CARMEN SMITH, DDS, MBA 2025 GOLD MEDAL FOR DISTINGUISHED SERVICE AWARD WINNER
NICOLE SCOTT, MANAGING EDITOR
467
ASK THE POWERS CENTER
BRITTANY MOLETA, DDS
MARY YOUNAN-RAOUF, DDS, MPH
MENTOR: MARIA GONZALEZ, DDS, MS GUEST EDITOR RADE D. PARAVINA, DDS, MS, PHD
468
GENERALIZED PULP STONES IN A 44-YEAR-OLD FEMALE PATIENT WITH A HISTORY OF STEREOTACTIC RADIATION: A CASE REPORT AND LITERATURE REVIEW
SIMA HABRAWI, DDS, MBA (MAIN AUTHOR) SHEILA YAGHMAI, DDS, MPH (PRIMARY INVESTIGATOR) MOHAMMED HUSAIN, DDS THE UNIVERSITY OF CALIFORNIA, LOS ANGELES, SCHOOL OF DENTISTRY
476
THE TDA MEETING PREVIEW
SPEAKER: ALEXANDRA OTTO, DDS, FAGD, FACD, FPFA, FICD
480
TEXAS MISSION OF MERCY, INC. 2025 ANNUAL REPORT
488
TDA SMILES FOUNDATION 2025 ANNUAL REPORT
490 FBI: FOUND BUT NOT IDENTIFIED (YET)
KATHLEEN A. KASPER, DDS, D-ABFO
What’s the big difference between purchasing insurance through TDA Financial Services Insurance Program and somewhere else? TDA members own the agency!
You’ll always have attentive customer service from a team dedicated to making insurance easier for TDA members and staff.
Beginning Nov. 1:
2026 Rates Are Available, Open Enrollment Begins. Review, compare, and buy health insurance through the portal at tdamemberinsure.com.
Special Enrollment for New Small Groups Begins. If you sign up during special enrollment, mandatory employer contribution towards employee premiums—and other requirements—are waived. Small group plans are less expensive than unsubsidized individual plans and enable you to have a PPO.
or learn
As a TDA member, you now have access to a new healthcare member benefit that utilizes a national PPO
Coverage cannot be denied.
Members can enroll THE FIRST DAY OF ANY MONTH with open enrollment. Enrollment needs to be completed no later than 30 days in advance.
or learn
for TDA Members
As dental insurance companies continue to lower reimbursement rates and more Americans are losing or not renewing their insurance, dental membership plans are emerging as a necessary solution for practices.
With DentalHQ, you can bring in more revenue per patient and create consistent, predictable revenue.
Managing plans is unbelievably easy because DentalHQ is automated. Your staff won’t have to spend time on payment collection, patient communication, and enrollment.
Create flexible plans that include services you wish to include andbcharge what you want to charge.
Nicole Scott, Managing Editor
467 ASK THE POWERS CENTER
Brittany Moleta, DDS
Mary Younan-Raouf, DDS, MPH
Mentor: Maria Gonzalez DDS, MS
Guest Editor Rade D. Paravina, DDS, MS, PhD
468 GENERALIZED PULP STONES IN A 44-YEAR-OLD FEMALE PATIENT WITH A HISTORY OF STEREOTACTIC RADIATION A CASE REPORT AND LITERATURE REVIEW
Sima Habrawi, DDS, MBA
Sheila Yaghmai, DDS, MPH
Mohammed Husain, DDS
476 THE TDA MEETING PREVIEW
SPEAKER: Alexandra Otto, DDS, FAGD, FACD, FPFA, FICD
480 TEXAS MISSION OF MERCY, INC. 2025 ANNUAL REPORT
488 TDA SMILES FOUNDATION 2025 ANNUAL REPORT
490 FBI: FOUND BUT NOT IDENTIFIED (YET)
Kathleen A. Kasper, DDS, D-ABFO
HIGHLIGHTS
464 In Memoriam
496 Value for Your Profession: Staffing in a Competitive Market: How to Attract and Retain the Best Dental Talent
500 Classifieds
503 Index to Advertisers ,
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 142 | No. 8
Texas Dental Journal (ISSN 0040-4284) is published monthly, except January-February, March-April, July-August, and November-December, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2025 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement at tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available):
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and 4
Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
Board
PRESIDENT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PRESIDENT-ELECT Elizabeth Goldman, DDS 214-585-0268, texasredbuddental@gmail.com
PAST PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
VICE PRESIDENT, SOUTHEAST Matthew J. Heck, DDS 512-280-8800, matthewjheckdds@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN**
Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR** Jacqueline M. Plemons, DDS, MS 214-507-0815, drplemons@yahoo.com
LEGAL COUNSEL** Carl R. Galant
INTERIM EXECUTIVE DIRECTOR** Lee Ann Johnson, CAE 512-443-3675, ljohnson@tda.org
*Non-voting member **Non-voting
Malpractice insurance that’s all about you .
As a dentist, you face unique challenges every day. That’s why at MedPro Group, we created an industry-leading malpractice policy that keeps you safe. Here’s what else you can expect with MedPro on your side.
Get unmatched coverage. Practice more safely. Protect your good name.
You’ll get great coverage at a great price. We also offer policy options that others don’t — including Occurrence and a pure consent clause, which gives you more control during a claim.
With 24/7 access to our free risk resources and on-staff experts, you and your practice will be better prepared for every day challenges. We don’t just defend claims, we help you avoid them.
The average dentist is sued at least once in their career, which is why we’re in your corner when it matters most. We lead the industry with a 95% dental trial win rate (plus 8 out of 10 claims close without payment).
CARMEN SMITH, DDS, MBA
2025 Gold Medal for Distinguished Service Award Winner
By Nicole Scott, Managing Editor
Drs Alicia Gray, Smith, and Ashla Martin.
Pictured at the TDA House of Delegates are Drs Eva Boldridde, Tameka Nickleberry, and Smith.
Members of the Dallas County Dental Society (District 5).
Are you following your Personal Legend? If you have read The Alchemist by Paulo Coelho, you know that your Personal Legend is your true purpose in life, and once you determine it and commit to its pursuit, the universe helps orchestrate it into place.
The Alchemist happens to be one of Dr Carmen Smith’s favorite books, and one could say that dentistry is her Personal Legend. Dr Smith was awarded the TDA’s highest honor, the 2025 TDA Gold Medal for Distinguished Service, at the House of Delegates in May.
Akin to Santiago’s quest in the book, Dr Smith has taken her life’s journey into her own hands to manifest her dream, which is right where she started—in Dallas.
“I am actually not sure where the inspiration came from; however, from the 11th grade, I decided I wanted to become a dentist or medical doctor,” says Dr Smith. “While both fields would afford me the opportunity to fulfill my desire to make the community healthy, dentistry seemed to provide more flexibility and autonomy when wanting to have a career, a family, and own a business.”
She is the 29th recipient of the prestigious award, the Association’s highest honor. “Receiving this award was a means to pay homage to those who paved the way for
Drs Eva Boldridge and Smith at the TDA Leadership Institute.
TDA Past President Dr Georganne McCandless and Dr Smith.
TDA Leadership Institute participants gather for dinner in Rockwall, Texas.
DCDS Executive Director Jane Evans (front), Dr Carmen Smith (back) TDA Director of Member Services Lee Ann Johnson and Dr Jodi Danna of Dallas enjoy time together in San Antonio.
Drs Duc Ho and Smith.
me to be a part of this incredible profession,” says Dr Smith. “God, ancestors, parents, friends, teachers, professors, colleagues, mentors, patients, and the community all played a role in shaping who I am today, and receiving the Gold Medal award meant that their work and my work has made a difference.”
Dr Smith graduated from Baylor College of Dentistry in 1996 and started her practice, Smith Family Dentistry, 24 years ago, which she says is her proudest accomplishment. “I have built long lasting relationships and friendships with patients and mentored high school, college, and dental students,” says Dr Smith.
Being a dentist and business owner have allowed her to make an impact on her community. One of Dr Smith’s patients is an assistant district attorney for Dallas County who works with women and girls who are trafficked or incarcerated. Now, Dr Smith uses her office to provide free dental services to some of those women through a recovery program.
“Through my partnership with the Dallas DA’s office, I provide free services to women who are recently released from incarceration, helping them to reengage with society with more confidence. This and a host of other philanthropic endeavors were made possible because of Smith Family Dentistry.”
Born and raised in Dallas with her brother Carlton, her parents were both elementary educators—mom Eretta was a second-grade teacher, and dad Cecil taught social studies and was the PE coach. She credits her dad for sparking her interest in gymnastics and sometimes serving as her coach. Carlton is now her office manager, and staying close to her family is important. “Dallas is home...I am very close to my family and knew that I would probably have a patient base already when I opened my practice.”
Growing up Dr Smith was a gymnast and played soccer, which she continued to do as an adult until she was sidelined by injury. She was on the drill team and worked as a math consultant in high school, and like a lot of teenagers her age, she loved New Edition and volunteered through her church.
Dr Smith’s favorite hobby is traveling, and she has lately taken up golf. She’s a foodie and an avid reader, and although she loves a good fiction novel
Dr Smith is pictured with students from Great Expectations at TAMU College of Dentistry.
ADA 15th District Delegation Women in Leadership Reception.
Pictured at the Southwest Dental Conference Chairman’s Dinner are Dr Cody Graves, Dr Jodi Danna, Dr Georganne McCandless, Dr Rich Potter, Mrs Linda Brady (former TDA executive director), Dr Smith, and Dr Drew Vanderbrook.
by Grisham, Patterson, or McFadden, her favorite books are The Purpose Driven Life, Who Moved My Cheese?, The Let Them Theory, and The Alchemist, which she says is one of the best “life” books.
The book’s message is that everyone has a unique purpose in life: “To realize one’s destiny is a person’s only real obligation.”
Dr Smith’s has been one of leadership and involvement in organized dentistry. She is a past TDA treasurer and member of the TDA Board of Directors and has served on many committees and councils. At the American Dental Association, she was a member of the Council on Membership, Committee for Continuing Education, and the Institute for Diversity in Leadership, and she was a 15th District delegate and currently is an alternate delegate. Locally, she served as the Dallas County Dental Society president, chair of the Southwest Dental Conference, and developed the Diversity and Inclusion committee.
“Serving and volunteering have always been a part of my makeup. When I was first asked to serve in organized dentistry by Dr Danette McNew, it was with the Southwest Dental Conference. It was a great experience and allowed me to meet and get to know more of my colleagues in the Dallas area,” says Dr Smith. “As I continued to participate and show a genuine interest in our organization, I was asked to take on more leadership roles, of which I gladly accepted. With each role, I feel like my leadership skills grew because I was becoming more aware of who I was and my capabilities. I felt like my voice was needed, and my voice was being heard.”
In her community, she is a member of the Delta Sigma Theta Sorority, Inc., the Dallas Black Chamber of Commerce, the Village Giving Circle, Attitudes and Attire, and Concord Church. She has previously been a member of the Junior League of Dallas, the Dallas Running Club and served as a CASA Volunteer.
Dr Smith’s high school goal to become a dentist came true and has paid off in dividends. As Coelho famously wrote, “It’s the possibility of having a dream come true that makes life interesting...”
and Wayne Woods.
About the Gold Medal Presentation
Owing to its stature, the TDA president presents the award before the House of Delegates. The name of the recipient is not revealed to anyone, including the recipient, until the actual presentation takes place. The Awards Committee works behind the scenes with the recipient’s family members to make sure they are in attendance without alerting the recipient. In 2006 the TDA commissioned nationally renowned Texas artist Ronadró to design a unique award piece to represent the Association. The result is a beautiful bronze relief depicting a dentist caring for a patient. This sculpture was adopted for the Gold Medal award in 2008. Inset into the shadowbox are custom designed medallions: the TDA seal and the gold medal.
About the Past Recipients
To date, there have been 28 previous recipients of the Gold Medal: Drs John D. Wilbanks, Michael D. Vaclav, O.V. Cartwright, H.M. “Mit” Sorrels, Jack H. Harris, James E. Bauerle, Robert V. Walker, Frank K. Eggleston, Robert M. Anderton, Rene M. Rosas, Richard M. Smith, Sam W. Rogers Jr, Stephen F. Schwartz, John S. Findley, S. Jerry Long, Patricia L. Blanton, Paul E. Stubbs, Richard C. Black, Michael L. Stuart, Hilton Israelson, Thomas Harrison, J. Preston Coleman, Larry W. Spradley, Rita M. Cammarata, John Purdy, Jacqueline M. Plemons, Rise’ Martin, and Craig Armstrong. By the judgment of their colleagues, they represent the best of the TDA; dentists who have dedicated their lives to the Association and profession, and have advanced both through their commitment, strength, and vision.
Dallas County Dental Society Executive Director Jane Evans and Drs Jodi Danna, Smith,
Luis O. Regueira, Sr., D.M.D.
Asra S. Hashmi, D.D.S. and has acquired the practice of Cleveland, Texas
Practices For Sale
FANTASTIC PLANO RETAIL LOCATION: Well-established 4-op general practice in excellent condition, located in a highly visible retail center. Open 7 days a week, the office is run by the owner and a part-time associate, providing both routine dental care and emergency services. The practice has over 1,750 active patients (approximately 20% FFS, 70% PPO, and less than 10% Medicaid) and produced $784,000 in the past year. Opened just over six years ago, this practice offers great potential for growth by building on the strong patient base and expanding available services. Opportunity ID: TX-02650
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Very real opportunity for growth by adding: a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02656
Alexandre R. Canevet, D.D.S.
Benjamin C. Edmunds, D.D.S.
Zayd M. Hashmi, D.M.D. has acquired the practice of Frisco, Texas
We are pleased to have assisted in these transitions.
David Mark Chapman Corpus Christi
9/27/1952–8/28/2025
Good Fellow: 2003 Life: 2017
Owen Dee Dillard McKinney
6/25/1935–9/6/2025
Good Fellow: 1992
Life: 2000
Fifty Year: 2017
William Paul Bennett
Sulphur Springs
4/12/1944–9/13/2025
Good Fellow: 1999
Life: 2009
Fifty Year: 2020
Ronald Treman Oglesby Ennis
9/5/1946–9/16/2025
Good Fellow: 1998
Life: 2011
Fifty Year: 2022
Rural West Texas – PRIME GROWTH OPPORTUNITY: 2,000 sq. ft. fully digital GP with 4 equipped ops and over 2,500 active patients. Grossing $789K, the practice currently runs just 3–3.5 days per week without a hygienist, leaving immediate room for growth. Patient base is primarily PPO with some FFS and Medicaid. Ideal for a hands-on owner ready to expand services and capture significant upside. Opportunity ID: TX-02692
REAL ESTATE AVAILABLE – SOUTHWEST OF ODESSA: 2,000 sq. ft. GP in converted residence with 3 ops (room to expand). $631K gross, 2,600+ active patients (mostly PPO, 25% FFS, 7% Medicaid). Eaglesoft, digital X-rays, Pano. No hygienist—strong growth potential. Opportunity ID: TX-02693
Go to our website or call to request information on other available practice opportunities!
Gregory Lee Baber
Uvalde
6/19/1948–9/24/2025
Life: 2019
James Henry Atkinson
Fort Worth
5/27/1930–9/8/2025
Good Fellow: 1989
Life: 1995
Fifty Year: 2014
John Levi Estes III
Abilene
4/8/1951–9/26/2025
Good Fellow: 2001
Life: 2016
Vencen Wayne McEntire
Amarillo
9/24/1948–9/24/2025
Good Fellow: 2001
Life: 2013
Fifty Year: 2025
Robert P Kennedy Jr
Kerens
10/19/1928–9/25/2025
Good Fellow: 1988
Life: 1996
Fifty Year: 2013
Jack Joseph Tucker
Dallas 7/23/1929–10/5/2025
Life: 1994
Fifty Year: 2010
Thomas Michael Riggs
Bryan 4/23/1947–10/11/2025
Good Fellow: 1999
Life: 2012
Fifty Year: 2024
Justin Carter Ramsey Spring 7/21/1983–10/21/2025
John Robert Goad
Irving 10/16/1930–9/01/2025
Good Fellow: 1982
Life: 1995
Fifty Year: 2008
Thomas W Daniels
Conroe 12/3/1945–9/22/2025
Good Fellow: 1998
Life: 2010
Guest Editor Rade D. Paravina, DDS, MS, PhD
Prosthetic Alternative to Restoring Facially Angulated Implants in the Anterior Esthetic Zone
Brittany
The purpose of this case report is to describe a novel approach to restoring challenging implant angulations in the esthetic zone. This method aims to optimize esthetics, retrievability of the screw channel, and biologic outcomes.
Case Report
This case involves a 55-year-old female patient presenting with healing abutments on osseointegrated implants #7 and #8 with a distofacially angulated implant #7 (Figure A). Following diagnostic casts and clinical evaluation, it was determined that the restorative options were limited. Screwretained implant provisional restorations were fabricated in the laboratory and carefully modified chairside over time until proper soft tissue contour was achieved (Figure B). To avoid a fully cement retained restoration that may later cause biologic concerns or an angled screw channel restoration that often experiences screw loosening, a zirconia custom abutment with a lithium disilicate veneer to plug the screw access channel was chosen as the alternative option for this
patient (Figure C and D).
Outcome
The final restorations were fabricated to closely match the existing shade and contours of the adjacent teeth. The patient elected not to veneer the remaining maxillary anterior dentition, prioritizing a natural appearance over complete elimination of the black triangles and perfect shade uniformity. The zirconia custom abutments were fabricated in 3Y-TZP zirconia for both increased strength and to mask the underlying gray hue of the titanium portion of the abutments (Figure D). The veneer segment of the restoration was fabricated in lithium disilicate for
enhanced esthetics and translucency (Figure C) with a 0.5mm subgingival margin. Also incorporated into the design of the veneers was a post or plug that served as both a block out for the screw access channel and as a prosthetic positional feature during intraoral cementation.
This restorative method resulted in an esthetically acceptable outcome and a satisfied patient. Clinically, it decreases the chances of biologic peri-implant health concerns due to excess cement that might be seen in a fully cement retained restoration, allows the provider to preserve the custom abutment by simple veneer removal in the future, and more friendly screw channel retrievability.
Conclusions
In conclusion, when the restorative dentist is presented with an esthetic challenge due to improperly angulated implants in the anterior esthetic zone, a veneered custom zirconia abutment can be considered as an effective alternative to a fully cement retained restoration.
Moleta, DDS; Mary Younan-Raouf, DDS, MPH. Mentor: Maria Gonzalez DDS, MS
Figure A: Distofacially angulated implant #7 and facially angulated implant #8; Figure B: Soft tissue contours following provisional period; Figure C: Lithium disilicate veneer plugs; Figure D: Zirconia custom abutment; Figure E: Final restorations. A
B
Generalized pulp stones in a 44-year-old female patient with a history of stereotactic radiation
A case report and literature review
Sima Habrawi, DDS, MBA (main author)
Sheila Yaghmai, DDS, MPH (primary investigator)
Mohammed Husain, DDS
University of California, Los Angeles, School of Dentistry
Abstract
Pulpal calcifications, also known as pulp stones, appear radiographically as dense, radiopaque masses. Several correlations have been made between pulp stones in teeth and systemic disorders like diabetes, hypertension, hyperlipidemia, and ischemic heart disease. At times, generalized pulp calcifications may also be a manifestation of an underlying genetic condition, as in dentin dysplasia or dentinogenesis imperfecta. Overall, very few reports exist on generalized pulp calcifications affecting most or the entire dentition. This case report adds to the literature by describing a case of generalized pulp stones in a patient with a history of Stereotactic Radiation Therapy (SRT) to treat cerebral arteriovenous malformation, suggesting a potential role of head and neck radiation therapy in the genesis of pulp stones. A literature review is also included discussing the etiology of pulp stones and their correlation to underlying systemic conditions.
Professional Program for International Dentists graduate UCLA School of Dentistry
Sheila Yaghmai, DDS,MPH
Assistant Clinical Professor Section of Interdisciplinary Dentistry
UCLA School of Dentistry
Mohammed A. Husain, DDS
Associate Clinical Professor Section of Oral and Maxillofacial Radiology
UCLA School of Dentistry
Sima Habrawi, DDS, MBA
Sheila Yaghmai, DDS, MPH
Mohammed Husain, DDS
Introduction
Pulpal calcified structures, often known as denticles, pulp stones, or dystrophic calcification, have been studied for over a decade. These discrete calcified structures are observed in the coronal or, less frequently, radicular pulp cavity of teeth; with a prevalence ranging from 8–90%, depending on the study type, design, and radiographic technique employed. They appear radiographically as dense, radiopaque masses.1,2
Pulp calcifications can be found in the dental pulp of teeth in the primary or permanent dentition; and can be detected in sound, infected or even impacted teeth. They can be embedded, attached to dentin walls or free within the pulp tissue.3 A single tooth may have from 1 to 12 or even more calcifications, with sizes varying from minute particles to large masses that occlude the pulp space completely; which greatly complicates root canal treatments.4 According to the literature, pulp calcifications occur more frequently in the pulp chamber rather than radicular pulp, and more frequently in maxillary teeth than in the mandibular teeth. They also occur most commonly in molars.5-7
The formation of pulpal calcifications is not completely understood. However, several factors have been implicated in their formation; including but not limited to impaired pulpal blood supply, chronic irritation from deep caries, fillings, or abrasion, and genetics. Pulpal obliteration from pulp stones is most often caused by trauma , orthodontic treatment, or transplantation.8-11 Some studies did not find any difference in pulp calcification occurrence between genders, while others found females to be more prone to their formation.12-16
We present a rare case of generalized pulp stones in a patient with a history of stereotactic radiation therapy (SRT) for cerebral arteriovenous malformation. The pulp calcifications were distinctly visualized on both intraoral radiography and cone beam computed tomography (CBCT). We further discuss the clinical significance of pulp stones and their implications for root canal treatment.
Pulp calcifications can be found in the dental pulp of teeth in the primary or permanent dentition; and can be detected in sound, infected or even impacted teeth.
Case report
A 44-year-old female patient presented to the general dentistry clinic at the University of California, Los Angeles with a chief complaint of wanting to replace her missing posterior teeth. Her last dental visit was more than 10 years ago. Past medical/surgical history was significant for right sided brain arteriovenous malformation (AVM), seizure disorder secondary to the AVM, stroke, endometrial cancer, and an SRT regimen of 30 Gy in 5 fractions over the span of 6 years. On extraoral examination, the patient reported non-painful clicking on the right temporomandibular joint with mild tenderness of the masseter muscles bilaterally. Intraoral
Radiographic examination:
examination revealed multiple moderately deep carious lesions, abrasion and attrition on the posterior molars and a non-restorable upper right first molar.
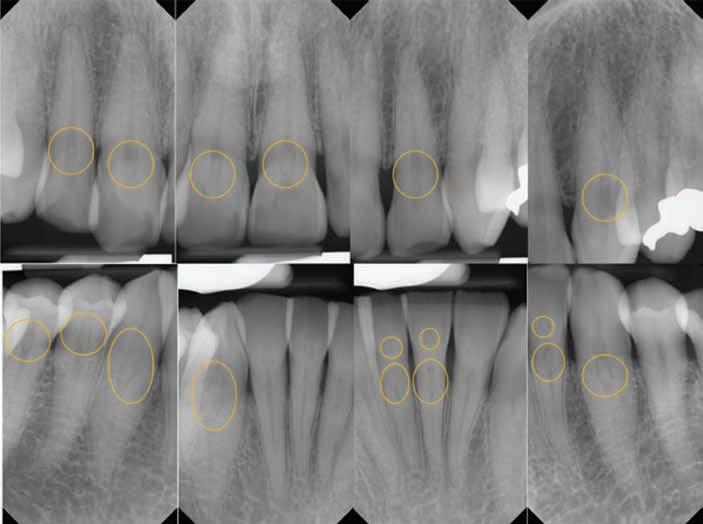
Her full mouth intraoral radiographs revealed generalized pulpal calcifications of various dimensions in the pulp chambers and root canals. In at least one tooth, multiple discrete pulpal calcifications were observed. All teeth with existing pulpal calcifications were asymptomatic, and did not show any radiographic signs of periapical bone loss or periodontal ligament (PDL) widening.
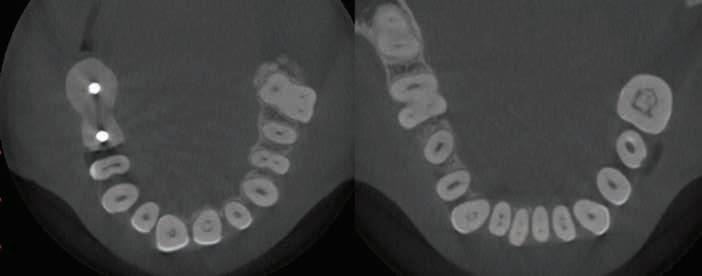
Figure 1. Full mouth radiographic survey reveals multiple pulpal calcifications of various dimensions affecting the pulp chamber and radicular pulp of patient’s remaining dentition.
Figure 2. Full mouth radiographic survey reveals multiple pulpal calcifications of various dimensions affecting the pulp chamber and radicular pulp of patient’s remaining dentition. Multiple discrete pulpal calcifications can be noted on upper left first molar pulp chamber.
Figure 3. Mounted casts showing lack of posterior support in the upper right side, anterior attrition and crowding.
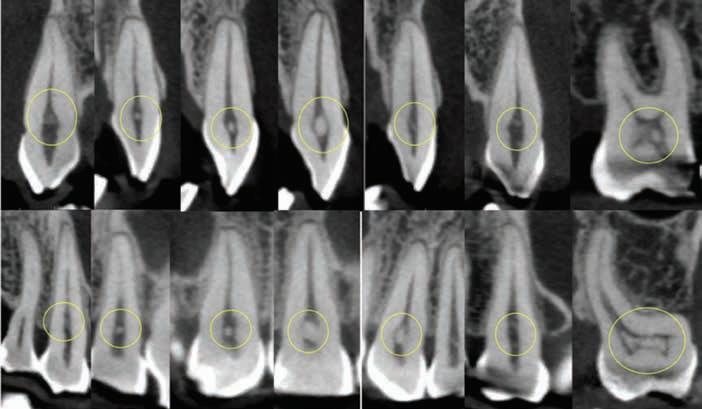
showing distinct pulp stones in canals of teeth #8, 9, 19, 23, 24,
4B. 8X8 CM MORITA ACCUITOMO 170 CONE BEAM CT SCAN—Sagittal and coronal view showing distinct pulp stones in canals of teeth #6, 7, 8, 9, 10, 11, 14. Multiple stones are noticed in the pulp chamber of 14.
While isolated pulp calcifications or pulp stones are a common incidental radiographic finding, the presence of generalized pulpal calcification is relatively rare and raises concerns about underlying systemic or metabolic disorders. To investigate this further, we conducted a review of the literature to assess the potential significance of our finding.
One might hypothesize that pulpal calcifications are a type of age-related degenerative change. However, there has been no correlation between age and the prevalence of pulpal calcifications.16,17 Given the absence of such correlations and the middle age of our patient, it is not likely be a factor in our case. Several studies, however, have reported a higher prevalence of pulp calcifications in females, suggesting that the sex of our patient is relevant to the development of this dental finding.18,19
A correlation between statins and pulp calcifications was noted by Pettiette et
al.20 Another case of generalized pulp canal obliteration was reported in 2022 by Jiandong et al. in a patient on longterm glucocorticoids.21 However, our patient has no history of medications associated with the formation of pulp stones.
Studies have demonstrated a correlation between pulp calcification and nephrolithiasis, hypertension, hyperlipidemia, and diabetes mellitus.22-24 Furthermore, a positive correlation between pulp stones and Ischemic Heart Diseases (IHD) has been suggested, highlighting a potential medical significance of this finding and a possible benefit for further workup to detect latent IHD.25 Nevertheless, the patient’s history was not significant for any of these conditions known to have a correlation with pulp stones.
At the ultrastructural level, several studies on pulp stones have highlighted similarities between these calcifications and those found in various other tissues throughout the body. Cardiac researchers have established that calcium phosphate
crystals contribute to inflammation in the arteries and play a significant role in acute myocardial infarctions (MIs), which can lead to sudden death.26 Ninomiya et al. reported an even distribution of type I collagen in pulp stones, while osteopontin was identified as playing a crucial role in the calcification process, particularly in the peripheral regions of the stones.25 Similarly, Hirota et al. found osteopontin in their immunohistochemical study of atherosclerotic plaques and urinary stones.27 This suggests a potential relationship between the formation of pulp stones and the calcifications observed in other tissues, such as arterial plaques, renal calculi (nephrolithiasis), gallstones (cholelithiasis), and various degenerative joint diseases (DJDs). This connection supports the hypothesis that pulp stones may be part of the broader systemic biomineralization process affecting multiple tissues throughout the body. The incidental finding of pulp stones in routine radiographic examinations at dental clinics could be considered an indication for further workup to detect latent IHD.
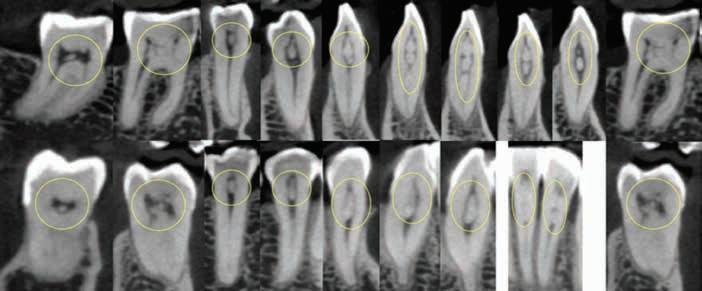
Figure 4C. 8X8 CM MORITA ACCUITOMO 170 CONE BEAM CT SCAN—Sagittal and coronal view showing distinct multiple pulp stones in canals of teeth #19, 22, 23, 24, 25, 26, 30. Single stones noticed in #27, 28, 31.
While numerous reports have addressed pulp calcifications, there are only a few that focus on generalized pulp calcifications affecting the majority or entire dentition, as these cases are rare. The differential diagnosis in such rare cases may include genetic disorders such as dentin dysplasia type II, Saethre-Chotzen syndrome, Ehlers-Danlos syndrome, and Otodental syndrome.28-31 However, our patient does not fit the diagnostic criteria of any of these genetic conditions.
Bahetwar Et al. reported generalized pulp stones found radiographically in a non-syndromic 13-year-old female; suggesting this unusual case may be of idiopathic origin.17 Our patient was evaluated for any syndromic or genetic involvement, but it was noncontributory.
Our patient’s medical history was significant for a cerebral arteriovenous malformation (AVM) on the right side of her brain. While the exact pathogenesis of AVM lesions remains poorly understood, they are primarily characterized by an abnormal connection between an artery and a vein, which can be either congenital or acquired. The consequences of AVMs can range from cosmetic issues to lifethreatening complications. As a result, several treatment options are available, including conservative management, open surgery, radiation (either as a single-stage or multistage procedure), and embolization.32 SRT doses for brain AVMs typically range from 16 to 25 Gy, with 16 Gy resulting in an obliteration rate of approximately 70%.33 Our patient underwent embolization procedures along with an SRT regimen of 30 Gy in 5 fractions over the span of 6 years.
Numerous studies have reported that radiation therapy can affect dental tissues, including promoting the formation of pulp stones. For example, the study by Vier-Pelisser et al. (2007) showed that fractionated teletherapy (radiotherapy) can induce nuclear alterations in the dental pulp tissue of rats, which may play a role in pulp stone formation.34 Furthermore, a systematic review by Weissheimer et al. (2022) highlighted that radiotherapy for head and neck cancer causes significant changes in pulp responses, potentially leading to the development of pulp stones.35 Tunc et al. found that the prevalence of pulp stones was notably higher in patients who underwent radiotherapy in the head and neck region compared to healthy individuals who did not receive radiation. As a result, patients receiving radiation in these areas are at an increased risk for developing pulp stones. It is recommended that these patients undergo a thorough dental examination for pulp stones before starting root canal treatment.36
Stereotactic radiation therapy (SRT) differs from conventional head and neck radiation in that it targets relatively small volumes with high doses per fraction, typically delivered in 1 to 5 sessions.37 To date, there is no substantial evidence directly linking SRT with the formation of pulp stones. Although a definitive or strong correlation between SRT and pulp stone formation has not been established, radiation’s impact on tissue calcification and chronic inflammation may create conditions that could contribute to pulp stone development. This case of a patient with generalized pulp stones detected following SRT suggests a possible link between the 2.
While the exact pathogenesis of AVM lesions remains poorly understood, they are primarily characterized by an abnormal connection between an artery and a vein, which can be either congenital or acquired.
From a clinical perspective, pulp stones typically do not have a significant impact on pulp vitality unless they are large enough to compress blood vessels and nerves. Therefore, a tooth with pulp stones can still be considered vital despite their presence.36 In most cases, pulp stones are incidental findings on dental radiographs and do not require specific treatment, unless they interfere with a planned dental procedure, such as a root canal treatment (RCT). In such cases, advanced imaging with CBCT may offer utility in visualizing the full extent of pulp stones and/or pulpal calcification with its high resolution and ability to overcome anatomic superimposition. During RCT, pulp stones can obstruct the file in a clear root canal, cause deformation of file tips, and hinder proper irrigation and disinfection, complicating the procedure and potentially leading to failure.37 While burs can be used to fragment large pulp stones, ultrasonic tips are generally preferred as they offer greater precision in breaking down calcified tissue while minimizing damage to surrounding tooth structure.38
Conclusion
We present a rare case of generalized pulpal calcifications affecting the entire dentition in a 44-year-old white female detected after receiving SRT to treat cerebral AVM. Given our patient’s absence of any known medical conditions, genetic syndromes, or medications linked to the formation of pulp stones, and given the pulpal alterations known to occur secondary to radiotherapy, we suggest that her history of SRT may be associated with her finding of generalized pulp stones. This case highlights the need for further investigation into the relationship between stereotactic radiotherapy and dental pulp calcifications, including further elucidation of physiological mechanisms, potential dose thresholds and time dependent effects.
Patient consent: Patient’s written consent was obtained.
Source of Support: Nil
Conflict of Interest: None declared.
References
1. Arys, A., C. Philippart, and N. Dourov, Microradiography and light microscopy of mineralization in the pulp of undemineralized human primary molars. J Oral Pathol Med, 1993. 22(2): p. 49-53.
2. Moss-Salentijn, L. and M. HendricksKlyvert, Calcified structures in human dental pulps. J Endod, 1988. 14(4): p. 184-9.
3. Goga, R., N.P. Chandler, and A.O. Oginni, Pulp stones: a review. Int Endod J, 2008. 41(6): p. 457-68.
4. Bevelander, G. and P.L. Johnson, Histogenesis and histochemistry of pulpal calcification. J Dent Res, 1956. 35(5): p. 71422.
5. Syryńska, M., M. Durka-Zajac, and J. Janiszewska-Olszowska, Prevalence and location of denticles on panoramic radiographs. Ann Acad Med Stetin, 2010. 56(2): p. 55-7.
6. Hsieh, C.Y., et al., The prevalence and distribution of radiopaque, calcified pulp stones: A cone-beam computed tomography study in a northern Taiwanese population. J Dent Sci, 2018. 13(2): p. 138144.
7. da Silva, E., et al., Assessing pulp stones by cone-beam computed tomography. Clin Oral Investig, 2017. 21(7): p. 2327-2333.
8. Sundell, J.R., H.R. Stanley, and C.L. White,
The relationship of coronal pulp stone formation to experimental operative procedures. Oral Surg Oral Med Oral Pathol, 1968. 25(4): p. 579-89.
9. VanDenBerghe, J.M., B. Panther, and T.G. Gound, Pulp stones throughout the dentition of monozygotic twins: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1999. 87(6): p. 749-51.
10. Delivanis, H.P. and G.J. Sauer, Incidence of canal calcification in the orthodontic patient. Am J Orthod, 1982. 82(1): p. 58-61.
11. Bauss, O., et al., Autotransplantation of immature third molars: influence of different splinting methods and fixation periods. Dent Traumatol, 2002. 18(6): p. 322-8.
12. Tamse, A., et al., Statistical evaluation of radiologic survey of pulp stones. J Endod, 1982. 8(10): p. 455-8.
13. al-Hadi Hamasha, A. and A. Darwazeh, Prevalence of pulp stones in Jordanian adults. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1998. 86(6): p. 730-2.
14. Sisman, Y., et al., The prevalence of pulp stones in a Turkish population. A radiographic survey. Med Oral Patol Oral Cir Bucal, 2012. 17(2): p. e212-7.
15. Çolak, H., et al., Assessment of the Prevalence of Pulp Stones in a Sample of Turkish Central Anatolian Population. The Scientific World Journal, 2012. 2012(1): p. 804278.
16. Alamoudi, R.A., et al., Assessment of the Correlation Between Systemic Conditions and Pulp Canal Calcification: A CaseControl Study. Cureus, 2023. 15(9): p. e45484.
17. Bahetwar, S.K. and R.K. Pandey, An unusual case report of generalized pulp stones in young permanent dentition. Contemporary Clinical Dentistry, 2010. 1(4): p. 281-283.
18. Turkal, M., et al., Incidence and distribution of pulp stones found in radiographic dental examination of adult Turkish dental patients. Ann Med Health Sci Res, 2013. 3(4): p. 572-6.
19. Kumar, P., et al., Prevalence of Pulp Stones in the Population of Rajasthan: A CrossSectional Study in a Tertiary Care Hospital. Cureus, 2024. 16(1): p. e51623.
20. Ideo, F., et al., The role of systemic statins in the inception and healing of apical periodontitis: a systematic review. BMC Oral Health, 2023. 23(1): p. 730.
21. Jiandong, B., et al., Generalized pulp canal obliteration in a patient on long-term glucocorticoids: a case report and literature review. BMC Oral Health, 2022. 22(1): p. 352.
22. Gabardo, M.C.L., et al., Association between Pulp Stones and Kidney Stones: A Systematic Review and Meta-analysis. J Endod, 2019. 45(9): p. 1099-1105.e2.
23. Jawahar, G., et al., Clinicopathological Correlation of Pulp Stones and Its Association with Hypertension and Hyperlipidemia: An Hospital-based Prevalence Study. J Pharm Bioallied Sci, 2021. 13(Suppl 2): p. S1268-s1274.
24. Srivastava, K.C., et al., Assessing the Prevalence and Association of Pulp Stones with Cardiovascular Diseases and Diabetes Mellitus in the Saudi Arabian Population-A CBCT Based Study. Int J Environ Res Public Health, 2020. 17(24).
25. S, N., et al., Pulp Stones: Diagnostic Significance in Early Diagnosis and Radiographic Correlation with Ischemic Heart Diseases. Indian J Radiol Imaging, 2021. 31(2): p. 277-283.
26. Aleksova, P. Dental Pulp Calcification in Patients with Cardiovascular Diseases : A Review. 2015.
27. Hirota, S., et al., Expression of osteopontin messenger RNA by macrophages in atherosclerotic plaques. A possible association with calcification. Am J Pathol, 1993. 143(4): p. 1003-8.
28. MK, O.C., W.K. Duncan, and T.M. Perkins, Dentin dysplasia: review of the literature and a proposed subclassification based on radiographic findings. Oral Surg Oral Med Oral Pathol, 1991. 72(1): p. 119-25.
29. Goho, C., Dental findings in SaethreChotzen syndrome (acrocephalosyndactyly type III): report of case. ASDC J Dent Child, 1998. 65(2): p. 136-7.
30. De Coster, P.J., L.C. Martens, and A. De Paepe, Oral health in prevalent types of Ehlers-Danlos syndromes. J Oral Pathol Med, 2005. 34(5): p. 298-307.
31. Kapferer-Seebacher, I., et al., Dental Manifestations of Ehlers-Danlos Syndromes: A Systematic Review. Acta Derm Venereol, 2020. 100(7): p. adv00092.
32. Naranbhai, N. and R. Pérez, Management of Brain Arteriovenous Malformations: A Review. Cureus, 2023. 15(1): p. e34053.
33. Patibandla, M.R., et al., Effect of treatment period on outcomes after stereotactic radiosurgery for brain arteriovenous malformations: an international multicenter study. Journal of neurosurgery, 2018. 130(2): p. 579-588.
34. Vier-Pelisser, F.V., et al., The effect of head-fractioned teletherapy on pulp tissue. International Endodontic Journal, 2007. 40(11): p. 859-865.
35. Weissheimer, T., et al., Head and neck radiotherapy effects on the dental pulp vitality and response to sensitivity tests: A systematic review with meta-analysis. Int Endod J, 2022. 55(6): p. 563-578.
36. Tunç, F. and K. Yılan, Radiographic Assessment of Pulp Stone Prevalence in Patients Undergoing Head and Neck Radiotherapy. ADO Klinik Bilimler Dergisi, 2024. 13(3): p. 490-495.
37. Song, C.W., et al., Biological Principles of Stereotactic Body Radiation Therapy (SBRT) and Stereotactic Radiation Surgery (SRS): Indirect Cell Death. International Journal of Radiation Oncology, Biology, Physics, 2021. 110(1): p. 21-34.
38. Stamos, D.G., et al., Endosonics: clinical impressions. J Endod, 1985. 11(4): p. 181-7.
P R E V I E W SPEAKER
About the Speaker
Alexandra Otto, DDS, FAGD, FACD, FPFA, FICD
will be presenting 3 sessions at the TDA Meeting:
Yes to Comprehensive Care
Friday, May 8, 9:30 AM – 11:30 AM • Event #F25
Unlocking Pediatric Dentistry
1:00 PM – 4:00 PM, Event #F26
Unleashing the Power of AI in Dentistry
Saturday, May 9, 8:30 AM – 11:00 AM • Event #S08
Dr Alexandra Otto is a board-certified pediatric dentist, president of the Texas Academy of Pediatric Dentistry, and Chair of the Texas Dental Association Council on Professions and Trends. She is the co-founder of Alcan Dental Cooperative, Kids Tooth Team Pediatric Dentistry, and Kids Tooth Team Outreach. Dr Otto also serves as the pediatric dentist on the Texas Children’s Hospital North Austin Craniofacial Team and manages the hospital’s pediatric dental service line.
Nationally recognized for her clinical and leadership excellence, Dr Otto has been honored as one of the American Dental Association’s “10 Under 10” and Incisal Edge’s “40 Under 40” award recipients. She serves as the national Private Practice Expert Consultant to the American Academy of Pediatric Dentistry Safety Committee, is a member of Sprig Oral Health Technologies’ Scientific Advisory Board, and lectures nationally for the ADA, AGD, AAPD, Sprig, CareStack, and Elevate Oral Care.
Dr Otto is a Fellow of the Academy of General Dentistry (AGD), American College of Dentists (ACD), Pierre Fauchard Academy (PFA), and International College of Dentists (ICD), and is a Diplomate of the American Board of Pediatric Dentistry (ABPD).
When she’s not in the clinic or on stage, Dr Otto enjoys traveling with her husband, Tim, and their two children Max (3) and Adaline (1.5), exploring the country in their RV, and finding creative ways to blend dentistry, leadership, and community impact.
Hello everyone! I’m Dr Alexandra Otto, a board-certified pediatric dentist and private practitioner based out of Buda, Texas. My husband, Tim, and I are the founders of Kids Tooth Team Pediatric Dentistry, a 6-location pediatric specialty practice serving Texas and Michigan. We also lead Alcan Dental Cooperative—a multi-location, multi-state partnership organization helping practices grow with integrity and innovation—and Kids Tooth Team Outreach, a 501(c)(3) nonprofit mobile dental unit that has donated over $700,000 in free dental care to underserved children across central Texas.
As president of the Texas Academy of Pediatric Dentistry and Chair for the TDA Council on Professions and Trends, I’m deeply passionate about bridging clinical excellence with real-world practicality.
I’m honored to be one of the featured speakers at the 2026 Texas Dental Association Annual Meeting, where I’ll be presenting 3 sessions designed to help every member of the dental team—doctor, hygienist, assistant, and office administrative teams—walk away with actionable strategies they can implement immediately.
Unleashing the Power of AI in Dentistry
Saturday, May 9
8:30 AM – 11:00 AM
Artificial intelligence (AI) has become one of the most transformative tools in modern dentistry— and yet, it remains one of the most misunderstood. My session, “Unleashing the Power of AI in Dentistry,” dives into the everyday ways AI can enhance diagnostics, streamline operations, and elevate patient care.
We’ll explore how platforms like Overjet, Pearl, and VoiceStack are revolutionizing clinical and administrative workflows—from radiographic analysis and caries detection to insurance processing, scheduling efficiency, and team communication.
But here’s my main message: AI isn’t replacing dentists—it’s amplifying us. It helps us make more consistent, data-driven decisions and communicate those decisions more clearly to our patients and teams. And just as importantly, it’s not replacing our teams—it’s streamlining operations to make us more efficient, polished, and professional.
Before the conference, I encourage you to download the Pro version of ChatGPT and experiment with it. Try it out in some of the following scenarios:
• Draft your next team email more clearly and concisely
• Create an agenda for your next important team meeting
• Summarize your office manual into digestible onboarding pieces
The more you play with these tools, the more you’ll see that AI can help every role in the practice—including the doctor—work smarter, faster, and with more confidence.
Unlocking Pediatric Dentistry
Friday, May 8
1:00 PM – 4:00 PM
My second session, “Unlocking Pediatric Dentistry,” focuses on helping dentists and team members think and treatment plan like pediatric specialists.
In pediatric dentistry, the phrase “minimally invasive” is often used, but its meaning can easily be oversimplified. True minimally invasive care isn’t about doing less—it’s about doing the right thing at the right time, using sound judgment and the best tools available. In this session, we’ll unpack how to blend preventive, restorative, and behavioral approaches to create meaningful outcomes for our youngest patients.
We’ll discuss:
• Modern restorative materials and minimally invasive techniques—how to use them and why
• Updated guidelines for caries management
• Behavior management strategies that promote smooth, positive appointments instead of stressful encounters.
We’ll also highlight how pediatric-specific techniques are now shaping broader trends in dentistry—and how bioactive materials, techniques like the Hall crown and esthetic preformed zirconia crowns are becoming the new standard of care.
Ultimately, treating children isn’t just about technical skill—it’s about perspective. It’s about keeping care patient-focused and family-centered. When we approach care with empathy, playfulness, and purpose, the dental chair becomes a place of safety and empowerment.
Yes to Comprehensive Care
Friday, May 8
9:30 AM – 11:30 AM
The third session, “Yes to Comprehensive Care,” is all about the heart of what we do: helping patients say yes to the care they need.
In a time when dentistry often swings between extremes—over-treatment or supervised neglect—our challenge is to deliver balanced, comprehensive care that’s both clinically responsible and patient-centered.
This course will equip you and your team with the communication skills, coaching, and tracking tools to improve case acceptance rates and patient trust. We’ll discuss:
• How to overcome “approval addiction” and stop seeking permission to do what’s right for the patient.
• How to coach patients through tough decisions with empathy and authority.
• How to use team-based communication—from the front desk to the back office—to reinforce confidence and consistency.
• How to measure your success with case acceptance analytics and patient outcomes.
I’ll also share practical scripting examples your team can start using the very next day—phrases that replace hesitation with clarity and turn difficult conversations into educational ones.
Because if we don’t understand a patient’s why—their motivations, fears, and goals—we can’t communicate our why in a way that connects. And when that connection is missing, treatment doesn’t move forward, and care doesn’t happen.
The Common Thread: Actionable, Human, and Honest Dentistry
Across all 3 sessions, my goal is simple: to make continuing education practical, relevant, and inspiring. Dentistry is evolving faster than ever—clinically, technologically, and culturally—and our ability to adapt depends on how we communicate, collaborate, and lead.
From AI-powered diagnostics to compassionate pediatric care to the art of case acceptance, these topics all share one theme: the intersection of innovation and intention.
If you leave my sessions feeling empowered to make even one meaningful change—whether that’s implementing AI into your workflow, revamping your pediatric protocols, or rethinking how your team presents treatment—that’s where real progress begins.
I can’t wait to see you at the 2026 TDA Annual Meeting and share this journey toward smarter, safer, and more connected dentistry.
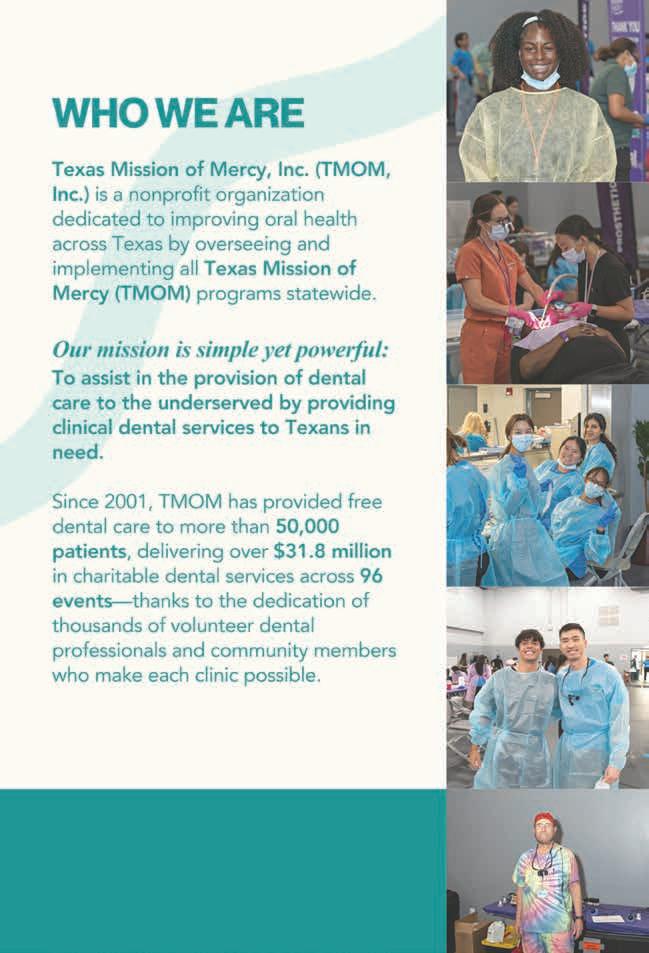
WHO WE ARE
2025 ANNUAL REPORT
The Texas Dental Association Smiles Foundation (TDASF) is the nonprofit affiliate of the Texas Dental Association (TDA) dedicated to creating healthier communities by expanding access to oral health care, educating the public and profession, and supporting initiatives that advance overall wellness.
2025 HIGHLIGHTS
TDASF VISION
To be recognized across Texas as a trusted leader in improving oral health through compassionate care, education, and community support, ensuring stronger and healthier communities for generations to come.
New Website & Brand Refresh: TDASF launched a newly redesigned website and refreshed brand identity to better communicate our mission and make it easier for donors, dental professionals and students to engage with our mission.
Scholarships: We remain dedicated to supporting the next generation of dental professionals. In 2025, two $2,000 scholarships were awarded to outstanding second-year dental students at each of Texas’s four dental schools.
Beverly Bain Memorial Speaker: Continuing our commitment to education and leadership, TDASF proudly sponsors a featured speaker at the TDA Annual Meeting in honor of Beverly Bain, recognizing her lasting impact on organized dentistry and community service.
Grant Initiatives: TDASF is preparing to open applications for new grants that align with the Foundation’s mission supporting innovative programs that advance dental care, education, and public outreach across Texas.
Strategic Planning: On October 11, the Foundation conducted a strategic planning session with Event Garde, setting the stage for enhanced focus, growth, and future program development.
THE 100 CLUB
One of the most impactful ways to support the Smiles Foundation is by joining the 100 Club—a community of dedicated donors who contribute monthly to sustain our mission. Membership in the 100 Club directly enables TDASF to:
Award scholarships to deserving dental students
Fund grants that expand access to care
Support outreach initiatives that make a lasting difference in communities across Texas
Every contribution helps transform smiles, fund education, and build a healthier future for Texans in need.
Continuing our mission for years to come...
With renewed direction from our recent strategic planning and a stronger brand presence, 2026 promises to be a year of focus and growth. We look forward to launching new grant opportunities, deepening our partnerships, and continuing to empower the dental community to make a difference one smile at a time.
FBI: Found But not Identified (yet)
A series of articles intended to assist Texas Medical Examiners in giving a name to “unidentified” individuals using postmortem dental evidence.
Do you recognize the dental work/conditions presented?
Kathleen A Kasper, DDS, D-ABFO
The Extent of the Problem
Over 600,000 individuals go missing in the United States every year. Fortunately, many missing children and adults are quickly found, alive and well. However, tens of thousands of individuals remain missing for more than one year—what many agencies consider “cold cases”.1
It is estimated that 4,400 unidentified bodies are recovered each year, with approximately 1,000 of those bodies remaining unidentified after one year.2
Medical examiner and coroner offices reported 11,380 unidentified remains on record as of 2018.3
The challenge in giving a name to these unidentified decedents is that the research and time invested can be extensive, expensive and after normal protocols have been exhausted, many individuals still remain unidentified. The hope in writing this series of articles on long term unidentified cases in Texas is that one of the many Texas dentists who read the TDA Journal will recognize the dental work presented as theirs or possibly remember a dental condition or feature that can give a name to the unidentified and help bring closure to the family.
The Medical Examiner’s Protocol to Legally Identify Individuals
Medical examiners follow a specific protocol to identify individuals who are found without any presumptive identity. This protocol is described below and, in this order, depending on the condition of the body.
By far Latent Prints (finger, palm, sole), are the fastest and least expensive way to make a positive identification. This method of identification is not always possible if remains are severely decomposed, charred, or skeletonized.
Medically Implanted Devices (hip/joint replacements, pacemakers), require knowing what hospital/physician placed the device to get the matching serial number and can be difficult.
Dental Records are also an easy, fast, and inexpensive way to identify a decedent; however, success depends on a presumptive identity and availability/existence/quality of those antemortem (before death) dental records. If all leads for a presumptive identity are exhausted, then a postmortem (after death) dental charting/profile is created and entered in the NamUs (National Missing and Unidentified Persons System) and NCIC (National Crime Information Center) databases.
Anthropologic Methods will use skeletal features to generate a biological profile that can support positive identification efforts.
DNA samples are collected. This takes the longest period of time and is most expensive. Depending upon the individual, it may involve obtaining DNA samples not only from the decedent but also from genealogically appropriate family members or select personal hygiene products of the decedent’s, if available. If no matches are obtained, then:
DNA samples are submitted to CODIS (Combine DNA Index System) which is a computer program that operates local, state, and national databases of DNA profiles from convicted offenders, unsolved crime scene evidence, unidentified remains and missing persons. This is maintained by the Federal Bureau of Investigation. If this search fails then, the State of Texas requires medical examiners to submit a DNA sample from long term unidentified decedents to the University of North Texas Center for Human Identification for additional genetic testing and comparison. This comparison may take up to a year to process, and a decedent may remain unidentified once completed.
Author
Kathleen A. Kasper, DDS, D-ABFO
Dr Kasper has been practicing general dentistry in Carrollton, Texas, since 1994. She is a graduate of the University of Iowa College of Dentistry.
She provides 3 counties in the Dallas-Ft. Worth Area with forensic dental services. These include Collin, Dallas, and Tarrant Counties. She is currently the only active board certified forensic dentist in north Texas.
She received her formal forensic odontology training at the University of Texas Health Science Center San Antonio, Texas, Center for Education and Research in Forensics (CERF) in 2003-2004.
Dr Kasper obtained Board Certification from the American Board of Forensic Odontology in 2010.
She is a fellow of the American Academy of Forensic Sciences, a member of the American Board of Forensic Odontology, and a member of the American Society of Forensic Odontology.
She is the current American Board of Forensic Odontology Dental Age Assessment Committee Chair.
Dr Kasper is also a published author in the Journal of Forensic Sciences and coauthor of a chapter in each of 3 forensic textbooks.
Perhaps one of her greatest undertakings was chairing a working group for the American Dental Association that has published the “Technical Report” for Forensic Dental Age Estimation which went on to become a “standard” for the Organization of Scientific Area Committees (OSAC) for Forensic Science.
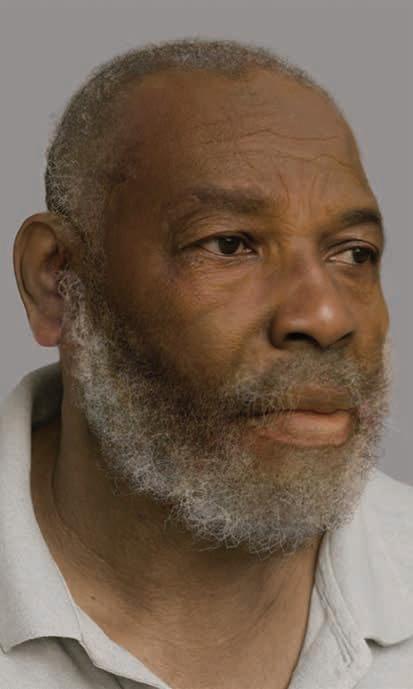
This is the proverbial end of the road; therefore, all Texas Dentists, Dental Auxiliaries and Staff; Can you help the Dallas County Medical Examiner’s Office give a name to the unidentified Black male decedent described below?
The
Unidentified Individual: Dallas County Medical Examiner (DCME) Case #25-06904, NamUs #UP144096
Date of Death: April 21, 2025
Body Condition: Fresh at time of death
Sex: Male
Ancestry: Black
Age: Approximately 60 years old
Height: 6’ 1”
DNA analysis completed: Yes; Profile entered in the Combined DNA Index System (CODIS) with no results or hits.
Details of Incident:
The decedent is an adult, black male, who was found by a passerby unresponsive in a ditch at 1610 St. Malcolm X. Blvd, in Dallas, Texas on 4/15/2025. He was transported to Baylor University Medical Center (BUMC) in Dallas, where he remained unidentified as an inpatient. His death was pronounced as an inpatient at BUMC on 4/21/2025.
Efforts to identify the decedent via fingerprint searches and comparisons have been unsuccessful.
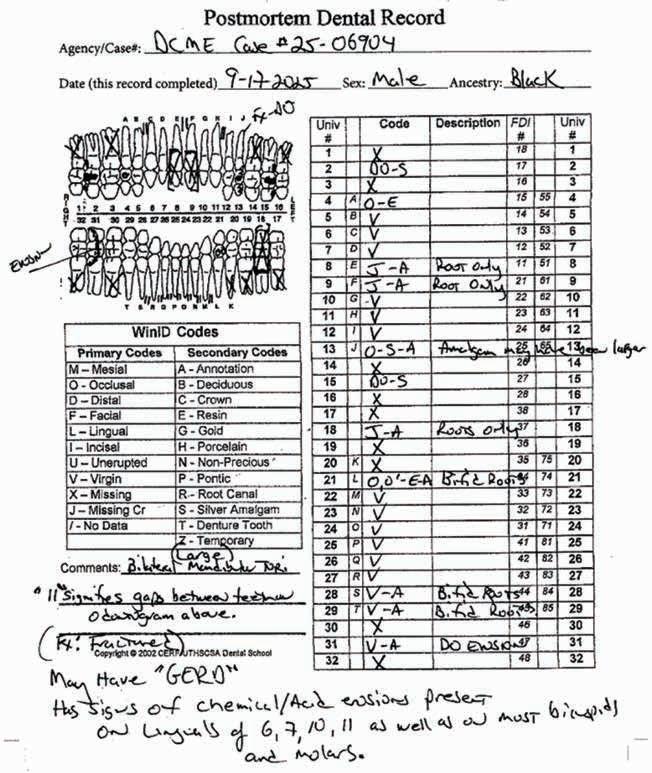
Dental Evidence Recovered: Maxilla and Mandible
To the left is a postmortem rendering created from remains recovered for DCME Case #25-06904/ NamUs #UP144096.
Maxilla Occlusal View
Mandible Occlusal View
Right Left
Right Lateral View
Left Lateral View
Right Left Left Right
Dental Postmortem Radiographs
DCME Case #25-06904:
Closing
If you believe you have any dental records, dental radiographs, intraoral/extraoral dental photographs, dental scans or other dental information regarding the unidentified Black male decedent described above as DCME Case #25-06904/ NamUs #UP144096, please contact the Dallas County Medical Examiner’s Office, 214-920-5900, ask for Steven Kurtz, chief medicolegal death investigator or Keara St Louis, deputy chief medicolegal death investigator.
Let’s give this individual a name!
References
1. Between 2007 and 2020, an average of 664,776 missing persons records annually were entered into the National Crime Information Center. See https://www.fbi.gov/services/cjis/ncic.
2. Medical Examiners And Coroners’ Offices, 2004. Matthew J. Hickman, Ph.D., Kristen A. Hughes, M.P.A., Bureau of Justice Statistics, Kevin J. Strom, Ph.D., Jeri D. Ropero-Miller, Ph.D., DABFT, RTI International.
3. Medical Examiner and Coroner Offices, 2018. Connor Brooks, Bureau of Justice Statistics, November 2021.
By Cloud Dentistry
The dental job market has changed dramatically in recent years. With increased demand for skilled professionals and a growing preference for workplace flexibility, dentists and practice managers must rethink their hiring strategies. Today’s dental professionals have more options than ever, making it essential for practices to stand out as employers of choice.
Attracting and retaining top talent goes beyond offering a paycheck—it requires a mix of competitive compensation, work-life balance, and a supportive office culture. Here’s what dental practices need to know to stay competitive.
Competitive Pay: The Foundation of Retention
It’s no secret that salary remains one of the most influential factors in a job seeker’s decision. According to the American Dental Association’s (ADA) Health Policy Institute, wages for dental hygienists and assistants have risen significantly in response to workforce shortages.1 If your compensation package isn’t keeping up with regional trends, attracting qualified candidates may become increasingly difficult (American Dental Association).
How to Stay Competitive:
• Research Salary Benchmarks: Utilize industry reports and local job postings to gather data on average salaries for similar positions. This information not only helps you set fair wages but also aids in attracting top talent who might be comparing offers from different employers.
• Offer Incentives: Offering sign-on bonuses or retention incentives can significantly enhance your recruitment efforts. A sign-on bonus can draw in candidates who may have multiple offers, while retention incentives can ensure that employees feel valued and remain with the company for the long haul.
• Consider Comprehensive Benefits: Consider benefits that go beyond salary. Incorporating comprehensive benefits such as elevated health insurance, retirement plans, and student loan assistance can greatly enhance your compensation package.
While competitive pay is a must, it’s not the only factor candidates consider. Many dental professionals prioritize flexibility and work-life balance as much as financial compensation. Dental practices that understand and address these needs will likely have a competitive edge in attracting and retaining top talent.
Work-Life Balance: A Growing Priority
Work-life balance is no longer just a perk—it’s quickly becoming an expectation. Many dedicated dental professionals are increasingly prioritizing schedules that accommodate their personal lives. As the demands of work increase, so does the desire for flexible schedules that allow for quality time with family, hobbies, and self-care. This shift reflects a broader cultural change where personal well-being is increasingly valued alongside professional success.
While competitive pay is a must, it’s not the only factor candidates consider. Many dental professionals prioritize flexibility and work-life balance as much as financial compensation.
Dental practices that understand and address these needs will likely have a competitive edge in attracting and retaining top talent.
Ways to Improve Work-Life Balance in Your Office:
• Offer flexible scheduling options, such as part-time or temp work.
• Ensure lunch breaks and downtime between patients are respected.
• Actively promote the importance of taking time off to recharge and prevent burnout.
• Do your best to avoid last-minute scheduling changes that disrupt personal plans.
By actively showing that you care about their time and personal lives, you create an environment where employees want to stay and grow. Investing in how you value your employees’ time is not just about creating a more harmonious work environment; it’s also a strategic approach to retaining talent and ensuring long-term success for your organization.
Office Culture:
The Key to LongTerm Retention
Pay and scheduling certainly matter, but a positive and supportive work environment is what keeps employees engaged in the long term. Toxic or high-stress workplaces can push even well-compensated staff to seek opportunities elsewhere.
What Makes a Strong Office Culture?
• Respect and Communication: Encourage open dialogue between team members and leadership. Employees should feel comfortable voicing concerns or suggesting improvements.
• Professional Growth: Offer mentorship, skills training, and opportunities for advancement. A 2023 survey by DentalPost found that career development is a top priority for dental professionals looking for long-term roles (DentalPost).2
• Team Recognition: Celebrate achievements, whether it’s a simple shoutout at morning huddles or an annual team appreciation event.
• Acts of Kindness: Small, unexpected gestures can make a big impact. Take note of team members’ go-to coffee orders, snacks, or lunches—then use it to surprise them every now and then. A little thoughtfulness goes a long way in creating a workplace people love.
Creating a workplace where employees feel valued will naturally lead to higher job satisfaction and lower turnover. By focusing on respect, communication, professional growth, and team recognition, businesses can create an engaging work environment that motivates employees and drives company performance. A commitment to these values not only attracts top talent but also cultivates a workforce that is enthusiastic, resilient, and ready to take on day-to-day challenges.
Adapting to a Changing Workforce
The modern workforce has different expectations than it did even five years ago. Dental professionals now have more employment options than ever, from traditional full-time roles to temp work and independent contracting.
Practices that embrace these changes— whether by offering more flexibility or improving workplace culture—will have an easier time attracting and keeping top talent.
By focusing on competitive compensation, work-life balance, and a supportive culture, your practice can become the kind of workplace that professionals seek out—not just for a job, but for a career.
Dental offices that join TDA Perks Program-endorsed Cloud Dentistry can significantly broaden their outreach to a diverse pool of dental professionals. Creating a Cloud Dentistry account is free; and after upgrading, TDA members receive 10% off their monthly subscription. Learn more at tdaperks. com (Insurance & HR) or by calling (844) 643-3128.
References
1. American Dental Association. The State of the Dental Workforce. Health Policy Institute, 2023. 2. DentalPost. 2023 Dental Salary Report. DentalPost, 2023.
APP-SOLUTELY RE-IMAGINED!
Designed for dentists, with dentists, the new ADA Member App is here and ready to put the resources you need in the palm of your hand.
• Chat 1:1 or with your network
• Newsfeed customized to your interests
• Digital wallet to store your important documents
• Stream the new “Dental Sound Bites” podcast
Tap into possibility at ADA.org/App
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/MemberResources/TDA-Classified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN (ID #745): Established, two-location GD practice in the Austin area. The practice serves a large, diverse, FFS/PPO patient base with excellent new patient flow, a combined 14 equipped operatories across both locations (with substantial room for expansion at one of the locations). The practice comes fully equipped with digital radiography, digital sensors, digital scanners, digital pano, CBCT, and paperless charts. AUSTIN (ID #749): Established GD office located in the heart of central Austin. The practice has an impeccable online reputation in the community and features a strong hygiene recall program with multiple avenues for future growth. 3,000+ sq ft office, 4 active operatories, ample room for expansion, equipped with a digital scanner, intra oral cameras, digital X-ray sensors, and paperless charts. AUSTIN (ID #762): Established GD office in the heart of central Austin with a majority PPO patient base, 1000+ active patients, a robust hygiene recall program, and a strong reputation online and in the community they serve. The 1,500 sq ft office space contains 3 total operatories, computers throughout, a digital X-ray scanner, and intra-oral cameras. The practice has consistently generated revenue of mid-6 figures with abundant upside opportunities to expand production/cash flow through launching strategic marketing and advertising initiatives, driving new patient flow, and offering additional advanced procedures in-house.
HOUSTON-SOUTH (ID #682):
Established, multi-specialty dental office in a suburb approximately 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout,
CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose.
HOUSTON-EAST
(ID #769): Unique opportunity to purchase an established, GD practice approximately 80 miles east of Houston. Large office containing 9 total chairs, advanced modern technology including computers throughout, digital X-ray sensors, digital pano, 3D cone beam CT, digital scanner, intra oral cameras and paperless charts. The large 5,000+ active patient base lays the foundation for exceptional growth opportunities by expanding the procedure mix and focusing on restorative procedures as well as adding in basic specialty procedures.
HOUSTON (ID #772):
Legacy GD practice and free-standing real estate located north of downtown Houston. Majority PPO patient base, 1,300+ active patients, and 20+ new patients visiting the office per month. Approximate 3,000 sq ft facility contains 6 total operatories (5 equipped), computers in each operatory, digital X-ray sensors, pano, digital scanner, dental laser, and paperless charts. The practice has consistently realized revenue mid-6 figures with robust net cash flow (45-55% on average) and upside opportunities to expand production through adding additional specialty procedures, equipping the open operatory, and implementing a strategic marketing initiative.
SAN ANTONIO-TX HILL COUNTRY (ID #685): Well-established dental practice and real estate
nestled in the hill country north of San Antonio. The office relies mostly on word-of-mouth- referrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023, and the trend continued into 2024. SAN ANTONIO-EAST (ID #716): Legacy GD practice and real estate in a rural community east of San Antonio. The large office space offers ample room for expansion and features 5 fully equipped operatories with computers in each op, digital X-ray sensors, a digital pano, a digital scanner, intraoral cameras and paperless
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
DSO C S PRACTICE SALES
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com PRACTICE APPRAISALS
www.dentaltransitions.com
classifieds
charts. This practice has strong profit margins and serves a large, multi-generation 100% FFS patient base. SOUTH TEXAS COAST (ID #754): Exceptional GD practice located in a serene coastal town. Rare opportunity to acquire a thriving, well-established business in an underserved area with consistent collections of 7 figures with a primarily FFS active patient base and strong new patient flow. Hygiene production is robust, having exceeded 25% each of the last 3 years. The spacious, modern facility is outfitted with state-of-the-art technology and is also available for purchase. The owner will be retiring at some point over the next few years but is available to stay for a transition of the buyer’s preference. WEST TEXAS—OMS (ID #771): One of the premier oral surgery practices in Texas. The practice serves a large FFS/PPO patient base supported by a dedicated and diverse referral base. 2,300 sq ft office in an easily accessible office park. State-of-the-art technology includes 5 fully equipped operatories, digital X-ray sensors, a 3D Cone Beam CT, a digital scanner, intra oral cameras and paperless charts. This practice is one of the strongest oral surgery practices to come to market in recent years. The doctor is available for a potential transition period with the incoming buyer. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www. dentaltransitions.com or contact us at 512-9007989 or info@dentaltransitions.com.
CENTRAL TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural four operatory dental practice for sale in the heart of the beautiful Texas hill country. This all-digital practice with a new pano produces
mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@ gmail.com for more information and showings.
DALLAS: Thriving north Texas OMS practice for sale: 3 surgical suites, 2 consult rooms, and 40 new patients/month, 7 figures in collections, $600K SDE, and real estate available. Established 20+ years with minimal advertising. Within 150 miles of Dallas. Contact PTS to learn more: bailey@ professionaltransition.com—Ref #TX30625.
MANSFIELD: Explore a remarkably unique dental practice for sale in the DFW area. Great startup opportunity for GP or specialist. Discover the possibilities online at www.yournewdentalpractice. com.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states. For more information and current listings please visit our website at www.adstexas.com or call us at 469-2223200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.