December 2020 | Vol 25 Issue 12
January 2021 | Vol 26 Issue 1
THE BEST OF THE ESCRS
VIRTUAL CONGRESS

SPECIAL FOCUS
CATARACT & REFRACTIVE | CORNEA | RETINA | GLAUCOMA PAEDIATRIC OPHTHALMOLOGY | GLOBAL OPHTHALMOLOGY
ESCRS 2020 by Numbers
5,612 Total number of visits to the Relaxation Lounge (yoga, meditation, Virtual Rijksmuseum tour, musical memories)
It was amazing resembling the actual meeting”

1,443 Presenters from all over the world
Oral Presentations in 4 Parallel Session Rooms with 48 LIVE sessions 1,797 On Demand Presentations of Free Papers, Posters,

2-4 October 2020 www.escrs.org Online. Live. Interactive. 38th Congress of the ESCRS 1st ever live Virtual Congress Attendees joined us online Countries were represented Exhibition Booths in 4 Halls Exhibitors Participated Total live-stream viewers at Industy Sessions of live & on demand sessions CME Credits Awarded
Scientific Programme Other Congress Highlights Breakdown of Attendees by Location 3 days 16 4,089 108 64 1,412 6,438 60% 1% 26% 8% Europe Australia Asia Africa 3% N. America 2% S. America
“
Reports, Videos Impressions on Twitter feeds Impressions on Instagram feeds 1.163m
J&J
Lucas & Steve
DJ
Friday evening Royal
Saturday evening
267
Case
61,207
Networking Lounge
Live
Set
Concertgebouw Orchestra
Publisher Carol Fitzpatrick
Executive Editor
Colin Kerr
Editors
Sean Henahan
Paul McGinn
Managing Editor Caroline Brick
Content Editor
Aidan Hanratty
Senior Designer


Lara Fitzgibbon
Designer


Ria Pollock
Circulation Manager
Angela Morrissey
Contributing Editors
Howard Larkin
Dermot McGrath
Roibeard Ó hÉineacháin
Contributors
Maryalicia Post
Leigh Spielberg
Gearóid Tuohy
Priscilla Lynch
Soosan Jacob
Colour and Print

W&G Baird Printers
Advertising Sales
Amy Bartlett ESCRS
Tel: 353 1 209 1100

email: amy.bartlett@escrs.org
Published by the European Society of Cataract and Refractive


Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the managing editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Surgeons,
As certified by ABC, the EuroTimes average net circulation for the 10 issues distributed between February and December 2019 was 47,863 P.40 CONTENTS A EUROPEAN OUTLOOK ON THE WORLD OF OPHTHALMOLOGY global pandemic REGULARS 38 My Mentor 39 Outlook on Industry 40 Random Thoughts 41 Industry News 42 Inside Ophthalmology 43 Calendar SPECIAL FOCUS BEST OF THE BEST 4 How Aravind Hospitals do more with less and save sight in the process 6 Plotting the history of laser vision correction 7 All the award winners from the 38th Congress of the ESCRS 8 The future of artificial intelligence and ophthalmology 9 Taking a deeper look inside the lens 12 Can SMILE compete with custom LASIK? 14 Strategies for saving vision in trauma cases 15 Normal vision with normal aberrations – the ultimate goal? 16 The bag-in-the-lens and young patients 17 Using the femtosecond laser for keratoconus CATARACT & REFRACTIVE 18 Benefits of preloaded IOL inserters 19 Computer-based method for measuring cyclorotation 20 Measuring long-term regression in refractive patients 21 JCRS highlights CORNEA 22 Hyaluronic acid drops for 23 New grafting technique promise for flattening curvature 24 Cell therapy for endothelial cell dysfunction 25 Using KPro surgery in ocular surface disease RETINA 26 Retinal complications anterior segment surgeries 28 Cataract surgery in patients with AMD 29 Complement 5 inhibition for geographic atrophy GLAUCOMA 30 Monitoring progression after phacoemulsification 31 Interpreting visual field loss 32 Getting the most out of optical coherence tomography PAEDIATRIC OPHTHALMOLOGY 33 Infectious keratitis in children 34 Endothelial keratoplasty in cases of corneal clouding EUROTIMES | DECEMBER 2020/JANUARY 2021
MEDICAL EDITORS


Re-inventing gatherings
While the congress is officially over, it remains online until the end of 2020
It is 2020, and we’ve all had to re-invent gatherings. ESCRS is no exception.
The old adage that ‘you can’t be in two places at once’ suddenly no longer applies. Over the course of the weekend at the ESCRS Virtual Congress, there were four live streams and Q&A sessions. And you can watch all of them. Because anything you missed live is available online for you to peruse at your own convenience.
The congress officially opened on the Friday afternoon and one of the standouts for me was the Ridley Medal Lecture by David F. Chang. It was an amazing and humble presentation given by one of the world’s best surgeons on how we can learn about efficiency, safety and sustainability in cataract surgery from the incredible work in Aravind Eye Hospital. I can’t look at disposable instruments the same way since!
This was followed by a great session on dealing with the traumatised cornea. At the same time, I was speaking at a really engaging ESCRS/WSPOS session about paediatric intraocular lenses. Normally I would have to miss the parallel sessions but with the virtual platform I could just watch what I missed.
Bruce Allan’s approach to corneal perforations was a real “must see” for me. Another standout moment was the Heritage Lecture, this year given by Theo Seiler. He walked us through the history of Laser Vision Correction and to hear it from someone so key in its development and seeing how far we have come from the “horrors of the past” was a treat.
But the sessions I keep coming back to are the instructional courses. The density of information here meant that it took me a few views to absorb it all. It’s like having a library at your disposal. Tricky surgical approaches are easier to learn when you can slow the presentation down and for me the course “Strategies and techniques for IOL exchange” really benefited from this.
INTERNATIONAL EDITORIAL BOARD



Noel Alpins (Australia), Bekir Aslan (Turkey), Roberto Bellucci (Italy), Hiroko Bissen-Miyajima (Japan), John Chang (China), Béatrice Cochener-Lamard (France), Oliver Findl (Austria), Nino Hirnschall (Austria), Soosan Jacob (India), Vikentia Katsanevaki (Greece), Daniel Kook (Germany), Boris Malyugin (Russia), Marguerite McDonald (USA), Cyres Mehta (India), Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands), Leigh Spielberg (The Netherlands), Sathish Srinivasan (UK), Robert Stegmann (South Africa), Ulf Stenevi (Sweden), Marie-José Tassignon (Belgium), Manfred Tetz (Germany), Carlo Enrico Traverso (Italy)
So while the congress is officially over, its remains online until the end of 2020. Make use of it in your own time because it really is a superb way to absorb all the material.
That being said, it would be nice to see each other in person again in 2021.
GUEST EDITORIAL
Emanuel Rosen Chief Medical Editor
José Güell
EDITORIAL 2
Thomas Kohnen
Paul Rosen
Sorcha Ní Dhubhghaill
Sorcha Ní Dhubhghaill is Professor of Anterior Segment Surgery at Antwerp University Hospital (UZA) and a Consultant Surgeon at the Netherlands Institute for Innovative Ocular Surgery (NIIOS)
A WORD
The old adage that ‘you can’t be in two places at once’ suddenly no longer applies
FROM SORCHA NÍ DHUBHGHAILL MB, PhD, FEBOS-CR
EUROTIMES | DECEMBER 2020/JANUARY 2021
Research Education Innovation
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.

Fighting blindness in the developing world
Aravind Hospitals do more with less and save sight in the process. Dermot McGrath reports

From humble beginnings as a small clinic with just 11 beds and the audacious goal of curing preventable blindness, the Aravind Eye Care System in southern India has grown into the largest eye care provider in the world and serves as a model for how cataract blindness might effectively be eliminated in the developing world, said David F. Chang in his Ridley Medal Lecture at the 38th Congress of the ESCRS.
“I have long felt that our single greatest challenge in cataracy surgery was not the invention of an accommodating IOL but rather reversing the rapidly increasing backlog of cataract blindness in the developing world, which accounts for half
of all global blindness,” he said.
One of the major stumbling blocks to tackling the caseload is the shortage of qualified cataract surgeons in developing countries, said Dr Chang.
“We need to maximise their productivity by allowing them to do rapid surgery at a very high volume. But it has to work well with the advanced cataracts that they face and to be performed with a very low complication rate. And then it also has to be cost effective and affordable,” he said.
Remarkably, the Aravind Eye Care System in India has managed to achieve all of these goals since it was first established in 1976 by Dr Govindappa Venkataswamy, or Dr V as he came to be known, said Dr Chang.
“After reaching the mandatory age of
retirement from the government hospital at 58, Dr V needed something new to do. So, he founded this modest family eye clinic, financed it himself and grew the system with the help of his family.”
HIGH-QUALITY AND COMPASSIONATE EYE CARE
Dr V’s goal in setting up Aravind was to eliminate needless blindness by providing high-quality and compassionate eye care that was affordable for all.
“It’s a proven model that is now emulated in so many countries and settings around the world, and this has given hope to all of us,” added Dr Chang.
Reflecting on his own association with
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 4
Courtesy of Aravind Eye Care System
The inpatient building at the Aravind Eye Hospital, Madurai, India
Aravind, which dates back to 2003, Dr Chang, Clinical Professor at the University of California, San Francisco, said that there are many lessons to be learnt from the Aravind model of providing large-volume, high-quality and affordable care through its network of 13 eye hospitals and 75 primary eye care facilities.

“I made the observation a few years ago that resource-rich countries like mine in the United States can still learn a lot from resource-poor settings such as in southern India. And I wanted to highlight some of the lessons that we can take from the Aravind model, the most important of which is that there is a proven way to eradicate global cataract blindness,” he said.
ASSEMBLY-LINE APPROACH
A critical component of Aravind’s model is high patient volume, which brings with it the benefits of economies of scale, noted Dr Chang.
Aravind’s unique assembly-line approach, with rates often exceeding 14-to-16 cases per hour per surgeon, increases productivity but without compromising on safety or quality.
“When I first saw this, I marvelled at how well choreographed it all was. Around 40% of private paying patients subsidise eye care for the other 60%, who receive services either free of cost or at a steeply subsidised rate, yet the organisation remains financially selfsustainable. The message is that we can use this type of cost-recovery model to reduce and eventually eliminate global cataract blindness,” he said.
At the heart of Aravind’s approach to cataract surgery in the indigent is the use of suture-less manual small-incision cataract surgery (MSICS) explained Dr Chang. The technique uses a long, temporal, scleralpocket incision that is wide enough to enable manual extraction of the undivided nucleus, after which a low-cost PMMA IOL is implanted. The incision is self-sealing, requires no sutures and is very fast to perform for an experienced surgeon. The private pay patients receive phacoemulsification with foldable IOLs.
CONTROLLING COSTS
The system is designed to keep expenses to an absolute minimum without compromising on safety or quality, said Dr Chang.
“In order to control costs, Aravind has its own manufacturing company that produces all consumables such as intraocular lenses, surgical sutures, pharmaceutical products,
surgical blades and equipment. An IOL costs less than $2 (US) and the entire cost of disposables per case is just $10. They also reuse as many supplies as possible such as tubing, gowns, gloves and drugs to cut down on wastage. Despite this and operating on multiple patients simultaneously in the same large OR, their infection rates are no higher than in the West,” he said.
Large-scale studies at Aravind show that the MSICS complication rate is lower than that with phacoemulsification for less experienced surgeons, and comparable for the most experienced surgeons. Furthermore, Dr Chang noted that indigent populations have a significant burden of ultra-brunescent and mature cataracts, increasing the risk of complications with phacoemulsification.
“Our studies at Aravind concluded that MSICS is a safer procedure than phaco for many surgeons unless they are very experienced with advanced hard cataracts. I now use MSICS in my own practice for the most advanced cataracts and I would maintain that many of us in the West would benefit by doing more of this as well,” he said.
SQUARE-EDGE IOLS TO TACKLE PCO
Published studies from Aravind have also shown that a squared posterior optic edge reduces PCO regardless of IOL material, said Dr Chang. This is important in developing countries where posterior capsular opacification (PCO) is a leading
cause of visual impairment due to a preponderance of PMMA IOLs.
“PCO is an inconvenience for us in the West but a leading cause of visual disability in developing countries due to poor access to care. We showed in long-term studies with up to nine years of follow-up that adding a square edge to the PMMA optic is an inexpensive modification that greatly reduces PCO rates,” he said.
Another key lesson to emerge from the Aravind experience is that intracameral moxifloxacin is safe and effective for endophthalmitis prophylaxis.
“The data is very robust and is based on 2 million consecutive surgeries over an eight-year period. The rate of postoperative endophthalmitis dropped from seven per 10,000 cases to two per 10,000 with the introduction of low-cost intracameral moxifloxacin,” he said.
A final lesson to be drawn from the Aravind experience is that inflexible operating room regulations in developed countries mandating single-use of most drugs and supplies may be of unproven benefit in reducing infection rates, said Dr Chang.
“The single-use rationale is supposedly to lower the infection rate. And yet our phacoemulsification infection rate in the US, where we dispose of everything after one use, is four times higher than the Aravind hospitals, where supply reuse and intracameral moxifloxacin are routine,” he said.
Dr Chang added that both the financial and environmental sustainability of cataract surgery is threatened by excessive surgical waste as the volume of surgery increases worldwide.
“We need to learn from systems such as Aravind’s how to be more efficient, reduce waste and reduce our carbon footprint while performing the most common operation in the world,” he concluded.
David F. Chang: dceye@earthlink.net

EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 5
Assembly line for cataract surgery. One surgeon alternates between two operating tables with one patient prepped and draped while the other is undergoing surgery through a temporal incision
Courtesy of David F. Chang
When I first saw this, I marvelled at how well choreographed it all was. Around 40% of private paying patients subsidise eye care for the other 60%...
David F. Chang
Evolution of LVC & cataract surgery
Professor Theo Seiler covered the origins of laser vision correction during his Heritage Lecture at 38th Congress of the ESCRS. Dermot McGrath reports
The history, development and complex implications of laser vision correction (LVC) both before and after cataract surgery were all addressed in a fascinating 2020 ESCRS Heritage Lecture delivered by Theo Seiler MD, PhD.
In his talk, Prof Seiler discussed the overlap between LVC and cataract surgery, the difficulty of obtaining consistently predictable refractive outcomes now that the first-generation of LVC patients has reached cataract age and the ways in which LVC can successfully improve the outcomes of cataract surgery.
“We are all aware that laser vision correction jeopardises the precision of cataract surgery. But on the other hand, LVC creates a kind of compensation because we can enhance the optical performance postoperatively of the operated eye and increase patient satisfaction,” he said.
The early history of laser vision correction (LVC) was a far cry from the high-tech technological precision that refractive surgeons today take for granted, said Prof Seiler.
“The first PRK surgeries that I performed were quite rudimentary by modern standards. The eye tracking and centration were performed using only my hands and my eyes so you can imagine that safety suffered accordingly, “he said.
Turning to modern cataract surgery, Prof Seiler noted that while significant improvements have been achieved in IOL power calculations due to advances in optical biometry, there is still considerable inaccuracy when it comes to keratometry measurements for post-LVC eyes.
“Studies have shown that despite better preoperative diagnostics that the chance of postoperative refractive surprise is still greater than 20%,” he said.
The primary reason for these refractive surprises is the irregularity of the cornea after previous refractive surgery, noted Prof Seiler.
“The corneal curvature or corneal power is significantly altered by LVC. Prof Seitz was one of the first to publish on this back in 1999 and he figured out if you use standard formulas and algorithms in these eyes you will end up with a postoperative hyperopia of up to +3 or +4 dioptres,” he said.
Almost 20 years after Prof Seitz’s study, modern biometry has still not resolved the problem of IOL power calculations in eyes with previous corneal
refractive surgery, said Prof Seiler. He cited a recent study by Koch et al that looked at the accuracy of several of the most popular methods currently used for IOL power calculation including the Haigis-L, the Shammas-PL and the Barrett True-K formulas.

“We see that the accuracy is not significantly better because between only 40% and 70% of the patients postoperatively were within 0.5D of their target refraction. So that still seems to be an unsolved problem,” said Prof Seiler.
Tools such as the ASCRS post-refractive IOL calculator, which incorporate a variety of formulas, may prove helpful in increasing the likelihood of attaining the target postoperative refraction in eyes that have undergone previous PRK, LASIK or RK, he added.
Careful preoperative counselling of the patient can also help in the event of a refractive surprise. “In Zurich we try to avoid this dilemma and explain to them that the predictability is not as good for post-refractive surgery eyes but that we can compensate for this by performing a laser enhancement treatment using a flap re-lift or we can change the intraocular lens. That is also why we select an IOL type that can be easily exchanged,” he said.
FINE-TUNING CATARACT SURGERY OUTCOMES
In the final part of his lecture, Prof Seiler discussed how laser vision correction can be used to improve the outcomes of cataract surgery. Specifically, Prof Seiler said that selective wavefront-guided LASIK may increase the success rate of multifocal and toric IOL implantations.
Prof Seiler cited recent studies (Maurino et al, Ophthalmology 2015;122:700-10; Rodov et al, J Refract Surg 2019; Jul 1;35(7):434440) that looked at the quality of vision after bilateral multifocal and trifocal IOL implantation.
“Maurino et al. showed that only 77% of patients never wore glasses for any purpose and only 68% said that they were very satisfied with their vision, which is not very impressive. Another study by Rodov et al. found that only 76% of patients would choose the same IOL again,” he said.
Prof Seiler’s own group carried out a prospective study of 213 eyes of 108 patients implanted with a trifocal IOL and found that 56 eyes (26%) were dissatisfied after surgery. The refractive reasons for their dissatisfaction were astigmatism in 63%, myopia in 45%, hyperopia in 20% and higher-order aberrations greater than 0.5 microns in 13%. After selective wavefront-guided LASIK, there was a significant increase of satisfaction from 2.1 preoperatively to 3.6 postoperatively on a scale of 1 (not satisfied) to 4 (totally satisfied), said Prof Seiler.
“Of the unsatisfied 42 patients, 38 said they would choose the same procedure of trifocal IOL and femto-LASIK again. In total, the satisfaction degree increased from 74% to 96% of the patients due to selective wavefront-guided LASIK. Of the four patients who were dissatisfied, all of them suffered from dry eye. This is why we now do selective wavefront-guided PRK in patients with significant dry eye preoperatively in order to re-establish the tear film faster,” he concluded.
Theo Seiler: c/o claudia.kindler@iroc.ch
EUROTIMES | DECEMBER 2020/JANUARY 2021
SPECIAL FOCUS: BEST OF THE BEST 6
Studies have shown that despite better preoperative diagnostics that the chance of postoperative refractive surprise is still greater than 20%
Theo Seiler MD, PhD
Changing the world
MICHAEL BLUMENTHAL AWARD
Dr Hisaharu Suzuki, Japan, won the Michael Blumenthal Award for overall winner in the 2020 ESCRS video competition.

Entitled “Hydrogen will change the world of ophthalmology”, Dr Suzuki impressed the judges with his research showing that hydrogen’s ability to selectively scavenge free radicals, and in particular cytotoxic hydroxyl, can improve outcomes in the treatment of retinal ischaemia as well as in cataract surgery.
Dr Suzuki’s study examined the effect of hydrogen in an irrigation solution in an animal study and a clinical trial and demonstrated its usefulness as a new method for protecting corneal endothelium in phacoemulsification.
Dr Suzuki graduated from Nippon Medical School in 2001 and joined the faculty in the Department of Ophthalmology at Nippon Medical School. He obtained a PhD in Medicine in 2009. In 2016, he became Associate professor in the Department of Ophthalmology at Nippon Medical School Musashikosugi Hospital. He opened the private clinic “Zengyo Suzuki Eye Clinic” in 2018. He is currently Visiting Assistant professor in the Department of Ophthalmology at Nippon Medical School.

ESCRS POSTER AWARD: REFRACTIVE
First prize for best refractive poster was awarded to Emilio TorresNetto, Switzerland, for his poster “Corneal cross-linking for treating infectious keratitis: final results of the prospective randomized controlled multicentre trial”.
Dr Torres-Netto’s prospective, randomised phase III study set out to analyse the time to corneal epithelisation with photoactivated chromophore for infectious keratitis-corneal cross-linking (PACK-CXL) as a first-line treatment in early infectious corneal ulcers, and compare it to antimicrobial therapy, which is the current standard of care.
A total of 42 patients were included in the study, 23 in the medication group and 19 in the PACK-CXL group. Grampositive cocci were the most commonly identified pathogens in the study. Cases of fungal infection were shown to have worse visual acuity both at presentation and at discharge. No significant differences in corneal re-epithelisation time were observed between the medication and PACK-CXL groups.
“Our results suggest a role for PACK-CXL as an alternative to antimicrobials as primary treatment for infectious corneal infiltrates and early corneal ulcers,” concluded Dr Torres-Netto.
ESCRS POSTER AWARD: CATARACT
Helene Bailleul from France won first prize for best cataract poster for her poster on the “Rate of re-intervention in paediatric cataract surgery with ‘bag-inthe-lens’ fixation: ten years of experience”.

Dr Bailleul’s retrospective study looked at the rate and reasons of secondary surgery in 76 paediatric patients implanted between 2009 and 2019 using Marie-José Tassignon’s bag-in-the-lens (BIL) technique.

The results reported just nine reoperations over the 10-year period.
“The prevalence of posterior capsule opacification tends to be close to 0% if both the posterior and anterior capsulorhexis are well calibrated and if the BIL implant is well positioned in both capsules,” Dr Bailleul concluded.
JOHN HENAHAN PRIZE
The winner of the 2020 John Henahan Prize was Dr Jennifer Kim, UK. The topic for this year’s essay was “Will Clinicians Be Replaced By A Robot
To Perform Cataract Surgery?”
Dr Kim studied medicine at Manchester Medical School, United Kingdom. She has recently completed her training at Manchester Royal Eye Hospital and is due to start her Corneal Fellowship at Birmingham and Midland Eye Centre. She has a special interest in Cornea and ocular surface diseases and after her fellowship, she hopes to pursue a career in this field.
“Winning this prize has allowed me to connect with colleagues and the ophthalmic community worldwide during this difficult time,” said Dr Kim. “When working in a clinical environment we have to keep a poker face whilst carrying a huge amount of emotion, and this can be difficult to balance as a trainee. Many of us are feeling additional stress from change in, or lack of, routine and overall uncertainty around COVID-19. Jotting down my thoughts regularly during this time has helped me to clear my mind and stay grounded. I would like to thank all the frontline healthcare workers in every corner of the world and also the ESCRS for giving me this prestigious award,” she said.
Emanuel Rosen, chief medical editor of EuroTimes and chairman of the judging panel, congratulated Dr Kim on winning the prize and said that all the submissions were of the highest quality.
“All of the entries were very well written even if I did not always agree with the content. In summary, no writer believes that robots in anterior segment ophthalmic surgery will be anything but a companion device for anterior segment ophthalmic surgery.”
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 7
Congratulations to all the prize winners at the 38th Congress of the ESCRS
AI & ophthalmology
The future of artificial intelligence (AI) looks exciting to assist but not replace ophthalmologists, concluded speakers during a dedicated Clinical Research Symposium on AI at the 38th Congress of the ESCRS.
Béatrice Cochener-Lamard MD, PhD, France, outlined the development of AI in ophthalmology and the role of deep learning to assist in diagnosis, citing its successful use in diabetic retinopathy.
Looking at the latest developments, she said that AI technology is now well on the road to automatic image classification, with AI to soon become a widespread tool in all imaging modalities (2D and 3D and beyond).
Thanks to the creation of more refined algorithms, the use of ‘big data’ is not always necessary now in AI and there are “multiple additional applications” on the way, she said. These include using AI as an integrated part of “screening, diagnosis, decision support and maybe even surgical help”.
“So the future looks very exciting [for AI] to help ophthalmologists for sure, but never to replace us,” Prof CochenerLamard concluded.
Although progress in deep learning no longer requires big data, it is crucial to emphasise that the development and validation of image recognition software relies on the number and quality of images and their interpretation, which condition the training of the algorithms.
Also speaking during this session, Bruce Allan MD, UK, gave a practical presentation on the development of a machine learning accessible electronic healthcare record suitable for a patient registry.
“All machine learning studies require the same thing; high-quality labelled data, usually collected for routine clinical practice,” he explained.
Data for machine learning and registry studies has four essential attributes, Dr Allan said.
“First of all it has to be legal, in line with GDPR legislation. It has to be high quality, it has to be accessible and searchable, and it has to be secure.”
Healthcare data does qualify for certain GDPR exemptions to the strict requirement for prior consent to research use. Data does not always have to be anonymised, rather “pseudo-anonymisation”, in which personally identifiable elements are held
at arms’ length from other healthcare data using an encryption key, can be sufficient, “but it is useful to have clear advice about this”, Dr Allan said.
ESCRS has now commissioned legal expertise on this topic, “which should help us in each member state to know where we stand, and remove some of the obstacles to research progress”.
In terms of collecting good-quality data, there are some generally applicable criteria that can be applied, including averaging key measurements across a sequence of three scans to improve precision, and labelling poor-quality scans that are still deemed to be clinically useful.
“ESCRS can help by setting standards for doing this and standards for simple aspects of data acquisition, like, for example, measuring intermediate visual acuity of 63cm. These kind of standards are not well defined at the moment,” Dr Allan said.
Also speaking during this session, Robert Wisse MD, PhD, the Netherlands, who discussed the use of digital eye testing, including on smartphones, in cataract and refractive care and the use of telemonitoring.

He explained that by 2040, older people will make up half of the population in Europe, and an estimated 40% of these will have three or more chronic conditions. This will create a significant extra demand on healthcare services and strengthens the need to increasingly utilise AI and telemedicine. “A paradigm shift in healthcare delivery is needed,” Dr Wisse maintained, adding that digital transition is not a goal per se but as a means to an end.
A prospective international RCT is one of eight research programmes to assess the true clinical validity and safety of this novel method for testing visual function. Easee BV (http://easeee.online) is a medtech start-up and the private partner in a public-private Digital Eye Health consortium that develops the web-based test. The tool will be integrated in several hospitals and Electronic Health Records.
IOL POWER CALCULATION
Warren Hill MD, USA, gave an update on IOL power calculation driven by AI.
He explained how the use of pattern recognition based on AI data calculations, rather than the more common theoretical formula approach, could help achieve more accurate IOL power calculation results.
“A ±0.50D accuracy of around 78% [with traditional formulas], which is where most surgeons are now, but with AI we can routinely get to 90% provided the measurements are good. A critical aspect of the best possible refractive outcomes is validating the measurements and making sure the ocular surface has been optimised.”
Dr Hill’s quoted positive comparison data from a number of international centres on the AI-based Hill-radial basis function (RBF) calculator, of which he is the author. The latest validated data on the updated RBF calculator show results of over 91% accuracy within ±0.5D of the intended target.
Renato Ambrósio MD, PhD, Brazil, discussed the detection of corneal ectasia using AI, noting that while laser vision correction and eye rubbing are the primary environmental culprits in the development of ectasia, detection of other risk factors is key to reducing cases and ensuring early diagnosis which AI is proving useful in.
The final speaker in this session was Jodhbir S Mehta MD, Singapore, who spoke about the use of AI for classification of corneal dystrophies. He said that while retinal disease is currently leading the way in AI-related ophthalmic applications, there are plenty of anterior segment classification uses; “I see this as a platform technology we can use for multiple things.”
For stromal dystrophies he has helped create validated AI software that can monitor disease progression, recurrence after transplantation, and monitor the effect of various treatments.
Concluding, Dr Mehta said AI offers much promise in any field where there is large data and good imaging, thus it is here to stay in ophthalmology.
AI set to be used in more eyecare applications. Priscilla Lynch reports
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 8
All machine learning studies require the same thing; high-quality labelled data, usually collected for routine clinical practice
Bruce Allan MD
A deeper look at the lens
How visual outcomes can be optimised in cataract patients. Priscilla Lynch reports
Despite all the advances in technology and surgical techniques, post-cataract surgery visual issues persist in some patients and must be dealt with honestly and practically while continuously striving to improve outcomes, said speakers during the ‘20/20 in 2020: The Lens’ symposium during the 38th Congress of the ESCRS.
Dr Béatrice Cochener-Lamard MD, France, spoke about the goal of “super vision”, which she explained goes far beyond just visual acuity: “It is not about 20/20 and zero refraction vision but rather good quality vision whatever the surrounding light conditions.”
She stressed the importance of choosing the right lens for the right patient and gathering the necessary data about their visual needs, noting that smartphone and computer usage have increased substantially in recent years.
Beyond the key metric of spectacle independence post-surgery, Prof CochenerLamard said it is important to conduct an objective, wide-ranging evaluation when assessing post-op eyes. She outlined a number of useful assessments and questionnaires (eg, contrast sensitivity, reading speed, halometry etc): “There are now a wide range of options to quantify the quality of vision, which have allowed a better understanding of optical aberrations.”
Prof Cochener-Lamard added that ocular surface issues are also an important consideration, with thorough pre-op assessment key to explain risks to the patient and to avoid post-op complications, with presbyopia correction more challenging in this regard than corneal refractive surgery. Indeed, with ageing, risk factors for ocular dryness accumulate, whereas multifocal optics and even EDOF are more sensitive to the degradation of light diffusion and the sensitivity of contrasts that can be induced by an unstable tear film.
Similarly, Giacomo Savini, Italy, warned against overpromising results to patients before surgery, during his talk entitled ‘The Quest for Emmetropia’. About 15% of eyes after surgery will have a prediction error of
>0.5D and patients with multifocal lenses should be advised that laser touch-up may be necessary in about 10% of cases to reach emmetropia, he said, so “if this happens then patients will not complain”
There is very little difference among the refractive results based on measurements from the current range of optical biometers: “the prediction error of <0.5D is generally between 80-85%. This is not surprising as all manufacturers follow the measurements of the original IOLMaster to be able to use the ULIB constants,” Dr Savini said. However, the newer optical biometers have other advantages, such as swept source OCT having the ability to penetrate through dense and subcapsular cataracts he noted.
Scott MacRae MD, USA, highlighted the success of early studies on novel femtosecond laser-induced refractive index change for IOL touch-ups, which he explained is biocompatible, relatively non-invasive and can treat refractive error, presbyopia and high-order aberrations. “We are very, very excited about this technology and look forward to presenting more information in the future.”
Gerd Auffarth MD, Germany, discussed restoring accommodation with IOLs. The reality is that there are not any real accommodative lens in use currently, but there are some promising developments, including fluid lenses that change curvature; “which is more rewarding than changing the position of the lens as you can achieve a real amount of accommodation with that,” he said.
Looking further into the future, Dr Auffarth said work is ongoing on lenses utilising artificial intelligence (AI) and ‘bionic IOLs’ that looks interesting, but clinical data is awaited, while he also questioned the use of the capsular bag as the standard location for accommodative lenses.
Also speaking during this session, Gregorius Luyten MD, the Netherlands, said that positive and negative dysphotopsia can occur in up to 20% of patients following uncomplicated cataract surgery, and “and I think it is important that we acknowledge to the patient that their symptoms are real”.
Positive dysphotopsia is more likely to occur with multifocal lenses while negative dysphotopsia occurs immediately after uncomplicated cataract surgery, with normal in-the-bag implantation, he explained.
Quoting the recent ESCRS vRESPOND study, Dr Luyten said the root causes of negative dysphotopsia could be due to significant geometrical differences – these patients tend to have a smaller pupil diameter, decentred pupil centres and tilted iris plane than controls.
Treatments for persistent pseudophakic dysphotopsia include piggyback IOL implantation and secondary reverse capture, but mostly involve exchanging the IOL, he said.
In terms of avoidance, perfect centration of the lens is key, as is putting haptics in the horizontal position, and using larger optics (6.5 or more), Dr Luyten recommended, reiterating that IOL exchange with a larger optic size has up to a 100% success rate.
Speaking about correcting astigmatism at the time of cataract surgery, Adi Abulafia MD, Israel, said toric lenses are becoming the standard of care for these patients but the results are not always predictable.
He outlined seven key tips to improve toric IOL outcomes including validating data, looking at the corneal topography and optimising the ocular surface; using several measuring devices, taking into account the posterior corneal astigmatism, being alert for unusual corneas; accounting for the corneal surgically induced astigmatism; optimising toric IOL alignment and having a low threshold for performing toric IOL calculations.
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 9
The reality is that there are not any real accommodative lens in use currently, but there are some promising developments
Gerd Auffarth MD
In conjunction with the Polish Society of Cataract and Refractive Surgery
19 – 21 February
Join us for an exciting Live Virtual Meeting , where expert speakers, chairpersons and panellists will deliver a scientifi c programme covering a range of hot topics, including lively discussion and interactive debate!
Main Symposia
Friday 19 February
Too Many Patients, Too Few Doctors, Better Eyecare
Chairpersons: J. Alio SPAIN , D. Spalton UK
Saturday 20 February
Optimizing Your Refractive Outcomes Before Cataract Surgery
Chairpersons: A. Abulafi a ISRAEL , N. Hirnschall AUSTRIA
Ocular Surface in Our Daily Surgical Practice
Chairpersons: B. Cochener-Lamard FRANCE , S. Barisic SERBIA
Sunday 21 February
Cataract Surgery in Special Conditions
Organised by the Young Ophthalmologists Committee
Chairpersons: B. Bostanci Ceran TURKEY , V. Qin BELGIUM
Included at the end of each Main Symposia is an Audience Q&A Session with the Experts ?
Other Sessions
Friday 19 February
Refractive Surgery Course
Free Paper Session Cataract
Saturday 20 February
Cornea Cases (Organised in conjuntion with EuCornea)
Young Ophthalmologists Programme
Surgical Video Symposium
Free Paper Session Refractive & Cornea
Cataract Surgery Courses
Cornea Medical Course
Experts Discuss the Latest Innovations from Industry
Sunday 21 February
Cornea Surgical Course
Refractive Surgery Course
Polish Society Sy mposium
On Demand Library including free papers, ePosters and Cornea Case Presentations +
This Meeting will Include:
Relaxation Lounge Meet the Experts Chat 3 Live Streams Live Q&A Sessions Interactive 3D Exhibition Networking Lounge Industry Supported Satellite Symposia Scientifi c Programme & Registration
www.escrs.org
SMILE vs custom LASIK
Debaters say the best choice depends on patients’ needs. Howard Larkin reports
Can SMILE® compete with topography-guided custom LASIK for most refractive surgery patients? The answer may depend upon the needs of individual patients, according to debaters at the JCRS Symposium at the 38th Congress of the ESCRS, held virtually for the first time.
Arguing for SMILE was Timothy J Archer MA (Oxon), DipCompSci (Cantab), PhD, of London Vision Clinic, London, UK. He allowed that topography-guided treatment gives excellent results for therapeutic purposes, such as correcting irregular astigmatism, enlarging optical zones and re-centring ablations. But it is a complex procedure that most patients don’t really need, and SMILE is a less-invasive alternative with equivalent visual outcomes.
Arguing for custom LASIK, Vance Thompson MD, of Vance Thompson Vision, Sioux Falls, South Dakota, USA, noted that it is necessary for some patients and can produce better low-contrast visual outcomes, making it a better choice for many patients. He agreed, though, that some patients require SMILE benefits such as reduced dry eye risk, and he prefers it for many patients who do not need topography or wave-front guided procedures.
LOW ABERRATIONS
Dr Archer pointed out that most patients have very low corneal aberrations with spherical aberration (SA) most common, averaging just 0.14 microns up to 0.42 at two standard deviations. Moreover, a small amount of SA is beneficial since it increases depth of field. For coma, the average is 0.19 and 95% of eyes have 0.42 micron or less.
“Topography-guided treatment might be an option for this 5%,” Dr Archer said.
For the other 95%, topography-guided procedures introduce complexities that potentially lead to errors. These include deciding which refraction and how much astigmatism to treat, since both are influenced not just by anterior corneal topography but also the posterior cornea, crystalline lens, retinal irregularities and neuroadaptation.
Corneal aberrations are often partially offset by internal aberrations leaving a low level of total aberrations.
“If you treat the corneal aberrations entirely you run the risk of unmasking
significant internal aberrations.”
Similarly, topographical coma can be measured as “pseudo” cylinder, so treatment based on manifest refractive cylinder can lead to significant overcorrection as both the coma and the pseudo-cylinder would be included in the treatment, Dr Archer said.
Tear film issues, contact lens use and measurement errors are other confounding factors.
“All this adds up to a lengthy and complex treatment planning process requiring trained and skilled operators.”
SMILE is a better alternative for most patients, Dr Archer said. As a less invasive “keyhole” surgery requiring no flap, SMILE is more attractive to patients, especially those participating in contact sports or other extreme activities.
Multiple studies also show that SMILE produces less dry eye than LASIK as measured by Schirmer’s test and tear break-up time (Singh Sambhi RD et al. Can J Ophthalmol. 2020 Apr;55(2):99-106). Symptoms are also significantly less three years out (Han T et al. Health and Quality of Life Outcomes. 2020; 18:107); and SMILE is less disruptive to corneal nerve fibres short term (Recchioni A et al. Cornea 2020 Jul; 39(7):851-857.). Furthermore, the biomechanical advantages of SMILE enables the use of larger optical zones, leading to less SA induction (Spiru B et al. J Refract Surg. 2018 Jun;34(6):419-423).
With 10 years’ history, SMILE is a mature procedure that produces visual outcomes similar to LASIK, according to data on nearly 4,000 patients with 12 months;’ follow-up at Dr Archer’s clinic. Of note is the importance of optimising the energy and spot spacing settings for each individual laser, and this goes some way to explain some of the reports of lower outcomes in SMILE compared to LASIK. This is most relevant in the US, where the energy and spot spacing settings were fixed until the second FDA approval in 2019. It is also highly predictable and stable, accurately corrects cylinder, and improves contrast sensitivity, even in patients with high myopia up to -13.00D spherical equivalent, he reported. And patient satisfaction is high. So, SMILE can compete with custom LASIK for eyes with normal visual aberrations, Dr Archer concluded.
Dr Thompson noted that he prefers
SMILE for many patients, but some require custom procedures. In addition to irregular astigmatism that can benefit from topography-guided treatment, patients with significant higher-order aberrations can benefit from wavefront-guided LASIK.
Custom LASIK can produce better vision results, Dr Thompson said. He referenced a study involving 80 patients by Edward E Manche of Stanford University presented at the ESCRS meeting comparing SMILE and wavefront-guided LASIK outcomes. More wavefront-guided LASIK patients had 20/20 uncorrected distance vision at one day after surgery, but visual outcomes were similar at one year. However, more LASIK patients gained one line of corrected VA and they had significantly better VA at 5% and 25% contrast than SMILE patients.
Some other studies show better accuracy with custom LASIK than current SMILE, Dr Thompson added (Kanellopoulos AJ. J Refract Surg. 2017 1;33(5):306-312. Khalifa MA et al. J Refract Surg. 2017 1;33(5):298-304). LASIK is also better for treating patients with astigmatism below 0.75D, he added.
However, while vision and optics are central, treatment decisions involve other factors as well. Patients are often well informed about dry eye and the impact of LASIK flaps on corneal biomechanics, Dr Thompson said. In addition to leaving a stronger cornea, SMILE does less damage to corneal nerve fibres, translating into less dry eye.
“When I have a patient concerned about the dry eye of LASIK, they are comforted by this fact,” he noted.
Timothy Archer: Timothy@londonvisionclinic.com
Vance Thompson: vance.thompson@ vancethompsonvision.com
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 12
All this adds up to a lengthy and complex treatment planning process requiring trained and skilled operators
Timothy J Archer MA










Saving vision
Strategies for reconstructing the anterior segment in trauma cases. Dermot McGrath reports
Avariety of different surgical strategies can be successfully deployed in the reconstruction of the anterior segment to save vision and obtain satisfactory functional and anatomical results in challenging cases of traumatic or chemical injury, according to Claus Cursiefen MD, PhD, FEBO.
“There are options available for these complex cases involving post-traumatic corneal oedema and scars, iris defects, cyclodialysis with hypotony and epithelial invasion, among others,” he said.
Speaking at the joint ESCRS-EuCornea symposium held during the 38th Congress of the ESCRS, Dr Cursiefen, Chairman and Professor of the Department of Ophthalmology at the University of Cologne, Germany, gave a broad overview of various techniques that could be applied to different repair scenarios.
In cases of post-traumatic corneal oedema, Descemet membrane endothelial keratoplasty (DMEK) is the first-choice surgical option, said Dr Cursiefen.
“We can try Descemet stripping automated endothelial keratoplasty (DSAEK) if DMEK is not possible, for example in cases of poor visibility where no intraoperative OCT is available or in eyes with very irregular posterior surface. The next option is penetrating keratoplasty but only if corneal scarring and severe corneal neovascularisation is present,” he said.
DMEK may also prove helpful in vascularised high-risk eyes with stromal oedema, said Dr Cursiefen. He cited a


retrospective study carried out using data taken from Cologne’s database of more than 5,000 different DMEK cases between 2011 and 2020.
Of 24 vascularised high-risk eyes with stromal oedema identified, DMEK was shown to be a viable treatment option.
“Significant regression of corneal neovascularisation was observed. The final visual acuity was relatively worse than in normal DMEK and we had a graft rejection in one eye (4.2%), which is also higher than for normal DMEK,” he said. “Nonetheless, safety and efficacy is much better compared to penetrating keratoplasty in vascularised high-risk eyes!”
For eyes with large iris defects, Dr Cursiefen noted that DMEK combined with a safety suture has been successfully employed in severe trauma cases to avoid dislocation of the graft. In cases of post-traumatic scar with no visual acuity and where it is not possible to wear an iris print lens, intrastromal corneal tattooing may provide a cosmetically acceptable result, he said.
In cases of post-traumatic hypotony due to cyclodialysis, Dr Cursiefen advised firstly adopting a “watch and wait” policy treating with cycloplegics and topical steroids. The indications for direct cycloplexy surgery include cyclodialysis of more than 60% circumference, with hypotony persisting for more than six weeks, beginning functional changes and morphologic changes such as macular folds, cystoid macular oedema and papilloedema.
Success rates of around 80% success can be expected for direct cycloplexy, with re-interventions more common in larger cleft defects, he said. Care has to be taken with early postoperative pressure spikes. Although epithelial invasion is a common complication after trauma, block excision with tectonic corneoscleral grafting is an effective treatment in cases of cystic and/or diffuse sheet-like epithelial ingrowth, he concluded.
Claus Cursiefen: augenklinikchefarztsekretariat@uk-koeln.de
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 14 EuroTimes is your magazine! Contact EuroTimes Executive Editor Colin Kerr at colin@eurotimes.org Do you have ideas for any stories that might be of interest to our readers?
There are options available for these complex cases involving post-traumatic corneal oedema and scars, iris defects, cyclodialysis with hypotony and epithelial invasion...
Claus Cursiefen MD, PhD, FEBO
The quest for super vision
The goal of providing refractive surgery patients with un-aberrated vision with almost superhuman visual acuity is neither currently feasible nor desirable; instead the aim should be to emulate the compromises that the normal human eye has adopted throughout the millennia in response to human visual needs, said Jesper Hjortdal MD, Aarhus University Hospital, Denmark.
“Surgical efforts towards normalisation of refractive errors and age-related changes in our visual functions is the realistic main aim for the near future,” Dr Hjortdal told the 38th Congress of the ESCRS.

At the beginning of this century, wavefront-guided corneal refractive surgery became available, offering the prospect of patients achieving visual acuity of better than 20/20, perhaps up to the limit of the retina’s capabilities, with the elimination of all natural sources of optical blur.

However, the technologies available to date have fallen short of those aims. Moreover, a better understanding of the way the human visual system processes aberrations now calls into question the value of an aberration-free retinal image, he said.
PITFALLS IN THE QUEST FOR SUPER VISION
Dr Hjortdal noted that in several randomised trials, wavefront-guided refractive surgery has performed no better than wavefront-optimised refractive surgery in terms of visual outcomes. He added that in a series of 51 eyes treated at his centre, best spectacle-corrected vision (BSCVA) becomes slightly worse after SMILE with an ablation profile corrected for aberrations measured using adaptive optics.
Part of the loss in BSCVA in such cases may result from “neural insensitivity”, which can cause a person’s visual system to perform less well when presented with a diffractionlimited retinal image or an image blurred by an unfamiliar point-spread function. Natural optical aberrations in the normal human eye can compensate for the limits to the sharpness of a retinal image by providing the anti-aliasing needed to generate a softer view with blurred edges and lower contrast.
Aberrations can also reduce the effects of presbyopia onset. Many refractive surgery treatments for presbyopia are designed to add aberrations to increase the depth of field. Removing the cornea’s natural aberrations can make the loss in image quality with near focus more precipitous when the eye’s ability to accommodate begins to wane with age, he noted.
“Visual quality is much more than visual acuity. We want glare-free vision, normal peripheral vision, normal contrast vision, normal night vision, normal colour vision and most important of all, particularly in older patients, normal uncorrected visual acuity at all distances. And we need technology to achieve this somehow in the future,” Dr Hjortdal concluded.
 Jesper Hjortdal: jesper.hjortdal@dadlnet.dk
Jesper Hjortdal: jesper.hjortdal@dadlnet.dk
Medicel AG D ornierstrasse 1 1 9 4 23 Altenrhein S W ITZ E RLAND T +41 (0)71 727 10 50 www.medicel.com info@medicel.com ACCUJECT DUAL ™
techniques 2in1 Injector ACCUJECT™ DUAL supports any surgeon’s preference – push or screw mode. Scan the following QR code for further details:
2
Normal vision with normal aberrations may be ultimate goal. Roibeard Ó hÉineacháin reports
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 15
Jesper Hjortdal MD
Bag-in-lens in young eyes
Tips and tricks for successful implantation of the bag-in-the-lens IOL. Roibeard Ó hÉineacháin reports
The bag-in-the-lens (BIL) intraocular lens has many characteristics that make it ideal for children with cataracts and the learning curve with the technique is fairly smooth for an experienced cataract surgeon, Sorcha Ní Dhubhghaill told the ESCRS/WSPOS symposium at the 38th Congress of the ESCRS.
“The BIL prevents posterior capsule opacification PCO and visual axis re-opacification. The method also guarantees excellent centration and, by trapping the capsular bag, we can also prevent rhexis phimosis. Moreover, the lens has been designed with a view to being quite exchangeable and interoperable, something that is particularly helpful for the paediatric population,” said Prof Ní Dhubhghaill MB, PhD, FEBOS-CR, Antwerp University Hospital, Edegem, Belgium.
She explained that the BIL IOL is a hydrophilic acrylic implant with a central 5.0mm optic and elongated oval-shaped haptics that are perpendicular to each other and between which is an interhaptic groove. To implant the lens the surgeon first creates an anterior posterior capsulorhexis and uses the haptics to clasp the leaves of the two capsulorhexis edges together within inter-haptic groove.
“By trapping the peripheral lens epithelial cells between these grooves, we can see that although they continue to grow and form a Soemmering’s ring, they remain confined to the very periphery of the lens. Eventually that forms a kind of donut around the IOL and the visual axis remains clear and the lens is made more stable by this additional Soemmering’s ring support,” Prof Ní Dhubhghaill said.
She added that although the posterior capsule is generally removed in paediatric cataract procedures, with standard IOLs the lens epithelial cells can still migrate across the back of the lens and opacify the visual axis. Performing YAG laser procedures in such cases can be very challenging.
Several case series of paediatric patients who have undergone successful implantation of the BIL have demonstrated that the visual axis remains clear of visual axis re-opacification throughout 10 or more years

of follow-up. In addition, because of the success of the lens in preventing PCO, it has become the IOL of choice in adult cataract patients at the Antwerp University Hospital.
MASTERING THE TECHNIQUE
Because of the BIL IOL’s unique and unconventional design, surgeons must adapt their technique in three specific respects to implant it successfully. They are the anterior capsulorhexis (ACCC), posterior capsulorhexis (PCCC) and lens insertion. For a skilled surgeon, the learning curve usually takes around 25 cases, she said.
To accommodate the BIL IOL, the capsulorhexis has to be 5.0mm in diameter. To ensure precision, a flexible ring-shaped calliper can be inserted after filling the anterior chamber with an ophthalmic viscosurgical device (OVD). An external Eye Cage device can then be used to align the calliper with the Purkinje reflexes and the limbus. An additional injection of OVD will then stabilise the anterior chamber for performance of the capsulorhexis. The cataract can then be removed using standard technique, which in paediatric cases generally requires only simple aspiration.
Following cataract extraction, the anterior rhexis serves as a guide to ensure that the posterior capsulorhexis matches its dimensions and centration. The surgeon should first create a central puncture in in the posterior capsule and inject an OVD into the space of Berger, which serves as circular cushion that pushes back the anterior hyaloid face and prevents vitreous prolapse.
“Before performing the posterior
capsulorhexis, make sure the capsular bag is emptied of any OVD so that it will be very flat, which makes it easier to control the vectors of force when you’re making your rhexis. What you don’t want is a capsular bag that bows downward because it will make performing the capsulorhexis less controlled.
“The posterior capsulorhexis starts with a small scratch to puncture the posterior capsule in a sideways rather than a downward motion to avoid touching the anterior hyaloid face. Inject OVD into the hole created to make the cushion of OVD just a little bit wider than the anterior capsulorhexis, which should tamponade the vitreous body. Sometimes it is necessary to dissect the anterior hyaloid face away from adhesions there to free the posterior capsule,” said Prof Ní Dhubhghaill.
Upon completion of the posterior capsulorhexis, the IOL is then injected into the anterior chamber followed by an injection of OVD over the lens to stabilise it and push it flat down against the anterior and posterior capsules. Once it is in position, the lens is tilted to catch the edges of the two capsular leaves beneath one of the posterior haptics and the remaining capsule is gently teased with a sliding motion to capture the rest of the capsule within the groove. With one final push the second posterior haptic is secured beneath the two rhexes.
In paediatric cases, Miostat is then injected to prevent optic-haptic capture and an iridotomy is performed to prevent pupillary block, she added.
Sorcha Ní Dhubhghaill: nidhubhs@gmail.com
EUROTIMES | DECEMBER 2020/JANUARY 2021 SPECIAL FOCUS: BEST OF THE BEST 16





Practice Management & Development Rebuilding Your Practice in a Challenging Environment Sunday 17 January, 11.00am CET Paul Rosen UK Faculty Moderator Topics Include: Enhancing the Patient Experience after COVID-19, Reimagining a High Performing Practice, Marketing your Practice in a Challenging Environment, Back To Work – Lessons Learned Arthur
Cummings IRELAND
WEBINAR For further information visit www.eurotimes.org
Kris Morrill FRANCE Rod Solar UK Guy Sallet BELGIUM
FREE
ESCRS Membership
• Reduced Registration Fees for ESCRS Congresses

• Subscription to Journal of Cataract & Refractive Surgery
• Access to ESCRS Grants, Bursaries and Research Awards
Access to:
• ESCRS iLearn
Online CME accredited interactive courses
• ESCRS On Demand
Online library of presentations from ESCRS Congresses
• EUREQUO
European Registry of Quality Outcomes for Cataract and Refractive Surgery
• ECCTR
European Cornea and Cell Transplantation Registry
Automatic IOL inserters
Preloaded automatic intraocular lens (IOL) inserters appear to stretch corneal incisions less than manual inserters, presenters said at the ASCRS Virtual Annual Meeting 2020.
In a comparison of a preloaded automatic IOL inserter with three manual inserters, Thomas Kohnen MD, PhD, of Goethe University, Frankfurt, Germany, found that the AutonoMe (Alcon, Fort Worth, Texas, USA) automated delivery system provided the smallest incision enlargement of the four when inserted through a 2.2mm incision (Comparative assessment of the corneal incision enlargement of 4 preloaded IOL delivery systems. Liu, Jingbo; Wolfe, Patricia; Hernandez, Victor; More; Journal of Cataract & Refractive Surgery. 46(7):1041-1046, July 2020.).
The mean 0.29±0.03mm stretch observed with AutonoMe matched that of the preloaded manual UltraSert (Alcon) was slightly less than the 0.31±0.03mm seen with the preloaded manual Tecnis iTec (Johnson & Johnson Vision, Rochester, New York, USA), and was significantly less than the 0.36±0.08 of the preloaded manual Vivinex iSert (Hoya Surgical Optics, Chromos, Singapore), Dr Kohnen reported. The in-vitro model involved 15 of each device and subtracted pre-insertion incision size from post-insertion incision size as measured by Asico incision gauges.
“The automated delivery system design and depth-guard tip may facilitate IOL implantations through smaller incisions with less incision enlargement,” Dr Kohnen said.
Further clinical studies are needed to confirm the effect of incision enlargement on wound healing and post-operative cornea morphology, he added.
CORNEAL HEALING
Motorised injectors caused less wound damage than a manual injector, particularly at smaller incision sizes, but no difference in wound healing was noted one month after surgery, according to a clinical study by Eiichi Nishimura MD, PhD, of Showa University Fujigaoka Hospital, Yokohama, Japan. The study involved 193 eyes in 124 patients and compared wound characteristics from cataract surgeries using two automated IOL injectors, AutonoMe and AutoSert (Alcon), and the manual UltraSert injector.
Anterior segment OCT revealed significantly more wound damage, as measured by Descemet’s detachment, bulge and endothelial gaps, with the manual inserter at 2.2mm and 2.4mm incisions one day and one week after surgery. No significant difference was seen among the groups one month after surgery, Dr Nishimura reported. Wound expansion was also significantly more for the manual injector at a 2.0mm incision, but not at larger incisions up to 2.6mm.
“As concluded in previous reports, IOL insertion using motorised injectors can reduce damage to incisions,” Dr Nishimura said (Allen et al. J Cataract Refract Surg 2012; 38: 249-255. Yokahama Y, Nishimura E et al. IOL&RS 2015 (Japanese); 29:224-229). However, wound healing significantly improved in all groups after one month, and there was no significant difference among the groups at that point, he said.
5 year membership for trainees
www.escrs.org Join today.
Preloaded motorised devices may stretch incisions less than manual inserters. Howard Larkin reports
EUROTIMES | DECEMBER 2020/JANUARY 2021 CATARACT & REFRACTIVE 18
Measurement of cyclorotation
Acomputer-based method for automated measurement of cyclorotation incorporated in the Catalys Precision Laser System (Johnson & Johnson Surgical Vision) demonstrated a high rate of successful registration and accuracy when compared to cyclorotation determinations of human graders, according to research presented at ARVO 2020.
The laser’s algorithm for measuring cyclorotation registers the image of the preoperative undilated iris captured by the Cassini low-light topographer (Cassini Technologies, Inc.) with the patient sitting upright to the dilated iris imaged with the patient supine and with the eye docked with the Catalys’s liquid optics interface. In addition to calculating the angle of cyclorotation, the algorithm generates a quality score indicating the confidence of the returned angle’s accuracy.
An investigation was conducted using images from 49 eyes of cataract patients operated on at Baylor College of Medicine, Texas, USA (37 eyes) and the Eye Centre of New York, New York, USA (12 eyes). The results showed that the automated algorithm successfully registered image pairs for 47 (96%) of the 49 eyes. For 46 (98%) of the 47 registered eyes, the cyclorotation measurement calculated by the automated system was within 2 degrees of the average cyclorotation determined by three human graders.
Discussing the relevance of the findings with EuroTimes, Douglas D Koch, MD, Baylor College of Medicine, noted that his goal for astigmatic correction during cataract surgery is to reduce refractive astigmatism to less than 0.5D.
“This is especially important for patients receiving presbyopia-correcting IOLs. When using the femtosecond laser to make arcuate incisions or toric alignment marks, accurate registration is essential to achieving these outcomes, but it can be complicated by rotation of the eye between the preoperative measurement and the laser,” he said.
“Automated intraoperative registration by the femtosecond laser provides maximal accuracy and saves time by eliminating preoperative and intraoperative marking steps.”
A second objective of the study was to describe the amount of cyclorotation present in femtosecond laser cataract surgery, said David Dewey, Research Scientist, Johnson & Johnson Surgical Vision, who reported the research.
The analyses showed the range and distribution of measured cyclorotation was nearly identical for the human graders and automated algorithm and identified a difference of about 10º between left and right eyes.
Mr Dewey commented: “In order to cover the breadth of the distribution in a symmetric manner, the automated system needs to address a ±20º range of cyclorotation angles. Based on other research, the left-right eye difference is likely due to the docking induced portion of the measured cyclorotation and not the natural cyclorotation associated with change in patient position,” he said.
Cataract, Refractive and Patient Reported Outcomes in One Platform
The patient-reported outcome is linked to clinical data in EUREQUO. This enables better knowledge of indications for surgery and o ers a tool for clinical improvement work based on the patients’ outcome.
19
Convenient Web-Based Registry
Join Track the EUREQUO Platform your Surgical Results EUREQUO is free of charge for all ESCRS members www.eurequo.org
Femto laser’s automated measurement system reliable and accurate.
Cheryl Guttman Krader reports
EUROTIMES | DECEMBER 2020/JANUARY 2021 CATARACT & REFRACTIVE
...it can be complicated by rotation of the eye between the preoperative measurement and the laser
Douglas D Koch, MD
Regression after refractive surgery




A20-year review comparing the time to retreatment in eyes undergoing LASIK and LASEK suggests that regression occurs earlier in older patients’ eyes after LASIK but not after LASEK, said Ciara E Byrne MBBS, Mater Private Hospital, Dublin, Ireland.
“Laser refractive corneal surgery provides an effective treatment option for myopia. Over the past decade, techniques have improved resulting in safer and more successful outcomes. Retreatment remains a complication despite a decrease in rates,” Ms Byrne told the ASCRS Virtual Meeting 2020.
The study reviewed the medical records of all cases of regression requiring retreatment following laser in situ keratomileusis (LASIK) or laser-assisted subepithelial keratectomy (LASEK) from 1998 to 2018 in the Mater Private Hospital, Dublin, Ireland.





























The mean age of patients at initial treatment was 31.9 years. Nearly half, 48%, reported an occupation that was categorised as likely to involve high-intensity computer use. The analysis of spherical equivalent, astigmatism and visual acuity included 269 eyes of 198 patients. Patients were excluded if they were myopic in one eye and hyperopic in the other eye or if they had undergone LASIK on one eye and LASEK on the other.
The analysis showed no significant difference between LASIK and LASEK in terms of time to retreatment, which was 55.6 months on average overall in this study cohort. As in previous research reported by the same group, the analysis showed no significant difference between LASIK and LASEK in terms of the effect of high refractive error on regression associated with retreatments.
The mean cylindrical value preoperatively in those treated with LASEK was -0.73D. The mean cylindrical value for those treated with LASIK was -0.86D. Prior to retreatment, mean cylinder value was -0.42D in the LASEK group and -0.54D for those treated with LASIK.
A linear regression analysis, with months to retreatment in the first eye as the outcome variable and age as the explanatory variable, showed that age was not significantly associated with months to retreatment In the LASEK group, but it was in the LASIK group. When the researchers analysed the sexes separately, they found the same association between age and LASIK but not between age and LASEK. They also found that gender did not influence regression rate with either technique.
“Our study does not demonstrate a difference in time to regression between LASIK and LASEK refractive surgery. Further study with a larger patient population would be beneficial in accurately evaluating the relationship between age and LASEK refractive surgery,” Ms Byrne added.
20 forum.escrs.org A library of symposia, interviews, video discussions, supplements, articles and presentations Spotlight on: Toric IOLs and Presbyopia Glaucoma Ocular Surface Disease Corneal Therapeutics Refractive IOL Patient Journey
NEW CONTENT
Older patients more prone to regression after LASIK but not after LASEK. Roibeard Ó hÉineacháin reports
EUROTIMES | DECEMBER 2020/JANUARY 2021 CATARACT & REFRACTIVE
Laser refractive corneal surgery provides an effective treatment option for myopia
Ciara E Byrne MBBS
THOMAS KOHNEN European Editor of JCRS


JCRS HIGHLIGHTS







VOL: 46 ISSUE: 10 MONTH: OCTOBER 2020
ICL AND SUBCLINICAL KERATOCONUS
Patients with subclinical keratoconus who received the V4c ICL/toric implantable collamer lens (ICL) maintained stable refractive results with follow-up of up to two years, Chinese investigators report. A retrospective study evaluated 60 eyes of 60 patients with a mean age of 27 years. Ectasia was measured with Scheimpflug tomography (Pentacam) and Corvis ST instruments. Mean postoperative UDVA and CDVA were 20/20 and 20/18. The mean difference between the intended and achieved spherical equivalent was −0.08 ± 0.47D. The spherical equivalent was within ±1.00D of the intended correction in 57 eyes (95%), and 58 eyes (97%) had astigmatism less than 0.50D. The refractive results were stable two years postoperatively, and the corneal biomechanical parameters returned to their preoperative levels at three months. K Li et al., “Visual outcomes and corneal biomechanics after V4c implantable collamer lens implantation in subclinical keratoconus”, 46(10):1339-1345.


MICROMONOVISION WITH BILATERAL TORIC EDOF IOLS
Toric extended depth of focus IOLs targeted for micromonovision appear to produce good functional vision and high patient satisfaction, a new study suggests. The study included 52 eyes of 26 patients with regular corneal astigmatism from 0.75 to 2.60 dioptres. Postoperative corrected distance, uncorrected distance, uncorrected intermediate, and uncorrected near visual acuities were −0.10 (±0.12), −0.01 (±0.13), 0.01 (±0.14) and 0.13 (±0.14), respectively. Mean refractive cylinder of 0.47 ± 0.46D at the three-month mark. Rotational predictability and centration were both good. Seventy-seven percent of patients reported spectacle independence, while 95% of patients were satisfied with distance and intermediate visual results. Some 70% were satisfied with their near vision results. S Georgiev et al., “Visual performance after bilateral toric extended depth-of-focus IOL exchange targeted for micromonovision”, 46(10):1346-1352.

TANGENTIAL CURVATURE MAPS AND IOL CALCULATIONS
IOL calculation in eyes undergoing cataract surgery that have previously undergone refractive surgery continues to be a major clinical challenge. Identifying the type of ablation performed is a key step in improving outcomes in these cases. Researchers compared tangential and axial map utility in a study of 52 novice reviewers who looked at 60 total images from 30 eyes presenting for cataract surgery evaluation with known refractive surgery status. Tangential curvature maps more accurately demonstrated postoperative curvature patterns than did axial curvature maps and facilitated identification of myopic and hyperopic ablations for the novice ophthalmologists. No difference was seen in pattern recognition accuracy between Placido and Scheimpflug imaging devices, suggesting that, for pattern recognition, the devices should be equivalent. Ravi S Shah et al., “Comparative postoperative topography pattern recognition analysis using axial vs tangential curvature maps”, 46(10):1368-1373
JCRS is the official journal of ESCRS and ASCRS CATARACT & REFRACTIVE
EUROTIMES | DECEMBER 2020/JANUARY 2021 21
Beyond palliative relief for severe dry eye disease
Clinical trial shows high molecular weight hyaluronic acid drops improve symptoms and regenerate damaged corneal nerves. Cheryl Guttman Krader reports
Treatment with a preservativefree, lubricating eye drop containing 0.15% high molecular weight hyaluronic acid (HMWHA; Comfort Shield, i.com medical GmbH) provides better symptomatic relief for patients with severe dry eye disease (DED) than existing “optimum” lubricant drops and has a remarkable benefit for promoting corneal nerve growth, according to results of a multicentre, prospective, randomised clinical trial.
Jutta Horwath-Winter MD, Assistant Professor of Ophthalmology, Medical University Graz, Graz, Austria, was a principal investigator in the study. She told EuroTimes: “Although the TFOS DEWS II Management and Therapy Report states that tear replacement products do not target the underlying pathophysiology of DED, the results of the HYLAN M study show that it in addition to its lubricating properties and effect for increasing tear viscosity, HMWHA apparently has neurotrophic effects.”
Gysbert van Setten MD, PhD, Assistant Professor of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden, was also a principal investigator in the research study and lead author of the published report.
He commented: “HMWHA is nature’s own lubricant, and the 0.15% HMWHA drops closely mimic the features and functions of the natural tear film. Instead of a DED regimen incorporating a plethora of drops and ointments, 0.15% HMWHA could provide a simplified approach, which would be particularly beneficial for older patients.”
Both investigators emphasised that while there are other commercially available artificial tears containing hyaluronic acid, the products are not all equal.
“The benefits of a product containing hyaluronic acid depend more on the molecular weight of the hyaluronic acid than its concentration. There is currently no convincing evidence that any other ocular lubricants lead to neuronal regeneration in DED,” Dr van Setten said.
Dr Horwath-Winter agreed that the properties of hyaluronic acid depend
mainly on molecular weight.
“HMWHA has a high water-binding capacity, anti-inflammatory properties and wound healing effects,” she said.
HYLAN M DESIGN AND DATA
The eight-week HYLAN M study included adults who met published criteria for severe DED [Ocular Surface Disease Index (OSDI) ≥33, Oxford corneal fluorescein staining (CFS) score ≥3] and had been on a stable treatment regimen. They were randomised 1:1 to use the HMWHA drops or continue their existing artificial tears.
Eighty-four patients were included in the efficacy analysis. Change in CFS from baseline to week eight was assessed as the primary endpoint and did not show a statistically significant difference between groups.
“Oxford staining gradients are demanding and subjective, and we cannot rule out that these issues confounded the ability to demonstrate a statistically significant benefit of HMWHA treatment despite all of the standardisation implemented in the study. Furthermore, the eight-week treatment period may have been too short to show a benefit. Just as symptoms of DED often manifest before signs, symptoms may improve before DED-related anatomical changes,” said Dr van Setten.
Dr Horwath-Winter noted that the low sub-basal nerve fiber length found in the study population of patients with severe DED might also have been a confounding issue. Trophic support from corneal nerves is important for epithelial renewal, she explained.
The analysis of change in total OSDI score, the key secondary endpoint, showed a 13.5-point statistically significant difference favouring the HMWHA group (P = .001). The HMWHA treatment also had statistically significant benefits compared with the control for improving the OSDI pain subscore, OSDI vision subscore and BCVA.
Both investigators underscored the importance of symptomatic improvement.
“Symptom assessment is a key element
in evaluating a DED treatment because of the impact of symptoms on patient wellbeing,” Dr van Setten said.
Dr Horwath-Winter quoted a conclusion from the recently published Asia Dry Eye Society consensus report, stating: “Therapeutic efficacy should be evaluated by the symptoms such as dry eye-related pain, discomfort or visual disturbances. Functional visual acuity should also be included as an outcome measure in further studies in this field.”
NERVE REGENERATION
Corneal nerve changes were assessed through masked reader review of in vivo confocal laser scanning microscopy images in a subset of 16 patients. The analyses showed corneal nerve fibre length was similar in the two treatment subgroups at baseline, but at study end, it had increased by 51% (P=0.03) in the HMWHA group and was unchanged in the control group.
The investigators commented that the effect of HMWHA treatment on corneal nerve growth correlates well with its benefit for relieving pain. In the absence of significant changes in dry eye signs, they suggested that the therapeutic benefits of the HMWHA drops are likely due to pharmacological effects, including downregulation of ocular inflammation and support of corneal nerve recovery, rather than physical effects like hydration or lubrication.
FUTURE RESEARCH
Because nerve damage is increasingly recognised as a factor in DED pathophysiology, the investigators believe further studies are warranted to investigate the role of HMWHA for improving corneal innervation and function. Ongoing studies include other DED patient subgroups and patients with diabetic keratopathy. There is also interest in investigating its use in patients undergoing surgical procedures that can damage corneal nerves.
The HYLAN M clinical trial results appeared in the Journal of Clinical Medicine [J Clin Med. 2020;9(110:E3536; J. Clin. Med. 2020, 9(12), 3799]
EUROTIMES | DECEMBER 2020/JANUARY 2021 CORNEA 22
Novel approach to keratoconus
New Bowman’s layer grafting technique shows promise.
Roibeard Ó hÉineacháin reports
Placing a donor Bowman’s layer graft on to a thin keratoconic cornea can result in an immediate flattening of the corneal curvature and stabilisation or improvement in patients’ visual acuity, according to Isabel Dapena MD, The Netherlands Institute for Innovative Ocular Surgery, Rotterdam, The Netherlands.
“In progressive keratoconus, the Bowman’s layer onlay technique has potential as a means of flattening the corneal surface, halting progression and postponing more invasive keratoplasty techniques while also maintaining preoperative contact lens visual acuity,” Dr Dapena told the 24th ESCRS Winter Meeting in Marrakech, Morocco.
The new surgical technique involves first removing the epithelium and then placing a Bowman’s membrane graft on to the stroma and stretching it so that there are no folds. Afterwards it is covered with a bandage contact lens, she explained.
Dr Dapena and her associates performed Bowman’s layer onlay grafting in five patients with advanced progressive keratoconus, including one case that had undergone corneal cross-linking (CXL) immediately previously. The remaining four patients were unsuitable candidates for CXL.
She noted that all the surgeries were performed successfully and with an immediate postoperative flattening of the corneal curvature in all eyes. In addition, all eyes were completely re-epithelialised with a well-integrated graft by two-to-three weeks postoperatively. In one eye with a particularly steep cornea there was a partial dislocation of the Bowman’s layer graft. It was repositioned and sutured over with amniotic membrane tissue.
At one-to-six months follow-up, the average Kmax decreased from 74.9D preoperatively to 69.1D, but there were no changes in posterior corneal values. Furthermore, at six months, best spectacle-corrected visual acuity (BSCVA) had improved by at least two lines in three of five patients and best contact lens-corrected visual acuity remained unchanged. Patients also expressed high satisfaction with the procedure.
HIGH PATIENT SATISFACTION
Dr Dapena noted that the new Bowman’s layer onlay technique may help address the need that exists for treatment of eyes with progressive keratoconus and thin corneas. Such eyes are often unsuitable candidates for procedures like corneal cross-linking and intracorneal ring segments.
The onlay technique is based on the hypothesis that keratoconus results from a disruption of Bowman’s layer. The results so far are similar to those of the Bowman’s layer intrastromal inlay technique, also developed at the Rotterdam Institute.
“This onlay technique is theoretically much better because it is a completely extraocular approach and there is no risk for micro-perforation, allowing the treatment for a much larger group of patients,” Dr Dapena added.
European Union Web-Based Registry
The aim of the project is to build a common assessment methodology and establish an EU web-based registry and network for academics, health professionals and authorities to assess and verify the safety quality and efficacy of corneal transplantation.
the ECCTR Registry Join Track
your Surgical Results
www.ecctr.org
ECCTR is a project funded by the ESCRS with initial support from the EU
EUROTIMES | DECEMBER 2020/JANUARY 2021 CORNEA
23
Keep learning. Whenever, wherever.
Cell therapy for Fuchs’ dystrophy
Injection of cultured human corneal epithelial cells (hCECs) supplemented with a rho-associated protein kinase (ROCK) inhibitor into the anterior chamber may offer a potentially groundbreaking new treatment for corneal endothelial dysfunction, according to Shigeru Kinoshita MD, PhD.
“This injected cell therapy holds a lot of promise for corneal endothelial cell disorders such as Fuchs’ endothelial corneal dystrophy. Initial studies have shown minimal immunological reaction, normal corneal configuration and rejuvenated endothelial cells after injection of hCECs in a series of bullous keratopathy patients,” said Dr Kinoshita at the World Ophthalmology Congress 2020 Virtual.
Dr Kinoshita’s research group at the Kyoto Prefectural University of Medicine, Kyoto, Japan, has been working for some years on hCEC injection therapy using donor allogenic cells.
“The interest of this is that conceptually, just one donor cornea could be sufficient to create cells for up to 1,000 patients in a safe, quick and easy procedure,” said Dr Kinoshita.
Dr Kinoshita explained that human CEC cultures comprise a plurality of subpopulations, some of which are unsuitable and unsafe for injection into human eyes.
“Our research has led us to understand that mature fully differentiated cells hold the key to a successful and safe treatment,” he said.
Learn online in your own time, with self-paced and assessed ESCRS iLearn courses on:

∙ Cataract Surgery
∙ Cornea
∙ Refractive Surgery
∙ Visual Optics
Trainers: use the task list to assign courses for trainees and monitor their progress.
Surveying the clinical research data, Dr Kinoshita said that his team has now injected hCECs in about 65 patients overall with very good safety and efficacy outcomes.
The most recent single-group study involved 11 patients who had received a diagnosis of bullous keratopathy and had no detectable CECs. The patients received injections in the anterior chamber of hCECs cultured from a donor cornea and supplemented with a ROCK inhibitor. Immediately after the procedure, the patients were placed in a prone position for three hours in order to enhance the adhesion of the injected cells.
The results at 24 weeks showed that the injection therapy was effective, with repopulation of CECs on Descemet’s membrane and the posterior surface of the corneal stroma, attainment of normal corneal thickness and resolution of corneal epithelial oedema.
“The visual acuity of many of the patients also improved significantly and the corneas were still transparent up to two years after surgery,” added Dr Kinoshita.
Shigeru Kinoshita: shigeruk@koto.kpu-m.ac.jp
EUROTIMES | DECEMBER 2020/JANUARY 2021 CORNEA
Bright future ahead for treatment of corneal endothelial dysfunction. Dermot McGrath reports
Learn more at https://elearning.escrs.org
24
Conceptually, just one donor cornea could be sufficient to create cells for up to 1,000 patients in a safe, quick and easy procedure
Shigeru Kinoshita MD, PhD
Reconstructing the ocular surface
Although not traditionally considered a first-line surgical option for ocular surface reconstruction, keratoprosthesis (KPro) devices have the ability to achieve good visual outcomes in patients who are poor candidates for standard keratoplasty surgery, according to Sadeer B Hannush MD.
“Historically, permanent keratoprosthesis surgery has been offered only after multiple graft failures. However, in the setting of ocular surface disease that is not amenable to conventional reconstructive surgical modalities, permanent KPro may be considered as a primary surgical intervention for the purpose of visual rehabilitation,” he said at the World Ophthalmology Congress 2020 Virtual.
The Boston KPro is currently the most frequently used keratoprosthesis, consisting of a back plate and optical stem that are incorporated with a donor cornea at the time of surgery.
In trying to decide whether to offer a full-thickness graft or a KPro device, some considerations need to be borne in mind, said Dr Hannush, Wills Eye Hospital, Philadelphia, Pennsylvania, United States.

“We need to weigh the likelihood of subsequent graft survival with a graft versus KPro implantation, and also take on board issues such as visual rehabilitation, systemic immunosuppression and the age of the patient in making our decision,” he said.
Once the surgeon has decided to proceed with a KPro, there are further strategic choices to be made in terms of leaving the patient aphakic or pseudophakic, and selecting the type and size of posterior plate to be used.
“Glaucoma management is the Achilles’ heel of KPro surgeries, so we need to plan in advance if we are placing a glaucoma drainage device or planning endoscopic cyclophotocoagulation (ECP) or other options combined with the KPro device,” he said.
Dr Hannush illustrated the utility of the KPro in two case studies. The first patient was a 75-year-old male who had multiple failed full thickness and endothelial grafts in his only seeing eye. B-scan ultrasonography, however, showed a normal posterior segment, so the decision was taken to proceed with KPro surgery. After removing the previous failed grafts, the 8.5mm KPro with a titanium back plate embedded in a full thickness cornea graft was sutured in place. The final outcome was good, with the patient achieving 20/50 vision several days after surgery, said Dr Hannush.
The second case study highlighted by Dr Hannush was a 40-year-old female patient with congenital aniridia.
“The ocular surface was very irregular and vascularised with limbal stem cell deficiency, and the patient also had a cataract, so it was quite challenging,” he said.
After performing a partial vitrectomy, Dr Hannush successfully removed the cataract and implanted a threepiece IOL into the capsular bag prior to suturing the KPro device/corneal transplant complex into place.
“The patient achieved a good outcome and was very happy with her vision after the surgery,” he concluded.
EUROTIMES | DECEMBER 2020/JANUARY 2021 CORNEA
169
KPro can achieve good outcomes where standard keratoplasty is not appropriate. Dermot McGrath reports at a
Glance
Reach
47,863 * * Average net circulation for the 10 issues circulated between 1 February 2019 to 31 December 2019. See www.abc.org.uk
25
The number of countries in which EuroTimes is distributed
Sadeer B Hannush MD
Complications of the anterior segment
Dr
Peri-ocular blocks can be associated with a risk of globe perforation, with higher risk in high myopes, previously buckled eyes, use of sharp long needles, retro-bulbar injection, inexperienced anaesthetists and uncooperative patients. Recognised by sudden loss of vision, a hypotonic eye, localised retinal or sub-retinal haemorrhage and absent red reflex, it can be avoided by the use of topical, intracameral and/ or sub-Tenon anaesthesia, especially in high risk cases.
Posterior Capsular Rent (PCR), vitreous loss, nucleus or IOL drop and retained lens fragments occur even in the most skilled hands. Though small amounts of cortex may be tolerated, larger amounts as well as retained nuclear fragments cause severe inflammatory reaction, glaucoma, corneal oedema (CME) and even retinal detachment (RD). It requires management at primary surgery or at least within three weeks by vitreo-retinal (VR) backup. The IOL scaffold technique (Agarwal et al) can be used to prevent fragment drop by preplacing a three-piece foldable IOL above the iris and below the prolapsed nuclear fragments to plug the pupil and allow safe phacoemulsification. Vitrectomy and residual cortex removal is done with vitrector via pars-plana alternating between cutting and aspiration modes. The IOL is finally translocated as either sulcus with optic capture or as glued IOL depending on residual capsular support.
Retinal tears, RD and CME are increased with PCR, nucleus and IOL


drop, chamber fluctuations, postoperative inflammation, vitreous strands etc. They are more common in complex cataracts such as subluxated, brown, hypermature, posterior polar, small pupil, IFIS, shallow or deep anterior chamber (AC), high myopes, vitrectomised eyes, traumatic cataracts, secondary IOL fixation, eyes with co-morbidities such as pseudoexfoliation and in complicated surgeries.
Improper vitreous management such as aspirating with vitrector, phaco or I/A probe or even Symcoe cannula without first cutting vitreous; blind manoeuvres to save a sinking nucleus; checking for vitreous by sweeping the AC with a rod or using a Weck-Cel at the wound can all lead to vitreous base traction and giant retinal tears and hence, should be strictly avoided. Proper vitrectomy with use of preservative-free intravitreal triamcinolone acetonide (IVTA) to stain the vitreous should be employed. Though small, localised PCR with limited vitreous prolapse may be handled trans-limbally, generally pars-plana vitrectomy is preferred, especially with larger PCR. The correct technique should be learnt or VR backup requested. Using a fixed infusion cannula frees both hands for bimanual manoeuvres. With pars-plana infusion, the tip must be visualised in the vitreous cavity before starting infusion to prevent accidental suprachoroidal or subretinal infusion. Its position should be constantly checked as manipulations of the eye may cause some retraction of the cannula. A slightly shorter scleral tunnel or longer infusion trocar helps prevent the cannula
from slipping out, but longer trocars risk injury to the capsule. The Agarwal trocar anterior chamber maintainer (ACM) or even a routine ACM are alternate options for anterior segment surgeons not used to placing pars-plana infusion. Sclerotomies for secondary IOL fixation should be at the correct distance and intra-operative hypotony should be avoided to prevent ciliary body bleeding and vitreous haemorrhage.
Pseudophakic rhegmatogenous RD has a rate of about 1%, and 50% occur within the first year of surgery. Risk factors include young age, high myopia, peripheral retinal degenerations, past history of RD, PCR, vitreous loss, vitreous incarceration and YAG capsulotomy. Multiple breaks and poor visibility secondary to opacified capsule and IOL reflections may make surgery difficult. Pseudophakic cystoid macular oedema (CME) is one of the most common causes of visual loss after cataract surgery and is due to a blood aqueous barrier breakdown. Risk is higher in diabetics, uveitis, older patients and following complicated cataract surgery. Postoperative topical NSAIDs are helpful for prevention and treatment.
Suprachoroidal haemorrhage (SCH) is a devastating complication that may occur intra- or early postoperatively. Risk factors include older age, arteriosclerosis, hypertension, use of adrenaline, systemic anticoagulants, large incisions, intra- and extra-capsular cataract extraction, aphakia, glaucoma, vitreous loss, raised intra-orbital or intraocular pressure, myopia, pressure from speculum, uncooperative patient, Valsalva manoeuvre such as coughing, sneezing, squeezing lids, history of expulsive in other eye, postoperative hypotony etc. It is recognised as sudden hardening of the eye, shallowing of AC, forward movement of lens or posterior capsule, vitreous presenting at wound, appearance of dark uveal mounds, loss of
EUROTIMES | DECEMBER 2020/JANUARY 2021
The retina is mysterious and intimidating and retinal complications are dreaded by all ophthalmologists.
Soosan Jacob, MS, FRCS, DNB reports
RETINA 26
Though small, localised PCR with limited vitreous prolapse may be handled trans-limbally, generally pars-plana vitrectomy is preferred
red reflex, bleeding from eye and partial or complete extrusion of intraocular contents. Immediate recognition and sutural closure of all wounds is paramount. Posterior sclerotomies are not very effective in draining the rapidly clotting blood and besides, may increase bleeding by removing tamponading effect and are therefore no longer advocated. Prompt management can limit SCH to a localised, self-limiting haemorrhage with reasonably good visual potential. Small SCH are observed for spontaneous resolution. Larger ones with compressive effect need drainage once the clot liquefies and this together with any other definitive procedure required is performed between one and two weeks later.
Endophthalmitis, another dreaded complication, can cause irreversible loss of sight. Prevention includes careful preoperative examination of the eye, adnexa and lacrimal sac; preoperative topical antibiotics and povidone iodine asepsis; intra-cameral antibiotics, especially if posterior capsular rent (PCR) occurs; proper management of PCR and good wound closure without vitreous wicks and with, if required, sutures. Avoiding postoperative hypotony; confirming an adequately pressurised eye at end of surgery, especially after loosening speculum; use of postoperative antibiotics and maintenance of good hygiene are important. 23 or 25 gauge pars plana vitrectomy ports created for PCR should be self-sealing, tunnelled entries and conjunctiva should be displaced before entering. Cluster endophthalmitis can occur from contaminated intraocular fluids and medications. Early diagnosis and prompt VR referral and intervention are essential for any suspected endophthalmitis.
Finally, exacerbation of diabetic retinopathy and other retinal conditions may occur and needs pre-, intra- or postoperative treatment for the underlying condition.
RETINAL COMPLICATIONS OF REFRACTIVE SURGERY
Though the risk is quite low in corneabased refractive surgeries such as LASIK, changes in VR vector forces from application of suction ring or applanation cone can lead to vitreous base and posterior pole traction, PVD, retinal breaks and RD. These complications occur more frequently with lens-based refractive surgeries (refractive lens exchange [RLE] and phakic IOLs). High myopia, low scleral rigidity, pre-existing peripheral retinal degeneration, breaks and holes, AC depth fluctuations, transient IOP changes and other risk factors as discussed with cataract surgery increase risk. RLE has a higher risk of RD than even general cataract surgery, especially in young myopes who have premature vitreous liquefaction and strong VR adhesions. YAG laser capsulotomy for posterior
capsular opacification also predisposes to breaks, RD and CME. Capsular polishing and use of hydrophobic, square-edge IOLs decreases this risk. Patients with phakic IOLs and RLE can develop CME, similar to that discussed previously. Rare reports of macular haemorrhage, choroidal neovascular membrane (CNVM), macular holes and central retinal artery occlusion after refractive surgery exist, risk factors being pre-existing lacquer cracks, CNVM, high myopia, macular traction, PVD, hypercoagulable states etc. Before any refractive surgery, a comprehensive preoperative retinal examination, including the periphery with scleral indentation, is a must, together with treatment of all indicated lesions. Postoperative routine retinal examinations are also a must for all patients.
RETINAL COMPLICATIONS OF OTHER ANTERIOR SEGMENT SURGERIES
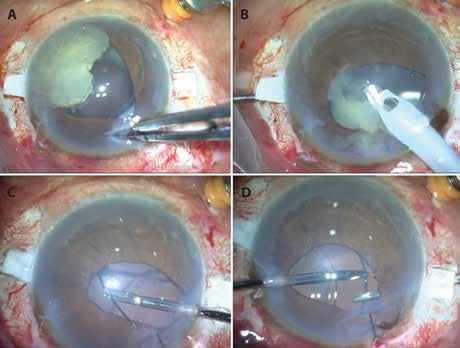
Complications discussed previously can occur here as well. Open-sky penetrating keratoplasty (PK) and glaucoma surgeries have a much higher risk of expulsive haemorrhage. Short open-sky time, use of general anaesthesia, head-end elevation and avoidance of all risk factors discussed previously is important. In PK, the opensky site should be immediately plugged with a finger (Osher M) until acute build-up in pressure subsides and a graft can be quickly sutured on. Preoperative uncontrolled IOP and postoperative hypotony both contribute to higher risk with glaucoma surgeries.
Glaucoma valves and strabismus
surgery may be associated with scleral and retinal perforation during needle pass, especially with thin scleras or if inadvertently passed deeply. This is generally ‘felt’ by the surgeon as having gone through and should also be suspected if uveal pigment or a vitreous bead is seen on the needle tip. Immediate retinal examination may identify it as localised retinal haemorrhage and retinal tear and laser or cryopexy at the site may be required. Mytomicin-C (MMC), which is often applied for glaucoma surgeriwes, or pterygium excision can cause scleral melt and necrosis, uveal show, retinal detachment and endophthalmitis if applied in too high a concentration or for too long. Inadvertent intraocular injection of MMC can cause retinal oedema, necrosis and atrophy.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
EUROTIMES | DECEMBER 2020/JANUARY 2021 RETINA 27
Glued IOL Scaffold: A, B: A three-piece foldable IOL placed as scaffold below nucleus and above iris prevents fragment drop during emulsification; C, D: After pars-plana vitrectomy and cortex aspiration with vitrector, the IOL is translocated as glued IOL using handshake technique
Endophthalmitis, another dreaded complication, can cause irreversible loss of sight
CATARACT SURGERY in patients with AMD
Experts review things to keep in mind with the cataract patient with retinal disease.
Leigh Spielberg reports
The ESCRS and EURETINA joined forces to broadcast an online symposium entitled “Cataract Surgery in Patients with AMD”. Chaired by Nic Reus MD, Breda, the Netherlands, and Carel Hoyng MD, Nijmegen, the Netherlands, the symposium covered various topics intended to help guide the decision-making process before, during and after cataract surgery in patients with age-related macular degeneration (AMD).
Dr Hoyng opened the symposium with an overview of the differential diagnosis of AMD. After all, what if your patient has a macular problem that isn’t AMD? His presentation, entitled “It’s AMD… Is it?” zoomed in on five important diseases that can closely mimic AMD. These monogenetic diseases, such as lateonset Stargardt’s disease and pattern dystrophy, might represent up to 10% of cases diagnosed as AMD, according to Dr Hoyng.
“You should suspect a retinal dystrophy in patients with AMD-like macular abnormalities who have an early age of onset, a positive family history, marked bilateral symmetry of the lesions, foveal sparing and distinct abnormalities on fundus autofluorescence,” said Dr Hoyng. He added that a correct diagnosis can help guide genetic counselling and can clarify the prognosis for the patient and his or her family.
José García-Arumí MD, Barcelona, Spain, reminded viewers that cataract and AMD are the two leading causes of blindness in high-income countries, and are often present in the same patient.
“When an AMD patient presents with cataract, how do we proceed?” he asked, with specific regards to whether cataract surgery increases the risk of AMD development or progression.
“Although cataract surgery induces iatrogenic inflammation and increases exposure to UV light postoperatively, recent studies do not indicate that there is a strong association between cataract surgery and the development or progression of AMD.” Dr GarcíaArumí concluded that the potential risk is outweighed by the benefits of improved visual acuity and better quality of life after cataract surgery.
“If an AMD patient presents with visually significant cataract, it is reasonable to offer cataract surgery as a treatment option,” he concluded. “In fact, although it is preferable to perform the surgery when the disease is under control, AMD patients may successfully undergo cataract extraction even with active exudative AMD.”
There are, however, no concrete recommendations regarding precisely when to plan the surgery in relation to the intravitreal injections, he added.
Ramin Tadayoni MD, Paris, France, gave an overview of the current state of affairs regarding the anti-VEGF treatment of neovascular AMD. He informed delegates of the three treatment regimens that have been extensively researched: fixed regimens, PRN regimens and treat-and-extend regimens.
The ophthalmologist treating patients with neovascular AMD is often faced with the question of when, during the course of active macular disease, to operate.
“The treat-and-extend regimens for intravitreal injections offer an extended window of time between injections during which
cataract surgery might be performed,” said Dr Tadayoni. In this regimen, the period between injections might increase to eight or more weeks.
“Another option is to administer an intravitreal anti-VEGF injection at the end of surgery,” added Dr Reus, which offers immediate effect during the postoperative period, when inflammation peaks.
Alex Day MD, London, England, offered insight into how to adapt the surgical procedure itself for patients with AMD.
“Previous intravitreal injections are a risk factor for posterior capsular rupture (PCR) during cataract surgery,” said Dr Day.
This risk can be up to 2.6 times higher for those patients who have received 10 or more injections, which can severely diminish the surgical outcome. The surgeon must pay especially close attention to the posterior lens during examination, in order to identify capsular compromise preoperatively.
Oliver Findl MD, Vienna, Austria, continued the topic of PCR in these patients, offering tips on how to perform the surgery in patients with a compromised posterior capsule.
“Careful hydrodelineation, rather than hydrodissection, will reduce the risk of extending the tear and dislocating the lens into the posterior segment, especially when combined with a low bottle height,” he recommended.
“Injecting an OVD through the paracentesis before removing the phaco tip or I/A instruments can also reduce the risk.”
Gabor Scharioth MD, Recklinghausen, Germany, offered his insights into the best choice of IOL in patients with AMD.
“My recommendation is to select a single-piece, hydrophobic acrylic IOL made of clear material for in-the-bag implantation,” said Dr Scharioth. If the visual acuity is worse than 0.4 due to AMD, a special, magnifying lens such as the Scharioth Macula Lens (SML) can be considered as a secondary implant in the sulcus.
Dr García-Arumí also offered further advice regarding IOL selection.
“We must remember that AMD patients have not only a compromised visual acuity, but also decreased contrast sensitivity,” he said. “Multifocal IOLs form a relative contraindication, as they also reduce contrast sensitivity.”
What about blue-blocking (yellow-tinted) IOLs? “These might protect the retina from blue-light damage, but might also negatively affect scotopic vision and circadian rhythms,” he concluded.
EUROTIMES | DECEMBER 2020/JANUARY 2021 RETINA 28
Previous intravitreal injections are a risk factor for posterior capsular rupture (PCR) during cataract surgery
Alex Day MD
New injections for late-stage AMD
Phase III trial shows efficacy for reducing GA area growth rate.
Cheryl Guttman Krader reports

Intravitreal avacincaptad pegol (Zimura, IVERIC bio) has shown signs of efficacy for the treatment of geographic atrophy (GA) due to age-related macular degeneration (AMD) in a Phase III clinical trial, reported Frank G Holz MD, at the 2020 EURETINA Virtual meeting.

“Zimura targets complement 5 in the complement pathway. Groups treated with either the 2mg or 4mg dose of Zimura in GATHER1 showed a statistically significant reduction in GA growth rate over 12 months of approximately 27% compared with sham-treated controls. The reduction in lesion growth was already present at six months in both dose groups, and both dosages were well tolerated over a period of 18 months,” said Dr Holz, Professor and Chair, Department of Ophthalmology, University of Bonn, Germany.
GATHER1 consisted of two parts and randomised 286 participants who were treated with sham or avacincaptad pegol 1mg, 2mg or 4mg. The 1mg dose was not included in the prespecified primary statistical
The study’s eligibility criteria required that subjects have nonfoveal GA secondary to dry AMD with a total GA lesion area between 2.5 and 17.5mm2 and at least one focal lesion of 1.25mm2 if the GA was multifocal. BCVA in the study eye had to be between 20/25 and 20/320 on the ETDRS chart. Patients with choroidal neovascularisation (CNV) in either eye were excluded.



REDUCTION IN LESION GROWTH RATE
The primary efficacy endpoint was mean rate of change in GA lesion size over 12 months measured by fundus autofluorescence imaging. Data collected at 18 months showed that compared with the sham group, there was a 28% reduction in lesion growth rate in the group treated with avacincaptad pegol 2mg and a 30% difference for the 4mg group.
The investigational treatment was well tolerated, without any drug-related adverse events or drug-related inflammation.
“The most frequently reported ocular adverse events were related to the injection procedure,” said Dr Holz.
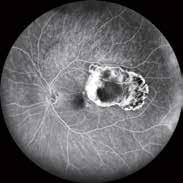


The rate of CNV development in study eyes in the sham, avacincaptad pegol 2mg, and avacincaptad pegol 4mg arms was 2.7%, 9% and 9.6%, respectively. The overall incidence of CNV development in untreated fellow eyes was 3.5%.
The GATHER1 results were recently published in the journal Ophthalmology (August 31, 2020).
GATHER2, a confirmatory pivotal trial, is now under way. GATHER2 has a planned enrolment of approximately 400 patients. Patients will receive their assigned treatment every four weeks. The primary efficacy endpoint is the same as in GATHER1.
Frank G Holz: frank.holz@ukb.uni-bonn.de
EUROTIMES | DECEMBER 2020/JANUARY 2021 RETINA
29
Frank G Holz MD
Glaucoma progression after cataract surgery
New baseline warranted postoperatively due to potential impact of cataract removal and IOL choice. Cheryl Guttman Krader reports
Findings on glaucoma diagnostic tests can change after phacoemulsification cataract surgery, said Carroll A B Webers, MD, at the 2020 ESCRS Virtual meeting.
Therefore, it is very important to have a new baseline measurement after phacoemulsification and IOL implantation in a glaucoma patient, he advised.
Addressing the question, “Does an IOL choice impact my glaucoma diagnostics”, during a session on glaucoma pearls for the cataract surgeon, Dr Webers reviewed changes in standard white-on-white perimetry parameters measured with the Humphrey Field Analyzer and on OCTmeasured peripapillary nerve fibre layer (PP NFL) thickness in glaucoma patients.
IMPACT ON VISUAL FIELD
His discussion of visual field changes focused on foveal sensitivity, mean deviation (MD) and the Visual Field Index (VFI). Dr Webers said that the fovea threshold, which is the retinal sensitivity in the fovea, is generally increased (improved) after phacoemulsification. The MD, which is a weighted average of the values presented in the total deviation plot (ie, the mean depression of the patient’s overall visual field), is also improved after cataract surgery. Similarly, the VFI, which is an enhancement of the MD, also generally improves.
“However, the VFI is less affected by cataract and it is more sensitive to changes near the centre in order to better correlate with the ganglion cell loss,” said Dr Webers, Professor and Chair, Department of Ophthalmology, Maastricht University, Maastricht, The Netherlands.
He also noted that the impact of phacoemulsification on the visual field
parameters will vary depending on the density and type of cataract and on the glaucoma stage, determined by the number of defects, the depth of the defects and their localisation. Dr Webers illustrated this point by discussing three case examples.
The first case involved a patient with a relatively dense cataract and mild glaucoma whose VF showed multiple changes, including improvements in foveal sensitivity, MD and VFI. He contrasted the visual field effects in that case with those of a case of a patient who had end-stage glaucoma. In this latter case, the visual field showed an increase in foveal sensitivity, but neither the MD nor VFI had changed.
“The MD and VFI values in this patient are mostly caused by the glaucoma and not affected so much by the cataract. The foveal sensitivity, however, increased since the cataract was removed,” Dr Webers explained.
The third example described a patient with moderate glaucoma in whom cataract density would be a more critical factor for predicting visual field changes. In such a case, any change can occur on the visual field, Dr Webers said.
“Normally the fovea sensitivity will stay the same or increase – it depends on how far the scotoma reaches. The MD change will depend on the intensity of the cataract, improving if there is a lot of cataract and staying the same if there is only little cataract,” he explained.
Discussing the impact of IOL choice on the VF parameters, Dr Webers noted there is little literature relating to this topic in normal eyes and even less pertaining to patients with glaucoma. Summarising the available information, he said that on average, a monofocal IOL will have
minimal to no effect on the MD value while a multifocal IOL will be associated with a significant nonspecific reduction of up to -3dB.
“This loss does not improve with time or neuroadaptation. The reduction seems to be related to the multifocal design of the implant rather than to pseudophakia, and is a generic property for all diffractive IOL types,” he said.
OCT IMPACT
Reports in the literature are relatively consistent in showing that PP NFL thickness in normal eyes increases following cataract extraction in the range of +4 to +19μm. Data on the change in patients with glaucoma are limited, but the available reports indicate that an increase in PP NFL thickness is also seen after cataract surgery in eyes with primary open angle glaucoma.
“I found a single study investigating patients with pseudoexfoliation glaucoma that found no change in PP NFL thickness, but it also found no change in normal control eyes,” Dr Webers said.
The postoperative increase in PP NFL thickness following phacoemulsification is seen regardless of the OCT machine used and is the result of an increase in signal strength following cataract removal, Dr Webers said.
“The cataract impedes signal transmission to and from the retina, and the delayed time-of-flight affects the delineation of the NFL, leading to a falsely low measurement,” he explained.
Information on potential differences relating to cataract type is variable.
“Some papers say the impact is greatest with nuclear cataracts, others say it is more with cortical cataracts, and even others say it is more with posterior subcapsular cataracts.”
Quotes cited from various papers addressing the impact of IOLs on OCT imaging show some lack of agreement. However, Dr Webers concluded that OCT image quality can be affected by multifocal IOLs.
Carroll A B Webers: c.webers@ maastrichtuniversity.nl
EUROTIMES | DECEMBER 2020/JANUARY 2021
GLAUCOMA 30
The MD and VFI values in this patient are mostly caused by the glaucoma and not affected so much by the cataract
Carroll A B Webers, MD
Interpreting visual FIELD LOSS
Attention to the right metrics overcomes confounding effects of cataract. Cheryl Guttman Krader reports
Assessing patients with glaucoma and cataract can be particularly challenging, since cataract formation can mimic visual field loss and progression, emphasised Hans G Lemij MD, PhD, during a session on glaucoma pearls for the cataract surgeon at the 2020 ESCRS Virtual meeting.
Dr Lemij, a glaucoma specialist at The Rotterdam Eye Hospital, Rotterdam, the Netherlands, began his presentation by showing street scene images to depict how patients with vision impairment from glaucoma with or without cataract perceive their vision in the real world. The examples demonstrated that patients with cataract and a centrally located scotoma from advanced glaucoma may be disappointed by their functional outcome after cataract surgery because of persisting glaucomarelated blurred central vision.
PEARLS FOR READING THE VISUAL FIELD TEST REPORT
Because a generalised depression of the entire visual field can be associated with glaucoma as well as with cataract, Dr Lemij recommended paying attention to the pattern deviation plot when interpreting the visual field printout in order to assess the potential functional outcome after cataract surgery in a patient with glaucoma.
The pattern deviation plot is based on the total deviation plot; it shows values that are corrected following a ranking of the field’s test locations. The seventh best point (i.e., the 85th percentile of the retinal sensitivities) is compared to the age-corrected normative database. The difference, intended to be caused by media opacities (such as cataract), a narrow pupil or refractive error, is then added to the values of retinal sensitivities for correction.
“By looking at the pattern deviation plot on the visual field printout, clinicians can get some insight into the contribution of cataract because the pattern deviation compensates for confounding from cataract,” Dr Lemij said.
In a case example, he demonstrated how this analysis can help clinicians parse out focal losses due to glaucoma in a patient with cataract. However, Dr Lemij also noted the need to consider the information in the context of the patient’s other findings.
Although the visual field of the patient in the case appeared greatly improved based on the pattern deviation analysis, closer inspection showed that some of the individual retinal sensitivity data points had a value less than 0, indicating that the patient failed to perceive even the brightest stimulus at those points during the testing.
“Retinal sensitivity data point values less than 0 would hardly ever occur because of cataract. Therefore, this case demonstrates why you cannot rely only on the pattern deviation value and instead need to factor in all other aspects collected during the examination,” Dr Lemij said.
“In this case, the patient had a visual acuity of 6/6, which is not consistent with cataract.”
DETECTING VISUAL FIELD PROGRESSION
Detection of progression is critical in managing patients with glaucoma, but when interpreting the visual field, clinicians must recognise that the ability to identify real progression can be confounded by measurement variability, which can mimic or mask true glaucomatous progression, and cataract formation, which can also mimic progression.
When trying to determine the rate of glaucomatous functional loss, repeating the visual fields will circumvent the confounding associated with measurement variability. Dr Lemij cited a paper by Chauhan and colleagues (Chauhan BC, et al. Br J Ophthalmol. 2008;92(4):569-573) that provided recommendations on the frequency of visual field examinations required to identify clinically meaningful rates of change in glaucoma.
“In this very important paper, the authors pointed out that you need to repeat the visual field tests very often to be certain or somewhat certain that you are dealing with true progression. Depending on your target, however, the required testing can be highly impractical and probably not realistic,” Dr Lemij said.
Illustrating the challenge, Dr. Lemij explained that to accurately detect an overall change in the mean deviation of -1.0 dB over two years (-0.50 dB/year) a patient would have to complete seven visual field tests per year. Detecting progression occurring at a rate of -1.0 dB/year over a three-year period would require that the patient undergo three visual field tests per year.
The information provided by progression software, and particularly the Glaucoma Progression Analysis, offers a helpful alternative. When assessing patients with cataract for glaucoma progression, Dr Lemij suggested focusing on the Visual Field Index (VFI) because unlike the mean deviation (MD), the VFI is relatively insensitive to confounding by cataract.
“Using the rate of change in the VFI in a patient with glaucoma and cataract, you can still monitor for glaucomatous visual field loss over time,” he said.
For interpreting the VFI rate of progression value, Dr Lemij noted that a decline of more than 1% per year would be considered clinically meaningful.
“In case of younger patients, with a longer life expectancy, one should obviously be stricter in accepting any progression than in very old patients,” he added.
Hans Lemij: H.Lemij@oogziekenhuis.nl
EUROTIMES | DECEMBER 2020/JANUARY 2021 GLAUCOMA 31
In case of younger patients, with a longer life expectancy, one should obviously be stricter in accepting any progression than in very old patients
Hans G Lemij MD, PhD
Glaucoma diagnosis using OCT
Step-by-step approach holds the key to accurate clinical application of OCT information. Cheryl Guttman Krader reports
Structural imaging with optical coherence tomography (OCT) is a core component of the evaluation for glaucoma diagnosis and monitoring, but the report needs to be interpreted carefully and with all of the patient’s clinical data taken into consideration, said David Garway-Heath MD, at the 2020 ESCRS Virtual meeting.
Dr Garway-Heath, Glaucoma UK Professor of Ophthalmology, University College London, London, England, underscored these points by adapting a quote from Mark Twain. The American author/humourist observed the hazard from not reading the newspaper but also from newspaper reading. Dr GarwayHeath said: “If you are not imaging with OCT, you will be relatively uninformed on glaucoma diagnosis, but if you just read the OCT report without interpreting it, you could be misinformed.”
Emphasising that OCT imaging is just part of the diagnostic workup, Dr Garway-Heath said: “Structure and function provide complementary information. Look for structure-structure and structure-function concordance, and remember you still need your clinical acumen because there are things that OCT cannot do. Look at the optic nerve for features such as optic nerve haemorrhage, which is an important prognostic factor for glaucoma and glaucoma progression, and for lesions in the retina and/or defects in the retinal nerve fibre layer that might explain visual field loss.”
He continued: “Even when there is structure-function concordance, you cannot necessarily make the diagnosis of glaucoma without excluding other potential causes. Finally, if you are uncertain of an abnormality, monitor for change over time that will tend to occur if the abnormality is due to glaucoma.”
REVIEWING THE OCT REPORT
Providing advice for interpreting the OCT report, he first acknowledged that the software generates “an overwhelming number of parameters” to look at. To
address this challenge, the first tip was to concentrate on the peripapillary nerve fibre layer (PP NFL) and the ganglion cell complex (GCC) thickness because those two anatomical structures provide the most information.
Next, he outlined a systematic approach to reviewing the OCT report, adding as a caveat that not all OCT devices provide all of the features he would be describing. The systematic approach is comprised of five steps and begins with a check of the retinal NFL segmentation, looking for segmentation errors and artifacts as a means of assessing the accuracy of the software’s segmentation.
“Some OCT devices allow the user to go back into the software and correct the segmentation. If that is not possible with your system, exercise caution when interpreting the result,” Dr GarwayHeath suggested.
The second step is to look for structureto-structure concordance between regions of retinal NFL thinning in the en face and PP NFL thickness maps. Here, Dr GarwayHeath advised caution, noting devicerelated differences in the displayed location of the temporal part of the PP NFL.
While there is a general movement towards showing the temporal part in the centre of the scan, with some machines it may still appear at the edge of the scan, he cautioned.
In addition, availability of the en face maps also varies. These maps, which are very useful for identifying the pattern of NFL thinning that is associated with glaucoma, are provided by all sweptsource OCT platforms, but not by all time-domain machines.
The third step in the systematic review of the OCT report is to look for topographical correspondence between the structural parameters (NFL thinning and ganglion cell loss) and visual field sensitivity loss. With some OCT devices, a map will be produced that aids in the check for concordance, Dr Garway-Heath said.
MACULA VULNERABILITY ZONE
Next, clinicians should look for damage in the macula vulnerability zone in both the PP NFL scan and the macula ganglion cell thickness scan. This information is particularly useful when assessing the OCT report for early glaucoma because it can show damage in the absence of any functional loss in the 24-2 visual field test.
“If there is thinning in the OCT scan, do a 10-2 visual field to pick up visual field loss in this region,” Dr GarwayHeath advised.
The last step is to look for correspondence between the macula and NFL maps and the visual field sensitivity loss to check for structure-to-structure and structure-to-function concordance.
He warned against automatically interpreting red in the report is a hallmark of glaucoma. The finding needs to be considered with particular caution in myopic eyes that have unique anatomic variations, he emphasised.
“In myopic eyes the thicker bundles in the superotemporal and inferotemporal parts of the nerve are closer to the temporal region. Consequently, parts of the NFL thickness sometimes fall outside normal ranges in an otherwise healthy eye without glaucoma. In addition, because the measurements are taken further away from the edge of the nerve in a myopic eye, the NFL measurements in the myopic eye are thinner than the average,” Dr Garway-Heath explained.

EUROTIMES | DECEMBER 2020/JANUARY 2021
GLAUCOMA 32
If you just read the OCT report without interpreting it, you could be misinformed on glaucoma diagnosis
David Garway-Heath MD
Infectious keratitis in children

Paediatric microbial keratitis requires special diagnostic considerations.
Roibeard Ó hÉineacháin reports
Infectious keratitis in children brings special challenges in diagnosis, and often require aggressive treatment to resolve, according to Vishal Jhanji MD, FRCS, FRCOphth, University of Pittsburgh School of Medicine Pittsburgh, USA.
“We face some real problems while managing infectious keratitis. Some of these include an uncooperative child, possible late presentation, lack of information prior to presentation, lack of information about previous treatments and use of traditional medicines in some parts of the world. And if you cross all these hurdles, you still have to deal with amblyopia in the recovery period,” Dr Jhanji told the 2020 WSPOS Virtual Meeting.
The main causes of infectious keratitis include contact lens use, inflammatory causes and ocular trauma, he noted.
Incomplete immunisation profile appears to contribute to its prevalence in the developing world. However, in developed countries where myopia has a high prevalence, the use of orthokeratology may be an additional risk factor. In a series of patients at tertiary care centre in Hong Kong, patients undergoing orthokeratology accounted for around 25% of microbial keratitis cases and 33% of contact lens-related keratitis cases.
SIGNS AND SYMPTOMS
The main signs and symptoms of keratitis include redness, pain, photophobia, conjunctival discharge and blurred vision. When examining the cornea, it is important to look at the location and size of the corneal infiltrate and epithelial defect, the degree of stromal oedema, corneal vascularisation and signs of corneal thinning and perforation. In addition, one should be careful not to overlook the presence of foreign bodies in the eye, Dr Jhanji advised.
He noted that corneal scrapings are more challenging in children, and general anaesthesia may therefore be required, especially in patients younger than five years. Cultures can also be obtained from contact lens cases and contact lens solutions. Bacterial isolates are more common than fungi and, unlike adult keratitis, can include coagulase negative staphylococci. Cultures for Acanthamoeba should be performed if indicated by clinical appearance or history.
Treatment of bacterial infections has to be aggressive, with frequent administration of antimicrobial agents. Fortified antibiotics are commonly used, although milder cases will often respond to topical moxifoxacin. Vancomycin eyedrops should only be used when absolutely necessary, due to their surface toxicity.
The spectrum of medications for fungal keratitis include topical natamycin (5%), fluconazole (0.5%) and amphotericin B (0.25%). Newer drugs with high corneal permeability such as voriconazole 1% eye drops can be used. Oral antifungals such as voricanazole are another option but baseline liver function testing is imperative, Dr Jhanji said.
Vishal Jhanji: jhanjiv@pitt.edu
At
believe that
Join
in the world.
EUROTIMES | DECEMBER 2020/JANUARY 2021 PAEDIATRIC OPHTHALMOLOGY
Free Membership
to WSPOS is available for FREE on www.wspos.org
Ophthalmology
Fax:
Membership
World Society of Paediatric
and Strabismus Contact Info: WSPOS, Temple House, Temple Road, Blackrock, Co. Dublin, Ireland Tel: +353 1 288 3630
+ 353 1 209 1112 Email: wspos@wspos.org
our
society and become part of one of the largest networks of paediatric ophthalmologists
WSPOS, we
“Expertise
You’ll gain access to our wide library of videos, including our “Masters in Surgery” archive and also get the chance to collaborate on our global case report quiz. 33
Resides ALL Over the World”
Endothelial keratoplasty in children
Endothelial keratoplasty may offer several distinct advantages over penetrating keratoplasty for children with visually significant corneal clouding due to endothelial dysfunction, according to Muralidhar Ramappa MD.
“Compared to PK, the advantages of a technique such as Descemet’s stripping endothelial keratoplasty (DSEK) include rapid visual recovery with predictable refractive outcome, minimised suture related events, less stringent follow-up postoperatively and reduced steroidrelated issues with the possibility of early tapering or weaning,” Dr Ramappa said at the World Ophthalmology Congress 2020 Virtual.
Dr Ramappa, a consultant ophthalmologist at the LV Prasad Eye Institute, Hyderabad, India, said that children with conditions such as congenital hereditary endothelial dystrophy (CHED) and other endothelial disorders could achieve excellent visual outcomes and realise a significant improvement in corneal transparency by undergoing DSEK or one of its variations.
“Our long-term clinical experience has shown that it is safe and effective and a superior surgical alternative to PK in children with endothelial disorders. However, some further study is justified to establish whether the use of superficial keratectomy with mitomycin C use may offer a substantial benefit in cases with dense anterior stromal opacification due to late presentation,” he said.
Dr Ramappa outlined the results of a retrospective study he carried out of 180 DSEAKs in 167 eyes of 111 children with corneal endothelial dysfunction treated with endothelial keratoplasty.
The median age at surgical intervention was 7.9 years (interquartile range IQR, 5.2 to 11.2 years), and the majority of indications were CHED (70%) followed by failed graft (12%), pseudophakic corneal oedema (7%) and xeroderma pigmentosa (6%). Cox proportional hazards regression analysis showed that the indication for DSAEK (p=0.007; hazards ratio: 2.17 ±
0.62), age at surgery (p= 0.02; hazards ratio: 0.87 ± 0.05) and any subsequent intervention following DSAEK (p=0.003; hazards ratio: 0.11 ± 0.08) were significant risk factors for DSAEK failure. Eyes with CHED had a significantly better graft survival than eyes with a prior failed PK.
Most of the cases (80%) were microkeratome assisted for donor preparation, with a push-through insertion technique used in 91%. “We have found this to be the most consistent approach and has shown the least amount of endothelial cell loss in our hands,” said Dr Ramappa. The ECD loss was 40.1% at six months, 45.4% at year one, 43.9% at year two, 51.6% at year three, 55.2% at year five and 61.9% at seven years from baseline.
The main complications included cataract formation, pupillary block, lenticule detachment and decentration and reversed lenticule. Primary graft failure was encountered in three cases, which Dr Ramappa surmised may have been related to the learning curve, and secondary glaucoma in five patients, which necessitated medical management. Repeat interventions included five for rebubbling, four repeat DSAEK, three PK surgeries, six for cataract, three glaucoma valve surgeries and one glaucoma filtering surgery.
The visual outcomes were excellent overall, said Dr Ramappa. The median BCVA improved from 1.45 ± 0.70 preoperatively to 0.90 ± 0.06 at the last follow-up visit (p<0.0001). The mean spherical equivalent refraction at the last visit had a median of 0.50D (IQR, -2.25 to +3.13).
“We report at a median postinterventional follow-up of 2.5 years (IQR, 0.9-3.4 years) 86.2% (144 of 167 eyes, 95% confidence interval 79.9% to 90.1%) maintained a clear graft.
“Factors affecting vision postoperatively included a late presentation, dense amblyopia, cataract and glaucoma. The cumulative overall long-term graft survival was 92.7%, 86.5%, and 77.7% at one, three and seven years respectively, which is very satisfactory,” he said. These longterm outcomes are much superior to in comparisons to conventional fill thickness corneal grafting.
The risk of allograft rejection and infection rates was significantly lower after an endothelial keratoplasty than conventional keratoplasty. Morphometric and densitometric analysis throughout the follow-up period showed an improvement of the graft-host thickness over time. These children were likely to be a bit hyperopic due to thicker graft host profiles.
Although DSEAK is more advantageous over conventional PK, it comes with specific intra and postoperatic challenges. The small, unstable anterior chamber, an underlying clear lens with poor visibility, makes it challenging to deal with intraoperatively and necessitates several modifications to avoid potential complications. Somewhat difficulty in strip thickened Descemet’s membrane, and there is potential risk of disturbing posterior stromal lamellae, thus results in a sub-optimal interface. Besides inadvertent lens or uveal trauma. Subsequent reinterventions again
EUROTIMES | DECEMBER 2020/JANUARY 2021
Paediatric keratoplasty possesses several distinct challenges in comparison to adults. Dermot McGrath reports
PAEDIATRIC OPHTHALMOLOGY 34
Our long-term clinical experience has shown that it is safe and effective and a superior surgical alternative to PK in children with endothelial disorders
Muralidhar Ramappa MD
requires general anaesthesia. Modifications in surgical technique can help to overcome most of these issues, he said.
“For instance, the problem of poor visibility and difficulty in stripping Descemet’s membrane can be taken care of using chandelier illumination, trypan blue, and fine micro forceps,” he said.
Other potential issues to be aware of include insertion difficulties with the unfolding of the donor lenticule in the small anterior chamber and preventing trauma to the crystalline lens.
Postoperatively, supine positioning under sedation for at least 30 minutes helps minimise the lenticule dislocation or decentration. A detailed postoperative evaluation is not technically easier to perform and may need multiple examinations under anaesthesia to ensure the graft is well attached and discern the graft host dynamic well. Postoperative cataract and glaucoma management also require special attention; each of these additional subsequent steps can put the graft under huge risk.
Based on their extensive experience with corneal grafts and keratoplasty over many years, Dr Ramappa and his colleagues have developed a treatment algorithm to help decide each pediatric
patient’s best course of action.
“The general rule of thumb is that where the corneal cloudiness is precluding the iris details due to significant anterior stromal alternations, it would be prudent to consider PK, and also to time the intervention as late as possible while caring amblyopia. If the case is mild to
moderate and the iris details are seen well, then explore endothelial keratoplasty options and try to expedite to circumvent irreversible stromal changes that typically occur in late interventions. Thus, end up with a superior outcome with a minimal post haze or sub-Bowman’s folds.
Summing up, Dr Ramappa said that DSEK helps eliminate suture-related events and graft-host dehiscence and offers other advantages over PK in younger patients.
“It makes the eye more robust against injuries, delivers early refractive stabilisation as it is more predictable, and significantly, it minimises the risk of cataract formation, secondary glaucoma, and the need for repeat interventions. Furthermore, allograft rejection is at least 10 times less frequent and more reversible.
In conclusion, DSAEK provides superior long-term clinical outcomes with low complication rates suggesting that DSAEK is a safe and effective surgical alternative in children with corneal endothelial disease. Notably, accelerated postoperative visual recovery helps in better long-term functional outcomes by minimising the risk of amblyopia.
Muralidhar Ramappa: muralidhar@lvpei.org
Continue your education online all year with our new range of online resources Ready when you are. Visit education.escrs.org EUROTIMES | DECEMBER 2020/JANUARY 2021 PAEDIATRIC OPHTHALMOLOGY 35
For instance, the problem of poor visibility and difficulty in stripping Descemet’s membrane can be taken care of using chandelier illumination, trypan blue, and fine micro forceps
Muralidhar Ramappa MD
Continuing vital care during the pandemic
ESCRS-supported charity working to eliminate avoidable blindness in under-developed countries. Priscilla Lynch reports

The impact of the COVID-19 pandemic continues to be wide-ranging and pervasive, including on the vital work of ophthalmology charity services in the developing world.
Eyes of the World, which receives support from the European Society of Cataract and Refractive Surgeons (ESCRS), is a non-profit organisation that works to eliminate avoidable blindness, through helping visually impaired people without economic resources living in some of the world’s most under-developed countries.
The foundation’s key focus involves providing long-term support to ensure that people receive qualified ophthalmological care from their local health services, at basic preventative and early diagnosis levels to specialised care.
Expert ophthalmology care, specialised training, equipment
provision and local public educational and awareness campaigns are among the key supports provided by Eyes of the World to help reduce pathological ocular incidence and create sustainable qualified ophthalmology services in each region.
The foundation also works at increasing global public awareness about the basic healthcare deficiencies in these areas.
ESCRS has provided important support to the foundation in recent years, most notably with its projects in Mali and Mozambique.
Since 2008 the Foundation has been providing eye care and support in the Mopti region in Mali, which has more than two million inhabitants and only a couple of ophthalmologists, under its Eyes of Mali programme. As a result of the lack of available care, it is estimated that more than 22,000 people are blind due to preventable causes or have curable eye conditions in this area.
EUROTIMES | DECEMBER 2020/JANUARY 2021 GLOBAL OPHTHALMOLOGY 36
Reference Health
Soap and water basins for the use of patients at the Koro
Centre
©Eyes of the world foundation
Similarly, the Eyes of Mozambique programme, started in 2002, is based in the south of the country in the Inhambane province, where there is a huge shortage of qualified ophthalmology professionals. There are almost 100,000 blind people and about 876,000 people with ocular problems, mostly due to corneal pathologies, glaucoma, trachoma, malnutrition and degenerative illnesses.
Some of the most notable recent results of the Mozambique project are the performance of 900 cataract operations by local ophthalmologists in a year, and the screening of more than 30,000 students from schools in the province of Inhambane, the foundation told Eurotimes.
Clearly maintaining and continuing its work in these countries despite COVID-19 is absolutely vital.
Speaking to Eurotimes, Núria Ramon i Garcia, General Manager of the Eyes of the World foundation, gave an update on both of these projects and the challenges they have faced because of the pandemic.
“Fortunately, after a few extremely complicated months due to restrictions on people’s access to health centres, the Eyes of the World project in Mozambique is functioning normally again. Consultation rooms have been fully opened and surgeries are being performed again. For this same month of October, we have planned a cataract surgery campaign in the district of Zabala. In addition, we have already resumed the training of 25 PMTs (Practitioners of Traditional Medicine).
“In Mali, all the purchases of prevention and protection materials and equipment foreseen in the project have already been made and the distribution of the last batch among the different

absence of data from the Koro district, Eyes of the World, with the support of the ESCRS, has already managed to attend 519 cases of eye emergencies (252 men, 182 women and 85 children under 14 years of age) and to realise 472 teleconsultations (241 men, 191 women and 40 children under 14 years of age).”

The contribution of ESCRS has been key to facilitating the safe care of urgent ophthalmic cases in these vulnerable and remote regions during the pandemic, Ms Ramon said. “That is people who otherwise would not have had any opportunity to receive treatment or eye care.”
“As for Mali, the support of ESCRS has made it possible for professionals in the region of Mopti, as well as patients, to have had the materials and equipment for the prevention of COVID-19 necessary for eye care. In this sense, all the ophthalmology units in the region have been strengthened, including the Sominé Dolo Hospital.”
She said that the continuing ESCRS support to the foundation is essential to ensure the eye care of the populations of Mali and Mozambique.
“Although thanks to the Eyes of the World projects and the support of our partners, the Mopti region (Mali) and the province of Inhambane (Mozambique) have ophthalmic care, there are still many needs to be covered; for instance: the training of more health personnel, the provision of equipment for eye health structures and the increasing of the quality and the ration of the cataract surgery, reaching the population of the most remote areas.
“Moreover, it is necessary to continue working with communities in order to raise awareness of eye hygiene and eye care guidelines; and to reach all schools to detect possible eye diseases at an early stage.” For more information and to support Eyes of the World go to
EUROTIMES | DECEMBER 2020/JANUARY 2021 GLOBAL OPHTHALMOLOGY 37
VISIT OUR WEBSITE FOR INDIAN OPHTHALMOLOGISTS www.eurotimesindia.org INDIA
Delivery of protective material to the ophthalmology team of the Koro Reference Health Centre Optical care at the Bankass Reference Health Centre
Compassionate care
It was love at first sight; a perfectly round graft right in the centre of the cornea with neatly aligned sutures.
On my first corneal operating list, I assisted Professor Fiona Carley in performing a corneal transplant surgery and I knew deep in my heart that this was the operation I wanted to carry out myself one day. Thinking back, it wasn’t just the surgery that made this experience so special.
A few years later, I performed my first corneal transplant surgery independently, this time with Prof Carley in the assistant’s seat. My heart was racing but with her encouragement and support, I knew that I would be able to complete the case safely and with a good outcome.
It is not an exaggeration to say that it takes blood, sweat and tears to nurture a trainee into a competent ophthalmologist and mentorship is increasingly becoming an integral tool in delivering medical training. Unfortunately, it is often overlooked in day-today medicine due to the enormous service commitment and time constraints that we all face. I was therefore incredibly lucky that Prof Carley had a special gift of turning every clinical encounter into a learning opportunity, whether it was in the midst of a busy ward round or packed clinic.
THE PATIENT BEHIND THE SLIT LAMP
For me, it was her actions that taught me more than the words. She encourages trainees to think about the patient behind the slit lamp, not just as eyes with pathology or another case

to operate on. With this new mindset, I was able to see the grandmother who desperately wanted her cataract removed so that she could see to write Christmas cards to her grandchildren, and a postman who was on the verge of losing his job as he struggled to see the address on letters due to dry eyes secondary to his graft versus host disease. Thanks to Prof Carley, I am now able to relate better to my patients and provide more compassionate care, a key skill that I will treasure for the rest of my career.
Whilst in training, it is easy to get caught up in the unending competition of chasing surgical numbers and meeting training competencies. However, this misses the point of training, which is to prepare you for a lifetime of caring, professional practice. Prof Carley pushes you to aim for excellence, not just competency and does this whilst making you feel comfortable within your own limits and capabilities.
As my career progresses each year, I increasingly find myself more in a trainer’s role, and I reflect back on how
Prof Carley shaped my own training and career aspirations. I feel strongly that it is up to us to inspire our younger colleagues and help them to become the best that they can be, as I was inspired as a junior trainee and continue to be now.
Dr Jennifer Kim is a Specialist Registrar at the Manchester Royal Eye Hospital, UK, and winner of the 2020 John Henahan Prize
Dr Jennifer Kim tells how her mentor, Professor Fiona Carley, taught her how to see the patient behind the slit lamp
EUROTIMES | DECEMBER 2020/JANUARY 2021 MY MENTOR 38
IllustrationbyClaireProuvost
J & J gets real
Functional device measures, support for practices bring innovative tech to life. Howard Larkin reports
Cataract surgery isn’t just about reading letters at six metres. It’s also about helping patients read their phones, shop, cook and avoid falls in their daily lives.
Measuring such functional and economic benefits of intraocular lenses (IOLs) and other devices is just one example of how Johnson & Johnson Surgical Vision is innovating to do a better job of meeting patient – and surgeon – needs, said Erin McEachren, J&J Surgical Vision’s new regional vice president for Europe, the Middle East and Africa.
Eyhance®, the TECNIS monofocal IOL that improves intermediate as well as distance vision, is a good example, McEachren said. “It’s not just innovation, but innovation at a cost that is not prohibitive. This really enables big institutions to use great technology in a way that delivers value that you can see, such as potentially reducing falls.”
To that end, J&J is developing registries and other survey tools that do a better job not only of quantifying patient benefits, but of also detecting and addressing unmet patient needs. “We are looking at it from a data-driven perspective; not just clinical outcomes but the whole picture so we can better understand functional outcomes and the healthcare economics of our products,” McEachren said.
McEachren sees this as a J&J strength due to its broad portfolio of businesses and resources, which include pharmaceutical development and non-surgical ocular products. “Pharma does a good job with value-based healthcare and we are applying that approach to medical device development, which is more dynamic. I won’t say we have it all figured out, but the data is driving it.”
Similarly, J&J Surgical Vision is innovating
to help surgeons be more effective and efficient. For example, new software for the Catalys Precision Laser System for femtosecond laser-assisted cataract surgery improves astigmatism correction in several ways.
Developed in collaboration with Cassini Technologies, the CATALYS™ System cOS 6.0 update adds iris registration for automatic cyclotorsion compensation. The software also reduces the need for intraoperative aberrometry for IOL alignment by allowing radial laser marks with a mean accuracy of 0.6°, or 5.5 times more precise than manual markers. Automated data entry increases accuracy and efficiency while built-in nomograms reduce time spent on calculations for arcuate incisions.
Combined with the TECNIS Synergy™ Toric II, introduced at this year’s Congress of the ESCRS, the update further strengthens J&J’s astigmatism platform. TECNIS Synergy™ Toric II is a newly designed lens with a flat defocus curve, which offers a broad range of continuous vision and superior low-light performance for reading in dim lighting. The new lens also features frosted haptics designed to improve rotational stability in the eye.
It’s all part of an overall corporate focus on improved effectiveness, efficiency and sustainability that includes professional education, research and clinic systems improvements. “One reason I joined J&J is there is so much development and a vision platform with a 2030 goal,” McEachren said.
COPING WITH COVID
As many ophthalmic practices have reported, COVID-19 has had one upside for J&J Surgical Vision, as it has enabled surgeons around the globe to collaborate more through video and webinars. “It has given us strategic time to reflect on our past and
plan our future, strengthening our organisation and our partnerships with clinicians,
private clinics, and public hospitals, and look at more-creative solutions,” McEachren said.
Throughout the pandemic, J&J has provided assistance in the hardest hit areas. In one UK case, J&J Surgical Vision donated a Tecnis Toric IOL and helped arrange surgery that allowed a critically needed consultant anaesthesiologist to return to work in London while elective surgeries were shut down. He had a first Tecnis lens implanted before the lockdown, and needed the second to correct anisometropia that left him barely able to function using PPE.
Fogged spectacles from mask wearing also appears to be driving an uptick in refractive surgery, McEachren noted. “It’s an opportunity for refractive lens exchange and to help younger patients transition to IOLs.” Overall, refractive centres have recovered a little quicker than cataract practices, though whether the trend holds remains to be seen.
Overall, the pandemic took a toll on J&J as well as practices, especially during the second quarter of 2020. Recovery has happened at different rates across the region, accordingly to lock down timings and local restrictions, McEachren said.
These unmet needs set the stage for a strong comeback, perhaps with more efficient processes and effective products, said McEachren, who is optimistic about the field’s prospects over the next few years. She believes J&J Surgical Vision has prepared and has the resources to change the trajectory of eye care going forward.
“I have been blown away by the great people at J&J and their commitment to our customers. I feel very lucky and supported as a business leader that we can focus on what really matters for our patients both now and in the future,” McEachren said.

EUROTIMES | DECEMBER 2020/JANUARY 2021 OUTLOOK ON INDUSTRY
39
One reason I joined J&J is there is so much development and a vision platform with a 2030 goal
Erin McEachren
Erin McEachren
It’s not just innovation, but innovation at a cost that is not prohibitive. This really enables big institutions to use great technology in a way that delivers value that you can see
Erin McEachren
Mind your language
The vast majority of ophthalmic surgery is performed under local anaesthesia and patients may be acutely aware of conversations that take place in theatre. Therefore, if the patient knows that the operation is being performed by a trainee surgeon, it is understandable that they may feel additional stress.
The success and ease of performing surgery requires both the trainee and the patient to feel relaxed. A key part of ensuring this is effective communication between the supervisor and trainee.

For example, during cataract surgery, my new trainees operate in a reverse modular fashion, starting with the last steps of surgery first. Performing each step repeatedly allows the trainee to build confidence in a particular step before proceeding to the next. Whilst I would have already discussed with the trainee which steps they would be expected to perform, it often becomes necessary to guide the trainee during surgery as well.
As such, it is desirable to have some form of coded communication between the supervisor and trainee. There is no one, absolute correct way, but it is imperative that both the supervisor and the trainee understand each other. It is also important that the supervisor’s statements or comments are not patronising or demoralising but at the same time clearly indicate when the trainee’s actions need modification.
LET ME HELP YOU
When I provide specific instructions, for example “hold the instrument horizontally”, it implies that I am happy for the trainee to proceed but keep in mind my suggestion. However, when I feel that the trainee is struggling or has had
a complication which they may be unable to handle, I use the phrase “Let me help you” to indicate that I wish to take over. In using these words, I neither discourage the trainee nor alarm the patient under the drape, thus allowing for a smooth change of hands. I never say “stop”, nor use any expletives or unprofessional language.
Theatre personnel talking to each other with reference to matters unrelated to the surgery being performed must be avoided. One must also be particularly vigilant about discussing other patients and the resultant risk of breaching patient confidentiality.
Equally important is debrief at the end of surgery. Video recording of surgery and reviewing it at the end of the list gives the supervisor and trainee an opportunity for critical appraisal to discuss what went well and how things could be improved.
Dr Jai Shankar is Consultant Ophthalmologist at Wrexham Maelor Hospital, United Kingdom
Jai Shankar: shobitha_jai@yahoo.co.uk

EUROTIMES | DECEMBER 2020/JANUARY 2021
A key part of ensuring successful surgery is effective communication between the supervisor and trainee, writes Dr Jai Shankar
RANDOM THOUGHTS 40
One must also be particularly vigilant about discussing other patients and the resultant risk of breaching patient confidentiality
Imaging Competition Winners
Haag-Streit has announced the winners of the 2020 Slit Lamp Imaging Competition. The judges selected 12 finalists from 300 entries, who delivered outstanding images.
Following a great deal of deliberation, the judges announced that the winner was Mel Yeneralski, Ophthalmic Photographer, Cambridge University Hospitals, UK, for her image of silicone oil bubbles.

John McCormick, Medical Photographer at the Tennent Institute of Ophthalmology, Gartnavel General Hospital, UK, received the prize for second place for his image of image of corneal endothelial pigment downgrowth.
Eva Steffan, University Clinic for Ophthalmology, Inselspital, University of Bern, Switzerland, received third prize for an image of a vitreous prolapse.
Haag-Streit Diagnostics also announced the nine runners up: Carmen Rodrigues, Katie Lachut, Kim Baxter, Nicole Mantel-Baerlocher, Dr Pablo Gili, Pia Lohri, Utpal Sarkar, Yajie Zheng and Zhang Yang.
All 12 images will feature in the Haag-Streit Diagnostics 2021 calendar. www.haag-streit.com/haag-streit-diagnostics
PREMIUM IOL CALCULATOR
Rayner have announced the launch of their updated web-based Premium IOL Calculator, Raytrace.

A company spokesperson said the new Raytrace version 3.5 was developed in line with surgeon feedback, includes the following improvements: Inclusion of Posterior Corneal Astigmatism (PCA) for more accurate toric IOL calculations; all biometric and IOL options now viewable on a single webpage for greater convenience; and addition of nominal values to compare with Raytrace results for verification; www.Raytrace.rayner.com
CHIEF DEVELOPMENT OFFICER
Oculis has appointed David Jacobs MD as Chief Development Officer. A company spokesperson said Dr Jacobs will be based in Oculis’ newly-established US office. In his new role, he will be responsible for leading all development plans and achieving market authorisations by coordinating all regulatory activities required for future New Drug Application submissions to the US Food and Drug Administration (FDA), and the equivalent for regulators in other territories.
www.oculis.com
Belong to something powerful . Join us. Visit www.escrs.org Take control of your future. for information about membership & benefits EUROTIMES | DECEMBER 2020/JANUARY 2021 INDUSTRY NEWS INDUSTRY NEWS
41
Lockdown Loco
Operating on patients during the COVID-19 pandemic is opening up new challenges for ophthalmologists. Dr Clare Quigley reports
Lockdown loco, we say. It’s our term for the creeping lockdown-induced cabin fever we are fighting; my husband and I are cutting each other some slack. He can go play games online with his friends, I am allowed to binge on Netflix occasionally. As it is, at the time of writing this article in October, we cannot move outside county Dublin.
We had plans. There was to be a trip to the west of Ireland to visit my mother, who would mind Michael while I logged into the ESCRS meeting. Trip cancelled due to evolving restrictions. At least we could still see family and friends in Dublin... for a while. The government has now advised against visiting other people’s homes. But we try to focus on the positives. Michael sleeps better now, a very welcome development. Also, we live near the Phoenix Park, an extensive urban park that’s home to Dublin zoo. In the zoo, an outdoor safari trail has remained open for now.
We brought Michael there for a visit – at 11 months he is a bit young for the zoo, maybe it was more ourselves we were taking for the outing – but he was captivated by one of the animals, a red panda. Red pandas are small, furry creatures native to the Himalayas, like a cross between a raccoon and a fox. One padded right by Michael as he followed it wide-eyed, watching through the glass until it was out of sight. Trips to the Phoenix park, and the other parks close by, feel precious at the moment. The trees are brilliantly lit up in shades of red, orange and yellow for another short while.
We had plans. There was to be a trip to the west of Ireland to visit my mother, who would mind Michael while I logged into the ESCRS meeting
with a drysdale instead of my usual chopper, minimal phaco required. In and out in under ten minutes.
The latter case was tricky. She was a 97-year-old lady, who was profoundly deaf, but seemed calm and able for surgery under local anaesthetic. I gave her written instructions, and she seemed to understand what was required. On the table though, after a promisingly quiet start, she did not stop moving her head and talking. Complicating matters, she had a tiny pupil that did not respond to intracameral phenylephrine, and a dense cataract. A Malyugin ring brought up her pupil to give adequate access, and I enlisted the scrub nurse to clamp his hands on her temples – I got through it okay in the end, after more than half an hour, but we both said we wouldn’t like to do it again.
Clinical activities in the Royal Victoria Eye and Ear Hospital – or the Eye and Ear as we call it – are still up and running, as a second wave of COVID is breaking. Patients attend for cataract surgery, and I’ve been getting back into the rhythm of operating. In one week I did my fastest, and one of my slowest cataract surgeries. The former case was a myopic woman in her fifties with posterior subcapsular cataract, who was quite nervous. The anaesthetist gave a good subtenons block and some sedation. I saw that the cataract looked soft, and that her anterior chamber was nice and deep; I could take my usual soft lens approach.
After making a generous rhexis I was able to pop up the lens on hydrodissection, so it sat vertically half in, half out of the bag. From there I aspirated in the iris plane, spinning the lens
Work is more than cataracts – until early next year I will be on the glaucoma team, training under Consultants Jeremy O’Connor and Aoife Doyle. The days begin with a ward round, followed by a mix of clinic and theatre sessions. I see complex patients in their clinics; my decision process about which patients need a trabeculectomy, and who could get by with laser or drops, is becoming more refined. Getting to know the visual field progression analysis software has helped, but more importantly the relatively quiet clinics mean I can have a good discussion on cases with the consultants; compared to normal times, the clinic numbers are halved, to comply with the social distancing measures. We don’t like to imagine how half the patients who used to attend regularly are getting on without a review... as a mitigating measure they have opened a new drive-through IOP clinic for suitable patients. Patients get a quick iCare pressure check, without even exiting their car. It’s not a clinic visit with a visual field, but it’s something. Infection rates may worsen, and elective surgeries and clinics may grind to a halt again. I try not to think about that. Or the health budget, and how much it will likely contract over the next few years – when I will be due to finish training – new consultant ophthalmologist jobs are already sporadic at best... Thinking about that too much, it would be easy to go lockdown loco.
Clare Quigley is a resident at the Royal Victoria Eye and Ear Hospital, Dublin, Ireland
EUROTIMES | DECEMBER 2020/JANUARY 2021 INSIDE OPHTHALMOLOGY 42
Illustration by Eoin Coveney
Due to the COVID-19 virus, a number of meetings have been cancelled or rescheduled. The information in this calendar is correct at the time of going to print; please check the meeting website or email the conference organisers to confirm all meeting dates.
↙ LAST CALL
DECEMBER 2020
14th EGS Congress
12 – 13 December
Online & in Brussels, Belgium www.egs2020.org/
JANUARY 2021
7th Annual Congress on Controversies in Ophthalmology: Asia-Australia (COPHy AA)
29 – 30 January
Bangkok, Thailand
http://cophyaa.comtecmed.com/
FEBRUARY
25th ESCRS
Winter Meeting
Virtual Meeting
19 – 21 February www.escrs.org
American-European Congress of Ophthalmic Surgery Winter Symposium 2021
21 – 24 February Aspen, USA

https://aecosurgery.org/ 2021-winter-symposium/
MARCH
6th San Raffaele OCT & Retina Forum
5 – 6 March Milan, Italy https://www.octforum2021.eu/
12th Annual Congress on Controversies in Ophthalmology: Europe (COPHy EU)
18 – 20 March
Lisbon, Portugal http://cophy.comtecmed.com/
APRIL
American Association for Pediatric Ophthalmology and Strabismus 2021 (AAPOS 2021)
Virtual Meeting
9 – 11 April
https://aapos.org/meetings/ meetings-future
MAY
ARVO 2021
2 – 6 May
San Francisco, USA https://www.arvo.org/
EUROTIMES | DECEMBER 2020/JANUARY 2021 CALENDAR 43
The American-European Congress of Ophthalmic Surgery Winter Symposium 2021 will take place in Aspen, USA
19↙
The 7th Annual Congress on Controversies in Ophthalmology: Asia-Australia (COPHy AA) will take place in Bangkok, Thailand
JUNE
AECOS 2021
European Symposium
3 – 6 June
Florence, Italy
https://aecosurgery.org/ 2021-european-symposium/
46th Meeting of the European Paediatric Ophthalmological Society (EPOS)
17 –19 June
Copenhagen, Denmark
https://epos2021.dk/
JULY
AECOS 2021 Summer Symposium
15 – 18 July
Utah, USA
https://aecosurgery.org/ 2020-summer-symposium/
33rd APACRS–
SNEC 30th Anniversary Joint Meeting
29 – 31 July
Suntec City, Singapore
https://apacrs-snec2020.org/
AUGUST
ASCRS Annual Meeting 2021
13 – 17 August
San Francisco, USA
https://ascrs.org/news/ascrs-news/ 2021-ascrs-annual-meeting-update

AUGUST
2nd World Congress on Ophthalmology and Optometry
23 – 24 August London, UK
https://ophthalmology. ophthalmologyconferences.com/
21st Global Ophthalmologists
Annual Meeting
23 – 24 August London, UK
https://annualmeeting.conferenceseries.com/ ophthalmologists/
EyeJC (ESCRS Journal Club)
Advanced Instructional Courses
Eye Contact Interviews
Video of the Month
Video Journal of Cataract, Refractive & Glaucoma Surgery
Young Ophthalmologists Videos: “My Early Surgeries”
the latest video content from ESCRS and
on the ESCRS Player
Watch
EuroTimes, FREE
player.escrs.org
The World Glaucoma Congress will take place in Kyoto, Japan
EUROTIMES | DECEMBER 2020/JANUARY 2021 CALENDAR 44
The 21st Global Ophthalmologists Annual Meeting will take place in London, UK
at a Glance 47,863 * * Average net circulation for the 10 issues circulated between 1 February 2019 to 31 December 2019. See www.abc.org.uk Reach 10 issues per year 27 Members on the editorial board 6 Subspecialities Available online 169 Countries eTimes newsletter Years in print 24
2020 Virtual ESCRS Congress




For indications, contraindications and warnings please refer to the relevant product’s instruction for use. © 2020 Alcon Inc. 11/20 EMEA-VIV-2000063 *The AcrySof® IQ Vivity® IOL clinically demonstrated monofocal visual disturbance profile1 References: 1. AcrySof® IQ Vivity® Extended Vision IOL Directions for Use. 2. Alcon Data on File, US Patent 9968440 B2, May 15, 2018. 3. Alcon Data on File, TDOC-0055575. 09 Apr 2019. 4. Alcon Data on File, TDOC-0056718. 18-Jun-2019. 5. Ligabue E, et al. ACRYSOF IQ VIVITY: Natural vision at a range of distances provided by a novel optical technology. Cataract & Refractive Surgery Today. April 2020 //. 6. Alcon Data on file. A02062-REP-043696, Optical Evaluations of Alcon Vivity®, Symfony*, and Zeiss* AT LARA* IOLs. 7. Lawless M. Insight news. “An IOL to change the cataract surgery paradigm?” available at “https://www.insightnews.com.au/an-iol-to-change-the-cataract-surgery-paradigm/”. Accessed July 17, 2020. Adva ncing CATARACT SURGERY PRESBYOPIA CORRECTION WITH MONOFOCAL SIMPLICITY
The AcrySof ® IQ Vivity® IOL X-WAVETM Technology allows you to leave halos and glare behind2* See the difference it can make for your patients. FIRST-OF-ITS-KIND
correction with monofocal simplicity: AcrySof® IQ Vivity®
Kjell Gunnar Gundersen (Norway) #VivaVivity NOW AVAILABLE ON-DEMAND Watch On-Demand at MyAlcon.com
1-7
Presbyopia
Moderator:















