Allegheny County Medical Society

Allegheny County Medical Society
Allegheny County Medical Society
February
Editorial
• Valentine's Day
Deval (Reshma) Paranjpe, MD, MBA, FACS
Editorial
• Medical History Vignette
Richard H. Daffner, MD, FACR
Society News
• Leadership Social January 2025
Advocacy
• Legislative Advocacy PAMED Advocacy Team
ACMS News
• An Update from the ACMS Board of Directors
Raymond E. Pontzer, MD & Keith T. Kanel, MD
ACMS News
• Specialty Group Updates
ACMS Staff: Nadine
Popovich, Melanie Mayer and Haley Thon

Foundation News
• Life-Changing Programs for Kids with Disabilities
Zach Marsh
Medical News
• Reportable Diseases 2022-2024
Allegheny County Health Department Selected Reportable Diseases/Conditions
Kristen Mertz, MD Allegheny County Health Department
Article
• Perspectives from Future Physicians MJ Lerma
Article
• Reviving Hearts
Erasmus Mutabi, MD, Alexandra Johnston, DO, Indu Poornima, MD, and Andrew Oehler, MD

2025
Executive Committee and Board of Directors
President
Keith T. Kanel, MD
President-elect
Kirsten D. Lin, MD
Secretary
Richard B. Hoffmaster, MD
Treasurer
William F. Coppula, MD
Board Chair
Raymond E. Pontzer, MD
Board of Directors
Term Expires 2025
Anuradha Anand, MD
Amber Elway, DO
Mark A. Goodman, MD
Elizabeth Ungerman, MD, MS
Alexander Yu, MD
Term Expires 2026
Michael M. Aziz, MD, MPH, FACOG
Michael W. Best, MD
Micah A. Jacobs, MD, FIDSA
Kevin G. Kotar, DO
Jody Leonardo, MD
Term Expires 2027:
David J. Deitrick, DO
Sharon L. Goldstein, MD
Prerna Mewawalla, MD
Raymond J. Pan, MD
Nicole F. Velez, MD
James Latronica, DO, DFASAM
Richard B. Hoffmaster, MD
Finance
William F. Coppula, MD
Nominating
Kirsten D. Lin, MD
Women’s Committee
Prerna Mewawalla, MD & Meilin Young, MD
Managing Editor
Sara C. Hussey, MBA, CAE ACMS Executive Director shussey@acms.org
Medical Editor
Deval (Reshma) Paranjpe, MD reshma_paranjpe@hotmail.com
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
The 2025 Bulletin Editorial Board will be announced after the February Board Meeting.
EDITORIAL/ADVERTISING
OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323.
USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Executive Director
Sara Hussey shussey@acms.org
Vice President - Member and Association Services
Nadine M. Popovich npopovich@acms.org
Manager - Member and Association Services
Haley Thon hthon@acms.org
Operations CoordinatorACMS & ACMS Foundation Melanie Mayer mmayer@acms.org
Manager - Operations and Finance
Elizabeth Yurkovich eyurkovich@acms.org
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.
Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorsement of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
COPYRIGHT 2025: ALLEGHENY COUNTY MEDICAL SOCIETY POSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212. ISSN: 0098-3772

By: Deval (Reshma) Paranjpe, MD, MBA, FACS
In a world full of weight and pain, drama and uncertainty, hate and violence--what constant can we cling to that will make everything better? Love.
Valentine’s Day has a bloody history— St. Valentine was a martyred priest who was sentenced to death for the crime of marrying couples in secret (to avoid living in sin) to evade an imperial decree forbidding soldiers from from getting married at all. He wrote kindly letters to his prosecutor’s daughter, signing them “your Valentine.” The holiday was established on Feb. 14 by a Pope of the Catholic church to celebrate the saint but also to replace the pagan holiday Lupercalia, which involved goat sacrifices, bacchanalia and fertility rituals.
The message of the holiday is clear though--a man disregards the threat of execution to marry couples who love each other and want to be wed. The same man, languishing in prison, soothes his own heart and that of the daughter of his persecutor with kindness and love. His signature becomes immortal.
Dr. Brian Weiss is a Yale and Columbia trained psychiatrist and hypotherapist who wrote a series of books beginning with “Many Lives, Many Masters” in the late 1980s based on his experiences regressing patients in his practice. I remembered hearing about these books when I was in school, and recently read them—they concern reincarnation and past life regression. Weiss writes about wondrous things—patients knowing their spouses through many past lives, lessons learned through repetition, and many more. If this is to be believed, one must ask—what is the purpose of life? What are we here to learn? We are here to learn to
love—only love is real.
Whatever you may think of reincarnation, think of your most powerful experiences with patients at work. How many times have we seen the power of love in action at the bedside, in the ED, in the field? The elderly parent who cares for their disabled child; the adult child who cares for their frail parent? The spouse in whose eyes you can read love and worry? The nurse who goes the extra mile, the IV team member who is extra gentle, the gentle technician who takes extra care? Our
own colleagues and ourselves when we stay up at night worrying about patients, or call each other to expedite care? All of this is love.
And love is the antidote to much worry, much trouble, and much care. Love is the only force that can stand against evil and the only force that will save the world from harm. Love is worth more than anything else, love overcomes, and love never dies. Love is the answer, and the cure.
I wish you all much love, today and always.

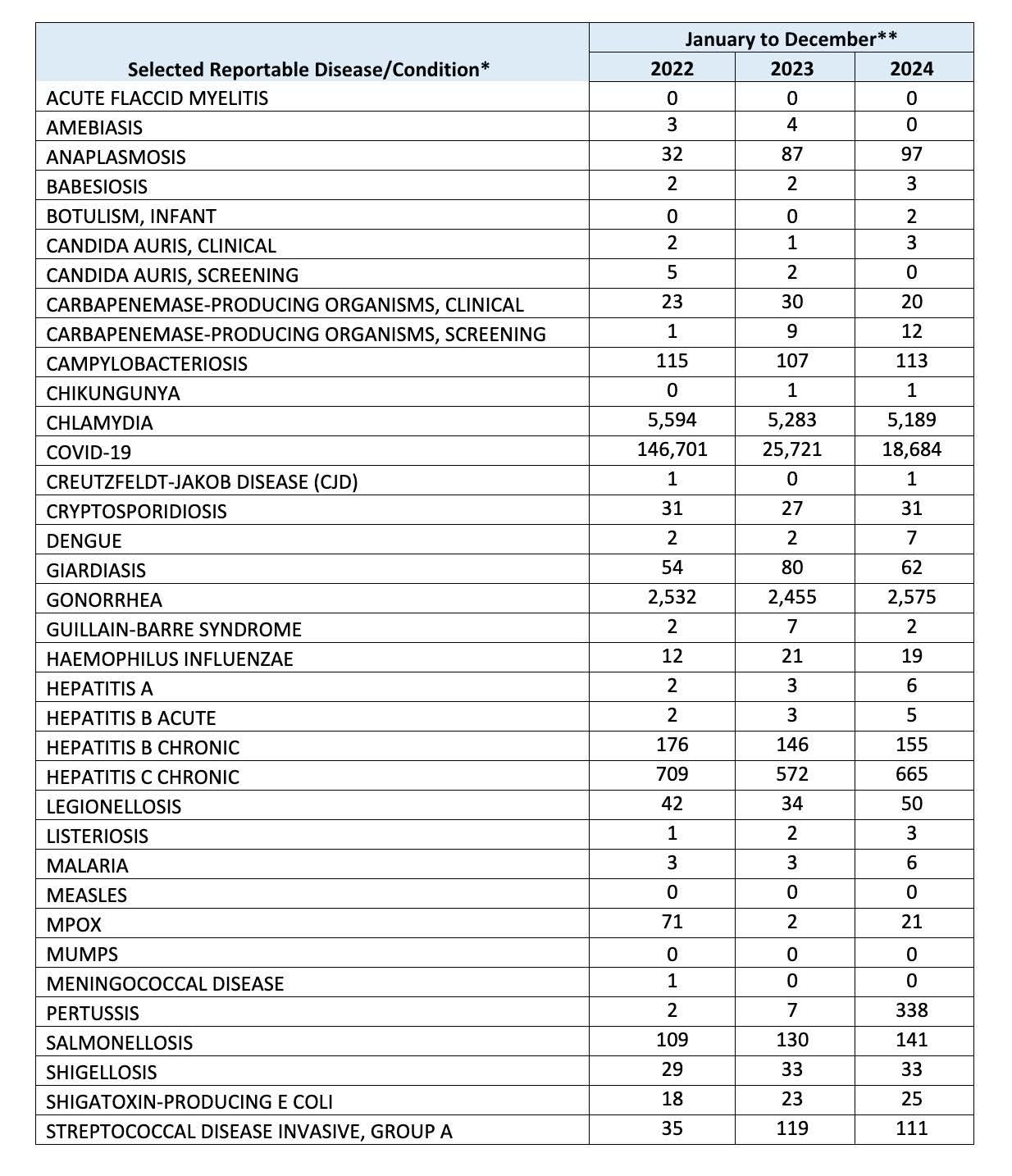
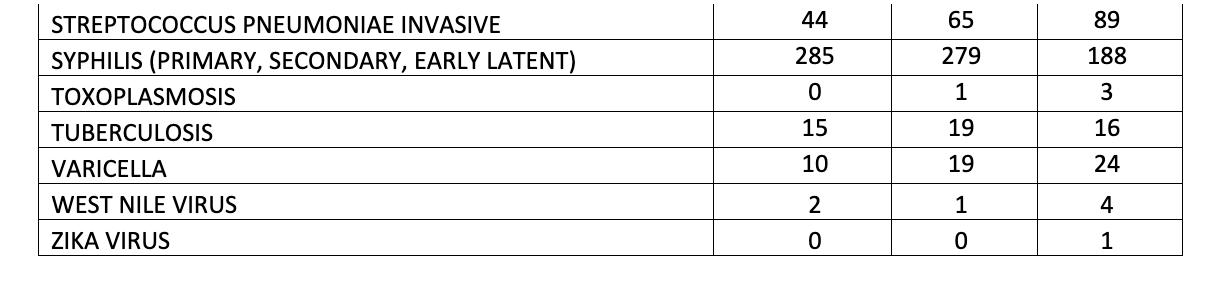
* Case classifications reflect definitions utilized by CDC’s Morbidity and Mortality Weekly Report.
** These counts do not reflect official case counts, as numbers for 2024 are not yet finalized. Inaccuracies in working case counts may be due to reporting/investigation lag.
NOTE: Disease reports may be filed electronically via PA-NEDSS. To register for PA-NEDSS, go to https://www.nedss. state.pa.us/NEDSS. To report outbreaks or diseases reportable within 24 hours, please call the Health Department’s 24-hour telephone line at 412-687-2243. For additional infections disease surveillance information, see ACHD’s “Disease Surveillance” webpage: Disease Surveillance - Allegheny County, PA
When your patients need specialty care, AHN has physicians with the right expertise — like our new hematologist/oncologist.
Dr. Curley offers some of the most advanced treatments and techniques, so your cancer patients can have the best possible outcomes.
To refer your patient, call (412) DOCTORS.
Thomas Curley, MD
Hematology and Oncology
Location:
AHN Cancer Institute
AHN West Penn Hospital 4800 Friendship Avenue Suite 311, Mellon Pavilion Pittsburgh, PA 15224
Specialties :
Skilled in diagnosing and treating leukemia, myeloproliferative neoplasm, and myelodysplastic syndrome
Clinical interest in survivorship in bone marrow transplant patients and clinical trials in leukemia

By: Richard H. Daffner, MD, FACR
A previous editorial of mine in the June 2023 Bulletin was devoted to our partners in the healing arts, pharmacists.1 In the editorial I described how pharmacy has changed since I earned my graduate degree in that time-honored profession 62 years ago. But what was pharmacy like before then? Step back in time with me as we tour an old apothecary shop (pharmacy) that is now a museum.
The Albany College of Pharmacy (now Albany College of Pharmacy and Health Sciences), founded in 1881, is one of the oldest pharmacy schools in the country. Upon entering the century-old O'Brien building of the College, visitors are greeted on the main floor by the oversized display windows of a 19th century apothecary shop. The windows are the front of the Throop (pronounced "troop"), Pharmacy Museum which stands in sharp contrast to the adjacent state-of-the-art 21st century laboratories where instruction and cutting-edge research take place, Step into the Throop Museum and you are transported back to another time, when standard therapy involved the use of various potions, herbal remedies, and yes, even some poisons to treat numerous ailments from syphilis to smallpox.2 The historic apothecary features an extensive mortar and pestle collection, medicine bottles, scales, and a variety of hand-operated devices such as pill grinders and suppository molds that were used to prepare the remedies that were commonly dispensed at that time (Figs.1, 2).
The apothecary was established by Jabez W. Throop in 1800 and was run by his family for 136 years in Schoharie,

NY, a quaint village an hour south of Albany nestled in the rolling foothills of the Catskill Mountains and the cascading valleys of the Schoharie Creek region. Throop was a prominent figure in 19th century Schoharie, serving his community as the town's first postmaster, working in the bucket brigade as a fire fighter, president of the local bank, and helping create the town's waterworks system. The museum also displays Throop's fire bucket, as well as the ledgers that were used to record payments at the drugstore.
When Jabez Throop retired, the store was taken over by his son, Origen Throop, who turned it from a general store into a full-service apothecary. When Origen died in 1883, the business passed to his son, Charles Throop, who operated it until 1930. (Charles became one of New York's first licensed pharmacists in 1884). Charles’ nephew, Charles Grant, managed the store
from 1930 through 1936, but he was not interested in the pharmacy business. In 1938, the Albany College of Pharmacy acquired the Throop apothecary shop with all its original contents. A state historic marker sits in front of the site of the shop (Fig. 3).
The apothecary was initially carefully photographed and then disassembled and reconstructed in its entirety in the basement of what is now the O’Brien building. It was subsequently moved to its current indoor location in 2001. During both moves, attention was paid to every detail to maintain the integrity of the original structure, which included the wooden floor, tin ceiling, original cabinets and shelves, millwork, and paint colors. Colorful show globes (more on them below) are featured in the windows and spittoons are located at each end of the main counter. Some of the meticulously labeled drawers, once filled with various herbs and medicinal ingredients, still contain residual
samples of their original contents from over a century ago.
The shop showcases the early evolution of pharmacy. Some of the medicine bottles on display date back to the 1700s, as evidenced by the company that printed their labels. There are numerous “patent medicines”, most of which made dubious claims to cure a variety of maladies from cirrhosis (Carter’s Little Liver Pills), renal failure (Doan’s Kidney’s Pills), and “female troubles” (Lydia Pinkham’s Herbal Compound).
There were also poisons, such as arsenic (used to treat syphilis) and cannabis tincture, which have been removed for safety and regulatory concerns. Mercury pills that are shaped like coffins or marked with skulland-crossbones symbols - the safety protocols of the time - are locked under glass. Dr, Lee Anna Obos, an ACP graduate and curator of the Throop Museum points out that poisons were kept in blue bottles, to make them more recognizable. In the 1800s, the four most prescribed medicines were mercury, arsenic, laudanum (opium) and antimony. This was the norm before the United States Food and Drug Administration (FDA) was first created to enforce the Pure Food and Drug Act of 1906.
The museum has received many donations of related pharmacy items over the years, including advertisements for cocaine toothache drops manufactured at

a factory in Albany in 1885. A flyer for it boasts "Cocaine is the new anesthetic now used so extensively throughout Europe and this country by Physicians, Surgeons and Dentists. This preparation of Toothache Drops contains Cocaine, and its wonderful properties are fully demonstrated by the many recommendations it is daily receiving."
The museum also owns an extensive collection of show globes – the ubiquitous symbols of pharmacies, which displayed colorful liquids in pharmacy windows. The origin of the show globes derives from the process of extracting the active ingredients from medicinal plants. One of the courses we took during my time as a student at ACP was "Manufacturing Pharmacy", where we extracted the drugs that were then used in the "Dispensing Pharmacy" lab. This was in the era when compounding was a major part of standard pharmacy practice. Would you believe that the active ingredient in Syrup of Wild Cherry comes from the bark of the cherry tree and not from the fruit (which is why the syrup tastes so bad). The old apothecaries would put bark, roots, or leaves of various drugcontaining plants in a large glass globe, fill the globe with water or alcohol (the menstruum) to extract the active ingredients, and place the globes in the windows of their shops, where they would be exposed to sunlight to aid the extraction process. As the extraction
process was occurring, the menstruum would turn colors, depending on what was placed in them. Apothecaries and early pharmacies were identified by such globes, similar to the way that striped poles announced the presence of a barbershop.
Dr Obos, now a lecturer at the college, maintains the museum and showcases its contents, opening each of her lessons with a bit of pharmacy history. When Dr. Obos gives tours, she allows visitors to test the cast-iron machinery, molding "pills" out of Play-Doh®, rolling corks and grinding cinnamon. Dr Obos says, "You need to have a history of where the profession has been so then you can see how far it's come and where it's going”. Indeed, pharmacy, like medicine, has come a long way.
References:
1. Daffner R. Our partners in the healing arts. ACMS Bulletin Jun 2023, pp 12 – 13.
2. Silberstein R. Poisons, potions and show globes: Historical treasures preserved at Throop Pharmacy Museum. Times Union, Dec 25, 2022.
Dr. Daffner is a retired radiologist who was a practicing pharmacist before and during medical school. He is also an amateur historian.

By: MJ Lerma – MPH Candidate Policy/Administrative Intern at ACMS
The Allegheny County Medical Society (ACMS) is home to a diverse membership, including MDs, DOs, medical students, and more. Each perspective is valued, bringing unique insights to the medical community. In this interview, we hear from two second-year medical students at the University of Pittsburgh, Nicky Don and Brady Grano-Mickelsen, who share their experiences with ACMS, their involvement in organized medicine, and their hopes for the future.
Nicky, a former government analyst with a passion for policy, is openminded about her future in medicine. Brady, a former lawyer, aspires to practice pediatric trauma surgery or pediatric emergency medicine, with the long-term goal of securing a political appointment at the FDA or HHS. Both have been active in ACMS, PAMED, and AMA for over a year and a half, leveraging their interdisciplinary backgrounds to contribute to discussions on medicine and policy. Questions and answers have been edited for clarity.
How would you describe your experience with ACMS so far?
Nicky: My real exposure to ACMS began at the House of Delegates (HOD) meeting in Hershey. Aside from enjoying hot chocolate—a bucket list item—I had the chance to comment on state-level resolutions. One resolution I provided written testimony about, on hospital data sharing, was approved before the HOD meeting began, but I hope to follow its development and see where it goes. The support I felt from practicing physicians at the meeting was incredible, and the conversations
provided a fascinating introduction to organized medicine.
Brady: ACMS has traditionally been very Pitt-centric, which makes sense. What I’m curious about in the coming year is how Duquesne’s new medical school will fit in. The DO perspective is somewhat lacking at ACMS, and incorporating that will be both exciting and a bit challenging. I’m eager to see how this develops.
Nicky: I totally agree. It was great to see a mix of physicians by specialty and background, including both MDs and DOs, at the HOD. I’m looking forward to seeing how that diversity grows within ACMS.
How has being part of ACMS benefited you as a medical student?
Brady: The House of Delegates has been a significant opportunity for Pitt students. We often send more students to the PAMED HOD than to the AMA, giving us a chance to learn about policy deliberation firsthand. It’s one thing to talk about policy in class, but experiencing it is entirely different. ACMS has shown interest in engaging more with students, and as Nicky and I step into leadership roles for the Pitt chapter, we’re prioritizing introducing students to ACMS and educating them on state and national advocacy work.
Nicky: I agree. The AMA student chapter at Pitt has been revitalized recently, and I hope the HOD meeting will be the first step toward regular student involvement and mentorship. We’ve had great turnout at meetings where organized medicine was discussed, even from students not previously involved with AMA or statelevel activities. It’s encouraging to see
that interest growing. There was also a resolution at the HOD about changes in student representation at the county level. ACMS allows more Pitt students to attend, which helps create continuity in our organization. Instead of sending just one delegate each year, we can build a community. I think that’s really valuable.
Brady: That resolution was ultimately voted down, but it was an interesting resolution that divided students. The division stemmed from differing perspectives on how to keep medical students involved in the House of Delegates for as long as possible. The resolution would have created permanent spots for students but with a more limited number of positions. In the short term, it would have significantly reduced the number of student members. However, there was concern among the medical student population about efforts by PAMED to make it more difficult for students to get involved, such as through increased fees and other barriers.
You mentioned that medical students were divided on this resolution. Where do you two stand?
Brady: I believe Nicky and I voted differently on this. She voted against it, and I voted in favor. My concern is that there’s a genuine effort to limit medical student participation in PAMED’s HOD. ACMS has done a lot to support students, like covering fees, but the resolution would have made it harder for PAMED to exclude students altogether, even if it reduced the number of student delegates. It’s a double-edged sword.
Nicky: I agree with that take. I had the
same understanding—the resolution was a compromise aimed at securing a medical student voice. However, many people who opposed it shared the same intentions as those who proposed it. The debate was really about how best to ensure that medical students remain involved, whether through funding allocation, seat allocation, or their placement within the organization.
What ultimately persuaded me to vote against it were concerns from counties without medical schools, especially rural ones. The fact that medical students aren't sequestered in their own section allows for more interaction between students and physicians. It felt like the resolution would isolate med students, putting them in a corner. I’d rather see fewer medical students integrated across counties, fostering institutional learning, than have them grouped together, which would limit interaction and simply count as the "medical student vote." It seemed counterproductive to building long-term engagement within these organizations. I think this is an issue that will need ongoing attention.
What Healthcare Policy Issue would you like to see ACMS/PAMED tackle?
Brady: Nicky’s passion for data sharing is shared by many medical students. For example, I seek care outside the UPMC system because I don’t want my advisors to access my records. This is an area that isn’t getting enough attention.
Nicky: A resolution that passed advocated for an opt-out system for data sharing, but I don’t think current IT systems can support that. At the AMA student level, I’m involved with the Committee on Health and Information Technology, where we address these issues and write reports for the medical student section.
What is something that you’re looking forward to this year?
Nicky: I'm excited for more opportunities to interact with physicians in the area and learn what it’s like to have both a clinical practice and a policy-oriented career—and how
it’s possible to balance both. Brady and I are nontraditional medical students; we’ve had work experience in other fields, and we want to integrate those experiences into our future careers. Seeing how physicians incorporate advocacy into their work has been incredibly helpful for me.
At the House of Delegates, for example, there are family medicine physicians running their own practices, discussing the challenges they face with today’s insurance and hospital systems, and how these issues impact patient care. Similar conversations happen around working within hospital systems and maintaining or exceeding standards of care. Learning about these different struggles and how physicians are either pushing back or finding solutions is really valuable.
I know it sounds cliché, but reading about these issues isn’t the same as experiencing them firsthand or engaging in conversations with those living it. It’s also incredibly motivating, as a medical student sitting at my desk, to see people actively leading and
shaping their careers. That’s been really inspiring for me.
Brady: Along those same lines, interprofessional education is frequently discussed in med school, but it usually refers to collaboration with nurses, physical therapists, and others within the healthcare sector. I think there’s a lot of room to broaden that scope to include fields like law and business. There’s a wealth of information to be shared between these areas of study.
I’m hoping to see more collaboration with Pitt’s law school. I want law students to gain a deeper understanding of the issues impacting healthcare, and I want medical students and physicians to learn how to be effective advocates when navigating the legal system. There’s so much information that could be shared, but it often isn’t because we’re stuck in silos. I hope that’s something we can begin to change this year. I know it’s a big task, but I believe it’s a direction we can move towards.


By: Erasmus Mutabi, MD, Alexandra Johnston, DO, Indu Poornima, MD, and Andrew Oehler, MD
1. Introduction to Cardiac Rehabilitation
Cardiac rehabilitation (CR) is a multidisciplinary, evidence-based intervention designed to optimize the cardiovascular health of individuals with heart disease. It includes exercise training, education on hearthealthy living, nutritional counseling, psychosocial support, and risk factor management. The primary goals are to enhance cardiovascular function, reduce morbidity and mortality, and improve patients' quality of life. Evidence consistently shows that CR reduces cardiovascular mortality and hospital readmissions, yet it remains underutilized, with less than 30% of eligible patients participating in these programs. Addressing this gap is vital for improving long-term outcomes in cardiovascular disease management.
2. Indications and Patient Selection CR is suitable for various cardiovascular conditions, including myocardial infarction, coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), heart failure with reduced ejection fraction (HFrEF), chronic stable angina, and valvular heart disease. Patients recovering from heart transplantation or congenital heart disease surgery also benefit significantly from CR. Eligibility for CR requires clinical stability, with no acute ischemia, uncontrolled arrhythmias, or severe symptoms limiting physical activity. Timely referrals by physicians are essential to ensure that eligible patients receive the full benefits of CR.
3. Components of Cardiac Rehabilitation
Cardiac rehabilitation is a multifaceted program designed to address various aspects of cardiovascular health. The core components include:
• Exercise Training: This is the cornerstone of CR, focusing on improving cardiovascular endurance and strength. Tailored aerobic and resistance exercises enhance functional capacity, reduce heart failure symptoms, and help patients regain independence. Studies show that regular exercise reduces hypertension and dyslipidemia, improves skeletal muscle conditioning, and ultimately increases the incidence of future cardiovascular events.
• Nutritional Counseling: A hearthealthy diet is critical for managing risk factors such as hyperlipidemia, obesity, and hypertension. The DASH (Dietary Approaches to Stop Hypertension) and Mediterranean diets are associated with lower LDL cholesterol, reduced blood pressure, and weight loss, which significantly lower cardiovascular risk.
• Psychosocial Support: Mental health support is crucial in CR, as many patients face depression, anxiety, or stress post-cardiac events. CR programs integrate cognitive-behavioral therapy and stress management to improve mental well-being and foster connections among patients for better disease navigation.
• Risk Factor Management: Managing modifiable risk factors, such as smoking, hypertension, hyperlipidemia, and diabetes,
is essential for preventing recurrent events. CR employs lifestyle changes, pharmacologic interventions, and regular monitoring to control these risks and enhance long-term cardiovascular health effectively..
4. Evidence-Based Benefits
CR offers significant benefits, including a 26% reduction in cardiovascular disease mortality and a 34% decrease in five-year all-cause mortality. It improves overall quality of life, enhances functional capacity and exercise tolerance by 20-30%, and decreases one-year hospital readmissions by 31%.1 In patients with chronic stable angina where medical therapy is comparable to percutaneous intervention, CR can enhance the effectiveness of medical therapy, leading to improvement in angina, lower complications, and lower cost of care. Additionally, CR reduces the incidence of depression, boosts medication compliance, and increases patient satisfaction while lowering hospital readmissions and associated healthcare expenses.
5. The Role of the Physician
Physicians are pivotal to the success of CR programs by being the initial contact for cardiovascular disease patients. They play a critical role in identifying eligible candidates and initiating referrals. Early referrals improve CR outcomes and reduce cardiovascular risks. It is essential for physicians to collaborate with the multidisciplinary CR team to customize programs for patients and monitor their progress. Regular follow-ups and encouragement from physicians
reinforce the importance of CR in maintaining heart health and preventing future events.
6. Medicare Coverage and Costs for Cardiac Rehabilitation
Medicare Part B covers cardiac rehabilitation (CR) and intensive cardiac rehabilitation (ICR) programs for eligible conditions like myocardial infarction within 12 months, stable angina, HFrEF, heart valve repair or replacement, CABG, PCI, and heart or heart-lung transplant. CR includes two one-hour sessions per day for up to 36 sessions over 36 weeks, while ICR offers up to six one-hour sessions per day for up to 72 sessions over 18 weeks. Medicare covers 80% of the costs after the deductible, with patients responsible for 20%, which supplemental insurance may offset. Some Medicare Advantage (Part C) plans offer additional benefits, including transportation and lower out-of-pocket costs. Services require a physician's referral and must be at approved facilities.
7. Barriers to Participation and Physician Strategies
Many patients encounter barriers to CR participation, including lack of awareness, misconceptions about its benefits, and logistical challenges like transportation and time constraints. Systemic issues, such as a shortage of CR centers in underserved areas, and financial barriers, such as inadequate reimbursement rates to institutions and high operational costs, also contribute to these disparities. Physicians can address these barriers by educating patients about the importance of CR and emphasizing its role in recovery and long-term health. Improving reimbursement policies, expanding insurance coverage, and offering alternative models such as home-based or virtual cardiac rehabilitation can enhance access to CR and increase participation rates.
Health disparities in cardiovascular outcomes significantly impact underrepresented populations,
particularly women, older adults, rural populations, and ethnic minorities, like African American and Hispanic patients, who experience lower referral and participation rates in CR despite higher risk levels.2,3 Contributing factors include socioeconomic status, access issues, cultural and language barriers, and healthcare biases.4 Addressing these disparities requires a multifaceted approach, including increased awareness among healthcare providers, culturally competent care, and policy reforms to ensure equitable access to CR. Communitybased interventions, such as mobile CR units or partnerships with local organizations, can improve access for underserved populations.
9. Advances in Cardiac Rehabilitation Technological advancements and telemedicine are transforming CR delivery. Virtual CR programs combining digital monitoring with home-based exercise demonstrate similar efficacy to traditional inperson programs, improving patients' exercise capacity and quality of life. Wearable devices and smartphone apps enable real-time monitoring, which encourages patient participation and adherence while providing valuable data to healthcare providers. Additionally, precision medicine offers the potential to tailor CR programs based on genetic profiles, enhancing their effectiveness.
10. Conclusion and Call to Action
Cardiac rehabilitation is a vital component of cardiovascular disease management, offering a comprehensive approach to recovery that reduces mortality, improves quality of life, and prevents recurrent events. Physicians are crucial in ensuring timely referrals and supporting patients through their rehabilitation journey. By addressing barriers to participation, advocating for policy changes, and intelligently embracing technological advancements, healthcare providers can improve access to CR and promote health equity. The evidence is undeniable: CR saves lives, improves outcomes, and is essential
for the holistic care of patients with cardiovascular disease. As healthcare providers, we are responsible for prioritizing CR integration into routine care and advocating for its broader implementation to benefit our patients with cardiovascular disease.
References:
1. McMahon S, Ades P, & Thompson P. The role of cardiac rehabilitation in patients with heart disease. Trends Cardiovasc Med. 2017;27(6):420-425. doi:10.1016/j.tcm.2017.02.005.
2. Keteyian S, Jackson S, Chang A, et al. Tracking Cardiac Rehabilitation Utilization in Medicare Beneficiaries: 2017 UPDATE. J Cardiopulm Rehabil Prev. 2022;42(4):235-245. doi:10.1097/ HCR.0000000000000675
3. Oehler A, Battel L, & Poornima I. Cardiac Rehabilitation and Health Care Disparities in the Post-COVID-19 Era. American College of Cardiology. https:// www.acc.org/Latest-in Cardiology/ Articles/2023/09/25/14/05/CardiacRehabilitation-and-Health-CareDisparities-in-the-Post-COVID-19-Era
4. Carew A, Taylor E, Pritchard I, et al. Ethnic Minorities' Experiences of Cardiac Rehabilitation: A Scoping Review. Healthcare (Basel). 2023;11(5):757. Published 2023 Mar 4. doi:10.3390/ healthcare11050757
By: Keith T. Kanel, MD & Raymond E. Pontzer, MD
The ACMS Board of Directors held their first board meeting of 2025 on Tuesday, February 11th. The meeting opened with a warm welcome from 2025 Board Chair, Raymond E. Pontzer, MD, who emphasized the critical role of the Executive Committee in ACMS operations, while reminding the Board that major decisions require full approval from the entire board. Joining the Board in 2025 are new directors Sharon Goldstein, MD, Kevin Kotar, DO, and Nicole Velez, MD, as well as reelected members Prerna Mewawalla, MD, Raymond Pan, MD, and David Dietrick DO.
Following the unanimous approval of the Consent Agenda, the meeting transitioned to committee updates.
Treasurer William Coppula, MD, and ACMS Executive Director Sara Hussey, MBA, CAE led the Finance Committee's presentation, offering a transparent review of the year's first-month financials. The committee set a clear goal: to strategically discuss how to best use our resources to support our membership initiatives.
The Bylaws Committee, represented by Richard Hoffmaster, MD, had no immediate updates but signaled potential revisions on the horizon. Similarly, Kirsten Lin, MD, from the Nominating Committee, noted a quieter season for nominations but promised updates in the spring.
The Executive Committee update expressed gratitude to board members accepting appointment to key ACMS Committees, including: Micah Jacobs, MD, Dr, Dietrick, and Dr. Goldstein to the Finance Committee; and Michael Best, MD, and Anu Anand, MD, to the Bylaws
Committee.
James Latronica, DO, provided an in-depth PAMED update, sharing that the ER Overcrowding Taskforce encountered a roadblock, with further developments expected in March. He also detailed the ongoing efforts of the Physician Unionization Task Force, which meets every five weeks. The task force is exploring various options, such as transforming PAMED into a union, spinning off a subsidiary, or affiliating with a guild. These discussions sparked lively conversations about models for local negotiations and the implications for physicians across Pennsylvania.
Michael Aziz, MD, the 2025 ACMS Delegation Chair, offered insights in the Delegation Update, focusing on harnessing current momentum to address members' needs. He encouraged engagement with PAMED Legislative staff to craft targeted resolutions, emphasizing the support available for those interested in drafting. With resolutions due by July 1, 2025, Dr. Aziz highlighted recent examples, including inclusive clothing in operating rooms and school vaccine requirements, to inspire participation.
Ad hoc committee updates brought attention to the Women in Healthcare Committee, with an update led by Dr. Velez who serves as a member on the Women in Healthcare committee. She shared excitement about the upcoming March 5th event at Ritual House, which includes dinner, drinks, and a one-hour CME session. With registration already halfway full, plans are also underway for a summer event and a fall conference in collaboration with AHN.
The Membership Task Force,
spearheaded by Dr. Lin and Keith Kanel, MD, has been particularly active, holding three meetings since late 2024. The task force introduced a Membership Map, featured in the board packet, and welcomed new student member Marissa Tremogli-Barkowski, who provided valuable insights on student engagement. The committee is dedicated to retaining full active members by showcasing the value of membership through initiatives like the Women in Healthcare events and new member benefits, such as discounts on travel, sports, and cultural events. A focus group will be launched to better understand why some full active members have left.
Membership growth is notable, with introductory rate numbers more than doubling compared to last year. The task force plans to engage new members through social events and is exploring subsidizing tickets for the Distinguished Awards. Discussions about scaling dues and setting ACMS dues will continue in the Finance Committee.
In her Executive Director Update, Ms. Hussey highlighted key upcoming events, including the Women in Healthcare event and a Legislative Update with Dr. Venkat. She shared the team's recent participation in the Variety “My Bike” program, a grant recipient of the ACMS Foundation, and reported increased utilization of the PWP program. A successful scrub drive resulted in over 100 women receiving scrubs.
Financially, ACMS ended the year strong, with investments surpassing
$1 million. Association services are expanding rapidly, with major conferences scheduled for March and April and potential partnerships with two additional associations on the horizon.
For the first time, Allegheny County will have the most delegates at the 2025 House of Delegates, driven by increased student and resident participation. Targeted marketing efforts will focus on advocacy, an area of keen interest for these groups.
Sara invited Board members to a Foundation breakfast event on February 28 at Babb and encouraged them to set up meetings with local legislators, emphasizing the importance of keeping ACMS informed for coordinated advocacy efforts.
In his President’s Update, Dr. Kanel outlined three key priorities for the year: Increasing member involvement in political advocacy, developing the ACMS contingent for the PAMED House of Delegates (HOD), and growing the Physician Wellness Program (PWP). He discussed Governor Shapiro’s recently announced 2025-26 Budget proposals, which includes the somewhat controversial granting of full practice authority to nurse practitioners—a development he urged physicians to monitor closely as it is debated by the state legislature.
ACMS has always worked closely with our colleagues at PAMED Government Relations in developing our policy priorities, and the new Board held a vigorous open discussion of how we
can best give our members voice in Harrisburg. Last year saw hard-fought successes in areas such as physician contracting, restrictive covenants, emergency room overcrowding, and prior authorization rules. Ahead lie new challenges, like scope of practice, support for our neighboring rural counties, and fair reimbursement to keep physician practices strong. The Board expressed excitement to engage in these important areas.
Dr. Aziz represents ACMS in PAMPAC, focusing on donations while PAMED leads advocacy efforts. Dr. Venkat will offer a virtual legislative update in February, with a fundraiser scheduled for May.
By: Sara C. Hussey, MBA, CAE — ACMS Executive Director
As physicians, one of your most critical roles is to empower our patients to make informed decisions about their health. An area often overlooked, yet profoundly impactful, is encouraging patients to complete an advanced directive. With the new year upon us, this is an ideal time to initiate these essential conversations with your patients.
What Are Advanced Directives?
Advanced directives are legal documents that allow individuals to outline their preferences for medical care in the event they cannot communicate their wishes. These documents include a living will and the designation of a healthcare power of attorney (POA). A living will specifies the types of life-sustaining treatments a patient may or may not want, such as mechanical ventilation or artificial nutrition. The healthcare POA identifies a trusted individual to make medical decisions on the patient’s behalf.
Why Are Advanced Directives Important?
Advanced directives provide clarity and guidance for healthcare teams and families during emotionally charged situations. By outlining preferences in advance, patients reduce the likelihood of family disputes, ensure their values and wishes are respected, and alleviate the emotional burden on loved ones forced to make difficult decisions.
From a clinical perspective, advanced directives facilitate better care coordination and decision-making. They provide a clear framework for implementing patient-centered care, particularly in critical care settings or at the end of life.
Physicians are uniquely positioned to guide patients in understanding and completing advanced directives. Here’s how we can take a proactive approach:
1. Start the Conversation Early: Discuss advanced directives during annual wellness visits or routine check-ups. Framing it as part of overall health planning helps normalize the discussion.
2. Educate Patients on the Process: Patients may feel overwhelmed by the prospect of completing legal documents. Provide resources, such as templates or links to reliable sources like the Allegheny County Bar Association’s guide to living wills (available at https:// www.acba.org/?pg=living-will).
3. Address Misconceptions: Many patients believe advanced directives are only for the elderly or terminally ill. Reinforce that these documents are essential for all adults, as unforeseen events can happen at any age.
4. Collaborate with Families: Encourage patients to discuss their wishes with family members and the individuals they plan to designate as healthcare POA. Open communication helps ensure everyone involved understands the patient’s choices.
5. Incorporate Advanced Directives into Practice Workflows: Documenting discussions about advanced directives in the patient’s medical record and regularly reviewing them ensures that preferences remain up-todate.
The start of a new year is a natural time to set goals and prioritize important tasks. Encourage your patients to include completing an advanced directive as one of their resolutions. By presenting this as a proactive and compassionate step, you can help patients feel empowered rather than apprehensive.
Consider utilizing your practice’s communication channels, such as newsletters, patient portals, or social media, to share information about the importance of advanced directives. Providing easy access to resources and emphasizing the benefits can inspire patients to take action.
Several years ago, the Allegheny County Medical Society and the Allegheny County Bar Association collaborated to create an Advanced Directive document. This resource, available as a public service, supports patients in recording their wishes for end-of-life healthcare decisions. Feel free to direct patients to this form on the ACMS website: https://www.acms. org/resources/advanced-directive/




On January 22, we kicked off the new year with a fantastic leadership social at Cadence + Cellar Speakeasy. It was a great opportunity to reconnect with familiar faces, meet new colleagues, mingle, and hear ACMS President Dr. Keith Kanel’s insights on the upcoming year. Thank you so much to all of the leaders from the ACMS Board, ACMS Delegation, ACMS Foundation, and PAMED leadership for attending.










By: PAMED Advocacy Team – Contact: Zachary Gates, Senior Director, Government Relations
It’s no secret that our political landscape is polarized. From school boards to the halls of congress everyone seems angry about something. Finger pointing, in most circles, has replaced collaboration and problem solving. The political noise is deafening. So, what’s the solution?
Relationships and mutual trust.
The most essential element to effective advocacy is relationship building and delivering a consistent message to legislators. Staying focused on legislative objectives while ignoring “political noise” can be daunting, but it’s not insurmountable. It takes patience and a little intestinal fortitude.
Organized medicine, be it the AMA, PAMED, specialty societies, or ACMS, has a full agenda, as established priorities are juxtaposed to the political reality of what is truly attainable. While physician issues are diverse and wide ranging, collectively we communicate a consistent message…giving physicians the clinical autonomy to do what is in the best interest of their patients. Of course, there are issues tangential to delivering quality patient care such as addressing the issue of non-compete agreements in physician contracts, further reforms to prior authorization, and ensuring that physicians remain leaders on healthcare teams.
At the state capitol, our General Assembly is a divided house with a republican majority in the State Senate and the House of Representatives narrowly controlled by democrats. One might view this division as universal gridlock from the perspective of attaining legislative goals. But it doesn’t have to be that way.
PAMED, through its legislative staff and physician engagement, maintains a steady hand in helping to shape sound public policy as it relates to patient care and the ability of physicians to provide care autonomously. Again, consistency in messaging and maintaining respectful lines of communication with lawmakers and their staff is imperative. Make no mistake, physician engage does have an impact.
Although the current legislative session is already underway, PAMED started late last year to identify credible pathways on priority issues such as Medicare and Medicaid reimbursement, scope of practice expansion, and non-compete physician contracts. Those efforts are ongoing along with the expectation that access to mental health services and Emergency Department overcrowding—two issues that frequently go hand-in-hand—will likely find their way to the front of the line as well.
What can you do to help? The simple answer is engage.
There is no downside to professional advocacy. The advocacy process can be challenging and at times, even downright frustrating. However, if you take the time to engage in the process, learn how the system works, and accept its limitations and potential outcomes, the process can be both productive and rewarding. To get started, use the following as your guide:
First, know your elected officials. Every physician should know who their elected representatives are. If you don’t know, here’s a link that will help identify them. Find Your Legislator
Second, are you registered to vote,
and do you vote consistently? Voter registration rolls are public information. When you meet with lawmakers there’s a strong likelihood that they’ve checked to see if you’re registered. If you’re not registered, here’s a link to facilitate that. Voter Registration Application Third, get to know your legislators. Make an appointment to meet them. You don’t have to discuss a legislative issue on your first visit, in fact, it’s better that you don’t. The important thing is to develop a trusting relationship. Offer to be a resource to them. If you’re in private practice, consider inviting them to visit your office to learn firsthand what happens behind the scenes…especially as it relates to insurance hassles like prior authorization, claim denials, or credentialing. If you need additional guidance, reach out to PAMED’s government relations staff.
Lastly, don’t shy away from “political” advocacy…supporting the Pennsylvania Medical Society’s political arm, PAMPAC. “Legislative” advocacy and “political” advocacy are interdependent. With financial support from physicians, PAMPAC helps to elect candidates that are sensitive to the concerns of physicians. Use this link to contribute to PAMPAC Join PAMPAC
Given the sheer volume of bills introduced each legislative session, legislators are unable to digest the details of every bill. While PAMED, through its legislative staff, works to inform and educate policy makers on legislative proposals, when a local physician engages with their representatives the result is far more effective. Personal relationships
between legislators and their physician constituents are the ultimate in legislative advocacy.
As a group, physicians have a unique ability to help shape legislative policy and sway public opinion. When appropriate, and at your discretion, discuss with patients’ legislative issues that impact your ability to appropriately care for them. Patients and legislators trust and respect your opinion. Give them the benefit of your knowledge.
So, be part of the solution to better government. Get involved. Meet your elected officials and develop a trusting relationship that will benefit both parties. With the right touch physicians can be a positive influence in helping to shape health care policy…and unlike organic chemistry, there’s no chance you’ll contaminate your product, use the wrong reagent, or ruin your synthesis!
You can do this!
Advocacy Resources
Stay informed & get involved with PAMED's advocacy resources!

By: Zach Marsh – Director of Communications, Development & Special Events at Variety
With a mission to empower children with disabilities to live life to the fullest, Variety the Children’s Charity provides social inclusion experiences and lifechanging mobility and communication equipment to ensure our most vulnerable kids are no longer left out, behind, or excluded.
Specifically, Variety kicked off its My Bike Program in November 2012 by providing Aubrey with the first adaptive bike after hearing that kids were missing this childhood milestone. Due to My Bike’s overwhelming success and impact, Variety listened to parents explain other critical needs of their kids that were not being met, and we launched My Stroller (adaptive strollers) and My Voice (communication devices) in 2014. Over the years, Variety has created an innovative program model that can easily be replicated to meet the needs of more kids, as we quickly expanded from 10 counties in southwestern Pa. to 59 counties throughout the state.
We know this equipment can provide transformative benefits for our most vulnerable population of kids, but for most families, the cost of this equipment is out of reach (i.e., $2,500 to sponsor one bike, $2,000 for one stroller, and $1,200 for one communication device – with costs expected to increase again soon). Without access to this equipment, many kids are automatically missing out on being included in the community, and as a result, the community is missing out on experiencing the beauty, joy, and uniqueness of the kids.
Due to the need and impact of the equipment, Variety’s programs have
become institutionalized throughout our service area, and with the incredible support of the community, My Bike, My Stroller, and My Voice have provided more than 8,200 adaptive bikes, adaptive strollers, and communication devices (worth more than $12.4 million in equipment) – with more than 19% going to youth in Allegheny County. These programs are meeting unmet needs and aim to improve the child’s social inclusion, health and wellbeing (including their safety), participation in the community or school setting, relationships with family and friends, as well as many more benefits on an individual level. The beauty is that receiving a new adaptive bike, adaptive stroller, or communication device is only the beginning for how that child and their family will ultimately be impacted.

5-year-old Lyla received her own communication device from Variety in 2023, and then in 2024, her mom, Rebecca shared this joyful update: “Lyla is doing so well with her communication device! When we last emailed, we were amazed with how quickly she started using it at age 3! She continues to thrive using the device. Now, she tells us her shapes, numbers, letters, colors, feelings, toys she wants, plays music, and listens to books on her tablet. She also lets her therapists know what activities she would like to do on that day. She loves picking out her snacks and meals as well on her tablet. It has been so helpful! She can even say “I love you on her tablet!!... Thank you again!” By listening to families and partners directly serving the kids, we’ve learned first-hand that riding an adaptive bike can provide transformative physical, mental, and emotional benefits; an adaptive stroller completely transforms the lives of the kids and their families, immediately; and a communication device opens up a whole new world of possibilities at home and school.
If you know of a child that could benefit from their own adaptive bike, adaptive stroller, or communication device, they can visit www. varietypittsburgh.org to learn more or get started on the process. Currently, My Bike and My Stroller are operating on a waitlist to ensure funding is confirmed before families complete a full application, but My Voice is actively accepting new applications.
More than anything, Variety needs funding to keep providing this equipment (especially bikes and strollers), as the need is great, and
Variety must raise the funds for every piece of equipment. By continuing to provide the equipment, we’re not only helping children, and their families live an inclusive, healthier quality of life, but within the community, we’re building a movement to rally behind the kids. If you or your organization want to get involved with Variety, please reach out to Tom Baker, Variety CEO at tom@ varietypittsburgh.org or (724) 933-0460.


By: Nadine Popovich, Melanie Mayer and Haley Thon
Allegheny County Immunization Coalition (ACIC) — 2024 Chair - Patrick Hussey, PharmD, MBA: The Allegheny County Immunization Coalition (ACIC) invites you to participate in our 2025 General Membership Meetings, held at the AIU Building and via Zoom from 9:00 AM – 11:00 AM on March 20, June 19, September 18, and December 11.
We’re also proud to support maternal and child health through Beverly's Babies Baby Shower Events in Monroeville on February 14 from 11:00 AM – 1:00 PM and Duquesne on February 26 from 11:00 AM – 1:00 PM. Both events are open to the public, and we encourage registration to ensure participation.
Allegheny County Immunization Coalition membership is free and funded by our grants. All healthcare professionals with an interest in vaccination are welcome. See our website for full details on membership and how to volunteer at our community events: http://www. immunizeallegheny.org
American College of Surgeons Southwestern Pennsylvania Chapter (ACS-SWPA) — 2024 President – Richard Fortunato, DO, FACS: The Southwestern PA Chapter of the American College of Surgeons continues to advance its initiatives for 2025. Planning is underway for the March Resident Event, "Debates and Dilemmas," with final details to be announced soon. The chapter remains committed to expanding engagement opportunities, including new networking and professional development initiatives for active surgeons. Efforts to fill leadership positions and recruit new
Fellows also remain a priority. Stay tuned for more updates as plans for the year take shape.
Pennsylvania Geriatric Society Western Division (PAGS-WD) — 2024 President - Heather Sakely, PharmD, BCPS, BCGP: Registration is live for 33rd Annual Virtual Clinical Update in Geriatric Medicine. https://cce.upmc. com/33rd-annual-clinical-updategeriatric-medicine
We invite you to attend the 33rd Annual Virtual Clinical Update in Geriatric Medicine conference scheduled for April 24-25, 2025. Although the program is presented in a virtual format, the goal is unchanged: to provide an evidence-based approach to help clinicians take exceptional care of these often complex and frail individuals. We’re excited to introduce a new format for this year’s course, emphasizing Fostering Age-Friendly Care through the 5Ms including mentation, medication, mobility, what matters most and multi-complexity
Join us from the comfort of your home or office for an outstanding agenda of lectures and panel discussions. This AGS award-winning course is a collaboration between The University of Pittsburgh, the AGS state chapter, and many healthcare organizations. Brochures are available to view on pagswd.org. Questions may be directed to Haley Thon, Administrator (hthon@acms.org).
The Pittsburgh Ophthalmology Society (POS) — 2024 President - Pamela P. Rath, MD: Pittsburgh Ophthalmology Society Hosts February 6 Meeting Featuring Dr. Mark Westcott

The Pittsburgh Ophthalmology Society (POS) welcomed a robust audience of 70 physicians to its February 6 meeting, featuring distinguished guest speaker Mark Westcott, MD, FRCOphth, Adjunct Professor in Ophthalmology, University of Pittsburgh; Consultant at Moorfields Eye Hospital, University College London and St. Bartholomew’s Hospital, London, UK.
Dr. Westcott, a globally recognized expert in uveitis, inflammatory eye disease, and glaucoma, delivered two insightful lectures: "The Challenge of Ocular TB – What Have We Learned from the COTS Study, and Its Relevance to North America" and "Tips and Tricks in Getting the Diagnosis in SightThreatening Uveitis – How to Get It Right." His presentations were met with enthusiasm, sparking engaging discussions among attendees. With over 22 years of experience as a Consultant Ophthalmologist at prestigious institutions, including
Moorfields Eye Hospital and St. Bartholomew’s Hospital, Dr. Westcott brought a wealth of knowledge to the evening.
The February meeting concludes the POS 2024-2025 Monthly meeting series. Planning for the 2025-2026 series is underway. Members will receive notification in May which will include the dates of each meeting and the guest presenter.
Registration Now Open for the 60th Annual Meeting and 45th Ophthalmic Personnel Meeting – March 21, 2025
Under the leadership of President Pamela P. Rath, MD, POS is proud to host the 60th Annual Meeting and the 45th Annual Meeting for Ophthalmic Personnel on Friday, March 21, 2025, at the Omni William Penn Hotel in Pittsburgh, PA. These premier events provide stellar opportunities for
education and networking in a collegial environment.
The Society is honored to welcome the 44th Annual Harvey E. Thorpe Lecturer, Ralph C. Eagle, Jr., MD, a world-renowned expert in ophthalmic pathology from Wills Eye Hospital. Dr. Eagle, known for his landmark textbook on eye pathology and numerous prestigious accolades, will deliver several highly anticipated lectures. Additional esteemed guest faculty members include Kendall E. Donaldson, MD, MS; Peter A. Netland, MD, PhD; and Mark A. Rolain, MD, who will share cutting-edge insights on various ophthalmic topics.
Running concurrently, the 45th Annual Meeting for Ophthalmic Personnel will provide attendees the opportunity to earn up to 7 IJCAHPO credit hours. Course directors Avni
Vyas, MD; Cari Lyle, MD; Jeffrey Wincko, MD; and Gideon Nkrumah, MD have planned a dynamic program featuring a skills workshop led by Jane Shuman, MSM, COT, COE, OSC, and a risk management course presented by Dr. Rolain on behalf of the Ophthalmic Mutual Insurance Company (OMIC).
Additional sessions will cover important topics such as diabetic retinopathy, ocular emergencies, and pediatric ophthalmology, with lectures from respected local faculty who are also POS members.
Registration is now open! For details on both events and to secure your spot, visit www.pghoph.org. Questions may be directed to Nadine Popovich, Administrator (npopovich@acms.org).