Can robots increase throughput and improve surgical outcomes?
Objective Cataract and Cornea Grading with OCT OCT imaging and machine learning suggest a new era of anterior chamber diagnostics.
ESCRS provides essential training in underserved areas.
Handling Inflammation with Care
Anticipating conditions that carry increased risk of inflammation after cataract surgery.
POWERFUL PREDICTABLE PROVEN
40+ PUBLICATIONS DEMONSTRATE ISTENT TECHNOLOGIES PROTECT AGAINST VISUAL FIELD LOSS † 81% OF PATIENTS BELOW 15MMHG AFTER 5 YEARS FOLLOW-UP2 97% OF 778 PATIENTS IN A METAANALYSIS OF STANDALONE ISTENT INJECT EYES DID NOT REQUIRE SECONDARY INCISIONAL SURGERY DURING FOLLOW-UP6
† Data on file.
1. Berdahl, J., Voskanyan, L., Myers, J. S., Katz, L. J., & Samuelson, T. W. (2020). iStent inject trabecular micro-bypass stents with topical prostaglandin as standalone treatment for open-angle glaucoma: 4-year outcomes. Clinical & Experimental Ophthalmology, 48(6), 767-774. 2. Hengerer, Fritz H., Gerd U. Auffarth, and Ina Conrad-Hengerer. “iStent inject Trabecular Micro-Bypass with or Without Cataract Surgery Yields Sustained 5-Year Glaucoma Control.” Advances in Therapy (2022): 1-15. 3. Ferguson, Tanner J., et al. “iStent trabecular micro-bypass stent implantation with phacoemulsification in patients with open-angle glaucoma: 6-year outcomes.” Clinical Ophthalmology (Auckland, NZ) 14 (2020): 1859. 4. Ziaei, Hadi, and Leon Au. “Manchester iStent study: long-term 7-year outcomes.” Eye 35.8 (2021): 2277- 2282. 5. Salimi, Ali, Harrison Watt, and Paul Harasymowycz. “Long-term outcomes of two first-generation trabecular microbypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results.” Eye and Vision 8.1 (2021): 1-12. *Consistent cohort. 6. Healey, Paul R., et al. "Standalone iStent trabecular micro-bypass glaucoma surgery: A systematic review and meta-analysis." Journal of Glaucoma 30.7 (2021): 606-620. 7. Samuelson TW, on behalf of the iStent inject Pivotal Trial Study Team. Three-Year Effectiveness and Safety of 2nd-Generation Trabecular MicroBypass (iStent inject). Paper at the Annual Meeting of the American Academy of Ophthalmology (AAO). Virtual Meeting: November 13-15 2020. 8. Samuelson, Thomas W., et al. "Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results." Ophthalmology 126.6 (2019): 811-821. iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATION FOR USE: The iStent inject ® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject ® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject ® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations.
• In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS:
• For prescription use only.
• This device has not been studied in patients with uveitic glaucoma.
• Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised.
• Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject ® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject ® W System.
• Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.”
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
08 Cover
A Force for Good in Global Eye Care ESCRS provides essential training in underserved areas.
Enters
Eric
Jean-Pierre
19 OmniVu Accommodating IOL Moving Forward
Dee G Stephenson MD
CORNEA
22 Cataract Surgery in Eyes with Keratoconus
Adi Abulafia MD
23 Treatment for Infectious Keratitis
Rohit Shetty MD, PhD
GLAUCOMA
24 Less is More in Angle-Closure Surgery
Andrew J Tatham MBChB Hons, FRCOphth, FRCSEd, FEBO, AFHEA
25 Are There Limits to MIGS?
Panayiota Founti MD, PhD
26 The Automated Future of Glaucoma Treatment
Matthias Elling MD and Professor Sir Peng Khaw
27 OSD and Glaucoma Drops Kjell Gunnar Gundersen MD, PhD
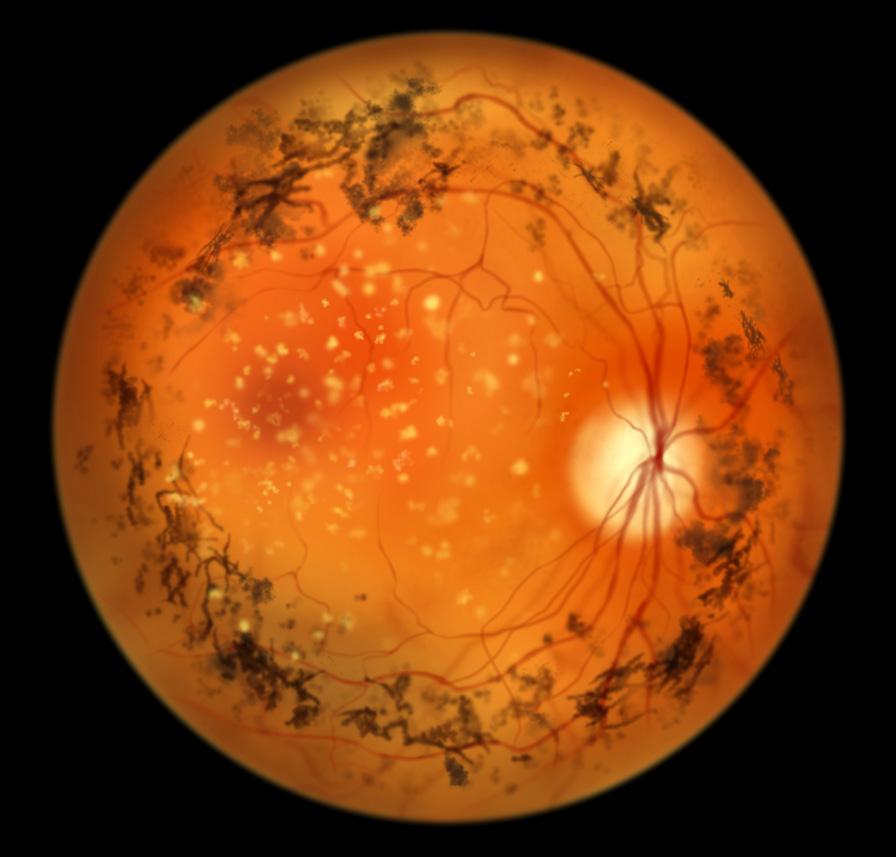
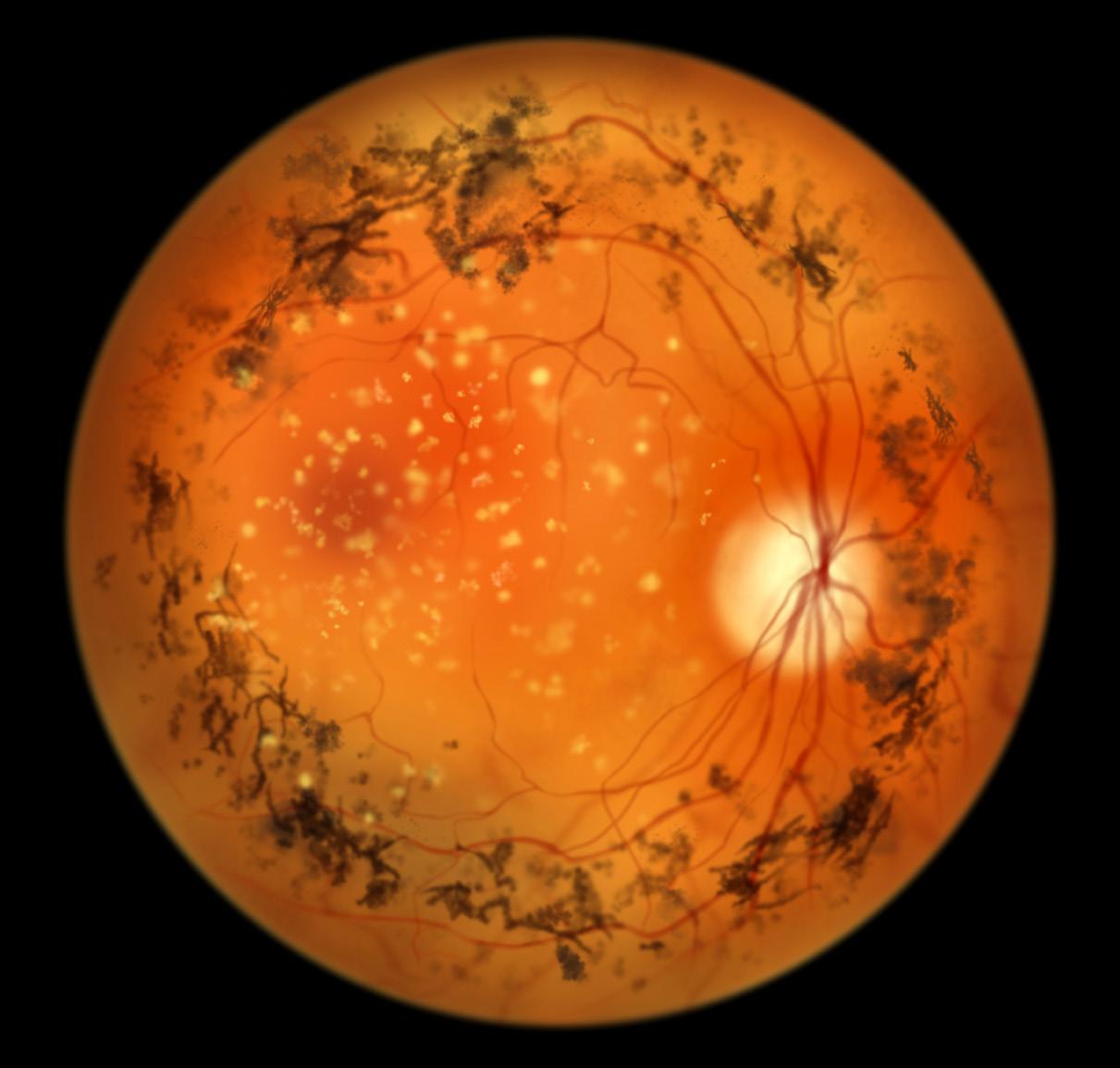
28 Gene Therapy for X-Linked Retinitis Pigmentosa
Robert MacLaren MD, PhD
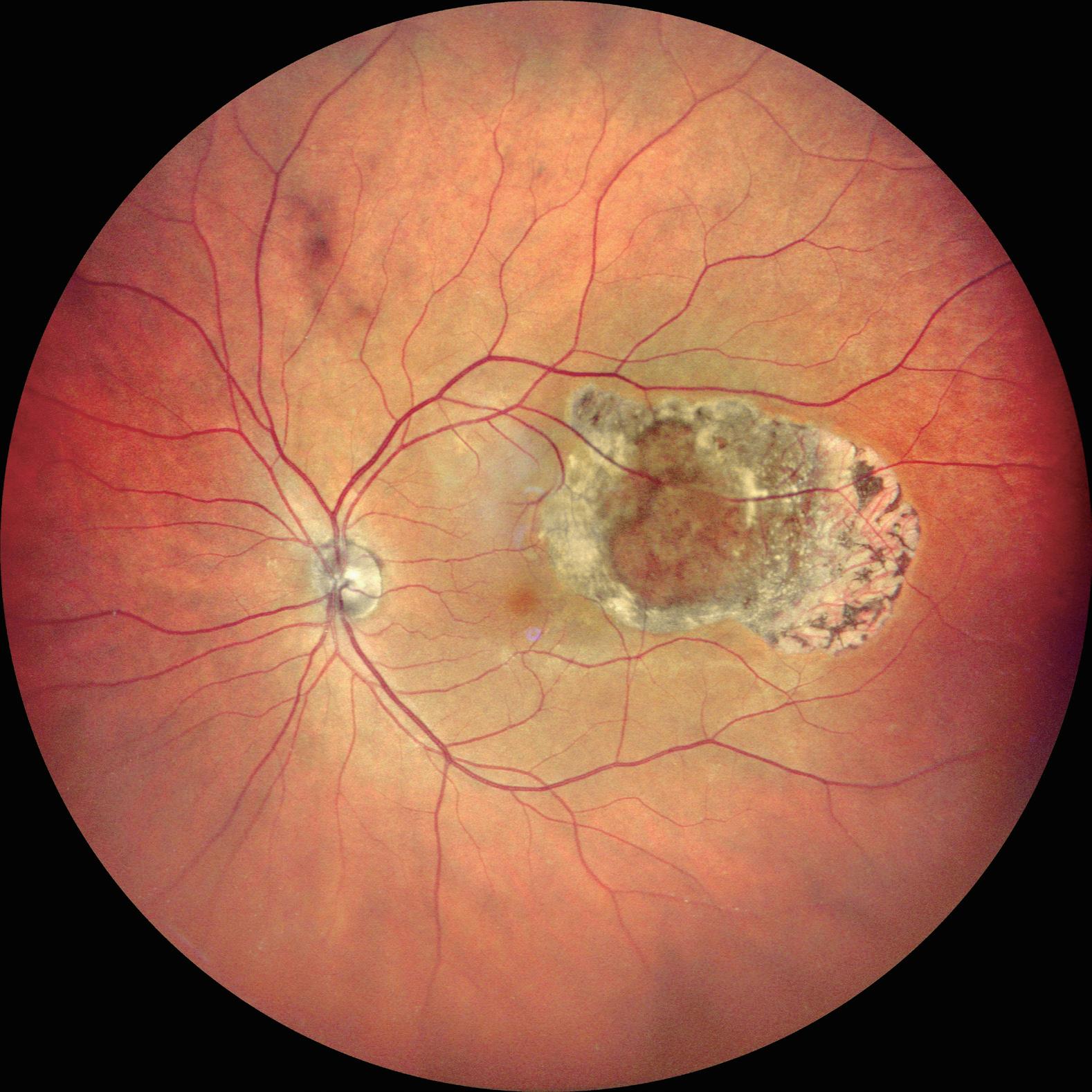
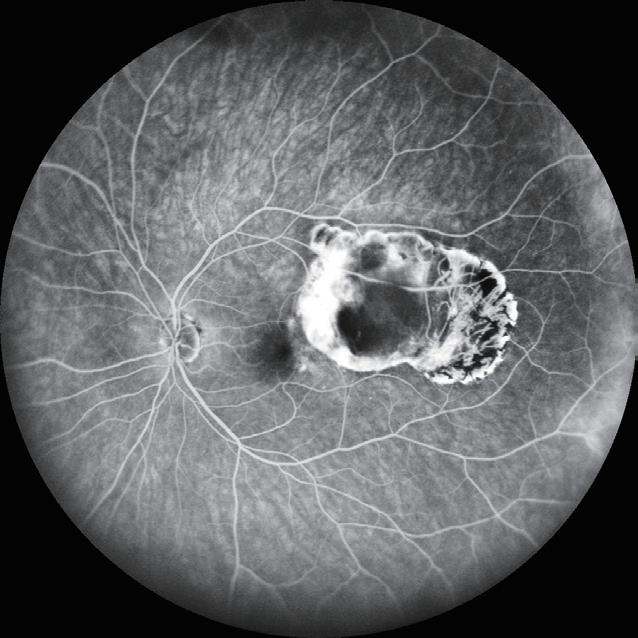
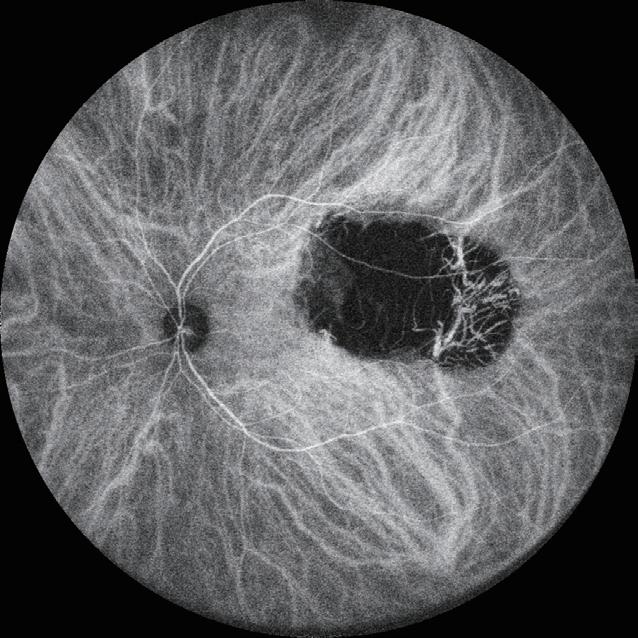
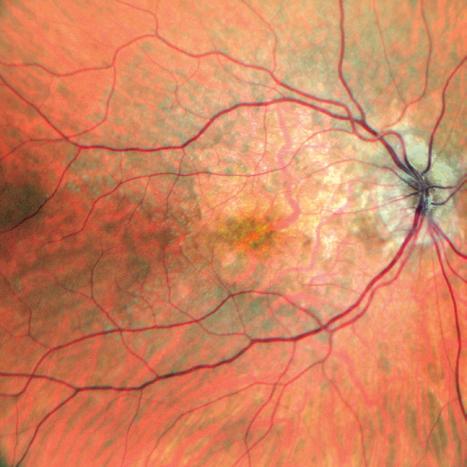
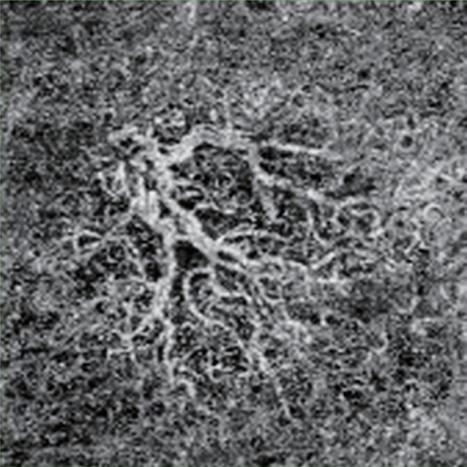
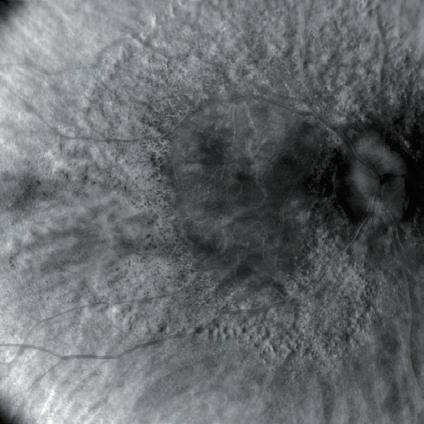
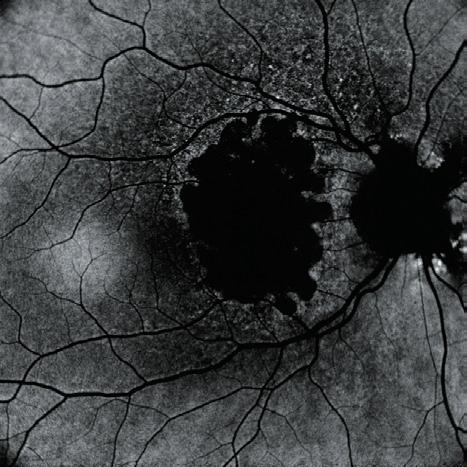
29 Preserving Foveal Function in Geographic Atrophy
Usha Chakravarthy MD, PhD
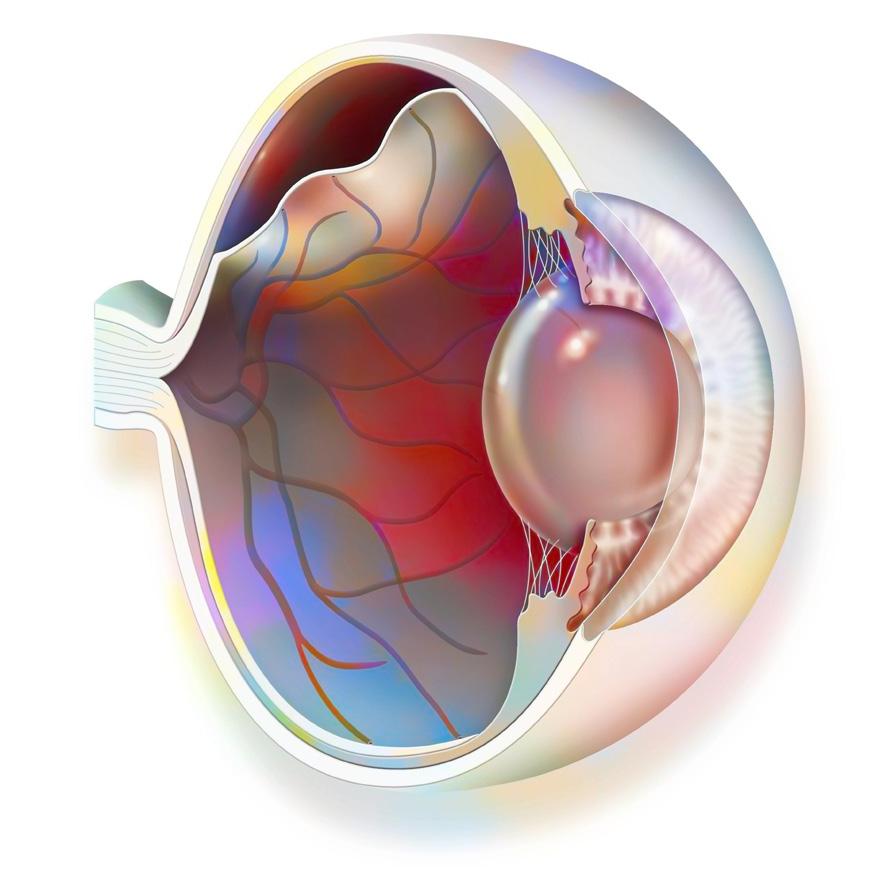
30 Hydrophilic Tamponade for Detached Retina
Kai Januschowski MD, PhD, FEBO
32 Identifying Progressive Keratoconus
Ingemar Gustafsson MD, PhD
34 Less Waste, More Vision
Victoria Liu MD and Kar Yen Phoong MBBS
Publisher Carey
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Nicola Lodge
Contributing Editors
Cheryl Guttman Krader
Howard Larkin
KLEX:
Dermot McGrath
Roibeárd O’hÉineacháin
Contributors
Soosan Jacob
Timothy Norris
Colour and Print
W&G Baird Printers
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Global Concerns, Local Solutions
It seems larger world events have encroached on our special world of ophthalmic surgery in recent years. The appearance of COVID-19 in 2019 brought about terrible global changes. Now, with vaccines and treatments in place, we can face this continuing challenge. We learned how to adapt and even benefit from these events by changing the way we handle patient care and surgical training. The pandemic was a setback for many young ophthalmologists just starting training. The ESCRS has responded by ramping up educational opportunities online and greatly expanding our training courses at our conferences.
The conflict in Eastern Europe was also felt in our clinical world. We were able to marshal our forces, providing much needed medical equipment to that embattled country while also extending opportunities to our Ukrainian colleagues at our conferences. These support efforts are ongoing.
In this issue, we take a closer look at the needs of underserved parts of the world in terms of ophthalmic care. Contributing editor Howard Larkin prepared this month’s cover article, taking a closer look at some of the programmes the ESCRS is collaborating with to provide local teaching resources in underserved countries in different parts of Africa.
Building local capacity multiplies the Society’s resources. When we build more local expertise, we can make sure we have a lasting impact and reduce dependence on external aid. It is a more significant and longer-term solution.
Indeed, the shift towards building local capacity is a cornerstone of ESCRS’s charitable strategy. We are collaborating with Eyes of the World in Mozambique in a programme guaranteeing the right to eye health through equitable
access to public health, using a human rights and gender approach. We also support the work of the Ridley Foundation in Nepal, ORBIS in Bangladesh, and others. Our events span continents, providing a platform for pioneering research, advanced surgical techniques, and continuous professional development.
The ESCRS Winter Meeting, held between 15 and 18 February in Frankfurt, is in conjunction with the DGII, the German Society of Cataract and Refractive Surgery.
In some ways, COVID-19 and the war in Ukraine drew attention away from perhaps the greatest existential threat to human existence—climate change. The ESCRS is taking a proactive role in advancing sustainability in our field. Improving the sustainability of the Winter Meeting is not only a moral duty but also a strategic opportunity to enhance our performance, reputation, and innovation.
This year, we are reinforcing our commitment to sustainability by placing a strong emphasis on social responsibility and promoting inclusivity through various initiatives. We will have a Focus Immersive Learning Programme and networking initiatives to address larger issues facing our field.
We are collaborating with our partners to work towards zero waste to landfill, zero net carbon emissions, and becoming a role model for social responsibility. We are implementing measures to support the wellness of our attendees, contribute to local and global causes, restore ecosystems, and foster sustainability leadership in our industry.
We invite you to join us on this journey. Together, we can make a difference. Together, we can make ESCRS a more sustainable Society.
EDITORIAL BOARD
Oliver Findl
ESCRS President
INTERNATIONAL EDITORIAL BOARD
Noel Alpins (Australia)
Bekir Aslan (Turkey)
Roberto Bellucci (Italy)
Hiroko Bissen-Miyajima (Japan)
John Chang (China)
Béatrice Cochener-Lamard (France)
Oliver Findl (Austria)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Vikentia Katsanevaki (Greece)
Daniel Kook (Germany)
Boris Malyugin (Russia)
Marguerite McDonald (US)
Cyres Mehta (India)
Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands)
Leigh Spielberg (The Netherlands)
Sathish Srinivasan (UK)
Robert Stegmann (South Africa)
Ulf Stenevi (Sweden)
Marie-José Tassignon (Belgium)
Manfred Tetz (Germany)
Carlo Enrico Traverso (Italy)
Thomas Kohnen Chief Medical Editor
José Güell Medical Editor
Paul Rosen Medical Editor
FILOMENA RIBEIRO MD, INCOMING PRESIDENT, ESCRS
Welcome to the Future of Glaucoma Laser Therapy
Introducing the Eagle™ by BELKIN Vision
Automation
Delightfully simple navigational guidance using an intuitve touch screen
Precision
120 automated treatments enabled by
delivered directly to the trabecular meshwork
FULL PAGE AD
Efficiency
Ergonomic patientand doctor- friendly set up for streamlined positioning and treatment
Innovative Programme Format Enhances LBI Learning Experience
BY STUART HALES, EXECUTIVE EDITOR
The field of cataract and refractive surgery has seen its share of innovations in recent years, including perioperative imaging, gene therapy, and intraocular lenses. In light of these advances, attendees at the 2023 ESCRS Leadership & Business Innovation Weekend in Frankfurt, Germany, could be forgiven for expecting they would learn about new technologies or surgical procedures being developed.
What they learned instead is innovation can be as simple as a new process to save time or a new approach to save money. It can even be as fundamental as a change in the way something is taught—which is exactly what happened this year in Frankfurt.
“At past LBI programmes, we stuck with the tried-and-true format of a lecture followed by audience questions,” says Colin Kerr, who worked with the ESCRS Leadership & Business Innovation Committee to design the programme schedule. “This was the first meeting where we tried to encourage the delegates to be active participants. We also put a lot of emphasis on small groups—we told them, ‘Based on what you heard in the last presentation, we want to give you an exercise.’ It was all very interactive.”
The format proved popular with the 20-plus trainees and ophthalmologists in public and private practice who attended the two-day event.
“I found it very interesting when we were split into small groups,” says Anna Slavík-Lenčová, consultant ophthalmic surgeon in Frankfurt. “It was a great opportunity to actively participate in different scenarios. And there were also excellent opportunities to get to know some colleagues from different countries.”
Also popular was the use of two moderators to keep the programme moving forward and on schedule.
“It was very well organised, especially the idea to invite moderators to keep the
programme moving and make sure it was not boring,” Slavík-Lenčová says. “And it was small, with not so many participants, so we had the opportunity to go more deeply into different topics and get to know the other participants.”
“There was a feeling that we are in this together,” says Ahmed Nahrawy, a consultant eye surgeon at Moorfields Eye Hospital in the United Kingdom. “Every struggle I’m facing now, someone has faced before, and I get to learn from their experience. So either I’m going to do it by myself—which means I’m going to make the same mistakes—or I’ll need to learn a smarter way of dealing with things. That’s why I went, to learn from others who have been there.”
A different view of innovation
Many attendees noted the emphasis on rethinking the concept of innovation helped them see their roles differently.
“The innovation part I found very interesting, because innovation was brought up in the context of process improvements in the patient journey or efficiency,” says Ruth Lapid-Gortzak, an ophthalmologist in academic and private practice in the Netherlands. “In my mind, innovation is a technological event, something we invent and develop and commercialise and bring to the market.”
Presenting innovation in a different light was one of the factors driving the selection of topics and speakers, according to Paul Rosen, a consultant
ophthalmic surgeon in the United Kingdom and chair of the Leadership & Business Innovation Committee.
“Innovation can be a new tech idea, it can be a new procedure, it can be a new way of delivering patient care that is cheaper or better but costs the same,” he says. “No matter what, it’s all about creating and developing value, whether you’re setting up a start-up or starting a practice. How did you go about it? What do you do? How do you get the funding?”
On hand to address those questions were a mix of physicians, healthcare administrators, and investors, including the following:
• David Lockington, a consultant ophthalmologist in the United Kingdom, discussed avoiding physician burnout.
• John Marshall, a pioneer in laser eye surgery and entrepreneurship in ophthalmology, presented on taking an innovation from conception to implementation.
• Arthur Cummings, an ophthalmic surgeon and recognised expert on laser eye surgery, and Daniel Kook, who runs a private ophthalmology practice in Germany, spoke about leading a team in a private ophthalmological practice.
• Celine Reibel, an ophthalmic administrator in France, presented on managing patient flow.
• Artemis Matsou, an ophthalmologist in the United Kingdom, discussed innovating to reduce costs in a public healthcare system.
Every struggle I’m facing now, someone has faced before, and I get to learn from their experience.
ESCRS Leadership, Business & Innovation
Helping facilitate the transitions between speakers and keep the programme moving were Matt Jensen, an investor in the United States, and Karl Thomas, a specialist in creativity and innovation in Ireland. In addition to serving as moderators, the two helped present some sessions and led a group project about creating a five-point plan for setting up a new private practice.
Complementing the weekend programme was a group dinner that allowed the attendees to interact with the presenters in a casual setting. The dinner was part networking event and part educational forum and provided an opportunity to share personal challenges and successes.
A follow-up survey of attendees revealed high ratings for both the programme content and format. Most attendees also indicated they would be interested in registering for future LBI weekends with new topics.
“I keep thinking—if I didn’t go, I would have no new insights,” says Nahrawy. “I would have had a great loss just by not attending.”
“As far as I’m concerned, it was very much a watershed,” says Kerr. “I think it should be the model for this programme going forward.”
AForce forGoodinGlobal yE
ESCRS provides essential training in underserved areas.
BY HOWARD LARKIN
espite two decades of progress reducing avoidable blindness, the need remains vast. Globally, about 1.1 billion people have unaddressed vision loss, according to the International Agency for the Prevention of Blindness. Of these, about 43 million are blind, with cataracts the leading cause. About 90% live in low- or middle-income countries, with the 46 countries of sub-Saharan Africa (SSA) making up
To address this critical need, the University of Cape Town in South Africa founded the Community Eye Health Institute in 2008, said Nagib du Toit PhD, who currently leads
“The idea was to create something international along the lines of the London School [of Hygiene and Tropical Medicine
Since then, the Institute has trained about 600 postgraduate professionals. Most now work in community eye health research and development, organising and managing services benefiting millions in Africa, the Middle East, and Asia,
In 2017, the institute added a surgical skills training programme focusing on small-incision cataract surgery, including simulation training, which was shown to improve surgical Based on courses developed by the UK Royal College of Ophthalmologists, it also offers training in
The institute launched a phacoemulsification wet lab in 2021 and acquired the only EyeSi Surgical simulator in SSA in
“There has been a big movement in Africa to upskill to phaco,” Prof du Toit said. However, the steep learning curve
So far, about 90 surgeons have trained at the simulation lab, Prof du Toit said. But training is a bottleneck. At full capacity, the programme’s six stations for manual small-incision cataract surgery (MSICs) and three to four stations for phaco can train just six or eight surgeons at a time. And while the programme has enough phaco machines, it still needs surgical microscopes. Even more critically, surgical trainers—as well as funds to sponsor travel and accommodations for the trainers and trainees at the three-day wet labs—are in short supply.
Those needs align with the resources and skills of ESCRS and its members. That is why the Society, through its Charity Committee, is partnering with the institute. “Collaborating with successful and experienced regional partners such as the Community Eye Health Institute (CEHI) maximises the impact of the Society’s funding to reduce avoidable blindness in sub-Saharan Africa,” said Mark Wevill, who is originally from South Africa and a graduate of the University of
“The benefit of ESCRS funding the CEHI surgical training unit is exponentially multiplied by training sub-Saharan African surgeons at the institute. Because not only are greater volumes of cataract surgery done better and more safely by each surgeon, improving the quality of life of blind people all over sub-Saharan Africa, but education builds a legacy. These graduates pass on the skills learned to other surgeons, and the graduates can return to the institute as trainers, sustaining the
great work of the institute,” added Dr Wevill, who has lived, travelled, and worked as an ophthalmologist in Africa for many years. In addition, ESCRS members are welcome to give some of their time and expertise to reducing avoidable blindness by becoming CEHI trainers—and, in so doing, meeting another need of the institute.
The benefit of ESCRS funding the CEHI surgical training unit is exponentially multiplied by training sub-Saharan African surgeons at the institute.
Indeed, the shift toward building local capacity is a cornerstone of ESCRS’s charitable strategy, Filomena Ribeiro MD, PhD said. She is working closely with another ESCRS grant programme supporting Eyes of the World in Mozambique.
“When we build more local expertise, we can make sure we have a lasting impact and reduce dependence on external aid,” she said. “It is a more significant and longer-term solution.”
Encouraging equitable access
Eyes of the World is a good example of a collaborative capacity-building programme. It has been operating in Africa and South America for 22 years, said Anna Barba i Giró. To date, it has trained more than 13,000 local professionals, including ophthalmologists, optometrists, eye technicians, traditional practitioners, and teachers in detecting, referring, and treating vision problems. ESCRS and its members have supported the agency in Mozambique for several years, including providing a vehicle to take supplies and staff to remote rural areas, she said.
The current ESCRS three-year grant campaign focuses on Inhambane province, where just two ophthalmologists serve a population of more than 1.5 million, and blindness affects more than 6 percent of the population over age 50. The goal is to deliver 3,300 cataract surgeries, of which 60 percent will be women. “If we don’t make a specific effort to reach women, it will increase inequality. Usually, more men get operated on,” Ms Barba i Giró said. In addition, 80,000 people will have eye consultations.
Training will play a major role. By the end of the project, two ophthalmologists and 15 technicians will be trained in cataract case selection and refraction techniques to promote better outcomes. Operating the same percentage of women and men diagnosed with cataracts is another important end goal.
“We are trying to address the gender gap,” Prof Ribeiro said. A surgical quality monitoring tool also will be implemented to help ophthalmologists improve their performance.
Community infrastructure
Building skills in refraction, case selection, and outcomes measurement and analysis is as critical to addressing vision
90%
About 90% of the world’s blind live in low- or middle-income countries, with the 46 countries of sub-Saharan Africa (SSA) making up about 10% of the world total.
loss as is direct surgical skills training, said Ype Henry MD, who has extensive experience working with eye health programmes in Africa, Asia, and Oceania. Currently working with an ESCRS-supported programme partnering with the Blantyre Institute for Community Outreach in Malawi, he noted, “Preand post-operation is often where the bottlenecks are.”
Often in underserved areas, surgeons do the surgery (and do it well), but there is no follow up to ensure residual refractive error and any complications are addressed, Dr Henry said. Measuring visual acuity before and after surgery—and using that data to improve performance—are essential for better refractive outcomes, he added. Along with screening and providing primary eye care, this is another reason why training technicians and other support personnel is so important.
Additionally, Dr Henry advised implementing outcomes registries as another important tool. The ESCRS grant supports registrar training, cataract skills refresher courses, and building systems to better supervise and track cataract surgery at four eye centres in Malawi. Integrating the extensive community and specialty eye care services the institute has fostered into the public health system is another programme goal.
Encouraging higher volume
Individual surgeons also should be encouraged and supported to perform more surgeries, Dr Henry said. Often, surgeons in SSA do only about 100 to 150 cataract cases per year.
“With such a limited supply of doctors, they should be doing 750 per person.”
On average, there are about 2.5 ophthalmologists per million population in SSA, with many low-income countries below 1.0 per million. By comparison, there is a mean of about 76 per million in high-income countries worldwide, according to the International Council of Ophthalmologists.2
St John Eye Hospital in Jerusalem is another programme ESCRS is supporting. A mobile outreach programme earlier this year provided 90 phaco operations in marginalised areas in Palestine. ESCRS supports young ophthalmologists training at St John, including some from Ukraine.
The ESCRS has also made major contributions to ophthalmology in Ukraine, including free attendance at the ESCRS Congress for Ukrainian delegates. ESCRS industry partners have contributed more than €1 million in supplies, and the Society has allocated €100,000 directly.
But as much as all this support helps, the need is greater still. Even in Cape Town, which is relatively well served, only about half of the WHO-recommended number of cataract surgeries are being performed—and the deficits are larger pretty much everywhere else in SSA, Prof du Toit said.
“We have a long way yet to go.”
ESCRS members are invited to donate to support global outreach programmes at https://donate.escrs.org. Surgeon trainers are also needed. Donations of equipment and
supplies in new or good condition to support capacity-building programmes are also welcome. Please contact escrs@mci-group.com for information.
For citation notes, see page 38.
Nagib du Toit MBChB(UCT), DipOphth(SA), FRCS(Ed), MMed(UCT), FCOphth(SA), PhD(UCT) is Chair of Ophthalmology at the University of Cape Town and head of ophthalmology at Groote Schuur Hospital and Red Cross Children’s Hospital in South Africa. nagib.dutoit@uct.ac.za
Mark Wevill MBChB, FRCS (Edinburgh), FCS (SA) is a cataract and refractive surgeon in Birmingham, UK, and ESCRS Charity Committee member, and a surgical trainer at the University of Cape Town Community Eye Health Institute Surgical Skills Laboratory. mark.wevill@gmail.com
Filomena Ribeiro MD, PhD, FEBO is chair of ophthalmology at Hospital da Luz Lisbon and professor of ophthalmology and biomedical engineering at the University of Lisbon, Portugal. She is ESCRS president-elect and associate editor of the Journal of Cataract and Refractive Surgery . filomenajribeiro@gmail.com
Anna Barba i Giró is director of Eyes of the World, a charity dedicated to reducing avoidable blindness based in Barcelona, Spain. abarba@ullsdelmon.org
Ype Henry MD, FEBO is a retired ophthalmologist in Amsterdam, Netherlands, and an ESCRS Charity Committee member. y.henry@hotmail.com
Images courtesy of
Sacco
Promising Presbyopia Option
Sulcus-based implant Lumina IOL overcomes the challenges of restoring accommodation.
CHERYL GUTTMAN KRADER REPORTS
The failure of multiple accommodative IOL designs begs whether achieving a working model is even a possibility. Prompted by the lack of success of previous implants, Jorge L Alió MD, PhD and colleagues set out 14 years ago on a novel path to create an IOL able to restore accommodation.
The product of their research—the Lumina IOL (Akkolens)—is placed in the sulcus, where the only force exerted on it comes from ciliary muscle contraction and relaxation. The action of the ciliary muscle, not the capsular bag, causes the optical elements of the dual-element varifocal lens system to shift across each other in the plane perpendicular to the optical axis, resulting in a change in focal power.
Highlighting published studies, Professor Alió said the Lumina is the only accommodative IOL with highly rated published evidence. Moreover, he proposed this safe and effective accommodating IOL will supplant the use of multifocal IOLs for presbyopia correction.
“Multifocality is not physiological, and multifocal optics will always require some degree of neuroadaptation,” he said. “Once accommodating IOLs are developed adequately, multifocal IOLs will be unable to compete, as happened with pseudophakic glasses and IOLs.”
The Lumina IOL was designed by Akkolens (Netherlands) based on knowledge of the mechanism of accommodation and understanding that the capsular bag becomes non-functional after cataract surgery.
98%
98% of patients reported not using reading glasses.
“The capsular bag seems to be the wrong location for accommodating IOLs due to its unavoidable decadence and fibrosis once the crystalline lens is emptied,” he explained. “Rather, the forces generated at the zonular-anterior capsule system are those for accommodating IOLs. Sulcus implantation is the only option.”
Proof of performance
Results from extensive testing performed in clinical trials comparing the Lumina IOL with monofocal controls provide evidence the sulcus-based accommodative IOL effectively restores visual performance for far distance and provides functional performance for intermediate and near vision, albeit with some interindividual variability.1,2 Mean decimal uncorrected visual acuity in a series of 44 eyes was 0.90 for distance, 0.89 for intermediate, and 0.85 for near; 98% of patients reported not using reading glasses.
“The near vision outcomes are justified, in part, by the accommodative range, which is variable between 1.0 and 3.0 D with accommodation and pseudoaccommodation. They also correlate well with high patient satisfaction,” Prof Alió said.
He reported that collected data show refractive predictability, contrast sensitivity, and visual quality with the accommodative IOL are comparable to a monofocal lens. Functional, refractive, and accommodative test results also show good stability at follow-up more than three years post-implantation. Bench testing shows image quality with the accommodative IOL is superior to multifocal and extended depth of focus lenses.3
Prof Alió noted that posterior capsule opacification occurs frequently in eyes implanted with the Lumina IOL. Nd:YAG laser capsulotomy is needed in about one-third of eyes by three months after implantation and restores near vision, he said.
“This experience shows not only that outcomes are good after capsulotomy—but it further proves the capsular bag is not necessary for accommodation and the Lumina IOL can be used successfully, even if the posterior capsule breaks,” he observed.
Prof Alió spoke at the 2023 ESCRS Congress in Vienna.
For citation notes, see page 38.
Jorge L Alió MD, PhD is Medical Director, Vissum Innovation, and Professor and Chairman of Ophthalmology, Universidad Miguel Hernández, Alicante, Spain. jlalio@vissum.com.
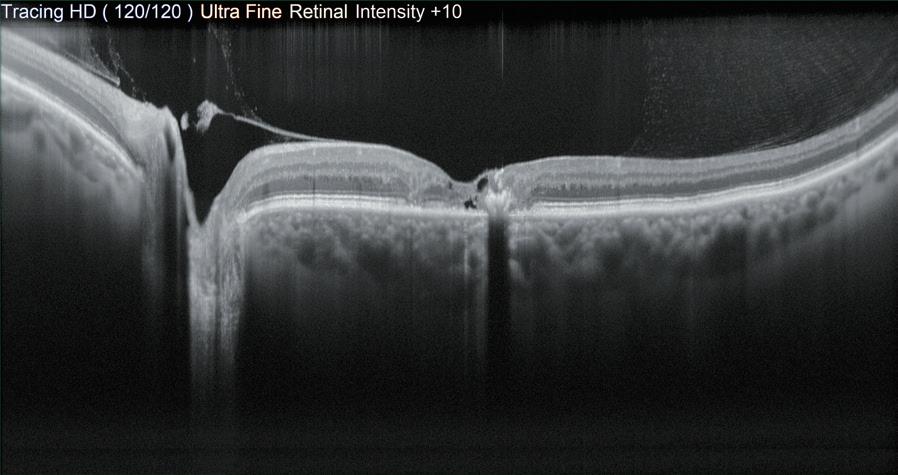
Universalising Intraoperative OCT Benefits
Cost-effectiveness research needed to justify wider use of intraoperative OCT.
Optical coherence tomography (OCT) has revolutionised ophthalmic imaging, providing invaluable diagnostic information for both posterior and anterior segment structures. More recently, intraoperative OCT systems developed to help guide surgery are now integrated with operating microscopes.
But does intraoperative OCT add enough value to justify its added cost? For corneal surgery, the answer is a qualified “yes,” but cataract surgery? There isn’t yet enough data, said Sorcha Ní Dhubhghaill MD, PhD.
To be sure, research shows intraoperative OCT is useful in cataract surgery, Dr Ní Dhubhghaill said. It can help visualise anterior chamber structures, evaluate lens tilt and capsular position after lens or capsular tension ring insertion, distinguish posterior polar cataracts from high-risk adhesions, and detect viscoelastics or lens particles left behind after lens implantation. And it is great for evaluating the retrolenticular space, including the anterior hyaloid and vitreous movement—which can be very helpful in posterior capsulotomy cases, such as in high myopes and delicate paediatric procedures.
“We can see previously invisible structures; we can see movement in real time,” Dr Ní Dhubhghaill said.
Combining OCT with low-flow fluidics could lead to better understanding of how surgical activity in the anterior chamber affects the posterior areas—possibly shedding light on why posterior complications such as macular oedema and retinal detachments develop.
“These kinds of applications are widely reported at clinical meetings. But when you get back to the clinic, the first response from management is, ‘prove to us that this is the wise investment,’” she noted. “So, we have a disconnection between this beautiful research and our ability to convince our providers to install this technology.”
What’s needed are cost-effectiveness studies. “To date, there are no cost [or] economic analyses to support increased efficiency or improved safety with intraoperative OCT in cataract surgery,” Dr Ní Dhubhghaill said. And though she believes intraoperative OCT does improve cataract surgery, more studies must be done to demonstrate it.
The situation is better for corneal surgery applications. “It’s a game changer in lamellar surgery,” Dr Ní Dhubhghaill said. OCT makes it possible to see various corneal layers and behind corneal grafts. It can be invaluable for positioning delicate grafts in Descemet membrane endothelial keratoplasty (DMEK). A Netherlands study found OCT information influenced surgical decisions in 40% of DMEK procedures.1
That same study also found using intraoperative OCT saved a mean of €107 per DMEK surgery. “When I discuss these options with decision makers at the financial level, I tell them there have been studies that can prove cost effectiveness. I don’t tell them it’s €107 per patient because of the number of DMEKs I’d have to do to offset the cost.”
The key is to universalise the benefits. “This is just one surgery. If we could find the cost effectiveness spread through all the different surgeries, we could really help each other to bring these technologies to our patients.”
Dr Ní Dhubhghaill presented at the 2023 ESCRS Congress in Vienna.
For citation notes, see page 38.
Sorcha Ní Dhubhghaill MD, PhD is Chair and Head of the Department of Ophthalmology, University Hospital Brussels/Vrije Universiteit Brussel, Belgium. nidhubhs@gmail.com
HOWARD LARKIN REPORTS
Ophthalmic Drug Delivery Enters New Era
Emerging products reduce the burden of conventional topical medications.
CHERYL GUTTMAN KRADER REPORTS
Innovations in drug delivery are leading to a new era in medication administration for patients undergoing cataract surgery, according to Eric D Donnenfeld MD.
“We are now in a transition period, but I predict that use of topical medications as it is known today will change greatly over the next several years,” he said. “The adoption of corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs) administered via external inserts, punctal plug systems, and intracamerally will address an important unmet need.”
The need for alternatives to topical medications relates to the issue of patient noncompliance with topical drop regimens and the adverse effects these products have on comfort, cosmesis, and the cornea. Several medications formulated in novel delivery systems with indications for controlling pain and/or inflammation after cataract surgery became available in 2023, and others are in development.
We are now in a transition period, but I predict that use of topical medications as it is known today will change greatly over the next several years.
A punctal plug device releasing the NSAID nepafenac over one month has also been investigated and shown in a placebo-controlled phase 2 study to be effective for reducing pain and inflammation after cataract surgery.2
“And as a surprise to me, 65% of patients in the punctal plug group and just 29% of controls had 20/20 or better BCVA at day 14,” Dr Donnenfeld reported.
Surgeons in the United States also have access to a commercially available intracameral product containing the NSAID ketorolac 0.3% and phenylephrine 1% (Omidria, Rayner), indicated for maintaining pupil size and reducing postoperative pain.
Within the corticosteroid category, two “dropless” sustained-release dexamethasone products are on the market— one is an intracanalicular hydrogel insert containing 0.4 mg dexamethasone (Dextenza, Ocular Therapeutix), and the other is an intraocular suspension containing 9% dexamethasone (Dexycu, EyePoint Pharmaceuticals) for injection into the posterior chamber behind the iris at the end of surgery.
A third dexamethasone product, OCS-01, is still under investigation, though results from a Phase 3 trial show it a promising option for allowing “less drops” surgery. OCS-01 is a preservative-free, high-concentration (15 mg/mL) dexamethasone drop formulated using nanoparticle technology that enhances corneal penetration in a vehicle with prolonged ocular surface residence time. In the Phase 3 trial, once-daily OCS-01 treatment demonstrated statistically significant superiority compared to vehicle in analyses of both the percentage of eyes with complete absence of anterior chamber cells on postoperative day 15 and the percentage with no pain on postoperative day 4.1
“One might postulate that the high pressure, forced infusion used in modern cataract surgery would force NSAID in the anterior chamber through the zonules into the vitreous. In fact, early results from a trial I am conducting show a very high level of ketorolac in the vitreous in procedures performed with intracameral ketorolac/phenylephrine,” Dr Donnenfeld said.
“I believe this finding could explain results of a published study showing a reduced incidence of cystoid macular oedema in eyes undergoing surgery with intracameral phenylephrine/ketorolac plus a topical NSAID compared with those treated with a topical NSAID and topical steroid.”3
Dr Donnenfeld spoke during the 2023 ESCRS Congress in Vienna.
For citation notes, see page 38.
Eric D Donnenfeld MD is Founding Partner, Ophthalmic Consultants of Long Island, Garden City, New York, US, and Clinical Professor of Ophthalmology, New York University Medical Center, New York, US. ericdonnenfeld@gmail.com
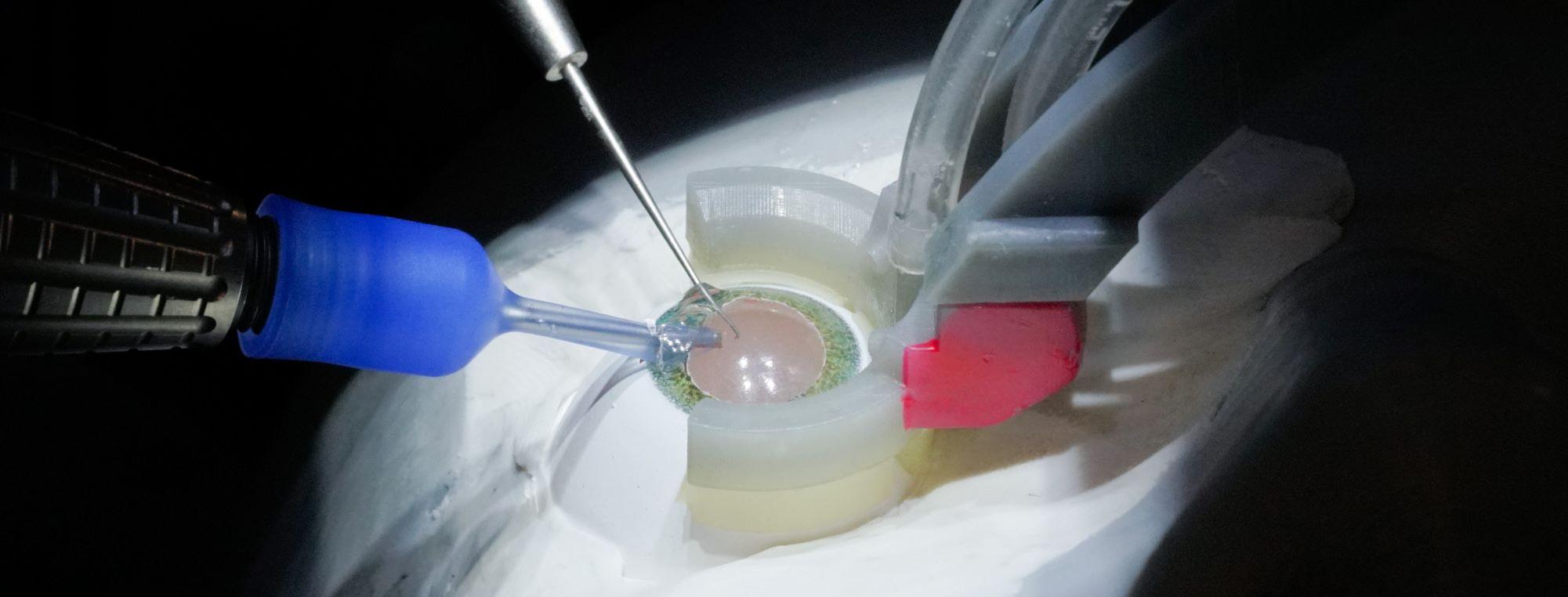
The Robotic Revolution in Cataract Surgery
Benefits from robotics system expected to have revolutionary impact on multiple fronts.
CHERYL GUTTMAN KRADER REPORTS
Robotics-assisted cataract surgery can lead to better surgical outcomes, improved surgeon performance, opened doors to new surgical manipulations, increased patient throughput, and eventually lower surgery costs, according to Jean-Pierre Hubschman MD.
“Although there is currently perfect visualisation and high manoeuvrability in cataract surgery, robotics technology can help address multiple existing challenges and improve every surgical step,” said Dr Hubschman.
“Robotics-assisted cataract surgery also provides a solution for overcoming the current and increasing gap in supply and demand for cataract surgery services, as well as democratise superior outcomes by negating the impact of differences in surgeon skill sets.”
Dr Hubschman is co-founder of a company developing a fully integrated, image-guided, artificial intelligence-enabled microsurgery platform for cataract surgery. Named Polaris, the system reconstructs anatomy in real time and proposes a trajectory supervised and validated by the surgeon before being executed autonomously by the robotic platform.
Technical groundwork for the system began 14 years ago at UCLA, where Dr Hubschman is a faculty member in the ophthalmology and engineering departments. The platform has demonstrated capability for performing cornea incision, viscoelastic injection, lens extraction, and IOL implantation and achieved promising outcomes in preclinical research conducted in cadaver and porcine eyes.
Although details about the system remain confidential, Dr Hubschman said it combines four major components— microsurgical robotic arms that allow for more precise and accurate manipulations; image guidance combining optical coherence tomography, a digital microscope, and other sensors that reconstruct anatomy in real time; machine learning allowing for real-time tissue differentiation and continuous improvement; and automation for increased throughput and consistent outcomes.
Outperform human surgeons?
“Whether considering sensing, processing, or precision, the robotics system can outperform human surgeons on every metric,” Dr Hubschman said.
Comparisons between human surgeons and the robotics system show the maximum achieved precision for humans is 80 microns versus less than 5 microns for the robotics system. The robotic technology’s reaction time of less than 20 milliseconds far exceeds the 250-millisecond time for humans. The robotics system also overcomes human limitations in visualising microanatomy and depth perception sensing through its ability to simultaneously process input from multimodal imaging and provide much better detection of all anatomy.
“With its level of visualisation and precision, we believe this technology can drastically reduce the rate of posterior capsule rupture, allow for much better cleaning of the capsular bag, and achieve better refractive outcomes through a more accurate selection and positioning of the IOL,” he said.
Assuring colleagues that a robotics platform will not circumvent their role, he noted that even though it performs all steps autonomously, it does so with human supervision.
“This technology will not replace surgeons but allow them to do a better job and [perform] more surgeries in a shorter period,” Dr Hubschman emphasised.
“Surgery is an art, and today, depending on the surgeon, the outcomes may be very different from one to another. With robotics technology, we can make cataract surgery a science and allow every patient and every surgeon to achieve the best care.”
Dr Hubschman spoke during the 2023 ESCRS Congress in Vienna.
Jean-Pierre Hubschman MD is Professor in Ophthalmology and Mechanical and Aerospace Engineering, UCLA and chief executive officer and co-founder of Horizon Surgical Systems, Los Angeles, California, US. jphubschman@horizonsurgicalsystems.com
Insertion of the tools with a plastic eye model.
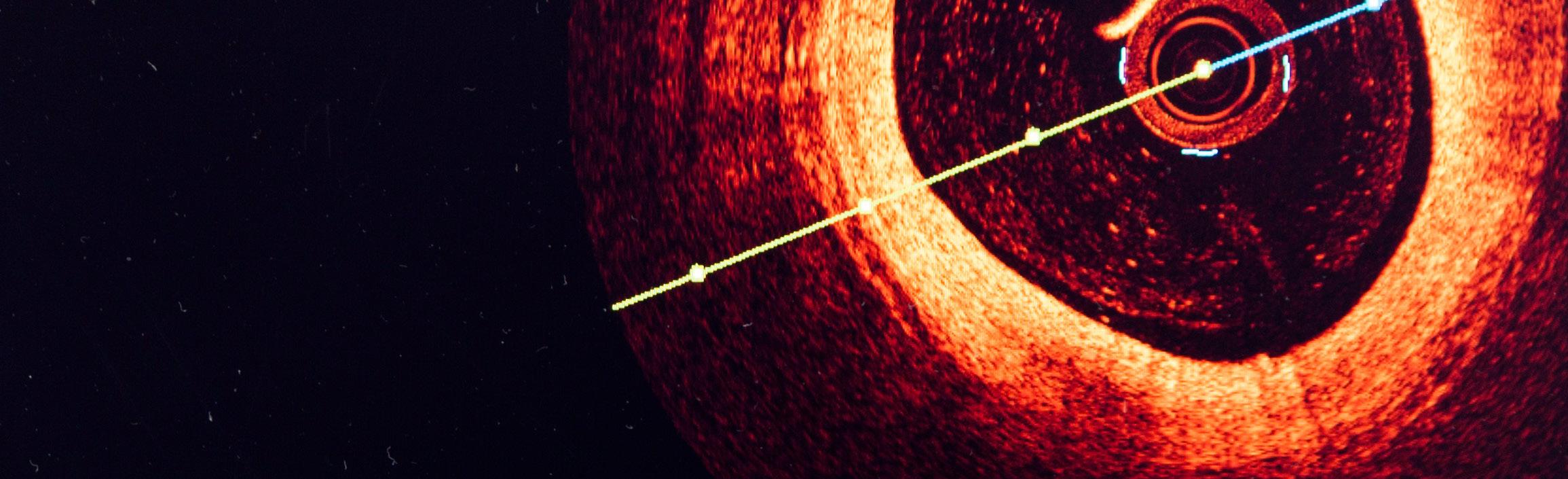
Deep Learning OCT
Advancements in OCT imaging and machine learning techniques for a new era of anterior chamber diagnosis.
TIMOTHY NORRIS REPORTS
Imaging advancements in OCT have reached extremely high standards in terms of quality and resolution, according to Pierre Zéboulon MD during the “OR Digitalisation: Truth and Myths” clinical research symposium at the ESCRS Congress, adding cutting-edge OCT potentiality is still under-exploited in clinical practice.
“We now have access to beautiful anterior segment OCT images with high levels of detail of the cornea and the lens,” he said. “We need to build new tools to take advantage of this advanced imaging.”
Using deep learning with OCT scans could be a very important step for ophthalmology, helping design new techniques and approaches to different diagnoses and bringing valuable insight to ocular pathology.
“With this, we will create new standards in the future, entering a new era of anterior segment diagnosis,” Dr Zéboulon said.
“Why do we need objective cataract grading? It is obviously better for the patient’s follow-up. It helps in complicated cases of visual activity loss. It will certainly be useful for the near future of telemedicine.”
Dr Zéboulon used Heidelberg’s Anterion for high-quality OCT scans of the anterior segment to show his cases. “We wanted to build something entirely new—that takes full advantage of the high-resolution images, a new approach not based on a calculated subjective clinical classification. We wanted it to be as objective as possible, with a clinically relevant output,” he said. “So, we went for individual continuous metrics for each lens layer with good interpretability.”
The cornerstone, he noted, is a deep learning model detecting pixel-wise cataracts on the OCT images, correctly and directly detecting any cataract type with great accuracy,
as demonstrated in a study published by the author in the Journal of Optometry in 2022.1
“And so, we built our grading solution on top of that model to access layer-wise information,” he said.
Global Cataract Score was created using linear discriminant analysis and the six variables on a development set of 331 eyes and tested on 217 eyes. “The output of this score is very simple,” Dr Zéboulon explained. “It’s a single value: If it’s positive, there’s clinically significant cataract.”
Deep learning-empowered OCT can also be used for the early detection of corneal oedema, a very useful tool given the constant growth of DMEK procedures worldwide. “Our solution is capable of detecting an oedema corresponding to a change of 20 μm with an AUC of 0.96, also providing an easy to read and en-face map,” Dr Zéboulon said.
Some limitations are still present in the model, especially in the en-face oedema map. “With a flat posterior surface, it can be a bit tricky to know if there’s a posterior displacement, and our model doesn’t fit the image. Also, if the posterior surface is prolate, such as in the case of keratoconus, it cancels out every feature of the presentation itself. The third limitation is in case of homogeneous thickness increase,” Dr Zéboulon explained.
Dr Zéboulon presented at the 2023 ESCRS Congress in Vienna.
For citation notes, please see page 38.
Pierre Zéboulon MD, MSc is a corneal surgeon in the Anterior and Refractive Surgery Department of the Rothschild Foundation Hospital, Paris. pierrezeboulon@gmail.com
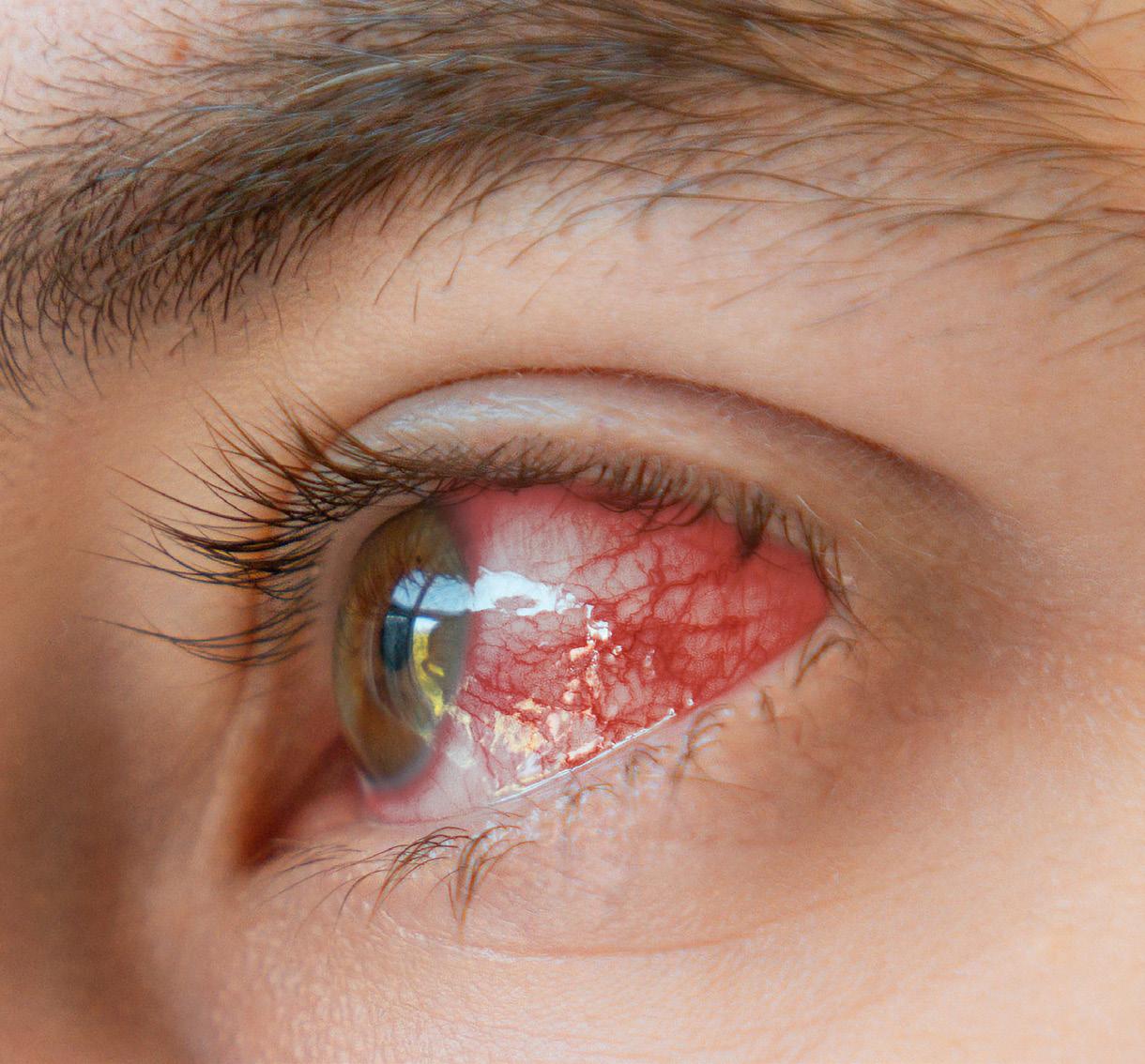
Handling Inflammation with Care
Knowledge of its interaction with cataract surgery guides surgical planning to optimise outcomes.
CHERYL GUTTMAN KRADER REPORTS
Even uncomplicated cataract surgery induces inflammation, but certain pre-existing conditions put patients at risk for developing a more exuberant and prolonged reaction. Understanding the aetiology for inflammation after cataract surgery can be infectious or non-infectious and arise from an exogenous or endogenous source is the foundation for implementing appropriate preventive and therapeutic strategies, according to Harminder S Dua MD, PhD.
“And, when thinking about the pathway to successful diagnosis and management, always remember that we must examine and treat the patient as a whole and not just the eye,” he said.
Professor Dua noted chronic or recurrent intraocular inflammation after cataract surgery reportedly occurs between 0.1% and 2.0% of cases. Risk factors for these events include prolonged/complicated surgery, retention of lens material, capsular bag infection, and pre-existing uveitis.
“It is very important to understand the cataract surgery age group is a population of patients who have a higher rate of uveitic conditions, and uveitis is commonly associated with cataract development,” he explained. “Therefore, patients with a history of uveitis must be identified so you can take the appropriate precautions to avoid serious complications.”
To illustrate, he discussed patients with collagen vascular disorders, such as rheumatoid arthritis, who can have ocular inflammation as a manifestation of their autoimmune disease. Even if the rheumatoid arthritis and any associated uveitis appear under control, these patients are at risk of developing corneal and scleral inflammation with subsequent melts after cataract surgery. In these cases, Prof Dua recommended considering operating through a sclerocorneal tunnel incision. He also encouraged involving the patient’s rheumatologist/ immunologist because these patients should also be treated with systemic steroids and immunosuppression.
Prof Dua also highlighted the need for caution when performing cataract surgery in patients with a history of ocular cicatricial pemphigoid, taking care not to manipulate the conjunctiva to avoid triggering a flare of the ocular surface autoimmune disease. He recommended placing a fixation ring to avoid using forceps to hold the conjunctiva, starting patients on immunosuppressive therapy preoperatively, and continuing steroid treatment for longer than usual after surgery.
Of other inflammatory ocular surface conditions possibly exacerbated by or capable of compromising cataract surgery outcomes, Prof Dua noted blepharitis is a risk factor for postoperative dry eye disease and infectious endophthalmitis—most commonly caused by entry into the eye through commensal bacteria on the lids and conjunctiva. He emphasised the importance of using povidone-iodine 5% preoperatively for disinfecting the ocular surface and periocular
skin along with appropriate draping. A temporal incision can be particularly beneficial in eyes with blepharitis because it avoids tangling with eyelashes that harbour bacteria.
Although anterior basement membrane dystrophy is not an inflammatory condition, when the epithelium is disturbed because of cataract surgery, eyes with this disorder are at risk for developing recurrent corneal erosion syndrome accompanied by chronic, recurrent inflammation.
“Recognise these eyes and handle them with care,” said Prof Dua, suggesting alcohol delamination is the simplest and most effective treatment for this dystrophy.
Prof Dua spoke at the 2023 ESCRS Congress in Vienna.
Harminder S Dua MD, PhD is Chair and Professor of Ophthalmology, University of Nottingham, England, United Kingdom. harminder.dua@nottingham.ac.uk
OmniVu Accommodating IOL Moving Forward
Novel AIOL showing promising results in early clinical study.
REPORTS
Amodular accommodating IOL has shown promising results in early clinical studies, with good visual results over a six-month follow-up period, according to Dee G Stephenson MD.
The OmniVu (Atia Vision) is a modular AIOL intended to simulate the natural accommodative action of the eye. It consists of a fluid-filled base optic that changes shape and refractive power in response to the contraction of the ciliary muscles and a fixed, exchangeable anterior optic targeting the patient’s refraction. The goals are to achieve refractive predictability and stability, restore full functional vision range, and preserve natural vision quality while reducing visual disturbances, Dr Stephenson added.
In a study involving 25 eyes of 18 patients, refractions were stable six months after surgery, with 95% of implanted eyes within 0.50 D of plano, Dr Stephenson reported. “That’s a really stable refraction.”
Visual acuity was also excellent at all distances, yielding vision of 20/32 or better over about 4.00 D of defocus binocularly and 2.75 D monocularly. Mean uncorrected distance visual acuity was 20/16, with distance-corrected intermediate vision of 20/20 and near vision of 20/32, or J2. Contrast sensitivity results are promising, and endothelial cell densities are comparable to existing lenses, he reported.
The lens is implanted in normal cataract surgery, with the base injected into the capsular bag through a manual capsulorhexis of 5.5 mm. Even though the base optic requires enlargement of the incision to 3.5 mm, the study did not detect
any clinically significant surgically induced astigmatism, Dr Stephenson said.
Composed of biocompatible silicone, the base optic completely fills the capsular bag and is designed to keep the platform stable. It has a groove into which the edge of the capsulotomy snaps and blue tabs along the periphery to help position it in surgery. No sutures are required to keep the lens stable afterwards or to close the wound.
The bag-filling design also reduces the risk of posterior capsule opacification (PCO). Only 1 of 25 eyes required a posterior capsulotomy for PCO during the study period. Dr Stephenson said the base optic stayed in position and continued to function after the capsulotomy.
The anterior optic is hydrophobic acrylic and can be replaced if the patient is unhappy with their vision. “Exchangeability is just an awesome part of this lens,” Dr Stephenson said.
Following these first-in-human trial results, Atia Vision aims to submit an application in the second half of 2024 to begin clinical trials for registration with the US Food and Drug Administration.
A toric anterior option is also in the works to correct astigmatism.
Dr Stephenson presented at the second ESCRS iNovation Day before the 2023 ESCRS Congress in Vienna.
Dee G Stephenson MD is the director of Stephenson Eye Associates in Venice, Florida, US. eyedrdee@aol.com
Preliminary First-in-Human Results
6 Month Follow-Up (n/N = 25 eyes/ 18 subjects)
STABLE REFRACTIVE OUTCOME
EXCELLENT VA AT ALL DISTANCES
KEY ADDITIONAL FINDINGS
NEXT MILESTONE
• 95% of eyes within 0 5 D of plano
• No clinically significant induced astigmatism
• Mean binocular UCVA = 6/4 8, UIVA = 6/6 and UNVA – 6/9 5 (J2)
• 100% achieved binocular CDVA & DCIVA of 6/6 and DCNVA of 6/9 5
• Maintains > 6/9.5 across 4.0 D of defocus, binocularly
• 3 5 mm incision without sutures, no wound leaks
• Promising preliminary contrast sensitivity data
• Endothelial cell density results comparable with standard cataract surgery procedures
• Early conversations with FDA, aiming for US IDE submission to the 2nd Half 2024
HOWARD LARKIN
SET YOUR SIGHTS ON FRANKFURT!
Mark your calendar now for the 2024 ESCRS Winter Meeting 15–18 February in Frankfurt!
The ESCRS Winter Meeting is a unique opportunity for ophthalmologists, researchers, and industry representatives to exchange ideas and insights about the latest advances and challenges in cataract and refractive surgery, whilst also providing an ideal setting to network with colleagues and forge new connections.
Review the Winter Meeting Programme
The 2024 Winter Meeting programme is now available online at https://wintermeeting.escrs.org/ programme/. It has been crafted for an immersive experience that promises to deepen your knowledge, expand your professional network, and shape the future of refractive expertise through its two main tracks, Intraocular Refractive Surgery and Corneal Refractive Surgery, running in parallel to the DGII Programme.
Register Now to Secure Your Space
Registration for the 2024 Winter Meeting is now open! Register now at https://wintermeeting.escrs.org/ registrations/ to ensure you take advantage of all the Winter Meeting has to offer, from symposia and free paper sessions to instructional courses and wetlabs to the young ophthalmologists programme. New networking features will also be offered.
Experience a Conference Like No Other
Prepare to immerse yourself in a groundbreaking experience at the ESCRS 2024 Winter Meeting in Frankfurt. You’ll experience a host of innovative initiatives that will revolutionize your conference journey. Spaces are limited, so secure your spot early to ensure you don’t miss out on these exclusive opportunities.
Collaborative Innovation in Action
Experience the unique “unconference” format, where you wield the power to shape sessions based on your interests. Dive into participant-driven discussions, ignite collaborations, and innovate within an open, dynamic environment. Be at the forefront of the agenda-setting process, fostering an engaging and personalized experience.
Share, Engage, and Learn
Participate in intimate roundtable discussions offering the perfect setting to share your ideas, experiences, and expertise with peers on relevant conference topics.
Guided Exhibition Tours with ESCRS Experts
Join guided exhibition tours led by members of the ESCRS Executive Committee. Gain firsthand insights and knowledge from industry veterans while exploring the latest advancements. It’s an ideal opportunity for young ophthalmologists to glean wisdom from seasoned professionals.
Escape Room Challenge: A Unique Learning Adventure
Embark on an immersive adventure in our Escape Room. Work together with your peers to solve intricate medical cases. You’ll foster teamwork, critical thinking, and problem-solving skills in an engaging and interactive setting.
Spotlight Theatre: Cutting-Edge Industry Presentations
Engage with exhibitors showcasing their latest innovations in an interactive Spotlight Theatre. Witness firsthand the advancements that are shaping the future of refractive surgery.
New Conference Tracks: Intraocular and Corneal Refractive Surgery
Ready to elevate your expertise in refractive surgery? Experience our new conference tracks focused on Intraocular and Corneal Refractive Surgery. Take a deep dive into these themed tracks covering essential topics across the entire educational programme.
Cataract Surgery in Eyes with Keratoconus
Overcoming the challenges of IOL power calculation and improving refractive accuracy.
CHERYL
GUTTMAN KRADER REPORTS
Using several devices for obtaining preoperative measurements and several keratoconus-specific formulas for IOL power calculation will help optimise refractive outcomes after cataract surgery in the challenging group of eyes with keratoconus, according to Adi Abulafia MD.
“Nevertheless, patient counselling is critical,” he said. “Importantly, therefore, underpromise and overdeliver.”
Prediction errors common
Whereas at least 80% of normal eyes generally achieve refractive outcome ±0.5 D of target, the prediction accuracy is dramatically lower when standard formulas calculate IOL power for eyes with keratoconus.
“When standard IOL power calculation formulas are used, eyes with keratoconus typically end up with a hyperopic error that increases with worsening of keratoconus stage,” Dr Abulafia said.
The challenges to achieving predictable refractive outcomes in eyes with keratoconus include difficulty obtaining
accurate corneal refractive power due to corneal curvature asymmetry. In addition, tear film irregularities in eyes with keratoconus limit measurement repeatability. Furthermore, a change in the ratio between the anterior and posterior corneal surfaces in eyes with keratoconus invalidates the use of the standard keratometric index.
“There are technologies for measuring the posterior cornea, but they are not perfect,” Dr Abulafia said. “Difficulty in predicting the effective lens position and obtaining a reliable subjective refraction in the multifocal corneal are other challenges.”
Achieving better accuracy
Currently, three keratoconus-adjusted formulas are available to calculate IOL power for monofocal lenses—the Holladay consulting software, Kane keratoconus, and Barrett True K for keratoconus, which is unique in its use of posterior cornea values. In cases of a planned implantation of a toric IOL, surgeons should use an IOL calculator developed specifically for toric IOL calculations in eyes with keratoconus; these options include the Kane and the Barrett True-K keratoconus toric calculators.
He noted while controversy remains about using toric IOLs to correct astigmatism in eyes with keratoconus, they can be suitable for select patients.
“The best candidates might be patients with mild to moderate stable keratoconus, no central corneal scarring, satisfactory vision with glasses prior to cataract development, and are contact lens intolerant or want not to wear hard or scleral contact lenses after surgery,” Dr Abulafia said.
Outlining his approach to toric IOL calculation in eyes with keratoconus, Dr Abulafia said he inputs the astigmatism data obtained from several measuring devices into the Barrett True K toric calculator to generate an integrated K value. Cylinder correction and axis are determined by entering the integrated K and measured posterior cornea data into the keratoconus-specific Barrett True K toric calculator. Then he decides on IOL power by considering the spherical equivalent prediction range generated by the Barrett True K with the measured or predicted posterior cornea, the SRK/T, and Kane keratoconus formulas.
Dr Abulafia spoke during Cornea Day of the 2023 ESCRS Congress in Vienna.
Adi Abulafia MD is the director of cataract surgery at Shaare Zedek Medical Center, Jerusalem, Israel. adi.abulafia@gmail.com
Treatment for Infectious Keratitis
PACK-CXL holds promise, but more evidence is needed from ongoing research.
CHERYL GUTTMAN KRADER REPORTS
Since corneal cross-linking (CXL) as a treatment for infectious keratitis (IK) was first reported in the literature 15 years ago, it has been the subject of more than 250 published articles and applied with different strategies across many clinical situations.1 Overall, evidence on the efficacy of this procedure known as Photoactivated Chromophore for Infectious Keratitis (PACK)-CXL is favourable.
Still, it is an area of ongoing evolution—the procedure is not without potential complications, and there remains a need for randomised controlled clinical trials using standardised outcome measures to determine the place of PACK-CXL in clinical practice, according to Rohit Shetty MD, PhD.
What is clear, however, is safe and effective PACK-CXL can address an unmet need, considering the prevalence and cost burdens of IK and the potential for blindness with failed antimicrobial therapy, he said.
Even if the infection is eradicated, the cornea may be left with a scar.
Highlighting some selected literature on PACK-CXL, Dr Shetty noted the published papers appear in both peer-reviewed and non-peer-reviewed journals, include a large number of retrospective case series and case reports, and discuss treatment for different pathogenic causes of IK at every stage using several treatment protocols. Initial investigations focused on PACK-CXL combined with antimicrobial treatment for infections that failed to respond to conventional maximal topical and systemic antimicrobial therapy. Additional research placed the technique as monotherapy for both primary treatment and rescue cases.
A systematic review and meta-analysis published in 2019 found PACK-CXL and antimicrobial therapy accelerated corneal healing compared to antimicrobial therapy alone.2
Results of a randomised, controlled trial—which Dr Shetty co-authored—found the treatment success rate was about 90% in groups treated with either antimicrobial therapy or PACKCXL with no difference in the mean time to corneal healing.3
“Even if the infection is eradicated, the cornea may be left with a scar,” Dr Shetty said. “If PACK-CXL shortens the time to healing, it could theoretically reduce scarring by minimising exposure to microbial-produced factors that promote fibrosis.”
As with any new therapy, the benefits must be weighed against the risks. Aside from lack of efficacy, reported PACKCXL complications include conjunctival injection, increased
uveitis and hypopyon, corneal endothelial cell loss, and herpes simplex keratitis exacerbation.
“It is important to understand the cause of the keratitis before using PACK-CXL for treatment,” said Dr Shetty, adding the technique appears to have better efficacy for treating bacterial infections compared to fungal and Acanthamoeba keratitis.
PACK-CXL for IK has been performed using different protocols that vary in terms of UV fluence and duration of irradiation. In addition, rose bengal-aided photodynamic therapy using a 532 nm light source has been explored.
Looking ahead, Dr Shetty expects to hear more about a new approach to CXL developed by Dr Farhad Hafezi in which patients are treated with a transepithelial procedure at the slit-lamp with the aid of a second-generation corneal penetration enhancer.
“This is a very exciting advance that I believe will shape the future,” Dr Shetty said.
Dr Shetty spoke during Cornea Day of the 2023 ESCRS Congress in Vienna.
For citation notes, see page 39.
Rohit Shetty MD, PhD is Vice Chairman of Narayana Nethralaya Eye Institute, Bangalore, India. drrohitshetty@yahoo.com
Less is More in Angle-Closure Surgery
Specialist urges keeping surgical approaches simple, weighing benefits and risks for these glaucoma patients.
DERMOT MCGRATH REPORTS
Surgeons should adhere to the basic principle of “less is more” in the surgical management of primary angle-closure glaucoma (PACG), according to Andrew J Tatham.
Dr Tatham reviewed the substantial evidence supporting phacoemulsification as a primary treatment modality for both acute angle-closure glaucoma and chronic angle-closure glaucoma.
“With primary angle-closure glaucoma, we know that the crystalline lens is central to the mechanism because it causes pupil block and blocks the angle,” he said. “So, if we remove the lens, that can help reverse the pupil block and open the angle, which is very effective.”
Dr Tatham said he adheres to the principle of “less is more” by avoiding combined procedures in angle-closure patients unless there are compelling reasons to do so.
“Phacoemulsification alone is preferred as the initial surgical treatment for the majority of patients,” he said. “The advice is to keep things simple, as phacoemulsification alone minimises the risk of surgical complications, reverses iridotrabecular contact, and often provides substantial reductions in intraocular pressure (IOP).”
There may also be certain instances where clear lens extraction is warranted.
“Even if a person does not yet have a cataract, clear lens extraction can be effective for those patients at high risk for primary angle closure,” he noted. “But of course, we need to balance the potential benefits of early lens extraction against the risks and can only be done on a case-by-case basis.”
Looking at scenarios where combined procedures may be justified, Dr Tatham said combined phacotrabeculectomy may be an option for advanced PACG, but exercise extreme caution with small and “hot” eyes (patients with acute primary angle-closure glaucoma).
To consider trabeculectomy before performing phacoemulsification in PACG, iridotrabecular contact (ITC) must be addressed first, advised Dr Tatham.
“There may be rare cases where laser iridotomy has reversed ITC, but further IOP lowering is warranted. However, it is best to avoid bleb-forming procedures in nanophthalmos eyes.”
The reality, he said, is cataract surgery in small eyes with angle closure is inherently risky.
“The national ophthalmology database in the UK has shown that shorter axial length eyes have a significantly higher risk of complications,” he said. “And for patients with very small eyes, the risk is even higher.”
Due to the unique ocular anatomy of small eyes, the surgery itself is more complicated to perform, with a high
incidence of complex complications such as angle-closure glaucoma, fluid misdirection syndrome, and uveal effusion syndrome (UES), Dr Tatham pointed out.
If the surgeon has performed initial phacoemulsification— but the pressure-lowering impact is insufficient, and a filtering procedure is envisaged—it is advisable to leave as long a gap as possible between the procedures.
“This is because anterior chamber flare has been shown to persist for up to six months after phaco, potentially reducing the success of the filtering procedure,” he said.
There are also some arguments in favour of combining minimally invasive glaucoma surgery (MIGS) with phacoemulsification in PACG, but Dr Tatham said the benefit-risk profile needs careful consideration.
“Iridotrabecular contact may cause direct trabecular meshwork dysfunction, which could be overcome by bypassing the trabecular meshwork. And there is a potential for additional IOP lowering with these approaches,” he said. “I think endoscopic cyclophotocoagulation (ECP) is also something that is potentially interesting because of the anatomical changes it induces. However, we need to bear in mind there is a lack of high-quality evidence concerning MIGS in PACG—and their off-label use—and phacoemulsification alone is often very effective in angle closure. There is also a high risk of synechiae formation where people use implants.”
Dr Tatham presented at Glaucoma Day at the 2023 ESCRS Congress in Vienna.
Andrew J Tatham MBChB Hons, FRCOphth, FRCSEd, FEBO, AFHEA is a Consultant Ophthalmic Surgeon, Princess Alexandra Eye Pavilion, Edinburgh, Scotland, UK. andrewjtatham@gmail.com
Are There Limits to MIGS?
Data shows sticking to tried-and-trusted options for angle-closure surgery is best, for now.
DERMOT MCGRATH REPORTS
Although minimally invasive glaucoma surgery (MIGS) has expanded the options for primary open-angle glaucoma (POAG), its indications and benefits in primary angle-closure glaucoma (PACG) are less clear and should be approached with caution, according to Panayiota Founti MD, PhD.
“The evidence at this point for surgical treatment of angle closure supports the use of laser peripheral iridotomy (LPI), lens extraction, and incisional surgery,” she said. “There is no high-quality evidence to support the use of MIGS devices or newer bleb-forming procedures in angle closure disease.”
Compared to POAG, the field of angle closure has been somewhat neglected in recent decades.
“When it comes to landmark trials, if you look at the studies that have considerably changed clinical practice, up until 2016, there was no study on angle closure,” she said. “We had to wait until the Effectiveness of Early Lens Extraction for the Treatment of Primary Angle-closure Glaucoma study (EAGLE study) and the Zhongshan Angle Closure Prevention trial (ZAP trial) to change the way we think about angle closure in general and how we approach that in a hospital setting.”
Based on the EAGLE and ZAP trials, the PACG guidelines were updated to reflect the current thinking.
“There is broad agreement that, beyond LPI and lens extraction, incisional filtration surgery is the appropriate course of action for uncontrolled PACG—although the technique should be modified, compared to what we do in POAG, to minimise the risk of complications,” she said.
Turning to MIGS, Dr Founti cited the new guidance on surgical innovation by the European Glaucoma Society, which defines it as only the ab interno non-bleb-forming procedures rather than newer sub-conjunctival bleb-forming techniques, such as Xen Gel Stent and PreserFlo MicroShunt.
Regarding MIGS, while it may be possible to use some of these devices in angle-closure disease, Dr Founti advised it is perhaps wiser to err on the side of caution.
“If you have a patient in front of you with PACG and you want to be open with them about the potential benefits and risks of a MIGS procedure, you need to let them know there is no evidence to support this intervention for the type of glaucoma they have,” she said.
In terms of newer bleb-forming techniques—such as the Xen Gel Stent and PreserFlo MicroShunt—a lot more clinical evidence is needed to properly assess their safety and efficacy in angle-closure glaucoma.
She noted the randomised trials comparing the Xen Gel Stent and PreserFlo MicroShunt versus trabeculectomy have shown substantial rates of hypotony using both approaches (23% and 26%, respectively).
“Of course, not all that hypotony will necessarily lead to devastating complications, but it occurs in about one in four patients, and we need to be aware of that,” she said. “While this hypotony may not cause problems to most patients with POAG, it may lead to severe complications in patients with PACG.”
With a trabeculectomy, Dr Founti said such hypotony can be avoided with appropriate modifications intra- and postoperatively, to bypass low eye pressure in the early postoperative period.
“Trabeculectomy is the most commonly performed procedure in China for PACG and is usually combined with phacoemulsification,” she noted. “According to published data, when using the appropriate technique, the complication rate is not that different from POAG. This busts the myth trabeculectomy in primary angle-closure glaucoma is associated with high rates of aqueous misdirection.”
Dr Founti presented at Glaucoma Day at the 2023 ESCRS Congress in Vienna.
Panayiota Founti MD, PhD is a Consultant Ophthalmic Surgeon at Moorfields Eye Hospital, London, United Kingdom. pfounti@gmail.com
The Automated Future of Glaucoma Treatment
Direct selective laser trabeculoplasty is easy, fast, and user and patient friendly.
TIMOTHY NORRIS REPORTS
Roughly 140 million patients suffer from glaucoma. Not all of them have access to a glaucoma specialist, and the eye drop treatment does not have high adherence due to side effects, with the patients often unhappy.
“So, we eye doctors are happy the European Glaucoma Society considers SLT as a first-line therapy in glaucoma,” said Matthias Elling MD during a free paper session at the ESCRS Congress in Vienna. “Conventional SLT is dependent on glaucoma specialists and time consuming, and the question is if that is the real best first-line treatment.”
Direct selective laser trabeculoplasty (DSLT) is a recent addition for glaucoma specialists looking for different first-line treatment options.
“We are glad to now have, at the University Eye Hospital of Bochum, the DSLT—in commercial use since November 2022—which has already treated 400 eyes,” Dr Elling said. “It is a very user and patient friendly automated treatment with an integrated algorithm that recognises the treatment area and an integrated eye tracker.”
As Professor Peng Tee Khaw explained, the process is rapid: the patients come in, lid speculums are placed, then eye drops, before they walk to the laser. “You focus on the limbus, and after the three seconds the actual treatment takes, they walk off, and you can do the second eye. This is an extraordinary type of innovative treatment.”
“It is a drop-free, easy, repeatable, and efficient alternative for a first-line therapy, and we can treat the patient only with a touch of one button, applying 120 laser spots in a 180-degree or 360-degree treatment area,” Dr Elling observed.
As demonstrated in the GLAUrious study, DSLT is safe and effective in providing a clinically meaningful reduction in IOP sustained out to 12 months.
“At six months, we had a washout comparison of mean IOP; then at 12 months, the results were similar,” Prof Khaw said. “A slight difference can be observed in the mean IOP reduction of -0.7 mmHG for the DSLT, not a huge amount.”
“After 12 months, we have in both groups nearly an identical IOP lowering effect of 3.4 mmHg,” Dr Elling added.
The standard evaluator-masked, randomised, controlled, non-inferiority trial was conducted on 99 and 93 patients in 14 study sites across the UK, Italy, Israel, and Georgia.
“Although you see there are some differences in the patients, there are no differences that would obviously burst the direct or the standard SLT,” Prof Khaw observed. “Of all patients with one medication, 70% were off all treatments at 12 months, and 50% of patients under three medications were also off at 12 months, compared to 39% of the standard SLT.”
According to Dr Elling, careful patient selection is essential. “Most of the glaucoma patients are really suitable for DSLT treatment, not only in naive eyes as a first-line therapy but also in eyes with advanced diseases and even after glaucoma surgery,” he explained.
We eye doctors are happy the European Glaucoma Society considers SLT as a first-line therapy in glaucoma.
Exclusion criteria for DSLT are very forgiving. “We can treat patients in a sitting or standing position but not in a lying position, and eyes with a previous surgery like a trabeculectomy could give some difficulty for the algorithm to find the limbus, making the treatment difficult to perform,” Dr Elling said.
Regarding safety results, only minor adverse effects were underlined in the study, with an identical safety profile compared to conventional SLT (with only one slight exception). “There are small punctuates of the conjunctival haemorrhages in 20% of cases, and they are very mild and reabsorb shortly,” Prof Khaw observed.
Both presenters said DSLT is a very safe and simple procedure.
“DSLT definitely provides a meaningful reduction in IOP at six months that sustains out at 12 months,” Prof Khaw said. “The pressure lowering is very similar to SLT, and 70% of the naive patients are still drop free, not dissimilar to the LiGHT study at a longer period. The extraordinary ease and speed of use—the patient walking in, lid speculum, drops chin up, laser and treatment done in a couple of seconds—may considerably improve efficiency and access to care, which is a resource that today tackles one of the biggest issues in glaucoma worldwide.”
“The future is automated,” Dr Elling concluded. “DSLT can be used as a first-line therapy, as mentioned by the European Glaucoma Society. It is an effective and gentle treatment that can optimise the adherence of treatment and the care of an increasing number of glaucoma patients.”
Matthias Elling MD is assistant medical director, Ruhr University, Bochum, Germany. Matthias.elling@kk-bochum.de
Professor Sir Peng Khaw is a consultant ophthalmic surgeon at Moorfields Eye Hospital, London, UK. p.khaw@ucl.ac.uk
OSD and Glaucoma Drops
Reduction of the number of glaucoma medications improves ocular surface status.
TIMOTHY NORRIS REPORTS
Cataract surgery and iStent (Glaukos) implantation in primary open-angle glaucoma (POAG) patients allow reduction of the number of IOP lowering medications, leading to improvement of ocular surface disease signs and symptoms, according to a study presented at the 2023 ESCRS Congress in Vienna.
Presented by Kjell Gunnar Gundersen MD, PhD, the study inspiration came from a master’s degree thesis by Andrea Mihovilovic, in which a high occurrence of ocular surface disease (OSD) signs was observed in POAG patients under treatment with unpreserved prostaglandin analogues and beta blockers.
“We then made a further literature review, looking at what has been written and studied on ocular surface and glaucoma,” he said. “To our surprise, there were relatively few publications—despite glaucoma being a frequent disease and its known impact on the ocular surface.”
A subsequent contralateral randomised interventional study further investigated the effect of reduced or stopped medication on OSD in patients with POAG on long-standing bilateral medical therapy. As of today, 19 patients with glaucoma were analysed six months after cataract surgery. One eye was randomised with the iStent, and the fellow eye had cataract surgery only.
“The primary outcome measurement was the change in subjective and objective signs of OSD between study and control eyes,” Dr Gundersen said. “The secondary outcome was to look at IOP control and the reduction of medications.”
Study results considered subjective and objective primary outcomes, with data collected through OSDI and SPEED questionnaires for the former.
“One could not expect a clear difference between both questionnaires because one eye was treated and one was not,” he explained. “But, we see a trend both in the OSDI measurements and the SPEED—a score reduction during the six months of observation. A clear but not statistically significant trend.”
Objective results were graded based on the corneal staining score. “We saw a significant drop among the patients receiving both iStent and cataract surgery compared to the control eyes. This was highly significant.”
Secondary outcomes showed both groups had a significantly reduced number of glaucoma medications from the start to the end of the study. “The difference between the study eye and the control eye was also significant. Moreover, from the beginning to the end of the study, the IOP was higher in the control group and higher in the study group: this is mainly because we chose the worst eye for the iStent implantation.”
Primary outcome measurements showed a highly significant difference in objective corneal staining score between study eyes and control eyes. “In only six months, we found an expected non-statistically significant trend in our OSDI and SPEED scores. The number of medications dropped significantly in both groups—and much more in the study group compared to the control group,” Dr Gundersen explained.
“Reducing the number of glaucoma medications significantly improves the ocular surface status, represented by the ocular staining score.”
Kjell Gunnar Gundersen MD, PhD is an ophthalmic surgeon at the Ifocus Eye Clinic in Haugesund, Norway. kg@ifocus.no
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.
Gene Therapy for X-Linked Retinitis Pigmentosa
Follow-up shows evidence of a biological response with few safety concerns.
CHERYL GUTTMAN KRADER REPORTS
An interim analysis conducted after 24 months of follow-up in the HORIZON phase 1/2 clinical trial shows AGTC-501 subretinal gene therapy for X-linked retinitis pigmentosa (XLRP)—caused by RPGR mutations—has a favourable safety profile and demonstrates efficacy for improving visual function, reported Robert MacLaren MD, PhD.
“AGTC-501 is intended to be a one-time therapy targeting the genetic cause of XLRP that uses a proven vector to replace the mutated RPGR,” he said. “The encouraging findings achieved so far in HORIZON strongly support continued clinical development of AGTC-501, and the sponsor (Beacon Therapeutics) plans to initiate two more clinical studies by the first quarter of 2024.”
HORIZON is an open-label dose-escalation study that enrolled 29 male patients into six dosing groups. Researchers evaluated central (subfoveal) and peripheral (extrafoveal) injections in the first two dosing groups, only peripheral in the third dosing group, and only central delivery in the subsequent dosing groups.
Safety is being evaluated as the primary endpoint in the phase 1/2 trial, and there were no clinically significant safety events related to the study agent. No eye showed significant vision loss or cone dysfunction, and there were no cases of endophthalmitis or suspected unexpected serious adverse reactions deemed related to the study agent.
“The overall safety profile of AGTC-501 gene therapy is consistent with a subretinal procedure, vitrectomy procedure, and concomitant corticosteroid treatment,” Dr MacLaren said.
The potential efficacy of AGTC-501 therapy was evaluated using Macular Integrity Assessment microperimetry, which reflects cone function, and BCVA testing. Compared with the fellow untreated eyes, the microperimetry results showed AGTC-501 had a significant benefit for improving visual sensitivity across the central 36 loci. The treatment effect was observed by month 3 post-injection and sustained through follow-up to 24 months—even extending to 36 months in the earliest treated patients.
“Interestingly, when we looked at patients who had a clinically significant response, defined as an improvement in 7 dB or more in 5 or more of the 36 central loci of the microperimetry grid, we see a very close correlation to the mean retinal sensitivity,” Dr MacLaren said.
“In addition, low luminance VA data also provided supportive evidence of a biological response and correlated with improvements in retinal sensitivity, both of which are subtle measures of cone function.”
Dr MacLaren underscored that in contrast to another investigational gene therapy under investigation for XLRP caused by RPGR mutations, AGTC-501 uses a stable, full-length RPGRORF15 gene therapy vector—not a version containing a large deletion in a critical region. Therefore, AGTC-501 is thought to have a higher probability of restoring the natural function of cone photoreceptors, yielding a greater and more sustained visual improvement.
The two AGTC-501 trials expected to begin in 2024 include DAWN, an open-label study conducted in the US treating the fellow untreated eye of patients previously dosed with an AAV vector-based full-length RPGR gene therapy. The second trial, VISTA, is a phase 2/3 randomised, controlled, masked multicentre study that will enrol patients in the US and Europe. It will evaluate two doses of AGTC-501 and have an untreated control group.
Dr MacLaren presented the HORIZON results at the 2023 EURETINA Congress in Amsterdam.
Robert MacLaren MD, PhD is Professor of Ophthalmology, University of Oxford, England, United Kingdom. maclaren@eye.ox.ac.uk
Preserving Foveal Function in Geographic Atrophy
Phase 3 OAKS trial follow-up shows benefit of C3 and C3b inhibition with pegcetacoplan.
CHERYL GUTTMAN KRADER REPORTS
Findings from a post hoc analysis assessing the effect of pegcetacoplan treatment on foveal light sensitivity in eyes with geographic atrophy (GA) secondary to age-related macular degeneration show a benefit of complement C3 and C3b inhibition in decreasing the hazard of progression to development of an absolute scotoma at the fovea, reported Usha Chakravarthy MD, PhD.
“Maintaining foveal light sensitivity is crucial for macular functionality and thus central visual function,” Dr Chakravarthy said. “These results from the analysis of microperimetry data demonstrate that treatment with pegcetacoplan was associated with additional time in maintaining foveal function and supports the hypothesis that intravitreal pegcetacoplan treatment provides a functional benefit in addition to slowing GA lesion growth.”
The phase 3 OAKS trial enrolled 637 patients aged 60 years and older with nonsubfoveal and/or subfoveal GA measuring between 2.5 to 17.5 mm2 in area (at least one focal lesion ≥1.25 mm2 in eyes with multifocal GA), BCVA ≥24 ETDRS letters (20/320 Snellen equivalent), and presence of perilesional hyperautofluorescence, which is an indicator for faster progression. Study participants were randomised into four groups (2:2:1:1) to receive pegcetacoplan 15 mg monthly or every other month, or sham monthly or every other month, respectively.
Maintaining foveal light sensitivity is crucial for macular functionality and thus central visual function.
Categorisation of eyes by number of central absolute scotomatous points showed at baseline, 18.3% had no foveal light sensitivity (four scotomatous foveal loci), 34.9% two or three scotomatous points, and 46.8% zero or one scotomatous points. Corresponding mean baseline BCVA (ETDRS letters) in the three subgroups was 47.1 (approximately 20/125 Snellen equivalent), 56.8 (approximately 20/80), and 65.3 (approximately 20/50), respectively.
“These data show clearly that having an increasing number of central scotomatous points negatively affects the BCVA of patients with GA,” Dr Chakravarthy said.
To measure longitudinal visual function, the study team conducted microperimetry at baseline and 6, 12, 18, and 24 months using the 10-2 MAIA grid (CenterVue, Padua, Italy) that tests the central 10 degrees of the visual field. The current analysis is focused on the central four microperimetry points. For inclusion, there had to be at least one non-scotomatous point in the central four loci at baseline with at least one post-baseline microperimetry assessment. The team recorded the number of foveal loci that became absolute scotomata at each visit and performed a time-to-event analysis for the two pegcetacoplan dosing groups and pooled sham groups. They defined an event as onset of absolute scotomata at all four foveal loci in the study eye.
At baseline, the Kaplan-Meier survival analysis of progression to foveal light insensitivity included 155 eyes in the pegcetacoplan monthly group, 152 eyes in the pegcetacoplan every other month group, and 148 sham-treated eyes. The event analysis showed fewer events occurred in the pegcetacoplan monthly group than in the sham group at month 6. At subsequent visits, there were fewer events in both pegcetacoplan treatment groups than sham. At 24 months, the hazard ratio for progression to an event in the pegcetacoplan monthly and every other month groups compared to sham was 0.66 (P = 0.0282) and 0.64 (P = 0.0164), respectively.
Dr Chakravarthy spoke at the 2023 EURETINA Congress in Amsterdam.
Usha Chakravarthy MD, PhD is Honorary and Emerita Professor of Ophthalmology and Vision Science, Queen’s University of Belfast, Northern Ireland, United Kingdom. u.chakravarthy@qub.ac.uk
Hydrophilic Tamponade for Detached Retina
Encouraging results for artificial vitreous substitute.
DERMOT MCGRATH REPORTS
Anovel hyaluronic acid-based hydrogel has shown promise as a safe and effective vitreous substitute in vitreoretinal surgery and may help to overcome some of the limitations of gas or silicone oil as a tamponade agent, according to Kai Januschowski MD, PhD.
“Our study demonstrates hydrophilic tamponades have a superior mechanism when it comes to reattaching the retina, and they have superior physical characteristics when it comes to the refractive index and swelling capacity,” he said. “The biocompatibility has been proven both ex vivo and in vivo, and we didn’t see any signs of emulsification yet.”
Professor Januschowski presented the data from a retrospective interventional study of 21 eyes from 21 patients with phthisis bulbi treated at the Eye Clinic Sulzbach, Germany, between August 2011 and June 2021.
Our study demonstrates hydrophilic tamponades have a superior mechanism when it comes to reattaching the retina.
More than 60% of the eyes treated with the non-crosslinked hyaluronic acid had an IOP increase above 5 mmHG that endured for 80 days but no emulsification or corneal transparency issues. With the cross-linked hydrogel, 83% of treated eyes recorded an increase of more than 5 mmHG, enduring for 100 days with no emulsification or corneal problems such as opacification or neovascularization.
“This is a long period where we collected patients [with] very heavily impacted eyes,” he explained. “These were patients going into hypotony, and we feared there would be the need for enucleation at some point, which is why the numbers are relatively small over that time period.”
Patients who underwent a 23-gauge pars plana vitrectomy received a vitreous substitute composed of one of three substances: a non-cross-linked hyaluronic acid (Healon GV, Johnson & Johnson Vision), the novel cross-linked hyaluronic acid-based hydrogel (UVHA), or silicone oil (SO-5000). The main outcome measures were intraocular pressure (IOP), visual acuity, and the structural integrity of the retina and choroid assessed by optical coherence tomography.
Results showed stabilized hypotony in five of the eight eyes treated with silicone oil, with an increase in IOP of about 5 mmHg for about 40 days. However, six of the eight eyes experienced emulsification with corneal opacities, oedema, and neovascularization of the cornea.
“Well, that’s not surprising because we all know that’s what happens when you put silicone oil in these catastrophic eyes,” Prof Januschowski noted.
One patient in the hydrogel group received a corneal transplant some 700 days after the initial treatment, said Prof Januschowski.
“Interestingly, as we performed the corneal transplant in an open sky vitrectomy setting, we could still find vitreous remnants, underlining the durability of the hydrogel in the eye.”
Summing up, Prof Januschowski said the hyaluronic acid-based hydrogel has demonstrated its safety and effectiveness in vivo, stabilizing IOP in patients with phthisis bulbi for about three months.
“I think the hydrogel holds a lot of promise, and we are excited by the possibility of having a viable, safe, and effective alternative to current tamponade methods, which have a lot of limitations,” he said. “The next steps will be looking into manufacturing the hydrogel and hopefully taking it to the next stage.”
Prof Januschowski presented this study at the EURETINA Congress in Amsterdam.
Kai Januschowski MD, PhD, FEBO is an ophthalmologist practising at the Augenklink Petrisberg in Trier, Germany. Kai.Januschowski@augenklinik-petrisberg.de
ESCRS AT A GLANCE
We are a society of surgeons who specialise in improving vision and restoring clarity. Since 1991, ESCRS has promoted the education and research of implant and refractive surgery. With over 7,500 members from 130 countries worldwide, ESCRS is a vital global platform for the field of ophthalmology.
Identifying Progressive Keratoconus
New tool designed on principles underlying accurate diagnosis.
CHERYL
GUTTMAN KRADER REPORTS
Anew application for identifying keratoconus progression in eyes with Amsler-Krumeich Stages 1 and 2 is expected to optimise and facilitate the accurate diagnosis of truly progressive disease, according to Ingemar Gustafsson MD, PhD.
Named the Scandinavian Keratoconus Progression Application (SKPA), it is a non-invasive tool developed for the Pentacam HR that simply reads the instrument’s data on the computer server. By optimising accurate diagnosis of keratoconus progression, the SKPA has implications for improving the quality of both clinical care and scientific research, Dr Gustafsson said.
“Progression of keratoconus is often defined as an increase in Kmax of 1.0 D—but using this single detection limit will underdiagnose progression in patients with less advanced keratoconus and overdiagnose it in those with more advanced disease,” he explained.
“The clinical consequence is cross-linking (CXL) will be underused in patients who have the most to gain from it and overused in those less likely to benefit. The issue from a scientific perspective is the potential for enrolling patients into CXL clinical trials erroneously identified as having progressive disease because of measurement error.”
Available for download as open access, the SKPA was developed based on the idea there is not a single best parameter for detecting keratoconus progression and the focus should be on the detection limits rather than a single parameter per se.1
The SKPA includes K2, Kmax, A, B, and C measurements and uses detection limits for each stratified according to disease severity. It also considers inter-day repeatability of measurements and whether single or replicate measurements are available.
Explaining these design principles, Dr Gustafsson reviewed studies showing that for keratoconus, the measurement error of parameters commonly used for assessing progression increases with advancing disease severity. This information underscores the need for stratified detection limits when considering disease severity to avoid progression underdiagnosis, undertreatment of eyes with earlier disease, and overdiagnosis of those with more advanced keratoconus (leading to CXL overtreatment).
Research also highlights the importance of considering the inter-day repeatability of the measurements used in assessing keratoconus progression since measurements taken on different days determine it. Used parameter detection limits often derive from studies analysing same-day measurements.
Adjusting the detection limits used in the SKPA depends on whether values for a single measurement or replicates reflect differences in clinical practice and the effect of the two approaches on the ability to detect progression.
“Using a mean of multiple measurements rather than a single measurement improves precision and makes diagnosis of progression more reliable, but it requires different detection limits,” Dr Gustafsson said.
“In a survey sent to clinical centres [performing] CXL, we found most respondents used a single measurement for assessing progression, but a significant proportion used a mean of replicates.2 The SKPA automatically calculates the mean of replicate measurements, thereby eliminating what was otherwise a time-consuming manual task. It then compares the difference between serial single or mean measurements using the appropriate detection limit.”
In addition to calculating the mean of replicate measurements, the SKPA facilitates clinical efficiency by showing the results in a single user-friendly interface featuring numerical, graphic, and colour-coded displays.
Dr Gustafsson spoke at Cornea Day of the 2023 ESCRS Congress in Vienna.
For citation notes, see page 39.
Ingemar Gustafsson MD, PhD is a consultant in the cornea service at Skåne University Hospital, Lund, Sweden. ingemar.gustafsson@med.lu.se
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
Less Waste, More Vision
Managing surgical tools and waste could cut costs and carbon emissions.
HOWARD LARKIN REPORTS
Reducing and properly managing surgical tools and waste could save significant money while reducing environmental impact, two young ophthalmologists report.
In a formal audit of 85 cataract surgeries by multiple surgeons at the University of Ottawa Eye Institute (Canada), Victoria Liu MD found about half of the tools in cataract surgery trays typically went unused. Overall, surgeons used a median of 46% of the tools per surgery, ranging from 32% to 59%. Seven of 22 tools on the tray were used in fewer than 2% of surgeries, with three going entirely unused.
Dr Liu estimated the total cost of these instruments, which did not include phacoemulsification tools, at more than $6,800 Canadian. Removing the eight tools used in less than 10% of surgeries would cut that total by about $2,470. Over just 50 trays, savings on the upfront cost of instruments would
exceed $120,000. Even more savings would accrue through reduced handling, sterilisation, and replacement costs. Cataract surgery volume at her centre is about 8,500 cases per year.
An audit of corneal surgery trays for Descemet stripping automated endothelial keratoplasty (DSAEK) produced similar results, Dr Liu reported. A mean of just 32% of 32 tools on the tray was used per surgery, ranging from 22% to 38%, with 41%—or 13 instruments—used in no surgeries at all. The total cost of these 32 instruments is more than $12,000 (€8,234), so eliminating the unused tools for the more than 110 annual DSAEK procedures could save significant money.
However, Dr Liu acknowledged the study samples were small, adding result confirmation and their impact in the OR need evaluation. “We are pending further feedback prior to making corneal tray changes.”
85
In a formal audit of 85 cataract surgeries by multiple surgeons at the University of Ottawa Eye Institute (Canada), Dr Victoria Liu found about half of the tools in cataract surgery trays typically went unused.
46%
Overall, surgeons used a median of 46% of the tools per surgery, ranging from 32% to 59%.
The 5 Rs
Reducing the volume of recyclable or reusable waste disposed of as clinical waste could cut the cost and environmental impact of ophthalmic surgery, said Kar Yen Phoong. Incinerating clinical waste emits four times more carbon dioxide than recycling and costs more than twice as much.
In a study of 24 cataract surgeries and 6 oculoplastic procedures, phacoemulsification cases generated a mean 1.20 kg of clinical waste, of which 0.72 kg—or 60%—was unnecessary. By contrast, major oculoplastic surgeries generated 0.20 kg of clinical waste, with 0.11 kg unnecessary, while minor oculoplastic surgeries produced just 0.15 kg of clinical waste, with 0.05 kg unnecessary. The costs of incinerating clinical waste and the amount of carbon dioxide generated were three times higher per cataract case than per major oculoplastic case.
Promoting awareness of recycling, including educating staff on the cost and carbon dioxide emissions of unnecessary clinical waste and placing laminated posters on waste disposal bins in the operating theatre, can also help improve performance, Dr Phoong said. More research to reduce the amount of plastic and other unnecessary disposables used in customised cataract packs is also important, she noted, adding most instruments used in oculoplastic surgery are reusable after sterilisation.
Reuse, reduce, recycle, rethink, and research are the five keys to improvement, Dr Phoong concluded. “Small steps can make a huge difference.”
Both doctors presented at the 2023 ESCRS Congress in Vienna.
Victoria Liu MD is an ophthalmology resident at the University of Ottawa Eye Institute, Ottawa, Canada.
Kar Yen Phoong MBBS is an ophthalmology resident at East Lancashire Hospitals NHS Trust, Blackburn, UK.
New allogeneic cell therapy for endothelial disease
Aurion Biotech has announced it has dosed the first subject in its Phase 1/2 US clinical trial (ABA-1, CLARA) of AURN001, a nonsurgical treatment of corneal oedema secondary to corneal endothelial dysfunction. The treatment involves the intracameral injection of neltependocel (allogeneic human corneal endothelial cells [CECs]) and Y-27632 (an inhibitor of Rho-associated, coiled-coil containing protein kinase [ROCK]). The company says it may provide an alternative to endothelial keratoplasty, reducing the currently unmet need for donor corneas. The prospective, multicentre, randomised, double-masked trial will evaluate three different doses in 100 corneal endothelial disease patients.
Streamlined surgical planning software
Bausch + Lomb has introduced new surgical planning software for the Eyetelligence platform designed to streamline surgical planning and information flow and enable electronic medical record (EMR) and diagnostic device integration. Its design intends to deliver a seamless, secure flow of information from the office to the operating room—without the need for multiple documents, sources, and folders. The Eyetelligence surgical planning software will offer both a surgeon-focused app and a nursing-focused app to enhance communication and improve workflow.
EMA PRIME designation for new geographic atrophy treatment
Annexon has announced the European Medicines Agency (EMA) granted Priority Medicine (PRIME) designation to ANX007 for the treatment of geographic atrophy (GA) secondary to age-related macular degeneration (AMD) as well as preclinical data supporting the protective effect of ANX007 against photoreceptor damage. ANX007 is a fragment antigen-binding (fab) antibody designed to selectively inhibit C1q, the initiating molecule of the classical complement pathway and a key driver of neurodegeneration. The EMA granted the PRIME designation based on Phase 2 ARCHER trial data showing statistically significant, durable, and dose-dependent preservation of visual function in patients with GA.
FDA approves Vabysmo for retinal vein occlusion (RVO)
The US Food and Drug Administration (FDA) has approved faricimab-svoa (Vabysmo®, Genentech) for treating macular oedema following retinal vein occlusion (RVO). Vabysmo is the first and only bispecific antibody approved for the eye. Two Phase III studies showed that in eyes with RVO, intravitreal injection of Vabysmo resulted in early and sustained vision improvements non-inferior to aflibercept, in addition to rapid and robust drying of retinal fluid. The therapy previously received FDA approval for treating neovascular age-related macular degeneration (AMD) and diabetic macular oedema (DME).
FDA issues eye drop warning
The FDA has issued an alert to customers and manufacturers regarding 26 over-the-counter eye drops. The brands in question are CVS Health, Leader (Cardinal Health), Rugby (Cardinal Health), Rite Aid, Target Up&Up, and Velocity Pharma. Although none of the eye drops have caused adverse effects in consumers, the FDA warned customers against using them and advised the manufacturers to recall the subject products because their investigators found bacterial contamination in critical drug production areas of a manufacturing facility.
KLEX: A NEW COMPREHENSIVE TERM FOR REFRACTIVE LENTICULE EXTRACTION
JCRS editors have issued a statement calling for the industry to adopt keratorefractive lenticule extraction (KLex) as a scientific and generic nomenclature for refractive lenticule extraction procedures. They note refractive lenticule s extraction has undergone several name changes depending on the proprietary technique used, starting with femtosecond lenticule extraction (FLE or Flex), then ReLex, then small-incision lenticule extraction (SMILE) when the procedure involved removing the lenticule through small incision instead of a LASIK-style flap. Companies have continued to add new proprietary terminologies for their variations in the procedure. The editors therefore deliberated on a term that would be descriptively accurate and inclusive of future variations while avoiding any proprietary names. They settled on keratorefractive lenticule extraction (KLex), noting: “KLex avoids proprietary terms, both past and present, and represents a consistent common denominator that is easily expressed phonetically as an acronym (‘kay-lex’).”
W J Dupps, et al., “Scientific nomenclature for keratorefractive lenticule extraction (KLEx) procedures: a joint editorial statement,” 49(11): 1085.
RISK OF PCD INCREASES WITH LENS THICKNESS
Lens thickness is another factor predictive of posterior capsular defects (PCD) occurring during cataract surgery, in addition to shallow anterior chamber depth (ACD), according to a population study. The study included 1,967 patients with a mean age of 70.56 years who underwent cataract surgery during an inpatient stay. The study’s authors measured their biometric parameters using SS-OCT (IOL Master 700, Carl Zeiss Meditec AG). Of the included patients, 59 (2.53%) had PCDs. The study showed significant associations between the incidence of PCDs and lens thickness LT and ACD. Other biometric parameters such as axial length, keratometry, white-towhite value, and corneal thickness were not significantly associated with the incidence of PCDs.
T Arad, “Association between anterior chamber biometry and posterior capsular defects,” 49(11): 1086–1091.
META-ANALYSIS CONFIRMS SAFETY OF IMMEDIATE BILATERAL CATARACT SURGERY
A new systematic review and meta-analysis comparing the safety and efficacy profile of immediate sequential bilateral cataract surgery (ISBCS) and delayed sequential bilateral cataract surgery (DSBCS) found no statistically significant differences between the two approaches. The authors searched MEDLINE (Ovid), EMBASE, and CENTRAL databases for relevant studies. They identified 13 articles in which a total of 11,068,622 participants (18,802,043 eyes) met the criteria for final inclusion—all published between 2006 and 2022. Outcome measures were postoperative visual acuity, postoperative spherical equivalent (refractive outcome), endophthalmitis, corneal oedema, pseudophakic macular oedema, and posterior capsule rupture (PCR). No statistically significant differences between ISBCS and DSBCS were identified in all the postoperative outcomes evaluated. However, a higher risk for posterior capsule rupture was identified in the ISBCS group from the pooled analysis of non-randomised studies.
F Aiello, et al., “Immediate sequential vs delayed sequential bilateral cataract surgery: systematic review and meta-analysis,” 49(11): 1168–1179.
GLOBAL REACH
As a renowned authority in the field of cataract and refractive surgery, ESCRS facilitates global connections amongst ophthalmic professionals, fostering collaboration and the exchange of knowledge.
Our events span across continents, providing a platform for pioneering research, advanced surgical techniques, and continuous professional development.
Using the interactive map on our website, we invite you to explore our global presence by viewing upcoming events and academies.
Join us to network with esteemed experts, access the latest advancements, and contribute to the enhancement of eye care on a worldwide scale.
escrs.org/meetings-and-events/global-reach/
Cited in this Issue
A Force for Good in Global Eye Care
Page 08
1. JAMA Ophthalmol. 2021 Jan 1; 139(1): 9–15.
2. Br J Ophthalmol. 2020 Apr; 104(4): 588–592.
Promising Presbyopia Option
Page 12
1. Alió JL, Simonov AN, Romero D, et al. “Analysis of accommodative performance of a new accommodative intraocular lens,” J Refract Surg., 2018; 34(2): 78–83.
2. Alió JL, Simonov A, Plaza-Puche, et al. “Visual outcomes and accommodative response of the Lumina accommodative intraocular lens,” Am J Ophthalmol., 2016; 164: 37–48.
3. Alió JL, D’Oria F, Toto F, et al. “Retinal image quality with multifocal, EDoF, and accommodative intraocular lenses as studied by pyramidal aberrometry,” Eye Vis (Lond)., 2021; 8(1): 37.
Universalising Intraoperative OCT Benefits Page 13
1. Acta Ophthalmol. 2023 Jun 20.
Ophthalmic Drug Delivery Enters New Era Page 14
1. Oculis. “OCS-01, first investigational eye drop for front and back of the eye, met both primary endpoints in phase 3 OPTIMIZE trial with a once daily regimen for the treatment of inflammation and pain following cataract surgery.” August 8, 2023. https://investors.oculis.com/news-releases/news-release-details/ocs-01-first-investigational-eye-drop-front-andback-eye-met. Accessed September 28, 2023.
2. Donnenfeld ED, Holland EJ, Solomon KD. “Safety and efficacy of nepafenac punctal plug delivery system in controlling postoperative ocular pain and inflammation after cataract surgery,” J Cataract Refract Surg., 2021 Feb 1; 47(2): 158–164.
ESCRS Academies
Committee representatives of ESCRS organise and present sessions at meetings organised by our national and sister societies. These sessions are typically delivered by a group of speakers on a current topic selected by ESCRS in person or virtually.
These sessions provide useful education as well as collaboration between societies promoting and sharing benefits across both memberships.
escrs.org/education/academies/
3. Visco DM, Bedi R. “Effect of intracameral phenylephrine 1.0%-ketorolac 0.3% on postoperative cystoid macular edema, iritis, pain, and photophobia after cataract surgery,” J Cataract Refract Surg. 2020 Jun; 46(6): 867–872.
Deep Learning OCT
Page 17
1. José M González-Méijome et al., J Optom., 2022; 15: 1–2.
Treatment for Infectious Keratitis
Page 21
1. Iseli HP, Thiel MA, Hafezi F, Kampmeier J, Seiler T. “Ultraviolet A/riboflavin corneal cross-linking for infectious keratitis associated with corneal melts,” Cornea. 2008; 27(5): 590–594.
2. Ting DSJ, Henein C, Said DG, Dua HS. “Photoactivated chromophore for infectious keratitis—Corneal cross-linking (PACK-CXL): A systematic review and meta-analysis,” Ocul
Surf. 2019; 17(4): 624–634.
3. Hafezi F, Hosny M, Shetty R, et al. PACK-CXL Working Group. “PACK-CXL vs. antimicrobial therapy for bacterial, fungal, and mixed infectious keratitis: a prospective randomized phase 3 trial,” Eye Vis (Lond). 2022; 9(1): 2.
Identifying Progressive Keratoconus
Page 30
1. Gustafsson I, Neumann O, Bizios D, et al. “Introducing a new tool for the assessment of progressive keratoconus: the Scandinavian Keratoconus Progression Application,” Journal of EuCornea. 2022; 11(3): 1–9.
2. Gustafsson I, Vicente A, Bergström A, et al. “Current clinical practice in corneal crosslinking for treatment of progressive keratoconus in four Nordic countries,” Acta Ophthalmol. 2023; 101(1): 109–116.
Upcoming Events
February 15–18
2024 ESCRS Winter Meeting in conjunction with the 38th Congress of the DGII Frankfurt, Germany
April 5–8
2024 ASCRS Annual Meeting Boston, United States
May 5–9
2024 ARVO Annual Meeting Seattle, United States
May 24–26
2024 EuCornea Annual Congress Paris, France
June 1–4
2024 European Glaucoma Society Congress Dublin, Ireland
September 6–10
2024 ESCRS Congress Barcelona, Spain
Feb 15
May 24
Sep 6
Research. Education. Innovation.
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.