BEFORE YOU SAYAAAH
AND AFTER

THE BEST GUIDE YOU WILL EVER READ TO MAKING YOUR NEXT DOCTOR APPOINTMENT EVERYTHING IT SHOULD BE
your personal information.
Your experience at the doctor’s office can be pleasant and rewarding or not. It depends on several things. When you visit any medical care facility, the ball is in your court. Whether it is a doctor, PA, NP or other person, they cannot read your mind. You have to be very clear about what your medical issue is.
As a patient, your job is communicating clearly and concisely with whomever you come in contact. This begins when you reach the office and go through the check-in process. You may be asked to complete paperwork or just to answer questions regarding
When you are taken to the treatment room, you are asked questions concerning why you are there, your medications, and related information. Vital signs are taken and the results entered in a computer. Ask what the results are. For example, if you take your blood pressure at home, you need to know if it corresponds to the current reading.
I suggest that you record your blood pressure readings for at least two weeks prior to your appointment and bring them with you.
The same thing applies if you are diabetic. Record your blood sugars so the doctor will get an idea of any fluctuations.
Explain in detail why you are there. You will probably have to repeat this information
BULLIES
October is National Bullying Prevention Month, a fact we were unaware of until the tragic death of an 11-year-old Harlem Middle School 6th grader a few weeks ago who was bullied by classmates. Our headline above is meant to suggest one of the recognized strategies for dealing with bullies: ignore them; make them disappear. But as the image below also suggests, that is a very difficult assignment.
However, bullying doesn’t always look like the picture shown. Sometimes the target gets the silent treatment, delivering the message that the victim is an outcast, excluded from the company of others. Other times it’s just the opposite: the victim is talked about constantly and maliciously, online and in person (often just within earshot), as the subject of gossip and rumors designed to hurt.
Why do people do this, when clearly they would hate to be treated the same way? Why do some people seem to be bully magnets? And how can people deal with bullies or avoid being bullied altogether?
The reasons bullies exist are numerous and complicated. Some people live miserable lives and they can’t stand to see others enjoying life. Others have an insatiable thirst for power, and it never goes away. They belittle people from kindergarten through adulthood. Sometimes the power display is their key to climb a group hierarchy, or gain entrance in the first place.
Please see BULLIES page 7






by guest columnist
Lucy Dianne Sharp, RN, BSN
Augusta, Georgia


PARENTHOOD
by Dr. Warren Umansky, PhD
It’s time to take stock. Over the past months, this column has addressed many issues and experiences that you are likely to have faced as a parent. Now, let’s see what you have done in response.
A. I read the column more for entertainment than for advice. Once I’ve skimmed the column, I move quickly to the jokes and puzzles.
B. I read, think about, and discuss the column with my spouse and friends. I usually go with what they think is the best thing to do.
C. I use the column as one source of information and guidance. I also consult other dependable sources and weigh all the information before applying a strategy.
D. I haven’t read the column before. I look forward to it becoming a source of information to make decisions about my parenting role.
If you answered:
A. No doubt you either have no children or your children are perfect. Congratulations! We are very pleased that you enjoy other aspects of the publication too.
B. You are wise to get other opinions, but you and your spouse probably know more about your children than do your friends. Whether you follow the advice you receive from this column certainly is up to you. The bottom line is to do what works. This column provides guidance based on what research says works and what is gleaned from decades of experience with hundreds of children and parents. What you decide to do to help your children and family be more successful is up to you and your definition of success. It sounds like you have a good vision for what kind of people you want your children to become.
C. You are thoughtful and wise to weigh different sources of information. That word “dependable” is important, since there is a lot of bad information easily accessible to those who use the internet as their primary source. The key phrases to remember are “do no harm” and “do what works.” This column does not advocate using approaches that hurt children (our definition of discipline is teaching, not punishment), so the use of spanking, yelling, physical punishments like standing with arms out for long periods of time, pinching, biting back, and the like are never advocated. Gather your information. Do what works. Do no harm.
D. We hope you will continue to find this column helpful for you and your family in the future. Columns from past issues can be found online at www.issuu.com/medicalexaminer. Dr. Umansky has a child behavioral health practice in Augusta.
NEXTISSUENOV7
• Recognizing that behaviors are excessive, but feeling powerless to stop them
What Causes OCD?
There is no one cause for OCD, but several factors can contribute:
THOUGHTS ABOUT THOUGHTS THOUGHTS
OBSESSIVE COMPULSIVE DISORDER When Worry Becomes a Ritual
Editor’s note: Written by local mental healthcare professionals, this series shares explores how people may think and act when affected by common and lesser-known mental health conditions.
“I used to spend hours every night before going to bed or before going out, checking that the stove was off,” says Rachel, 34. “Even after I’d double-checked it, I’d drive back home just to make sure again. I knew it didn’t make sense, but if I didn’t do it, the anxiety was unbearable.”
Rachel isn’t alone. She was experiencing Obsessive-Compulsive Disorder (OCD)—a mental health condition where intrusive thoughts and repetitive behaviors can take over daily life.
What is OCD?
Obsessive-Compulsive Disorder is a chronic mental health disorder where a person has persistent, unwanted thoughts (obsessions) and feels they must perform repetitive actions or mental rituals (compulsions).
These behaviors may relieve anxiety for a little while but ultimately strengthen the cycle of fear and repetition.
Common examples include:
• Obsessive fear of contamination, leading to excessive cleaning or handwashing
• Intrusive thoughts about harm, prompting repeated checking (doors, appliances, locks)
• Need for order or symmetry, resulting in counting, arranging, or repeating behaviors
Signs and Symptoms
• Intrusive, unwanted thoughts that cause distress
MEDICAL MYTHOLOGY MEDICAL MYTHOLOGY
1. “We’re all a little OCD.” Being neat or organized isn’t OCD. This disorder causes intense distress and disrupts daily life.
2. “People with OCD can stop if they just try harder.”
OCD is not about willpower; it involves complex neurological and psychological mechanisms.
3. “Medication can cure OCD.”
While medication is helpful, therapy, particularly ERP, is often needed for lasting change.
4. “Just being extra clean? Or double-checking things? That’s no big deal.”
OCD can include countless themes, including being overtaken by taboo thoughts, obsession with numbers or symetry, and fear of harm.
or anxiety
• Compulsive behaviors aimed at reducing that distress
• Spending an hour or more each day on obsessions or compulsions
• Avoiding triggers that might provoke obsessive thoughts
• Biological: Brain differences in serotonin regulation and hyperactivity in certain neural circuits
• Genetic: Family history can increase vulnerability
• Psychological: Perfectionism, heightened sense of responsibility, or intolerance of uncertainty
• Environmental: Stressful life events, trauma, or learned behaviors may trigger or worsen symptoms
Treatment and Management
The good news is that OCD is highly treatable with the right combination of therapy and support.
• Cognitive Behavioral Therapy (CBT), especially Exposure and Response Prevention (ERP), is the gold standard—helping patients face fears and resist compulsive responses.
• Medication such as SSRIs (selective serotonin reuptake inhibitors) can reduce obsessive thinking and compulsive urges.
• Mindfulness-based strategies and support groups help individuals manage ongoing anxiety and reduce relapse risk.
• Family education promotes understanding and reduces unintentional reinforcement of compulsive behavior.
Prognosis
With proper treatment, many people can see huge improvement or remission of symptoms.
Early intervention also boosts success. Without help, symptoms may continue or get worse—affecting work, relationships, and quality of life.
Need Support?
Integrated Psych Solutions (IPS) provides comprehensive behavioral health services including assessment, therapy, and treatment planning for individuals and families managing both common and complex mental health conditions. To schedule an appointment, call 706-204-1366 or visit integratedpsych.care.

Most doctor visits are scheduled every 15-20 minutes. That is an office problem, not yours. Take your time. You and/or your insurance are paying for this visit. You are a customer. Don’t let them rush you. Ask as many questions as you need to. If you get vague or unclear responses, ask them to find someone who can give you a clearer answer. Sometimes, doctors explain something and the patient downplays their issues so as not to appear dumb. Please don’t do this. You can ask them to write down anything you don’t understand or may forget. By the time you leave the office, and drive home, you may have forgotten valuable information.
When medication is changed or new medication ordered, ask questions. Should you notify someone at the office if you have problems? Ask for a specific person or number to call. If you just call the office, it might be 24-48 hours before you get a response. Regardless of how long a medication has been on the market or the low chance of side effects, anything could happen. Often it occurs when there is an interaction between your current meds and the new/changed med. Not all doctors check for interaction problems. You can go online to a site called Drug Interaction Checker. Be sure to include any vitamins or over the counter meds. I use this site often.
It tells you everything you need to know about your medications and any interaction you need to be aware of.
If bloodwork is ordered, ask why and how you can get the results. Most doctors today are part of an online network where you can find results on your own. Take advantage of this. You will often see the results before the doctor does.
If a referral to another medical professional is made, ask if they will contact you or if you need to contact them. Ask them to write down the name/office where the referral is sent. If you are referred to a specialist, like a cardiologist, you need to know the name of the practice office. There are numerous offices for all specialties. You don’t want to go to the wrong office. Ensure that any and all visits to a medical office, tests, referrals, etc. are covered by your insurance carrier. If you are scheduled by the office, ask if they know whether they are in your insurance network and have gotten approval for your visit. If they aren’t in network, contact your insurance for an alternate provider. Ask about your copay.
One last suggestion is that you keep on your person a list of your medications, allergies, and diagnoses. Update it after each visit. I know folks can do this digitally, but I keep a paper copy in case I am ever in an unconscious state and the emergency personnel need the info quickly.
IMPLEMENT • MONITOR SAY AAAH… from page 1 again to the PA, NP or doctor. Your explanation is influenced by your age, gender, culture, education, etc. That is okay. Keep talking until they fully understand your symptoms/concerns. I suggest you write down anything you need to speak to the doctor about and bring it with you. If you have access to an online network, submit your questions/concerns prior to your visit.
I hope this information has been helpful.
— Lucy Dianne Sharp, RN, BSN



WHAT IS CARDIAC CATH?
Most of us are familiar with the word catheter (or “cath” for short). It’s a thin flexible tube inserted into the body for various purposes, and the purpose often defines the type of catheter used. After surgery, for instance, it is not uncommon for a urinary (or “Foley”) catheter to be inserted into the bladder to drain urine.
Although simple catheters made from plant stalks and reeds date back to ancient times, the modern medical catheter was invented in 1752 by none other than Benjamin Franklin, although Franklin may have merely modified another’s invention from around 1720.
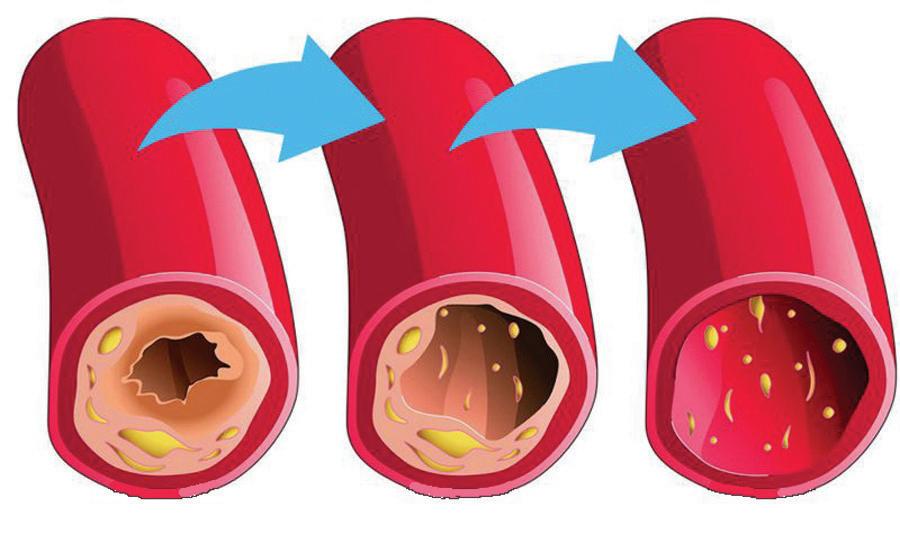
“Catheterization” is the process of inserting a catheter. In the case of cardiac catheterization (see why people say cardiac cath?), the catheter is inserted in a vein and threaded up into the heart. Once there, the catheter can get down to business. A contrast dye can be injected through the catheter that will make blood flow readily apparent, and more to the point, where any blockages from plaque or cholesterol are preventing normal and adequate blood flow. Pictures taken at this point are known as coronary angiography, or simply an angiogram. Measurements can be taken inside the heart to gauge its pumping efficiency in all four heart chambers, as well as how heart valves are performing. Oxygenation levels can be measured too, and tissue samples can be taken to later be biopsied in the lab.
Cardiac cath isn’t all diagnostic. Problems identified during catheterization can be immediately fixed. A blocked artery identified by contrast dye can be fixed by angioplasty, a procedure where a tiny balloon inserted by catheter is inflated to restore better bloodflow at that spot. As long as all the equipment is already there anyway, a stent — a small tubular scaffold to help keep the vein open — can also be inserted to decrease the chance of a future blockage at that spot.
Considering everything performed, inside a beating heart at that, cardiac cath is generally considered an extremely lowrisk procedure that can eliminate or prevent some very highrisk events like stroke and heart attack. +


Who is this?
Just as there were several doctors responsible for perpetrating the Tuskegee Syphilis Study upon trusting and unsuspecting participants (see “Who is this? ” page 5), there were likewise several public health advocates whose combined efforts brought the shameful study to its long-overdue end.
Launched in 1932, the study and its questionable protocols were known and accepted without question for decades, at least within the Public Health Service. It was not until 1955 that anyone outside the PHS raised ethical and moral objections to the study. Count Gibson, an Emory-trained MD born in Covington, Georgia, who was by 1955 a professor at the Medical College of Virginia, heard about the study from a speech by an Emory colleague. He later wrote the speaker to say that, from everything he could learn about the study, it “cannot be justified on the basis of any accepted moral standard.” He was advised by more senior faculty members to drop the matter, and he did.
Fast forward ten years, when 28-year-old epidemiologist Peter Buxtun (above) was hired by the PHS in San Francisco to interview patients with sexually transmitted diseases. Through this project he learned of the Tuskegee Experiment. He was to later write, “I didn’t want to believe it. This was the Public Health Service. We didn’t do things like that.” But the more he investigated, the clearer the picture became.
In 1966, he filed an internal complaint with the PHS’ Division of Venereal Diseases. The complaint was rejected on the grounds that the study was not yet complete (translation: all the participants were not dead yet*), so the merits of the study could not yet be properly judged.
Undeterred, Buxton filed another protest in 1968, and like the first one, this one too was quashed, its allegations ignored.
Buxton finally decided that outside intervention would be required. In the summer of 1972 he became a whistleblower and leaked the details of the Tuskegee Experiment to awardwinning investigative reporter Jean Heller of the Associated Press, who was to later describe the story as “one of the grossest violations of human rights I can imagine.” She broke the story in the Washington Star on July 25, 1972. On July 26, it was splashed across the front page of The New York Times. The ball was finally rolling. Congressional hearings were convened, at which Peter Buxton and numerous other officials from the U.S. Department of Health, Education, and Welfare testified. The experiment was terminated within days.
The following year, a $1.8 billion class action suit was filed in behalf of the study’s victims. It was settled out of court in 1974, awarding each still-living participant $37,500 in damages.
Over the years, unfavorable comparisons have been drawn between the Tuskegee Study and the inhumane experiments by Nazi doctors during World War II. One of the ironies of the Tuskegee story is that Peter Buxton was born in Czechoslovakia and fled to the US to escape Nazi oppression and some of the same cruelties he was to later discover here. +
ADVENTURES IN
Middle Age
BY J.B. COLLUM
Have you ever been cornered by a friend or relative who told you all about their health issues in minute detail? Was it intriguing and fun? Probably not. Unfortunately, I have been on both sides of such interactions. Perspective changes things drastically. When I am telling others about my health problems, I imagine them as deeply interested and awaiting my every word with bated breath. But when I am on the receiving end, I’m thinking about what I did wrong to deserve this. I ask myself what I could do next time to avoid their eyes if we’re face to face. If it’s a phone call, I wonder if I messed up when I answered the phone even though I saw the name on the caller ID and knew what they would be talking about.
I recognize that I might sound cold and uncaring by saying that, but part of my job is to shine a spotlight on unsaid and deeply embarrassing parts. To call out things we are afraid to talk about. I also recognize my hypocrisy since I am always telling you about my health problems in this column. There is a difference, however. You have chosen to read this and you probably don’t have anything better to do right now. Maybe at this very moment you are sitting in the waiting room of your doctor’s office, waiting patiently to be called back. Plus, I try to make my droning health updates as entertaining as possible. Why do we do this? Why do we feel the need to over-share about our ailments? I don’t know. Maybe because our health is probably, or at least should be, something we are intensely aware of and interested in. Sometimes we can get so caught up in it though, that it dominates our thoughts and our lives. If this is the case for you, then the friends who will still answer your calls should be counted as true friends of the highest degree. Now, show your appreciation for them by cutting back on the health talk. Even if they ask how you are, just give a quick synopsis and move on to talking about the Braves. Oh wait. Not them. That is too depressing this year. Pick a happy subject. Also, for your own sake, don’t let struggling with your health problems dominate your life. Set aside time to deal with them but live your life the best you can, while you still have it. Perhaps some of you are wondering about how I closed out the last edition of this column thinking I might have a pulmonary embolism. Short version: I don’t.
Long version: They don’t know what’s wrong with me, but I have some upcoming appointments for more testing, and the blood tests I got just last week are now showing other conditions that are of concern. I am now taking Ozempic because I can’t seem to get my diabetes or weight under control. We’ll see how it goes. Even with insurance it is costing me enough money to pay a nice motorcycle or boat payment. I tried to convince Lorie to let me get the motorcycle or boat instead of the meds if I promise to do better about my diet and exercise, but she knows me too well. She paid for the prescription over my vociferous protestations, and then watched while I injected myself with it to make sure I did it, or perhaps she was hoping to enjoy seeing me suffer. If that was the case she was disappointed. The needle is so small, I barely felt it. In fact, after I did it, she said, “That’s it?”
medicine costs $1,000 +
Another medicine they want to put me on costs $1000 a month. I said no thank you, but she is trying to see how we can also get that at a lower price with a coupon or through some other means. If she gets this prescription at $1000, it will be a waste of money because I’ll have a stroke if we spend that much money every month. If she does that, she had better invest in some life insurance first.
She fussed at me, saying I have no qualms about spending hundreds or even thousands of dollars on gadgets or toys, but balk at spending that much or less to perhaps save my life. I really didn’t have a good rebuttal for that, so I did the honorable thing and just quickly and quietly escaped to my office and locked the door, to use some of my gadgets and toys to help distract me from the truth.
Until next time, give all this some thought. Listen to your friends when they talk about their health problems, but try not to reciprocate. Also, be more balanced and focus your resources on extending your life, because no matter how many gadgets or toys you have when you die, you can’t take them with you. In the meantime, live life to the fullest extent you can.
J.B. Collum, author of this column and Special Forces Parenting, is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com

Special Forces Parenting
In dealing with the ever escalating “war” with Freyja (some of you have asked about pronunciation: it’s fray-uh) and her ability to get around any blocked or locked door and any other type of device designed to keep her safe, I am often reminded of a scene from the original 1993 Jurassic Park movie. You know, the good one. The game warden, Robert Muldoon, realized that the raptor had fooled him and just before he uttered his famous last words, “clever girl.” Even as he knew he had been bested and was about to meet his maker, he had begrudging respect for his foe. I feel the same way about Freyja. She is unable to speak, but she is perhaps the most clever kid I have ever come across. I recently shored up some weak boards in the ceiling of her playhouse that she had managed to pull completely out. I was sure it was now secure. Why? Because I went overboard with it. I added more screws to the boards and added three large cross-bracing boards that ran the full length of the playhouse and tied these to each of the other boards. I was sure this would make it impossible for her to break any more of the boards in this area and that no other areas presented any weaknesses. She proved me wrong. No, she wasn’t able to break the boards I shored up, but she systematically moved around in her playhouse until she found other boards that she began to attack. So far, they are holding up, but I can already see that it is only a matter of time. I didn’t even think she could reach them, but she managed to. She is like a Cirque De Soleil acrobat and contortionist all in one. She

manages to do well in the Special Olympics too. If we can ever get her to focus on wining the games, instead of getting distracted by a bug or pretty much anything that catches her eye, she will be unstoppable.
In fact, I am rethinking her playhouse altogether. She is outgrowing it, and I have learned lessons that will allow me to build it better if I can start from scratch. For one thing, next time I will only build two walls and use two real walls as the other sides. I’ll also build all the way to the ceiling so she can’t climb on top, which she does now, despite me giving her no handholds or horizontal places to put her feet below about four feet. She has grown and her arms are also strong enough to allow her to pull up her entire weight, while swinging her feet well above her head to catch hold. Of course, I will make each floor taller for her and expand the size of the playhouse as well. Instead of most of the living room, we are ready to give her all of it, except for a path from the front door to the rest of the house.
Yes, Freyja presents many challenges, but she is worth every one of them many times over. I’m sure that the vast majority of parents and grandparents of special needs children whole-heartedly join me in that opinion.
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
Every installment of this series so far, this side of the page, focusing on the bad eggs of medicine, has been about a murderer. This one will be different, although in some ways, sadly, it’s just more of the same.
The man to the right, you see, was one of the primary doctors running the infamous Tuskegee Syphilis Study, a 40year initiative (1932 to 1972) conducted by the United States Public Health Service and the Centers for Disease Control and Prevention.
To say the study was despicable, racist, deceptive and malicious barely begins to describe its depravity. It involved enrolling some 600 black men in poverty-stricken Macon County, Alabama. 400 of the men had syphilis, and 200 uninfected men were a supposed control group. On the surface, that could describe the basic structure of a legitimate study.
In this case, however, the whole point of the study was to deliberately withhold treatment: its purpose was to observe the effects of the untreated disease, all the way to death and autopsy. The study was true to its purpose, but the participants were never even informed of their syphilis diagnosis. They were instead told they had “bad blood” and were given placebos or ineffective treatments for conditions unrelated to syphilis.
There is plenty of blame to go around in the design and execution of this dark chapter in medical history. A doctor named Taliaferro Clark with the Public Health Service identified the need for the study and crafted its approach. Dr. Raymond Vonderlehr was the on-site director of the study and designed many of its deceptions in order to attract volunteers and fraudulently obtain the “consent” of participants.
We singled out Dr. John R. Heller (pictured) because, to be honest, he just looks hateable somehow, and because one of his main responsibilities was to make sure none of the study participants found out about penicillin, a drug that was known since the 1920s to effectively treat syphilis and was widely available even in the early years of the study. Not a single participant in the study was treated with penicillin.
The program finally came crashing down in 1972 due to the actions of a persistent whistleblower (see “Who is this?” page 4), but by then 28 patients had died from the direct effects of syphilis, another 100 were dead from complications related to the disease, 40 of the patients’ wives were infected, and 19 children of study participants were born with congenital syphilis. Heller continued to defend the study even then.
Heinous Nazi doctors deserve all the criticism leveled against them for their cruel experiments on unwilling patients, but some say the Tuskegee study is even worse. It has been called “the longest non-therapeutic experiment on human beings in medical history.”
+
Photography: Amber Rose. Poster Art: Valerie Steen

I WAS THINKING
by Pat Tante
RUG CREEP
Before I begin writing about rug creep, I want to say that if you have it, you should consult the Advice Doctor who writes a column in this very paper. I must confess here and now, I do have a problem with rug creep.
No, not that guy you knew in college. I’m talking about the actual heartbreak of rug creep – and I have it.
I have had it a long time, but until recently I did not know what caused it. I shall explain. I had placed a throw rug on top of my carpet, attempting to add depth and scale to my carpeted living room. It’s very “in” doncha know.
Over time, the rug began to creep or walk toward the front door. Why was that? Was it shy? Do they have some tiny feet to move them outdoors? I would
often have to pull the rug back into the living room to keep it off the front porch! And why didn’t it ever creep toward the back door?
Well, after a great deal of scientific research, I have learned why rugs do this.
They don’t like living here! Ha ha. Just kidding.
It seems that carpet fibers lean a certain way (who knew?) so that when a rug is placed atop your carpet and people walk on it, the rug will be pushed in the direction of the carpet pile by the force of walking on the rug.
Supposedly, every decent carpet installer knows about this phenomenon (but they never shared it with me). They will lay the
carpet pile pointing towards the main doorway to make the carpet colors more “vibrant” when visitors come over and track mud into your living room.
Please note that it is difficult for amateurs to tell which way the pile is pointing. Not to worry, the direction of the rug creep will let you know.
If your new imported oriental rug heads under the dining room table, you know which way your pile is pointed. Too late to change by then, but at least you’ll know. Sorry about that.
So now, you are probably wondering if there are remedies to stall rug creep and keep your rug in the house where it belongs, or if this

disease is incurable.
Surely no one would forego the opportunity to go down in history as the person who found the cure to rug creep.
So, yes! There are nonslip rubber mats (so that the rug has a mat, over a carpet, over another mat). There are also sprays and double-sided tape.
To save money, you could get someone to help slide grandmother’s halfton armoire on top of it as an anchor, but that would interfere with your traffic pattern.
Or, you could just roll up that wandering rug and put it in the closet.
— Pat Tante +

MEDICALEXAMINER
FALL FORWARD
In just a few weeks (Nov. 2, to be exact), we will be turning our clocks back an hour. The old adage about the beginning and end of Daylight Saving Time is “spring forward, fall back.”
So why is our headline fall forward?
For many of us in this part of the world, summer is not our favorite time to exercise. When you can get sweaty just walking to the mailbox at 9 a.m., you know it’s summertime in the South.
But the brutal heat of summer is behind us, making right now the perfect time to start (or restart) an exercise program. (Please read the next paragraph.)
Plenty of people stop reading when they see the E word. We know that. But please give us a few moments to plead our case.
Exercise is not just a way to be fit. Exercise itself is a fit word, as in one-size-fits-all.
For the twenty-something people among us, exercise might mean playing tennis a few times a week, or running a mile or two before work most mornings.
But what about forty- or fifty-somethings? Or even seventy- or eighty-somethings? With a few noteworthy exceptions (and congratulations to them), this demographic isn’t going to be literally running anywhere.
This is where the definition of the word “exercise” reveals
its flexibility. Each one of us gets to define it for ourselves.
For instance, at an assisted living facility their most popular exercise program might be called Sitercize. Participants never leave their chairs, but they definitely enjoy an age-appropriate workout.
That well illustrates that each of us can and should design the exercise program that perfectly fits our own situation.
As that applies to the illustration below, exercise can involve anything, even raking
leaves. And as the picture also suggests, it might be a little more like exercise if you use a rake rather than a blower. It’s quiet, carbon-neutral and all those other ecological factors.
Raking as exercise also makes another important point: exercise can be different every season, every week, even every day. The important thing is regularity.
And the many options — going for a walk, riding a bike or a thousand other choices — are so much more pleasant this time of year.

BULLIES from page 1
When it comes to stirring around for our health, remember: fall forward! +
In the same way that bullies share some general traits, so do their targets. Bullies look for people who exude low self-confidence as easy marks. Loners are another easy target, but not because the bully wants to do his cruelty in private. They want and need an audience, but they also want victims who have no support system or defenders. And bullies are shallow enough to victimize people simply because they’re “different,” whether that’s their hairstyle, clothing, nationality, religion, skin color, weight, income level, good grades, bad grades, or something else. Virtually anything can be a trigger if a bully is mean enough.
Before examining some strategies to prevent and or cope, let’s take a short detour to address the comment above about bullies needing an audience. Bystanders must realize that being a silent and complacent observer to bullying is really a form of participation in tormenting the victim. Think of any crime that will scar its victim for years to come and imagine having the ability to intervene and stop the crime but failing to do so. Bullying is no different. It is a crime, and it is also a crime (morally, if not legally) to give it tacit approval by failing to intervene if that is possible (and why wouldn’t it be?). Silence is viewed, in the mind of a bully, as a green light, encouraging the performance to continue for his audience. The intervention of a single person can break the spell, and who knows? Could the death of Aiden Lee in Harlem have been prevented by a few more kind words and actions of support and intervention?
What’s something fun for the whole family?
NOBODY OUT-SALUBRIOUSNESSES THE MEDICAL EXAMINER
In other words, bullying prevention can and should involve anyone and everyone, not just the victims. Parents can teach their kids by example that bullying is unacceptable. Going into “Karen mode” and berating a hapless store clerk in front of your kids sends exactly the wrong message. Parents can educate their kids on what bullying looks like and why it’s wrong to be a bully, and they can make sure their kids know that silence is not the way to respond when victimized by a bully. Kids need to know that the problem is with the bully, not them, and that speaking up to teachers, parents, coaches, counselors, and family members will help stop the bullying and provide protection.
Every bully will naturally threaten escalation and retaliation if their victim tattles. Of course they say that. They don’t want to face consequences for their actions. Sorry, Charlie... you brought this on yourself, so don’t blame anyone else, and don’t expect the very people you prey upon to help hide your crimes. As if!
In the moment, experts recommend a strong, firm, self-confident, even courteous response, perhaps with a little humor.
An article in Psychology Today cautioned that a simple, unemotional response works best. It sends the message that the target does not intend to be victimized without throwing down a challenge, which the bully may feel compelled to react to in order to save face. Practicing responses that are emotionally neutral will help prepare for the next confrontation. Staying cool lets the bully know that he isn’t getting under your skin. When he can’t do that, he will often lose interest.
It should be noted that we’ve been using male pronouns for the sake of simplicity, but girls and women can be just as vicious in the bully department as boys and men.
All of us can share in bullying prevention — every day.
DEE DEE KNEW WHAT TO DO
Dee Dee was a somewhat typical girl growing up about 4 decades ago. Her family was hard-working folks. Her mother had a job as well as her father.
She lived near Parris Island, South Carolina, one of the deepest ports on the East Coast. Ships from all over the world disgorged cargo there, including hundreds of tons of powdered white clay. With international ships going in and out daily, Dee Dee was exposed to more international flavors than was common for people in the low country of South Carolina.
Most international sailors did not have the proper documentation to get off the ship and enter the US. However, during those pre-9/11 times, this did not prevent American citizens from wondering on the ship, if invited by the crew.
When Dee Dee was about 10 years old, she and her younger sister were baby sat by a 15-year-old girl while their mothers worked. The 15-year-old baby sitter stood out because her “hormones had already hit and she carried a lot of her cargo on her upper deck.”
One nameless day, the 3 barefoot girls wandered

down the dock and were hailed by Russian sailorsmwho no doubt were attracted to the 15-year-old’s obvious assets. They yell back and forth in broken English for a while, and then the girls boldly walked up the gangplank.
After a quick tour of the upper deck, 2 sailors took the 3 girls to their quarters. The room was tiny and had double bunks. The walls were covered with nude and semi-nude posters in assorted poses. Dee Dee had never seen a Playboy poster before. And certainly not French posters.
After a few minutes of wide-eyed gawking, the sailors told the two younger girls to explore the ship on their own. They walked around the deck for about half an hour while the 15-year-old remained in the cabin with the two sailors for what one would assume to be more private and personal explorations.
After they left the ship, the 15-year-old never discussed what did -- or did not -- happen in the cabin. It might have been inappropriate for young ears. After all, she was the baby sitter and had responsibilities for their care.
BASED ON A TRUE STORY
did she become psychotic and rob a string of liquor stores to support a drug habit. No, she went on to be a normal person.
in psychological counseling forever for PTSD (Post Traumatic Stress Disorder).
(most of the time) A series by Bad
Times are different now.
Billy Laveau
The next night after midnight, the 3 girls snuck out and went back down to the ship.
The following morning, Dee Dee’s mother discovered white powdered clay footprints on the floor leaving no doubt that her daughters had walked the pier at night. Saying they were with the 15 year old baby sitter did not dissuade her mother’s righteous wrath. Dee Dee’s mother went into a flying fit and grounded her daughters for a month and forbade him to speak to the 15-year-old for 2 months.
Rumors were that the 15-year-old developed a somewhat lasting relationship one of the sailors, corresponding with him for a few years and occasionally seeing him in person when he was in port.
She did not get pregnant. Nor did she defect to Russia. Nor did she get a sexually transmitted disease. Nor did she become suicidal. Nor
Had this happened decades later, that would an international incident. The sailor would be charged with false imprisonment, statutory rape, aiding in the delinquency of a minor, and a litany of other ugly legal procedures.
The 15-year-old girl would have been on Oprah or Jerry Springer tearfully airing her horrible ordeal of imprisonment and sexual torture. That would probably be followed by either a reality series, a made-for-TV movie, or at least an internet sex video.
Nancy Grace would fiercely portray this as a communist plot to overthrow the US and an assault on the sacred virginity of Southern womanhood, a stand only she could take because she understands, being from international hotspot known as Macon, GA.
Ken Nugent’s new ad would have him standing atop a ship swearing to sue the Russian government and the shipping company for all sorts all dastardly damages and unimaginable amounts of money.
All three girls would be
Either separately or jointly, while proclaiming the moral high ground, Al Sharpton, Hell’s Angles, Augusta Pride, the KKK, and any other group desiring TV exposure and new contributors would stage demonstrations proclaiming all manner of alleged personal insults and injuries as well as foreign conspiracy.
Every Democrat and Republican presidential candidate would hold a press conference tearfully declaring how they “personally feel the pain and the shame of the families so horribly disrespected.”
On a less humorous note, virtually every teenage girl has her first sexual encounter in a manner that her father would not approve of and her mother would be horrified by. Assuming the act was voluntary and consensual, most survive this adventure without lasting psychologically horrifying implications.
And Dee Dee today? She came along through it all just fine. She is the beautiful caregiver of her invalid parents, the mother of a college student, the go-to person in the family when something must be done right, and votes for the best candidate in every election

Probably not.
Questions. And answers. On page 13.










CRASH COURSE

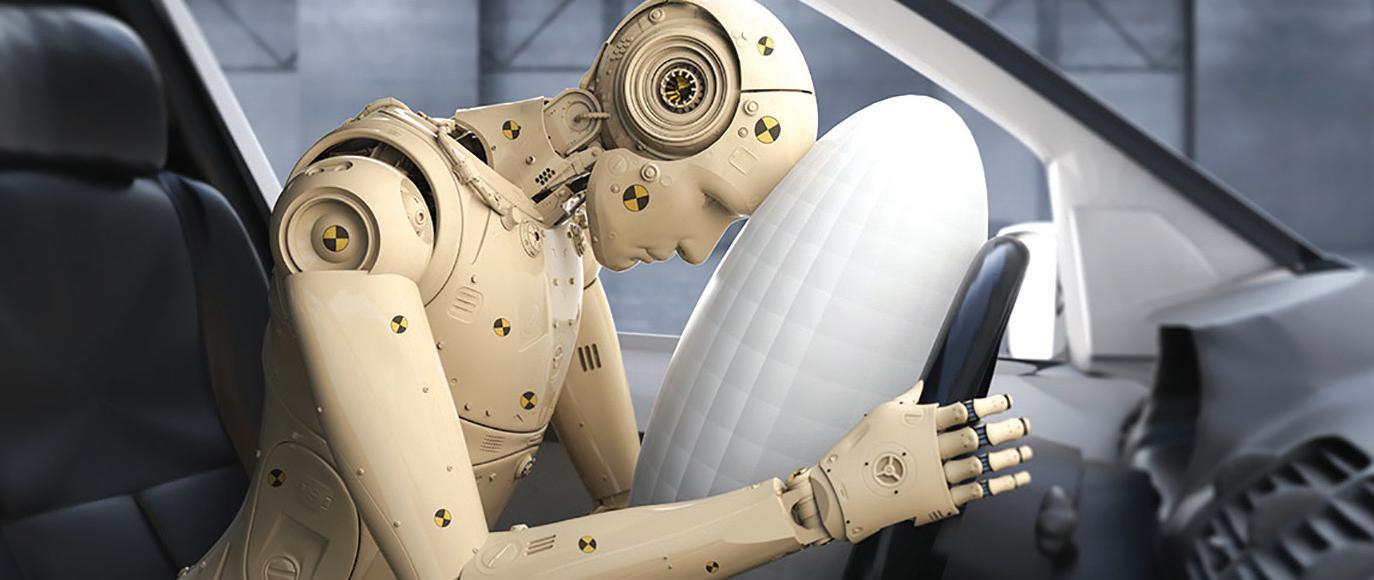
irbags are a pretty amazing invention, both in terms of what they do and how blindingly fast they do it.
They are comprised of a complex system that starts with sophisticated crash sensors that decide whether seat belts offer sufficient protection, and if not, which airbags to deploy.
The deployment itself happens in less than the blink of an eye: 1/20th of a second, give or take a few milliseconds.
In other words, an airbag inflates so rapidly that its speed as it expands can be as high as 200 mph. It has to be that fast so that it’s sitting there waiting for you to slam into it from the force of the crash a split second earlier.
Airbags might look like pillows, but they are anything but soft and fluffy. Very few things feel soft and fluffy when they hit us at 200 mph. But it’s far better to hit an airbag than a steering wheel, a dashboard, or a windshield.
Safety enhancements provided by airbags, required equipment on US vehicles since 1999, have saved more than 50,000 lives as of 2017, according to the National Highway Traffic Safety Administration (NHTSA).
At the same time, airbags have caused injuries, even deaths. According to NHTSA, more
than 290 deaths were caused by airbag inflation between 1990 (when airbags were optional equipment) and 2008. 90% of the deaths were in older vehicles, and more than 80% of those killed were unbelted or improperly restrained. First generation airbags deployed with greater force than today’s versions, and today’s advanced airbags even modify their deployment pattern if weight sensors detect a small driver or passenger, or a child safety seat.
Even so, airbags are known as a supplemental restraint system. That means they need to work along with seatbelts for maximum safety and effectiveness.
Because of their super-fast deployment, sitting very close to the steering wheel (which contains an airbag in most vehicles) is also dangerous. 10 inches is the minimum safe distance (including for pregnant drivers).
These are the same reasons kids under 13 are supposed to sit in the back seat and wear seat belts and/or be safely restrained in a car seat of the appropriate size and design for the child’s age and weight.
Airbags are not reusable, so if yours have deployed, they need to be replaced as part of the repairs made.


5 RED FLAGS
ABOUT THE ACCURACY OF MEDICAL INFORMATION
Red flags don’t necessarily mean that whatever they’re poking out of needs to be categorically rejected. But they do suggest that further investigation and caution would be prudent until the advice can be checked and verified. Since no two patients or cases are alike, even “green flag” medical advice should be checked and double-checked. Here are 5 examples of red flags.

SOURCE WEAKNESS
• Red flag: The advice doesn’t come from a recognized, credible source, or only offers vague references like “Doctors say...” or “Studies show...”
• Green flag: Look for specific information that comes from a known and respected source: “Studies at the Mayo Clinic...” or “Research earlier this year from the National Institutes of Health...”
AMATEUR HEALERS
• Red flag: Related to the above, reliable advice should come from those with solid medical or scientific backgrounds. Anonymous blogs and social media posts from random people should be viewed with skepticism. Articles written without attribution could come from an unqualified source or someone with a financial incentive to recommend a given treatment.
• Green flag: Good medicine and good medical advice is transparent.
PRODUCT-DRIVEN ADVICE
• Red flag: You have to buy this product to get relief. No other product (or doctor) can offer the relief this can. It offers a cure that the medical community is unaware of (or knows but wants to hide from you).
• Green flag: Trustworthy advice is independent and evidence-based. And the source of that evidence? See above.
MIRACLE CLAIMS
• Red flag: “Guaranteed to work!” “100% safe!” “Zero side effects!” are all red flags. Even aspirin can’t make claims like those.
• Green flag: The absence of exaggerated promises and extreme claims is a step in the right direction.
EVIDENCE BY TESTIMONIAL
• Red flag: Rather than medical research and clinical studies, recommendations are based on unverifiable testimonials from unknown individuals, outrage against the medical industry or “Big Pharma,” or the influence of viral accounts and videos.
• Green flag: Testimonials can be instructive and inspiring, but there has to be solid evidence behind them. If it’s all emotion and no science, it’s time to dig deeper. +


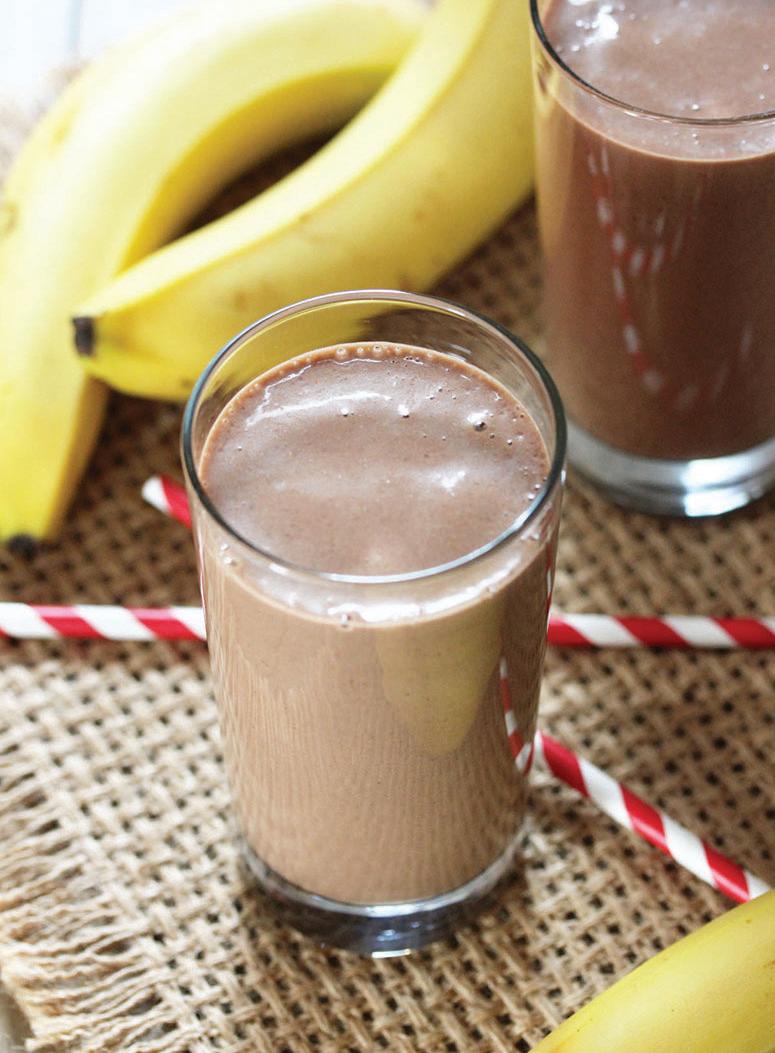
TRYTHISDISH
CHOCOLATE BANANA FRAPPÉ
Satisfy your sweet tooth with this protein-filled, energy-boosting chocolate treat.
Ingredients
• 1 cup (8-ounces) low-fat chocolate milk
• 1 cup 2% milk
• 2 (6-ounce) containers
vanilla Greek yogurt
• 1 large ripe banana, peeled
• 1 tablespoon unsweetened cocoa powder
• 1 cup ice cubes
• Chocolate sprinkles (optional)
Instructions
Slice banana and freeze for 30 minutes. Combine milk, yogurt, banana, cocoa powder and ice cubes in blender. Blend until smooth and frothy. Top with chocolate sprinkles, if desired.
Yield: 4 Servings (serving size: 8 ounces)
Nutrition Breakdown: Calories 140, Fat 2g (1g saturated fat), Cholesterol 5mg, Sodium 100mg, Carbohydrate 20g, Fiber 1g, Protein 12g. Diabetes Plate Plan: ¼
used with








Have you ever heard ads for a Name Your Price tool?


ACROSS
1. Stay at Mistletoe
5. Salt of uric acid
10. Dumb-dumb
14. Minerals
15. More pleasant
16. Republic in SW Asia
17. Alpha follower
18. Dew, for instance
20. Sheep’s bleat
21. Dust particle
22. Map collection
23. Former Russian rulers
25. Stroke, in short
26. Danzig’s name in Poland
28. Most-decorated Olympian of all time
31. A rich tapestry
32. Flower segment
34. Tree of the genus Ulmus
36. Fight for breath
37. Shankar’s instrument
38. New York canal
39. Doc’s org.
40. With “The,” an Augusta golf course
41. Swelling of tissues
42. Dougherty County (GA) seat
44. Type of school
45. Cover
46. Ambulance feature
47. Indian, for example
50. Augusta _____
51. Nickname of the 34th US president
54. Confederate facility in Augusta
57. Bucket
58. Fencing sword
59. Research deeply
60. Old cloth measures
61. He brought down Capone
62. Congressman Rick
63. _____ of Man
DOWN
1. #1 player for the Augusta Tourists
2. Part of CSRA
3. Of the foot bones
4. An ad for raising awareness (abbrev)
5. Open a wine bottle
6. Violent protests
7. Teen skin eruption
8. Mr. Turner
9. Before (to a poet)
10. Proximal’s opposite 11. Like most thermometers
12. Word with bank or base
13. Singles
19. Abdominal landmark
21. Spectrometer intro
24. Crack
25. Blacken
26. Very enthusiastic lady?
27. Stage play
by Dan Pearson

The Mystery Word for this issue: ENADTIME
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
28. Egyptian deity
29. Plants that live from year to year
30. Ball prefix?
32. Feel compassion for
33. Abbrev. for “and the rest”
35. Type of market
37. Castle-building material
38. Verge
40. Local college
41. English nobleman ranking above a viscount
43. Shoulder bones
44. Jenkins County (GA) seat
46. Medicinal ointment
47. Sign on many doors
48. Deal with
49. Female sheep
50. Enterprise follower
52. While away, as time
53. Otherwise
55. Food label abbrev.
56. Famed Brooks
57. Noted architect
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.

THEBESTMEDICINE

ha... ha...

Aman and his teenage son have a running argument going about the kid’s long hair. One day the kid asks his dad if he can borrow the car.
“Only if you get a haircut,” says the dad.
“Dad!” counters the frustrated son. “Did you ever stop to think that Jesus himself had long hair?”
“That’s true,” said the dad. “And he walked everywhere he went.”
Moe: Do you know what they would call a dolphin in Germany?
Joe: Adolphin, probably.
Moe: What does Arnold Schwarzenegger call a colonoscopy?
Joe: I give. What?
Moe: A Cameron Diaz.
Moe: Supposedly the easiest word to spell in the entire English language is “icy.”
Joe: Well, looking at it, I see why.
Moe: How was your weekend?
Joe: It was awesome because of one very special moment.
Moe: Do tell.
Joe: I was grilling some steaks out on the patio and my boy came out, watched me for awhile, and then said, “Dad, some day I will help you pay all your bills, buy groceries for you, and pay our rent.”
Moe: Aww. That is so sweet. How old is the little fellow?
Joe: He’ll be 37 next month.
Moe: I finally bought a pair of shoes that have memory foam insoles.
Joe: Are they comfortable?
Moe: Not really. I only bought them so I’ll stop forgetting why I walked into a room.
Moe: Don’t ever challenge Death to a pillow fight!
Joe: Right! Unless you’re prepared to deal with the reaper cushions.
Moe: Did I tell you my pizza joke yet?
Joe: Yeah. It was pretty cheesy.
Two cannibals are sitting at the table eating dinner when one suddenly says, “Geez, I hate my mother!”
“Well then try the salad,” says the other one.
A stapler, a file folder, and a tape dispenser walk into a bar. They order a pitcher of beer.
The bartender comes back with the pitcher and glasses and says, “That will be 16 dollars.”
“Put it on my tab,” says the file folder.
Staring at my phone all day has certainly had no Effect on ME!
By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME ADDRESS
Choose six months for $26 or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397
Dear Advice Doctor,

Dear Dating,
The Advice Doctor

Before I address the main point you’ve raised, let me first take a minor detour. I’m not sure you’re even aware of one of the serious problems you may be facing. You mention being unable to “find the words.” This is a matter of some concern. Known as aphasia, it’s an inability to comprehend or formulate language. The typical causes include stroke and trauma to the head, in short, some kind of brain damage.
Have you been evaluated by a neurologist? The fact that you could write this letter suggests your condition may be mild, but it never hurts to check.
Now on to your main issue.
This too is a potentially serious problem. The medical term for a heart that goes “pitter-patter” is arrhythmia. As a side note, 99 percent of the population would spell it “arrythmia,” so it can be useful in winning bar bets, etc. Ah, but I digress.
Arrhythmia is a fancy word for an irregular or abnormal heart beat. They can range from harmless to potentially fatal depending on the type of arrhythmia, its cause, where it originates in the heart (in the atria versus the ventricles), how long it lasts, and other factors such as your overall heart and vascular health.
Arrhythmias are often long term problems, but sometimes they are the result of some underlying problem (medication side effects or overactive thyroid, to name two examples). When that problem is removed or effectively managed, the arrhythmia may go away.
The short answer to any question about arrhythmias, however, is to see a doctor about the condition as soon as possible, or go the nearest emergency room. A heart arrhythmia is not something to take casually.
I’m seeing this guy at work that is — I can barely find the words! I love him! He makes my heart go all pitter-patter just walking through the room. The problem is, our company has a policy against dating co-workers. I guess we have two choices: one of us has to quit, or we can date on the sly until we’re sure it’s going to work out and hope no one finds out. Unless you can think of another good option. — Dating Dilemma +
I hope this answers your question.
Do you have a question for The Advice Doctor about life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.


THE MYSTERY SOLVED
The Celebrated MYSTERY WORD CONTEST
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.
WORDS BY NUMBER



PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC
Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC

DERMATOLOGY
Dermatology &



Parks Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com

Evans Chiropractic Health Center Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net

Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901 706-396-0600 www.augustadevelopmentalspecialists.com



Nursing|Companion 706-426-5967 www.zenahomecare.com

Bashir Chaudhary,
Jason H. Lee, DMD 116 Davis Road Augusta 30907 706-860-4048 Floss ‘em or lose ‘em!