Catholic health care providers brace for impact of budget bill
By LISA EISENHAUER
McPherson remembers the patients undergoing cancer care alongside her years ago who, unlike her, did not have private health insurance. She saw them drop out of treatment because they couldn’t afford the care or they lost access to insurance programs such as Medicaid.
“I had a little bit of survivor’s remorse, because the only reason why I was there and they weren’t was because I was insured,” McPherson recalls. “I did not have to have that hanging over my head, that somebody somewhere was going to pull my benefits from up under me, and I was going to have
CHRISTUS Children’s invests in pediatric heart care for region with high need
By JULIE MINDA
SAN ANTONIO — Because of multiple complex factors, cardiac disease is more common among children in South Texas than elsewhere in the state.
To help address this long-standing concern, CHRISTUS Health and philanthropic partners have been making strategic investments that have expanded the breadth and quality of the pediatric cardiovascular program at CHRISTUS Children’s in San Antonio. This has increased care access and improved heart health outcomes for South Texas kids,
Pacific Northwest collaborative formed to assess community needs explores how to address findings
By JULIE MINDA
Around 2010, the leaders of multiple health organizations in the Pacific Northwest began noting that, because of new or evolving government requirements, they were expending significant time and resources conducting community health needs assessments and developing plans to address the needs. They also were making requests for the same information from community members and organizations. They wondered whether they could pool their expertise and resources to share the costs and burdens of creating these assessments.
The health organizations decided to form the Healthy Columbia Willamette Collaborative and have since achieved results that illustrate the power of partnership. Now they want to build on their success in partnering on the assessments. They are looking for more ways to address community needs together.
Joseph Ichter is senior director of community health investment for Providence
Ascension credits Recognize and Rescue initiative with saving more than 4,000 lives in hospitals
By VALERIE SCHREMP HAHN
At one of the country’s largest nonprofit health systems, it may seem like a daunting task to get clinicians on the same page. But Ascension, with facilities in 16 states and the District of Columbia, credits the Recognize and Rescue initiative it started about five years ago with preventing more than 4,000 deaths in 88 hospitals over a threeyear study period, reducing risk-adjusted mortality by 20%.
The Recognize portion of the initiative is focused on optimizing the care of high-risk conditions and preventing the deterioration of the patient’s condition. It includes early identification of serious conditions such as sepsis and breathing problems; preventing health care-associated infections; monitoring and minimizing the side effects of certain medications; and engaging in goals-of-care discussions with patients and families. The Rescue portion of the
Dr. Ravi Ashwath tends to cardiology patient Quincy Riffle at CHRISTUS Children’s in San Antonio. Ashwath is division chief of pediatric cardiology, endowed chair in pediatric cardiology at CHRISTUS Children’s and a pediatrics professor at Baylor College of Medicine.
Danielle
CHA has created resources for its members to use in advocating for preservation of the advance premium tax credits that help millions of Americans afford health insurance. The resources are online at chausa.org/APTC.
New hospital
Trinity Health System of Steubenville, Ohio, has opened St. Clairsville Neighborhood Hospital less than a year after the closure of a regional hospital left a void.
Technology review
Two CommonSpirit Health executives share the system’s process for reviewing clinical and ethical concerns related to use of its data and artificial intelligence tools.
Maternal health
Sr. Mary Haddad, CHA president and CEO, writes that geography determines health outcomes for millions of rural residents, especially when it comes to maternal care.
‘Everybody deserves the best it can be’ Holy Cross Family Health Center opens in underserved Florida neighborhood
By VALERIE SCHREMP HAHN
The Holy Cross Health medical building in the Oakland Park neighborhood of Fort Lauderdale, Florida, had been underutilized for years. Medical offices occupied only about a third of the space, and the building hadn’t been updated since it was built in the early 1970s.
Meanwhile, a community health needs assessment showed that people wanted more access to health and social services. They had trouble affording and accessing fresh foods. They wanted help with personal finance issues and with finding and keeping a job.
They wanted a place to belong.
In early June, a ribbon cutting ceremony marked the opening of the Holy Cross Family Health Center, a 15,000-squarefoot space on the first floor of the medical building.
The health center is part of Holy Cross Health, a member of Trinity Health.
The center, made possible through $4.9 million in donations, includes 11 exam rooms, a teaching kitchen, a laboratory, a pediatric therapy center, a low-stimulation room for pediatric patients to calm themselves, office space for community health workers, and classroom and meeting spaces. In addition to primary care, wellness checkups and immunizations, patients can get medical nutrition therapy and access to culinary medicine to help them manage and prevent chronic diseases.
Kim Saiswick, Holy Cross vice president for community health and well-being, referred to how the system’s sponsor, the Sisters of Mercy, and their foundress, Catherine McAuley, are often associated with the symbol of a “comfortable cup of tea.”
“And so that’s what we wanted,” she said. “We wanted people to feel when they are here, it’s a comforting environment. We’re here for you.”
And at the ribbon cutting, she noted, the hosts offered visitors tea in porcelain cups.
Serving diverse needs
Saiswick and Kristen Schroeder-Brown, healthy living program manager, joked that even though both are nurses, they became architects to decide what they wanted in the family center and how everything should look. Through the needs assessment, they had a good blueprint. The building is in a “high-priority” ZIP code, which means 40% or more of its population is Black or Hispanic and many people are on Medicaid. Broward County, where Fort Lauderdale is located, has residents from more than 200 countries speaking
Lauderdale,
colorful space for pediatric therapy.
more than 130 languages. About a third of residents reported they are often or sometimes worried about running out of food. They also said they needed job skills training and support groups for things like domestic violence and healthy eating.
“So we thought, in a perfect world, let’s build a one-stop where the whole first floor is everything you would need to get things going, and so that’s what we envisioned, and worked very hard on,” Saiswick said.
In response to gaps identified in the needs assessment, in 2023 Holy Cross opened a smaller clinic in the historically Black Sistrunk neighborhood, about 7 miles away. Many of its patients report they hadn’t seen a primary caregiver in at least 10 years. That clinic’s décor features artwork done by African, Caribbean and Black Americans.
“We feel that the people who are coming in need to feel comfortable in the space that they’re in,” Saiswick said.
They built on that experience to plan for the family clinic.
Creating a welcoming space
Soothing ocean-themed artwork and frosted glass doors in the new clinic lend airiness and privacy. One multifunctional space has different seating options, including rockers, gliders, couches, and high-top tables to accommodate diverse needs and preferences.
A teaching kitchen is adjacent to a conference space, ideal for when one spouse is cooking during a diabetes education class while the other watches.
A pediatric therapy center includes equipment for children to work on motor skills. A tree centered in the room has swings hanging from its branches.
“We really wanted it to be a space that kids wanted to come, where kids were excited to learn, and a place that would also be calming,” Schroeder-Brown said. Par-
ents are thrilled because there is ordinarily a six-month minimum waiting list for pediatric therapy, but the center’s first patients were able to get in right away. “They were so excited and so thankful,” she said.
A low-stimulation room, for children to calm themselves or relax for therapy, includes a custom ceiling with a cloudshaped cutout that can be lit in different colors. Children can play with thin strands of rope lighting or a light-up pegboard or watch bubbles and small toy animals floating in bubble towers.
‘This is the space for me’
Plans include setting up workshops on resume writing, interviewing skills, personal finance, and budgeting. Center organizers also would like to set up more support groups for parents of neurodivergent children, domestic violence survivors, and seniors, specifically for LGBTQ+ seniors and those with HIV. About half of the people living with HIV in Broward County are aged 50 or older, and the center is a few miles from Wilton Manors, a city that is a LGBTQ+ hub.
The building’s additional three floors are being renovated for a variety of specialty medical practices, in a strategic move to bring specialty care closer to the community.
Saiswick and Schroeder-Brown said that at the open house, they took note of the astounded faces of visitors. They have tried to extend the same hospitality to those who have visited since. Too often in other places that serve vulnerable communities, people don’t feel safe or the furnishings aren’t the nicest, Saiswick pointed out.
“Everybody deserves the best it can be,” Saiswick said. “What we hope is that when folks walk in, they can feel: I belong here, and this is the space for me.”
Opinions, quotes and views appearing in Catholic Health World do not necessarily reflect those of CHA and do not represent an endorsement by CHA. Acceptance of advertising for publication does not constitute approval or endorsement by the publication or CHA. All advertising is subject to review before acceptance.
Vice President Communications and Marketing Brian P. Reardon Editor Lisa Eisenhauer leisenhauer@chausa.org 314-253-3437
CHA’s online platform helps ministry facilities assess fidelity to mission
By JULIE MINDA
Since CHA launched the online iteration of its Ministry Identity Assessment about three years ago, most of the largest Catholic health systems have signed on to use the platform. CHA has helped more than 170 health care facilities within those systems to complete the assessments.
Using this assessment, systems and their facilities have been able to evaluate their work — including policies, practices, community partnerships and treatment of patients and staff — to ensure they are adhering to their core commitments as Catholic health care facilities.
The tool has helped them standardize this work, benchmark their efforts alongside other Catholic health facilities, identify what needs improvement, and make and carry out plans to improve.
The core commitments
The seven core commitments that are derived from the “Shared Statement of Identity” are:
Serve as a ministry of the church
Promote and defend human dignity
Promote the common good
Attend to the whole person
Care for poor and vulnerable persons
Act on behalf of justice
Steward resources
Much of the work that is done through the Ministry Identity Assessment is based on adherence to these commitments.
from across the organization are asked to serve on core commitment committees, a wide range of information is being brought to the committee meetings that not everyone may be aware of,” she said.
She added that the assessment process provides opportunities for continuous quality improvement and “a formative experience that celebrates the ministry’s good work and commitment to continuing Jesus’ healing mission.”
Ministry mission leaders say the platform has become a vital tool.
A
In a video CHA created to share the impact of the tool, Rachelle Barina, chief mission officer of Hospital Sisters Health System, said, “The Ministry Identity Assessment really allowed us to do some deep and even transformative reflection on what it really means to live the values of Catholic identity.”
She added, “In addition to that deep reflection … the Ministry Identity Assessment challenged us to think about how can we live these commitments even further?”
A member need
CHA created the Ministry Identity Assessment in response to member demand. During a 2016 “Critical Conversations” gathering, CHA members — including CEOs, sponsors and mission leaders — discussed the need to maintain institutional integrity and ministry identity amid the rapid changes in health care. The group tasked CHA with identifying essential elements for a ministry identity assessment process and coming up with key performance indicators to evaluate how well a facility is maintaining its Catholic identity.
At the time that members made this ask, several large Catholic health systems already had their own internal tools for gauging mission effectiveness, but there were no standardized tools for use across the ministry.
In developing the Ministry Identity Assessment, CHA drew from the best practices of members and the expertise of task forces of ministry leaders. The assessment involves members completing a comprehensive evaluation of how they deliver
IN BRIEF
HSHS hospital’s helipad is part of $90 million renovation project Colleagues and leaders at HSHS St. Mary’s Hospital in Decatur, Illinois, joined in prayer during a blessing ceremony for the hospital’s new helipad on Aug. 15. Led by Fr. Amal Roche and Central Illinois Market Supervisor of Mission Integration and Spiritual Care Karla Marshall, the group laid hands on the pad, asking for protection and healing for all who will arrive and depart by air medical transport.
The new helipad is part of a $90 million infrastructure renovation project that also includes four new surgical suites, updated clinical spaces, improved patient room amenities, a new chapel design and the addition of other advanced technologies and equipment.
Our Lady of the Lake to start $55 million renovation project
This fall, Our Lady of the Lake Health in Baton Rouge, Louisiana, will begin a $55 million renovation of the emergency department at its flagship hospital, the
patient care, carry out their operational work and make decisions. They make their assessments in light of the seven core commitments of Catholic health care facilities as delineated in the ministry’s “Shared Statement of Identity.” The assessments also are based on the Baldrige Health Care Criteria for Performance Excellence.
CHA debuted its paper booklet format of the Ministry Identity Assessment in 2018.
The Baldrige Maturity Framework
CHA has incorporated measures into its Ministry Identity Assessment based on the Baldrige Health Care Criteria for Performance Excellence. The related Baldrige Maturity Framework includes these six focus areas: Planning Alignment Process Training Measurement Impact
New and improved
In recent years, members have asked for enhancements to the tool, especially to have it available digitally.
prepare people for the work, undertake it, check on progress, and meet with external experts to review it before finalization. CHA encourages ministry systems to share widely the report generated through this process, including with sponsors and bishops and to use the report for continual quality improvement. CHA recommends repeating the process every three years.
Dennis Gonzales is CHA’s senior director of mission innovation and integration, and Angela Henderson is CHA’s Ministry Identity Assessment coordinator. They said leaders of systems using the tool say it’s a very effective way to gain a thorough understanding of what is happening at their facilities and how well that work is aligned with the core commitments.
The online tool is sophisticated, allowing analysis of the data and multiple levels of benchmarking. Future plans call for users to be able to easily identify top performers in various categories of the assessment and receive their contact information so they can learn from them.
A significant investment
A Shared Statement of Identity for the
“One of the largest benefits has been the ability to standardize the work throughout the system market by market,” Mark Repenshek said in the CHA video on the assessment. He is Ascension vice president of ethics and church relations.
Shared Statement of Identity for the Catholic Health Ministry
He added that the tool also “has allowed us to … communicate to our sponsor in a way that says we are taking the idea of Catholic identity assessments extremely seriously and giving you the information you need to be able to say we can see that.”
Fr. Joseph Cardone, Bon Secours Mercy Health chief mission officer, said in the video that the Ministry Identity Assessment “helped us to quantify what we do” when it comes to mission.
He added that conversations that occurred throughout the assessment process “helped us see that everything we do is related to our mission and is an embodiment of our mission.”
This is the sixth article in a series on how CHA’s sponsorship and mission services department is reimagining its work.
CHA’s Ministry Identity Assessment is the focus of a podcast posted at www.chausa. org/ministryidentity.
jminda@chausa.org
Who’s using the tool?
A
Among the large health systems using the Ministry Identity Assessment are:
Catholic Health Ministry
After consultation with members and work with task forces of experts, CHA in 2022 launched the online platform and new protocols for completing the assessment. The platform guides users through all stages of what is typically a four- to six-month process. This includes pre-assessment work to educate people, gain leadership buy-in and identify the leaders and committee members responsible for coordinating the assessment. It also includes meetings to
Gonzales said CHA has made a significant investment over the years into this tool and platform because “everything in a Catholic hospital is connected to their Catholic identity.”
Henderson, who supports members who use the platform, said she has been hearing from them that “beyond the quantitative data being assessed, there is also great value in the conversations” that take place throughout the assessment process. “Because a broad range of professionals
The project will expand the emergency department’s capacity,
incorporate advanced technology and improve patient and staff experience. The department is the region’s only Level 1
Ascension
Shared Statement of Identity for the Catholic Health Ministry
Avera Health
Bon Secours Mercy Health
CHRISTUS Health
CommonSpirit Health
Covenant Health
Franciscan Missionaries of Our Lady Health System
Hospital Sisters Health System
Intermountain Health
Providence St. Joseph Health
SSM Health
Trinity Health
trauma center and one of the region’s busiest emergency departments.
The renovation will add 20 new treatment spaces to reduce wait times, and it will enhance patient flow for faster triage and intervention, upgrade diagnostic technology and improve design for greater comfort and privacy. The renovation also will improve way-finding.
The current emergency department will remain open around the clock during the construction.
Our Lady of the Lake President Chuck Spicer said in a release that the construction will “elevate and enhance our physical facility to the level of clinical excellence our team members and physicians provide in the delivery of emergency care every day.”
Our Lady of the Lake is part of Franciscan Missionaries of Our Lady Health System. That parent system’s president and CEO, E. J. Kuiper, said in the release that the emergency department renovation is part of FMOLHS’s broader strategic plan to modernize facilities, expand capabilities and elevate emergency care regionally.
Barina
Gonzales
Henderson
800-bed Our Lady of the Lake Regional Medical Center.
A blessing ceremony for the new helipad brings staff and leaders together at HSHS St. Mary's Hospital in Decatur, Illinois. The helipad is part of an infrastructure renovation project.
SSM, university partnership is expected to graduate 400-plus nurses annually
By JULIE MINDA
SSM Health and Chamberlain University are partnering to address the nationwide nursing shortage through an initiative to recruit and train nursing students from communities within SSM Health’s catchment area.
These students will pursue degrees through Chamberlain University while getting clinical experience at an SSM Health facility. The program includes financial support.
A key concept behind the initiative, called the Aspiring Nurse Program, is to train and educate students close to where they live, and incentivize them to stay within their hometown SSM Health facility after graduation.
Amy Wilson, SSM Health chief nurse executive, says, “We believe we’ll deliver better health care if people who live in our communities are trained in our communities. We believe that having local nurses on staff creates and improves trust with community members. And research says this also improves outcomes and addresses disparities.”
The Aspiring Nurse Program is expected to add more than 400 new nurse graduates annually in the four states where SSM Health operates and beyond. Those states are Oklahoma, Missouri, Illinois and Wisconsin.
Mission alignment
Chamberlain University is a college of nursing and public health based in Chicago. Its flagship campus in Addison, Illinois, is one of 23 campuses in 15 states. The college also has online learning courses. It has over 40,000 students in its bachelor’s and master’s programs. It is part of Adtalem Global Education.
SSM Health was familiar with Chamberlain through an earlier and more traditional relationship in which Chamberlain students receive prelicensure training at SSM Health facilities in the St. Louis area. Chamberlain graduate students also have trained at the health system’s facilities. Also, some of SSM Health’s clinicians went to school at Chamberlain’s campus in St. Louis (the only Chamberlain campus in a city where SSM Health has a presence). When the two started talking about how best to partner to address the nursing shortage crisis, SSM Health already knew of Chamberlain’s quality and success, notes Wilson.
Karen Cox, president of Chamberlain, adds that it is difficult to get into, stay in and complete nursing school. Cox attributes this challenge to what she refers to as the social determinants of learning for deterring prospective students. These are social factors, such as financial constraints, life stressors, transportation and living conditions that stand in the way of success at school.
Cox adds that both organizations have found common ground around mission, vision and values, including the fact that both prioritize increasing access to education.
Hometown nurses
Under the partnership SSM Health and Chamberlain announced July 9, they are putting in place a direct-placement training model that cultivates nursing talent in communities in SSM Health’s catchment area, creating “a sustainable pipeline of practiceready nurses committed to serving their local communities.”
People who live within 50 miles of an SSM Health facility will be eligible for the three-year prelicensure Aspiring Nurse Program. Those who live in a community
without a Chamberlain campus will pursue online courses. The others will have a choice between online and in-person study. All of the program’s participants will complete the hands-on, clinical aspects of their studies at their local SSM Health facility.
Aspiring Nurse participants will have access to student loans. SSM Health will
repay the loans of the nurses who become SSM Health employees until the loan is paid off or until the nurse is no longer an SSM Health employee. Unlike with some reimbursement programs, students will not have to enter into highly restrictive contractual relationships with SSM Health to access this aid.
As they near the end of their bachelor
of nursing studies, the students will have the option for additional coursework and clinical education and training through Chamberlain’s “Practice Ready. Specialty Focused.” program. This program lets students explore high-demand nursing specialties such as emergency, home health, nephrology and perioperative care. This training will be at no extra cost to the students.
Plans call for mission and ethics staffers from SSM Health to serve as visiting professors, teaching Aspiring Nurse participants from a Catholic bioethical perspective and preparing them to work in a faith-based environment that focuses on caring for the whole person – mind, body and spirit.
The program starts this fall, with prospective nurses in SSM Health’s Oklahoma market studying online and will expand over the next year across SSM Health’s markets. SSM Health and Chamberlain plan to involve more SSM Health staff as visiting professors and mentors in the program. Plans also call for Chamberlain to establish new campuses near or on SSM Health campuses.
jminda@chausa.org
2, 2026
Nurse Melody Sessler, left, a clinical educator at SSM Health St. Mary's Hospital in Jefferson City, Missouri, instructs nurse resident Taylor Bullock. SSM Health leaders say the system's new partnership with Chamberlain University will create broader opportunities for nursing students to get hands-on training in SSM Health facilities.
Wilson Cox
Medicaid
From page 1
to fend for myself.”
Now, as vice president of Medicaid managed care organizations and state government programs at Chesterfield, Missouribased Mercy, McPherson worries that looming cuts to Medicaid that are part of the new federal budget bill will mean more Americans won’t get needed health care.
“The unfortunate thing is that the people that are most impacted are the people who are most vulnerable,” she says.
Mercy is among many Catholic health care and social service providers that are bracing for the drop in federal funding and looking to help people who will likely lose benefits figure out how to cope.
Millions expected to lose insurance
The Congressional Budget Office estimates that over the next decade, the One Big Beautiful Bill signed July 4 by President Donald Trump will mean about $1 trillion less in health care funding — much of it for Medicaid and the Children’s Health Insurance Program — and increase the number of people without health insurance by 10 million.
If Congress doesn’t extend the enhanced premium tax credits for low-income people who buy insurance on the federal marketplace, the office estimates 4.2 million more people will lose coverage. Those credits, available since early in the COVID pandemic, are set to expire at the end of the year.
Congress is still working on the appropriations bills that will reflect the tightened budget and regulators are still formulating the policies that will put the changes in place. Nevertheless, the bill is starting to have an impact. For example, in August Providence St. Joseph Health cited the expected cuts in federal funding as one factor in announcing the closure of several programs and the loss of about 60 jobs in Northwest Washington.
Once the Medicaid cuts are fully in place, which is expected to take about 18 months, Trinity Health projects its bottom line will take an annual hit of about $1 billion. On average, Medicaid covers about 20% of Trinity Health’s patients across its 26-state catchment area.
“We estimate about 105,000 of the Medicaid recipients that we serve now will be without coverage,” says Mike Slubowski, the system’s president and CEO.
He points out that besides the Medicaid cuts, Trinity Health is grappling with or
Budget
monitoring other factors that are impacting its budget or could, such as:
A $1 billion annual budget gap due to cost increases from vendors and reimbursement rates from federal, state and commercial payers that are generally below the inflation rate.
A proposal by the Centers for Medicare & Medicaid Services to institute siteneutral reimbursements that would lower rates for procedures performed at hospitals. Pressure by drug companies to end the 340B program that allows hospitals to purchase medication at discounted rates.
“It’s sort of death by a thousand cuts,” Slubowski says.
Repositioning
To deal with the financial pressures and figure out how best to maintain services, Slubowski said Trinity Health is “repositioning the ministry.” The system’s leaders
“
With 80% of our reimbursement coming from Medicare and Medicaid, the magnitude of financial loss means fewer services, longer wait times, staff reductions, and the potential closure of programs and facilities.”
— Mike Slubowski
Other provisions of federal budget bill
Along with tax cuts that will be covered in part by decreasing funding for health care and food assistance programs, the federal budget bill has many other provisions that have drawn less media coverage. Catholic health care and social service providers point out that while they oppose hits to social safety net programs, some of those other provisions are welcome.
Brian Corbin, executive vice president of member services at Catholic Charities USA, and Paulo Pontemayor, senior director of government relations at CHA, cite four: Expansion of the low-income housing credit. The bill doubles the amount that federal agencies can invest in lowincome housing properties to a total of $4 billion per year. Catholic Charities agencies have partnered with other organizations, including Catholic health care
are looking for areas where they can create more access and increase patient volume as well as where they can reduce costs and become more efficient.
“With 80% of our reimbursement coming from Medicare and Medicaid, the magnitude of financial loss means fewer services, longer wait times, staff reductions, and the potential closure of programs and facilities,” Slubowski says. “When people lose coverage, they turn to the ED for basic care. Overwhelmed ERs become even more crowded, delaying care for everyone and straining staff who are already stretched. Our entire health system and every community we serve will feel the effects.”
Trinity Health’s advocacy team is partnering with other care providers and advocacy groups, including CHA, to make its concerns known as regulations are drafted enacting the budget bill’s policy charges.
Assessing downstream effects
Paulo Pontemayor, senior director of government relations at CHA, says the association is focused on “understanding the downstream effects” of the budget bill on CHA members. As the regulations related to the budget bill take shape, he says CHA is using its voice in hopes of keeping the rules from being overly burdensome for care providers and recipients.
Pontemayor points out that Medicaid is a federal-state partnership, so within the federal guidelines, each state or territory adopts its own rules for the program. That means there are about 55 sets of rule revisions underway over the next 18 months and CHA hopes to have a say in them.
“We like to think we have more than a year to do this, but in terms of law and policy, a year is definitely not a long time,” Pontemayor says.
CHA and others see work requirements, one new provision that will go into the regulations, as particularly concerning. States will need to verify every six months that adults without young children who are covered by Medicaid are working or doing community service at least 80 hours per month. CHA is updating and adding to its Medicaid Makes It Possible campaign to offer members more resources. This includes information on how to prepare for and respond to the work requirement, which is expected to mean more paperwork for care providers.
In addition to its members, CHA is working with several groups to influence the revised regulations. They include Catholic Charities USA, the United States Conference of Catholic Bishops and a coalition called The Partnership for Medicaid, which members elected CHA to chair this year and includes clinicians, health care providers, safety net health plans, and counties.
Preparing for more in need
Brian Corbin, executive vice president of member services at Catholic Charities USA, says his organization is bracing for both direct and indirect effects from the federal budget cuts. Catholic Charities agencies that provide behavioral health care and long-term nursing care likely will face funding cuts. Meanwhile, Corbin says people who lose their health insurance and benefits through the Supplemental Nutrition Assistance Program, which is also set to shrink, will turn to Catholic Charities and social service providers for help.
“With these potential cuts in Medicaid and in SNAP logistics, we’re preparing to see a lot more people who are going to need a lot more case management and or immediate help,” he says.
How will Catholic Charities continue its work and perhaps meet an increased need? “We’re hoping that philanthropy will be increased,” Corbin says. “Our people are beginning to appeal already to the hearts and wallets of people to prepare. Hopefully, Catholic Charities agencies can work in closer collaboration with Catholic health systems to prepare together how local communities can respond to persons and families in need.”
‘The time for us to really shine’ As for educating recipients about new requirements for federal assistance, Slubowski says Trinity Health plans to redirect the focus of some of its community health workers to help Medicaid enrollees understand and meet new federal requirements for coverage.
McPherson says Mercy will call on its community health workers in the same way as well as rely on its playbook from the Medicaid redetermination process. That process was mandated by the federal government at the end of the pandemic, to determine which enrollees still qualified for coverage. Mercy created various tools — including a website linked to resources for enrollees and a dashboard that tracked retentions for caregivers — to smooth the redetermination process. In the end, McPherson says, over 78% of Mercy patients who relied on Medicaid were able to prove that they still qualified for the program, compared to a rate of about 69% nationally.
McPherson admits being worried about the changes the budget cuts and related regulations will bring. “Unfortunately, we’re in a dark moment, but it still means that we should rise to the occasion. It doesn’t mean that we stop,” she says. “I think this is an opportunity for us, especially Mercy, that is centered in doing the right thing for people, centered in dignity. For our patients, I believe this is the time for us to really shine.” leisenhauer@chausa.org
systems, to tap the credits for affordable housing projects.
Increased child tax credit. The bill raises the maximum credit for each child under 17 by $200 to $2,200. Also, the credit will be adjusted for inflation each year starting in 2026.
Donations to private schools. A new credit will reimburse taxpayers for donations of up to $1,700 to groups that hand out tuition vouchers to attend private schools. The scholarships funded by those donations must only be available to students whose family household incomes were at or below 300% of the median income level in their area.
Corbin says the credit will help “the Catholic education system to be in communities and neighborhoods that are struggling and gives kids an opportunity to go to private school.”
delayed for
that
McPherson
Slubowski
Sources: Congressional Budget Office, KFF, Urban Institute
Corbin
Pontemayor
Nursing home staffing. The federal staffing mandate for nursing homes was
10 years. While CHA strongly agreed
adequate nurse staffing is essential for the well-being of nursing
home residents, the association was deeply concerned about the final rules imposing a staffing mandate because of the nursing workforce shortage.
A screenshot from a video that is part of CHA's Medicaid Makes It Possible campaign. The campaign provides resources that explain the insurance program’s importance to low-income Americans and the program's expanse, including covering 63% of nursing home residents.
In butterfly releases, HSHS Hospice offers hope at transformative time
By JILL MOON
Grief has parallels to the life cycle of a butterfly, says Valerie Engelbart, explaining in part why Hospital Sisters Health System Hospice has found releases of the delicate creatures to be comforting and popular events.
People in the early stages of grief are in something of a cocoon, like a caterpillar, trying to shield themselves from painful feelings while a loved one is transitioning from life to death, explains Engelbart, volunteer/ bereavement services supervisor for HSHS Home Care, which includes HSHS Hospice. “It’s a dark time,” she notes.
Just as the caterpillar is building up for change, the grief-stricken are building up resilience and preparing for what’s ahead, Engelbart says. And, like the way the caterpillar eventually emerges from the cocoon and transforms into a butterfly, she says
Recognize and Rescue
From page 1
initiative calls for prompt management of events. It includes guidance on standardization of rapid response and on code team process and protocols; escalation and use of the chain of command for resolving concerns; promoting teamwork while assessing and managing patients; and prioritizing frontline worker education through simulations.
Ascension leaders provided tool kits on the initiative to each market, which started their work in January 2022. The initiative ultimately involved more than 2 million patients over the first three years, and the results were published in the February edition of The Joint Commission Journal on Quality and Patient Safety Catholic Health World spoke with Dr. Mohamad Fakih, Ascension chief quality officer, about why the system started the initiative and why it has been successful. His responses have been edited for length and clarity.
What brought this on?
With the COVID pandemic, we witnessed many changes in health care. We had sicker patients, disruptions in the operational and clinical processes, and unprecedented pressure on the workforce. The big element for us was how to support our health care workers, to ensure that we have the optimal treatment for patients, not just COVID, but anyone who’s coming to a hospital. How do we treat them in the best way possible, with no gaps in care, and how can we assure that these patients don’t get exposed to any harm when they are in our facilities?
During the pandemic, the workforce was extremely exhausted. A lot of very seasoned health care workers left and newer people were coming in. We needed to also make sure that they have the best competencies to do their jobs. So that was also part of our focus, to have a standardized approach.
This sounded like the ultimate playbook. Was it a matter of putting it together and then communicating it?
I can buy a cookbook, but it does not mean I’ll become the best chef, right? It’s how we follow that recipe. We created a standardized tool kit that we shared with leaders of each market. We also underscored the importance of including key disciplines, ensuring multidisciplinary collaboration. We involved the clinical arms, both physician and nursing, in addition to
mourners can emerge from grief and learn to cope with their loss and the change in their lives.
“But we must come through the experience to be healed,” she says.
In addition, Engelbart says, the release of butterflies represents “the transformation of the spirit as our loved ones transition from this life.”
Grief support
HSHS Home Care, which serves 37 counties in Illinois, holds annual butterfly releases at all nine HSHS Illinois locations.
Its first release was in 2016 at HSHS St. Anthony’s Memorial Hospital in Effingham.
Over the years, the butterfly releases have evolved from events for the loved ones of hospice patients who have died into memorial services to support and honor anyone in the communities that HSHS serves.
pharmacy and other supporting services. The tool kit had concrete actions for processes and outcomes, how to do things to get to your goal.
We engaged every market. Initially it was monthly, and then after a year, we dropped it to every two months. We were supporting them technically on how to establish processes and adopt best practices, but also pushed for accountability of the leaders. We had additional focus on facilities that had high opportunities, or those that may need more support.
Were people on board and happy to get clear direction? Were there questions or resistance?
People become much less skeptical when they see improvement happen. When they see their numbers improve, then they believe more because they’re seeing it. We had a mix, initially. We had people doubting that it’s going to be effective, but we had others that embraced it.
I remember one of our market teams was very excited to embrace it. They had big opportunities, and they started working on it. What was really nice is that they shared their experience and findings with other markets.
So it wasn’t just the system pushing stuff at you, but also the learnings from each of the markets was shared, either we shared it from the system perspective or directly engaging each other. When you’re in these calls, it’s very collaborative. It has some accountability, but the main focus is pushing learning and how you improve your processes.
You’ve tied this work to Catholic social teaching. How so?
Almost 25 years ago, the Institute of Medicine (now the National Academy of Medicine) recommended addressing quality based on six domains, or STEEEP: Safe, Timely, Effective, Efficient, and Equitable, centered around the Patient. We’ve worked on how to marry the STEEEP framework with some of the principles of Catholic social teaching.
For example, promoting and defending human dignity and attending to the whole person requires us to be person centered. Acting on behalf of justice steers us to provide effective, timely and equitable care. Stewardship of resources translates into efficient care. Finally, advocating and caring for the poor and vulnerable speaks to equitable care. This brings the value of Catholic social teaching in optimizing care for our patients.
I think connecting it with these values is very, very important. I think it resonates with those that are doing the care, too.
Releases generally occur between Mother’s Day and Father’s Day. HSHS Hospice releases about 400 butterflies annually.
Are other systems reaching out to you about this?
We’ve had calls from a few different leaders from other organizations about this. I believe it is a generalizable initiative or product. It has been one of the most successful efforts I have been a part of, and I’m so proud of the work that has been done within our ministry.
What kinds of new problems are you tackling?
I don’t want to call it Recognize and Rescue 2.0, but we are evolving to address other important quality elements postpandemic. We were able to bring in other disciplines. We’ve been doing a lot of work on diagnostic stewardship, which is the right test for the right patient.
Putting a message in flight
When preparing to release the butterflies, the hospice team presents a reading and then encourages participants to think of their loved one, whisper a message of love, and envision the butterflies carrying that message on.
Karla Marshall, HSHS Central Illinois Market supervisor of mission integration and spiritual care, says the butterflies remind people of their loved one and give them an opportunity to touch their loved one, one more time.
She notes that each butterfly responds differently when released. “Some butterflies take off quickly, ready to go out and spread their wings. We might feel joy as we see them flying high and free. Sometimes they linger, which provides us with a longer time to hold them and talk with them,” Marshall says. “Whether our butterfly flies high or lingers around, it is a reminder, our loved one is always there.”
Looking back, what is the general feeling about the work you and others at Ascension have achieved?
I’m so, so proud of all the teams at Ascension from the front line to the managers to directors, leaders at the market level, at the system level, and the passion we have as a system to keep quality and safety in the forefront. That means so much to me. I truly believe if you have the collaboration and the focus and the drive, you can be number one in whatever you want to do.
A lot of the folks did it because they had the drive and the passion to do the work right. This is probably one of the best things I’ve ever been involved in and I’m so proud to be part of that team. I give a lot of credit to those that did the work on the front line. vhahn@chausa.org
Fakih
Crystal Habing, left, and her sister Ronda Flowers release butterflies in memory of Michael Habing, Crystal’s son, at HSHS St. Anthony’s Memorial Hospital in Effingham, Illinois, in May. The hospital is part of Hospital Sisters Health System.
Health care systems join others in urging extension of Medicare telehealth coverage
Ascension, SSM Health, Intermountain Health and Essentia Health are among more than 400 health care systems and organizations that have called on Congress to extend Medicare coverage for telehealth services before it expires on Sept. 30.
The organizations urged a permanent or the longest possible extension and said that a minimum of two years “is needed to ensure stability and provide clarity for patients, providers and the health care system as a whole,” according to a letter sent to congressional leaders Aug. 11.
Medicare has covered most telehealth services for the last five years. The letter pointed out that it is a bipartisan issue, and that “access to telehealth services serve as a lifeline to Medicare beneficiaries around the country,” allowing care even if they have barriers to care for things like weakened immune systems, neurodegenerative disorders, and chronic conditions, which can make in-person visits and travel particularly difficult.
The letter also outlined other benefits of extending this coverage:
Certainty for Medicare enrollees, because patients might otherwise lose access to clinicians and services.
Strengthening the health care workforce, because telehealth enables more clinicians to provide care and address workforce shortages.
Stability for rural health care systems, which allows smaller and rural organizations to plan for and invest in the tools and infrastructure they need to provide virtual care.
“Telehealth has transformed the way we deliver care at Essentia Health. By providing a virtual care option to our patients, we’ve removed barriers and made it easier and more convenient for patients to receive the care they need,” Essentia Health CEO Dr. David Herman said in a statement about the letter. The system provides care in Minnesota, North Dakota and Wisconsin.
Pediatric heart program
From page 1
says Dr. Ravi Ashwath, who is division chief of pediatric cardiology, the Richard S. Wayne, M.D. endowed chair in pediatric cardiology at CHRISTUS Children’s and a pediatrics professor at Baylor College of Medicine.
“Recognizing the critical demand for specialized heart care, CHRISTUS Children’s aimed to create a comprehensive heart center that could serve as a central hub for pediatric cardiovascular services in the region,” Ashwath says.
CHRISTUS Children’s has made much progress toward this goal, he says, and its “strategy not only addresses immediate health needs, but also fosters long-term health and well-being for the community.”
Myriad risk factors
Ashwath says South Texas children — and particularly those in marginalized communities — are at heightened risk of cardiovascular disease because of several factors. Among them:
A high prevalence of obesity and diabetes, which are significant risk factors for heart disease.
Health care access barriers that can lead to delayed diagnosis and treatment.
Socioeconomic factors such as lack of access to healthy foods and safe places to exercise and play.
Cultural and language differences that can lead to misunderstandings of medical information.
Ashwath says CHRISTUS Children’s has been “actively working to address these
Young Adult Center gets start
Archbishop Timothy Dolan of New York leads a blessing Aug. 15 at a grotto on the future site of the Young Adult Center in White Plains, New York, planned by Elizabeth Seton Children’s. In attendance is one of the future residents, Stephanie Gabaud, in wheelchair, who is holding hands with Lisa Alteri, left, a former board member of Elizabeth Seton Children’s, and Patricia Tursi, CEO of the care provider that serves medically complex children. The center, to open in early 2028, will offer essential care for young adults who are no longer eligible for pediatric services but still require intensive medical support.
pediatric services, the hospital also has invested in advanced imaging capabilities and other new technologies that no other provider in South Texas offers. This includes stress cardiac MRIs, 4D flows, fetal cardiac MRI capabilities, cardiac CTs for all ages including newborns, 3D modeling and printing, and virtual and augmented reality for various uses to diagnose and treat complex congenital heart disease. The hospital also offers full-service cardiothoracic surgery with ECMO capabilities that no other local provider offers for kids.
Ashwath notes that, in line with the CHRISTUS Health mission, this advanced care is available to anyone, regardless of ability to pay.
KEEPING UP
PRESIDENTS/CEOS
Matt Brown to president of CommonSpirit Health’s south region, from interim president. That region covers six of the 21 states where CommonSpirit operates: Arkansas, Georgia, Kentucky, Ohio, Tennessee and Texas.
gaps by expanding its cardiovascular services and developing comprehensive programs to serve the less privileged children in the region.”
Cris Daskevich, CEO of CHRISTUS Children’s and senior vice president of pediatric and maternal services for CHRISTUS Health, notes that while cardiovascular services are reimbursed by private and government insurance, the significant, multiyear capital infusion by CHRISTUS Health and the support of philanthropists have accelerated the growth and advancement of the pediatric cardiology program. She notes that CHRISTUS Health and the philanthropic community have similarly invested in CHRISTUS Children’s other five pillars of excellence: the Center for Surgical Innovation, the Maternal and Fetal Care Center, the Center for Neurosciences, the Cancer Center and the Mission and Ministry division.
No others in area
CHRISTUS Health’s San Antonio ministry began in 1869 with a downtown infirmary and has grown to include 10 hospitals and a network of outpatient sites around Central and South Texas. The children’s hospital branched off as a freestanding facility in 2012, and, in 2020, CHRISTUS Children’s implemented a strategic expansion plan to respond to population growth.
The Heart Center at the children’s hospital has grown significantly along the way, and it now offers a wide range of services, including congenital heart surgery, cardiac catheterization, electrophysiology, fetal cardiology, advanced cardiac imaging, cardiac intensive care, cardiovascular genetic testing and exercise stress testing.
Ashwath notes that beyond being the sole or one of the few providers of these
Just as with the other five pillars of CHRISTUS Children’s, the Heart Center offers wraparound assistance, such as services from child life specialists, dieticians, occupational and physical therapists, geneticists, pharmacists, behavioral health providers and social workers.
Ashwath adds that CHRISTUS Health is continually pursuing community outreach, education and policy work to further improve access and promote better health outcomes. He notes that in this way, the Heart Center is aiming to provide holistic care that gets at the core of the problems South Texas children and their families face.
Looming challenges
Despite the progress CHRISTUS Children’s has made in building out its pediatric heart program, there are persistent challenges.
One is a critical shortage of pediatric cardiologists and subspecialists in South Texas that leads to long wait times and care delays for children, especially kids with complex conditions. Also, for many families there are disparities such as lack of insurance, transportation and other basics that interfere with their ability to get pediatric care. Also, there is a gap in prevention and early intervention around obesity and diabetes, conditions closely related to cardiovascular health. There is also a need for better care coordination around pediatric services as well as for more community outreach and education.
Ashwath says CHRISTUS Health is mindful of these needs as it continues to develop its pediatric cardiology program.
“Overcoming these challenges will enable us to provide consistent, high-level care for this fragile and vulnerable population,” Ashwath says. “Ultimately, our goal is to improve health outcomes, set new standards for pediatric cardiovascular care and positively impact the lives of children and their families in South Texas.” jminda@chausa.org
Monte Wilson, who is CEO of CHRISTUS St. Frances Cabrini Hospital in Alexandria, Louisiana, will expand his role. He now is also CEO of CHRISTUS Ochsner Southwestern Louisiana in Lake Charles.
ADMINISTRATIVE CHANGES
Dr. José J. López to chief operating officer of Holy Cross Health in Fort Lauderdale, Florida, part of Trinity Health. He also will remain chief medical officer.
Mary Williams to vice president of marketing and communications for the central region of CommonSpirit Health. That region includes facilities in Nebraska, Iowa, North Dakota, Minnesota, Arizona and Nevada.
GRANTS
Holy Cross Health of Fort Lauderdale, Florida, part of Trinity Health, recently announced receiving two multimillion-dollar gifts:
Philanthropists Charles and Jacqueline Frasier have named Holy Cross in their estate plans, committing nearly $5 million to heart and vascular care. That is one of the single largest planned gifts the facility has received in its 70-year history. Earlier this year, the couple also made a $250,000 multiyear pledge to strengthen heart and vascular care at Holy Cross. Charles Frasier is a retired packaging industry entrepreneur who founded and led companies focused on engineering and logistics.
Jon and Helaine Ayers have given Holy Cross a $2 million gift to benefit its outpatient rehabilitation center. Holy Cross is naming the facility the Jon & Helaine Ayers Rehabilitation Center. Holy Cross is using the gift for state-of-the-art physical rehabilitation equipment. Jon Ayers, the former chairman and CEO of pet health care company IDEXX Laboratories, is a member of the Holy Cross board of directors. In June 2019, he was seriously injured in a bike crash, leaving him a quadriplegic. He said receiving care for his spinal cord injury gave him a great appreciation for physical and occupational therapy.
Brown López Williams
Ashwath
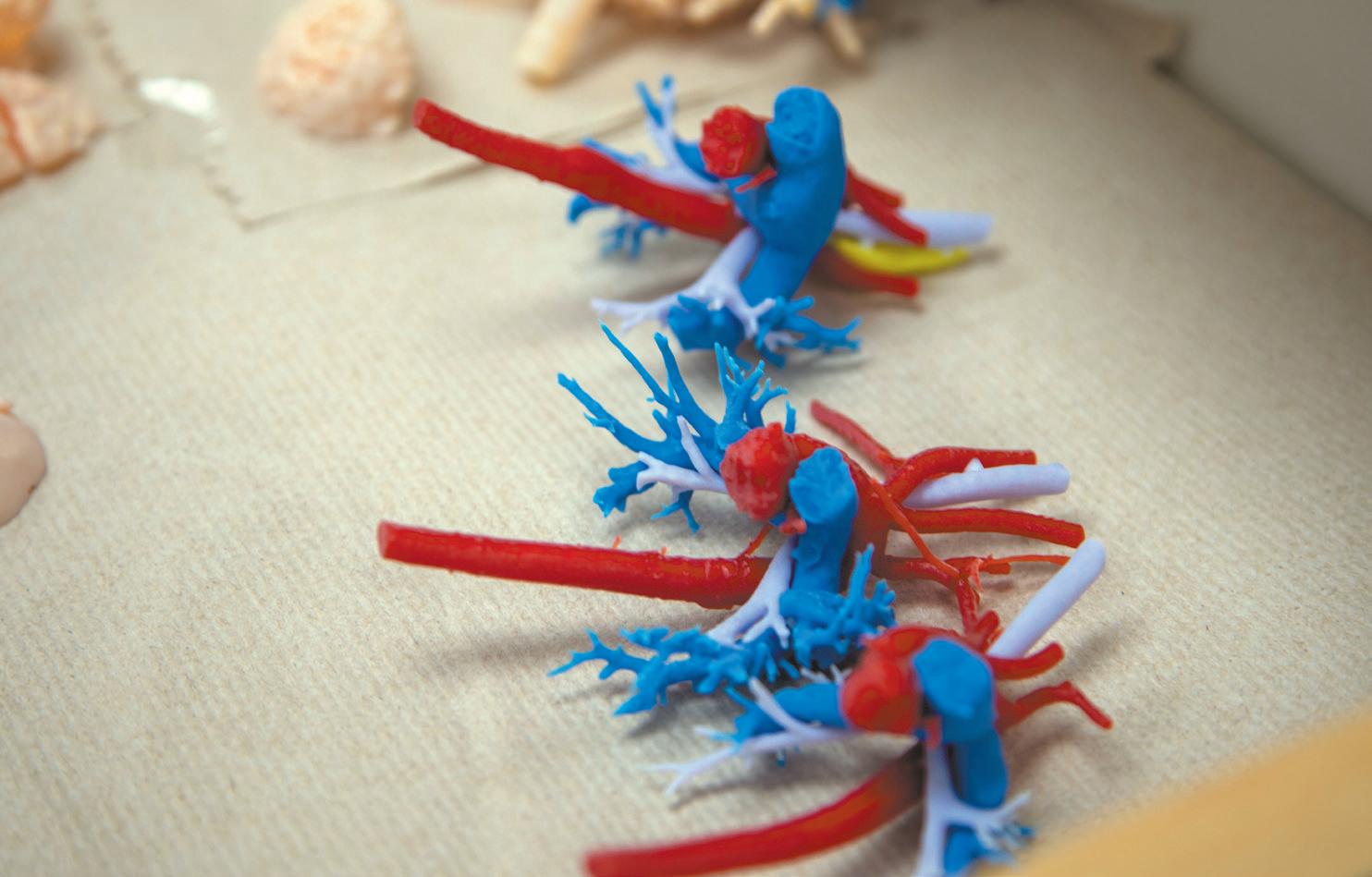
Among the advanced technologies that CHRISTUS Children’s has embraced in its Heart Center is 3D printing. These 3D-printed heart models can be used to plan and practice cardiology procedures.
CommonSpirit’s anti-stigma initiative seeks to teach, train caregivers about substance use disorders
By VALERIE SCHREMP HAHN
Caregivers are trained not to refer to patients as “the gallbladder” or “the heart attack,” so why would they refer to someone with a substance use disorder as a junkie, user or addict?
A group of caregivers with CommonSpirit Health are teaching their peers to use language that helps reduce the stigma surrounding substance use disorders.
The CommonSpirit Anti-Stigma Initiative started last year. About 60 staffers are now certified trainers and more than 300 of their peers have been trained.
The Centers for Disease Control and Prevention says more than one in six Americans above age 12 is living with a substance dependence.
“Our anti-stigma campaign is all about supporting patients that are impacted by substance use disorder, alcohol and drug addiction, and really creating more compassionate care and more awareness
Northwest collaborative
From page 1
Oregon, which is part of Providence St. Joseph Health. He says through the Healthy Columbia Willamette Collaborative, “we build networks and connections with organizations that have relationships that we may not have. We rely on the communitybased organizations and other partners to do lots of outreach and help us gather data, because you need trusted partners to get the data.”
around the fact that addiction is a medical condition that’s treatable and not a moral failing or a personal choice,” said Kathy Krebs-Dean, the system’s director of behavioral health, expansion and development who is leading the anti-stigma effort.
The effort ties with CommonSpirit’s mission to provide care for vulnerable populations and to advance social justice, said Krebs-Dean, evoking the system’s “Hello humankindness” slogan and related campaign.
The initiative uses a curriculum from the nonprofit Addiction Policy Forum called Responding to Addiction. The instruction covers the science of addiction, its signs and symptoms, evidence-based treatment options, medication interventions, and engagement strategies.
The instruction covers research that suggests genetic factors account for about half
of a person’s likelihood of developing a substance use disorder, and that substance use disorders get worse over time.
CommonSpirit also is partnering with the American Hospital Association on its People Matter, Words Matter campaign, which emphasizes that person-first and respectful communication is a powerful way to reduce stigma and increase compassion.
One challenge is responding to the different cultures and attitudes toward substance use and disorders across the country. More than 150,000 caregivers are employed by CommonSpirit across 21 states, and the sheer numbers alone are daunting in terms of training.
In December, the group presented their anti-stigma initiative work at the California Hospital Association Behavioral Health Symposium to over 200 health care professionals from various health systems.
Karen Frank is a nurse and the market
director of quality at CHI Memorial Hospital in Chattanooga, Tennessee. She is also a certified anti-stigma instructor. One patient with substance use disorder presented her with a poem he wrote about her called “The Lady Who Cares.”
The poem read in part: “She shared with me a lot of love and what she knew, which was the road I should take for me to live, what I had to do, and that’s why I’ll always remember and never forget, the most caring person I’ve ever met.”
Frank says instructors learn and convey why caregivers, who bring their own experiences or beliefs to their work, might use stigmatizing language or have stigmatizing feelings. “It’s a delicate balance,” she said. “It’s exciting to share the work and the difference it can make.”
with the group’s needs. If we are not aligned in what we are doing, it can erode trust,” and cause group dissention.
Another challenge to this collaborative approach, says Ichter, is that there are “a lot of cooks in the kitchen” so it can be difficult to arrive at a single report. Most of the participating organizations tailor their own individual reports, using the collaborative’s findings as a foundation, which can help solve for this problem. Providence tailors its local hospitals’ community health needs assessments in this way.
Strong foundation
Phyusin Myint is chief health equity and impact officer of Health Share of Oregon, a coordinated care organization that is part of the collaborative. She says the collaborative is “very visionary.” She adds, “HCWC really is centered in the power of collective impact. We believe that the interestholders coming together in collaboration creates the best outcomes for our community to address health disparities. To be able to support this work feels really impactful and exciting.”
Erin Jolly is a public health strategy supervisor with the Washington County Public Health agency, which also is part of the collaborative. “Our intent is to move towards similar goals and outcomes,” she says.
Advancing health equity
According to the Healthy Columbia Willamette Collaborative website, the group is “dedicated to advancing health equity in the quad-county region” that is made up of Clark County in Washington state and Clackamas, Multnomah and Washington counties in Oregon. Portland is the county seat of Multnomah County. The collaborative bills itself as a “platform for collaboration around health improvement plans and activities that use combined resources to improve the health and well-being of local communities.”
This public-private partnership is made up of a dozen organizations in the quadcounty region, including public health authorities, coordinated care organizations, and health systems and facilities. A coordinated care organization is a health plan designed to serve people insured under Medicaid.
Each of the dozen members is represented on the collaborative’s executive committee as well as on subgroups with specific functions.
With the help of community organiza-
tions, the collaborative produces a regionwide community health needs assessment every three years. One is underway now.
Key to the process are multiple focus groups and listening sessions as well as a community health survey and analysis of data.
Community leaders help both to develop the focus groups and community surveys and to facilitate them. The collaborative uses this vital input from hundreds of community members, leaders and communitybased organizations to learn the region’s needs.
Maria Tafolla, Health Share of Oregon director of community health partnerships, sums up that the community health needs assessment process “is driven by community.” The collaborative does “resonance checks” with community-based organizations and leaders throughout the process to ensure that the assessment accurately reflects the reality on the ground.
Each cycle, the collaborative members or sometimes a consultant uses the findings to write up the community health needs assessment. The members use that assessment as the basis for the reports they submit to the government and make public under federal law every three years. They also use the reports to develop plans to address the identified needs.
Michael Anderson-Nathe has been involved in this process since 2014 in a variety of roles, most recently as a consultant. He says that moving beyond describing needs to also addressing them as a cohesive group will mean that the group will be able to take a more regional approach to issues and have more impact through shared financial responsibility.
Focus on prevention
The collaborative will release its next iteration of the assessment later this year.
Some top priorities the collaborative identified in the 2022 report included mental health and substance use disorders, health-related social needs, economic security, and access to care and services. Members of the collaborative have since implemented their plans to address these needs.
Ichter notes that in addressing needs, Providence facilities ensure they remain aware of the impact of racism, discrimination and inclusion; culturally responsive care and services; and trauma-informed care and services.
Myint adds that there is a long-standing legacy of barriers related to health inequities, and that is reflected in these reports. She says it’s essential for all the organizations that address the needs to get upstream and prioritize prevention.
A family of organizations
Uniting a dozen organizations to create a comprehensive and useful needs assessment has been challenging, those involved acknowledge.
“We’re trying to address everyone’s needs, and like it is in a family, that is not always the easiest thing to do,” Ichter says. “We’re seeing that we need to listen and act to keep all our partners engaged and willing to continue.”
Jolly notes that some challenges arise from the organizations having different partnerships, catchment areas, health needs reporting requirements and timelines, and ways of addressing identified needs.
Myint adds that “it is a challenge to balance our organizations’ individual needs
Despite the challenges, the participants say the collaborative presents them with a great opportunity and there are many successes to point to.
They are saving time and resources by working together, Ichter says. He notes that the shared approach reduces the amount of research that each collaborative member must do and the burden on partner organizations, such as community-based organizations that assist with gathering input from their clients through focus groups and other methods.
And they are building strong relationships that benefit all the participants well beyond their work on the assessments.
Myint says the group members also can coordinate their efforts more easily, with all working from the same page to address community needs.
Jolly agrees, noting that collaborative members have been able to work toward similar goals because they’re responding to a common data set pointing toward the same community concerns. The collaborative members’ pursuit of strategies in their plans are impacting real concerns, such mental health conditions, addictions, housing instability and lack of access to health services.
Jolly notes that several members of the collaborative have been partnering on some of the strategies that they’ve outlined in their community health improvement plans.
But so far, Ichter says, there’s been no unified effort by the collaborative to develop and implement a joint community health improvement plan.
Now that their collaborative is in a mature phase, the organizations are exploring how to build upon this strong foundation to also work together on solutions to the issues raised.
While this effort to partner on solutions is in its infancy, those involved have high hopes.
“We’re putting process improvements in place to continually improve and learn from our prior experiences,” Jolly says She adds, “There’s just a really engaged, passionate, collaborative group right now, and there’s a lot of energy going into really making this as strong as it can be.”
Krebs-Dean Frank
Community leaders from throughout the catchment area of the Healthy Columbia Willamette Collaborative take part in an event hosted by Health Share of Oregon at Portland Community College. The event was to provide input on the collaborative's community health improvement plan. At the table is Rachel Schutz, executive director of the Family Center of Washington County, Oregon, left, and Natasha Davy, a senior program specialist for Multnomah County, Oregon.