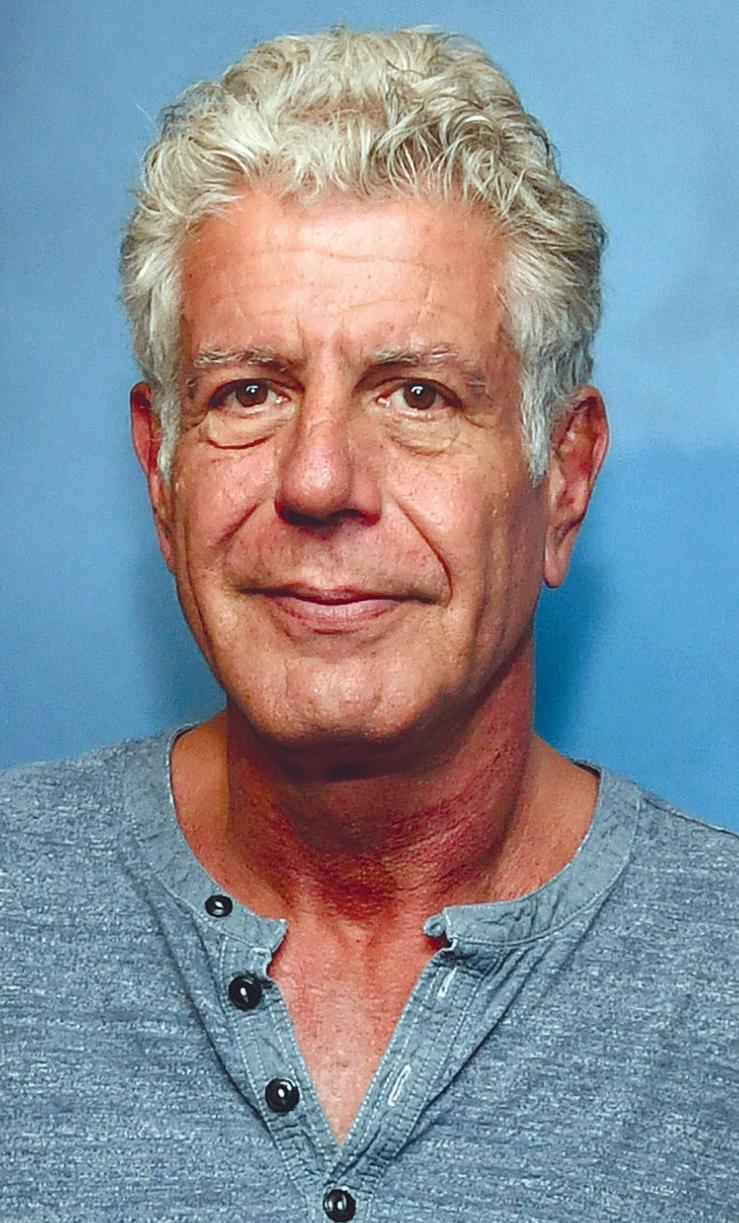
The late great chef and journalist Anthony Bourdain once hosted a culinary and cultural show on the Travel Channel called No Reservations. Although he went on to bigger and better things before his untimely death in 2018, there is perhaps no better term to describe Bourdain’s ability to cut through to the heart of the matter and say what needed to be said, at least in his opinion, without reservation.
Would you like an example? Of course you would. The remainder of this article is going to contain dozens of them, and is offered in lieu of the “Food is Medicine” column that would normally appear in this issue.
Wherever Bourdain went in his extensive travels for No Reservations and later for Parts Unknown, he ate what locals ate: sheep testicles in Morocco, a raw seal eyeball after an Inuit seal hunt, the still-beating heart of a cobra in Vietnam. And yet he famously said the most disgusting thing he had ever eaten was a Chicken McNugget. See why No Reservations was so appropriate? Here are more direct-quote examples of the culinary wit and wisdom of Anthony Bourdain:
An ounce of sauce covers a multitude of sins.
Pp
Margarine? That’s not food.
I Can’t Believe It’s Not Butter? I can. If you’re planning on using margarine in anything, you can stop reading now, because I won’t be able to help you.
Pp
Your body is not a temple, it’s an amusement park. Enjoy the ride.
Pp
PAGE 3
America’s most dangerous export was, is, and always will be, our fast-food.
I won’t eat in a restaurant with filthy bathrooms. This isn’t a hard call. They let you see the bathrooms. If they can’t be bothered to replace the puck in the urinal or keep the toilets and floors clean, then just imagine what their refrigeration and work spaces look like.
Pp
Barbecue may not be the road to world peace, but it’s a start. Pp
I’ve seen zero evidence of any nation on Earth other than Mexico even remotely having the slightest clue what Mexican food is about or even come close to reproducing it. It is perhaps the most misunderstood country and cuisine on Earth. Pp
A proper saute pan should cause serious head injury if brought down hard against someone else’s skull. If you have any doubts about which will dent, the victim’s head or your pan, then throw that pan right in the trash.
Pp
Never try to get your kid to eat anything she doesn’t already want to eat. Just eat interesting stuff in front of her while completely ignor-
PARENTHOOD
by Dr. Warren Umansky, PhD
Someone told you recently about a show she had heard on the radio that talked about RLEs – real life experiences – that should be the focus of a child’s life. The program proposed a ratio of 3 to 1 of real life experiences versus screen time. That is, for every hour of screen time during a day, multiply that time by three to determine how long your child engages in RLEs. To put it a more manageable way, your child gets to be on screens one-third the amount of time that he or she spends in RLEs. This does not include the amount of time in school. It does, however, include homework and studying, sports practice, playing outdoors, doing chores, working on a hobby, and running errands with or for you.
What do you think?
A. This sounds like punishing my child. She would never go for this.
B. It might be okay for young children, but it’s not fair for my teenager.
C. We already limit screen time to three hours a day and everything has to shut down by 11PM.
D. It’s a great idea. What a good way to teach the proper balance in life.
If you answered:
A. Your response indicates that your child is in charge. That is great if she is a responsible teenager who does well in school, is respectful, is mentally healthy, and has a good vision of her future. If none of these is true, you have to be the responsible parent who provides a structure at home for your child’s success. That’s your job and it brings great rewards!
B. It certainly is okay for younger children and is even more critical for teenagers, especially those who isolate themselves in their room with electronics. It is hard to say what your definition of “fair” is. Shouldn’t everything that makes your child more productive, more successful, and more mentally healthy be considered “fair”?
C. Ouch! With so much out there these days about the importance of children getting enough sleep, an 11:00 bedtime almost guarantees that your child is not doing well in school, is not very helpful at home, and/or has behavior that frustrates you. And how does one squeeze in three hours of screen time on school days without ignoring chores, homework and studying, outdoor play and exercise, and electronics-free meal time? Time to take better charge, parents! As an important aside, a recent review of research studies on parental technology use in a child’s presence shows a negative association with cognitive and psychosocial performance.
D. Children do best when involved in productive activities. As many children talk about becoming influencers and YouTube celebrities today as being NFL or NBA stars in the future. These visions usually come from sitting and playing video games and live streaming. A vision becomes a reality by doing and creating. It’s the time away from screens that is more likely to lead to a promising future. Invested parents realize that. For them, the 3:1 RLE:screentime is a good way to exercise their responsible role as parents.
Dr. Umansky has a child behavioral health practice in Augusta.
Treatment and Management
Many people with kleptomania do not seek help until they face legal or personal consequences. However, with the right treatment, it is possible to manage the condition and reduce impulsive urges. Common treatment approaches include:
THOUGHTS ABOUT THOUGHTS THOUGHTS
KLEPTOMANIA
Editor’s note: Written by local mental healthcare professionals, this series shares thoughts on how people think and act when affected by common and not-so-common mental health conditions.
Jenna is a 29-year-old accountant with no history of legal trouble—until now.
She was recently stopped by store security for attempting to take a bottle of lotion without paying. The incident left her confused and ashamed. She had no financial need to steal and wasn’t sure why she had done it.
This wasn’t the first time. Over the past year, Jenna had taken various small items from stores—things she didn’t particularly need or even use. Each time, she felt a brief sense of relief, quickly followed by guilt. Despite her best efforts to resist the urge, she found herself repeating the behavior.
Jenna has kleptomania, a mental health disorder that causes an overwhelming, compulsive urge to steal. Unlike theft driven by necessity or personal gain, kleptomania is rooted in impulse control issues.
What Is Kleptomania?
Kleptomania is classified as an impulse control disorder, similar to compulsive gambling or pyromania. It is characterized by the repeated inability to resist the urge to steal, even when the stolen items have little or no value to the individual.
People with kleptomania often experience:
• A mounting sense of tension before stealing
• A temporary feeling of relief or gratification immediately after
• Guilt, shame, or remorse once the act is complete
• Repeated episodes of stealing, despite efforts to stop
Unlike planned shoplifting, kleptomania-driven theft is typically unplanned and impulsive. Those affected do not steal out of financial need, revenge, or thrill-seeking but rather to relieve internal distress.
Who’s at Risk?
Kleptomania is a relatively rare condition, but can affect people from all walks of life. Research suggests that it is more common in women and often first appears in late adolescence or early adulthood.
While the exact cause is unknown, several factors may increase the likelihood of developing kleptomania:
• Family history of mental health disorders, particularly mood disorders and substance use disorders
• Underlying psychiatric conditions, such as anxiety, depression, or obsessive-compulsive disorder (OCD).
• Imbalances in brain chemistry, particularly involving dopamine, a neurotransmitter linked to pleasure and impulse control Kleptomania is often misunderstood. People may assume that those with the disorder are simply dishonest or lack self-control. In reality, it is a recognized psychiatric condition that requires treatment.
• Cognitive Behavioral Therapy (CBT): CBT helps individuals recognize the thought patterns that drive their compulsive stealing and develop healthier coping strategies. For instance, therapists may guide patients through exercises to help them pause and reassess their impulses before acting on them.
• Medication: Selective serotonin reuptake inhibitors (SSRIs) and other medications may help regulate impulse control and reduce the urge to steal. In some cases, mood stabilizers or opioid antagonists (which block the brain’s reward response) are also prescribed.
• Support Groups: Programs such as Kleptomaniacs and Shoplifters Anonymous (KASA) provide a structured support system for individuals seeking recovery.
• Behavioral Strategies: Avoiding high-risk situations, identifying triggers, and using distraction techniques can help prevent impulsive behavior.
Can Kleptomania Be Treated Successfully?
Kleptomania is a chronic condition, but long-term management is possible. Many individuals see significant improvement with therapy, medication, and behavioral strategies. However, relapses can occur, making ongoing support and treatment an important part of recovery.
For those struggling with kleptomania, seeking professional help is a crucial first step. The condition is not about lack of willpower. It’s about addressing an underlying mental health issue to regain control.
Integrated Psych Solutions provides inpatient and outpatient mental health services, with or without a referral, to help patients and their families progress through the care journey. To make an appointment, call 706-204-1366 or visit integratedpsych.care.
POURDECISION-MAKING
The most-abused drug on the planet also happens to be legal. There might be a correlation between those two facts.
People do enjoy drinking, there is no doubt. The National Center for Drug Abuse Statistics (NCDAS) reports that just over half of all Americans report having a drink within the past month. The statistic for within the past year is 67%, while 84% say they have consumed alcohol at some point n their lifetime.
As ubiquitous as alcohol may be, it is far from innocuous. Public health officials are concerned about a number of factors related to alcohol use.
Booze clues
As a broad-brush overview, NCDAS cites research that finds nearly 178,000 Americans are killed every year in ways that are in one way or another alcohol-related. The breakdown is approximately 117,000 deaths from chronic causes related to long-term drinking (liver disease, certain cancers, etc.) and another 61,000 or so who die from acute incidents like drunk driving crashes, violence, suicide, and alcohol poisoning. Because many of these deaths strike people at relatively young ages, the Centers for Disease Control says that alcohol-related deaths shorten lives by an average of 24 years.
Per person! Times 178,000! That translates to millions of years of potential life lost annually.
Millen, MD
Backing up the lost years of life numbers, doctors are seeing an alarming surge in alcohol-induced liver disease (AILD) among people in their 20s and 30s.
Between 2005 and 2021, hospitalizations for AILD among younger men rose by 169%, while liver transplants increased some 684%. As startling as those numbers are, they are even more dramatic for younger women: AILD hospitalizations soared by 283% from 2005 to 2021, and liver transplants jumped by 2,284%.
It is sobering — no pun intended — to contemplate massive numbers of people being hospitalized for essentially selfinduced organ transplants at any age, let alone in their 20s and 30s.
Last call
How can this growing problem be addressed? Given that “unhealthy alcohol use is a major cause of death and serious illness,” earlier this month the U.S. Preventive Services Task Force (USPSTF) urged doctors to take action when they see evidence of alcohol abuse, even if it’s only a simple, brief comment. It might make a difference to that patient. There is no potential for harm from a simple moment of counseling, but there is the potential for helpful assistance and a reduced risk of prolonged disease and premature death. That’s a good return on investment any day.
They are, indeed, although that doesn’t mean they’re a good idea for everyone. They are safe for most people to wear, but they are especially helpful for certain groups, including those with circulatory problems like deep vein thrombosis (DVT), varicose veins or lymphedema (fluid buildup in lower extremities), people who sit or stand all day at work, those who are diabetic, pregnant, or recovering from surgery. But they aren’t only for people with medical issues. Athletes of all kinds, from pros to weekend warriors, can also benefit from compression socks
Compression socks are built in various levels of tightness, but all types are the most snug around ankles, and the pressure lessens as the socks go up toward the knees. The design helps support better blood flow and prevent so-called pooling of blood and fluid buildup or edema. Better circulation also helps reduce the risk of blood clots. Also, some athletes say they recover faster after workouts when they wear compression socks. The benefit seems to come from reducing the buildup of lactic acid generated by strenuous exercise. And at the other end of the activity spectrum, people who are inactive for long hours or are generally immobile also benefit from the circulatory assist provided by compression stockings.
That’s not to say they are without drawbacks or side effects. People normally find them to be uncomfortable, especially at first. However, if you’re wearing them at your doctor’s direction, he or she will no doubt tell you the discomfort will go away soon enough, and the benefits outweigh the disadvantages. Speaking of doctors, they will specify the strength or tightness of the socks. They are also available in over the counter strengths, but anyone with circulatory disorders should check with their doctor about which socks to wear (if any).
Incidentally, copper-infused socks are touted as the premium option, especially for pain relief. Those claims have little to no scientific support, and one brand (Tommie Copper) was fined millions by the FTC for false and misleading pain relief claims. +
AIKEN-AUGUSTA’S MOST SALUBRIOUS NEWSPAPER
www.AugustaRx.com
The Medical Examiner’s mission: to provide information on topics of health and wellness of interest to general readers, to offer information to assist readers in wisely choosing their healthcare providers, and to serve as a central source of salubrious news within every part of the Augusta medical community.
Direct editorial and advertising inquiries to: Daniel R. Pearson, Publisher & Editor E-mail: Dan@AugustaRx.com
AUGUSTA MEDiCAL EXAMINER P.O. Box 397, Augusta, GA 30903-0397 (706) 860-5455
www.AugustaRx.com • E-mail: Dan@AugustaRX.com
www.Facebook.com/AugustaRX
Who is this?
The smiling face above belonged to a giant in medicine. How great were his achievements? Well, you just might be alive to read this very article because of him.
Born on April 1, 1919, in Milford, Massachusetts, Joseph E, Murray was a star athlete at Milford High. He entered college with the goal of a career in major league baseball, but class schedules conflicted with baseball practice, so he put sports on hold and put his energies into academics. With the encouragement of a family doctor, Murray decided to pursue a career in surgery. After college he attended Harvard Medical School, graduating with a medical degree in 1943.
A plane crash in India the following year marked an unexpected turning point in Dr. Murray’s career. His internship was interrupted when he was inducted into the U.S. Army Medical Corps, assigned to Valley Forge General Hospital in Pennsylvania under an accomplished plastic surgeon. His unit treated thousands of soldiers wounded during World War II, but one stood out: Charles Woods, a 22-year-old pilot burned over 70% of his body when his plane and its 12 tons of aviation fuel crashed upon takeoff in India. Six weeks and 10,000 miles later, Woods was at Valley Forge under the care of Dr. Murray, poised to undergo the first of some two dozen operations.
Woods’ situation was dire. He needed massive skin grafts, and with the permission of the family of a soldier who had just died, Woods was liberally draped with cadaver skin. It was a desperate act since foreign skin was normally rejected by the host within as little as 10 days, not enough time for Woods to grow new skin. Surprisingly, however, the new skin survived for more than a month, buying Woods enough time for his own skin to grow, saving his life. He went on to become a successful businessman and prominent political activist in Alabama.
That’s all well and good, you may be thinking, but how does that rather obscure case translate to the possibility that people could be reading this article whose lives were saved by Murray’s work?
As it turns out, plastic surgery was just a stepping stone in Murrays final career destination. As Murray later said, “the lessons learned in trying to help Charles [Woods] would determine the course of the rest of my professional life.” In short, the cadaver tissue that was not immediately rejected suggested a possible pathway to eliminate that same obstacle in transplant surgery.
Dr. Murray and colleagues went on to develop immunosuppressive drugs, and with their help in 1959 he performed the world’s first successful organ transplant, a kidney transplant. Within six years, the survival rate for kidney transplant recipients stood at 65%, a number that is closer to 95% today.
As far back as 2013, it was estimated that more than a million patients had already benefitted from organ transplant operations worldwide. For his pioneering efforts, Murray was awarded the Nobel Prize in Physiology or Medicine in 1990.
Dr. Murray was married to his college sweetheart for 67 years, and died in 2012 at age 93. +
Middle Age
BY J.B. COLLUM
What a few weeks we’ve had; peppered with loss, sorrow, unexpected joy, and discovery. These are things that we become more familiar with as we age. It’s a package deal.
If you read the previous column, you know that I was on the cusp of losing my cousin. He had already been in the hospital for over a week, and we were told not to expect his recovery. The past couple of weeks have been a roller-coaster ride of high hopes and deep despair as he cycled from good to bad and back again. He is still around though and I have been visiting him as often as possible ever since I found out. I am happy to say that, despite him still being in the hospital, he is on the road to recovery now. This is one of the joys I spoke of at the beginning. He and I grew up together and were nearly inseparable up until our late teens when he got married and had better things to do, which I understood. We had drifted apart for a while, but this sudden intense companionship brought on by the anticipation of losing him is bringing me great happiness. We have promised each other that we will spend much more time together for whatever years we have left. Our rekindled friendship is a wonderful and wholly unexpected outcome that came from this near tragedy.
ing a wife and child behind. His mother and I have known each other all our lives and she and her husband are pillars of the community. When older folks die after full, rich lives, we aren’t taken by surprise, but when younger ones make an early and sudden exit, it is a reminder of how fragile life is and how we aren’t guaranteed more than right now.
Life is fragile. Who knew?
On the dark side of things though, we lost two dear friends in the past month. One in his seventies, seemingly healthy and going in for a fairly routine catheterization before he took an international trip with his extended family. Tragically, he died during that procedure and left a large community of friends and family mourning his loss on the cusp of what was to be a once-in-a-lifetime trip. I am happy to say that, as we are all sure he would have wanted, his family did go ahead with their trip, but I am sure it will not be what it could have been. I hope they are able to lose themselves in this time and not spend every waking moment thinking of the loss.
We also lost a relatively young friend, someone at 40 close to the age of our own children. He died in a car accident, leav-
All of this really has me thinking, and some of the side-effects are that I have been up later and eating later suppers since I have spent a lot of time at the hospital. I’ve ended up eating less once I got home because it was late and I know what late eating can cause for me. Namely, acid reflux. Due to this, I ate my chicken wings without blue cheese dressing for the first time ever… and I liked it. I’ve decided that’s a good way to avoid stomach issues and calories moving forward. I did similarly with baked potatoes over this past week or so and ate them without sour cream. I ended up liking them just as much. I’ve even eaten salad without blue cheese! I’ve always said that lettuce was created only to add crunch to a burger or as a medium to eat blue cheese off of, yet here I am eating a salad with Italian dressing instead and I love it. I didn’t even order sour cream on the side for my last two visits to Mexican restaurants! My wife is looking for the pod under our bed and asking where her real husband is.
Yes, I am letting a concern for my health and desire for uninterrupted sleep overpower my long-standing eating choices and I’m happy about it. I won’t bore you with all of the diet choices I have changed recently, but I really feel like this time, the changes will stick. Only time will tell for sure, but I feel like they won’t just be something I try and quickly give up on.
+
J.B. Collum, author of this column and Special Forces Parenting, is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com
Special Forces Parenting
I thought I’d cover a couple of different aspects of raising special needs kids this time. I’ll start with the perils in regard to your expensive electronics along with how to mitigate them, and end on some rather promising advancements in Freyja’s ability to communicate.
I’ve always thought of insurance on phones as a bit of an extravagance, but with phone prices getting as high as $2,000 and the fact that most of them are encased front and back with glass, perhaps it is time to rethink that. Add the fact that we have a certified phone destroyer living in our home, and the rationale for having phone insurance suddenly becomes crystal clear. It is a no-brainer.
We have experienced that acutely this past week. Freyja has decided that she likes picking up phones near the pool and throwing them in the pool. It’s like she thinks they wanted to get into the pool, but their mean owners left them poolside as they taunted them from the cool water, just inches away. Of course, she has never bothered to ask them if they can swim before she unceremoniously tosses them head over heels into the water. No, she gives you that look while her hand is on your phone, and before you can take one slow slogging step towards her, the phone has done a triple flip followed by a belly flop right into the pool as you scream no! so loud that neighbor kids two blocks away stop whatever they were doing. But it is too late. She did that twice in the last week or so. Fortunately it was Kate’s phone both times. Well, fortunate for Lorie and me anyway, not so great for Kate.
Many phones these days claim to be water-proof or water resistant, but it seems that
they are only slightly more water resistant than a diaper in a pool. I even had a friend that had a phone fail because of steam from his shower.
With all of that out of the way, let’s just say that we have decided to keep insurance for our phones and to use dry bags for them when around the pool from now on. If you can’t change your child’s behavior, or can’t change it yet, change what you do or how you do it to find a way around the problem.
Now, it is time to talk about how Freyja is improving in her communication skills, and how we too are too, because it is a two-way street. We have to carefully observe her to perceive what she is trying to tell us when she can’t actually just say it. She has been doing some things for quite a while, like opening the refrigerator and taking out the milk or the tea pitcher to show us that she is thirsty, or throwing her sippy cups across the room when they are empty or she is just done with them. For quite a while now she has also pushed her plate away when she is not hungry or is full. This is a practice I should probably learn too, but that is another story for another day and page in this publication.
Lately, she has been able to communicate what she wants to watch on her TV. She really only has six or seven movies she likes, so as we cycle through the title screens, she puts her hands on her ears, which means “no,” and she sits down and smiles or starts playing with her toys when it is the one she wants. This is a big improvement from when she would let the wrong one start without a clue, and then start throwing things and generally pitching a fit a minute or so in.
We also recently received a new communication device through her school. It is an iPad with a clear thick plastic cover over the screen with small finger-sized holes to limit her touches to individual choices. Each choice has some image that is a clue to what it means. This is a wonderful device and it has already revealed some insights into her personality. We already knew she often liked going somewhere in the car, but now that she has this device, she says, “I go” over and over and over again. She really does love getting out of the house both for just
Please see SPECIAL FORCES page 6
GREG
LEOPARD PC ATTORNEY AT LAW
“Leopard Law is spot on.”
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
Depending on your source of information, this woman, Lucy Letby, is either the most prolific baby killer in British history, or is the victim of one of the worst miscarriages of justice on record.
A registered nurse, Letby began working in a neonatal unit in January 2012 when she was 22 years old. Over the next four and a half years, there were no significant red flags, although there were a few errors and lapses in care. Finally, one “minor” error too many resulted in her transfer from patient care to a desk job.
After her transfer, there was a thorough review of patient records from the neonatal unit which revealed some troubling facts. For example, in one month (June 2015) three infants died in the unit, which normally saw only two or three deaths in an entire year. Over the coming year, through June 2016, a high number of unexpected deaths occurred in the unit. The investigations found that Letby was on shift for virtually every one of the serious incidents identified, whether or not the death of an infant resulted.
Initially, that was not considered significant: Letby often worked extra shifts due to staffing shortages, and there was only one other nurse on the unit more senior than her.
The investigation involved many separate phases and employed a number of expert medical consultants. Its findings were far from unanimous, but when prosecutors reviewed the information, they arrested Letby in July 2018 on suspicion of eight counts of murder and six counts of attempted murder. By the time her trial convened in October 2022, the charges had been amended to seven counts of murder and 15 counts of attempted murder. She pleaded not guilty to all charges.
Prosecutors alleged that she injected babies with insulin, air embolisms, and in some cases by force feeding them or causing injury through physical violence. The victims ranged in age from a mere 24 hours to a few days old.
The trial held some elements destined to fuel post-verdict speculation, and there has been plenty of that. For instance, other than Letby herself, there was only one witness for the defense, a plumber; and the prosecution never presented any evidence about a possible motive for the crimes.
Even so, in August of 2023, Letby was convicted on most of the charges and sentenced to life without the possibility of parole. It is the most severe sentence possible under British law, and Letby is only the fourth woman in British history to be so sentenced.
While several attempted appeals have so far been rejected, a member of Parliament and a number of medical experts (including a neonatologist who is the former president of the Royal College of Paediatrics, and a doctor who said his research about infant deaths was used at Letby’s trial without his permission, and misinterpreted to boot) have joined her defense team in calling for her immediate release pending a new trial.
+
This case continues to unfold. It may not be over.
spending time outdoors or going for a car ride. I think she really likes Publix because she gets a free cookie every time and gets to ride in the cart and soak up a different environment. She even likes going to school as long as she wakes up early enough to get past her usual morning mood.
One thing we haven’t figured out yet is that she also taps the icon for “conditioner” almost as much as “I go.” We haven’t figured that one out yet, except maybe she wants to do something regarding her hair. Hopefully, this little mystery will get cleared up over time.
The main takeaway is that we are all making progress in communicating with one another, and this is bringing greater peace and harmony to the family. It gives us hope for ever-improving communication down the road.
TRYTHISDISH
by Kim Beavers, MS, RDN, CDCES
Registered Dietitian Nutritionist, Chef Coach, Author Follow Kim
on Facebook: facebook.com/eatingwellwithkimb
STEAK & POTATO SALAD
This recipe is great for dinner and then great again for lunch the next day! It is a perfect balance of steak, potatoes, and veggies!
Steak:
• 1 pound flatiron steak
• 1 tablespoon Worcestershire sauce
• 1 teaspoon cider vinegar
• 2 cloves minced garlic
• ½ teaspoon coarse salt (kosher salt)
• ½ teaspoon coarsely ground black pepper
Directions:
Trim any extra fat from the flat iron steak and place it in a shallow baking dish. Combine the remaining ingredients in a small bowl and then rub over both sides of the steak.
Allow to marinate for at least 15 minutes. Meanwhile prepare salad and potatoes. To cook the steak, spray a grill pan with vegetable oil cooking spray or lightly oil grill grates of an outdoor grill. Grill steak over medium high heat for 6-8 minutes on each side until the desired degree of doneness has been achieved. Cover loosely with foil and allow meat to rest for 10 minutes. Slice steak across the grain into thin strips and serve on top of salad.
Potatoes:
• 1 pound Yukon gold potatoes (about 4 medium)
• 1 large onion
• 1 tablespoon olive oil
• 1/8 teaspoon coarse black pepper
• 1/8 teaspoon salt
• Vegetable oil cooking spray
Directions
Preheat the oven to 400 degrees. Cut the potatoes into bite size pieces (about 1/2 –inch cubes). Cut the onion into slightly larger pieces (onions will cook faster than the potatoes so they need to be cut larger).
Toss vegetables with oil, salt and pepper and place on an aluminum foil lined baking sheet that has been coated with cooking spray. Spread vegetables out single layer and spray the tops with vegetable oil cooking spray. Roast for 15 minutes, turn the vegetables and roast an additional 10 to 15 minutes until the potatoes are tender.
Salad base:
• 8 cups Romaine lettuce
• 2 cups quartered cherry tomatoes
• ¼ cup light Caesar dressing.
Toss salad ingredients together in a bowl. Divide evenly among 4 plates.
Top each salad evenly with potatoes and steak (about 1 cup of potatoes and 3 ounces sliced steak). Enjoy!
The “Just a Few Dollars More” scam is more common than you might think. It comes in various forms, but here are common variations.
A presentable man is targeted by a younger presentable woman who is struggling. Her manners are good. She is not overly sexy. Her clothes are clean, but not high end. Hair neat and self-styled. No extensions. No store-bought nails. No high heels. Car is not new, but functional. They meet accidentally, purely at random. Conversations is pleasant. She smiles a lot, but with a slight edge. A few extra wrinkles in her brow. Kind of a worried daughter-ish presentation. They communicate on several levels. She is nice. He is nice. A connection slowly
BASED ON A TRUE STORY
(most of the time) A series by Bad Billy Laveau
forms. They exchange mi
ey. She doesn’t. Life is not always fair.
How can a caring Knight in Shining Armor not help a maiden in distress who has already scraped together 90% of the money? She has done most of it herself. Clearly a self-providing lady who just needs a little help
essary. She is grateful. He feels a fullness of accomplishment in his heart. It is the Christian thing to do. Money is gone. She most likely is gone. Unless she feels she can squeeze out another “few dollars more” deal next month. Don’t rush it. Don’t push. Don’t ask for it. Float a little chum on the water. fAnd read the tides. Is the tide coming in? Or going out? She is an expert. She will know.
yer will call you in a few minutes. Help me, Grandpa.”
He doesn’t even know he has been had.
Another Saturday morning form is, “Hello, Grandpa. This is your granddaughter. I hit another car and broke my nose so I don’t sound right. I’m in jail and need $1200 to get me out. I have $900 and need $300 more. (Just a few dollars more). I’m scared. My appointed law-
The lawyer calls and needs money on a gift card to get granddaughter out quickly. It is dangerous in the county jail. Grandpa’s eyes are still trying focus on the world. Thoughts are not clear. $300 is a small price to pay to get granddaughter out of that horrible jail. See the pattern? It is hard to resist if you are a reputable person and love your grandkids. If you even hear the word “gift card,” run away like a scalded house cat.
Whenever you hear the phrase “a few dollars more” and it is not referring to the Clint Eastwood movie, trouble lurks about, targeting your bank account. Hang up the phone and run faster than a speeding bullet.
CRASH COURSE
More Americans have died on US roads since 2009 than in World Wars I & II combined
You might be surprised to learn that “road rage” is not just a fairly new term; it’s a relatively new phenomenon altogether.
The term dates back only as far as the late 1980s, and was coined to describe a specific outbreak of California freeway shootings.
The broader application of the term to describe roadway temper tantrums on Main Street USA didn’t evolve for another decade.
It got serious in a hurry. These days, there are an aveage of 373 driver deaths and 662 passenger deaths per year (2019 numbers) according to the National Highway Trafic Safety Administration’s Fatality Analysis Reporting System (FARS).
That’s quite a jump from a trend so uncommon that it didn’t even have a name, to hundreds of deaths from that cause just a couple decades later.
Yes, boys and girls, it didn’t used to be like this.
Road rage incidents would be bad enough if all they amounted to was grownups (allegedly, that is) screaming obscenities at each other, laying on their horns, deliberately rear-ending other cars, brake-checking to try to deliberately cause accidents, ramming other vehicles, following people all the way home to exact some kind of revenge later, and tailgating, among other actions.
But no, those reactions are inadequate responses to someone not using their blinker or pulling out in front of you or failing to move over so you can pass them.
More is apparently required to respond sufficiently, and as the Gun Violence Archive reports, road rage shootings have surged from 83 incidents nationwide in 2014 to 456 in 2023. That is a 450% jump in ten years, and represents one person shot
approximately every 18 hours.
Keep in mind a couple of factors that should concern everyone who drives or is a passenger.
One is that there is no single uniform definition of road rage. Reporting varies widely from state to state and city to city based on local statutues, so there is no way to accurately tally the numbers involved. Some places legally separate road rage and aggressive driving. It usually takes a crash or an assault or an attempted murder to get an incident officially counted in one category or the other. Secondly, the vast majority of road rage incidents almost by definition go unreported. Those two factors combined mean that whatever the numbers are, they represent only the tip of the iceberg.
Solutions
The #1 way to prevent road rage is sex. It’s true. Or perhaps we should say gender: a number of studies have found that road ragers are predominantly male (96.6% to be exact) and young (average age: 33).
Another solution, also probably quite a challenge to bring about, is for road ragers to see a psychiatrist. The official term often invoked is “intermittent explosive disorder.” It’s not insignificant that this mental illness shares its acronym with actual bombs.
Misplaced anger and frustration play a part, as some drivers display their emotional immaturity by taking out frustrations over their job, family, finances, etc., on random strangers.
They personalize other drivers’ actions as a direct personal affront to them, a challenge that must be answered.
The more a rational person thinks about road rage, the more irrational it seems.
The blog spot
— posted by Grant Wallenfelsz on June 20, 2019 (edited for space)
A MED STUDENT’S COLLECTION OF FIRSTS
First day of third year — the year most medical students take a sigh of relief as they put their Step 1 book on the shelf and prepare to face the wards.
AT FIRST
I FELT GUILTY
I happened to draw the short straw by having my surgical rotation first, one that often brings an extra level of anxiety due to the unfamiliarity of the field. Before I knew it, I was fully scrubbed in side by side with my preceptor. All of a sudden, the textbooks turned into reality. Somewhere around the middle of the third day in the OR, we received a call over the intercom for an ER consult about a 52-year-old woman with abdominal pain. My preceptor, clearly busy, told me to un-scrub and get a jump start on seeing the patient
First ER consult — Pacing down the hallway, I rattled through differentials in my head, trying to prepare for what I was to encounter. As I approached the room, I saw through the door a thin woman lying in the fetal position barely visible under the blankets. As I timidly came to the bedside, I met Ms. D for the first time. In a soft voice, she began to explain an odd history of abdominal pain with months of agony upon eating, reaching an unbearable limit. Before I could finish, my preceptor arrived and stated that the CT revealed some sort of mesenteric mass leading to a bowel obstruction, a presentation that left both the surgeon and ER physician somewhat puzzled. Regardless, her name was added to the OR schedule for that afternoon.
First open case — an exploratory laparotomy at that. Excited at the opportunity, I assisted my preceptor in removing a golf-ball sized mass from her small bowel mesentery, which had subsequently led to a severe stricture, hence the bowel obstruction and pain. The procedure ran smoothly, and we shipped her off to post-op recovery, satisfied that we had likely removed the source of her suffering.
First day of pre-rounding — The following morning I wandered the halls and eventually found my way into Ms. D’s room. I couldn’t believe my eyes when I opened the door to a huge grin and a “Good morning!” The woman whose abdomen I was practically inside of no less than 24 hours prior was beaming with gratitude. We had eliminated her pain. I’m not sure that anything made her more excited than when she was finally eating solid food — pain-free — for the first time in months. Each morning, as I crept into the room no later than 6 a.m., I was greeted with a smile, another thanks and warm conversation. She progressed exceptionally well, and we were hopeful that she would be discharged within the next two or three days.
First day of call — I sat in the surgeon’s lounge the next morning eating egg soup and questionable coffee as my preceptor ran through the patient list. We had our hands full for the day. As we were wrapping up breakfast, over the intercom, we heard: “Code blue, rapid response room 637. Code blue, rapid response, room 637.” Room 637? I knew that room. Before I could say anything, my preceptor had arrived to the same realization. We had to go.
First code — As we walk up to Ms. D’s room, I saw a flurry of scrubs with orders being shouted left and right and a crash cart open with a nurse performing CPR. As my preceptor rapidly discussed the events leading up to her cardiopulmonary arrest with the hospitalist and nurse, I poked my head in to witness the poetic chaos of running a code. I look over to see Ms. D’s body stripped of clothing, pale and limp as chest compressions bounced her off the bed. As I stood in disbelief, I hear my name called. “Take off your coat and help with compressions.”
First time doing CPR — I stare down at the woman who I had come to know as I stepped to the edge of the bed to
begin compressions. Two minutes felt like a mere moment, and before I knew it, the nurse tapped me on the shoulder to trade out. Thirty-two total minutes of CPR. After all the medications, pulse checks and orders shouted, we finally stopped
First time of death — The hospitalist called the time, and the room fell eerily silent. I, with a couple of nurses, stood panting heavily, sweating, after countless rounds of compressions each. Our efforts were futile; it was her time. As everyone began to clean up, I followed my preceptor in silence back to the nurse’s station. We scoured through her chart, discussing and searching for clues as to what could have happened, deep down hoping we didn’t miss something. There were no answers to be found. Likely a postoperative MI my preceptor mumbled. Once done, we logged off the computer, pulled out our rounding sheet, and off to the next room we went. And that was it.
After all of these firsts and new experiences, I felt guilty because I did not feel the remorse that I thought would accompany the first loss of a patient. Aside from the obvious sorrow felt from the unexpected death of a woman who I had come to know, I was perplexed by how little I was I phased, especially since my emotions mirrored that of
my preceptor. Classmates asked if I was OK after telling them of my week, which further increased my guilt. Should I have been more upset by this?
I ultimately came to a realization that put my worry at ease. We had done all that we could for Ms. D. I know this for I took part in her care from the moment she came through the door to the moment her heart stopped beating. As physicians we have poured our entire lives into medical training to do just that; all that we can do. Training that gives our patients the best fighting chance at overcoming whatever disease process that they may face. Since it is nearly guaranteed that these firsts will not be my last, it is imperative that I remind myself and my colleagues that we are merely human. That sometimes our efforts might not be enough. As long as the efforts for continuous improvement never cease, both in medical knowledge and patient care, medical professionals can take solace in their chosen career. It is honorable to fight a battle in the face of an inevitable ending, meanwhile not knowing when that end may come. With that knowledge, we strive to buy patients time, by doing just that — all that we can do.
Grant Wallenfelsz is a medical student.
IS THERE A MYSTERY WORD IN THIS ISSUE?
OF COURSE!
WE’RE BEGGING YOU
We’re never too proud to beg. What we’re begging for is “Everybody Has a Story” articles. With your help, this could be (should be) in every issue of the Medical Examiner. After all, everybody has a story of something health- or medicine-related, and lots of people have many stories. See the No Rules Rules below, then send your interesting (or even semi-interesting) stories to the Medical Examiner, PO Box 397, Augusta, GA 30903 or e-mail to Dan@AugustaRx.com Thanks!
“And that’s when I fell.”
“He doesn’t remember a thing.”
“It was a terrible tragedy.”
“I retired from medicine seven years ago.”
“She saved my life.”
“I thought, ‘Well, this is it’.”
“They took me to the hospital by helicopter.”
“Now THAT hurt!”
“OUCH!” NOTHING SEEMED TO HELP, UNTIL...
“The cause was a mystery for a long time.”
“The nearest hospital was 30 miles away.”
“I was a battlefield medic.” “We had triplets.”
“He was just two when he died.”
“I sure learned my lesson.”
“It seemed like a miracle.”
“It was my first year of medical school.”
“It took 48 stitches.”
“The ambulance crashed.”
“I’m not supposed to be alive.”
“This was on my third day in Afghanistan.”
“I lost 23 pounds.”
“At first I thought it was something I ate.”
“My leg was broken in three places.”
“Turned out it was just indigestion.”
“The smoke detector woke me up.”
Everybody has a story. Tell us yours.
I think it happens to every couple from time to time.
ACROSS
1. Pleat
5. Tear down
9. Old anesthetic
14. Woodwind
15. Anti (Dialect)
16. Rasp; shred
17. Ceremony
18. Tie up
19. Haggard
20. Unexplored or undiscovered land
23. Brain wave activity (abbrev)
24. Flash start
25. People who are experts
29. Boast
31. ____play
34. Cloth woven from flax
35. Voice of Princess Fiona
36. Quantity of medicine
37. Like sports in high school
40. Mondrian’s first name
41. Network of nerves
42. Fragrance
43. 2013 sci-fi film
44. Big party
45. Title of reverence for God
46. Clumsy person
47. Type of boat
48. Sharp spending cuts
56. Trunk of the human body
57. Meter prefix
58. Western state
59. Extraterrestrial
60. Partner of zeroes in code
61. Chip additives
62. 7 numbers above 12
63. Regard or consider
64. Jacob’s twin
DOWN
1. Kid’s cardboard structure
2. Off-Broadway theater award
3. Tolkien ltrs.
4. Animal on road signs
5. Viral disease afflicting dogs
6. We’re always doing it
7. Element in some skin ointments
8. Prefix meaning internal
9. Holiday drink
10. Distinguishing quality
11. High-class; elegant
12. Volcano in Sicily
13. Veteran’s abbrev.
21. Healthcare insurer
22. Muslim fighter (and “Ben” follower)
25. “A” of the Hebrew alphabet
26. Augusta is in it
27. Word on many doors
28. Green bottle shampoo
29. Word before control or weight
by Dan Pearson
THE MYSTERY WORD
The Mystery Word for this issue: PSBCEI
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
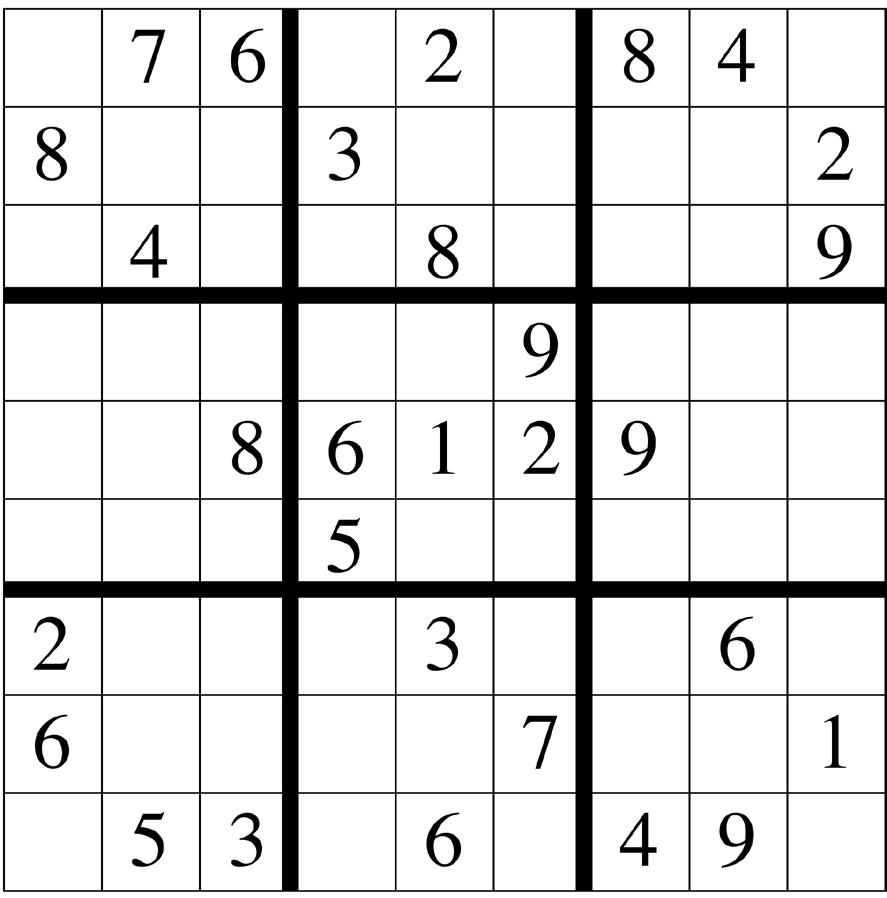
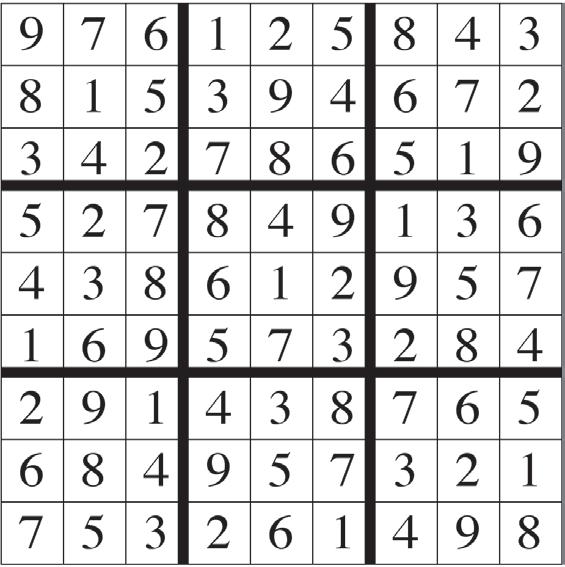
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
30. Infrequent
31. Part of the large intestine
32. Man killed on May 2, 2011
33. Inn for caravans
35. Membership fees
36. Former 5 peseta coin of Spain
38. _______ beer
39. Get something by begging
44. They’re used by conductors
45. Condition characterized by difficulty using language
46. Coworker of Kent and Lane
47. Number of rings in a circus?
48. Trunk of a tree
49. Great Lake
50. Apple music player
51. Mr. Sarazen
52. Au naturel
53. Inflammatory suffix
54. California valley
55. Old AU acronym
56. Make lace
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
— Fran Lebowitz
THEBESTMEDICINE
ha... ha...
Learning English can be difficult. But it can be taught through tough, thorough thought, though.
Moe: I got carded at the liquor store the other night.
Joe: At your age?
Moe: For real. So when I pulled out my ID, my Blockbuster card fell out. The cashier saw that and said never mind, we’re good.
Moe: Yeah, the years do fly by. Do you know my grandmother is 93, and to this day she doesn’t need glasses.
Joe: That is amazing. What’s her secret?
Moe: She just drinks straight from the bottle.
Moe: Do you ever wonder what happens after we die?
Joe: All the time.
Moe: I guess there’s really no way to know for sure.
Joe: Actually, I asked a nurse at a hospice
facility about it just the other day.
Moe: That’s a brilliant idea. They deal with death all the time. What did she say happens?
Joe: She said they clean the bed and get ready for a new patient.
Moe: What did 50 Cent do when he got hungry?
Joe: 58.
Moe: I’ve been getting into poetry lately, even writing some poems.
Joe: Oh yeah? Let’s hear one.
Moe: Ok, here goes: I dig. He digs. She digs. We dig. They dig. Everyone digs.
Moe: That is not a very good poem.
Joe: I’m still learning. But you have to admit, it’s deep.
Moe: Why do surgeons make patients count down as soon as they administer anesthesia?
Joe: To make them number.
Moe: They should use clocks in relay races instead of batons.
Joe: Why?
Moe: I don’t know...just seems like a good way to pass the time.
Staring at my phone all day has certainly had no Effect on ME!
If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
Dear Advice Doctor,
About a year ago I had a career in a field I loved, working a dream job. I had just been given a huge raise to boot, but honestly, I would have done this job for half the pay. I loved it that much. Then the rug was abruptly pulled out from under me when the CEO’s nephew appeared out of thin air and was given my position. He had no experience in the field. It was a bitter pill to swallow, and was the worst case of nepotism I’ve ever known. I’m still reeling. Should I sue, or just move on?
Dear Bouncing,
Choose six months for $26 or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397
— Bouncing back - or maybe not
Thank you for writing, and as I often say here, the beauty of your question is that countless others wondering the same thing who didn’t take the time to write will get the answer right along with you.
And there are countless others. Ask around and you will find that many among us have trouble swallowing pills — and whether they’re bitter or not doesn’t really matter.
What does matter are the various reasons (and there are many) and what we can do about them. It’s important; we aren’t taking medicines just for fun, right?
Sometimes difficulty swallowing a pill can be as simple as dry mouth which, ironically, some drugs cause. Some pills are notoriously large, big enough to give anyone a hard time getting them down the hatch. Anyone who has had trouble, especially soemthing serious like choking on a pill, can have enough anxiety to interfere with the natural swallowing reflex. There is a definite mental element to this question because most of us routinely swallow foods bigger than the pills that give us trouble.
Fortunately, there are plenty of patient-friendly solutions. The simplest: make sure to take pills with sufficient water or other liquid. Ask your doctor or pharmacist if a liquid version of the medication is available, or a different pill formulation (smaller, or gel-coated) is available. Do not cut or crush pills without checking with your pharmacist, but if permitted that may be a helpful option. Some people actually practice swalloing with hard candies about the size of their medication.
One thing you definitely do not want to do: skip needed medications due to swallowing issues. If it gets to that point, discuss it with your doctor as soon as possible.
Thanks for your question. I hope my advice has been helpful.
Do you have a question for The Advice Doctor about life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in Examiner issues.
THE MYSTERY SOLVED
The Celebrated MYSTERY WORD CONTEST
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.
PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC
Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC
DERMATOLOGY
Dermatology &
Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com
Evans Chiropractic Health Center Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net
Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901 706-396-0600 www.augustadevelopmentalspecialists.com
Jason H. Lee, DMD 116 Davis Road Augusta 30907 706-860-4048 Floss ‘em or lose ‘em!
BOURDAIN
ing her. Never, ever suggest “try it.” Never say those dreaded words “try it, it’s good.” Or worse, “It’s good for you.” That’ll poison the well.
Pp
Garlic is divine. Few food items can taste so many distinct ways, handled correctly. Misuse of garlic is a crime. Please, treat your garlic with respect. Avoid at all costs that vile spew you see rotting in oil in screwtop jars. Too lazy to peel fresh? You don’t deserve to eat garlic. Pp
Good food is very often, even most often, simple food. Pp
For their own good, vegetarians should never be allowed near fine beers and ales. It will only make them loud and belligerent, and they lack the physical strength and aggressive nature to back up any drunken assertions.
Pp
I don’t snack. I don’t generally eat sweets or drink soda. I never eat between meals.
Pp
Always entertain the possibility that something, no matter how squiggly and scary looking, just might be good.
Pp
Vegetarians, and their Hezbollah-like splinter faction, the vegans, are the enemy of everything good and decent in the human spirit.
Pp
Understand, when you eat meat, that something did die. You have an obligation to value it.
Pp
Street food, I believe, is the salvation of the human race.
We know that there is a direct, inverse relationship between frequency of family meals and social problems. Bluntly stated, members of families who eat together regularly are statistically less likely to stick up liquor stores, blow up meth labs, give birth to crack babies, commit suicide, or make donkey porn. If
Little Timmy had just had more meatloaf, he might not have grown up to fill chest freezers with Cub Scout parts.
Pp
The perfect meal, or the best meals, occur in a context that frequently has very little to do with the food itself.
Pp
I would think twice before telling an already obese nation that it’s OK to eat food that is killing us.
Pp
Only Texans and Jews understand brisket.
Pp
I think of [street food] as the antidote to fast food; it’s the clear alternative to the king, the clown and the colonel.
Pp
Wholesome food is wholesome food anywhere. I may not like something, but generally speaking, if it’s a busy street food stall serving mystery meat in India [or wherever], they’re in the business of serving their neighbors. They’re not targeted toward a transient crowd of tourists that won’t be around tomorrow. They’re not in the business of poisoning their neighbors.
Pp
Fast food is about as destructive and evil as it gets. It celebrates a mentality of sloth, convenience, and a cheerful embrace of food we know is hurting us.
Pp
Tokyo would probably be the foreign city if I had to eat one city’s food for the rest of my life, every day. It would have to be Tokyo, and I think the majority of chefs you ask would answer the same way.
Pp
[Of his first visit to Charleston] More important than anything, I discovered the glories of Waffle House, [a place for] the hungry, the lost, the seriously hammered all across the South to come inside a place of safety and nourishment.” [He wrote that it was a culinary experience “better than the French Laundry,” a threestar Michelin restaurant.]
At Seniors Helping Seniors®, we match older adults who need a hand with friendly, mature caregivers—people who understand, share their interests, and bring joy to everyday moments. Whether it's help around the house, getting to appointments, or just sharing a laugh, our caregivers offer support with daily living in a way that feels natural and uplifting.