


EMPLOYEE BENEFITS GUIDE Plan Year | 2023-24 Rusty Freeman & Associates, LLC 245 Landa Street New Braunfels, Texas 78130 (830)606-5100 www.usebsg.com www.mybenefitshub.com/copperascovecisd

Medical Insurance –
CCISD Alternate Plan – If you do not elect medical coverage through CCISD, the district will provide employee only dental, vision at no cost.

TeleMedicine – TelaDoc, Access to physicians for non-emergency treatment/prescriptions is currently available with TRS Aetna Health Plans only.
Ameritas Dental – Coverage for preventive, basic, major, and ortho services. The plan does not contain waiting periods. Remember that annual maximums reset on September 1st. All employees will receive new ID cards
Davis Vision – Plan includes coverage for eye exams, materials (such as frames and lenses), and discounts for laser vision correction. The plan has a defined network of providers. Out of network benefits are available on a reimbursement basis only. For more information, including a list of providers visit www.davisvision.com. The client code for CCISD is 3797.
Disability – Plan includes both short and long term disability coverage. Plan is designed to protect 60% of your gross CCISD income.
Texas Life Permanent Life – Portable, permanent life insurance available for employees, their spouses and dependents. Employees can keep the coverage upon termination or retirement from CCISD.
MetLife Group Life –Group term life insurance that ends when you terminate employment with CCISD. Coverage is also available for spouses and dependent children.
Lincoln Critical Illness – Critical Illness pays a lump sum benefit if the insured is diagnosed with a covered critical illness.
Allstate Cancer – Pays benefits for internal cancer diagnosis. Includes an annual cancer screening benefit.
Allstate Accident – Pays benefits for off the job accidents and related treatments. Includes a physical/wellness exam reimbursement.
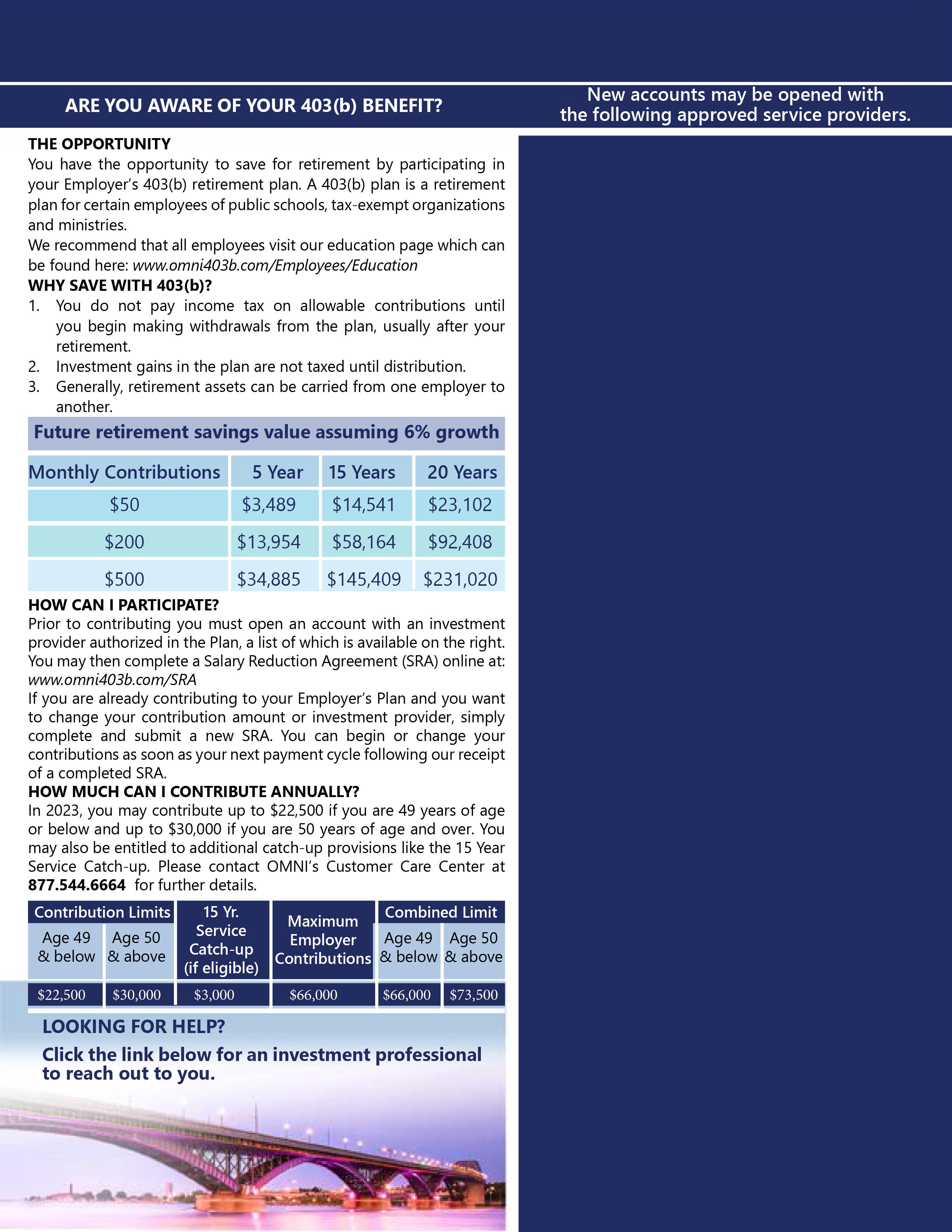
OMNI Retirement Plans – CCISD offers tax advantaged retirement plans designed to help supplement your TRS retirement benefits. Visit www.omni403b.com for more information.
If you cover dependents on any of your coverages through CCISD you must provide the dependents name, date of birth, and social security number. You must have all of this information before dependents can be added to the system.
Choose your benefits carefully. Several of the employee benefits plan contributions are made on a pre-tax basis and per IRS regulations, contribution amounts cannot be changed unless you experience a qualified life event. Qualifying life events include:
Marriage, divorce, legal separation;
Death of spouse or dependent;
Birth or adoption of a child;
Changes in employment for spouse or dependents; Significant cost or coverage changes;

You must submit your benefit change requests and include required documentation within 30 days of the event. Also note that per the IRS, only changes consistent with the life event are allowed.
New employees must enroll within 30 days of their hire date. If employees fail to enroll within the 30 days, all voluntary benefits will be waived and employees will automatically be placed on the CCISD alternate plan. Except for health insurance, plans will be effective on the first of the month following the date of hire. Health Insurance can be effective the date of hire or the first of the month following date of hire. Please be aware that if you choose date of hire as effective date for health insurance, you will be charged for the entire month.
Please carefully review your paycheck(s) to ensure all deductions are correct. If you find a discrepancy in your paycheck, please contact U.S. Employee Benefits immediately at (830)606-5100. Discrepancies must be identified within the first 30 days from the effective date of the policy.
For contact information, claim forms, benefits guides and more please visit the www.ccisd.com website. Once on the website select “Departments” followed by “Employee Benefits/Insurance”.
This guide contains a summary of the benefits offered by Copperas Cove ISD. If there is a conflict between the terms of this outline of benefi ts and the actual contracts, the terms of the contracts will prevail.

Critical Illness - Lincoln
Phone: Website: 800.423.2765
www.lincolnfinancial.com
Flexible Spending Accounts -
Phone: Website:
HSA Bank - Health Savings Account
Phone:800.357.6247
Website www.hsabank.com
877.5 .
Phone: Website:
Retirement Plan Information - The Omni Group
Phone: Website:
877.544.6664
www.omni403b.com
TRS ActiveCare -
Phone: Website: 800.222.9205 www. .com
TRS ActiveCare - Scott & White
Phone:800.321.7947
Website:www.trs.swhp.org
U.S. Employee Benefits Services Group
Phone: Website:
888.836.5100
www. .com
This guide contains a summary of the benefits offered by Copperas Cove ISD. If there is a conflict between the terms of this outline of benefi ts and the actual contracts, the terms of the contracts will prevail.
mployee ame Robert Smith, SS# 123-45-6789
Default Password
User Name: smith 6789
Password password once you enter the site.

• Premium: The monthly amount you pay for health care coverage.

• Deductible: The annual amount for medical expenses you’re responsible to pay before your plan begins to pay its portion.
• Copay: The set amount you pay for a covered service at the time you receive it. The amount can vary by the type of service.

• Coinsurance: The portion you’re required to pay for services after you meet your deductible. It’s often a specified percentage of the costs; i.e. you pay 20% while the health care plan pays 80%.
• Out-of-Pocket Maximum: The maximum amount you pay each year for medical costs. After reaching the out-of-pocket maximum, the plan pays 100% of allowable charges for covered services.
While you can’t see Dr. Pepper for your annual check-up, you can find a great one in TRS-ActiveCare’s largest network of doctors.
*Available for all plans. See the benefits guide for more details.
New Rx Benefits!
• Express Scripts is your new pharmacy benefits manager! CVS pharmacies and most of your preferred pharmacies and medication are still included.
•Certain specialty drugs are still $0 through SaveOnSP
*Pre-certification for genetic and specialty testing may apply. Contact a PHG at
questions.
TRS contracts with HMOs in certain regions to bring participants in those areas additional options. HMOs set their own rates and premiums. They’re fully insured products who pay their own claims.
You can choose this plan if you live in one of these counties: Austin, Bastrop, Bell, Blanco, Bosque, Brazos, Burleson, Burnet, Caldwell, Collin, Coryell, Dallas, Denton, Ellis, Erath, Falls, Freestone, Grimes, Hamilton, Hays, Hill, Hood, Houston, Johnson, Lampasas, Lee, Leon, Limestone, Madison, McLennan, Milam, Mills, Navarro, Robertson, Rockwall, Somervell, Tarrant, Travis, Walker, Waller, Washington, Williamson
You can choose this plan if you live in one of these counties: Cameron, Hildalgo, Starr, Willacy
You can choose this plan if you live in one of these counties: Andrews, Armstrong, Bailey, Borden, Brewster, Briscoe, Callahan, Carson, Castro, Childress, Cochran, Coke, Coleman, Collingsworth, Comanche, Concho, Cottle, Crane, Crockett, Crosby, Dallam, Dawson, Deaf Smith, Dickens, Donley, Eastland, Ector, Fisher, Floyd, Gaines, Garza, Glasscock, Gray, Hale, Hall, Hansford, Hartley, Haskell, Hemphill, Hockley, Howard, Hutchinson, Irion, Jones, Kent, Kimble, King, Knox, Lamb, Lipscomb, Llano, Loving, Lubbock, Lynn, Martin, Mason, McCulloch, Menard, Midland, Mitchell, Moore, Motley, Nolan, Ochiltree, Oldham, Parmer, Pecos, Potter, Randall, Reagan, Reeves, Roberts, Runnels, San Saba, Schleicher, Scurry, Shackelford, Sherman, Stephens, Sterling, Stonewall, Sutton, Swisher, Taylor, Terry, Throckmorton, Tom Green, Upton, Ward, Wheeler, Winkler, Yoakum
Bitewing
Fluoride for Children 13 and under (1 per benefit period)
Sealants (age 13 and under)
Full Mouth/Panoramic X-rays (1 in 5 years)
Periapical X-rays
Space Maintainers
Restorative Amalgams
Restorative Composites (anterior and posterior teeth) Simple Extractions
Onlays
Crowns (1 in 10 years per tooth)
Crown Repair
Endodontics (nonsurgical)
Endodontics (surgical)
Periodontics (nonsurgical)

Periodontics (surgical)
Denture Repair
Prosthodontics (fixed bridge; removable complete/partial dentures)
(1 in 10 years)
Complex Extractions
Anesthesia
Monthly Rates
Employee Only (EE)
EE + Spouse $
EE + Children $
EE + Spouse & Children $
Ameritas Information
We're Here to Help
This plan was designed specifically for the associates of COPPERAS COVE INDEPENDENT SCHOOL DISTRICT DBA COPPERAS COVE ISD. At Ameritas Group, we do more than provide coverage - we make sure there's always a friendly voice to explain your benefits, listen to your concerns, and answer your questions. Our customer relations associates will be pleased to assist you 7 a.m. to midnight (Central Time) Monday through Thursday, and 7 a.m. to 6:30 p.m. on Friday. You can speak to them by calling toll-free: 800-487-5553. For plan information any time, access our automated voice response system or go online to ameritas.com.
How would you rate your dental health?
In 2016, you can receive your Dental Health Report Card by signing into your secure member account online. Your assessment is based on claims submitted. The report card also offers suggestions if you strive to improve your dental health. Ameritas members can access the personalized report card by going to ameritas.com, click Account Access in the top right corner and choose the Dental/Vision/Hearing drop down. Select the Secure Member Account link and sign in to see your report.
Our valued plan members and their covered dependents can save on prescription medications at over 60,000 pharmacies across the nation including CVS, Walgreens, Rite Aid and Walmart. This Rx discount is offered at no additional cost, and it is not insurance.
To receive this Rx discount, Ameritas plan members just need to visit us at ameritas.com and sign into (or create) a secure member account where they can access and print an online-only Rx discount savings ID card.
Ameritas plan members may receive up to 10% off eyewear frames and lenses purchased at any Walmart Vision Center nationwide. Members may also bring in their current vision prescription from any vision care provider and purchase eyewear at Walmart. This savings arrangement is not insurance: it is available to members at no additional cost to their plan premium.
To receive the eyewear savings identification card, Ameritas plan members can visit ameritas.com and sign-in (or create) a secure member account. Members must present the Ameritas Eyewear Savings Card at time of purchase to receive the discount.
This dental plan includes a valuable feature that allows qualifying plan members to carryover part of their unused annual maximum. A member earns dental rewards by submitting at least one claim for dental expenses incurred during the benefit year, while staying at or under the threshold amount for benefits received for that year. Employees and their covered dependents may accumulate rewards up to the stated maximum carryover amount, and then use those rewards for any covered dental procedures subject to applicable coinsurance and plan provisions. If a plan member doesn't submit a dental claim during a benefit year, all accumulated rewards are lost. But he or she can begin earning rewar ds again the very next year.
To find a provider, visit ameritas.com and select F F IND A PROVIDER, then D DENTAL. Enter your criteria to search by location or for a specific dentist or practice. California Residents: When prompted to select your network, choose the Ameritas Network found on your ID Card or contact Customer Connections at 800-487-5553.
While we don't require a pretreatment authorization form for any procedure, we recommend them for any dental work you consider expensive. As a smart consumer, it's best for you to know your share of the cost up front. Simply ask your dentist to submit the information for a pretreatment estimate to our customer relations department. We'll inform both you and your dentist of the exact amount your insurance will cover and the amount that you will be responsible for. That way, there won't be any surprises once the work has been completed.
If a member does not elect to participate when initially eligible, the member may elect to participate at the policyholder's next enrollment period. This enrollment period will be held each year and those who elect to participate in this policy at that time will have their insurance become effective on September 1. If you do not enroll during your company's open enrollment period, then you will be subject to the Late Entrant Provision.
This plan is provided as part of the Policyholder's Section 125 Plan. Each employee has the option under the Section 125 Plan of participating or not participating in this plan. If an employee does not elect to participate when initially eligible, he/she may elect to participate at the Policyholder's next Annual Election Period.
Ever wonder what a dental procedure usually costs? The answer can be found using the Ameritas group division’s Dental Cost Estimator tool located in our Secure Member Account portal.
Members can search by ZIP Code for a specific dental procedure and see fee range estimates for out-of-network general dentists in that area. Of course, we always suggest that members partner with their dentists, so they know what’s involved in any recommended treatment plan.
The estimator tool is powered by Go2Dental and uses FAIR Health data that is updated annually. Please note, cost estimates do not reflect discounted rates available through provider networks, and the estimator does not include orthodontic estimates at this time.
In addition, when members are in their Secure Member Account, they can:
Go paperless with electronic Explanation of Benefits statements and reduce the clutter in their mailboxes
View their certificate of insurance and specific plan benefits information
Access value-added extras like the Rx discount ID card
When our members travel abroad, they’ll have peace of mind knowing that should a dental or vision need arise, help is just a phone call away. Through AXA Assistance, Ameritas offers its dental and vision plan members 24-hour access to dental or vision provider referrals when traveling outside the U.S.
Immediately after a call is made to AXA, an assistance coordinator assesses the situation, provides credible provider referrals and can even assist with making the appointment. Within 48 hours following the appointment, the coordinator calls the member to find out if additional assistance is needed. If all is well, the case is closed. Then, the plan member may submit a claim to Ameritas for reimbursement consideration based on applicable plan benefits. Contact AXA Assistance USA toll free by calling 866-662-2731, or call collect from anywhere in the world by dialing 1-312-935-3727.
We recognize the importance of communicating with our growing number of multilingual customers. That is why we offer a language assistance program that gives you access to: Spanish-speaking claims contact center representatives, telephone interpretation services in a wide range of languages, online dental network provider search in Spanish and a variety of Spanish documents such as enrollment forms, claim forms and certificates of insurance.
This document is a highlight of plan benefits provided by Ameritas Life Insurance Corp as selected by your employe r It is not a certificate of insurance and does not include exclusions and limitations For exclusions and limitations, or a complete list of covered procedures, contact your b enefits administrator
Healthy eyes and clear vision are an important part of your overall health and quality of life. Your vision plan helps you care for your eyes while saving you money by offering:
Paid-in-full eye examinations, eyeglasses and contacts!
Frame Collection: Your plan includes a selection of designer, name brand frames that are completely covered in full./1
Contact Lens Collection: Select from the most popular contact lenses on the market today with Davis Vision’s Contact Lens Collection./1
One-year eyeglass breakage warranty included on plan eyewear at no additional cost!
Just log on to the Open Enrollment section of our Member site at davisvision.com and click “Find a Provider” to locate a provider near you including:
Eye Examination
Eyeglasses
Spectacle Lenses
Every 12 months, Covered in full after $10 copayment
Every 12 months, Covered in full
For standard single-vision, lined bifocal, or trifocal lenses after $25 copayment
Every 24 months, Covered in full
Any Fashion or Designer frame from Davis Vision’s Collection/1 (value up to $160) OR
Frames
$130 retail allowance toward any frame from provider, plus 20% off balance/2 OR
$180 allowance, plus 20% off balance/2 to go toward any frame from a Visionworks family of store locations./4
Contact Lenses
Every 12 months Collection Contacts: Covered in full after $25 copayment
Contact Lens Evaluation, Fitting & Follow Up Care
Non Collection Contacts:
Standard Contacts: Covered in full after $25 copay Specialty Contacts/5: $60 allowance with 15% off balance/2 less $25 copay

Every 12 months, Covered in full
Contact Lenses (in lieu of eyeglasses)
Any contact lenses from Davis Vision’s Contact Lens Collection/1 OR

$130 retail allowance toward provider supplied contact lenses, plus 15% off balance/2
Standard Progressives (no-line bifocal)$198$50 Photochromic Lenses (i.e. Transitions®, etc.)/3 $110$65
3797.
and
Fashion Frame (from the Davis Vision Collection)$100$0 Designer Frame (from the Davis Vision Collection)$160$0 Premier Frame (from the Davis Vision Collection)$195$25
Value for our Members
pocket cost to members and their families. Our goal is 100% member satisfaction.
Convenient Network Locations
A national network of credentialed preferred providers throughout the 50 states.
Freedom of Choice
Access to care through either our network of independent, private practice doctors (optometrists and ophthalmologists) or select retail partners.

Value-Added Features:
• Mail Order Contact Lenses Replacement
DavisVisionContacts.com mail-order service ensures easy, convenient, purchasing online and quick, direct shipping to your door. Log on to our member Web site for details.
• Davis Vision provides you and your eligible dependents with the opportunity to receive discounted laser vision correction, often referred to as LASIK. For more information, visit www.davisvision.com.
For more details about the plan, just log on to the Open Enrollment section of our Member site at davisvision.com or call 1.877.923.2847 and enter Client Code 3797.
1/ Polycarbonate lenses are covered in full for dependent children, monocular patients and patients with prescriptions 6.00 diopters or greater.
2/ Transitions® is a registered trademark of Transitions Optical, Inc.
You may receive services from an out-of-network provider, although you will provider who participates in the network. If you choose an out-of-network provider, you must pay the provider directly for all charges and then submit a claim for reimbursement to:
Vision Care Processing Unit
P.O. Box 1525 Latham, NY 12110
Eye Examination up to $40 | Frame up to $50 Spectacle Lenses (per pair) up to: Single Vision $40, Bifocal $60, Trifocal $80, Lenticular $100 Elective Contacts up to $130, Visually Required Contacts up to $225
Employee-Paid SHORT-TERMDISABILITYINSURANCE

























































Employee-Paid LONG-TERMDISABILITYINSURANCE



























SUMMARYOFBENEFITS




































purelife-plus
Life insurance can be an ideal way to provide money for your family when they need it most. purelife-plus offers permanent insurance with a high death benefit and long guarantees1 that can provide financial peace of mind for you and your loved ones. purelife-plus is an ideal complement to any group term and optional term life insurance your employer might provide and has the following features:

You
You own it
You
QUICK QUESTIONS 3
You can qualify by answering just 3 questions – no exams or needles.
Been actively at work on a full time basis, performing usual duties?
Been absent from work due to illness or medical treatment for a period of more than 5 consecutive working days?

1.Aftertheguaranteeperiod,premiumsmaygodown,staythesameorgoup.



2.CoveragenotavailableonchildreninWAorongrandchildreninWAorMD. InMD,childrenmustresidewiththeapplicanttobeeligibleforcoverage.
3.Conditionsapply.
FlexiblePremiumAdjustableLifeInsurancetoage121.PolicyFormICC18PRFNG-NI-18orFormSeriesPRFNG-NI-18.Somelimitationsapply.Seethe PureLife-plusbrochurefordetails.TexasLifeislicensedtodobusinessinthe DistrictofColumbiaandeverystatebutNewYork.

19M016-C1092(exp0321)

Been disabled or received tests, treatment or care of any kind in a hospital or nursing home or received chemotherapy, hormonal therapy for cancer, radiation, dialysis treatment, or treatment for alcohol or drug abuse?

PureLife-plusispermanentlifeinsurancetoAttainedAge121thatcanneverbecancelledaslongasyoupaythenecessarypremiums.Afterthe GuaranteedPeriod,thepremiumscanbelower,thesame,orhigherthantheTablePremium.Seethebrochureunder”PermanentCoverage”.
PureLife-plusispermanentlifeinsurancetoAttainedAge121thatcanneverbecancelledaslongasyoupaythenecessarypremiums.Afterthe GuaranteedPeriod,thepremiumscanbelower,thesame,orhigherthantheTablePremium.Seethebrochureunder”PermanentCoverage”.
Your employer provides you withBasic Term Life and Accidental Death and Dismemberment insurance coverage in the amount of:
For You
For Your Spouse
For Your Dependent Children*
$10,000 increments to a maximum of the lesser of 5 times pay or $150,000.
$5,000 increments to a maximum of $50,000, not to exceed 50% of employees Optional Life Benefit.
Child under 15 days: $100 Child 15 days to 6 months: $500 Child over 6 months old: $10,000
*Child(ren)’s Eligibility: Dependent children ages from birth to 25 years old, are eligible for coverage. In TX, regardless of student status, child(ren) are covered until age 25.
You have the option to purchase Optional Term Life Insurance. Listed below are your monthly rates (based on your age as of your last birthday on the Plan Anniversary each year) as well as those for your spouse (based on your age of your last birthday on the Plan Anniversary each year). Rates to cover your child(ren) are also shown.
† Covers all eligible children.
*Note: rates are subject to the policy’s right to change premium rates, and the employer’s right to change employee contributions.

Are you protected from life’s accidents?

There are things that you or your family do outside of work that may lead to an accidental injury.







Group Voluntary Accident coverage from Allstate Benefits pays cash benefits for expenses associated with an accidental injury and can help protect hard-earned savings should an off-the-job accidental injury occur.
THE POLICY IS NOT A POLICY OF WORKERS’ COMPENSATION INSURANCE. THE EMPLOYER DOES NOT BECOME A SUBSCRIBER TO THE WORKERS’ COMPENSATION SYSTEM BY PURCHASING THIS POLICY, AND IF THE EMPLOYER IS A NON-SUBSCRIBER, THE EMPLOYER LOSES THOSE BENEFITS WHICH WOULD OTHERWISE ACCRUE UNDER THE WORKERS’ COMPENSATION LAWS. THE EMPLOYER MUST COMPLY WITH THE WORKERS’ COMPENSATION LAW AS IT PERTAINS TO NON-SUBSCRIBERS AND THE REQUIRED NOTIFICATION THAT MUST BE FILED AND POSTED – TX only.
No one plans to have an accident. But it can happen at any moment throughout the day, whether at home or at play. Most major medical insurance plans only pay a portion of the bills. Our coverage can help pick up where other insurance leaves off and provide cash to help cover the expenses. Our accident coverage helps offer peace of mind when an accidental injury occurs. Below is an example of how benefits are paid.*
Employee chooses benefit coverage under his Employer
Approved Plan
Employee incurred expenses for services in and out of the hospital. In addition to what major medical insurance paid, our accident benefits paid for:
With Accident Coverage
Additional dollars to pay for copay, deductible and other costs
Benefits paid: $3,530

2 i a l

2 years later the employee is going out to dinner, is in a car accident, and is air lifted to the hospital
Our accident coverage helps offer peace of mind when an accidental injury occurs.
• Coverage that is guaranteed issue; there are no medical exams or tests to take


• Benefits that correspond with treatment for off-the-job accidental injuries including hospitalization, emergency treatment, intensive care, fractures, plus more
• Off-the-job accident coverage for yourself or your entire family
• Affordable premiums
• Benefits paid directly to you, unless you assign them to someone else
• An additional benefit has been added to the plan to enhance your coverage
• Continuation of coverage
Without Accident Coverage
No additional dollars to pay for copay, deductible or other out-of-pocket costs
Benefits paid: $0
Accidental Death - Pays a benefit for accidental death.
Common Carrier Accidental Death – Pays a benefit for death while riding as a fare-paying passenger on a scheduled common carrier.
Dismemberment – Pays a benefit for dismemberment. Multiple dismemberments during the same injury are limited to the principal amount listed on page 2a.

Dislocation or Fracture – Pays a benefit for dislocation or fracture. Multiple dislocations or fractures during the same injury are limited to the principal amount listed on page 2a.
Hospital Confinement – Pays a benefit when you are confined in a hospital for the first time after your effective date. Paid once per year.
Daily Hospital Confinement – Pays a benefit when you are confined in a hospital up to 90 days for each accident.
Intensive Care – Pays a benefit when you are confined in a hospital intensive-care unit up to 90 days for each accident.
Ambulance – Pays a benefit for you to be transferred by ambulance service to or from a hospital.
Accident Physician Treatment – Pays a benefit when you receive treatment by a physician.

X-ray – Pays a benefit when X-rays are taken.
Emergency Room Services – Pays a benefit when emergency room services are received.
†Pays stated amounts for accidents only. Benefit amounts are shown on pages 2a and/or 2b. See page 4 for limits and conditions and pages 4 and 5 for state variations.



Lacerations – Pays a benefit when you receive treatment for 1 or more cuts within 3 days after an accident. Paid once per year.
Burns – Pays a benefit when you receive treatment for burns, other than sun burns, within 3 days after an accident.
Skin Graft** – Pays a benefit when you receive a skin graft for a covered burn.
Brain Injury Diagnosis – Pays a one-time benefit when you are diagnosed with 1 of these within 30 days after an accident: concussion, cerebral laceration, cerebral contusion, or intracranial hemorrhage. Must be first treated by a physician within 3 days after the accident.
Computed Tomography (CT) Scan and Magnetic Resonance Imaging (MRI)* – Pays a benefit when you receive a CT scan or MRI. Must be first treated by a physician within 30 days after the accident. Paid once per year.
Paralysis – Pays a one-time benefit when you are paralyzed from a spinal cord injury for at least 90 days. Must be confirmed by a physician within 3 days after the accident.
Coma with Respiratory Assistance – Pays a one-time benefit when you are in a coma for at least 7 days. Medically induced comas are not covered.
Open Abdominal or Thoracic Surgery – Pays a benefit when you have surgery for internal injuries within 3 days after the accident.
Tendon, Ligament, Rotator Cuff or Knee Cartilage Surgery* – Pays a benefit when you have surgery to repair a tendon, ligament, rotator cuff or knee cartilage; or for exploratory arthroscopic surgery.
Ruptured Disc Surgery* – Pays a benefit when you have a surgical procedure to repair a ruptured spinal disc.
Eye Surgery** – Pays a benefit when you have surgery or a foreign object removed from the eye.


General Anesthesia* – Pays a benefit for general anesthesia for a covered surgery.

Blood and Plasma – Pays a benefit for a blood or plasma transfusion within 3 days after an accident.
Appliance** – Pays a benefit for 1 of the following: wheelchair, crutches, or walker.
Medical Supplies** – Pays a benefit for over-the-counter medical supplies.†
Medicine** – Pays a benefit for prescription or overthe-counter medicine.†
Prosthesis* – Pays a benefit for a physician-prescribed prosthetic arm, leg, hand, foot or eye when a benefit is also paid under the Dismemberment benefit.
Physical Therapy** – Pays a benefit for physician-prescribed physical therapy (up to 6 treatments per accident) within 6 months after the accident. Not payable for chiropractic services or for the same visit that the Accident Follow-Up Treatment benefit is paid.†
Rehabilitation Unit – Pays a benefit when you are confined in a rehabilitation unit after a hospital stay. Paid up to 30 days per confinement (maximum 60 days per year). Not payable for days that the Daily Hospital Confinement benefit is paid.
Non-Local Transportation – Pays a benefit when you have physician-prescribed treatment at a hospital or treatment center more than 100 miles from your home. Paid up to 3 times per accident.
Family Member Lodging – Pays a benefit when one adult family member acc ompanies you to receive treatment at a hospital or treatment center more than 100 miles from the family member’s home.
Post-Accident Transportation – Pays a benefit when you are confined in a hospital for at least 3 days in a row more than 250 miles from your home, and you are brought home by a common carrier.
Accident Follow-Up Treatment** – Pays a benefit when you receive follow-up treatment from a physician in his or her office or in a hospital as an outpatient (up to 2 treatments per accident) within 6 months after the accident. Not payable for the same visit for which the Physical Therapy benefit is paid.†
Outpatient Physician’s Benefit – Pays a daily benefit when you receive treatment by a physician outside of a hospital for any reason. The benefit is limited to 2 days per covered person per calendar year, not to exceed 4 days per calendar year if coverage includes eligible dependents.
*Must begin or be received within 180 days of the accident.
**Must begin, be received, or performed within 90 days of the accident.
†Provided a benefit is paid under the Accident Physician Treatment or X-ray benefit.
Conditions and Limits – When an injury results in a covered loss within 90 days (180 days for dismemberment or accidental death), unless otherwise stated, from the date of an accident, and is diagnosed by a physician, Allstate Benefits will pay benefits as stated. Treatment must be received in the United States or its territories.
Your Eligibility – Your employer decides who is eligible for your group (such as length of service and hours worked each week). Issue ages are 18 and over.
Dependent Eligibility/Termination – (a) Coverage may include you, your spouse or domestic partner, and your children. (b) Coverage for children ends when the child reaches age 26, unless he or she continues to meet the requirements of an eligible dependent. (c) Spouse coverage ends upon valid decree of divorce or your death. (d)Domestic partner coverage ends upon termination of domestic partnership or your death.
When Coverage Ends – Coverage under the policy ends on the earliest of: (a) the date the policy is canceled; (b) the last day of the period for which you made any required contributions; (c) the last day you are in active employment, except as provided under the Temporary Layoff, Leave of Absence, or Family and Medical Leave of Absence provision; (d)the date you are no longer in an eligible class; (e) the date your class is no longer eligible; or (f) upon discovery of fraud or material misrepresentation when filing a claim.
Continuation of Coverage – You may be eligible to continue coverage when coverage under the policy ends. You have 60 days after coverage under the policy ends to let us know if you wish to continue coverage.
Accident and Benefit Enhancement Exclusions and Limitations – Benefits are not paid for: (a) injury incurred before the effective date; (b) injury as a result of an on-the-job accident; (c) any act of war or participation in a riot, insurrection or rebellion; (d) self-inflicted injury; (e) suicide or attempted suicide; (f) being under the influence of alcohol or narcotics unless taken on the advice of a physician; (g) bacterial infection (except pyogenic infections from an accidental cut or wound); (h) participation in aeronautics unless a fare-paying passenger on a licensed common-carrier aircraft; (i) engaging in an illegal occupation, assault or felony; (j) driving in any race or speed test or testing any vehicle on any racetrack or speedway; (k) serving as an active member of the Military, Naval, or Air Forces of any country; and (l) hernia, including complications.
Outpatient Physician’s Benefit Rider Exclusions and Limitations – Benefits are not paid for: (a) losses incurred before the effective date; (b) a loss as a result of an onthe-job accident; (c) any act of war or part icipation in a riot, insurrection or rebellion; (d) suicide or attempted suicide; (e) self-inflicted action; (f) being under the influence of alcohol or narcotics unless taken on the advice of a physician; (g) participation in aeronautics unless a farepaying passenger on a licensed common-carrier aircraft; (h)engaging in an illegal occupation, assault or felony; (i)driving in any race or speed test or testing any vehicle on any racetrack or speedway; (j) serving as an active member of the Military, Naval, or Air Forces of any country.
Arkansas (changes affect page 4) – In the Accident and Benefit Enhancement Exclusions and Limitations paragraph, item (f) is replaced with: injury resulting from being intoxicated or under the influence of any controlled substance unless taken on the advice of a physician; items (g) and (l) are deleted. In the Outpatient Physician’s Benefit Rider Exclusions and Limitations paragraph, item (f) is replaced with: loss resulting from being intoxicated or under the influence of any controlled substance, unless taken on the advice of a physician.
Georgia (changes affect pages 3 and 4) – In the Benefit Enhancements, the Coma with Respiratory Assistance benefit is deleted. The When Coverage Ends paragraph, specification includes: (g) the date you request to discontinue coverage in writing
Louisiana (changes affect pages 3 and 4) – In the Physical Therapy benefit, chiropractic services are payable. In the Accident and Benefit Enhancement Exclusions and Limitations paragraph, item (f) is replaced with: injury resulting from being intoxicated or under the influence of any narcotic not prescribed or recommended by a physician. In the Outpatient Physician’s Benefit Rider Exclusions and Limitations paragraph, item (f) is replaced with: loss resulting from being intoxicated or under the influence of any narcotic not prescribed or recommended by a physician.
New Mexico (change affects page 2) – The Accident Physician Treatment benefit includes coverage for Temporomandibular joint disorders and Craniomandibular joint disorders if a result of injury. We will not pay for orthodontic appliances and treatment, crowns, bridges and dentures, unless the disorder results from an injury.
*Benefits are payable once/covered accident/ covered person
1based on amounts shown in the Injury Benefit Schedule on reverse 2once/covered person/year
3per day, max. 90 days/injury
4payable once/covered person
5payable once/covered person/accident/year
62 or more procedures through same entry point are considered 1 operation
7per day, max. 6 treatments/accident/ covered person
8per trip, max. 3 times/ accident
9per day, max. 30 days
10per day, max. 30 days/covered person/ confinement, max. 60 days/year
11per day, max. 2 treatments/accident/ covered person
12per day, max. 2 days/ covered person/year, 4 if dependents are covered
Benefit amounts for coverage and one occurrence are shown below.
Covered spouse gets 50% of the amounts shown and children 25%.
LOSS OF LIFE OR LIMB PLAN
Life, or both eyes, hands, arms, feet, or legs, or one hand or arm and one foot or leg
One eye, hand, arm, foot, or leg
One or more entire toes or fingers
COMPLETE DISLOCATION PLAN
Hip joint $4,000
Knee or ankle joint*, bone or bones of the foot* $1,600
Wrist joint $1,400
Elbow joint $1,200
Shoulder joint $800
Bone or bones of the hand*, collarbone $600
Two or more fingers or toes $280
One finger or toe $120
COMPLETE, SIMPLE OR CLOSED FRACTURE PLAN
Hip, thigh (femur), pelvis** $4,000
Skull** $3,800
Arm, between shoulder and elbow (shaft), shoulder blade (scapula), leg (tibia or fibula) $2,200
Ankle, knee cap (patella), forearm (radius or ulna), collarbone (clavicle) $1,600
Foot**, hand or wrist** $1,400
Lower jaw** $800
Two or more ribs, fingers or toes, bones of face or nose $600
One rib, finger or toe, coccyx $280
*Knee joint (except patella). Bone or bones of the foot (except toes). Bone or bones of the hand (except fingers). **Pelvis (except coccyx). Skull (except bones of face or nose). Foot (except toes). Hand or wrist (except fingers). Lower jaw (except alveolar process).
premiums
EE = Employee; EE + SP = Employee + Spouse; EE + CH = Employee + Child(ren); and F = Family Issue Ages: 18 and over if Actively at Work
This insert is for use in: TX
This insert is part of brochure ABJ23842-3 and is not to be used on its own. Allstate Benefits is the marketing name used by American Heritage Life Insurance Company (Home Office, Jacksonville, FL), a subsidiary of The Allstate Corporation. ©2015 Allstate Insurance Company. www.allstate.com or allstatebenefits.com.
ABJ23842-3-Insert-Luddeke
Are you protected from a diagnosis of cancer?
There are daily living expenses you must pay for even if you are sick and cannot work.










Supplements existing coverage and can provide cash to help with medical and living expenses
Group Voluntary Cancer coverage from Allstate Benefits pays cash benefits for cancer and 29 specified diseases to help with the costs associated with treatments and expenses as they happen.
THIS IS NOT A POLICY OF WORKERS’ COMPENSATION INSURANCE. THE EMPLOYER DOES NOT BECOME A SUBSCRIBER TO THE WORKERS’ COMPENSATION SYSTEM BY PURCHASING THE POLICY, AND IF THE EMPLOYER IS A NON-SUBSCRIBER, THE EMPLOYER LOSES THOSE BENEFITS WHICH WOULD OTHERWISE ACCRUE UNDER THE WORKERS’ COMPENSATION LAWS. THE EMPLOYER MUST COMPLY WITH THE WORKERS’ COMPENSATION LAW AS IT PERTAINS TO NON-SUBSCRIBERS AND THE REQUIRED NOTIFICATIONS THAT MUST BE FILED AND POSTED.
Receiving a diagnosis of cancer or a specified disease can be difficult on anyone, both emotionally and financially. Having the right coverage to help when undergoing treatments for cancer or a specified disease is important. Our coverage can help provide added financial support when it is needed most.
Our coverage helps offer peace of mind when a diagnosis of cancer or a specified disease occurs. Below is an example of how benefits might be paid. *
Jane chooses benefit coverage under her Employer Approved Plan
Jane’s doctor recommends pre-op testing and provides her with the location of the hospital. Jane must travel 200 miles to have pre-op testing (medical imaging) and is admitted to the hospital for surgery.
Jane undergoes her annual wellness test and is diagnosed with cancer.
Jane undergoes surgery, anesthesia, radiation/chemo, and is visited by a doctor during a 3-day hospital stay. And every 2 weeks she has radiation/ chemotherapy at a local facility, is given anti-nausea medication, and sees her doctor during her follow-up visits.
Our cancer insurance policy paid Jane the following:


Wellness Exam $50
Hospital Confinement $600
Cancer Initial Diagnosis $3,000


Non-Local Transportation $160
Surgery $4,500
Anesthesia $1,125
Radiation/Chemo $5,000
Medical Imaging $250



Inpatient Medicine $75
Physician Visits $150
Anti-Nausea $200
Total Benefits: $15,110
*The example shown may vary from the plan your employer is offering. Your individual experience may also vary. Please see pages 2a and/or 2b for your plan details.
Our cancer coverage can help offer you and your family financial support.
• Benefits paid directly to you unless otherwise assigned
• Coverage for you or your entire family
• No evidence of insurability required at initial enrollment†
• Waiver of premium after 90 days of disability due to cancer for as long as your disability lasts**
• Portable
† Enrolling after your initial enrollment period requires evidence of insurability.
**Primary insured only.
Cancer and specified disease benefits can help cover the costs of specific treatments and expenses as they happen. Terms and conditions for each benefit will vary. Benefit amounts are shown on pages 2a and/or 2b.
Specified Diseases - Amyotrophic Lateral Sclerosis (Lou Gehrig’s Disease), Muscular Dystrophy, Poliomyelitis, Multiple Sclerosis, Encephalitis, Rabies, Tetanus, Tuberculosis, Osteomyelitis, Diphtheria, Scarlet Fever, Cerebrospinal Meningitis, Brucellosis, Sickle Cell Anemia, Thalassemia, Rocky Mountain Spotted Fever, Legionnaires’ Disease, Addison’s Disease, Hansen’s Disease, Tularemia, Hepatitis (Chronic B or C), Typhoid Fever, Myasthenia Gravis, Reye’s Syndrome, Primary Sclerosing Cholangitis (Walter Payton’s Disease), Lyme Disease, Systemic Lupus Erythematosus, Cystic Fibrosis, and Primary Biliary Cirrhosis.
Continuous Hospital Confinement - Pays a benefit for each day of inpatient confinement.
Government or Charity Hospital - Pays a benefit for each day of inpatient confinement to a U.S. government hospital or a hospital that does not charge for its services. In lieu of all other benefits.
Private Duty Nursing Services - Pays a daily benefit when receiving physician-authorized inpatient private nursing services.
Extended Care Facility - Pays a daily benefit for physician-authorized inpatient confinement (within 14 days of a hospital stay).
At Home Nursing - Pays a daily benefit for p hysician- authorized private nursing care (up to the number of days of the previous hospital stay).
Hospice Care - Pays a benefit when a physician determines terminal illness and approves hospice care at home (1 visit per day) or in a freestanding hospice care center.
RADIATION, CHEMOTHERAPY AND RELATED BENEFITS
Radiation/Chemotherapy for Cancer - Pays a benefit for covered treatment to destroy or modify cancerous tissue.
Blood, Plasma, and Platelets - Pays a benefit for blood, plasma, and platelets. Includes charges for transfusions, administration, processing, procurement and cross-matching. Does not include donor replaced blood or immunoglobulins.
Medical Imaging - Pays a benefit for an initial diagnosis or follow-up evaluation.
Hematological Drugs - Pays a benefit for drugs to boost cell lines when Radiation/Chemotherapy for Cancer benefit is paid.
Surgery*- Pays a benefit for an inpatient or outpatient operation listed in the Schedule of Surgical Procedures.
Anesthesia - Pays 25% of surgery benefit.
Ambulatory Surgical Center - Pays a benefit for surgery at an ambulatory surgical center.

Second Opinion - Pays a benefit for a second surgical opinion.
Bone Marrow or Stem Cell Transplant - Pays a benefit for transplants.



Inpatient Drugs and Medicine - Pays a daily benefit for inpatient drugs and medicine.
Physician’s Attendance - Pays a daily benefit for one inpatient visit.
Ambulance - Pays a benefit for transfer by ambulance service to or from a hospital.
Non-Local Transportation - Pays a benefit for transportation for treatment not available locally (up to 700 miles).
Outpatient Lodging - Pays a daily benefit for lodging when receiving radiation or chemotherapy on an outpatient basis non-locally (more than 100 miles from home).
Family Member Lodging and Transportation - Pays a benefit for one adult family member when confined at a non-local hospital for specialized treatment (more than 100 miles from family member’s home).
Physical or Speech Therapy - Pays a daily benefit for physical or speech therapy to restore normal body function.
New or Experimental Treatment - Pays a benefit for physician- approved new or experimental treatments not paid under other benefits.
Prosthesis - Pays a benefit for a prosthetic device that requires surgical implanting.
Hair Prosthesis - Pays a benefit for a wig or hairpiece when hair loss is experienced.
Nonsurgical External Breast Prosthesis - Pays a benefit for the initial nonsurgical breast prosthesis after a covered mastectomy.
Anti-Nausea Benefit - Pays a benefit for prescribed antinausea medication administered on an outpatient basis.
Waiver of Premium (primary insured only) - Pays premiums after disabled 90 days in a row due to cancer, for as long as disability lasts.
Cancer Initial Diagnosis - Pays a one-time benefit if diagnosed for the first time with cancer (except skin cancer).
Wellness - Pays a benefit each calendar year for one of the following: Biopsy for skin cancer; Blood tests for triglycerides, CA15-3 (breast cancer), CA125 (ovarian cancer), CEA (colon cancer) and PSA (prostate cancer); Bone Marrow Testing; Chest X-ray; Colonoscopy; Doppler screening for carotids or peripheral vascular disease; Echocardiogram; EKG; Flexible sigmoidoscopy; Hemoccult stool analysis; HPV (Human Papillomavirus) Vaccination; Lipid panel (total cholesterol count); Mammography, including Breast Ultrasound; Pap Smear, including ThinPrep Pap Test; Serum Protein Electrophoresis (test for myeloma); Stress test on bike or treadmill; Thermography; and Ultrasound screening for abdominal aortic aneurysms.
Intensive Care - Pays a daily benefit for Intensive Care Unit Confinements for any illness or accident (up to 45 days for each stay), Step-down Intensive Care Unit Confinements (up to 45 days for each stay) and air or surface ambulance to a hospital intensive-care unit.
Wellness tests A doctor visit is scheduled annually
You get paid cash Tests are run and results received T
Eligibility - Coverage may include you, your spouse or domestic partner and children under age 26.
Termination of Coverage - (a) Coverage under the policy ends on the date the policy is canceled; the last day premium payments were made; the last day of active employment, unless coverage is continued due to Temporary Layoff, Leave of Absence or Family and Medical Leave of Absence; the date you or your class is no longer eligible. (b) Spouse/domestic partner coverage ends upon divorce/termination of partnership or your death. (c) Coverage for children ends when the child reaches age 26, unless he or she continues to meet the requirements of an eligible dependent.
Portability Privilege - Coverage may be continued under the Portability Provision when coverage under the policy ends.
Pre-Existing Condition - (a) Allstate Benefits does not pay benefits for a pre-existing condition during the 12-month period beginning on the date that person’s coverage starts.
(b)A pre-existing condition is a disease or condition for which symptoms existed within the 12-month period prior to the effective date; or (c) medical advice or treatment was recommended or received from a medical professional within the 12-month period prior to the effective date.
(d)A pre-existing condition can exist even though a diagnosis has not yet been made.
Cancer and Specified Disease Benefits Exclusions and Limitations - (a) Allstate Benefits does not pay for any loss, except for losses due to cancer or a specified disease.
(b) Benefits are not paid for conditions caused or aggravated by cancer or a specified disease.
Treatment and services must be needed due to cancer or a specified disease and be received in the United States or its territories.
For the Surgery, New or Experimental Treatment and Prosthesis benefits, Allstate Benefits pays 50% of the applicable maximum when specific charges are not obtainable as proof of loss.
For the Radiation/Chemotherapy for Cancer benefit, Allstate Benefits does not pay for: (a) any other chemical substance which may be administered with or in conjunction with radiation/chemotherapy; or (b) treatment planning consultation; management; or the design and construction of treatment devices; or basic radiation dosimetry calculation; or any type of laboratory tests; X-ray or other imaging used for diagnosis or monitoring; or the diagnostic tests related to these treatments; or (c) any devices or supplies including intravenous solutions and needles related to these treatments.
Intensive Care Benefits Exclusions and Limitations(a)Benefits are not paid for: (1) attempted suicide or intentional self-inflicted injury; (2) intoxication or being under the influence of drugs not prescribed by a physician; or (3) alcoholism or drug addiction. (b) Benefits are not paid for confinements to a care unit that does not qualify as a hospital intensive-care unit including progressive care, subacute intensive care, intermediate care, private rooms with monitoring, step-down and other lesser care units. (c)Benefits are not paid for step-down confinements in the following units: telemetry or surgical recovery rooms; post-anesthesia care; progressive care; intermediate care; private monitored rooms; observation units in emergency rooms or outpatient surgery units; beds, wards, or private or semi-private rooms; emergency, labor or delivery rooms; or other facilities that do not meet the standards for a step-down hospital intensive-care unit. (d) Benefits are not paid for confinements occurring during a hospitalization prior to the effective date. (e) Children born within 10 months of the effective date are not covered for confinement occurring or beginning during the first 30 days of the child’s life. (f) We do not pay for ambulance if paid under the cancer and specified disease ambulance benefit.
Physical or Speech Therapy (daily)
New or Experimental Treatment (every 12 mos.)
Prosthesis
Hair Prosthesis (every 2 years)
Nonsurgical External Breast Prosthesis
3 $25 $25 $50* $50* $200* $200*
Listed to the left are benefit amounts associated with the benefits described in the brochure.
*Benefitpaysfor charges/costs up to amount listed 1 Limit $2,000/ 12 mo. period
2 Based on procedure up to maximum shown
Sponsored by:Copperas Cove ISD

Critical Illness insurance coverage provides a cash benefit to the policyholder when an insured person has a covered illness or event.
Eligibility All employees in an eligible class.Issue Ages 17-70
Non-Tobacco Monthly Premium per benefit amount for Employee
*Child Dependent coverage offered at no additional cost.
Tobacco Monthly Premium per benefit amount for Employee
Non-Tobacco Monthly Premium per benefit amount for Spouse
Tobacco Monthly Premium per benefit amount for Spouse
* The policy is guaranteed renewable. The insurer has the right to increase premium rates on any policy anniversary after the Policy’s first anniversary, for all policies of like class. Any insurance continued under the portability provision terminates at age 90.
** This is an estimate of premium cost. Actual deductions may vary slightly due to rounding and payroll frequency
A benefit will not be paid under this policy when:
A category maximum has been reached (for that Category, coverage will automatically terminate). If Lincoln CareCompass SM is the only remaining Category, coverage will be terminated.
A new Category Occurrence happens within 90 days of another payable event in a different category.
A Category Recurrence happens within 180 days of another payable event in the same category.
The diagnosis is deemed a pre-existing condition.
An event was caused by self-inflicted injury, self destructive, suicide or attempting any of these, whether sane or insane.
An event occurs during the attempt or commission of a felony, whether charged or not.
An event occurs during an act of war (which is not terrorism), participation ina riot, insurrection or rebellion of any kind.
An event occurs while serving as a member of any armed forces or auxiliary unit.
An event occurs after the insured had resided outside of the US, Mexico, or Canada for 12 or more months. An event occurs whilethe insured was incarcerated in any type of penal facility.
Accident Exclusions:
Additionally, a benefit will not be paid under this policy amendment when injury occurs due to: Bungee jumping, parachuting, base jumping, or mountaineering.
Cosmetic or elective surgery. Being intoxicated.
Having any sickness, illness (physical or mental), or infection independent of accident. Deliberate use of drugs, poison, gas or fumes, by ingestion, injection, inhalation, or absorption. Injury at work or in the course ofemployment.
Participating in, practicing for, or officiating a semiprofessional or professional sport. Riding in or driving any motor-driven vehicle for race, stunt show, or speed test.
For assistance or additional information Contact Lincoln Financial Group at (800)423-2765; reference ID: COPPERSCIS www.LincolnFinancial.com
NOTE: This is not intended as a complete description of the insurance coverage offered. While benefit amounts stated in this summary are specific to your coverage, other items may summarize our standard product features and not the specific features of your coverage. Controlling provisions are provided in the policy, and this summary does not modify those provisions or the insurance in any way. This is not a binding contract. A policy will be made available to you that describes the benefits in greater details. Should there be a difference between this summary and the policy, the policy will govern.
©2014
Insurance products GL51 are issued by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicit business in New York, nor is it licensed to do so. In New York, insurance products are issued by Lincoln Life & Annuity Company of New York (Syracuse, NY). Both are Lincoln Financial Group® com panies. Product availability and/or features may vary by state. Limitations and exclusions may apply.
Lincoln Financial Group is the marketing name for Lincoln National Corporation and its affiliates. Affiliates are separately responsible for their own financial and contractual obligations.
















A Health Savings Account (HSA) is an individually-owned, tax‐advantaged account that you can use to pay for current or future IRS‐qualified medical expenses. With an HSA, you’ll have the potential to build more savings for healthcare expenses or additional retirement savings through self-directed investment options¹ .
•You can contribute to your HSA via payroll deduction, online banking transfer, or by sending a personal check to HSA Bank. Your employer or third parties, such as a spouse or parent, may contribute to your account as well.
•You can pay for qualified medical expenses with your Health Benefits Debit Card directly to your medical provider or pay out-of-pocket. You can either choose to reimburse yourself or keep the funds in your HSA to grow your savings.
•Unused funds will roll over year to year. After age 65, funds can be withdrawn for any purpose without penalty (subject to ordinary income taxes).
•Check balances and account information via HSA Bank’s Member Website or mobile device 24/7.

If you have a qualified High Deductible Health Plan (HDHP) - either through your employer, through your spouse, or one you’ve purchased on your own - chances are you can open an HSA. Additionally:
•You cannot be covered by any other non-HSA-compatible health plan, including Medicare Parts A and B.
•You cannot be covered by TriCare.
•You cannot be claimed as a dependent on another person’s tax return (unless it’s your spouse).

•You must be covered by the qualified HDHP on the first day of the month. When you open an account, HSA Bank will request certain information to verify your identity and to process your application.

Contributions made by all parties to an HSA cannot exceed the annual HSA limit set by the Internal Revenue Service (IRS). Anyone can contribute to your HSA, but only the accountholder and employer can receive tax deductions on those contributions. Combined annual contributions for the accountholder, employer, and third parties (i.e., parent, spouse, or anyone else) must not exceed these limits.2
2023-2024
According to IRS guidelines, each year you have until the tax filing deadline to contribute to your HSA (typically April 15 of the following year). Online contributions must be submitted by 2:00 p.m., Central Time, the business day before the tax filing deadline. Wire contributions must be received by noon, Central Time, on the tax filing deadline, and contribution forms with checks must be received by the tax filing deadline.
Accountholders who meet these qualifications are eligible to make an HSA catch-up contribution of $1,000: Health Savings accountholder; age 55 or older (regardless of when in the year an accountholder turns 55); not enrolled in Medicare (if an accountholder enrolls in Medicare mid-year, catch-up contributions should be prorated). Authorized signers who are 55 or older must have their own HSA in order to make the catch-up contribution.
An HSA provides triple tax savings.3 Here’s how:
•Contributions to your HSA can be made with pre-tax dollars and any after-tax contributions that you make to your HSA are tax deductible.
•HSA funds earn interest and investment earnings are tax free.
•When used for IRS-qualified medical expenses, distributions are free from tax.
You can use your HSA to pay for a wide range of IRS-qualified medical expenses for yourself, your spouse, or tax dependents. An IRSqualified medical expense is defined as an expense that pays for healthcare services, equipment, or medications. Funds used to pay for IRS-qualified medical expenses are always tax-free.
HSA funds can be used to reimburse yourself for past medical expenses if the expense was incurred after your HSA was established. While you do not need to submit any receipts to HSA Bank, you must save your bills and receipts for tax purposes.
Examples of IRS-Qualified Medical Expenses4:
Acupuncture
Alcoholism treatment
Ambulance services
Annual physical examination
Artificial limb or prosthesis
Birth control pills (by prescription)
Chiropractor
Childbirth/delivery
Convalescent home (for medical treatment only)
Crutches
Doctor’s fees
Dental treatments (including x-rays, braces, dentures, fillings, oral surgery)
Dermatologist
Diagnostic services
Disabled dependent care
Drug addiction therapy
Fertility enhancement (including in-vitro fertilization)
Guide dog (or other service animal)
Gynecologist
Hearing aids and batteries
Hospital bills
Insurance premiums5
Laboratory fees
Lactation expenses
Lodging (away from home for outpatient care)
Nursing home
Nursing services
Obstetrician
Osteopath
Oxygen
Pregnancy test kit
Podiatrist
Prescription drugs and medicines (over-the-counter drugs are not IRS-qualified medical expenses unless prescribed by a doctor)
Prenatal care & postnatal treatments
Psychiatrist
Psychologist
Smoking cessation programs
Special education tutoring
Surgery
Telephone or TV equipment to assist the hearing or vision
impaired
Therapy or counseling
Medical transportation expenses
Transplants
Vaccines
Vasectomy
Vision care (including eyeglasses, contact lenses, lasik surgery)
Weight loss programs (for a specific disease diagnosed by a physician – such as obesity, hypertension, or heart disease)
Wheelchairs
X-rays
¹ Investment accounts are not FDIC insured, may lose value and are not a deposit or other obligation of, or guarantee by the bank. Investment losses which are replaced are subject to the annual contribution limits of the HSA.
2 HSA funds contributed in excess of these limits are subject to penalty and tax unless the excess and earnings are withdrawn prior to the due date, including any extensions for filing Federal Tax returns. Accountholders should consult with a qualified tax advisor in connection with excess contribution removal. The Internal Revenue Service requires HSA Bank to report withdrawals that are considered refunds of excess contributions. In order for the withdrawal to be accurately reported, accountholders may not withdraw the excess directly. Instead, an excess contribution refund must be requested from HSA Bank and an Excess Contribution Removal Form completed.
3 Federal Tax savings are available no matter where you live and HSAs are taxable in AL, CA, and NJ. HSA Bank does not provide tax advice. Consult your tax professional for tax‐related questions.
4 This list is not comprehensive. It is provided to you with the understanding that HSA Bank is not engaged in rendering tax advice. The information provided is not intended to be used to avoid Federal tax penalties. For more detailed information, please refer to IRS Publication 502 titled, “Medical and Dental Expenses”. Publications can be ordered directly from the IRS by calling 1-800-TAXFORM. If tax advice is required, you should seek the services of a professional.
5 Insurance premiums only qualify as an IRS-qualified medical expense: while continuing coverage under COBRA; for qualified long-term care coverage; coverage while receiving unemployment compensation; for any healthcare coverage for those over age 65 including Medicare (except Medicare supplemental coverage).
Please call the number on the back of your HSA Bank debit card or visit us at www.hsabank.com











MASA MTS is here toprotect its members and their families from the shortcomings of health insurance coverage by providing them with comprehensive financial protection for lifesaving emergencytransportationservices, bothathome andaway fromhome.
ManyAmericanemployersandemployees believethattheirhealthinsurancepolicies covermost,ifnotallambulanceexpenses. The truth is, they DONOT!

Even after insurance payments for emergency transportation, you couldreceive abillupto$5,000forgroundambulanceand as high as $70,000 for air ambulance. The financial burdens for medical transportation costs are veryreal.

AcrosstheUStherearethousandsofground ambulance providers andhundreds of air ambulance carriers. ONLY MASA offers comprehensive coverage since MASA is a PAYER andnotaPROVIDER!



ONLY MASA provides over 1.6million members with coverage for BOTH ground ambulance and air ambulance transport, REGARDLESS ofwhich provider transportsthem.


Members are covered ANYWHERE in all50 states andCanada!
Additionally, MASA provides arepatriation benefit:ifamemberishospitalizedmorethan 100miles from home, MASA can arrangeand pay tohave them transported toahospital closer totheir place ofresidence.
•American Century Services LLC
•American Fund/Capital Guardian
•Aspire Financial Services
•Equitable (formerly AXA)
•Fidelity Security Life Ins. Co.
•Franklin Templeton Funds
•General American
•GWN/Employee Deposit Acct
•Industrial Alliance - (Sec.Ben.)
•Invesco OppenheimerFunds
•Lincoln National
•National Life Group (LSW)
•PlanMember Services Corp.
•ROTH - Horace Mann Life Ins. Co.
•Thrivent Financial for Lutherans
•Vanguard Fiduciary Trust Co.
•Victory Capital (USAA Mutual Funds)