In-ovo vaccination
pr ot
ec
te
d
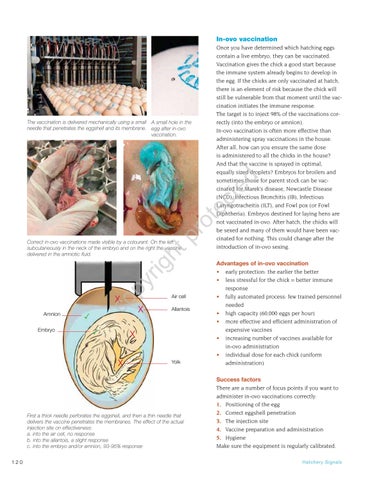
The vaccination is delivered mechanically using a small A small hole in the needle that penetrates the eggshell and its membrane. egg after in-ovo vaccination.
Once you have determined which hatching eggs contain a live embryo, they can be vaccinated. Vaccination gives the chick a good start because the immune system already begins to develop in the egg. If the chicks are only vaccinated at hatch, there is an element of risk because the chick will still be vulnerable from that moment until the vaccination initiates the immune response. The target is to inject 98% of the vaccinations correctly (into the embryo or amnion). In-ovo vaccination is often more effective than administering spray vaccinations in the house. After all, how can you ensure the same dose is administered to all the chicks in the house? And that the vaccine is sprayed in optimal, equally sized droplets? Embryos for broilers and sometimes those for parent stock can be vaccinated for Marek’s disease, Newcastle Disease (NCD), Infectious Bronchitis (IB), Infectious Laryngotracheitis (ILT), and Fowl pox (or Fowl Diphtheria). Embryos destined for laying hens are not vaccinated in-ovo. After hatch, the chicks will be sexed and many of them would have been vaccinated for nothing. This could change after the introduction of in-ovo sexing.
py
rig
ht
Correct in-ovo vaccinations made visible by a colourant. On the left subcutaneously in the neck of the embryo and on the right the vaccine delivered in the amniotic fluid.
Amnion Embryo
ᅚ
co
X
ᅚ
X
Air cell Allantois
X X
Yolk
First a thick needle perforates the eggshell, and then a thin needle that delivers the vaccine penetrates the membranes. The effect of the actual injection site on effectiveness: a. into the air cell, no response b. into the allantois, a slight response c. into the embryo and/or amnion, 93-95% response 120
Advantages of in-ovo vaccination • early protection: the earlier the better • less stressful for the chick = better immune response • fully automated process: few trained personnel needed • high capacity (60,000 eggs per hour) • more effective and efficient administration of expensive vaccines • increasing number of vaccines available for in-ovo administration • individual dose for each chick (uniform administration) Success factors There are a number of focus points if you want to administer in-ovo vaccinations correctly: 1. Positioning of the egg 2. Correct eggshell penetration 3. The injection site 4. Vaccine preparation and administration 5. Hygiene Make sure the equipment is regularly calibrated. Ha tc he ry S i gnal s







































































































