Seeking consensus on functional classification of simultaneous vision IOLs.
Big Advantages to SmallAperture IOLs
Small-aperture IOLs offer superior image quality with increased range of focus.
Prioritising Self Care
Benefits of maintaining physical, emotional, and mental health extend beyond the personal sphere.
Functional outcomes of an enhanced monofocal IOL based on spherical aberration modulation
Prof Daniele Tognetto, University Eye Clinic of Trieste (Italy)
Achieving high-quality intermediate vision is being increasingly prioritised as an outcome by cataract surgery patients, driven by the trend of individuals maintaining an active lifestyle as they age and their dependence on digital technologies. EVOLUX®, an innovative enhanced monofocal IOL from SIFI (Italy), was developed to address this goal.
EVOLUX® incorporates a unique, patented, non-diffractive optical profile based on spherical aberration technology optimisation that aims to enhance intermediate vision while maintaining the excellent distance acuity and low incidence of photic phenomena associated with standard monofocal IOLs.
The centre of the optic zone, which is the largest active zone among leading extended monofocal IOLs, features a unique combination of positive and negative spherical aberrations that stretches the distribution of incoming light (Figure 1), elongating the depth of focus to improve intermediate vision without compromising distance vision. The optic’s outer zone has a monofocal design that ensures consistent distance vision, mimicking the optical quality of standard monofocal IOLs.
EVOLUX® is designed to deliver predictable, stable visual outcomes, conferring tolerance to residual refractive errors and resistance to tilt and decentration as shown by pre-clinical data. It is constructed of a time-tested hydrophobic acrylic material that has been shown to minimise glistening and maintain long-term optical clarity.
The results of the prospective clinical trial we conducted highlighted the performance and benefits of EVOLUX® IOL. The study assessed outcomes of patients implanted with EVOLUX® extended monofocal IOL (SIFI), Tecnis 1-piece standard monofocal aspheric IOL (ZCB00, Johnson & Johnson), and Tecnis Eyhance extended monofocal IOL (ICB00, Johnson & Johnson).
We found uncorrected and distance-corrected intermediate visual acuity at one month in the EVOLUX® group were significantly better than in patients implanted with the Tecnis 1-piece monofocal IOL and comparable to outcomes in the Tecnis Eyhance extended monofocal IOL group. Uncorrected and best-corrected distance visual acuity results were similar in all groups, confirming EVOLUX® provides distance vision performance equivalent to a high-quality monofocal IOL.
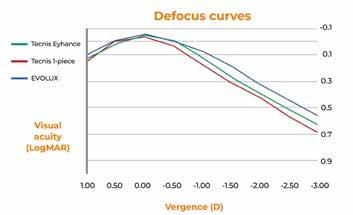
Defocus curve analysis showed EVOLUX® provided enhanced intermediate vision performance versus the monofocal Tecnis 1-piece (Figure 2). Compared to the Tecnis Eyhance, however, EVOLUX® had a smoother defocus curve and showed slightly better logMAR visual acuity at the intermediate viewing distance (66 cm, -1.50 D defocus).
These findings suggest that EVOLUX® may offer a more stable and continuous range of functional vision at intermediate distances compared to the Tecnis Eyhance and support its ability to provide a smooth transition between distance and intermediate visual tasks— which is a significant advantage for daily activities such as computer work, reading, and social interactions.
Scanning electron microscopy of the EVOLUX® optic showed it had no diffractive profile or distinct optical zones. These findings confirm its non-diffractive design principle and are consistent with patient-reported outcomes exploring the unwanted visual phenomena often associated with diffractive optics.
Conclusion
Our study supports EVOLUX® as a promising option for surgeons aiming to meet the visual goals commonly held by today’s cataract surgery patients. Its findings demonstrate that by leveraging spherical aberration modulation without introducing diffractive elements, EVOLUX® extends the visual range and preserves optical quality while minimising unwanted visual disturbances. Based on this information, I encourage my colleagues to explore the benefits of EVOLUX® in their practices and contribute to the growing body of evidence supporting this innovative technology.
Figure 1. The central zone of the EVOLUX® IOL optic uses optimised spherical aberration modulation to elongate the focal point, extending depth of focus.
Figure 2. Defocus curves for the EVOLUX®, Tecnis 1-piece, and Tecnis Eyhance IOLs.
Cover Story
Marie-José
20 Understanding Negotiating Know-How
Anne Louise Coleman MD, PhD
22 ESCRS Talks Technology at AAO
H Burkhard Dick MD, PhD, FEBOS-CR; Filomena Ribeiro MD, PhD, FEBO; Oliver Findl MD, MBA, FEBO; and Thomas Kohnen MD, PhD, FEBO
A New Focus on Intermediate Vision
Mayank Nanavaty MBBS, DO, FRCOphth, PhD
25 Inspiring Collaborative Excellence
Dan Z Reinstein MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO
26 Sorting Out Simultaneous Vision IOLs
Artemis Matsou MD, MRCP(UK), FEBOS-CR, FEBO, PgDip CRS; Alfredo Borgia MD, FEBO; Douglas Koch MD; H Burkhard Dick MD, PhD, FEBOS-CR; Daniel Chang MD; and Joaquín Fernández Pérez MD, PhD
28 Big Advantages to Small-Aperture IOLs
Elizabeth Yeu MD
CORNEA
30 Exploring the Expanded Array of KLEx Procedures
Alexander Chen MD
31 Refining Indications for CXL
Jose de la Cruz MD, MS
32 Knowing Iris Repair: Using Iridodiathermy in Iris Surgery
Soosan Jacob MS, FRCS, DNB
GLAUCOMA
34 NT-501 Encapsulated Cell Therapy for Glaucoma
Alexandria M Dominguez MS and Jeffrey L Goldberg MD, PhD
35 Understanding Glaucoma and Cataract Surgeries
Steven J Gedde MD
RETINA
36 Neuroprotectant Treatment for MacTel Type 2
Emily Y Chew MD
37 Targeting the Pathogenic Pathway
Christine Nichols Kay MD
38 Reducing the Treatment Burden for Neovascular AMD
Rishi P Singh MD
DIGITAL OPHTHALMOLOGY
40 Robotic Eye Surgery Could Expand Surgical Possibilities
Robert K Maloney MD, MA(Oxon)
INDUSTRY INSIGHTS
42 A Look at Innovative Treatments in Late-Stage Development
Philippe Sourdille MD and Karsten Klabe MD
Publisher Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin Roibeárd O’hÉineacháin
Contributors
Lauren Blanchard
Laura Gaspari
Soosan Jacob
Timothy Norris
Andrew Sweeney
Colour and Print
CitiPost
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Celebrating Women in Ophthalmology
Since 1911, 8 March has marked International Women’s Day, ‘a global occasion celebrating the social, economic, cultural, and political achievements of women.’1 This issue of EuroTimes extends that celebration to recognise the many achievements of women in ophthalmology, past and present.
And there is much to celebrate. In our cover story, Laura Gaspari notes women now comprise nearly half of those entering medical school, ophthalmology training, and residency. Moreover, women currently lead the majority of professional ophthalmology organisations, starting with the ESCRS, and including EURETINA, EuCornea, the European Glaucoma Society, along with the outgoing presidents of both the American Academy of Ophthalmology and the American Society of Cataract and Refractive Surgery. Most recently, Soosan Jacob, a frequent contributor to EuroTimes, has become president-elect of the International Society of Refractive Surgery.
We also look at the brilliant contributions of pioneering women ophthalmologists, including Marie-José Tassignon MD, PhD, the first female president of the ESCRS, and refractive surgery pioneer Marguerite McDonald MD.
Our cover article and related pieces also acknowledge that obstacles remain to be overcome before gender equality is achieved. Women ophthalmologists are underrepresented in leadership positions in academia and more likely to experience burnout.2 Female ophthalmology trainees in Europe continue to experience apparent gender bias.3 Bullying and harassment continue to plague the profession. A recent article
EDITORIAL BOARD
Adi Abulafia (Israel)
Bruce Allan (UK)
Noel Alpins (Australia)
Juan Alvarez de Toledo (Spain)
Gerd Auffarth (Germany)
Başak Bostanci (Turkey)
John Chang (Hong Kong SAR, China)
Béatrice Cochener-Lamard (France)
Burkhard Dick (Germany)
Mor Dickman (The Netherlands)
in JAMA Ophthalmology reveals two-thirds of women participating in a survey reported sexual harassment in the workplace, and fewer than 25% of serious incidents were reported to an authority.4
On the research front, there is room for improvement in diversifying clinical trial protocols.5 A related article in this issue looks at the problem of bias and lack of diversity in clinical trial design, and how improving clinical trial design can improve everything from surgical outcomes to patient relationships. This issue becomes even more urgent with the increasing use of AI in ophthalmology research.
Adding to these challenges are the political winds that threaten existing efforts to improve representation and reduce discrimination. The ESCRS recognises this and will continue to offer programmes to educate and raise awareness in our profession. One example is the Building Our Inclusive, Sustainable Society (BoSS) programme, which is dedicated to this cause and will feature at our Winter Meeting in Athens and our Annual Congress in Copenhagen. We also offer a growing selection of BoSS podcasts and videos at escrs.org.
We can reach the goal of gender equity in our profession and our society at large, but it will take the ongoing commitment and participation of all of us, women and men alike.
Filomena Ribeiro MD, PhD, FEBO President, ESCRS
For citation notes, see page 46.
Joaquín Fernández (Spain)
Oliver Findl (Austria)
Nicole Fram (US)
Sri Ganesh (India)
Fahrad Hafezi (Switzerland)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Jack Kane (Australia)
Yao Ke (China)
Mika Kotimäki (Finland)
David Lockington (UK)
Artemis Matsou (Greece)
Cyres Mehta (India)
Jod Mehta (Singapore)
Sorcha Ní Dhubhghaill (Belgium)
Rudy Nuijts (The Netherlands)
Catarina Pedrosa (Portugal)
Konrad Pesudovs (Australia)
Nic Reus (The Netherlands)
Filomena Ribeiro (Portugal)
Andreia Rosa (Portugal)
Giacomo Savini (Italy)
Julie Schallhorn (US)
Sathish Srinivasan (UK)
Paola Vinciguerra (Italy)
Shin Yamane (Japan)
Ron Yeoh (Singapore)
Mihail Zemba (Romania)
Thomas Kohnen
José Güell
Paul Rosen
Apply for the
John Henahan Writing Prize
Applicants to the 2025 contest must answer this prompt:
Diversity, equity, and inclusion (DEI) programmes, however well-intentioned, stir a variety of responses in the corporate and political worlds and in the scientific and medical spheres.
What DEI and unconscious bias issues are present in the current culture of ophthalmology training, practice, and clinical research? What are the potential benefits of addressing these issues for patients and ophthalmologists? What kind of meaningful changes need to happen to move beyond ‘talking the talk’ to ‘walking the walk’?
The competition is open to ESCRS members (including the free membership available to trainees) age 40 or younger on 1 January 2025. Submit your essay no later than 20 June 2025 to seanh@eurotimes.org.
Cover page: All essays must include a cover page with the following information:
• Author’s name
• Contact information (email and phone)
• Institution/affiliation
• Stage of ophthalmology training
• Date of birth
• ESCRS member number
Writing tips: Submit your essay in Microsoft Word or a similar text format (no PDFs, please). The punctuation, syntax, and grammar should reflect the high standard of content published in EuroTimes. Please remember to limit your essay to 800 words. We encourage you to have a colleague read your essay before you send it to check for style and grammar mistakes. Please include citations for any studies mentioned and state whether AI tools were used in the production of the essay.
Deadline: The closing date for entries is 20 June 2025. Send your essay with cover page to seanh@eurotimes.org.
Winning essays: Past winners have all shown some original insight and personal style in their essays. You can read the recent winning essays on our website .
iNovation
Day to Showcase Ideas to Improve Future of Ophthalmology
ESCRS has long been a source of new ideas to improve the practice of ophthalmology. With the launch of iNovation® Day at its 2022 Annual Congress, ESCRS took the next step: inviting business leaders to join medical experts in brainstorming ways to bring these new ideas to fruition.
At the 2025 Annual Congress in Copenhagen, ESCRS will host its fourth iNovation Day with a programme featuring as many as 20 presentations by emerging companies, a variety of guest speakers, and survey data on attendee interests, trends, and concerns. The day-long event will bring together doctors, corporate executives, emerging companies, and financial community leaders from across Europe and other parts of the world.
“In 2025, we will cover technology innovations to address barriers and urgent clinical needs within the next 5–10 years, with a special focus on artificial intelligence and how it will impact everyday practice,” says ESCRS President Filomena Ribeiro. “Unique perspectives will be shared by guest speakers from the European investment, regulatory, and research communities. We will also continue unique components, including a panel with leaders of all the major anterior segment associations and the Innovators Den, which features key doctor innovations.”
In 2025, we will cover technology innovations to address barriers and urgent clinical needs within the next 5–10 years.
The programme will be highly interactive, with a live chat for comments as well as audience polling to complement the focused panel discussions. The event will include two components with the potential for lasting consequences: (1) the Innovators Den and (2) the Emerging Company Showcase.
Innovators Den: The Innovators Den is an opportunity for entrepreneurs who have personally developed unique ideas to address some of the biggest unmet needs of ESCRS members. Innovators whose proposals are accepted will be paired with knowledgeable mentors who will help them create a compelling pitch and commercialisation plan to submit to a panel of judges. The three finalists will be officially recognised and have the chance to present their ideas during iNovation Day to a large ophthalmic audience, where the winner will be selected. Emerging Company Showcase: This competition seeks to identify smaller companies with emerging technologies to present to a large ophthalmic audience of doctors and industry to accelerate market introduction. Company applications will be reviewed by the ESCRS iNovation Day Programme Committee; presentations will be reviewed and discussed with a panel of ESCRS doctor leadership and key industry leads.
“iNovation Day is a truly unique meeting,” Prof Ribeiro says. “Not only because it brings together doctors, corporate
executives, emerging companies, and financial community leaders from across Europe and other parts of the world, but because it is ‘the innovation meeting for doctors’ to review, discuss, and shape the future of our industry!”
Workshop to Share Financial Tools, AI Insights
ESCRS is partnering with the Trinity College (Dublin) Business School executive education programme to present a practice management workshop in Zurich in late June.
The weekend workshop, taking place 27–29 June in Zurich, will cover two topics of critical importance to ophthalmologists in clinical practice or considering such a career: finance and artificial intelligence (AI).
Finance for ophthalmologists: On Saturday, 28 June, Trinity Adjunct Professor Hilary Hough will lead this session, which is based on Trinity’s workshop on Finance for Healthcare Professionals. There will also be a joint discussion between Prof Hough and Vanessa Foser, co-founder and chief commercial officer of the AI Business School in Switzerland, on the intersection between finance and AI.
What you really need to know about AI right now: Vanessa Foser will cut through all of the noise and hype about AI and focus on what ophthalmologists need to know today about using AI in their clinical practice. Members of the ESCRS Leadership Development and Business Innovation Committee will also share the AI tools that they are currently using in their daily practice to improve efficiency and effectiveness.
The application deadline is 15 May.
Adapting Aid from Conflict to Recovery
The ESCRS continues to provide valuable support to its Ukrainian colleagues while also learning from them.
ANDREW SWEENEY REPORTS
Since the start of Russia’s full-scale invasion of Ukraine in 2022, the WHO has recorded more than 1,900 attacks on medical facilities. Total damage to Ukrainian healthcare infrastructure reached at least US$3 billion by the end of 2024.
Hundreds of medical workers have died, and the ophthalmology sector has borne its share. The Okhmatdyt Children’s Hospital in Kyiv, which housed an ophthalmology department, was destroyed in a missile attack in June 2024, killing two. A private ophthalmology clinic in Zaporizhzhia was hit by rockets in December last year, killing three.
Throughout the war, the ESCRS has provided valuable support to its Ukrainian colleagues. Since February 2022, the Society has released funds from its reserves to purchase more than €1 million in essential logistics and equipment, primarily for treating ocular trauma.
The ESCRS has directly assisted 26 clinics and ophthalmic departments (several of which are situated near the front line), arranged seminars on ocular trauma, and provided bursaries for young Ukrainian ophthalmologists to study abroad. For the Society’s managing director, Tom Ogilvie-Graham MD, assistance to Ukraine is a duty the organisation can be proud of.
“The Ukrainians are our colleagues and, as a European society, it is our duty to support them during this difficult period,” Dr Ogilvie-Graham said. “The pressure on them is relentless; they’re working without respite to provide the best possible care to their patients under very difficult circumstances.”
He is keen to point out the persisting challenges faced by Ukrainian ophthalmologists. The number of soldiers (many of whom were civilians until recently) presenting with complex, bilateral polytrauma remains high, and there is an ongoing need for specialist equipment and materials.
One of those Ukrainian ophthalmologists who received this support is president of the Ukrainian Vitreoretinal Society, Andrii Ruban MD, PhD. Despite managing a private clinic in Kyiv and working on complex trauma cases pro bono, Dr Ruban still finds the time to work with the society.
“From the first days of the war, the ESCRS has been a key donor of humanitarian and ophthalmological aid to Ukraine, both in consumables and equipment. This help was intended not only for anterior segment trauma but also for posterior eye injury and adnexal trauma,” Dr Ruban said.
“I would like to express my deep gratitude and respect to Dr Ogilvie-Graham for his exceptional participation in helping Ukrainian ophthalmologists and patients. He made several visits to the National Military Hospital in Kyiv and showed personal courage while visiting a clinic a few kilometres from the front line in Izyum.”
Evolving support will help Ukraine long term
The ESCRS originally expected to provide considerable support in the form of tutorials but has learned much from its Ukrainian colleagues. Dr Ruban has frequently had to operate without main electricity, even during air raids in some cases. His experience and those of his fellows, particularly in treating trauma injuries, is valuable.
Some recommendations include focusing on minimal eye surgery to stabilise critical structures, as this will set a good foundation for later repair. Understanding what not to do is as important as understanding what to do too; for example, primary keratoplasty should not be performed if the injury is likely to progress.
Unfortunately, Ukrainian ophthalmology will continue to accumulate experience in dealing with severe ocular trauma. As such, Dr Ruban expects that much of the assistance provided to the country’s healthcare system should focus on this area.
“Blast injury evolves and can lead to other problems such as glaucoma, optical neuropathy, retinal detachment, corneal decompensation, and so on. That is why we must be prepared to increase the need for keratoplasty, secondary intraocular lens implantation, and secondary glaucoma surgery in the coming years,” Dr Ruban said.
“Therefore, cooperation with ESCRS will be very necessary in the future.”
The ESCRS is ready to provide that support, according to Dr Ogilvie-Graham, and will continue assisting in education and training. The Society will adapt its support when needed and is currently aiding the setup of the first Ukrainian public eye bank in Lviv.
“Whether through support by ESCRS leadership for academies or by other means (such as participating in seminars relating to war trauma injuries), we shall support our Ukrainian colleagues for as long as the conflict continues, as well as in the aftermath. We will also continue to support individual trainees with observerships and travel bursaries whilst offering substantial discounts on registration fees,” Dr Ogilvie-Graham said.
“Many Ukrainian surgeons will also have to catch up on training and education, and the ESCRS can provide specific support. As members of our Society, our Ukrainian colleagues can expect us to help with all the challenges likely to be there during the recovery period—just as we were there from the beginning.”
Tom Ogilvie-Graham MD is managing director of the ESCRS. tog@md.escrs.org
Andrii Ruban MD, PhD is president of the Ukrainian Vitreoretinal Society. ruban33@gmail.com
The conversation around women’s representation in ophthalmology has shifted from whispers to thunderous debates at global conferences and symposia. Society is evolving, and the rising tide of awareness has delivered real change.
On the bright side, the profession is nearing a balance in ophthalmology training, with women comprising 35–45% of residents.1 This surge in female applicants to medical schools signals a transformative era. A retrospective study in Ophthalmology revealed female representation in US ophthalmological societies skyrocketed from 29% in 2000 to 41% in 2020—a trend mirrored around the globe.2
Yet, the path remains steep. Despite these gains, only 20–30% of specialised ophthalmologists are women. An invisible bottleneck stifles their career advancement, with many struggling to break into surgical specialties or ascend to leadership roles. While the glass ceiling persists, new strategies are emerging to bridge the gap and foster a more inclusive field.
Diamonds Rough in the
The push for inclusivity in ophthalmology.
BY LAURA GASPARI
WOMEN IN OPHTHALMOLOGY
The challenges women still face
Like other surgical specialties, ophthalmology battles a significant gender gap in leadership. “Progress is evident, but women are still outnumbered—we still often see panel discussions where only one out of five or six speakers is a woman,” said Nivine Woods, president of Ophthalmic World Leaders (OWL).
Even though women have led many societies in recent years—including the ESCRS with Professor Filomena Ribeiro— women role models are still a minority compared to their male counterparts. Also, fewer of them complete their surgical training, establishing themselves as surgeons.
“There are certain areas where women are massively underrepresented, like refractive surgery as well as retinal surgery, and a little bit in cataract surgery,” said Sorcha Ní Dhubhghaill MD, PhD, Head of Department, Ophthalmology, at the Brussels University Hospital (UZ Brussel).
Women face more career obstacles than their male counterparts, especially during residency training, as the programmes are tough, demanding, and require a lot of personal sacrifices to achieve this higher level of training. Being in their late 20s or early 30s, an age in which many aspects of one’s future are determined, it is sometimes difficult to balance career and private life, making these decisions particularly tough.
According to Artemis Matsou MD, ophthalmic surgeon at Queen Victoria Hospital, East Grinstead, UK, this a multifactorial issue with two main roots: how the training programmes are structured and the need of some women to balance the extra pressure of pregnancy, motherhood, or family responsibilities.
“Some women may have been discouraged from pursuing a very surgery-heavy path [because the] training is very intense,” she stressed. “It takes away a lot of personal time and has an impact on someone who has a family. The structure of such programmes does not accommodate that; they are not really family or women friendly.”
Male residents do not usually feel the same burden, even if times are changing, with new generations of ophthalmologists more concerned about families and work-life balance. Yet it is still mainly women making the tough decision of renouncing their aspirations, with no equal opportunities discouraging this.
Harassment and bullying
Balance between work and private life is not the only reason women are discouraged or led to interrupt their advancements. Women unfortunately suffer more unwelcome and uncomfortable comments that can ruin a workday or performance in the OR, microaggressions, physical and psychological harassment and bullying, as well as being affected by unconscious bias, even from patients.
Women themselves could sometimes have implicit biases about their colleagues triggered by competition, jealousy, or the stereotypes shaped by social norms.
“We all have implicit biases. It is like a shadow—it never goes away and it never gets acknowledged,” Dr Matsou said. These biases extend to the operating theatre, as women are
generally still thought to be less capable than men in performing surgery and receive fewer opportunities.
“In countless fields—from surgeons and engineers to electricians and hairdressers—we see a deeply ingrained belief that men are inherently more capable,” Nivine Woods explained. “As a result, it takes a lot more effort, determination, and resilience for women—not only to prove their worth, but to shatter preconceived notions.”
There are certain areas where women are massively underrepresented, like refractive surgery as well as retinal surgery, and a little bit in cataract surgery.
As Professor Ní Dhubhghaill underlined, even women in higher positions are still required to demonstrate their capabilities more than their male colleagues, adapting themselves to situations. “We do not have the luxury to be unprepared, emotional, or not ready.”
This constant struggle—the fear of losing opportunities, the disadvantages, and the vulnerability—is difficult to overcome, she said, advocating for real and sustained solutions to take place, and not only some sporadic symposia or courses on the subject.
Catalysts for change
While change is structural and takes time, some solutions can help speed up the process. First, continuing to raise awareness is crucial because, as Dr Matsou noted, it should not be assumed that everyone knows or understands the situation for women in ophthalmology. Open discussions are very important for raising awareness, and the ESCRS is among the leaders providing such an avenue. Created by Prof Ribeiro and including Dr Matsou and Prof Ní Dhubhghaill as members, the ESCRS Building Our Sustainable Society (BoSS) programme maintains open discussion as a primary goal.
Collaboration with organisations like OWL is essential for building structured mentorship programmes and advocating for more inclusive policies. Women need support from institutions and scientific societies to create equal opportunities, make choices, and minimise the sacrifices that sometimes weigh on women’s shoulders.
Societies need to reflect on their overt and implicit biases to deconstruct them and place solid defence mechanisms from harassment. Importantly, male colleagues must be included in the discussions to advance the cause. For example, BoSS is open to everybody, with male leaders among the main team, and OWL rebranded from Ophthalmic Women Leaders to Ophthalmic World Leaders to reflect this inclusivity. According to both groups, men can be crucial sponsors, mentors, and drivers of change alongside women.
New technologies could serve well in this regard, as apart
from quickly connecting people all around the world, technology offers more opportunities—such as surgical training, thanks to the implementation of surgical simulators, as Prof Ní Dhubhghaill pointed out.
Mentorship has been recognised as another powerful tool to foster this change. It constitutes a continuous and sustained exchange between the mentor and the mentored, passing knowledge, contacts, and networks. In a competitive environment such as ophthalmology, finding a mentor could open many doors for ambitious people to unlock their full potential and shape future role models, leaders, and mentors.
“Mentors are not only effective, but they are also transformative,” Dr Matsou said. “It is a healthy cycle, being mentored and giving back. Having structured mentorship programmes is very significant, and ESCRS is providing that now through the BoSS platform.”
Mentorship is good not only for females but for male ophthalmologists as well, to shape a more desirable society. Being a mentor is no easy job, but Prof Ní Dhubhghaill believes it is worth it in the long run.
“We, as mentors, need to be sure our juniors are better than we are, which is how the evolution of the medical field needs to be,” she observed.
A bright future ahead
Despite improvements, much work remains. Ignoring the current disparities would squander opportunities for the next generation of female ophthalmologists, impacting research and patient care. “Women in ophthalmology are like diamonds in the rough—they’re brilliant, but it takes a bit of time and work to uncover,” Nivine Woods concluded. “With time and dedication, we can unveil this hidden treasure and cultivate the vibrant, inclusive future we all envision.”
For citation notes, see page 46.
Nivine Woods PharmD, MBA is President of Ophthalmic World Leaders (OWL), US.
Sorcha Ní Dhubhghaill MBBCh, BaO, PhD, Dip (stats), FEBO, FEBOS-CR, MRCSI(ophth) is Head of Department, Ophthalmology, at the Brussels University Hospital (UZ Brussel), Belgium. sorcha.ni.dhubhghaill@uzbrussel.be
Artemis Matsou MD, MRCP(UK), FEBOS-CR, FEBO, PgDip CRS is ophthalmic surgeon at Queen Victoria Hospital, East Grinstead, UK. art.mat sou@gmail.com
Making Female Leadership More than a Moment
A remarkable global confluence of women in key positions.
The two-year period 2024–2025 marked a pivotal moment for women’s leadership in global ophthalmology. Many ophthalmological societies around the globe saw the election of important female physicians and role models as presidents, leading the ophthalmological community.
Starting in Europe with the ESCRS, Professor Filomena Ribeiro, Head of the Ophthalmology Department at the Hospital da Luz in Lisbon and Professor of Ophthalmology and Biomedical Engineering at the University of Lisbon, became the third woman to lead the Society after Profs Marie-José Tassignon and Béatrice Cochener-Lamard. From the very beginning, Prof Ribeiro committed herself to more inclusivity, equity, and social awareness within the scientific society and in every aspect of ophthalmology, adding a focus on research and charity projects.
Prof Cochener-Lamard currently serves as president of EuCornea, the European scientific society uniting cornea and ocular surface specialists. Prof Cochener-Lamard is Professor and Chairperson of the Ophthalmology Department at the University Hospital of Brest in France. One of the most renowned experts on anterior segment, refractive surgery, and corneal surgery, she was awarded the French Legion of Honour in 2013.
The European Glaucoma Society has Prof Ingeborg Stalmans at the helm, Head of the Laboratory of Ophthalmology at the Catholic University of Leuven (KU Leuven) and of the Glaucoma Unit of the University Hospitals in Leuven (UZ Leuven), Belgium. The esteemed glaucoma specialist has devoted her career to research.
In the realm of the posterior segment, Anat Loewenstein, Professor of Ophthalmology at Tel Aviv University, Israel, leads as president of EURETINA. Prof Loewenstein is a globally recognised retina specialist and surgeon who advocates for women’s visibility in ophthalmology. She will be succeeded by Prof Nicole Eter of the University of Münster, Germany.
Globally, Dr Jane C Edmond is the outgoing president of the American Academy of Ophthalmology (AAO) after serving a one-year term. Dr Edmond specialises in paediatric and neuro-ophthalmology and she is chair of the Department of Ophthalmology at the Dell Medical School, Director of the Mitchel and Shannon Wong Eye Institute, and Vice Dean of Professional Practice, all of the University of Texas, Austin, US. She is the sixth woman ophthalmologist serving as AAO president.
Dr Elizabeth Yeu, renowned anterior segment surgeon and key opinion leader in global ophthalmology, is the immediate past president of the American Society of Cataract and Refractive Surgery (ASCRS). Dr Yeu is a consultant
at Virginia Eye Consultants and Assistant Professor at the Eastern Virginia Medical School, both of Norfolk, Virginia, US, and serves as Medical Director of the CVP Mid-Atlantic Surgery Center.
Rounding out this list is Dr Soosan Jacob, Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation (DARCF), Chennai, India, a regular EuroTimes contributor, and the first to describe CAIRS as a treatment for keratoconus. Dr Jacob has been nominated president-elect of the International Society of Refractive Surgery, succeeding Dr Deepinder K Dhaliwal, another female leader in ophthalmology.
Valuing Clinical Trial Design
How inclusivity and diversity can enhance scientific accuracy in research.
LAURA GASPARI REPORTS
The global scientific community is committed to reducing biases in clinical research, and while the situation is improving, there is still a lot of work to be done to foster inclusivity and diversity, according to Filomena Ribeiro MD, PhD, president of the ESCRS.
“Historically, many clinical trials have been dominated by participants from specific demographic groups, and these often exclude diverse populations, such as ethnic minorities, women, or older individuals,” Professor Ribeiro said.
A lack of diversity in the patient recruitment process can arise from systemic barriers which prevent them from participating in clinical trials, such as limited access to healthcare due to transportation or climate issues, mistrust in medical science, or language barriers. Bias and exclusion can also affect investigators.
“Lacking figures from underrepresented groups, in a non-intentional way, can have an impact and influence on the design of studies, recruitment strategies, and interpretation of results,” Prof Ribeiro said.
Diversity and inclusion in clinical research really matter— the consequences of their shortage can have a huge impact on the clinical research itself.
“It can be a limit to the ability to generalise our findings on the research,” Prof Ribeiro remarked.
She pointed out that the scarcity is in the non-heterogeneity of the population—not considering specific subgroups— which affects the safety and effectiveness of the object under study. For example, the ophthalmological community is already aware ethnicity, gender, and age impact the modelling for IOL power calculation and that there are some anatomical and treatment reaction differences in eyes from different geographic areas.
This bias could also lead to some problems when artificial intelligence is applied to provide insights on treatment since these programs use existing data sets. If clinical trials suffer from some biases, these can be transferred to algorithms, generating models that consider only a part of the population. Luckily, several developments are in place to avoid biases in information on clinical trials using AI, Prof Ribeiro explained.
However, she noted greater sensitivity on the topic arrived during the COVID pandemic, and the EMA and the FDA have begun to address it through global guidelines to encourage diversity, community engagement, and building trust in the research process.
While a good start, Prof Ribeiro believes more strategies and efforts should be put in place to tackle issues that prevent a more inclusive research process. For example, there should be a particular focus in reducing logistic barriers, offering more decentralised trial options, providing financial support for transportation, or supplying materials in different
languages. Research teams should be more diversified, with investigators trained to recognise possible existing biases. Researchers also need to model the results to have an appropriate representation across ethnic, gender, and sociodemographic dimensions and combine them to improve treatment safety and efficacy of treatments—which she said is true not only for pharmaceuticals but also medical devices.
Enhancing and fostering inclusivity can lead to improved quality in scientific research, increasing its applicability and ensuring findings are more representative of the broader population.
“This leads to more equitable healthcare solutions, and we can determine how treatments work for different groups, ensuring better outcomes for everyone,” Prof Ribeiro concluded. “Inclusivity builds trust in science, and as doctors and researchers, we want to serve the whole community, so we need to have this commitment.”
Filomena Ribeiro MD, PhD, FEBO is head of ophthalmology at Hospital da Luz, Lisbon, Portugal, and ESCRS president. filomenajribeiro@gmail.com
Progress and Promise for Women in Ophthalmology
Laser surgery pioneer Marguerite McDonald discusses her career and the ongoing issues women face in ophthalmology.
CHERYL
GUTTMAN KRADER REPORTS
Ask any ophthalmologist to name a leading woman within their field, and certainly Marguerite B McDonald MD will be top of mind. Well-known for performing the first laser vision correction procedure in the world, a photorefractive keratectomy (PRK), Dr McDonald continues to be a trailblazing researcher, adding many other ‘firsts’ to her curriculum vitae and serving as an inspiration to other women in ophthalmology.
In an interview with EuroTimes, Dr McDonald shared her professional motivations, the challenges she encountered as a woman trying to advance her career, and her perspectives on the current state of gender parity in ophthalmology.
Why did you choose to pursue a career in ophthalmology with a particular focus on the cornea?
My father was an orthopaedic surgeon who tried to dissuade me from going into medicine, but he was unsuccessful because I saw how much he loved what he did. I knew I wanted to be a surgeon like him, but seeing the physical toll he endured from being on his feet for hours each day, I decided to operate in a seated position, and I was interested in microsurgery. My specific interest in ophthalmology stemmed from the fact I had extreme myopia as a child, and it was the care from an ophthalmologist that greatly improved my life. I sought a cornea fellowship because I believed cornea-based treatments were the key to better strategies for addressing refractive error.
In 1980, I was very fortunate to land the cornea and external disease fellowship at Louisiana State University (LSU). This was a highly coveted position because it was directed by Dr Herbert E Kaufman, and it marked the start of my journey developing keratorefractive surgery: On my first day, I joined the research group working to perfect what became known as the Kaufman McDonald Epikeratophakia procedure. After completing my fellowship, I was hired as an assistant professor at LSU. In that position, at age 31, I became the only female and youngest of nine surgeon investigators in the Prospective Evaluation of Radial Keratotomy study. Of course, it was also at LSU where I was the first to perform PRK.
Have you met any gender-related challenges during your career?
I can share numerous stories about situations where I experienced or witnessed gender bias or discrimination. To give a few examples, when interviewing for residency programmes, I was routinely asked personal questions about my plans for marriage and a family. Then, as a new ophthalmology faculty member at LSU and the only female, I rose in protest at a department meeting where there was a discussion about firing the chief resident who had announced her pregnancy. She was our best resident, and her position was saved, but she was given just two weeks off after giving birth to her child in a complicated delivery.
What is the current status of gender parity in ophthalmology?
The treatment of women and opportunities for advancement are much improved. Overall, there are almost as many women as men in residency programmes, and women are well represented in leadership and executive committee positions in our professional societies as well as in roles as planners and speakers at scientific meetings. In fact, the current presidents of the American Academy of Ophthalmology, EURETINA, European Society of Cataract and Refractive Surgeons, and EuCornea are all women.
Unfortunately, there are still very few women holding the position of ophthalmology department chair in the academic world. In addition, a large pay gap remains between men and women in ophthalmology. For example, a recent study of practising ophthalmologists in the US found that during the first year of clinical practice, the mean salary with bonus earned was more than $33,000 less for women compared to their male colleagues.1 Another US study of academic ophthalmologists’ salaries showed women were paid more than $50,000 less on average than men. 2
So, clearly, there remains a need to address the gender-based disparity in pay and give women more opportunities to assume leadership positions at our universities. I am not suggesting that women be given chair positions simply for the purpose of achieving equality, but rather that the decision-makers keep an open mind and make themselves blind to gender when interviewing candidates for these positions.
What would you say to women today about choosing a career in ophthalmology?
Go for it because ophthalmology is a fantastic and fulfilling career. It provides intellectual and professional stimulation because it encompasses numerous areas of knowledge and involves multiple skills, and it is an exciting field in which advances are occurring rapidly. Importantly, ophthalmology is extremely rewarding from an emotional perspective. By restoring or preserving patient vision, ophthalmologists can find gratification in knowing we have a positive impact on the quality of life for our patients. At the same time, we are fortunate to be largely spared the sadness experienced by physicians caring for patients with terminal diseases.
For citation notes, see page 46.
GLOBAL REACH
As a renowned authority in the field of cataract and refractive surgery, ESCRS facilitates global connections amongst ophthalmic professionals, fostering collaboration and the exchange of knowledge.
Our events span across continents, providing a platform for pioneering research, advanced surgical techniques, and continuous professional development.
Using the interactive map on our website, we invite you to explore our global presence by viewing upcoming events and academies.
Join us to network with esteemed experts, access the latest advancements, and contribute to the enhancement of eye care on a worldwide scale.
Marguerite B McDonald MD is a Clinical Professor of Ophthalmology at both NYU Langone Medical Center, New York, New York, and Tulane University Health Sciences Center, New Orleans, Louisiana, and in private practice at OCLI Vision, Oceanside, New York, US.
Prioritising Self-Care
Benefits of maintaining physical, emotional, and mental health extend beyond the personal sphere.
CHERYL GUTTMAN KRADER REPORTS
With responsibility for taking care of their patients and families, women ophthalmologists may be neglecting their own physical, emotional, and mental health. Speaking at the Women in Ophthalmology symposium, Melissa Summerfield MD emphasised the importance of maintaining personal well-being and aimed to convince her female colleagues to begin paying more attention to their self-care needs.
“When you start prioritising your wellness, you will be able to take better care of those who are important to and depend on you,” Dr Summerfield said.
Survey results underscore the multiple work-related stresses affecting ophthalmologists, including problems with pain from overuse injuries and symptoms of burnout. Noting these issues may be more prominent among women than men, Dr Summerfield offered her perspective on why women are so dedicated to their jobs that they compromise their health. She proposed the answer is found in messaging from multiple sources, including society, colleagues, and medical culture— and guilt-laden messages women place on themselves.
Self-care solutions
Stating that self-care is any activity for increasing physical, mental, or emotional health, Dr Summerfield shared ideas about easy ways women can begin to “up their self-care game.”
Her first suggestion was to harness the physiological benefits of taking deep cleansing breaths to relieve feelings of stress during a demanding clinic day.
“Breath is a powerful tool because it is one of the few bodily functions under both conscious and autonomic control. When we consciously control our breath, it engages the parasympathetic nervous system, which resets our emotional thermostat back towards neutral and brings the front lobe back online,” Dr Summerfield said.
When you start prioritising your wellness, you will be able to take better care of those who are important to and depend on you.
“Taking a few cleansing breaths before entering the exam room leaves us feeling calmer when we begin the next patient encounter and also gives us the ability to make the best decisions for that individual.”
Exercise was the focus of Dr Summerfield’s next tip, accompanied by suggestions on how to find the necessary time.
“You knew you would not get out of a lecture on self-care without hearing about exercise,” Dr Summerfield quipped. “And I know everyone is busy. But what if I asked you to spend just 10 minutes three times a week?”
She advocated for weight training, considering women start to lose muscle mass at age 39 with consequences of decreased metabolism, which increases risk for obesity, and decreased core strength, which increases susceptibility to musculoskeletal injuries. While encouraging women to begin “lifting heavy stuff,” she also said taking time for a 10-minute walk during the lunch break 3 days a week was a good start.
For women who felt they didn’t even have that much time to spare, Dr Summerfield proposed carefully considering the many requests they receive to serve in professional, charitable, or family-related activities and declining involvement with obligations that do not fulfil a core desire or need.
“Saying no to things that do not add meaning or purpose to our lives gives us time, space, and energy to dedicate to the things that do,” she said.
Dr Summerfield spoke on this topic at AAO 2024 in Chicago, US.
Melissa Summerfield MD is a private practice ophthalmologist at North Iowa Eye Clinic in Mason City, Iowa, US. summerfield.melissa@gmail.com
Madam President
The first female ESCRS president reflects on her ophthalmic inspirations, achievements, and future.
LAURA GASPARI REPORTS
Marie-José Tassignon MD, PhD became the first female ESCRS president in 2004, serving through 2005. The career of the Belgian-born professor was marked by a lot of research, inventions, and innovations, which earned her the esteem and recognition of the European and global ophthalmological world. She trained as a doctor at the Vrije Universiteit Brussel, then specialised in ophthalmology at the University Hospital Brussels, obtaining her PhD at the University of Leiden, Netherlands. She served as Head and Chief of the Department of Ophthalmology of the Antwerp University Hospital and University of Antwerp in Belgium. She was also president of the EBO and Academia Ophthalmologica Internationalis.
Regarding her mentors, the names she brings up are those of the greats of ophthalmology of the last century.
“My career has been built thanks to people to whom I am still grateful because they have helped me a lot,” she said. Among them is Professor Jan Worst, with whom she discovered the Berger’s space, an essential part of one of her greatest achievements, the bag-in-the-lens technique. She also had the privilege to work alongside Charles Kelman and meet Sir Harold Ridley and the French resistance hero Charles Schepens—all of whom she described as great and strong influences in her career.
Prof Tassignon started as a vitreoretinal surgeon before moving, in her own words, “more and more anteriorly,” first
discovering interest in the lens and then the cornea. In recent years, she returned to the posterior segment, mainly in the vitreous, especially regarding paediatric cataracts.
As previously mentioned, one of her greatest achievements is the bag-in-the-lens (BIL), a surgical technique for cataract surgery she created in 2000. She published the results in adults in the Journal of Cataract and Refractive Surgery that year, where she later published the results in children in 2007. The rationale behind this technique, as she recalled, is to solve the problem of posterior capsular opacification (PCO) secondary to cataract surgery. It consists of doing a surgeon-controlled capsulorhexis and inserting the edge of both capsules into the groove of a special biconvex acrylic hydrophilic intraocular lens she designed specifically for this technique. Prof Tassignon subsequently designed and developed tools to improve the surgery and its results.
The hard-working ophthalmologist also distinguished herself as a teacher, leading and mentoring generations of ophthalmologists and acting as a role model for female specialists.
“My career has been a turning point for the role of women in ophthalmology, but I do not really like the idea of being chosen because I am a woman, but rather for my merit,” she said.
I do not really like the idea of being chosen because I am a woman, but rather for my merit.
Case in point: Prof Tassignon was the only candidate in a pool of ten proposed as Head of Department at the University of Antwerp. She gave herself a small chance to succeed but earned the job in the end. This was also true for the ESCRS presidency, where she was chosen for her merits and visionary work to enlarge the Society to include eastern EU countries.
In her free time, Prof Tassignon enjoys family, creates jewellery, and follows her interest in fashion. She said that when she was younger, she enjoyed painting and fashion designing, which made her choice for medicine quite hard. She is still in the field to make patients’ lives easier, still working on avoiding PCO, but now in babies and children.
Marie-José Tassignon MD, PhD, FEBO is emeritus chair and chief of the department of ophthalmology at the University Hospital of Antwerp, Belgium.
Understanding Negotiating Know-How
Learning negotiation skills and self-advocacy strategies emerge as fundamental for career success and satisfaction.
CHERYL GUTTMAN KRADER REPORTS
Self-advocacy and negotiation success can help pave the path to career growth and fulfilment but can be difficult for many people—particularly women, said Anne Louise Coleman MD, PhD.
Offering ideas for empowering effectiveness as a negotiator and self-advocate, Dr Coleman emphasised trust is crucial because it creates a psychologically safe environment where individuals feel comfortable expressing their needs, concerns, and ideas without fear of negative repercussions. Reflecting on her experience as chair of the department of ophthalmology at UCLA School of Medicine, Dr Coleman said when negotiations with candidates for a faculty position have fallen apart, a common reason is the individual does not trust her or the institution.
“Remember that you cannot negotiate in good faith or effectively advocate for yourself or your career development without trust,” Dr Coleman said.
Knowing one’s worth is another critical element for attaining success in negotiations, and for that, individuals may need to work on self-awareness, understanding the value they bring and how they are perceived by others.
“Think about your pros—the contributions and skills you bring to the table—but also the areas where you are not so strong,” Dr Coleman said.
Owning up to one’s weaknesses can be difficult for physicians who have a history of being overachievers throughout life, so it is important to accept the need for making changes and working towards self-improvement.
“It can be hard to not be the ‘straight A’ student in everything, but you need to become comfortable hearing honest feedback about yourself and realise you might not get everything you ask for,” she explained. “You have to be comfortable with putting in the time and effort to achieve your goals. This may also require changes that will hopefully be empowering.”
Even before entering into negotiations affecting one’s career path, individuals need to be honest with themselves about their priorities. Recognising what one values is a fundamental step, Dr Coleman said.
“Do you want an opportunity to pursue a mission, to pursue a position that will provide access to prestige, or fulfil an ambition to rise up the ladder, or to pursue a financially rewarding
career? The answers to these questions set the foundation for guiding life choices,” she stressed. “If money is important to you, there is nothing wrong with that, but be honest with yourself about it. If you are interested in money, then maybe an academic career is not the right way to go.”
She also cautioned that making threats and giving ultimatums is not an effective negotiating strategy. Not only can it change the environment from a positive discussion to an adversarial situation, but it can often backfire.
“The other party may not respond the way you think or hope they will,” Dr Coleman noted. “When negotiating, remember you may be unique and have special skills, but you are not irreplaceable.”
At the same time, self-confidence about one’s unique characteristics is an important trait for achieving negotiation success because it facilitates the ability to express needs and desires. Self-confident people are aware of their strengths and weaknesses and can articulate this information along with goals and motivations. Unfortunately, for a variety of reasons and depending on the environment, women may find it particularly difficult to advocate for themselves.
“Women are often expected to be more modest than men, so self-advocacy by a woman may be seen as excessive and make her less effective,” Dr Coleman said.
Recognising it can be difficult to overcome discomfort with self-advocacy, Dr Coleman suggested women may find it easier to use advocacy for their group or a project as a surrogate approach. The other side of the coin of not directly advocating for themselves, however, is women risk being perceived as uninterested in an opportunity or lacking motivation. To circumvent such misinterpretations, Dr Coleman advised being alert to opportunities to self-nominate and outlining one’s accomplishments and career goals in an annual written report, which benefits individuals involved in both sides of a negotiation.
“Sometimes people advocating for themselves assume others know everything about them, but that is not necessarily true. For example, although I conduct faceto-face reviews with faculty members, there is not a lot of time for each individual to share everything about what they are doing and their goals,” Dr Coleman said.
She also encouraged “being yourself” and offered a few tips that can enable authenticity.
“Focus on gaining respect of others rather than likeability. In addition, identify what matters most to you, and let those values guide your decisions and actions. Then surround yourself with a network of supportive friends, mentors, and/or colleagues who encourage you to be your authentic self.”
Dr Coleman spoke during the Women in Ophthalmology symposium at AAO 2024 in Chicago, US.
Anne Louise Coleman MD, PhD is the Bradley R Straatsma, MD Endowed Chair in Ophthalmology and Director of the Jules Stein Eye Institute at the University of California, Los Angeles, US. acoleman@mednet.ucla.edu
ESCRS Talks Technology at AAO
Europe adopts technological advances, US still waiting for lenses and lasers.
HOWARD LARKIN REPORTS
Four ESCRS leaders presented the latest in European eye surgery technology at Refractive Surgery Subspecialty Day during the American Academy of Ophthalmology annual meeting in Chicago, US.
Innovations
H Burkhard Dick MD, PhD led off featuring three breakthroughs that are not available in the US, despite greater funding and marketing opportunities and a more relaxed regulatory regimen.
“In Europe, MDR is like walking a tightrope over a river full of crocodiles while juggling with checklists,” he said. “The FDA looks like a moonwalk through the approval process, but I know you have to spend $32 million if you want to bring an IOL to the market.”
Laser-induced refractive index change (LIRIC) uses a femtosecond laser to break the bonds of monomers in hydrogel lenses to change their refractive power. LIRIC is being developed by Schwind and University Eye Clinic in Bochum, Germany, for use in corneal tissues to treat refractive errors. In animal trials it is proving feasible, effective, and safe, and human trials could begin in 2026, Professor Dick said.
A handheld, battery-powered femtosecond laser for cutting perfectly centred anterior capsulotomies is now available in Europe from Helix Surgical. It requires no suction, takes 4 seconds, and integrates well into patient workflow, Prof Dick said. “The results are very consistent.”
A small-aperture mask from Morcher that can be placed in the capsular bag or sulcus on top of any intraocular lens (IOL)
is succeeding in clinical tests. Implantable through a 2.0-mm incision, the removable device can be used with any lens to add depth of focus, making it more flexible than a dedicated small-aperture IOL.
“The future is undeniably bright, with more breakthrough moments and Europe’s ongoing role in co-shaping the future,” Prof Dick concluded.
Choosing an IOL
A huge array of IOLs is now available in Europe, and choosing among them requires careful evaluation of their characteristics, said Filomena Ribeiro MD, PhD.
The future is undeniably bright, with more breakthrough moments and Europe’s ongoing role in co-shaping the future.
Materials—whether hydrophobic or hydrophilic acrylic— influence everything from posterior capsule opacification to flexibility, centration, and quality of vision, Prof Ribeiro noted. Recently, improvements have been made in hydrophobic acrylic lens materials to address issues, including spherical aberrations and glistenings, she added.
Platforms also vary widely, with lens stability influenced by factors such as haptic design and lens diameter versus capsular bag size. These influence decentration, rotation, tilt, and axial displacement, all of which affect vision outcomes. Designs range from the classic C-loop to open C-loops to four-haptic and plate designs. Some are available in multiple sizes to fit the capsular bag.
And then there is optical design. IOLs can be classified as refractive, diffractive, or small aperture, but also by number of focal points, extended depth of focus (EDOF), or enhanced monofocal, Prof Ribeiro said. Trifocals are evolving toward fewer light-splitting rings and providing more light to intermediate vision, with some even incorporating refractive qualities or entirely refractive designs.
Generally, EDOF lenses provide less spectacle independence but better quality of vision and higher contrast sensitivity, Prof Ribeiro said. But as new lenses develop, distinctions among them blur, and the design alone tells little about how they function in patients’ eyes. ESCRS has compiled a functional classification system to help guide lens choices.
“Sometimes it’s not easy because we have diffractive IOLs that are considered EDOF, EDOF that perform like a bifocal, etc., so everything is right now very complex,” she said. “We have a very large catalogue of IOLs.”
Improving refractive outcomes
In the 75 years since the IOL was invented, refractive outcomes for cataract and now refractive lens exchange have steadily improved. That’s thanks in large part to improved technology and lens power calculation formulas that have addressed the main sources of error, said Oliver Findl MD. Current and near-future innovations hold promise for further improvement.
The 1990s saw the start of optical biometry used to help minimise the impact of axial length measurement errors on refractive error. Swept-source optical coherence tomography (OCT) further improved accuracy, allowing measurement of axial length, corneal thickness, anterior chamber depth, and lens thickness, enabling more accurate prediction of postoperative effective lens position.
But OCT remains expensive. Using surface-emitting laser diodes similar to those in laser printers and mobile phones soon could reduce OCT cost by as much as 100-fold, making it more available in limited resource settings, Prof Findl noted. “Cheaper technology is on the horizon.”
Accurate keratometry is also critical, Prof Findl said. Dry eye is particularly problematic, but treating it for weeks before surgery is cumbersome, unreliable, and may not improve keratometry accuracy much. Having patients close their eyes for 5 minutes before scanning can significantly improve surface hydration and scan quality. He added scans should be assessed for mire distortion before proceeding.
Accurate postoperative refractions also remain a significant source of error, and more robust measurement is needed.
“Unaided 20/20 is not enough,” Prof Findl said, noting measurements down to 0.25 D and better reproducibility would improve outcomes.
Last, he said accurate IOL power calculation is critical to estimating effective lens position. The ESCRS online calcula-
tor enables users access to several formulas with data entered just once. Variations in predictions can help identify potential refractive surprises in advance, allowing for patient counselling and effective treatment planning.
Phakic IOLs
Rapid increases in myopia and high myopia over the next 25 years will drive greater interest in phakic IOLs (PIOL), said Thomas Kohnen MD, PhD. Available in Europe since the mid-1980s, various angle-supported and iris-fixated anterior chamber PIOLs have evolved.
However, angle-supported lenses were pulled from the market due to problems with pupil ovalisation and long-term endothelial cell loss. Iris-claw lenses are also associated with long-term endothelial cell loss, especially in patients with shallow anterior chambers, so these must be monitored over the long term, Prof Kohnen noted.
Ciliary sulcus-fixated PIOLs, such as the posterior chamber implantable collamer lens (ICL, Staar Surgical), are also associated with mild endothelial cell loss. Recent models with a central hole have nearly eliminated cataract formation, making them attractive for high myopia correction, Prof Kohnen said.
An aspheric presbyopia-correcting ICL is now available, providing 0.1 logMAR visual acuity across roughly 2.00 D. “It is a good alternative for high myopia patients from age 45 to 55 years,” Prof Kohnen said. Another available option is a multizone refractive iris-fixated presbyopia-correcting PIOL that offers a full range of vision (Artiplus, Ophtec).
Current German guidelines, updated in 2022, call for PIOL use for myopia of -1.00 D or more and presbyopia of +1.00 or more. Astigmatism may be treated with a toric IOL or laser surgery, Prof Kohnen said. Upcoming ESCRS refractive surgery PIOL guidelines will be similar but add minimum anterior chamber depths of 2.8 mm for myopia and 3.0 mm for hyperopia, with astigmatism correction for 1.00 D or more.
In conclusion, Prof Kohnen noted that anterior chamber angle-supported lenses are no longer sold, though iris-fixated lenses are available in both Europe and the US. But “the winner at the moment seems to be ciliary sulcus-fixated lenses, going back to Fyodorov in 1993, also in presbyopia correction.”
H Burkhard Dick MD, PhD, FEBOS-CR is professor and chairman of the Ruhr University Eye Hospital in Bochum, Germany, and ESCRS president elect. dickburkhard@aol.com
Filomena Ribeiro MD, PhD, FEBO is head of ophthalmology at Hospital da Luz, Lisbon, Portugal, associate editor of the Journal of Cataract and Refractive Surgery , and ESCRS president. filomenajribeiro@gmail.com
Oliver Findl MD, MBA, FEBO is professor and chair of ophthalmology at Hanusch Hospital in Vienna, Austria, and past president of the ESCRS. oliver@findl.at
Thomas Kohnen MD, PhD, FEBO is professor and chair, Department of Ophthalmology, Goethe University, Frankfurt, Germany, and past treasurer of the ESCRS. kohnen@em.uni-frankfurt.de
A New Focus on Intermediate Vision
Careful planning of spherical aberration can provide higher spectacle independence.
TIMOTHY NORRIS REPORTS
The importance of intermediate vision has been increasingly recognised in recent years as an important part of functional vision for pseudophakic patients. As recognised by ESCRS in a position statement, several working distances are needed to perform many daily tasks such as cooking, seeing the speedometer in a car, or walking on uneven ground.
According to Mayank Nanavaty PhD, this has led the whole world of ophthalmology to focus on intermediate vision, with the industry taking a stride towards new and enhanced technologies and better lenses, with the promise of spectacle independence. However, the bottom line is “horses for courses,” he said. It is important to select the right technology for the right patient.
He added the path to achieving better visual acuity at all distances may be found in the infusion of negative spherical aberration, an important finding from the MERoV (Monofocal Extended Range of Vision) study, which he led.1 Focusing on the incidence and factors for pseudoaccommodation after monofocal lens implantation, the study collected data on 301 patients from the 412 initially included, observing a 9.4% incidence of patients achieving spectacle independence. Finding the factors responsible for pseudoaccommodation was the primary goal, and the primary outcome was to look at the number of patients achieving 6/12 and J4 for distance and near.
To further investigate this observation, Dr Nanavaty and his co-investigators David J Spalton and Catey Bunce approached data using univariate and multivariate analysis. The univariate analysis found four important factors involved with pseudoaccommodation: preoperative anterior chamber depth, spherical equivalent, spherical aberration, and mesopic pupil size.
A subsequent multivariate analysis showed similar results, with the exception of preoperative axial length instead of preoperative anterior chamber depth. Multivariate analysis is more important because it considers all the factors together in the eye and how they interact, Dr Nanavaty said, adding the statistics were quite complex for this reason, with a lot of interdependencies involved.
The results showed that pseudoaccommodation is a multifactorial combination of low myopic spherical equivalent, lower total eye spherical aberration, shorter preoperative axial length, and smaller pupil size. With the help of co-investigator and statistician Caty Bunce, an equation was formulated considering the four factors involved. Of the four factors, axial length and mesopic pupil size are considered non-modifiable, Dr Nanavaty observed. Therefore, it can be possible to act on
spherical aberration and spherical equivalent to effectively predict pseudoaccommodation in any scenario.
“What we are now finding is that changing the total eye spherical aberration between -0.30 and 0.50 µm gives more predictability in achieving spectacle independence for distance and near,” Dr Nanavaty said, concluding this can be achieved with careful planning of surgery on the cornea or the lens.
Dr Nanavaty spoke at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 46.
Mayank Nanavaty MBBS, DO, FRCOphth, PhD is Consultant Ophthalmologist and surgeon at the University Hospitals Sussex NHS Foundation Trust, Brighton, UK. mayank.nanavaty@nhs.net
Inspiring Collaborative Excellence
Dan Reinstein shares stories of his journeys pursuing multiple research interests.
CHERYL GUTTMAN KRADER REPORTS
The International Society of Refractive Surgery honoured Dan Z Reinstein MD as the recipient of the Barraquer Award at AAO 2024.
Dr Reinstein prefaced his lecture by explaining he chose its title—“The Jose I Ignacio Barraquer Factor: Combining scientifically driven clinical practice with pioneering innovation, collaborative excellence, and educational leadership in refractive surgery”—and its content to pay tribute to Dr Barraquer, recognising him as the quintessential clinician, scientist, and teacher.
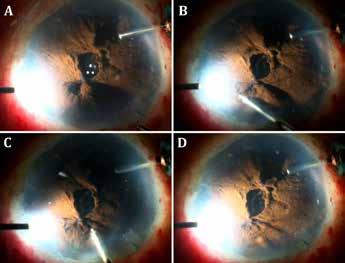
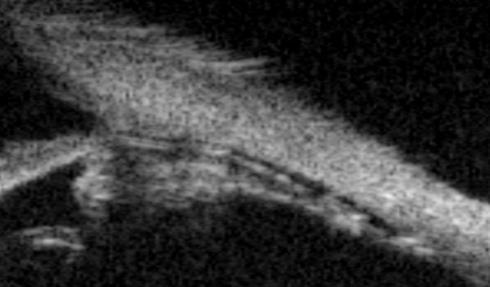
In his lecture, Dr Reinstein provided an overview of his major research interests and accomplishments that represent important contributions. He discussed his work leading to the development and applications of very high frequency digital ultrasound (VHFU) for scanning the cornea and anterior segment, an approach for better sizing of the implantable collamer lens (ICL), PRESBYOND for correcting presbyopia, and SMILE for refractive surgery.
“I will go through areas of research that were particularly difficult and, if I can say so, made me proud to have achieved some small steps,” Dr Reinstein said. “Now, I am looking forward to the rest of my career and seeing what more I can do for the specialty.”
Throughout his lecture and its conclusion, Dr Reinstein identified and credited those who taught, inspired, supported, and worked with him.
“We are a part of everyone who surrounds us. It is the interactions, relationships, and collaborations that make a difference.”
Measuring and mapping the corneal epithelium
Dr Reinstein recounted his first exposure to VHFU in 1991 as a research fellow at the Cornell Bioacoustic Research Facility, where the scanner was being used for evaluating ocular tumours. Staying late one night, he decided to scan a formalin-fixed rabbit eye and was excited to think he had discovered that the VHFU image revealed the front and back surfaces of the corneal epithelium.
Although he was told by one respected cornea specialist the information had no practical value, Dr Reinstein was not discouraged. With a team of collaborators, his continued research culminated in ARTEMIS, the first commercially available VHFU device, and the development of multiple applications that improve the safety and success of corneal and lens-based refractive surgery.1
Screening for keratoconus was the first application, and VHFU measurement of epithelial thickness had value for avoiding both false negatives and false positives. Dr Reinstein also used the information to develop rules for epithelial remodelling and showed how VHFU-enabled
analysis of corneal anatomy provided the diagnostic information key to repairing irregular astigmatism after corneal refractive surgery.
Predicting and monitoring ICL vault
Dr Reinstein also described the work done using VHFU to improve the science of ICL sizing. The research first showed a formula incorporating sulcus diameter versus the white-towhite measurement was far superior for predicting postoperative vault height.2 Subsequent work led to a new and better model using the ciliary body’s inner diameter instead of the sulcus diameter.3
Additionally, VHFU has a role in postoperative ICL vault monitoring.
“The thickest part of the lens in myopia is behind the iris, and the only way to see it is to dilate the eye, but that makes the lens go forward,” he explained. “Ultrasound is the only way to know how close the ICL is to the crystalline lens.”
Surgical innovations
Reflecting on his contributions to the field, Dr Reinstein described his work developing PRESBYOND as having the greatest impact—although he did note serendipity played a part. PRESBYOND introduces a controlled amount of spherical aberration to increase depth of field, and Dr Reinstein shared that it was while working on addressing night vision disturbances occurring after wavefront-guided LASIK he bumped into the idea of harnessing a ‘therapeutic’ amount of spherical aberration to manage presbyopia.
“According to this principle, presbyopia can be addressed by controlling spherical aberration on the cornea or with an intraocular lens. But which should you do?” he queried.
As support for PRESBYOND, Dr Reinstein said its results benefit from the extraordinary refractive accuracy of LASIK, which is much more accurate than lens calculations. Although he faced many challenges at the beginning of his work to develop SMILE, Dr Reinstein said every facet of the technique has been successfully addressed.
“SMILE is an incredibly mature procedure, and from the time of its release in 2011, it has been performed in more than 10 million eyes and is one of the most published procedures in medicine,” he said.
For citation notes, see page 46.
Dan Z Reinstein MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO is the medical director of the London Vision Clinic, London, UK. dzr@londonvisionclinic.com
Sorting Out Simultaneous Vision IOLs
The ESCRS Eye Journal Club discuss a new landmark paper on IOL classification and the need for harmonisation of terminology for presbyopic IOLs.
ROIBEÁRD O’HÉINEACHÁIN REPORTS
The ESCRS Eye Journal Club held a webinar hosted by Artemis Matsou MD and Alfredo Borgia MD to discuss the landmark paper, “Evidence-based functional classification of simultaneous vision intraocular lenses: seeking a global consensus by the ESCRS Functional Vision Working Group.”1 The expert panel included Douglas Koch MD, Daniel Chang MD, H Burkhard Dick MD, PhD, and Joaquín Fernández MD, PhD, lead author of the article under discussion.
Dr Matsou provided a summary of the paper, noting the International Organization for Standardization (ISO) offers the current IOL definitions. However, regarding the simultaneous vision intraocular lens (SVL) categories, the terminology remains ambiguous, with terms like multifocal and EDOF comprising a broad range of lens designs with varying optical designs and functional outcomes. Additionally, there are no defined endpoints for the new enhanced monofocal/monofocal-plus IOLs.
The ESCRS Vision Working Group reviewed scientific literature on SVLs using outcome data. They used cluster analysis to classify SVL IOLs into two main categories: partial range of field (ROF) and full ROF IOLs. Partial ROF is further divided into narrow range (standard monofocal IOLs), enhanced ROF (monofocal-plus IOLs), and extended range of field (EDOF IOLs). Full ROF IOLs are divided based on transition: continuous, smooth, and steep transition.
“The advantages of this classification system are that it focuses on the visual acuity the lenses can achieve across a range of distances based on patients’ experience. And while it recognises an overlap between optical and functional classifications, it is trying to bridge those metrics. There are some limitations,” Dr Matsou said. “For example, it does not include reports on dysphotopsias and patient-reported out-
comes, but that is mainly because of the inconsistent reporting of these parameters in the current literature.”
In the discussion that followed, Professor Koch noted the classification system the paper proposes adds further clarity to SVL IOL descriptions, particularly the functional distinctions between monofocal, monofocal plus, and EDOF IOLs, as well as the distinction between steep transition full ROF IOLs versus the smooth and continuous versions. However, he suggested the distinction between the smooth and continuous ROF IOLs may be less clinically relevant.
“Rather than range of field, I would ask that we consider the term depth of field,” he said. “Range of field might invite confusion with some of the newer IOLs, like Pablo Artal’s new lenses, designed to improve range of field in terms of perimetry.”
Dr Chang lauded the ESCRS Functional Vision Working Group’s achievement of adding clarity to IOL definitions amidst a rapidly evolving technology. He noted some factors may require closer consideration, including the conditions under which visual function testing is performed. Variations in testing conditions such as room lighting can influence visual acuity testing, as can the choice of vision charts and the duration and order of testing.
“The most important thing is for us to communicate and, in some ways, think about these things in a consistent fashion because our language doesn’t necessarily define how we think,” he added. “But it helps shape how we think, and how we think shapes what we say.”
Prof Dick noted that when he speaks at German society meetings, the nomenclature for the different IOLs becomes lost in translation. He added an overly complex classification system can be difficult to remember over time, while EDOF
and multifocal are well-established terms. However, he noted scientifically basing the nomenclature using de focus curves has the advantage of remaining applicable to new IOL technologies as they become available.
“It is also important to get a sufficient and reliable database,” he said. “And although there is variation in results between individuals that you never will be able to rule out, from a basic point of view, this is a very good step.”
Dr Matsou asked the panel how the scientific societ ies can work together with industry to convince them to accurately classify the IOLs based on functional outcome data.
“The FDA has strict rules about how to market a par ticular IOL. Companies do not have as much latitude in how they describe these IOLs as in Europe,” Prof Koch said. “Therefore, we need the ESCRS and the ASCRS to get together and request the manufacturers accurately describe these IOLs in terms of their depth of field.”
“I think most companies work hand in hand with physicians. And I think if we start using the terminology, they will start coming along,” Dr Chang said. “But if we do not agree as physicians, then they will take the reins and use the terminology they want.”
Prof Fernández noted the present landmark paper represents the first step in bringing the classification of simultaneous vision IOLs into accordance with evidence-based medicine.
“A bigger step will be to bring the ASCRS on board with a shared committee to not only consolidate the classifications but [collaborate] in the future as industries introduce new IOL technologies,” he added.
For citation notes, see page 46.
Artemis Matsou MD, MRCP(UK), FEBOS-CR, FEBO, PgDip CRS is a consultant ophthalmologist and cataract lead at Queen Victoria Hospital, East Grinstead, UK. art.matsou@gmail.com
Alfredo Borgia MD, FEBO is based at Royal Liverpool and Broadgreen University Hospitals, Liverpool, UK. alfr.borgia@gmail.com
Douglas Koch MD is Professor and Allen, Mosbacher, and Law Chair in Ophthalmology at The Cullen Eye Institute, Baylor College of Medicine, Houston, Texas, US. dkoch@bcm.edu
H Burkhard Dick MD, PhD, FEBOS-CR is Professor of Ophthalmology and Chairman, Ruhr University Eye Hospital Bochum, Germany. He is also Secretary of the ESCRS. dickburkhard@aol.com
Daniel Chang MD is based at Empire Eye and Laser, Bakersfield, California, US. dchang@empireeyeandlaser.com
Joaquín Fernández Pérez MD, PhD is based at Qvision, Department of Ophthalmology of Vithas Almería Hospital, Spain. He is the inco ming Secretary of the ESCRS. joaquinfernandezoft@qvision.es
ophthalmologist moderators from ESCRS.
Every two months, we release an insightful conversation—available as a video or podcast—so you can watch, listen, and learn, anytime and anywhere. Don’t miss out on cutting-edge conversations in ophthalmology. Tune in now and stay ahead of the latest research!
Big Advantages to Small-Aperture IOLs
Small-aperture IOLs offer superior image quality with increased range of focus.
HOWARD LARKIN REPORTS
Asmall-aperture intraocular lens (IOL) implanted in the non-dominant eye offers about 2.00 D additional depth of focus over a monofocal lens with image quality superior to other extended depth of focus and multifocal lenses, reported Elizabeth Yeu MD. Small-aperture lenses can also mask up to 1.50 D of corneal astigmatism and substantially improve vision in some patients with irregular corneas.
Dr Yeu reported on a prospective non-randomised open-label trial comparing 343 patients implanted with a monofocal lens targeting plano in the dominant eye and a small-aperture IC-8 lens (Bausch + Lomb) targeting -0.75 D in the non-dominant eye with 110 implanted with monofocals targeting plano in both eyes. At 12 months, mean monocular visual acuity was 20/32 at about -2.00 D defocus and 20/40 at -2.50 D in the IC-8 eyes compared with 20/40 at about -1.00 D in the monofocal eyes.
Binocularly, the two groups had comparable distance vision while the small-aperture group had superior intermediate and near vision, she said. Binocular contrast sensitivity was comparable with and without glare. Small-aperture patients also rated their severity of visual symptoms as very low or comparable to monofocal patients, with only about 3.0–3.6% of small-aperture patients reporting severe glare, halos, or starbursts.1
Irregular corneas
Dr Yeu noted that implantation in the non-dominant eye is the label indication for the IC-8. However, small-aperture lenses can be used to treat some aberrated corneas due to irregular astigmatism, previous refractive surgery, or even keratoconus. “Where it really shines is in these irregular corneas.”
Research by Nicole Fram MD and others shows an improvement of about seven lines of uncorrected distance vision in patients with irregular astigmatism when implanted with a small-aperture lens. In some cases, it can mitigate corneal astigmatism and higher-order aberrations by blocking peripheral aberrations, improving vision quality.2 Patients with worse uncorrected vision from aberrated corneas—from keratoconus or previous RK, for example—often experience a surprising level of satisfaction, Dr Yeu added.
Where it really shines is in these irregular corneas.
Dilation beyond 6.5 mm can help minimise dimness and aid in Nd:YAG posterior capsulotomy, Dr Yeu said. If dimming is not an issue on the first eye, the IC-8 can be implanted bilaterally off-label for irregular cornea patients.
However, “not all irregular corneas can benefit from seeing through a small aperture,” Dr Yeu said. Preoperative tests can help. Raytracing can simulate small aperture performance over a 1.0–2.0 mm pupil, which can help determine if the lens will be useful. Range of vision of a small-aperture lens can be tested preoperatively with pilocarpine.
Patients with previous hyperopic LASIK may complain of vision quality issues, though those with previous myopic LASIK or prior monovision adaptation with contact lenses are generally happy. Glare may be worse when more than -1.25 D is targeted, so the goal should stay between -0.75 to -1.25 D, she concluded.
Dr Yeu made her comments at AAO 2024 in Chicago, US.
For citation notes, see page 46.
Elizabeth Yeu MD is an ophthalmologist in private practice and assistant professor at the Eastern Virginia Medical School in Norfolk, Virginia, US, and past president of the ASCRS. eyeulin@gmail.com
for the Peter Barry Fellowship 2025 are
NOW OPEN! Applications
The Fellowship of €60,000 will allow a trainee to work abroad at a centre of excellence for clinical experience or research in the field of cataract and refractive surgery, anywhere in the world, for 1 year.
The application deadline is 2 May 2025.
Exploring the Expanded Array of KLEx Procedures
Comparative study highlights similarities and differences.
CHERYL GUTTMAN KRADER REPORTS
Astudy evaluating four different keratorefractive lenticule exchange (KLEx) platforms found they performed similarly for correcting myopic and astigmatic refractive errors and were associated with similarly good visual acuity outcomes at one month. However, the research also identified differences in ease of lenticule separation and visual recovery speed.
Conducted by refractive surgeons at Nobel Eye Clinics, Taiwan, the retrospective study analysed data for 55 eyes treated with SMILE (VisuMax laser), 40 eyes treated with SMILE Pro (VISUMAX 800 laser), 20 eyes treated with Smart Sight (ATOS laser), and 12 eyes treated with Smart Clear (Z8 laser). Multiple surgeons at multiple centres performed the procedures. Baseline demographics, refractive errors, central corneal thickness, and programmed optical zone size were similar in the four groups, reported Alexander Chen MD.
Outcomes at one month for residual spherical and astigmatic error, UDVA, contrast sensitivity in daylight and low light conditions, and change in higher-order aberrations were similar across all platforms. At one week postoperatively, however, both UDVA and low-light contrast sensitivity were significantly lower in eyes treated with Clear Sight and Smart Clear compared to the SMILE and SMILE Pro groups.
The mean score for ease of lenticule separation (rated on a scale of 0 to 100 [easiest]) was significantly lower for SMILE than the other three groups (81 versus 90 to 91). Analyses of other outcome measures showed the four platforms similarly overestimated central corneal stromal reduction and produced an optical zone about 1 mm smaller than programmed.
Personal perspectives
Dr Chen suggested the poorer early vision outcomes after Clear Sight and Smart Clear might be attributed, in part, to less surgeon experience with those two procedures and fewer patients in those groups. Nevertheless, when asked to compare the four KLEx procedures based on his personal experience, Dr Chen said he favoured the SMILE Pro because of the speed of the VISUMAX 800 laser.
“Operating at a repetition rate of 2 MHz, the VISUMAX 800 is the fastest laser. It completes lenticule creation in just 8 to 10 seconds compared with 23 seconds using the VisuMax, 33 seconds with the ATOS, and 45 seconds with the Z8. The faster speed leads to increased comfort for both patients and surgeons,” he explained.
“Faster speed may also be a factor for enhancing lenticule dissection, which I find is easiest in procedures done with the
VISUMAX 800, and it might reduce the risk of suction loss, although there were no cases of suction loss in our small study.”
Dr Chen identified other differences between the four femtosecond lasers/KLEx procedures that could influence surgeon choice. Compared to the other platforms, Smart Sight is approved for treating the largest range of spherical and cylinder errors, and the ATOS is the only laser with automated cyclotorsion compensation. Centration using the VisuMax must be done manually but is computer-guided with the other lasers. Only the Z8 laser has a flat corneal interface that Dr Chen said in theory may increase the accuracy of astigmatic correction compared to a curved interface.
Dr Chen presented the study at AAO 2024 in Chicago, US.
Alexander Chen MD is a cataract and refractive surgeon at Nobel Eye Clinics, Taipei, Taiwan. a1050276@hotmail.com
Refining Indications for CXL
Dresden protocol remains time-proven standard, but modifications help address its limitations.
CHERYL GUTTMAN KRADER REPORTS
Corneal cross-linking (CXL) for treating eyes with progressive keratoconus or ectasia after excimer laser refractive surgery is safe using either the standard Dresden protocol or an accelerated approach, and overall, the two techniques appear to provide clinically equivalent results, said Jose de la Cruz MD, based on a review of the literature.
“Outcomes of CXL may be affected by several variables, including age, risk and speed of progression, family history, coincident allergic conjunctivitis/eye rubbing, and follow-up,” he added. “And, due to the risk of damaging the endothelium, both the standard and accelerated approaches suffer the major limitation of being confined to use in eyes with a corneal thickness of at least 400 microns after epithelial debridement.”
Discussing standard and accelerated CXL techniques, Dr de la Cruz reviewed the parameters of the Dresden protocol, including a 30-minute period for applying the photosensitising agent (riboflavin 0.1%) and a 30-minute exposure time with ultraviolet A light (UVA) at an energy of 3 mW/cm2
“The effectiveness of this technique has been proven over time, but it is a long and arduous protocol for both the patient and physician,” he said.
Various accelerated protocols have been introduced that deliver the same cumulative energy dose as the Dresden protocol (5.4 J/cm2) but use higher UV irradiation intensities of 9, 18, or 30 mW/cm2 and shortened exposure times of 10, 5, or 3 minutes, respectively.
Dr de la Cruz discussed two published papers comparing outcomes of standard and accelerated CXL treatments, including a meta-analysis of six randomised controlled trials with 1 year of follow-up and another analysing 5-year outcomes for 100 eyes that had standard CXL and 76 treated with an accelerated protocol using data from the Save Sight Keratoconus Registry.1,2
Based on the findings of these and other publications, he concluded standard CXL may result in better VA outcomes, a greater decrease in Kmax, and a deeper demarcation line compared with accelerated CXL—but may have a higher rate of transient haze. Dr de la Cruz suggested the advantages and disadvantages of standard CXL versus accelerated CXL may be explained by their differences in duration and irradiation intensity.
CXL for thinner corneas
Discussing CXL for eyes with a central corneal thickness of less than 400 microns, Dr de la Cruz said various modified protocols have been introduced to enable a safe procedure. They include transiently thickening the cornea by application of a contact lens or hyperosmolar riboflavin. Another approach leaves islands of epithelium over the cornea’s thinnest regions.
“However, these protocols have limitations or have not been standardised,” he said.
Another technique developed by Hafezi (et al.) was designed to individualise fluence by adapting irradiation time to stromal thickness in 10-micron increments while keeping irradiance fixed at 3 mW/cm2 3 Data from a series of eyes followed for 1 year showed no significant changes in corrected distance visual acuity, sphere, or Kmax values, halting progression in 90% of eyes, and no signs of endothelial decompensation. A direct correlation was found between demarcation line depth and irradiation, although the investigators noted the algorithm underestimated the demarcation depth.
Dr de la Cruz spoke on this topic at the 2024 ESCRS Congress in Barcelona.
For citation notes, see page 47.
Jose de la Cruz MD, MS is Clinical Professor, Department of Ophthalmology and Visual Sciences, University of Illinois at Chicago, US. josedlc@uic.edu
Knowing Iris Repair: Using Iridodiathermy in Iris Surgery
Prepare for decentred pupils and uneven irides in multiple situations.
BY SOOSAN JACOB MS, FRCS, DNB
An uneven iris and a decentred or not round pupil can be addressed in different ways. This article discusses the problems that such situations lead to and what can be done.
Irregular anterior chamber
During pupilloplasty, taking the needle bites too close to the iris edge on either side can cause a gap between two consecutive pupilloplasty knots along a stretch of iris repair. The suture may also sometimes cheese-wire if too close to the edge.
On the other hand, if the needle bites are at a distance from the iris edge, bunching may be seen at the site where the knot tightens to bring the two limbs of iris tissue together. The amount of bunching depends on the distance between the edge and the needle bite—the greater the distance, the greater the bunching.
This bunching can sometimes not be avoided and can lead to the iris tenting upwards locally, causing an asymmetry in the anterior chamber (AC) volume and resulting in an AC that is shallower over the area of pupilloplasty. Though this may not cause problems in most cases, it can become an issue whenever air is to be left in the AC, e.g., post-air injection for a detached Descemet’s membrane (DM) or after endothelial keratoplasty.
FIGURE: Iris repair performed prior to pre-Descemet’s endothelial keratoplasty: A) Bunched-up iris seen on either side of the pupilloplasty knot and visualized well using oblique light from an endoilluminator; B,C) Iris diathermy is done using the endodiathermy probe applied to the mid-periphery on either side of the bunchedup iris stroma; D) A flat iris surface leads to better and more stable anterior chamber dynamics and a non-migratory air bubble.
The uneven AC can result in an irregular air bubble that is not uniform and may easily migrate partially or completely behind the iris, leading to localized or circumferential iridocorneal touch with an increased risk of peripheral anterior synechiae formation. In such cases, and especially if the eye is also monocameral (e.g., post intrascleral haptic fixation or after iris fixation of IOL), posterior migration of air into the vitreous cavity can occur, resulting in an increased risk of graft detachment.
Floppy iris
Certain eyes may have a floppy iris, which again becomes significant when air bubble dynamics are important. A floppy iris has excess mobility and can result in intra- and postoperative fluctuations in the AC depth, pupillary block, anterior iris bowing, shallow AC, and increased intraocular pressure. A shallow AC can result in difficulty in intraoperative manoeuvring of instruments and damage to ocular structures. This again becomes significant in endothelial keratoplasty, where air is left in the AC to hold the graft up against the host stroma. It also makes it easier for the air to migrate to the posterior chamber or the vitreous cavity in monocameral eyes, resulting in loss of support for the graft.
Decentred, non-circular pupil
The optical and neural axes of the eye are generally well aligned to allow good-quality foveal image formation. The pupil may be found decentred in some patients as a result of previous surgery, trauma, or inflammation, among others. A round and cantered pupil is important for good quality of vision. Prismatic effects can come with a tilted optical system. Decentration of the pupil induces higher-order aberrations and astigmatism, decreased light sensitivity, decreased contrast, changes in refractive error, and distortions in colour, depth, and size perception. When light rays fall obliquely on photoreceptors, each ray may stimulate more than one cone, resulting in acuity loss due to a retinal directional acuity effect. In addition, if performing iris repair, it is important to ensure a well-cantered and round pupil at the end of surgery.
Iridodiathermy
Endodiathermy has been used for many years in vitrectomy surgeries to arrest bleeding, mark the retina around holes or tears, and create retinotomies. More recently, it has been used in iris surgery. A full vitrectomy machine is not required for using the endodiathermy probe, and it can con-
nect to the phaco machine or a cautery unit through its connecting wires. The probe is available as a 23, 25, and 27 gauge and can be inserted through a paracentesis. The effect is activated only at the tip.
I have described iridodiathermy for treating localized iris bunching adjacent to pupilloplasty knots. The AC is irrigated with BSS via an anterior chamber maintainer. The tip of the endodiathermy probe is applied directly over the bunched-up iris and power activated. This results in contraction of the iris stroma and flattening. The power is kept low and test burns are applied, followed by slow titration upwards until the desired effect is obtained. Spots may be applied until the iris becomes flat and the AC is regular and of even depth again.
A floppy iris is similarly treated by placing spots on the mid-peripheral iris stroma. This causes the iris stroma to contract and tighten, thus tautening the floppiness. Going too close to the pupil should be avoided as this can result in distortion and drawing of the pupil to the side with the spots.
Ahmed (et al.) described the use of endodiathermy for cantering the pupil.1 It may be performed primarily in a case where the pupil is decentred secondary to disease, congenitally, or secondary to surgery/after pupilloplasty. Primary endodiathermal pupillary repositioning is done by simply using the endodiathermy probe. In this case, power is applied close to the pupillary margin and not at the iris, mid-periphery. The iris is drawn towards the endodiathermy application side. It can also be used to round up a non-circular iris using a short application very close to the iris border.
Eyes undergoing penetrating keratoplasty may sometimes need extensive anterior segment reconstruction to improve vision, decrease photic phenomena, release peripheral anterior synechiae, and improve AC dynamics. Suture pupilloplasty is often used to bring iris tissue together into as physiological a position as possible. Open sky endodiathermy can be applied in these cases to flatten the bunched-up iris.
Other uses for the endodiathermy probe in the anterior segment include creating a rhexis or creating a pupil in eyes with an occluded or fully updrawn pupil. The endodiathermy gives a greater effect on a darkly pigmented iris than on light-coloured irides. Also, with time, a mild depigmentation may be seen at the site of application of spots.
This is the seventh article in a series on iris repair. Please see past issues of EuroTimes for related columns.
For citation notes, see page 47.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
One-stop-shop Registries in Ophthalmology
EUREQUO
European Registry of Quality Outcomes for Cataract and Refractive Surgery
CNTF-secreting intravitreal implant shows promise in phase 2 clinical trial.
CHERYL GUTTMAN KRADER REPORTS
Long-term clinical trial results suggest NT-501, an intravitreal implant releasing soluble ciliary neurotrophic factor (CNTF), is safe and has promising biological activity in open-angle glaucoma patients, reported Alexandria M Dominguez.
She reported the results from 24 months of follow-up in a phase 2 randomised, sham-controlled clinical trial investigating NT-501. The implant contains an internal scaffold of bioengineered CNTF-secreting cells encapsulated within a semipermeable membrane that allows inflow of nutrients and oxygen to support the CNTF-secreting cells while protecting them from exposure to immune cells. CNTF is a potent neuroprotective protein that promotes the survival and maintenance of photoreceptors.
“The analyses showed enhancements in thickness of both the retinal nerve fibre layer (RNFL) and ganglion cell layer in eyes with the NT-501 implant compared to the sham group, but the study was underpowered to show efficacy based on functional assessment,” she said. “To better assess functional efficacy, the study’s cohort size has been increased, and dual implants are being evaluated.”
The phase 2 study is a multicentre trial with three investigational sites (Stanford University, Palo Alto, California; Columbia University, New York; and Glaucoma Associates of Texas, Dallas). A total of 55 patients were enrolled from 2016 to 2021. Eligible patients had stable IOP control and BCVA greater than 20/200 in both eyes. Patients were excluded if they had ophthalmic disease other than glaucoma, were pregnant, or had a history of past or current immunosuppression.
One eye of each patient was randomised to receive the implant or a sham procedure, and patients were followed every 3 months. Based on positive findings in an analysis of data at 1 year and a pre-specified crossover plan, 19 patients in the sham group subsequently received the NT-501 implant at the 12- or 24-month visit. Fifty-four of the 55 enrolled patients were evaluated at month 24, representing a high retention rate for the trial.
Change in Humphrey visual field at 12 months was assessed as one primary outcome measure. Ms Dominguez presented data collected from the subset of 27 patients enrolled at Stanford University, and the results showed stability of the visual field in the implant and sham groups.
“There were also no significant changes in BCVA throughout the trial in either the sham group or eyes with the implant,” Ms Dominguez said. “IOP was also stable in both the sham group and eyes that received the implant.”
Secondary endpoints included assessing changes from baseline to 6, 12, and 24 months in RNFL and ganglion cell layer thickness measured by spectral domain OCT. Results from follow-up at 2 years showed a significant increase in both structural measures in eyes with the implant relative to the sham group. The increases were often seen within 1 month after patients received the implant, plateaued at around month 12, and remained stable through month 24.
Study participants also completed the 25-item Visual Function Questionnaire. Analyses of data collected at baseline and month 12 showed no significant differences comparing the implant and sham groups.
“However, there was an interesting trend for the sham group to report worsening peripheral vision at month 12 relative to their baseline peripheral vision, and the opposite—an increase—was detected in the group that received the implant,” Ms Dominguez said.
There were no serious adverse events associated with the NT-501 implant. The most commonly reported adverse event was temporary postoperative conjunctival injection.
The NT-501 implant is being evaluated for the treatment of chronic retinal diseases. A clinical study is underway in patients with macular telangiectasia type 2.
Ms Dominguez presented the study findings on behalf of the investigators at AAO 2024 in Chicago, US.
Alexandria M Dominguez MS is a medical student at Howard University College of Medicine, Washington, DC, US.
Jeffrey L Goldberg MD, PhD is Professor and Chair of Ophthalmology, Byers Eye Institute, Stanford University, California, US, and is the principal investigator.
Understanding Glaucoma and Cataract Surgeries
Prospective, randomised PTVT Study provides evidence-based insights into the relationship.
CHERYL GUTTMAN KRADER REPORTS
As a prospective study enrolling only phakic patients and following them for up to 5 years, the Primary Tube Versus Trabeculectomy (PTVT) Study provided a unique opportunity for understanding how the two glaucoma procedures affect cataract development/ progression and how the IOP lowering effect of each is impacted by subsequently performed phacoemulsification.
Consistent with previous studies suggesting glaucoma surgery accelerates cataract development, the PTVT results showed cataract procedures were commonly performed after both trabeculectomy and tube shunt surgery. Findings from analyses of IOP control, glaucoma medication use, and glaucoma surgery failure rates also seemed to support available evidence indicating that compared to trabeculectomy blebs, tube function may be more resilient and resistant to failure after phacoemulsification, said Steven J Gedde MD.
“There are many published reports showing cataract surgery has a detrimental effect on bleb function in eyes with pre-existing trabeculectomy, but the evidence is mostly from retrospective case series,” Dr Gedde said. “Available reports on eyes with tube shunts suggest IOP control is not impacted by subsequent cataract extraction, but the information on that topic is much more limited.”
The PTVT Study randomised 242 eyes of 242 patients 1:1 to undergo trabeculectomy with mitomycin-C or tube shunt surgery. All study eyes were phakic because a history of ocular surgery was an exclusion criterion.
During 5 years of follow-up, the cumulative probability of phacoemulsification was higher in the tube shunt group than in the trabeculectomy group (57.2% vs 42.3%). The difference, however, was not statistically significant, Dr Gedde said.
Results from analyses of changes in IOP and IOP-lowering medication use after phacoemulsification showed there were
no significant changes in either endpoint through the last follow-up in eyes with a tube shunt. In the trabeculectomy group, however, there was a trend for an increase in IOP and a statistically significant increase in glaucoma medical therapy use at 1 year that remained statistically significant after 18 months, 2 years, and the last follow-up after phacoemulsification.
“Before phacoemulsification, however, mean daily use of medical therapy was much higher in the tube shunt group than the trabeculectomy group (2.3 vs 0.9), and so overall usage in the two groups equalised after cataract surgery,” Dr Gedde said.
Glaucoma surgery failure rates comparing eyes that did and did not have phacoemulsification showed a twofold higher risk of failure after phacoemulsification in the trabeculectomy group and a 30% increased risk of failure after phacoemulsification in the tube shunt group. The increased risk after phacoemulsification was not statistically significant in either glaucoma surgery group—but there was a trend towards a higher rate of failure after phacoemulsification in the eyes that had trabeculectomy.
Additional analyses of outcomes after phacoemulsification showed that complications were uncommon and occurred with similar frequency in the trabeculectomy and tube shunt groups. In addition, visual outcomes after phacoemulsification were favourable overall. Visual acuity in both the trabeculectomy and tube shunt groups improved after phacoemulsification.
Dr Gedde spoke at AAO 2024 in Chicago, US.
Steven J Gedde MD is Professor of Ophthalmology at Bascom Palmer Eye Institute, University of Miami, Florida, US, and chairman of the PTVT Study. sgedde@med.miami.edu
Neuroprotectant Treatment for MacTel Type 2
Intravitreal implant releasing ciliary neurotrophic factor found safe and effective in pivotal trials.
CHERYL GUTTMAN KRADER REPORTS
Sustained intraocular delivery of ciliary neurotrophic factor (CNTF) using NT-501 encapsulated cell therapy (revakinagene taroretcel) is safe and effective for treating macular telangiectasia (MacTel) type 2, suggest the results of two phase 3 clinical trials.
The NT-501 implant is inserted into the vitreous and sutured to the sclera. Reviewing the outcomes of the two phase 3 studies, Emily Y Chew MD reported both investigations met their primary endpoint, showing significantly greater photoreceptor preservation after 2 years in eyes receiving the first-in-class therapy compared to control eyes that underwent a sham operation. Analyses of secondary efficacy measures showed preserved retinal sensitivity within the ellipsoid zone break line in participants receiving NT-501, but the treatment effect was not statistically significant in either study.
“MacTel type 2 was the first disease to demonstrate benefit from treatment with NT-501, partly because of the availability of a good outcome measure for quantifying the structural change that occurs with disease progression,” Dr Chew said. “We believe that results of a pooled analysis of retinal sensitivity data may show a significant difference favouring NT-501 versus sham therapy.”
The two phase 3 trials involved more than 200 participants enrolled at 47 international sites. Patients aged 21 to 80 were eligible if they had a MacTel type 2 diagnosis, an ellipsoid zone break in the study eye and en face ellipsoid zone between 0.16 and 2.00 mm2, and BCVA ≥54 ETDRS letters (Snellen equivalent ≥20/80).
The study participants were primarily white and female, with a mean age of about 60 years and a baseline BCVA of about 20/40.
Data on change in ellipsoid zone area from baseline to 24 months showed that compared to sham, NT-501 reduced the loss rate by 55% in one study and 31% in the second.
“The treatment effect was statistically significant in both studies,” Dr Chew said. “Reasons for the difference between
studies in magnitude of the effect might be related to differences in the participants’ baseline lesion size and other patient characteristics.”
Microperimetry measured the retinal sensitivity, and Dr Chew suggested that differences between the two studies in lesion size and the quality of microperimetry data might explain why only one study demonstrated the benefit of better retinal sensitivity preservation.
“We don’t know for sure why the retinal sensitivity results varied, but it is well known that microperimetry testing can be very difficult for patients,” she said.
“We will be looking at various factors and hopefully doing an extension study to continue following patients. Examination of explanted NT-501 implants shows CNTF release remains durable for at least 14 years.”
Dr Chew described the safety profile of NT-501 as “excellent,” adding it was very well tolerated. Ocular treatment-emergent adverse events were uncommon and mostly mild and transient. There were a few serious ocular treatment-emergent adverse events, but most were related to surgery and, therefore, expected.
There were no serious treatment-emergent adverse events of endophthalmitis or ischemic optic neuropathy nor any instances of clinically significant intraocular inflammation.
“The rates of delayed dark adaptation and miosis were higher in the NT-501 groups compared to sham, but even some sham patients had delayed dark adaptation,” Dr Chew said.
Dr Chew presented the results at AAO 2024 in Chicago, US.
Emily Y Chew MD is Director of the Division of Epidemiology and Clinical Applications at the National Eye Institute/National Institutes of Health, Bethesda, Maryland, US. echew@nei.nih.gov
Targeting the Pathogenic Pathway
Oral gildeuretinol shows promising efficacy and safety in clinical trials for treating Stargardt disease.
Results from TEASE, an ongoing clinical trial programme, show that oral treatment with gildeuretinol is well-tolerated and significantly slows progression of Stargardt disease type 1 (STGD1), said Christine Nichols Kay MD.
“Stargardt disease is the most common form of inherited juvenile macular degeneration and associated with pathogenic variants in the ABCA4 gene,” said Dr Kay.
“Gildeuretinol is the first treatment to show efficacy in STGD1 in a double-masked, randomised, placebo-controlled clinical trial called TEASE-1, and topline results from a second randomised clinical trial called TEASE-2 are expected in 2025.”
Serving as a vitamin A replacement, gildeuretinol is a new chemical entity that reduces toxic vitamin A dimer formation in the eyes, as these cause damage to the retinal pigment epithelium and photoreceptors in patients with STGD1. While the molecule acts to slow disease progression, gildeuretinol does not interfere with the vitamin A cycle function.
TEASE-1 was the first of four clinical trials comprising the TEASE programme. Patients with advanced STGD1 were randomised to receive treatment with either gildeuretinol (30 patients) or placebo (20 patients). Based on early pharmacokinetic data, the 14 mg dose was chosen for further clinical development.
At 24 months, TEASE-1 met its primary endpoint, showing that gildeuretinol slowed the growth rate of retinal atrophic lesions by 21.6% based on the linear estimate, 29.5% based on untransformed areas (P < 0.001 for both) compared to the control group that included both placebo-treated participants and a little more than 50 natural history cases. Including only randomised patients and excluding natural history cases, the results remained significant (P = 0.006)
Treating STGD1 with gildeuretinol for younger patients with milder disease is being investigated in TEASE-2, the
fully enrolled 24-month study that randomised 80 patients 1:1 to gildeuretinol 14 mg or placebo taken once daily.
TEASE-3 is an open-label study evaluating gildeuretinol in patients with STGD1 and early signs of maculopathy, enrolling up to 10 patients expected to progress based on knowledge of natural history. Disease progression is evaluated from baseline to month 24 and compared to data from historical findings of untreated siblings when age-matched available. Dr Kay shared the overall stability of visual acuity and retinal imaging through the outcomes of three participants, showing no progression after 24 months of gildeuretinol treatment. When age matched, untreated siblings experienced significant vision decline and lesion growth.
Dr Kay reported that safety data from TEASE-1 and TEASE-3 are encouraging. “There have been no serious adverse events, clinically significant changes in liver function tests, adverse events related to hyper- or hypovitaminosis A, anterior segment manifestations of xerophthalmia, or reports of chromatopsia, dark adaptation delay, or night blindness,” she said.
TEASE-4 is a 24-month open-label clinical trial enrolling approximately 170 patients (from 8 years of age), including participants from other TEASE studies as well as treatment-naïve patients.
Dr Kay spoke on this topic at AAO 2024 in Chicago, US.
Christine Nichols Kay MD is Director of Retinal Genetics and Director of Clinical Research at Vitreo Retinal Associates, Gainesville, Florida, US. christine@vra-pa.com
CHERYL GUTTMAN KRADER REPORTS
Reducing the Treatment Burden for Neovascular AMD
Tyrosine kinase inhibitors emerging as promising new class of drugs.
CHERYL GUTTMAN KRADER REPORTS
Tyrosine kinase inhibitors (TKIs) represent a potential improvement for managing neovascular age-related macular degeneration (nAMD), phase 2 clinical trials suggest. Phase 3 studies will provide a better understanding of the efficacy of the modalities in this new class of drugs— although the findings will need to be considered cautiously, recognising the treatment protocols in the pivotal trials may not reflect real-world care, said Rishi P Singh MD.
Eight TKI products are being developed to treat retinal vascular diseases.1 Of those, three have completed phase 2 nAMD clinical trials and are the subject of phase 3 trials that are either underway or in the planning stage. The three products are sustained release axitinib intravitreal implant (Axpaxli, formerly OTX-TKI; Ocular Therapeutix); axitinib suspension for suprachoroidal injection (CLS-AX; Clearside Biomedical); and sustained release vorolanib in a rigid bioerodible insert (Duravyu, formerly EYP-1901; EyePoint).
“These drugs differ in their platform delivery mechanism and delivery time periods, and their study protocols differ with respect to front-end anti-VEGF injection regimens and retreatment criteria. Therefore, it is difficult to make any comparisons,” Dr Singh said.
“Preclinical data also suggest differences in potency, but the findings probably cannot be extrapolated to doses that are used clinically.”
OTX-TKI
The axitinib intravitreal implant is a hydrogel device that releases the drug at a fixed rate over about 5.5 months followed by terminal release upon implant bioresorption for a flexible redosing period.
A phase 1 study enrolled patients who had controlled nAMD after receiving an average of 8 anti-VEGF injections in the 12 months prior to study enrolment and randomised them to OTX-TKI or aflibercept 2 mg every 8 weeks (Q8W) after initial loading doses of aflibercept. After 12 months, visual acuity (VA) and central subfield thickness (CSFT) values were stable in the OTX-TKI recipients and comparable to the control group. Injection frequency in the OTX-TKI group was reduced by an average of 92% compared to the previous year, and at month 12, 60% of OTX-TKI recipients had received no rescue treatment.2
“The data on durability here and in the other studies are promising, but we must keep in mind that previous retreatments based on physician discretion may have led to earlier intervention than mandated by the study retreatment criteria,” Dr Singh said.
Preclinical data also suggest differences in potency, but the findings probably cannot be extrapolated to doses that are used clinically.
OTX-TKI is now being investigated in two pivotal trials. SOL-1 plans to enrol about 300 treatment-naïve patients, randomised to receive a single injection of the implant or aflibercept 2 mg after demonstrating response to two initial doses of aflibercept. The trial is unique in its design to demonstrate the implant’s superiority, Dr Singh said.
The primary endpoint in SOL-1 is analysing the proportion of patients who maintain BCVA (loss of ≤15 ETDRS letters) at week 36. A second study, SOL-R, is a 48-week trial designed to demonstrate OTX-TKI Q24W is noninferior to fixed dose aflibercept 2 mg Q8W. Patients who fail to respond to the aflibercept loading doses in SOL-1 are eligible for SOL-R, which is randomising 825 patients 2:2:1 to OTX-TKI, aflibercept 2 mg Q8W, or aflibercept 8 mg Q24W. All patients are receiving two loading doses of aflibercept 2 mg.
CLS-AX
CLS-AX administered as two suprachoroidal injections at baseline, and then at least Q24W, was compared with aflibercept Q8W in the phase 2b ODYSSEY trial that enrolled difficult-to-treat patients with nAMD. All patients received three aflibercept loading doses. Positive topline results showed the study met its primary endpoint assessing BCVA stability through 9 months. Patients treated with CLS-AX also had a >80% reduction in injection frequency compared to the 24 weeks prior to screening, and 67% had not received additional treatment at the 24-week redosing visit.3
“Data on repeat dosing in ODYSSEY will inform design of the phase 3 studies that will likely aim to produce findings that support a dosing interval of between 3 and 6 months,” Dr Singh said.
EYP-1901
The bioerodible platform used for EYP-1901 releases the drug immediately, allowing voralonib to reach target tissues within hours of implantation and then by zeroorder kinetics for at least 6 months.
The phase 2 DAVIO 2 clinical trial randomised patients with active nAMD controlled by anti-VEGF therapy to aflibercept Q2W or one of two doses of EYP-1901. Results through 12 months showed EYP-1901 maintained stable control of VA and CSFT while reducing treatment burden relative to the period before enrolment.4
Two phase 3 studies are investigating EYP-1901— LUGANO and LUCIA. These are noninferiority studies comparing EYP-1901 Q24W or aflibercept 2 mg Q8W. They will each enrol about 400 patients with active nAMD, including treatment-naïve and treatment-experienced patients. All patients are receiving three loading doses of aflibercept 2 mg. Mean change in BCVA from baseline to weeks 52 and 56 is the primary endpoint.
Dr Singh spoke at AAO 2024 in Chicago, US.
For citation notes, see page 47.
Rishi
P
Singh
MD is Staff Physician, Vice President, and Chief Medical Officer at Cleveland Clinic Martin Health, Stuart, Florida, US, and Professor of Ophthalmology Cleveland Clinic Lerner College of Medicine, Cleveland,
Ohio, US. drrishisingh@gmail.com
ESCRS Patient Portal
Patients are understandably curious to learn as much as they can about their upcoming cataract or refractive surgery. ESCRS has developed a Patient Portal on its website to help inform patients about these surgeries.
The Portal is split into two sections: Cataract and Refractive. Each section provides an easy-to-understand summary of the different types of conditions, including the benefits, risks, procedures, and aftercare of common conditions. Each section is easily navigable, with clear diagrams and a glossary to convey all the information patients might need to help prepare for surgery or during aftercare.
Robotic Eye Surgery Could Expand Surgical Possibilities
Safety and accuracy are the strong points for robotic assistance.
Robotic eye surgery is no longer in the realm of science fiction. It’s already here and could offer surgeons new capabilities and efficiencies, according to Robert K Maloney MD.
“Robots can dance and robots can drive cars safely. It’s not surprising that someone would think about using robots for eye surgery,” Dr Maloney noted. In fact, four companies have created robotic eye surgery systems—AcuSurgical, ForSight Robotics, Zeiss Exchange Robotics, and Horizon Surgical Systems, for which Dr Maloney is a consultant and equity holder.
One major advantage of robotic eye surgery is greater precision, Dr Maloney said. Millimetre movements of the human hand translate into micron instrument movements by the robot. Human hand tremors, which typically exceed 100 microns, can be reduced or eliminated. Doing away with such tremors could create new treatment possibilities, such as delivering clot-breaking medications into blocked 80-micron retinal arteries. Injecting subretinal medications could be more precise, accurately placing medication into the subretinal space.
The surgeon’s role
Robotic eye surgery systems come in two operating modes. The first is surgeon controlled. Similar to the Da Vinci system for general surgery, the surgeon sits at a console and controls the robot using joysticks while watching on a monitor.
Live robotic retinal surgery on humans is already happening, and the technology could also be used for cataract surgery with its offer of safety. If the patient moves, the robot can be out of the eye in 20 milliseconds, compared with about 250 milliseconds for a human.
The robot can also create ‘no fly’ zones, preventing instruments from getting too close to the endothelium or posterior capsule, Dr Maloney added. “It may offer surgery that is safer, and then you can be a little more aggressive and faster because the robot will keep you out of danger.”
The second possible mode is autonomous, in which artificial intelligence controls the robot under close surgeon supervision. “It’s very similar to the self-driving mode on a Tesla,” he said. “The car drives itself, but the driver remains alert and ultimately in control.”
Furthermore, Dr Maloney said autonomous robots could multiply surgeon productivity by allowing one surgeon to monitor multiple surgeries from a single console. “It’s much easier to train 100 robots than 100 surgeons.” Such efficiency gains could help offset the looming ophthalmologist shortage as patient demand grows while surgeon supply shrinks.
Autonomous systems are already operating successfully on animal cataracts. Surgeons preview and approve instrument trajectory, carried out under OCT guidance, so the robot knows exactly where the posterior capsule is during the procedure.
The surgical technique does have limitations, Dr Maloney observed. It’s more expensive, at least right now. It’s also slower, but as surgeons gain experience, it will likely get faster. And the surgeon will still be needed to manually intervene for complications, such as loose zonules or other ‘long tail’ events.
“So, the good news is we are nowhere near being obsolete,” Dr Maloney said. He sees robotic surgery not as part of a dystopian future, but as an opportunity to increase capabilities and efficiency that should be embraced.
Dr Maloney made his comments at AAO 2024 in Chicago, US.
Robert K Maloney MD, MA(Oxon) is clinical professor of ophthalmology at UCLA and a founding partner of the Maloney-Shamie Vision Institute, both in Los Angeles, US. rm@maloneyvision.com
HOWARD LARKIN REPORTS
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
A Look at Innovative Treatments in Late-Stage Development
Ciliary-scleral implant for glaucoma achieves European release.
HOWARD LARKIN REPORTS
An innovative glaucoma implant that lowers mean intraocular pressure (IOP) by one-third or more— without penetrating the anterior chamber—is now available in Europe.
Based on two- and three-year data from more than 100 patients with both open- and narrow-angle disease, the Intercil® uveal spacer device from the French medtech start-up Ciliatech recently won the CE mark. A launch in select European and UK centres will extend throughout the European Union later this year. Since Intercil may also treat angle-closure glaucoma, Ciliatech will eventually release the device across Asia.
As an ab externo device inserted between the sclera and ciliary body below the limbus, Intercil uveal spacer provides reliable IOP reduction while lowering the risk of damaging the corneal endothelium, as well as hyphaema and postoperative inflammation, compared with procedures that penetrate the iris root, according to Ciliatech’s co-founder and medical director Philippe Sourdille MD.
“Ciliatech was created to develop an approach to glaucoma treatment that had never been considered: to lower IOP without entering the anterior chamber or creating subconjunctival filtration. This makes Ciliatech’s approach significantly different from existing surgical propositions,” Dr Sourdille said. “It provides procedural simplicity with a fast learning curve. It does not inhibit future treatment options.”
Intercil might be especially appropriate for phakic glaucoma patients, said Karsten Klabe MD, a member of Ciliatech’s key opinion leader advisory board. “In addition to reducing the risk to the corneal endothelial cells, by not opening the anterior chamber, there is less risk of cataract or damaging the iris. It might be safer [than angle-based or filtering glaucoma surgery] for such a group of patients.”
Insight to invention
Observation in cases of low IOP showed a thin ciliary body detachment often appeared with ultrasound, sparking the development of the Intercil device, Dr Sourdille said. The resulting gap apparently reduces pressure in the supraciliary space, enhancing aqueous outflow.
“We aimed to change this passive IOP lowering mechanism to an active increase of uveoscleral outflow. This was done with a 400 micron-thick hydrophilic acrylic implant, 6.0 x 3.5 mm, inserted between the sclera and the ciliary body,” he said.
The device is inserted through a penetrating 3.5 mm radial scleral incision 2.0 mm away from the limbus. This full scleral incision gives the surgeon clear access to the supraciliary space to inject some OVD for a tunnel between the sclera and the ciliary body before inserting the device. It will prevent any intraciliary placement, Dr Sourdille added.
Current use of the device has been to treat mild to moderate glaucoma. In the first two standalone studies involving 42 patients with open-angle disease, SAFARI 1 and 2, mean IOP dropped 33% after three years, with 84% of patients achieving less than 18 mmHg and 68% becoming drug-free.1
A third standalone study involving 58 patients—half with open-angle and half with narrow-angle glaucoma—was conducted using a slightly modified device to increase uveoscleral and ciliochoroidal outflow, Dr Sourdille said. At two years, this improved outcomes to a 44% mean IOP decrease with 94% drug-free in both open- and narrow-angle cases. The study is ongoing to assess longer-term outcomes.2
So far, no cases have required explantation or additional surgery for IOP control, and no cases of encapsulation or fibrosis have been seen in follow-ups of up to four years. The device does not move in the eye. “It’s remarkably painless,” Dr Sourdille remarked. “Some patients can feel the sutures, but they are resorbable. The eyes are very quiet, and there is no flare, [creating no further] need for steroids.”
The procedure takes about 15 minutes, but Ciliatech’s approach leaves space if filtration surgery is necessary.
The road to market
Moving an innovation from concept to clinic requires a wide range of skills and resources beyond medical expertise: an understanding of engineering, manufacturing, regulatory affairs, marketing, education, and attracting investors are all needed.
So, to develop the Intercil concept, Dr Sourdille partnered with Olivier Benoit, an engineer with 25 years of experience leading medtech companies, to found Ciliatech in 2017. “He also helped develop the design. It was really the mixing of two minds,” Dr Sourdille said.
We are ready to sell thousands of this device.
At first, the idea was greeted with scepticism. “People would ask, ‘how do you think you can lower IOP without going into the anterior chamber?’,” Dr Sourdille said. But the results speak for themselves.
Clinical trials, which began in 2019, were disrupted by the pandemic and continue today. “Dozens of surgeons have already been trained on artificial eyes with our approach. Our education plan will continue to spread the technique and the indications,” Dr Sourdille said, adding a manufacturing facility experienced in IOL production is in place. “We are ready to sell thousands of this device.”
He also intends to continue innovating. “The need for new treatments in a very wide spectrum is continuous. As a clinician and surgeon, I can only mention the search of improvements in our daily practice as a reliable source of innovation, followed by patent filing and campaign funding.”
For citation notes, see page 47.
Philippe Sourdille MD is an ophthalmologist, researcher, inventor, and medical director and co-founder of Ciliatech in Chavanod, France. p.sourdille@cilia.tech
Karsten Klabe MD is an ophthalmologist specialising in glaucoma surgery at Breyer, Kaymak & Klabe Augenchirurgie in Düsseldorf, Germany. studien.k.klabe@augenchirurgie.clinic
Safety
• Very few and very mild adverse events
• UBM review: implant in place, no implant movement detected, no foreign body reaction
• Very good patient comfort, no pain reported
The Top 3 most c ommon complications repor ted for intracameral stents are all AC related (corneal damage, hyphema and AC inflammation)
Wit h Intercil® no single AC related comp lication was reported
Accelerated review for RP therapy
The European Commission has received a positive opinion on Ocugen’s OCU400 gene-agnostic therapy for retinitis pigmentosa (RP) from the EMA Committee for Advanced Therapies, granting it Advanced Therapy Medicinal Product (ATMP) classification. This classification accelerates regulatory review for groundbreaking therapies. OCU400 is the first agnostic gene therapy for retinitis pigmentosa to enter a phase 3 study, now actively enrolling participants. Instead of targeting specific RP variants, OCU400 addresses the NR2E3 gene, which regulates retinal functions, resetting altered cellular gene networks. ocugen.com
SUSVIMO approved for DME
The US FDA has approved Genentech’s Susvimo ocular implant (ranibizumab) 100 mg/mL for diabetic macular oedema (DME). Approval was based on one-year results from the phase 3 Pagoda study, showing similar visual improvements in DME patients receiving six monthly aflibercept refills of the Susvimo implant and those getting monthly 0.5 mg ranibizumab injections. Susvimo received FDA approval for treating wet age-related macular degeneration (AMD) in 2021. gene.com
FDA clearance for Sentinel Camera
AI Optics has received US FDA 510(k) clearance for its Sentinel Camera, a handheld retinal imaging system that captures high-quality eye images. The device supports non-dilated imaging and is designed to be suitable for use in primary care, optometry, retail clinics, and at home. The device uses DICOM-compliant formats for integration with electronic health record (EHR) systems. AI Optics is also developing AI-based software for the device to detect diabetic retinopathy, glaucoma, and macular degeneration. aioptics.ai
Virtual visual acuity testing
Virtual Vision Health announced the launch of visual acuity testing on their Virtual Eye VR platform. The FDA-registered device now measures visual acuity, adding to its previous capabilities: visual field testing, progression analysis, and colour sensitivity testing. The portable Virtual Eye headset provides analytics via cloud-based software on any computer, tablet, or mobile device with Wi-Fi. virtualvision.health/
PRISM Award for Norlase LYNX
Norlase has received the prestigious PRISM Award in the biomedical category for its latest innovation, LYNX™, the world’s first pattern laser indirect ophthalmoscope (LIO). The device integrates advanced laser and pattern-scanning technology into a lightweight, wearable headset. norlase.com
Gene therapy for AMD showing positive results
4D Molecular Therapeutics (4DMT) announced positive initial interim 52-week data from the phase 2b population extension cohort of the PRISM clinical trial of 4D150 gene therapy for wet age-related macular degeneration (AMD). The trial’s findings indicated that patients experienced sustained improvement in best-corrected visual acuity and reductions in central subfield thickness (CST). Additionally, 53% of patients of a general wet AMD cohort and 80% of the newly diagnosed cohort required no supplemental aflibercept injections, and no patient required more than one injection during the oneyear follow-up. The 4D-150 gene therapy is designed for administration as a single, low-dose intravitreal injection to induce continuous expression of therapeutic transgenes and suppress vascular endothelial factors (VEGFs) at the site of disease activity. 4dmoleculartherapeutics.com
VIRTUAL FOLLOW-UP OF CATARACT SURGERY SAFE AND PREFERRED
For patients who undergo uneventful cataract surgery, virtual telephone or video follow-ups appear to be a safe alternative to in-person visits and were generally preferred by patients, according to a recent systematic review. A comprehensive database search yielded 1,710 records, including seven studies involving 2,113 cataract surgeries in 1,994 patients who had virtual postoperative appointments. Virtual follow-up calls, conducted primarily by telephone, took place on postoperative day one in three studies, day seven in two studies, and day fourteen in one study. None of the studies reported serious adverse outcomes from substituting in-person follow-ups with telephone follow-ups. Two observational studies directly comparing the telephone and in-person follow-ups showed no significant differences in complication rates or visual acuity between the groups. One study combined the techniques for elderly patients, finding additional telephone follow-ups were associated with reduced surgical recovery times and decreased patient anxiety. A common theme observed was patients preferred telephone reviews, finding them more convenient than in-person follow-ups.
William J Dupps Jr MD, PhD noted the study contributes to the growing body of evidence suggesting telephone follow-up after routine cataract surgery does not negatively affect outcomes compared to the in-person version. He mentioned advances in digital communications and the widespread availability of smartphones offer the potential for improved virtual postoperative patient management while reducing costs, carbon footprint, and the burden on patients and caregivers.
A Hanna, et al. “Virtual follow-up after cataract surgery: systematic review,” 51(2): 167–174.; W Dupps, “Virtual postoperative visits in cataract,” 51(2): 89–90.
VITRECTOMY ELEVATES ENDOPHTHALMITIS RISK FACTORS AFTER SECONDARY IOL
IMPLANTATION
Preoperative aphakia and anterior vitrectomy are the greatest risk factors for postoperative endophthalmitis (POE) after secondary intraocular lens implantation, according to the findings of a retrospective study. The authors reviewed the records of 97,152 Medicare fee-for-service beneficiaries who underwent IOL exchange or secondary IOL implantation for preoperative aphakia between 1 January 2011 and 19 November 2022. The overall POE rate for all secondary IOL surgeries was 0.31% during those 11 years. Multivariate analysis showed a lower incidence of 42-day POE for eyes undergoing IOL exchange (0.28%), compared with secondary IOL surgery for aphakia 0.35%, especially if a concurrent vitrectomy was performed with the secondary IOL procedure (84%).
C H Kerrison, et al. “Endophthalmitis rates after secondary intraocular lens surgeries: 11-year Medicare fee-for-service analysis,” 51(2): 91–97.
KLEX OUTCOME SIMILAR TO PRK AND LASIK
Keratorefractive lenticule extraction (KLEx) shows similar outcomes to PRK and LASIK, according to a retrospective study. Data was collected from patients treated between 2019 and 2022. Of the 4,466 eyes, 737 (16.5%) underwent KLEx, 2,801 (62.7%) underwent PRK, and 928 (20.8%) underwent LASIK. At postoperative month six, there was no significant difference in the percentage of eyes achieving uncorrected distance visual acuity of 20/20 or better among the three procedures. The efficacy indexes (postoperative UCVA/preoperative BCVA) were 1.09 for KLEx, 1.10 for PRK, and 0.97 for LASIK. The safety indexes (postoperative BSCVA/preoperative BSCVA) were 0.96, 1.01, and 0.81, respectively.
C Evangelista, et al. “Comparing visual outcomes of keratorefractive lenticule extraction, PRK, and LASIK procedures in the military population,” 51(2): 98–105.
Cited in this Issue
Celebrating Women in Ophthalmology
Page 4
1. International Women’s Day. www.internationalwomensday.com
2. Sedhom JA, et al. “Physician Burnout in Ophthalmology: US Survey,” JCRS, 2022 June; 48(6): 723–729.
3. Ní Dhubhghaill S, et al. “Cataract Surgical Training in Europe: European Board of Ophthalmology Survey,” JCRS, 2023 November; 49(11): 1120–1127.
4. Killeen OJ, et al. “#MeToo in Ophthalmology,” JAMA Ophthalmol, Published online 20 February 2025. doi:10.1001/ jamaophthalmol.2024.6491
5. Tao BK, et al. JCRS, 2024 May; 50(5): 460–467.
Diamonds in the Rough
Page 10
1. Azad A D, et al. “Representation of Women in Ophthalmology Subspecialty Societies over 20 Years,” Ophthalmology, 2022; 129(5): 587–590.
2. Gill HK, Niederer RL, Shriver EM, Gordon LK, Coleman AL, Danesh-Meyer HV. “An Eye on Gender Equality: A Review of the Evolving Role and Representation of Women in Ophthalmology,” Am J Ophthalmol, 2022; 236: 232–240. doi:10.1016/j.ajo.2021.07.006
Progress and Promise for Women in Ophthalmology
Page 16
1. Jia JS, Lazzaro A, Lidder AK, et al. “Gender Compensation Gap for Ophthalmologists in the First Year of Clinical Practice,” Ophthalmology, 2021; 128(7): 971–980.
2. Emami-Naeini P, Lieng MK, Chen J. “Sex Differences in Salaries of Academic Ophthalmologists in the United States,” JAMA Ophthalmol, 2022; 140(5): 519–522.
An New Focus on Intermediate Vision
Page 24
1. Nanavaty MA, Mukhija R, Ashena Z, Bunce C, Spalton DJ. “Incidence and factors for pseudoaccommodation after monofocal lens implantation: the Monofocal Extended Range of Vision study,” J Cataract Refract Surg, 2023; 49: 1229–1235.
Inspiring Collaborative Excellence
Page 25
1. Reinstein DZ, Archer TJ, Vida RS. “Applications of epithelial thickness mapping in corneal refractive surgery,” Saudi J Ophthalmol, 2022; 36(1): 25–35.
2. Reinstein DZ, Lovisolo CF, Archer TJ, Gobbe M. “Comparison of postoperative vault height predictability using white-to-white or sulcus diameter-based sizing for the Visian implantable collamer lens,” J Refract Surg, 2013; 29(1): 30–35.
3. Reinstein DZ, Archer TJ, Vida RS, Piparia V, Potter JG. “New sizing parameters and model for predicting postoperative vault for the Implantable Collamer Lens posterior chamber phakic intraocular lens,” J Refract Surg, 2022; 38(5): 272–279.
Sorting Out Simultaneous Vision IOLs
Page 26
1. Ribeiro F, et al. “Evidence-based functional classification of simultaneous vision intraocular lenses: seeking a global consensus by the ESCRS Functional Vision Working Group,” J Cataract Refract Surg, 50(8): 794–798.
Big Advantages to Small-Aperture IOLs
Page 28
1. Vukich J, et al. JCRS, 50(11): 1165–1172, November 2024.
2. Fram N, “Clinical Outcomes of a Small Aperture IOL for Complex Corneas,” presented at ASCRS annual meeting 2024.
Refining Indications for CXL
Page 31
1. Kobashi H, Tsubota K. “Accelerated versus standard corneal cross-linking for progressive keratoconus: a meta-analysis of randomized controlled trials,” Cornea, 2020; 39(2): 172–180.
2. Kandel H, Abbondanza M, Gupta A, et al. “Comparison of standard versus accelerated corneal collagen cross-linking for keratoconus: 5-year outcomes from the Save Sight Keratoconus Registry,” Eye (Lond), 2024; 38(1): 95–102.
3. Hafezi F, Kling S, Gilardoni F, et al. “Individualized corneal cross-linking with riboflavin and UV-A in ultrathin corneas: the Sub400 protocol,” Am J Ophthalmol, 2021; 224: 133–142.
Knowing Iris Repair: Using Iridodiathermy in Iris Surgery
Page 32
1. Ahmed I, et al. “Endothermal pupilloplasty to optimize pupil centration, size, and contour,” J Cataract Refract Surg, 2021 Dec 1; 47(12): e80–e83.
Reducing the Treatment Burden for Neovascular AMD
Page 38
1. Das N, Chaurasia S, Singh RP. “A review of emerging tyrosine kinase inhibitors as durable treatment of neovascular age-related macular degeneration,” Expert Opin Emerg Drugs, 2023; 28(3): 203–211.
2. Moshfeghi A, et al. “US Phase 1 Study of Intravitreal Axitinib Implant (OTX-TKI) for Neovascular Age-related Macular Degeneration,” IOVS, June 2023; 64: 936.
3. Clearside Biomedical. “Clearside Biomedical Reports Significant Progress in ODYSSEY Phase 2b Trial of CLS-AX in Wet AMD,” company press release, 14 Dec 2023, https:// ir.clearsidebio.com/news-releases/news-release-details/ clearside-biomedical-reports-significant-progress-odysseyphase
4. Eichenbaum D, et al. “The DAVIO 2 trial: a phase 2, randomized, double-masked, controlled multicenter study of EYP-1901 vs aflibercept in previously treated wet age-related macular degeneration,” IOVS, June 2024; 65: 4401.
A Look at Innovative Treatments in Late-Stage Development
Page 42
1. Voskanyan L, et al. “3 Year Outcomes of a Novel Cilio-Scleral Interposition Device (Cid Sv13): Managing IOP Without Entering the Anterior Chamber,” poster presented at the European Society of Cataract and Refractive Surgeons Annual Congress, Barcelona, Spain, September 2024.
2. Benoit O. “Let’s take glaucoma surgery to a different space,” presentation at EyeCelerator during the American Academy of Ophthalmology annual meeting, Chicago, US, October 2024.
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.
Research. Education. Innovation.
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
Upcoming Events
April 25–28
ASCRS
Los Angeles, US
May 23–25
EuCornea
Prague, Czech Republic
June 7–9
European Society of Ophthalmology (SOE) Lisbon, Portugal
June 12–14
2nd World Keratoconus Congress (WKC 2025) Athens, Greece
September 4–7
EURETINA
Paris, France
September 12–16
2025 ESCRS Congress
Copenhagen, Denmark
23 May
September 25–28
German Ophthalmology Society Berlin, Germany
October 18–20
American Academy of Ophthalmology
Orlando, Florida, US
25 Apr
7 Jun
12 Sept 4 Sept
1-4
THE ONLY TRULY MICROINVASIVE GLAUCOMA TECHNOLOGY RAPIDRECOVERY
• Myopic shift
• Cyclodialysis
• Hypotony
• Significant hyphema ZERO
• Stent dislocation
SAFETY1,2
IMPROVES OCULAR SURFACE HEALTH6,9
OVERALL SAFETY PROFILE SIMILAR TO CATARACT SURGERY ALONE3 REDUCTION IN PATIENTS WITH SEVERE OSD SYMPTOMS5 72%
SIGNIFICANT IMPROVEMENTS IN VISION-RELATED QUALITY OF LIFE5
1. 7-Year Efficacy and Safety of iStent inject® Trabecular Micro-Bypass in Combined and Standalone Usage. Fritz H. Hengerer . Gerd U. Auffarth . Ina Conrad-Hengerer. 2. Ten-Year Effectiveness and Safety of Trabecular Micro-Bypass Stent Implantation with Cataract Surgery in Patients with Glaucoma or Ocular Hypertension. Tobias H. Neuhann, Raphael T. Neuhann, Dana M. Hornbeak. 3. Samuelson, Thomas W., et al. “Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results.” Ophthalmology 126.6 (2019): 811-821. 4. Rodriguez-Una, Ignacio, Augusto Azuara-Blanco, and Anthony J. King. “Survey of glaucoma surgical preferences and post-operative care in the United Kingdom.” Clinical & Experimental Ophthalmology 45.3 (2017): 232-240. 5. Samuelson, Thomas W., et al. “Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the iStent inject® pivotal trial.” American Journal of Ophthalmology 229 (2021): 220-229. 6. Schweitzer, Justin A., et al. “Prospective interventional cohort study of ocular surface disease changes in eyes after trabecular micro-bypass stent (s) implantation (iStent or iStent inject) with phacoemulsification.” Ophthalmology and Therapy 9 (2020): 941-953. 7. Jones, Lee, et al. “Impact of minimally invasive glaucoma surgery on the ocular surface and quality of life in patients with glaucoma.” Therapeutic Advances in Ophthalmology 15 (2023): 25158414231152765. 8. Ioannidis, Alexandros S., et al. “Refractive outcomes after trabecular micro-bypass stents (iStent inject®) with cataract extraction in open-angle glaucoma.” Clinical Ophthalmology (2020): 517-524. 9- Biela, Katarzyna, et al. “Dry eye disease as a cause of refractive errors after cataract surgery–A systematic review.” Clinical Ophthalmology (2023): 1629-1638.
iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATIONS FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body.