Ophthalmology at the Baylor College of Medicine, Houston, Texas, US. dkoch@bcm.edu
Extending Depth of Satisfaction
The ESCRS Eye Journal Club discuss a new study reviewing the causes and management of dissatisfaction after implantation of an EDOF IOL.
ROIBEARD O’HÉINEACHÁIN REPORTS
The ESCRS Eye Journal Club held a webinar hosted by Artemis Matsou MD, Alfredo Borgia MD, and Victoria Till MD to discuss the paper “Dissatisfaction after implantation of EDOF intraocular lenses,” published in the May 2025 issue of the Journal of Cataract & Refractive Surgery.1
The panellists were Andreia Rosa MD, PhD and Rudy MMA Nuijts MD, PhD, lead author of the article under discussion.
Providing a summary of the study, Dr Till noted the single-centre retrospective study reviewed medical records of patients who received an extended depth of focus (EDOF) lens at the University Eye Clinic of Maastricht University Medical Center between July 2020 and July 2022. It identified patients reporting dissatisfaction, the aetiology of the dissatisfaction, treatment responses, and final outcomes.
All patients underwent implantation of the AcrySof IQ Vivity (Alcon) single-piece foldable non-diffractive EDOF IOL. The lens is made from a hydrophobic acrylate/methacrylate copolymer material. It features a biconvex optic with an aspheric anterior surface and a spherical posterior surface, designed to provide a continuous range of focus from distant to intermediate vision as well as functional near visual acuity.
The target refraction was either bilateral emmetropia or minimonovision, with the dominant eye targeted for emmetropia and the non-dominant eye for residual myopia between -0.25 D and -0.75 D, aiming for a difference of 0.50 D between the two eyes. Eyes with an expected postoperative astigmatism greater than 1.00 D received toric IOLs.
You can improve the satisfaction of these patients really dramatically by doing it.
including interventions such as artificial tears, spectacles, or refractive surgery enhancement.
Treatment was successful in 57 of 83 eyes (68.7%) among 35 patients. However, 12 patients (21 eyes, 25.3%) remained dissatisfied despite treatment, and 5 patients were lost to follow-up. The main causes of dissatisfaction after unsuccessful treatment were waxy vision syndrome (6 eyes), DED (6 eyes), and expectation mismatch (4 eyes). Two patients had pre-existing ocular conditions, with one patient having age-related macular degeneration in both eyes and another having a history of retinal detachment in one eye.
Best for minimonovision?
In the discussion that followed, Dr Matsou noted that the minimonovision patients made up the highest proportion of dissatisfied patients. She asked the panel if the results challenged the practice of using EDOF IOLS in a minimonovision strategy, on the basis that they would be a safer option than multifocal lenses.
Professor Nuijts said that the dissatisfaction among minimonovision patients is usually due to poor distance vision. His treatment in such cases involves leaving the dominant eye slightly myopic and using laser-assisted sub-epithelial keratectomy (LASEK) on the non-dominant eye to target emmetropia. Patients often report significantly higher satisfaction with their vision in these cases with only slight refractive adjustments.
“If you implant these types of lenses, or even monofocal IOLs, it can really become a problem if you don’t have access to excimer laser surgery,” he said. “You can improve the satisfaction of these patients really dramatically by doing it.”
Dry eye considerations
Among 354 eyes of 202 patients, 52 patients reported dissatisfaction regarding 83 eyes (22.8%). They included 53 eyes (64%) that received a non-toric Vivity IOL and 30 eyes (36%) that received the toric version. The refractive target was minimonovision in 43 patients and emmetropia in 9 patients. Patients reported blurred vision in 78 eyes (94%), photic phenomena in 21 eyes (25.3%), and both conditions in 16 eyes (19%).
The primary causes of dissatisfaction were residual ametropia (51.8%), dry eye disease (DED, 26.5%), and posterior capsular opacification (12.0%). Additionally, 4 patients experienced expectation mismatches, with their dissatisfaction mainly attributed to their uncorrected near visual acuity (UNVA). Treatments were administered to 85.5% of the eyes,
Prof Nuijts also pointed out that the eyes in the study represented a complete case series of patients and included all causes of dissatisfaction. Similar rates of dry eye after cataract surgery were found in other studies where patients were proactively asked to report complaints, such as the PREMED study.
“The dry eye complaint [seen] here is, therefore, probably not really different from a control situation with a normal lens,” he said. “But the effect of the dry eye is probably different in this particular situation where you have an advanced technology IOL—in this case, an EDOF lens—because the condition causes more problems in the quality of vision domain.”
Dr Matsou asked the panel if they take any specific measures when implanting an EDOF lens to avoid postoperative dry eye and the resulting dissatisfaction.
Prof Rosa said she will not treat asymptomatic patients pre-emptively but will treat blepharitis when it is present. As
with all cataract surgery, she will take all necessary measures to ensure a normal ocular surface with good tear break-up times and without any punctate keratopathy. Postoperative management of dry eye is also crucial due to the disruption of the ocular surface induced by factors such as povidone iodine, corneal incisions, and NSAID eye drops.
“It’s important to tell patients they may need some sort of lubrication afterwards, to think about which drops they really need, and avoid over-medication, because it can also disrupt the ocular surface,” she added.
EDOF and ocular comorbidities
Dr Borgia asked whether persisting ocular conditions—such as previous corneal refractive surgery, macular atrophy, and epiretinal membrane—should be considered contraindications for an EDOF IOL.
Prof Nuijts said he would generally not consider patients with significant ocular comorbidities as candidates for EDOF IOLs, citing a UK registry study that showed eyes with epiretinal membranes had an incidence of CME after cataract surgery six times that of eyes without the condition.2 On the other hand, patients with primary open-angle glaucoma and those undergoing phacovitrectomy for epiretinal membrane reported very satisfactory outcomes with the Vivity EDOF lens in studies presented at the 2024 ESCRS Congress in Barcelona, he pointed out.3,4
For citation notes, see page 40.
Artemis Matsou MD, MRCP(UK), FEBOS-CR, FEBO, PgDip CRS is a consultant ophthalmologist and cataract lead at Queen Victoria Hospital, East Grinstead, UK. art.matsou@gmail.com
Alfredo Borgia MD, FEBO is a cornea, cataract, and refractive surgery consultant at “Mons. Dimiccoli” Teaching Hospital, Barletta, Italy. alfr.borgia@gmail.com
Victoria Till MD is based at Hanusch Hospital, Vienna, Austria. victoria.kauer@gmx.at
Rudy MMA Nuijts MD, PhD is Full Professor of Ophthalmology and Director of the Cornea Clinic and the Center for Refractive Surgery at the Department of Ophthalmology, University of Maastricht, Netherlands. rudy.nuijts@mumc.nl
Andreia Rosa MD, PhD is Assistant Professor of Ophthalmology at the Faculty of Medicine of the University of Coimbra, Portugal.
The full ESCRS Eye Journal Club episode is available on the ESCRS website or by scanning the QR code.
Conventional Versus Laser-Assisted Cataract Surgery
Evidence favours conventional technique in most cases.
CHERYL GUTTMAN KRADER REPORTS
Taking into consideration effectiveness, cost-effectiveness, and versatility, Joaquín Fernández MD, PhD highlighted reasons surgeons may prefer conventional cataract surgery, but he emphasised that he does not rely on it exclusively.
Speaking at the 2025 ASCRS meeting in Los Angeles, Professor Fernández reviewed the evidence supporting his practices.
“We are people of science, and we have to evaluate our decisions based on scientific evidence,” Prof Fernández said.
Information about the real-world effectiveness of the two procedures came from recent meta-analyses. Authors of a 2023 Cochrane meta-analysis, which reviewed 42 studies, identified some differences between conventional cataract surgery and a femtosecond laser-assisted approach in various endpoints, concluding any difference in postoperative visual outcomes would expected to be small.1 Another meta-analysis published in 2025 of 41 studies also found no difference between the procedures in visual outcomes at middle-term follow-up and concluded both are safe and effective.2
“There are some differences between the two procedures, such as the consistency of the shape and size of the capsulotomy; and there may be differences in safety, but these are minimal. When it comes to effectiveness, final visual acuity and quality of vision are the same,” Prof Fernández said.
While multiple groups have undertaken economic evaluations of femtosecond laser-assisted cataract surgery, the key when reviewing this research is to consider the type of analysis, the perspective under investigation, and the data source, Prof Fernández said.
He explained that economic evaluations can use a value-health concept linked to the individual or a cost-utility approach linked to health systems. The evaluation can be orchestrated from the perspective of the patient, provider, payer, or society, and the findings can differ from country to country.
Prof Fernández illustrated this information by discussing several studies. Although most research in this area finds that a laser-assisted approach is not cost-effective, an analysis conducted by Prof Fernández and colleagues assessing the cost-effectiveness of treating low corneal astigmatism from the patient’s perspective determined that in situations where a spherical IOL is implanted, correcting astigmatism with femtosecond laser-arcuate keratotomies was generally the most cost effective.3
When it comes to versatility, Prof Fernández mentioned a variety of situations where using a conventional approach could be safer or where using a femtosecond laser may not be feasible. The examples included eyes with tremor, dense
or white cataracts, zonular weakness or instability, posttraumatic cataract, or certain anterior segment abnormalities. However, he stated that he considers a femtosecond laser-assisted approach the better option in eyes with a shallow anterior chamber.
“We must also consider that phacoemulsification is more adaptable,” Prof Fernández said. “It can be used in high-resource settings with advanced machines and in low- and middle-income countries where manual small-incision cataract surgery or only basic phaco systems are used.”
He mentioned that in a world where there is growing concern about the environmental impact arising from the healthcare sector, sustainability is another issue necessary to consider. Currently, however, evidence comparing the sustainability of conventional cataract surgery to femtosecond laser-assisted methods is limited.
“Key questions that require further investigation include the environmental footprint associated with disposable versus reusable equipment, energy consumption differences between procedures, and long-term resource use, including the frequency of complications or reoperations that may indirectly impact sustainability,” Prof Fernández said.
For citation notes, see page 40.
Joaquín Fernández Pérez MD, PhD is CEO and Medical Director in the Ophthalmology Department at Qvisión in Vithas Virgen del Mar Hospital, Almería, Spain. joaquinfernandezoft@qvision.es
Need a quick introduction or refresher about a surgical procedure? Have a tip to share about a technique or approach you use that makes surgery easier?
The ESCRS 100 is the place to go. It’s a library of short (roughly 100 seconds), high-quality instructional videos about all fields of cataract and refractive surgery.
More than three dozen videos have already been created, and additional videos are being uploaded each month. Current videos include the following topics:
• Nodule removal
• Inserting the DMEK graft
• Descemet membrane stripping
• 4-flanged fixation of an artificial iris and closed-loop IOL
MAKE EVERY SECOND COUNT
—PUT THE ESCRS 100 VIDEO SERIES ON YOUR LIST OF MUST-WATCH EDUCATIONAL RESOURCES ! ESCRS 100
Need to Know: Spherical Aberration
Part three of this series examines spherical aberration and its influence on higher-order aberrations.
BY SOOSAN JACOB MS, FRCS, DNB
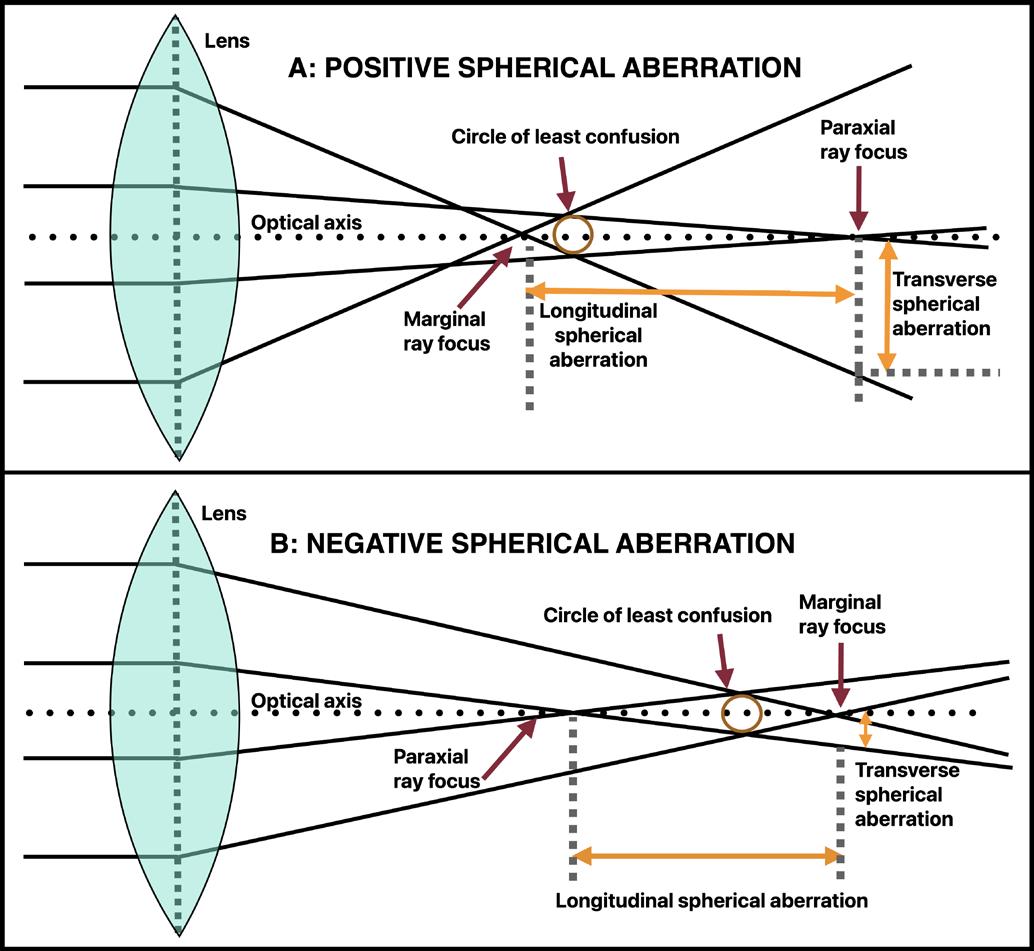
Spherical aberration (SA) is a rotationally symmetrical aberration belonging to the fourth order, together with secondary astigmatism and quadrafoil. SA occurs secondary to the lens refracting peripheral rays differently than the central paraxial rays. In a convex lens, the peripheral rays come to a focus before the rays close to the optical axis. This results in multiple foci, preventing a clear image from forming on the retina.
The distance between the focal points is known as axial or longitudinal spherical aberration (LSA). Transverse spherical aberration (TSA) refers to the perpendicular distance from the optical axis by which peripheral rays miss the ideal focal point. The direction of focus error in TSA is therefore perpendicular to the optical axis, unlike LSA, where the direction of focus error is along the optical axis (see figure).
LSA is due to peripheral rays focusing at different depths, causing a depth shift and resulting in defocus blur or axial blurring (depth related). Small amounts of LSA under certain conditions can give an increased depth of focus (DOF). In TSA, on the other hand, peripheral rays spread laterally. Blur is perpendicular in TSA and causes a lateral shift, resulting in light spreading around a point image—thereby reducing image sharpness and causing lateral blurring (spatial spread). Therefore, TSA is an indicator of image blur. It also results in reduced contrast and night vision problems.
In general, LSA is typically referred to as SA in ophthalmological practice. LSA can have a positive or negative value. In positive SA (PSA), peripheral rays focus in front of central rays (more anterior along the optical axis), leading to a myopic shift in refraction (Seidel’s classical optics) and causing halos, glare, and reduced contrast, especially in dim light. Myopic LASIK (oblate cornea) tends to create PSA. In negative SA (NSA) in an emmetropic eye, peripheral rays focus behind
central rays (more posterior along the optical axis), which can cause a peripheral hyperopic shift in refraction (Seidel’s classical optics) and affect depth perception. Creating a central myopic refraction (helping near vision) and a negative Seidel SA can provide good distance and near uncorrected visual acuity.
PSA has a ‘sombrero’ configuration in Zernike optics from the hidden second-order defocus, unlike the Gatinel–Malet mode’s flat centre and truer depiction of pure SA (as explained in part two of this series).
SA (LSA) is the ocular aberration with the greatest representation in the human eye. The average total value of Zernike SA for a 6 mm pupil is +0.10 ± 0.10 µm. Slightly positive total residual SA (+0.10 μm) may correlate with better visual acuity. A normal cornea has mild PSA, counteracting the lens’ NSA. The cornea contributes +0.28 ± 0.09 µm while the crystalline lens contributes -0.20 µm for a 6 mm pupil. During accommodation, NSA from the crystalline lens increases by approximately -0.04 µm per dioptre accommodation in a 5 mm pupil. The normal eye shifts from a PSA state at rest to an increasing NSA state with increasing accommodation. Lenticular SA goes from negative to positive as cataracts develop. Hyperopic LASIK (prolate cornea) induces NSA. Keratoconus progression can also increase NSA due to corneal steepening. Some aspheric IOLs are designed to induce NSA to balance corneal PSA, and decentration and tilt can be deleterious in these IOLs.
The human cornea has an aspheric shape, meaning it flattens towards the periphery. This shape reduces PSA and helps maintain better image focus by minimising the difference in focal points for central and peripheral rays. In oblate corneas, peripheral light rays converge in front of central rays, creating PSA. In prolate corneas, peripheral light rays converge posterior to central rays, creating NSA. SA comes into play when pupil size is more than 4 mm (low light).
FIGURE: A) Positive spherical aberration. Peripheral rays focus in front of paraxial rays; B) Negative spherical aberration. Peripheral rays focus behind paraxial rays. www.oculus.de
Clinical relevance of SA
Excessive SA significantly impacts visual quality. It also leads to reduced contrast sensitivity and decreased sharpness.
LSA and night vision disturbances In low light, the pupil allows more peripheral rays to enter. With positive LSA, peripheral rays focus in front of the retina, causing blur, halos, and reduced contrast sensitivity. Because SA is produced by the difference between peripheral and paracentral keratometry, its effect declines with smaller pupils. It contributes almost nothing to total aberrometry for pupil sizes less than or equal to 3 mm.
Keratoconus and irregular corneas Keratoconus produces inferior steepening, resulting in coma. The corneal steepening also increases LSA, which cause multiple focal points, blurred vision, visual distortions, ghosting, and halos (particularly in low-light conditions), ultimately impacting visual quality. LSA changes with disease progression and cone position, making it an important parameter for tracking severity and planning interventions. Many other aberrations also increase in keratoconus.
Double Down On Your Decision
Screening for ectasia with double safety
The Tomographic Biomechanical Index, or TBI, provides a unique combined expression of Corvis® ST und Pentacam® measurement data. It allows the risk of corneal ectasia to be assessed with greater reliability than ever before. The TBI assists you in selecting the optimal treatment based on sound reasoning. More safety for you and your patients!
LSA in refractive surgery (LASIK, PRK, SMILE) Myopic LASIK, especially standard LASIK with large optic zones, induces PSA and positive secondary astigmatism and can cause night vision problems (halos, glare). Wavefrontguided LASIK and aspheric ablation profiles aim to minimise LSA, improving post-surgical visual quality. Hyperopic LASIK induces NSA and negative secondary astigmatism. LASIK can introduce other aberrations as well.
LSA in cataract surgery and IOL selection
The human cornea is aspheric and slightly prolate (Q is less than 0). The natural crystalline lens contributes to NSA, which increases with age. Aspheric IOLs compensate for corneal LSA and improve contrast sensitivity after cataract surgery. Thus, spherical aberration can be corrected with appropriate IOL selection. IOLs can be neutral or induce PSA or NSA. Selecting an IOL that accounts for the patient’s corneal LSA is crucial for achieving optimal vision. However, these may not be a significant advantage with smaller pupil sizes.
IOLs inducing PSA Traditional spherical IOLs increase PSA. They are used in hyperprolate corneas (post-hyperopic LASIK) with NSA. Examples are the MA60AT (Alcon), CT Spheris 204 (Carl Zeiss), and Sensar (Johnson & Johnson) lenses.
IOLs that do not modify SA IOLs with prolate anterior and posterior surfaces that do not modify SA include Akreos, SofPort LI61AO (both Bausch + Lomb), and CT Asphina 409M (Carl Zeiss). These IOLs are less sensitive to tilt, decentration, and pupil eccentricity than aspheric IOLs and have better image quality than spherical IOLs. Zero SA IOLs may also have the advantage of residual SA, improving depth of field.
IOLs inducing NSA IOLs inducing NSA include aspheric IOLs with a prolate anterior surface (Tecnis, Johnson & Johnson), a prolate posterior surface (AcrySof IQ, Alcon), and both prolate surfaces (FineVision, PhysIOL [BVI] and CT Asphina 509M, Carl Zeiss). Depending on the amount of NSA, they provide better contrast sensitivity when correcting corneal PSA but less depth of focus than spherical lenses. They compensate positive aberrations of the average cornea almost completely (Tecnis with -0.27 microns NSA) or partially (AcrySof IQ Aspheric with -0.20 microns NSA). However, it is important to keep in mind SA interacts with residual sphere. Performance also depends on pupil size which needs to be more than 3 mm to see effect. IOL decentration and large angle alpha can induce other aberrations, such as coma, potentially compromising vision. Myopic LASIK patients benefit from NSA IOLs, which may also be better in patients with larger mesopic pupils and those with night-time driving needs.
Bi-sign IOLs These IOLs combine the advantages of neutral and correcting aspherical IOLs, like CT LUCIA
(Carl Zeiss), for example. Aspherical profile tolerates greater lens offset. This is good for most patients and ideal when angle alpha is greater than 0.5 mm or in patients at risk of decentred IOL.
Monofocal-plus IOLs Monofocal-plus IOLs mostly function as monofocal IOLs but with slightly increased DOF (between 0.25 D and 0.50 D), which is just enough to provide small improvement at intermediate distances. Increasing SA does not produce a noticeable drop in acuity but does slightly degrade contrast sensitivity. Examples include the Tecnis Eyhance (Johnson & Johnson), which combines NSA with increased central curvature; Isopure (BVI PhysIOL), which uses NSA customised to dioptric power; and RayOne (Rayner), which uses PSA.
Correcting/modifying SA Wavefront-guided LASIK, aspheric IOLs, and customised contact lenses can all modify SA. Controlled induction of HOA in refractive and cataract surgery can enhance DOF. SA can also compensate for loss of accommodation associated with presbyopia. NSA is used in PresbyLASIK and EDOF IOLs. However, all of these work better with a slight myopic central refraction. Custom contact lenses (scleral, hybrid) to reduce LSA and aspheric corneal cross-linking (CXL) protocols to stabilise LSA have been used in keratoconus.
Gatinel’s LD/ HD decomposition NSA creates a series of focal points with central rays focusing closer and peripheral rays farther down. Though NSA decreases visual quality, it remains stable across different defocus values. Depending on the maximum tolerable blur spot, the DOF can thus increase. However, the Zernike formula for SA also contains hidden defocus. For 0.25 microns of NSA with a 6 mm pupil, the amount of defocus present (about 1 micron) corresponds to at least +0.75 D of positive defocus (myopia). Therefore, the myopic shift caused by negative Zernike SA results in an improvement in intermediate and near visual acuity while the central hyperopic shift caused by positive Zernike SA leads to a degradation in intermediate and near visual acuity. This creates the misleading impression that only negative SA enhances DOF, while, in reality, both PSA and NSA can enhance DOF when used appropriately together with manipulation of paraxial defocus.
This is the third in a multipart tutorial on higher-order aberrations. Previous articles in the series can be found at escrs.org/eurotimes.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
The True Cost of Shingles Shots
Increasing access to vaccines that prevent ophthalmic shingles could save taxpayers money.
ANDREW SWEENEY REPORTS
What is the true value of a vaccine: the initial cost or the expense of long-term treatment of the unvaccinated? That was the question posed by “Vaccination Against Shingles and Prevention of Long-Term Ocular Morbidity—a Retrospective Study of Cost Implications to the National Health Service (NHS) of the UK.”
According to Bita Manzouri MBBS, PhD, herpes zoster ophthalmicus affects up to 20% of patients with shingles. Most ophthalmic manifestations involve the upper eyelid and the orbit of the eye. Up to a further 25% of these cases involve patients presenting with severe complications like keratitis, uveitis, and optic nerve palsies.
Shingles is caused by the reactivation of the herpes zoster virus, which is initially acquired as chickenpox. In the UK, vaccines are available on the NHS to those older than 65, using the Shingrix vaccine that superseded Zostavax in September 2023. The former is available privately to patients older than 50 years of age.
Dr Manzouri, along with her colleagues, wanted to discover the cost implications of not vaccinating patients between the ages of 50 and 65. Would the British taxpayer save money by vaccinating more patients or simply treating ophthalmic shingles patients?
Her retrospective study of patients, conducted over 28 months (April 2022–July 2024), examined the cost of treating ophthalmic shingles patients who would have been eligible for the vaccine if the age limit was lowered to 50. The baseline of the research was that the average cost of admission to NHS hospitals was £1,699 during this period, with in-patient treatment costing £423 per day, per patient.
The cost of vaccines was given as follows: one dose of Zostavax at £99.96 for those patients treated before September 2023 (placed into Group 1), and two doses of Shingrix at a total of £320 for patients treated after that date (Group 2).
Thirty-one patients were included in Group 1 and 17 in Group 2, with an average age of 59.3 years and an average hospital visit rate of 3.8 per patient. Mean eye drops administered per patient was 2.67, and around one-fifth went on to develop complications.
The team found the total cost of treating these 48 patients on the NHS to be £42,981.98, which included attendance, imaging, and medications. When examined per group, Group 1 cost £31,396.81 and Group 2 cost £11,612.27.
For the same cost as Group 1, 314 people could have been vaccinated against shingles and 36 people for Group 2. Dr Manzouri pointed out this does not include the added costs of lost time at work and treating the complications of the disease.
For the same cost as treating one group of patients, 314 people could have been vaccinated against shingles.
Dr Manzouri concluded that lowering the minimum age of the shingle vaccine to 50 would be more cost-effective for the NHS. This is especially important, she said, as the potential introduction of a chickenpox vaccine could reduce adult immunity to shingles.
Dr Manzouri presented at the 2025 EuCornea congress in Prague.
Bita Manzouri BSc, MBBS, MRCP, FRCOphth, PhD is a consultant corneal and cataract surgeon at Queen’s Hospital Romford, Essex, UK. bita.manzouri@nhs.net
Endothelial Keratoplasty in Vitrectomised Eyes
Retrospective study finds higher rate of post-EK CME.
CHERYL GUTTMAN KRADER REPORTS
Vitrectomised eyes are at increased risk of developing cystoid macular oedema (CME) after endothelial keratoplasty (EK), a new retrospective cohort study suggests.
“Based on the results of our study, we recommend closely monitoring the status of the macula during the first 6 months after EK in vitrectomised eyes,” said Ibrahim Qozat MD. “In addition, to try to prevent the development of CME, we propose using topical anti-inflammatory medication for an extended duration or giving dexamethasone by subconjunctival injection at the end of the keratoplasty procedure. Of course, additional studies are needed to assess the effectiveness of these approaches for prophylaxis.”
The study was undertaken recognising the growth of EK procedures performed in eyes with endothelial dysfunction requiring corneal transplantation.
“The number of EK procedures now exceeds that of penetrating keratoplasty,” he explained. “Therefore, it is important to understand the incidence of surgical complications after EK, including CME.”
Drawing from the TriNetX database, the retrospective study identified patients who underwent EK between 2004 and 2024, searching for patients with ICD-10 procedure codes for Descemet stripping automated endothelial keratoplasty (DSAEK) or Descemet membrane endothelial keratoplasty (DMEK). Patients were excluded if their history included conditions known to be associated with CME (e.g., uveitis, retinal vascular occlusion, diabetic macular oedema).
Propensity score—matching controls for age at index, sex, race, ethnicity, and the diagnosis of Fuchs’ dystrophy—was used to create cohorts with and without prior vitrectomy.
“Prior to propensity score matching, we had identified 526 patients with prior vitrectomy and 9,121 patients without [it],” Dr Qozat noted. “Comparing these two groups, we found statistically significant differences in age at event, sex, and history of endothelial corneal dystrophy.”
The final analysis included 522 patients in the vitrectomised and non-vitrectomised cohorts. The incidence of CME was significantly higher in the vitrectomised versus non-vitrectomised eyes (6.13% and 3.25%, respectively).
Discussing the research, Dr Qozat proposed several factors that could explain the higher rate of CME after EK in vitrectomised eyes. He cited a study that reported vitrectomised eyes undergoing DMEK appeared to have higher rates of intraoperative complications, graft failure, and endothelial cell loss.1
“Although the pathophysiology of postoperative CME remains incompletely understood, one of the most popular theories suggests that tissue manipulation during surgery stimulates the release of inflammatory mediators that enhance vascular permeability, leading to the accumulation of albumin and fluid in the inner nuclear and outer plexiform layers of the retina,” Dr Qozat said.
“[The research] suggested the more challenging anatomy of vitrectomised eyes led to longer surgical times causing more anterior segment inflammation and increased release of inflammatory mediators. In addition, absence of vitreous gel in vitrectomised eyes may facilitate diffusion of the surgery-induced inflammatory mediators from the anterior chamber through the posterior segment to the macula.”
Dr Qozat also identified limitations of the retrospective cohort study conducted by his group, including its retrospective design and potential inaccuracies of the diagnostic coding in the TriNetX database.
Dr Qozat presented at the 2025 ASCRS annual meeting in Los Angeles.
For citation notes, see page 40.
Ibrahim Qozat MD is a glaucoma fellow in the department of ophthalmology, Mayo Clinic, Jacksonville, Florida, US. qozat.ibrahim@mayo.edu
DMEK Following AC-IOL Explantation
Follow-up shows improvements in vision and anatomy but notable risk for secondary glaucoma.
CHERYL GUTTMAN KRADER REPORTS
Patients undergoing Descemet membrane endothelial keratoplasty (DMEK) for bullous keratopathy after explantation of an anterior chamber IOL (AC-IOL) achieve significant improvement in vision and corneal anatomy, albeit with a notable risk of postoperative complications, according to Ayça Bulut Ustael MD.
“Long-term presence of an AC-IOL can lead to corneal endothelial damage, corneal decompensation, and secondary glaucoma,” she explained. “As DMEK has gained popularity in treating corneal endothelial dysfunction and can be applied in eyes with different anterior segment abnormalities, we were interested in assessing the outcomes of DMEK after AC-IOL removal and identifying factors influencing surgical success and complications.”
In a retrospective study, Dr Ustael and colleagues identified 18 eyes with a minimum follow-up of 12 months after DMEK. The AC-IOL was implanted following complicated cataract surgery in 12 eyes, and the others had a phakic AC-IOL for myopic correction. Pars plana vitrectomy was performed before DMEK in most cases. All eyes that did not undergo vitrectomy had a phakic iris-claw AC-IOL. Patients left aphakic after AC-IOL explantation underwent IOL implantation, with the majority receiving a scleral-fixated IOL and the rest receiving a secondary sulcus-placed IOL. Anterior segment surgeons Ozlem Evren Kemer MD and Emine Esra Karaca MD performed the procedures in collaboration with Mehmet Onen MD, a vitreoretinal surgeon.
“In these complex cases, we prefer to remove the AC-IOL through a scleral tunnel to avoid further endothelial damage,” Dr Ustael said. “Depending on the case, a three-piece IOL is then fixated intrasclerally or in the sulcus.”
Since DMEK is often performed in eyes vitrectomised after AC-IOL removal, the anterior chamber is unusually deep, making graft unfolding and positioning particularly challenging. Special care is taken to control chamber depth and maintain graft stability.
Follow-up at 12 months after DMEK showed a statistically significant improvement in mean best-corrected visual acuity (BCVA) from 1.30 ± 0.62 logMAR to 0.48 ± 0.34 logMAR. Importantly, 61% of eyes achieved a BCVA of 20/40 or better. Mean central corneal thickness (CCT) decreased significantly in the same time frame, from 652 ± 162 µm preoperatively to 538 ± 52 µm.
“This change reflects improvement in endothelial function and a reduction in corneal oedema,” Dr Ustael said.
After DMEK, five eyes achieved and maintained a clear cornea and did not undergo additional surgery during the
available follow-up. Graft detachment occurred in eight eyes, of which three had successful graft reattachment with rebubbling. Repeat DMEK and penetrating keratoplasty were each performed in four eyes. Secondary glaucoma developed in eight eyes, of which three required survival intervention for management.
Prior to DMEK, eyes with pre-existing glaucoma had worse baseline BCVA and higher CCT than eyes without glaucoma. An analysis performed with eyes divided into two groups based on the duration of AC-IOL retention before explantation (≤ 7.5 versus > 7.5 years) showed the incidence of secondary glaucoma was significantly higher in the group with the longer period of AC-IOL retention.
“The sample size of our study was small. Larger prospective studies are needed to confirm our findings,” Dr Ustael said. “However, our data suggest that while DMEK after AC-IOL explantation significantly improves both vision and corneal structure, careful patient selection for DMEK and close postoperative monitoring are essential, particularly for eyes with prolonged AC-IOL retention and pre-existing glaucoma.”
Dr Ustael presented at the 2025 ASCRS annual meeting in Los Angeles.
Ayça Bulut Ustael MD is an ophthalmology resident at University of Health Sciences, Ankara Bilkent City Hospital, Ankara, Turkey. aycabulut96@gmail.com
Pharmacological Treatment for Corneal Oedema
Researchers report functional and anatomical improvements using topical Rho-kinase inhibitor.
CHERYL GUTTMAN KRADER REPORTS
Arecent open-label investigation appears to provide evidence supporting the topical use of the Rho-kinase inhibitor ripasudil for managing corneal oedema.
The study included 17 eyes of 16 patients who were candidates for cornea transplantation. The mean duration of corneal oedema prior to starting ripasudil was 3.250 weeks (range 1 to 12 weeks), and the mean duration of ripasudil treatment was 4.875 months.
Data collected at the last available follow-up showed treatment with the Rho-kinase inhibitor was associated with significant improvements in best-corrected visual acuity (BCVA) and central cornea thickness (CCT), allowing patients to postpone undergoing endothelial keratoplasty. Results were similar in an updated analysis that included data from an expanded cohort of eyes with corneal oedema post-cataract surgery, said Itay Lavy MD.
“Clearly, our study has limitations, including its small sample size, lack of a control group, and relatively short treatment duration,” he said. “In addition, most eyes treated with topical ripasudil at our centre were excluded from this study because data on pretreatment CCT was not available. However, we believe that our findings support further longterm studies investigating topical Rho-kinase inhibition for management of corneal oedema.”
We believe that our findings support further long-term studies investigating topical Rho-kinase inhibition for management of corneal oedema.
The aetiology of corneal oedema in the eyes included in the study comprised multiple conditions, the most common being oedema post-cataract surgery (31%) and failing corneal grafts (post-penetrating keratoplasty [25%] and post-Descemet membrane endothelial keratoplasty [19%]). Other eyes had corneal oedema associated with the presence of an Ahmed glaucoma valve or a history of trabeculectomy, among other conditions.
Pretreatment measurements showed the 17 eyes had a mean BCVA (logMAR) of 1.106, mean CCT of 619.50 µm, and mean endothelial cell count (ECC) of 849.0 cells/mm2. At last follow-up, mean BCVA was 0.560, mean CCT was 572.50, and mean ECC was 874.7 cells/mm2.
“While the changes in BCVA and CCT were statistically significant, mean ECC did not change significantly, which makes sense because we know that ripasudil does not cause cell division or increase the number of cells,” Dr Lavy said.
The expanded cohort of eyes with corneal oedema post-cataract surgery included 21 eyes, of which 17 had Fuchs’ endothelial dystrophy. Mean duration of ripasudil treatment in this cohort was 3.5 months. Mean BCVA (logMAR) improved significantly from 0.62 to 0.23, and mean CCT decreased significantly from 601.50 to 552.50. Mean ECC decreased from 1,654 to 1,574, but the change was not statistically significant.
Topical ripasudil is currently on the market in Japan, where it received approval in 2014 for treating glaucoma or ocular hypertension. Most of the research investigating its efficacy for treating endothelial dysfunction has been led by Japanese ophthalmologist Shigeru Kinoshita MD, PhD, Dr Lavy said.
“Rho-kinase inhibitors affect cell shape and movement through effects on the actin cytoskeleton,” Dr Lavy explained. “They have been shown to increase cell proliferation and migration, prevent apoptosis, and promote cell adhesion, all of which have relevance for managing corneal endothelial dysfunction.”
“Pretreatment ECC was known for all eyes in this subgroup because ECC is measured routinely before cataract surgery,” Dr Lavy said. “The improvements in CCT and BCVA in these eyes are much higher than in the population with mixed aetiologies for cornea oedema. The reduction in ECC is attributable to their having cataract surgery.”
Dr Lavy spoke at the 2025 ASCRS annual meeting in Los Angeles.
Itay Lavy MD is a senior ophthalmologist and Director of the Anterior Segment Surgical Unit at Hadassah Medical Center, Jerusalem, Israel, and specializes in corneal diseases and transplants. itaylavy@gmail.com
Amphotericin B-Supplemented Corneal Storage Media
Retrospective study examines benefit and risk.
CHERYL GUTTMAN KRADER REPORTS
Supplementation of corneal storage media with amphotericin B significantly decreases the rate of post-transplantation fungal infections and provides this benefit without significantly adversely affecting endothelial keratoplasty (EK) graft survival, according to the results of a retrospective study.
“Fungal infection after keratoplasty is a devastating, difficult-to-treat, sight-threatening complication, and its rate is higher for endothelial keratoplasty procedures that are growing in popularity. Given the rise in post-transplant fungal infections, CorneaGen began supplementing with amphotericin B in 2017 in hopes of preventing fungal keratitis,” said Nicole Fram MD.
“We conducted this study because it is not good enough to say that supplementing corneal storage media with this antifungal agent effectively decreases the risk of fungal infection. We also need to know that it is safe, and we have demonstrated that in our cohort. Now we are planning to conduct a prospective study to confirm the findings from our retrospective investigation and encourage others to perform studies using data from other eye banks so we can see if our findings can be generalized.”
The retrospective study included data from almost 53,400 transplants that represented all transplants performed in the United States over a 4-year period (2021–2024) using tissue from a single eye bank. Penetrating keratoplasty (PK) accounted for approximately 30% of the procedures, while 38% were Descemet stripping automated EK (DSAEK) and about 32% Descemet membrane EK (DMEK). Adverse event reports were reviewed for cases of infection (bacterial and fungal) and primary graft failure/early regraft (PGF/ER).
The analysis of fungal infections showed a statistically significant, 10-fold lower rate in cases performed using tissue from the amphotericin B-supplemented storage media compared to those using tissue from unsupplemented storage media. In the overall cohort, use of tissue stored in media
supplemented with amphotericin B was associated with a significantly higher rate of PGF/ER. Subgroup analyses of eyes categorized by type of keratoplasty showed the vast majority of tissue-related graft failures were in EK procedures, as the tissue is manipulated more before implantation. However, among eyes that underwent DSAEK or DMEK, there was not a statistically significant difference in the rate of PGF/ER comparing groups that used tissue stored in amphotericin B-supplemented media versus those stored in unsupplemented media. Interestingly, when all comers (including PKP) were included in the analysis, there was a statistical difference in PGF with amphotericin B, which will be investigated further as the sample size is increased.
“Anecdotally, we have heard from the Eye Bank of America that EK has a higher primary graft failure rate than penetrating keratoplasty. This makes sense knowing that EK procedures involve more tissue processing and handling,” Dr Fram said. “And with DMEK in particular, there can be more tissue manipulation. Therefore, it was very comforting to see that at least in the cohort in our study, the rate of PGF/ER within the DMEK subgroup was not increased when procedures were performed with tissue stored in the antifungal-supplemented storage media.”
Discussing study limitations, Dr Fram noted the possibility of outcome adverse event underreporting.
“We need accurate data to determine efficacy and safety of interventions. It is possible that not all cases of infection or PGF/ER were reported,” she said. “Having a better system of reporting outcomes is certainly desirable.”
Dr Fram presented at the 2025 ASCRS annual meeting in Los Angeles.
Nicole R Fram MD specializes in refractive, cataract, and corneal surgery in private practice at Advanced Vision Care in Los Angeles, US. nicfram@yahoo.com; drfram@avceye.com
A combination of better imaging and AI deep learning could significantly improve corneal imaging and diagnosis.
ANDREW SWEENEY REPORTS
AI-driven widefield specular microscopy promises an unprecedented improvement in imaging for Fuchs’ corneal endothelial dystrophy (FCED), recent studies from Singapore suggest.
Specular microscopy, the current standard practice for imaging FCED and the cornea in general, is too inaccurate and can be influenced by too many factors, according to Marcus Ang MBBS, PhD.
“Specular microscopy is the current standard, but this involves a central, less than 0.05 mm² endothelial scan, which covers less than 1% of the cornea. This can also be affected by corneal clarity, optical quality, artefacts, and patient cooperation,” he said.
“Widefield specular microscopy imaging could therefore provide real benefit, as it captures multiple images of the central, paracentral, and peripheral corneal epithelium. It can provide a map of the cornea within seconds, and the operator can then select the best quality images multiple times—from the central to the peripheral regions.”
Professor Ang discussed several studies based at the Singapore National Eye Centre, the first of which confirmed the quality of images taken by the widefield approach. One hundred FCED patients had 15 images taken of each eye,
divided accordingly: 1 central, 8 paracentral, and 6 peripheral. Image quality was graded as follows: (Grade 1) less than 25%, (Grade 2) 25–50%, (Grade 3) 50–75%, and (Grade 4) greater than 75%.
These images were then analysed and graded by a deep learning AI algorithm called DenseNet-121. They were also assessed by an independent clinician using a Bland–Altman plot and Kappa coefficient to act as a control.
Deep learning, wide imaging
Deep learning is a form of AI that creates artificial neural networks with multiple layers that are designed to mimic the structure and function of the human brain. It can analyse large volumes of high-resolution digital images, generated from various ophthalmic modalities, to create large data sets on a particular target.
Prof Ang reported DenseNet-121 was able to identify and grade each image correctly, and the accuracy level of both methods was identical. In total, 72.9% of the images were classified Grade 3 or above, and the image quality of the paracentral and peripheral regions was better in eyes with higher endothelial cell density, which he said was “a marker of FCED severity.”
al cell density correlated well with corneal oedema, meaning the images can also be used to ascertain cell loss in the paracentral and peripheral regions. As such, he recommended using widefield imaging combined with AI-driven analysis as an alternative to specular microscopy.
AI-driven widefield imaging could also help guide treatments such as Descemet stripping only (DSO). As the technique is primarily used in eyes with good pe ripheral cell counts, he believed he could use AI-driven widefield imaging to identify which eyes would make good candidates for DSO.
differentiate specular images of FCED and those with other types of endothelial damage, such as uveitis, from normal eyes. An independent data set of 752 paracen tral and 557 peripheral images of patients with mild to moderate FCED was examined.
Specular microscopy covers less than 1% of the cornea— AI-driven widefield imaging changes that.
“Our accuracies were pretty good, ranging from 0.77 to 0.99, and the AI could also identify eyes with cell densities of more than 1,000,” Prof Ang said. “This could be developed into software or an app designed for the treatment of DSO.”
Lastly, Prof Ang reported on a prospective study examining the role AI can play for FCED patients undergoing femtosecond laser-assisted cataract surgery (FLACS). He said he hopes to use AI to mitigate the impact of cataract surgery on the cornea’s endothelium, which can have differential effects on the central, paracentral, and peripheral areas.
Using deep learning again, Prof Ang plans to investigate how an AI detection tool could help improve cell shape detection and create regional maps of cell density in the cornea. Such maps could also include data on hexagonality and coefficient variation viewed both preand postoperatively to ascertain the impact of FLACS on corneas.
Prof Ang spoke at the EuCornea 2025 congress in Prague.
Marcus Ang MBBS, MMed(Ophth), MCI, FRCS(Ed), FAMS, PhD is a Senior Consultant at the Singapore Eye Centre and an associate professor at the Duke National University of Singapore Medical School. gmsahnm@nus.edu.sg
LEADERSHIP AND BUSINESS RESOURCES at Your Fingertips
What is the one leadership skill you would like to improve? What is the one business management challenge you would like to overcome?
The ESCRS Leadership, Business, and Innovation (LBI) programme provides ophthalmologists, clinic managers, and administrators and their teams with a variety of content to enable both online and in-person learning. Podcasts, webinars, video interviews, and more are available in the LBI library to help answer questions about topics such as selling a practice, finding a good work-life balance, facilitating patient decision making, and more.
AI and Gene Therapy as the Next Frontier
Effective new treatments are entering the clinic for uveitis.
PRISCILLA LYNCH REPORTS
The use of artificial intelligence (AI) and taking a ‘cross-sciences’ research approach holds the key to unlocking better future treatment pathways for uveitis, according to Andrew Dick MD.
He said uveitis is now on the cusp of achieving major further treatment progress in terms of sustained disease control with fewer systemic side effects. This technique will take an increasingly individualised treatment approach, using more precisely targeted agents to treat earlier detected disease and eventually introducing gene therapy into uveitis treatment protocols.
Evolution of treatment
“Despite being a leading cause of preventable blindness, uveitis remains underdiagnosed and undertreated,” Professor Dick said. “However, we have made significant inroads (treatment-wise) in the last two decades.”
Historically, treatment for uveitis has relied heavily on the use of corticosteroids—but these carry the risk of both shortterm and long-term side effects and increased morbidity and mortality rates, he noted.
“We know steroids are fantastic at inducing remission of acute inflammation, but you shouldn’t have patients on them for longer than three months as they start accruing side-effects, short term with change of mood and looks. Furthermore, the longer-term data is deeply worrying on cardiovascular, diabetes, and osteoporosis risks, as well as increased glaucoma and cataracts.”
However, increased disease understanding, particularly around cytokine inflammatory pathways, and recent advancements in treatment have significantly improved outcomes in uveitis. The use of disease-modifying antirheumatic drugs as first-line therapy, as well as biologic therapies (e.g., anti-TNF drugs such as adalimumab) for patients with severe or recurrent cases of uveitis has proven highly effective. While these treatments mark a significant step forward, ensuring global access, Prof Dick acknowledged optimising treatment protocols for the best responses and predicting non-responders remains a challenge.
“There has certainly been a lot of progress [but] there is a lot more to do. Among the key things we need to do [is] identify patients [who] are going to fail current very successful treatments, particularly anti-TNFs,” he told EuroTimes. “We know about 30–40% of patients do not respond adequately to anti-TNF therapies, but why is this? We need to know from the get-go who those patients are and have the necessary biomarkers to predict treatment response.”
Despite being a leading cause of preventable blindness, uveitis remains underdiagnosed and undertreated.
Prof Dick and others are currently working on identifying the molecular and cellular signature driving each case of uveitis disease. “If we can find that, then we could offer them earlier better treatment, so they don’t fail their first treatment.”
His talk stressed the importance of a tailored treatment approach specific to the cause of the inflammation driving the uveitis, as different subtypes require distinct management strategies. While non-infectious uveitis often involves immunosuppressive medications to control inflammation, infectious cases must be treated with targeted antimicrobial therapies.
“By tailoring treatment approaches, we can significantly decrease the likelihood of vision loss, which is the most serious potential outcome of untreated eye inflammation,” Prof Dick said.
The need for a multidisciplinary approach
Prof Dick also strongly advocated a multidisciplinary approach to managing uveitis, as it is frequently linked to underlying systemic diseases. Collaboration between ophthalmologists, rheumatologists, and infectious disease specialists is essential
for delivering comprehensive care and improving earlier detection and targeted treatment of uveitis.
Regarding research, he highlighted the advantages of a ‘cross sciences’ approach to tackling the remaining uveitis challenges.
Prof Dick is a co-investigator on CLUSTER, a consortium between four UK institutions combining the disciplines of immunology, clinical, genomic medicine and bioinformatics, and AI through computer science to define distinct ‘endotypes’ or ‘strata’ in juvenile idiopathic arthritis (JIA) uveitis, reflecting treatment response and disease course.
“Now we are engaging much more with computational biologists and mathematicians and bringing in deep learning and artificial intelligence because we need to unravel a huge amount of data—patient or biological data—that we are getting from the lab or patient.”
Beyond the ongoing development of “far better targeted treatments,” the next frontier of uveitis treatment will be gene therapy, Prof Dick explained. Ongoing research aims to refine vector designs, delivery methods, and patient selection criteria to maximise benefits and minimise risks.
“We are pushing really hard,” he said. “We are now in the process of developing a human-ready gene therapy and will see where we get to. There have been some setbacks, but we are close.”
With all of these ongoing advancements, Prof Dick concluded the future is bright for uveitis treatment.
Prof Dick presented the annual Mooney Lecture at the 2025 ICO annual conference in Kilkenny, Ireland.
Andrew Dick BSc, MBBS, MD, MRCP, FRCS, FRCP, FRCOphth, FMedSci is Director of the Institute of Ophthalmology at University College London and Professor of Ophthalmology at the University of Bristol, UK. A.Dick@bristol.ac.uk
Research Education Innovation
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
Opportunities for Enhancing Glaucoma Care with AI
Expanding array of tools cover applications inside and outside the clinic.
CHERYL GUTTMAN KRADER REPORTS
Artificial intelligence (AI) is expected to address a variety of unmet needs in glaucoma care by enhancing workflow efficiency, patient education, and clinical decision making, report a panel of experts.
Robert T Chang MD discussed significant AI use for patient education. He predicted realistic voice AI chatbot avatars would assist technicians and nurses as patient educators.
Dr Chang showcased this application through an AI-generated video about glaucoma geared towards patients. He emphasised the ease of the endeavour and its advantage of allowing practices to develop custom presentations more affordably than acquiring materials from outside sources.
AI can also enhance workflow efficiency in the clinic by serving as a ‘virtual scribe,’ listening to the doctor–patient conversation and then summarising the visit, coding, and billing, with the doctor then closing the encounter to verify the work. Dr Chang said his institution has already rolled out an enterprise-wide AI solution for all doctors and predicted it will be used more often as AI adoption and trust increases.
Highlighting areas outside of direct patient care where clinicians can benefit from modern large language models, Dr Chang discussed the utility for performing deep research. He demonstrated the reasoning process from a prompt asking, “Which FDA-cleared MIGS device has the best clinical studies proving its efficacy?
“AI now has a thinking step which also accesses digital sources for up-to-date information. This is a game changer since the models do not just rely on pre-trained data but can access most information humans can access,” he said.
“I predict traditional web searching will be replaced by AI agents that autonomously perform tasks on behalf of the user. These agents not only search information faster and more thoroughly, but they can actually make decisions and adapt
over time, allowing them to handle more complex tasks and improve their performance.”
AI now has a thinking step... This is a game changer.
Dr Chang also demonstrated how AI can help clinicians prepare polished slides for scientific presentations. “Granted, you still have to fact-check everything because AI can still make mistakes and choose from the wrong sources. However, reasoning AI models with proper prompting use a mixture of agents to double check actions, which improves the accuracy of the output,” he said.
Turning the topic to AI-based tools that support clinical decision making and teleglaucoma screening, Benjamin Y Xu MD, PhD described work he was involved with to streamline gonioscopy by leveraging AI.
“The AAO Preferred Practice Pattern recommends performing gonioscopy in all patients with newly diagnosed glaucoma, but our recent study of nearly 200,000 patients found that only 30% had received gonioscopy within the first six months after their initial glaucoma evaluation1,” he said.
As an alternative for detecting angle closure, anterior segment OCT (AS-OCT) overcomes several limitations of gonioscopy that limit its use and effectiveness. Nevertheless, the utility of AS-OCT is restricted by the need for manual interpretation of its images.
To address the drawback, Dr Xu and colleagues developed a deep learning classifier for automated detection of angle closure on AS-OCT images. Validation testing proved it performed consistently across two independent patient cohorts.2
“AI-based analysis of AS-OCT reduces the burden of performing gonioscopy and allows eye care providers to have the information about angle structure at the time the patient is dilated and ready for the ophthalmic examination,” Dr Xu said.
Discussing the application of AI for teleglaucoma screening, Dr Xu described a program that aims to help standardise glaucoma referrals and optimise resource use.
“We know a lot of patients who are referred through screening programmes as glaucoma suspects are not found to have glaucoma. In fact, we recently documented this inefficiency in a study where we found that only 8% of adults aged 18 to 40 years referred for glaucoma evaluation were diagnosed with glaucoma within a two-year period.3 Furthermore, using a very simple risk stratification method, we identified that more than half of the patients had less than a 5% risk for glaucoma based on age and cup-to-disc ratio.”
Now, through ATLAS (AI + Teleophthalmology in Los AngeleS), an initiative involving collaboration between Dr Xu, researchers from other departments at USC, and the Los Angeles County Department of Health Services, a deep learning algorithm will be used for automated screening of teleretinal fundus photographs to identify patients with referable glaucoma (i.e., those with a cup-to-disc ratio greater than or equal to 0.6).
“Human evaluation of cup-to-disc ratio is highly subjective. This makes it poorly suited for standardising referral and leads to over- and underdetection of at-risk patients,” he said. “Inserting AI into the task of cup-to-disc ratio analysis is a prime example of how AI can improve care.”
The deep learning algorithm was trained using approximately 13,000 images from patients with referable glaucoma and those without glaucoma. Then, its performance was validated by demonstrating its accuracy and reproducibility of detecting referable glaucoma, determining whether it matched or exceeded grades from a panel of 13 clinicians.
“Since our plan is to implement this algorithm into our clinical workflow, we need to have high-level evidence comparing its performance against the current standard of care, which is human grading,” Dr Xu said.
Drs Chang and Xu spoke on this topic at the 2025 ASCRS Glaucoma Day in Los Angeles.
For citation notes, see page 40.
Robert T Chang MD is Associate Professor of Ophthalmology and Glaucoma Fellowship Codirector, Byers Eye Institute, Stanford University School of Medicine, Palo Alto, California, US. viroptic@gmail.com
Benjamin Y Xu MD, PhD is Associate Professor of Ophthalmology and Chief of the Glaucoma Service, Keck School of Medicine of USC, Los Angeles, California, US. benjamix@usc.edu
Apply for the New Sustainability Research Award!
Ophthalmologists and researchers (MD and/or PhD) as well as experienced ophthalmic nurses are encouraged to apply for the new ESCRS Sustainability Research (SURE) Award, which will fund projects that investigate meaningful, practical ways to promote environmental responsibility in ophthalmic care.
Two awards will be granted; each award will provide up to €10,000 per project. Applicants must be active ESCRS members at the time of application and must hold a current full- or part-time clinical or research position at a clinical or academic institution. Early-career researchers and young ophthalmologists are especially encouraged to apply.
The application period opens 28 July and closes 01 November. Award recipients must submit an article to a peer-reviewed journal within six months after the research period concludes. The article should be made open access if accepted and submitted to the Journal of Cataract & Refractive Surgery in the first instance.
Get funding for projects to promote environmental responsibility in ophthalmic care.
Novel Strategy for Lowering Nocturnal IOP
Wearable device creates localized decrease in atmospheric pressure over the eye.
CHERYL GUTTMAN KRADER REPORTS
Apressurized goggle system for reducing IOP during night-time wear addresses unmet needs in glaucoma for lowering nocturnal IOP elevations and managing patients whose IOP is no more than 21 mmHg, according to Leon W Herndon Jr MD.
The device (FSYX Ocular Pressure Adjusting Pump [OPAP], Balance Ophthalmics) received approval from the US Food and Drug Administration in June 2024 for use in patients with normal-tension glaucoma (NTG) or open-angle glaucoma (OAG) whose IOP levels are no greater than 21 mmHg. It is expected to become commercially available in the US in the second quarter or early third quarter of 2026.
This novel technology represents a bilateral, non-invasive, non-surgical, non-pharmacological approach to lowering IOP, intended to serve as an adjunct to other therapies. Based on physics principles, the device uses a programmable vacuum pump to apply negative pressure, thereby reducing atmospheric pressure over the anterior eye.
“Atmospheric pressure pressurizes the entire body, and lowering the pressure only over the eye [decreases] the pressure inside the eye relative to the rest of the body,” Dr Herndon explained.“IOP is reduced by about 50% of the applied negative pressure. The device can be set to achieve a specific target IOP reduction, and clinicians receive data on negative pressure levels and patient compliance with device use.”
Dr Herndon discussed results from two multicentre controlled clinical trials investigating the safety and efficacy of the OPAP system. APOLLO was a three-month study of 64 patients who had one eye (study eye) randomized to receive negative pressure application.1 The fellow eye served as a control. Eligible patients had primary OAG, NTG, ocular hypertension, or were glaucoma suspects with a baseline IOP of 13 mmHg to 32 mmHg.
The results for the study eyes showed IOP reduced in all eyes and by more than 20% in approximately 90% of eyes. Mean IOP decreased by an average of 34% from 19.4 mmHg to 12.9 mmHg. HERCULES was a one-year, contralateral eye-controlled study enrolling 91 patients with NTG and an IOP less than or equal to 21 mmHg. Patients remained on existing therapy. The primary endpoint analyzed IOP measured overnight while patients slept in a sleep lab. The results showed that 98% of eyes exposed to the negative pressure met the primary endpoint, achieving greater than 20% IOP reduction. Mean IOP measured in the sleep lab decreased by 39% from 20.2 mmHg to 12.2 mmHg.
Temporary lid oedema, occurring in 17% to 20% of eyes exposed to negative pressure, was the most common side effect
in both studies. Data from HERCULES showed compliance with OPAP use declined somewhat over time but remained good throughout the one-year study, Dr Herndon said.
“Overall, patients wore the goggles on an average of 5.6 days per week for an average nightly wear time of 5.8 hours. The percentage of nights with OPAP use was about 86% during the first three months of the study and declined to about 79% during the last three months,” he reported.
Dr Herndon spoke at the 2025 ASCRS Glaucoma Day in Los Angeles.
For citation notes, see page 40.
Leon W Herndon Jr MD is Professor of Ophthalmology and Chief of the Glaucoma Division at Duke University School of Medicine, Durham, North Carolina, US. leon.herndon@duke.edu
AI Scribing and Telephone Management
Automating note-taking and call centres could boost practice efficiency.
HOWARD LARKIN REPORTS
The days of ‘press one for scheduling, press two for billing’ are over.” Or soon may be, according to an AI avatar created by Robert T Chang MD.
Using technology already available, phone menus could be replaced by generative AI call agents—human-sounding programs that respond appropriately and in context to natural language questions, giving better service to callers while reducing staffing needs.
“They do what is needed, like making an appointment, scheduling a refill, whatever,” Dr Chang said. Agents can be programmed with different personas, languages, and behaviours, such as casual, formal, or direct. General guidelines, such as coding the agent as a receptionist for a physician’s office, can be established. Also included are detailed workflows, such as which questions to ask in response to specific scenarios and prompts and when to alert a nurse or other provider.
AI is kind of a superpower. There are some things you can do with the click of a button that could take hours to do without AI.
an AI program. It prepares the clinical summary and notifies the physician for review. Once approved, the scribe sends the records and orders on their way. The whole process takes about 30 seconds, he said.
The system can also translate questions and answers into several languages in real time, Dr Chang noted. Templates can be customised to write notes in whatever format individual physicians prefer. The systems can handle a great deal of detail, which subspecialists such as neuro-ophthalmologists love, he said.
Some systems also automatically generate patient instruction notes written at a young adolescent reading level, which a clinician can review and edit if needed. “They’re getting better all the time,” Dr Chang added.
“You can see where we’re going here, with the variability of language, patient instructions, foreign languages—how can you make that visit better, faster, with fewer call-backs, better instructions? It’s AI,” he said. “AI is going to be doing a lot of those tasks for us.”
Dr Chang spoke in an AI Symposium at the 2025 ASCRS annual meeting in Los Angeles.
“You can program your agent to do whatever you want, whether [describing] premium lenses when you are scheduling cataract surgery or immediately directing you to a nurse if you have new flashes or floaters—all this is going to be worked into the AI,” Dr Chang said.
Speaking the patient’s language
And taking over the phones is just one way generative AI agents can improve practice efficiency, Dr Chang said. “AI is kind of a superpower. There are some things you can do with the click of a button that could take hours to do without AI.”
Virtual scribing is another example. Software already exists capable of handling many tasks that currently draw physicians’ time and attention away from patients, simply by listening to the doctor–patient conversation. These include creating summary notes, suggesting diagnosis and procedure codes, pre-charting test orders and prescription refills, creating after-visit summaries, and pre-writing answers to patient messages.
In Dr Chang’s clinic, the virtual scribe looks like a cell phone. It connects to the practice’s medical records system via
Robert T Chang MD is associate professor of ophthalmology at Stanford University, Stanford, California, US. viroptic@gmail.com
Generating AI’s Potential
How generative AI impacts medicine, society, and the environment.
In healthcare—and more precisely, in the field of ophthalmology—the use of generative AI may bring some important benefits to everyday clinical practice. However, there is a flip side to consider. A panel of key opinion leaders in ophthalmology discussed its many aspects from the perspective of efficiency and effectiveness, as well as ethical and legal concerns.
“What we have to keep in mind is what is the data we train the system with,” Nino Hirnschall MD, PhD said. “It must be the absolute truth, or we will face some problems in the future.”
According to Dr Hirnschall, as human beings suffer the cognitive bias of the Dunning–Kruger effect, so too does AI. As a black box, he observed, it is very difficult to trace the way it processes information, and the technology always considers its output as the absolute truth, despite its sensitivity to limitations such as culture, language, and computational mistakes.
“If you talk to clinicians, they will tell you that patients would never find AI replacing their doctor as a positive thing. However, large language models are shown to increase patient satisfaction—with a better bedside manner than the average doctor,” Sorcha Ní Dhubhghaill MBBCh, PhD observed.
“The real problem of AI in healthcare is sycophancy, because these programs are built to please the human user,” she added, considering the scenario where a patient might be more likely to seek a truth that pleases them rather than one that might consider the harsh reality of a diagnosis and treatment.
However, as underlined by Ernest Lim MBBS, PhD, there are some applications of generative AI in healthcare that might increase efficiency without the risk of sycophancy or mistakes. After four years of research, Dr Lim created a conversational AI assistant for the sole purpose of automating preoperative checks and collecting patient surgical outcomes, and he plans to expand it on generative AI, with a pinch of caution.
TIMOTHY NORRIS REPORTS
“There is a lot of amazing potential, but there’s a lot that can go wrong,” Dr Lim admitted.
While considering ethics and legality, Mor Dickman MD, PhD observed generative AI represents a constant breach of intellectual propriety and copyright, something that demands serious attention.
“AI principles are directly in [opposition to] the principles of data protection expressed in the GDPR, in complete violation of many basic human rights,” he stressed.
Such an oversight, according to Dr Dickman, will soon be tackled by the European Union AI Act, which will provide a single, harmonious system for European use that will directly impact the world of ophthalmology.
However, such a standpoint from the EU already dramatically differs from some of the ways of thinking expressed in other countries. As Bruce Allan MD observed, the cautionary angle of the EU stands in stark contrast to the more disruptive position of the US and its stakeholders.
It must be the absolute truth, or we will face some problems in the future.
So, what is AI for? Dr Ní Dhubhghaill asked. Agentic AI programs make preliminary medical decisions now considered an effortless way to cut personnel costs, demonstrating the technology’s social complexities. Still, Dr Hirnschall said the power of a tool providing helpful indications to the physician is undeniable. Nic Reus MD, PhD, noted that some programs are already capable of making very precise diagnoses, such as spotting signs and symptoms of diabetic retinopathy previously undetectable by the human eye, and this may represent a real opportunity to improve health in patients.
AI technology, however, comes at a great cost. According to Dr Ní Dhubhghaill, the consumption from data centres
in Ireland jumped from 5% of the overall national energy consumption in 2015 up to 21% in 2023. As she observed, the energy consumed to create an image in DALL-E mini, the least advanced generative AI, would charge a cell phone for a day. A video generated with AI consumes the energy equal to more than half a million views of a single episode of Friends on Netflix.
“The data consumption is enormous, and we must think very carefully about the environmental cost of this technology. Who is really paying for this?” she asked.
Dr Allan said only the future will tell. “Hopefully, we are not spiralling downwards. I am cautiously hoping for more efficient and less power-hungry models, for a golden period within a data revolution that will make our lives as doctors better,” he concluded.
The presenters spoke during the Generative AI in Ophthalmology TOGA Session at the 2025 ESCRS Winter Meeting in Athens.
Bruce Allan MD, FRCS is consultant ophthalmic surgeon at Moorfields Eye Hospital and Professor of Anterior Segment and Refractive Surgery at University College London, UK. bruce.allan@ucl.ac.uk
Nino Hirnschall MD, PhD (med Physics), MBA, FEBO is senior surgeon at the Kepler University Clinic, Linz, Austria. nino@hirnschall.at
Sorcha Ní Dhubhghaill MBBCh, PhD, MRCSI(Ophth), FEBO, FEBOS-CR, BaO, Dip(stats) is chair and head of the Department of Ophthalmology at University Hospital Brussels, Belgium. nidhubhs@gmail.com
Mor Dickman MD, PhD is Professor of Ophthalmology, University Eye Clinic, Maastricht University, Netherlands. mor.dickman@mumc.nl
Ernest Lim MBBS, BSc(Hons), PhD is an ophthalmic surgeon based in London and Science Director of Ufonia, UK.
Nic J Reus MD, PhD is an independent ophthalmologist at Amphia Hospital, Breda, Netherlands. nreus@amphia.nl
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.
Atropine drops approved for paediatric myopia
The European Commission has granted marketing authorization for Sydnexis’ SYD-101 (Ryjunea), a lowdose atropine ophthalmic solution, as the first pharmaceutical treatment for paediatric myopia progression in EU countries. Ryjunea is indicated for children aged 3 to 14 years and has shown a 30% reduction in annual myopia progression over 2 years in the STAR phase 3 trial. It is recommended for cases where myopia ranges from -0.5 D to -6.0 D with a yearly progression of 0.5 D or more. Santen SA licensed the rights from Sydnexis to commercialize SYD-101 under the brand name Ryjunea in Europe, the Middle East, and Africa. Santen SA is the Switzerland-based affiliate of Santen Pharmaceutical Co. of Japan. sydnexis.com; santen.com
FDA accepts NDA for miotic presbyopia combo
Tenpoint Therapeutics has announced the US Food and Drug Administration (FDA) has accepted the New Drug Application for BRIMOCHOL™ PF, intended for the treatment of presbyopia. This proprietary eye drop formulation combines two miotic agents, carbachol and brimonidine tartrate, which aim to enhance depth of focus through a ‘pinhole effect.’ The Phase 3 clinical trials are nearing completion, with a Prescription Drug User Fee Act (PDUFA) date scheduled for 28 January 2026. The FDA has indicated it does not intend to convene an advisory committee meeting regarding this application. tenpointtherapeutics.com
Nerve-stimulating drops approved for dry eye
The US FDA has approved TRYPTYR® (acoltremon ophthalmic solution, 0.003%, Alcon), formerly known as AR15512, for the treatment of signs and symptoms of dry eye disease (DED). TRYPTYR is a first-in-class TRPM8 receptor agonist (neuromodulator) that stimulates corneal sensory nerves to increase natural tear production. alcon.com
IND application for non-atropine paediatric myopia treatment
iVeena has filed an Investigational New Drug (IND) application with the US FDA for IVMED-85, a non-atropine daily eye drop for paediatric myopia. IVMED-85 aims to tackle myopia by boosting scleral and corneal collagen cross-linking through lysyl oxidase (LOX) activation, flattening the cornea, stiffening the sclera, and reducing axial elongation. Pending approval, multinational clinical trials are set to begin in 2025. iveenamed.com
CE mark for deepeye AI
deepeye Medical announces that its AI platform, deepeye® TPS¹ (Therapy Planning Support), has received a CE mark (Class IIa) under the EU Medical Device Regulation (MDR 2017/745). Certified by Kiwa Assurance, deepeye TPS1 aids in managing retinal disease and was trained on thousands of cases from more than 200 retina centres. Clinically validated with Novartis, Bayer, and Roche, physicians can access it via the Heidelberg HEYEX2 AppWay, with future integrations for Topcon Harmony, ZEISS FORUM, and other OCT platforms. deepeye-medical.com
UPDATED STEP KERATOCONUS GRADING SYSTEM FOR SS-OCT
An updated STEP system optimised for swept-source OCT (SS-OCT) aligns well with the Pentacam-based ABCD system for diagnosing and staging keratoconus (KC), according to a retrospective case-control study. Researchers used rotating Scheimpflug tomography (RSC, Pentacam) and SS-OCT (ANTERION) to examine 152 normal and 314 KC eyes from a German cohort. They compared the OCT-generated STEP system with the RSC-based ABC grading system. Using data from a Chinese cohort of 236 normal and 331 KC eyes, they assessed inter-device agreement between SS-OCT and spectral-domain OCT (SD-OCT). The study found consistent agreement between the two grading systems for the thinnest corneal thickness (TCT) among normal patients but only 30% agreement among those with keratoconus due to discrepancies between SS-OCT and SDOCT measurements. However, there were no differences between SS-OCT and RSC in measuring TCT. External validation of the updated STEP system in SS-OCT showed excellent agreement with RSC thinnest corneal pachymetry (98.61%) and high staging agreement (80.87%) in patients with keratoconus.
N-Ji Lu. “New keratoconus grading system based on OCT: threshold adjustment for SS-OCT,” 51(6): 511–519.
ENHANCED MONOFOCAL COMPARISON
The new Vivinex Impress XY1-E enhanced monofocal IOL demonstrated significantly better intermediate visual acuity and higher spectacle independence rates compared with conventional monofocal IOLs. It also showed comparable or slightly superior intermediate visual acuity and higher patient satisfaction compared to the other enhanced monofocal IOL, according to the findings of a retrospective study. The study included 130 eyes of 75 patients: 46 eyes of 27 patients implanted with the Vivinex Impress, 47 eyes of 26 patients implanted with the Eyhance IOL, and 37 eyes of 22 patients implanted with the Vivinex monofocal IOL. Corrected distance visual acuity (CDVA) was comparable across all three groups. Both enhanced monofocal IOLs demonstrated significantly superior distance-corrected intermediate visual acuity (DCIVA) and spectacle independence compared to the conventional monofocal IOL. In a direct comparison between the two enhanced monofocal IOLs, eyes with the Vivinex Impress exhibited a significantly better defocus curve at -1.5 D and higher subjective satisfaction for ‘reading a newspaper’ than those with the Eyhance.
R Kabura, et al. “Comparative evaluation of clinical results and patient-reported outcomes of enhanced monofocal and conventional monofocal intraocular lenses,” 51(6): 520–524.
ESCRS IOL POWER CALCULATOR MORE ACCURATE
A new study found the ESCRS calculator outperforms older biometric formulas. In 337 patients with monofocal IOL implants, researchers compared traditional formulas (Barrett Universal II [BUII], Haigis, SRK/T, and Hoffer Q) with modern formulas in the ESCRS calculator (BUII, Cooke K6, EVO, Hill-RBF, Hoffer QST, Kane, and Pearl-DGS). The best-performing formulas were Kane, EVO, and BUII. While the ESCRS formulas had a slightly lower mean absolute error (MAE), it was not significant. However, there was a notable difference between Hoffer QST and all other formulas. Excluding Hoffer QST, significant differences emerged between ESCRS and biometry formulas.
L Pomberger, et al. “Clinical feasibility of the ESCRS IOL power calculator,” 51(6): 504–510.
ESCRS Patient Portal
Patients are understandably curious to learn as much as they can about their upcoming cataract or refractive surgery. ESCRS has developed a Patient Portal on its website to help inform patients about these surgeries.
The Portal is split into two sections: Cataract and Refractive. Each section provides an easy-to-understand summary of the different types of conditions, including the benefits, risks, procedures, and aftercare of common conditions. Each section is easily navigable, with clear diagrams and a glossary to convey all the information patients might need to help prepare for surgery or during aftercare.
Cited in this Issue
Nutrition and the Eye: Recipe for Success
Page 8
1. Niu H, et al. Food & Medicine Homology, 2024 Sept; 1(1).
2. Li J, et al. “Health benefits of docosahexaenoic acid and its bioavailability: A review,” Food Sci Nutr, 2021 Jul 23; 9(9): 5229–5243.
4. Chew E, et al. “Lutein + Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration,” JAMA, 2013; 309(19): 2005–2015.
5. Wang W-X, et al. “Efficacy of Omega-3 Intake in Managing Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Control Trials,” J Clin Med, 2023 Nov 10; 12(22): 7026.
6. Bhargava R, et al. “Omega-3 fatty acid supplements for dry eye—Are they effective or ineffective?” Indian Journal of Ophthalmology, 2023 Apr; 71(4): 1619–1625.
7. Walter K. “What Is Dry Eye Disease?” JAMA, 2022; 328: 84. doi:https://jamanetwork.com/journals/jama/ fullarticle/2793824
Accurately Aligning Toric IOLs
Page 15
1. Koch D, et al. “Accuracy of toric intraocular lens axis alignment using a 3-dimensional computer-guided visualization system,” J Cataract Refract Surg, 2016; 42: 550–555.
2. Al-Mohtaseb Z, et al., “Toric Monofocal Intraocular Lenses for the Correction of Astigmatism during Cataract Surgery,” Ophthalmology, 2024; 131: 383–392.
Extending Depth of Satisfaction
Page 16
1. Wanten JC, et al. “Dissatisfaction after implantation of EDOF intraocular lenses,” J Cataract Refract Surg, 2025 May; 51(5): 399–405.
2. Hardin JS, et al. “Cataract Surgery Outcomes in Eyes with Primary Epiretinal Membrane,” JAMA Ophthalmol, 2018; 136(2): 148–154.
3. Urcola JA, et al. “Evaluation of visual outcomes after implantation of an extended depth-of-focus intraocular lens in patients with mild glaucoma,” presented at the European Society of Cataract and Refractive Surgeons Annual Meeting, 6–10 Sept 2024, Barcelona, Spain.
4. Sararols L. “A prospective study of the bilateral implantation of an extended depth-of-focus intraocular lens in patients undergoing phacoemulsification in one eye and phacovitrectomy for epiretinal membrane in the fellow eye,” presented at the European Society of Cataract and Refractive Surgeons Annual Meeting, 6–10 Sept 2024, Barcelona, Spain.
Conventional Versus Laser-Assisted Cataract Surgery
Page 18
1. Narayan A, Evans JR, O’Brart D, et al. “Laserassisted cataract surgery versus standard ultrasound phacoemulsification cataract surgery,” Cochrane Database Syst Rev, 2023; 6(6): CD010735.
2. Song X, Li L, Zhang X, Ma J. “Comparing the efficacy and safety between femtosecond laser-assisted cataract surgery and conventional phacoemulsification cataract surgery: systematic review and meta-analysis,” Can J Ophthalmol, 2025; 60(1): e1–e10.
3. Ginel J, Rodríguez-Vallejo M, Piñero D, et al. “Costeffectiveness of low-astigmatism correction with toric or spherical intraocular lenses combined with corneal incisions: an economic evaluation,” J Cataract Refract Surg, 2024; 50(10): 1012–1019.
1. Lee JH, Yoo K, Lung K, Apolo G, Toy B, Sanvicente C, Xu B. “Patterns and disparities in recorded gonioscopy during initial glaucoma evaluations in the United States,” Am J Ophthalmol, 2024; 264: 90–98.
2. Randhawa J, Chiang M, Porporato N, et al. “Generalisability and performance of an OCT-based deep learning classifier for community-based and hospital-based detection of gonioscopic angle closure,” Br J Ophthalmol, 2023; 107(4): 511–517.
3. Frediani T, Yoo K, Cho A, et al. “Outcomes of glaucoma referrals in adults aged 18 to 40 years,” JAMA Netw Open, 2025; 8(2): e2457843.
4. Nguyen V, Iyengar S, Rasheed H, et al. “Comparison of deep learning and clinician performance for detecting referable glaucoma from fundus photographs in a safety net population,” Ophthalmol Sci, 2025; 5(4): 100751.
Novel Strategy for Lowering Nocturnal IOP
Page 34
1. Ferguson TJ, et al. “Application of Negative Pressure by the Ocular Pressure Adjusting Pump to Provide a Sustained Reduction in IOP,” Clin Ophthalmol, 2024 Nov 6; 18: 3171–3178.
2. Ferguson TJ, et al. “Negative Pressure Application by the Ocular Pressure Adjusting Pump to Lower Intraocular Pressure in Normal-Tension Glaucoma: HERCULES Study,” Am J Ophthalmol, 2025 Mar 25; 275: 121–134.
Upcoming Events
September 4–7
EURETINA
Paris, France
September 12–16
2025 ESCRS Congress Copenhagen, Denmark
September 12
ESCRS iNovation Day Copenhagen, Denmark
September 25–28
German Ophthalmology Society Berlin, Germany
October 18–20
American Academy of Ophthalmology
Orlando, Florida, US
4 Sept
12 Sept 25 Sept
18 Oct
1-4
THE ONLY TRULY MICROINVASIVE GLAUCOMA TECHNOLOGY RAPIDRECOVERY
• Myopic shift
• Cyclodialysis
• Hypotony
• Significant hyphema ZERO
• Stent dislocation
SAFETY1,2
IMPROVES OCULAR SURFACE HEALTH6,9
OVERALL SAFETY PROFILE SIMILAR TO CATARACT SURGERY ALONE3 REDUCTION IN PATIENTS WITH SEVERE OSD SYMPTOMS5 72%
SIGNIFICANT IMPROVEMENTS IN VISION-RELATED QUALITY OF LIFE5
1. 7-Year Efficacy and Safety of iStent inject® Trabecular Micro-Bypass in Combined and Standalone Usage. Fritz H. Hengerer . Gerd U. Auffarth . Ina Conrad-Hengerer. 2. Ten-Year Effectiveness and Safety of Trabecular Micro-Bypass Stent Implantation with Cataract Surgery in Patients with Glaucoma or Ocular Hypertension. Tobias H. Neuhann, Raphael T. Neuhann, Dana M. Hornbeak. 3. Samuelson, Thomas W., et al. “Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results.” Ophthalmology 126.6 (2019): 811-821. 4. Rodriguez-Una, Ignacio, Augusto Azuara-Blanco, and Anthony J. King. “Survey of glaucoma surgical preferences and post-operative care in the United Kingdom.” Clinical & Experimental Ophthalmology 45.3 (2017): 232-240. 5. Samuelson, Thomas W., et al. “Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial.” American Journal of Ophthalmology 229 (2021): 220-229. 6. Schweitzer, Justin A., et al. “Prospective interventional cohort study of ocular surface disease changes in eyes after trabecular micro-bypass stent (s) implantation (iStent or iStent inject) with phacoemulsification.” Ophthalmology and Therapy 9 (2020): 941-953. 7. Jones, Lee, et al. “Impact of minimally invasive glaucoma surgery on the ocular surface and quality of life in patients with glaucoma.” Therapeutic Advances in Ophthalmology 15 (2023): 25158414231152765. 8. Ioannidis, Alexandros S., et al. “Refractive outcomes after trabecular micro-bypass stents (iStent inject®) with cataract extraction in open-angle glaucoma.” Clinical Ophthalmology (2020): 517-524. 9- Biela, Katarzyna, et al. “Dry eye disease as a cause of refractive errors after cataract surgery–A systematic review.” Clinical Ophthalmology (2023): 1629-1638.
iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATIONS FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body.