ALSO IN THIS ISSUE
Still a Place for Postoperative Drops?
Experts debate the pros and cons of best ways to prevent endophthalmitis.

ALSO IN THIS ISSUE
Still a Place for Postoperative Drops?
Experts debate the pros and cons of best ways to prevent endophthalmitis.
Multiple benefits include better training and surgical outcomes.
Detecting Subclinical Keratoconus
Motion-tracking Brillouin microscopy could solve this perennial challenge.
Keeping Track of Refractive Surgery Results
Free software tools to graph and compare in standardised format.


Leadership, Business & Innovation


27–29 June
Zurich, Switzerland
Want a better handle on the financial operations of your department or clinical practice? Wondering how to evaluate AI tools and incorporate them into your daily work?
Join Hilary Hough, Vanessa Foser, and the ESCRS Leadership, Business & Innovation (LBI) team for a Practice Management Weekend Workshop in Zurich on 27–29 June!
In this workshop, ESCRS will be partnering with the Trinity College (Dublin) Business School Executive Education programme. Trinity College offers one of the top-ranked MBA programmes in Europe and will be delivering business and practice management courses and workshops that are geared specifically for ESCRS members. In addition, it means Weekend Workshop attendees will earn continuing education credits for their participation.
Led by Trinity Adjunct Professor Hilary Hough, this session is based on Trinity’s workshop on Finance for Healthcare Professionals. Prof Hough is a certified accountant and chartered director with a wide range of corporate finance, accounting, and general management experience. He lectures in the full-time and executive Trinity MBA courses and a range of other executive education programmes.
Gain an understanding of fundamental financial principles.
Develop the skills to analyse and interpret key financial statements, including balance sheets, income statements, and cash flow statements.
Learn to create, manage, and optimise budgets to ensure the efficient use of resources within your department/ clinical practice.
Apply financial knowledge to improve operational efficiency, streamline processes, and achieve better patient outcomes.
Engage in peer-to-peer learning to share insights, best practices, and innovative financial solutions.
Join AI Business School Co-Founder/Chief Commercial Officer Vanessa Foser as she cuts through all the noise and hype about AI and focuses on what ophthalmologists need to know about using AI in clinical practice. Based in Zurich, the AI Business School supports organisations in their digital transformation. Ms Foser and her team are leaders in making workforces literate in (Generative) AI and its everyday use/application. In addition, members of the LBI Committee will share the AI tools they currently use in daily practice/daily life to improve efficiency and effectiveness.
Gain a better understanding of what exactly AI means.
Learn how to evaluate if an AI tool is valuable to incorporate into use.
Understand how to begin implementing AI into your clinical practice.
Attendance is limited to 30
Register for the workshop and save 50% on ESCRS Congress registration! Plus: ESCRS members enjoy an extra 15% off the LBI Workshop!
Anders
Bonnie An Henderson MD
Avi Wallerstein MD, FRCSC; Mathieu Gauvin B Eng, PhD; and Michael Mimouni MD
J Bradley Randleman MD
Eric D Donnenfeld MD
Knowing Iris Repair: Modified Trifold Technique Soosan Jacob MS, FRCS, DNB
Improving Clinical Management for nAMD and DME
Anat Loewenstein MD, MHA
Defining AMD Treatment Protocol
Luis Arias Barquet MD, PhD





























Publisher
Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy











Graphic Designer
Jennifer Lacey
Circulation Manager




Lucy Matthews
Contributing Editors

Cheryl Guttman Krader
Howard Larkin
Roibeárd O’hÉineacháin
Contributors
Laura Gaspari
Soosan Jacob

Timothy Norris
Andrew Sweeney
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983










ESCRS chose a location steeped in history for its 2025 Winter Meeting, but the more than 1,900 ophthalmologists, trainees, exhibitors, and others who filled the Megaron Conference Centre in Athens were mostly interested in looking ahead to the future and engaging in new experiences.
The Winter Meeting programme included several events that have debuted in recent years, such as speed mentoring sessions, World Café roundtable discussions, and a medical writing workshop. The Winter Meeting also featured some new events, including a podium presentation skills workshop and several ‘TOGA Sessions,’ which consisted of facilitated discussions among 20–30 people in an open environment.
Education and training opportunities, the traditional backbone of ESCRS meetings, were abundant. Six didactic courses were presented, three pertaining to the cornea, two devoted to cataract surgery, and one about basic visual optics. A near-live surgery programme offered eight sessions on topics including ICL implantation for high astigmatism correction and corneal stromal augmentation with an artificial collagen implant in patients with advanced keratoconus. The ESCRS moving simulator, which has now visited nine countries and helped more than 300 students hone their surgery skills, was on hand at the ESCRS booth and was frequently in use.
For those interested in history, EuroTimes Editor-in-Chief Sean Henahan led a heritage interview with Ioannis Pallikaris, a Greek ophthalmologist who performed the first LASIK procedure on a human eye (in 1990) and also developed Epi-LASIK.
The Winter Meeting closed with a traditional ‘best of the best’ session and a main symposium on handling posterior capsule ruptures when they occur.
Athens is known as the birthplace of Western democracy, a society in which citizens were encouraged to participate directly in shaping daily life. The 2025 ESCRS Winter Meeting drew on this tradition by offering ‘TOGA Sessions’ that placed presenters in intimate settings with small audiences to discuss various topics.
The sessions were scheduled to run 20 minutes apiece, but several lasted longer because the topics generated a lot of back-and-forth conversation. The topics were as follows:
• Conflict, Poverty, and Ophthalmology in South Sudan: Personal Perspectives
• Translating Evidence into Clinical Practice
• Optimising Cataract Surgery: How to Save Carbon—and Cash
• Toward a Unified IOL Classification: Collaboration, Consensus, and Future Directions
• Should Simulator Training be a Must Before Starting Cataract Surgery?
• Are There Differences Between Female and Male Eyes?
• Leadership, Business, and Innovation: Breaking Down the ESCRS Practice
Management Programme
• Generative AI in Ophthalmology
• Advancing Team Excellence in Refractive Surgery Practice
Although the sessions featured a microphone and a screen to display slides, some presenters chose to come down from the stage and sit among the attendees to facilitate interaction. The sessions took place in an open area of the convention centre, allowing attendees who were walking from one room to another to join the discussions for a few minutes before proceeding onward.
“The TOGA Sessions were designed to create an open, dynamic space where participants could actively shape discussions based on their interests,” said ESCRS President Filomena Ribeiro. “By sitting down with the audience rather than standing on a stage, we aimed to foster a more interactive and inclusive dialogue. This format encouraged collaboration, allowed for the exchange of valuable insights, and helped raise awareness of ESCRS initiatives among delegates.”
Increasing the pool of patients eligible for refractive surgery.
LAURA GASPARI REPORTS
Understanding corneal biomechanics and customised cross-linking protocols are crucial to allow more patients to be eligible for corneal refractive surgery and avoid over-and undertreatment, according to Ingemar Gustafsson MD, PhD. As clinical studies demonstrate, corneal biomechanical decompensation and weakness can lead to the formation of ectatic diseases, and this can also happen after corneal refractive surgery as tissue is ablated, leading to a lower biomechanical strength.
Reviewing biomechanical characteristics, ex vivo and in vivo experiments showed a weak central area of the ectatic cornea but a quite normal-looking outside, with few differences in a healthy cornea.1,2 As Dr Gustafsson remarked, if there is a focal problem, it should be addressed focally, and that is the purpose of customised cross-linking—dedicating more irradiance to the central part before gradually decreasing it.
“This has an important biomechanical impact because you have a strong flattening over the cone and an increased curvature outside,” he said. “So, you have a regularisation of the eye—which is good for visual acuity—but also increased survival of keratocytes and nerve regeneration that can be interesting in refractive surgery.”
The ophthalmology literature demonstrated the superiority of customised cross-linking over the standard one in visual outcomes, benefits for the epithelium, and clarity of the cornea in patients with keratoconus.3,4 It can also be considered an additive treatment (Xtra) to refractive surgery because it enhances corneal biomechanics.
Looking at the refractive surgical techniques (PRK, LASIK, and KLEx), there is minimal risk of ectasia, but Dr Gustafsson said this depends on the inclusion criteria considered by the surgeon as well as the factors beyond the known risk factors. A recent longitudinal investigation demonstrated that after 20 years of follow-up, 1.2% patients had keratoconus, and another 2.2% developed it between year 20 and 28.5
“In these cases, we need biomechanical assessment because the disease was already present in the eye, but we cannot see it yet and corneal tomography results [show as] normal,” he remarked.
Additionally, key ectasia risk factors to evaluate are ethnic and geographic differences, age, and hormones, which are difficult to include in an algorithm and are another reason why, according to Dr Gustafsson, the field needs new ways to assess corneal biomechanics objectively.
He further explained Xtra protocols are generally safe, given some reservations with PRK Xtra, which has some risks of haze and reduction in visual acuity, most likely due to the epi-off nature of the protocol. This is not the case in LASIK Xtra and KLEx Xtra, which use epi-on protocols, sometimes with an adapted fluence strategy.
Dr Gustafsson recently published a randomised trial showing that 75% of patients treated with isoosmolar riboflavin and 15% of those treated with hypoosmolar riboflavin had a significant reduction in corneal thickness below the commonly used safety limit of 400 µm.6 “What I suggest is to check the intrastromal thickness, add sterile water when appropriate, or convert to sub400 protocol to reduce the risk of over-cross-linking if an epi-off strategy is used,” he said.
Moreover, additive cross-linking protocols to refractive surgery have been shown to be beneficial in high myopia compared to corneal laser refractive surgery alone. This could be due to a stronger and regularised stroma, which consequently leads to a regularised epithelium—essential for the quality of vision.
Assessing corneal biomechanics and customised cross-linking use would be beneficial in the future, as Dr Gustafsson stressed.
“We know we have myopic times ahead, and there will be a significant increase also in high myopia,” he said. “And the refractive surgery industry is growing. So, these are relevant topics to understand and address in the future.”
Dr Gustafsson spoke at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 24.
Ingemar Gustafsson MD, PhD is senior consultant at the cornea service at Skåne University Hospital and researcher at Lund University, both of Sweden. ingemar. gustafsson@med.lu.se






















































































Cataract surgeons debate the benefits of intracameral cefuroxime prophylaxis.
LAURA GASPARI REPORTS
Is there still a need for topical antibiotic drops after cataract surgery? Anders Behndig MD, PhD and Andrzej Grzybowski MD, PhD debated this question at the 2024 ESCRS Congress in Barcelona.
When using intracameral antibiotics, omitting postoperative eye drops after cataract surgery does not increase the rate of endophthalmitis, Professor Behndig asserted. However, this procedure may have some caveats that can weigh the scales in favour of antibiotic topical treatment options, Prof Grzybowski countered.
“Since we started using intracameral antibiotics in Sweden, our rates of endophthalmitis went down, and it keeps going down,” Prof Behndig observed. “Very few in our country now use postoperative antibiotic eye drops.”
Only 23 cases of suspected endophthalmitis were recorded in 151,000 cataract procedures in 2023, with only 10 cultures positive. According to Prof Behndig, these were most commonly caused by an Enterococci infection that is notably resistant to cefuroxime, used in 64% of intracameral injections.
Limits of cefuroxime
“There are important limitations to cefuroxime,” argued Prof Grzybowski. “This antibiotic is not active not only against Enterococci but also against methicillin-resistant Staphylococcus aureus, Staphylococcus epidermis, and Pseudomonas aeruginosa.”
Citing data from multiple studies, Prof Grzybowski observed different rates of postoperative endophthalmitis, from 0.05% to 0.68%. These variations can be explained by many variables, starting with the patient’s country, ocular surface microbiome, presence of blepharitis and other infections, and especially surgical instrument contamination—all of which he stressed need careful consideration when administering antibiotics intracamerally.
Other considerations include not operating on patients with a background infection and ensuring the provision of appropriate antiseptics and good sterilisation of the surgical instruments. Finally, it is crucial to avoid a leaking surgical wound. A leaking corneal wound, if untreated with topical antibiotics, can increase the risk of endophthalmitis 44-fold, Prof Grzybowski explained.
Topical antibiotics could certainly be used as a complement in selected, complicated cases, Prof Behndig said. However, they represent consumption of a different sort.
“For every 7 million cataract surgeries done each year in Europe, intracameral cefuroxime already prevents 1,400 endophthalmites,” he observed. “How many antibiotic drops do we use? For the same number of surgeries, we require

35,000 kg of levofloxacin eye drops, equal to 175 kgs of the substance alone.” Performing a prospective randomised study to answer this question once and for all would require enormous resources, he added.
According to Prof Grzybowski, there is no clear legal support in both national and international societies—with widely varying positions between countries.
“To prevent postoperative endophthalmitis, the surgeon should consider preoperative irrigation of povidone iodine, with no topical antibiotics. Surely the surgery needs to be uncomplicated, with a sealed wound,” he observed. “If the use of intracameral antibiotics is associated postoperatively with a topical treatment, it is very important to use them in high concentration for a relatively short time; no longer than 5–7 days and certainly with no tapering.”
Profs Behndig and Grzybowski spoke during the Journal of Cataract and Refractive Surgery symposium at the 2024 ESCRS Congress in Barcelona.
Anders Behndig MD, PhD is the co-chair of EUREQUO, former President of the Swedish National Cataract Register and Swedish Ophthalmological Society, and Professor at Umeå University Hospital, Sweden. anders.behndig@umu.se
Andrzej Grzybowski MD, PhD is the past-president of EVER; Professor at the University of Warmia and Mazury, Olsztyn, Poland; and Head of Institute for Research in Ophthalmology, Foundation for Ophthalmology Development, Poznań, Poland.

Helping young surgeons build confidence and expertise.
LAURA GASPARI REPORTS
Simulators are extremely beneficial to young surgeons who want to learn to perform better cataract surgery, according to Alja Črnej MD.
“In an ideal world, every ophthalmological teaching facility would have a simulator, because the patients would benefit from it,” she said.
Approaching cataract surgery as a resident is not easy. Dr Črnej recalled how residents used to prepare for the capsulorhexis procedure by training using tomatoes or foil or spending a lot of their own money to access a wet lab abroad for just one week. Since ophthalmology is a highly surgical specialisation, providing residents access to good training before they start operating on human eyes is particularly important, she emphasised.
Dr Črnej’s experience with simulators started while she was in Boston, and it helped her a lot. “I spent three years doing research and not performing surgery, but I was lucky enough to have a simulator there, so when I returned to Slovenia, my home country, it was no hassle,” she said.
Adding simulators to teaching facilities is mainly beneficial because they are always accessible in the hospital, and the residents can repeat surgical steps until they fully master them, developing such skills gradually. Furthermore, simulators do not need disposables, so there is no need for pig eyes or instruments, and residents can practise their skills without time pressure, stress, or colleagues watching them.
“You can fail as many times as you want from the beginning and you can practise every step of the cataract surgery with the simulator at your own pace,” she said.
And how do simulators benefit the patients as well? Surgeons with simulator practice have been shown to experience reduced complications during surgery. Working with simulators that create the look and feel of real cataract surgery makes them more confident and self-assured of their skills.
Simulators allow trainees to track skills and performance improvement, helping them understand how far they went with their training. Such devices in training programmes could lead to standardisation, setting obligatory surgery step numbers before going to the next training level or entering the OR.
However, this is not an ideal world: simulators are expensive, and not all countries and facilities have them at their disposal, she said. ESCRS has been able to assist by offering a simulator area during its conferences and providing a Moving Simulator that travels all over Europe, which has already supported more than 300 students. The Society also sent the simulator to the Polish border to be at the disposal of Ukrainian surgeons.
“We asked participants for feedback,” Dr Črnej said. “And we got valuable feedback, especially from beginner surgeons. This was their first touch with cataract surgery, and most of them enjoyed it.”
Dr Črnej spoke at the Ophthalmology Foundation Symposium at the 2024 ESCRS Congress in Barcelona.
Alja Črnej MD, FEBO is an anterior surgeon specialist at the Pfeifer Eye Surgery Centre, Ljubljana, Slovenia.
Patient history and diabetes status among many factors to consider.
TIMOTHY NORRIS REPORTS
The association between cataract surgery and DME progression in diabetic patients may worsen outcomes and negatively impact the patient’s quality of life. According to Patricia Udaondo Mirete MD, PhD, knowing how to deal with the patient’s condition with the correct procedure is imperative to decrease the risk of onset and avoid the worsening of pre-existing oedema.
“We have patients with macular oedema who need cataract surgery; we have patients with a cataract and a high risk of developing oedema for the first time, and we must understand what to do in each case,” she said. “Do we have to do prevention if an oedema is already present, or if there is a history of treatment? Do we have to treat it if there are no signs of oedema but only a risk factor?”
Trying to find a precise answer to these questions may not be an easy task. Dr Udaondo pointed out that the literature on the subject is still scarce and far from a solid consensus. Reading the first papers from the 2010s, she noted a wide variation in the risk of progression of diabetic retinopathy in diabetic patients, going from 23% to 57%. However, the association between high glycosylated haemoglobin, the long evolution of the patient’s diabetes, and retinopathy is strong—despite the degree of the disease. In this way, the release of proinflammatory factors and cytokines in the eye triggered by cataract surgery plays a central role, she observed.
Macular oedema and diabetes can both be considered inflammatory processes, with the former being easily triggered or aggravated by a surgical insult. Diabetes is a multifactorial disease but also a systemic inflammatory disease that predisposes the patient to further inflammation, Dr Udaondo said. So, what is the correct prophylactic treatment for a cataract patient with diabetes?
It is imperative to correctly assess the status and the patient’s anamnesis before cataract surgery. Frequent and thorough examinations of the diabetic patient are needed, especially considering the increasing difficulty of performing a fundus exam in a cataract patient. Duration and control of the disease are very important factors, she emphasised. Topical treatment with either steroids or NSAIDs (or both) is still recommended, but if in doubt, Dr Udaondo suggested considering an additional intravitreal treatment immediately before or after surgery. If a patient is already under intravitreal treatment, there is no reason to change an ongoing regimen if DME is under control. Citing data from the VIVID and VISTA studies, Dr Udaondo showed how, despite a slight increase in macular thickness, BCVA in patients under aflibercept 2 mg anti-VEGF treatment that underwent
cataract surgery improved more than 10 letters, confirming the importance of a strict regimen protocol. Keeping previous treatments active, controlling inflammation, and performing thorough follow-ups are key to preventing postoperative DME, thus ensuring a good outcome, she said.
“Prophylaxis should be performed, and we need careful control one year after cataract surgery to be sure the patient will not develop macular oedema,” she concluded.
Dr Udaondo spoke at the 2024 ESCRS Congress in Barcelona.
Patricia Udaondo Mirete MD, PhD, FEBO is Co-founder and Medical Director of the Aiken Clinic, Valencia, Spain. patricia.udaondo@uv.es

Different strategies, such as PresbyLASIK, can offer presbyopes good outcomes.
LAURA GASPARI REPORTS
PresbyLASIK is a useful option to correct ametropia and presbyopia, and it is important to know every available option, according to Jaime Aramberri MD.
As the most prevalent visual condition in adulthood, presbyopia has been forecast to increase through 2030 before decreasing due to the incorporation of myopia epidemics. “Presbyopia has a significant impact on quality of life, and it is the main reason to seek refractive surgery today,” Dr Aramberri said.
PresbyLASIK applies a multifocal or EDOF profile to the cornea to achieve an increased depth of field. The attractiveness of this technique is its many advantages over multifocal IOLs: it is not an intraocular technique, it has a better safety profile, and it is a quick surgery under topical anaesthesia with a speedy recovery, which preserves the lens for future surgeries, he explained.
The technique offers two main strategies for near vision— the central option, which adds more power in a central area of the cornea, and the peripheral option, where more power is given to a paracentral-mid area of the cornea.
Dr Aramberri suggested the central PresbyLASIK approach seems to be better because there is a synergy with near miosis.
Central corneal higher power, plus its induced spherical aberration, and the small aperture all play in favour of a good near vision. Moreover, he added spherical aberration is natural and easily processed by the brain, there is less tissue ablation, and the surgery is easier to revert.
He observed that an increase in depth of focus of more than 1.5 to 2.0 D impairs visual quality and decreases BCVA. Therefore, focus can only be extended safely up to that limit.
“This is why we have to use micromonovision to add something to the eye—playing more in near—so this addition of refraction, plus the spherical aberration, will achieve a functional near vision,” he said.
Because of pupil dependency, especially the central profiles, understanding pupil dynamics and pupillometry is also essential in the preoperative study to achieve the best results, he added.
There are three popular platforms for PresbyLASIK using micromonovision as a strategy to correct presbyopia with the dominant eye for far and the non-dominant eye for near: PresbyMAX by Schwind, Supracor by Bausch + Lomb, and Presbyond by Zeiss. Even though there are differences in functioning, accuracy, and safety among the platforms, the long-term results show the quality of vision has improved through the years, and patients’ near-vision task performance is comparable to the preoperative situation. Yet, there is a learning curve in the outcomes.
“Results are much better now than they were 10 years ago, and there is some regression of the near effect through time, and this must be explained to the patient,” Dr Aramberri said. “Also, postoperative surveys show a high degree of satisfaction with the outcome.”
Dr Aramberri spoke at the 2024 ESCRS Congress in Barcelona.
Jaime Aramberri MD is ophthalmic surgeon specialised in cataract, refractive, and corneal surgery at Miranza Begitek, Donostia-San Sebastián, Spain, and Miranza Ókular, Vitoria-Gasteiz, Spain. jaimearamberri@telefonica.net

Goldmann may not be the gold standard, especially with PGA drops.
LAURA GASPARI
REPORTS
Goldmann applanation tonometry (GAT) use should not be advised when measuring IOP in patients treated with prostaglandin analogues (PGAs) who have undergone refractive surgery, as it could lead to inaccurate readings, Cynthia J Roberts PhD warned.
It is well known that central corneal thickness can cause measurement errors using Goldmann tonometry; moreover, one Goldmann assumption is ocular rigidity is offset by the tear film surface tension, she explained. A thin cornea requires less force to applanate than a thicker cornea, and that is independent of the IOP. If a high measured pressure is found, it may be that the cornea is thick. Conversely, if there is a low measured pressure, it may be that the cornea is thin. But looking at the IOP after refractive surgery and the differences in measurement, is corneal thickness the only thing affecting measurement accuracy?
“If you look at Goldmann tonometry, there are assumptions regarding curvature and thickness,” Professor Roberts explained. “But also, what has not yet been resolved is the involvement of biomechanical properties.”
In a paper she published in 2005, Prof Roberts demonstrated how there are huge differences in IOP measurement when biomechanical properties (the modulus of elasticity related to corneal stiffness) vary.1 Considering the same corneal thickness and two different stiffnesses, Prof Roberts demonstrated the measurement may vary, as a stiffer cornea has a stronger relationship between thickness and IOP measurement error—while a softer cornea has less impact. This is particularly important in considering PGAs, which

increase uveoscleral outflow and upregulate the expression of matrix metalloproteinases—degrading the extracellular matrix, increasing tissue permeability, and decreasing the resistance to outflow, leading to a decrease in corneal and scleral stiffness which can cause increased IOP measurement errors with applanation tonometry.
Yet refractive surgery is not the same situation as a thin cornea, Prof Roberts emphasised, because there is an ablation profile to consider. The common belief is the IOP measurement, on average, reduces by about two millimetres of mercury after refractive surgery. However, she stressed this is not the most significant insight when there is so much variability in the change of measured IOP with the same thickness reduction.
Prof Roberts does not recommend using GAT because there is no predictability in the IOP measurement error after refractive surgery, and the probe would get lost in the LASIK flap if IOP increased. The intact residual stromal bed would carry all the increased stress. “You might be able to do it with PRK or some kind of surface treatments because you have a uniform stress distribution through what is left there,” she said. Instead, using non-contact tonometry is not subject to the same errors with increased IOP because it inverts the cornea—so does pushing directly against the IOP.
The systematic errors in IOP measurements with applanation tonometry after refractive surgery are not only caused by cornea biomechanical properties but also by the resulting modified pachymetry profile.
Dr Roberts noted there are two alternatives, both using air puffs to indent the cornea: (1) with the corneal compensated IOP from the Ocular Response Analyzer, showing the same measurements before and after refractive surgery, and (2) with a biomechanically corrected IOP from the Corvis ST.
Dr Roberts spoke at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 24.
Cynthia J Roberts PhD is Professor of Ophthalmology and Visual Sciences, Biomedical Engineering, and Martha G and Milton Staub Chair for Research in Ophthalmology, The Ohio State University, US.
Internet, labs, simulators, and assisting surgery all contribute.
LAURA GASPARI REPORTS
There is no real, absolute, and universally accepted number of surgeries to perform that grants surgical proficiency while in ophthalmology training—but practice with wet labs, dry labs, and even new technologies such as simulators or having structured curricula is really useful, according to Bonnie An Henderson MD.
Some countries, like the US or the UK, require a minimum number of performed cataract surgeries during residency training. In any training programme, two things are paramount: skills and safety.
“The steps of proficiency are learning about cataract surgery and observing both experienced surgeons and people who are learning, practising, and finally performing,” she explained.
Learning surgery has become easier because of the internet, where online resources are easily accessible to trainees, no matter the location. Observation and assisting during surgery are also fundamental to the learning process. While residents in many European countries do not perform so many surgeries, they extensively observe other surgeons in the OR.
“I could always tell who is going to be a good surgeon by how they assist, how they anticipate the next step or complication, or which instrument to get ready to hand over. I know that person is already thinking two steps ahead,” Professor Henderson commented.
Practice is where innovative technologies really come into play. Wet labs, dry labs, and artificial eyes help the resident become familiar with the microscope and instruments, work both feet and both hands simultaneously, and repeat the
process to train muscle memory. Simulators allow trainees to repeat the steps of the surgery as many times as they want or learn how to manage complications they may not encounter when operating on real patients during residency training.
Prof Henderson suggested having the residents start with the last stages of the surgery, such as removing the OVD, and gradually having them do the other steps backwards—because if the learner makes mistakes at the very beginning, the whole case will be complicated. She also stressed the importance of making trainees do several surgeries on the same day so they do not forget the steps and what they previously learned.
With this reasoning, it is impossible to determine an exact, standard number of cataract surgeries required for each trainee to become fully proficient and competent, but implementing other strategies could help standardisation.
“I think there could be a minimum number we can really agree on, and it is important to have a structured curriculum,” she concluded. “Also, you really need particularly good supervision and intentional practice, and surgery needs to be performed again and again.”
Prof Henderson spoke at the 2024 ESCRS Congress in Barcelona.
Bonnie An Henderson MD is a Clinical Professor at Tufts University School of Medicine in Boston, US. She is past president of the ASCRS.


mEYEstro: Free software for analysing and graphing refractive surgery outcomes.
HOWARD LARKIN REPORTS
Afew years back, Avi Wallerstein MD and Mathieu Gauvin PhD consistently experienced problems analysing refractive surgery results at a large Canadian centre.
“It was frustrating looking at the published research to compare the outcomes of our surgeons [because] it was hard to find studies respecting the [reporting] standards,” Professor Gauvin said.
These inconsistencies were somewhat surprising given Excel spreadsheets incorporating the standards had been published by Professor Dan Reinstein (and others) years earlier. However, using macro-enabled spreadsheets is cumbersome, requiring manually entering and formatting data, conducting statistical calculations, and setting up charts.
“You are likely to make at least one mistake, and if you want to compare two groups, you have to do it outside Excel,”
Prof Gauvin explained.
Professor Wallerstein teamed up with Prof Gauvin, an experienced programmer, to develop a software package that would simplify the task. The result was mEYEstro. First developed for internal use, mEYEstro was later refined and released in 2023 as a free software download (see QR code) and regularly receives updates. A detailed software description appeared in a 2023 BMC Ophthalmology article.1
Research and outcomes improvement
mEYEstro reports and graphs refractive surgery outcomes in a standardised format required by leading ophthalmology journals, including the Journal of Cataract and Refractive Surgery, the Journal of Refractive Surgery, and Cornea. Its format is recommended by Ophthalmology, among others, and for presentations at scientific meetings. Standardisation simplifies comparisons between clinical studies and enhances reproducibility, Prof Gauvin said.
The program can analyse any kind of refractive surgery, including corneal and lens replacement procedures and
Download the free software
phakic IOLs. It is a freestanding desktop application that runs on Windows 10 or later computers with a MATLAB runtime compiler installed. Data on pre- and postoperative refraction and visual acuity are entered using formatted data files. Outputs are in nine standardised charts covering efficacy, safety, spherical equivalent accuracy, stability, and astigmatism accuracy, including vector analysis. The program performs regression analyses automatically.
While primarily intended for use in outcomes research for publishing and presentations, mEYEstro is also useful for improving outcomes internally by performing A/B comparisons between groups of patients receiving alternative treatments or nomograms.
“If you want to know if it improved outcomes, you get an immediate answer. It has been a huge benefit for the way we perform surgery on our patients,” said Michael Mimouni MD, who also uses it for published research.
“Ever since [mEYEstro] came out, it has been my go-to for analysing refractive surgery outcomes. I used to spend days making these graphs. Now, with the click of a few buttons, it can be done automatically in half an hour to an hour.”
For citation notes, see page 24.
Avi Wallerstein MD, FRCSC is assistant professor of ophthalmology at McGill University and co-founder and co-medical director of LASIK MD and Vision Group, all in Montréal, Canada. awallerstein@lasikmd.com
Mathieu Gauvin B Eng, PhD is associate professor at McGill University and director of research and development at the McGill Refractive Surgery Research Unit and LASIK MD and Vision Group. mgauvin@lasikmd.com
Michael Mimouni MD is associate professor at Technion-Israel Institute of Technology and director of the cornea unit at Rambam Health Care Campus, both in Haifa, Israel. He is chairman of the Israeli Cornea Society. michael@intername.co.il
Brillouin microscopy shows promise in clinical studies.
HOWARD LARKIN REPORTS
In screening laser refractive surgery candidates, distinguishing normal corneas from those with subclinical keratoconus is challenging. Ongoing studies suggest motion-tracking Brillouin microscopy may eventually provide a more reliable method for doing so, says J Bradley Randleman MD. This optical technology takes advantage of Brillouin light scattering, which detects shifts in optical reflections that correspond with biomechanical differences in tissues. It can measure corneal stiffness in three dimensions without making contact. Motion tracking enables measurement at focal points across the entire cornea, Professor Randleman explained.
In Brillouin microscopy, subclinical keratoconus reveals itself as a softer area in the cornea even though the surrounding tissue is similar to normal corneas. This focal softness may not be enough to show up as differences in corneal steepness or thickness on more conventional topographic or tomographic imaging or air-puff tonometry tests. However, over time, the weaker area will likely deform more under strain than the surrounding stiffer tissue, precipitating ectasia.
Prof Randleman and colleagues demonstrated the potential for motion-tracking Brillouin microscopy metrics to distinguish subclinical keratoconus in a study comparing 15

eyes with subclinical keratoconus with 15 normal control eyes. All patients underwent Scheimpflug tomography and motion-tracking Brillouin microscopy using a custom-built device. Metrics for each method—as well as specificity and sensitivity for each variable—were then compared for area under the receiver operating characteristic curves.
For the Scheimpflug metrics, significant differences were found between the two groups for thinnest corneal thickness, inferior-superior values, index of vertical asymmetry, and keratoconus index, but for no other metric. The keratoconus index had the highest area under the curve at 0.91, followed by inferior-superior values at 0.89 and index of vertical asymmetry at 0.88.
By contrast, all motion-tracking Brillouin metrics yielded statistically significant differences and fully differentiated between subclinical keratoconus and normal eyes, with areas under the curve of 1.0 and specificity and sensitivity of 100% for each. These included Brillouin mean and minimum values for the anterior plateau and anterior 150 microns.1
Even individual metrics, such as identifying the softest point on the cornea, reliably distinguished between normal and subclinical keratoconus eyes. “The Brillouin metrics outperformed all the Scheimpflug metrics in this cohort,” Prof Randleman observed.
Moreover, these differences were clearly and consistently visible on two-dimensional Brillouin shift maps. “I would argue it’s fairly easy to tell visually the difference between the normal cornea and the cornea with focal softening, as in the subclinical eyes,” he said.
Prof Randleman and colleagues are conducting further research to develop motion-tracking Brillouin scanning for detecting subclinical keratoconus. Key challenges include increasing the speed of scanning, which takes several minutes with the current device. Nonetheless, the technology shows promise for future clinical use.
Prof Randleman made his comments at Refractive Surgery Day at AAO 2024.
For citation notes, see page 24.
J Bradley Randleman MD is professor of ophthalmology at Case Western Reserve University and co-director of refractive surgery at the Cleveland Clinic, both in Cleveland, Ohio, US, and editor-in-chief of the Journal of Refractive Surgery . randlej@ccf.org
Improving visual acuity in patients with keratoconus.
HOWARD LARKIN REPORTS
Combining corneal cross-linking (CXL) with topography-guided photorefractive keratectomy (TPK) can greatly improve visual acuity in patients with keratoconus, often allowing correction with soft contact lenses or spectacles rather than gas-permeable hard lenses. But how and when to combine them is a matter of some debate, said Eric D Donnenfeld MD.
Combining the two procedures on the same day is the preferred method of A John Kanellopoulos MD, who pioneered the practice now known as the Athens Protocol. But Dr Donnenfeld follows a different approach.
CXL alters the corneal refractive index in sometimes unpredictable ways, Dr Donnenfeld pointed out. So, it is better to see where the cross-linked cornea settles before performing a refractive ablation.
Healing is also an issue, Dr Donnenfeld said. “My experience in cross-linking and laser ablation is when you do them at the same time, you end up having more healing problems—there’s more damage, there’s more risk of scarring. I almost always [perform] cross-linking and then wait three months [before] topographic ablation.”
The severity of corneal irregularities affects what kind of ablation to use, Dr Donnenfeld noted. For mild cases, it may be possible to conduct a wavefront-guided ablation, which has the advantage of considering both the anterior and posterior corneal surfaces.
However, in the majority of more severe cases, it is not possible to get a usable wavefront image, so topographic ablation is extraordinarily helpful.
“This changes lives,” Dr Donnenfeld said. “We’ve prevented hundreds of corneal transplants—we’ve moved people from gas-permeable lenses to soft lenses.”
However, he emphasised topography-guided procedures rely on a successful topographic image capture.
“We are looking for topography where you see a steep area and a flat area, and this has to coincide with the Topolyzer wavefront evaluation.”
The steep area receives a hyperopic ablation treatment and the flat area a myopic treatment.
“I find you can treat up to 10.0 D irregularity pretty regularly,” Dr Donnenfeld said.
Yet stromal thickness can limit tissue ablation. Dr Donnenfeld likes to leave behind at least 350 microns to ensure stability. If the ablation zones are too deep, the optical zone can be shrunk to remove less tissue.

Also, patients must be informed the goal is to achieve emmetropia.
“Never promise the patient they will get rid of glasses,” Dr Donnenfeld said. “You are trying to improve visual acuity, and the results can be very unpredictable.”
However, it’s not always possible to generate a usable topographic image. For example, pellucid marginal degeneration corneas tend not to do well with topographic imaging. If a treatable topographic image cannot be taken, patients do well with intrastromal ring implants followed by cross-linking, he added.
For patients who cannot have topical ablation (usually those with K values exceeding 55), Dr Donnenfeld recommends employing the volcano technique, which involves removing thickened epithelium that can add steepness. Ablating where it is thickest can reduce irregularity by up to 5.0 D. This can be enough to get patients into soft contact lenses. Alternatively, after six months, a topographic ablation may be possible.
“This is anything but cosmetic. This is visually rehabilitating some of the most difficult patients we see in our practices,” Dr Donnenfeld concluded. “While this is a wonderful treatment today, I’m absolutely certain the technology will continue to evolve.”
Dr Donnenfeld made his comments at Refractive Surgery Day at AAO 2024.
For citation notes, see page 24.
Eric D Donnenfeld MD is clinical professor of ophthalmology at New York University, US; trustee of Dartmouth Medical School in Hanover, New Hampshire, US; and in private practice in New York State, US. ericdonnenfeld@gmail.com
Part eight of our series covers the modified trifold technique for large iris defects.
BY SOOSAN JACOB MS, FRCS, DNB
Large iris defects are often seen post injury or secondary to iatrogenic iris trauma. These are challenging to close due to the shortage of iris tissue. The shortage results in excessive opposing vector forces when trying to bring opposite pedicles of the iris in a conventional pupilloplasty technique (Fig A, green arrows), leading either to an inability to suture the pedicles together or sometimes an iris root tear/iridodialysis secondary to the excessive pressure or pull on the iris root. In such cases, two pupilloplasty techniques can be used sequentially to close large iris defects with less tractional force. This article discusses the trifold technique, which is a combination of trocar-assisted iris repair and single-pass, four-throw pupilloplasty (SFT). Dr Agarwal and I described the trifold technique for repairing non-apposable large iris defects, and I modified it further to circularize and centralize the pupil. In the trifold technique, two initial iris repair sutures are used to appose the unapposed iris ends to the sclera (Fig A [red arrows], B). A subsequent SFT seals the now-smaller iris defect (Fig C). In the modified trifold technique, the initial repair is followed by centralizing and circularizing the pupil using a combination of microscissors, vitrector-assisted pupillectomy, and iridodiathermy (Fig D). This combination of an iridodialysis-style repair of the iris pedicles to the sclera, SFT, and pupil circularization is less manipulative and carries fewer complication risks for both the iris diaphragm and the pupil.
Let us understand this technique in greater detail:
Trifold technique
As previously mentioned, ocular trauma, iatrogenic iris damage, and (rarely) iris colobomas can lead to large, nonapposable iris defects. In such clinical scenarios, closing the iris using a series of SFT/other pupilloplasty knots starting from the pupil margin and proceeding towards the iris base is challenging due to abnormal directional vectors. The trifold technique involves three steps: the initial two steps are mainly to reduce the distance between the two disinserted iris pedicles by attaching the ends to the sclera, and the third step is pupil reformation by SFT pupilloplasty.
Under peribulbar anaesthesia, a narrow, partial thickness lamellar scleral incision is initially made in the clock hours of the expected iris reattachment. A Hoffman pocket may also avoid conjunctival dissection. A 25-gauge (G) trocar is introduced from the limbus in the direction diagonally opposite to the required zone of iris insertion. Once in position, a double-armed 9-0 polypropylene suture needle is guided through the trocar to engage the peripheral end of
the disinserted iris. A 30-G needle is then passed through the scleral incision into the anterior chamber (AC) and used to railroad the prolene suture out. The other arm of the suture is passed in the same method through the trocar into the adjacent iris stroma. With both sutures thus externalized, the suture knot is tied down, apposing the iris to the opposite sclera.
The second step repeats the same technique with the iris pedicle on the other side. Both iris pedicles are sutured as close as possible to each other onto the sclera while taking care to avoid excess traction on the opposite attached iris root, reducing the gap in the iris defect. A Snyder hang-back technique may also be similarly used in case of greater tissue shortage. Here, the detached peripheral iris is suspended by a suture from the scleral wall, helping to reduce corectopia while also avoiding inadvertent coverage of the trabecular meshwork by the peripheral iris.
In the third step, the residual vertical defect is closed with SFT pupilloplasty. A single-armed 9-0 or 10-0 polypropylene suture is passed through the proximal iris and docked through a 30-G needle that travelled through the distal iris via paracentesis, rail-
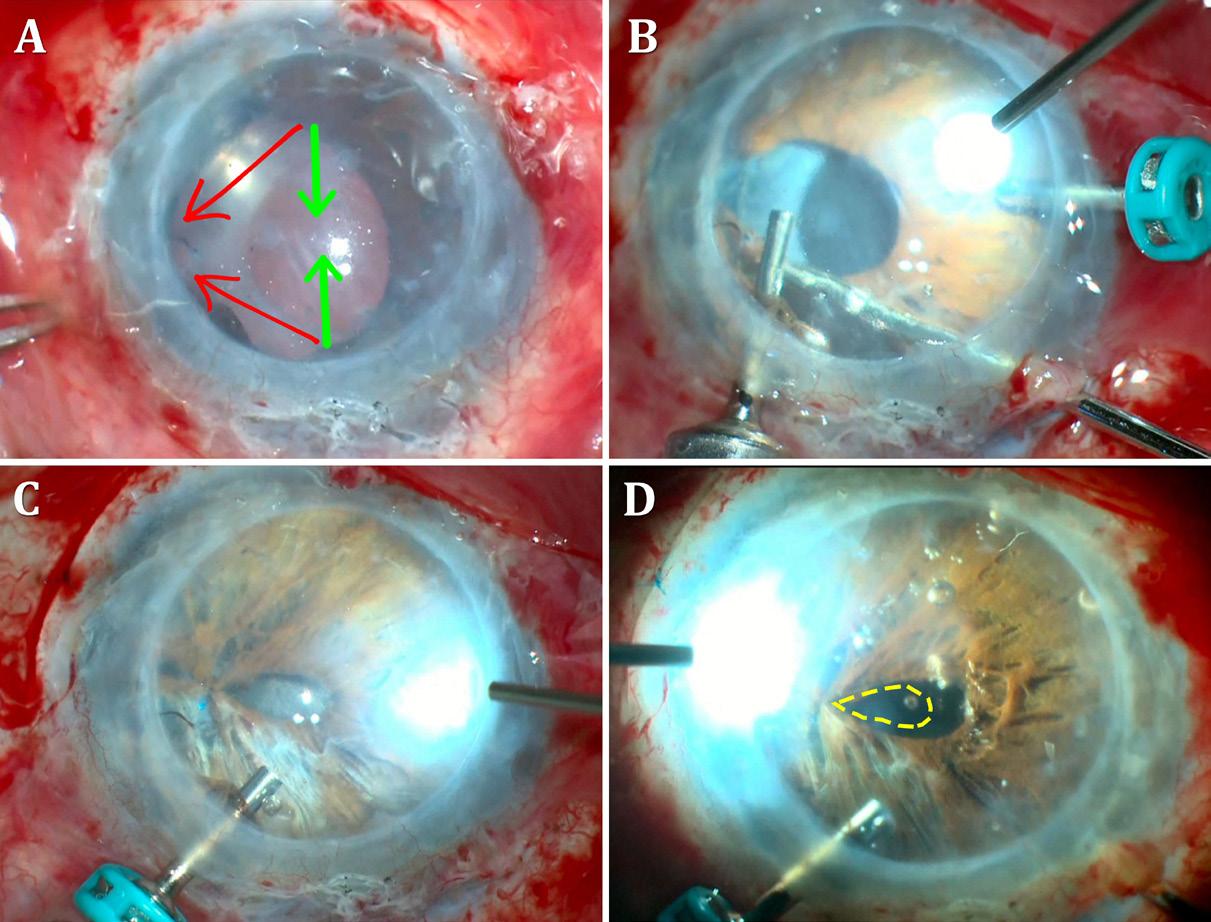
FIGURE: A) Large gap seen in iris. Green arrows show excess vector forces created in direct repair which if performed, can cause iridodialysis. Red arrows show modified direction of repair; B) After trocar-assisted iris repair of both iris pedicles, the gap is seen to decrease; C) SFT closure of the vertical defect; D) Corectopia correction with microscissor, vitrector, and iridodiathermy. The dotted yellow line marks the old pupil location.
roading the suture out. A Sinskey or Kuglen hook is introduced inside the AC through the paracentesis, and the formed suture loop is then pulled out through the paracentesis. The other end of the suture is cut and passed four times through the loop. The two suture ends on either side of the limbus are pulled apart to draw the loop back into the AC and to tighten the knot, bringing the two ends of the iris into apposition. The suture ends are then cut close to the knot using microscissors. Placing a series of such knots can close the vertical defect.
Care should be taken during every manoeuvre to avoid iris root traction and disinsertion. Any hyphaema that occurs can be controlled by washing the blood out and temporarily increasing the AC pressure.
The trocar facilitates passage of the long straight or curved needle of the polypropylene suture smoothly through the paracentesis without engaging corneal stroma at the incision. Accidental engagement of incisional stroma tethers the loop at the incision and prevents it from being pulled in. Therefore, the knot cannot be tied, and the entire needle pass needs redoing. The trocar allows the needles to enter the AC smoothly without engaging the incisional corneal stroma. The use of valved trocars generally does not create a problem. However, the valve may be removed prior to use, if needed.
The trifold technique may result in the pupil displacing towards the scleral attachment. This modification further enhances the functional and cosmetic outcome by circularizing and centralizing the pupil—performed by assessing the pupil position, and if displaced, a microscissor creates a vertical cut on the opposite intact pupillary margin. The vitrector is then used at a low cut rate and a 300 mm Hg vacuum to carefully cut the pupil into a round, centralized shape. The pupil can be further centralized and made more circular with iridodiathermy. An additional SFT may be added just ahead of the previous ones if required.
Good functional and cosmetic outcomes can be obtained using the modified trifold technique for large, non-apposable iris defects. These eyes often have other complex anterior segment
defects, and this technique can be used with others—for example, after glued intraocular lens in eyes with deficient posterior capsule or before endothelial keratoplasty, where stable air tamponade to the graft is imperative intra- and postoperatively to decrease the risk of air migration and graft detachment.
Iris defects can result in glare, photosensitivity, and diplopia. They may also be cosmetically concerning, especially in patients with light-coloured irides, and often need to be sutured or repaired. However, not all iris defects are apposable, and the risk of associated dialysis from the iris root is a barrier at times—especially in large defects of more than 90 degrees where the force and changed vectors caused by pulling the iris to the opposite direction while suturing can lead to further iris tear and damage. Managing this with a single surgical technique may not be possible. Therefore, to overcome this obstacle of intraoperative suturing, multiple procedures are required to change vector forces and manage the magnitude of defect.
The modified trifold technique for repairing large iris defects seems to involve less manipulation and is associated with fewer complications than other iris suturing techniques. It also does not need expensive iris prosthetic devices and can be done anywhere. In my experience, the modified trifold method of combined trocar-assisted iris repair with SFT and corectopia correction in large iris defects has shown satisfactory outcomes in large non-apposable iris defects. The modified trifold technique is a valuable method for iris diaphragm and pupil reformation. Alternative non-suturing methods for managing iris or pupil defects include coloured contact lenses, corneal tattooing, iris prosthesis, aniridia rings, aniridia IOLs, and iris prosthetic devices—which may have their own benefits and limitations.
This is the eighth article in a series on iris repair. Please see past issues of EuroTimes for related columns.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.


CHERYL GUTTMAN KRADER REPORTS
Findings from global surveys conducted to understand the challenges associated with neovascular age-related macular degeneration (nAMD), diabetic retinopathy (DR), and diabetic macular oedema (DME) management will provide a roadmap to practical policy and clinical practice solutions that could improve care delivery, treatment adherence, and patient outcomes, said Anat Loewenstein MD.
The research, conducted as an initiative of the Barometer Program, analysed surveys completed by more than 8,300 patients, 650 physicians, and 1,200 clinic staff from 78 clinics in 24 countries across 6 continents.1,2
Overall, the findings reinforced that patients needing antiVEGF therapy for their retinal disease experience considerable burdens relating to treatment frequency, long wait times in the clinic, travel difficulties, and costs. Patient responses also revealed high interest in having more time for dialogue with their provider and receiving more educational materials about their condition and treatment.
Treating physicians and clinic staff identified solutions that could reduce the frequency of clinic appointments without risking vision loss as an opportunity to best support patients. According to the healthcare providers, constrained clinic capacity was a leading impediment to providing the best outcomes for patients. Insufficient available educational materials designed to help patients understand their disease and its treatment also emerged as a challenge, in their opinion.
“We know from randomised clinical trials that anti-VEGF therapy for nAMD and DME is associated with anatomical and functional improvements that can be sustained with ongoing proactive treatment. However, we also know from real-world studies that adherence to continued treatment can be poor, [leading] to suboptimal outcomes,” said Dr
Loewenstein, a member of the nAMD Barometer Leadership Coalition and lead author of the published paper reporting findings from the nAMD survey.
“We thank all participants and clinics contributing to the survey and believe the findings will enable the development of interventions to support patient-centred care and improved outcomes to ultimately improve vision health and quality of life for patients with these sight-threatening retinal diseases,” she said. “The Barometer Program has now developed a series of educational resources to support addressing some of the challenges identified in the surveys, which can be found [on the site’s resources page].”
Although patients generally prioritised their anti-VEGF treatments, the finding that about one-fourth of those in both the nAMD and DME cohorts wondered whether their anti-VEGF treatment was necessary underscored a need for more education. Furthermore, patients with DME/DR and nAMD alike wanted better educational materials about their disease and its treatment—although patients with DME/DR also wanted an information pack that would help them explain their disease and need for regular treatment to their employers.
Patients also expressed a desire to have more time with a healthcare provider so they could ask questions, discuss concerns, and better understand their disease, its treatments, and expected outcomes. High proportions of providers and clinic staff concurred there was a need to be able to spend more time in the clinic to discuss care and answer patient questions. Consistent with these findings, responses from providers highlighted clinic capacity constraints hampered the ability to provide optimal patient care and is an issue that can
compromise anti-VEGF treatment adherence and persistence.
The survey responses from patients with DME highlighted the unique issues they face in adhering to anti-VEGF therapy. Often, patients with DME need to attend appointments with other medical specialists to manage their diabetes and its comorbidities. In addition, patients with DME are younger on average than those with nAMD and, therefore, are often still working.
Not surprisingly, responses from patients in treat ment for DME/DR indicated the need to take time off work and attend appointments with other medical spe cialists compounded the burdens associated with having to make regular visits to the retina clinic. Corresponding with these issues, the patients being treated for DME/ DR showed a high level of interest in clinics where they could access multidisciplinary services.
Physicians cited having other chronic health condi tions as the leading challenge patients faced in manag ing their diabetic eye disease and agreed clinics offering broader diabetic care services could address the frustra tion and difficulties patients experienced from having to see so many different providers.
Dr Loewenstein noted that while there has been previous research exploring barriers to optimising clinical management for patients needing anti-VEGF therapy for DME and nAMD, those projects tended to have a narrow scope, focusing on single countries or only on patients.
“The Barometer Program’s survey is unique because it has a global focus, sought perspectives from patients, physicians, and clinic staff, and the included clinics were diverse with respect to healthcare systems, settings, and reimbursement models,” she said.
The Barometer Program is an international coali tion of experts in retinal disease, vision care, diabetes, and ageing working to optimise clinical practice and improve treatment outcomes for patients with nAMD, DME, and diabetic retinopathy. Its members represent the International Agency for the Prevention of Blindness, International Federation on Ageing, Vision Academy, and Bayer Consumer Care AG. The activities of the Barometer Program and Vision Academy are funded and facilitated by Bayer, where the clinicians, scientists, and representa tives from the International Federation on Ageing and the International Agency for the Prevention of Blindness re tain decision authority over the research scope, methods analysis of findings, and dissemination of the outputs.
For citation notes, see page 24.
Anat Loewenstein MD, MHA is Professor and Chair of the Department of Ophthalmology at the Tel Aviv Medical Center, Tel Aviv, Israel. anatl@tlvmc.gov.il
Applicants to the 2025 contest must answer this prompt:
Diversity, equity, and inclusion (DEI) programmes, however well-intentioned, stir a variety of responses in the corporate and political worlds and in the scientific and medical spheres.
What DEI and unconscious bias issues are present in the current culture of ophthalmology training, practice, and clinical research? What are the potential benefits of addressing these issues for patients and ophthalmologists? What kind of meaningful changes need to happen to move beyond ‘talking the talk’ to ‘walking the walk’?
The competition is open to ESCRS members (including the free membership available to trainees) age 40 or younger on 1 January 2025. Submit your essay no later than 20 June 2025 to seanh@eurotimes.org.
Cover page: All essays must include a cover page with the following information:
• Author’s name
• Contact information (email and phone)
• Institution/affiliation
• Stage of ophthalmology training
• Date of birth
• ESCRS member number
Writing tips: Submit your essay in Microsoft Word or a similar text format (no PDFs, please). The punctuation, syntax, and grammar should reflect the high standard of content published in EuroTimes. Please remember to limit your essay to 800 words. We encourage you to have a colleague read your essay before you send it to check for style and grammar mistakes. Please include citations for any studies mentioned and state whether AI tools were used in the production of the essay.

Deadline: The closing date for entries is 20 June 2025. Send your essay with cover page to seanh@eurotimes.org.
Winning essays: Past winners have all shown some original insight and personal style in their essays. You can read the 2024 winning essay and recent winning essays here. https://www.escrs.org/eurotimes/john-henahan-writing-prize/
Treatments trending to fewer injections for better results.
TIMOTHY NORRIS REPORTS
Intravitreal injections are the gold standard for the treatment of exudative macular disorders such as neovascular AMD, DME, and RVO, granting a high intraocular concentration with a low systemic exposure. However, according to Luis Arias Barquet MD, PhD, some key questions still need to be answered: “What is the best drug to treat our patients? Which is the best treatment protocol? Do we need to apply the same treatment for all patients? What will future treatments be?”
To identify the best drugs available for the patient, Dr Arias explained it is important to observe the many different pathways that can be targeted by a drug for treating retinal disorders, adding the anti-VEGF blockade remains the most effective pathway for treating these conditions.
The first generation of anti-VEGF agents, such as ranibizumab and aflibercept 2 mg—while effective—needed a high frequency of injections to obtain good visual and anatomical results. The need for multiple monitoring follow-ups and treatments contributed to a huge socio-economic burden for the patient and the healthcare system and risked compromising treatment efficacy due to a lack of compliance.
The latest generation of anti-VEGF agents moved efforts a step further: Faricimab is the first bispecific antibody designed to target both VEGF and angiopoietin-2, used in a 6 mg clinical dose. Aflibercept 8 mg is the same fusion protein of the previous generation but with a modified molar concentration to enhance clinical effectiveness. Brolucizumab is a small antibody fragment with a very low molecular weight in a 6 mg dose.
Dr Arias observed these drugs have very similar visual results compared to the previous generation but with better anatomical results, resulting in longer durability that translates into fewer injections and longer treatment intervals—a breakthrough for the management of these conditions.
The high potency of brolucizumab, for example, keeps the macula dry for up to 6 months, Dr Arias said. Even so, the drug has had some safety issues regarding intraocular inflammation in 4% of cases, sometimes severe, requiring a balance of the risks and benefits.
Given this need for balance, no one treatment stands out as the best treatment protocol. Every treatment protocol can be helpful if done correctly, he explained, showing the results of a multicentre study he conducted that compared reactive (fixed, PRN) and proactive treat-and-extend (T&E) regimens.1
There are no clinical differences, he stated.
However, while the T&E approach was more popular with drugs such as aflibercept 2 mg, the tendency with the new drugs is a move towards a fixed regimen with longer intervals of up to 16 weeks. Besides anti-VEGF, the efficacy of treatments such as Ozurdex (INN-dexamethasone) and Iluvien (fluocinolone acetonide) is indisputable, he added.
Regarding new incoming treatments, Dr Arias highlighted the potential of port delivery systems that can be surgically implanted once and eventually refilled directly in the office. He said gene therapy is also extremely promising, explaining that the rationale is “to teach retinal cells to produce their own anti-VEGF molecules, a very promising alternative to intravitreal injections.”
Dr Arias spoke at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 24.
Luis Arias Barquet MD, PhD is Head of the Retina Department of Ophthalmology at Bellvitge University Hospital in Barcelona, Spain. luisariasbarquet@gmail.com


Alcon announced the Clareon® Vivity® lens received a CE Mark from the European Commission and will start commercial distribution in early Q2 2025. The initial rollout will feature Clareon Vivity lenses with the Monarch IV manual delivery system, while it will also be available with the AutonoMe system in Q3. The Clareon Vivity provides presbyopia correction with a monofocal visual disturbance profile.
alcon.com
Alcon and LENSAR have entered into an agreement in which Alcon plans to acquire LENSAR. The acquisition will include the ALLY Robotic Cataract Laser Treatment System and LENSAR’s proprietary Streamline software technology and legacy laser system. According to the terms of the agreement, Alcon will purchase all outstanding LENSAR shares for approximately $356 million and an additional $2.75 per share in cash, contingent upon achieving 614,000 cumulative procedures with LENSAR’s products between 1 January 2026 and 31 December 2027.
alcon.com, lensar.com
Opthea announced their anti-CEGF agent sozinibercept did not meet its primary endpoint from baseline to week 52 in the COAST (Combination OPT-302 with Aflibercept Study) phase 3 clinical trial, involving patients with vascular age-related macular degeneration (AMD). The trial showed no significant difference in mean change in best-corrected visual acuity (BCVA) between those receiving sozinibercept in combination with aflibercept and those receiving aflibercept alone and no numerical difference in the key secondary endpoints. “There remains material uncertainty as to Opthea’s ability to continue as a going concern,” the company stated. opthea.com
Haag-Streit announced the launch of their new METIS Ophthalmic Microscope System. Designed for glaucoma surgeons, the METIS system incorporates Haag-Streit’s optics—optimized with a coaxial red reflex to ensure accurate colour reproduction, high light transmission, and a large depth of field for clear visualization during procedures. Additionally, surgeons can control tilt, filter, focus, and zoom using programmable hand or foot switches, and the system has a modular design for potential upgrades such as 3D heads-up displays.
haag-streit.com
The FDA has approved Iluvien® fluocinolone acetonide implant for chronic non-infectious uveitis in the posterior eye segment. The implant initially releases 0.25 mcg/ day of fluocinolone acetonide and is designed to last 36 months. Previously approved for diabetic macular oedema in 2014, Iluvien’s approval for uveitis was supported by Phase 3 studies showing fewer recurrences at 6 months compared to a sham injection.
hcp.iluvien.com
Topcon Healthcare, RadiusXR, and Glaukos announced their partnership to launch RadiusXR’s new wearable vision testing platform, Inspire. The lightweight device, weighing just 6 ounces, allows patients to perform self-guided vision tests with minimal supervision. Topcon will be its exclusive global distributor and collaborate with RadiusXR, and Glaukos will manage commercialization, research, and education efforts.
topconhealthcare.eu, radiusxr.com, glaukos.com
Guest editorial contributors observed that advances in laser technology and the stromal response have made keratorefractive lenticule extraction (KLEx) roughly as safe and accurate as LASIK. But they also emphasized the need for further technological developments to fully harness KLEx’s potential.
Walter Sekundo reported success with femtosecond lenticule extraction (FLEx) in 2010, achieving 98.1% of eyes within 1.0 D of the target. Rupal Shah improved the technique, refining the laser-firing sequence. Dr Sekundo introduced small incision lenticule extraction (SMILE) the following year, initially showing delayed visual recovery, but later improvements significantly enhanced outcomes. SMILE is now widely used. Meta-analyses show no significant difference between SMILE and LASIK in clinical outcomes or higher-order aberrations.
Second-generation machines have addressed earlier issues, demonstrating lower suction loss rates through faster procedures and improved machine-controlled suction. Automated centration and torsional control are being implemented, with full automation on the Schwind ATOS. Hyperopic correction will soon be available on the VISUMAX 800, expanding treatment options.
Meanwhile, innovative technology linking lasers and diagnostic devices is under development for topography-guided KLEx for asymmetric corneas. Pre-clinical research suggests applanation-free KLEx, minimizing corneal stress, is achievable using a liquid system interface. Software enhancements for dynamic depth adjustment and equal arc lengths—with continued research and investment— are crucial for improving precision using attosecond pulses.
J S Mehta, et al. “Second-generation keratorefractive lenticule extraction: will there be a third?” 51(3): 179–181.
Recent years have seen an increase in immediate sequential bilateral cataract surgery (ISBCS). A higher volume of surgeons, recent graduates, and those practising in the Western US are more likely to perform ISBCS. The study used a cross-sectional analysis of Medicare and Medicaid data of patients undergoing bilateral cataract surgery between 2018 and 2022. The proportion of surgeons performing ISBCS increased from 15.63 per 1,000 in early 2018 to 26.55 per 1,000 in late 2022. Among 10,290 surgeons, the proportion of ISBCS cases per 1,000 bilateral surgeries doubled from 17.20 in 2018 to 35.50 in 2022.
M Ali, et al. “Surgeon adoption of immediate sequential bilateral cataract surgery in the United States from 2018 to 2022,” 51(3): 210–217.
A meta-analysis of 15 studies involving 1,247 cataract patients with poor capsular support indicates iris-fixated IOLs may have fewer complications than anterior chamber IOLs or sclerally fixated IOLs. The study showed the overall complication rate was not significantly lower in the iris fixation group (4.4%) compared to anterior chamber (7.4%) and scleral fixation groups (7.4%). Transient corneal oedema was most common in anterior chamber placement (29.9%), followed by scleral fixation (11.9%) and iris fixation (4.1%). Vitreous haemorrhages were more frequent after scleral fixation (8.5%) than anterior chamber placement (5.4%) or iris fixation (1.4%). IOL decentration/ dislocation occurred more often after scleral fixation (8.9%) than after anterior chamber placement (1.1%) or iris fixation (4.0%).
P Kanclerz, et al. “Postoperative complication rates in intraocular lens placement and fixation methods for inadequate capsular bag support: review and meta-analysis,” 51(3): 257–266.
ESCRS is now accepting applications for the 2025 Systematic Research Award (SRA) programme. The SRA is open to all ophthalmologists and researchers (MD and/or PhD or experienced ophthalmic nurses) who currently hold a full- or part-time clinical/research position at a clinical or academic institution.
Established in 2022, the SRA aims to encourage high-quality research that documents and codifies existing knowledge in cataract, refractive, and cornea medicine or surgery. The goal of the SRA is to provide new scholarly output in the field of cataract, refractive, and cornea medicine or surgery, focused on the methodology created by the Cochrane Library.
Up to six (6) awards are available, with a total maximum of €10,000 per award.
Preliminary applications will be accepted until 31 May 2025. Applicants are encouraged to refer to online resources at the Cochrane Library and/ or at PROSPERO and/or with PRISMA. The lead applicant should be an ESCRS member.
It’s All About Biomechanics!
Page 6
1. Scarcelli G, et al. “Biomechanical characterization of keratoconus corneas ex vivo with Brillouin microscopy,” Invest Ophthalmol Vis Sci, 2014 June 17; 55(7): 4490–4495.
2. Scarcelli G, et al. “In vivo biomechanical mapping of normal and keratoconus corneas,” JAMA Ophthalmol, 2015 April; 133(4): 480–482.
3. Cassagne M, et al. “Customized Topography-Guided Corneal Collagen Cross-linking for Keratoconus,” J Refract Surg, 2017 May 1; 35(5): 290–297.
4. Nordström M, et al. “Refractive improvements and safety with topography-guided corneal crosslinking for keratoconus: 1-year results,” Br J Ophthalmol, 2017 Jul; 101(7): 920–925.
5. Chan E, et al. Ophthalmology, 2023 April; 130(4): 445–448.
6. Gustafsson I, et al. “Early findings in a randomised controlled trial on crosslinking protocols using isoosmolar and hypoosmolar riboflavin for the treatment of progressive keratoconus,” Acta Ophthalmologica, 2025; 103(1): 23–32. Published online early 2024 July 5.
IOP Measurement Errors After Refractive Surgery
Page 11
1. C Roberts, et al. J Cataract Refract Surg, 2005 Jan; 31(1): 146–155.
Maintaining Standards with Refractive Surgery
Page 13
1. Gauvin M, et al. “mEYEstro software: an automatic tool for standardized refractive surgery outcomes reporting,” BMC Ophthalmology, 21 April 2023, doi:10.1186/s12886-02302904-6.
Emerging Technology for Detecting Subclinical Keratoconus
Page 14
1. Randleman JB, et al. “Subclinical Keratoconus Detection and Characterization Using Motion-Tracking Brillouin Microscopy,” Ophthalmology, 2024; 131(3): 310–321.
Topography-Guided PRK for Keratoconus
Page 15
1. A Nattis, et al. JCRS, 46(4): 507–516.
Improving Clinical Management for nAMD and DME
Page 18
1. Loewenstein A, Sylvanowicz M, Amoaku WM, et al. “Global Insights from Patients, Providers, and Staff on Challenges and Solutions in Managing Neovascular Age-Related Macular Degeneration,” Ophthalmol Ther, 2025; 14(1): 211–228.
2. Ziemssen F, Sylvanowicz M, Amoaku WM, et al. “Improving Clinical Management of Diabetic Macular Edema: Insights from a Global Survey of Patients, Healthcare Providers, and Clinic Staff,” Ophthalmol Ther, 2025; 14(1): 229–246.
Defining AMD Treatment Protocol
Page 20
1. López-Gávez MI, Arias-Barquet L, Figueora MS, García-Layana A, Ruiz-Moreno JM, In-Eye Study Group. “Bimonthly, treat-and-extend and as-needed ranibizumab in naïve neovascular age-related macular degeneration patients: 12-month outcomes of a randomized study,” Acta Ophthalmol, 2020; 98(7): e820–e829.

The leading community and trusted source for SCIENCE, EDUCATION & PROFESSIONAL DEVELOPMENT in the fields of cataract and refractive surgery.
April 25–28
ASCRS
Los Angeles, US
May 23–25
EuCornea
Prague, Czech Republic
June 7–9
European Society of Ophthalmology (SOE) Lisbon, Portugal
June 12–14
2nd World Keratoconus Congress (WKC 2025) Athens, Greece
September 4–7
EURETINA
Paris, France
September 12–16
2025 ESCRS Congress
Copenhagen, Denmark

23 May
September 25–28
German Ophthalmology Society Berlin, Germany
October 18–20
American Academy of Ophthalmology
Orlando, Florida, US


4 Sept
25 Apr
7 Jun


12 Sept



1-4
• Myopic shift
• Cyclodialysis
• Hypotony
• Significant hyphema ZERO
• Stent dislocation
SAFETY1,2
OVERALL SAFETY PROFILE SIMILAR TO CATARACT SURGERY ALONE3
SIGNIFICANT IMPROVEMENTS IN VISION-RELATED QUALITY OF LIFE5
REFRACTIVELY NEUTRAL5,6,8,9 FEWER FOLLOW-UP VISITS4 DAILY ACTIVITIES7 MENTAL HEALTH7
IMPROVES OCULAR SURFACE HEALTH6,9
REDUCTION IN PATIENTS WITH SEVERE OSD SYMPTOMS5 72%
WITHIN ± 1.0D OF REFRACTIVE TARGET8 99%
1. 7-Year Efficacy and Safety of iStent inject® Trabecular Micro-Bypass in Combined and Standalone Usage. Fritz H. Hengerer . Gerd U. Auffarth . Ina Conrad-Hengerer. 2. Ten-Year Effectiveness and Safety of Trabecular Micro-Bypass Stent Implantation with Cataract Surgery in Patients with Glaucoma or Ocular Hypertension. Tobias H. Neuhann, Raphael T. Neuhann, Dana M. Hornbeak. 3. Samuelson, Thomas W., et al. “Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results.” Ophthalmology 126.6 (2019): 811-821. 4. Rodriguez-Una, Ignacio, Augusto Azuara-Blanco, and Anthony J. King. “Survey of glaucoma surgical preferences and post-operative care in the United Kingdom.” Clinical & Experimental Ophthalmology 45.3 (2017): 232-240. 5. Samuelson, Thomas W., et al. “Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial.” American Journal of Ophthalmology 229 (2021): 220-229. 6. Schweitzer, Justin A., et al. “Prospective interventional cohort study of ocular surface disease changes in eyes after trabecular micro-bypass stent (s) implantation (iStent or iStent inject) with phacoemulsification.” Ophthalmology and Therapy 9 (2020): 941-953. 7. Jones, Lee, et al. “Impact of minimally invasive glaucoma surgery on the ocular surface and quality of life in patients with glaucoma.” Therapeutic Advances in Ophthalmology 15 (2023): 25158414231152765. 8. Ioannidis, Alexandros S., et al. “Refractive outcomes after trabecular micro-bypass stents (iStent inject®) with cataract extraction in open-angle glaucoma.” Clinical Ophthalmology (2020): 517-524. 9- Biela, Katarzyna, et al. “Dry eye disease as a cause of refractive errors after cataract surgery–A systematic review.” Clinical Ophthalmology (2023): 1629-1638.
iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATIONS FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body.