Age Alone is Not Associated with Increased Mortality Following Ruptured AAA Repair Christian Leung 1, Amit Rao MD 2, Jeffrey Silpe MD 2, Yana Etkin MD 1,2 1Donald and Barbara Zucker School of Medicine at Hofstra/Northwell 2Division of Vascular & Endovascular Surgery at Northshore University Hospital-Long Island Jewish Medical Center
Background • • • •
• •
Ruptured abdominal aortic aneurysm (rAAA) is a common vascular emergency with high mortality. Risk factors for perioperative mortality, such as age, have been proposed but there is no consensus on their predictive value Various risk scores have been developed but have limited utility or have not been validated In 2018, the Harborview Medical Center (HMC) preoperative risk score was developed to help predict mortality based on 4 preoperative factors: age > 76 years, creatinine > 2mg/dL, systolic BP < 70mmHg, pH < 7.2 HMC score has been validated in 2 previous studies and may provide valuable prognostic information The goal of our study was to analyze what factors predict perioperative mortality following rAAA repair.
Methods • A retrospective review was performed for all patients who presented with rAAA to a tertiary academic medical center from 2014 to 2020. • Patients’ comorbidities and procedural factors were analyzed using univariate and multivariate logistic regression to determine their association with perioperative mortality.
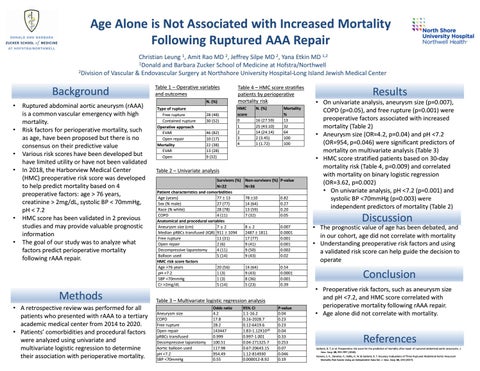
Table 1 – Operative variables and outcomes N. (%) Type of rupture Free rupture Contained rupture Operative approach EVAR Open repair Mortality EVAR Open
28 (48) 30 (52) 46 (82) 10 (17) 22 (38) 13 (28) 9 (32)
Table 4 – HMC score stratifies patients by perioperative mortality risk HMC score 0 1 2 3 4
N. (%) 16 (27.59) 25 (43.10) 14 (24.14) 2 (3.45) 1 (1.72)
Mortality % 13 32 64 100 100
Table 2 – Univariate analysis Survivors (%) N=22 Patient characteristics and comorbidities Age (years) 77 13 Sex (% male) 27 (77) Race (% white) 28 (78) COPD 4 (11) Anatomical and procedural variables Aneurysm size (cm) 7±2 Median pRBCs transfused (IQR) 911 1094 Free rupture 11 (31) Open repair 2 (6) Decompressive laparotomy 4 (11) Balloon used 5 (14) HMC risk score factors Age >76 years 20 (56) pH <7.2 1 (3) SBP <70mmHg 1 (3) Cr >2mg/dL 5 (14)
Non-survivors (%) P-value N=36 78 10 14 (64) 13 (59) 7 (32)
0.82 0.27 0.20 0.05
8±2 2487 1811 17 (77) 9 (41) 9 (50) 9 (43)
0.007 0.0001 0.001 0.001 0.002 0.02
14 (64) 9 (43) 8 (36) 5 (23)
0.54 0.0001 0.001 0.39
Table 3 – Multivariate logistic regression analysis Aneurysm size COPD Free rupture Open repair pRBCs transfused Decompressive laparotomy Aortic balloon used pH <7.2 SBP <70mmHg
Odds ratio 4.2 17.8 28.2 143447 0.999 100.51 117.98 954.49 0.55
95% CI 1.1-16.2 0.16-2028.7 0.12-6419.6 1.83-1.12X1010 0.997-1.001 0.04-271325.7 0.67-20643.15 1.12-814930 0.000012-8.92
P-value 0.04 0.23 0.23 0.04 0.33 0.253 0.07 0.046 0.19
Results
• On univariate analysis, aneurysm size (p=0.007), COPD (p=0.05), and free rupture (p=0.001) were preoperative factors associated with increased mortality (Table 2) • Aneurysm size (OR=4.2, p=0.04) and pH <7.2 (OR=954, p=0.046) were significant predictors of mortality on multivariate analysis (Table 3) • HMC score stratified patients based on 30-day mortality risk (Table 4, p=0.009) and correlated with mortality on binary logistic regression (OR=3.62, p=0.002) • On univariate analysis, pH <7.2 (p=0.001) and systolic BP <70mmHg (p=0.003) were independent predictors of mortality (Table 2)
Discussion
• The prognostic value of age has been debated, and in our cohort, age did not correlate with mortality • Understanding preoperative risk factors and using a validated risk score can help guide the decision to operate
Conclusion • Preoperative risk factors, such as aneurysm size and pH <7.2, and HMC score correlated with perioperative mortality following rAAA repair. • Age alone did not correlate with mortality.
References Garland, B. T. et al. Preoperative risk score for the prediction of mortality after repair of ruptured abdominal aortic aneurysms. J. Vasc. Surg. 68, 991–997 (2018). Hansen, S. K., Danaher, P., Hollis, H. W. & Garland, B. T. Accuracy Evaluations of Three Ruptured Abdominal Aortic Aneurysm Mortality Risk Scores Using an Independent Data Set. J. Vasc. Surg. 66, e53 (2017).