MEDICALEXAMINER
I REMEMBER
Memories of a Little Boy with Polio
by Warren B. Karp, Ph.D., D.M.D.
I was born in 1944, about 11 years before the first polio vaccine was available. It was the Salk vaccine, administered by the injection of an inactivated polio virus. That was 1955. Unfortunately, I was diagnosed with polio about 2 or 3 years prior to the vaccine. So, I remember feeling the panic and anxiety that surrounded each summer when polio cases skyrocketed. Parents were afraid to let their children play with other children, especially afraid of visiting pools and parks in the summer. In 1952, there were approximately 60,000 cases of polio in the United States and approximately 3000 deaths, many children. The Salk vaccine was made widely available in 1955, and I remember the very long lines of people clamoring to get the vaccine. By 1957, polio cases dropped to about 6000/yr and, by 1979, thanks to the polio vaccine, polio was all but eliminated in the United States.
Today, most parents have grown up with no memory of the devastation, anxiety and fear that parents faced each summer, prior to the vaccine. Today’s parents do not know the heartbreak of having a child diagnosed with polio and, even worse, losing the child. However, grandparents, like me, remember it well, especially grandparents, like me, who had polio and survived. I was extremely fortunate to have very minor effects of the disease. No, my breathing was never paralyzed. No, I never had to be in an iron lung. No, I never had to use crutches or a wheelchair. In fact, today, if you cast a cursory glance my way, you’d never even know I even had polio as a child. I was one of the lucky ones. Yes, one muscle group on my left side was permanently damaged by the disease. Years of over-compensation for this have made that particular marker of polio in my body almost undetectable. I never told any classmates or teammates what I had experienced. I was just content and thankful that those were the only minor inconveniences that polio had on my body.
For me, polio is a distant memory. I have forgotten many of the hard facts behind my bout with polio. The year I was diagnosed or the hospital I was in, how long was I sick with the acute phase of the disease? All distant, forgotten memories. In those days, people did not dwell on the unpleasantries of life. Once polio was “cured,” people rushed to forget the horror of the disease. My polio was never discussed again in my family.
Even so, I am left with strong emotional memories of having the disease, triggered now and then by environmental clues.
• Personal, local answers and assistance
• Review your current plan for optimum benefits
• Call to see if there is an enrollment for you
• All services provided at no cost to you



WHAT’S IN A

Some people think the most difficult words in the entire lexicon of the English language — which includes as many as a million words — must be the chemical names of drugs. Most of them are virtually unpronounceable. How do you pronounce empagliflozin, adalimumab, ubrogepant, or risankizumab-rzaa?
You know these drugs! For the record, those are the chemical names for the brand names Jardiance, Humira, Ubrelvy, and Skyrizi, in that order. Our reader contest in every issue shouldn’t be finding the Mystery Word. It should be How Do You Correctly Pronounce the Name of This Drug? It would be quite the challenge.
Even television commercials for semaglutide, one of the hottest drugs around, can’t seem to get it right. Some pronounce the drug seh-MAG-luh-tide, and others say semaGLOO-tide — keep in mind, these are originating from the pharmaceutical companies themselves. (For the record, the National Library of Medicine says sema-GLOO-tide is the correct option.)
To make things even more complicated, most drugs have three names, used for three different purposes. There are the chemical names, like the unpronounceable examples






PARENTHOOD
by Dr. Warren Umansky, PhD
You wander into your 10-year-old daughter’s room. She is staring at her phone with a big smile on her face. “What going on?” you ask. “I have a boyfriend!” she responds. You inquire further and find out that she met this boy on line and has never met him in person. She doesn’t have very much information about him either: where he lives, where he goes to school, how old he is. What do you do?
A. She’s just a kid and all the kids are doing that. It’s puppy love. No problem.
B. You’re taken aback and pretty speechless. “We’ll talk about this later,” you say.
C. “Let me have the phone, please, and let’s talk.”
D. “Get me a phone number for his parents. I need to talk with them to find out more about this boy.”
If you answered:
A. No, all the kids are not doing it. It really is a function of how careful a parent you are. Ten-year-olds should be focused on school and home life and athletics/art/music. Have you missed something along the way that allows her to be sitting in her room with a phone communicating with strangers?
B. Taken aback, indeed, but you don’t have the luxury in this situation of being speechless. Is what she is doing okay in your eyes? It’s dangerous and way beyond what she should be doing at her age. And, it’s proof that she is not mature and responsible enough to have a phone.
C. The phone needs to be in your possession and you need to begin a talk with her about how she is going to be better supervised and scheduled. The fault is yours, so no need to get angry with your daughter. She was given a phone before she was ready. She doesn’t understand the danger of communicating with strangers. She has a need in her life for a “boyfriend” at her very young age. You have to change your priorities so she changes hers.
D. I suspect your daughter does not have that information and won’t be able to get it. That makes the situation even more frightening at this time. This might be a case of two needy young kids seeking companionship on line. It also might be a predator grooming your child for much worse things (i.e., sexting or meeting up somewhere). All of this should be a serious wakeup call for you.
Children should not have phones until they prove that they are responsible. Indicators are good grades, respectfulness, doing assigned chores regularly, caring for their personal hygiene, getting enough sleep so they can wake up easily in the morning, and being kind to siblings. Even when you can check all those boxes, using a phone alone in their room should be reserved for older children only. As the parent who pays the phone bills, you also have a right and duty to monitor your children’s phone activity. It’s the safe thing to do!
Dr. Umansky has a child behavioral health practice in Augusta.
THOUGHTS ABOUT THOUGHTS THOUGHTS
WHEN THE WORLD FEELS UNREAL
Depersonalization/Derealization Disorder
Editor’s note: Written by local mental healthcare professionals, this series shares thoughts on how people may think and act when affected by common and lesser-known mental health conditions.
Maria, a 32-year-old mother of two, describes her experience as if she is “watching life happen from outside her body.” During moments of stress, she suddenly feels detached from herself; her voice sounds distant, or her surroundings appear foggy and dreamlike. These unsettling episodes leave her questioning her sanity and withdrawing from loved ones who don’t understand what she is going through.
Maria has Depersonalization/Derealization Disorder (DDD), a dissociative condition where a person persistently or repeatedly experiences feelings of detachment from themselves (depersonalization) or from their environment (derealization).
What is Depersonalization/ Derealization Disorder?
While many people may experience brief, fleeting episodes of feeling detached— often during stress, trauma, or fatigue—DDD is diagnosed when these symptoms are persistent, distressing, and interfere with daily life.
Signs and Symptoms
Depersonalization symptoms may include:
• Feeling like you are observing yourself from outside your body
• Numbness or lack of control over speech or movement
• Emotional disconnection from memories or identity
Derealization symptoms may include:
• Surroundings appearing unreal, blurry, or distorted
• Distorted sense of time or space
• Feeling like the world is a dream or movie
Individuals may experience one or both sets of symptoms, often alongside anxiety, depression, or trauma-related disorders.
Causes and Risk Factors Research suggests that
24/7, free, confidential mental health hot-line that connects individuals in need of support with counselors across the United States and its territories. People do not have to be suicidal to call. Reasons to call include: substance use disorder, economic worries, relationships, culture and identity, illness, intimate partner violence, depression, mental and physical illness, and loneliness. + 988

DDD is often triggered by severe stress, trauma, or substance use. It is more common in individuals who experienced childhood emotional abuse or neglect. While occasional dissociation is a normal response to stress, DDD develops when the brain’s coping mechanisms become stuck in this mode.
Treatments
Treatment for DDD often involves psychotherapy, with Cognitive Behavioral Therapy (CBT) and grounding techniques shown to help patients reconnect with their bodies and environments. Other effective approaches may include trauma-focused therapy, mindfulness practices, and in some cases, medication to address co-occurring anxiety or depression. Lifestyle supports, such as stress management, good sleep, and reducing stimulants, can also reduce episodes.
Prognosis
The outlook for DDD is generally positive with early recognition and treatment. While some people may experience recurring symptoms, many learn to manage and significantly reduce the impact on their daily life. Education and reducing stigma are crucial— DDD is not a sign of “going crazy,” but a treatable mental health condition.
Debunking Misconceptions
A common misconception is that people with DDD are “psychotic” or detached from reality. In truth, individuals with DDD remain aware that their experiences are unusual—this insight actually distinguishes the condition from psychotic disorders.
Need Support?
IPS provides comprehensive behavioral health services including assessment, therapy, and treatment planning for individuals and families navigating both common and lesser-known mental health conditions. To schedule an appointment, call 706-204-1366 or visit integratedpsych.care.
above. These are useful because they describe a drug’s chemical or molecular makeup, and help to identify its broader family. More about that in a minute.
Next up is the generic name, usually a simple, non-promotional name often reflecting the drug’s active ingredient.
Finally comes the proprietary brand name used to market the drug.
One review found that generic names average 14.4 letters and 5 syllables, while name brands average 10.4 letters and 3.5 syllables.
Here’s an example of the three names: Tylenol is the brand name for the generic drug acetaminophen, whose chemical name is N-acetyl-para-aminophenol.
Coming up with drug names, even generic ones, is a long, complicated, and expensive process. Oversight of the process is the job of the United States Adopted Names (USAN) Council. USAN choices also have to be approved by a naming committee of the World Health Organization. The pharmaceutical industry is international, so the naming process includes as many as 130 countries to make sure a name isn’t already in use elsewhere, or doesn’t mean something inappropriate in another language.
Interestingly, generic drugs cannot begin with the letters H, J, K, or W because those letters either do not exist in some languages or have different sounds in various languages, and there is a moratorium on using X and Z as the first letter in generic names; since those letters can have the same pronunciation, confusion could be the result. Drug names beginning with A have been popular so doctors scanning drug lists will see those products first. About a third of all the names drug companies propose for new products are rejected by USAN and the FDA. Another factor in name selection: a few years ago the number of brand name drugs in the US stood above 33,000, with 9,000 generic names registered. That number has undoubtedly grown. Further highlighting the importance of the naming process one study which found that between 1995 and 2000, 15% of all reported drug errors resulted from name confusion of some sort.
Judging by the opening examples, one might think drugs names are just a random string of letters. Actually, it is a meticulous process that starts with a “stem.”

Like a last name that brands you and all your relatives together, stems describe specific drug classes and functions. For instance, cholesterol-lowering drugs all end in -statin. ACE inhibitors, like lisinopril, end in -pril. The stem for many migraine medicines is -triptan.
Stems sometimes have a linguistic source: -statin comes from the Latin root “stat,” meaning to stop or inhibit; -caine, as in lidocaine, novocaine, and other local anesthetics, originated from cocaine. Other stems are devised from scratch to create distinctive labels that help doctors, patients, and pharmacists to instantly recognize various drug classes and their use.
If you wondered about the weird name of one of the drugs mentioned at the start of this article — risankizumab-rzaa — the FDA requires biosimilar drugs to have a 4-letter lowercase suffix — like rzaa — that is “devoid of meaning” added on to help identify such pharmaceutical cousins.
Would you like to see examples of how crazy drug names really aren’t so crazy after all? Of course you would.
Monoclonal antibodies are a good class to illustrate the point. “But I don’t know any!” you say. Actually, you do.
A good abbreviation for monoclonal antibodies would be -mab, so let’s use that as the stem in drugs like risankizu mab-rzaa. Look familiar? What about adalimu mab? Better known as Humira, that was one of the drugs we began with in the intro. What is the source of the antibodies in the particular drug being examined? One of the syllables identifies that. In the case of both drugs in the previous paragraph, the source is human, signified by u, as in risankiz umab-rzaa and adalim umab. Other single or double letters are used to denote other sources.
A third syllable identifies the target disease or condition for the particular MAB. The tu in rastuzumab and ri tuxumab stands for tumor; other MABs will include vir for virus, cir for cardiovascular, les for infectious lesions, or in the case of ada limumab we’ve been seeing in this article, lim denotes that this MAB is an immunomodulator.
So yes, drug names are quite a mouthful. But there is a careful system involved in the naming process, even when the result is practically unpronounceable.


I WAS THINKING
by Pat Tante
WOMEN’S LIB AND CHICKEN NECKS
Women’s Lib. Feminism. Equal Rights. We read these terms less often these days and there is just a bit of hohum in us whenever we do run across them. Can we even remember that momentous passage of ERA in 1982? Do we take it for granted that we are liberated and can achieve anything that we desire with nothing to hold us back?
Damn right we do!
But…could you kill a chicken, clean it, and cook it for Sunday dinner? I say Sunday dinner because back in the day it would take a long time to get your hands on a chicken in the yard or pen. This certainly added to the preparation time. Chickens are notorious for being able to make the quick right turn, the flying leap and the stinging peck.
I personally do not think that chickens are all that smart, but they are wary beasts when threatened with being dredged in flour and dipped into hot fat. Let’s get back to the prep time. Have you noticed that recipes today include the preparation time? How many recipes are you going to cut out of Southern Living magazine with a prep time that includes a chase and dismemberment?
“Why bring something like that up?” you say. “These days, you don’t even have to cook it yourself, much less kill it.” That’s my whole point. I want you to appreciate being able to go to the grocery and in about five minutes select a pile of fried chicken without any recognizable parts.
As a child, I saw my mother and grandmother kill chickens with my own eyes. Talk about your basic “from scratch” recipe; this was it. Each of them had her own method of dispatch and I would watch from a distance, ready to run at the slightest hint that the chicken might come my way while they were chasing it down.
My mother’s method of execution, while not exactly humane, was less terrorizing than Grandma’s. Once Mama got her hands on that chicken (which was no small feat, as I have already mentioned), she would quickly tie its legs to the clothesline pole, pull its neck taut and saw away with the butcher knife. Actually, I am glad that she used a knife.

www.AugustaRx.com
Direct editorial and advertising inquiries to: Daniel R. Pearson, Publisher & Editor E-mail: Dan@AugustaRx.com AUGUSTA MEDiCAL EXAMINER P.O. Box 397, Augusta, GA 30903-0397 (706) 860-5455 www.AugustaRx.com • E-mail: Dan@AugustaRX.com

Who is this?
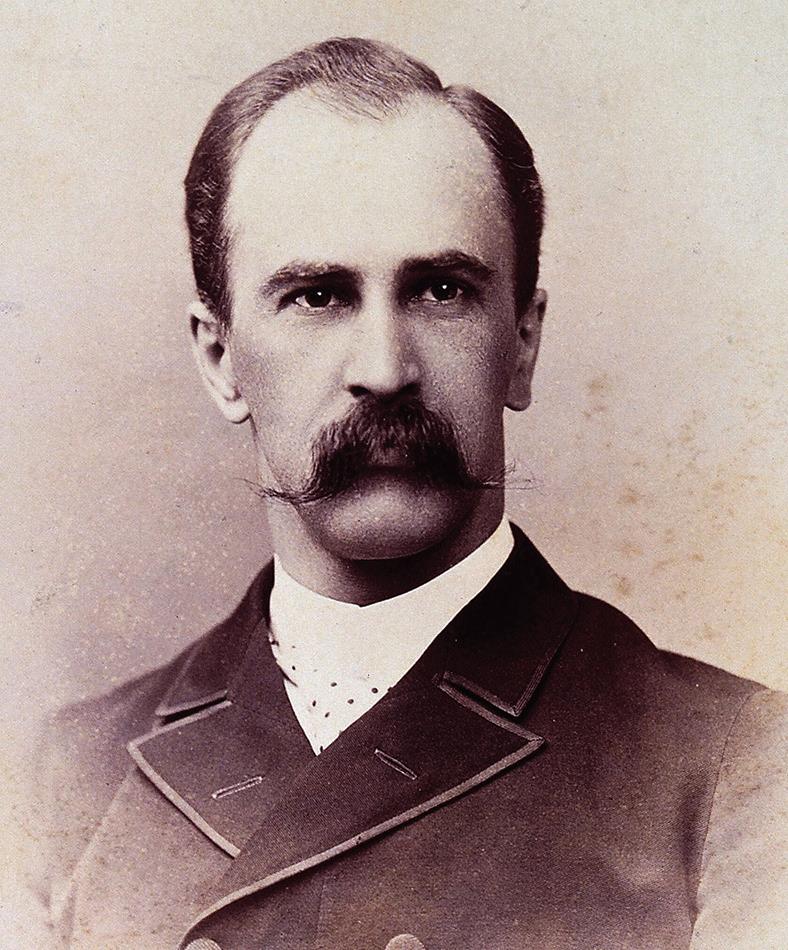
As promised in our previous issue, here is another of the founders of Johns Hopkins School of Medicine, the third of the so-called Big Four: William Halsted, Howard Kelly, and this man, William Osler (we’ll complete the set with a profile of William Henry Welch in our next issue).
William Osler was a brilliant doctor with a fascinating history. His wife’s great-grandfather was Paul Revere. His own great-grandfather, depending on who was telling the story, was either an ordinary sailor or a bona fide pirate. His father, Featherstone Osler (yes, Featherstone) served in the Royal Navy aboard the HMS Victory, a ship commissioned in 1778 and still in service today, 247 years later. Featherstone was invited to be the science officer aboard the HMS Beagle for Darwin’s voyage to the Galapagos Islands, but reluctantly declined because his father was dying.
As for son William, after initially deciding upon a career in the ministry, he switched to medicine within a year and forged a path that changed the course of medical history.
Simply put, Osler was a phenomenal doctor, “one of the greatest diagnosticians ever to wield a stethoscope.” He practiced precepts so elementary that people are sometimes shocked that they hadn’t been in practice for centuries. For example, Osler famously said, “Listen to your patient; he is telling you the diagnosis.” It is a principle nearly always true, but not easy to apply for a number of reasons. Osler underscored the principle when he wrote, “He who studies medicine without books sails an uncharted sea, but he who studies medicine without patients does not go to sea at all.”
Osler put these ideals into practice, pioneering the practice of bedside teaching, making rounds through the wards with a handful of students, performing what one student called “incomparably thorough physical examinations.”
A natural byproduct of this method of teaching was another Osler innovation: medical residency for students in teaching hospitals like Johns Hopkins. The term is no accident. As established by Osler, the system was a fulltime, live-in, sleep-in arrangement. Residents resided at the hospital; it was a 24/7 assignment, and was originally openended: some residencies lasted as long as eight years, during which residents led an almost monastic life. Osler viewed this innovation as so basic and so important that he hoped his tombstone would read, “He brought medical students into the wards for bedside teaching.” He also said, “I desire no other epitaph ... than the statement that I taught medical students in the wards, as I regard this as by far the most useful and important work I have been called upon to do.”
Osler has been called the Father of Modern Medicine, and although he helped found Johns Hopkins, he ended his career at Oxford University in England.
The Oslers had two sons, one who died shortly after birth. The other, Edward Revere Osler, died in World War I combat at age 21. Osler was crushed by the loss, and died at age 70 in 1919 during the global Spanish flu epidemic. +
Middle Age
BY J.B. COLLUM
Are you old? Are you young? If you answered no to both questions, then you are middle-aged. Then again, can I really trust you with the definition of middle-aged? I mean, I know folks in their eighties who say I’m still young and think they are middle-aged. I usually don’t hurt their feelings by telling themthey left middle-age in the rearview mirror quite a fewmiles back, but sometimes I do, depending on whether or not they irritated me. When I hear someone in their late seventies, eighties, or even older, tell me I’m still a young’un, it is a bit irritating because I certainly don’t feel young. At least physically. On the other hand, when a younger person says I’m still young or even seem young, I beam with pride! Why is that? Well, I’ve given this a lot of thought. Yes, it may seem like I have too much time on my hands, or at least that’s what two of my buddies (Chuck & Louie) say to me whenever I start pontificating about some ideas that are deeper than a kiddie pool. But they are wrong. I come up with these ideas right in the middle of when I’m supposed to be doing other stuff. Enough of that. Let me explain.
I think I get irritated when an elderly person says I’m still a young’un because it feels like I spent the first two decades of my adult life trying to get these same older people to take me seriously. Around forty is when it usually happens. I can see it from both sides too. I catch myself still thinking of people I’ve known since they were babies, as kids. Then reality hits and I remember that they are in their late forties or even early fifties! Regrettably, I do recall saying things about them still being young. I’m going to make a concerted effort to not do that and I encourage you all to follow suit. Those “young” folks I’m referring to probably already have the starter kit of middle age in their possession. You know what I’m talking about. They wake



up in the middle of the night and don’t know why. They suddenly have a pain in their back, side, or neck and don’t even remember hurting it. They need more coffee to wake up than an average police precinct needs on the nightshift. They have a subscription for Voltaren deliveries from their pharmacy, and they are already saying “what?” so much to their spouse that they both get mad at each other over things neither said. They also have to watch how much they drink before bed, or what they eat for supper so as to be able to sleep. So, to close this section, let’s respect, not just our elders, but the “freshmen” middle-aged folks too, and not belittle their newfound decrepitness. Speaking of getting up to go to the bathroom multiple times a night, I wanted to share something useful with you, as opposed to the rest of this article. For me, it has gotten to the point where I wake up every 90 minutes or so like clockwork and immediately feel the need to void my bladder. I may lie there for a few minutes trying to will it to stop bugging me, but it never listens. I did some reading and watched some videos from doctor’s who had some good suggestions on how to alleviate this problem and it has been working well for me. Now the caveat: I am not a physician and you should always check on these things yourself and/or talk to your medical practitioner, but here are the five things that have allowed me to sleep for six or more hours without waking to urinate. Remember, this is what is working for me. Your mileage may vary:
1. Don’t drink ANYTHING within three hours of bedtime. You might get away with less time, but this is the consensus safe limit. Don’t get dehydrated though. Front-load your liquid intake earlier in the day to be sure you get enough. How much is that? It depends, which means: I don’t

Special Forces
Parenting
We had another turdnado* strike this week. It feels like it was our fault. We got complacent. Thinking she was perhaps over that stage, we weren’t using the special clothing that she can’t take off, and we took our eye off the ball, or in this case, off Freyja. Come to think of it, calling her a ball is apt since she seems to bounce off the walls randomly and is very hard to catch.
If you, like us, have to cope with issues like this or any other difficult problem with your special needs child, don’t despair or beat yourself up about it when you fail to stop it or to handle it the way you hoped you would. Some challenges aren’t as much about the ones facing it as we’d like to think. The best example I can think of is climbing Mount Everest. Even if you prepare as well as you can and even if you do everything right, you can still fail. Except that, failing to climb Everest has a good chance of killing you.
Too macabre? Since we are back into football season again, maybe this will serve as a more fitting and less morbid example. Even when the coach and players thoroughly prepare for a game and execute their game plan perfectly, an exceptional player can still beat them. Think back to guys like Herschel Walker and Bo Jackson. Nothing

and no one was able to consistently stop them. They were freaks of nature, but in the best way possible.
Similarly, even if you read every book there is to read about how to handle your child and their special needs. Even if you do everything the physicians and therapists tell you to do. Even if you never take a break and constantly work at being the best parent or guardian you can be, you will fail sometimes, maybe even more often than not, but the failure won’t be on you.
Some mountains are just that hard to climb. They are unpredictable and capricious. Some people with special talents are indomitable. You may stymie them once or twice, but not with any consistency.
Similarly, raising a special needs child and coping with their sometimes difficult behavior can feel like you are on a treadmill with someone else controlling the speed, incline, and even the power switch. But unlike a regular treadmill you can get on and off of at will, this is a treadmill you live on 24/7 or nearly so. Can you imagine being asleep on a treadmill and then someone turns it on and sets it to the highest speed with no warning? Sure you can, it has essentially happened to you before in the form of some situation in the middle of the night or some other inopportune time. Things are nice and peaceful one moment, and the next you feel like you are living Mad Max Beyond Thunderdome
Just remember that you are not alone. There are lots of others out there like you. Don’t be afraid to reach out for help from support groups, friends, people in faith, and family. Praying certainly has helped us too.
* Turdnado definition: When our special needs granddaughter decides to use the contents of her diaper to get all artistic on the walls, floor, her toys, and/or herself.
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
Some people who are bullied just shrug it off and keep living their lives. Others turn into bullies themselves. And still others become absolute monsters.
Take the case of this man, Frans Hooijmaijers. That last name is quite a mouthful, so you might prefer to go by his nickname, which was Fat Frans.
(Helpful hint: as near as we can tell, his last name is pronounced HOY-myers.)
Not many details of his childhood are known, but he was an outcast at school thanks to being overweight and having a speech impediment caused by a cleft lip. His father regularly beat him, although when he became seriously ill, Frans was good enough to care for his father until his death.

In 1970 at age 35, Hooijmaijers got a job in a hospital’s so-called “Nightingale Ward,” reserved for elderly patients. He became known as the Good Samaritan for his devotion to his Catholic faith, praying for patients, and placing statues of the Virgin Mary at their bedsides. Ominously, he claimed to have the supernatural ability to accurately predict when patients would die.
That’s never a good sign.
Things went along quietly, at least for Fat Frans, for five years, and then things quickly unraveled in a big way. In 1975, the family of an 89-year-old woman who died at the hospital where Hooijmaijers worked filed a complaint, requesting an investigation. Within days the probe quickly uncovered various irregularities, all pointing to Hooijmaijers. When police went to his home to ask a few questions, they found jewelry and other valuables that had belonged to a number of patients who died under his care. He and his wife were both arrested.
A records review revealed that over the five years of Hooijmaijers’ tenure at the hospital, 78 patients died in other wards, but in what we’ll call the Fat Frans wards, hundreds of patients died. Of the total, 259 of were considered questionable at the very least, and 112 of them highly suspicious.
Under questioning, Hooijmaijers confessed to killing 15 of his patients, but later retracted that confession, admitting only to administering non-fatal doses of valium or insulin without medical authorization. Hooijmaijers blamed the hospital for inadequate staffing, forcing Good Samaritans like him to take action to help patients who were in pain when no doctors could be found to issue proper orders.
The Netherlands jury didn’t buy that defense, convicting Hooijmaijers of five murders and handing down a sentence of two life terms, along with a 23-year ban on practicing as a nurse. Prosecutors had planned to bring more charges later, but his attorneys launched an appeal in 1977 which resulted in a sentence reduction down to 18 years. He was released in 1987 and lived as a free man until his death from natural causes in 2006.
If Hooijmaijers committed all 259 murders for which police suspect that he’s responsible, that would mean he served a little over two weeks in prison for each patient he killed.
+
REMEMBER from page 1
Similar to PTSD, I guess. Did that repetitive sound I just hear really sound like the iron lung sounds that terrified me in the hospital? Was my last headache really like the severe headaches I had that signaled the invasion of the polio virus into my little boy body?
I thought it might be important for us grandparents of today to remind our children who are parents about what it was like prior to vaccines. What it was like for parents back then to fear polio, measles, whooping cough, and mumps. Today’s parents need to understand the devastation that polio had on the life of a little child, on the whole family and on the community. Here are some of my emotional memories of having polio as a child.
My earliest memory of polio was the severe headaches that kept me home from school, in bed, staring at the Hopalong Cassidy curtains that covered the window. I remember Dr. Copulsky, our neighborhood physician, coming to visit me in my bed. Yes, doctors made house calls in those days. I still feel the emotion of him telling my mother that it looked like I had polio. I remember her crying and I remember that I cried, too, not about the polio, but about my mother crying. I remember Dr. Copulsky asking my mother to stop crying because it made me cry.
I remember Dr. Copulsky telling my mother that the only way of reaching a definite conclusion about my polio was for me to have a spinal tap to see if the virus was present in my spinal fluid. How was a spinal tap done in those days? My emotional memory of that is vivid to this day. I remember Dr. Copulsky asking my parents to find four very strong men in the Brooklyn apartment building where we lived. We needed them to volunteer to hold me down on our dining room table, while he was doing the spinal tap. I remember my screams of fear, being held down on my stomach on our dining room table while Dr. Copulsky took spinal fluid from me. I remember being so terrified that I pooped and peed during the procedure, right on the table!
I remember Dr. Copulsky telling my parents that the results were positive for polio and that I had to be rushed to the hospital. I remember the speeding car ride to the hospital in the back seat with my parents. I remember speeding through every red light, the car horn blaring to warn other cars. I remember a motorcycle policeman stopping the car, finding out what was happening and then accompanying the car to the hospital, with sirens blaring through the red lights. I remember
Would I survive? If I did, would I be paralyzed?
feeling the anxiety of my parents in the back seat of that car and I remember that severe headache I had.
I remember having a second spinal tap in the hospital and then being put in a crib, which I hated. I was about 8 years old, and I certainly did not want to be in a crib. I was not allowed out of that crib during my entire hospital stay. I remember how odd it felt when I was finally discharged from the hospital and was allowed to walk again. I remember telling my parents that it felt like I was walking on air, like the feeling you get if you roller skate all day (a common childhood activity in Brooklyn in the early 50’s) and then take the skates off.
I remember that my hospital crib was near a small window that looked into the room next door, a hospital ward filled with children in iron lungs. I remember wondering if I would end up in that room. The sound of those iron lungs expanding and contracting is a vivid emotional memory. I could easily hear those iron lungs through the wall of my hospital room, 24 hours a day, seven days a week. My parents would go next door to speak to parents with children in the iron lungs and come back looking very scared and worried. Chil-
dren died in that room.
There was no treatment for polio in those days. I was isolated in the hospital room. I was observed. The treatment was “wait and see.” Would I die? Would I be paralyzed for life? What was going to happen? Wait and see… wait and see…
I remember that parents in our apartment building would not let their children play with my brother, Allen, fearing that he was a carrier of the polio virus. He never got polio. I remember that nobody was allowed to visit me in the hospital except my parents. I remember waving to my brother, to my grandparents, to my aunts and uncles, through my hospital window about 5 stories up. They looked so small. They sent me lots of little toys and books, which I kept in my crib. How disappointed I was when I was finally discharged but none of the toys and books were allowed to come home with me for fear they were contaminated.
What is the point of all of this? Polio is very real, very dangerous and very contagious. It is totally preventable with the polio vaccine. So are other childhood diseases which were very common when I was growing up. Significantly, they are all exceedingly rare now. With vaccine hesitancy spreading amongst parents today, I implore all grandparents who remember how it was before vaccines to tell their children, the parents of their grandchildren, what it was like. Parents, I urge you to follow the vaccine recommendations of The American Academy of Pediatrics and get your children vaccinated. It is very important. You can find the recommendations here: publications. aap.org/redbook/resources/15585/AAP-Immunization-Schedule
About the author: Dr. Karp is a Professor Emeritus of The Medical College of Georgia at Augusta University. He has had a distinguished career in research, teaching, and public service, especially in the area of preventive health. He is former vice chairman of The Columbia County Board of Health. You can find out more about Dr. Karp at wbkarp.com. +
SINCE YOU LOVE TO READ...
A recent study discussed in our last issue identified a troubling decline in reading for pleasure, not for work or school, but for sheer enjoyment. Our previous issue also listed many of the mental and physical benefits that reading provides. Since we want our readers to enjoy the maximum amount of salubriousness possible, we are giving away free books. Enter today! Time is running out!
WIN FREE BOOKS!

NORTH AUGUSTA 105 E Hugh St., Suite 103 North Augusta, SC 29841 (803) 441-3937 AIKEN 39-A Varden Drive Aiken, SC 29803 (803) 641-6104









FROM VERSUS WITH BASED
As we perhaps should be, we are obsessed with disorders, diseases, conditions, illness, and other things that can lead to our demise. In this era of 24-hour cable TV, we are inundated with information and advertisements. Some of it is true.
Carefully listening and understanding words is required for meaningful education and useful knowledge.
Take the use of “from” verses “with” as related to death. The two cannot be used interchangeably. I am bald. I will die with a bald head, but not from a bald head.
A lady friend has been diagnosed with fibromyalgia. She will die with fibromyalgia. She will not die from fibromyalgia.
Focus on these words when listening to news regarding Covid. Because someone died with Covid does not mean they died from Covid.
ON A TRUE STORY
(most of the time)
A series by Bad Billy Laveau
Should data of these two be co-mingled? Clearly not. It is a misservice to the public. The same is true with AIDS. Or HIV.
If you have atrial fibrillation and suffer an acute cardiac arrest while driving, are you an automotive fatality? True, you might have died in a car wreck, but not from a car wreck. Would banning cars prevent the cardiac arrest secondary to atrial fibrillation? Clearly not.
Someone drank 8 ounces of water yesterday and then died. He died after drinking 8 ounces of water, not from drinking 8 ounce of water. If you use the word from


indiscriminately, you would conclude that drinking 8 ounces of water should be banned for health reasons. That would be a stupid and invalid conclusion.
Cause and effect are not equivalent to coincidental occurrence. A rock in the hand of Cain killed Abel. A bad thing. A rock in the hand of David killed Goliath. A good thing. Should we ban rocks? Clearly not.
Another misleading term in advertising is that the product “supports heart health.”
If you have a heart problem, will taking a TV-advertised product improve your heart? Probably not. Not even the advertiser tells you it “will make your heart healthier.” They only say it “supports heart health.” Water supports heart health. So does breathing air. So does sunlight.
When you see or hear the phrase “supports thus-andso,” beware. That is a phrase


that misleads you to view a given product favorably. It has virtually no beneficial claim.
Has TV advertising become the modern-day traveling medicine snake oil show? It is not quite that bad, but they giving you 3 sentences that have been lawyer-approved that are frequently unrelated to the conclusion the advertiser wishes you to reach.
Many ads follow this fictionalized script. “Goats are pretty. Goats are vegetarian. Goats are environmentally friendly. I take Jeremiah Peabody’s Green and Purple Goat Pills, and I’m doing just great. Get Jeremiah Peabody’s Green and Purple Goat Pills online. Not sold in stores.”
Everything in the ad is true and accurate, if he has taken at least one goat pill. But there is no useful logic therein. No proof of anything. Of course, the speaker is doing




BAD BILLY from page 8
just great. He got paid a lot of money and has the prettiest girl friend his money can buy. But his proclamations have nothing to do with benefiting your health.
Put your brain in its skeptical gear before accepting what you are served to you as meaningful facts. Celebrity endorsements mean nothing more than that a famous face got paid a lot of money for one day of reading a script.
Be careful what you read or hear. Carefully analyze what a word actually means. The English language is complex. Many terms are similar, but necessarily the same.
Because something is “plant based” does not mean it is good for you. Alcohol is plant based. Cocaine is plant based. Marijuana is plant based. Tobacco is plant based. Hemlock is plant based. Sugar is plant based. Mushrooms are plant based. A quick Google search listed 25 plants that are poisonous or dangerous to human. Clearly, the list is much longer.
Pay attention to what you read and hear. Your health and your bank account depend upon your understanding of the English language. Always think: I hear him or her. It sounds good. But did it actually mean anything?
Am I going to die with a brain full of unrelated facts? Or die from a brain full of unrelated facts?
Clearly the former.





CRASH COURSE

More Americans have died on US roads since 2009 than in World Wars I & II combined
sAwe mentioned in our last issue to introduce these very instructive pointers, our intention is not to offend anyone. As we pointed out, so many people are already doing a fantastic job of bad driving without our help. We’re just hoping to offer a tiny bit of performance-boosting information — for other people, not even those reading this article. Why do we say that? Statistically, the vast majority of all motorists believe they are excellent drivers. To put that in math terms, nearly all drivers think they are above average.
Ponder that statement for a moment before reading on.
Now for more handy pointers.
they’re being polite! That is so cute! Readers of this column know the real purpose of blinkers, of course. And if you don’t, well, that’s why you’re reading.
It’s kind of a semi-carefully guarded secret and not something we want everyone to know, but one of the often overlooked purposes of blinkers is to give you the opportunity to block the driver using them. They are about to merge into your lane — and they tell you in advance? It doesn’t take a brain surgeon to realize that’s when you speed up to block them.
{ { How to be a bad driver, Part 2
Have you noticed how many people are looking at their phones while barreling down the highway or navigating our crowded city streets?
Of course, it is illegal in both Georgia and South Carolina to so much as touch a phone while driving unless it’s for navigation or emergency purposes. Still, if you’re observant enough it isn’t difficult to even see people texting behind the wheel.
Let’s just state the obvious right here: that is kindergarten-level bad driving. To graduate to the big leagues of bad driving you have to transition from texting while driving (where driving seems to be the main focus) to driving while texting That may seem like a subtle change, but it shows which activity is the main focus — the texting, obviously — and which is the extracurricular addition — driving.
We briefly touched upon the subject of turn signals last time. We have barely scratched the surface of that topic.
Over the years we have heard many people lament, “If only there was some way to indicate that I am about to turn or change lanes.”
What an adorable, innocent sentiment! They think the purpose of blinkers is to notify other motorists that they’re going to do some kind of turn maneuver. Like
Intersections provide a golden opportunity to tell the world that you aren’t an everyday garden variety bad driver. You aspire to greatness.
How can you step up to the next level? It isn’t difficult with the following two excellent pointers. Keep in mind, all this advice is provided free of charge. Is this a great country or what?
Step one is to stop for a red light in the left turn lane at an intersection, preferably one with a flashing yellow left turn arrow. As soon as you get the flashing yellow left turn arrow, here’s what you do: nothing. Why?
One of two reasons. The first might be that you’re posting something on Facebook, TikTok, or Instagram. Perhaps you’re watching a video on YouTube. In short, you’re busy at the moment. You don’t need to apologize to anyone for that. Another reason might simply be that you’re cautious. Every time you’re about to pull forward into the intersection, there’s another car visible a few hundred yards down the road. Better to stay put and wait until the light goes red and then you can try again. Sometimes it can take two, three, or more lights to find a safe opportunity to ease forward a few feet and possibly make a turn. No wonder so many people are texting and posting on IG in their cars!
from page 4
know. I don’t know if anybody knows.
2. Don’t eat ANYTHING within three hours of bedtime. This one may not be so obvious, but if you eat close to bedtime, your body works to digest the food and this can interrupt your sleep. Plus, if you eat something with a lot of sugar or starches, it will kick your kidneys into overdrive which results in more bathroom trips.
3. This is my favorite one as evidenced by my wife calling me a polar bear quite often. I love going into convenience store beer caves and the cooler rooms at Costco, Sam’s, and Chef’s Store. There are at least a half dozen store cooler sections I have been banned from for spending too much time in there. It was either that or maybe they didn’t like it when I brought a cot in, put on my pajamas and slept in there. Back to the subject. Keep your bedroom between 65 and 68 degrees. If it is much cooler than this you may cause blood to draw up and away from your extremities to warm your core. When this happens, your blood pressure rises and that is a trigger for your kidneys to… you guessed it, start making more urine. If your bedroom is warmer than 68, your body reacts in ways that stimulate your kidneys to… I think you get it.
4. Really empty your bladder. Whether you are male or female, sit on the toilet right before you go to bed. Don’t bring a phone or reading material. Just take deep breaths and relax. After you have gone once, just sit there and lower your upper body down over your knees by resting your forearms on your thighs. Hold that pose and relax. Give yourself some time. You might be surprised how much more urine was waiting to be sent downstream. I sure was. Sometimes, there is more the second time than the first.
5.Sleep on your side with your upper body elevated and put a pillow between your legs to help reduce pressure on your bladder.
Well, that wraps up this edition. There are several akeaways here so I will list them for your convenience:
A. Welcome our “freshmen” middle-agers and don’t belittle them.
B. Don’t eat anywhere near bedtime.
C. Don’t drink anything anywhere near bedtime.
D. Sleep in a room with the temperature between 65 and 68 degrees.
E. Completely empty your bladder right before bed.
F. Sleep on your side with a pillow between your legs.
G. Don’t bring a cot into a beer cave or cooler section at a store and try to sleep on it. If you do, just leave when they ask. And don’t chain yourself in there either. Not a good idea. Don’t ask me how I know that.

J.B. Collum, author of this column and Special Forces Parenting, is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com


TRYTHISDISH
by Kim Beavers, MS, RDN, CDCES
Registered Dietitian Nutritionist, Chef Coach, Author Follow Kim on Facebook: facebook.com/eatingwellwithkimb
CHICKEN VEGGIE RISOTTO
This is a flavorful and quick one-pot meal! Enjoy anytime you need dinner on the fly.
Ingredients
• 1 tablespoon extra-virgin olive oil
• 1 pound boneless, skinless chicken breast, cut into small pieces
• 1 teaspoon garlic-herb seasoning (salt-free)
• ¼ teaspoon salt
• ½ teaspoon black pepper
• ¼ teaspoon red pepper flakes
• 1 small onion, thinly sliced
• 1 can (10.5 ounces) reduced sodium chicken broth
• ¼ cup water
• 1½ cup instant brown rice, uncooked
• 1½ cup grape tomatoes, halved
• 4 cups baby spinach leaves, washed and patted dry
Directions
Heat oil in a large skillet over medium heat. Add the chicken pieces and season-

ings; cover and cook for about 10 minutes, stirring frequently until chicken is done.
Add onion and stir--fry for about 1 minute. Stir in broth, water, rice, tomatoes, and spinach. Bring to a boil. Reduce heat to low and cover. Simmer about 10 minutes. Turn burner off and let stand for 5 more minutes or until rice absorbs most of the liquid.





Yield: 4 Servings (Serving size: 1½ cup)
Nutrition Breakdown: Calories 280, Fat 8g (1g saturated fat), Cholesterol 70mg, Carbohydrate 25g, Fiber 4g fiber, Sodium 450mg, Protein 25g.
Diabetes Exchanges: 1 Vegetable, 2 Starches, 3 Lean Meats
Recipe modified from Produce for Better Health Foundation at: www.morematters.com
DOWNTOWN 990 Telfair St 706-724-0900
AUGUSTA W. AUGUSTA 3954 Wrightsboro Rd 706-863-9318
MARTINEZ 4014 Washington Rd 762-685-5555



1213
706-986-5427

How did your kids do the first week back at school?
Not all that great. My second-grader’s teacher called and said he had been disrupting the class all day.
What happened?


by Dan Pearson
Uh oh. So then what?

THE MYSTERY WORD
The Mystery Word for this issue: MIYALF
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
1. Type of apple? 6. Quintet number 10. Mountain range 14. Prince of India
Unlock 16. Hawaiian goose
17. Large wading bird
18. Breathe hard
19. Pre-Masters Week org.
20. Messenger
22. Large black beetle
23. Slippery fish
24. A small amount of somthing
26. Bird symbol in heraldry
28. Seasickness (French)
33. _____ scan
34. Willow genus 35. Artists’ ______
37. Lowest pulse location
41. Tinged with a slight trace (abbrev.) 42. Might 43. Wear away 44. Tidal bore
45. Where the Wild Things ___ 46. Indian tent
47. A canon has two
Grating, harsh
Lyric poems
SEC rival
DOWN
1. Rivalry lead-in
2. Challenge
3. Partly open 4. ________ from heaven (var. spelling)
5. Portable canvas refuge
6. Dandy 7. Apple product
8. Snake poison 9. Catch
10. Poorly or self-educated
11. Drive back
12. One could be acute or right
38. Very good (in slang)
39. Capital of Yemen 40. Historical English court 48. Rescue partner 50. Mr. Rogers
Harbor towns
52. Northwest state
53. Russian revolutionary leader 54. One can be tipped 58. Pal 60. Scottish Gaelic
Type of dancing
Feat
Kill
Natal beginning ACROSS
Produces (in farming)
Wife of a 14-A
One-time MCG head Dan
Bay window
Lean
Hint 70. Pale green mossy lichen
Tune
Blood prefix
Sordid and disreputable
13. Smallest
21. Block up 25. Skin root
27. Monotonous; unvarying 28. Small particle
Huge continent 30. This is Life host Lisa
Growing less 32. Lion sounds 36. Artist Andrew
A M I N E R S U D O K U
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
QUOTATIONPUZZLE
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
the puzzle above. All the listed letters following #1 are the first letters of the various words; the letters following #2 are the second letters of each word, and so on. Try solving words with letter clues or numbers with minimal choices listed. A sample is shown. Solution on page 14.

THEBESTMEDICINE

ha... ha...

Aproud mother was in the stands at Sanford Stadium, loudly and frequently cheering on the Dawgs during a big game.
At one point she gestured toward the field and said to the woman sitting next to her, “I guess it’s pretty obvious, but that’s my son down there.”
“I can tell you’re very proud,” the woman said. “What number is he?”
“He’s our third,” she said proudly.
Moe: Guess what? I can turn anything into a boomerang.
Joe: No way. How?
Moe: Throw it straight up.
Moe: I am dying to buy a motorcycle!
Joe: What’s stopping you?
Moe: Money! I’m only going to buy the best — Harley-Davidson — so I can’t afford a bike until I save up more cash.
Joe: Why don’t you buy one of those look-alike bikes? They’re half the price.
Moe: Look-alike bike? What look-alike?
Joe: Hardly-Davidson.
Moe: My teenage daughter thinks the school year is like being pregnant.
Joe: How so?
Moe: Because it lasts nine months, but you start to feel sick after just a few weeks.
Moe: Hey, wanna hear a bad joke?
Joe: Not particularly.
Moe: Here goes: what do extremely skeptical people use to blow their nose?
Joe: I give. What?
Moe: Truss Tissues.
Moe: Are you going to sign up for that 401k they’re offering at work?
Joe: There’s no way I can run that far.
Moe: They say you shouldn’t brush your teeth with your left hand.
Joe: That is correct. It’s better to use a toothbrush.
Moe: Do you have a favorite little-known fact?
Joe: Let’s see...it’s probably about that Cat in the Hat author. He was Hispanic.
Moe: His real name was Theodore Geisel. I’m pretty sure he was of German descent.
Joe: I saw him in a bar one time and somebody called to him. They said “Hey Seuss!”
Moe: What’s worse than finding a worm in your apple?
Joe: Getting hit by a bus.
Staring at my phone all day has certainly had no Effect on ME!
By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME
ADDRESS
CITY STATE ZIP
Choose six months for $26 or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397

Dear Advice Doctor,

Dear Too,
You are certainly not the only person who grapples with this issue. We live in a fast-paced world, and many people eat on the run, in a rush, while driving, at their desk, etc. Anyone trying to eat in a hurry is at risk of biting off more than they can chew in the interests of speed. Another related problem in rush-rush eating is not chewing food adequately. Why are these matters of concern?
The process of digestion is how our bodies access the nutrients in the food we eat. Shortchanging that process is like stealing from our own body and shortchanging our own health.
It’s easy to forget that digestion is not something that starts after we swallow. There are chemicals and enzymes in our saliva that start the process of digesting food as we’re chewing it. What you describe is one of two ways people interrupt this important step in digestion. First, what you do: take bites that are too big. It’s almost impossible to properly chew a huge bite of food, which leads to the second issue: chewing too fast and too briefly. For many people, this is how they eat all the time, big bites or small.
There are all kinds of ridiculous strategies offered as solutions, like counting how many times you chew each bite of food. Can you imagine? You can’t even have a conversation with friends or family because you’re counting your chews!
A better answer is to focus on the enjoyment of eating. Slow down. Savor the flavor. Set your fork or your sandwich down after every bite. Take your time. Don’t talk on the phone or do work while eating that divides your attention. Your job for those few minutes is eating, and doing so mindfully (not mindlessly). Bon appetit!
I’ve always had a hard time saying no. It’s a skill I need to learn, but so far, it’s still mission impossible. Take a neighbor to a doctor appointment and wait with them for two hours when I’m already slammed? Sure. Provide snacks for the kids’ entire class? No problem. Do a co-worker’s job for them and then watch them take credit for it? Just ask. I know what I need to do. But I knew that five years ago and here I am still biting off more than I can chew almost every day. What’s the secret to making this change? — Too Agreeable +
I hope this answers your question.
Do you have a question for The Advice Doctor about life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.

THE MYSTERY SOLVED
The Celebrated MYSTERY WORD CONTEST
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.



PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC
Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC

DERMATOLOGY
Dermatology



Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com

Evans Chiropractic Health Center Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net

Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901 706-396-0600 www.augustadevelopmentalspecialists.com



Nursing|Companion 706-426-5967 www.zenahomecare.com

Bashir Chaudhary,
Jason H. Lee, DMD 116 Davis Road Augusta 30907 706-860-4048 Floss ‘em or lose ‘em!












from page 3
If she had used a hatchet, I may have been called on to assist in the operation. Help me, Jesus!
I watched and tried to keep my skin from crawling completely off my body as she severed its head. I shudder today just to think of it. After a few jerky, splashy moments, the carcass was ready to clean. I’ll let you think about the next steps in the cleaning process.
Grandma, on the other hand, had a more grisly approach. It would make a spectacular scene for inclusion in any of today’s horror movies. She would walk up behind some unsuspecting hen on the pretense of scattering some corn, snatch her up by the neck, give her several twirls in the air and wring that chicken’s neck. I would stare in amazement as my sweet ol’ Grandma turned into Mr. Hyde of the chicken yard.
She turned the doomed creature loose to flop about the yard in its death throes. Even at death’s door, that yardbird could see and would chase me through the garden, determined to splash me with some foul fluid. “Help, Grandma! The chicken is trying to get me!”
I could never understand why the chickens never chased her. Although, as I recall, she was a very imposing figure who always wore a corset with metal stays. No soft, squishy Grandma, she – but that’s another story. I had every reason to believe that the chicken could live long enough to get revenge. You do know, don’t you, that a cockroach can live for days without its head? Couldn’t a chicken?
I would never stay around for the cleaning and plucking festivities because I had watched once before and it ruined Sunday dinners for a whole month.
Dinner came around and I would be parked at the table as usual, waiting on that golden fried chicken. Here came the platter! Papa got dibs and helped himself to his favorite piece. Grandma
did not believe in wasting any part and we always joked about who would get “the parson’s nose” or the “last part over the fence.” They certainly did not have to fight me for it. I probably should include the gizzard here too. I do not remember anyone at the table being particularly interested in it, but my friend, Sue, told me that her parents would say that eating the gizzard would make her hair
curly. It never helped as far as I could see.
The platter continued its way around the table and it finally got to me – the neck, back, gizzard and parson’s nose stared up at me. “Grandma, could I have a baloney sandwich?”
Well, we all know about baloney ingredients – baloney ranks right up there with potted meat. That’s another story. Don’t get me started.