What’s the big difference between purchasing insurance through TDA Financial Services Insurance Program and somewhere else? TDA members own the agency!
You’ll always have attentive customer service from a team dedicated to making insurance easier for TDA members and staff.
Beginning Nov. 1:
2026 Rates Are Available, Open Enrollment Begins. Review, compare, and buy health insurance through the portal at tdamemberinsure.com
Special Enrollment for New Small Groups Begins. If you sign up during special enrollment, mandatory employer contribution towards employee premiums—and other requirements—are waived. Small group plans are less expensive than unsubsidized individual plans and enable you to have a PPO.
or learn more at
As a TDA member, you now have access to a new healthcare member benefit that utilizes a
Coverage cannot be denied.
Members can enroll THE FIRST DAY OF ANY MONTH with open enrollment. Enrollment needs to be completed no later than 30 days in advance.
or learn
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available):
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
Mashael Alqahtani, DDS
Mentors: Maria Gonzalez, DDS, MS, Donald Belles, DDS, MS, The University of Texas School of Dentistry at Houston Guest Editor Rade D. Paravina, DDS, MS, PhD
HIGHLIGHTS
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 142 | No. 7
Texas Dental Journal (ISSN 0040-4284) is published monthly, except January-February, March-April, July-August, and November-December, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2025 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement at tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
PRESIDENT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PRESIDENT-ELECT Elizabeth Goldman, DDS 214-585-0268, texasredbuddental@gmail.com
PAST PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
VICE PRESIDENT, SOUTHEAST Matthew J. Heck, DDS 512-280-8800, matthewjheckdds@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN**
Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR** Jacqueline M. Plemons, DDS, MS 214-507-0815, drplemons@yahoo.com
LEGAL COUNSEL** Carl R. Galant
EXECUTIVE DIRECTOR** Greta Zeimetz, DBA, CAE, SHRM-SCP 512-443-3675, gzeimetz@tda.org
*Non-voting member **Non-voting Board of Directors
.
Your dental practice is more than a business—it’s your legacy. At Henry Schein Dental Practice Transitions, we specialize in helping practice owners with seamless, stress-free transitions tailored to personal, professional, and financial goals.
Why Choose Us for Your Practice Transition?
• Unlock your practice’s true value with expert, data-driven valuations to unlock your practice’s true value
• Gain access to 36,000+ purchasers
• Full-service support from your first consultation to final closing
• Unmatched expertise backed by local insights and deep industry connections
• Over 500 closings with over $400MM in sales price since 2023.
Start your journey to a rewarding retirement today. Contact us or scan the QR code to schedule a complimentary consultation.
2025 LEGISLATIVE Landscape
Dr
2025 Legislative Review:
89th Regular Legislative Session Summary
2025 Legislative Landscape
Dr Matt Roberts, Chair
TDA Council on Legislative, Regulatory, Government Affairs
Introduction
The October issue of the Texas Dental Journal focuses on organized dentistry’s efforts in the legislative and regulatory arenas. Much of what dentists do every day in their practices is controlled by the Texas legislature, made up of 150 members of the Texas House of Representatives and 31 members of the Texas Senate. The Texas State Board of Dental Examiners (TSBDE), made up of 11 members including six dentists, three dental hygienists, and two members of the public, also plays a significant role in regulating dentistry in Texas. In addition, Texas statewide officials—including the governor, lieutenant governor, attorney general, and comptroller—have significant roles in the oversight, regulation, and funding to programs impacting dentistry.
The practice and regulation of dentistry and dental hygiene are governed in state statute (law) by the Dental Practice Act (DPA) contained in the Texas Occupations Code. The DPA commits almost 20 chapters with over 200 sections to the practice and oversight of dentistry. The TSBDE is charged with interpreting and enforcing the DPA and the other statutes/laws affecting dentistry, as well as promulgating and implementing rules to protect public health and safety.
Dr Matt Roberts
Given the depth and complexity of the laws, regulations, and oversight of dentistry, it is imperative that the TDA commit adequate resources and personnel toward ensuring dentistry’s voice is not only present in Austin but heard in all legislative and regulatory forums where dentistry is considered.
The TDA’s Council on Legislative, Regulatory, and Governmental Affairs (or CLRA) is made up of TDA member dentists from around the state who have experience and expertise in the legislative and regulatory fields. CLRA is charged with working with the legislature and the regulatory entities to represent the Association and implementing its policies as set by the House of Delegates and Board of Directors.
The TDA legislative “team” (the TDA Department of Legislative and Regulatory Affairs staff and legislative consultants) work closely alongside CLRA members and the TDA leadership to assist with achieving organized dentistry’s goals.
The 89th Session of the Texas Legislature convened January 14, 2025 and concluded June 2. Like the previous three sessions, the 89th began with significant change, particularly in the Texas House where 31 new members were sworn in. There was also change at the leadership position in the House where incumbent speaker Dade Phelan (R–Beaumont) was replaced by Dustin Burrows (R– Lubbock).
Leadership change, combined with a significant number of new members and staff, results in a slow start, which is an understatement of how the 89th began. House committees weren’t named until day 31 of the session, leaving only 109 days to get the work done. The first Local/Consent/Resolutions calendar was not passed until April 25 in the House.
Things were up and running in the Senate much quicker, which is normal. With only 31 members in the chamber, only three freshmen, and no change in the leadership post, the Senate began its work soon after gaveling in.
The budget once again took center stage as an over-arching issue as did school choice (vouchers), the energy grid, public school funding, water infrastructure, border security, cell phone ban in public schools and many more topics that dominated lawmakers’ time.
The TDA came to the 89th with an aggressive agenda. TDA worked to increase funding to Medicaid dental, to further safeguard standards with DIY ortho appliances, to expand insurance coverage to vulnerable pediatric patients, to block unfair insurance tactics, to prevent banning of community water fluoridation, and more.
Each of these important oral health topics, and more, will be highlighted in this issue of the Journal
On behalf of CLRA and the legislative team, thank you for being a member of the TDA and if your TDA legislative team can be of any assistance to you, please do not hesitate to contact me, Jess Calvert, Diane Rhodes, or Staci Rives in the legislative department.
The TDA came to the 89th with an aggressive agenda. TDA worked to increase funding to Medicaid dental, to further safeguard standards with DIY ortho appliances, to expand insurance coverage to vulnerable pediatric patients, to block unfair insurance tactics, to prevent banning of community water fluoridation, and more.
Texas Legislature — Overview
The Texas Legislature is the chief policymaking branch of state government that the Texas Constitution vests with all legislative power in the state. It is a bicameral body composed of an upper chamber, the Texas Senate, and a lower chamber, the Texas House. The 181 members of the legislature are elected from districts throughout the state (31 senators, 150 representatives). The legislature enacts thousands of laws each session that govern behavior, allocate resources, and define the duties of government institutions. The only bill lawmakers are constitutionally required to pass every regular session, however, is the biennial state budget.
In addition to legislative powers, the legislature exercises other types of authority. Constituent powers include the ability to alter the state Constitution, and members have authority to exercise powers of attorney on behalf of their constituents. The legislature is also allowed by statute to create and regulate the state’s administrative system, which comprises boards, commissions and departments that oversee state agencies. The legislature establishes and funds the departments and agencies—such as the Texas State Board of Dental Examiners (TSBDE)—and defines their powers and functions.
Texas Legislative Sessions
The Texas Constitution limits the regular legislative session to a maximum of 140 days every two years, but the governor has authority to call special sessions when necessary. Regular sessions begin on the second Tuesday of January in oddnumbered years. Special sessions are limited to 30 days each and are limited to a specific “call,” or subject matter, determined by the governor.
Governor Abbott has called two special sessions of the 89th Legislature. The focus of both was primarily congressional redistricting although additional topics such as disaster preparedness and response, regulation of hemp-derived products, water infrastructure, and elimination of the STAAR test were also included.
Terms of Office — Texas House and Senate
House members serve two-year terms. To qualify to run for the office, representatives must be at least 21 years old, have been Texas residents for at least two years and residents of the district they wish to represent for at least one year. There is no limit on the number of terms a member can be reelected.
Senate members are elected to four-year terms. To run for Texas Senate, candidates must be at least 26 years old, have been residents of Texas for five years preceding their election and residents of the district they are seeking for at least one year.
Senate/House Membership — 89th Legislature
Each election cycle brings change. Members of the Senate and House change each cycle—voluntarily, meaning some choose to leave, and involuntarily, meaning some are defeated.
In the last election, there was no significant change in terms of the overall party make-up of the chambers. The Senate added one republican—20 republicans and 11 democrats, and the House added two—88 republicans and 62 democrats.
However, as previously stated, there was significant change in the members themselves, particularly in House with 31 freshmen.
In terms of leadership, Lt Governor Dan Patrick (R–Houston) was re-elected by Texas voters in 2022 as presiding officer of the Senate and Dustin Burrows (R–Lubbock) was elected by his House colleagues at the beginning of the 89th as Speaker of the House of Representatives.
The TDA spends a majority of its time working with lawmakers on the Senate Health and Human Services Committee, House Public Health Committee, and House Insurance Committee. Senator Lois Kolkhorst (R–Brenham) was again appointed chair of Senate Health and Human Services, and a new Speaker meant new chairs to Public Health with Gary Vandeaver (R–New Boston) replacing Stephanie Klick (R–Fort Worth), and Jay Dean (R–Longview) replacing Tom Oliverson (R–Cypress) as chair of Insurance.
89th Legislative Session
As previously stated, the TDA had an aggressive agenda in the 89th. Your legislative team worked around the clock every day in support of the issues we had on offense, and against the issues we had on defense.
It is important to note and highlight that your TDA legislative team has been together for decades. That continuity and consistency benefit our efforts. Lawmakers and staff know your team well and your team knows them well. Your team also knows dentistry.
Whether pursuing an issue on offense or defense, navigating the legislative process requires knowledge that only comes with experience, relationships with lawmakers and staff, instincts, strategy, communication, professionalism, camaraderie, and much more. Your team functions at a high level on your behalf and they are respected at the Capitol.
TDA Priority Issues
Medicaid Dental—Funding Increase
TDA achieved the first Medicaid dental funding increase since the 2007 Frew settlement agreement—a major victory for dental patients and dentists.
Through collaboration with the Texas Academy of Pediatric Dentistry and other Medicaid dental stakeholders, TDA secured approximately $140 million in reallocated funding to enhance reimbursement to 48 critical Medicaid dental codes.
This funding will improve reimbursement for procedure codes spanning diagnostic, radiographic, preventive, restorative, surgical, and supplemental dental services.
Enhanced reimbursement helps strengthen provider participation in the Medicaid program and expands access to care for patients who need it most.
Unfair Insurance Tactics Defeated
TDA protected dentists—and their patients—from harmful insurance legislation. TDA successfully defeated HB 335 that would have eliminated equal payment protection for dentists treating patients outside their insurance network.
Thanks to previously successful TDA advocacy, existing Insurance Code protections remain in place. These safeguards
ensure that state-regulated health insurance companies reimburse dentists at the same rates for the same services, regardless of whether the dentist is in-network or out-ofnetwork. This uniform payment standard preserves fairness, transparency, and patient choice—allowing Texans to select the dentist who best meets their needs without facing surprise costs or reduced coverage.
Do-It-Yourself Orthodontic Safeguards Passed
TDA worked in support of legislation to enhance patient safety in the orthodontic marketplace. In partnership with the Texas Association of Orthodontists, TDA helped to advocate and pass HB 4070, which requires an in-person exam by a Texaslicensed dentist before any orthodontic appliance is sold or prescribed.
This common-sense legislation ensures that all Texans— regardless of how they access orthodontic care—receive a thorough clinical evaluation by a qualified professional.
The law mandates an in-person exam by a Texas-licensed dentist that includes imaging review and patient counseling before treatment begins. These protections uphold high standards of care and safety in an increasingly digital and direct-to-consumer market.
TDA helped secure a life-changing victory for children requiring medically necessary dental care under general anesthesia. Supporting the Texas Academy of Pediatric Dentistry, TDA helped pass SB 527, which requires stateregulated insurance plans to cover general anesthesia for dental treatment in children under 13 when medically necessary.
This critical reform ensures that children with documented physical, mental, or medical conditions receive safe, effective, and equitable dental care—without unnecessary financial barriers. The law prohibits insurers from excluding this coverage, protecting vulnerable pediatric patients and supporting Texas families.
Community Water Fluoridation Ban Defeated
TDA successfully preserved one of the most effective public health measures for preventing tooth decay. TDA defeated proposals that would ban community water fluoridation in Texas.
Misinformation about fluoride continues to spread, but the science is clear: fluoridation is safe, effective, and essential for preventing tooth decay across all populations.
Adjusting naturally occurring fluoride levels to the recommended 0.7 parts per million is akin to fortifying salt with iodine or milk with Vitamin D. It is a proven, equitable strategy that benefits every Texan, regardless of income or access to dental care.
Aesthetic Botox Administration by Dentists
TDA will continue fighting to expand practice rights for Texas dentists. While SB 1117 did not pass both chambers this session, the bill would have authorized any Texas-licensed dentist to administer botulinum toxin (and its equivalents) for aesthetic purposes—contingent on completing a TSBDEapproved training program.
TDA remains committed to advancing this reform. Dentists possess deep expertise in the anatomy of the face and perioral areas, making them exceptionally qualified to safely perform these procedures. Texans deserve expanded access to safe aesthetic care.
Funding for Loan Repayment
TDA will continue working to restore a proven tool for addressing workforce distribution problems.
Due to state budget constraints, funding for DELRP was not reinstated during this session. The program would have provided $200,000 in loan repayment assistance over 4 years for 100 dentists to practice in rural and underserved areas.
With just 378 dentists needed to eliminate Dental Health Professional Shortage Areas statewide, restoring DELRP funding is a smart investment in public health. TDA will renew this effort in the next legislative session to help bring dental care to rural and underserved Texas.
Dental Insurance Reform
TDA will continue pursuing essential insurance reforms. Although SB 1090 did not advance, this bill would have curbed harmful bundling and downcoding practices by state-regulated dental insurers.
Bundling and downcoding lower payments to dentists and increase out-of-pocket costs for patients, making dental care less affordable and accessible. TDA remains steadfast in its commitment to advancing this reform and will reintroduce the bill in 2027 to protect both dentists and their patients.
Conclusion
The 89th Legislative Session was an incredible success for Texas dentists and their patients. The TDA accomplished its aggressive goals in large part due to the grassroots involvement of member dentists from across the state and the diligent, highly strategic work of the Association’s legislative team.
Now more than ever, dentistry needs all members to be active in the legislative and regulatory arenas. Get to know your state senator and state representative and their staff, educate yourself on the issues, support DENPAC, and respond to TDA calls to action. The success of the TDA is dependent upon each and every member!
Alexandre R. Canevet, D.D.S. Zayd M. Hashmi, D.M.D.
Practices For Sale
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a well-located professional building with 3 ops in good condition. Currently paper-based and non-digital, operating 4 doctor days per week. Growth potential by adding a hygienist, expanding services, marketing, or extending hours. Over 1,200 active patients (10% FFS, 50% PPO, 40% Medicaid). Ideal for a satellite office or first practice. Call AFTCO today! Opportunity ID: TX-02453
FANTASTIC TEXARKANA LOCATION: GP is in a bustling retail center with great visibility. The office is equipped with 3 ops, digital X-ray, and paperless patient charts. The practice has over 1,200 active patients that are a mixture of 20% FFS and 80% PPO. The seller refers out most specialties, and the practice operates on 3.5 doctor days and 4 hygiene days, leaving ample room for growth. Don’t wait, call AFTCO today! Opportunity ID: TX-02459
PRIME LOCATION IN RURAL WEST TEXAS: Well-located GP in the heart of town near residential and retail areas with strong visibility is grossing $789,000.00. The 2,000 sq. ft. digital office has 4 ops and room to expand. Operating 3–3.5 days/week with no hygienist, this practice sees 2,500+ active patients (mostly PPO). Major growth potential. Call AFTCO today! Opportunity ID: TX-02553
REAL ESTATE AVAILABLE: Southwest of Odessa, this GP is in a converted residence in the center of the town grossing $631,000.00. The office is 2,000 sq. ft. with 3 ops and room to expand. This computerized office, that utilizes Eaglesoft, is fully equipped with digital X-rays and Pano. The practice has over 2,600 active patients who are a blend of mostly PPO, with approximately 25% FFS, & 7% Medicaid. The practice is currently associatedriven with no hygienist, giving great room for growth or a simple way to have a satellite location. Don’t wait, call AFTCO today! Opportunity ID: TX-02554 Go to our website or call to request information on other available practice opportunities!
The Council ON Legislative, Regulatory, and Governmental Affairs
The Council on Legislative, Regulatory, and Governmental Affairs (CLRA) makes certain that the Texas Dental Association (TDA) has an effective voice in the legislative process and state government. CLRA works with the legislative and regulatory affairs staff and TDA contract legislative consultants to implement TDA’s legislative agenda and maintain positive working relationships with legislators, state officials, and allied professional groups. In conjunction with component societies, the council informs members about governmental actions and mobilizes the TDA’s grassroots organization. The council also works with regulatory agencies to help ensure a competitive marketplace for dentists and quality dental care for all Texans.
DR MATTHEW B. ROBERTS, CHAIR
General dentist from Crockett, former TDA president, former member of the American Dental Association (ADA) Council on Government Affairs, former member of the ADA Council on Access, Prevention and Interprofessional Relations, and former member of the Commission on Dental Accreditation. Dr Roberts is serving his 22nd year on CLRA.
DR JAY C. ADKINS, MEMBER
General dentist from Lubbock, former TDA Board of Directors member, former member of the Texas State Board of Dental Examiners Dental Hygiene Advisory Committee, current TDA Smiles Foundation Board member (21st year), past regent for Texas in the International College of Dentists (ICD), and current chair of ICD Fellowship Orientation Program. Dr Adkins is serving his 14th year on CLRA.
DR PAUL A. KENNEDY, III, MEMBER
Pediatric dentist from Corpus Christi, past president of the Nueces Valley District Dental Society, former adjunct professor in the department of pediatric dentistry at UT Health San Antonio. Dr Kennedy is serving his 8th year on CLRA.
DR DEBRAH J. WORSHAM, MEMBER
General dentist from Center, former TDA president, former DENPAC chair, current DENPAC board member, former ADPAC vice-chair, former TDA board member. Dr Worsham is serving her 23rd year on CLRA.
DR ELIZABETH S. GOLDMAN, PRESIDENT-ELECT
General dentist from McKinney, current TDA president-elect, current member ADA Council on Ethics, Bylaws, and Judicial Affairs, consultant to TDA Council on Public Health and Access to Care, former chair TDA Council on Peer Review, current member Collin College Dental Hygiene Advisory Board. Dr Goldman is serving her 1st year on CLRA.
DR GEORGANNE P. MCCANDLESS, PAST PRESIDENT
Pediatric dentist from Tomball, current TDA past president, former member of Council on Dental Licensing, Standards, and Education, current LAC member 8th district. Dr McCandless is serving her 3rd year on CLRA.
DR AUSTIN R. GREEN,
NEW DENTIST
General dentist from Waco, former president Central Texas Dental Society, current DENPAC board member, former Pathway to Fellowship Director for TAGD. Dr Green is serving his 2nd year on CLRA.
DR DAVID A. DUNCAN, CONSULTANT
General dentist from Amarillo, former TDA president, former TDA board member, former Panhandle Dental Society president, former member ADA Council on Dental Practice, former board member ADA’s political action committee (ADPAC). Dr Duncan is serving his 16th year on CLRA.
DR DUC “DUKE” M. HO, CONSULTANT
General dentist from Katy, former TDA past president, current member ADA Council on Government Affairs, former chair ADA Council on Dental Practice, former chair TDA Strategic Affairs Committee, former president Greater Houston Dental Society, served on the ADA Fight Insurance Interference Strategic Task Force, the ADA Dental Practice Recovery (COVID) Task Force, and the ADA ERISA Special Committee. Dr Ho is serving his 7th year on CLRA.
DR MARK PEPPARD, CONSULTANT
General dentist from Austin, served on the ADA’s political action committee (ADPAC), former TDA board member, former TDA delegate, former ADA delegate, current DENPAC board member. Dr Peppard is serving his 20th year on CLRA.
DR MICHAEL NAJERA, DENPAC
Periodontist from El Paso, former president 16th District, current chair Legislative Action Committee 16th District, current DENPAC chair, chair of 16th District for past 19 years, past TDA and ADA delegate. Dr Najera is serving his 6th year on CLRA.
MS JANET CROW, ALLIANCE
From Spicewood, current Alliance of the TDA (ATDA) treasurer, former ATDA president, former ATDA liaison to DENPAC and TDASF. Ms Crow is serving her 12th year on CLRA.
Row 1 (L-R)
Dr Matthew B. Roberts, Chair (Crockett)
Dr Jay C. Adkins (Lubbock)
Dr Paul A. Kennedy III (Corpus Christi)
Row 2 (L-R)
Dr Debrah Worsham (Center)
Dr Elizabeth S. Goldman (McKinney)
Dr Georganne P. McCandless (Tomball)
Row 3 (L-R)
Dr Austin R. Green (Waco)
Dr David A. Duncan (Amarillo)
Dr Duc “Duke” M. Ho (Katy)
Row 4 (L-R)
Dr Mark Peppard (Austin)
Dr Michael Najera (El Paso)
Ms Janet Crow (Spicewood)
TDA LEGISLATIVE
JESS CALVERT
is TDA’s director of public affairs. He serves as TDA’s in-house legislative consultant and oversees the day-to-day operations of the TDA Department of Legislative, Regulatory, and Governmental Affairs, including policy, DENPAC, and the contract legislative consultants. He began his career as an analyst at the Legislative Budget Board (LBB), where he was assigned to general government and natural resource agencies. After leaving the LBB, he served on the staff of the Texas House of Representatives Committee on Appropriations as an analyst assigned to education, criminal justice, and the judiciary. Prior to coming to work at the TDA, Jess was employed at General Motors Acceptance Corporation, where he managed several residential finance programs. A native of Austin, Jess earned a BA degree from Texas Tech University and a master of public administration from Texas State University.
NORA DEL BOSQUE
is a contract legislative consultant to TDA. Nora formerly worked as an associate to past TDA legislative consultant Dick Brown. Prior to that, she worked in public affairs and public relations for the Miller Brewing Company, serving as an industry lobbyist in Arizona, Colorado, New Mexico, and Texas. Before joining Miller Brewing Company, she worked in the Texas Legislature as chief clerk for the House Committee on Appropriations and as a legislative aide to the House Ways and Means Committee and for the late Representative James Hury (D-Galveston). A native of Abilene, Nora earned a BA degree from the University of Texas at Austin.
TEAM
SUSAN ROSS
is a contract legislative consultant to TDA and a former director of public affairs for the Association. Prior to representing TDA, she represented the nursing home industry for the Texas Health Care Association and worked as an aide to two influential legislative consultants, Bill Pewitt and Jack Gullahorn. Susan first came to the Capitol in 1993 as an aide to Senator Dan Shelley (R-Crosby). A native of Crosby, she earned a BS degree from Texas A&M University.
DIANE RHODES
is TDA’s senior policy manager. She works on legislative and regulatory issues and serves as staff liaison to the Texas State Board of Dental Examiners, the Council on Legislative, Regulatory, and Governmental Affairs (CLRA), the Council on Dental Licensing, Standards, and Education (CDLSE), and the Council on Public Health and Access to Care (CPHAC).
Prior to coming to TDA, Diane worked in the Division of State Grants in the governor’s office and as a legislative aide to Representative Tom Ramsay (D-Mount Pleasant). A native of Waco, Diane earned a BA degree from Baylor University.
STACI RIVES
is TDA’s policy analyst and DENPAC coordinator. She serves as staff liaison to DENPAC, the TDA Oral Health PAC (TOHPAC), the Council on Professions and Trends (CPT), and the Community Fluoride Committee (CFC). She worked six legislative sessions for various members of the Texas House of Representatives, most recently serving as chief of staff for Representative Ed Thompson (R-Pearland). She also spent time working as an insurance specialist for the Texas Department of Insurance. A native of Houston, Staci earned a BA degree from Southwestern University.
Regulating Smiles:
The Texas Dental Board’s Mission to Protect Patients and the Profession
Every 2 years, the Texas Legislature embarks on an intense 140-day session to review and debate thousands of proposed bills. Only a limited few successfully pass and become law. In dentistry, most relevant legislation is found within the Occupations Code. Specifically, the Texas Dental Practice Act—contained in Chapters 251 through 267 of the Texas Occupations Code—establishes the legal framework and regulations governing the practice of dentistry in Texas.
While the Texas State Board of Dental Examiners (TSBDE) implements and enforces regulations, TDA serves as the profession’s primary advocate—working to ensure those regulations remain fair, practical, and patient-centered.
According to the Texas Constitution, the authority to create laws—such as the Dental Practice Act (DPA)—belongs exclusively to the state legislature. The DPA grants the TSBDE the responsibility of enforcing state dental laws and its own administrative rules. The TSBDE holds the power to investigate dental licensees, issue disciplinary actions, and establish binding regulations that govern the dental profession.
Unlike the Texas Legislature, which convenes every two years, the TSBDE operates on an ongoing rulemaking schedule. This means Texas dentists must stay alert to new or revised rules that could impact how they practice. Keeping up with these developments can be challenging, but members of the Texas Dental Association (TDA) enjoy a significant advantage. Through its advocacy efforts, the TDA represents dentists before both the state legislature and the TSBDE, ensuring their concerns and interests are effectively communicated.
TDA helps its members remain up to date on TSBDE regulatory changes through multiple communication channels, including newsletters, email alerts, and social media updates. The organization also provides one-onone assistance for questions related to laws, regulations, and compliance matters. Members can easily contact the TDA by phone or email for guidance. Additionally, a dedicated webpage on
tda.org—found under Advocacy > Texas State Board of Dental Examiners— serves as a centralized resource for all TSBDE-related information.
Individual TSBDE Regulatory Compliance Assistance
TDA provides individualized help for member dentists who need TSBDE assistance. Call or email Senior Policy Manager Diane Rhodes at drhodes@ tda.org or 512-443-3675 ext 122.
Governor Appoints
New Dental Board
Governor Greg Abbott appointed Dr Bryan Henderson, a dentist anesthesiologist from Dallas, to serve as the TSBDE’s Presiding Officer. He also selected Janessa Bock, RDH, and Dr Lisa Masters, a periodontist from San Antonio, as new members and reappointed Dr Linda Burke, a pediatric dentist from Harlingen, to continue serving on the Dental Board. Their terms will run through February 1, 2031.
Important TSBDE Rule Changes for 2025
Throughout 2025, the TSBDE adopted several amendments to its rules, published in the Texas Register, to align state dental regulations with current professional standards and administrative practices. These updates affect various areas of dental practice, licensure, education, and reporting.
Individual TSBDE Regulatory Compliance Assistance
TDA provides individualized help for member dentists who need TSBDE assistance. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
March 2025 Rule Adoptions
The first set of rule changes was published on March 7, 2025, with an effective date of March 13, 2025.
The Dental Board amended this rule to eliminate the requirement that dental patients be covered with a lead apron and thyroid collar during X-rays. This change follows updated guidelines from the American Academy of Oral and Maxillofacial Radiology (AAOMR) titled “Patient Shielding During Dentomaxillofacial Radiography,” which advises discontinuing the use of lead shielding in dental radiography. A stakeholder meeting held on September 27, 2024, revealed broad support for aligning state regulations with the AAOMR recommendations.
Obtaining a Permit – 22 TAC §108.42
Similarly, the rule regarding mobile dental facilities and portable dental units was amended to remove the requirement for lead aprons and thyroid shields when conducting X-rays. The update mirrors the rationale behind the amendment to §113.2 and reflects the same national radiology guidelines and stakeholder feedback.
Additional Continuing Education Required – 22
TAC §111.1
This amendment deletes outdated sections (subsection (a) and paragraph (b)(1)) that are no longer applicable. The continuing education requirement for controlled substances remains under paragraph (1) and in §104.1(2)(B). The rule also updates the reference title for §104.1 to reflect current terminology.
Continuing Education for Certificate Holders – 22
TAC §114.12
The updated rule now clarifies that dental assistant registrations follow a biennial renewal cycle, aligning with the current administrative process.
May 2025 Rule Adoptions
A second group of amendments was published on May 16, 2025, taking effect on May 22, 2025.
Collection and Reporting of Enforcement and Licensing Data – 22 TAC §107.400
The Dental Board now requires licensees to submit enforcement and licensing data reports annually rather than quarterly, offering a more comprehensive overview of statewide data trends. The amendment also replaces references to “administrative citations” with “administrative penalties” and corrects a minor punctuation issue.
Records of the Dentist – 22 TAC
§108.8
Language referencing the American Dental Association guidelines on radiograph use was removed. Instead, dentists must now adhere to the minimum standard of care when determining radiographic needs.
Names and Responsibilities – 22 TAC §108.52
This revision specifies that recognized dental specialties must be approved by the National Commission on Recognition of Dental Specialties and Certifying Boards. The rule also includes minor grammatical updates for clarity.
August 2025 Rule Adoptions
A final set of amendments was published on August 22, 2025, and became effective August 28, 2025.
General Qualifications for Licensure – 22
TAC §101.1
Dentist licensure applicants are now required to submit a National Practitioner Data Bank (NPDB) self-query report at the time of initial application. This update formalizes a practice already followed by the Board.
Licensure by Examination – 22 TAC §101.2
The amendment reflects the merger between the Central Regional Dental Testing Service (CRDTS) and the States Resources for Testing and Assessments (SRTA). It also introduces flexibility in remediation requirements, allowing applicants to complete a remediation course either before or after passing an examination, with Board staff authorized to approve such courses.
General Qualifications for Licensure (Dental Hygiene) – 22 TAC §103.1
Dental hygiene applicants must also submit an NPDB selfquery report upon initial licensure, aligning dental hygiene requirements with those for dentists.
Licensure by Examination (Dental Hygiene) – 22 TAC §103.2
This rule is updated to reflect the CRDTS–SRTA merger.
Both sections were revised to incorporate the CRDTS–SRTA merger and ensure consistency across related continuing education provisions.
General Qualifications for Registration or Certification – 22 TAC §114.6
Applicants for dental assistant registration must now submit an NPDB self-query report with their initial application, formalizing the Board’s existing practice.
Dental Faculty Licensure – 22 TAC §117.2
Faculty license holders are now required to submit an employment affidavit form at renewal to confirm ongoing employment with their sponsoring educational institution. The amendment also includes a grammatical correction.
Dental Hygiene Faculty Licensure – 22 TAC §117.3
This rule was revised to align with Texas Occupations Code §267.003 and to require submission of an employment affidavit form at renewal. Additional grammatical and punctuation corrections were also made.
The 2025 TSBDE rule changes update Texas dental regulations to better reflect current clinical standards, simplify administrative procedures, and ensure consistency across licensure and renewal processes. From the discontinuation of lead aprons in X-ray procedures to new reporting and documentation requirements, these updates demonstrate the Dental Board’s commitment to evidence-based regulation and professional accountability in Texas dentistry. As the Dental Board continues to modernize its regulations, TDA remains closely engaged to ensure the voice of Texas dentists is represented at every stage of the rulemaking process.
Post 89th Regular
Legislative Session
HB 1700 (Teledentistry Recordkeeping)
The TSBDE proposed amendments to Rule 108.16 clarifying the informed consent documentation required for teledentistry services. Published in the Texas Register on September 12, 2025, the amendments outline the specific consent documentation that licensees must obtain when providing teledentistry care.
HB 4070 (Sale, Design, and Manufacture of Orthodontic Devices)
The TSBDE does not plan to introduce new rules, choosing instead to rely on the statutory language of HB 4070. The Dental Board maintains that its existing teledentistry rule (22 TAC §108.16) already fulfills the intent of HB 4070.
Additional Possible Rules
At its November meeting, the TSBDE will propose rules to implement HB 5629 and SB 1818, which address licensing for military service members, veterans, and their spouses. The Dental Board will also present a rule proposal for SB 912, establishing continuing education (CE) tracking systems to verify health care practitioners’ compliance with CE requirements
In addition, the Dental Board will introduce a rule proposal for SB 912, which establishes a continuing education (CE) tracking system to monitor compliance with CE requirements among health care professionals.
Stay Up to Date: Why Active and Visible Dental Licenses Matter
During the year, the TSBDE reviewed a concerning case involving a dental hygienist who continued working after their license had been canceled. This incident not only jeopardized the hygienist’s professional standing but also placed the supervising dentist at serious legal and ethical risk.
Dentists are legally obligated to verify that all dental hygienists and registered dental assistants under their supervision maintain current and valid licenses or registrations. Allowing anyone to practice with an expired credential is not just unwise—it’s against the law. If a license or registration remains expired for more than 365 days, it is officially canceled, and the individual must typically go through the reapplication process to regain licensure. To prevent these complications, both dentists and their team members must take proactive steps to ensure all credentials remain active and in good standing.
Although every dental professional is responsible for maintaining their own licensure or registration, supervising dentists have a legal duty to confirm that every team member is properly credentialed. Overlooking this responsibility can lead to serious legal, professional, and reputational consequences.
Equally important is the requirement to make licenses and registrations clearly visible within the dental office. According to TSBDE regulations, licenses for dentists, dental hygienists, and registered dental assistants must be publicly displayed in the area where patient care is provided. The only exception applies to the first 30 days after a new license or registration is issued. Posting credentials in a staff lounge or private office does not meet this requirement—they must be easily viewable by patients and the public within the treatment area.
Maintaining and displaying an active license isn’t just about regulatory compliance—it’s about protecting your practice and earning patient trust. Visible, up-to-date credentials reassure patients that they are receiving care from qualified professionals. In short, stay current, stay compliant, and keep your credentials in clear view.
New
Fingerprint Background
Check Requirement Begins January 1, 2026
Starting January 1, 2026, the TSBDE will require all license holders who do not have a State Identification (SID) number on file to complete a fingerprint-based criminal background check before they can renew their licenses.
The SID number serves as a unique identifier that links an individual’s fingerprints to their criminal history record. This helps state agencies, including the TSBDE, monitor and receive notifications about any criminal activity associated with a licensee.
Who This Applies To
This new requirement affects license renewals submitted on or after January 1, 2026. If you were licensed before 2016, it is likely that you do not have a SID number in the TSBDE system. Because fingerprints are not shared between agencies, having fingerprints on file with another state or licensing agency does not fulfill this requirement—you must complete the fingerprinting process specifically for the TSBDE.
How You’ll Be Notified
If your licensing record does not include fingerprint data, you will automatically receive a notification 90 days before your license expiration date through the Dental Board’s online licensing portal. This alert will include instructions for completing the fingerprintbased background check.
Do not contact the TSBDE to find out if your fingerprints or SID are already on file. The system will notify you if action is required.
Advisory Committee on Dental Anesthesia 2025 Report
The Advisory Committee on Dental Anesthesia (ACDA) published its latest annual report, summarizing the review of 16 cases from Fiscal Year 2024 (September 1, 2023 – August 31, 2024). Each case involved a sedation- or anesthesia-related death or incident, as defined under 22 Texas Administrative Code §100.12(c)(1). The patients affected ranged in age from 4 to 79 years.
The Committee noted that the trends identified this year closely mirror those seen in previous reports, emphasizing three major areas that continue to warrant attention:
1. Patient Selection
In 5 of the 16 cases, negative outcomes were linked to inappropriate patient selection. The report identified several contributing issues, including:
• Proceeding with dental procedures despite patients having uncontrolled medical conditions.
• Overdependence on medical consultations for clearance, rather than integrating those evaluations into a broader risk assessment.
• Incomplete consultation records, missing vital information such as treatment duration, anesthetic dosages, and prescribed postoperative medications.
New Fingerprint Background Check Requirement Begins January 1, 2026
Beginning January 1, 2026, all TSBDE licensees without a State Identification (SID) number on file must complete a fingerprint-based background check before renewing their license. Licensees will be automatically notified 90 days before expiration of their license after January 1, 2026, if fingerprinting is required do not contact the TSBDE.
• Lack of adequate training or improper delegation of consultation-related communications to nonclinical staff.
2. Local Anesthetic Dosage
Two of the reviewed cases involved the administration of local anesthetic beyond the maximum recommended dose, which led to adverse patient reactions.
3. Recordkeeping
The Committee found deficiencies in clinical documentation across several cases, reinforcing the need for more thorough and consistent recordkeeping within dental practices.
The ACDA’s report serves as a reminder of the ongoing importance of careful patient assessment, accurate dosage calculation, and comprehensive documentation in preventing anesthesia-related complications. The complete report is available online.
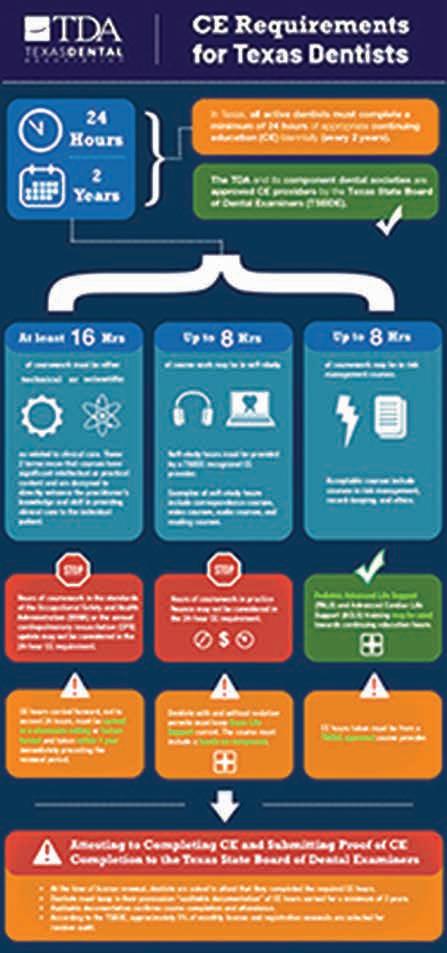
Simplifying CE Tracking for Texas Dentists
To renew a dental license in Texas, dentists must complete a designated number of CE hours. The required amount—and sometimes the specific subject areas—can differ based on a dentist’s professional role and the type of work they perform. But how can dental professionals easily keep track of what’s required, where to focus their efforts, and which CE courses are accepted by the TSBDE?
TDA’s CE Infographic: Your Quick Reference Guide
TDA developed a clear, easy-to-follow infographic to help. To access it, visit tda.org > Member Center > CE Requirements for Texas Dentists and Staff.
This resource allows dentists to quickly confirm their CE requirements, while dental hygienists and registered dental assistants
can also find information specific to their credentials. The infographic is regularly updated to reflect the latest CE rules and TSBDE changes—making it a reliable reference tool yearround.
Track CE Hours with the Dental Concierge App
For even greater convenience, the TDA offers the Dental Concierge app—a digital CE tracker designed specifically for Texas dental professionals. The app lets users:
• Track CE hours and store certificates securely in the cloud.
• View a personalized dashboard that displays completed and pending CE requirements.
• Access affordable, high-quality CE courses directly within the app.
• Set reminders for important deadlines, including license renewal and non-TSBDE obligations like X-ray equipment inspections.
Dentists can register at tdadentalconcierge.com and download the app from the Apple App Store or Google Play to get started.
By using these tools, Texas dentists and their teams can stay organized, meet CE requirements with confidence, and ensure they remain in full compliance with TSBDE regulations.
Dentists, hygienists, and RDAs can track and submit CE hours with the TDA Dental Concierge app.
And you can start right now.
Scan here:
tdadentalconcierge.com
Your Voice Matters: TDA Advocates for Texas Dentistry
TDA is committed to representing and protecting the interests of its members by championing legislation and regulations that support the dental profession. TDA continuously monitors and participates in state regulatory and legislative activities that influence how dentistry is practiced in Texas— making sure that dentists have a strong voice in every discussion.
TDA remains the unified voice of Texas dentistry—actively engaging with lawmakers, regulators, and the TSBDE to protect your right to practice, promote patient safety, and shape the future of oral health care in Texas.
References
1. Texas Occupations Code §258.003, Responsibility of Delegating Dentist
Now, state-regulated insurers are prohibited from recovering an overpayment made to a dentist unless the carrier notifies the dentist in writing no later than 180 days after the dentist received the overpayment.
Texas Dental Association (TDA) members identify dental benefits and third-party payer issues as their top concerns. TDA has a proven track record of achieving insurance victories for its members. Working closely with the various insurance plans (including Medicaid managed-care plans), the Texas Department of Insurance (TDI), and the Texas Health and Human Services Commission (HHSC), TDA successfully addresses issues members are facing every day.
In 2023, TDA passed HB 1527, a landmark reform package targeting three major pain points: retroactive denials, disallowable clauses, and silent network leasing. Under the first provision in the bill, insurance companies are held to a 180-day timeframe to engage in payment
recovery efforts, also known as retroactive denials. Retroactive denial allows insurance companies to require dentists to repay claims already paid to them when insurers discover they paid a claim mistakenly, even if the claim was processed years ago. This results in surprise billing at the expense of patients.
Now, state-regulated insurers are prohibited from recovering an overpayment made to a dentist unless the carrier notifies the dentist in writing no later than 180 days after the dentist received the overpayment. The dentist will have 45 days after receiving the written notice of overpayment to agree or challenge the request. If the dentist disagrees with the recovery of funds request, the applicable plan or policy must provide the dentist with an opportunity to challenge or appeal the recovery attempt.
The second provision of the bill targeted disallowable clauses, which can be found in most provider network agreements in place today. These clauses allow the insurer to both deny a dental benefit and prohibit the dentist from collecting fees for the dental services provided. This practice undermines the purpose of dental benefits, which exist to help patients with the cost of dental care, not to determine clinical decisions made by dentists and their patients. Disallowable clauses are now prohibited by state-regulated insurers, ensuring that healthcare decisions remain transparent, fair, and personal between the patient and their dentist.
The final provision addressed silent network leasing, a practice where insurance companies can pawn dentists off to different insurance networks without the provider’s knowledge or consent. When a network is leased without complete transparency, it can significantly impact the insurance benefits available to a dentist’s patients and result in an erosion of trust in the dentist-patient relationship. State-regulated insurers are now required to follow fair and accurate network leasing laws, allowing dentists to review contracts and decide whether to opt-out before an insurance network is leased.
In 2019, TDA secured passage of historic comprehensive reform for state-regulated insurance that brought much needed relief to dentists through HB 2486. The bill required state-regulated insurance plans to have a free website available for patients and dentists that includes information about the patient’s plan or policy. It also prohibited these plans from mandating payment methods to dentists. HB 2486 required state-regulated insurance plans to pay for dental treatment that has prior authorization. It also prevented the insurers from collecting an “overpayment” from a dentist who did not treat the patient where the overpayment occurred.
In 2015, TDA achieved coordination of benefits (COB) protection for dentists with the passage of HB 3024. That bill required state-regulated insurance plans to coordinate a patient’s primary and secondary insurance so that the secondary insurer also pays on a dental claim up to, but not exceeding, 100 percent of the total amount of the claim. When both plans have COB provisions, the plan in which the patient is enrolled as an employee or the main policyholder is primary. The plan in which the patient is enrolled as a dependent would be secondary.
In 2011, TDA attained non-covered services protection for dentists through the passage of SB 554. Stateregulated dental plans are prohibited from setting fees for dental services not covered by the plan. The only fees a dental plan may cap are fees for services the plan covers.
In 2003, TDA accomplished assignment of benefits protection for dentists, preventing state-regulated insurance plans from prohibiting or restricting a patient from making a written assignment of benefits to a dentist.
TDA will continue working with legislators and regulators to eliminate insurance issues plaguing dentists. Your involvement in advocacy and grassroots efforts is crucial to TDA’s success at the Capitol, and with your help TDA will continue to make significant insurance improvements for Texas dentists.
The Personal Side of Politics
DR MICHAEL NAJERA, DENPAC CHAIR
In my more than 20 years in leadership in the El Paso District Dental Society, I’ve learned a lot. As the new Chair of DENPAC, I have one main point I want to share with you: DENPAC isn’t just politics, it’s personal.
You’ve read about the many victories TDA had in this last legislative session. That kind of success doesn’t happen by accident. We have a hardworking legislative team with a great reputation and even better relationships inside the Capitol. TDA is a trusted voice for dentistry and oral health, and we always have a seat at the table when important decisions are getting made. But that’s not enough either—we still need DENPAC and we need YOU.
The more people who invest in DENPAC, the stronger impact we can make. Let’s work together to continue protecting your patients, your profession, and your practice.
TDA has member dentists in almost every legislative district with a personal connection to their legislators. We refer to those members as “key contact dentists”—members who volunteer their time and resources to help
L-R: former NVDDS president Dr Jenn Loftin, Rep. Todd Hunter, Dr Keely Hunsaker
advance TDA’s legislative and regulatory agendas. These key contacts may be asked to reach out to the legislator in their district when legislative issues affecting dentistry arise. And because these key contacts have already established a relationship with their legislator, they are more effective at influencing and achieving success.
Dr Keely Hunsaker, down in the Nueces Valley District Dental Society, has a longstanding relationship with Representative Todd Hunter. As Chair of the House Calendars Committee, Rep. Hunter is the gatekeeper for every major bill getting to the House floor. He’s a key influencer in the legislature, and Dr Hunsaker relationship plays a big role in our ability to contact him when we need something.
Dr Ralph Cooley in the Brazos Valley Dental Society occasionally meets up with Senator Brandon Creighton for breakfast at one of his favorite local spots. Getting engaged with your local elected officials doesn’t always have to look like campaign events and political fundraisers.
Representative Tom Oliverson has been one of TDA’s strongest champions in the Texas House. He’s carried dental insurance reform bills for us, and most recently carried the bill requiring medical insurance to cover general anesthesia in pediatric patients when
L-R: Dr. Ralph Cooley, Sen. Brandon Creighton
medically necessary. Being from the Houston area, many dentists from the Greater Houston Dental Society love to show up to his events and support him. They may not be constituents, but they know how important his leadership is and how much he’s done for dentistry!
As a political advocacy arm of the TDA, DENPAC uses voluntary contributions from member dentists to support campaigns of state candidates who are friends to TDA—meaning they are supportive of access to care, oral health, and organized dentistry. The financial support that DENPAC provides allows TDA’s legislative team to foster close relationships with these lawmakers and is a crucial part of the continued legislative achievements TDA has been able to attain.
But DENPAC can’t continue to foster political relationships without contributions from members like you. We need you. Every contribution, regardless of size, makes a difference. Will you donate today? Visit denpac.org to learn more and make an investment now.
Make a personal investment in your profession HERE
2026 will be a big election year in Texas, as most statewide and senate offices are on the ballot, and all 150 house seats are up as well. We predict there will be a lot of turnover, so we need boots on the ground in these districts to get to know these candidates. Want to learn more about being a key contact dentist? Email Staci Rives at srives@tda.org for more information.
Thank you to all our current DENPAC members and key contact dentists. Your investments and involvement are making a difference in our profession both now and for future generations!
L-R: Dr Duke Ho, Dr Rita Cammarata, Rep. Tom Oliverson, Dr Craig Armstrong, Dr Tommy Harrison
Those in the dental community who have recently passed
Richard Mark Linden Jr
Dallas 1/29/43–7/27/25
Good Fellow: 1999
Life: 2008
Fifty Year: 2023
Thomas D Bourland Jr
Willis 7/4/31–7/26/25
Good Fellow: 1998
Life: 2000
Robert Bagnell Kelly
Lake Jackson
11/21/29–7/4/25
Good Fellow: 1980
Life: 1994
Fifty Year: 2005
Walter August Brinkman Jr
Fort Worth
2/2/48–8/12/25
Good Fellow: 1999
Life: 2013
Fifty Year: 2024
Robert Randolph Debes
Houston 6/14/27–7/9/25
Good Fellow: 1978
Life: 1992
Fifty Year: 2002
Thomas Wayne Bohannan
Hurst
4/12/31–8/20/25
Good Fellow: 1983
Life: 1996
Fifty Year: 2008
Joe Weldon Christina
Corpus Christi 10/16/32–8/22/25
Good Fellow: 1987
Life: 1997
Fifty Year: 2012
Modernizing Medicaid Oversight in Chapter 32
Improvements are coming to Medicaid oversight that aim to better support providers and strengthen program integrity. With the passage of Senate Bill 1038 during the 89th Texas Legislative Session, Chapter 32 of the Human Resources Code has been updated to better align with today’s health care environment.
The purpose of this article is to help Medicaid dental providers understand what’s changing, why it matters, and how the updates promote fairness, clarity, and consistency. These changes reflect a shared commitment to high-quality care and responsible stewardship of Medicaid resources.
Why was it needed?
Medicaid has changed significantly over the past few decades with the rise of managed care, digital health records, and evolving health care delivery models. These significant changes required that the law governing Medicaid fraud and abuse evolve as well.
Chapter 32 had not been substantively revised in nearly 40 years. SB 1038 addressed the need to reflect the realities of health care today by aligning Chapter 32 with the violations outlined in Human Resources Code Chapter 36 and the Penal Code Chapter 35A, enabling consistent pursuit of misconduct across criminal, civil and administrative domains. SB 1038 also provided additional clarity to the administrative remedies available to the OIG under Chapter 32.
What’s new in Chapter 32?
The updated law includes several improvements and clarifications:
• Clearer definitions. Terms such as “claim,” “material,” and “knowingly” have been updated to better reflect current legal and health care standards, helping providers understand what constitutes a violation and creating greater consistency across the criminal, civil and administrative domains.
• Modernized enforcement tools. The law now clarifies impermissible activities, such as submitting false claims, failing to disclose material facts or obstructing an OIG investigation, and ensures OIG’s authority applies across different healthcare delivery systems to include managed care.
• Stronger penalties to deter misconduct. Updates clarify that penalties can include up to three times the amount improperly paid by Medicaid – including any benefits received directly, indirectly or to a third party. For violations involving elderly individuals, persons with disabilities, or individuals under age 18, the cap on the additional penalty amount is raised from $15,000 to the federal maximum under the False Claims Act if that amount exceeds $15,000. Ongoing violations may also result in daily penalties.
What this means for dental providers
For the vast majority of dental providers—those who follow the rules and serve their Medicaid patients with compassion, care, and integrity—the updates to Chapter 32 ensure that the rules are applied consistently across all providers, reinforcing the high standards that most dental providers already meet.
The law adds clarity with respect to particular administrative violations to improve compliance. It also protects the reputation of honest providers by equipping the OIG with a tool to hold bad actors accountable. The provisions in Chapter 32 are intended for providers who knowingly violated,
or who should have known they were violating Medicaid rules, unlike errors or good faith differences of interpretation, which will continue to fall under other statutes.
Looking ahead
SB 1038 went into effect on September 1, 2025. It is a muchneeded amendment that protects the integrity of the Medicaid program. By modernizing Chapter 32, the law ensures consistent and fair enforcement, deters fraudulent behavior and supports providers who are committed to doing things the right way.
To help providers stay informed, the OIG offers a variety of online resources. We encourage all Medicaid dental providers to visit the OIG website for
provider resources such as an overview video for Medicaid providers, dental solicitation one-pager and the selfdisclosure protocol.
Stay connected with the OIG
Facebook: www.facebook.com/TxOIG
X: www.x.com/TexasOIG
LinkedIn: www.linkedin.com/company/ txhhs-oig
TDA Legislative Resource Guide
Resources
The staff at the Texas Dental Association are ready to assist you. Please use this guide to identify staff members who are knowledgeable in areas of legislative and regulatory affairs. If you have questions or need assistance with any of these entities, or others not listed, please give us a call.
General Legislative & Regulatory Questions
8701 W Hwy 71, Ste 201-M Austin, TX 78735
512-443-3675, ext. 270
Director of Public Affairs
Jess Calvert
512-443-3675, ext. 132 jcalvert@tda.org
Senior Policy Manager
Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Policy Analyst/PAC Coordinator
Staci Rives
512-443-3675, ext. 123 srives@tda.org
DENPAC
8701 W Hwy 71, Ste 201-M Austin, TX 78735
512-443-3675, ext. 123
Texas State Board of Dental Examiners
1801 Congress Ave, Ste 8.600 Austin, TX 78701
P 512-463-6400
F 512-649-0797
www.tsbde.texas.gov
TDA Staff:
Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Office of Inspector General
Texas Health and Human Services
Chief Dental Officer
Dr Janice E. Reardon PO Box 85200 MC-1300
Austin, TX 78708
512-491-2060
janice.reardon@hhsc.state.tx.us
TDA Staff:
Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Texas Health and Human Services
Medicaid and CHIP Division 4601 W Guadalupe St Austin, TX 78711
Occupational Safety and Health Administration (OSHA)
US Department of Labor Occupational Safety and Health Administration 200 Constitution Ave NW Room Number N3626 Washington, DC 20210
1-800-321-6742
www.osha.gov/dentistry
TDA Staff:
Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Area OSHA Offices: Austin: 512-374-0271
Corpus Christi: 361-888-3420
Dallas: 972-952-1330
El Paso: 915-534-6251
Fort Worth: 817-428-2470
Houston (North): 936-760-3800
Houston (South): 281-286-0583
Lubbock: 806-472-7681
San Antonio: 210-472-5040
Environmental Regulations
Texas Commission on Environmental Quality (TCEQ) 512-239-1000
www.tceq.texas.gov
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Tax Issues
Texas Comptroller of Public Accounts PO Box 13528, Capitol Station Austin, TX 78711
111 E 17th St Austin, TX 78774
888-334-4112
www.comptroller.texas.gov
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
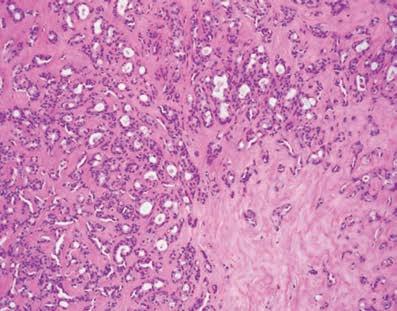
Innovative Approach of Fabricating Reduction Stents to Correct Misaligned Teeth Prior Crown Preparations
Mashael Alqahtani, DDS
Background
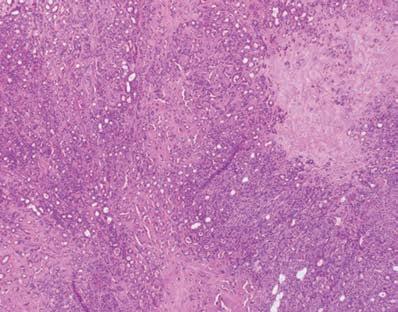
Dental misalignment is prevalent in adult patients especially patients who are diagnosed with Amelogenesis Imperfecta (AI) (Fig. 1).1-3 Malocclusions, especially dental open bite, appeared to be present in higher proportions in AI.1-3
Orthodontic correction should be the primary focus for correcting dental misalignment, yet only 15% of the 66% to 75% of adults who have malocclusion seek orthodontic treatment. The low motivation is due to lack of awareness, fear of discomfort,and seeking social acceptance.4
The longevity of dental restorations in patients with AI significantly decreases which inversely correlates with the severity of AI. Extensive coronal restorations of anterior and posterior teeth are often indicated.2,6 Full mouth rehabilitation is the optimal choice for individuals with amelogenesis imperfecta. In situations where parts of the
anterior teeth protrude beyond the dental arch, making the procedure of preparing a full arch rather difficult with an increased potential for extensive preparation which compromise the teeth vitality. Proclined teeth, if not addressed in advance, can result in flawed trial restorations, heightened necessity for endodontic treatments, and ultimately impact the patient’s satisfaction with the treatment.5
Utilizing reduction guides to correct the teeth alignment is seldom discussed in the literature for cases where orthodontic treatment is not viable or desired by the patient.5 Traditionally, practitioners relied on the mockup technique or using auto-polymerizing acrylic resin guides on stone casts.7-9 Both approaches fail to address the dilemma for the need for misalignment correction first before doing the necessary reduction for the crown preparation.
Aim
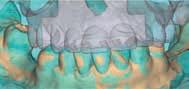
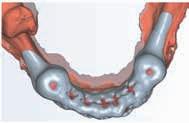
In this poster, a fabrication of two sets of 3D guides for a guided reduction technique is described to correct teeth misalignment utilizing (exocad DentalCAD;exocad GmbH). The first set is for the removal of the proclined sections of the teeth (misalignments correcting guide) 10 The second guide serves as a measuring stent, designed to verify that the tooth reduction remains within the planned limits (Measuring guide) 11
Mentors: Maria Gonzalez, DDS, MS*, Donald Belles, DDS, MS, The University of Texas School of Dentistry at Houston
Guest Editor Rade D. Paravina, DDS, MS, PhD
Fig. 1
Methodology
1. Standard Tessellation Language (STL) files for the maxillary and mandibular teeth is acquired using an intraoral digital scanner. The digital casts are mounted and a digital diagnostic wax-up at the reestablished VDO is made (Fig. 2).
2. The windows of the protruded portions are created by superimposing the two meshes in Exocad using the best fit matching function (Fig. 3). Visualize the prominent sections of the diagnostic cast through a diagnostic waxup.
Alqahtani, DDS teeth literature for viable or (7)(8) guides on address utilizing first set of the (10). The remains ). (11).
Methodology:
1.Standard Tessellation Language (STL) files for the maxillary and mandibular teeth is acquired using an intraoral digital scanner. The digital casts are mounted and a digital diagnostic wax-up at the reestablished VDO is made (Fig.2).
2.The windows of the protruded portions are created by superimposing the two meshes in Exocad using the best fit matching function(Fig.3). Visualize the prominent sections of the diagnostic cast through a diagnostic waxup.
3.Using the Crown mode Draw the margins of the protruding area. Align the insertion axis towards the facial surface. Proceed and finish the custom objects. Export the windows created as an STL file (Fig.4).
4.Using the Bite splint mode, proceed with the fabrication of the splint. The windows created are imported in the same position as the initial cast and subtracted from the splint creating a window in the misalignments correcting guide (Fig.5,7). Export the STL file and digitally print it. (Fig.9).
5.Using the Bite splint mode, proceed with the fabrication of another splint. Using the Freeform feature, create windows on a modified cast that represent the dentition after the correction using the misalignments correcting guide (Fig.6,8). Export the STL file of the Measuring guide and digitally print it. (Fig.10).
6. To verify prior to mouth preparation, position the first guide on the stone cast and grind the protruded sections accordingly. To ensure the passive fit of the second guide, place the second guide over the stone cast and proceed with the crown preparation (Fig.11)
7.Position the first guide on the teeth and reduce the protruded sections. Next, place the second guide (Measuring guide) to confirm the reduction to be within the planned limit (Fig.12,13), then continue with the definitive preparations followed by the fabrication of the trial restorations (Fig.14,15).
14
References:
Fig. 2
Fig. 3
Fig. 6
Fig. 8
Fig. 9
Fig. 10
Fig. 11
Donald Belles, DDS, MS.
Fig.
Fig. 15
Fig. 12
Fig. 13
Fig. 14
Fig. 15
Fig. 5
Fig. 7
Fig. 4
By Eric Tiedtke
A lot has happened in a year! TDA now has a member-owned insurance agency, a new executive director, and a new member healthcare option.
Much is going on with the Affordable Care Act (ACA), as previous legislation will expire at the end of 2025. Specifically, subsidies and eligibility are reverting to previous levels for ACA individual plans at the end of the year. There are also fewer companies offering plans in Texas.
As it has in the past, TDA Financial Services Insurance Program is here to keep you informed on the changing dynamics of health insurance for 2026 in the individual and small group markets.
Rates
If you have individual or small group coverage now, changes are coming with big rate increases in the individual HMO market and moderate increases in small group plans.
Filed rates are being reviewed to determine if proposed increases are based on reasonable cost assumptions and solid evidence. You won’t be able to compare rates until final rates are available, which will be sometime between the middle of October and before Nov. 1 when open enrollment starts.
Individual Plans
Statewide
There are no ACA-compliant individual PPO plans available statewide in Texas.
Blue Cross is the only company offering individual plans statewide in Texas. These are HMO only however their Plus plans (or POS Plans) provide coverage outside of the network, but with higher deductibles than the in-network HMO and no out-of-pocket caps.
Regional and Local
There are regional or market specific local ACA-compliant plans—available in limited areas of Texas where a hospital system, such United Healthcare, Baylor Scott & White or Memorial Hermann, has several facilities. Companies such as Molina, Oscar, Community Health, Imperial Health, and Sendero are also offering plans in select regions of the State. All the plans offered in Texas have filed for rate increases effective Jan. 1, 2026—some as high as 42%, so keep an eye out for your renewal.
Features
Most plans are incorporating tele-med, direct primary care, or concierge medicine as part of the coverage.
• Tele-med allows for virtual visits with your physician that may or may not have a copay.
• Direct primary care and concierge arrangements typically provide certain services (such as an annual physical exam and specified treatment for a specific condition) and often don’t qualify as insurance, as essentially, you’re prepaying for a service.
• Virtual primary care sessions can include some prescriptions, durable medical equipment, lab tests, and diagnostic imaging.
Critical Advice
It’s very important to understand the scope of the networks, the coverage, and limitations—especially if you’re seeing specialists for an ongoing medical condition. The network could have limited or no coverage in parts of the state.
About Subsidies (Premium Credits)
The ACA’s health insurance premium subsidies—also known as premium tax credits—normally adjust each year to keep pace with premiums. For 2026, significant changes to the ACA will take effect, including eliminating the enhanced premium subsidies and stricter eligibility requirements for subsidies.
The new rules make you ineligible for subsidies if you don’t file your federal income tax return or reconcile your income with your subsidy amount annually. Additionally, the year-round Special Enrollment Period for individuals with income below 150% of the poverty line is being ended.
Many individuals covered under the ACA for 2025 will no longer be eligible for any subsidy or will have the subsidy significantly reduced for 2026. This will result in them paying a much higher amount of the actual premium.
Small Group Plans
Small group plans continue to be the only option for getting true PPO plan options under the ACA.
Rate changes filed for small group plans range from less than 5% to 15%, depending on the company. For 2026, it appears small group:
• PPO rates will again be slightly lower than individual HMO rates.
• HMO group rates will be 5-15% lower than individual plans (non-subsidized).
Of the major companies, we anticipate Blue Cross will have the lowest rates; their filed rate increase for the PPO and HMO is around 13.4%, followed closely by United Healthcare, Baylor Scott & White, and Memorial Hermann. Aetna will no longer be in the small group market in Texas.
Coverage Options
PPO access is available to employees, contractors, and sole proprietors.
TDA members have access to a Healthcare Member Benefits Program that utilizes a national PPO network and is available in all 50 states. Some of the many benefits of the program include:
• Guaranteed Issue
• Availability of ACA-compliant health benefits
• Availability to W-2 employees, 1099 contractors, and sole proprietors
• Availability to Staff
To be eligible for the program, you must be a TDA member in good standing and actively working. For more information, contact the Concierge Team at 833-287-4765.
Small group plans are less expensive than individual plans and have more options.
If you have a practice with at least one other full or part time employee, you should consider a small group plan. Depending on how your practice is structured, the other employee could be your spouse.
Additional paperwork and effort are necessary start a small group plan, but they can be worth it for several reasons.
• Small group plans will be less expensive than unsubsidized individual plans; and you can still get a PPO.
• If you sign up during the special enrollment for new small groups (starting Nov. 1), the mandatory employer contribution towards employee premiums—as well as other requirements—are waived. This is a good way to attract and retain high-quality employees while offering a lot of flexibility on plan designs.
• If you deduct employee premiums from payroll on a pretax basis, it can lead to tax savings for the practice and employees.
• You can offer more than one plan, such as a base plan that’s less expensive for employees (e.g., an HMO with an RX and office copay), and a PPO plan for you and your family.
TDA Financial Services Insurance Program can help you compare rates for small group plans beginning October.
Here are the maximum out-of-pocket amounts for small group plans coverage in 2026:
In-network ACA maximums
• $10,600 for an individual
• $21,200 for a family
HSA-compatible high-deductible health plans (HDHP) are subject to these out-of-pocket maximums:
• $8,500 for individual coverage
• $17,000 for family coverage
Out-of-network maximums
If you have out-of-network expenses, the maximum can be double or more what’s listed above; or the expenses may not even be covered. The plans with the lowest premiums will have the highest out-of-pocket expenses.
Contact TDA Financial Services Insurance Program at (800) 677-8644 for details.
A Critical Consideration
Rates are important, but so are providers.
It’s essential you check the network of the insurance company you select for 2026, and make sure your providers and hospitals are in-network. You need to know the company name and the network name. Some providers, for instance, might take a Blue Cross PPO, but not Blue Cross HMO or United Healthcare Choice Plus but not the Choice Network.
Other Options
Level-Funded Plans
If your practice and its employees are generally healthy and not big users of health care, you might consider a level-funded plan. These are underwritten based on the health of the group and can be as much as 10–25% lower than regular ACA small-group plans.
Only about 50% of small groups will qualify based on underwriting, but the rate savings can be significant, so they’re worth considering. Also, these plans don’t typically qualify for the special enrollment, so the practice must pay 50% of the employee premium and meet a participation requirement regarding the number of eligible employees that participate. There are other considerations, such as
the different PPO networks, stop loss coverage, and just understanding how the plans work and what’s covered. United Healthcare is going all in on level-funded plans and has changed some of the requirements for smaller groups.
Faith-Based, Medi Share and Health-Share Groups
These types of plans are not insurance and should not be considered a substitute for insurance; but they can be an option if you understand how they work. With these types of arrangements, you join a group and pay or contribute a monthly amount to a plan. After your deductible is met, you submit your medical bills and are reimbursed from the funds available or through others making additional contributions to cover your bill. Many have incorporated a PPO network so you can get the discounted amount when you have treatment. However, you are still responsible for the bill, even if the health-share plan might reimburse you.
These arrangements have stricter guidelines than traditional insurance companies and on which procedures are eligible for reimbursement or cost sharing. There’s normally a lifestyle guideline where a member agrees to live a certain way (abstain from illegal drug consumption, sex outside of marriage, tobacco use, and abuse of alcohol or prescription drugs).
Payment of medical bills through these arrangements is not guaranteed in any way; and each member is solely responsible for the payment of his or her own medical bills. If you understand how the plans work and their limitations, these can be a less expensive option than ACA plans.
Short Term Medical
We don’t recommend you go without insurance, so short-term health insurance can be an option if you’re without coverage because of a waiting period, transitioning from one plan or coverage to another (e.g., in-between jobs); or it’s outside the open enrollment period or you’re close to being eligible for Medicare.
These plans are exempt from the definition of individual health insurance coverage under ACA provisions and usually don’t pay for pre-existing conditions. They’re designed to cover a new sickness or accident (with no treatment in the previous 5 years).
These plans have limitations on coverage (e.g., no maternity coverage) and don’t have all the same mandates, such as
unlimited-benefits maximums. These duration limits (how long you can keep the plan) have changed significantly from Administration to Administration. For new plans sold in Texas since September 1, 2024, the duration limit is an initial term of up to 3 months, with a maximum total duration of 4 months, including renewals. It was announced August 7 that the agencies including HHS, will not prioritize enforcement actions as they reconsider the definition of these types of plans.
Limited Benefit Sickness-and-Accident Plans
These plans are sometimes called “mini-med plans,” and are marketed as an ACA alternative with a PPO.
They may offer copays and RX benefits however they don’t include the “essential minimum health benefits” required by the ACA.
These types of plans may include a PPO and provide a schedule of benefits that pay a certain amount per day or treatment; and are limited to a maximum amount. A company selling these plans will often address this limitation by selling additional coverage for critical or specified illness or accidents.
These plans are underwritten based on good health and have some form of preexisting condition limitation, which means anything you’ve previously been treated for is not covered for a period—normally 12 months. If the plan is guaranteed issue with no pßre-existing condition, make sure you’re not just buying a discount plan.
These plans can be an option, but you really need to understand the limitations and coverage, as you could be responsible for tens of thousands of dollars—even though you are covered—if you have a major accident or illness.
Additional Options and Considerations
If you are concerned about having a high deductible, limited, or no out-of-network coverage, you might consider a supplemental product for accidents or hospital confinements. These types of plans pay you directly and in addition to your other coverage. They tend to be relatively less expensive and are a good option if you don’t want to self-insure high-deductible and out-of-pocket expenses.
Health Savings Accounts (HSA) Plans
When picking a plan, keep the above numbers in mind, but also consider the following. Prescription-drug and office-visit copays are convenient plan features, but you need to know the combined cost of your total out-of-pocket exposure and your plan (the premium). If you haven’t looked at HSA Plans or didn’t think they made sense previously, you should revisit them.
• HSA plans generally offer the lowest premium and can be a great way to build up a self-funding account for current and future medical expenses. This can be especially important if you have to go out-of-network.
• Contributions are tax deductible (as much as $4,400 for an individual and $8,750 for a family (excluding catch-up contribution).
If
you are concerned about having a high deductible, limited, or no out-ofnetwork coverage, you might consider a supplemental product for accidents or hospital confinements.
• Individuals with Bronze or Catastrophic Affordable Care Act (ACA) plans are now eligible to contribute to an HSA.
• In 2026, Direct Primary Care (DPC) arrangements with specific monthly fee limits will be considered qualified medical expenses, and having a DPC arrangement won’t prevent HSA contributions. Also, first-dollar coverage for telehealth in HDHPs will be permanently allowed for plan years starting after December 31, 2024, making virtual care HSA-compatible
• Earnings and interest accumulate tax-free.
• You own and control the funds.
• HSA plans are not a use-it or-lose-it vehicle.
ICRA
An Individual Coverage Health Reimbursement Arrangement (ICHRA) presents an opportunity for employers to take more control over their benefits spend. ICHRA allows them to set aside tax-advantaged dollars to reimburse their employees for individual health insurance plans that are inflation-resistant compared to group plan premiums. ICHRA brings more cost control and less risk for the employer and more purchasing power and choice for employees.
Keep in mind that the individual health insurance plans offered are going to probably be HMO only, and the individual HMO plans rates are going to be higher 15-25% higher than the group HMO plan, if unsubsidized. There is also the administration and set-up involved with ICHRA which is not particularly burdensome but does add additional administration on behalf of the practice.
HRA
Use of Health Reimbursement Accounts (HRAs) has expanded because new regulations issued by the Departments of Labor, Treasury, and Health and Human Services allow reimbursements for individual-market insurance premiums. Before employers offer a benefit that includes individual HRAs, they should consider the implications related to the (ACA) employer shared-responsibility mandate, and the ability of their employees to obtain a premium tax credit (PTC) or subsidy on the ACA marketplace.
The maximum new contribution for an excepted benefit HRA was indexed for inflation. The IRS announced that for plan years beginning in 2026, the maximum is $2,200, an increase from $2,150 in 2025.
Conclusion
Key Takeaways
If you want or need full coverage, the small group market is still the best way to get coverage with more options available at lower cost than in the unsubsidized individual market. The Member Healthcare option is also worth considering if you need a PPO, especially if you work as a contractor (1099 vs W-2) or just don’t want to go through the process of offering plans to staff.
The alternative options discussed all have a place at the table, but you need to make sure you understand plan limitations and risks before making a change to something less expensive.
Important Dates
The open enrollment period for health plans offered under ACA begins Nov. 1, 2025, and ends Jan. 15, 2026. For individual plans, you will have until Dec. 15 to pick or change to a new plan with a Jan. 1 effective date; or until Dec. 31, if your plan terminates Dec. 31.
You will be able to review individual plans and rates no later than Nov. 1, and small group plans and rates in early October. Stay informed and get ready to review and compare your options and decide as soon as possible.
Disclaimer: This article was submitted in late August, so some information may have changed by the time this article is published.
If you would like to receive more information or discuss available insurance options, please feel free to contact TDA Financial Services Insurance Program at (800) 677-8644 or visit www. tdamemberinsure.com.
ORAL and
maxillofacial pathology
case of the month
Clinical History
A 64-year-old male was referred to the Oral and Maxillofacial Surgery department by his primary care physician for a “cheek mass.” The patient’s medical history consisted of hypertension, Parkinson disease, gout, and a history of myocardial infarction status post coronary artery bypass graft in 2021. The patient presented with a well-circumscribed, firm, mobile, nontender, submucosal mass of the left buccal mucosa approximately 1.5 cm in diameter. The overlying mucosa was intact and slightly yellow in color, with no ulceration or induration. Small telangiectatic vessels were noted on the overlying surface mucosa. (Figure 1). The patient reported the mass had been present for 6-7 years and had recently increased in size, although he was
AUTHORS
Isabelle M. Hornung, BS Fourth-Year Dental Student, School of Dentistry, UT San Antonio, San Antonio, Texas
Gabriella S. Ward, BS Fourth-Year Dental Student, School of Dentistry, UT San Antonio, San Antonio, Texas
Anne Cale Jones, DDS UT System Distinguished Teaching Professor Department of Pathology and Laboratory Medicine, UT San Antonio, San Antonio, Texas
Rebeca Rodriguez, DDS Oral and Maxillofacial Surgery Resident Department of Oral and Maxillofacial Surgery, University Medical Center of El Paso, El Paso, Texas
Juliana Robledo, DDS Assistant Professor/Clinical, Department of Pathology and Laboratory Medicine, UT San Antonio, San Antonio, Texas
Figure 1. Clinical photograph of a firm, mobile, nontender, submucosal mass of the left buccal mucosa with surface telangietatic vessels.
unable to specify exactly when the increase began. The patient denied purulent drainage and facial swelling, and there was no sign of an acute odontogenic infection. No imaging studies were taken during the initial consultation. The initial clinical impression was that of either an adenoma or a calcifying mucocele. The oral and maxillofacial surgery intern (RR) had no concerns for malignancy given the mobile, well-circumscribed nature of the mass. The patient underwent an excisional biopsy under local anesthesia, with a submucosal blunt dissection performed to completely remove a welldelineated, encapsulated mass measuring 1.5 cm in diameter (Figure 2). The mass was submitted to oral and maxillofacial pathology for histopathologic examination.
Pathological Findings
Received is a bottle of formalin was a tan nodular mass of soft tissue measuring 1.2 cm x 1.2 cm x 0.9 cm. The specimen was sectioned and microscopic examination revealed sections of a well-delineated specimen composed of numerous ductal structures in a focally myxomatous to predominantly hyalinized stroma (Figure 3). The ductal structures were double-layered consisting of an inner layer of cuboidal cells with an eosinophilic cytoplasm and an outer layer of flattened myoepithelial cells with an eosinophilic to clear cytoplasm. The lumina of the ductal structures contained an eosinophilic coagulum (Figure 4). Scattered plasmacytoid shaped myoepithelial cells were noted throughout the neoplasm. Foci of chronic inflammation was seen at the peripheral of the neoplasm. The neoplasm was surrounded by a fibrous connective tissue capsule. Adjacent mucous gland lobules and striated muscle bundles were also noted.
What is the most likely diagnosis?
See page 446 for the answer and discussion.
Figure 2. Gross photograph of a well-delineated, encapsulated mass of the left buccal mucosa measuring 1.5 cm in diameter.
Figure 3. Benign neoplasm composed of numerous ductal structures in a hyalinized stroma (H&E: original magnification 4x).
Figure 4. Double layered ductal structures containing an eosinophilic coagulum (H&E: original magnification 20x).
ORAL and
maxillofacial pathology
diagnosis and management—from page 445
Diagnosis: Pleomorphic Adenoma
Discussion
Based on the clinical findings, the differential diagnosis is most appropriately categorized into two groups: benign salivary gland tumors and soft tissue tumors. This includes but is not limited to: pleomorphic adenoma, canalicular adenoma, schwannoma, and lipoma.
A pleomorphic adenoma (benign mixed tumor) is the most common salivary neoplasm, accounting for the majority of parotid and submandibular tumors, as well as 31%-44% of minor salivary gland tumors.1,2 Among minor salivary gland tumors, the palate is the most common site accounting for 50%-65% of intraoral examples followed by the upper lip (19%-27%).2 Pleomorphic adenoma may occur at any age but most frequently presents between the ages of 30 and 60, with a slight female predilection.1 Clinically, these tumors present as a slow-growing, painless, firm mass that may persist for years before diagnosis.2 Surgical excision with wide margins is the treatment of choice, as incomplete removal or simple enucleation may lead to local recurrence.1,3 Histologically, pleomorphic adenomas are typically wellcircumscribed and encapsulated; however, the capsule may be incomplete or show infiltration of tumor cells, increasing the risk of recurrence.1,2 The tumor is composed of a mix of glandular epithelium and myoepithelial cells within a mesenchyme-like stroma, hence the term pleomorphic.2 The epithelial component often forms sheets or ductal structures, with an outer layer of myoepithelial cells surrounding an inner layer of cuboidal cells.³ The prognosis for pleomorphic adenoma is favorable with cure rates reaching 95%.1 Malignant transformation occurs in 3%–4% of cases, with the risk increasing in proportion to tumor duration.²
A canalicular adenoma is the third most common benign tumor of the minor salivary glands.4 It is often classified as a subtype of the broader category known as monomorphic adenomas, originally termed due to a uniform microscopic pattern.² A canalicular adenoma is an uncommon tumor, representing roughly 1%-3% of salivary neoplasms.4 These tumors demonstrate a high predilection for older female adults, with the highest prevalence occurring during the seventh decade of life.² Nearly 75% of canalicular adenomas occur in the upper lip, followed by the buccal mucosa and hard palate as the next most common locations.2,4 Clinically, this neoplasm presents as a painless, slow-growing mass ranging from a few millimeters to 2 centimeters in
size.2 Upon palpation, the mass may feel firm or slightly fluctuant with a mucosa colored or bluish hue. Histologically, the canalicular adenoma consists of columnar and cuboidal epithelial cells aligned in anastomosing cords within a vascularized stroma.4 These cords often enclose ductal structures, forming long canals and cystic spaces.2,4 The tumor is typically well circumscribed and encapsulated by fibrous tissue. The microscopic appearance demonstrates a monomorphic pattern, lacking stromal alterations that are seen in a pleomorphic adenoma.2 Definitive treatment for the canalicular adenoma involves local surgical excision.2,4 Recurrence is rare, occurring primarily in multifocal cases.2
A schwannoma is a rare, benign tumor of Schwann cell origin.2,5 Schwannomas account for just 5% of benign, soft tissue tumors, with approximately 45% of schwannomas occurring in the head and neck region.5 The lesion most commonly affects young and middleaged adults, typically presenting as a well-circumscribed, slow-growing, asymptomatic, solitary mass.2,5,6 The tumor usually arises in association with a nerve trunk, which is displaced as the lesion enlarges.2 Within the oral cavity, the tongue is the most common site, followed by the palate and buccal mucosa. In some cases, schwannomas may occur centrally within the mandible, where pain and paresthesia may be reported.6 Complete surgical resection with preservation of the originating nerve is the recommended treatment for these tumors and recurrence is low.2,5 Histologically, a schwannoma is encapsulated and can demonstrate two characteristic patterns: Antoni A and Antoni B.2 Antoni A consists of closely packed Schwann cells arranged in bundles or rows with elongated, palisaded nuclei surrounding
central eosinophilic, amorphous areas known as Verocay bodies.2,6 Antoni B tissue is less cellular and organized, composed of spindle cells that are widely separated and irregularly distributed.6 The tumor cells will show positive immunohistochemical reaction to s-100 protein.2 The prognosis following surgical excision is excellent, with rare recurrence and malignant transformation.6
A lipoma is a benign tumor of fat and represents the most common mesenchymal neoplasm.7 They typically occur on the trunk and proximal extremities, with oral involvement being rare, accounting for less than 4% of benign mesenchymal neoplasms.2,7 An oral lipoma usually presents as asymptomatic, soft, smooth, and fluctuant mass that may be sessile or pedunculated, with the overlying mucosa appearing normal or slightly yellow.2,8 The buccal mucosa and vestibule account for nearly 50% of intraoral cases, while less common sites include the lips, tongue, floor of the mouth, and palate.⁷ In extremely rare cases, they have been reported in the buccal fat pad.8 Lipomas generally occur in adults over the age of 40.2,7 Most studies report no sex predilection, although some note solitary lipomas are more common in women and multiple lipomas in men.2,8 Size does not usually exceed 3 cm, although variation may occur.8 Histologically, a lipoma consists of mature adipocytes arranged in lobules, resembling normal fat tissue.2,7,8 Variants include a fibrolipoma, angiolipoma, spindle cell lipoma, pleomorphic lipoma, and intramuscular (infiltrating) lipoma, all containing mature adipocytes with additional components as indicated by their names.2,7
The treatment of choice is local excision, with rare recurrence, although infiltrating lipomas have a higher risk of recurrence.²
Based on histopathologic examination, the definitive diagnosis for our case was a pleomorphic adenoma. At the 2-week follow-up, a small, non-tender lump was noted, consistent with normal healing. By the 1-month visit, the excision site had healed, with mild erythema and palpable scar noted. An intraoral photograph at that time (Figure 5) demonstrated complete healing with no signs of infection or dehiscence.
References
1. Almeslet AS. Pleomorphic Adenoma: A Systematic Review. Int J Clin Pediatr Dent. 2020;13(3):284-287. doi:10.5005/jp-journals-10005-1776
2. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 4th ed. Elsevier; 2016.
3. Kalwaniya DS, Meena R, Kumar D, Tolat A, Arya SV. A Review of the Current Literature on Pleomorphic Adenoma. Cureus. Published online July 22, 2023. doi:10.7759/ cureus.42311
4. Peraza A, Wright J, Gómez R. Canalicular Adenoma: A systematic review. Journal of Cranio-Maxillofacial Surgery. 2017;45(10):1754-1758. doi:10.1016/j.jcms.2017.07.020
5. Biswas D, Marnane CN, Mal R, Baldwin D. Extracranial Head and Neck Schwannomas—A 10-Year Review. Auris Nasus Larynx. 2007;34(3):353-359. doi:10.1016/j. anl.2007.01.006
6. Martins M, Anunciato de Jesus L, Fernandes KS, Bussadori S, Taghloubi S, Martins MA. Intra-Oral Schwannoma: Case report and Literature Review. Indian Journal of Dental Research. 2009;20(1):121-125. doi:10.4103/0970-9290.49059
Figure 5. Clinical photograph at one month follow-up. Complete healing noted.
7. Naruse T, Yanamoto S, Yamada SI, Rokutanda S, Kawakita A, Takahashi H, Matsushita Y, Hayashida S, Imayama N, Morishita K, Yamashita K, Kawasaki G, Umeda M. Lipomas of the oral cavity: clinicopathological and immunohistochemical study of 24 cases and review of the literature. Indian J Otolaryngol Head Neck Surg. 2015;67(1):67-73. doi:10.1007/ s12070-014-0765-8
8. D’Agostino S, Valentini G, Dolci M. Lipoma of the buccal fat pad: Systematic review and report of a case. Oral Surg. 2025; [Epub ahead of print]. doi:10.1111/ors.12996
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/MemberResources/TDA-Classified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN (ID #745): Established, 2-location GD practice in the Austin area. The practice serves a large, diverse, FFS/ PPO patient base with excellent new patient flow, a combined 14 equipped operatories across both locations (with substantial room for expansion at one of the locations). The practice comes fully equipped with digital radiography, digital sensors, digital scanners, digital pano, CBCT, and paperless charts. AUSTIN (ID #749): Established GD office located in the heart of central Austin. The practice has an impeccable online reputation in the community and features a strong hygiene recall program with multiple avenues for future growth. 3,000+ sq ft office, 4 active operatories, ample room for expansion, equipped with a digital scanner, intra oral cameras, digital X-ray sensors, and paperless charts. AUSTIN (ID #762): Established GD office in the heart of central Austin with a majority PPO patient base, 1000+ active patients, a robust hygiene recall program, and a strong reputation online and in the community they serve. The 1,500 sq ft office space contains 3 total operatories, computers throughout, a digital X-ray scanner, and intra-oral cameras. The practice has consistently generated revenue of mid-6 figures with abundant upside opportunities to expand production/cash flow through launching strategic marketing and advertising initiatives,
driving new patient flow, and offering additional advanced procedures in-house. HOUSTONSOUTH (ID #682): Established, multi-specialty dental office in a suburb about 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose.
SAN ANTONIO-TX HILL COUNTRY (ID #685):
Well-established dental practice and real estate nestled in the hill country north of San Antonio. The office relies mostly on word-of-mouthreferrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023, and the trend continued into 2024. SAN ANTONIOEAST (ID #716): Legacy GD practice and real estate in a rural community east of San Antonio. The large office space offers ample room for expansion and features 5 fully equipped operatories with computers in each op, digital
X-ray sensors, a digital pano, a digital scanner, intraoral cameras and paperless charts. This practice has strong profit margins and serves a large, multi-generation 100% FFS patient base.
SOUTH TEXAS COAST (ID #754): Exceptional GD practice located in a serene coastal town. Rare opportunity to acquire a thriving, wellestablished business in an underserved area with consistent collections of 7 figures with a primarily FFS active patient base and strong new patient flow. Hygiene production is robust, having exceeded 25% each of the last 3 years. The spacious, modern facility is outfitted with
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
PRACTICE SALES
DSO C S
PRACTICE APPRAISALS
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com
www.dentaltransitions.com
classifieds
state-of-the-art technology and is also available for purchase. The owner will be retiring at some point over the next few years but is available to stay for a transition of the buyerís preference. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@ dentaltransitions.com.
CENTRAL TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural four operatory dental practice for sale in the heart of the beautiful Texas hill country. This all-digital practice with a new pano produces mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@gmail. com for more information and showings.
DALLAS: Thriving north Texas OMS practice for sale: 3 surgical suites, 2 consult rooms, and 40 new patients/month, 7 figures in collections and SDE, and real estate available. Established 20+ years with minimal advertising. Within
150 miles of Dallas. Contact PTS to learn more: bailey@professionaltransition.com—Ref #TX30625.
HOUSTON: General dental practice for sale in east Houston, just 15 miles from downtown. This thriving, 7-op practice averages 45ñ50 new patients per month and generates high-6 figures in collections with mid-6 figures in true take-home. The owner seeks a full transition post-sale. Ideal for a dentist or group seeking growth in a rapidly developing suburban corridor. Reference #HWT71425. Email, bailey@ professionaltransition.com.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.