MEDICALEXAMINER

4 MISUNDERSTOOD
MEDICAL WORDS AND TERMS
Medical terminology usually does an admirable job of conveying information precisely and accurately. But not always. Sometimes we hear a perfectly benign word and draw conclusions in exactly the opposite direction from the intended meaning. For example, what about benign?


BENIGN TUMORS
• What we might think it means: Harmless; ignorable.
• What it actually means: Non-cancerous, yes — but may still cause problems depending on size or location.
NEGATIVE TEST RESULTS
• What we might think it means: Uh oh. Negative. Not good! Something bad happened. I like positive things.
• What it actually means: No signs of the condition were found. In this situation, negative is good; positive is bad.
UNREMARKABLE, AS IN A SCAN
• What we might think it means: It doesn’t exactly sound bad, but it sure doesn’t sound good either.
• What it actually means: Everything looks normal. No abnormalities were detected. Nothing is worth remarking about. Everything’s cool.
STABLE CONDITION
• What we might think it means: Great! The patient is improving.
• What it actually means: There are no major changes; not getting worse, but not getting better either. It could mean staying the same when improvement was expectated, or it could mean holding steady in a critical state when it was feared things would get worse.


HUH?

The big question in medicine these days — on both sides of the stethoscope — is simple: “Huh?” But that’s not the only question. Another one is: who can you believe?
In olden times (like this time last year), longstanding fixtures in the healthcare world like the Centers for Disease Control (CDC) and the World Health Organization (WHO) were viewed as reliable sources for solid information on all things medical. Throw in the American Medical Association (AMA), the federal government’s Department of Health and Human Services (HHS), the National Institutes of Health (NIH), the Food and Drug Administration (FDA), plus numerous professional healthcare organizations representing physicians of every stripe.
Today, the entire healthcare landscape has been turned upside-down. People don’t know who to believe. Or should that be whom?
Either way, the most uncomplicated solutions to problems are often the best. The formula in this case is simple enough that this oh-so-brief article contains the complete answer to the who-can-you-believe question. Ready?
If you are a doctor, continue to trust your training and your years of real-world, handson experience. It’s that simple. And if you are a patient, do not get medical advice from social media, like Facebook, TikTok, or NextDoor and similar apps, or from publications like this one. Do not get medical advice from politicians or impersonal government agencies, nor from talk radio or TV news personalities. Do not get medical advice from anyone who has not performed at least a basic physical exam on you. That reduces your options considerably, leading to a simple conclusion: get medical advice from your doctor
Definitions: “Medical advice” refers to direction and guidance about healthcare concerns significant enough to require medical treatment. “Doctor” refers to an M.D. or another trained healthcare provider working under the direction of an M.D., such as a PA, NP, etc.









PARENTHOOD
by Dr. Warren Umansky, PhD
You received an email from your child’s high school today saying that a student at the school threatened to shoot up the school. It went on to describe the actions that the school took to address the threat and deal with the unnamed student. When your son arrived home, you asked him what he knew about it. He chuckled and said it was a friend of his and that he probably was just kidding.
“Yeah, a group of us have been talking on line about what would happen if a kid shot up our school. At least we wouldn’t have to go to school for a while if something like that happened!” What do you do?
A. It’s just a bunch of teenagers talking and fantasizing. How could they not think this way with all the stuff in the news these days?
B. You decide you want to look at your child’s phone to see what kind of conversations he’s been having. You walk into your child’s room to talk to him. You haven’t been in there much since he told you he didn’t want you prying. He refuses to give you his phone and your eyes are drawn to violent pictures he has posted on his walls.
C. You tell your child not to talk that way and you go about your business, as your child heads off to his room.
D. You tell your current husband what happened when he gets home a few hours later. He says he might check to see that the guns at home are locked up, but not to worry.
If you answered:
A. Have you been having conversations with your children about safety in schools and consequences for making threats? Are you confident about the emotional health of your children? This revelation by your child should be a wakeup call. Conversations need to start; careful monitoring of electronic devices needs to start, and talking with the school counselor, your pediatrician, and/or a mental professional should happen immediately.
B. This is not something that waits until tomorrow. As disappointing, surprising, eye-opening this might be for you and as much as you have to evaluate your parenting skills, getting help for your child must happen now. Connect your child with the school counselor immediately and contact your pediatrician for a referral to a mental health professional. Family therapy might be beneficial, as well, to help with communication at home.
C. This laissez-faire approach may suggest why you now are having to deal with this problem now. You’re not just a mother or father. As parent, you are responsible for shaping your children’s actions and for dealing with the consequences. Being an involved parent from the start makes it more likely that those consequences will be positive.
D. Worry. Your son’s situation could get a lot worse without acting now, which means your situation will get a lot worse. Logically, firearms must be secured at home. But your son and all the family need help. Dr. Umansky has a child behavioral health practice in Augusta.
THOUGHTS ABOUT THOUGHTS THOUGHTS
MUNCHAUSEN SYNDROME When Illness Becomes One’s Identity
Editor’s note: Written by local mental healthcare professionals, this series shares thoughts on how people may think and act when affected by common and lesser-known mental health conditions.
“I spent years bouncing between hospitals, convinced something was wrong with me,” Alex admitted. “I’d describe symptoms that didn’t exist, exaggerate test results, and even tamper with medications to convince doctors I was sick. For a while, the attention from medical staff made me feel cared for—but eventually, the lies caught up with me.”
Alex was not battling a hidden physical disease but a complex psychological condition known as Munchausen Syndrome, now more often called Factitious Disorder Imposed on Self.
What is Munchausen Syndrome?
Munchausen Syndrome is a rare but serious mental health disorder in which a person deliberately makes up, exaggerates, or causes illness or injury in themselves.
Unlike “malingering”— where someone fakes being sick for personal gain (such as money, drugs, or avoiding responsibility)—Munchausen’s primary motive is to get attention, sympathy, or care. Individuals may go to extremes, including falsifying medical records, self-harming to cause symptoms, or frequently changing doctors to avoid being found out.
Signs and Symptoms
• Dramatic but inconsistent medical history
• Symptoms that get worse when under observation but improve when unobserved
• Eagerness to undergo tests, surgeries, or painful procedures
• Extensive knowledge of
understood, but contributing factors may include:
• Psychological factors: These can include a history of childhood trauma, neglect, or prolonged illness, as well as feelings of low selfworth or need for control.
• Personality disorders: Traits such as borderline or narcissistic tendencies may overlap.
• Biological factors: Possible differences in brain functioning can be related to stress and attachment.
• Social factors: When the person receives care and attention, it reinforces their identity as a “sick patient.”
Treatment and Management
MEDICAL MYTHOLOGY MEDICAL MYTHOLOGY
1. “They’re just faking to get attention.”
While behaviors are deceptive, they stem from deep psychological distress—not simple manipulation.
2. “It’s no different than malingering.”
Malingering seeks external rewards; Munchausen is driven by psychological needs.
3. “People with Munchausen need to just stop lying.”
It is not about willpower— professional intervention is often necessary.
4. “It’s extremely rare, so it doesn’t matter.”
Though uncommon, the consequences for individuals and the healthcare system are significant.
medical terminology and hospital routines
• Frequent hospitalizations or doctor visits with vague or unexplained symptoms
• Reluctance to share prior medical records or contact past providers
• Evidence of self-inflicted injury or tampering with lab tests
What Causes Munchausen Syndrome?
The exact c ause isn’t fully
Treating Munchausen Syndrome can be difficult since many people with it refuse to acknowledge their condition. Effective approaches may include:
• Psychotherapy – Cognitive Behavioral Therapy (CBT) and trauma-focused therapy can address underlying emotional pain and unhealthy coping mechanisms.
• Medication – Antidepressants or antianxiety medications may help if co-occurring mood or anxiety disorders are present.
• Supportive care – Establishing trust with a consistent healthcare provider is essential to reduce unnecessary procedures while addressing psychological needs.
• Family involvement –Educating loved ones about the disorder reduces unintentional reinforcement of sick-role behaviors.
Prognosis
Outcomes vary widely. With proper treatment and support, some individuals can reduce harmful behaviors and build healthier coping strategies. But without intervention, Munchausen Syndrome can lead to repeated medical complications, damaged relationships, financial strain, and increased risk of serious harm.
Need Support?
IPS provides comprehensive behavioral health services including assessment, therapy, and treatment planning for individuals and families navigating both common and lesser-known mental health conditions. To schedule an appointment, call 706-204-1366 or visit integratedpsych.care.
ON BEING PREPARED
Editor’s note: A version of article first appeared a year ago in the immediate aftermath of Hurricane Helene. Its message bears repeating. Maybe it should be an annual feature.
Everybody talks about the weather but nobody does anything about it, as Mark Twain allegedly observed. Since that’s what everybody else is doing, let’s talk about something else. Hurricane Helene is so last year.
But surely there are valuable lessons we can learn from the disaster we have endured. Were you among the majority who felt unprepared, not only for the ferocity of the storm, but to deal with its aftermath?
Odds are we won’t be seeing anything like Helene anytime soon. But we might. Or there might be another ice storm, high winds and torrential rains, floods, a tornado, or a massive heat wave that results in power outages.
What can we do to be ready for the next natural disaster, whatever and whenever it might be?
Step one: make sure you have an emergency kit ready to go. Here is a checklist of some of the basic ingredients it should contain:
_ flashlight _ batteries
_ first aid kit
_ non-perishable food (freeze dried, for example)
_ eating utensils _ matches or a lighter _ tarps or plastic sheeting _ toilet paper _ manual can opener _ soap/hand sanitizer _ medications _ eyeglasses _ water
As we saw last year, the smooth gears of civilization can start to grind and completely shut down literally overnight. Availability of even the most basic human needs — like clean water — was interrupted in Richmond County, and countless other communities between here are North Carolina. Humans can’t live long without water, but there is a remedy.
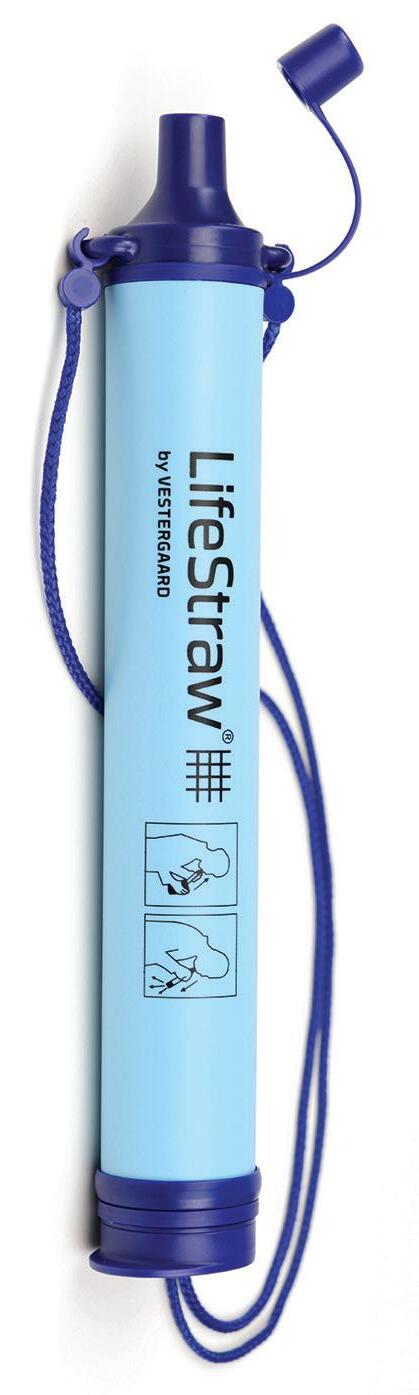
One of the best and most ingenious solutions to any interruption in safe water supplies is provided by LifeStraw. This inexpensive device (about $20) removes 99.999999% of waterborne bacteria, and 99.999% of waterborne parasites, as verified by independent lab tests. LifeStraw also filters out the tiniest of microplastics and foreign matter floating in water. A person could literally stick it into
a mud puddle in the middle of the street and suck out perfectly clean drinking water, and keep doing so for the duration of an extended emergency: the device’s filtration system is rated for 1,000 gallons of use before needing to be replaced.
A LifeStraw could come in handy on a camping trip, or the next time you’re pinned for a day or two in the wreckage of your partially submerged car that isn’t visible from the road.
Other important items for successfully weathering the next storm: a few basic tools, like a pocket knife, a crescent wrench, and screwdriver with multiple heads.
While tarps and plastic sheeting can be used for basic shelter, a tent is a better option, and it’s amazing how compact some very roomy tens can be when they are stowed. Experience tells us that tent could very well be set up in our own yard. Things happen. Hurricanes, for example.

One of the items in the checklist is matches or a lighter. That’s for building a fire to prepare food or stay warm. But what will you burn? After all, any and all available wood or other fuel could be soaking wet. Outdoor suppliers sell canned fuels like Sterno that are designed for easy portability, easy lighting, and safe cooking. Candles are nice to have in an emergency kit too.
The more a person meditates on potential emergency needs, the longer the list can grow. What about rope? A compass. Tote bags and ZipLoc bags. Don’t forget toothpaste, toothbrushes, and other toiletries. Many lists of must-haves include a whistle for emergency signaling, and some recommend including simple entertainment items like a deck or two of cards for those long nights withour power.
Locally, stores like Cabela’s, Camping World and others can help build an emergency kit that is portable and practical and includes all the important items.


I WAS THINKING
by Pat Tante
BEAGLING AS I SEE IT
(Definition of Beagling: the hunting of rabbits by beagles using their strong sense of smell. A beagle pack is usually followed on foot as beagles will follow a scent wherever it leads with no thought to roads or distance.)
Last fall I was invited to my first Beagling. Wanting to appear sophisticated and worldly, I replied – a what?
You know, a Beagling, where beagle owners and admirers of hounds get together to run the hounds through the woods where they follow scent trails and have a jolly old time running hither and thither. Meanwhile, the owners and admirers follow along on foot trying to keep track of where the hounds are by their baying (not barking).
Well of course, I said, that sounds like great fun. And I don’t have to get on a horse. What does one wear to a beagling? I have not a bit of camo clothing in my closet. I was secretly hoping that this lack of appropriate wear might provide a reason to demur. This could be one of those times when not having a thing to wear might provide a good excuse.
“Not to worry” my friend assured me. “Just wear good walking shoes and something warm, and I’ll bring you a stick.” A stick? Will there be snakes! “Oh no,” he replied. “The stick will help with walking the trails through the woods. Lots of ups and downs and a few mud bogs, you know.”
The Beagling Day arrives and we join a group of interesting people in a cleared area out in the woods of South Carolina somewhere. There were no hounds that I could see. Perhaps they had gone on ahead.
Everyone begins to walk toward a more densely wooded area. Lots of chitchat. They all know each other. Each is wearing some piece of appropriate Beagling clothing –boots, plaid jackets or wide brimmed hats. Suddenly I hear the hounds far off in the woods, possibly chasing a rabbit. I realized that this is not a spectator sport.
The scattered group heads down a rough road toward the baying of the hounds somewhere in the distance. Then the

Direct editorial and advertising inquiries to: Daniel R. Pearson, Publisher & Editor E-mail: Dan@AugustaRx.com
AUGUSTA MEDiCAL EXAMINER P.O. Box 397, Augusta, GA 30903-0397 (706) 860-5455 www.AugustaRx.com • E-mail: Dan@AugustaRX.com
Who is this?
Here (above) is the fourth of the four doctors who were the founders of Johns Hopkins School of Medicine (William Halsted, Howard Kelly, William Osler, and this man), William Henry Welch).
William H. Welch could have become just another rich kid living off the wealth of his family. But things certainly did not start off that way for the Welch family. Their arrival in the New World was anything but auspicious.
In 1636, Oliver Cromwell’s British soldiers, in raids across Ireland, drove some two-thirds of the Irish population from their homes. Many were captured and sold as slaves, including one 11-year-old boy, Philip Welch. He ended up sold into servitude under Samuel Symonds, the governor of Massachusetts. Fast forward a century and a half or so, and Philip’s great-great-grandson Benjamin apprenticed under a doctor in Windsor, Connecticut, and became a doctor himself, the first in the family’s history.
By the time William H. Welch was born on April 8, 1850, the Welch family had sired enough physicians and surgeons to staff a decent-sized hospital. In addition to his grandfather, Welch’s father and four uncles were also physicians. His nephew was a United States senator. This was a prominent, powerful and well-connected family. So naturally, William decided to become a high school teacher. What?
Rest easy; the man who was to become “The Dean of American Medicine” was just going through a phase. He soon went back to school, and five years after starting his teaching career he started his medical career with a brand new MD degree from Columbia University College of Physicians and Surgeons in Manhattan. For the next two years (1876-1877) he studied medicine in Europe, and returned to the US with an idea for a new hands-on medical teaching institute modeled on what he had seen at the University of Leipzig in Germany.
That was a choice based on experience — theirs, not his. The university was founded in 1409, making it one of the oldest institutions of higher education in the world. He put his European experience to work by launching a pathology laboratory in New York’s Bellevue Medical College, which led to an invitation to join the faculty at the then-fledgling Johns Hopkins Hospital and Medical School. Anyone who closely examined Welch’s career at Bellevue would not be particularly impressed. Welch himself was depressed and disappointed about that chapter of his career. Even so, the interview with Welch about a possible position at Johns Hopkins led to this assessment: “Upon the whole I think he is the best man in this country for the Hopkins.”
William Henry Welch has been called the foundation upon which the modern medical school was built. His colleague William Osler said of him, “In addition to a threestory intellect, Welch has an attic on top.”
A lifelong bachelor, Welch died in 1934 at age 84. +
ADVENTURES IN
Middle Age
BY J.B. COLLUM
We have a wealth of information at our fingertips these days. That’s good and bad depending on the accuracy of the information source. I’ve recently recounted some health issues I’ve been having here in this column in regard to blood pressure dropping very low and even some fainting episodes. I put my symptoms in some internet health websites yesterday and I don’t like what came back, but I am so dubious of anything I read online that I’m not sure whether I should laugh it off or go straight to the emergency room, not pass go, and not collect $200. Wait, I think I’m a little confused. That can a symptom too. Hmm.
What am I talking about? you ask. I’ll tell you. I’ve had an increasing number of episodes where, even with just a tiny amount of exertion, I have chest pain, irregular heartbeat, shortness of breath, I feel faint, sweat profusely, and sometimes lose consciousness. It started a few months back with only an occasional episode but now it is every day and even multiple times a day. I’ve fallen asleep while on a teleconference call with a co-worker even. When I woke up, I asked if I had not responded for a while, and he said it had been a few minutes. I tried to play it off by telling him he was boring and he agreed and said he has that affect on people.
So what did the internet experts spit back out at me? Pulmonary embolism. Scary stuff. My symptoms plus my age, and risk factors for this (like sitting a lot, being overweight, having heart disease, etc.) make this potential diagnosis seem more likely. That said, I will withhold judgement until I’ve seen a physician. I plan on calling them as soon as they open on Monday morning and get in to see someone about this one way or another because this is scary stuff.
A little over a week ago when I made one of my occasional trips to work in

the office, as I was getting my computer plugged in and set up, I felt what I call “the spell” coming on. It was a bit embarrassing, but I ended up voluntarily lying on the floor and putting my legs in the chair because I felt like I was about to faint. My boss walked in and nearly had a cow. He was worried about me because I had a lot of work to get done. I’m joking about that part, mostly. I have known him for 40 years and worked for him off and on throughout that time. He was genuinely concerned about me. Another co-worker ran to the nearby grocery store and got me some Powerade in case what I needed was some electrolytes. I’ve been super-conscious of this since I nearly lost a dear friend and cousin because of him getting dangerously low on sodium in particular. Now I don’t think that is the problem for me anymore.
What causes pulmonary embolisms? I read about that, and though I am going to share what I learned, remember that I am not a physician or an expert of any kind. This is just what I found. Sitting a lot can cause blood clots in the legs and these can migrate to your lungs where they can greatly increase blood pressure in the affected lung and cause them to not do well at their function of oxygenating blood. That’s what causes the shortness of breath. Your body is increasing your breathing to compensate for lower oxygen in the blood. It is sort of like a heart attack in your lungs, similar to how one of my kids once told me he had a headache in his tummy. The lung is not getting enough blood and parts of it can die if this lasts long enough. So, just like a heart attack where a blockage can kill part of your heart, a pulmonary embolism can kill part of your lung, and by extension, it can kill you. They can also be caused by tumors, air bubbles, or fat from the inside of a
Please see ADVENTURES page 6

Special Forces Parenting
How impatient I was as a young person! Of course now, I am the epitome of patience. Well, maybe that’s going too far. In fact, I’m sure it is. I’m still impatient, but I’m too tired and lazy to worry about it or even complain about it. In addition to that, time seems to fly by so quickly at my age now that it comes across as patience when in reality it is just that a year doesn’t seem that long to me.
When it comes to patience when looking for progress in our special needs children and grandchildren, you need it if you want to avoid frustration. I will once again use football for an analogy. If your team is like Alabama, Georgia, Clemson, Ohio State or some other blue blood program, you have been at the pinnacle of success and even rather recently. If your team loses a game early in a season, you get all worked up over it. You don’t expect them to lose. Your expectation is for greatness. National Championships or bust, right? I know the feeling. On the other hand, if your team has never won any kind of championship or hasn’t in decades or even in your entire life (Perhaps even ever), then you don’t expect much. I won’t name any regional teams that fit this bill. You fans of them know who they are. Fans of teams that don’t have championship winning histories are happy to enjoy the game experience. Perhaps to them it is mostly about the tailgating, the time with friends and family, the bands, or the excitement of the crowd.
So to put it in a nutshell, your problem isn’t what is happening in a game you have no control over. Your problem is your

expectations. The happiest people I’ve ever known weren’t rich and they didn’t expect much at all. What they came by in their life was fully appreciated by them. My mother is a good example of this. She was the valedictorian when she graduated from high school and had scholarship offers for college, but what she really wanted more than anything else was a family. Her mother had been ill most of her life and had passed away when my mother was 15 years old. She had two homes burn down. She had multiple cousins die very young and under tragic circumstances. They didn’t have much materially either. Her father, my grandfather, or grandpa as I called him, had a heart attack in his thirties while in the army and so then lost his job there. He had multiple jobs to make up for it over the years, many simultaneously. He was a sheriff’s deputy. He was the iceman who brought blocks of ice to your house before refrigerators were around or at least common for average people. He smoked and salted meat. He managed ponds for a rich family. He also fished in those ponds to help feed his family, in addition to getting portions of the meat he salted or smoked in exchange for his services. He also didn’t complain. To my mother, she didn’t feel poor, but they were. They had plenty of good food to eat. They had a roof over their head. They had something to wear and she didn’t care if they were hand me downs from one of her approximately 150 first cousins. She had an aunt she especially loved who took an interest in her too. Aunt Iola was a scandalous member of the family as she didn’t marry, but did well for herself and had lots of men vying for her attention. She loved to dance and have a good time, and she really loved my mom. She bought her and her siblings things they needed and spent time with them. My mother felt rich. Why?
Because of her expectations. She once even pined for a baby doll to play with, but when that didn’t happen, she took a piece of a pipe she found and dressed it up and treated it like her doll. Her expectations allowed her to have a good attitude despite all of the challenges she faced.
Please see SPECIAL FORCES page 5
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
The infamous career of this man is so twisted that historians have a difficult task sorting out the crimes he actually committed from those merely suspected to be his evil handiwork. One fact is uncontested: he was a serial scammer and conman.
Born Herman Webster Mudgett in 1861, he was an outstanding student at the prestigious Phillips Exeter Academy in New Hampshire, and graduated from another highly regarded private school at age 16. His father was a heavy drinker who often beat Herman and his two siblings, and he also endured bullying from classmates due to his high grades.

One incident might have been the match that ignited his dark side: he was forced to stand in front of a human skeleton with the skeleton’s bony hands on his face. Rather than terrify him, it sparked an interest in anatomy; he began dissecting animals.
He enrolled at the University of Vermont, but after a year transferred to the University of Michigan’s Department of Medicine and Surgery in 1882. There, he and the professor who was the chief anatomy instructor collaborated on a grave robbing scheme to supply medical cadavers.
After leaving Michigan, Mudgett moved to Chicago in 1885 and began using the name H. H. Holmes. It’s unclear whether he ever earned a medical degree, but in Chicago he passed himself off as a doctor. He found a job working in a pharmacy.
He built a three-story house nearby that was later dubbed his “Murder Castle,” replete with trap doors, airtight cells, torture chambers and body disposal chutes to easily move fresh victims to the basement for easy dismemberment and incineration.
Over time, investigators have come to believe that very little of the reporting of the day about the Castle was factual. The more outrageous the stories, the more newspapers could be sold. But take away all the legend of this man, who supposedly preyed on visitors to the nearby Chicago World’s Fair & Columbian Exposition of 1983, and what was left was more than enough to send him to his final destination: the gallows.
As just one example, Holmes and a partner in many scams cooked up one to score a $10,000 life insurance payout. The partner would supposedly be burned to death, but the burned corpse, supplied by Holmes would be someone else. Holmes was the beneficiary of the insurance policy, and when he was paid the two would split the payout. Holmes uncomplicated the plan greatly by simply killing the partner. He followed that up with a scam perpetrated on the widow and her five children (resulting in three of their deaths).
Holmes married women with regularity, at one point having three wives (none of whom knew about the others). He ultimately confessed to 27 murders (and was paid $7,500 by Hearst newspapers for doing so).
Holmes’ 1896 hanging did not result in a broken neck, so he twitched at the end of the rope for more than 15 minutes before finally dying.
+
READY OR NOT, HERE I COME!
by Ken Wilson Steppingstones to Recovery
Remember some childhood games you played that required you to close your eyes? I remember one that required a lot of trust – standing with my hands on my hips and falling backwards with closed eyes into the arms of a larger and stronger buddy who would catch me at the last moment! The rush was exhilarating!
By far the more common and sensible game was closing my eyes, counting to 30 or so, then opening my eyes and yelling out “Ready or not, here I come!” and trying to find my friends who had hidden themselves from me. The hunt was fun but not as exciting as free falling!
Last month we talked about the necessity of open eyes in recovery. This time I’ll talk
ADVENTURES
about the nature of closed eyes when open eyes are what’s needed. It is a myth to think you have to wait until someone is ready to have open eyes all on their own schedule.
I am reminded of the story of a wealthy man who announced to a group of swimmers on a small island not far offshore, “I’ll give a million dollars to anyone who can swim to shore!”
Only problem was, the water was infested with large alligators. After painful silence, the wealthy man heard someone splashing his way to shore – frantically but speedily – and safely making it to shore in short order! The benefactor handed over the money and asked, “How were you able to take such a risk?” and the swimmer replied, “I didn’t choose to – somebody pushed me!”
from page 4
Very few clients I’ve known for the past 40 years have come to treatment with eyes opened on their own. Most were pushed. Your friend could die while you are waiting for them to open their eyes on their own volition. In fact, studies have shown that the mandated client has a better chance of a positive treatment outcome than a self-admission. Go figure. Addicts or alcoholics with closed eyes truly do not think they can stop their self-destructive behavior. By the time treatment is necessary, most drink because they have to, not because they want to. The fear of giving up such a “friend” is overwhelming. Usually, though, they come around to open eyes when they see others who have successfully achieved sobriety. They will trust that one overcomer more than a hun-
SPECIAL FORCES
dred non-alcoholics cheering them from the island to swim through the alligators.
That’s how I lost 51.8 lbs over the past 10 months in the Weight Watchers program. I followed others who were successful before me and never got hungry, which was the biggest fear that kept my weight-loss eyes closed over the past few years while Covid allowed me to isolate and eat too many pastries!
Before getting on the recovery road, it is normal for the alcoholic to see nothing but bogey-men and alligators out to rain on their parade, to lick the red right off their candy. The excuses that accompany closed eyes are ad infinitum and ad nauseam…I wish I had logged them over the years. As the loved one of an addict or alcoholic, please do not play verbal tennis with them. There are better ways to get
… from page 4 large bone that gets broken. If you have heart disease, as I do, or you have or have had Covid, then you are also at a higher risk.
I’ll let you know how things turn out for me, but keep in mind that if this happens to you or a loved one, take it seriously and get it looked at right away. After all, I can’t afford to lose any of my dozen or so readers. Oh, and also because I genuinely care about all of you. Seriously. Yes, mom, especially you. No, Lorie, my dear wife, I meant both you and my mom.
Maybe I should just call an ambulance now.

J.B. Collum, author of this column and Special Forces Parenting, is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@ gmail.com +

If we parents, grandparents or guardians of special needs children will set our expectations realistically, while still holding out hope, we too can be happy despite the challenges. Instead of setting unrealistic expectations only to have them dashed, instead treasure every small bit of progress you see. Let me give you some examples from our life. Freyja hasn’t made what you could call rapid progress, but it is still promising. Here are some of the examples:
• She puts her hands over her ears when she is trying to tell us she doesn’t like the show or movie we are playing for her, or just doesn’t want to watch it now.
• When she is ready for bed, she will either just lie down where she is with a blanket and sleep, or she will come lie down beside one of us on the couch. When she is very tired and wants to get in her bed, she will start annoying everyone in the room by picking up their things beside them like phones, tablets, tissue boxes, or whatever is there and throw them. If you are lucky, she doesn’t throw them far, but just picks them up in sequence and drops them.
• She opens the refrigerator when she
your point across. I might suggest going to a self-help program, for instance, such as Al-Anon. Go for a good while until you begin to understand their predicament and your role in helping before you make any overtures. You will discover that you have had closed eyes, too, and sometimes they open very slowly. If you’re the afflicted one reading this column, get ready for a big push! Open your eyes and swim like crazy. Those gators will part the water for you! What a rush!
wants something to drink.
• If she wants milk, she also pulls the milk jug out. She does the same for other drinks sometimes.
• She will pick up her toys if you patiently get her started, though she will need to be supervised through it and mostly just encouraged.
• She is vocalizing though no words are understandable except perhaps when we read a little too much into them.
• She also sings along with some of her favorite movies. It may not always be in key or sound anything like what is playing on the TV, but it is singing, and practice makes perfect, right?
I urge you to give this some thought and find a way to celebrate even minor progress.
There may come a day when they reach their best and no more real progress will come, so enjoy these milestones when they happen. Our children can usually sense if we are pleased or not, so let’s change our attitudes, if needed, to help show them that they are loved and we are proud of them, not based on what some other kid has done, but just focused on them and their abilities.
+
NORTH AUGUSTA
105 E Hugh St., Suite 103 North Augusta, SC 29841 (803) 441-3937 AIKEN 39-A Varden Drive
Aiken, SC 29803 (803) 641-6104 AikenHearing.com









AI...MIRACLE OR DISASTER?
AI: It is all over the news. What is it? What will it do? No one is sure at the moment.
Artificial Intelligence. Is it new? Or is it the latest splurge designed to extract money from the public? Remember acid rain? Was going to destroy the world in 10 years? That was back in the 90s. It still rains and we are still here.
My first encounter with AI was in the early 80s when Canadian Jacque Benoit, MD wrote a computer program that, based on history and lab work, made medical diag-

JEWELRY REPAIR
nosis. Revolutionary? Well, that depends upon who you ask. Medical schools and the medical communitybasically said, “Phooey. Won’t work. Dangerous.” His idea went nowhere fast.
Now, 40 years later, AI is supposedly the panacea that will save the world, so says today’s medical industry.
Before we let AI tell us what to do and when, let’s look at the latest AI news. A California 16-year-old male committed suicide after being encouraged by AI. AI helped him write his suicide note. His parents are suing ChatGPT.
An AI apologist argued that AI is not really intelligence, but a computerized program that predicts what the next word should will be based on what has already been wrote and published.
A reasonable conclusion would be that AI is fun and useful, but requires human logic, thought, and restraint before application
AI would say the US Consitituion grants you the right be wrong or stupid. That does not mean you should be wrong or stupid if you can avoid it. Just because you can legally do something doesn’t mean that you should. You could sit in the middle of the street at midnight and set your hair on fire. Because you can does not mean it is a good idea.
friends.




In the suicide case above, the teenager had a legal right to kill himself. AI said he could. It helped him with encouragement. No consideration for the pain and damage to his family, his
Remember the Pro Life (abortionist) slogan? “My body. My decision.” That doesn’t always work out well.
If AI is our savior for the future, we no longer need medical school and highly trained doctors. Just some kid computer technician clicking keys. I am not ready for that yet.
No act is entirely isolated. Newton’s Third Law of Motion states: for every action, there is an equal and opposite reaction. Beware of the reaction portion of Newton’s Law, regardless of what AI says.








HCRASH COURSE

opefully you have been enjoying the handy pointers provided in this brief series so far. You have probably seen a number of bad habits described that you see often in other drivers, but probably very very few that you are ever guilty of — and that’s good. That’s very good.
This installment will probably offer more of the same.
For instance, isn’t it annoying when a driver is confused for some reason? Maybe they’re looking for an address or they’re lost. Driving more slowly than the normal flow of traffic is understandable in those circumstances.
But here’s what happens: let’s say they’re slowly tooling along in — what else? — the fast lane. They suddenly see the address they’re looking for, or maybe they realize — oops! that was my turn! And it’s three lanes over!
You might think that they would just drive on ahead a short distance until there’s a safe and convenient place to turn around and go back.
Instead, they will employ any one of several options. If they aren’t quite past their newly-discovered destination yet, they may veer across those three lanes to get to their intended turn. Another option is to slow down or stop — right in the middle of traffic — and wait for a clear and safe opportunity to glide across the lanes and make their turn.
Another version of this phenomenon sometimes happens at traffic lights. Let’s say someone is stopped by a red light in the rightturn-only lane when they suddenly realize they don’t want to turn after all; they want to go straight.
What they could do is just go ahead and make the right turn and then a block or two away make some compensatory turns to get back on track in their desired direction.
That approach keeps traffic flowing and doesn’t inconvenience anyone else.
What many drivers do instead is to angle their car over to the left toward cars in the adjoining straight-thru lane, wedging their front
left bumper into the gap between two cars if possible and entirely blocking the right-turn lane. Then they sit.
The line of drivers behind this person who could have turned right have no choice but to sit and wait through the red until the light goes green and someone lets in the blocking car.
Sometimes the blockees get annoyed by the blockers and take their frustrations out on their horns, gas pedals, middle fingers, and so on.
In other words, bad drivers often spawn other bad drivers.
As if we didn’t have enough already!
We haven’t talked much about one of the foundation principles of Bad Driving 101, which is tailgating.
One of the great ironies of tailgating is that tailgaters hate it — with a passion — when people tailgate them.
Does that tell you anything about the practice?
The same puzzling phenomenon is a trademark of drivers who camp out in the left lane and refuse to move for anyone. They don’t mind at all if 14 cars are stacked up behind them, but when they come up behind a driver who refuses to get over to the right for them — in other words, when they encounter someone who drives exactly like they do — it is infuriating.
After tailgating the offender down the interstate for a few hundred yards — or a mile or two if they are especially patient or mean — they will often perform the patented How Dare You Inhabit My Lane Maneuver, which consists of speeding around the offender as recklessly as possible, then cutting in front of them with an inch or two to spare, reclaiming the lane that is rightfully theirs.
Considering just the few Bad Driver moves we have considered in these three articles alone, it’s completely understandable that in just over two decades, American roads have been deadlier than the two most catastrophic global wars in human history.
BEAGLING
from page 3
baying seems to come from a different area.
This must have been some kind of signal because the Beaglers (my word) began to leave the road and walk through the woods and underbrush. Another group turns and walks back the way we came.
Meanwhile, I am trying to figure out the Beagling rules in my head. If the baying comes from over yonder, some of the group goes yonder. However, some of the group turns and goes back the way we came. Some free thinkers just stand in one spot and chat. Occasionally, I hear the hounds baying from somewhere near Atlanta. If there are Beagling rules, I’m having a hard time figuring them out.
Then I begin to notice some very officious people wearing green jackets (not Master’s jackets). They seem to have some destination in mind, but I have no idea what or where it is. They stride about looking very straight-backed and important. I figure that one is most certainly the Head Beagler, and there are two Lieutenant Beaglers. One is also the Beagle Bugler to call the dogs. I mean hounds. I deduced this on my own just by seeing the hunting horn in her hand. I have not seen the rule book so I don’t know when the Beagle Bugler does this.
So, the participants (Beaglers) continue walking here and there – to the pond – back – turn around, etc. I follow along trying to appear that I’m a quick learner in the art of Beagling. I am really getting into this to and fro business, and once in a while I see a hound running through the woods, or maybe hear them on their way back from Atlanta.
This all continues for the better part of two hours. Time enough to make some new friends as we go up the hills and down again.
Finally, we all begin to collect in a clearing. I am trying to decide if there will be a finale of some sort, so I am full of anticipation. However, there are no dogs — I mean hounds — in sight.
Then, I spy the Head Beagler - not a hair out of place –and we trudge behind him up a hill. Lo and behold, we are back where we started. Who knew! I had had too much toing and froing to even know where I was.
And now here come the rest of the designated Official Beaglers, regular Beaglers, and all of the beagle hounds –so many! I could have sworn there were only a handful, but what did I know?
What a happy crowd of puppy dogs! I mean beagle hounds. Time for treats! And, I see that a table of snacks and libations for the happy Toers and Froers has magically materialized.
I am definitely getting the hang of this Beagling sport! +

to all our advertisers and readers
More Americans have died on US roads since 2000 than in World Wars I & II combined

TRYTHISDISH
SUNFLOWER SEED WRAPS (WITH CHERRIES)
Bring out the kid in everyone with this flavorful little wrap that’s perfect in a bag lunch for all ages. Get a heart-healthy nutrient and antioxidant boost from the almond butter, sunflower seeds, and cherries in this crunchy wrap.
Ingredients
• 2 8-inch whole grain tortillas or wraps
• 2 tablespoons almond butter
• 2/3 cup sprouts
• 2 tablespoons sunflower seeds
• 2 tablespoons raisins
• 2 tablespoons dried cherries
Directions Spread one tablespoon almond butter evenly over each tortilla. Sprinkle 1/3 cup sprouts evenly over the almond butter on each tortilla, then sprinkle with one tablespoon sunflower seeds, 1 tablespoon raisins, and 1 tablespoon dried cherries. Tightly roll up each tortilla, then slice in half. Serve immediately or wrap in plastic to prevent the wrap from drying out.
Yield: 2 wraps
Nutrition Breakdown: Calories 362, Carbohydrate 48g, Fiber 7g, Protein 9g, Fat

17g, Saturated fat 1g, Sodium 195g.
Variations: Substitute hemp butter, tahini, and peanut butter or walnut butter for the almond butter. Try substituting dried apricot slices, dried blueberries, dried cranberries, or dried apple slices for the cherries. And you could replace the sun-





flower seeds with chopped walnuts, pistachios, almonds, pecans, or hazelnuts. The possibilities are endless.
Recipe used with permission: The Plant-Powered Diet: the lifelong eating plan for achieving optimal health beginning today by Sharon Palmer, RD. For more information visit www.sharonpalmer.com



I sure am sick of all this hot weather. I’m ready for fall. Are you serious? It’s been boiling. What else could it be??
I don’t think it’s been all that bad. I think you should consider that maybe it isn’t the weather.


ACROSS
1. Communicate on social media
5. Mr. Newton, familiarly
8. Remember this state
13. Continuous dull pain
14. Having wings
16. Abalone
17. Inflammation suffix
18. West ___ Virus
19. Amounts owed
20. Noted resort island
22. Glass container
23. South African golfer
24. Sign made by Churchhill
25. He shared a cabin here
27. It gets misspelled often
30. Paddle
31. Greek god of war
32. Policeman
33. Regional abbrev.
36. Search for
37. Chopping tool
38. Breastbone
42. Flexible; stretchy
44. Container used for frying
45. Bedouin
47. Set of 52
48. Consumed
49. Biblical weed
50. Braod Street architect
52. Not pos.
53. Sick
54. Plant
55. Possesses
58. Fuss
60. Tool
63. Broaden
65. _____-biter
66. Slang for an alcoholic
67. Tissue swelling
68. Trigonometric function
by Dan Pearson
Have you considered that it could be manopause?

The Mystery Word for this issue: RIYBARL
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
M I N E R S U D O K U
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
69. Exchange for money
70. Cooking herb
71. Lair
72. Joint above 56-D
DOWN
1. Local college
2. Number system with 8 as its base (adj.)
3. They’re between 72-A and 56-D
4. Exam
5. Oncologist’s focus
6. Similar
7. Curiously, this sometimes comes before nurse and model
8. Downtown theater
9. Part of 33-A
10. Overlap, like scales or petals
11. Take-home
12. Trauma pt. destinations
15. Pension collector
21. Cavaliers’ school (abbrev.)
26. Retired AU president
28. Some so-called friends are said to be this
29. Tiny particle, as of dust
30. Paddle
31. Similar to
33. Senatorial channel
34. Declare
35. Rebels
39. Hills of Augusta
40. River and mountain range
41. Florida team
43. Cable abbreviation
46. It can come before “careful”
50. Augusta springtime visitor
51. Female sheep
54. Group of connected bones
55. “Georgia’s Alpine Village”
56. Joint below 72-A
57. Genre
59. Prefix meaning half
61. Female servant
62. Surgeons wear one at work
63. One w of www
64. Former Gem State abbrev.
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
solve the puzzle above. All the listed letters following #1 are the first letters of the various words; the letters following #2 are the second letters of each word, and so on. Try solving words with letter clues or numbers with minimal choices listed. A sample is shown. Solution on page 14.

THEBESTMEDICINE

ha... ha...

Anun approaches her priest and says, “Excuse me father, but I noticed a spot where the roof of your church is leaking.”
“My daughter,” says the kindly priest, “you have served here for many years. It is not my church. It is our church, our roof.”
“Yes, father,” she says.
Later that day she again approached the priest with another comment. “Excuse me again, father, but I noticed that your chur — I mean our church — has a broken window.”
“Thank you my child,” said the priest. “I will have our window repaired.”.
The next day the priest was preparing for a visit by the bishop, sprucing up some flowers near the front of the church, when he cut his hand.
The nun happened to be nearby, so he called to her and asked her to go into his quarters and fetch a small bottle of rubbing alcohol there.
She hurried off on her errand, and while she was gone the bishop arrived.
When she returned she called out before noticing the bishop, “Father, I got the alcohol from under our bed!”
Moe: How do you feel about juggling? Joe: Just thinking about it makes me want to throw up.
Moe: I watched a friend of mine do 100 pushups. You think you could do that?
Joe: I don’t like to brag, but I feel pretty sure I could watch someone do 200 pushups.
Moe: I was reading that Mississippi has more S’s than any other word.
Joe: I suppose that could be true. Do you know what word has the most B’s?
Moe: I do not. Tell me.
Joe: Hive.
Moe: People criticize gambling, but it sure has brought our family closer together.
Joe: True. But that’s because you lost your home and you’re living in that tiny little place now.
Moe: Do you know if you turn a canoe over you can wear it as a hat?
Joe: Uh, no I did not.
Moe: Sure. Upside down they’re capsized.
Moe: On average, what’s the earliest age babies talk?
Joe: I don’t know about average, but I can tell you the earliest‚ and it wasn’t good!
Moe: Do tell, do tell.
Joe: The Bible says that Job cursed the day he was born.
Staring at my phone all day has certainly had no Effect on ME!
By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME ADDRESS
Choose six months for $26 or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903-
Dear Advice Doctor,

The Advice Doctor
©

I have three teenagers, and I have to say, they’re great kids. They have never rebelled or been disrespectful to us as their parents. They get good grades and are obedient. They do chores promptly and without complaining. Sounds perfect, right? I keep thinking maybe they’re too perfect. What if they’re only acting like model kids to get more freedom so they can do things they know we wouldn’t approve? How can I determine what their true charcter is?
— No Real Proof, Just a Gut Feeling
Dear No Real Proof,
I applaud your courage in bringing up this subject. For some reason it’s an awkward or uncomfortable topic for many people to admit to having, even though tens of millions of Americans have gut feelings ranging from ulcers and ulcerative colitis to irritable bowel syndrome, chronic indigestion, diarrhea, heartburn (gastroesophageal reflux disease or GERD), hemorrhoids, diverticular disease, abdominal pain, chronic constipation and more.
Some of the conditions in this list afflict up to 75 percent of the population of certain age groups; chronic constipation alone is a problem for more than 60 million people in the U.S. according to the American Journal of Gastroenterology
There are a number of good reasons to listen to what your body is telling you by its various gastrointestinal symptoms. First, help is available. Why suffer through months or years of discomfort unnecessarily? Answer: as stated above, because people are often embarrassed to talk about these issues. There’s no reason for that. Doctors have seen practically everything before they even graduate from medical school. Specialists like gastroenterologists make digestive issues their everyday life, so it certainly isn’t embarrassing to them.
Secondly, sometimes we imagine the problem (or the cure) to be far worse than it actually is. And so, in a true twist of irony, we do what makes zero sense: nothing. But what if a doctor told you to simply slow down and chew more thoroughly? Or to avoid one certain food that’s causing all your problems? Either one or both are realistic possibilities, and are about as non-invasive as it gets.
So the next time someone tells you, “follow your gut,” take them up on the invitation and follow your gut right into your doctor’s office. Get some help. Get some relief.
Do you have a question for The Advice Doctor about life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.

THE MYSTERY SOLVED
The Celebrated MYSTERY WORD CONTEST
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.
Of
— Janet Lane
WORDS BY NUMBER
The

— Kin Hubbard (1868-1930)

PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC
Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC

DERMATOLOGY
Georgia Dermatology &



Parks Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com

Evans Chiropractic Health Center Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net

Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901 706-396-0600 www.augustadevelopmentalspecialists.com



Nursing|Companion 706-426-5967 www.zenahomecare.com

Bashir Chaudhary,
Jason H. Lee, DMD 116 Davis Road Augusta 30907 706-860-4048 Floss ‘em or lose ‘em!