Antoine Pierre Brézin MD, PhD 23 Presbyopia-Correcting Cataract Surgery in the Post-LVC Patient
Ruth Lapid-Gortzak MD, PhD
Zaina
24 Building Databases, Building Networks
Mor M Dickman MD, PhD
35 Timing Keratoconus Treatment
Beatrice E Frueh MD RETINA
36 Revolutionising Retinal Imaging
Marion R Munk MD, PhD, FEBO
37 AI and the Macula
Ursula Schmidt-Erfurth MD, PhD
38 Optogenetic Therapy for Stargardt Disease
Victor H Gonzalez MD DIGITAL OPHTHALMOLOGIST
40 Robot-guided Cataract Surgery
Marvin Bende MSc
OCULAR UPDATE
42 Diagnostic Dilemmas in Neuro-ophthalmology
Misha Pless MD and Karl Golnik MD
Publisher
Carey Earle
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Nicola Lodge
Contributing Editors
Cheryl Guttman Krader
Howard Larkin
Dermot McGrath
Roibeárd O’hÉineacháin
Contributors
Soosan Jacob
Timothy Norris
Colour and Print
W&G Baird Printers
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Learn more about EuroTimes or connect with ESCRS at ESCRS.org
A Memorable Presidency
When Oliver Findl, president of the European Society of Cataract and Refractive Surgeons (ESCRS), steps down at the end of this year, the Society shall remember his tenure as a time of both challenges and achievements—and, most certainly, will look back on the Viennese ophthalmologist’s two years at the helm with gratitude.
Not only did the 2023 ESCRS Congress see record numbers of attendees, but its programme featured comprehensive insight into tomorrow’s ophthalmology, such as the iNovation Day. This is only the second year for the hugely successful initiative in bringing ophthalmic surgeons and industry together to highlight and debate the most recent innovations in ophthalmic surgery. And the Vienna delegates had a social blast that can hardly be topped: a Grand Ball held in the Hofburg, the palace where the Habsburgs ruled over a vast empire. This and much more was Oliver Findl’s doing.
Professor Findl, chief of the Department of Ophthalmology at Hanusch Hospital in Vienna, is one of Europe’s most experienced cataract surgeons with more than 18,000 surgeries under his belt (not to speak of his retinal and corneal interventions). He completed post-doctoral research at Harvard University and is a constant on The Ophthalmologist’s “Power List”.
He has left his mark on the ESCRS in several fields. Regarding ongoing education—one of the Society’s primary aims—he has contributed not only as co-chair of the Clinical Guidelines Development Group for cataract surgery but has also encouraged many other initiatives, such as setting up a common e-learning platform to improve access to educational material.
Oliver Findl supported the creation of a new Digital Health Award that recently made its first grant. He helped establish an online IOL calculator that now includes toric lenses. Under his guidance, the ESCRS purchased a stateof-the-art surgical simulator from Haag-Streit that has already supported skills development to scores of trainees in Romania, Poland, and now, Austria (for Ukrainian trainees). The uptake and feedback are beyond expectations, and that splendid machine’s next stop on its “Tour of Europe” is the combined ESCRS Winter Meeting/Annual Congress of the
EDITORIAL BOARD
Findl ESCRS President
Noel Alpins (Australia)
Bekir Aslan (Turkey)
Roberto Bellucci (Italy)
Hiroko Bissen-Miyajima (Japan)
John Chang (China)
Béatrice Cochener-Lamard (France)
German Society of Cataract and Refractive Surgery (DGII) in February 2024 in Frankfurt.
Under his leadership, the ESCRS has become a force for environmental and social conscience, as sustainability and fighting climate change have been a driving force for the Austrian ophthalmologist for many years. He was instrumental in making the ESCRS Congress carbon neutral and in promoting sustainability as a central theme internationally. Prof Findl played a vital role in establishing EyeSustain with ASCRS and AAO, where key issues such as reducing OR waste can be investigated. He has also established the Sustainability Index for Disposables in Cataract Surgery (SIDICS) project—a tool developed to assist users in evaluating the sustainability of customised cataract packs used in medical facilities and provides insights into the environmental impact of different product configurations.
Current events have kept him moving—rapidly and effectively responding according to circumstance. For example, Oliver Findl led the ESCRS in supporting Ukraine, encouraging industry partners to donate crucial surgical supplies. In addition to allocating a six-figure sum from its own reserves, ESCRS reached out to fellow societies to donate funds. He led the initiative to provide free congress registration for Ukrainian surgeons and emphasised the importance of relieving hardship in developing countries. Under his leadership, ESCRS funding for projects in developing countries has increased fivefold. In addition to major projects in Mozambique, Malawi, and Jerusalem, ESCRS has supported smaller cataract projects in South Sudan, Nepal, and Bangladesh.
Since stagnation means regression—as the saying goes— there will be several tasks for Prof Findl’s successor and the ESCRS council to pursue and complete. Among other things, the Society plans to provide patients (the “lay public”) with a website on cataract surgery. And the heritage website is under construction—things to accomplish after a presidential term that will surely be remembered for decades to come.
H Burkhard Dick MD, secretary of the ESCRS and chair of the department of ophthalmology at Bochum University, Germany.
Kohnen Chief Medical Editor
Oliver Findl (Austria)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Vikentia Katsanevaki (Greece)
Daniel Kook (Germany)
Boris Malyugin (Russia)
Güell Medical Editor
Marguerite McDonald (US)
Cyres Mehta (India)
Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands)
Leigh Spielberg (The Netherlands)
Sathish Srinivasan (UK)
Editor
Robert Stegmann (South Africa)
Ulf Stenevi (Sweden)
Marie-José Tassignon (Belgium)
Manfred Tetz (Germany)
Carlo Enrico Traverso (Italy)
Paul Rosen Medical
José
Thomas
Oliver
MEMBERS APPROVE BYLAWS CHANGES
At this year’s Annual Congress in Vienna, chang es were approved to the ESCRS bylaws during the annual General Meeting. These changes are designed to strengthen the four key pillars of ESCRS cor porate governance: accountability, transparency, responsi bility, and fairness.
These bylaws changes will help ensure a balance between (1) maintaining the institutional knowledge and expertise of senior members of the ESCRS and (2) opening committees to new members.
This will, in part, be achieved by establishing term limits for the Council of Management (a maximum of two terms of four years each), the Secretary and Treasurer (a maximum of two terms of two years each for each posi tion), and the European editor of the Journal of Cataract & Refractive Surgery (a maximum of two terms of four years each).
The ESCRS membership also decided the bylaws will be reviewed every two years so they can be amended regularly if considered necessary.
The ESCRS is now in a very good position, as we believe the approved changes will improve corporate governance and set the Society on a trajectory for growth over the years to come.
Yours sincerely,
H Burkhard Dick Secretary of the ESCRS
Since its founding in 2007, the European Registry of Quality Outcomes for Cataract and Refractive Surgery (EUREQUO) has grown to encompass three registries that contain data for more than 4 million surgeries.
FERNANDEZ, HAFEZI JOIN MANAGING COUNCIL
ESCRS members elected Joaquín Fernández (Spain) and Farhad Hafezi (Switzerland) and re-elected Bruce Allan (United Kingdom) and Nic Reus (the Netherlands) to the Council of Management, the Society’s governing body.
Each elected and re-elected member will serve a fouryear term. Fernandez and Hafezi will be eligible to run for a second four-year term in 2027; Allan and Reus will rotate off the Council when their current term expires. Fernandez and Hafezi will replace Jorge Alió (Spain) and Vikentia Katsanevaki (Greece), who are rotating off the Council.
In 2022, the Registries Steering Group worked to integrate additional data from national registries sharing common data models and centrally from individual sites committed to quality improvement enrolled in the registries.
DOWNLOAD YOUR FREE COPY TODAY:
Research Awards Drive Quest for Better Patient Care
BY STUART HALES, EXECUTIVE EDITOR
Funding for medical research comes from a variety of sources. Industry is the leading source of funding for applied biomedical research and development, while governments are key supporters of basic and translational research—the type that generates medical breakthroughs.
Non-profits and charities also play a funding role, especially large organisations such as the Wellcome Trust (UK), the Bill and Melinda Gates Foundation (US), the Howard Hughes Medical Institute (US), and the Knut and Alice Wallenberg Foundation (Sweden). The Wellcome Trust alone has an active grant portfolio of more than £7 billion spread across roughly 3,200 research awards.
In this vast pool of research funding, what difference can an organisation like ESCRS make? Quite a lot, judging from the variety of research awards the Society funds, the research topics, and the number of applicants.
“We expect that we can derive new solutions for better patient care,” says Burkhard Dick, chair of the ESCRS Research Committee, which oversees the Society’s awards for clinical research, pioneering studies, open access data sets, and systematic reviews.
“All the pieces are really coming together for ESCRS’s investment in clinical research to help benefit ophthalmology in a meaningful way,” agrees Kris Morrill, founder and president of Medevise Consulting and a consultant to ESCRS on research programmes.
As proof, Morrill cites the ongoing EPICAT study (Effectiveness of Periocular drug Injection in CATaract surgery), led by Nienke Visser of the Netherlands. Backed by approximately €750,000 in ESCRS funding, the study aims to investigate the effectiveness of anti-inflammatory drug delivery in or around the eye during cataract surgery to prevent postoperative inflammation.
“This study has the potential to change the standard of care in cataract surgery,” Morrill says.
‘Great things coming’
The EPICAT study is one of four ESCRS research projects in progress or recently completed. The other projects are as follows:
• Influence of posterior vitreous attachment on retinal detachment after lens surgery in myopic eyes (Oliver Findl, Austria)
• Monofocal extended range of vision (Mayank Nanavaty, UK)
Together, these studies have received approximately €650,000 in research funding from ESCRS.
More research studies are forthcoming. Earlier this year, ESCRS issued a “directed call” for the Clinical Research Awards (CRA), which supports
and encourages independent clinical research. For 2023, ESCRS requested applications on the topic of a comparative, controlled trial evaluating different types of presbyopia-correcting IOLs for post-keratorefractive surgery patients undergoing lens surgery.
“This topic was one of two identified during a series of think tank sessions,” Dick says. “Think tank sessions will now occur every other year to identify key research topics for Society support.”
The call for CRA applications closed in mid-October. Applications for two other ESCRS research programmes—the Pioneer Research Award, which funds young oph thalmologists pursuing new initiatives, and the Systematic Review Award, an initiative to support the preparation, collation, analy sis, synthesis, and reporting of high-quality medical research—are closed at the moment but will reopen in 2024.
“The Pioneer Research Award is working really well,” Morrill says. “They’re younger and hungrier. And the Systematic Review Award is an ideal forum to teach young ophthalmologists the value of conducting a well-constructed literature review.”
For more information about the ESCRS research awards, visit https://www.escrs.org/research/.
ESCRS WINS AWARD FOR WEBSITE EXCELLENCE
ESCRS has been honoured for the quality and usability of its website, beating out sites from seven other organisations to win the “Best Website or App” category at the Memcom 2023 Excellence Awards.
Other finalists for the award included the British Psychological Society, the Royal College of General Practitioners, and the Chartered Institute of Patent Attorneys.
“A good user experience is critical for ESCRS as we seek to grow our membership and cement our role as a leader in the ophthalmic community,” says Prof Dr Burkhard Dick, chair of the
ESCRS General Purposes Committee. “This award is proof we are delivering that experience.”
The ESCRS website has added several new features since its redesign last year, including a tool for evaluating the sustainability of cataract packs, a tool to compare results from four online toric IOL calculators, a calendar of events and webinars hosted by affiliated national societies, and a global reach map. More new content is expected soon, including clinical guidelines, a patient portal, and an enhanced learning management system.
A glimpse into the exciting events that unfolded at ESCRS 2023 in Vienna.
Saving Sight on the Frontlines
Ukrainian ophthalmologists hone in on common injuries they see, techniques to provide the best care, and the challenges that remain.
Ukrainian ophthalmologists continue to push their medical and surgical skills to the limit in dealing with the devastating impact of eye injuries incurred among both the civilian population and military personnel in the ongoing war with Russia.
The horrific extent of those injuries—and the various strategies employed by Ukrainian ophthalmologists to deal with them—were brought forcibly home to delegates during a special session on ocular trauma at the 2023 ESCRS Congress in Vienna.
Eye trauma is estimated to account for up to 13% of all injuries in modern warfare, and the war in Ukraine is no exception, said Dr Valerii Serdiuk, who recounted his experience of combat surgery over the past nine years.
“Evolution in warfare tactics means that anti-personnel mines and various explosive devices—both improvised and produced by industry—have become the main causes of eye combat trauma in all military conflicts,” he said. “Other causes include wounds from firearms and accidents.”
Thousands of military and civilian patients have been treated by the eye specialists at Dnipropetrovsk Hospital since the outbreak of conflict, said Dr Serdiuk, adding his teams typically encounter a high level of complex ocular polytrauma, often in association with other head, neck, face, or systemic injuries.
The advanced fragmentation weapons used in modern conflicts result in a high rate of ocular trauma, with binocular injuries in 34% and penetrating injuries in 42% of cases.
“The high percentage of eye injuries in the first months of the war was related to the shortage of protective eyewear and a lack of awareness on the part of military personnel about the threat to their visual health,” he said.
In this regard, he noted eight eviscerations/enucleations were performed from 2014 to 2021, but seven of those were carried out before September 2014, when protective eyewear use became widespread.
Dealing with ocular polytrauma requires a clear strategy on the part of the surgeon, Dr Serdiuk said. In penetrating and blunt eye injuries, there is usually combined damage to the anterior and posterior segments, including the cornea, iris, and retina, causing significant and diverse clinical and functional disorders in the injured eye.
Rapid intervention is also important to improve the prospects of saving sight in patients with severe ocular polytrauma, Dr Serdiuk added.
The complex nature of the ocular injuries facing surgeons in Ukraine was also described in detail by Professor Nadiia Ulianova, who reported on her experience treating combat victims at the Filatov Institute of Eye Diseases and Tissue Therapy in Odesa.
“Modern combat trauma is particularly severe and requires complex reconstructive treatment,” she said. “The optimal timing for pars plana vitrectomy (PPV) for open globe injury varies from one to four weeks from the moment of injury, and eight weeks postinjury for keratoplasty.”
DERMOT MCGRATH REPORTS
Prof Ulianova outlined the challenges of performing vitrectomy in traumatic injury cases.
“The most common indications for vitrectomy in cases of ocular trauma are vitreal haemorrhage, retinal detachment, intraocular foreign bodies, and macular holes,” she said. “All these indications are usually present in severe combat injuries.”
Although vitrectomy in trauma cases should ideally be performed as soon as possible, the reality is logistical difficulties in displacing wounded individuals from the frontlines and ensuring treatment of other life-threatening injuries often affect the timing of ocular surgery, she added.
Prof Ulianova listed some specific features of eye trauma due to modern combat, including extensive open globe injuries and multiple foreign bodies in the cornea. She highlighted strategies to deal with some of these scenarios, including using keratoprostheses, amniotic membrane, and soft contact lenses—either individually or in combination with PPV to try to rehabilitate the ocular structures and save vision.
Removing intraocular foreign bodies (IOFB) is common in combat-induced ocular trauma, requiring surgeons to call upon a wide range of techniques to achieve a successful outcome, noted Professor Ihor Novytskyy.
He recounted his experience at Lviv Military Hospital operating on 81 patients, 45 of whom had IOFBs.
“We encounter several problems in removing large IOFB,” he explained. “The bigger the size of the object, the bigger the tips of the forceps we must use. We must be careful to avoid retinal damage when manipulating the IOFB and trying to remove it safely and effectively from the eye without incurring further damage to the ocular structures.”
Small metallic IOFBs can be removed using intraocular magnets, but those larger than 3 mm and non-metallic fragments require specialised grasping forceps for removal, he said. To minimise retinal damage during grasping and lifting, perfluorocarbon fluids or viscoelastic in the vitreous cavity use is recommended.
Prof Novytskyy added IOFBs can be displaced from the vitreous cavity through a posterior capsulorhexis into the anterior chamber, followed by removal through a corneal incision.
“This technique usually works quite well, but the problem to be aware of is the possibility of the object retreating into the vitreous cavity,” he concluded.
Valerii Serdiuk MD, PhD, Professor of the Department of Ophthalmology and Neurology of the Dnipropetrovsk Medical Academy of the Ministry of Health of Ukraine. ophthalmologygroup.ukraine@gmail.com
Nadiia Ulianova MD, PhD, Head of the Department of Post-traumatic Eye Pathology, Filatov Institute of Eye Diseases and Tissue Therapy, Odesa, Ukraine.
Ihor Novytskyy MD, PhD, Professor of Ophthalmology, Lviv National Medical University, Ukraine. inovytskyy@gmail.com
One-stop-shop Registries in Ophthalmology
EUREQUO
European Registry of Quality Outcomes for Cataract and Refractive Surgery ECCTR
There is no doubt. The AI wave is here. We just have to learn how to surf.
Clearer View of a High-Tech Future Getting a
Addressing the challenges to adopting new technologies in cataract and refractive surgery.
“Clearly, there is a lot of work that needs to be done,” Dr Day told attendees, explaining that currently, femtosecond lasers perform only 5 of the 10 steps needed to complete cataract surgery and only do some of the 5 steps well.
“In brief, FLACS platforms are expensive devices for capsulotomy and astigmatic keratotomy,” he said.
Reviewing evidence from large randomised controlled trials showing no true advantages of FLACS versus phacoemulsification, he noted that while the FLACS systems are well-established platforms, there has generally been very little industry investment recently in its research and development.
Dr Day observed several research questions need to be answered to establish the role of FLACS versus phacoemulsification, mostly relating to the need for evidence on specific clinical outcomes—e.g., effects on dysphotopsia rates and presbyopia-correcting IOL outcomes. He also cited a need to investigate potential novel applications.
Waiting for the robots
Addressing robotics as the future of cataract surgery, Dr Jean-Pierre Hubschman said that although there is currently perfect visualisation and high manoeuvrability,
robotics technology can help address existing challenges on multiple fronts.
“We are still facing a shortage of surgeons and staff and increasing demand for surgery,” he said. “There are also current technological and human limitations and inconsistent outcomes impacted by different surgeon skill sets.”
Dr Hubschman briefly reviewed the two robotics platforms developed for ophthalmology and successfully tested in humans, both with retinal applications. He went on to describe a fully integrated, image-guided, AI-enabled microsurgery platform in development specifically for cataract surgery. This system has demonstrated a capability for performing every surgical step and promising outcomes in cadaver and porcine eye models.
Concluding, Dr Hubschman said robotics will improve every surgical step in cataract surgery, provide surgeons AI-driven insights for peak performance, significantly reduce complications, and increase throughput.
“Surgery is an art, and today, depending on the surgeon, the outcomes may be very different from one to another,” he observed. “With robotics technology, we can make cataract surgery a science and allow every patient and every surgeon to achieve the best care.”
An accommodating IOL in 2024?
Professor Jorge L Alió set expectations for the future of presbyopia-correcting IOL technology in his talk, “A working accommodative IOL: fact or fiction?”.
“Once accommodating IOLs are developed adequately, multifocal IOLs will be unable to compete, as happened with pseudophakic glasses and IOLs,” Prof Alió said.
He focused on the research surrounding the Lumina accommodating IOL his group developed, which will be commercially available in 2024.
Explaining the rationale for the sulcus location of this lens, Prof Alió said, “The capsular bag seems to be a wrong location for accommodating IOLs due to its unavoidable decadence and fibrosis once the crystalline lens is emptied. The forces generated at the zonular-anterior capsule system are those to be used for accommodating IOLs. Sulcus implantation is the only option.”
To demonstrate, Prof Alió presented a video of the IOL implantation, which is performed through a 2.75 to 3.00 mm incision and reviewed outcomes, including data on accommodative range and stability, visual acuity and refraction, contrast sensitivity, visual quality, patient satisfaction, and results after YAG laser capsulotomy.
Prof Alió said the Lumina accommodative IOL effectively restores the visual performance for far distance vision with functional performance for intermediate and near vision with good contrast sensitivity in presbyopic patients after cataract surgery. The accommodative range is variable, between 1.0 and 3.0 D, with accommodation and pseudo-accommodation justifying part of the near-vision outcomes. Its vision performance is a continuous range of distance from far to intermediate and near distances, with interindividual variability. Near-vision outcomes correlate well with high satisfaction levels of the implanted patients. It appears that an intact posterior capsule is not necessary for pseudophakic accommodation. Therefore, the Lumina can be implanted safely and successfully following a capsular break.
Flap versus lenticule
Turning to refractive surgery, former ESCRS President Professor Béatrice Cochener-Lamard offered her thoughts on the future of flap or lenticule-based refractive procedures.
She noted that femto-LASIK is the gold standard even though lenticular surgery was “born” to overcome the
limitations of the flap-based procedure. A portion of her talk reviewed the advantages, limitations, and outcomes of SMILE, which she referred to as the “pioneer” in lenticule-based procedures. This procedure has expanded over the years and has advanced with the development of a new-generation femtosecond laser.
Prof Cochener-Lamard also described three new upcoming platforms for lenticular surgery and suggested the new competitors may attract more surgeons to try lenticular refractive surgery. She anticipates more data on lenticular implantation surgical procedures for treating hyperopia, presbyopia, ectasia, and aphakia and correcting pathological corneal thinning.
“In 10 years, I guarantee surface ablations will not be obsolete because we will still have some specific indications for these procedures,” Prof Cochener-Lamard observed.
“[Lenticular surgery] does have a promising future, and it may be competitive for LASIK, but I cannot guess if it can replace it.”
AI
assistant
The future of AI for guiding surgeon decision-making was discussed by Dr David Smadja, who proposed that through its ability to process a large amount of data, AI will be especially helpful when choosing appropriate candidates for surgical procedures and the right procedure for each. He cautioned surgeons to be aware of its limitations because its performance depends on the training data set.
Dr Smadja also explained how AI could help in predicting and improving surgery outcomes, improve knowledge, save time, and assist with some aspects of manuscript preparation.
“There is no doubt. The AI wave is here,” Dr Smadja said. “We just have to learn how to surf.”
EuroTimes will provide detailed coverage of the specific issues and topics raised here in separate articles in this and future issues.
Alex Day PhD, FRCOphth is a consultant ophthalmic surgeon at Moorfields Eye Hospital, London, UK. alex.day@ucl.ac.uk
Jean-Pierre Hubschman MD is Professor in Ophthalmology and Mechanical and Aerospace Engineering, Los Angeles, California, US. jphubschman@horizonsurgicalsystems.com; Hubschman@jsei.ucla.edu
Jorge L Alió MD, PhD is Medical Director at Vissum Innovation and Professor and Chairman of Ophthalmology at Universidad Miguel Hernández, Alicante, Spain. jlalio@vissum.com; jlalio@vissum.com
Béatrice Cochener-Lamard MD, PhD is the Head of the Ophthalmology Department at Brest University, France. She is a former president of the ESCRS. beatrice.cochener-lamard@chu-brest.fr
David Smadja MD, PhD is the Director of the Refractive Surgery Unit at Hadassah Medical Center, Tel Aviv, Israel. smadj.david@gmail.com
Cataract Surgery Outcomes in Uveitis Patients
Steroid management key to success.
PRISCILLA LYNCH REPORTS
Cataract surgery in uveitis patients improves vision successfully in the majority of cases, despite the challenges posed by operating on these patients, according to a five-year Irish study.
“The key message really is that while cataract surgery in uveitis patients requires more intensive preoperative, perioperative, and postoperative management than non-uveitic patients, it is safe and effective in this patient cohort,” Dr Sarah Powell told EuroTimes.
Dr Powell and her colleagues carried out an analysis of cataract surgery outcomes in uveitis patients at a single centre— the Royal Victoria Eye and Ear Hospital (RVEEH), Dublin, Ireland—over five years.
They performed a retrospective review of electronic patient medical records of patients diagnosed with uveitis who underwent cataract surgery between January 2018 and January 2023. Patient data was analysed preoperatively, intraoperatively, and up to three months postoperatively. A total of 52 eyes from 41 patients were included in this study (54 eyes in total).
The most common type of uveitis in the study population was anterior uveitis, which accounted for 50% of the patients.
Steroid management
One-fifth of the uveitis patients were taking systemic immunosuppressive therapy, with 70% prescribed a course of oral steroids before surgery, Dr Powell reported.
A total of 39% of patients received an intravitreal Ozurdex® (Allergan) implant preoperatively and 15% a combination of Ozurdex and Iluvien® (Alimera Sciences) implants before their cataract surgery.
Intravitreal methylprednisolone (IVMP) was given to 45% of the patients perioperatively, 50% received subconjunctival dexamethasone intraoperatively, and 19% received both IVMP and subconjunctival dexamethasone.
Intraoperatively, the team noted posterior synechiae in 25% of the patients, 26% required iris hooks, and 10% of cases required trypan blue use. No intraoperative complications occurred.
The most common intraocular lens implanted was the Zeiss CT Asphina lens (58%), followed by the Alcon Clareon® IOL (31%).
Postoperatively, 73% of the patients were prescribed a tapering course of oral steroids and all patients an intensive topical steroid routine—21% starting with once-hourly prednisolone forte drops and 79% with twice-hourly prednisolone forte drops.
Results
Three months following cataract surgery, 94% of patients demonstrated an objective improvement their best-corrected visual acuity, and 67% had visual acuities of 6/12 or better, she said.
The most common postoperative complication reported was cystoid macular oedema, occurring in 17% of patients.
So, while cataract surgery in uveitis patients may pose a clinical challenge to ophthalmologists, in this study, visual acuity improved in 94% of the uveitis patients following surgery, highlighting its success, Dr Powell noted.
“The most important thing is to get the preoperative, perioperative, and postoperative steroid management right and closely follow these patients to look for any postoperative complications,” she said. “Because while uveitis patients don’t tend to experience more intraoperative complications than non-uveitis patients, they do have higher rates of postoperative inflammation and complications such as cystoid macular oedema, uveitis reactivation, and high intraocular pressures.”
Dr Powell presented her research at the Irish College of Ophthalmologists 2023 annual conference in Killarney, Ireland.
Sarah
Powell MB BCh, BAO BA is Ophthalmology Senior House Officer at the Royal Victoria Eye and Ear Hospital, Dublin, Ireland. powellsk@tcd.ie
Premium IOLs After Refractive Surgery
Patient screening, education, and expectation management are key.
HOWARD LARKIN REPORTS
With proper precautions, implanting premium intraocular lenses (IOL) in patients after they have had corneal refractive surgery is safe, said Dr Zaina Al-Mohtaseb.
She outlined the steps contributing to this success in a session at the 2023 ASCRS annual meeting in San Diego, US.
Expect high expectations – Patients had LASIK or other refractive surgery because they didn’t want to wear glasses, and they will seek spectacle independence after cataract or lens replacement surgery, Dr Al-Mohtaseb said. To avoid misunderstandings, manage these expectations upfront.
She advised educating patients on the trade-offs with presbyopia-correcting technologies, including multifocal lenses, extended depth of focus (EDOF) lenses, and monovision. Let them know what to expect—glare, halos, night vision problems, and limited near vision—focusing on outcomes in post-refractive surgery patients. Educating patients multiple times using multiple formats helps.
Rule out ocular pathology – Dr Al-Mohtaseb does topography and optical coherence tomography (OCT) macula on all post-refractive surgery cataract patients.
“You definitely want to pick up if there is [epithelial basement membrane dystrophy], Fuchs’ dystrophy, corneal oedema, ocular surface disease, epiretinal membrane, or retinal irregularities because you want that perfect patient. The only thing that has to be different is they have had previous refractive surgery.”
Select appropriate patients – Other factors to consider in selecting patients are the condition of the previous refractive surgery and personality. Make sure any ablation is well-centred, and be wary of perfectionists or patients with unrealistic expectations.
Ensure accurate biometry, keratometry, and IOL calculations – Standard data for calculating IOL power are derived from virgin eyes, making it much more difficult to pick the right lens power for post-corneal refractive surgery patients.
“If you put a premium lens in a patient who has had myopic LASIK and you miss the target, they are not going to be happy, even if it is not a premium lens,” Dr Al-Mohtaseb said.
Pre- and post-refractive surgery topography helps guide IOL power calculations. She finds the Barrett True-K TK formula helpful for patients with previous myopic or hyperopic LASIK. The ASCRS post-refractive IOL power calculator, developed by Dr Warren Hill, Dr Li Wang, and Dr Douglas Koch, is another powerful tool.
Allow for enhancement – When implanting a non-adjustable lens in a post-refractive patient, Dr Al-Mohtaseb suggest-
ed ensuring enough tissue remains if ablative enhancement becomes necessary.
The Light-Adjustable Lens™ (LAL, RxSight) is another option. “For me, the LAL has really changed my practice in terms of post-refractive patients.”
Toric lenses may be appropriate for post-refractive surgical patients with residual astigmatism, focusing on regular astigmatism across a 3.0 mm refractive zone, Dr Al-Mohtaseb said. And despite more dysphotopsias and less contrast sensitivity, patient satisfaction may also be higher for multifocal and EDOF lenses than monofocal lenses in post-refractive surgery patients.
“Uncorrected near vision matters to these patients,” Dr Al-Mohtaseb said.
“If you pick the right patient and everything else is perfect, it really ends up being a discussion between you and the patient about what they can tolerate.”
Zaina Al-Mohtaseb MD is a cataract, refractive, and cornea surgeon and director of research at Whitsett Vision Group, and clinical associate professor at Baylor College of Medicine, both in Houston, Texas, US. zaina1225@gmail.com
Sizing up for Successful Surgery
Challenges for sizing short eyes include IOL calculation and selection.
Cataract surgery is more challenging in short eyes, with increased complication rates and poorer postoperative refractive predictability. Nevertheless, careful preoperative planning, rigorous surgery, appropriate intraocular lens (IOL) selection, and meticulous postoperative follow-up will increase the likelihood of a successful outcome for such cases.
There is no universal definition of “short eyes,” an umbrella term that includes simple microphthalmos, complex microphthalmos, anophthalmos, and nanophthalmos, points out Professor Dr Isabelle Saelens.
“There is a broad clinical spectrum of the small eye, so it is important to be aware of the biological parameters and well prepared when planning surgery,” she said.
In microphthalmos (MO), the axial length is at least two standard deviations smaller than the mean axial length of a control group (typically less than 21.0 mm), with different phenotypes and a 2–14 individual prevalence in every 100,000. The clinical spectrum for MO can be divided into simple (nanophthalmos) or complex, she explained.
You need to anticipate these issues, plan ahead, inform the patient, and manage their expectations.
“Nanophthalmos is a small, organised eye with essentially normal structure: an axial length less than 20.5 mm and scleral thickness more than 1.7 mm,” Prof Dr Saelens noted. “In the scientific literature, however, there is no consensus on how short the eye should be to be called nanophthalmic. This makes a difference in describing the complication rate after cataract surgery, for instance.”
Biological parameters in nanophthalmos include increased scleral thickness (the main cause of choroidal effusion syndrome), a steep cornea above 46.0 D, and a small corneal diameter less than 11.0 mm.
“All of these patients have high hyperopia, so amblyopia is also common. The lens/eye volume ratio is very high, so they are prone to developing posterior or anterior synechiae,” she said. “They also tend to develop early angle closure glaucoma—which can be treated with laser iridotomy and peripheral iridoplasty in the early stage and vitrectomy and lensectomy at a later stage.”
Cataract surgery in nanophthalmos carries a higher risk of complications such as expulsive haemorrhage, persistent shallow anterior chamber, and aqueous misdirection syndrome, among others.
“Even if the surgery is uneventful, refractive surprises are common because of the short axial length. I always prefer to give a little bit of Mannitol intravenously just to dehydrate the vitreous and create a little bit more space that can help during the surgery,” she advised.
Refractive surprise
Short eyes requiring a higher IOL power are at higher risk of a refractive surprise, so it is important to plan accordingly before commencing surgery, points out Dr Nino Hirnschall.
Although 2019 data from the EUREQUO database of 171,930 cataract extractions showed an average spherical equivalent error of -0.04 D with 74% of patients within 0.5 D of target refraction, such refractive consistency does not typically extend to short eyes.
Dr Hirnschall cited a 2011 study that showed of a subset of patients with an axial length of 20.0 mm to 22.0 mm, less than half were within 0.5 D of target refraction.1
“That means, for these patients, we really do not perform refractive surgery after cataract surgery,” he said. “And especially for short eyes—if these patients are very demanding and want a multifocal or a toric IOL, it is very tricky because we don’t even completely correct the spherical equivalent for them.”
He added studies have shown preoperative estimation of postoperative IOL position, postoperative refraction determination, and preoperative axial length (AL) measurement are the largest contributors of IOL power calculation errors, with a mean absolute error (MAE) of 0.6 D for an eye of average dimensions.
“This a problem for every eye, no matter if it is emmetropic, hyperopic, or myopic,” Dr Hirnschall said. “The problem is that 1.0 mm of error in the prediction of the lens position results in different refractive errors. For an emmetropic eye, a difference or error of 1.0 mm results in a refractive error of 2.5 D. In
a short eye, this may be even 4.0 D or 6.0 D depending on the axial length. It is why even a slight error in prediction results in a significantly higher refractive error in short eyes.”
In terms of the best IOL power calculation formulas to use, Dr Hirnschall said that while popular ones such as Hoffer Q, SRK II, Holladay I and II, and SRK/T are acceptable for normal eyes, it is best to avoid them in short eyes.
“Studies have shown modern formulas such as Castrop-Rauxel, Kane, Okulix (raytracing), and EVO 2.0. perform better in short eyes,” he said.2
IOL selection
Although picking the right IOL in short eyes is challenging, ophthalmologists can employ some strategies to increase the chances of a successful outcome, said Dr Gerd Auffarth.
“Prediction errors increase with decreasing axial length, and there is limited availability of high-power IOLs over the range of 30.0 D,” he said. “Another aspect to bear in mind is the increase in spherical aberration in higher power lenses, but there are not so many aspheric lens designs available.”
One possible approach is to combine two IOLs if the anterior chamber depth is in the normal range of about 2.0 mm to 2.2 mm and there is adequate space for two lenses, Dr Auffarth said.
“The idea is to implant a high-power lens in the anterior chamber and then add a monofocal IOL or a Sulcoflex aspheric add-on lens (Rayner) in the sulcus, which goes up to 10.0 D,”
Precizon.
he explained. “If the surgeon doubts the IOL calculation, the basic lens can be implanted and then wait two months to correct the final refraction with the supplementary IOL.”
In addition to refractive surprise, Dr Auffarth said the surgery also carries a higher risk of complications, including uveal effusion, postoperative oedema, posterior capsule rupture, and elevated IOP after surgery.
“You need to anticipate these issues, plan ahead, inform the patient, and manage their expectations,” he concluded.
This article is based on presentations at the 2023 ESCRS Winter Meeting in Vilamoura, Portugal.
For citation notes, see page 48.
Isabelle Saelens MD, PhD is an ophthalmologist at the University Hospitals of Leuven, Belgium. isabelle.saelens@uzleuven.be
Nino Hirnschall MD, PhD is a clinician and researcher at the Kepler University Clinic, Linz, Austria. nino.hirnschall@googlemail.com
Gerd Auffarth MD, PhD, FEBO is Chairman of the Department of Ophthalmology at the Heidelberg University Eye Hospital, Germany. Gerd.Auffarth@med.uni-heidelberg.de
Meet the Precizon Family: best-in-class IOLs for any cataract challenge. Monofocal, enhanced intermediate vision and full range of vision lenses with patented CTF technology. Regular and Toric. With a natural fit and ingenious optics that deliver extraordinary results. For successful surgery and perfect natural vision. ophtec.com/precizon-family
Precizon Family
IOL Match is a Surgeon’s Helping Hand
A free app for iOS and Android to enhance the patient care journey.
TIMOTHY NORRIS REPORTS
Afree-to-use, simple, and constantly updated application for iOS and Android could soon be available as a helping hand in selecting the best IOL based on a patient’s needs.
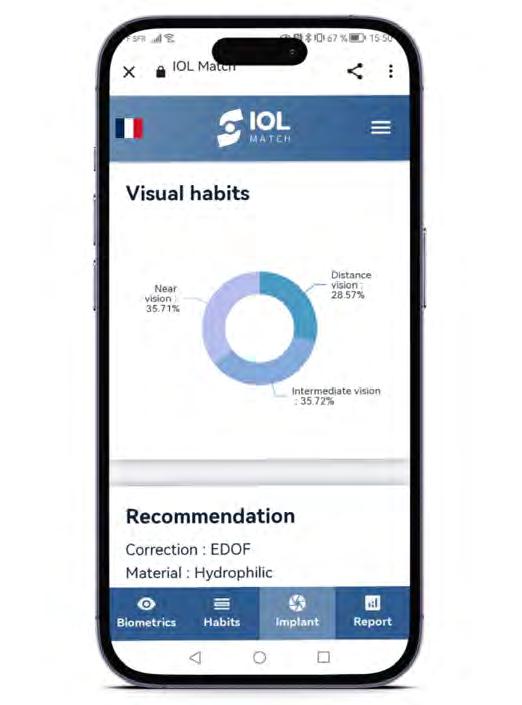
Created by Dr Gilles Lesieur and Mr Paul Dupeyre, IOL Match is a straightforward application that selects and compares the best options amongst several types of intraocular lenses based on patient parameters.
“It started with a defocus curve on an Excel sheet,” Dr Lesieur said. “We wanted to develop something to give our patients the best choice for the best results, so at the beginning of 2022, we decided to take a step forward from the spreadsheet phase and create an application out of it.”
“There is a jungle of different optics on the market, and this could make it difficult to choose the best lens for a patient,” Mr Dupeyre explained. “Our goal is straightforward: we want to identify the best-fit IOL for each patient’s ocular parameters and visual behaviours.”
According to the duo, automating the decision-making procedure through algorithms makes it possible to enhance the patient care journey.
“One of the main features of IOL Match is a decision-making protocol functioning as a comprehensive checklist, with a very precise lifestyle questionnaire and some crucial parameters that are generally overlooked,” Mr Dupeyre explained. “The application will then provide some intelligent recommendations of the most suitable implants based on the data collected, comparing different defocus curves for different IOLs,” Dr Lesieur added.
Finished with beta development, IOL Match will undergo beta testing to gain enough feedback for an optimised definitive version.
“This application will benefit from collaborative development, with surgeons from France and around the world helping to improve the application,” Dr Lesieur said. “We are also developing a protocol for collecting user experience data.”
The official release does not mark the end of the updates. Mr Dupeyre explained each surgeon will have a dedicated user account, allowing them to personalise specific parameters based on their practices. “The data will then be anonymised and implemented, while the application will constantly improve to keep up with the most recent advancements.”
Set to release in Q1 2024, IOL Match will be completely free on Android and iOS platforms. Once released, Dr Lesieur observed it will only refine its abilities—as more data comes in, the more data will improve the program. This data “is crucial to keep the application updated.”
“We want to improve the quality of life of patients, so we want this app to be as widespread as possible,” Mr Dupeyre added.
“It is the twenty-first century: if you want to have an impact and contribute to the evolution of ophthalmology, you will need to go collaborative. Freely. This is my way of thinking and why I decided to provide the app for free,” Dr Lesieur concluded.
Dr Lesieur and Mr Dupeyre presented this information at the 2023 ESCRS Congress in Vienna.
Gilles Lesieur MD is Founder, Owner, Chairman, and Medical Director of the Centre Ophtalmologique IRIDIS. g.lesieur@centre-iridis.fr
Paul Dupeyre MSc is an optometrist at the Centre Ophtalmologique IRIDIS. p.dupeyre@iridis-robotics.fr
Handheld FS Laser Closer to Market
Preliminary study results find handheld FS laser for capsulotomy safe, effective, and easy to use.
HOWARD LARKIN REPORTS
Precise and reproducible anterior capsulotomies are a hallmark of femtosecond (FS) laser-assisted cataract surgery (FLACS). Yet more than a decade after its introduction, many surgeons do not take advantage of the perfectly centred and circular capsulotomies FLACS offers, often due to cost and workflow issues.
Now, a handheld FS laser designed to be more affordable, efficient, and comfortable for patients is nearing the market. A preliminary study for CE marking found it easy to use, highly effective, and safe, reported Dr Francois J Lignereux.
Frugal system
The Rx laser system (Helix Surgical) is a small-footprint, portable, battery-operated FS laser with a handheld interface for pre-cutting capsulotomies. Because it uses a curved eyepiece without suction for docking and before corneal incisions, it can be used preoperatively or in the sterile OR without disrupting surgical flow. “No time is wasted,” Dr Lignereux said.
The study involved an experienced cataract surgeon who used the device on one eye from each of the 78 cataract patients who received manual capsulorhexes in the fellow eye. The surgeon filled out a usability survey to report their feelings at different steps for each case, ranking them as very easy, rather easy, rather difficult, or difficult.
Rx provides a solution to the contradictory conjunction between the desire for perfection
and economic constraints.
Preparation and handling were considered very easy in more than 98% of cases, reflecting the design intent to lower the operational burden of using FS capsulotomies. Visualisation through the system was considered easy in 70% of cases and very easy in 30%.
Centration was more challenging, ranking very difficult in 3% of cases, rather difficult in 35%, rather easy in 46%, and very easy in 16%, though the ratings improved with increased experience, Dr Lignereux reported. “This is due to the learning curve. Once this is over it becomes much easier.” Once centred by looking through a reticule on the top of the laser handpiece, holding the device steadily in place during firing was considered very easy in 92% of cases.
78
The study involved an experienced cataract surgeon who used the device on one eye from each of the 78 cataract patients who received manual capsulorhexes in the fellow eye.
70%
Visualisation through the system was considered easy in 70% of cases and very easy in 30%.
Patients were also surveyed on their experience. They expressed no significant pain during the laser or discomfort after, with 93% reporting none for either and 7% a little pain or discomfort. Patients were also satisfied, with 89% very satisfied and 11% rather satisfied—and 90% said they would do it again.
Safe and effective
Efficacy was excellent, with continuous precuts achieved in 96% and an R2 value of 98% for circularity. Centration relative to pupil within 360 microns was achieved in all cases, suggesting that while more difficult at first, it was readily achieved. These results exceeded the study objective of achieving 95% perfect capsulorhexis, Dr Lignereux said. Refractive outcomes were excellent as well, with 96% achieving a spherical equivalent refractive outcome within 0.50 D of target.
Safety was also excellent, although problems included two cuts requiring two strokes, two uncompleted cuts, one anterior tear, and one posterior rupture unrelated to laser use. There were no reported cases of myosis, inflammation, or excess endothelial cell loss.
“This laser is based on frugality,” Dr Lignereux said. “Rx provides a solution to the contradictory conjunction between the desire for perfection and economic constraints.”
Dr Lignereux presented these findings at the 2023 ESCRS Congress in Vienna.
Francois J Lignereux MD is an ophthalmologist at the Institut Ophtalmologique Sourdille Atlantique, Nantes, France. sec.lignereux@sourdille-atlantique.fr
Pressure Sensor in Phaco Handpiece Tested
Ultrasound energy and surgery time cut, potentially improving safety.
HOWARD LARKIN REPORTS
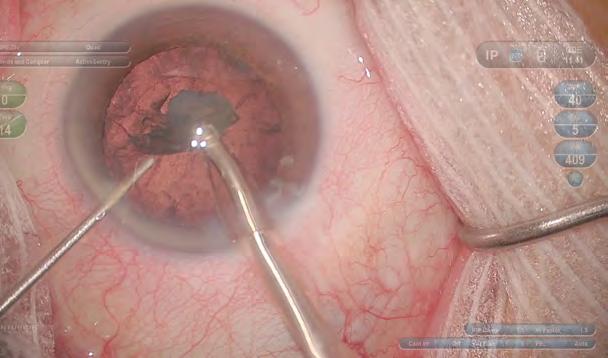
Aphacoemulsification handpiece with a built-in pressure sensor significantly reduced the cumulative dissipated energy (CDE) and surgical time in cataract surgery compared to an identical system with the pressure sensor in the phaco machine body, said Professor Antoine Pierre Brézin. Reducing the CDE could be important for protecting the corneal endothelium and other delicate ocular tissues.
Placing the pressure sensor in the phaco handpiece rather than farther away in the machine body makes the system more responsive to tip occlusions, reducing pressure surges, Prof Brézin said. As a result, surgeons can use a higher vacuum more of the time, reducing the need for ultrasound energy to fragment the lens.
Real-life study
The Study of Active Sentry in Cataract Surgery (SASCA) involved 1,432 cases by six surgeons in five centres in France, with 800 using the built-in Active Sentry (AS, Alcon) handpiece and 632 using a non-AS machine. All surgeons used the Centurion (Alcon) phaco machine in all cases, and patient characteristics were similar for the two treatment groups. Because SASCA was a real-life study, there were no fixed surgical parameters, leaving surgeons free to adjust them to their preferences and patient needs, Prof Brézin said. “The only comparative factor was Active Sentry or non-Active sentry.”
Mean CDE for the AS group was lower, at 8.0—ranging from 0.0 to 70.4—than in the non-AS group, at 9.3, ranging from 0.0 to 77.6 (p=0.0001). CDE was consistently lower for the AS group in each cataract grade. Both torsional and
longitudinal ultrasound energy and time were lower in the AS group, with a torsional median of 661.4 versus 725.0 (p=0.0074), and longitudinal median of 49.3 versus 74.4 (p=0.0001). Ultrasound times were significantly reduced with AS. No adverse events were recorded in either group.
At 9.8 minutes, surgical duration was also shorter in the AS group than in the non-AS group, at 11.0 minutes (p=0.002), Prof Brézin reported. The more immediate fluidic response with the AS to prevent pressure surges might be the cause. “This means the surgeon was sufficiently confident to press the pedal and use high vacuum rather than high ultrasound to complete the phaco cases.”
More detailed data analysis showed longitudinal energy cut back 34% and torsional energy 9%, which Prof Brézin said provides further evidence of surgeon confidence in the ability of the handpiece-mounted sensor to better mitigate pressure surges.
“Overall, you deliver less energy to the eye, we use less ultrasound, especially less longitudinal ultrasound,” which is known to be more harmful to the corneal endothelium than torsional energy, he explained, adding shorter surgery increases patient comfort.
Although neither group presented any complications, on a larger scale, Prof Brézin anticipates the significant energy reduction linked to using the AS system will increase the overall safety of cataract surgery. The benefits of the AS-based, low-energy strategy for phacoemulsification will be further investigated.
This work was supported by an investigator-initiated study grant funded by Alcon. Prof Brézin told EuroTimes an article reporting the results of the SASCA trial has been submitted to a peer-reviewed journal.
Prof Brézin presented at the 2023 ESCRS Congress in Vienna.
Antoine Pierre Brézin MD, PhD heads the Cochin Eye Care Centre and is professor of ophthalmology at the University Paris-Descartes, both in Paris, France. antoine.brezin@aphp.fr
Presbyopia-Correcting Cataract Surgery in the Post-LVC Patient
Complex situation mandates careful consideration for IOL decision-making.
CHERYL GUTTMAN KRADER REPORTS
Evidence on cataract surgery outcomes in eyes that have undergone laser vision correction (LVC) surgery clearly shows poorer refractive predictability compared to cohorts without the same history. Furthermore, studies support selecting a negative spherical aberration (SA) IOL in eyes that had LVC for myopia and a neutral SA lens for previously hyperopic eyes. However, there are no data from randomised trials to guide decisions for choosing presbyopia-correcting IOLs in post-LVC patients, said Dr Ruth Lapid-Gortzak.
“After considering the corneal topography plus a number of other issues, we might implant one of these premium IOLs and achieve good results,” she said. “But no matter how hard the patient tries to persuade you, saying no to someone who is not a good candidate is also sound advice.”
One strategy Dr Lapid-Gortzak suggested for approaching cataract surgery with a presbyopia-correcting IOL in a postLVC patient is restoring the corneal asphericity first before performing the cataract surgery. Advocated by Dr Paolo Vinciguerra, this solution might provide more control over the outcome, but it subjects patients to an extra procedure that may be unnecessary and carries risks.
“The alternative, which I tend to do, is to deal with these patients within the limitations of what our daily practices allow,” Dr Lapid-Gortzak observed. “Although this is not academic, it is practical, has wider applicability, and only involves a second procedure (a touch-up) if needed.”
Lens
decisions
The vast array of available presbyopia-correcting IOLs creates a challenge in selecting a specific lens. Factors to consider aside from asphericity include the type of material (hydrophobic or hydrophilic) and the optical design (diffractive or refractive). Citing a bench study analysing retinal image quality that showed diffractive multifocal IOLs perform better than refractive and asymmetrical IOLs, Dr Lapid-Gortzak said the finding was consistent with her experience.1
She emphasised extended depth of focus (EDOF) lenses as a heterogeneous group that includes diffractive, refractive, small aperture, and wavefront-adjusted optical designs. Diffractive EDOF IOLs, she added, are primarily bifocal diffractive IOLs, which have the same visual side effects as other diffractive trifocal or pentafocal lenses.
Patient considerations
Patients with a cataract who have already lost vision may be easier to please than persons wanting refractive lens exchange, she said. Also, with the aim of avoiding patient dissatisfaction, she cautioned about choosing presbyopia-correcting IOLs in men aged 40 to 50 years whose distance uncorrected visual acuity is greater than 1.0 and anyone in the midst of a major, difficult life event.
Dr Lapid-Gortzak said she is also careful about implanting a multifocal IOL in patients who underwent LVC for myopia greater than 5.0 D or greater than 3.0 D hyperopia. She is more willing to consider a true EDOF IOL (not a pseudo-diffractive or refractive type) for patients who are not ideal candidates for a multifocal lens.
In all cases, the informed consent discussion is critical.
“Whenever performing cataract surgery after LVC, warn about the likelihood of needing a touch-up and discuss its feasibility along with the possibility of dissatisfaction after the procedure,” she said.
“If you feel the patient does not understand, don’t opt for any complex solution to a complex problem.”
Dr Lapid-Gortzak spoke at the 2023 ESCRS Congress Cornea Day in Vienna.
For citation notes, see page 48.
Ruth Lapid-Gortzak MD, PhD is a Medical Specialist in Ophthalmology, Amsterdam University Medical Centers, Amsterdam, Netherlands. r.lapid@amsterdamumc.nl
Building Databases, Building Networks
EUREQUO and ECCTR registries yield a rich harvest of valuable data.
DERMOT MCGRATH REPORTS
National and international registries such as the European Registry of Quality Outcomes for Cataract and Refractive Surgery (EUREQUO) and the European Cornea and Cell Transplantation Registry (ECCTR) are extremely valuable resources in determining the real-world success rates of different surgical practices and enabling benchmarking to drive quality improvement and reduce healthcare costs, among many other benefits, noted Professor Mor M Dickman.
Starting with EUREQUO, Prof Dickman said this registry now holds more than 4.1 million cataract cases and over 227,000 refractive surgeries since its launch in 2008.
“This makes it one of the largest international IT platforms in ophthalmology, connecting surgeons all over the world and building a network to facilitate the exchange of expertise,” he said.
Among the key trends identified in 2022, Prof Dickman noted a total of 271,347 surgeries, with 57% of the patients being women and 43% men. The majority of intraocular lenses (IOLs), 92%, were hydrophobic acrylic. Additionally, 4% of IOLs used were toric, multifocal, or extended depth of focus.
“When we attend a congress like the ESCRS, we see a lot of focus on toric and presbyopic lenses; yet in the real world, we see that around 96% of our patients do not receive these IOLs, which underlines why registry data is so important,” he said.
Approximately a quarter of patients (24%) had ocular comorbidities, a figure which has been increasing in recent years. Femtosecond laser-assisted cataract surgery was employed in only 0.13% of cases. Notably, 2% of patients exhibited a vision of 0.1 or worse, while a significant portion (48%) had a baseline vision of 0.5 or better.
The mean best-corrected distance visual acuity (BCDVA) was 0.46 before surgery and 0.95 after. A final BCVA of 1.0 or better was achieved in 68% of cases, and 93% achieved a final BCVA of 0.5 or better. Improvement by two lines or more was observed in 90% of cases, while 53% improved by five lines or more. In 2022, the most frequently registered perioperative complications were posterior capsule rupture (PCR) in 0.45%, dropped nucleus in 0.01%, iris damage in 0.06%, and other complications in 0.94%.
Some 220,000 accumulated refractive surgery cases have now been recorded in the database, Prof Dickman noted. The average age of refractive patients was 47 years, with a standard deviation of 14 years. The mean preoperative vision measured was 0.03 logMAR. Among the patients, 58% were myopic, 40% were hyperopic, and 1% were emmetropic. In 71% of eyes, the final uncorrected distance visual acuity was 1.0 (6/6) or better. In 81% of cases, the final refraction was between -0.5 D and +0.5 D.
Corneal transplant registry
Turning to the corneal registry, Prof Dickman said the ECCTR now has data on more than 20,000 transplants from 15 European countries since its 2016 establishment, including information on the recipient, donor and eye bank processing, transplant procedure and two-year follow-up data such as graft survival and failure, and patient-reported outcome measures (PROMs).
Some key findings from its latest report include a mean recipient age of 70 for a corneal graft—with Fuchs’ endothelial dystrophy the primary reason for corneal transplantation, followed by graft failure, pseudophakic bullous keratopathy, and keratoconus.
“The registry data gives us a valuable reality check—since if our transplants are so successful, how do we explain that the second most common indication for transplants in Europe is graft failure?” he asked.
Although historically, Descemet’s stripping automated endothelial keratoplasty (DSAEK) was the dominant transplant procedure, followed by penetrating keratoplasty and Descemet membrane endothelial keratoplasty (DMEK), the landscape has changed in recent years with DMEK now in the lead.
“The adoption of deep anterior lamellar keratoplasty (DALK) remains limited, primarily due to increased cross-linking for keratoconus and the lack of specialized expertise in many centres,” he said.
While the registry notes an overall two-year transplant survival of 89%, Prof Dickman said survival is dominated by recipient diagnosis.
“Grafts performed for Fuchs’ dystrophy have better survival rates than grafts performed for bullous keratopathy,” he said. “Repeated grafts have a relatively poor prognosis, unfortunately.” Other poor prognostic factors are neovascularisation and a history of rejection.
Prof Dickman observed the past decades have seen a profound shift to endothelial keratoplasty (EK). Never theless, the real-world data emerging from the registry indicates survival rates may not be as impressive as initially thought.
“EK outcomes vary a lot. Looking at data from the Netherlands, we see that the graft survival rate increas es significantly with the adoption of DMEK by more surgeons as they go through their learning curve,” he said. “And DMEK performs very well in the long term because there is less rejection. Studies show that if you train the surgeons in centres [specializing] in DMEK, you can overcome this learning curve, but not at the expense of the patients.”
Prof Dickman provided these updates at the 2023 ESCRS Con gress in Vienna.
Mor M Dickman MD, PhD is professor of ophthalmology, University Eye Clinic, Maastricht UMC, Netherlands. m.dickman@maastrichtuniversity.nl
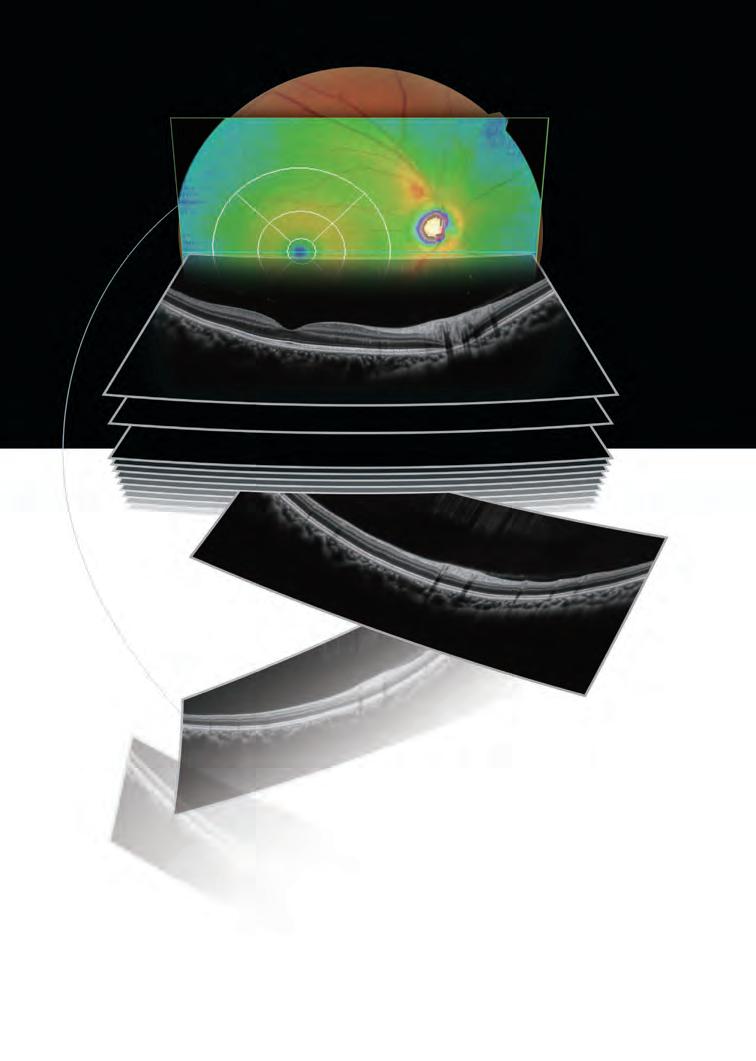
Fundus image acquisition with macula and disc capture in one image on OCT, for enhanced screening and clinical efficiency
Retina map
Denoising technique
Widefield image capture in a single shot High definition OCT image for all scans
Placement of Corneal Allogenic Intrastromal Ring Segments (CAIRS) is a technique I first started in 2015 and refers to the placement of allogenic tissue of any source within the host cornea. CAIRS works on the principle of Barraquer’s law of thickness, which states the thickness increasing in the mid-periphery of the cornea results in a flattening of the central cornea and vice versa. Thus, implanting CAIRS in the para-central and mid-peripheral zones gives the desired effect of flattening the cone in an ectatic patient.
Synthetic ICRS have already been used to achieve a central cornea flattening in keratoconic patients. These have been successful in bringing moderate visual improvement. Disadvantages include a limitation to the upper limit of achievable improvement, an inability to treat advanced cases, and a lack of individualised customisation. There is also a higher risk of complications such as anterior stromal necrosis, extrusion, intrusion, and migration, which hinders the use of these synthetic rings, especially in patients with advanced cones, eye rubbers, and those with the potential to progress.
Compared to synthetic ICRS, CAIRS has significant advantages—allogenicity, superior biocompatibility, and a refractive index similar to the rest of the cornea. These reduce the risk of complications, such as anterior stromal necrosis, associated with synthetic segments while allowing the ability to implant in much thinner and steeper corneas. At the same time, though our implantation of CAIRS is most commonly performed at 4.6 mm, we have also implanted it in optic zones up to 4.0 mm without the patient complaining of a ring or halo effect. These advantages allow for harnessing a large amount of flattening effect—even up to 30 D.
CAIRS can also be implanted more superficially than the traditional 70–80% depth for synthetic ICRS. We have been implanting CAIRS at about 50% depth and this superficial implantation—together with the greater thickness and volume of implanted tissue as well as the ability to use small optic zones—allow for a greater effect, thus becoming suitable for very advanced cones as well.
Customisation
Customisation is probably one of the greatest advancements in CAIRS surgery. Like synthetic segments, CAIRS can be cut to any arc length, thickness or volume, and optic zone. Implementation depth can be changed, and, most importantly, the shape can be customised. Therefore, it can have variable or progressive thickness and/or width.
Progressive thickness synthetic ICRS are available only in fixed arc lengths and optic zones and with a fixed and progressive gradation of thickness or width from one end of the segment to the other or from the centre to the edges. However, we know well that each keratoconic patient is unique
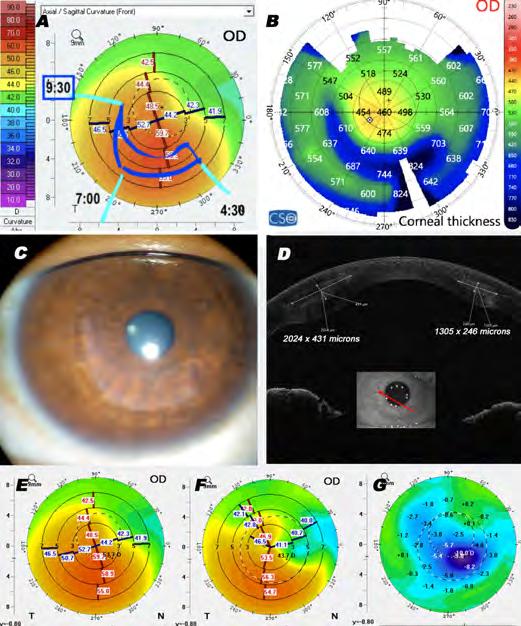
Figure 1, Customised CAIRS: A—Topographic plan drawn on the keratometric map as per steepness gradient shows a taper starting from 07:00 till 09:30 clock hours; B—Postoperative ASOCT pachymetric map showing the tapered segment in situ; C—Postoperative slit lamp image shows the customised CAIRS; D—ASOCT showing the varying thickness and volume along the length of the segment; E—Preoperative keratometric map; F—Postoperative keratometric map; G—Difference map showing a gradient in the amount of flattening achieved that follows the topographic plan.
concerning the cone pattern, its position and extent, thickness, refractive error, etc.
In addition, the internal gradient of keratometry can vary widely within the cone, so the same type of progressively tapered ICRS does not suit even phenotypically matching keratoconic patients. CAIRS allows exquisite surgeon customisation to exactly match to each patient’s topographic map and can be further customised based on the refractive error.
The taper gradient in customised CAIRS does not need to start at one end and progress smoothly to the other. Instead, the taper can be initiated anywhere within the arc, so there are tapered and non-tapered parts in the same segment—the length and thickness of the tapered part varied per patient. In addition, the taper can be gradual or sudden and can start from the centre towards both sides in a U- or V-shape or from
one side and progress to the other. Tapered segments, U- or V-shaped segments, and many other possibilities are possible depending on the patient’s topography.
Technique
Surgeons can easily customise on the table using the double-bladed Jacob CAIRS trephine™ (Madhu Instruments, India) and the CAIRS Customizer™ (Epsilon Instruments, US).
Any allogenic tissue source can be used to prepare CAIRS: for example, a donor corneal rim with the epithelium and endothelium removed. The Jacob CAIRS trephine then cuts circular CAIRS from the corneal stromal rim, which is placed on the CAIRS Customizer and aligned along the desired optic zone mark. The plan marked on the patient’s keratometric map is then amended on the CAIRS segment with a fine tipped marker pen. The segment is then placed on a Teflon cutting block and cut. Marks are also placed on the patient’s eye to transfer the plan accurately. The customised CAIRS is then inserted into the patient’s eye using CAIRS inserters. In progressive cases and young patients, this is combined with corneal cross-linking (CXL, Figure 1).
Real-world experience
We have more than 600 patients with all grades of keratoconus—from very mild to advanced disease—who have undergone CAIRS. The patient experience has been very positive, with patients reporting a decrease in distortion, improvement in visual acuity, decrease in spectacle power, decreased contact lens dependency, and, when required, improved contact lens fitting. Most patients have bilateral disease and undergo sequential bilateral surgery, and many refer their friends from support groups or other known contacts who suffer from ectasia.
CAIRS has numerous advantages over not just synthetic segments but DALK as well, as a minimally invasive, quick, and easy surgery with a smooth learning curve, quick rehabilitation, and low risk of intra- or postoperative complications, unlike DALK. It is also more advantageous than subtractive procedures such as topography-guided photorefractive or phototherapeutic keratectomy combined with CXL in obtaining a much larger effect and not running the risk of disease destabilisation. Unlike these procedures—which remove corneal tissue—CAIRS adds tissue, thereby increasing corneal thickness and redistributing corneal stress forces, helping decrease progression. Compared to other allogenic technology, CAIRS leaves the visual axis untouched and thus does not carry the risk of decreased vision from haze or rejection. Other synergistic techniques can follow to further decrease spectacle dependency if required.
Research Education Innovation
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
Dr Soosan Jacob MS, FRCS, DNB is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
A New Era in Treating Corneal Disease
Binkhorst Medal Lecture outlines a future with better outcomes, fewer burdens, and improved quality of life for patients.
The treatment of corneal diseases is undergoing a paradigm shift, which will overcome many of the shortcomings of current approaches to dealing with corneal dystrophies and other potentially blinding conditions, said Professor Jorge L Alió in his Binkhorst Medal Lecture at the 2023 ESCRS Congress in Vienna.
“We are at the forefront of an exciting revolution in the treatment of corneal blindness, moving from the old paradigm of cornea tissue substitution to one where cornea tissue regeneration becomes the new standard,” Prof Alió said.
The need for new treatments is pressing, he stressed, noting that corneal blindness is the second most common cause of blindness worldwide, with treatment limited by the number of donors for corneal transplants.
“The shortage of corneas results in over 40,000 visually impaired people waiting for corneal transplants every year in Europe alone, with 10 million untreated corneal blindness patients globally and 1.5 million new cases of corneal blindness annually,” he said.
This number is rising due to the ageing population and corneal graft failure, which often occurs due to rejection, becoming even more likely with each successive graft and new indication.
New solutions needed
“There is a need for new solutions to avoid tissue substitution, preferably immunologically neutral ones, independent
from human donor tissue, with unlimited accessibility that will probably be more cost effective than corneal grafts in the long term,” he said.
Advanced stem cell therapies may be the game-changer everyone has been waiting for, added Prof Alió, who outlined some of the latest research in regenerative techniques for a wide range of corneal diseases.
Adipose-derived adult mesenchymal stem cells (ADASCs), for instance, have been shown to provide a viable cell source for stromal regeneration and repopulation in diseased corneas. ADASCs are typically isolated from adipose (fat) tissue obtained from the patient’s body, which reduces the risk of rejection or immune-related complications.
ADASCs can be induced to differentiate into epithelial cells or stromal cells in the laboratory and can help repair the corneal epithelium, stroma, or endothelium, depending on the specific corneal injury or disease.
These cells have demonstrated anti-inflammatory and immunomodulatory properties, which can be beneficial for reducing inflammation and immune responses in the damaged cornea. They may also stimulate endogenous repair mechanisms in the cornea by releasing growth factors and cytokines that promote tissue healing.
Mesenchymal stem cells (MSCs) are suitable extraocular stem cells for corneal regenerative therapy. “They can differentiate into other cell types; they have anti-fibrotic, anti-apoptotic,
DERMOT MCGRATH REPORTS
and anti-inflammatory capacities; and they are non-immunogenic, so they do not require immunosuppressive therapy,” Prof Alió said.
Stem cell deficiency
MSCs have shown promise for the treatment of ocular surface diseases such as dry eye, corneal burns, ulcers, and limbal stem cell deficiency (LSCD).
Prof Alió highlighted the pioneering work of Dr Margarita Calonge, who reported the first proof-of-concept clinical trial using MSCs for treating corneal epithelial stem cell deficiency in 22 patients.
“MSCs have a present and future critical role in the management of corneal epithelial failure due to limbal stem cell deficiency. Severe forms of dry eye disease have already been improved with MSC therapy in open-label clinical trials, with randomised controlled clinical trials to follow,” he said. “Cell-free therapy such as PRP—especially with MSC-extracellular vesicles (such as exosomes)—could be a future better option than MSCs, provided the many existing challenges can be solved.”
As well as epithelial repair, MSCs can be differentiated into corneal stromal cells in vitro and then transplanted into the corneal stroma to promote tissue regeneration. The cells can also be incorporated into tissue-engineered constructs or biodegradable scaffolds for corneal transplantation in thin
corneas or cases where injection alone is insufficient to promote corneal regeneration.
The technique using ADASCs implanted into corneal stroma has already been successfully tested in the first human phase 1 and 2 trials in five patients with advanced keratoconus.
“The safety of the procedure has been demonstrated with local production of collagen by ADASCs in situ confirmed and recovery of the transparency of the implanted laminas confirmed,” he said. “The cases are stable after three years, opening the door for further clinical studies of this new therapy for keratoconus and other corneal dystrophies.”
Looking to the future, Prof Alió predicted corneal organoids could potentially solve the corneal graft tissue shortages.
He explained the corneal organoids are bio-constructs made with corneal epithelium tissue, stromal laminas from non-human origin, and endothelial tissue shaped with 5D printing techniques to deliver customised corneal optical power.
“This will improve patient quality of life and reduce the economic burden of corneal transplants on healthcare,” he said. “Furthermore, we expect these bio-constructs to provide better therapeutic outcomes over donor corneas, such as avoiding allograft rejection.”
ESCRS Academies
Committee representatives of ESCRS organise and present sessions at meetings organised by our national and sister societies. These sessions are typically delivered by a group of speakers on a current topic selected by ESCRS in person or virtually.
These sessions provide useful education as well as collaboration between societies promoting and sharing benefits across both memberships.
escrs.org/education/academies/
Jorge L Alió MD, PhD, FEBOphth is based at the Universidad Miguel Hernandez, Alicante, Spain. jlalio@vissum.com
Mitochondrial Function— A Modifiable Risk Factor?
Potential glaucoma treatment oral nicotinamide now in trials.
PRISCILLA LYNCH REPORTS
Mitochondrial dysfunction has been confirmed as a substantial risk factor for glaucoma, and clinical trials on using an oral vitamin supplement to modify that risk could hopefully yield positive results, according to Professor David Garway-Heath.
“We’re heading towards a stratified medicine approach,” he said. “Glaucoma is multifactorial. Mitochondrial function won’t underlie glaucoma in everybody, but I believe there will be a substantial subset of the glaucoma population where it is important, and this sort of intervention would be important.”
IOP reduction is currently the only proven method shown to slow glaucoma progression. However, a significant subset of patients (15–20%) still lose vision despite the best treatment, suggesting other factors are involved, Prof Garway-Heath noted.
Previously implicated in the pathophysiology of several neurodegenerative diseases, mitochondrial dysfunction has now been shown to play a role in the pathogenesis of glaucoma. Retinal ganglion cells (RGC), because of their high energy requirement, are heavily dependent on mitochondria for survival and function. Several studies of glaucoma patients
have shown higher levels of mitochondrial dysfunction, thus indicating that “mitochondrial function is an important risk factor [in glaucoma] that is possibly modifiable,” he said.
“What we have so far is mitochondrial function is implicated in glaucoma by genetic evidence, experimental evidence, and clinical evidence.”
So, can prevention or reversal of mitochondrial dysfunction reduce glaucoma risk and improve vision outcomes in glaucoma patients?
Prof Garway-Heath discussed ongoing work, including his own substantial research, focusing on the role of nicotinamide, a water-soluble form of vitamin B3 (niacin) that replenishes important molecules for mitochondria function. Studies have found nicotinamide levels lower in glaucoma patients than controls.
“Nicotinamide is cheap, safe, and well tolerated, but we are not encouraging people to use vitamin B3 yet, as we need the evidence it is effective before we can recommend it,” he told EuroTimes. “But it is looking like a good candidate treatment.”
The results to date “look very promising indeed”, with significant positive effects in lab and animal models.
“Then there is the short-term trial looking at improvement in vision in glaucoma patients on nicotinamide, [which] also seems to show some activity,” Prof Garway-Heath said. “But that doesn’t necessarily tell us it [will] affect the long-term course, and that is what the next trial is about, to look at affecting the long-term course of the disease.”
He is currently leading a major four-year randomised controlled clinical trial to discover whether taking oral nicotinamide with standard IOP treatment can reduce the amount of sight loss in recently diagnosed patients with open-angle glaucoma, and evaluate its long-term safety and effectiveness.
His research also seeks to identify biomarkers to determine who would benefit from the treatment.
If successful, the results could significantly improve treatment results in the future.
Prof Garway-Heath’s comments were made as part of the Annual Mooney Lecture during the Irish College of Ophthalmologists 2023 annual conference in Killarney, Ireland.
David Garway-Heath FRCOphth is a Consultant Ophthalmic Surgeon at Moorfields Eye Hospital London, and Glaucoma UK Professor of Ophthalmology for Glaucoma and Allied Studies at the Institute of Ophthalmology, University College London, UK. d.garwayheath@nhs.net
New EGS Guide Updates Options
Specialists hope the up-to-date information will provide research standards, raising the bar for future clinical trials.
SEAN HENAHAN REPORTS
Glaucoma Day at the 2023 ESCRS Congress offered a full range of topics, from innovations in glaucoma surgery to how to handle post-phaco complications. The European Glaucoma Society used the occasion to debut a new book, A Guide on Surgical Innovation for Glaucoma, giving all attendees a free copy.
Two years in the making, the book is the result of systematic work by a panel of European glaucoma specialists led by three editors—Dr Luís Abegão Pinto (Lisbon), Dr Ingeborg Stalmans
Critically, it also aims to provide the standard for research on the field, hopefully raising the bar for future clinical trials.
(Leuven), and Dr Gordana Sunaric Mégevand (Geneva).
The book is a response to the many innovations in glaucoma surgery in recent years. It allows readers to familiarize themselves with current procedures—both the minimally invasive glaucoma surgeries (MIGS) and bleb-forming devices—providing detailed descriptions of each, a summary of existing literature, and information on complications and caveats. In addition to telling readers what is out there, it addresses a need to create benchmarks for clinical trials to provide better data for comparing the risks and benefits of traditional and novel surgical interventions.
“The Guide offers an overview of the existing minimally invasive glaucoma surgery techniques but also aims to provide the reader with the tools for interpreting surgical studies,” said Dr Pinto, EGS Secretary. “Finally, or should I say, critically, it also aims to provide the standard for research on the field, hopefully raising the bar for future clinical trials.”
The editors gathered more than 250 questions from 50 European glaucoma specialists in 18 countries to name the top 10 clinical questions facing glaucoma surgery, which then went under systematic review. Where sufficient high-quality data was available, the editors included it but provided consensus statements based on clinical experience when sufficient data could not be found.
“We are not telling people what to do. We want to provide doctors with the data and the tools to make their own decisions,” Dr Pinto explained. “This book is intended to offer guidance for interventions popular enough to be widely used while avoiding bias towards techniques that are currently niche techniques.”
An important goal of the book is to create a framework of common standards for surgical trial design and reporting, making it easier to compare and judge future clinical studies using established benchmarks, he added.
The book will soon be available on the EGS website, www.eugs.org
Luís Abegão Pinto MD, PhD is Head of the Glaucoma Unit and Assistant Professor of Ophthalmology, Lisbon University, Portugal, and EGS Secretary. abegao.pinto@gmail.com
MIGS and SLT Slug It Out in Bruising Arena Contest
Two industry specialists consider which technique reigns supreme in the inaugural ESCRS Congress event.
DERMOT MCGRATH REPORTS
When a jackal is confronted with a jackhammer, the only possible outcome is a violent struggle for dominance.
And while there was thankfully no blood left on the canvas, the audience at the 2023 ESCRS Congress Arena debate in Vienna on minimally invasive glaucoma surgery (MIGS) versus selective laser trabeculoplasty (SLT) were still treated to a fiery contest as Karl “The Jackal” Mercieca from Germany slugged it out against Carlo “Jackhammer” Traverso from Italy.
Making the case for MIGS, Karl Mercieca came hurtling out of the blue corner with a volley of persuasive arguments.
“MIGS is way better than SLT. It can be combined with phacoemulsification, and the IOP lowering potential is way better than SLT,” he said. “If you look at the long-term results,
with one procedure, you can get consistent pressures over a much longer period. With SLT, you need to repeat and repeat and repeat, and not all patients respond.”
Barely pausing for breath, Dr Mercieca followed up with another devastating combination.
“People say that SLT is cost effective and non-invasive, and so forth. But actually, it’s not that cost effective at all. If you look at MIGS combined with phaco, for example, the quality of life is better for your patient, and it’s actually more cost effective.”
The real appeal of MIGS is its versatility, argued Dr Mercieca.
“MIGS doesn’t mean one procedure—you have got so many options to choose from. The other thing is it doesn’t depend on having a nice open angle, whereas SLT can only be used in eyes with large, wide angles. MIGS can be used in other situations,
especially combined with phaco, whereas SLT is not indicated in uveitis, narrower angles, and so forth. But the true beauty of MIGS is you can really tailor it. It’s truly personalised medicine for your glaucoma patients,” he concluded.
The Jackhammer fights back
In the red corner, Carlo the “Jackhammer” Traverso took the blows without complaint and decided to come out all guns blazing.
“First of all, what is the spelling for MIGS? If you are using MIGS, this means ‘my income grows steadily,’” he said to laughter from the assembled audience.
After this opening uppercut, Professor Traverso continued his verbal assault.
“Let us face it—MIGS are minimally effective. There is no comparable risk when we look at SLT,” he said. “With MIGS, we have seen endophthalmitis, choroidal issues, [etc.]. SLT is also doable without using the gonioscope. SLT is really not expensive, it is somewhat repeatable, and as a primary treatment, it is not only effective, it’s ethical. It is evident that there is no evidence whatsoever that trabecular MIGS are really working.”
Dr Mercieca responded that Prof Traverso’s arguments were strictly in the featherweight category.
“You are in the wrong boxing category because SLT is comparable to drops,” he said. “We are here at ESCRS with cataract surgeons who want to combine something with a cataract removal to get effective results, not something which they have to wait six weeks to see something positive.”
Prof Traverso was having none of it, delivering another stinging financial argument to his opponent: “Yes, of course, combine MIGS with phaco, so you get two surgical fees in 30 seconds. Who is going to pay for this?” he asked.
Dr Mercieca was quick to respond, adding long-term data showed that MIGS is a cost-effective procedure. “I would like
to quote one Carlos Traverso back in 2014 who said, ‘MIGS is definitely the way forward and an alternative to current treatment with really expanding horizons’,” he said.
However, Prof Traverso wasn’t taking this potential hammer blow lying down.
“Yes, but those were the early data. We were part of the very first trial on this trabecular stent, and we participated enthusiastically. But what are the long-term results published in the literature? If it’s not confirmed by data, what is that for? My income grows steadily if I use MIGS, but I’m not there for income. I’m there for the patient’s well-being. So, I think that as a first step, SLT is really the only way out,” he said.
Dr Mercieca said the scientific literature shows that MIGS prevents people from needing further surgery and saves vision.
“MIGS is effective, and of course it’s invasive. But if you are doing phacoemulsification and have a patient on drops, why not do something extra to give them a better quality of life?” he asked.
After some more lively trading of verbal blows in a hugely entertaining contest, both contestants retreated bloodied but unbowed to their corners and awaited the verdict of the audience present.
Summing up, the referee, Leon “The Lion” Au thanked both opponents for a lively debate and announced Dr Mercieca as the winner on points in a tight contest.
Carlo E Traverso MD is the Director of Eye Clinic, Department of Neurosciences, Ophthalmology and Genetics, University of Genoa, Italy. carloenrico.t raverso@hsanmartino.it
Karl Mercieca MD, FRCOphth is a consultant ophthalmic surgeon at the University of Bonn Eye Clinic, Germany. Karl.Mercieca@ukbonn.de
Keratoconus Screening in Children with Down Syndrome
Early screening leads to early intervention.
PRISCILLA LYNCH REPORTS
Children with Down syndrome (DS) should be screened for keratoconus, as the condition is much more common in this cohort, and diagnosis and treatment are often delayed, reported Mr Barry Power.
“These children have a much higher risk of development of keratoconus,” he told EuroTimes. “It happens earlier than the non-DS population, and we know early intervention is best— surgical rehabilitation in these cases is very, very challenging.”
The link between keratoconus and DS is well documented—a Norwegian study estimated the incidence to be 30 times that of the general population.
“Individuals with Down syndrome present with advanced disease to our clinics far too often,” he said. “Cross-linking is a highly effective early treatment and reduces the risk of further intervention and preventable sight loss.”
Mr Power and colleagues launched a pilot DS keratoconus screening programme at the Royal Victoria Eye and Ear Hospital (RVEEH), Dublin, Ireland, in 2020 in conjunction with the National DS Clinic at Tallaght University Hospital, Ireland.
Children with DS were invited to the RVEEH cornea clinic for assessment, where the clinic team recorded medical history, risk factors, BCDVA, and corneal topography. The data was then compared to a control group of adults with DS referred to the clinic by standard pathways.
The screening group included 22 children with DS; complete topographic data was available in 19 patients with an average age of 13.6 years (9–18). The control group included nine individuals with topographic data available from eight patients and an average age of 34.8 years (21–48).
The average K, Kmax, and CCT in the screening and control
groups were 46.6, 49.5, 470 and 55.7, 66.7, and 395, respectively.
In the screening group (N=44), 29 eyes (65%) were kept under review, 10 (22%) discharged, and 5 (11%) treated (all with cross-linking). In the non-screening control group (N=18), 8 eyes (44%) were kept under review, none discharged, and 10 (55%) needed intervention (1 penetrating keratoplasty [PKP], 2 EUA, 7 cross-linking). Several eyes in the non-screening cohort were too advanced at presentation for any form of intervention.
Mr Power reported the study found steep Ks, high levels of astigmatism, and corneal thinning in children with DS, which he believes supports the case for screening children with DS for keratoconus.
While there is no established optimum age to screen, Mr Power said, based on the pilot study: “We believe the optimum age for this to be the mid-teens to maximise the ability to undergo topography and minimise disease progression. Our data shows, unsurprisingly, that younger screened patients have milder disease levels and a lower requirement for intervention than an older, non-screened control group.”
He recommended using a Pentacam (Oculus) as a screening tool in this cohort, noting its good tolerability among those who participated in the pilot study.
Mr Power presented his research at the Irish College of Ophthalmologists 2023 annual conference in Killarney, Ireland.
Barry Power MSc, FRCOphth is an Ophthalmic Surgical Fellow at the Royal Victoria Eye and Ear Hospital, Dublin, Ireland. barryjapower@gmail.com
Timing Keratoconus Treatment
Faster progression underscores the importance of timely intervention for keratoconus in children.
CHERYL GUTTMAN KRADER REPORTS
Because keratoconus progresses faster in children than adults, treatment with corneal cross-linking (CXL) to achieve stabilisation should be performed in every child with keratoconus, with a few exceptions, said Dr Beatrice E Frueh.
“Often, the family may want to postpone the treatment until after summer vacation or for some other reason,” Dr Frueh said. “Nevertheless, we must be firm and tell the parents that young children should not wait months for the procedure.”
Being more specific about patient selection for prompt intervention with CXL, Dr Frueh advised treating every child with symptomatic keratoconus at presentation or with documented progression. On the other hand, watchful waiting can be appropriate for a child with early, asymptomatic keratoconus detected as an incidental finding through screening done because of a positive family history. In that situation, the child could have forme fruste keratoconus. As another exception, there is no reason to perform CXL if the central cornea is already scarred.
“CXL will not help, and keratoplasty is indicated instead,” Dr Frueh said.
She also urged ophthalmologists to keep in mind children with atopy, vernal keratoconjunctivitis, or Down syndrome are frequent eye rubbers, which puts them at risk for rapid progression.
“These children in particular have to be treated right away or followed very closely.”
Diagnostic challenges
Diagnosing keratoconus in children can be more difficult than in adults, partly because children do not complain about losing sight. In addition, it can be difficult to obtain reliably good measurements in children due to poor cooperation with topography imaging. These issues can contribute to the fact that keratoconus is often diagnosed later and at a more advanced stage in children than adults.
“However, if you are good at retinoscopy, you can already see the scissoring reflex early on, and topography can be done very well in children if you have a good operator,” Dr Frueh said.
Another issue to consider when identifying keratoconus progression is normal corneas serve as the basis for the widely used definition of a Kmax increase ≥1.0 D over 12 months.
“For very steep corneas, a 1.0 D increase in a year is not very significant,” she said.
Choosing the CXL procedure
The standard Dresden protocol, which is an epithelium-off technique using topical riboflavin and dextran followed by 30 minutes of irradiation with ultraviolet A at 3 mW/cm2,
remains the standard of care for performing CXL in paediatric patients. However, Dr Frueh suggested an accelerated CXL technique applying higher energy for a shorter duration, considering available evidence showing it provides similar results in children compared to the Dresden protocol.
“There are also epi-on protocols that would be very nice to use in children,” she said. “However, epi-on CXL should not be recommended because studies show it is followed by too much progression, and we also do not have enough follow-up data.”
Dr Frueh presented at Cornea Day at the 2023 ESCRS Congress in Vienna.
Beatrice E Frueh MD is Professor and Chief of the University Clinic for Ophthalmology, University of Bern, Inselspital, Bern, Switzerland. beatrice.frueh@insel.ch
Revolutionising Retinal Imaging
The rise of AI in ophthalmic practice follows a steep trajectory.
ROIBEÁRD O’HÉINEACHÁIN REPORTS
Artificial intelligence-based algorithms offer the prospect of improved efficiency in delivering care and reduced cost, but translating that potential into clinical practice will require a colossal effort, said Professor Marion R Munk.
“You see a lot of hurdles, but nonetheless AI will definitely make its way into our clinic—and already has. And as always, great revolutions need some time,” she said.
The past few decades have seen growing interest and research in artificial intelligence in medicine. A search on PubMed shows only one article on the subject in 1996, compared to more than 22,700 at present. There has likewise been substantial investment in the field with the EU contributing 1.5 billion through 2020 and France alone contributing a further 22,700 published articles, up from almost nothing in the 1990s.
As always, great revolutions need some time.
Moreover, there has been a corresponding explosion in the number of medical AI algorithms and machine learning-enabled devices gaining FDA clearance for clinical use. While most are in fields such as radiology and cardiology, there are also a few cleared for use in ophthalmic diagnostics, such as the LumineticsCore (formerly known as IDx-DR) for diabetic retinopathy screening and the EyeArt (Eyenuk)—previously approved for age-related macular degeneration (AMD) and now approved for diabetic retinopathy screening.
Quantity and quality
Prof Munk noted since the European Medicines Agency’s guidelines are less strict than the US FDA’s, there are currently more algorithms and AI-enabled ophthalmic devices available for clinical use in Europe than the US. The FDA requires companies submitting AI and AI-enabled devices to always use independent prospective data for the training and testing stages to ensure the data from these cohorts will not overlap. In contrast, the EMA allows the use of retrospective data, which greatly reduces the expense and amount of work involved.
The prediction accuracy of an AI algorithm always depends directly on the quantity and quality of the data used, she said. To create an AI algorithm that can distinguish between the presence, absence, and severity of proliferative and non-proliferative diabetic retinopathy requires around 50,000 to 60,000 images. In addition, for maximum performance, 4.5 graders are needed to label each one. Validating the algorithm
requires a separate, though smaller, set of images likewise labelled by a similar number of graders. The gold standard for FDA approval is a sensitivity of 0.85 and a specificity of 0.825. Another challenge is ensuring devices from different manufacturers are properly trained on the algorithms. It will also be essential to ensure using the AI devices will not complicate clinician workflow. The desired return from AI technology, she added, is improved efficiency in delivering care and reduced cost. Those benefits have yet to be proven. An additional question is how AI-enhanced diagnostic services will be remunerated—particularly in the EU, where, unlike the US, there are no general billing codes.
Prof Munk spoke during an EURETINA educational webinar, “AIBased Developments in Retinal Imaging”.
Marion R Munk MD, PhD, FEBO is a Uveitis and Medical Retina specialist and Chief Scientific Officer at Augenarzt-Praxisgemeinschaft Gutblick AG, Pfäffikon, Switzerland, and adjunct professor at Northwestern University, Feinberg School of Medicine, Chicago, US. marion_munk@hotmail.com
AI and the Macula
OCT device enhanced with AI takes AMD diagnosis and monitoring to a new level.
ROIBEÁRD O’HÉINEACHÁIN REPORTS
Artificial intelligence (AI) can markedly enhance the capabilities of optical coherence tomography in diagnosing and monitoring geographic atrophy and neovascular age-related macular degeneration, according to Professor Ursula Schmidt-Erfurth.
“It’s very important to use AI tools because they allow us to go from a subjective qualitative management to an objective quantitative one, significantly enhancing reliability and precision of the treatment,” she said. “It also answers a need of eye doctors who need to manage the huge task of treating more than 200 million individuals with AMD.”
AI helps us significantly in understanding disease activity.
Prof Schmidt-Erfurth noted geographic atrophy is characterised by retinal pigment epithelium (RPE) and photoreceptor loss. Research has shown photoreceptor loss exceeds and precedes RPE loss, and a high ratio of photoreceptor loss versus RPE
degeneration predicts a worsening of the lesions. She and her associates created a deep learning-based algorithm to extract and compare the RPE and photoreceptor layers obtained from the full Heidelberg Spectralis OCT device 3D volumetric image.
They applied their algorithm to the Oaks and Derby Phase 3 trials of pegcetacoplan (Syfovre, Apellis Pharmaceuticals) geographic atrophy treatment. They found, as predicted, a linear correlation between the rate of disease progression and the ratio of RPE loss and photoreceptor loss in the sham arms. In addition, a point-to-point comparison with microperimetry clearly showed retinal sensitivity correlated consistently and linearly with photoreceptor thickness. In the treatment arms, the rate of photoreceptor loss exceeded the RPE loss.
She noted clinicians can now measure these disease activity parameters on any regular OCT. For example, the RetinAI app on the Heidelberg Spectralis OCT uploads the retinal images to the cloud, returning a detailed, AI-powered analysis of disease activity and therapeutic benefits.
“AI helps us significantly in understanding disease activity,” she said. “It provides accuracy in detecting subclinical features and gives us parameters that can make predictions and allow us to visualise disease progression.”
Macular fluid quantification in neovascular AMD
Prof Schmidt-Erfurth and her associates have also developed an AI algorithm-based app for their OCT device to detect and quantify macular fluid in eyes with neovascular AMD. It uses a segmentation process similar to the one they developed for geographic atrophy, distinguishing between intraretinal fluid and subretinal fluid—which is helpful from a clinical perspective since research has shown eyes with a high volume of intraretinal fluid also have a high amount of photoreceptor loss. The same is not true for subretinal fluid, except where a high volume can lead to pigment epithelial detachment.
As with geographic atrophy, an app on the Heidelberg Spectralis called RetInSight allows clinicians to upload OCT images and obtain a precise fluid activity meter that converts pixels into nanolitres in a reliable, objective, and quantitative manner.
“At one glance, such a report significantly enhances workflow,” she observed. “It increases the precision of your personalised treatment and gives you a beautiful overview of the disease profile—like the biography of the disease in every single patient.”
Prof Schmidt-Erfurth presented during an EURETINA educational webinar, “AI-Based Developments in Retinal Imaging”.
Ursula Schmidt-Erfurth MD, PhD is Head of the Department of Ophthalmology and Optometry, Medical University of Vienna, Austria. ursula.schmidt-erfurth@meduniwien.ac.at
Optogenetic Therapy for Stargardt Disease
Safety and efficacy outcomes encouraging in clinical trial.
CHERYL GUTTMAN KRADER REPORTS
An intravitreally delivered, adeno-associated virus 2 (AAV2)-packaged optogenetic therapy has shown promise in treating patients with severe vision loss due to Stargardt disease.
The open-label, phase 2 clinical known as STARLIGHT enrolled six participants with a documented clinical diagnosis of Stargardt disease or genetic diagnosis with pathogenic variants ABCA4, ELOVL4, or PROM1. Three study subjects had a macular degeneration phenotype, and the other three patients had panretinal degeneration.
All patients received a single intravitreal injection of MCO-010 1.2E11 gc, an intravitreally delivered AAV2-packaged optogenetic therapy (sonpiretigene isteparvovec, Nanoscope Therapeutics), into one eye. The primary study objective was to evaluate ocular and systemic safety, but visual function tests also assessed efficacy.
Data from follow-up to week 24 showed MCO-010 had an exceptional safety profile and was associated with improved visual acuity (VA), stable or improved static perimetry, and improved electroretinogram results. Patients with the macular degeneration phenotype, however, showed a much higher propensity for gaining vision, reported Dr Victor H Gonzalez.
“Follow-up is continuing, and we look forward to seeing whether the early treatment benefit is maintained,” he told EuroTimes. “However, it is clear from this first clinical study of patients with Stargardt disease that individuals with the macular degeneration phenotype will be targeted for enrolment in the next study phase.”
In the study, ETDRS best corrected visual acuity (BCVA) ranged from 13 to 34 letters at baseline (mean 23 letters, approximately 1.8 logMAR), and patients with the macular degeneration phenotype achieved clinically meaningful improvements. The changes in this subgroup peaked with gains of 11 to 21 letters and showed some decline thereafter, although mean BCVA at week 24 remained higher than at baseline.
“As we look how long the treatment benefit is maintained, we [must] consider that this initial study assessed a single injection of a single dose of MCO-010,” Dr Gonzalez said. “Further research will be designed to help determine what may be an optimal regimen.”
Patients in the macular degeneration subgroup scored well on vision-guided mobility and near object recognition tests at baseline, which the study team expected because they do not have significant loss of peripheral vision, and they maintained their test performance throughout follow-up. Key domain scores of patient-reported outcome measures (PROMs), including reading and colour contrast, were also significantly improved.
Lack of serious safety signals
The safety profile of MCO-010 in patients with Stargardt disease was consistent with experience from other studies investigating it as a treatment for patients with retinitis pigmentosa. The only adverse events recorded were related to the injection procedure itself.
“Unlike other modalities that use AAV2 as a vector for delivery, we saw no evidence of a significant inflammatory response,” Dr Gonzalez said. A few patients developed mild inflammation that was easily controlled with topical medications,” Dr Gonzalez said.
The study was presented at ARVO 2023 in New Orleans, Louisiana, US.
Victor H Gonzalez MD is a retina specialist in private practice at Valley Retina Institute, McAllen, Texas, US. maculadoc@aol.com
https://escrs.org/special-interest-groups/yos/
Robot-guided Cataract Surgery
Researchers encouraged by technical performance in early testing.
CHERYL GUTTMAN KRADER REPORTS
Aprototype system using a 3D camera-guided robotic arm demonstrated promising results in initial technical feasibility studies investigating its potential for performing robot-assisted cataract surgery.
“Advancements in robotics and computing technology have enabled the development of robotic-enhanced surgeries in many medical sectors, but there are special challenges for adopting robotics in ophthalmic surgery,” said Mr Marvin Bende. “High precision in both tracking and positioning of the robotic arm is key. What sets our system apart from other efforts in this field is instead of relying on fixating the eye, we are using real-time stereo-tracking to follow the eye and the instrument simultaneously.”
Following a design goal focused on keeping the system as simple as possible, the model was built with mostly offthe-shelf parts. Its components include an industrial robotic arm fitted with a special attachment for instrument mounting. Instead of using an external laser, the robotic system is equipped with an electric high-frequency instrument for the capsulotomy. The optimized software enables very fine tasks with the necessary acceleration and stopping performance, Mr Bende said.
A stereo camera system achieves tracking and imaging, replacing the surgical microscope. It incorporates two syn-
chronized global shutters, colour cameras, and a light source in the centre to provide the red reflex. In addition to monitoring the eye’s position and rotation, the tracking system can extract some data that allows compensation for surgically induced changes, such as deformation resulting from the introduction of instruments.
Measuring performance
The studies assessing technical feasibility used mechanical eye models to evaluate instrument guidance, photorealistic dummy eyes to gauge tracking, and porcine eyes for assessing whole system performance in completing surgical tasks. So far, the system has only been evaluated for making corneal incisions and capsulotomies, which showed it operated with sufficient precision, motion fluidity, and speed.
“The 3D camera was able to triangulate a point in the 3D working space with accuracy of ±0.05 mm, and positioning any part of the instruments was achieved with the same level of accuracy,” he said. “With this level of performance, the robot can guide instruments within the anterior chamber using a small opening at the limbus as the access and pivot point. Comparisons to recordings of human-performed surgeries showed the robotic arm moved with human-like speed and smoothness.”
Further refinements
The prototype tested features a fast-swap single instrument mount, requiring the arm to come out of the eye for instruments to be exchanged manually or via an automated system where the robot selects from a bank of tools. An alternative design under consideration would use an automated, revolver-style instrument changer fitted with multiple surgical tools.
Marvin Bende spoke at ARVO 2023 in New Orleans, Louisiana, US.
Marvin Bende MSc is a researcher and project manager in the Department of Ophthalmology, Eberhard Karls University of Tübingen, Tübingen, Germany. marvin.bende@uni-tuebingen.de
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
Diagnostic Dilemmas in Neuro-ophthalmology
Still catching up after the pandemic.
DR CLARE QUIGLEY REPORTS
The European Neuro-Ophthalmology Society (EUNOS) and the North American Neuro-Ophthalmology Society (NANOS) presented a lively session on diagnostic dilemmas at the biannual European Society of Ophthalmology (SOE) meeting in Prague.
“In the time of COVID, we have missed a lot of neurological disease. We did not examine patients properly, and a mask is the neurologist’s enemy,” Professor Misha Pless explained.
He discussed double vision and his model for working through potential causes of double vision, which involves systematically considering the potential cause from the cerebral cortex, through brainstem, to the cranial nerves, and onto the neuromuscular junction and the orbit.
“If you suspect myasthenia gravis in a patient,” he said, “test the saccades.”
Only testing pursuit movements can lead to false reassurance; detecting abnormally slowed movements may only happen by testing fast eye movements.
“Another helpful test is the sleep test, the five-minute sleep test,” Prof Pless said, adding it is an alternative to the icepack test in myasthenia gravis. After measuring margin reflex distance and eye movements, the patient is asked to take a five-minute nap.
“You will see a difference in the examination,” Prof Pless said.
Bilateral visual acuity loss—this is a lot more difficult than unilateral.
Ophthalmologists cannot miss two underlying diagnoses, he said, as they can be deadly. Subarachnoid haemorrhage typically presents with severe, sudden headaches patients describe as “the worst of their life” and double vision resulting from an associated third nerve palsy. Pituitary apoplexy may present with double vision as a pituitary tumour expands rapidly due to a bleed.
Organic vs non-organic
Professor Karl Golnik had practical advice for differentiating organic from non-organic vision loss.
“My favourite trick for sure is the vertical prism test,” he said.
A patient reporting reduced vision in one eye is one such example of where the vertical prism test can be useful in
differentiating organic from non-organic vision loss. The test involves holding a vertical four-dioptre prism, base down, in front of the better eye. If the patient reports vertical diplopia, seeing two letters of equal clarity, the test has shown equal vision in the symptomatic eye. However, if the patient reports seeing one image or vertical diplopia with a blurry lower letter, it reveals true monocular reduced vision.
“Bilateral visual acuity loss—this is a lot more difficult than unilateral,” Prof Golnik said. He recommended observing ambulation and using the optokinetic nystagmus (OKN) drum. If the patient reports they cannot see the black and white stripes but then exhibits nystagmus on rotating the drum, their vision must be better than claimed.
Another potential non-organic presentation is a complaint of tunnel vision. Prof Golnik advised uncovering clinical findings that are not compatible with the optics of the visual field, whether that field is reduced or not.
“The further away you test the patient, no matter how small that visual field is, it expands,” he said.
When assessing a patient with a visual field deficit, non-expansion of a narrowed field on greater testing distance, done quickly and easily on confrontation, can support a functional vision loss diagnosis.
Misha Pless MD is a Professor of Ophthalmology at the Mayo Clinic, Jacksonville, Florida, US. pless.misha@mayo.edu
Karl Golnik MD is Chairman of the Ophthalmology Department at the University of Cincinnati and the Cincinnati Eye Institute, Ohio, US. golnikkc@ucmail.uc.edu
ESCRS AT A GLANCE
We are a society of surgeons who specialise in improving vision and restoring clarity. Since 1991, ESCRS has promoted the education and research of implant and refractive surgery. With over 7,500 members from 130 countries worldwide, ESCRS is a vital global platform for the field of ophthalmology.
LEARNING FROM THE EXPERIENCE OF OTHERS
Business skills can help young ophthalmologists make better practice decisions.
After years of intensive clinical training, it wasn’t until the last few months of her fellowship that Dr Artemis Matsou devoted much thought to moving from training into practice.
“All these questions suddenly came to mind: Do I want to go private? Do I want to stay in the public sector?” Dr Matsou said. And she realised she was ill-prepared to make a decision that would profoundly affect her career— and her private life.
Dr Matsou is not alone. As well prepared as surgeons are clinically, most have no training for the business challenges they will confront as they move into practice, she said in the Leadership and Business Innovation programme at the 2023 ESCRS Congress in Vienna.
As a result, management-related stress often replaces clinical work stress, even in public systems. Business tasks physician leaders routinely face include managing finances to increase revenues and reduce costs, managing supplies and supply chains, making business cases for new equipment or services, and constantly negotiating with operational managers, financial managers, and other hospital departments.
“These things were unknown to me until I got to the senior role I have,” Dr Matsou said. She has since learned much more about the business of medicine. While she successfully transitioned to a consultant role in a public hospital, she now plans to focus on a niche practice she believes will advance her career and professional and personal interests.
Noting it is easier to learn from the experience of others than from your own mistakes, Dr Matsou outlined business-related skills medical schools and postgraduate training ought to teach. But while few formal curricula currently include these skills, seminars, conferences, and business courses can fill in many of the gaps.
And it is not just about money, Dr Matsou emphasised. “We can offer better care to our patients by incorporating those business principles in our practice. Doctors are probably the best to marry clinical quality of care with an efficient, well-run, and profitable practice.”
Developing leadership skills
Surgeons interested in private practice should keep in mind they will need to act as the CEO and develop the leadership and management skills to do so. Dr Matsou recommended training classes, conferences, and leadership skill-building retreats, which are common in other professions.
Residency and fellowship programmes should incorporate business training through hands-on experience, observation, and visiting other institutions and private practices. Collaboration with administrators and medical directors should be encouraged to infuse their perspective and challenges, such as managing limited budgets, she added.
She encouraged young ophthalmologists to take a proactive approach by asking questions, seeking insights, and exploring solutions to learn from the experiences of others. “If you learn from other people’s mistakes, you learn much faster—you don’t have to make all those mistakes yourself.”
Among the specific skills, Dr Matsou advised cultivating:
Financial planning – Learning how to allocate resources wisely and budget for practice growth is essential. Dr Matsou recommended thinking about this early, especially when considering private practice, which requires significant money, research, planning, and lead time.
Continuous learning and networking – Staying up to date on clinical skills and industry trends is critical. Dr Matsou recommended attending conferences and workshops
and joining professional organisations. Seek mentoring and network to build connections and observe and learn from other practitioners, she said.
Contract negotiation – Learning, then practising, effective negotiating skills is an everyday competency— especially when considering contracts. Always check terms to ensure they are suitable, seeking legal advice when needed.
Time management – Mastering how to prioritise tasks and delegate—and using tools for efficient scheduling—go a long way towards heading off the frustration of trying to do everything alone and avoiding burnout.
Marketing and patient acquisition –Establishing an online presence and providing excellent patient experiences are crucial for building a practice. Dr Matsou noted many doctors undersell themselves in interviews and in public. “We aren’t very good at marketing ourselves.”
Other questions to consider before making a practice decision include whether there is a market for the services planned for the chosen area, the qualities valued in potential colleagues or partners, and how family situations fit into career plans.
Above all, make a plan and have a long-term vision, Dr Matsou advised. “We’ve thought about where we want to be in five years’ time; it should be 10or 15-years’ time. And very importantly, incorporate your personal life as well.”
Artemis Matsou MD, FEBO, MRCP(UK) is a consultant ophthalmic surgeon at Queen Victoria Hospital, East Grinstead, UK. art.matsou@gmail.com
Industrial leaders in ophthalmology premiered a range of innovations at the 2023 ESCRS Congress in Vienna.
Smooth as SILK
Johnson & Johnson announced their next-generation laser vision correction solution, the ELITA™ Platform, which enables surgeons to perform the new SILK (Smooth Incision Lenticule Keratomileusis) procedure for myopia correction, with or without astigmatism. The system’s ultra-precise laser pulse and fast laser delivery are designed to provide surgeons with consistently smooth and easy lenticule creation and removal. The formed lenticules have an industry-first biconvex shape designed for better quality of vision and a reduced cutting of corneal nerves to provide fast regeneration for a healthy ocular surface, the company reports.
www.jnj.com
Digital platform provides IOL insights
Rayner announced major enhancements to RayPRO, the company’s digital insights tool. Designed to harness the power of big data to support decision-making and long-term follow-up, RayPRO’s new enhancements include seamless patient registration on RayPRO at online IOL calculation and the ability to upload up to 200 patients’ data via a simple CSV file. In addition, surgeons can now compare key performance indicators such as spectacle independence and dysphotopsia—at both three months and one year postoperatively—for up to three IOLs with any manufacturer and model.
www.rayner.com
Open-access peer-to-peer education
Also unveiled at the ESCRS Congress was an upgrade to Rayner’s Peer2Peer clinical education platform for ophthalmic surgeons wishing to enhance their cataract and refractive surgery skills. Since its launch in 2022, the open-access Peer2Peer website has generated 5,000 hours of viewing across 20 webinars, 8 symposiums, 20 podcasts, and 100 surgeon interviews. Its latest iteration allows visitors to search through all Peer2Peer content in a simple and intuitive way, ensuring the insights are accessible to all who visit the website.
www.rayner.com/peer2peer
Multimodal corneal topography system
ZEISS showcased the new ZEISS ATLAS® 500, a next-generation corneal topography system. The system is a state-of-the-art, multimodality solution for the anterior eye segment and offers precise corneal topography, pupillometry, and dry eye assessment—all in a single device. It has an integrated, intuitive, and well-organised interface for efficient operation and is designed to fit into any modern clinic or practice environment. The new ZEISS ATLAS 500 integrates into both the ZEISS corneal refractive and cataract workflows.
www.zeiss.com
Indirect ophthalmoscope simulator for ROP
Attendees at the Vienna Congress also got a sneak peek at Haag-Streit’s Eyesi Indirect Ophthalmoscope retinopathy of prematurity (ROP) simulator for training retinal surgeons in examining premature babies and ROP classification. Based on its Eyesi Indirect Ophthalmoscope simulator technology platform, Haag-Streit is developing the new device to provide residents with the ability to practise device handling and decision-making in a lifelike yet risk-free environment.
www.haag-streit.com
EDOF IOLS BECOMING BETTER DEFINED, ENHANCED MONOFOCAL IOLS LESS SO
Greater standardisation in defining intraocular lenses (IOLs) as extended depth of focus (EDOF) and enhanced monofocal will depend on the clinical outcome evaluation rather than only the optical characteristics of new lens designs, said Sathish Srinivasan FRCSEd, FRCOphth, FACS. He noted that EDOF lenses are a new technology, which, in contrast to the discrete focal points provided by multifocal IOLs, create a single elongated focal point to provide a continuous range of focus from distance to intermediate and some near vision functionality. To achieve this, they employ a range of optical principles, including refractive aspheric, diffractive aspheric, small aperture, and wavefront aspheric. In their 2018 task force consensus statement, the American Academy of Ophthalmology established the American National Standards Institute (ANSI) standard to differentiate between monofocal and EDOF IOLs on a clinical basis. The ANSI standard requires a comparison between the six-month outcomes of 100 patients receiving EDOF IOLs and 100 patients receiving monofocal IOLs. The criteria for an IOL to achieve EDOF status include a mean visual acuity of at least 0.2 logMAR at a defocus of 0.5 D or greater, a mean distance-corrected intermediate visual acuity (DCIVA) superior to monofocal controls, a median DCIVA of 0.2 logMAR or better at 66 cm, and a mean best-corrected distance visual acuity non-inferior to controls. Although well-established in the United States, the ANSI EDOF standard has not yet achieved worldwide adoption. However, the ISO 11979-7 committee is due to publish its own EDOF clinical criteria by the end of 2023.
Meanwhile, a new wave of monofocal IOLs is entering the market. Like the EDOF lenses, their design provides an enhanced intermediate distance vision but with less range and less consistency of in-focus vision. Unfortunately, there is no international consensus on the testing and comparison criteria for this new generation of monofocal IOLs, increasing the difficulty of matching the technology to patients’ visual needs, demands, personalities, and lifestyles. Clinicians should therefore encourage IOL manufacturers to provide robust clinical data on these lenses. Randomised controlled trials provide the best evidence quality to gauge the value of a new lens. But, in the absence of such studies, clinical defocus curves obtained by measuring visual acuity through a range of spectacle lenses is the gold standard for assessing the ability of an IOL to correct refractive error at a range of focal points.
S Srinivasan, “Newer generation of intraocular lenses: time for better clarity and understanding”, 49: 903–904.
Cited in this Issue
Sizing Up for Successful Surgery
Page 18
1. Aristodemou P, et al. “Formula Choice: Hoffer Q, Holladay 1, or SRK/T and Refractive Outcomes in 8108 Eyes after Cataract Surgery with Biometry by Partial Coherence Interferometry,” J Cataract Refract Surg., 2011; 37: 63–71. doi: 10.1016/j. jcrs.2010.07.032.
2. Wendelstein J, Hoffmann P, Hirnschall N, et al. “Project hyperopic power prediction: accuracy of 13 different concepts for intraocular lens calculation in short eyes.” Br J Ophthalmol., 2022 Jun; 106(6): 795–801. doi: 10.1136/bjophthalmol-2020-318272.
Presbyopia-Correcting Cataract Surgery in the Post-LVC Patient
Page 23
1. Alio JL, D’Oria F, Toto F, et al. “Retinal image quality with multifocal, EDoF, and accommodative intraocular lenses as studied by pyramidal aberrometry,” Eye Vis (Lond). 2021; 8(1): 37.
JOIN the leading community and trusted source for SCIENCE, EDUCATION & PROFESSIONAL DEVELOPMENT in the fields of cataract and refractive surgery. learn more about membership at escrs.org
Upcoming Events
November 3–6
American Academy of Ophthalmology
San Francisco, United States
November 24–26
Italian Society of Ophthalmology
Rome, Italy
February 15–18
2024 ESCRS Winter Meeting in conjunction with the 38th Congress of the DGII Frankfurt, Germany
May 24–26
2024 EuCornea Annual Congress Paris, France
September 6–10
2024 ESCRS Congress Barcelona, Spain
Nov 3
Nov 24
Feb 15
Research. Education. Innovation.
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.