FORENSIC ODONTOLOGY FIRSTS: THE HISTORY OF HOW IT BEGAN DENISE C. MURMANN, DDS, D-ABF0
FORENSIC DENTAL IDENTIFICATION
SHANETHA L. COLLIER, DDS, MS, D-ABFO
FBI: FOUND BUT NOT IDENTIFIED (YET)
A. KASPER, DDS, D-ABFO
FORENSIC ANTHROPOLOGY—AN INTRODUCTION FOR DENTISTRY
JAMES P. FANCHER, DDS, MA, PHD, D-ABFO
DENTAL AGE ASSESSMENT IN CHILDREN, ADOLESCENTS, AND ADULTS—AN OVERVIEW
JOHN B. NASE, DDS, D-ABFO
THE EVOLUTION OF BITE MARK ANALYSIS AND THE ROLE OF THE ABFO DEREK M. DRAFT, DDS, D-ABFO
HUMAN ABUSE AND NEGLECT ROBIN A. AINSWORTH, DDS, MS, D-ABFO, ABGD, FAGD, CAPT (RET) USPHS
ARTIFICIAL AND AUGMENTED INTELLIGENCE IN FORENSIC ODONTOLOGY
KENNETH ASCHHEIM, DDS, D-ABFO
CIVIL AND CRIMINAL LITIGATION
TOM DAVID, DDS, D-ABFO
BECOMING INVOLVED IN FORENSIC ODONTOLOGY: UNVEILING THE MYSTERY
KAREN WILLIAMSON, DDS
An All-in-One Isolation System
Loved by Patients and Staff
A high-suction evacuator, bite block, tongue shield, and oral pathway protector in one easy-to-use device
DryShield leads the market in providing clinicians with isolation technology that provides maximum protection from potentially harmful aerosols—and maximizes ease, comfort, safety, and productivity.
TDA members have access to these specials: Buy 3 boxes of autoclavable mouthpieces and get the Isolation System free. Max: 1 time per year, per office.
Buy 2 boxes of autoclavable mouthpieces and get 1 bottle of PowerSonic Cleaning Solution free. Max: 1 time per year, per office.
• Autoclavable!
• Keeps work environment dry and clean
• Enhances patient and staff safety
• Enables 2-quadrant dentistry
• Increases visibility
• Allows for mobility with its portable kit
• Installs in seconds
316 INTRODUCTION TO FORENSIC DENTISTRY
Kathleen A. Kasper, DDS, D-ABFO
318 FORENSIC ODONTOLOGY FIRSTS: THE HISTORY OF HOW IT BEGAN
Denise C. Murmann, DDS, D-ABFO
328 FORENSIC DENTAL IDENTIFICATION
Shanetha L. Collier, DDS, MS, D-ABFO
338 FBI: FOUND BUT NOT IDENTIFIED (YET)
Kathleen A. Kasper, DDS, D-ABFO
344 FORENSIC ANTHROPOLOGY— AN INTRODUCTION FOR DENTISTRY
James P. Fancher, DDS, MA, PhD, D-ABFO
350 DENTAL AGE ASSESSMENT IN CHILDREN, ADOLESCENTS, AND ADULTS— AN OVERVIEW
John B. Nase, DDS, D-ABFO
360 THE EVOLUTION OF BITE MARK ANALYSIS AND THE ROLE OF THE ABFO
Derek M. Draft, DDS, D-ABFO
364 HUMAN ABUSE AND NEGLECT
Robin A. Ainsworth, DDS, MS, D-ABFO, ABGD, FAGD, CAPT (Ret) USPHS
370 ARTIFICIAL AND AUGMENTED INTELLIGENCE IN FORENSIC ODONTOLOGY: AN INTRODUCTORY OVERVIEW
Kenneth Aschheim, DDS, D-ABFO
380 CIVIL AND CRIMINAL LITIGATION
Tom David, DDS, D-ABFO
384 BECOMING INVOLVED IN FORENSIC ODONTOLOGY: UNVEILING THE MYSTERY
Karen Williamson, DDS
387 ASK THE POWERS CENTER
Fady Ibrahim, Udo Plaster, Petra C. Gierthmuehlen Guest Editor Rade D. Paravina, DDS, MS, PhD
HIGHLIGHTS
379 In Memoriam
388 Value for Your Profession: Biofilm, Bacteria, and CFU Counts: Understanding Waterline Contamination in Dentistry
390 Classifieds
395 Index to Advertisers ,
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 142 | No. 6
Texas Dental Journal (ISSN 0040-4284) is published monthly, except January-February, March-April, July-August, and November-December, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2025 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement at tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE!
(Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available):
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
PRESIDENT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PRESIDENT-ELECT Elizabeth Goldman, DDS 214-585-0268, texasredbuddental@gmail.com
PAST PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
VICE PRESIDENT, SOUTHEAST Matthew J. Heck, DDS 512-280-8800, matthewjheckdds@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN**
Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR** Jacqueline M. Plemons, DDS, MS 214-507-0815, drplemons@yahoo.com
LEGAL COUNSEL** Carl R. Galant
EXECUTIVE DIRECTOR** Greta Zeimetz, DBA, CAE, SHRM-SCP 512-443-3675, gzeimetz@tda.org
*Non-voting member **Non-voting Board of Directors
Kathleen A. Kasper, DDS, D-ABFO
This issue of the Texas Dental
Journal
is devoted entirely to the discipline of forensic dentistry.
In August 2024, the Texas Dental Journal Editor Jacqueline Plemons DDS, MS, invited me to serve as co-editor for this special publication. In short, this compilation has been a year in the making. The contributing authors are actively engaged with forensic organizations at both national and international levels—most of them recognized as leading voices in forensic odontology. I’m honored they agreed to participate, and I hope this issue deepens your understanding of a field we consider more a calling than a career.
Introduction to Forensic Dentistry
Forensic dentistry, also known as forensic odontology, stands at the intersection of dental science and the legal system. This specialized discipline employs the distinctive characteristics of the human dentition to facilitate the identification of individuals and to address legal issues. Teeth, recognized for their durability against decomposition, fire, and trauma, often persist when other anatomical features have been compromised, thereby proving indispensable in circumstances in which conventional identification methods prove inadequate. The value of forensic dentistry is extensive and is not limited to dental identification. It also encompasses contributions to criminal investigations, civil litigations, malpractice, mass victim identification, patterned injury/bitemark analysis, human abuse and neglect, oral/facial trauma, and the analysis of historical remains.
FORENSICDentistry
Scope and Applications
Forensic dentistry includes a broad spectrum of responsibilities within the legal system and related domains. Principal applications include:
• Human Identification: Forensic odontologists compare dental records to establish the identity of individuals in cases involving crime, accidents or natural calamities.
• Patterned Injury/Bite Mark Analysis: The analysis of bite marks on victims or objects can facilitate the connection of a suspect to a crime or serve to exonerate individuals from suspicion.
• Age Assessment: Examination of the dentition, which enables the estimation of age in both living and deceased individuals. This may involve developing or developed teeth as well as post developmental degenerative changes that occur with aging.
• Oral/Facial Injuries: Oral and facial injuries constitute another domain within forensic dentistry. Meticulous documentation of wounds, lacerations, and dental trauma can help determine the circumstances under which injuries occurred.
• Human Abuse and Neglect: Forensic dentists play a pivotal role in detecting and documenting evidence of abuse, especially among children, elders, or other vulnerable populations. Distinctive injury patterns with the head and neck and the oral cavity may provide critical evidence of neglect or violence.
• Litigation: Forensic dentists frequently act as expert witnesses, presenting dental evidence in judicial proceedings. This can include criminal, civil, fraud, personal injury, and malpractice cases.
The Future of Forensic Dentistry
Forensic dentistry continues to evolve through technological innovation, scholarly research, and international collaboration. As methodologies are refined and evidence-based practice becomes further entrenched, the discipline’s importance within the forensic sciences and the legal system will expand. The contributions of forensic odontologists not only assist in identification but also support the pursuit of justice for affected families and communities. We are often witness to the best of humanity and the worst.
Forensic dentistry is a vital branch of forensic science. Its applications are diverse, and the field is poised for continued progress. If dental documentation is maintained and the imperative for justice endures, forensic dentistry will remain an indispensable element of the forensic sciences for years to come.
A Call to Action
Despite growing demand, the number of qualified forensic dentists is declining. More young, passionate, and motivated dentists are needed in this unique and essential area.
Currently, the United States has fewer than 70 dentists certified by the American Board of Forensic Odontology (ABFO), the governing body responsible for setting standards and certifying practitioners in the field. The ABFO’s mission is to establish and refine qualification criteria, and to certify those who meet them as specialists in forensic odontology. In doing so, the board provides a transparent and trustworthy system for recognizing competent forensic dental professionals.
There is an urgent need for more qualified forensic dentists across the country. It is my sincere hope that this collection of articles inspires some of you to explore a future with forensic dentistry.
If you’re interested in getting involved, feel free to email me at exfiles11@aol.com. If you’re located outside the Dallas–Fort Worth area, another ABFO diplomate may be closer to you. You can find a list of active diplomates on the ABFO’s website under the “Resources” tab at www.abfo.org—look for ABFO diplomates information.
about the Author
Kathleen A. Kasper, DDS, D-ABFO
Dr Kasper has been practicing general dentistry in Carrollton, Texas, for 31 years. She is a graduate of the University of Iowa College of Dentistry.
She provides 3 counties in the Dallas-Ft. Worth area with forensic dental services. These include Collin, Dallas, and Tarrant Counties. She is currently the only active board certified forensic dentist in north Texas.
She received her formal forensic odontology training at the University of Texas Health Science Center San Antonio, Texas, Center for Education and Research in Forensics (CERF) in 2003-2004.
Dr Kasper obtained Board Certification from the American Board of Forensic Odontology in 2010.
She is a fellow of the American Academy of Forensic Sciences, a member of the American Board of Forensic Odontology, and a member of the American Society of Forensic Odontology.
She is the current American Board of Forensic Odontology Dental Age Assessment Committee Chair.
Dr Kasper is also a published author in the Journal of Forensic Sciences and coauthor of a chapter in each of 3 forensic textbooks.
Perhaps one of her greatest undertakings was chairing a working group for the American Dental Association that has published the “Technical Report” for Forensic Dental Age Estimation which went on to become a “standard” for forensic science with the Organization of Scientific Area Committees (OSAC).
Denise C. Murmann, DDS, D-abfo
Forensic Odontology Firsts: The History of How it Began
Denise C. Murmann, DDS, D-ABFO graduated from University of Illinois at Chicago School of Dentistry, 50 years after her grandfather (1992 and 1942, respectively). Colonel William Morlang’s course on Mass Disaster inspired more education in forensic odontology and to join the federal Disaster Mortuary Operational Response Team (DMORT). In 2001, she was deployed with many DMORT members to help with the dental identification of the victims of September 11. That deployment inspired more education, this time the Fellowship in Forensic Odontology with the University of Texas Health Science Center (UTHSC). The result of the Fellowship was a research project, “A Comparison of Animal Jaws and Bite Mark Patterns” that was presented at the American Academy of Forensic Sciences Scientific Session in 2005 and published in the Journal of Forensic Sciences in 2006. Later in 2005, Dr Murmann and many other DMORT members were deployed after Hurricane Katrina to help with dental identification in Gulfport, MS. In 2011, she became a diplomate of the American Board of Forensic Odontology (ABFO). Interest in the history of forensic odontology started when she was asked to contribute to the chapter on the history of forensic dentistry in the Manual of Forensic Odontology, 5th edition, published in 2013. Dr Murmann is a consultant to the coroner’s office for DuPage, Will, Kendall and Grundy Counties as a forensic odontologist and owns a private dental practice in Naperville, Illinois.
FORENSICOdontology
Abstract
It is said that the only things that are constant are death and taxes. As far back as we have history, the tragedy of death is recorded, as well as the grief of those who remain after they are gone. This grief is made worse if the beloved dead (or despised, as our first story will show) are not able to be identified. There was a small window of time for people who lived before refrigeration and embalming, to identify their dead by sight. Other methods were then necessary. One of those methods was by evaluating their teeth. The skeletal system, due to its mineral content, remains for a much longer period of time. The teeth are the only part of the skeletal system that is visible during life, so that could give clues in death. The following are the first known recorded stories of how people were identified by their teeth. We recognize that in the future, earlier examples may yet be discovered. Modern ways of recording the information (X-rays, photographs, digital impressions) make the process more accurate and easier to archive. However, the ingenuity and persistence of those who figured out how to identify someone by their teeth, is inspiring.
Thefirst time in history, that we are aware of, when teeth were used to identify someone who was dead, happened in the Roman Empire in the first century. This story does not involve coroners, physicians, nor dentists. It involves 2 women who were rivals, politically and romantically. Both wanted to become the wife of the Roman emperor Claudius. He had been married 3 times before. The first 2 wives he had divorced. His third wife was put to death for not only cheating on him, but having an expensive wedding to her lover, while still married to Claudius.1 Now he needed a new wife, and a few were suggested; 2 of them are the ladies in our story.
The first woman was Julia Agrippina, also known as Agrippina the Younger. She had excellent family connections that provided a political advantage. She was related to the first 5 Roman Emperors: Augustus (great-grandfather), Tiberius (great-uncle), Caligula (brother), Claudius (uncle) and Nero (son). Agrippina was recorded as being beautiful and that she had the habit of consulting with Claudius frequently.1 Another asset was that she had a son, who could be adopted to provide an heir, the 12-year-old Nero. To summarize, she was a well-connected, gorgeous woman who respected his opinion and already had a suitable successor for him. This was impressive but let us consider her competitor.
Lollia Paulina did not have as much political connection, but she had been married to the emperor Caligula (Agrippina’s brother). That means, for a time, Lollia Paulina and Agrippina had been sisters-in-law. The time, however, was short, as Caligula soon divorced her. She had no children thus could provide no heir. Why then was she a contender? Money, lots and lots of money. Pliny the Elder gives a firsthand account:
I once saw Lollia Paulina, the wife of the Emperor [Caligula] —it was not at any public festival, or any solemn ceremonial, but only at an ordinary wedding entertainment—covered with emeralds and pearls, which shone in alternate layers upon her head, in her hair, in her wreaths, in her ears, upon her neck, in her bracelets, and on her fingers, and the value of which amounted in all to 40 millions of sesterces.2 (Somewhere between $6-20 million US dollars.)
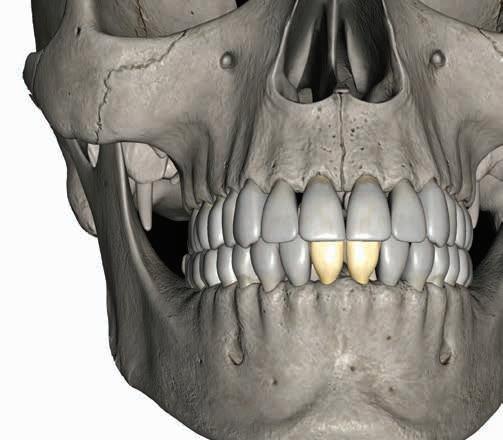
Ultimately, he decided upon Agrippina, his niece. After, of course, the Senate changed a law forbidding incest. Perhaps this is why she was considered fortunate. How do we know? Because of her teeth! Pliny the Elder wrote:
Those females who happen to have two canine teeth on the right side of the upper jaw, have promise of being the favorites of fortune, as was with the case Agrippina, the mother of Domitius Nero: When they are on the left side, it is just the contrary.3
Agrippina was savvy enough to know that just because she was the empress now, that it would last forever. This was Claudius’ fourth marriage and her third. If she wanted to keep her political power, she would need to act, and she did. Tacitus tells of how Agrippina handled the situation; she had an informer accuse Lollia Paulina of consulting astrologers and magicians to use magic to get Claudius to choose her to be his wife. In the trial, Claudius did not allow Lollia Paulina to speak or defend herself in any way. The verdict was that her property, including most of her money, should be confiscated, and she was to be banished from Italy.
Apparently, exile was not good enough. Agrippina and her sisters had been sent into exile when they were younger and they had come back, so she knew it was possible for Lollia too. To prevent this, a tribune, or Roman soldier was sent to force her to commit suicide.4 To make certain that it was Lollia that was dead, Agrippina gave the command that her head be cut off and brought back for her to examine. This was accomplished after a long journey, thus ensuring that there was advanced decomposition by the time the soldier returned to Rome. Indeed, we know from Cassius Dio.
“As she did not recognize the woman’s head when it was brought to her, she opened the mouth with her own hand and inspected the teeth, which had certain peculiarities.”5 Thus she confirmed her rival was dead.
1776
PaulThe First Known Dental Identification by a Dentist, Paul Revere (yes, THAT Paul Revere)
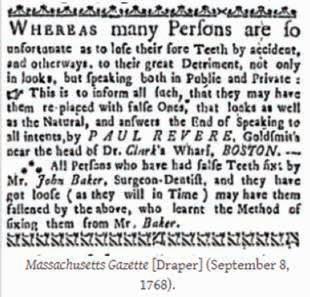
Revere was a hard worker. He was a soldier, silversmith, goldsmith, silver shop owner, and engraver. Even so, this did not protect his business from a stagnant economy that was hurt by a recession, and then the Stamp Act of 1765. To expand his business, he learned dentistry from the English Surgeon-Dentist, Mr John Baker. It was logical, because dentistry at that time used gold wire, which he was already proficient with. Baker was so well known that when Paul Revere put an advertisement about his dental skills in the Massachusetts Gazette on September 8, 1768, he states that it was Baker that taught him.6
When Baker left the area, Paul Revere could now see his patients. His dental career went so well, that by July 30, 1770, he placed another advertisement, this time in the Boston Gazette, expressing “his most sincere thanks to the Gentlemen and Ladies who had employed him in the care of their Teeth. He went on to, “inform them and all others…that he still continues in the Business of a Dentist.7”
One of his patients was Dr Joseph Warren. It was he who sent Paul Revere on his “midnight ride,” on April 18, 1775. Not only did they work together for the American Revolution, but they were also in the same Freemason Lodge, and Revere had wired in a false tooth for Warren. Historians consider Joseph Warren as one of the Founding Fathers of the United States, but he is largely forgotten as he died in the battle of Bunker (Breeds) Hill, on June 17, 1775. The British won and kept control of the battlefield after the fighting was over. They did not let the American colonists have access to the bodies of those who perished, but instead, buried them on the battlefield. When the British left Boston on March 17, 1776, the families of those who had been slain went to find their loved ones, about 10 months after they had died. Abigail Adams, in a letter to her husband, John Adams, dated April 7, 1776, reports that “Yesterday, the Remains of our Worthy General Warren were dug up on Bunker Hill and carried into Town and on Monday are to be interred with all the Honors of War.8 The funeral for Joseph Warren was an important enough event to make it into the newspapers.
“Last Monday, the remains of the brave General Warren were reinterred at Boston…The General’s remains were known by two artificial teeth fastened in with gold wire.9”
On July 4, 1825, General William Sumner interviewed soldiers in honor of the 50th anniversary of the Battle of Bunker Hill. Two of the soldiers that were
present at the exhumation of Warren in 1776 told Sumner what they saw.
“Mr. Clark, above named (Mr. Jonathan Clark) as well as another soldier whose name I have forgotten, was here on the 17th, who assisted at the exhumation on the presence of the doctor’s 2 brothers, who were satisfied of the
identity of the body, by many circumstances which they detailed. If stronger evidence of its identity were wanting, that afforded by Col. Paul Revere who set the artificial tooth… and who recollected the wire he used in fastening it in, would afford it.10”
1849
The First Homicide Case in the US Where Dental Evidence and Testimony Were Used Involved Harvard
Professors, and One of Them Was the Murderer
DrGeorge Parkman was a Harvardtrained physician, author, and businessman. Dr John White Webster was a teacher at Harvard Medical School and author of a chemistry book. Parkman came from a very wealthy Boston family and lived frugally. Webster was in debt to several people (including Parkman) and still lived beyond his means.
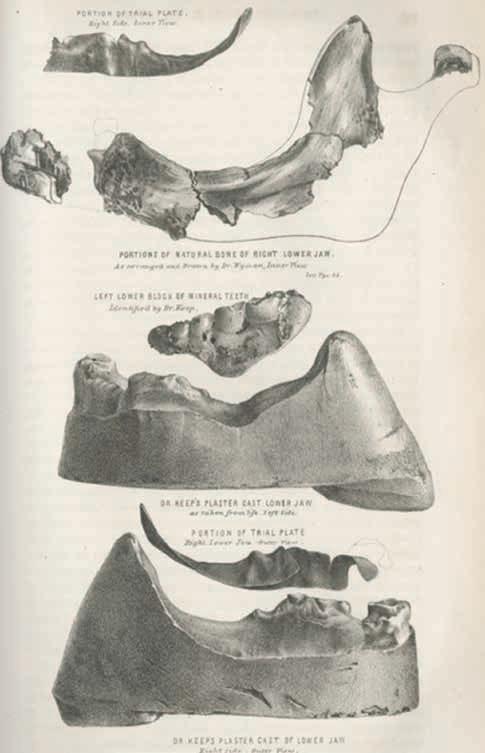
Parkman was last seen on November 23, 1849, heading toward the Medical College. The next day, Parkman’s family and the police started looking for him and placing fliers around Boston. Ephraim Littlefield, the janitor at Harvard Medical College, had seen Dr Webster behaving oddly and heard Webster in his locked office running the furnace much more than normal. During the Thanksgiving break, when no one was at the school, Littlefield took it upon himself to excavate through a wall into Webster’s office and saw body parts. He left quickly and went to get another professor from the university. He confirmed they were human and the police were called. Dismembered legs and a pelvis were found in the privy, a chest contained a partially burned torso, and bone fragments were found in the furnace, the most important of which was the right side of the mandible and a block of “mineral teeth” (denture teeth). Dr John White Webster was arrested on the charge of murder.
On March 19, 1850, the 12-day trial began; Webster pleaded not guilty. It was an international spectacle, with reporters coming from Europe and tickets handed out for people to be able to take their turn to watch part of the proceedings. On the third day of the trial, Dr Nathan C. Keep was called to the witness stand because he was the decedent’s dentist and had made him some teeth in 1846. Before the trial, Keep had been shown the block of mineral teeth found in the furnace and was asked if they were from the teeth that he had made Parkman. He testified that they were. Dr Keep’s assistant, Dr Lester Noble, also worked on Parkman’s teeth and testified that the mineral block of teeth that were found were indeed the teeth that they had made for Dr Parkman.
and lower jaw so peculiarly, that the impression left upon my mind was very distinct. I remember the peculiarity of the lower jaw, with great exactness.11” He described that later in his testimony as, “a great irregularity on the left side of the lower jaw.
When Dr Keep was first shown the mineral teeth, he retrieved the mould [sic] that he had used when making the teeth. He “put the metal upon its proper place, and it fitted exactly. There is sufficient left of these blocks to identify the place where they belonged. There is no mistake. [He then showed the mould [sic] and remains of the teeth, etc.] …During the progress of Dr Keep’s testimony, the Court and the spectators were affected even to tears, and Dr Keep, particularly, was overcome with emotion.” 11
Dr William T. G. Morton was famous for being the first person to use ether during a dental extraction in 1846. In addition, he had learned how to make false teeth from Dr Keep. He testified for the defense, but his testimony seems to contradict himself.
They had reason to remember the case. First, Dr Parkman had asked them to rush making the teeth, and they were able to finish the case, just 30 minutes before the program he needed them for started. In addition, “Dr Parkman’s mouth was a very peculiar mouth, in many respects; differing in the relation that existed between the upper
On the eighth day, a dental expert for the defense was sworn in and testified. Dr William T. G. Morton was famous for being the first person to use ether during a dental extraction in 1846. In addition, he had learned how to make false teeth from Dr Keep. He testified for the defense, but during his testimony he seemed to contradict himself.
Dr Daniel Harwood was a dentist that testified about the mineral teeth. At this time, they did not set denture teeth as we do in modern times. They MADE them.
“All mineral teeth are made of nearly the same substances—quartz, felspar, and fine white clay; but they differ in their proportions of the materials. Dr Keep’s teeth are almost destitute of white clay. This work appears to have been done by Dr Keep. I am quite confident that it is Dr Keep’s style and composition. When he manufactures blocks of teeth, he does not separate each tooth down to the gum, as I do, but he leaves them connected together, probably for the purpose of giving them greater strength.11”
On the 11th day of the trial, the verdict came back as guilty. The next day, the judge, Chief Justice Lemuel Shaw, pronounced the sentence of death by hanging. Webster appeared shocked at both the verdict and the sentence. However, later he confessed to the crime, explaining that it was done in a fit of rage because of the debt he owed Parkman. In addition, he wrote to Parkman’s brother, asking for forgiveness. The sentence was carried out on August 30, 1850.12
1897 The First Recorded Multiple Fatality Incident Where Dental Records Were Used, and it
Inspired the First Forensic Textbook
DrOscar Amoëdo is considered the Father of Forensic Odontology. We are fortunate to be able to claim him as such, for he was an amazing man. He was born in and completed dental school in Cuba, then went to the US to study at the New York Dental College and graduated with a second dental degree. He went back to Cuba and settled into private practice.
When he heard about the first Paris Dental Congress in 1889, he wrote a paper and submitted it to give a presentation. It was accepted, and Amoëdo went to Paris as the official representative of Cuba.13 When he finished his presentation on “mortified teeth,” he received a standing ovation. He was so impressed with the professional and academic culture of Paris that he decided to stay. Taking advantage of the education available, he enrolled in medical school, but also worked in private practice, as well as taught at the Paris School of Odontology. He was a prolific author of over 120 scholarly articles and inventor of 23 dental instruments.13
On May 4, 1897, there was a fire at the Bazar de la Charité in Paris. As the name implied, the Bazar was a charity event that was to raise money from wealthy women, to help the needs of the poor. A temporary wooden structure was set up and decorated with cloth and papier-mâché. A cinematograph (early form of motion picture film) was one of the main attractions. It used ether lamps and when a match was struck nearby, a fire started. It spread quickly through the wooden structure and onto the women themselves, due to their fashionable, yet highly flammable crinoline petticoats. There were not enough exits so many were trapped and 126
people died. Many of those people were aristocratic women, the most famous was Duchess Sophie Charlotte Aguste of Bavaria, who was the sister of Empress Elisabeth of Austria and Queen Maria Sophia of the Two Sicilies. Because of this, the fire drew international attention. The newspapers were poured over to get details of the fire, and how the victims were being returned to the families. It was noted in at least one paper that Duchess Sophie Charlotte was identified by her dentist, M. Lavanport, after he was able to find some gold fillings that he had placed.14
That tragic incident helped create the new field that Amoëdo would champion: Forensic Odontology. He was moved with compassion for the victims and the suffering of their families as they waited for their loved ones to be identified. He wanted to educate more dentists to the possibilities and expand the field to help more people. To that end, he interviewed those involved in the infamous fire and set forth protocols to be used going forward.
In November 1897, his article, “The Role of the Dentist in the Identification of the Victims of the Catastrophe of the ‘Bazar De La Charite,‘ Paris, 4th of May, 1897” was published in the journal, Dental Cosmos 14 Amoëdo named 5 dentists, “Drs Burt, Brault, Davenport, Ducourneau, Godon, and some others,” who had done the identifications. He also hinted that there was more to come about this topic. “From my confréres I obtained much information as to the precise results obtained by these examinations, and I am in possession of numerous documents and the greater part of the registers that they used. These I am keeping for a work I have in preparation.15”
That work was the defense of his medical thesis, “Dentistry in Legal Medicine,” (L’art dentaire en médecine légale), on July 7, 1898. He was successful and now also had the title of Doctor of Medicine.13 His thesis was also published in 1898, the first textbook on forensic odontology.
Dr Oscar Amoëdo
1954
The First Reported Case in the US When Bite Mark Evidence Was Used Was When a Thief Got Hungry During a Burglary
Perhaps,for a short time, James A. Doyle thought December 15, 1953, had been a good day for him. He robbed a grocery store scoring 2 bottles of booze, some change, several silver dollars and a meal. Even though he had taken the time to eat at the scene of the crime, he had still gotten away without anyone noticing. Doyle had lived in the city of Aspermont, Texas, for some time prior to that night, so he knew this was a small town; the 1950 census lists the population at 1,062.16 Thus, he should have known better, but the 2 bottles of liquor were utilized to their fullest potential instead of his reasoning. Inebriation was the inevitable result, so badly so, that the police were called. Sheriff Frazier arrived at the scene and arrested Doyle at 3:00 AM on December 16 for being intoxicated in a public place. Sheriff Frazier searched Doyle and found “thirteen silver dollars, some small change, and a few bills.17”
While Doyle was able to sleep it off in jail, Sheriff Frazier was still on the job. Poor Mr Peacock had gone to work at his grocery store in the morning on December 16. He found that “two windows had been broken, the store had been ransacked, two bottles of whiskey had been taken from his filing cabinet, thirteen silver dollars and some small change were missing; and that it was obvious that someone had been eating at his meat counter because some of the cold meat and cheese were not in their accustomed places.16” Indeed, when Sheriff Frazier examined the crime scene he found, “on the meat counter a large piece of cheese bearing pronounced teeth marks.17”
The 13 silver dollars and 2 bottles of whiskey made Sheriff Frazier think of Doyle, who he had arrested just a few hours earlier. “Sheriff Frazier testified that during the course of the morning he and Ranger Paulk interrogated the appellant, who was still in jail, that they asked the appellant to bite into a piece of cheese which they offered him, and that he voluntarily did so.”17
…“it was obvious that, someone, had been, eating at his meat counter, because some of the cold meat and cheese were not [sic] in their accustomed places.” when Sheriff Frazier examined the crime scene, “on the meat counter a large piece of cheese bearing pronounced teeth marks.”
“The 2 pieces of cheese were taken to the Texas Department of Public Safety at Austin, and Firearms Examiner Taylor testified that he had photographed both and had made plaster of Paris impressions of each and gave his opinion from caliper measurements that both pieces of cheese had been bitten by the same set of teeth.“17
“Dr Kemp, a dentist of Haskell, testified that he had examined the plaster casts and the photographs and gave his opinion that all were made by the same set of teeth.”17
Doyle was found guilty of burglary and was given the punishment of 2 years in prison.
The case was appealed and came before Judge William Arthur Morrison, Court of Criminal Appeals of Texas, on January 20, 1954. The appeals process is what made Doyle v. Texas the first reported case in the US when bitemark evidence was used. After the appeals process was completed, the judge’s opinion was published in a legal journal.
Doyle’s attorney, Clay Coggins, who appealed the case, did so on the grounds that when Doyle bit into the cheese, he had unwittingly made a confession of his guilt, and “the statutory warning had not been given him.”16 Judge Morrison did not agree. He listed cases to prove his point, then summed up by stating, “In fact, we fail to perceive any material distinction between the case at bar and the footprint and fingerprint cases so long recognized by this court.”17 Thus, the verdict of the trial court was affirmed.
References
1. Cassius Dio, Roman History. Book LXI.31. Cassius Dio — Epitome of Book 61 Retrieved July 20, 2025.
2. Pliny the Elder, Natural History. Book 9. Chapter 58. Pliny the Elder, The Natural History, BOOK IX. THE NATURAL HISTORY OF FISHES., CHAP. 58.—INSTANCES OF THE USE OF PEARLS. Retrieved July 20, 2025.
3. Pliny the Elder, Book 7. Chapter 15. https://www.perseus.tufts.edu/ hopper/text?doc=Perseus%3Atext% 3A1999.02.0137%3Abook%3D7%3 Achapter%3D15. Retrieved July 20, 2025.
4. Tacitus. Tacitus’ Annals. Book 12.22. https://www.perseus.tufts.edu/ hopper/text?doc=Perseus%3Atext% 3A1999.02.0078%3Abook%3D12%3 Achapter%3D22. Retrieved July 20, 2025.
5. Cassius Dio, Dio’s Rome. Volume 4.32. https://www.gutenberg.org/ cache/epub/10883/pg10883.txt Retrieved July 20, 2025.
6. Keyes, Carl Robert. The Adverts 250 Project: An Exploration of Advertising During the Era of the American Revolution, 250 Years Ago This Week. Paul Revere. September 8, 2018. https://adverts250project. org/tag/paul-revere/ Retrieved July 20, 2025.
7. Keyes, Carl Roberts. The Adverts 250 Project: An Exploration of Advertising During the Era of the American Revolution, 250 Years Ago This Week. Paul Revere. Guest Curator Kolbe Bell. August 1, 2020. https://adverts250project.org/ tag/paul-revere/ Retrieved July 20, 2025.
8. “Abigail Adams to John Adams, 7 April 1776,” Founders Online, National Archives, https:// founders.archives.gov/documents/ Adams/04-01-02-0244. [Original source: The Adams Papers, Adams Family Correspondence, vol. 1, December 1761 – May 1776, ed. Lyman H. Butterfield. Cambridge, MA: Harvard University Press, 1963, pp. 374–376.] Abigail Adams to John Adams, 7 April 1776 Retrieved July 20, 2025.
9. The Pennsylvania Evening Post. April 25, 1776. Page 180 of 450. The Pennsylvania Evening Post - State Library of Pennsylvania
10. Sumner, W.H. Reminiscences relating to General Warren and Bunker Hill. New England Historic Genealogical Register and Antiquarian Journal. 12. SG Drake, 1858: Page 119. The New England Historical & Genealogical Register and Antiquarian Journal - Google Books Retrieved July 20, 2025.
11. Stone, JW. Report of the Trial of Prof. John W. Webster, Indicted for the Murder of Dr George Parkman Before the Supreme Judicial Court of Massachusetts, Holden at Boston, on Tuesday, March 19, 1850. Phonographic Report. Boston: Phillips, Sampson & Company, 1850.
12. Martin, S. https://www.masshist. org/beehiveblog/2015/04/thelong-agony-is-over-the-trial-ofjohn-white-webster. Retrieved 07/19/2025.
13. Georget, C. and Labyt-Leroy, AS. Societe francaise d’hisotire de l’are dentaire’s article on Dr Oscar Amoëdo Y Valdes (1863-1945) An eclectic practitioner. https:// numerabilis.u-paris.fr/partenaires/ sfhad/actes/le-docteur-oscaramoado-y-valdes-1863-1945-unpraticien-eclectique/ Retrieved 07/04/2025.
14. The Future of Roubaix-Tourcoing Daily Republican Journal (L’Avenir de Roubaix-Tourcoing Journal Republicain Quotidien). http:// www.bn-r.fr/presse/pdf/PRA_AVE/ PDF/1897/PRA_AVE_18970507_001. pdf Retrieved 07/14/2025 and used Google Translate to translate from French to English.
15. “The Role of the Dentists in the Identification of the Victims of the Catastrophe of the “Bazar de la Charite,” Paris, 4th of May, 1897. [Volume: 39, Issue: 11, November, 1897, pp. 905-912].” In the digital collection Dental Cosmos. https://name.umdl.umich.edu/ acf8385.0039.001. University of Michigan Library Digital Collections. Accessed July 13, 2025.
16. 1950 Census, Texas, Enumeration District 217-1, Stonewall County. https://1950census.archives.gov/ search/?county=Stonewall&page= 1&state=TX. [Click “(View Original ED Description)”]. Retrieved July 20, 2025
17. Doyle v. State, 159 Tex. C.R. 310, 263 SW2d 779. 1954 as documented on the website Doyle v. State – CourtListener.com. Retrieved July 20, 2025.
Shanetha L. Collier, DDS, MS, D-ABFO
FORENSIC DENTAL IDENTIFICATION
Disclaimer: Photographs of real forensic dental identification cases are utilized in this article. These images can be graphic and may cause distress upon viewing.
Dr Shanetha Collier was born and raised in Durant, Oklahoma (so almost a Texan!). She earned her BS in chemistry from Oklahoma State University, her DDS from the University of Oklahoma College of Dentistry, and her MS in Forensic Dentistry from the University of Tennessee Health Science Center. She became a diplomate of the American Board of Forensic Dentistry (ABFO) in 2024. Since becoming board certified, she serves the ABFO as a member of the Board of Directors, the Dental Age Assessment Committee, the Civil Litigation Committee, and is also the chair of the Diplomate Development Committee. Currently residing and practicing general dentistry in Oklahoma City, Dr Collier spends her free time reading, traveling, watching/ attending sporting events, hanging out with friends and family, and, of course, doing all things forensic dentistry. She is an avid Disney fan, a proud dog mom, and an awesome aunt.
FORENSICIdentification
Forensic dental identification has been a source of curiosity amongst dental professionals for years. Cases can come from a wide range of circumstances: homicide, suicide, natural deaths, mass disasters, missing persons, immigration cases, and on occasion, cases with living individuals. This case variety certainly helps lend to the intrigue. In addition, forensic dental identifications are an area in which non-forensically trained dental professionals play a critical role in the outcome of the process. The following frequently asked questions and case examples will be used to provide education into what has become the “bread and butter” work of the forensic dentist and show how dental professionals contribute to their work.
Why do we need forensic dental identifications?
Identification of the deceased is important for several reasons. Criminal investigations often require positive identification of the victim for the case to proceed and bring about prosecution.1 For many family members, their ability to receive closure and progress through the grieving process depends on the positive identification that the deceased individual is their loved one. This is especially true in cases of missing persons, mass fatalities, and even victims of natural disasters. In addition to the grieving process, many family members cannot begin to settle affairs such as life insurance disbursements, estate transfers, execution of wills, and child custody issues without a legal death certificate issued upon positive identification of a decedent.2 Certain circumstances with living individuals can also utilize a forensic dental identification. For example, an individual with a medical issue such as dementia could potentially become lost, and being unable to positively identify themselves upon recovery, may need identification through other means.1 A forensic dental identification could also be used in cases of undocumented immigrants when proper supporting identification documentation is lacking.
Who is responsible for the forensic dental identification?
Identification of the deceased is the legal responsibility of the medical examiners and/or coroners while identification of a living individual who is not able to confirm their identity is the legal responsibility of local, state, or federal law enforcement.2 These agencies will rely upon proven scientific means of identification to fulfill this responsibility. There are 5 widely accepted methods of identification: visual, DNA, fingerprints, anthropology/radiology, and dental.1 While the legal responsibility falls on those agencies, if a dental identification is requested, it is the responsibility of the forensic dentist to provide an expert opinion and conclusion concerning the dental comparison and subsequent identification based on that comparison. It is important to remember that it is not the forensic dentist who “makes” the identification, but rather the legally responsible agency conferring an identification based on the expert opinion of the forensic dentist.
What makes dental identifications so reliable and widely used?
Firstly, the dentition is highly resistant to many biological, chemical, and traumatic processes to which other tissues are susceptible. These processes include decomposition, burning up to 1000ºF, water immersion, mummification, extreme trauma (such as encountered with mass disasters or natural disasters), and other postmortem (after-death) changes. So, while other
Acronyms in this article:
PA = Periapical
Pano = Panoramic radiograph
CBCT or CT = Cone Beam
Computed
Tomography
BW = Bitewing
Radiograph
FMX = Full Mouth
Series of radiographs
ID = Identification
AM = Antemortem
PM = Postmortem
tissues may be too degraded for identification purposes, the teeth are often still in good to excellent condition. Secondly, the dental features of an individual are unique due to tooth morphology, dental restorative treatment, missing teeth, pathology, the presence of supernumerary teeth, maxillary sinus morphology, bone trabeculation pattern, and many other features. Dental features in terms of forensic dental identifications are not just limited to the teeth and the bones of the maxilla and mandible. There are many structures available for a dental comparison. As such, the likelihood that 2 individuals have
Figure 1. (L and below): The ability of teeth to withstand many extreme circumstances is one reason forensic dental identifications are used. As seen here, this individual was severely burned in a house fire. However, despite the severe degradation of the other tissues, many of the teeth are still in very good condition.
identical dental features is extremely low, leading to the high reliability of forensic dental identifications. Thirdly, most individuals have been to a dentist at some point in their life resulting in antemortem (pre-death) dental records being more prevalent throughout the general population as compared to fingerprints, DNA records, and other radiographs. Lastly, dental identifications can often be performed quickly and cost-effectively. With most family members anxious to proceed with next steps and the identifying agencies having to operate within a specified budget, utilizing a method of identification that is scientific, reliable, quick, and low-cost is advantageous to all (Figure 1).
What type of cases with deceased individuals use dental forensic identification?
Cases in which the individual cannot be visually identified, does not have records for other means of ID, whose remains are too degraded for other means of
identification, and/or are victims of criminal acts (for which a scientific means of identification is usually preferred) make up the bulk of the forensic dentists’ workload. Cases that are not visually identifiable often include remains that are burned, decomposed, skeletonized, or have suffered large amounts of trauma. Sometimes first line attempts to identify an individual through fingerprints or other radiographic techniques (anthropology) are unsuccessful. This can be due to lack of antemortem records or degradation of the tissues needed for these identification techniques. DNA, while certainly precise, can be expensive, time consuming to obtain results, and requires tissues samples that have not been degraded—all factors that do not often apply in a forensic dental identification. In criminal cases, law enforcement and prosecutors desire high quality, scientific evidence in all aspects of the case, including the identification of the victim. In instances of mass disasters or mass fatalities, manifests or other documentation exist that help narrow the list of potential victims. Dental records can then be readily obtained for these individuals allowing for an
efficient means of identification when there are many victims and families awaiting confirmation of identities. For these reasons, dental is a preferred identification method for many of the aforementioned case types and situations (Figure 2).
How is a forensic dental comparison/ identification carried out?
Dental identifications are performed by comparing antemortem records to postmortem records and identifying any unique points of comparison. To obtain the antemortem records, a presumptive/presumed identity of the individual must exist. It is not the responsibility of the forensic dentist to determine the presumptive identity nor to acquire the antemortem records for that identity. A medico-legal death investigator is usually the forensic team member responsible for these tasks. Presumptive identities are obtained through talking with family members, contextual evidence at scenes (drivers licenses, car registrations, property deeds, etc), travel manifests, and other
investigative leads. Once antemortem records have been obtained, the forensic dentist will conduct a postmortem examination for use in comparison to those antemortem records. Depending on the quality of the features being compared and the level of certainty in that comparison, a conclusion statement for the dental identification will be issued. This conclusionary statement is reported to the medical examiner/coroner for use in their official determination of identity.
What are the conclusion statement options for a dental identification?
The American Board of Forensic Odontology is the accrediting organization in the United States for forensic dentistry, and as such, is responsible for providing standards and guidelines for the field. In these standards and guidelines, there are 4 separate conclusion statements for expressing the outcome of a forensic dental comparison for identification purposes: Exclusion, Insufficient
Figure 2. Examples of cases in which forensic dental identifications can be utilized. A) Skeletonized remains found in remote location; B) Burned remains due to a house fire; C) Decomposed remains found at residence during a requested welfare check; D) Traumatized remains due to motor vehicle accident.
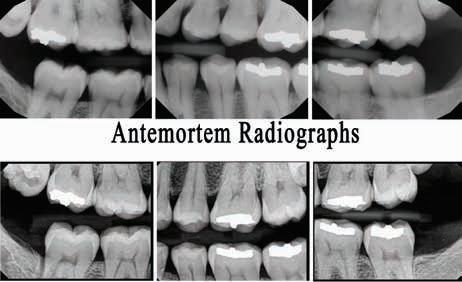
Antemortem Radiographs
Postmortem Radiographs
Figure 3. Comparison of antemortem bitewings with postmortem bitewings; Positive dental identification concluded based on restorations on teeth #2, #14, #18, and #19.
Antemortem Radiographs
Postmortem Radiographs
Figure 4. Comparison of antemortem full mouth and pano radiographs with postmortem full mouth radiographs for an individual who was burned in a motor vehicle accident; Positive dental identification concluded based on anatomic relationship of #10 to #11, pulp morphology #13, root morphology #14, left maxillary sinus floor morphology, root morphology #31, and anatomic position of #32. This case shows how other non-restorative dental features can be used to conclude a positive dental identification.
Evidence, Possible Identification, and Positive Identification.3 An exclusion designation means the individual represented by the antemortem records is NOT the same individual for whom postmortem records were collected. Insufficient evidence is used in situations where a forensic dental comparison cannot be performed. Common reasons for not being able to perform a comparison include, but are not limited to, lack of proper dental evidence, low quality records, or poor condition of the remains. A possible identification is given to individuals who have many similar points of comparison between the antemortem and postmortem records, but these points are not specific enough to give 100% certainty in the matching of the records. A Positive Identification is reported when there are no unexplainable inconsistencies noted between the antemortem and postmortem records, as well as the points of comparison are specific and unique enough to have no doubt that they are from the same individual (Figures 3 and 4).
What type of antemortem records can be used for a forensic dental identification?
All types of dental records can be used. Traditional dental radiographs (FMX, pano, BWs, PAs,) along with the written treatment record are the most common antemortem records used in the comparison process. However, other types of records such as CBCTs, digital intraoral scans, photographs, dental models, and any other head and neck radiographs can provide needed information for comparison. Removable
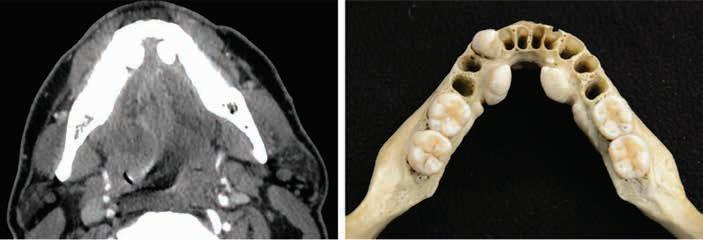
Antemortem Postmortem
Figure 5. Comparison of mandibular tori similarities using an antemortem record from a medical head CT horizontal slice and a postmortem photograph.
Figure 6. Comparison of maxillary restorations in teeth #3 (yellow arrow) and #14 (blue arrow) using an antemortem record from a medical head CT scout image and postmortem periapical radiographs. Note: the postmortem PA of #14 has been mirrored to match the orientation of the antemortem image.
Figure 7. When antemortem radiographic data is scarce or of poor quality, photographic comparisons can be utilized. This figure shows how an antemortem intraoral scan and postmortem photograph can be useful for visual comparison.
prosthetics, orthodontic appliances, surgical guides, and/or other oral health appliances can also be useful by fitting these appliances in an individual’s mouth to check for fit. If it has information concerning an individual’s oral, head, and/or neck status, it can potentially be used for a forensic dental identification (Figures 5, 6, and 7).
What are the components of a postmortem dental examination, and how is it completed?
Think of a postmortem dental examination like a new patient comprehensive work up. Records include, but are not limited to, photographs of the remains and their oral condition, dental charting of all findings, and a full mouth series of dental radiographs. The goal is to acquire enough information to have a representation of the decedent’s head, neck, and oral condition even after access to the remains or individual is not available. These examinations are carried out much like they would be on that new patient in your dental office, but sometimes the condition of the remains
Figure 8. This individual was found in a state of mummification in their home. This process results in the soft tissue being leathery, difficult to manipulate, and limited in elasticity. Soft tissue incisions were made from the commissures bilaterally to gain access to the oral structures. The TMJ was then able to be manipulated enough to achieve opening without needing further resection.
Figure 9. This individual was burned in a house fire leaving access to the oral cavity limited. Jaw resection was completed by making bilateral incisions through the soft tissues and using a bone saw to cut through the ascending ramus of the mandible. The second and third photograph show how much better the visibility and access is to the oral structures after the resection.
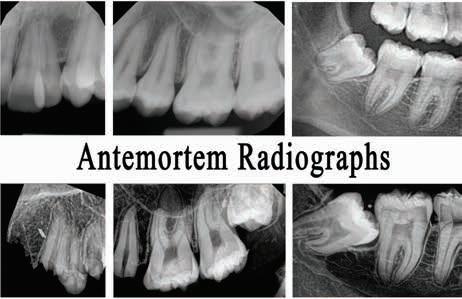
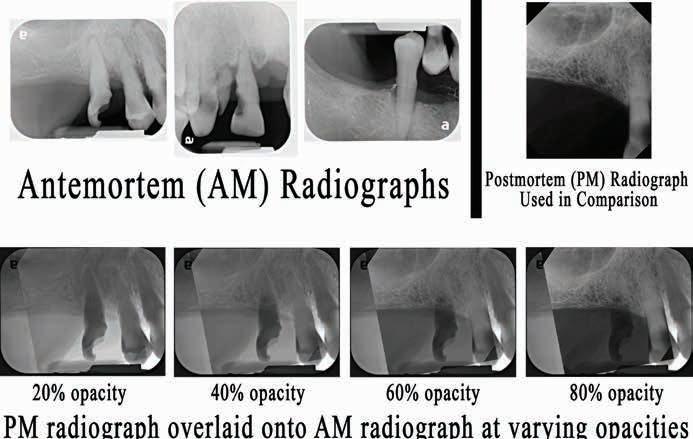
Antemortem (AM) Radiographs
Postmortem (PM) Radiograph Used in Comparison
PM Radiograph Overlaid onto AM Radiograph at Varying Opacities
Figure 10. In this decomposition case, only 3 antemortem radiographs were received. The individual had lost all teeth from the antemortem radiographs except teeth #5 and #6, with #6 being a retained root at the time of the postmortem dental examination. Despite minimal antemortem dental information, comparison of the right maxillary sinus morphology resulted in the use of this single feature to conclude a positive dental identification. A digital overlay of the postmortem radiograph onto the antemortem radiograph shows the unique morphology of this feature and the alignment between the 2 sets of radiographs.
does require additional care and/or aids to properly acquire the desired information. Jaw resections are sometimes needed in order to gain full access to the oral structures. These resections can involve only needing to incise some of the soft tissue to full separation of the bony structures through use of a Stryker saw or garden shears. Burned remains are brittle and require extreme care not to damage or lose critical postmortem information. Sometimes spraying the oral structures with hairspray or applying a cyanoacrylate adhesive can help hold the burned oral structures in place. Skeletal remains do not have soft tissue and as such, “donut” pillows or other stabilizers are used to keep these remains stationary while obtaining the photographs and radiographs. Outside of these often-needed modifications, acquisition of photographs, charting, and radiographs is carried out as it would be on a living individual (Figures 8 and 9).
How many points of comparison are needed for the
conclusion of a positive dental ID?
The more unique points of comparison there are between the antemortem and postmortem records, the more certain the identification can usually be. However, it only takes one unique point of comparison with no unexplainable inconsistencies in the remainder of the records to earn a conclusion of a positive identification. While the forensic dentist always wants to
have as many unique features for comparison as possible, a single unique enough feature can be all that is needed to say with full certainty the 2 sets of records are from the same individual (Figure 10).
I’ve gotten a request for records from law enforcement or a medical examiner. Won’t I be in violation of HIPAA laws if I provide records without proper release?
According to the HIPAA Act 45 CFR 164.512, if you are a dental provider and an agency requests records for use in identification of a deceased individual or records for a suspected victim of a crime, you will not violate any HIPAA laws by providing records without a release from the patient.4 Given this, if you are provided a subpoena for records, you should comply with the subpoena and submit all the requested records to the address provided.
How can I make the forensic dental identification process easier for the forensic dentist?
High quality records provided in a timely manner is the best way for a dental professional to help the forensic dentist. If you are a digital office, providing copies of those records digitally is what is desired. If you still have paper records and film x-rays, please send the original records/x-rays via mail
with a return address. These records can then be returned to you upon completion of the identification process. Photocopies of analog radiographs and printed copies of digital radiographs are often not high quality enough for a good forensic dental comparison. Also, proper charting of existing restorations on the odontogram and good documentation in the progress notes of treatment rendered can provide crucial information for any discrepancies noted between the antemortem records and the postmortem records. Even if you think a part of your records will provide no useful information, it is still better to send all antemortem dental data as the forensic dentist never knows what feature(s) will lead to the best comparison. Having the proper antemortem information can be the difference between not being able to perform a forensic dental identification, rendering a possible identification, or assigning a positive dental identification. There is nothing more heartbreaking to a forensic dentist than being able to obtain high quality postmortem records with many identifying features but being unable to complete the dental comparison due to poor quality or incomplete antemortem records. Ultimately, the higher quality the antemortem information available to the forensic dentist, the easier and more successful the comparison will be. If you are ever contacted about submitting records for a forensic dental identification but have questions concerning the process, do not hesitate to reach out to the requesting agency so they can get you in contact with the forensic dentist if needed. Remember, the goal of all parties involved is simply identification of the individual in question, and therefore any information you can provide to help achieve that goal accurately and efficiently is greatly appreciated.
ACKNOWLEDGMENTS
The author acknowledges that the Texas Dental Association assumes no responsibility or liability for any injury and/or damage to persons or property from any content within this article. The author also has no conflicts of interest, financial or otherwise, to disclose. Case photographs have been shared for educational purposes with permission from the appropriate case agencies. It is requested these photographs not be shared with individuals outside the dental profession in order to maintain the honor and dignity of those represented within the photographs. Lastly, the author would like to thank Dr Kathy Kasper for her request to contribute to this issue of the Texas Dental Journal.
REFERENCES
1. Berman GM, Bush MA, Bush PJ, Freeman AJ, Loomis PW, Miller RG. Dental Identification. In: Senn Dr, Weems RA, eds. Manual of Forensic Odontology, Fifth Edition. Boca Raton: CRC Press, 2013: 75-127.
2. Loomis PW, Reid JS, Tabor MP, Weems RA. Dental Identification and Radiographic Pitfalls. In David TJ, Lewis JM, eds. Forensic Odontology: Principles and Practice. London: Academic Press, 2018: 25-46.
3. American Board of Forensic Odontology. Body Identification Information & Guidelines. Nevada: American Board of Forensic Odontology, 2017.
4. Government of the United States of America. Health Insurance Portability and Accountability Act of 1996, 45 CFR §§160, 162, 164. Washington, DC: United States Department of Health and Human Services, 2023.
FBI: Found But not Identified (yet)
A series of articles intended to assist Texas Medical Examiners in giving a name to “unidentified” individuals using postmortem dental evidence.
Do you recognize the dental work/conditions presented?
Kathleen A Kasper, DDS, D-ABFO
The Extent of the Problem
Over 600,000 individuals go missing in the United States every year. Fortunately, many missing children and adults are quickly found, alive and well. However, tens of thousands of individuals remain missing for more than 1 year—what many agencies consider “cold cases”.1
It is estimated that 4,400 unidentified bodies are recovered each year, with approximately 1,000 of those bodies remaining unidentified after 1 year.2
Medical examiner and coroner offices reported 11,380 unidentified remains on record as of 2018.3
The challenge in giving a name to these unidentified decedents is that the research and time invested can be extensive and expensive, and after normal protocols have been exhausted, many individuals still remain unidentified. The hope in writing this series of articles on long-term unidentified in Texas is that one of the many Texas dentists who read the Texas Dental Journal will recognize the dental work presented as theirs or possibly remember a dental condition or feature that can give a name to the unidentified and help bring closure to the family.
The Medical Examiner’s Protocol to Legally Identify Individuals
Medical examiners follow a specific protocol to identify individuals who are found without any presumptive identity. This protocol is described below and, in this order, depending on the condition of the body.
Latent Prints (finger, palm, sole) are the fastest and least expensive way to make a positive identification. This method of identification is not always possible if remains are severely decomposed, incinerated, or skeletonized.
Medically Implanted Devices (hip/joint replacements, pacemakers) require knowing what hospital/physician placed the device to get the matching serial number, which can be difficult.
Dental Records are also an easy, fast, and inexpensive way to identify a decedent; however, success depends on a presumptive identity and availability/existence/ quality of those antemortem (before death) dental records. If all leads for a presumptive identity are exhausted, then a postmortem (after death) dental charting/ profile is created and entered in the NamUs (National Missing and Unidentified Persons System) and NCIC (National Crime Information Center) databases.
Anthropologic Methods will use skeletal features to make a positive identification. DNA samples are collected. This takes the longest period of time and is most expensive. Depending upon the individual, it may involve obtaining DNA samples not only from the decedent but also from family members or multiple family members if known. If no matches are obtained, then:
DNA Samples are submitted to CODIS (Combine DNA Index System), which is a computer program that operates local, state, and national databases of DNA profiles from convicted offenders, unsolved crime scene evidence, unidentified remains and missing persons. This is maintained by the Federal Bureau of Investigation. If this search fails then, the State of Texas requires medical examiners to submit a DNA sample from long-term unidentified decedents to the University of North Texas Center for Human Identification for additional genetic testing and comparison. This comparison may take up to a year to process, and a decedent may still remain unidentified once completed. This is the proverbial end of the road; therefore, all Texas dentists, dental auxiliaries and staff; Can you help the Dallas County Medical Examiner’s Office give a name to the unidentified Hispanic male decedent described on the next page?
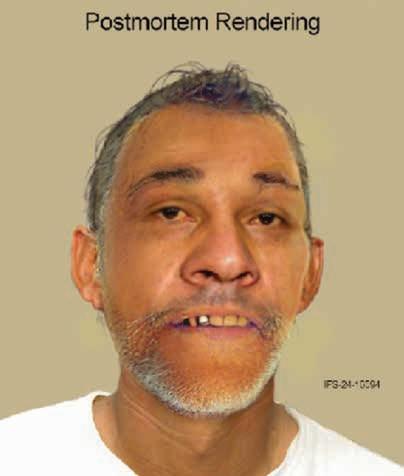
The Unidentified Individual:
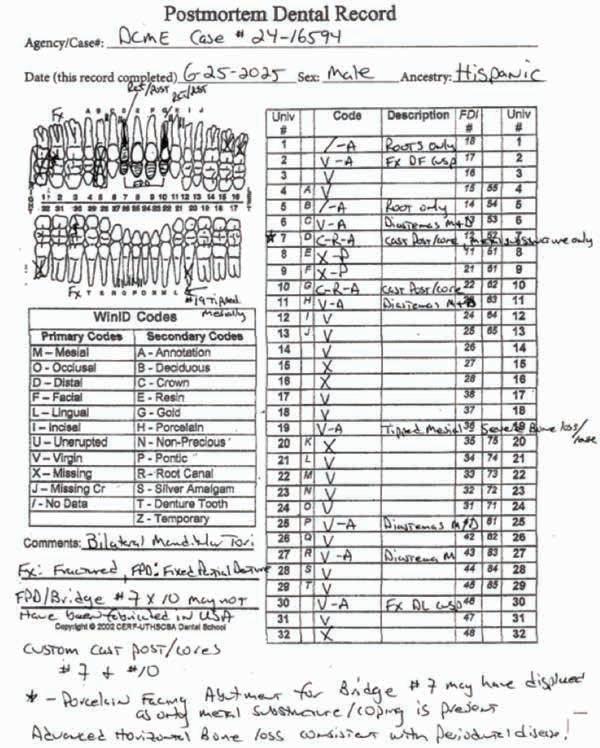
Dallas County Medical Examiner (DCME) Case #24-16594, NamUs #UP142230
Date of Death (Decedent found): September 26, 2024
Body Condition: Fresh at time of death
Sex: Male
Ancestry: Hispanic
Age Interval: TBD (pending forensic anthropology consult)
Height: 66 inches (5’ 6”)
DNA analysis completed: Yes—Profile entered in the Combined DNA Index System (CODIS)
Details of Incident:
On 09/26/2024 at approximately 6:54 PM, the decedent was attempting to cross the roadway near 1900 Record Crossing Road in Dallas when he was struck by a Honda Civic that was traveling in the far-right lane. The decedent was transported to Parkland Hospital via EMS where his death was pronounced at 7:22 PM. Paperwork was recovered from the decedent’s pocket providing a name of “Gabriel Martinez”; however, the decedent’s identification was unable to be verified.
Dental Evidence Recovered: Maxilla and Mandible
Below is a postmortem rendering created from remains recovered for DCME Case #24-16594/ NamUs #UP142230.
Right
Right Lateral View
Left Lateral View
Fixed Partial Denture #s 7 x 10
Maxilla Occlusal View
Right Left
Mandible Occlusal View
Left Right
[Fixed Bridge #s 7 x 10 may not have been fabricated in the USA]
Dental Existing Conditions DCME Case #24-16594:
Closing
If you believe you have any dental records, dental radiographs, intraoral/extraoral dental photographs, dental scans, or other dental information regarding the unidentified Hispanic male decedent described above as DCME Case #24-16594, please contact the Dallas County Medical Examiner’s Office, 214-920-5900, ask for Steven Kurtz, chief medicolegal death investigator.
Let’s give this individual a name!
References
1. Between 2007 and 2020, an average of 664,776 missing persons records annually were entered into the National Crime Information Center. See https://www.fbi.gov/ services/cjis/ncic.
2. Medical Examiners And Coroners’ Offices, 2004. Matthew J. Hickman, Ph.D., Kristen A. Hughes, M.P.A., Bureau of Justice Statistics, Kevin J. Strom, Ph.D., Jeri D. Ropero-Miller, Ph.D., DABFT, RTI International.
3. Medical Examiner and Coroner Offices, 2018. Connor Brooks, Bureau of Justice Statistics, November 2021.
James P. Fancher, DDS, MA, PhD, D-ABFO
Forensic Anthropology— An Introduction for Dentistry
Dr Fancher is a graduate of The UTDB, Houston (DDS), the University of Washington Dental School (Periodontics), Texas A&M University (PhD, Education), and Texas State University (MA, Biological Anthropology). He also completed a fellowship in Forensic Odontology at The UT San Antonio Dental School. He is an active diplomate of the American Board of Forensic Odontology, and a retired diplomate of the American Board of Periodontology.
He got his start in forensic odontology as an active duty dental officer in the Air Force where he completed several postmortem identifications and he presented on topics related to the commander and the law.
The most significant event that solidified his interest in forensics was working on the team that identified the 183 peopled murdered by terrorists at the Pentagon on 9/11. He has worked on numerous other mass casualty incidents including the 2015 Wimberley flood incident, the 2016 Caldwell County balloon incident, and the 2025 Guadalupe River flood incident. He has also contributed as an odontologist and/or anthropologist on numerous death investigations primarily in central and south Texas.
He is affiliated with the Forensic Anthropology Center at Texas State University, and he teaches a course in dental anthropology. He recently worked as an odontologist at Defense POW/MIA Accounting Agency, Hickam Field, HI.
FORENSICIdentification
Background Scenario
Imagine that you are a dentist in any town in the state of Texas, or any other part of the world. As part of your civic duties you have volunteered for the local law enforcement office to offer your professional assistance in any way possible. Early one weekend you get a call to assist on a confidential matter of importance, and you are told simply to report to the local law enforcement office as soon as possible, which you choose to do. You are told only that assistance is needed to excavate a site that potentially has human remains, and a dentist is needed to make sure that all dental evidence is collected for analysis. You are escorted to a remote cattle pasture in your county on a familiar country road, and you find a group of law enforcement officers and people in civilian working clothes that are gathered around one side of the field that has been cordoned off with official barriers. Obviously, there is a serious matter of concern in your community, and there is a story to be told, but you must treat all information and experiences as confidential. You ask few questions and strive to remain as unbiased as possible for this investigation.
On the edge of the field you note that a small oval depression in the soil is marked with utility flags, identifying an area that is peculiarly different from the surrounding terrain (Figure 1). The sunken soil appears turned over, compacted, and smooth when compared to the adjacent surface soil. It measures about 0.5 meter by 2 meters in a rectangular/
Abstract
Forensic anthropology is the academic and scientific field that operates at the intersection of biological anthropology and forensic science. Training and experience required to work in this field is extensive and usually includes many years of postgraduate education, advanced degrees, and practical experience. Dentists may interact with forensic anthropologists in many ways in working with forensic cases, and this article presents a common field-based scenario that may lead to professional associations. The education and training, scope of practice, certifications available, and employment opportunities for forensic anthropologists are discussed.
Figure 1. A site of potential forensic interest that has been identified in the field. There is disturbed surface soil that is sunken with altered foliage cover. The rectangular/oval dimensions are approximately 0.5 meter by 2 meters.
oval dimension. The 6 to 10 people in civilian clothes are working as a team under the direction of a determined and professional person that is identified as the forensic anthropologist (FA) from a local medical examiner’s office. The other team members are identified as death investigators plus students from a nearby university’s anthropology department. Your job as the dentist is to verify that dental elements are present and recovered, and you may volunteer to help with some of the excavation and physical labor.
A Total Station theodolite instrument is set up, and precise measurements with GPS coordinates to locate the boundaries of the site are made by the team before any excavation work begins. A team member continuously takes photographs of the site and makes detailed time-based notes about
all activities. The excavation team measures out a precise 1-meter by 2-meter rectangle on the ground that includes the entire depressed area, and the boundaries are marked with corner stakes with brightly colored carpenter’s string tightly strung to show the site boundaries. Under the close supervision of the FA they begin a delicate process of removing the covering foliage and then excavating the soil with shovels and hand trowels one 5-gallon bucket at a time. The going is slow, with only a few centimeters (~1 inch) removed at a time, and all soil removed is taken to an adjacent site for screening through a ¼-inch mesh box sieve to find any artifacts that may be of interest (Figure 2). Finally, after 2-3 hours of careful excavation, the form of a human skeleton emerges from the soil at a shallow depth of about 0.5 meter (about 19 inches).
During the excavation, the FA periodically stops the work while photographs are taken, survey measurements by the Total Station are made, and site notes are updated. The FA continually directs the team to avoid damage to the skeletal remains and closely examines and supervises bagging and labeling of all artifacts found during excavation or in the sieving process. When the exposure of the skeleton is completed (Figure 3), a detailed site map of the remains is made by hand drawing, and a digital map is made using GPS coordinates generated from the Total Station. Then the FA personally works with a team member to remove each skeletal element that is found, and a complete inventory of all 206 bones associated with a human skeleton is completed. Once the excavation is complete, the remains and other bagged artifacts are securely transferred to a
2. A box
All dirt and debris from the excavation site must be sieved through this ¼-inch mesh to screen for bone fragments, teeth, clothing remnants, metal fragments, firearm evidence, and any other artifact that has evidentiary value. Often there are scores or hundreds of 5-gallon buckets that must be examined.
Figure
sieve.
laboratory for analysis and potential identification. From the start to finish, the field work is completely documented by photography, highly accurate survey measurements, and field notes.
The next week you go to the medical examiner’s office to complete the postmortem dental exam for potential identification (charting, radiographs, and photographs). The FA meets with you and shows you the recovered human skeleton that is assembled in an anatomic position on a lab table. All osteological elements, or bones, are set out as close as possible to the normal anatomical relationship as though the individual were lying flat on the back, and a complete set of standard measurements and interpretations have been completed following classical and updated methods.1 The FA gives a summary of the skeletal analysis,
which is called the biological profile that includes the estimated sex, ancestry, stature (height), and age of the individual.2-5 Observations also are made about any skeletal trauma that may have been observed, as well as any pathological conditions that may exist in the bones. Other details that may be included are surgical artifacts such as prosthetic devices, healed bone trauma, degenerations such as osteoarthritis, and any other bony abnormality that may give a clue about the individual’s identity or experiences during their life history. There are some sites of surgical block cut outs from long bone shafts such as the upper arm (humerus) or legs (femur or tibia) that represent bone sections that have been removed for submission for DNA analysis. You are told that the set of remains is relatively complete except for a few small bones that were not recovered from the
hands and feet, and that there are no duplications of each individual bone recovered, so that this case represents a minimum number of one individual (MNI=1).
The FA may or may not be able to estimate a potential time of death by interpreting data related to the postmortem interval evident in the condition of the remains, artifacts recovered, and/or changes since death and burial (taphonomic changes).6
Other questions that are evaluated concern the context of the burial site; i.e., is this a recent versus historical/ prehistorical site; were the remains treated with elements of respect or haphazardly disposed of; is this a primary burial site, or have the remains been moved and reburied; or have other similar sites been found under similar circumstances? Most importantly, the FA
Figure 3. Excavation completed for a human skeleton buried at a depth of approximately 0.5 meter. After site documentation of this stage of excavation, the remains are methodically removed, inventoried, and taken to a forensic laboratory for further evaluation by a forensic anthropologist and other analysts, including a forensic odontologist. The human skeleton image shown in Figure 3 is an anonymous donor of the willed body program at the Forensic Anthropology Center at Texas State University.
has been able to take all the data from the analysis and use these data points to create a list of missing persons with similar biological profiles from local records and national data bases such as The National Missing and Unidentified Persons System (NamUs) and the National Crime Information Center (NCIC) Missing Person File.7 When you complete the postmortem dental exam, hopefully you will now have a list of individuals with antemortem dental records that may lead to an identification, possibly long before a comparative DNA analysis can be completed.
The Profession of Forensic Anthropology
This scenario is typical of some of the work that most forensic anthropologists (FA’s) complete on a routine basis, and it is somewhat typical of how dentists may encounter the professional field of this group of forensic scientists. An excellent general review of the history and science of forensic anthropology can be found in the edited publication “Forensic Anthropology—An Introduction.8 According to the American Board of Forensic Anthropology”, the profession is considered to be one of the applied fields of physical or biological anthropology that uses anthropological and associated science, methodology, and technology to help address medicolegal issues such as personal identification and circumstances surrounding death.9 Classically, FAs use clues from osseous structures to assist in the investigation of a variety of cases that involve skeletal remains, fragmented and/or decomposing remains, burned and charred bodies, burial recoveries of remains, child abuse, trauma analysis, and human rights violations. Developing a dental
profile is part of their training that can always be assisted by the dental community, especially since the dental profile may be considered an essential part of the biological profile that may lead to identification of human remains, as well as a deeper understanding of their clinical and life history.10 Dirkmaat and colleagues (2008) proposed a broader definition that forensic anthropology is “the scientific discipline that focuses on the life, the death, and the postlife history of a specific individual, as reflected primarily in their skeletal remains and the physical and forensic context in which they are emplaced”.11 Forensic anthropology is also defined by the interplay of concepts of human variation and secular change, developmental and evolutionary changes and adaptations, interpretation of the forensic record or context of the remains (who, what, where, when, and how questions), the required use of precise archaeological techniques, and metric and statistical interpretations that give a more precise base to the field than the detailed observational osteological knowledge.12
Besides playing the primary role in gathering and interpreting the traditional data for the biological profile, the FA also collects or facilitates collecting advanced biological, chemical, and anatomical data from hard and soft tissues that require analysis by other forensic specialists such as odontologists and DNA scientists. There has been tremendous progress in the practice of forensic anthropology based on much scholarly research and practice experience, but the modern mass media often portrays the field with many misconceptions about the true nature of criminal science. Forensic cases quite often are not solved quickly and may take many years and decades to find justice and final resolution.13 The advent
of molecular genetic methods (i.e., DNA technology) and other biochemical analyses such as stable isotope profiles have all led to great advances that can tell much about the genetic identity and biological history of an individual’s growth and development, but they also require expensive, time-consuming, and technically demanding methodologies that do not often meet the publics expectations of immediate or quick results.14-16 The gathering of basic data for genetic and advanced testing may be a routine part of the anthropological exam, but getting forensically meaningful results can take months and years.
The qualifications of a forensic anthropologist are based on many years of professional training and experience. The classical central component of education is to become an expert in osteology with an extensive knowledge of the bony anatomy and skeletal functions of the human body. These osseous elements, including teeth, tend to persist long after death (postmortem), and they carry a record of life and death events that provide long-lasting clues of existence. Although board certification is not required to do the work of a forensic anthropologist, it is reserved for those that have been examined and found to possess the highest recognized level of knowledge, skill, and abilities. The American Board of Forensic Anthropology (ABFA) offers a multilevel certification at 2 stages that begin as an analyst and may progress to diplomate status, all depending on education, training, experience, moral character, and passing of formal examinations.17 The entry academic level is usually earning a master’s degree or PhD in biological anthropology with a focus on forensics. During this 2–6+-year postgraduate education, the student must focus on developing
advanced skills in osteology, methods of forensic anthropology investigations, archaeological techniques and field experience, research methods, statistics, ethics, and education in cultural aspects of anthropology. A research project must be proposed and completed that results in a published thesis or dissertation that must be publicly defended. Many graduate programs also require extensive experience working with donated human body collections and actual forensic cases in the field and laboratory analysis.
Progressing to the diplomate level currently requires a prerequisite PhD and previous attainment of the analyst level. Additional experience and more rigorous evaluation are also required. Most people that attain diplomate status also have many years of experience in academic positions, and/or practical experience in field archaeology, death investigations, morgue assistance, legal clerical work, and research. Work sites for the experienced FA are very competitive and vary from academic university and college positions; employment in a medical examiner’s office as an anthropologist or death investigator; working in human rights investigations to document and identify humans that have suffered from official or criminal oppression such as war crimes, human trafficking, and political abuse; and supporting mass disaster response planning and relief efforts.18-20 The largest single employer of FAs in the United States is the federal agency Defense POW/MIA Accounting Agency (DPAA) that is responsible for accounting for and returning the remains of American service members who have been lost in foreign wars (visit the following site for more details: https:// www.dpaa.mil/).21
Summary
Forensic anthropology is the academic and professional field that functions at the intersection of biological anthropology and forensic sciences. It was once seen as a laboratory based subfield of biological anthropology that centered on the osteology of the human skeleton, but it has broadened its base to include the scientific study of an individual’s (or group of individuals) pre- and postlife history, as well as the physical and forensic context in which they are found.12 The basic skills of the FA include a mastery of human osteology, competence in archaeological methods and interpretations, recovery and analysis of human remains, ability to apply scientific inquiry and reasoning, a deep understanding of human genetics for individuals and populations, an understanding of cultural and social factors of human existence, and familiarity with newdeveloping biochemical and biological principles and techniques. The dental community may interact with FAs in academic communities, medico-legal investigations, mass disaster planning and incidents, and investigations of human rights cases.
References
1. Buikstra JE, Ubelaker DH, editors. Standards for Data Collection from Human Skeletal Remains: Proceedings of a Seminar at The Field Museum of Natural History. Fayetteville: Arkansas Archaeological Research Series; 1994.
2. Moore MK. Sex estimation and assessment. In: DiGangi EA, Moore MK, editors. Research methods in human skeletal biology. Boston: Elsevier; 2013. p. 91–116.
3. DiGangi EA, Hefner JT. Ancestry estimation. In: DiGangi EA, Moore MK, editors. Research methods in human skeletal biology. New York: Elsevier; 2013. p. 117–50.
4. Moore MK, Ross AH. Stature estimation. In: DiGangi EA, Moore MK, editors. Research methods in human skeletal biology. New York: Elsevier; 2013. p. 151–80.
5. Uhl NM. Age at Death Estimation. In: DiGangi EA, Moore MK, editors. Research
Methods in Human Skeletal Biology. New York: Elsevier; 2013. p. 63–90.
6. Haglund WD, Sorg MH, editors. Forensic Taphonomy: The Postmortem Fate of Human Remains. New York: CRC Press; 2006.
7. Fancher JP, Hampl P. Missing and unidentified persons. In: David TJ, Lewis JM, editors. Forensic odontology: Principles and practice. London, UK: Elsevier; 2018. p. 103–20.
8. Tersigni-Tarrant MA, Shirley NR, editors. Forensic Anthropology, An Introduction. New York: CRC; 2013.
9. ABFA. American Board of Forensic Anthropology - General Information [Accessed 7/13/2025]. Available from: https:// www.theabfa.org/general-information.
10. Adserias-Garriga J, Thomas C, Ubelaker DH, C. Zapico S. When forensic odontology met biochemistry: Multidisciplinary approach in forensic human identification. Archives of Oral Biology. 2018;87:7–14.
11. Dirkmaat DC, Cabo LL, Ousley SD, Symes SA. New perspectives in forensic anthropology. American Journal of Physical Anthropology. 2008;137(S47):33–52.
12. Boyd C, Boyd DC. Theory and the Scientific Basis for Forensic Anthropology. Journal of Forensic Sciences. 2011;56(6):1407–15.
13. Tersigni-Tarrant MA, Shirley NR. Brief History of Forensic Anthropology. In: TersigniTarrant MA, Shirley NR, editors. Forensic Anthropology, An Introduction. New York: CRC; 2013. p. 1–16.
14. Cabana GS, Hulsey BI, Pack FL. Molecular Methods. In: DiGangi EA, Moore MK, editors. Research Methods in Human Skeletal Biology. New York: Elsevier; 2013. p. 449–82.
15. Bethard JD. Isotopes. In: DiGangi EA, Moore MK, editors. Research Methods in Human Skeletal Biology. New York: Elsevier; 2013. p. 425–48.
16. Chesson LA, Berg GE, Megyesi M. Disaster victim identification: Stable isotope analysis and the identification of unknown decedents. J Forensic Sci. 2024;69(5):1658–70.
17. ABFA. American Board of Forensic Anthropology Multilevel Certification Program 2025 [Accessed 7/13/2025]. Available from: https://www.theabfa.org/multilevel.
18. Kimmerle EH. Forensic Anthropology: A Human Rights Approach. In: TersigniTarrant MTA, Shirley NR, editors. Forensic Anthropology - An Introduction. New York: CRC; 2013. p. 421–38.
19. Spradley KM, Herrmann NP, Siegert CB, McDaneld CP. Identifying Migrant Remains in South Texas: Policy and Practice. Forensic Sciences Research. 2018;4(1):60–8.
20. Sledzik PS. Forensic Anthropology in Mass Disasters. In: Tersigni-Tarrant MTA, Shirley NR, editors. Forensic Anthropology - An Introduction. New York: CRC; 2013. p. 439–50.
21. Holland TD, Tersigni-Tarrant MTA. Joint POW/MIA Accounting Command/Central Identification Laboratory (JPAC/CIL) History. In: Tersigni-Tarrant MTA, Shirley NR, editors. Forensic Anthropology - An Introduction. New York: CRC; 2013. p. 17–24.
John B. Nase, DDS, D-ABFO
Dental Age Assessment in Children, Adolescents, and Adults—An Overview
Dr John Nase is a practicing forensic odontologist, board certified by the American Board of Forensic Odontology (ABFO), and is an instructor for the ABFO Dental Age Assessment Workshop and an ABFO Board Examiner. He is the chief odontology consultant for the coroner’s offices in Montgomery, Bucks, and Chester Counties, as well as the medical examiner’s offices of Philadelphia and Delaware County, Pennsylvania. He is also the lead forensic dentist for Disaster Mortuary Operational Response Teams Region III. Dr Nase has been licensed to practice dentistry since 1992 and maintains a private general dentistry practice in Harleysville, Pennsylvania.
DENTAL Age Assessment
Introduction
Dental Age Assessment (DAA) is the process of approximating an individual’s chronological age at any given point before birth, during life, or their age at death through analyzing predictable patterns of tooth changes (growth, maturation, deterioration, etc.). The result of DAA generally is a Dental Age Estimation (DAE).
Even before birth, neonates begin to have visible tooth buds as early as 14 weeks in utero, which signals the beginning of the ability to determine the time since conception.1 The biological events surrounding birth are also recorded as the neonatal line that can be seen in thin cross section microscopically.2
The childhood period starts at birth and goes to the end of the period with a mixed primary and secondary dentition (loss of the last primary tooth). Age assessment for these periods relies on the predictable growth patterns seen in teeth. The techniques utilized within this age interval rely upon radiographic evaluation of the stages of tooth formation of the primary and permanent dentitions.3-6 These tooth stages are generally defined by mineralization, crown development, and root development. Accuracy of analysis in the childhood period can vary widely dependent on age, sex, and technique, but can still be as accurate as within 3 months of actual age.7
Adolescent dental growth is a bit less predictable but still can render results to within 5 years of actual age.8 Adolescent and young adult analysis is based mostly on the growth of the third molars. Through decades of research, it is also possible to use sex and population specific comparative data and techniques to render the most accurate results, specifically as the individual surpasses about 10 years of age.9
One might think that dental age assessment stops once all the teeth are fully formed, but what has been found is that there remain predictable changes in teeth as we age through adulthood. These predictors of age are called post-formational changes.10 Although not as specific as in the sub-adult, the accuracy of these analyses is generally within a decade or 2 of life.11
It is worth noting that there is another category of DAA called biochemical techniques. These include amino acid racemization and radiocarbon dating which are not described here.12-13
Scientific Rational for DAA
DAA has been extensively studied and used since the 1940s.14 In addition, evaluation of tooth development is easily done through intraoral and extraoral radiography.
Dental growth and development are largely genetically driven. Early in life, genetic factors predominate, and environmental factors tend to have minimal effects on the rate of tooth maturation. This is especially true in younger age groups (birth to 10 years).11 Further, it has been shown that common endocrine and maturational diseases affect tooth development at about one quarter pace compared to most other body tissues.15
Four basic evaluation criteria are used in child and adolescent age estimation.
Gingival emergence is a tooth’s initial appearance through the gingival soft tissue. Alveolar emergence is defined as the moment the most coronal portion of a tooth
Abstract
Dental Age Assessment (DAA) is the process of approximating an individual’s chronological age at any given point before birth, during life, or their age at death through analyzing predictable patterns of tooth changes. The result of DAA generally is a Dental Age Estimation (DAE).
Dental growth and development are largely genetically driven, especially early in life. Environmental factors tend to have minimal effects on the rate of tooth maturation. Further, it has been shown that common endocrine and maturational diseases affect tooth development at about one quarter pace compared to most other body tissues. There are many methods of DAA and have been extensively studied and used since the 1940s.
Some of the most popular and studied methods of DAA are outlined for the 3 main phases of life: infant/child, adolescent, and adult. Charts & atlas, morphological staging, and post-formational changes are explained. Specific methods, including The London Atlas of Human Tooth Development (2010), Moorrees, Fanning and Hunt (1963), Demirjian and Goldstein (1973), Cameriere et al. (2006), Mincer et al. (1993), Kvaal et al. (1995), and Cameriere et al. (2004 and 2007) are described.
Lastly, digital DAA tools are described as well as words of caution for the new user are offered.
makes its initial appearance through the alveolar bone. Together, gingival emergence and alveolar emergence define the eruption pattern of a tooth. Evaluation of the eruption pattern is the least accurate means of estimating an individual’s age.16 However, gingival emergence is considered less predictable than alveolar emergence due to its greater sensitivity to environmental factors such as premature tooth loss, caries, nutritional deficiencies, and genetic developmental disorders.17
Resorption refers to the progression of root disappearance from primary teeth as they prepare for exfoliation. Resorption patterns of the deciduous teeth have been found to be fairly consistent and can be used alongside other methods from ages 5 to 12.18
Both eruption and resorption techniques are limited because they can only be used when these processes are actively occurring.
Morphological development entails the scoring of teeth to identify their stage of growth as compared to a standard set of pictographs and/or written descriptors. Tooth morphology is considered the most accurate means of correlating growth and development to true chronologic age because it is the least affected by environmental and congenital factors.19 In addition, tooth mineralization spans a much longer age interval, making it more broadly applicable than either eruption or resorption.
Adolescent tooth development, as well as adult post-formational and biochemical changes in teeth have also been found to be predictable over time but can be more difficult to assess without specialized experience and training. Several parameters can be used.8
Infant and Child Methods of DAA
The are currently 2 categories of techniques for age assessment in infants and children, Charts & Atlases and Morphological Staging. All of these methods necessitate the use of good quality dental radiographs and are non-destructive.
Staging techniques account for differences in sex, although most systems also include a combined dataset when the sex is unknown. These staging systems also have a growing number of ancestry specific datasets to account for differences in populations.20 Staging evaluates individual teeth for their state of morphological development against a standard stage of growth.10 The teeth generally used are from the mandibular left side, however the methods allow use of a contralateral tooth instead if it is absent or not useable. A standardized graph or an average of the means is then used to calculate one estimated mean age using several teeth, which also includes a confidence interval based on statistical studies. All of these factors will produce the most accurate estimates of human dental chronologic age possible.11 It should be noted that there are many studies that use some type of staging; however, only the most used are described here.
The last technique outlined in this section (see “OPEN APICES”) uses morphometric analysis, which is related to morphological staging, but different.21 Two linear measurements per tooth are performed on a digital radiograph relative to each other and then used with a linear regression formula to calculate a data point that equates to actual estimated age. It is sex specific and has a growing number of ancestryspecific sub-studies with corresponding regression formulas.
ATLASES
Atlases utilize pictograms of developing tooth structures with their associated eruption pattern (usually the right side). A chart is simply a table outlining key events of dental development and can be found in several formats, primarily sourced from dental anatomy textbooks.1 Atlases and charts can be useful for a quick and easy age assessment of neonates, infants and children often used to determine the path
of further detailed analysis. However, they are not ancestry or sex driven and therefore the least accurate. Dental developmental atlases have been used by odontologists for decades to predict the chronologic age of infants and children; Schour and Masseler is no longer used, Ubelaker can still be useful with limitations, and the London Atlas of Human Tooth Development is currently preferred.6,15,22 The London Atlas underwent a meta-analysis in 2023 which determined a standardized mean age difference of 0.02 years from actual age of the study participants and is the easiest to use.19
MFH
Moorrees, Fanning, and Hunt (MFH) in 1963 developed the first morphologic staging system with drawings and corresponding written descriptors for subjects ranging from birth to 21 years old.3 Subsequent radiographic representations of the stages are also available.23 This system consists of 13 stages for single rooted teeth and 14 stages for multirooted teeth (an additional cleft stage added). Teeth should not be utilized if they have signs of periapical pathology, extensive caries, are extensively restored, or exhibit dental morphologic abnormality. When possible, multiple developing teeth from both sides of the mouth should
be included in the age assessment by averaging the data , as this will improve accuracy.24 When presented with a choice of teeth to analyze, it has been found that the mandibular canines and all maxillary teeth are the most unreliable but still can be used if needed. Further, it has been thought that including the third molar is not recommended due to growth variability. However, recent research has disproven this assumption.25 This technique can be used in 4 ways; primary mandibular canines and molars only, any permanent mandibular teeth plus permanent maxillary incisors (Figure 1), primary and permanent teeth in mixed dentition, and resorption of
Figure 1. Presented is a DAA that was performed for a young victim of a house fire to establish an identification versus her older sister who was also found. a) Work began on this case by taking specialized intra-oral radiographs that capture all of the developing teeth. Two aging methods were used: b) The first method utilized the London Atlas (6). This survey showed that the dental appearance is most like the 4.5-year-old glyph on the Atlas. c) Next, the radiographs were compared to MFH staging (23). d) The calculation yielded 4.5 years (4 years, 6 months) ± 1.0 years old at 95% confidence interval (2SD). The actual chronological age of this child was 4.45 years old (4 years, 5 months).
deciduous teeth. Unlike other systems, the number of teeth analyzed may vary. It is permissible to use only one tooth; however more accurate results are obtained using several teeth. This feature of MFH makes it very usable with fragmented or incomplete remains.
DEMIRJIAN
Demirjian and Goldstein, in 1973 studied a French-Canadian population of 2,407 boys and 2,349 girls. They developed a dental morphologic staging system that consists of only 8 stages, A through H, and then added Stage 0 (zero) for a beginning “no calcification” stage. They reduced the number of stages from the 14 used in MFH, because they claimed that it improves inter-operator agreement. The original technique requires staging of all 7 teeth on the mandibular left except the third molar.4 If one or all of these teeth are not available, then the same tooth from the contralateral side of mandible can be substituted. They expanded their technique to also allow for use of only 4 permanent teeth on the mandibular left in one of the following 2 combinations; all molars and premolars (“Method I”) or the second molar, premolars, and central Incisor (“Method II”).5
This technique is based on subjects with ages 2.5-17 years old. However, it is recommended that the classic 4-tooth and 7-tooth techniques should only be used on subjects between 2.5 and 14 years old because accuracy is seen to decrease with this method after age 14.10
As with MFH, teeth should not be utilized in this assessment if they have periapical pathology, extensive caries, extensively restored, or exhibit dental morphologic abnormality. The 1976 Demirjian technique has a
number of population-specific studies including American Blacks, whites, and Hispanics.26,27
After all teeth have been staged, each tooth is assigned a “self-weighted score” based upon the stage selected. These values are found in tables separated by method (7 or 4 tooth) and sex of the individual. The sum of the individual self-weighted scores results in the maturity score for that individual. This maturity score is then analyzed on a dental maturity percentiles graph specific to each technique and sex to find the corresponding age estimate. If the sex is unknown, the entire process is performed twice, using both boys’ and girls’ data, then averaged to yield the androgenous result.
Limitations of this technique include the following. It must be used with teeth specified in the analysis. If a needed tooth is not available, the analysis cannot be done. Likewise, if the remains are fragmented then needed teeth may not be present. Also, there is no way to deviate from the combinations presented, because the teeth used are weighted equally versus given toothspecific data sets (as in MFH). The age range starts at 2.5 years, versus at birth as in MFH.10 The graphs from the Demirjian publications are somewhat difficult to interpret due to a lack of detail and over-reproduction of “analog” journals from almost 50 years ago, although enhanced versions of the originals and Quicksheets™ reverseengineered values (see discussion section) are available. Lastly, it is worthy to note that the Demirjian system uses percentiles instead of standard deviation from the mean, which modifies the statistical reporting of results.
OPEN APICES
Cameriere et al. in 2006 devised a novel way to assess tooth development without having to assign a developmental stage to any teeth.21 He looked at 455 Italian Caucasian children initially, then the original study was expanded in 2007 to include 2,652 European Caucasian children between ages 5 and 15. The method is based on the observation that there is a correlation between age and the measurement of open apices in developing teeth. Several studies since then have re-validated his results on populations from around the world, including the United States. Cameriere was able to correlate this measurement to age through the use of a linear regression formula. In this study, a scatter plot of predicted age vs. observed (actual) age using variables involved with open apices was constructed. Then, a “best fit” line was mathematically calculated. This regression formula is able to predict age in a way unlike any other method. His original mathematical calculation is now called the “European regression”.
The system uses a simplified numbering system using 1 to 7, anterior to posterior in the mandibular left (similar to the Palmer Notation System). Like Demirjian, this system can only be used if all 7 teeth are present, however it is acceptable to use the contralateral tooth if one or more are absent. Only 2 measurements on 7 teeth from the mandibular left side are required. “A” is the distance between the inner sides of the developing apices and “L” is the overall tooth length. “A” is divided by “L” to yield “X” in the calculation to form a normalized ratio, so that different exposure angles and the unit of measure are inconsequential. “S” then is the sum of all of the normalized open
apices (X1, X2,…X7). Other variables that are considered are sex and the number of teeth that are fully formed with closed apices.
The calculated uncertainty in this method is a Standard Error of Estimate (SEE). In this method, one SEE is equal to 0.93 years. For practical purposes, SEE can be considered comparable to Standard Deviation (SD). Therefore, ± 2 x SEE approximates the 95% confidence interval (CI).
Adolescent Methods of DAA
As an individual approaches age 18, the only teeth yet to form completely are the third molars. To that end, late adolescent DAA techniques retool Demirjian staging to determine third molars’ stage of development and estimate chronological age.24 Alternatively, the London Atlas discussed earlier includes glyphs representing third molar development, up to age 23.5. However, atlas methods in general at this stage of human development can be inaccurate, primarily because it does not account for sex or race.20
MINCER
The seminal study in this area was introduced by Mincer et al. in 1993.28 The Mincer technique is best utilized between the ages of 14-21 years, relating to active morphological development timing of the third molars. Any or all of the 4 third molars can be studied, as long as they have adequate imaging, no pathology including extensive caries or perceived abnormalities. Fully formed teeth (stage H) are said to be “censored” and should not be used , because it is impossible to determine how far in the past their growth had been completed.29 It is a non-destructive method that can be used with both periapical and panorex radiographs.
Due to sexual dimorphism and cultural differences in the rate of development of the third molars, it is very important to consider these factors when accurately determining chronological age. It is recommended to use sex and population specific datasets whenever possible.20 The original Mincer dataset is sourced from 80% Caucasians as censored by Moore and should be used for White-American and European populations.28,30 However, there exist several sub-studies from other worldwide populations, including
Black-Americans, Asian, and AmericanHispanic, all with slightly different datasets than the original.9,31-33
UT-AGE
The UT-Age Dental Assessment Database was developed in 2002 with subsequent updates in 2008 and 2018.34 This organizational software was designed to assist the odontologist in analyzing the third molars, reporting results and archiving individual cases. It is currently available for download and is run locally on the personal computer (PC). It utilizes several of the population datasets and adds an additional “pooled” dataset to use when the ancestry is unknown. Another useful tool included in UT-Age is the determination and reporting of empirical probability of attaining a certain age, based on the DAA results (Figure 2). This is widely used by the U.S. Immigration and Naturalization Service in conjunction with the legal system to facilitate proper placement of individuals during the immigration process, as well as an aid to assist authorities in prosecution of undocumented individuals and human trafficking.20
Figure 2. An excerpt from an UT-Age report on a male Asian adolescent victim of a plane crash showing DAA of the mandibular third molars.34 (Left) As is the case with many, the maxillary third molars did not have adequate imaging to utilize in the DAA. (Middle) The mandibular right and left thirds’ growth was determined to be “F” and “E” respectively using Demirjian staging. (Right) Results of the analysis show Estimated Mean Age, the standard deviation with the corresponding age interval, and the Empirical Probability (EP) that the victim had reached the age of 18 years.
Adult Methods of DAA
POST FORMATIONAL STUDIES
After all of the teeth have completed formation, the adult period begins. DAA for the remainder of life focuses on what are called post-formational changes. There exist several predictable changing characteristics of aging teeth that have been studied including (but not limited to) root transparency, periodontal attachment, cementum apposition, attrition, and secondary dentin formation, collectively known as the Gustafson method.35-40 Sexual dimorphism and ancestral differences do not play a significant role in adult DAA, so both sexes and all populations are not differentiated or excluded in most techniques (a few exceptions exist). Some of the techniques are destructive (requiring tooth removal and/or sectioning) and others are not, requiring only adequate radiography. Research in this area is ongoing, and proposals have been made to incorporate modern modes of imaging, such as standard and micro computed tomography for DAA.41,42 The 2 methods described below are both non-destructive, easily reproducible and have some of the smallest CIs in their statistics, translating to relatively narrow DAE ranges. Both are based on the deposition of secondary dentin and its affect on the appearance of pulpal tissue.
KVAAL
In 1995, Kvaal et al. developed a systematic method for analyzing the secondary dentin deposition of single-rooted teeth.39 It can utilize one tooth, specified, or unspecified combinations of multiple teeth. However, those selected must be virgin with no trauma, pathology, rotations, and in normal function. The studied individuals were between 20 and 87 years old, and the technique is not sex-specific unless mandibular laterals are used. In order to eliminate the variables associated with radiographic angulation and magnification, ratios of width to length (instead of measured values) are used. Ratios also eliminate the significance of the unit of measure utilized; it makes no difference if using inches, millimeters, or pixel length (from a digital film) as long as the unit used is consistent. Essentially, the state of secondary dentin deposition is analyzed by establishing the ratio of root width to the width of the pulp at three reproducible points along the length of the tooth. Regression formulas for each tooth were devised to calculate an average mean age for any individual in the studied age range. The calculated uncertainty in this method is a SEE and is variable depending on the teeth chosen to study. However, the 95% CI is generally plus or minus around 2 decades of life.
CAMERIERE
In 2004 and again in 2007, Cameriere et al. developed another method of analyzing the progression of secondary dentin deposition by examining area volume ratios, instead of Kvaal’s linear measurements.
Cameriere et al. 2004 simplifies the analysis to only maxillary canines because they are readily visible along their entire length on radiographs and have a generally large pulpal chamber.43 The 2004 method is non-destructive and only requires standard dental radiography in situ. The studied population was between 18 and 72 years of age and is not sex or ethnicity specific. The technique involves defining 2 area volumes and 2 linear measurements and requires the use of imaging software, such as Photoshop™. First, the total tooth volume is found using imaging software tools to circumscribe the entire tooth image and recording its area in any square unit (inches, millimeters, pixels, etc.). Similarly, the pulpal volume is then determined. These measurements are then divided to find the pulp/tooth volume ratio. Similar to Kvaal, the ratio of pulp to tooth width at mid root is then determined. A regression formula can finally be used to determine estimated mean age. Use of the mid root calculation is optional and has a separate
regression formula. Both have a SEE of 5.35 years, translating to an age range of ± 10.7 years at 95% CI.
Expanding on his work, Cameriere et al. 2007 refines the method of determining the pulp/tooth ratio by imaging each tooth in 2 perpendicular planes.44 However, this requires extraction of teeth being studied, so it is not practical for use on the living. Further, it can be used on all 4 canines (Figure 3). The studied population was between 20 and 79 years of age and is not sex or ethnicity specific. The mid root calculation is also eliminated. Otherwise, the study parameters and technique are similar to 2004.
Improvement of results with the 2007 method is seen in its statistics; the SEE can be as low as 3.62 years, which translates to ± 7.24 years at 95% CI.
Discussion
Digitization of dental radiographs and the use of imaging software has advanced the precision and accuracy of DAA because of image optimization and enhancement when deciphering dental morphology. In addition, the ability to consistently and easily measure distances and calculate area volumes greatly improves DAA workflow.
DRAFT SHEETS
Another aid available are the Draft Age Estimation (DAE) Quicksheets™. The DAE Quicksheets™ are a series of proprietary Microsoft Excel™ spreadsheets which are designed to be used with many DAA methods to record data, perform the multitude of calculations involved, and report results. However, as explained in its readme file, “They are not designed to replace your knowledge” and should only supplement one’s familiarity with the particular method being used. There are currently 15 DAA methods included in the DAE Quicksheets™ set, which is only currently available directly from its creator Dr Derek Draft (DAEquicksheets@gmail.com).
Figure 3. This unknown adult decedent was found skeletonized in the woods with no presumed identity. A DAA was performed to add to the overall biological profile that was formulated. Teeth #6 and #22 were found to be appropriate for DAA. These teeth were extracted from their alveolar sockets and radiographed in both the facial-lingual and the mesial-distal planes. The Cameriere 2007 method estimated the decedent’s age as 24.73 ± 7.24 years.44 This yields a range of possible ages of 17 years, 6 months to 32 years, 0 months at a 95% confidence interval. The case was solved after 2 years of investigation. The victim’s actual age at death was approximately 32 years.
Conclusions
DAA can be performed through a large tacklebox of different techniques. Only a few of the most popular and current techniques have been outlined. It is worthy to mention that all DAA techniques have their specific applicability and pitfalls, therefore it is advisable to have adequate training in their use before application in practice.
References
1. Ash, M.M., Nelson, S.J. Development and eruption of teeth. In: Rudolf P, Pendill J, eds. Wheeler’s Dental Anatomy, Physiology and Occlusion Eighth Edition. USA:Elsevier Science, 2003:29-63.
2. Eli I, Sarnat H, Talmi E. Effect of the birth process on the neonatal line in primary tooth enamel. Pediatr Dent. 1989;11(3):220-223.
3. MOORREES CF, FANNING EA, HUNT EE Jr. AGE VARIATION OF FORMATION STAGES FOR TEN PERMANENT TEETH. J Dent Res. 1963;42:1490-1502. doi:1.1177/00220345630420062701
4. Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. 1973;45(2):211-227.
5. Demirjian A, Goldstein H. New systems for dental maturity based on seven and four teeth. Ann Hum Biol. 1976;3(5):411-421. doi:10.1080/03014467600001671
6. AlQahtani SJ, Hector MP, Liversidge HM. Brief communication: The London atlas of human tooth development and eruption. Am J Phys Anthropol. 2010;142(3):481-490. doi:10.1002/ajpa.21258
7. Al-Juhani A, Binshalhoub A, Showail S, et al. Comparative Analysis of Dental Age Estimation: A Systematic Review and Meta-analysis Assessing Gender-Specific Accuracy of the Demirjian and Nolla Methods Across Different Age Groups. Cureus. 2024;16(12):e75031. Published 2024 Dec 3. doi:10.7759/cureus.75031
8. Nortjé CJ. The permanent mandibular third molar. Its value in age determination. J Forensic Odontostomatol. 1983;1(1):27-31.
9. Lewis JM, Senn DR. Dental age estimation utilizing third molar
development: A review of principles, methods, and population studies used in the United States. Forensic Sci Int. 2010;201(1-3):79-83. doi:10.1016/j.forsciint.2010.04.042
10. Lewis, J.M., Senn D.R., Dental Age Estimation. In: Greene, D., & Williams, D. Manual of Forensic Odontology (D.R. Senn, & R.A. Weems, eds. (5th ed.). CRC Press, 2013:211-255. https://doi.org/10.1201/b13744
11. Taylor, J. and Blenkin, M. Age evaluation and odontology in the living. In: Black A, Aggrawal A, Payne-James J, eds. Age Estimation in the Living. West Sussex, U.K.:WileyBlackwell, 2010:176-201.
12. Ohtani S, Yamamoto T. Age estimation by amino acid racemization in human teeth. J Forensic Sci. 2010;55(6):16301633. doi:10.1111/j.15564029.2010.01472.x
13. Spalding KL, Buchholz BA, Bergman LE, Druid H, Frisén J. Forensics: age written in teeth by nuclear tests. Nature. 2005;437(7057):333-334. doi:10.1038/437333a
14. Schour, I., and M. Massler. The development of the human dentition. Journal of the American Dental Association. 1941;28:1153-1160.
15. Ubelaker, D.H. Human skeletal remains, excavation analysis, interpretation (2nd ed.). Washington D.C.: Taraxacum, 1989:44 -95.
16. Maber M, Liversidge HM, Hector MP. Accuracy of age estimation of radiographic methods using developing teeth. Forensic Sci Int. 2006;159 Suppl 1:S68-S73. doi:10.1016/j.forsciint.2006.02.019
17. Suri L, Gagari E, Vastardis H. Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004;126(4):432-445. doi:10.1016/j.ajodo.2003.10.031
18. Moorrees CF, Fanning EA, Hunt EE Jr. FORMATION AND RESORPTION OF THREE DECIDUOUS TEETH IN CHILDREN. Am J Phys Anthropol. 1963;21(2):205-213. doi:10.1002/ ajpa.1330210212
19. AlQahtani SJ, Hector MP, Liversidge HM. Accuracy of dental age estimation charts: Schour and Massler, Ubelaker and the London Atlas. Am J Phys Anthropol. 2014;154(1):70-78. doi:10.1002/ ajpa.22473
20. Lewis JM, and Kasper KA. Assessment of Dental Age. In: David TJ, and Lewis
JM, editors. Forensic Odontology: Principles and Practice.Elsivier: San Diego, CA, 2018:145-173.
21. Cameriere R, Ferrante L, Cingolani M. Age estimation in children by measurement of open apices in teeth. Int J Legal Med. 2006;120(1):4952. doi:10.1007/s00414-005-0047-9
22. Schour, I., and M. Massler. The development of the human dentition chart (2nd ed.). Chicago: American Dental Association, 1944.
23. Draft, D. M., Kasper, K. A., Fancher, J. P., & AlQahtani, S. J. Illustrated Moorrees, Fanning, and Hunt Dental Development Staging Charts. In: MFH Staging (Ed.). Open Source:Open Source, 2019.
24. Harris, E.F., Mincer H.H., Anderson K.M., Senn D.R. Age estimation from oral and dental structures. In: Senn, D.R., Stimpson, P.G., eds. Forensic Dentistry, 2nd ed. Boca Raton, FL: Taylor and Frances Group, 2010:263303.
25. Collier SL, Lewis JM, Kasper KA, Marks MK, Heidel RE. Dental Age Assessment of United States Black and White Children: Performance Reliability of Harris and McKee (1990). Am J Forensic Med Pathol. 2023;44(1):33-41. doi:10.1097/ PAF.0000000000000797
26. Harris EF, McKee JH. Tooth mineralization standards for blacks and whites from the middle southern United States. J Forensic Sci. 1990;35(4):859-872.
27. Jayaraman J, Mendez MJC, Gakunga PT, Roberts G. Age estimation of Hispanic children in the United States: Development and validation of dental reference dataset based on two staging systems. Leg Med (Tokyo). 2022;56:102033. doi:10.1016/j. legalmed.2022.102033
28. Mincer HH, Harris EF, Berryman HE. The A.B.F.O. study of third molar development and its use as an estimator of chronological age [published correction appears in J Forensic Sci 1993 Nov;38(6):1524]. J Forensic Sci. 1993;38(2):379-390.
29. Roberts GJ, McDonald F, Andiappan M, Lucas VS. Dental Age Estimation (DAE): Data management for tooth development stages including the third molar. Appropriate censoring of Stage H, the final stage of tooth development. J Forensic Leg Med. 2015;36:177-184. doi:10.1016/j. jflm.2015.08.013
30. Moore, J.A., Lewis J.M., Senn D.R. Third molar age estimation: appropriately censoring stage “H” using the data from two previously published studies: Blankenship et al. (2007) & Kasper et al. (2009). Presented at the Annual American Academy of Forensic Sciences Meeting, February 22-27, 2016, Las Vegas.
31. Blankenship JA, Mincer HH, Anderson KM, Woods MA, Burton EL. Third molar development in the estimation of chronologic age in american blacks as compared with whites. J Forensic Sci. 2007;52(2):428-433. doi:10.1111/ j.1556-4029.2006.00356.x
32. Arany S, Iino M, Yoshioka N. Radiographic survey of third molar development in relation to chronological age among Japanese juveniles. J Forensic Sci. 2004;49(3):534-538.
33. Kasper KA, Austin D, Kvanli AH, Rios TR, Senn DR. Reliability of third molar development for age estimation in a Texas Hispanic population: a comparison study. J Forensic Sci. 2009;54(3):651-657. doi:10.1111/ j.1556-4029.2009.01031.x
34. Lewis JM, Schuerman LA, Senn DR, Silvaggi J. UT-AGE 2018 (Version 2.2.23). Available from URL: http://
www.logisys-consulting.com/UTAge/ install.html
35. Bang G, Ramm E. Determination of age in humans from root dentin transparency. Acta Odontol Scand. 1970;28(1):3-35. doi:10.3109/00016357009033130
36. Lamendin H. Observations on teeth roots in the estimation of age. Int J Forensic Dent. 1973;1(1):4-7.
37. Bocutoğlu O, Yakan B. Coronal displacement of cementum: correlation between age and coronal movement of cementum in impacted teeth. Aust Dent J. 1997;42(3):185188. doi:10.1111/j.1834-7819.1997. tb00119.x
38. Smith, B.H. Standards of human tooth formation and dental age assessment. In: Kelly M.A., Larsen C.S., eds. Advances in dental anthropology. New York: Wiley-Liss, 1991:143-168.
39. Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T. Age estimation of adults from dental radiographs. Forensic Sci Int. 1995;74(3):175-185. doi:10.1016/0379-0738(95)01760-g
40. GUSTAFSON G. Age determination on teeth. J Am Dent Assoc. 1950;41(1):45-54. doi:10.14219/jada. archive.1950.0132
Practices For Sale
Luis O. Regueira, Sr., D.M.D.
Alexandre R. Canevet, D.D.S. Zayd M. Hashmi, D.M.D.
We
41. Pires AC, Vargas de Sousa Santos RF, Pereira CP. Dental age assessment by the pulp/tooth area proportion in cone beam computed tomography: is medico-legal application for age estimation reliable?. J Forensic Odontostomatol. 2021;39(2):2-14. Published 2021 Aug 30.
42. Zainuddin MZ, Mohamad NS, Su Keng T, Mohd Yusof MYP. The applications of MicroCT in studying age-related tooth morphological change and dental age estimation: A scoping review. J Forensic Sci. 2023;68(6):2048-2056. doi:10.1111/1556-4029.15352
43. Cameriere R, Ferrante L, Cingolani M. Variations in pulp/tooth area ratio as an indicator of age: a preliminary study. J Forensic Sci. 2004;49(2):317319.
44. Cameriere R, Ferrante L, Belcastro MG, Bonfiglioli B, Rastelli E, Cingolani M. Age estimation by pulp/tooth ratio in canines by peri-apical X-rays. J Forensic Sci. 2007;52(1):166170. doi:10.1111/j.15564029.2006.00336.x
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a well-located professional building with 3 ops in good condition. Currently paper-based and non-digital, operating 4 doctor days per week. Growth potential by adding a hygienist, expanding services, marketing, or extending hours. Over 1,200 active patients (10% FFS, 50% PPO, 40% Medicaid). Ideal for a satellite office or first practice. Call AFTCO today! Opportunity ID: TX-02453
FANTASTIC TEXARKANA LOCATION: GP is in a bustling retail center with great visibility. The office is equipped with 3 ops, digital X-ray, and paperless patient charts. The practice has over 1,200 active patients that are a mixture of 20% FFS and 80% PPO. The seller refers out most specialties, and the practice operates on 3.5 doctor days and 4 hygiene days, leaving ample room for growth. Don’t wait, call AFTCO today! Opportunity ID: TX-02459
PRIME LOCATION IN RURAL WEST TEXAS: Well-located GP in the heart of town near residential and retail areas with strong visibility is grossing $789,000.00. The 2,000 sq. ft. digital office has 4 ops and room to expand. Operating 3–3.5 days/week with no hygienist, this practice sees 2,500+ active patients (mostly PPO). Major growth potential. Call AFTCO today! Opportunity ID: TX-02553
REAL ESTATE AVAILABLE: Southwest of Odessa, this GP is in a converted residence in the center of the town grossing $631,000.00. The office is 2,000 sq. ft. with 3 ops and room to expand. This computerized office, that utilizes Eaglesoft, is fully equipped with digital X-rays and Pano. The practice has over 2,600 active patients who are a blend of mostly PPO, with approximately 25% FFS, & 7% Medicaid. The practice is currently associatedriven with no hygienist, giving great room for growth or a simple way to have a satellite location. Don’t wait, call AFTCO today! Opportunity ID: TX-02554 Go
Derek M. Draft, DDS, D-ABFO
The Evolution of Bite Mark Analysis and the Role of the ABFO
Abstract
Bite mark analysis has played a longstanding role in forensic odontology, contributing to criminal investigations and courtroom proceedings across the United States. While early applications helped establish public and judicial confidence in the field, the limitations of the technique, especially regarding human skin as a recording medium, drew increasing scrutiny in the 2000s. In response, the American Board of Forensic Odontology (ABFO) initiated a comprehensive effort to improve guidelines, clarify limitations, and promote responsible practice. Today, ABFO diplomates follow clear directives prohibiting identification of a specific biter and are required to offer qualified, well documented evaluations that reflect the constraints of the evidence. This article traces the evolution of bite mark analysis, highlights landmark cases and national reviews, and outlines the ABFO’s commitment to reform, accountability, and mentorship.
FORENSIC Bite Mark Analysis
Origins and Early Use of Bite Mark Analysis
Bite mark analysis has a long and complex history in forensic science. Its earliest documented use dates to the 19th century, but the practice gained widespread attention in the United States during the 1970s and 1980s. Forensic odontologists were increasingly called upon in criminal cases to compare bite marks on victims to the dentition of suspects. At the time, such evidence was often presented with high confidence, sometimes even as conclusive proof of identification.
Foundational assumptions, such as the uniqueness of dental patterns and the reliability of skin as a recording surface, were widely accepted. Early convictions bolstered confidence in the method and fueled its growth within forensic odontology.
Recent investigations into enamel microstructure have underscored its adjunctive role in bite mark comparisons, suggesting that enamel morphology, while not definitive, can provide corroborative evidence in support of injury analysis.1
However, the methods used were often unstandardized and heavily reliant on individual interpretation. Experts frequently disagreed on whether a mark was a bite at all, let alone who might have made it. Despite these limitations, bite mark analysis became a routine element of criminal investigations, built on a foundation that had yet to be rigorously tested.
Landmark Cases and Shifting Perceptions
Several high profile cases in the late 20th and early 21st centuries brought bite mark evidence to the forefront, initially reinforcing its legitimacy, but ultimately revealing its vulnerabilities.
People v. Marx (1975) in California is often cited as the first modern U.S. case to admit bite mark evidence. A forensic odontologist matched a bite mark on a victim’s nose to the defendant’s dental cast. The court deemed the evidence persuasive, paving the way for bite mark testimony to gain broader acceptance.
Another widely known case is that of Ted Bundy, where bite marks found on a victim served as a key piece of evidence in his conviction. The high profile nature of the case amplified public confidence in the technique, especially in an era preceding widespread DNA use.
But confidence began to erode as wrongful convictions came to light. Ray Krone was twice convicted of murder in Arizona based heavily on bite mark testimony. He spent over a decade in prison, including time on death row, before DNA evidence exonerated him. His case became a touchstone for critics of forensic pattern evidence.
about the Author
Derek M. Draft, DDS, D-ABFO
Dr Derek Draft received his DDS degree from the University of Michigan Dental School in 1998 and currently practices as a general dentist in both the US and Canada. Dr Draft joined the State of Michigan Forensic Dentistry ID Team in 2000 and he joined Disaster Mortuary Operational Response Team (DMORT) Region V in 2001. He was deployed to Joplin, Missouri, with DMORT after the devastating tornado in May 2011. Dr Draft has furthered his forensic education by attending multiple forensic courses including Forensic Odontology in a Medical Examiner’s Office, and the 21st Southwest Symposium on Forensic Dentistry and graduated from the Forensic Odontology fellowship at the University of Texas Health Science Center. He is a fellow of the American Academy of Forensic Sciences (AAFS) Odontology Section and a diplomate with the American Board of Forensic Odontology where he is the current president. Dr Draft developed the Draft Age Estimation Quicksheets™ which was presented at the 2016 AAFS meeting in Las Vegas.
Dr Draft provides forensic odontology services at the Le Laboratoire de sciences judiciaires et de médecine légale du Québec in Montreal and is also a clinical associate professor in the Pathology Department at the Western Michigan University Homer Stryker M.D. School of Medicine as a forensic odontology consultant.
Dr Draft lives in St. Lambert, Quebec, with his wife, Corinne D’Anjou, who is also a forensic odontologist. Together they have 5 children, Jasper, Hayden, Alex, Oli, and Anabelle. He enjoys time with his family snow skiing in the winter and playing volleyball in the summer. He also builds and runs 1/8th scale trains with his son, Hayden, and father, Tom.
Similarly, Keith Harward served 33 years for rape and murder based on bite mark analysis before being cleared by DNA in 2016. His exoneration drew national attention and reignited criticism of forensic disciplines lacking strong empirical validation.
These and other cases catalyzed public and professional reflection, highlighting the risks of overconfidence in bite mark interpretation. The ABFO responded with reforms aimed at strengthening guidelines, testimony standards, and practitioner accountability.
Standardization and the ABFO Guidelines
As forensic odontology matured, the need for consistency, objectivity, and procedural rigor became increasingly clear. The ABFO, established in 1976, positioned itself as a certifying authority and advocate for higher standards in the field. Recognizing both the potential and limitations of bite mark analysis, the ABFO worked to formalize methods that would promote transparency, consistency, and accountability.
Early case reports had varied widely in technique, documentation, and terminology. To address these inconsistencies, the ABFO began publishing detailed guidelines in the 1980s. These documents standardized key aspects of casework, including evidence collection, photographic documentation, impression techniques, and report language.
Critically, the ABFO’s guidelines promoted the use of qualified terminology that avoided absolute conclusions. Practitioners were instructed to account for the variability of human skin and the limitations inherent in bite mark evidence. This marked a turning point, encouraging forensic odontologists to frame their conclusions with caution and clarity.
The ABFO also advanced professionalization through its requirements for peer review, case documentation, and certification. By establishing expectations for thorough recordkeeping, such as including scale calibrated photographs, using transparent overlays, and providing detailed written analyses, the organization aimed to bring greater rigor to forensic odontology. While challenges remained, these steps reflected a growing commitment to learning from the past and improving the reliability of the discipline.
Challenges and Criticism of Bite Mark Analysis
Despite these efforts, bite mark analysis continued to face growing criticism in the early 2000s. The emergence of DNA exonerations brought renewed scrutiny to forensic disciplines that had long operated without strong empirical foundations.
Critics, ranging from defense attorneys to scientific researchers, raised concerns about skin’s reliability as a medium for comparison, the potential for distortion, and the influence of cognitive bias.6 Studies revealed inconsistent results among seasoned odontologists when interpreting the same evidence, undermining confidence
in the field’s objectivity. Nevertheless, although human skin is an imperfect recording medium subject to variable distortion, bite mark patterns can still provide investigatory value, yielding insights into directionality, relative tooth arrangement, and potential links between bite sequence and crime scene evidence.1,6
A pivotal moment came with the 2009 report by the National Academy of Sciences (NAS), which criticized several forensic practices, including bite mark analysis, for lacking sufficient scientific validation. The report urged further empirical testing and methodological reform.2
This was echoed by the 2016 report from the President’s Council of Advisors on Science and Technology (PCAST), which concluded that bite mark analysis had not demonstrated foundational validity or reproducibility. These assessments called into question the method’s continued use in criminal courts and intensified pressure for change.3
Reform and Reevaluation
Within the ABFO
In response to this scrutiny, the ABFO took clear and deliberate steps to modernize its approach. Central to this reform, first codified in the ABFO’s 2000 Standards and Guidelines, was the directive that diplomates may not identify or name a specific individual as the biter.4 This directive represented a fundamental break from past testimony practices and aligned with a growing recognition of the limitations of the evidence.
Under current guidelines, odontologists are limited to offering opinions of inclusion, exclusion, or inconclusive, clearly defining the boundaries of what the evidence can and cannot support. Notably, a “dentition cannot be excluded” opinion represents the strongest linkage that the questioned dentition could have produced the observed bite marks, without asserting unique identification. Reports and testimony must now reflect this approach, using appropriately qualified language and comprehensive documentation.
The ABFO also encouraged procedures aimed at reducing cognitive bias, including blinded analysis when feasible and peer review of conclusions. Additionally, educational initiatives and certification processes were updated to reflect these priorities.
Importantly, since the ABFO’s initial reforms roughly 20 years ago, there have been no known wrongful convictions overturned based on bite mark evidence introduced under its revised guidelines. While debate about the discipline’s future continues, this record suggests that reform efforts have contributed to more cautious and principled practice.
Looking Forward:
The Evolving Role of Bite Mark Analysis
The trajectory of bite mark analysis reflects a broader evolution in forensic science, from confident beginnings through scientific scrutiny to responsible reform. The ABFO’s leadership in promoting caution, transparency, and ethical restraint has
helped steer the field through these challenges.
Despite the scrutiny and reforms, one truth remains constant: humans will always bite each other. From assaults to child abuse cases, bite marks continue to appear in medicolegal contexts, and the justice system will continue to need expert interpretation of these injuries. Forensic odontologists, with their unique training in dental anatomy, injury patterns, and scientific methodology, are best positioned to provide this expertise. It is therefore essential that our discipline maintains its role in assisting courts and investigators, ensuring that when bite mark evidence is encountered, it is evaluated responsibly, ethically, and within scientifically grounded limits.
Today, bite mark evidence is applied more selectively and within well defined boundaries. Rather than claiming identification, odontologists offer measured opinions that reflect the true limits of the medium. When supported by other evidence and interpreted responsibly, bite marks can still offer investigatory value.
Forensic odontology’s contributions extend well beyond bite mark analysis, encompassing human identification, disaster victim recovery, and age assessment. These areas remain vital to forensic science and continue to benefit from the ABFO’s commitment to education, certification, and ongoing professional development.
As president of the ABFO, I am proud of the organization’s progress and mindful of the responsibility that comes with it. Our mission is not only to promote technical excellence but to serve justice with humility and integrity. Looking ahead, the ABFO remains committed
to mentoring the next generation of forensic odontologists, practitioners grounded in science, ethics, and a deep respect for their role in the legal system.
Through continued education, critical self reflection, and adherence to our core values, the ABFO will ensure that forensic odontology continues to evolve responsibly in service of truth and justice.
References
1. Barsley RE, Bernstein ML, Brumit PC, et al. Epidermis and enamel: insights into gnawing criticisms of human bitemark evidence. Am J Forensic Med Pathol. 2018.
2. National Research Council, Committee on Identifying the Needs of the Forensic Sciences Community. Strengthening Forensic Science in the United States: A Path Forward. Washington, DC: National Academies Press; 2009.
3. President’s Council of Advisors on Science and Technology. Forensic Science in Criminal Courts: Ensuring Scientific Validity of Feature Comparison Methods. Washington, DC: Executive Office of the President; 2016.
4. American Board of Forensic Odontology, Inc. ABFO Reference Manual. ABFO website. 2017. Available at: https://abfo.org/ resources/abfo-manual/. Accessed August 1, 2017.
5. Bowers CM. Identification from bitemarks. In: Faigman DL, Saks MJ, Sanders J, et al, eds. Modern Scientific Evidence: The Law and Science of Expert Testimony. Vol. 5. St. Paul, MN: Thomson-West; 2010:1–96.
6. Saks MJ, Albright T, Bohan TL, et al. Forensic bitemark identification: weak foundations, exaggerated claims. J Law Biosci. 2016;3(3):538–575.
Robin A. Ainsworth, DDS, MS, D-ABFO, ABGD, FAGD, CAPT (Ret) USPHS
Human Abuse and Neglect
Robin A. Ainsworth, DDS, MS, D-ABFO, ABGD, FAGD, CAPT (Ret) USPHS, currently practices general dentistry with the US Coast Guard as a USCG Auxiliarist and does forensic casework with the Pinellas County (FL) Medical Examiner’s Office. She also serves as the US Air Force Civilian Consultant for Forensic Dentistry. Dr Ainsworth served on active duty with the United States Public Health Service for 21 years. She is board certified with the American Board of Forensic Odontology and the American Board of General Dentistry. Dr Ainsworth earned a MS in Oral Biology from Uniformed Services University of the Heath Sciences, completed a Fellowship in Forensic Odontology from the University of Texas Health Science Center, and earned her DDS from The Ohio State University.
Human abuse and neglect are not new in our society. While the literature emphasizes that most violence is against women and children, no one is immune from potentially becoming a victim of this global problem.
There are 4 main recognized types of abuse: neglect, physical, sexual, and psychological. According to National Child Abuse and Neglect Data System (NCANDS) reports, neglect has
HUMAN Abuse and Neglect
been, and continues to be, the most common type of abuse reported.1 Abuse and neglect are not accidents. It does not happen because someone is stressed out, drinking, or using drugs. They are intentional acts that one person uses in a relationship to control the other.
In its most basic definition, neglect is a passive form of abuse in which a caregiver is responsible for, but fails to provide, adequate care for a dependent person (victim). It is a failure to provide for anything from food and shelter, to education, to health care. The latter is when caregivers repeatedly ignore recommendations of health care providers. Caregivers may acknowledge that a medical emergency or chronic condition exists; however, they may site religious beliefs in their decision to not seek necessary care. When these issues are resolved through the legal system, it is most often the decision of the court that the right to life and health of the victim supersedes the caregiver’s constitutional right to religious freedom.
Abuse is improper usage or treatment of an entity to unfairly or improperly gain benefit. Physical abuse is described as a person intentionally inflicting harm or injury upon someone else. It has been estimated that 30%-75% of physical abuse occurs in the head and neck area (elder abuse and child abuse, respectively).2,3 Soft and hard tissue physical injuries can take the form of bruises, lacerations, contusions, broken bones, bitemarks, and/or fractured, subluxated, avulsed teeth. There may be intraoral lacerations of the frenula, lacerations or contusions of the labial mucosa, buccal mucosa, floor of mouth, oropharynx, or soft palate. These lesions may also be found on the lips, nasal tissues, orbital and periorbital areas. Other injuries to the head and neck may include fractures of various bones of the skull, eyes, to include trauma to the globe, hyphemia and retinal hemorrhages, subdural hematomas, and traumatic alopecia.4
Sexual abuse is any sexual activity that is undesired, or has not been consented to, by one participant. The force is immediate, of short duration, or infrequent but is chronic in nature. It is comprised of any involuntary sexual act in which a person is threatened, coerced, forced to engage against their will, or assist others to engage against their will. This conduct includes rape, incest, prostitution, sexual exploitation, and human trafficking. Sexual abuse is a crime against another person and has nothing to do with employment and/or work performance (sexual harassment). Sexual harassment is unwelcome sexual advances, requests for sexual favors, and other verbal or physical conduct of a sexual nature. It is connected to employment or work performance and is a civil rights issue. It may be described as an action taken by a supervisor, such as hiring, firing, promotion or failure to promote, demotion, undesirable assignment, significant change in benefits or pay, or work assignment. It may also be considered a hostile environment where the offender is either a supervisor or a coworker. To meet the definition of a hostile environment, the harassment must be so severe that a reasonable person would view the environment as hostile, offensive, or abusive.
Psychological abuse, or emotional maltreatment, involves a pattern of controlling or humiliating behavior in an attempt to impact a person’s self-esteem or mental health. It may also be described as caregivers who interfere with a dependent person’s cognitive, emotional, or social development. Psychological maltreatment is persistent and chronic in nature. It may include passive behaviors such as ignoring (the caregiver is neither physically nor psychologically present; does not look at or acknowledge the victim), or active behaviors to include rejecting (active refusal to respond to victim’s needs), isolating (consistently
Neglect has been, and continues to be, the most common type of abuse reported. Abuse and neglect are not accidents. It does not happen because someone is stressed out, drinking, or using drugs. They are intentional acts that one person uses in a relationship to control the other.
prevents the victim from having normal social interactions), exploiting or corrupting (victim is encouraged or forced to develop inappropriate or illegal behaviors), verbally assaulting (constant belittling, shaming, or ridiculing), and terrorizing (threatens, creates a climate of fear).5
Although neglect and psychological abuse are not criminal behaviors, they are forms of abuse and can lead to criminal violence.
There are further subsets of neglect and abuse that describe certain populations, to include the following: child, elder, intimate partner, and special needs.
CHILD ABUSE
In 1874 there was an abused child, Mary Ellen, in New York City. Neighbors noticed her wandering the streets looking disheveled, unclean, and with bruises on her body. There were no legal protections for children in place at the time. The neighbors went to the authorities and had her removed from her foster home under the Society for the Prevention of Cruelty to Animals (SPCA), as she was a member of the animal kingdom. In April 1875, because of Mary Ellen, the first child protective agency, the New York Society for the Prevention of Cruelty to Children, was incorporated.3 During the ensuing quarter century, more than 150 similar societies emerged. Such agencies aim to protect abused and neglected children. Child protective agencies investigate accusations of child neglect or abuse and offers services to correct home conditions and, in appropriate situations, secures protection of the child by legal proceedings. Child protective services now exist in every state.6
On the medical front, in 1946, pediatric radiologist, Dr John Caffey documented common radiographic occurrences of spiral bone fractures and subdural hematomas in infants. Prior to that, in 1962, the Battered Child Syndrome (BCS) was described by Dr C. Henry Kempe in his paper published in the Journal of the American Medical Association. Similar to Caffey, Kempe documented unexplained clinical fractures and speculated that the injuries were nonaccidental, hence, the victim suffered abuse.3 In 1972, the phrase Shaken Baby Syndrome (SBS) was coined.4 SBS was the most frequent cause of permanent disability and death among abused infants. In 1969, Drs Kempe and Ray Helfer authored “The Battered Child.” It indicated a strong correlation between physical injuries to the oral, perioral and facial structures and
victims of abuse.4,7 In 2009, SBS became known as Abusive Head Trauma (AHT). Today, it is the leading cause of serious head injury and/or death among children.8
Prior to 1974 the federal government played a minor role in child protection. The Children’s Bureau was founded in 1912, but the Bureau paid little attention to maltreatment until the 1960s. In 1935, as part of President Franklin Roosevelt’s New Deal to save the nation from economic ruin, Congress passed the Social Security Act (SSA). In addition to old age pensions, unemployment insurance, and vocational services, the SSA created Aid to Dependent Children, which provided millions of dollars to states to support poor families. Within the SSA was a provision that authorized the Children’s Bureau “to cooperate with state public-welfare agencies in establishing, extending, and strengthening, especially in predominantly rural areas, [child welfare services] for the protection and care of homeless, dependent, and neglected children, and children in danger of becoming delinquent.”6 The SSA, as amended in 1962, provided money to expand child welfare services. This provision was very important for the emerging social work specialty of child welfare and a step toward becoming a central role for the federal government in efforts to protect children from abuse and neglect. In 1973, Senator Walter Mondale wrote, “Nowhere in the Federal Government could we find one official assigned full time to the prevention, identification and treatment of child abuse and neglect.” Due to Mondale’s efforts, Congress assumed a leadership role with passage of the Child Abuse Prevention and Treatment Act of 1974 (CAPTA).6,7 CAPTA authorized federal funds to improve states’ response to physical abuse, neglect, and sexual abuse. CAPTA focused on improved investigating and reporting. In addition, CAPTA provides funds for training, for regional multidisciplinary centers focused on child abuse and neglect, and provides grants to public agencies and nonprofit organizations, including Indian Tribes and Tribal organizations, for demonstration programs and projects. When first authorized, CAPTA played a major role in shaping the nationwide system of governmental child protective services that are still in place today. In addition, CAPTA marked the final passing of privately funded, nongovernmental child protection societies. Congress periodically renews CAPTA, and was most recently amended and reauthorized again in 2024, Pub. L. No. 118-193.9
One of the missions of the Children’s Bureau, which is under the Agency for Children and Families (ACF), is to collect data on abuse and neglect. One of the programs is the National Child Abuse and Neglect Data System (NCANDS).1 This is a data collection system that gathers information from all 50 states, plus the District of Columbia, and Puerto Rico, about reports of child abuse and neglect. States submit NCANDS data annually and voluntarily. Submissions are received during the NCANDS reporting period of October 1 to September 30. During federal fiscal year (FFY) 2023, 52 states reported over 3 million children received either an investigation or alternative response at a rate of 42.0 children per 1,000 in the population. For the same reporting period, 52 states reported over a half of a million victims of child abuse and neglect. This equates to a national rate of 7.4 victims per 1,000 children in the population. It is estimated that in FFY 23, 1,968 children died from abuse and neglect, at a rate of 2.73 per 100,000 children in the population. That is up from a report of 1,585 child deaths in FFY 2015 and 1,640 child deaths in FFY 2012. Of those children who died in FFY 2023, 59% were boys, 41% were girls, 74% were under the age of 4 years old. Of those 74%, 44% were under the age of one.10
ELDER ABUSE
According to the Centers for Disease Control and Prevention, elder abuse is “any action or inaction that harms, endangers, or causes distress to a person over age of 60.”11 It may also include psychological abuse, neglect, sexual abuse, or financial exploitation. There are 3 types of abuse amongst the elderly. The first is selfneglect, which is when an elderly, self-sufficient person loses autonomy. The next is unintentional, or passive, neglect. This is when a person is incapable of caring for another. The third is intentional, or active neglect. This constitutes a deliberate withholding of essential services, medications, or support necessary to maintain a good quality of life. According to the National Center on Elder Abuse (NECA), it is estimated that 10% of older adults who live in community living facilities are abused each year. They also site that 33% of older adults who are cognitively impaired experience abuse. Only one in 24 (4%) incidents of elder abuse comes to the attention of authorities.2 The National Committee for the Prevention of Elder Abuse states that the following should raise concerns for the oral health care professional: Injuries that are unexplained or implausible; family members providing different explanations of how injuries were sustained; a history of similar injuries or numerous hospitalizations, or both; victims brought to different medical facilities for treatment; delay between onset of injury and seeking medical care.12 However, a diagnosis of intentional trauma can be difficult in older adults due to systemic diseases and medications that can lead to increase bruising and hypotension. In addition, visual deficiencies, arrhythmias, and vertigo can lead to falls. Common signs of elder abuse include injuries to head and neck (30%), oral soft tissues, jaw fractures, fractured or avulsed teeth; traumatic hair and tooth loss, rope or strap marks (physical restraint); multicolored bruises; injuries suggesting healing “by secondary intention” (indicating
inappropriate or delayed presentation for care).3 Oral health care professionals may be legally required to report known or suspected abuse. It is important to know the relevant state and jurisdictional requirements and how to make a report.
In 1871, Alabama was the first state to rescind the legal right of men to beat their wives. In 1985, U.S. Surgeon General C. Everett Koop identified domestic violence/IPV as a public health issue that cannot be dealt by the police alone.13 IPV and emotional abuse are behaviors used by one person in a relationship to control the other. It is a crime of power and intimidation. Partners in a IPV situation may be married or not, living together, separated or dating. Children in homes where there is IPV are more likely to be abused and/or neglected. Most children in these homes know about the violence. Even if a child is not physically harmed, they may experience emotional and behavior problems. According to the Department of Justice, 95% of the victims of IPV are women, with 4 million American women being battered each year by a spouse or partner. However, only 10% of episodes of IPV are reported. The term Battered Woman Syndrome was first coined in 1979 by Dr Lenore Walker in her book, “The Battered Woman”, and is classified as International Classification of Diseases (ICD)-9 code.13 Battered women comprise 20-30% of ambulatory patients in emergency departments, yet only 5% are correctly identified/diagnosed as abuse by practitioners. In 2005, the first-ever World Health Organization (WHO) study on domestic violence revealed that IPV is the most common form of violence in women’s lives, much more so than assault or rape by strangers or acquaintances. The study also found very few women seek help from formal services. Those who do tend to be more severely abused.14
There are 3 recognized phases of abuse. During the first phase tension between partners escalates. There may be an excessive dependence on alcohol, drug abuse and/or jealousy that leads to tension and hostility. It is during this time that the abused partner becomes more nurturing or compliant. They avoid recognizing that an interpersonal problem or situation exists and they often direct blame for the problem on themselves. The second phase is when direct violent behavior begins. The abusive partner wants to “teach (them) a lesson.” The abused victim will often decline to prosecute for fear of later retaliation or loss of financial or emotional support from abuser. The third phase is considered the honeymoon phase. In this phase the abusive partner becomes loving and contrite. This emotional swing is precipitated by the abusive partner’s fear that the abused partner will end the relationship. There are sometimes promises made during this “making-up” phase that the abused partner wants to believe; they hope that the abuse is over. Without intervention, however, the cycle repeats itself. 15
SPECIAL NEEDS
There are 2 types of disabilities: developmental and intellectual. Developmental disability is classified as a group of conditions with an impairment in physical, learning, language, or behavior areas. Examples of this type of disability is down syndrome, cerebral palsy, autism, and intellectual disability.16 Intellectual disability is a condition that limits intelligence and disrupts abilities necessary for living independently. It was previously called ‘mental retardation.’17
People with disabilities are often victims of sexual abuse, specifically. According to research, they are at a greater risk for victimization of sexual assault or sexual abuse because of lack of understanding (Sobsey & Varnhagen, 1989). The rate of sexual abuse is shocking, yet most of these cases will go unnoticed. It is estimated that these individuals are victimized at 4 to 10 times the rate of the general population. Studies document that between 25% and 85% of those with intellectual disabilities are victims of sexual abuse; such a variance in percentage underscores the clandestine and subtle nature of such abuse. Furthermore, Sobsey estimates that between 15,000 and 19,000 individuals with developmental disabilities experience rape each year. There are several reasons why the intellectually disabled are especially prone to sexual abuse, the most significant of which is the ingrained reliance on the caregiver authority figure. Also, naivete and the underlying need to be accepted by peers, as they tend to be nonassertive and to agree to participate in sexual acts if directed to do so, possessing poor judgement in assessing other people’s motives. The sexual abuse offender is most likely to be known and trusted by the victim.18
MANDATED REPORTING
In 1996 the American Dental Association (ADA) published a statement on abuse and neglect: ADA Efforts to Educate Dental Professionals in Recognizing and Reporting Abuse and Neglect (1996:683). It “supports educating dental professionals to recognize abuse and neglect in children, women, elders, people with developmental disabilities, the physically challenged and any other person who might be the object of abuse or neglect.” It also encourages training programs on how to report such abuse and neglect to the proper authorities as required by state law.
In addition, in 2000, the ADA issued and adopted a report of the Council on Ethics, Bylaws and Judicial Affairs on Advisory Opinion 3.E.1. It states: “The public and the profession are best served by dentists who are familiar with identifying the signs of abuse and neglect and knowledgeable about the appropriate intervention resources for all populations.”
It is important to stress that oral health care professionals are mandated reporters of child abuse. In fact, there is a potential for both criminal liability and civil lawsuit for failure to report a suspicion of child abuse. Although lawsuits can be brought against a reporter of suspected cases, they are likely to be dismissed under “good faith reporting.” Regarding reporting suspected cases of adult victims of abuse and neglect, it is recommended to review your respective state’s/jurisdiction’s dental practice laws.
We know that violence is a learned behavior. Unfortunately, without some kind of help, the violence usually gets worse. However, with intervention, constructive alternatives to violence can be learned.5 The goal of intervention is to stop the battering, but safety is always the first consideration.
REFERENCES
1. https://acf.gov/cb/data-research/ ncands
2. https://ncea.acl.gov
3. Hershcaft; Manual of Forensic Odontology; Fourth edition, 2007
4. DiMaio; Handbook of Forensic Pathology, Second edition, 2006
Artificial and Augmented Intelligence in Forensic Odontology: An
Introductory Overview
Dr Kenneth W. Aschheim, a board-certified forensic odontologist, is a leader in integrating forensic odontology with advanced software. With over 20 years of experience, he developed the UDIM dental module for NYC’s Unified Victim Identification System (UVIS) and co-created OdontoSearch with Dr Bradley Adams. Expanding into AI, he partnered with Bright Forensics to develop AI-based dental identification software and led a machine learning project for assessing dental age. He also co-leads an oral pathology initiative with International Telecommunication Untion (ITU) and World Health Organization (WHO) and helped draft the first ISO standard for AI in 2D radiograph interpretation. Holding academic positions at NYU College of Dentistry and Mount Sinai Medical Center, he serves as assistant chief forensic odontologist for NYC’s Medical Examiner’s Office, as well as consulting for the National Center for Missing & Exploited Children.
FORENSIC Artificial Intelligence
Introduction
Artificial intelligence is becoming increasingly important in the field of forensic odontology. It offers new tools that can aid in identifying individuals, assessing age ranges, and interpreting data. However, many odontologists have reservations about these developments. They worry that the excitement surrounding innovative technologies might distract from their actual value and careful implementation. Other concerns include being overly dependent on these tools, the potential for misuse, unrealistic expectations, and even the fear of being replaced. To maximize the benefits of these advancements in forensic odontology, it is essential to have a comprehensive understanding of the technologies and their distinguishing features.
Defining Artificial Intelligence and Augmented Intelligence
To understand AI, it is crucial to recognize the difference between traditional programming and AI programming. A common analogy is that conventional programming is like giving someone an exact recipe, with each ingredient and step clearly defined. This approach mirrors the way a programmer provides precise instructions for a computer to execute.
However, AI programming is more analogous to giving someone several example recipes and a list of ingredients and then asking them, or the AI, to use that information to create new recipes. The AI learns from how the final result should look and taste, allowing it to generate new “recipes” in the future using different combinations of ingredients.
In addition to understanding how AI differs from traditional programming, it is crucial to distinguish between artificial intelligence (AI) and augmented intelligence (AuI). While advanced AI can operate entirely on its own, such as identifying a person from dental records and managing all follow-up tasks without human input, augmented intelligence is designed to assist professionals. For instance, AuI tools might rank potential dental matches or assess tooth development for age estimation, but a qualified odontologist still makes the final decision. These tools often employ advanced analytical techniques that were previously impossible with traditional programming.
Understanding the difference between AI and AuI is critical in forensic odontology, where legal and ethical accountability cannot be assigned to a machine. All current systems still require human
Abstract
Artificial intelligence (AI) is slowly emerging as a valuable tool in forensic odontology, assisting in human identification, age range assessment, and case documentation. However, many odontologists are unfamiliar with even the fundamental differences between artificial intelligence and augmented intelligence. Many are fearful of these technologies, even though they are designed to support professionals rather than replace them. To evaluate AI more effectively, it is important to understand the key stages of AI software development, such as data collection, labeling, supervised and unsupervised learning, and validation (proving it works). However, even before development begins, clearly defining “ground truth” is essential for training and evaluating AI, particularly in challenging areas like age estimation and suspect pattern injury analysis. AI is also important in fields such as DVI, where managing one-to-many comparisons and generating ranked candidate lists requires advanced algorithms and intuitive user interfaces. AI has the potential to open up new fields such as ancestry estimation and the analysis of dental treatment patterns. In addition, generative AI large language models have the potential to become essential tools for forensic odontologists since they simplify tasks such as report writing and organizing case information. However, the incorporation of this technology requires ethical, legal, cybersecurity, and regulatory considerations. Additional formal approval may be required, as AI-based dental tools are currently classified by the FDA as medical devices. Understanding AI and its need for consistent human oversight and professional accountability will be essential for creating systems that are safe, effective, and legally sound for use in forensic practice.1
oversight. However, many are marketed simply as AI, ignoring the fact that they function as decision-support tools. In this paper, the term AI is used for simplicity, though most systems operate within an AuI framework.1
The AI Learning Processes
Before using AI in forensic dentistry, it is important to understand the basic steps involved in how the technology learns and is developed. An everyday use of AI is to compare dental X-rays to help identify people. This process begins by collecting a large, diverse set of X-rays, preferably from individuals who have undergone multiple X-ray examinations over time. However, postmortem radiographs, particularly of skeletal remains, are especially useful because the absence of soft tissue reduces soft tissue scattering and improves the visualization of anatomical structures. The goal is to capture how dental features naturally change over time due to age, dental work, or injury.
Once the data is collected, the radiographs are processed through a step called preprocessing. This step corrects for variations in image quality, equipment, and technique, allowing the system to focus on relevant anatomical features rather than inconsistencies in image capture. Preprocessing helps
make the input data more uniform, which improves the accuracy and efficiency of the learning process (Figure 1).
After preprocessing is complete, the AI model begins its training phase. In supervised learning, the image pairs are labeled to indicate whether they are from the same individual (a match) or 2 different individuals (a non-match). Additionally, points of concordance can be highlighted. These labels serve as a reference that the model uses to learn how to identify relevant patterns. For instance, if 2 X-rays belong to the same person, the system is trained to associate similar patterns of tooth shape, spacing, or restorations. If they are from different people, they learn to detect distinguishing features. Over time, the system gets better at identifying whether 2 images are likely to match.
In certain situations, models may use an approach called unsupervised learning, which does not rely on labeled data. Instead, the system analyzes the image to discover hidden patterns or groupings that are not immediately obvious to the human eye. This technique, often used for exploring unknown structures in data, may require significantly more computing power.
The training process begins by feeding the model thousands of labeled examples, such as pairs of dental radiographs marked as matching or not matching. To analyze these images, AI converts them into numerical data by scanning them as pixel grids, tiny dots assigned a number based on their level of light or darkness. The software then examines these numerical groups and pattern sequences to detect edges, shapes, and features within the image, such as crown shape, tooth alignment, root length, and dental work. This process is similar to ASCII art, where symbols like “.”, ““ or “@” represent different shades to form a picture. As the AI processes thousands of examples, it improves its accuracy in making predictions. The more varied and well-labeled the training data, the better the model becomes at identifying key dental features across different image types.
To analyze images, AI converts pixel values into numerical data and compares patterns such as crown shape, tooth alignment, root length, and dental work. It processes thousands of examples to improve its accuracy in making predictions. The more varied and well-labeled the training data, the better the model can identify key dental features across different image types (Figures 2, 3).
As the training progresses, the test data—a subset of the training data that was segregated and not shown to the model—is used to determine the model’s ability to process unseen data. After each round of training, the model is evaluated on this segregated test data, which has been kept separate from the training set. Adjustments can be made to improve performance by comparing the model’s predictions with the actual outcomes in the test data.
Figure 1. AI Model Lifecycle
If it performs poorly, adjustments can be made. These adjustments may include changing the algorithm’s parameters, incorporating more diverse training data, or employing data augmentation techniques. Data augmentation involves slightly modifying existing images by rotating, resizing, or adjusting brightness to simulate a broader range of conditions.
Once training is complete, the model must be validated. Validation is the process of evaluating the model on new, unseen data to evaluate its real-world performance. Unlike the test data,
which is a subset of the training data on which the model was trained, the validation data is new data from diverse sources and is used to evaluate how well the model performs. This helps ensure that the model is not simply memorizing patterns from the training data but can make accurate predictions on new, previously unseen data.
Once the model has been validated, it must be integrated into forensic odontology software. It requires designing a user-friendly interface that is secure and seamlessly integrates with forensic workflows. Even with a
highly effective model, human oversight is essential. In the example, although the AI can identify likely matches, it cannot make decisions or provide legal determinations. A qualified forensic odontologist must review all AI-generated suggestions, apply expert judgment, and make the final decision to ensure accuracy, address context, and manage ethical concerns. AI is a tool that supports, not replaces, professional accountability, with legal responsibility remaining with the dentist or odontologist.
Labeling, Ground Truth, and Bias in AI Training
The most critical component of training AI models is the labeling of the data. The accurate labeling of data is commonly referred to as establishing ground truth. Ground truth refers to objectively verified data used as a reference for the training of the AI model.
In dental identification, ground truth in training data is typically straightforward. This clarity arises either because the radiographs are known to originate from the same individual or, in the case of disaster victim identification (DVI)
Figure 2. Portrait and ASCII art representation demonstrating image to text transformation.
Figure 3. Dental radiograph and its ASCII and grayscale numeric encodings illustrating image to text transformation.
(DVI) data, because the identification has been verified through a second scientific method, such as fingerprint or DNA analysis. Therefore, establishing ground truth in dental identification is relatively straightforward.
However, in age assessment, establishing ground truth is more challenging, as both the assignment of tooth developmental stages and the calibration of graders, trained experts who evaluate and score the radiographs, can be difficult. Additionally, even if the software can accurately assign a stage, meaning it consistently assigns the same stage to different radiographs that show the same stage of tooth bud development, further testing is needed to determine whether those assignments align with established historical tables.
In addition, training data that contains inconsistent or biased labels may cause the model to reinforce those flaws. For example, limited imaging variations or underrepresentation of certain demographic groups can lead to biased results.
These issues underscore the importance of well-rounded, highquality data and consistent labeling practices. They also emphasize the need for human oversight, not only for technical accuracy but also to ensure the system operates fairly and ethically in real-world clinical and forensic settings.
Generative AI
Generative AI is a type of artificial intelligence that creates new content, such as text, images, audio, or video, by learning from existing data. Models like generative pre-trained transformer (GPT) work by predicting what comes next, whether it is a word in a sentence or a section of an image. Unlike traditional AI, which mainly sorts or analyzes data, generative AI produces original content that can closely mimic human creativity and communication.
Generative AI is increasingly valuable in forensics, particularly through advanced language tools known as large language models (LLMs). Models such as ChatGPT, Claude, Perplexity, and Gemini generate content by predicting what comes next based on patterns learned from extensive datasets. These tools can summarize case notes, draft reports, translate documents, and efficiently organize large volumes of text. While they do not understand language like humans, their training enables them to produce coherent, context-aware, and human-like responses.
Their effectiveness stems from capturing deeper elements of language—such as tone, sentence structure, intent, and formality, not just grammar and vocabulary. For example, they can infer whether “That is great” is sincere or sarcastic based on previous context. By analyzing full conversations and identifying key cues, these models maintain consistency and relevance even in complex exchanges.
Although LLMs do not truly understand content, they simulate understanding by recognizing and responding to patterns in language. In forensic work, they serve as helpful support tools; however, trained professionals must
review their outputs to ensure accuracy, accountability, and adherence to established standards.
Applications of Forensic Odontology
Current AI forensic odontology software primarily focuses on dental identification and age assessment, both of which rely on comparing radiograph images. The image comparison process involves either matching a set of dental radiographs for points of concordance to facilitate identification or using templates to estimate age range by assessing tooth developmental stages in radiographs. However, with advances in artificial intelligence, new tools have the potential to expand on these core tasks. AI can be applied as a key research tool to determine if the transfer of class characteristics of the jaw can be observed in suspected patterns of dental origin. Given the historical challenges and controversies surrounding this type of analysis, including issues with subjectivity, inconsistency among experts, and limited empirical support, the integration of AI offers a promising avenue for introducing greater objectivity, reproducibility, and data-driven validation into the evaluation. AI can also save experts significant time on labeling (coding) and provide greater precision by matching structural features in addition to dental treatments, which are typically the primary focus of human analysis. AI can also serve as a key tool in disaster victim identification (DVI), ancestry and geographic origin estimation, and detecting patterns of dental work that may assist in narrowing down identity or likely background in forensic investigations.
Practical Applications in Forensic Odontology
1. Human Identification by Dental Means: AI can streamline forensic odontology by automating the comparison of antemortem and postmortem dental records. Using image recognition and machine learning, it quickly analyzes radiographs to detect unique patterns, not just missing teeth or restorations, thereby reducing time and minimizing human error. Generative AI tools can also assist with drafting reports, summarizing findings, and organizing case
2. Dental Age assessment: AI helps estimate dental age by analyzing tooth development, root length, pulp size, and apex closure. Trained in large datasets, machine learning models can assess wear patterns and anatomical markers to produce accurate demographic estimates. These tools provide consistent and objective results, making them especially useful in cases involving juvenile remains or incomplete skeletons (Figure 5).
3. Research into the Analysis of Suspected Dental Patterns: AI serves as a valuable research tool for examining whether jaw class characteristics are reliably reflected
in dental pattern evidence. Despite historical challenges, AI offers the potential for greater objectivity and reproducibility. However, the absence of a clear ground truth limits current applications, highlighting the need for further foundational research.
4. Disaster Victim Identification (DVI): While routine identification relies on one-to-one comparisons, DVI requires one-to-many comparisons across large databases. AI enhances this process by analyzing dental data, extracting features, and generating ranked match lists. With greater algorithmic sophistication and user-friendly interfaces, AI can improve the speed and scalability
Figure 4. Bright’s system uses AI to rank potential matches without the need for human labeling (coding) using a streamlined odontogram and software interface for the comparison of antemortem and postmortem dental radiographs. (Courtesy: Bright Forensics).
of identification during mass casualty events.
5. Ancestry and Geographic Origin Estimation: AI can support ancestry and geographic origin estimation by analyzing dental traits using radiographic or photographic methods. Models trained on global dental morphology datasets can help estimate a person’s background, especially in cases involving unidentified remains where other biological markers are unavailable or degraded.
6. Detection of Dental Work Patterns: AI can analyze dental
treatment patterns to identify region-specific techniques and distinguish between historical and modern dental work. Analyzing these patterns may provide valuable context in forensic investigations where other identifying details are limited.
Ethical
Considerations
With great power comes great responsibility. The ethical and legal dimensions of AI in dentistry cannot be overemphasized. Patient data used
for training must be anonymized and stored securely. Systems must comply with healthcare regulations, such as HIPAA. Moreover, as AI begins to influence diagnosis and treatment, there must be clarity regarding accountability. If an AI model makes a flawed suggestion that a clinician follows, who is liable for the outcome? These are the considerations regulators are beginning to grapple with. In the meantime, dentists must maintain transparency with patients, include AI disclosures in informed consent, and always apply their professional judgment.
Figure 5. DentiAgeAI interface displaying dental radiograph input, age estimation workflow, and automated staging results. (Courtesy: Dentisys.com).
Cybersecurity Considerations
As AI systems become more common, cybersecurity threats are growing. An example is data poisoning attacks, where misleading information is introduced into training data, causing models to produce faulty or unreliable results. Another threat is model invasions, which involve unauthorized access to sensitive data, such as patient information, leading to privacy violations or identity theft. AI-generated deepfakes, which are synthetic media created using artificial intelligence to mimic real people’s appearance, voice, or actions, can create fake images, videos, or audio clips. It is also theoretically possible to use a postmortem radiograph to generate a fake antemortem radiograph, potentially allowing an individual to fake their death for fraudulent purposes. These possibilities underscore the growing risks of AI misuse in creating deceptive and harmful content, making it essential to implement robust cybersecurity measures and remain vigilant against deepfakes to protect against emerging threats.
Legal Considerations
As AI becomes increasingly prevalent in the criminal justice system, it raises critical questions about its appropriateness and potential impact. Prosecutors, defense attorneys, judges, and expert witnesses are increasingly relying on AI for research and in preparing materials presented in court. However, concerns persist about how AI aligns with constitutional rights, particularly regarding due process and the Confrontation Clause. In Arizona v. Smith, the court reinforced a
defendant’s right to confront witnesses, raising doubts about whether AIgenerated evidence, lacking a clear person to cross-examine, can meet constitutional standards.
AI has the potential to amplify existing flaws in forensic science. Attorneys are already challenged to find qualified experts, and AI adds complexity that few are equipped to manage. Since forensic experts may not fully understand the AI tools they use, they will be unable to explain them clearly in court. Finally, because AI companies restrict access to how their proprietary systems work, these tools may fail to meet the transparency and reliability required under Daubert or Frye, which set the standards for admitting scientific evidence in court. Beyond the courtroom, AI in forensics raises broader concerns. Legal standards, such as Federal Rule of Evidence 702, require that expert testimony be based on reliable methods and solid data; however, these standards are continually evolving.
AI challenges traditional ideas of expertise and admissibility. To ensure fairness and protect constitutional rights, legal stakeholders must understand how these tools work and their limitations. AI should support, not replace, the rigorous legal and scientific processes that uphold justice and public trust.
Oversight Considerations
As AI becomes more ubiquitous, standards development organizations are actively working to establish clear guidelines and guardrails for the ethical and practical use of AI in dentistry and forensic odontology. The American Dental Association
The ethical and legal dimensions of AI in dentistry cannot be overlooked. Patient data used for training must be anonymized and stored securely. Systems must comply with healthcare regulations, such as HIPAA. Moreover, as AI begins to influence diagnosis and treatment, there must be clarity regarding accountability.
Standard Board (ANSI/ADA), in collaboration with the International Organization for Standardization (ISO), is playing a pivotal role in both national and international efforts to define and advance AI standards. Notably, ISO 18374:2025 is a newly published international standard that specifies requirements for data generation, annotation, processing, and documentation in AI and AuI enabled 2D dental radiograph analysis. Meanwhile, in the U.S., the ADA has also spearheaded efforts, including ADA White Paper No. 1106:2022 Dentistry—Overview of Augmented and Artificial Intelligence Uses in Dentistry, which provides an overview of AI/AuI applications in clinical care and administration, while emphasizing ethics, privacy, and clinician support. New technical reports and white papers are helping to define best practices for data collection, model training, validation, and clinical implementation. These frameworks aim to ensure that AI supports, rather than replaces, professional judgment and that its integration maintains high standards of care and accuracy. In the United States, the Food and Drug Administration (FDA) currently classifies many AI-driven dental tools as medical devices, requiring them to undergo the formal regulatory process for approval. This oversight is essential to ensure that AI applications are safe, effective, and appropriately tailored to support clinical and forensic decision-making.
Conclusion
The integration of AI into forensic odontology marks a paradigm shift requiring an understanding of the technology and an openness to revising traditional methods. However, while AI can offer valuable support, forensic odontologists must remain
at the center of analysis. Users of the technology must be informed about the technologies strengths and weaknesses and be aware of how it should properly be used. As AI technology evolves, the forensic odontology community must assume the responsibility of ensuring that these innovations meet not only scientific standards but legal and ethical standards as well. Integrating AI will help forensic odontology stay at the forefront of innovation in forensic science.
REFERENCES
1. Ahmed N, Abbasi MS, Zuberi F, et al. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry-A Systematic Review. Biomed Res Int. 2021;2021:9751564. Published 2021 Jun 22. doi:10.1155/2021/9751564
2. Alam MK, Alftaikhah SAA, Issrani R, et al. Applications of artificial intelligence in the utilisation of imaging modalities in dentistry: A systematic review and metaanalysis of in-vitro studies. Heliyon. 2024;10(3):e24221. Published 2024 Jan 14. doi:10.1016/j.heliyon.2024. e24221
3. Aldakhil S, Alkhurayji K, Albarrak S, Almihbash A, Aldalan R, Alshehri K, Alrusaini S, Asiri A. Awareness and Approaches Regarding Artificial Intelligence in Dentistry: A Scoping Review. Cureus. 2024;16(1):e51825. doi:10.7759/cureus.51825.
4. Ardila CM, Vivares-Builes AM. Artificial Intelligence through Wireless Sensors Applied in Restorative Dentistry: A Systematic Review. Dent J (Basel). 2024;12(5):120. Published 2024 Apr 24. doi:10.3390/dj12050120
5. Arjumand B. The Application of artificial intelligence in restorative Dentistry: A narrative review of
current research. Saudi Dent J. 2024;36(6):835-840. doi:10.1016/j. sdentj.2024.03.017
6. Aziz AM, Hamdoon Z, Husein AB, Dheyab S, Obaid F. Applications of artificial intelligence in restorative dentistry: a scoping review. Quintessence Int. 2024;55(6):430440. doi:10.3290/j.qi.b5437507
7. Baaj RE, Alangari TA. Artificial intelligence applications in smile design dentistry: A scoping review. J Prosthodont. 2025;34(4):341-349. doi:10.1111/jopr.14000
8. Bonny T, Al Nassan W, Obaideen K, Al Mallahi MN, Mohammad Y, El-Damanhoury HM. Contemporary Role and Applications of Artificial Intelligence in Dentistry. F1000Res. 2023;12:1179. Published 2023 Sep 20. doi:10.12688/ f1000research.140204.1
9. Carrillo-Perez F, Pecho OE, Morales JC, et al. Applications of artificial intelligence in dentistry: A comprehensive review. J Esthet Restor Dent. 2022;34(1):259-280. doi:10.1111/jerd.12844
10. Chakravorty S, Aulakh BK, Shil M, Nepale M, Puthenkandathil R, Syed W. Role of Artificial Intelligence (AI) in Dentistry: A Literature Review. J Pharm Bioallied Sci. 2024;16(Suppl 1):S14-S16. doi:10.4103/jpbs. jpbs_466_23
11. Gao S, Wang X, Xia Z, Zhang H, Yu J, Yang F. Artificial Intelligence in Dentistry: A Narrative Review of Diagnostic and Therapeutic Applications. Med Sci Monit. 2025;31:e946676. Published 2025 Apr 8. doi:10.12659/MSM.946676
12. Grischke J, Johannsmeier L, Eich L, Griga L, Haddadin S. Dentronics: Towards robotics and artificial intelligence in dentistry. Dent Mater. 2020;36(6):765-778. doi:10.1016/j.dental.2020.03.021
13. Hartman H, Nurdin D, Akbar S,
Cahyanto A, Setiawan AS. Exploring the potential of artificial intelligence in paediatric dentistry: A systematic review on deep learning algorithms for dental anomaly detection. Int J Paediatr Dent. 2024;34(5):639-652. doi:10.1111/ipd.13164
14. Karobari MI, Adil AH, Basheer SN, et al. Evaluation of the Diagnostic and Prognostic Accuracy of Artificial Intelligence in Endodontic Dentistry: A Comprehensive Review of Literature. Comput Math Methods Med. 2023;2023:7049360. Published 2023 Jan 31. doi:10.1155/2023/7049360
15. Lee SJ, Poon J, Jindarojanakul A, et al. Artificial intelligence in dentistry: Exploring emerging applications and future prospects. J Dent. 2025;155:105648. doi:10.1016/j. jdent.2025.105648.
16. Mörch CM, Atsu S, Cai W, et al. Artificial Intelligence and Ethics in Dentistry: A Scoping Review. J Dent Res. 2021;100(13):1452-1460.
doi:10.1177/00220345211013808
17. Naeimi SM, Darvish S, Salman BN, Luchian I. Artificial Intelligence in Adult and Pediatric Dentistry: A Narrative Review. Bioengineering (Basel). 2024;11(5):431. Published 2024 Apr 27. doi:10.3390/ bioengineering11050431
18. Nordblom NF, Büttner M, Schwendicke F. Artificial Intelligence in Orthodontics: Critical Review. J Dent Res. 2024;103(6):577-584. doi:10.1177/00220345241235606
19. Pethani F. Promises and perils of artificial intelligence in dentistry. Aust Dent J. 2021;66(2):124-135.
doi:10.1111/adj.12812
20. Revilla-León M, Gómez-Polo M, Vyas S, et al. Artificial intelligence applications in implant dentistry: A systematic review. J Prosthet Dent. 2023;129(2):293-300. doi:10.1016/j. prosdent.2021.05.008
21. Rokhshad R, Zhang P, MohammadRahimi H, Shobeiri P, Schwendicke F. Current Applications of
Artificial Intelligence for Pediatric Dentistry: A Systematic Review and Meta-Analysis. Pediatr Dent. 2024;46(1):27-35.
22. Shan T, Tay FR, Gu L. Application of Artificial Intelligence in Dentistry. J Dent Res. 2021;100(3):232-244. doi:10.1177/0022034520969115
23. Schwendicke F, Samek W, Krois J. Artificial Intelligence in Dentistry: Chances and Challenges. J Dent Res. 2020;99(7):769-774. doi:10.1177/0022034520915714
24. Tabatabaian F, Vora SR, Mirabbasi S. Applications, functions, and accuracy of artificial intelligence in restorative dentistry: A literature review. J Esthet Restor Dent. 2023;35(6):842-859. doi:10.1111/ jerd.13079
25. Vodanović M, Subašić M, Milošević DP, Galić I, Brkić H. Artificial intelligence in forensic medicine and forensic dentistry. J Forensic Odontostomatol. 2023;41(2):30-41. Published 2023 Aug 27.
Those in the dental community who have recently passed
Arthur Steve Baker
Longview
9/27/55–5/31/25
Good Fellow: 2006
Life: 2020
John Joseph Hempfling
Wichita Falls
9/24/49–6/11/25
Life: 2014
James Harry Ratliff
Austin 4/10/33–6/25/25
Good Fellow: 1984
Life: 1998
Fifty Year: 2010
George Riley Clark
Plano
3/14/40–6/22/25
Good Fellow: 1990
Life: 2005
Fifty Year: 2015
William Emerson Wyatt Sr
Glen Rose
4/28/28–7/22/25
Good Fellow: 1979
Life: 1993
Fifty Year: 2010
Richard John Campbell
Springtown
10/11/39–6/22/25
Good Fellow: 1996
Life: 2004
Fifty Year: 2019
Carter Edmond Karr
Amarillo
3/5/34–11/3/24
Good Fellow: 1984
Life: 2000
Fifty Year: 2009
Daniel Philip Urban
Houston 8/31/33–7/17/25
Life: 1998
tom david, DDS, D-ABFO
civil and criminal litigation
Thomas J. David, DDS, D-ABFO, earned his dental degree from Emory University School of Dentistry in 1977. He has maintained a dental practice since that time in the Atlanta metropolitan area. He is a member of the American Society of Forensic Odontology (ASFO), a Fellow of the American Academy of Forensic Sciences (AAFS) and a diplomate of the American Board of Forensic Odontology (ABFO). He has served as chair of the Odontology Section of AAFS and president of the ABFO and has also served on the Editorial Board of the Journal of Forensic Sciences (JFS). He has authored articles in various periodicals, including the JFS. He has also authored chapters in a number of textbooks, including multiple editions of the “Manual of Forensic Odontology” as well as the “2nd Edition of Forensic Dentistry”. He also co-edited the book “Forensic Odontology: Principles and Practice”, which was released in 2018.
Dr David is a consultant in Forensic Odontology to the Georgia Bureau of Investigation (GBI), Division of Forensic Sciences and the State of Georgia Medical Examiner’s Office. He also holds a faculty appointment as a Adjunct Professor at Lincoln Memorial University (LMU) , College of Dental Medicine. He provides instruction for the Forensic Odontology Fellowship program at LMU as well.
DENTISTRY Litigation
Introduction
Whether you are a forensic odontologist (dentist) or a clinical practitioner (either a general dentist or specialist), it is likely that you may become involved in litigation at some point in your professional career. Forensic dentists are more likely to become involved in criminal litigation based on their training and education, while practicing clinical dentists are more likely to become involved in civil litigation. In either case, it is important to understand the legal background of what you are about to encounter. Litigation is defined as “the act, process, or practice of settling a dispute in a court of law.” There are 3 primary types of litigation: criminal law, civil law, and administrative law. Knowledge of the legal system and how it works is essential to comprehension of your role as a dentist and what you may be asked to do to assist in the resolution of a legal matter. Your involvement may include writing a report or testifying as a fact witness or expert witness.
Criminal Law
A system of laws concerned with crimes and the punishment of individuals who commit crimes. Penal codes are a collection of laws that define criminal offenses and their corresponding punishments. Punishments for criminal offenses are called “sentences” and they range from incarceration (prison), probation, fine(s), restitution, community service and rarely death (capital punishment). The burden of proof in criminal courts is “beyond a reasonable doubt”.
Administrative Law
Administrative law encompasses laws and legal principles governing the administration and regulation of government agencies (both federal and state). Examples of administrative law concerning dentistry would be issues that pertain to licensure and participation in government health programs such as Medicaid and Medicare. The burden of proof in administrative courts is “a preponderance of the evidence”.
Civil Law
Civil law primarily focuses on resolving disputes and conflicts between individuals or entities (both corporate and private). There are 4 primary types of civil law: contract law, property law, domestic relations law, and tort law. A tort is defined
as an act or omission that gives rise to injury or harm to another and amounts to a civil wrong for which courts impose liability. A simpler definition of tort is a civil wrong. The only compensation in civil court is monetary. There are 2 areas of dentistry that pertain to tort law in civil litigation: standard of care (malpractice) and personal injury. The burden of proof in civil court is “a preponderance of the evidence”.
Standard of Care
Standard of care cases are essentially professional negligence cases. The plaintiff in these cases is typically the patient of the dentist (defendant) who is being sued. The complaint filed with the court of jurisdiction on behalf of the patient must specify what actions (or inactions) were negligent on the part of the dentist (or his/her employees). The complaint must also specify what damages occurred as a result of the negligent conduct of the dentist as well as the amount of monetary damages that are being requested. The defendant dentist must be served in person by a designated official of the court (usually the sheriff).
Once the defendant dentist is served, there must be a formal response to the complaint within a specified period of time (usually 30 days). After a formal response to the complaint by the defendant (through their attorney), the discovery process begins. The discovery process allows both the plaintiff and defendant to “discover” what evidence may be used to prove or disprove the allegations made in the complaint. The discovery process includes interrogatories (written questions posed by both sides to each other), depositions (sworn testimony) and mediation (either binding or non-binding) in a final attempt to resolve the case prior to trial.
If the case proceeds to trial, the plaintiff (patient) has the burden of proof and must present their case first, followed by the defendant (dentist). Both sides call witnesses that they believe will prove their case. In a civil trial, both the plaintiff and defendant must testify.
In addition to witness testimony, the jury will also hear about deposition testimony as well as records related to the treatment of the plaintiff (patient). After testimony has concluded, the judge will instruct the jury what to consider as well as what to not consider in rendering their verdict. After deliberation, the jury will render a verdict based on the “preponderance of the evidence”. The jury verdict must find for the plaintiff or the defendant. If the verdict is for the plaintiff, the jury must also decide how much money to award the plaintiff as compensation. If the verdict is for the defendant, there is no monetary compensation.
Dentists may be involved in these cases as either defendants or expert witnesses. In order to be retained by either side as an expert in a standard of care case, the dentist must have professional knowledge of the issues that pertain to the particular case. In addition, this knowledge must be reliable and provide relevant information to the jury in rendering a decision. An expert witness must be qualified by the court (judge) to show they have the requisite knowledge and skills. Their qualification by the court may be challenged by means of “voir dire” questioning by the opposite side.
Personal Injury
Personal injury involves physical injury inflicted on someone’s body as opposed to damage to property or reputation. With respect to a dentist’s involvement in personal injury cases, there are typically allegations of oral or dental injuries caused by a third party. In these cases, a dentist may be asked to testify as a fact or expert witness. If they are testifying as a fact witness, they may only testify about the particular details of dental treatment that was rendered as a result of the alleged dental injuries. However, they may not offer an opinion as to the cause of the alleged injuries. In order to offer an opinion about the cause of the injuries, a dentist must qualify as an expert with the same stipulations outlined above under Standard of Care. Many dentists testify as fact witnesses on behalf of patients they have treated. However, testifying as an expert on behalf of a patient you have treated can create a conflict of interest. A conflict of interest is created because as a treating dentist, your duty is to act in the best interest of your patient. Nevertheless, as an expert you must be unbiased and not act in the best interest of your patient. The complaint and discovery process is the same as outlined
…knowledge of relevant standards of care (SOC) is essential in civil litigation. Equally important is understanding the difference between SOC and professional judgment (PJ). Standard of Care is defined as “what a reasonable and prudent dentist would do under the same or similar circumstances”. In addition, professional judgment is defined as “making the best decision under a given set of circumstances”.
above in Standard of Care, except that the defendant is not the dentist who rendered the treatment, but rather a third party. If no settlement is reached, a trial proceeds as outlined above including the jury verdict.
Expert Witness Consultation & Testimony
The primary skills required to become an effective expert witness are proficiencies in report writing and expert witness testimony.
Writing an effective report entails providing appropriate information for the individual or entity (court) requesting the report. In some cases, the court of jurisdiction may require certain information or opinions in the report. Nevertheless, expert witness reports should use a specific template to insure that essential information is included as a basis for any opinions rendered. The specific template that is recommended is as follows: 1) Introduction—the 5 Ws as appropriate – who, what, when, where and why; 2) Inventory of Evidence Received—a specific list of all evidence provided that was the basis of your opinion(s); 3) Analysis of
Evidence—A detailed discussion of what specific evidence was relevant in forming your opinion(s) (records, depositions, imaging, testing, etc.). This discussion should include the reason certain evidence was relevant in forming an opinion; 4) Opinions—a specific listing of your opinion(s) that correlates relevance from your analyses with your opinion(s); 5) Disclaimer—A statement that indicates your opinion(s) may change if additional evidence becomes available at a later date. In some cases, the expert may need to collect additional evidence. If so, there should be a separate section in the report called Inventory of Evidence Collected and this section should be included after Inventory of Evidence Received.
Effective expert witness testimony is more complicated. However, knowledge of relevant standards of care (SOC) is essential in civil litigation. Equally important is understanding the difference between SOC and professional judgment (PJ). Standard of Care is defined as “what a reasonable and prudent dentist would do under the same or similar circumstances”. In addition, professional judgment is defined as “making the best decision under a given set of circumstances”. Unlike standard of care, there is no right or wrong answer as concerns professional judgment, but rather the “best” decision under the circumstances. It is important to understand that every decision made by a dentist concerning patient care is either SOC or PJ. In other words, it must be one or the other, but cannot be both.
Standards of care in dentistry as defined above include: 1) Failure to diagnose; 2) Failure to refer; 3) Failure to provide after-hours care; 4) Failure to provide post-operative care; 5) Failure to provide informed consent; 6) Failure to advise patients of undesirable treatment outcomes; 7) Failure to protect against aspirated/swallowed objects; 8) Patient abandonment; 9) Failure to maintain records; 10) Improper surgical/clinical technique. Opinions concerning breaches of SOC should be related to one or more of the SOC outlined above.
Summary
If you are not an attorney, knowledge of the legal system and how it may impact you and your professional career is important. Your professional reputation may be affected by how you handle a request for litigation related services by either a court or an attorney. Awareness of appropriate interaction with the legal system can help you avoid improper actions or professional consequences.
Karen Williamson, DDS
Becoming Involved in Forensic Odontology: Unveiling the Mystery
Dr Karen Williamson graduated from Baylor College of Dentistry in 1990), completing her GPR at the VA Hospital in Dallas, Texas, in 1991. In addition, she completed her Forensic Fellowship at the University of Tennessee in 2021. She currently assists Dr Kathleen Kasper (D-ABFO) with forensic cases for Tarrant, Collin, and Dallas Counties. Her private dental practice in Rockwall, Texas, has been a source of joy for many years. She and her husband, Bruce, have 4 children and they enjoy exploring the courthouses of small Texas towns as well as hiking in Canada. Dr Williamson is currently working on her board certification with the American Board of Forensic Odontology.
Sitting in a dental school lecture in the late 1980s, I briefly heard a thing or two about forensic dentistry. But enough of what I heard intrigued me to the point that many years later, I wanted to become involved. I just didn’t have a clue where to start. So, what does a reasonable person do? They google it. One Google search result was for a week-long overview course on forensic dentistry which I attended, entitled “All That Remains”, held at the University of Tennessee Graduate School of Medicine in Knoxville. I was exposed to multiple facets of forensic odontology and was highly encouraged to apply for the forensics fellowship the next year. I completed the fellowship in 2021 and have enjoyed assisting
BECOMING
Involved
Kathleen Kasper, DDS, D-ABFO, at the Dallas County and Tarrant County Medical Examiner’s offices. Most cases are not television show dramatics. Most are a death from driving too fast, a death from a fire. Some are age-estimation cases. Some are skulls/dentitions sitting at the morgue waiting to be entered into NamUs (unidentified and missing persons’ cases). Some are abuse cases. Some are quite interesting as to the circumstances. The real work is at the morgue taking the radiographs of all of the teeth, and charting existing conditions. Before I became a forensic dentist, I thought it must be really easy. Look at the radiographs, look at the teeth and the fillings and voilá—they match! After my fellowship, I realized, there is so much more to it. First of all, it is not easy taking radiographs on a deceased person—you can tell a patient to open and close and turn their head. Secondly, the radiographs the morgue receives from the dentists are often very outdated, not in good condition, and blurry. And lastly, the radiographs we take need to be as complete and as accurate as possible, because you never know what other antemortem evidence will turn up. Sometimes just figuring out the sequence of taking the radiographs is very important. For instance, in burn cases, the front teeth may be very fragile, and so it might be best to take those radiographs first before the teeth crumble. Even if a person is skeletonized, degraded, burned, or dismembered, dental structures are frequently retained. Some victims would never be identified without the forensic odontologist. The most rewarding part of forensics to me is knowing that you have helped a loved-one settle in their hearts the identity of their family member. In addition, the camaraderie that forensic dentists have is unique. I’ve made life-long friendships through forensic dentistry. If I’ve piqued your interest and you have a passion for dentistry and forensic science, here’s how you can become involved and the qualifications:
• Shadow an Experienced Forensic Dentist: Some forensic dentists would welcome your assistance on cases at the morgue. In addition, dental hygienists, dental assistants, and other medically-related professionals have been great assets at the morgue on cases, so their help is often welcome. Contact your local medical examiner’s office to explore opportunities, and if they have a forensic dentist on staff, they can guide you further.
• Forensic-related Electives or Continuing Education Classes: While not always available, some dental schools offer electives or courses in forensic dentistry. This is a great way to become exposed to the basics of the field. It is very important to understand the difference between TV forensics and the actual hands-on work involved. Organizations like the American Society of Forensic
Odontology (ASFO) are excellent resources for finding these courses. The ASFO is an entry-level organization that welcomes anyone with an interest in the field. Visit asfo.org.
• Network by becoming involved in organizations/ attending conferences: The American Academy of Forensic Sciences (AAFS) has some levels of membership that are entry-level as you work toward full membership. The AAFS yearly conference will be in New Orleans, Louisiana, February 9-14, 2026, and in Orlando, Florida, February 15-20, 2027. Visit asfo.org.
• Attend a Forensic Odontology Fellowship: Currently, an in-person, 15-month forensic fellowship is being offered at Lincoln Memorial University in Knoxville, Tennessee, with associations with the Knox County Regional Forensic Center. Attendees attend once a month for 3-day weekends, studying pattern analysis, age identification, disaster victim identification, recognition of human abuse, expert jurisprudence and testimony, forensic report writing, and clandestine grave recovery of human remains. A DDS, DMD, or equivalent degree is required. It is specifically designed to meet the educational requirement and to prepare individuals for board certification by the American Board of Forensic Odontology (ABFO). Contact Martha Gale at martha.gale@ imunet.edu for more information.
• Attend an online Forensic Odontology Program: Currently, an online course of approximately 9 months is available through the McGill University, Faculty of Dental Medicine, Quebec, Canada. Contact Dr Robert Dorion (rdorion@abfo.org) for further information.
• Become a board certified forensic odontologist: Visit the ABFO website (abfo.org) for further information. Board certification takes a minimum of 4-5 years to complete the requirements with subsequent passage of written and oral tests.
• Join a Disaster Mortuary Operational Response Team (DMORT): DMORT teams are deployed to supplement federal, state, and local territorial resources at the request of local authorities during natural disasters, terrorist attacks, and transportation accidents. They focus on the recovery, decontamination, examination, identification, and return of deceased victims to help families, friends, and communities find closure. Members have to join to be a part of DMORT and participate in training activities. Visit aspr.hhs.gov.
Hopefully, the resources in this article will get you going on your own forensic journey, and may your forensic journey, like mine, be ever-rewarding.
We’re Hiring: Endodontist
Are you a dentist passionate about endodontics and skilled in root canal treatments? Join our team and help transform patients’ oral health!
Position: Dentist with Expertise in Root Canals
Location: Vista Hills Family Dental, 1713 Weston Brent Ln, El Paso, TX 79935
Employment Type: Part-time / Full-time
Requirements:
• Licensed dentist in Texas
• Expertise and experience in performing root canal procedures.
• Dedication to patient care, comfort, and long-term oral health.
• More than five years of experience
What We Offer:
• Competitive salary and benefits package $200,000 - $300,000
• Supportive work environment with modern technology.
• Opportunities for growth and specialization.
• Flexible schedule
We’d love to hear from you if this sounds like the right fit for you! Send your resume to jvega@vistahillsfamilydental.com.
Designed for dentists, with dentists, the new ADA Member App is here and ready to put the resources you need in the palm of your hand.
• Chat 1:1 or with your network
• Newsfeed customized to your interests
• Digital wallet to store your important documents
• Stream the new “Dental Sound Bites” podcast
Tap into possibility at ADA.org/App
Guest Editor Rade D. Paravina, DDS, MS, PhD
Digital Approach Provides Predictability in Increasing the VDO in Erosive Wear: Clinical Technique and 9-Year Follow-Up
Fady Ibrahim, Udo Plaster, Petra C. Gierthmuehlen
First published: 31 October 2024
Funding: The authors received no specific funding for this work.
Access the open-access article at: https://doi.org/10.1111/jerd.13354
ABSTRACT
Objective
This clinical case describes a digital workflow using face scans and CAD/CAM technology for a full-mouth rehabilitation with increased vertical dimension of occlusion (VDO) with adhesive lithium disilicate restorations after 9 years.
Clinical Considerations
A healthy, 46-year-old man displaying severe tooth wear, underwent an extensive full-mouth rehabilitation involving an increase of the VDO through laminate veneers and adhesive partial coverage lithium disilicate restorations. Anatomical landmarks of the face and reference planes were captured using a digital face scanning system. The anatomical position of the maxilla was registered with a transfer device. Digital data sets of the intraoral situation combined with a facial scan enabled precise virtual planning, guiding minimally invasive preparations. Long-term provisional restorations, milled from high-performance polycarbonate, were used to test the novel VDO before the final lithium disilicate restorations were fabricated. This approach provided a time- and cost-efficient treatment solution. No failures were observed at the 9-year follow-up.
Conclusions
Utilizing face scans and design software enable a virtual visualization and comprehensive quality control for patients with dental wear, resulting in significant time savings and increased predictability for the dental technician, dentist and patient.
Clinical Significance
The described digital workflow optimizes the planning and implementation of a comprehensive adhesive full-arch rehabilitation with an increase of the VDO. The clinical long-term follow up result of CAD/CAM assisted minimally invasive lithium disilicate restorations after 9 years demonstrates to clinicians a reliable treatment concept for patients with dental wear.
value for your profession
Provided by: PERKS
P R O G R A M
Biofilm, Bacteria, and CFU Counts: Understanding Waterline Contamination in Dentistry
Provided by Solmetex
Summary
This article explores how biofilms form, how they affect colony-forming unit (CFU) counts, and why water testing should be a regular part of dental office protocols.
• Biofilm in dental waterlines can harbor harmful bacteria and is difficult to remove once established.
• Routine waterline maintenance and regular testing are essential to keeping CFU counts below the EPA limit of 500 CFU/mL.
• Preventive care, like continuous treatment and early detection, helps ensure safe water quality for both patients and providers.
Biofilm Buildup: A Hidden Risk in Dental Unit Waterlines
Dental unit waterlines (DUWLs) are an essential part of everyday practice, but they’re vulnerable to microbial contamination that’s often invisible to the naked eye.
Left unchecked, the buildup of biofilm—a complex community of microorganisms that adheres to surfaces in moist environments—in DUWLs can compromise water quality, create infection risks for patients and staff, and lead to regulatory non-compliance.
Why Does Biofilm Form in DUWLs?
Biofilm develops in dental unit waterlines when bacteria introduced from source water or oral fluids adhere to inner surfaces of the tubing.
Several factors make DUWLs especially vulnerable:
• Narrow tubing provides a large surface area for bacterial attachment.
• Water stagnation, especially overnight, gives microbes time to multiply.
• Low flow rates reduce turbulence, allowing bacteria to settle.
• Suck-back of oral fluids can occur during high-speed procedures, introducing additional organic material.
How Biofilms Contribute to High CFU Counts
The bacteria residing in biofilms are not just passive inhabitants. They actively reproduce and release cells into the water flowing through the DUWLs. These free-floating bacteria are what lab tests detect as CFUs, or colony-forming units. CFUs represent the number of viable bacteria present in a given volume of water. Regulatory guidelines, such as those from the EPA and CDC, recommend keeping DUWL water at or below 500 CFU/mL to prevent infections, especially in patients with compromised immune systems.
Once CFU counts begin to rise, it can be a warning sign that biofilm is establishing and that the routine maintenance protocols in place may not be sufficient.
Over time, the bacteria secrete a slimy matrix that forms a protective barrier, making the biofilm resistant to disinfectants and increasingly difficult to eliminate once established.
Poor Water Quality’s Implications on Health
During dental procedures, the use of ultrasonic scalers, air/water syringes, and high-speed handpieces generates aerosols that can carry waterborne bacteria into the air. This not only poses a risk to the patient in the chair, but also to staff and others in the operatory.
In rare cases, contaminated dental water has been linked to serious infections. Pediatric cases of Mycobacterium abscessus outbreaks have occurred when DUWLs were not properly maintained. While these are exceptions, they highlight the importance of consistent prevention and monitoring.
Prevention Strategies: Test, Treat, and Maintain
The best way to control bacterial growth in DUWLs is to implement a comprehensive waterline maintenance protocol that includes:
• Regular disinfection: Weekly or daily treatment helps prevent biofilm from forming.
• Daily maintenance products: These can reduce microbial load between disinfections.
• Flushing lines: Running water before and after procedures reduces stagnation.
• Water testing: Quarterly lab testing provides a clear picture of whether current practices are working, but the frequency may vary depending on the product and protocol used.
A standardized approach—such as a “test, treat, and maintain” protocol—ensures water quality is routinely assessed and adjusted before biofilm becomes entrenched.
Why Water Testing Matters
Visual inspections or self-contained water systems don’t guarantee safety. Water may look clear and still be teeming with bacteria. That’s why periodic microbial testing is so critical.
Testing provides 2 key benefits:
1. Verification confirms your treatment methods are effectively reducing bacteria to safe levels.
2. Early detection helps identify when bacterial loads begin to rise, giving you time to act before a compliance or health issue arises.
The Takeaway: Routine Testing Supports Safe Dentistry
Understanding how biofilm forms and how CFU counts reflect bacterial load is critical for any dental professional responsible for waterline maintenance. With the right combination of treatment, maintenance, and testing, water can easily be kept within safe, compliant limits.
Focusing on biofilm prevention and early detection is an investment in safety for your patients, staff, and practice reputation.
Perks Program Discount:
As a TDA member, you have access to exclusive deals for Solmetex, Sterisil, and DryShield products that will help ensure dental water safety and compliance.
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/MemberResources/TDA-Classified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN (ID #743): Legacy
GD office located in a suburb just north of Austin. 100% FFS patient base, 1500+ active patients, and a robust hygiene recall program. The office contains 5 equipped operatories, with computers throughout, digital x-rays, CBCT, and a digital scanner. The practice offers opportunities for additional growth via expanding current marketing activities and keeping additional specialty procedures in-house. AUSTIN (ID #745): Established, 2-location GD practice in the Austin area. The practice serves a large, diverse, FFS/ PPO patient base with excellent new patient flow, a combined 14 equipped operatories across both locations (with substantial room for expansion at one of the locations). The practice comes fully equipped with digital radiography, digital sensors, digital scanners, digital Pano, CBCT, and paperless charts.
AUSTIN (ID #749): Established GD office located in the heart of central Austin. The practice has an impeccable online reputation in the community and features a strong
hygiene recall program with multiple avenues for future growth. 3,000+ sq ft office, four active operatories, ample room for expansion, equipped with a digital scanner, intra oral cameras, digital x-ray sensors, and paperless charts.
DALLAS (ID #741): Established, multi-specialty dental practice and freestanding real estate in the heart of the DFW Mid-Cities. The newly renovated 3,100 sq ft office contains 6 fully equipped operatories with advanced modern technology including computers throughout, digital x-ray sensors, 3D CBCT, digital scanner, dental laser, intraoral cameras, and paperless charts. With approximately 65% of the production being focused on restorative/advanced general procedures and hygiene, 20% pediatrics, and 15% ortho, the office is built on a stable foundation with the opportunity to take it any direction you choose.
DALLAS/FORT
WORTH (ID #744): Well-established GD office located in a growing suburb of DFW. Impeccable reputation in the community, treats a majority PPO patient base with 1,900+ active patients. The 2,500 sq ft high-visibility retail location contains 5 fully equipped operatories (with the opportunity
to expand into a 6th) with computers throughout, digital x-ray sensors, panoramic x-ray, digital scanner, and intra-oral cameras.
HOUSTON-SOUTH (ID #682): Established, multi-specialty dental office in a suburb about 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
PRACTICE SALES
DSO C S
PRACTICE APPRAISALS
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com
www.dentaltransitions.com
classifieds
over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose.
SAN ANTONIO-TX
HILL COUNTRY (ID #685): Well-established dental practice and real estate nestled in the Hill Country north of San Antonio. The office relies mostly on word-of-mouth- referrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023, and the trend continued into 2024. SAN ANTONIOEAST (ID #716): Legacy GD practice and real estate in a rural community east of
San Antonio. The large office space offers ample room for expansion and features 5 fully equipped operatories with computers in each op, digital x-ray sensors, a digital Pano, a digital scanner, intraoral cameras and paperless charts. This practice has strong profit margins and serves a large, multigeneration 100% FFS patient base. SOUTH TEXAS COAST (ID #754): Exceptional GD practice located in a serene coastal town. Rare opportunity to acquire a thriving, wellestablished business in an underserved area with consistent collections of 7 figures with a primarily FFS active patient base and strong new patient flow. Hygiene production is robust, having exceeded 25% each of the last 3 years. The spacious, modern facility is outfitted with state-of-the-art technology and is also available for purchase. The owner will be retiring at some point over the next few years but is available to stay for a transition of the buyer’s preference. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATESí LISTINGS: Please register at www.dentaltransitions.com or contact us
at 512-900-7989 or info@dentaltransitions. com.
CENTRAL SAN ANTONIO: San Antonio family practice for sale in the desired Alamo Heights neighborhood. Low 6-figure production, 3+1 operatories, 700 patients of record. Practice is ideal for growth, startup, or satellite clinic. Contact my broker at ddsmatch.com.
CENTRAL TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural four operatory dental practice for sale in the heart of the beautiful Texas Hill Country. This all-digital practice with a new pano produces mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact
dentalofficesale2024@gmail.com for more information and showings.
DALLAS: Dental practice for sale in north Dallas. Located in a sought-after north Dallas community, this 100% FFS general dental practice features 5 operatories (with room for a 6th), 1,800 active patients, and 10-15 new patients/month. Collections reach 7 figures with $515K in EBITDA. Contact PTS: bailey@ professionaltransition.com or 719-694-8320. Reference #TX61725.
DALLAS: Thriving north Texas OMS practice for sale: 3 surgical suites, 2 consult rooms, and 40 new patients/month, 7 figures in collections, $600K SDE, and real estate available. Established 20+ years with minimal advertising. Within 150 miles of Dallas. Contact PTS to learn more: bailey@ professionaltransition.com—Ref #TX30625.
classifieds
HOUSTON: General dental practice for sale in east Houston, just 15 miles from downtown. This thriving, 7-op practice averages 45-50 new patients per month and generates high6 figures in collections with mid-6 figures in true take-home. The owner seeks a full transition post-sale. Ideal for a dentist or group seeking growth in a rapidly developing suburban corridor. Reference #HWT71425. Email, bailey@professionaltransition.com.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states. For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.