Indiana physician at Ascension hospital focuses on spiritual care in retirement
By JULIE MINDA
Faith and medicine long have been central throughlines of Dr. Tony Schapker’s life.
He says from the start of his 40-year medical career, he recognized the critical importance of spirituality to healing. But it is only now, as a volunteer in retirement, that he has been able to invest significant time and energy into learning how best to provide pastoral care to people in his Southern Indiana community.
Throughout his time at what is now Ascension St. Vincent in Evansville, Schapker was intentional not just about advancing his skills as a physician but also about forming himself in his Catholic faith and
Continued on 8
“
As I have witnessed the delivery of spiritual care in different departments in the hospital, I could see that people felt they were receiving better care when their spiritual needs were addressed.”
— Dr. Tony Schapker
Through collaboratives, CHRISTUS Santa Rosa helps ensure unhoused people get health care
By JULIE MINDA
SAN ANTONIO — There are many organizations in San Antonio — the nation’s seventh largest city — that long have been working to address the needs of its homeless population of more than 3,000.
But community and civic leaders grew concerned more than a decade ago that the community organizations’ responses were often disconnected, uncoordinated and sometimes duplicative, so collaboratives have formed to help ensure a more efficient and effective response. CHRISTUS
SSM Health and regional partners work to ease
vulnerable
patients’ access to specialty care
By JULIE MINDA
Representatives of multiple health care facilities serving the safety net population in St. Louis say that working together through the St. Louis Integrated Health Network has helped them to coordinate specialty care effectively. And this in turn has enabled them to address the health care
needs of marginalized people in a patientcentered way.
SSM Health is part of the network.
Dr. Saida Kent, a hospitalist with SSM Health Saint Louis University Hospital, said the network is a great resource for directing her patients to the help they need.
She said that most of her patients are
Avera
Dignity Health clinic staffer honored for helping woman escape sex trafficker
By JULIE MINDA
A Sacramento, California, mom who was being trafficked for sex escaped the abuse due largely to the intervention of a staff member of the Dignity Health Medical Safe Haven clinic, part of CommonSpirit Health. Since then, the woman has helped secure her abuser’s conviction, and she is rebuilding her life with her two small children.
Courtney Martin is deputy district attorney with the Sacramento County District Attorney’s Office, which gave the clinic staffer, Gigi Barrios, an award earlier this year for her actions. Martin credits the trafficker’s conviction to how well Barrios and the Medical Safe Haven, along with law enforcement and the court system, worked together.
That successful collaboration, Martin says, “is reflected in the relationships that Gigi builds with human trafficking victims and with the organizations that help them. The victim knew Gigi and trusted her, and she knew Gigi was safe.”
doctor who has a son with Down syndrome serves families at clinic focused on the disorder
By VALERIE SCHREMP HAHN
Sixteen years ago, Dr. Jennifer Tegethoff didn’t know her son Aaron would be born with Down syndrome. But on the evening of his birth, after a difficult day of grasping the fact that he had the disorder, she went over to the warmer in the nursery to hold his tiny hand.
In her head, she heard what she believed was God’s voice saying: “This is my plan,
girl, not yours.”
“It was a wake-up moment,” Tegethoff recalled. “I remember thinking, this is going to be OK.”
Tegethoff, a pediatrician in Mitchell, South Dakota, is one of the co-founders of the Avera Down Syndrome Clinic, which she runs with another pediatrician, Dr. Christiane Maroun.
The clinic opened in 2014 and operates
Dr. Tony Schapker prepares to enter a patient’s room at Ascension St. Vincent, where he retired from practicing medicine. He remains a volunteer Eucharistic minister at the hospital in Evansville, Indiana.
Rebekah Valdez, left, a clinical outreach coordinator with the San Antonio Homeless Services and Strategy Department, follows up with a client.
of the San Antonio Department of Human Services
Barrios
Sustainability recognition
St. Patrick Hospital in Montana is one of five hospitals across Providence that are among the top 2025 honorees of a national health care organization focused on environmental issues. Staff voices propelled the effort.
Shutdown Q and A
As the government shutdown lingers, concerns grow about the impact on health care. Lucas Swanepoel, CHA's senior director of government relations, discusses the importance of ending the impasse.
Essential source
CHA's 340-page guide for reporting and planning community benefit includes an easier-to-navigate layout and updates on definitions and community benefit categories.
Q and A: CHA’s Darren Henson explores what Pope Leo’s Dilexi Te means for those in Catholic health care
By VALERIE SCHREMP HAHN
Pope Leo XIV’s first apostolic exhortation, Dilexi Te, reaffirms that faith cannot be separated from love of the poor, and he specifically calls out the Catholic health care ministry for continuing to serve them.
“The Christian presence among the sick reveals that salvation is not an abstract idea, but a concrete action,” he wrote in the document released Oct. 9. “In the act of healing a wound, the Church proclaims that the Kingdom of God begins among the most vulnerable.”
Darren Henson, CHA senior director of ministry formation, spoke with Catholic Health World about the lessons for Catholic health care providers in the exhortation and how they can use those teachings to advance human flourishing. His responses have been edited for length and clarity.
What should Catholic health care providers take from this document?
It’s intended to push us. It’s not an encyclical; it’s not a formal teaching that must be adhered to. But he’s urging us, he’s exhorting us, to use this lens of the experience of poverty and suffering to help us see where we might go with our ministry. It’s like an executive leader telling their team: I need you to stay focused on this.
What were your first impressions of the document?
This concept of a preferential option for the poor was popularized and first articulated in the 1970s by Gustavo Gutiérrez, a Dominican priest who was Peruvian. And it was very contentious at the time and received a lot of pushback. Now we have our second pope from South America, Pope Leo, who is American and is also a Peruvian citizen like Gutiérrez. Pope Leo starts his pontificate off saying, “We’re going to highlight this preferential option for the poor.” So I find that lovely.
I find it also really appropriate and fitting that, by all accounts, this was being drafted previously by Pope Francis. I think Pope Leo’s demonstrating his clear continuity with his predecessors. I think he’s signaling he’s squarely in the mainstream of the tradition, with a topic that can sometimes be difficult, especially for those of us in a very affluent society.
There is a very specific section on health care. What are your thoughts on that?
I think there’s room for those of us who do this work — whether it’s in a formation program, whether it’s among folks in mission departments — to look at that section and see, what is it that we would add to it?
I appreciate that he’s saying that this legacy of caring for those who are sick and poor continues today in Catholic hospitals and health care facilities. In the very act of heal-
ing a wound, the church is proclaiming the reign of God amongst those who are poor and vulnerable.
He also rightly reiterated aspects of Catholic social tradition that articulate how the state or the government is responsible for the common good. This is where our efforts in policy and advocacy are important, which is to help our civil servants and leaders of nation states to maintain their focus and their commitments, their responsibilities to the common good. More specifically, he addressed housing and environmental issues as two topical areas that are pressing matters for those who are poor.
He speaks broadly about other matters that apply to Catholic health care. What can we take from that?
Underneath all this, of course, is the bedrock of the Catholic social tradition — the fundamental dignity of all human life — and that this dignity then becomes the basis for human rights, and some of those rights, as the church has taught, are the right to health care, the right to be cared for in old age, the right to be cared for in times of widowhood, and when one is not employed.
He’s reiterating for us this fundamental right to be cared for, especially for those who are poor and most in need of care.
From a mission formation perspective, we bring this aspect of Catholic identity into our formation programs, so that our leaders are deeply immersed in this vision and integrate it into our policies and operations.
Pope Leo is saying we have to be mindful of how we are shaped, or I would say, formed by secular ideologies, and then the need to be also formed by the Gospel specifically. He does an exquisite job of going through a lot of the Gospel text, showing Jesus’s own experience of poverty, which I think is a real gift of this document. But I think it tells us that we have to return to those Gospel stories, in particular the parable of the Last Judgment and the parable of the Good Samaritan.
Poverty is both about and not about money in this document, correct?
It certainly is a critique of the wealthiest of the world, of the growing inequalities in societies and globally. And it could be seen as a critique of the government defunding things like USAID and other programs that have aided some of the poorest of the world with regard to their health, food, water, shelter, safety.
There are different kinds of poverty that we need to be aware of, and he specifically says there “is no longer a single, uniform reality, but now involves multiple forms of economic and social impoverishment, reflecting the spread of inequality even in largely affluent contexts.” He then talks about new forms of poverty that are emerging. Lack of access to electricity used to not be considered a sign of poverty, nor was it a source of hardship, but that very well might be for many people around the world. In our United States context, access to the internet can create new forms of poverty. I think it would be a really rich opportunity in a formation program, where you have some space and time to do some table exercises, to ask: What do we think of when we hear the word poverty?
Leaders and people in power have many things to learn from the poor, as Pope Leo points out.
He reminds us that, and this part of what liberation theologian Gustavo Gutiérrez and his collaborators say, we also have to recognize the uniqueness and the subjectivity of the poor and involve them, allow their voice and their experiences to be part of the creating of something new. He has this beautiful reflection and a reminder that it’s not just what the rich do for the poor, but let’s also reflect upon and take seriously what the poor do for the rich, or what the poor can offer the rich.
The example he uses comes from health care, where he talks about the elderly and our experiences of accompanying our elders. They offer us so much in return. And I think that could even be an inroad in approaching some of this with our clinicians. Really good clinicians, nurses, or a good physician preceptor will help other caregivers see how their patients will teach them a lot.
There are a lot of challenges out there. How do we take these lessons and do something?
I think a lot of our type A, left brain functioning jumps to ideas for solving the experience of poverty.
The exhortation links poverty with suffering, and we are called to enter into one another’s suffering. We journey with one another and bear each other’s burdens, as Jesus did for the least of us.
But that doesn’t mean we shouldn’t work towards greater expressions of God’s justice, peace and love.
Pope Leo XIV issued his first apostolic exhortation, Dilexi Te, on Oct. 9. The phrase means “I have loved you” in Latin. The document focuses on the church’s love and care for the poor.
CommonSpirit peer-to-peer support helps reduce physician burnout
Program encourages doctors, advanced practice providers to ‘share their struggles’
By JILL MOON
CommonSpirit Health is seeing success in responding to the high rate of physician burnout through peer-to-peer support.
Heather Chambers, medical director of advanced practice providers for CHI Health, a CommonSpirit member system, co-chairs the support program that offers doctors and advanced practice providers a safe place for open communications.
“They can share their struggles and peers can acknowledge their experience,” she says.
One of the metrics that CommonSpirit tracks to monitor physician stress is the scores from an annual burnout assessment.
“Based on last year’s score of 9% burnout for physicians and advanced practice providers, we decreased to 5% this year,” Chambers notes.
Chambers says the peer supporters are not counselors or therapists.
“It’s about learning together how to handle a situation and feeling confident discussing it,” she explains.
Chambers is based in Omaha, Nebraska. Her cochair for the peer support program is psychiatrist Dr. Jyostna Ranga.
‘We need this’
A study cited in May by the American Medical Association found that in 2023, 45.2% of physicians reported at least one symptom of burnout. That figure has remained stubbornly high. It was 62.8% in 2021, 43.9% in 2017, 54.4% in 2014 and 45.5% in 2011.
CommonSpirit has about 170 peer sup-
Physician burnout
Rates improved between 2021 and 2023, but U.S. physicians remain at a higher risk for burnout relative to other U.S. workers.
Percentage of physicians who experienced at least one symptom of burnout over the years.
porters for doctors and advanced practice providers across the 24 states where it operates, more than half of them in the Midwest market.
having colleagues to lean on when challenging situations arise is absolutely crucial,” Vivekanandan says.
awareness of the program.
Referrals also help connect staff to the peer support program. “Anyone can refer a physician or APP for peer support if they observe signs of struggle, whether in their professional or personal life,” Chambers says. “The primary goal of this support is not to offer therapy, but to lend a compassionate ear and provide assistance as they navigate their challenges.”
The program also provides additional resources, if needed, based on what the provider shares. “Sometimes it’s more about the issue at hand,” Chambers says. “If they are struggling with something specific that we actually know about, then we try to connect them with someone who maybe has gone through that situation.”
CommonSpirit holds monthly checkins for the doctors’ peer supporters to talk through their experiences. “We don’t want our peer supporters to take on this heavy load and not support them, as well,” Chambers says.
CommonSpirit intranets have links for any staffer to reach out for peer support. Compared to the peer-to-peer support program for doctors and APPs, peer support programs for other roles go “through a different route, but it’s parallel and we work closely together,” Chambers says.
Dr. Renuga Vivekanandan, CHI Health Midwest’s chief medical officer and vice president for medical operations, and Chambers started a conversation with national leaders about provider burnout four years ago, during the COVID pandemic.
Vivekanandan says the urgency of providing assistance to overstressed clinicians didn’t end with the pandemic. “We need this for our providers, not just because of COVID, but what we experience every day,” Vivekanandan says.
She says CommonSpirit became committed to addressing burnout and to creating “an engaged well culture.”
“Given the daily difficulties in medicine,
in the Darkness
A CHA ADVENT RESOURCE
The Catholic Health Association invites you to experience Finding Hope in the Darkness — a beautifully curated daily Advent resource designed to inspire prayer, reflection and connection throughout this sacred season.
Available digitally and as a self-standing coil-bound calendar with an accompanying poster set for display in your ministry.
chausa.org/advent
An example of when peer support can be needed is when a patient dies unexpectedly, when a patient has a poor outcome or during a personal struggle like divorce.
“To have another colleague who they can talk to and debrief in a confidential manner is really helpful,” Vivekanandan says. “This is not counseling or mental health support. This is more of a peer-to-peer confidential support.”
Vivekanandan says peer support “speaks to our culture at CommonSpirit Health and CHI Health of how we value our providers and their well-being.”
Becoming a peer supporter
Peer supporters go through a two- to three-hour training program, typically on Zoom.
The training goes over what it means to be a peer supporter and provides tools to use in talking to colleagues, such as questions to assess their stress level. It also covers how to offer more resources for caregivers in need of help beyond peer support.
The training is based on American Medical Association peer support guidance, as well as programs developed in CommonSpirit’s Tennessee and Arizona markets.
Peer supporters wear badges that identify them. The badges sometimes prompt colleagues to ask what being a peer supporter means, which in turn helps spread
Holy Name’s
Measure of success
The physician peer support program is funded by a community health and well-being grant, which is administered by CommonSpirit’s mission and ministry departments. In December, the program’s three-year grant will lapse. The directors plan to seek funding for an extension.
Chambers says the program’s initial cost included setting up the training protocol, but now mainly is the pay for an administrator. The administrator manages logistics for several different projects related to the peer support program, including arranging meetings, conferences and speakers and developing agendas.
Chambers compares the peer support program to “code kindness rounding” in which compassionate and empathetic practices are subtly incorporated into traditional rounding.
“We try to be sensitive to how others are feeling and truly live our CommonSpirit values, which shows up in our tagline, ‘Hello Humankindness,’” she says. “In our peer support program, the focus is on direct, unconditional support. We don’t gauge burnout or administer assessments. When a peer requires support, a provider proactively reaches out to assist them with their present concerns.”
nursing school in Teaneck, New Jersey, announces $2 million gift from founding sisters
The Sisters of St. Joseph of Peace, the founding congregation of Holy Name’s Sister Claire Tynan School of Nursing in Teaneck, New Jersey, recently announced a $2 million pledge to endow a scholars program at the school.
The congregation announced the donation following a Eucharistic celebration on Oct. 12. The donation will endow the Mother Agatha Browne Spirit of Holy Name Scholar Program, which will help students pursuing degrees as registered nurses and licensed practical nurses.
Mother Browne founded Holy Name Medical Center and nursing school 100 years ago.
“She is remembered as a woman with great zeal, courage, and love for the congregation,” Congregation Leader Sr. Andrea Nenzel said in a press release about the gift.
The endowment will provide four full scholarships annually and each will be named for a member of the Sisters of St. Joseph of Peace who graduated from the
nursing school.
After graduation, the recipients will have the opportunity to transition into staff positions at the medical center.
“The state of New Jersey predicts a shortage of 11,400 nurses by 2030, the third highest in the nation,” Sr. Susan Francois, assistant congregation leader and member of the medical center and foundation board of trustees, said in the release. She explained that the Holy Name program is strong, with 205 students enrolled this fall. She said graduates have high nursing licensure exam pass rates.
“We are extremely grateful to the Congregation of the Sisters of St. Joseph of Peace for their generous and visionary support of our nursing students,” said Holy Name’s President and CEO Michael Maron. “With approximately 80% of these students relying on financial aid, we appreciate that the congregation recognizes the urgent need to assist talented and deserving students to pursue their calling in nursing.”
Source: American Medical Association
Chambers
Ranga
Vivekanandan
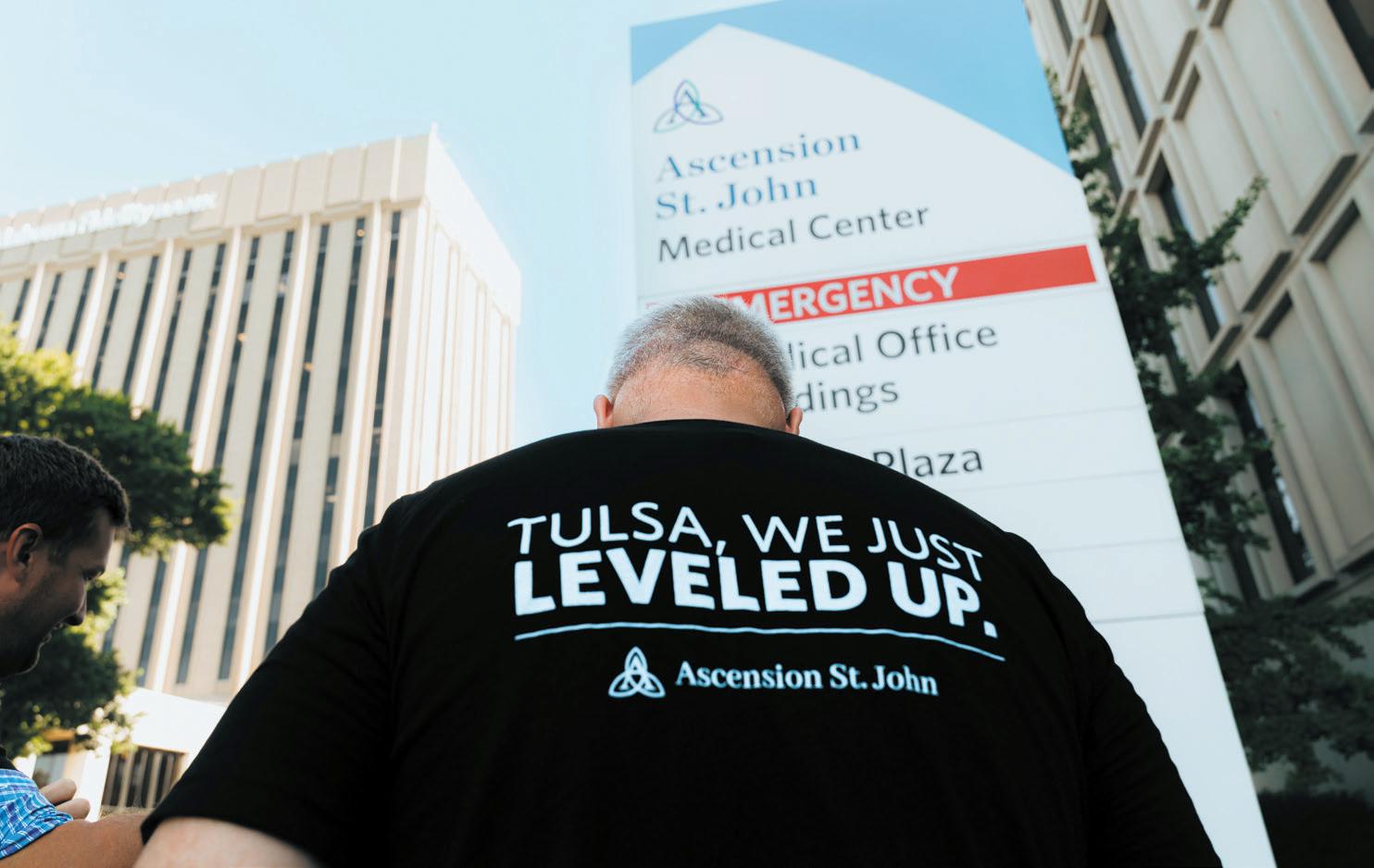
Ascension St. John Medical Center becomes Tulsa’s first Level 1 trauma center
By VALERIE SCHREMP HAHN
It’s “beautiful timing” that as Ascension St. John Medical Center ramps up to celebrate its centennial in 2026 in the growing community of Tulsa, Oklahoma, it is already celebrating its new verification as the city’s first Level 1 trauma center, CEO Bo Beaudry said.
“This status really means that we can take care of anyone with any injury that walks through our doors,” Beaudry said. “With trauma, you think car accidents, gun violence, issues on the oil field, or really any kind of traumatic injury — we can take care of those patients.”
The verification by the American College of Surgeons became official in July. Until then, the closest Level 1 trauma center to Tulsa had been in Oklahoma City.
“You definitely hear more helicopters,” Beaudry said during an interview in early September. “No kidding, I think that we hear one right now.”
Five other Ascension hospitals nationwide have Level 1 trauma care verifications. The American Trauma Society says the verification means a hospital’s trauma center “is capable of providing total care for every aspect of injury — from prevention through rehabilitation.”
Leveling up
Beaudry started at Ascension St. John in fall 2023 as market CEO. Leaders already were talking about what it would take to reach Level 1 status as a trauma center. The hospital had operated at Level 2 since 2009.
The leaders laid out a plan to achieve the next level, making sure the hospital had surgical subspecialists available around the clock to cover emergencies in all areas,
including neurosurgery, orthopedics, cardiothoracic surgery, vascular surgery, hand surgery and obstetrics/gynecology.
The certification also required setting up a more robust research component involving trauma care, which allows doctors to share best practices with the broader medical community.
Tulsa is a growing area, with about 937,000 residents in 2010 and an estimated 1.6 million in 2024. Beaudry said Ascension St. John also gets patients from western Arkansas and southern Kansas. He said that the trauma center status could attract more growth and new business for the city.
“Access to top-tier trauma care is a critical component of a thriving city.”
— Mike Neal
Mercy’s online screening tool flags people with heightened risk of certain genetic conditions
By JULIE MINDA
Chesterfield, Missouri-based Mercy is offering a free online assessment for people to determine their level of risk for genetic mutations, particularly those related to lifethreatening cancers.
Mercy says it is one of the first U.S. health systems to make such an assessment widely and proactively available, according to a press release on the new tool. Mercy partnered with genetic testing company Tempus to offer the assessment, which is available at mercy.net/service/ hereditary-cancer-test/.
Anyone aged 18 and up can take the screening.
The screening tool identifies patients who may have an inherited risk for a mutation and who meet guidelines to be eligible for genetic testing focused on hereditary, or germline, mutations of DNA. The mutations are inherited from a parent and increase the chances of developing hereditary cancers and other health conditions. Breast, ovarian, prostate and pancreatic cancers are some conditions that are associated with genetic risk.
If positive for a mutation, test results can alert patients to a heightened risk of disease, allow for earlier-than-usual detection and treatment of conditions, help inform treatment plans for patients, and enable family members of people with genetic mutations to know if they, too, are at risk.
The germline test can help patients with a detected mutation avoid more taxing treatments and worsened prognoses that can come with delayed diagnosis and help people gain better control of their health, according to Mercy.
Some Mercy markets are texting the assessment link to patients who are sched-
uled for mammograms. This practice will roll out to other communities served by Mercy in the future. Mercy’s catchment area spans parts of Arkansas, Illinois, Kansas, Missouri and Oklahoma.
People who are found to be at heightened risk for a condition based on their responses to the screening will be contacted by a Mercy representative, who will provide counseling prior to scheduling the blood test. That blood testing covers 77 genes.
The germline testing helps clinicians recommend a path for diagnosis or treatment. For instance, if the screening and genetic testing reveal a patient has a high risk of breast cancer, the clinician may recommend earlier-than-planned mammograms, magnetic resonance imaging or testing for family members, and riskreduction measures. The screening and testing information can help clinicians understand what medicines or procedures would be most promising for treatment.
The new screening tool is coordinated through Mercy’s Center for Precision Medicine, a virtual team offering treatment recommendations based on people’s particular genetic characteristics. According to the center’s website, precision medicine examines people’s genes, environment and lifestyle to provide a better understanding of their overall health. The center offers personalized care plans to help ensure patients receive the most appropriate treatment.
The center’s services include early detection tests for more than 50 types of cancer; tests for inherited gene mutations that increase the risk for cancer; pharmacogenomics to predict people’s likely response to medication; testing of tumors for cancerous cells; and genetic testing for senior executive leaders. jminda@chausa.org
“I think it’s great for Tulsa and the broader community. Companies know that if they move here, they have access to Level 1 care for their employees and their families,” he said.
Community milestone
“This achievement is not just a medical milestone, it’s a community milestone,” Mike Neal, president and CEO of the Tulsa Regional Chamber, said in a statement. “Access to top-tier trauma care is a critical component of a thriving city. It strengthens our region’s infrastructure, supports workforce readiness, and gives families and businesses the confidence that Tulsa is a place where their health and well-being are prioritized.”
Beaudry said that working for and maintaining the Level 1 status helps Ascension St. John fulfill its mission as a Catholic health care ministry. “We commit ourselves to serving all persons, with attention to those who are poor and vulnerable. This really is us opening our doors to all people across eastern Oklahoma, and adjacent states, and saying that we can take care of you,” he said.
“Any patient, with any injury, on any day, at any time can receive world-class care right in Tulsa, Oklahoma, at Ascension St. John Medical Center.” vhahn@chausa.org
CHA BOARD OF TRUSTEES — CALL FOR NOMINATIONS
CHA is seeking ministry leaders who are passionate about Catholic health care to serve on its Board of Trustees. As CHA advances its strategic plan focused on the pillars of Care for All, Health Reimagined, and United for Change, we are especially interested in nominees with expertise in:
Church relations
Communications, marketing, and public/media relations
Managed care, health care payment models, and/or population health
CHAUSA.ORG/BOARDNOMINATIONS
NOMINATIONS ARE DUE BY NOV. 21. USE THIS QR CODE TO ACCESS THE NOMINATIONS FORM.
Beaudry
Ascension St. John Medical Center in Tulsa, Oklahoma, recently celebrated its new verification as the city’s first Level 1 trauma center.
California social and health care ministries shine at conference
By VALERIE SCHREMP HAHN
GARDEN GROVE, Calif.— About 275 people from California and beyond recently came here for the Pilgrims of Hope: Serving the Vulnerable conference that celebrated the state’s Catholic social and health care ministries.
The title of the conference reflected Pope Francis’ theme for the Jubilee Year 2025. Organized by Catholic Charities of California, the Alliance of Catholic Health Care, the Knights of Columbus, Mercy Housing, and the Society of St. Vincent de Paul Los Angeles, the conference was a first and highlighted contributions of those and other organizations.
Participants heard from leaders at the forefront of Catholic services, including health care, nutrition security, immigration, housing and disaster relief. The gathering was Oct. 9-10 at the Christ Cathedral campus of the Diocese of Orange.
In his welcoming remarks, Msgr. Gregory Cox, the president of the executive committee of Catholic Charities of California and executive director of Catholic Charities of Los Angeles, pointed out that California, with a population of more than 39 million, has 49 Catholic health care systems and hospitals, which served more than 9.9 million people last year. Catholic Charities of California served more than 1.2 million people in 2023, according to its website.
Msgr. Cox talked about how the giant sequoias in Northern California have roots that go barely below the surface, yet they withstand strong winds. The trees grow only in groves, and their roots intertwine underneath the surface.
“Like the sequoias that grow in groves, Catholic health care and Catholic social services grow in communities of faith,” he said. “Together, our roots of faith and love for the poor and vulnerable are intertwined with each other, so that when the strong winds of lack of resources, legal battles and challenges and despair come, we hold each other up.”
Here are some takeaways from Catholic health care providers at the conference: Erik Wexler, president and CEO of Providence St. Joseph Health, and Julie Sprengel, president and CEO of CommonSpirit Health California Region, interviewed one another during a session on the history, mission and challenges of Catholic health care. Wexler spoke about health care facing a “poly-crisis” of issues, including cutbacks from federal programs, commercial payers reimbursing at low rates and the workforce shortage. But these are also the best of times, Wexler said. “This is when we can truly transform, but we’ve got
to keep ourselves focused in a way that we continue to serve those who are vulnerable,” he said. Sprengel said she was concerned about new work requirements for Medicaid recipients, and the administrative burden that will require. “All of us are going to have to think differently, and I think that’s one important way where we can collectively come together,” she said. “How do we ensure that those who are eligible for coverage are able to make that happen?”
Kenya Beckmann, chief philanthropy and health equity officer of the Providence South Division, pointed out that 90% of new information has been generated in the past few years, and that she, like others, is overwhelmed. “When I think about the value proposition of Catholic health care and why that’s important, and of Catholic social services, is that there’s a permanency about it,” she said. “Those aren’t things of the day. Those are things of eternal, right? Those are things of human dignity. Those are how we work together and how we show up.”
Rachelle Reyes Wenger, system vice president of public policy and advocacy engagement at CommonSpirit Health, encouraged all present to see each other as not just as an arm of Catholic health care, but also as one body that is the healing ministry. “The world needs us so very badly right now,” she said. “Julie and Erik have very
right now, and
our body is so strong when we are doing things together.”
Gabriela Robles is president and chief executive of the St. Joseph Community Partnership Fund, the grant-making foundation of Providence, and chief mission integration officer for the Providence South Division. She spoke about growing up in the 1980s in a large immigrant community in Los Angeles, where the challenges of legal status, poverty and language barriers were similar to those of today. The church was the center of everything, she said. “So while we had challenges, we had assets: We had
faith, we had hope,” she said. The charisms of Providence’s founding sisters have influenced how she handles her dual roles, she said. “It’s about bringing people together. It’s about setting the table and having people come to the table. It’s really identifying challenges in partnership with others.”
Tammy Shaff, director of community health at Dignity Health St. Joseph’s Medical Center in Stockton, California, spoke about a program called the Connected Community Network that helps clinicians easily link patients to resources such as housing and food assistance. The closed loop referral system allows everyone to see if a service provider has followed up with a family or individual. There are nearly 1,000 different programs in the network, she said. “The beauty of the CCN is that it brings the community together, because collaboration is key,” she said.
Jennifer Tanner, system director of real estate growth for CommonSpirit, said the system partners with organizations like Mercy Housing to address the need for affordable and senior housing. Rising construction costs challenge everyone, but she finds hope in the fact that she’s hearing more people outside the health care setting talking about social determinants of health, and that others are learning that having stable housing is the best preventive health care. “There are a lot of minds trying to get creative,” she said. “And I do like when real estate minds get around and start talking about it, so that gives me hope that something’s going to happen.”
vhahn@chausa.org
much told you, in a very nice way, how much we are in peril. You guys are feeling it. It’s real. The pain is so real
Participants at the Pilgrims of Hope: Serving the Vulnerable conference on Oct. 9-10 in Garden Grove, California, attended Mass each day at the Christ Cathedral of the Diocese of Orange.
Julie Sprengel, president and CEO of CommonSpirit Health California Region, and Erik Wexler, president and CEO of Providence St. Joseph Health, showed a video and interviewed one another during a session on the history, mission and challenges of Catholic health care.
The conference took place on the Christ Cathedral campus of the Diocese of Orange.
Valerie Schremp Hahn/@CHA
Event
Image
Services
‘Faith is at the heart of what we do’
While health care got a spotlight at the conference, many social service leaders spoke about their ministries that address homelessness, nutrition security, immigration, housing and disaster services. Scan to read more:
Homeless outreach
From page 1
Santa Rosa Health System of San Antonio has been a key player in these collaboratives, says Esmeralda “Mela” Perez, community health director of CHRISTUS Santa Rosa, a four-hospital subsystem of CHRISTUS Health.
Perez says two of the most effective efforts to streamline and improve community response to homelessness have been San Antonio’s Homeless Outreach effort and the Southwest Texas Regional Advisory Council’s homelessness services mapping approach. As part of a broader effort, that advisory council convenes the county’s health care facilities and law enforcement agencies to ensure it is clear where police should take people with behavioral health needs, including people who are homeless.
“We had been seeing that there was a population of people who were homeless, and in some cases undocumented, who were not getting the access they needed to services,” Perez says. “So we have been collaborating with other community organizations. We want to address the social determinants of health.”
Homeless Outreach
Members of the city of San Antonio’s Homeless Outreach team locate and engage daily with people who are experiencing homelessness. The team is part of the Homeless Services and Strategy Department that the city launched in October. The Homeless Outreach team members establish trust with the individuals, get to know them, collect their biographical information if shared, learn their social and health needs, and work to connect them with services.
The team members are trained to approach their work in a person-centered, trauma-informed and culturally responsive way.
The outreach team uses a mapping process to document where people who are experiencing homelessness live, where they are at any given time and what they need.
The city outreach team connects the people who have health needs with CHRISTUS Santa Rosa and other health care providers in the collaborative. CHRISTUS Santa Rosa’s clinical team members assess these patients and provide treatment. Additionally, CHRISTUS Santa Rosa refers patients who are experiencing homelessness but who are not yet connected with the city’s homeless response system. CHRISTUS Santa Rosa’s community health program remains in touch with patients who are experiencing homelessness after their discharge, to help them navigate the social service system to obtain shelter, prescriptions, follow-up care and other services.
Checking on coverage
CHRISTUS Santa Rosa partners with the company Elevate Patient Financial Solutions to meet with patients who are uninsured, including those referred by the Homeless Outreach team, to provide free financial information and advocacy. Elevate identifies what financial assistance may be available to these patients to cover medical bills. If patients qualify as disabled or for Medicare or Medicaid, Elevate representatives help them access that coverage.
Additionally, CHRISTUS Santa Rosa has trained staff who work with these vulnerable patients on how to ask about social determinants of health. This way, the clinical team can fully understand these patients’ situations and help connect them to social service providers, if the Homeless Outreach team has not already helped the patients address those needs.
Perez says working together, the Homeless Outreach team, CHRISTUS Santa Rosa and other San Antonio health and social
service providers have helped many people, including with housing, transportation, food and immigration services.
Regional Advisory Council
The Southwest Texas Regional Advisory Council is a nonprofit agency founded in 1998 to convene Bexar County health care providers and other organizations to ensure it is clear where frontline responders and law enforcement officers should take individuals who are in a medical trauma or emergency. This ensures a more efficient use of local resources and that people get the right care at the right location. In 2016 the council convened providers to determine the care paths for individuals in behavioral health crisis, including homeless people. CHRISTUS Santa Rosa is among the Bexar County medical providers that annually fund the network that was created to ensure individuals get to the right place to get the right care.
Perez explains that law enforcement and other frontline responders and health care facility representatives came together through the council’s efforts after seeing that police officers frequently brought homeless individuals who were in behavioral health crisis to emergency rooms for treatment, when they did not have an acute medical need. It took much time and effort to get the individuals to the appropriate site of care. And there was no consistency of care. Some people were just circulating through these facilities with no lasting resolution of their behavioral health and other needs, and little or no communication among the organizations.
The council, which goes by the acronym STRAC, linked health and social service providers serving this vulnerable population into a network called the Southwest Texas Crisis Collaborative. All organizations in the network have access to a central electronic record system. This way, they all can document their interactions with each individual who comes to them through this system and keep a record of the health care and social services those patients receive.
Continuity of care
The approach promotes continuity of care. Providers avoid duplicating services and they are aware of past services received.
The Homeless Outreach team members establish trust with the individuals, get to know them, collect their biographical information if shared, learn their social and health needs, and work to connect them with services.
Perez says working through this interconnected network, CHRISTUS Santa Rosa clinicians can avoid overprescribing medicine that other health care providers dispensed to patients. The network also flags concerning trends, she adds. For instance, health care providers learned that an unscrupulous insurance provider was selling very high-premium, high-deductible plans to vulnerable populations. The plans failed to cover the health conditions of the patients. Having this knowledge enabled the members of the network to intervene.
According to the STRAC website, the system has been used to help law enforcement better understand where they should take people who are unhoused and have acute psychiatric needs.
Perez says that the San Antonio Home-
less Outreach program and STRAC are examples that illustrate how vital it is for all the organizations working together in a community to be closely connected and in continual communication. She says being linked so closely has resulted in homeless individuals getting more seamless access to services.
She adds that since the responding organizations have limited resources, it has made sense to work together to figure out the best way, as a collaborative, to meet the needs of vulnerable populations.
She says it is all linked to a goal that is right in line with CHRISTUS’ mission to extend the healing ministry of Jesus Christ. She says: “We want people to have a better quality of life.”
jminda@chausa.org
AI Ethics in Catholic Health
sponsored
MARCH 20-21, 2026, AT BOSTON COLLEGE
The “Artificial Intelligence, Authentic Mercy: Navigating AI Ethics in Catholic Health” conference will bring together physicians, nurses, health care administrators, biomedical engineers, technologists, theologians and ethicists to explore the opportunities and challenges presented by AI in Catholic health care settings.
Perez
Stephanie Bracely, left, a homeless outreach specialist, and Rebekah Valdez, a clinical outreach coordinator, talk with a veteran experiencing homelessness. Both are with the San Antonio Homeless Services and Strategy Department.
Photo courtesy of the San Antonio Department of Human Services
In St. Louis, SSM Health partners with other providers to assess and address barriers
By JULIE MINDA
Uninsured and underinsured people face significant barriers to accessing specialty care. In St. Louis, specialty care access has improved for many people since Missouri expanded Medicaid in 2021. Yet, many patients still fall through the cracks.
SSM Health, which has eight hospitals and a network of outpatient facilities in the St. Louis area, is part of the St. Louis Integrated Health Network, a regional collaborative of safety net providers. The providers work together to better understand the health care needs — including specialty care needs — of marginalized St. Louisans and the barriers they face to accessing that care. The network also coordinates care for these patients.
Members of the network agree that the specialty care access challenges that marginalized people face are complex, multilayered and intractable. They say it’s essential for the partners in the network to be intentional and dogged in ensuring they provide extensive support.
“There is not always a clear path for everyone to be able to access specialty care,” said Karen Bradshaw, regional director of community health for SSM Health — St. Louis and Southern Illinois. She said in large part the issues are related to the “complexity of the health care system in the U.S. It’s hard to navigate that complexity.”
But, nonetheless, it’s essential to help patients with that navigation, said Aramide Ayorinde, because “for the whole system to
Specialty care
From page 1
uninsured or underinsured, and it’s usual for her to talk extensively with them about the barriers they face to care and to point them to solutions.
“It’s our role as physicians that — even though we can’t solve all the issues — we need to acknowledge the issues patients have,” Kent said. “I need to view my patients as a whole — not just as a body. It’s important to know your patient and to, at a bare minimum, see the person in front of you.”
Need for care coordination
The Integrated Health Network is the result of efforts by the St. Louis Regional Health Commission to better coordinate the care of vulnerable patients. The commission wanted the providers to collaborate to improve care access, enhance care quality, achieve cost efficiencies, and improve patient outcomes.
In November 2003, the commission launched the Integrated Health Network. The network has evolved over the years and now includes four federally qualified health centers, three hospital systems, two medical schools and two public health departments.
One of the Integrated Health Network’s programs is the Care Transitions Initiative, which in turn has its own program called the Community Referral Coordinator Program. Through that initiative, 12 community referral coordinators work on-site at hospitals and two work in the community.
The hospital-based coordinators meet with acute care patients to help them navigate their movement between inpatient units, the emergency department and outpatient providers.
The coordinators focus on patient education and preventive care. They help patients find a primary care home, schedule appointments, and set up transportation and connections to social services.
work, we need both primary care and specialty care.” Ayorinde is CEO of the Family Care Health Centers, a system of federally qualified health centers that is part of the Integrated Health Network.
Expansion eases access
According to the Centers for Medicare & Medicaid Services, specialties are areas of medicine or groups of patients with specific symptoms and conditions. Some examples are oncology, cardiology, orthopedics, obstetrics, endocrinology, gastroenterology, and neurology, among numerous others. Bradshaw noted that she considers behavioral medicine to be a specialty.
The “Access to Care Data Book” from the St. Louis Regional Health Commission says in 2020 about 262,000 people from a population of about 1.3 million in St. Louis and St. Louis County were in the safety net population. This included uninsured and underinsured St. Louisans.
For more than a dozen years, Bradshaw has worked in various capacities addressing the health care needs of this population. She said, as has been common nationwide, it long has been extremely difficult for people in St. Louis’ safety net population to access specialty care. That is in part because there has been a perpetual shortage of providers in many specialties.
Since Missouri expanded Medicaid eligibility four years ago, Bradshaw said, more people have a reimbursement source for specialty care, which has improved their access. But, she said, even those insured under Medicaid still face barriers; and people with no insurance — including undocumented immigrants — face formidable
challenges to specialty care access.
Prohibitive costs
Getting and keeping Medicaid is an ongoing challenge. Bradshaw said many people do not know they are eligible to receive Medicaid, and so they go without insurance when they don’t have to. For those who are enrolled in Medicaid, if their income rises, they can lose coverage. Meanwhile, federal funding cuts are targeting the Medicaid program, so access could be further threatened.
Dr. Melissa Tepe is vice president and chief medical officer of Affinia Healthcare, a St. Louis FQHC that is part of the Integrated Health Network. “There can be high deductibles and high co-pays, and that can lead to patients struggling with financial challenges,” she said. “The challenges can be overwhelming for patients.”
Fear of these costs can cause patients to delay getting specialty care. Tepe said the delay can cause people to be less engaged with the system, which can mean that health conditions can fester dangerously.
Moreover, it can be difficult for uninsured and underinsured people to find specialists who are taking new patients, and especially those without insurance.
‘Fog of poverty’
Dwayne Butler, who is CEO of the Betty Jean Kerr People’s Health Centers FQHC, said another category of challenges relates to “the socioeconomic issues of patients, which are most prominent when they are
The Integrated Health Network’s website says the coordinators have had more than 220,000 patient encounters in the hospitals and community since 2007.
The Integrated Health Network also offers programs to educate patients on the levels of care available to them, including primary care, urgent care, living well, specialty care and emergency care.
‘A team sport’
A main reason the network is successful is that the safety net providers take a systems approach to improving care delivery, making sure that they function as a whole rather than as separate facilities, explained Aramide Ayorinde, CEO of the Family Care Health Centers, a federally qualified health center that is part of the network.
Karen Bradshaw, regional director of community health for SSM Health — St. Louis and Southern Illinois, said the organizations in the network all are represented on a board of directors and a task force. Between these groups, the network members meet regularly to talk about how to improve the way patients move through the system.
The network members connect through
dealing with the fog of poverty.”
He explained that for impoverished people, “it is difficult to predict what tomorrow will bring. Their lives are unstable.” They are dealing with issues connected with so many social determinants of health that they are unable to prioritize seeking care.
Dr. Saida Kent is a hospitalist at SSM Health Saint Louis University Hospital. Most of the patients she sees are uninsured or underinsured. She said they face an almost inexhaustible list of social determinants that can interfere with their ability to seek specialty care and to comply with the medical guidance and self-care instructions of specialists. For instance, if people have no reliable transportation, they can struggle to get to appointments. If they are food insecure, they may not be able to comply with healthy eating instructions. If they don’t have walkable sidewalks, they may not be able to follow clinicians’ advice to exercise. “It can be emotionally draining for patients,” Kent said.
Tepe pointed out that the working poor may not have a job that allows for paid time off to go to medical appointments.
Butler said that the safety net population already has worse health indicators than the privately insured population. So, they are more vulnerable to the impacts of missing out on specialty care. “They are much sicker” than the broader population, he said.
He added that “it is hard to get a lot of the people in the safety net population into primary care, and even more difficult to get them in specialty care. But it is really important that we do get them into that specialty care.”
patients can move more smoothly through the St. Louis safety net system, as a physician with SSM Health Saint Louis University Hospital, she has access to other resources and approaches to ensure patients’ needs are addressed holistically, including when they get specialty care.
First, she said, is that SSM Health Saint Louis University Hospital prioritizes daily face-to-face huddles by the teams treating specialty care patients. In these multidisciplinary huddles, clinicians and other staff flag and address issues patients are facing.
electronic health records, jointly develop community health needs assessments, partner on programming, and share resources including grant dollars in some cases.
“Health care is a team sport,” said Dr. Melissa Tepe, vice president and chief medical officer of Affinia Healthcare, a St. Louis FQHC that is part of the network.
Dwayne Butler, CEO of the Betty Jean Kerr People’s Health Centers FQHC, said the coordination happening through the network can have a profound impact on patient health outcomes as well as on the metrics on quality care.
For example, he said that care coordination can lead to patients keeping their primary care follow-up appointments after specialty care. Keeping such appointments and adhering to post-care instructions can help people recover better and quicker. And it can lead to lower hospital readmission rates.
Patient empowerment
Kent said in addition to relying upon the Integrated Health Network to ensure
Second, Kent said, is a transitional care clinic, also known as a BRIDGE clinic, which has a staff that meets with patients after their discharge from inpatient care to ensure their needs are met. BRIDGE stands for Bridging Recovery, Informing Decisions and Guiding Empowerment. This navigation includes making sure patients who have transportation needs receive help with that and that patients are set up for followup appointments and have all the prescriptions they need and understand how to take them, understand posttreatment care instructions and are equipped to follow them, and that any socioeconomic barriers to recovery are addressed. Kent said this transitional care clinic has been essential to helping patients with the many concerns that can stand in the way of successful specialty care treatment and recovery.
The last key element she mentioned is patient education, which she said should be woven into the entire approach. She said providers must take the time to confirm patients fully understand the path they are on with specialty care. Verifying patient understanding can make a life-or-death difference in their outcomes, she said.
Coordinating care and taking the time to get to know patients and comprehend their struggles and help them address those concerns are key to effective specialty care delivery, Kent said. “When you take care of them in this way, they still have barriers, but you’ve given them ways to get help. They can feel empowered. As a provider, I’m saying that I can’t remove all your barriers, but I can help empower you.” jminda@chausa.org
Patients visit a pharmacy connected with the Betty Jean Kerr People’s Health Centers in the St. Louis area.
That federally qualified health center is among the eastern Missouri health facilities and related organizations that make up the Integrated Health Network.
Kent
Butler
Bradshaw
Tepe
Down syndrome clinic
From page 1
about once every two months out of the Avera McKennan Hospital & University Health Center campus in Sioux Falls, South Dakota. At the clinic, families and their children with the genetic disorder can see a general pediatrician and several other experts, including pediatric subspecialists and speech, occupational and physical therapists.
About one in every 775 babies in the United States — or about 5,000 a year — is born with Down syndrome, according to the Centers for Disease Control and Prevention. It is the most common chromosomal condition diagnosed in the country.
The disorder can cause developmental and physical challenges, such as speech delays, congenital heart defects, hearing loss, obstructive sleep apnea, poor muscle tone, and loose joints, according to the CDC. Many people with Down syndrome develop thyroid issues.
always just keep her like our safe place (during) the whole situation,” Bellefeuille said.
After Havyn spent some time in the Sioux Falls hospital’s neonatal intensive care unit, the Bellefeuilles learned about the Avera Down Syndrome Clinic. It would become a safe place for the young family.
They have traveled there about four times since Havyn, now 2, was born. The family lives in Aberdeen, about 200 miles from Sioux Falls.
MiKayla Bellefeuille feels confident that the doctors and specialists work and communicate with one another and are familiar with patients with Down syndrome. Havyn has had surgeries for a cleft palate and has cervical instability issues. She sees Avera specialists for monitoring and treatment.
Bellefeuille also feels reassured when she talks with Tegethoff, and knows that her spunky, sassy toddler will someday be a teenager like Aaron. She and her husband also have a baby boy, who is neurotypical.
There are evaluations that children with Down syndrome should have at certain ages, said Tegethoff. She said her job at the Down syndrome clinic “is to make sure that all those appropriate evaluations are getting done, and to incorporate (patients’) subspecialties as much as we can into all one visit.”
Stewarding, sharing resources
Tegethoff remembers taking Aaron to 32 medical appointments in the first three months of his life. Navigating the system and arranging the trips, often a 75-mile drive from Mitchell to Sioux Falls, was at times overwhelming.
“I think that helping to combine services and helping to provide everything all in one place really is being a good steward of our services,” Tegethoff said.
Spiritual care
From page 1
looking for ways to bring that faith to his work. Ordained a deacon in 2009, he long has been an active member of the Eucharistic ministry volunteer corps at the hospital and of his church’s visitation program for sick parishioners. Around the time of his 2022 retirement, when a member of the pastoral care department of Ascension St. Vincent suggested Schapker pursue clinical pastoral education, he was intrigued, though not quite ready to act.
The seed of the idea took root, and late last year, Schapker enrolled in the Ascension St. Vincent Hospital Clinical Pastoral Education program. Since then, he has taken CPE classes there and elsewhere to deepen his knowledge of how to provide spiritual support to patients.
He says this new era of his life reconfirms for him how essential it is for ministry clinicians to embrace holistic care. “The emphasis is that healing takes place not just in the body, but in the mind, body and soul,” he says. “As I have witnessed the delivery of spiritual care in different departments in the hospital, I could see that people felt they were receiving better care when their spiritual needs were addressed.”
Inspired by the Daughters
After medical school, Schapker served in private practice before accepting a position at what was then St. Mary’s Medical Center in his hometown of Evansville.
He was hired to work with St. Mary’s family medicine residency program and concurrently supervised a pediatric clinic for indigent children. He transitioned into
Tegethoff and Maroun stay up to date on research and recommendations for patients with Down syndrome and inform parents and other caregivers.
The clinic sees about 30 patients a year, or about five every other month. It has seen more in the past and has hosted the clinic monthly to meet the need. Families come from South Dakota, Iowa, Minnesota and Nebraska.
Because she has a child with Down syn-
“ I hope that the advice that I’m giving is helping parents see the positive and helping them navigate the journey. Even if I didn’t have that problem, I often know where to look for those resources.”
— Dr. Jennifer Tegethoff
private practice in Evansville in the early 2000s before his medical group joined St. Mary’s as a managed practice. He finished his medical career at that Ascension hospital. Founded by the Daughters of Charity, St. Mary’s was part of the Daughters of Charity National Health System, which merged with another system in 1999 to form Ascension Health, the predecessor of Ascension. In 2017, St. Mary’s was renamed Ascension St. Vincent; it is part of the St. Vincent Health subsystem of Ascension.
Schapker says that from the time he started at St. Mary’s, he valued the presence of the Daughters of Charity at the hospital, as well as the colleagues in the pastoral care department. “I worked alongside some of the Daughters — they had a presence at St. Mary’s,” he says. “They showed how spirituality was important, and gradually I added it more to what I was doing. My main emphasis was patients’ physical health, but the Daughters showed me how to utilize spiritual health, too.”
Taking action
During much of Schapker’s early tenure at the hospital, Sr. Catherine Kelly, a Daughter of Charity, headed the spiritual care department. Due in large part to her encouragement, Schapker found many ways to act on his faith to improve patients’ health in a holistic way. He became a volunteer in the hospital’s Eucharistic ministry, a role he continues to this day. He came to better understand the social determinants of health, and that drove him to go on more than a dozen medical missions to provide care in Jamaica, as well as to volunteer at a mobile health clinic in Evansville.
He also took on some transformative roles that drew upon his medical expertise
drome, Tegethoff is able to reassure families and give them advice, such as how to navigate the individualized education program process at school or search for other treatment options, such as additional therapy services and resources.
“I hope that the advice that I’m giving is helping parents see the positive and helping them navigate the journey,” she said. “Even if I didn’t have that problem, I often know where to look for those resources.”
A safe place
MiKayla and Alex Bellefeuille found out their baby girl had Down syndrome when MiKayla was pregnant.
“We kind of felt like the world was over,” MiKayla Bellefeuille said. “I know that sounds so terrible. But we were 27, and all of our friends were having healthy babies, and we’re like, why don’t we get that?”
While they were absorbing the news, they picked out a name for their daughter — Havyn, pronounced the same as the word for a safe place.
“We were able to talk about her, and we kept the name to ourselves, and we could
but also enabled him to advocate for and help vulnerable people. This included volunteering to staff outreach clinics at affordable housing complexes, assisting with lead screenings, and helping conduct evaluations of abused children to help them get the care they needed.
He also joined the Catholic Medical Association, a professional organization for physicians. He helped establish a CMA guild in Evansville that remains active today. He drew upon CMA resources to host seminars and reading groups around hot ethical topics, such as natural family planning and brain death. He served on his hospital’s ethics committee.
“My Catholic faith has informed and influenced me in what I’ve done in medicine. I knew it was important. Because of my upbringing and education, I knew holistic care was important. I knew there was more to medicine than the physical health of a person.”
He adds, “There’s so much more enjoyment (for clinicians) when we become involved in different aspects of patients’ lives beyond just the medical.”
New vocation
Schapker’s wife of 40 years died of pancreatic cancer in 2020. Retirement has opened up more time to visit his three children and five grandchildren, who all live out of state, as well as to indulge his joy of gardening, reading and hiking. In 2023, he and a group of friends spent more than a month trekking the Camino de Santiago, a 500-mile hike across northern Spain.
Since late last year, Schapker, 70, has been building up his pastoral care capabilities through the CPE courses and other educational programs. He says he has been
Bellefeuille wishes she could offer her younger self encouragement. “It’s going to be a better place when you actually get to see her and smile and snuggle her,” she said she would say. “Really, the world was nowhere near ending for us.”
More typical than different
Tegethoff tells parents what she wished she would have known during those first days after delivering Aaron: Yes, this is going to be hard at times, but life is going to be a lot more typical than you think it is.
Aaron goes to high school and is involved in sports and activities. He’s one of six children, and the family’s time is spent navigating typical kid activities instead of medical and therapy appointments. And that is also normal: As many children with Down syndrome age, they need less monitoring for medical and developmental issues.
“I hope the main things that I’m honestly doing are saving families time and resources, helping people see the beauty of this situation, and giving parents places and people to turn to when they have struggles,” Tegethoff said.
vhahn@chausa.org
learning how to better listen to patients and their loved ones to understand their spiritual needs and what resources could help. In addition to those courses, he’s enrolled in learning opportunities from the Formation and Education for the Life of the Church program from Saint Meinrad Seminary and School of Theology in St. Meinrad, Indiana.
“I’m learning to listen to people in a different way than when I was a physician listening to patients,” he says.
He is considering applying to join the pastoral care staff on an as needed basis.
No ‘separate boxes’
Schapker says that when he visits patients in his volunteer roles, he sometimes is invited to huddle with care teams. He says that if it’s appropriate, he makes a point of raising people’s emotional and spiritual struggles with the medical team. For instance, he once informed a patient’s team that the person feared being homeless upon discharge, and that was causing stress that could impact their physical health.
He notes that many clinicians he sees at the hospital in his spiritual care volunteer role approach him to ask about this new era of his life.
He is eager to share how clear it’s always been to him that spiritual and physical health are intertwined. He encourages them to explore their own faith and bring it to bear on their work. He says compartmentalizing different aspects of life can contribute to burnout among health care workers.
He says, for him, “I’ve always known, there’s no putting the different things I do in separate boxes. I want to bring them together.”
jminda@chausa.org
MiKayla and Alex Bellefeuille with their 2-year-old daughter Havyn visit Dr. Jennifer Tegethoff at the Avera Down Syndrome Clinic in Sioux Falls, South Dakota. Tegethoff co-founded the clinic.
Tegethoff
Maroun
Safe Haven
From page 1
The trafficking survivor is named Precious. Senior caseworker Vanessa Velarde says the Medical Safe Haven collaboration and Barrios’ expertise were key to Precious getting to safety. “It’s about Gigi knowing who to call — it’s much more than just a referral,” Velarde says.
‘I wanted to give back’
Barrios has been helping vulnerable women and their families since college. “I wanted to give back,” she says.
During college, Barrios interned at City of Refuge Sacramento, a community-based social services organization, and took a job there after graduation. The nonprofit is based near “The Blade,” a high-crime area in Sacramento where human traffickers operate. Barrios was among the caseworkers helping extract women from sex trafficking and into City of Refuge’s shelter. “I loved doing that work,” she says.
She was one of many frontline professionals who Dignity Health Methodist Hospital of Sacramento consulted about a decade ago as it was developing its pioneering Medical Safe Haven, a clinic that provides trauma-informed medical care to identified victims and survivors of human trafficking. Barrios says that until she heard Dignity Health’s ideas for the clinic, she’d never considered the importance of having preventive care tailored to traumatized people. She and the other professionals involved in the discussions enthusiastically supported the establishment of the clinic, which opened around 2016.
The facility, which operates under a family medicine residency, trains clinicians to provide care in a way that is particularly compassionate and gentle for traumatized people.
Barrios became a familiar face at the Medical Safe Haven as she accompanied City of Refuge clients to the clinic. Five years ago, when the Medical Safe Haven was recruiting a senior program coordinator, she was a natural fit. In this role, Barrios supports the growing network of Medical Safe Haven clinics, which now are at five Dignity Health campuses in California.
‘Something wasn’t right’
Barrios regularly scans the Medical Safe Haven clinics’ patient schedules for familiar names, so she can catch up with past
clients. On Nov. 18, 2022, she spotted her former City of Refuge client Precious on the schedule and saw a note in the medical record that she had been struggling. Barrios decided to meet with Precious in the clinic’s waiting room to help her prepare mentally for her first trimester prenatal exam.
Barrios recalls that while chatting, she saw Precious become agitated and increasingly fearful as texts popped up on her phone. “I picked up that something wasn’t right. … Because we had that past relationship, I was able to ask her, ‘Tell me, how are you really doing?’”
Precious broke down and confided that Dominick Roberson — her boyfriend and the father of the baby she was carrying — was in the parking lot, armed with a gun and threatening her via texts. She revealed that during the couple of months she’d been with Roberson, he’d assaulted her, repeatedly said he would hurt her and her year-old son if she did not do as he said, and forced her into prostitution.
“I said to her, ‘Are you ready to get help?’” Barrios recalls.
Safe exit
Precious’ assent set Barrios into motion. Barrios reached out to her contacts in law enforcement to get Precious’ son to a safe location and to have Roberson apprehended at the clinic. She coordinated with other contacts to ensure Precious and her son could enter a safe house network and have all their basic needs met while there.
With the support of clinic management, police safely detained Roberson.
Since then, the collaborative — including Barrios and her Medical Safe Haven colleagues, law enforcement, the Sacramento County attorney’s office and a network of social service providers — have accompanied Precious along a fraught process. She gave her statement and provided evidence at the clinic, then cooperated during Roberson’s July 2023 criminal trial, where Barrios testified.
Roberson was convicted and sentenced to 71 years to life and is now in prison.
Velarde was among those who helped Precious and her son — and, in time, her infant daughter — move through the safe house network and begin to build a new life. Though Velarde now is with a different nonprofit that helps trafficking victims, she remains in touch with Precious. Velarde reports that Precious “is doing very well, working on getting her education and pursuing stable housing” for herself and her two children. She is leaning on her faith.
Velarde calls Precious “a strong, amazing survivor who made her voice heard very
Include your organization’s Christmas message in the December issue of
Catholic Health World invites you to extend a seasonal greeting to your employees and to colleagues in the Catholic health ministry. Visit chausa.org/Christmas for more details. Send an email to ads@chausa.org to reserve your ad space.
Dignity Health Medical Safe Haven clinics provide trauma-informed care to victims and survivors
According to a study from the Polaris nonprofit anti-trafficking organization, 69% of human trafficking survivors report they had access to health services at some time during their exploitation.
To help ensure that health care staff know how to identify these patients and aid them, CommonSpirit Health has developed numerous educational materials and training opportunities under its Human Trafficking Response Program.
Inspired by that initiative, staff of one of CommonSpirit’s programs — the Dignity Health Methodist Hospital of Sacramento Family Medicine Residency Program in California — developed the Medical Safe Haven clinic network.
That network trains medical professionals to provide gentle, traumainformed care to vulnerable people, particularly those who have been exploited through human trafficking.
In the Medical Safe Haven clinics, providers “build a relationship with patients — it’s like a family. The physicians give the patients the space and time they need for their medical visits. They walk them through. It’s very special,” says Gigi Barrios, a senior program coordinator for the Medical Safe Haven program at Dignity Health Methodist Hospital’s residency program.
Funded in part by the CommonSpirit Foundation, the Human Trafficking Response Program seeks to address the issue that health care professionals are “too often unprepared to identify and assist trafficked persons,” according to the response program’s website.
Through the Human Trafficking
loudly” in seeking justice.
‘In a healthier place’
In April, Barrios received an Outstanding Citizen Award. The Sacramento County District Attorney’s Office annually bestows the honor on “victims and witnesses who have shown uncommon courage by participating in the criminal justice process under extraordinarily challenging circumstances,” according to the office’s website.
Precious attended the ceremony. Barrios says of her, “she looks good, she’s doing well, and she’s in a healthier place.”
Velarde says it’s because Barrios invested the time throughout her career to learn how best to help vulnerable people
Response Program, CommonSpirit provides health care staff — both at CommonSpirit facilities and external systems and facilities — with information about how to respond to the trafficking phenomenon.
Building off the work of the Human Trafficking Response Program, Dr. Ron Chambers and Jennifer Cox of Methodist’s Family Medicine Residency Program led the 2016 creation of a Medical Safe Haven there.
At the Medical Safe Haven in the residency practice, medical residents learn how to provide trauma-informed care to vulnerable patients. They hold clinics during specific time blocks on the family medicine practice’s calendar, and human trafficking victims can come in during those appointment times to see medical providers who are well-equipped to tend to their medical needs.
The Medical Safe Haven clinics are in Sacramento, Redding, Northridge, Santa Maria, and San Francisco. They are part of CommonSpirit Health’s physician enterprise.
Among the services the Medical Safe Haven clinics provide are primary care, women’s health, prenatal and obstetrics care, infant and pediatric care, mental health support, medicated-assisted substance use treatment, vaccinations, testing and treatment for sexually transmitted conditions, contraception, referrals to social services, gender-affirming care and laser tattoo removal.
CommonSpirit is replicating its Medical Safe Haven network in Arizona.
— JULIE MINDA
and because she was compassionate and intentional when talking to Precious at that clinic appointment that she was able to intervene in such an impactful way.
Martin
Martin agrees. “Gigi was able to read the signs that something was wrong because she had a relationship with Precious, and building that type of relationship takes passion, empathy and thoughtfulness, and that is who Gigi has been all along,” she says. Barrios defers credit. “I identified the issue, but it took a village to get Precious safe,” she says. jminda@chausa.org
Researcher at Providence-affiliated institute receives Nobel Prize for medicine
By LISA EISENHAUER
A researcher from a nonprofit institute affiliated with Providence St. Joseph Health was among the three winners of this year’s Nobel Prize in medicine for their combined groundbreaking discoveries related to the immune system.
Mary E. Brunkow of the Seattle-based Institute for Systems Biology, Fred Ramsdell of Sonoma Biotherapeutics in California and Dr. Shimon Sakaguchi of Osaka University in Japan were honored with the award on Oct. 6.
In a press release about the award, the Nobel committee lauded the trio of researchers for identifying “the immune system’s security guards, regulatory T cells, which prevent immune cells from attacking our own body.”
The Nobel committee said the researchers’ foundational discoveries launched the field of peripheral tolerance, which studies
what prevents immune cells from damaging the body. The committee said the discoveries have spurred “the development of medical treatments for cancer and autoimmune diseases. This may also lead to more successful transplantations. Several of these treatments are now undergoing clinical trials.”
At a press conference, Brunkow credited other scientific advances, including human genome sequencing, with helping pave the way for her Nobel Prizewinning work. Of her team’s research, she said, “ultimately it led to really new insights into a very exciting and previously unknown piece of the immune system, which is, how is the immune response regulated or tamped down.”
Scan to read an extended version of this story.
The Institute for Systems Biology has been affiliated with Providence since 2016.
Velarde
Brunkow
PeaceHealth therapist continues care in rural Oregon school after 2020 wildfire
By NANCY FOWLER
Every year as fall approaches, a deep unease settles into the McKenzie River valley in Western Oregon. This year is perhaps even more distressing. It’s been five years since the Holiday Farm Fire blazed through the region, killing one person and destroying hundreds of homes and businesses. The anniversary is a grim reminder of a tragedy that raises fears about whether it could happen again.
But thanks to an arrangement between PeaceHealth and the local school district, help is nearby for the community’s young residents. Kelly Shaw, a licensed professional counselor with PeaceHealth, has an office inside McKenzie River Community School in Finn Rock, which serves preschool through high school students. From there, she can offer counseling to every student in the district, helping them and their families cope.
Shaw, who graduated from the school as did her mother and other relatives, jumped at the chance to help children and families at her alma mater.
“The fire brought a lot of terror for folks — to be so close to it, to feel the heat through the car as they fled,” Shaw says. “People were in genuine fear for their lives.”
Working through emotions
Shaw understands the terror firsthand. She vividly remembers the Labor Day 2020 exodus when she fled her home with her elderly mother and aunt. It was two weeks before Shaw and her family, along with the rest of the community, could return to the blackened region.
Unlike many of her neighbors’ homes, Shaw’s home, which had once belonged to her grandparents, remained standing. That her house was spared seems inexplicable to her, given that the heat was intense enough to melt her blinds and that four surrounding homes were destroyed.
In the aftermath, a cascade of emotions washed over the community.
“There was a lot of gratitude and relief, and because there was a death, we were in wonder about how so many people got out safely and alive,” Shaw says. “And then the devastation of it all started to trickle in.”
At McKenzie River Community School, Shaw helped students work through initial feelings through doll play and puppetry, building with LEGO blocks, and playing card games. Talking while walking helped many students open up.
Children and adolescents, who already were dealing with COVID restrictions, grieved for friends whose families moved away after the fire. They picked up on the stress of their parents, some of whom struggled with post-traumatic stress disorder from the fire and evacuation.
“How do you get back in the car and drive someplace after the car was both your rescue and also the place where you felt trapped?” Shaw says.
A lot of work with parents involved managing panic attacks and helping them cope with persistent emotions such as survivor’s guilt, and feeling unable to help others despite wanting to. Shaw understood all too well.
“I was in it with them, trying to figure out my own feelings while holding space for them to have their own,” Shaw says. “I was grateful to have my work and to be a support.”
‘A mental health desert’
Superintendent Lane Tompkins says the
McKenzie School District, with fewer than 200 students, long had been in need of an accessible therapist. Even before the fire and pandemic, Tompkins was concerned with his students’ ability to regulate emotions and the lack of a school counselor or any other nearby options.
“It was kind of a mental health desert,” Tompkins says.
Not only are mental health providers some 45 minutes away, the cost is prohibitive for many families. All students in the district receive free breakfast and lunch. “They’re great kids but they just don’t have a lot of the resources that some families do,” Tompkins says.
The district secured funds for mental health counseling through Oregon’s 2019 Student Success Act, which created a corporate activity tax to support schools. But figuring out how to successfully execute the idea proved difficult until PeaceHealth — a more robust health care system than the one the district initially partnered with — offered to provide supervision and billing services along with a therapist.
“We appreciate PeaceHealth coming out to an underserved rural area,” Tompkins
says. “It’s definitely in line with their mission of helping those in need.”
Money from the special tax covers all copays so there is no cost for families. Those families “really respond to Kelly and really respect her,” Tompkins says.
“And I’m not saying our classrooms are problem-free, but a lot of the kids who’ve worked with her have been able to find a much better path forward,” he says.
‘A big, collective breath’
Since January 2021, Shaw’s office has been conveniently located inside the school. Teachers keep an eye out for students they might refer. Those who spend a lot of time with comfort objects such as weighted blankets, or whose parents have brought up concerns, are potential candidates.
Shaw frequently attends Individual Education Program meetings for kids who need extra support. She also goes to parentteacher events, making sure to keep her office door open or mingle with parents in the halls.
“Sometimes the idea of seeing a counselor can come with a lot of stigma or past experiences that might not always be positive,” Shaw says. “When people come into my room and meet me, maybe I can show that I might not live up to whatever stereotype they had.”
In the years since the Holiday Farm Fire, other nearby fires have blanketed the area with thick, black smoke. Some have been close enough that firefighting operations were based at the school. “In my head, I know the fire is far away and I’m safe,” Shaw says. “But physically, I feel a tightness in my chest and I’m edgy and irritable.”
It’s hard to ever forget the danger.
“Every fire season, it seems like the valley just takes a big, collective breath and holds it,” Shaw says. “We’re all praying and crossing our fingers.”
This year, she imagines even former students may make appointments with her outside of her school hours and obligations.
“Those who were freshmen the year of the fire have all graduated,” Shaw says. “Now they’re in a different developmental stage than they were five years ago, so they might need to talk about it again.”
Catholic bishops renew mental health campaign to raise awareness, end stigma
By LISA EISENHAUER
The United States Conference of Catholic Bishops is renewing and refreshing its National Catholic Mental Health Campaign.
The bishops say the campaign is meant “to encourage all people of goodwill to respond to the ongoing mental health crisis.” CHA is part of a national coalition that helped the USCCB develop and create the bishops’ initiative, which launched in 2023. Paul Jarzembowski has a lead role in the campaign in his position as associate director for the laity in the USCCB’s Secretariat of Laity, Marriage, Family Life and Youth. He says in its first two years the campaign has succeeded in raising awareness of mental illness among Catholics.
For example, he says more dioceses have put information about mental illness and links to resources for care on their websites and many parish priests have addressed the topic, including planning Mental Health Sunday services in mid-October using USCCB-created resources. A key resource is the Novena for Mental Health. The novena’s prayers stretch over nine days. Each one has a focus, such as poverty and mental health, removing stigmas, and suicide awareness. Jarzembowski credits the campaign for encouraging open discussions about an
often-sensitive topic. “Anyone who finds out about it is very enthused about the fact that the bishops are really engaged in this issue,” he says. “So that inspires the conference to keep building and growing.”
Reinvigoration
In what Jarzembowski calls a reinvigoration of the campaign, the bishops added a component this year called Healing and Hope. The USCCB describes the component as “focused on amplifying local engagement on mental health and the accompaniment of people struggling with mental illness.” The initiative includes a revitalized social media campaign with new reflections by bishops that invite conversations on the realities and stigmas of mental illness and plans for state conferences focused on mental health.
“Part of the reinvigoration is looking at ways in which this campaign can go from being an idea that the bishops have in their national capacity to actually affecting and engaging people in their local parishes and dioceses,” Jarzembowski says.
In spotlighting mental health, he says the bishops are being intentional in framing it as both a spiritual issue that should be met with understanding, compassion and prayer as well as a clinical one that can require medical interventions.
A call to action for Catholic health care in the campaign, he says, is “to recognize that we all need to work together more and to be
more collaborative in how we address mental health from a Catholic perspective, that it’s not just spiritual or clinical. Instead, it is about all of us working together.”
Advocacy
Clay O’Dell, CHA director of advocacy, serves on the council that advises the bishops’ conference on health and social issues and that helped initiate the campaign.
O’Dell says CHA’s advocacy work includes encouraging policymakers to continue to cover and expand access to mental health care.
“CHA’s policy perspective is an important one, making sure that the government and Congress are doing what they can to support mental health initiatives in the country,” O’Dell says. “But that is really based on having awareness among people of the importance of mental health and where to go to get mental health services.”
Like Jarzembowski, O’Dell says the efforts of both health care providers — and groups like CHA that advocate for them — and spiritual care providers are vital to ensuring that mental health care is seen as essential and that funding is available to support it.
“I think that all of the coalition members would agree that within Catholic teaching is the importance of good health, and that includes physical health and mental
health,” he says. “For CHA, that’s our number one issue and priority is making sure that people get the quality and affordable health care, physical and mental, that they need.”
Workforce issue
Jill Fisk, director of mission services for CHA, says the organization recognizes mental health care as a basic and essential human need and part of holistic care. She says providing this care aligns with Catholic tradition, teachings and scripture that calls for meeting the needs of the whole person.
She notes that mental health care also is critical for health care workers themselves. She points to work to address this need from CHA’s well-being advisory council and other organizations such as the Harvard Human Flourishing Program and the Coalition for Physician and APP Well-being.
“It’s encouraging to see the church’s commitment to this, because it’s one of the most pressing needs upon our workforce,” Fisk says. “To not only see the good work that’s happening within our systems, and the strategic emphasis upon a healthy workforce, but also to see the church equally be committed, really is helping to support human dignity.” leisenhauer@chausa.org
Kelly Shaw, with her furry companion Charlie, works from an office inside the McKenzie River Community School in Finn Rock, Oregon. A licensed professional counselor with PeaceHealth, Shaw offers her services to any student. Shaw says Charlie is the school’s unofficial support dog.
Tompkins
Jarzembowski
O’Dell
Fisk
PRESIDENTS/CEOS
Organizations within CommonSpirit Health have made these changes:
Mario Garner to president of Dignity Health East Valley, which includes Dignity Health Chandler Regional and Mercy Gilbert Medical Centers, and Arizona General Hospital — Mesa, all in Arizona. Garner was president of St. Luke’s Health — The Vintage Hospital, in Houston.
Jarrett B. Millsaps Jr. to president of Saint Joseph East in Lexington and Saint Joseph Mount Sterling, both in Kentucky. The facilities are part of Saint Joseph Health of Lexington. Millsaps was a consultant with Bancroft Trust Health Partners in Chattanooga, Tennessee.
Organizations within Trinity Health have made these changes:
Sarah Hunter to president of Gottlieb Memorial Hospital of Melrose Park, Illinois. She was chief operating officer at Northwest Health in Valparaiso, Indiana.
Robert Ritz is retiring as president and CEO of MercyOne of Des Moines, Iowa, effective Jan. 2. Trinity Health will begin recruiting for his successor in the coming months.
ADMINISTRATIVE CHANGES
Organizations within CommonSpirit Health have made these administrative changes: Michael P. Browning to system senior executive vice president and chief financial officer of CommonSpirit Health, effective Jan. 2. Tadren Kennedy to chief operating officer of Dignity Health Mercy General Hospital in Sacramento, California.
Subsidiaries of Trinity Health of Livonia, Michigan, have made these administrative changes: Michelle Peña to regional chief nursing officer of Trinity Health Michigan; Tommy Starr to chief nursing officer for
Saint Joseph Health System of Mishawaka, Indiana; and Alicia Wolfe to mission leader at Saint Agnes Medical Center in Fresno, California.
Dr. Matthew Fox to chief medical officer of Mercy Medical Center of Cedar Rapids, Iowa, effective in December.
OBITUARY
Dr. Patricia Maryland, who spent about 20 years as an executive with Ascension or its predecessors, died Oct. 24. In her last position with the St. Louis-based system, Maryland served as executive vice president of Ascension and president and CEO of Ascension Healthcare from July 2017 to July 2019. She served on the CHA Board of Trustees for two years, leaving in June 2019.
ANNIVERSARIES
Dignity Health — Northridge Hospital Medical Center, part of CommonSpirit Health, 70 years.
Holy Cross Health, Fort Lauderdale, Florida, part of Trinity Health, 70 years.
Foundations of Catholic Health Care Leadership
JANUARY 29 — MARCH 19, 2026
Foundations Live is an interactive eight-week engaging virtual program with sessions each Thursday from 1–3:30 p.m. ET.
AN ESSENTIAL PRIMER FOR NEW AND CURRENT LEADERS
Deepens understanding of the pivotal role leaders play in carrying out the healing mission of Catholic health care.
By JULIE MINDA
When a Portland, Oregon, day shelter called Rose Haven started a mental health program several years ago that offered support groups, one-on-one therapy and drop-in mental health care, facility leaders wanted to make sure they were implementing the program as well as they could to have the best possible impact on clients’ lives.
Data can provide key insights to accomplish a goal like this, but it can be difficult for a small independent nonprofit like Rose Haven to harness and use data in this way. That’s where the Portland-based Providence Center for Outcomes Research and Education, or CORE for short, came in.
Through its Data for Change program, CORE worked with Rose Haven to clarify the desired outcomes for the mental health program, used surveys and other data collection tools to gauge progress, and helped the shelter learn from the data to shape the program for maximum effectiveness. Such data services have enabled shelter leaders to continually evolve their programming to meet clients’ needs.
Rose Haven is one of dozens of organizations that are working with CORE. CORE’s goal is to make important data understandable and usable, so that insights gained through research can help build and sustain effective systems, policies and programs.
Keri Vartanian, CORE’s director, says, “There is so much to learn from data, and this information can advance organizations and their work and help the people they serve. You need to collect data to understand a program and its impact. You can tell a story with data.”
Broadening scope of services
One of Providence St. Joseph Health’s predecessors, Providence Health System, founded the Center for Outcomes Research and Education nearly 40 years ago to use data to improve health care, primarily by evaluating promising medical treatments and programs. In time, leadership decided that CORE should focus more upstream to understand how systems and policies shape health and to determine ways to improve outcomes for everyone. In the early 2000s, that work included research on the effects of Medicaid policies enacted by Oregon. CORE leadership then decided to broaden the organization’s purview to get at root causes of health issues and concentrate on the social determinants of health. This includes research on topics such as how housing and food access relate to health.
A current priority for CORE is research that engages community members and that informs action.
Today, CORE, part of Providence, has a multidisciplinary staff of nearly 30 researchers, scientists and data experts. Their several dozen clients include health systems and community-based organizations as well as social service providers, health plans and government agencies. Some of CORE’s clients are subsidiaries of Providence, most are not. CORE is independently funded through its clients’ projects and grants.
No cookie cutter
CORE conducts a range of research projects, including on equity, health services, population health, housing, and social and economic factors. It’s now working on about 30 projects.
Vartanian says many of the smaller organizations CORE works with have limited resources and lack the internal capacity or expertise to conduct research and evaluation, to collect and analyze data, or
to use data to build capacity. CORE gives them access to staff with deep skillsets in all these areas.
Hannah Cohen-Cline, CORE’s program director of research and evaluation, adds that CORE is independent from its clients, so it can conduct research with less bias, which lends credibility to its findings.
Lisa Angus, CORE’s program director for analytics and strategic consulting, says that with decades of experience researching health and social service issues primarily along the West Coast, “We’re pretty locally grounded and understand the context of the work. We understand what’s going on here, and we meet (our clients) where they are.”
Additionally, Angus notes, the center’s approach is “not cookie cutter. We are flexible and adaptable, but we also bring a sophistication and rigor to our work without being over the top for what is needed.”
A deeper understanding
Clients have employed CORE for many ends. This includes research to get a deeper understanding of the changing landscape in which the client operates, or of the population the client serves, or of the needs that population has, or of the ways that programming can be carried out. Some clients such as state Medicaid programs and plans have worked with CORE to track metrics on the impact of their work and to meet the reporting requirements of grantors or government agencies. Some clients have used CORE’s services to refine community benefit programming, and some to further their advocacy work. Some have used it to improve their partnerships with other organizations.
“From a very basic level,” Cohen-Cline explains, “when we think about program evaluation, you want to know your program is working and, if not, how to improve it and whether and how to scale it to help the communities you serve.”
Angus adds, “It’s an opportunity to get better at what you do, to make better decisions and to better understand the needs of the populations you serve and what people are responding to.”
Data for Change
CORE’s leadership says Data for Change, launched in 2021, has been a big success for everyone involved — CORE, Providence and the community-based partners.
Through this effort, CORE has supported more than 30 small Oregon-based community organizations with data collection and analysis so that they can enhance and grow their work. Many of the clients in the Data for Change program — the Rose Haven shelter included — are recipients of grants from Providence.
CORE works with its Data for Change clients in a cohort, providing individualized technical assistance, webinars and data summits. One main goal is to help these clients to build their capacity to use data.
Vartanian says CORE supports community-based organizations that provide much-needed services.
Cohen-Cline says CORE helps those providers to take a look at the value they add from many different perspectives, and then to demonstrate that value to others.
“It can be fun to dive into data,” Angus says. “Data can bring some really good insights. Data can be engaging and motivating and sense-making. It can help organizations to build their capacity.”
jminda@chausa.org
Millsaps Peña
Maryland
Browning
Wolfe Hunter Starr
Vartanian
Cohen-Cline
Angus
IN BRIEF
Catholic Medical Center announces nearly $100 million in upgrades
Catholic Medical Center of Manchester, New Hampshire, is planning nearly $100 million in infrastructure upgrades and a new freestanding emergency room in Nashua, about 20 miles away from the main facility.
A core part of the medical center’s plan is a $43.3 million renovation of its central energy plant, which will modernize the hospital’s power, heating and cooling systems.
“For years, CMC’s facilities team worked tirelessly to extend the life of the aging plant, but a complete overhaul was long overdue,” a press release about the project says.
Catholic Medical Center will spend an additional $46.5 million on equipment upgrades, facility renovations and patient care enhancements. This includes nursing unit refreshes, operating room modernization, a new hybrid operating room and interventional radiology suite, an electrophysiology lab renovation, and public space renovations.
Catholic Medical Center expects to complete most of the projects within the next two years.
Officials broke ground Oct. 28 on the emergency room in Nashua, with a projected opening in mid-2026. The $16 million, nearly-10,000-square-foot facility will be open around the clock. It will be staffed by emergency physicians and other clinical professionals.
The building will have 11 emergency
bays, including a trauma bay, and will be equipped to handle high-acuity cases such as cardiac arrest, stroke and severe injuries.
ArchCare’s new PACE center in Harlem is its own neighborhood
ArchCare is opening a Program of AllInclusive Care for the Elderly center in New York modeled on a neighborhood setting, complete with a movie theater, beauty salon and library.
ArchCare, the continuing care community of the Archdiocese of New York, cut the ribbon on the ArchCare Senior Life PACE Harlem Center in early October. The center opens this month.
The site combines an adult day center
with a fully equipped medical clinic. It will provide the medical, social and other services seniors would otherwise receive in a nursing home but let them continue to live in their own homes or with relatives. Inside the center, participants also will find a range of familiar and engaging spaces designed to spark connection and comfort:
A movie theater
A full-service beauty salon
An arts and crafts workshop
A café and social lounge
A library for quiet reflection
Communal spaces for music, conversation and recreation
ArchCare said the center’s design reflects research in eldercare showing that sensory-rich environments with spaces
for leisure, creativity and social interaction can improve quality of life, reduce isolation, and enhance well-being among older adults.
“We set out to design a space that honors the whole person, not just their medical needs, but their social, emotional, spiritual, and cultural lives,” said Scott LaRue, president and CEO of ArchCare.
CHI Health Good Samaritan receives $12.6 million gift for women’s health
The foundation of CHI Health Good Samaritan in Kearney, Nebraska, has received a $12.6 million donation to advance women’s health in south central Nebraska. The anonymous gift from a private foundation is the largest single donation in the CommonSpirit Health hospital’s history.
The funds will benefit cardiovascular and maternity care at Good Samaritan.
A phased renovation will update the hospital’s interventional cardiology suites. Work will begin in the spring with the installation of advanced imaging and guidance equipment. In addition to the cath lab, the hospital’s cardiac care program includes noninvasive cardiology, vascular surgery, cardiothoracic surgery and cardiopulmonary rehabilitation.
Construction to update the hospital’s maternity center will begin in the spring as well. The redesigned space will include a surgical suite and 11 birthing suites with a large whirlpool bath and sleeping accommodations for family members. Updates also will include a new waiting room and refreshment center for visitors. The renovation also will create a private entrance and add a surgical suite.
Clinicians face complex ethical challenges in the novel virtual emergency care space
By JULIE MINDA
Given the challenges to providing inperson emergency care, many health care systems and facilities have expanded into — or are looking to expand into — virtual emergency care.
Providing emergency care via telehealth can help address many concerns, including clinician and resource shortages and financial constraints. But virtual emergency care is an emerging field, and entrants into this novel space are facing some complex challenges in establishing protocols and practices. This includes ethical challenges having to do with trust, justice and dignity.
During an October CHA webinar, Dr. Marija Kirjanenko spoke on the topic. Kirjanenko is a lecturer in philosophical bioethics at Australian Catholic University as well as an emergency physician. The webinar, “Ethical Challenges in the Novel Space of Virtual Emergency Care,” is the latest in CHA’s series, Emerging Topics in Catholic Health Care Ethics.
“Virtual emergency departments fill a gap, but they are not quite like in-person care,” Kirjanenko said. “It will take time to establish standards, and in the meantime, we’ll aim for best practices and avoiding harm.”
She said virtual emergency departments “are a very high-risk environment, and this is a very different model” compared to inperson care and virtual, nonemergency care.
63-fold increase
The growing use of virtual emergency care has followed the dramatic increase in telehealth use generally since the pandemic’s onset. A late 2021 report from the U.S. Department of Health and Human Services found that “massive increases in the use of telehealth helped maintain some health care access during the COVID-19 pandemic.” The report said, for instance, that
Medicare visits conducted through telehealth increased 63-fold in one year — from 840,000 in 2019 to 52.7 million in 2020.
According to an online HHS resource, some ways that providers are using telehealth for emergency care include:
Tele-triage, which involves screening patients remotely to determine their condition and the care needed
Tele-emergency care, in which clinicians at a central hub connect with providers and patients at hospitals on the “spokes” of the hub
Virtual rounds, in which health care providers check on emergency department patients virtually, including to avoid exposure to contagions
E-consults, in which specialists provide recommendations to providers remotely
Telehealth follow-up care, or care delivered remotely to patients who have been triaged before emergency care or to those who have been discharged from the emergency department
A May 2025 study in the Annals of Emergency Medicine showed the potential for growth in virtual emergency care. It found that telehealth could be an option in up to 10% of U.S. emergency department visits.
Skyrocketing use in Australia
Kirjanenko said the use of telehealth has been skyrocketing in Australia since the pandemic, with a variety of models evolving in the last several years. The main models are: outpatient general practitioner care delivered remotely, inpatient consultation between hospital hubs and satellite locations, specialist consultations to fellow providers, and virtual emergency departments.
She explained that unlike in the other three models, in virtual emergency care, the patients’ location, the clinicians involved, the tasks that need to be performed, and the structure of the relationships among the clinicians and patients can be very unpredictable and fluid. The providers and patients may not know each other. Instability or uncertainty in patients’ conditions can make virtual emergency consultations extra
risky, as can off-kilter family dynamics.
Trust, justice, dignity
Kirjanenko used two case studies to illustrate what virtual emergency care might look like. She talked through how ethical concerns around such priorities as trust, justice and dignity could be at play in these cases.
The first case was Anna, an 80-year-old woman in long-term care with abdominal pain, vomiting and heavy perspiration. The staff at her facility call an ambulance, and the paramedic connects remotely to a physician for an emergency consult.
For Anna, Kirjanenko raised these questions: If the remote physician is asking the paramedic to perform some basic physical examinations on the patient, to what extent does the physician trust the paramedic, particularly if they’ve never worked together? And to what degree do the paramedic and patient trust a potentially unfamiliar physician? How does the physician’s lack of physical presence impact the situation? Being unable to have in-person eye contact and to observe other in-person cues can impact the interaction. Additionally, the artificial environment of communicating through an electronic screen can impact the situation. If Anna is cognitively impaired, she may react negatively to a physician talking through a virtual connection. And does the patient get full justice and preserve her full dignity if a physician is making a judgment call on her care based on information received through a mode of connection that may lack the quality of an in-person interaction?
The second case was Tony, a 45-year-old who arrives at an urgent care center after severely cutting his thumb with a chainsaw. A nurse at the center consults remotely with a physician. Tony tells the nurse and remote physician he just wants his thumb sutured, he does not want to travel the two hours to go to a hospital in case the laceration has done significant damage to his thumb. Kirjanenko said that a physician consulting remotely could experience significant moral distress from trying to make deci-
sions based on the limited information he is receiving and from potentially agreeing to the suturing, which could have grave implications if the thumb injury is worse than what it appears to be. The bedside nurse likewise could experience moral distress from the situation.
Speaking up
Kirjanenko said as emergencies unfold — with unacquainted physicians working together virtually, limited information and evolving standards of care — there are many ethical quandaries to consider even beyond those explored in the Anna and Tony case studies. For instance, what is the hierarchy among providers who are not used to working together? What is the team structure, when the team members and dynamics may be constantly changing? What is the duty to care? How is harm defined in the imperfect world of virtual care? What risk are providers taking on in the way they are carrying out their roles over telehealth connections?
She encouraged intentionality around communication and team-building among providers as possible steps. She said all team members must know their limits and be comfortable speaking up and expressing what they are thinking without shame or stigma. She also advised relationshipbuilding outside of the virtual care environment. She said in Australia’s Queensland, for instance, providers have organized a hub system, and those involved in the care hub gather in-person periodically to build their connections and assess how they are doing on the job.
Kirjanenko acknowledged that there are more questions than answers now when it comes to virtual care. But she said it’s important to work through the issues. “We need ways to get out of these dilemmas. How do we provide compassionate care in virtual spaces without causing distress to patients and families” as well as the providers caring for them? she asked. jminda@chausa.org
Guests explore the Crafter's Corner at the ribbon cutting of ArchCare Senior Life PACE Harlem Center in New York. The space is dedicated to creativity and connection for program participants.