

GUIDE 2023-2024 BENEFITS Rusty Freeman & Associates, LLC. U.S. Employee Benefits Services Group 245 Landa Street New Braunfels, TX 78130 (830) 606-5100 www.usebsg.com www.mybenefitshub.com/palestineisd
Palestine Independent School District


TableofContents

Uow to Enroll �edical-TRSActivecare 1800MD -Tele-Medicine MedicalTransport-MASA �ellfleet-Accident Unum-CriticalIllness
ColonialLife- Cancer
& EAP
superiorVision Group & VoluntaryLife- Unum
K
I Page 3 - 6 7 8 - 9 10 - 11 12 - 18 19 - 24 25 - 27 28 - 29 30 - 37 38 - 41 42 43 - 48 49 - 50 51 - 52 53 - 56 57
�urich/SIS-GapPlan
rfheStandard-Disabiltiy
�eam-Dental
rrexasLife-PermanentLife �ealthSavings-HSABA
�BS-FlexibleSpending 03(B) RETIREMENT- Group




Customer Service Contact Phone Mobile Email Marlene Freeman(830)606-5100 (830)708-1112 mfreeman@usebsg.com Tracy Hamel (830)606-5100 thamel@usebsg.com Gemma Funai gfunai@palestineschools.org (830) 500-9025 (903) 731-8048 usebsg.com
Enrollment Instructions for THEbenefitsHUB

Site Access: To access your employer online enrollment site, THEbenefitsHUB, you can login to the following website


www.mybenefitshub.com/palestineisd

Braunfels,Texas
3
245 Landa Street New
78130 Phone: (830) 606-5100
Know Your Benefits! Below is a summary of benefits offered through PISD.

Medical Transport - MASA Provides Emergency Transportation for ground, emergency air, and non-emergency hospital to hospital transportation anywhere in the US/Canada.
Employee Assistance Program - Employee Assistant Program that provides support, guidance, and resources. A helping hand when you need it. *Palestine ISD provides this benefit to all eligible employees at no cost.
TeleMedicine - 1.800MD, provides access to physicians for non-emergency treatment/prescriptions. For questions, please contact 1.800MD directly at 1-800-530-8666
Gap Plan - A low cost program designed to help you pay for covered out-of-pocket expenses you may incur while you are either confined in a hospital or being treated as an outpatient for an injury or illness.
Critical Illness UNUM - no Evidence of Insurability required, guaranteed issue. ** Includes $50 wellness benefit.
Standard Disability - Plan includes long term disability coverage. Plan is designed to protect up to 66 2/3% of your gross PISD income.
Texas Life Permanent Life - Portable, permanent life insurance available for employees, their spouses, and dependents. Employees can keep the coverage upon termination or retirement from PISD.
UNUM Group Life - Group term life that ends when you terminate employment with PISD. Coverage is also available for spouses and dependent children.
Colonial Life Cancer - Pays benefits for internal cancer diagnosis. ** Includes $50 wellness benefit.
BEAM Dental - Coverage for preventative, basic, major, and orthodontia services.
** All employee that enroll will receive a Beam toothbrush kit and perks throughout the year for regular use.
Superior Vision - Plan includes coverage for eye exams, materials (such as frames and lenses). This plan has a list of defined network providers. For more information, including a list of providers, visit www.superiorvision.com.
Wellfleet Accident - Pays benefits for off-the-job accidents and related treatments. Includes a physical/wellness exam reimbursement. ** Includes a $200 health screening Benefit per year, per covered member.
NBS Flexible Spending - Make sure to spend/claim the money in your current reimbursement account by 8/31/2023 Visit fsa.nbsbenefits.com to check account balances or request information.
HSA Bank - Participants in the TRS-ActiveCare HD health plan are eligible to contribute to a health savings account.


2023-2024 OPEN ENROLLMENT INFORMATION
year begins 09/01/2023 and ends 08/31/2024. All benefits elected during the annual open enrollment will be effective 09/01/2023.
The 2023-2024 Section 125 Cafeteria Plan
4
ENROLLMENT FAQ
INTRODUCTION
Providing great benefit choices to you and your family is just one of the many ways PISD looks after the health and financial welfare of the people who make our district work so well. Our goal at PISD is to provide you with an array of benefit options that will meet your personal needs as part of your total compensation and rewards.
HOW DO I ENROLL?
Visit www.mybenefitshub.com/palestineisd
USERNAME: Enter the first 6 letters of your last name, followed by the first letter of your first name, and then the last 4 digits of your SSN. (EX: John Sanderson SSN: xxxxx-1234



USERNAME: sanderj1234)
PASSWORD: Complete last name (excluding any special characters or spaces) followed by the last 4 digits of your SSN. (Ex: sanderson1234)
WHO IS ELIGIBLE?
You are eligible to enroll in the PISD Benefits Program if you are a regular employee working at least 15 hours per week in a permanent position. All other employees, to include substitutes, who work less than 15 hours per week, are eligible to enroll in medical insurance at full cost.
WHO IS AN ELIGIBLE DEPENDENT?
Your legal spouse
Children under the age of 26, yours OR your spouse’s Dependent children of any age who are disabled
Children under your legal guardianship

When adding dependents for the first time, please provide date of birth, gender and social security number.
NEW HIRE ENROLLMENT
Online benefit enrollment must be completed within 30 days of your active at work date. Elected benefits will take effect on the 1st of the following month.

MID-YEAR CHANGES
The benefits you choose will remain in effect throughout the plan year (from September 1 - August 31). You may only add or cancel coverage during the year if you have a qualifying change in the family or employment status that causes you to gain or lose eligibility for benefits. Qualifying changes may include:

A change in your legal marital status
A change in your number of dependents as a result of birth, adoption, legal custody, or if your dependent child satisfies or ceases to satisfy eligibility requirements for coverage, or the death of a dependent child or spouse
A change in employment status for you or your spouse loss or gain of eligibility for other insurance (including CHIP & Medicaid)
You must notify the Palestine ISD payroll office of the requested change within 30 calendar days of the change in status. There are no exceptions to this rule.
WHEN WILL I RECEIVE ID CARDS?
Everyone enrolled in Medical will receive a new Medical Card. Enrolled participants will receive HSA and FSA cards prior to the effective date of the new coverage. For most plans, you can login to the carrier website and print a temporary ID card or give your provider the insurance company’s phone number to call and verify your coverage if you do not have an ID card at the time of service.
WHO DO I CONTACT WITH QUESTIONS?
For questions, you can contact your PISD Benefits Department
Gemma Funai
Office: 903-731-8048
Email: Gfunai@palestineschools.org
Marlene Freeman
Office: 830-606-5100
Email: Mfreeman@usebsg.com
• • •
• • • •
• •
@
�
5
Covering Dependents?
If you cover dependents on any of your coverages through PISD you must provide the dependents name, date of birth, and social security number. You must have all of this information before dependents can be added to the system.
Making Changes During the Year
Choose your benefits carefully. Several of the employee benefits plan contributions are made on a pre-tax basis and per IRS regulations, contribution amounts cannot be changed unless you experience a qualified life event. Qualifying life events include:
Marriage, divorce, legal separation; Death of spouse or dependent;
Birth or adoption of a child;
Changes in employment for spouse or dependents; Coverage changes;
You must submit your benefit change requests and include required documentation within 30 days of the event. Also note that per the IRS, only changes consistent with the life event are allowed.
New Employees
New employees must enroll within 30 days of their start date. If employees fail to enroll within 30 days, all benefits will be waived. Except for health insurance, plans will be effective on the first of the month following the date of start. Health Insurance can be effective the date of start or the first month following date of start. Please be aware that if you choose date of start as effective date for health insurance, you will be charged for the entire month.
Very Important
Please carefully review your paycheck(s) to ensure all deductions are correct. If you find a discrepancy in your paycheck, please contact Gemma Funai immediately at 903-731-8048. Discrepancies must be identified within the first 30 days from the effective date of the policy to be considered.
Benefit Related Documents
For contact information, claim forms, benefits guides, and more, please visit palestineschools.org.
• • • • •
2023-2024 MORE
MPORTANT
NFORMATION 6
I
I
2023-24 TRS-ActiveCare Plan Highlights
All TRS-ActiveCare participants have three plan options. Each includes a wide range of wellness benefits.
*Available for all plans. See the benefits guide for more details.
This plan is closed and not accepting new enrollees. If you’re currently enrolled in TRS-ActiveCare 2, you can remain in this plan. TRS-ActiveCare 2 • Closed to new enrollees • Current enrollees can choose to stay in plan • Lower deductible • Copays for many services and drugs • Nationwide network with out-of-network coverage • No requirement for PCPs or referrals TRS-ActiveCare Primary TRS-ActiveCare Primary+ TRS-ActiveCare HD Plan Summary • Lowest premium of all three plans • Copays for doctor visits before you meet your deductible • Statewide network • Primary Care Provider (PCP) referrals required to see specialists • Not compatible with a Health Savings Account (HSA) • No out-of-network coverage • Lower deductible than the HD and Primary plans • Copays for many services and drugs • Higher premium • Statewide network • PCP referrals required to see specialists • Not compatible with a Health Savings Account (HSA) • No out-of-network coverage • Compatible with a Health Savings Account (HSA) • Nationwide network with out-of-network coverage • No requirement for PCPs or referrals • Must meet your deductible before plan pays for non-preventive care Monthly Premiums Employee Only $442 $ $519 $ $456 $ Employee and Spouse $1,194 $ $1,350 $ $1,232 $ Employee and Children $752 $ $883 $ $776 $ Employee and Family $1,503 $ $1,713 $ $1,551 $ Total Premium Total Premium Total Premium Your Premium Your Premium Your Premium Total Premium Your Premium $1,013 $ $2,402 $ $1,507 $ $2,841 $ How to Calculate Your Monthly Premium Total Monthly Premium Your District and State Contributions Your Premium Ask your Benefits Administrator for your district’s specific premiums. Wellness Benefits at No Extra Cost* Being healthy is easy with: •$0 preventive care •24/7 customer service •One-on-one health coaches •Weight loss programs
programs
pregnancy support
TRS Virtual Health
•Nutrition
•OviaTM
•
•Mental health benefits
•And much more!
Immediate Care Urgent Care $50 copay $50 copay You pay 30% after deductibleYou pay 50% after deductible Emergency Care You pay 30% after deductible You pay 20% after deductible You pay 30% after deductible TRS Virtual Health-RediMD (TM) $0 per medical consultation $0 per medical consultation $30 per medical consultation TRS Virtual Health-Teladoc® $12 per medical consultation $12 per medical consultation $42 per medical consultation $50 copay You pay 40% after deductible You pay a $250 copay plus 20% after deductible $0 per medical consultation $12 per medical consultation
Sept. 1, 2023 – Aug. 31, 2024 New Rx Benefits!
Express Scripts is your new pharmacy benefits manager! CVS pharmacies and most of your preferred pharmacies and medication are still included.
Certain specialty drugs are still $0 through SaveOnSP. Doctor Visits Primary Care $30 copay $15 copay You pay 30% after deductibleYou pay 50% after deductible Specialist $70 copay $70 copay You pay 30% after deductibleYou pay 50% after deductible $30 copay You pay 40% after deductible $70 copay You pay 40% after deductible Plan Features Type of Coverage In-Network Coverage Only In-Network Coverage Only In-Network Out-of-Network Individual/Family Deductible $2,500/$5,000 $1,200/$2,400 $3,000/$6,000 $5,500/$11,000 Coinsurance You pay 30% after deductible You pay 20% after deductible You pay 30% after deductibleYou pay 50% after deductible Individual/Family Maximum Out of Pocket $7,500/$15,000 $6,900/$13,800 $7,500/$15,000 $20,250/$40,500 Network Statewide Network Statewide Network Nationwide Network PCP Required Yes Yes No In-Network Out-of-Network $1,000/$3,000 $2,000/$6,000 You pay 20% after deductibleYou pay 40% after deductible $7,900/$15,800 $23,700/$47,400 Nationwide Network No Prescription Drugs Drug Deductible Integrated with medical $200 deductible per participant (brand drugs only) Integrated with medical Generics (31-Day Supply/90-Day Supply)$15/$45 copay; $0 copay for certain generics $15/$45 copay You pay 20% after deductible; $0 coinsurance for certain generics Preferred You pay 30% after deductible You pay 25% after deductible You pay 25% after deductible Non-preferred You pay 50% after deductible You pay 50% after deductible You pay 50% after deductible Specialty (31-Day Max) $0 if SaveOnSP eligible; You pay 30% after deductible $0 if SaveOnSP eligible; You pay 30% after deductible You pay 20% after deductible Insulin Out-of-Pocket Costs$25 copay for 31-day supply; $75 for 61-90 day supply$25 copay for 31-day supply; $75 for 61-90 day supply You pay 25% after deductible $200 brand deductible $20/$45 copay You pay 25% after deductible ($40 min/$80 max)/ You pay 25% after deductible ($105 min/$210 max) You pay 50% after deductible ($100 min/$200 max)/ You pay 50% after deductible ($215 min/$430 max) $0 if SaveOnSP eligible; You pay 30% after deductible ($200 min/$900 max)/ No 90-day supply of specialty medications $25 copay for 31-day supply; $75 for 61-90 day supply 117.00 869.00 427.00 1178.00 194.00 1025.00 558.00 1388.00 131.00 907.00 451.00 1226.00 688.00 2077.00 1182.00 2516.00 7
•
•
HOW IT WORKS

MEMBER INFORMATION Providing Fast And Convenient Care For Your Medical Needs…
•Access to licensed, board-certified physicians • Little or no time missed from work •No crowded waiting rooms or appointment times • Allergies • Arthritic Pain • Cold & Flu • Tonsillitis • Laryngitis • Pharyngitis • Skin Infections
Gastroenteritis
Ear Infection
Pink Eye
Insect Bites
Minor Burns
Respiratory Infections
Sinusitis
Sprains and Strains
Urinary tract Infection
Consulting for International and Domestic Travel
AND MUCH MORE!
COMMONLY TREATED CONDITIONS
•
•
•
•
•
•
•
•
•
•
•
Activate your account online at www.1800MD.com or by calling member services at 1.800.530.8666. Once activated, you will need to setup your member profile and complete your electronic health record. Activate 1 Login to your account online or call member services at 1.800.530.8666 to request a consult anytime 24/7. Request a Consult 2 Receive diagnosis and treatment. 1.800MD provides quality care and peace of mind wherever you are. Receive Care 3 Health and pharmacy information must be completed before requesting a consultation. 8
What is 1.800MD?
1.800MD is a national telehealth company specializing in convenient, quality medical care. With board-certified physicians in all 50 states*, those in need can obtain diagnosis, treatment and a prescription, when necessary, through the convenience of a telephone and digital communications.

*Subjecttostateregulations.
I have a pre-existing condition. Will 1.800MD still accept me?
Absolutely! 1.800MD is not insurance. We do not deny access to quality care because of pre-existing conditions.
Can I get a consultation after hours or on weekends?
Yes. 1.800MD is available 24 hours a day, seven days a week and 365 days a year.
CONVENIENCE
Talk to a doctor any time, day or night, on the weekend or when traveling away from home. No inconvenience or hassle of traveling to the doctor’s office, urgent care or ER and waiting to be seen.
SAVES MONEY
1.800MD reduces unnecessary doctor’s office and emergency room visits. Up to 70 percent of all urgent care and emergency room visits are unneeded, costly and can be handled with a 1.800MD telephone or video consultation.
QUALITY CARE
With an average of 15 years of internal medicine, family practice or pediatrics experience, you can rest assured each physician is properly licensed in your state, board-certified and verified by the National Physician Data Base and the American Medical Association.
CONTINUITY OF CARE
Real-time access to medical records, and the ability to send them to your primary care physi-cian or other providers.
WELLNESS AND PREVENTATIVE HEALTH TOOLS
The 1.800MD member portal contains information and tools to help you make informed health care decisions.
E-PRESCRIPTIONS
If a 1.800MD physician recommends medication as part of your treatment plan, the prescription will be digitally sent to the local pharmacy of your choice.
BENEFITS TO YOU
www.1800md.com CALL 1.800.530.8666 l.800MD does not replace the primary care physician. l800MD does not guarantee that a prescription will be written. l800MD operates subject to State regulations and may not be available in certain States. l800MD does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. l800MD physicians reserve the right to deny care for potentialmisuseofservices. 9
The Ultimate Peace of Mind for Employees and Their Families
The Harrison’s Story
• Jim and his family were at a local festival when his daughter, Sara, suddenly began experiencing horrible abdominal and back pain, after a fall from earlier in the day.
• His wife, Heather, called 911 and Sara was transported to a local hospital, when it was decided that she needed to be flown to another hospital.
• Upon arrival, Sara underwent multiple procedures and her condition was stabilized.

• After further testing, it was discovered that Sara needed additional specialized treatment at another hospital requiring transport on a non-emergent basis.
And then, the Bills came!
Any Ground. Any Air. Anywhere.TM
No matter how comprehensive your local in-network coverage may be, you still have significant exposure to out-of-network emergency transportation. Moreover, when you and your family travel outside your area, there is an 80% chance of being picked up by an out-of-network provider.
A MASA Membership prepares you for the unexpected. ONLY MASA MTS provides you with:
• Coverage ANYWHERE in all 50 states and Canada whether at home or away
• Coverage for BOTH emergent ground ambulance and air ambulance transport REGARDLESS of the provider

• Non-emergent transport services, which are frequently covered inadequately by your insurance, if at all
For more information, please contact your local MASA MTS representative or visit www.masamts.com
As a MASA Member If a Non-MASA Member Sara would pay*If In-Network**If Out-of-Network** 911 Ground Ambulance Cost: $1,800 $0$300$1,600 Emergent Air Ambulance Cost: $45,000 $0$4,000$30,000 Non-Emergent Air Transport† Cost: $20,000 $0$20,000 $20,000 Total Out-of-Pocket Cost $0$24,300$51,600 *Benefit is dependent on Membership Enrolled. **Out-of-pocket dollars vary dependent on provider, distance, health plan design, current status of deductible and out-of pocket max. These figures are an example of the costs one may incur. †More and more health plans are not covering interfacility transports on a non-emergent basis.
FLYER_COMP_B2B
Based on a true story. Names were changed to protect identities in compliance with HIPAA.
10
EMERGENCY TRANSPORTATIONCOSTS

MASA MTS is hereto protect its members andtheir families from the shortcomings of health insurance coverageby providingthem with comprehensivefinancial protectionfor lifesaving emergencytransportationservices, both at home and away fromhome.
ManyAmericanemployers and employees believe that theirhealthinsurancepolicies covermost, if notallambulanceexpenses. Thetruth is, they DONOT!

Even after insurance payments for emergency transportation, you couldreceive abill up to $5,000 forgroundambulanceand as high as $70,000 for air ambulance. The financial burdens for medical transportation costs are veryreal.

HOW MASA ISDIFFERENT
Across the US therearethousands of ground ambulance providers and hundreds of air ambulance carriers. ONLYMASA offers comprehensive coverage since MASA is a PAYERand not aPROVIDER!

ONLY MASA provides over 1.6million members with coverage for BOTH ground ambulance and air ambulance transport, REGARDLESS ofwhich provider transportsthem.
Members are covered ANYWHEREin all50 states andCanada!
Additionally, MASA provides a repatriation benefit: if amember is hospitalizedmore than 100 miles from home, MASA can arrangeand pay to have them transported to a hospital closer to their place of residence.
A MASA Membership prepares you for the unexpectedandgives you the peaceof mind to access vital emergency medical transportation no matter where you live, for a minimal monthlyfee.
• Onelow fee for the entire family
• NO deductibles
• NO healthquestions
• Easy claims process
For more information, pleasecontact Your Broker or MASA Representative
EmergentGround Transportation EmergentAir Transportation Non-EmergentAir Transportation Repatriation U.S./Canada U.S./Canada U.S./Canada U.S./Canada Emergent Plus $14/mo.
EVERY FAMILY DESERVES AMASA MEMBERSHIP OURBENEFITS Benefit*
Ground. Any Air. Anywhere.™ * Please refer to the MSA for a detailed explanation of benefits and eligibility, 11
Any
ACCIDENT INSURANCE for Palestine Independent School District
A personalized guide to understanding your plan
What is Accident Insurance?
This coverage pays benefits for injuries, such as cuts, broken bones, concussions and related expenses. Accident Insurance is supplemental coverage that can complement your health insurance and help cover your out-of-pocket expenses.
When you carry this coverage, if you have a covered accident, you are paid a total cash benefit that is based on the amount listed for each covered benefit and/or treatment. See the benefit schedule for additional details.
Use your benefits any way you like.
Use your benefit proceeds however you want. Whether it is toward your mortgage, medical bills or student loans, it is up to you.
Coverage highlights
• No health questions asked
• Affordable premiums

• Simplified claims-filing
How does the coverage work?
When you carry Accident Insurance and have a covered accident, simply file an Accident claim with our Claims Care Team online, or via mail or fax You’ll be paid a total cash benefit based on the amount listed for each covered benefit and/ or treatment.
Benefit snapshot: Luis’ goal
One night while playing a game with his local soccer league, Luis went for a goal that left him with a broken leg and concussion. Fortunately, he carried Accident Insurance. The benefits Luis received helped offset his medical bills and cover other expenses, like time away from work, while he recovered.
Ground ambulance:
Emergency room treatment:
Fracture (thigh, non-surgical):
Luis’ Accident policy paid these benefits*: $200 $200 $4,000
Concussion: $300
Total benefits paid: $4,700
*This example is for illustrative purposes only. Your plan details may vary. See your enrollment guide for more information around the benefits covered under your group’s plan.
1212 12
What benefits are included in my coverage?
ACCIDENT PLAN BENEFITS BENEFIT AMOUNT Emergency and Initial Accident Treatment Benefits Ambulance Ground $200.00 Air $600.00 Water $600.00 EmergencyRoom Treatment $200.00 UrgentCare $75.00 Major Diagnostic Imaging $200.00 X-ray $75 00 Hospital Benefits Hospital Admission $1,000.00 Hospital Confinement $200.00 Maximum per accident 365 days Intensive Care Admission $1,000.00 ICU Confinement $200.00 Maximum per accident 365 days Observation Unit $100.00 Specific Injury Benefit Fractures Closed/Non-Surgical Treatment Skull (except Bones of Face or Nose) Depressed $4,000.00 Hip, Thigh (Femur) $4,000.00 Vertebrae, Body of (excluding Vertebral Process) $4,000.00 Pelvis $4,000.00 Leg (Tibia and/or Fibula) $4,000.00 Upper Arm (Humerus) $3,000.00 Shoulder Blade $3,000.00 Collarbone $3,000.00 Upper Jaw, Maxilla (except Alveolar Process) $2,500.00 13
Lower Jaw, Mandible (except Alveolar Process) $2,500.00 Vertebral Process $1,600.00 Forearm (Ulna and/or Radius) $1,600.00 Hand, Wrist (except Fingers) $1,600.00 Kneecap $1,600.00 Foot (except Toes) $1,600.00 Ankle $1,600.00 Rib $300.00 Coccyx $300.00 Finger, Toe $300.00 Enhancement for Open/Surgical Reduction 2X Chip Fractures 25% Dislocations Closed/Non-Surgical Treatment Hip $4,000.00 Knee (other than Kneecap) $2,250.00 Shoulder $2,250.00 Kneecap $1,000.00 Ankle bone or bones of the foot $1,000.00 Elbow $1,000.00 Wrist $1,000.00 Bone or bones of the hand $1,000.00 Jawbone $1,000.00 Collarbone $1,000.00 One toe or finger $300.00 Enhancement for Open/Surgical Reduction 2X Partial Dislocations 25% Lacerations No Repair $50.00 Repair - up to 2 inches $50.00 Repair - over 2 inches, up to 6 inches $200.00 Repair - over 6 inches $400.00 Burns 2nd Degree Burns At least 1%, but less than 20% of skin surface $100.00 20% or greater of skin surface $500.00 3rd Degree Burns Less than 5% of skin surface $500.00 At least 5%, but less than 20% of skin surface $5,000.00 20% or greater of skin surface $10,000.00 Skin Graft 14
Due to Burns (% of applicable Burn benefit)
50% Not due to Burns At least 1%, but less than 20% of skin surface $100.00 20% or greater of skin surface $200.00 Concussion and Other Brain Injuries $300.00 Dental Benefit $250.00 Eye Injury Benefit $200.00 Surgery Benefits Outpatient Surgery Benefit Facilities other than Physician Office or Emergency Room $300.00 Physician Office or Emergency Room $300.00 Internal Injuries Surgical Benefits Open Abdominal & Thoracic $2,000.00 Hernia $200.00 Exploratory without Repair $150.00 Tendon/Ligament/Rotator Cuff Surgical Benefit Single $700.00 Multiple $1,050.00 Exploratory without Repair $150.00 Torn Knee Cartilage Surgery Benefit Torn with Surgical Repair $600.00 Exploratory without Repair $225.00 Diagnosis only with no surgery or repair $100.00 Ruptured Disc with Surgical Repair $600.00 Anesthesia Benefit General Anesthesia $200.00 Epidural or Regional Anesthesia $200.00 Medical Benefits Blood, Plasma & Platelets Benefit $500.00 Prosthetic Device Benefit One only $1,000.00 Two or more $2,000.00 Appliances $300.00 Pain Management Benefit $200.00 Follow-Up Care and Transportation Benefits Physician Office Visit $75.00 Maximum number of visits 4 Therapy Services Benefit (Occupational, Physical, Speech Therapy) $60.00 Maximum number of visits 12 Rehabilitation Unit Confinement $200.00 15
Maximum number of days 90 Residence/Vehicle Modification Benefit $1,000 00 Transportation (minimum of 100 miles from residence, up to 3 round trips) $.60/mile Lodging $200.00 Maximum number of days 30 Accidental Death Benefits Accidental Death Employee $40,000.00 Spouse $20,000.00 Child(ren) $20,000.00 Common Carrier Accidental Death Employee $200,000.00 Spouse $100,000.00 Child(ren) $100,000.00 Organ Donor Benefit $5,000.00 Accidental Dismemberment Benefits Dismemberment Loss of Both Hands, or Loss of Both Feet, or Loss of One Hand and One Foot $40,000.00 Loss of One Hand or Loss of One Foot $20,000.00 Partial Dismemberment Loss of One or More Fingers or Toes $600 00 Partial Amputation of Finger or Toe $200 00 Catastrophic Benefits Catastrophic Loss Loss of Sight in both eyes or Hearing in both ears $20,000.00 Loss of Speech or Sight in one eye or Hearing in one ear $5,000.00 Coma $20,000.00 Paralysis Paraplegia $15,000.00 Quadriplegia $30,000.00 Riders Health Screening Benefit Rider: $200.00 16
member,
1 per covered
per annual year
Blood tests for triglycerides
Annual exam for adults
Bone density screening
Breast MRI
Carotid ultrasound
Concussion baseline testing
How much does it cost?
Examples of Eligible Screening Events
Colonoscopy
Bone marrow testing
Chicken pox immunization
Fasting blood glucose test
Flu vaccination
Dermatological screening for skin cancer
Hepatitis B immunization
HPV immunization
Mammography
Pap smear
Pneumonia immunization
Genetic screening for medical diagnosis & treatment
Sports physicals
Stress test
Tetanus
Virtual colonoscopy
Well child visits
Serum cholesterol
HDL/LDL
See the rate chart below to calculate your coverage costs.
Employee Only Employee & Spouse Employee & Child(ren) Family Monthly Rate $13.85 $25.48 $27.34 $34.14 17
Exclusions & limitations
This is not a complete disclosure of plan qualifications and limitations. Benefits and riders may vary and may not be available in all states. In addition to any benefit-specific exclusion, benefits will not be paid for any loss which, directly or indirectly, in whole or in part, is caused by or results from any of the following, unless coverage is specifically provided for by name in the insurance certificate.
• An injury incurred while working for pay or profit;
• Intentionally self-inflicted injury, suicide, or any attempt or threat while sane or insane;
• Participating in war or any act of war whether declared or undeclared;
• Commission or attempt to commit a felony;
• Commission of or active participation in a riot, insurrection, or terrorist activity;
• Engaging in an illegal activity or occupation;
• Flight in, boarding, or alighting from an aircraft or any craft designed to fly above the earth’s surface, including any travel beyond the earth’s atmosphere except a fare-paying passenger on a regularly scheduled commercial or charter airline;
• Travel in or on any on-road and off-road motorized vehicle except a golf cart that does not require licensing as a motor vehicle;
• Practicing for or participating in any semi-professional or professional competitive athletic contest, including officiating or coaching, for which the covered person receives any compensation or remuneration;
• Sickness, except for any bacterial infection resulting from an accidental external cut or wound or accidental ingestion of contaminated food;
• Voluntary ingestion or inhalation of any narcotic, drug, poison, gas or fumes, unless prescribed or taken under the direction of a physician and taken in accordance with the prescribed dosage;
• Operating any type of vehicle while under the influence of alcohol or any drug, narcotic or other intoxicant including any prescribed drug for which the covered person has been provided a written warning against operating a vehicle while taking it. Under the influence of alcohol, for purposes of this exclusion, means intoxicated, as defined by the law of the State in which the covered accident occurred;
• Care that is not recommended and approved by a physician.
Questions?
Contact your plan administrator with questions about the offered Accident coverage.
This document is meant to highlight some, but not all the features Wellfleet coverage provides. It is not an insurance contract. Wellfleet Workplace benefits provide limited benefits and are not a substitute for mandated ACA healthcare coverage. Like most supplemental offerings, these benefits may have state-specific variations, and some product offerings and details may not be available in all states. Rates are subject to change. Wellfleet reserves the right to raise premium with proper notice, as noted in the policy. For complete details, see your certificate. Wellfleet is the marketing name used to refer to the insurance and administrative operations of Wellfleet Insurance Company, Wellfleet New York Insurance Company and Wellfleet Group, LLC. All insurance products are administered or managed by Wellfleet Group, LLC.
©2022 Wellfleet Group, LLC. All rights reserved.
18
Palestine Independent School District UNUM Critical Illness Plan Highlights
Policy Number 474777
Critical Illness insurance provides financial protection by paying a lump sum benefit if you are diagnosed with a covered critical illness.
Who is eligible for this coverage?
What are the Critical Illness coverage amounts?
All employees in active employment in the United States working at least 15 hours per week and their eligible spouses and children (up to age 26 regardless of student or marital status).
The following coverage amounts are available.
For you: Select one of the following $10,000, $15,000 or $20,000
For your Spouse: 100% of employee coverage amount
For your Children: 50% of employee coverage amount Can I be denied coverage?
When is coverage effective?
Coverage is guarantee issue.
Please see your Plan Administrator for your effective date of coverage.
Insurance coverage will be delayed if you are not in active employment because of an injury, sickness, temporary layoff, or leave of absence on the date that insurance would otherwise become effective.
What critical illness conditions are covered? Covered Conditions* Percentage of Coverage Amount Critical Illnesses Coronary Artery Disease (major) 50% Coronary Artery Disease (minor) 10% End Stage Renal (Kidney) Failure 100% Heart Attack (Myocardial Infarction) 100% Major Organ Failure Requiring Transplant 100% Stroke 100% Cancer Invasive Cancer (including all Breast Cancer) 100% Non-Invasive Cancer 25% Skin Cancer $500 Supplemental Critical Illnesses Benign Brain Tumor 100% Coma 100% Loss of Hearing 100% Loss of Sight 100% Loss of Speech 100% Infectious Disease 25% Occupational Human Immunodeficiency Virus (HIV) or Hepatitis 100% Permanent Paralysis 100%
19
Are wellness screenings covered?
*Please refer to the policy for complete definitions of covered conditions.
Covered Condition Benefit
The covered condition benefit is payable once per covered condition per insured.
Unum will pay a covered condition benefit for a different covered condition if: - the new covered condition is medically unrelated to the first covered condition; or
- the dates of diagnosis are separated by more than 180 days.
Reoccurring Condition Benefit
We will pay the reoccurring condition benefit for the diagnosis of the same covered condition if the covered condition benefit was previously paid and the new date of diagnosis is more than 180 days after the prior date of diagnosis.
The benefit amount for any reoccurring condition benefit is 100% of the percentage of coverage amount for that condition.
The following Covered Conditions are eligible for a reoccurring condition benefit:
Benign Brain Tumor Heart Attack (Myocardial Infarction)
Coma
Invasive Cancer (includes all Breast Cancer)
Coronary Artery Disease (Major) Major Organ Failure Requiring Transplant
Coronary Artery Disease (Minor) Non-Invasive Cancer
End Stage Renal (Kidney) Failure Stroke
Each insured is eligible to receive one Be Well Benefit per calendar year.
Be Well Benefit
For you, your spouse and your children: $50
If the employee’s Critical Illness Coverage Amount is: The Be Well Benefit Amount for you, your spouse and your children is:
Be Well Screenings include tests for the following: cholesterol and diabetes, cancer and cardiovascular function. They also include imaging studies, immunizations and annual examinations by a Physician. See certificate for details.
Progressive Diseases Amyotrophic Lateral Sclerosis (ALS) 100% Dementia (including Alzheimer’s Disease) 100% Functional Loss 100% Multiple Sclerosis (MS) 100% Parkinson’s Disease 100% Additional Critical Illnesses for your Children Cerebral Palsy 100% Cleft Lip or Palate 100% Cystic Fibrosis 100% Down Syndrome 100% Spina Bifida 100%
$10,000 $50 $15,000 $50 $20,000 $50
20
does the coverage cost? Option 1 Monthly Critical Illness Cost $10,000 EE, $10,000 SP, $50 Be Well Benefit Age Employee Cost Spouse Cost Less than age 25 $3.84 $3.84 25-29 $4.74 $4.74 30-34 $5.84 $5.84 35-39 $7.84 $7.84 40-44 $10.24 $10.24 45-49 $13.34 $13.34 50-54 $16.94 $16.94 55-59 $22.84 $22.84 60-64 $31.84 $31.84 65-69 $45.94 $45.94 70-74 $71.04 $71.04 75-79 $104.24 $104.24 80-84 $151.14 $151.14 85 or over $242.94 $242.94 Option 2 Monthly Critical Illness Cost $15,000 EE, $15,000 SP, $50 Be Well Benefit Age Employee Cost Spouse Cost Less than age 25 $4.84 $4.84 25-29 $6.19 $6.19 30-34 $7.84 $7.84 35-39 $10.84 $10.84 40-44 $14.44 $14.44 45-49 $19.09 $19.09 50-54 $24.49 $24.49 55-59 $33.34 $33.34 60-64 $46.84 $46.84 65-69 $67.99 $67.99 70-74 $105.64 $105.64 75-79 $155.44 $155.44 80-84 $225.79 $225.79 85 or over $363.49 $363.49 21
How much
Do my critical illness insurance benefits decrease with age?
Are there any exclusions or limitations?
Option 3
Your rate is based on your insurance age, which is your age immediately prior to and including the anniversary/effective date.
Spouse rate is based on your Spouse’s insurance age, which is their age immediately prior to and including the anniversary/effective date.
Critical Illness benefits do not decrease due to age.
We will not pay benefits for a claim that is caused by, contributed to by, or occurs as a result of any of the following:
- committing or attempting to commit a felony;
- being engaged in an illegal occupation or activity;
- injuring oneself intentionally or attempting or committing suicide, whether sane or not;
- active participation in a riot, insurrection, or terrorist activity. This does not include civil commotion or disorder, injury as an innocent bystander, or Injury for self-defense;
- participating in war or any act of war, whether declared or undeclared;
- combat or training for combat while serving in the armed forces of any nation or authority, including the National Guard, or similar government organizations;
- voluntary use of or treatment for voluntary use of any prescription or nonprescription drug, alcohol, poison, fume, or other chemical substance unless taken as prescribed or directed by the Insured’s Physician;
- being intoxicated; and
- a Date of Diagnosis that occurs while an Insured is legally incarcerated in a penal or correctional institution.
Additionally, no benefits will be paid for a Date of Diagnosis that occurs prior to the coverage effective date.
Monthly Critical Illness Cost $20,000 EE, $20,000 SP, $50 Be Well Benefit Age Employee Cost Spouse Cost Less than age 25 $5.84 $5.84 25-29 $7.64 $7.64 30-34 $9.84 $9.84 35-39 $13.84 $13.84 40-44 $18.64 $18.64 45-49 $24.84 $24.84 50-54 $32.04 $32.04 55-59 $43.84 $43.84 60-64 $61.84 $61.84 65-69 $90.04 $90.04 70-74 $140.24 $140.24 75-79 $206.64 $206.64 80-84 $300.44 $300.44 85 or over $484.04 $484.04
22
Is the coverage portable (can I keep it if I leave my employer)?
Pre-existing Conditions
We will not pay benefits for a claim when the covered loss occurs in the first 12 months following an insured’s coverage effective date and the covered loss is caused by, contributed to by, or occurs as a result of any of the following:
- a pre-existing condition; or
- complications arising from treatment or surgery for, or medications taken for, a pre-existing condition.
An insured has a pre-existing condition if, within the 3 months just prior to their coverage effective date, they have an injury or sickness, whether diagnosed or not, for which:
- medical treatment, consultation, care or services, or diagnostic measures were received or recommended to be received during that period;
- drugs or medications were taken, or prescribed to be taken during that period; or
- symptoms existed.
Pre-existing Condition requirements are not applicable to children who are newly acquired after your Coverage Effective Date.
The pre-existing condition provision applies to any Insured’s initial coverage and any increases in coverage. Coverage effective date refers to the date any initial coverage or increases in coverage become effective.
If your employment with your employer ends or you are no longer in an eligible group you can apply for ported coverage and pay the first premium within 31 days to continue coverage for yourself, your spouse and your children.
If your spouse’s coverage ends as a result of your death, divorce or annulment, your spouse may elect to continue spouse and children coverage, as long as premium is paid as required.
When does my coverage end?
If you choose to cancel coverage, it will end on the first of the month following the date you provide notification to your employer.
Otherwise, coverage ends on the earliest of:
- the date the policy is cancelled by your employer;
- the date you no longer are in an eligible group;
- the date your eligible group is no longer covered;
- the date of your death
- the last day of the period any required contributions are made;
- the last day you are in active employment
If you choose to cancel your Spouse’s coverage, it will end on the first of the month following the date you provide notification to your employer.
Otherwise, your spouse’s coverage will end on the earliest of:
- the date your coverage ends;
- the date your spouse is no longer eligible for coverage;
- the date your spouse no longer meets the definition of a spouse;
- the date of your spouse’s death; or
- the date of divorce or annulment.
23
Your children’s coverage will end on the earliest of:
- the date your coverage ends;
- the date your children are no longer eligible for coverage; or
- the date your children no longer meet the definition of children.
The limited benefits provided are a supplement to major medical coverage and are not a substitute for major medical coverage or other minimal essential coverage as required by federal law. Lack of minimal essential coverage may result in an additional tax payment being due.
This information is not intended to be a complete description of the insurance coverage available. The policy or its provisions may vary or be unavailable in some states. The policy has exclusions and limitations which may affect any benefits payable. For complete details of coverage and availability, please refer to Policy Form GCIP16-1 et al or contact your Unum representative.
© 2018 Unum Group. All rights reserved. Unum is a registered trademark and marketing brand of Unum Group and its insuring subsidiaries.
Underwritten by Unum Insurance Company, Portland, Maine
AE-1226 FOR EMPLOYEES
24
Zurich Specialty Health Supplemental
GAP Medical
*This maximum applies to the entire family unit, regardless of the number of covered persons within the family unit. An “occurrence” is the treatment, or series of treatments, for a specific sickness or injury. All expenses related to the treatment of the same or related sickness or injury will accrue toward the out-patient maximum for one occurrence, regardless of whether such treatment is received in more than one calendar year period. If, however, a Covered Person is treatment-free, at any time, for at least 30 consecutive days, they may qualify for an additional outpatient maximum benefit if the family maximum per calendar year has not been met.
Monthly Rates*
Employees and dependents enrolled in the company sponsored Major Medical Plan may enroll for coverage in the Zurich Supplemental GAP Medical Plan.
– Plan 1 Inpatient Expense Benefit Per Covered Person $1,500 per Plan Year Per Family N/A Outpatient Expense Benefit I Per Covered Person $1,000 per Injury or Sickness per Plan Year Maximum Per Family* 4 outpatient occurrences per Family per Plan Year
Coverage Summary
Four-Tier Rates Under 40 Age 40-49 Age 50+ Composite Employee Only N/A N/A N/A $41.30 Employee & Spouse N/A N/A N/A $75.89 Employee & Children N/A N/A N/A $95.83 Employee & Family N/A N/A N/A $123.27
25
Serving customers for almost 150 years
Zurich Insurance Group





Founded in Switzerland in 1872, we are one of the world’s most experienced global insurers
Providing a wide range of property and casualty, and life insurance products and services in more than 215 countries and territories
Strong investor proposition; resilient business model, clear strategy, and responsible and impactful business
Doing business in the U.S. since 1912
Approximately 55,000 experienced professionals worldwide
Approximately 9,000 employees in North America
North America contributed approximately $1.43 billion toward Zurich’s $4.2 billion in operating profit in 2020
Insurance a broad range of Middle Market customers as well as more than 95 percent of the Fortune 500
Providing multinational solutions in the U.S. for almost 50 years
Zurich North America is one of the largest providers of insurance solutions and services to businesses and individuals.
To learn more, visit www.zurichna.com
• Eligibility
• Employees enrolled in the company’s sponsored Major Medical Plan are eligible for Gap medical coverage. Employee’s dependents are also eligible for coverage.
• Eligibility waiting period
• Same as Major Medical Plan.
• Inpatient Expense Benefit – Benefits will be paid if a covered person is confined to a hospital as a direct result of an injury sustained in an accident or sickness. Benefits are limited to out-of-pocket expenses incurred by the covered person, including the deductible and coinsurance amounts the covered person is required to pay under the Major Medical Plan.
• Outpatient Expense Benefit – Benefits will be paid for outpatient treatment of an injury sustained in an accident or sickness. Benefits are limited to out-of-pocket expenses incurred by the covered person, including the deductible and coinsurance amounts the covered person is required to pay under the Major Medical Plan.
• Combined Inpatient and Outpatient Expense Benefit –Benefits will be paid if a covered person is confined to a hospital or receives outpatient treatment as a direct result of an injury sustained in an accident or sickness. Benefits are limited to out-of-pocket expenses incurred by the covered person, including the deductible and coinsurance amounts the covered person is required to pay under the Major Medical Plan. All benefits are subject to the Policy Deductible and the Supplemental Medical Coinsurance percentage for the Plan Year shown on the following pages:
• Policy Deductible – Benefits will be payable after the Covered Person has met the “Per Covered Person” Policy Deductible or after the “Per Family” Policy Deductible has been met, whichever occurs first.
• Supplemental Medical Co-insurance – The maximum percentage that will be paid under this Policy for covered expenses incurred by a covered person.
• Plan Year – A consecutive 12-month period during which a covered person’s coverage under the policy is in force.
Zurich 1299 Zurich Way, Schaumburg, Illinois 60196-1056 800.382.2150 www.zurichna.com
26
General exclusions and limitations
This coverage does not cover any loss, treatment, or services resulting from any of the following:
1. Suicide or any attempt at suicide
2. Intentionally self-inflicted Injury or Sickness, while sane or insane
3. Declared or undeclared war, or any act of declared or undeclared war
4. Full-time active duty in the armed forces of any country or international authority
5. Any Injury or Sickness for which the Covered Person is entitled to benefits pursuant to any workers’ compensation law or other similar legislation
6. The Covered Person’s commission of or attempt to commit a felony, assault, sexual assault, riot or insurrection or any Injury resulting from the Covered Person’s provocation of an attack against them
7. Travel or flight in or on (including getting in or out of, or on or off of) any vehicle used for aerial navigation, if the Covered Person is
a. Riding as a passenger in any aircraft not intended or licensed for the transportation of passengers
b. Performing, learning to perform or instructing others to perform as a pilot or crew member of any aircraft
c. Riding as a passenger in an aircraft owned, leased or operated by the Policyholder or the Covered Person
8. Skydiving, parasailing, parachuting, hang-gliding, bungee-jumping and participation in a contest of speed in power driven vehicles
9. Dental or vision services, including treatment, surgery, extractions, or x-rays, unless: (a) resulting from an Accident occurring while the Covered Person’s coverage is in force and if performed within 12 months of the date of such Accident; or (b) due to congenital disease or anomaly of a covered newborn child
10. Treatment or services for Injury and Sickness provided outside of the United States
11. Rest care or rehabilitative care and treatment (this does not include rehabilitation for treatment of physical disability)
12. Voluntary abortion except, with respect to the Covered Person: (a) where the Insured or the Insured’s Dependent’s life would be endangered if the fetus were carried to term; or (b) where medical complications have arisen from abortion
13. Elective cosmetic surgery (except newborn circumcision)
14. Sterilization and reversal of sterilization
15. Any expense which is not Medically Necessary
16. Prescription drugs
17. Any loss for which the Covered Person is not required to pay a Health Benefit Plan Deductible, co-payment and/or Health Benefit Plan Coinsurance under the Covered Person’s Health Benefit Plan; and
18. Any expense or benefit that is excluded under the Covered Person’s Health Benefit Plan
Health Benefit Plan Limitation
If a Covered Person does not have a Health Benefit Plan on the Covered Person’s Effective Date under this coverage, the Company’s sole obligation will then be to refund all premiums paid for that Covered Person.
27
Nearly everyone has experienced or knows somebody who has experienced a cancer diagnosis in their family. The good news is that cancer screenings and cancer-fighting technologies have gotten a lot better in recent years. However, with advanced technology come high costs. Major medical health insurance is a great start, but even with this essential safety net, cancer sufferers can still be hit with unexpected medical and non-medical expenses.
Cancer coverage from Colonial Life offers the protection you need to concentrate on what is most important — your care.
Features of Colonial Life’s Cancer Insurance:

1. Pays benefits to help with the cost of cancer screening and cancertreatment.
2. Provides benefits to help pay for the indirect costs associated with cancer, such as:
l Loss of wages or salary
l Deductibles and coinsurance
l Travel expenses to and from treatment centers

l Lodging and meals
l Child care
3. Pays regardless of any other insurance you have with other insurance companies.
4. Provides a cancer screening benefit that you can use even if you are never diagnosed with cancer.
5. Benefits paid directly to you unless you specify otherwise.
6. Flexible coverage options for employees and theirfamilies.
Group Cancer 1000 With Additional Benefits 28
This is a brief description of some available benefits.
We will pay benefits if one of the following routine cancer screening tests is performed or if cancer is diagnosed while your coverage is in force.

Cancer Screening Benefit Tests
This benefit is payable once per calendar year per covered person.
l Pap Smear
l ThinPrep Pap Test1
l CA125 (Blood test for ovarian cancer)
l Mammography
l Breast Ultrasound
l CA15-3(Bloodtestforbreastcancer)
l PSA(Bloodtest for prostate cancer)
l Chest X-ray
l Biopsy of Skin Lesion
l Colonoscopy
l Virtual Colonoscopy
l Hemoccult Stool Analysis
l Flexible Sigmoidoscopy
l CEA (Blood test for colon cancer)
l Bone Marrow Aspiration/Biopsy
l Thermography
l Serum Protein Electrophoresis (Blood test for Myeloma)
To file a claim for a covered cancer screening/wellness test, it is not necessary to complete a claim form. Call our toll-free Customer Service number, 1.800.325.4368, with the medical information
Inpatient Benefits
l Hospital andHospitalIntensiveCare Unit Confinement
l Ambulance
l Private Full-Time Nursing Services
l Attending Physician
Treatment Benefits (In-or Outpatient)
l Radiation/Chemotherapy
l Antinausea Medication
l Blood/Plasma/Platelets/Immunoglobulins
l Experimental Treatment
l HairProsthesis/ExternalBreast/VoiceBoxProsthesis
l Supportive/Protective Care Drugs and Colony
Stimulating Factors
l Bone Marrow Stem Cell Transplant
l Peripheral Stem Cell Transplant
Surgery Benefits
l Surgery Procedures (including skin cancer)
l Anesthesia (including skin cancer)
l Second Medical Opinion
l Reconstructive Surgery
l Prosthesis/ArtificialLimb
l Outpatient Surgical Center
Transportation/Lodging Benefits
l Transportation
l Transportation for Companion
l Lodging
Extended Care Benefits
l Skilled Nursing Care Facility
l Hospice
l Home Health Care Service
Waiver of Premium
THIS IS A CANCER ONLY POLICY.
This policy has exclusions and limitations. For cost and complete details of the coverage, see your Colonial Life benefits counselor. Coverage may vary by state and may not be available in all states. Applicable to policy form GCAN-MP and certificate form GCAN-C (including state abbreviations where used, for example GCAN-C-TX.)
1ThinPrep is a registered trademark of Cytyc Corporation.
Colonial Life 1200 Colonial Life Boulevard Columbia, South Carolina 29210 coloniallife.com Group Cancer 1000 With Additional Benefits 29
Educator Options Voluntary Long Term Disability Coverage Highlights – Texas Palestine Independent School District

Voluntary Long Term Disability Insurance
Standard Insurance Company has developed this document to provide you with information about the optional insurance coverage you may select through Palestine Independent School District. Written in non-technical language, this is not intended as a complete description of the coverage. If you have additional questions, please check with your human resources representative.
Employer Plan Effective Date
The group policy effective date is October 1, 2013.
Eligibility
To become insured, you must be:
• A regular employee of Palestine Independent School District, excluding temporary or seasonal employees, fulltime members of the armed forces, leased employees or independent contractors

• Actively at work at least 15 hours each week
• A citizen or resident of the United States or Canada
Employee Coverage Effective Date
Please contact your human resources representative for more information regarding the following requirements that must be satisfied for your insurance to become effective. You must satisfy:
• Eligibility requirements
• An evidence of insurability requirement, if applicable
• An active work requirement. This means that if you are not actively at work on the day before the scheduled effective date of insurance, your insurance will not become effective until the day after you complete one full day of active work as an eligible employee.
Benefit Amount
You may select a monthly benefit amount in $100 increments from $200 to $8,000; based on the tables and guidelines presented in the Rates section of these Coverage Highlights. The monthly benefit amount must not exceed 66 2/3 percent of your monthly earnings.
Benefits are payable for non-occupational disabilities only. Occupational disabilities are not covered.
Plan Maximum Monthly Benefit: 66 2/3 percent of predisability earnings
Plan Minimum Monthly Benefit: 10 percent of your LTD benefit before reduction by deductible income
SI 14494-156607 (4/16)
30
Benefit Waiting Period and Maximum Benefit Period
The benefit waiting period is the period of time that you must be continuously disabled before benefits become payable. Benefits are not payable during the benefit waiting period. The maximum benefit period is the period for which benefits are payable. The benefit waiting period and maximum benefit period associated with your plan options are shown below:
Options 1-6: Maximum Benefit Period To Age 65 for Sickness and Accident
If you become disabled before age 62, LTD benefits may continue during disability until you reach age 65. If you become disabled at age 62 or older, the benefit duration is determined by your age when disability begins:
First Day Hospital Benefit
With this benefit, if an insured employee is hospital confined for at least four hours, is admitted as an inpatient and is charged room and board during the benefit waiting period, the benefit waiting period will be satisfied. Benefits become payable on the date of hospitalization; the maximum benefit period also begins on that date. This feature is included only on LTD plans with benefit waiting periods of 30 days or less.
Preexisting Condition Exclusion
A general description of the preexisting condition exclusion is included in the Group Voluntary Long Term Disability Insurance for Educators and Administrators brochure. If you have questions, please check with your human resources representative.
Preexisting Condition Period: The 90-day period just before your insurance becomes effective Exclusion Period: 12 months
Insurance Company Educator Options Voluntary Long Term Disability Coverage Highlights – Texas Palestine Independent School District SI 14494-156607 (4/16)
Standard
Option Accidental Injury Other Disability Maximum Benefit Period 1 7 days 7 days To age 65 for both Sickness and Accident 2 14 days 14 days To age 65 for both Sickness and Accident 3 30 days 30 days To age 65 for both Sickness and Accident 4 60 days 60 days To age 65 for both Sickness and Accident
90 days 90 days
age 65 for both Sickness and Accident
180 days 180 days
age 65 for both Sickness and Accident
5
To
6
To
Age Maximum Benefit Period 62 3 years 6 months 63 3 years 64 2 years 6 months
2 years 66 1 year 9 months
1 year 6 months
1 year 3 months
1 year
65
67
68
69+
31
Preexisting Condition Waiver
If your insurance has been in force for 12 months or more, for the first 90 days of disability after the benefit waiting period, the Preexisting Condition provision will not be applied to an increase in your benefit amount. After 90 days of benefits, the Preexisting Condition provision will apply to increases of more than $300. The Preexisting Condition Provision applies immediately if you:
• Decrease your Benefit Waiting Period by more than one level; or
• Increase your Maximum Benefit Period
If your insurance has been in force for less than 12 months and your disability is found to be a Preexisting Condition, you may be eligible for up to 90 days of benefits if you are disabled and meet all applicable policy provisions. If the Benefit Waiting Period you elect under this policy is less than the Benefit Waiting Period you were insured for under the Prior Plan, your benefits will begin on the later of these two plans.
If a disability is deemed to be a Preexisting Condition, benefits are payable under your prior elections, if any.
Own Occupation Period
For the plan’s definition of disability, as described in your brochure, the own occupation period is the first 24 months for which LTD benefits are paid.
Any Occupation Period
The any occupation period begins at the end of the own occupation period and continues until the end of the maximum benefit period.
Other LTD Features
• Employee Assistance Program (EAP) – This program offers support, guidance and resources that can help an employee resolve personal issues and meet life’s challenges.
• Family Care Expense Adjustment – Disabled employees faced with the added expense of family care when returning to work may receive combined income from LTD benefits and work earnings in excess of 100 percent of indexed predisability earnings during the first 12 months immediately after a disabled employee’s return to work.
• Special Dismemberment Provision – If an employee suffers a lost as a result of an accident, the employee will be considered disabled for the applicable Minimum Benefit Period and can extend beyond the end of the Maximum Benefit Period
• Reasonable Accommodation Expense Benefit – Subject to The Standard’s prior approval, this benefit allows us to pay up to $25,000 of an employer’s expenses toward work-site modifications that result in a disabled employee’s return to work.
• Survivor Benefit – A Survivor Benefit may also be payable. This benefit can help to address a family’s financial need in the event of the employee’s death.
• Return to Work (RTW) Incentive – The Standard’s RTW Incentive is one of the most comprehensive in the employee benefits history. For the first 12 months after returning to work, the employee’s LTD benefit will not be reduced by work earnings until work earnings plus the LTD benefit exceed 100 percent of predisability earnings. After that period, only 50 percent of work earnings are deducted.
• Rehabilitation Plan Provision – Subject to The Standard’s prior approval, rehabilitation incentives may include training and education expense, family (child and elder) care expenses, and job-related and job search expenses.
Standard Insurance Company Educator Options Voluntary Long Term Disability Coverage Highlights – Texas Palestine Independent School District SI 14494-156607 32 (4/16)
When Benefits End
LTD benefits end automatically on the earliest of:
• The date you are no longer disabled
• The date your maximum benefit period ends
• The date you die
• The date benefits become payable under any other LTD plan under which you become insured through employment during a period of temporary recovery
• The date you fail to provide proof of continued disability and entitlement to benefits
Rates
Employees can select a monthly LTD benefit ranging from a minimum of $200 to a maximum amount based on how much they earn. Referencing the appropriate attached charts, follow these steps to find the monthly cost for your desired level of monthly LTD benefit and benefit waiting period:
1.Find the maximum LTD benefit by locating the amount of your earnings in either the Annual Earnings or Monthly Earnings column. The LTD benefit amount shown associated with these earnings is the maximum amount you can receive. If your earnings fall between two amounts, you must select the lower amount.
2. Select the desired monthly LTD benefit between the minimum of $200 and the determined maximum amount, making sure not to exceed the maximum for your earnings.
3. In the same row, select the desired benefit waiting period to see the monthly cost for that selection. If you have questions regarding how to determine your monthly LTD benefit, the benefit waiting period, or the premium payment of your desired benefit, please contact your human resources representative.
Group Insurance Certificate
If you become insured, you will receive a group insurance certificate containing a detailed description of the insurance coverage. The information presented above is controlled by the group policy and does not modify it in any way. The controlling provisions are in the group policy issued by Standard Insurance Company.
Standard Insurance Company Educator Options Voluntary Long Term Disability Coverage Highlights – Texas Palestine Independent School District SI 14494-156607 33 (4/16)
Disability
– Texas Palestine Independent School District SI 14494-156607 34 (4/16) Annual Earnings Monthly Earnings Monthly Disability Benefit Accident/Sickness Benefit Waiting Period Cost Per Month 7 and 7 14-14 30-30 60-60 90-90 180-180 3,600 300 200 6.84 6.29 5.34 3.46 2.99 2.19 5,400 450 300 10.25 9.43 8.01 5.19 4.49 3.29 7,200 600 400 13.67 12.57 10.68 6.92 5.99 4.39 9,000 750 500 17.09 15.72 13.35 8.65 7.49 5.49 10,800 900 600 20.51 18.86 16.01 10.38 8.98 6.58 12,600 1,050 700 23.92 22 18.68 12.11 10.48 7.68 14,400 1,200 800 27.34 25.15 21.35 13.84 11.98 8.78 16,200 1,350 900 30.76 28.29 24.02 15.57 13.48 9.88 18,000 1,500 1,000 34.18 31.43 26.69 17.3 14.97 10.97 19,800 1,650 1,100 37.59 34.58 29.36 19.03 16.47 12.07 21,600 1,800 1,200 41.01 37.72 32.03 20.76 17.97 13.17 23,400 1,950 1,300 44.43 40.86 34.7 22.49 19.46 14.27 25,200 2,100 1,400 47.85 44.01 37.37 24.22 20.96 15.36 27,000 2,250 1,500 51.26 47.15 40.04 25.95 22.46 16.46 28,800 2,400 1,600 54.68 50.29 42.71 27.68 23.96 17.56 30,600 2,550 1,700 58.1 53.44 45.37 29.41 25.45 18.66 32,400 2,700 1,800 61.52 56.58 48.04 31.14 26.95 19.75 34,200 2,850 1,900 64.93 59.72 50.71 32.87 28.45 20.85 36,000 3,000 2,000 68.35 62.87 53.38 34.6 29.95 21.95 37,800 3,150 2,100 71.77 66.01 56.05 36.33 31.44 23.05 39,600 3,300 2,200 75.19 69.15 58.72 38.06 32.94 24.14 41,400 3,450 2,300 78.6 72.3 61.39 39.79 34.44 25.24 43,200 3,600 2,400 82.02 75.44 64.06 41.52 35.94 26.34 45,000 3,750 2,500 85.44 78.59 66.73 43.25 37.43 27.44 46,800 3,900 2,600 88.86 81.73 69.4 44.97 38.93 28.53 48,600 4,050 2,700 92.28 84.87 72.07 46.7 40.43 29.63 50,400 4,200 2,800 95.69 88.02 74.73 48.43 41.92 30.73 52,200 4,350 2,900 99.11 91.16 77.4 50.16 43.42 31.82 54,000 4,500 3,000 102.53 94.3 80.07 51.89 44.92 32.92 55,800 4,650 3,100 105.95 97.45 82.74 53.62 46.42 34.02 57,600 4,800 3,200 109.36 100.59 85.41 55.35 47.91 35.12 59,400 4,950 3,300 112.78 103.73 88.08 57.08 49.41 36.21 61,200 5,100 3,400 116.2 106.88 90.75 58.81 50.91 37.31 63,000 5,250 3,500 119.62 110.02 93.42 60.54 52.41 38.41 64,800 5,400 3,600 123.03 113.16 96.09 62.27 53.9 39.51 66,600 5,550 3,700 126.45 116.31 98.76 64 55.4 40.6 68,400 5,700 3,800 129.87 119.45 101.43 65.73 56.9 41.7 70,200 5,850 3,900 133.29 122.59 104.09 67.46 58.39 42.8 72,000 6,000 4,000 136.7 125.74 106.76 69.19 59.89 43.9
Standard Insurance Company Educator Options Voluntary Long Term
Coverage Highlights
– Texas Palestine Independent School District SI 14494-156607 35 (4/16) Annual Earnings Monthly Earnings Monthly Disability Benefit Accident/Sickness Benefit Waiting Period Cost Per Month 7 and 7 14-14 30-30 60-60 90-90 180-180 73,800 6,150 4,100 140.12 128.88 109.43 70.92 61.39 44.99 75,600 6,300 4,200 143.54 132.02 112.1 72.65 62.89 46.09 77,400 6,450 4,300 146.96 135.17 114.77 74.38 64.38 47.19 79,200 6,600 4,400 150.37 138.31 117.44 76.11 65.88 48.29 81,000 6,750 4,500 153.79 141.45 120.11 77.84 67.38 49.38 82,800 6,900 4,600 157.21 144.6 122.78 79.57 68.88 50.48 84,600 7,050 4,700 160.63 147.74 125.45 81.3 70.37 51.58 86,400 7,200 4,800 164.04 150.88 128.12 83.03 71.87 52.68 88,200 7,350 4,900 167.46 154.03 130.79 84.76 73.37 53.77 90,000 7,500 5,000 170.88 157.17 133.46 86.49 74.87 54.87 91,800 7,650 5,100 174.3 160.31 136.12 88.22 76.36 55.97 93,600 7,800 5,200 177.72 163.46 138.79 89.95 77.86 57.06 95,400 7,950 5,300 181.13 166.6 141.46 91.68 79.36 58.16 97,200 8,100 5,400 184.55 169.74 144.13 93.41 80.85 59.26 99,000 8,250 5,500 187.97 172.89 146.8 95.14 82.35 60.36 100,800 8,400 5,600 191.39 176.03 149.47 96.87 83.85 61.45 102,600 8,550 5,700 194.8 179.17 152.14 98.6 85.35 62.55 104,400 8,700 5,800 198.22 182.32 154.81 100.33 86.84 63.65 106,200 8,850 5,900 201.64 185.46 157.48 102.06 88.34 64.75 108,000 9,000 6,000 205.06 188.6 160.15 103.79 89.84 65.84 109,800 9,150 6,100 208.47 191.75 162.82 105.52 91.34 66.94 111,600 9,300 6,200 211.89 194.89 165.48 107.25 92.83 68.04 113,400 9,450 6,300 215.31 198.03 168.15 108.98 94.33 69.14 115,200 9,600 6,400 218.73 201.18 170.82 110.71 95.83 70.23 117,000 9,750 6,500 222.14 204.32 173.49 112.44 97.32 71.33 118,800 9,900 6,600 225.56 207.46 176.16 114.17 98.82 72.43 120,600 10,050 6,700 228.98 210.61 178.83 115.9 100.32 73.53 122,400 10,200 6,800 232.4 213.75 181.5 117.63 101.82 74.62 124,200 10,350 6,900 235.81 216.89 184.17 119.36 103.31 75.72 126,000 10,500 7,000 239.23 220.04 186.84 121.09 104.81 76.82 127,800 10,650 7,100 242.65 223.18 189.51 122.82 106.31 77.92 129,600 10,800 7,200 246.07 226.32 192.18 124.55 107.81 79.01 131,400 10,950 7,300 249.48 229.47 194.84 126.28 109.3 80.11 133,200 11,100 7,400 252.9 232.61 197.51 128.01 110.8 81.21 135,000 11,250 7,500 256.32 235.76 200.18 129.74 112.3 82.31 136,800 11,400 7,600 259.74 238.9 202.85 131.46 113.79 83.4 138,600 11,550 7,700 263.16 242.04 205.52 133.19 115.29 84.5 140,400 11,700 7,800 266.57 245.19 208.19 134.92 116.79 85.6 142,200 11,850 7,900 269.99 248.33 210.86 136.65 118.29 86.69 144,000 12,000 8,000 273.41 251.47 213.53 138.38 119.78 87.79
Standard Insurance Company Educator Options Voluntary Long Term Disability Coverage Highlights

36

37
PLAN: SmartPremium 100/80/50/50-1250-1000
POLICY EFFECTIVE DATE: 2022-09-01
POLICY LENGTH: 24 months
MINIMUM EMPLOYER CONTRIBUTIONS: 0.0% for employee and 0.0% for dependent(s).
EMPLOYEE $30.44 monthly
EMPLOYEE + SPOUSE $65.38 monthly
EMPLOYEE + CHILDREN $70.64 monthly
FAMILY $108.72 monthly
WHY BEAM
Beam is the future of group dental insurance, for employers large and small. We’re pairing innovative tech with personal service to deliver an insurance experience unlike any other.








90th Percentile UCR OON
Nationwide network (Over 400,000 access points) Digital implementation and admin


Beam Perks included
BEAM PERKS
Plans ship with the Beam Brush included.
Beam Brush Smart, electric toothbrush.
Beam Paste

High-quality, custom formulated toothpaste.
Free shipping Delivered to your door, right when you need it.
DENTAL INSURANCE QUOTE
BM-GRQ-0005-202203 FIND A DENTIST https://dentists.beam.dental ? QUESTIONS? support@beam.dental CHECK ELIGIBILITY https://providers.beam.dental 1 of 5 38
Palestine ISD
PLAN COVERAGE
PREVENTIVE & DIAGNOSTIC
Diagnostic and preventive: exams, cleanings, fluoride, space maintainers, x-rays, and sealants
BASIC
Minor restorative: fillings
Emergency palliative treatment: to temporarily relieve pain
Oral surgery: extractions and dental surgery
Prosthetic maintenance: relines and repairs to bridges and dentures
MAJOR
Endodontics: root canals
Periodontics: to treat gum disease
Implants: endosteal in lieu of a 2 or 3 unit bridge
Major restorative: crowns, inlays, and onlays
Prosthetics: bridges
Prosthodontics: dentures
ORTHODONTIA
100% 100%
80% 80%
50% 50%
Child Orthodontics: braces with age limit of 19 50% 50%
PLAN MAXES
Annual maximum applies to diagnostic & preventive, basic services, and major services. Lifetime maximum applies to orthodontic services.
Annual max based on Calendar Year ANNUAL MAX
PLAN DEDUCTIBLE
The deductible is waived for diagnostic & preventive services. INDIVIDUAL
IN-NETWORK (PPO Fee) OUT-OF-NETWORK (90TH PERCENTILE UCR)
$1,250 /yr ANNUAL
$1,250
(In network)
MAX (Out of network)
/yr ORTHO LIFETIME MAX $1,000 /lifetime
FAMILY
BM-GRQ-0005-202203 FIND A DENTIST https://dentists.beam.dental ? QUESTIONS? support@beam.dental CHECK ELIGIBILITY https://providers.beam.dental 2 of 5 39
$50 /yr
$150 /yr
CLAIMS INFORMATION
Beam Dental PPO Standard coverages, as of August 1, 2019
SMART PREMIUM
HOW LOWERING YOUR PREMIUM WORKS
Using the Beam Brush earns you a Beam score. The better your group’s Beam score, the bigger potential drop in your premium at your renewal.*
Brush better, get a lower premium—pretty simple. Don’t worry, your rates will not increase based on your group Beam score alone. Just get rewarded for good brushing by your group.
*Premium reduction occurs at renewal (plan year or calendar year) and is based on Beam score aggregate of your group, prior year claims data analysis, and changes in dentist reimbursement contracts. The reduction stated above nor any reduction in premiums is guaranteed. Premium rates can be increased based on the factors previously stated, if determined in the underwriting process. Increases in premium will not occur based on group aggregate Beam score alone.
ADDITIONAL DETAILS
SEE ANY DENTIST
Our PPO plans allow you to see any licensed dentist. Savings in plan cost and member out of pocket expenses may be obtained by utilizing participating network dentists.
Beam has partnered with leading regional and national PPO network partners through Dental Benefit Providers, Careington PPO Dental, and DenteMax Plus Network to provide you with the most choices possible.
Note: The information contained in this proposal is not intended to be contractually binding without a written agreement executed by both parties memorializing the terms and conditions of dental benefit underwriting and/or administration anticipated to be provided by Beam and its partners. We and our partners reserve the right to withdraw this proposal at any time.
RATING REQUIREMENTS
Minimum employer contributions: 0.0% for employee and 0.0% for dependent(s).
Minimum employee enrollment: 20% of eligible employees
Maximum number of subgroups: 10
Rates are valid for 90 days after 06/03/22
This proposal is based on information provided with the proposal request. If accepted, final rates and benefits will be based on verification of the information provided with the rate request.
Once eligible, Certificate Holders and their Eligible Dependents must enroll for coverage under this policy within 30 days from the date upon which such Certificate Holder or Eligible Dependents become eligible for Benefits.
A Certificate Holder properly enrolls for coverage by completing all enrollment forms required by Beam and NGL and submitting such forms to the Policyholder.
If the Certificate Holder or Eligible Dependent is not properly enrolled for coverage within 30 days from the date upon which he/she becomes eligible for Benefits, then such Certificate Holder or Eligible Dependent must wait until the next Open Enrollment Period to enroll.
Electronic payer ID BEAM1 NEA ID BEAM1 Fax number (844)688-4821 Phone number (800)648-1179 Claim form accepted ADA form 2006 or later
Beam Insurance Administrators PO Box 75372 Cincinnati, OH 45275
BM-GRQ-0005-202203 FIND A DENTIST https://dentists.beam.dental ? QUESTIONS? support@beam.dental CHECK ELIGIBILITY https://providers.beam.dental 3 of 5 40
COVERAGE RULES
CODE PROCEDURE
COVERED UNDERFREQUENCY
D0120, D0150, D9310 Periodic oral exam, Comprehensive oral exam, Consultation Diagnostic Limit of three per 12 months
D0140 Limited oral exam Diagnostic Two per 12 months
D0210 Radiographs-FMX Diagnostic One per 60 months
D0220 Radiographs-periapical (first) Diagnostic Not covered if inclusive of a procedure with x-rays.
D0230 Radiographs-periapical (each additional)Diagnostic Not covered if inclusive of a procedure with x-rays.
D0270-D0274Radiographs-bitewings Diagnostic Every 6 months
D0330 Radiographs-panoramic
D1110 Prophylaxis
D1206, D1208Fluoride
D1351, D1352Sealants, Resins
D2140-D2161Fillings
D2330-D2394Fillings
D2740, D2750 ...Crowns (N,X,A)
D2950 Core Build-up (X)
Diagnostic One per 60 months
Preventive Two per benefit period
Preventive One per 12 months
Preventive One per 36 months, per tooth
Minor RestorativeOne per 24 months, per tooth
Minor RestorativeOne per 24 months, per tooth
Major One per 60 months, paid on seat date; seat date required
Major One per 60 months
D4341-D4342Periodontal scaling and root planing (N, P, X)PeriodonticsOne per 24 months, per quadrant
D4910 Periodontal maintenance (H) Periodontics Two per year unless pregnant (3) or diabetes (4)
D6010 Endosteal Implants (N,M,X2)
Major One per lifetime
Not covered: D0350, D0364, D0470, D1330, D2962, D3110, D3120, D8093, D9230, D9248
NOTES
Limited to 3 oral evaluation procedures, in any combination (D0120, D0150, D9310) per 12 month period
Can do treatment on same day; no shared freq with D0120; shared freq with D0170
Shared freq with D0330; not reimbursed within 6 months of Bitewing Radiographs
Bitewings and 7 or more periapicals will be reimbursed as FMX. Not covered on same day as D0210, D0330 or if considered a part of billed procedures
Bitewings and 7 or more periapicals will be reimbursed as FMX. Not covered on same day as D0210, D0330 or if considered a part of billed procedures
Can perform 6 months after D0210
Shared freq with D0210
Three per 12 months if pregnant 2nd/3rd trimester, four per 12 months if diabetic (N, V); not covered within 3 months of D4910
Covered under age 16
Covered under age 16, 1st & 2nd permanent molars
Multiple restorations on one surface are payable as one surface. Multiple surfaces on a single tooth will not be paid as separate restorations.
Multiple restorations on one surface are payable as one surface. Multiple surfaces on a single tooth will not be paid as separate restorations. Posterior composites covered.
See * note below for details
See * note below for details
Can perform all 4 quads in one day
After peridontal treatment; can be alternated with D1110 for one per three months
In lieu of a single tooth replacement when a 2 or 3 unit bridge has been approved for coverage when adjacent teeth are not in need of crowns on their own merit; if there are no additional teeth missing throughout the arch. Alternate benefit of a partial denture will be considered if criteria is not met.
*Exclusions include, but are not limited to: correction of attrition, abrasion, erosion, or abfraction; for teeth that are not broken down by extensive decay or accidental injury; to restore teeth with microfractures fracture lines, undermined cusps, or existing large restorations without overt pathology.
FREQUENTLY ASKED QUESTIONS
Continuation of service? Covered starting on patient's effective date
Continuation of benefits? Earlier effective date is primary
Frequency of ortho payments? Monthly – submit claims for on-going treatment
Are prior extractions covered? Yes – no missing tooth clause
N = Narrative of medical necessity
P = Perio charting
X = Labeled & dated, pre-op x-rays
X2 = Labeled & dated, pre-op and post op x-rays
Timely Filing limit? 12 months from date of service unless otherwise specified by state law. Please refer to your CertificateH = Periodontal history
Is pre-authorization mandatory? No – but estimates recommended for $300+ services
A = date of prior insertion of existing crown
M = panoramic x-ray or FMX (if available), all missing teeth
V = Verification from physician (if pregnant requires due date)
DISCLAIMER: Depending on the coverage you selected, your benefits may differ from those outlined above. Please review your Certificate of Insurance for full benefit descriptions and limitations. If there are any discrepancies between this summary and the plan documents, the plan documents will prevail.
BM-CSD-0002-051021 FIND A DENTIST https://dentists.beam.dental ? QUESTIONS? support@beam.dental CHECK ELIGIBILITY https://providers.beam.dental 5 of 5 41
Vision Plan Benefits for Palestine ISD
Co-Pays Monthly Premiums Services/Frequency
Benefits through Superior Select Southwest Network
Co-pays apply to in-network benefits; co-pays for out-of-network visits are deducted from reimbursements
1Covered to provider’s in-office standard retail lined trifocal amount; member pays difference between progressive and standard retail lined trifocal, plus applicable co-pay
2 Contact lenses and related professional services (fitting, evaluation and follow-up) are covered in lieu of eyeglass lenses and frames benefit
3 Lasik Vision Correction is in lieu of eyewear benefit, subject to routine regulatory filings and certain exclusions and limitations

Discount Features
Non-Covered Eyewear Discount: Members may also receive a discount of 20% from a participating provider’s usual and customary fees for eyewear purchases which exceed the benefit coverage (except disposable contact lenses, for which no discount applies). This includes eyeglass frames which exceed the selected benefit coverage, specialty lenses (i.e. progressives) and lens “extras” such as tints and coatings. Eyewear purchased from a Walmart Vision Center does not qualify for this additional discount because of Walmart’s “Always Low Prices” policy.
The Plan discount features are not insurance.
All allowances are retail; the member is responsible for paying the provider directly for all non-covered items and/or any amount over the allowances, minus available discounts. These are not covered by the plan.
Discounts are subject to change without notice.
Disclaimer: All final determinations of benefits, administrative duties, and definitions are governed by the Certificate of Insurance for your vision plan. Please check with your Human Resources department if you have any questions
Superior Vision of Texas P.O. Box 967 Rancho Cordova, CA 95741 800.507.3800 SuperiorVision.com 0715-BSv2/TX
Exam $10 Emp. only $7.88 Exam 12 months Materials $25 Emp. + spouse $13.54 Frame 24 months Emp. + child(ren) $14.22 Lenses 12 months Emp. + family $21.42 Contact Lenses 12 months (Based on date of service)
In-Network Out-of-Network Exam Covered in full Up to $35 retail Frames $150 retail allowance Up to $70 retail Lenses (standard) per pair Single Vision Covered in full Up to $25 retail Bifocal Covered in full Up to $40 retail Trifocal Covered in full Up to $45 retail Tints Covered in full Up to $15 retail Polycarbonate Covered in full Up to $20 retail Scratch resistant coating Covered in full Up to $25 retail Progressive See description1 Up to $45 retail Lenticular Covered in full Up to $80 retail Contact Lenses2 $175 retail allowance Up to $80 retail Medically Necessary Contact Lenses Covered in full Up to $150 retail Lasik Vision Correction $200 allowance3
SuperiorVision.com Customer Service 800.507.3800
42
Learn more about your annual Be Well Benefit
Your Unum plan pays a Be Well Benefit for one Be Well screening each year.
With Unum’s Be Well Benefit, you and other covered family members can receive a valuable incentive for important tests and screenings. Many of these tests are routinely performed, so it’s easy to take advantage of this benefit.
Your Critical Illness Be Well benefit is $50.
Be Well screenings
• Annual exams by a physician including sports physicals and well-child visits
• Cancer screenings including pap smear, colonoscopy
• Cardiovascular function screenings
• Cholesterol and diabetes screenings
• Imaging studies, including chest X-ray, mammography
• Immunizations including HPV, MMR, tetanus, influenza
It’s easy to file a claim.
You can receive a benefit for tests that are performed after your initial coverage date. Follow these simple steps:
File your claim by mail or over the phone. Simply call 1-800-635-5597 to learn more.
You will need to provide the following:
•First and last names of the employee and claimant (the employee might not be the claimant)
•Employee’s Social Security number or policy number
• Name and date of the test
•Name of physician and the facility where the test was performed.
Each year, you can earn a valuable incentive just for taking care of your health. And so can each of your covered family members.
For more information, please contact your HR representative.
Unum will pay Be Well benefits for all eligible policies according to policy terms. THESE POLICIES OFFER LIMITED BENEFITS
The policies or their provisions may vary or be unavailable in some states. The policies have exclusions and limitations which may affect any benefits payable. See the actual policy or your Unum representative for specific provisions and details of availability.
EN-1911-BeWell (1-20) FOR EMPLOYEES Underwritten by: Unum Insurance Company, Portland, Maine; In New York, underwritten by: Provident Life and Casualty Insurance Company, Chattanooga, Tennessee unum.com © 2020 Unum Group. All rights reserved. Unum is a registered trademark and marketing brand of Unum Group and its insuring subsidiaries.
43
Palestine Independent School District
Who is eligible for this coverage?
What is the coverage amount?
Is it portable (can I keep it if I leave my employer)?
When is coverage effective?*
What does my AD&D insurance pay for?
Palestine Independent School District UNUM Life and
Do my life insurance benefits decrease with age?
Insurance Plan Highlights
AD&D
Policy Number 474775
All actively employed employees working at least 15 hours each week for your employer in the U.S.
Your employer is providing you with $10,000 of term life insurance. You will also receive $10,000 of Accidental Death and Dismemberment insurance
If you retire, reduce your hours or leave your employer, you can continue coverage at the group rate. Portability is not available for people who have a medical condition that could shorten their life expectancy — but they may be able to convert their term life policy to an individual life insurance policy.
Please see your plan administrator for your effective date.
The full benefit amount is paid for loss of:
- Life
- Both hands or both feet or sight of both eyes
- One hand and one foot
- One hand and the sight of one eye
- Speech and hearing
Coverage amounts will reduce according to the following schedule:
amount reduces to:
Coverage may not be increased after a reduction.
*Delayed effective date of coverage
Insurance coverage will be delayed if you are not an active employee because of an injury, sickness, temporary layoff, or leave of absence on the date that insurance would otherwise become effective.
The policy provisions may vary or not be available in all states. The policy has exclusions and limitations which may affect any benefits payable. For complete details of coverage, please refer to Policy Form C.FP-1 et al or contact your Unum representative.
Underwritten by Unum Life Insurance Company of America, Portland, Maine
© 2018 Unum Group. All rights reserved. Unum is a registered trademark and marketing brand of Unum Group and its insuring subsidiaries.
EN-1771 (6-18) FOR EMPLOYEES
Age: Insurance
65 65%
original
70 45% of original amount 75 30% of the
of
amount
original amount
44
Who is eligible for this coverage?
What are the Life coverage amounts?
Palestine Independent School District
UNUM Voluntary Life and AD&D Insurance Plan Highlights Policy Number 474776
All actively employed employees working at least 15 hours each week for your employer in the U.S. and their eligible spouses and children to 26.
Employee: up to 5 times salary in increments of $10,000; not to exceed $500,000. Spouse: up to 100% of employee amount in increments of $5,000; not to exceed $250,000
Child: $10,000. The maximum death benefit for a child between the ages of live birth and six months is $1,000.
What are the AD&D coverage amounts?
Employee: up to 5 times salary in increments of $10,000; not to exceed $500,000. Spouse: up to 100% of employee amount in increments of $5,000; not to exceed $250,000.
Note: In order to purchase life and AD&D coverage for your dependents, you must buy coverage for yourself.
Can I be denied coverage?
Current employees: If you and your eligible dependents are enrolled in the plan and wish to increase your life insurance coverage, you may apply on or before the enrollment deadline for any amount of additional coverage up to $150,000 for yourself and any amount of additional coverage up to $50,000 for your spouse. Any life insurance coverage over the guaranteed amount(s) will be subject to answers to health questions.
If you and your eligible dependents are not currently enrolled in the plan, you may apply for coverage on or before the enrollment deadline and will be required to answer health questions for any amount of coverage.
New employees: To apply for coverage, complete your enrollment within 31 days of your eligibility period. If you apply for coverage after 31 days, or if you choose coverage over the amount you are guaranteed, you will need to complete a medical questionnaire which you can get from your plan administrator. You may also be required to take certain medical tests at Unum’s expense.
How do I apply? Please see your plan administrator.
When is coverage effective?
Please see your plan administrator for your effective date.
Insurance coverage will be delayed if you are not in active employment because of an injury, sickness, temporary layoff, or leave of absence on the date that insurance would otherwise become effective.
For your dependent spouse and children, insurance coverage will be delayed if that dependent is totally disabled on the date that insurance would otherwise be effective. Totally disabled means that as a result of an injury, sickness, or disorder, your dependent spouse and children: are confined in a hospital or similar institution; or are confined at home under the care of a physician for a sickness or injury. Exception: Infants are insured from live birth.
45
How much does the coverage cost?
Do my life insurance benefits decrease with age?
Your rate is based on your insurance age, which is your age immediately prior to and including the anniversary/effective date.
Spouse rate is based on employee’s insurance age.
Coverage amounts will reduce according to the following schedule:
Is the coverage portable (can I keep it if I leave my employer)?
Are there any life insurance exclusions or limitations?
Will my premiums be waived if I’m disabled?
What does my AD&D insurance pay for?
Coverage may not be increased after a reduction.
If you retire, reduce your hours or leave your employer, you can continue coverage for yourself your spouse and your dependent children at the group rate. Portability is not available for people who have a medical condition that could shorten their life expectancy — but they may be able to convert their term life policy to an individual life insurance policy.
Life insurance benefits will not be paid for deaths caused by suicide within the first 24 months after the date your coverage becomes effective. If you increase or add coverage, these enhancements will not be paid for deaths caused by suicide within the first 24 months after you make these changes.
If you become disabled (as defined by your plan) and are no longer able to work, your life premium payments will be waived until your disability period ends.
The full benefit amount is paid for loss of:
• life;
• both hands or both feet or sight of both eyes;
• one hand and one foot;
• one hand or one foot and the sight of one eye;
• speech and hearing.
Other losses may be covered as well. Please contact your plan administrator.
Monthly Rates Age band Employee Life/AD&D rate per $10,000 Spouse Life/AD&D rate per $5,000 <25 $0.80 $0.40 25-29 $0.90 $0.45 30-34 $1.10 $0.55 35-39 $1.30 $0.65 40-44 $1.80 $0.90 45-49 $2.80 $1.40 50-54 $4.40 $2.20 55-59 $7.00 $3.50 60-64 $8.70 $4.35 65-69 $14.90 $7.45 70-74 $7.00 $7.45 75+ $8.70 $7.45 Child Life monthly rate is $1.00 for $10,000. One life
children.
premium covers all
Age: Insurance amount
to: 65 65% of original amount 70 45% of original amount 75 30% of original
reduces
amount
46
Are there any AD&D exclusions or limitations?
Accidental death and dismemberment benefits will not be paid for losses caused by, contributed to by, or resulting from:
• disease of the body; diagnostic, medical or surgical treatment or mental disorder as set forth in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM);
• suicide, self-destruction while sane, intentionally self-inflicted injury while sane or self-inflicted injury while insane;
• war, declared or undeclared, or any act of war;
• active participation in a riot;
• committing or attempting to commit a crime under state or federal law;
• the voluntary use of any prescription or non-prescription drug, poison, fume or other chemical substance unless used according to the prescription or direction of your or your dependent’s doctor. This exclusion does not apply to you or your dependent if the chemical substance is ethanol;
• intoxication – “being intoxicated” means you or your dependent’s blood alcohol level equals or exceeds the legal limit for operating a motor vehicle in the state or jurisdiction where the accident occurred.
When does my coverage end?
You and your dependents’ coverage under the Summary of Benefits ends on the earliest of:
• the date the policy or plan is cancelled;
• the date you no longer are in an eligible group;
• the date your eligible group is no longer covered;
• the last day of the period for which you made any required contributions;
• the last day you are in active employment unless continued due to a covered layoff or leave of absence or due to an injury or sickness, as described in the certificate of coverage.
In addition, coverage for any one dependent will end on the earliest of:
• the date your coverage under a plan ends;
• the date your dependent ceases to be an eligible dependent;
• for a spouse, the date of a divorce or annulment;
• for dependent coverage, the date of your death.
Unum will provide coverage for a payable claim that occurs while you and your dependents are covered under the policy or plan.
This information is not intended to be a complete description of the insurance coverage available. The policy or its provisions may vary or be unavailable in some states. The policy has exclusions and limitations which may affect any benefits payable. For complete details of coverage and availability, please refer to Policy Form C.FP-1 et al or contact your Unum representative.
© 2017 Unum Group. All rights reserved. Unum is a registered trademark and marketing brand of Unum Group and its insuring subsidiaries.
Underwritten by Unum Life Insurance Company of America, Portland, Maine
EN-1773 (8-17) FOR EMPLOYEES
47
Find clarity and comfort during trying times
Life planning financial & legal resources
When a loved one is terminally ill, or passes away, you may need help with the personal, financial and legal decisions that need to be made. Support is always available when you are protected by Unum Group Life Insurance.
When a loved one is terminally ill, or passes away, you may need help with the personal, financial and legal decisions that need to be made. Support is always available when you are protected by Unum Group Life Insurance.
LIFE PLANNING FINANCIAL & LEGAL RESOURCES WILL BE THERE
With Unum group life coverage, you have automatic access to Life Planning Financial & Legal Resources. This service is provided at no extra cost for employees, spouses and beneficiaries who need help during a terminal illness, or after the loss of a covered employee.
CARING CONSULTANTS CAN PROVIDE THE ASSISTANCE YOU NEED
When a life claim is submitted and approved, a speciallytrained consultant will reach out to the employee or beneficiary to provide support. Each consultant holds a Master’s degree in the mental health field, and is highly skilled at assisting those who need help dealing with the emotional challenges of a terminal illness or the loss of a loved one.
Life Planning consultants are also able to provide financial and legal support regarding estate settlement, Social Security, cash flow, taxes and investment planning. They can help you develop a customized financial plan to preserve your quality of life, protect resources and build future security.
These consultants are available to assist you in your time of need, and their services are designed to coordinate with the efforts of a family attorney, accountant, or broker. Their services are strictly confidential, and they do not work on commission and will not try to sell any product or service.
YOU MAY HAVE QUESTIONS LIKE THESE:
• There’s so much paperwork. Where do I begin?
• Do I need to pay outstanding bills?
• How should I manage retirement accounts?
• How should I invest the insurance money?
• What do I do with the will?
• Do I need to file probate?
Answers to these questions and more are available at no charge as part of your life insurance coverage from Unum.
ASSISTANCE IS ONLY A CALL OR CLICK AWAY
Whenever you need support, a Master’s level consultant can be reached by phone 24 hours a day, 365 days of the year.
To speak to a counselor or for more information:
• Call 1-800-854-1446 (multi-lingual)
• Visit members.healthadvocate.com (Enter Unum - Life Planning)
48
PureLife-plusispermanentlifeinsurancetoAttainedAge121that canneverbecancelledaslongasyoupaythenecessarypremiums.Afterthe GuaranteedPeriod,thepremiumscanbelower,thesame,orhigherthantheTablePremium.Seethebrochureunder”PermanentCoverage”.
monthlypremiums
ExpressIssue GUARANTEED MonthlyPremiumsforLifeInsuranceFaceAmountsShown PERIOD AgetoWhich Issue Coverageis Age Guaranteedat (ALB) $10,000 $15,000 $25,000 $40,000 $50,000 $75,000 $100,000 $125,000 $150,000 TablePremium 15D-1 9.25 81 2-4 9.50 80 5-8 9.75 79 9-10 10.00 79 11-16 10.25 77 17-20 10.25 15.05 18.25 26.25 34.25 42.25 50.25 75 21-22 10.50 15.45 18.75 27.00 35.25 43.50 51.75 74 23 10.75 15.85 19.25 27.75 36.25 44.75 53.25 75 24-25 11.00 16.25 19.75 28.50 37.25 46.00 54.75 74 26 11.50 17.05 20.75 30.00 39.25 48.50 57.75 75 27-28 11.75 17.45 21.25 30.75 40.25 49.75 59.25 74 29 12.00 17.85 21.75 31.50 41.25 51.00 60.75 74 30-31 12.25 18.25 22.25 32.25 42.25 52.25 62.25 73 32 13.00 19.45 23.75 34.50 45.25 56.00 66.75 74 33 13.50 20.25 24.75 36.00 47.25 58.50 69.75 74 34 14.25 21.45 26.25 38.25 50.25 62.25 74.25 75 35 10.05 15.25 23.05 28.25 41.25 54.25 67.25 80.25 76 36 10.35 15.75 23.85 29.25 42.75 56.25 69.75 83.25 76 37 10.80 16.50 25.05 30.75 45.00 59.25 73.50 87.75 77 38 11.25 17.25 26.25 32.25 47.25 62.25 77.25 92.25 77 39 12.00 18.50 28.25 34.75 51.00 67.25 83.50 99.75 78 40 9.25 12.75 19.75 30.25 37.25 54.75 72.25 89.75 107.25 79 41 9.95 13.80 21.50 33.05 40.75 60.00 79.25 98.50 117.75 80 42 10.75 15.00 23.50 36.25 44.75 66.00 87.25 108.50 129.75 81 43 11.45 16.05 25.25 39.05 48.25 71.25 94.25 117.25 140.25 82 44 12.15 17.10 27.00 41.85 51.75 76.50 101.25 126.00 150.75 83 45 12.85 18.15 28.75 44.65 55.25 81.75 108.25 134.75 161.25 83 46 13.65 19.35 30.75 47.85 59.25 87.75 116.25 144.75 173.25 84 47 14.35 20.40 32.50 50.65 62.75 93.00 123.25 153.50 183.75 84 48 15.05 21.45 34.25 53.45 66.25 98.25 130.25 162.25 194.25 85 49 15.95 22.80 36.50 57.05 70.75 105.00 139.25 173.50 207.75 85 50 16.95 24.30 39.00 61.05 75.75 112.50 86 51 18.15 26.10 42.00 65.85 81.75 121.50 87 52 19.45 28.05 45.25 71.05 88.25 131.25 88 53 20.45 29.55 47.75 75.05 93.25 138.75 88 54 21.45 31.05 50.25 79.05 98.25 146.25 88 55 22.55 32.70 53.00 83.45 103.75 154.50 89 56 23.55 34.20 55.50 87.45 108.75 162.00 89 57 24.75 36.00 58.50 92.25 114.75 171.00 89 58 25.85 37.65 61.25 96.65 120.25 179.25 89 59 27.05 39.45 64.25 101.45 126.25 188.25 89 60 28.55 41.70 68.00 107.45 133.75 199.50 90 61 29.85 43.65 71.25 112.65 140.25 209.25 90 62 31.45 46.05 75.25 119.05 148.25 221.25 90 63 33.05 48.45 79.25 125.45 156.25 233.25 90 64 34.75 51.00 83.50 132.25 164.75 246.00 90 65 36.65 53.85 88.25 139.85 174.25 260.25 90 66 38.75 90 67 41.05 91 68 43.55 91 69 46.05 91 70 48.65 91
Non-Tobacco
PureLife-plus StandardRiskTablePremiums Non-Tobacco
Form:21M013-ICCEXP-A-M-1LO 49
Tobacco monthlypremiums
GUARANTEED MonthlyPremiumsforLifeInsuranceFaceAmountsShown PERIOD AgetoWhich Issue Coverageis Age Guaranteedat (ALB) $10,000 $15,000 $25,000 $40,000 $50,000 $75,000 $100,000 $125,000 $150,000 TablePremium 15D-1 81 2-4 80 5-8 79 9-10 79 11-16 77 17-20 15.25 23.05 28.25 41.25 54.25 67.25 80.25 71 21-22 16.00 24.25 29.75 43.50 57.25 71.00 84.75 71 23 16.75 25.45 31.25 45.75 60.25 74.75 89.25 72 24-25 17.25 26.25 32.25 47.25 62.25 77.25 92.25 71 26 17.75 27.05 33.25 48.75 64.25 79.75 95.25 72 27-28 18.25 27.85 34.25 50.25 66.25 82.25 98.25 71 29 18.50 28.25 34.75 51.00 67.25 83.50 99.75 71 30-31 21.00 32.25 39.75 58.50 77.25 96.00 114.75 72 32 21.75 33.45 41.25 60.75 80.25 99.75 119.25 72 33 22.00 33.85 41.75 61.50 81.25 101.00 120.75 72 34 22.25 34.25 42.25 62.25 82.25 102.25 122.25 71 35 15.30 24.00 37.05 45.75 67.50 89.25 111.00 132.75 72 36 15.75 24.75 38.25 47.25 69.75 92.25 114.75 137.25 72 37 16.80 26.50 41.05 50.75 75.00 99.25 123.50 147.75 73 38 17.25 27.25 42.25 52.25 77.25 102.25 127.25 152.25 73 39 18.45 29.25 45.45 56.25 83.25 110.25 137.25 164.25 74 40 14.15 20.10 32.00 49.85 61.75 91.50 121.25 151.00 180.75 76 41 15.05 21.45 34.25 53.45 66.25 98.25 130.25 162.25 194.25 77 42 16.15 23.10 37.00 57.85 71.75 106.50 141.25 176.00 210.75 78 43 17.55 25.20 40.50 63.45 78.75 117.00 155.25 193.50 231.75 80 44 18.25 26.25 42.25 66.25 82.25 122.25 162.25 202.25 242.25 80 45 19.25 27.75 44.75 70.25 87.25 129.75 172.25 214.75 257.25 81 46 20.05 28.95 46.75 73.45 91.25 135.75 180.25 224.75 269.25 81 47 21.05 30.45 49.25 77.45 96.25 143.25 190.25 237.25 284.25 82 48 21.95 31.80 51.50 81.05 100.75 150.00 199.25 248.50 297.75 82 49 23.25 33.75 54.75 86.25 107.25 159.75 212.25 264.75 317.25 83 50 24.35 35.40 57.50 90.65 112.75 168.00 83 51 25.45 37.05 60.25 95.05 118.25 176.25 83 52 27.05 39.45 64.25 101.45 126.25 188.25 84 53 28.45 41.55 67.75 107.05 133.25 198.75 85 54 29.75 43.50 71.00 112.25 139.75 208.50 85 55 31.15 45.60 74.50 117.85 146.75 219.00 85 56 32.75 48.00 78.50 124.25 154.75 231.00 85 57 34.35 50.40 82.50 130.65 162.75 243.00 86 58 36.05 52.95 86.75 137.45 171.25 255.75 86 59 37.75 55.50 91.00 144.25 179.75 268.50 86 60 39.55 58.20 95.50 151.45 188.75 282.00 86 61 41.85 61.65 101.25 160.65 200.25 299.25 86 62 44.05 64.95 106.75 169.45 211.25 315.75 87 63 46.25 68.25 112.25 178.25 222.25 332.25 87 64 48.45 71.55 117.75 187.05 233.25 348.75 87 65 50.85 75.15 123.75 196.65 245.25 366.75 87 66 53.45 88 67 56.25 88 68 59.15 88 69 62.25 88 70 65.55 89 PureLife-plusispermanentlifeinsurancetoAttainedAge121that canneverbecancelledaslongasyoupaythenecessarypremiums.Afterthe GuaranteedPeriod,thepremiumscanbelower,thesame,orhigherthan theTablePremium.Seethebrochureunder”PermanentCoverage”. Form:21M013-ICCEXP-A-M-1LO 50
PureLife-plus StandardRiskTablePremiums Tobacco ExpressIssue
Health Savings Accounts
Maximize your savings
A Health Savings Account, or HSA, is a tax-advantaged savings account you can use for healthcare expenses. Along with saving you money on taxes, HSAs can help you grow your nest egg for retirement.

How an HSA works:
• Contribute to your HSA by payroll deduction, online banking transfer or personal check.
• Pay for qualified medical expenses for yourself, your spouse and your dependents. Both current and past expenses are covered if they’re from after you opened your HSA.
• Use your HSA Bank Health Benefits Debit Card to pay directly, or pay out of pocket for reimbursement or to grow your HSA funds.
• Roll over any unused funds year to year. It’s your money — for life.
• Invest your HSA funds and potentially grow your savings.¹
What’s covered?
You can use your HSA funds to pay for any IRS-qualified medical expenses, like doctor visits, hospital fees, prescriptions, dental exams, vision appointments, over-the-counter medications and more. Visit hsabank.com/QME for a full list.
Am I eligible for an HSA?
You’re most likely eligible to open an HSA if:
• You have a qualified high-deductible health plan (HDHP).
• You’re not covered by any other non-HSA-compatible health plan, like Medicare Parts A and B.
• You’re not covered by TriCare.
• No one (other than your spouse) claims you as a dependent on their tax return.
51
How much can I contribute?
The IRS limits how much you can contribute to your HSA every year. This includes contributions from your employer, spouse, parents and anyone else.2 Maximum contribution limit
Catch-up contributions
You may be eligible to make a $1,000 HSA catch-up contribution if you’re:
• Over 55.
• An HSA accountholder.
• Not enrolled in Medicare (if you enroll mid-year, annual contributions are prorated).
A huge way that HSAs can benefit you is they let you save on taxes in three ways.
1 You don’t pay federal taxes on contributions to your HSA.3
2 Earnings from interest and investments are tax-free.
3
Distributions are tax free when used for qualified medical expenses.
¹ Investment accounts are not FDIC insured, may lose value and are not a deposit or other obligation of, or guarantee by the bank. Investment losses which are replaced are subject to the annual contribution limits of the HSA.
2 HSA contributions in excess of IRS limits are subject to penalty and tax unless the excess and earnings are withdrawn prior to the tax filing deadline as explained in IRS Publication 969.
3 Federal tax savings are available regardless of your state. State tax laws may vary. Consult a tax professional for more information.
© 2022 HSA Bank. HSA Bank is a division of Webster
N.A., Member FDIC. Plan Administrative Services and Benefit Services
Webster Servicing LLC. HSA_Overview_050522
Bank,
are administered by
Triple tax savings
SINGLE PLAN SINGLE PLAN FAMILY PLAN FAMILY PLAN Visit www.hsabank.com
52
Maximum contribution limit
orcallthe numberonthebackofyourdebit cardformoreinformation. $8,300 $4,150 $7,750 $3,850 2024 2023

What is a Flexible Spending Account (FSA)? Help Make Medical Costs Painless. Visit fsa.nbsbenefits.com for more info or call one of our Benefit Specialists at 800-274-0503 Salt Lake City, UT - Headquarters Dallas, TX | San Diego, CA | Honolulu, HI 800-274-0503 fsa@nbsbenefits.com How Much Can I Save with an FSA? FSANo FSA Annual Taxable Income $24,000$24,000 Health FSA$1,500 $0 Dependent Care FSA $1,500 $0 Total Pre-tax Contributions -$3,000 $0 Taxable Income after FSA $21,000$24,000 Income Taxes-$6,300-$7,200 After-tax Income$14,700$16,800 After-tax Health and Welfare Expenses $0 -$3,000 Take-home Pay$14,700$13,800 You Saved $900$0 57 FSA Annual Limit $3050.00
Flexible Spending Account (FSA)
Partial List of Eligible Expenses:
Medical/Dental/Vision Copays and Deductibles
Prescription Drugs
Physical Therapy
Chiropractor
First-Aid Supplies
Two Types of FSAs
To take advantage of a health FSA, start by choosing an annual election amount. This amount will be available on day one of your plan year for eligible medical expenses.
Payroll deductions will then be made throughout the plan year to fund your account.
A dependent care FSA works differently than a health FSA. Money only becomes available as it is contributed and can only be used for dependent care expenses.
Both are pre-tax benefits your employer offers through a cafeteria plan. Choose one or both — whichever is right for you.
What is a Cafeteria Plan?
A cafeteria plan enables you to save money on group insurance, healthcare expenses, and dependent care expenses. Your contributions are deducted from your paycheck by your employer before taxes are withheld. These deductions lower your taxable income which can save you up to 35% on income taxes!
How to Spend
Spending is easy

Our convenient NBS Smart Card allows you to avoid out-of-pocket expenses, cumbersome claim forms and reimbursement delays. You may also utilize the “pay a provider” option on our web portal.
Lab Fees
Psychiatrist/Psychologist
Vaccinations
Dental Work/Orthodontia
Eye Exams
Laser Eye Surgery


Eyeglasses, Contact Lenses, Lens Solution


Prescribed OTC Medication
Account access is easy
Get account information from our easy-to-use online portal and mobile app. See your account balance, contributions and account history in real time.
Life’s not always flexible, but your money can be.
Enrollment Consideration
After the enrollment period ends, you may increase, decrease, or stop your contribution only when you experience a qualifying “change of status” (e.g. marriage, divorce, employment change, dependent change).
Be conservative in the total amount you elect to avoid forfeiting money at the end of the plan year.
From baby care to pain relief, shop the largest selection of guaranteed FSA-eligible products with zero guesswork at FSA Store. Is your health need FSA-eligible? Find out using our comprehensive Eligibility List.
Get $10 off using code NBS1819.
Shop FSA Store at fsastore.com/nbs
58
What is a Dependent Care Assistance Program (DCAP)?
The Dependent Care Assistance Program (DCAP) allows you to use tax-free dollars to pay for child day care or elder day care expenses that you incur because you and your spouse are both gainfully employed.
To participate, determine the annual amount that you want to deduct from your paycheck before taxes. The maximum amount you can elect depends on your federal tax filing status ($5,000 if you are married and filing a joint return or if you are a single parent, $2,500 if you are married but filing separately)
Your annual amount will be divided by the number of pay periods in the plan year and that amount will be deducted from each paycheck.
Who is an eligible dependent?
You can use the DCAP for expenses incurred for:
•Your qualifying child who is age twelve or younger for whom you claim a dependency exemption on your income tax return.

•Your qualifying relative (e.g. a child over twelve, your parent, a spouse’s parent) who is physically or mentally incapable of caring for himself or herself and has the same principal place of abode as you for more than half of the year.
•Your spouse who is physically or mentally incapable of caring for himself or herself and has the same principal place of abode as you for more than half of the year.
Special Rule for Parents Who Are Divorced, Separated, or Living Apart
Only the custodial parent can claim expenses from the DCAP. The custodial parent is generally the parent with whom the child resides for the greater number of nights during the calendar year. Additionally, the custodial parent cannot be reimbursed from the DCAP for child-care expenses while the child lives with the non-custodial parent because such expenses are not incurred to enable the custodial parent to be gainfully employed.
What are eligible expenses for the DCAP?
The expenses which are eligible for reimbursement must have been incurred during the plan year and in connection with you and your spouse to remain gainfully employed.
Examples of eligible expenses:
•Before and After School and/or Extended Day Programs
•Daycare in your home or elsewhere so long as the dependent regularly spends at least 8 hours a day in your home.
•Base cost of day camps or similar programs.
Examples of ineligible expenses:
•Schooling for a child in kindergarten or above
•Babysitter while you go to the movies or out to eat
•Cost of overnight camps
Salt Lake City, UT - Headquarters | Dallas, TX | San Diego, CA |onolulu, HI (800)274-0503 | service@nbsbenefits.com | www.nbsbenefits.com H 55
What does it mean to be “gainfully employed”?
This means that you are working and earning an income (i.e. not doing volunteer work). You are not considered gainfully employed during paid vacation time or sick days. Gainful employment is determined on a daily basis.
If you are married, then your spouse would also need to be gainfully employed for your day care expenses to be eligible for reimbursement.

You are also considered gainfully employed if you are unemployed but actively looking for work, you are self-employed, you are physically or mentally not capable of self-care, or you are a full-time student (must attend for the number of hours that the school considers full-time, must have been a student for some part of each of 5 calendar months during the year, cannot be attending school only at night, does not include on-the-job training courses or correspondence schools).
What are some other important IRS regulations?
•You cannot be reimbursed for dependent care expenses that were paid to (1) one of your dependents, (2) your spouse, or (3) one of your children who is under the age of nineteen.
•In the event that you use a day care center that cares for more than six children, the center must be licensed.
• You must provide the day care provider’s Social Security Number/Tax Identification Number (EIN) on form 2441 when you file your taxes.
What are some other important IRS regulations?
The IRS allows you to take a tax credit for your dependent care expenses. The tax credit may provide you with a greater benefit than the DCAP if you are in a lower tax bracket. To determine whether the tax credit or the DCAP is best for you, you will need to review your individual tax circumstances. You cannot use the same expenses for both the tax credit and the DCAP, however, you may be able to coordinate the federal dependent care tax credit with participation in the DCAP for expenses not reimbursed through DCAP. For more information, please call 1(800) 274-0503
Salt Lake City, UT - Headquarters Dallas, TX | San Diego, CA | Honolulu, HI www.nbsbenefits.com
service@nbsbenefits.com 56
800-274-0503
•American Fund/Capital Guardian
•Corebridge Financial (formerly AIG/VALIC)
•Equitable (formerly AXA)
•Horace Mann Life Ins. Co.
•Industrial Alliance - (Sec.Ben.)
•Invesco OppenheimerFunds
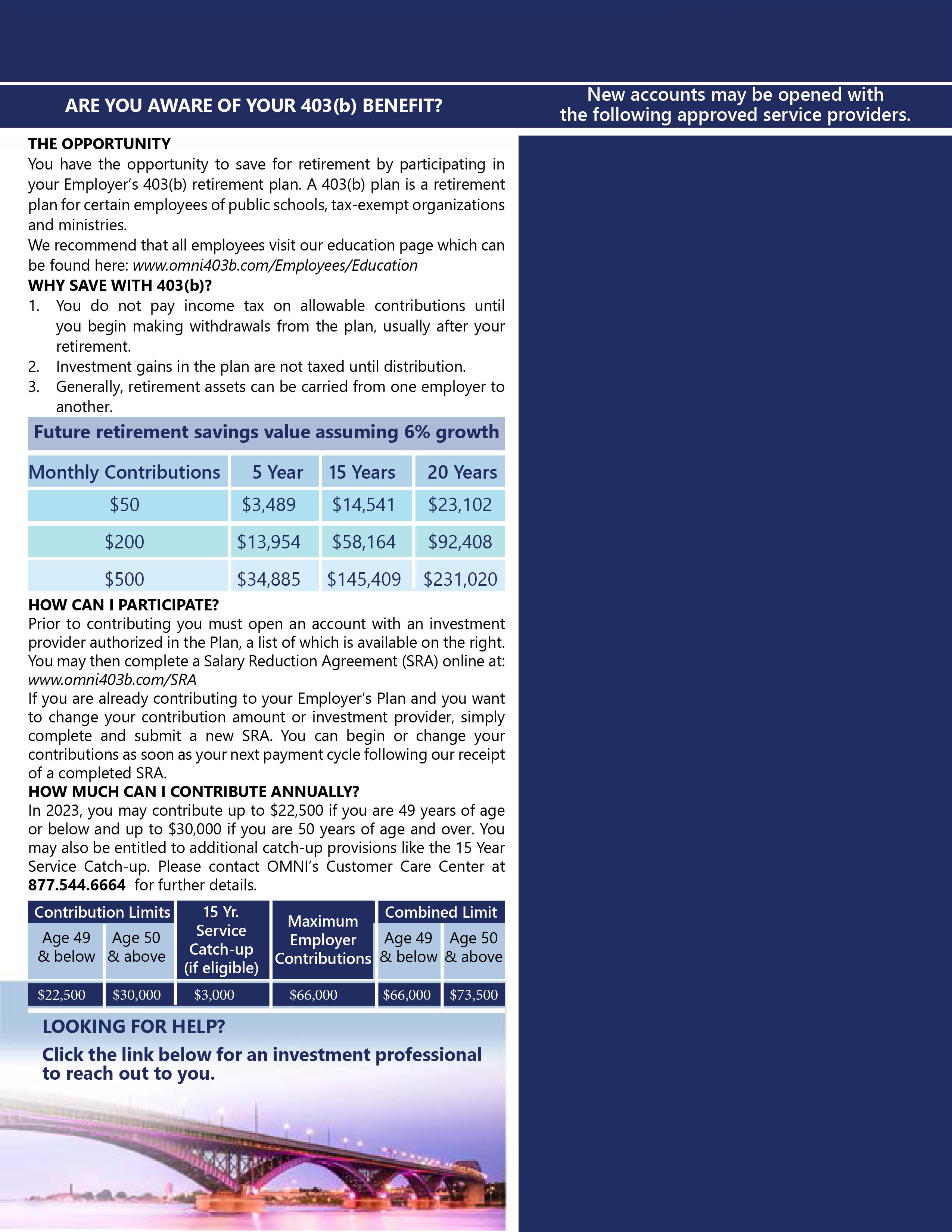
•Jefferson National Life
•National Life Group (LSW)
•PlanMember Services Corp.
•Putnam Investments
•ROTH - Equitable (formerly AXA)
•ROTH - National Life Group (LSW)
•ROTH - PlanMember Services Corp.
•Vanguard Fiduciary Trust Co.
•Voya Financial (North.)
•Voya Financial (Reliastar)
•Voya Financial (VRIAC)
Palestine ISD Plan Detail Page
Palestine ISD
57

