
Allegheny County Medical Society

Allegheny County Medical Society
Allegheny County Medical Society
Editorial
• Reunion
Deval (Reshma) Paranjpe, MD, MBA, FACS
Editorial
• Avoiding Rash Decisions
Charles Mount, MD
Editorial
• 2025 Pittsburgh Marathon Anthony Kovatch, MD
Membership
• Q&A with Rachel Toney, MD
ACMS News
• Call For Nominations
ACMS News
• Member Acknowledgements
ACMS News
• Specialty Group Updates
ACMS Staff: Nadine
Popovich, Melanie Mayer and Haley Thon

Article
• What We're Losing in the Storm Keith T. Kanel, MD
Medical News
• Reportable Diseases 2025: Q1 Allegheny County Health Department Selected Reportable Diseases/Conditions
Kristen Mertz, MD Allegheny County Health Department
Article
• MJ's Q&A MJ Lerma, MPH
Materia medica
• Aprocitentan (Tryvio®)
Chaise Stiteler, PharmD and Alexa Wardoclip, PharmD, BCPS

2025
Executive Committee and Board of Directors
President
Keith T. Kanel, MD
President-elect
Kirsten D. Lin, MD
Secretary
Richard B. Hoffmaster, MD
Treasurer
William F. Coppula, MD
Board Chair
Raymond E. Pontzer, MD
Board of Directors
Term Expires 2025
Anuradha Anand, MD
Amber Elway, DO
Mark A. Goodman, MD
Elizabeth Ungerman, MD, MS
Alexander Yu, MD
Term Expires 2026
Michael M. Aziz, MD, MPH, FACOG
Michael W. Best, MD
Micah A. Jacobs, MD, FIDSA
Kevin G. Kotar, DO
Jody Leonardo, MD
Term Expires 2027:
David J. Deitrick, DO
Sharon L. Goldstein, MD
Prerna Mewawalla, MD
Raymond J. Pan, MD
Nicole F. Velez, MD
James Latronica, DO, DFASAM
Richard B. Hoffmaster, MD
Finance
William F. Coppula, MD
Nominating
Kirsten D. Lin, MD
Women’s Committee
Prerna Mewawalla, MD & Meilin Young, MD
Managing Editor
Sara C. Hussey, MBA, CAE
ACMS Executive Director shussey@acms.org
Medical Editor
Deval (Reshma) Paranjpe, MD reshma_paranjpe@hotmail.com
Bulletin Designer
Victoria Gricks victoria@thecorcorancollective.com
2025 Bulletin Editorial Board
Richard Daffner, MD, FACR
Robert Howland, MD
Anthony Kovatch, MD
Charles E. Mount, MD, FAAD
Alexandra Johnston, DO
John P. Williams, MD
Executive Director
Sara Hussey shussey@acms.org
Vice President - Member and Association Services
Nadine M. Popovich npopovich@acms.org
Manager - Member and Association Services
Haley Thon hthon@acms.org
Operations CoordinatorACMS & ACMS Foundation
Melanie Mayer mmayer@acms.org
Manager - Operations and Finance
Elizabeth Yurkovich eyurkovich@acms.org
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
EDITORIAL/ADVERTISING
OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323.
USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.
Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorsement of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
COPYRIGHT 2025: ALLEGHENY COUNTY MEDICAL SOCIETY POSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212. ISSN: 0098-3772

By: Deval (Reshma) Paranjpe, MD, MBA, FACS
In a few weeks, I’m going back to a beautiful little city—Providence—where over the course of eight years I grew up. I started out as a kid without a driver’s license, knowing no one, scared of my own shadow. I ended up as a graduating medical student who had seen birth, terror, suffering, tears and death. I was now capable of putting in lines, retracting, drawing ABGs doing rectal exams, doing a killer H+P, and acing scutwork. (None of which I do now as an ophthalmologist. Well, maybe the H+P and the scutwork.)
Providence carries a lot of memories— cold sea winds, endless rain, and those brutally bright blue New England skies. Memories of nights spent in the library, of maniacal Orgo professors, of endless thesis work in a roomful of computers and a small Komodo dragon that wouldn’t stop staring at me, of the comforting clatter of the dining halls, of spare and spartan dorm rooms, and of battling through blizzards on the way to exams.
Memories of medical school also come flooding back--the smell of the anatomy lab, the inability to eat chicken on the bone for a full year for fear of being able to identify structures, the endless pathology slides, pathophysiology sessions where we were all convinced we had every disease we studied…until the next unit came along. Long days and nights studying for Step 1, ice cream treats, pizza parties, the arduous and nerve wracking process of applying for an early match. So much emotion compressed into four years.
But what I miss and remember most of all are the people. Everyone in college was a jewel waiting to be discovered, with a myriad of glittering and exotic
facets. Everyone had something to teach you in spite of themselves. I remember such a sense of wonder as I met new people and imagined what their lives were like. There were students from all over the country and from all over the world who had grown up in every conceivable way.
When I think of this, I try to summon some of that excitement back to today’s reality and apply that same attitude to people I meet now. How must their backgrounds have shaped their experience and the prism through which they view the world? Asking these questions is a skill that may be needed more today than yesterday.
I remember how lost I was when I left Providence and ventured into the real world of residency. Gone were familiar people; gone was home. I wondered what lives my classmates were living and what they were discovering.
The first college reunion was an exciting time—people were getting married, a few were having children, many were forging ahead in their careers, still uncertain of where life would take them. The next reunion’s theme was weddings--so many new partners to meet. The next one was full of babies—in strollers, in carriers, on hips and toddling everywhere.
The reunions after started to bring divorces, physical transformations, career changes, and anxiety. Some people who had gone into tech in Silicon Valley were actually retired, and some of those people moved on to second careers doing things they loved. Everyone else still struggling on the hamster wheel suddenly felt slightly inadequate or behind the eight ball, but
also relieved and happy for the ones who made it out. Now there was a goal to attain; the finish line was suddenly announcing itself and in sight.
Then came the pandemic, and the reunions were cancelled. Everyone connected over Zoom reunions, and the jobs and the titles and the family angst melted away. We were all kids again having deep conversations at 2 am in dorm hallways and having online dance parties in our pajamas (except this time kids and spouses joined in). My college, which is known for its do-gooders and can-do attitude, delivered via its alumni. I watched as a newly-elected state attorney general offered a veteran public school teacher a civics and law lesson for his students—in person. I saw others offer internships to kids who needed them and put together charitable efforts. None of these people knew each other in college, but none of that mattered now. We were all siblings, forged from the same crucible.
I’m looking forward to embracing old friends and making new ones. I’m looking forward to remembering who I was, figuring out who I’ve become, and setting goals about whom to become as I continue to grow.
I’m looking forward to ice cream and coffee and cheap eats on the main drag, seeing the memorial to a dear old friend, and feeling that all-pervasive, all-knowing Providence wind coming off the water and through my bones once again. I’m looking forward to a renewed sense of purpose.
You can go home again, but it will have changed, and may change you.
Wishing you all wonderful reunions of your own.

If employed by a health system or in private practice.
Contact John Fenner Cell: 412-638-1846
Email: fenner@fennercorp.com
Three Penn Center West Pittsburgh, PA 15276 fennercorp.com Specializing in Hospital and Physician Consulting and Billing Since 1991


By: Keith T. Kanel, MD – President, Allegheny County Medical Society
From Washington to Pittsburgh, ACMS President Keith Kanel reflects on recent disruptions – and loss – in federal medical research.
Bloated. Duplicative. Wasteful. Politicized. Those are but a few of the terms used to justify the rampant and lamentable dismantling of the U.S. Department of Health and Human Services (DHHS), a process unfolding as I write this article. Things are moving at breakneck speed. The cuts appear deep and durable, and distressingly wanton. Alas, in the pursuit of government efficiency, we may be breaking apart one of the finest health care research and quality networks in the world.
In 2021, I left Pittsburgh to become Director of the Division of Practice Improvement at the Agency for Healthcare Research and Quality (AHRQ) in Washington, DC. AHRQ is one of the 13 branches of DHHS, alongside the National Institutes of Health, the Center for Disease Control, the Food and Drug Administration, and the Center for Medicare and Medicaid Services. AHRQ is the part of government that directly supports doctors, nurses, and practitioners of all disciplines in ensuring that medical care is safe, effective, reported, and backed up by the best scientific evidence.

AHRQ had funded early research I led a decade ago to embed depression and substance abuse screening in a cohort of Allegheny County primary

care practices, a model that we rapidly disseminated to three other states, ultimately screening over 60,000 patients. It directly impacted the way we provide care in this community and beyond.
In moving my career to AHRQ, I had the privilege of working alongside some of the premier health researchers in the country. My team coordinated national projects to reduce opioid abuse, improve cardiovascular risk reduction, expand telehealth access, and empower community practices to fast-track evidence-based medical advances directly to the frontline of care. I joined AHRQ during the first Trump administration and left in the Biden administration.
Politics rarely influenced what we did. We worked by convening and cooperation. Through strategic grantmaking, we built partnerships
between federal agencies, with universities and public health entities, and directly with neighborhood hospitals and practices to “move the needle” in making healthcare better, safer, and more accessible for Americans.
Many of you may never have even heard of AHRQ. But if you are a practicing physician, you benefit from its work every day:
Do you recommend your patients receive mammograms, colonoscopies, and immunizations on a schedule? If so, you are likely using guidelines from the U.S. Preventive Services Task Force, an independent advisory managed by AHRQ. In it, leading physicians from around the country are selected to scour the literature to update guidelines we use daily, from whether 50-year-old men should take a daily aspirin to prevent heart attack and
stroke, to the effectiveness of Apple watches in detecting paroxysmal atrial fibrillation.
Have you noticed hospitals proudly marketing their “5-star” ratings? They are likely citing a sophisticated scorecard system from CMS Hospital Compare, publicly available without charge, which allows consumers to shop for care based on quality metrics. The core of Hospital Compare is AHRQ’s HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) surveys of patient experience, which collects and collates the opinions of thousands of patients every year.
Nursing checklists to codify best practices at the bedside have nearly eliminated central-line associated bacteremia and ventilator associated pneumonia in ICUs. How to build and customize these simple tools, efficiently train staff, and deploy them to the frontline was the result of the AHRQ-funded CUSP (Comprehensive Unit-based Safety Program) Initiative, a collaboration of multi-disciplinary patient-safety experts across dozens of research sites who sought to understand what works and what doesn’t, and then engaged hospital

The division I led – whose mission was to support providers in improving medical practice – is completely gone.
partners in ensuring that the evidence was translated into routine practice. This commitment to quality science has saved countless lives.
The very antibiotics used to manage community-acquired pneumonia were worked out by the AHRQ-sponsored PORT (Pneumonia Outcomes Research Team) trial, pridefully based at our own University of Pittsburgh School of Medicine. The clinical prediction tool developed helps physicians decide whether to admit to the hospital, transfer to the ICU, or discharge home, and to this day can be found on the smart phones of many emergency medicine physicians.
These are but a few of the important but too-often unheralded accomplishments of AHRQ since its inception in 1989.
Not every AHRQ initiative was successful or useful. Many flopped. Such is the nature of science; we design experiments to test our intuition in the real world. A negative result can be as important as a positive one in steering us away from ineffective investments of time or resources. Sometimes what is learned is neither groundbreaking nor transformative, but rather just “a drop in the bucket” that, when added to a multitude of other drops points us in an important new direction. Medical science has always been built brick-by-brick, by singleshitters with tenacity to keep trying, in it for the long haul. AHRQ exemplified that ethos, and we as physicians benefited.
But in April 2025, this all changed.
AHRQ, as well as many parts of DHHS, was deemed “expendable”. If you went to the home offices of AHRQ today, you’d see a sea of empty desks. Much of its incredible staff is being scattered through reorganization, early retirement, and furlough. The division I led – whose mission was to support providers in improving medical practice
– is completely gone. What is left of the agency is expected to be absorbed into an entirely new division at DHHS with a different, as-yet-to-be fully defined mission. Ongoing research all over the country is losing its backing, and the fate of decades of invaluable, taxpayerfunded intellectual property is unclear.
The demise of AHRQ is being replicated throughout government. From cancer research to food security to vaccine development, we’re seeing the suspension of programs that support our everyday work as doctors. What is happening in Washington today has the fury of a storm. As with a storm, we had little warning, and our infrastructure has been compromised. And like any community hit by a storm, it will be a while before we can fully assess the damage, as well as the full extent of the rebuilding that will be needed. Make no mistake; in medicine we’ve lost things that will take years – if not decades – to restore.
Our commitment at the Allegheny County Medical Society is, as it has always been, to speak on behalf of our doctors, our patients, and our community. We need to keep our collective finger on the political pulse of the country, to be an active participant in the process, and be prepared to respond when our foundational institutions are under siege. Although we pause to lament what we’ve lost in the storm, we have work to do.









By: Charles E. Mount III, MD, FAAD - Associate Director of Allegheny Health Network Cancer Institute Skin Cancer Center
With May being Skin Cancer Awareness Month the annual ritual would be to remind everyone of the importance of sun protection. However, this year I have opted to try to provide some user-friendly guidance on the evaluation of rashes to improve the efficiency and accuracy of patients’ workups and to preserve your sanity in the process. According to a 2016 study by the American Academy of Dermatology (AAD) one in four Americans were impacted by skin disease yet only one in three of those Americans saw a dermatologist1 Perhaps in your real life experience it seems obvious, but the likelihood of patients being worked up for rash prior to or without dermatology evaluation is more likely than not.
When first evaluating a rash you don’t have to be an expert, but you can exclude or include low hanging fruit to narrow your quest. Remember that eczematous conditions are the most common class of dermatoses after infections so if you’re a betting person if it isn’t infection statistically it is likely eczema or a form of it. Eczema affects approximately 10% of US citizens whereas psoriasis affects 1-2%2 and other diseases are even less common. Whereas children typically have congenital elements of atopic dermatitis adults with new onset eczema typically often have acquired forms such as irritant or allergic contact dermatitis (ICD/ACD) from their longstanding skin and hair products or other external contact sources. In the elderly many patients suffer from eczematous conditions at least in part due to the natural degradation of the
skin barrier with age. Anecdotally, in our Autoimmune Institute I would argue over half of patients who are self-referred for chronic rashes have some form of an eczematous condition and not an autoimmune (AI) skin disease. Even many patients referred by other specialists for Rash NOS also have eczematous conditions as their sole issue or complicating their primary AI disease. Many patients have had hundreds to thousands of dollars in blood tests, yet no one has questioned their skin products or cosmetics as a potential factor. The common misconception I still see in many medical records refers to “no new products or exposures.” Remember that type IV hypersensitivity skin disease (contact dermatitis) almost exclusively develops from chronic exposure, i.e. products that have been used for years. When I’m evaluating a new patient with a suspected non-eczematous disease I still always delve into their personal products as an ICD/ACD component may be complicating their primary condition. Organic, clean, natural based products often contain high levels of fragrance which are among the most common contact dermatitis culprits. I cannot stress this enough, but during your rash exams encourage patients to wear a gown for their examination. You may find areas of their rash hidden under clothing that are helpful in their diagnosis of which they were unaware or they felt irrelevant to their condition. What appears nonspecific on the face or hands may be obviously something else on their trunk or proximal extremities. In addition, you might also spot an asymptomatic skin cancer in
patients who have never had a formal skin cancer screening exam. Especially prudent to consider this summer when phytodermatitis cases are likely to be common, remember with very few exceptions the human body does not like to make linear rashes or those in a geometric shape. So first rule out ACD or another exogenous etiology when you see straight lines, triangles, circles, rectangles, etc.
On the topic of antinuclear antibody (ANA) tests, lupus, and other AI rash workups often our first instinct is to check an ANA when a patient has an impressive facial rash or a photosensitive rash. While over 95% of systemic lupus (SLE) patients have a positive ANA, up to 20% of healthy adults also have a positive ANA and only 11-13% of them might have lupus and some sources suggest even lower numbers3. Furthermore, thyroid disease and some medications may cause an elevated ANA. If you are ordering an ANA for a rash workup it is important to always complete the serology workup with an extractable nuclear antibody (ENA) panel as an isolated ANA often only leads to more questions and anxiety for patient and provider alike. Only about 50% of patients with subacute cutaneous lupus (SCLE) and 10-15% of adult discoid lupus (DLE) patients will have SLE so their ANA results are likely to be normal. Many patients with SCLE, however, will have a positive SSA/Ro antibody which demonstrates the importance of always getting an ENA panel.
If you are doing your own biopsies or reviewing pathology reports for your patients helpful buzz words for
a potential AI etiology are going to be “basovacuolar” and/or “interface” dermatitis often with mucin. The presence of mucin does not rule in lupus (can be a product of chronic sun damage) nor does its absence rule lupus. There can sometimes be a lichenoid pattern reported similar to lichen planus, but there will often be differences on histology and physical exam. Bottom line, regardless of blood tests and antibody profiles rely on your physical exam and a quality skin biopsy result ready by dermatopathology to direct diagnosis and management of complex and/or recalcitrant inflammatory skin conditions.
Lastly, a few words on skin biopsies and pathology results:
1. If you see rashes as part of your practice consider doing biopsies if you don’t already. Complex dermatoses often require multiple biopsies for definitive diagnosis and an early biopsy may avoid delays in appropriate treatment and unnecessary testing. Rashes are often spontaneously resolved or clear with steroids by the time patients see a dermatologist. If you do biopsy know your options of dermatopathology labs you can send to for interpretation as inflammatory specimens are extremely challenging to interpret without experience. Many oral and vulvar biopsies are not read by dermatopathology, but ensure your specimens are if they are biopsies for an inflammatory process instead of a neoplastic one.
2. If your pathology result doesn’t match your clinical concern REBIOPSY and/or of course send for dermatology evaluation. Not all pink papules in an anatomic field are necessarily the same thing. One could easily biopsy lesions consistent with folliculitis, Grover disease, and papular eczema on the same patient within a few square centimeters. If you biopsy eczema in a patient that has lupus you will not uncommonly see concurrent or background histologic lupus changes with spongiotic/eczema changes while the primary problem is still eczema.
Flushing red cheeks in a lupus patient could show patterns consistent with rosacea and lupus, but it’s their rosacea that is flaring with the typical triggers and needs appropriate treatment for such instead of lupus treatment escalation.
3. Inflammatory dermatoses can evolve over time and anatomic site can influence the pathology findings. Early psoriasis looks eczematous and chronic eczema looks psoriatic on histology. Eczema biopsied on the elbow, knee, or acral skin can look psoriasiform. Proceed with caution using the term “biopsy proven” when referring to rashes. Furthermore, always be a critic when you hear a biopsy was “negative” or “nonspecific”. There are often microscopic findings in their report that can aid a provider familiar with dermatopathology to exclude or include certain conditions. A skin biopsy, at least in inflammatory conditions, like any blood test is a just that: a test and not a diagnosis. Furthermore, it is not a positive-negative or black-or-white test result. It is an interpretation of microscopic findings dependent upon the experience and training of your pathologist and the quality of the tiny piece of tissue and clinical history provided to them. A truly daunting task and responsibility of our pathologists of which I am not envious, but eternally grateful. Finally, trust your clinical suspicion over the biopsy result if the patient is not responding to treatment.
The last topic I wanted to cover briefly was the growing role of oncodermatology as a resource for your patients undergoing cancer treatment. An oncodermatologist focuses on the care of skin, hair, and nail concerns and complications of patients undergoing cancer treatment4, 5. Cutaneous adverse effects (AEs) are extremely common in patients undergoing chemo-, immuno-, and radiation therapy. Such side effects not only cause significant reductions in quality of life in patients already suffering from a terrible disease, but when serious enough these complications also threaten to
be a factor in stopping their otherwise effective cancer treatment. Oncologists are often forced to pause or discontinue treatment when cutaneous AEs reach a certain threshold potentially threatening their survival. While it may seem contradictory to use medications classified as “immunosuppressive” many biologics and systemic agents including jak inhibitors used in the management of psoriasis, eczema, and lichenoid conditions are suitable to use in the setting of active cancer/ cancer treatment. They are often more effective and safer when treating cutaneous AEs versus traditional DMARDs and long-term systemic steroids. I would encourage you to be familiar with your dermatologists that are comfortable and experienced in managing cutaneous AEs of cancer treatment to reduce the morbidity of cancer treatment and provide our patients the best quality of life in what time they have left.
References
1. The burden of skin disease in the United States. Lim, Henry W. et al. Journal of the American Academy of Dermatology, Volume 76, Issue 5, 958 - 972.e2
2. Eczema stats. National Eczema Association. (2025, February 27). https://nationaleczema.org/ eczema-facts/
3. American College of Rheumatology. Antinuclear antibodies. https://rheumatology.org/ patients/antinuclear-antibodies-ana
4. Bang AS, Anadkat MJ, Choi JN, LeBoeuf NR, Jung JY, Markova A, Gordon A, Rossi AM, Noor SJ, Sibaud V, Lacouture ME. Oncodermatology: Advancing the Science and Care of Cancer Patients and Survivors. Am J Clin Dermatol. 2022 Jul;23(4):587-589. doi: 10.1007/s40257-02200705-z. Epub 2022 Jul 5. PMID: 35788536; PMCID: PMC10569770.
5. Oncodermatology Society, www. oncodermatologysociety.org/.

Dr. Rachel Toney is an Attending Physician with the Allegheny Center for Digestive Health, part of the Allegheny Health Network. She is also Assistant Professor in the Department of Medicine at Drexel University College of Medicine. She has 15 years of experience in general Gastroenterology, and is passionate about education, mentorship and advocacy.
She is Vice President and has been nominated to be the next President of the Gateway Medical Society in Pittsburgh, a 501c(3) organization and component of the National Medical Association whose Mission is to reduce health care disparities in Western Pennsylvania. Gateway Medical Society (GMS) provides health care symposia to educate healthcare professionals and the community about medical

conditions that disproportionately affect the underserved. It also provides a boy’s mentorship program called ‘Journey to Medicine’ with the goal that some of the students will enter the field of medicine.
Q: CAN YOU SHARE A LITTLE ABOUT YOUR BACKGROUND AND WHAT LED YOU TO A CAREER IN MEDICINE?
A: I was the first person in my family to become a physician and am very proud that my cousin is now the second doctor. As the only child of an Army Colonel father and a Licensed Clinical Psychiatric Social Worker mother, I learned the value of being in service to others and the responsibility associated with being part of something larger than yourself. This background, along with my inspirational high school science teacher, Ms. Pearson, led me to pursue medicine.
Q: WHAT INSPIRED YOU TO PURSUE YOUR CURRENT SPECIALTY?
A: During my Internal Medicine rotation in medical school, I most enjoyed thinking about the digestive system. Gastroenterology is such an innovative and diverse field that there is always something new to learn! Plus, I enjoy the instant gratification of being able to solve a problem using a procedural approach. My work in health care advocacy taught me that only 3.7% of academic gastroenterology
faculty were Black, while Black people represent 13% of the United States population. This has heightened my purpose, since Black people are 20% more likely to be diagnosed with colorectal cancer and 40% more likely to die once diagnosed compared to other groups.
Q: CAN YOU TELL US ABOUT YOUR CURRENT ROLE AND WHAT A TYPICAL WORKDAY OR WEEK LOOKS LIKE FOR YOU?
A: I have a clinical and academic role. An average week consists of three procedural days and two office days, usually at either West Penn Hospital or Allegheny General Hospital, where I will often have a GI Fellow or physician in training with me. Periodically my work is more like a private practice model at our locations in Wexford, McCandless, Forbes, Jefferson and Bethel Park, where our APPs are a vital part of the team. I mentor residents interested in Gastroenterology and work with our Research Fellow to provide them opportunities to publish and present case reports drawn from my clinical practice.
Q: WHAT HAS BEEN THE MOST REWARDING ASPECT OF BEING AN ACMS MEMBER?
A: I enjoy the opportunities to meet other physicians outside of my practice through the multiple ACMS social

events, like the Women’s Networking Event at the Pittsburgh Winery. The monthly Bulletins are informative, especially Dr. Deval (Reshma) Paranjpe’s restaurant recommendations, since I’m a bit of a foodie! ACMS is also a great resource for learning about legislation that affects healthcare and having our voices heard.
Q: WHAT DO YOU THINK IS THE BIGGEST CHALLENGE FACING HEALTHCARE TODAY?
A: Medical mistrust is one of the biggest challenges today. It is partly the result of rising healthcare costs, shortened patient encounters, and the politicizing of the scientific method. But, in the African-American community, this mistrust is informed by medicine's history of unethical practices. A few examples include the Tuskegee syphilis experiment; Dr. James Marion Sims' surgical research conducted on enslaved Black women without anesthesia; and the cervical cancer cells from Henrietta Lacks, taken without her consent, that became HeLa cells which revolutionized cancer research. It is important we address these concerns with our patients but also to engage in community outreach to reassure them that we have their best interests in mind.
Q: WHAT ADVICE WOULD YOU GIVE TO MEDICAL STUDENTS OR EARLYCAREER PHYSICIANS?
A: Build healthy habits now! Schedule rest and play like a doctor's appointment, because it is restorative
to engage your brain in activities other than work. It is easy to fall into the "arrival fallacy" when our medical training is a series of steps. Find joy in the present not just the future. Don't shy away from leadership roles thinking that you are not qualified. You have already demonstrated your ability to learn new things and work well with people. Join a local volunteer or nonprofit organization to raise your sense of belonging to a community. You will make lasting friendships with energetic and positive people outside of medicine who share your altruism.
Q: OUTSIDE OF MEDICINE, WHAT ARE YOUR HOBBIES OR INTERESTS?
A: I enjoy anything that allows me to be creative. This includes sewing, crafting and gardening. City Grows in the Strip or Cavacini Garden Center in Lawrenceville are great local businesses for buying plants. I find many handmade treasures at the annual Shadyside Arts Festival. As an undergraduate, I sang in an a cappella group and am a trained dancer so I regularly attend performances in the Cultural District. I am on the garden committee of the Pittsburgh Alumnae Chapter of Delta Sigma Theta Sorority, Incorporated, founded in 1913. We partner with the Western Pennsylvania Conservancy to plant and maintain the Homewood Brushton neighborhood garden. I also serve on the Board of Directors of Attack Theatre - a 501(c) (3) modern dance company that works with numerous arts organizations throughout Pittsburgh and develops arts education programs for Pittsburgh Public Schools.
Q: HOW DO YOU MAINTAIN WORKLIFE BALANCE?
A: The Apple TV series Severance wonderfully explored the disastrous consequences of having two completely separate lives at work and at home. I think it’s important to accept that, as a physician, our work/life balance is more fluid than in other professions. Nevertheless, you still have to prioritize
the things in your life that are important to you. The “rocks, pebbles, sand, water” analogy comes to mind. My rocks are my close relationships and my health. Without those things being harmonious, my work cannot be productive.
Q: HOW CAN FELLOW ACMS MEMBERS CONNECT WITH YOU OR SUPPORT YOUR WORK?
A: Gateway Medical Society is always looking for speakers for our programming to raise health awareness. Additionally, we want to increase our membership, which also includes physicians in training, dentists, nurses, and allied health professionals. While fulfilling our mission to reduce health care disparities, our goal is also to be a resource for underrepresented minority physicians and physicians in training looking for community, mentorship, and more social outlets in Pittsburgh. My involvement with Gateway has helped to make Pittsburgh my home, and I look forward to amplifying that experience. I can be reached at racheltoney@comcast.net. For official Gateway inquiries, please email our executive assistant, Tamara Lunsford-Reese, at administration@ gatewaymedicalsociety.org.















www.acms.org/nominations/
Join the Board of Directors & ACMS House of Delegates! Nominations are due by: July 15, 2025.
The ACMS Nominating Committee is thrilled to announce six exciting opportunities to join the 2026 Board of Directors! We’re looking for enthusiastic, forward-thinking members to fill (5) three-year term seats.
• Influence and Impact: Shape the future of healthcare and make your voice heard in crucial decisions.
• Networking: Connect with leading professionals and create invaluable relationships.
• Professional Development: Gain leadership experience and new skills that will propel your career forward.
• Personal Fulfillment: Make a difference in your community and be part of something bigger.
Key Details:
• Meetings: Four times a year (quarterly) with a preference for in-person attendance.
• Special Meetings: Occasionally, extra meetings may arise, adding a dynamic twist to your role.
• Eligibility: Open to all ACMS physician members in good standing.
Join the ACMS Delegation to the PA Medical Society House of Delegates on October 22 - 25, 2026.
• Make a Difference: Play a key role in shaping policies that affect the medical community.
• Grow Your Network: Meet and collaborate with peers and leaders in the field.
• Boost Your Career: Enhance your resume and gain valuable experience in governance.
Key Details:
• Delegates: Serve for two years (up to three consecutive terms).
• Alternate Delegates: Serve for one year with unlimited consecutive terms.
• Attendance: In-person participation is highly encouraged to make the most of this experience.
To nominate yourself or a colleague, use our easy online submission portal by visiting www. acms.org/nominations/. For any questions, reach out to ACMS Executive Director, Sara Hussey at shussey@acms.org or Kirsten D. Lin, MD – Nominating Committee Chair and ACMS President-Elect kdlin8@gmail.com.
Don’t miss this chance to elevate your career and contribute to the medical community in a meaningful way. Step up and make a difference. This next seat could be yours!

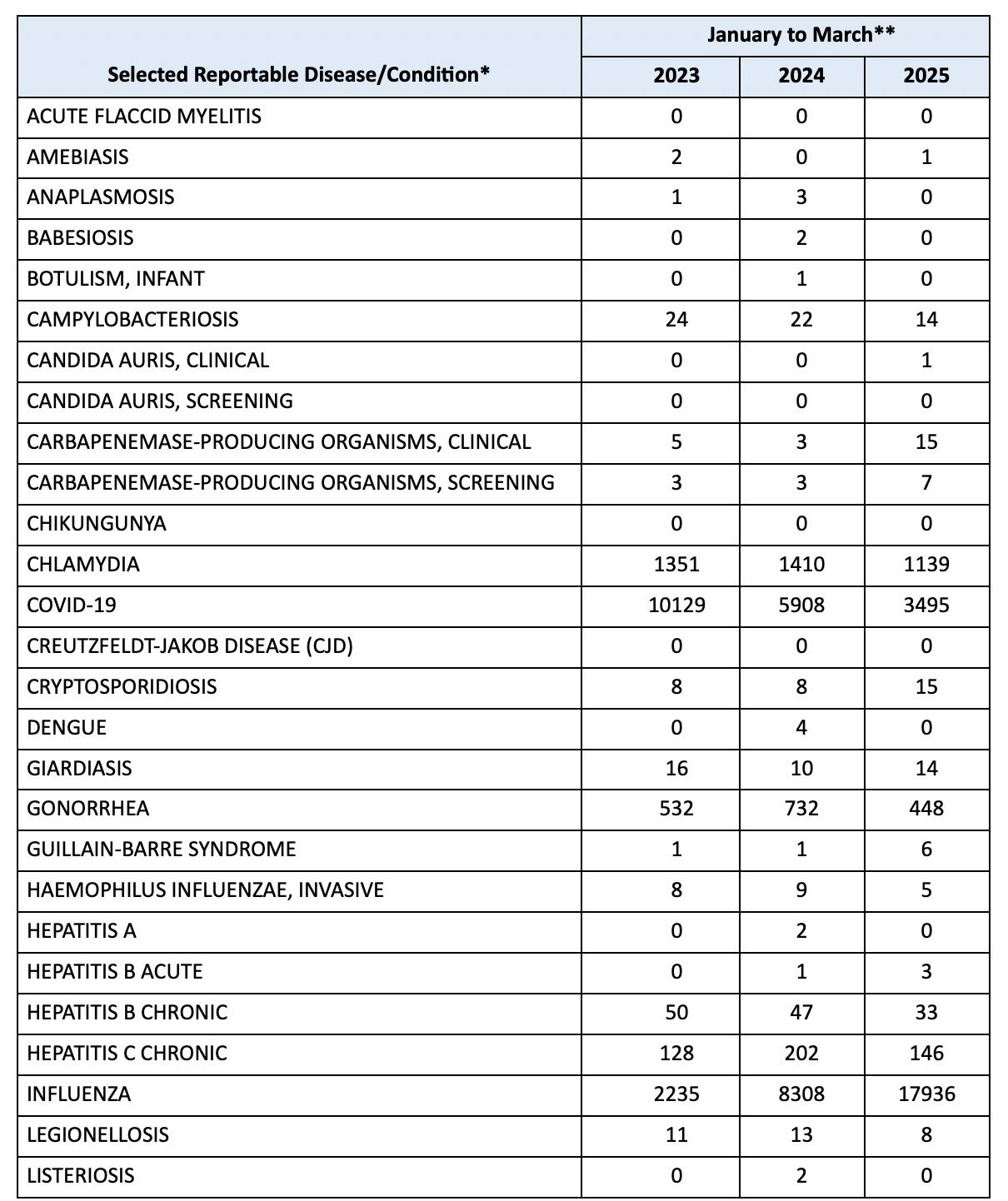

* Case classifications reflect definitions utilized by CDC Morbidity and Mortality Weekly Report.
** These counts do not reflect official case counts, as current year numbers are not yet finalized. Inaccuracies in working case counts may be due to reporting/investigation lag.
NOTE: Disease reports may be filed electronically via PA-NEDSS. To register for PA-NEDSS, go to https://www.nedss. state.pa.us/NEDSS. To report outbreaks or diseases reportable within 24 hours, please call the Health Department’s 24-hour telephone line at 412-687-2243.
For more complete surveillance information, see the Respiratory Virus, Infectious Disease and HIV/STI dashboards.
The Elizabeth R. Sagan, MD, Endowed Chair of Female Urology Established at Pitt
The University of Pittsburgh School of Medicine has announced the establishment of the Elizabeth R. Sagan, MD, Endowed Chair of Female Urology, honoring a trailblazing physician whose career changed the landscape of urology in Western Pennsylvania.
Dr. Elizabeth Sagan, who passed away earlier this year, graduated from the University of Pittsburgh School of Medicine in 1979 and went on to become the region’s first female urologist. In 1990, she founded Pittsburgh’s first women-exclusive urology practice, cementing her legacy as a pioneer in her field. Dr. Sagan was a past ACMS member and a past officer of the Pittsburgh Urological Association.
This newly established endowed chair will strengthen the female urology program within the Department of Urology at Pitt while advancing one of Dr. Sagan’s greatest passions— mentoring the next generation of women in medicine.
To date, $2.1 million has been raised for the initiative, including a generous
$1 million match from UPMC, surpassing the minimum threshold required to establish an endowed chair. The ultimate goal is to recruit a mid-career academic female urologist with a proven commitment to mentorship and advancing women in urology.
You can support this important legacy by contributing to the fund: https:// lnkd.in/g8-y4gSq
Dr. Sagan’s full obituary can be read at: bit.ly/sagan-obit
Dr. G. Alan Yeasted Honored
In April, G. Alan Yeasted, MD, Chief Medical Officer Emeritus of St. Clair Health was officially elected to Mastership with the American College of Physicians (MACP)! One of the field's most prestigious awards, Master status signals integrity, the utmost professional behavior, excellence in the practice of internal medicine, and significant impact on the profession.
Throughout his tenure as a physician, Dr. Yeasted has balanced his commitment to patient care with a passion for service and advocacy.
Please join us in congratulating Dr. Yeasted!


The Pennsylvania Medical Society (PAMED) has recognized Dr. Aaron Grand, of the Hand & Should Center in Wexford, PA, with their Everyday Hero Award. This award celebrates physicians who exemplify extraordinary commitment, compassion, and resilience in their daily practice, often going above and beyond to improve patient lives and community well-being.
Dr. Grand’s peers have consistently recognized his excellence, with Castle Connolly and Pittsburgh Magazine naming him a “Top Doctor” in Hand Surgery annually since 2021.
The Everyday Hero Award underscores Dr. Grand’s unwavering dedication to patient care, medical education, and humanitarian efforts. His multifaceted contributions embody the very essence of the award, highlighting the profound impact one physician can have both locally and globally.
To learn more about the Everyday Hero Award and to nominate a colleague visit: https://www.pamedsoc.org/ membership/awards

By: MJ Lerma, MPH – Policy/Administrative Intern
Over the past several months, MJ Lerma—a recent graduate from Pitt Public Health with a Master’s in Health Policy and Management—has brought energy, insight, and a fresh perspective to ACMS through her internship. Her column, MJ’s Q&As, featured interviews with a wide range of healthcare professionals, highlighting voices and experiences that matter to our physician community. As her internship wraps up, we’re flipping the script: in this special edition, MJ reflects on her time at ACMS, what she’s learned, and her hopes for the future of public health. You can connect with her at www.linkedin.com/in/mjlerma
What part of your internship are you most proud of?
I am the most proud of the interviews and articles. Highlighting diverse voices in healthcare, from high school students to physicians, and bringing policy discussions into a space where they resonated with physicians was incredibly rewarding. Performing these interviews and reflecting on the conversation I had while writing reinforced why I’m passionate about bridging policy with real-world impact.
What’s one challenge you encountered during your time at ACMS, and how did you navigate it?
One challenge was distilling complex health policy topics into accessible, engaging content for ACMS members. Talking in person and reading exactly what they have said written down doesn’t always make a lot of sense, but there is always a story in their words. I navigated this by focusing on practical
takeaways, prioritizing clarity, and always being open to feedback
Which interview from your Q&A series stood out to you the most, and why?
One of my favorite interviews was one I had with Dr. Iulia Vann. During these times of what feels like constant flux, it was very comforting to hear from one of the leading public health professionals in Allegheny County about hope. I remember being a little nervous going to her office, but she was so kind and personable once we met. She gave me great insight into the Allegheny Health Department and what their priorities are—from clean air to transparency in messaging.
Another interview that stands out to me is the last one that I conducted with the Avonworth High School seniors and their teacher. Educating the youth and opening different pathways and opportunities for them is so valuable. I liked this interview because the students and their teacher were so much fun to talk to and so obviously passionate about what they were learning and where they were heading.
How has this experience shaped your vision for your future in public health?
Working with ACMS has reinforced the importance of bridging policy with the everyday realities of physicians and patients. One of the things that surprised me most was just how connected medical societies are to advocacy work and how much influence they can have beyond individual patient care. Seeing firsthand how physicians engage with systemic challenges
deepened my commitment to making health policy both practical and equitable. It also solidified my desire to work at the intersection of policy and implementation—where real impact happens.
What’s one issue in public health you’re especially passionate about tackling in your career?
One issue in public health I am especially passionate about tackling is health misinformation. Right now, especially on social media platforms, health misinformation is prevalent and dangerous. I hope to improve health and well-being by increasing trust and focusing on resilience in communities.
How would you describe your growth—from your first day at ACMS to now?
This internship has been really educational and fun. One of my favorite events was the ACMS Awards Night at Acrisure Stadium. The venue was, of course, my favorite part, but it was also nice to meet so many passionate people. I would definitely recommend pursuing an internship at a medical society or professional organization. My time at ACMS has been fruitful with experiences working with different types of people on a variety of projects. I had the flexibility and agency to choose what I wanted to work on and what skills I wanted to develop. I have grown so much professionally and personally in my role, and it’s been a lot of fun working with Sara, Mel, Haley, Liz, and Nadine. They are all so intelligent and strong, and I have learned a lot working with them.

By: Anthony Kovatch, MD
"In the future, everyone will be world famous for 15 minutes."
--quote misattributed to Pittsburgh native and Pop icon Andy Warhol; in actuality, the phrase “15 minutes of fame" was first printed in the program for a 1968 exhibition of Warhol’s work in Stockholm, Sweden
The race had an ominous takeoff for me as I was dead last to cross the starting line, bidding farewell to the port-a-johns lining the starting corals and internally reciting a brief prayer for safety. I argued to myself that 80% of success is just showing up and that I had “only” 7 hours equivalent to a 16 minute per mile “turtle” pace from this point to fulfill my intention of pounding the pavement to the finish line as inconspicuously as possible in my old age.
I would bet my bottom dollar that the thousands of runners (and walkers) who participated in the 2025 Pittsburgh Marathon and Half Marathon on May 4th would agree that the most humorous and inspiring moment of the race was reading the banner displayed in the Southside that read:
The marathon distance has officially been changed to 28.8 miles (rather than 26.2 miles) due to the recent tariffs imposed by President Trump!!
For most of us, this assertion provided some comic relief to the physical and psychological stress; however, little did this 73-year-old veteran of TNTC half and whole marathons know that his career as a competitor was still in its formative stage! What was to transpire would
add new meaning to the conviction of Brazilian author Paulo Coello voiced in “The Alchemist”:
"And when you want something, all the universe conspires in helping you to achieve it."
It would be more than I could imagine, even in my wildest dreams something of strange magic, inscrutable synchronicity perhaps even in the realm of the miraculous! Because of anticipatory anxiety about not running a full marathon in 1 ½ years, I signed up only about a month before the event but was assigned the low number 711—the so-called lucky “angel number,” that signifies a positive new beginning, good fortune, individuality, and appreciation for blessings. Despite this “blessing,” I was disappointed that my submission for identification on my bib “Slowvatch” (a self-invented moniker and feeble attempt at humor) was rejected by some computer. I argued to myself that technology is my sworn enemy and simply changed it to the mundane equivalent “Slow Tony”! Little did I know this change to something more easily readable would “make all the difference”!
I likewise was disappointed when the crowd of half marathon runners that had previously surrounded me during the first half of the race veered to the left on the bridge over the Mon River and I was immediately exposed as the lone runner (some might say “walker” at that point) on the right lane of the bridge heading up the imposing “hill to Magee” to proceed to the second leg of the marathon. As I crossed the halfway marker as a “lone wolf” with the rest of the field well ahead of me, the “sweeper”

motorcade---an ambulance, the yellow bus that picks up those who “run out of steam,” and several cop cars that marshal the reopening of the roads planted itself at my heels and escorted me the final 13.1 miles to the finish line! I often was startled from my running “slumber” by the revving of the vehicles’ engines. “Was that intentional?” I mused to myself.
This entourage and the “Slow Tony” designation on my lucky bib made me stand out like a monkey that had escaped his cage at the zoo in Hiland Park, and I was accosted by an explosion of high-fives and shoutouts by the remaining thousands of spectators who were compelled to verbally propel this hobbling underdog to the finish line before he might bail out and take a seat on the bus—a gesture of resignation! The cheering magnified during the last mile; despite all this inspiration, I was unable to sprint
and pass any of my fellow travelers and indeed crossed the finish line dead last—as my “game face” transmogrified into an almost psychopathic smile. Even the bananas and oranges had been depleted. Fortunately, there was still one of the elaborate, dazzling medals left for yours truly!
I completed my personal 28.8-mile race as I wearily lumbered an extra mile or more back to my car in the Northside ....at the same 15 (or rather 16) minute pace that I had maintained throughout the true marathon. I had no idea when I trudged past the Warhol Museum that my “15 minutes” of fame would be eagerly waiting for me in the ensuing days. I finally found my car thanks to the kindness of strangers who pointed out to me the location of the Croatian Center which I had used as a reminder; I had not realized that its signage was hidden from street view!
The rest is history! Why the smiling face of the last runner to waddle across the finish line “went viral” remains a mystery to me. Perhaps it was the remembrance of pugilistic New York Yankees manager Leo Durocher’s infamous quote “Nice guys finish last” that truly went viral in a world that is in the process of recovering its kindness! Whether I wanted it or not, I was miraculously blessed with celebrity status, which no doubt will be fleeting. I must effusively thank everybody who graciously offered their inspiring cheers and kind social media comments. If the Divine Powers are willing, I will see you all on the same course in 2026. Until

that time, we must continue to believe in miracles:
“The whole world is a series of miracles, but we’re so used to them we call them ordinary things.”
--Danish master of the fairytale Hans Christian Anderson
….and equally to believe in the solemn conviction of George Sheehan (1918-1993) cardiologist, writer, father of 12, and running guru who remains an inspiration to many of us who took up the physical, mental, and spiritual challenges of long-distance running in our 40’s and 50’s and beyond:
“No matter how old I get, the race remains one of life's most rewarding experiences. My times become slower and slower, but the experience of the race is unchanged: each race a drama, each race a challenge, each race stretching me in one way or another, and each race telling me more about myself and others.”
“The distance runner is mysteriously reconciling the separation of body and mind, of pain and pleasure, of the conscious and the unconscious. He is repairing the rent and healing the wound in his divided self. He has found a way to make the ordinary extraordinary; the commonplace unique; the everyday eternal.
--from “Running and Being: The Total Experience” by George Sheehan




By: Chaise Stiteler, PharmD and Alexa Wardoclip, PharmD, BCPS
Background
It is estimated that approximately 10% of adults living with hypertension, are suffering from resistant hypertension.1 Aprocitentan (Tryvio®) is the first and only dual endothelin antagonist that has undergone FDA-approval for resistant hypertension, where blood pressure cannot be controlled with first line antihypertensives agents.2 This approved medication works by blocking the endothelin pathway, which is a new mechanism for an antihypertensive medication approved in over 40 years . The current ACC/ AHA guidelines recommend utilizing a mineralocorticoid receptor antagonist, such as spironolactone or eplerenone, in patients with uncontrolled hypertension that are on 3 different antihypertensives, one of which including a thiazide diuretic.3 The mineralocorticoid receptor antagonists carry adverse reactions, such as hyperkalemia, which need to be considered when prescribing these medications to patients. It is theorized that the endothelin pathway is activated in resistant hypertension. This is especially true in African American patients, patients with obesity, obstructive sleep apnea, diabetes, or chronic kidney disease. Aprocitentan was developed and approved as an alternative approach to treat resistant hypertension.
The endothelin pathway focuses on enhancing previous pathways that are a part of the current standard of care, such as regulation of salt and water retention, as well as in preventing cardiac remodeling. This medication
works on both the endothelin (ET- A and B) receptors to prevent endothelin-1 (ET-1) from binding.4 ET-1 contributes to the development of hypertension by regulating vascular tone and blood pressure. It is a known vasoconstrictor peptide that causes activation with neurohormonal and sympathetic systems. It is known in human patients with hypertension that vascular ET-1 expression is increased which leaves the endothelin mechanism one of the only pathways left to target hypertension.
Although this is the first endothelin antagonist that has been approved for resistant hypertension, it is not the first that has shown to be efficacious in lowering blood pressure. Previously, endothelin antagonist bosentan and darusentan have shown a promising blood pressure lowering effect as an add on therapy to both resistant and chronic hypertension. By antagonizing the endothelial pathway, it is believed that the blood pressure lowering effect will show no neurohormonal reflux activation.
Based on data that was obtained from animal reproductive studies within this class of medications, aprocitentan has a black box warning for fetal toxicity, and is contraindicated in pregnancy. As of March 17, 2025, patients are no longer required to enroll in a risk evaluation and mitigation strategy (REMS) program and obtain a negative pregnancy test prior to starting, monthly during treatment, and one month after discontinuation of the medication. However, healthcare providers must enroll in a the Tryvio®
REMS program in order to prescribe the medication. There is a chance of decreased sperm count in males and is recommended that healthcare providers discuss this with patients prior to initiation.
Hepatotoxicity is an established risk with this class of medications, which includes aprocitentan. It is recommended to avoid this medication if AST/ALT are elevated >3 times the upper limit of normal, or if a patient has moderate/severe liver impairment (Child-Pugh Class B or C). The phase 3 clinical trial noted a potential decrease in hemoglobin and hematocrit in patients receiving the medication when compared to placebo but resolved once the medication was discontinued. The manufacturer does not recommend initiating aprocitentan in severely anemic patients. They also recommend checking hemoglobin prior to initiation of aprocitentan.
The most commonly reported adverse effect was fluid retention, which is dose-dependent and requires diuretic use to resolve. Fluid retention was most common in the older adult population and patients with chronic kidney disease. The manufacturer does not recommend aprocitentan in patients with heart failure NYHA stage III-IV, unstable cardiac function, or NTproBNP ≥ 500 pg/mL. It is not recommended to start this medication in patients with ESRD (eGFR < 15 mL/ min) or on dialysis.
Aprocitentan is proposed to be a well-tolerated oral medication. With the approved dose, the most common adverse effect of fluid retention
occurred in 9% of patients that received the medication, as compared to 2% of patients that received placebo. The second most common adverse effect that patients experienced was decreases in hemoglobin, which occurred in <4% of patients receiving the FDA-approved dosing.
Efficacy
The approval of aprocitentan in resistant hypertension was based on a multicenter, blinded, randomized, parallel-group, phase 3 trial. The current FDA-approved dose is 12.5 mg once daily given a previous dose-finding phase-2 trial, however, the PRECISION trial investigated placebo, aprocitentan 12.5 mg once daily and aprocitentan 25 mg once daily. This study investigated the use of aprocitentan as a fourth-line agent, in patients receiving amlodipine, valsartan, and hydrochlorothiazide.
A statically significant difference in office visit systolic blood pressure readings between aprocitentan 12.5 mg and placebo was found over a 4-week double-blind portion of the trial -15.3 mmHg vs -11.5 mmHg, (97.5% CI -6.76 to -0.82; p = 0.0042). Patients were placed in a 4-week withdrawal period, then received aprocitentan 25 mg daily or placebo for 12 weeks. Patients who received aprocitentan had lower inoffice systolic blood pressure readings (-1.5 mmHg) compared to placebo who had higher systolic blood pressure readings (4.4 mmHg), (95% CI, -7.94 to -3.71, p<0.0001). Patients did not experience hyperkalemia as a result of receiving aprocitentan.
Price
Aprocitentan’s retail price for a 30day supply is $926.59. However, there is a Tryvio® saving card available on the manufacturer's website that may be an option for patients with commercial insurance to pay as little as $10 for a 30-day supply. The prescriptions must be sent through Walgreens Specialty Pharmacy.
Aprocitentan is a once daily medication, dosed at 12.5 mg.This medication can be taken with or without food and must be swallowed
whole. Due to the long half-life of ~41 hours, if a patient does miss a dose, it is recommended to skip the missed dose and not take two doses in the same day. This medication lacks clinically significant drug-drug interactions.
Bottom Line
The endothelin pathway is a new mechanistic pathway for targeting uncontrolled hypertension. Aprocitentan (Tryvio®) has received the first FDA approval within this drug class. As hypertension is a leading cause of cardiovascular disease and mortality, it is important to control hypertension to reduce this risk. Aprocitentan is the first approved medication for hypertension treatment in the last 40 years, and the first antihypertensive medication that acts on the endothelin pathway. Aprocitentan is recommended for patients who are not adequately controlled on other antihypertensive drugs. Although this medication is welltolerated and taken once daily, patients of child-bearing potential require more extensive monitoring. There were statistically significant benefits in systolic blood pressure reductions in aprocitentan as compared to placebo in the PRECISION trial. While effective, this medication remains costly, but a one-time $10 discount card is available for a 30-day supply. The current treatment for resistant hypertension, mineralocorticoid receptor antagonist, comes with known risk of hyperkalemia which may make providers hesitant to prescribe based on patient’s potassium level. Therefore, patients in need of additional blood pressure lowering while on optimal therapy and with a risk of developing hyperkalemia, may benefit from aprocitentan due to the lack of hyperkalemia found in the phase 3 PRICISION clinical trial.
At the time of authorship, Chaise Stiteler, PharmD is a PGY-1 Pharmacy Resident at UPMC St Margaret and can be reached at stitelerc@upmc.edu. Alexa Wardoclip, PharmD, BCPS is a PGY-2 Ambulatory Care Pharmacy Resident at UPMC St Margaret and can be reached at wardoclipam@upmc.edu. Heather Sakely, PharmD, BCPS, BCGP provided editing and mentoring for this article and can be reached at sakelyh@upmc.edu.
1. Schlaich MP, Bellet M, Weber MA, et al. Dual endothelin antagonist aprocitentan for resistant hypertension (PRECISION): a multicentre, blinded, randomised, parallel-group, phase 3 trial [published correction appears in Lancet. 2023 Jan 28;401(10373):268. doi: 10.1016/S0140-6736(23)00119-8]. Lancet. 2022;400(10367):1927-1937. doi:10.1016/ S0140-6736(22)02034-7
2. Tryvio (aprocitentan) prescribing information. Radnor, PA: Idorsia Pharmaceutical, Lts; 2024, Sep
3. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2018 May 15;71(19):2275-2279. doi: 10.1016/j.jacc.2018.03.016]. J Am Coll Cardiol. 2018;71(19):e127-e248. doi:10.1016/j.jacc.2017.11.006
4. Angeli F, Verdecchia P, Reboldi G. Aprocitentan, A Dual Endothelin Receptor Antagonist Under Development for the Treatment of Resistant Hypertension. Cardiol Ther. 2021;10(2):397-406. doi:10.1007/s40119-021-00233-7
By: Nadine Popovich, Melanie Mayer and Haley Thon
Allegheny County Immunization Coalition (ACIC) — 2024-2025 Chair - Patrick Hussey, PharmD, MBA: This spring, ACIC proudly participated in several community outreach events, including the Health and Mental Health Family Wellness Event in Homestead, the August Wilson Birthday Celebration Block Party in the Hill District, and the Bible Chapel & Cornerstone Baptist Church Health Fair in Wilkinsburg. These events allowed us to engage directly with families, share vaccine education, and build trust in local communities.
Looking ahead, ACIC invites members and partners to our Quarterly Membership Meeting on Wednesday, June 19, 2025, from 9:00–11:00 AM, featuring guest speaker Biyanka Patel, MSL of Bavarian Nordic, who will present “Chikungunya – An Emerging Threat.” Registration opens May 8. We’re also excited to announce the 20th Annual Immunization Conference, happening Wednesday, November 5, 2025, at the Regional Learning Alliance in Cranberry Township. Stay tuned to www.immunizeallegheny.org for updates, registration, and sponsorship opportunities.
American College of Surgeons Southwestern Pennsylvania Chapter (ACS-SWPA) — 2025 President –Richard Fortunato, DO, FACS: The ACS Southwestern Pennsylvania Chapter is gearing up for its annual “Most Interesting Cases” event, taking place Wednesday, May 28, 2025, at the Kimpton Hotel Monaco in downtown Pittsburgh. This evening program features challenging and unique surgical cases presented by local
residents and reviewed by a panel of ACS Fellows. It’s a long-standing tradition that supports surgical education, peer connection, and professional development across our region.
Abstract submissions are due by May 16, and registration is open through May 23. While the event is primarily designed for surgeons and trainees, all ACMS members are welcome to attend and connect with the surgical community. Registration is free for residents, $25 for ACS members, and $50 for non-members.
To register or learn more, visit: https://alleghenycountymedicalsociety. regfox.com/acs-swpa-mostinteresting-cases
Pennsylvania Geriatric Society Western Division (PAGS-WD) — 2025 President - Heather Sakely, PharmD, BCPS, BCGP: The 33rd Annual Virtual Clinical Update in Geriatric Medicine was a tremendous success, with over 200 geriatricians joining online to learn, share insights, and connect with colleagues. This year, the course directors introduced a new thematic framework to guide the lectures and discussions: Fostering Age-Friendly Care through the 5Ms—Mentation, Medication, Mobility, What Matters Most, and Multicomplexity. Within each of these domains, expert speakers provided practical, clinically relevant insights across a wide range of topics essential to the care of older adults. Interactive Q&A sessions further enriched the learning experience. To review the CME/CEU process, please visit pagswd.org. CME credit will be available through May 28, but all
registered attendees will retain access to presentation materials until July 1.
We’re also excited to announce that the 34th Annual Clinical Update in Geriatric Medicine will return in person in 2026! The date and location are TBD but once finalized, all past attendees will be notified by email once details are confirmed.
The David C. Martin Award | The Awards Committee is pleased to announce that four outstanding students have been selected to receive honoraria to help offset the cost of attending the virtual AGS Annual Scientific Meeting, taking place May 8–10, 2025. Each recipient will present a poster based on the abstract they submitted. Congratulations to Anjana Mahesh, Joseph Shin, Naomi Shin, and Rutvi Chahal!




The Pittsburgh Ophthalmology Society (POS) — 2025 PresidentLaurie A. Roba, MD: POS Announces Appointment of Officers
The Pittsburgh Ophthalmology Society (POS) is pleased to announce the installation of Laurie A. Roba, MD, as President during the Society’s Annual Banquet held on March 20, 2025, at Hotel Monaco in Pittsburgh, PA. Dr. Roba will serve a two-year term (20252027).
An active member of the POS since 2004, Dr. Roba has previously served as Course Director for the Ophthalmic Personnel Program (2016–2019) and as Treasurer (2020–2025). She has been in private practice for 30 years in Fox Chapel, PA, performing a broad range of ophthalmic procedures including refractive cataract surgery, penetrating keratoplasty, PRK, PTK, and LASIK. Dr. Roba looks forward to working with the POS Board of Directors to uphold the Society’s tradition of excellence in providing high-level educational programming for its members through both the monthly meeting series and the annual meeting.
The Society also congratulates Eric
A. Pennock, MD, on his appointment as President-Elect. Dr. Pennock, a dedicated member since 2009, was elected at the January 2025 POS monthly meeting and will also serve a two-year term. He has significantly contributed to the organization, most notably as Membership Chair since 2018, and has been a frequent speaker at the Ophthalmic Personnel programs, most recently presenting in 2025. Dr. Pennock practices at Pediatric Ophthalmology and Adult Strabismus in Cranberry Township, PA.
Additionally, Jared E. Knickelbein, MD, PhD, has been appointed Treasurer, also for a two-year term. A longstanding member of the Society since 2016, Dr. Knickelbein previously served as Chair of Public Relations (2021–2023) and Chair of Provider Relations (2024–2025). He is a retina and uveitis specialist with Retina Vitreous Consultants, with locations in Monroeville, Bethel Park, Cranberry, Johnstown, Altoona, and Triadelphia, WV. Dr. Knickelbein received his BS in Biochemistry from Duquesne University and earned both his MD and PhD through the Medical Scientist Training
Program at the University of Pittsburgh School of Medicine. He completed his ophthalmology residency at the University of Pittsburgh Medical Center, where he served as Chief Resident, and pursued fellowship training in Uveitis, Ocular Immunology, and Medical Retina at the National Eye Institute. The Pittsburgh Ophthalmology Society is proud to recognize these outstanding leaders and looks forward to continued success under their direction and leadership.
